
VOLUME 8/ISSUE 6 - MAY 2021 Marketing Summer Treatments Sales director Graham Clarke discusses summer marketing Treating Lip Lines Dr Ellen Selkon and Dr Sarah Hart explore addressing photodamaged lips Choosing SPF for Your Patients Three practitioners share considerations for recommending SPF CPD: Artistic Appreciation Mr Paul Banwell and Nina Prisk discuss the concept of beauty and aesthetics S I LY M A R I N C F ENVIRONMENTAL PROTECTION FOR OILY, BLEMISH-PRONE SKIN. FIGHTS AGAINST VISIBLE SKIN AGEING. *CLINICAL STUDY 35 SUBJECTS (CHINA 2020) OUR ANTIOXIDANT ANSWER REDUCES OILINESS REFINES SKIN TEXTURE IMPROVES SKIN CLARITY CLINICALLY PROVEN TO REDUCE OIL OXIDATION BY UP TO 76% * REGISTERNOW!AWARDS CEREMONYVIRTUAL MAY28!

THEIR LOOK
We believe natural-looking, long lasting results are achieved by enhancing your client’s features, not changing them.
The Juvéderm® Vycross® range of fillers includes five tailored products designed for a specific area of the face at the optimum dermal level. Which means you can offer your clients a bespoke and tailored treatment to help suit their needs.
Produced and Funded by Juvéderm®. UK-JUV-2150067 March 2021 ©2021 Allergan. All rights reserved. Model treated with Juvéderm®. Individual patient results may vary.
Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk/ Adverse events should also be reported to Allergan Ltd. UK_Medinfo@allergan.com or 01628 494026.

To find out why Juvéderm® could work for your clients and your clinic on every level, visit juvederm.co.uk
*Juvéderm® offers a range of facial fillers to answer a variety of needs, each of which is administered at a different dermal layer.































Case Study: The Teoxane Approach
Mrs Sabrina Shah-Desai explains how she uses the Teoxane range
Register for the Virtual Aesthetics Awards Don’t miss out on this year’s exciting and free-to-attend digital ceremony 48 Treating the Perioral Area
Jennie Hawkins explains the importance of treating the whole perioral area 49 Preventing the Signs of Ageing
Dr Vincent Wong and colleagues explore maintaining a youthful appearance 53 Case Study: Managing a Vascular Occlusion Two practitioners manage a complication following non-surgical rhinoplasty
Beauty is No Longer Skin Deep Discover the EMERALD non-thermal body sculpting laser
Dr Sieuming Ng assesses the controversy of the Fox Eye trend
Special Feature: Choosing SPF for Your Patients Page 21

Clinical Contributors
Mr Paul Banwell is a consultant plastic and cosmetic surgeon in London and the South-East. He is the founder of the Banwell Collective and a visiting professor of plastic surgery to Harvard Medical School. Mr Banwell is the co-founder of Banwell.Prisk School of Medicine.

Nina Prisk is an aesthetic nurse prescriber. She practises from her clinic Update Aesthetics in Cornwall, as well as in Harley Street as part of the Banwell Collective. Prisk is the co-founder of Banwell.Prisk School of Medicine.
Dr Ellen Selkon has been practising aesthetic medicine in New Zealand for 15 years. She is on the executive committee of the NZ Society of Cosmetic Medicine and the NZ conference organising committee.

Dr Selkon is a trainer for Galderma Pharmaceuticals.
Dr Sarah Hart has been practising cosmetic medicine since 2002. She serves on the NZ Society of Cosmetic Medicine’s executive and education board as censor and education faculty member. Dr Hart has been an Allergan Advisory board member since 2007.

Dr Manika Rajput is an aesthetics practitioner and director of Aeon Aesthetics in Surrey. She completed her honours dental degree at King’s College London. She has more than 10 years’ experience in dentistry and was trained by the Avanti Aesthetics Training Academy.

Dr Vincent Wong is an aesthetic practitioner and founder of VinDoc Aesthetics. He has a Bachelor of Science in Medicine from the University of St Andrews and a Bachelor of Medicine and Surgery from the University of Aberdeen.

Marie Line El Helou has a Doctor of Pharmacy degree from the Lebanese American University and a Master of Science in Pharmacology from Paris-Sud University. She has been working in pharmacovigilance in the investigational and post-marketing settings.


Marie-Elizabeth Ragi is a licensed clinical dietitian. She has a Bachelor of Science in Nutrition and Dietetics from Saint Joseph University and a Master of Science in Human Nutrition from the American University of Beirut.
Mikala Foster is a registered nurse and founder of Essex Cosmetics. She began her nursing career in an NHS emergency department, before starting her aesthetic career in 2015. Foster is currently undergoing her prescribing qualifications at university.


Dr Manav Bawa is an aesthetic practitioner and GP with a surgical background. He is the medical director of Time Clinic in London and has completed a Diploma in Aesthetic Injectable Therapies. Dr Bawa is an associate member of BCAM.

Contents • May 2021
NEXT MONTH IN FOCUS: TREATING MEN • Transgender Patients • Defining Male Beauty 08 News The latest product and industry news 18 News Special: Taking Care of Your Mental Health
the ways practitioners
20 Introducing
CLINICAL PRACTICE 21 Special
for Your Patients Three
28 CPD:
Aesthetics explores
can look after their wellbeing
Ultherapy How technology under the skin can optimise lifting results
Feature: Choosing SPF
practitioners share considerations for recommending sunscreen
Understanding Artistic Appreciation
35 Treating Lip Lines
38 The
41
45
Mr Paul Banwell and Nina Prisk discuss concepts in beauty and aesthetics
Two practitioners explore how to address photodamaged lip lines
Trends of Today RELIFE brand ambassadors provide insights on the latest treatment trends
Exploring Hyperpigmentation in Skin of Colour Dr Manika Rajput discusses common causes of hyperpigmentation
47
61
Pricing
65
58
59 Abstracts A round-up and summary of useful clinical papers IN PRACTICE
Updating Your Clinic’s
Structure Business coach Alan S. Adams outlines the benefits of a pricing structure
Communicating with Existing Patients Dr MJ Rowland-Warmann provides tips for engaging current patients 69 Marketing Summer Treatments Sales director Graham Clarke discusses marketing in the summer months 72 In Profile: Annie Cartwright The Merz Innovation Partner shares her journey into aesthetics 73 In The Life Of: Dr Uliana Gout The BCAM president gives us an insight into her everyday life 74 The Last Word: Fox Eye Trend
The revolutionary new collagen stimulating injectable
Lanluma is a highly effective collagen stimulating injectable range that smoothes, shapes and sculpts both face and body.

www.lanluma.com


The device is suitable for increasing the volume of depressed areas, particularly to correct skin depressions.

UK-LAN-AD-02/2021-B
Chloé Gronow Editor & Content Manager @chloe_aestheticseditor
It’s the Aesthetics Awards month! On May 28, you’re invited to join us for a spectacular afternoon/evening of celebration and recognition after one of the hardest years. While we’re disappointed we don’t get to celebrate in real life, we’re hosting a virtual ceremony via Zoom from 4pm with all the usual glitz and glamour you’d expect!
There’ll be a best-dressed competition, cocktails and decorations, as well as celebrity host Cherry Healey. You’ll recognise her from presenting 10 Years Younger in 10 Days on Channel 5, as well as BBC 2’s Inside the Factory and lots of other fantastic documentaries! The Awards will be free to attend for anyone in the specialty, so there’s no excuse not to be there! You should register in advance via aestheticsawards.com. Don’t forget to tag @aestheticsjournaluk in all your fabulous pics and videos on Instagram, which we’ll be sharing throughout the evening to bring the aesthetics community together for this special event!
Clinical Advisory Board
Summertime – it’s almost upon us. SPF is of course a must all year round, but even more so across the next few months. On p.21 you can find vital advice for educating your patients on sunscreen use, as well as tips to help you choose which products to stock.
Also explored in this issue is your mental health. How are you feeling? After more than a year of on and off clinic closures, and now high demand from patients as you return to business, it’ll come as no surprise that you may feel stressed, anxious and exhausted. In our News Special on p.18, we explore recent statistics that indicate 62% of nurses felt their mental health was much worse now than at the start of the pandemic, while 71% of physicians noted that they felt burnt out. So if this is you, how do you manage? Thankfully, the British Association of Cosmetic Nurses and the British College of Aesthetic Medicine are there for support. Both organisations have implemented strategies to help their members, from recommending mindfulness techniques to providing a network to communicate with others in similar situations. Check them out to get back to business confidently and positively!
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content
Mr Dalvi Humzah is a consultant plastic, reconstructive and aesthetic surgeon with more than 20 years’ experience and is director of P&D Surgery. He is an international presenter, as well as the medical director and lead tutor of the multi-award-winning Dalvi Humzah Aesthetic Training courses. Mr Humzah is founding member of the Academy of Clinical Educators at the Royal College of Physicians and Surgeons of Glasgow.


Dr Raj Acquilla is a cosmetic dermatologist with more than 12 years’ experience in facial aesthetic medicine. In 2015 he won the Aesthetics Award for Aesthetic Medical Practitioner of the Year and in 2012 he was named Speaker of the Year. Dr Acquilla is a UK ambassador, global KOL and masterclass trainer for botulinum toxin and dermal fillers.
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon at the Cadogan Clinic in Chelsea. She specialises in blepharoplasty surgery and facial aesthetics. Miss Hawkes was clinical lead for the emergency eye care service for the Royal Berkshire NHS Foundation Trust. She is an examiner for the Royal College of Ophthalmologists.
Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.

PORTFOLIO
Alison Willis Director
T: 07747 761198 | alison.willis@easyfairs.com
EDITORIAL
Chloé Gronow Editor & Content Manager
T: 0203 196 4350 | M: 07788 712 615
chloe@aestheticsjournal.com
Shannon Kilgariff Deputy Editor T: 0203 196 4351 | M: 07557 359 257
shannon@aestheticsjournal.com
Holly Carver Journalist | T: 0203 196 4427 holly.carver@easyfairs.com
Ellie Holden Editorial Intern | T: 0203 196 4427 ellie.holden@easyfairs.com
Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN) and the UK lead on the BSI committee for aesthetic nonsurgical medical standards. She is a registered university mentor in cosmetic medicine and has completed the Northumbria University Master’s course in non-surgical cosmetic interventions.

Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the clinical director of Revivify London, an honorary clinical teacher at King’s College London and a visiting associate professor at Shanghai Jiao Tong University.


ADVERTISING & SPONSORSHIP
Courtney Baldwin • Event Manager
T: 0203 196 4300 | M: 07818 118 741
courtney.baldwin@easyfairs.com
Judith Nowell • Business Development Manager
T: 0203 196 4352 | M: 07494 179535
judith@aestheticsjournal.com
Chloe Carville • Sales Executive
T: 0203 196 4367 | chloe.carville@aestheticsjournal.com
MARKETING
Aleiya Lonsdale
Head of Marketing
T: 0203 196 4375 | aleiya.lonsdale@easyfairs.com
Katie Gray • Marketing Manager

T: 0203 1964 366 | katie.gray@easyfairs.com
DESIGN
Peter Johnson • Senior Designer
T: 0203 196 4359 | peter@aestheticsjournal.com
WE WANT TO HEAR FROM YOU!
Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email editorial@aestheticsjournal.com
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 AntiAgeing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Dr Stefanie Williams is a dermatologist with special interest in aesthetic medicine. She is the founder and medical director of the multi-award winning EUDELO Dermatology & Skin Wellbeing in London. She lectures in the Division of Cosmetic Science and has published more than 100 scientific articles, book chapters and abstracts.


ARTICLE PDFs AND REPRO
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com
Aesthetics Media
© Copyright 2021 Aesthetics. All rights reserved. Aesthetics is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final.
Editor’s letter
DISCLAIMER:
Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
The
PUBLISHED BY
Mr Dalvi Humzah, Clinical Lead
MANAGEMENT
Talk #Aesthetics
Follow
#Panel
Dr Kathryn Taylor-Barnes
@realyouclinic
It was a pleasure to be on the panel at the #Sculptra interactive launch webinar! I hope everyone felt informed and furthered their knowledge to enhance their practice #launch #webinar
#BeyondBeauty
Sharon Bennett
@sharonbennettskin
Wow! The first edition of Beyond Beauty is published and I’m honoured to be part of it! #magazine #aesthetics

#Filming
Dr Raul Cetto
@drcetto
Wrapping up three days of filming and live streaming in London with the big man himself @leewalker_academy! Thank you for the support @teoxanepro #socials
#Technology
Miss Sherina Balaratnam @sthetics_clinic
A fantastic day training with the super Kelly & Ruth from @btlaestheticsuk on our incredible new EMSCULPT NEO technology! #training


Sinclair Pharma introduces new HA filler
Pharmaceutical company Sinclair Pharma is launching a new hyaluronic acid (HA) facial filler called MaiLi. The company explains that MaiLi has four products in its portfolio: Precise, Define, Volume and Extreme. Precise is designed to treat fine lines, reconstruct structural defects from scar tissue, and treat the periorbital area. Define is designed for filling deep wrinkles and for volumising the lips. Volume is designed for facial volumisation and subdermal fat pad injection. Extreme is formulated with the highest concentration of HA within the MaiLi product range and is created to sculpt and shape the face.
According to Sinclair Pharma, MaiLi patented the world’s first OxiFree technology, which preserves long molecular HA chains. The company states that the crosslinking of HA with 1,4-Butanediol diglycidyl ether (BDDE) has created a supple, spring-like gel with volume, projection power and longevity.
Chloé Antunes, Sinclair Pharma marketing manager, said, “Through identifying a sizeable gap in the market for fillers to maximise volume, suppleness and longevity combined, MaiLi utilised a unique opportunity to design a premium line of HA gels to meet this demand. When partnering with MaiLi, treatment possibilities are elevated with a premium portfolio of high-performing HA gels, promising supreme volume, suppleness, projection power and longevity, for technically-gifted professionals to refine their craft with precision and care.”
Collaboration
Cutera and SkinCeuticals announce UK partnership
Professional skincare and antioxidant company SkinCeuticals has formed a commercial partnership with aesthetic technology manufacturer Cutera. Focused on the UK aesthetics market, Cutera explains that the new collaboration will see both brands work to develop a specialist treatment protocol that will help optimise clinical outcomes for patients. According to Cutera both companies will be holding workshops in the second half of 2021, where they will showcase and discuss the newly developed protocol and evaluate the clinical outcomes observed through this combination.
#Aestheticsjournal
Dr Jemma Gewargis
@dr.jemma.g
So chuffed to see my article in print this month’s @aestheticsjournaluk. Thank you so much to the brilliant team! #publication #necklift
Tim Taylor, UK country manager for Cutera, commented, “I am delighted to announce this partnership alongside professional skincare company SkinCeuticals. I feel both brands complement each other perfectly with our shared ambition for innovation, together with results-driven treatments backed up by science and research.”
National sales manager UKI at SkinCeuticals, Michelle Goulbourne, said, “Together we share an aligned vision that puts the consumer and the business account at the heart of everything we do, to ensure patients’ optimal skin health, maximum treatment efficacy and safe results.”


Injectables
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
us on Twitter @aestheticsgroup and Instagram @aestheticsjournaluk
Beyond Beauty magazine comes to life
Easyfairs, the owner of the Aesthetics portfolio and the recently launched Beyond Beauty magazine, is introducing a new consumerfacing event bringing the publication to life called Beyond Beauty Live.
The event will provide a platform for members of the public to learn about aesthetic treatments and cosmetic surgery from medically qualified practitioners and discover the newest products, treatments and technologies. There will be live demonstrations of the newest devices and treatments, and debates and presentations on topical subjects.
Aesthetics & CCR events manager, Courtney Baldwin, said, “The team behind Beyond Beauty Live are working with the world’s leading medical aesthetic practitioners to provide an opportunity for the public to meet with and learn from the best of the best, encouraging patients to choose safe, qualified practitioners who have the skills and experience to achieve exquisite, natural results. Topics that will be covered include aesthetic gynaecology, the Brazilian Butt Lift, body dysmorphic disorder and how to spot it, the perfect lips, body contouring, and real-life patient case studies to portray ‘before and after’ results.”
Launch partners of Beyond Beauty Live include: AestheticSource, Church Pharmacy, Clinisoothe, HydraFacial, InMode, Medical-Up, Teoxane, Totally Derma, Sebbin, Solta Medical, Sciton, Venus Concept, WOW Facial, and Zemits.
Beyond Beauty Live will take place at the Business Design Centre on May 7 and 8, 2022. If you’re a clinic/company that’s interested in exhibiting, please email courtney.baldwin@easyfairs.com for more information. Sun damage
Merz introduces Belotero Revive
Global pharmaceutical company Merz Aesthetics has launched Belotero Revive, an injectable resorbable implant indicated for the revitalisation of early onset photodamaged skin.
The company explains that the implant uses patented cohesive polydensified matrix technology which allows for homogeneous dermal integration. The company states that the implant also includes the addition of 17.5mg/ml of glycerol, which has highly hydrophilic properties. According to Merz, this aims to treat the early signs of sun damage by rehydrating the skin, improving elasticity and firmness, and smoothing superficial fine lines.
Vital Statistics
The number of new melanoma cases diagnosed in 2021 will increase by 5.8% (American Cancer Society, 2021) 20.3 million antidepressant drugs were prescribed between October and December 2020 (NHS Business Services Authority, 2021)
In a survey of 1,543 consumers, 38% require at least a 4-star average rating to consider engaging with a business (Podium, 2021)
In a survey of 2,200 facial plastic surgeons, 70% experienced an increase in bookings and treatments due to the pandemic (AAFPRS, 2021)
In a survey of 1,013 participants aged 20 years or older, 73% reported having acne (Journal of the American Academy of Dermatology, 2021)
71% of 2,000 UK consumers do not think brands and retailers are doing enough to make their beauty purchases more sustainable (The Pull Agency, 2021)
Patient education
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
JOIN THE VIRTUAL CEREMONY
Awards
Cherry Healey to host the Aesthetics Awards

Skincare AestheticSource introduces new brand to its portfolio
AestheticSource has been appointed as the UK distributor of cosmeceutical brand Revision Skincare. Originating from the US, the company explains that Revision Skincare products are formulated using bioavailable peptides, which aim to combat visible signs of ageing, and prebiotic technology to harness skin’s natural microbiome.
AestheticSource notes that the range will debut with an initial 12 products, including the Brightening Facial Wash, Gentle Cleansing Lotion, D·E·J Face Cream, D·E·J Night Face Cream, C+ Correcting Complex 30%, Hydrating Serum, Nectifirm ADVANCED, Retinol Complete, Revox7, Vitamin C Lotion 15%, Vitamin C Lotion 30%, and the Pore Purifying Clay Mask. Another 12 products are set to follow throughout 2021.
Lorna McDonnell-Bowes, CEO of AestheticSource, said, “The addition of Revision Skincare to our portfolio represents a very exciting development for new clinic partners looking for a brand that resonates with current consumer demand for innovative technology and multi-tasking products, presented in an easy to communicate and stunning package. With an exceptional success story in the US, we are ready to share the science, marketing, PR, training and commercial opportunities with clinics who relish the idea of carrying a top US brand during the launch phase.”
Hyaluronic acid
New dermal filler range launches
TV presenter Cherry Healey will be the host of this year’s glamorous Aesthetics Awards, taking place on May 28. Healy began her onscreen career with numerous immersive documentary series on BBC Three. She now presents 10 Years Younger in 10 Days for Channel 5, where she details the latest beauty advice and non-invasive cosmetic techniques, alongside experts in their field. Due to the pandemic, the Awards will take place as a virtual ceremony at 4pm to recognise the remarkable achievements of clinics, individuals, teams and product manufacturers.
To register for the free event go to www.aestheticsawards.com
A new filler range called UTH has been released in the UK. Developed by UTH Aesthetics Ltd, part of CST Group of Companies, the UTH range comprises of four products: Hydrate, Fine, Deep and Sub-Q. The company explains that Hydrate is a skin booster that acts as a sub-dermal moisturiser, stimulating the fibroblasts to produce collagen; Fine is a soft hyaluronic acid filler used for correcting wrinkles and volume loss; Deep is a thicker gel for treating moderate to deep wrinkles and the lips; and Sub-Q has the thickest properties of the range, designed for tissue augmentation, volume restoration and facial contouring. Neil Clarkson, director of UTH Aesthetics Ltd, said, “This product is the culmination of 18 years of research. We wanted to create a dermal filler range that is second to none when it comes to quality and safety, while also being competitively priced. The product ingredients are unrivalled in their quality and our glass syringe delivery system guarantees no plastic contamination of hyaluronic acid.”
According to the company, all practitioners who stock the product will receive a comprehensive marketing pack, which will include collateral and selling tools as well as consent and aftercare forms.

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
New social network introduced

A new app for the medical aesthetic community has been introduced.
Comma is a global social network designed for practitioners to share knowledge and discuss topics related to aesthetic medicine within a secure, private and dedicated community. The app organises the global conversation into sub-groups, or ‘Commas’, which aim to help practitioners find their niche and network with like-minded clinicians who can provide them with support. Comma has partnered with global key opinion leaders (KOLs) to create educational content showcased in a library of high-definition videos. Subscribers can also access exclusive live events and stay up to date through in-app video courses. Dr Tapan Patel, the first KOL to join Comma, commented, “Comma fills a muchneeded gap in creating a professional online environment in which our specialty can communicate and network. I very much look forward to speaking with my colleagues on Comma!”
Careers
Aesthetic recruitment agency launches
Directors of Cosmetic Courses, Jim Savin and plastic and reconstructive surgeon Mr Adrian Richards, have partnered with recruitment consultant Chris Parsons to launch a new recruitment agency specialising in aesthetics. They explain that Clinic People has been created to help clinics get the best and most qualified candidates. Mr Richards commented, “We created Clinic People because we saw a need for a specialist recruitment agency in the industry, led by people who knew just what qualities are needed to create a successful clinic team. Overseeing aesthetic recruitment helps us ensure a safer future by working with well-trained and passionate injectors.”
Savin said, “By working with pharmaceutical companies and training providers we can provide well-trained medical professionals along with support staff for all clinics, regardless of size. We have seen that there is a need for a reliable source of safe and reliable injectors. We can now fulfil that need with Clinic People.” Expansion
Sinclair Pharma acquires Cocoon Medical
Pharmaceutical company Sinclair Pharma has announced the acquisition of the group of companies forming the Cocoon Medical business.
Based in Barcelona, Spain, Cocoon has a portfolio of non-invasive lasers and cryolipolysis devices, with direct commercial operations in Europe, Latin America, Hong Kong and the US, and manages a network of more than 60 distributors. Cocoon’s leading cryolipolysis brands include Cooltech and Cooltech Define, as well as the laser hair removal device Primelase.
Chris Spooner, CEO of Sinclair, commented, “Non-invasive aesthetic therapy regimens frequently involve the use of both injectables and energy-based devices, and it is Sinclair’s vision to service this need by offering our customers a full range of treatment options. Cocoon’s products combine outstanding technology, build quality and user flexibility with competitive pricing to generate an industry-leading value proposition.”
BACN UPDATES
A roundup of the latest news and events from the British Association of Cosmetic Nurses

CLINIC REOPENING
It was fantastic to speak with so many members who were opening their clinics from mid-April and beyond. We know how long it’s been, and it was truly wonderful to see members prioritise patient safety and follow COVID-19 guidelines upon reopening. For the BACN, it is imperative to ensure wellbeing of all practitioners, and wellbeing guidance has been sent out to all members. Every month, the BACN holds a Peer Review and Social, and these are great opportunities to come together and discuss any worries or issues members have been having within their practice. It’s also a chance to de-stress and catch up with members across the UK who are going through similar experiences.
INTERNATIONAL NURSES’ DAY
May 12th is International Nurses’ Day, led by the International Council of Nurses. In 2021, the theme for IND will be ‘Nurses: A Voice to Lead – A vision for future healthcare’. #IND2021 will focus on the changes to and innovations in nursing and how this will ultimately shape the future of healthcare.
APRIL ROUND-UP
In April, the BACN focused on ‘Prescribing within Aesthetic Medicine’ with a range of digital events, offering guidance, updates, and discussion for prescribers and non-prescribers Members are reminded that they can access the digital content post-event by logging into the BACN Member’s Area and going to ‘Resources’, ‘Digital Webinars’.
MAY DIGITAL EVENTS
The BACN will be working with Allergan Aesthetics, an AbbVie Company, throughout May to offer three digital events to members. This month will be about consultation and assessment, with some great speakers and innovative content lined up. Full details, agenda, and list of speakers can be found on the BACN events page.
• In Conversation With – Instagram Live @BACNurses – 18th May 6.00pm
• In Focus Live Webinar – Consultation and Assessment – 25th May 6.00pm
• Peer Review and Social – Zoom Catchup –27th May 6.00pm
This column is written and supported by the BACN
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Social media

Education
Latest patient trends to be revealed in RELIFE webinar
Discover what aesthetic trends you should be watching out for this year by attending the RELIFE webinar, hosted exclusively by the Aesthetics journal. The session will be hosted by award-winning beauty and health journalist, Ingeborg van Lotingen. RELIFE’s key opinion leaders, Dr Martyn King, Dr Simon Zokaie and Dr Vincent Wong will then highlight how clinicians can incorporate the RELIFE Definisse range of fillers, peels and threads into their clinics. The webinar will take place on May 10 at 6:30pm GMT, and practitioners can register for free via the Aesthetics website. To learn more about RELIFE turn to p.38

 Coronavirus
Coronavirus

Hypersensitivity reaction to COVID-19 reported
Aesthetic practitioner Dr MJ Rowland-Warmann has recorded a hypersensitivity reaction to hyaluronic acid dermal filler following contraction of COVID-19. Her case report published in the Journal of Cosmetic Dermatology describes a 22-year-old woman who experienced a delayed reaction after hyaluronic acid dermal filler treatment on her nose. The patient subsequently contracted a moderate case of COVID-19.
According to the report, three weeks after her successful filler treatment the patient found that her nose was red, swollen, hardened, tender, and the skin felt tight. There was no other reason why her nose should have become inflamed, and she had no other symptoms, according to Dr Rowland-Warmann. Dr Rowland-Warmann explains that she offered the young woman oral steroids to treat the inflammation, but the patient declined this and over the next week, the swelling and other symptoms subsided without the need for medical intervention. However, the hump on her nose, which had been completely masked by the HA filler, appeared prominently once again when the swelling went down.
Although this case resolved without the need for intervention, Dr Rowland-Warmann advises that clinicians should be aware of the risk of a hypersensitivity reaction to hyaluronic acid dermal filler in light of the pandemic. The Aesthetic Complications Expert (ACE) Group World has released guidance which recommends that practitioners should not be performing soft tissue filler treatments either two weeks before or three weeks after COVID-19 infection. This guidance applies to all current COVID-19 vaccinations.
Lips
iS Clinical launches two new skincare sets
Skincare brand iS Clinical has introduced the Liperfection Trio and the Extreme Protect Duo to its portfolio. The company explains that the Liperfection Trio includes the Lip Polish for exfoliating dry skin, the Youth Lip Elixir for hydration, and the new Liprotect SPF 35 for UVA/UVB protection. The set will only be available until May 31.

iS Clinical explains that the Extreme Protect Duo includes the Extreme Protect SPF 40, a broad-spectrum UVA/UVB sunscreen and the Liprotect SPF 35.
Your Photoshoot Checklist
Things you need to know before booking photography
•
Know your brand
By this I don’t only mean your logo and colours (have a read of my January column for a more in-depth dive into your branding). But more importantly your core brand values – what is it your brand stands for? What is your brand’s voice; how do you want customers to perceive you from your photographs?
• Your strategy
What are your services or products? What specific image requirements do you have for social platforms, your website and other marketing? What action do you want people to take when they see your images?
• Identify your dream
customers
Who is your ideal customer/patient? Think of the type of people you want to be booking and buying from you. We can work out together how to appeal to them in your images.
• Research photographers
Who is it you are drawn to – is it dark, dramatic images or light, relaxed shots? Is it a lifestyle or studio approach?
Next month’s column: how to prepare for your brand photoshoot
This column is written and supported by Hannah McClune, owner of brand photography company Visible by Hannah www.visiblebyhannah.com

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Photographer Hannah McClune’s monthly tips on how to strengthen your business through branding
Dr Bob Khanna Training Institute gets RSPH approval
The Dr Bob Khanna Training Institute has received approval from the Royal Society for Public Health (RSPH) to deliver a regulated qualification, whilst retaining the core structure and content of its courses.
As a result of this achievement, the Dr Bob Khanna Training Institute is now permitted to offer delegates the chance to obtain the Qualification Council for Cosmetic Procedures (QCCP) medical aesthetic certificates.
Dr Bob Khanna commented, “I am absolutely thrilled that the Dr Khanna Training Institute has become the first in the UK to be approved by the Royal Society of Public Health! We have always been committed to providing a learning pathway that above all promotes patient safety and predictable results. Being recognised as leaders in this area by the RSPH is a direct reflection of the high standards that we have always strived for here at the Training Institute, and we are honoured to have received this accreditation.”
The Skin Cream Parlour Experience Day, Hove
On April 15, private label cosmeceutical provider 5 Squirrels held its first customer experience day at its new manufacturing site in Hove.
The award-winning company enables practitioners to launch their own branded skincare, as well as develop bespoke formulations through The Skin Cream Parlour.
Esther Fieldgrass, founder of EF Medispa, was invited to meet the scientific team to create new formulations to add to her current product offering – also developed with the support of 5 Squirrels – as well as to update her existing branding ready to
Charity Acquisition Aesthetics supports Operation Smile UK
Training provider Acquisition
Aesthetics has launched a partnership with the global medical charity Operation Smile. The charity provides opportunities for safe surgeries for those born with a cleft lip and cleft palate.
CEOs of Acquisition Aesthetics and Operation Smile business ambassadors Miss Lara Watson and Miss Priyanka Chadha say they hope to change at least 17 children’s lives around the world with the target funds raised.

