AUGUST 2024 – JULY 2025
+ incorporating the OTC products guide
AUGUST 2024 – JULY 2025
+ incorporating the OTC products guide


A broad spectrum first aid cream with no known bacterial resistance, 1 unlike topical antibiotics.
MAKE CRYSTADERM® THE FIRST CHOICE FOR FIRST AID
Unique Hydrogen Peroxide cream formula – a little goes a long way!
Preservative free
Treats and prevents minor skin infections such as cuts, scrapes, burns and school sores
Effectively treats mild to moderate acne by killing acne-causing bacteria
Keeps killing bacteria no matter how often it’s used2

Reference: 1. Lipsky, B. A., and Hoey, C., Topical Antimicrobial Therapy for Treating Chronic Wounds, 2009, 49:1541–1549. 2. AFT Pharmaceuticals Ltd. (2015) “Microbiological Efficacy on Crystaderm®” (unpublished - data on file). 2. Lipsky, B. A., and
C., Topical Antimicrobial Therapy for Treating Chronic Wounds, 2009, 49:1541-1549. Crystaderm® First Aid Cream (Hydrogen Peroxide 1% w/w, 10g) is for the treatment and prevention of minor skin infections such as acne, cuts, scrapes, burns or school sores. Please refer to the Product Packaging for information on precautions, Contra-indications, Adverse events, Interactions and Dosage. AFT Pharmaceuticals, Auckland. TAPS PP8881.
AUGUST 2024 – JULY 2025
PUBLISHER
The Health Media
TECHNICAL EDITOR
Carmen Pope BPharm, PG.Dip.Clin.Pharm, PG.Cert.Psych.Pharm, RegPharmNZ, MPS
EDITOR, PHARMACY TODAY KAITIAKI RONGOA O TE WA
Jonathan Chilton-Towle
ADVISORY PANEL
Carmen Pope BPharm, PG.Dip.Clin.Pharm, PG.Cert.Psych.Pharm, RegPharmNZ, MPS
Phil Rasmusen MPharm, MPS, Dip.Herb.Med, MNIMH, MNHAA, MNZAMH
DESIGN / PRODUCTION
Annabelle Wong
Doreen Yandall
Tao Jiang
PRODUCTION MANAGER
Annabelle Wong
SUBSCRIPTIONS
Fiona Hewitt
2024-2025 Healthcare Handbook is published in association with Pharmacy Today Kaitiaki Rongoa o Te Wa. Online access is distributed free per full-priced Pharmacy Today subscription. For advertising queries contact Annabelle Wong: Phone: 09-488 4286 Email: awong@thehealthmedia.co.nz
The Health Media Ltd Phone: 09-488 4286
Email: enquiries@thehealthmedia.co.nz Website: www.pharmacytoday.co.nz
ISSN 1176-2241
some love with a to Pharmacy Today Kaitiaki o te Wā Group Subscription
New Zealand’s best-loved source of independent news, opinion and education for the pharmacy sector.
What’s in it for your pharmacy team?
• Award-winning journalists with an eye on what matters.
• Timely clinical content including Everybody Patient Sheets and the Healthcare Handbook.
• News editorials and education including the CLASS professional development suite.
With a personal account manager, we make it easy with set-up in minutes.
Show your team you care by opening up the world of Pharmacy Today.
To find out more visit pharmacytoday.co.nz or contact Subscriptions Manager: Fiona Hewitt M 027 404 4054 E fhewitt@thehealthmedia.co.nz
Every month in print, every day online


Welcome to the Healthcare Handbook 2024-2025, which is aimed at pharmacy technicians, pharmacy assistants, retail assistants, and intern pharmacists. It also provides a way for pharmacists to quickly refresh their knowledge about common medical conditions and their treatments.
The Healthcare Handbook should be read in conjunction with the Healthcare Handbook Education articles that feature in Pharmacy Today. These focus on one chapter each month and go into more depth about symptoms, causes, treatment options, and advice. The Healthcare Handbook Education article quiz has moved online to pharmacytoday.co.nz and has become an informal way for readers to check their understanding of topics covered in the magazine.
CAPTURE is a tool developed by Pharmacy Today to help online subscribers keep track of their favourite articles and to help pharmacists keep a record of their reading and learning as they work towards their requirements under the Pharmacy Council’s recertification framework.
At the end of each article there is a CAPTURE button which records your visit to the article and gives you the opportunity to write notes. This is saved to your personal account and the CAPTURE record can be downloaded at a later time and uploaded to MyRecert if necessary.
CLASS is Pharmacy Today’s new suite of educational activities that allow pharmacists to build on their professional knowledge and improve their practice. CLASS activities are accessed from the banner on Pharmacy Today’s home page, and for each CLASS topic there are three elements you can choose to complete:
• CLASStime
• CLASSact
• CLASSmates.
CLASStime is how you keep up to date, by reading, watching, or listening to CLASStime content. Once you have finished reading the article, you can CAPTURE it for your record of learning. CLASSact means assessing your knowledge by completing the CLASSact worksheet and reflecting on it.
CLASSmates refers to sharing your newfound knowledge with your profesional peers, and implementing it in your practice. Files recorded during CLASS can be uploaded to MyRecert as evidence of action.







Each common condition includes:
• Key points
• Your customer
• Refer to a pharmacist
• Treatment options
• Need to know
• Customer advice




they do, then you should refer the customer to a pharmacist.



The front section of this handbook gives an overview of 76 of the most common conditions customers seek advice about from a pharmacy.
These conditions are presented in alphabetical order and are usually in a twopage format (see above).
These give a brief overview of the topic or a quick summary of the most important aspects of that topic.
When talking to a customer about a condition, it is important to be observant and not to bombard them with too many questions, especially if the answers are obvious. The “Your customer” paragraph for each condition offers guidance about how to approach a customer or what specific symptoms to look for. A full explanation about how to conduct an initial assessment is given on page 8.
You should ask questions to determine if any of the bullet points in the Refer to a pharmacist text box apply to your customer. If
The Treatment paragraph explains how the condition is usually treated and the Treatment Options Table lists most of the currently available products for that condition. Products with an asterisk have abridged, but more detailed, product information in the OTC Products section (see left, for an example).
This section provides general information about each condition, including a description of the actual condition, and possible causes, risk factors, and symptoms if appropriate.
Knowing some basic information about each condition can help you engage with your customer better.
This provides some helpful, usually nonpharmacological advice, that you can give your customers regarding their condition, or the treatment of their condition.
Every day, complete strangers walk into a pharmacy to purchase products off the shelf. While many happily self-select what they need, pay for it, and then leave, often without discussing their purchase with anybody, as a staff member working on the shop floor there are times when it may be in your customer’s best interest that you intervene, or at least offer some advice about their purchase.
But deciding who does and who doesn’t need extra assistance and advice can be a challenge. In addition, some customers quickly brush aside all offers of help, although the time of purchase always allows another opportunity to try to engage with them. Try to always remain friendly and open, instead of “Can I help you?”, tailor your approach to what they are looking for, for example “Would you like me to explain what each ingredient does in this cough medicine”, or “Would you be interested in some more information about head lice”.
An initial visual assessment can tell you a lot about a person and provide a good basis for asking a few questions, but always be mindful that it is your own subjective opinion and you need to be careful not to come across as judgemental or offensive in your questioning.
When somebody approaches you in the pharmacy, or if you see somebody looking at medicines on the shelf, have a guess at their approximate age, take note of their body shape and stature, mood, and overall look and involve yourself in their purchase if you have any concerns. The heading Your customer within each chapter offers some pointers about approaching customers or key symptoms to look for, for that particular topic. Frame your questions tactfully. Instead of jumping in with “You look pregnant. Are you?”, ask instead “Is there a possibility you could be pregnant?”.
As a rule, any purchases for infants under the age of two should be referred to a pharmacist. Many products are not recommended for babies, and babies are often more susceptible to the side effects of medicines, so even if the parent has self-selected a product for their child, ask if they are happy for you to check with the pharmacist for suitability.
Older people are more likely to have reduced kidney function, other health conditions, and be on other medications. Side effects are therefore more likely with medicines such as non-steroidal
anti-inflammatory drugs (eg, ibuprofen, aspirin) and sedating antihistamines, and a pharmacist’s involvement is necessary.
People who carry excess weight are at higher risk of cancer, heart disease, high blood pressure, high cholesterol, gout, reproductive problems, sleep apnoea, type 2 diabetes, and osteoarthritis.
Overeating is best viewed as an addiction, and it can be very difficult for some people to lose weight, so ensure you are empathetic in your approach without being condescending. Some pain-relieving medications, cough and cold remedies, and motion sickness treatments may not be suitable with some of the conditions listed above.
A person’s posture may give some clues as to what other underlying medical conditions they may have. For example, osteoporosis is the most likely cause of a stooped posture in elderly people, pain may be a reason younger people appear doubled over. A shuffling or slowness of movement may be caused by conditions such as Parkinson’s disease; involuntary movements of the tongue may reflect a side-effect of antipsychotics.
We all feel anxious or a bit down at times, but, while we readily admit to having a cold or the flu, most of us tend to hide our times of emotional fragility. Recognising a low mood in a customer and sensitively asking “Are you under any stress at the moment?”, or “You don’t seem your normal self today”, shows compassion, and you may well be the only person who has reached out to them that day. Listen to what they have to say, and talk with a pharmacist if you have any serious concerns about their mental health.
Most people who look unwell, are unwell, and this can provide a lead-in to ask about their health, particularly if your customer is a regular who usually appears healthy. Take note of the colour and condition of somebody’s skin. A grey or a blue tinge suggests a lack of oxygenated blood that could be caused by a breathing problem, cancer or late-stage disease such as heart failure or kidney failure. A yellowish discolouration (jaundice) may indicate a
This infographic summarises key features to note during an initial assessment
Always invite your customer to talk in a private area of the pharmacy
problem with the liver or with bile flow. In newborns, jaundice is relatively common and usually improves with phototherapy. Very pale skin or mucous membranes could signal anaemia. Be careful not to assume your customer has a specific underlying condition, because it may just be their natural colouring. However, you could ask if they have any underlying health issues that may impact on what products they buy. Be observant for any skin rashes or significant blemishes. Seniors and people with fair skin are prone to skin cancers, such as basal or squamous cell carcinomas, and melanoma. Most skin cancers can be successfully treated if found early, and with regular customers you may like to point out any blemishes of concern and ask if they have seen a doctor about them. Many creams and topical products sold over the counter may irritate some people’s skin, particularly those with eczema, allergies, or psoriasis so refer people with sensitive skin to a pharmacist.
Once you have conducted your initial assessment, you need to make a decision about whether to refer the customer to a pharmacist or sell them a product yourself. ALWAYS refer customers to the pharmacist in the following situations:
• the customer asks to talk to a pharmacist
• the customer requires a pharmacist only product (eg, for vaginal thrush)
• the customer has had no success with other treatment products
• the customer has other medical conditions or takes other medicines
• the customer is particularly unwell
• the customer is pregnant or breastfeeding
• the medicine sought is for an infant or an elderly person
• there are symptoms of concern
• you have concerns about the customer’s behaviour or intentions.
• Condition of hair and scalp: dandruff, dermatitis, hair loss, itching, oiliness.
• Ears: discharge, hearing loss, pain.
• Eyes: discharge, itchiness, pain, presence of contact lenses, reactivity to light, redness.
• Face: acne, cold sores, dermatitis, facial droop, shingles-like rash (typically occurs around one eye).
• Mouth and throat: difficulty swallowing, enlargement of the thyroid gland, lesions, odour, pain, presence of dentures, sore neck, swelling, thrush on tongue.
• Nose: congestion, difficulty breathing, discharge, sneezing.
• General: confusion, dizziness, headache, sedation.
• Colour: blue-grey, flushed, jaundiced (yellow), pale.
• Quality: calloused, numerous veins, paper-thin, rough, sundamaged.
• Temperature: clammy, cold, hot, sweaty.
• Wounds and lesions: discharge, infection, state of healing, swelling, tenderness.
• General: bruising, irritated, itchy, moisture content, rash.
• Breathing: heavy, noisy, shallow, wheezing.
• Mood: anxious, depressed, friendly, reserved, stand-offish, suspicious, tired.
• Movement: difficult, limping, painful, shaking, shuffling, uncoordinated.
• Posture: clutching abdomen, curvature of spine, deformities, stooped.
• Size: frail, overweight, pregnant, underweight.
• General: smells of cigarette smoke or alcohol.

Building a rapport with your customers is one of the most important things you can do for the pharmacy you work for. Customers are more likely to come back if they feel listened to, valued, and if you give good advice. In some circumstances, foregoing a sale in favour of referring somebody to a doctor or other health professional is more likely to result in repeat business from that customer than just selling them something for the sake of it.
Make sure you are well presented before you even walk on the shop floor. Pharmacies are viewed by the public as professional businesses, so it is important that your own personal grooming reflects this. Hair, nails and make-up (if worn) should be neat; and uniforms, clean, and ironed. Keep your body language open and friendly and greet all customers with a smile.
Pharmacy staff are expected to have good product knowledge and be able to explain key differences between a wide range of products that look and sound the same and are used for a similar purpose. Consider
enrolling in a pharmacy assistant or technician training programme to gain this knowledge in a structured way or use this handbook and online resources to educate yourself about the most common ingredients used in over-the-counter products. Determine which ingredients are used for particular symptoms; for example, phenylephrine and oxymetazoline relieve nasal congestion, and some herbal products are good for a dry cough. This saves you from having to remember confusing brand names and allows you to pick up any product box and read and explain the ingredients off the label.
Once you have conducted your initial visual assessment (see previous page) use the information you have gained and your product knowledge to select the best product for that particular customer. If at any time you feel unsure about your advice or out of your depth, refer the customer to a pharmacist or senior staff member, whoever is the most appropriate.
When you have chosen a product for your customer, or if a customer has self-
selected an appropriate product, cover the following points:
• discuss the DOSE, FREQUENCY OF ADMINISTRATION, and HOW LONG each product should be used
• reiterate the NAME of the product and mention OTHER NAMES that the product may be called to avoid therapy duplication
• offer ADVICE (refer to the “Advice for customers” section for each condition)
• encourage FOLLOW-UP, and advise customers to return, or seek medical advice if the problem persists for more than a few days, despite treatment
• suggest customers TELL THEIR DOCTOR, or any other pharmacy they visit, that they are using this product so as to avoid possible interactions or duplications
• THANK the customer for their purchase and finish off the sale with a smile! Lastly, confidentiality is another key aspect of pharmacy, and one that customers expect you to uphold. Never discuss specific sales, conversations, or medication histories with other people outside of your pharmacy. Act respectfully when told sensitive information and do not judge.
This publication is not intended to provide definitive product advice. For further product details of prescription and most OTC products refer to www.medsafe.govt.nz or contact the company that manufactures the product.

New Zealand is unique in the way that it classifies medicines. Overseas, medicines tend to be either available through a doctor on prescription and dispensed in a pharmacy or available unrestricted, through a general retail outlet, supermarket, or gas station.
New Zealand has four broad categories of medicine classifications:
• [GENERAL SALE] can be sold through other retail outlets not just pharmacies
• [PHARMACY ONLY MEDICINE] only available in pharmacies
• [PHARMACIST ONLY MEDICINE] can only be sold by a pharmacist
• [PRESCRIPTION MEDICINE] only available on a doctor’s prescription but dispensed by a pharmacist.
Medicine classifications can change after the Healthcare Handbook goes to print, so it is important you are alert to updates circulated by the Medicines Classification Committee regarding classification changes. The current classification of any medicine can be found on the Medsafe website at medsafe.govt.nz/profs/class/classintro.asp
Alternatively go to medsafe.govt.nz and click on the medicines tab and choose
classification. Click on classification database and enter the generic name of the medicine whose classification you wish to check in the search box provided.
Be mindful of certain products that may be a challenge to administer to specific populations; for example, eye drops in the very old; liquid medicines for an uncooperative toddler; nit combs on very curly, thick hair.
People with limited mobility or arthritis may have difficulty opening foil packaging or correctly applying fungal nail products. Seek advice from your pharmacist or more experienced staff members about ways people can overcome these difficulties.
Complementary therapies have been included in many treatment options tables, in the row headed “Natural/ herbal products/ supplements”.
In most instances, only those with evidence for an effect as cited by a reputable natural medicines database have been included.
The Healthcare Handbook also includes general information on a few common medical conditions, such as asthma, diabetes, and gout. Although most of the medicines prescribed for these conditions are only available on a prescription, customers with these conditions may request OTC products for other conditions from time to time.
Always involve a pharmacist in any discussion about OTC product use in people with chronic conditions, such as arthritis, asthma, blood pressure, cancer, depression, glaucoma, gout, heart disease, osteoporosis and pain.
The Ministry of Health also provides free pamphlets, stickers, and posters covering a wide range of topics (eg, head lice, HPV vaccination) for consumers. These are available online from healthed.govt.nz



• Mostly caused by hormone fluctuations, most commonly during puberty.
• Treatment success relies on regular skin cleansing and product application.
• Over-the-counter products are only effective for treating mild-to-moderate acne.
• Untreated or undertreated severe acne may lead to permanent skin discolouration and scarring.
Look at the person’s face and decide if their acne looks mild, moderate or severe. Ask if they have it elsewhere, such as their back or shoulders, and how it impacts on their day-to-day life. Severe acne with big or angry-looking nodules does not really respond to over-the-counter treatments and you should refer these customers to a doctor.
Mild-to-moderate acne usually responds to a good cleansing routine and topical anti-acne products. Without proper treatment, severe acne can lead to skin discolouration and permanent scarring.
Over-the-counter treatment is effective for mild to slightly moderate acne, but refer teenagers and adults with more severe acne to a doctor or dermatologist for stronger treatments such as oral antibiotics, hormonal contraceptives, and retinoids. There are also various laser and light therapy treatments available.
Effective early treatment will reduce the risk of acne permanently scarring the face.
Anti-acne products should be applied to skin that has been gently cleansed, not scrubbed raw. The aim is to wash away excess sebum and dead skin cells, not to irritate the skin further. A mild
Category
Soap-free face washes [GENERAL SALE] eg, AZClear Action, Benzac AC Wash, DermaLab range
Keratolytic + antibacterial action
Antibacterial, anti-inflammatory or keratolytic action
[GENERAL SALE] Contains benzoyl or hydrogen peroxide eg, Benzac AC range, Crystaderm cream* Contains salicylic acid eg, Clean & Clear
[GENERAL SALE] IDP eg, Epiology Superoxidised solutions eg, Gramaderm Antiacne Hydrogel [PHARMACY ONLY] Contains azaleic acid eg, AZClear Action, Skinoren
Other [GENERAL SALE] eg, Mebo Acne, glycolic acid, kawakawa, manuka, tea tree, totarol, willowherb, zinc
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• Younger than 12 or older than 30.
• Taking medicines or supplements known to exacerbate acne.
• Previous acne treatments used for at least three months have been unsuccessful.
• Atypical features (some other skin conditions may appear similar to acne but
soap-free or specific anti-acne wash should be used twice a day, every day. Teenagers and adults who play a lot of sport or work in a greasy or humid environment should also be advised to wash their skin as soon as they finish training or work.
Tell your customers that acne products don’t work magically overnight. It will likely take six to eight weeks of twice-daily skin cleansing and product application before a real change in the skin is noticed, although some differences should be seen within a week or two. Even after the acne has cleared, it is important to maintain the same skin regimen, otherwise the acne will come back.
Benzoyl peroxide (BPO) has historically been the preferred treatment for mild acne but it can cause irritation and skin peeling initially and newer ingredients may be preferred. BPO is antibacterial, anti-inflammatory, and anticomedogenic (prevents pimple formation) and accumulates in the sebaceous ducts because it is fat soluble, making it highly effective. Research has shown 2.5% BPO is just as effective as 5% or 10% BPO, with fewer side effects. Advise customers to avoid excessive sunlight which can exacerbate irritation.
need different treatment).
• Extensive, moderately-severe or severe acne.
• Unable to avoid exposure to acneexacerbating substances (such as car mechanics exposed to motor oil).
• Women with excessive facial hair, irregular periods or prone to weight gain.
• People with sensitive skin or allergies to topical products.
Stabilised hydrogen peroxide (HP) contains a stabilising ingredient which means that it lacks the tissue-destroying properties unstabilised hydrogen peroxide is renowned for. It works in a similar way to BPO and research has found it just as effective but with fewer side effects.
Azelaic acid is a naturally occurring acid found in grains such as barley, wheat, and rye that has antibacterial, keratolytic, comedolytic, and anti-inflammatory effects. Trials have compared azelaic acid to BPO, retinoids, and antibiotics and found similar efficacy with generally less redness, peeling, and irritation. It may also improve uneven skin tone
Salicylic acid is an effective keratolytic and is usually found in combination with other ingredients in a wide range of anti-acne products. Skin peeling is a common side effect.
Superoxidised solutions (SOS) are made by passing an electric current through a solution of salt and water. This produces charged hydrogen, oxygen, and chlorine particles which undergo chemical reactions with proteins and molecules, destroying the cell walls of bacteria and interfering with other cellular processes. A small trial showed it was more effective at
Face washes degrease the skin and help to reduce skin bacteria. Use at least twice daily before applying treatment products for best effect. Some products contain cetrimide or chlorhexidine for their antibacterial action. Others include benzoyl peroxide or salicyclic acid for their keratolytic effect.
Dryness and skin peeling common. Some reddening, dryness, and worsening of acne may occur initially. Discontinue use if skin becomes too inflamed or sore. Some improvement may be seen in five days but may take several weeks or months to have the maximum effect. HP or 2.5% BPO is as effective as 5-10% BPO with fewer side effects. Peroxides can bleach clothing, bedding and, rarely, hair and eyebrows.
IPD are naturally occurring milk proteins with antibacterial and anti-inflammatory properties. Superoxidised solutions are considered a safe, effective alternative to antibiotics and hydrogen peroxide. Apply azaleic acid products to the entire affected area twice daily and rub in well. Avoid contact with the eyes as products will sting. Make-up can be applied over the application. If irritation occurs reduce frequency of application until the skin settles. May improve uneven skin tone. Research shows is as effective as BPO, antibiotics, and retinoids with less redness, peeling, and irritation.
Mebo contains cactus extracts and other ingredients to help fight bacteria and stimulate the natural regrowth of skin tissue. Glycolic acid peels can help remove comedones after two to three treatments. Kawakawa, tea tree, manuka, totarol, zinc and other herbs and supplements may reduce acne.
improving inflammatory lesions in people with acne compared with BPO.
Immune Defence Proteins (IDP) are naturally occurring milk proteins that have antimicrobial and anti-inflammatory properties that help reduce acne and redness.
Phycosaccharide ACP is a marine sugar compound that is combined with zinc and has anti-inflammatory, antibacterial, and sebum regulating properties.
Glycolic acid is a naturally occurring alpha hydroxy acid found in fruits, sugar cane, and milk. It is present in many cosmetics, and glycolic acid face peels can help remove comedones after two or three treatments.
Between peels, low concentrations of glycolic acid in a facial cleanser can help prevent acne from returning.
Acne is mostly caused by hormone fluctuations, most commonly those that occur during puberty, which is why it is more prevalent in those aged 12 to 18, affecting up to 80% of adolescents.
Androgens are the main hormones responsible. Even though we refer to oestrogen as the female hormone and testosterone as the male hormone,
this is not entirely correct as females and males have both oestrogen and testosterone in their bodies, as well as other hormones, just in different amounts.
During puberty, the pituitary gland increases its release of two gonadotrophins: follicle stimulating hormone (FSH) and luteinising hormones (LH). FSH and LH act on the gonads (the ovaries in girls and the testes in boys) to produce the sex hormones, oestrogen in females and testosterone in males. The ovaries also produce small amounts of androgens, androstenedione and testosterone, and excess testosterone in males is converted by a process called aromatisation to a type of oestrogen called oestradiol. Oestradiol in males determines bone growth during puberty, epiphyseal closure (growth plate fusion), harmonic skeletal proportions, and bone mass, in addition to modulating libido, erectile function and spermatogenesis in adult men.
The pituitary gland also releases adrenocorticotropic hormone (ACTH) which regulates cortisol and androgen production in both males and females from the adrenal glands – these are small glands located above each kidney. The main androgens released by the adrenal cortex (the outer part of the adrenal gland) are called androstenedione and DHEA (dehydroepiandrosterone).
Androgens are the main regulators of sebaceous
• Wash the face and neck area gently with a mild acne cleansing lotion twice a day.
• Apply a thin smear of treatment product to the whole area of affected skin, not just to individual spots or pimples.
• Some treatments may cause dryness, particularly in the first month of use. Apply an oil-free moisturiser between treatments if the skin is obviously peeling.
gland function. Sebaceous glands are microscopic glands within the skin that open into a hair follicle. They secrete an oily substance called sebum into the sebaceous duct where the hair follicle sits, to lubricate our hair and skin. These glands have receptors for androgens on their surface, which means production of sebum is increased when levels of androgens increase.
Acne is the result of a cascade of processes, that occur in response to increased androgen levels, as follows:
• an increase in the production of sebum by the sebaceous glands
• skin cells block the hair follicle because of the increased sebum and extra skin cell shedding
• overgrowth of naturally occurring bacteria Propionibacterium acnes within the blocked follicles
• inflammation of the follicles because of P. acnes overgrowth.
Clogged pores become blackheads or pimples. If bacteria are also present, redness and swelling can occur, resulting in the progression of the pimple into a papule (solid lumps less than 1cm), pustules (elevated lesions that contain pus), or nodules (solid, painful lumps bigger than 1cm).
• Use sunscreens that are non-acnegenic and, if using foundation, choose an oil-free one specific for acne-prone skin and apply it lightly. Apply sunscreen before going outside.
• Do not pick or squeeze acne because this can cause scarring.
• High-glycaemic diets and dairy may exacerbate acne. Low-glycaemic, low-dairy diets that contain plenty of vegetables may improve acne. Avoid protein or amino acid supplements, particularly if they contain leucine.
• An allergic reaction is the result of the immune system mistaking a normally harmless substance for a dangerous invader.
• An allergy is a chronic condition where a person’s immune system regularly reacts to an allergen.
• An allergen is the name given to a substance that has the potential to cause an allergic reaction.
• Symptoms depend on how the allergen entered the body and how the immune system reacts.
• Antihistamines are effective for most mild-tomoderate allergic reactions.
• Anaphylaxis is a medical emergency requiring adrenaline and urgent professional care.
Symptoms of an allergic reaction vary depending on how reactive an individual’s immune system is to that allergen and how the allergen entered the body. For example, a mosquito bite on the skin may cause a minor red bump in some people or significant redness and swelling in another.
Ask your cutomer to describe their symptoms and what they suspect was the cause.
Airborne allergens (such as pollen) can cause sneezing, a blocked and runny nose, a tickly throat and itchy eyes (see also Hay Fever).
Food or medication allergies may cause facial swelling, mouth tingling or itching, abdominal pain, hives or welts on the skin (see also Urticaria), wheezing, or anaphylaxis.
Insect bites or stings (see also Bites and Stings) may cause a large area of swelling at the sting site, a body-wide rash or itching, cough or wheezing, or anaphylaxis.
Cellulitis is a potential complication of insect bites, and symptoms include redness, swelling, and inflammation around the bite area. Refer anyone with suspected cellulitis or a severe allergic reaction to a doctor.
Adrenaline [PHARMACIST ONLY] eg, adrenaline auto-injector device (EpiPen Adult, EpiPen Junior)
Oral antihistamines [PHARMACY ONLY MEDICINE]
• People with other health conditions, immunosuppressed, or pregnant/ breastfeeding.
• Younger than 12 or older than 65.
• Previous treatments are not effective.
• Taking supplements that may exacerbate allergy symptoms (eg, chamomile).
Non-sedating
• Requesting an adrenaline injector.
• With symptoms of cellulitis.
• With a history of serious symptoms, such as shortness of breath, facial swelling, or an extensive rash. Ring 111 if serious symptoms are currently present.
• With allergies to medicines.
Bilastine Rapid onset, long-lasting, low risk of drug interactions, may be used in kidney disease
Cetirizine May cause drowsiness in susceptible individuals
Desloratadine Less potent than some other antihistamines. Long duration of action. Rarely causes drowsiness
Fexofenadine
Levocetirizine
One of the most potent. Relatively short duration of action. Higher potential for interactions
One of the most potent. Also relieves nasal congestion May cause drowsiness in susceptible individuals (but less than cetirizine)
Loratadine Slower onset of action (requires metabolism to be active)
Sedating
Dexchlorpheniramine
Promethazine
First-generation antihistamines, potent. Discourage use except if sleep wanted May cause sedation, fatigue, and impaired concentration. Pharmacist only.
Treatment of the allergy depends on the cause and the person’s response.
Antihistamines stabilise histamine receptors in their inactive state and are considered the treatment of choice for mild-to-moderate reactions (see the table above for a comparison of different antihistamines).
Decongestants reduce congestion and swelling in the nasal passages but should not be used for longer than three days.
Antihistamine or corticosteroid skin creams can be used if only a small area of skin has been bitten or stung; otherwise oral antihistamines are preferred. Some people with moderateto-severe allergic reactions may require oral corticosteroids prescribed by a doctor.
Immunotherapy (also called desensitisation
Non-sedating, eg, bilastine (Labixten), cetirizine (Razene), desloratadine (Aerius), fexofenadine (Fexofast), levocetirizine (Levrix), loratadine (Loraclear) [PHARMACIST ONLY] Sedating, eg, dexchlorpheniramine (Polaramine), promethazine (Phenergan)
Oral combination products [PHARMACY ONLY MEDICINE] eg, phenylephrine + loratadine (Maxiclear Cold & Nasal Relief/Hayfever & Sinus Relief*)
or hyposensitisation) may be considered in people with allergies to food, insects, or with multiple allergies. It involves the administration of gradually increasing amounts of an allergen over a long period of time (up to five years in some cases) which stimulates the immune system to develop a resistance to that allergen. The best management for allergies is to avoid the allergen if possible. In some people, oral antihistamines taken before a known exposure to an antigen can reduce symptoms.
An allergic reaction occurs when the body’s immune system overreacts to a normally harmless substance called an allergen. A person whose immune system responds like this regularly is said to have an allergy.
Offer training. Free training pens are available on joining EpiClub (www.epiclub.co.nz). Inject into the upper thigh not the buttock. Call an ambulance following administration for follow-up. Fully subsidised on prescription with Special Authority number (max. 2 per script).
Suitable for mild to moderate reactions due to food or drug allergies, allergic rhinitis, or insect bites. Help to control body-wide symptoms including itch, swelling, and inflammation. Generally, non-sedating medicines do not cause drowsiness; however, some people may be more sensitive than others. Customers need to be warned about the risks of driving or operating machinery if they do get drowsy (see also Hay Fever). May be given to treat allergic rhinitis, drug or food allergies, hay fever, or insect bites.
See also Bites and Sting for a complete list of treatment options in this category.
Combination products that contain a decongestant as well as an antihistamine relieve congestion and help dry up a runny nose.
Oral and topical (nasal and ocular) antihistamines, nasal corticosteroids and decongestants. See Hay Fever for a complete list of treatment options in this category Emollients and topical corticosteroids. See Dermatitis/Eczema for a complete list of treatment options in this category
• Allergy NZ www.allergy.org.nz
• Australasian Society of Clinical Immunology and Allergy www.allergy.org.au
Reactions may range from mild to potentially life-threatening. People with hay fever, eczema and asthma commonly have allergies.
Allergens may be airborne, present in food, or on surfaces that are touched. Environmental allergens can be seasonal (for example, pollens and moulds) or present year round (eg, house dust mites, pet dander). Other allergens include:
• foods – cow’s milk, eggs, fish, nuts, soy, and wheat account for over 90% of all food allergies
• insect stings or bites
• latex or medicines (eg, penicillin, sulfa drugs).
• Advise people with allergies to wear a medical alert bracelet or necklace (such as Mediband, Medic Alert, St. John’s) that states details of their allergy(ies) and to inform all health professionals of their allergic status before starting any new treatment, including complementary medicines.
• Caregivers of children with serious allergies should consider providing a poster that clearly outlines their child’s condition and treatment to their school or daycare. Training for staff on how to use auto-injector devices may also be needed. See www.allergy.org.nz for more information.






While allergies are not directly inherited, people do inherit the tendency to be allergic. A person prone to allergies is called atopic, and these individuals have a tendency to develop new allergies, often to things they have not been allergic to in the past.
Why does an allergic reaction happen?
When a person encounters an allergen, their body responds by overproducing immunoglobulin E (IgE) antibodies. These attach themselves to immune system cells, called mast cells, and trigger the release of histamine and other chemicals.
Mast cells are most commonly found in the skin, conjunctiva of the eye, and the mucosa of the nose, mouth, lung, and digestive tract. The release of histamine causes allergic symptoms such as itching, redness, sneezing, and swelling.
Anaphylaxis is the most severe form of allergic reaction and potentially lifethreatening. It is a medical emergency requiring immediate medical care and treatment. Anaphylaxis is rare, but can occur in anybody, even people who have never reacted to an allergen before. Signs and symptoms occur within the first 20 minutes of exposure and may include:
• breathing difficulties, wheezing, cough
• loss of consciousness or fainting
• nausea or vomiting
• a rapid heartbeat
• tongue swelling or throat tightness. Adrenaline is the first-line treatment for anaphylaxis. Other medications (eg, corticosteroids, antihistamines) may also be administered. Adrenaline is available in an automatic device (eg, EpiPen).
Animal dander Keep pets out of your bedroom and off carpet and furniture.
Dust mites Use allergen-proof bed covers and wash bedding weekly.
Keep humidity low and ensure good house ventilation. Dust with a wet rag, wash stuffed toys regularly and vacuum with a double-layered microfilter bag or HEPA filter.
Replace carpet with wood or vinyl flooring. Remove clutter.
Food allergies Keep a diary of what you eat and subsequent reaction to help identify food allergens. Experts no longer recommend delaying the introduction of allergenic foods in babies. Seek further advice from a doctor or allergy specialist.
Insect bites and stings
Wear footwear outdoors and cover body with clothes.
Be alert for the presence of wasps around camp-sites or bins.
Wear gloves and insect repellent when gardening.
Pollen Keep the garden free of highly allergenic plants.
Stay indoors when pollen count is high (eg, hot or windy days) and shut windows. Get someone else to mow your lawn, or wear a good mask and wraparound sunglasses. Shower and wash hair at night to wash away any pollen.
Skin allergies Avoid strong soaps, perfumes and products that may irritate.






• Asthma affects one in seven children and one in eight adults in New Zealand.
• Lung function can deteriorate quickly.
• New Zealand has one of the highest hospital admission rates for asthma of OECD countires.
• Asthma mortality rates are 4.3 times higher for Māori and 3.2 times higher for Pacific peoples.
• Check the person’s metered dose inhaler (MDI) technique.
The majority of customers with asthma or COPD require life-long medications and will regularly come into your pharmacy to collect these.
Pay attention to the way they usually look, and if you notice any deterioration in their health, breathing, or if talking or walking appears difficult, ask if they would like to talk to a pharmacist.
Always involve a pharmacist in cold or flu medicine requests by people with asthma or COPD, because lung function can quickly become compromised with illness.
Category
Relievers/ bronchodilators: shortacting beta-agonists (SABA)
If someone appears to have difficulty breathing, CALL 111 IMMEDIATELY, whether or not the person is known to have asthma or COPD. Refer all other people with less severe breathing difficulties to a pharmacist, who should:
• ASSESS the severity of the episode and call 111 if severe
• SIT the person down and get them to lean forward
• TREAT with six puffs of a blue “reliever” inhaler through a spacer if already prescribed (use the patient’s own if available)
• HELP by calling an ambulance if the person does not improve
• MONITOR for improvement and repeat reliever doses every six minutes if needed
• ALL OK. Stay with them until they are OK then refer them to their doctor.
Metered dose inhalers (MDIs) – also called “puffers” – are the most common type of treatment prescribed for asthma or COPD. There are lots of different types available and you should ensure customers understand which inhaler(s) help breathlessness and which ones keep the airway free of inflammation. Younger and older patients may find MDIs difficult to use because they require good
coordination between activation of the MDI and inhalation. Other types of devices such as dry powder inhalers which are breath-activated may be more suitable. Most MDIs require regular cleaning, preferably weekly, and many need to be shaken before use.
Nebulisers are machines that convert liquid into a mist that can be inhaled into the lungs. They are common in hospitals and medical centres and some people may have one at home.
Examples
Beta2-agonists [PRESCRIPTION MEDICINE] eg, salbutamol inhaler (Asthalin, SalAir, Respigen, Ventolin) eg, salbutamol liquid (Ventolin) eg, terbutaline (Bricanyl)
Preventers Inhaled corticosteroids (ICS) [PRESCRIPTION MEDICINE] eg, beclomethasone (Beclazone, Qvar), budesonide (Pulmicort), fluticasone propionate (Flixotide)
Mast cell stabilisers and others [PRESCRIPTION MEDICINE] eg, montelukast (Montelukast Mylan)
Short-acting muscarinic antagonists (SAMA) or long-acting muscarinic antagonists (LAMA)
Symptom controllers: long-acting beta2 agonists (LABA)
[PRESCRIPTION MEDICINE]
SAMA: eg, ipratropium (Atrovent, Univent) LAMA: eg, glycopyrronium (Seebri Breezhaler), tiotropium (Spiriva), umeclidinium (Incruse)
[PRESCRIPTION MEDICINE] eg, eformoterol (Foradil, Oxis), indacaterol (Onbrez), salmeterol (Serevent)
Combination therapy [PRESCRIPTION MEDICINE]
SABA + SAMA: eg, ipratropium + salbutamol (Duolin HFA)
LABA + ICS: eg, eformoterol/formoterol + budesonide (DuoResp Spiromax, Symbicort, Vannair), salmeterol + fluticasone propionate (Seretide), vilanterol + fluticasone furoate (Breo Ellipta)
LABA + LAMA: eg, glycopyrronium + indacaterol (Ultibro Breezhaler), tiotropium + olodaterol (Spiolto Respimat), umeclidinium + vilanterol (Anoro Ellipta)
Spacers eg, e-chamber Turbo/ La Grande Children aged six or less eg, e-chamber mask
Comments
Reliever inhalers are used to treat the acute symptoms of asthma (ie, the difficulty in breathing). They provide relief within a couple of minutes. Most reliever inhalers are blue. Current guidelines recommend using with an inhaled corticosteroid.
Anyone using a reliever more than three times a week or waking at night short of breath should go to the doctor. If a person finds their bronchodilator has become less effective, it may indicate worsening asthma and the need to initiate an action plan or to visit the doctor to review therapy.
Preventer inhalers contain ICS. They do not have an immediate effect, so nothing is felt after inhalation; however, when used regularly they reduce the underlying inflammation of the airways and help reduce the incidence and severity of asthma attacks and hospitalisations. Most preventer inhalers are either brown, orange or dark red. Reduce risk of oral thrush by using a spacer and rinsing the mouth with water after use.
Montelukast is a leukotriene receptor antagonist that may be used in addition to ICS for an additive effect. Can be of benefit in exercise-induced asthma and in people who also have rhinitis.
Ipratropium reduces mucous secretions and relaxes airway muscle. It is a SAMA bronchodilator and has a slower onset of action than beta2-agonists so is used more in COPD, although certain asthma patients may benefit. Glycopyrronium, tiotropium, and umeclidinium are subsidised by endorsement.
Do not relieve underlying inflammation, but may be an alternative in mild-to-moderate asthma to higher dosages of ICS. Used in conjunction with an ICS. Only eformoterol can be used for immediate relief of asthma symptoms due to its fast action. Indacaterol is an ultra long-acting bronchodilator for COPD.
Budesonide + eformoterol/formoterol is the preferred treatment for all adolescents and adults with asthma. This can be used for the relief of symptoms and as maintenance treatment. Please refer to the 2020 New Zealand Adolescent and Asthma Guidelines for more detailed information.
Fluticasone propionate 250mcg twice daily is approximately equivalent to fluticasone furoate 100mcg once daily.
A Special Authority is required in some instances.
For safe management of asthma, eformoterol/formoterol, salmeterol, and vilanterol must be used only in combination with an inhaled corticosteroid.
Indacaterol and olodaterol are indicated for the maintenance treatment of COPD. Not indicated for asthma.
Help to improve delivery of MDIs to the lungs, reduce adverse effects of ICS. Wash once a week with warm water and a squirt of detergent and allow to completely drip dry. This leaves a slight residue of detergent on the inside of the spacer which reduces static and stops the medicine in the inhaler sticking to the sides. Replace every six to 12 months (tiny abrasions can prevent the spacer working as effectively).
Spacers are specially designed plastic tubes that are used with MDIs. They bypass the need for patients to coordinate activation of the inhaler with inhalation, and also help prevent the occurrence of oral thrush. Spacers can be helpful during an acute asthma episode and some are available fully funded on a PSO (practitioner supply order) ( see Treatment options)
New Zealand has one of the highest prevalences of asthma in the world and nearly 600,000 people regularly take medication for asthma. An estimated one in seven children and one in eight adults are affected, and only a small number of children appear to grow out of the condition. Māori and Pasifika are three to four times more likely to be admitted to hospital with asthma than other people.
Common symptoms include wheezing (a whistling sound most obvious when breathing out), shortness of breath, tightness in the chest, difficulty speaking, and a persistent dry cough (usually at night or after exercise). Over time this cough may become more productive. A cough may be the only symptom in young children. These symptoms may occur suddenly as an asthma “attack”, or they can be present most of the time. During an “attack”, breathing becomes very difficult due to inflammation and contraction of the smooth muscle within the airway, excessive mucus secretion, and swelling of the smaller airways. Permanent damage of the airways can result from untreated asthma.
It is common for asthmatics to also be prone
to hay fever or eczema, and/or to have a family history of these conditions.
The cause of asthma is unknown; however, common triggers of asthma attacks include animal dander (especially from cats), cigarette smoke, cold air, exercise, house dust mites, perfume, pollen, stress, viral infections (eg, a cold) and some medicines (eg, aspirin and NSAIDs).
Asthma cannot be cured but most people are able to manage it with medicine so that it does not interfere with their day-to-day life.
Education is vital to help people know how and when to use their inhalers or other treatments and what symptoms mean they should start their Asthma Self-Management Plan. Symptoms that indicate worsening asthma include a dry, persistent cough, usually at night and after exercise, and increasing use of a “reliever” medicine. Daily use of a peak flow meter (a device that measures maximum air flow from the lungs) may help people recognise worsening asthma.
NZ Asthma and COPD Guidelines Guidelines for Child, Adolescent and Adult Asthma, as well as for COPD are available from:
nzrespiratoryguidelines.co.nz
COPD is an umbrella term used to describe progressive lung diseases, such as emphysema, chronic bronchitis, and chronic asthma. COPD is more likely to develop in people over the age of 40 and symptoms include breathlessness, coughing, and increased phelgm.
The major difference between COPD and asthma is that COPD is generally irreversible, although most symptoms can be controlled and further deterioration in lung function prevented with early treatment. Some people have both COPD and asthma.
Ninety per cent of people with COPD have previously smoked; other causes include air pollutants and genetic deficiencies (eg, Alpha-1 Antitrypsin Deficiency).
• Ensure customers know what each inhaler is for and how to use them.
• Advise people with asthma to use paracetamol instead of NSAIDs because NSAIDs may precipitate an asthma attack in some people.
• Ensure they have talked with their doctor about what to do if their asthma worsens and they have an Asthma Self-Management Plan.
• Treat allergies and avoid known asthma triggers wherever possible.
• People with exercise-induced asthma should warm up and use a reliever before exercising.
• Refer any baby with worrying signs or symptoms to a doctor or pharmacist.
• Nappy rash is common and can be prevented with barrier creams, frequent nappy changing, and nappy-free times.
• Teething may cause babies to drool, be irritable or fussy with food, or restless.
It can be stressful caring for a new baby and many parents feel overwhelmed especially if their baby is unwell or not feeding properly.
Many parents will just be seeking reassurance that they are doing the right thing for their baby; however, always listen carefully to their description of their baby’s symptoms and ask appropriate questions to determine if you should refer the baby to a pharmacist or a doctor.
Treatment varies depending on what ailment the baby has (see each subtopic).
In addition to feeding problems (see Baby Feeding) some common health concerns in new babies include: teething, colic, cradle cap, nappy rash, and seborrhoeic dermatitis.
Baby teeth start to erupt through the gums between the ages of six months and two-and-ahalf years. This may cause irritability, drooling, swollen red gums and cheeks, and the child may
• All babies with a medical condition (eg, gastro-oesophageal reflux disease [GORD], immunosuppression) or with a fever.
• Babies currently being given medicines or supplements.
• Babies with a severe rash or one that extends beyond the groin area, is oozing or blistering or looks swollen.
be fussy with food or restless. All 20 baby teeth will have erupted by age three or four.
Permanent teeth start to come through around six or seven years of age. Baby teeth should be cared for as soon as they have erupted, to prevent tooth decay (see Dental Pain).
Relieve the pain of teething by giving the baby something cold to chew on (eg, a frozen banana wrapped in muslin, a cold teething ring) or oral pain relief (eg, paracetamol) if necessary.
Colic may affect up to one in five babies older than two weeks, before resolving at around three to four months of age.
Symptoms include excessive, inconsolable crying, for no apparent reason. The cause is not known but it may be due to an immature digestive system, an imbalance in the gut microbiome, food intolerances or allergies, or an early form of childhood migraine.
Soothing strategies, such as wrapping the baby snuggly in a soft cotton sheet (swaddling),
Soap alternatives eg, Aveeno Baby wash, Baby Goat Skincare, Biohoney Baby Soap, Dr Bronner’s, Sebamed
Antifungal preparations [PHARMACY ONLY MEDICINE] eg, bifonazole (Canesten Bifonazole), clotrimazole (Canesten range), miconazole (Daktarin, Resolve), miconazole and zinc oxide (Daktozin)
Antifungal + hydrocortisone combinations
[PHARMACY ONLY MEDICINE] eg, Resolve Plus 0.5% [PHARMACIST ONLY MEDICINE] eg, Canesten Plus, Resolve Plus 1%
Healing/soothing preparations eg, Bepanthen Nappy Rash, Lucas Papaw, Mustela range, Weleda Nappy Change, Sudocream Baby
Oral and topical oral analgesics for baby/child teething
[PHARMACY ONLY MEDICINE] eg, Pamol Infant, Paracare for Babies & Young Children 3 months–6 years [GENERAL SALE] eg, choline salicylate (Bonjela Teething Gel)
• Previous treatment has not been successful or has worsened the rash.
• If a similar rash is present elsewhere on the body (such as the scalp or other skin folds).
• Babies with feeding difficulties.
• Babies with allergies or previous reactions to topical products.
shushing (white noise, such as audio static or a vacuum cleaner), carrying in a baby sling or carrier, offering the baby a pacifier, or lying the baby across their caregiver’s legs, may help soothe the baby.
Colic powder, gripe water, probiotics, or rhubarb and ginger mixture are all possible

