
Helen Schneider, Mndebele Jabulani, Ramphelane Morewane, Gio Perez
Primary health care (PHC), as envisioned by the 1978 Alma-Ata Declaration, has been a key pillar of South Africa’s health system since the advent of democracy. After the political transition in 1994, a number of PHC-related health policy measures were prioritised, most notably removing user fees for women and children under six years of age, subsequently extended to all public PHC services. During its first two terms of office (1994–2004), the new government also implemented an extensive programme of public PHC facility upgrading. The PHC approach was also enshrined in key health policy statements and legislation, starting with the White Paper on the Transformation of the Health System in 1997 and the National Health Act of 2003, which established the district health system (DHS) as the decentralised building block of the health system.
These measures established a sound basis in policy for the PHC system in South Africa, offering a comprehensive package of basic services including maternal, child and reproductive health, HIV and tuberculosis (TB) testing and treatment, screening and care for non-communicable diseases (NCDs) and treatment of common ailments1 South Africa is an outlier amongst low- and middle-income countries (LMICs) in having low levels of out-of-pocket health expenditure2.
Despite these gains, the rapid emergence of a catastrophic HIV/AIDS epidemic in the mid-1990s impacted severely on health system development. For at least a decade, HIV became an all-consuming and singular focus in South Africa, displacing attention away from the earlier processes of health system reform. The first critical gap was in the human resource dimensions of PHC – the failure to realign health professional education towards PHC, weak management and leadership, and inconsistent policy on mid-level and community-based cadres3. The second gap was in the establishment of a coherent and standardised DHS as the governance
mechanism for PHC and district hospitals. Overall, in this period, the PHC system offered an important safety net but was still characterised by highly uneven quality of care, low public participation and accountability, and a focus on disease treatment rather than prevention.
In 2010, following a visit to the Brazilian health system, the Department of Health adopted the national ‘PHC Re-engineering Strategy’ which, amongst others, formalised a national community health worker (CHW) programme referred to as the Ward-Based Primary Health Care Outreach Team (WBPHCOT) strategy4. The PHC re-engineering strategy became an integral part of a further set of comprehensive reforms in the National Health Insurance (NHI) proposals, which once again placed PHC and the DHS at the centre of the health system. An NHI Green Paper was issued in 2011, followed by a White Paper in 2015 and finally an NHI Bill5 tabled in Parliament in 2019. In the period 2012–2017, 11 (of 52) health districts were designated as NHI pilots across the country, where interventions targeting PHC system strengthening were implemented through conditional grants6, and are currently being scaled up to other districts. Reflecting emerging global agendas on the Sustainable Development Goals (SDGs), the social determinants of health also received attention in this period, with regulations on salt in processed foods and a sugar tax introduced.
These interventions formed the main elements of national policy and programming in the period under review (2015–2020). While these national processes were being implemented, nodes of PHC system innovations were emerging in districts and provinces across the country. These sub-national, bottom-up initiatives are rich in system learning that can inform and complement top-down system development and are reported as case studies of promising practices in this chapter.
The advent of the COVID-19 pandemic in March 2020 had major implications for the PHC system, diverting staff and services away from routine prevention and care and reversing health gains7. The pandemic also precipitated a severe economic and fiscal crisis that will impact on future funding. At the same time, the COVID-19 responses have promoted system innovation and catalysed new relationships and intersectoral action on health and new forms of working (including use of technology), which could be leveraged in future.
The chapter examines the significant contextual factors impacting on PHC in the period, key programmes and interventions implemented and the elements they address. Evidence on PHC performance and sub-national case studies of promising practices are then presented. These include the sub-district model in KwaZulu-Natal (KZN), community-oriented primary care, the 3-feet model in Mpumalanga and Limpopo, and a community-led clinic monitoring programme, Ritshidze. The chapter concludes with a summative assessment of PHC in South Africa, based on the core strategic levers of the World Health Organization (WHO), and the way forward.
Developments in South Africa have occurred against a backdrop of renewed global impetus for PHC as part of Universal Health Coverage (UHC) and the SDGs, culminating in the Astana Conference and Declaration on PHC in 2018, commemorating the 40th anniversary of the landmark 1978 Alma-Ata Conference and Declaration. The Astana Declaration reaffirmed the founding values and principles of the Alma-Ata Declaration, asserting health as a human right and PHC as ‘the cornerstone of a sustainable health system for universal health coverage and health-related Sustainable Development Goals’8. The Declaration recognised a vastly changed context and the ongoing challenges confronting PHC systems9, including:
• new disease burdens – while maternal and child mortality has declined, NCDs, mental health, violence and emergence of new pandemics have increased;
• rapid developments in information technology;
• growing environmental pressures from climate change and urbanisation;
• increasingly pluralistic health systems; and
• deepening inequities – between and within countries.
In 2020, the WHO and the United Nations Children’s Fund (UNICEF) launched a follow-up ‘Operational Framework for Primary Health Care’ proposing three factors as the basis of health and well-being (Figure 4.1): (i) integrated primary care and essential public health functions resulting in improved access, utilisation and quality; (ii) empowered people and communities resulting in improved health literacy, participation and care seeking; and (iii) multisectoral policy and action resulting in improved determinants of health10.

4.1 Primary health care components (copied from: WHO/UNICEF, 2020)
These components are made possible by fourteen ‘core strategic and operational levers’ outlined in Table 4.1.
Figure 4.1 Core strategic and operational levers for PHC (Source: WHO & UNICEF, 2020)
Core strategic levers
• Political commitment and leadership
• Governance and policy frameworks
• Funding and allocation of resources
• Engagement of community and other stakeholders
Operational levers
• Models of care
• Primary Health Care workforce
• Physical infrastructure
• Medicines and other health products
• Engagement with private sector providers
• Purchasing and payment systems
• Digital technologies
• Systems for improving quality of care
• PHC-oriented research
• Monitoring and evaluation
This chapter reviews progress and challenges of PHC in South Africa since 2015, taking the Astana Declaration and the PHC Operational Framework as its starting points, namely, that PHC:
• is the core pivot around which the rest of the health system turns;
• has a population orientation – starting with the smallest political unit, the ward;
• includes community-based services, PHC facilities and hospitals in coordinated systems of integrated delivery;
• provides essential public health functions;
• relates to the sub-district and district structures and processes, which provide the governance and support mechanisms, and which are coterminous with local government and other sectors;
• is mandated to interact with other sectors in a place-based approach; and
• is held accountable through community participation.
