Neck
























































VOLUME 6/ISSUE 4 - MARCH 2019
of
Restylane
you
freedom to personalise your
Good comes to those who SWAGGER STYLE FORTUNE KARMA ADVENTURE CHAOS DREAM CHEAT DARE FLIRT REBEL SIN RES19-02-0048a Date of preparation Feb 2019
With the broadest choice
fıllers,
gives
complete
patient’s treatment to fulfıl their every need and bring out their true individuality. Choice Matters
Knowing Your Competition
explains how competition can boost your business
Clinic owner Kerri Lewis
Threads
Patients
Ruth
provides tips for suture insertion when treating patients over 60 Special Feature: Adding New Clinic Services Practitioners discuss working with specialist service providers Dr Tiina Orasmae-Meder describes pre and probiotics in skincare Pre & Probiotics in Topicals CPD ACEENJOY MARCH2019! 1&2 AESTHETICSCONFERENCE.COM
& Older
Dr
Harker

1 & 2 MARCH 2019 / LONDON SEE US AT
Dr Tiina Orasmae-Meder details the use of pre and probiotics in cosmeceuticals

Treating Lips Using a Cannula
Aesthetic nurse prescriber Jackie Partridge shares advice for treating the lips and perioral area using a cannula
Mr Arturo Almeida presents an overview of fat-dissolving injections 41 Understanding Menopausal Hormones
Dr Aarti Narayan-Denning explains how women’s hormones impact physiology, anatomy and ageing 47 Treating
Older Necks Using Threads
Dr Ruth Harker explores the use of sutures in patients over 60 undergoing a non-surgical neck lift 53 Approaches to Treating the Submental Area
Mr Marc Pacifico outlines different options for treating the submental area and shares a successful case study 57 Abstracts
A round-up and summary of useful clinical papers IN PRACTICE 59 Understanding Facebook Advert Audiences
Marketing and PR professional James Dempster details the ways practitioners can target patients using Facebook advertising 63 Knowing Your Competition

Clinic owner Kerri Lewis discusses the benefits of recognising your competition to improve your business 67

Boosting Your Social Media Profile
Mr Olivier Branford shares his social media journey and explains how to educate and attract patients online 71

In Profile: Esther Fieldgrass
EF Medispa founder and entrepreneur Esther Fieldgrass reflects on her success as a multiple clinic owner in the aesthetics specialty 72 The Last Word
Dr Tatiana Lapa questions whether aesthetic practitioners are promoting a ‘do-it-yourself’ culture
NEXT
Dr Tiina Orasmae-Meder has specialised in dermatology and skincare for the past 20 years, working in clinical research and product development for numerous companies. She is the founder of Meder Beauty Science.
Jackie Partridge is an award-winning independent nurse prescriber and clinical director of Dermal Clinic in Edinburgh. Partridge is a KOL and member of the Galderma Global Nurse Faculty and represents the BACN to improve regulation standards in Scotland.


Mr Arturo Almeida is a consultant surgeon in general surgery who trained in the US and Europe. He has been practising aesthetic medicine for 12 years. His expertise lies in varicose vein treatments and fatdissolving injections.

Dr Aarti Narayan-Denning is an aesthetic practitioner and independent GP with more than 20 years’ experience. She has a diploma in Obstetrics and Gynaecology and specialises in aesthetic medicine for mature women.

Dr Ruth Harker is medical director of Erme Clinic in the South West, works for the NHS in the Skin Cancer Clinic at her local direct general hospital and is a procedural GP. She is finance and conference director of BCAM.
Mr Marc Pacifico is an aesthetic consultant plastic surgeon based in Tunbridge Wells. He was awarded the Gold Medal in the FRCS (Plast) exam, has published more than 50 international peer-reviewed papers and is regularly invited to speak at conferences.
Enjoy ACE 2019 on March 1 & 2! aestheticsconference.com Contents • March 2019 Subscribe Free to Aesthetics Subscribe to Aesthetics, the UK’s leading free-of-charge journal for medical aesthetic professionals. Visit aestheticsjournal.com or call
1228 Special Feature Integrating New Services into your Clinic Page 21 In Practice Knowing Your Competition Page 63
0203 096
Clinical Contributors
News
MONTH IN FOCUS: Fat • Radiotherapy on the Skin • Eyelash Enhancers • Botulinum Toxin Update 06
The latest product and industry news 16 ACE Overview
18
21
26
The exciting happenings at the Aesthetics Conference & Exhibition on March 1 and 2
News Special: Westminster Debate Aesthetics reports on the recent Westminster Hall debate on non-surgical cosmetic procedures CLINICAL PRACTICE
Special Feature: Integrating New Services into Your Clinic Aesthetic practitioners and specialist service providers discuss how they work collaboratively to enhance patient experience
CPD: Prebiotics and Probiotics in Topical Solutions
31
35
Utilising Fat-dissolving Injections
The Benefits of Clinisept+
+ Optimum cleansing. Clinisept+ is a highly effective cleansing solution with antimicrobial properties.



+ Optimum skin compatibility. Clinisept+ is gentle. It has a skin neutral pH and has been proven non-toxic, non-mutagenic, non-irritant to skin, non-irritant to eyes and noncytotoxic to re-growing skin cells.

Cleans, Calms and
Cares.
+ Client benefits. Clinisept+ calms and soothes the skin. It reduces the appearance of redness and swelling, and provides the optimum conditions for skin to flourish.
+ Revolutionary. Clinisept + technology is revolutionary: it contains no alcohol petroleum, lanolin, or oils and is nonsensitising, even to sensitive skin.
Clinisept delivers significant benefits in client outcomes.
“Clinisept+ has been a great substitute for chlorhexidine for me in both my injectable and laser based procedures. I have noticed reduced skin irritation and erythema with its use versus chlorhexidine both during and after treatments”
Dr. Benji Dhillon
Meeting the needs of your business, delivering high satisfaction to your patients Call us on 01234 313130 | info@aestheticsource.com www.aestheticsource.com

NEW 500ML PUMP BOTTLE COMING SOON WINNER 2017 THE BARRY KNAPP AWARD FOR PRODUCT INNOVATION OF THE YEAR, SUPPORTED BY MEDICAL AESTHETIC GROUP HIGHLY COMMENDED 2017 Winner Product Innovation of the Year Highly Commended Best UK Manufacturer
Professional Use Professional Use Patient Use
Amanda Cameron Editor


If you are reading this letter at ACE 2019, welcome! Much planning and months of hard work went into the event you are now experiencing! We hope you enjoy and learn a great deal, making the most of all the opportunities available. CPD points will be available on your Training Record on the Aesthetics website following the conference, so make sure you get scanned into each session to claim your important professional development points. March – Brexit deadline! What is it going to mean to all of us? Only time will tell. In the meantime, many of you will have heard about the debate in parliament in regards to aesthetic regulation. It’s positive to see that Government is taking our concerns seriously, even at such a critical time for the UK, so find out what was discussed and what this means for our specialty on p.18 What is new in aesthetics as we approach springtime? This month we look at ways of growing your practice in 2019. Our Special Feature focuses on integrating other services to your clinic and how this can
benefit your practice and your patients. Find out how this works for three clinics, now also offering semi-permanent makeup, nutritional advice and a wellness service, on p.21. How important is it to know what your competition is up to? Clinic owner Kerri Lewis believes it is extremely important and can influence the actions you take on a daily basis; find out how she monitors competition and grows her practice as a result on p.63. Our other March business articles offer advice on enhancing your online presence to ultimately attract new patients and retain those existing. Digital marketer James Dempster provides valuable advice on Facebook advertising and identifying relevant audiences on p.59, while Dr Olivier Branford who has combined social following of 250,000, talks us through his growth strategy tips on p.67. One person who has had huge success in growing her clinic is the founder of EF Medispa Esther Fieldgrass, who now runs four practices and offers clinic franchise opportunities. Find out how Fieldgrass built her business in her In Profile on p.71 As always, we encourage you to share your feedback and get in touch if you’d like to contribute to Aesthetics by emailing editorial@aestheticsjournal.com.

Editorial advisory board
We are honoured that a number of leading figures from the medical aesthetic community have joined the Aesthetics journal’s editorial advisory board to help steer the direction of our educational, clinical and business content

Mr Dalvi Humzah is a consultant plastic, reconstructive and aesthetic surgeon with over 20 years’ experience. He is an international presenter, as well as the medical director and lead tutor of Medicos Rx.
Mr Humzah also runs the multi-award winning Dalvi Humzah Aesthetic Training courses. He is a founding member of the Academy of Clinical Educators at the Royal College of Physicians and Surgeons of Glasgow.



Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN) and the UK lead on the BSI committee for aesthetic non-surgical medical standards. She is a registered university mentor in cosmetic medicine and currently a second year student on the Northumbria University Masters course in non-surgical cosmetic interventions. Bennett has been developing her practice in aesthetics for 25 years.


Mr Adrian Richards is a plastic and cosmetic surgeon with 12 years of specialism in plastic surgery at both NHS and private clinics. He is a member of the British Association of Plastic and Reconstructive Surgeons (BAPRAS) and the British Association of Aesthetic Plastic Surgeons (BAAPS). He has won numerous awards and has written a best-selling textbook.
Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Dr Christopher Rowland Payne is a consultant dermatologist and internationally recognised expert in cosmetic dermatology. As well as being a co-founder of the European Society for Cosmetic and Aesthetic Dermatology (ESCAD), he was also the founding editor of the Journal of Cosmetic Dermatology and has authored numerous scientific papers and studies.

Aesthetics
Dr Raj Acquilla is a cosmetic dermatologist with more than 12 years' experience in facial aesthetic medicine. In 2015 he won the Aesthetics Award for Aesthetic Medical Practitioner of the Year and in 2012 he was named Speaker of the Year. Dr Acquilla is a UK ambassador, global KOL and masterclass trainer in the cosmetic use of botulinum toxin and dermal fillers.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 Anti-Ageing Experts. Dr Patel is passionate about standards in aesthetic medicine and ensures that along with day-to-day clinic work he also attends and speaks at numerous conferences.
Dr Maria Gonzalez has worked in the field of dermatology for the past 22 years, dividing her time between academic work at Cardiff University and clinical work at the University Hospital of Wales. Dr Gonzalez’s areas of special interest include acne, dermatologic and laser surgery, pigmentary disorders and the treatment of skin cancers.
Dr Stefanie Williams is a dermatologist with special interest in aesthetic medicine. She is the founder and medical director of the multiaward winning EUDELO Dermatology & Skin Wellbeing in London. She lectures in the Division of Cosmetic Science and has published more than 100 scientific articles, book chapters and abstracts. Dr Williams is also author of Amazon-No-1 Bestseller ‘Look great, not done’.
Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the clinical director of Revivify London, an honorary clinical teacher at King’s College London and a visiting associate professor at Shanghai Jiao Tong University. Dr Samizadeh frequently presents at international conferences and is passionate about raising industry standards.

Editor’s letter
ARTICLE PDFs AND REPRO Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com © Copyright 2019 Aesthetics. All rights reserved. Aesthetics Journal is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184 DISCLAIMER: The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final. ABC accredited publication PUBLISHED BY PORTFOLIO MANAGEMENT Chris Edmonds • Chairman T: 0203 096 1228 chris@aestheticsjournal.com Suzy Allinson • Brand Director T: 0207 148 1292 | M: 07500 007 013 suzy@aestheticsjournal.com Jenny Claridge • Commercial Director T: 0203 096 1228 | jenny@aestheticsjournal.com ADVERTISING & SPONSORSHIP Hollie Dunwell • Business Development Manager T: 0203 096 1228 | M: 07557 359 257 hollie@aestheticsjournal com EDITORIAL Amanda Cameron • Editor T: 0207 148 1292 | M: 07810
401
Gronow • Deputy Editor
Communications Manager
|
758
mandy@aestheticsjournal.com Chloé
&
T: 0207 148 1292
M: 07788 712 615 chloe@aestheticsjournal.com
• Senior Journalist
•
•
Shannon Kilgariff
T: 0207 148 1292 shannon@aestheticsjournal.com Megan Close
Journalist T: 0207 148 1292 megan@aestheticsjournal.com Sophie Thompson
Content Executive T: 0207 148 1292 sophie@aestheticsjournal.com
•
•
CUSTOMER LIAISON Chloe Carville
Customer Liaison Executive T: 0203 096 1228 | contact@aestheticsjournal.com EVENTS Kirsty Shanks
Events Manager T: 0203 096 1228 | kirsty@aestheticsjournal.com
•
FOLLOW US Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
DESIGN Peter Johnson
Senior Designer T: 0203 096 1228 | peter@aestheticsjournal.com Chiara Mariani • Designer T: 0203 096 1228 | chiara@aestheticsjournal.com
Talk #Aesthetics
Rejuvenation AestheticSource introduces PEEL2GLOW
#Conference
Mr Marc Pacifico
@marcpacifico
Great to be in #Paris at #IMCAS with @olivierbranford & @ashmosahebisurgeon. Looking forward to catching up with friends from all corners of the globe!

#Regulation
Health & Aesthetics @DrRekhaTailor
We are so pleased to see @AlbertoCostaMP push for change in our industry and welcome much stricter regulations.
#Training
FTT Skin Clinics @ftt_skin_clinic_scotland
We had the best time in Dublin, thank you to our hosts #ObagiMedical. Great to see our Obagi ambassador friends again, in particular Aine, Deirdra and Elaine and of course Mary. Can’t wait to tell you what’s coming to @ftt_skin_ clinic_scotland

#Education
Dr Ruth Harker @Ermeclinic Dr Ruth Harker of the Erme Skin Clinic lecturing on Benign Skin Lesions at the Royal College of General Practitioners

Aesthetic distributor AestheticSource has launched the new PEEL2GLOW under its SkinTech brand. According to the company, the two-step peel kit can be incorporated into existing treatments as well as retailed in-clinic for regular home use. The PEEL2GLOW is presented in two 1.5ml glass ampoules with an ampoule opener. AestheticSource explains that step one is the peel, containing glycolic and mandelic acid, which aims to exfoliate the superficial layer of the skin, removing dead skin cells and impurities and aid in the penetration of actives for the second step, the glow. The company explains that the second ampoule contains propylene glycol, glycerine, vitamin C, A and E as well as tocopheryl acetate, and is designed to moisturise and protect the skin against external aggressors and pollutants to enhance skin texture, tone and radiance. Dr Mayoni Gooneratne who trialled the newly-launched product said, “I have enjoyed using PEEL2GLOW and have found that it is an innovative home skincare peel suitable for all patients and is also great for those who have regular peels to use between or after a treatment.”


Devices
Dermalux LED launches two new devices
#Empowerment
Dr Kate Goldie @drkategoldie
Don’t mess with us! Merz empowerment tour great night in Hollywood, LA

#MerzAesthetics #MerzInstitute #DrSabrinaFabi
#Essentials
Dr Fiona Durban
@drfiona_durban
Aesthetic Technology Ltd, manufacturer of the Dermalux LED systems, has launched two new products; the Tri-Wave MD and the Flex. The Tri-Wave MD delivers LED technology with wavelengths of 415 nm, 633 nm and 830 nm and, according to the company, is the only medical device to deliver all three wavelengths simultaneously at an amplified optical power. Key features include a zero-gravity arm for flexible positioning, an articulated four-panel LED head, 20 pre-set programmes, custom protocols and photodynamic therapy (PDT), used specifically for dermatological conditions. In addition, the system is operated via a full-colour capacitive touch screen which enables the system to be upgraded remotely. The second product to launch, the Dermalux Flex, is targeted as an entry-level device which is fully portable, suitable for in-clinic and mobile use. It delivers the same three wavelengths as the Tri-Wave MD and can be used for the face and the body. As of February, the company obtained the ISO13485:2016 and ISO9001:2015 certification to become a fully accredited medical device manufacturer.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Essentials
#Aesthetics
#Dermalfiller
for the day, treating at The Private Clinic, Bucks
#Voluma
#CoffeeandChocolate #DaytimeEssentials
Follow us on Twitter @aestheticsgroup and Instagram @aestheticsjournalUK
Botulinum toxin
FDA approves new toxin for glabellar lines
The Food and Drug Administration (FDA) has approved Jeuveau, a botulinum toxin type A, for the temporary improvement in the appearance of moderate to severe glabellar lines. Jeuveau is manufactured by the US-based medical aesthetic company Evolus Inc and is the company’s first and only product. The FDA approval was supported by clinical data from US Phase III randomised, multi-centre, double-blind placebo-controlled clinical trials. It was reported that 67.5% of subjects in study one and 70.4% of subjects in study two met the primary endpoint, compared to 1.2% and 1.3% of patients in each placebo arm, respectively. David Moatazedi, president and chief executive officer of Evolus, stated, “What makes Evolus unique is our focus on delivering performance beauty products with a customer-centric approach. We are pleased to introduce Jeuveau, the first FDA approved neurotoxin dedicated to aesthetics.” Mr Dalvi Humzah, consultant plastic, reconstructive and aesthetic surgeon said he welcomes the introduction of a new toxin to the market. “I think the FDA approval of Jeuveau is good news for the aesthetic specialty. Having another toxin on the market will encourage good competition and further the development in this area. I would urge practitioners who are interested in using this new product to become fully aware of the pharmacology before treating their patients.” Since the FDA approval, it has been reported that global pharmaceutical company Allergan is seeking to block imports of the rival treatment, claiming it was developed by former employees and therefore includes various manufacturing secrets. Evolus responded to this stating, “This represents another legal manoeuvre in a long-litany of attempts by Allergan and Medytox to stifle competition and limit physician and consumer choice. This does not change our plans for a successful US commercial launch of Jeuveau in the spring of 2019.” A release date for the UK market is yet to be confirmed.
PCA Skin releases antioxidant formula

Skincare company PCA Skin has released a new formula called the C&E Advanced with Hexylresorcinol and Silymarin. The product aims to repair, protect and prevent free radical damage through the combination of 20% l-ascorbic acid and 5% tocopherol. The pairing works to protect the aqueous and lipid environments in the skin, while supporting one another against oxidation, the company claims. The PCA Skin C&E Advanced also includes 1% hexylresorcinol and 1% silymarin to reduce inflammation. PCA Skin advise that patients should apply the product to the face and neck in the morning after cleansing and toning. Lizzie Shaw, PCA Skin UK brand manager said, “I believe the C&E Advanced is the most sophisticated product in the industry, due to the unique water-free formula paired with the high levels of pure antioxidants.” Medical aesthetic supplier Church Pharmacy is the exclusive distributor of the new PCA Skin C&E Advanced with Hexylresorcinol and Silymarin.
Vital Statistics
41% of people considering cosmetic treatments stated their top concern was having an unnatural appearance (AAFPRS, 2018)
A 2018 survey demonstrated that 76% of people in the UK did not know that botulinum toxin was a prescriptiononly medicine (SaveFace, 2018)
46% of people in the UK agree that social media has made getting nonsurgical procedures more commonplace (Mintel, 2018)
A 2018 report showed a 24% increase in cosmetic surgery and injectable treatments in patients under the age of 30 since 2013 (AAFPRS, 2018)
YouTube has the second highest online traffic, while Google remains the most visited website worldwide (Amazon, 2018)
Non-surgical fat reduction treatments have increased by 10% since 2017 (ISAPS, 2018)
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Skincare
Events diary
4th-6th April 2019
Aesthetic & Anti-aging Medicine World Congress, Monte Carlo www.euromedicom.com
1st May 2019
Aesthetics Awards 2019 entry opens www.aestheticsawards.com
8th-10th May 2019
37th Annual Conference of the British Medical Laser Association, London www.bmla.co.uk/bmla-conference-2019
14th May 2019
British Association of Sclerotherapists Annual Conference, Windsor www.bassclerotherapy.com
5th-8th June
Vegas Cosmetic Surgery and Aesthetic Dermatology Conference, Las Vegas www.vegascosmeticsurgery.info
21st September
British College of Aesthetic Medicine Conference, London www.bcam.ac.uk
Acquisition sk:n announces new ownership
Medical skincare clinic group sk:n, which operates 51 clinics across the UK, has been acquired by private equity company Tri Span. It was bought for an estimated £35 million from fellow private equity company Graphite Capital. Commenting on the deal, CEO of sk:n Darren Grassby said, “We’re very excited to take sk:n to the next level and we are confident that the combination of our highly experienced team with TriSpan’s experience in rollouts, plus its network and its international exposure, will enable us to propel the business forward.” TriSpan’s European private equity partners, Fady Michel Abouchalache and Joseph-Patrick Dib said in a combined statement, “We’re excited to support the brand’s strong management team to consolidate its leadership position and drive growth across multiple avenues.”
Television New surgical TV programme receives criticism from BAPRAS
A new show will air on Channel 4 that will allow patients to pitch their desired surgery to a panel of judges, called ‘The Surjury’. However, professionals in the aesthetic field have criticised the production because they believe it could glamourise surgery. In this production, patients will stand before a jury and pitch their ideal cosmetic surgery, the jury will then vote on whether they should undergo the procedure. The patients must secure 75% of the panel to vote for them to receive the treatment. Mr Mark Henley, president of the British Association of Plastic, Reconstructive and Aesthetic Surgeons said, “We are extremely concerned about the message this programme portrays and its particular focus on young people. Based on the promotional material alone, we believe the show will trivialise the serious decision all should take when considering aesthetic procedures. It is disappointing that, in 2019, we are still having to remind large broadcasters of the potential harm caused by glamourising cosmetic surgery – particularly when targeting young adults or those with self-esteem issues.” The creator of ‘The Surjury’, Gobstopper Television, has also commissioned another series for BBC Three, called ‘Surgery on Show’. During the programme, patients will observe the cosmetic surgery procedure they are interested in prior to having the treatment. Each patient will be joined by a friend or family member to watch the procedure being performed. Throughout the process, the group will debate the positive and negatives of cosmetic surgery, while studio guests with experience of the procedure will offer information surrounding the operation.
Hyaluronic
acid
mesoestetic releases hyaluronic acid concentrate
Pharmaceutical and skincare manufacturer mesoestetic released the ha densimatrix, a hyaluronic acid (HA) concentrate that aims to promote a moisturising, antiageing and filling action to the skin. mesoestetic explains that the product includes a combination of HA in several forms and molecular weights with an active ingredient that enhances its endogenous synthesis. It also features a plant extract and potent antioxidant that protects HA from degradation and blocks the oxidation from external aggressors. As well as this, it promotes collagen and elastin synthesis to provide firmness and elasticity to tissues. The company advises that the ha densimatrix is suitable for all skin types and, to use, three to four drops should be applied to dry skin and massaged in with an ascending motion.

Conference
New speakers confirmed for ACE
The Aesthetics Conference and Exhibition (ACE) taking place on March 1 and 2, held at London’s Business Design Centre will welcome some of the best speakers within the speciality to its clinical agenda. Amongst some of the newly confirmed presenters are aesthetic practitioners Dr Sach Mohan, Dr Beatriz Molina, Dr Uliana Gout and Dr Claudio Urbani. As well as this, implant and cosmetic dental surgeon Dr Ian Hallam, physician Professor Syed Haq, obstetrician and gynaecologist Dr Alexander Bader and German board-certified dermatologist Dr Stefanie Williams will all be part of the unmissable line-up. Hosting the Teoxane Symposiums are aesthetic practitioners Dr Lee Walker, Dr Benji Dhillon, Dr Raul Cetto, Mr Ayad Harb and Dr Tahera Bhojani-Lynch. Companies recently added to the 30-minute Expert Clinic sessions are Medira Ltd, Novonordisk, Venus Concept and Belle. To find out more about the agenda visit aestheticsconference.com
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Rejuvenation Study shows positive results for SkinCeuticals H.A. Intensifier

A new study has suggested that the use of cosmeceutical company SkinCeuticals’ H.A. Intensifier on eyes and lips has demonstrated visible improvement in lip plumpness and reduction of under-eye hollows. An eight-week, single-centre clinical study was conducted on 50 females, aged 35-60 with Fitzpatrick skin type I-VI, with mild to moderate undereye hollows and thin lips. H.A. Intensifier was applied twice a day and efficacy evaluations were conducted after four and eight weeks. According to SkinCeuticals, the study demonstrated visible improvement in lip plumpness and reduction of under-eye hollows, and suggested that H.A. Intensifier is well tolerated for use in these new indications. The H.A. Intensifier is a corrective serum aiming to boost the skin’s hyaluronic acid levels to support the skin’s matrix, resulting in improved firmness and plumpness, according to the company.
Tanning MP calls for ban on sunbeds
Last month, Mid Derbyshire MP Pauline Latham called for the ban of sunbed use across the UK in a Westminster Hall debate. Sunbeds are currently restricted to users over 18 years of age, but MP Latham believes more needs to be done, expressing concern about the rising levels of melanoma every year. She suggested following suit with countries such as Australia and Brazil where sunbed use is already banned. She stated, “Statistics show that people who have used a sunbed at least once, have a 20% higher risk of developing melanoma than those who have never used a sunbed.” Rhondda MP Chris Bryant referred to sunbeds as ‘death machines’ and agreed that the use should be banned. MP Steve Brine, parliamentary undersecretary of state for health and social care concluded the debate stating, “The Government’s ambitions outlined in the long-term plan for the NHS, the Secretary of State’s prevention strategy, and the Green Paper will ensure that we strive to do even better over the next decade. In conclusion, I agree completely.”
Sinclair Pharma introduces four new thread-lift protocols
Pharmaceutical company Sinclair Pharma has introduced four new protocols, titled the Recontour, Redefine, Reshape and Reshape Plus, all under the umbrella term of the Ultimate Reshaping Solution. The protocols are designed to improve overall results and enhance facial contouring by using the Silhouette Soft sutures. The new techniques use an increased number of sutures, which in turn increases the stimulation of type one collagen, the company explains. The mid-face lift, the Recontour, uses six sutures of eight cones and treats mild sagging and volume loss in the cheek area and the nasolabial folds. The lower-face lift, Redefine, uses two sutures of 12 cones and four sutures of eight cones to treat mild sagging to the lower face and jawline laxity. In addition, the full-face lift, called the Reshape, uses 10 sutures of eight cones and 10 sutures of 12 cones to reshape moderate tissue sagging and the full-face and neck treatment, while the Reshape Plus uses four sutures of 12 cones and eight sutures of eight cones to lift tissue sagging.
BACN UPDATES
A roundup of the latest news and events from the British Association of Cosmetic Nurses

ACE 2019
If you’re reading this at ACE then pop by Stand 69 to catch up with the team and find out more about being a part of the BACN! As always, it’s great to see so many members and catch up with familiar faces, while also meeting those new to aesthetics and new to the BACN. Thanks to everyone who keeps us busy!
BACN RENEWALS
Once again, it’s time to renew membership. The BACN membership year runs from April until the end of March and we’re encouraging members to renew to remain a part of the largest professional association for aesthetic nurses in the UK, as well as welcoming new members into our support network. 2018 was a fantastic year for the BACN, with professional initiatives being launched, a larger conference than ever before, while continuing to support aesthetic nurses with a range of experience and individual needs. Information on how to renew will be sent to all members throughout March and the renewals process should be quicker and smoother than it ever has before. The BACN has also launched a digital certificate section in the members’ area, so you won’t need to worry about waiting for certificates and marketing material to be sent, as everything can be downloaded. For more information, contact Gareth Lewis, membership and marketing manager at glewis@bacn.org.uk
BACN REGIONAL EVENTS
We have our meetings and events calendar live on the BACN website, and members are encouraged to book online for the next round of regional meetings taking place throughout April and May, with a wide range of presenters and demonstrations. All our meetings are tailored to benefit those who have been practising for years and also our newer members. BACN events are CPD accredited and really invaluable learning experiences, offering the chance to meet others, so nurses do not feel isolated working in aesthetics. To book your place at one of our events please go to the website and click the events tab – if you have any questions please contact Tara our events manager at tglover@bacn.org.uk We look forward to seeing you all over the UK!
This column is written and supported by the BACN
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Threads

NMC appoints new chief executive and registrar

Andrea Sutcliffe has been appointed as chief executive and registrar for the Nursing and Midwifery Council (NMC). Sutcliffe has more than 30 years’ experience in health and social care and was previously chief inspector of adult social care for the Care Quality Commission. She was awarded a CBE for services to adult social care in the 2018 New Year’s Honours’ list. Sutcliffe said, “I’m thrilled to finally join the NMC. It’s a privilege to take on this role at such an important time, not only for the organisation, but for health and social care in the UK.”
LED therapy
Enoura Aesthetics introduces first LED device
Medical equipment manufacturer Enoura Aesthetics has launched the Levura LED, the company’s first LED device. Enoura Aesthetics explains that the Levura LED is a multi-platform photodynamic therapy device, featuring three interchangeable heads, one for red and blue light, one for yellow light and the other for infrared. The company states that it also has a medical Class IIb CE mark. Levura LED is designed to reduce the appearance of fine lines and wrinkles, rejuvenate skin, treat common skin conditions such as pigmentation, and promote healing after aesthetic treatments. Aesthetic practitioner Dr Asher Siddiqi, director of Enoura Aesthetics, said, “Levura LED is the latest product to be introduced alongside our successful HIFU range. We take pride in offering one of the latest high quality and affordable medical devices, which offers an excellent return on investment for your clinic.” The product is assembled in the UK and is distributed directly by Enoura Aesthetics.
Skincare iS Clinical launches the Prodigy peel system


Skincare company iS Clinical has launched a three-step peel system designed to rejuvenate skin. The first step, Prodigy Prep features witch hazel to prepare the skin for step two, the peel solution. There are two grades of peels available, the superficial Prodigy Peel and the superficial to medium-depth Prodigy Peel Pro. The first grade is formulated with lactic, salicylic, citric acids and resorcinol and aims to rejuvenate dull, rough skin concerns and can be used on all skin types. The second grade features higher percentages of lactic acid, resorcinol and an advanced form of salicylic acid, which is designed to maximise cellular renewal at a deeper level. The third step in the system involves the use of the Prodigy Boost solution, which contains retinol, capryloyl salicylic acid and hexylresorcinol to encourage collagen and protect against UVB and UVA. iS Clinical products are distributed by Harpar Grace.
Sharon Bennett, aesthetic nurse prescriber

How did it feel to win The Schuco Aesthetics Award for Outstanding Achievement in Medical Aesthetics at the Aesthetics Awards?
I was genuinely surprised but
naturally delighted. My aesthetic career began in Harley Street 30 years ago working alongside plastic surgeons and developing an interest in non-surgical treatments. I knew immediately it was the area of practice in which I wanted to develop my career as it combined two things I enjoy enormously – medicine and art. I am proud that I was involved in bringing Restylane, the first hyaluronic acid (HA) dermal filler, into the UK and, since then, I have watched the evolution and launch of many other fillers as they vie for a position in this hugely competitive market.
What’s new in the world of injectables?
Dermal fillers have evolved greatly since 1996 Products are extremely advanced and can adapt to every tissue type to integrate seamlessly, enhancing expression. My filler of choice is still Restylane, which holds the data to support its position as the gold standard of HA dermal filler
The large portfolio of products suits my patient base, which ranges from millennials through to mature men and women. Whilst filler technologies have advanced, injection technique has also vastly improved. Practitioners can be very creative with the needle and cannula, layering techniques to achieve amazing results. There is a heavy emphasis on knowledge of the anatomy and complications management which I believe is making aesthetic treatments much safer
What do you see as the big trends for the year ahead?
The pan-perioral zone and an emphasis on balancing the face by looking at the profile, reshaping noses, chins and jawlines in order to achieve a desirable outcome. I see more and more patients benefit from outstanding results due to using a combination treatment approach I work on enhancing the upper layers of the skin with hydrating Skinboosters, meanwhile restoring and enhancing features with Restylane gels. With innovative placement techniques the patient experiences low levels of discomfort and downtime.
RES19-01-0027 DOP February 2019
This article is supported by
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
60
11 Insider News @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Appointment
Business development
Cynosure establishes service initiative

To celebrate 20 years in the UK aesthetic medical laser industry, Cynosure has launched a customer service initiative in association with its learning and development platform, Aesthetic Exchange. The company explains that it will be hosting a series of specialised customer training and educational events and workshops, featuring knowledgeable speakers and covering technological advances, best clinical practice and business growth tips. The company has also released four mini videos which outline what they believe sets Cynosure apart from other manufacturers.
Fiona Comport, UK marketing communications manager commented, “At Cynosure we are passionate about truly going above and beyond for our customers; this means not just manufacturing and servicing our award-winning devices, but delivering high-quality clinical training alongside industry-leading sales and marketing support.” She continued, “For us, it’s about helping our customers secure their own success, which is why we are so excited to be launching this celebration of customer service in our 20th year.”
MarketingAllergan launches new campaign for Juvéderm
Global pharmaceutical company Allergan will launch a new international advertising campaign for its dermal filler Juvéderm in Spring 2019.
According to the company, the campaign is designed for different patient needs, rather than a ‘one size fits all’ approach and is created to empower a new generation of customers. Anna Edwards, executive director for facial aesthetics international strategic marketing at Allergan said, “This bold and high-impact campaign marks a new era for consumers; it is a celebration of empowerment and confidence which is what we think beauty is about. It’s also really good fun, with a sassy and humorous attitude behind it all!
The approach is bold and will energise the Juvéderm brand, encouraging more consumers to become engaged and informed about this growing category.”
The company explains that the campaign has a ‘modernised logo and bright poppy colour scheme with refreshed talent, imagery and edgy soundtrack’.
The shoot took place at landmark venues around London, including the Tate Modern art museum, and all models received Juvéderm treatment.
UK supplement company introduces vegan collagen booster
A new vegan collagen booster has been introduced by vitamin supplement company Rejuvenated, called Botani-col. According to the company, it has developed a plant amino acid protein in the same ratio as those within collagens. Botani-col aims to support the fascia, promote healing and wound repair, improve digestion, promote a healthy metabolism, and support cardiovascular and joint health. In addition, it aims to alleviate a number of skin conditions such as acne, rosacea and eczema, while preventing oxidative stress. Rejuvenated currently offers Botani-col in capsule form, called the Skin Perfecting Complex. The company intends to introduce further collagen-boosting supplements that can be added to a number of products including creams and drinks. Kathryn Danzey, founder of Rejuvenated said, “We had already sourced a vegetarian collagen from egg protein. However, the demand for consumers wanting animal-free products has increased dramatically. Many are opting for a flexitarian diet where they opt to cut out animal protein in certain areas of their life and beauty is one of these areas. We are excited to have the first product to offer a solution for these customers.”