Use instead of soap to wash away urine and faeces from the area, without stripping oils off the skin.
Use antifungal creams to treat the fungal infection and continue for one week after the rash has cleared.
Use in combination with a barrier cream to protect and soothe the skin.
For skin that is inflamed, or if there is concurrent dermatitis and only after talking to a pharmacist. Advise two to three days use only unless under medical supervision. Always use corticosteroids in combination with an antifungal when used in the nappy area. Apply sparingly and change to a formulation without hydrocortisone as soon as possible.
Reduce redness, soothe, heal and protect the skin. Most contain a barrier-like agent.
Liquid preparations containing paracetamol should be used only occasionally and only as directed.
Do not use topical choline salicylate in babies younger than four months. Do not use more than every three hours. Apply sparingly to the gums.
Colic remedies eg, Rhuger, Weleda Colic powder, Gripe water May help relieve colic; also consider probiotics, dill, ginger, or kiwifruit extract.
Hypoallergenic pH-balanced wipes eg, Clear Eyes, Little Eyes*
Use single-use wipes to keep eyes clean.
Natural / herbal products / supplements Aloe vera, calendula, chamomile, vitamin A, B & E, zinc Natural products with soothing properties help heal nappy rash.
• Babies should be exclusively breastfed until they are around six months old.
• Do not offer advice about breastfeeding unless you really know what you are talking about. Refer the mother to an expert (eg, a lactation consultant or Plunket) instead.
• Babies with suspected reflux should be referred to a doctor for a proper diagnosis.
Be mindful that new mums and dads may be exhausted and fragile. Becoming a parent for the first time can be both joyous and stressful, so make life easier for them by keeping your aisles free of clutter and wide enough to fit a buggy or pram through. Keep baby products in an easy to reach location and provide a small box of toys for any accompanying toddlers to play with.
Greet them with a smile and ask how you can help. Ensure you can confidently talk about the baby products you stock and be sensitive to different cultures, but refer any new parent with anything other than a basic request to a pharmacist.
Do not offer advice about breastfeeding unless you really know what you are talking about – incorrect advice in this area may affect milk production, feeding, or a mother’s confidence. Instead, refer the woman to her midwife, Plunket, a local lactation consultant, or suggest she talk with whānau that have breastfed recently.
Most pharmacies stock a range of bottles, teats, breast pumps and sterilising units,
Category Examples
Products for cracked nipples and breastcare while breastfeeding
• Any mother with symptoms of mastitis, such as breast pain, redness, swelling, fever or flu-like symptoms.
• Any baby who is not gaining weight, has few wet nappies, or appears unwell.
• Anybody planning to take or buy any medicine, supplement or herbal remedy for a
although some may not stock formula because of its limited shelf life and availability in supermarkets. However, you should still know the basics about infant formulas (see opposite page). Keep products for cracked nipples in the same area as other general baby care items, such as nappy rash creams.
Breastfeeding is best for babies and recommended by the World Health Organization, the New Zealand Ministry of Health, the New Zealand Breastfeeding Alliance (babyfriendly.org.nz), and other services in New Zealand and globally. Breast milk is nutritionally well-balanced, easily absorbed, economical, safe and always at the right temperature. For the mother it is a time saver compared with cleaning, sterilising, and mixing formula.
It is also protective against breast and ovarian cancer and may help a woman return to her pre-pregnancy weight sooner. Breastfeeding allows close body contact with the baby which encourages bonding and gives the baby vital antibodies (especially colostrum which is
[GENERAL SALE] eg, creams (Lansinoh HPA Lanolin, Medela PureLan 100 Nipple Cream) eg, breast-care (Lansinoh Breast Pads, Manuka Health Breast Pads [contain manuka honey]), NUK Breast Gel Cushions, NUK Nursing Pads)
Products for thrush on the nipples [PHARMACY ONLY MEDICINE] eg, clotrimazole (Canesten cream), miconazole cream
Products for reflux [GENERAL SALE] eg, Gaviscon infant sachets
Sterilising products eg, Avent 3 in 1 Electric/Microwave Steam Steriliser, Milton tablets, NUK microwave/electric sterilising equipment
Products for expressing milk eg, NUK manual pump, NUK electric pump, NUK Breast Milk Containers
Other products eg, Lansinoh range (gel packs, nursing pads, pour spouts, storage bages) NUK Orthodontic Shaped Teats/Soothers, NUK Glass and BPAfree bottles
woman who is breastfeeding or for a baby.
• Any mother with possible signs of depression (eg, crying, feelings of helplessness, inability to cope, or difficulty sleeping).
• Babies with feeding difficulties.
produced in the first few days after birth) that helps protect against infections.
Babies who are breastfed are less likely to develop allergies, eczema, childhood diabetes, or die from sudden infant death syndrome (SIDS).
Beginning breastfeeding
There is more to breastfeeding than most people think and sometimes the belief that breastfeeding is easy can undermine a new mother’s confidence if she discovers it is not. Many women need a lot of support and help to start with.
Each feed should start on the opposite breast to the one used at the beginning of the last feed. The baby should not suck on the nipple alone, but take in part or all of the areola (the pigmented area around the nipple) as well. This allows the nipple and areola to be drawn right to the top of the baby’s mouth for effective feeding. Incorrect latching causes damage (cracked nipples) and makes feeding less effective.
Babies may make audible swallowing sounds when breast milk flows fast at the start of the feed. Allow the baby to completely empty one breast before swapping to the other. To release
Comments
Cracked nipples are usually caused by poor latching or from comfort sucking (slipping back onto the nipple for long periods after nutritional feeding has slowed). Do not stop feeding but try to get a better latch – contact a midwife, Plunket nurse, La Leche League or a lactation consultant for help.
Nipple shields are not generally recommended except for women with inverted nipples or on the advice of a lactation consultant. Breast pads containing manuka honey relieve nipple discomfort as well as absorbing excess milk. Nursing pads absorb any leakage between feeds.
Treat mother and baby simultaneously. Use a regular topical antifungal cream, such as clotrimazole or miconazole, on the mother’s nipples and wipe off before breastfeeding. Apply nystatin oral drops to the inside of the baby’s mouth (see Oral Health) and an antifungal cream to their bottom if necessary.
Mixes with and stabilises stomach contents preventing reflux and regurgitation. Each sachet contains 21mg of sodium. Best given under medical supervision. Not to be used in infants under one year.
Clean all equipment that goes in a baby’s mouth, such as feeding bottles, nipple shields and pacifiers (dummies) using detergent, hot water and a brush. Sterilise all equipment used for babies under three months in addition to washing.
Expressing can be done by hand, manual pump, battery pump or electric pump. Expressed milk can be refrigerated or frozen.
Specialised teats (eg, for babies with cleft palates) are also available. Pacifiers (soothers) may reduce the risk of sudden unexpected death in infancy but are best used after breastfeeding has been established. Keep clean, sterilise frequently and check for loose parts or cracks regularly.
the baby’s latch (eg, to change sides) the mother can gently slide a clean little finger into the corner of baby’s mouth.
Exclusive breastfeeding is recommended until a baby is around six months old. At this time, a baby should be started on plain, smooth, and soft solid foods in addition to breastfeeding. Encourage mothers to continue breastfeeding until their baby is at least one year old.
Advise mothers wishing to wean to reduce feeding gradually, for example, drop one feed a day, then, after a while, drop another feed. If breasts become engorged, expressing a little milk will make them more comfortable. Tablets are rarely recommended to stop breastfeeding due to side effects.
Sometimes breasts can become engorged, causing pain and difficulty in “latching” the baby. Expressing a little milk just before a feed may make latching easier.
Mastitis (infected, blocked milk ducts) may follow engorgement. Symptoms usually include breast pain, warmth, redness and swelling in one area of the breast with fever and flu-like symptoms. Antibiotics prescribed by a doctor or midwife are often needed if symptoms persist for longer than 24 hours. Women should continue to breastfeed during mastitis and encourage the baby to completely drain the affected breast at each feed. This will lead to a quicker recovery than if a woman stops feeding.

For cracked nipples apply a soothing cream (see Treatment options previous page) and get help with technique – the baby is probably latching incorrectly.
Some mothers worry that they do not have enough milk, often in response to a baby feeding more often than normal. Reassure the mother that babies naturally go through growth periods, and will feed more frequently during this time.
Generally, if a baby appears healthy and active AND is gaining weight AND having six or more very wet nappies a day, then the milk supply is fine. In most cases, the mother’s supply adjusts to this increased demand within a couple of days and the baby resorts back to its regular feeding schedule.
Occasionally, a baby may not be getting enough milk due to incorrect latching or sucking, or, rarely, milk underproduction. Encourage the mother to contact her midwife or lactation consultant for further advice; to rest and relax whenever she can; and to make sure she is eating and drinking well. Pasteurised (heat-treated), donated breast milk is available through certain hospitals or through mothersmilknz.org.nz
Reflux in babies is common and is thought to be caused by an immature lower oesophageal sphincter (the band of tissue that prevents the contents of the stomach from rising up the oesophagus). Symptoms include distress or arching of the back when feeding, irritability, coughing and frequent hiccups. Colic may also coexist with reflux (see Baby Care previous
topic). Parents should take their baby to a doctor for a proper diagnosis if reflux is suspected.
Although health professionals have a responsibility to promote and support breastfeeding, if a woman decides to bottle-feed, she will need support and advice.
Most infant formulas are derived from cow’s milk, although goat’s milk, soy-based, lactosefree, and hypoallergenic formulas are available. Advice must be sought from Plunket, a midwife, or a doctor before giving thickened formulas, lactose-free or non-dairy formulas long-term.
Infant formulas are formulated to contain differing levels of whey and casein depending on the baby’s age, as well as all of the recommended essential vitamins and minerals. Regular cow’s milk must not be used for infants aged less than one because it contains higher levels of protein and salt and not enough iron and other nutrients necessary for a growing baby.
Standard formulas contain all the nutrients specified in infant formula regulations, whereas ‘gold’ formulas contain extra ingredients allowed by the regulations to be added. Formulas are usually age-based, falling into the categories 0-6 months (stage 1); 6-12 months (stage 1, follow-on or progress formulas); and over 12 months (stage 2 or toddler’s milk).
Keep powdered formula covered and use within four weeks of opening. Wash hands and clean all feeding equipment thoroughly before preparing formula; sterilise it if a baby is less than three months old. See Feeding Your Baby Infant Formula at www.healthed.govt.nz
• Oral antihistamines relieve redness and itching from widespread bites. • Offer advice on how customers can reduce their risk of getting bitten in the future.
Although treatment is mostly similar, identifying the cause of the bite can help prevent them in the future. Ask your customer to show you the sting or bite mark if they are comfortable doing so in a private area.
The appearance, location, and quantity of bite or sting marks should give you some idea of the culprit (for example, single bite: wasp or spider; multiple bites: bed bug, mosquito, flea, or sandfly; itchy rash after swimming: duck itch [fresh water] or hydromedusae [sea water]).
Watch for cellulitis which can quickly develop after a bite or sting. Symptoms include swelling and redness in the affected area which may feel hot to the touch. Without antibiotics, cellulitis can be life-threatening, so refer to a doctor.
Wasp, bee or hornet stings
Most people will have successfully
Category Examples
Oral antihistamines
Non-sedating
[PHARMACY ONLY MEDICINE]
• If someone appears to be having a severe allergic reaction (see Allergies) to a bite or sting CALL 111 IMMEDIATELY
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• Children younger than six.
• If the bite or sting looks infected (eg, pus
removed the stinger by the time they present to your pharmacy. If not, carefully scrape away the stinger with the side of your fingernail or a plastic card rather than grasping it, as this can accidentally squeeze more venom into the patient.
Ice should be applied to the affected area and an oral non-sedating antihistamine tablet (such as fexofenadine) considered. For very minor stings, a topical corticosteroid cream may be used. Seek urgent medical help for anybody with signs of anaphylaxis (see also Allergies for an antihistamine comparison).
Insect bites
Suggest use of topical or oral antihistamines,
eg, bilastine (Labixten), cetirizine (Razene, Zyrtec), desloratadine (Aerius), fexofenadine (Fexofast), levocetirizine (Levrix), loratadine (Claratyne)
Sedating [PHARMACIST ONLY MEDICINE] eg, dexchlorpheniramine (Polaramine), promethazine (Phenergan)
Topical antihistamines [PHARMACY ONLY MEDICINE] eg, mepyramine (Anthisan cream)
Anti-pruritic (anti-itch) preparations [GENERAL SALE] eg, Calamine, Pinetarsol, Eurax
Topical corticosteroids [PHARMACY ONLY MEDICINE] eg, hydrocortisone 0.5% (DermAid) [PHARMACIST ONLY MEDICINE] eg, hydrocortisone 1% (DermAid)
Topical anaesthetics [PHARMACY ONLY MEDICINE] eg, lignocaine (Ethics 4 Way Antiseptic Cream, Soov Bite Gel [with cetrimide])
Anti-sting preparations [GENERAL SALE] eg, AfterBite, Ozone Anti-itch, Stingose Spray/Gel, Weleda Stings & Bites
PREVENTION Insect repellents Anti-insect bands eg, Para'Kito Mosquito-band Topical insect repellents eg, picardin (eg, Repel New Era) eg, DEET (eg, Aerogard, Bushman, Repel) eg, Oil of lemon eucalyptus (eg, 2B Repellent)
Natural / herbal / supplements Citronella, clove, coconut oil, eucalyptus, lemon grass, neem oil or cream, soybean, tea tree
or crusting at the site of injury.
• Past reactions have been severe.
• With bites caused by an overseas or unknown source.
• With extensive swelling or redness around the site of the bite or sting.
• With allergies to medicines.
anti-pruritics, topical corticosteroids, or creams containing anaesthetics for itching (see Treatment Options table below). If the cause is thought to be due to scabies or head lice, treatment products should be used (see Scabies or Head Lice).
Refer the customer to a pharmacist if they have recently been overseas and there is a possibility they may have been bitten by a disease-carrying insect. Discuss ways to protect against future bites (see text box opposite page).
New Zealand has many species of spider but only the red-back and katipo are considered poisonous. An anti-venom effective for both
Comments
Helps control total body itch and inflammation after a bite or sting. More convenient for multiple bites/stings than topical antihistamines. Generally, non-sedating medicines do not cause drowsiness; however, some people may be more sensitive than others. Customers need to be warned about the risks of driving or operating machinery if they do get drowsy. For a comparison of antihistamines, see Allergies
Purpose is similar to non-sedating antihistamines (above) but can cause drowsiness which may be useful to improve sleep quality at night but not if alertness (ie, for driving or operating machinery) is required. Warn about sedating effects and advise customers to avoid alcohol. Not suitable for everybody (see Reference Section, OTC Medicine Precautions). Not suitable for young children.
Relieves local itch and inflammation. Some people may develop skin sensitisation if used too extensively. Use for only two to three days to help relieve itchy bites.
Tar products (eg, Pinetarsol) help relieve generalised skin itching. Calamine lotion has a soothing, cooling effect and contains 0.5% phenol, which also provides a local anaesthetic action, but may dry out skin.
Relieves local itch and inflammation. Apply a thin layer to skin. Do not use for more than one week unless under medical supervision. Avoid the face and genital area unless directed by a doctor.
Early use may help relieve the initial sharp pain caused by stings. Not suitable for those with eczema. May cause contact dermatitis.
Ozone Anti-itch contains ammonia, zinc and other ingredients to neutralise the bite area and soothe skin. Stingose contains aluminium sulphate and inactivates proteins in venom. Arnica and essential oils can help relieve itch.
Anti-insect bands contain natural oils. Protection against mosquitoes and other insects is provided over several days (see individual products) with continuous band wearing.
DEET (N,N-diethyl-m-toluamide), picaridin, IR 3535 and synthetic oil of lemon eucalyptus are all effective at repelling disease-carrying mosquitoes. Recommend to people travelling overseas to at-risk countries. Products containing >30% DEET have been banned in some countries.
Plant-based insect repellents (eg, citronella, soybean, eucalyptus) are suitable for use in countries not at risk of mosquito-borne diseases (eg, New Zealand).
these spiders is available throughout NZ. No deaths from katipo spiders have been reported here since the 19th century.
Although white-tailed spiders are known to bite, their venom rarely causes harm, although some people do develop an allergic reaction and need an oral antihistamine.
Seek urgent medical help if the person has difficulty breathing or a severe reaction.
Bluebottles Wash the stung area in fresh or salt water and remove any stings or tentacles attached to the skin (but not with bare hands). Immerse affected area in warm water for 20 minutes then leave to dry without towelling. DO NOT apply vinegar (increases toxin release).
Lion’s mane jellyfish/mauve stingers Apply wet sand or a towel soaked in sea water initially, then flush the area with warm sea water. Vinegar is effective for these types of jellyfish (but fresh water is not). Wipe remaining tentacles off with a dry towel after five minutes. Cold packs may help relieve pain.
Hydromedusae Microscopic, semi-transparent jellyfish that invade upper North Island beaches during summer causing an itchy rash on skin covered by swimwear. Remove togs as soon as possible after leaving the water. Shower in preferably salt water.
Follow-up treatment Lignocaine, calamine lotion, or hydrocortisone cream may be applied to the skin and an oral antihistamine taken if the skin is itchy. Refer extensive jellyfish stings to a doctor.
Duck itch develops when immature larval forms
of parasitic flatworms penetrate the skin of swimmers. Ducks are the normal hosts of these flatworms and aquatic snails an intermediate host. The condition is common in summer when water temperatures aid snail reproduction, aquatic birds return to full activity, and people swim in shallow water.
Symptoms consist of a rash limited to areas exposed to water, that progresses from tiny red spots to pimple-like bumps, with intense itching. Rinsing the skin with isopropyl alcohol followed by application of calamine lotion or 1% hydrocortisone cream or oral antihistamines may help relieve symptoms. Sunscreen containing phenoxyethanol or DEET may help prevent the condition.
Bites and stings can be either venomous or non-venomous. Bees, hornets, wasps, jellyfish, and the katipo and red-back spider are venomous. Bed bugs, fleas, lice, mosquitoes, sandflies, scabies and ticks are non-venomous. Venomous stingers or biters inject a toxic and often painful venom into their victim as a defence mechanism to ward off attack. A stinging sensation or pain is felt in the area which becomes inflamed, swollen, and sometimes itchy. Certain wasp or jellyfish stings are particularly painful
• Customers with severe reactions to a bite or sting should carry adrenaline at all times and wear medical alert jewellery that states what they react to and what happens.
• Avoid scratching the area (this also
and the pain may persist for several hours even after first aid has been applied.
Non-venomous biters pierce the skin and feed on blood, resulting in a small raised red spot and often intense itching. Infection of the open sore commonly occurs due to scratching. Outside of New Zealand, many non-venomous biting insects carry diseases, for example, malaria, zika, or dengue fever (see Travel Health)
Tips to avoid getting bitten
• Use insect repellents and cover arms and legs if in an area prone to insects.
• Avoid perfume or wearing brightcoloured clothing around bees; mosquitoes like dark clothing.
• Cover food and rubbish and try to minimise odours at picnics. Destroy wasp nests.
• Drain pools of stagnating water or add household bleach to them to eliminate mosquito larvae.
• Repel mosquitoes with electrical insect-repelling devices or citronella products when outside.
• De-flea cats, dogs and other household pets regularly.
reduces the risk of infection).
• Cover-up and take extra precautions if travelling to an area at risk of tick or mosquito-borne illnesses (see Travel Health).
• Minor bruises are not dangerous but serious bruises need to be referred.
• Keep wounds covered during the initial healing period and maintain good skin hydration afterwards to minimise scarring.
• Vein creams may reduce redness.
Always be tactful when helping customers with obvious scars or spider veins as some may be self-conscious about them. If you notice unusual bruising, or significant bruising in an older person, ask the customer if they are taking any other medications or are prone to bleeding, particularly if they are buying NSAIDs or aspirin, as further advice may be needed from a pharmacist.
Bruising
Apply ice to the bruise as soon as it forms to reduce blood flow to the area and reduce swelling. Apply a bag of frozen peas or an ice pack wrapped in a towel for 20 minutes at a time throughout the first two days. Then place a heating pad or warm compress on the injured area and elevate, if possible, above the heart. Paracetamol or ibuprofen may be given to relieve pain, if needed.
Most bruises will resolve within two weeks.
Category Examples
Bruises
• A bruise which is swollen, hard to the touch, affects vision, or appears on the abdomen, head, or trunk with no known cause
• A bruise that persists for almost two weeks without fading.
• A particularly painful bruise, numbness, or difficulty moving the affected area (may be damage, such as a fracture or sprain underneath).
• The customer takes medicines that may increase the risk of bruising.
• The person states they bruise easily for no apparent reason.
Heparinoid creams dissolve clots and improve blood supply to the skin and may be used to reduce bruising. Arnica has anti-inflammatory effects and also reduces bruising. Refer anyone with a serious bruise to a doctor.
Scars usually fade over time but never go away completely. Scars should be covered with tape for three months following the initial healing period then creams or oils applied regularly to the scarred area to keep the skin moist. This
Bruises eg, arnica (eg, Anti-Flamme range, Natures Kiss Arnica cream) eg, mucopolysaccharide polysulphate (MPS) (eg, Hirudoid)
Scars Essential oils and vitamins eg, Derma Oil, Hiruscar Gel, Palmers Skin Therapy Oil, Skybright Rosehip Oil, Trilogy Organic Rosehip Oil
Support stem-cell regeneration eg, Mebo Skin Restore, Mebo Wound Repair
Topical silicone gel eg, Bepanthen Scar Treatment, DermaScar, Dermatix, Epicyn Scar Reducing Silicone Gel
Silicone gel sheets eg, Cica-Care Adhesive Silicone Gel Sheet
Veins eg, heparinoids (eg, Hirudoid) eg, essential oils and vitamins (eg, Bio-Oil) eg, Couperose Thread & Spider Veins Balm eg, Rucus extract (Avene Antirougeurs Fort Relief)
Natural / herbal products / supplements Spider veins
Horse chestnut (Aesculus hippocastanum), eg, Venotrex
Bilberry extract
Scars
Alphahydroxy acids
Rosehip or Tea Tree oil
Vitamin E
Bruises
Arnica, comfrey (eg, Kiwiherb Comfrey), frankincense, helichrysum, kawakawa, rosemary, St. John’s Wort
• Bruises that cover a large area.
• Other symptoms are present in addition to the bruising (eg, feeling unwell, headaches). Scars
• Extensive scarring.
• Oozing, pus or blood from the scar.
• Scars that are painful, very red, or extremely thick.
Spider veins
• The customer has a history of steroid cream use. This may be the cause.
• The customer has been unwell or has a condition that might increase their risk of spider veins.
can help minimise their appearance. Other treatments, such as surgery, dermabrasion, laser treatments, injections, and chemical peels may reduce scarring that has already developed.
Keloid scars (lumpy and large overgrowths of scar tissue) may be treated with surgery, steroid injections, pressure and silicone gel sheets (eg, Cica-Care, see Treatment options). Even old scars can respond to treatment.
Creams to reduce redness are available but
Comments
Arnica reduces bruising, relieves pain, and helps restore normal skin tone. MPS is a naturally occurring heparinoid compound that is antiinflammatory and antithrombotic. It can soften hematomas, improve the appearrance of bruises, relieve pain, and help disperse excess fluid in swollen areas. Avoid naked flames.
These help reduce the appearance of scars and stretch marks.
Helps return elasticity to damaged skin and fades scars and blemishes. It also protects newly healed skin.
Forms a flexible and transparent silicone sheet that acts like a second layer on the skin. Helps to flatten, soften and smooth hypertrophic and keloid scars. Recommended treatment duration: two months.
Softens, flattens and fades red, dark or raised scars. Use on fresh or old hypertrophic or keloid scars. Prevents hypertrophic scars and keloids. Use after stitches have been removed.
Spider veins can be treated with laser treatment, Intense Pulsed Light (IPL) therapy and sclerotherapy, although often other spider veins can develop in the same area. Hirudoid cream may be used to reduce vein inflammation under medical supervision.
Bio-Oil may help reduce the appearance of spider veins. Rucus extract may reduce redness.
Oral horse chestnut seed extracts or bilberry extracts have been used in the treatment of vein conditions.
Alphahydroxy acids applied as a facial peel appears to improve the appearance of atrophic acne scars.
Rosehip oil, diluted Tea Tree oil and vitamin E cream or capsules may help reduce scarring.
Topical comfrey improves pain and tenderness of bruises.
Arnica may help reduce bruising.
Frankincense (also known as olibanum) is an aromatic resin obtained from the Boswellia tree. It has an anti-inflammatory effect and can reduce bruise appearance and size more quickly.
vein clinics may be able to offer more effective treatments.
Bruises are common and are usually caused by an impact or injury that breaks or bursts the small blood vessels, called capillaries, that lie near the skin’s surface. Because the skin has not broken, the blood contained inside these vessels does not have anywhere to go and pools near the skin’s surface and forms clots.
Right after the injury, the bruised area looks dark red. Within a day or two, it will turn a bluish or purple colour on fair skin or dark purple, brownish or black colour on dark skin. Within five to 10 days the bruise may be green or yellow, then fades to yellowy-brown or light brown within two weeks, before disappearing completely once all the blood has been reabsorbed.
This change in colour is due to haemoglobin breaking down. Haemoglobin is the iron-rich protein contained in red blood cells that carries oxygen around the body and transports carbon dioxide back to the lungs.
Most bruises feel swollen and tender initially, but the pain usually subsides within a few days. The majority are not typically something to worry about and can be safely treated at home. Refer people with concerns identified by the Refer to a pharmacist checklist. Spontaneous bruising may be the sign of a bleeding disorder or bone marrow problem.
People who are more likely to bruise include those with thinner skin (women, elderly), with certain medical conditions such as liver disease, or taking medications that affect clotting (eg, warfarin, aspirin or NSAIDs). Bruises are also
more likely to occur in areas where there is less fat, such as around the knees.
A haematoma is a hard lump that is caused by blood pooling in a muscle or small vein and these may need to be drained off.
Scars are permanent areas of fibrous tissue that grow over a wound. Part of the natural healing process, they can occur from surgery, burns, cuts and grazes, acne, skin infection, chickenpox and scratches. Scars are often thicker, pinker, redder, or shinier than normal skin.
Scars do not contain sweat glands or hair follicles and are also more prone to sunburn. How much of a scar remains long term depends on how deep the wound is, where it is, how long it takes to heal, the age and health of the person, and the person’s inherited tendency to scar.
Cover wounds initially to allow deeper and more consistent healing, then tape with medical grade paper tape for at least eight to 12 weeks.
Keloid scars are raised, often red and can be bigger than the injury, surgery or acne causing
Bruising
• Use PRICED treatment (Protect, Rest, Ice, Compression, Elevation and Diagnosis) straight after the soft tissue injury (see Strains and Sprains). Do not massage a bruise.
Scarring
• Use moist wound dressings and, if necessary, wound closure strips to help reduce scarring. Continue until the wound
them. Excess collagen forms as an abnormal response to the injury.
Hypertrophic scars are similar to keloid scars but are no bigger than the injury. They can be treated with silicone gel sheets. Contracture scars may come from a burn. The skin becomes tight and can also affect mobility.
Spider veins, also known as starbursts or telangiectasia, indicate an underlying circulation problem known as venous insufficiency. They are similar to varicose veins but much smaller. They may be red, blue or purple and are closer to the surface of the skin than varicose veins (see Varicose Veins and Support Stockings). They usually occur in a group and look like a tree branch or spider web, and are commonly found on the legs and face. They can cover a very small or very large area of skin and can be painful.
Reticular veins are bigger blue veins and lie deeper in the skin than spider veins. Spider veins often come from reticular veins, so these may need treating as well.
heals then tape for at least three months. Do not pick at wounds. Minimise movement of the area while healing.
• Do not expose new scars to the sun –cover or apply sunblock.
Veins
• Wearing support hose, maintaining an ideal body weight, exercise and avoiding prolonged standing may help to prevent spider veins.
• Do not dismiss a caregiver’s perception that their child seems unwell. Refer them to a pharmacist.
• The benefits of immunisation far outweigh any risks for the majority of children.
• Keep up to date with vaccination information so that you can offer informed and accurate advice (see also www.immune.org.nz). Slight changes to the vaccination schedule happen most years.
The majority of children who are unwell, look unwell, but it can be difficult to tell whether a child is seriously ill or not. Always encourage caregivers with unwell children to talk to the pharmacist, unless they have already seen a doctor and are comfortable with looking after the child.
Any child with difficulty breathing, with a blue tinge around their lips or tongue, having difficulty feeding or refusing to drink, who is overly sleepy or floppy, feels cold to the touch, is not urinating, or is under three months old and looks unwell needs urgent medical attention.
Always be mindful that most childhood diseases are contagious, and pharmacy staff have a high likelihood of being exposed to many of these conditions, particularly during epidemics. Unimmunised pharmacy staff without natural immunity to common infections need to be particularly careful, and should be encouraged to bring their immunisation status up-to-date.
The majority of childhood diseases are caused by viruses, and treatment usually
Category Examples
includes maintaining a good fluid intake to ensure dehydration does not develop, occasional pain relief when needed, and antibiotics to prevent or treat secondary bacterial infections. Many childhood diseases are potentially fatal, and caregivers should be encouraged to vaccinate their children (and ensure their own vaccination status is up-to-date), to prevent contracting the disease.
Infectious diseases tend to be more prevalent in children than in adults; however, non-immune adults are still susceptible to infection.
Immunisation is the process by which a child or adult is made resistant to a specific disease, typically by administration of a vaccine. It is a proven tool for controlling and eliminating life-
Refer all children with a suspected infectious disease to a pharmacist for further advice and evaluation. For each infectious disease on the following pages, guidance is offered on when pharmacists should refer customers to their doctor.
threatening infectious diseases and the World Health Organization estimates it averts between two million and three million deaths per year. Benefits of immunisation far outweigh risks but customers seeking reassurance about the safety and effectiveness of specific vaccines are best referred to the Immunisation Advisory Centre (www.immune.org.nz or 0800 IMMUNE). This organisation is based

