Plump up the volume
Discover a safe and highly effective* dermal filler for buttocks that quickly contours, reshapes and activates the skin’s natural collagen. Give your patients the curves and confidence they crave.


Discover a safe and highly effective* dermal filler for buttocks that quickly contours, reshapes and activates the skin’s natural collagen. Give your patients the curves and confidence they crave.
Dr Ahmed El Houssieny discusses non-invasive neck treatments
Practitioners propose a way to classify labial vascular compromise
Dr Raquel Amado details the anatomy of deep fat pads
Gary Monaghan offers advice on establishing a clinic


Bocouture® (botulinum toxin type A (150 kD), free from complexing proteins) 50/100 unit vials*. Prescribing information: M-BOC-UK-0432. Please refer to the Summary of Product Characteristics (SmPC) before prescribing. Presentation: 50/100 units of Clostridium Botulinum Neurotoxin type A, free from complexing proteins as a powder for solution for injection. Indications: Temporary improvement in the appearance of moderate to severe upper facial lines (glabellar frown lines, crow’s feet lines, horizontal forehead lines) in adults ≥18 and <65 years when the severity of these lines has an important psychological impact for the patient. Dosage and administration: For intramuscular use only. Unit doses recommended for Bocouture are not interchangeable with those for other preparations of botulinum toxin. BOCOUTURE should only be administered by an appropriately qualified healthcare practitioner with expertise in the treatment of the relevant indication and the use of the required equipment, in accordance with national guidelines . The intervals between treatments should not be shorter than 3 months. Reconstitute with 0.9% sodium chloride. Glabellar Frown Lines: Total recommended standard dose is 20 units. 4 units into 5 injection sites (2 injections in each corrugator muscle and 1 injection in the procerus muscle). May be increased to up to 30 units. Injections near the levator palpebrae superioris and into the cranial portion of the orbicularis oculi should be avoided. Crow’s Feet lines: Total recommended standard dosing is 12 units per side (overall total dose: 24 units); 4 units injected bilaterally into each of the 3 injection sites. Injections too close to the Zygomaticus major muscle should be avoided to prevent lip ptosis. Horizontal Forehead Lines: The recommended total dose range is 10 to 20 units; a total injection volume of 10 units to 20 units is injected into the frontalis muscle in five horizontally aligned injection sites at least 2 cm above the orbital rim. An injection volume of 2 units, 3 units or 4 units is applied per injection point, respectively. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Generalised disorders of muscle activity (e.g. myasthenia gravis, Lambert-Eaton syndrome). Infection or inflammation at the proposed injection site. Special warnings and precautions: It should be taken into consideration that horizontal forehead lines may not only be dynamic, but may also result from the loss of dermal elasticity (e.g. associated with ageing or photo damage). In this case, patients may not respond to botulinum toxin products. Should not be injected into a blood vessel. Not recommended for patients with a history of dysphagia and aspiration. Caution in patients with botulinum toxin hypersensitivity, amyotrophic lateral sclerosis, peripheral neuromuscular dysfunction, or in targeted muscles displaying pronounced weakness or atrophy. Bocouture should be used with

caution in patients receiving therapy that could have an anticoagulant effect, or if bleeding disorders of any type occur. Too frequent or too high dosing of botulinum toxin type A may increase the risk of antibodies forming. Should not be used during pregnancy unless clearly necessary. Should not be used during breastfeeding. Interactions: Concomitant use with aminoglycosides or spectinomycin requires special care. Peripheral muscle relaxants should be used with caution. 4-aminoquinolines may reduce the effect. Undesirable effects: Usually, undesirable effects are observed within the first week after treatment and are temporary in nature. Undesirable effects independent of indication include; application related undesirable effects (localised pain, inflammation, swelling), class related undesirable effects (localised muscle weakness, blepharoptosis), and toxin spread (very rare - exaggerated muscle weakness, dysphagia, aspiration pneumonia). Hypersensitivity reactions have been reported with botulinum toxin products. Glabellar Frown Lines: Common: headache, muscle disorders (elevation of eyebrow). Crow’s Feet Lines: Common: eyelid oedema, dry eye, injection site haematoma. Upper Facial Lines: Very common: headache. Common: hypoaesthesia, injection site haematoma, application site pain, application site erythema, discomfort (heavy feeling of frontal area), eyelid ptosis, dry eye, facial asymmetry, nausea. For a full list of adverse reactions, please consult the SmPC. Overdose: May result in pronounced neuromuscular paralysis distant from the injection site. Symptoms are not immediately apparent post-injection. Legal Category: POM. List Price: 50 U/vial £72.00, 50 U twin pack £144.00, 100 U/vial £229.90, 100 U twin pack £459.80. Product Licence Number: PL 29978/0002, PL 29978/0005 Marketing Authorisation Holder: Merz Pharmaceuticals GmbH, Eckenheimer Landstraße 100,60318 Frankfurt/Main, Germany. Date of Preparation:August 2021. Further information available from:. Ground Floor Suite B, Breakspear Park, Breakspear Way, Hemel Hempstead, Hertfordshire, HP2 4TZ Tel: +44 (0) 333 200 4143
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard for the UK. Adverse events should also be reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143.
For information about dates and locations and to reserve your place, scan the QR code.
Free from complexing proteins

















































CCR 2022 will bring you 5 theatres, 80 speakers, 16 CPD points and 1 unmissable party
PRACTICE
Special Feature: Celebrating 10 Years of Aesthetics
We reflect on a decade of the Aesthetics journal and the development of the specialty 28 Meet Evolus
Evolus invites you to evolve the future of beauty with them 31 CPD: Rejuvenating the Neck
Dr Ahmed El Houssieny discusses treatments for the ageing neck 37 Classifying Labial Vascular Compromise
Practitioners propose a classification system for labial vascular compromise 41 Taking a Holistic Approach Towards Aesthetics
Turn your AART into a HIT with the Galderma aesthetics portfolio 45 Managing Photodamage

Anna Baker provides an overview of the treatment options for photodamage 51 The Evolution of RF Microneedling
Discover the next generation of radiofrequency microneedling treatments 53 Case Study: Treating Superior Sulcus Hollows
Dr Joshua Van der Aa explains how using fillers can improve the position of the brows and upper eyelids 58 Understanding the Deep Fat Pads
Dr Raquel Amado details the structure of the deep fat pads in the mid-face 61 Supporting Patients with Excess Weight
A spotlight on weight management to implement into your practice 63 Using Subcision to Treat Acne Scarring
Lucy Williams explores the use of subcision for treating acne scars 68 Case Study: Non-Surgical Rhinoplasty
Dr Thuha Jabbar provides a case study using Stylage XXL 69 Abstracts
A round-up and summary of useful clinical papers IN PRACTICE 71 Attracting Your Ideal Patient
James Dempster offers insight on marketing to attract your perfect clientele 74
Integrating Aesthetic Medicine into Dentistry
Dr Martin Nimmo provides his advice for dentists moving into aesthetics 77 Building an Aesthetic Clinic
Gary Monaghan gives advice on establishing a clinic from the ground up 81 In Profile: Dr Jean Carruthers

Dr Jean Carruthers reflects on her journey to discovering botulinum toxin for wrinkles 82 The Last Word: Specialising in Aesthetics
Mr Amir Sadri debates whether practitioners should be specialists or generalists
Special Feature: Celebrating 10 Years of Aesthetics Page 23
Dr Ahmed El Houssieny is an anaesthetist with a passion for aesthetics. He is an honorary lecturer at the University of Chester and an education provider on cosmetic procedures. Dr El Houssieny is an associate member of the British College of Aesthetic Medicine.


Mr Mark Devlin is a consultant cleft and maxillofacial surgeon based at the Royal Hospital for Children in Glasgow. For many years he maintained a facial aesthetic surgical practice, but now concentrates his non-NHS time to medicolegal work.
Mr Jeff Downie is a consultant oral and maxillofacial surgeon who has a specialist interest in facial aesthetic and reconstructive surgery. He practises facial surgery in Glasgow and his NHS sub-speciality is facial deformity and post-traumatic facial reconstruction.

Anna Baker is an aesthetic prescribing nurse, trainer and qualified educator. She is a board member for the British Association of Cosmetic Nurses (BACN), and jointly leads on their Education & Training Committee.


Dr Joshua Van der Aa is an injection-focused cosmetic practitioner specialising in rejuvenation of the periorbital area. Before opening his own clinic, Dr Joshua Harley Street Aesthetics, he worked in several clinics based in London and the Netherlands.
Dr Raquel Amado has 21 years’ experience as a practising dentist, is a Level 7 qualified aesthetic injector and clinical trainer. She runs a successful clinic in Kent and has a passion for anatomy and full-face rejuvenation.
Lucy Williams is the founder and director of Aurielle Aesthetics in Wiltshire. She has more than 12 years’ experience as a nurse and five years’ experience as an aesthetic injector. Williams is registered with the ACE Group World and Save Face.

















With the leaves turning into a beautiful carpet of red and orange, it is a sign that it’s time for our Autumn show – CCR London! If you’re reading this before October 13-14, then make sure you register. If you’re reading this at CCR, then welcome! There is so much going on for you to take advantage of – you can learn, network, explore, share ideas, and more (p.20 has the highlights).
This month in the journal, we have a big CCR focus to coincide with the event – we’ve worked with some of our 80+ speakers who have written fantastic clinical and business articles for you to enjoy! Some of my personal favourites are Dr Ahmed El Houssieny’s CPD on neck ageing (p.31), nurse prescriber Anna Baker’s introduction to treatments for photodamage (p.45), plus all the In Practice business articles covering marketing, building a clinic and moving from dentistry into aesthetics (from p.71). Outside of our CCR speaker articles, a very interesting read this month is an article by Mr Mark Devlin and Mr Jeff Downie (p.37), who propose
a new classification system for labial vascular compromise. We at Aesthetics are very excited that the journal is also going into its tenth year! After working at the journal for seven years, I have had the privilege of getting to know so many of you and watch the industry flourish. So, our Special Feature article this month looks at some of the developments I have observed, as well as input from our Clinical Advisory Board Members (p.23). To coincide with this, we have launched an exciting new Aesthetics Membership, which you can read about on p.9. I look forward to welcoming you to our community!
Finally, the team were delighted to meet the one and only Dr Jean Carruthers – the pioneer of botulinum toxin for wrinkle reduction – at the recent BCAM conference. You can learn more about her at the end of the journal, she really is a fascinating person. Of course, producing this journal would not be possible without our fantastic editorial team. We are all going to be at CCR and would love to meet as many of you as possible! We are on the lookout for new article contributors and we would love to hear about what you enjoy reading, so come and say hello or get in touch any time –editorial@aestheticsjournal.com! See you at CCR!
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content

Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN), previous UK lead of the BSI committee for aesthetic non-surgical standards, and member of the Clinical Advisory Group for the JCCP. She is a trainer and registered university mentor in cosmetic medical practice, and is finishing her MSc at Northumbria University. Bennett has won the Aesthetics Award for Nurse Practitioner of the Year and the Award for Outstanding Achievement.
Mr Naveen Cavale has been a consultant plastic, reconstructive and aesthetic surgeon since 2009. He has his own private clinic and hospital, REAL, in London’s Battersea. Mr Cavale is the national secretary for the ISAPS, president of the Royal Society of Medicine, and vice-chair for the British Foundation for International Reconstructive Surgery.

Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also a member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.
PORTFOLIO
Alison Willis • Director
T: 07747 761198 | alison.willis@easyfairs.com
EDITORIAL
Shannon
shannon@aestheticsjournal.com
Holly Carver • Senior Journalist | T: 0203 196 4427 holly.carver@easyfairs.com
Ellie Holden • Journalist | T: 0203 196 4265 ellie.holden@easyfairs.com
Kate Byng-Hall • Journalist | T: 0203 196 4265 kate.byng-hall@easyfairs.com
DESIGN
Peter Johnson • Senior Designer T: 0203 196 4359 | peter@aestheticsjournal.com
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon. She is the lead oculoplastic surgeon at the Cadogan Clinic, specialising in blepharoplasty and advanced facial aesthetics. Miss Hawkes is a full member of the BOPSS and the ESOPRS and is an examiner and fellow of the Royal College of Ophthalmologists.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 Anti-Ageing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the founder of the Great British Academy of Medicine and Revivify London Clinic. Dr Samizadeh is a Visiting Teaching Fellow at University College London and King’s College London.


ADVERTISING & SPONSORSHIP
Courtney Baldwin • Event Director T: 0203 196 4300 | M: 07818 118 741 courtney.baldwin@easyfairs.com
Judith Nowell • Business Development Manager T: 0203 196 4352 | M: 07494 179535 judith@aestheticsjournal.com



Chloe Carville • Sales Executive T: 0203 196 4367 | chloe.carville@aestheticsjournal.com
Emma Coyne • Sales Executive T: 020 3196 4372 | emma.coyne@easyfairs.com
MARKETING
Aimee Moore • Marketing Manager
T: 020 3196 4370 | aimee.moore@easyfairs.com
Abigail Larkin • Marketing Executive T: 020 3196 4306 | abigail.larkin@easyfairs.com

Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email: editorial@aestheticsjournal.com
Dr Stefanie Williams is a dermatologist with a special interest in adult acne, rosacea and aesthetic medicine. She is the founder and medical director of multi-award winning EUDELO Dermatology & Skin Wellbeing in London, and creator of Delo Rx skincare. She is the author of three books and has published more than 100 scientific articles, book chapters and abstracts.
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com
© Copyright
Aesthetics.
rights reserved.
Ltd, which is registered as
in England; No 9887184
Dr James Olding
@dr_jamesolding
Reading the Aesthetics journal at this weekend’s advanced injectables course.
Dr David Eccleston
@drdavidecceleston
Privilege to be in the presence of the great Dr Jean Carruthers, pioneer of Botox in cosmetic and ophthalmic applications. She hasn’t frowned since 1987!
Dr Lee Walker
@leewalker_academy
Great couple of days sharing knowledge with colleagues from Croatia, Ukraine and Slovenia.
A new survey has revealed that nearly half of junior doctors are considering leaving their profession.
According to a new Medscape UK survey completed by 1,012 UK doctors, 36% of GPs and 25% of specialty doctors are considering leaving medicine to pursue an alternative career. Doctors under 45 were more likely to be considering the change than doctors over 45. The results revealed that ‘burnout’ not tied to the COVID-19 pandemic was the top reason (37%) so many are considering a career change.
Popular alternative career choices included working for healthcare business companies (33%), in education or teaching (32%), working for pharmaceutical companies (22%), writing (20%), in technology (17%) or switching to law (9%).
Despite this, for those considering changing careers, 34% felt no guilt or regret about the time or money spent getting a medical degree, compared to 21% who felt guilty or regretful about leaving medicine. This was especially strong in women doctors and in those under 45.
Skincare distributor AestheticSource has launched its new skinbetter science antioxidant defence serum.
#Wellness
Lauren Gibson
@lauren_hydrafacialuk
Fabulous morning with UK press at our Biohacking Beauty morning with biohacking queen Davinia Taylor and host extraordinaire Paul Wharton.

Dr Saleena Zimri
@drsaleenazimri
I’ve had the pleasure of welcoming many of you in clinic for shadowing days. This year we’ve had professionals from Canada, Portugal, Spain, Wales and London!


According to the company, the Alto Advanced Defense and Repair serum offers the benefits of the Alto Defense serum combined with a new antioxidant. The serum includes WEL technology, which has a patented complex of antioxidants that aim to defend against environmental assaults, as well as TAP technology, which has a patented, new antioxidant protection targeting intrinsic oxidative stress to support the skin’s renewal process.
The serum aims to improve brightness and redness, along with overall skin tone and texture, as well as address intrinsic and extrinsic stressors, explains AestheticSource.
In a clinical study by board-certified physicians, 39 subjects of varying skin tones used the serum twice daily for 12 weeks. Results showed that >90% of subjects reported an overall improvement in the appearance of their skin, saying it was brighter looking, more radiant, softer, smoother and more hydrated. Lorna Bowes, CEO of skinbetter science’s distributor AestheticSource, said, “I love seeing the launch of a new product when the science is such a significant step forwards, as is the case with Alto Advanced. I get doubly excited given the current economic climate and the consumer need for evidence-based, trusted products. We think we’ve got a really great opportunity here for our clinics to support their growth.”
Both AestheticSource and skinbetter science are exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Aesthetics has launched a Membership community for subscribers to access exclusive content and benefits.
By joining the Aesthetics community through our new Membership, you will have full access to top educational content and monthly CPD points, as well as crucial tips and advice from industry experts, companies and suppliers through the monthly Aesthetics journal and annual ACE and CCR events, plus free submission to the prestigious Aesthetics Awards.
There are three Membership structures available which include a plethora of benefits: Aesthetics Full Member for £130 a year, Aesthetics Print Member for £100 a year and Aesthetics Digital Member for £60 a year.
If you are an existing subscriber, this new Membership will upgrade what you already receive, giving you the benefit of exclusive industry updates, discounts, partnerships and more, alongside the journal every month. Courtney LeBorgne, event director at Aesthetics and CCR, commented, “We’re really excited to welcome our readers to our new Membership community. We’re sure you will love the Special Member ticket price for The Aesthetics Awards, invitations to exclusive Aesthetics events and much more to come! Watch this space for even more incredible content.” To continue receiving your monthly journal, please renew as a Member at Aesthetics online today, or email editorial@aestheticsjournal.com with any questions. We look forward to welcoming you to the community!
Pharmaceutical company Galderma has developed a new holistic approach through its HIT methodology. According to the company, the methodology aims to help patients discover how different treatments can work in conjunction to achieve individualised natural and balanced results. The method teaches the use of AART – Assessment, Anatomy, Range and Treatment in order to deliver these ‘Holistic Individualised Treatments’, also known as HITs. Galderma explains that this provides a simplified approach to facial aesthetic needs, based on cross-usage of products for different areas of concern. Galderma will be showcasing its HIT approach at CCR on October 13-14 at ExCeL, London, with continued content scheduled for 2023. Galderma will be launching this with two symposiums at CCR. The first will be Shape Up, a methodology to lift the mid-face using the Restylane portfolio, and the second will be Kiss & Smile, a methodology to rejuvenate the lips and perioral region with the Restylane portfolio.
Galderma is the Headline Sponsor at CCR on October 13-14 at ExCeL, London. Turn to p.20 to register for free.
Of 1,500 women, 47% said their mental health was affecting their confidence, but only 7% were addressing it (WooWoo, 2022)
Approximately 85% of people between the ages of 12 and 24 experience at least minor acne (AAD, 2022)

There was a 44% increase in botched cosmetic surgeries performed abroad in 2021 compared to the previous year (BAAPS, 2022)
In the UK, 2% of the population experience body dysmorphic disorder (BDD) at any point in time (Health and Social Care Committee, 2022)
The global chemical peel facial rejuvenation market is expected to grow from US $2 billion in 2016 to about US $3.1 billion by 2026 (Statistica, 2022)
Breast procedures such as breast augmentations, breast lifts and breast reductions increased by 48% in the US in 2021 (The Aesthetic Society, 2022)
13th-14th October
CCR ccrlondon.com
13th October
ACE Group World Conference ccrlondon.com/visit/ace-group-world-2022 14th October
ISAPS Symposium UK ccrlondon.com/visit/ccr-2022-isaps
12th November
Aesthetics United Charity Conference aucc.co.uk
19th November
IAAFA Conference & Ball iaafa.net 19th-20th November
CMAC Conference cmac.world/conference
Skincare brand SkinCeuticals has been unveiled as the networking drinks sponsor at this year’s CCR conference. SkinCeuticals will be hosting a networking drinks event for delegates on October 13 – the first day of CCR – from 5-7pm GMT at ExCeL, London. Sinead Mayne, medical relations manager at SkinCeuticals, said, “We at SkinCeuticals are passionate about aesthetics and the aesthetics community, and we are delighted to be sponsoring the CCR networking drinks which are always a high point of the expo. It’s great to be in pride of place at the biggest and best aesthetics expo in the UK with the who’s who of practitioners.”

Turn to p.20 to learn how to register free for CCR to attend this great networking opportunity.
Education
Aesthetic training provider Acquisition Aesthetics is opening its first Scottish location in Glasgow.
‘Send Nudes: Body SOS’ documentary debuts on Channel 4 TV personality Vogue Williams is hosting a new programme on Channel 4 – ‘Send Nudes: Body SOS’. The programme follows members of the public who are considering plastic surgery, generating simulated images of their bodies after the procedure they are contemplating and asking the public whether they prefer the before or after image. Williams says the premise is designed to be “empowering” for those struggling with body image.
The hashtag #babybotox is trending on video-sharing platform TikTok as people seek minimal non-surgical cosmetic procedures. ‘Baby Botox’ refers to small amounts of botulinum toxin used to smooth the face and improve the skin. However, Aesthetics Clinical Advisory Board Member Jackie Partridge highlights that the term merely refers to a smaller dose of toxin rather than a different treatment altogether.
Acquisition Aesthetics explains that the Glasgow centre is its sixth training location and will begin by providing foundation botulinum toxin and dermal filler courses before eventually expanding to offer the complete training portfolio, including advanced courses and the Level 7 Diploma.
Miss Lara Watson, co-director at Acquisition Aesthetics, said, “In response to the continued rise in demand for high quality aesthetics training in the North, Acquisition Aesthetics is thrilled to introduce their award-winning portfolio of CPD and Level 7 accredited training courses to Glasgow! The foundation course launches on December 3 and will feature members of the academy’s nationally renowned faculty of trainers which we have been celebrated for.”
Acquisition Aesthetics is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Aesthetic laser company Lynton has announced the opening of a new training academy in London to cater for southern England, alongside their existing location in Cheshire. Located in London’s Docklands area, the training centre will offer education on Lynton’s devices, as well as providing Ofqual regulated qualifications in energy-based devices.
Dr Samantha Hills, clinical director at Lynton, said, “With further regulation of the aesthetic industry expected in the coming years, there is a pressing requirement for quality and regulatory-compliant training in energy-based devices.”

Hills continued, “Our qualifications are delivered by our team of experienced clinical trainers and assessors, using an array of high-quality aesthetic equipment, ensuring that our students can go out into the industry being able to offer their clients the very best results with an exceptional safety profile.”
Lynton is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
The fifth International Society of Aesthetic Plastic Surgery (ISAPS) Symposium UK will take place at CCR in October. Curated by consultant plastic, reconstructive and aesthetic surgeon Mr Naveen Cavale, the agenda focuses on techniques for the breast and face, as well as tips for business success in your practice. Speakers include surgical director Dr Francisco Bravo, consultant plastic and aesthetic surgeon Mr Daniel Saleh, consultant plastic surgeon Mr Tunc Tiryaki and plastic surgery registrar Miss Priya Chadha. Meet the sponsors of the symposium – Specialist Cosmetic Care, Incision indemnity, Sebbin, Macom Medical and Triangle Surgical - while you’re there!

The symposium will offer a private meeting, lunch sponsored by Incision Indemnity and CCR VIP privileges including canapés and cocktails in the VIP lounge. Tickets to the symposium are limited and are open to both ISAPS members and non-members. Members can receive a special discount code by emailing info@ccrlondon.com. The ISAPS symposium will take place at CCR on October 14. Turn to p.20 to register. Conference
The Aesthetics United Charity Conference (AUCC) has announced its line-up of speakers taking to the stage in November.

AUCC is a non-profit organisation bringing members of the aesthetics community together to learn, grow and raise money for chosen charities. This year, the conference is supporting Operation Smile and the Ukrainian Red Cross to better the lives of children affected by cleft lip palate and respond to the humanitarian crisis that is occurring because of the eastern conflict.
Speakers at this year’s conference include aesthetic practitioners Miss Sherina Balaratnam, Dr Raj Acquilla, Dr Ifeoma Ejikeme, Dr Tapan Patel, Dr Lee Walker, Dr Nina Bal, Dr Sabika Karim, Dr Raul Cetto, Dr Yusra Al-Mukhtar, nurse prescriber Sharon Bennett, consultant plastic reconstructive and aesthetic surgeon Mr Dalvi Humzah and oculoplastic surgeon Miss Sabrina Shah-Desai.