Team update
Sinclair Pharma recruits new team members
Pharmaceutical company Sinclair Pharma has recruited two new members to join the account management team. Sinead Foran, who previously worked at Merz Aesthetics for three years as an aesthetic account manager, has been appointed as sales representative for Ireland. Nicola Grimwood, who also worked for Merz Aesthetics as an aesthetics account manager, will be joining Blair Stevens, who has recently been promoted to regional business manager, to cover the north London and Essex territory from March 4. In addition, members of the UK team were recognised at the Sinclair European sales and marketing meeting in Lisbon in January. Blair Stevens was awarded Best Sinclair College Practitioner Engagement, Best Silhouette Soft Sales and Best Perfectha Sales. Joanne O’Connor, who manages the North West region was recognised as having Best Perfectha Sales Growth and Nicola Lord, sales representative for Midlands, East Anglia and Hertfordshire was presented with the award for Best Ellansé Sales Growth. Jo Neal, brand manager for Sinclair Pharma, said “Sinclair is delighted to announce that we have a full sales team supporting our customers in the UK and Ireland. This enables us to be able to provide our current and new users with continued training and marketing support along with regular update meetings which are planned to take place on each territory this year. Our account managers were recognised as some of the best at Sinclair at the recent European sales and marketing meeting, we would encourage all of our customers to utilise their account manager and work in partnership with them.”
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Collagen
Please join us for a Symposium with Dr. Carl Thornfeldt, the worldwide leader of barrier repair and innovator of the awardwinning skincare line Epionce, to learn about the future of skin health. Don’t miss this fantastic opportunity to hear him speak during a rare visit to the UK and Ireland. New and existing customers welcome.
About Founder Dr Thornfeldt
Dr Thornfeldt is a practising dermatologist with more than 30 years of skin research experience and 22 US patents granted. He has spent over 25 years focusing on researching abnormalities of the skin barrier, cutaneous inflammation, drug delivery, herbs and disease therapies.

Join Dr Carl Thornfeldt for an in-depth insight covering:

The Epionce philosophy for skin health
The power of clinical results
Hot trends in skincare and your practice
The science of anti-ageing by inhibiting inflammation and repairing the skin barrier

Delivering clinical results WITHOUT compromising barrier function


The new way to understand adult acne
Plus Unmissable Epionce Offers

When & Where:
2nd April: 41 Portland Place, London. 10.00am – 3.00pm
4th April: MacDonald Hotel, Manchester. 10.00am – 3.00pm
5th April: Malone House, Belfast. 8.30am - 1.00pm
5th April: The Alex Hotel, Dublin. 3.30pm – 7.00pm
For more information or to book your FREE place email carly@edenaesthetics.com or call 01245 227752.
AESTHETICSJOURNAL.COM VISIT WWW.AESTHETICSJOURNAL.COM TO JOIN FREE TODAY
up-to-date on the latest aesthetics developments and best practice guidance
your
tablet
our Library for a
of categorised
and tools relating
your specialism and interests Add training to your personal Training Record for easy reference Complete accredited CPD articles and receive digital certification Advertise and search for job opportunities and clinic equipment for sale in the Marketplace Explore the Aesthetics website
Keep
on
desktop,
or phone Search
huge range
content
to
•
•
•
•
•
•
To reserve your space and to receive your Epionce
Discovery Set. COME SEE US AT ACE ON STAND 64
Anti-Ageing
Discover the Epionce Revolution.
Digital Mr Adrian Richards launches live streaming service for practitioners
Consultant plastic and reconstructive surgeon, and clinical director of training provider Cosmetic Courses, Mr Adrian Richards has launched a live streaming service to offer a range of tips and advice to those in the specialty. The first live stream was broadcast on the Cosmetic Courses Facebook page and YouTube channel, where Mr Richards was joined by director of Consulting Room and MediZen, Ron Myers and cosmetic manager of Hamilton Fraser Insurance, Naomi Di-Scala.
During the live stream, Mr Richards discussed the different approaches to setting up a business in the aesthetics specialty, including pricing strategies, patient journey and industry legislations, as well as marketing tools to expand a clinic’s practice. This was followed by a discussion outlining the importance of cosmetic insurance, how to deal with claims and how GDPR regulations can impact a practitioners’ routine. There was also a live question and answer session. This service is free and is available for public viewing, the next live stream will take place on March 1.
Injection delivery
New dermal filler syringe launches

Global medical technology company Becton Dickinson (BD) has launched a glass, pre-fillable syringe for the administration of viscous solutions such as dermal fillers, called the BD Hylok. According to the company, the BD Hylok luer-lok adaptor (LLA) is strongly affixed, using new bonding technology, and reduces the risk of LLA rotation or disconnection that could potentially cause leakage. The new BD Hylok syringe is currently available in 1ml and additional sizes will be introduced in the future. BD also states that the new syringe is compatible with intravenous (IV) connectors.
Peter Nolan, worldwide president of pharmaceutical systems at BD said, “The recent launch of BD Hylok exemplifies BD’s ability to continuously innovate. By offering a stronger and better connection with needles and IV connectors, this new syringe has an array of medical uses and benefits that will suit multiple needs across the healthcare and medical aesthetic markets.”
IMCAS Academy app launches
The International Master Course on Ageing Science (IMCAS) Academy has launched a mobile app for its e-learning platform. The app encompasses three components: Library, Webinars and the Alert. According to IMCAS, the library contains a video collection of 3,000 recent lectures and demonstrations that can be viewed anytime, anywhere. The videos cover a wide range of topics including injections, lasers, energy-based devices, cosmeceuticals, clinical dermatology, plastic surgery, threads, hair restoration and practice management. The webinars, aired from the IMCAS studio each month, allow viewers to ask questions directly through the platform to the presenters who can then answer immediately. IMCAS Alert allows physician members to receive expert advice on complications, cases or procedures from the Scientific Board. They can first select the relevant topic that relates to the case, and then submit the case details anonymously. Once published, the community will aim to share their advice for the case within 24 hours. A spokesperson from IMCAS explains that the Academy also encompasses a social aspect where you can contact IMCAS professionals and the 15,000 other members all year long. Members can manage their connections, follow their progress on courses and update their profile and professional data at any time online. The IMCAS Academy app is available to download app stores.
News in Brief
IQ signs agreement with JCCP
Awarding organisation Industry Qualifications (IQ) has joined EduQual as the second awarding body to sign a memorandum of understanding with the Joint Council of Cosmetic Practitioners (JCCP). Through signing this memorandum of understanding, the JCCP has confirmed that the IQ Level 7 Certificate in Injectables for Aesthetic Medicine meets all necessary guidelines. Laurence Clarke, IQ qualification development and sector lead for aesthetic medicine, said, “Following the signing of this memorandum of understanding, the JCCP will continue to work closely with IQ to ensure that IQ aesthetic qualifications remain the hallmark of quality within the sector.”
TruCryo appoints cryotherapy trainer
Cryotherapy device manufacturer, TruCryo, has appointed a new key opinion leader (KOL), who will provide training for the use of its cryotherapy devices. Laura Huggett is a registered dental nurse and phlebotomist with more than 20 years’ experience in aesthetics. As the new KOL for TruCryo, Huggett will be lecturing and demonstrating the benefits and techniques used in targeted cryotherapy treatments during workshops and industry events.
DHAT expands team
Multiple award-winning training provider Dalvi Humzah Aesthetic Training (DHAT) has expanded its team and appointed a new admin coordinator. Nina Doherty will be responsible for the day-to-day organisation of the DHAT courses and will also assist in the production of new course materials and logistics for future courses. Consultant plastic, aesthetic and reconstructive surgeon, Mr Dalvi Humzah, said, “I am delighted to welcome Nina to the DHAT team – she will be helping the rest of the team to develop our new and exciting 2019 programme.”
Alice Hart-Davis launches book and website for consumers
Journalist Alice Hart-Davis has released a book titled, ‘The Tweakments Guide’ that discusses an array of non-surgical procedures and treatment reviews aimed at consumers. To support the launch of the book, there will also be a website which Hart-Davis explains will have an interactive practitioner finder as well as a ‘tweakment’ finder.
Amongst those practitioners that have been confirmed to be listed on the website are aesthetic practitioners Dr Tracy Mountford, Dr Tapan Patel, Dr Galyna Selezneva and aesthetic nurse prescriber Sharon Bennett. In addition, consumers will be able to search for practitioners with specific accreditations, for example a member of the BCAM.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
App
Obagi Ambassador Awards
From January 29 to 31, aesthetic distributor Healthxchange Pharmacy hosted the Obagi Ambassador Awards in London, Manchester and Dublin. The Awards celebrated the achievements of those on the Obagi Ambassador Programme, which was launched in 2016 to further clinical education, share best practice and network with fellow Obagi skincare clients. The Award for Best Patient Result was won by aesthetic nurse prescriber Angela Brennan, clinic director Emma Beddow won Best Use of Marketing, Most Improved Clinic Sales was awarded to aesthetic practitioner Dr Marwa Ali and aesthetic nurse practitioner, Julie Goldsmith, won Ambassador of the Year. Before the awards were handed out, guests learnt

about updates to the Obagi skincare line and the Obagi consultation prescribing service, which is a free service that sees nurse prescribers assist clinics in patient consultations. Nurse prescriber Amanda Wilson, who attended the event said, “The Obagi Ambassador meeting was thoroughly enjoyed by staff and delegates alike. It was a well-deserved celebration of the achievements of the Obagi Ambassadors over the last 12 months.”
Production and Research at Aesthetic Technology Ltd

Aesthetics visits the headquarters of Aesthetic Technology Ltd, the manufacturer of Dermalux LED, to learn more about the company’s development process
Aesthetic Technology Ltd was founded in 2012 by Huw Anthony and Louise Taylor. The pairing of Huw’s background in product development and Louise’s personal experience of using LED phototherapy saw the start of what is now a multiple Aesthetics Award-winning company with a portfolio of four devices, serving more than 20 countries worldwide and employing 14 members of staff. The entire design and development process of the Warringtonbased LED company’s products is undertaken in the UK, which is something that is very important to both Huw and Louise. Something that is just as essential to the pair is producing quality products and delivering sound education to their customers. So much so that when the company first began, the Taylors decided to invest profit back into the research and development (R&D) division, which they believe has influenced their success so far. Huw says, “Right from the very early days, we decided to invest significantly into the innovation of our proprietary technology with the aim of delivering best in class and the most advanced LED phototherapy systems possible. Louise adds, “One of our main focuses has always been the education behind LED technology and in my experience, I have found that LED phototherapy is quite misunderstood in the industry, so we provide
continuous support and training to our customers to ensure the best possible service.” In 2018, the company also introduced a 3D printing system to create prototypes of components before they go into full manufacture, which Dale Needham, managing director, explains ‘revolutionised internal R&D activities’. He continues, “What started as a low-level requirement has now turned out to be one of the best tools in the design development cycle. The facility enables us to offer a full turnkey solution to our clients in addition to rapidly improving our own internal processes. We have the ability to replicate all of the plastic and rubber components enabling us to test and trial the product in its end form before committing to tooling.” Aesthetic Technology Ltd has now expanded its product range to include two new medical devices, the Tri-Wave MD and the Flex. This is done through obtaining ISO13485 certification (a quality management system designed for regulatory compliance). Chris Ashworth, quality operations director, explains, “Currently there is no requirement to have the ISO13485 but with new laws from the Medical Device Directive that are due to come into place next year, LED phototherapy devices will be required to be manufactured as a medical device and CE marked as such. To obtain a Medical CE mark the manufacturer must be certified to ISO13485. A big part is traceability, so there are a number of components within our machines that have a unique serial numbers that go through a heightened testing process, which means that we can track all of our machines to ensure they are working optimally.” Needham concludes, “It’s very easy to get consumed in the development process, which has taken a number of years, but the most rewarding thing for all of us is to see that we have created huge opportunities for so many businesses worldwide and that is something that I am very proud of.”

Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
ACE HEADLINE SPONSOR ADVERTORIAL STAND 20
Managing director Dale Needham with Aesthetics journalist Megan Close
On the Scene
Technicians at Aesthetic Technology Ltd
If, like thousands of your peers, you take education and learning seriously, then there’s a good chance you’re reading the Aesthetics journal whilst exploring the Aesthetics Conference and Exhibition (ACE) in London! This year’s event is more comprehensive than ever, with the introduction of a whole new clinical agenda, expert speakers never before seen at ACE and more exhibition space for eager delegates to explore.


Last year ACE was recognised as one of the best free to attend conferences in the whole of the UK and won silver at the Conference Awards 2018. So, what does award-winning learning look like at ACE?
First-class clinical education
See live treatment demonstrations, discover new techniques and protocols and enhance your learning on the science behind the most effective modalities at the Expert Clinic, Masterclass and Symposium agendas. All from the industry’s most reputable and experienced speakers!
Injectable innovations
Injectables are among the most popular non-surgical procedures in the aesthetics field, but there are hundreds of products to choose from, and even more techniques for successful outcomes. Speaking on the latest injectable procedures and providing advice on treatments such as dermal fillers, botulinum toxin and platelet-rich plasma will be Dr Raul Cetto, Dr Priyanka Chadha, Dr Benji Dhillon, Dr Tahera Bhojani-Lynch, Mr Ayad Harb, Dr Syed Haq, Dr Max Malik, Dr Beatriz Molina, Dr Gabriel Siquier Dameto, Dr Lee Walker, injectable sales manager Frank Ward and Dr Lara Watson.
Skin science
Of course, the importance of skin quality and health is constantly highlighted in this sector. From skin rejuvenation and scar revision to at-home cosmeceuticals, these presenters will cover the lot! You will discover the latest advice from aesthetic trainer Luciano De Min, Dr Xavier Goodarzian, Dr Mayoni Gooneratne, Dr Uliana Gout, aesthetic distributor David Gower, Mr Dalvi Humzah, Dr Beatriz Molina, Dr David Rouse and Dr Stefanie Williams.
Your ACE 2019 Experience
See what award-winning learning looks like at the long-awaited Aesthetics Conference & Exhibition on March 1 and 2
Device developments
Machines and devices are technologies that can not only provide outstanding results for patients, but also provide lucrative business success. A huge range of devices are available to learn about at ACE, which treat skin, fat and feminine health concerns, among many other indications. The innovative discussions will be hosted by Dr Alexander Bader, Dr Alicia Baptista, Dr Ian Hallam, Dr David Jack, Dr Sabika Karim, Dr Alex Karkhi, Dr Shirin Lakhani, medical aesthetician Renée Lapino, Dr Joanna Lovatt, Dr Sach Mohan, Dr Beatriz Molina, LED specialist Dale Needham, Dr Simon Ravichandran, aesthetic distributor Ben Sharples, and Dr Claudio Urbani. Other treatments and advancements to help you develop your product offering will also be discussed by nurse prescriber Sandy Green and Dr Matthew Capehorn.
Business building advice
Of course, boosting your clinical skills and knowledge isn’t the only thing that will help you gain and retain patients to further progress your aesthetic career. That’s why the business topics are so important! How can you increase your turnover? Gain effective press coverage? Set achievable KPIs? Or keep you employees happy? The most effective practical tips to help grow your practice will be revealed by industry leaders on the Business Track agenda. Providing their best business tips and industry updates will be lawyer Rohana Abeywardana, business coach and author Alan Adams, aesthetician and directory website founder Dija Ayodele, travel law specialist Sarah Barnes, aesthetic nurse and clinic owner
Exhibition opening times Friday 1 March: 9:00-18:00 (Networking Event 18:00-19:00) Saturday 2 March: 9:30-16:00 (Some educational sessions continue until 17:00) Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Cheryl Barton, digital marketer Danny Bermant, plastic surgeon and social media guru Mr Olivier Branford, VAT and TAX consultant Veronica Donnelly, digital marketing consultant Adam Hampson, beauty journalist and author Alice Hart-Davis, sales leader and marketer Jean Johnston, aesthetician and marketer Nikki Jones, PR consultant Julia Kendrick, clinic software specialist Mark Lainchbury, aesthetic practitioner and clinic owner Dr Victoria Manning, aesthetic practitioner and clinic owner Dr Rita Rakus, surgeon and clinic owner Mr Adrian Richards, chair of the JCCP Professor David Sines and marketer and aesthetic practitioner Dr Harry Singh.
An Elite Training Experience
Enhance your consultation skills, improve your injection techniques, expand your anatomy knowledge and increase your understanding of complication management with guidance and demonstrations from expert training providers in medical aesthetics. Attend the comprehensive Elite Training Experience agenda with half-day sessions from Drs Emma and Simon Ravichandran from Advanced Training Academy, Mr Dalvi Humzah, nurse prescriber Anna Baker and Dr Rajan Sharma from Dalvi Humzah Aesthetic Training and Professor Bob Khanna from Dr Bob Khanna Training Institute. Dr Beatriz Molina from the International Association for Prevention of Complications in Aesthetic Medicine (IAPCAM) will also host a complications workshop, which will also feature nurse prescriber Sharon Bennett and Dr Sophie Shotter, as well as Mr Jeff Downie. For only £195 +VAT you can learn from the most experienced internationally-renowned speakers from the UK and gain 10% off future training with your chosen Elite Trainer!
A buzzing Exhibition
It’s where connections are made, the latest innovations are showcased, live demonstrations are performed and lifelong friends and colleagues share experiences. Set across an impressive 2,500m2 space, the Exhibition Floor really is the beating heart of ACE. The learning opportunities here are endless; discover the latest innovations and product launches from 80+ aesthetic companies and meet valuable new contacts to further develop your business. You can even take advantage of exclusive show offers and discounts, with some companies advertising hundreds of pounds off their products and services!
ACE 2019 agenda overview
SYMPOSIUM (NEW)
Two-hour sessions, 8 learning hours, 8 CPD points available
EXPERT CLINIC
Half-hour sessions, 17.5 learning hours, 17.5 CPD points available
MASTERCLASSES
One-hour sessions, 8 learning hours, 8 CPD points available
BUSINESS TRACK
Half-hour sessions, 9 5 learning hours, 9.5 CPD points available
ELITE TRAINING EXPERIENCE
Three-hour sessions, 12 learning hours, 12 CPD points available
NETWORKING EVENT
Join delegates and speakers for the free Networking Event at 6pm on Friday March 1, supported by Enhance Insurance

Join the aesthetics community
It’s not too late to join hundreds of your peers for award-winning learning at ACE 2019. Simply visit the Business Design Centre in Islington, London and register for free at the registration desk. For those already joining us, we welcome you to ACE 2019 and encourage you to make the most out of the endless free opportunities!
Please note that access to some of the clinical sessions is restricted to certain professionals and you will have been required to supply your professional number upon registration. Check the session information via the website or conference guide beforehand. If you have not already supplied your professional number, you can visit the Registration Desk to do so.
HEADLINE SPONSOR Group REGISTRATION, FLOORPLAN & WIFI SPONSOR Enhance Insurance Advice | Support BUSINESS TRACK & NETWORKING SPONSOR CONSUMABLES PARTNER AESTHETICS LANYARD SPONSOR 1 & 2 MARCH 2019 / LONDON T RAI N IN G EX PERI EN C E ELIT E 2 0 1 9 2019
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Westminster Regulation Debate
Aesthetics reports on the recent debate in Westminster Hall on the regulation of non-surgical aesthetic procedures

On February 12, the regulation of the non-surgical cosmetic industry was discussed in a Westminster Hall debate, with MPs stating that regulation does not go far enough to protect the public.1,2 The debate was tabled by South Leicestershire MP Alberto Costa following concerns raised to Prime Minister Theresa May in the House of Commons in January regarding MP Costa’s constituent, Rachael Knappier. Last year, Knappier suffered a complication after a lip filler treatment from an unregulated beauty therapist at a party.1-3 Many of the concerns raised by MPs in the debate included the lack of formal, recognised training for administering procedures such as dermal fillers and botulinum toxin, the vulnerability of young patients who have access to treatment, issues surrounding social media and advertising, the influence of celebrities, the types of products used, and the screening of patients with body dysmorphic disorder. One of MP Costa’s main concerns was the type of practitioners administering non-surgical cosmetic procedures as they may not be held accountable by any regulatory body. He said, “The mark of a professional in our society is somebody that is regulated, that is trained, qualified, licensed and that has ongoing regulation development. In addition, in the private sector, they must carry professional indemnity insurance so that people have someone to sue when things go wrong.”
MP Costa added that he believes the lack of regulation is an issue that affects all constituents, as well as the National Health Service, and stated that although there is voluntary regulation in place, it does not go far enough. He said, “I agree that regulation is required and
it shouldn’t be voluntary regulation. I also think a regulator should identify the training, expertise and qualifications that are required and what products should be permitted in the market.” He added, “It is beyond belief that anyone can inject someone with a foreign substance and have no medical expertise whatsoever.”
Central Suffolk and North Ipswich MP Dr Daniel Poulter highlighted the points made in the 2013 Keogh review on the unregulated nature of the industry. He explained, “If you are performing operations on the body you should have the prerequisite knowledge and training on the anatomy involved and understand the consequences of what goes on. Far too often, unregulated practitioners do not have the skills or the knowledge to understand what can go wrong, or indeed have the skills and the knowledge to advise people about the potential adverse consequences. It is time, I agree, for some proper regulation.”
MP Costa added that more needs to be done to educate the public on the dangers behind non-surgical cosmetic procedures, and the importance of going to a reputable, qualified practitioner.
The introduction of the voluntary practitioner and training registers by the Joint Council for Cosmetic Practitioners (JCCP) was also discussed.
MP Costa commented, “In the absence of an obligatory statutory register, as a minimum I say to the Government that there should be clear public information about the need to seek a practitioner who is at the very least registered with the independent voluntary regulator. However, a voluntary and independent register does not go far enough.” He continued, “I would like to ask the Government to at least consider setting up a cohesive and compressive plan to properly regulate the non-surgical cosmetics industry.”
MP Jackie Doyle-Price, Secretary of State for Mental Health,
responded to MP Costa’s concerns, agreeing that it is important consumers are properly educated on this issue and emphasising that adequate regulation is needed in the sector. MP Doyle-Price also mentioned that dermal fillers will be soon regulated as a medical device,1,4 which she hopes will remove some of the risks associated with the treatment.
“I think we need to make much more rapid and substantial progress if we are going to protect consumers. This is not like going to have a haircut and we need to make sure we are properly looking after consumers and improving safety. Within the Department of Health our priority has to be the safety of people facing these procedures,” MP Doyle-Price said.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
“I am looking at a time scale of about two to three years to get to a point where the Government will propose legislation. My job is to encourage the Government to do that”
MP Alberto Costa
The debate was followed closely by many professionals working within the non-surgical aesthetic sector. Independent nurse prescriber Sharon King, co-founder of the Aesthetic Complications Expert (ACE) Group and vice-chair of the British Association of Cosmetic Nurses, thought the debate was a step in the right direction. She explains, “It was great to see the MPs taking an interest, particularly from MP Costa. The arguments raised were not anything new, but there were a few points that they did pick up on that was good to see, for example how the media is portraying the treatments to the young and vulnerable. They also said that although voluntary regulation is a step in the right direction, we do need some formal regulation – it’s good to see that this, as well as training and education needs, was actually raised.”
Dr Paul Charlson, president of the British College of Aesthetic Medicine also felt positive about the debate. “I think the more exposure we get the better, and all we can do is keep lobbying to keep it in the public mind,” he says. Consultant plastic surgeon Mr Rajan Uppa, council member of the British Association of Aesthetic Plastic Surgeons, adds, “In the debate, the Keogh review was mentioned again, but I think the lack of implementation of its recommendations for regulation is a failure by our politicians. The fact that there is no regulation is scandalous, but this debate is extremely important in raising public awareness because most people assume that the people doing these treatments are qualified, until something goes wrong.” King emphasises, “Overall, I think the debate was all very good and very positive, but how it’s going to go forward I don’t know.” In an exclusive interview following the debate,
MP Costa confirmed to Aesthetics that his aim is to see Government propose legislation within the next few years. He says, “Whilst the country is getting on with things like Brexit, that doesn’t mean that other concerns of importance shouldn’t be dealt with, particularly when constituents are bringing their concerns to us. Laws are not changed overnight. I am looking at a time scale of about two to three years to get to a point where the Government will propose legislation. My job is to encourage the Government to do that.”
To help him achieve this, MP Costa calls for all involved in the specialty to help. He explains, “I encourage anyone with a view on this area, whether they are a patient or practitioner, to email or write to their local MP and very simply say that they support the debate in Parliament and that they would like to see non-surgical cosmetic procedures properly regulated. The more MPs hear about this, the higher the likelihood that the Government will listen.” As well as this, there are also petitions in action, which the public can take part in.5
REFERENCES
1. Westminister Hall, Non-surgical Cosmetic Procedures: Regulation, February 12 2019.<https://hansard. parliament.uk/Commons/2019-02-12/debates/C5F01389-9B2F-4867-BFF8-0B85376CFBFD/Non-Sur gicalCosmeticProceduresRegulation>
2. Parliament TV, Westminster Hall – EXTRACT, February 12, 2019. <https://parliamentlive.tv/event/index/ d4945cee-b71b-4b21-97e5-230627f00fb7?in=11:00:00&out=11:30:30>
3. Prime Minister addresses regulation issues of non-surgical treatments, January 24, 2019, Aesthetics <https://aestheticsjournal.com/news/prime-minister-addresses-regulation-issue-of-non-surgicaltreatments>
4. MHRA confirms no plans to make fillers prescription only, January 2018, Aesthetics. <https:// aestheticsjournal.com/news/mhra-confirms-no-plans-to-make-fillers-prescription-only>
5. UK Government of Parliament, Petitions, Aesthetic medical treatments to only be performed by Doctors, Nurses & Dentists. Deadline 21 March. <https://petition.parliament.uk/petitions/228515>
Unique Oxygenating Foundations and Moisturisers that work like a virtual breathable second skin
Oxygenating Foundation I SPF 25+
Containing the patented Ceravitae™ Complex it stimulates skin cell production and helps the healing process following most procedures. Soothes, heals and protects damaged skin thanks to its oxygen-enriched, natural components making it virtually a second skin. Available in 14 shades.