Comments
Simple analgesics [GENERAL SALE] eg, paracetamol – less than 20 tablets, (Panadol, Paracare) [PHARMACY ONLY MEDICINE] eg, paracetamol – greater than 20 tablets, suspension (Pamol range, Paracare range)
Non-steroidal antiinflammatory drugs (NSAIDs) [PHARMACY ONLY MEDICINE] eg, ibuprofen (Advil, Fenpaed, Nurofen)
Topical anaesthetics [PHARMACY ONLY MEDICINE] eg, lignocaine/prilocaine (Emla)
Anti-pruritics [GENERAL SALE] eg, Calamine, Pinetarsol, PoxClin
Vaccinations: COVID-19, influenza, tetanus/ diphtheria/ pertussis (Tdap), HPV, meningococcal, zoster, measles/mumps/rubella (MMR)
[PRESCRIPTION] – except when administered by a pharmacist who has successfully completed an approved vaccinator training course (some are funded for eligible people)
Natural / herbal products / supplements Honey, calendula ointment, zinc cream, vitamin A ointment
Paracetamol has few side effects and is safe for occasional use at recommended dosages. Take care to avoid overdose. Advise customers to check strength, formulation and dosage instructions on the back of the product packet, and to never exceed these. Given to relieve discomfort rather than to bring down a fever (for more information see Fever). Paracetamol is not recommended for routine use before or after vaccination as it may decrease the antibody response to vaccines and affect the duration of immunity.
Avoid NSAIDs in chickenpox due to the rare possibility of complications. Ibuprofen may not be suitable for some children (see Childhood Pain).
Emla patches and cream numb small areas of skin prior to needle insertion, vaccination, and superficial surgical procedures. Apply at least an hour before the procedure.
Calamine can help relieve itch. Tar-based pine oil products are useful in the bath to help reduce itching. PoxClin has a natural cooling action and helps enhance the skin's protective barrier. Also relieves itch.
Appropriately trained pharmacists may administer influenza vaccines (see Influenza) to those 3 years +, COVID-19 vaccines to those 5 years +, Tdap vaccine to those 18 years + or pregnant women aged 13 + HPV vaccine to those 9 +, meningococcal vaccine to those 16 years +, and MMR vaccine to those 3 years +. Herpes zoster vaccines (see Shingles) may be administered to those 50 +, and Dukoral (see Travel Health) to those travelling overseas. Intern pharmacist vaccinators may administer influenza, COVID-19, HPV, and MMR. For updates and more information see www.immune.org.nz search: pharmacists and intern vaccinators. .
One to two teaspoonfuls of honey taken at night can be effective at relieving cough associated with some childhood diseases. Calendula, vitamin A ointment or zinc cream may help relieve irritated skin and reduce scarring (ie, from chickenpox).
at the University of Auckland and provides independent factual information based on international research regarding the benefits and risks of immunisation.
The National Immunisation Schedule (NIS) is the series of vaccines that are generally offered free to babies, children, adolescents and adults of certain ages in New Zealand, although some vaccines have restrictions on their use.
Revaccination of children following significant immunosuppression (eg, as a result of chemotherapy) is also funded for most vaccines on the NIS, as long as eligibility rules apply. The current schedule can be found on the Ministry of Health’s website at www.health.govt.nz, search Immunisation
Detailed consumer information on diseases and vaccines, including diseases not covered by the National Immunisation Schedule, can be found in the YourHealth section of this website.
Pharmacy staff can help improve overall immunisation rates by displaying and discussing
information on the relative risks and benefits of immunisation and informing customers about current epidemics and checking their immunisation status.
Some immunisations can cause pain and fever. While the use of paracetamol or ibuprofen to relieve pain or discomfort immediately prior to or following vaccination is not contraindicated, experts do not recommend that painrelieving medicines be routinely used because their use has been associated with a lower immune response (the exception is vaccination with Bexsero for meningococcal B). However, if a child is distressed by fever, discomfort, or pain following immunisation, they may be given.
Injection pain may be reduced by applying a topical anaesthetic patch or cream to the area at least one hour prior to vaccination.
Report any adverse vaccination reactions to the Centre for Adverse Reactions Monitoring (see Medicines Safety, page 193).
• Keep children at home until they are no longer infectious (see individual conditions for exclusion periods).
• Keep sick children away from pregnant women, newborn babies or any person who is immunocompromised (eg, with cancer, HIV, or organ transplant recipients), whenever possible.
• Advise caregivers to observe their child frequently and to seek urgent medical advice if they are worried or the child seems in distress.
• Fluids should be offered regularly in order to avoid dehydration in the sick child. If their child refuses even small sips, caregivers should seek medical advice urgently.
• Caregivers should wash and dry their hands frequently, especially before and after tending to a sick child.
• Well Child/Tamariki Ora: A series of free health visits and support for most children aged around six weeks to five years. Available to all children enrolled in the Well Child/Tamariki Ora programme.
• Triple P: Tips to manage a child’s behaviour from babies to teens (triplep-parenting.net.nz)
• Kia matua rautia: Parenting information and resources (takai.nz)
• Kiwi Families: Practical parenting advice (kiwifamilies.co.nz)
• Parent Help NZ: Deals with all parenting issues (parenthelp.org.nz)
• Dress children in light, loose-fitting clothing or pyjamas and encourage them to rest in a half-darkened room.
• Only administer pain relief, such as paracetamol, occasionally if needed to relieve a child’s discomfort (see Fever for more detailed information).
• Aspirin should not be given to children under 16 years (unless under medical advice) due to the risk of Reye’s syndrome (see Childhood Pain for more information).
• Trim children’s fingernails short to discourage scratching which may lead to infection.
• Some diseases may require specific medicines prescribed by a doctor (see individual conditions for details).
CHICKENPOX (varicella)
COVID-19 (current at the time of going to print)
Chickenpox is a common, contagious disease caused by the varicella zoster virus. Varicella vaccine (Varivax) is funded on the NIS for children at 15 months old, and at least one injection is given. The second dose (if given, not funded for all) should be administered at least 3 months after the first dose. The vaccine is also funded for children and adults with reduced immunity or at very high risk of contracting the disease (two doses recommended). Children who have had chickenpox disease previously do not need to be vaccinated. People who have had chickenpox are also at risk of developing shingles later in life (see Shingles).
COVID-19 is an infectious disease caused by a coronavirus – SARS-CoV-2. The number of COVID-attributed deaths in New Zealand, since the pandemic was declared in March, 2020, has exceeded 2600, at the time of publishing. The majority of cases reported have been mild. Everyone in New Zealand over the age of 5 is eligible to get a free COVID-19 vaccine, regardless of visa or citizenship status. Vaccination is voluntary.
Symptoms
Initially, fever, headache, tiredness or sore throat for up to three days before the rash appears (adults may develop a flu-like illness). The rash begins as red itchy spots, usually in crops of three to five that eventually become blisters. Most commonly begin on the head and neck before moving to the trunk and limbs. May also appear inside the mouth or on the genitals. Blisters crust over after three to five days and are extremely itchy. Number of blisters can range from a few to several hundred. Secondary bacterial infection is common.
Cough, fever, sore throat, anosmia (loss of sense of smell), shortness of breath, sneezing, a runny nose, fatigue, diarrhoea, and abdominal cramps are the more common symptoms, depending on the variant. Some people may present with headache, muscle pain, nausea or vomiting, confusion, or irritability.
If the blisters become infected. If there are spots in the eyes, ears, or mouth.
If the child has another illness affecting their immune system. If the child seems particularly unwell. If the diagnosis is uncertain.
HAEMOPHILUS INFLUENZAE TYPE B
Diphtheria is a serious, often fatal disease caused by Corynebacterium diphtheriae. Diphtheria is included in the NIS as part of the Infanrix-hexa (diphtheria, tetanus, pertussis, polio, hepatitis B, Haemophilus influenzae type b) vaccine. It is also a component of Boostrix (tetanus/diphtheria/pertussis) and some other vaccines (ie, Infanrix-IPV).
Diphtheria is extremely rare in New Zealand but is endemic in many developing countries.
Haemophilus influenzae type b (Hib) is caused by a bacterium. Humans are the only hosts of these bacteria and children aged less than five years are especially at risk. Hib vaccine (as Hiberix or Infanrix-hexa) is funded on the NIS for all children aged less than five years and for older children and adults meeting certain criteria.
The bacteria cause mucous membrane inflammation so the most common symptom is a sore throat, hoarseness, painful swallowing and the development of a bluishgreyish membrane that covers the inside of the throat and tonsils. Other symptoms include a nasal discharge, fever and chills. Some people have no symptoms.
Before immunisation, most common presentations were meningitis and epiglottitis.
Meningitis tends to occur in younger children aged less than three years. Symptoms include fever, loss of appetite, vomiting, bulging fontanelle (babies), drowsiness, light sensitivity. Epiglottitis usually occurs in children aged two to four years. Symptoms include difficulty breathing and swallowing, and drooling. May extend neck and stick tongue out. Rapid onset.
HEPATITIS A Hepatitis A is a virus that is more common in areas with low living standards, poor hygiene and high population density. In countries where the disease is endemic, almost all adults are immune. Three notable outbreaks in New Zealand have occurred in 2013, 2015, and 2022/2023. Havrix and Havrix Junior are funded on the NIS for transplant patients, children with chronic liver disease, and close contacts of known hepatitis A carriers. In infants and preschool children most infections are either asymptomatic or cause mild nonspecific symptoms without jaundice. Adults typically develop symptomatic disease (eg, jaundice, weight loss, abdominal discomfort, dark urine), the severity of which increases with age.
HEPATITIS B Hepatitis B is a very infectious viral disease that infects liver cells. The subsequent host’s immune response leads to infected liver cell death. Hepatitis B is included in the NIS as part of the Infanrix-hexa (diphtheria, tetanus, pertussis, polio, hepatitis B, Haemophilus influenzae type b) vaccine. Engerix-B is also funded for other people meeting certain criteria.
Symptoms of acute hepatitis B include nausea and vomiting, jaundice, dark urine, pale faeces, tiredness, anorexia, stomach and muscle aches and fever. Some people are infected with the virus but do not show symptoms for a long time (chronic hepatitis).
Be concerned about anybody with problems breathing, chest pain, sudden confusion, or with bluish lips or face.
Call a doctor or Healthline (0800 611 116) (if appropriate) first for advice.
Protect yourself and other people from possible infection. Consider asking the person who is potentially infected to return to their car, if you are serving them in a shop.
Anybody with suspected diphtheria as the diphtheria toxin can affect the lungs, heart, peripheral nerves, and kidneys. Fatality rate is 2%–10%.
Anybody with suspected Hib infection. Hospitalisation may be required.
Anybody with suspected hepatitis A infection.
Anybody with suspected hepatitis B.
Transmitted either by droplet inhalation (through the infectious person coughing or sneezing) or by direct contact with the blister exudate (fluid). Incubation is 10–20 days. Contagious period is one to two days before the rash appears and until all the blisters have formed scabs – may take between five and 10 days. Keep children away from school or childcare facilities throughout this contagious period. Immunocompromised people can develop the disease more than once.
Depends on the variant. With Omicron it is considered to be one to two days before symptoms appear, to two to three days after symptoms appear. Research shows COVID-19 is primarily spread by droplets when a person coughs, breathes, or sneezes, but there have been some studies that show it can spread on surfaces.
People at higher risk include those over the age of 65, or who are obese, smokers, of certain ethnicities (Asian, Caribbean, or African), or with underlying health conditions, such as chronic lung disease, serious heart conditions, liver or kidney disease, poorly controlled diabetes, or who are immunocompromised.
Transmission is by respiratory droplets or by direct contact with skin lesions or articles soiled by infected individuals. Diphtheria can be spread through contaminated food, such as milk. Untreated people are infectious for up to a month. Once appropriately treated the contagious period can be limited to four days. Incubation period: two to five days.
Spread by infectious droplets through coughing and sneezing.
Incubation period: unknown, probably two to four days.
Scarring as a result of chickenpox infection occurs in approximately one in five children with an average of three scars per child, often on the face. Secondary bacterial infection as a result of scratching is common. Antibiotics may be needed. People with asthma may get a worsening of their asthma symptoms or develop a viral pneumonia. Other more severe complications (eg, encephalitis, Guillain-Barré syndrome, Reye’s syndrome) are rare and more likely in immunocompromised and adult chickenpox cases.
Foetal abnormalities, premature labour and delivery and, rarely, maternal or neonatal death (2%–5% risk) can occur if a pregnant woman contracts chickenpox at eight to 20 weeks' gestation. Newborns are at risk of serious disease if their mother contracts chickenpox between the 5th day before delivery and the 2nd day after the baby is born. Other cases of chickenpox acquired in utero may cause no symptoms in the foetus but may present later as shingles at a young age.
One dose of vaccine gives good protection; two doses gives optimal protection. Up to five out of 100 vaccinees may develop a vaccinerelated rash after immunisation. Although transmission of the virus is unlikely, vaccinees with a rash should avoid contact with susceptible people. Avoid NSAIDs in chickenpox due to the rare possibility of complications. Varicella-zoster immune globulin given within 96 hours of initial contact can also reduce disease severity.
As of 31 March, 2023, the following vaccines have been approved for use in New Zealand: the Pfizer–BioNTech (Comirnaty) vaccine (RNA) pediatric (for ages 5 to 11 years), original, and bivalent (Pfizer BA.4/5) vaccines, and the Novavax (Nuvaxovid) vaccine (protein subunit) – available as a primary course for people aged 12 years and older (not recommended during pregnancy). Can also be used as a booster for anyone over 18 years old.
The Oxford/AstraZeneca (Vaxzevria) vaccine (non-replicating viral vector) is no longer available in New Zealand. Alternatives include the Pfizer or Novavax vaccine.
Provisional approval has been granted by Medsafe for Jcovden (previously Janssen) vaccine for primary courses and boosters for ages 18 and over. Jcovden is a single-dose viral vector vaccine.
Treatment is with diphtheria antitoxin and antibiotics.
Recommended in combination with other vaccines to children aged 6 weeks, 3 months, 5 months, 4 years, and 11 or 12 years. Recommended for pregnant women from 16 weeks of pregnancy.
Booster doses should be considered by adults every 10 years particularly if travelling overseas to developing countries (usually given as a combined tetanus and diphtheria vaccine). Boostrix is funded on the NIS for adults aged 45 and 65 years old needing a catch-up tetanus and diphtheria immunisation and booster immunisation, or for individuals needing a tetanus booster because of a wound.
The infection is treated with antibiotics and additional treatments may be required for associated illnesses. Before the introduction of the Hib vaccine in 1994, Hib disease was the most common cause of life-threatening bacterial infection in children aged less than five years. Since 1994, hospitalisations due to Hib have decreased by approximately 90%.
Avoid overcrowded conditions and sharing food and utensils. Practise good hygiene measures.
Can survive outside the body for prolonged periods in food and water.
Incubation period: 15–50 days.
Transmitted either through person-to-person contact or through food or drink contaminated with faeces from an infected person.
Signs and symptoms usually last less than two months, although can last up to six.
Usually transmitted through contact with infected blood or body fluids during childbirth, contact with broken skin in childhood, or during sexual intercourse or intravenous drug use.
Hepatitis B virus in desiccated blood remains infective for at least one week.
Incubation period: six weeks to six months.
Thoroughly wash hands before and after using the toilet, before preparing and serving food, and after changing nappies.
The number of notified cases has steadily decreased since 1980; however, outbreaks frequently occur, most notably in the Ashburton district in 2013 with over 28 confirmed cases reported, and in 2015 and 2022/2023 linked to imported frozen berries. Complications of hepatitis A are rare but can include cholestasis (a build-up of bile inside the liver) and liver failure which is potentially fatal.
No specific treatment. Chronic hepatitis B infection can be treated with interferon and anti-viral medication. Contacts and family members of infected persons should be vaccinated against hepatitis B and practise strict hygiene measures. As there is no cure, preventing infection with the disease through vaccination, not sharing needles and practising safe sex using condoms is recommended.
People with chronic hepatitis B are at higher risk for liver disease or liver cancer.
HUMAN PAPILLOMA
VIRUS (HPV)
HPV viruses are a group of more than 200 related viruses. At least 40 different types can be spread through sexual contact and HPV infections are the most commonly sexually transmitted infections.
The HPV vaccine Gardasil 9 (protects against HPV types 6, 11,16,18, 31, 33, 45, 52 and 58) is funded on the NIS for both males and females from age nine to under 27.Two doses are recommended for those aged 14 and under; three doses for those aged 15 to 26 or aged 9 to 26 years with confirmed HIV infection or transplant patients. Refer to www.immune.org.nz for further information about administration and funding.
INFLUENZA See the Influenza chapter for details about influenza immunisation.
MEASLES Measles is a highly contagious disease caused by a paramyxovirus of the genus Morbillivirus. Vaccinations against measles are funded on the NIS and given as a combined measles, mumps and rubella vaccine (MMR II, Priorix); see NIS for administration recommendations. Last reported epidemic in New Zealand and the Pacific Islands was 2019/2020 (2193+ cases [1736 in Auckland] in NZ, 2 deaths of unborn foetuses; 5697+ cases, 83 deaths in Samoa). Current low vaccination rates suggest another epidemic is imminent. Measles is endemic in many countries overseas and more than a million children die from the virus each year. Travellers to countries experiencing outbreaks may need to show evidence of vaccination.
MENINGOCOCCAL DISEASE
Meningococcal disease is a bacterial infection caused by the bacterium Neisseria meningitidis, of which several different groups exist (A, B, C, E, W, X, Y). Between 40 and 150 cases of meningococcal disease occur in New Zealand each year, with most cases being caused by group B bacteria. Group W and group C are also common. Group W and Y are the cause of bacteraemia and pneumonia in the elderly. Humans are the only hosts of these bacteria. Although there are a number of meningococcal vaccines available, only Menactra, MenQuadfi, and NeisVac-C are publicly funded for certain groups of people at high risk (see the Pharmaceutical Schedule for criteria). During outbreaks, other meningococcal vaccines may be funded for local communities. Customers may choose to purchase these privately.
NeisVac-C only protects against Group C bacteria and Menactra and MenQuadfi protect against Groups A, C, Y and W. Conjugate vaccines are considered superior to polysaccharide vaccines.
Meningococcal B bacteria vaccines are difficult to develop; however, Bexsero was approved in New Zealand in 2018 and protects against Group B only.
MUMPS Mumps (epidemic parotitis) is caused by a paramyxovirus of the genus Paromyxovirus. Most reported cases are in children aged five to nine years. Mumps is funded on the NIS and is given as a combined measles, mumps and rubella vaccine (MMR II, Priorix). A significant mumps outbreak affecting more than 1200 people occurred mostly in the Auckland region in 2018, and another outbreak occurred at the end of 2019.
Symptoms
HPV is very common with four out of five people becoming infected with HPV during their lifetime. In most people, the infection clears by itself without causing any symptoms or long-lasting health problems. Low-risk HPVs 6 and 11 cause approximately 90% of genital warts. Genital warts appear as a small bump or cluster of bumps in the genital area. They may be raised or flat, small or large, or shaped like a cauliflower. High-risk HPVs cause cancer, including cancer of the cervix and anus and oropharyngeal cancer. HPVs 16 and 18 are the most commonly implicated viruses. Cancer often takes years to develop after a person gets HPV.
First three days: high temperature, cough, cold, runny nose, sore throat, swollen neck glands. Red, sore, watery eyes and an inability to tolerate light. Day three: Koplik’s spots may appear (small red spots on inner surfaces of cheeks and soft palate). These are transient and not seen in every case of measles. Days four and five: blotchy, flat red rash, first appearing on the face then progressing down the trunk and limbs, with or without itch.
If there is any suspicion of genital warts.
For any abnormal bleeding, pain, or discharge in the genital area. Women aged 20 to 70 should undergo cervical screening at least every three years.
Symptoms can develop suddenly and include: a high fever, headache, sleepiness, joint and muscle pains. More specific symptoms include: a stiff neck, photophobia (cannot tolerate light), vomiting, crying, and a reddish-purple, pinprick, spotty rash or bruises that do not blanch (go white) when pressed.
In babies and very young children, the signs may be more subtle.
Infants may refuse to feed.
The child may be listless or strangely quiet, irritable, or have a very high-pitched cry.
The child may have a bulging or tight fontanelle (top of the head).
Neck stiffness may be absent in infants.
Mothers are usually very instinctive about their children and, if they believe there is “something not quite right”, the child should be referred to a doctor.
If there is ear pain. If the child is unwell after the rash subsides. If the diagnosis is uncertain.
Some people do not experience any symptoms.
Both parotid (salivary) glands on the side of the neck enlarge and become tender although one usually swells one to two days before the other.
The glands become increasingly sore, especially when swallowing, talking, chewing and drinking.
Dry mouth, fever, stiff neck, loss of appetite, nausea, vomiting, tiredness and convulsions may occur.
Be alert for the signs and symptoms of meningococcal disease and seek urgent medical treatment if it is suspected or cannot be ruled out. For more information go to the YourHealth topics on the New Zealand Ministry of Health’s website www.health.govt.nz (or phone Healthline: 0800 611 116 or 111 if it is an emergency).
If your customer has already seen a doctor and been sent home but is still concerned, advise them to call the medical centre or hospital again, or to phone a different doctor, and insist on further tests or observation.
If customer is going through puberty. If the customer has repeated vomiting, headache and a stiff neck. If the customer is an adult or adolescent male with the disease. If the diagnosis is uncertain.
HPV can be transmitted through skin-to-skin contact, although it is most commonly spread during vaginal or oral sex. Transmission can occur even when condoms are used and without penetrative intercourse.
Incubation period: typically one to 20 months; however, in some people, symptoms do not develop until years after having sex with somebody who is infected.
In most infections, a person’s own immune system eradicates cells infected with HPV within five years.
Low-risk HPVs do not cause cancer but can cause skin warts on or around the genitals, anus, mouth and throat. HPV types 6 and 11 can also cause respiratory papillomatosis (a condition where bengin tumors grow within the respiratory system).
More than 10 high-risk HPVs have been identified that cause cancer, including HPV types 16, 18, 31, 33, 45, 52, and 58. HPV types 16 and 18 cause the majority of cancers, including 70% of all cervical cancers. HPV viruses also cause 95% of anal cancers, 70% of oropharyngeal cancers, 65% of vaginal cancers, 50% of vulvar cancers, and 35% of penile cancers.
Vaccination should ideally be administered to children aged nine to 14, before the onset of sexual activity, and the course completed within six to 12 months. Cervical cancer screening is still recommended in women between the ages of 20 and 70, even if they have received the vaccine.
Transmission of the virus is by inhalation or ingestion of infected droplets that have become airborne when a person with measles coughs or sneezes.
Incubation period: four to 12 days. There are usually no symptoms until the rash appears.
An infected person is contagious from two days before any symptoms show to at least five days after the onset of rash. Children should stay away from school or childcare facilities throughout this contagious period.
Transmission is by close or lengthy contact with an infected person's saliva or respiratory secretions; the bacteria are transferred during coughing or kissing. Transmission is more likely to occur between people living in the same household or in shared accommodation.
Meningococcal bacteria are not as contagious as viruses that cause the cold and flu so a person is unlikely to become infected during casual contact or by breathing the same air as an infected person.
Meningococcal disease is more common in infants, adolescents, and young adults; in people without a spleen, with HIV, or with persistent complement component deficiencies; and in sub-Saharan Africa.
Risk of complications from contracting measles are far greater than risks associated with vaccination with the MMR vaccine. Those at risk of complications include those who are malnourished (particularly vitamin A deficient), immunocompromised and pregnant women. Diarrhoea leading to severe dehydration is the most common complication of measles. Other complications include otitis media which may lead to deafness, pneumonia which may be fatal, bronchitis, croup, conjunctivitis and/or corneal ulceration leading to blindness (especially if vitamin A deficient), mouth ulceration, acute glomerulonephritis (inflammation of kidneys) and acute renal failure. Measles infection during pregnancy increases the risk of premature labour and delivery, and foetal loss. There is also a risk of maternal death. There is no causal link between receiving the MMR vaccine and developing autism or bowel disease. An acute infection of measles almost always gives lifelong immunity. Vaccination induces probably lifelong immunity in most individuals. Although New Zealand gained verification from the World Health Organization for eliminating endemic measles in 2017, an epidemic still occurred in 2019/2020, linked to people bringing in the disease from overseas. Given the currently low vaccination rates, another epidemic is likely soon. Other management: Severe cases of measles usually require hospitalisation and antibiotic administration for secondary bacterial infections. Antiviral medication may be prescribed to adults or those with severe infection.
Infection can cause two very serious illnesses: meningitis (an infection in the brain) and septicaemia (blood poisoning). Both are medical emergencies and can occur suddenly causing a person to deteriorate rapidly. Haemorrhage, shock, coma and death can occur within several hours despite antibiotic therapy. People who survive may be left with permanent disability or hearing loss.
Parenteral antibiotics should be administered to all cases as soon as meningococcal disease is suspected. Vaccination and/or prophylactic oral antibiotics should be considered for all people who qualify as close-contacts of a person with meningococcal disease.
About one in 10 people harbour the bacterium that causes meningococcal disease in the back of their nose and throat without any signs or symptoms of the disease.
Meningitis may also be caused by viruses and fungi.
General health measures (such as covering the nose and mouth when sneezing or coughing, washing hands before eating, and not sharing eating or drinking utensils, toothbrushes, or pacifiers) should be practised by everybody to limit the risk of contracting Meningococcal disease, particularly those living in shared accommodation such as university hostels, flats or army barracks.
In late 2018, an outbreak of a new, virulent strain of meningitis W (MenW) occurred throughout New Zealand, with the highest number of deaths reported in Northland before widespread vaccination. MenW may present with the typical symptoms of meningitis as well as other symptoms, such as gastrointestinal complaints, pneumonia, septic arthritis, and endocarditis. Antibiotics may be needed (ceftriaxone is preferred but use benzyl-penicillin if ceftriaxone not available).
In 2019, 139 cases of meningococcal disease were reported with 10 deaths. Cases per group were: B (62), W (36), Y (16), C (7) and E (1). 69 cases of meningococcal disease were reported in New Zealand in 2022.
Requires close personal contact for transmission to occur.
Incubation period: 12–25 days.
People with mumps are infectious from about one week before the onset of mumps to up to nine days after the swellings appear. Children should stay away from school or childcare facilities throughout this contagious period.
Unvaccinated adolescents and adults are most at risk of severe mumps disease. Postpubertal males are at risk of sterility if the disease affects the testicles. Mumps in pregnant women in their first trimester is associated with an increased rate of miscarriage. Complications include viral meningitis (15% of cases), encephalitis (1:6000 cases, of whom 1:100 die) and deafness (1:15,000 cases). Orchitis (testicle inflammation) affects one in five adult males, may be a risk factor for testicular cancer. Usually affects one testicle, sterility rare unless both testicles affected. Ovary inflammation affects one in 20 females. For most people one infection confers lifelong immunity. Vaccination with MMR vaccine is 85% effective at preventing mumps.
PERTUSSIS
PNEUMOCOCCAL DISEASE
Pertussis (whooping cough) is a highly contagious bacterial disease caused by Bordetella pertussis. Pertussis is one of the leading causes of vaccine-preventable deaths worldwide, with most deaths occurring in unvaccinated or incompletely vaccinated young infants. Pertussis is a component of several combination vaccines (such as Boostrix, Infanrix IPV, and Infanrix-Hexa) and is funded on the NIS in children.
Tetanus/diphtheria/pertussis (Boostrix) is also recommended for pregnant women in their second or third trimester, as well as caregivers of infants admitted to a specialised baby care unit for more than three days. Several other groups of people are eligible, see the Pharmaceutical Schedule for eligibility rules.
Pneumococcal disease is caused by the Streptococcus pneumoniae bacterium. More than 90 types of this bacterium exist and infections can vary from minor to severe. The pneumococcal 10-valent protein conjugate vaccine (Synflorix) is recommended at ages 6 weeks and 5 months followed by a booster at 12 months. The 13-valent vaccine (Prevenar 13) and 23-valent Pneumovax 23 is funded for high-risk patients children and adults only. See the Pharmaceutical Schedule for eligibility rules
POLIO
Poliomyelitis is a highly contagious viral disease caused by three types of polio virus (types 1,2 and 3). Prior to the development of polio vaccines, nearly every person became infected, especially infants and young children. Humans are the only hosts for polioviruses. Inactivated poliomyelitis vaccine (as either Infanrix IPV or InfanrixHexa) is funded on the NIS for unvaccinated individuals and for revaccination following immunosuppression. The first dose is usually given at six weeks of age as part of Infanrix-Hexa.
ROTAVIRUS Rotavirus is the leading cause of severe vomiting and diarrhoea in babies and young children in New Zealand. More than 90% of all unvaccinated children will have been infected by age three. Oral Rotarix is funded on the NIS. Two doses are recommended (6 weeks and 3 months). First dose must be given before 15 weeks of age and course must be completed before 25 weeks of age.
RUBELLA Rubella (German measles or three-day measles) is caused by a togavirus.
Rubella is funded on the NIS and is given as a combined measles, mumps and rubella vaccine (MMR II, Priorix).
SHINGLES (herpes zoster) See the Shingles chapter for details about immunisation for shingles (herpes zoster).
TETANUS Tetanus is a serious infection caused by the bacillus Clostridium tetani – found worldwide in soil. Tetanus is funded on the NIS and contained in several combination vaccines (such as Boostrix, Infanrix IPV, Infanrix-Hexa).
Booster doses are given to children aged four and 11, to pregnant women from 16 weeks of pregnancy, adults aged 45 who have not already received four doses of tetanus vaccine and adults aged 65. People in certain occupations and travellers may benefit from tetanus booster doses every 10 years.
Symptoms
Disease is more severe in infants and young children.
Catarrhal stage: Lasts one to two weeks and includes a runny nose, sneezing, fever, and mild cough.
Paroxysmal stage: Usually lasts one to six weeks, but can persist for up to 10. Burst, or paroxysm, of numerous, rapid coughs occurs followed by a long inhaling effort characterised by a high-pitched whoop. Some babies may not “whoop”.
Convalescent stage: The cough may persist for up to three months although usually disappears after two to three weeks. Paroxysms may recur with subsequent respiratory infections.
Major cause of ear infections and sinusitis. Pneumococcal pneumonia is the most common form of serious pneumococcal disease (fever, chills, cough, shortness of breath, rapid breathing). Pneumococcal meningitis and bacteraemia can also occur.
If the child is aged less than six months old.
If the disease is in its early stages, since antibiotics prescribed by a doctor can be effective.
If there is ear pain.
If there is vomiting, convulsions, exhaustion, dehydration, or the person is not eating.
If the diagnosis is uncertain.
Hospitalisation may be necessary for infants under six months – about half of older children may also need hospital care.
Anybody with suspected serious pneumococcal disease.
Ninety-five per cent of infected people have no symptoms; 4%–8% have mild symptoms such as a low-grade fever, headache, fatigue, vomiting, neck stiffness, sore throat, muscle pain. Some may develop aseptic meningitis a few days after, but most recover fully. Two per cent develop acute irreversible flaccid paralysis with loss of reflexes, which may also affect the breathing muscles.
Most common symptoms include diarrhoea, vomiting, and fever. In severe cases, children can have diarrhoea up to 20 times in one day. Symptoms can begin suddenly and last up to seven days.
Symptoms are often mild and may be absent or missed in 30%–50% of cases. A pink macular rash occurs on the forehead and face about seven days following infection. This spreads rapidly to the body, especially the chest and lasts two to three days. There may also be a slight fever, a runny nose, mild conjunctivitis, cervical lymphadenopathy and aching joints. Small petechial lesions (forchheimer spots) may be seen on the palate.
Bacteria in the wound produce a toxin which causes the muscles to stiffen around the jaw, neck, back, chest, abdomen and limbs; causing painful muscle spasms and lockjaw. Food may be difficult to chew or swallow. Some people may develop fever and sweating, and have difficulty breathing.
Anybody with suspected polio. Since 1962 only seven cases of polio have been reported in New Zealand. Six were vaccine or probably vaccine-associated before New Zealand changed to the inactivated polio vaccine in 2002. One case was acquired in Tonga and imported to New Zealand.
Seek medical advice immediately if child becomes dehydrated –symptoms include drowsiness or floppiness in children, a sunken fontanelle, sunken eyes or no tears.
All suspected cases of rubella should be notified so that public health control programmes can limit the spread.
Anybody with suspected tetanus needs to go to hospital immediately. The disease can be fatal (one in 10 people die). Children and the elderly are most at risk.
Spread by inhalation of infected droplets from a cough or sneeze.
Incubation period: six to 20 days.
Highly infectious and around 90% of nonimmune household contacts will contract it.
Infectious period: seven days after exposure until three weeks after the cough begins. Children should stay away from school or childcare facilities throughout this contagious period.
Babies aged less than six months are most at risk (75% require hospitalisation). Almost no maternal protection against pertussis is passed to the newborn from the mother. Children under 12 months who are ill enough to be admitted to hospital have a one in 200 chance of dying of whooping cough. In one to three per 1000 children whooping cough leads to permanent brain damage, paralysis, deafness or blindness (mortality rate of approximately 1%). Adolescents and adults may just present with a persistent cough similar to that found in other upper respiratory infections (but still infectious).
Other management: Antibiotics do not cure pertussis, but may be given to reduce spread of infection to others. Cough medicines provide little relief and should never be used in children under six. A mist vaporiser may soothe dry, irritated airways. Keep the room free of irritants such as dust and smoke. Maintain a good fluid intake – keep meals small and more frequent. Ensure sick children get plenty of bedrest.
Additional notes: Pertussis immunity wanes over time; both following natural disease and vaccination (immunity lasts five to 10 years). Pertussis is estimated to be responsible for up to 20% of severe coughs in adults lasting one to three months. These could be a significant reservoir of infection. Reinfection may present as a persistent cough, rather than typical pertussis. Currently available vaccines prevent disease much better than they prevent infection, so outbreaks still occur in countries with widespread vaccination, although mortality and morbidity is greatly reduced.
Pneumococcal bacteria are carried in the nose and throat of healthy adults and children. Transmitted through infected droplets released into the air by coughing or sneezing.
Incubation period: varies, may be as short as one to three days.
Transmitted by the faecal-oral route or by ingestion of pharyngeal secretions.
Asymptomatic people will shed the virus in their stool and through poor hygiene will spread the infection to others.
Incubation period: three to 21 days. Virus persists in the pharynx for approximately one week and in the faeces for three to six weeks.
Highly contagious. Virus is able to survive a long time on surfaces such as taps, bench tops and toys. Main route of infection is contamination of hands, utensils and other objects with faeces from an infected person.
Incubation period: 24–72 hours.
Transmission is through direct or droplet contact with infected nasopharyngeal secretions (through a cough or sneeze). Infants with congenital rubella shed virus in their pharyngeal secretions and urine for months after birth and should be considered infectious until they are 12 months old.
Incubation period: 14–21 days.
Humans are the only source of rubella infection.
Soil is the most common source of Clostridium tetani spores and bacilli. Animals also carry the bacilli and spores in their intestine and release it in their faeces. Entry can be gained into the body through a relatively minor cut, graze or puncture wound.
Incubation period: three to 21 days.
A person with tetanus is not infectious to other people.
Pneumococcal disease is more common in autumn and winter and is the leading cause of bacterial pneumonia in young children and adults older than 65. Maori and Pacific children are affected by pneumococcal disease more than other ethnicities in New Zealand. Vaccination provides protection against pneumococcal pneumonia and invasive disease, meningitis and septicaemia. Evidence suggests Synflorix may reduce the incidence of acute otitis media in children who start their vaccination course at the recommended time (at 6 weeks of age). Synflorix covers the 10 most common serotypes (1, 4, 5, 6B, 7F, 9V, 14,18C,19F, 23F) and provides cross-protection against 6A and 19A. Prevenar 13 covers the same 10 serotypes as Synflorix as well as 3, 6A, and 19A. Pneumovax 23 covers the same 10 serotypes as Prevenar 13 (except 6A) as well as 2, 8, 9N, 10A, 11A, 12F, 15B, 17F, 20, 22F, and 33F.
The disease is incurable. While the person is acutely unwell only supportive care can be provided to reduce complications associated with paralysis. Once recovered, rehabilitation can prevent or reduce post-polio deformities and increase independence.
The Global Polio Eradication Initiative aims to immunise every last child on the globe with polio vaccine and ensure a polio-free world for future generations. Until eradication throughout the world is confirmed, there is a risk of polio returning to New Zealand. New Zealand started immunising against polio in 1961 using the oral polio vaccine, which was replaced in 2002 by the inactivated polio vaccine. Worldwide rates of polio have decreased by 99% since 1988. Polio is still endemic in Afghanistan and Pakistan. Most years, several previously polio-free countries are reinfected due to imports of the virus from endemic countries infecting non-immune people, for example, polio virus was detected in New York’s wastewater in 2022 and several cases of paralysis caused by the polio virus were reported.
Strict hygiene is vital in preventing transmission. Hands should be thoroughly washed after changing nappies or cleaning up diarrhoea or vomit. Vaccination with the oral rotavirus vaccine is the most effective way to prevent infection. There is no specific treatment for rotavirus infection. The most important thing is to prevent dehydration by replacing fluid lost through diarrhoea and vomiting.
Rubella is usually a mild disease in children; adults tend to have more complications. The most serious complication of rubella infection is Congenital Rubella Syndrome (CRS), which results when the rubella virus attacks a developing foetus. When infection occurs during the first trimester of pregnancy, up to 85% of infants will be born with some type of birth defect, including deafness, eye defects, heart defects, mental retardation and more. Defects are rare when infection occurs after 20 weeks’ gestation.
Rubella vaccine, as contained in the combined measles, mumps, and rubella vaccine, is 95%–96% effective at preventing disease. Those who are not protected after the first dose almost always develop protection after the second dose.
The last significant rubella outbreak in New Zealand was 1995/96 where 1600 cases were notified. In 2017, New Zealand gained verification from the World Health Organization for eliminating endemic rubella; however, people may still bring in the disease from overseas.
Intensive care treatment is required and recovery can take months.
Almost all of the recent cases of tetanus reported in New Zealand occurred in individuals who had not received their primary immunisation course of a tetanus-containing vaccine. Between 1997 and 2016, 33 cases of tetanus were reported. Seven cases were reported in 2010, the highest number since 1992 and one person died. One case had received a primary course of tetanus vaccines but had not received a booster dose for 15 years. Most years, between zero and two cases are notified.
Boostrix is funded on the NIS for adults aged 45 and 65 years old needing a catch-up tetanus and diphtheria immunisation and booster immunisation, or for individuals needing a tetanus booster because of a wound.
• Young children are not very good at verbalising pain but asking them to point to a happy or sad face may help.
• Pain is not only a physical sensation; learned behaviour as well as psychological, social, and spiritual elements contribute to it as well.
• Pharmacy staff should not be telling caregivers to give their children regular paracetamol or ibuprofen - only a doctor should be doing this.
Young children may find it difficult to verbalise their pain, but they can usually indicate the severity of their pain by using the FACES pain scale which uses a series of faces ranging from a happy face at zero to a crying face at 10.
Changes in behaviour can indicate that babies or young children with disabilities are in pain. This may be observed as changes in movement of the whole body or certain body parts, crying, agitation or irritability, facial expressions, or a reluctance to eat or drink.
Listen carefully to a caregiver’s description of their child’s pain and observe the child’s behaviour. If the child is young are they:
• difficult to comfort or distract?
• quiet, withdrawn or very still?
• crying constantly or appear angry, agitated, or anxious?
• holding part of their body or favouring one limb over another?
• refusing food, milk, or other liquids?
• tugging at their ears?
• awakening frequently?
Always involve the pharmacist in any discussion about pain relief for a child.
Category Examples
Simple analgesics [GENERAL SALE]
• Seek urgent medical advice for children who are floppy, pale, hard to wake or unresponsive, with an unusual cry or who develop a rash or complain of a stiff neck.
• Children with other health conditions (such as asthma, diabetes, immunosuppression), or taking other medicines.
• Children younger than six.
• Children who are crying, grizzling and tugging their ears (ear infection).
• Children with an unknown source of pain.
• Children with persistent or worsening
Paracetamol or ibuprofen are considered first-line treatments for mild-tomoderate pain in children. Aspirin should be avoided in children under the age of 16 unless it is on the advice of a doctor, because of the risk of Reye’s syndrome.
Reye’s syndrome is a rare and serious condition which most commonly occurs after viral infections that have been treated with aspirin. Symptoms include vomiting or constant nausea, drowsiness, confusion, hallucinations, agitation and seizures. Urgent medical attention is required.
Although paracetamol is often perceived by parents and health professionals as being safer than ibuprofen, a meta-analysis of 19 trials found no significant differences in the incidence of adverse effects between the two agents in paediatric patients. Pharmacy staff should advise against regular administration of either paracetamol or ibuprofen in young children, unless a doctor has specifically stated to do so. Be alert for any caregiver who may be giving their child paracetamol or ibuprofen
eg, paracetamol – less than 20 tablets, (Panadol, Paracare) [PHARMACY ONLY MEDICINE] eg, paracetamol – greater than 20 tablets, suspension (Pamol All Ages, Paracare range)
Non-steroidal antiinflammatory drugs (NSAIDs) [PHARMACY ONLY MEDICINE] eg, ibuprofen (Nurofen for Children Soft Chewable Capsules*, Nurofen for Children
3 Months - 5 Years* and Nurofen for Children
5 - 12 Years*)
Topical anaesthetics [GENERAL SALE] eg, lignocaine (Soov cream) [PHARMACY ONLY MEDICINE] eg, lignocaine/prilocaine (Emla cream/patch)
Comments
pain, despite 24-hour treatment with OTC pain relievers.
• Children complaining of a very sore throat.
• Children who are refusing to eat or drink fluids or vomiting.
• When you or the caregiver feel “things are not quite right” (pain relievers can cover up symptoms of serious pain).
• Children with a history of seizures related to fever.
• Children with allergies to medicines.
for extended periods of time, and refer them to your pharmacist. Any child with pain that is not being controlled by occasional use of either of these analgesics should be referred to a doctor for further investigations.
It is important to remember that integrative, non-pharmacological treatments, such as aromatherapy, controlled abdominal breathing, distraction techniques, and heat and cold therapy all have a place in the mangement of children’s pain, especially for chronic or recurring pain.
Pain is essentially a signal about a threat to our bodies from the external world or sometimes an internal issue. When we burn our finger on the toaster or hit our shin on a table we immediately experience a pain withdrawal reflex, then a fast, acute sensation of pain, followed by a slow, duller, pain sensation.
Pain is generally classified as acute or chronic. Acute pain is a useful alarm system. Its purpose is to stop us from doing things that damage
Although paracetamol appears to have few side effects, regular use should be discouraged in young children unless on the advice of a doctor. Weight-based dosing may be more appropriate for underweight children. Age-based dosing or dosing based on ideal body weight may be more appropriate for overweight children. Always refer children with jaundice, hepatic or renal impairment to a pharmacist. The risk of liver toxicity is increased with higher dosages, in children with a family history of liver disease, and with dehydration. Take care to avoid overdose. Check strength, formulation and dosage instructions.
Ibuprofen is the NSAID least likely to cause stomach irritation. Always refer children who are dehydrated, with asthma, coagulation defects, hepatic or renal impairment to a pharmacist. Discontinue use if stomach upsets, increased bruising or prolonged bleeding occur. Ensure children stay well hydrated. Short-term ibuprofen is well tolerated and does not need to be given with food.
Lignocaine can be used to relieve skin pain due to sunburn, minor scalds or burns, and cuts and grazes. Lignocaine/prilocaine creams can be used before procedures (eg, injections or taking blood samples). Apply to the skin 60 minutes before the procedure to allow time for the lignocaine to numb the pain response. Lignocaine creams should be used with caution in infants up to three months of age because adverse effects are more likely in this age group. Products
• There are two types of herpes simplex virus: HSV-1 (usually associated with facial infections) and HSV-2 (usually associated with genital or rectal infections).
• HSV-1 causes the majority of cold sores; however, infections with HSV-2 are becoming more common.
• Cold sore treatments reduce the duration of symptoms and may improve the appearance of a cold sore; however, they are not a cure.
• Always give your customers advice on how to avoid transmission of HSVs.
Take a look at the cold sore and ask the customer if they have experienced cold sores in the past. If you are not sure if it is actually a cold sore, or if they have any other features of concern, refer them to a pharmacist. For all other customers, explain the treatment options available to them.
Although herpes viruses are incurable, treatment products can shorten the duration of symptoms and improve the appearance of the cold sore. Left untreated, most cold sores heal within seven to 10 days. Topical antivirals such as aciclovir and penciclovir help shorten symptom duration if started early (at the first tingle). Effectiveness of iodine-based preparations such as idoxuridine and povidone-iodine is questionable; however, one product also contains an anaesthetic that can help relieve pain and itching associated with the sore. Hydrocolloid patches create a benefi-
Category Examples
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• Young children.
• Cold sores inside the mouth.
• Cold sore-like lesions elsewhere on the body.
• Cold sores that are located near or on the edge of the eyes.
• Cold sores that have lasted more than 10 days or persisted despite treatment.
cial healing environment for the cold sore, help reduce viral transmission, and also keep nerve endings moist, helping to relieve pain. Make-up can also be applied over the patch, helping to hide the cold sore. Laboratory studies have shown an antiviral effect for propolis that may be enhanced when combined with aciclovir.
Famciclovir, three tablets taken together as a single dose, is available as a Pharmacist only medicine for the treatment of recurrent cold sores.
Prescription oral antiviral agents such as aciclovir and valaciclovir are more likely to be prescribed for people with genital herpes, although may be used to treat severe facial infection or infection in immunocompromised people. They stop HSV from multiplying so can shorten and prevent attacks; however, cannot eradicate it from its resting state within the nerve cells. Valaciclovir is converted into aciclovir in the body and has the advantage of two to three times daily
Medicated ointments [GENERAL SALE] eg, Blistex Medicated Relief (contains camphor, padimate and oxybenzone)
Antiviral agents (topical) [GENERAL SALE] eg, aciclovir (Viraban, Viratac, Zovirax) idoxuridine + lignocaine (Virasolve) povidone iodine (Betadine Cold Sore Paint) [PHARMACY ONLY MEDICINE] eg. penciclovir (Vectavir)
Antiviral agents (oral) [PHARMACIST ONLY MEDICINE] eg. famciclovir (Famciclovir Once)
Healing/protective plasters [GENERAL SALE] eg, Compeed Invisible Cold Sore Patch
Natural/herbal products/ supplements Calendula/ hypericum perforatum (eg, Weleda Hypercal), honey (Honevo Cold Sore), lemon balm, rhubarb & sage, lysine (Nutralife Cold Sore Formula), pelargonium, propolis (Herstat Lip Care)
• Cold sores that look infected (eg, with pus or swollen).
• Frequently recurring cold sores.
• Large cold sores (for example, as big as a 10 cent piece) or people having multiple cold sores.
• People who also have dermatitis or other skin conditions near the cold sore.
• People with other symptoms such as fever or who feel unwell.
• People with allergies to topical medicines.
dosing instead of the five times daily dosing required for aciclovir.
Lysine (also called L-lysine) is an essential amino acid that is necessary for growth and tissue development. It also has antiviral properties; however, trials investigating the effectiveness of lysine for HSV infections have yielded conflicting results. In some people, regular lysine may reduce cold sore recurrences and improve symptoms.
Cold sores are fluid-filled blisters caused by HSV that commonly appear on the lips or the bottom edge of the nose. Most start with a tingling sensation in the affected area, followed by the appearance of a blister or blisters that pop soon after to form clusters of fluid-filled pockets. Some people may also complain of a sore throat, fever, or swollen lymph nodes in the neck.
There are two types of herpes simplex virus:
Comments
Helps protects the lips from sun, wind and cold. May help prevent recurrence of cold sores induced by the sun. Relieves cold sore discomfort.
May prevent the cold sore appearing when applied at the first signs of a cold sore (the tingling stage). Even if used after this, topical antivirals can reduce healing time; however, they do not eradicate the virus from its resting state within the nerve cells so will not prevent future attacks. Apply treatments exactly as directed by the manufacturer (some may specify as frequently as every two hours while awake).
Famciclovir is a prodrug of penciclovir. It inhibits viral DNA replication and reduces time to resolution of symptoms such as pain and tenderness. Suitable for adults aged 18 years and older to treat recurrent outbreaks of cold sores. All three tablets should be taken as a single dose.
Keeps cold sores moist, creating a beneficial wound-healing environment. Relieves pain, burning and itching, and prevents scabbing. Hides and protects the cold sore and stops the spread to other people. Change patch when it starts to detach from the skin (usually after eight to 12 hours).
Oral lysine can reduce recurrences of cold sores, and both oral and topical lysine can reduce the duration and symptoms of developed cold sores. Honey keeps the area hydrated and acidic, helping wound healing. Pelargonium has some antiviral activity. Propolis has antiviral activity and may help shorten the duration of a cold sore and relieve cracked lips.
Type 1 (HSV-1) and Type 2 (HSV-2). Although HSV-1 is mainly associated with facial herpes (cold sores), and HSV-2 with genital and rectal infections, either virus can infect almost any area of the skin or mucous membrane.
The World Health Organization (WHO) estimates two-thirds of the world’s population under 50 are infected with HSV-1. Most people first acquire HSV-1 during childhood; in crowded, undeveloped areas of the world most children have been infected by age five.
Gingivostomatitis (an inflammation of the oral palate and gums) is the most common way HSV-1 presents the first time a person (usually a child) is infected. Symptoms include a high fever, excessive dribbling, red and swollen gums which bleed easily, and whitish-yellowish ulcers may be present on the tongue or inside cheeks or roof of the mouth. The fever usually subsides within three to five days, although recovery may take two weeks. Some children may have no noticeable
symptoms at all.
HSV-2 infections are mainly transmitted through sexual contact and these are more likely to occur after puberty.
Once acquired, HSV remains in the body for the person’s lifetime in a latent state in the spinal dorsal root nerves. Certain environmental or individual factors can cause the virus to reactivate.
Common triggers include other viral infections (such as the cold or flu), stress, dental work, the sun, or hormonal changes in women.
Recurrences are more common in people with a weakened immune system and outbreaks tend to become less frequent as people get older, as the body makes antibodies to the virus. During an attack, the virus can be inoculated into new areas of skin or transferred directly or indirectly to other people. For example, a thumb-sucker may transmit the virus from their mouth to their thumb or an infected rugby player may infect others during a scrum (“scrum pox” ).
• Use a lip balm containing sunscreen on your lips before going outside if you find sunlight tends to reactivate the virus.
• Have treatment on hand, ready to use at the first “tingle”.
• Keep the cold sore moisturised to prevent the affected area drying out and cracking, and do not pick off the scab.
• People who get repeat attacks of severe cold sores despite use of a 3-day course of famciclovir should see their doctor for prescription antivirals.
• Cold sores are easily spread from person to person, especially when the sore is still weeping. Advise your customers that while they have the cold sore they should:
➤ avoid kissing or other intimate contact
Concern has been expressed by the WHO regarding the rise in the number of cases of genital herpes attributable to HSV-1. In certain regions, such as the Americas, Europe, and the Western Pacific (including Australia and New Zealand), there has been a decrease in the number of childhood HSV-1 infections (which confer some degree of immunity to genital HSV-1 infection), and a rise in the practice of orogenital sex. Although HSV-1 genital herpes is less likely than HSV-2 genital herpes to recur, it carries a higher risk of causing neonatal herpes and has been associated with an increase in the risk of HIV acquisition.
People with a weakened immune system are more prone to developing severe and recurrent cold sores.
➤ avoid sharing towels, face flannels, or eating and drinking utensils
➤ take care not to touch the cold sore, then touch or rub their eyes. Extra care should be taken if they wear contact lenses
➤ wash their hands before and after applying cold sore products, before preparing food or eating, and before attending to other people
➤ avoid using the same finger when applying cold sore products as they may contaminate the cream
➤ not share their cold sore cream with other people
➤ not share cosmetics, especially lipsticks.
Bloomin’ Great Learning just got easier
Bloomin’ Great Learning just got easier
Class - pharmacist education to guide your recertification
Class - pharmacist education to guide your recertification
Capture - your ‘keeping up to date’ reading record
Capture - your ‘keeping up to date’ reading record
• Distinguishing between a typical cold, COVID-19, the flu, and hay fever can sometimes be difficult.
• COVID-19 is very contagious and deadly for some. Follow recommended guidelines to ensure you are not inadvertently exposed to the virus.
• Over-the-counter treatments only temporarily relieve cold symptoms.
Customers with suspected COVID-19 should ideally not enter the pharmacy; however, you should still respectfully attend to
their requests by talking with them over the phone, outside, or through a representative, and arranging delivery if needed.
For other customers, maintain a safe distance to reduce your risk of infection and listen to their description of their symptoms. What is their most obvious symptom? Do their eyes appear red or watery or look sore? Are they sneezing a lot or is their nose just runny? Do they actually look unwell and are complaining of a sore throat or body aches and pains?
Symptoms of a cold, COVID-19, the flu (influenza), and hay fever (allergic rhinitis) can be similar but there are some key differences (see
Category Examples Comments
Simple analgesics [GENERAL SALE] eg, paracetamol (Pamol range, Paracare range, Panadol, Lemsip Cold & Flu Hot Drink*)
Saline nasal spray/drops [GENERAL SALE] eg, saline products (Bosistos, Fess Saline, NeilMed, Otrivin Saline Plus, XClear)
Decongestant nasal sprays [PHARMACY ONLY MEDICINE] eg, oxymetazoline (Sudafed Nasal Decongestant, Vicks Sinex), xylometazoline (Otrivin Junior, Otrivin Adult, Otrivin Plus [+ ipratropium])
Single and combination products [GENERAL SALE]
eg, paracetamol (Lemsip Max Hot Drink*) eg, phenylephrine + ibuprofen (Maxigesic PE* [+ paracetamol] [20’s], Nurofen Cold & Flu*)
eg, phenylephrine + paracetamol (Lemsip Max Cold & Flu Capsules with Decongestant*, Lemsip Max Hot Drink with Decongestant*)
eg, phenylephrine + paracetamol + caffeine (Lemsip Max Cold & Flu Day & Night Capsules*)
eg, phenylephrine + paracetamol + guaiphenesin (Lemsip Cough Max For Mucus Cough & Cold capsules*, Lemsip Cough Max For Mucus Cough & Cold Hot Drink*) [PHARMACY ONLY MEDICINE]
eg, phenylephrine + paracetamol (Codral Cold & Flu), Maxiclear Cold & Flu Relief Sinus & Pain Relief)
eg, phenylephrine + paracetamol + ibuprofen (Maxigesic PE* [30’s])
eg, phenylephrine + paracetamol + antihistamine (Codral Nightime Cold & Flu)
eg, phenylephrine + loratadine (Maxiclear Cold & Nasal Relief Hayfever & Sinus Relief*) [PHARMACIST ONLY]
eg, phenylephrine + paracetamol + antihistamine + dextromethorphan (Codral Cold & Flu + Cough, Coldrex PE Cold & Flu Day & Night)
eg, phenylephrine + paracetamol + antihistamine (at night) (Codral Day & Night Cold and Flu)
eg, pholcodine linctus
eg, pseudoephedrine + paracetamol (Codral Original Day & Night)
eg, pseudoephedrine + ibuprofen (Nurofen Cold & Flu with Decongestant*)
Inhalations [GENERAL SALE] eg, combinations of volatile oils (Olbas Oil Inhalant Decongestant, Vicks Vapo Steam Inhalant)
Antibacterial prophylaxis [PHARMACIST ONLY] eg, Buccaline
Other products eg, Bonnington's Irish Moss eg, Neil Med Naspira Nasal-Oral Aspirator
Natural / herbal products / supplements
Andrographis, echinacea, garlic, honey, ivy leaf, olive leaf, probiotics, propolis, Saccharomyces cerevisia, Siberian ginseng, vitamin C, zinc eg, vitamin C (Lipo-Sachets*), vitamin D (Lipo-Sachets*)
the Table: Differentiating Cold, COVID-19, Flu, and Hay Fever Symptoms, opposite page). Symptoms of COVID-19 typically include a sore throat, cough, fever, abdominal pains, fatigue, or a loss of taste or smell; however, other symptoms, such as a headache, a runny nose, aches and pains, or diarrhoea may also be present. Symptoms can vary depending on the variant. Always consider it as a possibility.
Colds generally get better by themselves, but over-the-counter medicines may be taken to improve symptoms. Ask the customer
Use for headache or general sinus pain relief.
Saline drops/spray help liquefy mucus and soothe irritated nasal membranes. Safe for infants, toddlers, pregnant women or those with chronic congestion.
The topical decongestants oxymetazoline and xylometazoline are effective at unblocking congested nasal passages. Decongestants should not be used for longer than three days at one time because they may cause rebound congestion when discontinued.
Products may include a decongestant to unblock a congested nose (eg, phenylephrine), an analgesic (eg, ibuprofen, paracetamol), an antihistamine to dry up a runny nose (eg, loratadine, chlorpheniramine), a cough suppressant to stop a dry cough (eg, pholcodine), an expectorant to help expel mucus from the lungs (eg, guaiphenesin), or a mucolytic (eg, bromhexine) to liquefy mucus and phlegm. Coughs associated with colds are more likely to be productive.
Analgesics (eg, paracetamol, ibuprofen) can help make a person feel more comfortable if they are in pain. Watch for double-ups with other analgesic medicines. Combination codeine products are PRESCRIPTION only because the harms associated with codeine were considered to outweigh its benefits.
Some antihistamines may cause drowsiness and affect a person’s ability to drive or operate machinery. Avoid alcohol.
Cough suppressants (eg, pholcodine, dextromethorphan) control or suppress the cough reflex and can provide relief from a dry, unproductive cough. These are both classified PHARMACIST ONLY. Dextromethorphan can interact with medicines that have serotonergic activity (eg, antidepressants, tramadol, lithium, St John’s wort), and pholcodine has been linked to an increased risk of allergic reactions following anaesthesia. Do not supply pholcodine to people with surgery scheduled within the next 6 to 12 months.
Cough expectorants (eg, guaiphenesin) loosen mucus and phlegm, allowing it to be coughed up more easily and can help a chesty cough.
Mucolytics (eg, bromhexine) help liquefy mucus and phlegm aiding its passage from the lungs to the mouth.
Most cold and flu medicines require a pharmacist’s advice before using them in children aged less than 12 years.
Place a few drops in a bowl of hot water and inhale the steam, or on a tissue tucked inside a pillow case at night. Avoid in very young children.
May help protect against bacterial complications from a cold.
Combination menthol, camphor, liquorice extract and carrageenan (a seaweed extract) help loosen phlegm and relieve congestion. Nasal-oral aspirators allow removal of nasal mucus.
Andrographis, garlic, and Siberian ginseng may reduce cold symptoms if started within 72 hours of a cold. Note: allergic reactions, including anaphylaxis, have been reported with andrographis use. Zinc lozenges may decrease cold duration.
Echinacea may reduce cold severity and duration by 10%–30%; long-term use not recommended. Honey can soothe a dry throat and relieve cough in children older than one year – a single nighttime dose of 2.5–10ml was as effective in children as dextromethorphan.
Ivy leaf is an expectorant and is commonly used in Germany alongside conventional medicines for asthma/bronchitis. Olive leaf can help boost the immune system. Probiotics may reduce cold frequency. Propolis may decrease cold duration.
Vitamin C (1–3g/day) may decrease cold symptom duration by 24 to 36 hours. Lipo-sachets contain vitamin C encapsulated in Liposhell liposomes to enhance absorption.
which symptom(s) they find most troublesome, and choose a product that contains ingredients to suit (see Treatment Options, opposite page). To reduce the risk of side effects or interactions, avoid selling products that contain unnecessary or unwanted ingredients.
Refer any children under 12 to a pharmacist. Most cold remedies are not recommended for children, although saline drops may help relieve irritated nasal passages and paracetamol may be used occasionally to relieve general discomfort.
Ask anybody with suspected COVID-19 to wait outside and obtain their phone number to give to the pharmacist.
Colds are contagious and affect the mucous membranes of the head and chest, including the nose, throat, sinuses and ears. More than 50% of colds are caused by rhinoviruses but other common viruses include coronaviruses and respiratory syncytial virus.
Some people may get a bacterial infection after a cold (such as an ear or sinus infection) or
• People with suspected COVID-19, other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People who take regular medications, including herbal/complementary medicines.
• Children younger than 12.
develop pneumonia.
Colds are easily transmitted through direct contact with infected people, surfaces or objects; or by breathing in infectious droplets made airborne through sneezing and coughing.
The most common cold symptoms are a runny, congested nose with sneezing. Cough, sore throat, a slight fever, headache, earache and red, watery eyes may also occur.
COVID-19 is caused by the SARS-CoV-2
Sore
• People with a high temperature, body chills, joint aches or pains or who feel extremely unwell.
• People who complain of earache or facial/ sinus pain.
• Colds that have lasted more than a week.
• People with allergies to medicines.
virus, a coronavirus identified in January 2020. Most people develop a mild illness and some are symptomless. People more at risk of developing severe disease include Māori and Pasifika, smokers, people who are immunosuppressed or with underlying medical conditions (such as diabetes, heart disease, lung disease), and those older than 65. See also Childhood Diseases and Immunisations: COVID-19 for COVID-19 vaccination information. Treatment with antivirals is available for eligible people from doctors or from suitably qualified and trained pharmacists.
• Constipation is defined as the infrequent passing of stools, or difficulty in passing stools.
• What constitutes “infrequent” varies from person to person.
• Mild constipation may respond to exercise and increasing fluid and fibre in their diet.
• Long-term use of stimulant laxatives should be avoided unless on a doctor’s advice.
Ask your customer to describe their symptoms and ask how frequently they go to the toilet. Do they appear well hydrated or does their skin look dry? Could they possibly be pregnant?
Try to determine how severe the person’s constipation is, if it is caused by an underlying condition (such as dehydration, pregnancy, or some medicines), if the person seems to have an unusual preoccupation with their bowels, and to identify those customers who need to be referred to a pharmacist.
Despite pharmacies selling a wide range of laxatives, only mild cases of constipation, with a duration of less than one
Category
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People taking medication, including herbal/complementary medications.
• Babies and young children.
• Constipation that has lasted longer than seven days.
• People who you suspect may be abusing or misusing laxatives, or who have an unusual preoccupation with their bowels.
week, should be treated without being under medical supervision. This is because longterm constipation can have serious health consequences.
Straining to pass a stool can affect both the brain and the heart, and up to 8% of sudden cardiac deaths in those with existing cardiovascular disease are associated with straining or trying to force hard faeces out.
Products used to treat constipation are called laxatives and several different types are available. Most need to be given for a few doses in a row before they begin to work (see Table: Laxative types and mode of action, opposite page).
Bulk-forming laxatives [GENERAL SALE] eg, psyllium husk (Metamucil [sugar-free available]) eg, sterculia (Normacol, Normacol Plus [also contains frangula bark, a stimulant laxative])
Faecal softeners [GENERAL SALE] eg, docusate sodium (Coloxyl, Laxofast), poloxamer (Coloxyl Drops)
Osmotic laxatives [PHARMACY ONLY MEDICINE] eg, glycerol suppositories, lactulose (Laevolac)
Iso-osmotic laxatives [GENERAL SALE] eg, macrogol 3350 with electrolytes (Molaxole, Movicol, Movicol-Half)
Stimulant laxatives [PHARMACY ONLY MEDICINE] eg, bisacodyl (Dulcolax) eg, sennosides (Senokot*)
Combination products eg, senna + docusate (Coloxyl with Senna, Laxsol) eg, Microlax
• People with other symptoms such as abdominal pain, bloating, a fever, vomiting, or weight loss.
• Bowel motions that contain blood or are very dark or look like tar.
• Constipation that alternates with diarrhoea.
• Recurrent, persistent or worsening constipation.
• People with allergies to medicines.
Regular, daily exercise and an increased intake of fluids should be suggested initially to people trying to relieve mild constipation. In addition, prune or pear juice, and an increased intake of vegetables and fibre can help soften the stool. Lactulose is generally preferred in children with chronic constipation and bulking agents may be considered by women who are pregnant.
Constipation is defined as the infrequent passage of stools, or difficulty in passing stools. What constitutes “infrequent” varies from person to person and there is no right
Good as first-line agents because they have few interactions with medicines or long-term side effects. Avoid in people with bowel obstructions or when faecal matter is impacted, in bed-ridden patients, and in people unable to drink the required amount of fluid. Most are safe in pregnancy, except Normacol Plus because it contains a stimulant – frangula.
Most effective for mild constipation that has recently occurred and may be beneficial for people with haemorrhoids (piles).
Lactulose is not absorbed from the gastrointestinal tract and may be considered in children and pregnant women requiring regular laxatives.
Macrogols (also called polyethelene glycols) are virtually unabsorbed and are indentified by a number that represents their molecular weight (for example macrogol 3350). They are mixed with water before taking and may cause less dehydration than other osmotic laxatives.
Long-term use not recommended. Avoid in pregnancy unless under medical advice.
Senna and docusate combine a stimulant laxative with a faecal softener. The onset of effect is eight to 10 hours for tablets (one to two hours for suppositories). Microlax contains a combination of ingredients with osmotic and stool-softening effects.
Food supplements eg, gluten-free wheat dextrin (eg, Benefiber) Fine powder with minimum taste. Can be sprinkled on foods to increase fibre in diet. Safe long-term. Best for mild constipation and for people unable to eat fibrous food.
Probiotics eg, Bifidobacterium lactis, Lactobacillus reuteri
Bifidobacteria + lactobacilli (Inner Health, Lifestream BowelBiotics, Nutralife Probiotic)
Natural / herbal products / supplements eg, cape aloes, cascara, chia, European buckthorn, flaxseed oil, glycerol, magnesium, psyllium, senna leaf, olive oil eg, kiwifruit extract (Kiwi Crush, Phloe Bowel Health)
Contain probiotics +/- prebiotics (see Probiotics and Prebiotics). Help restore levels of naturally occurring bacteria in the bowel. An imbalance in bacteria may lead to constipation, diarrhoea, or bloating. Useful following a course of antibiotics. For daily use in adults.
Many commercial products for constipation are based on natural ingredients. Psyllium works as a bulk laxative, senna as a stimulant, glycerol as a softener, and magnesium can help soften faeces. European buckthorn has a stimulant effect, and olive oil softens stools. Kiwifruit extract contains prebiotics, enzymes and dietary fibre to optimise bowel health.
answer for how many times a person should defecate each week. Internal factors, such as age, physiology, and current mood, as well as external factors such as diet, social and cultural practices, and medications, all play a role in the frequency of a person’s bowel movement. In Western society, normal stool frequency ranges from two to three times per day to two to three times per week.The most common reasons for constipation are:
• being immobile – forced bedrest or disability
• dehydration – drinking too little fluid, vomiting or excessive sweating
• diet – eating too little, or eating low bulk or milky foods
• pain or other medical conditions (such as irritable bowel syndrome, Parkinson’s disease)
• pregnancy
• medicines such as diuretics, iron supplements, and opioid pain relievers.
Chronic constipation is estimated to affect up to 18% of the population and females are twice as likely as males to be affected. People with no apparent reason for their constipation should be referred to a doctor for further advice if it persists. Some people are found to have a generally underactive bowel, and may need long-term laxatives prescribed.
Occasionally, some people complaining of diarrhoea as well as constipation may in fact have “overflow” diarrhoea as a result of severe constipation (refer to a pharmacist).
People who suffer from constipation may also complain of stomach cramps, frequent passing of wind (flatulence) or bloating. Haemorrhoids can also occur with constipation as a result of straining when passing a bowel motion (see Haemorrhoids).
Bulking agent (fibre supplements)
Faecal softener
Psyllium
Sterculia
Methylcellulose
Polycarbophil
Docusate
2–3 days Contains soluble fibre which swells on contact with fluid, bulking out the stool and encouraging peristalsis (the symmetrical contraction and relaxation of the muscles in the bowel).
12–72h (oral) 15–20 min (rectal)
Poloxamer 12–24h
These act like detergents, lowering surface tension and encouraging a mixture of dietary fat and water to penetrate hard stools. This allows the stools to pass through the bowel more easily.
Docusate also has some stimulant activity.
Iso-osmotic Macrogol 3350 1–3 days Deliver liquid to the bowel rather than drawing it in from the surrounding tissue. Hydrate and soften the stool.
Osmotic Glycerol 15–60 min (rectal) Attract large amounts of water into the bowel, making the stool soft, loose, and easier to pass.
Lactulose Up to 48h
Microlax 15–20 mins Contains ingredients which have both an osmotic and stool-softening effect.
Stimulant Bisacodyl Sodium picosulfate
10–12h (oral) 20–60 min (rectal) Speed up peristalsis which moves the stool along by contraction.
Sennosides 8–12h
• Fibre is important for our health, and highfibre diets should be recommended for most, although they may not be appropriate for the very young or very old.
➤ Wholegrain breads and cereals, nuts, beans, lentils, fresh and dried fruits (not fruit juices) and vegetables are high in fibre.
➤ Men should aim for around 38g/day of fibre and women 28g/day.
➤ Children aged between four and 18 need about 18–28g/day.
➤ Increase fibre intake once constipation has resolved.
May cause cramping and abdominal discomfort. Do not use if intestinal obstruction is suspected.
• Don’t put off going to the toilet if you feel the urge as this can lead to constipation or make it worse.
• Regular exercise and sufficient fluid intake – at least six glasses of water a day – also prevents constipation.
• Not everyone has a daily bowel motion.
• Offer advice about haemorrhoids (see Haemorrhoids) if these are also present.
• Avoid long-term use of stimulant laxatives unless under medical advice.
• Seek medical advice if problems with bowel motions persist.
• Refer ALL women seeking information about oral or emergency contraception to a pharmacist.
• The effectiveness of the emergency contraceptive pill (ECP) may be decreased in women weighing more than 70kg (a copper IUD or 3mg of levonorgestrel is recommended for these women).
• Pharmacists can sell oral contraceptives to women meeting certain criteria.
While some women may confidently ask for the ECP, others may not. Politely asking female customers if they have something they would like to talk to the pharmacist about may be the best approach in women who appear embarrassed or shy.
All women wishing to purchase a supply of the ECP or an oral contraceptive must be referred to a pharmacist.
Only pharmacists who have completed and passed the required training can sell the ECP.
The ECP prevents pregnancy by interrupting follicular development and ovulation, and hindering the ability of sperm and ova to move through the fallopian tubes. It may also alter the lining of the uterus but recent studies suggest it does not affect implantation. The ECP cannot interrupt or harm an established pregnancy and may be used more than once in a menstrual cycle; however, this should not be encouraged. Instead, women should be referred to a doctor to discuss more consistent methods of contraception.
• Discuss the possibility of a double-dose (3mg levonorgestrel), or refer to a doctor or family planning clinic, women who are over 70kg OR with a BMI of 26 kg/m2 or more, or those taking medications that induce hepatic enzymes or with malabsorption syndromes.
• The ECP is considered safe to take while breastfeeding, although a woman should talk further with a doctor if she is concerned.
• Women with a BMI of 26 kg/m2 or more.
• Women with acute porphyria, severe liver disease, severe hypertension, diabetes, stroke, heart disease, or a past history of breast cancer requesting the ECP.
• A woman who has had the ECP and then has a period that is more than five days late,
• Around 14% of women taking the ECP feel nauseous and 1% may vomit. Taking the medicine with food may help. The pharmacist supplying the ECP may also sell up to 10 prochlorperazine tablets to prevent nausea and vomiting associated with taking the ECP.
• Advise the customer that her next period may be later or earlier than usual, or there may be spotting or irregular bleeding before her period occurs. She should see her doctor if her next period is late or lighter than usual.
• Other side effects of the ECP include tender breasts, headaches, lower abdominal pain, dizziness and fatigue.
• Do not give the ECP to any woman who is allergic to levonorgestrel or to any of the inactive ingredients in the tablet.
Oral contraceptives (OC) – also called birth control pills – contain hormones that prevent pregnancy.
The combined OC (COC) contains an oestrogen and a progestogen to prevent ovulation (the release of eggs from the ovaries), thin the uterine lining, and thicken cervical mucus making it impenetrable to sperm.
The progestogen-only pill (POP) – also called the mini-pill – contains just one hormone, progestogen. Most POPs work by thickening cervical mucus, preventing sperm from entering the womb. Some POPs (eg, desogestrel) also prevent ovulation, and offer a higher level of contraceptive efficacy than other POPs, and may be preferred in women unable to tolerate oestrogens or who are breastfeeding.
Although oral contraceptives are a very
Category Examples Comments
Emergency Contraceptive Pill (ECP) [PHARMACIST ONLY] (Accredited ECP pharmacists) eg, levonorgestrel 1.5mg (Levonorgestrel BNM)
Antiemetics [PRESCRIPTION] (Except when sold for the treatment of nausea associated with the ECP) eg, prochlorperazine (Nausafix)
Oral contraceptives (OC) (desogestrel, ethinylestradiol, levonorgestrel, norethisterone)
[RESTRICTED when sold by suitably trained pharmacists for women over the age of 16 previously prescribed an OC within the last three years]
unusually light or heavy, or is painful.
• A woman who thinks she may be pregnant or who has erratic periods.
• Women who may be at risk of contracting a sexually transmitted infection (STI).
• Women who need to consider long-term contraception.
effective method of birth control they do not prevent the spread of diseases (such as HIV or other STIs), so use with condoms should be encouraged.
Only pharmacists who have passed approved training can sell a select range of oral contraceptives, and only to women meeting strict criteria (see Treatment Options table).
Emergency contraception is a way of preventing pregnancy after unprotected sex or when contraception has failed. It is also called the “morning after pill”, although a woman does not need to wait until the morning after to take it. It is not intended for use as a regular way of preventing pregnancy.
There are two main types of emergency contraception – the emergency hormonal contraceptive pill (ECP) and the intrauterine contraceptive device (IUD). A copper IUD inserted within five days of unprotected intercourse has almost 100% effectiveness but must be fitted by a doctor. It has the advantage of providing long-term contraception and being effective for heavier women.
Pregnancy is most likely to occur if intercourse happens up to five to seven days before, or one day after ovulation. This is because some sperm can survive up to seven days (average three to four days) inside a woman, whereas the ovum (egg) has a life span of only about 12–24 hours.
However, many women have irregular cycles or are unsure of the date of their last period, so, unless they have periods like clockwork, or are taking a contraceptive pill, it is best to assume
Advise customers to take the tablet as soon as possible (and no later than 72 hours) after unprotected sex.
Up to 10 tablets may be supplied by an accredited pharmacist for nausea associated with the ECP.
Must be in an approved pack containing no more than six months’ supply. Refer women with newly identified contraindications to the OC to a doctor. Encourage regular cervical screenings and cardiovascular risk assessments.
• Pregnancy risk depends on pill type, duration of use, and at what point in the cycle the pill was missed.
• COC, 21-day continuous hormones (no hormone-free days, >3 month usage): Up to seven in a row could be missed because it is the same as having a week of inactive pills.
• COC 28-day pill cycle (three weeks of active pills and one week of inactive/no pills): Inactive tablet missed = no risk. Active tablet = some risk, especially if the missed pill was at the start or end of the inactive tablets.
• POP 28-day continuous hormones (no hormone-free days): More than three hours late (except for desogestrel: more than 12 hours late), risk of pregnancy.
• If there is a risk, condoms should be used or sex avoided:
➤ For seven days for COCs
➤ For two days for most POPs.
unprotected sex on any day of the cycle might result in pregnancy.
Emergency contraception should be made available to any woman who feels she needs it.
Refer to the Pharmacy Council of New Zealand website (www.pharmacycouncil. org.nz) for the nine standards prescribed by the council for the non-prescription supply by pharmacists of the levonorgestrel ECP. Nurses
Timing of use
When to use
Preferably within 12 hours but no later than 72 hours after sexual intercourse.*
Repeat the dose if vomiting occurs within 3 hours of taking the ECP.
Heterosexual sex that occurs without any form of contraception.
Incorrect condom usage or condom breakage.
Part or complete expulsion of an IUD.
Vomiting or severe diarrhoea while taking an oral contraceptive.
Missed Depo-Provera injection or missed critical oral contraceptive pills.
Who can sell Only accredited pharmacists who have successfully completed an approved ECP training programme.
Pharmacies may display an ECP decal indicating the ECP is available from an accredited pharmacist working there.
Who can buy Women of any age.
Preferably the woman requiring it; however, it may be sold to a representative.
Effectiveness Between 96% to 99% in healthy women of less than 70kg taking no interacting medicines. (Note: effectiveness rates vary depending on reference source).
Effectiveness reduced when taken with medications that induce hepatic enzymes (eg, carbamazepine, phenytoin, topiramate, St John’s wort, rifampicin, rifabutin, ritonavir), or with malabsorption syndromes.
Effectiveness may be decreased in women weighing more than 70kg or with a BMI of 26kg/m2 or more.
Other information Speak in a private area where the conversation cannot be overheard.
Pharmacists must attend to the request personally, and not just oversee the sale.
Details should be recorded; however, the woman can refuse to supply identifying details.
Reasonable efforts must be made to inform the woman about the limitations of the ECP as an ongoing method of contraception, and refer her if further investigations or long-term contraception is required.
Women must be advised that the ECP is not 100% effective and they should seek further advice if their next period is lighter than usual, late or different in any way, or if unusual bleeding or lower abdominal pain occurs.
The ECP may be supplied for future use.
*According to the World Health Organization, the ECP can be used up to five days after unprotected sex; however, failure rates are higher.
• Advise customers that the ECP: ➤ is not 100% effective. The woman should carry out a pregnancy test if her next period is late
➤ does not protect the woman from STIs ➤ is not recommended as an ongoing
method of contraception.
• Women seeking multiple dispensings of the ECP should be referred to a doctor or family planning clinic for other methods of regular contraception.
• A cough is a symptom, not a disease.
• Dry coughs cause a tickly throat.
• Viral infections are a common cause of coughs but consider other causes.
• Follow recommended guidelines to ensure you are not inadvertently exposed to droplets emitted by a person coughing. A dry cough is a common symptom of COVID-19 (see Colds and COVID-19).
• Dextromethorphan and pholcodine [both Pharmacist only] are used as cough suppressants. Honey may also be effective.
• Refer children under 12 to a pharmacist.
When talking to a customer with a cough ensure you keep a two metre distance and wear a mask. People with suspected COVID-19 should not enter the pharmacy (see Colds and COVID-19 for more information).
Dry coughs are how our body responds to an irritated airway and most people describe having a dry or tickly throat, or wanting to ah-hem all the time. Their voice may also sound hoarse or raspy and they may find it difficult to talk without having a coughing fit. No mucus is produced or coughed up.
Generally, if a person states that their chest also feels congested and/or their breathing is
Category
• People with suspected COVID-19, other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People taking regular medication, including herbal/complementary medications.
• Children aged less than 12 or the elderly.
• With other symptoms of concern (eg, breathing problems, chest pain, high fever,
tight or impaired, then the cough is probably productive in nature and should be treated as such (see Coughs: Productive).
Coughing is a symptom of an underlying problem and you should ask questions to try and determine the likely cause. Refer customers (especially young children) to a doctor if need be. If there is no identifiable cause, or the cough is a result of a viral infection, then a cough suppressant may be appropriate to provide relief and to lessen sleep disturbance. Be mindful that suppressing a cough may be detrimental in certain circumstances (such as with a productive cough or asthma).
Address known or suspected underlying
Cough suppressants [PHARMACIST ONLY] eg, dextromethorphan (Robitussin Dry Cough, Strepsils Dry Cough Lozenges) eg, pholcodine (Durotuss Dry Cough Regular/Forte, Pharmacy Health Stubborn Dry Tickly Cough), Difflam Cough Lozenges (+ benzydamine hydrochloride)
Demulcents and other [GENERAL SALE] eg, glycerol (Lemsip Dry Cough*) eg, Bonnington's Irish Moss
Combination liquids and tablets [PHARMACIST ONLY] eg, pholcodine + phenylephrine (Duro-Tuss PE Dry Cough Plus Nasal Decongestant)
pholcodine + bromhexine (Duro-Tuss Expectorant) eg, dextromethorphan + phenylephrine (Benadryl PE Dry Cough & Nasal Congestion)
dextromethorphan + phenylephrine + brompheniramine (Pharmacy Health Congested Cold & Cough)
dextromethorphan + phenylephrine + paracetamol + chlorpheniramine (at night) (Codral Cold & Flu + Cough) dextromethorphan + guaiphenesin (Robitussin Cough & Chest)
honey, Ivy leaf, marshmallow root, olive leaf, peppermint, probiotics, vitamin C, zinc
Comments
severe headache, rash, weight loss).
• Coughing up blood or pink-tinged mucus (phlegm).
• A cough that only occurs at night.
• A cough that has lasted longer than 10 days or goes away for a period of time only to recur.
• Customers who smoke.
• Customers with allergies to medicines.
disorders (such as asthma, gastro-oesophageal reflux disease [GORD], ACE inhibitors, or post-nasal drip), if possible, first. This may involve referral to a doctor.
Dextromethorphan and pholcodine are cough suppressants (also called anti-tussives) that act directly in the brain to suppress the urge to cough (see Table: Common Ingredients in Dry Cough Products opposite page). However, studies have shown that neither is particularly effective at doing this, although a strong placebo effect has been noted and some adults may find them useful. Research has shown 2.5 to 10mL of honey was as effective as dextromethorphan at relieving cough. Combination products containing other ingredients such as decongestants should only be used if other troublesome symptoms are
Linctuses (eg, pholcodine) are best taken in warm water and sipped slowly. Dextromethorphan can interact with medicines that have serotonergic activity (eg, antidepressants, tramadol, lithium, St John’s wort), and pholcodine has been linked to an increased risk of allergic reactions following anaesthesia. Do not supply pholcodine to people with surgery scheduled within the next 6 to 12 months.
Lozenges are easier to carry around than bottles of syrup.
Sucking lozenges helps stimulate saliva flow to lubricate irritated throats.
Demulcents, such as glycerol, or sugar-free alternatives (eg, isomalt, maltitol) coat the inside of the throat and relieve irritation that promotes coughing. Bonnington's Irish Moss contains menthol, camphor, liquorice extract and carrageenan (a seaweed extract).
Cough suppressants (eg, pholcodine, dextromethorphan) control or suppress the cough reflex and can provide relief from a dry, unproductive cough. Dextromethorphan can interact with medicines (see comments above) and pholcodine has been linked to an increased risk of allergic reactions following anaesthesia. Do not supply pholcodine to people with surgery scheduled within the next 6 to 12 months.
Phenylephrine is a decongestant that can help relieve congestion in the nose and sinuses.
Antihistamines (such as doxylamine, chlorpheniramine) may cause drowsiness and affect a person’s ability to drive or operate machinery. They may also dry out the mucous membranes and have the potential to irritate a dry cough further. Avoid alcohol with sedating antihistamines
Supplements may help moisten airways or boost the immune response; however, most have limited evidence of effectiveness. Honey can help soothe a dry throat and relieve cough – a single night-time dose of 2.5–10ml was as effective in children as dextromethorphan. Do not give honey to children under one due to the increased risk of botulism due to their immature digestive systems.
• A cough is a symptom, not a disease.
• Productive coughs are associated with mucus or phlegm.
• Viral infections are a common cause of cough but enquire about other possible causes.
• Follow recommended guidelines to ensure you are not inadvertently exposed to droplets emitted by a person coughing. Cough is a common symptom of COVID-19 (see Colds and COVID-19).
• Guaiphenesin and bromhexine may help relieve symptoms of a productive cough.
• Refer children under 12 to a pharmacist.
When talking to a customer with a cough ensure you keep a two metre distance and wear a mask. People with suspected COVID-19 should not enter the pharmacy (see Colds and COVID-19 for more information).
Secretions such as phlegm or mucus are the hallmarks of productive (wet or chesty) coughs. These are usually coughed up from the lungs or drain from the sinuses. Most people also feel congested, tight, or sore in their chest. Symptoms are typically worse on awakening, while talking, or during exercise. Young children with a productive cough may vomit because they are more likely to swallow sputum than cough it up. Ask your customer to cough into a tissue for you and listen to the sound their cough makes. With productive coughs, you should hear a rattling sound and some people may wheeze slightly when they breathe. People with dry coughs have nothing to cough up, so their voice may sound hoarse or raspy and it may be difficult for them to talk without having a coughing fit.
Category Examples
• People with suspected COVID-19, other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People taking regular medication, including herbal/complementary medications.
• Children aged less than 12 or the elderly.
• With other symptoms of concern (eg, breathing difficulties, chest pain, high fever,
severe headache, a rash, weight loss).
• Coughing up blood or pink-tinged mucus (phlegm).
• A cough that only occurs at night.
• A cough that has lasted longer than five days or goes away for a period of time only to recur.
• Customers who smoke.
• Customers with allergies to medicines.

