
Dr. Mitchell Corey Sanders
CEO, ProDevLabs, LLC Southborough, MA

Nikole Siegmund
VP of Preclinical Development, ProDevLabs, LLC
Southborough, MA

Dr. Akram M. Salam
Scientist, ProDevLabs, LLC
Southborough, MA

Dr. Mitchell Corey Sanders
CEO, ProDevLabs, LLC Southborough, MA
Nikole Siegmund
VP of Preclinical Development, ProDevLabs, LLC
Southborough, MA
Dr. Akram M. Salam
Scientist, ProDevLabs, LLC
Southborough, MA
This preclinical study evaluates soft and rigid porous matrices for wound healing in a diabetic mouse model, addressing the critical need for e ective treatments for large surface area wounds. While allogeneic and xenogeneic matrices have shown promise, they face limitations in cost, durability, and variability. Recent years have seen a push towards novel biodegradable or absorbable synthetic matrices to overcome these challenges. The study compares the wound healing properties of a soft, porous, single-layered, bioabsorbable polyurethane matrix (MTX) with a rigid Bilayer matrix in a diabetic mouse model. The research aims to elucidate the mechanisms of action and di erentiate these products from other o erings in the eld. Key aspects of the study include gene expression analysis, proteomics, biomechanical properties, and histology to understand how these synthetic products heal chronic wounds. The investigation employs a delayed healing model in diabetic mice to simulate real-world clinical conditions. This research has signi cant implications for clinical practice, potentially guiding the development and application of advanced wound healing products for patients with challenging wounds, such as those associated with diabetes.

HMia Hanna Scientist, ProDevLabs, LLC Southborough, MA

Dr. Joshua Cheetham
Director of Research and Development, PolyNovo Limited Melbourne, Australia
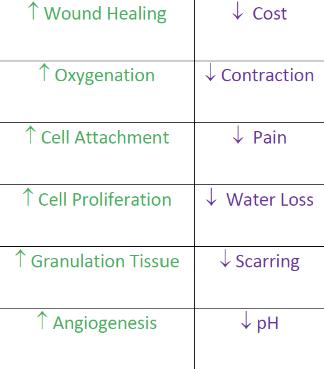
ealing large surface area wounds is a very challenging unmet need in clinical practice. Although there has been a surge in the development of allogenec and xenogenic matrices for healing wounds, these products have signi cant limitations including, but not limited to, cost, durability, longevity, and donor and process variability. In the last ve years there has been a push in the marketplace to provide novel biodegradable or absorbable synthetic matrices that reduce these limitations of the naturally derived products. Some examples of the current biodegradable and resorbable matrices on the market include NovoSorb® BTM, Suprathel®, Supra SDRM®, Altrazeal®, AC5, Integra® Bilayer (Bilayer), G4Derm, Restrata®, Phoenix Wound Matrix®, Spincare™ Microlyte®, Mirrage® and NovoSorb® MTX (MTX). The clinical indications for use of these products have been provided in recent reviews.1-3 Each of these porous matrices have their inherent bene ts and limitations, but few studies have compared the products in clinical or even preclinical studies to provide a direct comparison of the potential bene ts and weaknesses. Some of the features of an ideal biosynthetic dressing are provided in Table 1. One obvious feature is that the products need to enhance wound healing at a reasonable cost. Limited clinical studies suggest that this novel class of wound matrices may also improve wound oxygenation, cell attachment and proliferation, fresh granulation tissue formation, and accelerate angiogenesis. Some of these products also have the added bene t of potentially reducing pain, wound contraction, water loss, and scarring, as well as lowering pH, which is known to control bacterial bioburden in a wound. One new product that recently received 510(K) clearance is a soft, porous, single-layered, bioabsorbable polyurethane matrix referred to as MTX. Although case studies with this resorbable matrix seem to suggest a lot of promise for its use in the clinical setting, the mechanism of action of how this product accelerates wound healing and how this product di erentiates itself from other product o erings in this class is poorly understood. The primary goal of this was study was to compare the wound healing properties of the soft and porous MTX matrix with that of a rigid Bilayer matrix which is a competing product in the same class of bioabsorbable matrices. Our hypothesis was that a delayed healing model in the diabetic mouse may elucidate some of the indications for use of these products to help guide clinical practice. Our secondary goal was to analyze wound gene expression, proteomics, biomechanical properties, and histology to better understand the mechanism of action of how these synthetic products heal chronic wounds.