These are enabled through core strategic and operational system levers outlined in Table 4.1.
The assessment of progress and performance of PHC in the period draws on several sources. We conducted a non-exhaustive search of publications on PHC in South Africa since 2015, consulted websites and submissions to the NHI parliamentary hearings, and reviewed major strategies developed or evaluations conducted in the period. A key report in the period was the evaluation of PHC system strengthening in the NHI pilot sites6. The chapter also draws on a case study of South Africa’s PHC system conducted for WHO’s Alliance for Health Policy and Systems Research in 20161, which formed part of a subsequent multi-country comparative analysis2 .
Developments related to NHI have been the most significant macro-level factor impacting on PHC. The 2015 White Paper considered PHC as the ‘heartbeat of NHI’, and proposed Contracting Units for Primary Health Care (CUPS) and District Management Offices as the basic building blocks of the new health system11. With the NHI Bill still currently under consideration by Parliament, these system reforms remain paper proposals but will have major implications if eventually implemented. The 11 NHI pilot districts referred to earlier were established while these policy and legislative processes were unfolding. Importantly, the NHI pilot sites ‘did not involve developing new funding arrangements for health care in South Africa, but rather piloted various health system strengthening interventions focused at the primary health care (PHC) level’6
The second key development was the announcement of a universal HIV ‘test and treat’ policy in 2016, with expanded budget allocations, and the deployment of donor-funded (principally the United States President’s Emergency Plan For AIDS Relief (PEPFAR) and the United States Agency for International Development (USAID)) partners to support districts. Several of the health system strengthening interventions implemented in the pilot districts were enabled through these partnerships, aimed at mainstreaming the HIV programme while benefiting the PHC system more generally.
After a 15-year period of expanding budgets and per capita expenditure on public sector PHC, the introduction of austerity measures from 2019/20 onwards reversed this pattern of growth. Declining budgetary allocations pose a significant threat to the future development of PHC, especially in the stabilisation of components such as the WBPHCOT, and in ensuring greater equity. Community health workers emerged as key players in the public health response to COVID-19, yet remain poorly managed and remunerated1
A key development in the period was the widely consulted 2030 Human Resources for Health (HRH) Strategy and associated 2020/21–2024/5 HRH Strategic Plan12. This Strategy makes extensive recommendations on all aspects of HRH development in South Africa, emphasising the critical importance of this core system function for the future development of an NHI. The report specifically assesses current availability and distribution of, and models future HRH needs for HRH public PHC, identifying significant shortfalls and inequities.
In 2017, a South African Lancet National Commission on quality of care was launched following the Lancet Global Health Commission on High-Quality Health Systems in the Sustainable Development Goals (SDG) Era. The report13 has helped to elevate the focus on quality in the health system, highlighting, in particular, the role of people in health systems, i.e. their availability, management and motivations.
In 2019 the president launched the District Development Model (DDM). The DDM is ‘an approach by which the three spheres of government and state entities work in unison in an impact-oriented way, and where there is higher performance and accountability for coherent service delivery and development outcomes’, in order to better respond to the major structural challenges of inequality and poverty. The COVID-19 emergency revealed the necessity for intersectoral collaboration and in some localities, mandated mechanisms such as the Joint Operation Centres catalysed local relationships which could serve as a resource for future place-based approaches to the social determinants of health14.
An overarching feature of the period, compounding fiscal constraints, was a general crisis of governance at provincial level, a high turnover of political and senior administrative leadership, and loss of institutional memory and capacity for stewardship of the health system15. This unstable provincial context resulted in the selective centralisation of decision-making to the national level, notably in the systems interventions linked to NHI pilots, but also hampered the coherence, coordination and integration of initiatives in PHC described in the next section.
In this section we review key initiatives to strengthen PHC over the period, including a centrally funded portfolio of interventions introduced through the PHC Re-engineering Strategy and subsequently as part of the NHI pilot sites and other processes.
Over the last decade the WBPHCOTs have emerged as a central component of the PHC system in South Africa. In 2019, there were 54 000 CHWs in the public health system, constituting 22% of the total and 47% of the PHC workforce, respectively12. These CHWs have a comprehensive scope, fulfilling promotive, preventive and adherence support functions, are supervised by nursing cadres (outreach team leaders) and relate closely to the nurse-based PHC system. The CHWs have become a vital part of new systems of community-based distribution and follow-up for chronic diseases (communicable and non-communicable) and are credited in part for the pattern of reduced PHC facility utilisation over the last five years. Community health workers were a highly visible part of the early COVID-19 pandemic response, as the mainstay of community screening and testing, and supporting the home delivery of chronic medication to patients in households to limit their exposure through health facilities16
The WBPHCOTs grew into a CHW programme from an initially unregulated, highly diverse and fluid community-based care and support system that emerged as part of the HIV/AIDS response from the mid-1990s onwards. However, over the ensuing years the community-based sector struggled to shift from a loose and relatively informal, disease-specific infrastructure to a comprehensive CHW programme, adequately funded, supported and integrated into the health system. In the context of a widening fiscal crisis, frequent lip service to the value of CHWs has not been matched by political, budgetary and organisational commitments. Thus, despite their numerical importance (nearly half of all PHC workers), CHWs constituted only one-tenth of the total PHC health workforce expenditure in 2019, coordinated national and provincial governance of the programme has remained weak, and levels of coverage, recognition, training and supervisory and support systems are highly uneven across the country17
Nevertheless, over the 2015–2019 period, a number of developments signalled that the status of WBPHCOTs may be shifting towards greater formalisation and integration into the health system. The teams formed one of the key components of the intervention package in NHI pilot sites, benefitting from additional resources to expand coverage and team leader support. In 2018, the National Department of Health (NDoH) issued, for the first time, a ‘policy framework and strategy’ for WBPHCOTs, seeking to create
a standardised programme design, laying out norms, scopes of work, roles of different players, mandates and monitoring systems for the country18. The training curricula and processes were redeveloped and a CHW unit established within the DHS cluster to steer the programme nationally.