Miss Lara Watson, co-founder of AUCC, said, “The AUCC returns this year bringing together some of the biggest names of the industry for another agenda of unparalleled content intended to educate and entertain delegates like never before, while raising money for Operation Smile and the Ukrainian Red Cross. The event will be attended by key suppliers and manufacturers, however, AUCC is an independent conference, granting speakers the freedom to discuss subjects that matter most to them.”
The Aesthetics & CCR team will be exhibiting at the AUCC on November 12 at Sofitel, St James, London.
A round-up of the latest news and events from the British Association of Cosmetic Nurses

On September 15-16, 2022, Birmingham’s The Eastside Rooms saw the return of the BACN Autumn Aesthetic Conference. The annual event showcased the very best in medical aesthetics, providing a place for nurses from all over the UK to come together and network.


Thursday began with BACN chair Sharon Bennett and BACN CEO Paul Burgess welcoming new and longstanding members to the first conference since 2019, providing crucial updates about the specialty. A moving tribute was then paid to the late Queen Elizabeth II, looking back on her relationship with nurses over the last century.
Dr Andrew Greenwood and Dr Vikram Swaminathan kicked off the day of talks, followed by Miss Elizabeth Hawkes, Julie Scott, Dr Steve Harris, Lou Sommereux, Dr Nina Bal, Dr Emily Mehta and Lorna Bowes. Talks ranged from consultation skills to lip anatomy, included two live demonstrations.
Members then gathered in the evening at the BACN drinks reception, where fizz, canapés, a live DJ and Instagram-ready photobooth (kindly sponsored by Aesthetics) awaited them.
The next day featured more talks and live demos, with Freya Carlsen, Rachel Goddard, Karen Burgess, Gillian Murray, Dr Priya Chadha, Tracey Jones, Veronica Donnelly, Julie Scott, Dawn Attewell and Alexandra Mills all presenting. Members have since shared how much they enjoyed the event, and how beneficial they found the exhibitors, speakers topics, and of course, the numerous networking opportunities. The BACN HQ team want to thank all our sponsors, exhibitors, speakers and attendees for another successful conference – roll on 2023!
This column is written and supported by the BACN
Skincare platform GetHarley has teamed up with iS Clinical to offer its range of medical-grade products. According to the company, medical practitioners using the GetHarley service can add iS Clinical products to their digital shelves, following full training with the brand. The companies will be teaming up for a joint webinar event to introduce the best products to the GetHarley community and to those who currently sell iS Clinical products but are interested to learn more about the platform. Charmaine Chow, founder and CEO of GetHarley, said, “iS Clinical is an impressive, botanical brand, popular with the medical community. We are thrilled to welcome the brand to our community and look forward to servicing our clinicians who desire to sell the products to their patients, and welcoming those who want to start selling iS Clinical via GetHarley.” The webinar will be taking place on November 17. GetHarley will be exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Aesthetic manufacturer Cutera has announced the third annual Cutera University Clinical Forum (CUCF) taking place in November. The aim of the event is to connect clinicians in the UK and Ireland to explore the latest clinical trends and developments and share best practices, explains Cutera.
The forum will provide an eight-point CPD-accredited agenda, featuring talks, panel discussions and live demonstrations focusing on some of the company’s newest product launches.
The conference will include talks from aesthetic practitioners Dr Tapan Patel, Dr Nestor Demosthenous, Dr Tatiana Lapa, Mr Rishi Mandavia, Dr Nima Mahmood, dental surgeon Dr Yusra Al-Mukhtar and ENT consultant and facial plastic surgeon Mr Kambiz Golchin.

In addition to the conference, the company will be hosting a black-tie charity ball with Dr Patel to help support and raise funds for the Great Ormond Street Hospital Children’s charity.
Leighannah Tickner, country manager of UK and Ireland, said, “CUCF is a fantastic opportunity to learn from some of the best in the industry, and I am so excited to bring together top industry professionals to share their unique experiences and best practices. Driven by a passion to support our clients and partners, we have put CUCF on the map to celebrate and reflect on what has been achieved in such a short amount of time.”
The event will be taking place on November 27 at the De Vere Beaumont Estate. Cutera is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Skincare brand IMAGE Skincare has released an SPF primer and a restoring eye mask.
The PREVENTION+ Daily Perfecting Primer SPF 50 is available for consumers now, with the company saying the product features a ferment-based ingredient to mitigate environmental factors such as sun and wind, providing a sheer finish for most skin tones.
The IMAGE MD Restoring Eye Masks are available to professionals only, with the company claiming the hydro-gel formulation reduces signs of fatigue through an antioxidant and tetrapeptide blend, and a triple HA complex.

Leigh Wilson, UK regional skin manager, said, “We are delighted to launch our latest innovative, clean and clinical products within our best-selling Prevention Plus collection and our high performance, doctor-developed IMAGE MD line. We look forward to both becoming staple homecare products recommended by IMAGE skincare professionals nationwide.”

Aesthetics distributor Eden Aesthetics has announced the launch of the new version of its DermaFrac device. The treatment combines microdermabrasion and microneedling with simultaneous infusion of targeted serums, aiming to address concerns including fine lines and hyperpigmentation, according to the company. Dr Preema Vig, who will be offering the treatment in her London clinic, said, “My patients want results-driven treatments that deliver in minimal time. DermaFrac is an ideal option. It uses a range of proven technologies and delivers high-grade active ingredients to the dermal layer to target a range of skin concerns. It also eliminates potential problems associated with traditional microneedling roller treatment, where variations in pressure applied can produce uneven and unpredictable results.”
Eden Aesthetics is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Aesthetic device manufacturer Prollenium has unveiled a new dermal filler to its portfolio. The hyaluronic acid filler Outline is suitable for treating the lips as it can help build definition and structure. The filler can also be used to treat areas which require more structure such as the chin or cheeks, or projection for more voluminous lip desires by using larger quantities, explains Prollenium.
Canadian plastic surgeon Dr Arthur Swift, said, “Outline is amazingly versatile for lip enhancement and restoration. It can be used structurally for creating beautiful architecture, more robustly for lip augmentation with smooth contours, or delicately to define the vermillion border by strengthening the white roll. I’ve been extremely impressed with the natural results obtained both in repose and with animation, and the minimal post-procedural swelling.” Prollenium is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
The Aesthetic Complications Expert (ACE) Group World conference will be taking place at CCR for the second year.
With informative talks and renowned speakers, the conference aims to help and advise practitioners who encounter a complication, as well as improve patient safety by producing evidence-based guidelines for the management of complications.
Sessions include delayed onset nodules with aesthetic practitioner Dr Martyn King and body dysmorphic disorder and mental health assessment in aesthetic practice with nurse prescriber Lou Sommereux.
Consultant orthopaedic surgeon Mr Ansar Mahmood will be discussing management of filler complications using ultrasound and consultant ophthalmic plastic, reconstructive and cosmetic surgeon Dr Julia Sen will be speaking on vascular occlusions. Dr King commented, “We are very excited to be teaming up with CCR to make our conference possible and will have a packed agenda of well-renowned key speakers from our expert faculty. We welcome new and existing members to attend, to learn more about the latest evidence and guidelines on the management of non-surgical aesthetic complications.”

The ACE Group World Conference will be taking place at CCR on October 13. Passes to the conference are £125 with limited tickets available. Turn to p.20 to register for CCR and purchase tickets via the registration form.
The entry period for The Aesthetics Awards has closed and we have received so many great entries. The meticulous shortlisting process has begun and Finalists will be announced on January 3 2023. Read further details about how you can attend the ceremony and celebrate our industry’s success at the dazzling Grosvenor House below!

Aesthetics Awards tickets are out now – don’t miss out on the early-bird rate!
If you and your team thrive on the celebration of excellence in aesthetics, then The Aesthetics Awards 2023 is a night not to be missed. Join us at one of the biggest events on the aesthetics calendar where you’ll get to meet our celebrity host and British television presenter Cherry Healey, enjoy live music and have the opportunity to network with colleagues from across the UK and Ireland. The Aesthetics Awards will once again take place on the evening of the second day of ACE, to culminate the proceedings in a night of celebration at the after party of the year! Grab your Aesthetics Awards Early Bird Rate tickets before December 31 to be a part of the celebrations at the luxurious Grosvenor House, London.
What does the ticket include?
• Champagne reception
• Entry to The Aesthetics Awards ceremony
• A delicious three course meal including a ½ bottle of wine per person
• Live entertainment and dancing
• A professional photographer at the press board
• An evening with top brands and practitioners
Who is eligible to attend?
EVERYONE in the aesthetics specialty is welcome!
Whether you are:
• Practitioners working within medical aesthetics
• Marketing and business specialists in aesthetics
• Clinic teams
• Companies and organisations that endorse best practice
• PR teams and press who work within medical aesthetics
To learn more about the ceremony, or to take part in the glitz, glamour and fun with a celebrity host leading the proceedings, scan the QR code to book your early-bird tickets.

Skincare company Medik8 has launched a new salicylic acid tonic, Press & Clear.

According to the company, Press & Clear is a solution for providing blemish care with the aim of clarifying the skin in seven days. The tonic has a pH of 5.5 to ensure gentle use on the skin.
The product contains 2% encapsulated salicylic acid which exfoliates and decongests skin; 2% tranexamic acid to minimise the appearance of post-blemish imperfections; sake extract to support and nourish the skin barrier and aloe vera to soothe relief during breakouts and offset any dryness.
Daniel Isaacs, director of research at Medik8, said, “A true innovation within the beta hydroxy acid skincare space, Press & Clear recognises that blemish-prone skin is sensitive skin, and that it needs to be treated kindly to achieve the best long-term results.”
Artificial intelligence (AI) and augmented reality provider Perfect Corp has introduced a new simulation technology for practitioners and professionals.
The AI Face Reshape Simulator solution allows patients to visualise the results of various treatments through the technology. According to the company, the technology delivers simulations for eyebrow lifts, cheek and lip filler treatments, jaw reshaping, eyelid treatments and nose reshaping.

Alice Chang, CEO and founder of Perfect Corp, said, “Personalised consultations have become a major priority for today’s patients who are looking to receive tailored advice and recommendations before investing in a new product or service. We are thrilled to be bringing Perfect Corp’s AI technology to this new space and look forward to empowering the industry.”
Aesthetic device company 3D Aesthetics has unveiled a new skincare concept, Lesielle. The device offers a range of base creams and active ingredients which offers a personalised skincare routine in one product. Lesielle addresses every skincare concern and allows users to create the ideal skincare, which has been tailored specifically to their skin needs, explains the company. The device determines the patient’s skincare concerns through an online consultation questionnaire. Using an advanced algorithm, it identifies the products and ingredients that it can combine to best suit the patient’s skin. The device can adapt the formula depending on the skin concerns, and the patient is able to push the button allowing for the product to be available for use. The device will be available for practitioners to offer to their patients as well as free training for providing the correct advice to patients. Jon-Paul Hoy, 3D Aesthetics trainer, said, “Simplified skincare routines are really trending on social media at the moment, so having the easy select option via the website will help clients and businesses. People love technology-led gadgets, and it’s great for busy clients. Everything is 100% customisable, and you can change that seasonally, daily or environmentally.”
3D Aesthetics is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Aesthetic distributor Circa Skin has collaborated with aesthetic practitioner Dr Uche Aniagwu for his online course.
The Tear Trough Mastery and Dark Circles, Aetiology, Anatomy and Physiology courses help practitioners understand how to treat the tear trough, minimise risk, improve patient selection and increase patient satisfaction, explains the company.
As part of the partnership, customers of Circa Skin and users of KYSENSE dermal filler will get access to all of Dr Aniagwu’s online training courses for free via an exclusive code.
Clare Williams, CEO of Circa Skin, said, “Our collaboration with Dr Aniagwu really fits in with our educational ethos of wanting to elevate our practitioners to experts. We believe that education should be accessible price wise and be of very high quality.”
Circa Skin is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Skincare brand PCA Skin is holding an event in Manchester this month, providing a morning of skin education followed by the company’s first awards ceremony.
PCA Skin international educators and nurse prescribers Sue Young and Lauren Asquith will explore four common skin concerns –ageing, discolouration, acne and sensitivity –before the awards kick off in the afternoon. Lizzie Shaw, PCA Skin UK brand manager, said, “We are extremely excited to bring PCA Skin back on the road after two years with our Social Symposium event. We know our stockists love education, learning and meeting their peers, so we saw this as a great opportunity to combine those into a science-based social symposium.”
The event is being held at Menagerie Restaurant & Bar, Manchester on October 24.

With entry to The Aesthetics Awards now closed, Early Bird tickets to attend the prestigious ceremony are available to purchase. Tickets to the Awards include entry to the glamorous ceremony with celebrity host Cherry Healey, a delicious three course meal, live entertainment and dancing, networking drinks reception and professional photography throughout the Awards evening. Courtney LeBorgne, event director of Aesthetics and CCR, commented, “We have received hundreds of Awards entries from practitioners, suppliers, manufacturers and companies celebrating their achievements and progression over the past year, which has been amazing to see! With a bigger and grander Awards venue in 2023, now is the time to get your tickets! Tickets for The Aesthetics Awards completely sold out this year, so make sure to buy yours sooner rather than later, to avoid missing out.” We are also excited to announce new Aesthetics Awards sponsors including skincare brand SkinCeuticals supporting the Energy Device of the Year Award, aesthetic insurance provider Hamilton Fraser sponsoring the Best Clinic South Award aesthetic supplier Healthxchange will be supporting Best Non-Surgical Result and skincare company Dermalogica PRO for the Medical Aesthetic Practitioner of the Year Award. The Aesthetics Awards will be taking place on March 11, 2023, at Grosvenor House, London after the second day of ACE. Turn to p.40 to purchase your tickets.
BioPhotas Inc, manufacturers of the Celluma Series of light therapy devices, has unveiled a new hair restoration LED device.

The RESTORE device is FDA-cleared and CE-marked for over-the-counter use to treat four concerns in a single device including ageing skin, hair loss, dermal wound healing and general pain conditions, explains Celluma. The design permits customised placement over the head to effectively deliver light energy and promote hair regrowth. It can also be placed anywhere on the body to reduce pain and improve skin health according to the company.
BioPhotas president and chief executive officer Patrick Johnson said, “It’s great to add a hair restoration indication-for-use to our long list of treatment clearances. Providing a single device that treats whole body aches and pains, fine lines and wrinkles, dermal wounds and hair loss on the scalp is the ultimate antiageing device.”
Celluma will be exhibiting at CCR on October 13-14. Register for free on p.20.
Tell us about your current role… I have been representing the SkinPen Precision medical microneedling device for more than three years, working for Crown Aesthetics – a premier medical aesthetic company helping leading aesthetic practices worldwide grow their businesses, with dramatic results in rejuvenation and restoration. SkinPen Precision is the first FDA-cleared microneedling device.
What’s been happening for Crown Aesthetics recently?

In March 2022, we launched our first Global London Symposium, with clinical education and business development workshops for attendees. The event was live streamed to 400+ delegates of international partners and customers, and 150 delegates in attendance. The event was an overwhelming success. The next symposium is on October 1. Our focus has been on customer engagement, support and education, as well as growing the UK and Ireland team. We have partnered with leading aesthetic doctors and clinics to enhance patient results further with our device (S-Thetics clinic, PHI Clinic, Eudelo, DermaSpa).
What does the SkinPen device do?
SkinPen is an automated, non-surgical medical microneedling device designed for use by licensed healthcare professionals.
SkinPen delivers its results by creating millions of controlled micro-injuries in the skin, eliciting the body’s natural wound healing cascade. This process begins with injury/inflammation, progresses to tissue proliferation and results in tissue re-modelling with new collagen and elastin.
What makes the SkinPen medical device unique?
SkinPen is the world’s first FDA-cleared microneedling device and procedure. It is CE-marked, ISO certified and backed by more than 90 validation studies, making it clinically proven as a safe and effective treatment for skin remodelling/ microneedling. Our Advanced Needle Cartridge (ACU) is patented, FDA-cleared and validated for high performance and safety. The ACU is a one-time use per patient device.
This column is written and supplied by SkinPen UK

VIVACY
Aesthetic product manufacturer VIVACY UK has appointed Madeleine Farrant as its new marketing manager. Farrant has previously worked as a scientific coordinator for Euromedicom, the organiser of The Aesthetic and Anti-Aging Medicine World Congress (AMWC) in Monaco and FACE in London, since 2018. Farrant said, “I am delighted to have joined the VIVACY UK team as their marketing manager. The aesthetics industry is one that I love and know well, and VIVACY has always stood out to me as a brand full of innovation.”
VIVACY is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Dr Stephen Tristram retires as chair of the BAS
Founding member of the British Association of Sclerotherapists (BAS) Dr Stephen Tristram has retired as chairman of the Board after 10 years. Aesthetic practitioner Dr Martyn King will step in as Interim Chair for the next 12 months. Hilary Furber, operations manager and board secretary, said, “Dr Tristram has been a guiding light and the face of the BAS for almost 20 years. We are delighted that he will continue to support the BAS, albeit not as a board member; he is very much looking forward to May 2023 when the BAS will hold its first physical conference since lockdown.”
Promoitalia launches new hyperpigmentation treatment Medical cosmetic company Promoitalia has released V Bianco – a topical skin treatment to reduce the appearance of melanic spots with active ingredients including tranexamic acid, biomimetic glutathione and sym radiance resorcinol. CEO and founder of Promoitalia, Valerio Matanò, said, “As the new complete system for the treatment of hyperpigmentation suitable for all skin types, V Bianco is able to remove the formation of hypochromias and increase cell turnover, removing spots already present whilst promoting a strong antiageing effect.”
Promoitalia is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
AlumierMD launches new Colour Match Tool
Skincare brand AlumierMD has announced the release of their new Colour Match Tool, helping practitioners aid their patients in finding their perfect shade of tinted moisturiser. According to the company, the tool installed on practitioners’ phones or tablets finds the patient’s shade match within two minutes, taking into account the skin’s undertones.
Skincare brand Crystal Clear Skincare has announced the launch of the SKINSTORM personalised facial device, developed by the company’s founder and managing director Sharon Hilditch. The company says that the SKINSTORM machine combines several non-invasive treatments into one, supposedly addressing multiple different skin complaints.
According to Crystal Clear Skincare, the device incorporates cryotherapy, ice microneedling, vitamin infusion and high-pressure injection into six elements within one treatment, exfoliating, hydrating and collagen-boosting without the need for a needle. The procedure ends with an LED light bandage to balance the skin barrier, according to the company.

Hilditch said, “SKINSTORM is my most exciting development yet, simultaneously utilising six different technologies within one stand-alone device, practitioners can now offer a comprehensive treatment portfolio without the need for numerous devices.” Crystal Clear Skincare will be exhibiting at CCR on October 13-14. Register for free on p.20.
On the Scene
On September 8, HydraFacial UK held a biohacking breakfast talk with wellness author and former Hollyoaks actress Davinia Taylor.
Hosted by television personality Paul Wharton at HydraFacial’s London flagship store, Taylor shared her experience of tackling low mood and weight gain through diet and lifestyle changes such as exercise and intermittent fasting, alongside supplements and bespoke hormones.

Taylor commented, “I think that skincare actually starts on the inside, and I found a huge difference in my skin quality when I started adding collagen to my tea and coffee, and also increasing the fat content in my diet and removing of vegetables and seed oil which, to me, is worse than sugar.”
Lauren Gibson, HydraFacial country manager for the UK and Ireland, also spoke on how the brand is looking to embrace a holistic wellness approach to skin, hair and body health. Gibson said, “HydraFacial is all about how we approach 360-degree wellness and a holistic approach to skincare. You can have a HydraFacial on the face, back and arms or in the scalp, using our boosters to make sure we’re taking the skin to that next level. For example, our boosters have got peptides in, like Davinia said about taking collagen in your coffee. It’s all about mimicking the body to make sure that the treatment isn’t artificial or chemical. Watch this space for more boosters coming soon!”
HydraFacial is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
On September 10, the British College of Aesthetic Medicine (BCAM) held its annual conference at Church House in Westminster.
The day kicked off with a welcome from the association’s new president Dr Catherine Fairris, before the injectables stream began in the clinical portion of the conference.
The guest of honour was pioneer of botulinum toxin in aesthetics Dr Jean Carruthers, who spoke on knowledge and innovation in facial aesthetics, as well as answering questions in a live Q&A.

BCAM board member Dr Sophie Shotter said, “We have been headlined by the strongest pioneer of science in aesthetics in the world, so it has been a true privilege to have Dr Carruthers join us.”