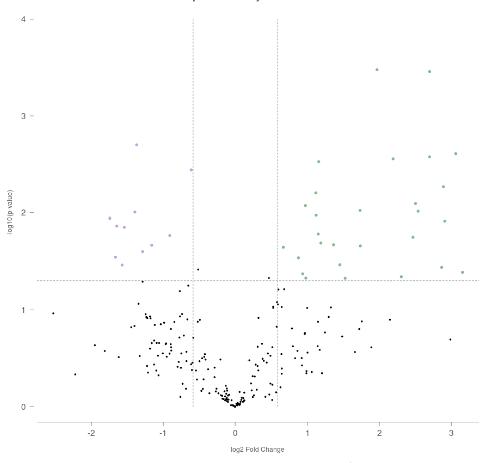
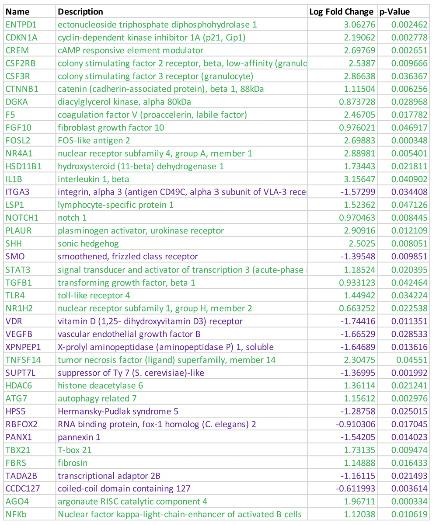
“From gene expression studies on Day 11, profound di erences in the MTX vs. the Bilayer treatment groups were observed. Table 2 shows the statistically signi cant gene expression pro le and fold changes in gene expression. Ten (10) genes were down regulated (highlighted in purple) and 29 genes (highlighted in green) were upregulated, as shown in the volcano plot in Figure 1. By Day 21, the expression pattern was very similar with only 2 genes di erentially expressed in the MTX treated group as compared to the Bilayer group.”
Methods
This study was performed under IACUC Protocol G2022-148, IBC registration 2022-G77, and in accordance with the O#ce of Laboratory Animal Welfare (OLAW), assured and registered with the United States Department of Agriculture (USDA) to conduct research in laboratory animals. All conditions of testing conformed with the Animal Welfare Act (CFR 9) and its amendments, the Public Health Service Policy on Humane Care and Use of Laboratory Animals, the Guide for the Care and Use of Laboratory Animals.4-5
Nine-week-old, male BKS.Cg-Dock7m +/+ Leprdb/J diabetic (db/db) mice (Stock # 000642) were obtained from Jackson Laboratories (Bar Harbor, ME), and acclimated for eight (8) days prior to study initiation and wound creation on Day 0. The strain, gender and age of the mice were chosen because the db/db strain of diabetes share comorbidities with the human disease phenotype and male mice tend to be more obese than females.6 The animals were randomly separated into two treatment groups: MTX (N=23) and Bilayer (N=23), and two control groups, Tegaderm alone (N=23) and Unwounded (N=3). On Day 0, animals were
anesthetized using iso urane with O2 (1 – 4%). Sterile, disposable, 10 mm skin biopsy punches were used to form a wound on the dorsal side of each animal. The wound was then covered with either MTX + Tegaderm, Bilayer + Tegaderm, or Tegaderm alone, as the negative control. On Days 11 and 21, a portion of the animals (3 per group per day) were euthanized in accordance with accepted American Veterinary Medical Association (AVMA) guidelines to isolate the tissue for mRNA processing.7-8
In this study, the wounds were examined on Days 0, 4, 7, 11, 14, 18, and 21 by digital photography and with digital calipers that measured the interaction of the wound bed perimeter with the synthetic matrices.
