
VOLUME 6/ISSUE 7 - JUNE 2019
& The Lower Face CPD
A PARTNERSHIP YOU CAN COUNT ON CELEBRATING OUR 10TH ANNIVERSARY IN AESTHETIC TREATMENTS Here’s to another decade of natural-looking results and high patient satisfaction.1 Prescribing information can be found overleaf References: 1.Molina B et al. J Eur Acad Dermatol Venereol 2015;29(7):1382–8. Date of Preparation: May 2019 Job code: AZZ19-05-0053
Gender
Dr Eleanor Reid, Miss Lara Watson and Miss Priyanka Chadha on gender differences
Dr Mayoni Gooneratne advises how to collaborate with bloggers Topical Formulations for the Neck Dr Loredana Nigro explores considerations for neck rhytids Special Feature: Treating the Lower Third Practitioners present informative case studies for jawline treatments ENTRYAWARDSCLOSES JUNE28
Working with Influencers
Azzalure Prescribing Information (UK & IRE)
Presentation: Botulinum toxin type A (Clostridium botulinum toxin A haemagglutinin complex) 125 Speywood units of reconstituted solution (powder for solution for injection)
Indications: Temporary improvement in appearance of moderate to severe:
• Glabellar lines seen at maximum frown, and/or
• lateral canthal lines (crow’s feet lines) seen at maximum smile in adult patients under 65 years, when severity of these lines has an important psychological impact on the patient.
Dosage & Administration: Azzalure should only be administered by physicians with appropriate qualifications and expertise in this treatment and having the required equipment. Botulinum toxin units are different depending on the medicinal products. Speywood units are specific to this preparation and are not interchangeable with other botulinum toxins. Reconstitute prior to injection. Intramuscular injections should be performed using a sterile suitable gauge needle.
Glabellar lines: recommended dose is 50 Speywood units divided equally into 5 injection sites, 10 Speywood units to be administered intramuscularly, at right angles to the skin; 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle.
Lateral canthal lines: recommended dose per side is 30 Speywood units divided into 3 injection sites; 10 Speywood units to be administered intramuscularly into each injection point, injected lateral (20 - 30° angle) to the skin and very superficial. All injection points should be at the external part of the orbicularis oculi muscle and sufficiently far from the orbital rim (approximately 1 - 2 cm); (See summary of product characteristics for full technique).
Treatment interval should not be more frequent than every three months. The efficacy and safety of repeat injections of Azzalure has been evaluated in Glabellar lines up to 24 months and up to 8 repeat treatment cycles and for Lateral Canthal lines up to 12 months and up to 5 repeat treatment cycles. Not recommended for use in individuals under 18 years of age.
Contraindications: In individuals with hypersensitivity to botulinum toxin A or to any of the excipients. In the presence of infection at the proposed injection sites, myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis.
Special warnings and precautions for use: Care should be taken to ensure that Azzalure is not injected into a blood vessel. Use with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission, in the presence of inflammation at the proposed injection site(s) or when the targeted muscle shows excessive weakness or atrophy. Patients treated with therapeutic doses may experience exaggerated muscle weakness. Not recommended in patients with history of dysphagia, aspiration or with prolonged bleeding time. Seek immediate medical care if swallowing, speech or respiratory difficulties arise.
Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to facial anatomy, as a result of previous surgical interventions should be taken into consideration prior to injection. Injections at more frequent intervals/higher doses can increase the risk of antibody formation. Avoid administering different botulinum neurotoxins during the course of treatment with Azzalure.
To be used for one single patient treatment only during a single session. There is a potential risk of localised muscle weakness or visual disturbances linked with the use of this medicinal product which may temporarily impair the ability to drive or operate machinery.
Interactions: Concomitant treatment with aminoglycosides or other agents interfering with neuromuscular transmission (e.g. curare-like agents) may potentiate effect of botulinum toxin.
Pregnancy, Lactation & Fertility: Not to be used during pregnancy or lactation. There are no clinical data from the use of Azzalure on fertility. There is no evidence of direct effect of Azzalure on fertility in animal studies
Side Effects: Most frequently occurring related reactions are headache and injection site reactions for glabellar lines and; headache, injection site reactions and eyelid oedema for lateral canthal lines. Generally treatment/injection technique related reactions occur within first week following injection and are transient. Undesirable effects may be related to the active substance, the injection procedure, or a combination of both.
For glabellar lines: Very Common (≥ 1/10): Headache, Injection site reactions (e.g. erythema, oedema, irritation, rash, pruritus, paraesthesia, pain, discomfort, stinging and haematoma). Common (≥ 1/100 to < 1/10): Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites, predominantly describes brow paresis), Asthenopia, Eyelid ptosis, Eyelid oedema, Lacrimation increase, Dry eye, Muscle twitching (twitching of muscles around the eyes). Uncommon (≥ 1/1,000 to <1/100): Dizziness, Visual impairment, Vision blurred, Diplopia, Pruritus, Rash, Hypersensitivity, Eye movement disorder. Rare (≥ 1/10,000 to < 1/1,000): Urticaria.
For lateral canthal lines: Common (≥ 1/100 to < 1/10): Headache, Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites), Eyelid ptosis, Eyelid oedema and Injection site disorders (e.g. haematoma, pruritus and oedema). Uncommon (≥ 1/1,000 to <1/100): Dry eye.
Adverse reactions resulting from distribution of the effects of the toxin to sites remote from the site of injection have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcome in some cases). Prescribers should consult the summary of product characteristics in relation to other side effects.
Packaging Quantities & Cost: UK 1 Vial Pack (1 x 125u) £64.00 (RRP), 2 Vial Pack (2 x 125u) £128.00 (RRP), IRE 1 Vial Pack (1 x 125u) €93.50, 2 Vial Pack (2 x 125u) €187.05 (RRP)
Marketing Authorisation Number: PL 06958/0031 (UK), PA 1613/001/001 (IRE)
Legal Category: POM
Further Information is Available From: Galderma (UK) Limited, Meridien House, 69-71 Clarendon Road, Watford, Herts. WD17 1DS, UK. Tel: +44 (0) 1923 208950 Fax: +44 (0) 1923 208998
Date of Revision: September 2018
Adverse events should be reported. For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard
For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: medsafety@hpra.ie
Adverse events should also be reported to Galderma (UK) Ltd.
AZZALURE® IS A TRADEMARK BELONGING TO NESTLE SKIN HEALTH S.A.

of Preparation: May 2019 Job code: AZZ19-05-0053
Date
CLINICAL PRACTICE
Dr Eleanor Reid, Miss Lara Watson and Miss Priyanka Chadha explore the gender differences in the lower facial third
Practice
Dr Paul Charlson discusses the use of cryotherapy for dermatologic concerns 32
Advertorial: Myths and Misconceptions around Toxins
Professor Syed Haq outlines considerations when selecting a botulinum toxin 34 Sleep and Ageing
Dr Mehvish Khan explores the impact of sleep deprivation on skin ageing 36 Celebrate Your Success at the Aesthetics Awards
Be a finalist at the most prestigious Awards ceremony in the specialty 39 Treating Neck Lines with Topicals
Dr Loredana Nigro outlines treatments to improve rhytids on the neck 42 Lymphatic Drainage in Facial Aesthetics

Aesthetic nurse Rose Poyner details the benefits of manual lymphatic drainage with facial aesthetic treatments 44 Case Study: Lip Vascular Occlusion

Nurse prescriber Lynn Lowery shares a case study of a lip complication 47
Advertorial: Supporting Aesthetic Practitioners
Spark innovation manager John Campbell presents the new Allergan Spark 48 Hand Rejuvenation Using Fillers
Dr Victoria Manning and Dr Charlotte Woodward discuss characteristics of ageing hands and detail their preferred treatment choice 52 Advertorial: Flexible Thread Technology
Thread treatments that can retain natural facial expression 53 Abstracts
A round-up and summary of useful clinical papers IN PRACTICE 55 Live Chat Functions
Web developer and marketer Alex Bugg outlines adding a live chat function to your website 59
Rebranding Your Website
Practice manager Hannah Betts discusses updating your website 63 Working with Influencers

Dr Mayoni Gooneratne advises on collaborating with social media influencers 67 In Profile: Dr Souphiyeh Samizadeh
Dental surgeon Dr Souphiyeh Samizadeh details her journey into aesthetics 68 The Last Word


Dr MJ Rowland-Warmann shares her views on when and why aesthetic practitioners should be saying no to patients

Special Feature Treating the Lower Face Page 19
Clinical Contributors
Dr Eleanor Reid is an aesthetic practitioner and dental surgeon who graduated from Newcastle University. Dr Reid is currently lead trainer in Newcastle-upon-Tyne for Acquisition Aesthetics and director of Paragon Aesthetics.

Miss Lara Watson is dual qualified in medicine and dentistry and is a faculty member for Galderma. She is currently on the only maxillofacial surgery themed core training pathway in London. Miss Watson is also a cofounding director of Acquisition Aesthetics.

Miss Priyanka Chadha currently works as a plastic surgery registrar in London and is co-founding director of Acquisition Aesthetics training academy. Her academic CV comprises national and international prizes, and she is a faculty member for Galderma.
Dr Paul Charlson is the president of the British College of Aesthetic Medicine. He has worked as a GPwER in dermatology for 14 years and is an assessor for the Royal College of General Practitioners with Extended Roles accreditation panel.

Dr Mehvish Khan is founder of MK Aesthetics in Wexford, Ireland. She completed her Master’s in Aesthetic Medicine with a distinction from Queen Mary University of London and also holds a degree in Biomedical Sciences and Medicine.
Dr Loredana Nigro graduated from WITS Medical School in Johannesburg in 2003. She is currently a senior aesthetic clinician at Riverbanks Clinic in Harpenden. Dr Nigro is also a KOL and clinical consultant for mesoestetic UK.

Rose Poyner is an aesthetic nurse practitioner based at Cosmedic Skin Clinic. She has received extensive training from aesthetic practitioners Dr Martyn and Sharon King, founders of the Cosmedic Skin Clinic, in all aspects of aesthetic medicine.
Lynn Lowery is an independent nurse prescriber with more than 10 years’ experience in medical aesthetics and is dual-qualified as a paramedic. Lowery has been an Allergan and Merz trainer and is currently a mentor for Northumbria University.
Dr Victoria Manning is an aesthetic practitioner and GP. She is the co-founder of River Aesthetics and also a threads trainer, a key opinion leader and an aesthetics industry media contributor, writer and speaker.
Dr Charlotte Woodward is a medical aesthetic practitioner and is the co-founder of River Aesthetics. She was also one of the first in the UK to perform a non-surgical breast lift using threads and is a national trainer for PDO threads.

Entry for the Aesthetics Awards closes this month! aestheticsawards.com Contents • June 2019 Subscribe Free to Aesthetics Subscribe to Aesthetics, the UK’s leading free-of-charge journal for medical aesthetic professionals. Visit aestheticsjournal.com or call 0203 096 1228
•
06 News The
15
16
NEXT MONTH
IN FOCUS: Complications • Stress and Ageing • Taking on Complications
latest product and industry news
On the Scene Out and about in aesthetics
News Special: Latest Statistics in Cosmetic Surgery Aesthetics reviews the data released from the BAAPS annual audit
19 Special Feature: Treating the Lower Third Practitioners present their case studies of successful jawline treatment 24 CPD: Gender & The Lower Face
29 Cryotherapy in Aesthetic



































Meeting the needs of your business, delivering high satisfaction to your patients Call us on 01234 313130 info@aestheticsource.com www.aestheticsource.com When Friday 6th September 2019 Where 30 Euston Square, London, NW1 2FB Attendance fees will be donated to Born to be Beautiful www.borntobebeautiful.org Pigmentation un-covered Symposium listSpeaker & full agenda released in June! We are excited to announce the first AestheticSource Symposium. A multitude of industry experts from the UK and overseas will be sharing their knowledge and experience of diagnosis, treatment and maintenance for Pigmentation... 50% of places reserved! To register your interest or book your place, please email becca@aestheticsource.com
It is with a mixture of sadness and pride that I announce my retirement from the Aesthetics editorship; sad to say goodbye, yet proud of everything we have achieved over the past five years. I feel the time has come for me to hand over to a very capable team to take our special publication to the next level. I have loved every moment and am privileged to have been involved with so many events and learning opportunities, which have kept me networked and very involved in the specialty I have come to love over 30 years. So time to let the team fly, thanks to all of you who have supported and engaged with me over the years. Onwards and upwards, as I hand the baton to Chloé Gronow, who I have worked with closely as an excellent deputy editor and I’m confident will continue to enhance the Aesthetics brand for years to come.
Amanda Cameron Former Editor
Gronow Editor & Communications Manager
It is a huge honour to take over the editorship of Aesthetics from Mandy, who so many of you will know as one of the pioneers of our specialty. Since I joined the team five years ago, Mandy has taught me so much about the wonderful world of medical aesthetics, fuelling my passion and instilling the importance of high quality education, which the editorial team and I will continue to deliver across all areas of the Aesthetics Media brand. Supporting me in the clinical direction of Aesthetics will be newly-appointed Clinical Lead Mr Dalvi Humzah, who has more than 20 years’ experience in aesthetics, as well as our other hugely valued Clinical Advisory Board members. By sharing their expertise and experiences, this dynamic group of professionals help us to continue to deliver engaging and, most importantly, educational content to you each month. Since joining Aesthetics I have met many inspiring key opinion leaders, contributors, clients and readers, and, as part of my new role, it will be fantastic to meet more of you in future. So if you see me at any conferences or events then please do come and say hello! Likewise, if you have any ideas of articles you would like to read or contribute to, then don’t hesitate to get in touch – you can email me via chloe@aestheticsjournal.com or call 0207 148 1292 I look forward to speaking to you soon!
Clinical Advisory Board
A number of leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content

Mr Dalvi Humzah is a consultant plastic, reconstructive and aesthetic surgeon with more than 20 years’ experience and is director of P&D Surgery. He is an international presenter, as well as the medical director and lead tutor of the multi-award-winning Dalvi Humzah Aesthetic Training courses. Mr Humzah is founding member of the Academy of Clinical Educators at the Royal College of Physicians and Surgeons of Glasgow.


Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN) and the UK lead on the BSI committee for aesthetic nonsurgical medical standards. She is a registered university mentor in cosmetic medicine and has completed the Northumbria University Master’s course in non-surgical cosmetic interventions.


Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.
Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Dr Christopher Rowland Payne is a consultant dermatologist and internationally recognised expert in cosmetic dermatology. As well as being a co-founder of the European Society for Cosmetic and Aesthetic Dermatology (ESCAD), he was also the founding editor of the Journal of Cosmetic Dermatology and has authored numerous scientific papers and studies.
Dr Raj Acquilla is a cosmetic dermatologist with more than 12 years’ experience in facial aesthetic medicine. In 2015 he won the Aesthetics Award for Aesthetic Medical Practitioner of the Year and in 2012 he was named Speaker of the Year. Dr Acquilla is a UK ambassador, global KOL and masterclass trainer for botulinum toxin and dermal fillers.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 AntiAgeing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email editorial@aestheticsjournal.com
Dr Stefanie Williams is a dermatologist with special interest in aesthetic medicine. She is the founder and medical director of the multi-award winning EUDELO Dermatology & Skin Wellbeing in London. She lectures in the Division of Cosmetic Science and has published more than 100 scientific articles, book chapters and abstracts.


Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the clinical director of Revivify London, an honorary clinical teacher at King’s College London and a visiting associate professor at Shanghai Jiao Tong University.

PDFs AND REPRO
Chloe Carville, contact@aestheticsjournal.com
T: 0207 148 1292 megan@aestheticsjournal.com
Sophie Thompson • Content Executive
T: 0207 148 1292 sophie@aestheticsjournal.com
CUSTOMER LIAISON
Chloe Carville • Customer Liaison Executive
T: 0203 096 1228 | contact@aestheticsjournal.com
Lian Graham • Customer Liaison Executive

T: 0203 096 1228 contact@aestheticsjournal.com
DESIGN
Peter Johnson • Senior Designer
T: 0203 096 1228 | peter@aestheticsjournal.com
© Copyright 2019 Aesthetics. All rights reserved. Aesthetics Journal is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
Chloé
Editor’s letter
ARTICLE
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact
DISCLAIMER: The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final. PUBLISHED BY PORTFOLIO MANAGEMENT
Edmonds • Chairman T:
096 1228
Suzy Allinson • Brand Director
1292 |
013
Claridge • Commercial Director
096 1228 | jenny@aestheticsjournal.com ADVERTISING & SPONSORSHIP Judith Nowell • Business Development Manager T: 0203 740 3886 | M: 07494 179535 judith@aestheticsjournal.com EDITORIAL & COMMUNICATIONS Chloé Gronow • Editor & Communications Manager T: 0207 148 1292 | M: 07788 712 615 chloe@aestheticsjournal.com Shannon Kilgariff • Deputy Editor T: 0207 148 1292 shannon@aestheticsjournal.com Megan Close • Journalist
Chris
0203
chris@aestheticsjournal.com
T: 0207 148
M: 07500 007
suzy@aestheticsjournal.com Jenny
T: 0203
Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
Mr Dalvi Humzah, Clinical Lead
ABC accredited publication
WE WANT TO HEAR FROM YOU!
Talk #Aesthetics
#ClinicOpening
The Clinic by Dr Mayoni
@drmayoni_clinic
A super proud moment for @mayonibyre as the second site in Crystal Palace opens! A fabulous day with @healthxchangeuk launching the new wellness clinic! Loved seeing old friends and new explore the new space, try out treatments and hear all about Mayoni’s plans for this space.

#Learning
BTL Aesthetics UK
@btlaestheticsuk
About to kick off the first of three BTL Cellulite workshops across the UK at the Royal Society of Medicine. We’re also very pleased to welcome @drarielhaus as our guest speaker. What a beautiful venue to talk about the 5 anatomical causes of cellulite and how to treat it using multiple technologies.

#Conference
Liz Harris
@eh.medicalcosmetics
What an amazing day at the Coastal Clinical Conference on No Man’s Fort. Another day of learning and Networking.

#CoastalClinicalConference
#Solentforts #AlwaysLearning
#International
Dr Kate Goldie
@drkategoldie
Honoured to be part of this esteemed faculty at the Merz symposium in Taipei, sharing our global consensus paper on the innovative uses of hyperdilute Radiesse and presenting the importance of Ultrasound and the SPT system for ultherapy.

#MerzInstitute #MerzAesthetics #Radiesse #Ultherapy
#Filming
Dr Ayad Harb @drayadharb Filming with the BBC crew and @queenmehreen in Bicester today. Talking noses, non-surgical treatments and the ethics of aesthetics. Amazing but exhausting day! Exciting things coming soon.

Patient safety UK Government launches patient safety campaign
The Department of Health and Social Care (DHSC) launched a consumer campaign on May 14, designed to ensure that members of the public are aware of the risks associated with cosmetic procedures. The campaign includes print and digital content featured in consumer publications Heat, Closer and Grazia, and aims to signpost people to advice and guidance on the NHS website when considering a cosmetic procedure. The updated advice published on the NHS website includes topics such as speaking to a professional about what to expect, choosing a qualified practitioner and what to do to avoid hasty decisions or feeling pressured.
The DHSC stated that it is also working with stakeholders, such as independent accreditation body Save Face and the Joint Council for Cosmetic Practitioners, to strengthen the regulation of cosmetic procedures and improve standards. Ashton Collins, director of Save Face, commented, “The campaign empowers people to take control and make a safe and informed choice about who they trust with their health and appearance. By supporting the campaign, we can make a real impact and significantly reduce the number of people who suffer unnecessary adverse events.”
PCA Skin introduces new skin brightening product
Skincare company PCA Skin has added a new skin brightening product to its portfolio, called the Enzymatic Treatment.
According to the company, the product combines enzymatic and alpha hydroxy acid with antioxidant action and anti-inflammatory benefits, aiming to exfoliate, brighten, and strengthen skin. The key ingredients for the Enzymatic Treatment include carica papaya fruit, tartaric acid, resveratrol ferment extract, and vitis vinifera fruit cell extract. Combined, these ingredients aim to improve skin texture and protect epidermal stem cells from damage, the company claims. Lizzie Shaw, PCA Skin UK brand manager, said, “The Enzymatic Treatment has come at a perfect time of year for us as patients tend to look at alternatives to chemical peels coming into the summer months.” She added, “This product is fully diverse and can be used as either a standalone treatment or to enhance our other professional treatment protocols. It is ideal for those wanting maximum results with minimal downtime.”

Twitter
and Instagram
Follow us on
@aestheticsgroup
@aestheticsjournaluk
Skincare
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Aesthetics appoints new Editor and Clinical Lead
Chloé Gronow has been appointed as Editor & Communications Manager at Aesthetics Media. Gronow joined the company five years ago in a journalist role, before being promoted to Deputy Editor & Communications Manager in 2016. She is an NCTJ Gold Standardqualified journalist, with a degree in English and Contemporary Media. The news comes following the retirement of Amanda Cameron, who has held the editor position for the past five years. Cameron said, “I have loved every moment and have felt privileged to have been involved with so many events and learning opportunities that have kept me networked and very involved in the specialty I have come to love over 30 years. Onwards and upwards now, as I hand the baton to Chloé, who I have worked with closely for the past five years as an excellent deputy editor and I’m confident will continue to enhance the Aesthetics brand for years to come.” Gronow added, “It is a huge honour to take over the editorship of Aesthetics from Amanda, who has taught me so much about the specialty and will be greatly missed by everyone. I am extremely excited to continue to develop the Aesthetics offering, particularly with our digital content, to deliver the highest level of education for our readers.”
To further support the clinical direction of Aesthetics, consultant plastic, reconstructive and aesthetic surgeon Mr Dalvi Humzah has been appointed Clinical Lead for the Advisory Board. Previously known as the Editorial Advisory Board, the renamed Clinical Advisory Board comprises members of various professions within the aesthetic specialty, who share their expertise and experiences with Aesthetics to ensure the latest clinical updates and standards are passed on to readers. The change will also see members have greater involvement across the brand, including the educational content of the Aesthetics Conference and Exhibition and the judging of the Aesthetics Awards. Gronow said, “Mr Humzah has worked with Aesthetics since its inception, sharing his expertise and vast knowledge of the specialty in both published material for readers and in an advisory capacity with the team. I am delighted he has accepted this position and look forward to working with him and other members of the Clinical Advisory Board to drive forward our clinical content.” Mr Humzah added, “It has always been a great pleasure to work with Amanda so I would like to thank her and wish her the very best for the future; I am deeply honoured to be offered the role as Clinical Lead of the Advisory Board. This is a significant development for Aesthetics and I am excited and looking forward to working with Chloé, the Aesthetics team and my respected colleagues on our future projects together.”

Botulinum toxin
Evolus receives backing for EU marketing of new toxin
The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) has issued a positive opinion on the marketing authorisation application for Evolus’ botulinum toxin type A formulation. By receiving scientific recommendation for marketing by the CHMP, the EU Commission will now review the advice and deliver its final decision on the company’s marketing authorisation application.
Vital Statistics
A 2018 survey demonstrated that 78% of aesthetic practitioners work part-time (Hamilton Fraser Cosmetic Insurance, 2019)
(Allergan, 2019)
As of January 2019, the average daily time spent by adults using the internet is 5 hours and 46 minutes (Hootsuite, 2019)
A survey conducted in the UK demonstrated that 64% of patients chose their practitioner based on the price of the treatments (SaveFace, 2019)

In a survey of 334 doctors and dentists, 25% had been practising aesthetic medicine for more than 13 years (BCAM, 2019)
In the UK, Facebook has an advertising audience of 40 million active users (Hootsuite, 2019)
A UK survey demonstrated that cosmetic dentistry is the top non-surgical treatment among adults (RealSelf, 2018)
Editorship
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
83% of 14,584 people are willing to invest in their appearance
Events diary
5th-8th June
Vegas Cosmetic Surgery and Aesthetic Dermatology Conference www.vegascosmeticsurgery.info
8th June
Cosmetic Courses 3rd Annual Conference www.cosmeticcourses.co.uk
21st September
British College of Aesthetic Medicine Conference www.bcam.ac.uk
7th-8th November
British Association of Cosmetic Nurses Conference www.bacn.org.uk
Training Cosmetic Courses named as Allergan’s first approved trainer
Global pharmaceutical company Allergan has appointed aesthetic training provider Cosmetic Courses as its first approved trainer for medical aesthetics. The appointment comes as a result of the newly-launched support website, Allergan Spark. According to the company, one of the ways to promote best practice amongst the next generation of aesthetic professionals is to provide details of local training providers. The aim of the initiative is to build the skills and confidence of those new to the specialty, to elevate the quality of treatment outcomes and to encourage the ethical growth of medical aesthetic careers and businesses. Mr Adrian Richards, consultant plastic and reconstructive surgeon and clinical director of Cosmetic Courses said, “We have developed our courses over the years to incorporate theory, practical and business to give delegates the best start to their new career. Working together with Allergan and being the first appointed provider is great news for Cosmetic Courses and we are really excited about the Spark initiative and the future this has.”
Events
Aesthetics Awards wins silver at Awards Awards 2019
7th December
The Aesthetics Awards 2019 www.aestheticsawards.com

Accreditation
Clinisept+ attains CE mark
UK aesthetic distributor AestheticSource has announced that Clinisept+ has attained CE accreditation.

According to the UK Government, a CE mark is not a general requirement for chemicals, pharmaceuticals or cosmetics, however Lorna McDonnell-Bowes, director of AestheticSource, believes that the CE mark helps to reinforce best practice to both patients and practitioners. She said, “Safety has always been at the heart of our product selection, alongside efficacy and marketleading clinic support, marketing and PR. The opportunities this CE Mark opens up for existing and new users of Clinisept+ are very exciting indeed.”
The Aesthetics Awards, hosted by Aesthetics Media, has been presented a silver award for the Best Business Awards Event at the annual Awards Awards, hosted on May 17. The event aims to acknowledge and celebrate the behind-the-scenes commitment of companies who are part of coordinating industry award ceremonies. As well as this, the Aesthetics Conference and Exhibition (ACE), also hosted by Aesthetics Media, has been shortlisted in the category for UK Conference of the Year over 1,500 Delegates at the Conference Awards 2019. Aesthetics Media brand director, Suzy Allinson commented, “We are thrilled to not only have won silver at the Awards Awards but also to be a finalist in this year’s Conference Awards and to be named amongst the best conferences in the UK. It’s fantastic to be recognised for all of our hard work, across both of our annual events, and something that, as a company, we are very proud of.” The winner will be announced at the Conference Awards ceremony on July 5.
Distribution
Galderma confirms Med-fx as preferred distributor
Pharmaceutical company Galderma (UK) Limited has confirmed that aesthetic and skincare product supplier Med-fx Ltd will become the company’s preferred distributor, subject to contract, for its aesthetics portfolio. Med-fx will service all customers who purchase under the Azzalure (abobotulinum toxin type A) and Restylane brands in the UK and Republic of Ireland, the company explains, with the aim of offering an enhanced level of customer service. Galderma has confirmed that the new proposals are due to come into play, subject to contract, from September 8. Existing distributors will continue to be able to purchase and sell Galderma products and services before and after this date. Toby Cooper, medical solutions business unit head of Galderma UK and Ireland commented, “We’re very pleased to be working with Med-fx on developing an improved proposition for our customers. They have a strong market standing and share our vision of being healthcare professionals’ trusted partners in making a positive difference in the lives of patients.”
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Ageing
SkinCeuticals releases three-step skin kits

Cosmeceutical company SkinCeuticals has released two retails kits; the Age Renewal System and the Clarifying Skin System. The three-step kits are designed to address the needs of two common skin concerns frequently seen in skin clinics; ageing skin and ageing, blemish prone skin, the company explains. The Age Renewal System includes the C E Ferulic antioxidant serum, H.A Intensifier serum and Retinol 0.3, all in 30ml sizes. The Clarifying Skin System features the Blemish + Age Cleanser Gel in 240ml, and the Blemish + Age Defense corrective serum and the Phyto Corrective moisturing serum; both in 30ml sizes.
Half of millennials compare aesthetic treatment to a haircut
A recent poll of 1,033 UK women aged between 18 and 30 has highlighted patient perceptions of non-surgical and surgical cosmetic treatments. The survey, which was carried out by Deltapoll and commissioned by the BBC, suggest that 48% believe that having a cosmetic procedure is a lot like having a haircut. There were 66% of 18 to 30-year-olds who indicated that they have either had a cosmetic procedure, or would consider one; however, only 7% admitted to already having something done. Of those that had undergone treatment, 27% had botulinum toxin, 28% had lip fillers and 20% had breast surgery. Most (77%) were happy with the results following treatment, while 69% said it made them feel more confident. When asked whether they think Britain is obsessed with cosmetic procedures, 47% agreed, while 45% believe it’s too easy to get cosmetic procedures in the UK. Aesthetic practitioner Dr Sophie Shotter said, “What worries me most is that 48% believe treatment is like having a haircut. It’s great that these treatments are becoming more acceptable, however, it’s worrying that aesthetic medical treatments are being trivialised and that people are not aware of the risks.”
Education
Harley Academy introduces advanced masterclasses
Aesthetic training provider Harley Academy has launched a new series of advanced training courses, called the Harley Academy Injectables and Complications Masterclasses. The classes will be led by aesthetic practitioner Dr Raul Cetto, and aesthetic practitioner, founder and CEO of Harley Academy, Dr Tristan Mehta. They consist of a series of five one-day courses that aim to provide an in-depth examination of the anatomy and injection techniques for five key facial zones using both toxin and fillers. Each masterclass will also cover complications that can arise when treating particular areas, as well as hands-on practical learning with patients selected in advance of the session. The masterclasses are available to Level 7 students/graduates and experienced injectors.
BACN UPDATES
A roundup of the latest news and events from the British Association of Cosmetic Nurses



BACN TRAINING
The BACN values the importance of continual professional development, and has worked with training companies in the past to offer courses which provide members with accessible learning that is in line with the BACN’s ethos of patient safety and support of aesthetic nurses. Previously, the BACN, in conjunction with other companies, has offered facial anatomy courses which involve cadaveric dissection. In September and December, the BACN will once more be supplying these opportunities with Oculo-Facial Aesthetic Academy (OFAA) under Miss Sabrina Shah-Desai in London, and La Belle Forme Training under Mr Taimur Shoaib in Glasgow. These courses provide a detailed analysis of facial anatomy, and allow BACN nurses to practise various injection techniques within a safe environment.
These courses are offered to BACN members at a highly discounted rate, with the hope that members who have not the financial capabilities otherwise are able to attend a day that provides a vital and unique understanding of facial anatomy and injection. Please contact Gareth Lewis at glewis@bacn.org.uk for more info.
BACN CONFERENCE
The BACN Autumn Aesthetic Conference 2019 on November 7 and 8 is now open for booking on the BACN website. Members are encouraged to book their space as last year sold out before the event took place. This year there will be a full agenda of expert presentations, demonstrations, and wide networking opportunities with exhibitors and other BACN nurses. More information can be found by going to the events page on the BACN website.
This column is written and supported by the BACN
Survey
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Patrick Johnson, CEO of BioPhotas

Tell us about your decision to enter the UK market with the Celluma SERIES of light therapy devices?

