
Veterinarian
Rare birth for world’s black rhino population
A rare black rhino calf was born in April, at Taronga Western Plains Zoo in Dubbo, NSW. The zoo celebrated the birth of the male calf, conceived using a world-first reproductive treatment for the critically endangered species, of which only 6500 remain in the wild.
The calf’s mother, Kufara, faced fertility issues after the birth of her first calf in April 2017; however, Taronga Western Plains Zoo has been involved in a collaborative rhino research program with other conservation partners including Omaha’s Henry Doorly Zoo and Aquarium, and SeaWorld USA’s Species Preservation Lab. The research, funded by the Institute of Museum and Library Services and the Taronga Foundation, assisted in the successful pregnancy.
“Knowledge of the species’ biology generated from this, and previous programs, was integrated into Kufara’s clinical treatment to address her infertility,” Taronga’s Manager of Conservation Science, Justine O’Brien said.
“This involved Kufara receiving a series of hormone treatments by our veterinary and rhino keeper teams and builds on a multi-decade program of rhino reproductive research at Taronga.”
The close monitoring of Kufara throughout the process also gleaned new information on the gestation length the species can experience, with her calf born 490 days after mating, which exceeds that of the longest reported length for black rhinos of 486 days.
The use of science to support best practice management of zoo-based rhino insurance populations forms part of the work at the newly
openedTaronga Western Plains Zoo Wildlife Hospital. The new hospital has been developed to facilitatethe highest level of care for both free-ranging and zoo-based animals, as well as advanced reproductive technologies aiding in the conservation and breeding of threatened species.
“This special birth is the result of an international research partnership in black rhino conservation and represents the fifth calf born into the conservation breeding program for
the species in the last eight years,” black rhino supervisor, Jennifer Conaghan, said.
“Zookeepers were given a rare treat when they actually witnessed the birth. Historically southern black rhinos here at the zoo have been born overnight after a 14 to 16-month gestation. This little calf was born feet first at 11:15am.” Kufara and her calf will continue to bond behind the scenes for several months, before making the move to the black rhino paddock, where they can be seen by the public.
Musician’s sanctuary story headed for the big screen Salmon farming a risk for marine life
A feature documentar y about the Ellis Park wildlife sanctuary is in production for a 2024 release.
Ellis Park follows Australian musician Warren Ellis (Dirty Three, Nick Cave and the Bad Seeds) and his co-founding of the Sumatran facility for animals rescued from human captivity.
Screen Australia announced production funding for the film and said in a statement
that it is about “hope, redemption and how even little efforts can make a big difference.”
Working on the project are director Justin Kurzel (Nitram, Snowtown), and producers Nick Batzias (The Australian Dream ) and Charlotte Wheaton (Clean).
Taking to social media, Ellis said “there’s never been a film like it.”
■ SAMWORRAD8
For several years concerns have been raised about Tasmania’s salmon farming industry and the impact it is having on the state’s coastal wildlife. With the Tasmanian government’s long-term Salmon Industry Plan due to be released in May, several leading scientists and professionals have spoken out about the viability of the industry’s plans for expansion.
Members of the Tasmanian Independent Science Council are dedicated to science-based policy reform that will safeguard the Tasmanian environment’s long-term health. The group has called for a pause on further growth of the salmon industry until more robust scientific and regulatory frameworks are established. TISC has produced a Plan B with To page 30
CLINICALREVIEW
Naomi Hansen■ May 2023 ■ www.theveterinarian.com.au NEWS Female koalas and stress NEWS Eastern barred bandicoot FEATURE Olivia Pozzan 19 KIWI POST 10 MANAGEMENT 12 ABSTRACTS 15 ADVERTORIAL 17 BUSINESS 29
ONTHE INSIDE >>>>>>>>
5
3
Picture Jake Williams
Infectious and Vector Borne Disease Testing
Introducing Heska® trūRapid the latest point-of-care infectious disease testing for all practices.









Focus on prevention and early detection with easy-to-use trūRapid tests. Fast, accurate and cost-e ective bloodborne and faecal infectious disease diagnostics - now in the palm of your hand.


trūRapid Heartworm (Dirofilaria)

Canine Antigen Lateral Flow Test Kit
trūRapid Parvovirus Canine Antigen
Lateral Flow Test Kit
trūRapid Giardia Canine Antigen


Lateral Flow Test Kit
trūRapid FIV Antibody




Lateral Flow Test Kit
trūRapid FeLV Feline Leukemia







Virus Antigen Lateral Flow Test Kit*

trūRapidFIV/ FeLV Combo




trūRapid Parvovirus Giardia Combo Lateral Flow Test Kit
Versatile Fast, accurate and easy-to-use 10
to results Tests available for
and
Room temperature storage Excellent speci city
www.heska.com.au Reliable
minutes
cats
dogs
and sensitivity
Lateral
$10/test $12/test $12/test $17/test $17/test $21/test $30/test FELINE CANINE / FELINE
Flow Test Kit
© 2023 Heska Corporation. All Rights Reserved. Heska is a registered trademark and trūRapid is a trademark of Heska Corporation in the U.S. and other countries. AU23AD0302
trūRapid Test Kits Prices shown exclude GST CANINE (diro laria)
Female koalas more impacted by stress
New research recently published in veterinary sciences journal MDPI has shown diseased or injured female koalas are impacted more by stress than their male counterparts.
The study, led by Australian koala researcher, Flavia Santamaria, from CQUniversity, analysed the faecal samples of 234 koalas for metabolites which indicated the level of stress in the animals, and was the fourth in a series that demonstrates the importance of using a targeted analytical tool to correctly assess stress in koalas.
“Using a koala-specific enzyme immunoassay called 50c as a non-invasive monitoring tool for the detection of faecal cortisol metabolites (FCMs), we were able to evaluate the impact of stress on hospitalised injured and diseased wild koalas,” Santamaria said.
The study found that diseased and injured koalas had significantly higher FCM values than clinically healthy control animals and
AVA, Apiam turn up the heat on HECS
TheAVA has escalated its calls for veterinarians working in regional communities to have their HECS debts removed.
AVA CEO David Andrews said he was disappointed that the Federal Government did not address the regional vet shortage in the recent 2023-24 budget, and said more communities were at risk of losing their veterinaryservices.
“Despite the important role of vets in animal agricultural industries, workforce shortages could see access to veterinary services in regional and rural areas collapse,” Andrews said in a statement.
“Governments bank on the $70 billion contribution of the agricultural sector to the Australian economy but it’s an industry which has been left exposed by chronic under investment in the veterinaryworkforce.”
Andrews added that this year veterinary practices have closed in Parkes and Wee Waa in New South Wales, Jamestown in South Australia and could be closing in Longford, Tasmania.
“[This leaves] major farming towns without access to veterinaryservices,” he said.
The AVA is hoping to work with Agriculture Minister Murray Watt to better support the vital industry.
“In 2022, the gross value of livestock was approximately $25 billion…therefore a situation where there are fewer and fewer vets available to service the industry presents a fundamental economic and animal welfare risk,” Andrews said.
“Given that it would cost just $4.8 million per year to provide dozens of willing veterinarians
to communities that so desperately need them, we are disappointed that the Government has overlooked this small but important investment.”
In addition to the AVA’s lobbying, rural veterinarybusiness Apiam Animal Health has introduced its own HECS forgiveness plan.
The HECS forgiveness plan is open to existing Apiam employees and new graduates and will be offered to 10 vets in its first year,with successful applicants each being assisted with grants of $65,000 paid across a four-year period.
Apiam Managing Director Chris Richards said the plan will ensure a “future pipeline” and retention of talented vets into rural and regional areas to meet a growing market.
“We have some vets several years into their careers still burdened by huge student debts in excess of $100,000,” Richards said.
“We are therefore offering the same support to these valuable team members to ensure that they remain in regional Australia and continue to apply their skills in under serviced regions.”
Aspokesperson for Apiam indicated there was “strong interest” in the program since it opened on the May 15.
Warragul-based vet Amy Hewitt works for the company and has been a vet for four years.
Hewitt’s HECS debt is currently around $50,000 which is causing financial stress and necessitating afterhours work.
“Depending on when and where they graduate, you’ll see vets with debts of $190,000, and some had to pay $30,000 out of their own money to pay for their tuition,” she said.
that while sick koalas stress more than healthy ones, females take on an even bigger emotional load than males.
While it has been documented that habitat loss, urbanisation and climate change can cause stress in wild koalas, this latest research proves that they also stress when they’re physically compromised.
“Stress is associated with higher plasma cortisol levels, reflected in the faeces with an increased excretion of cortisol metabolites, hence, the aim was to determine if diseases and injuries, as well as hospitalisation, would increase FCM values in wild koalas,” Santamaria said.
“The faeces of diseased and injured koalas collected on day one showed altered values due to the prolonged pain that the koalas may have experienced prior to being admitted to hospital.”
■ JULIA GARDINER“Things like getting house loans become difficult, and having a reduction in HECS debts would be a great help to vets (because) if you have to pay two, three, four grand off your debts at tax time you just can’t get ahead.”
The University of Queensland graduate said the financial concerns are common among her peers.
“One of my best friends from uni found the financial prospects post-graduation a bit of a deterrent, and that’s why she went into government work and graduated earlier,” she said.
“So it’squite difficult; of course veterinarians do it for the love of it, but we’ve got to be financially sound.”
Hewitt added that aspiring vets should be better briefed on what they’re up against.
“We need to be having these conversations before students sign up to have awareness of what will be involved, and factor it in when making the decision,” she said.
“It’s obviously a very worthwhile profession, but we need better schemes in place.”
■ SAM WORRADNews TheVeterinarian 3 MAY 2023 www.theveterinarian.com.au
Flavia Santamaria

Support for the eastern barred bandicoot
Although Easter remains firmly associated with rabbits in the public consciousness, the festival is increasingly being used by conservationists to highlight the plight of Australia’s critically endangered species. This year the focus was on the eastern barred bandicoot, (Perameles gunnii), a nocturnal marsupial endemic to the country’s south-east.
Habitat destruction and predation from introduced species led to the mainland bandicoot subspecies being declared extinct in the wild in 2013, a status that was reclassified in 2021 to being ‘critically endangered’ following an extensive captive breeding and release program in Victoria and South Australia. Although not formally recognised as a distinct species, Tasmania’s subpopulation of eastern barred bandicoots is also considered to be in steep decline, largely because of habitat loss through land clearance for agriculture, and vegetation degradation.
Bridgette Barnden, a PhD candidate at the University of Tasmania’s School of Natural Sciences, is studying an additional threat to bandicoots: cat predation. Her research involves discovering the influence that cats and the cat-borne parasite toxoplasma may be having on bandicoot populations, and it is being supported through a collaborative project that includes the federal government’s National Landcare Program, the Tasmanian Land Conservancy, and the state’s natural resource management organisation, NRM North.
“Although more abundant than their mainland cousins, Tasmania’s bandicoot population is receding into the north and south of the state. They’ve completely disappeared from the Midlands, an area which is Australia’s only nationally recognised biodiversity hotspot but where up to 80 per cent of native vegetation has been transformed into agricultural land,” Barnden explained.
Although the impact of land clearance and
Importance of poo for healthy oceans
Two studies published recently have focused on how marine animal waste can impact on ocean health, with results showing the important role faeces play in the maintenance of healthy ecosystems in the Southern Ocean, and on coral reefs.
Previously scientists believed coral-eating fish, or corallivores, weakened coral reefs through their consumption of coral tissue, while the grazer fish that feed on algae and detritus, were thought to keep reefs healthy. A study published in Frontiers of Marine Science and led by researchers from the Rice University in Houston, USA has found that the faeces from grazer fish leave large lesions on coral, possibly because they contain coral pathogens. In contrast the faeces from corallivores may provide a source of beneficial microbes that help coral thrive.
Lead author Carsten Grupstra explained that although corallivorous fish are generally regarded as harmful because they bite the corals, this was only part of the story.
“Corallivore faeces contain many of the bacterial taxa that are associated with healthy corals under normal conditions, potentially resulting in the natural dispersal of ‘coral probiotics’, analogous to faecal microbiota transplantation therapy in humans,” he said.
Tropical coral reefs are home to many fish species, all of which defecate. Although their faeces disperse nutrients which may help support a healthy reef, they also contain pathogens and sediments which can smother parts of living coral. Tobetter understand how the cycle of waste and nutrients works, and help protect delicate coral reef ecosystems, the researchers placed pieces of coral in jars with sterile seawater. They then applied faeces from corallivore and
grazer fish to different jars. Some samples were sterilised to determine whether the physical characteristics of the faeces alone caused the lesions. After the experiment each piece of coral was examined and categorised as apparently healthy,containing lesions, or dead.
The faeces of several corallivore and grazer species were then examined to find out what bacteria they contained. This enabled researchers to understand which bacteria might be contributing to the effects seen on the coral, whether the faeces contained specific coral pathogens, and whether results from the experiment could be generalised to other fish that also ate coral or algae and detritus.
Results showed that the addition of faeces to the jars sometimes caused lesions on coral pieces, and potentially even the death of the fragment, whereas fragments without any faeces remained healthy. Faeces from grazer fish caused lesions or death in all coral pieces, while faeces from corallivores caused fewer and smaller lesions and rarely caused death.
“Sterilised faeces from either type of fish caused little harm, comparable to low levels of damage caused by corallivore faeces. We suspect this is due to a greater abundance of coral pathogens found in the fresh faeces of grazers, and the higher abundance of beneficial microbes found in the fresh faeces of corallivores. The fish we assumed were harmful may actually be contributing to important processes that promote coral reef health, but more research is needed to test how fish faeces affect corals, and how we might use these in management efforts to support coral reef health,” Grupstra said.
degradation is well known, the impact of feral cats on bandicoot populations is less well understood. With little being known about bandicoot-cat interactions, 16 weeks of Barnden’s first PhD year was spent trapping the elusive marsupials across northern Tasmania’s West Tamar region, collecting ear biopsies for genetic sampling. This area is where NRM North has conducted a large-scale bandicoot-targeted monitoring and revegetation project.
Barnden’s fieldwork this year is in Ulverstone in the state’s northwest and will involve trapping bandicoots every two months. She will collect blood samples to find out if the animals are carrying toxoplasma from cats, and the impact it has on the bandicoot population. She will also investigate bandicoot behaviours and their responses to the presence of cats in foraging areas.
“The more we know about the needs and challenges of our eastern barred bandicoots the better we’ll be able to manage habitat fragmentation through targeted restoration. Any activity that brings to the forefront the plight of these tiny,very cute marsupials is great, and we need to convince Tasmanians that making a few smart choices in their gardens, such as planting small shrubs for bandicoots to hide and nest in, and ensuring their cats are contained, we can have a massive and positive impact on building the bandicoot population back up,” she said.
■ ANNE LAYTON-BENNETTHe said it was important to note that lesion effects in real-world conditions may not be so severe, or so evenly distributed in every territory given differences in fish behaviours and the presence of other organisms in the water.
“These findings result in a more nuanced understanding of the roles of fish on coral reefs. Both corallivores and grazers have important ecological roles and understanding these can help us better manage and conserve these important ecosystems,” he said.
Meanwhile in the Southern Ocean the research focus for scientists from Spain’s Institute of Marine Sciences in Andalusia was on the important role iron plays in an ecosystem that supports numerous marine species both large and small. Although krill and baleen whale excrement has previously been shown to play a large role in driving iron recycling in the upper Southern Ocean, the impact of seabirds, such as penguins, had not been examined. To page 30
News TheVeterinarian 5 MAY 2023 www.theveterinarian.com.au
Bridgette Barnden
PictureOleg Belyaev Korolev