The injectables session continued with talks from practitioners including Dr Xavier Goodarzian and Dr Shotter, before moving onto the body stream in the afternoon, featuring past president Dr Uliana Gout, Dr Elisabeth McCulloch and more, discussing a variety of treatments.
Business advice was also on hand, with talks from Dr Askari Townshend, Professor Benoit Hendrickx, Alice Hart-Davis, Lorna Bowes and more, covering topics including augmented reality, social media and focused consultations.
The day ended with a networking drinks reception for delegates. Reflecting on the day, Dr Fairris said, “The general feedback has been that everyone is happy with the calibre of the presentations. We want it to be very much an evidence-based conference with good science, that’s really the key.”
She also hinted at the future of BCAM under her leadership, commenting, “The biggest thing for BCAM at the moment is the need for a register of licensed professionals who can practise aesthetic medicine. At BCAM, we strongly believe we should be at the core of this conversation, driving legislation in a direction that promotes doctors and those who are medically trained to be protected by that register, and protecting patient safety.”
BCAM is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
On September 15-16, the British Association of Cosmetic Nurses (BACN) held its Autumn Aesthetic Conference at The Eastside Rooms in Birmingham. The two-day conference was opened by BACN CEO Sir Paul Burgess and BACN chair aesthetic nurse prescriber Sharon Bennett, who introduced the agenda of CPD-accredited clinical and business talks. Bennett said, “The BACN Autumn Aesthetic Conference is about understanding our chosen specialty more deeply, looking at issues that relate specifically to it, applying new-found learning into our practice, sharing our expert knowledge with each other and promoting the professionalism and position of specialist aesthetic nurses to a wide audience.”
On the first day, the content on offer included live demonstrations from oculoplastic surgeon Miss Elizabeth Hawkes, aesthetic practitioners Dr Nina Bal and Dr Emily Mehta and nurse prescriber Lou Sommereux, as well as further talks from psychologist Kimberley Cairns, aesthetic nurses Julie Scott and Lorna Bowes and more.
The day finished with a networking drinks reception for approximately 300 delegates, topped off with a fun photo booth sponsored by Aesthetics and CCR.
The second day brought content from nurse practitioner Karen Burgess speaking on skincare, pharmacist Gillian Murray on medicines in aesthetics and nurse prescriber Tracey Jones on registration with healthcare regulators, as well as a live injection demonstration from plastic surgeon Miss Priya Chadha.
BACN operations and communications manager Gareth Lewis said, “It
has been brilliant to get back together after a number of years apart, and this is now our biggest conference to date held over two days! We have a wide agenda full of nurse speakers and live demonstrations, which is everything that the nurses love.”
He continued, “We’re really keen on providing a platform for nurse speakers to get on stage, so it’s exciting that more than 70% of our speakers are nurses. Networking is also extremely important for nurses because they work in isolation, so it’s so important to hold events like the BACN Autumn Aesthetic Conference to get together.”
The BACN is exhibiting at CCR on October 13-14. Turn to p.20 to register for free.
Aesthetics looks at a new study on social media before and after photos and investigates why the standards of photography are low in the aesthetic specialty
Taking before and after photos is a common part of an aesthetic appointment. As well as being vital for medicolegal and insurance purposes, they also allow the patient to see areas of improvement and the end results of their treatment. Furthermore, with patient consent, the photos can benefit the practitioner as they can be used as a marketing tool on social media to highlight your work to prospective patients, and the results you can achieve.1,2,3 Despite this, a new study has shown that many before and after photos may be of substandard quality, taken with inconsistent photography parameters such as lighting, angles, facial expressions and more.
In the study, a total of 510 social media posts encompassing 2,020 clinical photographs published by 102 practitioner accounts on Instagram were audited for photographic quality. The images were evaluated using a newly proposed Standards for Evaluation of Photographs in Aesthetics (SEPIA) nine-point photograph scoring system.4 In the system, subject position, facial expression, lighting, background, camera zoom, makeup and styling, multiple views, timing and descriptive information were all assessed.4
The average score was four out of nine, with approximately 40% of posts scoring in the low-quality range. Camera zoom, lighting, timing and presentation of multiple views were the standards commonly disregarded. Low-quality photos were most often seen with rhinoplasty and lip filler treatments, compared with surgical and non-surgical procedures, due to a higher incidence of immediate photographs and selfies.4
The study concluded that before and after photos of cosmetic treatment outcomes on social media were frequently of substandard quality.4 In light of the study, we spoke to plastic surgeon Mr Dean Rhobaye and founder of photography lighting system Clinical PhotoPro Clint Singh to understand why the standards are so low in the industry, as well as their tips on how practitioners can improve their patient photography.
Although the study was conducted in the US, Singh believes patient photography to be a global issue. “The problem is industry wide. Clinics follow each other on social media and so trends and industry standards spread. The problem may also be technology-driven, as the use of smart devices is here to stay. Manufacturers are constantly improving devices for photography in clinics and patient management software producers are also making their systems available for smart devices. However, these are for general photography and using them for clinical images requires training, which is often not being provided or actively sought out by practitioners,” outlines Singh.
Achieving good quality clinical photography is pivotal to showcase patients’ results accurately and professionally, noted both Singh and Mr Rhobaye. In a recent study of 30 volunteers, photos with a 12-inch and 18-inch series with a front-facing smartphone camera and a five-foot clinical photography series with a digital single-lens reflex camera were taken. Nasal length was 6.4% longer in the 12-inch selfies compared to clinical photography and 4.3% longer in 18-inch selfies compared to clinical photography, highlighting that image quality can affect the patient’s perception of themselves.5
Singh notes that the introduction of smartphones has resulted in professional clinical photography taking a back seat. “Smart devices have given clinics a quick and easy, point-and-shoot option with no effort to photography needed. Unfortunately, with no training, standardisation or guidance on how to use these devices for the precision needed for clinical photography, we are seeing substandard quality before and afters,” Singh explains.
According to Mr Rhobaye, there are numerous reasons why photography standards are low in aesthetics. He explains, “Time constraints can have an impact – practitioners may feel they cannot commit to spending time acquiring higher-quality images, particularly if they have a busy practice.” Furthermore, Mr Rhobaye believes that a common practice on social media among practitioners is publishing non-standardised images that exaggerate the treatment changes. “An example of this practice is the use of perspective distortion in photography caused by taking a ‘before’ image with a wide-angled lens close to the patient. As a result, the perspective distortion warps the facial dimensions in the captured image versus reality, creating an unflattering image. In contrast, the ‘after’ image is taken further away or the distortion is reduced with no warping of facial features,” he notes. Other potentially misleading methods Mr Rhobaye identified include using different lighting, facial postures and tricks with makeup, which worsen the appearance in the before image but flatter the ‘after’. Many professionals are not aware they are intentionally doing this, however, this goes against the Advertising Standards Authority’s rulings as it is misleading.6
Singh also notes that smaller businesses may find taking photographs harder due to a lack of space. He explains, “A smaller business might not have the luxury of bigger premises with a room dedicated

to photography. A dedicated room can significantly improve the consistency of before and afters as the lighting can be left in place, and the distances and angles can be replicated.”
According to Mr Rhobaye, practitioners should optimise the duration of their appointments and invest in a quality camera, lens, lighting and accessories. He explains, “Allow time during patient appointments for photography, or another team member can be trained to take the images before and after seeing the practitioner. I would advise practitioners to carefully consider what colour background they would like. Colours, such as light blue, are better suited for medical photography, but also the colour needs to be consistent with the brand image.” Mr Rhobaye also recommended that practitioners invest in a 3D imaging system for clinics that want to practise more advanced facial aesthetics. He explained that they have additional benefits to 2D photography for patient education, monitoring treatment outcomes and collecting data for research studies. Producing good quality and accurate photography can be achieved through focusing on factors such as lighting, distances and angles and receiving adequate training if necessary, argues Singh. “Natural light is the biggest cause for the inconsistency in before and afters. The colour and strength of this light changes throughout the day and unless your photography area is protected from the outside by having closed blinds, a camera will react to these conditions, producing images of different exposure and colour. To improve consistency, mark out distances and angles - practitioners should have a consistent environment to photograph their patients in. Invest in training that is specific for photography in aesthetics with mobile devices. The training should consider the requirements of the SEPIA scale, which I think is a much-needed proposed scale for the industry,” he reflects.7
Patient photography is a pivotal practice for patient education and highlighting accurate outcomes. Mr Rhobaye concludes, “Photography can become complicated when practising at a professional level, dealing with different environments, subjects and lighting. However, in an aesthetic clinic, once the key settings are optimised for the environment, the process becomes, by and large, a ‘point and click’ exercise without having to worry about any further adjustments.”
There are many companies out there which can help increase the quality of clinical photography for your practice. Below are just a few to look into:
• Canfield
• QuantifiCare
• RxPhoto
• VISIA
• Clinical PhotoPro – check them out at CCR!
• oVio Technologies –check them out at CCR!



FEATURES
360 Images (12 seconds or less)
360 Video
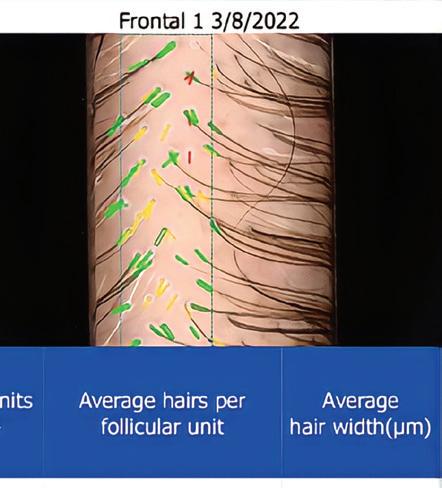
Top Down Capture for Hair (Overhead)
Live Motion Capture
Consistent Lighting Improved Workflow (Pre to Post Treatment)
Dynamic & Living Images Consistent and Standardised Images
Multi Image Comparison
Increased Patient Satisfaction
Others
Getting Consistent before and after photos has never been easier.

October is finally here, and with it comes CCR 2022, the UK’s flagship event in medical aesthetics uniting surgical, dermatological and aesthetic specialties. More than 3,000 medical professionals will attend ExCeL London on October 13-14 for the aesthetic event of the year. This year, as our industry has exploded back into action with a huge surge in patient demand, CCR 2022 will be an edition like no other, extending your learning opportunities further than the traditional expo. We have more specialised agendas than ever before and additional features which will enhance learning and development to make it a truly unmissable event for medical professionals.



As you can see from your Agenda at a Glance insert, the full agenda is now confirmed and promises to deliver high-level clinical education across two days, covering all aspects of the aesthetic specialty from injectable innovations to holistic treatments for patients. The five conference stages include Facial Aesthetics, ACE Group World Complications Conference, In Practice, Skin, ISAPS Symposium UK, Aesthetic Wellness, Galderma Symposiums, Masterclasses, Innovation, A Dentist’s Guide to Aesthetics, Allergan Lunchtime Takeovers, Dr Tapan Patel’s Live Injection Masterclass and so much more.
The new Aesthetics Arena brings the Aesthetics journal to CCR. This fully CPD-accredited agenda will take you on a journey through treating the full-face, with protocols for treating different areas of facial anatomy. Topics include, Innovations in Botulinum Toxin, Sculpting the Jawline, Stem Cell and Stromal-Enriched Nanofat Grafting for Volumisation and Rejuvenation, Mid-face Rejuvenation, Tear Trough Transformations and Innovative Uses of Ultrasound to name a few. Speakers include Professor Bob Khanna, Dr Souphiyeh Samizadeh, Dr Joshua Van Der Aa, Miss Rachna Murthy, Professor Jonathan Roos, Dr Raul Cetto, Dr Jeremy Isaac and Mr Dalvi Humzah. Headline Sponsor Galderma will host two symposiums: ‘Turn your AART into a HIT with the Galderma aesthetics portfolio. Part 1

SHAPE UP, Part 2 KISS & SMILE!’ as well as ‘A methodology to lift the mid-face and rejuvenate the lips and perioral region with the Restylane portfolio’. Speakers will include Michele Di Giacomo, Miss Priyanka Chadha, Jackie Partridge and Dr Rikin Parekh.
Dr Martyn King, Sharon King and their expert speakers return to CCR for the third annual ACE Group World Complications Conference. The agenda is set to cover Vascular Occlusions, Management of Filler Complications using Ultrasound, Delayed Onset Nodules and more with confirmed speakers including Dr Julia Sen, Mr Ansar Mahmood, Lou Sommereux and Professor David Sines. This is a paid for conference with limited tickets available to purchase via the CCR registration form.
As always, CCR dedicates agendas to the world leading brands as they share their latest products and launches, delivered by their esteemed medical faculty.
Highlights include:
• Allergan Lunchtime Takeovers – A Future with Hybrid Injectables – What is HArmonyCa? LIVE DEMONSTRATION with Dr Tapan Patel and Mr James Olding
• The launch of Evolus – UK exclusive with Dr Steve Fagien
• Rejuvenation, Lifting and Volumisation from Croma – a complete portfolio for addressing the modern patient’s needs with Professor Syed Haq and Dr Munir Somji
• Sofwave Next Generation Facial + Neck Treatment Workshop with Dr Munir Somji
• Medical Profiloplasty using STYLAGE dermal fillers* with Dr Magdalena Bejma
New for 2022 we are bringing you the CCR Innovation Trail showcasing the latest and most innovative products on the UK market. Do you want to hear about the best, industry-changing products to add to your practices? Then the CCR Innovation Trail will provide you a quick and straightforward way to find these products at the event. A total of 10 game-changing products will be highlighted on the trail.
The ISAPS UK Symposium returns to CCR for the second year. Curated by ISAPS UK national secretary and consultant plastic surgeon Mr Naveen Cavale, this meeting will cover a range of enlightening surgical topics, focusing on breast, face and non-surgical.
With a tidal shift of more surgeons setting up their own practices, the symposium will also provide unmissable business insights and advice from surgeons who have done just that. Speakers include Dr Francisco Bravo, Mr Stephen Hamilton, Mr Reza Nassab and Miss Priyanka Chadha
To deal with increased demand from the aesthetics boom, correctly managing your clinic, staff and patients is vital now more than ever. The In Practice Theatre features the latest business insights and advice from experts and individuals that are successfully running clinics and business, sharing their tips and lessons learnt. This year will cover:
• Getting Started: A Guide For Dentists curated by Professor Bob Khanna
• Patient Safety and Regulation with Samantha Senior and Professor David Sines
• Marketing with James Dempster and Cait McLaughlin
• Patient Relations with Mel Recchia, Dr Catherine Fairris and Dr Harry Singh
• Taking the Next Steps with Shannon Kilgariff, Gary Monaghan and Richard Crawford-Small
While the clinical agendas are at the heart of CCR, we understand the value of connecting and networking with your industry. This year we’ve introduced more networking opportunities than ever, so we really do hope you enjoy the experience!
After you have interacted with exhibitors, sourced the latest market-leading products
and increased your annual CPD points through attending the conferences, be sure to swing by the Networking Lounge sponsored by Galderma. This relaxed setting is the perfect place to catch up with peers and friends, enjoy a coffee and reflect on new techniques learnt in the conferences.
Once the conference sessions have finished at 5pm, head back to the Networking Lounge for Networking Drinks sponsored by SkinCeuticals.
Following on from the drinks, for the first time ever CCR are throwing you an official after party – The PHI Lanthropy Diwali Party with Dr Tapan Patel – on October 13 from 8pm at Trinity Bouy Wharf, just five minutes from the ExCeL. The evening will include luxurious Indian cuisine, unlimited drinks and of course celebration and dancing.
Get your suits, gowns, saris and lehengas ready, this is going to be an unmissable evening dedicated to some truly wonderful charities. Please show your support and book your ticket to join the after party of the year! All proceeds go directly to charity. Tickets are £150 and are available to purchase in the online shop via the CCR registration form. Scan to Register FREE now to be the first to find out more.
• Registration for CCR is free, but some sessions are paid for
• ACE Group World Conference –£125
• Dr Tapan Patel LIVE Injectable Masterclass – £120

• ISAPS 5th UK Symposium – £150 for members

• CCR PHI Lanthropy Diwali Party –£150
Please note: some sessions in the CCR Agendas are gated to medical professionals registered with the GMC, NMC and GDC only.













As we move into our tenth year in 2023, we take the opportunity to look back at the changes we have seen and consider how medical aesthetics will evolve over the next 10 years.
Editor and content manager Shannon Kilgariff comments on the trends she has seen over the years and shares her unique insight from working closely with both the companies developing new products, and the practitioners seeing the results in clinics throughout the UK. You’ll also be able to learn more about the latest products and treatments following our aesthetic conference CCR on October 13-14. Our annual Trends Report will be available to the community following the event.
According to research, the aesthetics injectable market has grown by more than 10% annually and could grow by 12-14% a year over the next five years. Forecasts suggest that this is largely expected due to the expanding portfolio of dermal fillers and biostimulators.1 Each year, we are seeing new products being introduced to the market and exciting new studies looking into ways to improve the skin from within.
Kilgariff says, “Focus has shifted from treating the symptoms of ageing and instead is aiming to address the cause. Over the past couple of years, it’s been fascinating to learn more about biostimulation products – each work in their unique way and provide practitioners with a new tool to tackle ageing. It’s going to be interesting to see which ones take off and become the most successful over the next few years. Some of the brands I’ve been keeping an eye on include HArmonyCA from Allergan, Juvenus from Croma-Pharma and Plenhyage XL from DermaFocus.
The toxin market has also been experiencing big changes. While not much progressed in the first half of the decade, new toxins have been under development for the past few years. Just last month, Daxxify from Revance Therapeutics was approved by the US Food and Drug Administration, with clinical studies suggesting that results can last up to nine months.2 We’ve also seen the introduction of Letybo from Croma-Pharma, Alluzience from Galderma and Nuceiva from Evolus.
“With topical toxins in the works as well, it’s going to be an interesting few years,” says Kilgariff, adding, “At the moment it seems practitioners are still unsure whether topical toxin will be as effective as the injectables we’re familiar with. I’ll be keen to see whether they stick to the brands that they know, and provide proven results, or try something new!” Threads have also grown in popularity. While they’ve been around since the 80s, better products and techniques have led to improved results with less pain and downtime. Serving a different
purpose to that of dermal fillers, practitioners highlight that threads can offer a decent amount of lift to anchor and reposition tissues, while stimulating collagen production.3
Kilgariff says, “It was great to see the introduction of tighter regulations for thread lifts back in 2018. Any medical-led clinic performing a thread lift must be registered with the Care Quality Commission (CQC) or their nation’s equivalent, which enhances safety for patients, and is something I’m sure we’d like to see much more of over the coming years.”4
Whether you want to tighten, rejuvenate, contour, heat or freeze, in 2022, there is an energy device for you.
The global market size was worth US $2,661.6 million in 2021, with forecasts suggesting this will rise to US $6,326.2 million in 2030 – a growth rate of 10.1%.5 “While huge numbers are mentioned here, this is unsurprising news. For the last few years, we have seen new devices launching regularly thanks to the rapid development of new technology and consumer awareness of these products increasing. Patients appreciate the minimal downtime and fantastic results that they can offer,” says Kilgariff.
As of 2021, lasers were the most popular energy-based device, holding around 40% of the market share. According to reports, this is largely attributed to the widening capabilities of lasers – from rejuvenating skin, to removing hair.5
The last few years have also seen electromagnetic devices increase in popularity, with a number of new devices, such as EMSculpt Neo and truSculpt Flex, launched here in the UK. Research suggests that this market is anticipated to see the highest growth over the next few years.6
Additionally, increased availability of home-use devices is expected. Kilgariff comments, “We are starting to see this, particularly with at-home light-based devices becoming available over the past few years. Some brands include Dermalux Flex MD and Celluma HOME. I just hope that companies don’t comprise safety for money when it comes to adapting their technology. It’s also imperative that, if being sold through clinics, practitioners are investing in and recommending well-researched products, rather than selling cheaper counterfeit devices that do not meet safety and result standards.”
In 2013, the global skincare market was worth US $103 billion, while in 2023 it is set to bring in US $ 171.7 billion.7 More locally, anecdotal reports suggest that lockdown led skincare sales to boom in the UK.
We reflect on a decade of publishing the Aesthetics journal and discuss the development of the specialty over this time
HArmonyCa™ is a Hybrid Injectable that combines hyaluronic acid (HA) with calcium hydroxyapatite (CaHA), which may give your patients the benefits of an immediate lift effect from HA and sustained collagen stimulation associated with CaHA, for a new way to facial harmony.1–3,*,†

Produced and funded by Allergan Aesthetics, an AbbVie company.
Please see HArmonyCa™ IFU for the full list of contraindications, warnings and precautions.1
* Results from a pre-clinical animal study of HArmonyCa™ with results demonstrated over 12 weeks.2
† Results from a pre-clinical animal study of HArmonyCa™ with results demonstrated over 8 weeks.3
HArmonyCa™ Lidocaine is referred to as HArmonyCa™.
HArmonyCa™ is a dermal filler intended for facial soft tissue augmentation and should be injected into the deep dermal and sub-dermal layers.1
For use in patients ≥ 18 years old only.
©AbbVie 2022. All rights reserved.
References
1. Allergan Aesthetics. HArmonyCa™ Lidocaine IFU. M032 V01. 2021.
2. Allergan Aesthetics. Data on File. INT-HAR-2150036. HArmonyCa™ Lidocaine. Lift capacity. Jul 2021.
Adverse events should be reported.
Reporting forms and information can be found at:
UK adverse events reporting https://yellowcard.mhra.gov.uk/
Adverse events should also be reported to Allergan Ltd.
UK_medinfo@allergan.com or 01628 494026
Irish adverse events reporting https://www.hpra.ie
Adverse events should also be reported to Allergan Ltd. UK_medinfo@allergan.com or 01628 494026
3. Allergan Aesthetics. Data on File. INT-HAR-2150040. HArmonyCa™ Lidocaine. Collagen stimulation. Jul 2021.
Kilgariff explains, “Reports from practitioners suggested that the ‘Zoom Boom’ led to consumers becoming more aware of their skin quality as they spent so much time looking at their face through video calling. Interest in aesthetic procedures soared, but of course clinics weren’t open to address concerns. Instead, practitioners were recommending skincare so patients could take action at home, which helped users recognise the value of sticking to a good skincare routine and investing in products that work.”
Alongside this, online consultations began to grow – saving time for both practitioners and patients. Moving forward, Kilgariff has heard from many practitioners who say this digital communication has transformed their practice. “It means practitioners can see patients from further afield, as well as fitting in more appointments. But practitioners don’t have to utilise the extra free time it allows specifically for work – the pandemic helped lots of people reset and consider what a good work/life balance means to them. I’ve seen many practitioners move towards prioritising their own wellness, as well as their patients’, which surely can only be a good thing,” she says. The last 10 years have seen the growth of skin analysis devices too; a useful tool to demonstrate to patients the extent of their skin damage, get them on board with treatment and review progress. Having one of these devices, such as VISIA Skin Analysis, OBSERV or LifeViz, can make a clinic stand out from the crowd. Kilgariff says, “As consumers, we don’t like to be sold to anymore! Instead, we want to conduct our own research, with the help of credible advice, and see the value of investing in something for ourselves. Skin analysis backs up a practitioner’s recommendations by showing us evidence and demonstrating results. I expect these devices to become more popular over the coming years.”
We all know that the most important part of everyone’s skincare routine should be SPF application. While this advice has not changed in the past 10 years, are consumers still getting the message? In 2012, a survey found that 13% of Brits regularly use tanning oils with SPF factors of 10 or less, while only one in four use SPF 30 or above.8
While we don’t have exact comparisons, research suggests that not much has changed – in 2022, 45% of over 50s said they rarely use sunscreen in the UK.9
Skin cancer rates continue to rise, according to Cancer Research UK, with a drop only seen in those aged 0-24. Since the early 90s, for those aged 25-49 rates have increased by 67%, in 50-59s they’ve increased by 102%, in 60-69s they’ve increased by 158%, in 70-79s they’ve increased by 236% and in 80+ skin cancer rates have increased by 218%.10
Kilgariff says, “Anecdotally, practitioners say that there is more appreciation for suncare, but these statistics suggest there’s more that needs to be done. Aesthetic practitioners are perfectly placed to educate patients on the importance of SPF, highlighting both the impact on ageing and, most importantly, the skin cancer risk.”
What were we doing to promote and champion diversity 10 years ago? Looking back, adverts, publications, events and marketing materials featured largely Caucasian faces and many noted that clinical research lacked representation of black, Asian and ethnic minority patients. The Black Lives Matter movement in 2020 had an impact. Along with the Black Aesthetics Advisory Board (BAAB) and the Black Skin Directory, we took matters into our own hands. We ran surveys to investigate the experiences of black practitioners and consumers, as well as practitioners from other ethnicities, to better understand their views on the representation and treatment of skin of colour in general.
Statistics were revealing. The majority of respondents (92%) said they felt comfortable approaching diversity in their clinics, despite the fact that comments suggested they were scared to say the wrong thing and felt they needed better training and guidance on treating skin of colour, and acknowledged that more literature on treating darker skin was needed.11
Sadly, 84% of black practitioners said they did not feel well represented when attending aesthetic conferences, 70% said they did not think they had a fair shot of becoming a key opinion leader, and seven out of 10 black patients said they had difficulties in finding practitioners confident in treating their skin.11
Kilgariff says, “Carrying out these surveys was absolutely necessary and really helped start an important conversation. To build further awareness, we published the results throughout the Aesthetics journal and website, turned the stats into serialised social media posts across our platforms, and hosted Instagram Lives discussing the outcome and actions with BAAB board members. Of course, we looked at changes we as an organisation could make, while providing guidance and training to our employees. Simple things like using stock images of patients of all races and ensuring clinical articles noted considerations for treating skin of colour were just small changes we made.”
She continues, “On a larger scale, we focused on reaching out and engaging with more diverse practitioners; ensuring we provide writing and speaking opportunities for all, while encouraging everyone to enter The Aesthetics Awards and gain the recognition they deserve. We endeavour to continue this work and hope that over the next 10 years, all practitioners feel represented, regardless of their skin colour!” Kilgariff adds that diversity is a key part of a wider conversation for parent company of Aesthetics & CCR, Easyfairs, which has initiated a huge focus on Environmental and Social Governance (ESG) and is treating this as a priority.
In our first issue in 2013, our Aesthetics journal headlines included ‘Stopping the Cosmetic Cowboys’ and ‘A Third of Brits Undergo Cosmetic Surgery Abroad’.12 You may read these and think, ‘Hey, not much has changed!’ But is that fair?
Of course, regulation isn’t where we want it, but the last 10 years have seen positive steps forward. Organisations such as the Joint Council for Cosmetic Practitioners, British College of Aesthetic Medicine and British Association of Cosmetic Nurses are working hard to provide guidance and support to enforce regulation, while Healthcare Improvement Scotland introduced regulation of private clinics in the country back in 2016.13
In 2021, the Botulinum Toxin and Cosmetic Fillers (Children) Act came into force,14 while earlier this year we saw the introduction of the Health and Care Bill 2022, which aims to apply a licensing scheme for practitioners working in England.15 Kilgariff comments, “For now, all this means is that the Government has the power to introduce a new licensing scheme to regulate premises and practitioners, but we have no timeline for when this will be developed and introduced. Regardless, it’s promising to see steps moving forward!”
Over the last 10 years and as we move forward into the next decade, we are seeing much greater focus on complication prevention and management from training providers, manufacturers, associations and organisations. There’s also now lots of discussion around using ultrasound to aid placement of injectables and support complication management. Although Kilgariff points out that the advice from experts in this area is that practitioners should not be relying on ultrasound to

We chat to three of our long-standing Clinical Advisory Board members for their thoughts on our specialty’s development...