The partnership also encapsulates an official partnership position at the Aesthetics United Charity Conference in 2022, run by Miss Watson and Miss Chadha. Miss Chadha commented, “It has been a longstanding ambition of mine and Lara’s to be involved with Operation Smile and we are absolutely honoured to be chosen as business ambassadors. We hope to raise awareness around the charity and the lives of those it impacts through fundraising events. We also hope to attend a medical mission when we are able to in the near future.”
retail from her clinics and online shop. The team behind 5 Squirrels talked passionately about how courageous it is to launch a skincare brand in such a saturated market, noting that this is why they have created a Wizard of Oz-themed Yellow Brick Road running through the entrance of the premises.
“From the moment customers enter, they can follow in the footsteps of the many skincare pioneers who came before them and lay their very own ‘brick’ on our 5 Squirrels Yellow Brick Road,” explained co-founder Gary Conroy.

Fieldgrass was given a personalised yellow sticker with the brand name and launch date of her skincare range, which she stuck to the ‘road’ and signed, commemorating her achievements. She was also presented with a yellow ‘brick’ trophy to display in her clinic, before being invited to officially open The Skin Cream Parlour with a bottle of bubbly and tour the site’s bespoke rooms for product
development. Conroy said, “We have an apothecary where visitors can work with our formulator to select the active ingredients for their skincare, a perfumery where they can select fragrances, a bottle shop to choose packaging, as well as a design studio for branding and photography.”
He added that customers can create samples of their own products to take home with them, before they go into testing and launch approximately six months later.
Fellow co-founder Amanda Cameron said, “This is the first time we’ve had a customer experience the fabulous Skin Cream Parlour that the team have been working so hard on over the last several months. It’s been so exciting to see it come to fruition and give customers the opportunity to experience creating their own skincare first-hand.”
For Fieldgrass, the experience was thrilling! She commented, “I was so excited to hear about this launch and seeing my ideas for new products come to life fills with me inspiration. I was blown away by the Yellow Brick Road – what can be more perfect?! My brick will take pride of place in my clinic! It’s also so positive to see skincare being manufactured here in the UK, as so much often comes from abroad.”
She added, “The team is so great to work with – I always come with lots of ideas, and I love how open and supportive they are of that.” The Skin Cream Parlour will be open for new customers from July 1.
Qualification
On the Scene
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021

Devices
Dr Tapan Patel announced as KOL for Endolift
Aesthetic practitioner and owner of PHI Clinic in London Dr Tapan Patel is a new UK key opinion leader for skin tightening laser treatment Endolift.
Dr Patel will be joining Dr Priya Verma, another KOL for the Endolift treatment, at MediOracle Consulting, a CPD accredited and recognised medical aesthetics training academy. Dr Patel stated that he was drawn to Endolift due to the many success stories and positive feedback he has received from patients.
Dr Tapan commented, “Endolift is a procedure which bridges the gap between traditional surgery and a non-invasive procedure. By delivering high impact results with minimal downtime, my patients and colleagues are reporting great satisfaction with the outcomes. Endolift is the future of facial tightening; a versatile technology with many applications for skin, dermatology, body contouring and beyond.”
Cutera confirms new brand ambassador
Aesthetic technology manufacturer Cutera has announced its latest UK brand ambassador as Dr David Eccleston, owner of MediZen clinic.

According to the company, the partnership will focus on its new radiofrequency microneedling device Secret RF and will see MediZen as an official ‘Centre of Excellence’ training centre for Cutera. Dr Eccleston commented, “I am pleased and proud to be working with Cutera as an expert and key opinion leader in this exciting new treatment. I am thrilled to be the first clinic in the Midlands to offer Secret RF, as well as being a national training centre. This is the first time I have been seriously impressed with the clinical results of combined needling and radiofrequency treatment. I believe this treatment is a game-changer for skin quality improvement, skin tightening, and the management of scarring and stretch marks, without the need for significant downtime.”
Cutera is set to announce training workshops at the Birmingham-based clinic this summer.
Interface Aesthetics receives VTCT Level 7 Diploma
Training academy Interface Aesthetics has received the VTCT qualification in Clinical Aesthetic Injectables, after the previous Level 7 certificate was withdrawn in 2020. The qualification is recognised and approved by the Joint Council of Cosmetic Practitioners (JCCP).
The company explains that the course incorporates the pre-existing e-Interface online material as well as more video-based content to cover advanced techniques, with the aim of increasing anatomical understanding and safety.
Founder and director of Interface, oral and maxillofacial surgery registrar, Mr James Olding, commented, “We have spent months working towards officially becoming a provider of this regulated and Ofqual-accredited qualification, as we believe that it is the future of injectables training in the UK. At Interface, we believe passionately in patient safety through stronger regulation. Regulating training is the key step in pushing forward this process, as training is the gateway to the industry.”
News in Brief
Intraline appoints country manager
Aesthetic company Intraline has announced Graeme Bryson as its UK country manager. Bryson has more than 15 years of experience as head of sales and commercial for Galderma, national strategic account manager at Novo Nordisk and director at GMCCB Consultancy Ltd, before his current role at Intraline.
Bryson said, “I look forward to working with and supporting our UK partners and clinics with their aesthetic business moving forward following the impact of COVID-19. We want to take our strengths and successes to work in partnership with businesses in the UK market to offer a range of products that will offer impressive results.”
Venus Concept partners with Venus Williams
Non-invasive aesthetic device manufacturer
Venus Concept has appointed tennis player
Venus Williams as its new global brand ambassador. The partnership will see Williams endorse the Venus Bliss device, released last July. Paul Talbot, sales director of Venus Concept UK, commented, “We are beyond excited to share the exciting news of our new global ambassador for Venus Bliss, tennis champion and entrepreneur Venus Williams! Her excellent reputation as an athlete and person is consistent with our company goals and vision.”
Vivacy releases CQC webinar
Aesthetic product manufacturer Vivacy has collaborated with the Care Quality Commission (CQC) to release a webinar. The session explains the purpose of the CQC, and its key issues such as patient safety, cleanliness, and management, as well as how practitioners can maximise becoming accredited.
Country director Camille Nadal commented, “We were delighted to collaborate with the CQC and assist on this webinar to have everyone’s CQC questions and doubts answered.” The webinar took place on April 8 but is now available on demand by emailing Vivacy UK.
JCCP appoints new trustees
The Joint Council for Cosmetic Practitioners (JCCP) has appointed aesthetic practitioner Dr Martyn King and Professor John Underwood as its two new trustees. Dr King has also accepted the role of JCCP vice chair. He commented, “I am extremely honoured to be appointed to the position of vice chair of the JCCP and will work professionally and diligently with the Board of Trustees, sub-committees and all stakeholders to help the JCCP achieve its goals to improve regulation, education, standards and most importantly, patient safety.”
Qualification
Ambassador
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Dramatic Results with Minimal Downtime

Secret RF is a novel fractional radiofrequency (RF) microneedling system that delivers precise, controlled energy at various depths to target patients’ most common skin concerns on the face and body, with little to no downtime.






ALL SKIN TYPES
A unique combination of non-insulated/semiinsulated needles that let you treat a wide range of applications for ALL skin types, avoiding pigmentary complications on darker skin types
IMPROVED PATIENT COMFORT
Precisely controlled RF energy directly into various depths of skin – from 0.5-3.5 mm - offering customised dermal remodelling based on the area and the depth of the condition being treated.


MINIMAL TO NO DOWNTIME
A unique ‘Smooth Motor’ Tip delivery combined with gold-plated needles, reduces discomfort and minimises damage and irritation to the skin’s surface.
Before After 1 Tx Before After 2 Tx Before After 1 Tx Photos courtesy of Clinic for Aesthetic Operative Dermatology, A Renta MD and Michael Sarti MD
Taking Care of Your Mental Wellbeing
Recent statistics released by the Nursing Times revealed that 44% of 1,200 nurses described their mental health and wellbeing as ‘bad’ or ‘very bad’ over the past year. In addition, 62% felt their mental health was much worse now than at the start of the pandemic.1 The decline in mental wellbeing is also reflected in a Physician Burnout Survey, where 71% of physicians reported feeling burnt out. When asked what caused their burnout, 31% of physicians said too much paperwork, 15% cited poor work-life balance, and 12% said the COVID-19 pandemic.2 As healthcare professionals, aesthetic practitioners too are feeling the effects of the pandemic, whether it’s working part time in the NHS, not being able to work at all, or clinic re-openings causing a hectic schedule. Industry associations are taking action, with the British College of Aesthetic Medicine (BCAM) creating a new mindfulness initiative3 and the British Association of Cosmetic Nurses (BACN) sending wellbeing guidance to practitioners. To find out how you can protect your mental health over the next few months, we spoke to aesthetic practitioner and BCAM board member Dr Bhavjit Kaur, and aesthetic nurse prescriber and committee member for the BACN Rachel Goddard.
Incorporating mindfulness
Dr Kaur has been involved in creating BCAM’s new mindfulness and wellbeing initiative. She explains that during doctor appraisals, the association found that there had been a significant negative impact on its members. She comments, “Our members are dealing with the stress of having to treat COVID patients, experiencing financial problems due to a reduced workload, or managing their clinics reopening. Something we’ve found when creating our initiative is that people are rarely focusing on the current moment. They’re always worrying about the past or the future and finding it hard to relax in the present.”
To help this, BCAM is recommending that members learn how to implement mindfulness techniques into their everyday lives. Dr Kaur comments, “We’ve been sharing some simple mindfulness techniques, which are hugely beneficial, however we recognise this doesn’t work for everyone. Instead, practitioners can implement mindfulness throughout their day simply by working on focusing their minds. For example, if you’re out on a walk, don’t be on your phone at the same time and focus on your steps. If you’re eating, focus solely on chewing the food and not also watching the TV. These are little things that can really help to refocus our minds and stop them from getting too overwhelmed.”
Setting your schedule
Goddard advises that practitioners should stick to their assigned clinic hours over the next few months. She comments, “We all have so many patients who haven’t had their treatments done over the last few months, and they’re desperate to have them as soon as possible. As practitioners, it can be really hard to say no to them, but this runs the risk of us working through our lunch and/or working late. In order for us to avoid the risk of burnout, it’s integral to ensure we have those breaks and have that relaxation time, so practitioners need to make sure they aren’t putting their needs above their own. Make sure that you decide what hours you’re going to work, and don’t go over that.”
Goddard also highlights the importance of delegating your workload to your other staff members. She comments, “When it comes to the admin or business activities, it’s okay to delegate that to your colleagues if you’re having a busy day. That way you can focus solely on the clinical side of things. If you have too much to do, you run the risk of rushing treatments or consultations, which can lead to ill-informed patients and complications.”
Dr Kaur notes that getting the correct
amount of sleep is important for a healthy mind. She advises, “As well as making sure your working day is regimented, your sleep schedule is also key for getting through the day. Everyone should be getting at least eight hours per night, which I know is easier said than done! Something important to note is that when practitioners are doing work from home, ensure that you’re working space isn’t in your bedroom – your brain needs to recognise that this is a place of sleep and not work.” The BCAM mindfulness initiative also recommended that members stay away from screens before bed, and instead spend time meditating or reading to relax their mind.
Stay connected
Both Dr Kaur and Goddard note that staying in touch with other people in similar positions to you will be helpful for keeping a positive mindset over the next few months.
Goddard comments, “Since the first lockdown, the BACN experienced a huge spike in new members. It was a time of confusion and upset for the specialty, and I think that associations really gave practitioners something to turn to. If anyone is finding something difficult or has any questions, they can put it onto our forum, which enables them to get responses from others having the same experiences. Associations are vital for giving people the support they need, particularly in a specialty that involves a lot of lone working.”
Dr Kaur also emphasises the importance of having a network of likeminded people, stating, “The reason we created the mindfulness initiative is because we’ve also lived through it, and we know how our members are feeling. It’s useful to have a community that can share their advice and coping mechanisms with you. Everyone in the industry has experienced the same feelings of isolation and loneliness over the last year and I think it’s important for aesthetic practitioners to realise that they aren’t alone. Something as simple as having a virtual coffee morning with other healthcare professionals will really help boost morale.”
REFERENCES
1. Megan Ford, The States of Nurses Mental Health One Year into the Pandemic, 2021, <https://www.nursingtimes.net/news/ mental-health/nursing-times-survey-reveals-state-of-nursesmental-health-one-year-into-pandemic-31-03-2021/>
2. Medical Economics Staff, 2021’s Top Challenges Facing Physicians, Dermatology Times, 2021 <https://www. dermatologytimes.com/view/2021-s-top-challenges-facingphysicians>
3. Holly Carver, BCAM Wellbeing Initiative Targets Pandemic Impact, 2021, < https://aestheticsjournal.com/news/bcamwellbeing-initiative-targets-pandemic-impact?authed>
Following the release of pandemic wellness guidance for aesthetic professionals, Aesthetics explores the ways practitioners can look after their mental health
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Before
After Before After Before After
The gold standard
An expert consensus acclaimed Ultherapy® as the gold standard in lifting and tightening (as published in the Journal of Drugs in Dermatology).
Introducing
The technologies that aesthetic practitioners now have at their disposal has seen the device-based skin rejuvenation market boom. Patients are now demanding more efficacious results but without the downtime required in the past, while physicians are recognising that individuallytargeted and customised treatments are a great way to facilitate this demand.

Every one of our patients has a unique anatomical landscape and, in order to provide them with the optimal clinical outcomes and results, we need to be accurate and targeted with our treatments. However, when it comes to stimulating collagen and elastin in order to facilitate skin lifting and tightening, it can sometimes feel like we are treating in the dark. So, what if you could really see what was going on under your patient’s skin during treatment and could stimulate new collagen and elastin with more precision and accuracy? Even a few years ago this may have seemed like the stuff of science fiction but today it is possible.
Ultherapy®’s Real-Time Visualisation allows clinicians to precisely deliver microfocused ultrasound energy at the correct layer for optimal results.1 And, what’s more, Ultherapy® is the only device of its kind indicated for imaging below the skin’s
surface.2 FDA-cleared and CE certified for non-invasive sculpting and lifting of the skin on the upper and lower face, under the chin, neck and on the eyebrows as well as improving the appearance of lines and wrinkles on the décolletage,2 Ultherapy® uses precise micro-focused ultrasound energy to target the deep structural layers of the skin without disrupting the skin’s surface.3
Seeing every detail matters
Microfocused ultrasound with visualisation (MFU-V) is the foundation of Ultherapy®. By imaging dermal tissues and subcutaneous structures, it allows you to truly see beneath the surface of the skin and feel confident that you are delivering the energy just where it’s needed to rebuild and trigger collagen synthesis while avoiding treating unwanted areas like, bone, fat or nerves.
This means the treatment can also be tailored according to different areas of the face and treatment plans can be customised to individual patient needs.4
Real-time visualisation allows providers to:
• Evaluate the anatomy of patients’ skin
• Select the proper transducer
• Target the desired tissue layer
• Ensure optimal device to skin coupling
• Avoid bone and vessel
• Minimise patient discomfort
Dr Tracy Mountford from the Cosmetic Skin Clinic in Buckinghamshire says, “Patients now recognise the benefits of Ultherapy® as a first line of treatment for skin maintenance and optimum skin health.
The results-driven non-surgical Ultherapy® treatment enables the skin to naturally lift and tighten, so patients can achieve a lifted midface, a more defined jawline and neck, or natural looking brow lift.”
Why choose Ultherapy®?
• The only FDA-cleared device of its kind
• 1.75 million treatments worldwide
• Most researched skin tightening device
• 6,000 systems sold globally
• 100+ patents
• 50+ clinical studies
• Supported by 90+ peer reviewed papers
With Ultherapy®’s unique visualisation technology you never have to treat your patients blindly again.
Want to find out more? Contact your Merz Aesthetics account manager for more information on Ultherapy® by visiting https://ultherapy.co.uk/contact-us/
This advertorial is sponsored by Merz Aesthetics UK & Ireland
REFERENCES
1. Fabi SG, Joseph J, Sevi J, Green JB, Peterson JD. Optimizing patient outcomes by customizing treatment with microfocused ultrasound with visualization: gold standard consensus guidelines from an expert panel. J Drugs Dermatol. 2019;18(5):426-432.
2. www.accessdata.fda.gov/cdrh_docs/pdf13/k134032.pdf. Acce
3. White WM, et al. Arch Facial Plast Surg Clin N Am. 2014;22;27ssed September 2019
4. Fabi SG and Goldman MP. Dermatol Surg. 2014;40;570
5. White WM, et al. Arch Facial Plast Surg Clin N Am. 2014;22
(0) 333 200 4143.
Aesthetics | May 2021 20 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Merz Aesthetics
Reporting
information
Ultherapy® How technology
that lets
you
see under the skin can optimise lifting and
tightening
results
Please consult your practitioner as individual results may vary. Adverse events should be reported. Reporting forms and information for United Kingdom can be found at www.mhra.gov.uk/yellowcard.
forms and
for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/report-an-issue/mdiur.Adverse events should also be reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44
M-ULT-UKI-0936 Date of preparation April 2021
Choosing SPF for Your Patients
Hot summer holidays abroad might be put on hold this year, but that doesn’t mean sun care shouldn’t be at the forefront of your patients’ minds. In fact, because they are more likely to be holidaying in the UK this summer, they might have the misconception that SPF isn’t needed!
Here, dermatology and aesthetic nurse prescriber Anna Baker, aesthetic practitioner Dr Dev Patel and consultant dermatologist Dr Maria Gonzalez share their advice for recommending sun protection to patients and detail their top tips for patient education.
The importance of SPF
First and foremost, sun protection factor (SPF) is crucial for melanoma skin cancer prevention, which has more than doubled (135% increase) in the UK since the early 1990s.1 Dr Gonzalez says, “Before you think about aesthetics, life-threatening skin cancer caused by UV rays is crucial to prevent and it’s probably the most important reason for recommending sun protection to your patients. From a cosmetic standpoint, excessive sun exposure is one of the most damaging things your patients can do to accelerate their skin ageing.”
According to a study involving 298 Caucasian women, UV exposure accounted for around 80% of the signs of ageing – known as photoageing.2
Baker adds, “UV can also lead to polymorphic light eruption, solar urticaria, and can aggravate symptoms of rosacea, as well as skin lesions of lupus erythematosus – even herpes simplex. The prolonged effects of unprotected sun exposure over time can include irreversible damage, such as skin cancers, as well as triggering photodamage dyschromias, the appearance of uneven pigmentation, textural skin changes (roughness), the appearance of visible pores, in addition to visible lines and wrinkles.”
With all of these factors to consider, Dr Patel reiterates that it’s no surprise aesthetic professionals are re-enforcing the importance of using an effective SPF formula every day to maximise skin health
and further enhance the impact of patients’ cosmetic interventions. He says, “SPF is also a critical part of the aftercare for so many treatments, including chemical peels, laser and intense pulsed light, to help prevent hyperpigmentation and encourage successful healing.”
Choosing sun protection
There are many different factors to consider when it comes to sun protection, the practitioners note. The UVA and UVB protection capacity, the type of filter, and cosmetic appeal are just some of the considerations they make when choosing products to stock in their clinics and recommend to patients.
UVB protection
Sunscreens contain substances which protect the skin from UVA and UVB radiation (Figures 1 & 2). Baker explains, “SPF provides an indication of the degree of protection offered against UVB specifically; the multiples of protection provided against burning, compared with unprotected skin.”
The SPF value will protect the skin from a certain percentage of the UVB rays. For example, Dr Patel explains, “SPF 15 will
Understanding UV wavelengths
Sunlight contains ultraviolet (UV) radiation, which is approximately 200-400 nm in wavelength. Short wavelengths (UVC) do not reach the skin as they are absorbed by the earth’s ozone. Medium wavelengths (UVB) are most associated with sunburn, while long wavelengths (UVA) enter the skin more deeply, can penetrate window glass, and play a major part in skin ageing. Both UVA and UVB contribute to skin cancer.3,4,5
protect the skin from 94% of the UVB rays. If we jump up to factor 30 it offers 97% protection, for factor 50 it is 98% and for SPF 100 it is 99%.6 What many people don’t realise is that although the factor number jumps to a higher value, realistically the percentage of protection increases at a much smaller percentage.”
Although a minimum of factor 15 is often recommended and is the lowest factor endorsed by the US Food and Drug Association,7 the British Association of Dermatologists (BAD) recommends a sunscreen with an SPF of 30 as a satisfactory form of sun protection, in addition to protective shade and clothing.8 This aligns with advice from the American Academy of Dermatology Association.7
According to The Australasian College of Dermatologists, individuals should use SPF 30 or 50 because sunscreens with higher SPF have been shown in real world settings to be more resistant to wearing off due to factors such as sweating, wiping off with towels, and not applying sunscreen thickly enough.9
Of course, SPF recommendation should also consider the Fitzpatrick skin type of patients. Dr Gonzalez suggests, “Those of higher Fitzpatrick skin types will require less SPF protection than those with lower types from a burning and skin cancer perspective due to the melanin in the skin, but application for all skin types, particularly those with pigmentation, will help reduce the signs of ageing.” According to the BAD, skin types V-VI should wear sunscreen during periods of prolonged or intense sun exposure, but it’s not needed routinely.10
Practitioners share their advice and considerations for recommending SPF to your patients
UVA Atmosphere ozone 400nm 320nm 280nm 100nm UVB UVC Dermis Epidermis Figure 1: Solar ultraviolet rays and their biologic effects on the skin5 Solar Radiation UVA biology effects Oxidative damage Abasic sites Base modifications Strand breaks UVB biology effects Cell cycle changes Cyclobutane pyrimidine dimers Mutations 6-4 photoproducts @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
BELIEVE IN THE POWER OF SEEING.
Ultherapy® is the only FDA cleared microfocused ultrasound technology that has real time visualisation (MFU-V).1,2
Real-time visualisation, enabling treatment customisation, precision targeting of tissues, and optimised patient outcomes 3
FDA-cleared and CE-marked so you can be confident of Ultherapy®’s good safety profile1
The Gold Standard for non-surgical lifting and skin tightening, as determined by an expert consensus panel3
For more information visit Ultherapy.co.uk

REAL-TIME VISUALISATION
REFERENCES:
1. www.accessdata.fda.gov/cdrh_docs/pdf13/k134032.pdf Accessed September 2019 2. Ulthera release: Ultherapy® décolletage treatment now FDA-cleared. BioSpace website. https://www.biospace.com/ article/releases/ulthera-release-ultherapy-and-0174-d%C3%A9colletage-treatment-now-fda-cleared-/. Accessed January 21, 2020. 3. Fabi SG, Joseph J, Sevi J, Green JB, Peterson JD. Optimizing patient outcomes by customizing treatment with microfocused ultrasound with visualization: gold standard consensus guidelines from an expert panel. J Drugs Dermatol. 2019;18(5):426-432
Adverse events should be reported. Reporting forms and information for United Kingdom can be found at www.mhra.gov.uk/yellowcard. Reporting forms and information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/report-anissue/mdiur. Adverse events should also be reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143.
Refer to the Instructions for Use (IFU) for complete instructions on operating the Ultherapy® System The non-invasive Ultherapy® procedure is U.S. FDA-cleared to lift skin on the neck, on the eyebrow and under the chin as well as to improve lines and wrinkles on the décolleté. The CE Mark indications for use for the Ulthera® System include non-invasive dermatological sculpting and lifting of the dermis on the upper face, lower face, neck and décolleté. Reported adverse events from postmarketing surveillance are available in the Instructions for Use (IFU ). Please see the available IFU in your country for product and safety information, including a full list of these events. © 2018 Ulthera, Inc. The Merz Aesthetics logo is a registered trademark of Merz Pharma GmbH & Co. Ulthera, Ultherapy, DeepSEE, SEE THE BEAUTY OF SOUND and the Ultherapy logo are trademarks or registered trademarks of Ulthera, Inc., in the U .S. and /or certain foreign countries.
Merz Pharma UK Ltd. 260 Centennial Park, Elstree Hill South, Elstree, Hertfordshire, WD6 3SR Tel: +44 (0) 333 200 4140
M-ULT-UKI-0914 Date of Preparation March 2021
1
@merzaesthetics.uki Merz
Aesthetics UK & Ireland
Inorganic








sunscreens have typically excelled. Dr Gonzalez also suggests that a combination of both organic and inorganic filters can be beneficial for patients with pigmentary problems. “Melasma for example is such a stubborn condition that it’s useful to try everything you can to prevent and further cause the discolouration, if there are no issues with sensitivity.”