Although the first goal of the WBPHCOT policy framework is to ‘Improve the working conditions of WBPHCOTs’, it remains silent on questions of CHW remuneration and the sources of funding for CHWs. In practice, CHWs have been paid through a variety of short-term contracting arrangements determined at provincial level – whether through non-governmental organisations (NGOs), third party ‘paymasters’ or the government payroll system. In 2018 the national Public Health and Social Development Sector Bargaining Council signed an agreement with the NDoH and unions to standardise remuneration of CHWs across the country at the minimum wage, with the view to eventually integrating CHWs into the public sector. These bottom-up pressures on conditions of service have been a key driver of formalisation.
In South Africa, an emerging evidence base has provided evidence on the effectiveness19, affordability20 and a high benefit-to-cost ratio of 3.421 of an adequately supported CHW programme. A nationally commissioned investment case estimated that ‘a properly resourced, scaled-up WBPHCOT programme could save 200 000 lives and more than five million productive disability-adjusted life years over 10 years. The multiplier effects of saved lives and employment creation would inject billions of rands of additional revenue into the economy’4
District Clinical Teams (DCSTs) were established as a system of clinical governance, mentorship and quality improvement of districts across the country in 2012, first as part of the PHC Re-engineering Strategy and then subsumed under NHI. These teams had a focus on maternal, newborn and child health, and were to include an obstetrician and gynaecologist, a paediatrician, a family physician, an anaesthetist, a midwife, and a professional nurse in each of the 52 districts. Establishment of DCSTs was slow – after 18 months only 56.4% of posts had been filled across the country, with particular challenges in filling medical specialist posts24. Experiences of the DCSTs have been uneven across the country. When linked to wider systems of clinical governance, DCSTs have been credited with significant gains in maternal and child health outcomes23-26. However, an evaluation of the DCST component in the NHI pilot sites found there was uncertainty of roles (especially with parallel maternal-child health programme structures), variable performance, questionable cost-effectiveness, and crowding out of systems of outreach and support from regional hospitals6,26. The teams were initially funded by conditional grants with the expectation that they would be absorbed into district budgets through the equitable share. One KZN district estimated that the seven members of the DCST constituted 15% of the District Health Management Office budget. Some provinces decided to do away with DCSTs, replacing these with specialist outreach and support through regional and tertiary hospitals, and absorbing nurse specialists into programme structures.
The Ideal Clinic Realisation and Maintenance (ICRM) programme is a PHC standardsetting and quality assurance programme, established in 2013 as a system of auditing and response, intended to improve the PHC infrastructure in preparation for NHI. The purpose is to ‘assure the public that the specific Health Establishment is safe and delivers minimum standard of care as measured against the norms and standards set by the NDoH’iii
In 2015, after an initial period of piloting, the highest health sector decision body – the National Health Council – mandated implementation of the ICRM across the public health system. By 2019, audits had been conducted in all districts and 1 501 (43%) of PHC facilities had retained Ideal Clinic status.
A five-year review of the ICRM conducted in 2020 reported the following achievements of the Ideal Clinic programme:iii
• More than 50% of PHC facilities had achieved Ideal Clinic status (even if some had not maintained this status)
• The programme had been aligned with other processes – notably the Office of Health Standards Compliance and District Health Plans
• The auditing processes are supported by software (including mobile applications), and regularly updated. The Ideal Clinic Manual is regularly updated (Version 19 appeared in May 2021)
• The Ideal Clinic portal provides links to a range of handbooks, guidelines and catalogues
• Resources were mobilised for equipment purchases
• Successes had spurred the development of an Ideal Hospital programme
• The process has been supported by funds from partners
The Ideal Clinic runs the risk of all externally mandated audit systems in organisations –that is, becoming a compliance mechanism rather than a driver of real change, especially if the mechanism does not reflect the reality of practice. The evaluation of the NHI pilot districts alluded to this phenomenon when it reported that ‘facilities would purchase equipment irrespective of the need, in order to reach ideal clinic status’6. Such ‘gaming’, producing ‘an illusion of compliance’, has been reported by others28,29 studying frontline practices associated with the Ideal Clinic. The transaction costs of repeated assessments are high with ‘short implementation windows in which facilities have to adapt to new requirements to achieve the desired ideal clinic status’6. The onus on facility managers to resolve problems of resourcing and infrastructure outside of their decision-space is demotivating28
The Ideal Clinic process reflects a general trend towards greater use of audits and expectations of transparency, which is likely to increase with the advent of the NHI
i See for example: https://www.iol.co.za/news/politics/community-health-workers-to-waitanother-year-for-permanent-employment-26cf6114-c3ba-48a0-a502-4c43bfe3bcac
ii Mkhize, NC and Msimango, P. Sub-District Model Presentation to DHMT, King Cetshwayo District, 30 September 2019 (PowerPoint provided by J Mndebele).
iii Morewane, R. ICRM 5-Year Review: Overview. PowerPoint presentation, 26 February 2020 [available at: www.idealhealthfacility.org.za/].
and the introduction of ‘purchaser–provider’ split arrangements. Intensification of audit and compliance can, however, be counterproductive. An inventory of accountability mechanisms for maternal, neonatal and child health in one district counted a total of 19 different direct or indirect mechanisms, often duplicating and generating accountability overloads29
As part of the NHI pilot site intervention package, in 2014, the NDoH introduced a Central Chronic Medicines Dispensing and Distribution (CCMDD) programme to support adherence and retention in care for HIV and other chronic NCDs. The CCMDD enables follow-up and distribution of medication to stable patients through facility fast queues, community adherence clubs, retail pharmacies and other novel ‘pick-up points’ (PUPs).
