Shawn "Joseph" Collier Resident Physician Family Medicine Residency Program & Sports Medicine Fellowship
FSU Student Representatives: Stephania Dzialo | Giselle Nicolas
Julie Grimm - Editor, Executive Director
President’s Message:
Amol K. Gupta, MD
Physical Medicine & Rehabilitation
Dear Colleagues,
It has been a great honor to serve as your president of the Volusia County Medical Society. For years, Volusia County has had an excellent reputation of providing top quality care to the community. As a society, VCMS, has unique relationships with the many accomplished physicians, hospital systems (Halifax and Advent), Universities (FSU, UF, ERAU, BCU, Stetson, DSC) that serve and take care of our community. As the settings of how physicians practice change, I believe it is even more vital to be part of and to support VCMS. Ultimately, our goal as physicians is to provide the best medical care to our patients and VCMS can serve as the bridge between various practice and hospital models.
At the beginning of the year I highlighted what I believed to be the 4 key pillars of VCMS: Networking, Social Connection, Advocacy/Education, and Service and would like to highlight some of what VCMS accomplished this year.
We started scholarship funds for FSU and UF medical students and for students entering college with a desire to pursue medicine. We also returned to judging at the Volusia County Regional Science Fair and provided awards to the middle and high school students.
We have continued our annual food drives and volunteering at the food kitchens and this year partnered with Habitat for Humanity for volunteering on service projects.
We started a spring and fall pickle ball event at Pictona and Trivia Night at Houligan’s for our members and their families. We have had networking meetings at ERAU basketball games, re-connected with the Dental Society, and shared a mixer with Halifax Hospital for new physicians. All the while, as a society we continued to advocate for our patients and our profession.
I would like to thank Julie Grimm (Executive Director) for her dedicated work to the VCMS. I have enjoyed my service on the VCMS Executive Board and wish much success to our incoming president Dr. Sandra Buchanan. I look forward to watching VCMS continue to thrive. Thank you for continuing to support the Volusia County Medical Society.
Sincerely,
Amol K. Gupta, MD
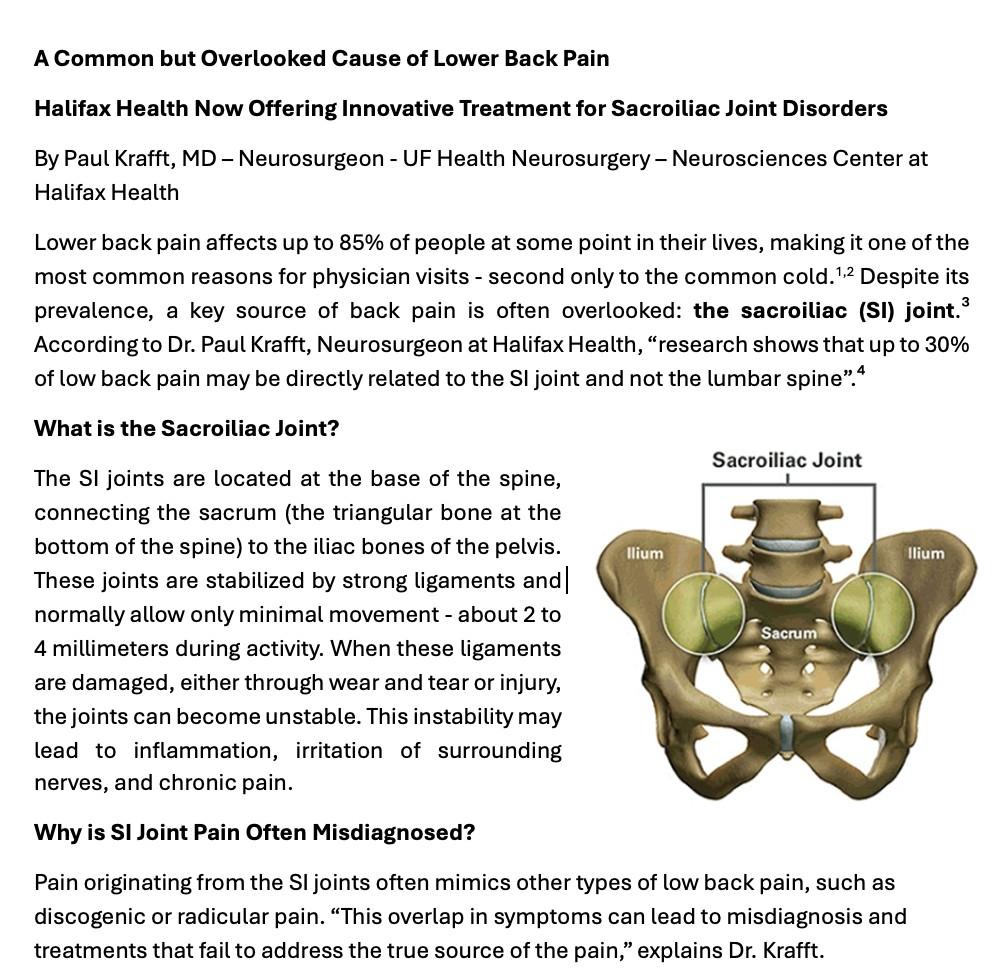
Diagnosing and Treating
SI Joint Dysfunction
Your physician may perform several tests to determine whether the SI joint is contributing to your symptoms. These include hands-on physical assessments (provocative tests) and diagnostic SI joint injections. Initial treatment may involve physical therapy and targeted injections. However, if conservative methods fail, a minimally invasive surgical option may be considered. “For patients who haven’t found relief through non-surgical treatments, we offer a minimally invasive procedure designed to stabilize the SI joint,” says Dr. Krafft. Minimally invasive SI joint fusion surgery involves several techniques designed to stabilize the SI joint while minimizing muscle disruption and recovery time. Each approach is tailored to the patients’ specific needs and underlying pathology. The surgery is performed under general anesthesia, and is usually an outpatient, same-day discharge procedure.
Sources:
1. Frymoyer JW (1988) Back pain and sciatica. N Engl J Med 318:291–300
2. Hart, et al. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine. 1995;20(1):11-9.
3. Weksler, Velan, et al. The role of SI joint dysfunction in the genesis of low back pain: the obvious is not always right. Archives of ortho and trauma surgery. 2007 Dec; 10(127) 858-8.
4. Szadek, et al. Diagnostic Validity of Criteria for Sacroiliac Joint Pain. Journal of Pain, 2009: 10(4) 354-368Deyo RA, Weinstein JN, Low Back Pain, N Engl J Med 2001: 344(5): 363-370
5. INSITE 2yr – Polly DW, et al. Two-Year Outcomes from a Randomized Controlled Trial of Minimally Invasive Sacroiliac Joint Fusion vs. Non-Surgical Management for Sacroiliac Joint Dysfunction. Int J Spine Surg. 2016;10.Article 28. DOI: 10.14444/3028.
6. iMIA 2yr – Dengler J, et al. Randomized Trial of Sacroiliac Joint Fusion vs. Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint. J Bone Joint Surg Am. 2019;101(5):400-411. DOI: 10.2106/JBJS.18.00022
Thursday, October 23, 2025 5:00 to 8:00 pm The Brannon Center 105 S. Riverside Dr. New Smyrna Beach, Florida
Presented by The Hub on Canal and Halifax Health, this elegant event will feature small signature plates from some of the area’s favorite restaurants, paired with captivating live artistic performances. hubsignatureevents.com/taste-for-the-arts
Cancer nor Technology can ever take away our Humanity
David Gorelov, MD
As the neurosurgeon lay on his deathbed, there was a peace and victory in his eyes that spoke defiantly amidst the cancer that prohibited him from swallowing and restricted the audibility of his voice. Dr. B, who was a patient of mine in hospice, was inching closer to his next home, and he was ready. At that moment, I could not bring any tools of technology that would comfort him. What I brought instead was my presence and listening ear. The happy tears of his two daughters and the joy of his answers to my curiosity about his long, full life taught me that my interest in his story - or any patient's story - meant more than anything else that I could do. I offered my time to him and he in return offered what little time he had in his last few days on earth. He gave me valuable advice and wisdom that only comes from the 90 years of time spent well. Time is the most valuable currency. We can never get it back and we can never increase it, but we can joyfully and sacrificially give it. Our humanism of how we give our time to others is simply revealed by the intentional presence we offer to our patients, family, friends, and everyone we meet.
Our giving presence is enriched by the human touch, the eye-level acknowledgment, and the listening ear which create an environment of receptiveness and humanism that breaks any barriers or walls existing before we as physicians encounter our patients. As physicians, we are called to connect and care for the person behind the plaguing illness. Patients want cures and healing, yet even if they do not know it, they thirst to drink from the cup of compassionate care. If we pour out our compassion, they will be filled with something that will make them feel whole, even while battling an incurable cancer.
“Be worthy to serve the suffering” is a statement that has captivated me since I heard it first in the AOA motto. I believe that technology will never be able to be worthy to serve the suffering even in an increasingly digital world. Technology and even artificial intelligence cannot truly empathize with human suffering because it will never experience suffering as we experience it. The fear of the unknown, the pain of sickness, the hope for a better tomorrow will never be understood unless humanly experienced. This is something that we all have experienced albeit on many different levels. The physician offers an empathetic response and can understand how much is required to serve the suffering. When we experience suffering in our lives, encountering similar trials and tribulations of life as others, then through our own experience with pain, we can offer to others our empathy, hope, and presence. That is the power of the human experience, and it will never be replaced. There is a lot of healing and power that comes with sharing in the pain and suffering with another person. It tells the patient that they are not alone. They are not unique to suffering. If we and so many others who have tasted defeat, sorrow, and pain can resiliently still stand, then the patient who lays on the hospital bed has hope that they too will one day stand against the adversity. Dr. B, who was now on the other side of the hospital bed as a patient, knew the power of generously giving time and presence, and he was looking forward to standing again as he crossed the finish line of his life.
The Great Physician offers us hope, peace, and healing to our restless souls. We too can model his example and selflessly share our cup of charity to the aching soul. May we never let technology take our time and presence away from our patients. Instead, may we use it to our advantage to make more time for our patients, giving them the most valuable thing we have: our time through presence. 9
Colon Cancer Doesn’t Wait Until 50
Alex Flynn-Hanlon, MD
Colorectal cancer has long been considered a disease of older adults, with the majority of cases diagnosed after age 50. For decades, screening guidelines reflected this, recommending colonoscopy and other tests starting in middle age. However, recent trends have highlighted a worrisome rise in colorectal cancer among younger adults. With that rising trend, the timing of colon cancer screening has been an evolving topic.
Colorectal cancer is one of the most common forms of cancer in humans. Most colorectal cancers begin as small polyps in the colon or rectum, which can be removed before they become malignant. Screening via colonoscopy not only detects cancer early, when treatment is most effective, but also prevents cancer by identifying and eliminating precancerous growths that might have turned into cancer in the future. Widespread screening is one of the reasons overall colorectal cancer rates have comparatively declined in older adults.
The troubling exception to this progress is among people under the age of 50. Studies have shown that rates of colorectal cancer in adults in their 20s, 30s, and 40s have been steadily increasing for decades. Many of these cancers are detected at advanced stages, partly because symptoms such as rectal bleeding, abdominal pain, or changes in bowel habits are overlooked or attributed to more benign causes. Younger patients are also less likely to undergo routine screening, which delays diagnosis.
Because of this trend, the U.S. Preventive Services Task Force and American Cancer Society have both lowered the recommended age for starting screening from 50 to 45. For individuals with a strong family history of colorectal cancer, inflammatory bowel disease, or certain genetic syndromes, screening may need to begin even earlier. Available screening options include colonoscopy, stool-based tests, and imaging, each with varying benefits, risks, and accessibility.
Despite updated guidelines, many younger adults are unaware of their risk. Misconceptions that colorectal cancer is an “older person’s disease” can delay both preventive screening and evaluation of symptoms. Barriers such as lack of insurance coverage, limited access to primary care, and fear or stigma around colonoscopy further contribute to under-screening.
The rise of colorectal cancer in younger populations underscores the importance of vigilance. Clinicians should maintain a high index of suspicion when younger patients report concerning symptoms. Public health efforts must focus on educating communities about screening options, lifestyle risk factors such as obesity and diet, and the need for timely evaluation. Colorectal cancer is one of the most preventable cancers, but only if screening occurs. With shifting trends in incidence, embracing earlier and broader screening is a critical step toward saving lives.
Florida State University College of Medicine
Pathographies
Medical student essays on patients from their third year rotations
All patient names are fictitious
A Spine of Support
ByTalaTello
He was a 45-year-old teacher, admitted for back pain that had become unrelenting pain that had chased him from classroom to clinic, until finally, it brought him to the hospital. We first met him sitting upright in bed, a wince stitched across his brow. He spoke gently, even through discomfort, like someone who’d spent his life choosing words carefully for the sake of others. What seemed at first like a straightforward case of musculoskeletal pain quickly unraveled into something deeper: osteomyelitis.