SS: Awareness of complication management was almost non-existent 10 years ago, whereas our knowledge now is outstanding. It’s great to see so many training companies prioritising this, as well as conferences and publications like the Aesthetics journal, educating attendees and readers on complication prevention, as well as management.
SW: Thankfully most good practitioners have come away from chasing isolated lines and wrinkles, as was the case 10 years ago, and are instead treating the face as a whole.
AR: This will sound a bit weird, but it was probably lockdown in 2020. I’ve been operating for 38 years and it’s been full on, all of the time. Lockdown gave me the opportunity to try new things and I spent a lot of time engaging with colleagues and sharing knowledge online – I did more than 150 Instagram Lives and started a podcast; it was a lot of fun and great to chat to practitioners from around the world in depth and learn new things.
SW: I’m glad to see us move away from trying to make our patients look younger at any cost, but instead try to make them look like the best version of themselves. Whatever their age, it’s good to embrace the changes that come with it, rather than fearing them. We still have a way to go though!
SS: The move towards regenerative medicine is really exciting. While it’s still in its infancy, it’s great to see new products coming to market using a combination of hyaluronic acid and various biostimulators, which move away from simply filling or correcting a concern, but instead focus on treating the cause.
SW: I’m excited about a more holistic approach to aesthetic medicine going forward. For example, the integration of mitochondria support treatments such as intermittent hypoxia/hyperoxia, rather than just treating the skin’s surface in isolation. Hopefully we will see many more systemic treatments appear that support both the skin and general health.
AR: For me as a breast surgeon, the advancements in imaging and ultrasound


are getting so much better. I do a lot of 3D simulations, so it’s fantastic that people can see how they may look with different types of implants and I’m excited to continue working with this. It’s also great to see techniques continually improving and implants becoming safer.
AR: New trends and ensure they think analytically. Don’t just go for the first thing that comes along. I always say, think if you or your family were the patient, what would you do? Never do anything that you wouldn’t want done to you.
SS: Always go back to basics. People sometimes get super excited about new treatments, without properly understanding what they do. Think first about patient care, anatomy and pharmacology; this way you will gain the respect and trust of your patients.
SW: Don’t blindly jump on the next bandwagon. Closely look at the evidence behind treatments, before exposing your patients to them. We should also be more aware of the high incidence of BDD in our patients and should protect them from treatments that they don’t benefit from.
help them with their work, she says, “Sound knowledge of anatomy and complication management should always come first – this is what I’m hearing at conferences on the subject.”
Kilgariff adds, “In general, the work being done by all to prevent complications is incredible,” says Kilgariff, highlighting that her team has also been committed to enhancing understanding and knowledge. She says, “All of our articles provide safe practice advice, with a discussion of potential side effects and complications as standard. We also host the Aesthetics Complications Expert (ACE) Group World conference at CCR, as well as seeking evidence of complication protocols for all Aesthetics Awards entries.”
As evidenced over the past 10 years, medical aesthetics is an ever-growing market with hundreds of exciting technologies being developed, and thousands of new practitioners emerging every year. While this brings opportunities for individual growth, Kilgariff emphasises that it is imperative we take the advice of the practitioners outlined earlier and be cautious before jumping into anything new too fast. She concludes, “The sentiment echoed by our Clinical Advisory
Board is to do your research, focus on your area of expertise and always stay safe. You don’t have to have the biggest clinic, offering every treatment under the sun – do what you do well, build trust and you will naturally gain loyal customers who recommend your services and keep coming back for more.”
From the get-go, we wanted Evolus to be different. We describe ourselves as a performance beauty company, taking learnings from the beauty sector and applying this within aesthetics. The beauty sector is great at capturing trends, understanding what consumers want, reacting quickly and creating desirable brands. And we also know that you need products that really perform.
Just as your practices have evolved over the last 15 to 20 years, so has the mindset and desires of consumers. Today, this category is booming. Many people, across the generations, view beauty treatments as a part of daily life. This can be especially true for those with a millennial mindset who are visiting clinics and fuelling the boom.
“After more than 20 years’ working with aesthetic practices, I’m excited to be building something different. I believe there is a gap in the market for a radically different type of company – one that is designed around our customers,” says Dan Stewart, vice president and general manager for Evolus International. “We invite you to evolve the future of beauty with us.”

Since our foundation, we have focused exclusively on aesthetics. This means we live and breathe beauty, whilst also being a pharmaceutical company.
We are a small start-up with a big vision. Our culture is designed around these three ideas: We want our work to disrupt the status quo. We want to make an impact. Yet most importantly, we want to be customer-centric – always. (P.S Please remind us if we aren’t!)
If you love what you do, you’ll never work a day in your life. This is a mantra we live and breathe. Transparent
At Evolus, we’re clear, open and honest –with each other and with our customers. Impact
As a team, we move quickly but also have enough time and space to listen and create broad, innovative ideas.
Evolus invites you to evolve the future of beauty with them
“I believe there is a gap in the market for a radically different type of company – one that is designed around our customers”Dan Stewart
Come meet our Evolusionaries at our booth at CCR
We’d love to see you.
THE WORLD 2021, over 1,400 new the total number of 7,500 in the US alone. operations outside of Britain, Germany and significant step in our strategy multi-product performance
Holly McDonald, London and the South East, also known as Hollywood



Amy Wood, Manchester and the North West, our Peloton junkie



In the last three years, we’ve had a lot of conversations and learned a lot from our North American customers about what works, and what doesn’t work. We’re taking these lessons, and evolving what we do in Europe and beyond to meet your needs.
We invite healthcare professionals to join us at our CCR symposium on October 13 at 12:30-13:30, with Dr David Eccleston, Dr Steve Fagien and guests. We’ll explore who is Evolus, what we are doing in Europe and share how we can help you evolve the future of performance beauty.
Yet there is one thing that comes across clearly. Our North American customers are delighted to have choices.
From our global corporate headquarters in Newport Beach, we have been growing since 2012. We have more than 170 associates with some amazing skills – from research and development experts to digital engineers and sales and marketing gurus, one thing unites us –we love being disruptive!
Now, we want to hear from the aesthetics community in the UK about the trends you are seeing and how your business is evolving.
thing that comes across clearly. Our North American customers are delighted to have choices. Now, we want to hear from the aesthetics community in the UK about the trends you are seeing and how your business is evolving.
We look forward to partnering with you as we launch a different type of company.
Visit www.hello-evolus.com to find out more.
As a company, we are flourishing. In 2021, more than 1,400 new practices joined Evolus, bringing the total number of customers we support to more than 8,000 in the US alone. Now, we are excited to expand our operations outside of North America. For us, this is another significant step in our strategy to become a leading, global, multi-product performance beauty company.


Visit www.hello-evolus.com to find out more.
We look forward to partnering with you as we launch a different type of company. CCR symposium
1230 – 1330, guests.
In the last three years, we’ve had a lot of conversations and learnt a lot from our North American customers about what works, and what doesn’t work. We’re taking these lessons, and evolving what we do in Europe and beyond to meet your needs. Yet there is one
Don’t stand still, evolve with us.
This advertorial was written and supplied by Evolus.
Date of preparation August 2022 UK-UNB-2200016
Suse Alexander, our UK general manager, and all-round superstar Jean Johnston, Scotland and the North, wearer of killer heels Hilary Gates, Southern and West England, equestrian Queen Nichola Smith, Central and Easternish England, outdoor enthusiast Samuel Oladiran, medical science liaison, and community champion Suse Alexander, our UK General Manager, and all-round superstar Jean Johnston, Scotland and the North, Wearer of Killer Heels Hilary Gates, Southern and West England, Equestrian Queen Nichola Smith, Central and Eastern-ish England, outdoor enthusiast Holly McDonald, London and the South East, also known as Hollywood Amy Wood, Manchester and the North West, our Peloton junkie Samuel Oladiran, Medical Science Liaison, and community champion

Patients requesting non-invasive aesthetic treatment for an ageing neck may report a range of unwanted signs. These include loose or sagging skin, changes in skin colour or texture, accumulation of fat between the chin and the neck, changes to the cervicomental angle, horizontal ‘necklace’ lines or vertical platysmal bands on the neck itself.1,2 It is no longer the case that surgery presents the only option for addressing these signs. Now a growing range of minimally invasive treatment options are available. Injectable agents, such as botulinum toxin and soft-tissue fillers have a key role to play, as do devices and techniques including energy-based treatments.2,3
This article takes a closer look at how to approach rejuvenation of the neck and some of the treatments that are appropriate, as well as the evidence for combinations of treatments in this delicate and complex area.
Several layers of the superficial anatomy of the skin may be implicated in non-invasive treatment for the effects of ageing.1 Dermal thinning can occur due to ageing or ultraviolet damage.4 Other indications of photodamage on the skin’s surface include lentigines, telangiectasia and dyschromia.5 Below the dermis and epidermis lie the planes of subcutaneous fat, the platysma muscle and the deeper subplatysmal fat with the digastric muscles and the submandibular glands.4,6 Fat may accumulate or be repositioned in the subcutaneous and subplatysmal layers as part of the ageing process (Figure 1).7 The platysma muscle extends from the collar bone to the musculoaponeurotic system of the face and pulls the skin of the neck in downward and lateral directions 8 It is important, therefore, to include the lower face in the physical examination as it too may require treatment to address signs of ageing in the neck (Figure 2).6 Hyperkinetic activity and loss of muscle tone with age can result in the appearance of vertical muscle bands as well as horizontal neck rhytides (necklace lines) and sagging skin.8,9 Interestingly, younger patients are also increasingly experiencing horizontal lines, possibly due to looking down at a computer screen or mobile device for extended periods.10
As a neuromodulator, botulinum toxin (BoNT-A) works by blocking the release of the neurotransmitter acetylcholine, which produces a temporary reduction in muscle contractions lasting for three months or more.11 The toxin is the first-line therapy in platysmal banding and is recommended for the prevention of or early intervention in the formation of prominent bands.4 In addition to showing efficacy in treating lines caused by movement of the platysma, BoNT-A has also shown improvement in re-contouring the jaw in a so-called Nefertiti lift.8 Of the 30 patients in a study by Jabbour et al., improvement in the appearance of both the neck and jaw was reported by respondents in 93.3% of patients with both platysmal bands at rest and when contracted, showing statistically significant improvement.8 A subsequent study also showed statistically significant improvement in platysmal banding at contraction, jowls and neck volume in 25 patients who had previously undergone a Nefertiti lift and were subsequently treated with BoNT-A using a microdroplet technique.12 However, in the Jabbour study, significant improvement in platysmal banding occurred at contraction and at rest (p<0.0001 and p = 0.022 respectively) but only at contraction and not at rest in the Awaida study (p<0.0001 and p = 0.6269 respectively), suggesting that the microdroplet technique may be more appropriate to address sagging skin caused by ptosis of the soft tissues.12
When targeting the platysmal bands, BoNT-A should be injected into the platysma intramuscularly or intracutaneously at three to six points in each band with a dose ranging from 6 to 12 units per band, with a maximum total dose of 60 U of onabotulinumtoxin A.13 Dose choice should reflect the requirements of the individual patient. Intracutaneous injection can be used in order to minimise the depth and magnitude of toxin administration.13 Doses greater than 50 U may impede the function of the neck flexor and deglutition muscles.4 Differences in doses between ona- and incobotulinumtoxin A and those for abobotulinumtoxin A should be noted.11 A conversion ratio of 1:2.5 (inco/onabotulinumtoixn A: abobotulinumtoxin A) has been suggested when treating the face based on the literature and clinical experience.14
Treating patients in the sitting position can make the platysmal banding more visible and asking the patient to clench their teeth enables the practitioner to target the bands and inject directly into the muscle.9 Injection deep into the structures of the neck should be avoided.9 Dysphagia, dyspnea, dry mouth and neck weakness are rare adverse effects of BoNT-A when injecting in the platysma.9,13 The risk can be minimised by careful monitoring of doses and avoidance of injection into the thyroid cartilage.9,13
Figure 1: Cross-section of superficial planes in the neckThe practitioner has a choice of dermal fillers for use in the rejuvenation of the neck including hyaluronic acid (HA), calcium hydroxylapatite (CaHa), polycaprolactone (PCL) and poly L-lactic acid (PLLA) fillers. Injections of HA fillers at different layers of tissue create volume, whereas biostimulatory fillers such as CaHa, PCL and PLLA fillers induce neocollagenesis, thus increasing volume, tightening the skin and lifting the tissue.3,15,16 While fillers have not been a mainstay treatment in the rejuvenation of the neck, HA fillers have been effective in the treatment of horizontal neck lines or ‘necklace’ lines.17,18 HA filler formulations with and without cross-linking have both shown good results.2,18 In a study of non-cross-linked HA, significantly improved horizontal neck lines (P = 0.000) were reported on follow-up visits up to 10 months in 25 patients who received two to three sessions of an HA compound filling plus mesotherapy when compared with one treatment of BoNT-A.2 Results were graded by blinded evaluators and levels of patient satisfaction were assessed.2 The authors conclude that the effect of the mesotherapy in addressing dryness and fine lines may be complementary to the efficacy of the filler.2 Analysis of a retrospective case series showed that treatment with a cross-linked, cohesive polydensified matrix HA filler with low elastic modulus, low viscous modulus and a high tan delta was also associated with improvement in wrinkle intensity in 64 lateral neck halves (from 32 women), as assessed by Horizontal Neck Wrinkle Severity Scale, from the second week onwards (1.352 ± 0.682, P<0.05).18
Further, diluted CaHa fillers are recommended as a treatment for skin laxity and skin quality without a volumising effect in areas, including the neck, where the skin is thin.4,19,20 Injections of CaHa fillers have shown efficacy in the neck when administered as a single therapy and in combination.21-23 CaHa fillers combined with microfocused ultrasound with visualisation (MFU-V) have been shown to reduce fine lines and improve the texture of the skin in two studies of 20 and 47 participants respectively.22,23 Diluted PLLA fillers have also demonstrated improvements to skin laxity and volume in the neck.24 A combination with microfocused ultrasound has been recommended based on

clinical practice.25 The administration of a multi-treatment approach to the rejuvenation of the neck using PCL filler with an HA filler and suspension sutures is suggested based on expert consensus.3 There is a need for further published studies in the use of CaHa, PLLA and PCL fillers alone and in combination with other treatment options in the neck.
HA fillers can also be injected more superficially when used as skin boosters in the neck, where the aim is to improve overall skin quality. Dehydration of the skin increases with age, but the injection of a small-particle HA filler in micro-aliquots in the neck in one small study (n=15) has been found to improve hydration levels.26,27 The recommended volume for the neck per injection of the skin boosting HA filler is the smallest injectable aliquot (0.05ml) with a total volume of 1ml, which should be injected into the deep dermis, targeting areas such as horizontal lines as needed.28 Stretching the skin of the neck while administering filler injections can help in identifying the depth of injection as well as reducing discomfort for the patient and minimising bruising.28 The most common adverse events associated with fillers post-injection are transient erythema, pruritus, ecchymosis and localised swelling.18,19
Deoxycholic acid, unlike other treatment options for the neck, is a lipolytic agent that addresses submental fat.5 Approved by the Food and Drug Administration (FDA) in the US in 2015, deoxycholic acid injection (ATX-101) has shown efficacy in significantly reducing submental fat deposits without increasing skin laxity in the area.29,30 Results of the randomised controlled studies showed a ≥1-point improvement in the Clinician-Reported Submental Fat Rating Scale in 62.3% of participants (n=122) receiving 2mg/cm2 of ATX-101 vs 34.5% (n=117) with placebo in the study by Ascher et al. and 65.3% (n=121) vs 23% (n=122) in the study by Rzany et al. (p<0.001 for both studies).29,30 The effects of the treatment are maintained more than five years without the need for maintenance treatments.31 Injections may be performed roughly every six weeks, but due to the fact that post-treatment swelling, erythema and bruising can cause repeated inflammation, they shouldn’t be performed more often than every four weeks.1,25 In most cases, adverse effects are mild and transient.31 Patients who are likely to benefit most from this
Figure 2: Extent of platysma muscleStretching the skin of the neck while administering filler injections can help in identifying the depth of injectionTrapezius Platysma Depressor anguli oris
treatment are those with a moderate to large amount of submental fat in the pre-platysmal layer, but with only moderate laxity of the submental skin.32 Injection into the fat of the pre-platysmal fat should be done with care to avoid nearby anatomic structures.32
The use of lasers to resurface the skin by removing epidermal and dermal layers has developed greatly over recent decades and now represents an effective and safe method for treating photoaged skin, dyschromia and facial rhytides.33 The advent of CO2 and erbium-doped yttrium aluminium garnet (Er:YAG) lasers has increased the practitioner’s control in targeting specific areas of skin and at different depths.33 Due to the thinness of the skin on the neck, it is suggested that fractionated (targeting a specific fraction of skin) may be preferable to non-fractionated (full-field) laser treatment in the neck and that it should go no deeper than the papillary layer of the dermis.1 This depth is indicated by pinpoint bleeding and a subtle yellowing in the colour of the skin.1 Laser resurfacing has been shown to be a low-risk procedure with possible adverse effects including scarring and dyspigmentation.33 Laser resurfacing is not recommended in patients with darker skin (Fitzpatrick skin types IV to VI), a history of keloidal scarring or prior radiation therapy.33
By emitting energy into the skin, laser resurfacing stimulates neocollagenesis, remodelling and skin tightness.33 A 2014 study with 20 participants of the long-term effects of treatment for the ageing neck with fractional CO2 lasering identified significant (p<0.0001)
improvements in skin laxity, jowling and horizontal neck lines after one month that were maintained after one year.7 Improved skin tightness also improved the appearance of fat tissue.7 Some studies of laser treatment in combination with MFU or HA fillers to address skin ageing in the neck are available and have demonstrated that combined treatment is able to address multiple signs of ageing.34-36 A retrospective analysis by Woodward and colleagues of 60 patients from three centres who had undergone treatment to the neck, for example, reported significant improvement in skin laxity and photodamage with combined ablative fractionated laser treatment with micro-focused ultrasound.34
As with other energy-based devices, radiofrequency (RF) uses thermal energy applied to the dermis to stimulate the generation of new collagen and elastin.37,38 Low fluence, multiple pass treatment is considered to be effective and safe.38,39 RF works in a different way to lasers, allowing epidermal protection while heating the dermal collagen to the optimal level.37 Monopolar and bipolar devices are available, the latter penetrating the skin less deeply, offering more control for the practitioner and less discomfort for patients.37
A study of hybrid bipolar RF in patients with neck and lower face laxity (n = 247) found a statistically significant improvement (P < 0.001) from pre- to post-treatment, and that larger effects were noted in the older patients (mean age 55.1 years).40 The modality is also effective in combination with other treatment modalities, with a significant improvement in a sagging neck shown in 158 patients who were given four sessions of treatment with RF and ultrasound hybrid device at each appointment.38
In RF microneedling, the application of microneedles to different depths of the skin at the same time as the release of RF energy stimulates the production of collagen and elastin. Administered alone or in combination with platelet-rich plasma, RF microneedling demonstrated in a 2022 study with 20 participants that significant improvement in dermal thickness and measurement of cervicomental angle was achieved with both treatment modalities.41
RF is considered to be most effective in patients with mild-to-moderate skin laxity and should not be used in individuals who have or have had a pacemaker or defibrillator, nor in those using oral isotretinoin, with keloids, or hypertrophic scarring.9
Intense pulsed light (IPL) is a non-laser, high-intensity light source that uses broad wavelengths to deliver pulses of light to the skin.42 IPL is effective in addressing age-related changes of the dermis.5 It has shown efficacy in disorders of pigmentation and telangiectasias, clearing more than 75% of telangiectasias and hyperpigmentation in a study of 135 participants with poikiloderma of Civatte.43 The thin skin of the neck requires IPL to be administered at lower settings than those used on the face in order to avoid adverse effects or slowing the healing process.5 IPL is reported to have a lower incidence of post-treatment hyperpigmentation in Fitzpatrick skin types IV to VI compared with laser treatment.44
Studies show the efficacy of IPL in combination with laser treatment in the face.45,46 In combination with ablative fractional laser treatment, for example, IPL showed significantly increased skin elasticity, reduced skin wrinkles and improved skin texture in
Given that there are many different factors in the ageing process, age-related changes to the neck may require multiple interventions in combination for optimal improvements
a population of 28 Chinese women with an average age of 51.4 years.45 However, further studies of IPL in combination with a range of other treatments for rejuvenating the neck are needed.
In some cases, the ageing neck may be successfully treated with one treatment option.1,10,47 However, given that there are many different factors in the ageing process, age-related changes to the neck may require multiple interventions in combination for optimal improvements.3,4,5 Indeed, many combination treatments in the ageing neck have been shown to be effective and well-tolerated with no increases in the incidence of adverse events.3,4,26,48 It is of note that, to date, the published literature of non-invasive treatments for the ageing neck is largely based on non-randomised control trials and case studies, and further research in this area of the body would be welcome.3,19,49
It has become possible to treat many signs of the ageing neck in a way which is more time-effective and less costly than surgery. The neck needs to be considered in relation to the face –rejuvenating one without the other can look uneven – yet the dermal thinness and the anatomical structure of the neck demand a specific treatment approach. More than one sign of ageing may be present and a combination of treatments may be required. It is an area of aesthetic practice that is developing quickly as technology becomes available and evidence is accrued for more treatment combinations. Non-surgical interventions are not suitable for all patients, and those with severe ageing are likely to require surgery, so practitioners should be doing appropriate assessments/patient selections.
Dr Ahmed El Houssieny is a trained anaesthetist with a passion for aesthetics. He is an honorary lecturer at the University of Chester and an education provider on cosmetic procedures. Dr El Houssieny is an associate member of the British College of Aesthetic Medicine. Qual: MBBCH


Dr Ahmed El Houssieny discusses non-surgical neck rejuvenation in this month’s CPD article. The article covers anatomy and the interplay of muscle and fat in the ageing neck. The neck is a challenging area to treat and often a common aesthetic concern, particularly now in the younger patient. The article covers non-surgical options such as botulinum toxin injections to the platysma muscle. There is a thorough discussion on the use of dermal fillers for rejuvenation, cross linked and non-crosslinked hyaluronic acid and the use of biostimulatory fillers. The use of deoxycholic acid to submental fat is briefly covered; this treatment will gain popularity over the next few years as techniques are refined. Finally, the article covers energy-based devices including the use of laser resurfacing, radiofrequency and intense pulsed light.
In clinical practice, a combination approach is required for optimal results and will vary according to the patient’s age and clinical findings. This article provides a foundation for further reading on non-surgical neck rejuvenation.
Answers: C,D,D,A,D









Blunt-tip reduces friction and glides through dermal tissue

Ultra-thin cannula wall increases lumen diameter and reduces injection forces
Premium quality single-use cannula used by clinical and industry leaders
Made in Britain for over 30 years

Firstly, we carried out a literature search using Medline. We inserted a variety of key words in combination, which included, ‘filler’, ‘lip’, ‘labial’, ‘compartment syndrome’ and ‘labial artery’. Our aim was to determine whether any classification system currently existed. We were also interested to ascertain whether CS had been considered and/or described as one of the specific pathological processes underlying the presentation of post-lip filler vascular compromise.
We also conducted a review of recent cases presented to our clinic in which the diagnosis of LVC was made following aesthetic injection with lip filler. We sought to classify the various presentation types in a simple clinical system. We also reviewed the recent literature on the management of CS to determine if there were areas of commonality which may contribute to the understanding and management of LVC and labial compartment syndrome (LCS), which we discuss later.
Post-filler LVC was reported in the literature, however, we found no current classification system. No comparisons of treatment modalities related to the potential underlying processes which may cause LVC were also found.
Labial vascular compromise (LVC) following lip filler injection is the subject of much discussion and anxiety amongst aesthetic clinicians. Most of the discussion centres on the avoidance and management of this complication, but little about the underlying pathogenesis and mechanisms.1 The aim of this paper is to expand the debate on this subject.