By 2019, the CCMDD programme had expanded to all the districts (except in the Western Cape which had an existing programme), was present in close to 3 500 facilities, had registered more than 2 000 external PUPs and more than 2 million patients were being followed up through the system30. Just over half of patients were collecting medication from fast lanes in PHC facilities, 13% through adherence clubs and 35% from external PUPs. Project Last Mile supported the development of external PUPs such as ‘smart lockers’ through private sector engagement. Successful implementation of the CCMDD has been attributed to ‘strong political leadership and will’ and ‘reliable data to support continued implementation’6 According to patient evaluations, the CCMDD facilitated access, reduced waiting times in health facilities and created new medicine collection options33. However, patients also indicated receiving inferior care in private facilities compared with paying patients. Another challenge of a contracted-out system of PUPs is the tracking of patients in two parallel systems and the lack of mechanisms to trace those lost to follow-up in the private sector. The reliance on a few central contractors is also regarded as a risk and requires capacity for managerial oversight and monitoring6
During the COVID-19 pandemic, health services in the Cape Town and Tshwane metros further extended their community-based distribution systems for chronic disease care to include home delivery through CHWs16,32. Within one month of the initial lockdown, the Cape Town metro had distributed 184 000 parcels to patients with chronic diseases who were ‘therefore protected from exposure to COVID-19 at health facilities and public transport’16.
In 2012, the national government launched an eHealth Strategy. In the first step, a Health Patient Registration System (HPRS) was developed and introduced into 657 NHI pilot site PHC facilities as part of a broader ehealth programme, that included installation of computers and Wi-Fi connectivity, rationalisation of existing registers and plans for interoperability between electronic systems (e.g. electronic antiretroviral therapy registers and the district health information system). By 2019 close to 3 000 PHC facilities and nearly 70% of the population was registered on the system33
However, at the time of writing, the HPSR has not progressed beyond patient registration in PHC facilities, and has yet to be integrated with other ehealth and hospital information systems or with the WBPHCOTs34. The WBPHCOTs conduct household registrations and are playing increasingly significant roles in chronic disease follow-up, but their activities are not captured in NHI. Other key infrastructural challenges associated with HPSR implementation include inadequate computer supplies and difficulties with maintenance, safety of equipment and poor network connectivity6. In a survey of facility managers in NHI pilot sites, only 30% reported reliable network connectivity, with the remainder reporting either ‘somewhat reliable’ (52%) or ‘completely unreliable’ (18%) network connections6
Another ehealth innovation – the Stock Visibility System (SVS) – was introduced in NHI pilot sites to support real-time monitoring and reporting of essential medicines and vaccines stocks. The SVS connects players across the supply chain and its purpose is ‘to improve oversight of stock through an electronic stock monitoring system, and thereby reduce stock-outs by allowing for appropriate and timely ordering’6. The SVS was scaled up nationally, reaching over 90% coverage of PHC facilities by 2017/18. Nearly half the 49 managers interviewed in NHI pilot sites reported ‘a substantial decrease in stock-outs as a result of SVS’. The SVS, as with the HPRS, remains a siloed innovation, and shares the same broader challenges of other ehealth interventions in PHC – ensuring stable and functioning infrastructure (in this case mobile phones), securing interoperability, and convergence of data sources into an ‘ehealth enterprise architecture’ for NHI33
Although focused on public sector systems strengthening in the first phase, the NHI ultimately aims to integrate private and public sector provisioning into one health system, funded by a single payer (the NHI fund). Primary care in the private sector is provided in the main through private general practitioners (GP), working in solo or small group practices. GPs are widely available in the private sector, estimated to be 3–4 fold that of the public sector35. Private GP practices typically cater to both insured and uninsured (cash paying) populations, and account in part for out-of-pocket payments for health care in South Africa.
The NHI pilot site interventions have experimented with forms of private sector contracting, which include the use of private sector supply chains and providers in the CCMDD programme. A second initiative was to contract-in private GPs to provide care in public sector PHC facilities. By 2018, 330 GPs had been contracted to work in PHC facilities in the pilot sites6. Three contracting mechanisms emerged – direct contracting with the NDoH, contracting via an intermediary (a national GP organisation) and contracting with the district authority35. Despite the establishment of a dedicated national contracting unit, capacity for oversight and monitoring from this level proved to be limited. Uptake of GP contracts was low in many sites, and the monitoring of claims poor, resulting in over-expenditure on this component of the NHI grants6. The most decentralised model worked best but rested on a pre-existing track record of successful contracting by districts35. The GP contracting initiative was thus not extended beyond the pilot phases.
The experiences with GP contracting highlight the inherent complexity of contracting for health care, and the risks facing a future NHI premised on the purchaser–provider spilt model. Engaging the private sector – in whatever capacity –requires high levels of decentralised capacity for monitoring and oversight in public authorities, which is as yet not present at district level.
During the period under consideration, PHC in South Africa benefitted from significant system strengthening initiatives, supported by ring-fenced budgets under the umbrella of NHI. The consolidation of initiatives in NHI pilot sites, considerable technical and other support from partners and ring-fenced funding through conditional grants resulted in successful implementation of many of the interventions, some beyond the pilot sites. Collectively, these interventions engaged all the operational levers proposed by WHO/UNICEF (Table 4.2) and have contributed to improved access, quality and standardisation of PHC.
This considerable portfolio of new technology and systems was however constrained by weak strategic levers, in particular, the growing fiscal constraints and budgetary and governance crises besetting many provinces. While the centralisation of funding, planning and donor support meant that provinces could be bypassed, this is unlikely to be sustained in the long run. The ultimate success of the interventions rests on background capacity (staffing, infrastructures, governance, etc.) of provincial health systems. In this regard, the next section discusses metrics of overall performance of the PHC system.
The orientations of interventions of this period also reflected the central preoccupations of NHI – namely ensuring the provision of essential primary care. There were no strategies specifically focused on strengthening public participation and accountability or advancing intersectoral collaboration, despite national initiatives such as the DDM. However, while the national strategies described above were being introduced, nodes of innovation and development were emerging across the country that engaged both strategic and operational levers holistically and which themselves provide important lessons for a future NHI (see bottom-up health system strengthening below).
In this section, we review indicators of PHC performance in three areas: financing, health workforce and utilisation of PHC. The indicators are drawn from routine data sources (collated by the Health System Trust and reported annually in the District Health Barometer36), and a modelling exercise on PHC personnel conducted for the 2030 HRH Strategy. The reported indicators are all for the public s ector and for uninsured populations and exclude curative ambulatory services by private providers (GPs, dentists, pharmacies, therapists, traditional healers and others). The public sector is the majority provider (86% of the population), and despite significant resources within the private sector, these have not contributed in any significant manner to PHC for this majority. Indicators of quality and health outcomes are reported in other chapters.