On Days 11 and 21, we isolated the tissue and puri ed mRNA using the RNeasy Micro Kit (QIAGEN). The puri ed RNA was normalized to 20 ng/%L then analyzed with a Pro 5s nCounter Prep Station and Digital Analyzer (NanoString). A custom mouse wound healing code set was used with 282 probes that cover genes in the di erent phases of wound healing (hemostasis, in ammation, proliferation, tissue remodeling),
“This study demonstrated that the MTX matrix is tightly integrated into the periwound bed and regulates 39 genes to accelerate wound healing early in the proliferative phase (Day 11). MTX does so by regulating growth factors and important cytokines (VEGF, TGF-&, FGF, and Fibrosin) in addition to several other genes that are involved in regulating in ammation (IL1&), macrophage defense and activation (CSF3R, CSFR&, PLAUR, NR4A1), transcription factors (FOSL2), autophagy (ATG7), gene silencing (AGO4), keratinocyte proliferation (CDKN1A), collagen deposition (KPNPEP2), and re-epithelialization (SHH, SMO, RBFOX2, ENTPD1, VDR).”
brosis, and macrophage plasticity. The detailed bioinformatics analysis is provided in the supplemental methods section.
Proteins were isolated from the tissue harvested for mass spectrometry on Day 21, and the samples were processed with urea/ thiourea to denature the proteins, reduced with dithiothreitol (DTT) and alkylated with iodoacetamide prior to a 6 fold dilution with water and digestion with sequencing-grade trypsin (as described by the manufacturer, Thermo Scienti c). After an overnight digestion at 37oC, the peptides were concentrated and puri ed using C-18 spin columns, and the puri ed samples were analyzed using an Easy nanoLC1000 UHPLC system coupled to a Fusion Orbitrap Tribrid mass spectrometer (Thermo Scienti c) utilizing the Proteome Discoverer v. 2.2 processing software.
Biomechanical Testing:
Tissue integrity (Max Force and Tensile Strength) testing was performed on an ADMET tabletop 1kN expert 7601 Universal Test System with a 10 lbf load cell and MTESTQuattro® Software (ADMET Inc. Norwood, MA). For Max force (N) determination, each of the samples was pulled at a constant speed of 10 mm/s until the tissue was completely disrupted and sample broke within the middle of the the wound in millimeters (mm) generates a standardized stress measurement (N/mm), automatically calculated by the MTESTQuattro® software.
Tissues harvested on Day 21 were xed in 4% paraformaldehyde in PHEM (60 mm PIPES, 25 mm HEPES, 10 mm EGTA, and 2 mm MgCl2 at pH 6.9), embedded in para#n, and then sliced into 5 %m sections. Para#n sections were dewaxed and rehydrated with xylene and an alcohol gradient prior to staining with hematoxylin and eosin (H&E). Histology was performed at HistoWiz, Inc. (Brooklyn, NY) using standard operating procedures with a fully automated work ow.
Statistical Analysis:
Statistical analysis for biomechanical testing and mass spectrometry was analyzed with either Two-Way ANOVA or One-Way ANOVA using GraphPad Prism 9.2; p-values <0.05 were indicative of statistical signi cance. Statistical analysis of the gene expression data was performed using Rosalind Bioinformatic Software. Normalization, fold changes, and p-values were calculated using criteria provided by NanoString. Housekeeping probes were used for normalization and selected based on the
“Our evidence suggests that the soft and porous MTX matrix may have several bene ts over the rigid biosynthetic matrices including improved wound healing, cell attachment, cell proliferation, and re-epithelialization. Clinical studies may further elucidate the bene ts of this MTX matrix which were not examinable in the immediate study due to the limitations of the study design. We predict that the soft and porous MTX matrix may also reduce pain, provide enhanced barrier function (prevent water loss), and reduce scarring, and these will be investigated in future clinical studies.”