In considering LVC we have also examined the potential underlying process of compartment syndrome (CS). This is a well-recognised clinical phenomenon occurring when the pressure within a tissue compartment rises to exceed perfusion pressure.2 Therefore, it results in vascular compromise with tissue ischaemia and potential necrosis. The syndrome itself represents a spectrum of severity and can present in both acute and chronic forms.2
Whilst CS occurs in many anatomical areas of the body, the vascular compromise specifically seen following labial injection of filler has never been considered, or defined, as a form of this syndrome. In this article, we review the presentation of vascular compromise following lip filler and consider what anatomical, technical and pathogenic considerations may be contributory. In considering CS as a potential endpoint of swelling and inflammation within the aesthetic lip compartment/subunit, we also seek to consider what lessons may be learnt from the management of CS elsewhere in the body. This article represents a theoretical proposal regarding the underlying pathogenesis of LVC. Understanding the potential subtypes of LVC may help in directing treatment algorithms or be beneficial if treatment modalities were to be compared.
In terms of CS, this represents a spectrum of clinical presentations with a consistent underlying pathogenesis.2,3 Typically, CS occurs following trauma or bleeding. Whilst it affects the limbs in most cases, variants within the head and neck have been described, for example, the superior orbital fissure syndrome.4,5 The consistent anatomical elements can be considered as neurovascular anatomy that traverses and is contained within muscular compartments. Any cause of muscle swelling or increased pressure within the compartment may result in a rise in pressure which, if it exceeds the perfusion pressure, will result in vascular compromise and give rise to a predictable pattern of signs and symptoms.
The signs and symptoms of CS are traditionally described as being the ‘six Ps’. These are described as pain, pallor, pulselessness, paraesthesia, paralysis and perishing cold (poikilothermia). The lower limb is the most common site for this to occur and trauma is cited as the most common cause of acute CS. Chronic variants of CS are described, for instance, in relation to exercise. There are acute and chronic presentations of this condition. It does not seem that the definition of CS has been specifically used to define or describe any of the pathological processes underlying the vascular compromise seen in association with lip filler, although the diagnosis has been defined in the head and neck, most notably the orbit.4,5 In the case of vascular compromise following lip injections, the signs and symptoms are somewhat consistent with the above. Immediate pain and blanching of the tissues are commonly described by patients suffering this complication.
Mr Mark Devlin and Mr Jeff Downie outline a proposed classification system related to labial vascular compromise
The general effects of lip filler on the capillary vasculature have been reviewed and the impact on the capillary system have been suggested as critical.6 This effect on the microvasculature is in keeping with a more general issue with perfusion, rather than that of simple direct intravascular injection.
From our own clinical experience, LVC presents in either one of two ways. For clarity, we have considered these as either Type 1 or Type 2. These can be further subclassified and described as below described, as summarised in Table 1
Type 1 typically presents as soon as the injection begins. There is usually severe pain and immediate blanching of the skin and vermillion. Patients who have had treatments before will state that this was unlike any previous experience. Anecdotally, this may be more often seen in patients who are having a first treatment of this region. The following are the potential mechanisms for this presentation:
1. Intravascular injection – this would cause immediate vascular occlusion. The dimensions of the labial artery are such that this is not likely but does remain a possibility. There is evidence of this occurrence in the literature.
2. Intramural injection (mural damage) – this could occur in association with the above but could also occur without intravascular ingress of material. Arterial spasms would result as well as almost immediate mural and extramural swelling.
3. Extramural – in this case the vascular occlusion would be related to external pressure. This is perhaps most likely in the case of smaller diameter vessels or where there is an intramuscular course at the point of the injection, leading to an immediate compression of this ‘compartment’.
This type typically presents at some point beyond the initiation of the injection itself (hours or even days). It may be preceded by increasing pain, swelling and bruising. The signs and symptoms tend to be initially milder than those seen in Type 1. If these processes continue, then we postulate that a common end point may be LCS.
1. Haematoma formation – this could result from direct injury to the labial artery or a branch of this, which falls short of causing an immediate vascular compromise.
2. Oedema – any tissue damage may result in swelling post-treatment. If this is significant, in the lip, a CS may result within the aesthetic compartment.
3. Secondary infection – this could be either viral or bacterial. This is more likely in the presence of a relative vascular compromise and may worsen the symptoms.
Type 2 pathogenesis may result in a milder form of vascular occlusion. We would expect simple conservative management, with no active intervention, to result in a complete resolution. There would be a risk of sudden deterioration of this group resulting in signs and symptoms of a Type 1 presentation.
This type of variable presentation has been described previously and the role of hyaluronidase as a treatment modality reviewed for its efficacy.7 We have also considered the various independent factors that may influence the risk of either type of LVC. These factors include labial artery anatomy, volume of injection, depth of injection, speed of injection or concurrent pathology/infection, such as herpes simplex or staph aureus, all seem likely to contribute to the relative risk for any patient or treatment episode.
Labial artery anatomy has been the subject of considerable interest in literature. Studies have described these variations topographically and in cadavers, whilst others have used imaging (surface and cross-sectional) to describe the course of the arteries within the lip.8-11 The practical clinical question raised by these studies is whether these variations are contributory to the underlying risk of LVC or even subsequent LCS.
CS is most likely when the neurovascular structures are at risk to the effects of increased pressure within a relatively fixed compartment. The one variant of the labial artery that would seem to increase the theoretical risk of both Type 1 and Type 2 is LVC being the intramuscular variant. Where the artery lies in the loose areolar tissue deep (oral mucosal side) to the orbicularis oris muscle, the risk of LCS would theoretically be significantly lower, especially to Type 1. LVC could still develop in this situation if large volumes are injected or if significant post-treatment swelling were to occur. Bleeding and haematoma formation might also contribute to the development of LVC. In this sense, the depth of injection may have an influence in the development of LVC. The speed of injection may also be significant
Type 1 typically presents as soon as the injection begins. There is usually severe pain and immediate blanching of the skin and vermillion
in relation to trauma and subsequent tissue oedema, thus constituting a relative contributory factor. Any factor contributing to inflammation and swelling would also be seen as a risk factor for Type 2 LVC. These would include traumatic technique, infection and haemorrhage. It is clearly good practice to avoid filler injections in the presence of active infection, but there may be pathogens present without any obvious signs or symptoms. The delayed presentation may therefore be due to the reduction in perfusion pressure within a compartment of the facial anatomy. Given the various compartments of the face, it seems possible that a CS could develop. We also reviewed the published treatment algorithms, but only found the Aesthetic Complications Expert (ACE) Group World guidance.12 This provided a sensible approach to the management of LVC and potential lip necrosis. It has been developed from current published evidence, but does not seek to classify the underlying mechanism of VC. As we have considered the possibility of LCS being a common endpoint of untreated LVC of either main subtype, we sought lessons in relation to possible treatments of LVC and LCS from the general scientific literature. Whilst these lessons need careful consideration, it does seem clear that any treatment algorithm to manage LVC and potential lip necrosis should bear these in mind. To that end, we would think it appropriate to add corticosteroids, botulinum toxin-A and surgery to any future debate regarding the treatment of LVC.2,3
LVC can occur following injection of filler in the lip. The exact mechanism in each individual case is unknown, but there would appear to be a small, predictable number of these which we might define from first principles. The mechanism of injury is significant when considering treatment/management options, but no current classification exists.
In proposing this classification system, we hope that it may expand the debate regarding the management of LVC given the anxiety and morbidity caused. CS has not yet been proposed as an endpoint in cases of delayed onset LVC, and by doing so in this
article, we also seek to expand the debate regarding the true pathogenesis of LVC in this subset of patients. By considering this possible underlying process, we can extrapolate from the evidence-based treatment options of CS elsewhere in the body.
Mr Mark Devlin is a consultant cleft and maxillofacial surgeon. He is based at the Royal Hospital for Children on the Queen Elizabeth University Hospital campus in Glasgow. For many years he maintained a facial aesthetic surgical practice but now concentrates his non-NHS time to medicolegal work. Aside from his clinical work, he is involved in medical education and training for undergraduates and postgraduates.
Qual: FRCSEd(OMFS), FRCSEd(CSiG), FRCSRCPSG, FDSRCPS, FFSTEd, PGDipClinEd(RCPSG), MBChB, BDS, MEWI
Mr Jeff Downie is a consultant oral and maxillofacial surgeon who has a specialist interest in facial aesthetic and reconstructive surgery. He practises facial surgery in Glasgow and his NHS sub-speciality is facial deformity and post-traumatic facial reconstruction. In addition, he treats skin cancers, salivary gland disease and is trained in all aspects of hard and soft tissue oral-facial surgery.

Qual: FRCSEd(OMFS), FDSRCSEd, FDSRCSEng, FDSRCPS
1. Cohen JL, ‘Understanding, avoiding, and managing dermal filler complications’, Dermatol Surg, 2008.

2. Garner M, Taylor S, et al., ‘Compartment Syndrome: Diagnosis, Management, and Unique Concerns in the Twenty-First Century’, 2014.
3. Guo J, Yin Y, et al., ‘Acute compartment syndrome Cause, diagnosis, and new viewpoint’, 2019.
4. Colon M, El Khoury L, ‘Orbital compartment syndrome as the first manifestation of SLE’, Clinical Rheumatology, 2020.
5. Kansakar P, Sundar G, ‘Vision loss associated with orbital surgery - a major review’, Orbit, 2020.
6. Hirsch P, Infanger M, Kraus A, ‘A case of upper lip necrosis after cosmetic injection of hyaluronic acid soft-tissue filler-Does capillary infarction play a role in the development of vascular compromise, and what are the implications?’, Journal of Cosmetic Dermatology, 2020.
7. Ors S, ‘The Effect of Hyaluronidase on Depth of Necrosis in Hyaluronic Acid Filling-Related Skin Complications’, Aesthetic Plastic Surgery, 2020.
8. Pinar YA, Bilge O, Govsa F, ‘Anatomic study of the blood supply of the perioral region’, Clin Anat, 2005.
9. Cotofana S, Pretterklieber B, et al, ‘Distribution pattern of the superior and inferior labial arteries: impact for safe upper and lower lip augmentation procedures’, Plast Reconstrue Surg, 2017.
10. Phumyoo T, Tansatit T, Rachkeaw N, ‘The Soft Tissue Landmarks to Avoid Injury to the Facial Artery During Filler and Neurotoxin Injection at the Nasolabial Region’, J Craniofac Surg, 2014.
11. Lee S-H, Gil Y-C, et al., ‘Topographic Anatomy of the Superior Labial Artery for Dermal Filler Injection’, Plast Reconstr Surg, 2015.
12. King M, ‘Management of Necrosis’, J Clin Aesthet Dermatol, 2018.
Bleeding and haematoma formation might also contribute to the development of LVC. In this sense, the depth of injection may have an influence in the development of LVC
Catch up with friends and colleagues, get photographed at our press board and meet leading aesthetic professionals at the glamorous drinks reception

Recognise your achievements and celebrate the specialty’s successes at the UK’s most prestigious ceremony for medical aesthetics

Indulge in a delicious three-course meal in the dazzling Grosvenor House before the main ceremony gets underway

Believing every patient’s skin story is unique, Galderma embraces these differences by offering several premium brands to suit a patient’s individual needs through aesthetics. Known for its innovative and effective aesthetic solutions, Galderma provides its customers with the treatments, services, and education to help its clients achieve optimal results that enhance their skin and meet their individual needs.

With this in mind, Galderma will be taking a new, increasingly holistic approach towards aesthetics, following a methodology that helps patients discover how different treatments can work in conjunction, to garner individualised natural, balanced, and beautiful results. Their method teaches the use of AART™ – Assessment, Anatomy, Range and Treatment in order to deliver these ‘Holistic Individualised Treatments’ (HITs), that provide a simplified approach to facial aesthetic needs, based on cross-usage of products for different areas of concern.
Galderma will be begin showcasing its HITs approach at CCR this year, with roll out of content scheduled from 2023 onwards. Galderma will be launching this with two symposiums at CCR as part of its education programme. Firstly showcasing SHAPE UP – a methodology to lift the mid-face using the Restylane portfolio, as well as KISS & SMILE – a methodology to rejuvenate the lips and perioral region with the Restylane portfolio.
Galderma KOL and advanced trainer in aesthetics, Dr Priya Chadha says, “Using CCR as a launchpad, Galderma is introducing HITs to the aesthetics world, a holistic approach towards treatment for patients. Following a methodology that helps patients discover how treatments can work in conjunction to achieve natural and beautiful results. As a practitioner with many years of experience, I think this more universal approach is very beneficial to our patients and helps us meet our patients needs and deliver excellent, robust results.”

• Bright Eyes – Hyaluronic acid fillers Restylane Eyelight and Restylane Volyme from the Galderma portfolio, to treat the delicate eye area.
• Profile – Hyaluronic acid fillers from the Restylane range, including Restylane Lyft, Defyne, Volyme and Kysse for treating facial structure and proportions.

• Kiss & Smile – Hyaluronic acid fillers from the Restylane range including Restylane Kysse, Defyne and Refyne, combined with Skinboosters for dynamic treatment of lips and perioral area.
• Glow On – Combining Restylane Skinboosters and Sculptra to treat dull, dehydrated or ageing skin.

• Shape Up – For a non-surgical lifting effect, Shape Up combines the use of Restylane Volyme, Lyft and Defyne hyaluronic acid with collagen stimulation using Sculptra.
Dr Chadha continues, “The pace of aesthetics is picking up again and CCR is a fantastic time to catch up with my peers and discuss new innovations in the industry, which I can bring to my patients. I am also partnering in a live treatment demonstration with Galderma, focusing on how to use AART™ – Assessment, Anatomy, Range and Treatment – to deliver a Holistic Individualised Treatment (HIT) for each patient.”














Nurse prescriber Anna Baker provides an introductory overview of the treatment options for photodamage
Skin ageing is a complex multifactorial phenomenon with many intrinsic and extrinsic influences.1 Cutaneous changes can also be influenced by ethnic origin in light of underlying structural and functional differences.2 Intrinsic ageing reflects the genetic background of an individual and occurs progressively with time. Chronologically aged skin manifests thinning, fine lines, soft tissue descent and fat atrophy.3
Skin of colour demonstrates less severe intrinsic facial ageing, often with visible signs appearing approximately a decade later than lighter skin types.2 Consistent with other organs, the skin undergoes a gradual decline to the accumulation of molecular damage.4 During menopause, women may experience accelerated skin ageing due to declining oestrogen levels, which greatly influence the skin’s appearance.5 Flattening of the epidermal/dermal junction influences the structural integrity of the epidermis and can reduce nutrient flux between the epidermis and dermis which can negatively impact keratinocyte proliferation.6
Melanocyte number, as well as activity, are altered which triggers a cascade of pigmentary changes across different skin types.7 The dermis loses volume and density, alongside decreased collagen production and deranged organisation of the elastin content in the skin.8 Extrinsic skin ageing arises mainly from UV light exposure.9 Approximately 80% of facial skin ageing can
be attributed to UV exposure.10 The effects of UV radiation are based on light absorption in chromophores and the conversion of energy in chemical reactions.11 Cumulative UVA and UVB radiation contributes to potentially irreversible and detrimental effects, resulting in skin ageing and photocarcinogenesis.10 Short wave UVB is mainly absorbed in the epidermis, causing DNA damage by producing cyclobutene pyrimidine dimers (CPDs).12
Extrinsic ageing is also influenced by individual health status, amount of sun exposure, tobacco inhalation and diet.13 Cumulative sun exposure is one of the detrimental factors in ageing skin, and in skin types III-VI, dyspigmentation is one of the most common features of photoageing.14 Common clinical signs of photoageing include lentigines, rhytides, telangiectasias, dark spots and loss of elasticity.15 Skin of colour is less susceptible to sun-induced damage, and therefore these age-related changes are less severe and may occur 10-20 years later than Caucasian skin of a similar age.16 Mechanistically, photodamaged skin is affected by elevated matrix metalloproteinases (MMPs), which degrade collagen fibrils in the skin. In addition, there are significant alterations in collagen, characterised as damaged and disorganised fibrils with an accumulation of elastic material (solar elastosis).17

Taking time to explore and educate patients around the contributing factors is key to achieving the best outcomes, as well as maintaining and preventing future damage. Many modalities and approaches are described in the literature to counteract the different attributes of photodamage.18 It is increasingly acknowledged that a combined approach utilising a bespoke regimen can provide the best possible treatment outcomes but may be influenced by individual compliance. A prescribed regimen can be tailored to include the following key factors: the degree of photodamage, willingness to adopt/compromise with lifestyle choices (such as sun exposure or diet), anatomical area to be treated, frequency of attending clinic appointments and specified budget, as well as expected time frame to achieve desired results.19
The treatments that are briefly summarised are not intended to be exhaustive, but can be considered some of the more popular modalities, both as standalone and as combination approaches.
LED phototherapy provides an affordable and effective treatment option for all skin types, as well as a diverse range of skin conditions on the face and body.20 Near infrared (830 nm) and red (633 nm) provide a powerful antiageing combination which collectively energises cells to repair, regenerate, boost collagen and elastin production, promoting healthy skin and reducing signs of pigmentation.21 The mechanisms of action are based on the same principles as photosynthesis, known as photobiomodulation, which means that the light is absorbed by target cells to activate specific biological functions.22
A number of critical factors are key considerations with regard to achieving successful treatment outcomes with LED: principally, the correct wavelength, dose, energy and treatment time.20 LED provides an excellent standalone or combination treatment with any regimen to target signs of photodamage and overall antiageing.23
Mesotherapy is a type of injectable skin biorevitalisation treatment which combines linear (non-stabilised) hyaluronic acid (HA)







maximum versatility and effectiveness with clinically proven results

Discover the next generation of radiofrequency microneedling treatments
Radiofrequency microneedling is constantly growing in popularity within the aesthetic specialty, and there are continued advancements in its technology. With four radiofrequency modes, nine different needle configurations and customisable energy, the Potenza device is the world’s first radiofrequency microneedling (RFM) system that combines monopolar and bipolar RF at 1 or 2MHz frequencies in a single device. The four RF modes allow you to treat a larger variety of conditions both superficial and deep, producing clinically superior results for almost all ageing concerns.
The Potenza device combines the mechanical injuries created by its ultrafine needles with the radiofrequency dose delivered into the dermis where it will trigger a natural repair mechanism inducing the creation of both collagen and elastin. Both deep tissue and more superficial concerns can be targeted by adjusting the needle depth in .25mm increments. Potenza offers a greater variety of needle arrays to attach onto the handpiece, meaning that it is more customisable in treating a bigger variety of scars on the face and the body.
Potenza is a highly versatile treatment offering for all Fitzpatrick skin types for the face and the body. Sun exposure isn’t a limiting factor to this treatment in the way that laser therapy is, making it a more flexible option for patients of all skin types, all year round.
Improvement in the skin can be observed from the first or second treatment, however the patient may need three to five treatments dependent on the desired result. The treatment interval is four to six weeks apart to allow more time for healing.
The device is minimally invasive, so pinpoint bleeding is expected at the time of treatment and patients experience a sunburn sensation with some swelling. However, this typically resolves in 24-48 hours and mineral makeup can be worn from the next day to cover any residual redness.
Potenza’s Tiger tip is a semi-insulated needle array which allows delivery of the energy at two depths simultaneously. This means that fewer passes are needed, as two layers are treated in one pass, resulting in shorter treatment times.
Potenza also offers a unique tip designed to enhance topical penetration by up to 67%.1 The Fusion tip operates in monopolar at 1MHz for deep and wide RF delivery and enhanced tissue engagement and topical penetration, with 21 insulated needle arrays and an adjustable depth of 0.5-2.5mm.
Dr Kaywaan Khan, aesthetic practitioner and founder of Hannah London Medispa, commented, “Potenza is a cut above older technology. It provides practitioners with the ultimate freedom and flexibility as it has a unique propensity to customise the intensity and distribution of energy for different parts of the body or face. This means not only can multiple concerns be addressed, but there are also fewer passes needed – resulting in minimal downtime for the patient and maximum return on investment for the user.”

This article was funded by Cynosure
For more information on the device visit www.cynosureuk.com
REFERENCES
1. Cynosure, Potenza the new standard in RF microneedling, <https://www.cynosureaustralia.com/potenza-the-new-standardin-rf-microneedling/#:~:text=Cynosure%E2%80%99s%20 Potenza%20takes%20the%20world%E2%80%99s%20next%20 step%20towards,penetration%20up%20to%2067%25%20 with%20the%20Fusion%20Tip.>
The four RF modes allow you to treat a larger variety of conditions both superficial and deep


the upper eyelid area so she could look fresher, more awake and less downcast in aspect. This was to be a finishing touch to an aesthetic journey, which included a facelift, separate lip lift and upper blepharoplasty procedures performed by other practitioners. A previous brow lift had come down again, if only slightly.
On assessment, I could immediately see that she was a good candidate for InclinEyes, a customisable, filler-only treatment I designed to enhance the eyebrow apex and subtly scoop and reposition drooping brow tails so that eyes appear more open and youthful. I also believed that she would benefit from toxin injections to smooth out her crow’s feet. She had some hollowing medially and laterally of the temporal crest, which is typical with ageing. There was no obvious flatness above the apex of the brow; this was more prevalent on either side where the injections could be administered. I noted the slight volume deficit in her fat pads, indicating a lack of sufficient support for the skin below the brow rim. The quality of her skin was notably firm, smooth, hydrated and free of congestion or irregularities – all of which factor in a better result. She was particularly expressive in conversation and was in overall good health with no underlying issues to give concern.
Our eyes tell stories. But as we grow older, people can often become less comfortable with their message. In the outer areas, the appearance of excess skin, dark circles, puffiness, wrinkles or recesses are signs to others that we’re looking tired, aged and lacklustre; even though that’s not how we feel inside.
‘Tired-looking eyes’ is the single biggest frustration that drives patients through my doors for the first time. And, in approximately two-thirds of these cases, the most bothersome region is the lower lid. But for the remaining third – still a sizeable number – the issue impacting their self-image is the upper eyelids, sometimes in combination with the lower.
The treatments I administer here will usually address flattened brows, upper eyelid hollows, A-frame deformities, eyelid asymmetries or folds in the upper eyelid crease caused by volume depletion. Where surgical intervention is indicated – soft tissue laxity or ptosis causing skin to droop on to the lashes, for example – referral to an oculoplastic surgeon is typically appropriate.

