CANCER PREVENTION & CONTROL PROGRAM RETREAT





8:30–9 AM Breakfast and Registration
9–9:15 AM Opening Remarks from CPC Program Leadership
Jennifer Bea, PhD
Co-Leader, Cancer Prevention & Control Program, University of Arizona Cancer Center
Heidi Hamann, PhD
Co-Leader, Cancer Prevention & Control Program, University of Arizona Cancer Center
9:15–9:25 AM UACC Director’s Remarks
Dan Theodorescu, MD, PhD
Nancy C. and Craig M. Berge Endowed Chair for the Director of the Cancer Center Professor, College of Medicine
9:25–9:50 AM New Member Lightning Round
9:50–11:20 AM Strategic Fund Sourcing with breakout sessions to follow Bekah Coşkun, DrPH Research Development University of Arizona Cancer Center
11:20–11:30 AM Scavenger Hunt + Break
11:30AM–12:30 PM Hot Topic: Early Onset Cancer
Caitlin C. Murphy, PhD, MPH Associate Professor UTHealth Houston School of Public Health
12:30–1:30 PM Lunch + Poster Session
1:30–1:55 PM CRTEC Trainee Lightning Round
1:55–2:40 PM Cooking Demo with Tucson Village Farms
2:40–2:55 PM Awards + Celebrations
2:55–3 PM Closing Remarks


Opening Remarks from CPC Program Leadership

Jennifer Bea, PhD

Heidi Hamann, PhD
UACC Director’s Remarks

New CPCP Member Lightning Round 9:25 AM 9:00 AM
Julie Armin
Stephen Adamo
Rachel Adler
Dan Theodorescu, MD, PhD
Nancy C. and Craig M. Berge Endowed Chair for the Director of the Cancer Center Professor, College of Medicine 9:15 AM
Adriana Maldonado
Anna Morenz
Patricia Thompson

Research Development
University of Arizona Cancer Center bekahc@arizona.edu

Associate Professor
UTHealth Houston School of Public Health
Caitlin Murphy, PhD, MPH is Associate Professor in the Department of Health Promotion & Behavioral Sciences at UTHealth Houston School of Public Health. Dr. Murphy is a cancer epidemiologist with internationally-recognized expertise in adolescents and young adults with cancer. A cancer diagnosis at this pivotal life stage disrupts growth and development, and adolescents and young adults must navigate these challenges while simultaneously managing long-term and late effects of cancer. Her research has been supported by grant awards from the National Institutes of Health, U.S. Department of Defense, and American Cancer Society and has been featured in The New York Times and Scientific American. Dr. Murphy has an MPH in Health Promotion from UTHealth Houston School of Public Health and a PhD in Epidemiology from the University of North Carolina at Chapel Hill (go Tar Heels!).
Lunch + Poster Session 12:30-1:30 PM

University of Arizona
College
of Medicine
Koenraad Van Doorslaer
Cross-Sectional Analysis of Physical Health in Hispanic Prostate Cancer Survivors and their Caregivers Participating in a Pilot Dyadic Exercise Program
Clinical Translational Sciences College of Health Sciences
Meghan Skiba
Rina S. Fox
Expectations, self-reported adherence, and perceived benefit of sleep/circadian intervention among gynecologic cancer survivors
• Patient expectations prior to treatment initiation have been associated with treatment effects in various clinical populations
• We explored the relationship of treatment expectancies with perceived benefit and treatment adherence among gynecologic cancer survivors receiving a a behavioral sleep/circadian intervention
Early-stage gynecologic cancer survivors completed a 6week behavioral sleep/circadian intervention that included 3 components:
• Measuring treatment expectations could inform predictions about:
• Treatment engagement
Measures
• Treatment expectations measured at baseline with the Credibility/Expectancy Questionnaire
• Credibility: cognitively-driven beliefs regarding treatment credibility
• Expectancy: emotionally-driven beliefs regarding anticipated improvements
• Subscale scores range from 3 to 27, higher=greater credibility/expectancy
• Perceived treatment benefit measured at postintervention
• 1 (not at all) to 5 (very much) how much believed each invention components improved their sleep.
• Participants that rated ≥1 component ≥3 (somewhat) were considered to perceive benefit
• Self-reported adherence measured at postintervention
• Asked how many days per week, on average, followed instructions for each component
We would like to thank the participants for their contributions to this study. This research was supported by the National Cancer Institute under Grant Numbers K08CA247973 and P30CA023074, the University of Arizona College of Nursing, and the National Institutes of Health’s National Center for Advancing Translational Sciences under Grant Number UL1TR001422. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors would like to thank Bettina Hofacre, Eva Crudo, Margaret Dolan, and Alice Tu for their contributions to this work. Methods
• Perceived benefit

