12 minute read
Treating Lip Lines


Advertisement
Dr Ellen Selkon and Dr Sarah Hart explore their method for treating aged and photodamaged lip lines using filler, toxin and subcision
the perioral musculature, and an underlying resorption of the maxillary and mandibular bone.4 The vermillion border loses its definition and rhytids extend from the upper lip into the tissue above the lip. Although sun exposure is a contributing factor for ageing across the world, in countries like New Zealand and Australia, practitioners hypothesise that solar damage from the high UV environment causes a higher degree of damage and ageing of the perioral skin. A study by dermatologist Professor Greg Goodman showed that Australian women noticed signs of ageing such as facial lines one to two decades earlier than their counterparts in the northern hemisphere.5 Each of these factors contributes to a varying degree to the ageing of patients. Some patients have strong muscle action and lesser volume loss, leading to multiple fine lines. Alternatively, a relatively weaker muscle and greater volume loss appears to be associated with fewer, deeper lines (Figure 1). The Selkon Subcision Slurry technique is well suited to patients with the first pattern. Women frequently present with concerns about fine or deep Treatment for lip lines lines and wrinkles in the lip and perioral area, which may give an Lip lines can be improved with hyaluronic acid filler placed appearance of anger or disapproval, and often appear prior to directly into the line superficially in the dermal plane. If there is ageing signs elsewhere in the face. The lips are a focus of attention perioral volume loss, dermal filler can also be used to restore on the face, communicating both emotion and speech, and are loss of fat in the subcutaneous and/or submuscular planes, using therefore a priority for treatment for many patients. a cannula. However, an excess volume of dermal filler can also Treating lip lines remain a challenge for most injectors, as a full cause unwanted convexity of the upper cutaneous lip, commonly correction of lines in this dynamic area is usually difficult to achieve. termed the ‘monkey muzzle’ or ‘Marge Simpson’. This abnormal Overuse of dermal filler can cause an unnaturally protruding contour is disliked by patients and injectors and can occur even appearance of the upper cutaneous lip. Even more difficult are patients when the lines themselves are not fully corrected. with well-established static lines accompanied by solar damage to the skin of the upper cutaneous lip, a common occurrence in the high UV Botulinum toxin is a useful additional tool for improving lip environment of the southern hemisphere. The cause of lip lines are lines when injected to weaken the orbicularis oris muscle lying multifactorial and are thought to be a combination of the loss of deep beneath the lip lines. However, used on its own it is rarely enough and subcutaneous perioral fat, thinning of the dermis, and the effects of to restore a full correction, and higher doses can cause too much repeated muscle contraction over time.1 interference with oral function for the patient to tolerate. The Selkon Subcision Slurry technique is a new approach that Laser resurfacing, such as fractionated CO2, is useful to improve addresses these multiple causes of lip lines by combining three superficial lines once volume loss has been corrected. However, treatment modalities – filler, toxin and subcision – in one treatment. many patients are unwilling to contemplate downtime, and these It is designed to minimise convexity of the upper cutaneous lip devices can be expensive and are not universally available at all arising from over-volumisation of the area with filler and weaken the clinics. influence of the orbicularis oris muscle on the skin, without excessive loss of function. Patient A Patient B How do lip lines occur? During ageing, the upper lip undergoes vertical lengthening and inversion with the thinning of the vermillion and loss of anterior projection. As a result, the philtral columns and cupid’s bow become ill-defined.2 This causes vertical and horizontal rhytids to appear on the lips. The perioral lines develop at the edge of the white roll of the lip where the orbicularis oris muscle is attached to the dermis with no interposed fatty layer.3 It is believed that these lines develop because of perioral soft tissue volume loss, lip atrophy, hyperdynamic contractions of
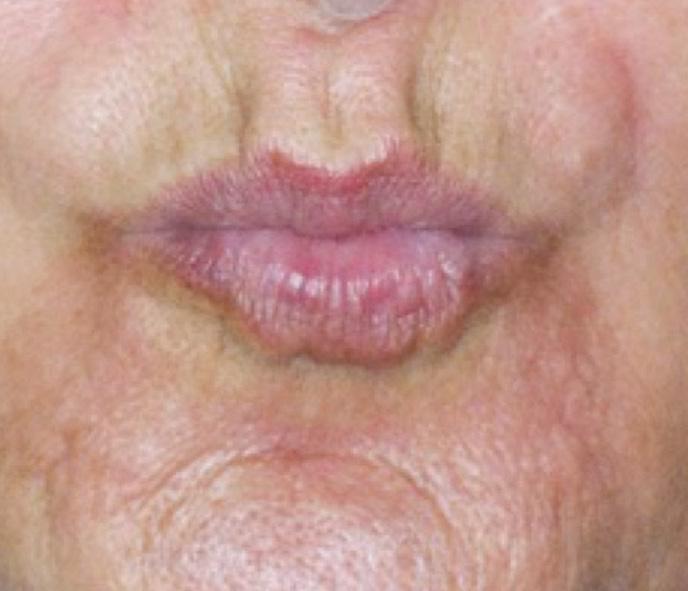
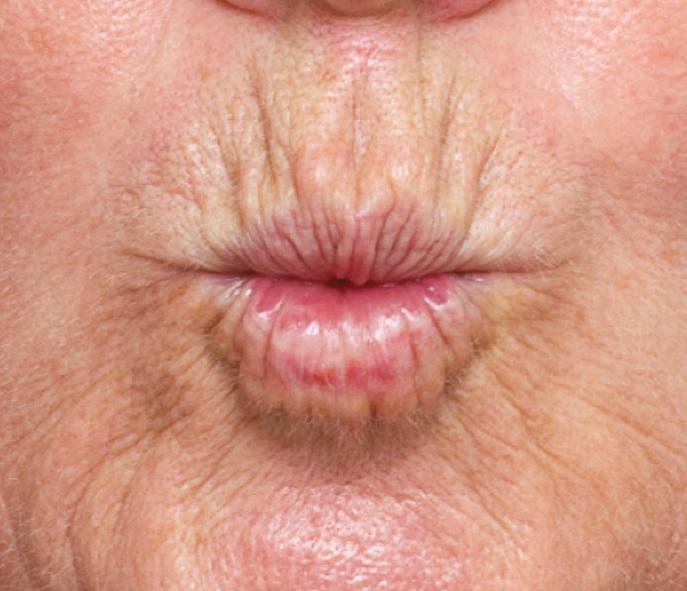
Figure 1: Difference in fine lines between two patients based on muscle strength and volume. Patient A has a strong muscle and minimal volume loss with multiple shallow lines, while Patient B has weaker muscle and more volume loss with fewer deeper lines.
Cannula Insertion Point
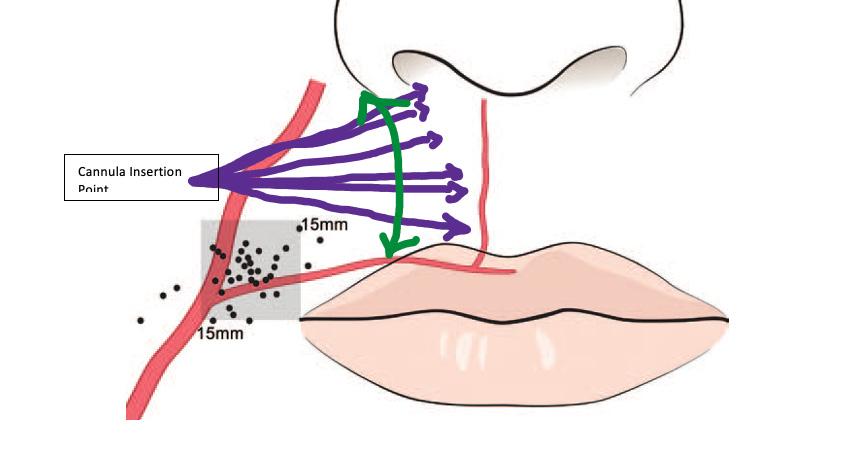