the geNorm algorithm, as described by Perkens et l., 2012.9
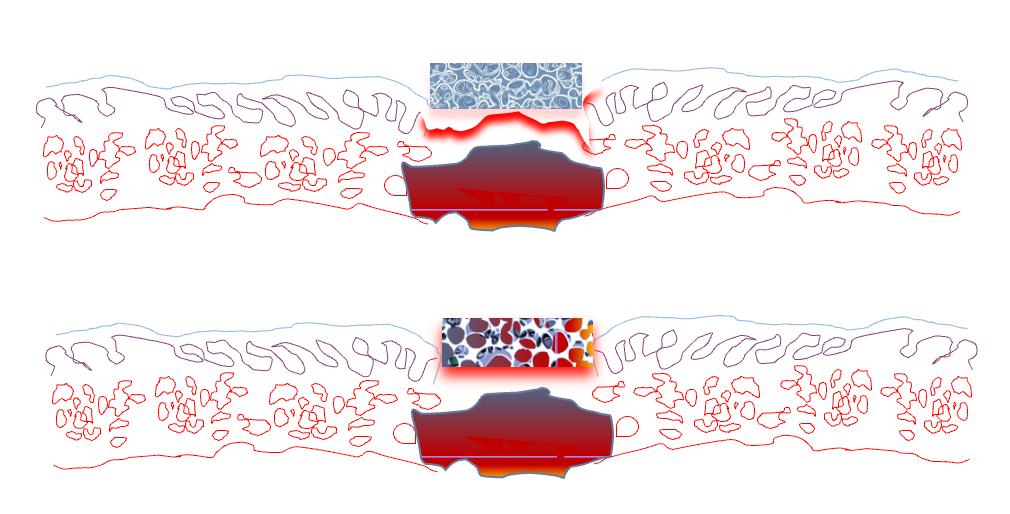
The mice in this study were examined on Days 0, 4, 7, 11, 14, 18, 21 by digital photography and with digital calipers to test the interaction of the perimeter of the wound bed with the synthetic and biosynthetic matrices. Most interestingly, the cells in the wound beds were found to react di erently to soft and rigid porous matrices. Immediately after punch biopsies, the soft MTX matrix conformed to the wound shape and took up the in ltrating white and red blood cells.
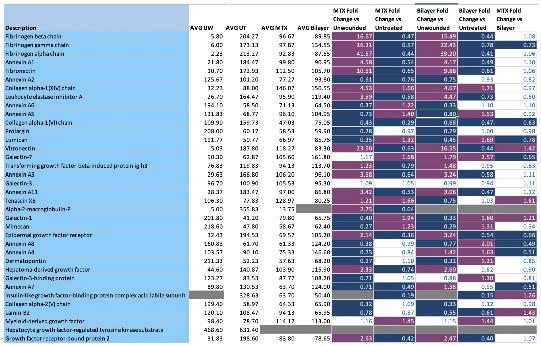
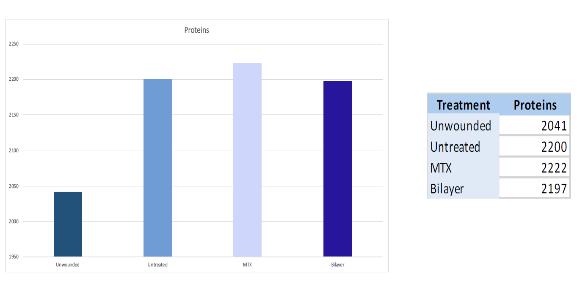
In contrast, the Bilayer matrix did not absorb the cells or conform to the depth of the wound bed. At the conclusion of the 21-day time period in the MTX treatment group, the perimeter of the wound beds was still tightly adhered to the MTX matrices, and in the last 4 days the dressing became convex, e ectively “bubbling up” as the migrating cell perimeter pushed in the matrix. In contrast, the edges of the Bilayer dressing began to bio-absorb and seemed to interact less with the perimeter of the wound bed. By Day 21, most of the MTX matrices were still tightly associated with the proliferating wound while only a few of the Bilayers were physically attached to the encompassing wound perimeter (5 MTX vs. 3 Bilayer). From gene expression studies on Day 11, profound di erences in the MTX vs. the Bilayer treatment groups were observed. Table 2 shows the statistically signi cant gene expression pro le and fold changes in gene expression. Ten (11) genes were down regulated (highlighted in purple) and 28 genes (highlighted in green) were upregulated, as shown in the volcano plot in Figure 1. By Day 21, the expression pattern was very similar with only 2 genes di erentially expressed in the MTX treated group as compared to the Bilayer group. Figure 3 tabulates the ECM protein di erences between the unwounded, untreated, MTX and
“One limitation to this study was that we did not measure gene expression during the in ammatory phase of wound healing due to a limited number of samples. The other limitation of this study was that the MTX product was tightly associated with the wound bed over the course of healing, which made it impossible to measure the percentage of wound area reduction (PAR) over time during each dressing change. Lastly, the diabetic mouse skin is much thinner than human skin and may not fully re ect the clinical bene ts and pitfalls of these soft and rigid matrices.”