After becoming the recognised leader in the US, coming into the UK market was like returning to the birthplace of light therapy. More than 15 years ago, Omnilux introduced the first FDA-cleared LowLevel Light Therapy (LLLT) device, conducting their own clinical studies and doing the ‘heavy lifting’ to gain regulatory credentials as a medical device. Since then, many other similar LLLT devices have entered the market. For us, it was time for innovation and for light therapy to enter the digital age, so we took a different path with the Celluma.
Please explain that ‘different path’. In the early stages of developing the Celluma, we were surprised that the majority of the LLLT devices on the market were rigid arrays of LEDs positioned several inches from the surface of the skin. Intuitively, this didn’t make sense to us. Positioning a source of light energy away from the skin generally requires a larger more powerful device that takes up a lot of space in the treatment room and can cost up to £20,000. We realised that if we could design a device that was flexible and shape-taking, one that could be contoured to the area of treatment, then we could potentially deliver superior clinical results at a dramatically lower price.
So that’s the Celluma difference? Exactly! The Celluma shapes to the area of treatment and stays where you put it without any stands or retention devices. When we were designing the Celluma, we selected technical characteristics that were clinically proven to be beneficial in the scientific literature and validated those benefits with our own peerreviewed and published studies. We used those studies to ensure the Celluma is an extremely well medically-credentialed LLLT device.
This column is written and supported by
Approval Aesthetics Awards receives Trust Mark
The Aesthetics Awards has been approved for an Awards Trust Mark, designed to enhance trust between those entering awards schemes and the companies organising them. The Awards Trust Mark scheme is a not-for-profit accreditation programme run by the Independent Awards Standards Council that requires the awards organisers to commit to a voluntary code of conduct. Suzy Allinson, brand director at Aesthetics Media commented, “Receiving the Awards Trust Mark is yet another mark of credibility for the leading Awards ceremony in the specialty. It showcases our dedication to providing a high-quality process from start to finish.” The Aesthetics Awards is also delighted to announce sponsorship for this year and already confirmed is: The Healthxchange Group Award for Sales Representative of the Year, The AestheticSource Award for Best New Clinic, UK and Ireland, The Sinclair Pharma Award for Best Independent Training Provider, The Venus Concept Award for Best Clinic Ireland, The SpringPharm Award for Aesthetic Nurse Practitioner of the Year, The ClinicSoftware.com Award for Aesthetic Product Distributor of the Year, The Dalvi Humzah Aesthetic Training Award for Best Supplier Training Provider of the Year, The Celluma Award for Best Clinic London, The John Bannon Award for Medical Aesthetic Practitioner of the Year and The Schuco Aesthetics Award for Outstanding Achievement in Medical Aesthetics
Training MATA introduces Level 7 injectables diploma
Aesthetic training provider Medical Aesthetic Training Academy (MATA) has introduced a Level 7 Postgraduate Diploma in Facial Aesthetics, regulated by Ofqual. The Level 7 Diploma in Facial Aesthetics qualification incorporates the OTHM Level 7 Certificate/Diploma in Clinical Aesthetic Injectable Therapies. OTHM is an awarding organisation regulated by Ofqual. The course comprises foundation, advanced, and mentorships days, and includes four units of theory learning, covering anatomy, physiology, patient medical assessment including body dysmorphia, principles of practice, and injectable therapies for the management of hyperhidrosis. According to MATA, delegates are assessed continually with direct observational practice, virtual learning environment quizzes, critical essays, short answer questions and a clinical log book. Delegates must also complete observed and delivered dermal filler and botulinum toxin treatments. The new qualification is mapped to the new JCCP/CPSA guidelines.
Diversity
Obagi launches global campaign
Global skincare company Obagi Medical has launched a worldwide initiative that is designed to celebrate diversity, titled SKINCLUSION. According to the company, the initiative is designed to elevate the global dialogue about diversity and how to see beauty in differences, specifically surrounding skin tone. Aesthetic clinics are encouraged by Obagi Medical to visit the Healthxchange portal, the exclusive UK Obagi supplier, and download information and campaign marketing materials. These materials include a campaign guide, social media images, an infographic and a brochure, as well as an exclusive video with celebrity and campaign ambassador Priyanka Chopra-Jonas. Professionals within the specialty are also encouraged to join the dialogue on social media by using the hashtag #SKINCLUSION.
FDA-Cleared Medical CE Mark
Wound Healing • Pain Management • Skin Care
60
INDEPENDENT AWARDS STANDARDS COUNCIL
2019 AWARD
AWARDS TRUSTMARK
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Device Alma adds applicator for Accent Prime
Laser and light-based device manufacturer Alma, has introduced a new applicator for its skin tightening and body contouring device, the Accent Prime. The applicator, called the Colibri, offers dual ablative and thermal modes for the treatment of sagging eyelids and facial wrinkles and unlike previous applicators for the Accent Prime, the Colibri is smaller and needle shaped, according to the company. The Colibri uses unipolar radiofrequency-based technology to produce microplasma sparks, which the company explains creates microperforations on the skin leading to skin contraction, aiming to tighten and smooth the skin. The Accent Prime and its applicators are distributed through ABC Lasers.

Campaign
JCCP announces petition to make fillers prescription only
A national petition to make dermal fillers prescription only and the relevant insurance required to access them mandatory has been launched by the Joint Council of Cosmetic Practitioner (JCCP).
Currently, dermal fillers are classified as a class III medical device in the UK and do not require a prescription. As a result of this, they can be purchased and administered by anyone, whether or not they have relevant training in the treatment or the insurance to support their use. The JCCP launched the petition, supported by JCCP patient trustee Dawn Knight, to coincide with the launch of the UK Government public awareness campaign. Professor David Sines, chair of the JCCP, commented, “There is a large acceptance that fillers are a major problem regarding complications based on evidence and case studies published in the media. By restricting fillers to be prescription devices only, you would provide professional oversight for non-prescriber practitioners who can access them.”
Nutrition
Post-procedure nutritional supplement released
Nutritional supplement company, Advanced Nutrition Programme, has introduced a supplement that aims to specifically target the healing of skin following an aesthetic treatment. According to the distributor, the International Institute for Anti-Ageing (iiaa), the supplement supports the skin’s recovery process following non-surgical aesthetic treatments such as chemical peels, microdermabrasion, laser treatments injectables and skin needling. The Skin Aesthetic Recovery Pack contains vitamin C, Coenzyme Q10, lutein, vitamin A, pine bark extract, omegas 3 and 6 and lycopene, which aims to calm and sooth irritated and sensitive skin to help restore skin health. Lorraine Perretta, head of nutrition at Advanced Nutrition Programme, said, “The Skin Aesthetic Recovery pack works in synergy with aesthetic treatments and would be an added bonus for the patients in every clinic practice. Practitioners would be able to support their treatments by giving their patients nutritional support from the inside for a holistic approach.”
Body dysmorphia
Save Face launches BDD training for practitioners
Independent accreditation body Save Face has confirmed that it has launched a series of training events to help aesthetic practitioners more easily recognise and diagnose body dysmorphic disorder (BDD). The training will be provided by mental health charity Mind and will cover a number of topics including; an overview of mental health problems, support and treatments available, recognising the signs and how to respond and manage challenging situations. Clinical director at Save Face and registered nurse Emma Davies commented, “We are very excited to be able to offer this training which we hope will equip our practitioners with the skills and expertise they need to support the many people they are likely to come across who may be experiencing difficulties with their mental health.”
Medik8 introduces vitamin A products
Global skincare brand Medik8 has launched two new vitamin A night serums, the Crystal Retinal 1 and the Crystal Retinal 3. According to the company, the serums aim to minimise fine lines and wrinkles whilst plumping and resurfacing the skin. Crystal Retinal 1 contains 0.01% crystal-encapsulated retinaldehyde and Crystal Retinal 3 contains 0.03% crystal-encapsulated retinaldehyde.
The Crystal Retinal 1 is a gentle strength vitamin A for patients who have sensitive skin or those who are looking to incorporate a low strength but highly effective vitamin A serum into their skincare regime, according to Medik8. The Crystal Retinal 3 is a medium strength vitamin A, for those who are new to vitamin A or have previously tried mild retinol formulas, the company claims.
 Skincare
Skincare
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
‘ABOBOTULINUM TOXIN IN ACTION: KEY PRINCIPLES & TREATMENT FOR GLABELLAR LINES’

IT WILL BE HELD ON MONDAY JUNE 17 AT 7PM.
How do I guarantee my place on ‘Abobotulinum toxin in Action: Key Principles & Treatment for Glabellar Lines’ Webinar’?
1. Visit www.aestheticsjournal.com/ Webinar_GaldermaJune2019
2. Login OR join as a member for free
3. You will then be prompted to use your DocCheck* password to confirm that you are a Doctor, Nurse or Dentist and able to access this webinar (if you registered for the last Aesthetics webinar, your DocCheck account will be valid)
4. Tick the box to confirm that you would like to sign up for the webinar. You’ll then receive reminder emails for the event closer to the time to ensure you don’t miss out!
*What if I don’t have a DocCheck login?
Register with DocCheck for free www.doccheck.com/register
Please note that you will need to provide the following when you have registered your contact details:
- A PDF of your record on the register downloaded from the GMC/NMC/GDC website as appropriate AND proof of ID (passport or driving licence)
- OR your personal certificate from your medical qualification
Your information will be checked and once it has been verified you can then visit the Aesthetics webinar page, use your DocCheck password and confirm you would like to sign up for the webinar by ticking the box. If you have any issues with your DocCheck verification please contact cream@doccheck.com
IMPORTANT: You will need to register and provide proof of your medical qualification to DocCheck by Thursday June 13 in order to guarantee that your registration will be processed in time for access to the webinar
PLEASE LOOK OUT FOR THE NEXT GALDERMA WEBINAR...
Botulinum toxin
are different
on the
Speywood units are specific to this preparation and are not interchangeable with other botulinum toxins. Reconstitute prior to injection. Intramuscular injections should be performed using a sterile suitable gauge needle. Glabellar lines: recommended dose is 50 Speywood units divided equally into 5 injection sites, 10 Speywood units to be administered intramuscularly, at right angles to the skin; 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle. Lateral canthal lines: recommended dose per side is 30 Speywood units divided into 3 injection sites; 10 Speywood units to be administered intramuscularly into each injection point, injected lateral (20 - 30° angle) to the skin and very superficial. All injection points should be at the external part of the orbicularis oculi muscle and sufficiently far from the orbital rim (approximately 1 - 2 cm); (See summary of product characteristics for full technique). Treatment interval should not be more frequent than every three months. The efficacy and safety of repeat injections of Azzalure has been evaluated in Glabellar lines up to 24 months and up to 8 repeat treatment cycles and for Lateral Canthal lines up to 12 months and up to 5 repeat treatment cycles. Not recommended for use in individuals under 18 years of age. Contraindications: In individuals with hypersensitivity to botulinum toxin A or to any of the excipients. In the presence of infection at the proposed injection sites, myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis. Special warnings and precautions for use: Care should be taken to ensure that Azzalure is not injected into a blood vessel. Use with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission, in the presence of inflammation at the proposed injection site(s) or when the targeted muscle shows excessive weakness or atrophy. Patients treated with therapeutic doses may experience exaggerated muscle weakness. Not recommended in patients with history of dysphagia, aspiration or with prolonged bleeding time. Seek immediate medical care if swallowing, speech or respiratory difficulties arise. Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to facial anatomy, as a result of previous surgical interventions should be taken into consideration prior to injection. Injections at more frequent intervals/higher doses can increase the risk of antibody formation. Avoid administering different botulinum neurotoxins during the course of treatment with Azzalure. To be used for one single patient treatment only during a single session. There is a potential risk of localised muscle weakness or visual disturbances linked with the use of this medicinal product which may temporarily impair the
ability to drive or operate machinery. Interactions: Concomitant treatment with aminoglycosides or other agents interfering with neuromuscular transmission (e.g. curare-like agents) may potentiate effect of botulinum toxin. Pregnancy, Lactation & Fertility: Not to be used during pregnancy or lactation. There are no clinical data from the use of Azzalure on fertility. There is no evidence of direct effect of Azzalure on fertility in animal studies. Side Effects: Most frequently occurring related reactions are headache and injection site reactions for glabellar lines and; headache, injection site reactions and eyelid oedema for lateral canthal lines. Generally treatment/injection technique related reactions occur within first week following injection and are transient. Undesirable effects may be related to the active substance, the injection procedure, or a combination of both. For glabellar lines: Very Common (≥ 1/10): Headache, Injection site reactions (e.g. erythema, oedema, irritation, rash, pruritus, paraesthesia, pain, discomfort, stinging and haematoma). Common (≥ 1/100 to < 1/10): Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites, predominantly describes brow paresis), Asthenopia, Eyelid ptosis, Eyelid oedema, Lacrimation increase, Dry eye, Muscle twitching (twitching of muscles around the eyes). Uncommon (≥ 1/1,000 to <1/100): Dizziness, Visual impairment, Vision blurred, Diplopia, Pruritus, Rash, Hypersensitivity, Eye movement disorder. Rare (≥ 1/10,000 to < 1/1,000): Urticaria. For lateral canthal lines: Common (≥ 1/100 to < 1/10): Headache, Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites), Eyelid ptosis, Eyelid oedema and Injection site disorders (e.g. haematoma, pruritus and oedema). Uncommon (≥ 1/1,000 to <1/100): Dry eye. Adverse reactions resulting from distribution of the effects of the toxin to sites remote from the site of injection have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcome in some cases). Prescribers should consult the summary of product characteristics in relation to other side effects. Packaging Quantities & Cost: UK 1 Vial Pack (1 x 125u) £64.00 (RRP), 2 Vial Pack (2 x 125u) £128.00 (RRP), IRE 1 Vial Pack (1 x 125u) €93.50, 2 Vial Pack (2 x 125u) €187.05 (RRP) Marketing Authorisation Number: PL 06958/0031 (UK), PA 1613/001/001 (IRE) Legal Category: POM Further Information is Available From: Galderma (UK) Limited, Meridien House, 69-71 Clarendon Road, Watford, Herts. WD17 1DS, UK. Tel: +44 (0) 1923 208950 Fax: +44 (0) 1923 208998 Date of Revision: September 2018
Adverse events should be reported.
For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard
For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: medsafety@hpra.ie. Adverse events should also be reported to Galderma
Ltd.
Date of Preparation: April 2019 Job code: AZZ19-04-0034e
(UK)
Azzalure Prescribing Information (UK & IRE) Presentation: Botulinum toxin type A (Clostridium botulinum toxin A haemagglutinin complex) 125 Speywood units of reconstituted solution (powder for solution for injection) Indications: Temporary improvement in appearance of moderate to severe: • Glabellar lines seen at maximum frown, and/or • lateral canthal lines (crow’s feet lines) seen at maximum smile in adult patients under 65 years, when severity of these lines has an important psychological impact on the patient. Dosage & Administration: Azzalure should only be administered by physicians with appropriate qualifications and expertise in this treatment and having the required equipment.
units
depending
medicinal products.
WEBINAR
HEALTHCARE PROFESSIONALS
AESTHETICS
THE NEXT
FOR
HOSTED BY
JOURNAL IN ASSOCIATION WITH GALDERMA WILL BE
iS Clinical introduces lip care duo

Skincare company iS Clinical, has released two additions to its product portfolio, specifically designed to target the lip area. The first is the Lip Polish, a scrub with key ingredients including sucrose, cocoa butter, tetrahexyldecyl ascorbate (vitamin C), and tocopherol (vitamin E), which aims to smooth and hydrate lips. The second half of the duo is the Youth Lip Elixir, a cream aimed at softening, hydrating and plumping the overall appearance of the lips. The formulation includes hyaluronic acid, cocoa butter, vitamin E and C. Available to purchase through the iS Clinical exclusive UK distributor, Harpar Grace International, the products can be used for all skin types to treat dehydration, poor elasticity and ageing skin, the company claims. From June 6, iS Clinical will also be forming a partnership with laser developer and manufacturer Cynosure.

AestheticSource expands team

UK aesthetic distributor AestheticSource has recruited two new members to join the team. Kerry Stewart will be joining as the new business development manager for the London region, supporting practitioners and clinics that stock brands across the whole AestheticSource portfolio. In addition, Clarissa Burke will be joining the company’s customer service team based at the head office in Bedford. According to AestheticSource, Burke will be ensuring that the experience throughout the company is synonymous, working across the portfolio of brands and departments to achieve this. Lorna McDonnell-Bowes, director of AestheticSource, said, “The London area is a key territory for AestheticSource and so we are delighted to have Kerry join us. Clarissa joined us in April and became the youngest member of this growing company. A warm welcome to both!”

Aesthetics confirms next Galderma webinar on June 17
The highly anticipated Aesthetics Media webinar, titled Azzalure (abobotulinum toxin type A) in Action: Key Principles and Treatment for Glabellar Lines in association with pharmaceutical company Galderma UK, is taking place on June 17 from 7 to 9pm. Professor Syed Haq will present on the key principles and science behind toxins, detailing different toxins on the market, their field of effect, safety and efficacy, as well the key questions that aesthetic practitioners should be asking when purchasing a toxin. Aesthetic nurse prescriber Lou Sommereux will then discuss the treatment of the glabellar lines specifically. She will explore the anatomy, reference points for injections, share best practice and provide advice on minimising risks. This will then be supported with several treatment demonstrations on an older female, younger female and a male patient. The webinar is only available for doctors, surgeons, nurses and dentists with a valid professional licence. You must submit your licence (GMC/NMC/GDC certificate) and proof of identity certificates (e.g. driving licence/passport) to DocCheck by June 13. For those who registered for the previous Anatomy of the Smile webinar, you will not be required to do this again. This webinar is supported by Galderma. For prescribing information for Azzalure (abobotulinum toxin type A) see p.12. AZZ19-04-0043h and DoP: May 2019
News in Brief
NMC confirms increase in register numbers
A report published by the Nursing and Midwifery Council (NMC) indicates a rise in the number of nurses and midwifes that have joined the register in the last year. On March 31, there were 698,237 people on its register, an increase of 7,959 (1.2%) from the previous year. There was also a 126% increase in the number of nurses and midwifes from outside of the EU registering for the first time, totalling 6,157.
Cocoon
Medical
releases
primelase in UK Aesthetic manufacturer Cocoon Medical has introduced hair removal device primelase to the UK market. The primelase is a diode laser that features three different wavelengths; 755 nm, 810 nm and 1060 nm. The applicator also has combined wavelengths of 810 nm, 940 nm and 1060 nm. Peter McGuinness, managing director of Cocoon Medical said, “primelase allows clinics to offer fast pain-free hair removal for all skin types and can treat full legs in 10 minutes. This means that clinics can take on a high volume of patients and achieve maximum profitability.”
Harpar Grace appoints trainer for iS Clinical Distribution company Harpar Grace International has appointed aesthetic nurse and clinic owner Sally Frank as a clinical trainer for the iS Clinical brand. The company has confirmed that Frank will be joining the team to assist with national training days and lead the training for the newly-launched Prodigy Peel in the north of England.
FILLMED launches NANOSOFT intradermal device
FILLMED, formerly Filorga Medical, has launched the NANOSOFT, an intradermal implantation device that the company explains sits in between a mesotherapy and microneedling device. According to the company, the NANOSOFT delivers the company’s patented formula NCTF which contains 59 active ingredients plus hyaluronic acid. It features three microneedles of 0.6mm depth made from crystal silicone which creates micro wounds to stimulate cellulate communication and the wound healing response. During this, NCTF is delivered to treat indications such as fine lines, wrinkles, tonicity, pigmentation and pore size reduction, the company states. The product is distributed exclusively by FILLMED and laboratory Cosmedi Ltd.
Advertorial
Recruitment
Product launch
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Upcoming Training Dates
Loughborough
Monday 24th June
Monday 15th July Monday 12th August Monday 9th September Monday 14th October
London
Monday 17th June Monday 22nd July Monday 19th August Tuesday 24th September Monday 21st October
Cardiff Tuesday 4th June Tuesday 13th August Thursday 24th October
Dublin Tuesday 3rd September Monday 11th November
Aberdeen Thursday 1st August Thursday 31st October
Manchester Wednesday 19th June Tuesday 15th October
Bristol
Wednesday 10th July Monday 30th September
Glasgow
Tuesday 11th June Monday 4th November
Belfast Monday 18th November
Professional Peel Training
• Discover the science behind the brand
• Learn about the most sophisticated retinols
• Find out how to treat common skin concerns with our daily and professional range
• Take a deeper look into our chemical peel system, including our 6% Pure Retinol

• See the results for yourself, perform and receive a PCA SKIN treatment on the day
• Become PCA SKIN certified
/pcaskinuk info@churchpharmacy.co.uk @pcaskin_uk +44 (0)1509 357 300
EXCLUSIVE TO Healthcare
professionals only.
On the Scene
Out and about in the specialty BMLA Conference, London
Clinic by Dr Mayoni second site opening, London
On May 15, aesthetic practitioner Dr Mayoni Gooneratne opened her second clinic, based in Crystal Palace in South London. Dr Gooneratne, who opened her flagship clinic in south London in 2016, celebrated the official opening of her second clinic with a launch event for family, friends and colleagues. During the interactive event, there were live demonstrations of the Obagi Medical skin systems, including the Blue Radiance peel, as well as different treatments that will be offered in the clinic. Dr Gooneratne also discussed her plans for her new concepts titled Skinfit, MindFit, BodyFit; which are holistic treatment packages for the skin, mind and body. Those who attended were offered a limited number of free consultations, as well as discounts and vouchers for future treatments.

The annual British Medical Laser Association (BMLA) conference took place from May 8-10 at the Park Inn by Radisson hotel in Heathrow, London, designed for medical and aesthetic laser enthusiasts.

The two-day event featured dedicated sessions for skin laser treatments, photodynamic therapy and biophotonics, the use of lasers in surgery, lasers in dentistry and a session dedicated for nurses and therapists. Following this, the BMLA then launched its latest guidelines, designed to act as a reference to all individuals or organisations creating laser or IPL treatment protocols. Speakers throughout the event included laser clinical nurse specialist Natalie Allen, consultant dermatologist Dr Firas Al-Niaimi, clinical director at Lynton Samantha Hills and independent nurse prescriber Andrew Rankin, amongst many others. Dr Vishal Madan, president of the BMLA and consultant dermatologist commented on the event, “It was, yet again, a fantastic conference for anyone interested in medical lasers as the event offered a unique blend of science and medicine all with a high level of academic rigor so often missing from other forums.” Delegates were also able to meet aesthetic businesses at a small exhibition, which included Candela, SkinCeuticals and in Venus Concept, amongst others. Dr Tom Lister, consultant clinical scientist and laser protection advisor added, “This year was a considerable success. Particular highlights included the launch of the BMLA treatment guidelines, a debate session covering contraindications to treatment, a multitude of experts talking on lasers in dentistry and many exciting advances in laser treatments, laser safety and photodynamic therapy.”
Candela Vascular Day, Amsterdam
Practitioners met at the Amsterdam Universitair Medische Centra Department of Dermatology in the Netherlands on May 18 to learn about the latest developments in laser technologies for vascular conditions from device manufacturer, Candela. Delegates were welcomed by Hamish McNair, director of clinical education EMEA at Candela, before Perry Tomasetti, senior director of medical aesthetics for global business unit at Candela, then enlightened delegates on Candela’s journey from its early beginnings in pulsed dye laser (PDL) technology in 1970 to present, with the launch of its newest technology, the Vbeam Prima PDL and Nd:YAG platform. Dermatologist Dr Albert Wolkerstorfer, from the Netherlands, followed with a presentation on vascular indications, showcasing the types of results that can be achieved using lasers on capillary malformations such as port wine stains (PWS), highlighting the importance of treating patients as early as possible. UK-based consultant dermatologist Dr Firas Al-Niaimi, who was the first to use the new Vbeam Prima in Europe, focused his presentation
on his experiences using the device. He said, “What excites me is the versatility and the choices I can provide to my patients with having the Vbeam Prima. One of the key mistakes that practitioners make is to rely on a standard set of parameters to treat patients with the same pathological condition, as there are huge varieties between patients.”
The vascular theme continued with dermatologist Professor Peter Bjerring from Denmark exploring the use of IPL technology for effective treatment.
Following lunch, Dr Al-Niaimi and Dr Wolkerstorfer provided a literature review presentation, highlighting studies around laser efficacy for certain conditions and discussed and debated their findings with the audience. Speakers then invited delegates to view the Vbeam Prima and Ellipse devices, and explained the mechanisms behind their use in practice. A round table discussion then followed, where audience members were engaged in discussions around the efficacy and use of PDL, IPL and Nd:YAG, as well as CO2 lasers.
Tim Stevens, product manager for EMEA at Candela, said the event was a huge success. “We got great feedback from our customers and one of the best things about it was that we had a really good forum for discussion with some of the greatest minds about vascular issues and applications of our new and existing technologies. It was also the first time we have ever parallel presented both the Vbeam Prima and the Nordlys Ellipse IPL together so physicians can really think about what platform is best for their practice and patients,” he concluded.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The Latest Statistics in Cosmetic Surgery
plays a significant part, surgery may be the only option for some patients and there is definitely less of a stigma around surgery these days.”
A drop in browlifts
The number of procedures performed and recorded by cosmetic surgeons has been declining for the last two years,1,2 however the annual audit conducted by the British Association of Aesthetic Plastic Surgeons (BAAPS) indicates that the number of treatments carried out in 2018 has seen a small increase of 0.1% compared to 2017, in addition to the rise in non-surgical treatments.3
The statistics released indicate that 28,347 surgical procedures took place in 2018, a small uplift of 32 surgeries from the previous year.4
The most notable rise was in liposuction procedures, with a 12% increase in women having this procedure compared to 2017. Surgical browlifts saw the biggest decline, now at an all-time low, with just 383 procedures being performed in 2018 compared to 2,138 in 2013 when the treatment was at its peak.4
Consultant plastic surgeon and former BAAPS president, Mr Rajiv Grover, who compiles the statistics each year, says, “The 2018 BAAPS audit shows that demand for cosmetic surgery remains buoyant, despite a year when the high street has struggled.5 While demand for non-surgical treatments such as fillers and skin tightening is rising,3 it’s important to note that, once there is actual loose skin, only surgery is likely to make a significant long-term improvement.”
Aesthetics interviews consultant plastic surgeon and BAAPS member Mr Ali Juma and aesthetic practitioner Dr Vincent Wong about their thoughts on the results, examining some of the potential influences behind the key variations in statistics.
What’s stopped the decrease?
“I would postulate that the very small increase in the BAAPS cosmetic surgery figures is multi-factorial,” shares Mr Juma.
“The report shows a very small increase against a difficult and uncertain economy, particularly with the ambiguity around Brexit, as well as competition from independent companies and overseas providers. However, I believe that BAAPS members have managed to buck the trend and maintain the share of a difficult market by being able and visible to those seeking their expertise to achieve the highest of outcomes. All of this has been achieved against a tough economy and strong competition with much bigger spending power,” he explains. Dr Wong agrees that the figures reflect a more educated and accepting market, “I think surgical procedures are much more acceptable and readily available these days. The fear of looking ‘frozen’ or ‘overdone’ is slowing decreasing too, primarily down to the expertise of those performing the treatments. We all know that the nonsurgical specialty has been a factor in the previous drops in statistics and the lack of regulation has been highlighted in recent news. I think patients are slowly becoming more and more aware of this too, even though we are not quite there yet, it’s definitely a step in the right direction.” Mr Juma highlights, “Although the rise of non-surgical procedures
From 2009, when BAAPS released the results of its first ever annual audit, this particular procedure saw a steady increase until 2015. However, from then on, browlifts dropped significantly. It was reported that there was a 71% decrease in 2016, a 27% decrease in 2017 and now a further 14% drop, with just 383 browlift procedures performed in 2018, compared to 2,138 in 2013 when the treatment was at its most popular (Figure 1). Both Mr Juma and Dr Wong believe that this significant decrease is primarily due to the growth in popularity and recognition that botulinum toxin, dermal filler and thread treatments can work for both preventative and corrective measures. “I see patients in their 30s requesting non-surgical browlifts on a regular basis in my practice, when very minimal signs of ageing are starting to appear. The good thing about offering these types of treatments is that they’re really subtle,” says Dr Wong. Mr Juma echoes, “Here we are talking about a significant decline in this procedure. Patients nowadays tend to be more inclined to have treatments that allow them to walk out of a clinic with no telltale signs that they have undergone treatment and continue their day. When carried out by a medical expert, non-surgical treatments can achieve excellent results in correctly-selected patients, although the outcomes do not have the longevity of surgery. However, patients simply find it more convenient and the minimal to no scarring, with almost no down time, are certain attractions.”
A rise in liposuction
The biggest increase in treatments amongst women was liposuction, up 12% from the previous year and 9% for both men and women combined, something which Mr Juma found to be particularly interesting. He says, “I would have thought the number of liposuction procedures would have stayed the same or seen a very small increase due to the volume of non-surgical body contouring devices on the market, which don’t need to be
2009 0 500 1,000 1,500 2,000 2,500 2010 2011 2012 2013 2014 2015 2016 2017 2018 Figure
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Aesthetics reviews the data released from the BAAPS annual audit and highlights some of the most notable changes during 2018
1: The rise and fall in surgical browlift procedures
administered by a medical professional.”



Dr Wong suggests that this spike may be due to the popularity in athleisure, the fashion trend which sees workout clothing worn in other settings. In 2017, the athleisure market was worth £2.5 billion and the trend is predicted to increase by 22.6% by 2020.6 He comments, “We know already that social media and reality TV shows could be playing a part in the rise of these types of procedures, however I believe that fashion is also having an influence more so than ever before. It’s never been so trendy to wear sportswear and people think that you have to have an athletic body to look good in it.” Dr Wong adds, “Generally, the results from non-surgical body-contouring devices can be fairly slow and can become expensive due to needing repeat sessions, which is why patients may be turning to liposuction.”






Mr Juma agrees that needing repeat sessions could be a contributing factor, “The statistics show us that many people are looking for more than what the current devices can manage. In the majority of surgical cases, a patient has one treatment, the results are visible immediately and they continue to improve for up to six months.”

The practitioners also agree that surgery should never be portrayed as the ‘easier’ option. Mr Grover emphasises the risks around the procedures, adding, “The danger of cosmetic surgery becoming too closely linked to reality TV or celebrity endorsement is that it can make surgery seem like a commodity, which should never be the case. An operation is not something that can simply be returned to the shop if you have second thoughts.”
Working in tandem
Both Mr Juma and Dr Wong recognise that the gap between nonsurgical and surgical treatments is now closer than ever and agree that it is one of the many ways that the industry is evolving.
Dr Wong says, “I work with a surgeon in my practice and it’s a great partnership. There is absolutely space for both categories; it’s just about finding what is right for the patient.”

Mr Juma concludes, “I’m hoping that we will see an increase in the non-surgical treatments performed by BAAPS members and that in due course we will see official audit reports around the two areas working in harmony. This will, of course, take time but would be a great step forward for our specialty.”
REFERENCES
1. Gronow C, Cosmetics Surgey’s Decline in 2016, Aesthetics journal, March 2017, <https:// aestheticsjournal.com/feature/cosmetic-surgery-s-decline-in-2016>
2. Cooke K, The Decline in Cosmetic Surgery – a healthier perception or a struggling economy? Aesthetics journal, March 2018 < https://aestheticsjournal.com/feature/the-decline-in-cosmeticsurgery-a-healthier-perception-or-a-struggling-economy>
3. American Society for Aesthetic Plastic Surgery, 2018 Trends, 2018 <https://www.surgery.org/sites/ default/files/ASAPS-Stats2018-Trends.pdf>
4. BAAPS, Cosmetic surgery stats: number of surgeries remains stable amid calls for greater regulation of quick fix solutioins, May 2019 <https://baaps.org.uk/media/press_releases/1708/cosmetic_surgery_ stats_number_of_surgeries_remains_stable_amid_calls_for_greater_regulation_of_quick_fix_ solutions>

















5. BBC News, What went wrong on the high street in 2018?, December 2018 < https://www.bbc.co.uk/ news/business-46646990>
6. Growth Funders, The growth of athleisure, July 2018 <https://blog.growthfunders.com/the-growth-ofathleisure>

Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 799-74EMCHPFMA2ENGB100; Emsculpt_AD_Half-page-180x125mm_FMA2_ENGB100 Results and patient experience may vary. Patients shown in the B&A pictures are within +/- 5 lbs of their original weight unless specifi ed. As with any medical procedure, ask your doctor if the Emsculpt procedure is right for you. The Emsculpt procedure is U.S. FDA cleared for improvement of abdominal tone, strengthening of the abdominal muscles, development of fi rmer abdomen, strengthening, toning and fi rming of buttocks. ©2018 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® are registered trademarks in the United States of America, the European Union and/or other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. CONTACT INFO@BTLAESTHETICS.CO.UK BUILD MUSCLE & BURN FAT NO SURGERY – NO DOWNTIME Emsculpt_AD_Half-page-180x125mm_FMA2_ENGB100.indd 1 11.10.2018 8:50:08




info@breitaesthetics.com | www.dermafill.eu | 020 7193 2128
is the first of a new 4th generation of safer and more effective pure Monophasic injectable dermal fillers which exceed the stricter standards of the FDA very low level BDDE controls. The DERMAFILL range is presented as 3 products, each specific to the indications being treated Available from £56 per 1ml on Prescription DERMAFILL Global Xtra For fine lines and wrinkles DERMAFILL Volume Ultra For the correction of deep wrinkles and restoration of facial volume DERMAFILL Lips To redraw the lip contour and enhance volume
DERMAFILL
Treating the Lower Third
Regardless of patient demographic, the jawline is an aesthetic concern for many. Both men and women will experience agerelated changes that include bone resorption, decreased tissue elasticity, and redistribution of subcutaneous fullness.1 According to practitioners interviewed for this article, younger patients are also now recognising how aesthetic treatments can create a more defined jawline, which will enhance their profile and overall facial features. So how should aesthetic practitioners approach treatment?
37-year-old male patient
Consultation
This 37-year-old patient initially presented to my clinic with concerns regarding his lower face, in particular a weak chin and poorly-defined jawline. He had previously undergone mid-face and undereye dermal filler treatment. During the consultation, the patient told me that he had always been concerned with the lack of definition of his lower face and what he described as a ‘weak chin’. He explained that he even grooms his beard so that it is longer in certain areas to simulate a welldefined jawline and a projected chin. I had to convince the patient to shave before coming to see me, as he hasn’t had a clean shave for years. following a two-week cooling-off period, the patient attended my clinic for treatment. I ran through all the points in the consent form, which informed him of potential risks, as well as what to expect from treatment immediately and in the following days.