Children with whooping cough (also called Pertussis) usually cough continuously for several seconds, followed by a “whoop” sound as they attempt to breathe in air. Croup causes more of a “barking” cough that gets worse at night and it can be very serious in babies less than six months old. Vaccination against Pertussis is included in the National Immunisation Schedule.
Croup is another common type of cough in children under the age of three. The cough sounds like a bark and it commonly follows a cold.
Expectorants & mucolytics [GENERAL SALE] eg, guaiphenesin (Mucinex Chesty Cough*, Mucinex Maximum Strength Chesty Cough*, Robitussin Chesty Cough) eg, irish moss extract, camphor, + ipecac (Bonnington’s Irish Moss)
[PHARMACY ONLY MEDICINE] eg, bromhexine (Bisolvon Chesty Forte) eg, bromhexine + guaiphenesin (Benadryl Chesty Forte, DuroTuss Chesty Cough Forte, Robitussin Chesty Cough Forte) eg, guaiphenesin + phenylephrine (Benadryl PE Chesty Cough & Nasal Congestion)
Steam inhalations [GENERAL SALE]
eg, combinations of volatile oils (Olbas Oil Inhalant Decongestant, Vicks Vapo Steam Inhalant)
Natural / herbal products / supplements eg, camphor, honey, Ivy leaf, marshmallow root, olive leaf, probiotics, vitamin C, zinc
Comments
Humidified air or standing with the child in a steam-filled bathroom may help relieve the cough. Coughing is a symptom of an underlying problem and you should ask questions to try and determine the likely cause. Refer customers (especially young children) to a doctor if need be. If there is no identifiable cause, or the cough is a result of a viral infection, then a cough expectorant can water down mucus and clear secretions from the airways.
Expectorants (eg, guaiphenesin) help expel mucus from the lungs. Mucolytics (eg, bromhexine) help break down thick, sticky chest phlegm, making it easier to cough up.
Products containing other ingredients, such as decongestants (eg, phenylephrine), should only be used if nasal symptoms (ie, blocked nose, sinus congestion) are present and troublesome.
Products containing guaiphenesin, bromhexine, ipecacuanha, or phenylephrine should NOT be given to children aged less than six years and pharmacist advice should be sought before using them in children aged less than 12 years.
Steam helps break down mucus and also aids in expectoration (coughing it up). Avoid inhalants in very young children as the ingredients may be irritating to the airways.
Supplements may help moisten airways or boost the immune response; however, most have limited evidence of effectiveness. Camphor used in a topical rub can reduce chest pain caused by coughing. Ivy leaf is an expectorant and is commonly used in Germany alongside conventional medicines for asthma and bronchitis. Olive leaf boosts the immune system.
Since coughing is the body’s way of removing excess secretions from the airways, a productive cough should generally not be suppressed.
Treatment may be considered with an expectorant to help expel secretions from the lungs (eg, guaiphenesin) and/or a mucolytic (eg, bromhexine) which helps liquefy mucous, allowing easier clearance (see Table: Common Ingredients in Productive Cough Products, opposite).
Herbal chest syrups contain ingredients to support the respiratory tract such as carrageenan, honey, ivy, liquorice, marshmallow root, and can help relieve symptoms in adults or children. Increasing a person’s fluid intake can help thin out secretions and paracetamol or ibuprofen may be given to relieve overall discomfort.
Combination products (such as those containing decongestants) should be used only if other troublesome symptoms are present. Avoid antihistamines, since these tend to dry up and thicken secretions, making it difficult to
• Keep warm and rest.
Cough expectorant Guaiphenesin
Ipecacuanha (ipecac)
Mucolytics Bromhexine
Increases volume and decreases viscosity of secretions.
May cause nausea, vomiting, constipation, and, rarely, allergic reactions. Extra fluids enhance effect.
Thins mucus.
May cause nausea, vomiting, stomach irritation.
Can be toxic at high dosages.
Thins mucus by disrupting the formation of mucopolysaccharide fibres within mucus.
May cause transient rises in liver enzymes, headache, dizziness, sweating, and, rarely, allergic reactions.
cough them up. Cough suppressants are also not recommended for a productive cough because they suppress the cough reflex, taking away a person’s ability to cough up excessive secretions.
Refer anybody with a productive cough lasting longer than five days to a pharmacist, who should refer them to a doctor, as it is highly suggestive of an underlying condition.
Coughing helps to protect the airways and the lungs, and provides a way for us to clear inhaled allergens, irritants, and
• Drink plenty of fluids such as water, diluted non-sweetened fruit juice and clear, warm soups. Liquids help thin the mucus in the throat and lungs and make it easier to cough up.
• Gargle with plain water for one minute, three times a day – this can ease symptoms.
• Humidify the air if it is dry. If a humidifier is not available, steam from a hot shower will also help break down mucus.
• Combination cough suppressant/expectorant cough mixtures are
excess secretions. But a cough can also spread infections or decrease a person’s quality of life.
See Coughs: Dry for a discussion about the mechanism of cough.
Common causes of a productive cough include:
• viral infections (eg, a cold, COVID-19)
• bacterial and other infections (eg, pneumonia, bronchitis, rarely tuberculosis)
• chronic lung disease (eg, bronchiectasis, chronic obstructive pulmonary disease [COPD])
• congestive heart failure
• cystic fibrosis
• smoking or other tobacco use.
not recommended for productive coughs; however, may be soothing for unproductive coughs (see Coughs: Dry).
• Always cover your mouth when you cough, preferably with a tissue, or cough into the crook of your arm.
• Wash your hands after coughing, before preparing food, and before touching other people to reduce spread if the cough is from an infectious source.
• Always use tissues (not handkerchiefs) and dispose of them hygienically following a single use.
• Refer all large or dirty wounds that cannot be cleaned properly to a doctor.
• Clean wounds with water, saline, or a lowtoxicity antiseptic solution. Apply a low-toxicity antiseptic before dressing the wound.
• Any break in the skin puts a person at risk of skin infections such as erysipelas and cellulitis.
• Keep wounds covered to lower the risk of scarring.
“What is the chance of infection” and “Is there any risk of significant blood loss” are two questions you should find out if somebody comes into your pharmacy with any type of wound, especially if you are unable to look at it yourself.
Immediately refer any severe wounds, very dirty wounds, or ones that are bleeding profusely to a doctor or pharmacist. Run through the Refer to a pharmacist checklist and decide who else needs referring. For all other customers, discuss the appropriate treatment options.
Most cuts, abrasions and blisters can be treated with simple first aid. Clean the affected area with water, saline, or a low-toxicity antiseptic and cover with a breathable dressing that encourages moisture retention. This allows the area to heal properly with less scarring. See the Table: First Aid Treatment for Abrasions, Blisters and Cuts, opposite page.
This topic deals with minor cuts,
Blisters
Cuts and abrasions
• People who are immunosuppressed, with diabetes, or with circulation problems.
• People who are very old or very young.
• People who have not had a tetanus vaccination in the past five years.
• People with fever or flu-like symptoms in addition to their wound.
• If foreign objects or particles are
abrasions (grazes) and blisters. For information about more serious wounds, see Wound Care
Cuts are usually caused by sharp objects and usually heal faster if the edges of the wound are brought together with wound closure strips.
Some people may require a booster tetanus shot for wounds considered a high tetanus risk if their last tetanus vaccination was more than five years ago. Tetanus-prone wounds include those that involve a puncture-type injury (including animal bites) particularly when there has been contact with soil or manure; compound fractures; or wounds containing a foreign body.
Abrasions (grazes) occur when the upper layers of the skin get damaged and broken, usually as a result of friction or rubbing against a hard rough surface. They commonly happen in children and on thin-skinned, bony parts of the body (eg, knees, ankles and elbows). Once the bleeding has stopped they should be thoroughly but gently cleaned.
Hydrocolloid dressings (Compeed Blister Pack range,
Nexcare Blister Waterproof Plaster)
Dressing strips (Elastoplast, Nexcare)
Dry, non-stick wound pads (Cutilin, Melolin, Telfa)
Blister prevention (Engo, Scholl, Spenco range)
Saline 0.9% (GP Wound Wash Saline, Saline ampoules)
Dressing strips (Elastoplast, Nexcare)
Wound closure strips (Leukostrip, Steri-strips)
Dry non-stick pad dressings (Cutilin, Melolin, Telfa)
Dry self-adhesive pad island dressings (Cutiplast Sterile, Primapore, Tegaderm with pad)
Film dressings (Cutifilm Plus, Opsite Flexigrid, Tegaderm)
Dressings impregnated with honey (ApiNate Dressing)
Topical antiseptics eg, Crystaderm cream*(see Wound
Care for detailed information)
Natural / herbal products / supplements Honey, trypsin, St John’s wort, tea-tree, zinc cream, vitamin A cream, calendula ointment
embedded in the cut and unable to be removed easily.
• Large, deep, or dirty wounds.
• Severe bleeding.
• Very inflamed wounds or wounds that contain pus.
• People with allergies to topical agents, such as iodine.
Blisters are fluid-filled sacs which form when the skin has been damaged (either by friction, rubbing, poor-fitting shoes, heat, cold or chemical exposure), if the skin is crushed or pinched (eg, blood blister) or as a result of a medical condition (eg, chickenpox).
Most experts recommend small blisters are left intact if possible, rather than popping them. This is because the blister fluid protects the delicate skin underneath, which promotes healing and the top of the blister protects against infection.
Most blisters heal themselves after three to seven days; but covering them with a hydrocolloid dressing relieves pain, aids healing and protects the skin.
People with diabetes or poor circulation have a higher risk of infection from minor wounds and should see a doctor.
For information about recommended topical antiseptics see Wound Care
Hydrocolloid dressings keep the blister moist, easing pain and protecting from further damage and infection. Dry, non-stick pads absorb any discharging fluid without sticking to skin. Blister prevention dressings either cushion an area prone to rubbing or prevent friction.
Normal saline (sodium chloride 0.9%), tap water, or a low-toxicity antiseptic solution may be used to clean wounds. Wound closures keep wound edges together to help healing and reduce scarring and are hypoallergenic.
Island dressings are self-adhesive and have a non-stick wound pad. Film dressings are made of a clear waterproof film which is applied and left on until the dressing falls off, leaving the wound moist and undisturbed, but are only effective if there is no exudate (discharge) from the wound.
Topical antiseptics reduce the risk of infection. Lignocaine, a local anaesthetic, helps reduce pain.
Modern wound dressings aim to maintain a good moisture balance in the wound. This allows optimal healing as well as providing a low oxygen and low pH environment, reducing the risk of infection.
Honey improves skin healing and reduces odours, exudate, pain and risk of infection. Topical trypsin or St John’s wort may improve wound healing and reduce scar formation. Other natural ingredients may also help healing.
Cut
• Apply pressure to the cut with a clean dressing pad, cloth, or non-linting tissue.
• Elevate the wound if necessary to stop the bleeding.
• Seek immediate medical attention if the wound is serious, extensive, or won’t stop bleeding after 15 to 20 minutes of continuous pressure.
➤ Do not remove blood-soaked dressings but keep putting new ones on top and renewing the pressure.
• Once the bleeding has subsided or stopped, apply wound closure strips and cover minor cuts with a dressing strip or dry non-stick wound pad.
➤ Before applying a dressing, make sure the cut is clean. Clean carefully with warm water, saline, or a low-toxicity antiseptic solution if necessary, but be careful not to encourage further bleeding. Apply a topical antiseptic (see Wound Care for detailed information).
➤ Cover deeper cuts with island or film dressings (if there is no exudate) and seek medical advice as stitches may be needed.
Abrasion
• Gently rinse the area clean using tap water, saline solution, or a low-toxicity antiseptic solution.
➤ Use tweezers to remove surface debris but seek medical attention if anything is embedded in the wound or the wound cannot be cleaned properly.
• Apply a topical antiseptic to the area before covering minor abrasions with a sterile dressing strip or non-stick wound pad.
➤ Cover more extensive abrasions with island or film dressings to keep the area moist and undisturbed.
Blister
• Apply a hydrocolloid dressing. Leave the dressing on until it falls off by itself.
• If pain persists despite a hydrocolloid dressing, a clean, sharp needle sterilised over an open flame or with boiling water may be used to carefully prick the blister near its edge. Press the blister carefully to allow the fluid to drain but leave the overlying skin intact.
• If the blister is already broken, clean with warm water and allow to dry.
• If hydrocolloid plasters are not available, a dressing strip (plaster) or dry non-stick wound pad may be used to protect the area from further damage.
Cuts and abrasions
• Any break in the skin puts a person at risk of erysipelas and cellulitis – these are infections of the superficial and deeper layers of the skin respectively. The risk is increased in people who are immunosuppressed, from low socioeconomic areas, or who have had cellulitis previously. Seek medical advice if the area is very red, swollen, or hot to the touch.
• Do not pick scabs off as the wound heals – this can cause scarring. Keep scabs moist with film dressings.

• Watch for signs of infection and seek medical advice if this occurs.
• Wear proper fitting shoes to avoid blisters on the feet.
• Ensure the heel does not slip during walking. Select socks that fit the foot without being too tight or too loose. Choose ones made of soft wicking fabric.
• Do not wear untested socks on a long walk and never wear unwashed socks. Follow the manufacturer’s instructions for laundering.
• Consider applying moleskin, hydrocolloid plasters or duct tape to foot areas prone to rubbing prior to long walks.




• Cystitis is another name for a lower urinary tract infection that affects the bladder and urethra.
• Refer anybody with suspected cystitis to a pharmacist.
• Nitrofurantoin (or sometimes trimethoprim) may be sold to women meeting certain criteria by pharmacists who have completed the Urinary Tract Infections Accreditation Programme.
• Urinary alkalisers can reduce the effectiveness of some antibiotics (eg, nitrofurantoin).
All men, children, and pregnant women with suspected cystitis will need to be referred to a doctor, and all women should be referred to a pharmacist who can decide what treatment is appropriate for them.
Cystitis can often resolve on its own; however, antibiotics are recommended for women with classic cystitis symptoms who meet the criteria and can be sold by a pharmacist who has successfully completed the Urinary Tract Infections (UTIs) Accreditation Programme (see Table: Conditions for the Sale of UTI Antibiotics by Pharmacists, opposite page). NSAIDs, such as ibuprofen can be considered as an add-on to antibiotic treatment for pain relief. Both the New Zealand Formulary and BPACnz recommend nitrofurantoin as the firstline treatment for cystitis because of increasing trimethoprim resistance in New Zealand, and this is the preferred antibiotic for pharmacists to choose. Advise customers to see their doctor if antibiotics sold by a pharmacist do not resolve their cystitis.
Category Examples
• People with other health conditions or who are immunosuppressed or pregnant.
• Children aged less than 16 years or adults aged over 65 years.
• Men.
• If trimethoprim or urinary alkalisers are not suitable.
• If vaginal symptoms are also present, such as itch or discharge (there may be a fungal or sexually transmitted infection), and over-the-counter treatment is not available or appropriate.
• People with abnormal urinary tracts or
A Cochrane review could not recommend the use of urinary alkalisers for UTI symptoms because there were few good quality trials; however, they may help relieve pain while urinating. Urinary alkalisers can reduce the effectiveness of nitrofurantoin and methenamine hippurate, because they increase urinary pH.
Cystitis is an infection of the bladder and urethra, usually caused by bacteria, which causes the bladder and urethral walls to become inflamed.
The term urinary tract infection (UTI) may be used interchangeably with cystitis; however, a UTI technically means an infection in some part of the urinary tract system (ie, ureters, kidneys, urethra or bladder), not just the bladder. Common symptoms of cystitis include a burning pain or stinging sensation on urination and a frequent urge to pass small volumes of urine. The urine may also be cloudy and strong
Urinary alkalisers [GENERAL SALE] eg, contain a mixture of sodium and potassium salts (eg, Ural)
Preventive [GENERAL SALE] eg, methenamine hippurate (eg, Hiprex)
Preventive/Treatment eg, d-mannose (UroFem D-mannose)
Antibiotics (treatment)
[PRESCRIPTION] Unless sold by an accredited pharmacist ie, Nitrofurantoin, Trimethoprim
Natural / herbal products / supplements eg, cranberry supplements, Lactobacillus probiotics
who have a urinary catheter in place.
• People with other symptoms, such as fever, nausea, vomiting, or pain on the sides of the lower back over the kidney area (likely to be a kidney infection).
• With recurrent cystitis (repeated UTIs can lead to kidney infection).
• With haematuria (blood in the urine).
• With symptoms that have lasted longer than two to three days or persisted despite treatment.
• With allergies to trimethoprim.

smelling. Lower back pain, discomfort just above the pubic area, nocturia (getting up repeatedly during the night to urinate) and haematuria (blood in the urine) may also occur.
Comments
Dissolve sachets in a glass of water and drink up to four times a day. There is a lack of good quality trials regarding the safety and effectiveness of urinary alkalisers. Should not be used in pregnancy, renal impairment, cardiac disease, and with some medicines. Contain sodium and potassium; exercise caution when giving to people on potassium-sparing medicine or a sodium-restricted diet. May help relieve painful urination. Do not take with nitrofurantoin or methenamine hippurate because an acidic urine is needed for methenamine to work.
Methenamine hippurate has bacteriostatic properties and is converted into formaldehyde within an acidic environment (do not use with urinary alkalisers). 1g every 12 hours has been used to prevent recurrent UTIs.
D-mannose may prevent bacteria from adhering to the bladder wall. D-mannose powder (2g) was as effective as nitrofurantoin at preventing recurrent UTIs over 6 months. May also reduce symptoms of an acute UTI such as dysuria, urgency, and supra-pubic pain.
See Treatment for conditions under which a pharmacist may dispense nitrofurantoin or trimethoprim. Dosage: Nitrofurantoin MR,100mg TWICE daily with food for 5 days. Trimethoprim one tablet at bedtime for three days. Drink plenty of fluid.
Concentrated cranberry products (>18%) are more likely to be effective than dilute formulations (2-4%). Some studies suggest taking at night. Probiotics may help support urinary health.
Cystitis is caused in most cases by the person’s own bowel flora ascending the urethra from the perineal and perianal areas. The bacteria most often involved are Escherichia coli (responsible for up to 80% of uncomplicated cystitis), Staphylococcus and Enterococci. If the infection spreads to the kidneys (this is called pyelonephritis), it can damage the kidneys or spread to the bloodstream and cause sepsis, which can be life-threatening.
Women are more prone to cystitis than men because they have a shorter urethra which makes it easier for bacteria to reach the bladder. Women at higher risk include those aged 15–40 and elderly women living in aged-care facilities. Cystitis is rare in men, but may occur in men aged over 50 due to prostate enlargement. Refer all men with suspected cystitis to a doctor.
Children or adults with recurrent UTIs may require further investigations to look for abnormalities in their urinary tract.
Age and sex
Treatment must be for a woman aged between 16 and 65 years
Exclusions Pregnancy
Symptoms Symptoms must be consistent with those of uncomplicated cystitis and include two or more of:
• painful urination
• urinary frequency
• urinary urgency
• suprapubic pain
Refer to a doctor
Breastfeeding if infant <6 weeks old or G6PD deficiency
Vaginal symptoms such as itch or discharge (may be vaginal thrush or a sexually transmitted infection [STI]). Treatment for vaginal thrush may be sold by a pharmacist if the woman has had it before.
Known history of STI or risk factors for an STI (eg, recent change in partner, unprotected sex).
Systemic symptoms (eg, fever, chills, nausea, vomiting, feeling particularly unwell, pain in one or both sides of the trunk or back).
3 or more UTIs in last 12 months or 2 or more UTIs in past 6 months or treated within the past two weeks.
Immunocompromised or other medical conditions, including diabetes and moderate to severe pulmonary disease (see algorithm)
Any risk for resistant bacteria (eg, history of hospitalisation in the past four weeks)
Previous nitrofurantoin hypersensitivity (including pulmonary, liver, blood or skin reactions)
Change choice of antibiotic or management
• Keep up your fluid intake, although there is no evidence that drinking more fluids than normal decreases the duration of a UTI.
• Rest and a hot water bottle placed on the stomach may help relieve pain. Paracetamol or ibuprofen may be taken. Avoid aspirin.
• Vaginal lubricants may reduce the risk of “Honeymoon cystitis”, caused by repeated trauma in the genital area.
• Bath products and vaginal deodorants may cause irritation.
• Some medications may result in inefficient emptying of the bladder. Talk to your doctor if the cystitis seems to have coincided with a recently started medicine.
• Incorrect toileting may cause cystitis. Wipe “front to back”, preferably using a “blotting” technique. Respond to the urge to urinate
On clozapine, probenecid, a quinolone antibiotic
On antacids or urinary alkalisers
Known renal impairment or conditions that may affect renal imapirment
– do not “hold on” as this can cause urine to concentrate and give bacteria an opportunity to multiply.
• Acidic drinks (eg, fruit juices, fizzy drinks) and spicy foods may irritate the bladder in some people.
• Wear loose-fitting cotton underpants and trousers. Tight clothing can encourage bacterial growth.
• If antibiotics are prescribed, take them exactly as directed and complete the course. Some antibiotics may interact with other medicines. Once-daily doses are best taken before bed after emptying the bladder.
• Higher concentrations of cranberry products are more effective than lower concentrations.