To find the perfect Cubex solution for your practice, scan the QR Code or visit therian.com.au/cubex AU: 1800 251 766 | NZ: +61 7 5657 6777 | technology@therian.com.au CUBEX WORKS FOR PRACTICES OF ALL SIZES.
We automate every aspect of inventory management to maximize safety, profitability, and efficiency.
CUBEX YOUR INVENTORY EXPERT Discover Kontak Retriever, a NEW cloud-based phone system built for vets! Visit us at AVA conference 2023, Stand 129 to learn more.
Cubex integrates with your practice management software and can grow into a full practice solution, connecting everything from wireless controllers in your supply room to smart cabinets in your pharmacy and treatment areas; to fit each practice’s needs, regardless of size.
New arrivals for quoll double breeding program
The quest to protect the endangered Chuditch has reached a new milestone, with 10 individuals successfully translocated from Southern and Western Australia to Taronga Western Plains Zoo in Dubbo to expand a critical conservation breeding program.
Also known as Idnya or Western Quoll, the Chuditch was once found across 70% of mainland Australia but has been reduced to just five per cent of its former range and is extinct in the wild in NSW.
Taronga Conservation Society Australia’s conservation breeding program to restore the Chuditch to its former range commenced in 2022 in Dubbo, thanks to a generous philanthropic donation from the Kinghorn Foundation. Within the first year of the program, 17 offspring were born from just four breeding pairs, and 15 individuals were released into the wild at South Australia’s Vulkathunha-Gammon Ranges National Park.
“Chuditch are one of the top 20
priority mammals listed under the Federal Species Strategy, and this year we will double our breeding capacity at the Taronga Sanctuary in Dubbo as we strive to improve the plight of this endangered carnivorous marsupial,” Taronga Wildlife Conservation Officer Rachael Schildkraut said.
“We had such an amazing year last year. We’re aiming to successfully breed eight pairs but in order to dothat we needed to translocate new founders and introduce fresh genetics to ensure genetically robust individuals for release to the wild.”
Working in collaboration with the Western Australian Department of Biodiversity, Conservation and Attractions (DBCA), and the South Australian Department for Environment and Water (DEW), Taronga Conservation Officers and Specialist Keepers recently selected four males and six females to join the conservation breeding program from Ikara-Flinders Ranges National Park in South Australia and healthy populations in southwest Western Australia.
Five animals were flown directly from South Australia to Dubbo airport, while the remaining five were driven from Sydney to Dubbo after a red-eye flight from the west coast.
Animals a focus in Domestic Violence Awareness month
May is Domestic Violence Awareness month, and this year
$400,000 of donations will be made to organisations with programs that provide support for survivors of domestic violence to access vet care and emergency accommodation for their pets.
Recent data from the Australian Bureau of Statistics (ABS) reports an estimated eight million Australians have experienced violence since the age of 15, with one Australian study reporting 33 per cent of female pet owners living in crisis accommodation delayed leaving a violent relationship because of concern for their pet’s welfare.
The funding has been provided by the Petbarn Foundation, which, since its inception in 2012, has donated over $25 million to help animal welfare groups and rescue organisations through Australia, this year donating a total of $ 400,000 to Pet Medical Crisis, RSPCA Tasmania, and RSPCA Queensland.
“Pets are an important part of the family. Unfortunately, individuals who commit acts of violence often exploit this close bond, causing harm to pets as a means of targeting their victims.
“The Petbarn Foundation recognises the importance of these programs and know the donations will help provide veterinary care and refuge for beloved pets until
they can be reunited with their owners in a safe environment,” Petbarn Foundation National Manager Janelle Bloxsom said.
The organisations which have received the donations said the funding comes at a time where their services are stretched.
Pet Medical Crisis is a charity that helps vulnerable Victorians fund lifesaving veterinary care for their pets, with 73 per cent of their cases related to domestic violence situations.
“The rising cost of living is really being felt hard by our clients, and the demand for our services is growing year-on-year. Last year, we assisted vulnerable pet owners in 81 suburbs across Victoria and that’s just one state. We would love to be able to expand and help as many vulnerable pet owners across the country as we can,” Pet Medical Crisis founder Jennifer Hunt said.
RSPCA QLD’s Pets in Crisis program will use the donation to extend their animal refuge services, which has provided accommodation and care for over 70 animals in 2023 already.
“Pets in Crisis program ensures that beloved family pets are safe and protected while their owners get themselves to safety,” Nanda Ten-Gorenhuis, Head of Animal Experience at RSPCA QLD said.
■ JULIA GARDINER
“South Australia and our project partner, the Foundation for Australia’s Most Endangered Species (FAME), are grateful for the opportunity to further the recovery of Chuditch beyond our borders,” Bounceback Program manager Rob Brandle said.
“The successful reintroduction program in South Australia, without the use of fences, has only been possible through the 11-year partnership with FAME Inc. and demonstrates the importance of public-private partnerships in delivering high impact conservation projects.
“The amazing response of the Flinders Ranges population to consecutive La Niña seasons enabled us to provide Taronga To page 30
News TheVeterinarian 7 MAY2023 www.theveterinarian.com.au
PictureRick Stevens
Facinating felines
My cat, Pepper, recently celebrated his 22nd birthday. Although Pepper suffers from renal disease, diabetes and arthritis he manages to have a contented life. He might not be the agile ninja he once was and he’s a bit stiff and slow to walk but he’s the undisputed king of his domain. He can still climb the elaborate staircase to his throne (i.e., the daybed) where he enjoys napping in the sun and watching butterflies flit in the garden. He snores when he sleeps, purrs when cuddled and chirrups when he wants amassage.
For a cat to reach the age of 22 is an extraordinary achievement but, of course, cats are extraordinary creatures. Watching Pepper snooze in the sun Iremembered his younger years and the impressive array of senses and abilities he once possessed but that age has dimmed. In honour of his birthday I felt compelled to pay homage to the cat world and catalogue some remarkable features of feline physiology.
Cats have eyes that are specifically adapted for hunting in low light conditions, which is why they are often considered to be crepuscular animals (i.e., active during twilight). Their pupils can dilate much larger than human pupils, allowing more light to enter the eye. They have a reflective layer at the back of their eyes called the tapetum lucidum which amplifies available light, enhancing their ability to see in the dark. Also, cats have a larger number of rod cells in their retina, which are responsible for detecting light and motion. This gives them incredible visual acuity and allows them to track the movement of prey with outstanding speed and accuracy Pepper, I recalled, would gaze sphinx-like at grasshoppers in the garden then suddenly strike out, catching them at lightning speed.
But it's not just feline vision that's impressive. Cats also have a phenomenal sense of hearing, and their ears are able to swivel independently of each other to pinpoint the source of a sound with amazing accuracy. Their ears are so sensitive that they can hear the sound of a grasshopper rustling in the leaves from several meters away and can even hear the click of a butterfly’s wings. Pepper’shearing and vision has waned over the years, but his sense of smell is as strong as ever. He loves prawns and if there are any in the house -like on his birthday - his nose will start twitching even while he’s asleep. It’s no surprise considering a cat’s sense of smell is up to 14 times more powerful than our own, thanks to the presence of a specialized organ called the Jacobson's organ.
This organ, also called the vomeronasal organ, is located in the roof of the mouth and is responsible for detecting pheromones and other chemical signals that can't be detected by a cat’s regular olfactory system. When a cat detects these chemical signals, they will often display the Flehmen response, curling back their upper lip to draw the odor directly into the Jacobson's organ for more detailed analysis. With such a finely-tuned nose it’s no wonder Pepper can detect even the faintest whiff of his favourite dish.
Another intriguing (and cute) feature of cats is their long delicate whiskers. These long, stiff hairs, or vibrissae, are super sensitive and located on either side of the nose, above the eyes, and on the chin. They help cats navigate their surroundings and detect changes in their environment.
particular!
exceptional climbers and acrobats with incredible agility and lightning-fast reflexes. They can jump several times their own height, run at speeds up to 48 kph and change direction quickly and effortlessly. When I see Pepper hesitantly negotiate the doorstep I wonder if he laments the vagaries of an ageing body.
Maybe, as an old cat’s physiological senses wane, he comes to rely more on his extrasensory or supernatural abilities. Of course, some people dismiss a cat’s uncanny knowing as superstition or myth. But the ancient Egyptians revered cats as sacred animals, believing them to have magical powers. In those times, cats were treated with the utmost care and respect as representatives of the goddess, Bastet. Modern-day felines seem to channel this god-like quality with ease, along with their reputed sixth sense. Anyone who lives with a cat has a tale to tell of telepathy, clairvoyance or mystic encounters.
There are many reported instances where cats have apparently predicted events before they happened, such as sensing when their owners are about to come home or anticipating a change in their routine. Cats have been known to predict earthquakes, tsunamis, and other natural disasters, either by acting agitated or hiding in a safe place before the event occurs. Some cats have alerted their owners to an impending hypoglycemic attack, epileptic seizure or pre-cancerous state.
But it's not just their whiskers that are sensitive –their paw pads are covered in tiny receptors called mechanoreceptors that help them feel texture, temperature, and pressure. This is important for gripping surfaces, detecting prey, and communicating with other cats through physical contact.
Cats use their sense of touch in all sorts of ways, from grooming themselves and each other to communicating with other cats. Pepper rubs his face against me to convey affection and pats me lightly with his paw to gain attention.
Arthritis is the bane of any oldie – whether human or animal – and especially for a former ninja. Cats have a flexible spine, allowing them to contort their bodies in ways that would be impossible for other animals. Combined with powerful leg muscles, this makes them
Acat’sextraordinarysenses can explain some of these seemingly psychic acts. They can pick up on subtle changes in body language and scent, detect changes in air pressure, see and hear beyond our limited range and react to stimuli we don’t even cognize. But a lot of what they do is still wonderfully inexplicable. When a cat stares fixedly into space and then suddenly pounces into action, has he seen a ghost or is he just messing with us?
Pepper has taught me a lot about cats and their exceptional senses and abilities. But perhaps their greatest talent is the way these tiny fur-balls have managed to domesticate humans with their playful, affectionate, independent and quirky personalities. Most cat lovers freely admit to being willing slaves to their pets. For sure, in my home, Pepper is king. So, next time a cat deigns to let you into his world, take a moment to appreciate just how extraordinary these animals truly are.
■ OLIVIAPOZZANFEATURE
TheVeterinarian MAY 2023 8 ■ www.theveterinarian.com.au
Veterinarian and author Olivia Pozzan shares some thoughts about cats – one in