Product choice
For the treatment itself, I used a combination of two hyaluronic acid (HA) dermal fillers. These were Teosyal Ultra Deep, which is used on the periosteum to project the overlying tissue to create volume from deep within.2 I find that it’s very good, especially if you want to give the chin projection as, in my experience, it gives quite a lot of lift of
And what results can be achieved? Four clinicians share their techniques and best practice advice.
Concerns
“The main concern patients present with is a lack of definition of the jawline,” explains aesthetic practitioner Dr Raul Cetto. “Having a straight line from the corner of the mandible to the chin is a sign of youth, but as we age there is a redistribution of volume so we end up having things like a double chin or a heavy jowl,” he explains.
For women particularly, jowling is often their number one concern in this area, according to dentist and aesthetic practitioner Dr Heather Muir. “Very few older ladies will come in saying they need bigger cheeks, but they will tug on their jowl to try and lift their face; pulling it upwards and backwards to take the jowls away,” she explains, adding, “It’s often the first place they tend to go when you ask them to point out their concerns.” Aesthetic practitioner Dr Paul Baines agrees, emphasising that this is a valuable treatment for ageing patients and those seeking stronger definition.
the overlying structures. For this case, it was particularly useful because it created a more masculine ‘bone structure’, with a broader chin which is more anteriorly projected. I then used Teosyal RHA 4, injected superficially. The product is also a volumiser, but because of its viscoelastic properties, it’s actually very strong but malleable.2 I find that it works well when you want to create a straight mandibular and chin line. Most importantly, when patients are speaking or eating and the mouth is moving, the product won’t be visible. It looks natural, whereas if I used a stiff volumiser injected deeply you would be able to see the implant upon animation.
Technique
To start, I injected a 0.2ml bolus of Ultra Deep into the chin in three points, down to the bone, using a needle to achieve a broader chin and anterior projection. I then injected a 0.1ml bolus on each side of the pre-jowl sulcus, medial to the mandibular ligament to further broaden the mandible and camouflage the jowl fat, followed by a 0.2ml bolus on each side of the gonial angle, deep onto the bone, which gave lateral projection and definition of the lower face. The total amount of Ultra Deep used was one syringe of 1.2ml. RHA 4 was then injected at the level of the superficial fat using a 25 gauge 50mm cannula, with a total of 0.3ml per side to the lateral lower face at the gonial angle. For the chin and the jowl, a secondary entry point was made and 0.3ml of RHA 4 was injected
again at the level of the superficial fat to reduce the marionette lines, labio-mental crease and enhance the chin line. The same procedure was repeated on the other side, using a total of one syringe of 1.2ml of RHA 4. Overall, this patient had two syringes for his treatment.
Results
The patient did not experience any side effects and was very happy with his results when I followed up two weeks later. It’s extremely satisfying to be able to use these tools not only for addressing the ageing process, but also to correct or create structure where it has always been deficient. Undesirable anatomical variants such as a retrognathic chin or an underdeveloped mandible could previously only be treated with surgery, so the fact that we have these non-surgical implants which can also correct with little to no downtime is amazing.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Four practitioners present their case studies of successful jawline treatment using hyaluronic acid
Dr Raul Cetto Before After






@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com www.cambridgestratum.com Email: info@cambridgestratum.com CALL 01223 846881 Four skin treatments - one slim machine Dermalux FlexTM LED bundle from £51/week +VAT HydroMedi Refreshes and brightens skin Removes and kills acne bacteria OxyNrich Exfoliates and nourishes Bohr effect to oxygenate skin QuadPolar RF Gently tightens face/neck skin Comfortable treatment Ultra Serum—ultrasound meizo therapy Hydrates and nourishes Serum penetrates the skin without needles Finance options from £46/week + VAT Stratum Synergy TOTAL SKIN MANAGEMENT www.cambridgestratum.com Email: info@cambridgestratum.com CALL 01223 846881 Four skin treatments - one slim machine Dermalux FlexTM LED bundle from £51/week +VAT HydroMedi Refreshes and brightens skin Removes and kills acne bacteria OxyNrich Exfoliates and nourishes Bohr effect to oxygenate skin QuadPolar RF Gently tightens face/neck skin Comfortable treatment Ultra Serum—ultrasound meizo therapy Hydrates and nourishes Serum penetrates the skin without needles Finance options from £46/week + VAT Stratum Synergy TOTAL SKIN MANAGEMENT
62-year-old female patient
Consultation
I’ve been treating this 62-year-old patient for about eight years with HA, toxin and skin-tightening procedures. While she’s had a few treatments and looks great anyway, the general loss of definition in her jawline was something that really bothered her. Addressing the patient’s concerns in the lower face was the next phase in her overall treatment plan – I had started in the upper face and worked my way down. The patient was informed and aware of the risks of bruising, swelling, asymmetry, and lumps and bumps, as well as more serious complications. I also discussed alternative treatments for the lower face, such as surgery and thread lifts; the patient chose to go ahead with fillers as she considered them less invasive and valued the minimal downtime. I used Clinisept Plus to thoroughly cleanse the skin and remove traces of makeup before the treatment, and covered the patient’s hair with a hairnet. I find this is particularly important when treating the jawline as it’s easy for hair to fall into that area if it isn’t tied back.
Product choice
The main product I used was Restylane Lyft, which I find beneficial particularly in the posterior area of the mandible because it’s got a high G prime,3 which means I can use a small amount of product injected in a bolus to lift the tissue quickly and provide structure. More anteriorly in the pre-jowl sulcus I used Restylane Defyne; in my experience this integrates well with the tissues, which is especially important in this area of animation. It still has a good G prime and is crosslinked so will be quite robust, but it is just a little bit smoother.4
Technique
For this patient, I injected a 0.5ml bolus deeply down to the bone using a needle on either side of the mandible. Next I used a 25 gauge cannula for my two other injection points in the border of the
mandible; my insertion point was at least 1cm in front of the anterior border of the masseter muscle. When injecting, I looked out for the facial artery – it tends to traverse up in front of the masseter muscle – I marked that point to ensure I avoided it. I ensured I marked the patient while she was sitting upright to ensure I don’t add volume to the region. From that point I worked back, creating a line with a 25 gauge cannula along the mandible and then came up from the anterior point in the mental region. Again, I used a cannula along the border of the mandible, injecting 0.5ml in a fanning motion upwards in the prejowl sulcus on either side – this time using Restylane Defyne. I started posteriorly first, with deep injections, then linearly threading using a cannula, before linear threading with a fanning technique in the pre-jowl sulcus. I did this because by pulling back the tissues in this area, I did not need as much product. I also addressed the patient’s ‘orange peel’ dimpling appearance on her chin. For this I adopted a fanning technique, putting extra support between the skin and mentalis muscle. This meant that when the muscle is active and you can particularly notice the dimpling, there’s a little bit more cushioning and support there so it doesn’t quite pucker the same.
Results
The patient experienced a small bruise in the pre-jowl sulcus, which was not of concern and disappeared within a couple of days. I reviewed the patient two weeks later and everything had settled beautifully, so she was very happy with the results.
52-year-old female patient
Consultation
This 52-year-old lady has been a patient of mine for approximately seven years. Her original concerns were feeling tired and saggy, so she wanted to look and feel her best for her age. She has regular botulinum toxin treatments and is on a full-face dermal filler treatment plan, in which we have treated her cheeks, jawline, chin, lips, nasolabial folds, marionette lines and given her an eyebrow lift. The patient is happy with what we have achieved, so we are simply maintaining her results when appropriate, which is usually every 18 months. About two months prior to this particular treatment, she had 2ml of Juvéderm Voluma injected into her cheeks




in total. As such, treatment of her chin was now on the agenda so I invited her to try the new Juvéderm Volux product.


Product choice
Juvéderm Volux has been specifically formulated for chin and jawline treatment, and shouldn’t be used anywhere else.
It is a high elasticity and high cohesivity product, with a high lift capacity, which basically means you get a better result with less product. Clinical data has
suggested that it will last for up to two years.4 Previously I would have used Juvéderm Voluma to treat this area, however that would usually require an average of 4ml of product, compared to the 2ml used in this treatment.
Injecting Juvéderm Volux feels the same as Juvéderm Voluma, however it is important to note that practitioners require specific training and need to be mindful of depth, placement and volume of product used.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Heather Muir
Rachel Goddard
Before
Before
After After
Technique
The patient has a bulky mentalis muscle, with a deep labiomental sulcus. Lack of bone support in the chin has resulted in hyperactivity of mentalis, causing the chin to rotate, giving a masculine appearance. I treated the labiomental sulcus directly with cannula, using a total of 0.3ml. Myomodulation with dermal fillers can be used to either support muscle movement or to stop overaction of muscle. Treating the labiomental crease myomudulated mentalis by reducing muscle movement, everting the chin and making the lower lip appear more enhanced. Then I treated the chin apex with a total of 1ml for further chin eversion and to create a softer,
more feminine point. To complete the treatment, a total of 0.7ml was injected via cannula into the soft tissue pogonion, giving support to the anterior chin. I used a cannula to administer the product as it improved the comfort for the patient without me needing to create multiple punctures in the area, as the chin can be a very sensitive area to inject.
Results
The patient did not experience any side effects such as swelling or bruising, however it has been reported that patients can have some tenderness in the treatment area for a couple of days. The patient did not have any topical
anaesthetic cream prior to treatment and found it very comfortable. I advised her to avoid makeup, exercise and alcohol for 24 hours and told her to not touch the area for the same period of time – I always spray patients hands with Clinisept Plus just in case they do accidentally touch the area. I also tell patients to avoid facials or other treatments in the area for a minimum of seven to 10 days. I followed up with the patient two weeks later, as I usually do with all my patients, and we discussed the next stages of her treatment plan, which involves creating further support in the marionette lines.
41-year-old female patient
Consultation
My 41-year-old patient presented in clinic requesting a subtle lift to the whole face, without being able to identify which areas had been treated. The plan to achieve this was to target all three of the lifting vectors of the face; namely, the cheek, chin and behind the jowl towards the angle of the mandible. The patient was satisfied with my rationale behind this approach, encouraged by the prospect of achieving maximum lift whilst maintaining a natural look.


Product choice
In the mid-face I used Restylane Volyme, which is a softer product and, in my experience, produces better contouring and allows for greater expression in this area. In the lower face, along the jawline and in the chin, I used Restylane Lyft as it has a higher G prime to achieve projection. I also used Lyft behind the angle of the mandible because again this allowed precise lifting without lateral volumisation.
Technique
For the chin I used approximately 1ml of Restylane Lyft spread over six injections, at three points either side of the midline. I injected below the mental ligament to extend the vertical length of the chin, as well as achieve anterior projection. Injections were placed immediately above the periosteum. Due to the inevitable blunting of the needles with this technique, I prefer to change needle with every injection to reduce the likelihood of bruising. A very small amount of product is lost with the needle change, but as only very small doses are required using Lyft, the benefits to patients makes this sacrifice worthwhile. The posterior injection point varies between individuals, but for this particular patient I placed a single bolus of 0.5ml of Lyft directly onto the periosteum, behind the angle of the mandible. I recommend opening the jaw and very clearly palpating the contour of the posterior aspect of
the angle of the mandible. Placing the needle directly onto the angle, I placed my thumb below the mandibular margin to prevent inferior displacement. Aspirating prior to injection, I then placed 0.5ml of Lyft. This creates an immediate retraction of soft tissues with tightening of the jawline. The process was then repeated on the other side.
Results
The patient did not experience side effects or complications and returned to work the next day, very happy with her results. I arranged to see her four weeks following the treatment, at which point the products had fully integrated into the tissues.
I would anticipate this sort of treatment lasting for about nine to 12 months but we would plan a review around six months when a top-up can be considered. I like to let the product integrate into the tissue before adding more to minimise the risk of biofilms, which can be associated with larger boluses.5

Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Paul Baines
Before After
I injected below the mental ligament to extend the vertical length of the chin
Considerations
Side effects and complications
Dr Cetto explains that the first thing patients will notice following HA treatment is the anaesthetic from the product wearing off. “Especially around the mouth, it can feel a bit funny,” he explains, noting that this will usually go away in half an hour or so. While patients tend to be impressed with the instant results, the skin tends to be a little red, he says, adding, “Thanks to the microcannulas we use, patients can barely see the entry points as they’re so small.”
The practitioners emphasise that bruising can be expected, but will disappear within a few days. “I advise my patients that they can use arnica or vitamin K to reduce a bruise, but most will just wait for it to disappear,” says Dr Muir. Warning patients of the risk of redness, bruising and inflammation is essential, agree the practitioners, as is enquiring about upcoming social arrangements to plan suitable treatment dates.
“Tell them to keep the area clean for a day and do a gentle wash at night,” says Dr Cetto, adding, “I ask them to avoid massaging the area, as I find this tends to increase inflammation and swelling. I also ask patients to avoid anything that would increase their heart rate or make their face flush because that tends to aggravate swelling; for example, excessive drinking or heavy exercise.”
The clinicians agree that it is imperative to reduce the risk of infection by thoroughly cleansing the skin prior to treatment and working in an aseptic environment. Dr Muir performs all her injectable treatments with the assistance of a nurse, specifically to reduce the risk of infection. “When I’m working with a cannula I never place it back down onto a surface; it’s always passed to person to person, keeping it nice and clean,” she says. As Dr Baines highlights, a vascular occlusion is the most catastrophic complication that could occur following injection of HA. “The number one rule when performing these treatments is to have full awareness of where the blood vessels are,” he says, adding that, it is particularly vital that practitioners recognise the route of the facial artery, remembering it runs deeply over the border of the mandible, anterior to the masseter. Dr Baines advises to inject superficially and always use a cannula in this area to reduce risk.
Dr Cetto adds, “Luckily, vascular events are rare but it is definitely something we must point out to patients. Something I learnt when working as a surgical registrar is when
you’re consenting a patient, for every single potential complication you mention you should say what you’re going to do to try and prevent it. For example, with bruising and vascular complication, I’ll explain that I’m going to use a cannula, which will be less likely to bruise and inject into a blood vessel. For infection, I’ll sterilise the skin and ask the patient to keep it clean after the treatment.” Dr Cetto says that by adopting this approach, it will builds patients’ trust in you as a practitioner.
Gender variations
Recognising anatomical gender differences is vital, says Dr Cetto. “Practitioners should note the lower facial third differences in men and women in terms of angle and the width of the chin. The female lower face tends to become heavier in the lower third as we age, and becomes squarer,” he explains, noting, “Adding more volume on the lateral aspect where it’s already heavy usually has little to no improvement and can potentially make things look worse.”
From Dr Muir’s perspective, assessment is the most important part of a consultation.
“I think practitioners have to look at jawline positioning and consider the maxillary and mandibular position,” she says, explaining, “If they don’t and the patient already has a class three mandible that protrudes more than the maxilla, they may be exaggerating the angle of the mandible or the mental region, which can make that look more predominant.” In female patients, this is not always aesthetically pleasing as it is generally regarded as a more masculine trait, she adds.
Managing expectations
Cost of jawline treatment with HA can be expensive due to the amount of product needed, says Dr Muir, so ensuring patients know what results they can expect is particularly important. “A lot of patients think that because of the money involved, it’s going to give the same results as facelift, but it’s not, unfortunately. HA will give a good result but it won’t be as clean cut as being able to pull all the tissues back,” she says, advising, “Some patients will be over the moon with the immediate result when there is a degree of inflammation, but slightly disappointed when this decreases over the next few days. Choosing products that don’t tend to have a large degree of inflammation and making sure patients are fully aware of what to expect is therefore vital,” she says.
To breakdown the treatment process and
expected results, Dr Baines says he uses the analogy of a tent with patients. “I explain that the structure of the face can be compared to the frame of a tent,” he says, detailing, “The ‘ridge pole’ of the tent is the mandible itself, the jawbone. As we age, that ‘ridge pole’ gets shorter as the bones are resorbed. As the ‘ridge pole’ gets shorter, the effect is that the ‘tent material’, which represents your skin, starts to gather, resulting in the appearance of the jowl. We address this by making the mandible ‘ridge pole’ longer again by reinforcing the projection anteriorly at the chin and posteriorly behind the angle of mandible or by increasing the height of the ‘tent’, by augmenting the cheek.”
Dr Baines adds that the lower face is two thirds of the structural support of the ‘tent’. He explains, “A lot of practitioners fall into the trap of over-reliance on the cheek as the only lifting vector – all too often leading to over-treatment in this area. By incorporating the lower-face vectors of the chin and posterior mandible, volumisation can be shared between these sites and a more natural result achieved.
For Dr Cetto, it’s important practitioners know the limitations of their tools. He says, “We should discuss with patients the treatments that we don’t personally offer so they have a clear choice of options – it’s therefore important that we know what a facelift or necklift involves, the approximate cost, associated downtime and who to refer to if patients wanted to go down that route.”
As always, the practitioners agree that it’s very important that we treat aesthetic treatment as a medical procedure. Dr Cetto concludes, “We should treat injectable procedures with even with more seriousness because they are usually an unnecessary medical procedure – we’re not doing it for medical reasons – we have to be extremely careful and take as little risk as possible.”
To read more about gender differences in the lower facial third and gain a CPD point for your learning, turn to p.24.
REFERENCES
1. Coleman SR, Grover R, ‘The anatomy of the aging face: volume loss and changes in 3-dimensional topography’, Aesthetic Surgery Journal (2006) <https://www.ncbi.nlm.nih.gov/ pubmed/19338976>
2. Teoxane, Teosyal Products, (UK: Teoxane, 2019) https://teoxane. com/dermal-fillers/teosyalr-products
3. Baines P, Advertorial: The Secret to a Sharper, Chiselled Jawline with Restylane Lyft (UK: Aesthetics, 2019( <https:// aestheticsjournal.com/feature/advertorial-the-secret-to-asharper-chiselled-jawline?authed>
4. Data available on file.
5. Heydenrych et al., ‘A 10-point plan for avoiding hyaluronic acid dermal filler-realted complications during facial aesthetic procedures and algorithms for management’, Cli Cosmet Investig Dermatol (2018) <https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC6257077/>
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Gender & The Lower Face
Trends published in the press and social media, as well as our own combined clinical experience, suggest that the demand for treatment of the lower facial third has become increasingly popular in recent years for both male and female patients. When planning treatment, gender differences with regards to the anatomy, histology of the hard and soft tissues, surface contours and soft tissue features should be considered, as well as how these evolve through the distinctive male and female patterns of ageing.
Anatomical differences in males and female
In the developmental stages, all faces phenotypically start ‘female’, regardless of biological gender. Approaching adulthood, however, the male face forms a more masculine appearance through changes driven by testosterone, including adaptations in skeletal shape, subcutaneous fat distribution and cutaneous physiology.1,2 The facial height to width ratio gives the overall facial type – the proportion of which in males is typically 1.35:1 and 1.31:1 in females.3 The vertical facial thirds are typically equal in women, however in men, the anterior lower facial height is often slightly greater than the middle third.3
Bone
At a bony level, the Caucasian female facial skeleton is more oval and v-shaped, compared to the male skeleton, which is typically more angular and square in formation. The male mandible has a more prominent flexure, resulting in a stronger, wider and more anteriorly projected chin, a more defined jawline with greater definition at the ramus and angle of mandible.4 In one study, orthopantomographs of 2,699 individuals were analysed, which demonstrated the average gonial angle (angle of the mandible) in female participants to be significantly larger than that of male participants (P<0.0002). Additionally, ramus height and bigonial width were shown to be greater in males compared to females (P<0.0001).5
Histological
The skin plays a key role in the perception of beauty and wellness. Knowledge of the physiological and chemical differences between male and female skin can help practitioners devise tailored treatment plans to deliver optimal cosmetic results. Studies have shown that male skin comprises larger pores and produces more sebum, making it more prone to congestion, the formation of pustules (spots) and the development of acne at a pre-adolescent age.6-9 In post adolescent groups, clinical acne is, however, more prevalent in females; oppose to physiological variables in skin this may be related to the use of low-dose oral contraceptives.10 Furthermore, skin pigmentation and cross-sectional thickness are significantly higher in men.6 Male skin naturally has a high collagen
content and demonstrates higher levels of lactic acid production.7 At the subcutaneous level, female skin is shown to contain higher relative quantities of adipose tissue.11
Muscle
With regards to the facial musculature, men and women differ in terms of both anatomical size and dynamic function (movement). It is well documented that female muscle bulk, including that of the facial musculature, is significantly lower than in men.4,12 In the lower third, for instance, this is demonstrated in the masseter muscles, where the mean thickness in females is reported as 13mm +/- 1.8mm and in males it is 15.1mm +/- 1.9mm.13 The kinetic energy generated by these muscles is comparably greater in men than in women, resulting in larger movements of surface features and dimensionally greater facial expressions. These differences have an impact upon the formation of rhytides (wrinkles) and the gender-specific patterns that can occur.4 In one study of 173 Japanese men and women, measures of wrinkle formation and severity using 3D analysis techniques were found to be significantly greater in men compared with women for most sites including the nasolabial groove and mouth corner.14
Soft tissue features
When considering the soft tissues of the lower face, anatomical studies have shown that the female chin and jaws are narrower and less prominent compared to that of the male.1,2,15 Assessment of the female face in profile shows that the chin sits slightly posterior to the lower lip, whereas in men they are in line.1,2 A deeper labiomental groove is observed in men, typically measuring 6mm compared to the average 4mm seen in women. The literature also reports that men tend to have larger mouths (intercommissural distance), but smaller lips (particularly the upper lip) with wider and thicker philtral columns.1,11
Ageing of the face in the lower third
It is clear that unique patterns of ageing occur in men and women at every histological level, including the skin, subcutaneous tissues, muscle layer and bone. Practitioners should be aware of the distinct characteristics of gender-specific ageing in order to deliver effective and appropriate treatment. While men experience gradual and progressive reductions in testosterone production with age, women demonstrate abrupt declines in oestrogen production around the time of menopause in the fifth decade of life.16,17 With age, men can lose the masculine features of the lower third with reduction in the overall bony dimensions of the mandible (jawbone) through skeletal resorption, loss of the angular shape and definition of the jawline and sagging of the overlying skin to create pre-jowls.4 On the contrary, women complain of the face becoming masculinised and adopting the typical male ‘square’ shaped lower
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Eleanor Reid, Miss Lara Watson and Miss Priyanka Chadha explore the gender differences in the lower facial third and discuss treatment considerations
face. This occurs through a loss of relative width in the mid-face, gravitational descent of soft tissues, progressive laxity of the retaining ligaments and dentoalveolar resorption.4,5
Computerised tomography (CT) scans such as those described by Mendelson and Wong show clear radiographic evidence that the facial skeleton undergoes selective resorption with age.18 Both male and female mandibles show no change in the bigonial width and breadth of the ramus; however, with age, the height of the ramus and mandibular body decrease and the mandibular angle increases. The result creates a more obtuse mandibular angle and retraction of the chin. This occurs even with the presence of a full dentition, although tooth loss significantly accelerates maxillary and mandibular resorption.15,18 Ageing at the bony level has a subsequent effect on the overlying soft tissues in the lower face region. In this area, the lack of bony projection creates a relative concavity and contributes to the presence of jowls.18 It is well reported that age changes in the mid-face have an effect on the lower third. Major loss of the bony projection of the maxilla, which contributes to the edge of the pyriform aperture, results in the undermining of structural support to the alar base and upper lip, resulting in the development of nasolabial folds (amongst other lower facial folds) in both sexes.4,18 At a skin level, facial ageing can be more apparent in women than men. Due to a higher level of adipose tissue at the subcutaneous level, women are more likely to develop fine surface lines, opposed to the deeper rhytides seen in men.11 Deeper lines in men are also attributed to a greater skin thickness. Higher rates of sebum and lactic acid production, however, assist in the lubrication of the stratum corneum, aiding natural moisturisation of the male skin and making it less prone to surface dryness.11
In terms of the dynamism of the lower face, men have a greater upward vertical movement of the facial muscles when puckering the lips and smiling, which should be considered to select a product of appropriate rheology. Both men and women can be prone to masseteric hypertrophy through bruxism and other parafunctional habits, but the resulting cosmetic impact of this is distinctively different between the sexes; masculinising the female face and creating an irregular contour and aggressive appearance in the male face.4
In youth, men tend to have deeper rhytids in the perioral region than women of the corresponding age due to the differences in dynamic movement and gender specific skin characteristics discussed above. In the ageing face, however, this region is the one exception to where older women develop deeper rhytides than men.4,11 Across both sexes, thinning of the lips and blunting of the vermillion border and philtral columns are observed.4
Lower face ideals: male vs. female

Although the perception of beauty and facial ideals are very much subjective to societal trends and individual opinion, the physical attributes that are conventionally considered ‘attractive’ differ between the sexes. Features that contribute to an overall aesthetic appearance are variable from one race to another; however, consideration should be made that the norms of any population should be considered as
a guide and not an absolute value, which may vary depending upon age, gender and ethnicity. Furthermore, the practitioner should never make assumptions as to what the patient’s treatment goals are based on their sex or any other demographic measure.
In women, facial attractiveness is mostly attributed to the cheekbones and prominent upper facial features. The ‘inverted triangle of youth’ that describes a gradual taper in the facial contour from upper to lower is considered a feminine feature of youth across all ethnicities.1,2,4 A chin width that is equal to the flare of the nostrils that descends into an apex and sits at or just posterior to the Riedel line – a line connecting the most anterior point of the upper lip, lower lip and chin in a balanced face – is perceived as a feminine facial appearance.19 This also denotes where the maximum lip volume should be concentrated. In Caucasian women, traditional ‘golden ratio’ of upper to lower lip is 1:1.6; however, a shift in recent trends tends to favour the 1:1 ratio.19 Alternatively, male attractiveness is mostly attributed to the masculine appearance that can be created with a strong jawline and chin.1,2,20 In men, the ideal facial shape has a chin width that corresponds to the width of the mouth. It is flatter and more projected with two squaredoff tubercles.2,4 Emphasis is also placed on the lateral flare of the mandible, with the maximum width of the lateral projection of the zygomas equalling the lateral flare of the mandibular angle, in order to create an equally balanced middle and lower third that creates the ideal ‘square’ male facial shape.11 In profile, both upper and lower lip should project anteriorly to satisfy the Riedel line.4
Before After

In youth, men tend to have deeper rhytids in the perioral region than women of the corresponding age due to the differences in dynamic movement and gender specific skin characteristics
Figure 1: Pre- and post-treatment photographs of a male patient receiving chin and jawline augmentation. Pre-treatment photograph demonstrates poorly defined mandibular angle and a rounded chin. A total of 4ml of Restylane Volyme was used to increase width of the lower third and enhance the definition of the jawline.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 3: Immediate post-treatment photographs. The profile has been corrected with an increased anterior projection of the chin. The squareness of the lower third has been softened to create a curved point and feminise the lower third. 2ml of Restylane Volyme was injected for chin augmentation, 2.2ml of Restylane Volyme administered along the jawline and angle of the mandible. Patient also received treatment to the mid-face (cheeks) and temples.


Treatment motivations
Typically, the motivation for men to seek aesthetic treatments is not only to look younger and more rejuvenated, but also to improve their competitiveness in the workforce.11 The literature shows that in the lower facial third, enhancing the masculine features improves the perception of masculinity and can also be associated with negative attributions, including dishonesty and coldness. Over-exaggerated masculine features such as an overly broad chin can be perceived as being aggressive or threatening.4,18 When carrying out aesthetic enhancements, across all cultures it is deemed that a more feminised face on a man is considered to be more attractive than a more masculinised face.4,18 It is likely that male attractiveness is more a balance between masculinity and femininity. When applying this into aesthetic practice, augmentation should be performed conservatively, using sufficient volume to restore a youthful contour, but avoiding exaggerated augmentations. Conversely, a global survey of 7,700 women by Allergan in 2016 showed the main motivation for females to seek non-surgical facial aesthetics procedure was to ‘look good’, primarily for themselves.21 The desire to improve their aesthetic appearance ranked more highly than to address the signs of ageing.21 As previously described, female attractiveness is typically attributed to the mid-face and the literature suggests that the eye area is highly ranked by women as area of concern with regards to facial ageing.21,22
Treating the lower facial third
When treating both male and female patients, the fundamental principles of thorough patient assessment, knowledge and understanding of anatomy, correct product selection and safe practice apply. Patients may select from a variety of treatment modalities including laser technology, threads and skin resurfacing techniques. This article, however, will focus on the use of injectables (botulinum toxin and dermal fillers) to augment the lower third through the regulation of muscle activity and the volumisation and rehydration of the soft tissues.
When using hyaluronic acid (HA) filler, a high viscosity product is preferable when augmenting the chin and jawline to simulate the bony architecture and provide the desired structural enhancement.2,20,23,24 Selecting a product with a high G prime is recommended to facilitate the appropriate rheology (resistance to the number of deforming forces that may be applied to the HA filler) and the resulting cosmetic effects in function and expression.2,20,24
Treatment of the female patient may focus more on dermal filler placement to accentuate the inferior projection of the chin and enhance the feminine contracture of the lower facial third and comply with the ‘inverted triangle of youth’ concept.19 Treatment in this area may be performed by injecting a bolus of product on to the menton in front of the bony mental protuberance at the midline of the jaw, with a further two more injections either side to taper the product and create a chin apex.23 A square or box-like pattern of administration may be preferable in a male patient with two injection sites anteriorly (either side of the midline), which can be supplemented by a further lateral injection site on either side. This helps preserve the masculine squareness of a chin and jawline, and avoids creating an overly soft and rounded appearance.4,11,23 When treating the chin in both sexes, small boluses of product may be placed deep on to the supraperiosteum to aid compartmentalisation of the filler in the tight fat compartment. Due to the relatively tight tissues in the chin, slow conservative HA filler placement is recommended, pinching the tissues whilst placing the product to encourage good anterior projection, whilst avoiding unwanted lateralising volumisation. With consideration to the mental artery and vein, aspiration is recommended with every injection.23,25


Treating the mandibular body and angle will create a more defined contour to the jawline in both sexes. Injections along the body are placed more superficially in the subcutaneous layer where the use of a microcannula is advisable with careful consideration of the facial vein and artery that ascends the face on the medial portion of the masseter muscle.20,23
When treating the female patient, placement of filler along the inferior border of the mandible is preferred to add definition and contour without increasing the bigonial width, which could alter the width ratios of the vertical facial thirds and masculinise a face. Conversely, the filler should be placed more laterally along the body in the male patient to add definition and a masculine lateral flare to the mandible. For this same reason, a much more conservative volume of filler is indicated when placing deep bolus injections onto the angle of the mandible in women to avoid creating a masculine appearance.23
In both sexes, the use of botulinum toxin type A injections in hypertrophic masseter muscles can offer a non-invasive alternative for improving the zygomatic-bigonial ratio, as well as the ratio of the bigonial distance to total face height (trichion to gnathion ratio).13,26
Figure 2: Pre-treatment photographs demonstrating a mild-moderate skeletal class II relationship (retrognathic mandible or ‘overbite’) and a squaring of the lower facial third. The jawline is also under defined.
Before
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
After Before After
The use of botulinum toxin can assist in temporarily reducing muscle activity in the masseter muscle, thus reducing muscle mass, with the aesthetic outcome of creating a more slender angle of the mandible. Dosing can range from 20-40 units per side, though higher doses in general are associated with a greater incidence of complications.13,26
A physiological consideration when treating men is that they tend to have a greater number of microvessels present, coupled with a dense vascular plexus to support hair follicles that product thicker facial hair.11 As a result, men are more prone to bruising after facial injections. Although no one single injection protocol can be applied to each individual sex, it is widely accepted that due to the presence of larger facial muscles, men require higher doses of botulinum toxin injections to create the same cosmetic effect as in women. In any case, a dynamic assessment of each individual patient should be made to determine potential areas of stronger contraction that may be indicated by deeper lines, larger visible and palpable muscle mass and greater dynamic movement.12
Conclusion
While this article has discussed the typical dimorphic approaches to the treatment of the lower facial third in the male and female, sensitive consideration should be made to the fact that society in general and young people in particular are increasingly challenging conventional gender stereotypes. The subject of gender has become a topical source of interest and debate as societal interpretation of gender and its implications on the identity of an individual are continuing to shift and evolve. As with any non-surgical aesthetic treatment, a thorough consultation, systematic assessment of soft and hard tissues and their functional behaviour is essential to understanding the individual’s treatment goals and achieving outcomes that support and enhance the patient’s sense of self including that of gender identity.
Dr Eleanor Reid is an aesthetic practitioner and dental surgeon graduating from Newcastle University. Dr Reid has a background in maxillofacial surgery, hospital and practice based dentistry and is lead trainer in Newcastleupon-Tyne for Acquisition Aesthetics and director of Paragon Aesthetics.