• Dandruff is the name given to small pieces of dry skin that flake off the scalp.
• Check the scalp to ensure the symptoms are actually dandruff and not eczema or psoriasis.
• Control relies on regular use of anti-dandruff shampoos or treatments.
• Dandruff tends to recur once treatment stops.
Examine the scalp to ensure that the symptoms the customer is describing are
Category
Examples
Medicated shampoos [GENERAL SALE] eg, zinc pyrithione (Head & Shoulders Dry Scalp), eg, coal tar (Neutrogena T Gel, Sebitar Scalp Treatment) eg, piroctone olamine (Sebamed Anti-Dandruff Shampoo) eg, selenium sulphide (Selsun Blue Shampoo range)
Antifungal shampoos [GENERAL SALE] eg, ketoconazole 1% (Nizoral Blue 1%, Sebizole Dandruff 1%) [PHARMACY ONLY MEDICINE] eg, ketoconazole 2% (Nizoral 2%, Sebizole Dandruff 2%)
Topical applications [GENERAL SALE] eg, Coco-Scalp*
Mild cleansing shampoos eg, lauryl polyglucose (Dermasoft Moisturising)
Natural / herbal products / supplements Apple cider vinegar, calendula, coconut oil, licorice, malaleuca oil (tea-tree oil)
• People who are immunosuppressed, pregnant or breastfeeding.
• Young children or the elderly.
• People with hair loss associated with dandruff.
• With sores, crusts, or very inflamed-looking scalps; or if there are thick silvery scales
the result of dandruff. Dandruff flakes are small and white and typically found where the hair parts or dotted on the shoulders.
A pink inflamed-looking scalp with greasylooking flakes is most likely seborrhoeic dermatitis (see Dermatitis/Eczema), or the presence of thick silvery scales may indicate psoriasis (see Psoriasis). Both should be referred to a pharmacist.
Ask about any concurrent skin conditions and if symptoms seem related to the recent use of hair products.
Dandruff is usually very responsive to treatment but often returns after treatment stops. Mild cases usually respond to daily shampooing with a gentle cleanser. More noticeable cases will require regular and ongoing treatment with a medicated or antifungal shampoo. Use dandruff shampoo twice a week, and regular shampoo at other times if needed (see Table: Common Anti-Dandruff Product Ingredients).
Comments
present on the scalp.
• When anti-dandruff shampoos have been tried before without success.
• With symptoms that extend to other parts of the body (eg, eyebrows, forehead or ears).
• With allergies to topical medicines.
The majority of treatment products have antifungal properties which control the presence of the yeast Malassezia. Reduction in this yeast reduces the presence of fatty acids thereby reducing the flaking and the itch of Malasseziaassociated dandruff.
Dandruff is generally more of a cosmetic problem than a medical problem but it can affect a person’s self-esteem so treatment is warranted.
Dandruff is a common condition in which numerous small flakes of dry skin are shed from the scalp and are visible in the hair or on the shoulders. Dandruff affects around 15%–20% of the population.
Dandruff may be caused by hair products, over or under-shampooing, not enough hair brushing, a poor diet, illnesses such as Parkinson’s disease or HIV, a weakened immune system, stress, or an overgrowth of the yeast Malassezia Malassezia feeds on the natural oils of the scalp and excretes a fatty acid byproduct which irritates the scalp
When using coal tar-based products it is important to use the accompanying rinse/conditioner as this helps remove the coal tar smell. Coal tar can also cause staining. Use treatment products exactly as directed on the label or by a doctor. Avoid the eyes. Most products are toxic if swallowed, so keep products out of reach of children. Discontinue use if scalp irritation or stinging occurs.
Use according to the instructions on the packet. Generally the 1% ketoconazole product is for regular use, up to twice a week, while the 2% strength is used twice a week for two to four weeks, with at least a four-week gap before repeating the course. There is more evidence of an effect for the 2% formulation.
Mild cleansing shampoos can be used in between shampooing with antifungal products.
Contains coal tar, sulphur and salicylic acid in a coconut oil base. Has antifungal and keratolytic (sloughs off dead skin cells) properties. Apply to affected areas of scalp and remove after one hour using warm water and a shampoo. Repeat daily for three to seven days. Not for children under six.
Lauryl polyglucose provides gentle yet effective cleansing without irritation. The neutral pH of 5.5 helps preserve the protective acid mantle of the scalp. May benefit eczema sufferers.
Apple cider vinegar and tea-tree oil have antifungal properties. Coconut oil aids in the removal of dandruff, and also moisturises and strengthens hair. Aloe vera and calendula help calm itchy, sensitive scalps. Daily shampooing with a teatree oil shampoo may help reduce dandruff.
causing flaking and itching and a faster-thannormal shedding of skin cells. Skin cells are shed as quickly as every two to seven days, as opposed to people without dandruff, who shed skin cells only monthly. Dandruff is not infectious.
Certain skin conditions (such as dry skin, psoriasis, or eczema/dermatitis) can also cause dandruff. Seborrhoeic dermatitis of the scalp is a severe, inflamed form of dandruff which causes larger, greasier flakes than other causes of dandruff. Seborrhoeic dermatitis usually affects skin on other parts of the body as well, such as the eyebrows (see Dermatitis/Eczema).
Dandruff is more common after puberty and is rare in children, although most newborns get cradle cap, which looks like dandruff (see Baby Care).
Dandruff tends to come and go over time but may worsen in autumn and winter when indoor heating can dry out skin and people are not exposed to as much sunlight (UVA is effective at counteracting the effects of the yeast).
EFFECT
INGREDIENT COMMENTS
Antifungal Ketoconazole
Medicated Coal tar
Piroctone olamine
Salicylic acid
Selenium sulphide
Zinc pyrithione
Other Coconut oil
Tea tree
Broad spectrum antifungal. Works by blocking the synthesis of ergosterol, a vital component of fungal cell membrane.
Active against Malassezia and Candida species
Reduces epithelial skin cell turnover rate; relieves scaling and itching.
Makes the scalp more susceptible to sunburn.
Can stain clothes and discolour blonde, grey or white hair.
Strong-smelling.
Antifungal and antibacterial properties.
Gentle with few side effects.
Loosens and softens scaly skin making it easier to remove.
May cause a slight burning and skin redness.
Reduces the rate of epithelial skin cell turnover, relieving scaling and itching.
Can discolour hair and metallic jewellery and stain clothes.
May cause unusual scalp oiliness or dryness and hair loss.
Fungistatic and bacteriostatic.
May irritate the scalp.
Moisturises scalp which controls itching and scaling. Antifungal effect.
Gentle with few side effects.
Anti-inflammatory, antifungal, and anti-bacterial effects.
May irritate the scalp. Strong-smelling.
May cause an allergic reaction in some people.
• Regular hair washing (at least twice weekly) with a treatment shampoos will reduce dandruff.
➤ Follow directions exactly as directed on the shampoo label. If the product irritates or burns your scalp, rinse it away thoroughly and do not use it again. Ask a pharmacist about alternative products.
➤ If one product does not appear to work, relief may be gained by using a different type of anti-dandruff product.
➤ Do not use dandruff products if your skin is broken, and avoid getting it into your eyes.
➤ Use regular shampoo on other days of the week if needed and rinse out thoroughly.
• Dandruff is more visible on dark clothing compared to light clothing.
• Stress may trigger dandruff or worsen existing symptoms. Take time out to relax and try to manage stress.
• Cut back on the use of styling products. Hair sprays, styling gels, mousses, and hair waxes can all build up and irritate the scalp.
• Eat a healthy, well-balanced diet.
• A little bit of sun on the hair is good for dandruff but avoid overexposure. Wear a hat if outside for prolonged periods to avoid sunburn.
• Daily shampooing with shampoo containing tea-tree oil has been shown to reduce the incidence of dandruff.
• Treatment reduces symptoms but does not cure the problem long term – customers may need to repeat treatment periodically.
• Oral analgesics only temporarily relieve dental pain; most customers will need to see a dentist.
• Thorough, twice-daily toothcare combined with a low-sugar diet helps prevent tooth decay.
Visually, there is not usually anything to see when somebody complains of dental pain. Ask the customer (or their caregiver if they are a child) to describe their symptoms including onset of pain and any history of teeth problems. Also ask them to describe how they care for their teeth.
Run through the Refer to a Pharmacist checklist and refer any customers with concerns.
Oral analgesics such as paracetamol or ibuprofen may be sold to temporarily relieve dental pain until the customer sees a dentist; however, ultimately professional dental care is required. Topical pain-relieving preparations such as clove oil are also available; however, these are not suitable for everyone. For people prone to cavities or with concerns about their teeth, offer advice about good oral hygiene (see Oral Health), and consider the use of probiotics (see Probiotics and Prebiotics) such as S.salivarius K12 and M18. Mouthwashes may also help, but these should not be used as a substitute for good tooth brushing and should only be used short-term.
• People who are immunosuppressed, have diabetes, a nerve-related disease such as trigeminal neuralgia, shingles, or women who are pregnant or breastfeeding.
• People who you suspect may misuse drugs or alcohol.
• Children aged less than 16 years.
• If the tooth pain is due to a facial injury.
Dental pain is the term used to describe pain that occurs in and around the teeth and jaws. The pain usually starts suddenly and it can vary from mild discomfort to a severe throbbing, often worse at night, and may be aggravated by hot or cold food or drinks.
Teeth have two main anatomical parts. The crown of a tooth is covered with enamel and is visible in our mouths. The root is the part embedded in the jaw that anchors the tooth into its bony socket. It is normally not visible.
Beneath the enamel lies a layer of dentine. Dentine is much softer than enamel, forms the bulk of the tooth, and becomes sensitive if the protection of the enamel is lost.The pulp is the innermost part of the tooth. It is made up of soft, sensitive tissue that contains the blood and nerve supply to the tooth. The pulp extends from the crown to the tip of the root.
Toothache happens when the innermost layer
Category Examples Comments
Simple analgesics [GENERAL SALE] eg, paracetamol (Panadol, Paracare, Pamol suspension)
Oral non-steroidal anti-inflammatory agents (NSAIDs)
[GENERAL SALE] eg, aspirin (Aspro Clear), ibuprofen <25s (Advil tablets, Nurofen range) [PHARMACY ONLY MEDICINE]
eg, diclofenac 12.5mg (Voltaren Rapid 12.5), ibuprofen >25s (Advil tablets, Nurofen range), ibuprofen suspension (Fenpaed) eg, ibuprofen + paracetamol (Maxigesic*, Nuromol) [PHARMACIST ONLY MEDICINE] eg, diclofenac 25mg (Voltaren Rapid 25) [PRESCRIPTION MEDICINE] eg, ibuprofen + codeine (Ibucode Plus, Nurofen Plus), paracetamol + codeine (Panadeine, Panadeine Extra)
Oral hygiene products eg, interdental brushes, dental floss, mouthwashes, personal water jets, toothbrushes, toothpastes, xylitol or fluoride-containing products, sugar-free gum
Natural / herbal products / supplements Clove oil, S. salivarius K12 and M18 (Bliss Probiotics
• People who drink unfluoridated water.
• People who report prior dental extractions.
• People with other symptoms such as nasal congestion or a fever.
• With swelling around the tooth, jaw or face; or an abscess.
• People with allergies to medicines.
of the tooth – the pulp – becomes inflamed. The most common reason for dental pulp inflammation is tooth decay (dental caries).
Tooth decay is caused by the action of acids on the enamel surface. The acid is produced when sugars (ie, fructose, glucose, sucrose) in foods or drinks react with bacteria present in the plaque on the tooth surface. This acid encourages the leaching of calcium and phosphate from the enamel by a process called demineralisation. Saliva acts to dilute and neutralise the acid that causes demineralisation and is an important natural defence against caries. Saliva also has the ability to remineralise areas of destroyed enamel once the acids have been neutralised. However, if the process of demineralisation exceeds remineralisation, the erosion progresses and a breakdown in the enamel surface occurs leading to a cavity. Other causes of dental pain include:
Effective at relieving pain but are not anti-inflammatory so will not relieve swelling or inflammation in the area. Suitable for people with contraindications to NSAIDs.
Ibuprofen is the NSAID least likely to cause stomach irritation. NSAIDs may not be suitable for people on certain other medications or with some medical conditions (eg, asthma, kidney disease – see Refer to Pharmacist). Advise customer to stop taking if stomach upsets, increased bruising or prolonged bleeding occur.
Aspirin is not recommended for adolescents or children under 16 years old due to the risk of Reye’s syndrome. Avoid aspirin following dental surgery (may prolong bleeding time). Combination codeine analgesics are PRESCRIPTION medicines because the harms associated with codeine are considered to outweigh its benefits.
Interdental brushes help remove plaque and food from between teeth and are an alternative to dental floss. Products containg xylitol or fluoride can decrease the risk of dental caries. Mouthwashes (antiseptics) temporarily lower the number of bacteria in the saliva but are not a substitute for regular teeth brushing.
Chewing sugar-free gum stimulates saliva production which is important for buffering food acids, supplying minerals for remineralisation, and diluting and increasing clearance of food debris from around the teeth. See Oral Health: Treatment options, for product details.
Clove oil contains eugenol which acts as an anaesthetic and an antibacterial agent. Apply directly to tooth with a cotton bud but do not overuse. Can be fatal if swallowed so keep out of reach of children.
S. salivarius K12 and M18 are oral cavity probiotics which have activity against bacteria implicated in bad breath, gingivitis, and tooth decay.
• Dermatitis and eczema are interchangeable terms.
• Identifying and eliminating contributing factors as well as keeping skin moisturised help with dermatitis control.
• People with atopic dermatitis are more likely to suffer from hay fever, asthma, or food allergies.
Ask your customer if you can look at their dermatitis (in a private area if necessary) and run through the Refer to a Pharmacist checklist to decide which customers should be referred.
Take note of the location of the dermatitis (eg, skin flexures, hands) and ask about any possible aggravating factors (for example, jewellery, occupation, new clothes, co-existing conditions). If your customer does not need to be referred to a pharmacist, discuss what treatment options are available, such as soap-free cleansers, soothing creams, topical corticosteroids, and moisturisers.
Identifying and eliminating (if possible)
Category Examples
• People who are immunosuppressed, pregnant or breastfeeding.
• Young children.
• People with skin that is broken, inflamed or has signs of infection (ie, pus).
• If the affected area is covered with white patches or silvery scales.
• If vesicles (little pimples with clear fluid) are present in the rash.
• With dermatitis that has spread or worsened despite treatment.
• People with allergies to topical medicines.
any contributing factors to the dermatitis is an important component of treatment.
Most people with dermatitis have a tendency towards dry skin, so regular daily moisturising and a good fluid intake are important.
Emollients soften the skin and include fats or oils such as lanolin. Moisturisers add moisture to the skin and usually contain a humectant such as glycerin or urea that pulls water from the dermis or the atmosphere into the epidermis (the outermost layer of skin).
Finding a product that makes a difference may take trial and error. Tell the customer to stop using any product that seems to irritate the skin more and talk to a pharmacist. Some people may be allergic to preservatives or fragrances used in topical products but this is uncommon.
Soap substitutes [GENERAL SALE] eg, Aveeno Body Wash, Cetaphil Gentle Skin Cleanser, Dermalab Gentle Cleansing, Dermasoft, Dermaveen, Dove Unscented Bar, Hopes Relief Cleansing Bar, QV Gentle Wash
Moisturisers [GENERAL SALE] eg, Dermalab Stay Hydrated, Dermasoft, Hope’s Relief Moisturising Cream/Derma Lotion, Lipobase Cream, Lucas Papaw ointment, QV Skin Lotion, Weleda Rash Relief
Barrier creams [GENERAL SALE] eg, dimethicone (DU IT Tough Hands, Plunkett’s Working Hands), zinc (Sudocream), zinc and castor oil
Anti-pruritics (anti-itch) [GENERAL SALE] eg, Pinetarsol range
Itchy scalp [GENERAL SALE] eg, Coco-Scalp*
Bath/shower products [GENERAL SALE] eg, E45 Moisturising Shower Cream, Scratchy & Itchy Soothing Bath, QV range
Anti-inflammatory products [GENERAL SALE] eg, Ichthammol, (Egoderm Cream, Egoderm Ointment [with zinc])
Topical corticosteroids [PHARMACY ONLY MEDICINE] eg, hydrocortisone 0.5% (Derm-Aid Soft 0.5%, Skincalm 0.5%)
[PHARMACIST ONLY MEDICINE] eg, hydrocortisone 1% (Derm-Aid Soft 1%, Skincalm 1%), Clobetasone 0.05% (Eumovate)
Products for cradle cap [GENERAL SALE] eg, Egozite Cradle Cap, Mustela Cradle Cap Cream, Kiwiherb Baby Balm
Natural / herbal products / supplements eg, Artemis Itch Calm, Weleda Eczema Comp, Mebo Anti-itch, Omega 3/6, Bifidobacterium, Lactobacillus
Comments
Dermatitis is the term used to describe a group of inflammatory skin conditions. The word “eczema” may be used interchangeably with dermatitis. Dermatitis is common.
Symptoms include an intense redness of the skin or scalp, with raised bumpy areas and sometimes bleeding, blistered, or weepy patches. These patches can be incredibly itchy and may interfere with sleep and other activities. Constant scratching can cause skin changes and affect pigmentation.
Dermatitis may flare-up occasionally or be present all the time. It is usually classified according to its known or suspected cause, for example, allergic contact dermatitis, atopic dermatitis, irritant contact dermatitis, and seborrhoeic dermatitis.
People with dermatitis should always use a gentle cleanser that removes dirt without compromising the integrity of the skin barrier. Aqueous cream is not recommended as a cleanser or moisturiser because it contains sodium lauryl sulphate (a detergent) which may aggravate dermatitis.
Regular use of a moisturiser improves the skin’s function as a barrier. The base used to make the cream and dissolve any ingredients plays just as important a role as the active ingredients themselves. Humectants (eg, glycerin, oatmeal, propylene glycol, phospholipids) hold water in the skin. Ointments containing petrolatum or lanolin tend to be greasier than creams.
Provide a barrier between the skin and outside influences (eg, water, detergent). Apply regularly, especially on hands just before immersing them in water.
Tar-based pine oil products are useful to help reduce itching. Some people may be allergic.
Contains ingredients that break down scalp scale, relieve itch, and condition the hair.
Bath oils containing antiseptics may be useful in dermatitis to reduce flare-ups due to bacterial colonisation. Use no more than the recommended amount. Warn about slipping. Half a cup of regular bleach added to a 20cm deep bath twice a week can help prevent infection and improve dermatitis.
Can reduce flare-ups associated with eczema.
Do not apply to broken skin or to face. Apply a small amount no more than twice daily, and limit use to one week at a time. Long-term use may result in skin thinning and stretch marks.
Loosens and removes the crusts due to cradle cap.
Natural ingredients soothe the skin and reduce the urge to scratch. Oral Bifidobacterium or Lactobacillus can reduce atopic eczema severity in infants.
This is a skin reaction which results from contact with an allergen (eg, ingredients in cosmetics, dyes in clothing or footwear, hair dyes, latex gloves or condoms, nail polish, nickel in jewellery, plants, sticking plasters, or sunscreen). A rash featuring red, raised welts on the area contacted by the allergen is the most typical symptom.
Atopic dermatitis (AD) is the most common inflammatory skin condition worldwide and causes symptoms such as dry skin, itch, and rash. AD usually affects people with a predisposition to hypersensitivity-type conditions such as hay fever, asthma, chronic urticaria, or food allergies. It tends to run in families and most commonly presents in children under the age of six, although may occur at any age.
AD tends to come and go with periods of activity (called flares) and periods of relative skin normality in between, although in most people the skin always appears slightly dry. Flares in AD usually occur following exposure to certain allergens or trigger factors including grasses, pollen, animal dander, dust mites, stress or temperature/climate change.
Skin flexures (eg, inside the elbows or behind the knees) are more commonly affected and usually symmetrically. Broken areas of skin are prone to infection, and raw or weepy looking rashes should be referred to the pharmacist.
Barrier defects such as filaggrin gene mutations (filaggrin is a protein responsible for maintaining an effective skin barrier) appear to be a key factor of AD. Environmental factors (eg, weather, temperature, allergens), defective keratinocytes (skin cells), commensal microbes, and irregularities with the immune and digestive systems also play a role.
Treatment may be required for many months, possibly years, and should include avoidance of trigger factors (where possible), regular moisturisers, and intermittent, short-course (five to 15 days) topical corticosteroids. Topical calcineurin inhibitors (pimecrolimus, tacrolimus), antibiotics, antihistamines, phototherapy or oral corticosteroids may also be needed.
This is the most common form of dermatitis and frequently occurs in people in occupations such as hairdressing or cleaning that expose them to irritants that strip natural oils from the skin. The
• Have showers instead of baths and use lukewarm water. Keep shower-time to under five minutes and use a soap-free cleanser.
• Wear gloves or use barrier creams to protect hands from detergents or solvents. Do not moisturise hands before putting gloves on and avoid prolonged glove-wearing as this can also cause dermatitis.
• Moisturise the whole body at least twice daily with a fragrance-free emollient and always after bathing (see also Dry Skin).
skin may take on a glazed or scalded appearance and hands are most commonly affected.
Other conditions such as dribble rash (a bright red rash around the lips and chin caused by saliva) and napkin dermatitis (see Baby Care) are also forms of irritant dermatitis.
Healing is usually quick if the irritating agent or practice is avoided or exposure is reduced (such as by wearing gloves). Emollients, compresses, and/or topical steroids can also assist healing. Sometimes antibiotics may be needed if there is a secondary bacterial infection.
This is a common, harmless, salmon pink, scaling rash which can affect the face, scalp, eyebrows, eyelid edges and other areas. Topical antifungals, occasional topical corticosteroids, and combination scalp products containing coal tar, coconut oil and other ingredients may help control the condition but it can be quite persistent. Scalp seborrhoeic dermatitis can be a cause of dandruff.
Cradle cap
Cradle cap is a scaly, crusty, patchy, greasy, skin rash that occurs on the scalp of recently born babies (see Baby Care).
• Avoid scratchy fabrics or coarse fibres such as wool or synthetics.
• Protect the skin as much as possible from dust, harsh chemicals or water and avoid excessive sun exposure.
• Stress can also aggravate eczema and it is a good idea to have some stress-relieving techniques on hand.
• Zinc-based sunscreens are less likely to aggravate dermatitis.
• There are three main types of diabetes: type 1, type 2, and gestational diabetes.
• Depending on the type of diabetes, either not enough insulin is produced by the body to allow proper glucose uptake by muscle, adipose, and other cells OR cells are unable to recognise insulin and use it properly.
• People with type 1 diabetes require daily insulin, whereas most people with type 2 diabetes can be initially managed with diet, weight loss, or oral tablets. Many people with type 2 diabetes will eventually require insulin.
Treatment of type 1 diabetes is with multiple daily injections of insulin or a continuous insulin pump which is tailored to each individual around waking, activity, and eating times.
Some people are able to manage their type 2 diabetes by altering their diet and losing weight. Most people will need to take oral medicines which stimulate the production of insulin or help cells uptake glucose. Many eventually require insulin injections as the disease progresses.
In most cases, gestational diabetes is able to be managed by diet and exercise during the pregnancy; however, some women will require insulin injections. Insulin is considered safe during pregnancy.
Diabetes is a condition in which the body fails to produce enough insulin to keep blood glucose (sugar) levels in the normal range. In some people insulin is produced but the cells of the body do not recognise it properly.
Insulin is a hormone that is produced by special cells (called beta cells) in the pancreas. It facilitates the entry of glucose into muscle, adipose (fat) and several other tissue types, where it can be used for energy, and also switches off the release of glucose by the liver.
Glucose comes from the carbohydrates we eat, and is present in the blood as an energy source. Glucose also comes from our liver, where it is stored in order to provide a constant supply for when we are not eating.
In people without diabetes, insulin keeps blood glucose levels fairly stable (between 4.0mmol/L and 7.5mmol/L). In people with untreated diabetes, blood glucose levels can regularly go high (11mmol/L and higher). There are three different types of diabetes.
Type 1 diabetes is most commonly diagnosed in children aged seven to 12 years, although it can
occur at any age. It is an autoimmune condition where the immune system of the body rejects or destroys its own insulin-producing cells.
People with type 1 diabetes produce very little or no insulin hormone, resulting in a lifelong dependence on exogenous insulin. It is unknown what first starts this cascade of immune events, but evidence suggests that both a genetic predisposition and environmental factors, such as a viral infection, are involved. Of all the people with diabetes about 10% of them have type 1 diabetes.
Symptoms include excessive or constant thirst (polydipsia), excessive and frequent urination (polyuria), tiredness or weakness and mood changes. People with type 1 diabetes often experience rapid weight loss because their body is actually being starved. Some people may also experience abdominal pain, nausea or vomiting, skin infections (eg, thrush), extreme hunger or have difficulty concentrating. Symptoms usually develop quickly and urgent hospitalisation may be necessary. Diagnosis is by blood and urine tests.
This is the most common type of diabetes and usually affects people who are middle-aged or older, although can occur earlier in people who carry excess weight, do limited exercise, or who are of certain ethnicities.
Unlike people with type 1 diabetes, people with type 2 diabetes still produce insulin; however, it is either not enough to mop up all the glucose in the blood or their body is unable to recognise the insulin and use it properly (insulin resistance).
Type 2 diabetes comes on gradually and symptoms may be so subtle that many people are unaware that they have the condition. In addition to feeling thirsty and going to the toilet often, people with type 2 diabetes get tired, feel hungry and lack energy. Other common symptoms include more frequent infections and infections which are hard to heal, and some may notice a deterioration or blurring of their vision.
About one-third of people with type 2 diabetes also have hypertension (high blood pressure) and dyslipidaemia (see also Heart Health). This combination of conditions is often referred to as “the metabolic syndrome”.
Gestational diabetes happens when a pregnant woman cannot produce enough insulin to cope with her body’s increased needs during pregnancy (a pregnant woman’s insulin needs are two to three times that of someone who is not pregnant). It affects around 4%–8% of pregnant women, and is routinely screened for during pregnancy
at around 26 to 28 weeks’ gestation. Although gestational diabetes usually disappears after the baby is born, women who have had it are at greater risk of developing type 2 diabetes later in life.
When sugar levels in the blood remain high for a long period of time, permanent damage can occur to most of the blood vessels in the body, leading to an increased risk of heart attack and stroke, erectile dysfunction, foot problems, gum disease, infections, kidney disease, nerve damage and visual problems.
There are certain factors that increase the risk of type 2 diabetes, although not everybody with these risk factors goes on to develop the disease. Type 2 diabetes is more common in people who are overweight – especially if the extra weight is around the waist; in those who are inactive; and in people of an older age.
Māori, Asian, Middle Eastern or Pacific Island people tend to develop type 2 diabetes at a younger age than those of European descent. People with a family history of diabetes or women who had gestational diabetes or gave birth to baby weighing more than 4kg are also more likely to develop the condition.
Some over-the-counter medicines such as NSAIDs (for example, ibuprofen) and sugarcontaining cough syrups may not be suitable for people with diabetes. If you don’t know the medical history of the customer, and they have obvious risk factors for the disease, tactfully ask if they have any known medical conditions, such as diabetes. Refer anybody with suspected diabetes to a pharmacist.
Doctors may order a glycated haemoglobin (HbA1c) test if they suspect diabetes. The test indicates how good a person’s blood glucose control has been over the past two to three months and has less biological variability than a fasting plasma glucose (FPG) test. It also does not require fasting. However, an FPG remains a valuable test.
An HbA1c of greater than or equal to 50 mmol/ mol is considered the threshold for the diagnosis of diabetes by the New Zealand Society for the Study of Diabetes (NZSSD) and the Ministry of Health. In people with symptoms (eg, polyuria, polydipsia), a single HbA1c of >/=50 mmol/
mol is considered diagnostic of diabetes for the majority of people (though some exceptions exist).
In people without symptoms, an HbA1c of >/=50 mmol/mol strongly indicates diabetes; however, a second test (ideally another HbA1c at least three months later or an FPG) is needed for confirmation. Lifestyle interventions should be encouraged during the three-month wait for a second test.
Home blood glucose testing allows customers with diabetes to better manage their diabetes at home. If your pharmacy offers a blood glucose testing service your standard operating procedure (SOP) should clearly outline how to conduct the test and when to refer people to a doctor for an HbA1c.
Customers reporting frequent high blood sugar readings (hyperglycaemia) should be referred to their doctor for further investigation. Reasons for high blood glucose recordings in known
• Ensure customers:
➤ Know how to use their blood glucose meter and to contact a pharmacist or diabetes educator if the equipment is not working correctly.
➤ Wear a personalised medical bracelet (eg, Bupa, Mediband, MedicAlert) stating that they have diabetes and their usual treatment.
diabetics include increased carbohydrate intake, inadequate diabetes medicine or insulin, illness or decreased exercise.
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycaemic state (HHS) are acute and potentially life-threatening complications of hyperglycaemia that can occur with either type 1 or type 2 diabetes. Both require urgent medical attention. Symptoms of DKA and HHS are generally preceded by a few days of unwellness but may develop suddenly and include:
• signs of dehydration (thirst, dry mouth, lack of skin elasticity)
• abdominal pain, nausea and vomiting
• polydipsia
• deep and laboured breathing
• ketones on the breath (fruity, acetone smell)
• confusion, an alteration in consciousness or unconsciousness.
HHS is less common than DKA but more deadly. It is most commonly seen in people with type 2 diabetes who have an infection or illness that leads to a reduced fluid intake. Advise
people with diabetes to discuss with their doctor a “sick-day plan” which details what changes to make to their insulin regimen and how frequently to measure their blood glucose.
Hypoglycaemia (low blood glucose)
Low blood glucose levels (usually less than 4mmol/L) in a diabetic may indicate the dosage of their diabetes medicine or insulin is too high or that a meal has been missed.
Symptoms of hypoglycaemia include blurred vision, sweating, feeling light-headed, confusion, trembling, tingling fingers and lips, and loss of consciousness.
Management of suspected hypoglycaemia includes giving simple sugars (two to three glucose tablets, half a glass of fruit juice, two to three teaspoons of jam, honey or sugar in water, seven to eight jelly beans) every 10 minutes until the blood glucose reading is satisfactory. Follow with a meal or complex carbohydrate (slice of bread, piece of raw fruit, two crackers or biscuits). If a person has lost consciousness consult a doctor immediately.
CareSens N
CareSens N POP
CareSens N Premier
CareSens Dual
CareSens N Strips
CareSens N Strips
CareSens N Strips
CareSensPro
Sensocard Plus Talking Meter SensoCard Test Strips
• Refer all children or elderly people with diarrhoea or vomiting to a pharmacist.
• Dehydration can occur rapidly in people with severe vomiting and/or diarrhoea.
• Electrolyte replacement fluids help with recovery and should be given as frequent small sips.
If the person with the diarrhoea or vomiting is a child or older adult, talk to a pharmacist.
For other customers, ask what symptoms they have and how long they have had them for.
Check for signs of dehydration (see Dehydration subtopic, opposite page) including dry mouth and thirst. Run through the Refer to a Pharmacist checklist and refer anyone else with concerns.
People with diarrhoea should be given fluids, preferably electrolyte replacement solutions to prevent dehydration, and, if they have no contraindications, anti-diarrhoeal medicines to stop or slow the diarrhoea, such as loperamide. Anti-diarrhoeal medicines are not recommended for young children.
Antiemetics are medicines which can be used to control vomiting, but these can only be sold by a pharmacist under special circumstances. People with vomiting can also easily become dehydrated, and electrolyte replacement solutions should be given. People with severe dehydration may need to go to hospital for intravenous fluids.
TREATMENT OPTIONS
Category Examples
Electrolyte replacement therapy (ERT)
Anti-diarrhoea (antimotility) medications
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People taking other medication, including herbal/complementary medications.
• Children, frail, or elderly people.
• Diarrhoea or vomiting that has lasted longer than 48 hours in adults.
• People who are refusing to drink fluids or are unable to keep them down.
• Anybody with blood or mucus in their faeces (these look dark or like tar).
• People whose vomit contains blood or dark brown flecks.
• People whose faeces are pale, greasy, or difficult to flush.
• If other significant symptoms are present such as severe abdominal pain or fever.
• Anyone who has recently returned from overseas.
• People with a history of recurrent diarrhoea or constipation.
• People who appear to be underweight.
• People with allergies to medicines.