UVA protection
Practitioners note that it’s also important patients are using a product containing UVA protection, not just UVB. The UVA ingredients are shown in Figure 2
In the UK, many sunscreen manufacturers use the UVA star rating on the packaging to demonstrate it also protects against the rays commonly causing the signs of ageing. It ranges from 0-5 stars and refers to the ratio of UVA protection compared with UVB. Baker says, “Star rating systems have become contentious regarding their usefulness. It’s important to remain mindful that in using a low SPF, it may still have a high level of stars – not because it is providing lots of UVA protection, but because the ratio between the UVA and UVB protection is about the same.”

Sunscreens which comply to this stipulation can be labelled with a UVA logo alongside the SPF classification, she says. “Evidence suggests that formulations which contain reflective substances, such as titanium dioxide, provide superior levels of protection against UVA. Current evidence supports the recommendation to consider choosing a high SPF as well as a high UVA protection – for example a product with a high number of stars. SPFs providing both UVA and UVB protection are called ‘broad spectrum’.”
Organic vs. inorganic filters
There are two different types of filters that will be included in a sunscreen – organic/ chemical and inorganic/physical – see Figure 2 for more information on filter ingredients. Baker explains, “Organic filters absorb harmful UV radiation, convert it and give this energy back out as infrared. These are sometimes referred to as ‘absorbers’, or ‘chemical’ sunscreens, such as avobenzone
and octisalate-organic. It does not mean ‘organic’ in the environmental sense, which can be confusing for patients!” She adds, “Inorganic filters (often described as ‘physical’, ‘natural’, ‘reflective’ or ‘zinc’) reflect the UV rays.”
When Baker educates patients about the difference, she says organic/chemical filters can be considered as sponges that mop up the UV radiation, and inorganic/physical filters can be thought of as mirrors, which bounce UV straight back off the skin, which she says resonates well with them.
So, should you choose or recommend organic or inorganic filters for your patients? The practitioners reiterate that it depends on their skin.
Dr Patel says, “As organic/chemical filters release energy as heat or light, this may have a pro-inflammatory effect on the skin and encourage inflammation.”
Dr Gonzalez adds that this is particularly crucial to consider from a dermatology perspective. “There is a higher possibility of causing skin sensitivity with organic/ chemical sunscreens so for patients with any skin condition, such as rosacea who report sensitive skin, I would avoid. In my clinic, I see a lot of patients with rosacea, and these patients tend to have very dry, sensitive skin so it can be tricky to find sun protection which they can tolerant, so it is important to make sure you have sun protection which includes more inorganic components. In my experience, inorganic/physical sunblocks tends to be better tolerated by patients of all skin types, whether they are sensitive or not sensitive. For acne-prone patients, I also tend to avoid oil-based sunscreens.” Of course, she notes, the cosmetic appeal of the product also needs to be considered for maximum compliance, which is where organic/chemical
Dr Patel prefers to recommend inorganic/ physical filters to his patients for the above reasons, because he finds them less irritating following cosmetic interventions. “I think a combination of the two filters is ok, but I would always look at the ingredients’ list to identify if there is a decent percentage of the physical filter.” If the percentage is not specified, Dr Patel says you can have an idea of the amount according to where it appears in the ingredients’ list – with the top usually appearing first, and lowest last. He adds, “The most important thing for me is a product which has zinc oxide in it as this protects from UVA as well as the UVB rays. I also check that the product is free of fragrance to avoid irritation.”

Another consideration Dr Patel says, is the longevity of the product. “Organic/ chemical sunscreen also tends to not be as photostable, so may deplete quicker than inorganic/physical which tends to last longer on the skin. If you have a patient who is less likely to reapply their sunscreen then I would recommend they use inorganic/physical,” Dr Patel explains.
Product cosmetic appeal
It’s easy to recommend an SPF to your patients and educate them in its use, but they also need to like using the product from a cosmetic standpoint, otherwise they just won’t bother. “This is a big consideration. What I have found is that one SPF product does not fit the needs of all my patients as there are lots of different preferences when it comes to the cosmetic appeal of the product,” says Dr Patel, adding that patients must enjoy using the product and be happy to use it longterm. “This is why I choose to include several different brands of SPFs in my clinic.”
Although Dr Patel prefers to recommend inorganic/physical SPFs, they have traditionally had a thick, chalky appearance, which can cause the skin to look white or have a greyish hue. “We tend to sell a lot of tinted sunscreens to compensate for this. Nanotechnology has been an advancement to reduce the particle size of the filters, which
2.
3.
4.
5. Diethylamino hydroxybenzoyl
benzoate 6. Ecamsule 7. Methyl
1. PABA
•
2.
•
•
3.
•
•
4.
5. Ensulizole 6.
1.
2.
3.
4.
1.
2.
3.
4.
•
•
•
•
•
•
Figure 2: The key ingredients in topical sunscreens5,11 UVA filters 1. Benzophenones • Oxybenzone Sulisobenzone • Dioxybenzone
Avobenzone
Meradimate
Bisdisulizole disodium
hexyl
anthranilate UVB filters
derivatives:
Padimate O
Cinnamates
Octinoxates
Cinoxate
Salicylates
Octisalate
Homosalate Trolamine salicylate
Octocrylene
Ethylhexyl triazone Broad spectrum filters
Ecamsule
Silatriazole
Bemotrizinol
Bisoctrizole Broad spectrum filters
ZnO
TiO₂
CeO₂
Others:
Iron oxide
Red veterinary petrolatum
Kaolin
Calamine Ichthammol
Talc
1.
2.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Organic Hybrid (Organic/Inorganic)
Bisoctrizole
Inorganic + organic agent
THE WORLD LEADER JUST RAISED THE BAR
*Referring to the original CoolSculpting® system, CoolSculpting® is the world's number one body contouring treatment, based on HCP tracking market research in the US, UK, Germany, Canada, Brazil, China and Australia (N=526), and global market research of the overall body shaping and skin tightening market.2

During or immediately after the procedure you may experience pulling, tugging, mild pinching, intense cold, tingling, stinging, aching, cramping, redness, swelling, blanching, bruising, firmness, tenderness, cramping, itching, skin sensitivity, and numbness that can persist for several weeks. After submental treatment you may feel fullness in the back of the throat. Rare side effects include paradoxical hyperplasia, late-onset pain, freeze burn, vasovagal symptoms, subcutaneous induration, hyperpigmentation and hernia. The procedure should only be undertaken with physician advice, and not for those with cryoglobulinaemia, cold agglutinin disease or paroxysmal cold haemoglobinuria. It is not a treatment for obesity, weight loss, or a replacement for a healthy diet and active lifestyle.1
1. Allergan. CoolSculpting® system (CoolSculpting® ELITE) user manual. CS-UM-CM3-04-EN-A. 2020. 2. Allergan. Unpublished data. INT-CSC-1950062. CoolSculpting® market research. July 2019.
3. FDA. K193566. ZELTIQ® CoolSculpting® System. January 2020.
CoolSculpting®, the CoolSculpting® logo, the CoolSculpting® ELITE logo, and the Snowflake design are registered trademarks of Allergan Aesthetics. CoolSculpting® systems, applicators and cards are medical devices Class I or Class IIa CE0197. ZELTIQ® is part of Allergan Aesthetics, an AbbVie company. © 2020 AbbVie. All rights reserved.
UK-CSC-2050439 Date
Material
Adverse
THE NUMBER 1 BODY CONTOURING TREATMENT PROUDLY INTRODUCES THE NEXT-LEVEL COOLSCULPTING® ELITE* 1–3 TO MEET YOUR POTENTIAL WITH COOLSCULPTING® ELITE GET IN TOUCH WITH YOUR LOCAL REPRESENTATIVE INT.COOLSCULPTINGHCP.COM/UK
The suitability of CoolSculpting® treatment on an individual patient basis should always be considered as part of the assessment and consultation process. CoolSculpting® is not suitable for all patients. Please consult the Directions for Use prior to the procedure. Patient results may vary.
of preparation: December 2020.
produced and funded by Allergan Aesthetics an AbbVie Company.
events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov.uk Adverse events should also be reported to Allergan Ltd. UK_Medinfo@allergan.com or 01628 494026
Products in practice
We know there are hundreds of sunscreens available, so it can be hard to find the right products for your patients. Here practitioners share what they are recommending to their patients at the moment.
Anna Baker: A product my patients are really loving at the moment is Tancream because it offers the option to develop a gradual self-tan with advanced antiageing benefits. When patients want some good tinted coverage I also like to recommend the Skinbetter Tone Smart SPF 50, which provides advanced mineral protection in an elegant compact formulation.
Dr Dev Patel: For many years I have had the Tebiskin and Synchrorose ranges in my clinic. Their SPFs incorporate ingredients that also help support and restore the skin’s integrity, so I find they are excellent for conditions like rosacea and acne, as well as helping inflammation post procedure. Another brand I like to recommend is AlumierMD, which boasts a purely physical filter SPF range. I also recently introduced my own skincare line called CellDerma and we are about to launch three new SPFs, which includes two pure mineral-based formulae and an ultralight cream that goes on perfectly under make-up as well as on darker skin types.
Dr Maria Gonzalez: The most commonly sold SPF in my clinic is SunSense, which is an Australian brand. I find that it’s not terribly expensive and most people seem to tolerate it well. I also recommend the NeoStrata Defend Sheer Physical Protection SPF 50 and Universkin Nexultra Dermaheal SPF 50+, which are cosmetically acceptable formulations offering good sun protection that patients tend to like.
is improving the thickness and chalkiness, but there are still advances to be made in this area.” Dr Gonzalez says that patients with darker skin often don’t like to use inorganic/ physical sunscreens because they are cosmetically unacceptable appearing very white on darker skin. This is challenging and should be considered, but notes that tinted sunscreens can help.
Educating patients
Firstly, studies looking into the application of sunscreen emphasises the importance of educating patients about using it generously and frequently.
According to one study of 16 participants, sunscreen users received less than half the sun protection they think based on their topical use.12 Other research involving 57 participants found that when applying sunscreen people miss, on average, 10% of their face, with the most commonly missed areas being the eyelids (13%) and the area between the inner corner of the eye and the bridge of the nose (77%).13
The BAD notes that with so many different types of sun protection products available (including lotions, mousses, sprays and gels) it’s difficult to give set guidance on application. However, it recommends that when using lotions, patients should apply at least six full teaspoons to cover the body of an average adult, which is more than half a teaspoon of sunscreen to each arm and the face/neck (including ears). It should
be reapplied at least every two hours, and immediately after swimming, perspiring and towel drying, or if it has rubbed off.14
Whilst Baker emphasises that practitioners should work to gold standard UK and international dermatology guidelines,7,8 a bespoke approach to education is key. “Patients should be counselled on an individual basis with regard to Fitzpatrick skin type, and condition of their skin when deciding the specific SPF that’s most suited to them, with advice on frequency of application/reapplication depending on their medical history and day-to-day lifestyle considerations,” she says.
Educating patients on the impact of the sun and ageing really encourages compliance, according to Dr Patel. “Patients still don’t often understand the relationship between the sun and pigmentation, for example. When you explain that pigmentation from the sun causes a loss of skin vitality and an aged appearance, and utilising SPF religiously will help slow down the process of pigmentation in their skin, it helps motivate them,” he notes. Of course, it’s also important to educate yourself and your patients on the importance of vitamin D and the fact that supplementation might be needed, especially in the winter months and for those with a high Fitzpatrick skin type, practitioners highlight.
SPF in makeup and moisturisers
There is a huge misconception that SPF in makeup and moisturisers is the same as
regular sunscreen, practitioners say. “It’s important to remain mindful that an SPF in a moisturiser is not considered sufficient broadspectrum protection and may not contain any UVA protection. SPF used in moisturisers is usually tested the same way as sunscreens, however, many formulations are less likely to be water resistant, rub-resistant, and are likely to be applied more thinly than SPF,” Baker states. This point is also emphasised by the BAD.15
When it comes to makeup, Dr Patel says that many patients believe their SPF 15 foundation is sufficient protection for burning and ageing prevention. “It’s better to educate patients to apply makeup after their sunscreen because makeup is very dose dependent; someone might want light makeup, for example. We know that most people don’t apply SPF properly and don’t use enough, but interestingly, it has been reported in the past that the average person needs to use seven to 14 times the normal amount of powder or foundation to get the SPF coverage required.”16 Of course, tinted SPFs can also be recommended as a substitute to makeup, as long as they apply enough for sufficient protection, practitioners note. A new study suggests that combining the two might be a good approach, finding that layering sunscreen with makeup containing SPF may compensate for insufficient sunscreen application in real-life conditions by providing an additional source of UV protection and improving the homogeneity of coverage.17
Shining light on sun protection
Choosing the right sun care for your patients will help increase compliance, and thus reduce their chances of skin cancer and photoageing. Educating patients is key and due to different cosmetic aspects of products, it might be useful to integrate and recommend several brands in your practice. Outside the scope of this article is the evolving understanding and research around sunscreens to protect the skin against blue light, as well as the inclusion of ingredients such as antioxidants and vitamins to further support skin health.
VIEW THE REFERENCES ONLINE! WWW.AESTHETICSJOURNAL.COM @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021

YOUR LOOK THE EXCELLENCE OF SWISS SCIENCE
LIGHT UP
RHA 4
DYNAMIC & SOFT VOLUMIZING
Manufactured to boast resilience and strength when placed within dynamic anatomical zones, this volumizer will provide soft volume within the superficial fat to naturally enhance and contour the mid cheek.
•High strength & stretch
•Low BDDE + High Molecular Weight
A TWO
-
STEP APPROACH
By combining two complementary HA fillers: Redensity 2, the first and only HA gel specifically designed to treat the under-eye hollows, alongside RHA 4, a dynamic HA filler that offers soft volume enhancement in the mid cheek region, Teoxane can provide a holistic treatment approach to target the infraorbital area.


These two products are perfectly positioned to combine for optimal outcomes, offering your patient visibly brighter, refreshed and hydrated under eye and mid face treatment.
REDENSITY 2
FIRST AND ONLY HYALURONIC ACID GEL DESIGNED FOR UNDER EYES HOLLOWS
A rheological profile that has been specifically designed to treat the infraorbital hollows.
• Low hygroscopy for decreased risk of adverse events & reliable correction
• High spreadability for improved gel positioning & efficient filling of the under-eye cavity
• Manufactured with a mix of crosslinked & non crosslinked HA with essential nutrients
Understanding Artistic Appreciation
A deep understanding of beauty and aesthetics is implicit when forging a career in aesthetic medicine and yet perhaps this is not given the attention it should receive when in training.
There is quite rightly a focus on patient assessment, anatomy, technical skills, product knowledge, safety and avoidance of complications, but the study of aesthetics and artistic appreciation is generally considered to be an area of expertise developed over time. In this article we will explore some of the historical and contemporary concepts of beauty, the psychology of beauty in the modern world and the importance of artistic appreciation within a successful aesthetic practice.
Why is artistic appreciation important?
Understanding and learning about artistic appreciation is a fundamental concept within aesthetic practice. However, we recognise it is considered a relatively nebulous concept and usually only grasped and embraced after years in practice.
The concepts behind beauty, including its representation, articulation and modification are part of a complex sociological dynamic spanning thousands of years. However, regardless of fads and fashions, we wish to present a few ideas and inspirations that practitioners may find useful and incorporate into their own thought processes when assessing and treating patients.
It is also important to constantly examine what we are trying to achieve for any one patient and to listen carefully to their aspirations and wishes – are we improving beauty, treating their insecurities and psychology, are we contouring, improving proportions, minimising asymmetry or making patients look younger? Or indeed all of the above? Whilst we need to be sensitive to what the patient wants and not necessarily what the aesthetic practitioner wants, an understanding of beauty and artistic appreciation will help evolve the best treatment programme for that patient.
Historical concepts of beauty
The notion that beauty is ever changing is certainly true but to understand where we are today, we must first understand where our concepts of beauty are derived. Western standards of beauty were generally considered to be set 2,400 years ago in Greece and Rome.
The ancient Greeks believed that a beautiful woman’s face was defined by perfect, harmonious proportions and symmetry. Maths played a significant role in this, with early mathematicians such as Euclid formulating a pattern known as the ‘Golden Ratio’ (also termed the Fibonacci Ratio, Phi Ratio and, sometimes, the Divine Proportion), which has a constant value of Phi=1.618.1
This ratio was later used by artists, such as Leonardo Da Vinci when drawing the human body, as a way of creating perfect symmetry and form. The width of the mouth is ‘Phi’ times the width
of the nose. The distance between the lateral canthi is ‘Phi’ times the width of the mouth. The height of the face from the pupils to the chin is ‘Phi’ times the height from the hairline to the pupils (Figure 1). “The secret to beauty, by Greek standards, was in the harmonious proportions of facial features,” confirmed art historian and painter Carol Ravenal in a Washington Post article, who added, “There was both a rationale as well as mystical appeal. Mathematics was the key to form.”2 In a similar vein the Greek philosopher Plato viewed the structure of the human body and face as a system of triads; for Greek mathematicians, the number three had special significance. The perfect face was divided into three sections: from hairline to eyes, from eyes to upper lip, and from upper lip to chin. The ideal face was two thirds as wide as it was high. Even today, plastic surgeons divide the face into thirds during their routine examinations and we would encourage all aesthetic practitioners to do likewise.3


Concepts of feminine beauty then definitely entered a new era and changed subtly with advent of the 15th-century Italian Renaissance. Famous artists like Botticelli, Raphael and Leonardo Da Vinci painted a procession of exquisitely varied faces and yet all were united by a certain aesthetic. Ravenal explained, “Botticelli’s Madonnas are lovely… because they appear delicate and destructible. Leonardo’s paintings of the Virgin show a woman who is beautiful not because her features are perfect in the Greek sense but because her face conveys a sense of tenderness and mystery,” – i.e. is less objective and more subjective.2 However, many commentators believe it is Raphael’s standard of beauty that shaped the work of artists for centuries after. “His image of beauty is exquisite,” said Ravenal, “It’s not threatening. While less monumental than the Greeks, it’s still harmonic.
Figure 2: Raphael – Young Woman with Unicorn. Concepts of feminine beauty and aesthetics entered a new era with the Renaissance. Raphael was considered to be one of the most influential artists in this regard.

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Consultant plastic surgeon Mr Paul Banwell and nurse prescriber Nina Prisk discuss the essential concepts in beauty and aesthetics
Figure 1: Diagram illustrating the concept of the Fibonacci Ratio and the Golden Ratio in a beautiful face
Raphael understood the feminine psyche.”2 These comments start to give us a flavour of the different approaches to beauty and aesthetics – they give credence to the importance of both the complexities of mathematical ratios, symmetry and facial harmony from the Greeks, but also the more erudite and nebulous subjective concepts of beauty developed during the Renaissance. Both these concepts are very much evident today in our aesthetic practices. In essence, history suggests that whilst a beautiful face is one with harmonious proportions and symmetry, other factors come into play too.
Contemporary concepts of beauty
The modern idea of beauty draws richly from these past influences, with one commentator summarising four emerging concepts that are now widely acknowledged as being the major determinants of attractiveness.3,4 These are:
• Averageness (prototypicality) – this draws on the concept that humans are actually attracted to ‘average’ faces as they are easier on the eye and on the mind
• Sexual dimorphism – femininity is considered more desirable as it is a signal of fertility in human female faces because it is associated with oestrogens which in turn is a sign of reproductive health
• Youthfulness – a young face that doesn’t show the signs of ageing is generally considered most attractive
• Symmetry – facial features in proportion with one another are often regarded as a signal of beauty5
Inspired by the concepts of symmetry and patterns from the Greeks, in 2001 board-certified plastic surgeon Dr Stephen Marquardt adapted these ideas and created a template called the Marquardt Beauty Mask, which is made up of a primary and secondary ‘Decagon Golden Matrix’ (geometrically and mathematically all multiples of Phi).6 He believes this concept identifies facial characteristics that are universally perceived as beautiful. This ‘mask’ has often been applied to various actresses and individuals considered to represent the pinnacle of a beautiful face. Whilst beauty is subjective and in the eye of the beholder as well as determined by culture, fashion and many other influences, the Marquardt Beauty Mask was formulated on the concept that certain aspects of beauty remain consistent throughout history. However, not all commentators subscribe to the importance of symmetry and one London author, Alexander Walker, considered further definitions of beauty in his 1836 book Beauty: An Analysis and Classification. He countered the importance of the idea of symmetry and instead identified the need for asymmetry, saying that it is, “The first character of beauty in thinking beings. An occasional irregularity makes us better appreciate symmetry.”2 This is perhaps something to bear in mind in every day aesthetic practice as it is not always wise or correct to chase the quest for symmetry.
The psychology of beauty
Like it or not, there is a beauty bias. Scientists discovered long ago that people for better or worse show favour to those with a pretty face.7 Attractive people are also more likely to get jobs and we even unconsciously think attractive people are smarter and friendlier than less attractive people. This so-called ‘Beauty Premium’ is a theory that people who are more attractive are more successful in life, in work and earn more money than those with
below average looks.7
This idea is also supported by Daniel Hamermesh, a US economist, and a professor of Economics at Royal Holloway, University of London. He contests that beauty is connected to financial success and has written a book called Beauty Pays, Why Attractive People Are More Successful looking at this correlation. The book also suggests that attractive people earn an average of 3-4% more than people with below-average looks.8 Even more well-known is Nancy Etcoff, a faculty member at Harvard Medical School and a practising psychologist, who has promoted similar concepts in her book – a must-read for all aesthetic practitioners – Survival of the Prettiest. She examines notions such as how beauty cannot be precisely defined, but how people recognise it instinctually (many parallels with our discussion on classical concepts of beauty above). Crucially, Etcoff supports the concept that it is an evolutionary and biological development of our species.9 In other words, our desire for beauty is hardwired in our brains.
Social media and modern influences on beauty idealism
Social media, influencers, celebrities, selfies, filters, Zoom and Snapchat dysmorphia are now all instantly recognisable terms highlighting how modern technology dominates and drives perceptions of beauty. However, clinical psychologists Mavis Henriques and Debasis Patnaik point out that, “Images on social media sites are idealised and unreal, due to digital alteration thereby setting high expectations from individuals in society.”10 The impact of social media has been further explored by author Autumn Whitefield-Madrano in her book Face Value: The Hidden Ways Beauty Shapes Women’s Lives 11 This diary of beauty examines in detail the relationship between appearance, beauty, science, social media, sex, friendship and more. The prevalence of photo-editing technology has also altered our perceptions of beauty and means the level of physical ‘perfection’ previously seen only in celebrity or beauty magazines is now commonplace on social media. Researchers from Boston in the US argue that as these images become the norm, people’s perceptions of beauty worldwide are changing and being distorted, which can inevitably take a toll on a person’s self-esteem and can trigger body dysmorphic disorder.12 Research published in 2018, consisting of 26 in-depth interviews with women aged 18-32, indicated that although female millennials do look up to celebrities to define their ideal body, they also experience equally intense negative feelings after the comparison of their selfies to those of attractive friends. It was also demonstrated that the number of likes and comments are as important to female millennials as the aesthetics of the selfie. Likes and comments therefore play a significant role in the construction of body image perception of beauty.13
Artistic appreciation and facial aesthetics
Whilst practitioners definitely need to be aware of classical and modern influences on beauty idealism as well as consideration of patient psychology, a focus and understanding of their application to artistic appreciation is clinically more relevant. No matter what stage you are at in your career, artistic appreciation encompasses a consideration and understanding of beauty, geometry, harmony and proportions. Whilst we have seen that concepts of beauty have changed over the years, there are constants that still remain and our contemporary understanding of the ageing
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
process to include bony, soft tissue, fat compartments and skin changes has reinforced our thoughts immensely in this regard.14,15 However, a systematic (and critical) full facial physical evaluation still remains a prerequisite regardless of whether you are at foundation level or an advanced injector – the assessment should always remain constant, but the treatment response/ technique/product
choice may vary depending upon experience. Splitting the face into thirds, as per the Greeks, still remains at the core of artistic appreciation (Figure 3). We recommend careful observation of the upper third (forehead, temples and eyes), middle third (nose, fat pads and cheeks) and lower third (mouth, chin and jaw) to visualise symmetries and asymmetries, before looking at the side profile with particular reference to the profile balance (relationship of the nose and chin). The age of the patient and their ‘skin age’ will also then influence choice of product and therapeutic approach. A younger patient in general will be looking for balance and harmony with refinements in structure and contour, in contrast to an older patient, where addressing volume loss is usually the key.
As part of our teaching programme at Banwell.Prisk School of Medicine we have formalised these steps into the following acronym to help focus thoughts of artistic appreciation: F.A.C.E. A.R.T.
• Full facial assessment
• Asymmetry
• Contour and curves
• Evaluate
• Artistic considerations
• Re-evaluate
• Treatment plan/Therapeutic approach
Thinking about the full face in a holistic manner, focusing on asymmetry, contours and curves leads to a complete evaluation; however, make a point of thinking about your patients as a canvas in an artistic way and then re-evaluate your plan before commencing treatment. Another simplistic observation which is often overlooked is not to be afraid to move around the patient – get yourself in the most comfortable position to perform your work, even if it means moving when injecting one side. Artists move around their work all the time and it is the same when thinking about artistic appreciation in aesthetics.
Focused anatomical approaches and artistic appreciation
Treatment of the ageing mid-face is increasingly recognised as a key component in aesthetic rejuvenation and is arguably one of the two main areas where artistic appreciation is particularly pertinent.
Board-certified plastic surgeon Dr Oscar Ramirez described the so-called zygomatic point,16 otherwise known as the malar eminence, while board-certified plastic surgeon Dr Arthur Swift and board-certified dermatologist
Dr Kent Remington have argued that clinicians should use the Phi relationships to apply to the mid-face.17 And, of course, boardcertified plastic surgeon Dr John Little described the ‘ogee’ curve – a curvilinear silhouette found in art and architecture and in the youthful human face (Figure 4).18
Figure 4: This clinical case demonstrates an ogee curve post cheek treatment, created in a natural fashion with artistic considerations.
The authors of a Juvéderm trial using Voluma also attempted to sub-classify the cheeks into zones,19 while Marianetti and colleagues described the so-called ‘beauty arch’ for the assessment of sagittal projection of the malar region.20
Linkov and colleagues also reported that having cheekbones that are as wide as the eyebrows is apparently the most desirable type of face and described as ‘mathematically beautiful’. Their conclusion was derived after analysing the average facial measurements from photographs of 55 female models using the WIZDOM (Width of the Interzygomatic Distance of the Midface) research tool.
They revealed that the ‘average inter-pupillary distance’ was a strict 59.2mm and the vertical distance between the eyes and the cheekbones should be 13.1mm to be classed as attractive. They believe these measurements add up to create a ‘heart-shaped’ attractive face, which can act as a guide to help plastic surgeons and aesthetic practitioners design their filler treatments.21

The second pertinent focused area for artistic appreciation are the lips, which also represent the most common anatomical area to be treated with dermal filler globally.