Concavity in the upper orbit is often genetic – I treat many 25-35-yearolds with this – or a natural and anatomical response to ageing due to diminishing soft tissue density and bone resorption in older recipients.1
The aim in both groups is to restore visible symmetry, youthful plumpness and tauter skin to the periorbital area.
My patient was a 57-year-old woman bothered by the droop in her brows and the obvious darkness and hollowness above her eyes. She asked me to assess her suitability for non-surgically rejuvenating
In addition to reviewing her full medical history, I explained the effects of filler in the periorbital area, the products I would use, the injection sites and the technique. We also discussed potential risks, downtime and aftercare, which included avoiding alcohol and exercise for at least two days prior to, and following, the appointment. The treatments were to be administered in the clinic on the same day. A bonus was that her extensive research, in relation to my own upper eyelid work – and her history of facial surgeries – meant she was very well informed. She listened intently and asked good questions and I was satisfied that, by also physically demonstrating for her what could be achieved above the eye and at the tail of the brow – a repositioning as opposed to a lift – her expectations were realistic.
In situations where this isn’t quite so evident, for example, if the patient expects a significant vertical lifting of the entire brow area or a reduction in the laxity of the upper eyelid skin, I recommend the patient takes more time to consider their options – generally a couple of weeks – or I will explain why I might decline treating at all. I also make it clear that my team or I can be contacted via email, WhatsApp or phone with any questions or concerns in the days and weeks that follow treatment.
Informed consent was given and the patient was guided to the studio area where the clinical photographs were taken. I ensure I get images from the front, oblique and side views. This area of the clinic includes studio directional lighting, voice-controlled shutoff of the lights during pictures and an automatic roller blind to block the window, ensuring that weather and time of day don’t affect the light – all of which


helps ensure consistency in the clarity and angles of the pictures.
I positioned her at 45-degrees on the treatment bed; my preferred angle for working, giving me ample access, as well as being very comfortable for the patient. I work under high-lumen LED twin bar lights so I can see everything and never work in my own shadow. After removing her makeup, I began by disinfecting the relevant areas of the upper third using a 10cm square gauze dampened with Clinisept+ Prep & Procedure No anaesthetic was used because it’s a surprisingly painless treatment that can sometimes feel a little uncomfortable or unfamiliar at worst, and there’s also lidocaine in the dermal fillers used.
To increase the volume and improve the contour of the upper eyelid and the way it drapes in the superior sulcus, I chose Teoxane’s Teosyal RHA 1, a soft and fluid-consistency filler ideally suited for this delicate area. I administered 0.9ml of the product using a TSK STERiGLIDE 27 gauge 5cm cannula. I chose a cannula over a needle here as it will remain in the anatomical space and there’s no scope for accidental damage to the eyeball. It also limits the chance of other accidental bruising and injury. Despite some scarring in the area post-upper blepharoplasty, it wasn’t an issue. The cannula went in smoothly. Sometimes, an aggressive upper blepharoplasty can exaggerate hollowing, but that wasn’t the case here.
To gently restore the arches of her brows, I revolumised the fat pads to achieve a more open appearance. Then I repeated the process in the fat pads near the tail of the brow. The product was injected with a 30 gauge needle slowly and precisely in very small aliquots supraperiosteally, for which a needle is a superior instrument over a cannula in my opinion. This is because a needle will more easily pierce the different layers down to the bone. There was little variation on my usual InclinEyes technique, but I always customise according to the patient’s individual need. In this case, I treated the very anterior aspect of the temples right behind the orbital rim and inferior of the temporal crest. I selected Teoxane’s Teosyal RHA 3 and used 0.6ml overall. This product is more of a volumiser, yet is not too heavy and it integrates well.
Once the doses were in, I asked her to sit upright and look directly into my eyes. A steady horizontal gaze like this facilitates careful examination of how the eyelids are draping. I can also feel for any minor remaining volume shortfalls. I made some markings using a readily available white liquid eyeliner, with each dot indicating a point where extra volume was needed so that I could subtly adjust and further improve her result. I then treated those for an optimal outcome. I also lightly massaged the upper eyelid to help blend the filler into the area. The crow’s feet were then treated using botulinum toxin.
A good result was visible immediately and the patient was amazed by the improvement she got, commenting that it exceeded her expectations. As can be seen in Figure 1, the eyes appear brighter and now catch the light evenly along the periorbital rim thanks to that smoother and fuller curve, lending an altogether more youthful appearance.
A typical recovery from InclinEyes – likewise for upper eyelid fillers without the brow tail adjustment – is very straightforward. Patients can expect to experience some puffiness, particularly on day one after treatment, but it’s otherwise unproblematic if the aftercare advice is followed. This includes not applying any pressure to the area for a couple of weeks.


Bruising here is rare but if it does occur, it can be covered up easily. If bruising were to be more pronounced, it would present as a black eye. Filler in this area will take four-to-six weeks to fully integrate and settle. Usually, one treatment is enough and, depending on the individual, will last between 12 to 18 months. The longevity of the treatment will usually extend beyond this time following subsequent maintenance treatments. If a follow-up treatment is required, I don’t recommend adding further product in the upper eyelid area before six weeks so that the initial filler has fully integrated and settled.
It’s important in facial analysis not to neglect volume depletion in the upper eye – too often the upper eyelid and brow area is neglected. I’d argue that facial rejuvenation is never complete if a patient is left with hollow eyes, as sometimes we see after facelifts, for example. The treatments should be as safe as possible, both in relation to the techniques and instruments used, with results that look so natural the patient could be born with them. Using fillers adds an extra safety feature because they’re reversible.
Eyes are the very first thing we see when we look at someone and the first area to show signs of ageing because of the fine nature of the external skin. They’re vital for human connection and communication, and one of the most challenging areas to get right because there’s zero margin for error. For me, working in the eye area is the most professionally rewarding; the aesthetic impact and importance is unquestionable and, technically, it’s exacting to get right.
Dr Joshua Van der Aa is an injection-focused cosmetic practitioner specialising in rejuvenation of the periorbital area. He is a graduate of Leuven University’s medical school. Before opening his own clinic, Dr Joshua Harley Street Aesthetics, in 2020, he worked in several reputable clinics based in London and the Netherlands.
Qual: Master’s Degree in Medicine, Belgium
1. Bryan Mendelson and Chin-Ho Wong, 2012, Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation, <https://pubmed.ncbi.nlm.nih.gov/22580543/>
13 & 14 Oct
ExCeL London, UK
Dr Joshua Van der Aa will be speaking at CCR, giving a live demo on jawline sculpting in the Aesthetics Arena. Register for free on p.20.

HydraFacial is for everyone. It’s suitable for all skin types and addresses all skincare needs. The HydraFacial delivers immediate, noticeable results, with no downtime, that keep your customers returning regularly.
HydraFacial is your connection to millions of believers that know that beauty is more than a physical attribute – it’s a feeling. Our customers’ want to give their clients the best experience possible.


The HydraFacial Company helps them deliver it.
Consumers want to be pro-actively offered personalised solutions for skin health and provide them with education on their ideal, easy-to-follow skin health regimen1.
And your clients needs are as individual as they are, which is why HydraFacial has partnered with the best brands in aesthetics to bring you advanced booster options that meet the emerging consumer trends that are influencing our industry more than ever before.
HydraFacial is scored as a ‘99% Worth It’ rating by www.realself.com and on average, somewhere in the world, a HydraFacial treatment is now carried out every 10 seconds!
1 EddieWouldGrow Facial Research 2018, n=2000; 2 Mintel Trends 2017



Only HydraFacial uses a unique, patented Vortex-Fusion delivery system to exfoliate, extract and hydrate skin. The spiral design of HydroPeel® Tips, used in conjunction with the HydraFacial proprietary vacuum technology and serums, creates a vortex effect to easily dislodge and remove impurities while simultaneously delivering hydrating skin solutions.
• Convenient, single use, saves time; eliminates the need for sterilisation equipment • Range of exfoliation levels allows for custom treatment results • Spiral design delivers painless extractions


Expand into a new category with HydraFacial Keravive scalp heath treatment that leads to fuller looking hair. HydraFacial Keravive is a first of its kind 3-step treatment that includes an in-clinic component, as well as a 30-day take-home spray.

Dr Raquel Amado details the anatomical structure of the deep fat pads in the mid-face
When addressing rejuvenation volume replacement, the mid-face is an important area to focus on. Despite it being an area of the face which is frequently discussed and educated on, I still find when delivering training to new or even more experienced practitioners alike, there remains a lot of confusion.
The mid-face is composed of five layers. The order of the layers is skin, subcutaneous fat, superficial musculoaponeurotic layer (SMAS), deep fat and spaces and the deep fascia/ periosteum.1 However, for the purpose of this article, I will be exploring the anatomy of the deep fat pads in the mid-face.
As the deep fat compartments have been shown to be relatively stable during ageing (they are not displaced inferiorly onto the bone), deep soft filler implantation in these compartments and in contact with the bone will provide support for the overlying structures and increase anterior projection.2
There are five deep fat compartments: lateral sub-orbicularis oculi fat (LSOOF), medial sub-orbicularis oculi fat (MSOOF), deep lateral cheek (DLCF), deep medial cheek (DMCF) and deep nasolabial fat (Figure 1). These fat pads adhere to the bone and provide support to the overlying soft tissue. The SMAS and superficial fat have an important role on the facial topography.2 In his cadaveric studies, plastic surgeon Dr Fabio Ingallina found that the MSOOF is a triangular fat compartment extending from the lateral canthal line onto the maxillary bone. It is separated from the lateral SOOF by a vertical septum, and from the inferior eyelid’s pre-septal space by the orbicularis retaining ligament (ORL). Inferiorly, the MSOOF also connects with the medial zygomatic cutaneous ligament (ZCL).2
The LSOOF lies laterally to the vertical septum and covers the prominence of the zygomatic bone. The lateral ZCL and the DLCF pad constitute its inferior border.2 The DMCF lies underneath the superficial medial cheek fat and the SMAS. It is triangular-shaped and directly overlies the maxillary bone.2
As we age, we see atrophy of these compartments, however they will still maintain their position, therefore we will witness a decrease in the cheek volume but not a descent of the upper cheeks. Subsequently, injecting soft filler deep into these fat compartments will give the projection required to rejuvenate the area.3,4

Without understanding and respecting the ageing face, we cannot predict our outcome and the safety of the procedure.
An article by Cotofana et al. explains how soft-tissue filler injections can result in different skin surface effects depending on the targeted facial fat compartment.5 It revealed that the SOOF compartment had the highest correlation coefficient and the highest surface-volume coefficient. In practical terms, this means that by using the lowest volume of soft filler, the most correction can be achieved. Therefore, practitioners have the anatomical knowledge to prioritise where they are going to place the filler to bring their patients the best aesthetic outcome.
Surmising from this study, we understand that the first deep fat pad that we should target to get the best outcome on a mid-face rejuvenation is the SOOF.5 However, we also need to consider that should the patient present with infraorbital hypertrophy, malar mounds, festoons or any kind of lymphatic compromise in this area, caution needs to be taken in order to not exacerbate and potentially compromise this area further. We also need to consider where in the SOOF we are going to place our soft filler. The SOOF is divided into two compartments (superior and inferior) by the malar septum.1 If we inject the soft filler into the superior SOOF compartment, the injected filler could possibly compromise the lymphatics by blocking them and inhibiting drainage. The other consideration that must be factored in is that due to the hydrophilic qualities of the HA filler, the lymphatic drainage system in this area could become overwhelmed, resulting in inactive lymph drainage and oedema. If this happens, then practitioners should avoiding treating the patient.
Each patient’s anatomy is slightly different in position and therefore there are no safe zones. Treating each patient as an individual and having a deeper knowledge of the anatomy is key. When treating the deep fat pad compartments, the main vasculatures that we need to be aware of are the infraorbital foramen (IFO), facial artery and facial vein. Dentists will be aware that the IFO location correlates with the second premolar on a vertical axis, however if this
tooth is missing or if you are not a dentist, this is probably not the easiest way of finding your IFO.6 According to a study, we know that the average distance between the IFO and the infraorbital rim is 10mm and 26mm from IFO to the lateral orbital rim.6
The facial artery supplies the lower anterior part of the cheek and there are a staggering 50 different variations of the facial artery.7 A study from Hong et al. demonstrates this rather articulately. So, when it comes to injection vasculature it’s more favourable to rely on depth rather than distribution. In the mid-face we know if the facial artery is present, it runs superficially in layer two.7
The facial vein is often located underneath the zygomaticus major and minor muscle, along the mid-cheek groove. This divides into the deep medial and lateral cheek fat pad, therefore we shouldn’t inject directly into the groove.8 As the harmonious veins accompany the arteries, we can conclude that the facial artery is likely to be in this area too.2,9
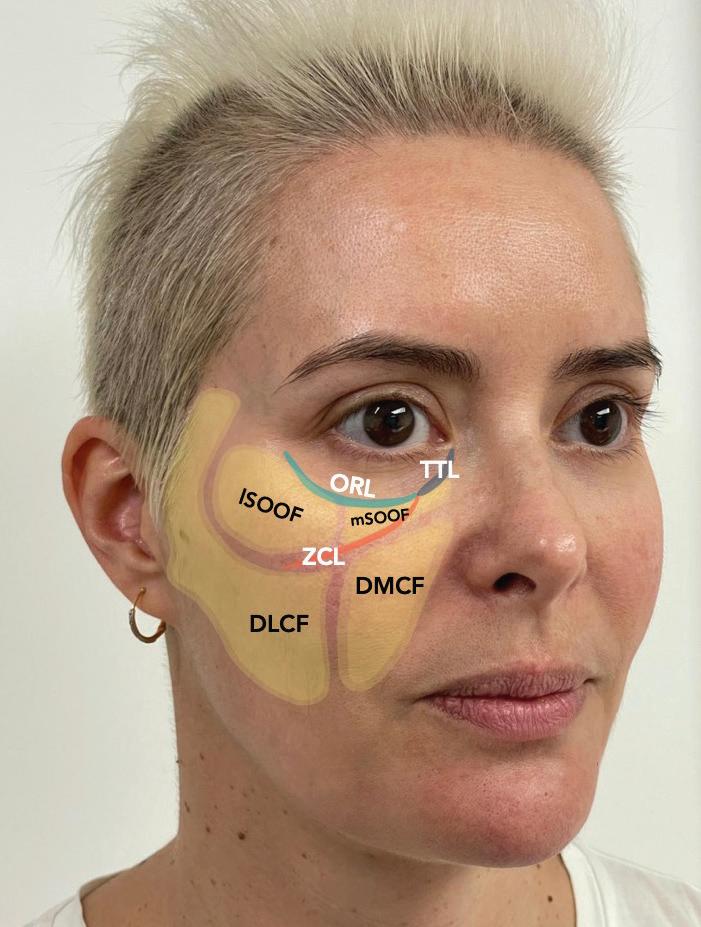
When it comes to injection techniques, this will depend on the injector’s experience and preference. You can find multiple techniques to treat this area. Therefore, the technique used will be dependent on the practitioner’s experience, patient presentation and the product selection.
Cannulas tend to be more comfortable for the patient and have less risk of complications, as they are less likely to penetrate the arterial
wall.10 However, they are more technique sensitive due to being longer and more flexible than needles.11
Needles offer more precision than cannulas as they are sharper; however, they can be more traumatic to the tissues and carry a higher risk of vascular compromise.10 My preferred way to inject the deep fat pads is by using a needle as opposed to a cannula because of the challenge of the accuracy in the SOOF, which is due to the presence of the malar septum, as explained above. Despite this, some practitioners may prefer to use cannulas in their technique.
When selecting products for this area, I focus on cohesive and viscoelastic products. Products I recommend are Neauvia Intense LV, Teosyal RHA 4 or Ultra Deep, but there are many other suitable reputable brands available. In my experience, these products are going to offer the projection required to lift the three layers above, but also allow patients to look natural in both static and dynamic movement as well as resist deformation.
It’s important to take into consideration the gender and ethnicity of your patients. When we know that female patients wish to achieve more anterior projection than males, and therefore care must be taken not to over feminise a masculine face.9 Consideration also needs to be taken in relation to a patient’s ethnicity and their features. For example, Asian faces are naturally flatter.12 This is why the consultation is important to determine what patients are after and manage their expectations.
It is vital to discuss all these considerations during the consultation and explain to the patient how the treatment will affect the outcome. You must respect heritage features and consult carefully, being sure to listen to what patients are seeking to achieve. Conversely, there are instances where patients are seeking treatments to enhance features and create a ‘westernised appearance’. The resounding message here is that consultation is the key before any treatment plan is carried out.
Age is also an important factor. Replacing volume in the deep fat compartments and on bone is where I begin my mid-face rejuvenation. You will generally find that in younger patients, replacing the deep fat compartments is often enough to create a
good clinical outcome. However, in cases of severe volume deficit, usually in older patients or patients that have had significant weight loss, additional treatment would be recommended. Often, a multi-layered technique is used to address the superficial fat pads to optimise the clinical outcome, however this is outside the remit of this article.
In summary, having an in-depth knowledge and understanding around the anatomy will make your treatments safer and more predictable. There are constantly new updates and studies being performed in this area. To be a progressive practitioner it’s crucial that we are aware of new findings. Registering with academic resources, undertaking cadaveric courses or attending aesthetic conferences such as ACE and CCR are all ways you can do this.
Dr Raquel Amado has 21 years’ experience as a practising dentist, is a Level 7 qualified aesthetic injector and clinical trainer. She runs a successful clinic in Kent and has a passion for anatomy and full-face rejuvenation. Recently, Dr Amado was shortlisted as a Finalist at the 2022 Aesthetics Awards in the ‘Rising Star’ category. Qual: LMD, PGC (sedation and pain management), PGC cosmetic dentistry, Level 7 Harley Academy

1. Walker L, Cetto C, ‘Facial ageing and injection anatomy’, 2021, p.1
2. Ingallina F, ‘Facial Anatomy and Volumizing Injections: Superior & Middle Third’ 2017, p.21-31.
3. Cotofana S, Gotkin R, et al., ‘The Functional Anatomy of the Deep Facial Fat Compartments: A Detailed Imaging-Based Investigation’, Plast Reconstr Surg, 2019.
4. Wen L, Wang J, et al., ‘Progress of mid-facial fat compartments and related clinical applications’, Chinese journal of reparative and reconstructive surgery, 2008.
5. Cotofana S, Koban K, et al., ‘The Surface-Volume Coefficient of the Superficial and Deep Facial Fat Compartments: A Cadaveric Three-Dimensional Volumetric Analysis’, Aesthetic Plast Surg, 2019.
6. Raschke R, Hazani R, Yaremchuk M, ‘Identifying a safe zone for midface augmentation using anatomic landmarks for the infraorbital foramen’, Aesthet Surg J, 2013.
7. Hong S, Park S, et al., ‘Variant facial artery anatomy revisited’, 2020.
8. Bagci B,’ A New Approach in the Correction of the Mid-cheek Groove: The Liquid Malar-lift Technique’, Plast Reconstr Surg Glob Open, 2020.
9. Von Arx T, Tamura K, et al., ‘The face – a vascular perspective. A literature review’, Swiss Dent J, 2018.
10. Pavicic, T, Webb K, et al., ‘Arterial Wall Penetration Forces in Needles versus Cannulas’, Plastic and Reconstructive Surgery 2019, p.504-512.
11. Mehta M, ‘Using Cannulas’, Aesthetics journal, 2022, <https:// aestheticsjournal.com/feature/using-cannulas>
12. Woffles TLW, Liew S, et al., ‘Consensus on Current Injectable Treatment Strategies in the Asian Face’, Aesthetic Plast Surg 2016.
The Stellar M22™ Photofabulous™ treatment is a complete skin rejuvenation solution that empowers physicians to offer remarkable results to their patients.

By combining both IPL and ResurFX™ technologies in the same treatment session, both skin pigmentation and texture can be treated at the same time.
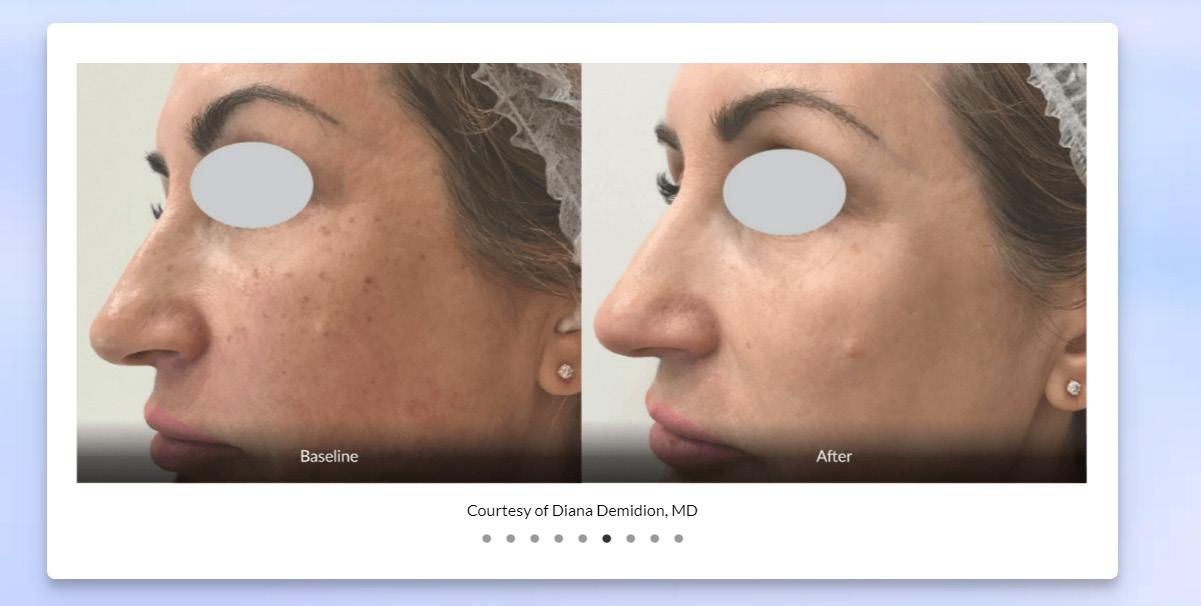

Leading Aesthetic Practitioner, Dr. Marwa Ali, of The Harrods Wellness Clinic, says:

“My patients love the Lumenis PhotoFabulous™ treatment, and are always more confident after their sessions.
There is no better option for non-invasive brightening and evening of skin tone. The results that we have seen are incredible and completely bespoke to each patient’s needs, skin type and lifestyle. A superb investment for our clinic that is already showing a healthy ROI.”
Lumenis.co.uk
To find out more, scan this code.
Before Before After After Courtesy of Diana Demidion, MD Courtesy of Matthew Knight, MD


Join Dr. Uche for a live Kysense® tear trough demonstration on the CCR innovation stage 13th October 10:30am. The premium high quality CE marked intelligent HA dermal filler harnesses advanced patented technology that leads to improvements in injection precision, tissue projection and patient satisfaction.