Diarrhoea and vomiting are two conditions that can occur either separately or at the same time. Viral gastroenteritis, which is easily spread from person to person through direct contact or through contaminated food or water, is
Comments
the most common cause of diarrhoea and vomiting that occur together.
[GENERAL SALE] eg, Enerlyte, Gastrolyte, Hydralyte*, Pedialyte
[GENERAL SALE] eg, diosmectite (DiaRelieve*) [PHARMACY ONLY MEDICINE] eg, loperamide (Diamide, Nodia, Imodium, Imodium Zapid), loperamide + simethicone (Imodium Advanced)
Combination products [PHARMACY ONLY] Rapid Restore Gastro Pack (Enerlyte + Nodia)
Vaccination [PRESCRIPTION] eg, rotavirus vaccine (Rotarix)
Other Lacteeze Extra Strength Chewable
Natural / herbal / supplements
Bifidobacterium lactis, Gastro Relief, Lactobacillus acidophillus, Psyllium hulls, Saccharomyces boulardii, Slippery Elm Bark, zinc
Electrolyte solutions replace fluid and electrolytes and prevent dehydration. They contain sodium, potassium, glucose and citrates/bicarbonates in concentrations easily absorbed by the body. Suitable for all ages. Mix exactly as directed and ONLY with water. Best given slightly chilled and drunk as frequent small sips.
Diosmectite is a natural clay that can absorb up to eight times its weight in water. Suitable for children from 1 year through to adults.
Loperamide normalises the speed of the digestive system, helping to reduce the number and frequency of bowel motions, and restore fluid resorption. Used to temporarily stop or slow diarrhoea. Should be used in conjunction with ERT.
Simethicone helps to disperse gas, relieving bloating and flatulence.
Contains both Enerlyte sachets to correct and prevent dehydration and Nodia tablets to stop diarrhoea.
Funded on National Immunisation Schedule for babies, first dose must be given by 15 weeks of age (see Childhood Diseases and Immunisation: Rotavirus).
Lacteeze replaces the enzyme lactase in people who are lactose intolerant. Use just before eating dairy products (eg, cheese, ice cream, milk) as effects only last an hour.
Psyllium hulls are useful for both diarrhoea and constipation. The bulk fibre absorbs the extra fluid in the bowel. Some probiotics can reduce the duration of diarrhoea. Zinc can reduce the duration and severity of persistent diarrhoea in zinc-deficient children. Slippery Elm Bark can help soothe gastrointestinal irritation and normalise bowel actions. Suitable for either diarrhoea or constipation.
The main symptom of diarrhoea is frequent, loose, watery bowel motions which are usually Products with
accompanied by an urgent need to go to the toilet. Abdominal pain or cramping may also occur, and sometimes nausea and/or vomiting. Common causes of diarrhoea include:
• viruses (eg, norovirus, rotavirus)
• bacteria or other non-viral infections (eg, salmonella, campylobacter, giardia, Escherichiacoli)
• certain medical conditions (eg, inflammatory bowel disease, coeliac disease)
• diet or food intolerance (eg, spicy food, lactose in milk, too much fruit juice)
• medicines (eg, antibiotics, antacids containing magnesium)
• excessive alcohol.
For more information about avoiding diarrhoea while travelling (see Travel Health and Vaccinations).
Rotavirus
Rotavirus is a highly contagious virus which is the leading cause of severe vomiting and diarrhoea in babies and young children in New Zealand.
Symptoms can range from a short period of mild, watery diarrhoea to severe diarrhoea with vomiting, fever, and shock. Profound dehydration is common. Before immunisation, more than 90% of all children were infected by this virus by the age of three.
Rotavirus vaccine is funded on the National Immunisation Schedule (see Childhood Diseases and Immunisation: Rotavirus) and the first dose should be given before a child is 15 weeks of age.
Vomiting
Vomiting (throwing up) is when the contents of the stomach are forcefully expelled by the body through the mouth, usually involuntarily.
Nausea is the term used to describe the feeling of being about to vomit.
Common causes of vomiting include gastroenteritis, viral illnesses such as influenza, overindulgence in alcohol, food allergies, food poisoning, migraines, pregnancy, and some medicines.
Motion may also cause temporary nausea or vomiting (see Travel Sickness).
The most common complication of diarrhoea and vomiting is dehydration, due to water loss through the bowel or mouth, which can be up to four times greater than usual. Important electrolytes, such as sodium and potassium, are also lost. Dehydration can be particularly serious in the very young or very old, or in people who have other illnesses, medical conditions or who
• Most infectious causes of diarrhoea and vomiting are easily spread.
➤ All household members and close contacts of the infectious person should wash their hands frequently and thoroughly.
➤ Alcohol-based hand gels are useful but should be used in addition to hand washing, not as a substitute, unless facilities to wash your hands are not available.
• Electrolyte solutions should be drunk to help prevent dehydration because water alone will not replace electrolytes lost through diarrhoea or vomiting.
take certain medicines.
Since up to 75% of the body’s weight is water, signs and symptoms of dehydration can occur quickly if water is not replaced adequately.
A dry mouth or mild thirst is a sign of mild dehydration and indicates that fluid intake is not good enough.
Signs of moderate-to-severe dehydration which require immediate medical help include:
• cold hands or feet, or mottled bluish skin
• confusion (especially in the elderly)
• dark-coloured urine
• drowsiness or “floppiness” in children, or difficulty waking them
• loss of skin elasticity – skin remains upright and does not flatten after being pinched
• Babies: a sunken fontanelle (soft spot on a baby’s head), sunken eyes, lack of tears, or unusually dry nappies.
• Undiluted fruit juices, soft drinks (eg, flat lemonade), sports drinks and cordials can worsen dehydration due to their high sugar content.
• Mothers with sick babies who are still breastfeeding should continue with feeds as normal. Any baby that is unable to keep fluids down (whether breastfed or bottle-fed) needs to be referred to a doctor.
• Food intake does not need to be restricted if the person feels like eating, although bland and dry foods may be preferred initially.
• Be particularly careful with food hygiene during summer and when cooking barbecues. Cook, Cover, Chill.
• Dry skin can be uncomfortable and itchy and gets more common with age.
• Advise customers to use a mild cleanser, exfoliate regularly, and moisturise daily.
• Sun protection and lifestyle changes, including diet, can improve skin.
Ask your customer for permission to look at and touch their skin. Very dry skin feels quite rough and tight. Redness and deep cracks, particularly on the hands, and large flaky scales, often on the legs, are usually also present when the skin is extremely dry. Run through the Refer to a Pharmacist checklist and refer any customers with concerns.
Oils, dirt, make-up and toxins from air pollution can build up our face and skin and contribute to acne breakouts and inflammation. These won’t dissolve away with water alone which is why everybody needs a mild cleanser to use every day.
Traditional soaps usually contain chemicals such as lye, parabens, sodium lauryl sulfate (SLS), sodium laureth sulfate (SLES), fragrances, alcohol, and other additives which can irritate skin and dry it out. Natural cleansers
Category
• People with other health conditions or who are immunosuppressed or pregnant.
• People with skin that is extremely dry, broken, inflamed or looks infected (ie, with redness or pus).
• If there are any thickened patches of skin and/or silvery scales visible, for example,
include oatmeal, honey, lemon, cucumber, coconut oil, and rose water.
Gentle exfoliation using a mild substance such as glycolic or lactic acid or a wet flannel two or three times per week removes dead skin cells from the surface of the epidermis allowing better penetration of moisturisers and removing dry flaky patches of skin.
Customers with dry skin benefit from hydrating creams (not lotions) that have a low to neutral pH that contain added ingredients such as:
• ceramides. These are found naturally in the skin and help form a protective layer that limits moisture loss. Products may be labelled ceramide AP, EOP, NG, NP, or NS, or contain ceramide precursors, such as phytosphingosine and sphingosine. These are most effective when combined with other
Soap substitutes [GENERAL SALE] eg, Aveeno Body Wash, Cetaphil Gentle Skin Cleanser, Dermalab Gentle Cleansing, Dermasoft, Dermaveen, Dove Unscented Bar, Hopes Relief Cleansing Bar, QV Gentle Wash
Moisturisers and emollients [GENERAL SALE] eg, Cetaphil Moisturising Cream/Lotion, Dermalab Stay Hydrated, Dermasoft, Hope’s Relief Moisturising Cream/Derma Lotion, Lipobase Cream, Lucas Papaw ointment, QV Skin Lotion, Weleda Rash Relief
Lip balms for dry lips/nasal gel for dry nasal passages
[GENERAL SALE] eg, Badger range, Carmex Lip Balm, Fess Nasal Gel, HayMax, Nivea range, QV Lip Balm
Barrier creams [GENERAL SALE] eg, dimethicone (DU IT Tough Hands, Plunkett’s NS Working Hands), zinc (Mustela Vitamin Barrier cream), zinc and castor oil
Anti-pruritic (anti-itch) preparations
[GENERAL SALE] eg, Pinetarsol
Bath/shower products [GENERAL SALE] eg, E45 Moisturising Shower Cream, Scratchy & Itchy Soothing Bath, QV range
Natural / herbal products / supplements Almond oil, Aloe Vera, alphahydroxy acids (AHAs), avocado, coconut oil, honey, lecithin, mango, oatmeal, sesame oil
icthyosis or psoriasis.
• People whose sleep is affected by their dry skin.
• If treatment has been tried before without success.
• Young children.
• People with allergies to topical medicines.
skin-replenishing ingredients like fatty acids, glycerin, and cholesterol. Ceramides help reinforce the skin barrier and increase hydration, giving the appearance of plumper, smoother, firmer-feeling skin with fewer visible lines and wrinkles
• hyaluronic acid. This is a clear, gel-like substance that is produced naturally by the body. It binds to water and helps retain moisture, reducing the appearance of fine lines, wrinkles, and redness
• antioxidants. Vitamin C is one of the most studied antioxidants which can protect the skin by limiting free radical production that occurs in response to sunlight, air pollution, or other factors. Daily use has been shown to reduce sunspots, calm inflammation, and improve skin hydration. Other antioxidants include niacinamide, linoleic acid, peptides, and retinol
Soap substitutes are mild cleansers which do not strip the skin of its natural oils. Use of a soap-free cleanser or soap substitute is important for people with dry skin to prevent further drying. Aqueous cream is not recommended as a cleanser or moisturiser because it contains sodium lauryl sulphate (a detergent) which may aggravate dermatitis.
Regular use of a moisturiser improves the skin’s ability to function properly and act as a barrier. Customers may need to try several products before they find one that they like with the right amount of greasiness. The base used to make the cream and dissolve any ingredients plays just as important a role as the active ingredients themselves. Humectants (eg, glycerin, oatmeal, propylene glycol, phospholipids) hold water in the skin. Ointments containing petrolatum or lanolin tend to be greasier than creams. Some people are allergic to lanolin.
Formulated to adhere to mucus membranes of the lips or inside of the nose. Contain moisturisers to help with chafing, cracking and soreness. HayMax moisturises and prevents dust, pet dander, and pollen from entering the nose.
Provide a barrier between the skin and outside influences (eg, water, detergent). Apply regularly, especially on hands just before immersing them in water.
Tar-based, pine-oil products are useful in the bath to help reduce itching. A few people are allergic to pine oil and should avoid it.
Bath oils containing antiseptics may be useful in people with dry skin and dermatitis to reduce flare-ups due to bacterial colonisation. Use no more than the recommended amount. Warn about the danger of slipping.
AHAs are natural acids found in foods that work by exfoliating the top layers of dead skin cells, improving the skin’s appearance and reducing blemishes and age spots. Coconut oil improves skin moisture and oil levels. Lecithin is used in topical products as a humectant. Several other natural ingredients help restore moisture to dry skin.
(which also functions as an exfoliant)
• keratolytics (eg, urea or ammonium lactate) –used to remove flakes of dead skin, but these may sting
• menthol – provides a cooling effect and reduces itching
• oatmeal – provides a protective barrier over the skin
• shea butter – a non-toxic, solid, fatty oil with skin healing and moisturising benefits
• sunscreens – in day creams to protect against UV rays.
Avoid products that contain charcoal or clay because these absorb excess oil from the skin’s surface. Calamine lotion contains zinc oxide and phenol 0.5% which can increase skin dryness and should not be recommended.
Our skin is the largest organ in our body with an average surface area of 2m2 The outer layers can be grouped into two regions – the epidermis and dermis. The epidermis is mostly composed of keratinocytes with a lipid barrier formed from ceramides (a type of lipid), fatty acids, and cholesterol that protects against water loss and penetration by allergens and irritants. Because it is devoid of blood vessels, the epidermis is entirely dependent on the underlying dermis for the delivery of nutrients and the removal of wastes or toxins.
Collagen and elastin are the main structural components of the dermis and these connective tissues give strength and flexibility to our skin. They are embedded in a gel-like substance that contains hyaluronic acid which has a high capacity for water-binding and helps to maintain the volume of our skin.
• Always apply an SPF 30 to 50+ sunscreen daily before going outside, even if it’s cloudy.
• Limit showers to 4 minutes or less and keep the water warm, not hot, because hot water can really dry out the skin. Pat the skin dry gently with a towel (do not rub) and apply a thick body moisturiser within 60 seconds of stepping out of the shower.
• Coat dry hands and cuticles with a thick moisturiser that contains ceramides or hyaluronic acid before bed, followed by cotton gloves if hands are particularly cracked.
• Some fabrics, such as wool, can exacerbate dry skin so recommend people wear a layer of breathable cotton underneath woollen clothes.
• Keep hydrated.
As we age, our natural production of collagen and elastin slows down and lifestyle factors such as sun exposure and temperature changes impact levels of collagen, elastin, and hyaluronic acid in our skin, decreasing the ability of the skin to bind water. As a result, our skin becomes dryer, less toned, and wrinkles appear. If a red rash is present, this may indicate dermatitis/eczema (see Dermatitis/Eczema).
Some people are born with a tendency towards dry skin, whereas others may develop it as a result of excessive bathing or swimming (particularly in water that is chlorinated), overuse of soap or other products that strip natural oils from the skin, spending too much time in dry or cold air, artificial heat exposure (such as heaters, fires, electric blankets), over exposure to the sun and wearing clothes that chafe the skin (eg, wool).
The existence of a “brain-gut-skin axis”, was initially proposed by John H. Stokes and Donald M. Pillsbury in 1930 who hypothesised that emotional states such as depression and anxiety alter both the function of the gut and the diversity of the bacteria within it,
which increases intestinal permeability and systemic inflammation, and disrupts our skin microbiome. Changes in the diversity of our gut have been associated with skin conditions such as acne, atopic dermatitis, and psoriasis. In addition, many gastrointestinal disorders such as Crohn’s disease, ulcerative colitis, and coeliac disease are often accompanied by skin manifestations.
Limiting processed, high-sugar, and high-fat foods; eating plenty of plant-based high-fibre foods (including walnuts and avocados that are rich in beneficial fats) and lean protein; the addition of fermented foods to the diet such as yogurt kefir, and sauerkraut which are great natural sources of probiotics; drinking six to eight glasses of water per day; avoiding alcohol and eliminating foods that you may be intolerant to can improve gut health and lead to a noticeable improvement in the skin.
• Ear conditions that are treatable with OTC products include swimmer’s ear and excessive earwax.
• Customers should be discouraged from cleaning their ears with cotton buds because this can damage the lining of the external ear canal and push more earwax into the ear. Instead, they should use an earwax softener or see an ear nurse for wax removal.
Specialised equipment is needed to look properly into the ear canal so a pharmacy only sells products that treat conditions that affect the external ear, such as earwax, swimmer’s ear, and contact dermatitis from sensitivity reactions (see also Dermatitis/Eczema). Use a torch to look as far into the ear as you can but asking the customer about their symptoms may give you a better idea about what their ear problem is. Refer those with concerns identified from the Refer to a Pharmacist checklist.
Treatment varies depending on the ear condition (see under each subtopic).
Earwax (cerumen)
The ears are typically self-cleansing and only a few people are genetically more prone to excessive earwax production. In these people, problematic wax should be removed with drops, by irrigation with warm water, with gentle suction, or by a ear nurse, doctor, or audiologist. OTC preparations that soften earwax or irrigate the ear work better for people with small to moderate amounts of wax. Ear candles are NOT recommended as there is no research that
Category Examples
• People who are immunosuppresssed, pregnant or breastfeeding.
• People who take medicines that may be associated with an ear condition (for example, aspirin and diuretics may cause tinnitus).
• Children.
• People who are feeling generally unwell or have a fever.
• People who describe trauma to the ear preceding the current problem (eg, insertion of a cotton bud or other cleaning tool).
• Whose hearing has suddenly become
says they are effective and the risk of burns high.
Swimmer’s ear is best prevented by drying the ears thoroughly after exposure to water and using a product containing a water-evaporating agent (see Treatment options: swimmer’s ear) to remove any moisture collected within the external ear canal. People prone to swimmer’s ear should also wear ear plugs during swimming or showering.
Referral to a doctor for antibiotics is often necessary if a bacterial infection has already developed.
It is important to refer children with otitis media to a doctor, who will investigate further because chronic unrelieved pressure within the ear may result in glue ear.
Antibiotics are not necessarily prescribed routinely for otitis media, but paracetamol or
Earwax removal drops [GENERAL SALE] eg, Audiclean, Waxsol [PHARMACY ONLY MEDICINE] eg, Auralgan, Cerumol, Ear Clear
Ear cleansing products [GENERAL SALE] eg, Audiclean, Ear Clear Ear Cleanser, Earigate Ear Cleaning
Swimmer’s ear products [GENERAL SALE] eg, isopropyl alcohol ear drops (Audiclean Swimmers Ear), propylene glycol/acetic acid (Vosol) eg, ear plugs (Otifleks, Macks range) eg, Swim Seal Ear Drops
Comments
impaired or has been gradually deteriorating.
• Whose symptoms have persisted despite treatment, or if the ear has become itchy with treatment.
• With a history of neck or head injury prior to the ear pain.
• With an unusual growth visible near the ear.
• With a suspected foreign object lodged in the ear.
• With pain, tinnitus (ringing in the ear), dizziness, or a discharge (such as pus or blood) from the ear.
• People with allergies to topical medicines.
ibuprofen may be given to help relieve pain.
A child who appears not to be hearing properly should be referred to a doctor. Signs may include inattention at school, ignoring instructions, naughtiness, or wanting the television very loud.
Our ears allow us to hear and keep our balance. Each ear consists of three parts: the outer, middle and inner ear. The outer ear collects sounds from the environment and funnels them through the rest of the ear. It is composed of the pinna (the flap of skin that channels sound), the external ear canal, and the tympanic membrane (eardrum).
The tympanic membrane separates the outer ear from the middle ear. The middle ear is an oval, air-filled space approximately 2cm3 in volume that contains three tiny bones (the hammer, anvil and stirrup) that form a chain
Helps soften or loosen earwax. Warming of drops prior to use may improve effectiveness. Once drops are administered, the patient should lie with the ear containing the solution uppermost for five to 10 minutes. Some drops contain a local anaesthetic to relieve ear pain. Prolonged use of these medicines may lead to hypersensitivity and irritation. Consult a doctor if pain occurs when using these medicines.
Contain fluids such as purified sea water to wash away dirt and excess wax instead of pushing it into the ear canal. These products are safer than cotton buds (cotton buds are not recommended for cleaning out ears).
Products may contain acetic acid, propylene glycol or isopropyl alcohol to dry up any water in the ear. These products are usually more effective at preventing rather than relieving swimmer’s ear.
Ear plugs help keep water out of the ears during swimming and showering.
Swim Seal ear drops contain a mixutre of polysiloxane and tea tree oil that coats the ear canal, providing a barrier against water. Self-removing.
Natural / herbal products / supplements Ear wax removal and swimmer’s ear
Warm olive oil (eg, Cerumol Olive Oil)
Glue ear
Echinacea (eg, Kiwiherb De-Stuff)
Tinnitus
Gingko biloba (eg, Tebonin EGb 761)
Olive oil may help soften wax aiding removal. One drop placed in the ears is also good for relieving an itch and is better than sticking cotton buds or other objects into the ear.
Echinacea root preparations may help prevent or relieve upper respiratory tract infections, reducing the risk of otitis media and the development of glue ear. There is no evidence that ear candling is effective and it may leave deposits of candle wax in the ear or burn skin.
Ginkgo biloba extract may help with balance and inner ear noise.
• Red eyes, conjunctivitis, dry eyes, styes, and blepharitis are common eye problems.
• Many eye products can be sold over the counter and chloramphenicol eye drops/ ointment can be sold by a pharmacist for conjunctivitis.
• Refer people with other serious eye concerns to a doctor or TPA-endorsed optometrist.
If the customer is unsure what is wrong with their eyes or you cannot easily see what is wrong yourself, involve a pharmacist. See over the page for symptoms of common eye conditions.
How to perform a basic eye examination (pharmacists)
• Wash your hands and ask the customer to sit down in a private area with good light.
• Ask the patient to look straight ahead and pull down the lower eyelid.
• Instruct the patient to look up, then down, to the left and right while you examine the conjunctiva.
➤ Look for signs of redness, dryness, foreign
• People with other health conditions that may cause eye problems, such as immunosuppression or diabetes.
• People taking medicines that may adversely affect the eyes (such as amiodarone, bisphosphonates, topiramate).
• People wearing contact lenses.
• People with a family history of eye problems (eg, glaucoma).
• Young children, women who are pregnant, or the elderly.
• People who report seeing halos or yellow/ green colours when they look at lights.
• Whose problem has persisted despite treatment or recurs frequently.
• With a cloudy cornea.
• With a coloured discharge or mucus from the eye.
bodies (eg, wood splinters), or infection.
➤ Use the information on the following pages to try and identify the most likely condition and recommended treatment.
• With swelling of the iris or eyeball, or of the tissues surrounding the eye.
• With a suspected herpes zoster infection (shingles), indicated by a painful rash near the affected eye.
• With pain in the eye(s), light sensitivity, a foreign object in the eye, or deterioration in vision.
• With pupils that are different sizes or an irregular shape or with redness localised around the pupil.
• With systemic symptoms such as a headache or vomiting.
• With allergies to topical eye products or certain preservatives.
➤ If there is a foreign object in the eye, consider using an eye wash to flush it out or refer the customer to a doctor if the object is strongly embedded or difficult to remove.

Category
Examples
Natural / herbal products / supplements Bilberry
Euphrasia (eyebright)
Ginkgo
Vitamin C with bioflavonoids
Age-related macular degeneration
Lutein
Zeaxanthin
Styes
Black tea
Pulsatilla
Dry eyes
Omega 3 & 6
Flaxseed oil
Comments
• Base your product recommendations or decision to refer on information gained during the examination.
• Refer any customer wearing contact lenses, with eye or eyelid swelling, pupils that do not react to light, reporting vision disturbances or with an uncertain diagnosis to a doctor or an optometrist holding a Therapeutic Pharmaceutical Agents (TPA) endorsement (these optometrists are able to prescribe a range of eye medicines).
Our eyes are structurally and functionally complex. Each eyeball sits in a pear-shaped, bony cavity within our skull called the orbit.
Each eyeball is covered by a tough, white layer called the sclera. The front part of the eye is covered by a thin, transparent membrane called the conjunctiva; this lines the inside of the eyelids and covers the sclera.
Bilberry is used for improving visual acuity including night vision, cataracts, degenerative retinal conditions. Coleus Euphrasia can help relieve sore and irritated eyes, and provide relief from conjunctivitis.
Ginkgo may improve blood flow to the retina.
Vitamin C may help decrease the risk of age-related macular degeneration.
Several herbs have infection-fighting properties; however, eye washes containing these ingredients should only be made by a herbal practitioner trained in botanical medicine.
Age-related macular degeneration
Lutein and zeaxanthin are antioxidants which may help protect the macula against damage.
Styes
Topically applied Pulsatilla may help with styes.
A tea bag applied to the stye may help reduce symptoms.
Dry eyes
Increasing omega 3 and 6 intake can lower risk of developing dry eye syndrome.
The cornea is a clear, curved layer which helps focus light on the retina at the back of the eye. Light passes through the pupil (the black centre of the eye), and the amount of light that reaches the retina is controlled by the iris muscles – the coloured part of the eye.
Conjunctivitis is the name given to
Applying eye drops
• Wash your hands first.
• Shake the container if it says to.
• Pull the lower eyelid down gently with the index finger to form a pocket. Tilt head slightly back and look up.
• Gently squeeze the bottle to release the recommended number of drops into the pouch.
• Do not touch eye with the dropper tip.
• Close eye and press the corner of the eye gently. Remove excess drops with a clean tissue.
• If this is difficult to do in young children, you can get them to lie flat, close their eyes, place the drop into the inner corner of their closed eye, then get them to open their eyes. The drop will drain into the eye.
• Wait 10 minutes before adding other eye products to the eyes. Put eye drops in before putting in eye ointment.
Applying eye ointment
• Hold the tube between your thumb and index finger and rest your hand against the base of your nose to position the
inflammation of the conjunctiva, which may be allergic, bacterial, or viral in origin. Dry eye is caused by a change in the composition or quantity of tears that bathe the cornea.
problem with the macula, which is located in the centre of the retina.
Some of the more common conditions encountered in pharmacy are discussed in more detail on the following pages
Blepharitis and styes occur on the eyelids. Age-related macular degeneration is caused by a
ointment tube tip.
• Apply a small blob of ointment into the lower eyelid pocket. Do not touch the eye with tube tip.
• Eye ointment may blur vision for a short time after use. Do not drive or operate machinery until vision is clear.
Eye mist sprays
• Spray directly onto closed eyelids. Moisturising particles are then swept into the eye with every blink.
• Easier to use and last longer than regular eye drops; however, may be more expensive.
Useful tips
• Our eyes damage easily and conditions such as dry eye need to be treated, otherwise the cornea can scratch easily which can result in infection, ulcers, or scarring.
• Some eye products contain preservatives or ingredients that can affect contact lenses, or they may cause a sensitivity with continued use.
➤ Preservative-free eye drops may be more suitable for customers who use eye drops regularly.
• Protect eyes from the wind and sun by

wearing sunglasses.
• Discard multi-use eye products one month after opening unless the label says otherwise. Single-use products are sterile until they are opened. Eye mist sprays are designed to keep the product sterile even when in use. Refer to their package instructions for the discard date.
• Replace eye make-up frequently and do not share with others.
• Contact lens wearers should always follow their optometrist’s instructions with regards to lens hygiene (see Eye Conditions: Contact Lenses)
• Most people should see an optometrist at least every two years for an eye examination.
➤ Eye problems are more likely as people age.
➤ An optometrist has the equipment to detect eye diseases earlier, eg, glaucoma is symptomless.
➤ Contact lens wearers should see an optometrist at least yearly.

Long-lasting


Preservative and phosphate-free
At least 300 sterile drops per 10ml bottle
Use for 6 months after opening
Use with contact lenses
Delivered through the unique COMOD® multi-dose application system
AGE-RELATED MACULAR DEGENERATION (AMD)
Loss of vision or a blurred area near the centre of vision in one or both eyes. Vision loss may occur gradually, or suddenly. Blurred area may become larger or blank spots may develop in the central vision.
Loss of vision may interfere with everyday activities. Objects may not appear as sharp or bright as they used to be.
AMD is common and the leading cause of vision loss among people over the age of 50.
AMD is more common in people over the age of 50, in Caucasians compared with AfricanAmericans or Hispanics/Latinos and in people with a family history of AMD.
Stop smoking if you smoke; smoking doubles the risk of AMD.
Exercise regularly, keep blood pressure and cholesterol under control, and eat a diet rich in green, leafy vegetables and fish. Get a comprehensive dilated eye exam at least once a year.
Consider taking supplements which have been shown in trials to reduce the risk of late AMD by 25%. Known as AREDS and AREDS2 these substances contained clinically effective dosages of vitamin C, vitamin E, zinc oxide, cupric oxide, and betacarotene, lutein, or zeaxanthin.
[GENERAL SALE]
eg, Blackmore’s Macu-Vision, Goodhealth Premium Vision, Macutec Once-Daily, Clinicians VisionCare with Lutein
BACTERIAL CONJUNCTIVITIS
ALLERGIC CONJUNCTIVITIS
Symptoms are red, burning, sore eyes often with puffy eyelids and a thick white/yellow discharge. Eyelids may be stuck together on awakening.
Symptoms come on suddenly and both eyes are usually infected (it is very contagious), although one eye may be affected a day or so before the other. Symptoms usually resolve themselves within about one to two weeks.
Antibiotic eye drops will hasten recovery.
Symptoms include very itchy, burning, sore red eyes with puffy eyelids and maybe dark pouches below the eyes, and a clear, copious discharge that may be watery or sticky. There is often a history of other allergy symptoms, such as sneezing and a runny or congested nose (see Hay Fever).
Bathe eyelids with warm water or saline solution and use warm compresses. Soak cloth in nappy solution and wash thoroughly after each use.
Do not share face cloths, towels or eye drops. Dispose of tissues carefully.
Do not use decongestant eye drops as they can mask redness and thereby mask a worsening infection. Wash your hands frequently and after any contact with the eyes.
Apply a cold flannel to soothe the eyes. Avoid triggers (eg, pollen, animal dander) where possible. Wash hands frequently and after any contact with the eyes.
Combination eye drops containing decongestants should not be used for more than three days, to avoid rebound congestion in the eyes.
Bacterial conjunctivitis can be treated with antibacterial/ antibiotic eye drops. Consider using single-use wipes to keep eyes clean.
Hypoallergenic pH-balanced wipes eg, Clear Eyes, Fess
Antibacterial eye drops
[PHARMACIST ONLY MEDICINES]
eg, Chloramphenicol eye drops 0.5% (Chlorafast), Chloramphenicol eye ointment 1% (Chlorsig)
Treat with antihistamine tablets or eye drops (see Hay Fever).
Hypoallergenic pH-balanced wipes
eg, Clear Eyes*, Fess
Mast cell stabilisers (eye drops)
[PHARMACY ONLY MEDICINE]
eg, cromoglycate (Cromo-Fresh), lodoxamide (Lomide)
These preventive medicines should be used four times daily on an ongoing basis.
Antihistamines (eye drops)
[PHARMACY ONLY MEDICINE]
eg, levocabastine (Livostin), ketotifen (Zaditen)
Decongestant combinations (eye drops)
[PHARMACY ONLY MEDICINE]
eg, naphazoline (+ antazoline: Albalon A Allergy; + pheniramine: Visine Allergy; + zinc: Clear Eyes Allergy)
VIRAL CONJUNCTIVITIS
MINOR EYE IRRITATIONS RED EYES
Symptoms are red, sore and gritty eyes with a clear watery discharge. Some itching and swelling may be present, with some crusting on the eyelids. One or both eyes may be infected.
Frequently caused by the common cold virus or adenoviruses; other viral symptoms may also be present (eg, fever, sore throat). Symptoms may last two to three weeks. If herpes simplex is involved, there will be no other viral symptoms but there may be cold sores elsewhere (see Cold Sores). Refer to a doctor immediately as herpes simplex can cause scarring and perforation of the cornea.
Symptoms are red, sore, watering eyes, with or without itch.
Causes are numerous, including allergies, late nights (“party eyes”), wind, dust, smoke, air conditioning, air pollution, chemicals, sunlamps, glare (snow, sand, sun, sea), staring at a computer.
A patch of bright red in the white of the eye is called a subconjunctival haemorrhage. It usually causes no pain and is self-limiting, clearing in about one week.
Viral conjunctivitis is contagious so do not share face cloths, towels or eye drops. Dispose of tissues carefully. Wash hands frequently and after any contact with the eyes. If symptoms do not improve or get worse seek medical advice.
Allergy is a common cause of red eye (see allergic conjunctivitis previous page). Avoid the cause if possible.
Eye drops containing decongestants should not be used for more than three days, to avoid rebound congestion in the eyes.
There are no OTC preparations available to treat viral conjunctivitis. Treat symptomatically using soothing lubricant eye drops and bathing the eyes. Consider using single-use wipes to keep eyes clean.
Hypoallergenic pH-balanced wipes eg, Clear Eyes Wipes, Fess Little Eyes Wipes
Lubricant eye drops/eye spray
[GENERAL SALE]
eg, Hylo-Fresh*(PF) Novatears*(PF), Optrex Actimist 2 in 1 Dry & Irritated Eye Spray*, Optrex Actimist Advanced Preservative Free Spray*(PF)
Treat minor eye irritations with lubricants or decongestant eye drops.
Lubricant eye drops/eye spray
[GENERAL SALE]
eg, Celluvisc(PF), Clear Eyes Redness, GenTeal(PF), Hylo-Fresh*(PF), Optrex ActiMist Eye Spray for Dry, Tired, & Irritated Eyes*, Optrex Actimist Advanced Preservative Free Spray*(PF), Optrex Red Eyes*, Optrex Sore Eyes*
Decongestant eye drops
[PHARMACY ONLY MEDICINE]
eg, Albalon A Allergy (with antihistamine), Albalon Relief(PF), Clear Eyes Allergy, Optrex RedEyes*, Visine range
Eye wash
[GENERAL SALE]
eg, Optrex Eye Wash with Eye Bath*
DRY EYES
Symptoms are dry and gritty eyes (feels like sand in the eye). Caused by an imbalance in the components that make up the tear film that lubricates the eye between blinks. This means that watery eyes is a common symptom because the tear film is now ineffective for lubrication. Eyes may look slightly pink or have a fine crusting on the lids. Contact lenses may not sit properly on the eye.
Caused by ageing, contact lens wear, hormone fluctuations (eg, with menopause, oral contraceptive use, pregnancy), medical conditions (eg, rheumatoid arthritis), irritants (eg, smoke, dust, wind), surgery, trauma, and certain medicines (eg, diuretics, antihistamines, decongestants and tricyclic antidepressants).
Eliminate or treat the cause if possible and keep well-hydrated. Damage to the eyes can occur if left untreated for too long, as the cornea can easily get scratched. Protect eyes from the wind and wear sunglasses when outside. Use an eye wash to soothe sore, irritated and tired eyes. Use lubricant eye drops (artificial tears) during the day and lubricant eye ointment at night. Throw multi-use eye drops away one month after opening unless otherwise stated. Consider using preservative-free eye drops long term as sensitivities can develop with regular use of preservative-containing drops. Omega-3 supplements may also help.
Lubricant eye products do not cure dry eyes but mimic the effect of natural tears so can relieve the symptoms. Regular eye washes may help improve symptoms.
Eye wash
[GENERAL SALE]
eg, Optrex Eye Wash with Eye Bath*
Lubricant eye drops/eye spray
[GENERAL SALE]
eg, Clear Eyes Dryness*, Hylo-Fresh*(PF), Novatears*(PF), Optrex ActiMist Eye Spray for Dry, Tired, & Irritated Eyes*, Optrex Actimist Advance For Dry Eyes Preservative Free Spray*(PF), Optrex Rehydrating Eye Drops for Dry Eyes*, VitA-PosPF)
[GENERAL SALE]
eg, lubricant eye ointment (Refresh Night Time Eye Ointment(PF), Viscotears Gel)
eg, Optimel Antibacterial Manuka + Eye Gel
These may temporarily blur vision after instillation.
Other eg, omega-3 (TheraTears Nutrition)
BLEPHARITIS Symptoms include inflammation of the eyelids, with crusting or scales at lid margins.
The eyelids are usually red, thickened, burning, sore and feel itchy, and may be stuck together in the mornings.
There may be photophobia (sensitivity to light).
The condition is often chronic and tends to be associated with dandruff and/or dry eye.
STYES A stye is an infected gland at the base of an eyelash. Symptoms include a localised, painful swelling in the upper or lower edge of the eyelid, which is sensitive to touch. The eyes may water and be sensitive to light. A person with a stye may report feeling as if they have a foreign body in the eye. Most styes resolve spontaneously.
Daily eyelid hygiene helps to control blepharitis.
Baby shampoo (not soap) may be used to wash the eyelids. Use half a teaspoon of baby shampoo into a bowl of hot, not boiling, water. Wet a clean cloth with the solution. Place the cloth over the eyes as a compress for two minutes. Clean around the eyelashes gently, using a cotton bud dipped in the hot baby shampoo solution. Use twice a day, then less often as the blepharitis settles. Rinse the cloth first in nappy wash solution and then fresh water before use to avoid bacterial contamination of the cloth.
Otherwise, pre-moistened wipes containing gentle lid cleansers can be used to wipe the eyelids.
Using a heated eye compress on the eyes for a few minutes before cleaning the lids can loosen any crusting at the gland openings and promote improved oil flow.
Treat any dandruff if also present(see Dandruff).
Most styes resolve themselves when they rupture and pus is released.
Warm-to-hot (but NOT boiling) compresses, using a clean cloth applied three to six times daily, can hasten the “pointing” of the stye. Avoid touching the stye, or squeezing it, or using make-up near it.
Some wipes for styes contain homeopathic ingredients that may provide relief.
Blepharitis is not curable but daily lid hygiene can help control the symptoms. Lubricating eye drops also help to supplement the inadequate natural tear film. Antibiotic drops are only required if the blepharitis is not kept under control with lid hygiene.
Lubricant eye drops
[GENERAL SALE]
eg, Celluvisc Drops(PF), Clear Eyes Eye Mist Spray(PF) GenTeal(PF)
Optive, Optrex ActiMist Eye Spray for Dry, Tired, & Irritated
Eyes* Refresh range
eg, Optimel Antibacterial Manuka + Eye Gel
Eyelid wipes and cleansers
eg, Blephadex Eyelid Wipes (tea tree oil and coconut), Blephadex Eyelid Foam Cleanser
Other
Eye pack (wheat bag)
Opti-Soothe Moist Heat Mask
Consider using single-use wipes to keep eyes clean. Topical antibacterial/antibiotic drops may prevent secondary infection occurring when the stye ruptures, but are usually not necessary.
Homeopathic treatments
eg, Similasan Stye Eye Relief
Other
Stye Away Reuseable Compress
• Contact lenses are an alternative to wearing glasses for poor eyesight, although some are worn for cosmetic reasons (eg, to change colour of the eyes).
• Disposable hydrogel contact lenses are the most popular type of contact lens. They are thrown away after one day’s use.
• Other contact lenses require careful daily cleaning unless they are the extended-wear type.
• Any contact lens wearer with an eye infection should be referred to a TPA-endorsed optometrist or a doctor.
All customers with contact lenses should be refered to a pharmacist as they are prone to more serious eye conditions.
Contact-lens wearing customers whose eyes are red, uncomfortable, painful, sensitive to light or who have abnormal vision should see a doctor or optometrist immediately.
When selling a lens cleaning or rewetting product, make sure that it is compatible with the customer’s lens type.
Hydrogel lenses are available as daily disposable and extended-wear types. Hydrogel lenses have a high water content and allow oxygen into the eye. Some also mimic the lipid layer of the tear film and have a UV filter.
Hydrogel lenses are quick to get used to wearing, so can be used occasionally (ie, just for sport) if necessary because they are stable on the eye during exercise and easy to remove. There are many different types of disposable and extended-wear lenses, but all are designed to be worn for a set period of time (eg, daily, two-weekly, monthly) then thrown away.
Daily disposable lenses remove the need for cleaning, while daily wear weekly or monthly
Category Examples

lenses require nightly care so should be removed each night.
Soft lenses are also available that enhance the colour of the eyes or add special effects (such as designs) to them. The middle of the lens is left clear so the person can still see; however, vision may be affected if the lens slips from its correct position.
Customers wanting advice about cosmetic lenses should always check with an optometrist before using them, as some people have eye conditions that make them unsuitable.
People who wear cosmetic lenses are prone to the same infections as vision-correcting lens wearers, so lenses must be cleaned and disposed of as instructed. Cosmetic lenses should never be shared.
Gas permeable lenses are made of durable plastic that has a high permeability to oxygen. They usually also contain silicone for flexibility and are smaller in diameter than the cornea (8–10mm).
They allow good oxygen transmission which maintains corneal health and reduces the risk of corneal infections and allergic reactions. GP lenses also provide better vision, durability, and
Disinfecting/cleaning products For soft lenses only eg, Bausch & Lomb ReNu Fresh, BioTrue Multipurpose, Complete Multipurpose, RevitaLens Multipurpose RGP lenses only eg, Total Care 1 Solution, Boston Advance Conditioning Solution
Saline solutions Suitable for both soft and RGP lenses eg, Lens Plus Saline
Protein removal tablets RGP lenses only eg, Menicon Progent
Lubricants, artificial tears, wetting agents Suitable for all types of lenses eg, Complete Blink-N-Clean, Blink Contacts, Refresh Contacts, TheraTears
Comments
deposit resistance than soft contact lenses. They usually take longer to get used to initially which is the main reason they are not as popular as soft contacts.
GP lenses may be better suited to people with astigmatism or those with presbyopia since bifocal and multifocal types are available. Patients with keratoconus (a cone-shaped cornea that causes severe visual disturbances) may require a GP lens to achieve reasonable vision, as may people requiring contact lenses after refractive surgery.
Although GP lenses are more expensive initially than soft lenses, they can last for years so can work out cheaper in the long run. An ophthalmologist may be able to apply for a government subsidy to help with the costs of contact lens wear in certain conditions.
Because they can last for years, GP lenses require scrupulous cleaning and disinfecting to keep the wearer safe from eye infections.
Photo-refractive keratectomy (PRK) and laser in situ keratomileusis (LASIK) are two laser eye surgery techniques that are commonly used for correcting short-sightedness (myopia), long-sightedness (hyperopia), astigmatism and presbyopia, but they are not without their risks and their popularity has
Cleaning products include multi-purpose solution, daily cleaner, hydrogen peroxide solution, cleaning/ disinfecting devices.
Immediately after removing lenses each day, clean them with a cleaning solution to remove eye-produced build-up such as protein, cosmetics and other debris. Place lens in the palm of the hand, put two or three drops of the cleaner on it and rub well for 20 to 30 seconds. Note some cleaners are ‘no rub’ cleaners. Leave for as long as recommended.
Useful for rinsing lenses or dissolving protein tablets.
Rinse lens for recommended time to remove cleaner and loosened debris.
Removes excess protein deposits from lenses that are worn for longer periods of time. If used with correct cleaning products some lenses do not require separate protein removal.
Lubricants can help improve dry eye in contact lens wearers although referral to an optometrist is recommended as dry eye in contact lens wearers can sometimes be resolved by changing the lens type or improving gland function around the eye.
diminished in recent years.
PRK is more suitable for treating mild degrees of myopia. A layer of cells covering the cornea is removed then a laser is used to alter the shape of the front of the cornea.
LASIK uses a highly specialised laser underneath a corneal flap to reshape the cornea, and provides improved results for people with greater degrees of myopia, hyperopia and astigmatism. Long-term problems include eye infections, chronic pain, and detached retinas.
Refractive lens exchange is identical to cataract surgery but is performed in people who do not have cataracts to allow them to see better without wearing glasses or contact lenses. The person’s natural lens is replaced with a clear artificial lens.
Orthokeratology (also called Corneal Refractive Therapy) is a non-surgical, non-invasive and reversible process of using a specially designed contact lens to reshape the cornea during sleep, allowing lens-free clear vision throughout the next day.
Research has shown that orthokeratology can slow down and even stop the progression of short-sightedness in children and teenagers. Effects are usually noticed after the first night, and lenses are worn nightly initially, reducing to two or three nights a week to maintain the effect long term. Orthokeratology is available throughout New Zealand; however, there are some concerns it may increase corneal irregularity and impair contrast sensitivity.
• See an optometrist for an eye check regularly (at least every 12 months).
• Always wash, rinse and dry hands before handling lenses.
• Do not use tap water or saliva on contact lenses.
➤ A naturally occurring amoeba found in water can cause an infection that can be difficult to treat and has the potential to lead to blindness.
➤ Dirty storage cases, incorrect cleaning of lenses and using tap water or saliva on lenses or lens cases are common sources of infection.
➤ Use an unused toothbrush to clean the lens case every week before rinsing with lens cleaner. Replace the case monthly.
➤ Never touch lens solution bottle tips to any surface as they may become contaminated.
➤ Dry lenses may be rehydrated with saline, rewetting solution, or lubricant drops before reinsertion. Soft lenses become brittle if they dry out.
➤ Do not exceed the recommended wearing time of your lenses.
➤ Never share contact lenses.
• If contact lenses make eyes drier than normal, lubricant eye drops are available that are compatible with contact lenses.
➤ Consider using preservative-free products long term.
• Insert lenses before applying make-up and remove them before removing it.
➤ Cream or gel eye shadows are less likely than powders to fall into the eye.
➤ Avoid mascara with lash-building fibres.
• Do not use lens-care products or eye products (especially make-up) past their expiry date.
• If you lose or drop a lens:
➤ For a GP lens, use a vacuum cleaner with pantyhose over the inlet to catch the lens
➤ For a soft lens, turn out the light and shine a torch around the room (the light will reflect off the lens).
Eye products and contact lenses
• Remove contact lenses before using eye drops or ointments, except when using lenswetting agents or when directed by the optometrist to keep the lenses in.
• Soft lenses in particular may become stained when exposed to chemicals in diagnostic eye drops, some medicated eye drops and some medicines taken by mouth that are then secreted in tears (eg, rifampicin, sulfasalazine).
• A fever is a temporary increase in body temperature (normal body temperature is considered to be 37°C).
• Fever is most commonly associated with infection although it may occur with a number of other conditions.
• Fever is considered an important part of the immune response and there is controversy about whether it should be treated with fever-lowering medicines.
Customers who have symptoms such as skin discolouration (pale, ashen, blue, or mottled skin), breathing changes (a faster breathing rate or visible use of chest muscles), reduced activity levels (difficulty in rousing, lack of response to social cues, continuous crying), a faster heart rate, or reduced skin turgor (how quickly the skin flattens after being pinched) are likely to have a serious underlying reason for their fever and should be referred to a doctor immediately. Slightly elevated temperatures in infants and toddlers can also indicate serious infection and should be referred.
For all other customers, run through the Refer to a Pharmacist checklist and refer those with concerns to a pharmacist.
Controversy surrounds the usefulness of fever and whether it should be treated with antipyretic (temperature-lowering) medicines (eg, paracetamol, ibuprofen) or not. Research has shown that fever can help fight infection by enhancing the body’s immunological response, and creating an unbearable environment for some pathogens. Most experts recommend that antipyretics be used only occasionally, if at all, in low-grade fevers to relieve discomfort rather than specifically to lower body
Category Examples
• People with other health conditions, or who are immunosuppressed, pregnant or breastfeeding.
• People who take medicines, including herbal/complementary medications.
• Children aged less than six years or any child who describes pain with the fever.
• Fever that is accompanied by a painful sore throat.
• Fever that is accompanied by a stiff neck, headache, sensitivity to light, irritability, rash and/or vomiting. This may indicate meningitis which can be fatal (see Childhood
temperature. These medicines will not shorten the duration of an illness.
Most people just need bedrest and supportive care (such as staying hydrated, keeping bedding light) to recover from a fever, although other treatments (such as antibiotics) may be needed depending on the cause.
Anybody with a particularly high fever (above 39°C), who is extremely sleepy or appears very unwell, is refusing fluids, aged under six months, or with symptoms suggestive of meningitis (see Childhood Diseases and Immunisation) should aways seek immediate medical attention.
About 2%–5% of children aged three months to six years will experience a tonic-clonic seizure during a fever. Children aged eight to 20 months are more at risk.
During a febrile seizure the child usually loses consciousness and the limbs on both sides of the body rapidly shake or convulse. Some children just become rigid with minor body twitches.
Febrile seizures are thought to be due to a sudden rise in body temperature, and often
Antipyretics (feverlowering medicines) [GENERAL SALE] eg, aspirin (Aspro, Disprin range) eg, ibuprofen <25s (Advil range, Nurofen range) eg, ibuprofen + paracetamol 16s (Maxigesic, Nuromol) eg, paracetamol (Paracare, Panadol) [PHARMACY ONLY MEDICINE] eg, ibuprofen >25s (Nurofen range) eg, ibuprofen suspensions (Fenpaed, Nurofen for Children) eg, ibuprofen + paracetamol >25s (Maxigesic, Nuromol) eg, paracetamol suspensions (Pamol, Panadol Colour Free, Paracare)
Diseases and Immunisation)
• People who appear quite unwell, or who describe feeling very lethargic or sleepy.
• People who are refusing fluids or are unable to keep any fluids down.
• People who have recently returned from overseas.
• People with a fever that has lasted more than 48 hours.
• Anybody with other symptoms of concern such as heavy night sweats or a rash.
• People with allergies to medicines.
occur before the caregiver even realises the child is ill. Cool compresses or fever-reducing medicines such as paracetamol or ibuprofen will not prevent a febrile seizure. Most of these seizures resolve themselves after one to five minutes, are harmless, do not require daily medication, and do not cause brain damage, although caregivers should seek further medical advice to establish the source of fever.
If a febrile seizure occurs, the caregiver should lay the child on their side, somewhere safe, and stay with them while they recover. Any sharp objects near the child should be removed, and tight clothing loosened. Objects (eg, pacifiers) should not be placed in the child’s mouth and attempts should not be made to stop the seizure. Although most seizures stop on their own, if the seizure persists for longer than five minutes, caregivers should ring for medical advice. Emergency medical assistance should be sought if a seizure lasts longer than 10 minutes. Although alarming for parents, the vast majority of febrile seizures cause no lasting effects.
Comments
Consider occasional antipyretic use to make the person feel more comfortable. Paracetamol is not recommended for routine use before or after vaccination as it may reduce the effectiveness of childhood vaccinations to stimulate lasting immunity (infection-fighting ability). If taking paracetamol for pain relief, be careful not to double-up with other combination medicines containing paracetamol.
Some non-steroidal anti-inflammatory drugs (NSAIDs) may not be suitable for people taking certain other medications or with some medical conditions (eg, asthma, kidney disease). Advise customers to stop taking if stomach upsets, increased bruising or prolonged bleeding occur. Aspirin has an increased risk compared with ibuprofen and is generally not the preferred NSAID. Aspirin is not recommended for children or adolescents under 16 years old (see Childhood Pain).
Ibuprofen may be used in children aged over three months.
Fever is defined as a rise in the normal body temperature and is generally considered present when body temperature rises above 38°C. Normal body temperature varies by person, age, activity, and time of day (usually lower in the morning and higher at night). Many other factors, such as the menstrual cycle, can also affect temperature.
The average normal body temperature in adults is considered to be 37°C, with a range of 36.1 to 37.2°C. Temperature measured under the arm or in the ear is usually about 0.5°C lower than oral body temperature, and that in the rectum about 0.5°C higher. It is important to remember that the reading on a thermometer is not the most important indication as to how sick a person is. Do not underestimate or dismiss a perception that a person feels hot when a hand is placed on their forehead or looks “off-colour”.
Depending on the cause of the fever, other symptoms may also be present such as aching
muscles, cough, earache, enlarged lymph glands, headache, loss of appetite, pain (which may cause irritability in a child), shivering, tiredness or a rash.
Fever is a common symptom that is most often associated with infection although it may occur with a number of other conditions such as:
• an allergic reaction
• cancer (most commonly leukaemia, lymphomas, renal cancer)
• cerebral haemorrhage (stroke)
• immunological disorders (eg, lupus erythematosus)
• metabolic disorders (eg, gout, porphyria)
• myocardial infarction (heart attack)
• thromboembolic events (eg, deep venous thrombosis, pulmonary embolism).
Vaccinations, some medicines, and extreme sunburn can also cause a fever.
Body temperature is controlled by an area of the
• Be alert for symptoms that may indicate meningitis and seek urgent medical attention if any worrying signs are present or if you are unsure (see Childhood Diseases and Immunisation).
➤ Classic signs include a fever, stiff neck, headache, sensitivity to light and nausea or vomiting. A rash may or may not be present.
• A luke-warm bath or cool compresses may provide comfort from a fever.
• Dress the person in light clothing and keep bedding light.
• Drink plenty of water and/or electrolyte replacement fluids since fever can cause dehydration.
brain called the hypothalamus which acts like a thermostat. Body temperature is normal when the heat produced within the body, particulary by the liver and muscles, is in balance with the heat lost by the body. A fever occurs when the hypothalamus resets body temperature in response to infection as part of the inflammatory response or another body condition.
Usually, as a person’s temperature is rising, there is a feeling of cold until it reaches the new set temperature, when there becomes a feeling of warmth. Later, when the thermostat is reset to its normal level, the body eliminates excess heat through sweating and shunting of blood to the skin.
• When using a mercury thermometer, always shake before use. Wait 10 minutes after eating anything hot or cold before taking the temperature.
➤ Tympanic thermometers measure the temperature of the eardrum, but may underestimate temperature if not used properly.
➤ Digital thermometers are preferred in children as there is a risk children may bite the glass bulb of a mercury thermometer, releasing its contents.
• Always refer people with foot problems and diabetes, poor circulation, or who are imunosuppressed, to a podiatrist.
• Jandals should be worn in communal changing areas to reduce the risk of contracting athlete’s foot or warts.
If necessary, offer to take the customer into a private area where they can sit down and you can have a proper look at their feet. Wear gloves and examine the affected area, noting what symptoms correspond to the conditions listed below.
Refer any customers with concerns identified from the Refer to a Pharmacist checklist. Also refer if you are unsure what the condition is, or do not know the appropriate treatment.
Treatment varies depending on the foot condition (see under each subtopic).
Athlete’s foot
Athlete’s foot is usually caused by a dermatophyte fungal infection which infects the skin between the toes and the soles of the feet.
Category Examples
• People with diabetes, circulatory problems, or who are immunosuppressed, or pregnant.
• If the person is aged over 50 and it is the first time they have experienced a wart.
• If the area involved is extensive; or for a toenail infection, if multiple toenails are infected.
• People whose feet are bleeding or if there are signs of infection (such as pus, redness) near the affected area.
• People with a foot condition that has
The skin may look white and soggy, or scaly, red and itchy. Cracks may be visible and there may be a slight odour.
Dermatophyte fungi live in shed skin scales and are easily transferred via direct contact with wet floors, shared footwear, or towels. Treatment is with topical antifungal creams, powders, or sprays.
Blisters can form on the feet where the skin has been damaged (either by friction, rubbing or poor-fitting shoes), see Cuts, Abrasions and Blisters. Fluid collects between the upper skin
Topical antifungals (athlete’s foot) [GENERAL SALE] eg, zinc undecenoate (Mycota) [PHARMACY ONLY MEDICINE] eg, bifonazole (Canesten Bifonazole), clotrimazole (Canesten), econazole (Pevaryl), ketoconazole (Daktagold), miconazole (Resolve), terbinafine (Lamisil, SolvEasy)
Antiperspirants and deodorants (for smelly feet)
eg, aluminium chlorohydrate (Neat Feet RollOn Foot Deodorant/Cool Foot Spray) eg, various ingredients (Actifresh Foot Spray, Gran’s Remedy Powder, Poo shoes)
Topical nail preparations See Fungal Nail Infections (Onychomycosis): Treatment options
Products for corns, calluses, verrucae and warts [PHARMACY ONLY MEDICINE] eg, salicylic acid products (Carnation Corn Caps, Duofilm [+ lactic acid], Scholl range), dimethyl ether propane spray (Wartner)
Cracked heels [GENERAL SALE] eg, DU’IT Foot & Heel Balm Plus, DU’IT Roll-A-Balm, Ellgy Plus, Eulactol range
Blisters [GENERAL SALE] eg, hydrocolloid (Compeed Blister Patch, Scholl range, Spenco range)
persisted or recurred despite treatment.
• With atypical symptoms (such as itching or a colour change in a suspected wart).
• With a condition that also affects other areas of the body (such as the face or scalp).
• With a foot condition that is inhibiting their ability to walk.
• With severely cracked or infected heels.
• With painful, soft corns.
• People with allergies to topical medicines.
layers and forms a small bubble or pocket. Most blisters will heal by themselves within three to seven days.
Puncturing the blister is generally not recommended unless it is very large, and then it should be done with a sharp sterilised needle.
Hydrocolloid dressings can be used to relieve pain, protect the area from further damage, and promote faster healing.
Corns and calluses are areas of hard, thickened skin which build up on areas of the feet subject to pressure and rubbing. They are
Comments
Terbinafine is fungicidal and can resolve athlete’s foot with once-daily applications. Most other antifungals are fungistatic and also effective, although more frequent application and longer treatment courses (continuing for one to two weeks after the infection has cleared) are required.
Creams are easy to apply. They are good if the skin is moist, because they are water-soluble. Spray powders can give even cover over the sole and between the toes. Non-spray powders may clump, but are good for putting in shoes or socks to help reduce reinfection.
Antifungal creams containing hydrocortisone (ie, Canesten Plus, Resolve Plus) also calm inflammation.
A strong antiperspirant deodorant will stop feet sweating, reduce foot odour, soggy skin, and help prevent athlete’s foot from developing. If athlete’s foot is present, treat. Do not use the same container on feet and underarms because of the risk of cross-infection.
Powders are long-lasting and may be used on the feet or put into socks.
Cushioned inner soles that contain charcoal may also be effective.
Do not use these products on moles or birthmarks. Soak corn or callus in warm water and remove dead skin with pumice. Protect unaffected skin around the corn, wart or verruca with Vaseline or a plaster before applying product. Some conditions may need four to 12 weeks’ treatment. Wartner is applied directly to the wart with a repeat treatment in 15 days if necessary.
Use heel balms regularly to treat or prevent cracked heels. Usually contain either urea, lactic acid or allantoin which are keratolytic, loosening surface skin cells. which then shed, exposing new skin. Electronic foot files make it easier to remove dead skin. Softening socks may speed recovery of cracked heels, particularly if used with a heel balm.
Protects blister from further rubbing, relieves pain and accelerates healing.
Other Orthotic inserts (eg, Scholl range) Correcting poor foot posture and alignment can improve heel and knee pain.
Natural / herbal / supplements Apricot kernel, Bitter orange, cider vinegar, garlic, Kolorex Horopito, tea-tree oil
Various natural topical products have been used in the treatment of athlete’s foot and related fungal infections.
common in people with toe deformities (such as hammertoes), bony prominences, gait abnormalities, or with footwear that is too tight.
Corns are typically smaller than calluses and found on the top or sides of the toes or soles of the feet. They can be hard or soft. Soft corns look white and rubbery and are characterised by a damp and peeling skin surface. They can be extremely painful and are more commonly found between toes. Anybody with a painful soft corn should be referred to a podiatrist.
Calluses can develop on any area of the body and are larger areas of thickened skin that are not as defined as a corn. They are painless and often found on the heel or ball of the foot, or on the fingers or palms.
Treatment consists of relieving pressure on the affected area and reducing skin thickness. Moleskin, lambswool, or thin podiatry felt may be used to relieve pressure and comfortable, well-fitting footwear should be worn. Soaking a hard corn in warm water for 10 minutes makes reducing its thickness easier with sandpaper or a pumice stone. Keratolytic creams containing urea or salicylic acid can also help soften hard corns.
Always refer people with diabetes or circulatory problems or wanting permanent corn or callous removal to a podiatrist.
Cracked heels are common in summer when people wear sandals or go barefoot and the feet dry out. Treat with a thick, oil-based moisturiser, applied twice daily, after using a pumice stone or foot file to remove any thickened skin. Wearing socks after treating the feet can speed up recovery.
Feet have more sweat glands than any other part of the body and feet can start to smell when the sweat cannot evaporate and becomes trapped inside footwear, providing a warm and moist environment for odour-producing fungi and bacteria to grow.
Customers should avoid wearing the same pair of shoes every day, and allow at least 24 hours for shoes to dry out. Socks should also be changed daily. People prone to more sweaty feet (see also Sweating: Excessive [Hyperhidrosis]) may need to use a foot antiperspirant. Treat athlete’s foot if present and use a shoe deodoriser for smelly shoes.
Infected toenails are common but can be difficult to treat. The nail looks thick and discoloured, white or yellowish. It may be brittle or crumbly and parts, or all of it, may fall off (see
Athlete’s foot, infected nails, warts
• Bleach the shower/bath area regularly to kill fungi and viruses.
• Wash socks and towels in hot water and allow to dry in the sun.
• Wear jandals in communal changing areas (ie, at public pools).
• Wash feet twice daily with an antibacterial soap and dry thoroughly, particularly between the toes. Use a clean towel.
Fungal Nail Infections [Onychomycosis] for more information).
Veruccas are warts that occur on the sole of the foot. They are caused by the human papilloma virus which causes an overgrowth of keratin and are easily caught from wet floors and carpet. Over time they can enlarge and multiply.
Most are found on the sole but some appear on the top of the foot. They are typically grey or brown and may appear spongy. Small black dots may be visible near the middle of the wart which is caused by bleeding.
Although they can disappear spontaneously, this may take up to two years. Products containing salicylic acid or volatile ingredients that “freeze” the wart can speed up the process. Follow the instructions to avoid damaging unaffected skin. People with multiple warts are best referred to a podiatrist.
• Change socks daily and wear cotton, not synthetic, socks. Wash socks and towels at a high temperature.
• Wear leather shoes or open shoes, such as sandals, to reduce sweating.
• Apply a foot antiperspirant daily if feet sweat a lot.
Cracked heels
• Inspect feet daily and apply a moisturising cream two to three times daily at the first signs of cracking.
• Fungal infections are common because our skin, nails, and scalp contain keratin, which fungi feed off.
• Dermatophyte fungal infections commonly occur in areas of high temperature and humidity, and are easily transferred to others through body contact, towels, and wet surfaces.
Ask your customer what symptoms they have and, if appropriate and not disrespectful, take a look for yourself.
Run through the Refer to a Pharmacist checklist, and refer customers with concerns or if you are unsure what the condition is. For all other customers, discuss the appropriate treatment options depending on the condition.
Treatment varies depending on what area of the body is affected by the fungal infection (see under each individual subtopic).
Superficial fungal infections can occur on the outer layers of the skin, nails, or scalp. These type of infections are generally mild in healthy people, but may become severe in people who are very sick or with lowered immunity.
The three main groups of fungi that cause these infections are dermatophytes, yeasts, and moulds. Most fungal infections are treated based on a person’s history and symptoms. A definite diagnosis requires skin scrapings or nail clippings to be sent to a laboratory but is usually not done unless there has been no response to typical antifungal therapy.
Dermatophyte infections
Dermatophytes feed off keratin and are the main group of fungi to cause infection of the skin, hair and nails. There are more than 40
• People with diabetes, circulatory problems, or who are immunosuppressed or pregnant.
• Young children.
• Fungal infections that are inside the mouth.
• If other symptoms are present (eg, flu-like symptoms, increased thirst or urination).
• If the area involved is extensive; or for a toenail infection, if multiple toenails are infected.
different species, and they can live for up to a year off the body in shed human skin scales. They are common in areas with high temperature and humidity, and may be transmitted either by direct body contact, via towels or clothing, or through wet surfaces (eg, swimming pool or bathroom floors).
Dermatophyte infections are commonly seen on the scalp (tinea capitis), body surfaces (tinea corporis), groin (tinea cruris), feet (tinea pedis), and nails (tinea unguium). Topical antifungals are effective for most dermatophyte infections.
Tinea capitis (ringworm of the scalp)
Symptoms of tinea capitis include scaling and loss of hair on the scalp. More common in children, it is usually due to contact with an infected kitten or, rarely, an older dog or cat.
Treatment is with an oral antifungal such as terbinafine or fluconazole, or an antifungal shampoo. If the customer has a pet with evidence of ringworm, then they should seek treatment for the pet from a vet.
Tinea corporis (ringworm of the body)
Tinea corporis infections usually occur on the trunk or limbs. It is often called ringworm as infection causes a circular, red and itchy rash that looks like a worm under the skin.
Edges of the rash are usually raised with an
Category Examples Comments
Topical antifungals [GENERAL SALE] eg, zinc undecenoate (Mycota) [PHARMACY ONLY MEDICINE] eg, bifonazole (Canesten Bifonazole), clotrimazole (Canesten range), ketoconazole (Daktagold), miconazole (Resolve Tinea), terbinafine (Dermafex, Lamisil Cream, Lamisil Derm Gel, SolvEasy Tinea Cream)
Topical nail preparations See Fungal Nail Infections (Onychomycosis): Treatment options
• If the condition has persisted or recurred despite treatment.
• If there are signs of a bacterial infection as well (such as oozing, crusting, or swelling), or the skin is broken or bleeding.
• Women with a suspected vaginal infection.
• People with allergies to topical medicines.