Figure 2: Insertion point for the cannula shown in purple
New technique using subcision Inspired by Rosengaus-Leizgold’s paper on subcision of the muscles of the lower face to weaken their effect without using toxin,8 Dr Ellen Selkon devised a new approach called ‘The Selkon Subcision Slurry technique’ to improve lip lines. It is important to note that this is an ‘off label’ technique and should only be attempted by experienced injectors. A cannula is used to subcise subcutaneously, loosening the attachments of the orbicularis oris muscle before a slurry of diluted dermal filler (for skin quality and subtle volume restoration) and botulinum toxin (for muscle relaxation) is placed in the subcutaneous plane. Adding both saline and reconstituted botulinum toxin to the filler reduces its volumising effect, which, in our experience, diminishes the chance of an abnormal contour of the upper cutaneous lip.
This technique appears to be especially helpful in cases where volume loss is present but not excessive, the dermis exhibits moderate solar damage, and the orbicularis oris muscle remains strong. Patient selection is vital to achieving a good result as this technique is not suitable for all patients. Although the volumising effect is milder than other filler techniques, patients with a protruding upper lip or convex upper cutaneous on profile view are not good candidates. Patients with very tethered lines and severe solar elastosis may only demonstrate limited improvement. As the main blood supply of the upper lip is the superior labial artery, which runs in the submuscular (78%) or intramuscular planes (18%), it is therefore safer to inject in the subcutaneous plane directly between the muscle and the skin, as the artery is least likely (3%) to be in this plane.6 The Selkon Subcision Slurry technique is designed for this safer plane. The origin of the superior labial artery is 85% of the time within a square 1.5cm superior and lateral to the oral commissure.7 The cannula entry point should lie superior to this area (Figure 2).
Preparation An aseptic technique should be used throughout preparation. Firstly, 0.6ml of a low G-prime filler is decanted into a 3ml syringe. Into a second 3ml syringe, 0.4ml normal saline is drawn up and 15 units of abobotulinum toxin or 6 units of onabotulinum toxin/ incobotulinum toxin is added. Both syringes are attached to a three-way tap and mixed well by depressing each plunger in turn, expelling the mixture from syringe to syringe. This will create 1ml of a well-mixed slurry of filler/saline/toxin. It should be decanted it into 2x1ml syringes ready for use.
Procedure During the procedure, an infraorbital nerve block is performed using lidocaine 2%. A 25 gauge 40mm firm cannula is inserted, just lateral to the nasolabial fold (Figure 2). Subcision is then performed.
The cannula should glide in the subcutaneous plane to the philtral column and should not advance medial to the philtral column. Without injecting any product, the area is subcised using the cannula as a
Before After