Oxygenating Foundation Acne Control I SPF 25+


This unique and revolutionary formula was three years in the making! Since having identified the need for a treatment foundation we started working hard to create the perfect acne control foundation that is also an oxygenating treatment foundation developed to simultaneously clear and conceal the frustrating conditions of acne.
NEW Oxygenating Hydro-Matrix


Much more than a simple moisturiser, this hydrating and healing post-treatment behaves like a ‘second skin’, containing Oxygenetix’s patent formula Ceravitae™, that allows oxygen to penetrate the skin and reinforce the natural healing process. It also beautifully primes the skin ready for the application of the Oxygenetix Oxygenating Foundation. Available in 30ml, 50ml and 100ml.
Award winning, flawless finish, breathable liquid foundations.
Exclusive to

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com









SUPERFICIAL STRETCHING indicated for the dynamic areas of the face (perioral, periocular & forehead) DEEP HYDRATION to improve elasticity, radiance and smoothness of the skin THE TWO EXPRESSIONS OF HYALURONIC ACID Exclusive UK & Ireland distributor / training provider of IBSA’s aesthetic products 0208 455 4896 | info@ha-derma.co.uk 3 months after the 2nd treatment Before SYMPOSIUM ACE CONFERENCE FRIDAY, MARCH 1 2:30 - 4:30PM
Integrating New Services into Your Clinic
With competition in the aesthetics field growing, business owners are finding new ways to add value. Journalist Allie Anderson speaks to aesthetic practitioners and specialist service providers who work together to further assist patients in their aesthetic journey
Working with a permanent makeup artist
In 2013, with business at her Wirral-based practice SDS Rejuvenate booming, aesthetic practitioner Dr Sally-Ann Dolan recognised an opportunity to expand her offering by

collaborating with a permanent makeup artist. Gemma Kennelly fitted the bill, and she has been working from one of the SDS clinic rooms ever since.

DR SALLY-ANN DOLAN SAYS, “My background is as a GP, but I started out in aesthetics more than 10 years ago and opened my first clinic around six years ago. We became busier doing non-surgical aesthetics and began offering beauty treatments as well, such as manicures, eyelash treatments, waxing and spray tanning. It became a one-stop shop, and permanent and semi-permanent makeup was a natural fit. Gemma and I met, and I was impressed by her work; it was appropriate for people of all ages, not just the younger clientele. She also had experience working with people who had lost their eyebrows and eyelashes after chemotherapy or due to alopecia. Gemma talked very passionately about it, and, as a doctor, that meant a lot to me. As she became established at the clinic, people started asking about her services. We often refer patients to her, and she brings some of her clients to us if they ask about aesthetics or beauty treatments. For example, if Gemma is seeing a patient who is due to have their next botulinum toxin treatment soon, she’ll suggest they come to me to have that done before she does their eyebrows. Also, if a client of hers has a skin condition, she might ask my clinical advice. Gemma holds her own diary, so if one of our patients is interested in having an appointment with her, they contact her directly and she will then check when the clinic room is free. Sometimes she will work from here once a week, but during busy times it might be more often. She is self-employed and pays to rent the clinic room, based on how long she uses it for. There is no other financial arrangement in place whereby, for example, there’s an incentive for either of us to cross-refer clients or patients. When aesthetic practitioners are considering integrating another service into their practice, you have to make sure anyone you allow to be associated with your brand or your clinic is reputable. See their work in real life, not just photographs of what they’ve done. Although, I also think you’ve got to give people a chance, particularly if they are just starting out and you know they are good at what they do. As they build their business, you get a return on that. Although Gemma is independent and works for herself, both at our clinic and elsewhere, she is part of our family. She gets on with everyone really well, and her services fit beautifully with ours. There is a natural crossover between the two, which benefits both parties.”
“ “
GEMMA
KENNELLY SAYS, “When I initially completed my training as a permanent makeup artist, I was advised by the training company that the best way to get started is to source multiple clinics to maximise client reach. So, I set about the task of trying to find clinics that would be interested in offering my services alongside their business. Approaching them by mail at first, I introduced myself and explained how what I do could be a great add-on to their business. It’s hard as a beginner to get people to believe in you and let you essentially tattoo their face. But with perseverance I managed to start building my business. I did work with some beauty salons to start with, as back then, there weren’t as many aesthetic clinics around. After gaining some experience I approached SDS and met with Dr Dolan. I really wanted to work with her and the team as their standards are so high. As a permanent makeup artist, I wanted to work with businesses that have the same professional approach to hygiene and safety standards, with a great reputation for the quality of their work, as that’s the kind of business I’m building. I’m happy to say I’ve been there ever since. I offer permanent makeup for brows, eyeliner and lip colour. I also offer microblading and permanent makeup removal. I absolutely love my job, and it’s extremely rewarding.
Permanent makeup is an aesthetic change to your face, it’s not a simple beauty treatment. Working in a highly respected clinic builds trust with your clientele. We share many crossover clients and patients, whereby I refer clients to the team at SDS and vice versa.
I take pride in what I do and having a base like SDS definitely enhances my business. I had worked previously in a high-end spa and am used to working to a high standard. So, SDS Rejuvenate is just perfect for me.”
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
” ”







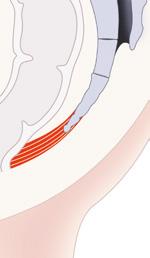
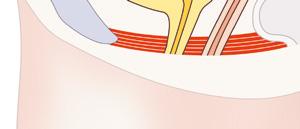


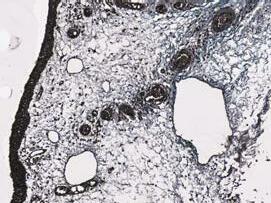
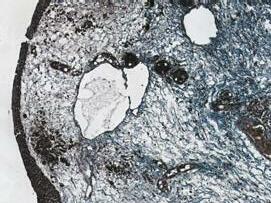
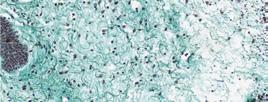
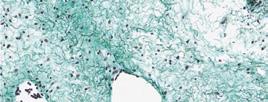
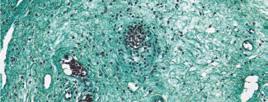
THE SOLUTION FOR INTIMATE HEALTH BY BTL *Data on file **Shortest Radio Frequency Intimate procedure ©2018 BTL Group of Companies. All rights reserved. BTL® and EMSELLA and HIFEM® are registered trademarks in the United States of America, the European Union and/or other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. Individual results may vary. 099-75EMUF360CRENGB100 BTL-Aesthetics_AD_Consulting-room_ENGB100 EMSELLA.COM | SALES@BTLNET.COM Restoration of collagen and elastin* Increasing blood fl ow
vaginal laxity and sexual
Histology after 3 TX* 1-WEEK FOLLOW-UP: elastin fibers 1-MONTH FOLLOW-UP: elastin fibers Histology after 3 TX* 1-WEEK FOLLOW-UP: collagen fibers 1-MONTH FOLLOW-UP: collagen fibers A frontal view of the pelvic floor muscles and bladder using ultrasound imaging. BEFORE: AFTER: BLADDER PELVIC FLOOR MUSCLES RELAXED AND LOOSENED PELVIC FLOOR BLADDER PELVIC FLOOR MUSCLES STIMULATED PELVIC FLOOR BY BTL EMSELLA REMAIN FULLY CLOTHED WALK-IN WALK-OUT PROCEDURE 95% PATIENT SATISFACTION* SHORTEST INTIMATE PROCEDURE** 360° TECHNOLOGY TREATMENT NON-SURGICAL NO DOWNTIME 95% 1 & 2 MARCH 2019 / LONDON SEE US AT
Muscle stimulation and strengthening Restoration of neuromuscular control* For urinary incontinence and pelvic floor muscles. For
dysfunction.
Working with a psychologist
Dr Rosh Ravindran, aesthetic practitioner and CEO of KLNIK in Cheshire, brought psychologist and body image specialist Kimberley Cairns on board when the clinic opened last year. She
DR ROSH RAVINDRAN

SAYS, “I
envisaged the concept of wellbeing and wellness being incorporated into KLNIK from its inception. As our personal wellness trainer, Kimberley is at the core of our ethos and acts in the pursuit of public health protection. Kimberley was introduced to me by my commercial director, who has worked with her over the years and knew that she would be a perfect fit. Working with her has broadened my knowledge and given me a vast understanding and compassionate approach in working with body image and its presenting difficulties.
The process begins with a bespoke, one-hour ‘Signature Consultation’ comprising 30 minutes with Kimberley, followed by 30 minutes with me. As a highly trained psychologist experienced in treating people in distress, Kimberley takes a full medical history, giving parity to physical and mental health. A confidential therapeutic narrative unfolds to allow a patient to share their concerns without judgement. This approach is not compulsory for patients; however, we use it as our default process and recommend it to all patients, as it works so well. Kimberley provides a safe, therapeutic space for patients to express their stories, which are often combined with significant emotional distress. Kimberley is competent in working with a range of psychological mood disturbances, including body dysmorphic disorder (BDD), which are often correlated to appearance anxiety that may create a conflict for aesthetic intervention. Recognising this fusion between our internal and external worlds, Kimberley and I developed an ‘Aesthetic Wellness Scale’ (AWS). Patients are invited to complete the AWS, which captures the impact of their concerns on their overall wellness. This is used to ensure the patient is guided on the wellness journey that suits their needs, and it may result in no aesthetic intervention.
If there was intervention, all our patients are brought back for timely reviews following their procedure, with the clinician and Kimberley, where we can identify if any problem has arisen. Kimberley effectively supports the patient’s individual wellness through various pathways. This includes more than 20 wellness modules, such as ‘Aesthetic Resilience’ and ‘Pain Management’. She has also led several safeguarding training sessions for our staff, which tackle difficult situations including treating vulnerable adults, BDD, patient confidentiality, professional boundaries. When integrating any new service, it is important to understand the implications it will have, and to thoroughly understand its capabilities. I’m absolutely delighted at the patient response to the personal wellness trainer initiative. It has proven to be a huge success, demonstrated by engagement and improvement of patient wellbeing outcomes.”
is employed by the clinic and works as a personal wellness trainer, supporting patients’ psychological wellbeing from their initial consultation and through a number of bespoke wellness modules.
KIMBERLEY
CAIRNS SAYS, “I have worked extensively with body image over the past 10 years in a range of settings, including intensive mental health services, education and crisis psychological intervention, where I worked closely with people psychologically and physically affected in the 2017 Manchester and London bombings.
This has shown me just how debilitating a negative body image can be. It really can affect all aspects of identity and the way a person relates to their social and physical environments. That being said, your body image also has the ability to uplift and transform your life and underpin your self-confidence.
There can be a lack of understanding of a patient’s motivation for treatment, and realistic outcomes are not always considered. From the outset, I was instantly committed to ensuring no psychological harm is done to those seeking aesthetics. A patient journey into aesthetics cannot be done without wellness; it is integral. Our consultation is robust and thorough, and allows the clinical team to measure objectively if there are any ‘red flags’. Saying ‘no’ as part of a consultation is to be expected as everybody is not automatically a suitable candidate for a treatment. It takes a lot of courage for some patients to share their private body talk and we are in a position of privilege and trust. Alternative pathways to wellness can be provided in the absence of aesthetic intervention. After the consultation, each patient is given a ‘Care Plan’, which may include a one-to-one personal wellness module. This involves ongoing consultation to address the patient’s concerns and continue their journey to wellbeing, both physically and psychologically. Modules are tailored to each individual, and can continue for two, three or six months, during which time I typically see the patient every week. I also often see patients before treatment for relaxation techniques to target pain relief or tackle needle phobia, for example. Unfortunately, we do see patients who have had negative, distressing and even traumatic experiences with aesthetic professionals during consultations and treatments at other clinics. I facilitate an ‘Aesthetic Resilience’ wellness module to address this specifically, to ensure we are reducing possible re-traumatisation to the patient seeking treatment. Embedding psychological wellbeing is fundamental to KLNIK’s vision of ensuring wellness is at the heart of what we do. It allows for a patient-centric, ethical service that builds patient satisfaction and patient retention while also improving industry standards.”
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
always
”
”
“
“
EMSCULPT is the only procedure to help both women and men burn fat, while toning the underlying muscle.
EMSCULPT is the only procedure to help both women and men burn fat, while toning the underlying muscle.
EMSCULPT is the only procedure to help both women and men burn fat, while toning the underlying muscle.

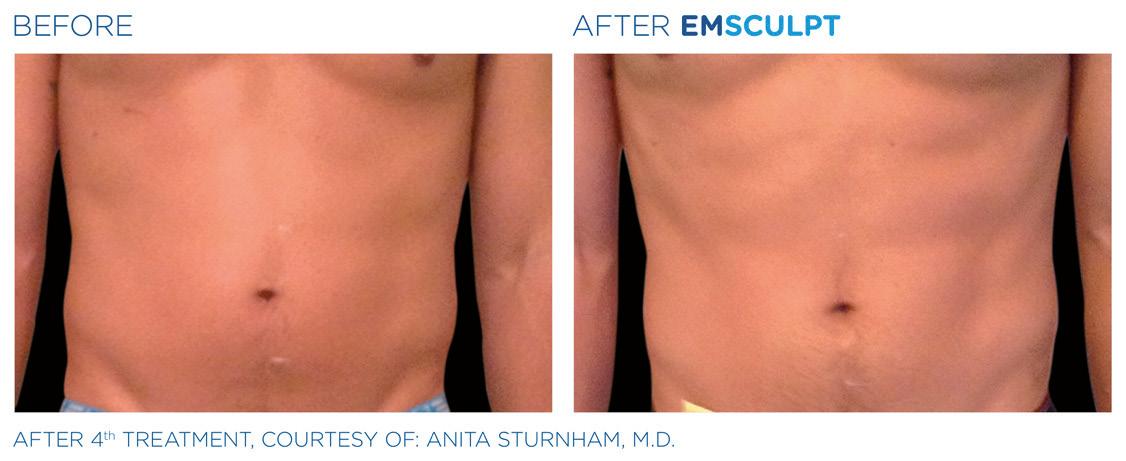

BUILD MUSCLE & BURN FAT SURGERY – NO DOWNTIME 799-79EMCLFFMA2EN100; Emsculpt_LF_FMA2_EN100 patient experience may vary. Patients shown in the B&A pictures are within +/- 5 lbs of their original weight unless specified. As with any medical procedure, ask your doctor if the Emsculpt procedure The Emsculpt procedure is U.S. FDA cleared for improvement of abdominal tone, strengthening of the abdominal muscles, development of firmer abdomen, strengthening, toning and firming ©2018 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® are registered trademarks in the United States of America, the European Union and/or other countries. The products, of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. EMSCULPT.COM | SALES@BTLNET.COM
VISIT EMSCULPT.COM FIND YOU PROVIDER BUILD MUSCLE & BURN FAT NO SURGERY – NO DOWNTIME 799-79EMCLFFMA2EN100; Emsculpt_LF_FMA2_EN100 Results and patient experience may vary. Patients shown in the B&A pictures are within +/- 5 lbs of their original weight unless specified. As with any medical procedure, ask your doctor if the Emsculpt procedure is right for you. The Emsculpt procedure is U.S. FDA cleared for improvement of abdominal tone, strengthening of the abdominal muscles, development of firmer abdomen, strengthening, toning and firming of buttocks. ©2018 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® are registered trademarks in the United States of America, the European Union and/or other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. EMSCULPT.COM | SALES@BTLNET.COM
SCULPT is the only procedure to help both women men burn fat, while toning the underlying muscle.
VISIT EMSCULPT.COM TO FIND YOU PROVIDER BUILD MUSCLE & BURN FAT NO SURGERY – NO DOWNTIME Results and patient experience may vary. Patients shown in the B&A pictures are within +/- 5 lbs of their original weight unless specified. As with any medical procedure, ask your doctor if the Emsculpt procedure is right for you. The Emsculpt procedure is U.S. FDA cleared for improvement of abdominal tone, strengthening of the abdominal muscles, development of firmer abdomen, strengthening, toning and firming of buttocks. ©2018 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® are registered trademarks in the United States of America, the European Union and/or other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. EMSCULPT.COM | SALES@BTLNET.COM
VISIT
.COM TO FIND YOU PROVIDER BUILD
NO SURGERY – NO DOWNTIME 799-79EMCLFFMA2EN100; Emsculpt_LF_FMA2_EN100 Results and patient experience may vary. Patients shown in the B&A pictures are within +/- 5 lbs of their original weight unless specified. As with any medical procedure, ask your doctor if the Emsculpt procedure is right for you. The Emsculpt procedure is U.S. FDA cleared for improvement of abdominal tone, strengthening of the abdominal muscles, development of firmer abdomen, strengthening, toning and firming of buttocks. ©2018 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® are registered trademarks in the United States of America, the European Union and/or other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. EMSCULPT.COM | SALES@BTLNET.COM
EMSCULPT
MUSCLE & BURN FAT
VISIT EMSCULPT.COM TO FIND YOU PROVIDER 1 & 2 MARCH 2019 / LONDON SEE US AT
Working with a nutritionist
Recognising the value of a healthy diet and nutritional support brings to overall health and wellbeing, aesthetic practitioner Dr Rita Rakus decided a nutrition professional would be a beneficial
DR RITA RAKUS SAYS, “Nutrition is a very important part of your general health and your skin health. If you have good nutrition, your skin will be in much better shape. Not only that, but we find that we get a better result from the treatments we perform. I’ve incorporated a nutritional aspect into my practice for the last five years or so. I knew of Karim through talking to colleagues and peers in the industry. He was at the forefront of nutrition and naturopathy, and I thought it would be a good opportunity to work with someone of that calibre.

When I see my patients, I suggest that we extend my advice to incorporate nutrition, and if they choose to, they can then book to see Karim for additional support. Generally speaking, they are all very interested in the concept. Karim comes into my clinic as a consultant on an ad-hoc basis, where we pay him per patient he sees. The service is offered to all patients who visit my clinic, regardless of what procedure or treatment they are coming for. We give details of Karim’s services in the consent forms and documents patients complete during their initial consultation, as well as in leaflets and newsletters, so patients let us know if they want to see him.
addition to her team. Naturopath and nutritionist Karim Chubin, who is based in Switzerland, visits Dr Rakus’s Knightsbridge clinic approximately once a month to see patients.
KARIM CHUBIN SAYS, “I began my private practice as a family naturopath almost 15 years ago. I still have a solo practice, but I wanted to join forces with a leading expert – such as Dr Rakus – who is at the cutting edge of aesthetic medicine using the ‘outsidein approach’. My interest is how you can support the individual by building health rather than fighting disease. From a naturopathic perspective, we have an ability to thrive but most of us don’t know what that means or looks like. Food and nutrition can have an impact on all the body’s systems: you start having more energy and better skin, recovering better, and feeling generally brighter and more vital.

Karim sees patients in my clinic in addition to running his own practice. Patients will have a consultation with him, and many will then undertake one of his programmes addressing their diet and nutrition. We also offer intravenous drips and supplements in combination with the nutrition consultations, so it works well together.
In terms of advice for integrating a new service, I would say go to all the conferences and lectures, find out what’s popular in the press, and talk to people in the industry to find out what will best suit your clinic.”
When a patient comes to me through Dr Rakus’s clinic, I meet them initially for up to a couple of hours. I really get to understand them by asking questions relating to their lifestyle and diet, as well as analysing their clinical signs, such as the shape of their body and where their body fat accumulates. I also focus on how our hormones interact with one another, deficiencies and stress. When we get to know our patients, we get to know where the weaker links are; for example, whether they are low in cortisol or serotonin. These are important elements that reveal invaluable data about a patient’s metabolic blueprint. I take that data and then run specific tests, using saliva, urine, stools and blood testing, to explore what’s happening inside the person’s gut to be able to personalise nutritional, herbal and essential oil compounds, before putting together a personalised plan for the patient. In the first four to six months following an initial appointment with a patient, I make myself very available and I commit to two or three remote conversations a week if they can’t come and see me in Dr Rakus’s practice. As I am based in Switzerland, I may fly to the UK for a day or two to visit a handful of individual patients. This may be in Dr Rakus’s clinic or at the patients’ own homes – either way, Dr Rakus is always informed. Dr Rakus and I have an agreement in place which takes into account both the patients she recommends to me, as well as the patients I bring to her clinic. Patients who see Dr Rakus come for non-invasive aesthetic treatments, and many are now realising that everything we are looking to solve on the outside comes from within. So, she will recommend my approach.”
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
“
The service is offered to all patients who visit my clinic
”
”
Many are now realising that everything we are looking to solve on the outside comes from within
“
Prebiotics and Probiotics in Topical Solutions
Dermatologist
discusses the use of pre and probiotics in cosmeceuticals
Dr Tiina Orasmae-Meder
Bacterial skin colonisation has long been of interest to dermatologists. The skin of an adult human is a complex ecosystem spread over a 1.8m2 area, which includes folds, invaginations and specific niches where the microbes’ living conditions can vary quite significantly. Most microorganisms living on the skin are harmless and, in some cases, they can perform certain functions without involving human genome.1
A shift in our understanding of the skin, moving on from the general consensus that ‘the skin is the biggest bodily organ providing barrier function by its specific structure and cell functions’ to ‘the skin is an ecosystem, a live biological complex of various microorganisms actively interacting with tissue cells’,1,7 helps us achieve a more profound understanding of how the skin functions are performed. This can allow us to discover new ways to prevent and treat various skin pathologies, including the ones that cause aesthetic discomfort. Skin colonisation is a completely normal process that refers to the growth of bacteria on the body when exposed to the environment, without causing infection. For decades, the gram-positive bacterium staphylococcus epidermidis was considered the major colonist of the skin but, with time, coryneform bacteria and micrococci were discovered.2 Further studies isolated fungi, primarily of the malassezia genus,3 and parasitic mites, primarily demodex folliculorum and demodex brevis,4 which are now viewed as part of normal flora. Newly developed research methods have allowed us to identify the skin’s microbiome, which describes the collective genome of microorganisms harboured by a human body. Microbiome is a very complex and diverse interaction among various microorganisms, including interspecies relations between viruses, fungi, bacteria and parasites.5
A qualitative identification of microorganisms was made possible by molecular techniques and it revolutionised our view of the skin.6 Microorganisms are identified by means of genome analysis based on sequence analysis of the 16S ribosomal RNA gene. This has revealed that most of skin microflora belongs to one of the four phyla: actinobacteria, firmicutes, bacteroidetes and proteobacteria; the same as in the gastrointestinal tract, but in different proportions. Both skin and gastrointestinal flora are uniform at the group level and diverse within the bacterial group.7
Understanding the skin microbiome
The microbiome forms a vital part of skin function. It makes skin not only an organ, but a unique and variable ecosystem, where host and microbiome interactions shape and influence skin health. This forms a skin immunity and helps to synthesise the variety of vital substances,
as well as create the structure of the epidermis.7
Skin colonisation starts at the moment of birth, when vaginal microflora is picked up by the baby moving through the birth canal,8 and continues in the lactation period.9 Most microorganisms living on the skin are harmless,1 while symbiotic microorganisms can protect the skin from pathogens and train billions of T-cells to respond to similarlymarked pathogenic flora.1
The skin is an ecosystem, rather than just an organ; it is a live biological complex of various microorganisms actively interacting with tissue cells. External factors, such as those discussed below, have a strong, and often negative, effect on the microbiome’s conditions and characteristics, reducing its diversity and richness, while decreasing the skin’s protective function. A number of studies confirm that physical injuries, stress, systemic and topical disease therapy can affect the skin’s microbiome and the pathogeny of certain microbes.10,11
Frequent washing disrupts the skin’s barrier function and brings about significant negative changes to the microbiome, increasing the risk of infections and dermatoses.12 Evidence points to the potential effect of hygiene solutions and skincare (including makeup)13 on the skin microbiome. For example, regular use of acid-containing products can affect the pH of the skin, disturbing the stability of the microbiome. This can be beneficial in some case like an acne patient, when Propionibacterium acnes is overgrown and the acidic environment helps to slow down the pathological process. However, it can be negative in cases of healthy skin with a healthy microbiome; when pH decreases, it can make the skin more vulnerable, affecting the staphylococcus epidermidis and other beneficial bacterial communities.14
As well as this, excessive use of antibiotics, both systemic and topical, always affects skin, as well as the gut microflora and can lead to the development of antibiotic-resistant bacterial strains, presenting a global challenge to the infectious disease therapy.15,16
Knowing that the skin’s functions are largely performed by a complex of mutually-active cells and a live biological conglomerate of microorganisms, we are faced with a necessity to reconsider our treatment of many skin diseases. We may be able to correct the skin’s condition (such as psoriasis, acne, atopic dermatitis) by changing the microbiome and actively restoring the balance of microorganisms, which make up the skin’s healthy flora.17
A recent paper by Chen et al. highlighted the fact that there is a scientific consensus that microbiome is important and affects health and disease. However, authors also pointed out that the extent of its affect is debated and strong evidence is limited. Furthermore, it is not exactly known what defines a ‘healthy’ microbiome; Chen et
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
al. suggests it’s possible that there isn’t one or there may be several profiles.18 The following information in this article will explore how we can change the skin microbiome to promote healthy flora through the introduction of topical prebiotics and probiotics.
The introduction of prebiotics and probiotics
In recent years, medical gastroenterology turned to the treatment strategies aimed at gut microbiome and underwent a notable change in the approach to antibiotics and other antibacterial solutions.19 The extrapolation of such methods to aesthetic skincare has demonstrated favourable preliminary results.20,21 Agents that can affect the microbiome are probiotics and prebiotics. Probiotics are cultures of live microorganisms found in healthy microbiome.22 Prebiotics are various agents that can serve as a nutrient medium for commensal and symbiotic microbes, increasing their growth and promoting successful colonisation.22 Both probiotics and prebiotics can be applied topically and taken orally.23 In 2010, Arck et al. put forward a theory of gut-brain-skin axis;24 which supported other research suggesting that probiotics and prebiotics taken orally can have a beneficial effect on the skin.25 In addition to oral intake, new emollients and daily care solutions have been described, containing bacterial lysates, particularly vitreoscilla filiformis and lactobacillus;26,27,28 these solutions were offered primarily to patients with atopic dermatitis and acne.29,30 For the purpose of this article, only topical application of prebiotics and probiotics will be explored.
Topical prebiotics and probiotics
Today, prebiotic and probiotic-based cosmetic ingredients are fairly common, both in professional and home-use cosmetic solutions. Skincare with probiotic and prebiotics were previously offered to care for sensitive or damaged skin; however, numerous studies have shown that prebiotic and probiotic therapy can be universal and generally beneficial for the skin, and even provide an antiageing effect.31,32,33
The use of prebiotics and probiotics in topical formulations has also been applied in dermatology, primarily in the therapy of atopic
Commercial name Manufacturer
BioEcolia Solabia
Biolin GOVA
PreBio Defence Vantage
Yogurtene Balance Givaudan
Seboclear-MP RAHN
Relipidium BASF
ALGACTIV BioSKN Greenaltech
Rice Phytmic Greenphyt
preBIULIN FOS GOVA
Fensebiome Peptide Solution Lipotec
dermatitis and acne.34 Encouraging results have been obtained with the use of cream containing the probiotic bifidobacterium longum on patients with increased skin reactivity; researchers noted a pronounced reduction of skin sensitivity and the skin’s increased resistance to physical and chemical aggression.35
Prebiotic and probiotic use topically excludes simultaneous use of antibacterial solutions such as alcohol, salicylic acid, triclosan, benzoyl peroxide or topical antibiotics.36 The elimination of staphylococcus epidermidis in the course of topical antibiotic therapy leads to a sharp drop in the number of antimicrobial peptides and the increased colonisation by staphylococcus aureus and other potential pathogens, which eventually results in dysbiosis and inflammation.37 Any solutions containing alcohol or salicylic acid and non-selective bacterial drugs will, most likely, negate the effect of prebiotic and probiotic therapy.38
Prebiotics in topicals
Prebiotics are relatively easy to introduce, as the agents with proven prebiotic activity are usually stable enough and easy to incorporate into a cosmetic formulation, while also being affordable and easily manufacturable. There are several studies suggesting the efficacy of prebiotics for skin health, although as previously mentioned they do have limitations.34,39,40,41 One study investigated the effect of α-Glucan on skin microflora, staphylococcus. Two strains of staphylococcus were incubated in a culture medium containing a carbonated substrate (α-Glucan vs glucose), at a concentration of 0.5%. After incubating for 24 hours, it was observed that α-Glucan stimulated the growth of beneficial resident flora, and the authors concluded that a product containing this material would have a potential benefit for skin health.42
Prebiotics present a much easier-to-use solution compared to probiotics, as the agents with proven prebiotic activity are usually stable enough, easy to incorporate into a cosmetic formulation, as well as being affordable and easy to manufacture.43
Table 1 provides an overview of some of the most popular prebiotic ingredients, which are useful for practitioners who are unsure of what ingredients are actually classified as a prebiotic. They can be
International Nomenclature of Cosmetic Ingredients (INCI)
Alpha-glucan oligosaccharide42
Inulin (and) Alpha-glucan oligosaccharide
Mannitol (and) cellulose (and) hydroxypropyl methyl cellulose (and) inulin (and) yeast beta glucan (and) undaria pinnatifida extract
Inulin (and) yogurt powder
Aqua (and) alcohol denat (and) sodium salicylate (and) plantago lanceolata leaf extract (and) mahonia aquifolium root extract
Hydrolsyed yeast protein (and) butylene glycol (and) pentylene glycol
Plankton extract (and) aqua
Oryza sativa extract
Inulin (and) fructose
Water (and) acetyl heptapeptide-4 (and) caprylyl glycol
ACTIBIOME GPA Codif Water (and) seawater (and) glycerin (and) laminaria digitata extract (and) Phenethyl alcohol (and) chlorella vulgaris extract (and) saccharide isomerate
Salixin Organic Extract 800 NP Salixin A/S
Pentavitin DSM
SYN-UP DSM
Revivyl Givaudan
Table 1: Types of prebiotic ingredients commonly used in topical formulations
Salix purpurea bark extract
Saccharide isomerate (and) aqua (and) citric acid (and) sodium citrate
Benzylsulfonyl D-Seryl Homophenylalanine Aminobenzamide Acetate45
Propanediol (and) orobanche rapum extract42
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
included in all kinds of cosmetic products, from cleansers to skincare or makeup formulations.42,44
Probiotics in topicals
The use of probiotics in topical formulations and for the treatment of skin conditions has been described in the literature; although, many of these are in vitro, and more detailed research should be performed in order to showcase the efficacy and safety of probiotics.33,46,47 Authors of one in vitro study concluded that many of the tested probiotics prevented biofilm formation, suggesting that they could be used as a complement to conventional therapies in treating skin disorders.46
The topical application of probiotics is problematic; the key difficulty being the preservation of live bacterial culture in a product for many months – only living microorganisms can colonise the skin.48 Microcapsulation technology is most often used for topical applications; however, it can be expensive and difficult to guarantee the standard shelf life of 36 and 12 months.49 It is also not an easy task to determine which bacteria are necessary to correct particular aesthetic concerns, and, most importantly, the baseline of healthy microbiome is not yet established, as the individual variability of microflora is too extensive. Other complicating factors are the patient’s general skin condition, their lifestyle and, most importantly, the use of cosmetic and hygienic solutions that can hinder the re-colonisation and restoration of healthy microbiome during the active therapy period.50
The practical use of the probiotic fermented bacterial lysates is less complicated than many forms. Lysates are obtained when beneficial bacteria cultures grow in an enriched medium, and the resulting mixture, consisting mostly of cytoplasmic gel, fragments of membranes and organelles, is used as an active ingredient.32 Bacterial lysates enhance the growth of commensal flora and generally act as prebiotics, even though technically they are closer to probiotics.51 Lactococcus ferment lysate is perhaps the most used – it relieves irritated and inflamed skin and is commonly used in sensitive skincare.35 Bacillus ferment, a lysate of Bacillus subtilis, is often used in exfoliators.52
Other considerations of probiotics
While prebiotics more or less have a universal effect, enhancing the growth of commensal flora and suppressing that of pathogenic or conditionally pathogenic, the use of probiotics implies successful colonisation of the skin by external bacteria, which isn’t always achievable. The study of probiotics is hindered by the fact that today’s
experimental models of human cell cultures are sterile and not suitable for bacterial interaction. Another problem that manufacturers would face with probiotics is the registration of such skincare products. According to EU legislation concerning the production and quality of cosmetic solutions, a required microbiological test must show no signs of bacterial contamination, otherwise it won’t be released to the market.53 Still, lactobacillus culture (a probiotic) is commonly explored for topical use for the treatment of the periodontal inflammation, second-degree burn wounds, acne and atopic dermatitis54 and the US Food and Drug Administration (FDA) classes it as Generally Regarded as Safe (GRAS).55
Conclusion
The development of microbiome-friendly skincare is an emerging area and has only just begun; therefore many questions remain unanswered with limitations to the scientific literature available. It is obvious that any development in this area will require certain changes in legislation, amendments and elaborations in marketing and claim regulations. The research base for prebiotics and probiotics is still insufficient and we are only just beginning to accumulate relevant knowledge. There is a need of more scientific literature to support the efficacy of such skincare and to identify its limitations.
Disclosure: Dr Tiina Orasmae-Meder is the founder of skincare range Meder Beauty Science, which contains prebiotics and probiotics in some products.