Public sector PHC is funded through taxation and is provided free at the point of use. In a recent comparative analysis of 20 LMIC PHC systems2, South Africa had the lowest out-of-pocket payments for health care, estimated as 8% of total health expenditure in 2018. The PHC system thus forms an important safety net, providing a comprehensive package of services, including a programme of Nurse-initiated and Managed Antiretroviral Treatment (NIMART) to over 5 million people in 2021.
In the 10-year period from 2010/11 to 2019/20, per capita public PHC expenditureiv increased by 40% in real terms, from R910 (US$60) to R1 272 (US$84) (Figure 4.2). In this period, the proportion of total government health expenditure on PHC increased from 25% to 29%, and all district health services increased from 41–45% of total expenditure. However, it is important to note that much of the growth in expenditure was driven by expansion of HIV/AIDS care over the period, which increased its share of total district expenditure from 14% to 22%36. In addition, the rate of growth in expenditure underwent a steady decline from 2017 onwards.
Figure 4.2 Per capita expenditure on PHC (rand real 2019/20 prices) (primary vertical axis) and percentage of total health expenditure on PHC, 2010/11 to 2019/20
Source: National Treasury and Health System Trust
iv Includes provincial and local government expenditure, conditional grants (e.g. HIV/AIDS, NHI), but excludes district hospitals and district management.
In 2019, there was a total of 244 000 health workers employed in the public health system, a ratio of 5/1 000 public sector dependent population (PSDP). This health workforce is predominantly nurse-based, constituting 56% of public sector workers, with doctors making up 8.6% of the total12. The combined availability of doctors and nurses in the public sector was 3.3/1 000 PSDP, which is below the WHO-recommended norm of 4/1 000 population37. However, when the private sector medical/nursing personnel is included, the ratio rises to 6.9/1 000 population, underscoring the considerable inequities in South Africa’s health system2
As part of the 2030 HRH Strategy, the current (2019) and five-year projected (2025) health workforce needs for PHC were determined. In 2019, nurses and CHWs constituted 90% of the workforce, at 43% and 47% of the total, respectively12. In order to achieve universal (equitable) coverage (as laid out in the PHC Re-engineering Strategy and assuming a PHC utilisation of 3.2), the gap in the public sector PHC health workforce was estimated to be 71 000 in 2019, rising to 88 000 in 2025. Bridging this gap would require an additional 34 billion rand.
The investments in PHC, accompanied by changing disease burdens (HIV/AIDS and NCDs), and introduction of new programmes in PHC are reflected in increased utilisation of services. Public PHC utilisation rates – measured as annual PHC head count per capita uninsured person – was 3.0 in 2010 but declined from 2015/16 onwards, reaching 2.2 in 2019/20, and below the target rate of 3.2 referred to in the previous section. Figure 4.3 shows 2019/2020 data reflecting significant inter-provincial variation (ranging from 1.6 to 2.8) but suggests a pro-equity pattern: wealthier provinces with a greater concentration of private ambulatory providers (Gauteng and Western Cape) have lower utilisation rates. These provinces also concentrate regional and tertiary hospitals, and patients may bypass PHC to access specialist care at higher levels36
Figure 4.3 2019/20 PHC utilisation rates and average annual change between 2015/16 and 2019/20 by province
Source: Copied from District Health Barometer 2019/2036
Plausible reasons for the decline in utilisation include the general shift towards community-based service delivery for stable patients on chronic medication – whether through the external PUPs in the CCMDD programme described above or through the Ward-based Outreach Teams (WBOTS)36. Lower demand for care due to improved health status of children and adults may be another factor. Finally, a factor also suggested is greater quality of data following the rationalisation of facility registers and less double counting of activity.
COVID-19 had a dramatic impact on PHC utilisation. PHC head counts dropped from 99.6 million in 2019 to 81.2 million 2020, an 18.4% decline7. Worryingly, HIV testing and GeneXpert tests for TB declined by 22% and 26%, respectively. The initial severe lockdowns, diversion of staff to the COVID-19 response, and closure of facilities because of staff illness and patient fears all played a role in these declines. However, there were also purposeful initiatives to ‘decongest’ PHC through the organisation of home delivery programmes16,32. The collateral impacts of COVID-19 on PHC programmes are likely to be felt for years to come.
In this section, we review significant innovations in the PHC system that have emerged at sub-national level. Some of these innovations build on or extend existing national strategies (community-oriented primary care and sub-district models), while others introduce novel approaches (community-level monitoring). All provide fresh, and to a large extent, holistic perspectives on the ‘what’ and the ‘how’ of PHC system strengthening and are thus uniquely positioned to inform and complement the ‘top-down’ national strategies reviewed earlier in the chapter.
Community-Oriented Primary Care, defined as ‘a continuous process by which primary health care is provided to a defined community on the basis of its assessed health needs, by the planned integration of primary care practice and public health’40 has a long history in South Africa, dating back to the 1940s. Supported by Departments of Family Medicine, a growing number of COPC nodes across the country have re-emerged over the last 10 years, combining the public health, managerial and primary care principles that inspired the original model. The most developed and articulated of the COPC models is in the Tshwane Metropolitan Municipality of Gauteng province. The core features of the Tshwane COPC model22,v, are:
• Community-based teams of CHWs, providing comprehensive care to households in defined and mapped geographical areas;
• Seamless integration between community-based and facility-based (i.e. clinic and hospital) multidisciplinary teams (including clinical associates and GPS), providing support and referral in defined patient care pathways;
• A locally developed ‘ICT-enabled’ (smart phones, tablets, facility ICT infrastructure) information system architecture, integrating community- with facility-based service activity, support functions (e.g. laboratories) and the district health information system; and providing real-time feedback to providers;
• Systems of local planning and resource allocation, based on population characteristics and disease profile for individual facility catchment areas; and
• A partnership with University of Pretoria of service learning, system development, continuing education, research and evaluation of the model.
The Tshwane COPC model is also the basis of community-based services in KZN.vi Although there are no published impact assessments of the Tshwane programme, economic modelling of its application in a rural district of Limpopo has shown a benefit cost ratio (BCR) of 3.4, with high net savings in averted clinic and hospital use21. The COPC model is also being implemented in the Cape Town metro, with a participatory co-design process, resulting in the formulation of a framework of 10 elements – see Figure 4.416.