The Selkon Subcision Slurry technique is a new approach that addresses the multiple causes of lip lines by combining filler, toxin and subcision in one treatment
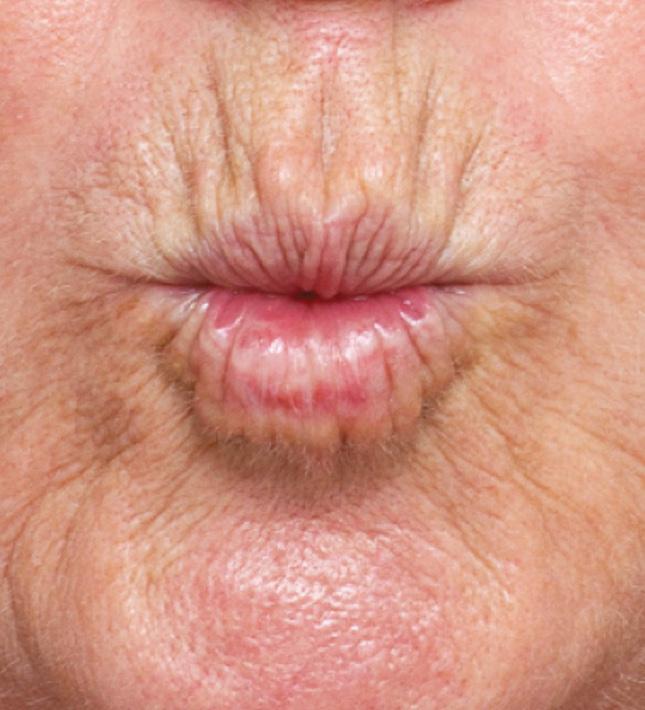
Figure 3: 49-year-old patient before and two weeks after. Images courtesy of Dr Sarah Hart.
Before After

Figure 4: A 49-year-old patient injected with just 0.3ml per side of slurry. This totalled 0.6mls of slurry, equating to a dose of about 4 units of onabotulinum toxin for the entire upper cutaneous lip. The remainder 0.4ml unadulterated filler was injected in very small aliquots into the oral commissures, mental crease and lips. Images courtesy of Dr Sarah Hart.