Dr Tiina Orasmae-Meder completed her postgraduate studies at St. Petersburg Medical Academy in Russia, where she worked as a teaching and clinical research assistant for the dermatology and plastic surgery department. Since then, she has gained more than 20 years’ experience in the professional beauty industry. Dr OrasmaeMeder is the founder of Meder Beauty Science and has worked for numerous professional brands on their product development.
REFERENCES
1. Nakamizo S, Egawa G, et al. Commensal bacteria and cutaneous immunity. Semin Immunopathol. 2015 Jan;37(1):73-80. Epub 2014 Oct 18
2. Roth RR, James WD Annu, Microbial ecology of the skin. Rev Microbiol. 1988; 42():441-64
3. Gao Z, Perez-Perez GI, Chen Y, Quantitation of major human cutaneous bacterial and fungal populations, Blaser MJ J Clin Microbiol. 2010 Oct; 48(10):3575-81.7
4. Elston DM, Demodex mites: facts and controversies. Clin Dermatol. 2010 Sep-Oct; 28(5):502-4.
5. Zilber-Rosenberg I, Rosenberg E. Role of microorganisms in the evolution of animals and plants: the hologenome theory of evolution. FEMS Microbiol Rev 2008; 32: 723–73
6. Davies CE, Wilson MJ, et al. Use of molecular techniques to study microbial diversity in the skin: chronic wounds reevaluated. Wound Repair Regen 2001 Sep-Oct; 9(5):332-40.
7. Elizabeth A. Grice and Julia A. Segre The skin microbiome, Nat Rev Microbiol. 2011 Apr; 9(4): 244–253.
8. Capone KA, Dowd SE, Stamatas GN, Nikolovski J. Diversity of the human skin microbiome early in life. J Invest Dermatol 2011; 131: 2026–2032
9. Latuga MS, Stuebe A, Seed PC. A review of the source and function of microbiota in breast milk. Semin Reprod Med 2014; 32:68–73.
10. Holmes CJ, Plichta JK, et al. Dynamic role of host stress responses in modulating the cutaneous microbiome: implications for wound healing and infection. Adv Wound Care (New Rochelle) 2015; 4:24–37.
11. Zapata HJ, Quagliarello VJ. The microbiota and microbiome in aging: potential implications in health and age-related diseases. J Am Geriatr Soc 2015; 63: 776–781
12. LA Rocha, EBL Ferreira de Almeida, PP Gontijo Filho, Changes in hands microbiota associated with skin damage because of hand hygiene procedures on the health care workers, Am J Infect Control, 2009
13. Staudinger T, Pipal A, Redl B. Molecular analysis of the prevalent microbiota of human male and female forehead skin compared to forearm skin and the influence of make-up. J Appl Microbiol 2011; 110: 1381–1389.
14. Studinger T, Pipal A, Redl B, Molecular analysis of the prevalent microbiota of human male and female forehead skin compared to forearm skin and the influence of make-up. J Appl Microbiol, (2011) 110:1381–1389.
15. A Langdon, N Crook, G Dantas, The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation, Genome Med, 2016.
16. MT Leccia, N Auffret, et al., Topical acne treatments in Europe and the issue of antimicrobial resistance, Eur Acad Dermatol Venereol, 2015
17. Belkaid Y, Tamoutounour S. The influence of skin microorganisms on cutaneous immunity. Nat Rev Immunol. 2016;16:353 366.
18. Ma Y, Chen H, Lan C, Ren J. Help, hope and hype: ethical considerations of human microbiome research and applications. Protein Cell. 2018;9(5):404-415.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Numerous studies have shown that prebiotic and probiotic therapy can be universal and generally beneficial for the skin, and even provide an antiageing effect
Award winning, flawless finish, breathable liquid foundations.
Unique Oxygenating Foundations and Moisturisers
Oxygenating Foundation I SPF 25+
Containing the patented Ceravitae™ Complex it stimulates skin cell production and helps the healing process following most procedures. Soothes, heals and protects damaged skin thanks to its oxygen-enriched, natural components making it virtually a second skin. Available in 14 shades.
Oxygenating Foundation Acne Control I SPF 25+
This unique and revolutionary formula was three years in the making! Since having identified the need for a treatment foundation we started working hard to create the perfect acne control foundation that is also an oxygenating treatment foundation developed to simultaneously clear and conceal the frustrating conditions of acne.
NEW Oxygenating Hydro-Matrix
Much more than a simple moisturiser, this hydrating and healing post-treatment behaves like a ‘second skin’, containing Oxygenetix’s patent formula Ceravitae™, that allows oxygen to penetrate the skin and reinforce the natural healing process. It also beautifully primes the skin ready for the application of the Oxygenetix Oxygenating Foundation. Available in 30ml, 50ml and 100ml.
Exclusive to
Available to order now
The active ingredient of NatraSan Skin is HOCI or hypochlorous acid, a highly effective weak acid that is naturally present in the human immune system.
Ingredients are water, salt and hypochlorous only. Contains no sodium hypochlorite, phosphoric acid or alcohol.
NatraSan Skin delivers ultimate levels of skin disinfection and is powerfully bactericidal, virucidal, fungicidal and sporicidal.

NatraSan Skin is also fast acting and kills pathogens on contact. Respects skin barrier and non-irritant.
The shelf life is 18 months (even after opening) Available in 500ml for clinic use and 100ml for patient use.
Recognised as one of the Leading UK Suppliers to the Aesthetic Medicine Professional Unit 3 Compass Point, Ensign Way Hamble, Southampton, Hampshire SO31 4RA
aestheticsjournal.com
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics
19. S Nishijima, W Suda, et al, The gut microbiome of healthy Japanese and its microbial and functional uniqueness, DNA Res, 2016 20. Gueniche A, Phillippe D, et al, Castiel-Higounenc I (2014) Randomised double-blind placebocontrolled properties and potential biotechnological applications. Current Pharmaceutical Biotechnology, 2009, 10: 38-61 38. Al-Ghazzewi FH Tester RF, Impact of prebiotics and probiotics on skin health, Benef Microbes. 2014
E: info@magroup T: 02380 676733 www.magroup.co.uk
that work like a virtual breathable second skin
n FDA-cleared1 and EU CE mark certified2
n Non-surgical, multiple treatment-indicated areas3











n Scientifically proven to stimulate new collagen growth3


n Lift that can last over a year with minimal downtime4,5
n Customised treatment with DeepSEE® visualisation technology (MFU-V)3,6
ultrasound
the full face, neck and décolletage with micro-focused
LIFT, SCULPT & TIGHTEN
Before After 3 Months Before After 3 Months After 6 Months After 6 Months
51 Before After 3 Months Before After 3 Months
39 After 6 Months After 6 Months All treatments were carried out by The Cosmetic Skin Clinic. Disclaimer: Please be aware that results and benefits may vary from patient to patient taking into consideration factors such as age, lifestyle and medical history. References: 1. http://www.accessdata.fda.gov/cdrh_docs/pdf13/k134032.pdf Accessed August 2018. 2. CE Certificate 3808396CE01, DEKRA March 2017. 3. Ulthera System Instructions for Use, 1001393IFU Rev L. 4. Sasaki GH & Tevez A. Journal of Cosmetics, Dermatological Sciences and _Applications. 2012; 2: 108-116. 5. Brobst RW, et al. Facial Plast Surg Clin N Am. 2014;22:191-202. 6. Fabi SG and Goldman MP. Dermatol Surg. 2014;40;569. M-ULT-UKI-0398 Date of Preparation September 2018 Choose the authentic Ultherapy® treatment ultherapy.co.uk
Tina, Stylist/Makeup Artist, Age
Amale, Actress, Age
Treating Lips Using a Cannula
Aesthetic nurse prescriber Jackie Partridge shares her tips and technique advice for treating the perioral area using a cannula
Lips are one of the most important features of the face and youthful, plump, full lips are something many people aspire to Lip augmentation has gained momentum in recent years and is one of the most popular facial volumisation treatments.1 Successful, natural lip augmentation is often about looking at the proportions of a patient’s face to determine which shape best complements their other facial features. There is no single technique that suits every lip, and each practitioner will have their own unique treatment approach to achieve the desired results. Many practitioners ask me whether I prefer to augment the perioral area using a needle or cannula. My answer is always that the decision depends on what is presented clinically, the area I am working on and the outcome I am looking for. However, the use of a cannula in this area does present its advantages.
Benefits of cannulas in the perioral area
Traditionally, dermal fillers were injected using sharp tip needles. I like to use Restylane Kysse in the lips and it comes pre-packaged with two needles, as do other dermal filler brands such as Juvéderm, but using a blunt-tipped cannula for the injection of dermal filler in the lip has many benefits.

Treatment with a cannula has been found to result in significantly fewer bruises and be less painful, so is gaining popularity with patients.2,3 A needle gives several sharp pricks, rather than just one or two pricks with a cannula, so this is very appealing for patients and increases patient retention rates; those who are less likely to bruise are more satisfied with their overall treatment and experience.2 There is also less downtime associated, meaning patients can return to work sooner. The perioral area is highly vascular and the labial artery has several branches coming off it, which makes it more prone to bruising than other areas of the face. In patients who are more likely to bruise or swell, using a cannula has been shown to lessen this risk.2 According to Manhattan-
based dermatologist Dr Anne Chapas, who was an investigator for a mid-face cannula study in the US, none of the 60 patients treated experienced arterial occlusion and the cannula reduced postinjection bruising and swelling.4 The safety profile of cannulas is considered higher than needles because the blunt end is more likely to glide past a vessel or a ligament rather than penetrate it, resulting in less trauma and bruising.5 The facial arterial system represents a danger zone for filler injections, as intra-arterial injection can potentially lead to widespread necrosis and even blindness.6 Minimising the risk of intra-arterial injection of fillers is therefore of paramount importance. There are also far fewer entry points with a cannula. By making one entry point lateral to the corner of the mouth, manoeuvrability is improved, and you can treat the whole perioral area, including the lips, the nasolabial folds and the oral commissures. By treating all these areas from one access point, the risk of bleeding, bruising and infection is reduced because there are less breaks in the skin.5 Additionally, when using a cannula, the practitioner can feel resistance from the structures that the cannula passes through. This enables you to judge when and how to apply pressure, and to clearly determine the direction of the cannula, as well as indicating which plane you are working in. If you are too deep, you will be injecting into subcutaneous fat and the product will not give as much projection.7
Advice for successful injections
A thorough understanding of the anatomy is essential for any successful aesthetic procedure. When treating the perioral area, an awareness of position and depth of the inferior and superior labial arteries is vital. However, every patient has anatomical variations, so to help me establish the position of the arteries before treatment, I always palpate the labial arteries before injecting. As with any procedure that breaks the skin’s surface, dermal fillers present a risk of infection, so an aseptic technique must be adopted. The mouth presents a higher risk of bacterial load than other areas on the face, so it is important to make sure that the field you are working in is as clean as possible.8 Do not drag the cannula across hair or other unclean surfaces as this can lead to contamination. The entry point is usually lateral to the corners of the mouth and I inject into the deep dermis. Each plane feels different; fat is very smooth, whereas more superficial planes feel slightly more resistant in places. You know that you’re in the right plane because it should feel effortless, with no pain or at the very most, slight discomfort for the patient.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
You know that you’re in the right plane because it should feel effortless, with no pain or at the very most, slight discomfort for the patient
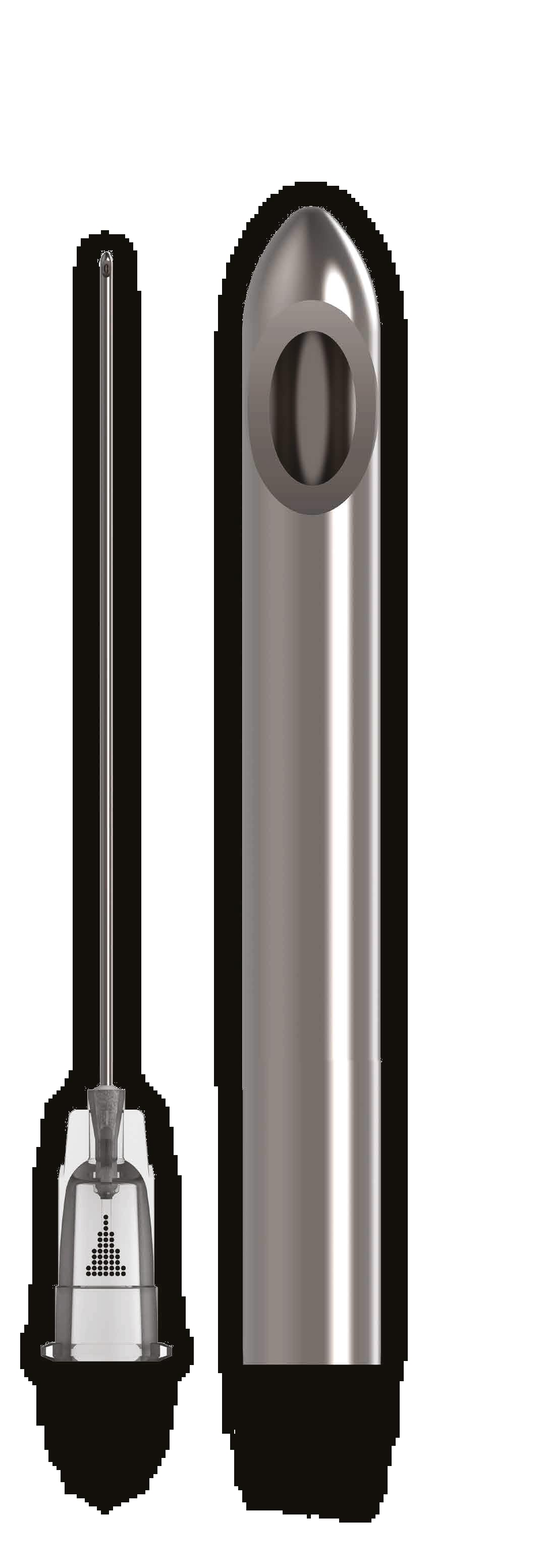
1 & 2 MARCH 2019 LONDON SEE US AT
Choosing a cannula
It is vital that the correct size and length of cannula is used. A cannula that is too fine will behave just like a needle, which can give the practitioner a false sense of security and could result in vessel penetration.10 I don’t use a cannula that is narrower than 25 gauge, and this is my standard approach for all areas. My length of choice is a 38mm cannula, which is slightly longer than a standard needle at around half an inch;9 however, I still feel that I can control it in a safe way. I find that a 25 gauge 38mm is less likely to puncture a vessel and is a good length to reach to the midline of the perioral area or lip from each side when entering from the side of the mouth. It is important to select the size of the access needle carefully – it must be the appropriate size to break the skin at the access point and should be a slightly larger gauge than the cannula; some companies supply both the cannula and the appropriate needle together. The length of the cannula doesn’t impact safety greatly, as its blunt tip coupled with a greater flexibility allows the cannula to glide under the dermis with less trauma.10 I would say that the most important factor for me is the confidence and the experience of the practitioner. However, if the cannula is too long it can change the plane into which you inject as it travels through the tissue. There are a variety of different brands of cannula on the market, so it is important that practitioners are knowledgeable about the brand they are using. Some brands have the bevel on the side of the cannula, while others have the bevel at the very end of the tip. The bevel should be in an upright position when injecting as the product will sit more superficially, ensuring that you are getting the benefit of the lift of the product within the dermis or subcutaneous tissue.
Drawbacks of cannula use
Although cannula injection methods offer many benefits to both patients and practitioners when treating the perioral area, there are still cases when needles are the best option of delivery. I find that I have more precision and control with a needle; however, one cadaver study by Humzah et al, which looked at the differences between needles and cannulas, concluded that the cannula showed more precision in the placement of product and a lower risk of intra-arterial injection complications.6 It’s my belief that as long as the plane that the cannula is positioned in is correct, needles and cannulas behave in the same way. In my hands, I find that needles are more precise than cannulas because when using cannulas, due to the longer length and flexibility, you are able to place a product up to 90mm away from the insertion point in some cases, which perhaps allows for a change in depth. It is also important to bear in mind the cost of cannulas. A cannula is around £7, while a needle will come free when purchasing the
product. From a business point of view, practitioners need to remember to think about costs when putting together their treatment pricing structure. However, the patients’ needs and the safety benefits of using a cannula or a needle should always be at the forefront of our priorities.
Conclusion
There will always be a place for injection methods using both cannula and needle depending on the technique, product and patient choice. It is well known that many patients appreciate the benefits of the cannula delivery method since there are generally fewer associated risks, less bruising and reduced downtime than with a sharp needle.6
It is essential that practitioners equip themselves with the essential anatomical knowledge, as well as familiarity with product types and injection techniques. This, combined with a clear examination and a thorough patient consultation, will determine the most appropriate modality of treatment to achieve the best aesthetic goals.
Jackie Partridge is an award-winning independent aesthetic nurse prescriber and is the clinical director and owner of Dermal Clinic in Edinburgh. Partridge is a KOL and member of the Galderma Global Nurse Faculty and works with the Scottish Government, representing the BACN, to strive for improvements in standards. Partridge has recently completed a Master’s in Aesthetic Medicine at Northumbria University.

REFERENCES
1. American Society of Plastic Surgeons, Complete Plastic Surgery Statistics Report (American Society of Plastic Surgeons, 2017), p7. <https://www.plasticsurgery.org/news/plastic-surgery-statistics>
2. Amit Luthra, ‘Shaping lips with fillers’, Journal of Cutaneous Aesthetic Surgery, 8 (2015) p.139-142. <http:// www.jcasonline.com/article.asp?issn=0974-2077;year=2015;volume=8;issue=3;spage=139;epage=142; aulast=Luthra>


3. James Fulton, Caroline Caperton, Susan Weinkle and Luc Dewandre, ‘Filler Injections With the Blunt-Tip Microcannula’, Journal of Drugs in Dermatology, 11 (2012) <http://jddonline.com/articles/dermatology/ S1545961612P1098X>
4. Lisette Hilton, ‘FDA approves HA filler for midface via cannula injection’ (The Aesthetic Channel, 2018) <https://www.aestheticchannel.com/facial-contouring/fda-approves-ha-filler-midface-cannula-injection>
5. Sabine Zenker, ‘Indication Specific Cannula Treatment’, Journal of Pigmentary Disorders, 3 (2016) < <https://www.omicsonline.org/open-access/indication-specific-cannula-treatment-2376-0427-1000247. pdf>
6. Jani A J van Loghem, Dalvi Humzah and Martina Kerscher, ‘Cannula Versus Sharp Needle for Placement of Soft Tissue Fillers: An Observational Cadaver Study’, Aesthetic Surgery Journal, 38 (2016).
7. Giovanni Salti and Raffaele Rauso, ‘Facial Rejuvenation with Fillers: The Dual Plane Technique’, Journal of Cutaneous Aesthetic Surgery, 8 (2015) p. 127-133.
8. David Funt and Tatjana Pavicic, ‘Dermal fillers in aesthetics: an overview of adverse events and treatment approaches’, Clinical, Cosmetic and Investigational Dermatology, 6 (2013) <https://www.ncbi. nlm.nih.gov/pmc/articles/PMC3865975/> [Accessed 21 January 2019](p. 295-316).
9. Nicole Galan, ‘Choosing the Best Syringe and Needle Size for an Injection’ (Verywell health, 2018) <https://www.verywellhealth.com/how-to-select-the-correct-needle-size-for-an-injection-2616536>
10. Carlos Roberto Antonio, João Roberto Antonio, Maria Gabriela Gonçalves Coura, Estela Ferreira David, Fernanda Tomé Alves and Ivan Rollemberg, ‘Microcannulas in dermatology specifications’, Surgery Cosmetic Dermatology, 3 (2015), (p. 241-244)
WANT TO LEARN MORE?
Jackie Partridge is performing a lip augmentation demonstration at the Anatomy of the Smile webinar hosted on the Aesthetics journal website on March 11 from 7-9pm.
The webinar is sponsored by Galderma For more information, go to www.aestheticsjournal.com/news/galderma-webinar-details
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Before After
Figure 1: Patient before and after lip augmentation. The patient was treated with 1ml of Restylane Kysse using a 25 gauge 38mm cannula.

Clinical Training You’re committed to being the best in your field. So are we. There’s never been a better time to invest with Cynosure Visit www.cynosureuk.com or call 01628 5222 52. 98% of customers felt ‘very confident’ after training Cynosure’s dedicated clinical team offer outstanding customer training as exemplified by the following stats. Cynosure’s dedicated team of engineers offer exceptional support to ensure your devices are well maintained and as powerful as ever. Percentage based on 462 customers surveyed. 93% of customers said our clinical trainers' knowledge was ‘Excellent’ or ‘Very Good’. 94% of customers said that our practical training was ‘Excellent’ or ‘Very Good’. 98% 93% 94% 92% first time fix rate All contract customers are attended within 2 working days Weekend support offered If on a service contract, unlimited clinical training Service 92%
Utilising Fat-dissolving Injections
Injectable methods for non-surgical fat reduction, such as mesotherapy or Lipodissolve1 have been researched for over two decades. After initial enthusiasm, these fat-reduction therapies lost popularity due to lack of controlled studies and unwanted side effects.2 Recently, however, the availability of new formulations, most of them based on deoxycholic acid, has produced an increase in their demand, particularly following the US Food and Drug Administration’s (FDA) approval of one of them in 2015, ATX-101, for reduction of submental fat.3
History of fat-dissolving injections
At the end of the 1980s, an Italian doctor began to use a mesotherapy preparation containing phosphatidylcholine (PC) for the infiltration of xanthelasmas. He achieved satisfactory results and presented his method at the 5th International Mesotherapy Congress in Paris in 1988.4 In 1995, Brazilian dermatologist Dr Patricia Rittes treated her lower eye pads with injections of PC (although this is not advised, as she performed the treatment herself). The product Dr Rittes used was Lipostabil Endovena, which was marketed in Europe, South America and South Africa and was originally developed to treat fat embolism after trauma.2 The active principle was PC with a small percentage of sodium deoxycholate (SDC) to act as a detergent, as PC is not water soluble.7 She reported good results, so started to treat patients with unwanted fat deposits, publishing her results in a 2001 peer-reviewed journal.5 This was followed by articles in popular magazines in the US6 and other countries, focusing on people who succeeded in having fat deposits, such as cellulite, back rolls and lower eyelid fat herniation, eliminated with ‘miraculous’ injections. However, despite its rampant use in Brazil, Lipostabil was banned for cosmetic use in December 2002 by ANVISA, the Brazilian equivalent to the FDA in the US. The FDA and the Medicines and Healthcare products Regulatory Agency (MHRA) in the UK subsequently issued strong warnings against its cosmetic use as there were no clinical trials supporting its efficacy.8,9
Fat-dissolving agents
Sodium deoxycholate
The description by Rotunda et al.10 and other authors11-12 on the pharmacologic effect of SDC originated an increased interest in this substance, and subsequently, a range of products became available in the market. SDC is a secondary bile acid and therefore, its role in the bile is to emulsify the fat to ease its digestion. SDC acts as a detergent, resulting in compromising the phospholipid bilayer and leading to cell lysis. SDC behaves as an ionic detergent, disrupting the cellular membrane by introducing their polar hydroxyl groups into the hydrophobic core of the bilayer. This will lead to solubilisation of the membrane-associated proteins, and the cell membrane finally collapses into mixed micelles of phospholipids and detergent molecules.12 However, one of the main problems with SDC is the lack of specificity regarding the detergent activity. In the past, aqueous solutions of SDC were used through mesotherapy, and a number of
cases of skin necrosis were reported.13 In vitro experiments revealed that mature adipocytes were more resistant to detergent-induced cellular lysis than other cell types, therefore raising concerns about the safety of using this substance in the fat compartment.14 Further studies showed that SDC is more effective if there is a lower protein content in the cell, as is the case for adipocytes (less than 5% protein content).15 One of the first SDC-containing products available in the EU market was a galactose-buffered, gelatinous substance known as Motolese’s solution or Aqualyx.16 It was released in 2008 and became available in the UK in 2014. Aqualyx was originally CE marked as a Class III medical device to be used as an adjuvant to ultrasound cavitation therapy;27 although, this CE mark is currently under review for non-medical reasons that are beyond the remit of this article, and therefore its use is regarded as off-label.
Other brands have also become available in the UK market, such as DesoBody/DesoFace or Celluform and Celluform Plus. They all have SDC in common, and differ in the concentration of SDC present per millilitre and/or the association with other substances.
The product that really has raised the awareness about these group of fat-dissolving agents is ATX-101, known as Kybella in the US Market and Belkyra in Canada and the EU.17 It was approved by the FDA as a first-in-class injectable drug for improvement in appearance of moderate to severe convexity or fullness associated with submental class.2 Its efficacy and clinical safety has been confirmed in four large Phase 3 trials, two conducted in Europe and two in the US and Canada.18-19 Although it is not yet available in the UK (at the time of publication), the experience in other European countries seems to be promising.
Phosphatidylcholine
In its early days, PC was thought to be the active fat-melting agent present in Lipostabil; however, its role on PC is currently unclear. PC is the most important phospholipid in the human body, and between 40-50% of cell membranes are composed of PC so it provides the main structural support.20 It is a dipolar ion with both lipophilic and hydrophilic properties, which makes it a natural emulsifier with the ability to emulsify blood lipids. It can reduce cholesterol levels to some extent, and its intravenous usage may prevent fat embolism in trauma patients or after major orthopaedic surgery.21 Although there have been several hypotheses of how PC acts as a fat dissolvent (one being that due to its emulsifying properties it can dissolve triglycerides and transport them), none of them actually explains it.12 It has also been hypothesised that the presence of PC within SDC-containing injectables help to control the detergent action of SDC.9 Another study suggests that the association of PC and SDC may regulate the expression of lipolysisrelated factors, and therefore, stimulate lipolysis.22 One of the products currently available has PC in the formulation (Celluform).
Other ingredients
Other active ingredients have been also described as fat-dissolving agents or as adjuvants to the action of SDC. L-carnitine is known to promote the transportation of fatty acids into the mitochondrial matrix of the adipocyte during the breakdown of lipids. It is available as a nutritional supplement but is present in some SDC-containing products (Sagoni Melt, which is not currently available in the UK) and mesotherapy formulations.23 Caffeine helps in the hydrolysation of triglycerides within the adipocytes. Readily available in different beverages and supplements, it is frequently used in combination within mesotherapy preparations.24
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Mr Arturo Almeida presents an overview of fat-dissolving injections
Lipolysis or adipocytolysis?
Lipolysis is the biological process for which the triglycerides (TG) are broken down into free fatty acids (FFA) and glycerol. This process can occur at both intracellular or extracellular levels. Intra-adipocyte lipolysis is carried out by hormone-dependant lipases and its goal is to use the lipid storage at the intracytoplasmic vacuole as a source for energy. The lipolytic cascade is triggered at the β-receptors by catecholamines or cortisol, and requires a second-messenger, mainly cAMP. However, at the extracellular level, lipolysis is mediated by lipoprotein lipases, both from muscular and adipocyte origin, and is responsible for the breakdown of circulating TG (in the form of chylomicrons or very-low density lipoproteins or VLDL) to FFA. This could be used as a form of energy or subsequently re-esterified as TG within the adipocyte.25 Adipocytolysis, on the contrary, is the destruction of the adipocyte cell, with the subsequent release of cell debris and TG that may, subsequently, be hydrolysed and eliminated via the lymphatic system or renal excretion.20
As mentioned above, at initial stages, the fat-dissolving properties were incorrectly attributed to PC – the main component of Lipostabil – but the research performed by Rotunda et al.10 in 2004 indicated that the real agent that actually produced the fat-dissolving effect was deoxycholic acid, the detergent used to solubilise PC. Therefore, in light of the mechanism of action described above, what we are in fact doing when using fat injection agents (SDC) is adipocytolysis, which is the basis behind these treatments.
Indications, side effects and contraindications
Fat-dissolving injections are mainly indicated to reduce and sometimes eliminate localised fat depots, which are defined as fatty areas present in normal-weight individuals that don’t go away despite intensive exercise and/or diet measures.26 Therefore, this is not a weight loss treatment, and this point should be clearly addressed to patients considering this kind of intervention. Almost any area with localised fat can be treated – in my experience the most popular are back rolls, saddle bags, ‘bra-roll’ and double chins. Another indication is for patients who present with small lumps of adipose tissue after undergoing liposuction or other surgical fat-reducing procedures.27 Fat-dissolving treatments have also been successfully used to treat lipomas; although in such cases, patients must be advised about lipoma recurrence, as the capsule cannot be eliminated.28 Undoubtedly, the occurrence of a number of scars, particularly in cases with multiple lipomatosis, is avoided. Such treatments have also been used to treat the so-called ‘buffalo hump deformity’ behind the shoulder, which may be often seen as a result of HIVrelated lipodystrophy.29 The most common side effects are swelling and bruising at the treated areas. Pain or discomfort is sometimes observed, but this rarely needs treatment. Swelling must be properly

addressed with patients, as it may last up to three weeks. Less commonly seen side effects are inflammatory nodules and numbness that sometimes last up to six weeks.27 Numbness has been reported more often when treating the submental area.30
Besides the normal contraindications for cosmetic treatments (such as pregnancy, lactation, acute infectious or autoimmune diseases), obesity – as mentioned earlier – is not an indication in itself. However, a bespoke treatment plan for such patients, which would include commitment to a dietary plan and exercise, can be offered and can have fantastic results, as the addition of fat-dissolving injections will speed up the volume reduction and increase their motivation to carry on with diet and exercise.
Patients without enough thickness of fat layer are not candidates for these treatments as this may increase the incidence of side effects. A minimum of 1.5cm thickness is desired,27 and this can be easily assessed by using a ‘pinch test’ (Figure 1).