As the diagnosis became clearer, so too did the complexity of his care. Each day during rounds, his room filled with a familiar rhythm: the nurse’s quiet updates, the infectious disease doctor’s assessment, my preceptor’s plan, and the review of radiology images glowing on the computer screen. There was a choreography to it all, each person stepping into the space with a specific role yet working toward the same outcome. The language of medicine wove through the conversation, but always grounded by the patient himself alert, engaged, asking questions not just for clarity, but to understandthe path ahead.
But his room wasn’t just filled with medical voices. His family was there always. A sister on speakerphone. A cousin sitting cross-legged on the visitor chair. Handwritten notes and children’s drawings lined the windowsill, as if to form a second team
of consultants: those who knew him not by labs or films, but bylaughter and stories. Then, on a Saturday, his mother finally arrived in person. When she entered the room, she looked at us and, with a smile, said, “It is so good to finally meet you two in person.” The weight of those wordsstruck me—here, in a place so foreign and sterile, was a mother grateful to meet the people caring for her son. She had followed his progress through phone calls, messages, and updates, but this moment, where the physical connection became tangible, was the culmination ofher own journey of support.
Over two weeks, I came to recognize a mirrored structure: our interdisciplinary team on one side, his family on the other. Specialists in care, and specialists in love. Each offering a unique perspective, each advocating fiercely for his well-being. There were disagreements, to be sure—debates over antibiotics, concerns about surgery risks—but through it all, there was a shared goal: to restore this man not just to health, but to his role as teacher, mentor, familymember.
Witnessing his care was a lesson in coordination, not only of medicine but of compassion. Just as osteomyelitis erodes bone at its core, chronic illness can threaten to hollow out one’s support systems. But in his case, both remained intact - fortified, even. The spine that was diseased was held together by invisible structures: collaboration, persistence, and love.
In a world where healthcare can sometimes feel fractured, this case reminded me of its potential for unity. The healing of one person became the work of many—each offering something vital, each reminded,
perhaps, of what it means to belong to someone.
By PavloKravchuk
I met her in a quiet exam room that smelled faintly of antiseptic and wintergreen lotion. She was already sitting when I walked into the room — back straight, eyes steady, purse clutched tight in her lap. Eighty-seven, with a laundry list of medical issues that could fill a textbook, but that’s not what I noticed first. It was the way she looked at me. Not angry. Not scared. Just tired.Tired in the way only chronic illness can make someone tired. Yet, her eyes said it all, before she even spoke. She smiled when I introduced myself and asked if I wanted to see the notebook where she kept all her appointments and medication.
“I don’t understand what they’re looking for,” she said, “but I can’t breathe like I usedto.”
She didn’t say it with panic. It was the kind of shortness of breath that had become background noise in her life — until it wasn’t.
Her breathing was labored, even just sitting still. She told me she used to walk across the room just fine. Now, she stopped midway to catch her breath. She was scared, not in a dramatic way, but in that quiet, familiar way people
She Deserved Better
get when used to being told, “We’re still figuring it out.”
Her grandson had driven her that day. She could no longer navigate the city on her own, and I could tell she hated the dependence more than the disease. When we discussed her shortness of breath and the long trail of inconclusive tests, she nodded with a sort of resigned grace. “They said I had a heart echo this year. But it got canceled. No one toldme why.”
That was the moment something in me shifted. I had been so focused on the pulmonary pressures, the medication algorithms, the pathology — it was like standing too close to a painting. Suddenly, I stepped back and sawher: a woman navigating a broken system, trying to breathe, literally and metaphorically, through the cracks.
She wasn’t asking for miracles. She wanted answers. Maybe a plan. Maybe just someone to notice that her care had stalled, that she had been scheduled, canceled, bounced around, and left wondering what had gone wrong.
And the thing is — she was right. The system had let her down.
An echo that was canceled months ago hadn’t been rescheduled. A third-party lab meant to monitor her posthospitalization labs never showed. The pulmonology appointment she waited weeks for ended with a shrug and a request to come back, after she repeated a test she thought she’d already done. It wasn’t malicious. It wasn’t anyone’s fault in particular. But the impact on her?It was huge.
It’s strange how easy it is to lose the plot in medicine. You get so used to flow sheets, labs, plans. But she reminded me there’s a story behind each of those. And if we don’t stop to listen—actually listen—we miss it
The irony is that her physiology was relatively stable: Pro-BNP reassuring, vitals unimpressive. But she was drowning in the inefficiencies around her. I thought of the echo not ordered in time, the lab not drawn posthospitalization, the pulmonologist forced to reschedule due to missing information. These weren’t just paperwork errors. They were missed opportunities for healing.
She wasn’t her CKD or her dyspnea or her labs. She was a full person with a life and grandsons who drove her to appointments and a voice that had started to go quiet from not being heard.
That silence botheredme.
Because I don’t want to be the kind of doctorwho forgetsthat distinction.
What she needed wasn’t complex. She needed someone to look ahead, to make sure the echo was actually scheduled before she showed up again. She needed someone to notice the gaps before they became consequences. And maybe, just maybe, she needed someone to sit down and say, “This isn’t yourfault.We see you.”
I don’t think I helped her in some dramatic, life-saving way. But I do think I heard her. And I think that matters.
This experience didn’t just show me the cracks in the system, it showed me the spaces where a little awareness and initiative can make a huge difference. We talk a lot about patient-centered care, but it’s easy to forget that means keeping track of the patient even when they’re not in the room.
And sure, I’m still a student. I’m learning. But I can already see the kind of physician I want to be.The kind that
catches things early — not just clinically, but in how people are slipping through the cracks. The kind that pays attention to what patients aren’t saying out loud. The kind that doesn’t confuse busywork with care. Medicine wasn’t just about knowing the right answer. Sometimes, it was about noticing when no one else was paying attention.
She deserved better.And I think a lot of patients do.
What I carry from that visit isn’t a brilliant diagnostic insight or a successful intervention. It’s the quiet conviction that systems must bend toward the patient, not the other way around. That no one should have to keep track of their medical care in a spiral-bound notebook and hope someone reads it.
I’ll carry her story with me, not as a clinical puzzle, but as a lesson in humanity. She reminded me that care isn't just what we prescribe; it's how we show up. It’s how we listen. It’s how we make someone feel seen, even when the answers are slow to come.
I don’t have all the answers yet. But I’ve learned to ask the right questions. And I’m not afraid to sit in the silence and listen.
Because that’s where the medicine starts.
Frank Is in Today
By John Searcy
I was on my emergency medicine
elective rotation when I first heard about Frank. That week, I was assigned to ride along with the local fire department. We were hanging out between calls, swapping stories about memorable patients, when one of the firefighters asked me, “Have you met Frank yet?” I told him no, and without missing a beat, he launched into a story about a well-known homeless man in Volusia County.
According to the crew, Frank was something of a local legend and celebrity amongst the medical community.They said they get multiple calls a month from him, always requesting a ride to the hospital. “He knows the game,” someone said. “Wait until it rains, say you’ve got chest pain, and boom—you get a warm bed and a sandwich.” Laughter followed. It was clear Frank was familiar to everyone in that room, and the conversation danced somewhere between annoyance and reluctant affection. They described him as someone who took advantage of the system. At the time, I listened and laughed along, trying to fit in, but deep down, I wondered who Frank really was beneath all thestories.
The following week, I was back in the emergency department. I was excited, hoping to see traumas, interesting diagnoses, and rare conditions. I threw myself into every case, trying to soak up as much as I could in this fastpaced, chaotic environment. Amidst all this learning, I started to hear the name Frank again—this time from nurses and techs.
“Oh, Frank’s in today,” one nurse said as she rolled her eyes. Another replied, “If we were a for-profit hospital, we could just turn him away.” I overheard more than a few grumblings— complaints about wasted resources, about patients like Frank “clogging up the system.” I tried not to let those comments bias me, but I’ll admit, it was hard. I began to question whether his constant visits were fair. Was he taking up a bed that could be used for someone truly in crisis? Was he, as many seemed to believe, gaming the system?
Then one rainy afternoon, my preceptor turned to me and said with a half-smile, “I wonder if Frank’s gonna come in today with chest pain.” Moments later, asifon cue, he arrived.
“You finally get to meet him,” my preceptor said. “See what he wants. We’ll give him a sandwich and get him out of here.”
I walked into the exam room expecting to find a man matching the stories I’d been told. Instead, I met someone who looked old enough to be my grandfather. His shoes were worn thin, the soles nearly detached. His clothes were tattered and layered, as though he was trying to wear everything he owned at once. His face was red and weathered from years spent outdoors, and he carried a faded felt bag containing all his belongings. On his head, a tattered ball cap clung tightly, the edgesfraying and stiff withage.
Frank said he had chest pain, but as I examined him, it became clear something else was going on. There was a large, angry patch of infected skin on the back of his head—hot, swollen, and tender to the touch. It was likely caused by pressure from the old hat he wore constantly, combined with poor hygiene andsleeping on rough
surfaces. It was a textbook case of cellulitis, and it needed treatment.
I told him he would need antibiotics and explained what was going on. He looked genuinely surprised—almost stunned—that someone had taken the time to thoroughly examine him and speak to him with care. He reached out, grabbed my hand, and with tears in his eyes, said “Thank you.” It was simple, but deeply sincere. In that moment, I felt the weight of his gratitude—not just for the medical care, but for being seen.
We sat and talked for a while. I asked about his medications and found out he had heart failure. He hadn’t been taking his medications consistently—not because he didn’t want to, but because they were too expensive, and he had no stable place to store them. I went through his prescriptions with him, explaining what each one did, and gave him a list of local pharmacies that offered discounted prices. He listened attentively, asked questions, and held onto the paper like it was something precious.
Walking out of the room that day, I felt something shift in me. Before meeting Frank, I had absorbed so many secondhand opinions. I had let the jaded perspectives of others shape my own assumptions. But now, having spent just a little time with him, I saw him for who he really was: a human being navigating an unimaginably difficult life, with dignity, resilience, and a capacity for gratitude that humbled me.
Frank wasn’t a burden. He was a person failed by countless systems— housing, mental health, social services —and showing up at the ER wasn’t manipulation; it was survival. He came to the hospital not just for food or shelter, but for something just as essential: human connection.
This experience challenged my biases and taught me more about medicine than any textbook could. I learned that empathy isn’t just a soft skill—it’s an essential tool. Taking the time to listen and connect can dramatically change the care a patient receives and the impact we have as providers. It also reminded me that every patient, no matter how many times they’ve been in the system, deserves to be treated with dignity and compassion.
I still think about Frank. I think about how quickly we label people as “frequent flyers” or “noncompliant,” and how those labels strip away their stories and humanity. Frank helped me grow—not just as a clinician, but as a person. He reminded me that behind every visit, every chief complaint, is a story worth hearing.
If I can carry that forward in my career —if I can remember to slow down, to listen, to treat each patient like it’s the first time they’ve been seen—then Frank will have given me one of the most valuable lessons of my training.
Empathy in Real Time
By KevinSalimi
visit. I recognized her name immediately. She had been a grade above me in high school, and I had known her husband's family for years. She was six months older than me—an age gap that, in high school, felt more distant than it does now. Today, it made her story hit closer to home than any case I had encountered in medical school.
A week postpartum, KJ’s visit was supposed to be routine. She was recovering well from a cesarean section, her baby was healthy, and she only reported mild diarrhea. But her story unraveled with quiet gravity.
During her labor, there had been confusion. She presented to the hospital with malaise and shortness of breath but was sent home after testing negative for viral illness and showing no signs of labor. Still not feeling well, she reached out to her sister-in-law, a nurse practitioner in Orlando, who encouraged her to come to a hospital with top-tier neonatal care. There, she tested positive for Influenza A, and an induction was initiated. Labor did not progress, partially due to an unexpected finding—a fibroid obstructing her cervix. A cesarean was performed, and her babywas delivered safely.
The biopsy came back: poorly differentiated cervical cancer. My attending had suspected as much during the exam under anesthesia, but I wasn’t prepared for the finality of that diagnosis. I was present when we diagnosed cancer for the first time, and it shook me. Not just because of the diagnosis, but because it was KJ. Someone my age. Someone I had known.
This was the first time I saw medicine not just from a clinical lens, but through the eyes of someone living it. As I watched her navigate her options —considering aggressive treatment like hysterectomy versus more conservative, fertility-preserving approaches—I couldn’t help but think about my own life. At the time, my wife and I were trying to conceive. As of writing this, we are eight weeks pregnant.
It was inevitable. Florida State University's community-based medical school structure meant returning home for clinical rotations. I had always known that, eventually, I would care for someone I knew personally. But nothing prepared me for what that wouldtruly feel like—until I met KJ.
KJ came into the clinic during my OB/GYN rotation for herpostpartum
It wasn’t until her postpartum visit that I began to understand how much more lay beneath the surface. A car accident shortly after discharge led to further testing, where norovirus and concerning uterine findings prompted her readmission. When I saw her again in the hospital, she was spiking fevers, and we began to suspect retained products of conception.Theplan was to perform a dilation and curettage (D&C) —a procedure that also allowed us to biopsy the fibroid.