Miss Lara Watson is dual qualified in medicine and dentistry and is currently on the only maxillofacial surgery themed core training pathway in London. Dr Watson is a faculty member for Galderma and is also a co-founding director of Acquisition Aesthetics, a training academy committed to raising the bar for standards of practice in aesthetic medicine.
Miss Priyanka Chadha currently works as a plastic surgery registrar in London and is co-director of Acquisition Aesthetics training academy. Her academic CV comprises national and international prizes and presentations, as well as higher degrees in surgical education and training. Dr Chadha is a faculty member for Galderma.

REFERENCES
1. Mauricio de Maio, Ethnic and Gender Considerations in the Use of Facial Injectables: Male Patients, Plast Reconstr Surg. 2015 Nov;136(5 Suppl):40S-43S.
2. Cetto R. Male chin and jawline Ageing. Aesthetics Journal 2019 31-33. <https://aestheticsjournal. com/feature/male-chin-and-jawline-ageing>
3. Farhad B A Naini, Daljit S Gill, Facial Aesthetics:2.Clincal Assessment. Dental Update 2008; 35:159-170.
4. Isabela T. Wieczorek, Brian P. Hibler, and Anthony M. Rossi, Injectable Cosmetic Procedures for the Male Patient, Journal of Drugs in Dermatology, September 2015, Volume 14, Issue 9.
5. J Leversha et al. 2016 ‘Age and gender correlation of gonial angle, ramus height and bigonial width in dentate subjects in a dental school in Far North Queensland’, J Clin Exp Dent. 2016 Feb; 8(1) e49-e54.
6. Rahrovan, F. Fanian, P. Mehryan, et al., Male versus female skin: What dermatologists and cosmeticians should know, Int J Womens Dermatol. 2018 Sep; 4(3): 122–130.
7. Dr Uma Jeyanathan, What men want. Eshtetics Dentistry Today, vol 11, no3, June 2017, pp. 36-37.
8. Joshua A. Farhadian, Bradley S. Bloom, and Jeremy A. Brauera, Male Aesthetics: A Review of Facial Anatomy and Pertinent Clinical Implications, Journal of Drugs in Dermatology, September 2015 Volume 14, Issue 9.
9. Grace K, Kim DO, Brent D. Post-adolescent Acne in Women: more common and more clinical considerations. Journal of Drugs and Dermatology. 2012(11) 708-713
10. Cunliffe WJ, Gould DJ. Prevalence of facial acne vulgarise in late adolescence and in adults. British Medical Journal, 1979 (1) 1109-1110.
11. Joshua A. Farhadian, Bradley S. Bloom, and Jeremy A. Brauera, Male Aesthetics: A Review of Facial Anatomy and Pertinent Clinical Implications, Journal of Drugs in Dermatology, September 2015 Volume 14, Issue 9.
12. Anido J et al. Tailored botulinum toxin type A injections in aesthetic medicine: consensus panel recommendations for treating the forehead based on individual facial anatomy and muscle tone. Clin Cosmet Investif Dermatol 2017 10 413-421.
13. Jaff, S. Culbard, A. The Use of Boutlinum Toxin Type A in the Hypertrophic Masster Mucscle. Aesthetic Dentistry Today, 2017. Pp.33-35.
14. Tsukahara K, Hotta M, Osanai O, Kawada H, Kitahara T, Takema, Y. Gender-dependent differences in degree of facial wrinkles. Skin Res Technol. 2013 Feb;19(1):e65-71.
15. Doual JM, Ferri J, Laude M. The influence of senescence on craniofacial and cervical morphology in humans. Sure Radio Anat 1997 (19) 175-183.
16. Harman SM, Metter EJ, Tobin JD, Pearson J Blacman MR. Longitudinal effects of ageing on serum total and free testosterone levels in healthy mean. Baltimore Longitudinal Studying of Aging. J Clin Endocrinol Metab 2001 86 (2) 724-31
17. Wysong A, Kim D, Joseph T, MacFarlane DF, Tang JY, Gladstone HB. Qualifying soft tissue loss in the aging male face using resonance Imaging, Dermal Surgery 2014 40 (7) 783-93.
18. Bryan Mendelson & Chin-Ho Wong, Changes in the Facial Skeleton with aging: Implications and clinical application in Facial Rejuvenation. Aesthetic Plastic Surgery 2012 36: 753 760
19. Swift A, Remington K. BeautiPHIcatiion: A global approach to facial beauty. Clin Plastic Surg 38 2011 347-377
20. Jack D Contouring the Male Jawline. Aesthetics Journal, 2017 43-45. <https://aestheticsjournal. com/feature/contouring-the-male-jawline>
21. New Global Research From Allergan Shows New Attitude To Beauty As Women Seek Confidence Over Youth, Jun 28, 2016. <https://www.newswire.ca/news-releases/new-globalresearch-from-allergan-shows-new-attitude-to-beauty-as-women-seek-confidence-overyouth-584655091.html>
22. Sobanko JF et al., Motivations for Seeking Minimally Invasive Cosmetic Procedures in an Academic Outpatient Setting, Aesthet Surg J. 2015 Nov;35(8):1014-20.
23. Maio M., Wu W.T.L., Goodman G.J., Monheit G. (2017). Facial Assessment and Injection Guide for Botulinum Toxin and Injectable Hyaluronic Acid Filler: Focus on the Lower Face. Plast. reconstr. Sur. 140: 393-404
24. Sundaram, H. and D.Cassuto, Biophysical characteristics of hyaluronic acid soft-tissues fillers and their relevance to aesthetic applications. Plastic and reconstructive surgery, 2013. 132(4s-2): p. 5s-21s.
25. Wang Q et al., Vascular Complications after chin augmentation using Hyaluronic acid. Aesth Last Surg 2018 42 553-59.
26. Chang, C-S. Kang, G. Achieving Ideal Lower Face Aesthetic Contours: Combination of Tridemensional Fat Grafting to the Chin with Master Boutlinum Toxin Injection. Aesthetic Surgery Journal (2016), p1093-1100.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The secret to full facial rejuvenation
Dr Kuldeep Minocha, Aesthetic Practitioner
DR KULDEEP MINOCHA
Do you have any tips for practitioners looking to treat the whole face?
Each time you see a patient, look at them with fresh eyes. Take the time to look at how the light is hitting the face and where the shadows are.
Which dermal fillers do you prefer?
I only ever use the Restylane® range. I’ve used Restylane® in over 30,000 treatments over twelve years. My reputation depends on using products I know and trust. There are eight fillers in the range and each one varies slightly in consistency, particle size and lift capacity. I like having a broad artistic palette to choose from and it means I can tailor the treatment for each patient.

What do you look for when assessing the face?

• Skin quality – assess skin hydration, sun damage, fine lines and wrinkles

• Facial shape and balance – is there too much weight in the lower third and can we recreate the heart-shaped or oval-shaped face?
• Proportions and contours – look at the frontal view, the profile view and the three-quarter view and assess the relationships between each subunit of the face
• Facial symmetry – are the features balanced and how do they change when animated?
• Emotion – does the face look sad, angry or tired and which areas are contributing to these emotions?
What products do you use for different parts of the face?
If I’m looking to fill a large area I use Restylane Volyme™, say for the temple or the sub-malar area. If I’m injecting more superficially I’d go for Restylane Refyne™ which has a smaller particle size and integrates nicely into the skin. Where I want definition and projection on the cheeks, nose, jaw or chin, I use Restylane Lyft™. If I’m reconstructing or restoring the lips I’ll use Restylane™, but if I’m looking to volumise, beautify and enhance the lip I’d use Restylane Kysse™ which is softer and integrates well.
If you could only choose one product what would you choose?
That’s easy. My go-to product would always be Restylane Lyft™. The high G-prime, precision and lift means you can get a impressive result with only one or two syringes. It’s really effective for countering the reabsorption of the bone and the descent of the fat pads that happens to all of us as we age. Not everyone can afford multiple syringes and I find more and more people want the biggest bang for their buck. With Restylane Lyft™ you get that.
About Dr Minocha
Dr Kuldeep Minocha qualified as a GP in 1996. After working for the NHS as GP principal in Essex for a number of years, he commenced training and practice in facial aesthetics in 2006.
Dr Minocha founded Minocha Health, his aesthetic practice, the same year, before concluding his NHS commitments in 2011 to take up a full-time career in aesthetics. Dr Minocha is a global brand ambassador and key opinion leader for Galderma.

RES19-03-0144 DoP: March 2019
BEFORE AFTER A patient treated with Restylane Lyft™ , Restylane Refyne™ , Restylane Volyme™ and Restylane Defyne™
“ My go-to product would always be Restylane Lyft™ ”
scope of practice, be trained and assessed as competent to assess, diagnose and treat some skin lesions.3,4
Of course, a verruca on a young person’s foot is likely to be fairly obvious, but an apparent wart in an elderly person may be a squamous cell carcinoma, a common form of skin cancer. Pigmented lesions are of particular concern as treating them inappropriately with cryotherapy can alter the histology and prolong overall time to diagnosis,5 which is crucial in melanomas. Practitioners must therefore be trained in recognising such lesions for safe diagnosis before treatment.
Performing the treatment
Cryotherapy in Aesthetic Practice
Cyrotherapy is an established treatment for dermatological lesions and can be used for a variety of conditions including benign lesions such as viral warts, seborrheic keratosis, sebaceous hyperplasia, haemangiomas and lentigo, and pre-malignant lesions including actinic keratosis and Bowen’s disease. Many, if not most, GPs in the UK will no longer provide cryotherapy through the NHS for benign lesions.1 In fact, in November 2018 the NHS released the Evidence-Based Interventions: Guidance for CCGs document, which states in its update description for the removal of benign skin lesions that they ‘cannot be offered for cosmetic reasons’ and should only be offered in situations where the lesion is causing symptoms outlined in at least one of its criteria. Some examples of criteria include: the lesion is unavoidably and significantly traumatised on a regular basis, repeated infection, regular bleeding, regular pain and impacts function.2

I have found that many GPs also don’t offer treatment on a private basis, so there is certainly a gap in the market for aesthetic practitioners to do so. I believe that cryotherapy has become a more common and popular treatment in non-surgical aesthetic clinics and is a useful addition to your current treatment portfolio. In this article, I will explore the clinical aspects behind its use for treating cosmetic benign lesions, and also touch on the benefits it can bring to you from a business perspective.
Training requirements
Firstly, it’s important to recognise that the training requirements needed to identify and diagnose appropriate lesions for cryotherapy are different to those required for performing the actual cryotherapy treatment.
Diagnosis
The practitioner must have the ability to make the correct clinical diagnosis of the lesion before treating it. This requires significant dermatological training to be considered safe and usually only general practitioners with extended roles (GPwER) or dermatologists can do this. Some dermatology nurse specialists and consultant dermatology nurses who have undertaken extensive post-graduate dermatology training may, as part of their extended
If you do not have the skills in diagnosing, you could ask your patient to obtain a diagnosis from their GP (with qualifications explained above) so that you can still perform the actual treatment in your clinic. If the lesion is diagnosed as benign, then the GP can refer to you for treatment. As mentioned, many GPs will not provide cryotherapy through the NHS nor on a private basis, so they will sometimes be relieved to have a provider they can trust to refer their patients onto.
As with many skin-related treatments that are classified as cosmetic, one does not need to be a medical professional, just trained in performing the procedure. Personally, however, I only endorse that medical professionals, with appropriate training, perform this procedure in a clinical environment as there are possible clinical side effects (Table 1).6 Practitioners must have
Dr Paul Charlson discusses the use of cryotherapy for benign dermatologic concerns in aesthetic practice and how it can benefit both your patients and business
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The practitioner must have the ability to make the correct clinical diagnosis of the lesion before treating it
‘ABOBOTULINUM TOXIN IN ACTION: KEY PRINCIPLES & TREATMENT FOR GLABELLAR LINES’
IT WILL BE HELD ON MONDAY JUNE 17 AT 7PM.
How do I guarantee my place on ‘Abobotulinum toxin in Action: Key Principles & Treatment for Glabellar Lines’ Webinar’?
1. Visit www.aestheticsjournal.com/ Webinar_GaldermaJune2019
2. Login OR join as a member for free
3. You will then be prompted to use your DocCheck* password to confirm that you are a Doctor, Nurse or Dentist and able to access this webinar (if you registered for the last Aesthetics webinar, your DocCheck account will be valid)
4. Tick the box to confirm that you would like to sign up for the webinar. You’ll then receive reminder emails for the event closer to the time to ensure you don’t miss out!
*What if I don’t have a DocCheck login?
Register with DocCheck for free www.doccheck.com/register
Please note that you will need to provide the following when you have registered your contact details:
- A PDF of your record on the register downloaded from the GMC/NMC/GDC website as appropriate AND proof of ID (passport or driving licence)
- OR your personal certificate from your medical qualification
Your information will be checked and once it has been verified you can then visit the Aesthetics webinar page, use your DocCheck password and confirm you would like to sign up for the webinar by ticking the box. If you have any issues with your DocCheck verification please contact cream@doccheck.com
IMPORTANT: You will need to register and provide proof of your medical qualification to DocCheck by Thursday June 13 in order to guarantee that your registration will be processed in time for access to the webinar
PLEASE LOOK OUT FOR THE NEXT GALDERMA WEBINAR...
Botulinum toxin
are different
on the
Speywood units are specific to this preparation and are not interchangeable with other botulinum toxins. Reconstitute prior to injection. Intramuscular injections should be performed using a sterile suitable gauge needle. Glabellar lines: recommended dose is 50 Speywood units divided equally into 5 injection sites, 10 Speywood units to be administered intramuscularly, at right angles to the skin; 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle. Lateral canthal lines: recommended dose per side is 30 Speywood units divided into 3 injection sites; 10 Speywood units to be administered intramuscularly into each injection point, injected lateral (20 - 30° angle) to the skin and very superficial. All injection points should be at the external part of the orbicularis oculi muscle and sufficiently far from the orbital rim (approximately 1 - 2 cm); (See summary of product characteristics for full technique). Treatment interval should not be more frequent than every three months. The efficacy and safety of repeat injections of Azzalure has been evaluated in Glabellar lines up to 24 months and up to 8 repeat treatment cycles and for Lateral Canthal lines up to 12 months and up to 5 repeat treatment cycles. Not recommended for use in individuals under 18 years of age. Contraindications: In individuals with hypersensitivity to botulinum toxin A or to any of the excipients. In the presence of infection at the proposed injection sites, myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis. Special warnings and precautions for use: Care should be taken to ensure that Azzalure is not injected into a blood vessel. Use with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission, in the presence of inflammation at the proposed injection site(s) or when the targeted muscle shows excessive weakness or atrophy. Patients treated with therapeutic doses may experience exaggerated muscle weakness. Not recommended in patients with history of dysphagia, aspiration or with prolonged bleeding time. Seek immediate medical care if swallowing, speech or respiratory difficulties arise. Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to facial anatomy, as a result of previous surgical interventions should be taken into consideration prior to injection. Injections at more frequent intervals/higher doses can increase the risk of antibody formation. Avoid administering different botulinum neurotoxins during the course of treatment with Azzalure. To be used for one single patient treatment only during a single session. There is a potential risk of localised muscle weakness or visual disturbances linked with the use of this medicinal product which may temporarily impair the
ability to drive or operate machinery. Interactions: Concomitant treatment with aminoglycosides or other agents interfering with neuromuscular transmission (e.g. curare-like agents) may potentiate effect of botulinum toxin. Pregnancy, Lactation & Fertility: Not to be used during pregnancy or lactation. There are no clinical data from the use of Azzalure on fertility. There is no evidence of direct effect of Azzalure on fertility in animal studies. Side Effects: Most frequently occurring related reactions are headache and injection site reactions for glabellar lines and; headache, injection site reactions and eyelid oedema for lateral canthal lines. Generally treatment/injection technique related reactions occur within first week following injection and are transient. Undesirable effects may be related to the active substance, the injection procedure, or a combination of both. For glabellar lines: Very Common (≥ 1/10): Headache, Injection site reactions (e.g. erythema, oedema, irritation, rash, pruritus, paraesthesia, pain, discomfort, stinging and haematoma). Common (≥ 1/100 to < 1/10): Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites, predominantly describes brow paresis), Asthenopia, Eyelid ptosis, Eyelid oedema, Lacrimation increase, Dry eye, Muscle twitching (twitching of muscles around the eyes). Uncommon (≥ 1/1,000 to <1/100): Dizziness, Visual impairment, Vision blurred, Diplopia, Pruritus, Rash, Hypersensitivity, Eye movement disorder. Rare (≥ 1/10,000 to < 1/1,000): Urticaria. For lateral canthal lines: Common (≥ 1/100 to < 1/10): Headache, Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites), Eyelid ptosis, Eyelid oedema and Injection site disorders (e.g. haematoma, pruritus and oedema). Uncommon (≥ 1/1,000 to <1/100): Dry eye. Adverse reactions resulting from distribution of the effects of the toxin to sites remote from the site of injection have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcome in some cases). Prescribers should consult the summary of product characteristics in relation to other side effects. Packaging Quantities & Cost: UK 1 Vial Pack (1 x 125u) £64.00 (RRP), 2 Vial Pack (2 x 125u) £128.00 (RRP), IRE 1 Vial Pack (1 x 125u) €93.50, 2 Vial Pack (2 x 125u) €187.05 (RRP) Marketing Authorisation Number: PL 06958/0031 (UK), PA 1613/001/001 (IRE) Legal Category: POM Further Information is Available From: Galderma (UK) Limited, Meridien House, 69-71 Clarendon Road, Watford, Herts. WD17 1DS, UK. Tel: +44 (0) 1923 208950 Fax: +44 (0) 1923 208998 Date of Revision: September 2018
Adverse events should be reported.
For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard
For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: medsafety@hpra.ie. Adverse events should also be reported to Galderma
Ltd.
Date of Preparation: April 2019 Job code: AZZ19-04-0034e
(UK)
Azzalure Prescribing Information (UK & IRE) Presentation: Botulinum toxin type A (Clostridium botulinum toxin A haemagglutinin complex) 125 Speywood units of reconstituted solution (powder for solution for injection) Indications: Temporary improvement in appearance of moderate to severe: • Glabellar lines seen at maximum frown, and/or • lateral canthal lines (crow’s feet lines) seen at maximum smile in adult patients under 65 years, when severity of these lines has an important psychological impact on the patient. Dosage & Administration: Azzalure should only be administered by physicians with appropriate qualifications and expertise in this treatment and having the required equipment.
units
depending
medicinal products.
WEBINAR
HEALTHCARE PROFESSIONALS
AESTHETICS
THE NEXT
FOR
HOSTED BY
JOURNAL IN ASSOCIATION WITH GALDERMA WILL BE
good knowledge and understanding of the equipment, treatment protocols and methods for the device employed, which can usually be obtained from your device provider. Like many treatments in aesthetics, insurance is what determines whether or not you are able to perform cryotherapy treatments, and there are several providers available.
How cryotherapy works
Cryotherapy is defined as the local or general use of low temperatures in medical therapy, and refers to the removal of skin lesions by freezing. The procedure works by cellular and vascular injury to the tissue.7 There are several methods for delivering cryotherapy, such as liquid nitrogen, those that employ vapourisation of a volatile liquid to create cooling, and others that use nitrous oxide. As my experience lies in liquid nitrogen, I will be discussing this approach. The advantage of liquid nitrogen cyrospray is that it reaches colder temperatures than other methods,8,9,10 which I find achieves superior results. However, the disadvantages are that it requires a large storage dewar and an appropriate safe storage space,11 while other methods are more
Cryotherapy side effects
ready to hand and economical for purchase. The clinic will also require regular deliveries of liquid nitrogen to utilise this approach. The treatment is usually delivered by a cryotherapy spray or probe that is connected to a reservoir of liquid nitrogen, which is at a temperature of -196°C. Using an open spray of liquid nitrogen creates an ice ball, the depth of which is roughly equal to the lateral spread.12 Much is known about the efficacy of liquid nitrogen,13,14 and guidelines for treatment are well established.15
What can be treated?
As mentioned above, many skin conditions can be treated using cryotherapy. The types of benign skin lesions that are suitable for this treatment include actinic keratosis, solar lentigo, seborrheic keratosis, viral wart, molluscum contagiosum, and dermatofibroma.16 It should be noted that the efficacy of treatment depends on the condition; cryotherapy for solar lentigo is considered by some to be the treatment of choice, for example,17 whilst others suggest laser may be better.18 Other lesions such as keloid scars that have been treated with cryotherapy plus steroid injection have shown positive results.19 Some conditions are easier to treat through cryotherapy than others – for example, some cells such as melanocytes are easily damaged by cold, whereas others such as fibroblasts are very resistant to cold. There is a comprehensive list of lesions that can be safely treated with cryotherapy in Cutaneous Cryosurgery 12
Immediate Subsequent Pain
Although usually well-tolerated, if a deep freeze has been used, then cryotherapy can cause some discomfort and pain both during and after the treatment. Taking painkillers an hour before the anticipated treatments and for the following 24 hours may relieve discomfort.
Swelling and redness
This is a common immediate response to skin freezing and usually settles after two to three days. The area might ooze watery fluid for a short time following the procedure and treatment close to the eyes may result in prominent puffiness of the lower eyelids, which settles within days.
Blistering
This is a common effect, but settles after a few days as the scab forms. Some patients are more prone to blistering than others and it does not necessarily mean the skin has been frozen too much. The blisters may occasionally become filled with blood and should only be punctured with a sterile needle if it is very uncomfortable/painful.
Infection
This is uncommon, but can occur. Infection can result in increased pain and pus formation, which may require topical antiseptic or antibiotic therapy.
1:
Scarring
A scar will rarely form, and is more common if a deep freeze has been necessary. Hypertrophic/keloid scarring is rare, and appears as a founded, hard growth on the skin. These are more common in those with dark skin.
Pigmentation changes
The area at or around the treatment site may darken or lighten in colour, which is more common in dark-skinned individuals. This can be permanent, however usually improves with time.
Numbness
This can occur if a superficial nerve is frozen. Normal feeling usually returns within a few months.
Treatment process
As diagnosis involves comprehensive assessment and training, and differs for each condition, I will not be discussing this in detail. Once a diagnosis has been made, cryotherapy treatment is fairly simple. An informed consent must be obtained and the side effects of cryotherapy outlined. These are outlined in the British Association of Dermatologists’ Patient Information Leaflets, which I issue to my patients (Table 1).6 Once consent is obtained, it is useful to apply a topical anaesthetic cream such as EMLA and de-bulk the most hyperkeratotic lesions before treatment. This removes the excess lesion; I often break a tongue depressor by twisting it and scraping off the excess material or use a scalpel. There are a variety of ways to treat with liquid nitrogen and the kits supplied usually have different nozzle sizes. I find that it is useful to use the disposable ear cones that come with otoscopes as they can be cut to a lesion size to funnel the spray.
Unideal treatment outcome
Treatment may not be effective, or the condition may recur.
The lesion is sprayed from about 1cm away until an ice ball forms around it, which should be maintained for the number of seconds required in the protocol, which are well-established and are different for each lesion. More information on these protocols can be found in Cutaneous Cyrosurgery 21 Feathering is a method I use to blend the edges of the treatment area, which is
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Table
The potential side effects of cryotherapy. Information obtained from the British Association of Dermatologists’ Patient Information Leaflets.6
Surface Imaging Solutions is the exclusive distributor partner in the UK and Ireland for Canfield Scientific (www.canfieldsci. com) , the market leader in healthcare imaging solutions. Our rich portfolio includes Aesthetic Systems such as the VISIA® complexion analysis system, the VECTRA®3D range and IntelliStudio® and in Medical Dermatology the VECTRA®3D WB360, VECTRA®3D H1 XP, IntelliStudio® and VEOS® products and DermaGraphix® application software. As a market leader in healthcare imaging solutions, we deliver outstanding photographic systems, software applications, consultancy and support services to consultant surgeons, physicians and practitioners in Aesthetic, Cosmetic, Plastic and Reconstructive Surgery across the NHS and Private practices and Aesthetic Clinics in our market space.



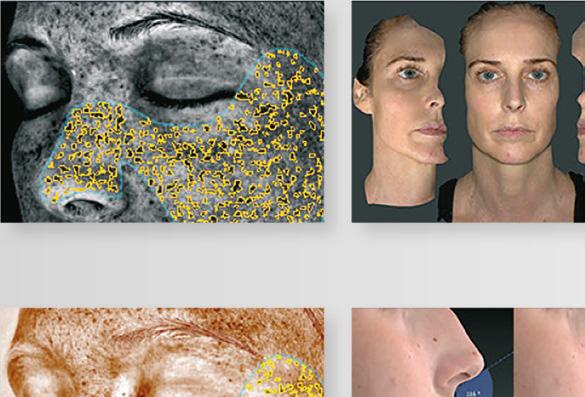
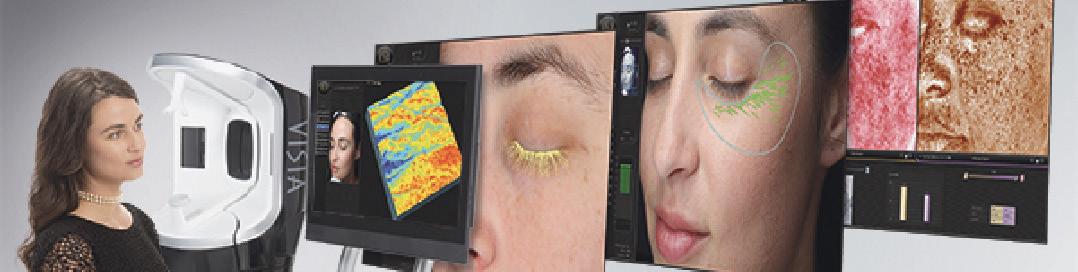



SIS ensure all healthcare professionals are provided the tools to offer the best services to their patients improving communication, planning and managing treatment outcomes across the continuum of care, combined with methods and services to support them in today’s regulatory environment.
Ready to Try?
Experience the latest 3D imaging technology that will enable your patients to clearly express, visualise and document their aesthetic desires. Using our FREE VectraView® 3D application, you have full camera and rotation control of your patients’ 3D data capture, right in your consulting room.


Ready to Buy?
 Lease VISIA or VECTRA H1 from £95 / week. Full warranty over lease purchase term
Lease VISIA or VECTRA H1 from £95 / week. Full warranty over lease purchase term
SU R FA C E I M AG I NG SOLUTIONS +44 (0) 77 7480 2409 surfaceimaging.co.uk
We offer a wide range of purchase options and support packages to help grow your practice, including
Increase patient satisfaction Differentiate your practice Communicate the possibilities
the ViewMyConsult® patient portal.
Why incorporate cryotherapy into your clinic?
From a business perspective, setting up a cryotherapy service is extremely rewarding as it can give your patients great satisfaction and can be extremely profitable and simple to set up, when you have the appropriate training.
Although there are other possible treatment approaches, such as lasers, for conditions like viral warts, seborrheic keratosis, sebaceous hyperplasia, haemangiomas and lentigo, cryotherapy can be a more economical option for you as a business.
Purchasing a dewar and canister costs about £2,000 and a year’s delivery of liquid nitrogen is around £400. I charge £150 for two treatments, which makes the system quickly profitable. After the initial consultation of around 20 minutes, the actual treatment takes only seconds and the follow-up consultation takes around 15 minutes, which I usually do a month later. Note that sometimes patients need repeat treatments and a second or third may be required.
Storage and handling of liquid nitrogen is straightforward and as long as you have a safe, locked, vented area in your clinic, it is reasonable to store the dewar there.11 Filling the canister reservoir requires gloves and eye protection, but is easy and quick. A good protocol for storage has been compiled by North Devon Hospitals.18
particularly important for pigmented lesions because a white centre and a pigmented edge can otherwise form. With most benign lesions, a single freeze thaw cycle, rather than several in one treatment, is all that is required. Other methods that can be used are cotton buds and artery forceps dipped in liquid nitrogen, or the use of a solid probe, which contacts the lesion directly. Repeat treatment intervals vary.21
Summary
I have found my cryotherapy equipment very useful as part of my clinic treatment portfolio and it’s a particularly good additional profit stream. When looking to offer this service in your clinic, the key point is that all skin lesions require a correct diagnosis before treatment; never treat if you do not know the diagnosis of the lesion and do not have sufficient training. It is important to be familiar with the equipment that you purchase, use the correct treatment protocol for the lesion, and ensure you obtain informed consent from your patient.
Dr Paul Charlson is the president of the British College of Aesthetic Medicine. He has worked as a GPwER in dermatology for 14 years and is an assessor for the Royal College of General Practitioners with Extended Roles accreditation panel. Dr Charlson is a Fellow of the Royal College of General Practitioners, and has Diplomas in Practical Dermatology and Occupational Medicine. He has several clinics providing cryotherapy and scar treatment as part of a wider aesthetic portfolio.
REFERENCES
1. NHS, Can I get a mole removed on the NHS? 2018. <https://www.nhs.uk/common-health-questions/ nhs-services-and-treatments/can-i-get-a-mole-removed-on-the-nhs/>
2. Evidence-Based Interventions: Guidance for CCGs Published by NHS England in partnership with NHS Clinical Commissioners, the Academy of Medical Royal Colleges, NHS Improvement and the National Institute for Health and Care Excellence. 28 November 2018. p.22. <https://www.england. nhs.uk/wp-content/uploads/2018/11/ebi-statutory-guidance-v2.pdf>
3. Quality standards for dermatology providing the right care for people with skin conditions, British Association of Dermatologists & The Department of Health. <http://www.bad.org.uk/library-media/ documents/Dermatology%20Standards%20FINAL%20-%20July%202011.pdf>
4. Models of Integrated Service Delivery in Dermatology, Dermatology Workforce Group Date: January 2007. <http://www.bad.org.uk/shared/get-file.ashx?itemtype=document&id=1610>
5. Weedon D., Skin Pathology. 3rd ed. London, Churchill Livingstone Elsevier, 2010.
6. BAD, Patient Information Leaflets (PILs) <http://www.bad.org.uk/for-the-public/patient-informationleaflets/cryotherapy/>
7. Jacob G Unger, MD Resident Physician, Department of Plastic Surgery, University of Texas Southwestern Medical Center at Dallas, Southwestern Medical School, Medscape, 2017. <https:// emedicine.medscape.com/article/1125851-overview>
8. Verruca Freeze, Verruca-Freeze is the Future of Cryosurgery Safe, Easy & Effective Cryotherapy. <https://cryosurgeryinc.com/compare/histofreezer/>
9. GP Supplies, Dermafreeze Cryotherapy. <https://www.gpsupplies.com/dermafreeze-cryotherapy>
10. Anthony Chu, Comparative study of cryopen and liquid nitrogen in actinic keratosis, NHS, 2014. <https://www.hra.nhs.uk/planning-and-improving-research/application-summaries/researchsummaries/comparative-study-of-cryopen-and-liquid-nitrogen-in-actinic-keratosis/>
11. CQC, Nigel’s surgery 86: Storing liquid nitrogen. <https://www.cqc.org.uk/guidance-providers/gps/ nigels-surgery-86-storing-liquid-nitrogen>
12. Rodney P. R. Dawber, Graham Colver, Arthur Jackson, Cutaneous Cryosurgery: Principles and Clinical Practice, 1992.
13. Herron, Bowen AR, Krueger GG. Seborrheic keratoses: a study comparing the standard cryosurgery with topical calcipotriene, topical tazarotene, and topical imiquimod. Int J Dermatol. 2004;43(4):30030215090020
14. Effectiveness of cryosurgery in xanthelasma palpebrarum, 7 Indian Journal of Dermatology and Venerology and leprosy, 1995, Vol 61, Issue 1.
15. Zimmerman EE, Crawford P. Cutaneous cryosurgery. Am Fam Physician. 2012 Dec 15;86(12):1118-24
16. Mark D. Andrews, Cryosurgery for Common Skin Conditions, Am Fam Physician. 2004 May 15;69(10):2365-2372. <https://www.aafp.org/afp/2004/0515/p2365.html>