The Fibonacci sequence/Golden Ratio/Phi proportions (1:1.6) greatly appertain to the appearance of ‘perfect lips’, where the lower lip should be 1.6 times thicker than the upper lip in Caucasian patients.22 Note that this will differ in other ethnicities. The lower lip should also be longer than the upper lip and the modiolus (corners of the mouth) should be straight and preferentially elevated. In keeping with the Golden Ratio, the distance between the nose and upper lip should represent 1 to the 1.6 of the distance from the lower lip to the chin – over recent years, surgical lip lifts have become increasingly popular which also help to adhere to this tenet.
Like the rest of the face, it is especially important to remember that lips are beautiful three-dimensional structures and, as mentioned above, aesthetic practitioners must assess the profile of patients before treatment. Consider the Steiner line – the line from the mid-nares to the chin – and ensure the lips just barely touch it. When they cross this line, the lips have been over projected. This is often ignored to the

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Figure 5: This patient’s before and after photographs demonstrate a natural lip augmentation.
Figure 3: Splitting the face into thirds and assessing individual components is a key step in facial aesthetic evaluation and artistic appreciation.
Upper Third Forehead Temple Brow
Middle Third Eyes, Temple Tear Trough Cheeks, Nose
Lower Third Lips Chin Jaw
detriment of natural-looking lips.23
Another important point to check when augmenting the lips is the nasolabial angle. Armijo and colleagues found this should be 93.4 to 98.5 degrees for men and 95.5 to 100.1 degrees for women.24 The angle/slope/concavity of the upper lip skin above the vermilion border should also be assessed. Conventionally there should be a ‘ski-jump’ appearance, with a slight elevation at the vermilion border of the upper lip along the whole length (the Glogau-Klein point – area of inflection as the lip turns from glabrous skin to mucosa).23 In accordance with these findings aesthetic practitioners should therefore be careful to avoid ‘shelving’, ‘trout pout’ or a ‘duck-lips’ look associated with over correction, poor technique or lack of artistic appreciation.
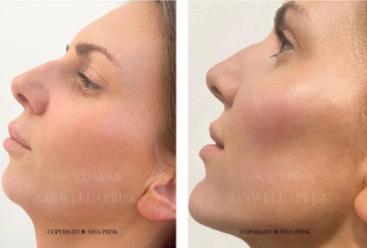
Style and artistic approaches
Not everyone can be a master artist, but it is expected that an aesthetic practitioner should be able to obtain excellent, reproducible results by following certain rules and structured approaches. Using the elements discussed in this paper, thinking about a sense of proportion should help injectors elevate their skills beyond a simplistic formulaic approach. However, the highest quality products, on-going training and mentorship should not be forgotten in this quest. Beyond foundation techniques, one particular and successful structured approach to artistic appreciation (albeit by another name) in contemporary aesthetic practice is the work of Dr Mauricio de Maio, who invented and popularised the ‘MD codes’. This is a systematic method to approach facial assessment and treatment and is derived from his earlier concepts of injecting eight specific anatomical areas to produce a non-surgical facelift.25
However, the highest elite level of technique, injectors will often abandon such structure and be seen to adopt a more ‘freestyle’ approach, which creates more of a mystique but is essentially a culmination of years of practice and a heightened awareness of artistic appreciation. A classic example of this is observing the markings and approach of Dr Raj Acquilla. Consider the following quote by Picasso to describe this approach which is relevant to both surgical and nonsurgical aesthetic practice alike, “Learn the rules like a pro, so you can break them like an artist.”
The last component that warrants discussion is the concept of style in aesthetics. Every practitioner will have their own style and some will have more flair than others. Many practitioners will follow wellaccepted approaches but others, as we have discussed, will go beyond these frameworks and freestyle within their treatment plans with patients.
The analogy is that we may start teaching with a painting by numbers approach but over time we expect practitioners to develop their own style, just like great artists with their own individualistic approaches.
Moving forward
Understanding the origins of beauty and how mathematicians, historical artists and modern perceptions perceive this, leads us to the idea of ‘artistic appreciation’. It is a simple yet complex subject but we believe it is a mandatory pre-requisite for aesthetic practice at the highest level. We believe it needs to be integrated into training programmes at foundation level and explored more deeply throughout one’s career so that clinicians may truly practise as an artist. In conclusion, always view your patient as a work of art: take time to step back, pause, appraise and appreciate – just like going to a museum to look at art.
Mr Paul Banwell is a consultant plastic and cosmetic surgeon based in London and the South-East. He is the founder of the Banwell Collective and a visiting professor of plastic surgery to Harvard Medical School. Mr Banwell is the co-founder of Banwell.Prisk School of Medicine and, along with Prisk, has formalised steps for artistic appreciation through their F.A.C.E. A.R.T concept.

Nina Prisk is an aesthetic nurse prescriber, who trained on Harley Street and now works full time in facial aesthetics, concentrating solely on injectables. She practises from her clinic Update Aesthetics in Cornwall, as well as in Harley Street as part of the Banwell Collective. Prisk is the co-founder of Banwell.Prisk School of Medicine and, along with Mr Banwell, has formalised steps for artistic appreciation through their F.A.C.E. A.R.T concept.

TO VIEW THE REFERENCES GO ONLINE AT WWW.AESTHETICSJOURNAL.COM
Test your knowledge!
Complete the multiple-choice questions below and go online to receive your CPD certificate!
Questions
1. What value is PHI?
5. What did Armijo et al. claim the ideal nasolabial angle to be in men?
Possible answers
1.618 b. 1.816
14.1mm b. 12.2mm c. 13.1mm d. 13.5mm
a. 95.5 to 100.1 degrees b. 93.4 to 98.5 degrees c. 92.6 to 95.4 degrees d. 97.8 to 100.3 degrees
Answers: 1a, 2d, 3b, 4c, 5,b
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Figure 6: Mid-face enhancement (and facial contouring) obeying the rules of artistic appreciation can create natural-looking, more youthful appearances.
a.
c. 1.182 d. 1.681 2. How much more money are ‘attractive people’ suggested to earn according to economist Daniel Hammermesh? a. 6-7% b. 2-3% c. 10-11% d. 3-4% 3. What does the R stand for in our F.A.CE. A.R.T concept? a. Rejuvenate b. Re-evaluate c. Redefine d. Relax 4. What did Linkov et al. deem to be the most attractive vertical distance between the eyes and cheekbones? a.
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or App Store Adverse events should also be reported to A. Menarini Farmaceutica Internazionale SRL. Phone no. 01628 531171 or email: DrugSafety@pharmalex.com


Model for illustrative purposes only.
Filler SKUs CE 0123 –
Threads CE
Assut
For more information, ask today at: info@relifecompany.co.uk To register for training, sign up today at: ukrelifemasterclass.com Available now from Church Pharmacy: 01509 357 300 www.churchpharmacy.co.uk A. MENARINI FARMACEUTICA INTERNAZIONALE SRL | Menarini House, Mercury Park, Wycombe Lane, Wooburn Green, Buckinghamshire, HP10 0HH. Incorporated in Italy with Limited Liability | Branch registered in England No BR016024 | Tel: 01628 531171 | Email: DrugSafety@pharmalex.com
CROMA-PHARMA GmbH, Industriezeile 6, 2100 Leobendorf, Austria
0373
Europe SpA, Via G.Gregoraci, 12 00173 Roma, Italia Hydrobooster CE 0459 CROMA GmbH, Industriezeile 6, 2100 Leobendorf, Austria Peel Program CE Mastelli S.r.l., Via Bussana Vecchia 32, 18038 Sanremo (IM)
Creative genius has long been part of our Florentine history, dating as far back as Michelangelo’s works of art. These values have inspired us to create RELIFE® – a growing portfolio of premium aesthetic medicine solutions built with innovative technology. See how our new Definisse™ range of peels, filler and threads, can transform your practice and your patients. Launching for the first time in the UK.
The beauty of the moment
Illustration does not show all packs available in the range


My

PP-RL-UK-0109 October 2020 GB20025
skin says how I feel Resurface, Restore, Reshape. The Definisse™ range from RELIFE. relifecompany.co.uk


Deliver impressive skin rejuvenation with little to no downtime Visit Lynton.co.uk to find out more @dekalaseruk CO 2 ... but cooler!
Supported in the UK by Lynton
Treating Lip Lines
Women frequently present with concerns about fine or deep lines and wrinkles in the lip and perioral area, which may give an appearance of anger or disapproval, and often appear prior to ageing signs elsewhere in the face. The lips are a focus of attention on the face, communicating both emotion and speech, and are therefore a priority for treatment for many patients.
Treating lip lines remain a challenge for most injectors, as a full correction of lines in this dynamic area is usually difficult to achieve. Overuse of dermal filler can cause an unnaturally protruding appearance of the upper cutaneous lip. Even more difficult are patients with well-established static lines accompanied by solar damage to the skin of the upper cutaneous lip, a common occurrence in the high UV environment of the southern hemisphere. The cause of lip lines are multifactorial and are thought to be a combination of the loss of deep and subcutaneous perioral fat, thinning of the dermis, and the effects of repeated muscle contraction over time.1
The Selkon Subcision Slurry technique is a new approach that addresses these multiple causes of lip lines by combining three treatment modalities – filler, toxin and subcision – in one treatment. It is designed to minimise convexity of the upper cutaneous lip arising from over-volumisation of the area with filler and weaken the influence of the orbicularis oris muscle on the skin, without excessive loss of function.
How do lip lines occur?
During ageing, the upper lip undergoes vertical lengthening and inversion with the thinning of the vermillion and loss of anterior projection. As a result, the philtral columns and cupid’s bow become ill-defined.2 This causes vertical and horizontal rhytids to appear on the lips. The perioral lines develop at the edge of the white roll of the lip where the orbicularis oris muscle is attached to the dermis with no interposed fatty layer.3
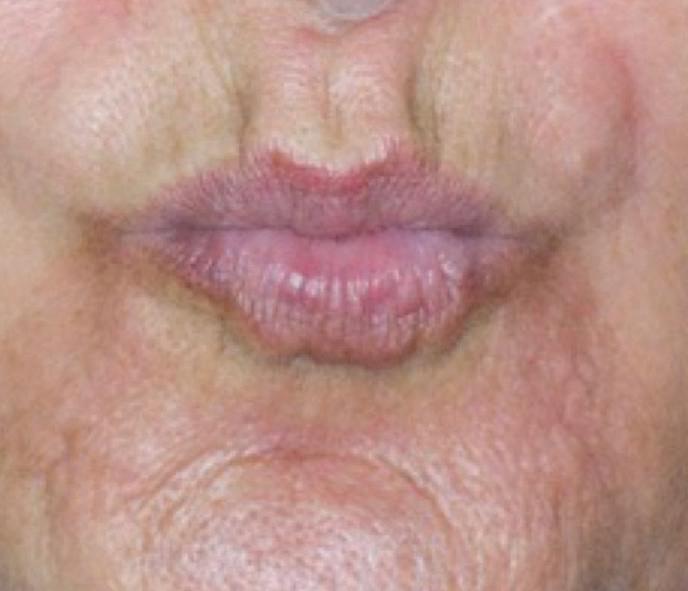
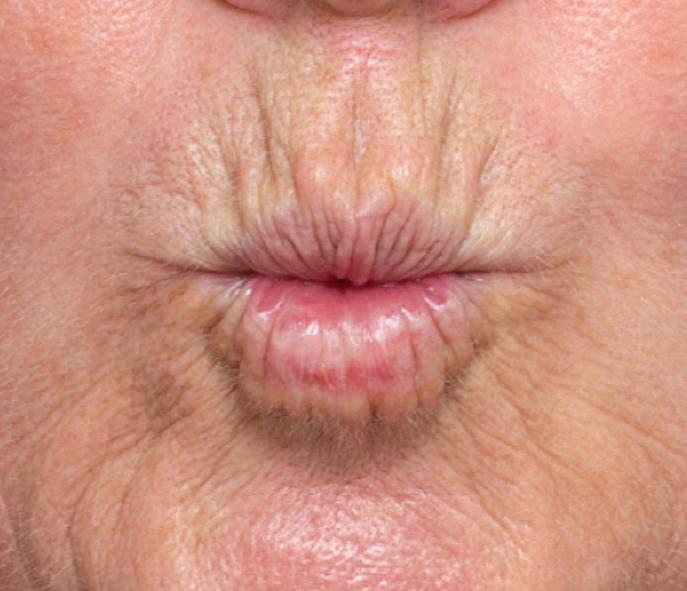
It is believed that these lines develop because of perioral soft tissue volume loss, lip atrophy, hyperdynamic contractions of
the perioral musculature, and an underlying resorption of the maxillary and mandibular bone.4 The vermillion border loses its definition and rhytids extend from the upper lip into the tissue above the lip. Although sun exposure is a contributing factor for ageing across the world, in countries like New Zealand and Australia, practitioners hypothesise that solar damage from the high UV environment causes a higher degree of damage and ageing of the perioral skin. A study by dermatologist Professor Greg Goodman showed that Australian women noticed signs of ageing such as facial lines one to two decades earlier than their counterparts in the northern hemisphere.5 Each of these factors contributes to a varying degree to the ageing of patients. Some patients have strong muscle action and lesser volume loss, leading to multiple fine lines. Alternatively, a relatively weaker muscle and greater volume loss appears to be associated with fewer, deeper lines (Figure 1). The Selkon Subcision Slurry technique is well suited to patients with the first pattern.
Treatment for lip lines
Lip lines can be improved with hyaluronic acid filler placed directly into the line superficially in the dermal plane. If there is perioral volume loss, dermal filler can also be used to restore loss of fat in the subcutaneous and/or submuscular planes, using a cannula. However, an excess volume of dermal filler can also cause unwanted convexity of the upper cutaneous lip, commonly termed the ‘monkey muzzle’ or ‘Marge Simpson’. This abnormal contour is disliked by patients and injectors and can occur even when the lines themselves are not fully corrected.
Botulinum toxin is a useful additional tool for improving lip lines when injected to weaken the orbicularis oris muscle lying beneath the lip lines. However, used on its own it is rarely enough to restore a full correction, and higher doses can cause too much interference with oral function for the patient to tolerate. Laser resurfacing, such as fractionated CO2, is useful to improve superficial lines once volume loss has been corrected. However, many patients are unwilling to contemplate downtime, and these devices can be expensive and are not universally available at all clinics.

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Dr Ellen Selkon and Dr Sarah Hart explore their method for treating aged and photodamaged lip lines using filler, toxin and subcision
Figure 1: Difference in fine lines between two patients based on muscle strength and volume. Patient A has a strong muscle and minimal volume loss with multiple shallow lines, while Patient B has weaker muscle and more volume loss with fewer deeper lines.
Patient A Patient B
New technique using subcision
Inspired by Rosengaus-Leizgold’s paper on subcision of the muscles of the lower face to weaken their effect without using toxin, Dr Ellen Selkon devised a new approach called ‘The Selkon Subcision Slurry technique’ to improve lip lines.

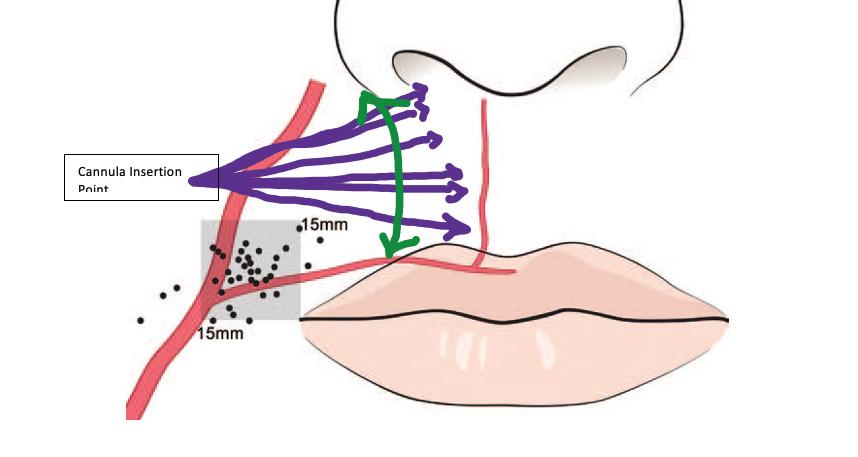
It is important to note that this is an ‘off label’ technique and should only be attempted by experienced injectors.
A cannula is used to subcise subcutaneously, loosening the attachments of the orbicularis oris muscle before a slurry of diluted dermal filler (for skin quality and subtle volume restoration) and botulinum toxin (for muscle relaxation) is placed in the subcutaneous plane.
Adding both saline and reconstituted botulinum toxin to the filler reduces its volumising effect, which, in our experience, diminishes the chance of an abnormal contour of the upper cutaneous lip.



The Selkon Subcision




plane directly between the muscle and the skin, as the artery is least likely (3%) to be in this plane.6 The Selkon Subcision Slurry technique is designed for this safer plane. The origin of the superior labial artery is 85% of the time within a square 1.5cm superior and lateral to the oral commissure.7 The cannula entry point should lie superior to this area (Figure 2)
Preparation
An aseptic technique should be used throughout preparation. Firstly, 0.6ml of a low G-prime filler is decanted into a 3ml syringe. Into a second 3ml syringe, 0.4ml normal saline is drawn up and 15 units of abobotulinum toxin or 6 units of onabotulinum toxin/ incobotulinum toxin is added. Both syringes are attached to a three-way tap and mixed well by depressing each plunger in turn, expelling the mixture from syringe to syringe. This will create 1ml of a well-mixed slurry of filler/saline/toxin. It should be decanted it into 2x1ml syringes ready for use.
Procedure

During the procedure, an infraorbital nerve block is performed using lidocaine 2%. A 25 gauge 40mm firm cannula is inserted, just lateral to the nasolabial fold (Figure 2). Subcision is then performed.
The cannula should glide in the subcutaneous plane to the philtral column and should not advance medial to the philtral column. Without injecting any product, the area is subcised using the cannula as a




































This technique appears to be especially helpful in cases where volume loss is present but not excessive, the dermis exhibits moderate solar damage, and the orbicularis oris muscle remains strong.
Patient selection is vital to achieving a good result as this technique is not suitable for all patients. Although the volumising effect is milder than other filler techniques, patients with a protruding upper lip or convex upper cutaneous on profile view are not good candidates. Patients with very tethered lines and severe solar elastosis may only demonstrate limited improvement.


As the main blood supply of the upper lip is the superior labial artery, which runs in the submuscular (78%) or intramuscular planes (18%), it is therefore safer to inject in the subcutaneous
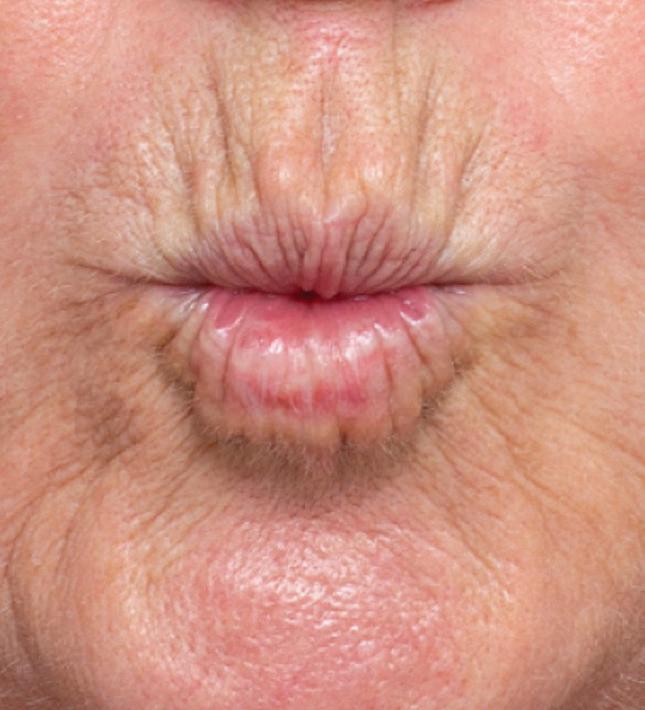
aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Figure 2: Insertion point for the cannula shown in purple
Figure 3: 49-year-old patient before and two weeks after. Images courtesy of Dr Sarah Hart.
Slurry technique is a new approach that addresses the multiple causes of lip lines by combining filler, toxin and subcision in one treatment
Figure 4: A 49-year-old patient injected with just 0.3ml per side of slurry. This totalled 0.6mls of slurry, equating to a dose of about 4 units of onabotulinum toxin for the entire upper cutaneous lip. The remainder 0.4ml unadulterated filler was injected in very small aliquots into the oral commissures, mental crease and lips. Images courtesy of Dr Sarah Hart.
After Before
After Before
Insertion
Cannula
Point
Figure 6: 55-year-old patient before and after treatment. She showed immediate swelling and convexity of the upper cutaneous lip which will resolve. Images courtesy of Dr Ellen Selkon.
subcision tool, breaking down the fibrous attachments from the dermal layers to the muscle. This will separate the soft tissue from the orbicularis oris muscle, creating a plane that can be filled with the slurry. Many passes with the cannula are required.
The injector should work in an orderly manner from just above the white roll to the sub-nasal area. Once subcising has finished, and the area is free of tethering, the cannula should move freely like a pendulum from the white roll to the sub-nasal tissue without interference (Figure 5)

Thin strands of approximately 0.01-0.05ml of slurry should be injected, to a total of approximately 0.3-0.5ml per side. By injecting horizontally, there is less chance of intravascular injection as the arterial branches in this region generally run vertically from the superior labial artery.9 No slurry should be injected medial to the philtral columns as this will lead to a flattening of the philtrum and loss of lip shape.
Once finished, the upper lip area will look full. It’s important to remember that almost half of what has been injected is saline and will therefore be absorbed over the next 24-48 hours. Therefore, it is important to warn patients prior that they will have downtime associated with this procedure. Firstly from the 48 hours of fullness and, secondly, from the bruising associated with the subcision technique.
The area should be gently massaged to ensure that there are no obvious lumps or accumulation of slurry. Practitioners should never use leftover slurry mixture in areas where toxin effect is not desired. However, the remaining 0.4ml of unadulterated filler can be used in other perioral areas such as the body of the lip or the mental crease.


Follow up
A follow-up session should be conducted in two weeks to ensure that the toxin has worked and that the patient is happy with the results. Results should always look natural and subtle, allowing you to repeat the procedure again in approximately six months. Possible complications to consider include those generally associated with dermal filler and toxin treatment. Bruising may be more significant than usual following the procedure and, in our experience, immediately post-procedure swelling is greater due to trauma from subcision and the added saline, which will be absorbed. Generally, results are optimal two to four weeks post procedure, after the swelling and bruising has subsided, and will last up to six months.
A multifactorial approach
The Selkon Subcision Slurry technique combines diluted filler, toxin and subcision in one treatment to address the multifactorial causes of lip lines. Results to date are anecdotal and we welcome further study on this technique. It is designed to minimise convexity of the upper cutaneous lip arising from over-volumisation of the area with filler and weaken the influence of the orbicularis muscle on the skin without excessive loss of function. We find it is particularly helpful for patients with minimal to moderate volume loss, moderate solar damage, and a strong orbicularis muscle. To achieve optimal results, it is essential to select your patient carefully, use a low G-prime dermal filler and a firm cannula, achieve good analgesia prior to subcision, and subcise the area well, prior to injecting.
Dr Ellen Selkon has been practising aesthetic medicine in New Zealand for 15 years. She is on the executive committee of the NZ Society of Cosmetic Medicine and the NZ conference organising committee. Dr Selkon is also an international teacher and speaker on dermal fillers and botulinum toxin and is an Australasian trainer for Galderma Pharmaceuticals, educating healthcare professionals through the GAIN programme.

Qual: MBChB, FRNZCGP, NZSCM
Dr Sarah Hart has been practising cosmetic medicine since 2002. She serves on the NZ Society of Cosmetic Medicine’s executive and education board as censor and education faculty member. Dr Hart has been an Allergan Advisory board member since 2007. She lectures on the use of dermal filler and botulinum toxin on the international stage and trains her colleagues across Australasia in facial rejuvenation techniques. As a KOL, Dr Hart has a particular focus on safety, is a published author on this topic and has featured on three seasons of the TV series ‘Ten Years Younger in Ten Days’ in New Zealand.
Qual: MBChB
REFERENCES
1. Rohrich RJ, Pessa JE, ‘The Anatomy and Clinical Implications of Perioral Submuscular Fat’, Plastic and Reconstructive Surgery, 124 (2009), pp. 266-271.
2. Tonnard PL, ‘Ageing of the Upper Lip: Part II. Evidence-Based Rejuvenation of the Upper Lip—A Review of 500 Consecutive Cases’, Plastic and Reconstructive Surgery, 143 (2019), pp.1333-1342.
3. Hotta TA, ‘Understanding perioral anatomy’, Plastic Surgical Nursing, 36 (2016), pp.12-18.
4. Maio M, DeBoulle K, et al., ‘Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: focus on the lower face’, Plastic Reconstructive Surgery, 140 (2017), pp. 540550.
5. Goodman GJ, Armour KS, et al., ‘Comparison of self-reported signs of facial ageing among Caucasian women in Australia versus those in the USA, the UK and Canada’, Australasian Journal of Dermatology, (2017).