That’swhen everything changed.
This connection made empathy effortless—but also painful. I saw KJ in my wife. I saw myself in her husband. I imagined the unimaginable: having to choose between fertility and life, or being the one asked to support that decision. It brought to life every TV trope I’ve ever seen—the dramatic moment when a partner has to decide between saving a mother or her child. But this wasn’t fiction. This was real. And I was standing in theroom.
I’ve always believed in the importance of empathy in patient care, but this experience gave that belief new meaning. Textbook definitions of empathy ask us to put ourselves in someone else’s shoes. I didn’t have to try with KJ—I was already there. I didn’t just understand her fear; I felt it. I didn’t just understand what was at stake; I recognized how closely her experiencemirrored a possibilityin
my own life.
It also forced me to confront the limits of medical science and the unpredictability of life. I remember watching OB/GYN lectures that said, thanks to HPV vaccination, we would likely never encounter cervical cancer in practice. That false sense of security was shatteredinone afternoon.
KJ’s case deepened my understanding of what it means to be a physician. We aren’t just diagnosticians or proceduralists—we are witnesses to our patients’ most vulnerable moments. We don’t always have answers. But we can always offer presence, compassion, and spacefor shareddecision-making.
I don’t know what KJ ultimately chose. My rotation ended, and I haven't kept in touch. But I do know she was surrounded by a team of empathetic, dedicated clinicians who honored her autonomy and walked with her through the complexity. I’m proud to have been part ofthat, even briefly.
More than anything, I learned that professional identity isn’t built only through technical skill—it’s shaped by moments that touch us, surprise us, and, at times, break our hearts a little. This experience didn’t just make me a better future physician. It made me a better human.
rotation doing pulmonology. It was during this rotation that I met somebody who reminded me why I am in school to become a physician. Before I describe the interaction I had with this individual, I would like to provide some context about how I was feeling before the interaction.
Having just taken USMLE Step 1, I must say that doing hundreds of practice questions that begin with something along the lines of “Axx year old patient presents with XX days of XX…” was not only exhausting, but also an extremely clinical way to view a patient. After doing hundreds of these, it has become burned into our brains and has veered us into a clinical way of thinking. I am not presenting this situation as a “black or white” matter, suggesting that this is entirely bad. It’s not. To an extent, there needs to be a level of objectivity when addressing the problem at hand. That being said, this way of thinking is our day in and day out. Furthermore, we remain busy in our learning that our time with the outside world is limited. Thus, we spend increasingly more time with our peers, who are all doing the same UWorld questions and Anki cards.
very interesting to me to see the conditions I read about in real life. To begin understanding real-world patient management was exciting to me, as a third-year medical student who just started rotations. I noticed a particularly younger male on our list, which stood out to me. He was in his 30s and all that was next to his name was “pulmonary edema”.When it came time to see him and we entered the room, he was sleeping. Before seeing him, I was confused as to what would have led him to be in the hospital of all places. I then saw in his chart that he was nearly 600 pounds with numerous comorbidities. He had such a difficult time breathing due to his weight and fluid in his lungs that he needed to be on BiPAP. I had never seen somebody in this sort of condition before. I felt a variety of emotions in that moment. My curiosity, inquisitiveness, and excitement from starting clinicals became overshadowed by concern. I was afraid for him. After we spoke to him briefly, and I listened to his heart and lungs, we had to move on to the next patient. At the end of the day, my preceptor let me pick which patients I wanted to pre-round on tomorrow. Obviously, I put him on my list.
By ImadRaza
My most memorable patient experience was during my first rotation of third year. I began with my Internal Medicine
Upon stepping foot in the hospital wards, it became apparent to me how much of a machine the hospital is. What I mean by this metaphor is that there is such an emphasis on productivity with dictation devices with set phrases and hearing someone saying “discharge” on my left and “admit” to my right. Watching providers go from room to room with large patient lists. I was shocked when I saw our patient list and just for the morning it was nearly 20 patients. Later during that rotation with a different physician, we would have 40 for the entire day. As we rounded on patients it was certainly
The next morning, I went to go see him. He was sleeping, as majority of the patients were at this time. At this time, I was just intending to get a brief update on how he was feeling, but he ended up deciding to fully wake up.As I was doing my physical exam, he said, “you know I wasn’t always like this man.” I had to wonder what even led him to get to this point. However, this was not the time for an extensive discussion especially since I still had to see a few more patients. It planted a seedin myhead though.
During rounds, we went togosee him.
Uplifting Moment
It was the same quick interaction as before. It was actually the following day after we rounded that I went to see him in the afternoon. I went to go ask how he was doing, and that conversation easily turned into him telling me about his life. In hindsight, I think he was wanting to tell me or perhaps somebody about his story. He then confided with me that he draws all of this to when he was a little kid, probably 6 or 7. I was intrigued. He said his memory is blurry at this point, but it was when his mother remarried, and the new stepfather loved to make fried foods. He stated that both him and his younger brother were overweight growing up. This stepfather he says expressed his love through cooking, but that was about it. He described him as being physically and mentally abusive. He hit both him and his younger brother and often called them expletives. He also loved taunting them. The way he described the environment was like “alpha male vs the betas”. Hearing this made me feel infuriated because this is no way to grow up. He stated that all of this ended up affecting him mentally for the rest of his life, and only realized the effects in hindsight so many years later. Eventually once he grew up and became physically stronger, he states he was able to “stand up to his father”. The whole story made me feel many different emotions. Not only did I have a baseline fear for his health, but his story also made me made me both mad and sad. I was mad because this was not fair for him to deal with this as a child growing up. I was sad because of what his life and mental well-being could have been. He then shared that he was able to move out of the house and work. He then suffered a leg injury that led him to be bed bound. Once that happened, he remained bed bound for an extended period of time due to the weight he gained. He draws back to not
only his eating habits acquired from his family, but also his lack of feeling like he could change anything due to the mental damage from his stepfather. He did say that one day he said enough was enough and started exercising from his bed to become able to fully walk again. However, he states that this time around, he suffered another injury and has been bed bound for years since. He states he was exhausted now and doesn’t have the drive he had before. I took the opportunity to draw upon his ability to make a change before to reassure him that he is still the same person and can do it again. I found that his initial feeling of hopelessness seemed to transform into “I do want to get better and get my life back.”At this point I looked at the time to realize that 2 hours had flown by. I asked him if he needed anything else. He politely asked me if I could hook up his PS5 to the TV. I had no idea people could play video games in the hospital. I chuckled a bit and did the favor.As I walked out of his room, I was back into the hustle and bustle of the rest of the floor. The feeling of exiting a soft-spoken deep conversation into the loud chatter and speed of the outside was an intense contrast of environment. I took a deep breath appreciating the moment I just experienced with him and carried on with my day.
The significance of this story for me is that it serves as such a vivid reminder how much is left out of our traditional clinical patient encounter. In my personal statement for medical school, I wrote about how I was inspired by a pediatric ER physician who not only took care of his patients medically, but also had a bedside manner that made the kids smile during times of suffering. While fixing their problem is fulfilling, it was equally fulfilling for me to see physicians take the opportunity they
have to be there during times of distress to uplift people. This was the day that I was able to actually do what inspired me to go down this path in the first place. It remains the most fulfilling experience I have had. Realizing this, I now do my best, as time permits, to understand and listen to my patients the best I can because that is what gives me the most gratification.
By JaredSaifman
Reflecting on my experiences in the hospital setting, one patient distinctly stands out, illuminating not only the profound psychosocial dimensions of care but also raising complex questions of clinical ethics and compassion. She was diagnosed with late-stage colorectal cancer. The cancer had metastasized beyond the reach of surgery, and treatment options had narrowed to palliative care. What unfolded in her final days taught me more than any textbook could; about dignity, autonomy, and the deeply human side of medicine.
From the beginning, it was clear that she understood her diagnosis. She asked pointed questions about her prognosis and treatments, not with desperation, but with a quiet resolve. She had made peace with her situation in a way that seemed foreign to those around her. There was a palpable contrast between her calm acceptance and her family's emotional turmoil. While she expressed a desire for peace, her family seemed gripped by denial, unable, or unwilling, to accept the terminal nature of her illness.
A Nice Cup of Tea
She voiced a simple yet profound wish: to leave the sterile confines of the hospital, return to the comfort of her own home, and savor a nice cup of tea. This statement struck me deeply; not for its poetic simplicity, but for the depth of meaning it carried.That cup of tea symbolized so much: her longing for normalcy, familiarity, dignity, and the autonomy to spend her remaining days as she chose. It was not about giving up; it was about reclaiming a life that was no longer defined by IV poles and lab results.
And yet, her family couldn’t see that. They advocated fiercely for continued tests, more scans, more consultations. I am sure their insistence stemmed from love and fear, perhaps even guilt, but it inadvertently silenced her voice. They were so focused on the fight that they forgot to listen to who they were fighting for. I found myself caught in the middle of this silent tension, an ethical and emotional dilemma that asked: Who is our duty ultimately to? The patient, or the family?
In clinical ethics, we often emphasize patient autonomy as a cornerstone of respectful care. But applying that principle in real life can be filled with emotional resistance. Here was a woman who had clearly expressed her wishes. Yet the well-intentioned interference of her family risked overriding her agency. It made me question: how do we, as providers, mediate these situations without alienating the people who care the most? How do we advocate for the patient while acknowledging the family'sgrief?
There’s a part of me that imagines what I would feel in her position.At first, I’d be overwhelmed by fear, uncertainty, and anger. But I hope, eventually, I’d arrive at the samesense of clarity and
acceptance she had found. The idea of facing mortality is terrifying. It is, by its nature, unanswerable. But the loss of control, that feels even more suffocating. In the hospital, patients surrender so much: their privacy, their routines, their independence. Watching her reclaim even a small part of that, simply by expressing a desire to return home, was a profound reminder of the power ofpersonal choice.
Her story also embodies a narrative of medicine: the patient’s voice, their story, and the context that gives their life meaning. She did not see herself as a diagnosis or a collection of symptoms. She had a clear sense of past and present, and of what she wanted her final chapter to look like. She spoke about her family, the smell of home cooked meals, the quiet evenings she spent with a good book in hand. These were not trivial details, they were markers of identity and peace. She saw her life as a whole, a continuum that didn’t end in the hospital but sought closure in the placesthat madeher feel most herself.
In speaking with her, I sensed that she had come to terms with her illness, not in resignation, but in acceptance. I couldn’t help but contrast her experience with my own previous understanding of death and dying. Coming from a family that often avoids direct conversations about mortality, I had rarely encountered such calm and clarity in the face of death. Her story forced me to re-evaluate my own discomfort with end-of-life discussions. I realized how important it is, not just clinically, but humanistically, to be present in these moments. To listen without the need to fix. To accompany, not to control.
Ultimately, this patient left the hospital. With the help of a dedicatedpalliative
care team, her wish was honored. She went home. I never saw her again, but I like to think she got her cup of tea; warm, familiar, and peaceful.
Her story has stayed with me, not because it marks the end, but because it affirms everything I hope to uphold in my medical journey: respect, empathy, humility, and the courage to let go.
Early Rounds and an Enduring Spirit
By Nick Kostrubsky
During my internal medicine rotation, I met a patient who challenged many of my assumptions -- not with words, but with the way he lived, the way he greeted each morning, and the surprising energy he brought to a hospital room. Mr. N was 81 years old and admitted for the prophylactic management of a new chemotherapy regimen for his chronic lymphocytic leukemia. Though his admission was precautionary, I initially expected a frail, quiet older gentlemen. What I found instead was someone who was vibrant, sharp, and more engaged with life than most people younger thanhim.
Mr. N had a military background, and it showed. He kept a routine, even in the hospital. While most of my patients were still asleep when I began morning rounds, Mr. N was always up and ready -- eating breakfast in the chair adjacent to the bed. This gave me the perfect opportunity to connect with him. “Great, you’re here!” he’d say, smiling as I entered his room, always the first stop of my day. He greeted me like an old friend, and I quickly came to look forward to thosequiet early morning
conversations.
The first day I met him, he was relaxed and upbeat. As I acquired his medical history, I also learned about the major events of his life. I learned he grew up in Wisconsin, and he was an engineer building boats on Lake Michigan. When I asked how he felt about starting his new chemotherapy, he replied, grinning, “This is nothing… I’ve been through worse - I’ve raised four kids!”. His charts showed anemia and some mildly elevated cholesterol, but otherwise he appeared healthy. He didn’t fit the image I had unconsciously carried with me about what an 81-yearold chemotherapy patient might be like.
What deepened our connection was football. On one of my visits, I noticed him wearing a Green Bay Packers sweater. I asked whether he was a fan and his eyes lit up. That opened the floodgates. Each day, before discussing his labs or medications, we’d talk about football -- about the Aaron Rodgers drama, about the recent dominance of the NFC North, and about the upcoming games for that respective weekend. It gave us a common ground that wasn’t clinical, and I began to see the man behind the diagnosis more clearly.