area of clear skin in the middle. Infection can originate from the feet (tinea pedis) or nails (tinea unguium) or from cats, dogs, or cattle.
Treatment is with antifungal creams.
Tinea cruris (jock itch)
Dermatophyte infections of the groin are more common in men than women. Symptoms typically include an intensely itchy, reddish/ brown rash with a scaly raised border that spreads
Terbinafine is fungicidal and can resolve superficial skin infections with once-daily applications. Most other antifungals are fungistatic and also effective, although more frequent application and longer treatment courses (continuing for one to two weeks after the infection has cleared) are required. Topical mycostatin preparations are not effective against dermatophytes and should only be used to treat candida infections. Each product should be used according to the manufacturer’s instructions. Creams are easy to apply. They are good if the skin is moist, because they are water soluble. Lotions are suitable for hairy areas. Spray powders can give even cover on difficult to reach places (eg, under breasts or groin). Non-spray powders may clump, but may be useful for putting in clothing (eg, bras, socks) to help reduce reinfection. Tinctures may sting if the skin is broken or irritated.
Antifungal creams containing hydrocortisone (ie, Canesten Plus, Resolve Plus) also calm inflammation.
Natural products Acetic acid, tea-tree oil, garlic Various natural topical products have antifungal properties.
down the inner thighs from the groin or scrotum. Infection often originates from the feet (tinea pedis) or nails (tinea unguium) and is transferred by scratching or when the person dries themselves with a towel. Treatment is with antifungal creams, lotions, or powders.
Tinea pedis (athlete’s foot)
Dermatophytes are the most common cause of athlete’s foot (see Foot Care for more information and treatment options).
Tinea unguium (fungal nail infections)
Dermatophytes are a common cause of fungal nail infections (also called tinea unguium or onychomycosis), although infection can also be caused by yeasts or moulds. Fungal nail infections are more common as people age and often spread from dermatophyte infections of the feet, or less commonly, the hands. Infection most commonly involves the big toenail or little toenail (see Fungal Nail Infections [Onychomycosis] for treatment information).
Yeast infections
Candida and Malassezia are two common types of yeast. Yeasts are a type of fungi.
Candida infections
Candida are white-coloured yeasts which normally live in our digestive tract. Usually, they cause no symptoms or disease, but sometimes environmental changes (such as humid weather or plastic overpants in babies) or low immunity can trigger an overgrowth of the yeast. Candida infections (also called candidiasis) can affect the mucosa (ie, the lining of the mouth, anus, and genitals), nail folds, skin, or
rarely, the whole body.
Symptoms of oral candidiasis (also called oral thrush) include soft, raised, creamy-white patches on the tongue or roof of the mouth that can be scraped off to reveal red-looking mucosa underneath. It more commonly occurs in babies, people prescribed inhaled corticosteroids, in women after menopause, or in those with low immunity (see Oral Health).
Vaginal candidiasis (also called vaginal thrush or a vaginal yeast infection) is common in females after puberty and before menopause (see Women’s Health).
Candida is also a common cause of chronic paronychia (inflammation of the nail fold). It causes the nail fold to become swollen and lifted off the nail plate. It may be red and tender and sometimes a little pus can be expressed. The nail plate becomes distorted and ridged as it grows. Treatment may take months and oral antifungal agents may be necessary if topical antifungal creams do not work (see Fungal Nail Infections [Onychomycosis] for more information).
Candida infections can also cause or exacerbate nappy rash (see Baby Care).
Malassezia infections
Malassezia are a normal inhabitant of the skin that are associated with several conditions such as dandruff (see Dandruff), seborrhoeic dermatitis (see Dermatitis/Eczema), and pityriasis versicolor.
In pityriasis versicolor, the Malassezia yeast causes pink, coppery brown or pale patches to form on the skin, typically on the trunk, neck, or shoulders. It may be mildly itchy and more noticeable in dark-skinned people. This infection is more common in hot, humid
climates or in those who sweat heavily, so may recur each summer.
Selenium sulfide (found in some antidandruff shampoos) or topical antifungal foaming products are usually effective if applied overnight for the required time. Oral antifungal agents prescribed by a doctor may be needed for extensive pityriasis versicolor or when topical treatments have failed.
Moulds are microscopic fungi and these occasionally infect the skin or nails after contact with soil. They can cause similar symptoms as dermatophyte infections although nail mould infections cause inflamed nail beds. They can be difficult to treat and should be suspected if antifungal treatment has not worked. Refer to the pharmacist.
Athlete’s foot, infected nails
• Bleach the shower/bath area regularly to kill fungi and viruses.
• Wash socks and towels in hot water and allow to dry in the sun.
• Wear jandals in communal changing areas (ie, at public pools).
Jock itch, ringworm
• Avoid sharing towels.
• Check pets for evidence of ringworm and get pets treated by a vet.
• Fungal nail infections can be difficult to treat.
• Filing or thinning down the affected nail before applying some topical antifungal products can help them work better because it helps the product to fully penetrate the nail and reach the nail bed.
• Topical treatments do not usually work if the infection involves the matrix or growth plate of the nail, or if more than three nails are infected.
If the customer thinks they have a fungal nail infection, offer to take them to a private area where they can sit down and you can have a proper look at their feet. See how many toenails are infected and if the infection covers all or just the end of the nail, because pharmacysold treatment products are unlikely to work for extensively infected toenails. The same applies for fingernail infections.
Sometimes it can be hard to distinguish fungal nail infections from other types of infections or medical conditions, such as psoriasis (usually affects all nails and tends to exist elsewhere on body), dermatitis (fingers or toes are typically also affected by dermatitis), or Lichen planus (this autoimmune disease causes thinning of the nail plate, and grooves and ridges in the nail. The nails may shed or stop growing altogether). If you are unsure if the infection is fungal, or if you have other concerns, identified by the Refer to a Pharmacist checklist, call over a pharmacist.
Unsightly nails can really affect a person’s quality of life and can cause significant discomfort, difficulty in walking or wearing footwear, embarrassment, and low selfesteem. Infected nails also serve as a reservoir for fungi with a potential to spread to the feet, hands, and groin, and to other members of the same household.
• People with diabetes, circulatory problems or who are immunosuppressed or pregnant.
• Infections that involve more than three nails or more than 50% of any one nail.
• Infections that involve the matrix (growth part of the nail).
• If there is any oozing, blisters, swelling, or a foul odour around the nail.
• Recurrent fungal nail infections or if previous treatment has not worked.
• People with other symptoms (including flu-like symptoms, or increased thirst or urination).
• People with allergies to topical medicines.
Interestingly, children rather than spouses of infected people are more likely to become infected, indicating genetic susceptibility.
Treatment of fungal nail infections, particularly toenail infections, can be difficult. Only topical antifungal products are available in a pharmacy, but doctors can prescribe oral antifungal agents, and podiatrists can offer chemical, surgical, laser and other treatments.
Pharmacy-available topical treatments should only be attempted if the fungal infection involves less than 50% of the distal part of the nail (not the matrix or growth centre), no more than three nails, and the cuticle is not affected.
Unfortunately, topical antifungal agents such as amorolfine 5% and ciclopirox 8% have a low clinical cure rate (clearing of nail symptoms) of only about 8%–38%. This low efficacy appears
to be due to an inability of the drug to penetrate through the nail plate to the nail bed where the infection resides. Although instructions advise filing of the nail before application, thickening of the nail is often extensive and filing may be physically impossible for some people with limited sight and flexibility.
One fungal nail treatment uses urea cream initially to debride the nail before topical bifonazole is applied. Reported clinical cure rates for this combined approach are higher, indicating the importance of thinning out the nail beforehand. Although some products claim that nails can be treated in two months or less, make customers aware that although the infection may be gone, it can take six to 18 months for toenails to grow back.
Other nail treatment solutions contain

Category Examples Comments
Topical nail preparations Fungal nails [PHARMACY ONLY MEDICINE] eg, amorolfine (Loceryl, MycoNail), bifonazole (Canesten Fungal Nail), ciclopirox (Rejuvenail), miconazole (Daktarin tincture), polyureaurethane (RestoraNail) eg, Excilor Fungal Nail, Nailclin Antifungal Nail Treatment, Pronail Fungal Nail Pen Discoloured and damaged nails eg, poly-ureaurethane (RestoraNail)
Products for infected nails usually work better if most of the infected part of the nail is removed or extensively thinned before application, unless they also contain an ingredient that enhances penetration of the active ingredient. Application needs to be regular and consistent and according to manufacturer’s instructions. RestoraNail contains poly-ureaurethane, a unique substance that covers and protects the nail, treating both the fungal infection and repairing damage. Excilor and Nailclin contain a mixture of ingredients designed to penetrate the nail plate and alter the pH of the nail bed preventing fungal growth. Pronail contains Olile-Active, an undisclosed ingredient that creates a hostile environment for the fungus.
• Refer all customers with suspected gout to a pharmacist.
• Regular administration of uric acid-lowering agents in people prone to gout reduces the risk of joint destruction, heart disease, and kidney damage.
• Gout is more common and typically more severe among Māori and Pacific Island peoples, compared to people of European descent.
Direct any customer who asks you about gout, or who you suspect may be selfmedicating an acute gout attack with NSAIDs, to a pharmacist who should advise them on the benefits of preventive medicine.
Among the Māori and Pacific Island communities in New Zealand, there tends to be a normalisation of gout, and those affected tend to just put up with the pain.
➤ Rarely do these patients present to a doctor for a formal diagnosis.
➤ Without the appropriate use of uric acid-lowering agents, their gout becomes progressive and chronic.
➤ Many of these patients would also benefit from a thorough cardiovascular risk assessment (see Heart Health).
Non-steroidal anti-inflammatory drugs (NSAIDs) are recommended first line (unless contraindicated) as pain relief for acute attacks of gout (see Treatment Options). Corticosteroids or low dose colchicine prescribed by a doctor may also be used as an alternative to NSAIDs in some people.
Category Examples
Acute gout [PHARMACY ONLY] or [PRESCRIPTION] (higher dosages)
Non-steroidal anti-inflammatory drugs (NSAIDs) eg, diclofenac, naproxen
[PRESCRIPTION] Oral corticosteroids eg, prednisone
Intra-articular corticosteroids, eg, methylprednisolone, triamcinolone
[PRESCRIPTION] eg, Colchicine (Colgout)
Prevention of gout [PRESCRIPTION] eg, allopurinol
[PRESCRIPTION] eg, febuxostat eg, benzbromarone
[PRESCRIPTION] eg, probenecid
Any medicine used to treat an acute attack should be taken at the first sign of the attack at an effective dose. In most people, pain and inflammation caused by the gout can be controlled within 12–24 hours and treatment discontinued after a few days.
Drugs used for gout attacks have no effect on reducing uric acid levels and all customers with symptoms suggestive of gout should be referred to a doctor for consideration of allopurinol or probenecid. Febuxostat and benzbromarone are also available on special authority. Early control of gout, before the onset of tophi, erosive disease and renal impairment, is vital.
Historically known as the “disease of kings” due to its association with rich foods, alcohol, and wealth, gout is common today among New Zealanders of a wide socioeconomic range, and affects just over 5% of the total population aged over 20.
Gout affects three times as many men than women, and Māori and Pacific Island peoples are two to three times more likely than those of European ancestry to be affected. Gout is uncommon in women until after menopause.
Gout is a form of arthritis that can easily be mistaken for a bacterial cellulitis (an infection in the first two layers of skin). An acute attack causes sudden intense swelling, redness, and warmth in a joint, most commonly the big toe, although it can occur in the ball of the foot, instep, ankle, knee, wrist, tip of the elbow, or fingers. Gout is considered the most painful of all types of arthritis with the affected person unable to weight-bear or wear shoes if the gout
Comments
is present in the foot. In addition to localised pain, a person with gout may also have a mild fever or feel unwell.
Left untreated, gout can lead to permanent joint destruction and kidney damage and can double the risk of a heart attack or stroke.
Although the most common reason gout occurs is due to high uric acid levels (hyperuricaemia) in the blood, the relationship between uric acid and gout is not clear-cut. Research has identified that 20% of people with hyperuricaemia develop gout, but 80%–90% of people with gout are hyperuricaemic. An inherited tendency to excrete less uric acid through the kidneys is the primary reason people have high uric acid levels (see Table opposite page for other common causes of hyperuricaemia).
Gout occurs when uric acid accumulates in a joint and saturates out to form tiny needle-shaped crystals. The body mounts an inflammatory response to the crystals in that joint, leading to the characteristic gout symptoms of inflammation and pain. Most early gout attacks resolve spontaneously after seven to 10 days, but severe pain typically forces people to seek treatment earlier.
The length of time between attacks can vary widely, with some patients only ever having one attack. For the majority of patients, a second attack will occur within a year. If a patient’s uric acid level remains high (>0.36mmol/L) despite the patient being symptom free, there can be ongoing joint inflammation which results in joint damage and tophi formation. High uric acid levels have also been identified as a
Give regularly until severe pain reduces then decrease dosage (ie, diclofenac 75mg bd or naproxen 500mg bd initially). May not be suitable for some people taking other medicines or with some medical conditions (eg, asthma, kidney disease), and should be discontinued if stomach upsets, increased bruising or prolonged bleeding occur.
See Reference section, OTC Medicines – Precautions
Alternative if NSAIDs are contraindicated. Infection should be excluded before using. Intra-articular corticosteroids may be considered if gout localised to single joints.
No longer considered first-line treatment for acute gout, but may be used as an alternative treatment, or as an adjunct to NSAID treatment. Can also be used as a prophylactic. Overdosage can cause diarrhoea.
Usually started at least two weeks after an acute gout attack. 1%–2% of people develop a rash (more common in patients with renal impairment). Regular allopurinol taken before the start of an acute attack should be continued.
Available on special authority for those with special conditions, contraindications, intolerance, or who have failed to respond to treatment with other preventive drugs.
Useful for patients with normal renal function and urate under-excretion. May be used in combination with allopurinol in certain people (ie, with persistent hyperuricaemia). Contraindicated in patients with a history of renal stones. Ensure good fluid intake (eight glasses of water per day). If a patient has been taking probenecid regularly at the time of an acute attack, it should be continued.
marker for a number of other metabolic and haemodynamic abnormalities, including high blood pressure and renal impairment.
Years of unresolved gout can lead to chronic tophaceous gout. Tophi are firm, white, translucent nodules that can occur around the joints or on the external ear and arise from the deposition of urate crystals. They usually take at least five to 10 years after the initial attack to develop.
As well as causing joint destruction, they are disfiguring and also cause physical hindrance. Although effective treatments can cause regression of tophi, they are far more difficult to manage once they have developed.
Research has located a specific genetic variant within a gene that doubles the risk of gout in Europeans and increases the risk by more than five times in people of Māori or Pacific ancestry.
People who drink soft drinks sweetened with high fructose corn syrup (HFCS) or consume diets rich in fruit or fruit juice are also at increased risk.
In addition, certain medical conditions (such as type 2 diabetes, kidney problems, or high blood pressure), some medicines (eg, diuretics, cytotoxics), large intakes of purine-rich foods or alcohol (particularly beer) and joint injury also contribute to the risk.
Most experts agree preventive therapies should aim to reduce serum uric acid concentration to below 0.36mmol/L. This is the target required for dissolution of uric acid crystals within the
• Advise people predisposed to high uric acid levels, or who have a history of gout attacks to:
➤ avoid HFCS-sweetened drinks, fruit juice, and limit intake of fruit
➤ drink at least five glasses of water each day
➤ eat only small amounts of red meat or
joints and subcutaneous tissues.
The two main drugs used are allopurinol (lowers uric acid production) or probenecid (helps the kidneys remove uric acid). While allopurinol is the most recommended drug, in certain people, probenecid or benzbromarone may be preferred.
These drugs should be started at least two weeks after an acute attack, and for the first three months should be prescribed with NSAIDs or colchicine to avoid the development
CAUSES OF HYPERURICAEMIA
seafood. Eat mainly chicken or white fish
➤ eat plenty of vegetables
➤ keep active and keep weight down
➤ restrict alcohol intake (especially beer, lager, port and RTDs)
➤ take all medicines as prescribed and see a doctor as early as possible if another gout attack occurs.
of further acute attacks. It is important that these medicines are not discontinued without a doctor’s advice, even if the person is feeling well, as the benefits of lowering uric acid levels take several years to occur.
Once serum uric acid is below 0.36mmol/L, monitoring can be reduced to three to six monthly. In most people, allopurinol is administered long-term, except in cases of allopurinol intolerance.
EXAMPLES AND COMMENTS
Dietary High fructose corn syrup beverages and foods
High intakes of fruit juices and fruit
High intakes of purine-rich foods – includes meat, organ-meats (eg, kidneys, liver, brains), seafood (eg, herring, mussels, oysters, sardines, scallops), certain types of alcohol. Purine-rich vegetables (eg, beans, cauliflower, lentils, mushrooms) or oatmeal are no longer thought to cause hyperuricaemia
Excessive production and destruction of cells
Associated with certain medical conditions including leukaemia, lymphoma, multiple myeloma, psoriasis, starvation, toxaemia of pregnancy
Genetic disorders Includes glucose-6-phosphatase deficiency and trisomy 21
Medicines
Metabolic diseases
Other
Aspirin and all diuretics except spironolactone (particularly thiazides)
Chemotherapy and radiation treatment
Acute renal failure, hyperlipidaemia, hypothyroidism
Alcoholism, dehydration, infectious mononucleosis, lead poisoning, sarcoidosis, tumour lysis syndrome
• People with rectal bleeding who have not been formerly diagnosed with haemorrhoids should be referred to a doctor.
• Products for haemorrhoids only temporarily relieve symptoms, they do not cure haemorrhoids.
• Haemorrhoids are often associated with constipation which should also be treated.
Many people with haemorrhoids are reluctant to discuss their condition and may prefer to self-select a product. However, a tactful enquiry such as “Are you managing your condition okay or would you like further information from a pharmacist”, may be appreciated. Always refer patients with rectal bleeding who have not yet seen a doctor to a pharmacist.
Treatment generally relieves symptoms such as itching, pain, and swelling, but will not cure haemorrhoids. The choice of treatment depends on the severity of symptoms and if the haemorrhoids are internal or external (see Need to Know)
Suppositories or topical ointments that are packaged with a nozzle for internal rectal use are used to treat internal haemorrhoids.
Initially it may be more comfortable to apply the ointment with a clean finger wrapped in cling film rather than use the nozzle, particularly if the haemorrhoids are very inflamed and painful. A clean finger can be used to apply topical ointments directly to external haemorrhoids.
Category Examples
• People with diabetes or circulatory problems, or who are immunosuppressed or pregnant.
• People who take medicines (including herbal/complementary products) that may be causing constipation.
• Children.
• If other symptoms are present (such as abdominal pain, fatigue, fever, vomiting, nausea, loss of appetite, unexplained weight loss).
• If the person has rectal bleeding that is unrelated to their bowel motions.
• If the person’s symptoms have lasted more than three weeks or the symptoms have not improved despite treatment.
• If there is blood mixed into the stool (not just sitting on top of it).
• If there is pus or any other signs of infection around the anal area.
• People who are unsure if they have haemorrhoids or not.
• People who describe a haemorrhoid that prolapses out of the anus.
• People whose bowel habits have changed recently after years of regularity.
• People with pain associated with their bowel movements or who feel like they are unable to completely empty their bowel.
• People with allergies to topical medicines.
Advise customers to wash their hands after application of the product.
Products are best applied after defecation once the anal area has been thoroughly cleaned (unfragranced wet wipes are usually more effective and kinder at cleaning the region than toilet paper).
If constipation is present it should be treated at the same time, preferably using a stool softener, such as docusate (see Constipation)
It can take up to one week for external haemorrhoids to disappear or improve. Many patients will require further specialised therapy, such as sclerotherapy (injection of a substance into the haemorrhoid), rubber-
Products for haemorrhoids [GENERAL SALE] eg, Anusol ointment and suppositories (zinc oxide, Peruvian balsam, benzyl benzoate) eg, Asteroid ointment(zinc, mentholum, honey)
[PHARMACY ONLY]
eg, Proctosedyl ointment and suppositories (contains cinchocaine and hydrocortisone)
[PHARMACIST ONLY]
eg, Rectogesic ointment* (contains glyceryl trinitrate)
[PRESCRIPTION]
eg, Ultraproct ointment and suppositories (contains fluocortolone and cinchocaine)
Natural / herbal products / supplements Artemis Vein Support, Calendula, grape seed extract, horse chestnut, witch hazel, Lucas Papaw ointment, Weleda Haemorrhoid ointment
Comments
band ligation therapy (small rubber bands are placed around the haemorrhoid causing it to shrink), laser or electrocoagulation (causes the haemorrhoid to harden and shrivel), stapled haemorrhoidopexy (staples are used to anchor the haemorrhoid in place) or surgery for persistent haemorrhoids.
Haemorrhoids (also called “piles”) are common, affecting around one in two adults at some point in their lives. They occur when the anal cushions (pillows of veincontaining tissues that seal the anal canal and maintain continence) become engorged and
Products are usually made up of a combination of different ingredients.
Anaesthetics (eg, cinchocaine) numb the area to relieve pain, burning and itching.
Astringents (eg, zinc oxide) reduce secretion of mucus and fluids from damaged skin cells and provide a protective barrier.
Mentholum provides a cooling effect. Honey soothes and has antimicrobial properties.
Anti-inflammatories (eg, hydrocortisone) reduce inflammation and swelling of the haemorrhoid, but are recommended only for short-term use as they can cause skin atrophy.
Skin protectants (eg, Peruvian balsam) provide a protective coating over the damaged skin, preventing further irritation and relieving itchiness.
Benzyl benzoate has weak antiseptic properties and is also used as a vehicle for dissolving other active ingredients.
Suppositories may be better for internal haemorrhoids. Remind customers to always remove the foil or plastic wrap before inserting the suppository. Products are best used after a bowel motion.
For some treatment products the dosage may change over days or weeks; always follow instructions. Most products are well tolerated but discontinue use if skin irritation or sensitivity develops.
Glyceryl trinitrate relaxes the internal and sphincter muscle, allowing anal fissures to heal.
Antioxidants (eg, grape seed extract) and astringents (eg, witch hazel) can help relieve haemorrhoids. Weleda ointment contains horse chestnut, witch hazel and calendula which can help temporarily relieve the itching, burning and discomfort associated with haemorrhoids. Papaw ointment can temporarily relieve the discomfort of haemorrhoids.
swollen. They can be classified into two types:
• internal haemorrhoids, which occur inside the lower rectum and are not usually visible. These can cause a feeling of pressure in the rectum and often bleed but are usually painless.
Occasionally, they may prolapse (pop out) through the rectum with a bowel motion, which can be quite painful. Some easily “pop back in”, either by themselves or when pushed with a finger, but others may remain prolapsed which can lead to complications.
• external haemorrhoids, which develop under the skin around the anus. These are typically visible and surround the anal sphincter. They look like small bunches of grapes and when inflamed become red, very tender, itchy, or painful and usually bleed with every bowel motion.
Occasionally a blood clot forms inside an external haemorrhoid, and can be felt as a firm,
tender mass in the anal area, about the size of a pea. It can cause severe pain. If the clot does not go away by itself with haemorrhoid creams, it can be removed by a doctor in a minor office procedure. When the clot dissolves, excess skin may be left behind which may itch or become easily irritated.
Haemorrhoids are thought to be caused by certain factors that increase pressure in the anal cushions or degenerate the elastic tissue around the anus. Chronic (long-lasting) constipation, straining during bowel movements, and prolonged sitting on the toilet all interfere with blood flow to and from the rectal area and carry the most risk.
Pressure or tissue degeneration in the anal region can also be due to ageing, obesity, heavy lifting, chronic diarrhoea, a low-fibre diet, poor posture, pregnancy or childbirth, sitting or standing for long
• Keeping the stools soft helps prevent haemorrhoids from occurring.
➤ Eat a diet high in fibre (fruit, vegetables, wholegrains).
➤ Maintain a reasonable fluid intake (six glasses of water a day).
➤ Treat any constipation if present (see Constipation) and avoid straining when passing a bowel motion if possible.
• Avoid foods and drinks that may make haemorrhoids worse, including spicy foods, nuts and seeds, and alcohol.
• Get plenty of exercise and avoid sitting for long periods.
• Do not ignore the urge to go to the toilet (“holding-on” can lead to increased pressure inside the anus).
• Use unfragranced wet wipes instead of toilet paper to clean the anal area.
➤ Avoid soap as this may further aggravate the problem.
periods of time, spinal cord injury, anal intercourse and, rarely, rectal or bowel tumours.
Some families may be genetically more susceptible to developing haemorrhoids.
The most reported symptom is bleeding from the rectal area, especially after a bowel motion. This may be visible either as bright red blood on toilet tissue, in the toilet bowl, or on the outside of the stools.
Constant wiping of protruding haemorrhoids can cause an irritation called pruritus ani, also known as anal itch.
Some people may also report a burning or dull pain in the rectal area, especially when trying to pass a bowel motion, or when sitting for long periods.
➤ Ensure used wipes are discarded appropriately and not flushed as they can easily block sanitary systems.
• Apply products only as directed and for the recommended time. If treatment fails to improve haemorrhoids, seek further medical advice.
• A cold compress applied to the area may help with symptoms.
➤ Alternatively sitting in a warm bath for 15–20 minutes at a time (a sitz bath) after each bowel movement may provide relief.
➤ Gently pat the area to dry afterward, or alternatively use a hairdryer.
• Wear cotton underwear to minimise discomfort.
• Avoid scratching the anal area.
• Sit on a cushion rather than a hard surface to reduce the swelling of existing haemorrhoids and prevent the formation of new ones.
• The pattern of hair loss together with an examination of the hair root can help identify the type of hair loss.
• Minoxidil may be used to treat both male and female pattern hair loss.
• Early treatment is the key to successful regrowth.
Take an empathic approach when talking with a customer about their hair loss, as it may be affecting their self-esteem. In a private area, with their permission, take a look at their hair and listen to their history of hair loss to determine if they have any of the more common conditions listed in this chapter. Reassurance that the hair should grow back may be all that is needed for customers with a temporary cause for their hair loss (such as illness, jet lag, childbirth).
Before selling minoxidil to men or women, make sure the product is appropriate for their pattern of hair loss and they are aware that longterm use is necessary to prevent the hair loss reverting to what it was prior to treatment. Refer any customers with concerns identified by the Refer to a Pharmacist checklist. Also refer if you are unsure what treatment is best.
Better results are achieved by people who seek help as soon as they notice their hair starting to thin, fall out, or they are unable to grow it as long as they used to. Early treatment is the key to successful regrowth. Treatment options vary according to the type of hair loss but may include minoxidil solution, finasteride tablets [PRESCRIPTION MEDICINE], hair replacement or transplantation, laser therapy, keratin treatment, hairpieces, or hormonal treatments.
Alopecia is the medical term for hair loss. Hair loss is common, with almost 60% of men and up to 40% of women experiencing it at some point in their lives. While genetic inheritance plays a major role
Category Examples
• People who have been diagnosed with a health condition that may contribute to hair loss (such as iron deficiency, thyroid disease, systemic lupus erythematosus).
• People who have had or are undergoing chemotherapy or who take any medicines that may contribute to hair loss (such as allopurinol, beta-blockers, or warfarin).
• People whose scalp looks flaky or scaly or itches.
• Adolescents and children younger than 18.
• People who compulsively twist or pull their own hair.
• If minoxidil has been used for 12 months without success.
• People with allergies to topical medicines.
in most cases, many other factors contribute to hair loss, some temporary. These are discussed under the common types of hair loss.
We are born with all the hair follicles we are ever going to have, and these usually continue to produce hair for the rest of our lives. However, as we age, some follicles start replacing long, thick hairs with finer, almost invisible hairs. This may look like we are losing hair, but in fact, the hair has just become thinner and shorter.
Human hair has three different growth phases: the anagen, catagen, and telogen phases. At any given time, hairs will be in various stages of growth or shedding.
The anagen phase is the active or growing stage of hair growth. On average, hair grows 0.3–0.4mm/day or around 12–15cm per year. During this phase, the hair root is long, white and tapered.
How long hair stays in this growing stage is genetically predetermined and explains why some people’s hair grows longer than others. Around 85% of hair follicles are in this phase at any given time, although hair on different parts of the body varies as to how long it stays in the anagen phase.
On the scalp, the anagen phase can last for two to seven years, whereas on the arms, legs, eyelashes, and eyebrows this anagen growth phase only lasts around 30–45 days. At some point in the anagen phase, an unknown signal causes hair to go into the catagen phase.
Products for hair regrowth [PHARMACY ONLY MEDICINE] eg, minoxidil 5% topical solution/foam (Regaine Extra Strength Foam/Solution, Regaine Women’s, Regro Hair Growth Spray)
Natural / herbal products / supplements Gingko biloba (Sebamed Anti-Hairloss Shampoo), lavender oil, thyme, rosemary, cedarwood, saw palmetto, zinc
Hair growth stops in the catagen phase as the hair root sheath begins to shrink and becomes rounded as the follicle prepares to enter the telogen phase. This phase lasts for about two to three weeks, but can be as short as two days.
This is the final stage of hair growth, also called the resting stage. The hair is fully grown and the root of the hair is now completely rounded. Pulling out a hair in this phase will reveal a solid, hard, dry, white material at the root.
This phase lasts about three to four months for scalp hair but much longer for hairs on other parts of the body – around nine months for eyebrow hair. Hair is shed when a new anagen hair begins to grow under the resting telogen hair. Fifty to 100 telogen hairs are shed daily from a normal scalp.
Hair loss can affect localised areas of the scalp or occur evenly over the whole area. Other hairy parts of the body may also be affected.
Male-pattern hair loss (androgenetic alopecia) is an inherited condition, caused by a genetically determined sensitivity to the effects of dihydrotestosterone (DHT). DHT is thought to shorten the anagen phase of the hair cycle, causing progressively finer hairs to be produced.
The disorder is characterised by a receding hairline and/or hair loss on the top of the head,
Comments
Minoxidil is recommended for men who have a general thinning of hair on the top of the scalp (vertex pattern only). Not intended for frontal baldness or a receding hairline. Hair shedding may temporarily increase during the first few weeks of use. Regrowth may take two to four months. Continued use is required. Minoxidil may also be used to treat FPHL in women aged 18 to 65 years.
Some oils and herbs may help maintain a healthy scalp, encouraging hair growth.
and male Caucasians are more likely to be affected.
The hereditary female-pattern of balding is characterised by a diffuse thinning of hair on the scalp due to an increase in hair shedding or a reduction in hair volume. It is more common during or after menopause with around 40% of women by age 50 showing signs of hair loss.
The hair loss process is not usually constant and there are often accelerated phases of hair loss for three to six months, followed by periods of stability lasting six to 18 months.
Excessive shedding of telogen hairs occurs. This may be acute and temporary or chronic and persistent. Although the thickness and length of the hair may be reduced, because new hair continues to grow, it does not result in baldness.
Acute telogen effluvium usually follows some major shock to the body and as many as 70% of the anagen hairs can be precipitated into the telogen phase. The telogen hairs remain firmly attached to the scalp at first. It is only about two months after the initial shock that the new anagen hairs growing up through the scalp push out the dead telogen hairs and increased hair shedding is noticed.
Causes are numerous, including accidents, childbirth, surgery, certain medicines (eg, discontinuing the oral contraceptive pill), excessive sun exposure, excessive weight loss or major dietary changes, illness (especially with fever), and jet lag. In most cases the condition is self-correcting and complete recovery occurs within six to nine months, although it may be
incomplete in some cases.
Chronic telogen effluvium is characterised by a persistent or cyclical diffuse hair loss and an inability to grow hair long. There may be fluctuations in shedding severity (eg, cyclical variations) similar to moulting that occurs in other mammals. Although chronic telogen effluvium does not cause baldness, bi-temporal recession of hair is common (high forehead).
In some cases, tests may be done to exclude thyroid disease and to check levels of iron, vitamin B12 and folic acid, as any deficiency in these can slow hair growth.
Hair shedding occurs due to interruption of the anagen phase of growth, and can result in baldness. Most common causes are chemotherapy, toxins or inflammation.
Round bald patches appear suddenly, most often on the scalp, although any hair-bearing areas can be affected (eg, eyebrows, eyelashes, beard). May occur at any age, including childhood. It is
thought to be due to an autoimmune disorder, and commonly affects more than one member of the family, or in people with chromosomal disorders such as Down syndrome.
Alopecia areata is often first noticed by hairdressers, as the initial bald patch may be small. This enlarges over time before new growth occurs. Complete regrowth may take months, or sometimes years to occur. One patch of hair may be falling out while another is regrowing.
Various forms of the condition can exist, including alopecia totalis when all scalp hair is lost, and alopecia universalis where the entire body hair is shed.
The following medicines have been associated with specific types of hair loss:
• anagen effluvium: chemotherapy; following poisoning with arsenic, bismuth, boric acid, or thallium; and, rarely, colchicine or gold
• telogen effluvium: ACE inhibitors, anticoagulants, anticonvulsants, antidepressants, beta-blockers, hormones, levothyroxine, lithium, NSAIDs, retinoids, statins, and many more.
• Handle hair gently and avoid over-vigorous combing, brushing, tying up and any type of scalp massage.
• Wash hair with a mild shampoo and avoid dyes and other chemicals.
• Treat dandruff or psoriasis if present.
• If using a hairdryer, use on a low setting to avoid damaging the hair shaft.
• Relaxation techniques may help with hair loss caused by stress.
• Eat a well-balanced diet and consider supplements with deficiencies.
• Cooling caps or scalp cooling systems may allow some people to keep some of their hair during chemotherapy.
• Symptoms of hay fever (seasonal allergic rhinitis) usually only occur during spring or summer; symptoms that occur all-year round are known as persistent allergic rhinitis.
• Oral antihistamines should be recommended for mild hay fever and corticosteroid nasal sprays for moderate or severe hay fever.
Ask your customer to describe their symptoms and look for key features that confirm their symptoms are the result of hay fever, and not from a viral infection, such as a cold, COVID-19, or the flu (see Colds;Table: Differentiating Cold, COVID-19, Flu, and Hay Fever Symptoms).
Itchiness of the eyes, mouth, or throat is typical of hay fever, and it is a seasonal condition, generally occurring during spring and summer each year. Run through the Refer to a Pharmacist checklist and refer any customers with concerns.
For other customers, base product selection on their most troublesome symptom. For example:
• itchy eyes – an antihistamine eye drop
• blocked nose – an oral or nasal decongestant
• runny nose – an oral antihistamine
• eye and nose symptoms – a nasal corticosteroid.
Encourage people who also have asthma-like symptoms to talk with their doctor at their next appointment about the association between hay fever and asthma.
Antihistamines and nasal corticosteroids are the main treatments for hay fever, alongside non-pharmacological measures (see Text box: Medication-free ways to manage Hay Fever). Usually, once nasal symptoms are under control, eye symptoms generally resolve as well. The New Zealand Formulary recommends:
• treatment should begin two to three weeks before the season commences in those people whose symptoms occur each year
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People who take medicines, including herbal/complementary medications.
• Children.
• People who complain of pain in their sinuses or tooth pain.
• People who are experiencing shortness of breath or wheeze.
• When only one eye or one side of the nose is affected.
• With a coloured or yellow discharge coming from the nose or eyes.
• With symptoms that have persisted despite treatment or occur all year round.
• People with allergies to medicines.
• use an oral antihistamine (see Allergies for an overview of common antihistamines), or nasal corticosteroid for mild hay fever
• nasal corticosteroids should be used for more persistent symptoms
• nasal decongestant sprays may be used for up to three days to relieve congestion and allow the nasal corticosteroid to have an effect
• ipratropium nasal spray may be useful in those with a runny nose
• the nasal antihistamine, azelastine may be useful for breakthrough symptoms
• oral nasal decongestants appear to be of doubtful value for allergic rhinitis
• montelukast (prescription) is considered less effective than nasal corticosteroids but may be a good option in those with hay fever as well as asthma
• short courses of oral steroids (such as prednisone) may be justified for those with very disabling symptoms (for example, students taking exams), or for a few days at the start of treatment to relieve severe congestion and allow the nasal corticosteroid to take effect
• treatment may need to be continued every day for several months
• during pregnancy, if symptoms cannot be tolerated, nasal beclomethasone, budesonide, fluticasone, or sodium cromoglicate may be considered, see Treatment Options page 90. Desensitisation or immunotherapy may be considered for people with particularly severe