6. Cotofana S, et al., ‘Distribution Pattern of the Superior and Inferior Labial Arteries: Impact for Safe Upper and Lower Lip Augmentation Procedures’, Plastic and Reconstructive Surgery, 139 (2017), pp.1075-1082.
7. Lee SH, et al., ‘Anatomy of the Superior Labial Artery’, Plastic Reconstructive Surgery, 135 (2015), pp.445-450.
8. Rozengaus-Leizgold R, et al., ‘The Happy Face Treatment’, Journal of Drugs in Dermatology, 17 (2018), pp.1226-1228.
9. Tansatit et al., A Typical Pattern of the Labial Arteries with Implication for Lip Augmentation with Injectable Fillers, Aesth Plast Surg (2014) 38: 1083-1089.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Figure 5: Cannula insertion point
After
Before
Beauty of the Moment: The Trends of Today
For aesthetic practitioners across the country the last year has been more than challenging and without doubt unexpected, with a rollercoaster of surprises and some real hardship. However, with the recent reopening of clinics, it has been somewhat of a relief to be worrying about the pent-up demand and how to fit clients in for their regular top up treatments. Following months of living predominantly indoors it is no surprise that clients are looking for something a little bit extra – something to give them a lift and feel ready for the new postpandemic world. Here, RELIFE talks to some of the UK’s leading aesthetic clinicians to get their insights as to what their clients are asking for, what ‘Beauty of the Moment’ means to them, and the trends that they are seeing coming through.
Skin rejuvenation
Following a stressful year, getting some vitamin D, eating healthily and exercising has been difficult for many. The result? Skin health overall has suffered and is evidenced by dehydrated, dark and dull appearances in patients. Dr Martyn King, aesthetic doctor and co-founder of Cosmedic Clinic, says, “The environmental effects of living indoors, especially during the winter, with cold weather, central heating, and limited exercise all take their toll and can lead to a slowdown of the skin’s natural regeneration process. As a result, we have seen an uplift in the demand for treatments that give a fresh, healthy and glowing look to the skin as our patients return to normal life.”
TREAT IT
Dr King says, “We’ve been using the Definisse Hydrobooster from RELIFE. It gives great naturally fresh-looking hydrated skin, which literally glows with health which our patients love. The pharmaceutical quality formulation refreshes the skin and boosts moisture levels using a homogenised, biorevitalising injectable gel which is really easy to use and there is little to no downtime.”
‘Mascne’
Face mask induced acne, or ‘Mascne’, is a frequent side effect of the daily mask-wearing that has become the norm with the arrival of COVID. “So called ‘mascne’ is triggered by excess heat, pressure, friction or rubbing of the skin, combined with sweat and oil under occlusion leading to clogged and inflamed pores,” says aesthetic nurse and co-founder of Cosmedic Clinic, Sharon King. “We’ve definitely seen a rise in the number of patients, both men and
women, who have come to the clinic looking for ways to treat acne on the lower face – a condition they have never suffered from previously,” she adds.
TREAT IT
King says, “There are numerous treatments for Mascne, including topical treatments, laser and chemical peels. The Definisse Peel Program from RELIFE gives us real flexibility as there are pre-peels as well as peels –formulated for specific skin types. They give great results, improving skin texture and quality as dry, old skin cells fall away to reveal new, fresher looking skin.”
‘ZOOM’ face
Dr King says, “We’ve seen a significant uplift in clients looking for advice on treatments which focus on improving jawline angles and reduce sagging skin to the chin, cheek and jaw.” He puts this down to the amount of time that clients have spent seeing themselves on screen while grappling with Zoom and Teams which have become part of everyday life.
TREAT IT
Dr King says, “One of the most effective treatments to lift and contour the face is threads. They give such great, natural-looking instant but long-lasting results which we have found has patients delighted. We use RELIFE Definisse Threads, to reshape facial contours and lift soft tissue using a unique, well tolerated thread which works in harmony with the face and can be used in conjunction with any of the RELIFE Fillers range if required.”

Sign up to the RELIFE ‘Beauty of the Moment’ Webinar
The RELIFE Beauty of the Moment webinar takes place on Monday 10th May, hosted by award-winning beauty journalist and skincare author Ingeborg van Lotringen, ex beauty director at Cosmopolitan and writer for Elle, Red, Good Housekeeping and national newspapers. She is also the author of ‘Great Skin’. Ingeborg will be putting questions to Dr Martyn King, aesthetic nurse Sharon King and Dr Simon Zokaie about what post lockdown trends they think will be take hold. Register today by visiting https://app. livestorm.co/aesthetics-and-ccr/beautyof-the-moment-webinar-with-relife

Aesthetics | May 2021 38 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial RELIFE
brand ambassadors provide insights on the latest treatment trends
RELIFE
Expert Q&A: Dr Simon Zokaie

Leading aesthetic doctor and RELIFE brand ambassador, Dr Simon Zokaie, shares his take on ‘Beauty of the Moment’ and how he uses RELIFE to deliver great results which get his clientele coming back again and again.
What does ‘Beauty of the Moment’ mean to you?
For me, ‘Beauty of the Moment’ right now is all about natural looking results – products which work with the body, not against it. When patients have come to us talking about wanting to wake up their skin and get rid of their ‘tired-looking’ complexions, we’ve been recommending treatments such as skin boosters, which have a biostimulating effect and hydrate the skin to look fresh and youthful. Our patients seem to be more interested in embracing their natural look and are seeking subtle tweakments rather than big changes, which will be there for all to see at the next Zoom call. It might also be that influencers have had a part to play, and younger patients especially are dissolving their filler and opting for a more natural appearance.
What trends do you predict for the summer?
After what has been pretty much 12 months of lockdown, we don’t expect people will want treatments which require long downtimes. From what we’ve seen already, we’re expecting an increased demand in natural-looking rejuvenation techniques and possibly longer lasting ‘lockdown proof’ treatments. This is where a range
like RELIFE really comes into its own as you can mix and match peels, fillers and threads to create really natural looking results which just get better over time.
What are the benefits of using RELIFE Definisse products?
The RELIFE Definisse range provides a one-stop-shop for practitioners like me. I feel totally at ease using their range of premium, pharmaceutical quality aesthetic products. The range comprises peels, filler and threads which work seamlessly together, and equally well on their own. I was first drawn to RELIFE Definisse after attending the IMCAS conference and seeing really impressive results, with a strong science backing and safety profile.
You provide training on the Definisse Filler range – what makes the Definisse Filler different to other brands out there?
The Definisse Filler uses RELIFE’s XTR technology to deliver the perfect mix of viscosity and elasticity, restoring volume safely and effectively, without migration. Whether clients are looking for a simple moisture boost, which can be achieved using the Definisse Hydrobooster, or a more longer lasting youthful plumpness, the range achieves excellent results and a naturally beautiful finish.
What can aesthetic practitioners expect from RELIFE training?
The training itself is really interactive and is run by a world-leading team of trainers. There are only four to five delegates per trainer, so it is an intimate setting and you become a close team. It is very hands on and there is no judgement at all – we encourage lots of questions to provide the best experience for everyone.
Register for RELIFE training
RELIFE provides free training from leading practitioners including Dr Vincent Wong, Dr Martyn King, Dr Simon Zokaie, Sharon King and Jackie Knight to keep practitioners up to speed on Definisse products and the latest techniques.
Dr Martyn King says, “I am a strong advocate of patient safety and the amount of support provided by RELIFE before, during and after training is one of the main reasons that I am proud to support them.”
Sign up now for RELIFE training at www.ukrelifemasterclass.com
This advertorial was written and supplied by RELIFE PP-RL-UK-0277 Date of preparation April 2021 GB21095
Aesthetics | May 2021 39 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial RELIFE
Adverse events should be reported.
For the UK, reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store.
For Ireland, suspected adverse events can be reported via HPRA Pharmacovigilance, www.hpra.ie Adverse events should also be reported to Galderma (UK) Ltd. E-mail: Medinfo.uk@galderma.com Tel: +44 1 923 208950
1. Gubanova El et al. J Drugs Dermatol 2015;14, 288-298.

2. Gubanova El et al. Poster presented at IMCAS 2015. *with three treatments
UKI-RES-2100052 Date of Preparation: April 2021

Hydrate from within for up to 12 months*1,2 with injectable HA microdroplets
Exploring Hyperpigmentation in Skin of Colour
Hyperpigmentation is defined as darkening patches of skin. This occurs when the skin produces more melanin; the pigment that gives skin its colour. Although hyperpigmentation occurs in all skin types, it is one of the main skin complaints of people with darker skin tones. Facial hyperpigmentation can cause significant cosmetic disfigurement with subsequent emotional impact.1,2,3
Darker skin types are generally classified as Fitzpatrick types IV-VI. There are structural and functional differences in the skin, which produces variances in skin conditions, presentation and treatments. These skin types are categorised by higher melanin content and more effective distribution of melanin, producing better protection against ultraviolet (UV) radiation. Melanin is generally classified into two types: eumelanin and pheomelanin. Darker skin types have a higher eumelanin to pheomelanin ratio, and higher amount of eumelanin than lighter-skinned individuals.4
The concentration of melanin in melanosomes within the epidermis is double in those with darker skin compared to lighter-pigmented individuals, although the number of melanocytes is the same. There is also a slower degradation of the melanosome within a keratinocyte in individuals with darker skin. These structural and functional differences mean special considerations need to be given when diagnosing and treating skin of colour.5
The process of melanin production
The process of melanin production is regulated by the enzyme tyrosinase. This enzyme converts L-tyrosine L-3,4-dihydroxyphenylalanine (L-DOPA), which is then oxidised to form L-dopauinone. This key compound can then follow two different pathways depending on the availability of cysteine to form eumelanin or pheomelanin (Figure 1).6 ,7
Melanocytes are cells within the basal layer of the epidermis responsible for producing melanin. Once formed, melanin is then packaged into small, round organelles called melanosomes which are transported to neighbouring keratinocytes via dendritic processes. They are deposited superficially to the cell nucleus to offer protection from UV radiation (Figure 1).8
When this process goes into overdrive, excess melanin is produced and can cause darkening of the skin in that area. This is known as hyperpigmentation and occurs in various forms, which happen all over the body in small patches, spots or larger areas. There are many reasons why this happens, which are discussed next.
Sun damage
This is the main cause of hyperpigmentation and can exacerbate existing hyperpigmentation. The initial melanin production from sun exposure acts as a natural sunscreen to protect from harmful UV rays. However, excess UVA and UVB exposure disrupts the melanin production, which leads to increased pigmentation. This pigmentation can be harder to treat as it is produced in the dermal layers of the skin. In fact, this result can happen from any UVA and UVB source, including sunbeds.5 Sun damage induced hyperpigmentation can present in multiple ways. Most commonly as ‘sunspots’, also known as ephelides and lentigines which presents as tan-dark brown macules or patches. Another presentation is melasma, which has multiple causes, one of which is intense sun exposure. This is visible as symmetrical light to dark brown patches with irregular borders and is most commonly seen on centrofacial, malar and mandibular regions. Many of our mature skin-of-colour patients will experience darkening of malar cheeks and the forehead which is diagnosed as maturational dyschromia and has developed from years of chronic sun exposure. A rare presentation of sun induced hyperpigmentation is Lichen planus pigmentosus which favours Fitzpatrick lll-V skin types. It presents on sun-exposed areas as greybrown to brown macules and its distribution indicates UV radiation as the cause.5
Hormones
It has been shown in a number of studies from across the world that increased levels of oestrogen constitute a risk factor for hyperpigmentation disorders.9 This change in oestrogen levels is commonly seen in pregnancy. When hyperpigmentation presents in this way it is known as the
Tyrosinase (TYR) Tyrosinase (TYR) Tyrosinase Related Protein 2 (TRP-2) Tyrosinase Related Protein 1 (TRP-1) Tyrosinase (TYR)
Dr Manika Rajput discusses common causes and management of hyperpigmentation in patients with skin of colour Figure 1: a) The biochemical pathway of melanin synthesis occurs within melanosomes or pheomelanosomes and b) the developmental stages of melanosomes (I-IV) during melanin synthesis.6,8 Stage IV (Melanin) Stage III (TYR + Melanin) Stage II (Finrillar matrix + TYR) Stage I Melanocyte Golgi Body Nucleus Tyrosinase Synthesis Rough Endoplasmic Reticulum (RER) L-Tyrosine 3,4-dihydroxyphenylananine (L-DOPA) L-DOPAquinone Glutathion or Cystein Leucodopachrome DOPAchrome 5,6dihydroxyindole -2-carboxylic acid (DHIGA) Indole-5-6-quinone -2-carboxylic acid 5,6dihydroxyindole (DHI) Indole-5-6quinone GlutathionylDOPA/ Cysteinyl DOPA 1,4Benzothiazinylalanine PHEOMELANIN EUMELANIN @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021







mask of pregnancy – a form of melasma. As mentioned above melasma has multiple causes. Fortunately, in most cases it resolves or fades itself after pregnancy, however it can reappear with exposure to UV rays.5 These hyperpigmentation changes can also be seen with hormone replacement therapy (HRT) and combined oral contraceptive pills. Due to the decrease of oestrogen in menopause, it has been shown to improve symptoms of melasma when not taking HRT.9
Skin injuries and inflammation
This is the main cause for post-inflammatory hyperpigmentation (PIH).10 Injuries such as cuts, burns, chemical exposure, infections or inflammation can lead to darkened patchy skin. Incorrect skin treatments which lead to damage and inflammation can also cause PIH. The long-term application and misuse of skin-lightening agents containing hydroquinone can lead to the formation of a blue-black pigmentation known as exogenous ochronosis. It is therefore important that prescription topical formulations of hydroquinone are used under clinician supervision.5 Allergens in cosmetics or textiles can induce pigmentated contact dermatitis also known as Riehl’s melanosis, which is characterised by a brown-grey appearance on areas of application.5
Genetics
Hyperpigmentation can also be a hereditary condition seen more commonly in darker-skinned patients. This typically presents itself as a brown-black pigmented area around the eyes, known as periorbital hyperpigmentation.5
Illnesses and medication
Systemic conditions such as Addison’s disease and hyperthyroidism cause a diffuse hyperpigmentation. It tends to be more pronounced in areas of sun exposure. Hemochromatosis, a disorder of iron storage and deposition, causes a slate-grey hyperpigmentation.11 Acanthosis nigricans typically affects Fitzpatrick Vl skin types and presents as thickened, hyperpigmented plaques. This is commonly associated with insulin resistance, obesity and polycystic ovary syndrome.5 A range of medications from chemotherapy drugs to antimalarials and anti-epileptic medication can also cause grey patches of pigmentation.12
Prevention
Educating and advising patients about sun protection is key in preventing hyperpigmentation in the first place. It is important patients understand that sun protection needs to be used 365 days a year and that the sun will cause damage even on cloudy days.12 A broad-spectrum SPF 30+ needs to be used daily to give adequate protection from UVA and UVB rays.13 Many sunscreens now come in tinted formulations to help camouflage pigmentation too.5
To help prevent hyperpigmentation, patients should:5,14
• Avoid peak hours of sunlight between 11am to 3pm when the sun’s UV rays are at their strongest
• Seek shade and wear protective clothing such as sun hats and sunglasses
• Use sun protection daily
• Avoid picking or scratching spots or scabs
• Avoid products or treatments that will cause irritation and inflammation of the skin
It is important when limiting sun exposure to note that vitamin D synthesis is very important for bone health. Darker-skinned patients tend to have lower levels of vitamin D especially if they live in less sunny climates or are strict about sun exposure.5 These patients will need counselling and monitoring for vitamin D supplementation, however the Scientific Advisory Committee on Nutrition (SACN) recommends everyone over the age of four of any skin colour should consider taking a daily supplement all year round.15,16 When it comes to treating pigmentation, it is important to first identify and eliminate the cause. A tailored skincare regime can then be developed which suits the patient’s skin type and condition. This can help reduce the appearance of pigmentation and also prevent it from forming. It is important to note here that treatment of hyperpigmentation can be a difficult and prolonged process. There have been better results seen with epidermal pigmentation compared to dermal pigmentation and the patient needs to be informed and have their expectations managed.
Topical treatments
Hydroquinone
This is considered the gold standard and most effective topical agent for treatment of pigmentation. Its mechanism of action is to inhibit tyrosinase and, in turn, the conversion of L-DOPA to melanin.13 Hydroquinone should be used with caution and for limited periods of time because if misused or used excessively it can lead to erythema, irritation, confetti-like depigmentation with higher concentrations, and exogenous ochronosis.5
Retinoids
These are a form of vitamin A. Common preparations are retinoic acid, tretinoin, adapalene and tazarotene. They work to reduce hyperpigmentation through multiple mechanisms: increasing cell turnover, reducing melanin transfer via melanosomes, and allowing increased penetration of other active ingredients.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
When it comes to treating pigmentation, it is important to first identify and eliminate the cause. A tailored skincare regime can then be developed which suits the patient’s skin type and condition
Ascorbic acid
Ascorbic acid, also known as vitamin C, decreases melanin production by interacting with copper ions at the tyrosinase-active site, which inhibits the action of the enzyme tyrosinase.17 Vitamin C is a powerful antioxidant and further reduces hyperpigmentation with its photoprotective properties.
Niacinamide
Niacinamide reduces pigmentation by reversibly preventing the transfer of melanosomes from melanocytes to the keratinocytes. It is an important component of many over-the-counter lightening creams.20
Kojic acid
This is a naturally-occurring fungal product derived from certain species of acetobacter, aspergillus and penicillium. It works by reducing the production of free tyrosinase and as a powerful antioxidant.21
Liquorice derivatives
Liquorice is a root extract from glycyrrhiza glabra. It has many important properties such as anti-inflammatory, antiviral, antimicrobial, and anti-carcinogenic.22 It contains two active ingredients – glabridin which inhibits tyrosinase and possesses anti-inflammatory effects23,24 and liquitrin, which causes melanin dispersion and removal.25
Azelaic acid
This was initially developed as an anti-acne agent but was also found to have inhibitory effects on tyrosinase. Its use has now been extended to hyperpigmentary disorders such as melasma and PIH.26
Cysteamine
This is a newer ingredient on the market that has promising outcomes. It has been shown that topical cysteamine 5% has considerable results in treating stubborn hyperpigmentation in ethnic populations.27,28 It also induces fewer side effects to other topical agents.
Many of these topical ingredients can be used in isolation or more commonly in combination. Topical agents work on different stages of melanogenesis so, when combined, can give better therapeutic results.
Physical treatments
Chemical peels
These are common procedures for reducing hyperpigmentation and can be used alone or combined with other modalities. For patients of a darker skin tone, it is best to be cautious and limit to superficial peels only, as medium and deep peels may be more likely to cause further irritation and pigmentation.5 A superficial peel combined with regular topical therapy can produce better results than chemical peels alone.10,16
Laser
Laser therapy can be an effective treatment for hyperpigmentation. However, this modality needs to be used cautiously in darker-skinned patients due to the higher melanin content. Melanin has a broad absorption range which unfortunately means that lasers targeted for the deeper dermal melanin can be absorbed by more superficial epidermal melanin leading to further pigmentation, blistering and scarring.29,30
Hyperpigmentation treatment with lasers has been associated with an
unpredictable response, frequent relapses and high risk of both postinflammatory hyper- and hypopigmentation.29 It is advisable that only experienced practitioners carry out this treatment and patients should be counselled about the side effects and results that can be achieved.
Microneedling
There are various studies to show that microneedling is a popular option for treating pigmentation in darker-skinned individuals, in particular, melasma and periorbital pigmentation.31,32 The microchannels produced during treatment not only induce collagen production, but also improve the transdermal drug absorption compared to topical treatments alone.33,34
Dermabrasion
A study from 2001 showed that in a mixed Fitzpatrick skin type group, dermabrasion produced successful results on more resistant melasma or dermal pigmentation.36 However, due to the depth of treatment it should be used with caution on darker-skinned patients as there is a higher risk of developing prolonged erythema, hyper/ hypopigmentation and hypertrophic scarring.37 Microdermabrasion on the other hand, is less invasive with reduced downtime and therefore less risks.39
Conclusion
The UK has a diverse population with the skin of colour proportion growing steadily. Hyperpigmentation is prevalent within this group and we are therefore more likely to treat this skin concern. As discussed in this review we have a challenge to correctly diagnose, effectively counsel and provide consistently successful treatments to all our patients. There are a number of ways to treat hyperpigmentation, but with varying degrees of success. It is important to select the correct treatment based on the patient’s skin type to prevent any further damage and manage expectations. Hyperpigmentation is a distressing condition and we have the ability to help these patients improve their concern and quality of life.
Dr Manika Rajput is an aesthetic practitioner and director of her own clinic, Aeon Aesthetics in Surrey. She completed her honours dental degree at King’s College London. Dr Rajput has more than 10 years’ experience in dentistry and has been trained by the Avanti Aesthetics Training Academy in Harley Street. She has a keen interest in antiageing treatments and improving skin health.
Qual: BDS (Hons), PGDip (PDC), MJDF Eng

TO VIEW THE REFERENCES GO ONLINE AT WWW.AESTHETICSJOURNAL.COM @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Case Study: The Teoxane Approach


Assessment, Ageing & Anatomy
A lady in her mid-40s presented to my clinic explaining that she felt she looked tired and older than her friends of the same age group. In any aesthetic assessment it’s important to consider the anatomy and ageing cycle, as well as lifestyle factors causing this ageing. I determined that the patient is a smoker, runner, has sun damage, is approaching the menopause, and doesn’t eat very healthily, which as well as the structural changes to the bone and the soft-tissue anatomy, contributes to thin and wrinkled skin, along with an aged appearance.
The patient’s tired look was the main factor for seeking treatment, so I considered at how I could best address this. The majority of the time, tiredness comes from shadows on the face, due to deflation of soft tissue volume. Her temples were more concave, the tail of the brow was angled down, and the under-eye hollow extended into the cheek.
In addition, the patient had shadows from deepening nasolabial folds and marionette lines. I also assessed her degree of sag; she had mild tissue sag and I could identify that it was mainly the volume loss that was contributing to this tired appearance. Through considering her ageing and anatomy, I determined that this patient
could have really significant improvement by treating her whole face with dermal filler, starting with the mid-face, before moving to the upper face, and finally the lower face. By opening up the eye frame and changing the light reflex you can immediately improve the negative emotional expression of tiredness and sadness, which is exactly what we wanted to achieve.

Technique and product selection
It’s important practitioners take a dynamic approach to treatment and choose products based on the skin layers and rheology. I started with the mid-face. The patient had very thin skin, likely due to smoking and sun damage, so I needed a product which would give her volume, but also be very forgiving, which is why I chose Teosyal® RHA 4. It’s a dynamic volumiser with great stretchability and dynamic strength, so it projects well to restore volume effectively but is also mouldable and forgiving under thin skin.1
I used a bi-planar technique using a needle, injecting both deep onto the bone to get projection, and then into the suborbicularis oculi fat (SOOF), as well as placing some product in the subcutaneous cheek fat pads. When you restore optimum volume both deep and superficially in this manner, you avoid alienising the face and getting those chipmunk cheeks!
I then addressed the patient’s periorbital area, treating her tear trough, palpebromalar groove and superior sulcus to support the brow using Redensity 2. I love this product because it is specifically designed for the periorbital area and has low hygroscopy, which means it doesn’t swell very much. As we know, the periorbital area is challenging to treat and complications can occur because of the type of product, technique, volume, or incorrect assessment. Redensity 2 is associated with a very low complication profile and its rheology means it is very spreadable,2,3 so I find Redensity 2 provides a very natural result.
Next was her temple. I used a gunshot technique with a needle, injecting RHA 4 onto the bone, which really helped support the tail of her brow. Finally, I moved to the lower face. I chose RHA 2 which is a robust filler with great stretchability, and ideal to treat my patient’s highly dynamic nasolabial folds, pre-jowl sulcus and marionette area in the subcutaneous plane using a cannula. I also supported her radial cheek smile lines by placing RHA 2 subcutaneously, which really helped improve her dynamic wrinkles and sagging jowls.
Top tips for success
The anatomy of the ageing face requires practitioners to employ bi-planar anatomical techniques using the rheological properties of dynamic fillers to give natural results, using both needle and cannulas. I believe they should move away from only injecting onto the bone. The TEOXANE dermal filler range is highly versatile, and the different products can be used well in combination for enhanced outcomes. Practitioners must assess the degree of sag – if treating an older patient with moderate to severe tissue sag, I advise combining filler with energy-based devices or surgery for natural outcomes.
Aesthetics | May 2021 45 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Teoxane
1. TEOSYAL® RHA 4 Instruction leaflet 08/12/15 2. TEOSYAL® PureSense Redensity II Instruction leaflet 27/01/16 3. TEOSYAL® PureSense Redensity II clinical trial result brochure. Multicentric and international study: 2012/2013. 33 practitioners,151 patients (86% of women and 14% of men). Visit 1 (T0): Injection, Visit 2 (T30days): Controlnand evaluation. Indications: 93% of patients
REFERENCES
were injected in the tear trough area.
Consultant aesthetic oculoplastic surgeon Mrs Sabrina Shah-Desai explains how she used the Teoxane range for successful full-face rejuvenation Teosyal® RHA 4: SOOF & supraperiosteal (0.4ml/hemiface), deep medial cheek fat compartment (0.2ml/ hemiface), temple (0.4ml/hemiface). RHA4 in subcutaneous cheek fat pad (0.2 ml/hemiface) Teosyal® PureSense Redensity 2: Tear trough (0.2mL/hemiface), palpebromalar groove (0.3ml/hemiface), superior sulcus (0.2ml/hemiface). Teosyal® RHA 2: Nasolabial fold (0.3 ml/hemiface), prejowl sulcus/marionette (0.2 ml/hemiface), radial smile lines (0.5 ml/hemiface) This advertorial was supplied by teoxane.com/uk Before Before After After
The beauty of the moment



A. MENARINI FARMACEUTICA INTERNAZIONALE SRL Menarini House, Mercury Park, Wycombe Lane, Wooburn Green, Buckinghamshire, HP10 0HH. Incorporated in Italy with Limited Liability Branch registered in England No BR016024 Tel: 01628 856400 | Email: menarini@medinformation.co.uk Model for illustrative purposes only. Material intended for Healthcare Professionals only. Scan QR code or visit bit.ly/RELIFEwebinar to register now. 210422_J3240_RELIFE_Webinar_Half_Pg_Ad_Journal of Aesthetic Nursing_180x125_v1-4.indd 1 22/04/2021 20:04
Live webinar Monday 10th May at 6.30 - 7.30pm Join us for discussions with international experts on what’s trending today as the beauty of the moment. My skin says how I feel relifecompany.co.uk PP-RL-UK-0293 April 2021 GB21101
Register for the Virtual Aesthetics Awards


Don’t miss out on this year’s exclusive free awards ceremony
Prepare for a glamorous afternoon on May 28 when the prestigious Aesthetics Awards will be taking place via Zoom at 4pm Despite being hosted remotely this year, the Awards will be as stylish and entertaining as ever, whilst recognising the remarkable achievements of clinics, individuals, teams, and product manufacturers over this past year.
HOST ANNOUNCED
Your celebrity host leading the celebrations is British television presenter Cherry Healey!

Currently presenting 10 Years Younger in 10 Days on Channel 5, Cherry has a keen interest in non-invasive cosmetic techniques and the beauty industry as a whole. It was important for us to have a presenter on board who is just as passionate about the aesthetics sector as ourselves, so we know she will be the perfect host for the evening – plus adding an extra sparkle!
A MONUMENTAL YEAR…
We believe it is essential to continue celebrating the fantastic achievements of the aesthetics specialty, even with a pandemic thrown in! It has been a monumental year for the industry with clinics being forced to close their doors, but we know how much you care about your patients.
As clinics reopen, practitioners can keep a watchful eye for award-winning products and devices which have launched over the year, learning what’s worth investing in for your own clinics to give patients the best of the best in aesthetic medicine.
WHAT CAN YOU EXPECT FROM THE EVENT…
• Mixology masterclass to make a delicious cocktail • Audience reactions – the perfect opportunity to get glammed up and send your reactions in • Exciting new categories for 2021 and the much-anticipated Outstanding Achievement Award • A digital party package sent to you – including cocktail recipes, Instagram filters, virtual backgrounds, and more • A fun-filled afternoon of entertainment and recognition
Following the ceremony, you can safely continue your celebration with colleagues into the evening and across the weekend!
REGISTER FREE WWW.AESTHETICSAWARDS.COM
“I think the Aesthetics Awards are fantastic –they are of the highest calibre and it’s great to celebrate together!”
DR IFEOMA EJIKEME, WINNER OF THE CELLUMA AWARD FOR BEST CLINIC LONDON 2019
Aesthetics | May 2021 Aesthetics Awards Special Focus @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 47
Treating the Perioral Area
When I first began injecting more than 11 years ago, like many other practitioners new to aesthetics I was trained in lip enhancement. What I didn’t quite appreciate at the time is that no structure on the face exists in isolation and this is particularly true for the lips. When I came across Dr Mauricio De Maio’s ‘8 point lift’ where a single treatment session addressed multiple areas of the face, it completely changed how I consulted with my patients. As I began widening discussions with them, I was able to educate them on how the lips are both directly and indirectly affected when we place filler in the cutaneous upper lip, oral commissures, marionettes, and indeed wider areas such as the nasolabial folds, chin and cheeks.1,2


presents as a line/volume loss/or a structural deficit for each patient.
I am looking for: consistent and reproducible results, seamless tissue integration, good longevity and natural-looking facial contouring at rest and on animation. My method to achieve this is with the full range of Juvéderm products using a full-face approach to treatment.