Medically, he tolerated the chemotherapy remarkably well. No significant nausea. No abnormal electrolyte shifts. He remained alert and in good spirits throughout. My attending often commented on how relaxed and polite he was. He always made an extra effort to ask how our days were going.
Three days after admission, he was ready for discharge. As I went to say goodbye, he smiled and shook my hand withan unexpected firmness. He
wished me good luck on my future endeavors and walked out like nothing ever happened.Again, this is not what I expected to see in someone with his medical condition.
Mr. N wasn’t a stubborn man -- he was aware of his age, his diagnoses, his immunosuppression. But he never let those realities define him. He chose, every day, to approach life with energy, curiosity, and gratitude. He didn’t see himself as someone being “taken care of.” He saw himself as someone still contributing -- to the conversations, the mood on the floor, and to the humanity of the people caringfor him.
Reflecting on those few days with Mr. N helped reshape my understanding of aging, illness, and the patient experience. Prior to that that patient experience, I would have expected to view a geriatric oncology patient primarily through a clinical lens: risk factors, prognosis, tolerance to chemotherapy. But Mr. N reminded me that patients are not their statistics. They are their stories. His identity was not “81-year-old with cancer.” It was veteran, father, Packers fan, early riser, happyhuman being.
His optimism was intentional. And I began to understand how powerful that perspective can be in the context of illness. It doesn't change lab values or outcomes, but it changes the experience of being sick. It changes how patients navigate their treatment, how they engage with us, and how they remind us why we do this work in the first place.
From Mr. N, I also learned the value of presence. He showed me that even short clinical encounters can be rich in meaning if we are fully present. We should not only ask, “How are you feeling today?” but also, “What’s your
favorite team?” or “What are you looking forward to?” Those questions may not be on the progress note, but they are essential to understanding the patient in the room.
In medical school it’s easy to get caught up in efficiency so that you can make it home at a reasonable hour and cram in an hour or two of studying. But Mr. N reminded me that slowing down, even for a few minutes, can make the difference between helping treat a patient and caring for a person.
Though our time together was brief, Mr. N left a lasting mark. He taught me that health isn’t always about being disease-free. Sometimes, it’s about maintaining dignity, finding joy, and staying connected to the parts of ourselves that mattermost.
He was the first patient I saw each morning, and in many ways, he was the one who taught me how to start my day - with purpose, with presence, and with a reminder of the resilience that lives within our patients, even in the face of uncertainty.
ByAmyTran
We were called to the hospital for two consults. The first patient was brought to the emergency department by her family for altered mental status. LG, who had been lying quietly in the intensive care unit, was found to have two enhancing masses in the basal ganglia and the hypothalamus, suspicious for primary CNS
The Two Consults Who Wanted to Go Home
lymphoma. We approached her bed, but she could not move or follow commands. She had not been eating. She muttered and mumbled in response to tactile stimulation. All we could make out was “I want to go back to France.”
Her family members disagreed with her goals of care. Some wanted to confirm the diagnosis with a brain biopsy, aggressively continue with high-dose Decadron, and treat her with chemotherapy; others were open to transferring her to hospice and pursuing comfort care. The truth is that several days prior, the steroids did help with her responsiveness, and this most likely provided a sliver of hope to her family. From our perspective, her age and performance status did not make her a candidate for surgery, chemotherapy, or radiation. But from theirs, they were not ready to let go of their once lively mother and grandmother. This is understandable. The most pressing matter was to do what she would have wanted and ultimately, the family switched her code status to DNR/DNI. They agreed to transfer her to hospice where she could be given the kindness and attention she needed at the end of her life.
We left the ICU and headed to the ED to meet the second patient, CH. He had a history of chronic lymphocytic leukemia, but this never required treatment and there had been minimal progression over the years. He presented to the ED for shortness of breath and recently left against medical advice after being diagnosed with hepatitis at a tertiary care center. He also had uncontrolled chronic pain.
“I want to go home and die.” he stated.
“What makes you think you are dying?” My preceptor asked.
We had a long discussion about each of his conditions and their prognosis. His CLL was under watchful waiting. His hepatitis could be managed with medications. But it was the pain from his arthritis that he felt made his life unbearable. His death was not imminent but by patient request, the admitting physician placed a transfer to hospice which unbeknownst to us at the time, had been accepted. We left him and his family with a suggestion to reconsider medical care and an offer to see him for a follow-up in the office, should hechangehismind.
Both ofthese patients were in their 80s. The first patient was dying but the family did not want her to. The second patient wished for death but was not actively dying. I interpreted LG’s words of wanting to go back home to where she grew up to mean that she was ready to go to a place of comfort. And where that is is certainly open to individual interpretation.
Neither she nor her loved ones asked or were ready for her passing. The option for her to continue with life while in the ICU initially seemed like the better choice but these efforts would have been uncomfortable for the patient and futile at best. In her final days, she was surrounded by her family who should not be morally faulted for struggling to accept the severity and permanence of her condition or for fearing what life wouldbelike without her presence.
CH makes a similar statement of wanting to go home and die. One might say that this was suicidal ideation that warranted a psychiatric evaluation. But would an involuntary admission at this time have helped him as a whole? And were we in any position to take away his capacity? To most of us, his words may seem like an exaggeration, but they illustrate how debilitating his
chronic pain was. He sees no better alternative to suffering than death, which is thought to end all suffering but is this actually true? No living person would know. His predicament is that due to the illusion of choice, death is seen as the more enticing option compared to what pain he experiences now, because he has never felt, or can know what it means to be dead. Nevertheless, he should not be morally faulted for asking for death because from his perspective, the weight of his mortality has gotten too abundantly heavy.
Physicians cannot save patients from their inevitable death. Nor can we prevent our own because we are as mortal as our patients. There is no life that exists on this earth without grief, loss, failure, pain, guilt, or suffering. But even in these darkest times, remember that the clouds are not necessarily whiter on the other side and that the time that we have on this side is never promised. That does not mean you should fear death and or dying either.You should only fear living a life that is unfulfilling.
As an existentialist, what I have learned from these two consults is the importance of a life that has meaning to you. Whether that be devoting your career to a rewarding job, spending precious time with family who care for you, or pursuing hobbies that bring you joy. Life should be lived with the values of integrity, authenticity, and gratitude.When on our deathbeds, what kind of person do we want to be remembered as? What kind of impact do we want to make on our patients? And looking back on our lives, what kind of memories will we hold onto when we meet our maker?
Privilege of Presence
By Daniella Devaney
It started like any other clinic day. Midway through my pediatrics rotation, the schedule was packed with wellchild visits. Vaccines, growth charts, developmental milestones—it was the rhythm of reassurance, and most visits ended with a smile, a sticker, and the words, “Everything looks great!” By late morning, I had settled into the comforting pattern of normalcy. That’s when I saw him—a quiet 6-year-old boy with his mother scheduled for a sick visit. There was no fever, no vomiting, no overt signs of illness. His mother’s concern was vague but firm: “Somethingjust feels off.”
My preceptor was finishing his previous note and sent me in to gather a history. I started my patient encounter and asked the usual questions. He was more tired than usual, not eating much, and not his usual playful self. He also had been having headaches. His mother had noticed more bruises lately, mostly on his legs. But he hadn’t had any big falls, and he was still going to school. On exam, he was pale and quiet, moving a bit more slowly than most kids his age. The bruises on his shins seemed easy to explain—he was a kid, after all. But the mother’s concern didn’t waver. As I reported back to my preceptor to present the case, I remember his face getting more visibly worrisome as I went down the list of symptoms. We quickly went back into the patient's room and my preceptor conducted a physical exam. The patient had hepatosplenomegaly and petechiae in his mouth.
Suddenly, the tone of the day shifted from wellness and reassurance to lifealtering reality. My preceptor looked back at me with an alarming look on his face. Everything else faded into the background as he said, almost solemnly, “I am going to send him to the hospital to get emergent labs.” The mother immediately panicked and questioned the doctor’s concerns. My preceptor firmly, yet empathetically said, “We must rule out leukemia.” The mother, who had walked into the clinic with an intuitive concern, was now being told her child may have a lifethreatening illness. I watched her face shift from confusion to devastation in seconds. She clutched her son to her chest as she asked, “Are you sure? This can’t be a real possibility, can it?” Unfortunately, it was not only a possibility, but it wasthereality.
While my preceptor coordinated care with the nearby Emergency Room, I remained in the room with the mother and her son. She was crying, and he sat quietly, confused by his mother’s emotions. She asked me questions — about what this might mean, about statistics and outcomes— but at that moment, all I could recall were scattered facts from my study materials on childhood leukemia. I realized then that I couldn’t offer her certainty or medical expertise. What I could offer, though, was presence. I sat with her, listened, and allowed her to feel everything she was feeling. At that moment, I wasn’t there as a student with answers, I was simply a fellow human being, bearing witness to her fear.
The patient eventually made it to the hospital and several hours later my preceptor received a call confirming the boy’s white blood cell count was critically elevated. His platelets were low and he hada significantly high
LDH. The patient was admitted for further evaluation, and within days, the diagnosis of acute lymphoblastic leukemia (ALL) was confirmed. He began chemotherapy almost immediately.
What struck me most about this experience wasn’t the rarity of the diagnosis or the complexity of treatment. It was how quickly a normal day, a routine clinic visit, became the worst day of someone’s life. I had entered the morning thinking about babbling milestones and which kids needed the MMR vaccination. By afternoon, I had witnessed a mother receive a diagnosis that would alter her child’s future.This experience reshaped how I think about the role of a physician. Medical school teaches us how to recognize disease, interpret lab values, and create treatment plans. But it’s only in these moments—when everything changes—that we learn what it truly means tobe adoctor.
Being a physician means being the person families turn to when their world falls apart. It means carrying the knowledge that at any moment, a simple complaint might uncover something devastating. It means knowing that your words and comfort can change someone’s life. That responsibility is enormous, but it is also a profound privilege. As a student, I wasn’t the one making the final calls or delivering the treatment plan. But I was there. I was present when a mother voiced her worry, and I was part of the team that listened. I saw firsthand how trust is built—not in grand moments, but in the quiet ones. A parent says, “I don’t know what it is, but I know something’s not right,” and we choose to believe them.
Since that day, I’ve thought often about what it means to holdspace for
someone’s pain. In medicine, we will be there for birthdays, checkups, and good news—but we’ll also be there for diagnoses, for grief, for life-altering moments. We are allowed into the most sacred, vulnerable places in a person’s life. And when we’re invited in, we must bring not just our knowledge, but our empathy, our humanity, and our strength. This experience reminded me that being a doctor isn’t about being the hero or having all the answers. It’s about being reliable in the chaos. It’s about standing steady when someone else’s world is collapsing. Sometimes that means having difficult conversations, delivering bad news, or holding a mother’s hand as she absorbs unthinkable information.
The child continues to receive care through the oncology team. His prognosis is good, and he’s responding well to treatment. But I know the road ahead will be long, filled with hospital visits, blood draws, side effects, and uncertainty. And yet, there’s something beautiful about being part of that journey—not because of what we do, but because of what it means to be invited into someone’s life during their most vulnerable moment. Now, as I move forward in my training, I approach each patient encounter with a deeper awareness. I no longer assume that any visit is “routine.” I’ve learned that what starts as a quiet concern in an outpatient clinic can unfold into something unimaginable. I carry the weight of that responsibility with humility, and I remind myself daily that at any moment, I could be the person a family remembers on the worst day of their life. And that is both a sacred privilege and a tremendous responsibility.
The Broken By Greggory Boatright
It is a strange concept to put myself in the shoes of the patient, due to the cognitive dissonance required to be objective in facilitating their care, but it is something I try to keep in mind in providing optimal care. The idea of allowing strangers to poke, prod, and operate on me is a foreign concept. I mean, I have worked on cars and flown planes, but I never expected the vehicle to figure out where I am going or when I am leaving. With being a patient, it is a bit foreign in the same way, since there is a disconnect between giving and receiving medical care. In the hospital experience, you really do not get the chance to get to know the members of the medical team before you put your treatment (and possibly your life) in their hands. So that is a bit scary for me to comprehend. How does one really expect an insurance-paid (or cash paid) medical person that you’ve never met be trusted to cure ailments? I am not trying to wax philosophically very heavily, but if I had no concept of medical treatment and I got sick, it is scary to imagine putting my life in someone else’s hands.
There was one patient that weighs heavily in my mind, due to him being so brash in his explanation of what had happened him. He was a man in his 50s that had the world on his shoulders after having a fight in with his son-inlaw. He had gotten into a spat about living conditions after his daughter was happy to have him stay at her home, but her husband was not happy about the predicament. The patient’s son-inlaw ended up pushing the patient down
flight of stairs after a heated conversation, leading to the patient needing to get an ambulance ride to the nearby hospital. He had 3 broken ribs, a dislocated shoulder, and a dislocated hip. He was in too much pain at first to piece together what had happened, but once he was in the hospital overnight, he understood the event more completely.