• Potential implications for both research and clinical practice

• Current work: exploring the impact of the 3 treatment components, individually and in combination, on sleep health
Actigraphy-measured sleep before and after engaging in a behavioral sleep/circadian intervention: Exploratory values among post-treatment gynecologic cancer survivors
Actigraphy-measured Sleep Before and After Engaging in a Behavioral Sleep/Circadian Intervention: Exploratory Values Among Post-treatment Gynecologic Cancer Survivors
•
•
•
We integrated wrist-worn actigraphy into a larger study investigating a behavioral sleep/circadian intervention among post-treatment gynecologic cancer survivors
•
•
• The
Integrating actigraphy allowed us to explore objectively-measured changes in sleep

Wrist-worn actigraphy is low cost
Incorporating actigraphy could enhance both research and clinical care
We would like to thank the participants for their contributions to this study. This research was supported by the National Cancer Institute under Grant Numbers K08CA247973 and P30CA023074, the University of Arizona College of Nursing, and the National Institutes of Health’s National Center for Advancing Translational Sciences under Grant Number UL1TR001422. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors would like to thank Bettina Hofacre, Eva Crudo, Margaret Dolan, and Alice Tu for their contributions to this work.
Structural features of the neopeptide-MHC complex are associated with immunogenicity in human cancer
College of Medicine - Phoenix
Dermatology
Karen Hastings
Background
Structural features of the neopeptide-MHC complex are associated with immunogenicity in human cancer
Emily Kaelin1, Jasmine Singh2, Elizabeth Borden1, Chad Brambley2, Brian
Mutated proteins in cancer cells can be recognized by T cells, contributing to anti-tumor immunity. Tumors have thousands of mutations, but only a fraction result in immunogenic neoantigens.
Understanding features that lead to TCR recognition of the neopeptide-MHC complex could improve selection of neoantigen targets for immunotherapy.

Previous work from our group showed that in mice, increased solvent-accessible surface area (SASA) of the mutated residue was associated with tumor rejection in neopeptides without improved MHC binding compared to the wild-type peptid. Other studies have suggested that peptide or residue hydrophobicity may influence TCR recognition.




Calculation of structural measurements and downstream analysis
In neopeptides without improved MHC binding compared to the wild-type, higher peptide HSASA change was associated with immunogenicity. These results suggest that structural features may influence immunogenicity and could improve the selection of target neoantigens for immunotherapy.
Additional features including mutant residue position and molecular weight change had interacting effects on peptide HSASA change, suggesting that these features should be considered in models that utilize HSASA to predict immunogenicity.
We plan to build on our previous work by developing a scoring system that considers structural features of the neopeptide-MHC complex, with the goal of improving immunogenic neoantigen prediction compared to existing models.
Hypothesis
We hypothesized that increased exposure of the mutated peptide and residue would promote T cell recognition and immunogenicity in human cancer.
This work
Voluntary wheel running controls hematological tumor progression in mice
University of Arizona Cancer Center
UACC - T32 Cancer Prevention and Control Program
Richard Simpson
Dr. Heidi Hamann
Community-Based Strategies to Decrease the Financial Burden of Cancer Care for Uninsured Patients in Pima County
Hatty Lara,1 Jonathan Smith,1 Julie Armin,1 Nancy Johnson,2 Ivana Klymko,1 Tara Radke,1 Andres Yubeta,2 Heidi Hamann,1
1. University of Arizona; 2. El Rio Health
Background
• High levels of Southern Arizona border county residents remain uninsured.
• Pima
• In Southern Arizona, uninsured patients experience unequal cancer disease burden and treatment barriers.
• This disparity is exacerbated by the lack of a dedicated health care safety net system in Arizona.
• The goal of the current study was to engage stakeholders in addressing cancer care burden among uninsured cancer patients in Pima County, Arizona, a U.S./Mexico border county with a high rate of uninsured individuals.
• This study is essential in light of the absence of a cancer care safety net for the uninsured in Arizona.