17. Journal of the American Academy of Dermatology Volume 54, Issue 5, Supplement 2, May 2006, Pages S262-S271.
18. Michael M. Todd, MD; Tena M. Rallis, MD; John W. Gerwels, MD; et al., A Comparison of 3 Lasers and Liquid Nitrogen in the Treatment of Solar Lentigines, A Randomized, Controlled, Comparative Trial. Arch Dermatol. 2000;136(7):841-846.
19. Simin Shamsi Meymandi, Mahmood Moosazadeh, and Azadeh Rezazadehc, Comparing Two Methods of Cryotherapy and Intense Pulsed Light with Triamcinolone Injection in the Treatment of Keloid and Hypertrophic Scars: A Clinical Trial. Osong Public Health Res Perspect. 2016 Oct; 7(5): 313–319.
20. NHS, Liquid Nitrogen Guideline. <https://www.northdevonhealth.nhs.uk/wp-content/uploads/2017/02/ Liquid-Nitrogen-Guidelines-Version-1.0-31Jan17.pdf>
21. Cutaneous Cyrosurgery Second Edition 1997 R Dowber G Colver A Jackson F Pringle p43.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Sleep and Ageing
Sleep deprivation has been recognised to be associated with an increased risk for many chronic diseases, such as hypertension, diabetes mellitus, obesity, cardiovascular disease, depression and even cancer.1 So, should skin health be added to the list of medical conditions that are affected by poor sleep?
When it comes to antiageing treatment or prevention, it is rare that one reflects upon their sleeping patterns or sleeping habits. This article shines light on the term ‘beauty sleep’ and explores the various mechanisms by which poor sleep quality can cause skin ageing and the clinical studies that have demonstrated this link.
Circadian rhythm
Sleep is vital for the growth and renewal of many physiological systems within the body and it is strictly controlled by the circadian system. The circadian system is an organism’s 24 hour oscillations of rhythmic expression of physiological functions and behaviour and is entrained by the ‘master clock’, which is located in the suprachiasmatic nucleus (SCN) of the hypothalamus.2 This master clock, in response to environmental cues, regulates a person’s sleep pattern, body temperature, cardiac activity, hormone secretion, oxygen intake and metabolic rate.2 It is also known to protect against systemic inflammation and DNA damage.3
In recent times, mammalian peripheral clocks and clock gene expression have been researched and it has been found that these clocks are present in all nucleated cells in our body. The skin, being the largest organ of the body, also possesses cycles, which receives timing information from the ‘master clock’ in the SCN via a combination of sympathetic innervation and secreted hormones.2
Given the role of the skin as a physical barrier between the body and the external environment, the skin carries out physiological functions in order to maintain homeostasis, despite external changes such as humidity, temperature and UV radiation, as well as internal changes such as stress or hormone levels.3 Evidence of
the existence of the skin circadian clock was presented in a study by Zanello et al. in 2000.4 Oscillators were found to be present not only in fibroblasts, but also in epidermal keratinocytes and melanocytes and coordinate together to carry out timely functions of the skin. It is likely that this multi-oscillatory system is vital in fine-tuning skin physiology in response to external and internal stimuli and, hence, allowing the skin to effectively carry its role.3 In addition, as the skin is an active endocrine tissue, it is suggested that this tissue may contribute to the humoral signals to synchronise the rhythms of the rest of the organism.4
Sleep deprivation effects on skin
Good quality sleep helps to regulate hormone levels and metabolism. When sleep is disrupted, hormone levels destabilise, the metabolism is affected and stress is induced on the body. The major hormones that are affected by poor sleep are cortisol, melatonin and insulin.5 Inflammation, damage to DNA and oxidative stress have also been linked to sleep deprivation. These adverse pathophysiologic consequences, in turn, contribute to signs of ageing such as wrinkling and alterations in pigmentation.5 A group of researchers from the Skin Research Center in Hamburg, discovered that a circadian transcription factor present in the human epidermis which controls keratinocyte proliferation, Kruppel-like factor 9, is affected by the hormone cortisol.6
Circulating levels of glucocorticoids are one of the main mechanisms by which the ‘master clock’ regulates and synchronises peripheral tissues. Glucocorticoid receptors, when bound to the glucocorticoids, mediate circadian clock entrainment in peripheral tissues that are not responsive to light. They are found to also be involved at the level of gene expression.2
In addition, it has been reported that overproduction of glucocorticoids triggered by sleep deprivation may alter the structure of lamellar bodies and collagen molecules, impairing the integrity of the skin as well as mucous membranes.7
Insulin is another hormone affected by sleep deprivation. An elevated level of serum glucose occurs following disturbed sleep due to a reduction in glucose clearance, and a decrease in the activity of insulin, partially due to high level of glucocorticoids. An increase in glucose level has been found to impair the proliferation of keratinocytes and fibroblasts. The morphology of keratinocytes is altered and terminally differentiated cells arrest without further generation of new cells, affecting the function and integrity of the skin.5 As part of the circadian rhythm, a higher level of melatonin is released from the pineal gland by stimulation from the suprachiasmatic nuclei (SCN) of the anterior-basal hypothalamus during the night. It is important in increasing sleep time, improving sleep maintenance and reducing sleep latency. The role of melatonin at the level of the skin has also been demonstrated. Its place in skin functions such as hair growth, hair pigmentation, antioxidant activity and protection against UV damage are compromised when its levels are dysregulated.5
Sleep deprivation has also been associated with DNA damage, oxidative stress, and a decline in immune function, according to studies performed on murine models.2,5 In fact, it has been reported that high levels of oxidative stress induce resetting of the clock and synchronisation in cultured murine fibroblasts, giving negative repercussions.2
Evidence of poor sleep quality on facial appearance
A study by Axelsson et al. in 2010 demonstrated the facial aesthetic effects of restricted sleep. It photographed 23 healthy participants (age 18-31) who were photographed after a normal night’s sleep (eight hours) and after sleep deprivation (31 hours of wakefulness after a night of reduced sleep). The photographs were rated by 65 untrained observers (age 18-61). It found that subjects who suffered disturbed sleep patterns appeared less healthy, less attractive and more tired with changes in skin colour.8 Another experimental study in 2013 more specifically noted paler skin, more skin wrinkling, dark circles, skin laxity around the mouth and swollen eyes as a result of sleep deprivation in 10 facial photographs after normal sleep and after 31 hours of sleep deprivation. In addition, sleep-deprived subjects appeared to look sadder, which was related to looking fatigued.9
A cross sectional study which was performed by Oyetakin et al. in 2015 evaluated if sleep quality in 60 women was associated with skin
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Mehvish Khan explores existing evidence on the impact of sleep deprivation and poor sleep quality on skin ageing
changes. The Pittsburgh Sleep Quality Index (PSQI) self-assessment questionnaire was used to assess sleep quality of the individuals. This evaluates seven components of sleep: duration, disturbances, latency, daytime dysfunction due to sleepiness, efficiency, subjective sleep quality, and medications needed for sleep. It was found that subjects who slept less than five hours per night exhibited greater signs of intrinsic ageing, which included: uneven pigmentation, fines line and wrinkles, skin laxity, loss of subcutaneous fat and the growth of benign lesions.10 A link was also established between good quality sleepers and better recovery from UV-induced erythema, and better selfperception of overall appearance.10
Conclusion
Good quality sleep can protect the skin from premature intrinsic ageing through hormonal balance, reducing oxidative stress, protecting against inflammation and DNA damage, and maintaining optimum immune function.3
Evidence has shown that disruption in the circadian rhythm of hormones through sleep deprivation results in skin damage and
accelerated ageing.2
Learning that the skin exhibits its own circadian rhythm allows us to understand a little better the complex behaviour of skin and its role as a major organ with precise regulation and systemic effects. More research is needed to explore the link between poor sleep quality and affected skin function and premature skin ageing. Mechanisms have been proposed, however high level of evidence to prove them is lacking. Additional research should be also encouraged to understand the coordination of the various clocks within the human system.
Dr Mehvish Khan is an aesthetic practitioner and founder of MK Aesthetics in Wexford, Ireland. She completed her Master’s in Aesthetic Medicine with a distinction from Queen Mary University of London and also holds a degree in Biomedical Sciences and Medicine. Dr Khan offers injectable treatments, skincare and medical peels at her clinic.

REFERENCES
1. Harding, K. and Feldman, M., 2008. Sleep Disorders and Sleep Deprivation. Journal of the American Academy of Child & Adolescent Psychiatry 47(4), pp.473-474.
2. Matsui, M., Pelle, E., Dong, K. and Pernodet, N., 2016. Biological rhythms in the skin. International journal of molecular sciences 17(6), p.801.
3. Oyetakin-White, P., Koo, B., Matsui, M., Yarosh, D., Fthenakis, C., Cooper, K. and Baron, E., 2013. Effects of sleep quality on skin aging and function. J. Invest. Dermatol, pp.S126-S126.
4. Zanello, S.B., Jackson, D.M. and Holick, M.F., 2000. Expression of the circadian clock genes clock and period1 in human skin. Journal of investigative dermatology, 115(4), pp.757-760.
5. Guan, L., Mehra, R. and Baron, E., 2017. Sleep and Aging Skin. Textbook of Aging Skin, pp.2161-2173.
6. Spörl, F., Korge, S., Jürchott, K., Wunderskirchner, M., Schellenberg, K., Heins, S., Specht, A., Stoll, C., Klemz, R., Maier, B. and Wenck, H., 2012. Krüppel-like factor 9 is a circadian transcription factor in human epidermis that controls proliferation of keratinocytes. Proceedings of the National Academy of Sciences, 109(27), pp.10903-10908.
7. Kahan, V., Andersen, M.L., Tomimori, J. and Tufik, S., 2010. Can poor sleep affect skin integrity?. Medical hypotheses, 75(6), pp.535-537.
8. Axelsson, J., Sundelin, T., Ingre, M., Van Someren, E.J., Olsson, A. and Lekander, M., 2010. Beauty sleep: experimental study on the perceived health and attractiveness of sleep deprived people. Bmj 341, p.c6614.
9. Sundelin, T., Lekander, M., Kecklund, G., Van Someren, E.J., Olsson, A. and Axelsson, J., 2013. Cues of fatigue: effects of sleep deprivation on facial appearance. Sleep, 36(9), pp.1355-1360.
10. Oyetakin White, P., Suggs, A., Koo, B., Matsui, M.S., Yarosh, D., Cooper, K.D. and Baron, E.D., 2015. Does poor sleep quality affect skin ageing?. Clinical and experimental dermatology, 40(1), pp.17-22.
Introducing Tor-bac
Alison Stevenson, managing director of manufacturer Tor Generics Ltd, introduces the new single-dose bacteriostatic saline
Practitioners offering injectable procedures will be familiar with the use of bacteriostatic saline solution to reconstitute medicinal products for intramuscular/intradermal injection. Those who use the Tor-bac brand will know that each millilitre of solution contains sodium chloride 9mg and 0.9% (9mg/ml) benzyl alcohol added as a bacteriostatic preservative, which is less

painful at the site of administration compared to an ordinary saline. Traditionally, however, bacteriostatic saline solution has only been available in 30ml vials. Until now. Practitioners can now purchase ten 5ml ampoules of Tor-bac, meaning they can use one ampoule per patient. In addition, they are easier to administer and compliant with both single-use botulinum toxin and hyaluronidase applications. With Tor-bac, there’s no risk of cross contamination and the single-use doses means they are cost effective too! Aesthetic nurse prescriber Emma Davies says, “Since a single patient treatment rarely requires more than 2.5ml of saline to reconstitute a single vial of toxin, either practitioners are wasting a great deal of product, or they are in breach of regulations, by reusing a 30ml multi-dose vial for multiple patients. As such, the new 5ml vials offer a valuable solution!” To find out more and purchase your 5ml ampoules, get in touch with:
Church Pharmacy: 01509 357 300 info@churchpharmacy.co.uk www.tor-generics.com
REFERENCE:
1. Centre for Disease Control, ‘Frequently Asked Questions (FAQs) regarding Safe Practices for Medical Injections’ < https://www.cdc.gov/ injectionsafety/providers/provider_faqs_multivials.html> Last accessed: 19 March 2018.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
solution
Advertorial
In such an evolving and fast-paced specialty, it is so important to be recognised for your achievements and stand out from the crowd. But what’s the best way to do this? By entering the Aesthetics Awards, the industry’s most respected Awards provider, you could be announced as among the best and most accomplished in your field by becoming a finalist, allowing you to be acknowledged by your current and future clients as well as industry peers.




If you or your exceptional aesthetic business becomes one of our esteemed finalists, you will also receive a range of coverage to boost your success. This includes a finalist announcement in the Aesthetics journal, your name and company description viewed an estimated 2,300 times on our website, weekly social media coverage to a combined following of 33,600+, your name read out to the guests at the dazzling Awards ceremony, and much more.

KEY DATES • Entry closes on June 28 • Finalists announced September 2 • Winners awarded at the ceremony on December 7 Visit aestheticsawards.com and get started today! Celebrate your success at the Aesthetics Awards! Be a finalist at the most prestigious awards ceremony the specialty 1
“It was amazing to be a finalist at the Awards, although we didn’t win, it gave our team a real boost!”
Aesthetics | June 2019 36 Aesthetics Awards Special Focus @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com YOUR ENTRY TIMELINE FIND YOUR CATEGORIES 2 DOWNLOAD YOUR QUESTIONS
Aesthetics Awards 2018 finalist







Celluma ELITE Celluma PRO Celluma LITE www.celluma.co.uk Tel: +44 (0) 203 981 3993 Celluma is an integral component of NYDG signature treatments like the Triad and Runway Facials which employ the regenerative and lifting effects of multi-layered energy waves and technologies in single sessions. The biophotonic waves of Celluma are implemented as the final step to accelerate recovery by providing the cells with the energy to heal from within. Quite often, recommend the device as an ongoing maintenance treatment at home to further optimise results. - The Wellness Clinic Harrods, London“ ” FIND YOUR CATEGORY! PROFESSIONALS CLINICS THE SPRINGPHARM AWARD FOR AESTHETIC NURSE PRACTITIONER OF THE YEAR 5 THE AESTHETICSOURCE AWARD FOR BEST NEW CLINIC, UK AND IRELAND Group CLINIC, COMPANY OR ORGANISATION PROFESSIONAL INITIATIVE OF THE YEAR PRODUCTS PRODUCT INNOVATION OF THE YEAR INJECTABLE PRODUCT OF THE YEAR ENERGY DEVICE OF THE YEAR TOPICAL SKIN PRODUCT/ RANGE OF THE YEAR TRAINING PROVIDERS THE SINCLAIR PHARMA AWARD FOR BEST INDEPENDENT TRAINING PROVIDER INDUSTRY THE HEALTHXCHANGE GROUP AWARD FOR SALES REPRESENTATIVE OF THE YEAR PHARMACY DISTRIBUTOR OF THE YEAR BEST UK SUBSIDIARY OF A GLOBAL MANUFACTURER BEST CLINIC SUPPORT PARTNER BEST MANUFACTURER IN THE UK CLINIC RECEPTION TEAM OF THE YEAR BEST CLINIC SCOTLAND BEST CLINIC NORTH ENGLAND BEST CLINIC MIDLANDS & WALES BEST CLINIC SOUTH ENGLAND BEST CLINIC GROUP, UK & IRELAND (3 CLINICS OR MORE) BEST CLINIC GROUP, UK & IRELAND (10 CLINICS OR MORE) THE SCHUCO AESTHETICS AWARD FOR OUTSTANDING ACHIEVEMENT IN MEDICAL AESTHETICS THE VENUS CONCEPT AWARD FOR BEST CLINIC IRELAND THE JOHN BANNON AWARD FOR MEDICAL AESTHETIC PRACTITIONER OF THE YEAR THE DALVI HUMZAH AESTHETIC TRAINING AWARD FOR BEST SUPPLIER TRAINING PROVIDER THE CLINICSOFTWARE.COM AWARD FOR AESTHETIC PRODUCT DISTRIBUTOR OF THE YEAR THE CELLUMA AWARD FOR BEST CLINIC LONDON Celluma ELITE Celluma PRO Celluma LITE Wound Healing Pain Management • Skin Care Experience Celluma at: ACE, London Stand #42 Mar 1-2 FDA-Cleared Medical CE Mark www.celluma.co.uk Tel: +44 (0) 203 981 3993 Celluma is an integral component of NYDG signature treatments like the Triad and Runway Facials which employ the regenerative and lifting effects of multi-layered energy waves and technologies in single sessions. The biophotonic waves of Celluma are implemented as the final step to accelerate recovery by providing the cells with the energy to heal from Quite often, recommend the device as an ongoing maintenance treatment at home to further optimise results. Dr Costas Papageorgiou MD FACS“ ” Aesthetics | June 2019 37 Aesthetics Awards Special Focus @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 3 GATHER YOUR EVIDENCE 4 DRAFT YOUR ENTRY PROOF READ YOUR ENTRY 6 SUBMIT BY JUNE 28!
new pack
dermamelan
depigmenting solution by mesoestetic
trust the leader*
®
the world’s leading professional depigmentation method




* Considering international distribution.
The new dermamelan® pack includes a patient’s home pack with two innovative complementary products specifically developed to achieve more efficient and lasting results.
 dermamelan® method efficacy has been demonstrated in numerous studies under medical supervision. More than 500,000 patients treated worldwide, in any skin phototype (I-VI) and in all ethnicities.
dermamelan® method efficacy has been demonstrated in numerous studies under medical supervision. More than 500,000 patients treated worldwide, in any skin phototype (I-VI) and in all ethnicities.
®
after
after before For more
visit
before
information
us at www.mesoestetic.com
Long term results obtained after 12 weeks demonstrates method’s efficacy on pigmentation reappearance control.
Treating Neck Lines with Topicals
The lines on the neck, also known as necklace lines or transverse neck lines, are regularly perceived by patients as a negative sign of ageing and ways to reduce the appearance of lines are often reported by consumer media.1,2 The lines commonly present as horizontal overlapping skin folds and can be seen in patients of any age, as there is some congenital occurrence. They are progressive in nature and there is a strong correlation between age and rhytid depth.1 In clinical practice, I find the reasons patients present for progressive conditions such as neck rhytids are multifactorial – including financial, social and life-event drivers. For instance, we often see patients present when they have self-observed a significant, rapid negative change, such as during periods of accelerated visible ageing around the peri-menopause. In many cases, an earlier preventative adjuvant therapy regime would delay the requirement for intervention. Although there are several in-clinic treatment approaches for this concern, such as dermal filler and botulinum toxin injections, energetic stimulation radiofrequency, micro-focused ultrasound and lasers to name a few,3-10 there are also out-of-clinic recommendations and lifestyle factors that patients can adopt to either complement treatment approaches or prevent further damage.
Aetiology
Neck lines are caused by the intrinsic skin and tissue changes associated with ageing. As with most facial lines, the main pathology is loss of collagen, along with elastin.11 However, the specific histology of the neck indicates greater propensity for structural degradation and permanent changes, including (when compared to the cheek) sparser adnexa in the reticular dermis and a thinner, stiffer stratum corneum, adhering to a more compliant and mobile dermis. Increases in extensibility, viscoelastic effect, and transepidermal water loss all drive earlier physical failure, compared to the face.1 An important structural component of the skin is the extracellular matrix (ECM), which is composed of glycosaminoglycans (GAGs), proteoglycans (PGs), collagen fibres and other large molecules. Together, these form a super-structure, which facilitates the biochemical function and structure of the skin as an organ. Degradation of the ECM is a key result of both chronological skin ageing and photoageing.2
Other contributing effects leading to the presentation and increasing severity of neck lines include gravity, skin laxity, body fat fluctuations, and the action of the platysma muscle. The causative factors often lead to co-occurrence of Poikiloderma of Civatte, a common skin condition that presents as red-brown skin with prominent hair follicles that mainly affects the skin on the sides of the neck.11
Patient awareness of visible neck ageing in women often coincides chronologically with menopause – this is likely due to accelerated collagen loss. Research has suggested that women lose an average of 30% of Type I and III collagen in the five years following menopause,
which naturally increases the severity of neck lines that may have been present but unobtrusive.12
Menopause in women and general ageing in both sexes is also associated with bony atrophy, which degrades and reduces the supporting structure of the jawbone, structurally deepening visible lines.12 The neck can be seen as a drape from the mental protuberance to the clavicles and, following bone resorption, the drape begins to sag, deepening existing lines and increasing intradermal shear forces.13
Classification
The condition of the neck can be classified according to its severity of presentation. The appropriate treatment approach will be determined by the class of neck line, which include:
0 – None: No transverse neck lines
1 – Minimal: Superficial transverse neck lines
2 – Moderate: Moderate, effaceable transverse neck lines
3 – Severe: Deep, non-effaceable transverse neck lines
4 – Extreme: Non-effaceable transverse neck furrows with redundant skin
As with many conditions involving structural degradation of tissue, surgery may provide the only practical solution for the most serious and extreme cases, for example where redundant skin is present.14 Multimodal, less-invasive approaches can help minimal to severe presentations. If practitioners incorporate a combination of lessinvasive treatments with the below adjuvant therapies, I believe optimum results can be achieved.
Adjuvant therapies
In addition to injectables and energy-based treatments, a number of topical and other adjunctive therapies are available, with demonstrated efficacy (Table 1).3-10 A key objective, particularly in younger patients, and patients entering menopause, is prevention. A regime of treatments that mitigate the damaging effects of photoageing is also very important.
Lifestyle modifications
The key to prevention of neck lines is preservation and support of structured collagen and elastin. Lifestyle modification to address these
Dr Loredana Nigro explores how lifestyle amendments and topical formulations can help prevent or improve rhytids on the neck
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
While budgets vary, patients concerned about necklines should be encouraged to include lifestyle modifications and topical barriers and antioxidants from as early in life as possible
biochemical and physical impacts can mitigate collagen degradation, structural failures and the formation of lines.
Smoking, excessive alcohol consumption, lack of sleep, inflammatory diet, and extended and unprotected sun exposure can all contribute to premature ageing and structural decline of the neck skin and tissue, through elevating levels of free radicals and reactive oxygen species.15 A significant problem susceptible to lifestyle modification, which is becoming more prevalent particularly in younger adults is ‘text neck’ or ‘tech neck’ – a syndrome of musculoskeletal pain, arthritis and disability related to awkward smartphone use.16 This is a newer structural driver of skin damage and can likely exacerbate neck lines in younger patients.16
Barrier
UV damage due to sun exposure can affect skin tissue and subsequently play a large part in the ageing process of the neck. Patients should be mindful that not all clothing forms an effective sun protection barrier, and I recommend that when in the sun, all patients should regularly reapply sun protection to the entire face area, neck and décolletage. Research also shows the degrading impacts of high energy visible (HEV) light. Blue light – ubiquitous in our modern existence of computers, tablets and smartphones – is shown to negatively impact pro-collagen I. Suspected to damage collagen through reduction of cutaneous carotenoids, its higher wavelength means deeper penetration (1mm against 0.2-0.4mm for UV wavelengths).17-19 Regular use of a full spectrum barrier is therefore recommended, even when spending a lot of time indoors.20 For all patients, I recommend an antiageing sun protection product which specifically mitigates UVA, UVB, IR and HEV light.
Menopause management
As mentioned, menopause and associated hormonal changes are extremely detrimental to collagen levels, elastin levels, and overall skin quality, including the neck area.21 Adjuvant therapies to mitigate menopause, include hormone replacement therapy, biophotomodulation or photodynamic therapy (PDT) with red/ near infrared (NIR) irradiation, and topical applications that will help build the ECM.22,23
Topical treatments
A variety of effective topical treatments exists to improve the appearance of transverse neck lines – which can work in isolation
and provide a beneficial adjuvant effect to the multi-modal approaches discussed above. Topical formulations or regimes comprise various combinations of synergistic ingredients; what I personally deem to be the most relevant components are described below. Evidence is becoming available of their efficacy in revision of existing lines, along with preventative functions relating to collagen and elastin maintenance.3,24 Manufacturers may provide specific application instructions that have been developed in conjunction with the product chemistry, and I generally recommend that these should be followed.
N-acetyl glucosamine (NAG)
NAG is a monosaccharide amide, which is demonstrated to increase hyaluronic acid production and to moderate uneven pigment. Application of NAG supports structure, integrity, growth and repair of the ECM. NAG supports the competence of the neck skin superstructure, preserving the adherence of the dermis and stratum corneum.24
Triethyl citrate
This is an ester of citric acid which is shown to increase dermal collagen with high efficacy.24 Ongoing replacement of dermal collagen is key to maintenance of the ECM and slowing or preventing progression of neck lines. 24
Antioxidants
Antioxidants improve the health, structure and integrity of the dermal ECM, and so support collagen and elastin maintenance. Vitamins are common components of topical formulations – vitamin B3 regulates cell regeneration and metabolism, vitamin C upregulates the production of collagen types I and III, and vitamin E has demonstrated anti-inflammatory and anti-proliferative effects. Vitamin C and E in combination have been shown to have synergistic benefits in terms of antioxidative protection. Pro-amino acids such as palmitoyl glycine also reduce inflammation and increase procollagen production.25
Other cell regulators
Vitamin A and derivatives such as tretinoin are antioxidants which upregulate collagen synthesis, and suppress the effects of collagenase, directly supporting the health of the ECM matrix through metabolic effects. Polypeptides can imitate matrix components, and stimulate dermal metabolism, including collagen synthesis, and certain botanical extracts (including polyphenols and stem cells extracts) have been demonstrated to provide similar metabolic upregulation.25 Pigmentation modulators and acid peels can also stimulate exfoliation, collagen biosynthesis, skin tautness, and eradication of effaceable lines.25
Topical hyaluronic acid
This can be applied directly to the skin in ultra-small particle formulations (also known as nano-HA), which allows deep penetration of the product into the dermal matrix, which has been shown to significantly improve the appearance of fine lines as per a minimal presentation of transverse neck lines.26
Efficacy of topical formulations
While conducting my research, I found many studies documenting the general benefits of topical treatments on skin rhytids, but I could only find one study that purely focussed on treating the neck with topicals. This 2015 study (P=42) recorded the effect of a multi-ingredient
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Lifestyle modification to address these biochemical and physical impacts can mitigate collagen degradation, structural failures and the formation of lines
The class of neck line
Relative
Therapy
Frequency
Cost None Minimal Moderate Severe Extreme
Behaviour modification √ √ √ √ √ Ongoing Zero
Topical barrier / photochemical protection √ √ √ √ √ Daily Low
Topical antioxidant √ √ √ √ √ Daily Low
Topical barrier with serum combo (NAG/HA/stem cells) √ √ √ √ Daily Moderate
Neuromodulators (toxin) √ √ √
Per 4-6 months. Suitability is anatomy-dependent Med-High
Dermal filler (HA-based) √ √ √ Per 9-15 months High
Ultrasound or radiofrequency √ √ √ Per 1-3 years High Laser √ √ √ Per 2-5 years High
Table 1: Description of the therapies I use for treating the neck in my clinic. The table is presented in ascending order of annualised cost seen in my clinical experience.3-10
topical cream over a 12-week daily application profile, without any additional multi-modal therapies. The cream comprised 8% N-acetyl glucosamine, 4% tri-ethyl citrate, along with various antioxidants and anti-inflammatory agents (vitamin E, palmitol glycine and swiss apple stem cell extract).27
Adjuvant treatment matrix
In my clinic, we treat each patient as their individual presentation and circumstances dictate. However, Table 1 reflects my own clinical decision-making process, which should factor in the treatments available, the classification of the neck lines, and of course the patient’s budget when deciding upon an appropriate combination regime. While budgets vary, patients concerned about neck lines should be encouraged to include lifestyle modifications, topical barriers and antioxidants from as early in life as possible.
Treat early and appropriately
Transverse necks lines present as a progressive condition, and therefore a regular intervention regime which supports the maintenance and rejuvenation of the skin and underlying ECM matrix is key to management. Particular care should be taken to consider the increased support requirements of metabolically significant life changes such as peri-menopause. The neck is a difficult area to treat and is an aesthetically sensitive part of the body. While surgery may be indicated for the most serious cases, there are a range of non-invasive procedures which can improve the area. Adjuvant to the available remediation therapies, a daily regime incorporating full-spectrum barrier protection, appropriate lifestyle choices, and supporting topical applications (including matrix builders, antioxidants and cell regulators) will minimise the emergence or worsening of this unwanted sign of ageing. To adequately address all issues, in-clinic and home care should be considered on an ongoing basis.
Dr Loredana Nigro graduated from WITS Medical School in Johannesburg in 2003. She worked in internal medicine in South Africa’s public health sector until 2009, and decided in 2010 to move into aesthetic and antiageing medicine in private practice. She is currently a senior aesthetic clinician at Riverbanks Clinic in Harpenden and works with patients of all ages and skin types. Dr Nigro is also a KOL and clinical consultant for mesoestetic UK.