the Bilayer groups to compare fold protein composition.
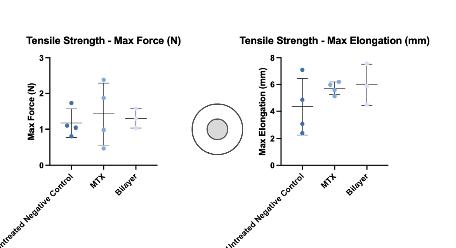
Biomechanical studies did not reveal any statistical signi cance in terms of max force or elasticity between the treatment groups. The MTX group had a much tighter standard deviation and may have been statistically signi cant with a larger sample size.
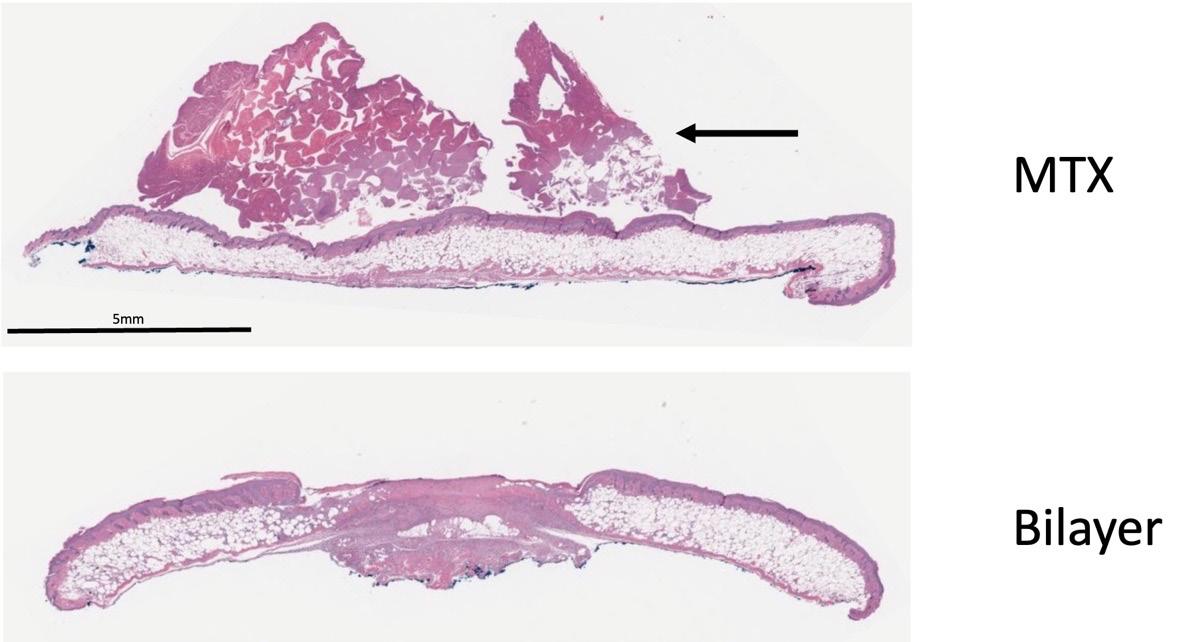
H&E staining on Day 21 revealed that MTXtreated wounds demonstrated markedly improved tissue integrity of the epithelial layer as compared to the untreated control or the Bilayer group. Although the untreated control and MTX wounds looked nearly healed by digital imaging, H&E staining revealed that there was not a complete epithelial layer present in the untreated control and Bilayer groups.