• Lips – Juvéderm Smile, Juvéderm 3 (mid and deep lines and lips), Juvéderm Volift, Juvéderm Volbella4,5,7,8

• Skin – Juvéderm Volbella (mid lines and soft volume to lips) and Juvéderm Volite (hydration and elasticity)4,9
• Chin – Juvéderm Voluma and Juvéderm Volux (structure/stability)6,10
• Nasolabial folds – Juvéderm Volift (deep lines, volume)7
• Cheeks – Juvéderm Voluma (volume and contour)6
Top tips for successful perioral treatments

Don’t treat in isolation! View the perioral area as an extension of the chin, cheeks, jawline and neck. Do not prioritise form over proportion and function, and utilise the bony plane of the face to help stabilise the perioral area. Always ensure you assess and treat on an individual basis because what is ideal for one patient will not be so for another. Remember, by considering the whole of the perioral area, and not just the lips, we are better able to respect the natural proportions and balance for each patient and, critically, respect the anatomical function of the mouth.
How can you enhance the whole perioral area?
As the structures around the lips are connected and have a direct correlation on how the lips look, when you assess these structures and improve them, they can have such an impact on the lips themselves that sometimes the lips don’t even need treating. Incredibly, we can reduce the action of a depressor muscle or that of a hypertonic elevator muscle, as well as help to re-establish the tone and lifting effect of an elevator muscle using filler – known as myomodulation.3 When it comes to the perioral area, there is a complex ‘tug of war’ with this buccolabial group of muscles. By understanding and utilising this, we can improve the position and function of the lips, and indeed beyond them. For this reason, the surrounding areas such as the chin, nasolabial folds and cheeks always form part of my treatment plan with patients who are considering perioral rejuvenation. I believe this is the key to truly delivering harmonious, individualised and seamless facial reshaping treatments.
Product selection
When treating the perioral area, I consider the full Juvéderm Vycross and Ultra ranges. My choice of product will depend on the target tissue and the impact I need to exert on them. I need to understand the dynamics of the skin, subcutaneous, muscle and bony layers and how this now
This article was produced and funded by Allergan Aesthetics, an AbbVie Company. For more information go to: www.juvederm.co.uk UK-JUV-2150182 Date of preparation: Apr 2021


REFERENCES
1. M. de Maio. MD Codes™ A Methodological Approach Aesthetic Plastic Surgery. 2020.
2. Allergan and M. de Maio. VYCROSS 2nd Edition. INT/0836/2016a. 2017.
3. M. de Maio. Myomodulation with Injectable Fillers. Aesthetic Plastic Surgery. 2018.
4. Juvéderm® VOLBELLA DFU. 73363JR10. 2020

5. Juvéderm® ULTRA SMILE DFU. 73664JR10. 2019.
6. Juvéderm® VOLUMA DFU. 73650JR10. 2019.
7. Juvéderm® VOLIFT DFU. 73652JR10. 2019.
8. Juvéderm® ULTRA 3 DFU. 72490JR12. 2016.
9. Juvéderm® VOLITE DFU. 73655JR10. 2019.
https://yellowcard.mhra.gov.uk/
Are you treating the lips in isolation? Aesthetic nurse prescriber Jennie Hawkins explains the importance of taking a step back to assess and treat the whole perioral area for optimum outcomes
Adverse events should be reported. Reporting forms and information can be found at
10. Juvéderm® VOLUX DFU. 73561JR10. 2019. Adverse events should also be reported to Allergan Ltd.
UK_Medinfo@allergan.com or 01628 494026.
Voluma (1ml) placed as a bolus to bone at the zygomaticotemporal region of the zygomatic arch. Voluma (1ml) was also placed as a bolus to bone, medial to the protuberance of the chin and then subcutaneously at the sublabial crease.
Aesthetics | May 2021 48 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Allergan Aesthetics
Before After
Preventing the Signs of Ageing
Vincent Wong,
techniques that stimulate collagen production (also called collagen-banking techniques) and interventions that prevent collagen breakdown.
Facial balance and harmony
pharmacist Marie Line
Marie-Elizabeth
The past decade has witnessed a significant global increase in the use of minimally-invasive cosmetic techniques for aesthetics and rejuvenation.1 Interestingly, this was also paralleled with a rise in the use of social media platforms with photo-filtering options like Snapchat, especially by younger adults.
Indeed, according to an online survey involving 2,092 participants, 77% of people aged between 18 and 24 and 38% of people aged between 35 and 44 reported using Snapchat in the UK, versus only 2% of people aged 75 and above.2 The advent of image-based social media has put photo editing and filters in everyone’s arsenal and has standardised the perception of beauty worldwide, such as creating smooth young-looking spotless skin.3 Skin health is indeed considered one of the principal factors indicating overall wellbeing in humans.4 The skin is altered with ageing due to the loss of elasticity and the appearance of expression lines and, later, wrinkles. In this article, we will explore and introduce many of the minimally-invasive techniques for age prevention and reversal, which include neurotoxin, fillers, skin peels, resurfacing treatments, medical-grade skincare, as well as modifications in lifestyle habits and nutrition.
Changes in hyaluronic acid and collagen bank with skin ageing
The phenomenon of ageing is a fundamental feature of life.5 Skin ageing is characterised by decreased synthesis and increased degradation of collagen, elastin, and hyaluronic acid (HA), the main components of the skin’s connective tissue, leading to reduced skin resilience and elasticity.6

Moreover, youthful skin seems to retain its turgor and pliability, due to its high content of water. The crucial molecule involved in skin moisture is HA, which has a distinctive capability to bind and retain water molecules. Skin ageing starts in the mid-20s with progressive hormonal changes, such as the gradual decrease in production of sex hormones and the latter decrease in oestrogens and progesterone associated with menopause in women.7 The production of collagen also slows down from around the age of 25, with a reported 1% loss of collagen production yearly.8
Meanwhile, collagen degradation is promoted by external factors such as UV-light exposure, smoking, vitamin C deficiency, and some diseases (e.g. osteoarthritis).9,10 Thus, maintaining a proper amount of collagen in the skin is of high importance to maintain skin health and relies on
The success of cosmetic procedures does not depend only on improving individual features, but also on establishing facial harmony and preventing or correcting ageing aspects.11 Symmetry, averageness, and gender-specific traits play important roles in determining the attractiveness of a face.12 In particular, smaller than the average chin, smaller than the average nose, and higher than the average forehead, all are traits associated with a female’s attractiveness according to male study participants.13 Female preferences for male faces are thought to be less specific. Preferred features were influenced by cultural, psychological and hormonal factors and included masculine eyes (narrower and more deep set than female eyes), but not particularly masculine facial outlines.13
However, the aim of cosmetic procedures should be to treat conservatively and not to give an unrecognisable appearance. Moreover, correction of the skeletal facial structure is increasingly regarded as the new objective in facial rejuvenation as certain areas of the facial skeleton such as the maxilla and the pre-jowl area of the mandible undergo resorption with ageing.14 Indeed, enhancing certain features can, at the same time, improve facial harmony and help prevent ageing. For instance, according to Dr
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
For those new to aesthetics, Dr
clinical
El Helou, and clinical dietitian
Ragi present an introduction to the modalities that can help your patients maintain a youthful appearance
Preventing ageing through skincare, lifestyle changes, and diet management is as important as cosmetic interventions
Wong’s experience, favouring a prominent chin and jawline can help prevent the development of jowls in older age. Similarly, correcting a negative vector in the cheeks with fillers can help restore harmony and youth to the face.15
Minimally-invasive modalities to help prevent ageing Countless minimally-invasive approaches are available to address skin ageing and enhance facial rejuvenation, with many of them acting on maintaining skin collagen and elastin. Infiltrative therapies, such as filler injections, employ filling substances (e.g. collagen, HA, or autologous fat) to target soft tissue augmentation and large wrinkle improvement.16 They have also been utilised to correct volume distribution and achieve balanced facial contouring.17
Conversely, mesotherapy uses microinjections in the superficial layer of the skin, to help improve skin brightness and texture, notably eye wrinkles and dermal thickness.18 Indeed, HA micro-injections have become very popular as a ‘youth booster’ thanks to their ease of use, efficacy to reverse early signs of ageing by improving skin elasticity and complexion radiance, and positive safety profile, including low immunogenicity.6,7,19,20
On the other hand, radiofrequency therapy as well as resurfacing procedures, such as chemical peeling, microdermabrasion, microneedling, laser, and intense pulsed light (IPL), have been applied to effectively protect existing collagen and stimulate new collagen synthesis, thus promoting skin repair, skin tightening, alleviating acne, scarring, wrinkles and photoageing, and correcting hyperpigmentation.17,21-23 The type of laser is chosen based on the degree and severity of defects, with ablative lasers being used for severe skin damages and deep creases,
and their non-ablative counterparts being favoured for moderate imperfections.21 Chemical peels, which contain varied strength of acids, are also popular as a means to exfoliate the superficial epidermis and correct superficial skin damages.21 Contrastingly, radiofrequency therapy uses radiowave energy to heat the deep layer of the skin (dermis and subcutaneous tissue) to stimulate collagen production for a natural rejuvenating effect.22,23 PRP treatments and stem cellderived therapy using growth factors are beneficial to promote collagen production and reduce hyperpigmentation.24,25 However, notable side effects might ensue from all these approaches such as procedure-related pain, scarring, discolouration, and infections.21,22 These modalities also vary in the degree of clinical changes and most often require multiple sessions, prolonged treatment and follow-ups to sustain their effects, although studies are needed to assess their longlasting outcomes.21 Finally, preventing ageing through skincare, lifestyle changes, and diet management is as important as cosmetic interventions.
Muscle modulation of the face
Botulinum toxin type A injection is one of the most frequently performed cosmetic procedures for the treatment of facial wrinkles. Wrinkles are formed by dermal atrophy and repetitive contraction of the underlying facial musculature. Injection of small quantities of neurotoxin into specific overactive muscles causes localised muscle relaxation that smooths the overlying skin and reduces wrinkles.26
Neurotoxin inhibits the release of the neurotransmitter acetylcholine from axon endings at the neuromuscular junction, thereby promoting muscle paralysis.26 In
clinical practice, neurotoxin is mainly used for wrinkles located in the upper one-third of the face, such as glabellar lines and lateral canthal lines, commonly called frown lines and crow’s feet, respectively.
Patients with dynamic wrinkles demonstrate the best improvements from neurotoxin compared to those with static wrinkles, who require a longer treatment duration and more frequent injections.27 Interestingly, clinicians’ experience and case studies have pointed out that repeated neurotoxin injections in targeted areas (particularly forehead, glabellar and periorbital areas) can prevent the development of expression wrinkles by promoting localised muscle relaxation, especially in younger patients before these wrinkles are definitively settled.28-31
However, overuse of neurotoxin may also result in undesirable outcomes such as a frozen look due to decreased facial expressions, or a skeletal look because of muscle atrophy due to prolonged muscle chemodenervation.32 It should be noted that muscle atrophy has been particularly reported in the masseter muscle after repeated neurotoxin injections for lower face contouring.33 Nevertheless, physicians can manage those side effects by minimising the dose and/or the frequency of neurotoxin injections and should reassure patients about the temporary and reversible effects of neurotoxin-induced muscle atrophy.34 Lately, the aesthetic practice has been favouring the combined use of dermal fillers and neurotoxin.35 Indeed, this appears to restore facial appearance by the dual mechanisms of reflation and relaxation, and by increasing the longevity of tissue dwell time of the filling agent.36 According to an open label clinical study with 57 participants conducted over six months, combination treatment resulted in high patient satisfaction (96.5 %) and good tolerability.37
Medical-grade
skincare and SPF
Patients possess individual control over the ability to maintain skin youth and rejuvenate damaged skin by adopting preventive measures. With the availability of various options that might create confusion to the patients, practitioners should be aware of the latest treatments and educate patients on the most appropriate products to adopt, and continuously follow-up to maintain a targeted treatment plan.
Indeed, numerous changes contributing to the aged appearance are attributed to modifiable factors. Among them, sun
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Sun exposure remains the predominant causative agent of skin cancer and photoageing, creating skin atrophy, pigmentary changes, wrinkling, and malignancy
exposure remains the predominant causative agent of skin cancer and photoageing, creating skin atrophy, pigmentary changes, wrinkling, and malignancy.38
Long-term continuous exposure to ultraviolet radiation has been shown to notably inhibit the synthesis of HA and stimulate the production of advanced glycation end products (AGEs), where collagen is rendered incapable of repair. It may also induce oxidative stress in epidermal cells, subsequently generating the production of reactive oxygen species (ROS), causing DNA damage, inflammation, impairment of collagen and elastin synthesis, and potentially leading to tissue destruction and dermal degeneration.9,39-41
However, UV-induced skin damage can be prevented by avoiding sun exposure and applying sunscreens, with a minimum SPF of 30.42,43 Topical vitamin A in the form of retinoids have also gained favour for the ability to prevent oxidative stress, and promote collagen and elastin production.44 Indeed, topical creams with antiageing properties have become very popular due to their ease of use, minimal adverse effects, and affordable price. They are reported to maintain skin smoothness, repair superficial skin damages and prevent photoageing by virtue of their sun protection (titanium dioxide or zinc oxide), prolonged moisturising effects, antioxidants components (coenzyme Q, vitamins C and E), and peeling properties (alpha or beta hydroxy acids).44
Recent concerns are also directed toward the increasing exposure to short-wavelength blue light emitted by electronic devices. Indeed, even short exposures may stimulate the production of ROS, increase oxidative stress, and induce skin damage, but more research is still needed on their long-term effect on skin ageing.45
Lifestyle habits
Many other lifestyle habits and nutritional components are closely involved in skin health: some hold antiageing properties, while others might contribute to skin damage.43 Smoking and excessive alcohol consumption have been linked to increased oxidative stress, facial ageing, wrinkling, and changes in skin thickness and pigmentation, as a result of elastic tissue breakdown, with the degree of facial skin damage proportional to the amount and time of exposure.9,10,40,41,46 Studies comparing twins have supported this, as higher tobacco and alcohol consumption, as well as sun exposure, were found to be associated with the perception of an older
appearance.47-49
While avoiding smoking and limiting alcohol consumption is crucial to delay facial ageing, it is however advised to indulge in moderate consumption of red wine, which contains resveratrol, a polyphenol with potent antioxidant properties.42 Indeed, food antioxidants and phytochemicals, majorly present in fruits and vegetables, of which flavonoids (red cabbage, berries), lycopene (tomatoes), proanthocyanidins (grape seeds), and polyphenols (green tea, coffee), have been reported to possess substantial skin photoprotective effects.50
Copper, zinc, selenium, and vitamins, specifically A, C, and E, are also powerful antioxidants that protect against skin ageing.9 For instance, according to a literary review, studies have shown that copper plays an important role in improving skin elasticity, reducing facial fine lines and wrinkles, and promoting wound healing.51 In contrast, excessive intake of sugars and fried food has been associated with the accelerated production of AGEs, while high-fat diets have been found to promote skin oxidative stress and inflammatory responses.9,52 Indeed, limiting dietary carbohydrates, same as caloric restriction, are reported to reduce the production of glycosylated collagen and delay ageing.9,52 These practices should, however, be avoided as they can compromise our health by generating malnutrition and deficiencies in essential nutrients.53,54 Instead, findings report that spices and herbs (cinnamon, cloves, oregano, and allspice) inhibit the production of AGEs,42 and are to be included in a balanced diet, rich in a colourful variety of fruits and vegetables, along with regular physical activity and adequate sleeping.55,56 Finally, consultations with specialists are necessary to help identify each patients’ nutritional needs, set up a targeted dietary plan and advise on the lifestyle changes to be followed.
Prevention is better than cure
With the rise of social media platforms and influencer movements, young millennial adults have been seeking approaches to preserve a younger-looking appearance and improve their facial features according to popular aesthetic standards.
Minimally invasive modalities such as neurotoxin, fillers, and resurfacing treatments, are being chosen thanks to their rapid satisfactory aesthetic outcomes and relatively favourable safety profile. These techniques should however be aimed at promoting facial balance and proportion, and effectively
correcting age-related skin features rather than changing one’s facial appearance. The resort to topical skincare and lifestyle modifications, including proper nutrition and regular exercise, are also key factors to maintain proper skin health and to age gracefully. With the successful integration of many of these modalities, a complete facial rejuvenation regimen can be established to ensure patients’ goals and maximise satisfaction.
Dr Vincent Wong is an aesthetic practitioner and founder of VinDoc Aesthetics. He has a Bachelor of Science in Medicine from the University of St Andrews and a Bachelor of Medicine and Surgery from the University of Aberdeen. Dr Wong has won a number of awards, is actively involved in research and has more than 35 scientific publications to his name.

Qual: BSc Medical Science (First Class Honours), MBChB
Marie Line El Helou has a Doctor of Pharmacy degree from the Lebanese American University and a Master of Science in Pharmacology from Paris-Sud University. She has been working in pharmacovigilance in the investigational and post-marketing settings, and has participated in several research projects in drug formulation and drug safety.
Qual: PharmD, M.Sc. Pharmacology
Marie-Elizabeth Ragi is a licensed clinical dietitian. She has a Bachelor of Science in Nutrition and Dietetics from Saint Joseph University and a Master of Science in Human Nutrition from the American University of Beirut. Ragi has been working as a researcher and conducting scientific studies for more than five years.

Qual: B.Sc. Nutrition and Dietetics, M.Sc. Human Nutrition

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM



NO FILTER. JUST YOU. @merzaesthetics.uki merz-aesthetics.co.uk Merz Aesthetics UK & Ireland Adverse events should be reported. Reporting forms and information for United Kingdom can be found at www.mhra.gov.uk/yellowcard. Reporting forms and information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/report-anissue/mdiur. Adverse events should also be reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143. 1. Belotero Revive IFU 2. BELOVE 2019 Facial skin revitalization with CPM-HA20G an effective and safe early intervention M-BEL-UKI-1071 Date of Preparation April 2021 BELOTERO® Revive is the newest product in the BELOTERO® portfolio of fillers indicated to revitalise the signs of early onset of photodamaged facial skin. • Improves skin hydration1 • Increases skin elasticity and firmness1 • Smooths skin texture1 • Reduces pigmentation2 NEW REGISTER NOW to attend the launch of BELOTERO® Revive at merzwebinars.com AVAILABLE FROM THE 10TH MAY
Case Study: Managing a Vascular Occlusion
Soft tissue augmentation using dermal filler has grown in popularity with hyaluronic acid (HA) based products comprising the most commonly used soft tissue filler.1 HA fillers are generally considered to be safe treatments with relatively rare and transient side effects,2 however rare complications can occur, such as vascular occlusion (VO) potentially leading to skin necrosis.3
If a VO is diagnosed and treated rapidly using an appropriate protocol, for example the Pulse Protocol4 (discussed later) skin necrosis can be prevented or reversed, and complete wound healing can be achieved.5 This may prevent long-term skin damage and longstanding deformity. If immediate reversal of vascular compromise is delayed and skin necrosis presents, there is evidence hyperbaric oxygen therapy (HBOT) can aid clinical improvement.6,7
In this case study we will present a patient who suffered a VO following a non-surgical rhinoplasty using HA dermal filler, how she was treated, including the use of hyperbaric oxygen therapy, and how full resolution was achieved following this complication.
Presentation
The 30-year-old female patient underwent a non-surgical rhinoplasty with EPTQ dermal filler at an undisclosed location by a non-medical professional. Around seven hours following the treatment, the patient noticed skin discolouration and contacted the initial injector, who subsequently reviewed her. The skin changes were deemed to be an
allergic reaction due to the skin preparation fluid. After a second opinion by the injector’s trainer via FaceTime, the patient was again advised this was a rash due to the skin preparation fluid.
The patient subsequently sought a second opinion by contacting aesthetic nurse Mikala Foster at Essex Cosmetics clinic via a WhatsApp image and asking for help, as she was extremely concerned this was more than just an allergic reaction. As soon as the image had been reviewed, the patient was advised by Foster to come in urgently for a face-to-face assessment, due to the likelihood of a VO following the procedure.
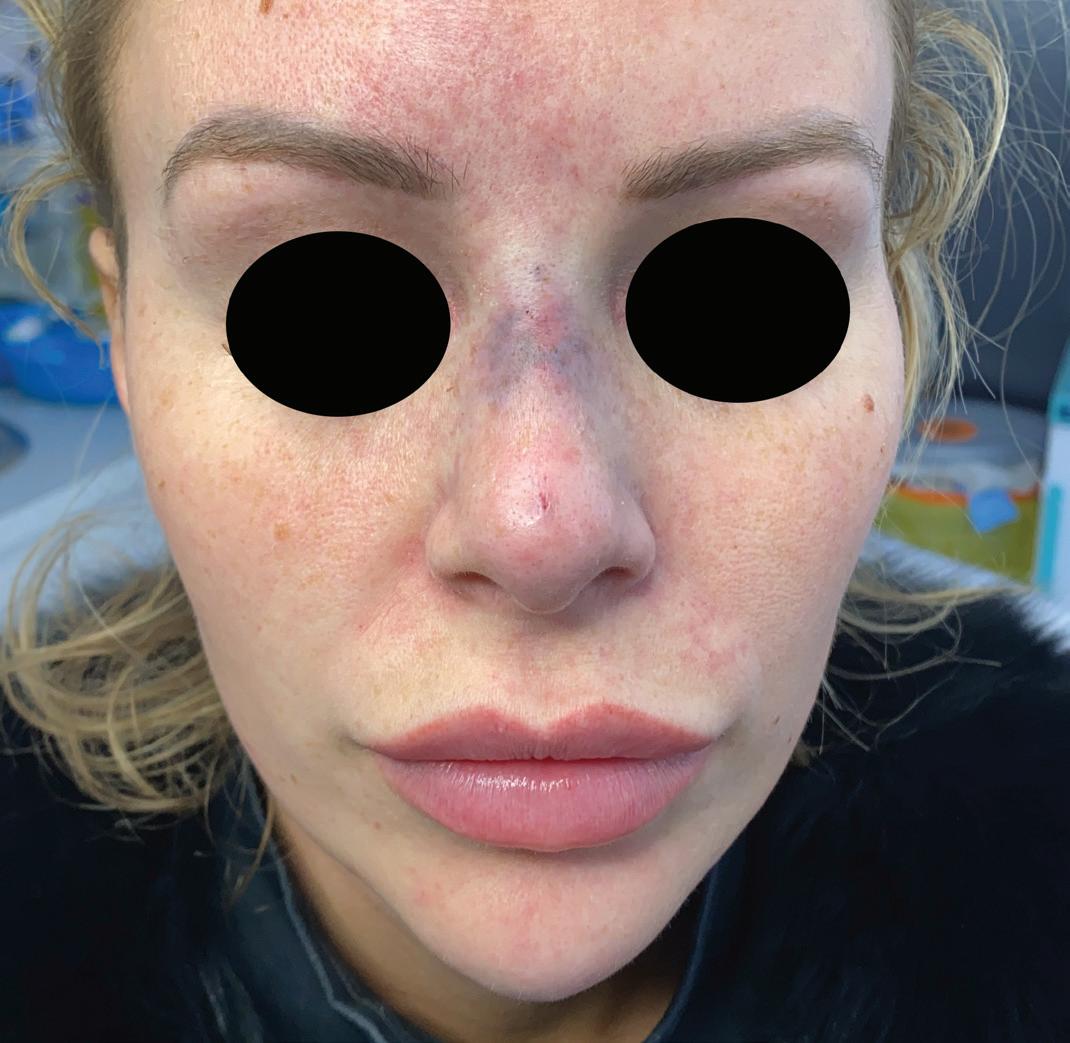
The initial injector was called to discuss exactly what had been injected and where – they claimed they were going on holiday that day so weren’t able to intervene. It was confirmed that the patient had been injected with approximately 0.3ml of dermal filler via two injection points, using a technique where the dermal filler was decanted into a BD Insulin syringe prior to injecting (there was no information regarding aspiration).
The patient complained of numbness to the bridge of the nose, as well as reporting a sharp sensation in her left inner nostril along with generalised pain, which she described as severe and rated 7/10. On examination, the nasal tissue was mottled and cool to touch, with an area of pallor present across the radix point. There was tenderness on palpation to the left side of the nose and nasolabial area. There was a delayed capillary refill of four to five seconds to the nasal tip and bridge (which should usually be equal to or less than two seconds), with significant livedo reticularis following the pattern of the facial, supratrochlear, angular and dorsal nasal arteries. Vision was intact.
Initial management
A warm compress was applied with massage to assess if any improvement would occur, while hyaluronidase was simultaneously prepared. As expected, there was no improvement or increased skin perfusion, so the Pulse Protocol4 – which involves continuous flooding of hyaluronidase to the occluded area, as established by the Aesthetics Complication Expert (ACE) Group World – was initiated immediately with the aim of dissolving the product and
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Aesthetic nurse Mikala Foster and Dr Manav Bawa outline how they successfully managed a complication following a non-surgical rhinoplasty
Figure 1: Patient upon presentation to the clinic, displaying signs of vascular occlusion.
The nasal tissue was mottled and cool to touch, with an area of pallor present across the radix point
subsequently achieving reperfusion the skin. 1,500iu of hyaluronidase was administered to the areas in 40 to 60-minute cycles as per the protocol, repeated four times.
Injection points from the previous injector were still obvious so hyaluronidase was flooded through these entry points both perpendicular to periosteum, and superficially with small boluses and liner threads. Hyaluronidase was administered to the nose, adjacent areas, around the nasolabial fold and forehead, following the pattern of the reticulated tissue. The hyaluronidase was administered using a combination of 32 gauge needles for precision. A 25 gauge blunt tip cannula was also used to cover a larger area with reduced trauma to the tissue, as well as comfort for the patient. This was important to minimise bruising and aid accurate capillary refill assessment. No topical lidocaine was used throughout the management to prevent a topical hue on the skin, and the patient tolerated treatment well so did not require it.
After each cycle, capillary refill was reassessed, and the skin was re-examined closely for positive tissue changes. Whilst the nasal tip was improving rapidly, the radix point continued to show pallor with a sluggish capillary refill. Four cycles were competed by 10pm that evening, when the patient was unable to tolerate further treatment due to exhaustion. It was explained we should continue, however the patient refused and agreed to return first thing in the morning.
In total 6,000iu of hyaluronidase were administered on day one and the patient was also prescribed 300mg aspirin stat and 50mg sildenafil stat, both with the aim of improving circulation and tissue perfusion. 30mg prednisolone once a day for five days was prescribed to reduce swelling and inflammation. The patient was also prescribed 500mg clarithromycin twice a day for seven days to prevent an infection to the hypoxic skin. The ACE Group World guidelines for vascular occlusion were followed throughout.
Hyperbaric oxygen therapy
During the treatment, it was deemed beneficial to discuss how hyperbaric oxygen could help, due to the widespread nature of the complication and skin changes.8 A referral was made to a local chamber, and the patient privately had five cycles of hyperbaric oxygen. When the patient returned the following morning, the delayed capillary refill and pallor remained present and a further 1,500iu of hyaluronidase was administered to the radix point. A clear improvement was made almost immediately and, reassuringly, the capillary refill time went back down to two seconds.
Following this, the patient subsequently received five hyperbaric oxygen treatment sessions over five days, with continued resolution of symptoms. Each session in the chamber took an hour but, with the preparation time involved, the patient was there for approximately three hours each day.