Procedure
• Identified community stakeholders and partners.
• Utilized Community-Engaged Framework (Simmons et al., 2015).
• Used community action research to identify gaps.
• Conducted focus groups and semi-structured in-depth interviews (Heath et al., 2018).
Analysis





Participants
• Community Health Workers (CHWs)
• Primary Care Physicians (PCPs)
• Health Care Administrators (HCAs)
• Policy Makers
• Faith-Leaders
• Uninsured cancer patients (N=5)
• Qualitative Data Translated, Transcribed, Coded, and Themes Identified using Thematic Analysis (Braun & Clarke, 2006).
Findings
Insurance Status
• Uninsured Immigration Status
• Undocumented Organizations providing low-cost cancer care
• El Rio (FQHC)
• Clinica Amistad Financial Barriers
• Extreme costs
• No insurance Financial Support
• El Rio Foundation
• Family & Friends


There is a need:
• for a cancer care healthcare safety net infrastructure to replace the existing “patchwork” of workarounds that lead to delayed, incomplete, inefficient and unaffordable cancer care.
• to establish multi-system level interventions at the community, county, and state levels to improve cancer care outcomes for uninsured patients in Arizona.
• to adequately fund Federally Qualified Heath Centers (FQHCs) for primary care coordination and early cancer detection.
• for continued engagement with community stakeholders to support patient level interventions.
• to develop community and state-wide system efforts to expand coverage policies, care coordination programs, and charity care programs.
• to increase capacity building in Pima County with primary, secondary, tertiary care providers to collaborate and share burden of care.
• for the development of a collaborative care model for policy makers.
Non-Financial Support
• Family & Friends Support from Medical Personnel
• Primary Care Physicians
• Oncologists
• Nurses
• Administrative Staff Missing Resources
• Additional funding for cancer care
• Nutrition for cancer patients
• Social Workers
• Navigators
• Utility & rental assistance
• Database for referral & resources

for a Multi-Behavior Change Text Message Intervention for Cancer Survivors and Caregivers: The Eat, Play, Sleep
• This study explored a digital approach to health behavior change for cancer survivors and caregivers.
• It can be difficult for cancer survivors and caregivers to access traditional health behavior interventions.
• This study evaluates the feasibility and acceptability of a text message-based intervention targeting dietary quality, physical activity, and sleep hygiene.
Participants: 21 cancer survivor-caregiver dyads (total N=42), English or Spanish-speaking.
Design: Three-arm, non-randomized pilot study.
Intervention: Based on self-reported health behavior challenges, participants received two daily texts for four weeks related to dietary quality, physical activity, or sleep hygiene.
Primary Endpoint
Feasibility
• Defined as successful receipt of ≥95% of SMS.
• Retention of ≥75% of the dyads. Acceptability
• Assessed via immediate follow-up rating questions sent after each message
• Acceptable content defined by an average satisfaction score ≥2 on a 0 -4 scale.
Secondary Endpoint Behavior Changes:
• Pre- and post-intervention assessments measuring improvements in dietary quality, physical activity, and sleep hygiene behaviors.