To discuss buying and training options email: info@circaskin.co.uk

Aesthetic nurse prescriber Lucy Williams explores the use of subcision for treating acne scars
The issue of acne scarring is one of the most common cosmetic concerns and can cause psychological distress, with post-acne scarring affecting up to 95% of patients with acne vulgaris.1,2 Acne scarring can prompt embarrassment, low self-esteem and even depression, as well as cause patients to feel socially isolated, therefore leading to a reduction in patients’ quality of life.3 Since the 1970s, a number of treatments have been used effectively for improving acne scarring such as microneedling, chemical peels and prescription medications.4 However, there is yet to be a treatment that works effectively across the board for all patients. At the time of writing this article, I was treating a patient for deep acne scarring using chemical peels and wanted to know what other treatment options were available as, although we were getting some minor improvement in her acne scarring with the chemical peels, they remained visible and very deep. Here, I will look into the evidence surrounding subcision as an effective treatment for acne scarring.
Acne scars are skin lesions that develop as a result of the healing of wounds after skin inflammation from acne. Scars consist of fibrous connective tissue, hair follicles, nerve endings and sebaceous glands. Acne scarring can range in appearance from indents, raised areas and pigmentation.5 Acne scars occur because the skin creates collagen to help heal the wound, but the body can go into overdrive, producing too much collagen to create new healthy tissue. If the body makes too much collagen too quickly, scars can form.6
Acne scars can be divided into two categories: hypertrophic or atrophic. Hypertrophic scars form above the skin – these scars appear as raised lesions and are a result of the overgrowth of fibrous tissue in the region where the acne lesion had developed. Atrophic type scars occur during the healing process when the skin loses its underlying support and develops fibrous bands of tissue between the skin and subcutaneous layer, which pull on the epidermis and causes scars such as rolling, ice pick and boxcar scars (Figure 1).7

Several treatment options have been utilised to improve acne scarring over the years, such as lasers, steroid injections, chemical peels, fillers, microneedling and subcision. Although subcision has been used for a number of years, with some research trials dating back to 1995, there was not a lot of supporting literature available until much more recently. Within the aesthetics specialty, it does not seem to be a common treatment option used for acne scarring. This may be due to people not knowing much about subcision as a potential treatment.
Subcision can be used to treat a variety of skin conditions including atrophic acne scars, depressed scars, wrinkles and cellulite.8
Subcision works by using a needle or cannula to break up and detach the fibrous strands that bind down the scar. By doing this, these strands get replaced with normal connective tissue. Releasing the fibrous tissue helps raise the scar, consequently helping to reduce its appearance.9
There are a number of studies that I will discuss below which show that subcision can be an efficient treatment for atrophic acne scars, particularly rolling type scars.10
There have been a lot of studies looking at the safety and efficacy of subcision for acne scarring, with a recent 2021 review article analysing more than 40 articles on subcision, with 21 being about subcision in the treatment of acne scarring and other scars. The article concluded that based on the evidence, subcision seems to be an effective treatment for acne and depressed scars. The article explained that as well as subcision being effective, it’s easy to apply, inexpensive and has a short downtime along with no significant complications.11
Subcision can be applied via a cannula or needle method. A study looked at more than 100 patients with rolling acne scars who were randomised into a standard technique of a 18 gauge cannula vs a 27 gauge needle. The outcomes of these procedures were assessed by three blinded dermatologists and by patients’ satisfaction. The results showed that subcision using the cannula showed good to very good improvement in 83% of patients with almost no side effects being observed compared to needle subcision. Overall, the authors concluded that cannula subcision appears to be a safe and practical technique that can enhance the efficacy of subcision without considerable complications.12
Another study evaluating at whether subcision is an effective method for treating acne scars looked at eight patients who suffered from mild to severe rolling acne scars. The patients underwent subcision via cannula and were followed up for three months. The outcomes were assessed by three dermatologists (blind) after two sessions of treatment. The patients’ satisfaction was considered to compare with dermatologists’ opinions. According to the dermatologists, they saw 88% improvement and 100% of patients said they believed they

had good or very good improvement. The study also used photographic data which showed 100% improvement in scar depth and the appearance of acne scars. The conclusion showed subcision with cannula is highly effective, with high satisfaction in patients. We observed an interesting cure rate (more than 50% after two sessions).13
This demonstrates it to be a safe procedure because it was performed by single perforation in each side instead of multiple perforations, helping to reduce the patients’ pain and risk of scars. Although the evidence in this trial was deemed to be good, it should be noted this was a very small trial and cannot be considered a comprehensive representation.13

As well as there being an array of research studies for acne subcision, there are several articles that state that combining treatments with subcision can give better results than subcision alone. It has been stated that hyaluronic acid filler (HA) along with subcision can also be used to treat acne scarring.
A recent 2022 split-face, blind, randomised placebo-controlled clinical trial investigated the efficacy and safety of a hyaluronic acid filler for atrophic facial scars. A total of 15 subjects were enrolled and randomised to receive either 1ml of HA acid or 1ml of saline via cannula to their cheek. The subjects were graded using the quantitative Global Scarring Grading System (QGSGS). The results showed that there was a significant reduction on the QGSGS at 90 days compared to saline alone, as well as an increase in the improvement of rolling box scars with filler combined to saline alone.14
Ebrahim et al. conducted a study to evaluate the efficacy of subcision alone versus its combination with cross-linked HA or poly-L-lactic acid threads in atrophic post-acne scars. The study consisted of 40 women and men, and all participants had
three sessions at four weekly intervals. The results showed that subcision combined with HA or threads gave a better clinical improvement than subcision alone.15 Deshmukh et al. used platelet-rich plasma (PRP) with the subcision method in their 40-person split face study. A total of 40 patients completed the split-face study. The right side of the face was treated with autologous PRP injected right after subcision, and the left side was the control side where only subcision was performed. After treatment, the right side showed better improvement in post-acne scars than subcision alone. This treatment performed better for rolling scars than for box scars. It indicates that synergic treatments are better for treating scars.16
A case series looked at 10 patients with moderate to severe acne scarring. The patients received three sequential subcision and microneedling treatments over a period of three months with an interval of four weeks between each session. The qualitative and quantitative acne scar grading system and photographs were used for assessment. The results showed that out of seven of the patients with grade 4 scars, 29% showed improvement by 2 grades and 71% showed improvement by 1 grade, while the other three patients with grade 3 scars showed improvement by 1 grade. Overall, 30% of patients had minimal improvement, 50% had moderate improvement and 20% had good improvement in scars.17
Subcision is classed as a minor surgical procedure.9 Therefore, as with any surgical procedure, patient selection along with safety should be a priority. Subcision should not be used in patients with a history of keloid who are on isotretinoin or who have an active infection.18,19
After a subcision treatment, patients should be able to resume normal activities but may have swelling and bruising. To reduce these
effects, practitioners should recommend applying ice to the treatment area following the treatment or may also prescribe antibiotics and anti-inflammatory drugs.18,19
Whilst there seems to be an array of literature confirming that subcision is a safe and effective treatment for acne scarring, there may be more effective methods that work alongside subcision rather than using it as a stand-alone treatment. Research has shown that cannula rather than needle is more effective and that combining already widely used treatments with subcision is more effective than subcision alone, however, there need to be more large-scale research trials to confirm what treatment is the most effective method for addressing acne scarring alongside subcision.
Lucy Williams is the founder and director of Aurielle Aesthetics in Wiltshire. She has more than 12 years’ experience as a nurse and five years’ experience as an aesthetic injector. Williams is registered with the ACE Group World and Save Face and has extensive training and expertise within aesthetics.
Qual: INP, RGN, DIP Nursing
 Figure 1: Types of acne scars
Figure 1: Types of acne scars












Cosmetic dentist Dr Thuha Jabbar provides a non-surgical rhinoplasty case study using Stylage® XXL

The non-surgical rhinoplasty is one of the most requested procedures in my practice. The increase in patient knowledge and awareness of non-surgical procedures, coupled with the advancement of dermal filler rheology and injection techniques, has led to a significant shift from surgical to non-surgical procedures. Having performed more than 1,000 non-surgical rhinoplasties, from simple cases to those that are more complex or even post-surgical, I have not only advanced my techniques, but have also witnessed the lifespan of the non-surgical rhinoplasty. I will be sharing a case study below.
A 21-year-old female presented in 2019, unhappy with the side profile of her nose. She had no history of previous non-surgical aesthetic procedures and no relevant medical history. She wanted the ‘bump’ softened, the nose to appear straighter and the tip to stop drooping, particularly when she smiled. The profile of the nose can be significantly enhanced using the non-surgical rhinoplasty, with very few exceptions. It is important to thoroughly assess numerous key anatomical features, such as the depth of the radix, the location of the dorsal hump and its relation to the glabella and the degree of nasal tip drooping on expression, to name a few. In this case, the patient presented with a very deep radix, a large dorsal hump, a flat and drooping nasal tip, little columella shows and an acute nasolabial angle.


The nose is not an area that needs ‘filling’ but rather requires a high-density dermal filler, which can support the areas to be augmented without requiring large volumes. Therefore, Stylage® XXL has been my product of choice for many years for this highly complex area of the face. The patented IPN-like technology of the product has created unique viscoelastic properties which allow it to
create excellent projection with minimal volume injected Clinically, this is very important. When augmenting a deep radix, care has to be taken to avoid widening the nose and thus creating the undesired and unnatural ‘avatar’ look. The same principles apply when lifting the nasal tip; good projection and elevation with as little volume as possible to avoid widening the tip. Again, this is achieved with ease using Stylage® XXL and in this case, despite its complexity, a total of 0.9ml was used.
Given the need for precise product placement in the nose, I used a 30-gauge needle at four main anatomical points, in varying depths relative to the anatomy. I injected slowly and inserted small micro boluses of filler, until the desired, pre-planned shape was achieved. I always start at the radix, followed by the anterior nasal spine and columella, middle crus, supratip lobule and upper lateral cartilages. Starting with the radix allows me to correct the dorsal hump. This is also the least uncomfortable area for the patient so a good place to start.
The purpose of injecting the anterior nasal spine is to create additional support at the base of the nose, which in turn will do two things. Firstly, it will project the columella, thus enhancing the columella show and, secondly, it will also lift and support the tip, preventing it from drooping on expression. This is achieved by an element of myomodulation of the depressor septi muscle, eliminating the need for botulinum toxin. Augmenting the middle crus allows you to alter the shape and position of the nasal tip. Raising the tip higher contributes to the appearance of a shorter nasal bridge and sharpens the tip, contributing to a nose that appears slimmer and softer. Finally, to treat the lower portion of the nose and to soften any irregularities/asymmetries, I placed small linear threads along the cartilage plates.
The patient returned after 18 months to have the treatment repeated. It is very interesting to see that despite the duration, the nose had not returned to its original form and had indeed retained some of the non-surgical augmentations. This is the case in all the noses I re-treat. My approach for the re-treatment is identical to the initial approach and what I often find is that even less product is required, and the results are usually even better as you are starting with essentially a simpler nose. In this case, on the second visit, only 0.5ml of Stylage® XXL was used.
The non-surgical rhinoplasty, in my opinion, is by far the most rewarding and life-enhancing area of the face to treat. Given the ability to create surgical results, with little downtime and the option of reversibility, the procedure will continue to be in high demand. It is important for practitioners to equip themselves with the ability to correctly assess treatment plans and execute this delicate procedure to the highest of standards, utilising premium products that will allow practitioners to achieve excellence.
Title: Patient Satisfaction and Clinical Effects of Platelet-Rich Plasma on Pattern Hair Loss in Male and Female Patients
Authors: Hetz S P, Martin J, Pototschnig H
Published: Cureus Journal of Medical Science, September 2022
Keywords: Hair Loss, Patient Satisfaction, Platelet-Rich Plasma
Abstract: Hair loss is a widespread condition in both genders. Over the past decade, platelet-rich plasma (PRP) has become a common treatment for hair loss. Our goal was to analyse patient satisfaction and the clinical effects of PRP on male and female pattern hair loss. Over a period of 12 months, we treated a total of 56 patients for androgenetic alopecia with a varying number of PRP injections. Follow-ups were conducted one month after the last treatment. A self-drawn questionnaire was used to assess the satisfaction and clinical results from the patient’s and clinician’s perspectives. The average age was 41 years (20-68 years). 57% of all patients were male and 43% female. In total, the patients were satisfied with the treatment results. The average score was 7.29 on a scale from 0 to 10. The clinician’s rating was similar (6.46). Moreover, with an average score of 8 on a scale from 0 to 10, it is very likely that the patients will recommend PRP treatments to friends. Our study revealed encouraging results for the treatment of male and female pattern hair loss with PRP. The autologous treatment was rated with high satisfaction scores and can be considered a safe and effective treatment modality.
Title: Clinical Evaluation of Anti-Ageing Effects of Combined Therapy – Azelaic Acid, Phytic Acid and Vitamin C Applied Layer by Layer in Females with Fitzpatrick Skin Types II and III
Authors: Markiewicz-Tomczyk A, Budzisz E, Erkiert-Polguj A
Published: Journal of Cosmetic Dermatology, September 2022 Keywords: Anti-Ageing, Combination Therapy, Skin Ageing Abstract: Vitamins C, E, A and substances of plant origin, including azelaic acid and phytic acid, are frequently used in cosmetic preparations to counteract oxidative stress and negative effects of free radicals. The aim of the study was to evaluate a novel combined therapy consisting of azelaic acid, ascorbic acid and phytic acid. 20 study participants received a series of eight treatments performed every seven days. 20% azelaic acid and then 30% phytic acid were applied to the entire face, with 40% l-ascorbic acid only on the left side. Skin parameters were measured before the series of treatments, after the series of eight treatments and one month after treatment ended. The combination resulted in a significant improvement in erythema and hyperpigmentation both on the forehead and cheeks; most pronounced effects were observed when all three active compounds were used. All the participants were satisfied with the effects of the treatment. A majority of them reported an improvement in skin hydration, firmness and elasticity, more uniform skin tone and a reduction of skin redness and wrinkles. Topical application of these active compounds resulted in improvement of skin elasticity and flexibility, reduction of wrinkles, hyperpigmentation, erythema and telangiectasia, as well as amelioration of skin tone.
Title: Aesthetic Evaluation of Breast Reconstruction with Autologous Fat Transfer vs. Implants
Authors: Wederfoort J L M, et al.
Published: Aesthetic Plastic Surgery, September 2022
Keywords: Breast Reconstruction, Fat Transfer, Implant Abstract: Autologous fat transfer (AFT) seems to be a new minimally invasive method for total breast reconstruction, yet, how patients, surgeons and laymen evaluate cosmesis is lacking. The aim of this study was to evaluate the aesthetic outcome of AFT (intervention group) for total breast reconstruction post-mastectomy, as compared to implant-based reconstruction (IBR) (control group). A random and blinded 3D photographic aesthetic outcome study was performed on a selection of 50 patients, scored by three panels: plastic surgeons, breast cancer patients and laymen. Secondary outcomes included agreement within groups and possible patient characteristics influencing scoring. Breast cancer patients and plastic surgeons did not differ in the aesthetic scores between the treatment groups. In contrast, the laymen group scored AFT patients lower than IBR patients (- 1.04, p < 0.001). Remarkably, mean given scores were low for all groups and overall agreement within groups was poor (ICC < 0.50). Higher scores were given when subjects underwent a bilateral reconstruction and if a mamilla was present. Evaluation of aesthetic outcomes varies greatly. Hence, aesthetic outcome remains a very personal measure and this emphasises the importance of thorough patient counselling, including information on achievable aesthetic results, before starting a reconstructive procedure.
Title: Treating Sunken Upper Eyelid with Hyaluronic Acid: Recommendations and Results
Authors: Spada J
Published: Journal of Drugs in Dermatology, September 2022
Keywords: Dermal Filler, Eyelid, Hyaluronic Acid
Abstract: Supraorbital hollowness is a feature that gives an aged aspect to the eyelids. This complex anatomic area is affected by different variables. Treating this area with dermal fillers poses a real challenge in terms of reducing risks and predicting natural results. We aimed to report outcomes observed in patients treated with injections of hyaluronic acid (HA) soft tissue fillers. Additionally, we have reviewed sunken upper eyelid (SUE) anatomy, aetiology and pathophysiology with the objectives of describing a new classification of SUE, showing a lower risk technique to fill the area, and explaining the importance of using a high cohesivity HA product. We included 32 adults without previous fillers in the area, who were injected with HA via a 25-gauge, 40 mm blunt cannula across two/three visits. The assessment was performed at day 0, day 14, day 30, and day 365. All patients showed natural results without significant edema on day 30. Only one patient required hyaluronidase injections to dissolve overcorrection of the area on day 14. No severe complications were observed. For most patients, obtained results remained stable on day 365. We present our results with a cohesive HA as a highly suitable filler for SUE. Given the high patient satisfaction, long-lasting results and reduced complication risk, our presented approach may represent a safe and effective novel treatment strategy.
In today’s world, everything is personal. From product recommendations at your supermarket to targeted adverts in your inbox, the more you know about your clientele, the more likely you are to succeed. With more than a decade’s experience in healthcare marketing, I’m going to be sharing some of my top marketing strategies that you can put into practice, enabling you to take a more personalised, human approach to attracting new patients.
Let’s start at the beginning: who is your ideal patient? It’s a big question and there’s no one-size-fits-all answer. With multiple treatment options, procedures and services, it’s likely that you’ll have a whole host of ideal patients, and you’re not going to be able to promote to all of them in one go. If this is the first time you’re looking to create defined marketing strategies or you think it’s time to refresh your plans, here’s how you should go about it.
Finding out what makes your audience tick can be challenging, but don’t underestimate what you already know. You have likely spent years working in your sector, and after all, you know your patients best. Get your team together and spend time building the big picture. Where do your customers shop? What other brands do they like? What do they normally wear when you see them? Do they care about the environment? Do they have families?
You could do this by picturing the three types of patients who most often come into your clinic, giving each of the three people a name
and then really delving into their interests. All these questions will help you develop key messages to use in your marketing activities, as well as areas to avoid. For example, if your target audience doesn’t have children, there’s no need to focus on messaging about being a family-friendly clinic.
Pick the treatments you want to promote I’m a big believer in quality over quantity! Rather than trying to create multiple marketing strategies across different treatments, start by focusing on one or two and take the time to ensure you’ve nailed the basics before launching multiple strategies. These could be the services with the fewest enquiries that need a boost, or you could focus on those that are your biggest revenue drivers. Either way, it’s best to start small and scale up, otherwise you’ll risk wasting time and budget on activities which don’t help your bottom line.
Consider data, data, data
Data tells stories, and stories are the foundation of strong marketing strategies. You will already have a pool of valuable data that can be used to craft meaningful marketing strategies. Existing patient data is the key to success. Take a look through your patient data filtered by service, and start to drill down into the data. To create meaningful strategies, we need to find out what makes your patients tick: where they spend their time, what motivates them and why they became your patients to begin with. This might sound like an onerous task, but it doesn’t have to be. If you do have the time, analysing your own data is always best (Google, Twitter and Facebook/Meta all have free access analytics), but if you don’t, each platform produces demographic numbers. This will help you unlock personalised strategies to target new patients. For too many years now, we’ve been building strategies around profiles like ‘Sarah, 25-30, lives in London’. In today’s personalised world, this isn’t enough to cut through the competition. Taking the time to gather extensive data to build real patient profiles will put you in the strongest position to build a strategy that generates new patient enquiries. An easy way to do this is via patient feedback forms. These can be included in email receipts, or on a good old-fashioned clipboard in a waiting area. Keep it short and easy to engage with.
you’ve delved deep into your target audiences, the next challenge is marketing to and engaging with them. Let’s look back on the basic principles of marketing, where strong strategies begin: awareness, consideration and acquisition. These three stages are key if you want to take a considered approach to your marketing strategy. Each stage offers the opportunity to directly engage with your audience through nuanced messaging that enhances their experience, positions you as the trusted choice and ultimately pushes them through to make an enquiry. For example, if we’re looking at targeting an audience of high-spending young professionals, it’s best to look at how you want
Once
Marketing professional James Dempster offers insight into how tailoring your marketing strategy can attract your perfect clientele

to communicate with that audience through these three stages. From our work with aesthetic clinics, we know that this particular audience engages visually. Polished, professional, creative assets will catch their eye, signal that your business is taking its brand seriously and show that your services are suited to them.
Instagram could be the perfect tool for this, with the largest share of users aged between 25 and 34 years old.1 This channel can be used throughout the marketing funnel. In the awareness phase, think about how you want to present your clinic and what key messages you want to promote. If you’re focusing on one service, visual before and after adverts are a great way to showcase your skill and expertise. This channel also offers a cost-effective way of advertising with sophisticated targeting options so you can ensure you’re reaching young professionals who match your persona. You will need to ensure that all your adverts meet the requirements of the Advertising Standards Authority (ASA) and the Committee of Advertising Practice (CAP).2
As the marketing world becomes more personal, we recommend using the consideration phase to introduce your potential customers to the staff they will be meeting face-to-face! Building trust and authenticity through videos, quick biographies and warm imagery is another way to position yourself as the best choice. You need to focus on how the patient will feel, taking the time to show you understand them by delivering content that addresses their needs.
Through the acquisition phase, this is where you really need to position yourself as best-in-class. Showcase your unique selling points (USPs), testimonials and further information about the customer experience to increase confidence in your service and clinic. Website landing pages are great for this, with your advert pushing people through to a dedicated page that answers their questions, gives a clear overview of what to expect and ultimately takes people to fill out a form, make an enquiry or pick up the phone.
Choosing your platforms
Taking a look at some other channels to utilise, Facebook is still an excellent option, particularly with a more mature demographic. The 60+ audience isn’t afraid of technology, but you do need to think carefully about the services you’re promoting, the language you use and the type of questions they would answer through the consideration phase.
a lookalike audience. From here, you can ensure the correct parameters are chosen, such as location, age and gender.3
Whilst the number of marketing channels can seem overwhelming, it’s important to choose wisely. If you don’t have a TikTok or Snapchat account already, it probably means your target audience doesn’t use them, so don’t create strategies on channels you don’t feel confident with. You’ll risk wasting budget for minimal reward. It’s better to spend your time really getting under the skin of your potential customers on a few channels which you know they engage with.
Taking a gendered approach
For aesthetics in particular, male customers are a growing audience, but they can be harder to engage with. Take time to think carefully about how this group differs from a female audience. Is there still stigma around cosmetic procedures for men? Are they more worried about confidentiality? Do they need reassurance that services are suitable for them too?

Tailor marketing to your clientele
With a whole host of channels, audiences and strategies available to you, it’s best to start small and ensure you’ve nailed the basics. Don’t run before you can walk, and invest time upfront to really grasp who your audience is. Knowing exactly who you’re marketing to will save you time and money in the future, and the more you can dive into that person’s values and motivations, the more you’ll be able to influence their decision-making, from awareness through to acquisition. It’s time to start attracting your ideal patients.
James Dempster is MD and co-founder of Fox&Bear, an award-winning marketing agency with many forward-thinking healthcare clients. Having worked in the healthcare sector for over a decade, he is experienced in telling stories on behalf of his clients that elicit emotional responses and ultimately make patients happier.
13 & 14 Oct ExCeL London, UK @aestheticsjournaluk Aesthetics @aestheticsgroup aestheticsjournal.com
1. Dixon S, Distribution of Instagram users in the United Kingdom (UK) as of March 2022, by age group (UK: Statista, 2022) <https://www.statista.com/statistics/1018012/instagram-users-unitedkingdom/#:~:text=In%20March%202022%2C%20Instagram%20had,old%2C%20at%20almost%20 31%20percent>
<https://www.facebook.com/business/help/465262276878947?id=401668390442328>
As a dentist now working solely in aesthetic medicine, if someone had told me this would have been my calling 10 years ago, I simply wouldn’t have believed them. When I embarked upon my initial botulinum toxin and dermal filler training back in 2011, I thought injectables would be a minor add-on to complement my general dental treatments.
Fast forward over a decade, and the evolution of aesthetic medicine has occurred at a tremendous rate. The increased understanding of the facial ageing process has coincided with improvements in both device-based treatments and the quality of injectable products and our utilisation of them. These developments have helped us optimise treatment plans to create global facial improvements.
The advancements have also been met by a surge in patient demand, and dentists are optimally positioned to capitalise on this by utilising their existing skills and expertise, working environments and patient bases. However, I’ve found that many dentists are anxious about making a move into aesthetics because they are apprehensive about treating extra-orally, opening up conversations about aesthetic concerns that are perceived to be awkward, or that they simply do not know where to start when it comes to finding reputable training courses and mentorship. Here, I will identify how dentists can experience a successful transition into aesthetic medicine.
Even in the early stages of a dentist’s career, due to the structure of the undergraduate curriculum, they exhibit a high degree of manual dexterity, excellent knowledge of head and neck anatomy and aesthetic proportionality, while simultaneously understanding pharmacology and materials science. These qualities lend themselves especially well to dermal filler and toxin treatments. Dentists can quickly acquire the assessment skills in order to adequately evaluate an individual’s concerns and treatment suitability to ultimately deliver safe treatments with good aesthetic outcomes, while respecting the functional anatomy. It’s easy to see why dentists are suitable to undertake this. The most obvious one is the fact that as a dentist, one of our main tasks is to assess patients, openly discuss their concerns and the treatment options suitable for them and then develop an integrated treatment plan addressing the ‘issues’ that have been discussed. Asking open questions and responding in an empathetic and caring manner is something all successful dentists will be skilled at. These basic communication skills are entirely transferrable
to aesthetic medicine and paramount to gathering information about patients facial concerns, treatment aspirations and discussing potential options.
That being said, many patients are apprehensive about embracing injectable treatments so answering questions clearly and concisely about patients’ perceived barriers to treatment goes a long way to converting them and retaining them in the longer term. At the end of the day, it comes down to trust. Apart from being highly skilled, the Care Quality Commission requirements call for dental surgeries to follow strict cross-infection control measures and provide good lighting, while also have provision to deal with medical emergencies.1 As such, these strict clinical conditions make them not only a desirable environment for safe practice, but also for fulfilling the potential future premises requirements recommended by the Joint Council for Cosmetic Practitioners (JCCP)2 which could come into force with a new licensing regime following an amendment in the Health and Social Care Act.3
Unlike many other healthcare professionals starting their careers in aesthetic medicine, dentists have a distinct advantage – an existing patient base. Many healthcare professionals who struggle to get their aesthetic medicine career off the ground do so as a result of the time and money taken to grow a sustainable list of patients.