Completion of care
The patient was seen again in the clinic 21 days following her presentation, where she had made a full recovery, with complete resolution of her VO and skin changes. Following her experience, the patient has not been put off further HA filler treatment but will now only see experienced and qualified medical professionals able to recognise and manage a complication.

Recommendations
As well as always using the safest technique possible, it is important to understand the anatomy of the face – especially the vascular supply – being aware that there are many anomalies. Remember there is no 100% safe technique, so reducing all risks as much as possible will increase the safety of the procedure. Also remember that the nose is one of the most advanced areas to treat with dermal filler, so we recommend gaining experience in general aesthetic medicine prior to undertaking this procedure. Being able to diagnose a VO is extremely important, as well as being

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Figure 2: One day following four cycles of hyaluronidase (6,000iu in total) and prescription medication.
Figure 3: Patient undergoing hyperbaric oxygen therapy.
Figure 4: Patient following 21 days, demonstrating full recovery.
competent to manage one, for example a complications course is always a good option, as well as reading or online learning on how to manage an emergency situation.
Have your protocols written up, easy to locate and follow, as during a complication such as a VO, stress and nerves may set in, therefore simple instructions would be much easier to follow in an emergency situation. Always ensure adequate stock of hyaluronidase in case you require multiple vials.
Also ensure to ask for help early – we discussed this case the day after the patient presented. As we all learn during our basic life support training, it is always wise to ask for help as early as possible if the situation may require additional support. In a case like this, time is of the essence, so it is worth asking early if you need it.
Create a local support network or join an association, where you can seek aid and advice if required, subsequently, a complications group to support you if you find yourself in a challenging situation. We also recommend collaborating with local teams such as the plastic surgeons, ophthalmologists and your local hyperbaric team, for situations such as this.
We must remember to communicate openly and honestly with the patient to ensure they understand what is happening, and why we recommend a particular emergency treatment. We have a duty of candour to our patients, which should be upheld at all times. It will likely be a stressful time for patients, and many will be very scared, so empathy and clear explanations will be greatly appreciated.
Photography is extremely important to continually assess and should be mandatory for the medical records. A consent form should be discussed and signed as well. Be aware of different types of dermal filler, and the effect of hyaluronidase on them, as different fillers are dissolved at different rates or quantities of hyaluronidase.9
Reflection on a complication is always worthwhile as it will allow you to see what you did well in that situation, and what could have been done differently if this were to reoccur.
Act quickly and safely
This case study highlights the importance of acting quickly to resolve a vascular occlusion, which is a medical aesthetics emergency. Having set protocols and being competent in managing complications is extremely important, as the more treatments we do, the more risk there is of occurring.
Also, patients may present to us having been treated from another clinic with an emergency complication, so it is important to be able to act appropriately and manage the situation, as well as understand how to escalate where required.
Note: This case was brought to aesthetic nurse Mikala Foster. All prescription-only medicines mentioned in this article were prescribed by aesthetic nurse prescriber Charlotte Page, who reviewed the patient and works alongside Foster at her clinic, Essex Cosmetics. Dr Manav Bawa was contacted the day after the event for further guidance and opinion on the management approach.
Mikala Foster is a registered nurse and founder of Essex Cosmetics. She began her nursing career in an NHS emergency department, before starting her aesthetic career in 2015. Foster is passionate on raising awareness, safety and regulation in the industry, and is currently undergoing her prescribing qualifications at university.

Qual: RN
Dr Manav Bawa is an aesthetic practitioner and GP with a surgical background. He is the medical director of Time Clinic in London, an injectables trainer, and has completed a Diploma in Aesthetic Injectable Therapies. Dr Bawa is an associate member of BCAM and is passionate about mentoring, education and patient safety.

Qual: MD, PGDip(ESSQ), MRCS(Eng), M Ed(SE) & DIC, MRCGP, PGDip(CAIT)
REFERENCES
1. Rod J Rohrich et al. ‘Practical Approach and Safety of Hyaluronic Acid Fillers’, Plast Reconstr Surg Glob Open, (2019), 14;7(6):e2172.
2. Kwok Thye David Loh et al. ‘Prevention and management of vision loss relating to facial filler injections’, Singapore Med J, (2016), 57:438-43.
3. Joel L Cohen et al. ‘Treatment of Hyaluronic Acid Filler-Induced Impending Necrosis With Hyaluronidase: Consensus Recommendations’, Aesthetic surgery journal (2015), 35,7:844-9.
4. Martyn King et al. ‘This month’s guideline: The Use of Hyaluronidase in Aesthetic Practice (v2.4)’, The Journal of clinical and aesthetic dermatology (2018), 11,6:E61-E68.
5. Ramtin Kassir et al. ‘Extensive necrosis after injection of hyaluronic acid filler: case report and review of the literature’, Journal of cosmetic dermatology, (2011), 10,3:224-31.
6. Raelene M Leach et al. ‘Hyperbaric oxygen therapy’, BMJ, (1998), 317(7166):1140-1143.
7. Raven Henderson et al. ‘Hyperbaric Oxygen for Ischemia due to Injection of Cosmetic Fillers: Case Report and Issues’, Plast Reconstr Surg Glob Open, (2018), 6(1):e1618.
8. Dr Ahmed El-Houisseny, Using Oxygen Therapy for Vascular Compromise (UK: Aesthetics, 2020) <https://aestheticsjournal.com/cpd/module/using-oxygen-therapy-for-vascular-compromise>
9. Veena Rao et al. ‘Reversing facial fillers: interactions between hyaluronidase and commercially available hyaluronic-acid based fillers’, Journal of drugs in dermatology: JDD, (2014), 13,9:1053-6.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
JOIN THE FREE CEREMONY




DO YOUR REVISION! Introducing Revision Skincare ® PROFESSIONAL MEDICAL-GRADE SKINCARE FOR VISIBLE RESULTS AT HOME PURPOSE We help skin care professionals around the world give people the best skin of their lives.






WHY REVISION Revision Skincare® was founded to change the way professional skincare results are achieved. We believe youthful-looking
can be accomplished without ever compromising skin’s
health. Our unique formulation
for better treatment methods and challenging
approaches to deliver powerful results. C OMPLETE PRODUCT OFFERING Full range of Skincare Solutions to help Achieve Healthy, Beautiful Skin™: Cleanse Tone Mask & Exfoliate Treat Moisturise & Protect ACHIEVE HEALTHY, BEAUTIFUL SKIN ™ revisionskincare.co.uk JOIN THE CONVERSATION • @revisionskincareUK • #revisionskincareUK • #healthybeautifulskin Distributed in the UK and Ireland by • 01234 313130 • info@aestheticsource.com • www.aestheticsource.com LATEST AWARD WINNING PRODUCTS MULTIPLE PATHWAYS SKIN NEUTRAL pH MICROBIOME TECHNOLOGY BIOAVAILABLE PEPTIDES SYNERGISTIC USAGE OUR FORMULATION PHILOSOPHY We use an array of industry-first technologies generating clinicallyvalidated results. We accomplish superior efficacy while nurturing long-term skin health using 5 formulation principles:
skin
long-term
philosophy is leading the way
traditional
Beauty is No Longer Skin Deep
Discover the EMERALD non-thermal body sculpting laser by Erchonia

Non-thermal low-level laser (NTLLL) has been in clinical use since the late 1960s, and for many years its method of action was not fully understood or appreciated.
NTLLL covers a broad medical spectrum which can be used to the benefit of your patients and the expansion of your clinical practice. Some patients are not just looking for ways to aesthetically modify their appearance, but many are also looking for ways of restoring, re-energising and revitalising their cells to restore health and wellness and using their own fat to get their health back.
How NTLLL works
The biochemical mechanism underlying the therapeutic results of NTLLL has a wide range of effects at the molecular, cellular, and tissue levels. There is strong evidence to suggest that within the cell, NTLLL acts on the mitochondria via cytochrome-c (COX) to increase adenosine triphosphate (ATP) production. This up-regulates mitochondrial respiration and is the energetic component that produces an energy cascade and electron transport.
Specific wavelengths of light can trigger mast cell degranulation, modulation of reactive oxygen species (ROS) and free nitric oxide (NO), and the induction of transcription factors. Numerous transcription factors are regulated by changes in cellular redox state. As a result, an increase is seen in cell proliferation and migration, and modulation in the levels of transcription factor. These
Case study
Before
transcription factors then cause protein synthesis that triggers further effects.1
The EMERALD LASER™, Europe’s latest revolutionary treatment for body sculpting


The EMERALD LASER™ works by empowering the body to repair and restore itself by harnessing the body’s ability to function at a higher level through cellular activity. This in turn leads to an ability to reduce fat by not harming the fat cell itself, and collagen reprofiling, thus improving the appearance of cellulite. The EMERALD LASER™ is currently the only device US FDA market cleared to treat those with a BMI of over 30 on overall body circumference. The EMERALD LASER™ experience causes our fat cells to release their fatty content for safe removal from the body by the lymphatic system. These fat cells now begin to act and function like healthy lean fat cells again, releasing the correct messages to your brain and, even more exciting, they begin a communication cascade throughout the fat organ causing other fat cells to react the same way, releasing their content and returning their hormone responses back to the positive!
How does the EMERALD LASER™ empower the body through fat and other processes?
We look at fat as being bad, but fat is good if correctly processed. It is food for the body
to use for energy and essential chemical processes. Through chemical actions, fat protects us and tell us when we are hungry, balances hormones and signals regulation.
The EMERALD LASER™ emulsifies the fat and turns it into free fatty acid, which our body can convert into energy to power and fuel activity. Once this fat is liberated from the fat cell through a transitory pore, a large part of it is used for energy. Some is removed from the body via phagocytosis and lymphatic action, and the remainder returns to any available fat cells. Non-Thermal Laser also empowers the body to create mtDNA and assist in mtRNA synthesis, and this releases usable energy into the body. As we age the viable number of mtDNA is greatly diminished as is our ability to produce stem cells.
What clinical studies have been conducted using the EMERALD LASER™?
The EMERALD LASER™ and Verju 532nm green diode lasers by Erchonia underwent multiple placebo-controlled, double blind, randomised, multi-centre clinical studies to gauge their efficacy and achieved unrivalled results. There were no adjunct therapies or lifestyle changes in the studies. Erchonia hold 18 of the 21 US FDA market clearances for Low Level Laser and have over $5 million invested in any one time into research. There have been no reported side effects or adverse reactions, and the system is truly inspired by the simplicity of nature.
What is the depth of penetration?
Erchonia non-thermal lasers use the minimum amount of power to generate a stable laser beam which delivers electromagnetic energy in the body. The body converts this energy into viable metabolic energy which fuels processes throughout the system creating a systemic effect of communication from cell to cell. It is important to say that this is a true laser i.e. collimated, monochromatic and unidirectional.
REFERENCES

After
1. Hamblin M and Demidova-Rice TN 2007 Cellular chromophores and signalling in LLLT
Aesthetics | May 2021 58 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Erchonia
This advertorial was written and supplied by Erchonia
The laser was applied 11-15cm from the skin surface, and the heads were distributed to cover the stomach area and thighs. As can be seen, there was well-dispersed cellulite deposits, large amounts of fat to the stomach, lateral flanks and mid torso. The after image shows improved skin tone, reduction in cellulite and fat. More info: +44 (0) 1491 821135 www.erchonia-emea.com
Lasers Ltd
A summary of the latest clinical studies
Title: Oil Thickening with Organoclay Enhances the Ultraviolet Absorption Ability of Sunscreen
Authors: Yamaguchi K, et al.
Published: Journal of Oleo Science, April 2021
Keywords: Skin-Mimicking Substrate, Oil Thickener, Sunscreen
Abstract: The performance of sunscreen products depends on their ultraviolet (UV) absorption ability through the film formed on the skin surface upon application. Therefore, it is important that a uniform film is formed on the uneven skin surface for effective sunscreen performance. Most UV filters are oil soluble; in this study the increasing viscosity of the oil phase of a sunscreen product can improve the performance of sunscreen. We examined the association between the concentration of the oil thickener and the UV absorption ability of the sunscreen product using a skin-mimicking substrate (SMS). Among all thickeners examined, organoclay and silica silylate increased the UV absorbance of sunscreen on the SMS in a concentration-dependent manner. Thereafter, we examined film uniformity to elucidate the mechanism underlying the observed increase in UV absorption. The uniformity of film thickness on the SMS increased with organoclay content. Our results showed that increasing the viscosity of the oil phase with organoclay resulted in the formation of a uniform film, thereby increasing UV absorbance. Thus, the use of thickeners, such as organoclay, increases the viscosity of the oil phase at a low shear rate after the high shear of application.
Title: Characteristics of Non-Ablative Resurfacing of Soft Tissues by Er:YAG Laser Pulse Irradiation
Authors: Lukac M, et al.
Published: Lasers in Surgery and Medicine, April 2021
Keywords: Er:YAG Laser, Non-Ablative Resurfacing, Rejuvenation
Abstract: Several minimally invasive gynaecological, ENT and aesthetic procedures have been introduced based on delivering ‘smooth’ sequences of Er:YAG laser pulses to mucosal tissue at moderate cumulative fluences not below the ablation threshold but typically do not require local anaesthesia. The observed clinical results using ‘smooth-resurfacing’, has suggested that in addition to the direct heat injury to deeper-lying connective tissues, there is an additional mechanism based on indirect triggering of tissue regeneration. This study is to improve understanding of the complex dynamics of the exposure of tissues to a series of Er:YAG laser pulses, during which the thermal exposure times transition from short to long durations. A physical model of laser-tissue interaction was used to calculate the temperature evolution. Two modalities of non-ablative resurfacing were explored: a ‘sub-resurfacing’ modality with cumulative fluences, and the ‘smooth-resurfacing’ modality with fluences below the patient’s pain threshold. A skin tightening situation was explored by measuring pain tolerance threshold fluences for treatments on abdominal skin with and without topical anaesthesia. Two preferred smooth-resurfacing treatment modalities were identified. One using optimally long pulse sequence durations with optimal number of pulses. For deeper coagulation, long pulse sequences with delivered pulses are used with topical anaesthesia.
Title: Factors Influencing the Unmet Effects of Alpha Hydroxy Acid Peels on Acne Vulgaris
Authors: Tang J, et al
Published: Dermatologic Therapy, April 2021
Keywords: Acne Vulgaris, Chemexfoliation, Hydroxyl Acids
Abstract: Alpha hydroxy acid (AHA) peels have been previously recommended as an option for patients with intolerance to first-line treatments especially for long-term use. The safety and efficacy of AHA peels for acne have been established, but factors influencing the effects are unknown. We recruited patients diagnosed with acne who were intolerant to or refused the first-line treatments and collected the medical and demographic information of patients treated with a full course of AHA peels; data collected included age, sex, treatment history, and efficacy after treatment. The efficacy score was defined by revised scales: 2 points indicated significant improvement, 1 point indicated mild improvement, and 0 point indicated no improvement. Additionally, only efficacy scores of 2 points were classified in the satisfactory group; the others were classified in the unmet effect group. A total of 141 patients (120 female, 21 male) were included. The patients in the satisfactory group were older and showed better compliance than the patients in the unmet effect group. Multiple analyses confirmed the effects of younger ages and poor compliance on the unmet effect. Unsatisfactory compliance and age might decrease the effects of AHA peels on acne.
Title: Clinical Experience of Poly-L-lactic Acid Injections For Body Contouring Treatment
Authors: Shridharani S, et al
Published: Journal of Cosmetic Dermatology, April 2021
Keywords: Body Contouring, Biostimulator, Poly-L-lactic Acid
Abstract: Clinical data on body contouring with injectable polyL-lactic acid are sparsely reported in published literature. This study describes the lead author’s clinical experience using injectable polyL-lactic acid for body contouring in various anatomic locations. 20 consecutive patients undergoing body contouring treatments with poly-L-lactic acid were prospectively followed. All treatments were performed at a single clinic. Treatment details such as reconstitution, injection volume and dosage were documented. Treatment response was assessed independently by patients and the treating physician. Twenty patients (85% women) received injectable poly-L-lactic acid for body contouring treatments such as buttocks volumization, cellulite, and skin quality treatment. In most patients (65%), polyL-lactic acid was administered to correct post-surgical soft tissue deformities. Overall, patients had a mean of 5.1 treatment sessions in a mean of 1.4 anatomic locations. The most treated anatomic locations were buttocks (58%), thighs (20%), and abdomen (9%). Most treatment sessions resulted in improvement of the treated area. Adverse events included bruising, edema, numbness, and tenderness. Nodule formation was recorded for one patient. According to the lead author’s clinical experience, poly-L-lactic acid injection is well tolerated and can achieve good aesthetic outcomes when used for body contouring in appropriate patients.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
The beauty of the moment
Illustration does not show all packs available in the range.
Creative genius has long been part of our Florentine history, dating as far back as Michelangelo’s works of art. These values have inspired us to create RELIFE® – a growing portfolio of premium aesthetic medicine solutions built with innovative technology. See how our new Definisse™ range of peels, filler and threads, can transform your practice and your patients. Launching for the first time in the UK.



Filler SKUs CE0123 – CROMA-PHARMA GmbH, Industriezeile 6, 2100 Leobendorf, Austria Threads CE0373 Assut Europe SpA, Via G.Gregoraci, 12 00173 Roma, Italia

Hydrobooster
CE0459 CROMA GmbH, Industriezeile 6, 2100 Leobendorf, Austria Peel Program CE Mastelli S.r.l., Via Bussana Vecchia 32, 18038 Sanremo (IM)
only.
or
A. MENARINI FARMACEUTICA INTERNAZIONALE SRL
Mercury Park, Wycombe Lane, Wooburn Green, Buckinghamshire,
with Limited Liability | Branch
My skin says how I feel REsurface, REstore, REshape. The Definisse™ range from RELIFE. relifecompany.co.uk PP-RL-UK-0115. August 2020. GB20002 Model for illustrative purposes
For more information, to register for training
place an order, ask today at: info@relifecompany.co.uk Available now from Church Pharmacy: +44 (0)1509 380 046 www.churchpharmacy.co.uk
Menarini House,
HP10 0HH. Incorporated in Italy
registered in England No BR016024. Tel: 01628 856400 | Email: menarini@medinformation.co.uk
Updating your Clinic’s Pricing Structure
Business coach Alan S. Adams outlines how practitioners can benefit by implementing
As with any business, the profit your clinic makes can be hugely impacted by various differentials, including your sales process, regular outgoings, product investments or staff salaries. Regularly reviewing your pricing model, revenue, and costs is a standard procedure of running any company. However, many clinic owners I work with do not give these areas enough attention and risk losing out on potentially higher profit margins.
Do your research
Pricing your services correctly is the key to a successful business venture. When I started working with clinic owners, some of the first questions I asked were: how often do you think about your pricing structure, and when was the last time it was adjusted?
New product innovations are quickly added to the service offered by clinics wishing to stay ahead of the game and offer their patients the latest trends. Despite this, pricing models are not adjusted nearly as much as they should be to ensure ongoing business success. As an absolute minimum, clinic owners should be increasing their prices once a year – even if that’s just in-line with inflation.
If you leave it longer than this – for example five years – you run the risk of two occurrences: a sudden realisation that you need to increase your prices a lot (which could be a potential turnoff for your patients), and lower profit margins for every year you’ve not updated your pricing. How frequently you need to review the packages you offer is entirely individual to your clinic and there is no correct answer, but as an owner you need to schedule time in to review and analyse your costs.
Know your worth
By pricing too low, you risk looking unprofessional and unable to deliver the calibre and quality of the services that some high-end patients may be seeking. Your profit margin will narrow, and you undervalue yourself as a company and as a respected professional. However, if you price too high (without the right positioning and a well-thought-out customer journey), you risk pricing yourself out of new patients, who might favour a more affordable competitor who offers the same perceived value.
Conducting in-depth market research will allow you to understand the industry price for a particular treatment, but almost as importantly, how long it will take for you or your staff to deliver it. You can easily wipe some profits from your business if you come in too low a price,
and an appointment takes longer than you anticipated.
Therefore, regularly think about how much your time is worth (considering your education, qualifications, and experience), as well as the industry ‘norm’ for a service, and adjust your prices accordingly to ensure that you’re making enough profit overall.
Customer psychology
Purchasing behaviour is influenced not only by the value attached to a product or service, but also by the way this value is presented to us. The process of setting a pricing structure is more nuanced than simply attaching a price to a treatment and then focusing on how many treatments you can carry out, and how many new and returning customers are coming through the door.
All of the processes you use to encourage patients to visit your clinic rather than a competitor’s are a vital part of running your clinic. By reviewing your pricing structure regularly and employing gentle and ethical persuasion techniques, which have been researched and proven to work by a raft of esteemed experts, is equally important. There are many different strategies which can prove beneficial to your profits and bolster your clinic to the next level but, to begin with, there are three considerations to focus on: the number of choices your potential patients have, the order in which those choices are presented, and approaching interactions with patients who are hesitant to commit to a highvalue treatment.
Offering multiple choices
Deciding how many choices to give patients within each specialised sub-category of treatments you offer can be tricky. You do not want to overwhelm them with a long list, but few options could lead potential patients to look elsewhere for a better variety.
A study showed students performed better and took less time to complete a multiplechoice test when given three potential answers rather than four or five.1 We also know too many choices can demotivate a person – shoppers were ten times less likely to buy jam when they were given 24 different options to try compared to six.2
How many choices should you offer? There is a lot of research on the subject but a three-tier system works especially well. The argument for this pricing structure is perhaps most succinctly described by distinguished author and therapist Virginia Satir: “To have one choice is no choice; to have two choices is a dilemma; and to have three choices
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
a pricing structure in their clinics


o uk
around the value of your treatments and time. If you are the kind of person who is motivated to steer away from loss rather than towards gain, then pricing fear could be withholding you from adjusting the costs of the services you offer. Comparisons between yourself and and reservations – it will give you a distinct
understand that value, and what they stand to gain, rather than focusing on the ‘loss’ of payment is pivotal. If a patient comes to you solely based on price, it is very likely they’ll go elsewhere based on this, and these aren’t the type of patients you want to attract because
discussed above, can reap huge benefits in in your clinic into you gaining a new patient
aesthetic clinic sector. He was a finalist in The Association of Professional Coaches, Trainers and Consultants’ Coach of the Year Awards
Nation in 2020 as a Top 50 Advisor in the UK
between three option, four option and five option multiple choice question tests for Lepper MR, Iyengar SS, ‘When Choice is Demotivating: Can one Personality Processes and ‘The Satir Model: Family Therapy and Beyond’,
K, Jiheon L,
of Price
‘Comparison
accelerators/2013/04/10/paul-lee-the-williams-sonoma-breadSuk
‘The Influence
Presentation Order on 49 (2012)
Singh S, ‘Anchoring should be a mainstay of pricing research’, https://www.research-live.com/article/ opinion/anchoring-should-be-a-mainstay-of-pricing-research/
Cialdini R, ‘The Principles of Persuasion aren’t just for business’,






FIND OUT MORE: BTLAESTHETICS.COM | 01782 579060 | INFO@BTLAESTHETICS.CO.UK TAUT TONED & Tone Up & Treat Cellulite Results and patient experience may vary. Patients shown in the B&A pictures are within +/- 2,25 kg of their original weight unless specified. As with any medical procedure, ask your doctor if the EMSCULPT® and EMTONE procedure is right for you. In the EU: EMSCULPT® is intended for the treatment of obesity by fat reduction through neuromuscular stimulation and increase of the blood flow. EMTONE is intended for treatment of obesity and localized obesity by fat reduction, skin laxity treatment, skin regeneration, treatment of gynoid lipodystrophy, alleviation of pain and alleviation of muscle spasms. ©2021 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® are registered trademarks in the United States of America, the European Union, and other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. Trademarks EMSCULPT®, EMSELLA®, EMTONE®, EMBODY®, and HIFEM® are parts of EM™ Family of products. *Data on File. 799-79TATEEMA4ENGB100 Emsculpt-Emtone_LF_Taut-and-tone-enjoy-every-moment_A4_ENGB100 # tautandtoned From Unflattering to Unbelievable Treat Skin, Muscle and Fat Results You Can See No Downtime, No Needles
Communicating with Existing Patients
manage or influence this will either help or hinder you. In order to set yourself up for an effective consultation you need to begin by setting the patient’s expectation. As practitioners we don’t want to be overpromising and under-delivering, but we also don’t want to be misdirecting our patients and confusing them. Setting and managing patient expectations will have a huge impact on your overall success.
The best way to set expectations is to ensure continuity from the first contact. When a patient makes first contact, walk them through exactly what you’ll discuss in your consultation, let them know a little bit about you and your areas of special interest. As an example, for dentists, telling your patient that your cosmetic dentistry consultation will contain an assessment of their teeth and their face prepares them for the type of discussions that you’ll be having, and gives them time to digest the information before they’re in the treatment room. It also gives the patient a chance to decide whether you are the type of clinician they want or not.
For practitioners looking to encourage their patients into trying other treatments in your offering, the clarity and a willingness to share information fosters trust and ensures that the relationship between patient and clinician is robust. Patients with whom you have built a strong relationship are more willing to open up to you, and explore the potential of getting other treatments. Similarly, meeting expectations means happy patients, and happy patients are more likely to return for further treatments and tell their friends and family about their experience.
When your new business or practice is just starting out, the likelihood is that you won’t have thousands of pounds to spend on press and marketing. You’ll need to think of creative ways of communicating with your patients and client base organically, without influencers, ad campaigns or magazine spreads. One of the most important and under-utilised forms of patient retention is engaging current patients and guiding them towards aesthetic procedures that they may not have tried yet which could be beneficial for them. This can apply to your current aesthetic patients who may only come in for the odd facial, but could benefit from having other treatments such as injectables. For practitioners who already have a private practice focusing on a different healthcare area, such as dentistry, you may be able to open the eyes of these patients to delve into the world of cosmetic procedures.
All medical practitioners have the skills needed to be successful, but we often overlook the soft skills needed to really push our businesses. For example, good communication, listening and confident selfpromotion are so important. These skills are brilliant combatants to the self-doubt many practitioners feel when trying to steer their existing patients towards aesthetics.
Setting the tone and managing expectations
The patient journey begins way before they step into the treatment room. This is the case for both new patients and dental patients who we are trying to transition into becoming aesthetics patients. Every patient will arrive at your practice with an expectation, so how you
A comprehensive consultation
When a patient steps into the treatment room it’s tempting to focus only on what they expressed was their primary concern when booking the appointment. At the Smileworks Aesthetics Hub, we teach that asking the right questions is integral to a successful consultation.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Moving away from selling and into educating the patient shows them the problem and allows them to explore the situation
Dr MJ Rowland-Warmann shares her top tips for engaging current patients and guiding them towards facial aesthetics procedures
STERILE FACE SOLUTIONS
Remodel, tone, rebuild, firm, counter and correct facial skin imperfections