Caution must be taken when treating delicate areas such as the submental, jowls and inner knee, and extensive anatomy knowledge and mastery of the technique is key to achieve the desired results and minimise unwanted side effects.31 Fat-dissolving injections are no longer indicated to treat eye fat pads. Practitioners using these treatments have to be particularly careful with patients with body dysmorphic disorder. As we all know, many of these patients have not yet been diagnosed and we should be mindful during a medical consultation to identify alert signs that may be evident.
Treatment delivery
As mentioned, in the early stages of fat-dissolving treatments, the only available technique was mesotherapy, which involves multiple intradermal or subdermal injections of small aliquots of substances. Some of the products currently available still use this method of injection but are always administered subdermally32 (Figure 2). With the advent of new SDC-containing formulations, and in particular with Aqualyx, a technique called intralipotherapy was developed.27 The main advantage is the use of only two or three opposite injection sites per treated area (Figure 3) versus numerous injection sites with mesotherapy. As well as this, there is the possibility of releasing the adipocytolytic agent directly into the fatty tissue homogenously and at different levels, therefore reducing the occurrence of nodules or irregularities of the skin. Patients are marked and photographed in a standing position, and preferably measured, to properly document the results of the treatment. A specially-designed needle that is between 70mm and 100mm long is then inserted and a retrograde fan technique is used to treat the entire surface of tissue. A small dose of 2% lidocaine is recommended to reduce discomfort during the injection, which is almost pain-free.27,33 ATX-101 is delivered with a very specific and standardised technique at the submental level.34 Key
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 1: Example of a ‘pinch test’. A minimum of 1.5cm fat thickness is desired for treatment.
Figure 2: Example of fat-dissolving treatment using deep mesotherapy technique.
Figure 3: Intralipotherapy technique allows to deliver fatdissolving treatments with just two opposite injection points.



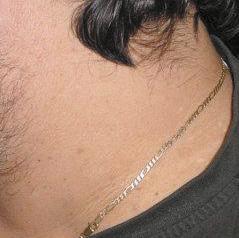























EXCLUSIVE TO the pursuit of skin perfection Ideal to treat: Skin tags, pigmentation, warts, age spots, sun spots, liver spots and verrucas Age spot treatment Hemangioma treatment For the removal of skin imperfections Get rid of unsightly warts, skin tags and benign lesions with CryoPen® SINCE THE NHS DOES NOT ALWAYS PROVIDES FREE REMOVAL OF SKIN LESIONS, CRYOPEN® IS A MUST IN ANY CLINIC! PRODUCES ULTRA-COLD N2O AT -89 C THAT RUPTURES THE CELL’S MEMBRANE DESTROYING THE CELLS PINPOINT ACCURACY THAT CAN TREAT LESIONS FROM 1MM-10MM IN SIZE SO CAN SAFELY TREAT LESIONS CLOSE TO EYE AREA DIFFERENT CARTRIDGE SIZES OF 8G AND 16G WHICH DELIVER CONSTANT FLOW OF 120-240 SECONDS QUICK TREATMENT TIMES AND LOW ONGOING RUNNING COSTS MEANS QUICK RETURN ON INVESTMENT QUICK RESULTS OF ONLY ONE TREATMENT ON COMMON WARTS WITH OTHER DEEPER WARTS REQUIRING MORE THAN ONE SMALL, PORTABLE PEN LIKE DEVICE MAKES TREATMENTS EASY TO PERFORM COMMENDED 2017 TREATMENT OF THE YEAR HIGHLY COMMENDED 2017 DISTRIBUTOR OF THE YEAR TREATMENT OF THE YEAR EQUIPMENT SUPPLIER OF THE YEAR DERMAPEN 0333 358 3904 info@naturastudios.co.uk naturastudios.co.uk Want to learn more? Come join us at our free demonstration sessions at our new Academy in Elstree, North London. Get the opportunity to see the package, meet with our rep to hear all about how CryoPen® can improve your clinic & ask any questions you may have. Call us today on 0333 358 3904 to book your demonstration or for more info! Demonstration dates Monday 18th March Monday 15th April Monday 20th May
Figure 4:
anatomical landmarks in this area are the inferior mandibular border, the antegonial notch (a bony landmark at the anterior masseter that approximates the location of the marginal mandibular nerve) and the thyroid cartilage.31 After the submental area is marked, a 1cm injection grid is used to mark the injection sites (Figure 4). A volume of 0.2ml of product is delivered at each site, using a 30 gauge 13mm needle. A similar approach is used by other formulations, such as Celluform Plus. In all cases, several sessions are required, spaced between three to four weeks apart to allow the normal inflammatory response, which occurs as a consequence of adipocytolysis, to subsidise. Approximately three sessions are usually required. An important point to address is the mandatory need of specific training before using any of these deoxycholate-containing products. This is to ensure the proper understanding of its mechanism of action and to make sure that the treatment is accurately delivered.
Results
Patients’ overall satisfaction is very good, although sometimes the degree of success is perceived differently by patients and practitioners. Besides the fact that practitioners have access to different evaluators such as photography, measurements and even ultrasound scans, another reason for this discrepancy is that patients often don’t remember the extent of their original concern, leading them to underestimate the results. Also, as with any aesthetic treatment, careful patient selection and proper management of expectations is key.33 In a multicentre study published on Aqualyx experience, the best results were seen on the hips, double chin and buffalo humps, and the worst results were observed on the arms and inner thighs.27 Android fat-type (abdomen and hips) shows increase responsiveness to treatment; therefore, a smaller number of sessions are required than gynoid fat-type depots (saddle bags, inner thighs and inner knee).33 In a recently published, single-centre study on the effectiveness of ATX-101 for the contouring of the neck, a statisticallysignificant improvement was seen in 88% of patients.35
Conclusion
There is enough scientific data proving the effectiveness of adipocytolytic injections to reduce unwanted fat depots. These treatments are safe, with minimum side effects and almost no interference with our patients’ daily activities. However, accurate knowledge of the mechanisms of action and proper training and certification, together with careful patient selection, are mandatory to achieve the desired outcome.
Disclosure: Mr Arturo Almeida is a UK trainer for Aqualyx and Celluform/Celluform Plus, as well as an international trainer for Sagoni Melt.
Mr Arturo Almeida is a consultant surgeon in general surgery who trained in the US and Europe. He has been practising aesthetic medicine for 12 years. His main areas of expertise are varicose vein treatments, minimally-invasive procedures and fat-dissolving injections, which he has been offering since 2009. Mr Almeida practices in Leeds and Manchester and serves as a KOL and global trainer for various companies.
REFERENCES
1. Mahmud K, Crutchfield III CE, Lipodissolve for body sculpting: Safety, effectiveness and patient satisfaction. J Clin Aesth Dermatol 2012; 5(10):16-19
2. Young VL. Lipostabil. The effects of phosphatidylcholine in subcutaneous fat. Aesth Surg J 2003;23(5):413-417
3. Kybella prescribing information. (Westlake CA, USA:2015) <www.accessdata.fda.gov/drugsatfda_ docs/label/2015/206333orig1s000lbl.pdf>
4. Maggiori S. Traitment mésotérapique des xanthelasmas à la phosphatidylcholine polyinsturèe (EPL). V Congrès International de Mésothérapie, Paris, 1988. Dermatologie. p. 364
5. Rittes PG. The use of phosphatidylcholine for correction of lower lid bulging due to prominent fat pads. Dermatol Surg 2001; 27: 391–2.

6. Neal, R. Burn fat away with an injection? (New York City, NY: CBS 2003) <https://www.cbsnews.com/ news/burn-fat-away-with-an-injection>
7. Lichtenberg d, Robson rj, Dennis EA. Solubilization of phospholipids by detergents: Structural and kinetic aspects. Biochem Biophys Acta 1983; 737:285-304
8. Medicine Health Regulatory Agency (MHRA). Questions and answers about Lipostabil, also markete as Flabjab; Lipomelt and Fat Away, which is being illegally promoted as a cosmetic in the UK. 14th April 2004. <webarchive.nationalarchives.gov.uk/20150110163657/http://www.mhra.gov. uk/Safetyinformation/Safetywarningsalertsandrecalls/Safetywarningsandmessagesformedicines/ CON1004243>
9. Kamalpour s, Leblanc K. Injection adipolysis: Mechanisms, agents and future directions. J Clin Aesth Dermatol 2016;9(12):44-50
10. Rotunda AM, Suzuki H, Moy RL, Kolodney MS. Detergent effects of sodium deoxycholate are a major feature of an injectable phosphatidylcholine formulation used for localized fat dissolution. Dermatol Surg 2004 July; 30: 1001–8
11. Yagima Odo ME, Cucé LC, Odo LM, Natrielli A. Action of sodium deoxicholate on subcutaneous human tissue. Local and systemics effects. Dermatolog Surg 2007;33:178-179
12. Motolese P. Phospholipids do not have lipolytic activity: A critical review. J Cosm Laser Therap 2008;10: 114-118
13. Yagima Odo ME, Cucé Lc, Odo LM et al. Action of sodium deoxycholate on subcutaneous human tissue: local and systemic effects. Dermatol Surg 2007;33:178-188
14. Janke J, Engeli S, Gorzelniak K, Luft FC, Jordan J. Compounds used for “injection lipolysis” destroy adipocytes and other cells found in adipose tissue. Obes Facts 2009;2 (1) : 36-39
15. Thuangtong R, Bentow JJ, Knopp K, et al. Tissue-selective effects of injected deoxycholate. Dermatol Surg 2010;36(6): 899-908
16. Salti G, Motolese P. Cavitational adipocitolysis with a new microgelatinous injectable for subcutaneous adipose tissue reduction: ex-vivo histological findings. Eur. J. Aesth Medicine and Dermatology 2012;2(2): 94-97
17. Dayan SH, Humphrey S, Jones DH, Lizzul PF, Gross TM et al. Overview of ATX-101 (deoxycholic acid): A non surgical approach for reduction of submental fat. Dermatol Surg 2016; 42:115S: S263-S270
18. Dayan SH, Jone DH, Carruthers J et al. A pooled analysis of the Safety and and Efficay results of a Multicenter, double-blind, randomized, placebo-controlled phase 3 REFINE-1 and REFINE-2 Trials of ATX-101, a submental contouring injectable drug for the reduction of submental fat. Plast Reconstr Surg 2014; 134 (4 Suppl 1):123
19. Jones DH, Carruthers J, Joseph JH et al. REFINE-1, a multicentre , randomized, double-blind, placebocontrolled , phase 3 trial with ATX-101, an injectable drug for submental fat reduction. Dermatol Surg 2016;42(1):38-49
20. Kramp G. Cellular and molecular biology. NY: John Wiley; 2002

21. Shepherd j. Lipids in health and disease. Biochem Soc Trans 2004;32:1051-6
22. Won TJ, Nam y, Lee HS, Chung S, et al. Injection of phosphatidylcholine and deoxycholic acid regulates gene expression of lipolysis-related factors, pro-inflammatory cytokines and hormones on mouse fat tissue. Food Chem Toxicol 2013;60:236-268
23. Hoppel C. The role of carnitine in normal and altered fatty acid metabolism. Am J Kidney Dis 2003; 41 (4 suppl 4):S4-12
24. Acheson KJ, Gremaud G, Meirim I, et al. Metabolic effects of caffeine in humans: lipid oxidation or futile cycling?. Am J Clin Nutr 2004;79:40-46
25. Santamaria-Fojo S, Dugi KA. Structure, function and role of of lipoprotein lipase in lipoprotein mechanism. Curr Opin Lipidol 1994;5:117-25
26. Pinto H. Local fat treatments: classification proposal. Adipocyte 2016;5:22-26
27. Amore R, Pinto H, Gritzalas K, Hernandez C, Skwara-Guzikowska K, Amuso D et al. Intralipotherapy: the state of the art. Plast ReconstrSurg Glob Open 2016;4:e1085
28. Rotunda AM, Ablon G, Kolodnet MS. Lipomas treated with subcutaneous deoxycholate injections. J Am Acad Dermatol 2005;53:973-8
29. Rausso R, Non surgical reduction of buffalo hump deformity: Case report and literature review. Eur J Aesth Medicine and Dermatology 2011;1(1): 29-34
30. Asher B, Hoffmann k, Walter p, et al. Efficacy, patient-reported outcomes and safety profile of ATX-101 (deoxycholic acid), an injectable drug for the reduction of unwanted submental fat. Results from a phase III, randomized, placebo-controlled study. J Eur Acad Dermatol Veneorol 2014;28:1707-15
31. Anatomical and clinical implications of the deep and superficial fat compartments of the neck. Plastic Reconstr Surg 2017;140:405e
32. Duncan D, Rubin JP, Golitz L, et al. Refinement of technique in injection lipolysis based on scientific studies and clinical evaluation. Clin Plast Surg 2009;36(2):195-209
33. Amore R, Amuso D, Leonardi V, Leva F, Carnovale Sibaud A, Guida A, Costa E et al. Evaluation of safe and effectiveness of an injectable solution acid deoxycholic based for reduction of localized adiposities. Plast Reconstr Surg Glob Open 2018;6:e1794
34. Jones DH, Kenkel JM, Fagien S, Glasser DA, Monheit GD, Stauffer K et al. Proper technique administration of ATX-101 (Deoxicholic acid injection): Insights from an injection practicum and roundtable discussion. Dermatolog Surg 2016; 42 (115S): S275-S281
35. Shridharani SM. Early experience in 100 consecutive patients with injection adipocytolysis for neck contouring with ATX-101 (deoxycholic acid). Dermatol Surg 2017;43:950-958
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The 1cm injection grid that is used to mark the injection sites when treating submental fat.
©2019 Allergan. treatment share in the
Model treated with JUVÉDERM®. Book a consultation to find out if JUVÉDERM® is appropriate for you. Individual patient results may vary.
Model treated with JUVÉDERM®. Book a consultation to find out if JUVÉDERM® is appropriate for you. Individual patient results may vary.




LIFT IT SMOOTH IT PLUMP IT
LIFT IT SMOOTH IT PLUMP IT
JUVÉDERM


It’s time to stop dreaming and start doing. Get the lasting and natural looking* results you want with the help of JUVÉDERM ®, the world’s leading brand of hyaluronic acid facial fillers. †
It’s time to stop dreaming and start doing. Get the lasting and natural looking* results you want with the help of JUVÉDERM ®, the world’s leading brand of hyaluronic acid facial fillers. †
Allergan. All rights reserved. All trademarks are the property of their respective owners. * Results with JUVÉDERM® can last from 9 to 24 months depending on the chosen. JUVÉDERM® products blend with the tissue underneath the skin, to give natural looking results. † The no.1 hyaluronic acid brand according to market the majority of markets where data is available (2018). UK/0569/2018. Date of preparation: December 2018.
©2019 Allergan. All rights reserved. All trademarks are the property of their respective owners. * Results with JUVÉDERM® can last from 9 to 24 months depending on the treatment chosen. JUVÉDERM® products blend with the tissue underneath the skin, to give natural looking results. † The no.1 hyaluronic acid brand according to market share in the majority of markets where data is available (2018). UK/0569/2018. Date of preparation: December 2018.


JUVÉDERM ® IT BOOK A CONSULTATION TO FIND OUT MORE JUVEDERM.CO.UK
® IT BOOK A CONSULTATION TO FIND OUT MORE JUVEDERM.CO.UK
Personalized Body Sculpting:

1 & 2 MARCH 2019 / LONDON SEE US AT
Understanding Menopausal Hormones
Female hormones change across stages of reproductive ageing, culminating in the menopausal transition, altering physiology and anatomy and accelerating signs of ageing in the process. Unlike most clinical articles in this subject area, which generally revolve around treatment of menopausal symptoms, this article is concerned with the endocrinology of the menopausal transition, leading up to the clinical features we recognise.
Understanding the menopause
Menopausal physiology was not researched as extensively as the menstrual cycle until these past 20 years. Only now do we benefit from standardised nomenclature for stages in the menopausal transition; improved knowledge of reproductive ageing physiology; and how it relates to the challenging symptoms experienced by women. The NHS website refers to menopause as ‘the cessation of menstruation following the loss of ovarian follicular activity’.1 The clinical diagnosis of menopause is made when 12 months of amenorrhoea (absence of a menstrual period) follow the final menstrual period (FMP); the average age of menopause in the UK is 51 years. Perimenopause (the transition) and menopause are collectively referred to as the ‘climacteric’.2 There are a number of statistics relating to menopause that are useful for practitioners to be aware of. First of all, the average life expectancy of a woman in the UK is 82.5 years, compared to 50 years in 1900 and about 46% of the UK female population (33 million in 2016) is above the age of 45.3,4 The Office for National Statistics also reported in July 2017 that around 4.3 million women aged 50 or over, including 75-80% of women of menopausal age, were in employment; of those, 75% experience symptoms, of which 25% experience serious symptoms.3,4 With that in mind, medical aesthetic treatments are frequently carried out to address
the medical and psychological needs of this demographic, so it is essential to understand this stage of patients’ life.3,4
Hormones pertinent to menopause
Hormones relevant to the menopause are the sex steroids (oestrogens, androgens and progestogens) and the hormones of the hypothalamic-pituitary-ovarian (HPO) axis. Sex steroids are the main steroid hormones produced by the ovaries. Each stage of their biosynthesis is used in diagnosis and treatment of hormonal imbalance – pregnenolone, DHEA, oestriol, progesterone, to name a few.8 The pituitary gland produces follicle-stimulating hormone (FSH) which acts on the ovaries to stimulate the development of a mature egg every 28 days, and luteinising hormone (LH) which stimulates ovulation. Pituitary function in turn is controlled by the hypothalamus, which acts as the master controller for reproductive function via luteinising hormone-releasing hormone (LHRH) and gonadotropinreleasing hormone (GnRH).8 It is vital to understand how the premenopausal cycling of female sex steroids is controlled and how they differ from hormones such as thyroxine and insulin, which is indicated in Figure 1. However, both steroid and peptide hormones are signalling molecules that regulate the physiology of organs. They are produced in endocrine glands and reach target organs via the bloodstream.
HPO axis
The HPO axis primarily acts as a negative feedback system (except for the mid-cycle gonadotropin surge which triggers ovulation), whereby peptide gonadotropins stimulate steroid hormone production in the ovaries. This in turn inhibits gonadotropin secretion, thus allowing menstrual cycles to occur.5-7 The feedback systems in the HPO axis in relation to premenopausal ovarian function and hormones are summarised below to refresh the memory before proceeding to hormonal changes of menopausal transition:

1. GnRH released from the hypothalamus stimulates the pituitary to secrete FSH
2. Negative feedback: FSH stimulates ovaries leading to follicular maturation. Follicles secrete oestradiol (commonly abbreviated as E2). This inhibits further secretion of the stimulating hormones FSH and GnRH
3. Positive feedback: LH stimulates the production of E2. This increases further secretion of LH. When LH levels reach a threshold, ovulation occurs, and oestrogen levels fall
4. After ovulation the ruptured follicle becomes the corpus luteum, secreting progesterone and decreasing levels of E2 during the luteal phase5-7
Menstrual cycle overview
Follicular phase
At the start of the menstrual cycle, the ovary contains several antral follicles, which contain oocytes enclosed in granulosa cells, basal membrane, and outer theca cell layers. The follicle most sensitive to FSH stimulation goes on to mature (dominant follicle) while others degenerate.5-7 The theca cells of the dominant follicle develop LH receptors, which produce androgens. Granulosa cells have FSH receptors. These cells absorb androgens and metabolise them to E2.5,7 Granulosa cells also produce the peptide hormone, inhibin (isoforms A and B).5,6 Increasing levels of E2 from the dominant follicle stimulate endometrial proliferation. At the pituitary gland, rising levels of E2 and inhibin B act to reduce FSH and LH secretion (negative feedback).5-7
Late follicular phase
About 36 hours prior to ovulation, E2 reaches levels that switch the negative feedback effect to a positive feedback effect. This leads to the LH surge (and a smaller FSH surge) over the 24 hours prior to ovulation, causing the dominant follicle to rupture, releasing its oocyte.6,7
Luteal phase (after ovulation)
E2 production from the ruptured follicle falls abruptly at the time of ovulation and continues falling through this phase. The follicle becomes the corpus luteum (Latin for yellow body), producing progesterone and diminishing amounts of E2, which now act on the endometrium to promote implantation.8
LH maintains the corpus luteum in the post-ovulatory week. If pregnancy does not occur, the corpus luteum degenerates. E2
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Aarti Narayan-Denning explains how a woman’s hormones alter in order for menopausal transition to take place and how this impacts physiology, anatomy and ageing

EFFECTIVELY NEUTRALISES free radical damage IMPROVES VISIBLE SIGNS of ageing TESTED SUITABLE FOR USE after laser treatment 30 YEARS OF RESEARCH IN EVERY DROP ANTIOXIDANT AUTHORITY STAND 32 INSTAGRAM @SKINCEUTICALS_UKI TWITTER @SKINCEUTICALSUK WEBSITE WWW.SKINCEUTICALS.CO.UK
Steroid hormones
Derived from cholesterol
Molecules are small and hydrophobic (lipid based)
Synthesised as and when needed, by the smooth endoplasmic reticulum
Bound to protein carriers to circulate in the bloodstream to the target issues
Peptide hormones
Derived from amino acids
Molecules are large or small, and hydrophilic
Synthesised in the rough endoplasmic reticulum and stored until signalled to secrete
Can circulate freely in the bloodstream
these are less reliable guides to menopausal status (the stage in the menopausal transition).
Symptoms of the menopause and underlying pathophysiology11
Symptoms of the climacteric are due to relative decline of E2 alongside health and psychosocial stressors. Commonly reported menopausal symptoms are:14-19
Have receptors located at the cell surface
Have receptors inside the cell, in the nucleus Act as second messengers
Have a slower but permanent effect
Examples are testosterone and oestrogen (these are also called the sex steroids)
Bind to DNA, modifying transcription
Fast acting, temporary action
Examples are insulin, thyroxine, calcitonin and anti-diuretic hormone
Figure 1: Differences between steroid and peptide hormones13
and progesterone production falls, as does the negative feedback on FSH. As a result of this, FSH rises and a new menstrual cycle commences.8
Physiology of menopausal transition
Follicle depletion
The ovaries of a 20-week female foetus contain about 7.5 million immature ova (germ cells) enclosed in follicles. This follicular pool depletes steadily, falling to two million at birth and about 300,000 by puberty. A 37-year old woman will have about 25,000 healthy ova left. At this point, follicle depletion accelerates, usually resulting in menopause around age 51.5,6,9,10 Environmental factors such as cigarette smoking and iatrogenic causes (ovarian surgery, chemotherapy) accelerate follicle depletion and the menopause occurs earlier.5,6,9,10 Early in the menopausal transition, menstrual cycles become shorter and irregular, increasing follicular loss from about 10 years pre-menopause. Eventually there is only occasional ovulation. Perimenopausal women have hypomenorrhea and oligomenorrhea (infrequent and light menstruation) and often more than 35 days between cycles.11 When follicular cells deteriorate to the extent that immature ova cannot be developed, the necessary sex hormones can no longer be produced and ovarian failure results.2 Oestrogen and progesterone levels fall, and deficiency symptoms may occur such as hot flushes, anxiety, joint and muscle pains.2
Inhibin feedback and cycle length
In the late reproductive stage and early menopausal transition, antral follicle numbers decline, and so does inhibin B production
by granulosa cells.6,2,12 As inhibin B falls, FSH levels rise.6,2 With follicle recruitment, E2 levels rise earlier and the LH surge occurs earlier. In some women entering perimenopause, this leads to shorter follicular phases, reducing the overall cycle length.5 Until later in the transition, the luteal phase remains constant.5 As women move into the late menopausal transition, menstrual cycles lengthen. Anovulatory cycles become more frequent as the HPO axis gets progressively deregulated.11 High mid-cycle E2 levels fail to elicit the LH surge, and the luteal phase drop in E2 fails to lower the LH levels. Sustained high FSH also prevents ovulation. Progesterone levels steadily fall, due to reduced ovulation and corpus luteal secretion.9,10
Changes in sex steroid profiles
E2 levels start falling in the two years preceding FMP, whilst FSH rises.10 Persistently low E2 levels occur only after the 12-month period of amenorrhea.9 The predominant oestrogen in postmenopausal women is estrone (commonly abbreviated as E1), unlike estriol in the premenopausal state. Androgens secreted by adrenals and postmenopausal ovaries are converted to E1 in adipose tissue and liver.5 In the late menopausal transition, FSH levels slowly decline,2 as do levels of sex hormone binding globulin (SHBG). This leads to a relative increase in free testosterone proportion.9 Androgen levels are not significantly affected by natural menopause, but ovarian androgen production will be lost in women having gonadotropin suppression treatment, whose ovaries were surgically removed, or damaged by chemotherapy or radiotherapy. Because E2 and FSH levels vary significantly over the menopausal transition, measuring
• Vasomotor symptoms: hot flushes, night sweats
• Insomnia: sleep disturbance
• Psychological symptoms: anxiety, irritability, emotional lability, depression
• Arthralgia: joint aches and pains
• Vaginal (urogenital) atrophy: structural and physiological changes
• Fatigue, diminished well-being
Physical consequences include: 16-19
• Bone loss due to increased bone resorption, osteoporosis
• Central abdominal fat increase, fall in adiponectin, increase in insulin resistance
• Transition from gynoid to android pattern of body fat distribution
• Conversion to a more adverse cardiovascular risk lipid profile, total cholesterol, LDL-cholesterol and apo-B levels increase
• Stress and urge urinary incontinence
Low levels of oestrogen can influence the appearance of facial contours, especially the perioral skin, lips and eyes. The speed of resorption of the bone structure is dependent on the level of oestrogen present.16 As well as this, change in sleep quality is common in menopause and may occur independent of vasomotor symptoms. Treatment of insomnia may be an important indication for hormone therapy. Arthralgia is also often incapacitating and increasingly frequent with progression of menopausal stages. It affects women treated with aromatase enzyme inhibitors after breast cancer, which is strong evidence that arthralgia is consequent to oestrogen depletion.17-19 More commonly, menstrual irregularity is an early indication of the perimenopause. Menopausal symptoms may start years before menopause, with no cut-off for start or end age.
Clinical considerations when treating patients in the climacteric Medical aesthetic professionals often
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
new pack
dermamelan
depigmenting solution by mesoestetic
trust the leader*
®
the world’s leading professional depigmentation method




* Considering international distribution.
The new dermamelan® pack includes a patient’s home pack with two innovative complementary products specifically developed to achieve more efficient and lasting results.
 dermamelan® method efficacy has been demonstrated in numerous studies under medical supervision. More than 500,000 patients treated worldwide, in any skin phototype (I-VI) and in all ethnicities.
dermamelan® method efficacy has been demonstrated in numerous studies under medical supervision. More than 500,000 patients treated worldwide, in any skin phototype (I-VI) and in all ethnicities.
®
after
after before For more
visit
before
information
us at www.mesoestetic.com
Long term results obtained after 12 weeks demonstrates method’s efficacy on pigmentation reappearance control.
Oestrogens Androgens Oestriol
Figure 2: Pre and post-menopausal concentrations for pituitary and steroid hormones. Levels shown represent averages. Adapted from Lentz, Comprehensive Gynecology, 7E8
encounter patients in the climacteric.20 We need to confidently advise these patients about the suitability (or not) of treatment, whether it is hormonal replacement therapy, skin rejuvenation, vaginal rejuvenation or medical aesthetic treatment, depending upon our areas of practice. It is helpful to identify the patient’s stage in the menopausal transition. For women with an intact uterus, this diagnosis is clinical; change in the cycles and eventually amenorrhea. For women who cannot report their cycles (history of hysterectomy, endometrial ablation or progestogen intrauterine device), hormonal measurement described above can help. Oestrogens modulate skin physiology by targeting keratinocytes, fibroblasts, melanocytes, hair follicles and sebaceous glands, encouraging angiogenesis and wound healing. Oestrogen deficiency accelerates skin ageing and causes atrophic skin changes.17 There are some important considerations when contemplating medical aesthetic procedures in menopausal women, particularly in relation to how the skin and subcutaneous tissues will respond and heal. If we consider the changes occurring in the body during this period (described above), we can see how they will impact healing and outcomes in these patients following medical aesthetic procedures.
For example:
• Oestrogen insufficiency decreases defence of menopausal skin against oxidative stress22
• Due to the compromised protective function of the skin’s outer layers,22 there is an increased risk of skin cancer21
• Greater risk of infection and inflammation means longer recovery and downtime should be expected
• Skin is thinner with less collagen and a decreased elasticity
• Increased wrinkling and dryness so exfoliating or resurfacing procedures need to be undertaken cautiously
• Vascularity is reduced, causing impaired wound healing, so extra care to minimise vascular compromise is necessary
• Greater risk of post-inflammatory pigmentation so protection from sun damage should be emphasised
Treatment plans for patients in menopausal transition should thus consider the extensive systemic changes going on. Outcomes will be impacted by healing times, psychological and physical wellbeing.
Conclusion
Women in the climacteric are a substantial, economically productive and a clinically significant cohort to aesthetic practitioners, so understanding this state and the resulting medical and psychosocial needs is essential. To summarise, the hormones relevant to the menopause are the sex steroids and the hormones of the HPO axis. There is progressive deregulation of the HPO axis alongside depletion of follicular reserve, resulting in ovarian failure. This is central to the pathophysiology of menopause. Because E2 and FSH levels vary markedly over the menopause transition, measuring these are less reliable as guides to the patient’s menopausal status. Before we treat patients, it is vital to understand the endocrinology of the menopausal transition, which should help us to recognise the clinical features that are often presented in clinic.
Dr Aarti Narayan-Denning is an aesthetic practitioner and independent GP with more than 20 years of medical and aesthetic experience. She provides integrated health and medical aesthetic treatment at Reverse Time in Hampshire. Dr Narayan-Denning has a diploma in medicine and Obstetrics and Gynaecology and is also a member of the Royal College of General Practitioners.