Discussion
Wound healing is a tightly regulated process that is a ected by multiple cytokines and growth factors including vascular endothelial growth factor (VEGF), broblast growth factor (FGF), and transforming growth factor & (TGF-&).10-13
This study demonstrated that the MTX matrix is tightly integrated into the periwound bed and regulates 39 genes to accelerate wound healing early in the proliferative phase (Day 11). MTX does so by regulating growth factors and important cytokines (VEGF, TGF-&, FGF, and Fibrosin) in addition to several other genes that are involved in regulating in ammation (IL1B), macrophage defense and activation (CSF3R, CSFRB, PLAUR, NR4A1), transcription factors (FOSL2), autophagy (ATG7), gene silencing (AGO4), keratinocyte proliferation (CDKN1A), collagen deposition (XPNPEP2), and re-epithelialization (SHH, SMO, RBFOX2, ENTPD1, VDR). By Day 21, mRNA and protein composition was similar between the MTX and the Bilayer group. Biomechanical testing of max force and tensile strength of the tissue did not achieve statistical signi cance. However, based on H&E staining, wounds treated with MTX had achieved complete re-epithelialization, which is in sharp contrast to the Bilayer group which had
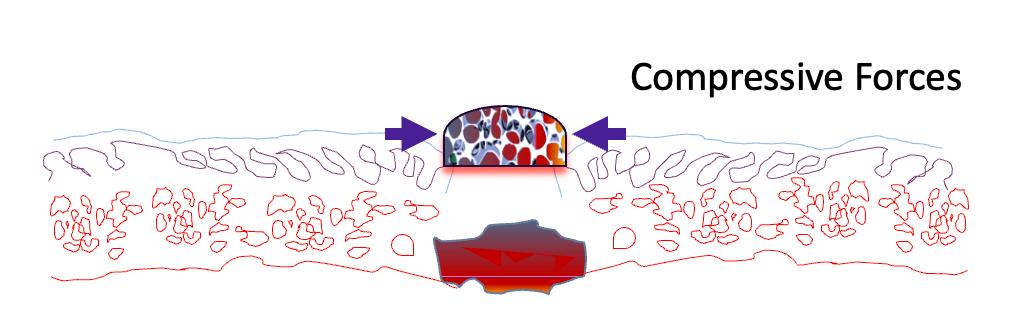
incomplete wound healing by Day 21. Our hypothesis is that the soft, porous, biodegradable MTX matrix provides just the right level of shielding or compressive forces on the perimeter of the wound bed to activate cell proliferation and re-epithelialization. Several groups, including Gurtner and colleagues, have demonstrated that mechanical forces play a critical role in stem cell proliferation, wound healing, and scar reduction.14-16 Our preclinical studies in a delayed healing model in the diabetic mouse suggest that soft matrices such as MTX may have better healing outcomes than rigid matrices.
One limitation to this study was that we did not measure gene expression during the in ammatory phase of wound healing due to a limited number of samples. The other limitation of this study was that the MTX product was tightly associated with the wound bed over the course of healing, which made it impossible to measure the percentage of wound area reduction (PAR) over time during each cover dressing change. Lastly, the diabetic mouse skin is much thinner than human skin and may not fully re ect the clinical bene ts and pitfalls of these soft and rigid matrices.
Our evidence suggests that the soft and porous MTX matrix may have several bene ts over the rigid biosynthetic matrices including improved wound healing, cell attachment, cell proliferation, and re-epithelialization. Clinical studies may show other bene ts of this MTX matrix which were not examinable in the immediate study due to the limitations of the study design. We predict that the soft and porous MTX matrix may also reduce pain, provide enhanced barrier function (prevent water loss), and reduce scarring, and these will be investigated in future clinical studies.
References: 1.Horn CP, Fierro AL, Lantis JC 2nd. The Shift to Synthetics: A Review of Novel Synthetic Matrices for Wound Closure. Surg Technol Int. 2023 Oct 7;42:sti42/1711. Epub ahead of print. PMID: 37802070.
2.Fernandez LG, Matthews MR, Kim PJ. A synthetic hybrid-scale ber matrix for complex surgical wounds: consensus guidelines. Wounds. 2023 May;35(5):E160-E168. doi: 10.25270/wnds/22067. PMID: 37256692.