See product label for full claim details and directions for use. For more information, contact Boehringer Ingelheim Customer Care on 1800 808 691. Boehringer Ingelheim Animal Health Australia Pty Ltd. Level 1, 78 Waterloo Road, North Ryde NSW 2113. ®ORAVET is a registered trademark of Boehringer Ingelheim. AU-PET-0027-2022 Scan the QR code below to watch an OraVet demonstration video Order through your wholesaler today oravet.com.au OraVet_FP_A4_Ad.indd 1 22/3/22 4:05 pm
Kiwi Post
So, I’m a student again! The digs and food are slightly better but there’s still a party in the room next door-the 20yos from my course are celebrating the arrival/departure of another 20yo with copious vodka and Redbull and D&B. Outside the piste groomers are beep-beeping asthey prepare for tomorrow.
I’m back at college- and out on externship. For a number of years I’d planned to take time out to learn to train as a Ski Patroller. And, after a brief COVID interruption of three years, I’m finally here in British Columbia making it happen.
There are nine of us on the nine week course. It’s a mixture of intensive human emergency medical training, risk management, avalanche training and field work with the Patrol. We are from NZ, Australia, UK, Sweden, Latvia. And we’re a neuropsychologist, a paramedic, acouple of students, a yachtie, a young jeweller, acouple of very young ski instructors. And an old vet.
The medical training should be the easiest for the old vet- but it’snot as straight forward as that. We take for granted how lucky we are to be able to do what we do to animals, with limited further training. There’sonly so many times the tutor can say, exasperated, ‘no, you can’t just do that Mark, it isn’tadog!’ You need separate qualifications for everything from administering aspirin to taking a blood prick for glucose.
Everyprocedure and approach is also accompanied by acronyms- to the point it becomes a ludicrous running joke amongst us. HEMPBC, OPQRST, SAILER, SMR, SAMPLE, FAST, AVPU, DCAP-BTLS….I kid you not. But there is merit in some of this, in formalising diagnostic processes that we probably all do intuitively but struggle to communicate perhaps to younger vets and new grads. I make a mental note…
The field work is physical, unsurprisingly cold and long hours. We start in the dark at 6.30am and finish in the dark at 5.30pm. In between seems to be mostly mist, snow, cold, wind. Temperature regulation is the first challengeyou’re either sweating under layers of Merino while shifting crash pads or 50kg sledges around; or shivering on a chairlift as your sweaty merino chills you to the bone.
Meanwhile, in the Patrol Clinic, I’m overcome with a huge feeling of empathy towards the vet students who attend our clinic. Being a student is quite scary! Our group assembles and starts sniffing each other out while we wait for the patrollers. We have lots of gear; we hover around awkwardly unsure where to put it or ourselves.
The patrollers arrive and bustle about busysome are nice and introduce themselves but others seem to scowl as they rush around doing serious things. The older ones appear pre-occupied; and the younger ones are….so young! They speak in acronyms and abbreviations and strange accents and I can’t really understand much of what they say.There is so much that is unfamiliar, and it’s all a bit overwhelming.
But, there is also much that is familiar. It’s a clinic- so they have masks and bandages and i/v lines and Oxygen and NO2. They have a drug room. They do stocktakes (weekly!!), and they have phones and radios that ring incessantly and interrupt them constantly. The patrollers need to stock up each day for what they may need- and, in case you’re still not convinced of the similarities- we’re introduced to the nurses and told ‘they run the place’.
There are various other support teams including ops people, and Despatchers who are really our receptionists who take all the calls and tryto find spare vets/patrollers to rush to the emergencies. Some patrollers are easy to manage and direct
while others are less accommodating… it’s all remarkably familiar!
The familiarity continues. Every morning a bunchof unkempt, overdressed, semi uniformed patrollers -who, when you get to know them, are not that scary and are actually diverse and fun- unload themselves into the clinic at 6.30am. Then they’re briefed for the dramas of the day, amixture of routine and whatever comes in and their Clinic Lead assigns them to various positions either in the clinic or out in the field.
Back at the clinic, people wander in unannounced alongside patients who have had the courtesy to call ahead. It can be weirdly quiet or stupidly busy. Workspaces are cluttered. There are mugs and water bottles and things where they shouldn’t be. Patrollers rush in to restock their packs with bandages, meds, gear; or to grab more specialised gear for the next call.
And at the end of each long day, everyone sweeps back in, jobs done, tired, cold, wet, knackered; or those who spent all day inside warmer but overrun with in-clinic dramas. A final review of the day at 5.30 and then home to do it all again. Oh, and there’s even a couple of patrollers and nurses who stay on till 8pm for the late shift.
And, to complete this strange mirror of our own professional world, any day could be long, hard, challenging, morally distressing, unsatisfactory, sad, wet, cold and unpleasant. You’d question your career choice. But then the next day you would literally be on top of the world at 7am, alone, as the sun rose, amongst unimaginable beauty,and you’d pinch yourself at how lucky you were to be doing and seeing this.
It was a good break. And it was both challenging and a great learning experience. But really, it was like holding a mirror up to our own profession. And, to murder a phrase, it was just the same shit, different species!
DOYOUHAVE SOMETHING TO SAY?
Is there a topic you’ve wanted to tell everyone about?
Have you ever thought you would like to write a clinical review but don’t know where to start?
Do you have a hobby or history that you think vets everywhere would like to learn more about?
Then don’t delay – email The Veterinarian at editor@vetmag.com.au and let us know –because your words could be in the pages of next month’s issue!
Mark Bryan qualified in Glasgow in 1988, and moved to New Zealand in 1995.TheVeterinarian MAY 2023 10 ■ www.theveterinarian.com.au
The first liquid solution for hypertension
Semintra® 10 mg/mL Oral Solution for Cats is the first angiotensin receptor blocker licensed for feline hypertension. Its unique, targeted mode of action provides reliable, long-term control of blood pressure.1 And, as Semintra® is an easy to give liquid formulation, it is well accepted by cats, making administration easy.2


References: 1. Glaus, T.M., et al. (2019) Efficacy of long‐term oral telmisartan treatment in cats with hypertension: results of a prospective European clinical trial. JVetInternMed, 33(2), 413-422. 2. Zimmering, T. et al. (2015) Effect of Semintra® and owner observations on quality of life in cats with Chronic Kidney Disease - update on cat owner feedback (“EASY Programme”). Poster presentation at SEVC 2015, Barcelona. Boehringer Ingelheim Animal Health Australia Pty. Ltd. Level 1, 78 Waterloo Road, North Ryde, NSW 2113. Semintra® is a registered trademark of Boehringer Ingelheim Vetmedica GmbH – used under licence. AU-FEL-0027-2022
Know when it’s time to go: the hidden art of quitting
Selling your practice is simply the divestment of an asset and the release of capital. The right time to do this is the same aswith any asset. We should aim to sell any asset when its value (usually reflected in its turnover, profit, and likely prospects) is at its peak.
When to quit clinical practice
The right time to quit clinical practice is more complex. Many veterinarians think of quitting clinical practice as the day when they put down their tools for the last time. In reality, veterinarians usually quit practicing slowly, by increments, over their last decade of practicing.
Either due to age, fatigue, health concerns or the desire to spend their time elsewhere, they start slowly quitting. They quit:
■ The number of hours per day that they work
Weare often told the secret to a successful career is hard work, determination, persistence, and resilience. What we aren’t told is that another crucial skill in determining the success of your overall career is the exact opposite…knowing when and how to quit.
There are many reasons to celebrate grit. The things that we value most will often require us to persist through challenging times.Despite its many virtues, though, it is possible to overvalue grittiness. Just as important as the discipline of grit, is the selfawareness toknow when to quit. For a veterinary practice owner, there are two crucial and veryseparate “quits” that they will need to time and sequence correctly in their career:
1. When to quit practice ownership
2. When to quit clinical practice
There is an epidemic in the veterinary industry of poorly timed quitters, veterinarians who hold onto their status as owners and clinicians far too long, past the point at which their financial capital, health and/or clinical reputation have been eroded and compromised.
When to quit practice ownership
It is important to make clear the that selling your practice is not the same thing as quitting clinical practice. Most vet practice owners will work for some time post sale, even if it is just to ensure a smooth transition of goodwill.
■ The number of weeks that they work
■ The number of consults per day
■ Clinical range
■ Innovation in their practice
Quitting slowly like this is often necessary. Physical and mental health, and relationships with loved ones, cannot be maintained if an owner needs to keep up the long hours andintense pace that they worked in their youth. Quitting clinical practice slowly is often necessaryfor clinical longevity.
Sequencing the two quits
Sequencing your two quits needs to be done carefully, such that the timing of the second quit doesn’t compromise the first.
In other words, a veterinary practice owner who is considering slowing down towards the end of their career should consider selling their practice before their reduction of their time/clinical range/speed in the practice compromises the practice’s value (reflected in turnover, profit, and likely prospects).
Veterinary practice owners should also realise that a purchaser will usually pay more for a practice where the vendor stays on clinically post sale (even if it is part time, with long holidays each year), to give the new owner an implied endorsement and ensure a smooth transition.
From a practice value perspective, it would be ideal for a veterinary practice owner to plan on working for the buyer of their practice in some capacity for at least a year.
Simon Palmer is the Managing Director of Practice Sale Search, Australia’s largest vet practice brokerage. If you’d like more information on practice sales or want to have a confidential discussion about your practice’s circumstances, email Simon Palmer at info@practicesalesearch. com.au or call 1300 282 042.Management TheVeterinarian MAY 2023 12 ■ www.theveterinarian.com.au
INSEPARABLE
PEXION® is the only targeted therapy developed specifically for dogs with idiopathic epilepsy, balancing seizure control whilst preserving quality of life in patients.1,2

RECOMMENDED BY SPECIALISTS
Scan to rediscover the role of PEXION in managing canine idiopathic epilepsy*

“PEXION has provided a vital new tool for the treatment of epilepsy in dogs. As a neurologist, I now use it as my first choice anticonvulsant in drug-naive patients, because of its improved side effect profile over more traditional drugs, its improved hepatic safety, and its short half-life (which means I know whether it’s working fairly quickly). It is also one of the few anticonvulsants that has a sound body of evidence to support its use and it gives us one more option to use in our never-ending quest for that most elusive of things: perfect seizure control.”