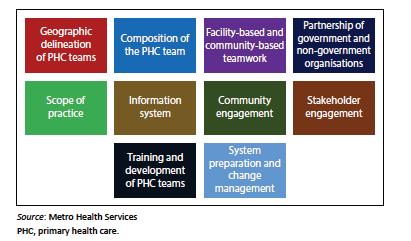
Source: 16
The COPC models address many of the current weaknesses in the WBPHCOTs programme, in centering populations and community health systems in PHC, rather than treating them as marginal add-ons; through systematic evidence-based public health and clinical approaches; supportive supervision; and ‘21st century’ ICT-enabled information systems.
Sub-district models
A health sub-district typically serves between 50 000 and 500 000 people and contains community-based services, clinics and a district hospital (public sector), and private and traditional providers (dependent on degree of rurality), that form a logical service delivery unit.
In practice, the sub-district as a governance and coordination mechanism is under-developed in South Africa, with reporting lines of the different elements running in parallel to district management teams. This creates a fragmented service delivery environment, compounded by the proliferation of vertical health programmes (HIV, TB, NCDs, etc.) extending from the district into facilities and communities. In such a system, implementation of integrated approaches in a continuum of care, as proposed in the COPC model above, is difficult.
v Marcus, TS. COPC integrated healthcare to and from the home = 21st Century UHC (PowerPoint). Presentation to the National UHC Dialogue, 21-22 November, 2019.
vi Shabangu, GC. Community-Based Model – A Service Delivery Model for KZN (PowerPoint). Presentation to the KZN Department of Health, February 2020.
In this section, we describe two initiatives seeking to formalise and strengthen the sub-district as the basic building block of South Africa’s health system:
• The sub-district management model proposed by the KZN provincial health department, variations of which are present or emerging in other parts of the country
• Achieving improved quality and outcomes through a coordinated sub-district approach in districts of Limpopo and Mpumalanga (referred to as the 3-feet model)
The KZN sub-district management model is premised on the rationale that successful implementation of ‘Community-Oriented Primary Care (COPC) with a responsive Community-Based Model’ requires a sub-district governance mechanism. The aim is ‘to develop a standardised, seamless and well-defined sub district management model, with clear boundaries and well-defined supervisory roles and responsibilities for improved efficiency and effectiveness on the health system’.vii The model defines core functions (roles and responsibilities) and a unified reporting line in the sub-district, through the district hospital Chief Executive Officer (or the most senior other manager if there is no hospital in the sub-district).
Echoing the COPC approach outlined above, Box 1 spells out the functions of the sub-district management.
Box 1: Roles and responsibilities of sub-district management
• Coordinate, oversee and manage service delivery for district hospitals, community health centres, clinics, midwifery obstetric units and community-based services
• Institutionalise COPC concept as a service delivery model
• Create an enabling environment for proper health information management and utilisation for decision-making
• Facilitate health programme coordination, integration and supportive supervision
• Ensure that there is a well-communicated referral system from household right up to the district hospitals
• Collaborate with all stakeholders in the promotion of quality of life of all individuals in the sub-district through Operation Sukuma Sakhe (intersectoral) Strategy.
The sub-district is envisaged to become the CUPS mechanism proposed in the NHI, with the CUPs ‘comprised of a district hospital, clinics and, or community health centers and ward-based outreach teams, and private primary service providers, organised in horizontal networks within a specified geographical sub-district area’.
vii Mkhize, NC and Msimango, P. Sub-District Model Presentation to DHMT, King Cetshwayo District, 30 September 2019 (PowerPoint provided by J Mndebele).
The formalisation of the sub-district will require:
• ‘Right sizing’ of district management structures to fulfil its new mandate of service planning, coordination, monitoring and evaluation
• Reconfiguration of organisational structures of district hospitals and community health centres to be aligned to the responsibility of supporting PHC management
• Integration of PHC and health programmes, with programme managers reassigned as PHC local area managers
• Strengthening the role of family physicians to provide oversight of the quality of clinical services in district health hospitals and PHC.
In 2013, in response to high maternal and child mortality, the NDoH prioritised a number of districts for targeted action. The 3-feet model was thus developed as an approach to improving quality and outcomes, centred on real-time mortality surveillance and responses in the basic unit of service delivery. A local governance mechanism – the Monitoring and Response Unit (MRU) – was established at sub-district level, creating functional coordination between community, clinic and district hospital services, and between line managers, clinicians, and health programme and information managers. The MRU focuses on outcomes and contributory factors, the development of whole systems thinking, integrating real-time evidence and building responses based on the principles of comprehensive PHC and local decision-making. The 3-feet model is supported by a number of reporting and decision-making tools and a training package39
The model was successfully trialed in the Waterberg and Gert Sibande Districts of Limpopo and Mpumalanga, respectively, and was associated with declines in mortality (most notably for severe acute malnutrition) in both these districts25,40. The approach complements well, and provides a methodology for actioning the sub-district structures and roles and responsibilities outlined in the previous section. The 3-feet model is currently being introduced into a number of other districts across the country, with the focus going beyond just maternal-child health and mortality to incorporate morbidity monitoring and response. The model of the MRU has also been incorporated into District Health Planning frameworks.
viii Ndivhuwo Rambau, Data Project Officer. The Ritshidze campaign: Civil society monitoring of PHC performance (PowerPoint). Presentation to the webinar: Revitalising primary health care: promising practices, 5 October 2021.
Social Accountability: Ritshidze Community-Led Monitoring of PHC
Ritshidze was established in 2018 as a consortium of organisations of people living with HIV to improve the experience and quality of care in PHC clinics across South Africa. Ritshidze is a rigorous and independent community-led monitoring and advocacy initiative involving over 400 clinics/community health centres across 29 districts of South Africa. The initiative was made possible through a formal Memorandum of Understanding with the NDoH and followed by negotiations with individual provincial governments.viii Using pre-designed tools and entering data onto tablets, Ritshidze members (‘monitors’) carry out structured quarterly interviews and observations of facilities, with a national team collating data on dashboards in real-time on facility, district, provincial and national levels. Indicators assessed include waiting times, medicine availability, patient treatment literacy and qualitative feedback, and are reported publicly on a web portal (http://data.ritshidze.org.za/). Local monitors engage patients, communities and health facility staff to generate solutions from the data, provide quarterly feedback to facility managers and clinic committees (where these exist), and to ‘duty bearers’ at provincial and national level. Over the period of implementation, a number of Ritshidze indicators – patient waiting times, availability of staff and medicines –have improveVIII Drawing on longstanding, home-grown forms of right-based activism, Ritshidze holds what may ultimately be more effective as a tool of participation and accountability than clinic committees and audit systems such as the Ideal Clinic.