REFERENCES
1. NHS.uk, Menopause Overview <https://www.nhs.uk/ conditions/menopause/>
2. Butler L, Santoro N. The reproductive endocrinology of the menopausal transition. Steroids. 2011 Jun. 76(7):627-35
3. Overview of the UK population: July 2017, Office for National Statistics <https://www.ons.gov.uk/ peoplepopulationandcommunity/populationandmigration/ populationestimates/articles/overviewoftheukpopulation/ july2017>
4. Research and analysis Menopause transition: effects on women’s economic participation Evidence review, covering 104 publications, of the extent to which menopause transition impacts on women’s economic participation, Gov.uk, July 2017 <https://www.gov.uk/government/publications/menopausetransition-effects-on-womens-economic-participation>
5. Bruce D, Rymer J. Symptoms of the menopause. Best Pract Res Clin Obstet Gynaecol 2009; 23: 25–32.
6. Devoto L, Palomino A, Céspedes P, Kohen P. Neuroendocrinology and ovarian aging. Gynecol Endocrinol 2012; 28 Suppl 1: 14–7.
7. Billings EL, Brown JB, Billings JJ, Burger HG. Symptoms and hormonal changes accompanying ovulation. Lancet 1972; 1: 282–4.
8. Comprehensive Gynecology 7th ed. Lobo R, Gershenson D, Lentz G,. Elsevier. Part 1: Basic Science, Chapter 4 Reproductive Endocrinology.
9. Prior JC, Hitchcock CL. The endocrinology of perimenopause: need for a paradigm shift. Front Biosci (Schol Ed) 2011; 3: 474–86.
10. Burger HG, Hale GE, Robertson DM, Dennerstein L. A review of hormonal changes during the menopausal transition: focus on findings from the Melbourne Women’s Midlife Health Project. Hum Reprod Update 2007; 13: 559–65.
11. Comprehensive Gynecology 7th ed. Lobo R, Gershenson D, Lentz G,. Elsevier. Part 2: Comprehensive Evaluation of the female, Chapter 14 Menopause and the care of the mature woman.
12. Edwards BJ, Li J. Endocrinology of menopause. Periodontol 2000 2013; 61: 177–94.
13. Textbook of Medical Physiology, Guyton & Hall 11e, Chapter 74 Introduction to Endocrinology Pg 906-915
14. MacBride MB, Rhodes DJ, Shuster LT (2010) Vulvovaginal atrophy. Mayo Clin Proc 85(1): 87–94. doi: 10.4065/ mcp.2009.0413
15. Rees M, Stevenson J, Hope S (2009) Management of the Menopause. Royal Society of Medicine Press, London
16. Sumino H, Ichikawa S, Abe M et al (2004) Effects of aging and postmenopausal hypoestrogenism on skin elasticity and bone mineral density in Japanese women. Endocr J 51(2): 159–64
17. Thornton M. J (2013) Estrogens and aging skin. Dermatoendocrinol. 2013 Apr 1; 5(2): 264–270. Published online 2013 Apr 1. doi: 10.4161/derm.23872 PMCID: PMC3772914
18. Davis et al, Understanding weight gain at menopause. Climacteric 2012;15:419-29
19. Carr M, The Emergence of the Metabolic Syndrome with Menopause. The Journal of Clinical Endocrinology & Metabolism, Volume 88, Issue 6, 1 June 2003, Pages 2404–2411, https://doi.org/10.1210/jc.2003-030242
20. Milothiridis P et al. A systematic review of the factors predicting interest in cosmetic plastic surgery, Indian journal of plastic surgery, 2016
21. Cancer Research UK, https://www.cancerresearchuk.org/ health-professional/cancer-statistics/statistics-by-cancertype/non-melanoma-skin-cancer/incidence#heading-One, Accessed January 2019
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Pituitary hormones (in mIU/mL) Steroid hormones (in pg/mL)
20 20 0 0 200 400 600 800 1000 1200 1400 1600 1800 2000 40 40 60 80
22. Thornton J, Estrogens and aging skin, Dermatoendocrinol. 2013 Apr 1; 5(2): 264–270. PMCID: PMC3772914 Follicle-stimulating
Oestrone Androstenedione Testosterone Luteinising hormone
hormone
Premenopause Postmenopause









OUR EXPERT RANGE ALLOWS YOU TO RESHAPE, REGENERATE AND REDEFINE
Rev A For more product and training information visit www.sinclairpharma.com sinclair_uk Silhouette Soft ®: 3D cone technology suspension sutures Ellansé ®: Collagen stimulating dermal filler Perfectha ®: Full range of Hyaluronic Acid fillers WORKING WITH YOU TO DELIVER NATURAL LOOKING RESULTS 1 & 2 MARCH 2019 / LONDON SEE US AT
Sinclair Pharma. 1st Floor Whitfield Court, 30-32 Whitfield Street, London W1T 2RQ. 0207 467 6920 Date of preparation: January 2019 COR04
Thread lifts using polydioxanone (PDO) or poly-L-lactic acid (PLLA) sutures have become mainstream procedures over the last five years in the UK. I believe this is because the risks and downtime are more favourable compared to plastic surgery, although the effect is more subtle. After the age of 40, most Caucasian women’s necks show ageing with thinner, coarsely wrinkled, textured skin. The degree of ageing is commonly related to the amount of UV exposure, Fitzpatrick skin type, and familial tendencies.1 Thread insertion in the neck can provide a pleasing and worthwhile result as patients find it an appealing option to improve their old, sagging necks, while avoiding the risks associated with surgery. In my experience, the ideal age group is the 40s and 50s. Although a good result is still possible for patients over 60 years old, more caution is needed for patient selection and management. This article discusses the challenges associated with treating patients over 60 and provides some tips for the assessment process. Incorrect patient selection for thread neck lifts will lead to patient dissatisfaction, as well as higher risks of side effects and complications.
The consultation and patient selection
As with all treatments, carefully listen to your patient during the consultation to fully understand what it is they really want. Is what they are asking achievable and are they being realistic? In my experience, good candidates for the thread neck lift are those who are fit and well, have robust, good quality skin and are not on any anti-coagulants.2-4 If they have requested a neck lift but you believe it to be unsuitable, explain tactfully why this is so. You should discuss alternatives that might help, such as radiofrequency skin tightening, chemical peels, dermal fillers, botulinum toxin and surgery. I advise my older patients that I never treat the neck with threads unless the jawline and area under the chin (the dewlap) have been treated first or if they
Treating Older Necks Using Threads

are open to treating that as well. This is because, in older patients, just treating the neck alone can create a peculiar appearance.4 The degree of neck and facial atrophy should be assessed; I believe that if there is no jawline and instead there is a 45 degree drop from the chin to the sternal notch, then a neck thread lift is unlikely to be beneficial. Usually the neck drooping has developed over many years and it is unrealistic to imagine that threads would be able to pull back this weight of flesh. The manufacturers advise the maximum pull-back for any thread is 1cm, and other authors have also reported this.5 If this isn’t enough for the patient, then they either need to approach a plastic surgeon or accept the neck as it is. It is crucial not to raise older patients’ expectations. When planning thread treatment, I use a soft cosmetic pencil and draw out the path of each thread and demonstrate what can be achieved by pulling back towards the scalp at the nape of the neck by 1cm. Ask if the patient is happy with this, as often 1cm may not be enough to make any appreciable difference with older patients. Unfortunately, in people over 60, the subcutaneous tissues can be very thin and fragile. In my experience, if the neck skin feels like you are grasping ‘turkey neck skin’, for example, then it is likely that the threads will not hold and may migrate and protrude through the skin, which is unsightly (Figure 1).

Adverse events
Thoroughly explain all possible side effects, adverse events and complications, which are always listed in the manufacturer’s leaflets for the product that you are using. In general, you need to explain that extensive bruising is common in the neck and can look alarming. Cannula methods using PDO anchored threads may be less likely to cause bleeding than the needle methods such as the PLLA threads. The visibility of the thread is a concern; the anchored (barbed) threads are often blue in colour and can be easily visible through thin skin.6 These also have a more rigid consistency, so can feel more uncomfortable. If using PLLA threads, the cones may be visible and palpable through very thin skin.7 I find this is more common if there is not 2cm from the last cone to the exit. Unsightly puckering is more common with older patients as they have more redundant folds of skin, but this should settle with time so patience is needed. Granulomas and infection are also a rare risk.2
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 1: Patient who is unsuitable for treatment as her neck atrophy is too severe.
Image courtesy of Sinclair Pharma.
Dr Ruth Harker explores the use of sutures in patients over 60 for a non-surgical neck lift and shares her experience performing this procedure

Tips for treatment success
The tips below are useful to maximise patient satisfaction and avoid problems, but are particularly important in the older, higher risk neck thread treatment patient.

• Product selection: personally, I often use PLLA threads (Silhouette Soft) as I find there is less pain with these threads than the anchored (barbed) threads, making them more tolerable by the older person. This procedure will last up to two years as the cones cause neocollagenesis.10 However, PDO threads are a cannula method so some practitioners may feel they are safer in the elderly, where blood vessels are more friable.2
• Provide treatment examples: show before and after photos of patients within their age group that demonstrates clearly the level of improvement possible. Make sure that you have written consent for your patients’ photographs, which allows you to show them to other patients.

• Prepare and provide patient resources: questionnaires, leaflets, contact details, side effects, complications, photographs, sample consent form, an aftercare advice sheet.
• Cooling-off period: insist on at least two weeks.11
• Warn of bruising: bruising in the neck area is often worse than a thread lift in the face, so even if a patient has had a previous facial lift, they may need warning that the bruising could be worse. Recommend Arnica tablets from the pharmacy; one three times a day for a week prior to the procedure to help bruising settle. Remember that old people tend to bruise worse.12
• Inflammatory reactions: ask if they react severely to insect bites as this may predict a tendency to a marked inflammatory reaction.
• Diet: recommend a preparatory high protein diet in to help strengthen and firm subcutaneous tissues and stop smoking.12,13
• Timing of procedure: leave at least six weeks before important events.
• Photography: take photos in good light against a plain white background with a good quality digital camera. Take one full face frontal, 90 degrees left and 90 degrees right and always take half-way stage photos.
Contraindications
Practitioners should always conduct a thorough medical history. For older patients, you must be diligent to consider their age, frailty and medication. Check their medication history carefully; underlying conditions like diabetes or epilepsy may need an adjustment of medications prior to the procedure. If the patient is a diabetic or is prone to soft tissue infections, consider a prophylactic prescription of antibiotics. With age, healing is slower and you should warn the patient of this.2 Anticoagulants are a relative contraindication and it would be wise to decline the case. Even if not taking any anticoagulants, older people often have more ineffective clotting systems and if you find that, on examination, they have spontaneous bruises then they are likely to bruise badly following thread placement. Allergy history, such as asthma, hay fever, contact allergies, drug allergies (particularly local anaesthetic) and suture allergies are also contraindications.4
As well as this, if the patient has experienced recent weight loss, I would recommend postponing the procedure until the patient is at a static weight. Request that they try not to lose any weight before the procedure or for 18 months following; weight is commonly lost off the face and neck after individuals are middle aged.2 An evaluation for body dysmorphic disorder should be made and if you gauge that they seem neurotic or highly anxious it is advisable to use the BDD questionnaire.8 As well as this, check for potential needle/blood phobia and assess the patient’s level of anxiety/ability to relax and lay still for up to one hour. The older person is more likely to have
musculo-skeletal aches and pains, meaning they may not be able to do this. Additionally, I recommend assessing their pain threshold generally – will they cope with the procedure? A useful question to ask is ‘how do you cope with local anaesthetic at the dentist?’ Explain that there are several small boluses compared to one large one at the dentist. From cardiology training, practitioners should remember that a raised venous jugular pressure, palpable carotid atherosclerosis, prominent carotid pulsation, canon waves or a carotid bruit all signify various cardiac pathologies.2 If any of these are found, I advise declining the case and refer the patient back to their GP. If there is any history of heart disease or arrhythmia, then you must ask yourself if it’s medically appropriate to perform the procedure as the risk of heart attack or stroke is there. Although this is a minimally-invasive procedure, one should not be complacent and there is a significant risk the older and frailer patient is. Remember this is not an essential treatment and the physician’s rule is ‘first do no harm’. When assessing patients, you should also examine the quality of connective tissue – is the skin like tissue paper? If so you will not get a good result. The thickness of connective tissue should also be considered. My rule is if you grasp skin over the neck, over the hyoid cartilage thumb and forefinger (or callipers), they should be approximately 1cm apart. If your thumb and forefinger are touching, then this is a case to decline because the connective tissue will be too thin to support the sutures and they may be palpable/visible or migrate and a disastrous outcome may result.9
The day of the procedure
Practitioners should revise the treatment outcomes again and explain what you are expecting to achieve; draw the path of threads to demonstrate this to the patient. A consent form must be signed, only if both patient and practitioner are happy that every aspect has been covered. In addition, check if the patient has eaten or drunk fluids recently and offer water and/or a glucose tablet if they are feeling hypoglycaemic. Do not proceed until you are sure they are
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 2: A 58-year-old patient before and six months after treatment using Silhouette Soft 16 cone. Images courtesy of Sinclair Pharma.














NUTRACEUTICAL SUPPLEMENT PREMIUM once-a-day Collagen DRINK Supplement Skin • Hair • Nails • Joints • Bones • Gut Health • Peri/Post Menopause FOR AGE MANAGEMENT Once a day supplement mixed with water, smoothie or fruit juice Expect results in 3-12 weeks CLINICALLY PROVEN SCIENCE www.totallyderma.com Tel: 020 3126 6795 | Email: info@totallyderma.com Tel: 020 3868 6242 | Email: enquiries@harpargrace.com • Added revenue stream • Full marketing support Also available from our distributing partner hair skin joints arteries gut bladder urethra vagina nails ligaments tendons bone Enhances the effect of topical medical aesthetic treatments Stimulates collagen and hyaluronic acid sites ALL OVER the body • evidence based and results-driven • pharmaceutical-grade ingredients • 95% bioavailable (pre-digested collagen amino acid peptides) • visible difference in skin firmness, elasticity and
longer, stronger hair and nails,
pain-free joints
key supplement
• promotes recovery post-procedure up to 200% more Collagen than current market players at least 300% more Hyaluronic acid up to 300% more L-Ascorbic Vitamin C Key antioxidants and anti-inflammatory ingredients: Grape Seed Extract, Green Tea Extract, Alpha Lipoic Acid, Zinc, Copper, Manganese
hydration,
more flexible,
•
for gynaecological menopausal dryness
feeling well. If the patient has any allergies or a swelling tendency, antihistamines may help on the day of procedure.14 Lastly, make the patient comfortable, with their neck supported with a comfortable pillow. Remember the patient may have to stay in this position for a prolonged time, which can be difficult for older patients. I find that it is best for the patient to be sitting as upright as they can manage comfortably; when the patient is supine it is easy to get the direction of the threads incorrect. The practitioner needs to see the neck at its worst.
Performing the treatment
The risk of infection is greater in the older person.2 A sterile technique is essential to prevent infection and a nursing assistant is necessary as one doesn’t want to desterilise the sterile field. Also, the assistant must wear sterile gloves and press on any bleeding point. I advise to keep local anaesthetic to a minimum as it may cause bruising in the neck, particularly under the chin, and also disguise the anatomy you are trying to correct.2 It goes without saying that you must follow the exact procedure that you have been taught on the courses you have attended to learn the particular thread system you are using. Note that only practitioners specially trained and certified are able to obtain Silhouette Soft threads from the manufacturer. Silhouette Soft is a needle system, whereas PDO threads are a cannula system, and the instructions for use are completely different; the number used and injection technique varies considerably. Generally speaking, in my experience, the practitioner must be gentle when inserting the sutures. Ask the patient to lift their chin up and stretch the skin, which helps keep in the superficial plane and enter at 45 degrees. Then, when you feel the ‘give’ of passing through the dermis, you must traverse the needle/cannula horizontally superficially, pinching the skin ahead of the needle/cannula, which should be approximately 4mm in depth. Always be absolutely sure that you know where the tip of the needle/cannula is, and keep checking where it is and where it is likely to come out and ensure this is the desired position. Check that the needle/cannula is not in the platysma muscle by palpation and not in the supra-tracheal tissues by asking the patient to swallow before pulling the needle.
Following the procedure
Following the procedure, I recommend ice packs, paracetamol or low dose codeine to ease the pain. I advise that the patient sleeps on their back for three to five days, using extra pillows. They should avoid saunas, steam rooms, UV exposure, dental treatments and sports. They should avoid any other activity that strains the neck up or forward for three weeks. Even pilates and yoga, which elderly
women often do, may be painful and strain the newly inserted threads. Swallowing may be uncomfortable for several days so softer foods may be preferred. Also make sure the patient abides by the necessary pre-procedural and aftercare instructions; for example, avoidance of non-steroidal anti-inflammatory drugs for two weeks before and two weeks after the procedure.16
Summary
Good, thorough treatment preparation and patient selection can prevent a lot of problems and a worthwhile neck thread lift can be achieved even in older patients. However, if what the patient desires is not achievable, don’t carry out the treatment and always stress that results cannot be guaranteed, outlining this in the consent form. Only practitioners who are specially trained and qualified in performing thread lifts should attempt this procedure. It is essential practitioners attend a course for the particular threads they have chosen to specialise in and repeat this course with live models until they are completely confident in their use. For optimal results, I recommend a cadaver anatomy course as it will help you learn how to stay in the right plane. A foundation of experience needs to be built before the practitioner tries this alone in their clinic.
Dr Ruth Harker is medical director of the Erme Clinic in the South West, which is a specialist centre for thread lifts and minor dermatological operations. Dr Harker also works for the NHS in the Skin Cancer Clinic at her local direct general hospital and is a procedural GP. She is finance and conference director of the British College of Aesthetic Medicine.
REFERENCES
1. Gilchrest BA, A review of skin ageing and its medical therapy, Br J Dermatol. 1996 Dec;135(6):867-75.
2. Townsend, Beauchamp, Evers, Mattox, Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, 20th Edition., p202, p207, p210, p241, p281, p327, p360.
3. Kiser, Kathryn, Oral Anticoagulation Therapy: Cases and Clinical Correlation, 2017.
4. John A. Heit, Perioperative Management of the Chronically Anticoagulated Patient, Journal of Thrombosis and Thrombolysis, September 2001, Volume 12, Issue 1, pp 81–87
5. Tonks, S, Understanding Threadlifting, Aesthetics journal, 2015. <https://aestheticsjournal.com/feature/ understanding-thread-lifting>
6. Moy et al, A Review of Sutures and Suturing Techniques, J Dermatol Surg Oncol 1992;18:785–795.
7. Information obtained from Sinclair Pharma’s World Experts Meeting, Barcelona in November 2018. More information is available from the author and Sinclair Pharma upon request.
8. Anthony Bewley & Dimitre Dimitrov, Recognising Body Dysmorphic Disorder in Aesthetic Practice, Aesthetics journal, 01 Dec 2015. <https://aestheticsjournal.com/feature/recognising-body-dysmorphic-disorder-in-aesthetic-practice>
9. Khavkin, Ellis, Aging Skin: Histology, Physiology, and Pathology Facial Plastic Surgery Clinics May 2011, Volume 19, Issue 2, Pages 229–234.

10. De Benito, J., et al., Facial rejuvenation and improvement of malar projection using sutures with absorbable cones: surgical technique and case studies. Aesthetic Plast Surg ,2011.35(2):p248-53
11. General Medical Council, Guidance for doctors who offer cosmetic interventions (April 2016) <http:// www.gmc-uk.org/guidance/ethical_guidance/28687.asp>
12. Hamman, Goldman,J Clin Aesthet Dermatol. 2013 Aug; 6(8): 16–18. Minimizing Bruising Following Fillers and Other Cosmetic Injectables Giner et al. Nutrition12,1, Jan1996, p 23-29.
13. Giner M1, Laviano A, Meguid MM, Gleason JR, In 1995 a correlation between malnutrition and poor outcome in critically ill patients still exists. Nutrition. 1996 Jan;12(1):23-9.
14. NHS, Treatment: Angioedema, 2019. <https://www.nhs.uk/conditions/angioedema/treatment/>
15. Arendt-Nielsen L, Egekvist H, Bjerring, Pain following controlled cutaneous insertion of needles with different diameter, Somatosens Mot Res. 2006 Mar-Jun;23(1-2):37-43.
16. Kearney et al ,Aus J Derm Volume42, Issue2 5/ 2001 p102-105 RESEARCH REPORT Long term patient satisfaction with cosmetic outcome of minor cutaneous surgery
FURTHER READING
• Suh, Dong Hye et al. Outcomes of Polydioxanone Knotless Thread Lifting for Facial Rejuvenation, Dermatologic Surgery: June 2015 - Volume 41 - Issue 6 - p 720–725
• Malcolm D. Paul, Barbed Sutures for Aesthetic Facial Plastic Surgery: Indications and Techniques, Clinic in Plastic Surgery, Volume 35, Issue 3, July 2008, Pages 451-461
• Rima F. Abraham, et al, Thread-lift for Facial Rejuvenation Assessment of Long-term Results, Arch Facial Plast Surg. 2009;11(3):178-183. doi:10.1001/archfacial.2009.10
• D. F. Horne, M. S. Kaminer Reduction of Face and Neck Laxity With Anchored, Barbed Polypropylene Sutures (Contour Threads).Skin Therapy Letter Volume 11 Number 1 February 1, 2006:p336
• Allen, D et al., Assessment of the biological safety of Silhouette Soft Suture: biological safety risk assessment,2015,Chorley Consulting: Alderley Edge, UK
• Palm, MD., et al., Cosmetic use of poly-l-lactic acid: a retrospective study of 130 patients. Dermatol Surg, 2010 36(2):p161-70
• Wei,Z.,et al., In vitro degradation, hemolysis, and cytocompatibility of PEO/PLLA composite coating on biogradable AZ31 alloy. J Biomed Mater Res B Appl Biomater,2015. 103(2):p342-54
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Unsightly puckering is more common with older patients as they have more redundant folds of skin, but this should settle with time so patience is needed
Wound Healing • Pain Management

Experience Celluma at: ACE, London Stand #42 Mar 1-2


FDA-Cleared Medical CE Mark
• Skin Care
Aesthetic Medicine London Stand #H36 Mar 23-24
Celluma is an integral component of NYDG signature treatments like the Triad and Runway Facials which employ the regenerative and lifting effects of multi-layered energy waves and technologies in single sessions. The biophotonic waves of Celluma are implemented as the final step to accelerate recovery by providing the cells with the energy to heal from within. Quite often, I recommend the device as an ongoing maintenance treatment at home to further optimise results.


Oculofacial
- The Wellness Clinic at Harrods, London - 119 5th Avenue, New York

Celluma ELITE Celluma PRO Celluma LITE
www.celluma.co.uk | Tel: +44 (0) 203 981 3993
Dr Costas Papageorgiou MD FACS
Plastic Surgeon New York Dermatology Group
“ ”
Treating the Submental Area
The submental area can be one of the most challenging areas of the head and neck to treat. This relates to both the underlying anatomy as well as various pre-existing factors; the principle being skin quality, but also including environmental insults (such as smoking and sun exposure), background genetic make-up and history of weight fluctuations. A typical patient presenting to clinic will either complain of a ‘double chin’ or a ‘turkey neck’, which in effect gives a clue to whether their problem is principally related to excess fat or skin, respectively. In some cases, there may be a combination of the two. In this overview, I look at assessment and treatment options for the submental area.
Surgical option
If the underlying issue relates to skin excess, usually as a result of ageing but sometimes associated with weight loss, I believe that surgery remains the gold standard in the form of a lower face/neck lift, with or without the addition of further direct access to the submental area via a submental incision to plicate the platysma muscle. Surgery also retains a strong role in addressing fat deposition in this area and has the advantage of allowing access to both deep and superficial fat compartments. Broadly speaking, the fat can be located superficially or deep to platysma. Superficial fat can easily be accessed using liposuction, as well as by a variety of non-surgical technologies, which I discuss in more detail below. Deep fat is more challenging to remove and can only be addressed via surgical means.




Non-surgical technologies
I would say that over the last 10 years, non-surgical technologies have been developed to address submental fat deposition through a variety of means. The non-surgical approaches offer a strategy to address pre-platysmal (subcutaneous) fat rather than sub-platysmal deep fat.1 They each offer potential advantages with varying side effects and are becoming an increasingly attractive alternative to surgery for many patients. Before discussing the various options
available to patients, it is vital to ensure that several key steps are taken during the assessment stage to adequately assess a patient for suitability for non-surgical submental approaches, as well as to determine whether surgery might be the more suitable option.
1. Skin assessment
First of all, the quality of the skin needs to be determined to assess whether there is a presence of skin excess or whether the morphology of the area is primarily due to fat deposition. If skin excess is present, this will have variable success in contraction once pre-platysmal fat is reduced. As a rule, the older and less elastic the skin is, the less predictable and less likely the skin is to retract. The risk in this situation is that fat reduction without skin removal leaves further excess, ptotic skin; much to the patient’s chagrin. In my experience, the best result with isolated fat reduction approaches are generally seen in younger, better quality skin that is generally thicker, non-sun damaged with more elasticity. If it is hard to determine whether the submental appearance is due to skin or fat, a good technique is to assess and compare the patient in lateral view standing and laying (Figure 1 and 2). If the patient retains submental fullness when laying supine, it indicates there is fat deposition in the area. If, however, the patient’s shape is significantly improved when supine with loss of submental fullness, then fat is not the underlying cause, but rather skin and platysmal laxity.
2. Fat distribution
It is key to determine whether submental fullness is a result of preplatysmal fat, or deep sub-platysmal fat (or a combination of the two). Isolated fat reduction techniques will not address sub-platysmal fat that resides between the platysma and floor of mouth. This can only be accessed surgically. To determine the location of the fat, a tip is to pinch the patient’s submental area and ensure a good hold of the soft tissue (Figure 3 and 4). Ask the patient to swallow. The tissue remaining in your pinch is subcutaneous/pre-platysmal. Any tissue that has been pulled away from between your pinch is sub-platysmal. It can be surprising in some cases how much of the submental fullness is actually sub-platysmal.
Non-surgical treatment options
Recently, novel technologies have gained traction to address this area non-surgically. There is an increasing desire to obtain a degree of improvement in the submental area without resorting to surgery, whilst patients are prepared to accept a more modest improvement with a non-surgical approach.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Mr Marc Pacifico outlines treatment options for addressing the submental area and shares a successful case study
Figure 1: Patient standing to observe submental fullness. Note at this stage it is not possible to determine whether the fat deposition is pre or post-platysmal.
Figure 3: Pinching of the submental fat.
Figure 2: Patient lying supine demonstrating maintenance of submental fullness, indicating the underlying issue is fat deposition, rather than skin excess.
Figure 4: Patient swallowing whilst submental fat pinched to assess preplatysmal component.












Low-level laser therapy
Rodrigo Neira et al. led initial studies1,2 providing evidence that the application of laser therapy at 635 nm with output intensity between 7 and 20 mw consistently induces the formation of a transitory pore within the membrane of adipocytes, provoking their collapse.2,3
The low-level laser therapy emulsified fat and encouraged its release from cells. This development initially led to it being used as an adjunct to surgical liposuction.2 Subsequently, Jackson et al. investigated using low-level laser as an independent isolated means of achieving fat reduction, without the use of additional liposuction.3,4 In the randomised control study, they demonstrated for the first time that the effects of lowlevel laser significantly achieved fat reduction. The same group reported an overall reduction in both triglyceride and total cholesterol levels following two weeks of laser therapy.5,6 Very few side effects of this treatment have been noticed, aside from localised redness, and a transient swelling of regional nodes, which is associated with the fat excretion.

Cryolipolysis
Case study
A 22-year old patient with underlying polycystic ovaries, presented in clinic complaining of submental fullness, which is not uncommon in those with this condition.11 It was something that she was particularly concerned with and as a result her confidence and self-esteem were very low. Examination revealed a significant area of pre-platysmal fat and good quality overlying skin. She underwent four treatments using the Strawberry Lift device, which uses low-level laser therapy, at two-week intervals. Over that time period she didn’t lose weight from the rest of her body, as she was just trying to focus on this area. The pictures below demonstrate her lateral view before undergoing any treatment, and then eight weeks after completing the course of four treatments. The patient was very pleased with the results and will be reassessed six months post treatment to see if any further treatments are indicated.
Before After
Since the ‘popsicle panniculitis’ observations, when buccal fat was noted to reduce in volume with cold exposure from ice-lolly sucking,8 a variety of cryolipolysis devices have been developed. This relies on controlled cold exposure to affect a gradual reduction of the subcutaneous fat layer using natural thermal diffusion, without damage to other tissues. Studies have demonstrated a 2-3.7 mm fat layer reduction, with no rise in serum lipid levels or derangement of liver function tests.7 Adverse effects include self-limiting effects such as erythema, numbness and sensitivity, and there have also been reports of paradoxical adipocyte hyperplasia requiring treatment with surgical liposuction.
Injection lipolysis
Using low dose formulations of a purified synthetic version of deoxycholic acid, focal adipocytolysis can be achieved, with the surround soft tissue being largely unaffected.8 A study held by Rotunda Am et al. using a combination of cell cultures and porcine skin treated with phosphatidylcholine demonstrated a significant loss of cell viability, cell membrane lysis, and disruption of fat.9 In my experience, these require a number of treatments (often two to three, but sometimes upwards of five) at one-month intervals. Adverse reactions tend to be localised and temporary, and can include injection site oedema, haematoma, numbness and, rarely, transient palsy to the marginal mandibular nerve.
Radiofrequency
Radiofrequency submental fat reduction relies on the deep heating of adipose tissue to stimulate destruction of adipocytes. A consensus statement published in 201710 suggested that subdermal radiofrequency treatment in the submental area was an effective means for disrupting fat volume and skin tightening. It also offered the potential for skin tightening of the face, neck, and jawline. However, in a similar way to most non-surgical approaches, the authors recognise that better results can be achieved in those with better skin quality and a mild to moderate degree of fat deposition. As with most of the other non-surgical options, most side effects are localised and self-limiting, such as erythema, pain, oedema and vesicle formation.
Summary
An accurate assessment is imperative to ensure that the treatment modality of choice is appropriate for the patient with concerns of their submental area. A non-surgical treatment being used to try to improve sub-platysmal fat will only lead to disappointment that could have been avoided. Whilst I believe that surgery remains the gold standard, the range of potential non-surgical treatments to address submental pre-platysmal fat is increasing, with few side effects or complications, and is becoming increasingly desirable to the patient population, partly due to the low to no downtime as well as being more cost effective.
Disclosure: Mr Marc Pacifico is a KOL for Laser Lipo, manufacturer of the Strawberry Lift.