3.Aderibigbe BA. Hybrid-Based Wound Dressings: Combination of Synthetic and Biopolymers. Polymers (Basel). 2022 Sep 12;14(18):3806. doi: 10.3390/polym14183806. PMID: 36145951; PMCID: PMC9502880.
4.O#ce of Laboratory Animal Welfare. Public Health Services Policy on Humane Care and Use of Laboratory Animals. Bethesda, Maryland: National Institutes of Health, Revised 2015.
5.National Research Council (NRC). Guide for the Care and Use of Laboratory Animals. Washington, D.C.: National Academy Press; 8th Ed. 2011.
6.Huynh P, Phie J, Krishna SM, Golledge J. Systematic review and meta-analysis of mouse models of diabetes-associated ulcers.BMJ Open Diabetes Res Care. 2020;8(1):e000982. doi:10.1136/bmjdrc-2019-000982.
7.American Veterinary Medical Association. AVMA Guidelines on Euthanasia. http:// www.avma.org/sites/default/files/2020-01/2020-Euthanasia-Final-1-17-20.pdf.
Published January 2020.
8.Report of the American Veterinary Medical Association (AVMA) Panel on Euthanasia. Journal of the American Veterinary Medical Association. 2001; 218:669–696.
9.Perkins, JR. et al. ReadqPCR and NormqPCR: R packages for the reading, quality checking and normalisation of RT-qPCR quanti cation cycle (Cq) data. BMC Genomics 13, 286+ (2012).
10.Gan MS, Yang B, Fang DL, Wu BL. IL-1B can serve as a healing process and is a critical regulator of diabetic foot ulcer. Ann Transl Med. 2022 Feb;10(4):179. doi: 10.21037/ atm-22-75. PMID: 35280410; PMCID: PMC8908170.
11.Castro-Dopico T, Fleming A, Dennison TW, Ferdinand JR, Harcourt K, Stewart BJ, Cader Z, Tuong ZK, Jing C, Lok LSC, Mathews RJ, Portet A, Kaser A, Clare S, Clatworthy MR. GM-CSF Calibrates Macrophage Defense and Wound Healing Programs during Intestinal Infection and In ammation. Cell Rep. 2020 Jul 7;32(1):107857. doi: 10.1016/j. celrep.2020.107857. PMID: 32640223; PMCID: PMC7351110.
12.Ågren MS, Litman T, Eriksen JO, Schjerling P, Bzorek M, Gjerdrum LMR. Gene Expression Linked to Reepithelialization of Human Skin Wounds. Int J Mol Sci. 2022 Dec 12;23(24):15746. doi: 10.3390/ijms232415746. PMID: 36555389; PMCID: PMC9779194.
13.Prakash S, Robbins PW. Fibrosin: a novel lymphokine in wound healing. Exp Mo Pathol. 2001 Dec;71(3):247-55. doi: 10.1006/exmp.2001.2402. PMID: 11733950.
14.Gurtner GC, Dauskardt RH, Wong VW, Bhatt KA, Wu K, Vial IN, et al. Improving cutaneous scar formation by controlling the mechanical environment: large animal and phase I studies. Ann Surg. (2011) 254(2):217–25. doi: 10.1097/ SLA.0b013e318220b159
15.Rodrigues M, Kosaric N, Bonham CA, Gurtner GC. Wound Healing: A Cellular Perspective. Physiol Rev. 2019 Jan 1;99(1):665-706. doi: 10.1152/physrev.00067.2017. PMID: 30475656; PMCID: PMC6442927.
16.Barnes LA, Marshall CD, Leavitt T, Hu MS, Moore AL, Gonzalez JG, Longaker MT, Gurtner GC. Mechanical Forces in Cutaneous Wound Healing: Emerging Therapies to Minimize Scar Formation. Adv Wound Care (New Rochelle). 2018 Feb 1;7(2):47-56. doi: 10.1089/wound.2016.0709. PMID: 29392093; PMCID: PMC5792236.
Supplementary data accessible at - https://rb.gy/zp07as