As indicated earlier, these various bottom-up systems strengthening innovations provide a rich basis for an approach to PHC in a future NHI. A key issue going forward will be how to ensure that national strategy development is informed by and engages these bottom-up perspectives, recognising that the priorities of NHI (such as public-private partnerships) may not always cohere with the rationales and approaches of these locally embedded models.
This chapter has shown how PHC remains a central organising idea in South Africa’s health system, and continues to receive concerted attention in policies, programmes and interventions, translating into budgetary commitments. However, we have also argued that investment in the operational levers of PHC have not been adequately matched by attention to the core strategic levers, in particular the structures and systems of governance at sub-district and district levels; or to the problems of unstable leadership, deepening fiscal crisis and corruption at provincial level. There is also a lack of alignment between developments in PHC and other strategic processes – such as human resources for health, quality improvement and the DDM. In such an environment, the introduction of a new mechanism such as the CUPS proposed in the NHI bill may compound system fragmentation (especially between PHC and other levels of the health system) and engender a further loss of coherence and accountability.
Another challenge is that the interventions in PHC have tended to be piecemeal and technical under NHI as the umbrella policy, rather than NHI being embedded in a whole system perspective that places communities and PHC at the strategic centre of the health system. The NHI bill also reinforces a curative view of PHC, defining it as ‘the first level of contact of individuals, the family and community with the national health system, bringing health care as close as possible to where people live and work,
and constitutes the first element of a continuing health care process’5. As a financing reform, NHI is naturally more concerned with technical and allocative efficiency, than with public participation and intersectoral action on the social determinants of health. This echoes global critiques of the UHC movement41
A final challenge is that policy-makers and the ‘political elite’ are typically not users of public sector primary care, which may be a disincentive to embarking on complex and politically difficult PHC-related governance or budgetary reforms.
Primary health care has to be approached as a wider system philosophy embracing participation, intersectoral action and comprehensive approaches to health, embedded within coherent sub-district and district systems. While achieving greater system efficiency is key, further development of the PHC system, especially components such as the WBPHCOTs, cannot occur in an environment of austerity and disinvestment. Emphasis also needs to shift from the ‘what’ of policy to the ‘how’ of implementation, focused on learning through deliberation and by doing, keeping a finger on the pulse of ground realities (‘at 3-feet’), adapting or de-implementing ineffective or harmful strategies, supported by partnerships and embedded and co-produced evaluation and research. The reasons for declining patterns of PHC utilisation need to be better understood.
Going forward, further development of PHC in South Africa will require:
1) A willingness to tackle the governance weaknesses in PHC, starting with the formulation of a coherent sub-district system, and beyond this, establishing meaningful community participation and intersectoral collaboration;
2) The shift from a curative, disease orientation (the focus of NHI proposals) to a more expansive approach, centred on prevention, promotion and action on the social determinants of health;
3) Aligning developments in PHC with other system developments, in particular around HRH development and financing;
4) A commitment to establishing stable, skilled and public-interested leadership in PHC and district health systems; and
5) Forms of health system learning that rely less on nationally defined audits than on co-produced approaches better able to harness bottom-up participation and innovation.
1. McKenzie A, Schneider H, Schaay N, Scott V, Sanders D. Primary Health Care Systems (PRIMASYS): Case Study from South Africa. Geneva; 2017. https:// www.who.int/alliance-hpsr/projects/alliancehpsr_southafricaprimasys.pdf?ua=1.
2. Langlois EV, Mckenzie A, Mecaskey JW. Measures to strengthen primary health-care systems in low- and middle-income countries. Bull World Health Organ. 2020;98:781–791. doi: http://dx.doi.org/10.2471/BLT.20.252742
3. Ryneveld M Van, Schneider H, Lehmann U. Looking back to look forward : A review of human resources for health governance in South Africa from 1994 to 2018. Hum Resour Health. 2020;18:92:1–10. doi:10.1186/ s12960-020-00536-1
4. Schneider H, Daviaud E, Besada D, Rhode S, Sanders D. Ward-based primary health care outreach teams in South Africa: developments, challenges and future directions. In: Rispel L, Padarath A, eds. South African Health Review 2018 Durban: Health Systems Trust; 2018:59–66.
5. Minister of Health Republic of South Africa. National Health Insurance Bill. South Africa: Government Gazette; 2019.
6. Genesis, The Centre for Health Policy, PWC. Evaluation of Phase 1 Implementation of Interventions in the National Health Insurance (NHI) Pilot Districts in South Africa. Johannesburg; 2019.
7. Pillay Y, Pienaar S, Barron P, Zondi T. Impact of COVID-19 on routine primary healthcare services in South Africa. South African Med J. 2020;epub ahead. doi:10.7196/SAMJ.2021.v111i8.15786
8. WHO; UNICEF. Declaration of Astana. Geneva; 2018. https://www.who.int/ docs/default-source/primary-health/declaration/gcphc-declaration.pdf.
9. Rasanathan K, Evans TG. Primary health care, the Declaration of Astana and COVID-19. Bull World Health Organ. 2020;98(February):801–808. doi:10.2471/ BLT.20.252932
10. WHO, UNICEF. Operational Framework for Primary Health Care: Transforming Vision into Action. Geneva; 2020.
11. National Department of Health. National Health Insurance for South Africa (White Paper). Pretoria: Department of Health, Republic of South Africa; 2015.
12. National Department of Health. 2030 Human Resources for Health Strategy: Investing in the Health Workforce for Universal Health Coverage. Pretoria: Department of Health, Republic of South Africa; 2020.
13. South African Lancet National Commission. Confronting the Right to Ethical and Accountable Quality Health Care in South Africa. Pretoria; 2019.
14. Schneider H, Okeyo I, du Toit A, et al. Intersectoral collaboration before and during the COVID-19 pandemic in the Western Cape: implications for future whole-of-society approaches to health and wellbeing. In: South African Health Review 2021. Durban: Health Systems Trust.