Mr Marc Pacifico is an aesthetic consultant plastic surgeon based in Tunbridge Wells. His academic, surgical and practice achievements include being awarded the Gold Medal in the FRCS (Plast) exam, the publication of over 50 international peer-reviewed papers, being a regular invited speaker at conferences and being the director of the aesthetic clinic Purity Bridge, alongside his private surgical practice.
N Engl J Med 1970;282(17):966-7.
8. Avram MM, Harry RS, Cryolipolysis for subcutaneous fat layer reduction. Lasers Surg Med 2009; 41(10):703-8
9. Rotunda Am et al., Detergent effects of sodium deoxycholate are a major feature of an injectable phosphatidylcholine formulation used for localized fat dissolution. Dermatol Surg 2004;30(7):1001-8
10. Kinney et al., Use of a controlled subdermal radio frequency thermistor for treating the aging neck: Consensus recommendations J Cosmet Laser Ther. 2017 Dec;19(8):444-450
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
REFERENCES 1. Saluja S & Avram M, Overview of non-invasive treatments for submental fat reduction, PMFA Journal, August/Setpember 2018 Vol 5 No 6 2. Neira et al. Am J Cosm Surg vol. 18 No 3 pp133-140, 2001 3. Neira R, Arroyave, Ramirez H, et al. Fat liquefication: Effect of low-level laser energy on adipose tissue, Plast Reconstr Surg 2002;110:912–922 4. Robert F Jackson et al, Low-Level Laser Therapy as a Non-Invasive Approach for Body Contouring: A Randomized, Controlled Study, Lasers in Surgery and Medicine 41:799–809 (2009) 5. Maloney R, Shanks S, Jenney E, The reduction in cholesterol and triglyceride serum levels following low-level laser irradiation: A non-controlled, non-randomized pilot study, Laser Surg Med 2009;21S:66. 6. Chardonneau JM, Evaluation of fat reduction with non invasive transdermal low level laser using the strawberry laser diode, Personal Communication 7. Epstein EH Jr, Oren ME, Popsicle panniculitis,
Figure 5: Before and after four Strawberry Lift treatments over an eight-week period






Safe and Effective on ALL Skin Types • 360° Cooling for Virtually Pain Free Treatments • Ultra-fast Treatments (man’s back in under 5 minutes) • High Peak Powerful Diode Laser • Easy pre-set treatment protocols for ease of use • Outstanding on-going after sales program An Advanced and Efficient High Powered Diode Laser for Permanent Hair Reduction Two preset modes of operation: Slide and Pulse Telephone: 0208 748 2221 info.uk@venusconcept.com www.venusconcept.com High Powered Diode Laser for Hair Removal 23-24 March 2019 Olympia London SEE US ON STAND K20 SEE US ON 1 & 2 MARCH 2019 L ONDON SEE US ON STAND 58
A summary of the latest clinical studies
Title: Evaluation of Changes in Selected Skin Parameters Under the Influence of Extremely Low Temperature
Authors: Skrzek A, Ciszek A, et al.

Published: Cryobiology, February 2019
Keywords: Cryotherapy, hydration, lubrication
Abstract: The aim of the work was to evaluate changes in selected skin parameters under the influence of low temperature. The tests were conducted on a group of 20 women using whole-body cryotherapy. The average age of participants was 58.7 ± 7.54 years; the average body weight 77.84 ± 16.01 kg, the mean BMI 30.14 ± 5.81, and the average body height 160.7 ± 6.48 cm. The tested parameters included hydration, lubrication, temperature, and pH of the skin. The skin measurements were made on the first and tenth treatment days, before and after leaving the whole-body cryo-chamber. After a series of ten treatment sessions, the greatest decrease was observed in skin hydration and skin temperature. No significant differences were noted for lubrication and skin pH. The analysis showed statistically significant differences in skin parameters between all measurement locations; the upper and lower limbs responded more significantly than other parts of the body. It was also found that the facial skin was more lubricated and hydrated compared to other measuring locations. We conclude that various skin parts respond differently to low temperature. Cryotherapy causes a significant decrease in temperature and hydration of the skin whereas differences in pH and lubrication of the skin remain insignificant.
Title: Three-Dimensional Evaluation of Static and Dynamic Effects of Botulinum Toxin A on Glabellar Frown Lines
Authors: Rappl T, Wurzer P, et al.
Published: Aesthetic Plastic Surgery, February 2019
Keywords: Botulinum toxin, wrinkles, toxin, ageing
Abstract: We aimed at assessing static and dynamic effects of botulinum toxin A (BoNTA) on glabellar lines by use of an objective three-dimensional methodology. We prospectively collected threedimensional stereographic photographs of two different facial expressions (pre-treatment, 30 and 90 days’ post-treatment) in 21 patients, receiving a total of 20 units of BoNTA in both corrugator supercilii muscles. The primary endpoint was the three-dimensional static and dynamic surface irregularity, and secondary endpoints were the glabellar line scale and overall patient satisfaction. Blinded retrospective data analysis and statistical evaluation were performed with p < 0.05 considered statistically significant. Static glabellar lines (neutral facial expression) were significantly reduced by - 17% and - 24% on day 30 and 90 post-treatment, respectively (vs. pretreatment; both p < 0.0001). Dynamic glabellar frown lines (firmest possible bilateral eye closure) demonstrated a reduction of surface irregularity by - 26% and - 21% on day 30 and 90 post-treatment, respectively (vs. pre-treatment; both p < 0.0001). The subjective dynamic glabellar line scale documented a statistically significant improvement on day 30 post-treatment (mean ± SD: 1.5 ± 0.8; p < 0.05) versus pre-treatment (2.8 ± 1.0). Polled patients confirmed a subjective wrinkle improvement 90 days post-treatment. The presented setup detected even subtle changes of BoNTA treatment for facial wrinkling.
Title: Anatomy of the Superficial Venous Structures of the Neck: A Cadaveric Study to Guide Superficial Injections
Authors: Lee HJ, Ryu SY, et al.
Published: Dermatologic Surgery, February 2019
Keywords: Superficial venous, neck, dermal fillers, cadaver, veins
Abstract: The aims of this study were to identify the locations and communication patterns of the anterior jugular vein and external jugular vein (AJV and EJV) and the communicating vein (CV) based on superficial anatomical landmarks and to determine dangerous areas for dermal filler injections into the neck. Thirty sides of the neck from Korean adult cadavers were dissected for this study. Four anatomical variants were identified. In Type Ia, the CV ran along the anterior border of the sternocleidomastoid muscle (SCM) (33.4%); in Type Ib, a single vein was observed connecting the CV and the EJV at the level of laryngeal prominence (23.3%); in Type Ic, the CV proceeded separately from the medial side of the anterior border of the SCM (13.3%); and in Type II, the CV was absent while the EJV and AJV were observed (30%). Given the four anatomical variants identified in this study, the authors recommend exerting caution when performing dermal filler injections approximately 10, 30, and 60mm lateral to the midsagittal line to avoid iatrogenic side effects.
Title: Effects of Lactobionic Acid Peel, Aluminum Oxide Crystal Microdermabrasion, and Both Procedures on Skin Hydration, Elasticity, and Transepidermal Water Loss
Authors: Algiert-Zielińska B, Mucha, P et al.

Published: Journal of Cosmetic Dermatology, January 2019
Keywords: Microdermabrasion, chemical peel, hydration, Abstract: Topical applications of alpha-hydroxy acids and poly hydroxy acids in the form of peels gained popularity. To enhance the effect of these substances, aluminum oxide crystal microdermabrasion can be used in one procedure. The assessment of skin hydration, elasticity, and TEWL after using lactobionic acid in the form of 20% peel and lactobionic acid in the form of 20% peel combined with aluminum oxide crystal microdermabrasion. The study involved 20 Caucasian female subjects. Six treatments were performed at weekly intervals, using the Split face method –20% LA was used on the left side of the face and aluminum oxide crystal microdermabrasion followed by 20% LA application on the right side of the face. Corneometric measurement showed statistically significant differences between the hydration level for sessions 1 and 3 and 1 and 6. A higher hydration level was found on the side with the combined procedure. Tewametric measurement showed that the TEWL values were different for sessions 1 and 3 and 1 and 6 – they decreased. There were no statistically significant differences between the two procedures. The cutometric measurement indicated statistically significant differences between skin elasticity for pairs in session 1 and 3 and 1 and 6. The results of the study indicate that the combination of LA peel with microdermabrasion increases its moisturising effect and improves skin elasticity. The use of both procedures also contributed to the decrease in TEWL; however, greater exfoliation of the epidermis in combined procedures resulted in slightly higher TEWL values.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
www.cosmeticdigital.co.uk

Blogging? Branding?
Brochure design? Clinic naming? Content?
Content managment systems?
Conversion rate optimisation?
Dedicated super fast hosting? Digital marketing campaigns? eCommerce websites? Email marketing?
Exhibition design? Film & videography? Google display? Google Ads? Google remarketing? Landing pages? Leaflets?
Logo design? Magazine advertising? Marketing strategies? Packaging design? Photography? Printing? Search Engine Optimisation? Stationery design? Signage & planning? Social media? Social paid Ads? Website design? Welcome packs? WordPress?
With so many marketing options out there, it’s good to know there’s one company you can trust ;) Our customers say Excellent 4.92 out of 5 on Your industry, Our expertise Come and see us at ACE Stand 56 to discuss your digital marketing.
Understanding Facebook Advert Audiences
Marketing and PR professional James Dempster explains how to use Facebook audiences
With more than 52% of consumers searching online for information about treatment options, and 21% using social media to research health concerns or healthcare providers, there has never been a better time to adopt digital marketing strategies to support business growth.1
For aesthetic clinics looking to attract new patients and raise the profile of their business, Facebook advertising can be extremely fruitful, whilst delivering excellent return on investment. In this article, I’ll explore how to get the most out of your Facebook audiences and teach you how to monitor your success. With more than two billion active users on Facebook daily, and an average use time of 35 minutes per user, Facebook advertising is a fantastic way to reach new patients, customers and new employees.2
What is a Facebook audience?
As you may know if you are involved with your clinic’s marketing, Facebook advertising allows you to choose and target who sees your advertisements. The ‘target’, ‘ideal patient’ or ‘market’ that you want to advertise to is called an ‘audience’ on Facebook. As well as targeting users by location, age and sex, Facebook also enables you to target by interest, behaviour and engagement. There are three audience selection tools that Facebook offers to help you find the people who are right for your business –core audiences, custom audiences and lookalike audiences.3 These audiences can be advertised to via Facebook, Instagram, Facebook Messenger, or through mobile apps with Audience Network. Audience Network is a way for advertisers to extend their campaigns beyond Facebook and into other mobile apps.4 Whilst it may seem like there are a lot of decisions to make around how to create your audience, it’s important to spend time ensuring that you get it right. After all, you don’t want to waste your budget targeting someone that has no
interest in aesthetics and will be unlikely to convert into a new patient.
Core audiences
Core audiences allows you to target adverts using Facebook data.5,6 This data is collected by Facebook every time you consent to share your data. Facebook sweeps your Facebook profile, your recent activity, and any changes to build a profile of you, what you’re interested in and what you’ve engaged with recently.7 Building a core audience lets you build an audience based around the following options:
• Location: reach people in the cities and towns where you want to do business. You can either choose everyone in a location, only people who live in a particular location, new residents who have updated their location recently or visitors who have checked into or been tagged in another place.
• Demographics: create your audience based on age, gender, education, relationship status, job title and more.
• Behaviour: choose people based on their prior purchase history, their device usage (desktop, tablet or mobile), and other activities such as the browser they’re using.
• Connections: reach people who are connected to your Facebook page or event and have either ‘liked’ or ‘followed’ your page or are ‘interested’ or ‘going’ to your events. You can also exclude them to ensure you’re reaching a new audience.
• Interests: target your adverts to people who are already engaged in your sector.
Custom audiences
Facebook custom audiences are built from patient data that you have and supply to Facebook. Custom audiences can be built with three key sets of data: contact lists, website visitors and app users. Uploading
this data to Facebook will allow you to create a potential audience based on people that have already shown an interest in your business. You can upload the data you collect from your own business to Facebook via a .csv file, but only if your patient has explicitly said that they are happy for their data to be used in this way.8 It is worth noting that although Facebook states that 100 people is the minimum audience size to target Facebook users, we would recommend an audience size of at least 1,000 for it to be truly effective. Custom audiences also allow you to use data from those who have visited your website, commonly known as remarketing. Whilst there is a common misconception that since GDPR remarketing isn’t allowed, so long as you have a robust cookie policy (you often see these pop up on websites), remarketing is allowed.9 This is a great way of connecting with people who have already shown interest in your website, but have not necessarily gone on to book a treatment with you. In order to set this up, you will have had to install a Facebook pixel on your website. A Facebook pixel is a piece of code that’s placed on your website that enables Facebook to gather the data of people who have visited your website.10,11 The pixel only tracks users that have opted in to allow cookies to be collected, so be mindful that it won’t track everyone. In order to create a pixel, if you don’t have one already, you’ll need to follow Facebook’s instructions or ask your digital marketing team for help.10,11
Lookalike audiences
Facebook’s lookalike audience function is a fantastic way to reach an audience that you are currently not engaged with, but who will very likely be interested in what you have to offer. A ‘lookalike’ audience is just that, an audience that quite literally ‘looks like’ another particular audience that you decide upon. This function takes on board information about the demographics and behaviours of your existing patient base, and Facebook will then automatically identify similar qualities of your chosen group and class this audience as ‘lookalikes’.12 For example, a very effective way of employing lookalike audiences within your Facebook advertising campaign is to create a custom audience (explained above) based on your most valuable patients, also known as a value-based lookalike. These could be the patients who booked three or more treatments in the last six months, for instance. You could upload their details on Facebook and create a ‘lookalike’ audience based on this information. As a result,
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com





AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
Top tips to ensure you’re targeting the right audience
1. Take time to understand what data you already have about your ideal patients. Rather than dive straight into Facebook to select your audience, work with your team to discover who your ideal patients are, what you know about them already, and what data you already hold about these patients.
2. Test, test and test again. Use A/B testing to really understand if your adverts are resonating with your audiences. It might be trial and error to begin with, but it’s worth the time and effort in the long run.
3. Use the Audience Insights tool.14 Audience Insights looks at trends relevant to your potential patients across Facebook, which means you can gather even more information about demographics, Facebook usage, page likes and past purchase behaviour. Using audience insights allows you to get aggregate information that includes demographic, Facebook usage, location and purchase history. Armed with this information you can decide whether Facebook advertising is an effective channel for you to be focusing on. If your target audience turns out to not be massively invested in their Facebook profile, it would be worth trialling other channels.
4. Be specific about who you want to reach. There’s no point serving adverts to audiences for the sake of it. To make the most of your investment, you’ll want to focus on the people who matter most to your business.
Facebook’s algorithm will start looking for users with interests and behaviours similar to the ones of your most loyal patients, who in turn are more likely to become loyal patients themselves. Essentially, you can create a lookalike audience from any audience you create on Facebook, making it easier for you to test varying adverts and offers based on a user’s previous habits.
How should I monitor the success of Facebook advertising?
Once you’ve spent time creating audiences, you need to make sure they’re working for you. If they aren’t, you need to be able to adapt and change it to get the best value for money, and importantly, get new patients through your doors. Once your adverts are up and running for at least seven to 10 days, you can begin to gather some insight into whether or not they’re working for your business. It’s important to understand what ‘good’ looks like, so here are my tips:
1. Concentrate on the advert’s objective – is it delivering the leads you want? (if leads are the main objective).
2. Look at interactions (likes, comments, shares) over the reach (how many people have seen the add). Interactions show that your advert is resonating with your chosen audience.
3. Relevancy score – does Facebook deem your advert to be relevant to your audience?
4. Frequency – you don’t want to bombard your audience. We suggest aiming for each advert to be shown no more than three
times throughout the campaign.
5. Cost per result – is it financially viable for the ads to continue? For example, if you make £20 per procedure and convert one in five appointments to a procedure, you’ll need to ensure that your cost per lead is £4 or less.
If you’re not seeing the engagement you expected, it could be that your target audience is too narrow and so is reducing the chances of spending your budget. This varies by case, but measure against your own results. If not enough people are reacting to the advert, try expanding the amount of people seeing it. Measuring success will depend on what your goal is, but let’s say it’s that you want to promote a new service your clinic offers. You’ll expect to see clicks through to your website from the advert, the users may spend significant time on the page, and then if there’s a relevant enquiry form on the site that you’re directing people to, you’ll want to see an increase in completed forms. This can all be tracked through Google Analytics so you can ensure that your adverts are delivering the traffic and interaction you expect.13 If you’re not seeing the uplift in enquiries that you’re expecting, you can optimise your Facebook adverts and improve their performance with A/B tests. This essentially means that you can show two or more versions of an ad to similar audiences to see which one performs better. This is great if you want to test a few different audiences to see which one is more engaged. Each group will have identical ad sets except one variable, in this case, the
chosen audience. This will then be measured against your campaign objectives and once complete, Facebook will notify you of the winning strategy.
Start engaging
Whether you’re looking to promote a new treatment your clinic offers, you’re opening a new practice and want to increase footfall, or you want to encourage people to engage with your social channels, Facebook advertising is a great way to do this. It can allow you to reach out to your current patients who may not have engaged with you in a while, or it can help you find whole new audiences. You don’t need to be a marketing expert to see brilliant results from Facebook advertising. As long as you’re carefully choosing your audience and monitoring your adverts, you’ll soon be able to make tweaks and amends that will propel your adverts to the next level.
James Dempster has worked in marketing and PR for more than 10 years. Previously a commercial director for a private hospital, in 2013 he formed a business partnership to found Cobb Healthcare, a full-service marketing and PR agency for healthcare professionals, and Cobb Digital, a digital marketing agency aimed at helping all sectors create powerful online campaigns.

REFERENCES
1. Chris Girardi, The Evolving Role of Digital Marketing in Healthcare (USA: Evariant, 2017) <https://www.evariant.com/ blog/evolving-role-digital-marketing-healthcare>
2. Maddy Osman, 28 Powerful Facebook Stats Your Brand Can’t Ignore in 2018 (USA: Sprout Social, 2018) <https://sproutsocial. com/insights/facebook-stats-for-marketers/>
3. Facebook Business, Help your ads find the people who will love your business. <https://www.facebook.com/business/ads/ ad-targeting>
4. Facebook, Introducing Facebook’s Audience Network, 2014. <https://www.facebook.com/business/news/audiencenetwork>
5. Facebook Business, Easier, More Effective Ways to Reach the Right People on Facebook. <https://www.facebook.com/ business/news/Core-Audiences>
6. Lister, M, All of Facebook’s Ad Targeting Options (in One Epic Infographic), WorldStream, 2018.<https://www.wordstream. com/blog/ws/2016/06/27/facebook-ad-targeting-optionsinfographic>
7. Facebook, Data Policy, 2019. <https://www.facebook.com/ full_data_use_policy>
8. Optimizely, Optimize your digital experiences and achieve the greatest return on investment in SaaS. <https://www.optimizely. com>
9. Facebook Business, What is the General Data Protection Regulation (GDPR)? <https://en-gb.facebook.com/business/ gdpr>
10. Hootsuite, The Facebook Pixel: What It Is and How to Use It, 2019. <https://blog.hootsuite.com/facebook-pixel/>
11. Facebook Business, Use Facebook pixel. <https://www. facebook.com/business/help/952192354843755>
12. Facebook Business, About Lookalike Audiences, 2019. <https://www.facebook.com/business/help/164749007013531>
13. Optimize Start, Complete Guide to Google Analytics for Facebook. <https://www.optimizesmart.com/tracking-facebooksocial-interactions-with-google-analytics-and-google-tagmanager/>
14. Facebook Business, Learn More About the People that Matter to Your Business with Facebook Audience Insights, 2014. <https://www.facebook.com/business/news/audience-insights>
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com




1 & 2 MARCH 2019 / LONDON SEE US AT
Knowing Your Competition
Having grown 200% since 2000,1 it’s fair to say that the aesthetics industry is bursting with competition and the range of skills, offerings and ethics is diverse. From experience, it’s very easy to get wrapped up in your own business, expertise and services, and not pay attention to what your competitors are doing, as those are of course very important aspects to you. Personally, I put a lot of emphasis on listening to patients and treating them well; I don’t let myself become too distracted by competition, however, I believe there is real merit in having a look at what your competition is and isn’t doing. By analysing your competition, your business can benefit by filling the gaps in their services and you can find ways to stand out from competitors. Healthy competition is positive, especially in an over-crowded industry as it keeps both you and your employees on your toes.2 Quite simply, competition forces you to assess what reasons you give patients to pick you over a competing clinic or practitioner and allows you to amend your offering and services accordingly. When analysing your competition, it’s best not to simply look at your perceived competitors in isolation. There are three main areas of focus you should evaluate if you want to use this activity to better your business; you, your patient and your competitors. The idea is not to emulate your competitors but to use this information to stand out from them.
1. What do you offer?
When distinguishing yourself from your competition you must first define your
unique selling points (USPs); a fundamental, key exercise as this will allow you to market your offerings and set yourself apart from any competition. Start by listing points about you and your business which motivate your patients to come to you, for example, good transport links to your premises, discreet or easily-found location, your specific qualifications and experience, so that you can start effectively selling yourself and your services.3 I know that medical professionals occasionally find it difficult to ‘sell’ themselves but it is important to get to grips with this skill. If you don’t give your potential patients strong enough reasons why they should use your services over others – your competitors will. If you are struggling to find your USPs go straight to your patients. Ask them why they first came to you and why they keep visiting you; you could do this either verbally or you may consider sending a survey to your patients. These are your strengths, use them. When defining your USPs, I would strongly discourage you to use cheap prices4 as one of your selling points because it not only cheapens your skills, experience and service, but gives you little flexibility with pricing your services in the future and can be easily matched by your competition.
2. Identifying your ideal patient
It’s not enough to say that your target patient is anyone who is interested in the services you offer.5 Narrow your view and be specific in identifying who your ideal patient is so you’re able to target them with your marketing efforts; this will save

you money and give you a better return on your investment. Ask yourself, what’s going to be most cost and time effective? Will it be shouting your message about treating ‘mummy tummies’ into a room of people of all ages, sexes, incomes and aesthetic needs? Or targeting a room of people who are mothers or soon-to-be mothers with an income that would allow them access to your services?
Who will use your services?
Start by asking yourself who will be using your service. If you’re not sure where to start, describe your ideal patient(s); perhaps they already come to you and you would like more of the same. This will generally be the patients who bring in the most business. This is an important step as it helps you to understand if you are dipping into the same pool of patients as other practitioners in a similar location. Define their sex, location, age, income, lifestyle, hobbies and services they’d benefit from. For example, female, aged between 45 and 55, located in Chelmsford or close surrounding area, ABC demographic, plays sports such as tennis and golf, socialises frequently with friends at local restaurants, non-smoker, goes on holiday at least once a year, has adult children and will be interested in rejuvenation treatments for the face and body. The more detailed your definition, the better, as we are currently living in an age where we can target potential customers online using these exact details, like Facebook advertising for example.6
Having a detailed image of your ideal patient should also help you keep on track with business decisions outside of marketing, such as what new treatments and products to bring into your business. If you’re not able to get into this level of detail, you may consider surveying your ideal patients and finding out these details directly from them; even if you think you know these answers, there’s no harm in doing this as well as there may be things that surprise you. Google Forms7 and Survey Monkey8 are useful tools to help you do this.
Why do your patients come to you?
When analysing why your patients come to you, break it down into two segments; the tangible reasons and the emotional reasons. These all make up the value in your offering.9
The tangible reasons should be reasonably clear to you and may include elements such as qualifications, amount of experience, ease of location, devices/treatments offered, customer service. Evaluating the emotional
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Clinic owner Kerri Lewis discusses the benefits of knowing your competition and how to act upon this to improve your business
Consent Required Face Up To It
Patient photographs form part of a patient’s medical record and should be treated with the utmost confidentiality.
If you don’t have the patient’s specific consent to use their images outside of their medical records, you could run the risk of legal action even if the images are anonymised.

At Enhance we can protect you against any alleged breach of confidentiality whether founded or otherwise.
If you require any further guidance regarding data protection issues call us today and we’ll help you implement the tools to mitigate future problems and help with compliance.
Call: 0800 980 3776 Visit: www.enhanceinsurance.co.uk Enhance Insurance is a trading name of Vantage Insurance Services Limited (VISL) registered in England (No 03441136)which is authorised and regulated by the Financial Conduct Authority.
aspect of what drives your patients to use your services will allow you to talk to them in a meaningful way rather than simply telling them about a device you have; in marketing the idea of describing the benefits, not the features of whatever it is you’re selling is a well-known concept and it’s important not to overlook the ‘emotional benefits’10 of your offering. Charles Revson, founder of cosmetic brand Revlon is well documented as saying, “In the factory we make cosmetics; in the drugstore we sell hope.”11 Ask your patients why they come to you and what they’ve gained from the treatments you’ve performed on them and/ or have a look at your patient reviews; the emotive reasons behind their visits and loyalty should become clear. When I look at the patient reviews for my business, roughly eight to nine out of 10 won’t even mention the treatment or the results they’ve achieved, they focus on how we’ve made them feel during their visits and the feelings associated with their results, for example, they feel they can now go out without makeup on. Speak to your target market in a way that they can identify with, so that they understand that by seeing you they’ll be moving away from the pain they’re experiencing and towards pleasure.12
By identifying and talking about the emotional benefits of your service you’ll also be able to try to overcome some of the preconceived ideas and hurdles about your services, such as controversial press coverage on dermal fillers.13 Once you have a solid definition of what makes you and your business special, you’ll be able to look at your competitors and make a direct comparison to help refine this further and give your business a competitive edge.
Scoping out your perceived competitors
I believe that by following the above steps you will have a better judgement on whether someone else is even a competitor in the first place; then you can define what it is you are competing on. I say ‘perceived’ here because the aim is to position yourself so that you have no real head-to-head competition
by making yourself stand out to those in a similar location to you, those who attract similar patients and those who have a similar treatment offering. In order to do this, you need to analyse your competition. I find listing competitors side-by-side is helpful, but I’ll discuss that later. First, figure out how you’d like to research your competitors:
• Internet search: you may be able to get much of the information you are looking for on your competitors’ website and social media.
• Mystery shop: pay your competitors a visit as a patient, you’ll be able to get a lot of information about their offering and customer service. You may wish to do this over the phone or in person. What was your journey like and is there anything you can learn from this experience, both positive and negative?
It almost goes without saying that you should conduct yourself in a respectful manner whilst doing this. If you think that you may be recognised, it could be uncomfortable for both parties, so task a colleague with this visit instead and give them a comprehensive list of what you’d like them to ask and pay attention to. I would strongly advise doing both; a bare minimum of internet research and mysteryshopper phone calls. You’ll probably know the relevant competitors you want to research, and I would put a limit on the amount you want to look at otherwise it may become very time consuming; I don’t tend to look at more than five or six.
Before you start your research, make a list of what exactly your ideal patients, as mentioned above, want and/or need and mark your competitors out of five for each of those points, one showing that you think that this aspect of their offering/service is very poor.
I’ve found using this chart (Figure 1) from D. Edwards et al 14 simple and easy.
To help you understand further, examples of things you may want to measure as suggested in the above table’s left hand column could include; non-surgical rejuvenation treatment options, female-only practitioner, dermatologist on site, weekend availability. As previously mentioned, you may find it useful to directly ask your patients why they use your business to help you define
these points. Once you’ve conducted your research, tally up each competitors’ score at the end of the row and you should get good idea of how well patient needs and wants are being addressed. Those needs/wants that tally the lowest scores give you an idea of the weakness in your overall competition and these are aspects that you should consider filling within your own business. It is important to note, this is not a one-time activity and should be part of an annual routine; your competitors’ businesses will be evolving and you’ll need to be aware of this as it will impact on yours.
Embrace the competition
In conclusion, healthy competition should be embraced because it forces your business to perform at its best. Rather than be overly concerned and preoccupied by your competitors, a simple, regular analysis of them can help you refocus and re-evaluate your business and patients, thus using your competitors’ weaknesses to strengthen your business offering.
Kerri Lewis opened her clinic, The Skin to Love Clinic, in St. Albans in 2013. She also won the SME Young Business Person of The Year award in 2017 and the Business Woman of the Year award in 2018.