Family is supposed to be everything. Right? Well, after a tumble down a staircase this patient was not really feeling the kumbaya feelings anymore. He was angry, felt betrayed, and was in so much pain he could barely stand to move an inch before receiving a jolt of electricity in hisbody. It wasbafflingto see how well he was handling the whole situation, considering the pain of the event.
I always comfort myself when I get in a car, a plane, etc., by understanding how it works and knowing that the likelihood of death is slim so long as I am careful. Applying that to being a patient sounds difficult, being most disease complexes are so intricately difficult to understand. With research, I could retroactively look up what the medical staff informs me of, but I am not really that good at learning when I am super sick. Trusting medical staff is really the only option when in excruciating pain, since the pain really does prevent clear thought. The idea of being blisteringly in pain after a horrible night is enough to make me a bit nauseous, so trying to imagine how this patient felt is baffling.
I am grateful for the trust that the patients I work with show in the American medical system. Even skeptics of medicine still trust the system enough to show up and ask for help when they need it. To be fair, I wouldnot really think that much about
the issues I had, I would be more focused on the care I got from the medical team. I mean, great nurses and kind doctors makes most of the patient experience bearable, making it almost as important as the treatment itself. I have seen patients check out of a hospital against medical advice to go to a different hospital just because of a disagreement with their medical team. I don’t think I would do that, but I can see why they feel so disgruntled when they feel like that trust they had for their providers is broken. So besides being scary and requiring a lot of trust, I guess the biggest thing I would be thinking of is how stir crazy I would get laying around all day if I hadtostay more than a few days. I guess that is partially why doctors can make the worst patients.
Trying to personify pain is difficult. How much painkillers is enough? How much should we worry about addiction when you can not stop grinding your teeth in a haze of pain and discomfort? I am not really sure the best answer to these, because truthfully I doubt much would be going through my mind other than the pain of the situation. Whether thinking that it could have been worse or understanding that simply being at the hospital means that there are probably sicker and more troubled people there than you may give a slight discomfort when contemplating getting the proper amount of care. Hard to catch the attention of a nearby nurse when the patient next door is coding (from a myocardial infarction), in my opinion anyways. It is pleasant to be respected by the staff, but they are people too. Should the patient be expected to leave a tip after the patient has received IV fluids or drugs? To be honest, I don’t know the answer to any of these questions directly through my personal experience, but the patient did
jokingly ask me these things when getting ahistory and physical exam.
Most importantly, this visit gave me a sense of duty. Throughout the hospital stay of this patient, I checked on him everyday. He was always happy to see me, because oddly, he got lonely during his hospital stay. With his son-in-law putting him in the hospital he did not get many family visits, other than from his daughter. His medical staff were focused on his health and well-being, but not trying to have extensive conversations. So, his greatest worry in the week he was there was actually not the pain, it was the loneliness of a medical hotel room without someone to keep him company. This is why he stood out from many of my other patients: with all of his hurting and medications, his loneliness during his inpatient stay was what bothered him the most.
An Unexpected First Day
By LucyWilkinson
crackles dispersed throughout her lungs, I feared what was going to happen to this woman and her baby. I had never met this woman before, knew very little about her history, and yet I was about to witness a terrifying moment her life.
I listened to the discussions between the anesthesia team, NICU providers, an intensivist, and the doctor as they considered the complications, risks, and how to best care for this mother and her baby. I tried to understand as much as I could about the medicine they were deliberating, but I felt like I was fumbling through darkness with little clue about what was happening around me. I watched as the patient’s mother cried while being told that the patient would be put under general anesthesia for the C-section and would likely be on a ventilator in the ICU after surgery. Her mother’s fear, the hectic rush of the L&D floor as they rolled her back, and the swarm of people converging on the OR to care for this woman and her baby terrified me. I was scared I was about to watch this woman andher baby die.
Patient X was a 35-year-old female who was about to be taken back to the OR for a STAT C-section due to preeclampsia with severe features complicated by acute respiratory decompensation. It was the very first morning of my OBGYN rotation and this was the first case of the day. I went into her room to introduce myself, but she couldn’t speak due to her difficulty breathing. Grasping an oxygen mask to her face, she looked tired and scared as nurses and surgical techs scrambled in and out of the room preparing to roll her backtothe OR.As I listened to the
While I had been nervous for days about being in the OR for the first time, I didn’t even have the time to be nervous as I scrubbed in, downed my gown and gloves, and stepped beside my preceptor in front of the patient on the table. I watched in awe as the OR was assembled around this patient. It was a well-oiled machine of controlled chaos and every person in the room was completely focused as they prepared for this delivery.As I watched my preceptor cut into the patient, move through the layers down to the uterus, and finally pull the baby into the world, I was shocked that this was my first delivery. I had not expected to walk in the first day and immediately be in the OR withinan hour. Ihad imagined a
simple delivery, with the opportunity to get to know the patient, and to be overwhelmed by the joy and excitement I was witnessing. I didn’t expect to be terrified forthe mother and the baby, and I didn’t expect to be witnessing, not one of the happiest moments of this mother’s life, but possibly one of the most terrifying days of her life. I didn’t expect that the mother wouldn’t even be awake for her baby’s delivery due to her being so sick and in such a dire situation.
The baby was blue and covered in goop as he popped out of the womb.The first thing that popped into my mind was that he looked like a little alien. It all felt surreal as the NICU team scooped him away after the cord was cut. The focus then returned to the mother, and I was flummoxed as my preceptor asked me to reach in and remove the placenta. I was awed to be a part of the delivery and I felt an adrenaline rush of excitement to be a part of the surgery. At the same moment, I felt guilty for being excited in the midst of this intense case.
Thankfully, the mother did well throughout the rest of the C-section and the baby was stable in the NICU over the next few days. My preceptor and I visited the mother everyday while she was in the ICU on the ventilator. After a few days, she was taken off the ventilator and continued to improve. Unlike other patient encounters, I got to know this patient not before, but after I was a part of her care. It was a unique experience to be able to hear about the patient’s story in retrospect and I was humbled that she was willing to open up to me and share her experience. She described the fogginess she experienced leading up to the C-section and her only fear being for her baby. She was tearful as she shared her thoughts with me.
This experience highlighted to me the balance between focusing on the medicine, which can sometimes separate the humanity of the patient from the acuity of the disease process you are treating, and tuning back into what the patient is feeling and experiencing throughout their care, especially when it comes to high-stress, high-acuity situations. During the moments leading up to the patient’s Csection, the entire healthcare team was laser focused on all the nuances of her care, from respiratory support to risks of the procedure to worse case scenarios. The focus was entirely on the medicine, and it almost felt as though the patient was removed from the situation. This was not a bad thing at all and what I learned was that this was necessary to provide the best care for the patient. The most important thing I learned was that afterwards, once all the dust settles, your care for the patient is not over. Talking to the patient and repeatedly checking in with her after her delivery was immensely important, not only for the patient so that she felt cared for and heard, but also for her providersto remindthem to ground themselves throughout the craziness that is medicine. Being in medicine day in and day out desensitizes us to how jarring and terrifying medicine can be for the patients. I learned the importance of always tuning back in to the humanity of the patient and being there to hear their stories, especially during the most challenging cases of medicine.
By SophieGorelov
“I first noticed it around 9 or 10 am, when I was sitting at home, eating breakfast.”
“Did you havepain in your chest?”
“No, it felt like…felt like this…this feeling that went across mychest.”
I waited patiently as he searched for the right words to describe this nonspecific, strange feeling in his chest.
“Do you mind if I listen to your heart?” I asked.
I placed my stethoscope on the chest of this 87-year-old man, listening intently as I watched the monitor with its meaningful squiggly lines.
As I finished my exam of his heart, lungs, and abdomen, interrogating his body with the tools of auscultation and palpation, Mr. P started to share his story – the details of his life absorbed by his body which could not be elucidated from any ECG or CT. “About 8 years ago, my wife started to have difficulty remembering how to get back home.” I didn’t know where this story was heading, but knew it was important. “We lived in Ocala 50+ years and raised two children there. When my wife began to get more lost at familiar places nearby, we were concerned and took her to our doctor. After doing all the tests, they told me, P, your wife has Alzheimer’s disease” Mr. P went on to share his experience over the last 8 years, as his wife became more and more dependent, needing to move into a long-term care
“Though she no longer recognized or remembered me, I would take her out for drives, and she loved to look out the window. We’d go get pizza and sit on the beach together.” Mr. P shared about her final moments of life on earth. He shared about the time they had together, the time spent travelling to 37 countries around the world and the 57 years they had together that nonetheless “went so fast.”
In his reflections out loud, he wondered if he had told his wife every night before bed that he loved her in those years which were “sobusy.”
He told me, “now, every day, all the time,” he thinks about how fast things go – “and you never get the moment, the conversation, the time back.” I shared that I was newly married, and he told me to cherish the time I have.
“March 22nd is the upcoming anniversary of her death. And…I’m wondering if how I’m feeling – if how my heart is feeling – is all related to this.”
I had read the notes in the chart, the numbers of his labs, but as he awaited further testing, I could not give him an answer about his heart.Yet, it reminded me, that while I did not have the expertise of a cardiologist, there was still something I could do – listen to his heart.
In the rush of rounding or the day of a long list of patients to be seen, the “why” behind it all can easily be threatened to get buried beneath the charts, checkboxes, and chock-full schedules.
Why medicine? This question demanded an answer on our medical school applications.Yet it remains
deeply relevant to the daily practice of medicine. My why was inspired – and continues to be driven – by the desire to devote my time to listening to my patients, entering their stories, and seeking to alleviate their suffering.
Like my patient, Mr. P, as I look back over 3rd year, I truly marvel at how fast the time has gone by.
In studying the classic signs of disease presentation, I have simultaneously witnessed throughout the year that the same disease presents differently in human beings as uniquely made individuals.
I have learned that the first tool of a physician is the ability to listen – with our ears and with our heart. This guides us in what to examine, order, test, or treat. It expands and narrows our differential.
It communicates to the patient that we truly care. It builds the bridge of sacred trust with our patient that enables us to take the next step together on the journey towards healing.
More Than the Numbers
By JoanneZhao
someone who is living through circumstances that can never be fully understoodfrom numbers alone.
Mrs. A was an 82-year-old female patient, with a known history of type 2 diabetes, hypertension, and chronic kidney disease. She was presenting to the clinic for her routine four-month follow-up. I had reviewed her chart beforehand, including her labs and recent notes. I noticed her hemoglobin A1c immediately, as it had increased from a stable 6% to 9.5% in just four months. Immediately, the questions started forming in my mind. Had she stopped taking her metformin? Was her diet less controlled? Had she been exercising regularly? Was there a new medication interfering with her glucose control? I made a mental note to ask these questions as I knocked on the door, ready tofind the root cause of this change. But as I stepped into the room, what I saw wasn't a patient failing to manage her chronic illness, but a frail, weary woman sitting quietly, her hands clasped in her lap, her eyes rimmed with fatigue. She looked up as I greeted her, offering afaint smile.
In medicine, numbers often dominate the conversation. They guide diagnoses, inform treatment plans, and measure progress. In medical school, we are taught to notice the trends – the rise in A1c, the drop in eGFR, and the uptick in blood pressure. But it is just as important to recognize that every number on a chart belongs to a person,
When I introduced myself and asked her how she was doing, there was a long pause. She opened her mouth to speak, then closed it again. Her eyes welled up, and she looked down at her hands. “I’ve been having a hard time, actually,” she said quietly. “It’s Jim, he’s not doing well.” I came to learn that Jim was Mrs. A’s husband of over 50 years. He had been diagnosed with dementia several years ago, but his condition had recently taken a turn for the worse. “These past few weeks, he doesn’t even recognize me anymore,” she said tearfully. “I knew it was coming, but nothing prepares you.” I reached out and held her hand as she cried. Her pain was palpable, heavy in
the air. I sat with her for a few moments in silence, wanting to give her the space to speak when she was ready. I said to her gently, “That must be so incredibly difficult. You’ve been taking care of him, but what about your own health? Is there anyone helping to take care of you?”
Mrs. A explained to me how her daughter lives up north and is only able to visit her and Jim a few times a year as she has to work. She and Jim used to take care of each other, but in the past few years, she has shouldered the caretaker role for both of them. She expressed her concerns about her husband not eating, and his overall deteriorating state. She has not had much of an appetite herself recently and has been getting about 3 to 4 hours of fragmented sleep each night. “I’m always worried he will wander off and fall or accidently hurt himself. Sometimes I forget to take my medications. I don’t mean to. It’s just been so overwhelming,” she said. With just a few minutes of conversation, it all made sense. Here was the context I had been looking for, though not one I could have discovered in any lab report or progress note. In that room, in those moments, I was reminded of something that all too often gets lost in clinical encounters – the immense power of humanconnection.
As physicians and medical students, we are taught to fix things. We look for the problem, identify the solution, and implement it. But some things cannot be fixed, at least not in the traditional sense. I could not reverse her husband’s dementia. I could not bring back the man who she had shared her life with for over 50 years. But I could sit with her, listen to her, and remind her, in that moment, that she was not alone. My encounter withMrs.Aprofoundly
shaped the way I think about medicine. It reminded me that empathy is not something we do in addition to providing care, but rather, it is the care. It is what allows us to understand the person behind the patient, and to tailor our medical decisions to their real-life context.