15. Presidential Health Summit. Strengthening the South African Health System towards an Integrated and Unified Health System. Pretoria; 2018.
16. Mash R, Goliath C, Perez G. Re-organising primary health care to respond to the Coronavirus epidemic in Cape Town, South Africa. African J Prim Heal Care Fam Med. 2020;12(1)(a2607):1–4.
17. Murphy JP, Moolla A, Kgowedi S, et al. Community health worker models in South Africa: A qualitative study on policy implementation of the 2018/19 revised framework. Health Policy Plan. 2021;36(4):384-396. doi:10.1093/heapol/ czaa172
18. National Department of Health. Policy Framework and Strategy for Ward-Based Primary Healthcare Outreach Teams. Pretoria; 2018.
19. Assegaai T, Reagon G, Schneider H. Evaluating the effect of ward-based outreach teams on primary healthcare performance in North West province, South Africa: A plausibility design using routine data. South African Med J. 2018;108(4):329–335. doi:10.7196/SAMJ.2018.v108i4.12755
20. Bennett R, Marcus TS, Abbott G, Hugo JF. Scaling community-based services in Gauteng, South Africa: A comparison of three workforce-planning scenarios. African J Prim Heal Care Fam Med. 2018;10(1):1–7. doi:10.4102/phcfm. v10i1.1748
21. Bennett R, Marcus TS, Abbott G, Hugo JF. Modelling cost benefit of community-oriented primary care in rural South Africa. African J Prim Heal Care Fam Med. 2020;12(1):1–8. doi:10.4102/phcfm.v12i1.2225
22. Voce A, Monticelli F, Pillay Y, et al. District Clinical Specialist Teams. In: Padarath A, English R, eds. South African Health Review 2013/2014. Durban: Health Systems Trust; 2014:45–58.
23. Caldwell RI, Grant M, Gaede B, Aldous C. Enabling factors for specialist outreach in western KwaZulu-Natal. African J Prim Heal Care Fam Med. 2018;10(1):1–10. doi:10.4102/phcfm.v10i1.1690
24. Feucht U, Marshall C, Kauchali S, et al. Innovations in the clinical care of mothers and children in South Africa: The contribution of district clinical specialist teams. South African Med J. 2018;108(3):S38–S43. doi:10.7196/SAMJ.2018. V108I3B.12808
25. Schneider H, George A, Mukinda F, Tabana H. District Governance and Improved Maternal, Neonatal and Child Health in South Africa: Pathways of Change. Heal Syst Reform. 2020;6:1(e1669943). doi:10.1080/23288604.2019.1669943
26. Oboirien K, Harris B, Goudge J, Eyles J. Implementation of district-based clinical specialist teams in South Africa: Analysing a new role in a transforming system. BMC Health Serv Res. 2018;18(1):1–14. doi:10.1186/s12913-018-3377-2
27. National Department of Health. Ideal Clinic Manual: Version 19. Pretoria; 2021.
28. Muthathi IS, Levin J, Rispel LC. Decision space and participation of primary healthcare facility managers in the Ideal Clinic Realisation and Maintenance programme in two South African provinces. Health Policy Plan. 2020;35(3):302–312. doi:10.1093/heapol/czz166
29. Mukinda FK, Van Belle S, George A, Schneider H. The crowded space of local accountability for maternal, newborn and child health: A case study of the South African health system. Health Policy Plan. 2020;35(3):279–290. doi:10.1093/ heapol/czz162
30. Liu L, Christie S, Munsamy M, et al. Expansion of a national differentiated service delivery model to support people living with HIV and other chronic conditions in South Africa: a descriptive analysis. BMC Health Serv Res. 2021;21:463:1–8. doi:10.1186/s12913-021-06561-7
31. Dorward J, Msimango L, Gibbs A, et al. Understanding how community antiretroviral delivery influences engagement in HIV care: A qualitative assessment of the Centralised Chronic Medication Dispensing and Distribution programme in South Africa. BMJ Open. 2020;10(5):1–10. doi:10.1136/bmjopen-2019-035412
32. Louw JM, Rantloane B, Ngcobo S, et al. Home delivery of medication as part of reducing congestion in primary healthcare in Tshwane District Health Services. South African J Public Heal (incorporating Strength Heal Syst) 2020;4(2):50. doi:10.7196/shs.2020.v4i2.124
33. Wolmarans M, Solomon W, Tanna G, et al. eHealth Programme reference implementation in primary health care facilities. In: Ashnie P, King G, English R, eds. South African Health Review. Durban: Health System Trust; 2015:35–44.
34. National Department of Health. Annual Report 2018–19. Pretoria: Department of Health, Republic of South Africa; 2018.
35. Mureithi L, Burnett JM, Bertscher A, English R. Emergence of three general practitioner contracting-in models in South Africa: A qualitative multi-case study Int J Equity Health. 2018;17(1):1–18. doi:10.1186/s12939-018-0830-0
36. Massyn N, Day C, Ndlovu N, Padayachee T, eds. District Health Barometer 2019/20. Durban: Health System Trust; 2020.
37. World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals. Geneva: World Health Organization; 2016. https://apps.who.int/iris/bitstream/hand le/10665/250330/9789241511407-eng.pdf.
38. Mash R, Ray S, Essuman A, Burgueño E. Community-orientated primary care: a scoping review of different models, and their effectiveness and feasibility in sub-Saharan Africa. BMJ Glob Heal. 2019;4(Suppl 8):e001489. doi:10.1136/bm jgh-2019-001489
39. Clinton Health Access Initiaitive. Health Systems Strengthening at the Sub-District Level : The Three Feet Model. An Implementation Guide. Johannesburg; 2021.
40. Schneider H, Van Der Merwe M, Marutla B, Cupido J, Kauchali S. The whole is more than the sum of the parts: Establishing an enabling health system environment for reducing acute child malnutrition in a rural South African district. Health Policy Plan. 2019;34(6):430–439. doi:10.1093/heapol/czz060
41. Sanders D, Nandi S, Labonté R, Vance C, Van Damme W. From primary health care to universal health coverage—one step forward and two steps back. Lancet. 2019;394(10199):619–621. doi:10.1016/S0140-6736(19)31831-8