– Dr Sam Long BVSc PhD DipECVN, Veterinary Referral Hospital.
*If you are registering with Animal Health Academy for the first time, please use access code: myAcademy For more information, please contact Boehringer Ingelheim Animal Health on 1800 808 691 References: 1. Bhatti, SFM, et al. (2015) International Veterinary Epilepsy Task Force consensus proposal: medical treatment of canine epilepsy in Europe. BMC Vet Res.;11:176. 2. Tipold A, et al. (2015) Clinical efficacy and safety of imepitoin in comparison with phenobarbital for the control of idiopathic epilepsy in dogs. J Vet Pharmacol Ther.;38(2):160-168. Boehringer Ingelheim Animal Health Australia Pty. Ltd. Level 1, 78 Waterloo Road, North Ryde, NSW 2113. Toll Free 1800 808 691. ®PEXION is a registered trademark of the Boehringer Ingelheim Group. All rights reserved. AU-CAN-0003-2023


The next generation in canine osteoarthritis pain relief is here INDICATION For the treatment of pain and inflammation associated with osteoarthritis in dogs. Read product leaflet for full instructions. The safety of Galliprant has not been established in dogs less than 3.6 kg or less than 9 months of age. Galliprant is a trademark of Elanco or its a liates. ©2021 Elanco or its a liates. PM-AU-21-0160 For more information contact Elanco Ph: 1800 995 709 or email: ANZCustomerAdviceLine@elanco.com Available now from your preferred wholesaler FIRST-IN-CLASS non-COX inhibiting NSAID UNIQUE MODE OF ACTION specifically blocks the EP4 receptor, a key mediator of OA pain, but does not interfere with homeostatic mechanisms mediated through other prostanoid receptors FOR ALL STAGES of OA from the earliest clinical signs Recommend Galliprant as first-line treatment
Epididymectomy as a novel
surgical procedure; application in the domestic cat
Feline overpopulation raises issues concerning health, ecology, economy, and ethics. Procedures to limit overpopulation should carefully address animal welfare, efficiency, costs, and feasibility. Vasectomy in unowned cats is suggested as preferable to standard neutering as it maintains male sexual behaviour which may induce ovulation and pseudopregnancy in intact females and may prevent immigration of other males. Vasectomy is not performed routinely because it is fastidious, time consuming and requires more material than standard neutering. We describe epididymectomy as an alternative. In a first experiment, we analysed semen, testosterone, behaviour and pain in six experimental cats before and after epididymectomy, and after castration two months later. Excised tissues were analysed histologically. Testosterone concentrations did not differ significantly between intact and epididymectomised animals but were significantly different after castration. Sexual behaviour and testicular spermatogenesis persisted after epididymectomy, but with a marked drop in the semen count after 7 days. The Glasgow pain scores did not differ significantly after epididymectomy and castration. In a subsequent experiment, 20 privately owned cats were epididymectomised and castrated immediately afterwards, to analyse the learning curve and perioperative complications. The time required for an epididymectomy was significantly shorter than for castration. The study confirms that epididymectomy is quicker and less invasive than castration, it is associated with minimal risks and post-operative pain while easy to learn and inexpensive. Further field studies are required to test its efficiency for feline feral population control or in other species such as in bears, lions or deer, where infertility is required, and castration not wanted.
Etienne Furthner1,Rosalie Fabian2,Anja Kipar2,Gerhard Schuler3, Fredi Janett4,Nicolas Nudelmann5,Annette P N Kutter6, Iris M Reichler7
Theriogenology.2023 Apr 1; 200:168-178. doi: 10.1016/j.therioge nology.2023.02.009.
1Clinic of Reproductive Medicine, Vetsuisse Faculty, University of Zurich, Zurich, Switzerland; Centre d'Etude en Reproduction des Carnivores, Ecole Nationale Vétérinaire d'Alfort, Maisons-Alfort, France. Electronic address: efurthner@gmail.com.
2Institute of Veterinary Pathology, Vetsuisse Faculty, University of Zurich, Zurich, Switzerland.
3Clinic for Obstetrics, Gynaecology and Andrology of Large and Small Animals, Faculty of Veterinary Medicine, Justus-Liebig-University Giessen, Giessen, Germany.
4Section of Andrology, Vetsuisse Faculty, University of Zurich, Zurich, Switzerland.
5Centre d'Etude en Reproduction des Carnivores, Ecole Nationale Vétérinaire d'Alfort, Maisons-Alfort, France.
6Section of Anaesthesiology, Vetsuisse Faculty, University of Zurich, Zurich, Switzerland.
7Clinic of Reproductive Medicine, Vetsuisse Faculty, University of Zurich, Zurich, Switzerland.
Euthanasia of dogs and cats by veterinarians in New Zealand: protocols, procedures, and experiences
Aims: Tocollect data on protocols used by New Zealand veterinarians to perform euthanasia of dogs and cats, and to explore opinions towards the training they received in euthanasia during veterinary school.
Methods: Across-sectional survey was administered to all veterinarians registered with the Veterinary Council of New Zealand. The survey asked respondents about their practices' policies for euthanasia; protocols for performing euthanasia of dogs and cats; opinions towards euthanasia training received in veterinary school; and subsequent experiences with euthanasia in practice. Descriptive statistics were provided for all quantitative study variables and thematic analysis was performed on the free-text comments.
Results: The survey was completed by 361/1,448 (24.9 per cent) veterinarians in companion or mixed animal practice. The mean number of dogs and cats euthanised each month were7.2 (median 5; min 0; max 60) and 7.9 (median 5; min 0; max 60), respectively. Fewer than half of respondents reported that their clinic had a standardprotocol for euthanising dogs (147/361; 40.7 per cent) and cats (157/361; 43.5 per cent). For euthanasia of dogs, 119/361 (32.9 per cent) always used sedation while 71/361 (19.7 per cent) indicated that they would not use sedation. For euthanasia of cats, 170/361 (47.1 per cent) always used sedation while 53/361 (14.7 per cent) indicated that they would not use sedation. Placement of IV catheters, methods for patient restraint, preferences towards the presence of owners during euthanasia, services provided with euthanasia, and discussions with owners were also highly variable and handled case-by-case depending on the client, patient, and clinical scenario. When asked about the euthanasia training received at veterinary school, it was generally ranked as below satisfactory, with approximately one third of respondents indicating that they received no training in dealing with emotional clients (113/361; 31.3 per cent), sedation protocols for euthanasia (107/361; 29.6 per cent), or managing compassion fatigue (132/361; 36.6 per cent). Most respondents (268/361; 74.2 per cent) received no formal training in euthanasia after graduation and learned from experience or discussions with colleagues. Providing animals and owners with a good experience during the euthanasia process was highlighted as important for managing compassion fatigue. Conclusions: Euthanasia is a common procedurein companion animal practice and there is considerable variation in how veterinarians approach both the technical and non-technical elements. Training provided during veterinary school was generally considered below satisfactory, particularly regarding managing compassion fatigue and clients' emotional needs.
Topage 30
The evolution of two transmissible cancers in Tasmanian devils
Tasmanian devils have spawned two transmissible cancer lineages, named devil facial tumour 1 (DFT1) and devil facial tumour 2 (DFT2). We investigated the genetic diversity and evolution of these clones by analysing 78 DFT1 and 41 DFT2 genomes relative to a newly assembled, chromosome-level reference. Time-resolved phylogenetic trees reveal that DFT1 first emerged in 1986 (1982 to 1989) and DFT2 in 2011 (2009 to 2012). Subclone analysis documents transmission of heterogeneous cell populations. DFT2 has faster mutation rates than DFT1 across all variant classes, including substitutions, indels, rearrangements, transposable element insertions, and copy number alterations, and we identify a hypermutated DFT1 lineage with defective DNA mismatch repair. Several loci show plausible evidence of positive selection in DFT1 or DFT2, including loss of chromosome Yand inactivation ofMGA, but none are common to both cancers.
This study reveals the parallel long-term evolution of two transmissible cancers inhabiting a common niche in Tasmanian devils.
Maximilian R.Stammnitz1,KevinGori1,Young MiKwon1,Edward Harry2,Fergal J.Martin3,KonstantinosBillis3,YuanyuanCheng , AdrianBaez-Ortega1,WilliamChow2,SebastienComte5,6,Hannes Eggertsson7 ,SamanthaFox8,9,RodrigoHamede5,10,Menna Jones5,BillieLazenby8,SarahPeck8,RuthPye11 ,Michael A. Quail2,KateSwift12,JinhongWang1,JonathanWood2,Kerstin Howe2,Michael R.Stratton2,ZeminNing2,andElizabeth P. Murchison1 Science, 2023 Apr 20,380 (6642):283-293, doi: 10.1126/science. abq6453
1Transmissible Cancer Group, Department of Veterinary Medicine, University of Cambridge, Cambridge, UK. Topage 30
■
EDITEDBYJENIHOODBSc(Hons)BVMSPhD
Abstracts TheVeterinarian 15 MAY 2023 www.theveterinarian.com.au



CVS Group: expanding our network
Established in 1999, and with over 500 Veterinary practices throughout the UK, Netherlands and the Republic of Ireland, CVS Group is one of the largest veterinary service providers in the UK.
Weare now looking to expand our network of quality, independent practices.
We focus on recommending and providing the best clinical care every time
At CVS Group, we focus on recommending and providing the best clinical care to every patient, every time, and we believe this is what drives the success of our practices.
Wedeliver the highest standard of healthcare, and we empower our colleagues to make the right clinical decisions for our patients.
We support and develop our teams to be the best in their role, which includes access to industry-leading learning, education, and development, supported by a diverse team of learning professionals and subject matter experts and an engaging educational platform.
CVS also shares best practice across our company and at the same time we give our veterinary
advantage and developing their career across our company – for example in more specialist roles, or in management. We have a track record of developing and promoting from within and encourage secondment and permanent opportunities across our network of clinics both nationally and internationally.
We are also proud to offer funding to colleagues for veterinary clinical research that aims to benefit the animals under veterinary care, and research that supports the veterinary profession in providing the best possible care to animals.
In addition, all our practices and people are supported by experts in IT,HR, Health & Safety, Recruitment and Procurement - leaving veterinary colleagues free to focus on caring for our patients.
We provide great facilities and equipment
In the UK, all our practices meet the rigorous standards of the Royal College of Veterinary Surgeons voluntary Practice Standards Scheme.
We are also investing up to AU $ 90m each year in our practice facilities, clinical
CVS places great importance on line manager conversations and has introduced check-ins to ensure all colleagues are getting the time and engagement needed from their manager. As well as providing feedback on performance and identifying development opportunities, these regular check-ins are designed to support colleagues’ wellbeing.
In addition to this, we have active Wellbeing Champions and managers trained in “Supporting the Wellbeing of Your Team” and have introduced a Wellbeing Calendar for colleagues featuring topics such as resilience, exercise, sleep, stress. We have also launched a new CVS Refresh reward scheme where teams receive a weekly allowance to spend on treats or classes.
Wetrack our performance by regularly measuring colleague engagement. Our employee Net Promoter Score (eNPS) reflects the number of people who would recommend us as a good place to work. It has increased significantly from June last year and has been increasing since 2019.
If you are interested
Wewould love to speak with you regarding your succession plans.
If you are interested in your practice joining CVS we offer partial and full sale options.
Vendors find us an attractive option because we don’t change their practice, practice name, clinical care, and culture.
professionals the independent freedom to make the best clinical decisions for their patients.
We are a great place to work and have a career
Our vision is that we want to be the veterinary company people most want to work for. This will help us attract the verybest people to enable us to achieve our purpose of delivering the best possible care to animals.
Our practices are backed by the strengths of operating within a group that is run at every level by vets, including on the Board of Directors.
Our General Practice Veterinarians are supported by a specialist team that offer unique expertise, experience, and advice to practices across the country,to continuously improve the standard of care that our patients receive.
Our unique Knowledge Hub gives our colleagues access to the industry’sbest learning, education and development platform - with a catalogue of over 450 courses, programmes and webinars. We also offer our colleagues free access to the British Small Animal Veterinary Association Library - home to all BSAVA publications, covering the spectrum of small animal veterinary practice.
The breadth of our business means there is also a vast range of career opportunities. We are pleased to see many of our people take
equipment, and technology to improve standards of clinical care and our colleague and client experience.
Inthe UK, this includes rolling out a brandnewCVS minimum practice facility standard –specifically designed by our veterinary surgeons, nurses, practice managers, receptionists, and patient care assistants – which includes well laid out clinical areas, modern office space and dedicated staff rooms.
It enables our vets to do the work they want to do, allows our vets to offer an increased range of services, and creates a nice place to work.
Wetake our responsibilities seriously including putting our people first Every important decision we make takes into consideration the impact it will have on our people in practice. We care about supporting our colleagues’ wellbeing and progress.
We have a network of pastoral support vets, mentors and wellbeing champions that help our colleagues to look after their mental health, their career and to do their best work.
We care about being a truly inclusive organisation and we have programmes around our business to ensure that all our colleagues feel welcome.
Wealso look after their team – maintaining and protecting their entitlements, wages, and conditions.
In addition, we offer a quick and efficient process with completion and transfer of funds in as little as six weeks.
As a stock market-listed company, we invest for the long-run, which means you can be assured that we are here for the long term. Being publicly listed on the London stock exchange, also means that CVS Group are held accountable to public scrutiny, and there is more transparency than some other large, privately held (PE backed) groups.
Come and meet us or get in contact
If you might like to know more or if you are interested in discussing any aspect of CVS Group –and whether we would be a favourable option for you, your practice, and your team – we would be very happy to meet with you for an initial, confidential chat.
You can come and visit us at our stand 108-111 at the Australian Veterinary Association Annual Conference (28 May to 2 June 2023, The Adelaide Convention Centre, North Terrace, Adelaide).
Alternatively,please contact Nathan Micallef at CVS Australia on 0418 754 853 or email Nathan.Micallef@cvsvets.com.
Advertorial TheVeterinarian 17 MAY 2023 www.theveterinarian.com.au



