The likelihood is that most dental clinics will have a good number of patients who can be informed of aesthetic medicine procedures through the clinic’s existing direct marketing channels, as long as the relevant advertising guidance from the General Dental Council4 and the Committee of Advertising Practice5 is adhered to.
Although discussion of the contents of these documents would exceed the remit of this article, it is worth noting that as botulinum toxin is a prescription-only medicine, it therefore cannot be advertised to the public by name. Any intervention using toxin should be referred to in non-specific terms, such as ‘a consultation for the treatment of lines and wrinkles’. Other notable points are that aesthetic procedures should not be marketed to those under 18 years of age, and that dentists should not refer to themselves as ‘specialists’ or ‘specialist in’ aesthetic medicine.4,5
In light of these regulations, marketing ‘solutions’ to common concerns rather than
the specific treatments themselves can often be a more engaging way to attract new and existing patients. Marketing emails or social media posts which, for example, discuss improvements in skin quality or reduction of lines can include references to broad treatment categories such as, ‘our latest injectable treatment’. Not only does this comply with marketing standards, it stimulates curiosity with the reader to find out which specific treatment can achieve these results. Having a call to action such as, ‘Would you like to see how we can help you? Book your consultation today’ can prompt the patient to make further enquires, hopefully resulting in a conversion to treatment.
Another way of raising awareness and starting conversations with patients is through an interests questionnaire, which includes both dental and facial aesthetic aspirations. As the questionnaire is completed prior to a patient’s appointment, it will indicate those who have a genuine interest in seeking interventions and allow the practitioner to discuss the subject without fear of potentially causing offence. Useful tools for the facial aesthetics component may be as simple as having a diagram of a face with tick boxes pointing to specific facial areas with common corresponding concerns, such as forehead lines or marionette lines. This is often easier for patients to understand and likely to achieve more engagement than an open question such as, ‘do you have any facial aesthetic concerns’, especially if the primary reason for attendance in the clinic is for dentistry. Asking about a patient’s previous aesthetic treatment history can also identify those who are already undertaking aesthetic interventions, allowing a conversation to start about treatments you may offer to complement their current regime.
There are a plethora of training courses in facial aesthetics on the market, ranging significantly in duration, price and unfortunately, quality. It is important to research the providers thoroughly and ensure they are registered healthcare providers (HCPs) with extensive experience in aesthetic medicine. Ultimately, there is currently no set requirement for the minimum level of training, however this may change given the potential amendments to the Health and Social Care Act as previously discussed. It is important that any training you undertake meets your own individual learning needs, while also understanding that a foundation course is the very beginning of a journey, which can take
years to master. It is pertinent to consider a training provider that can provide some form of mentorship and follow-up, especially if you are undertaking procedures in a clinic where you are the sole provider.
It is also wise to educate your wider dental team in the various aesthetic interventions you plan to undertake following training. Many patients’ initial inquiries will likely be with the reception team who may not have a significant degree of understanding of aesthetic procedures if they are from a purely dental background. It is essential that they are competent in their basic communication of procedures so patients have sufficient confidence in the clinic to proceed with booking a consultation.
Dental nurses can also be utilised to assist in facial aesthetic procedures. Having a second pair of hands is invaluable at improving the flow of treatment, assisting with aseptic technique and helping to stem any bleeding.
In order to undertake aesthetic treatments, it is a legal requirement to hold the appropriate level of indemnity for the procedures you wish to undertake.6 Some dental indemnity providers, such as the Dental Defence Union, will provide cover but require an additional supplement if you are a recently qualified dentist or if your gross earnings for this work exceed £8,000 per year.7 Other indemnity providers, such as Cosmetic Insure, Enhance Insurance or Hamilton Fraser Cosmetic Insurance, can provide separate indemnity cover. It is important to undertake personal research with the various providers to establish which cover will be most suitable for your individual needs.
Upon completion of initial training, like any other new clinical service, it is essential to build upon the basic fundamentals before embarking upon more complex treatments. Patient selection at this stage is key. It is important to choose patients who present with relatively easy-to-treat concerns away from higher risk areas such as the tear trough and nose. During the initial phases of administering injectables, it is important to focus on injection technique and hone skills such as hand stability, particularly when aspirating dermal filler with a needle, and aseptic technique. Dentists are ideally placed to offer treatments directly related to common functional issues and dental aesthetic
concerns. Toxin can achieve very good results in reducing masseteric tenderness as a result of parafunction and, in many cases, can offer a relatively straightforward solution to addressing ‘gummy smiles’ as opposed to surgical crown lengthening.
Although most dentists will commence their aesthetic medicine practice with injectable procedures such as botulinum toxin and dermal fillers, there is a growing demand for adjunctive treatments to improve skin quality and other aesthetic concerns. One of the benefits of modern aesthetic practice is that there are now a number of adjunctive devices on the market, such as radiofrequency and microneedling machines, which can be easily integrated into an aesthetic treatment plan in a dental practice. Most devices now do not take up a significant degree of physical clinical space, and can potentially attract more patients who are apprehensive about undertaking injectable treatments.
The field of aesthetic medicine is a rapidly growing and exciting area to be a part of. Although many dentists can be apprehensive about working outside of the intra-oral comfort zone, the transferable skills outlined in this article demonstrate the ease of integrating these treatments into a dental clinic, providing a high degree of patient and provider satisfaction.
Dr Martin Nimmo originally qualified as a dentist from the University of Dundee in 2008, and is now working full time in aesthetic medicine. He is the owner of The Nimmo Clinic and a trainer and member of the Allergan Medical Institute. Qual: BDS, MFDS RCS(Ed)



Business consultant Gary Monaghan gives some step-by-step advice on how to establish your own aesthetic clinic from the ground up
The rise in self pay market – namely patients self-funding their procedures – has paved the way for an increasing number of clinicians to pursue an entrepreneurial venture: setting up their own private clinics and hospitals. However, do you understand and appreciate what is involved? Most practitioners have never undertaken a project of this scale before so are asking where to start and what to think about. We will look at some of the key points you should consider in this article.
Having your own clinic carries great benefits, of course, but it also entails a certain amount of risk and stress. As an example, think of a problem receptionist in your current workplace… that person now becomes your concern! The bills that need paying, the staff who need a salary and the disputes that inevitably arise within teams all become yours. You will either be a building owner or a tenant, and each carries its own challenges to bear in mind. You will potentially become a manager of a Care Quality Commission (CQC) registered entity (or the Scottish, Welsh or Irish equivalents), responsible for all standards and processes therein. Having made you consider all the challenges, let’s readdress the balance. Your own place brings freedom: freedom to buy what equipment you want, open when you want and employ who you want. It also brings great value to your business. All the revenue that you spend renting rooms or facilities is now part of the income of your clinic. You also now have a facility associated with your brand, undoubtedly adding value when you come to expand and ultimately sell. In short, it gives you control, breeding a huge sense of ownership that brings pride, kudos to you and your brand and a sense of achievement.
With any project, the initial question is what do you want to achieve? More in-depth considerations incorporate the venue you want, what treatments you will offer onsite and how
many rooms and facilities you need. Only when these basics are established can you really start to look at the project in more detail. The key to any successful project is its financial viability. Nobody starts a business to lose money, but many do start without really considering the overheads, set-up costs and any unforeseen and potentially costly issues that might arise along the way. These could be industry and economic trends or one-off events. Once the type of venue for your clinic has been decided upon, the next step should be to form a business plan which might serve as an essential document to any investor or bank, and a cashflow. This will tell you a huge amount about what you will be letting yourself in for!
It is absolutely essential that a great deal of fact finding and planning is undertaken at the outset. All practitioners will have worked in premises owned by other people, but do you understand what is behind the structure of these venues? Do you understand the issues faced daily by a clinic owner? It just might be that these additional stresses on top of your clinical work are too much! Get to understand them first before you spend too much time on them, or worse still, commit to the project and incur unwanted financial costs.
The main costs are often underestimated. Most people have a rough idea of build costs (although this is frequently underestimated due to rising prices), but certain costs are quite frequently not even considered. Do you know that most landlords require a rent deposit of up to a year’s rent? This could equate to a six-figure sum which has to be part of the overall cost!
We also frequently see a tendency for practitioners to factor in the cost of larger pieces of equipment, but forget to consider the smaller costs which really do add up. Investment in basic disposable items such as needles, syringes, gloves, drapes, drugs and many other considerations easily add up to tens of thousands of pounds. Other factors such as legal costs, fees for registrations and so on, frequently run into the thousands too. There is also the question of VAT, which many practitioners are not registered for.1,2 As such, the huge amounts of VAT racked up in build costs, services and equipment purchases are not to be forgotten. It is vital that overall set-up costs are calculated. It is equally vital that a cash buffer is built in for any unforeseen areas of expenditure and to provide working capital while the project builds to a consistent break-even point.


On balance, opening a clinic seems like a good idea. So how can you fund it? Pure cash is necessary, of course. Many lenders will only lend if the borrower puts a certain amount in themselves. Bank loans are viable – even in the current climate of rising interest rates, good deals can be had. Investor finance is an option, although I always feel that the lower this is, the better for the clinic owner. There are a lot of caveats to this statement, but any project is at a weaker point at the outset to appeal to investors than at a later stage in its development. If you go for investment with nothing but a general idea or basic plan, you are likely to get an inferior deal compared to if you already have a part or fully built clinic. Think Dragons Den! Simple concepts are a total punt, whereas projects with existing sales are much more investable. Asset finance is a good option for funding these types of projects. This is a way of funding equipment and tangible items through an asset loan, whereby an asset finance company retains title of the goods until the loan is paid off, at which point it transfers to the borrower. Good rates can be found, and there is appetite within this sector for providing funding to healthcare projects. If you are considering entering this venture with a fellow practitioner, you need to think long and hard about the viability of this. Working in the same venue is one thing but having a colleague as a business partner is very different. Take care about who you invite to join your project, how things are structured and how they work between you and any colleagues you involve. A friend or even current colleague does not necessarily make a good business partner. These are lifelong projects – can you work daily with the person and manage disagreements when they occur? It could work very well indeed, or it could be the worst thing you have ever done.
By this stage, you’ve considered the pitfalls, costs and benefits of setting up your own clinic, and you want to progress. The venue location, type and size are now your key considerations. Note that until this point, we have not mentioned these specifics. Many people I see have chosen a venue before they have considered these, and I frequently reset clients to the start of the process to ensure they have indeed contemplated every detail involved.
The venue will define the lion’s share of the costs, as well as the overall likely success of the venture. It can be very difficult to envisage the outcome at a given venue as it’s hard to know what space is required to achieve a desired end result. Specialist help is very important here, owing to the rules and regulations that healthcare environments must adhere to such as Health Technical Memoranda (HTMs), CQC rules and fire regulations. Knowledge of how to adhere to or negotiate these is absolutely essential, so I highly recommend seeking the guidance of a specialist builder conversant with all the regulations specific to your desired venue. If you do not do this, these regulations may not be followed and in the worst-case scenario, you will not be permitted to trade.
As we have stressed before, planning is very important at this stage. Get your layout right, even if you have to amend it several times. You cannot do this once your clinic is built without incurring substantial costs and delays.
Another area I see real issues in is that of project planning. How long does something take? When should you apply to the CQC or equivalent regulators? When should you order a treatment couch? In recent years, these questions have become more and more difficult to manage as timeframes that used to be short and pretty predictable have
become elongated and wildly unpredictable. Each one could delay your project by many weeks if miscalculated or underestimated.
Timings are very difficult to get right, and with so many tasks to complete, it is a minefield where you really need to seek assistance from experienced business experts. Let us not forget, every hour you are working on the project rather than your clinical practice is an hour’s lost revenue for you. Do not take too much on yourself – these projects can be stressful and time consuming. Delegation and outsourcing are your friend!
I do not believe everyone wanting to open their own clinic should proceed to actually build or buy one without giving it careful thought! People have different attitudes to risk, stress and ambition, which will influence their strategies of project management. There is no doubt that a project like this is going to cost a lot of money. It is also almost impossible to do quickly – allow four months as a minimum from concept to completion.
Nevertheless, it is undeniable that if everything is considered, thought through and understood, then it is a viable and lucrative opportunity for an established practitioner. It can give real long-term stability, solid financial footing and a legacy. For many practitioners, this is too good an opportunity to pass by.
Gary Monaghan is an aesthetic clinic business consultant. He began his aesthetic career in sales for Nagor, before moving on to set up cosmetic insurance company Premium Medical Protection. After this he ventured into business consultancy for practitioners – The Cosmetic Consultants –which includes setting up clinics for surgeons.
1. Aesthetics, Understanding VAT Exemptions (UK: Aesthetics, 2020) <https://aestheticsjournal.com/feature/understanding-vatexemptions>
2. Aesthetics, VAT in Aesthetic Practice (UK: Aesthetics 2019) <https://aestheticsjournal.com/feature/vat-in-aesthetic-practice>
13 & 14 Oct ExCeL London, UK
Gary Monaghan will be speaking at CCR 2022 at ExCeL, London on October 13 and 14. Make sure to register for free now to catch his talk! Find out more on p.20

Your own clinic brings freedom to buy what equipment you want, open when you want and employ who you want



Having authored nearly 400 peer-reviewed scientific studies, published nine textbooks and spoken around the world, Dr Jean Carruthers continues to educate and conduct research on botulinum toxin today. Beginning her career at the University of British Columbia in Vancouver to study medicine in 1968, Dr Carruthers decided she wanted to travel to London to study ophthalmology. She undertook a primary fellowship in surgery at the Royal College of Surgeons where she worked as a higher scientific officer at a London hospital in Whitechapel. Afterwards, in 1972, Dr Carruthers was accepted onto the house at Moorfields Eye Hospital. She explains, “I think I was the second woman on the house at Moorfields so that was an amazing experience! I finished this in 1977 and decided to go back to Canada to work as an academic ophthalmologist at the University of British Columbia. Gradually, I started to work in paediatric ophthalmology and ocular genetics.” Dr Carruthers notes that this is where she began to take an interest in botulinum toxin, as another ophthalmologist Dr Alan Scott was treating patients suffering from misaligned eyes with an injection rather than surgery.
In 1982, Dr Carruthers travelled to San Francisco with her husband, dermatologist Dr Alastair Carruthers, to learn more about botulinum toxin. “It was a great learning experience as I worked alongside Dr Scott at the Smith-Kettlewell Eye Research Institute
for the summer and saw a remarkable way to use toxin to relax muscles. I brought all my learnings back to Canada and was approved by Health Canada to join Dr Scott’s multicentre world trial of botulinum toxin,” she adds. At her clinic in Vancouver, Dr Carruthers discovered the use of botulinum toxin for wrinkles while treating one of her patients for blepharospasms. She reflects, “Blepharospasms were a difficult condition to treat with surgery, however, with botulinum toxin, you could weaken the overactive muscles, so the patient looked normal. It was so exciting to see! While I was treating one of these patients, they got upset at me for not treating their inner brow. I apologised to them and explained that I didn’t realise they were spasming there. The patient replied that she wasn’t, but every time they were treated there, they got a beautiful, untroubled expression. That’s when the penny dropped!” Dr Carruthers told her husband about this discovery. They decided to start conducting studies on botulinum toxin for treating the signs of ageing.
In 1990, Dr Carruthers gave her first talk on the cosmetic usage of botulinum toxin to an audience at the annual meeting of the American Society for Dermatologic Surgery and, according to Dr Carruthers, they were horrified. “Usually, I would get lots of questions after a talk, but instead it was uncomfortable. People came up to me afterwards and said, ‘how could you use a terrible poison on something so frivolous as wrinkles’. Of course,
in large dosages, botulinum toxin is a poison, but what they didn’t realise was that there was nothing frivolous about wrinkles!” she explains. After the talk, Dr Carruthers realised that she had a lot of work to do to prove this to her colleagues. She conducted multiple studies and slowly started to get recognition of this indication in the medical community. In 1992, Dr Carruthers published her first medical paper called Treatment of Glabellar Frown Lines with C. Botulinum-A Exotoxin with her husband. She notes, “This was my biggest achievement as people started to get excited about our discovery. I think what most practitioners found revolutionary was how they could utilise botulinum toxin in their practices and how this would define aesthetic medicine in the future.” Throughout her career, Dr Carruthers has worked and conducted research with nearly all the neuromodulator companies, as well as being a member of many associations. “I’ve been a key opinion leader for many years. I belong to the American Society of Dermatologic Surgery, American Society of Plastic Surgeons and the Canadian Ophthalmological Society. I’ve just renewed my licence in the UK so that I could perform demonstrations at the recent British College of Aesthetic Medicine (BCAM) conference, which I loved.” Dr Carruthers believes that practitioners should take time to read the literature to better their medical outcomes. “I think one of the reasons why procedures can go wrong for practitioners is that they don’t understand the background and so heavy reading is a great suggestion as the literature is exceptional,” she notes. When looking back at her career, Dr Carruthers wishes that she had fought for a patent for botulinum toxin for the glabellar. She concludes, “We went to two different law firms and they both said that there was nothing to patent. Knowing what I know now, we would have gone to more law firms as obviously, we had our hands on something big!”

“What practitioners found revolutionary was how they could utilise botulinum toxin in their practices”
Dr Jean Carruthers reflects on her journey to discovering botulinum toxin for wrinkles and her advice for fellow practitioners in aesthetics What
The world of aesthetic medicine is constantly expanding and evolving. There are now a plethora of treatments available to our prospective patients. Alongside this sharp rise in cosmetic procedures, there has also been a noticeable rise in healthcare professionals becoming practitioners in the cosmetic field, practicing procedures outside of their core specialty. I have observed many examples recently, such as heart surgeons performing face lifts and dentists performing dermal filler injections. The medical requirements are met, but is this really the route we should be going down? Here I will debate the pros and cons of being a generalist or a specialist within the field of medical aesthetics and plastic surgery.
When entering the aesthetic world, it’s likely that practitioners may not know what their main interest is. So, it is indeed useful to partake in training and gain knowledge of all treatments in order to find out what you really love and where your core skillsets lie. Having the correct training in multiple procedures and treatments also means that you can advise patients accordingly when they come to you with questions, or refer them to more apt medical professionals.

Keeping yourself broad in terms of treatment offering can also be more commercially viable –it’s understandable that you don’t want to lose a patient who comes through the door willing to pay for your services. If you only specialise in injectables, a patient who is after a chemical peel will go elsewhere and you will lose that income. In the plastic surgery sector of the aesthetics world, the financial benefits of performing multiple surgeries are even greater, due to the higher price points. Therefore, in both the invasive and non-invasive aesthetics sectors, being a generalist may initially seem more financially beneficial.
Just being able to say ‘I can do this procedure’ doesn’t equal ‘I can do it well.’ Aesthetic practitioners and surgeons can often do multiple procedures and treatments competently, but if you look at the results of generalists compared to someone who has a singular specialty, the difference in results can be striking. Specialism can also lead to striving for, and attaining, perfection in your results. Those that have dedicated their lives to one specific treatment or procedure will have a higher understanding of the patient journey, aftercare and results. It can be argued that specialists also show greater focus and dedication to specific parts of the anatomy – that their specialism is a lifelong vocation and not simply a side interest to further commercial viability.
If you look at anyone who is a real leader within their field, they are usually specialists. Furthermore, specialism can also be beneficial to your marketing and public relations efforts.
If, for example, you are able to garner the nickname as the ‘body contouring queen’, or ‘the go-to rhinoplasty surgeon’, prospective patients will be able to find you more easily, in addition to increased confidence in your work. Similarly, if you publish new articles, techniques and do talks at aesthetic conferences on your specialism, aesthetic companies and brands will notice you. So, in the long run, this does also help the commercial side too.
In light of the above, in terms of noninvasive aesthetic treatments or ‘tweakments’ as they’ve been coined, generalism can be helpful early on in your career to further your knowledge and understand your true strengths. Once the latter has been attained, I believe it is then time to narrow down your offering and specialise – you can always employ others in your practice to fill the skill gaps so that you’d don’t lose out commercially. In regards to more invasive procedures such as cosmetic surgery, I believe that specialism here is of the utmost importance. Invasive aesthetic procedures are much riskier, the patient journey is longer and the aftercare is more complicated and as such, full dedication and expertise in the procedure is paramount. As healthcare professionals, our first duty of care is to the patient. So while you may see generalism as more financially beneficial, this should never be the main focus nor your main decision maker. The main focus should always be creating the best outcomes and results for your patients.
Of course, becoming a specialist takes time and it is not easy – it requires years of training, practice and dedication. Not only does it take time to become proficient at a procedure, but there also needs to be enough demand for that procedure by patients. However, in the long run, beautiful results and wonderful patient testimonials will lead to being an esteemed practitioner in your field.
Mr Amir Sadri undertook his medical studies at the University of Liverpool. During this time, he also gained an Honours degree in Anatomy. He graduated in 2007 and continued his surgical training in London to become a Member of the Royal College of Surgeons of England in 2008. He trained in plastic, reconstructive and cosmetic surgery at a number of plastic surgery units both in London and Liverpool.
Qual: BSc, MB ChB, MRCS






COOLSCULPTING® ELITE YOUR PARTNER FOR BODY-CONTOURING
PATIENT SAFETY FIRST: Dual applicators with consistent cooling, monitored by Freeze Detect ® and CoolControl sensors.1,2 Ergonomically-designed dual applicator cups to help optimise patient outcomes.3,4 Fast set-up, easy handling, simple clean-up.1,2






During the procedure patients may experience sensations of pulling, tugging, mild pinching, intense cold, tingling, stinging, aching and cramping at the treatment site.1 These sensations subside as the area becomes numb.1 Following the procedure, typical side effects include redness, swelling, blanching, bruising, firmness, tingling, stinging, tenderness, cramping, aching, itching, skin sensitivity and numbness. Numbness can persist for up to several weeks. A sensation of fullness in the back of the throat may occur after submental treatment.1 These rare and very rare adverse events have the following incidence rates (approximate occurrences per number of treatments): paradoxical hyperplasia (1/3000 [0.033%]), visibly enlarged tissue volume within the treatment area, which may develop two to five months after treatment, surgical intervention may be required; late-onset pain (1/6000 [0.017%]); severe pain (1/6000 [0.017%]); hyperpigmentation (1/11000 [0.009%]); freeze burn (1/15000 [0.006%]); treatment area demarcation (1/20000 [0.005%]); vasovagal symptoms (1/30000 [0 .003%]); subcutaneous induration (1/30000 [0.003%]); cold panniculitis (1/60000 [0.002%]) and hernia (1/185000 [0.001%]).1,5
The CoolSculpting® procedure is not for everyone. Patients should not have the CoolSculpting® procedure if they suffer from cryoglobulinaemia, cold agglutinin disease or paroxysmal cold haemoglobinuria.1
The CoolSculpting® procedure is not a treatment for obesity. 2 CoolSculpting® is not a weight loss procedure and should not replace a healthy diet and active lifestyle.
References:
1. Allergan. CoolSculpting® system (CoolSculpting® ELITE) user manual. CS-UM-CM3-04-EN-A. 2020. 2. FDA. K193566. ZELTIQ® CoolSculpting® System. January 2020. 3. Allergan. Unpublished data. INT-CSC-2050029. CoolSculpting® applicator dimensions and design information. May 2020. 4. Allergan. Unpublished data. INT-CSC-2050028. CoolSculpting® clinical fit and function study testing of VO03 cups. February 2020 5. Zeltiq Aesthetics, Inc., An AbbVie Company. Full safety information: https://www.coolsculpting.com/pdfs/CSC146039-v2-CoolSculpting_Elite_Full_Important_Safety_Information.pdf [Accessed September 2022].
Adverse events should be reported. Reporting forms and information can be found at: UK adverse events reporting https://yellowcard.mhra.gov.uk Adverse events should also be reported to Allergan Ltd. UK_medinfo@allergan.com or 01628 494026 Irish adverse events reporting https://www.hpra.ie Adverse events should also be reported to Allergan Ltd. UK_medinfo@allergan.com or 01628 494026
Material produced and funded by Allergan Aesthetics an AbbVie Company. UK-CSC-220140 Date of preparation: September 2022