REFERENCES
1. Medical Aesthetics Market By Product (Dental Implant, Breast Implant, Facial Aesthetics, Laser-Based Aesthetics, Body Contouring Aesthetics, Others), Credence Research, November 2018 < https://www.credenceresearch.com/report/ medical-aesthetics-market>
2. Forbes, 5 Reasons Why Competition is Good for Your Business, <https://www.forbes.com/pictures/emjl45fhdh/ innovation/#68c8c7243a76>
3. The Economic Times, Definition of Unique Selling Proposition <https://economictimes.indiatimes.com/definition/uniqueselling-proposition>
4. Machado R, Cassim S, Marketing for Entrepreneurs, 2nd edition, pg 10, 2002
5. Porta M, How to Define Your Target Market, Inc.com <https:// www.inc.com/guides/2010/06/defining-your-target-market. html>
6. Burke Z, The Beginner’s Guide to Facebook Marketing: Master Organic & Paid Reach, Digital Marketing Institute <https:// digitalmarketinginstitute.com/en-gb/blog/beginners-guidefacebook-marketing-master-organic-paid-reach>
7. Google, Google Forms <https://www.google.co.uk/forms/ about/>
8. Survery Monkey.co.uk <www.surveymonkey.co.uk>
9. Marketing Donut, Why value-based pricing works best <https:// www.marketingdonut.co.uk/marketing-strategy/pricing/whyvalue-based-pricing-works-best>
10. Simone S, Why Emotional Benefits Are The Key To Reader Response, Copyblogger.com <https://www.copyblogger.com/ emotional-benefits/>
11. Dowling G R, Winning the Reputation Game: Creating Stakeholder Value and Competitive Advantage, The MIT Press, April 2016
12. Higgins E T, Beyond Pleasure and Pain. American Psychologist, 1997 <https://doi.org/10.1037/0003-066X.52.12.1280>
13. Singh H, The Elevator Speech, Aesthetics journal, November 2016 <https://aestheticsjournal.com/feature/the-elevatorspeech?utm_sq=fsh73dxvja>
14. Hess E, Goetz C, So, You Want to Start a Business?: 8 Steps to Take Before Making the Leap, 2009
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 1: An example of a completed comparison table for your competitors14 Customer Needs/Wants Competitors A B C D E F G Total 1st Need/Want 4 1 3 5 2 4 5 24 2nd Need/Want 1 3 3 2 4 2 3 18









Official partners in UK and Ireland 01827 338115 www.johnbannonpharmacy.co.uk enquiries@johnbannonpharmacy.co.uk 00353 1678 9665 www.johnbannonpharma.co.uk info@johnbannon.ie
Boosting Your Social Media Profile
website. There are now one billion Instagram users and they’re an engaged user base; the average person spends one hour on the platform every day.5,6 Instagram users have the greatest engagement out of all platforms – 10 times that of Facebook for the same number of followers.7 I get far less patients coming to me from Twitter; however, all posts are index linked on Google, so it helps with search engine optimisation (SEO). I’m also on Facebook and LinkedIn; but Facebook is a more financially-driven platform, which means that your posts are shown to more people based on your spend and LinkedIn is mainly business to business so I don’t tend to get patients this way.
My keys to success
Social media (which I refer to as SoMe) is now an essential tool for business. In this article, I’m going to show you the possibilities that stem from using SoMe and how you’re limiting your business if you don’t. I’ll also share with you my SoMe journey, from zero to 250,000 followers on my various platforms from 2015 until now.
Why my focus is on social media
I find that these days, most patients do their homework via SoMe. In fact, according to the latest statistics from the aesthetic review website RealSelf, 97% of patients expect online engagement.1 The number one consistently trending healthcare hashtag in the world with four billion views per year is currently #PlasticSurgery and the public are turning to this to seek credible, medical information.2 SoMe is a visual medium so it is well suited to aesthetics. What I find patients want is two-way communication. They have questions and possible concerns, and they want to know that the practitioner they choose is communicative, accountable, approachable and competent and, in my experience, patients believe that practitioners who have successful SoMe accounts demonstrate this. SoMe also allows you to engage, educate and control your digital image. SoMe is the new language of plastic surgery and non-surgical aesthetics and it is quickly overtaking word-of-mouth as the most popular way of obtaining information.3 I believe that SoMe also assists you with your
consultation to treatment conversion rate. Although there is no published data on this yet, I have heard numerous times at conferences that approximately only 40% of patients who go to a consultation follow through with the actual treatment. My conversion rate is more than 95%, which I think is because my patients already feel they know me, my ethos and the treatment they want through SoMe. In addition, SoMe channels are saturated with relentless marketing from unscrupulous organisations and practitioners representing untrained, poorly-qualified individuals. This is why it’s so important for the genuine experts to make a huge effort to be visible on SoMe.
My SoMe journey
My journey started in 2015 when I opened my Twitter account. Today, I have 150,000 followers on Twitter as well as almost 100,000 followers on Instagram, where my focus has moved primarily for reasons described below. According to the Aesthetic Surgery Journal, my large following has led me to be one of the top global SoMe influencers in plastic surgery.4 My demographic (patients seeking breast augmentation, body contouring and non-surgical facial aesthetics) are huge users of SoMe; in particular, Instagram. Instagram is what I consider to be ‘the new website’ as 90% of my patients come via Instagram and most of the remaining 10% have checked out my work and approach to aesthetic treatments before getting in touch via my
From my experience, I think one of the key pillars for success on SoMe includes being positive and to never engage in arguments. Be social, be kind, support others and interact with them. As well as following marketing guidelines,8-15 I believe practitioners should always behave ethically and never target insecurities. They should focus on education, patient happiness and wellbeing, both physically and mentally, and the consequence of different treatments on outcomes. I strongly believe that SoMe should be used responsibly; I believe that we as medical practitioners shouldn’t promote a false ideal of beauty or overdone, exaggerated looks. As such, I use my voice to promote natural beauty, and I recommend that my colleagues to do the same.
Images
Don’t use stock photos or poor quality images, and remember that you must have full explicit consent to use clinical photos.16 I recommend avoiding overuse of before and after images because I believe that, to some extent, they have a negative aspect in that they celebrate how good someone looks now in relation to how ‘bad’ they may have looked before. As mentioned, I always try to advocate natural beauty on my SoMe feeds – indeed I use the hashtag #naturalbeauty in my posts and typically post photos of patients looking natural and refreshed, without wearing makeup, rather than before and after photos. Although, I do sometimes use before and after images because they are quite popular with patients. If using before and after images, be sure to follow the Advertising Standard Authority’s guidelines.14 I also find that re-sharing patients’ posts works well – I repost images that my patients send me to post after their treatment
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Mr Olivier Branford shares his social media journey and explains how he uses it as his primary way of educating and attracting patients

or images where they have recommended me. I want to emphasise that patient images should never be manipulated and I also advocate the avoidance of graphic surgical images – according to Realself, 8% of people are turned off by graphic/gory content.17
Content
I have coined the term ‘academic marketing’, which essentially means to use the evidence base as content – I have 50 PubMed cited publications which I share on SoMe. To make it easy for patients to understand, I mainly talk about my publications on breast beauty, SoMe and plastic surgery and do not go into too much detail about the actual paper. This is a form of content marketing – the process of creating and distributing relevant and valuable content to attract, acquire, and engage an audience with the objective of driving profitable customer action. It’s about educating, rather than selling.
Influencers
I have also found influencer marketing, the new buzz word, very successful for my business. This involves collaborating with prominent individuals to help produce and distribute content. People want to ‘buy’, but they don’t want to be sold to! So how do you sell without selling? As medical professionals we are familiar with the term ‘key opinion leaders’ (KOLs), but in the world of SoMe, these are known as ‘digital opinion leaders’ (DOLs).18 The fact is that most of the top aesthetic and beauty influencers are not practitioners – only 18% of top plastic surgery posts on SoMe are by boardcertified plastic surgeons.3 When working with influencers, I recommend the use of videos and even podcasts for different and interesting content. I recently recorded a podcast on breast augmentation with my patient Mimi Bouchard, who runs a lifestyle podcast. This sort of content makes a very useful resource for prospective patients, is good content for my SoMe, and my expertise was broadcast by an individual who has 162,000 Instagram followers.19
Other tips
I believe in posting about ‘hot’ and trending topics, such as the recent risks of buttock fat grafting that was highlighted in the media. Keep an eye on trending hashtags and news in the industry and be sure to comment about it. I believe that the future is all about video – and I am not alone. The latest Cisco Visual Networking Index Complete Forecast predicts that by 2022, 82% of all IP traffic
will be video.18 So, start thinking about how you can implement video into your SoMe. Another useful way to gather new followers, I find, is to follow the kinds of people you think could be potential patients. Social media is social; unless you are a celebrity, I feel that you can’t build your following without making new contacts, so follow new people and try to engage with them as much as possible so that they follow you back.
SoMe management
Of course, what must be noted is that SoMe does take time, effort and energy. I often hear from surgeons and other aesthetic professionals that they don’t have time to be on SoMe. What I simply say to them is that, really, you have to be. Treat it as any part of your daily commitment, like opening your emails, rather than an ‘extra’, which it’s not. Learn to be efficient with managing your SoMe and take your time – it’s a marathon, not a sprint. I mainly manage my SoMe on my commute and find that it matches the time that many of my followers are online. Talk to your following, even if it’s just one person at a time and remember that we all start somewhere. I personally advise to manage your SoMe yourself, although you can get some help from a third party. I manage it myself because I find that it’s possible to engage with your followers through conversations better this way. Although some people and businesses find it useful to automate posts, and they are very successful at doing so, I never do this as I believe that SoMe must be responsive and I don’t believe automation would work for my current follower base.
Conclusion
With the majority of my new patients finding me through Instagram, I see communication through this platform as being an essential skill for any aesthetic practitioner hoping to be successful in today’s society. I always recommend that you add a personal touch to your brand by engaging with individuals. Using SoMe successfully will help you to gain patients and build trust in your brand, and trust is marketing gold.
Mr Olivier Branford is an aesthetic plastic and reconstructive surgeon. He is one of the most followed consultants on social media globally. He is consulting editor for social media at PRS Global Open Journal, a member of the social media committee at the American Society of Plastic Surgery and also acts as a social media consultant for a number of aesthetic brands.

REFERENCES
1. RealSelf, What Patients Really Want, 2018. <https://www. slideshare.net/realselfinsights/what-patients-really-want>
2. OA Branford, P Kamali, RJ Rohrich, D Liu, DH Song, P Mallucci, K Sun, M Stubican, SJ Lin. #PlasticSurgery Plast Recon Surg 2016;138(6): 1354-65.
3. Dorfman RG, Vaca EE, Mahmood E, Fine NA, Schierle CF. Plastic Surgery-Related Hashtag Utilization on Instagram: Implications for Education and Marketing. Aesthet Surg J. 2018;15;38(3):332338.
4. A Chandawarkar, D Gould, W Stevens, ‘The Top 100 Social Media Influencers in Plastic Surgery on Twitter: Who Should You Be Following?’, Aesthetic Surgery Journal 38(4), March 2018.
5. Statista, Number of monthly active Instagram users from January 2013 to June 2018 (in millions). <https://www.statista.com/ statistics/253577/number-of-monthly-active-instagram-users/>
6. Rani Molla and Kurt Wagner, People spend almost as much time on Instagram as they do on Facebook, Jun 25, 2018. <https:// www.recode.net/2018/6/25/17501224/instagram-facebooksnapchat-time-spent-growth-data>
7. TrackMavan, What 51 Million Pieces of Content Say About Your Social Media Marketing Strategy, 2019. https://trackmaven.com/ blog/social-media-marketing-strategy-report/
8. Cosmetics Interventions Marketing (non-broadcast and broadcast), Committee for Advertising Practice, Marketing of Cosmetic Interventions, (2013). <https://www.asa.org.uk/adviceonline/cosmetic-surgery.html>
9. GMC, Guidance for Doctors Who Offer Cosmetic Procedures, General Medical Council. <http://www.gmc-uk.org/guidance/ ethical_guidance/28687.asp>
10. Medicines and Healthcare Products Regulatory Agency. Blue Guide: advertising and promotion of medicines in the UK. Third Edition, First revision (September 2014) <www.assets. publishing.service.gov. uk/government/uploads/system/uploads/ attachment_data/file/376398/Blue_Guide.pdf>
11. Nursing and Midwifery Council. Guidance (2018) <www.nmc.org. uk/standards/guidance/>
12. General Dental Council. Guidance on advertising (September 2013) < https://www.gdc-uk.org/api/files/Guidance%20on%20 advertising%20(Sept%202013).pdf>
13. Committee of Advertising Practice. The CAP Code; The UK Code of Non-Broadcast Advertising and Direct and Promotional Marketing (2014) <www.asa.org.uk/uploads/assets/uploaded/ cacc4b1f-5171- 4ba4-8679bb383a25aa2a.pdf>
14. Committee of Advertising Practice, Before and after photos (December 2014) <www.asa.org.uk/advice-online/before-andafter-photos.html>
15. Julia Kendrick, Maintaining Compliant Marketing in Aesthetics (UK: Aesthetics, February 2017). <https://aestheticsjournal.com/ cpd/module/maintaining-compliant-marketing-in-aesthetics>
16. Martin Swann, Patient Photography and Data, Aesthetics journal, 2018. <https://aestheticsjournal.com/feature/patientphotography-and-data>
17. CISCO, VNI Global Fixed and Mobile Internet Traffic Forecas. <https://www.cisco.com/c/en/us/solutions/service-provider/ visual-networking-index-vni/index.html>
18. Gregg Fisher and Kevin Michels-Kim, Digital opinion leaders (DOLs) and their role in pharma markets, 2017. <https://pharmaceuticalcommerce.com/brand-marketingcommunications/digital-opinion-leaders-dols-role-pharmamarkets/>
19. Mimibee Podcast, #47: Plastic Surgeon Olivier Branford Answers Your Boob Job + Filler Questions (Recorded Live At The Cadogan Clinic!) <https://www.mimibee.com/47-plasticsurgeon-olivier-branford-answers-your-boob-job-filler-questionsrecorded-live-at-the-cadogan-clinic/>
Mr Olivier Branford is speaking on boosting your social media profile at the Aesthetics Conference and Exhibition (ACE) 2019 at the Business Track on Friday March 1 at 10:50am. To attend, register free by visiting www.aestheticsconference.com
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
1 & 2 MARCH 2019 / LONDON
333 200 4143.

M-BEL-UKI-0474 Date of Preparation February 2019
forms and
A Natural Look is an EXACT SCIENCE ® www.lips.belotero.co.uk The new digital consumer campaign is now LIVE Want to get involved? Contact Church Pharmacy, Wigmore Medical or your Merz Aesthetics Account Manager The ONLY COMBINATION approach to lip enhancement, specifically designed to target the VERMILION BORDER AND BODY OF THE LIP BELOTERO® Lips Shape To volumise the body of the lip (0.6ml) BELOTERO® Lips Contour To create definition in the vermilion border (0.6ml) In partnership with www.wigmoremedical.com www.churchpharmacy.co.uk
Adverse events should be reported. Reporting forms and information for United Kingdom can be found at www.mhra.gov.uk/yellowcard. Reporting
information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/report-an-issue/mdiur. Adverse events should also be reported to Merz Pharma UK Ltd by email to UKdrugsafety@merz.com or on +44 (0)
As the owner of four clinics across London, two franchises and a career that spans more than three decades, Esther Fieldgrass’ approach to aesthetics has been unique, particularly in comparison to others in the specialty. It all began in the 1970s with training in beauty therapy, but since then she has developed an award-winning business in medical aesthetics. So how has she become the successful entrepreneur that she is today?

“In 1971, I opened and managed my first hairdressing salon before opening the second in 1973 where I decided to incorporate beauty rooms. It was then that I went to train in beauty to get my qualifications. I’ve always loved making people feel good about themselves so adding this service was the perfect addition to my offering,” she explains. It wasn’t until the early 2000s that Fieldgrass’ interest in antiageing and aesthetic treatments really rocketed. She spent 13 years living in Hong Kong from 1983, where she was introduced to traditional Chinese medicine, which focuses on ‘inner health for outer beauty’, a motto that she now lives by.
Fieldgrass says, “When I came back from Hong Kong I was that little bit older and became interested in how to make myself look younger and feel better. My background in manual beauty was never enough for lifting and firming the skin, and having travelled extensively, I soon realised that there was a lot of technology coming out that I wanted to learn more about.” Whilst working in beauty, and renting beauty rooms in Kensington, she noticed that there were limited places for patients to go who wanted to combine both non-surgical and surgical cosmetic procedures. In 2006, Fieldgrass opened the very first EF Medispa, where she explains medical professionals such as doctors, surgeons, nurses, as well as therapists, could collaborate to help a patient achieve all of their aesthetic goals. Fieldgrass explains, “My vision was to make the public more aware and more accepting of medical aesthetic treatments and to do this I recognised that I needed medical professionals working in my clinic, as well as therapists, to do so. In the early 2000s, the public lacked knowledge and education on the types of procedures available, as well as the practitioners that should be performing them. Although there is still an element of this today, I wanted to bring aesthetics to the high street and make it more reputable.”
She continues, “I believe that only medical professionals should be performing facial injectable treatments, like Botox and fillers, as they have extensive knowledge of the anatomy. Even the doctors that work with me have to have at least five years’ practise before they touch any of my patients’ faces.” Fieldgrass employs 70 practitioners and emphasises that she couldn’t succeed without them.
“I employ a whole range of professionals, such as plastic surgeons, gynaecologists, dermatologists, nutritionists and many more. They are a huge asset to my practice and because of them I am able to offer a complete holistic approach to my patients,” she highlights.
Fieldgrass shares that when she decided to open her second clinic, it was in the middle of a recession and everyone around her expressed concern. She explains, “Everyone thought I was absolutely crazy, but I just felt in my gut it was the right thing to do. You have to have confidence in yourself otherwise no one else will.” When asked what the key skills are to start and grow a successful business, Fieldgrass simply says, “Communication and education.” She elaborates, “First of all, you need to be completely passionate about your area of expertise. Continually educate yourself and be open to adapting with the ever-growing industry. I also believe that everyone needs a mentor. For me, that person was David Hicks who was head of a large aesthetic distribution company; he really helped me at the beginning with business advice and I don’t think I’d be here today without him!”
Fieldgrass adds, “To grow your practice, be confident that you have excellent senior management and recognise that you cannot do everything. Your management team should understand your ethos and be adept at training to maintain exceptional standards. As you open each new clinic, you begin to divide your attention and you need to make sure that each clinic maintains the same high standards across the board; a strong management team will help deliver this. Remember, a business is only as good as the people that work in it.” Whilst managing a successful chain of clinics is one of her biggest achievements, Fieldgrass is also proud of other accomplishments and opportunities that have presented themselves to her, making her the entrepreneur that she is today. Not only did Fieldgrass own a lingerie shop in 2013, but she recently started a patient-focused podcast called The Beauty Biz. She says, “I love my podcast, it just felt so right to do it and is so refreshing. My husband refers to me as a serial entrepreneur! I love the quote, ‘An entrepreneur is someone who jumps of a cliff and builds a plane on the way down’. I can relate to that.”
Fieldgrass concludes, “When I look back on my career, I’ve thoroughly enjoyed the ride. It’s been a huge learning curve, but I wouldn’t change it for the world.”
Do you have an industry pet hate?
Yes, people who try to poach my highly-trained staff.
What’s the best piece of career advice you’ve ever been given?
My father told me from a young age to ‘concentrate on what you’re good at’ and for me that’s listening. I love listening to people to find out exactly what it is that’s bothering them and work with them to find a solution.
Do you have any hobbies outside of aesthetics?
I’m fascinated by alternative medicine such as acupuncture and reiki; I think that this all stems from my time in the Far East and my passion for inner wellbeing.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
“Working in aesthetics has been a huge learning curve, but I wouldn’t change it for the world”
EF Medispa founder and entrepreneur Esther Fieldgrass reflects on her success as a multiple clinic owner in aesthetics
The Last Word
The last two decades have seen considerable growth in the non-surgical aesthetic sector. The demand for these treatments has increased by over 400%,1,2 and last year alone, non-surgical treatments were worth more than $8.5 billion in the US.2 This has been attributed to increasing numbers of people being dissatisfied with their appearance,3,4 as well as improved convenience, affordability and perceived safety of non-surgical treatments. I have noticed that this growth in non-surgical aesthetics has recently been accompanied by an apparent rise in ‘do-it-yourself’ (DIY) treatments. This term refers to members of the public treating themselves with medical therapies, ranging from chemical peels to self-injecting. One author has suggested that practitioners themselves are partly responsible for this trend.5
Social media and DIY
Practitioners are increasingly using social media platforms to engage with patients, provide education and promote their services. This has been accompanied by a recent trend in practitioners using these channels to share videos or photographs of themselves performing DIY cosmetic treatments. Instagram has more than 2,200 posts tagged with variations on the term ‘self-injection’; many of which are aesthetic practitioners such as doctors and nurses, demonstrating on themselves how to inject.22 Practitioners also use YouTube to share these videos, with some of them attracting more
than 100,000 public views.23 Of concern is the correlating trend for members of the public performing DIY medical treatments; a search using YouTube for ‘self-injection dermal filler’ returns several pages of videos where members of the public self-inject dermal filler with clear and worrying errors in administration.23 For example, individuals are re-using syringes,6 sharing syringes,7 over-injecting,8 injecting in unsafe zones8 and purchasing unverified products through forums and social media platforms.5
The risks of DIY Trained professionals are very well-aware that aesthetic treatments are not riskfree. Dermal fillers for example, even in the hands of trained professionals, can cause infection, anaphylaxis, local tissue necrosis and embolisation.9 In his report for the Department of Health (DoH) on the regulation of the cosmetic industry, Sir Bruce Keogh, the medical director of the NHS and director general of the DoH at the time, highlighted that ‘dermal fillers are a disaster waiting to happen’.10 In my opinion, dermal fillers in the hands of untrained members of the public, are a disaster that is already happening. A simple PubMed search for the term ‘selfinjection for cosmetic treatment’ identifies 14 case reports of self-injecting for cosmetic reasons and the complications that arose as a result. The reports describe individuals who have self-injected dermal filler,11-13 paraffin,14-16 oil,17-19 lipase20 and bovine fat.21

Almost all of these individuals were left with significant long-term morbidity as a result of their self-treatment.
Patients are watching us
It is important that we, as responsible practitioners, understand that the public are watching and learning from what we post on social media. A recent article by Brennan et al. has shed light on the growing DIY trend among members of the public.5 The authors collected data from four online forums and interviewed members of the public who had previously self-injected botulinum toxin or dermal filler, or those who were planning to self-inject. Reasons for choosing to self-inject included cutting cost and lack of confidence in practitioners. Those interviewed reported that they had found information about self-injection by watching YouTube tutorials and downloading instructional materials from the internet. I believe that professionals who post videos of self-injection are facilitating this DIY culture and enabling unsafe practice and are therefore partly responsible for serious risks to public safety. The selfinjection trend is not without considerable risks; even if it is a practitioner injecting themselves we should not consider them immune. A recent case report describes a 37-year-old practitioner who self-injected her temples using hyaluronic acid dermal filler.11 The practitioner developed occlusion of a branch of her left superficial temporal artery and required hospital admission and hyperbaric oxygen therapy. The authors comment that practitioners should adhere to local guidelines on self-treatment, but fall short of saying that self-injection should be avoided. Numerous professional bodies including the General Medical Council,22 Nursing and Midwifery Council,23 General Dental Council24 and the Medical Defence Union25 have provided guidance stating that medical professionals should, wherever possible, avoid providing medical care to themselves. The GMC states that a lack of independent assessment, lack of appropriate checks and measures (especially in drugs of addiction), possibility of inaccurate diagnosis, and potential impedance to further treatment, for example emergency treatment, are all reasons as to why clinicians should not self-treat. With present concerns about safety, ethics and regulation of the aesthetic sector,10 practitioners should ensure that they adhere to such guidance and follow gold standard practice.
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Tatiana Lapa questions whether aesthetic practitioners are promoting a ‘do-it-yourself’ culture
Conclusion
The rapid growth in non-surgical aesthetics has recently been accompanied by a trend in practitioners using social media to share videos or photographs performing DIY cosmetic treatments on themselves. Of concern is the correlating trend for members of the public following their example, with obvious safety concerns. As professionals, we must be more mindful of what the public are learning from the content we post online and we should work towards promoting safety and quality standards, rather than a DIY culture.
Dr Tatiana Lapa qualified as a doctor at St George’s Medical School, following a Bachelor’s of Science degree at King’s College London in Aerospace Medicine. Whilst attaining her membership to the Royal College of General Practitioners, Dr Lapa gained an interest in non-surgical aesthetics and was awarded a First-Class Master’s Degree in Aesthetic Medicine at Queen Mary University. She established the Dr Tatiana Clinic in London in 2014.


REFERENCES
1. Surgery ASFAP. ASAPS 1997 Statistics on Cosmetic Surgery 1997 <https://www.surgery.org/sites/default/files/ASAPS1997Stats_0.pdf>
2. Surgery ASFAP. Cosmetic Surgery National Data Bank Statistics 2017<https://surgery.org/sites/default/files/ASAPS-Stats2017.pdf>
3. Cash TF, Henry PE. Women’s body images: The results of a national survey in the USA. Sex Roles. 1995;33(1-2):19–28.
4. Frederick DA, Jafary AM, Gruys K, Daniels EA. Encylopedia of body image and human appearance. Cash TF, editor. Elsevier; 2012. 9 p.
5. Brennan R, Wells JSG, Van Hout M. “Saving Face”: An Online Study of the Injecting Use of DIY Botox and Dermal Filler Kits. Plast Surg (Oakv). 2018 Aug;26(3):154–9.
6. C AJFABK. Fillers self injection YouTube; 2017. <https://www. youtube.com/watch?v=ZM_obJn-_kE>
7. OBrien Z. REVEALED: lip filler frenzy leaving teenage girls with HORRIFIC damage. Sunday Express. 2016 Feb 25. <https://www. express.co.uk/news/uk/647566/REVEALED-Lip-filler-frenzy-leavingteenage-girls-with-HORRIFIC-damage>
8. Dermis DO. Dermal Filler Injection Technique on Yourself. YouTube; 2017. <https://www.youtube.com/watch?v=bUxBzN9XW8Q>
9. Urdiales-Galvez F, Delgado NE, Figueiredo V, Lajo-Plaza JV, Mira M, Moreno A, et al. Treatment of Soft Tissue Filler Complications: Expert Consensus Recommendations. Aesthetic Plast Surg. 2018 Apr;42(2):498–510.
10. Health DO. Review of the Regulation of Cosmetic Interventions. 2013. <https://www.gov.uk/government/uploads/system/uploads/ attachment_data/file/192028/Review_of_the_Regulation_of_ Cosmetic_Interventions.pdf>
11. Henderson R, Reilly DA, Cooper JS. Hyperbaric Oxygen for Ischemia due to Injection of Cosmetic Fillers: Case Report and Issues. Plast Reconstr Surg Glob Open. 2018 Jan;6(1):e1618.
12. Raoof N, Salvi SM. Self-injection of dermal filler: an underdiagnosed entity? Br J Dermatol. 2015 Mar;172(3):782–3.
13. Ono S, Hyakusoku H. Complications after self-injection of hyaluronic acid and phosphatidylcholine for aesthetic purposes. Aesthet Surg J. 2010 May;30(3):442–5.
14. De Siati M, Selvaggio O, Di Fino G, Liuzzi G, Massenio P, Sanguedolce F, et al. An unusual delayed complication of paraffin self-injection for penile girth augmentation. BMC Urol. 2013 Dec;13:66.
15. Iversen L, Lemcke A, Bitsch M, Karlsmark T. Compression bandage as treatment for ulcers induced by intramuscular self-injection of paraffin oil. Acta Derm Venereol. 2009;89(2):196–7.
16. Cohen JL, Keoleian CM, Krull EA. Penile paraffinoma: selfinjection with mineral oil. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S251–3.
17. De Gado F, Mazzocchi M, Chiummariello S, Gagliardi DN, Alfano C. Johnson’s baby oil, a new type of filler? Acta Chir Plast. 2006;48(4):123–6.
18. Darsow U, Bruckbauer H, Worret WI, Hofmann H, Ring J. Subcutaneous oleomas induced by self-injection of sesame seed oil for muscle augmentation. J Am Acad Dermatol. 2000 Feb;42(2 Pt 1):292–4.
19. Thomas P, Boussuges A, Gainnier M, Quenee V, Donati S, Ayem ML, et al. [Fat embolism after intrapenile injection of sweet almond oil]. Rev Mal Respir. 1998 Jun;15(3):307–8.
20. Khoo AAK-A, Branford OA, Javaid M. Self injection of lipase--an extreme case for regulation in non-surgical cosmetic procedures. J Plast Reconstr Aesthet Surg. 2010 Jan;63(1):e6–8.
21. Tumerdem B, Aydin A, Kesim SN. An unusual case of self-injected bovine fat in liquid form to the face for cosmetic reasons. Aesthetic Plast Surg. 2004 Jul;28(4):251–3.
22. GMC. Guidance on assessing the seriousness of concerns relating to self-prescribing, or prescribing to those in closer personal relationships with doctors. 2016 <https://www.gmc-uk.org/-/media/ documents/DC6649_Guidance_on_assessing_the_seriousness_ of_concerns_relating_to_prescribing.pdf_58666780.pdf>
23. Instagram, theenhancers, <https://www.instagram.com/p/ BmwIPlSH32i/>
24. YouTube, self-injection dermal filler. <https://www.youtube.com/ results?search_query=self-injection+dermal+filler>
25. NMC. The Code. 2015 Jan 29. <https://www.nmc.org.uk/ globalassets/sitedocuments/nmc-publications/nmc-code.pdf>
26. GDC. Guidance on prescribing medicines. 2013 <https://www.gdcuk.org/search?querytext=prescribing>
27. MDU. Self-prescribing, 2018 <https://www.themdu.com/guidanceand-advice/guides/self-prescribing>
Reproduced from Aesthetics | Volume 6/Issue 4 - March 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
This
first time that umbilical
cord lining stem cells
–or stem cells in general – are being truly utilized in a topical skincare to promote skin health.



”
- Prof. Mitchel P. Goldman MD, double-board certified cosmetic dermatologist
Contact us for training
WINNER 2018
Wholesaler of the Year
The one stop shop for all your medical aesthetic and clinic supplies.
London | Loughborough | Online
WINNER 2016
Best Customer Service
ChurchPharmacy 01509 357 300
ChurchPharmacyUK
ChurchPharmacy.co.uk skincare@churchpharmacy.co.uk
“
is the
The anatomy of the smile
Join us from 7-9pm 11th March 2019 on aestheticsjournal.com
How do I guarantee my place on ‘The Anatomy of the Smile’ Webinar?
1. First register for DocCheck – IMPORTANT please do this by 7th March 2019 in order to guarantee that your registration will be processed in time for access to the webinar
a. Visit the following link: https://www.doccheck.com/com/ account/register
b. Register and provide your medical certification as proof of your profession
c. Your information will be checked and once verified you will be provided with a DocCheck password

2. Register for the Webinar at https://aestheticsjournal.com/ Webinar_GaldermaMarch2019
3. Login or join for free as a member
4. You will then be prompted to use your DocCheck* password to confirm you are a doctor, nurse or dentist
5. Tick the box to confirm you would like to pre-register for the webinar
The Restylane Webinar
DoP February 2019 RES18-11-0842g