At the end of our conversation, Mrs. A and I explored ways to support her not just medically, but emotionally and practically. We talked about involving her daughter more, connecting her with caregiver resources in the community, and possibly arranging for respite care. We made a follow-up plan that prioritized both her physical health, as well as her emotional well-being. This interaction reinforced for me that the best medicine is rooted in listening. When we take the time to understand what is really happening in our patients’lives, we not only make better clinical decisions, but we also help patients feel seen, supported, and less alone in their struggles. And sometimes, that can make all the difference.
Humanism in medicine is not about heroic interventions or dramatic diagnoses. It is about being present, providing compassion, and creating space for patients like Mrs. A to share their stories and to feel heard. I still think about Mrs. A. I think about the strength it took for her to show up that day and to care for someone she loves while quietly falling apart. And I think about how many other individuals like her are out there, waiting not just for treatment, but for someone to really see them. We owe it to them to do more than manage disease. We owe it to them tocare.
The Person behind the Chart
By David Labissiere
When I first met Ms. Smith, I remember thinking that this elderly woman had the perfect balance of intensity and kindness in every word she spoke, and her Southern accent emphasized it all. The first thing she said as my preceptor and I walked into her room was, “Oh, I remember you!” referring to my preceptor, who had apparently encouraged her to ambulate more than she had wanted to after her last surgery a few years prior. She recalled that it wasn’t very nice at the time, but she respected it and thanked him for taking goodcare of her.
What I came to find out was that Ms. Smith’s last visit involved an extensive bowel resection due to gastric cancer, which she had been diagnosed with five years before I had the pleasure of meeting her. Since then, she had undergone chemotherapy and had been in remission. The reason we were seeing her this time was due to a suspected small bowel obstruction causing nauseaand vomiting.
I’ll never forget how, at 89 years old, she stopped my preceptor mid-sentence as he began to go over the assessment and plan. She pulled out her cell phone, called her daughter Jane Smith, and told her, “I’m with the doctor now. If you have any questions after listening, you can ask no more than three questions.”
After reviewing her CT scans, we discovered that there was, in fact, an obstruction in Ms. Smith’s small bowel. The surgeon was able to remove it a few days after our initial encounter, and
for a brief time, Ms. Smith was feeling and looking better. However, her nausea, vomiting, and pain continued as we advanced her diet to solids, and her bowel movements became less frequent. This prompted us to consult GI and proceed with an endoscopy. Unfortunately, the procedure took a turn for the worst when they discovered another obstructing mass. Further imaging revealed that Ms. Smith’s cancer had returned and metastasized to several areas throughout her GI tract. An NG tube was placed, which she despised, and she was adamant about not having a GJ tube placed.
Since meeting Ms. Smith happened within my first few days of internal medicine, I had no idea what to expect from her case. But her demeanor quickly made me a fan, and I was more than happy when my preceptor assigned her to my patient load. Every morning for those three weeks, I would round on Ms. Smith, either before or after formal rounds. I would review her labs and scans, and I even had the opportunity to observe some of her procedures. She became a constant for me during those weeks, and I gradually found myself cheering when there was good news and feeling down when there wasn’t. I also found myself making more and more time for Ms. Smith, because our interactions grew from a simple “How are you doing today?” and a physical exam to real conversations about her life.
I learned that Ms. Smith’s father was a miner, on an actual railroad, and that she had married her husband right out of high school and later became a teacher. She adored her one and only daughter, who was a lawyer and had passed the bar on her first try, despite beingvery nervous.
She also loved her grandchildren deeply. She encouraged me on my journey to becoming a physician and even told me that she had no doubt my mother was proud of me, as was she. I really came to enjoy my morning talks with Ms. Smith, and I think I’ll cherish them forthe rest of mylife.
As a last-ditch effort to give her some comfort, since she was absolutely against a GJ tube, we went through with one final procedure at her request: the placement of a duodenal stent. The procedure itself was a success, but her condition quickly declined. Seemingly overnight, the quick-witted, sweet elderly woman who had shared her life story with me could barely speak. As her husband and daughter tearfully decided that hospice would be the best option, I felt incredibly sad, knowing that she didn’t have much time left. But I also felt grateful to have met her and for everything she taught me about seeing a patient as more than just a chart.
Ms. Smith wasn’t just a vignette requiring a multiple-choice answer that I would move on from and forget days, weeks, or now, as I write this months later. Without me even realizing it at the time, Ms. Smith was my first “true” introduction to medicine.
By Macauley Mascarenhas
Today I walk into my primary care physician’s office for a 3-month checkup. This is a routine thing for me, as I see my physician quite frequently and I like him a lot. My daughter came with me for my appointment because I’ve been having some trouble lately driving through busy traffic. I like having her there because she helps me remember all the advice that the doctor tells me. Sometimes I feel like she speaks for me, but I’m okay with this because I know that she wantsthe best for me.
One of the nurses brings me back to one of the rooms and takes my vitals. One of the best parts of my doctor’s office is the wonderful staff who are always so welcoming. She says that my doctor has a medical student working with him and asks if it's alright if he comes in before the doctor. I say that’s fine, I’ve seen students at this clinic before and they are always very friendly.
A knock at the door. It opens, “Hello, my name is Macauley, I’m a 3rd year medical student working with Dr. McCollum today. I’m here to ask you a few questions and then perform a short physical exam. Then I’ll report back to the doctor, and he’ll come in and do your full visit. Is that alright?” I say sure and he sits down next to me. He asks me about general health and how I’ve been feeling since my last appointment.
I’ve been feeling well, and I don’t really have any complaints. I’ve always kept in good health, and I feel very proud of that. How often do you meet someone of my age who doesn’t have any health problems. Then he asks about my memory. I don’t think there’s anything wrong. I feel like my memory is fine. Sure, I forget a name now and then, or get confused when I’m driving, but who doesn’t? I’m 80-years-old, and I’ve been around long enough to know that there’s nothing wrong with me.
This is when my daughter chimes in. She says that I have been asking them to repeat themselves multiple times throughout the day. She says that it seems like I forget things almost immediately. She says that I can’t remember my way around town anymore, so they’ve taken away my car keys. And then she says that I sometimes forget to eat my meals unless someone tells me. I feel like she is exaggerating. I know that I am getting older but I don’t think that I am incapable.
And then she brings it up. A nursing home. I’ve already told my family I do not want to go there. We toured a couple places a few months ago because I felt like it would make them happy, but I knew I wasn’t going to agree to move in there. Those places feel like living mortuary. I have so much more of my life to live and I can’t do anything if I’m all cooped up in anursinghome.
I’ve lived in my home for the past 35 years. I sent my kids off to college from that home. I babysit my grandkids in that home. It was the last place that I lived in with my husband before he passed away. The idea of leaving that home, those memories, my safe place, feels unimaginable.
Would I be able to bring all my belongings if I went to a nursing home? Would my family still come check on me? What if I can’t afford to pay for the nursing home with my retirement. I don’t want to be a burden on my family.
I turn to my daughter, and I tell her “No. I will not go to a nursing home.” The medical student looks puzzled. “May I ask if there is a reason you don’t want to go to a nursing home?” I explain all the thoughts swirling in my head. I can see him listening intently, he seems like he really wants to get to know my feelings. He says he understands but just wants to remind me that my family and all my doctors just want me to be safe. They want me to have everything I need to be able to take care of myself and sometimes a nursing home is the best option. I know that what he’s saying is the truth. I just don’t feel ready to move out of my home yet.
He asks if I have any other questions. He leaves to go get my doctor. Soon they both return. We have a long discussion about possible options; nursing homes, home health aides, going to live with one my kids. We talk about my day, how I manage to take care of myself, cook my meals, clean my house. He does make some good points about how it would make my life easier if I had some help around the house. We come up with a plan for right now, where my daughter is going to come to the house more frequently to check on me and she will look into hiring someone to help around the house.
As I leave the office, I feel so much better knowing that I’m going to be well taken care of, and that for right now, I get to live in my beautiful home.
After my appointment today, I know that maybe someday I’ll have to reconsider a nursing home, but I’ll be more ready and happy to do it on my own terms.
“All” You Have to Do
ByMadeline Keenan
At 80 years old, Mr. B was still an active man. After growing tired of the cold winters, he and his wife had moved from up north several years ago to live in the Sunshine State. He was the main caretaker of his wife, who was in poor health and suffering from heart failure, but they were managing well. Mr. B went to his yearly checkups and followed up with specialists. However, on one visit to his primary care doctor, they noticed that Mr. B had lost a significant amount of weight. He appeared cachectic, and his abdomen was concave. His PCP ordered a CT scan, and Mr. B found himself sitting in the oncology office. Mr. B knew he had cancer, but that knowledge came with a slew of questions. Mr. B explained his situation. His whole life, he had been a very healthy man. He was the main caretaker for his wife. He said he had felt fine and been living life as usual. He had noticed weight loss but didn't think much of it. The weight loss continued, and now, sitting before me was a severely emaciated man with a diagnosis ofcancer.
He seemed stunned and overwhelmed with the questions and decisions that needed tobe made.
He wondered about the best treatment and how long he had to live, among millions of other questions. For Mr. B, it wasn’t a simple decision of whether to pursue treatment or not. He also had to consider his wife and his family up north. Who would take care of his wife? Who would take care of him? Would they have to hire assistance at home? How would that impact them financially? How would this impact his family? Should they move back up north? How long did he have to live? Should he pursue treatment or enjoy the time remaining? The questions swirling in Mr. B’s head were neverending. We discussed his diagnosis, possibilities, and potential outcomes.
Mr. B took time to consider his options. His son flew down to come to his next appointment. We reviewed the options again. Mr. B was still torn about pursuing treatment. He was also torn about whether he and his wife should move home to be with their family or remain in Florida surrounded by their familiar doctors and friends. After much deliberation, they decided that Mr. B and his wife should move home to be with family. Even after coming to this conclusion, Mr. B still had millions of decisions awaiting him. For now, they were not going to begin treatment, but Mr. B still wanted to explore options and couldn’t take pursuing treatment off the table completely.
I found myself wondering what the right answer was for Mr. B. Would treatment give him more time to live, or would it ruin the time he had left? Some may say pursuing treatment was futile, but in Mr. B’s eyes, he had been a healthy, active man. It appeared to pain him greatly to not consider treatment. There is no simple answer to all of Mr. B’s questions.
For me, at this point in my training, it’s terrifying to think about the implications that my future recommendations and guidance will have on these questions that carry such great gravity. Some answers are easy, but others are seemingly unanswerable. How can you ever know the exact right answer to some of the questions? I don’t know that some questions have correct answers. The complexity of the questions we are faced with is frightening. Of course, there is always shared decision-making, but in cases such as Mr. B’s, he was looking for definitive answers from his doctors that he knew andtrusted.
We are given such an intimate view into our patients' lives, and our guidance has a massive impact on their lives. It’s both exciting and terrifying. Mr. B emphasized to me the importance of taking time to consider every question attached to a patient's diagnosis because every answer to those questions can be life-altering for that patient. Every answer to every question affects not only the patient but also their spouses, family, and friends. Mr. B’s diagnosis changed everything for him and his wife. They must leave their life here in Florida. It changes everything for his family up north. They now must restructure their lives to help their ill grandparents. It changes the lives of Mr. B’s friends in Florida as they say goodbye. I hope to always remember the implications of the diagnosis I give and the domino effect they haveonso many lives.
As physicians, we give patients diagnoses daily. Some are minor, and others are detrimental. It is a part of our daily life, but for each patient, it’s a completelynew experience.
Not every diagnosis is as significant as cancer, but every diagnosis means something different to each patient. Every diagnosis attached to each patient carries numerous questions and implications into that person's life. Mr. B emphasized the importance and privilege of the patient-doctor relationship. He loved and trusted his doctors in Florida so much that he was unbelievably torn about whether to return to his family or stay with his doctors. That is an incredibly significant relationship. As I grow in my career, I hope to be a physician who carries that importance to a patient. Mr. B also emphasized the importance of remembering the strings attached to each diagnosis. The social and emotional web weaved with each diagnosis is extensive. Physicians have the honorable and daunting task of considering these webs every time we attach adiagnosis to a patient.
ByEvelyn Heimann
When I was assigned my first patient on inpatient psychiatry, I was asked to see him every morning, determine his treatment plan, and collaborate with case management to develop a safe discharge plan when appropriate. Before meeting him, I reviewed his chart and read that he was a 48-yearold white male with a history of Bipolar I disorder, recently released from jail after assaulting his father. He had been instructed to report to the probation office upon release but instead went to the store to purchase a knife.
Lessons from the Hallway
My heart sank as I read the emergency department note: a bystander had found him behind a bar after he had cut deeply down both arms from elbow to wrist, requiring emergency trauma surgery andlife-savingmeasures.