REFERENCES
1. Eunjoo Kim, Gayoung Cho, Nam Gae Won, Juncheol Cho, Age‐related changes in skin bio‐mechanical properties: the neck skin compared with the cheek and forearm skin in Korean females, Skin Research & Technology, 2013.
2. Dong-Hun Lee, Jang-Hee Oh & Jin Ho Chung, Glycosaminoglycan and proteoglycan in skin aging, Journal of dermatological science 83(3), May 2016.
3. Casabona, G, Nogueira Teixeira, D. Microfocused ultrasound in combination with diluted calcium hydroxylapatite for improving skin laxity and the appearance of lines in the neck and décolletage. J Cosmet Dermatol. 2018; 17: 66– 72.
4. Tamura, Bhertha. (2012). The Effect of Botulinum Toxin on the Platysma Muscle. Current Dermatology Reports. 1. 10.1007/s13671-012-0013-y.
5. Hruza, George & Taub, Amy & L Collier, Susannah & Mulholland, R. Stephen. (2009). Skin rejuvenation and wrinkle reduction using a fractional radiofrequency system. Journal of drugs in dermatology : JDD. 8. 259-65.
6. Hyun MY, Li K, Kim BJ, Kim MN, Hong CK, Kim H, Koh HJ, Park WS. Novel treatment of neck wrinkles with an intradermal radiofrequency device. Ann Dermatol. 2015 Feb;27(1):79-81.
7. Fabi, Sabrina. (2015). Noninvasive skin tightening: Focus on new ultrasound techniques. Clinical, Cosmetic and Investigational Dermatology. 8. 47. 10.2147/CCID.S69118.
8. Alster, Tina & Tanzi, EL. (2002). Treatment of transverse neck lines with a nonablative 1450 nm diode laser. Lasers in Surgery and Medicine. 33-33.
9. Nakashima, Yuya & Ohta, Shigeo & Wolf, Alexander. (2017). Blue light-induced oxidative stress in live skin. Free Radical Biology and Medicine. 108. 10.1016/j.freeradbiomed.2017.03.010.
10. Schlessinger, Joel & Green, Barbara & Edison, Brenda & Murphy, Lynn & Sabherwal, Yamini. (2016). A Firming Neck Cream Containing N-Acetyl Glucosamine Significantly Improves Signs of Aging on the Challenging Neck and Décolletage. Journal of drugs in dermatology : JDD. 15. 47-52.
11. Lemperle, Gottfried & E. Holmes, Ralph & Cohen, Steven & Lemperle, Stefan. (2001). A Classification of Facial Wrinkles. Plastic and reconstructive surgery. 108. 1735-50; discussion 1751.
12. Thornton MJ. Estrogens and aging skin. Dermatoendocrinol. 2013 Apr 1;5(2):264-70. doi: 10.4161/ derm.23872. Epub 2013 Apr 1.PubMed PMID: 24194966;
13. Munakata M, Tachikawa N, et al., Influence of menopause on mandibular bone quantity and quality in Japanese women receiving dental implants, Arch Osteoporos, 2011;6:51-7.
14. de Maio, Maurício. (2018). Myomodulation with Injectable Fillers: An Innovative Approach to Addressing Facial Muscle Movement. Aesthetic Plastic Surgery. 42. 10.1007/s00266-018-1116-z.
15. Addor, F. Beyond photoaging: additional factors involved in the process of skin aging. Clinical, Cosmetic and Investigational Dermatology, 2018, Volume 11, 437–443.
16. Ilja L. Kruglikov and Philipp E. Scherer, Skin aging as a mechanical phenomenon: The main weak links, Nutr Healthy Aging, 2018; 4(4): 291–307.
17. Vandersee S, Beyer M, Lademann J, Darvin ME. Blue-violet light irradiation dose dependently decreases carotenoids in human skin, which indicates the generation of free radicals. Oxid Med Cell Longev. 2015;2015:579675.
18. Mahmoud BH, Hexsel CL, et al., Effects of visible light on the skin, Photochem Photobiol. 2008 MarApr;84(2):450-62.
19. Manpreet Randhawa, InSeok Seo, Visible Light Induces Melanogenesis in Human Skin through a Photoadaptive Response, Published: June 29, 2015
20. Ganceviciene R, Liakou AI, Theodoridis A, Makrantonaki E, Zouboulis CC. Skin anti-aging strategies. Dermatoendocrinol. 2012 Jul 1;4(3):308-19.
21. Nick Raine-Fenning, Mark P Brincat, Yves Muscat Baron, Skin Aging and Menopause, American Journal of Clinical Dermatology, 4(6):371-8, February 2003.
22. Eero Varila Immo Rantala Aarne Oikarinen, et al., The effect of topical oestradiol on skin collagen of postmenopausal women, BJOG, 1995. <https://obgyn.onlinelibrary.wiley.com/doi/ abs/10.1111/j.1471-0528.1995.tb10906.x>
23. Maria Claudia Almeida Issa, et al., Photodynamic therapy in photoaging: literature review, Surgical and Cosmetic Dermatology 8(4) 2016.
24. Manjula Jegasothy, S & Zabolotniaia, Valentina & Bielfeldt, Stephan. (2014). Efficacy of a New Topical Nano-hyaluronic Acid in Humans. The Journal of clinical and aesthetic dermatology. 7. 27-9.
25. Crystal Martin, What to Do About Your Neck, The New York Times, 2017. <https://www.nytimes. com/2017/01/09/fashion/neck-chest-skin-care-solutions.html>
26. Lori Keong, Is There Anything (Non-Surgical) You Can Do About Your Neck?, The Strategist, 2018. <http://nymag.com/strategist/article/best-neck-creams.html>
27. Schlessinger, Joel & Green, Barbara & Edison, Brenda & Murphy, Lynn & Sabherwal, Yamini. (2016). A Firming Neck Cream Containing N-Acetyl Glucosamine Significantly Improves Signs of Aging on the Challenging Neck and Décolletage. Journal of drugs in dermatology: JDD. 15. 47-52.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Background of lymphatics
The lymphatic system was first described in the 17th century by Italian physician, Dr Gaspare Aselli and is made up of a network of tissues and organs that remove waste and other unwanted materials from the body.2 Its primary function is to support our immune system by transporting lymph through a network of larger vessels and smaller, thin-walled capillaries. Lymph is the name given to the fluid found in the lymphatic system, which is comprised of interstitial fluid and other substances that are continually exchanged through the highly permeable vessel walls.2
Lymphatic Drainage in Facial Aesthetics

There appears to be little acknowledgement of the importance of the lymphatic system in the medical aesthetics speciality and manual lymphatic drainage (MLD) is usually only used as practitioner’s preference. This may be down to the fact that anyone can perform MLD and it is used more frequently in holistic therapies and alternative medicine. However, when drawing upon both current and previous research, which is limited, there are benefits to adopting this approach as a routine part of future treatments.
The lymphatic system is important when considering the valuable role of the lymphatic vasculature during acute inflammation;1 often caused by a range of aesthetic treatments. This article will explore the lymphatic system and the benefits of MLD as a routine part of facial aesthetic treatments, primarily dermal fillers, and how it can minimise the side effects experienced by patients, thus increasing satisfaction with their treatment.
The lymph nodes are found at various points along the lymph vessels, for example, in the neck (Figure 1) and the role of the lymph nodes is to filter passing lymph from nearby parts of the body.3 The lymph nodes also contain immune cells which help fight infection by destroying germs carried in lymph fluid.4 The most significant role of the lymphatic system in aesthetics is the ability to drain excess interstitial fluid away from the extra-cellular tissue and return it to the venous circulation, thus reducing any oedema as a result of trauma and inflammation post treatment.3 There is a close structural and developmental relationship between the vascular and lymphatic systems and they are sometimes described as being developed in parallel; however, it is unclear what role the lymphatic vasculature plays in helping to reduce acute inflammation. A study in 2011 conducted by Huggenberger et al. explored the possibility that an expanded lymphatic network reduced dermal oedema formation and therefore, limited acute skin inflammation.5 It is important to note here that this study was conducted on murine; with that in mind it would be fair to say that more human-based clinical trials would be beneficial.
How can it be used in aesthetics?
Injecting dermal fillers for example, involves causing trauma to the skin and deeper tissues, triggering the body’s natural inflammatory response. The damaged cells release chemicals such as histamine and prostaglandins, which causes fluid to be leaked from blood vessels leading to localised swelling of the tissues.6 In addition, dermal fillers can cause a degree of lymphoedema by obstructing the lymph nodes and lymphatic vessels causing a build-up of lymph fluid in the affected area.7 Although there is little evidence to support the use of MLD in facial aesthetic treatments, there is a proven link between the injection of dermal fillers and oedema as a complication, due to the obstruction of lymphatic vessels and, furthermore, that manual compression is a suitable treatment for this side effect.8
There is also increasing discussion within the field of holistic therapies about the use of MLD for overall health and wellbeing and it is widely reported as being able to relieve fluid congestion, particularly around the eye area, as well as enhancing the woundhealing process by improving microcirculation to the area.9
There are additional benefits for patients which may make combining MLD with facial aesthetic treatments seem more appealing such as improved skin tone, reduced puffiness around the eye area and accelerated healing time.10 The natural ageing process
Aesthetic nurse Rose Poyner details the benefits of incorporating manual lymphatic drainage with facial aesthetic treatments Figure 1: Diagram of lymph nodes and lymphatic vessels in the head and neck3 Submental nodes Facial nodes Submandibular nodes Deep cervical nodes Clavicle Supraclavicular nodes Superficial cervical nodes Occipital nodes Posterior auricular nodes Pre-auricular nodes Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
contributes to deteriorating lymphatic function and promoting increased lymphatic flow can also be beneficial to patients, regardless of whether they are having aesthetic treatments or not.11
Technique
Manual lymphatic drainage is a specialised massage technique that was proposed in the 1930s by Dr Emil Vodder and his wife Dr Estrid Vodder. It works to stimulate the lymphatic system to promote resorption of the fluid from swollen tissues.12 Dr Vodder’s technique is characterised by gentle pumping, circular movements applying pressures of approximately 30mmHg (the unit of pressure, known as the millimetre of mercury) to the affected area. Other methods are described in the literature such as those pioneered by Foldi, CasleySmith and Leduc, all of which have slightly different techniques.13 For example, the Foldi method, is based upon the Vodder technique however lays emphasis on thrust and relaxation. The Casley-Smith technique involves the use of small and gentle movements with the side of the hand and the Leduc method involves use of enticing movements which reflect how lymph is absorbed in the initial lymphatics. I have found however that Vodder’s technique remains the most commonly used and widely recognised in practice. Although there has been further development of MLD techniques over the years, the overall aim remains the same; to promote variations in interstitial pressures by stretching the skin in specific directions incorporating slow, repetitive movements and allowing a brief resting phase where the skin can return to ‘normal’.14
Treatment considerations
When considering when MLD would be most useful for aesthetic practitioners it is important to carefully review the anatomy and physiology of the face. As mentioned, oedema is a very common side effect of most aesthetic treatments, regardless of the area injected, although it is more prevalent in the lips, the periorbital and malar regions.15 This could be due to the hydrophilic nature of some hyaluronic acid based fillers, but could equally be caused by the compression of lymphatic vessels or the temporary paralysis of facial musculature after anti-wrinkle injections causing lymphostasis.16 This emphasises the importance of MLD post-delivery of facial aesthetic treatments in anticipation of lymphostasis, hopefully reducing the amount of swelling experienced by the patient.
If the treating practitioner is using local anaesthetics during treatment, consideration should be given to secondary oedema as a result of this and, in my experience, MLD post procedure could be beneficial to
reduce this. If a patient experiences localised oedema post treatment it is reasonable to expect it to dissipate within two weeks, although most cases will resolve earlier than this.17 If swelling persists, the patient should be assessed face-to-face by the treating practitioner to determine the underlying cause of the problem.
It is important to be able to distinguish between straightforward oedema and other causes of swelling such as infection. The area affected by oedema should feel soft and be easily compressed when palpated and may feel tender due to the procedure itself; however, if there is a localised infection, the area may appear red, inflamed and hot to touch. MLD is generally suitable for the majority of aesthetic patients, however, the technique should not be performed on patients with lymphatic disorders such as Milroy disease which affects the way the lymphatic system functions.18
Conclusion
MLD is a well-established technique to aid the reduction of fluid build-up, which can be the cause of reduced patient satisfaction post treatment. With additional benefits as well as reducing oedema, there is an argument for combining MLD with facial aesthetic treatments routinely to maximise results and improve the overall appearance of the skin.
Rose Poyner is an aesthetic nurse practitioner based at Cosmedic Skin Clinic and has a particular passion for skincare. She has received extensive training from aesthetic practitioners Dr Martyn and Sharon King, founders of the Cosmedic Skin Clinic, in all aspects of aesthetic medicine and performs a range of treatments from skin peels and laser treatments to injectables.
REFERENCES
1. Huggenburger, R and others, ‘An important role of lymphatic vessel activation’, Blood: American Society of Haematology, 117 (2011) <http://www.bloodjournal.org/content/117/17/4667?ssochecked=true> (p.4667-4678)
2. Oliver, G, Lymphatic vasculature development, Nature Reviews: Immunology, 4 (2004) 35-34 (p.35)
3. Lymphoma Action, The Lymphatic System <https://lymphoma-action.org.uk/about-lymphoma-whatlymphoma/lymphatic-system>
4. Lymphoma Action, Lymph nodes and cancer: What is the lymph system? <https://lymphoma-action. org.uk/about-lymphoma-what-lymphoma/lymphatic-system>
5. Huggenburger, R and others, ‘An important role of lymphatic vessel activation’, Blood: American Society of Haematology, 117, 2011 <http://www.bloodjournal.org/content/117/17/4667?ssochecked=true> (p.4667-4678)
6. MedlinePLus.gov, Immune Repsonse, 2019 < https://medlineplus.gov/ency/article/000821.htm>
7. King, M, Management of Edema, The Journal of Clinical and Aesthetic Dermatology, 10 (2017) <https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC5300735/>
8. NHS Direct Wales, Oedema, 2016 <https://www.nhsdirect.wales.nhs.uk/Encyclopaedia/o/article/ oedema/> [15/05/2019]

9. Loskotova, A, Myofascial-manual lymphatic drainage for burn trauma: a service evaluation, British Journal of Community Nursing, (2017) S8-S12
10. Williams, A, ‘Manual Lymphatic Drainage: exploring the history and evidence base’, British Journal of Community Nursing, S18-S24
11. Neill, U. S, ‘Skin Care in the Ageing Female: Myths and Truths’, Journal of Clinical Investigation, 122 (2012) https://search-proquest-com.rcn.idm.oclc.org/health/docview/921471707/fulltext/ BB82574127854E9APQ/1?accountid=26447 (p.473-477)
12. Williams, A, ‘Manual Lymphatic Drainage: exploring the history and evidence base’, British Journal of Community Nursing, S18-S24
13. MLDUK.org.uk, MLD Courses, 2019 < http://www.mlduk.org.uk/courses-casley-smith/>
14. Williams, A, ‘Manual Lymphatic Drainage: exploring the history and evidence base’, British Journal of Community Nursing, S18-S24
15. King, M, ‘Management of Edema’, The Journal of Clinical and Aesthetic Dermatology, 10 (2017) <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5300735/>
16. Funt, D & Pavicic, T, Dermal fillers in aesthetics: an overview of adverse events and treatment approaches, Clinical Cosmgation Dermatol, 6 (2013) <https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC3865975/>
17. Funt, D & Pavicic, T, Dermal fillers in aesthetics: an overview of adverse events and treatment approaches, Clinical Cosmgation Dermatol, 6 (2013) <https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC3865975/>
18. U.S. National Library of Medicine, Milroy Disease, 2019 <https://ghr.nlm.nih.gov/condition/milroydisease>
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The lymphatic system is important when considering the valuable role of the lymphatic vasculature during acute inflammation; often caused by a range of aesthetic treatments
Case Study: Lip Vascular Occlusion

Nurse prescriber Lynn Lowery shares a case study of a lip complication that she successfully treated and describes how practitioners can avoid similar scenarios
Dealing with a complication is one of the most difficult experiences within the aesthetic setting. However, it presents even more of a challenge when the patient presents to you with a complication from another clinic, as you may not ever have the full clinical information of the previous treatment. In my professional opinion, best practice is to send the patient back to the treating practitioner. However, this is not always a possibility for a number of reasons: the patient may not have confidence in the original practitioner, they may feel worried that their complication may not be treated seriously by the practitioner, there is a potential for misdiagnosis if they do not have the training, or the practitioner may not be available. In addition, other patients may present to you following a referral from their treating practitioner as they feel unable to deal with the situation. Whatever the circumstances for a patient’s presentation to your clinic, it is important to gain as much valuable information as possible about the procedure from both the patient and practitioner. Complications are easier to manage if there are details of a full medical history, timeline of treatment, products used and the technique of delivery. These incidents are distressing for all parties and the patients are usually feeling generally unwell and distressed.
Patient journey
A 52-year-old female patient was injected by a different aesthetic practitioner with 1ml of a well-known hyaluronic acid (HA) dermal filler into the lips using a needle. A dental block was administered prior to the lip augmentation for pain management. At the time of the injection, what appeared to be a large haematoma appeared to the left superior lateral tubercle. The practitioner had massaged the ‘lump’ upwards and outwards and advised the patient that it may bruise. The following day, the patient became concerned about the appearance of her lip, which was causing her slight discomfort and had an appearance of a bruise, so she contacted her treating practitioner (Figure 1). After a review that day, the patient was told by the practitioner that it was just a bruise and the blood supply was fine and so she was sent home.

Two days following treatment, the patient was feeling very unwell with increased pain. She contacted her practitioner for a review and again she was informed that the blood supply was fine. Note that the Aesthetic Complications Expert (ACE) guidelines state that, ‘Severe pain is not a feature of dermal filler treatment and if the patient complains of severe pain in the subsequent hours after treatment, this should alert the practitioner to the risk of an impending necrosis’.1,2
The patient continued to worry for the days following because the pain was increasing and she was unable to eat or drink. She tried contacting her practitioner for the next two days but could not get through as they had gone on holiday.
Five days after her original dermal filler treatment, the patient decided to seek additional help and was seen by a nurse in her local GP surgery. She was prescribed doxycycline for five days as the nurse didn’t know what the problem was and suspected it could be an infection. They also advised that the patient go back to her original practitioner.
Patient presenting to my clinic
On the same day as visiting the local GP surgery, the patient came to my clinic after she was referred to me from the ACE Group forum, a closed Facebook group only available to ACE members. The patient allowed me to examine the lip, despite extreme pain; she was tearful and feeling generally unwell (Figure 2). Unfortunately, I had no access to her clinic notes so I had to take a comprehensive medical history and timeline of events from the patient, discussed above. The patient was able to determine that the practitioner had used a needle for the treatment.
Upon my examination, I noted extreme discolouration. This colour distribution was the biggest indicator to help me identify that she was experiencing impending necrosis due to the dermal filler injection, which had caused a vascular occlusion. I suspected that the vascular occlusion was due to the dermal filler being directly injected into the superior labial
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 1: One day following treatment the patient presented with haematoma to the left superior lateral tubercle
artery, which lies between the mucous membrane and the orbicularis oris. I determined that the only solution was to dissolve the filler to regain tissue perfusion as soon as possible and limit the depth of the necrosis. I explained at length the cause of the vascular occlusion, the use of hyaluronidase in vascular emergencies, and the fact that this was our best chance of limiting the tissue damage and subsequent skin discolouration post occlusion. The patient agreed with my advice and consented to the treatment.
A patch test was performed on the forearm of the patient prior to treatment, which was negative.3 Lidocaine was injected to the area of necrosis due to the extreme pain; necrotic skin tissue is characterised by extreme pain due to the interrupted blood supply causing the cells to be acidic.4
Once the patient felt the anaesthetic effect, I then examined the tissue damage more extensively. The tissue had partial thickness damage, meaning that it only extended into the first two layers of the skin epidermis and dermis, and the patient still had full muscle function to the orbicularis oris. Capillary refill time was extremely delayed and the





skin discolouration had started to develop slough to the superficial dermis, which was able to be debrided with ease. According to ACE Group guidelines, devitalised tissue must be removed to decrease wound bacterial bioburden and to allow healthy tissue to regrow.5 I administered 1500 units of hyaluronidase dissolved in 2.5mls of bacteriostatic saline to the necrotic area, including the oral mucosal surface, as per ACE Group guidelines.5 The patient was administered 300mg of aspirin immediately after the treatment as a precaution for any localised coagulation around the occlusion and to limit platelet aggregation; although this is anecdotal evidence, I felt it was appropriate due to the time delay. This hyaluronidase treatment was repeated twice and the patient was sent home with a prescription for analgesia. The patient had showed a good result to the first dose of hyaluronidase (Figure 3), although the patient didn’t feel any change to the aching or gum discomfort. In my experience, the patient is the best indicator if you have resolved the occlusion as the pain should be relieved. The morning of the following day, which was six days following the original filler procedure, I reviewed the patient and because she still had extreme pain and the skin was still discoloured, I administered another 1500 units of hyaluronidase. I also arranged for the patient to attend the local hyperbaric chamber following this treatment. Oxygen therapy has been used successfully to treat retinal artery occlusions, and is thought to be an efficacious adjunct in dermal filler complication scenarios due to a variety of mechanisms, including oxygenation of ischaemic tissues, reduction of oedema, amelioration of ischemic/reperfusion injury, and promotion of angiogenesis and collagen maturation.6 I have personally found it to be effective in the reperfusion of tissue, limiting its damage. In the evening of the same day, I saw the patient again and repeated the hyaluronidase treatment and another 1500 units were given. I also prescribed acyclovir for five days due to the patient’s history of herpes, because she said that she could feel the start of an outbreak. At this stage, the patient was feeling generally unwell, nauseous, tearful and tired (Figure 4), which,
 Figure 2: Patient when she presented to my clinic five days after dermal filler treatment
Figure 3: Patient immediately following the first hyaluronidase treatment, five days following her original dermal filler treatment
Figure 4: Patient in the evening after three hyaluronidase treatments, six days after original filler treatment
Figure 2: Patient when she presented to my clinic five days after dermal filler treatment
Figure 3: Patient immediately following the first hyaluronidase treatment, five days following her original dermal filler treatment
Figure 4: Patient in the evening after three hyaluronidase treatments, six days after original filler treatment
Early recognition and treatment is extremely important to limiting the subsequent damage to the tissue in the event of a vascular occlusion
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 5: Patient on day three of intervention. At this point the patient was healing and the slough is beginning to lift away from the lip due to the healing process
in my experience, is normal at this stage. The pain was still severe and was radiating to the eye and ear, eating was also a problem as any clenching or grinding of the teeth was also very painful. I advised the patient to consume high calorie drinks via a straw.
On the third day of intervention, seven days following the original treatment, the patient underwent another hyperbaric oxygen therapy session and I reviewed again (Figure 5). I decided that a transdermal drug delivery treatment would be beneficial to help the healing because it has anti-inflammatory and anti-bacterial properties. I used the Plasma Shower device, which I have used previously to minimise the build-up of toxins from necrosis.
The review eight days following the original procedure and four days after my interventions revealed a much healthier perfused tissue with limited slough (Figure 6). I decided that another Plasma Shower treatment would be beneficial to help with the bacteria and
inflammation. The patient’s pain was now minimal, although there was still some disruption to the nerve with the patient reporting a numb feeling to the superior border and perioral tissue.

The patient continued taking oral antibiotics and acyclovir and was reviewed six days later. As shown in Figure 7, the patient did not have any residual skin discolouration, although she continued to have sensation difficulties to the left perioral tissue. The patient continues to have open access to our clinic, should she require any further treatment.
Discussion
In my opinion, this patient’s complication worsened as it went undiagnosed for several days and was allowed to develop. Early recognition and treatment is extremely important to limiting the subsequent damage to the tissue in the event of a vascular occlusion. Practitioners should be confident in their understanding of the difference between bruising and the dusky discolouration of a vascular occlusion.7,8
The patient’s distress was unfortunately made worse as she could not get hold of the practitioner while they were on holiday. The GMC states, ‘You must make sure that your patients know how to contact you or another named suitably-qualified person if they experience complications outside your normal working hours’.2 While the practitioner had given the patient the name of someone to contact, this was over an hour away and the patient did not feel able to travel. I felt it was important to refer the patient back to her original practitioner on their return from holiday and recommend that others do so too; everyone can make a mistake and the practitioner was very concerned about the wellbeing of the patient. Unfortunately, the lines of communication had broken down and the patient will no longer communicate with the original treating practitioner, although I did make sure that they were updated with the patient’s journey and progress.
Practitioners need to ensure that they are trained in the management of complications, which include anatomy and management skills. They should also establish a good solid network of colleagues they can trust and rely on when needed to assist them in the event of a complication.
Lynn Lowery is an independent nurse prescriber with more than 10 years’ experience in medical aesthetics. She has been a registered nurse for more than 20 years and remains dual-qualified as a paramedic. Lowery is an active member of the global medical aesthetic community, regularly attending training seminars in order to enhance her skills and stay abreast of new developments. Lowery has been an Allergan and Merz trainer and is currently a mentor for Northumbria University.

REFERENCES
1. Martyn King, Management of Necrosis, ACE Group, 2014. <http://acegroup.online/wp-content/uploads/2016/01/Necrosis-v1.4.pdf>
2. Guidance for doctors who offer cosmetic interventions, GMC, 2016. <https://www.gmc-uk.org/-/media/ documents/Guidance_for_doctors_who_offer_cosmetic_interventions_210316.pdf_65254111.pdf>
3. Martyn King, The Use of Hyaluronidase in Aesthetic Practice, ACE Group, 2014. <http://acegroup. online/wp-content/uploads/2016/01/ACE-Group-Hyaluronidase-v1.2.pdf>
4. Adrienne J. Headley, Necrotizing Soft Tissue Infections: A Primary Care Review, American Family Physician, 2003. <https://www.aafp.org/afp/2003/0715/p323.html>
5. ACE Group, Guidelines. <http://acegroup.online/guidelines/>
6. Impending Necrosis After Injection of Hyaluronic Acid and Calcium Hydroxylapatite Fillers: Report of 2 Cases Treated With Hyperbaric Oxygen Therapy. American Society for Dermatologic Surgery. 2014; 40:9:1049-1052

7. Kenneth Beer, Jeanine Downie, & Jacob Beer, A Treatment Protocol for Vascular Occlusion from Particulate Soft Tissue Augmentation, J Clin Aesthet Dermatol. 2012 May; 5(5): 44–47 8. Bruna Souza Felix Bravo, Laila Klotz De Almeida Balassiano, et al., Delayed-type Necrosis after Soft-tissue Augmentation with Hyaluronic Acid, J Clin Aesthet Dermatol. 2015 Dec; 8(12): 42–47.
 Figure 6: Patient on day four of intervention, after four hyaluronidase treatments, two hyperbaric oxygen treatments and two Plasma Shower treatments
Figure 7: Patient 14 days following original dermal filler resulting in vascular occlusion and nine days following intervention with hyaluronidase
Figure 6: Patient on day four of intervention, after four hyaluronidase treatments, two hyperbaric oxygen treatments and two Plasma Shower treatments
Figure 7: Patient 14 days following original dermal filler resulting in vascular occlusion and nine days following intervention with hyaluronidase
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Practitioners need to ensure that they are trained in the management of complications, which include anatomy and management skills
Wanting to Ignite your medical aesthetics journey? Allergan may just have the answer
The journey towards becoming an aesthetic practitioner can be an overwhelming one at the beginning. Finishing a training course can leave you feeling excited and ready to start applying your newly learned skills yourself, but the reality can be a stark contrast when you are on your own with a patient for the very first time. Newlyqualified aesthetic healthcare professionals can often struggle to attract new patients, and it is at this period of time that we receive the most enquiries from clinicians reaching out for meaningful support.
Concrete resources can be hard to find and even harder to trust, so who do you reach out to for support?
Why SPARK for HCPs?
At Allergan we always strive to improve our offering to customers, and to the industry. Having piloted the Spark Service at the end of last year, it has given us the opportunity to gain feedback and test ideas. We are now ready to roll the Spark Service out wider to the industry and it is available to registered doctors, dentists and nurses in the UK and Ireland. The Spark Service centres around the online portal and it’s Knowledge Hub. The Knowledge Hub is the foundation that the other services built from.

Knowledge Hub
The aim is for the website and knowledge hub to be constantly growing to reflect the emerging needs of the industry, adapting to include updated information. We will be adapting many great tools and resources currently available and including them in the Knowledge Hub.
Account Executive
Our dedicated team will help our callers find the information they are looking for. They are available from Monday to Friday 10am4pm. They lead the charge in developing content and can assist in arranging contact with remote Product Specialists.
Did you ever want more support when you started in aesthetics?
Booster Training
Our Third Party Training Provider page will provide a clear path to choosing suitable external training with Allergan Appointed Training Providers who have worked directly with the company to create
enriching educational experiences. We have Allergan Faculty Providers and other Key Providers listed. To add to this, we also have the Allergan Medical Institute (AMI) Digital World linked with Spark Service, for more clinical-based information.
Events
SPARK will host events to introduce Allergan products, cover vital topics, and provide chances to network. These will be dedicated to sharing knowledge to help practitioners and their patients. If you are registered and have consented, you will receive invites to these events, which will provide a diverse range of opportunities.
Future
Currently, SPARK has launched and has big plans in the future to develop content according to the emerging needs of the industry.
John Campbell is the Spark Innovation Manager at Allergan. Having joined the industry in 2008, he has worked in various roles that include product specialist, key accounts and business consultancy. Campbell has a blend of both clinical and business knowledge of aesthetics, which puts him in a great place to lead the Spark project.

www.allergan-spark.com
The journey towards becoming an aesthetic practitioner can be an overwhelming one at the beginning. Finishing a training course can leave you feeling excited and ready to start applying your newly learned skills yourself, but the reality can be a stark contrast when you are on your own with a patient for the very first time. New healthcare professionals can often struggle to
Knowledge Hub
Produced and funded by Allergan UK/0301/2019 Date of Preparation: May 2019
Aesthetics | June 2019 47 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Allergan Spark
igniting medical aesthetics careers
Booster Training Account Executive Events Knowledge Hub
igniting medical aesthetics careers
Booster Training Account Executive Events Knowledge Hub
Aesthetics
Aesthetics aestheticsjournal.com
@aestheticsgroup
Journal
Aesthetics Awards Special Focus
igniting medical aesthetics careers Booster Training Account Executive Events igniting medical aesthetics careers Booster Training Account Executive Events Knowledge Hub igniting medical aesthetics careers Booster Training Account Executive Events Knowledge Hub
Hand Rejuvenation Using Fillers
Dr Victoria Manning and Dr Charlotte Woodward discuss characteristics of ageing hands and detail their preferred treatment choice, sharing a successful case study
The hands represent one of the most important functional parts of the human body. Although patients pay particular attention to facial rejuvenation, they often tend to neglect other parts of their body; notably the hands. Hand rejuvenation is becoming increasingly popular not only in our clinic, but across the specialty too. Just a few years ago, clinic operator Transform Cosmetic Surgery reported an 28% rise in the number of enquiries from patients wanting antiageing procedures on their hands.1,2
Treating ageing hands is of considerable importance to patients as, just like our face and neck, they are an area of the body that are almost always exposed, no matter the season. This in turn can mean that the hands can display a sense of one’s age. In fact, according to a study conducted by the American Society of Plastic Surgeons, a person’s age can be estimated by looking at the hands alone.3 We have found that potential patients become interested in hand rejuvenation when there is a discrepancy between the appearance of facial age and hand age. Treatment options for hand rejuvenation include dermal filler injections, laser therapy, sclerotherapy, and autologous fat grafting, amongst others. Each treatment option is dependent on the patient’s concern, for example pigmentation could be treated with lasers. However, in this article we will be focusing on our preferred technique, the use of dermal fillers to restore the threedimensional aspect of the ageing hand for volume loss.4 In general, volume loss of the hands occurs in the older population.5
Hand anatomy
Understanding the anatomy of the hand and identifying its vasculature is paramount for successful rejuvenation procedures. In addition, it is
important to recognise that the epidermis and dermis are thinner in the hands compared to most areas of the face.6
There is very little subcutaneous fat on the dorsum of the hands, so even small decreases in collagen or elastin fibres will cause a noticeable impact on the hands. The dorsum of the hand is the next most prominent exposed surface area after the face.7 Bidic et al. conducted a histological and ultrasound analysis of the dorsum of the hand and found three distinct layers that they called the dorsal superficial, the dorsal intermediate, and the dorsal deep lamina.8 The dorsal superficial lamina is found between the dermis and dorsal superficial fascia; this is our target plane for filler injections. The sensory nerves and dorsal veins are contained within the dorsal intermediate lamina and the extensor tendons reside in the dorsal deep lamina.8
Thus, targeted injection of dermal filler into the superficial lamina allows camouflage of the veins and tendons, making them less obvious. Importantly, there are no vital structures running in the superficial layer, making it a safer layer for injection.7 Therefore it is important to place the product in the right plane to give an optimal correction for the volume loss and a natural clinical result without risk of complications. Due to the thinness of the skin on the dorsum, the technique for product placement is important to consider.9
Rating Definition
or two tendons are slightly exposed
three central tendons are partially exposed
three central tendons are partially exposed, with one or two tendons fully exposed
All three central tendons are fully exposed
Figure 2: The Busso Hand Volume Severity Scale. Note: the hand should be laying prone on a level surface, fingers extended.10









Hand ageing is characterised by dermal and subcutaneous volume loss, resulting in wrinkle formation. It is also associated with increased visibility of tendons and veins as well as age spots, textural roughness, loss of elasticity and epidermal, dermal, and subcutaneous thinning, In the deeper planes, atrophy of the subcutaneous fat causes underlying tendons and bony
In comparison, youthful hands appear plump and firm and the skin maintains its elasticity and smoothness. With that in mind, there are two grading scales that we use in clinic to assess the severity of volume loss in the hand. The first is the Busso Hand Volume Severity which focuses on tendon exposure and visibility. published a validated grading scale for assessment of volume loss in ageing hands (Figure 3). We find that these are good tools for aesthetic practitioners to use because they allow us to monitor treatment outcomes and this in turn helps us
Figure 1: The anatomy of the hand, showing the different layers of the dorsum, fascial layers and fatty laminae, with cannula injection placed within the dorsal superficial lamina. Adapted from Bidec et al.8
Both intrinsic and extrinsic factors influence ageing of the hands and generally the speed and extent of the changes vary with the individual patient’s genetics. We find that some of the most common external
0 No
1 One
2 All
3
4
tendons are exposed
All
7
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 1 2 9 3 8 4 5 6









OUR EXPERT RANGE ALLOWS YOU TO RESHAPE, REGENERATE AND REDEFINE
Rev
For more product and training information visit www.sinclairpharma.com sinclair_uk
Soft ®: 3D cone technology suspension sutures Ellansé ®: Collagen stimulating dermal filler Perfectha ®: Full range of Hyaluronic Acid fillers WORKING WITH YOU TO DELIVER NATURAL LOOKING RESULTS
Sinclair Pharma. 1st Floor Whitfield Court, 30-32 Whitfield Street, London W1T 2RQ. 0207 467 6920 Date of preparation: January 2019 COR04
A
Silhouette
3: Carruthers et al. scale of ageing hands. (0= no volume loss to 4 = very severe volume loss).11
factors include smoking, alcohol abuse and photodamage.7 It is important to note that we always remind our patients that prevention truly is the best medicine, so recommend that they apply a broadspectrum sunscreen with an SPF 30 or more to all exposed areas of skin — including the backs of the hands.
Treatment using fillers
Although there are a number of treatment options available, we have found the use of dermal fillers to be most effective for treating volume loss and reducing the visibility of both tendons and veins.12
A dermal filler containing polycaprolactone is our product of choice as it will volumise and smooth the skin, whilst stimulating the production of collagen to provide a youthful look.12
Case Study
A 63-year-old female presented in clinic complaining that she felt her hands were ageing; she had recently inherited some rings that she felt too embarrassed to wear as her hands had such visible tendons and the skin looked crepey.