and warranty in
industry. Order Direct www.im3vet.com.au 02 9420 5766 | sales@im3vet.com TABLES HANDPIECES HAND INSTRUMENTS ADVANCED DENTISTRY SCALERS & MICROMOTORS CONSUMABLES DENTAL UNITS PREVENTATIVE TREATMENT DENTAL X-RAY
The iM3 name is your guarantee of quality veterinary dental products coupled with the very best after-sales support
the
BVSc MACVSc graduated from Queensland University in 1997. She worked in mixed animal practice in Queensland after graduation, before moving to Canberra to work for John Aspley Davis at Kippax Veterinary Hospital. She has completed aresidency in emergency and critical care at Melbourne University and was a resident in the same field at the Pennsylvania University Veterinary Hospital in the US. She is veterinary director of North Coast Veterinary Emergency and Critical Care (NCVECC) in Sippy Downs, Qld. Hansen is a member of the Emergency and Critical Care Chapter of the ACVS.
Respiratory emergencies: a review
A pet in respiratory distress is a common veterinary emergency presentation and one of the most distressing for the owners. Fortunately, most pet owners are aware of the importance of breathing and the serious implications associated with apet that is “having trouble breathing” so wesee these patients arriving with an urgency..
Triage of the patient in respiratory distress
The staff member attending the reception area is the first in contact with the patient in respiratory distress and should be alerted to the urgency of this patient’s condition.
The management of a patient with a life threatening condition should be addressed on several levels:
● The patient
● The owner
● The other clients
1.The patient
Triage (definition: to sort)
The initial triage (patient assessment) should be performed in a standardized manner to ensure rapid, accurate assessment of the patient. This will more than likely be happening on the crash table in the emergency treatment room so flow by oxygen can be provided to the patient.
a. INITIAL OBSERVATION/ EVALUATION: Observe the patient from a distance before commencing your physical examination will provide important information as to the respiratory rate and pattern before the patient becomes anxious/distressed by the emergency environment. Listen for any abnormal noises during breathing that may help localize the area of concern (i.e., an audible stridor is suggestive of upper respiratory tract disease)
■ Astanding/walking patient is far less concerning than a recumbent patient, and apatient that is in sternal recumbence is more comforting than one that is laterally recumbent.
b. AIRWAY: Assess the upper airway for patency and the presence of a gag reflex.
■ If there is an upper airway obstruction the patient should be sedated or anaesthetised, and the obstruction removed immediately.
■ Patients that present recumbent with no gag reflex should be intubated immediately.
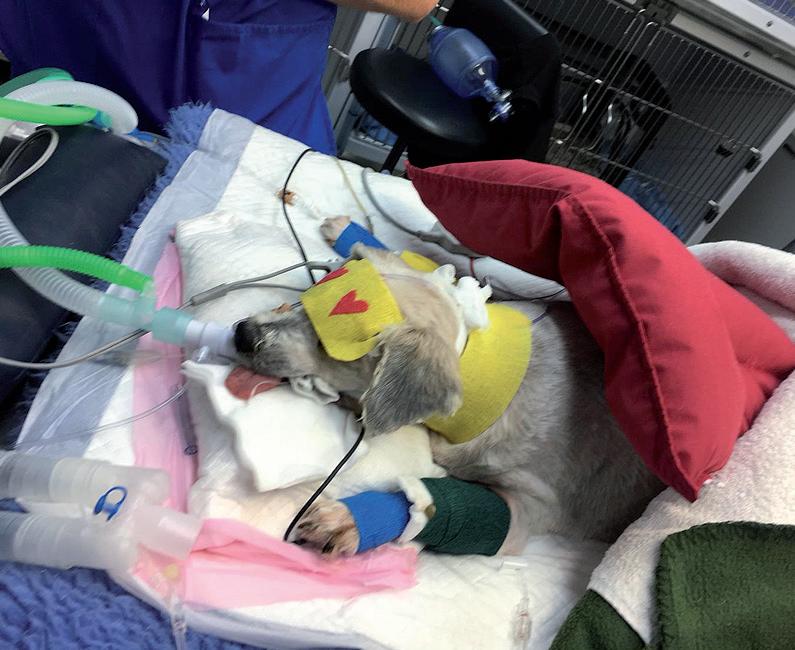
■ If an airway obstruction cannot be alleviated a tracheostomy should be performed (Figure 1).
c. BREATHING: A distant, visual assessment of the breathing effort and pattern will assist in localizing the respiratory problem (Table 1).
d. CIRCULATION: The circulatory status of the patient can be assessed through examination of the patients’ mentation, mucous membrane colour, capillar y refill time (CRT), heart
First Aid for the dyspneic patient
■ Rest reduces the body’s demand for oxygen
■ Gentle handling avoids distressing the patient
■ Oxygen support maximizes the amount of oxygen reaching the alveoli
■ Close observation: these patients can deteriorate rapidly
rate (HR), pulse quality and extremity temperature.
All emergency patients require a thorough examination of all organ systems following triage to ensure all disease processes are managed appropriately.
2.The owner
The owner will be extremely emotional by the time he/she reaches the clinic and will often require as much attention as their pet.


Itis a good idea to allocate a staff member to comfort the owner and keep him/her informed on the situation ‘out the back’ in the treatment room.
3. The other clients
The clients in the reception area will subconsciously assess management of the emergency situation. In their minds, it is a reflection of your competence as a veterinarian and cohesion as a clinic. Practicing emergency protocols and role-play of emergency situations will ensure your clinic is portrayed as a professional cohesive unit.
Preparedness for emergency situations:
•Establish clinic protocols for the triage and first aid of emergency patients
•Ensure all the staff members areawareof the protocols and know where the relevant equipment is located
• Practice......Practice......Practice. This may sound a little crazy but practice does ensure all emergencies are managed professionally.
Characterising dyspnea:
1. Tachypnea
Increased respiratory rate
2. Orthopnea
Difficulty breathing except in an upright position
3. Hyperpnea
Abnormal increase in depth and rate of respiratory movements
4. Apnea
Cessation of respiratory movements
5. Bradypnea
Low respiratoryrate
Dyspnea
Dyspnea describes a situation whereby there is difficult or laboured breathing. Dyspnea is further characterized by identifying abnormalities of respiratory rate, respiratory rhythm, respiratory character and/or altered behaviour.
■ Dyspnea may occur in paroxysms; it may be continuous or intermittent.
■ Dyspnea may or may not indicate a respiratory problem.
■ Chronic cardiac or chronic pulmonary disease may both present as acute dyspnea
Physical Examination
1.History
Documentation of an accurate patient history is extremely important and may be difficult depending on the emotional state of the owner.
Try to ascertain the following:
● Whether the dyspnea was acute or chronic in onset
● Whether there is an underlying disease process that may predispose an acute onset of respiratory difficulty (i.e., pre-existing respiratory disease, cardiac disease, endocrine disease, haematological or vascular disease)?
● Whether there is any potential for access to toxic or noxious substances prior to presentation. These may be inhaled, topical or ingested toxins.
● Whether the patient is on any medications that may affect your diagnostic and treatment plan.
2. Describe and classify the breathing pattern and/or the ventilation effort Observe the patient from a distance (‘hands off’)while he/she is at rest and document his/her breathing pattern. This allows an appreciation of the respiratory rate and effort without human intervention. Listen for externally audible respiratory noises (eg. stridor or stertor) which may help with anatomical localization of the underlying pathology.
Careful palpation of the neck and thorax followed by a thorough four quadrant auscultation of the thorax should be undertaken in a quietish environment. Careful cardiac auscultation and simultaneous palpation of the femoral or dorsal pedal arterywill help allude to any cardiovascular abnormalities (i.e., murmur, arrhythmia, pulse deficits, intensity of heart sounds). A thorough auscultation of the thoraxin multiple quadrants over both the left and right hemithorax is required, do not underestimate the value of this diagnostic tool.
TheVeterinarian 19 MAY 2023 ■ www.theveterinarian.com.au Clinical Review
Naomi Hansen
Increased inspiratory effort: upper airway and generally associated with an audible respiratory noise.
>Patients are predisposed to anxiety and hyperthermia
Increased expiratory effort: lower airway andgenerally associated with wheezes on thoracic auscultation
Restrictive breathing (rapid and shallow)
Increase in both inspiratory and expiratoryeffort
● Extra-thoracic lesion: nose, pharynx, larynx, cervical trachea
● Parenchymal disease
● Cardiac disease
● Neuromuscular disease
● Vascular disease (thromboembolic disease)
● Acute anaemia
● Intrathoracic lesion: small airways, bronchi, intrathoracic trachea
● Pleural space
● Thoracic wall
● Parenchymal disease
● Neuromuscular disease
● Parenchymal disease
● Vascular disease
● Medullary dysfunction (respiratory centre)
● Hypovolaemia
● Cardiac disease
● Acute anaemia
● Neuromuscular disease
● Acute anaemia
● Metabolic disease (acidosis)
● Tryand differentiate normal lung parenchyma from diseased lung parenchyma and normal pleura from diseased pleura.
● Document your findings in each quadrant and try and standardize/grade your findings to assist in monitoring the disease progression.
Ventilation physiology
Control of ventilation
The respiratory minute volume (RMV) is a function ofan animals’ acid/base status and blood gas partial pressure (oxygen and carbon dioxide).
RMV = tidal volume x respiratory rate
1.The central respiratory centre (medulla) responds to alterations in pH.
2. The peripheral chemoreceptors (carotid bodies) responds to pulmonary oxygenation levels.
3.The mechanoreceptors and stretch receptors alter the respiratory minute volume (RMV) to minimise muscular fatigue.
4. The sympathetic nervous system (b2 adrenergic receptors) innervation of the bronchial smooth muscle stimulates bronchodilation.
5. The parasympathetic nervous system (Vagus N.) innervation of bronchial smooth muscle stimulates bronchoconstriction.
Methods of evaluating pulmonaryfunction
1. Breathing pattern and ventilation effort
2. Blood gas analysis
Decreased ventilation effort
● Medullary dysfunction (respiratory centre)
● Spinal cord (efferent motor nerve dysfunction)
● Neuromuscular junction: NM blocking agents, myasthenia gravis, polyneuropathy
PaCO2 is a measureof ventilation
PaO2 is a measure of dissolved oxygen (irrespective of Hb levels)
SpO2 is a measureof haemoglobin saturation (irrespective of Hb levels)
Increased ventilation effort
● Large airway obstruction: pharyngeal masses, laryngeal oedema, recurrent laryngeal nerve paralysis, tracheal collapse, tracheal masses, peri-pharyngeal masses, peri-tracheal masses
● Small airway obstruction
● Chest wall disease
● Abdominal distension
● Pleural space disease
● Pulmonary parenchymal disease
● Pulmonary thromboembolism
● Hypotension, hyperthermia, anxiety, acidosis, anemia, opioids
Indicatory for ventilation support: PaCO2 >60mmHg, PaO2 <60mmHg, SpO2 <90%
3. Capnometry
Measureof expired CO2 (ETCO2 =32-40mmHg)
Anaesethesia and opioids shift the PaCO2 response curve to the right (increased resting PaCO2)
Differential diagnosis for ventilation failure (hypercarbia):
1. Neuromuscular disease
2. Airway obstruction
3. Abdominal enlargement
4. Thoracic wall disease
5. Pleural space disease
Cyanosis
Red
Oxygen desaturation (PCV>18%)
Peripheral vasodilation
Pale Anaemia or shock (cardiogenic, hypovolaemic or redistributive)
Jaundice Pre hepatic (i.e. haemolysis), intrahepatic (i.e. hepatopathy) or post hepatic (i.e. biliary duct system) dysfunction
Hemorrhage or petechiae
Then ask yourself “are the lung sounds appropriate?”
● Aunilateral or bilateral reduction in lung sounds in the presence of pronounced respiratory effort may suggest the presence of pleural disease.
● Crackles that are audible at the mouth without astethoscope are termed ‘harsh’ and indicated fluid movement between the throat ad more proximal airways (i.e tracheal hemorrhage).
● Crackles that are audible within the thorax are termed “fine” and indicate fluid or cells in the lung tissue. There are 5 differential causes for fine crackles as their presence suggests
Coagulopathy (primary or secondary haemostatic dysfunction)
alveolar disease: fluid which may be cardiogenic or non-cardiogenic, haemorrhage, cells which may be neoplastic or inflammatory.
● Wheezes are higher pitched sounds and support lower airway pathology.
4. Auscultation of the thorax
Auscultation of the thorax should be undertaken systematically.
● Divide the thorax into four quadrants and listen to each quadrant closely for the presence of lung sounds, crackles (alveolar disease) and/or wheezes (airway disease).
6. Mediastinal disease
Differential diagnosis for respiratory failure(hypoxemia):
1. Trauma (blunt/penetrating)
2. Pulmonaryinterstitial disease (inflammatory or neoplastic cellular infiltration)
3. Hydrostatic/oncotic force imbalance
Muscles of ventilation
Inspiration
Inspiration is the simultaneous contraction of the diaphragm and intercostal muscles. This action increases the thoracic volume and gen-erates a negative pressure within the thorax (‘Bellows Mechanism’). Air then enters the alveoli passively,along the pressure gradient established by respiratorymuscle contraction.
● Pleural pressure: -4cm H2O(-20cm H2Opeak inspiration).
● Innervation: Phrenic nerve (C5/C7) passes through the thoracic inlet and mediastinum to innervate the diaphragm and the intercostal nerves (C1-C5).
Table 1. Breathing and ventilation pattern classification 3. Assess the mucous membrane colour: Table 2. Mucous membrane colourTheVeterinarian MAY2023 20 ■ www.theveterinarian.com.au Breathing pattern Differential diagnosis Ventilation effort Differential diagnosis Mucus membrane colour Differential diagnosis
Clinical Review
- Dr Trevor Pavey Veterinarian & Practice Owner, Lakeside Vet Centre






































loyalty your clients with Unlock unique opportunities to build Vetplus provides veterinary business with a number of unique digital tools, including the Digital Pet Health Passport app and First Aid for Pets app to help foster deeper relationships between your clinic and clients. If you’re looking for an organic solution to price sensitivity and shopping around, scan the QR code or talk to your Boehringer Ingelheim Territory Manager to discover what Vetplus can offer your practice. Boehringer Ingelheim Animal Health Australia Pty. Ltd. Level 1, 78 Waterloo Road, North Ryde, NSW 2113. Toll Free 1800 808 691. Vetplus ® is a registered trademark of Boehringer Ingelheim Animal Health Australia Pty Ltd. Protech ®, Duramune ® and Fel-O-Vax ® are registered trademarks of Boehringer Vetmedica Inc. All rights reserved. BI1716TA-VAC-04/23. Proudly supported by Australia’s leading canine and feline vaccine range: Protech ® Duramune ® and Fel-O-Vax ® ... you can’t overstate the value of nurturing lifelong client relationships’ ‘
Treating urinary incontinence in dogs is easy with PROIN®