I would be lying if I said I wasn’t nervous to meet a man with such acute suicidality, a history of aggression, multiple assaults, and a criminal record. Still, I reminded myself that he deserved care just as much as any other patient—and that I needed to treat him with the same respect and dignity. I spoke with his nurse to get an update since his transfer tothe med-psych unit. She looked at me with concern and said, “Be careful.” When I asked what she meant, she admitted she hadn’t entered his room yet due to a shift change but had heard he was aggressive. She added that you never know what a patient “like him” might do. As I walked away, her skepticism lingered in my mind, but I reminded myself: this patient deserves a conversation before judgments are made.
I entered his room cautiously. The lights were off, and he was still asleep. A gentle knock and a quiet “Good morning” was enough to wake him. I introduced myself and told him to take his time. He had a roommate and requested to speak privately, so we met in the hallway a few moments later. He shuffled out slowly, his forearms completely wrapped from wrist to elbow. During our interview, he was calm but somnolent. His speech was slow and monotonous, and he made eye contact only a handful of times.
He was the most obvious example of major depression I had ever seen. He described his suicide attempt as an impulsive act, but carried out with full intent to die.
I asked him how he was feeling about still being here, to which he quickly responded “I wish I wasn’t.” I had known this man for only ten minutes, but his pain hit me deeply—especially when he told me all his family had disowned him and plainly stated, “I have no one.”
At the end of our conversation, I walked him back to his room and assured him I would see him again the next day. I presented his case to my preceptor, and we agreed to start him on Depakote and Latuda for bipolar depression. Over the next few days, he remained much the same—deeply depressed, filled with guilt and hopelessness, and still expressingregret about surviving his attempt. We adjusted his medications and monitored him closely. I met with his case manager and was relieved to learn he was attending group and individual therapy. Although he was not yet near discharge, we began to discuss a possible plan on where he may go once that time comes.
When we met at the start of the second week, I could sense some improvement had been made. During this visit, he cracked his first joke and even a slight smile. He told me he had spoken with his father and then with his brother and sister over the weekend. When I asked what they had talked about, he said, “They told me they love me and still care about me.” He began to prove that he was pulling himself out of the dark tunnel – noticing his surroundings and asking me how I was doing, rather than treating our encounters as aforcedtask.
On Tuesday of the second week, I no longer had to prompt him for information. In a quiet conference room, he opened up to me about his brother who had died while driving undertheinfluence.
He recalled his brother once telling him “I think we have the same problem.” He stated “I was never sure what he meant, but had always thought he was talking about the drinking.” He continued to explain how over the last few days, he has been reflecting on this. Maybe his brother was referencing something deeper—a shared struggle with mental illness and a tendency for it to take over. On Thursday of the second week, he used the word “hopeful” when I asked how he was feeling that day. The same day, his case manager told me his father had decided to give him another chance: he would be allowed to live with him while getting back on his feet, as long as he committed to takinghis medications.
The following week, I was no longer on inpatient psychiatry and at some point he was discharged. In just two weeks of knowing this patient, I not only witnessed the change in him, but also in myself and how I will practice medicine. I was profoundly impacted by the change the field of medicine can make in the lives of the patient’s burdened by mental illness. I also gained a deeper appreciation for the accountability, strength, and resilience each of these patients requires in order to not let their illness define them.
This patient had been a danger to himself and others, but he still deserved time, care, and compassion—and a chance to change the trajectory of his life. Being allowed to play a role in his recovery is something I will never forget. It has deeply shaped how I will approach my future patients—with openness, respect, and unwavering commitment to their dignity and potential for growth.
Still Solving Problems
By Peter Giannas
That sentence stayed with me. It wasn’t just humility—it was love. It was a connection that ran deeper than an obligation. It reminded me that what matters most in the relationships we build—whether as tutors, friends, or physicians—isn’t always how much we know, but how muchwe care.
I wish I didn’t know her by her diagnosis before I met her. I wish our first interaction had started with what she wanted to talk about. And what she wanted to talk about—what lit her up and gave me a glimpse of who she truly was—was the story of how she met her husband.
They met in a rehab facility. He was her medical assistant, the one assigned to take her vitals during every visit. It was routine, clinical even, but something in the repetition made room for connection. He lingered. He listened. He spent too much time in her room—enough to get in trouble for it. She noticed, of course. She liked it. And she found herself wondering, again and again, if it would be weird to ask him out. Eventually, she did. They went out for a beer. It was simple and yet it was the beginning of something beautiful — two people finding each other in a place no one expects love to bloom.
She went on to tell me that before all this, she was a tutor. She helped a young girl with math, guiding her from elementary school into middle school — fractions, decimals, pre-algebra. “She and her mom still visit me every day,” she said, not as a boast, but as a quiet truth. “You must have been a great tutor,” I said, smiling. She looked thoughtful, then replied, “I think they’d still visit even if I was a bad tutor.”
One afternoon on rounds with my preceptor, she told us she was taking online college courses—math classes. She asked if my preceptor and I could bring her a few things: a scientific calculator, a wide ruled notebook, and some new pens. It was a simple request, but it said so much about her. Despite everything, she was still working through math problems. Still learning. Still pushing forward. In a world that often focuses on what people with chronic illnesses can’t do, she quietly kept doing.
Only later in our visits did her diagnosis fully come into view. She’s 34 years old, living with Friedreich’s Ataxia—a rare, progressive neurodegenerative disease that slowly affects balance, coordination, speech, and mobility. She had to stop tutoring last year. Getting around is harder now. Her world has changed shape. She also has dysarthria, which makes speaking physically difficult. Our conversations took time. Sometimes words came slowly, sometimes we’d have to repeat things back to each other—but she never seemed frustrated. There was patience in the pauses, and something deeply human in the effort we both made to connect. What struck me most was how she never centered her illness in her story. She spokeinmemories and relationships, in laughter and small joys. She told love stories and solved math problems. Sheasked for pens.
She defined her life by the way she lived—by the warmth she radiates, by the people who return to her hospital room day after day, and by the quiet dignity of continuing to learn when no one would blame her for stopping. Her story was not about dying. It’s about the spaces where life persists: In long conversations and simple acts of care. In used notebooks and half-solved math problems. In love that began over a blood pressure cuff and never left her side.
Friedreich’s Ataxia may shape her body. But it hasn’t shaped who she is. And that iswhat I’ll remember most.
By Logan Franks
When we had the opportunity to sign up for an elective rotation at the beginning of third year, I knew I was interested in spending time with Emergency Medical Services (EMS). As a student interested in a career in emergency medicine, I thought it would be invaluable to gain firsthand experience in pre-hospital care. During my rotation, I had incredible conversations with paramedics who shared their insights on what they wished emergency medicine physicians knew. I gained a deep appreciation for their work, but the moment that affected me the most was one I had not anticipated.
During my second week, we were dispatched for an altered mental status call.
Hey Buddy
Aconcerned neighbor had not seen Mr. R in several days and, after failing to get a response at his door, decided to use her spare key to check on him. She knew he had bilateral above-knee amputations and often needed assistance. As soon as she opened the door, she was met with an overwhelming smell and immediately sensed that something was wrong. Inside, she found him sitting on the floor, staring out the window, rhythmically rocking and hitting his head against the wall. His clothes were soiled, and it was clear that he had been in the same position for days.
One of the paramedics gently tried to engage him. "Hey buddy," he said. "Buddy, buddy, buddy, buddy," Mr. R repeated back in a monotone voice.The paramedics continued their assessment, but he was largely unresponsive to their questions. “Buddy, buddy, buddy” his voice echoed through the small apartment, his words a hollow repetition rather thana response.
To gather more information, and possibly identify an underlying condition, I began scanning the room and eventually checked his medication bottles sitting on the counter. I saw his prescriptions - propranolol, hydrochlorothiazide, metformin - and in that moment, it struck me just how invasive this was. I was standing in a stranger’s home, rifling through his personal belongings. Medicine is inherently intrusive. We ask deeply personal questions, probe into people’s private lives, and expect honest answers from individuals who may have no reason to trust us. Perhaps I had grown desensitized to this reality during my third year but being physically present in his home made it feel so much more personal.
This wasn’t just another case presentation or a chart to review, this was someone in their most vulnerable state.
While preparing to transport him, we discovered a massive sacral ulcer, pretty much down to the bone. The paramedics exchanged a knowing look. "He’s not going to make it," one of them muttered. There was no doubt this patient was septic. We stabilized him as best we could and transported him to the emergency department, but it felt like we had arrivedtoo late.
The following week, I started my internal medicine rotation. On my first day, I was running late after getting lost in the hospital, but I caught up with my attending just in time for rounds.As we entered Room 1503, my jaw nearly hit the floor. There, sitting upright in bed and eating breakfast, was Mr. R. I was stunned. The man we had found nearly unresponsive in his apartment was now alert, talking, and seemingly doing well. A week of antibiotics, fluids, and electrolyte correction had transformed him.
He, unsurprisingly, had no memory of me but seeing him in this state was nothing short of remarkable. I had to pinch my arm - I couldn’t believe it. Just as I was getting excited about what appeared to be a miraculous recovery, my doctor asked a difficult questionone that is common but never easy. "What are your wishes if something like this happens again? Have you considered signing a Do Not Resuscitate (DNR) order?"
The weight of these questions never lessens, and the answers are never easy for patients to give. It was clear that Mr. R had been alone for a long time, and the thought of going through another similar episode without support was daunting.
In medicine, we often focus on clinical interventions - treating infections and stabilizing vitals. But cases like Mr. R’s reveal a deeper human element of healthcare. His recovery was not just about medicine; it was about dignity and trust. The hospital room looked different than his apartment, but I was still standing in the middle of one of his most vulnerable moments.
Reflecting on this experience, I realize that trust is one of the most profound gifts a patient can give a healthcare provider. Whether it’s allowing a paramedic to carry them out of their home, a physician to ask them about their final wishes, or a medical student to piece together their history, patients place themselves in our hands with an incredible amount of faith. This experience reinforced for me the immense responsibility we bear - not only to treat but to truly see and respect the individuals behind the medical conditions.
By Natalie Dix
It is Friday afternoon in the triage of the emergency department. The emergency room is bustling with activity, and despite the efforts of the healthcare team to maintain a brisk pace, there is a palpable sense of delay. With a constant flow of patients, the goal is to see an average of three patients per hour, but the feeling of being behind lingers. The typical mix of complaints is present — upper respiratory infections, chronic joint pain flare-ups, musculoskeletal injuries, chest pain, and superficial lacerations.
Triage and Tribulation
However, amidst this routine, my attending and I find ourselves unexpectedly delayed by a very agitated patient. He is yelling at us for offering imaging and non-narcotic pain management for his chronic back pain exacerbation. This disruption pushes back the schedule, but I quickly check for the next patient and realize it will not be a quickvisit either.
The next patient, an eighty-one-yearold female with stage 4 pancreatic cancer is here for worsening abdominal pain and ascites. Symptoms have become progressively more difficult for her to tolerate. The patient lies in bed, weak, and barely able to speak in more than short phrases. The pressure from the fluid buildup in her abdomen has made breathing, eating, sleeping, and even talking an agonizing challenge. Her husband sits at her bedside, visibly anxious and frustrated, having already waited all day to be seen after being told by their oncologist that a procedure would be arranged in outpatient interventional radiology for placement of an indwelling peritoneal catheter to manage her recurrent ascites. However, due to a scheduling mix-up, they were instructed to come to the emergency department for a paracentesis in the interim. Complicating matters, the emergency department is at capacity, with no available beds, and the triage rooms are not equipped to safely perform the procedure.
When the patient and her husband learn that their expectations for immediate relief cannot be met today, they are engulfed in a state of panic, worry, and frustration. The husband has watched his wife endure rounds of chemotherapy, been by her side through countless doctor visits, and witnessed the slow but inevitable progression of her disease. He struggles to manage his anger, desperate to find some way to alleviate her suffering.The patient, who is too tired and weak to intervene, pleads with her husband to stop shouting. She apologizes to us, asking that we not hold his outburst against him.
After a moment of silence, the husband, holding back tears, speaks. "You have to understand," he says, his voice breaking, "I’ve known her since we were kids. We’ve been married for 61 years. We’re a package deal. Her pain is my pain. The pain she feels, I feel ten times more because she is the love of my life." His eyes well up with emotion, and he continues, "She is already so thin and hasn’t had anything to eat or drink since yesterday morning."
As if the situation were not complex enough, it is nearing five o’clock on a Friday afternoon. Interventional radiology will be unavailable until after the weekend, and the hospice team is bound by strict protocols. If the patient were admitted for a paracentesis, she would lose her eligibility for hospice care. The hospice coordinator is contacted and confirms that while the mix-up with the outpatient procedure is acknowledged, the next available opportunity for intervention would be three days away, on Monday. The patient's current status complicates matters further, as an admission to the hospital would immediately disqualify her from the comfort of hospice care, an outcome both she and her husband dread.This leaves them caught between two painful choices, neither of which offers immediate relief.