• This study will provide crucial information about the feasibility and acceptability of multiple health behavior text message -based interventions.
• Feedback from participants will be used to refine message content, improving future digital health coaching protocols.
• Insights from this pilot could inform larger-scale implementation efforts.
• This approach supports equitable access to healthpromoting information for both English - and Spanishspeaking cancer survivors and caregivers.
This research was supported by the University of Arizona Cancer Prevention and Control Pilot Award (MPI:RSF/MBS), the Arizona Institute for Resilience Vertically Integrated Project Program (PI: MBS), and the University of Arizona Cancer Center Behavioral Measurement and Interventions Shared Resource (P30CA023074). RSF is supported by (K08CA247973) from the National Cancer Institute.
Advancing
College of Engineering
Biomedical Engineering
Dr. Dongkyun Kang
Dongkyun Kang
Introduction
Objective
• Develop a portable, real-time, and low-cost imaging tool for visualizing cellular features of skin in vivo with improved resolution and reduced speckle noise
Reflectance Confocal Microscopy (RCM)
• RCM is a non-invasive imaging technique that can visualize different skin layers in near-cellular resolution
• This improves skin cancer diagnosis and treatment by reducing unnecessary biopsy
• Limitations of the widespread clinical adoption of RCM include high device cost and bulkiness
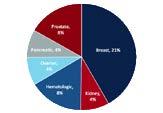
Portable Confocal Microscopy (PCM)
• PCM uses a broadband light source and cylindrical lens (or slit) to form line illumination, and diffraction grating to perform 2D scanning
• This scanning method replaces a laser and beamsteering mirrors, achieving low-cost, and highspeed imaging with less moving parts


Challenges in Previous Versions of PCM
• Superluminescent LED (sLED) based PCM can achieve high speed imaging (203 FPS) but exhibits speckles due to its high spatial coherence
• LED based PCM reduces the speckle but struggled with the imaging speed (20 FPS)

Methods

• sLED as a light source
• λ = 840nm, Δλ = 40nm, P = 10mW
• A line illumination is formed by a cylindrical lens
• The rotating diffuser continuously generates random illumination speckle patterns
• Summing all the speckle patterns during adequate exposure time creates speckle-free illumination.

Summary





Results
Specifications:
• Imaging Speed: 107 FPS
• Imaging Area: 700um x 500um
• Imaging Depth: 250um
• Resolution: Lateral 1 4/1 2µm and Axial 2 8µm
• Device cost: ~$5,000

Speckle Reduction

• Some detailed features become visible with speckle modulation


Skin Imaging



• Different layers of skin are imaged


SM-PCM device offers near-cellular resolution, high-speed capabilities, and speckle-free imaging This technology allows for fast, non-invasive skin imaging, all while keeping low device cost and ensuring portability.
Rina Fox Psychology College of Science
Integrating a Psychometrically Validated Assessment of Participant Satisfaction into Behavioral Intervention Research
Fiona R. Webb; Ana A. Morales, BA; Marjorie A. Nelson BA; Terry A. Badger PhD, RN, PMHCNS -BC; Sairam Parthasarathy MD; Rina S. Fox PhD, MPH University of Arizona
• Assessing patients’ experiences of treatment is valuable in research and clinical care
• We integrated a validated measure of participant satisfaction into a behavioral intervention study
• Participants were post-treatment survivors of stage I-II gynecologic cancer
• Completed a 6-week behavioral sleep/circadian intervention
• Participant satisfaction was measured at postintervention with FACIT-TS-G
More than 75% of participants agreed the 6-week behavioral sleep/circadian intervention was effective and satisfactory
Fewer said they would recommend the intervention to others or do it again
Most participants rated the intervention as good or better


Integrating a validated assessment of participant satisfaction enhanced understanding of intervention acceptability
RESULTS: FACIT-TS-G RESPONSES
University of Arizona Cancer Center
Gloria Coronado