A comprehensive medical and aesthetic history was taken and her expectations addressed. She felt her hands simply didn’t match her face. Examination showed them to be a Busso grade 3 and we felt we could improve her hands to a grade 1.10 Contraindications to treatment were explored, such as history of autoimmune conditions and any known allergy to polycaprolactone. Pre and post procedural photos were then taken and consent was obtained. A blunt-tipped 25-gauge cannula was used to inject the product. The cannula was inserted subcutaneously, superficial to the veins, into the superficial fat compartments, with an entry point just distal to the wrist crease. A cannula was used for this treatment because, in our experience, a more proximal site of entry is preferred to maximise the surface area filled with a single-entry point, hence reducing tissue trauma and preventing intravascular injection. At the cannula entry site, the patient was anaesthetised using lidocaine and then an entry point using a 23-gauge needle was created. Through that opening, the cannula was introduced. The preferred technique is to ensure that the skin is ‘tented’ upward (Figure 4) to allow the cannula to easily enter the dorsal superficial lamina; a safe plane to inject filler. Skin tenting helps to increase the injection space, which is the fatty plane between the dermis and the superficial dorsal fascia. Skin tenting also provides more separation between the cannula and the veins and
tendons that are located at the base of the ‘tent’.13 The filler was deposited directly above the fascial plane in a parallel fashion between the ligaments. The optimal place for the deposition of a filler is the under-surface of the dermis and we find that using a cannula scraping the deep side of the dermis is a good technique, which gives a perfect placement of product restricted to the fascial layer. To prevent lumps and bumps, we recommend a linear thread technique of 0.1ml per pass. The total amount of product used is really dependent on the degree of volume loss, however generally speaking you can expect to use 0.5ml to 1ml per hand. We like to use a filler that is moldable, has a long duration of action and is also durable to withstand repeated movements, which is essential to maintaining normal function of the hands. For this particular case 1ml was used in each hand and our product of choice was Ellansé. It is important to be aware that when using collagen-stimulating fillers, practitioners should under-correct to allow time for the neocollagenesis process to have an effect, especially in younger patients.14 The product was then massaged to ensure the precise contouring and an even spread. In this case, post-treatment instructions were given, namely hand hygiene. We asked her to ensure hands were washed frequently especially with pets in the house. This helps to reduce post-treatment infection. We also advised the use of an antihistamine for any post-procedural oedema, should it arise. She was reviewed two weeks following treatment very pleased with the results and a three month review is also scheduled. At this point, a further top-up treatment can be undertaken, but never before, due the collagen stimulation being maximal at 12 weeks.
Possible complications
Complications when using dermal fillers include erythema, contusions and tenderness, amongst others, however the most common issues that arise when treating the hands are oedema and ecchymosis.15
From personal experience, immediate post-treatment oedema can be reduced by asking the patients to sit on their hands for five minutes after injection, which has the same effects as compression. However, we are uncertain of the percentage of patients that
0 1 2 3
4
Figure 4: An example of the tenting technique
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 5: Before and two weeks following injection of 1ml per hand. Image courtesy of River Aesthetics.
Figure
Adapted by Aesthetics journal for publication.
actually experience swelling.16 Ecchymosis is minimal with this technique due to using only one entry point for cannula insertion. I find the presence of bumps are minimal too, as long as the practitioner massages post treatment to smooth the product.
Conclusion
Although the majority of patients requesting cosmetic procedures look to rejuvenate the face, ageing hands are a give-away of a patient’s age. When properly performed by a skilled practitioner, rejuvenation of the hands is a simple procedure with high patient satisfaction and in our experience, has a low rate of complications.
Dr Victoria Manning is an aesthetic practitioner and GP, with more than 20 years’ clinical experience. She is the co-founder of River Aesthetics which specialises in thread lifting and feminine rejuvenation. Dr Manning is also a threads trainer, a key opinion leader and an aesthetics industry media contributor, writer and speaker.
Dr Charlotte Woodward is a medical aesthetic practitioner with more than 25 years’ clinical experience. She is also the co-founder of River Aesthetics, which specialises in thread lifting and feminine rejuvenation. She was also one of the first in the UK to perform a nonsurgical breast lift using threads and is a national trainer for PDO threads.


REFERENCES
1. Female First, The rise of the ageing hands, August 2013 <http://www.femalefirst.co.uk/lifestylefashion/stylebeauty/the-rise-of-ageing-hands-327231.html>
2. Face Your Hands: National Survey from Nestlé Skin Health Reveals How US Women Feel about Their Aging Hands (US: PR Newswire, 2018) <https://www.prnewswire.com/news-releases/ faceyour-hands-national-survey-from-nestle-skin-health-reveals-how-us-women-feel-about-theiraginghands-300686196.html>

3. Bains RD, Thorpe H, Southern S. Hand aging: patients’ opinions. Plast Reconstr Surg. 2006;117:2212–2218
4. Hand: Clinical Anatomy and Regional Approaches with Injectable Fillers, Lefebvre-Vilardebo M, Trevidic P, Moradi A, Busso M, Sutton AB, Bucay VW, Plast Reconstr Surg. 2015 Nov; 136(5 Suppl):258S-275S.
5. Redaelli A. Cosmetic use of polylactic acid for hand rejuvenation: report on 27 patients. J Cosmet Dermatol. 2006;5:233–238.
6. Wiest L. Do we currently have ideal injectables for hand rejuvenation? In: Lefebvre-Vilardebo M, ed. Anatomy & Hand Medical Rejuvenation. Paris: E2e Medical Publishing; 2013:144
7. Shamban AT.Combination hand rejuvenation procedures. Aesthetic surg J/2009,29(5):409-513
8. Dorsal hand anatomy relevant to volumetric rejuvenation, Bidic SM, Hatef DA, Rohrich RJ: Plast Reconstr Surg. 2010 Jul; 126(1):163-8.
9. Wiest L. Do we currently have ideal injectables for hand rejuvenation? In: Lefebvre-Vilardebo M, ed. Anatomy & Hand Medical Rejuvenation. Paris: E2e Medical Publishing; 2013:144
10. Busso M, et al. Dermatol Surg. 2010;36(Suppl s1): 790-797
11. Carruthers A, Carruthers J, Hardas B, et al., A validated hand grading scale. Dermatol Surg. 2008;34(suppl 2):S179-S183.
12. Dove Press, Recommendations for volume augmentation and rejuvenation of the face and hands with the new generation polycaprolactone-based collagen stimulator (Ellanse), June 2017 <https://www.dovepress.com/recommendations-for-volume-augmentation-and-rejuvenation-ofthe-face-a-peer-reviewed-fulltext-article-CCID>

13. Rivkin A, Volume correction in the aging hand: role of dermal fillers, Clinical, Cosmetic and Investigational Dermatology, August 2016 <https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC5012627/>
14. De Melo, Nicolau P et al., Recommendations for volume augmentation and rejuvenation of the face and hands with the new generation polycaprolactone-based collagen stimulator, Clinical, Cosmetic and Investigational Dermatology, November 2017
15. Buso et al., Multicentre, randomised trial assessing the effectiveness and safety of calciumhydroxyapatite for hand rejuvenation, Dermatol Surg. 2010;36(Suppl s1):790-797
16. Leclere FM et al. Nonanimal stabilised hyaluronic acid for tissue augmentation of the dorsal hamnds :a prospective study on 38 patients. Aesthetic Plast Surg. 2012;36(6):1367-1375

AESTHETICSJOURNAL.COM VISIT WWW.AESTHETICSJOURNAL.COM TO JOIN FREE TODAY Keep up-to-date with the latest aesthetics developments and best practice guidance on your desktop, tablet or phone Search our Library for a huge range of categorised content and tools relating to your specialism and interests Add training to your personal Training Record for easy reference Complete accredited CPD articles and receive digital certification Advertise and search for job opportunities and clinic equipment for sale in the Marketplace Explore the Aesthetics website
Flexible Thread Technology for Natural Facial Expression
Spring Thread® is a totally innovative suspension thread for the treatment of ptosis


Before creating Spring Thread®, we went to doctors and asked, “When you administer threads, what are you looking for?”
They said they want long, blunt needles that can be manipulated easily. They also said they wanted a long and strong thread, which is reliable and simple to use. Doctors want something flexible, with elasticity, as they want to treat parts of the face which are moving a lot, and if they have a product that’s rigid, they’ll have a rigid aspect. We then went to patients and asked, “What do you want from your thread treatment?” They said, “We want something effective that will last a long time; we don’t want to go back and pay for the thread treatment every six months.” All of these characteristics have been included in Spring Thread®, to offer the advanced aesthetic doctor and surgeon, a new, reliable option for long-lasting tissue suspension and skin rejuvenation.

Product characteristics
Spring Thread® is a composite implant consisting of a silicone matrix that provides elasticity and flexibility, as well as a polyester helix core which offers resistance and control of the elasticity. Spring Thread® elasticity is similar to human skin (20%) and this flexibility leads to a better tolerance of the product:1
• The thread can lengthen or shorten during muscle movements
• It avoids the hard end extrusions
• It distributes tensions along the entire length of the thread
Results
• It absorb tensile stresses (like a shockabsorber of a car)
• The thread remains fixed and without pain due to excessive stress
In summary, Spring Thread® allows for dynamic stabilisation of tissues. They can ‘live’, lengthening and shortening, with muscle mobility preserved. The result is a natural effect. Spring Thread® cogs are rounded, non-aggressive, pointing in four directions and very close: 24 small cogs/cm. They provide a non-traumatic and effective anchorage and significant fibrosis.1 Spring Thread® is a very strong thread, which allows for good tissue suspension and extremely long-lasting results for three years plus, which can be extended as the thread can be repositioned over time.1 The thread is perfectly biocompatible, safe and neutral, and does not interfere with the body or cause negative reactions and side effects.2
Procedure
Spring Thread® is placed in the same way as current threads with the thread being implanted in the subcutaneous fat, before the SMAS (between 2mm and 3mm deep), but not too superficially to touch any hair follicles. Spring Thread® has a soft needle, so as not to damage nerves or vessels and reduces trauma. The best procedure is selected according to the patient profile (severity of sagging, asymmetry to correct), always choosing the most simple laying technique possible and allowing for easy adjustment with maximum safety. During procedure, it is possible to relax a thread which is too tight
and, if the thread has been placed incorrectly, in can be removed. Then, in a week, fibrosis produces an excellent fixation. Spring Thread® is very successful for applications on the cheeks, neck, the eyebrows, for the treatment of facial palsy, and body indications that include breast, buttock and thigh ptosis. Although Spring Thread® can be successfully utilised for various procedures intraoperatively, it is often considered for patients not quite needing, wanting or contraindicated for surgical face lifting, or indeed, patients who have already undergone surgery some years previously and have returned to the surgeon and are asking, ‘What can help me now?’


Product range
There is a range of two diameters and four references of threads:
• A thin thread, 300mm long for the face, neck and arms, with two 150mm long crimped needles
• The same thread without needle to place with a specific 200mm separate needle
• A thicker thread, 30mm long, for the treatment of the body (thigh, abdomen, buttocks and small breast ptosis)
• The same thread with a central part of 50mm without cogs, suitable for implementation in a U-shape under the breast
Spring Thread® is manufactured in France by 1st SurgiConcept, under CE mark and ISO 13485, and was implanted for the first time in October 2007. Distributed in more than 40 countries, there are now over 70,000 threads implanted.
Conclusion
Spring Thread® is a new, soft and elastic, suspension thread, which corresponds optimally to the biomechanical characteristics of recipients’ tissue and expected functions. It is an effective thread for ageing patients, with long-term results and limited side effects.
Spring Thread® is exclusively distributed in the UK and Eire by Mesostrata Ltd and is available through Springpharm. For more information telephone 0345 319 4000, see our website www.springthread.com or email info@springpharm.co.uk
REFERENCES 1. J.P Foumentezee, D Guillo, G Jeanblanc, ‘Multi-centric retrospective clinic study for suspension thread
Somerefs
2. Data on file. Available from Mesostrata Ltd. 3. Lifting via Permanent Suspension Threads. Five Rules for Beautiful Results, By Dr Denis Guillo,
of Medical Aesthetics and Surgical
SPRING THREAD’,
(2010).
Journal
Dermatology, December 2016.
Before Before After After
Spring Thread® users get very interesting results. Due to the characteristics of flexibility and elasticity, muscle mobility is preserved, which results in a natural effect. In addition to the immediate lifting effect, results improve during the months following the intervention.1
before and one year after
Aesthetics | June 2019 52 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Spring Thread®
Dominique Malard, CEO of 1st SurgiConcept Two
patients
treatment with Spring Thread®. Images courtesy of Dr Denis Guillo.3
A summary of the latest clinical studies
Title: A Double-Blind, Placebo-Controlled, Phase 3b Study of ATX-101 for Reduction of Mild or Extreme Submental Fat
Authors: Glogau RG, Glaser DA, et al.
Published: Dermatologic Surgery, April 2019
Keywords: Fat dissolving, ATX-101, deoxycholic acid
Abstract: Objective: to evaluate the efficacy and safety of ATX-101 in subjects with mild or mild or extreme submental fat (SMF). Adults with mild or extreme SMF (based on clinician assessment) were randomized to receive ≤6 treatments with ATX-101 or placebo. Efficacy end points, evaluated at 12 weeks after last treatment, included percentage of subjects who achieved ≥1-grade improvement in SMF from baseline based on both clinician and patient assessment (composite CR-1/PR-1 response) as well as multiple subject-reported outcomes. Safety end points included change in skin laxity and incidence of adverse events. Overall, 61.3% of ATX-101-treated subjects versus 6.7% of placebo-treated subjects with mild SMF and 89.3% versus 13.3% of subjects, respectively, with extreme SMF achieved a composite CR-1/PR-1 response (p < .001 for both). ATX-101-treated subjects also reported higher levels of satisfaction and greater reductions in the psychological impact of SMF versus placebo-treated subjects regardless of baseline SMF severity. Skin laxity was unchanged or improved in most of the subjects. Adverse events were mainly mild/moderate, transient, and associated with the injection site. ATX-101 was efficacious and well tolerated for reduction of mild or extreme SMF.
Title: Red Deer Umbilical Cord Lining Mesenchymal Stem Cell Extract Cream for Rejuvenation of the Face
Authors: Alhaddad M, Boen M, et al.
Published: Journal of Drugs in Dermatology, April 2019
Keywords: Stem cell, facial rejuvenation, ageing
Abstract: A new patented protein mix derived from red deer umbilical cord lining stem cell conditioned media (Calecim Multi Action Cream, CellResearch Corporation, Singapore) has been developed to improve the signs of aging. The extract is the conditioned media from umbilical cord lining mesenchymal stem cell culture in basal media and consists of a mixture, in specific proportions, of cytokines, growth factors, extracellular matrix proteins, amino acids, peptides, and other proteins. It has been developed to increase epidermal cell turnover and stimulate fibroblast function, reducing the appearance of pigmentation, fine lines, and redness, and to restore skin elasticity. The objective of this IRB-approved, prospective, randomized, double-blind, split-face, placebo-controlled clinical trial was to compare the efficacy of red deer mesenchymal stem cell extract (RCE) versus vehicle for facial rejuvenation. The trial involved 40 healthy subjects with moderate to severe facial wrinkling secondary to photodamage. One half of the face was randomized to receive topical RCE cream and vehicle cream to the other half of the face. Treatment was continued for three months, and evaluations were performed in a double-blind fashion. Both sides of the face achieved significant improvement. Blinded investigator assessments did not detect any statistically significant differences between the two halves of the face in terms of efficacy, safety,
or tolerability. Subject evaluations demonstrated superiority of the active treatment side. Red deer umbilical cord lining mesenchymal stem cell extract was effective in rejuvenating the aging face as demonstrated by investigator and subject measures.
Title: Hyperbaric Oxygen Therapy for Dermal Ischemia after Dermal Filler Injection with Calcium Hydroxylapatite
Authors: Uittenbogaard D, Lansdorp CA, et al.
Published: Journal of the Undersea and Hyperbaric Medical Society, May 2019
Keywords: Dermal filler, complications, vascular occlusion
Abstract: One of the most threatening complications after dermal filler injection is skin necrosis due to vascular occlusion. Different treatment options are available, including the use of hyperbaric oxygen (HBO2) therapy. A 46-year-old female received facial dermal filler injections with calcium hydroxylapatite at an aesthetic clinic. A few days after injection she developed a burning pain, numbness of the skin and white discoloration in the injected area. Two days after injection treatment was started with hyaluronidase and warm compresses. In addition, the patient received prednisolone, sildenafil and nifedipine. After the start of these treatments, the pain, numbness and discoloration of the skin persisted. Because of dermal ischemia and to improve healing she was referred for HBO2. Treatment consisted of 10 sessions of 100% oxygen for 90 minutes in a multiplace chamber at 2.5 atmospheres absolute pressure. During HBO2 the discoloration resolved, pain and numbness disappeared, and the tissue healed completely. After a six-month follow-up she had an excellent cosmetic outcome. Given the pathophysiologic mechanisms of vascular complications after dermal filler injection, HBO2 should be considered when treating these complications.
Title: Evaluation Of Platelet-rich Plasma vs Intralesional Steroid in Treatment of Alopecia Areata
Authors: Albalat W, Ebrahim H M


Published: Journal of Cosmetic Dermatology, May 2019
Keywords: PRP, alopecia, hair loss
Abstract: Objective: to evaluate the safety and efficacy of Platelet-rich plasma (PRP) vs intralesional corticosteroid (ILCs) in treatment of Alopecia areata (AA). This study was conducted on 80 patients of both sexes who had AA. Patients were classified into Group I treated by ILCs and group II treated by PRP. Results were assessed by dermoscopic evaluation and by hair re-growth score (RGS) at (baseline), 2, 4, 6, 8, and 12 weeks. Patients were followed up for 6 months. There was greater hair re-growth after treatment in both groups. In group I, (26) patients (65%) showed improvement >70% compared to 29 patients (72.5%) in group II. There was significant re-growth of pigmented hair and decrease in dystrophic hair (P < 0.001) by dermoscopic evaluation in both groups. The difference between both groups was insignificant (P = 0.57). At follow-up, two (5%) patients in group II had relapse compared to 10 (25%) patients in group I. PRP is a safe and promising therapeutic option in AA.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com


MATA Level 7 Post Graduate Diploma in Facial Aesthetics (Incorporating OTHM Level 7 Certificate/Diploma In Clinical Aesthetic Injectable Therapies) Our Diploma Provides – 150 Hours of Online Learning – 2 Days of Foundation Training – 2 Days of Advanced Training – (Including Hyperhydrosis) – Mentorship Days Up to date with the latest JCCP guidelines Learn Facial Aesthetics to a Higher Standard Call: 020 3126 4870 Discounted from £9000 + VAT to £5150 + VAT with the code AJ5150 for a limited time. 1 Harley Street, London, W1G 9QD www.matacourses.com Special price available for delegates who want to upgrade to the new 60 Credit MATA Diploma from the existing 28 Credit Level 7 Certificate Subject to RPL
Live Chat Functions
Web developer Alex Bugg discusses ways to effectively add a live chat function to your website
Patients are frequently asking questions before they even present to clinic for a consultation; where they once might have called via phone, the new norm is asking these questions through social media or website messaging. ‘Which brands of dermal filler do you use?’, ‘Are there any cancellation appointments with Dr Smith this week?’, ‘I had microneedling on Monday, can I put on a face mask now?’ are all examples of commonlyasked questions by patients. It has not just stemmed from the ‘fear’ of speaking on the phone, backed up by total outgoing phonecalls dropping by over one billion minutes last year despite a surge in smartphone use,1 but it’s also down to the sheer convenience of being able to message with the assurance you will receive a reply almost instantly that is so appealing. You are (hopefully) already engaging with existing and potential patients in your clinic with a whole selection of marketing materials and, through this, you are probably driving as many people as you can to your website to showcase your unique selling points (USPs), your talent and your latest offers. It was reported by marketer Tim Pickard that failure to respond via social channels can result in an extra 15% of customers leaving your site or service.2 He also stated that 53% of customers expect a response on social networking site Twitter within just one hour.2 I too believe this to be essential, no matter what the query; this potential or existing patient has taken the time to get in touch with your brand – so give them the time back. In this article, I’ll introduce live chat functions on websites and explore what
platforms you have to choose from. I’ll also outline some considerations when looking to commit to live chat, and how it can or cannot pay off for your business.
What is live chat?
Live chat is an additional software added to your website, allowing visitors to instantly message you. It’s fast, and when managed well, can provide a great user experience, hopefully leading to increased conversions. In my opinion, live chat is the modern way to communicate with companies as it is quick and convenient compared to telephone, email or in-person enquiries. Research conducted by social networking site Facebook has shown that 61% of those in the UK who use messenger services have made contact with a business and 53% of people said they are more likely to shop with a business they can message directly.3
Once someone has engaged with your live chat, it shows that they are interested in your business. Statistics from service provider Moneypenny indicate that 3.27% of visitors to websites with a live chat function engage with it, compared to just 0.5% of visitors filling in a web form.4 It was also concluded that customers using chat functions are 43% more likely to convert to a paying client.4
Benefits
A main benefit of adding a live chat function to your site is that you can answer short, simple enquiries that you would usually get via email/phone such as, ‘When is the next appointment for a facial with Jane?’ or ‘How
much is laser hair removal?’. It’s quicker to reply in this way as you can send across a link to the pricelist page for example, and by improving the user experience, you will hopefully find more browsers becoming patients. You will also have access to chat logs, allowing you to analyse your most common enquiries, without having to take notes during each phone call. This data will highlight your most frequent queries; which may mean that the information is not clearly highlighted on your website or across your social media and could be improved. You can also create valuable blog posts using your FAQs for the benefit of your website; your content now has context, and you can also use this content for social media.
Live chats can also maximise the benefit of your paid advertising such as pay-per-clicks and social media ads, such as those on Facebook for example. Paid-for advertising should hopefully increase traffic to your website,5 then once they’re there, having a new way to capture enquiries through live chat, alongside web forms, email and phone calls, gives your customer more choice. If they prefer to engage with you in this way, answering a simple question via your chat function could be the difference between a booking and a bounce away from your website.5 If you want to add the function but are worried about your response time, you can put together an auto-response to let people know your active hours, or take a step further and build ‘chat bots’6 so that your FAQs are answered via automation.
Selecting your live chat
There are dozens of customer service software applications on the market and each has its costs and benefits however, unless you are a software developer, you will likely require third party help.

Some follow a ‘freemium’ model, where you get the basic platform for free (for example, one log on, short chat history, limited message volume) and additional features incur a cost. Additional features that I find useful are extra user accounts, reporting, chat history and personalised auto-responders.
You should expect to pay monthly for your live chat, or annually for a potential discount. The website you have also plays a part in the live chat’s success, so make sure your platform can import the code/plugin. Speak to your web developer or provider if you are unsure, or you can ask the chat platform support team. Detailed below are some of the most common options available:
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com





AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
Questions to ask yourself when selecting live chat
Generally, I would advise that you take your time to research the software you’re going to go with. In my experience, making use of two or three ‘free trials’ from companies offering a chance to try it out is the best practice. Ask yourself:
• Has it got the features I am looking for? Am I paying too much, or not enough? Expect premium subscriptions to cost up to £50 per month if you manage your chat yourself; this should suit most small-medium clinic set ups
• Is it simple for me to use? Can the team navigate it?
• Is it easy for my patients to use? Trial this by testing it from a patient’s perspective
• Can I access it on all of the devices I want to use?
• Am I receiving the volume of messages I am expecting/paying for? Compare this to your website traffic and take a percentage. If 2% are messaging, in my experience, that’s a good use of your time
1. Facebook Messenger
It’s a familiar experience for your user due to the popularity of the site. Conversations are saved for the customer in their app as well as your business page inbox and it’s also a simple format.7 This free option relies on both your visitor and your clinic having a Facebook page. It is a good place to start trialling live chat. Our clients who have small to medium-sized clinics have opted for this and, in our experience, they have received an uplift in messages received through Facebook, ultimately leading to more business. For your patient, the interface is the same bubble in the bottom right corner, and they will feel familiar with sending the message. For your clinic, you will receive these messages in your Facebook inbox, not through your website, so make sure to stay logged in and switch notifications on!
2. Market-leading solutions
They are the most established platforms, have advanced rule-building for automation (such as an autoreply) and detailed customisation. Some of the most popular in my experience include Livechat, Zendesk, Manychat and Olark.8-11 If you Google ‘live chat software’ you will come across lots of options. Each site will lay out their features and pricing structure. You can expect to pay for features such as chat history, automation and the number of concurrent chats (or agents). One size does not fit all, so I advise to first consider what you want the software to do, then look for matches and decide if the value is worth the cost.
3. Managed chat via a virtual personal assistant
Many of the benefits for this option are the same as above, plus it is managed
for you by a contractor briefed by you or your clinic team. Examples of these are Moneypenny and Influx.12,13 Outsourcing your live chat has its potential if you have the budget. You provide them with as much information as possible on your clinic and they handle the chat either fulltime or simply when you are offline (away, out of hours, weekends for example). However, this can get expensive and difficult questions will be sent to your email by you to address yourself. Consider the time taken to educate the personal assistant, compared to utilising your already-there front-of-house staff.
Each platform will have its own installation and configuration process, but for the most part, it’s simple. The provider will give you a piece of code which is inserted into your clinic website; you will simply follow the instructions to install it or can ask your web agency/provider to install it for you. Premium platforms may even have a full ‘onboarding’ service, where they take you through the process of installing on your website and familiarising you with the interface, so you can navigate your software.
Considerations and challenges
One of the main considerations when adding this service is the type of information you are providing your patients. I’d strongly advise that you do not deliver medical advice over live chat,14 such as how patients should deal with a potential complication or whether or not they require injectable treatments. Training your staff to respond appropriately to these sorts of enquiries by recommending that they book a face-to-face consultation is very important. Time and resources is also a huge factor. If you or your front-of-house team cannot commit to managing the live chat and responding promptly, then it may not be worth it. In my experience, you will
want to respond to messages within just a few minutes of them arriving, even if its just an automated reponse acknowledging that the message has been recieved. Consider capacity; if your phone rings all day, and your receptionists are dealing with emails and social media enquiries, then can they handle live chat on your website too? The best way to know is to trial the service and get a feel for the volume of messages you receive. Lastly, I would advise that you don’t make the function pop-up repeatedly or make a loud noise. As with any pop-up, some visitors to your website may find it annoying and obstructive,15 so I would say that one, automated ‘Can we help?’ message on the home page will let customers know you have the feature, then leave them to reach out when required.
Conclusion
Discuss the feasibility and benefits of running a live chat with your team to ensure that they are on board with the introduction and feel confident in its use; once it’s implemented it can be a great tool for your business. Integrating live chat software to your clinic’s website can be a simple and straightforward way to increase engagement, patient satisfaction and return on ad spend.
Alex Bugg has worked with the Web Marketing Clinic since 2012 and has a key interest in developing strategies for cosmetic clinics and biotechnology firms across the UK and abroad. Bugg also has a Master’s in chronic disease and immunity from University of Leicester, graduating in 2016.

REFERENCES
1. Ofcom, The Communications Market 2018, Interactive Report, August 2018 < https://www.ofcom.org.uk/research-and-data/ multi-sector-research/cmr/cmr-2018/interactive>
2. Pickard T, Sixteen customer service statistics and what they mean for small companies, Small Business, May 2016 <https:// smallbusiness.co.uk/sixteen-customer-service-statistics-andwhat-they-mean-for-small-companies-2521451/>
3. Facebook, Facebook messenger for business <https://www. facebook.com/business/marketing/messenger>
4. Stringer H, Moneypenny Live Chat Statistics, 2018 < https://www. moneypenny.com/uk/resources/videos/live-chat-your-mostpowerful-website-tool/>
5. Hootsuite, How to advertise on Facebook: The Complete Guide, May 2015 <https://blog.hootsuite.com/how-to-advertiseon-facebook/>
6. Sprout Social, Chatbot <https://sproutsocial.com/glossary/ chatbots/>
7. Facebook, Why Messaging Businesses is the new normal, June 2018 < https://www.facebook.com/business/news/insights/whymessaging-businesses-is-the-new-normal>
8. LiveChatInc.com <https://www.livechatinc. com/?utm_expid=.eujnjFzZQoiYioAXkiknYQ.0&utm_ referrer=https%3A%2F%2Fwww.google.com%2F>
9. Zendesk.co.uk <https://www.zendesk.co.uk/>
10. ManyChat.com <https://manychat.com/>
11. Olark.com <https://www.olark.com/features>
12. MoneyPenny.com <https://www.moneypenny.com/uk/live-chat/>
13. Influx.com < https://influx.com/solutions/live-chat-support>
14. GMC, Remote Consultations <https://www.gmc-uk.org/ethicalguidance/ethical-hub/remote-consultations>
15. SEO training London, How do website visitors feel about pop-ups? < https://www.seotraininglondon.org/should-usepopups-website/>
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com




















BEAUTY BOOSTING REDENSIFICATION HYDRATION FIRMNESS RADIANCE
Rebranding Your Website
Practice manager Hannah Betts looks at considerations for updating or rebranding your website
As responsible practitioners, I believe that it is our obligation to ensure that our online presence offers a true representation of what both the industry and respective clinics offer so that we uphold the best in service and clinical excellence from the very first click. Your website is usually the first place that your existing and potential patients will learn about you, so make it a reflection of your company’s ethos and values. This article aims to address the general importance of a website as a brand communication tool, specifically looking at rebranding your website to coincide with a clinic refresh or update.
Reasons for rebranding
A website could easily be considered as an additional (and arguably the most important) employee. Often the first point of contact for prospective patients, it’s important that the website accurately reflects your brand image and values. We are fortunate to work in a constantly evolving industry that actively embraces and champions technological advancements and innovations. Given the very nature of our industry, it is inevitable that our business will also change and grow alongside it. Although a website may work for you for a considerable number of years, it doesn’t mean that it should infinitely remain the same. Reasons for rebranding your website may include (but are not necessarily limited to):
• Overall refresh: if the overall look of your business changes then it is a logical step for your website to be refreshed at the same time. This will ensure that your brand messages are consistently communicated.
• Technological advances: online appointment systems, increased retailing opportunities and the boom in social media and mobile device usage has garnered a need for websites to be mobile friendly. According to media company comScore, mobile devices now account for nearly two of every three minutes spent online,1 so it’s highly likely that prospective patients will be using their mobiles to conduct their initial research. In addition, video content is becoming increasingly important and with some statistics suggesting that embedding videos in landing pages can increase conversion rates by 80%;2 it’s certainly worth the consideration.
• To create a competitive edge: professional aesthetic clinics can often bare similarities to their competitors and this may lead to prospective patients missing your unique selling points (USPs). Therefore, rebranding your website can reinforce individuality and create a competitive edge.
• To reflect a change in the services that you offer: if you change the type of treatments that you offer or decide to specialise in a certain category of aesthetics, then you may want to change your website to reflect this. This can be done by re-organising your navigation categories, by changing your page layout or adding extra pages to an existing layout to help give the user clear options of what is on offer.
Whatever the reasons for rebranding your website, it’s important to not lose sight of your identity and to ensure that your tone of voice remains professional and inviting. Communicating changes to your clinic team and patients can be a challenging aspect of any rebrand process, but is essential to ensure that you do not lose custom. An example would be to update your customers through the use of emails and social media. It is always a good idea to plan ahead and if there is any chance that the website would be down, schedule this during a less popular time, such as late in the evening or first thing in the morning.
Requirements for your website
In order for you to fill the above requirements, you will more than likely need to find a partner to assist you. Whilst some clinics may employ someone in-house to do this, it is rare and the majority will outsource the work to a specialised agency. However, before you choose the right partner, you must decide what you want from your website. Spending time thinking about the appearance, usability and accessibility is crucial. This will help when both researching potential partners and compiling a brief to ensure that your needs are met and that you achieve the outcome that you want. Specific considerations include:
• Appearance: a visually appealing, polished and professional website is key to creating the right first impressions. Ensure that text is easy to read, the colours used are consistent with your brand and that images are of high-quality.
• Content: engaging content that is well written, informative, engaging and up-todate is essential. This will help to build trust in your clinic from the outset. In my experience, a combination of informative content, explaining the procedures in full, mixed with legitimate reviews and video content that is easy to access, has the lowest bounce rate meaning users spend more time on the page.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
• Functionality: your website should work quickly and correctly so make sure time is spent testing its functionality before going live. Poorly constructed components will simply direct potential patients elsewhere.
From contact forms and online booking facilities to site search, everything should work 100% as expected.
• Usability: similarly, good website usability is essential for ensuring that both existing and potential patients can use the site problem free. It should be easy to navigate with clear call-to-actions throughout.
• Search engine optimisation (SEO): ensure that your website can be found efficiently. I would advise that you work closely with an SEO agency to ensure that the best digital practices are used when developing content and changing any layout to the site. This can include the incorporation of videos, editorial pieces or more technical things such as conversionrate optimisation with placement of phone numbers and contact forms.
• GDPR compliance: as with other aspects of your business, if you manage patient records via your website then it’s essential that the latest General Data Protection Regulation (GDPR) legislation is adhered to.3
Choosing your partner
By deciding the above and creating a list of requirements, you will consequently be able to research potential partners. It is important here that you can do some of these things yourself, like writing and uploading content for example, but without appropriate coding knowledge for example, you will probably need to hire someone to do this for you. You should ask yourself a number of questions when going through this process which will help determine whether they are right for your business needs. I’d firstly recommend you check that any prospective partner has designed and built websites
that will at the very least meet (and ideally exceed) your expectations. Have they worked with similar businesses as this can be advantageous in terms of them understanding certain terminology and what customers might want? Don’t discount those that don’t have these credentials though, as they may bring a fresh approach and new ideas to help you stand out from your competitors.
You should also talk to current and former clients of any potential partners and ask them for their honest opinions. Are they easy to work with and do they possess effective project management and communication skills? Word of mouth is a great way of finding and deciding partners.
As well as this, honest two-way communication is essential for building a fruitful working relationship that will garner the best results for your business. Ask about how they like to communicate progress and agree decisions, and ensure that this suits the way in which you like to work. Our current agency uses a collaboration and organisational online tool to help us manage work flow with them, prioritise issues and help ensure all things are on record. It is helpful to choose a partner that has the ability to listen, as well as provide counsel, so that all of your opinions are given consideration.
Budget is also a huge consideration when outsourcing website design, be realistic with your budget and ensure that you take all cost elements into consideration. Costs will vary dramatically between a website being designed, built and tested from scratch to an existing site that has minimal updates. A well designed and executed website can bring significant return on investment so take this into account when deciding your project fees and budget.
Lastly, what are the timescales? It’s important to establish clear timescales of when the project can start, how long it will take and whether this fits with your deadlines. Websites
take a certain amount of time to plan, build and test properly, so ensure that you find out how long this will realistically take. In my experience, this is generally based on the size of website needed and its functionality required; if it is an ecommerce site, this will take longer as the content is much more substantial. In comparison, a website with a few treatments and a contact form is slightly more basic and therefore needs less time for layout planning and building. This will also be reflected in the cost of the build.
Conclusion
The importance of a website as a brand communication tool should not be underestimated and websites should regularly be reviewed and updated to reflect ongoing advancements in both the aesthetic and digital industries. Before embarking on a website rebrand, it is important to consider the needs of existing and potential patients, and that outstanding customer service and standards of excellence are clearly communicated and maintained. Researching any potential partners thoroughly is key to securing a successful return on investment.
Hannah Betts is the clinic manager at Health & Aesthetics and an aesthetician with more than 10 years’ experience, specialising in skin rejuvenation, laser treatments and body contouring. Betts recently managed the rebrand process and successful implementation of the new Health & Aesthetics website, and moved the clinic to Elstead.