NEW TREATMENT NEWREGISTRATION
✔ Clinically proven for urinary incontinence in female and male dogs
✔ High dose formulation for increased efficacy in female and male dogs
✔ Easy dosing flavoured chewable tablets – dogs like them
✔ Dogs lose weight when on PROIN treatment
✔ No issues in switching dogs from other treatments to PROIN Chewable Tablets

✔ Scored tablets for dosing accuracy
✔ 50mg tablets, in bottles of 60.
Ausrichter Pty Ltd (02) 9517 1166 www.ausrichter.com
Expiration
Expiration is the recoil/relaxation of the muscles of respiration, expelling the air from the lungs.
1.Neuromuscular disease: decreased breathing effort
● Central nervous system
The respiratory centre is located in the medulla oblongata. Medullary dysfunction reduces the respiratory centres’ responsiveness to elevations in blood carbon dioxide concentrations and/or instigates an abnormal ventilatory pattern associated with site of the lesion (i.e. apneustic breathing, Cheyne-stokes breathing, tachypnoea).
● Peripheral nervous system
Spinal nerve damage (C1-C7), peripheral nerve damage (Phrenic N. or Intercostal N.), neuromuscular junction disease and/or muscular disease/weakness.
2. Airway obstruction
Airway obstructions (intrathoracic or extrathoracic) increase the resistance to passive airflow and an increased inspiratory/expiratory effort is required to achieve the equivalent end inspiratory/expiratory volume. Airway obstructions are rarely circumferential and fixed, they are dynamic and alter with the ventilation cycle.
● Extra thoracic obstruction: Increased inspiratory effort resulting in collapse of the intrathoracic airways on inspiration (sucked in).
● Intrathoracic obstruction: Increased expiratory effort resulting in airway collapse and forced exhalation.
Anti-anxiety medications are beneficial in reducing ventilation effort and airway collapse
3. Abdominal enlargement
Generation of negative intrathoracic pressure relies on contraction and caudal displacement of the diaphragm.
● This action will be hampered by space occupying diseases of the abdomen (i.e. GDV, Ascites, Ileus, Intestinal foreign body).
4. Chest wall disease
Thoracic wall disease decreases the efficiency of the intercostal muscles and diaphragm in the generation of negative intrathoracic pressure. This means that the pressure gradient for passive air flow is reduced so an increase in respiratory effort will be required to achieve the same tidal volume.
● Open pneumothorax
The open pneumothorax provides an inlet for air to flow from the environment into the pleural space.
● The negative pressure gradient is reduced due to the communication between the pleural space and the atmospheric air so the inspiratory effort will be increased.
● Open pneumothorax may be self limiting if the rent in the lung/thoracic wall is small.
● Closed pneumothorax
Aclosed pneumothorax involves an internal defect within the bronchial tree or lungs allowing air to move into the pleural space.
● Tension pneumothorax
A tension pneumothorax develops when a one-way-valve ‘flap’ occurs in the skin. During inspiration the air rushes into the pleural space (along the pressure gradient generated by the inspiratory muscles) and is trapped on expiration. The rapid increase in thoracic pressure causes the lungs to collapse and decreases the venous return to the heart altering the ‘thoracic pump mechanism’.
A tension pneumothorax will rapidly result in respiratory arrest
● Flail chest
This occurs when successive rib segments are broken in two places giving rise to a floating rib
section and regional haemorrhage (pleura and pulmonary parenchyma).
● This condition is extremely painful and local infusion of Lignocaine (1-2mg/kg diluted to deliver 0.5mL at each injection site) or 0.5% Bupivicaine (0.5mL at each injection site) at the caudal border of each fractured rib, above and below the fracture may assist in improving ventilation function.
● The increased negative pressure in the chest ‘sucks’ the floating segment towards the pleura and pulmonary parenchyma and reduces the total negative pressure generated.
● There is a risk of rib fragments penetration the lung parenchyma so surgical/mechanical stabilization is advised.
5. Pleural space filling disease
Air, fluid or abdominal contents that occupy the pleural space reduce the pressure gradient generated during inspiration.
Transudate
Modified Transudate
Exudate
Chylothorax
● Pneumothorax
Air in the pleural space tends to be more debilitating than fluid.
● The air pocket will expand/compress with inspiration/expiration more than fluid so an increased is required effort for the equivalent tidal volume.
*Avoid positive pressure ventilation (PPV) or place achest drain prior to ventilating*
● Pleural effusions
The parietal pleura produces pleural fluid at a constant rate (the parietal pleura covers mediastinum, chest wall and diaphragm) and the visceral pleura absorbs pleural fluid via lymphatics (the visceral pleura covers the lung and vasculature).
Pleural fluid accumulates as a function of raised hydrostatic pressure, reduced capillary oncotic pressure, increased capillarypermeability and/or obstruction to lymphatic drainage
Imbalance of hydrostatic and osmotic pressure between pleural and pulmonary capillaries
Clear/pale colour,TP <25g/L, WCC <1,000/ml
Slightly higher protein concentrations and white cell count
TP 25-50g/L, WCC 1,000-5,000/ml
Inflammatorycondition of the parietal/visceral pleura
Cloudy,TP >25g/L, WCC > 5,000/ml
Interruption to lymphatic drainage (thoracic duct)
Opaque/milky white/pink
Triglyceride/cholesterol differential:
Triglyceride/content fluid > serum
Cholesterol/content fluid > serum
Stain chylomicrons with sudan III
Pyothorax
Generally obligate anaerobes (Pasteurella, Bacteoides, Fusobacterium)
Yellow/red/brown and +++neutrophils +/- bacteria
TheVeterinarian 23 MAY 2023 ■ www.theveterinarian.com.au Clinical Review
Figure1. Mechanical ventilation is required when a patient suffers from respiratory fatigue
Pleural effusion Effusion characteristics
Through innovation, invention, and strategic partnerships with worldwide leaders in diagnostics, Heska provides the bene ts of latest generation technologies to veterinary professionals. From our ever-growing and wide range of in-house lab and imaging solutions, to outstanding service and support, discover all the ways Heska helps you provide a voice










Internet BasedPACS HeskaView Cloud HDDigital Radiogr Cuattro DRHD SingleUse RapidTests trūRapid Telecytology Pathologists HeskaView Telecytology Scanner HeskaView ImmunodiagnosticAnalyser eterinaryHematologyAnalyse r Element HT5 Veterinary ChemistryAnalyser CX ArtificialIntelligenceMicroscopy Element AIM Your diagnosis, their voice. Find out what there is to discover. Call Heska today.
www.heska.com.au 1300 437 522 ©2022 Heska Corporation. All Rights Reserved. HESKA, Element AIM, Element i+, Element HT5 and Element DC5X are registered trademarks and Element DCX, Heskaview, Cuattro DRHD, Reset, and trūRapid are trademarks of Heska Corporation in the United States and other countries. AU22AD0902 DISCOVER HESKA
for your patients.
Stabilisation/management of patients with respiratory distress
Chemical restraint is usually titrated to effect
Mediastinal disease
● Mediastinal mass
Medistinal mass lesions may cause compression of the cranial intrathoracic trachea resulting in an expiratory dyspnea.
● Pneumomediastinum
Pneumomediastinum (free air in the mediastinum) occurs associated with a trauma and may progress to a pneumothorax or generalized emphysema (air migrates between fascial planes).
Radiographically, this is depicted by the presence of air outlining the great vessels and large airways and associated with an airway rupture, oesophageal perforation or penetrating neck wound.
● Mediastinitis
Ventilatory fatigue and failure
Ventilatory fatigue and failure are common sequalae to a patient having a prolonged period of increased respiratory effort. They can be monitored clinically by serial assessment of the patients’ blood gas values, specifically PCO2 (either arterial or venous are suitable).
This may occur in the following clinical situations:
1.Hyperthermia, dehydration, hypovolaemia and reduced peripheral perfusion.
2. Hypercarbia (Hypoventilation) and hypoxemia
3.Respiratory acidosis +/- metabolic acidosis (lactate production)
4. Muscular hypoxia and ischemia (lactate production)
5. SIRS
6. Respiratoryarrest
Positive pressure ventilation (PPV) should be considered if PaO2 < 60mmHg, PaCO2 > 60mmHg or SpO2 <90%
Bronchodilators (indicated for small airway disease)
● Beta adrenergic agents:
Stimulate β 2 adrenergic receptors in the bronchial and vascular smooth muscle bronchodilation and vasodilation and may stimulate β1 adrenergic receptors in the myocardium (positive ionotrope and positive chonotrope)
Albuterol (Salbutamol or Ventolin) can be administered via an inhaler/spacer and is handy to have in your crash cart.
Terbutaline 0.01mg/kg SC (3-5 ug/kg IV and 5-10 ug/kg IM)
Airway/breathing
Oxygen supplementation:
● Flow by flow oxygen 100-200mL/kg/min (FiO2 ~30-60%)
● Oxygen cage
● Face mask
● Nasal oxygen 100-200 mL/kg/min (FiO2 ~40%)
● Intubate and ventilate 100% oxygen (avoid FiO2 >60% for longer than 24 hours; wean to FiO2 <60% after 24 hours to avoid oxygen toxicity)
Positive pressure ventilation should be considered if PaO2 < 60mmHg despite oxygen support, PaCO2 > 60mmHg and/or SpO2 <90% despite oxygen support.
Therapeutic Thoracocentesis
Thoracocentesis is generally performed in the awake, restrained animal with or without local analgesia.
Equipment: sterile gloves, needle/catheter, 3-way-tap, extension tube, syringe (10-20mL) +/- scapel blade and 1-2 mL Lignocaine (2%)
A. The lateral thorax clipped and aseptically prepared in the vicinity of the 7th/8th intercostal space (if a pneumothorax is suspected the dorsal half of the thorax is clipped and ifan effusion is suspected the ventral half of the thorax is clipped):
Remember the intercostal vessels and nerves are located on the caudal aspect of the rib and avoid the heart and the internal thoracic artery when performing thoracocentesis ventrally
B. Positiong the patient is important: restrain the patient in sternal or lateral recumbency ensuring the limbs are controlled.
C.Needle thoracocentesis: Advance the needle perpendicular to the thorax, once the needle is within the pleural space direct the needle caudally against the rib cage with the bevel facing away from the lung. Thoracocentesis should always be performed with an extension set, a 3way-tap, asyringe and the operator should wear sterile gloves.
Diagnostic Thoracocentesis
A diagnostic thoracocentesis is indicated in patients that are suspected of having pleural space disease, it is a rapid, inexpensive, and very sensitive test for the confirmation of pneumothorax or pleural effusion. A diagnostic thoracocentesis can be performed with a 3mL syringe and a 22G hypodermic needle or butterfly catheter with the patient in a comfortable position and minimal preparation.