Sarah Yeo, Priyanka Ravi, Zeyad Abbker, Rogelio Robles-Morales, Purnima Madhivanan, Scott Carvajal, Gloria Coronado
• 43.7 million refugees (as of June 2024)
• More than 3.2 million refugees in the US since 1980
• Refugees tend to be less
• Familiar with preventive care
• Aware of cancer risks
• Screened for cancer
• Visible in health surveillance
To map literature on cancer research among refugee populations in the US using the Cancer Control Continuum
• Period: inception – April 2, 2024
• Databases: PubMed, CINAHL, PsycINFO, EMBASE, SCOPUS
• Inclusion criteria:
• Refugee populations in the US
• Empirical studies addressing any stage of cancer continuum
• Studies in the US
• Regardless of the designs
• Protocol: registered on Open Science Framework
• Screened and extracted through covidence
• 7648 screened -> 97 included


DISCUSSION
• Study design: 68% Quantitative (n=66), 20% qualitative (n=19), 12% mixed (n=12%)
• Study sites: MA(11), mixed(9), not clear (8), CA(7), MN(7), NE(6), WA(6), OH(5), TX(5), GA(4), PA(4), MI(3), NY(3), NC(3), RI(3), FL(2), ME(2), AZ/ID/IN/IA/MO/OR/UT/VA/WI(1) CANCER PREVENTION
• Hepatitis B: higher infection ranging from 2.8-14% with regional variations, low awareness of HBV or vaccination status, linkage to care ranged widely (13-89%)
• Diet/nutrition: higher acculturation or longer time in the US associated with a greater intake of sugar/sweet, lower fruit/vegetable intake among Somali/Sudan/Cuban, higher FV consumption among Burmese/Cambodian
• Obesity and physical activity: increase in BMI/overweight/obesity post-resettlement with regional variations, lower PA
• Smoking: different types, smoking prevalence greatly varied (66.4% among Bosnian 4% among Cambodian), lower perceived risk among smokers, Betel nut chewing considered as a social practice among Cambodian women
• Alcohol use: higher rates of problematic alcohol use among Nepali/Bhutanese/Karen, low rates among Arab/Cambodian
CANCER DETECTION & DIAGNOSIS
• Breast cancer screening: uptake of screening ranging from 15-63%
• Cervical cancer screening: Uptake ranging from 13.9-90.6%
• Barriers: language, culture, lack of knowledge/awareness, fear, male providers/interpreters, insurance, complex health care system, transportation, childcare, etc.
• Facilitators: recommendations/reminders from health care providers, family support/involvement, religion
• Recommendations: culturally and linguistically appropriate educational materials (e.g, videos), community-based culturally/linguistically tailored health education delivered by navigators, CHWs.
• No studies explored beyond cancer prevention and detection/diagnosis.
• Disproportionate attention (region, ethnicity)
• Heterogeneity among refugee populations
• Selection bias: Electronic medical records of refugee-serving clinics and lack of rigor in the study designs
CONCLUSION
• More attention on treatment/survivorship/end of life care and underrepresented populations, heterogeneity among them
• Disproportionate attention (region, ethnicity)
• Culturally and linguistically relevant education and navigation support
• Efforts to increase academic rigor
This research is supported in part by T32CA272303.
Chris Lim
Jeonggyo Yoon1, Rena R. Jones2, George D. Thurston3, Chris C. Lim1
1Department of Community, Environment, and Policy, Zuckerman College of Public Health, The University of Arizona, Tucson, Arizona, USA
2Occupational and Environmental Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, Rockville, MD, USA.
3Department of Environmental Medicine, New York University School of Medicine, New York, NY, USA
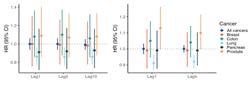
Ambient particulate matter (PM2.5, <2.5 µm) is a known human carcinogen, but research on associations with cancer survival remains limited. We sought to investigate the long-term effects of air pollution exposure on post-diagnosis cancer survival, utilizing data from the NIH-AARP Diet and Health Study.
• Study population & Mortality Ascertainment :
ü The NIH-AARP Diet and Health Study, aged 50–71 years, from 6 U.S. states (CA, FL, LA, NJ, NC, PA) and 2 metropolitan areas (Atlanta, GA; Detroit, MI), with follow-up from 1995 to 2011.
ü Vital status was determined through regular linkage of the cohort with multiple data sources: the Social Security Administration Death Master File, National Death Index Plus, cancer registry records, questionnaire responses, and other mailings.
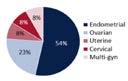
ü Analyzed associations with survival of all cancers combined (N=92,818), and lung (N=11,213), colon (N=6,389), prostate (N=25,686), breast (N=10,821), and pancreas cancer (N=1,901).
• Air Pollution Exposure Assessment:
ü Annual average PM2.5 concentrations (ug/m3) (1980–2010) were estimated at the census tract level using a spatio-temporal model based on geographic predictors, with extrapolation for pre-1999 levels before nationwide monitoring began.
ü Annual average NO₂ concentrations (ppb) (1990–2012) were estimated at the census tract level using a national land use regression model incorporating regulatory monitoring data, satellite-based measurements, and geographic predictors.
• Statistical Methods:
ü Cox proportional hazards models with time-varying exposures adjusted for demographic, socioeconomic, and behavioral factors (age, sex, race and ethnicity, education level, body mass index, diet, alcohol, and smoking history).
ü Different lag structures were examined to assess cumulative and delayed effects on survival outcomes.
Associations between air pollution and cancer survivorship varied by cancer type.
Our findings highlight the need for survivorship research that addresses cancer type-specific effects and identifies strategies to improve survivor outcomes.