Figure 5: Cannula insertion point
Before
After

Figure 6: 55-year-old patient before and after treatment. She showed immediate swelling and convexity of the upper cutaneous lip which will resolve. Images courtesy of Dr Ellen Selkon.
subcision tool, breaking down the fibrous attachments from the dermal layers to the muscle. This will separate the soft tissue from the orbicularis oris muscle, creating a plane that can be filled with the slurry. Many passes with the cannula are required. The injector should work in an orderly manner from just above the white roll to the sub-nasal area. Once subcising has finished, and the area is free of tethering, the cannula should move freely like a pendulum from the white roll to the sub-nasal tissue without interference (Figure 5). Thin strands of approximately 0.01-0.05ml of slurry should be injected, to a total of approximately 0.3-0.5ml per side. By injecting horizontally, there is less chance of intravascular injection as the arterial branches in this region generally run vertically from the superior labial artery.9 No slurry should be injected medial to the philtral columns as this will lead to a flattening of the philtrum and loss of lip shape. Once finished, the upper lip area will look full. It’s important to remember that almost half of what has been injected is saline and will therefore be absorbed over the next 24-48 hours. Therefore, it is important to warn patients prior that they will have downtime associated with this procedure. Firstly from the 48 hours of fullness and, secondly, from the bruising associated with the subcision technique. The area should be gently massaged to ensure that there are no obvious lumps or accumulation of slurry. Practitioners should never use leftover slurry mixture in areas where toxin effect is not desired. However, the remaining 0.4ml of unadulterated filler can be used in other perioral areas such as the body of the lip or the mental crease. Follow up A follow-up session should be conducted in two weeks to ensure that the toxin has worked and that the patient is happy with the results. Results should always look natural and subtle, allowing you to repeat the procedure again in approximately six months. Possible complications to consider include those generally associated with dermal filler and toxin treatment. Bruising may be more significant than usual following the procedure and, in our experience, immediately post-procedure swelling is greater due to trauma from subcision and the added saline, which will be absorbed. Generally, results are optimal two to four weeks post procedure, after the swelling and bruising has subsided, and will last up to six months.

A multifactorial approach The Selkon Subcision Slurry technique combines diluted filler, toxin and subcision in one treatment to address the multifactorial causes of lip lines. Results to date are anecdotal and we welcome further study on this technique. It is designed to minimise convexity of the upper cutaneous lip arising from over-volumisation of the area with filler and weaken the influence of the orbicularis muscle on the skin without excessive loss of function. We find it is particularly helpful for patients with minimal to moderate volume loss, moderate solar damage, and a strong orbicularis muscle. To achieve optimal results, it is essential to select your patient carefully, use a low G-prime dermal filler and a firm cannula, achieve good analgesia prior to subcision, and subcise the area well, prior to injecting.
Dr Ellen Selkon has been practising aesthetic medicine in New Zealand for 15 years. She is on the executive committee of the NZ Society of Cosmetic Medicine and the NZ conference organising committee. Dr Selkon is also an international teacher and speaker on dermal fillers and botulinum toxin and is an Australasian trainer for Galderma Pharmaceuticals, educating healthcare professionals through the GAIN programme. Qual: MBChB, FRNZCGP, NZSCM
Dr Sarah Hart has been practising cosmetic medicine since 2002. She serves on the NZ Society of Cosmetic Medicine’s executive and education board as censor and education faculty member. Dr Hart has been an Allergan Advisory board member since 2007. She lectures on the use of dermal filler and botulinum toxin on the international stage and trains her colleagues across Australasia in facial rejuvenation techniques. As a KOL, Dr Hart has a particular focus on safety, is a published author on this topic and has featured on three seasons of the TV series ‘Ten Years Younger in Ten Days’ in New Zealand. Qual: MBChB
REFERENCES
1. Rohrich RJ, Pessa JE, ‘The Anatomy and Clinical Implications of Perioral Submuscular Fat’, Plastic and
Reconstructive Surgery, 124 (2009), pp. 266-271. 2. Tonnard PL, ‘Ageing of the Upper Lip: Part II. Evidence-Based Rejuvenation of the Upper Lip—A
Review of 500 Consecutive Cases’, Plastic and Reconstructive Surgery, 143 (2019), pp.1333-1342. 3. Hotta TA, ‘Understanding perioral anatomy’, Plastic Surgical Nursing, 36 (2016), pp.12-18. 4. Maio M, DeBoulle K, et al., ‘Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: focus on the lower face’, Plastic Reconstructive Surgery, 140 (2017), pp. 540550. 5. Goodman GJ, Armour KS, et al., ‘Comparison of self-reported signs of facial ageing among
Caucasian women in Australia versus those in the USA, the UK and Canada’, Australasian Journal of
Dermatology, (2017). 6. Cotofana S, et al., ‘Distribution Pattern of the Superior and Inferior Labial Arteries: Impact for Safe
Upper and Lower Lip Augmentation Procedures’, Plastic and Reconstructive Surgery, 139 (2017), pp.1075-1082. 7. Lee SH, et al., ‘Anatomy of the Superior Labial Artery’, Plastic Reconstructive Surgery, 135 (2015), pp.445-450. 8. Rozengaus-Leizgold R, et al., ‘The Happy Face Treatment’, Journal of Drugs in Dermatology, 17 (2018), pp.1226-1228. 9. Tansatit et al., A Typical Pattern of the Labial Arteries with Implication for Lip Augmentation with
Injectable Fillers, Aesth Plast Surg (2014) 38: 1083-1089.