The ideal location to insert the needle for a diagnostic thoracocentesis is the cranial aspect (to avoid the neurovascular bundle) of the 7th to 9th intercostal spaces, around the level of the costochondral junction for a pleural effusion and more dorsally for a suspect pneumothorax. When the needle has entered the skin apply asmall amount of pressure on the syringe (i.e., 1mL) to create a vacuum while simultaneously advancing the needle (with confidence) into the pleural space (in a straight direction). Upon contacting the positive pressure of the pleural space, the vacuum will be lost and either fluid or air will enter the syringe.
In the event of a positive diagnostic thoracocentesis, a therapeutic thoracocentesis or placement of a thoracostomy tube can be performed toremove remaining air/fluid from the pleural space.
Ultrasonic evaluation (i.e. point-of-care ultrasound (POCUS) or focused assessment with sonography for trauma (FAST)
Five anatomical sited are examined with traditional T-FAST (thoracic imaging):
● Right and left ‘chest tube sites’ (i.e. 7th-9th intercostal spaces)
● Right and left ‘pericardial sites’ (i.e. 3rd-5th intercostal spaces)
● Sub-xiphoid ‘diaphragmaticohepatic’ site: The sub-xiphoid site is the most sensitive for the detection of pleural effusion. The pericardial sites are used to identify the presence/absence of pericardial effusion and can be used to attain some echocardiographic views.
The chest tube sites are used to assess the lung tissue, the interface between soft tissue structures and air (i.e. air filled lung) results in 99.9% of the ultrasound beam being reflected which means that aerated lung is impenetrable to
TheVeterinarian 25 MAY 2023 ■ www.theveterinarian.com.au Clinical Review Drug Dose Medetomidine 2-4ug/kg IV and can be infused as a CRI Buprenorphine 0.01-0.02mg/kg IV or IM Methadone 0.2-0.3mg/kg IV or IM Butorphanol 0.1-0.2mg/kg IV or IM Ketamine 0.25-0.5 mg/kg IV Alfaxalone 1-4mg/kg IV to effect Propofol 1-2mg/kg bolus IV to effect
Figure 2. TFAST image of the left lateral thorax (middle) in a patient with a significant pleural effusion

ultrasound. Lung pathology can be identified as lung surface artefacts where aerated lung exists alongside consolidated lung.
In veterinary medicine, the point of care lung ultrasound procedure is published for the identification of pneumothorax, pleural effusion and alveolar interstitial syndrome (AIS).
Sonographic lung appearance:
● Bat sign/Gator sign: When the probe is placed perpendicular to the ribs over the thorax the rib head, rib shadowing and pleural lines are visible. The ribs appear as curvilinear white lines with rib shadowing. The first white line below the rib head is the pleural line.
● Glide sign: The to-and-fro movement of the lung sliding along the chest wall during respiration. This is observed at the pulmonary/pleural interface (i.e. the pleural line).
● A-lines: The air below the pleural line (aerated lungs) reflects the majority of the ultrasound waves back to the transducer (the transducer is also a reflector) which then bounces the waves back to the pleural line. This bouncing creates horizontal artifacts known as A-lines.
● B-lines: Blines originate at the lung surface, they move with the Glide sign, they obliterate A-lines and they extend to the far field without fading. The presence of a small number (<3) B-lines maybe normal but the presence of a large number of coalescing B lines supports pulmonary pathology (i.e. alveolar interstitial syndrome, pulmonary contusions, pulmonary oedema, pneumonia, neoplasia etc.
● Curtain sign: The interface between the thorax and the abdomen (a vertical line).
Alines propagate through air so are present in normal aerates lung and in the presence of a
Temporary Tracheostomy
Atemporary tracheostomy is indicated inpatients with a severe upper airway obstruction that is unresponsive to medical management. This will involve rapid induction of general anaesthesia and intubation*.
The ventral neck is clipped from the rami of the mandibles to the manubrium and laterally to the middle of the neck. Positioning the patient is important: extend the neck cranially and strap the legs caudally (sandbags may assist with support).
Incise the ventral cervical region (midline) at the 2 nd-3rd cartilage ring below the thyroid cartilage (~ 4cm from the caudal border of the larynx).
Split the sternohyoideus muscle midline and retract laterally.
Remove the peritracheal connective tissue from the ventral trachea.
Place the temporary tracheostomy between the second and third or third and fourth tracheal rings; once selected stay sutures are placed around the tracheal rings either side of the planned incision.
Incise the annular ligament ~ 1/3 (no more than 1⁄2) of the circumference to form the tracheal stoma.
pneumothorax, the difference is the presence/absence
of the glide sign
Normal aerated lungs = A-lines and a Glide sign
Pneumothorax = A-lines and NO glide sign AIS = an increase in numbers of B-lines (>3 B-lines at any one location)
Radiographic evaluation
Radiographic evaluation is indicated in the STABLE respiratory patient only.

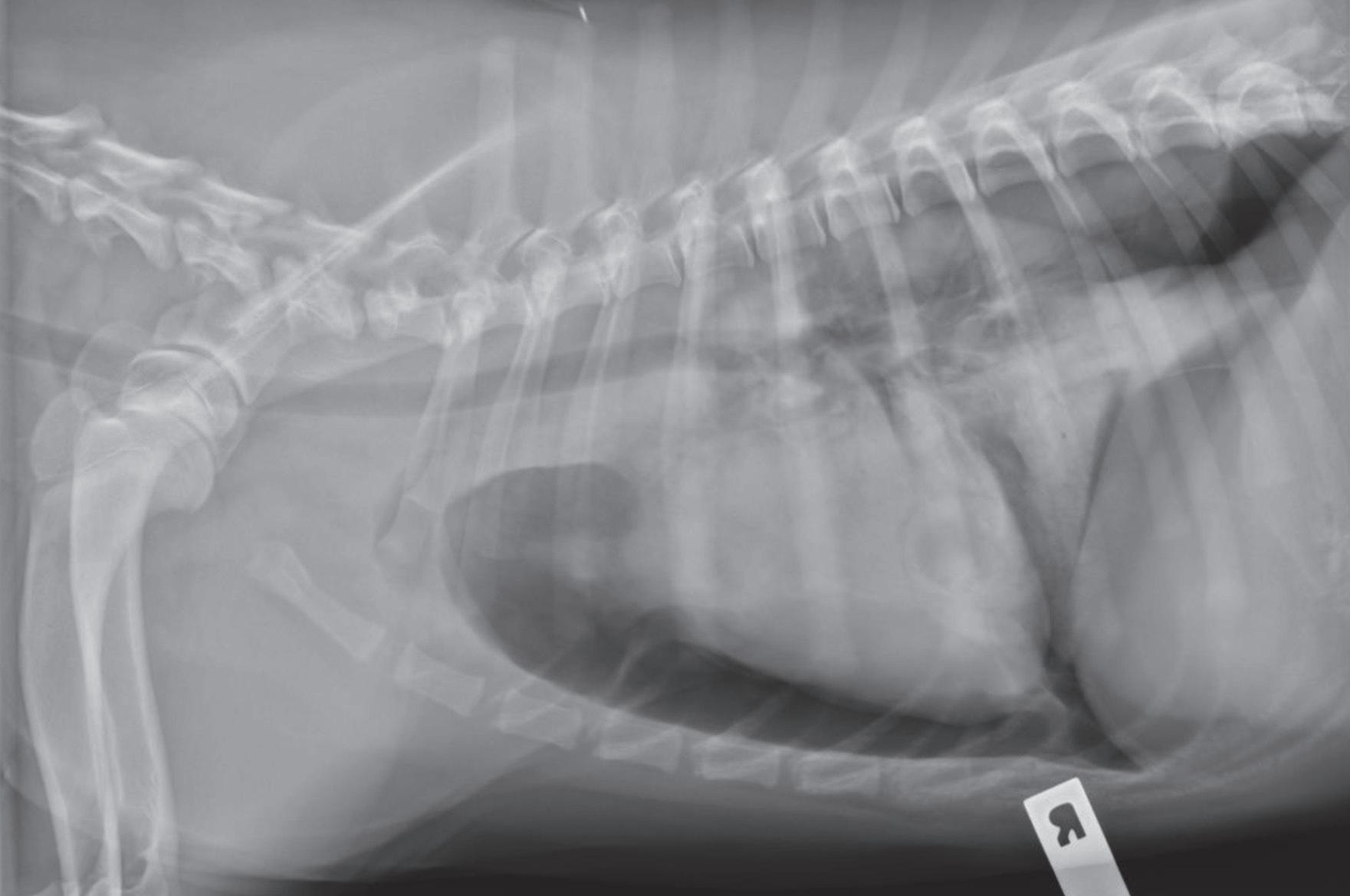

The initial management of the respiratory patient will be performed without the benefits of this diagnostic modality,hence the importance of a thorough clinical examination.
Rushing a respiratory patient to radiology without adequate initial stabilization will ensurea one way trip! Thoracic radiology is used as a confirmatory tool more often than a diagnostic tool.
Figure 3. Left lateral thoracic radiograph of a patient after a saltwater aspiration. This patient has significant alveolar disease in the right cranial and right middle lung lobesTheVeterinarian 27 MAY 2023 ■ www.theveterinarian.com.au
Figure4a and 4b. Right lateral and VD thorax of a patient presented following a motor vehicle accident. These images supportapneumothorax with associated pulmonary consolidation
Clinical Review
SUBSCRIBENOWTOTHE
No.1
AUSTRALIAN VETERINARY
MAGAZINE!
The Veterinarian provides product and industry news, expert columnists, clinical articles, practice management, research updates and nursing information together with lifestyle issues affecting your profession globally.
Send me The Veterinarian magazine by mail everyissue!
Mail POBox 305 Millthorpe NSW 2798

Phone (02) 9487 6627
www.theveterinarian.com.au
One year: $93.50 (incl GST)
Two years: $138.60 (incl GST)
Three years: $182.60 (incl GST)
Overseas rates (all prices Australian dollars)
New Zealand
$105 (AUD) 1 Year
$160 (AUD) 2 Years
$210 (AUD) 3 Years
Rest of the world: $135 (One year)
www.theveterinarian.com.au
Name:.....................................................................................................................................................
Company:...............................................................................................................................................
Address:..................................................................................................................................................
Suburb:..................................................................State:.......................................Postcode:.................
Telephone:.............................................................Fax:..........................................................................

Email:......................................................................................................................................................
Payment of $......................................... by cheque or money order made payable to Sydney Magazine Publishers Pty Ltd