Associations between DXA-derived visceral and subcutaneous adipose tissue and obesity-related cancer incidence in postmenopausal women
Ziller, S.G.1, Blew, R.2, Walker, E.,1 Archibeque, S.,1 Roe, D.,1 Odegaard, A.3, Caan, B.4, Chen, Z.1, Rohan, T.5, Lane, D.S.6, Felix, A7,
Department of Epidemiology and Biostatistics, University of Arizona1; Department of Health Promotion Sciences, University of Arizona2; University of California, Irvine3; Kaiser Permanente Division of
Einstein College of Medicine5; Department of Family, Population, & Preventive Medicine, Stony Brook University6; College of Public Health, Ohio State University7;
Introduction
• Obesity defined by BMI is a risk factor for 13-15 types of cancer called obesity-related cancers (ObRC)
• However, BMI is not as strongly related to adiposity in postmenopausal women
Purpose. We examined the relationships between first incident ObRC and dual-energy Xray absorptiometry (DXA) derived abdominal adipose tissue depots, specifically total (TAT), visceral (VAT) and subcutaneous (SAT), in postmenopausal women of the Women’s Health Initiative DXA Cohort (n=9,950).
Methods
Utilized the Women’s Health Initiative (WHI) DXA Cohort (n=11,405)
• Participants completed whole-body DXA scans (QDR2000, 2000+, or 4500W; Hologic Inc., Bedford, MA) at baseline
• APEX 4.0 software estimated abdominal VAT, SAT, and total adipose tissue (TAT) in 5cm wide section across the abdomen, above the iliac crest at approximately the 4th lumbar vertebrae (Figure 1)

Figure 1: Abdominal visceral and subcutaneous fat quantification in a DXA scan. ROI is illustrated by the red box at L4. Visible lateral subcutaneous adipose tissue (LSAT) is used to estimate total SAT.
Figure 2: Inclusion and exclusion criteria for WHI participants
Clinical Trial and Observation Study WHI participants (n =161,808)
WHI participants with DXA scans (n =11,405)
WHI participants with baseline DXA scans and complete data on prevalent cancer at baseline (n =10,681) At risk for first primary cancer (n=9,950)
Excluded: No DXA scan (n=150,403)
Excluded: No baseline DXA scan (n=579)
Excluded: missing prevalent cancer data at baseline (n=145) or had prevalent cancer at baseline (n=731)
Adjudicated cancer outcomes from enrollment to 27 years of follow-up
• Descriptive statistics stratified by quartiles of VAT were calculated Fine and Gray’s competing-risks regression was completed to estimate sub-hazard ratios (SHR; Figure 3) Multiple imputation using chained equations was used to address missing covariates
3: Fine and Gray’s competing-risks regression model components and corresponding mean years of follow-up
H8, Luo,
Epidemiology, Harvard University10
Figure 4: Adjusted Sub-Hazard ratio forest plot: association of baseline abdominal body composition with ObRC incidence in postmenopausal women (n=9,950)