REFERENCES
1. ComScore.com, US Cross Platform Future in Focus, 2016 <https://www.comscore.com/Insights/Presentations-andWhitepapers/2016/2016-US-Cross-Platform-Future-in-Focus>
2. Matt Bowman, Forbes Agency Council Video Marketing The Future Of Content Marketing (www.forbes. com, 3rd February 2017 (https://www.forbes.com/sites/ forbesagencycouncil/2017/02/03/video-marketing-the-future-ofcontent-marketing/#59485c36b535)
3. EU GDPR.org <https://eugdpr.org/>
Spending time thinking about the appearance, usability and accessibility is crucial
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com

THEY MANAGE E VERY THING WITH CLINICSOFT WARE.COM
Think inside the cell


Find out more at www.cynosureuk.com/picosure
revitalization
Array deliver energy
cell signaling
downtime.
ATTRACT NEW PATIENTS • 15 minute treatments • Minimal downtime; only 1-3 hours • Reduced pigment, increased collagen and elastin PicoSure 755 is FDA cleared to treat tattoos and pigmented lesions in skin types I-VI. PicoSure 755 with Focus is FDA cleared to treat pigmented lesions in skin types I-VI and acne scars and wrinkles in skin types I- IV. Patient results will vary. Cover model used for illustrative purposes and this depiction is not an actual before and after photo. © 2018 Hologic, Inc. Hologic and PicoSure are registered trademarks and Focus is a trademark of Cynosure, Inc. Signaling a new day in skin
Only PicoSure® 755nm and Focus™ Lens
that works with the body, uniquely activating natural
processes to create brighter, healthier, younger looking skin – with virtually no
Working with Influencers
Bloggers, or social media influencers, as they are now more commonly known, have become an established part of marketing strategies; and you can see why. According to 2018 statistics, 83% of the adult UK population is now active on social media, with the top networks, in order of usage, being Facebook, YouTube, Twitter and Instagram.1
Data also shows that 23% of UK consumers have clicked through to buy a product after seeing it featured by an influencer.2
A social media influencer is someone with a reputation for expertise and knowledge in an area because they post regularly about it. They have the power to influence their followers’ opinions, and this can also extend to their purchase decisions. This is where influencers really come into their own; their followers trust and respect their opinions and are usually very engaged with their content.
The average influencer engagement rate (the percentage of their followers that responds to their content, for example by clicking on a link or liking a post) is 5.7%, compared with just 2-3% for brands on Instagram.3
As such, working with influencers is now central to many branding campaigns across all major categories. The beauty category has become especially noteworthy. Although return on investment is hard to measure, a recent report found that for every £1 spent on influencers within the beauty industry in 2017, brands received an average return of £8.81.4
According to business magazine Marketing Week, nearly all beauty marketers say their budget for influencer marketing is likely to increase over the next 12 months and nearly two thirds (65%) are planning to increase spend in this area by at least 10%.3
If this is all sounding too good to be true, you’re right; it hasn’t all been plain sailing. Influencer fraud hit the headlines last year, with some high-profile cases of fake followers (influencers buying followers or having a large number of fake followers) and influencers not correctly flagging up paid promotions.5
The fall-out from this can be damaging – and expensive – for the brands involved. A recent
report has revealed that 11% of engagement with influencer-sponsored Instagram posts in 2017 was generated from fraudulent accounts.6 As an aesthetic clinic, this kind of thing could mean that you are not receiving the return on investment that you planned and can even hurt your brand if real accounts start associating you with fake influencers and no longer trust you because of it.
At the start of 2019, the Advertising Standards Authority (ASA) contacted more than 200 social media influencers about failing to state clearly in their posts if they were paid or received products, loans or gifts of the products they endorse.7 Following on from that, The Competition and Markets Authority (CMA) secured formal commitments from 16 celebrities to be more transparent when posting online.8
So, if you’re thinking about working with influencers, there are pitfalls to avoid and steps you can take to make sure that your relationship is successful and productive.
Are influencers right for my brand?
The first question to ask yourself is if influencers are appropriate for your target market, so you must firstly do research to determine how your patients use media. I have found that the Adults’ Media Use and Attitudes Report from Ofcom is very useful to understand our patients’ likely media habits.9
For example, Instagram has a younger user profile than Facebook and recent statistics show that only 10% of UK women aged between 55 and 64 years are using Instagram.10,11 So, there is little use in running a campaign on Instagram if very few of your target audience is using the app.
How do you find an influencer?
You need to find an influencer that your target audience will trust and respond to, for example, someone who has demonstrated knowledge and expertise within beauty and skincare. Be active on social media, follow local beauty and skin bloggers and look at the interaction between the influencer and
their followers. You may need to use your gut instinct to determine whether you think your target market would ‘fit in’ with this influencer. When I first started to work with influencers, I was lucky to know someone personally that really fitted the bill for The Clinic by Dr. Mayoni and her audience closely mirrored my core target market. Just as importantly, her outlook and attitude reflected my clinic’s brand values too; that looking good is just as much about feeling good and mental wellbeing. That was very fortunate – but there are other ways to find the right person for your needs. Good places to start are by identifying the hashtags and topics that are key to your business and seeing who is already active in this area. Ensure the individual you are researching is genuine; Influencer Marketing Hub has a useful free tool to analyse Instagram accounts for fake followers and their number of likes.12 Once you have identified someone you want to work with, contact them through the relevant social media platform or by email – many will include an address in the contact section of their profile. It’s also worth checking their website to see if they have any advice on how best to get in touch. From here, keep your tone professional and make sure you include details about yourself and your business so that they know that you are serious and can get a better idea of your offering. When selecting who to approach, you will need to keep your budget in mind too. As a general rule of thumb, the more followers a person has, the more you will pay. The price you will pay will vary enormously according to the influencer in question and the type of project you have in mind. For example, a one-off post about your brand will involve less commitment than a before and after treatment blog. Your deal may also include other elements; for example, offering free or discounted treatments that you want the influencer to write about, inviting them to your events, giving them first access to new treatments and products, and so on. Again, it is important that the influencer makes it clear if they have received free or discounted treatments. All these elements will be part of your negotiation, and the sky is the limit. In terms of costs, statistics in the US put Instagram posts at around $1,000 per 100,000 followers13 but Kylie Jenner reportedly makes around $1m per paid post!14 Finding your perfect partner can be a timeconsuming process, so you may want to consider using an agency to help. Specialist influencer agencies and many PR companies can help with this process, from finding your influencer to negotiating the terms of
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Mayoni Gooneratne provides her top tips to help practitioners work effectively with bloggers and social media influencers to grow your brand and business
 REF: Efficacy test of a serum with gold nanocomplex combined with radiofrequency to reduce the cellulite effects. Endor Technologies S.L., Instituto de Fotomedicina, Dr. Joaquin Querol, Gabriel Buendía Bordera M. Sc., Dr. Jorge Gaviria, Dr. Juan Bascones.
REF: Efficacy test of a serum with gold nanocomplex combined with radiofrequency to reduce the cellulite effects. Endor Technologies S.L., Instituto de Fotomedicina, Dr. Joaquin Querol, Gabriel Buendía Bordera M. Sc., Dr. Jorge Gaviria, Dr. Juan Bascones.
your relationship and planning the creative content. You can find a list of UK-based influencer marketing agencies at Influencer Marketing Hub.15 Industry publication PR Week also has a really useful section on Influencer Marketing and is well worth a look for tips and contacts.16
How can I work well with an influencer?
I think the best influencer campaigns work because of the synergy between them and the brand. You should already know a fair bit about them, but now is the time for your influencer to get to know you well. Nothing beats face-to-face meetings if possible, so you can really get your passion for your craft and your brand across. The other thing you should do is draw up a really detailed brief in writing so that you both fully understand what is expected.
Be clear about what you are prepared to do – and what you are not prepared to do. For example, appearing in video content or providing free treatments to the influencer. Think now, too, about what you expect in return and get this agreed and in the brief before you go any further. For example, you might ask to see insight data on individual posts, such as the reach, engagement and impressions they achieved.17 This is a very useful way to gauge how well your campaign is working. You should work out in advance how many posts you would like to see, how often they will appear and how long this campaign will last, for example. If you’ve found the right person you will hopefully be building a long-term relationship, so it is worth spending time now building solid foundations. As a rule of thumb, all your work with an influencer should be about building brand awareness and understanding rather than driving sales for individual products. Followers look to these accounts for advice and knowledge, not the hard sell. Your influencer is unlikely to want to be your salesperson in any case: this is not their job.
Once these things are in place, you will feel confident about my next piece of advice: allow your influencer creative freedom with the brief. According to research, nearly 40% of influencers feel that restrictive content guidelines are one of the biggest mistakes brands make when working with them.18 It stops them from integrating the posts successfully with their own content and presenting them in their own style. This inauthenticity will jar with their followers and isn’t good for the influencer or the brand in question. It’s important that your influencer’s
personality can come across in any work you do together. They know their medium inside and out, and more importantly, their audience, so trust their expertise.
Hopefully, if you’ve found the right person, you won’t have a problem in them being creative with the brief and putting their own unique spin on the content. If you think that their current content won’t work well for your brand, then it may be time to look again. Be sure not to burn any bridges; sometimes a relationship will not work out, but try to part on good terms and leave the door open for future collaboration.
How can I make the most out of influencers?
Another top tip is to make the most of all the content that is created by repurposing it on all of the platforms that make sense for your target audience. Ask influencers if they are active across more than one platform, and if so check that they will share your content across each of them. Agreeing the preferred platforms for your campaign should be part of your brief. Keeping on top of new techniques is also an important part of the influencer/ brand-owner relationship. For example, Instagram Stories are currently really popular, but it wouldn’t be surprising if something new comes along soon to shift our attention. When your campaign is underway, it is important to keep in close contact and review regularly with your blogger/ influencer. They will be able to tell you what resonated with their audience, and what missed the mark. Allow space and time for your campaign to evolve as you both learn more. Don’t be afraid to try something new; creativity can really help to cut through the noise. Getting people to engage with the content by sharing their own thoughts and pictures is also really impactful; for example, you could pose a question to encourage engagement.
Conclusion
If your target market is active on social media, influencer marketing is well worth spending time and devoting marketing budget to. Concentrate your efforts on finding the right influencer for you and your brand and put time into developing that relationship. Do your homework to make sure they are what they claim to be, and now more than ever make sure that all paid posts associated with your brand are clearly labelled as such. Have a professional relationship from the very beginning and allow influencers the freedom
to work creatively. They are the experts in their medium and are working to protect their brand too, so mutual trust is essential. Working together in partnership can reap huge rewards for brands, helping to build awareness and understanding.
Dr Mayoni Gooneratne is a graduate of St George’s Hospital and has been a member of the Royal College of Surgeons since 2002. She has completed extensive training in aesthetic techniques over the last few years which has culminated in the creation of private aesthetic clinic The Clinic by Dr Mayoni in 2016. She is accredited by Save Face and is an associate member of BCAM, and is part of the IAPCAM Faculty for 2019. She is an Ambassador for Geneveve by Viveve Medical.

REFERENCES
1. Alison Battisby, The Latest Uk Social Media Statistics For 2018 https://www.avocadosocial.com/the-latest-uk-social-media-statistics-for-2018/
2. Statista, Consumer attitude towards influencer marketing in the United Kingdom (UK) in 2018 <https://www.statista.com/statistics/822171/influencer-marketing-consumer-attitude-in-the-uk/>
3. Kevin Gallagher, The Influencer Marketing Report: Research, strategy & platforms for leveraging social media influencers, Business Insider. <https://www.businessinsider.com/the-influencer-marketing-report-2018-1?r=UK&IR=T%20:>
4. Molly Fleming, Beauty influencers deliver ROI of £8.81, report finds, Marketing Week, 2018. <https://www.marketingweek. com/2018/06/12/beauty-influencer-marketing-roi/?nocache=true&adfesuccess=1 >
5. Solberg Audunsson, 2019 will be the year influencer marketing shifts from who to how. Campaign Live, 2018. <https://www. campaignlive.co.uk/article/2019-will-year-influencer-marketing-shifts/1520478 >
6. http://www.cityam.com/271164/brands-waste-millions-extent-instagram-influencer-fraud >
7. Ali Fortescue, Ad watchdog has eyes on social media influencers, Sky News, 2019. <https://news.sky.com/story/ad-watchdoghas-eyes-on-social-media-influencers-11604806
8. Gov.uk, Celebrities pledge to clean up their act on social media, 2019. <https://www.gov.uk/government/news/celebrities-pledgeto-clean-up-their-act-on-social-media
9. Adults’ Media Use and Attitudes Report, OfCom, 2018. <https:// www.ofcom.org.uk/__data/assets/pdf_file/0011/113222/AdultsMedia-Use-and-Attitudes-Report-2018.pdf
10. eMarketer, Social Media Platforms Used by UK Internet Users, by Age, Sep 2017 (% of respondents in each group), 2018. <https://www.emarketer.com/Chart/Social-Media-PlatformsUsed-by-UK-Internet-Users-by-Age-Sep-2017-of-respondentseach-group/212173
11. Statista, Instagram usage in Great Britain (GB) as of May 2017, by age and gender, 2017. <https://www.statista.com/statistics/536697/instagram-usage-in-uk-by-age-and-gender/
12. Influencer Marketing Hub, How to Spot Fake Instagram Followers [Free Instagram Audit Tool & Fake Follower Check]. <https://influencermarketinghub.com/instagram-fake-follower-bot-checker-free/
13. Tara Johnson, How Much Do Influencers Charge?, Influencer Marketing, 2018. <https://www.cpcstrategy.com/blog/2018/06/ how-much-do-influencers-charge-paying-influencers-2018guide/
14. Zameena Mejia, Kylie Jenner reportedly makes $1 million per paid Instagram post—here’s how much other top influencers get, 2018. <https://www.cnbc.com/2018/07/31/kylie-jennermakes-1-million-per-paid-instagram-post-hopper-hq-says.html
15. Influencer Marketing Hub, Influencer Marketing Agencies in the UK You Should Know. <https://influencermarketinghub.com/ influencer-marketing-agencies-uk/
16. PR Week, PRWeek UK’s in-depth guide to social media influencers, <https://www.prweek.com/uk/influencers
17. Hopper: Instagram Insights: What do they mean? <https://www. hopperhq.com/blog/instagram-insights-meaning-2019/
18. Stuart Found, Virtual Polarity: Marketers Far from Consensus On Social Media Influencers, GDS Group. <https://gdsgroup.com/ insights/marketing/far-from-consensus-social-media-influencers/
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Contours & shape taking whilst staying in place, portable & stand-free

Class IIa medical devices, FDA-Cleared, medically CE Marked

Clinically proven wavelengths, powerful skin rejuvenation
Global market leader, registered for sale in 73 countries
Extensive post-sale marketing & educational support
Choose from 9 professional grade models

Don’t Settle for Imitations When You Can Have the
LED
Today!
◊
◊
◊
◊
◊
◊
◊
“Celluma
signature treatments like the Triad and
Facials which employ
energy
and technologies in single
recovery by providing
maintenance treatment
World-Leading
technology
Experience Celluma at: FACE @ QEII Centre London Stand #74 June 7-8 Aesthetic Medicine North Manchester Stand #A5 June 28-29
Globally recognised, clinically validated & multiple awarded professional LED
is an integral component of NYDG
Runway
the regenerative and lifting effects of multi-layered
waves
sessions. The biophotonic light waves of Celluma are implemented as the final step to accelerate
the cells with the energy to heal from within. Quite often, I recommend the device as an ongoing
at home to further optimise results.”
MEDICALLY CE MARKED FOR: Acne • Skin care • Dermal wound healing • Decreasing inflammation • Increasing micro circulation • General pain • Muscle & joint pain • Muscle tension, spasm & stiffness PROFESSIONAL ENQUIRY: www.celluma.co.uk +44 (0) 203 981 3993 +44 (0) 7767 367 070 Celluma: The Original Flexible LED Panel
Dr Costas Papageorgiou, MD FACS Oculofacial Plastic Surgeon New York Dermatology Group • The Wellness Clinic at Harrods, London
Even throughout her childhood, PersianBritish dental surgeon and aesthetic practitioner Dr Souphiyeh Samizadeh loved learning and had a natural flair for caring about others – fundamental qualities for the aesthetics field. “I was known for having a caring attitude towards everyone around me, even as a very young child. I would happily try to help ease their pain if anyone had a headache, and I’d love to observe people’s symptoms, body language and do my best to bring positivity and wellness to others,” she explains.
Dr Samizadeh started her journey by completing a Bachelor of Science in Medical Biochemistry in 2007 and graduated from King’s College London with a Bachelor of Dental Surgery in 2011. She started practising dental surgery at several clinics in London and soon after also started training in the field of medical aesthetics, which she says was just a natural progression. She explains, “I learnt how small positive physical changes can affect one’s confidence and wellbeing which, in turn, can change one’s outlook on life. I knew that offering facial aesthetic treatments would complement my primary skillset and in turn help more patients.”
Dr Samizadeh attended multiple aesthetic courses, and completed her Master’s in Aesthetic Medicine at Queen Mary University of London with distinction, as well as her Postgraduate Certificate in Clinical Education at King’s College London in 2015. Soon after she opened Revivify London Medical Aesthetic Clinic in Mayfair. “This was very exciting, but challenging, and scary all at the same time,” she says, adding, “When I got into aesthetics, I quickly became very passionate about learning, teaching and research in this field and have dedicated much of my life to it. I have been practising for eight years and over this time I have written many articles and papers that have been published in peer-reviewed journals and presented at many national and international conferences. I am also a
Dental surgeon and Aesthetics Clinical Advisory Board member Dr Souphiyeh Samizadeh shares her journey into the specialty

committee member of The Royal Society of Medicine Aesthetics Conference.”
But Dr Samizadeh didn’t stop there. In 2016 she founded the Great British Academy of Aesthetic Medicine (GBAAM) to help further the education and raise standards of training and practice. Recently, Dr Samizadeh has spent a particularly large amount of time providing injectable training in Asia, and is the visiting associate professor for Shanghai Jiao Tong University. “The differences in facial morphology, ideals of beauty, demand for targeted aesthetic treatments, the sheer number of patients, and the standards of practice in Asia is fascinating. With each country I travel to, every hospital I visit, every practitioner I meet, and every conference I attend, my knowledge and understanding of aesthetics evolves and my practise improves. The constant challenge and learning are immensely enjoyable to me and a huge motivator,” she says. When asked about the views of some in the industry who believe that dentists or dental surgeons may not fit in the aesthetics arena, Dr Samizadeh simply says that, “This is an ignorant view.” She explains, “In many countries, including many US states, dental surgeons have been successfully providing non-surgical aesthetic procedures for years. Dental surgeons have a unique position in that they have advanced knowledge of face and neck anatomy, facial assessment, excellent manual dexterity, good clinical diagnostic and communication skills. In addition, they see patients with bruxism, temporomandibular disorder or facial-oral-mandibular spasms, for example, who could benefit from such treatments and that could possibly be overlooked
by other practitioners.” The other thing, Dr Samizadeh explains, is that those with a dental background have a huge amount of knowledge of the dentofacial complex and the lower facial third. She says, “The lower face plays a key role on the perception of beauty and facial aesthetics and this area is, in turn, directly affected by the dentofacial complex,” she says. When asked about advice for success, Dr Samizadeh recommends, “Never look for shortcuts or cheaper ways of doing things.” Research and writing is also useful, she adds. When asked what the fundamental part of her aesthetic practice is, Dr Samizadeh shares, “Ethics, and to remember that these treatments are still medical procedures. Good patient-centred care should not be compromised and should be the core of our practice with the same ethics that we would carry out for other medical procedures.”
What’s it like being on the Aesthetics Clinical Advisory Board?
I am very pleased to be on the board. Aesthetics Media is well-respected and it provides support for the practitioners in the field, scientific articles and the latest news in the industry. It is great to be part of the Aesthetics family.
What interesting things have you learnt from teaching abroad?
One that stands out is that the experience of some Asian doctors is superb, as some see as many as 40 cosmetic patients for treatments a day!
What are your favourite treatments?
Helping patients with advanced facial volume loss, migraines, or bruxism. You can make dramatic improvements to quality of life, which is the most rewarding part of this job for me.
What brings you happiness outside work?
I am married and I have two cute dogs that bring so much joy to our life. I became a vegetarian approximately four years ago and the longer I do not eat meat, the more I become sensitive towards animals, their protection and wellbeing.
“I have dedicated my life to learning, teaching and research in medical aesthetics”
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The Last Word
Facial rejuvenation accounts for more than 10 million procedures worldwide with the global aesthetics market projected to reach over $17 billion by 2023; within this, the largest share is facial aesthetics.1,2 It’s therefore no surprise that practitioners want to be part of this developing industry. However, it seems that the aesthetics specialty in particular is subject to patients dictating more than they likely would in any other medical profession. For example, it is not uncommon for a patient to present in clinic asking for a specific amount of lip filler or asking for a particular product. I believe that this is possibly in part due to the fact that our discipline is exclusively elective and our patients are fee-paying.
When should we say no?
There is no denying that patients sometimes aren’t suitable for treatments and there are a number of reasons to say no. These include unrealistic expectations, signs of body dysmorphic disorder or an incompatibility with the patient and practitioner. However, within
Regulatory standards
Doctors, dentists and nurses answer to regulators who lay down rules by which professionals should conduct themselves. These regulatory bodies provide the framework for practitioner behaviour and patient care to ensure positive outcomes.3
There is an outright requirement to be appropriately qualified and have undertaken suitable training to obtain the requisite knowledge and skills to perform a treatment safely. If this is not the case, there is an absolute need to refer on to someone who has this skillset.3 The Keogh review published in 2013 made mention of the need to attain the necessary skills to perform aesthetic treatments safely and to a high standard.4
this article I will focus on why and how we should say no when the patient has asked for a treatment that is outside of the practitioner’s scope of practice or experience. I have found that it is often this which results in bad outcomes and conflict between patient and professional.
The difficult choice
The practitioner stands before a difficult decision when declining the patient for treatment; say no, and risk the patient going elsewhere, or say yes, and risk a bad outcome. The upshot of which may be serious harm to the patient, or a costly legal battle.
It’s difficult to be the practitioner who turns a patient down, knowing the patient may go to another practice and potentially put their health at risk.
It loses business and many practitioners think if someone should treat, it should be them. The patient is sitting there with a bag of money and someone should take it, right? Wrong.

Hubris may get the better of some practitioners, ignoring caution and ‘giving it a shot’ when they don’t have the experience. For example, a one-day training course may have left them ill-prepared not just technically, but also for selecting patients appropriate for the procedure. Likewise, they may have treated a similar area and think that they will be skilled in another area or may have observed a treatment and feel comfortable in replicating this. I believe that treating patients in these circumstances is not going to do anyone’s business any good. It’s likely to lead to dissatisfied patients and poor outcomes, both of which will have substantially negative consequences for business compared with the immediate win of a few hundred pounds gross margin. Many of us in this specialty would agree that an unhappy patient is a reputational landmine. According to a report by customer experience research company, the Temkin Group, after a good experience, 23% of people are likely to tell their friends. After a bad experience, this rises to 32% and the failure to manage negative outcomes can result in reputations being left in tatters.5 Bad publicity is simply more virulent than good publicity and can leave lasting damage to businesses.6
The solution
The solutions are easier said than done, as most will mean sacrificing immediate income for the sake of the long-term gain. Just remember, quick wins don’t build an Empire; meticulous planning, intensive training and careful execution do.
In my opinion, mentorship can significantly reduce risk whilst improving skill level. This is widely accepted in every branch of medicine and dentistry, however it is only recently coming to the fore in aesthetics. With that in mind, there are currently a number of associations that are offering these schemes and something that I would advise looking into. With a good mentor, practitioners can treat cases in their own setting, improve their skills and retain business.
I believe that the interplay between clinical ability and case selection can be rehearsed with an appropriately experienced guide, leading to fewer complications due to inappropriate treatment. A good mentor is not one who takes cases away from budding clinicians, but one who supports, guides and develops. I think I speak for most experienced colleagues when I say that I’d rather mentor practitioners to improve
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr MJ Rowland-Warmann shares her views on when and why aesthetic practitioners should be saying no to patients
skill and avoid complications than to have to receive the referrals when they’ve gone wrong due to inexperience.
It takes an enlightened practitioner to refer to someone else because the patient’s needs are beyond their scope of practice. In my opinion, it shows honesty and integrity as a practitioner. A recommendation against your interests and to someone outside your business creates an enormous amount of emotional capital and these referred individuals will value your honesty and not only refer their friends to you, but, in my experience, will likely return to you at some point.7
Proud of ‘no’
It’s ok to say no; after all, aesthetic treatments are largely elective and not having a treatment never hurt anyone. Reputationally, I would say that it’s actually better to be known as the practitioner who says ‘no’. Patients trust people who demonstrate authority and follow their suggestions. This is because it shows confidence, strong clinical judgement and creates credibility in the eyes of patients.8 In my personal experience, my patient base has been shaped as a result of me saying no and the patients that I do treat have become great ambassadors of my brand. I can also sleep at night knowing I am causing no harm.
Conclusion
In few other medical disciplines do patients dictate so much to professionals; it’s a problem endemic to aesthetics. It’s degrading and commoditising aesthetic medicine. I think that it’s time practitioners think about what direction our industry is heading in, and help correct
the course of patient perception to a more favourable and safer path. There is no reason why aesthetics should be any different to other branches of medicine. Practitioners should always stand their ground on what they believe is ethical, appropriate and defensible. They should be empowered to decline patients for treatment under suitable circumstances. I believe that the long-term benefits of saying no outweigh the short-term financial rewards.
Dr MJ Rowland-Warmann is a dentist, the founder and lead clinician at Smileworks in Liverpool. She is committed to continuing professional development, in 2016 completing her MSc in Aesthetic Medicine (with distinction) from Queen Mary University of London. She has a special interest in the management of complications, writing extensively on the subject.

REFERENCES
1. ISAPS, ISAPS internationals survey on aesthetic/cosmetic procedures performed in 2017. https://www. isaps.org/wp-content/uploads/2018/10/ISAPS_2017_International_Study_Cosmetic_Procedures.pdf, 2017.
2. Newswire, P., Medical Aesthetics Market worth $17.07 Billion by 2023. https://www.prnewswire.com/ news-releases/medical-aesthetics-market-worth-17-07-billion-by-2023-877401471.html, 2018.
3. General Dental Council, T., Standards for the Dental Team. https://www.gdc-uk.org/professionals/ standards, 2018.
4. Keogh, B., et al., Review of the Regulation of Cosmetic Interventions. Department of Health Publication, 2013.
5. TemkinGroup, What happens after a good or bad experience. https://experiencematters. blog/2018/06/04/report-happens-good-bad-experience-2018/, 2018.
6. ZenDesk, Poor service frightens away customers for years to come. https://www.zendesk.com/company/press/zendesk-study-shows-poor-service-frightens-away-customers-years-come-germany/, 2013.
7. Belfort, J., Way of the Wolf: Master the art of persuasion and build massive wealth. John Murray Learning, 2017.
8. Cialdini, R., Influence: The Psychology of Persuasion. HarperBusiness, 1984.
Reproduced from Aesthetics | Volume 6/Issue 7 - June 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com FLICK BACK TO P.36 FOR THE CATEGORIES OVERVIEW! ENTER TODAY
Susanne, actual Belotero® patient, 46
Be the Master of Your Art
Creative control to achieve that natural-look
Belotero® is not about painting by numbers for a generic look. The four products within the range have been specifically tailored to allow you to create natural-looking, lasting results, through your expertise and artistry in analysing the face, and by using the correct tools and techniques.


Adverse events should be reported. Reporting forms and information for United Kingdom can be found at www.mhra.gov.uk/yellowcard. Reporting forms and information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/report-an-issue/mdiur.

Adverse events should also be reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143.
Find out more
www.belotero.co.uk
Let your patients show their emotions with confidence OWN YOUR BEAUTY
M-BEL-UKI-0275 Date of Preparation December 2017
with Juvéderm® VOLUX 1,*
INT/0654/2018. Juvéderm® VOLUX final clinical study report & clinical evaluation report – efficacy and duration data. Oct 2018. 4. Allergan. Data on File. INT/0074/2019. Juvéderm® VOLUX final clinical evaluation report, July 2018. Jan 2019. 5. Raspaldo H etal.JCosmetDermatol. 2010;9:11–15. ©2019 Allergan. All rights reserved. Material developed and produced by Allergan. UK/0203/2019 Date of preparation: April 2019
Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk Adverse events should also be reported to Allergan Ltd. UK_Medinfo@allergan.com or 01628 494026.

When you want to define the lower face, there’s a new, structural gel that allows you to
the
and jaw
Juvéderm® VOLUX can restore and create facial volume 1,† in the chin and jaw area for 18–24 months.3,4,‡ Model treated with JUVÉDERM®. Results may vary. * Juvéderm® VOLUX contains lidocaine.1 The addition of lidocaine does not alter the physical properties of JUVÉDERM® products.5 † No available controlled clinical data on the effectiveness and tolerance of Juvéderm® VOLUX injection into anatomic regions other than the chin and jawline. ‡ Based on comparative preclinical testing and results from repeat treatment data, added to Juvéderm® VOLUX clinical study showing duration beyond 18 months after initial treatment or initial + top-up treatment in the chin and jaw, and based on clinical results for Juvéderm® VOLUMA with lidocaine showing 24 month duration in the mid-face establishes Juvéderm® VOLUX as having an
situ
months.4 1. Juvéderm® VOLUX DFU. 72778JR10. Revision 2018-07-26. 2. Allergan. Data on File. INT/0663/2018. Juvéderm® VOLUX final clinical evaluation report. Oct 2018. 3. Allergan. Data on File.
focus on
chin
area.1–3
in
duration of 18–24