Or please charge my Visa AmexMastercard
Card holder’s number:...........................................................................................................................
Card holder’s name:...............................................................................................................................
Signature:.......................................................................................Expiry Date:....................................
YOU CAN CHANGE YOUR DELIVERY POINT AS OFTEN AS YOU LIKE, HOWEVER NO REFUNDS AVAILABLE.
❏ ❏❏❏ ❏ ❏ ❏ ❏ ❏
Nobivac feline range: flexible vaccination options for cats
Are you looking for a feline vaccine range that aligns with expert guidelines, with flexible protocols to suit your practice?
When it comes to cat vaccination, expert groups such as the World Small Animal Veterinary Association’s (WSAVA) Vaccination Guidelines Group (VGG) agree that nonadjuvanted vaccines should be chosen when possible. Their guidelines state that all efforts should be made to minimise antigen administration while ensuring maximum protection.
WSAVA recommends that cats are vaccinated against feline panleucopaenia virus every three years where possible, with viral respiratory disease antigens being administered annually in most cases.1 Nonetheless, for some practices, an annual F3 vaccination protocol aligns best with client behaviour and staff preference.
The Nobivac Feline (MSD Animal Health Australia) range offers modified live virus (non-adjuvanted) vaccines with unique clinical benefits and flexible protocols to suit every practice.
Nobivac FLEX Tricat
A trivalent feline core vaccine containing feline panleucopaenia (FPV), feline calicivirus (FCV) and feline herpesvirus-1 (FHV-1) antigens. The FPV component is proven to provide 3 years’ protection following the primary course.
Nobivac Ducat
A bivalent feline core vaccine containing FHV-1 and FCV antigens.
Nobivac Feline Range Benefits
Together, the two vaccines allow alignment with WSAVA guidelines when it comes to using nonadjuvanted vaccines, minimising antigen administration and triennial vaccination against FPV.Benefits of the Nobivac Feline range include:
1. Flexibility to use Nobivac FLEX Tricat in either a triennial protocol with Nobivac Ducat in the interim years, or an annual protocol as astand-alone vaccine. These protocol options are illustrated in the tables below.This flexibility means that when following an annual
Water cremation for pets
With local governments banning backyard burials and an average size dog emitting approximately 45kg of CO2 during traditional cremation, greener alternatives, such as water cremation, now offer pet owners a gentler process, with minimal impact on the environment.
Blue Leaf Water Cremation, a WA familyowned and operated business, is offering a
protocol, a single missed vaccine does not jeopardise the feline patient’s immunity to FPV, nor does it negate the associated MSD Vaccine Guarantee for FPV (refer to point 5).
2. The benefits of modified live virus vaccination compared to killed vaccines. These include:
■ The absence of an adjuvant;
■ Ability to overcome maternally derived antibodies in kittens earlier2 and;
■ Rapid immunity with stimulation of both humoral and cell-mediated components, compared to killed vaccines.2
3. Option for early finish of kitten vaccination program. Nobivac FLEX Tricat has been proven to provide immunity after two doses, 4 weeks apart, at 8 weeks and 12 weeks of age.
4. Reduction of shedding of FPV: Nobivac FLEX Tricat is the only feline core vaccine currently available in Australia with a registered label claim for reduction of viral shedding following FPV infection. While FPV is generally of low prevalence in Australia, in recent years a number of outbreaks in areas such as Sydney’s West and Greater Melbourne had devastating effects in shelter populations.3
personal level of service, during a difficult and delicate time. As long-time pet owners, they wanted to offer a gentler and more respectful alternative in pet aftercare: one that was also environmentally friendlier than traditional options.
If you haven’theard of Water Cremation, you are not alone. Though patented 1888, it was only made available to the aftercare industry in 2011. The process has been adopted for both pet and human aftercare, in the US, Canada, UK and South Africa. It made worldwide headlines in 2022, when South African Archbishop Desmond Tutu, was cremated by water.
Water cremation, or alkaline hydrolysis, uses agentle flow of 95 per cent water and 5 per cent alkali, to mimic what would take place in nature, where the body is reduced to its essential elements, leaving behind bones as calcium phosphate, which is prepared and placed into an urn before returning to the family.
For many years, burial and flame cremation have been the most common and traditional animal aftercare options, however, they are far from environmentally friendly. Blue Leaf believes water cremation offers an alternative that;
■ Uses 90 per cent less energy
■ Does not burn fossil fuels
■ Does not emit harmful greenhouse gases
5. A Vaccine Guarantee against FPV infection for up to three years after a primary course or booster with Nobivac FLEX Tricat.
6. All Nobivac vaccines are Australian made in Bendigo, Victoria, benefitting local employment and reducing the carbon footprint when compared to products manufactured overseas.
Talk to your local MSD Animal Health Representative or contact us on 1800 033 461 for a confidential discussion on how we can partner with you for premium patient protection and profitability of your vaccine program.
This article was provided by MSD Animal Health.
1.Day MJ, Horzinek MC et al. WSAVA Guidelines for the Vaccination for Dogs and Cats. Journal of Small Animal Practice (2016); 57(1) E1-E45.
2. O’Brien C. Feline Vaccinations- A Review. The Veterinarian.March 2007; 27-28.
3. Westman M and Malik R. Cat Plague is back after nearly 40 years in Hiding- Here’s What You Need to Know. The Conversation. https://theconversation.com/cat-plagueis-back-after-nearly-40-years-in-hidingheres-what-youneed-to-know-91234
■ Does not release chemicals from animals that have been euthanised and buried
■ Does not contaminate soil with bacteria because of decomposition
■ Remains are 100% clean, sterile, and pathogen-free and can be safely returned to the earth
■ The remaining water is a sterile solution which can nourish soil and support plant growth. For further information, visit www.blueleaf.net.au. This content was provided by Blue Leaf.
TheVeterinarian 29 MAY 2023 ■ www.theveterinarian.com.au BUSINESS
Salmon farming a risk for marine life
From page 1 recommendations designed to transition the industry out of shallow coastal waterways and onto land and/or further offshore.
TISC’s leading water quality expert Christine Coughanowr said Tasmania boasts some of the largest salmon cages in the world but the untreated pollution from a typical farm’s 20 cages is contributing to the algal blooms and oxygen crashes that will also be exacerbated by climate change.
“Inland waters are also affected.
TISC member Lisa Gershwin, a marine biologist and ecologist, said another example of the science missing from the industry’s regulations involved south-eastern Australia’s endemic Burrunan dolphin, (Tursiops australis), a species that is found nowhere else in the world.
“The Tasmanian dolphin likely to bemost affected is now listed as Critically Endangered in Victoria but astonishingly it’s still not officially listed as Tasmanian fauna, and the species receives no special protection here,” Gershwin explained.
Support for the eastern barred bandicoot
From page 5
Much of the ocean’s iron comes from the poop of chinstrap penguins, one of Antarctic’s most abundant penguin species. Results of the study, published recently in Nature Communications, suggest the birds are responsible for supplying about 521 tonnes of iron each year, an amount that is approximately half that produced in the 1980s. The scientists are concerned the sharp decline in penguin numbers over forty years, largely due to climate change, and the subsequent reduction in the iron and nutrient cycle, could be creating a domino effect. This has prompted fears marine ecosystem health, phytoplankton growth and carbon storage may all be under threat.
Lead author of the study, Oleg
Belyaev said drone images of penguin colonies were collected to calculate guano volumes. Chemical analysis found the guano contained very high concentrations of iron, (about three milligrams per gram) suggesting that penguin guano, and potentially that from other penguin species, plays a crucial, and previously unaccounted for, role in iron recycling in the Southern Ocean.
“A deeper understanding of the chinstrap’s - and other penguins’life and prey-consumption cycles, migrations, and breeding-site guano export dynamics, would help improve their conservation status and their impact on iron recycling in the Antarctic marine ecosystem,” Belyaev said.
■ ANNE LAYTON-BENNETTNew arrivals for quoll double breeding program
From page 7 with the five animals they needed as well as translocating an extra 25 animals to our new population at Vulkathunha-Gammon Ranges National Park in the northern Flinders.”
After a visual vet check on arrival, the Chuditch have been released into specialised breeding enclosures within the Taronga Sanctuary in Dubbo. They will undergo a full health check in the coming weeks and then continue to be monitored remotely in the lead up to the breeding season, which commences in May,with birthing expected between May-September.
“These new individuals are showing positive behaviours and settling into their new habitat here in Dubbo,” Chuditch Keeper Morrigan Guinane said.
“As we’re able to provide ideal breeding conditions, we can increase their numbers at a faster rate than would occur in the wild.
“This allows us to return a high number of genetically robust individuals back to the wild in areas where they used to roam far and wide but are no longer found.
“It’s a real honour and a privilege tobe involved and be making a really meaningful contribution towards the conservation of this special native species.”
“Predation by feral cats and foxes continue to pose a significant threat to the survival of many WAnative species including the Chuditch,” Western Shield ecologist
Michelle Drew, from the WA DBCA, said.
“DBCA’s wildlife recovery program Western Shield, now in its 27th year, continues to recover native animals in the wild through fox and feral cat baiting across more than 3.8 million hectares of State Forest and reintroduce native animals to areas where they once existed.
“Western Shield is proud to collaborate with Taronga Western PlainsZoo on this interstate translocation to ensure the Chuditch has the best possible chance to establish new populations and thrive for generations to come.”
Chuditch are large, high order carnivorous marsupials, one of four species of quoll in Australia and related to the Tasmanian Devil. They have a relatively short life span of only three to four years and are generally solitary outside of the breeding season. Chuditch have a short gestation of only 17–18 days and are supernumerary breeders, producing up to 50 foetuses, of which up to six can survive.
The Chuditch breeding facility is located within the 110ha Taronga Sanctuary at Taronga Western Plains Zoo, Dubbo. Taronga is extremely grateful to The Kinghorn Foundation for making this species-saving conservation breeding program possible.
For moreinformation visit www.taronga.org.au/dubbo.
She said noise was a major factor for both dolphins and seals, but salmon farming had transformed previously quiet bays into permanently noisy industrial sites. It is an environment that creates serious health issues for marine mammals where echolocation is a crucial aspect of their lives, from finding food to social cohesion.
“Plan B recommends an immediate pause in expansion to let the science and regulation catch up so a major rethink of the fundamental principles of how and where salmon is farmed can be undertaken,” he said.
When it was first announced in
2021 former Primary Industries Minister Guy Barnett said the new plan would be guided by four guiding principles: no net increase in leased farming areas in Tasmanian waters; future growth to lie in landbased and offshore salmon farming; world-best practice through continuous improvement; and strict independent regulation.
■ ANNE LAYTON-BENNETT‘Plan B: An alter native vision for salmon aquaculture in Tasmania’ is available at site bp79amrv.dotezcdn.com/ uploads/397ef5f921854efca03a403e9 63c8672.pdf
Abstracts - Tasmanian devils
From page 15
2Wellcome Sanger Institute, Wellcome Genome Campus, Hinxton, Cambridge, UK.
3European Molecular Biology Laboratory, European Bioinformatics Institute, Wellcome Genome Campus, Hinxton, Cambridge, UK.
4School of Life and Environmental Sciences, University of Sydney, Sydney, NSW, Australia.
5School of Natural Sciences, University of Tasmania, Hobart, TAS, Australia.
6Vertebrate Pest Research Unit, NSW Department of Primary Industries, Orange, NSW,Australia.
7deCODE Genetics Inc., Reykjavik, Iceland.
8Save the Tasmanian Devil Program, Tasmanian Department of Natural Resources and Environment, Hobart, TAS, Australia.
9Toledo Zoo, Toledo, OH, USA.
10CANCEV,Centre de Recherches Ecologiques et Evolutives sur le Cancer,Montpellier,France.
11Menzies Institute for Medical Research, University of Tasmania, Hobart, TAS, Australia
12Mount Pleasant Laboratories, Tasmanian Department of Natural Resources and Environment, Prospect, TAS, Australia
Abstracts - Euthanasia of dogs
From page 15
Clinical relevance: Providing veterinarians with additional training on adapting their euthanasia protocols to different clinical scenarios may improve the experience for patients, owners, and veterinary staff.
MC Gates1,N J Kells1,K K Kongara1,K E Littlewood1
NZ Vet J.2023 Mar 22; 1-28.doi: 10.1080/00480169.2023.2194687.
1Tawharau Ora - School of Veterinar y Science, Massey University, Palmerston North, New Zealand.
TheVeterinarian
Sydney Magazine Publishers Pty Ltd
ACN 102752787 ISSN 1447-9768
PO Box 305 Millthorpe NSW 2798
Tel: 02 9487 6627
Director - Clem Martin
Email: clem.martin@vetmag.com.au
Editorial Advisory Board
Thomas Donnelly BVSc DipVP
DipACLAM
Nicholas Kannegieter BVSc
DipVetClinStud PhD FACVSc
David Lidbetter BVSc MVS FACVSc
DipECVS Dip ACVS
Angus Martin BVSc
Mary Porter BVSc (Hons) MACVSc
Jeffrey Smith BVSc FACVSc Dip ACVO
David Vella BSc BVSc (Hons) DABVP
Editor - Luke Martin
Tel: 0418 698 228
Email: luke.martin@vetmag.com.au
National Sales Manager
James Martin
Tel: 0432 575 877
Email: james.martin@vetmag.com.au
Designer - Anne Norrell
Email: annenorrelldesign@gmail.com
Printed by Newstyle Printing
41 Manchester St, Mile End SA 5031
Post Print Approved PP255003/06488
All material in The Veterinarian is subject to copyright and must not be reproduced wholly or in part without the written permission of the Editor. Views expressed in The Veterinarian are not necessarily those of The Veterinarian orSydney Magazine Publishers Pty Ltd.
Subscriptions - Clem Martin
Tel: 02 9487 6627
Email: clem.martin@vetmag.com.au
SUBSCRIBE NOW!
Mail POBox 305 Millthorpe NSW 2798
Phone (02) 9487 6627
www.theveterinarian.com.au
Subscriptions
Australia
$93.50 for 1 Year
$138.60 for 2 Years
$182.60 for 3 Years
New Zealand
$105 (AUD) 1 Year
$160 (AUD) 2 Years
$210 (AUD) 3 Years
USA/Canada (airmail) $135
UK/Europe
TheVeterinarian MAY 2023 30 ■ www.theveterinarian.com.au
rates arequoted in Australian dollars News
(airmail) $135 *All
CREATURE Feature
The largest extant species of guineafowl, this species is found in northeast Africa. It lives primarily on seeds and small invertebrates, is terrestrial, and will run – rather than fly – when alarmed.
Vulturine guineafowl (Acryllium vulturinum) Picture Manfred Werner


Just one dose Spread the word! Neptra can be used first-line for everyday otitis externa cases. Convenience and compliance – just got easier. Best clinical practice is to identify causative organism by cytology or culture and sensitivity before, or as soon as possible after treatment is commenced. For single application treatment of otitis externa in dogs associated with susceptible strains of yeast (Malassezia pachydermatis) and bacteria (S. pseudintermedius, S. canis, E. coli and Proteus spp). © 2021 Elanco or its affiliates. Elanco Australasia Pty Ltd (ABN 64 076 745 198), Level 3, 7 Eden Park Drive, Macquarie Park NSW 2113. All trade marks are the property of their respective owners. For further information contact: 1800 678 368 from anywhere in Australia Monday to Friday or email enquiries_au@elancoah.com. ELAN0146 11/21. PM-AU-21-0854.