Models adjusted for: Age at baseline, region, education, income, race and ethnicity, Hormone Replacement therapy trial arm, Diet Modification trial arm, Calcium and Vitamin D trial arm, height at baseline, alcohol intake, smoking status, Physical activity (MET-hrs/wk), Physical function (SF 36 score), total energy intake (kcal/day), HEI-2015 score, first-degree relatives with ObRC relevant medications, and reproductive factors
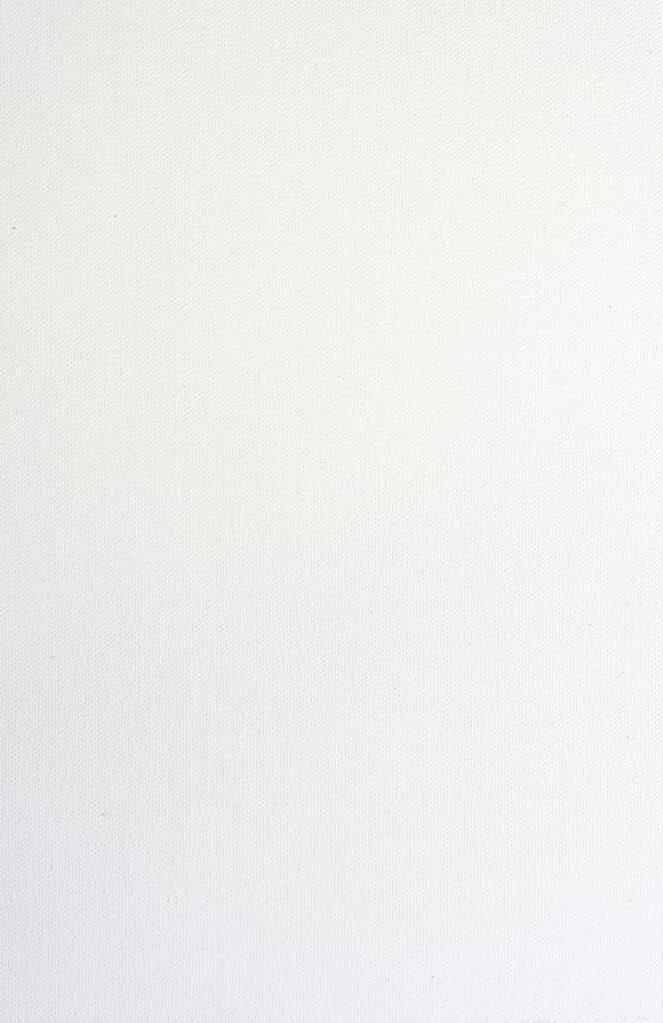
Figure 5: Distribution of obesity-related cancer types in cases (n=1,273)
• The majority of ObRC cases were breast cancer
All measures of abdominal adiposity were associated with increased risk of incident ObRC in postmenopausal women
• The risk associated with continuous VAT was twice as elevated compared to continuous SAT
In quartile models, VAT still showed higher SHRs than SAT
• Variables utilized in analyses are novel in the WHI population Further work required to examine time-varying and stratified analyses

This work was supported through R01CA253302, R01CA253302-02S1, and P30CA023074 from the National Cancer at the National Institutes of Health Project and abstract were reviewed and approved by the Women’s Health Initiative (WHI) Project and Proposal committee (MSID: 4850)
Get to know your fellow CPCP members and find opportunities for collaboration and ideas.

https://bit.ly/CPCPkumu