STERILE HAIR SOLUTIONS
Revitalize the scalp, support the hair growth and stimulate the development of the hair bulb


STERILE BODY SOLUTIONS

Combat fat deposits and cellulite, accelerate metabolism, and promote fluid drainage

“LITTLE, RARELY AND IN THE RIGHT PLACE”
Distributed exclusively by DermaFocus 02039941666 info@dermafocus.co.uk
Painless, Precise, Safe & Effective Mesotherapy Gun
www.dermafocus.co.uk
Instead of the typical introductory rigidity speaking about the specific area of concern the patient has outlined when booking the appointment, start off by simply saying something like ‘What brings you here today?’
Open and non-leading questions and making the interaction about them allows the patient to feel comfortable from the outset. You’ll be surprised by how much a shift in language can change the direction of a consultation. This question allows them to lead the conversation and share more about why they’ve really come to see you. You can determine whether it’s a very specific concern like ‘I have dark circles under my eyes’ – which may not be as effective for selling them on other aesthetic treatments – or a more generalised problem such as ‘I feel like I look very tired all the time’, which is a patient telling you it may not just be their eyes they are concerned about. This invites you to plan comprehensively. By sharing aspects of themselves which they’re unhappy with, they’re asking you for solutions to make them feel better. This is the first step in building your discussion about aesthetics and what treatments may benefit them.
Another question that invites sharing and a good jumping off point for aesthetics is ‘When you look in the mirror, how do you feel?’ It’s not specifically asking ‘How do you feel about your face?’, a question that could cause the patient to clam up. ‘How do you feel?’ is gentle but it often hits the crux of the matter, the real reason why they’re seeking treatment. It lets patients know that it’s okay to share the difficult thoughts and feelings that they’ve been having, and allows you, the practitioner, to listen to what they’re really saying. Opening a dialogue and learning to actually listen to what your patients are saying instead of asking closed questions from a list shows them that you are ready to work collaboratively with them in their journey. In my experience, open questions lead to a talking patient.
Using co-diagnosis
Co-diagnosis is about sharing the decision-making process with your patient and reaching a treatment plan with them. This may sound obvious to you, but consultations are still often paternalistic or authoritarian, where the clinician is rather prescriptive about proposed treatment. Co-diagnosis works in a three-step way to guide the patient through their discussions, explorations and engaging them in their treatment plan.
The first step is to recognise the problem together with the patient. Then, discussing options for treatment in a non-biased way,
remembering to explain what happens if they do nothing and thirdly, highlighting the benefits of having treatment and how the results can expect to look and feel. Incorporating this means assessments look more structured and you’re delivering consistency with a patient who feels in control. Most clinicians think they are doing this already, but really incorporating co-diagnosis is more nuanced than just coming up with multiple options and giving them select treatment plans to choose from. It’s about integrating exploration and choice and letting them discover options whilst you act as their guide.
Taking clinical pictures isn’t anything new, whether they’re used for social media, for portfolios or for medical records, but few practitioners actually use them with the patient. In my experience, this is one of the most powerful ways of converting patients into trying new treatments. Photographs, rather than mirrors, nudge the patient away from the subjective and towards an objective view of what is really there. Patients often become fixated on one part of their reflection, while their pictures somewhat neutralise this and the chance of you both seeing the same thing increases as the patient can become a little bit more removed and critical, seeing the bigger picture with you. When looking at the photos with the patient, ask them ‘What do you see?’ Instead of immediately noting all of the problem areas for them. This will engage them with the process, so they feel in control, more confident and less embarrassed when you come to a treatment conclusion.
The trick is to keep them constantly in the loop as you work your way through the different elements of their face, making sure they don’t feel lost or like you’re talking about something that is too complicated. The more accessible you make the consultation, the more collaborative it feels. Was it your idea or was it theirs? Moving away from selling and into educating the patient shows them the problem and allows them to explore the situation. Before you know it, they are asking for the solutions themselves.
Modifying your approach
A comprehensive examination means comprehensive treatment, which results in a comprehensive outcome. Fail to do the first, and the rest won’t happen. Get it right, and you have a trusting patient who always follows your lead. Of course, some people may not be open to extra aesthetic treatments, but some might be, and they could be too shy to ask about them or unsure what exactly it is they should be asking. It’s our job to let patients know their options and it’s up to them to choose from them; you’ll be doing both you and your patient a disservice to skirt around it for fear of offending them. Executing these skills isn’t something anybody can do. It takes time, practice and training. It also needs the courage to step outside of your comfort zone. However, if you are someone who is persistent, hardworking and ready to take this step towards incorporating facial aesthetics into your treatment portfolio then you will be rewarded tenfold.
Dr MJ Rowland-Warmann is the founder and CEO of Smileworks Liverpool, an eight surgery multi-disciplinary dental and aesthetics medicine practice. She is also the CEO of the Aesthetic Hub, a seven surgery training facility. Dr Rowland-Warmann has more than 10 years’ experience as a dentist and aesthetic injector, and holds an MSc in Aesthetic Medicine (with distinction) from QMUL.
Qual: BDS, BSc, MSc Aes.Med., MClinDent, Orthod., PGDip Endod., MJDF

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Patients with whom you have built a strong relationship are more willing to open up to you about, and explore the potential of, other treatments









• Retinol Youth Renewal Serum (15 mL NET VOL 0.5 FL OZ) • Retinol Youth Renewal Eye Serum (5 mL NET VOL 0.17 FL OZ) • Retinol Youth Renewal Night Serum (15 mL NET VOL 0.5 FL OZ) • Retinol Booster for HydraFacial (9 mL NET VOL 0.3 FL OZ) DELIVERED BY HYDRAFACIAL™ POWERED BY MURAD® Before After one HydraFacial Treatment with Murad Retinol Booster *In a Murad sponsored study. Individual results will vary. †After 2 Hydrafacial with Murad Retinol Booster treatments and daily application of Murad’s Retinol Youth Renewal system. Murad P/N: 653352/0220 HydraFacial P/N: 1900038−A Murad® Retinol Booster for HydraFacial We’re delighted to announce the launch of the Murad Retinol booster into the UK.
renewal,
wrinkles and
to
weeks*. Before After 4 Weeks† Retinol Rapid Renewal System with Murad Retinol Booster Enhance
HydraFacial treatments with Murad’s
and
wrinkles,
skin tone and
W: hydrafacial.co.uk E: infoUK@hydrafacial.com T: 01788 572 007 To see the HydraFacial in action follow us @hydrafacialuk
This potent serum accelerates skin’s surface
plumps to minimise the look of
evens tone
boost a youthful finish. Inspired by Murad’s Retinol Youth Renewal Serum: 93% saw a reduction in fine lines and wrinkles in just 2
results between
powerful yet gentle retinol trio to quickly
visibly smooth
even
boost radiance.
1) Are your posts summer smart? I find posts with photos have high levels of engagement, particularly strong before and after shots. In late spring/early summer I recommend using before and after body shots. This is a key area of focus in the summer months and your patients, prospective or otherwise, will be calling to book after seeing what visible results can be achieved. I also find that in all campaigns it’s a good idea to ask relevant questions on social media to increase audience engagement. In summer for example, you might ask: ‘what do you use to protect your skin against the sun’s rays?’ and then explain more about its impact on ageing.
Marketing Summer Treatments
The summer season is almost upon us and whilst not all treatments are best suited to this time of year (due to concerns such as post-inflammatory hyperpigmentation) there are some amazing services we can and should be marketing to your treatment starved patients.
A survey by Transform Hospital Group showed that people in the UK spend one third of their pre-holiday budget on beauty treatments,1 so it’s the perfect time to update your marketing strategies to reflect the season!
Following one of the longest winters and (enforced) hibernations we have seen for patients in our industry’s history, how do we market our services in these warmer, sunnier months and what are the best treatments to focus your marketing efforts on?
Changing your marketing strategy
The first thing that you should consider when adapting your marketing strategy is whether your social media is summer fit and working for you as a strong channel.
Throughout my time working in the aesthetics specialty, I have always liked to change things up with strategic marketing seasonally. But before this, whenever I work directly with businesses in a coaching capacity, I always ask the question: does your social
media audience match the number of clinic patients? If not, a perfect way to build on this is to encourage all patients to follow you in some way. This could be by using a teaser email sent out to your list of patients who have opted in, letting them know that you would love them to follow you on Instagram or Facebook, as they may be missing out on your summer promotions!
I also always recommend that clinics take time in the spring/summer to clean up or strategically change their angles and language for all available social media channels. So often in our industry we focus on the treatments, benefits, and results. Why not switch this up and ask your social followers what their main concerns are for the summer months? You can then respond with relevant posts, targeting these specific areas. You should always consider whether you are providing thoughtful content and speaking to the patient with real relevance to the season, if you’re truly engaging with patients, and whether you’re utilising these all-important business tools to educate and entice new patients.
When moving to a summer seasonal strategic marketing approach or changing things up with social media marketing, try having a look at the following:
2) Are you optimising your supplier’s assets? In my experience, high performing posts generally feature product shots, so you should always speak to your supplier about whether they have readymade summer seasonal assets that you can use. I find a good way to keep engagement is to feature a ‘product or treatment of the week’ specifically focusing on the benefit for the summer. If you do not have readymade assets, then perhaps when you are out on a long summer walk or a visit to the beach bring a skincare product or two and take a few pictures!
3) Can you create summer bundles? If a patient books in for two or more treatments, could you retail a seasonal product, trial kit, travel set or sample pack? Creating a value proposition is sure to pique interest, particularly if the gift reflects the season or summer skin needs. Your patients will travel this year, all be it planning summer trips or vacations in the UK, so think about providing a kit that is easy for them to take away.
4) What time are your patients/audience most active? Does your audience spend a lot of time commuting to work? If so, maybe schedule posts just before they do so your messages pop up on their feed as they travel to and from work. If you have a lot of busy mums as patients, maybe think about scheduling when they have time in between school runs to check their feeds. Remember this may well change in the summer months due to holidays with their children being at home so always check the analysis tools of your chosen social media platform which will show you when your followers are most active.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Sales director Graham Clarke discusses marketing strategies in the summer months and how businesses should promote different treatments



AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
Treatments to focus on
In my experience, part of getting your marketing strategy summer ready is looking at what kinds of treatments you should be focusing your marketing efforts on. Below are some treatments that will likely be beneficial to your business to market during the warmer months. Of course, it’s always a good idea to actually ask your current patients what they want to hear about, as this can help you to understand what their biggest needs are at specific times of the year.
Skin treatments
In the summer, patients want to ensure that their skin looks healthy and has a ‘summer glow.’ This is particularly important when there are days too hot for people to wear a full face of makeup and hide their skin concerns. In this regard, clinics can capitalise on various facials which can offer people deep hydration and cleansing, leaving their skin looking renewed. Clinics also have the option to create their own facials specifically designed for each season. This way, your patients know that what you’re offering can tackle their specific concerns during the summer period, for example sun protection, hydration and pigmentation.
Many of your patients will be used to getting chemical peels in the winter months, but high intensity deep chemical peels are not ideal for the summer as they can cause sun sensitivity and hyperpigmentation, as well as require a certain amount of downtime for the patient.2 However, this does not mean peels have to be avoided altogether. A superficial
peel, such as an amino fruit acid/enzyme peel, can be a good alternative as it only targets the epidermis and is well tolerated by dry and sensitive skin.3 These light peels can help bring that much desired summer glow to the skin following the dark winter months, as well as prep the skin for more intensive peels when the time is right.
Body treatments
Unlike traditional liposuction treatments that require some downtime and recovery, patients now have the option of nonsurgical body sculpting treatments such as cryolipolysis and muscle stimulation. Owing to the minimal recovery time, these are perfect for the summer months. Obviously, the patient will not see the results straight away but after as little as two to three treatments (depending on the technology used) the desired results can be achieved.
Smoother skin is also an absolute must in the summer period, particularly for those patients looking to improve the surface of their skin or who are concerned with the appearance of cellulite. Let your patients know that cellulite treatment devices, such as Endermologie or Thermage, can help improve their confidence and day-to-day interactions – they no longer need to fear wearing shorts in public or feel self-conscious to have their legs on show!
Homecare
As well as advertising in-clinic treatments, we also must consider what at-home products will benefit our patients the most in the summer months. The obvious one is SPF
and sun damage protection, although this should be a skincare staple in every patient’s routine every day of the year. Patients should always look to go for SPF 30 or above for sufficient protection.4 Prior to SPF application, the other topical formulation that should be recommended in the summer is a targeted vitamin C serum to assist with protection during the day, and keep the skin nourished. As mentioned above, these could be marketed together as a summer package for the ultimate skin protection.
Lips are an area that may get overlooked at this time but advising our patients to keep them protected and nourished is particularly important as they tend to dry out during the warmer months.
Start planning!
When creating your marketing strategy for the summer months, you need to think strategicially about what your patients main concerns will be and communicate with them effectively. Once your patients are engaged and booked for their summer experiences, the will return for the more intensive treatments when the autumn inevitably rolls around again.
Graham Clarke has worked in the professional skincare and aesthetics specialty for more than 20 years, with global market experience in the business of the aesthetic skincare industry, from manufacturing, business coaching, marketing and distribution. He is currently the sales director responsible for the distribution and expansion of Image Skincare across the UK.

REFERENCES
1. Sian Ranscombe, 2017, Brits spend up to a third of their holiday budget on beauty, < https://www.harpersbazaar.com/uk/beauty/ skincare/news/a41454/brits-spend-up-to-a-third-of-holidaybudget-on-beauty/>
2. Costa M, et al., Review in peeling complications, 2017, Journal of Cosmetic Dermatology, <https://pubmed.ncbi.nlm.nih. gov/28349655/>
3. Sarkar S. et al, Chemical Peels: A Global Perspective, 2019
4. British Association of Dermatologists, Suncreen Fact Sheet, 2013, <https://www.bad.org.uk/skin-cancer/sunscreen-factsheet#spf-in-moisturisers>
Creating a value proposition is sure to pique interest, particularly if the gift reflects the season or summer skin needs
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
in”
With 34 years’ experience in medicine, nurse prescriber Annie Cartwright has always had a strong interest in the science behind the health and beauty industry. Becoming a qualified nurse in 1987, Cartwright worked in the NHS before moving into the pharmaceutical sector where she worked for more than a decade. She then started her own consultancy business and worked for a spell in medical education. In 2003, Cartwright became fascinated by the rise in popularity of non-surgical procedures and wanted to be involved in this new and growing industry. “I loved the combination of the academic and medical understanding with a clinical application. I enjoyed the practical element of carrying out aesthetic treatments, but also the science behind it,” she explains, noting that she completed her prescribing course in 2008. After her injectables training course, Cartwright felt that she was not educated enough. She says, “The training made me question everything I had been taught as a nurse and there were a lot of ‘why’ questions that I asked myself. I wanted to know why I was using this needle and not a different one, or why I was choosing a certain product to inject over another brand, for example.”
During the next three years, Cartwright was mentored by a dentist who observed her treatments. She explains that this mentorship was integral for her success as a practitioner, stating, “It provided me with in-depth education on the anatomy, proportion and shape of the mouth, giving me a better understanding and knowledge of the perioral area. I was taught to consider the underlying anatomy and health conditions of a patient when examining. I always look at the bigger picture and ask these questions to myself now and advise those I teach to do the same.”
In 2011, Cartwright completed a Master’s in Advanced Practice, whilst she rented treatment rooms in other clinics. In 2014, she opened her own premises – Skin and Face Clinics – in Llandaff, Cardiff, whilst continuing to provide treatments for her Surrey-based patients every fortnight, and has been travelling between the two for more than ten years. She says, “I have always remained committed to taking on another clinic, knowing that the travel would be a big factor to consider.”

Cartwright is proud that the training programmes for new practitioners have been improved, commenting, “Some of the aesthetic training provided by companies, such as Merz Aesthetics, are excellent. There is a greater in-depth teaching now on the anatomy of the body and the possibilities of complications occurring, which was not a major component of training in the early days. Instead, education was more focused on the product and its uses, rather than patient safety,” she recalls.
Two years ago, Cartwright became a Merz Innovation Partner to assist in delivering training, educating others on the use of products, including the BELOTERO® range of dermal fillers, whilst raising standards in aesthetic medicine. Throughout the pandemic, Merz has focused
My hobbies outside of work…
Beekeeping. I have a colony of bees in my garden, and it is a great escape for me. I have so far only been stung once!
My favourite treatment to perform…
Tear trough rejuvenation. I love how complex the treatment is and it’s so transformative for my patients who struggle with shadows or hollows under the eye.
My favourite aspect of my job…
My patients! I love meeting all of humanity in my clinic. They all have a story to tell and deserve respect and honesty.
on delivering education through webinars to allow practitioners to increase their knowledge and insights into the portfolio. Cartwright comments, “It is hard to be successful in this business, but I would like to see more regulation to ensure practitioners have the appropriate medical background, experience and training. I’m delighted to help Merz increase practitioner education in the sector, which can only lead to safer treatments and more successful outcomes.” She adds that continuing education and staying updated is vital for success. “A lot of people describe themselves as passionate about aesthetics, including me, but I would question whether the level of specialist education and training they have sought out, and invested in, is adequate. It’s very easy to say you are passionate, but passion is reflected in the amount of time, effort, input and training you are prepared to invest in,” Cartwright explains. In the future, Cartwright wants to continue educating herself, as well as others, on the psychological aspects of aesthetics, which she discussed in her master’s dissertation. She concludes, “Currently, mental health is a pivotal topic and I think we will continue talking about it for many years. However, I think it is important to have medically-trained professionals who understand this and are able to respond appropriately to the mental health issues they recognise in their patients. A practitioner’s aesthetic treatments have got tremendous potential to boost their patients’ confidence, improving how they feel on the inside, as well as how they look on the outside.”
If you’re interested in attending a Merz webinar, visit www.merzwebinars.com This article is sponsored by Merz Aesthetics, UK & Ireland
“Passion is reflected by the amount of time, effort, input and education you have invested
Nurse prescriber and Merz Innovation Partner Annie Cartwright shares her journey into aesthetics and how she became an educator
M-MA-UKI-1404 – Date of Preparation: April 2021 Aesthetics | May 2021 72 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Merz Aesthetics
In The Life Of Dr Uliana Gout
The BCAM president gives us an insight into her everyday life
I start my mornings with…
A cup of tea! I love my herbal teas, and I have a huge collection of Japanese teas at home. After that I always take my dogs out for a walk – we have two little mini schnauzers Maple and Bubble, so it’s a great way to begin my day!
I set off for work at around 7:15am, and during this period I catch up on all of my emails and ensure that nothing has been missed. Once I get to the London Aesthetic Medicine (LAM) Clinic at around 8:15am, my team begins by having a group chat where we all discuss our plans for the day and have a look at what patients we have coming in. The rest of my day is then taken up by consultations and treatments!
I typically see no more than 20 people a day as I don’t like to rush things, especially consultations which can usually take between 45 minutes to an hour. In my opinion this time is necessary because you need to really get to know the patient and build a relationship with them, so that you can plan ahead for the next five or 10 years. I like to create a short and long-term strategy for my patients.
I typically finish work between 5-7pm, and go for another walk before I travel home. My clinic is on Harley Street, and I grew up at the end of this lovely street right next to Regent Street, so the park nearby gives me a lovely sense of nostalgia! Once I get back to my house I always try to do some power cardio – I’ve just invested in a rowing machine so I like to spend half an hour on that!
Fitting BCAM into my routine…
I became president of the British College of Aesthetic Medicine (BCAM) last year, so this introduced a new element into my career and gave me new responsibilities. Although it’s a big role it was an easy addition for me because I’m so passionate about it. I tend to weave it into the rest of my day, whenever I have small breaks or downtime during clinic hours.
COVID-19 has really highlighted how important an association like BCAM is for people, because I think everyone in the industry has been feeling quite isolated and confused at times. In particular, incorporating

different webinars and Zoom talks into the working week has enabled us all to connect with each other, and I probably now do a virtual lecture at least once every fortnight. Although I really do miss events and being around my colleagues, I feel we as a community have done very well with virtual learning and networking. I am very proud of how fast paced and dynamic everyone has been.
What would I change about my working routine?
Nothing! I love everything about my job and I love the UK aesthetics community, so I really wouldn’t change a thing.
If I wasn’t an aesthetic practitioner…
I always wanted to be an artist when I was growing up because I love painting and sketching. I do see aesthetics as being an art in itself though!
My favourite treatment...
I like to do several different treatments in one sitting! For example a chemical peel with a radiofrequency treatment, alongside followed by injectables. I always think it gives the patients optimal results.
In my spare time...
I’m really into history and archeology! I’m fascinated by the Roman era and I was actually meant to go on a dig in Pompeii last year, but unfortunately it was postponed because of the pandemic. I’ve always had a hobby for collecting antiques from different time periods, and I’ve recently started to decorate my home with them! I also take a lot of time to read up on recent developments and research on our specialty – I have so many books and journals. I actually have a collection of all the old Aesthetics journals in my office! I just think that it’s so important for all of us to keep up-to-date with what’s going on in the industry, as well as reflect on how things have changed, because it’s so fast paced and there are always so many new innovations, approaches and techniques. I strongly believe that no matter where we are in our careers, we can always learn from one another.
My most memorable day…
I think it has to be when I was going to Monaco for my first Aesthetic and Anti-Ageing Medicine World Congress (AMWC), which was during the time that I was transitioning from the NHS to aesthetic medicine. I’d written a huge thesis on hand rejuvenation and had actually submitted a poster to the AMWC which got accepted. As I drove into Monaco, I specifically remember that feeling of excitement and positivity knowing that I was on my way to learn new concepts, as well as getting to be around 10,000 other like-minded people from across the globe. The aesthetics industry is really great in that sense because countries from all over the world communicate so well with each other. I’m now a course director for that very conference!
My advice to anyone starting out in this industry is to make sure that you attend lots of these events, whether it’s international or local, because that’s how you’ll meet and connect with other people. I think that’s integral in order to be able to grow in your career, and we also have so many amazing personalities that we can all learn from. We’re so lucky to have such a great community of people!
the
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
The Last Word
Dr Sieuming Ng explores the controversy surrounding the ‘Fox Eye’ trend in aesthetics
The trend
The ‘Fox Eye’ look is one of the latest beauty trends, made popular by A-list celebrities such as models Bella Hadid, Kendall Jenner and Megan Fox. To date, the popular social media platform TikTok has amassed more than 129 million views with the trending hashtag #foxeye.1,2 The growing popularity of this trend has led to an increase in demand for the use of non-surgical aesthetic techniques to achieve it.3 The technique involved is typically a combination of the use of threads, dermal fillers and botulinum toxin. The aim is to use dermal filler to fill the hollowness of the temples, botulinum toxin to achieve a level of brow lift and to reduce periorbital movements, then finally use dissolvable threads to lift the distal portion of the eyebrow to achieve that straighter brow tail finish. The overall procedure takes between 45 to 60 minutes depending on the combination of techniques used, and the results typically last between 12 to 18 months.
Why is there controversy?
Unfortunately, this much-coveted current look has come with its fair share of backlash. The East Asian community are not all happy with the ‘Fox Eye’ trend now being a celebrated look and are calling it out for cultural appropriation. This is largely due to the fact that the trend is a replication of a particular East Asian facial feature which we have grown up being teased and bullied for. Moreover, celebrities, social media influencers or anyone imitating the hand gesture of pulling their eyes up next to
their eyebrows by the temple region, to exaggerate this facial effect in photos and videos, are mirroring the action historically used to ridicule the East Asian community. As such, this stereotype is a universally recognised symbol of xenophobia and can be extremely triggering to some. To add insult to injury, those who have spoken out about taking offence to this trend have been accused of overreaction, which has understandably not helped the situation.4-7
Managing patients
As an aesthetic practitioner and member of the Asian community I do, to a certain extent, believe in respecting the wishes of my patients. I certainly do not believe in stopping anyone from wanting to achieve a certain look, and neither is it my place to change their desired aesthetic. However, with regards to this particular trend, I believe there are steps that many practitioners can take to approach the situation more appropriately.
Understand the cultural connotations
In my opinion, many aesthetic practitioners need to be better informed when it comes to fashions such as the ‘Fox Eye’ trend before treating patients. Research and understand the connotation associated with the term ‘Fox Eye’ and consider if this is an aesthetic trend that you would like to promote in your aesthetic practice.
If it makes you uncomfortable providing this treatment for personal, social and/or any other reasons, the best approach is probably to be upfront in explaining this to your patients and also educating them about the
connotations. If they still wish to go ahead, consider referring them to a colleague who is offering this treatment.
If you are fully equipped with the knowledge of the ‘Fox Eye’ trend and decide you are happy to offer this treatment at the clinic, it may be an idea to consider whether you would be open to re-phrasing the colloquial ‘Fox Eye’ term in your aesthetic practice and in your marketing messages.
Manage expectations
It is also important to bear in mind that often patients may come in asking for a particular look but what they ask for might not necessarily reflect what they mean. For example, they might actually want a simple brow lift to brighten their face but may use the term ‘Fox Eye’ to describe it. Do they specifically want the almond-shaped eyes or are they actually more concerned about their eye bags? Or is it ptosis of the eyelids? Once you have established that it is indeed the almond-shaped eyes they are after, assess their suitability to decide if the nonsurgical approach is suitable in achieving those results.

Respecting cultural opinions
I personally feel pride and joy in the celebration of my East Asian features. However, I do not condone the use of hand gestures to exaggerate the ‘Fox Eye’ effect and can fully appreciate why the East Asian community may take offence with this trend. While it may not have stemmed from malicious racial intent, the bottom line remains that any discomfort expressed by the East Asian community around this trend should be heard and respected.
Dr Sieuming Ng is a GMCregistered member of the Royal College of Surgeons. After completing her medical studies at the University of Nottingham, she trained as a general surgeon in Cardiff and London. Dr Sieuming has completed advanced training in injectables such as botulinum toxin and dermal fillers, and runs her own aesthetic practice in London.
Qual: BMedSci, BMBS, MRCS

VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 8/Issue 6 - May 2021
Introducing the JCCP approved Level 7 Diploma in Clinical Aesthetic Injectable Treatments
The VTCT (iTEC) Level 7 Diploma in Clinical Aesthetic Injectable Treatments is designed for professionals who are registered with a healthcare statutory regulatory body.

This regulated qualification mitigates concerns for patient safety as it raises the standard for treatments performed in non-surgical aesthetics.
For more information, visit www.vtct.org.uk/level7-aesthetics