Despite the bureaucratic and logistical barriers, the situation is deeply personal. The couple’s anguish is palpable as they are faced with the harsh realities of an overburdened healthcare system. The patient and her husband struggle to understand why these rules, although rational in theory, seem callous in the face of their suffering. The emotional toll weighs heavily on them, and they ask what their options are. Several possibilities are discussed. One option is to manage her ascites conservatively, replace fluids while using diuretics to try and reduce fluid buildup until she can undergo the paracentesis on Monday. The alternative would be to admit the patient to the hospital, risking the loss of her hospice benefits to perform the procedure immediately.
This is not the first time the patient has needed a paracentesis due to the advanced nature of her pancreatic cancer. She has come to terms with the idea of her impending death, but the raw, unrelenting nature of her current suffering feels like a betrayal of the hope she held that some comfort might still be possible in her final days. She longs for relief, even if it is temporary, and so doesher husband.
After a quiet pause, the husband, ever the advocate for his wife’s care, asks her what she would like to do. The patient, exhausted and resigned to her fate, shakes her head firmly when it becomes clear that admitting her to the hospital would forfeit her hospice care. For the couple, the promise of hospice care represents a final sanctuary of comfort and dignity. Losing that would feel like losingeverything. This encounter is not one of simple solutions or clear-cut answers. It highlights the complexities of patient advocacy and the often painful realities of navigating a healthcare system that can sometimes seem indifferent to the needs of patients and their families. The tension between the desire to do everything to alleviate pain and the reality of limited resources is felt deeply by everyone involved. This experience was a stark reminder while clinical knowledge and technical skills are essential, the ability to listen with empathy, understand the emotional weight of a patient’s situation, and navigate the difficult bureaucratic landscape are just as critical. It is an illustration of the emotional weight that healthcare professionals carry when faced with decisions that do not have easyanswers.
The Toll of the Giver
By Daniel Gonzalez
A listening ear can be one of the most powerful tools in the field of medicine. Not long ago I had a patient named JS who was presenting to the clinic for a follow up of major depression treatment. He was a young man in his early twenties and well dressed for the appointment in his work uniform. When I first entered the room and introduced myself as a student, I asked what he had come to the clinic for and he told me that he was following up on some headaches he had been having. Seeing the indication in the chart, though, I followed up my exploratory questions about the headaches with a query of how he was feeling emotionally and his response was very interesting. He took long pauses in between his answers, clearly considering what he was going to say very carefully, but eventually he said that he was trying not to say anything that I might find “not relevant.”
I thought that was interesting because it seemed he was under the impression that his emotional issues weren’t something to be discussed here in the doctor’s office, or maybe he thought I was only concerned with his physical health and wouldn’t be willing to hear him out. I didn’t miss a beat in telling him that there was no such thing as an irrelevant topic if it was something important to him that he wanted to say. After that, he began to open up a little at a time.
He began to say that over the past 3 to 4 weeks he had been having significant issues with depression, describing the feeling as a kind of emptiness rather than simplesadness.
He said that he had been doing a lot of extracurricular volunteer work with the local community and found that the people he was helping had intense challenges that he found hard to get out of his mind. He dedicated his time to volunteering because he felt that this population was facing desperate struggles, having their rights taken from them and that he felt he had a responsibility to help them in any way he could. At the same time, however, he admitted that he was probably burning the candle at both ends. He had a full time position at his company and volunteered on the side as often as he could, leaving little room for much else. He had a hard time getting enough sleep both because of his workload and personal family issues. JS slept on a pullout couch that was very uncomfortable, meaning he got only around 5 hours of sleep per night. Things that he used to take pleasure in now held no appeal and he found it very difficult to keep his mind off his depressive thoughts.
Being a necessary step for patient safety, I asked him if he had any suicidal thoughts. He did, those being passive ideation to want to sleep “for a very long time” or otherwise just not to be alive. With some difficulty he also described self-harming behaviors from long in his past with the most recent episodes being afewmonthsago.
All the while he seemed almost pained to recount these things, taking long pauses to consider his words with an apologetic air. I made sure to remind him that he didn’t need to tell me anything if he found it too uncomfortable and he had no reason to feel obligated to. He said that he had never gone into detail like this about his issues with anyone before. I took this as a high honor and thanked him for his trust in me.
The rest of the appointment centered on increasing the dosage of his recently started medication and connecting him with services for therapy, but the weight ofthe meeting stuck with me.
I came to realize that he and I had many things in common when it came to our personal history, and I saw a lot of myself in the way that he struggled with describing his emotions. Even the way he described his feeling like he couldn’t tone back his hours volunteering due to the responsibility he felt for the people of the community was familiar to me. I believe that he was struggling with something any healthcare worker does, a feeling like we have to put our own issues aside for the greater goal of doing the right thing even if it is to ourdetriment.
I came away from that meeting with a renewed passion for mental healthcare, a field that is often overlooked in society and even within ourselves. We all to some degree put the needs of others before our own and while it leads to good outcomes for others it puts ourselves at risk. I hope to bring these revelations into the future and I also hope that this young man finds some peace in the course of his treatment. There was so much more under the surface that I could see just from the way we interacted and those are things that take time and effort to address. But I felt that I did my part to show him that he is not alone, building trust for the future so he knows that he doesn’t have to keep these things hidden and suppressed - but this meeting was only a step in the journey for him and for myself.
A
Cowboy’s Last Ride
By Lauren Frankle
Bay C-55, 65-year-old male, COPD exacerbation, metastatic melanoma. Sometimes inmedicine, that is all we
see when we meet a new patient: their age, sex, chief concern, and any relevant medical history. In our medical training, this is encouraged. The expectation of every good medical student is to be able to present a patient concisely, with all the pertinent information, in under 2 minutes. In our rush to recite all the details, not forgetting a single vital sign or lab finding, we sometimes forget to ask: who is this person in front of us? We forget to pause and appreciate the art of patient centered care and practicing medicine. In those moments, we are no longerhealers; we are data collectors.
When you are so focused on the medical information, you miss the real story of the person. 65-year-old male, COPD exacerbation, metastatic melanoma.What if that was all we ever knew about this person?What if we got so invested in the process that we lost the whole art of practicing medicine? What if we lost the ability to hear their story and truly connect with our patients?
The man in bay C-55 helped pull me out of the world of diagnoses and treatments and bring me back to reality, back to humanism. When I walked into his room, he was lying in the bed silently, comfortably now that he was receiving oxygen through a nasal cannula.
His skin was tan, painted with the sunspots we Floridians are so familiar with, and his hands were strong and calloused. He spoke deliberately, slowly, with a southern twang, and with the quiet confidence of someone who had faced death long before he ever stepped foot intothis hospital.
When I began to talk with him and gather the important medical information, he helped me remember the humanism in medicine by being eager to talk about who he was as a person, not just about his medical background. This man was not just a gentleman with metastatic melanoma and COPD; he was a world champion rodeo cowboy. Sitting in front of me was a man whose life was marked by courage.Aman who tamed wild horses and conquered the rodeo arena. His eyes gleamed with equal parts pride and nostalgia as he described his championship belt buckles and the arenas he once mastered. The way he described his life and his stories made me feel as though I was in the audience, reliving his glory days right alongside him.
His resilience was even more profound. After his parents could no longer manage the family ranch in Tennessee, he stepped up, taking on the responsibility of running it alone. And then, tragedy struck; he lost his wife, daughter, and grandchild in a devastating car accident.
Now, five months into a six-month prognosis after being diagnosed with metastatic melanoma, he had moved to Florida, saying simply that he had “come to Floridato die.”
His last wishes were simple: a regular diet in the hospital, his Marlboros, and to share with me his story. As we spoke, I wondered what it must be like for him in a place as foreign as a hospital. Instead of the familiar sounds of crickets singing him a lullaby as he went to bed, he was lulled to sleep by the rhythmic beeping of the monitors in his room. The familiar fragrance of the open fields now replaced by the sterile scent of the hospital. He had spent most of his life surrounded by nature and the freedom of the range and was now confined to this hospital room. From wide open skies to windowless walls.
With no family left and no one to carry on his legacy, I could feel the weight of his loneliness. Even though we do not talk about it, we all want to be remembered. We want to live a great life and leave a lasting legacy on this earth before we go. Whether that legacy is a championship belt buckle or simply a story passed on to a stranger in your hospital room, we all want the reassurance that our memory lives on and that our presence on this earth mattered.
He thanked me for listening, for allowing him to reflect on his life and share his story with another in his last days. In that moment, I understood how vital human connection is, even for the strongest among us. Talking with him made me rethink end of life care. It is not just physical but also profoundly emotional and spiritual. We all must remember that the privilege of practicing medicine lies not only in saving the lives in front of us, but in honoring them. Sometimes, the most healing thing we can offer a person is not some medication or life saving procedure, but simply our presence.
His wishes seemed focused only on simplicity and dignity. He had no grand requests, no need for elaborate interventions. He requested only comfort and the ability to hold on to two small pleasures: his cigarettes and a regular diet so he could eat a cheeseburger inthehospital.
The cowboy’s story serves as a powerful reminder that hospitals are not just places of healing, but also where the last chapters of life unfold. In those moments, true care goes beyond medicine. It is about listening, truly listening, to the person in front of you. It is about honoring their story, their dignity, and the quiet strength that carries them through their final days. This cowboy made me pause and reconnect with the privilege that is practicingmedicine.
The beauty of patient care is learning not just about the medical story of our patients, but about the true essence of who they are as a person and the life they lived.
It was a privilege to share in his closing chapter, even for a brief moment. Bay C-55, 65-year-old male, COPD exacerbation, metastatic melanoma, world champion rodeo cowboy. Behind every room number is a name.Alife.Alegacy.
Food For Thought Goes Fishing at Cast and Crew
Ahoy Mates, Daytona finally has its first upscale seafood restaurant extraordinaire, Cast and Crew!
This beacon of contemporary fine dining is the creation of Executive Chef Olivier Koster who works with the James Beard nominated Concentrics Restaurant Group. Chef Koster hails from the Netherlands and is specialized in Dutch, French, and Italian cuisines. His previous roles were head chef at Fuell Beach Club and executive sous chef at many other establishments.
Cast and Crew describes itself as “tide to table dining”. Located at the new Renaissance Daytona Beach Oceanfront Hotel at 640 North Atlantic Avenue, the restaurant has free complimentary valet parking and a separate entrance available for diners. The restaurant has both indoor and outdoor dining areas as well as seating by the futuristic attention drawing pool.
Lisa and I chose to sit indoors for our first gastronomic exploration. The aura of the room itself is quite romantic. The waitstaff are quite attentive and well dressed. The whole dinner ran smoothly as if rehearsed as a fine tuned operatic performance. They have a nice wine list as well as a full bar menu. We chose a luscious white Pinot Grigio from Italy – Il Valore Terre Siciliane.
The Overture- Before we knew it, our waiter came out with an amuse-bouche. This mouth watering chef preparation consisted of marinated fig with white chocolate goat cheese foam on a transparent butternut squash chip with chive oil. OMG! And that was just the preface to ACT 1, the appetizer. Lisa and I of course, shared everything.
ACT 1 The appetizer We chose Mussels served in a fine green coconut curry and grilled bread. These were some of the best I have ever tasted. One of Lisa’s mussels wasn’t open so after we finished the open ones we were served with a whole second order.
ACT 2 The Entrees Lisa opted for the succulent Scallops served on top of potato with a pickled cauliflower. WOW!! Unbelievably delicious and just bursting with a rainbow of flavors.
I chose a fresh pan roasted snapper with beluga lentil, eggplant, and melt in your mouth fingerling potatoes. More WOW!! We were stuffed but to be able to do this review for you, dear reader, we forced ourselves to indulge in dessert. And boy am I glad we did.
ACT 3 The Dessert Normally I do not enjoy profiteroles as they are usually small and remind me of a cream puff. Not this one. This was one enormous profiterole stuffed with cream on top of honeycomb and blackberries. OMG squared!!!
The ENCORE They just wouldn’t stop with the food. With the check came lemon zest squares made also with butter, flour, and sugar. I felt like I needed a wheelbarrow to roll me out.
Even though the price tag of this stupendous gastronomic extravaganza will cost you around $200/couple, it is so worth the experience.
The STANDING OVATION
Quality of food: 5 stethoscopes
Ambiance: 5 stethoscopes
Value: 5 stethoscopes
Service: 5 stethoscopes
PO Box 9595
Daytona Beach, FL 32120
Are you a physician in Volusia County seeking to explore the benefits of joining a medical society?
Membership Benefits:
● Physician referral service
● Online directory
● Legislative updates and voice
● 24/7 access to an on-call healthcare attorney
● Exclusive webinars and CME courses
● Access to free confidential mental health sessions
● Annual Daytona State College scholarship partnership
● The Stethoscope Journal, a member driven magazine with member articles
● Access to community banking, investing and insurance companies
● A monthly digital newsletter posting current articles, legislative news, and VCMS events
● Job postings and referral services
● Social networking events, outings and more…
VCMS memberships are also available to medical students and residents seeking to become involved! New or Returning Members – talk, type, or text for a membership application or visit us online www.vcms.org / vcmedsociety@gmail.com / (386) 255-3321