hay fever if none of the above treatment options work (see also Allergies).
Hay fever (also called intermittent or seasonal allergic rhinitis) is an allergic reaction that occurs seasonally, most commonly in spring and summer. Hay fever can have a huge impact on a person’s daily life, with 20% of those affected experiencing symptoms for more than nine months of the year. Customers with symptoms that happen continuously throughout the year are more likely to have another form of rhinitis, called persistent allergic rhinitis (see Sinus and Nasal Problems). Hay fever is mostly associated with grass or tree pollens which are only present for part of the year. People whose symptoms tend to come on in late winter or early spring are more likely to have an allergy to tree pollen. People whose symptoms present in late spring or early summer are typically allergic to grass or weed pollen. Pollen season at the top of the North Island usually starts in October and ends in February, approximately one month earlier than the lower South Island.
Wind pollinated plants are the ones most likely to cause hay fever symptoms because they produce high numbers of light and buoyant pollen grains which are easily distributed through the air. Plants that are brightly coloured or scented are unlikely to trigger hay fever because they attract bees and other insects to them to transfer pollen from flower to flower. The pollen season in New Zealand runs from October through to late March, with tree pollens typically prevalent from September to February, and grass and weed pollens more prevalent from October through to March. The annual pollen calendar issued by Allergy New Zealand lists nearly 40 different species and their pollination period. For example,
in February, the main pollinators are macrocarpa, Pohutukawa/Rata, plantain, privet, dock, chenopod weeds, and grasses (such as ryegrass, fescue, brown top, and timothy). Knowing what a person is allergic to may help them to work out what is triggering their allergy in a particular month and try to remove it from their garden or to avoid it in general. See allergy.org.nz for a free downloadable pollen calendar.
Perennial rye grass is the most widely sown turf and pasture grass in this country. It is the biggest pollen producer of all and the most common cause of springtime hay fever. The pollen is small and can remain windborne for many miles.
English plantain is an abundant weed in New Zealand, growing in parks, lawns and roadside verges. Although it produces only small amounts of pollen, the pollen is highly allergenic and is a common cause of hay fever.
Silver birch is a popular introduced species that produces copious amounts of pollen. It is the main cause of tree pollen allergies.
Privet is common throughout New Zealand and it produces a highly scented flower. But it is not a strong allergen and many people who think they are allergic to privet are actually allergic to ryegrass, which is not as visible as privet. Cupressusmacrocarpa is commonly cultivated as shelter belts on farms or individually in gardens. Although the tree produces a lot of
pollen it is not as allergenic as silver birch but may be responsible for a lot of early spring hay fever.
A huge amount of pine pollen comes from our widespread forestry plantations of pinus radiata. Thankfully it is not very allergenic and only a small proportion of people with hay fever will be sensitised to it.
Some fruit and vegetables have a similar molecular structure to pollen, so cross-reactivity can occur. This most frequently affects people with a silver birch allergy. Oral allergy symptoms (ie, itching or swelling of the lips, tongue, throat, or roof of the mouth) develop on exposure to raw apples, stone fruit, wheat, carrots and some other vegetables. Cooking or canning destroys the allergens causing these reactions.
Hay fever is a reaction to pollen. It is caused by an oversensitive immune system that perceives pollen as a harmful substance or allergen. The immune system overreacts by producing antibodies called immunoglobulin E (IgE) which combine with the pollen and cause the release of substances to counteract the
allergen, such as histamine from mast cells. Histamine irritates the tissues of the nose, throat, and eyes, causing hay fever symptoms. Grass pollen allergies usually develop in children aged three to four whereas tree pollen allergies typically develop about age seven. It is not unusual for adults to develop hay fever as it can take two to three seasons to become sensitised to pollen. This may occur in adults moving from relatively pollen-free coastal areas to inland farming areas. It is not known why some people are more atopic (genetically predisposed towards allergies) than others.
Up to 80% of people with asthma also have hay fever, and up to 40% of people with hay fever, will go on to develop asthma. All asthma patients should be evaluated for allergic rhinitis and vice versa, and in planning treatment, both conditions should be considered together.
• Close windows at night. Use air conditioning instead.
• Avoid outside activities between 5am to 10am when pollen is most usually emitted.
• Keep car windows closed and choose the ‘re-circulated air’ option.
• Pollen counts are higher on windy days or when humidity is high. Stay indoors when possible.
• Choose coastal holidays rather than inland holidays.
• Wear sunglasses outdoors and shower as soon as you come inside.
• Get someone else to mow your lawns or wear a mask when you mow them.
• Dry clothes and linen in a clothes dryer, not outside.
Category Examples
Oral antihistamines
Non-sedating [PHARMACY ONLY MEDICINE]
eg, bilastine (Labixten), cetirizine (Razene), desloratadine (Aerius), fexofenadine (Fexofast), levocetirizine (Levrix), loratadine (Loraclear)
Sedating
[PHARMACIST ONLY MEDICINE]
eg, dexchlorpheniramine (Polaramine), promethazine (Phenergan)
Topical (nasal and ocular) antihistamines [PHARMACY ONLY MEDICINE] eg, levocabastine (Livostin Eye Drops, Livostin Nasal Spray), naphazoline + pheniramine (Naphcon-A, Visine Allergy), naphazoline + zinc (Clear eyes-A), antazoline + naphazoline (Albalon A Allergy), ketotifen (Zaditen)
Nasal corticosteroids [PHARMACY ONLY MEDICINE] eg, beclomethasone (Alanase, Beconase Allergy & Hayfever), budesonide (Butacort), fluticasone (Flixonase), triamcinolone acetonide (Telnase)
Other nasal products eg, cellulose and peppermint powder (Nasaleze) eg, protective nasal balm (Botanica Hayfever Gel, HayMax) [PHARMACY ONLY MEDICINE] eg, ipratropium bromide (Univent Nasal Spray)
Decongestants Topical (nasal) [PHARMACY ONLY MEDICINE]
eg, oxymetazoline (Dimetapp 12 Hour Nasal Spray, Drixine No Drip), xylometazoline (Otrivin)
Oral eg, phenylephrine + paracetamol
[GENERAL SALE]
eg, Panadol Sinus Relief PE
[PHARMACY ONLY MEDICINE]
eg, Sudafed PE Sinus Day & Night Relief (contains chlorpheniramine in night tablet) eg, phenylephrine + loratadine (Dimetapp Elixir, Dimetapp Elixir Colour-free, Maxiclear Hayfever & Sinus Relief)
Mast cell stabilisers
Saline nasal products
Natural / herbal products / supplements
[PHARMACY ONLY MEDICINE]
eg, lodoxamide (Lomide eye drops)
eg, sodium cromoglicate (Allerfix)
[GENERAL SALE]
eg, Otrivin Clear Saline Plus, Fess Nasal range, NeilMed
Astragalus, bitter orange, bromelian, butterbur, ginger, magnolia, pycnogenol, Quail egg powder, quercetin, stinging nettle, tinospora cordifolia, vitamin C
Comments
Useful for symptoms that persist during the day.
May be taken before hay fever occurs to avoid any slight delay in response. All relieve sneezing, itching, and help dry up a runny nose but only levocetirizine has shown to relieve nasal congestion.
Although drowsiness with these products is rare, it may still occasionally occur in some people. Always warn customers about driving or operating machinery if feeling drowsy. May not be suitable for children of certain ages.
Sedating antihistamines may be considered when symptoms are more problematic at night, to aid sleep. Warn about drowsiness and the risk of driving or operating machinery the next day. Refer people on medications or with certain health conditions to the pharmacist since these products may not be suitable for them. (See Reference section, OTC Medicines – Precautions). Avoid alcohol.
Sedating antihistamines are prescription medicines for children under two.
Have a localised effect and a rapid onset of action.
Contact lenses may need to be removed before applying eye drops – check instructions. Use eye drops combining antihistamines with decongestants short term only (ie, less than three days).
Throw drops away one month after opening.
Stinging and a bitter taste after application have been reported.
Useful for treatment and prevention and as a first-line therapy for moderate-to-severe allergic rhinitis.
Use at the start of the hay fever season to prevent symptoms occurring. A decongestant or antihistamine may also be required initially as relief may be delayed two to three days.
Cellulose powder is delivered as a fine mist into the nasal passages where it forms an impermeable barrier to allergens. A 2018 study found it was as effective as mometasone nasal spray and may be used in young children or during pregnancy.
Protective balms help prevent pollen entering the nasal cavity and lessen allergic reactions. Ipratropium relieves a runny nose but does not treat sneezing or congestion.
Best reserved for when nasal congestion needs to be treated quickly. Useful for symptom relief while waiting for nasal corticosteroids to take effect. Rebound congestion can occur with extended use. Nasal decongestants should not be used for longer than three days. Children’s formulations of intranasal oxymetazoline and xylometazoline are still considered safe to give to children two years of age and older.
Combination tablets contain a variety of different ingredients. Refer to the packet for the list of ingredients which may include a decongestant (eg, phenylephrine), analgesic (eg, paracetamol) or antihistamine (to dry up runny noses). (See also Reference section, OTC Medicines –Precautions).
Stabilise mast cells to prevent histamine release. Frequent administration (four to six times daily) is needed. Can be used for prevention up to one week before allergy symptoms occur.
Saline thins nasal mucus and moisturises dry nasal passages. It allows mucus to break down faster and washes away pollen, animal dander and dust. Suitable for pregnant women.
May be effective at either stabilising the allergic response or relieving symptoms of hay fever.
It’s
• Head lice products with a physical effect rather than a chemical action generally have less potential side effects.
• Thoroughly explain the instructions to your customer, including repeating treatment.
If a customer asks you to check their head for head lice, move them to a private area, put on gloves, and start by looking for nits (the empty, white egg cases) which tend to be found firmly attached to hair shafts located behind the ears or at the nape of the neck.
Advise customers who wish to do their own checking that the most reliable way to check for head lice is by using a conditioner and a fine-toothed nit comb. The conditioner should be applied to the hair for 10 minutes before combing through.
The conditioner stuns the lice, forcing them to let go of the hair, and they readily show up against the white conditioner. Theoretically, if done meticulously (every three days until no lice are seen for three consecutive sessions), this method can be used as a non-pharmacological way to remove head lice. However, in practice, failure rates are high because of the heavy commitment involved and the high probability of missing at least one louse.
Hair should be treated for head lice if lice or viable eggs (opaque, and less than 1cm from the scalp) are found. Head lice treatments with a physical effect are readily
Category Examples
Egg removal products and combs
Products to detect head lice
Products with a physical action
• People who are immunosuppressed, pregnant or breastfeeding.
• People with sores on their scalp (may indicate a secondary bacterial infection).
• People who have a particularly heavy infestation or if their hair is thick or matted.
• If you are not sure if your customer actually does have head lice (itching may be due to another skin condition eg, dandruff).
• When treatment has been tried before without success.
• People who are unable to pay for treatment (dimeticone is fully funded).
• People with allergies to topical medicines.
available and considered safer than those with a chemical action. Pharmacies should stock and promote the safest, least toxic, and environmentally-friendly products. Treatment products can be grouped into those with a physical action, a chemical effect, or a combined physical/chemical effect. Products with a physical action tend to be less toxic (see Table: Head Lice Product Ingredients and Effects).
Few comparative trials between head lice treatment products exist, and resistance rates can vary widely. In addition, independent studies have shown that most products do not kill head lice eggs, even if they say they do.
Reassure customers that head lice are not a sign of dirty hair or poor hygiene, and are just as likely to be found in clean hair. Girls are more likely to get head lice if they have long hair and it is not tied back.
Head lice (pediculosis capitis) are small, brownish-grey, wingless insects, about the size of a sesame seed (2–3mm), which feed
[GENERAL SALE] eg, NeutraLice Conditioner Shampoo Lice Egg Remover, Neutralice Nitcomb, Robi Comb, TCJ-Kids Nit Comb
[GENERAL SALE] eg, Moov Combing Conditioner for Head Lice Detection
[GENERAL SALE] eg, benzyl alcohol 5% (eg, NeutraLice Advance), biococidine (eg, Parasidose Natural), dimethicone 4% (eg, Hedrin 15, Quitnits Once-Only), diisopropyl adipate (Moov Defence), isopropyl myristate (eg, Moov Sensitive)
Products with a chemical action
Products with both a physical and chemical action (usually contain essential oils)
[GENERAL SALE] eg, maldison (KP 24, permethrin (Lice Clear), d-Phenothrine (Parasidose Extra-Strength Shampoo)
[GENERAL SALE] eg, essential oils (Moov Head Lice Solution/Shampoo, NeutraLice Natural Spray, Nit-Enz Organic) eg, neem oil (Licener Single Treatment)
Preventive products [GENERAL SALE] eg, Euky Bear Bitz Nitz, Moov Head Lice Defence Spray, Nit-Enz Head Lice Repellant, NitWits
Comments
removal
allow eggs to be
on blood from the scalp. They are most common in children, but can also spread to adults.
They cannot jump or fly, instead they use their single claw and “opposing thumb” to grasp the hair shaft and quickly crawl from head to head. Most are grey, although some may look black and after feeding their body may take on a reddish colour. They spread easily among people in close contact.
Head lice only feed on human blood and only infect the scalp – they are a different species to body lice and pubic lice, and in the natural environment will not interbreed. Unlike body lice, they do not carry disease, and apart from a risk of secondary infection from scratching, are unlikely to cause medical harm.
An itchy scalp is the most common symptom of head lice, caused by a delayed allergic reaction to the lice’s saliva or faeces. This reaction may take between a week and three months to develop which means that many customers may have been infested for some time without knowing. Some people may not itch at all.
Female head lice can lay up to eight eggs per day. These egg cases are brown and hard to see
out
combs with rounded teeth are used to detect and remove head lice. Electric combs stun or kill lice and are used on dry hair. Hard to use on very thick and curly hair or on young children.
Combing conditioners stun lice and help detect the presence of head lice and eggs. These products do not kill lice or nits.
Some may be used in children as young as three months and in pregnant women (check product labels). Most are suitable for those with asthma.
Resistance is common. May cause skin, eye, nose, or throat irritation. May pose a risk to aquatic organisms, bees, beneficial insects, and birds.
Essential oils such as anise oil, cinnamon leaf, citronella, clove oil, eucalyptus oil, geranium, lavender oil, mint, tea-tree oil, and thyme can be toxic if misused, and strong evidence for their effectiveness at killing head lice or their eggs is lacking, although combinations with vegetable oils may be more effective.
Either contain essential oils that repel lice or coat the hair making it difficult for lice to attach. Usually used every two to three days or weekly to keep lice from infesting hair. Will not treat already established infestations.
• OTC analgesics, such as paracetamol or ibuprofen, can be used for mild headaches but should not be taken every day.
• Customers with Warning Signs should be referred to a doctor.
Ask your customer to describe which area of their head is painful and what the pain is like (eg, throbbing, like a band of pressure, extremely severe). The Table: Common Types of Headache opposite page, may help. Refer any customers with concerns identified by the Refer to a Pharmacist checklist. People with Warning Signs (see text box next page) should be immediately referred to a doctor.
Customers with a headache should be encouraged to go home and rest in a darkened room, with a hot or cold compress (depending on their preference) applied to the head or neck.
Analgesics such as paracetamol, aspirin, ibuprofen, and naproxen are available over the counter (OTC), and are usually effective for occasional tension-type headaches. However, customers should be discouraged from using these for more than two days a week because of the risk of developing medication overuse headache (MOH).
Caffeine may enhance the effectiveness of analgesics, but it can also trigger headaches, and has been implicated in MOH. Headaches caused by sinusitis may respond
Seek urgent medical advice for anybody with warning signs (see Headache Warning Signs).
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People who take medicines, including herbal/complementary medications.
• With symptoms that have persisted despite treatment with adequate doses of analgesics, or lasted longer than 24 hours.
• Children aged less than 12.
• Older people complaining of a recurring headache that originates from the temples (may be temporal arteritis).
• People who also have a fever, rash or a stiff or sore neck (see Childhood Diseases and Immunisation: Meningococcal Disease).
• Headaches accompanied by symptoms such as nausea or visual disturbances.
• People with frequent headaches (more than one a month) or attempting to purchase large quantities of analgesics.
• People with allergies to medicines.
to nasal or oral decongestants in addition to paracetamol or NSAIDs, but antibiotics may be needed if the cause is due to a bacterial infection. Migraine treatments relieve symptoms and preventive medications available from a doctor may help reduce the frequency of attacks (see Migraine for more in-depth information).
People with frequent, severe headaches that are affecting their quality of life should be referred to a doctor or to a headache clinic. Non-pharmacological treatments, such as acupuncture, cervical spine manipulation, cognitive behavioural therapy, hypnotherapy, massage, or stress management may also help.
Headache is a general term that is used to describe pain that occurs in the head
Simple analgesics [GENERAL SALE] eg, paracetamol (Panadol, Panadol Rapid, Paracare) [PHARMACY ONLY MEDICINE] eg, paracetamol (larger packs) (Panadol, Panadol Rapid, Paracare, Panadol Optizorb)
Non-steroidal antiinflammatory drugs (NSAIDs)
[GENERAL SALE] eg, aspirin (Aspro, Disprin), ibuprofen </=25s (Advil range, Nurofen*, Nurofen Quickzorb*, Nurofen Zavance Tablets and Caplets*, Nurofen Zavance Liquid Capsules*) [PHARMACY ONLY MEDICINE] eg, diclofenac (Voltaren Rapid 12.5), ibuprofen >25s (Advil range, Nurofen*, Nurofen Zavance Tablets and Capblets*, Nurofen Zavance Liquid Capsules*), naproxen (Sonaflam) [PHARMACIST ONLY] eg, diclofenac (Voltaren Rapid 25)
Combination analgesics [GENERAL SALE] eg, paracetamol + caffeine (Panadol Extra) eg, ibuprofen + paracetamol (Maxigesic* [16], Nuromol* [12]) [PHARMACY ONLY MEDICINE] eg, paracetamol + caffeine (Parafast Extra [36]), eg, ibuprofen + paracetamol (Maxigesic*, Nuromol*) [PRESCRIPTION] eg, paracetamol + codeine (Panadeine range), ibuprofen + codeine (Nurofen Plus), paracetamol + doxylamine + codeine (Mersyndol)
Natural / herbal products / supplements Butterbur, caffeine, cayenne, feverfew, magnesium, peppermint
or upper neck and more than 300 different types have been identified. They are common and can be triggered by many different factors. The seven most common triggers are:
• stress
• diet
• alcohol
• the environment
• hormones
• caffeine withdrawal
• lack of sleep.
Headaches are classified based on their severity, location of the pain, duration, frequency, triggers, and presence of other symptoms.
Knowing what type of headache a customer has can help in management and treatment.
Effective for most people with few adverse effects. Avoid duplication of paracetamol-containing medications (present in combination cold/flu and sinus products).
Ibuprofen is the NSAID least likely to cause stomach irritation, aspirin is the most. NSAIDs may not be suitable for people on certain other medications or with some medical conditions (eg, asthma, kidney disease). Advise customers to stop taking if stomach upsets, increased bruising or prolonged bleeding occur. Aspirin is not recommended for adolescents or children under 16 years old because of the risk of Reye’s syndrome. See also Reference Section, OTC Medicines – Precautions
Try simple analgesics or NSAIDs first before combination products. Codeine-containing preparations were reclassified in November 2020 to prescription-only. Mersyndol contains doxylamine which can cause drowsiness. See also Migraine
Some natural remedies have analgesic properties and may be considered for headache relief. Butterbur may cause liver toxicity. Evidence for magnesium and feverfew is mixed.
Most headaches are self-limiting and resolve themselves, with or without treatment.
A migraine typically occurs just on one side of the head, as a dull throb or tightening which then intensifies into a concentrated and severe pain (see Migraine for more information).
Tension headache
Tension headaches are the most common type of headache. Described as a mild, aching pain that occurs on the sides or back of the head, or as a tight band across the forehead, this headache tends to worsen as the day goes on, or with stress. Avoiding eye strain or bad posture and using massage or relaxation techniques may help reduce the frequency of these headaches.
Sinusitis
Blocked nasal passages can lead to sinusitis, where mucus is unable to drain, causing pressure
LIKELY CONDITION IDENTIFYING
Cluster headaches
Haemorrhage
Medication overuse headache
Migraine
Sinusitis
Temporal arteritis
Refer your customer to a doctor if any of the following apply:
A first headache in a person over 50. Headaches that:
➤ are brought on by lying down, a cough, bending or with certain activities (eg, weightlifting, jogging, sex)
➤ are described as “The worst headache of my life” (needs urgent medical attention, even if the person habitually suffers from headaches)
➤ are new or different
build-up and pain. Sinusitis is usually associated with a cold, and often causes a frontal headache or aching teeth.
Medication Overuse Headache
Rebound headaches (medication-overuse
Headaches are short lasting but painful and occur frequently (such as daily for weeks or months at a time)
Sudden pain like a blow to the head
Brought on by attempts to discontinue pain-relievers (eg, paracetamol, NSAIDs)
Severe throbbing pain or pulsing sensation, often just on one side of the head
May be accompanied by nausea or vomiting or sensitivity to light and sound
May or may not be accompanied by an aura
Pain, pressure, fullness in the forehead, cheek, or tooth area
Pain worsens when bending over or lying down
Throbbing headache that is usually located in the temples
May be associated with double vision or vision loss in one eye
Tension headache Dull, aching pain
May be felt as a band of pressure across the forehead, sides or back of the head
Scalp, neck and shoulder muscles may be tender
➤ are severe right from the start
➤ develop after a head injury or trauma
➤ worsen over time (months).
Headaches that are accompanied by other symptoms such as:
➤ fever, high blood pressure, muscle aches, or weight loss (may suggest a whole body disorder)
➤ changes in consciousness, confusion, gait disturbances, loss of balance, memory loss, seizures, or speech difficulties.
headaches) are caused by taking pain-relieving medicines too frequently for headaches. They are the third most common cause of headache after migraine and tension-type headaches.
Analgesics should be avoided for a period to revert the headaches back to a normal pattern. Non-medicine-related, self-help measures (see Customer Advice) may help during this period.
• Identify and avoid factors that trigger the headache if possible.
• Rest in a quiet, darkened room. Reusable heat pads may provide relief.
• Be careful not to overuse pain-relief medicines.
• Drink plenty of water, maintain regular exercise, and eat a healthy diet.
• Know what to do if a customer appears to be having a heart attack or a cardiac arrest in front of you.
• Know the risk factors for cardiovascular disease and be able to explain to customers what high cholesterol and high blood pressure are.
• Encourage people who are middle-aged and older or with risk factors to see their doctor for a Heart Check.
Know the difference between a heart attack and a sudden cardiac arrest (SCA), what symptoms to look for (see Signs of a heart attack and Signs of cardiac arrest subtopics in this chapter), and what to do. Encourage people who are middle-aged, particularly those with risk factors, to have a cardiovascular disease risk assessment from their doctor or talk to the pharmacist for more information.
Cardiovascular (CV) disease (which means everything that involves the heart and blood vessels, including those inside the brain) is the leading cause of death in New Zealand, accounting for more than 33% of deaths annually. Every 90 minutes one New Zealander dies as a result of CV disease. CV disease is the leading cause of death in both men and women in New Zealand. Risk factors that increase the likelihood that someone has or will develop CV disease include:
• older age
• diabetes or prediabetes or a family history of type 2 diabetes (see also Diabetes)
• diets high in trans fats, sodium, or alcohol; or low in fibre, fish, fruit, wholegrains or vegetables
• ethnicity (tendency to develop at a younger age in Māori, Pasifika, or South Asian peoples)
• high blood pressure (BP)
• high cholesterol/high density lipoprotein (HDL) ratio above 7 (the ideal is 3.5)
• kidney disease (eGFR less than 60 ml/ min/1.73m2)
• obesity – a BMI of 30 or more or truncal obesity (see Weight Loss)
• physical inactivity
• premature coronary heart disease or ischaemic stroke in a first-degree relative
• smoking or a history of smoking within the last 12 months
• women with a history of gestational diabetes or polycystic ovary syndrome.
Several non-traditional risk factors have also been identified including the ankle-brachial index (ABI), high-sensitivity C-reactive protein (hsCRP), and coronary artery calcium (CAC) score, and abnormal values of these are associated with poor outcomes.
A Heart Check (also called a cardiovascular disease risk assessment) should be carried out at the following ages in the following populations:
• people with diabetes: at the time of diagnosis
• people with severe mental illness: age 25
• Māori, Pasifika or South Asian peoples: men at age 30, women at age 40
• risk factors for CV disease present: men at age 35, women at age 45
• everybody else: men at age 45, women at age 55. These checks may be free for certain people and should be repeated annually in people at high risk. Successful interventions can dramatically reduce CV risk.
Category Examples Comments
Cholesterol and triglyceride treatments [PRESCRIPTION MEDICINE] eg, acipimox, atorvastatin, bezafibrate, colestipol, ezetimibe, gemfibrozil, nicotinic acid, pravastatin, simvastatin
Blood pressure treatments [PRESCRIPTION MEDICINE] Includes beta-blockers, diuretics, ACE inhibitors, angiotensin II antagonists, calcium channel blockers, alpha-blockers and nitrates
Antiplatelet agents [GENERAL SALE] eg, Aspirin (Ethics Aspirin) [PRESCRIPTION MEDICINE] eg, clopidogrel, dipyridamole, prasugrel, ticagrelor
Natural / herbal products / supplements Co-enzyme Q10, English walnut, fish oil, Ginkgo Biloba, omega 3, quercetin, red krill oil, resveratrol
• Seek urgent medical attention for all customers with chest pain.
• Refer all customers with CV risk factors for further investigations and ongoing monitoring and treatment.
Cholesterol is a white, waxy substance manufactured naturally, mainly by the liver and also obtained through our diet.
It is a vital building block of cells and plays a crucial role in the production of steroid hormones (eg, testosterone, oestrogen) and the absorption of fat-soluble vitamins. There are two types of cholesterol carriers: LDL (low density lipoprotein) which transports cholesterol around the body and through blood vessels, and HDL (high density lipoprotein) which transports cholesterol back to the liver where it is broken down. Traditionally, LDL cholesterol has been termed “bad cholesterol” and HDL cholesterol has been described as “good cholesterol”, but it is more complicated than that.
Cholesterol levels are measured as part of a Heart Check which takes into account other CV risk factors to determine a person’s overall risk of having a stroke or heart attack in the next five years. A Heart Check helps a doctor to decide if a person needs medication to lower their cholesterol.
A rise in cholesterol is normal in pregnancy and cholesterol levels should not be measured at this time.
Blood pressure (BP) is usually measured from the arm with a device called a sphygmomanometer. The first recording is called
Muscle aches and cramps are the most common side effects of statins, and appear to be more common in women than men. They should initially be reported to a doctor.
Colestipol binds cholesterol preventing its absorption into the blood. Mainly lowers LDL but can increase HDL slightly.
Most people will need more than one medicine to reduce their blood pressure sufficiently.
Despite the fact aspirin can be bought on general sale, it is important people discuss taking it with their doctor. Usual daily dosage is 100mg to help prevent heart attacks and stroke. Caution in those who are sensitive to aspirin or NSAIDs, have a peptic ulcer, have bleeding risks or have uncontrolled high blood pressure (See also Reference Section, OTC Medicines – Precautions).
Walnuts and other nuts may reduce risk of coronary heart disease. Fish oil may reduce mortality in some people with congestive heart failure. A higher dietary intake of quercetin has been associated with a reduced risk of death from coronary heart disease. Red krill oil is a source of phospholipids, omega-3 fatty acids and antioxidants.
the systolic pressure and it measures the force the heart has to pump against (resistance) to get the blood to flow around the body (indicated by the pressure around the arm, which stops the blood flow). The second sound recorded is the diastolic pressure. This measures the resting pressure when the heart relaxes.
An ideal BP for most people is 120/75 mmHg, or lower; however, this depends on many factors, such as a person’s overall risk of heart attack and stroke. For people already on blood pressure medication, an ideal BP is 130/80mmHg, or lower.
High BP (hypertension) is when BP is consistently around or above 140/90 mmHg. It affects nearly one in five New Zealanders and many people have no symptoms, although some may develop a headache or feel unwell.
Persistent high BP can cause the heart to enlarge and weaken. It also contributes to blood vessel damage, especially in people with diabetes, high cholesterol or who smoke. If blood vessels become narrowed or blocked, a heart attack or stroke may occur. High BP is also linked to kidney and eye damage, and poor circulation in the arteries of the legs.
A heart attack occurs when blood flow to the heart is blocked or significantly slowed. If the artery is not reopened quickly, the heart muscle nourished by that artery begins to die.
Symptoms may come on suddenly or start slowly and be mistaken for indigestion. A person may describe chest pain or a heaviness, tightness, pressure or discomfort in the upper half of the torso, neck, or arms. Symptoms in women may be more subtle than in men and
include shortness of breath, dizziness, extreme fatigue, and pressure in the upper abdomen or back. Women are less likely to report chest pain.
If you suspect somebody is having a heart attack, call 111 or seek urgent medical advice if it is close by (such as a next-door medical centre).
If a doctor is not nearby, give a non-enteric coated 325mg aspirin tablet unless the person has been advised previously not to take aspirin. Get the person to rest quietly and wait with them until the ambulance arrives.
A sudden cardiac arrest (SCA) is a condition in which the heart suddenly stops beating or starts beating abnormally. It is caused by an electrical malfunction in the heart and is not the same as a heart attack (which is a circulation problem), although having a heart attack increases the risk of having an SCA. It often occurs without warning and the main symptom is loss of consciousness and unresponsiveness.
Seconds count in people having an SCA. Call 111 and then get an automated external
• aedlocations.co.nz
➤ Location of nearest automated external defibrillator (AED)
• My Heart Check heartfoundation.org.nz
➤ A free online heart health check
defibrillator (AED) if one is available (see Helpful Websites textbox). Use it as soon as it arrives, and begin CPR until professional emergency services are able to take over.
All community pharmacists and those working in clinical roles in the community are required to have a first aid certificate which includes CPR training. CPR typically combines chest compressions with artificial ventilation to maintain blood flow during an SCA. In some countries, handsonly CPR is promoted. Immediate CPR can significantly increase a person’s chance of survival.
• Follow the Ministry of Health’s Eating and Activity Guidelines. Eat plenty of vegetables and fruit; grain foods; some milk and milk products (mostly low or reduced fat); some legumes, nuts, seeds, fish, poultry and lean meat.
➤ Cut back on foods high in sugar, salt, and trans fats.
➤ Make water your preferred drink.
• Partake in at least 150 minutes of moderate or 75 minutes of vigorous intensity physical activity throughout the week. Do muscle strengthening exercises on at least two days per week. Break up long periods of sitting with activity.
• Stop smoking, lose weight, keep alcohol intake low, and maintain good blood glucose control if you have diabetes.
• Some serious conditions can have similar symptoms to heartburn or indigestion. Always be alert for RED FLAGS
• Lifestyle changes can help reduce symptoms of heartburn and indigestion (also called dyspepsia).
• Refer people not responding to OTC heartburn/indigestion treatments within two to four weeks to a doctor.
Although many customers self-select their own indigestion and heartburn treatments; many would probably benefit from further information about the condition and some lifestyle advice. This could be offered at the point of sale by asking “Are you finding this helpful?”. You should also check that they are not in a high risk group (see RED FLAGS) or have symptoms of concern.
Refer any customers with obvious RED FLAGS to a doctor, as these increase the likelihood of a more serious or sinister condition. Also run through the Refer to a Pharmacist checklist.
Many people are able to manage their indigestion and heartburn by making simple lifestyle adjustments, such as including more vegetables and fibre in their diet; reducing fat intake; limiting caffeine, spicy or acidic foods; losing weight; stopping smoking; limiting
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People prescribed medicine that may be causing their indigestion (for example, bisphosphonates, NSAIDs, prednisone).
• People with persistent indigestion, despite treatment, even if they have recently seen a doctor.
• People whose symptoms raise concerns (see RED FLAGS opposite page).
• Children aged less than 12.
• People on a sodium-restricted diet.
• People with allergies to medicines.
alcohol intake or NSAID use; and staying upright for some time after a meal.
If your customer has a history of NSAID or full-dose aspirin use, but there are no other symptoms of concern and their symptoms are mild, you should tell them initially to stop the NSAID and then reassess their symptoms.
Antacid/alginate combination products may be used to relieve occasional symptoms when they occur or are expected. They neutralise stomach acid and increase the viscosity of stomach contents and form a viscous gel (a “raft”) on top of the stomach contents. This helps protect the lining of the oesophagus from acid reflux in people with gastro-oesophageal reflux disease (GORD).
Proton pump inhibitors (PPIs) may be used to treat persistent symptoms of dyspepsia or GORD. Customers who don’t respond or those whose symptoms still persist despite up to four weeks of treatment should be referred
Category Examples Comments
Antacids and alginates [GENERAL SALE]
eg, alginate sodium + calcium carbonate + sodium bicarbonate (eg, Gaviscon Dual Action Liquid/Liquid Sachets/Tablets*) eg, alginate sodium + calcium carbonate + potassium bicarbonate (Gaviscon Extra Strength Liquid / Tablets*)
eg, aginic acid + aluminium + calcium + magnesium + sodium bicarbonate (Mylanta Dual action, Mylanta Heartburn)
Alginates [GENERAL SALE] eg, Gaviscon Infant Sachets*
Proton pump inhibitors (PPIs) [PHARMACY ONLY MEDICINE] eg, omeprazole 10mg (Losec) eg, omeprazole 20mg (Losec Extra)
Anti-flatulence agents [GENERAL SALE] eg, simethicone (De-Gas)
Natural / herbal products / supplements eg, apple cider vinegar and manuka honey (Radiance ManukaGuard Nutralize) eg, kawakawa and hoheria (Kiwiherb Herbal Digestive) eg, ginger, slippery elm eg, digestive enzymes (Nutralife, Radiance DigestAid, Thompson's Digestion Manager)
to a doctor for evaluation and possible Helicobacter pylori testing (H.pylori is a bacteria commonly associated with stomach ulcers and gastritis).
Indigestion (dyspepsia), heartburn and gastritis are not actually medical conditions themselves, but rather symptoms common to several different conditions.
Indigestion (also called dyspepsia) is a term used to describe pain or discomfort centred in the upper abdomen, often after meals. It usually occurs soon after eating, particularly when people eat too much, too fast, or with certain types of foods.
People with indigestion may also feel full within a few minutes of beginning a meal, or experience bloating, belching, or nausea.
Antacids neutralise stomach acid and are recommended for people with mild, occasional, indigestion-like symptoms. Most contain two to four constituents with different onsets and durations of action.
Alginates precipitate out when in contact with gastric acid, thickening the contents or forming a raft that sits on top of the stomach contents. This protects the lining of the oesophagus when the contents regurgitate upwards. Most products contain an antacid as well (such as aluminium hydroxide, calcium carbonate, magnesium hydroxide, potassium bicarbonate, or sodium bicarbonate) and may be used to relieve indigestion symptoms (dyspepsia). Shake well. Do not lie down immediately after administration.
Symptoms of GORD in babies include poor weight gain, feeding difficulties, or frequent spilling. Only sell on the advice of a doctor because the baby will need ongoing monitoring.
Used for the short-term symptomatic relief of reflux-like symptoms in adults aged 18 years and over. Acts directly on gastric acid-releasing cells in stomach. Seek further medical advice if symptoms don’t improve after two weeks. Take in the morning, 30 minutes before food, for optimal acid suppression.
Simethicone breaks up large bubbles of air in the stomach and relieves burping and flatulence.
Apple cider vinegar has an acid/alkaline balancing effect and manuka honey has a natural antibacterial action.
Kawakawa and Hoheria may help soothe the digestive tract.
Slippery elm tablets may help soothe heartburn.
Ginger may help with the absorption of food and symptoms of indigestion.
Digestive enzymes help reduce symptoms of indigestion and bloating associated with low stomach acid. Take with food.
Symptoms can occur ocasionally or happen all the time.
The three most common conditions with indigestion as a symptom are gastroesophageal reflux disease (GORD), gastric ulcers, and gallbladder disease. Very rarely, indigestion can be a symptom of stomach cancer. Stomach cancer affects less than 0.5% of people with indigestion, and is mostly found in those aged older than 50. In 70% of people, no cause is found for the indigestion (this is called functional dyspepsia).
Heartburn is usually described as a burning sensation behind the sternum, often with a feeling of acid regurgitation. This burning feeling may extend to the neck and jaw and tends to worsen when bending over or lying down. Most cases are attributed to gastrooesophageal reflux disease (GORD), which is thought to be caused by an ineffective lower oesophageal sphincter muscle. This muscle is unable to prevent regurgitation of stomach acid contents up the oesophagus.
Symptoms generally occur after eating, exercising, bending over or lying down and are often associated with indigestion. Obesity is a risk factor and the condition is more common in women who are pregnant and in those who eat a high-fat diet, who smoke, or who are under stress. Although the term heartburn has nothing to do with the heart, it is important to realise that symptoms of a heart attack (chest pain or discomfort that radiates up the neck and jaw) may be similar. Refer to a pharmacist if unsure.
Babies can also get reflux, and symptoms include vomiting straight after a feed, failure to thrive, and prolonged bouts of crying. Refer any
Seek urgent medical advice for anybody whose symptoms suggest a heart attack (see Heart Health).
• Refer anybody with the following to a doctor:
➤ Aged 50 or older (or 40 years and older if of Māori, Pacific Island or Asian descent) and new indigestion/heartburn
➤ A chronic persistent cough
➤ Difficulty in swallowing
➤ A family history of gastric cancer with
children under 12 with symptoms of reflux or indigestion to the pharmacist.
Gastritis has similar symptoms to indigestion, except that symptoms persist for most of the day. Some people may feel nauseous or vomit. Gastritis can occur as a result of increased acid production, certain medicines, alcohol, stomach ulcers, or a bacterium called H.pylori
age of onset less than 50 years
➤ GORD that occurs at night
➤ A history of a stomach ulcer
➤ Aspirin, NSAID or prednisone use
➤ Persistent, protracted vomiting
➤ Severe or persistent symptoms
➤ Signs of bleeding from the rectum, black stools, or blood in vomit
➤ Suspected iron-deficiency anaemia
➤ Unexplained weight loss
➤ With a palpable lump in their stomach.
As with indigestion, very rarely it may be a symptom of stomach cancer. Refer anybody with suspected gastritis to the pharmacist.
• Stop smoking if you smoke and try to lose weight if you are overweight.
• Avoid tight waistbands, bending over or lying down soon after a meal.
• Watch what you eat and how much you eat. Try to eat small meals slowly and avoid overfilling your stomach. Reduce alcohol and coffee intake.
• Antacids and alginates may reduce the absorption of some medicines so need to be taken two hours apart from them – check with your pharmacist.
• Raise the head of the bed by 10cm and avoid eating two to three hours before lying down if you are prone to nocturnal symptoms.
• Avoid taking NSAIDs. Use paracetamol for pain relief.
• The flu is very contagious and can be deadly in some people. Maintain a safe distance when talking to customers and follow recommended guidelines to reduce your risk of infection.
• Annual flu vaccination is recommended because protection against flu viruses wanes with time and most years the composition of the vaccine changes to reflect the likely prevailing viruses.
Ask your customer what symptoms they are experiencing and clarify that these symptoms reflect those of the flu, and not from a viral infection, such as a cold, COVID-19, or hay fever (see Colds and COVID-19;Table: Differentiating Cold, COVID-19, Flu and Hay Fever Symptoms). People with suspected COVID-19 should not be allowed to enter the pharmacy (see Colds and COVID-19 for further information).
Sudden, excessive fatigue is a common first sign that a person is coming down with the flu. Body aches, joint pains or chills, a sore throat, high fever (38.8–40°C), headache, and a cough may develop a few hours later. Some flu strains may cause stomach pain, diarrhoea, nausea, or vomiting. Children may be difficult to rouse and refuse fluids and foods.
Always take precautions to protect your own health during flu season. Yearly vaccination is the best form of protection, and you should always wash your hands before and after direct contact with customers. Always wear a face mask when talking with customers who are actively coughing. Run through the Refer
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People taking regular or herbal/complementary medicines.
• Children aged less than 12 or the elderly.
• People whose symptoms include a rash or a stiff/sore neck (see Childhood Diseases and Immunisation: Meningococcal disease).
• People having trouble eating or drinking.
• People who have recently been overseas.
• People with a fever that has lasted a couple of days or with severe symptoms.
• With symptoms such as confusion, diarrhoea, difficulty breathing, skin discolouration, or vomiting.
• With symptoms that are worsening or that have persisted for longer than a week.
• People with allergies to medicines.
to a Pharmacist checklist to help you decide which customers have mild symptoms and can self-treat and who needs to be referred to the pharmacist.
Medicines are available over the counter to help make people with the flu feel more comfortable. Analgesics, such as paracetamol and ibuprofen relieve aches, pains and headaches; cough suppressants may help ease a dry cough; and lozenges may soothe a sore throat.
Over-the-counter flu remedies should not be used in children aged less than six years because few products are effective and some may be harmful. Paracetamol may be used to relieve discomfort and natural remedies, containing ingredients such as glycerol, honey, or lemon may help soothe irritated throats or coughs in children older than one year. Refer all children

aged less than 12 to a pharmacist.
Oseltamivir is an antiviral agent that may be used to treat infections caused by influenza A or B viruses in people who have been symptomatic for no more than 48 hours (see Treatment options over page).
Vaccination is the most effective way to prevent the flu. It takes approximately two weeks for a vaccine to reach full effectiveness.
Influenza (flu) is a common contagious viral infection that spreads quickly and can cause serious illness and sometimes death.
There are thousands of different strains of influenza virus and they have been classified as four types: A, B, C, D. Within these types are several different subtypes (for example, influenza A has 18 hemagglutinin subtypes [H1–H18] and 11 neuraminidase subtypes [N1–N11]). Only types A and B have been associated with seasonal outbreaks in humans.
Older people, young children, pregnant women and people with certain medical conditions (such as asthma, diabetes, heart disease, or an autoimmune disease) are at a higher risk of developing serious complications from influenza.
Influenza can be spread through the air via coughing or sneezing, or by direct contact with an infected person. People are infectious usually one day before the symptoms start and up to
Helpful website
• www.immune.org.nz –
Immunisation Advisory Centre (IMAC) Provides independent, factual information about vaccine-preventable diseases and the benefits and risks of immunisation.
• There are two funded quadrivalent vaccines for 2023, Afluria Quad for children and adults who meet the influenza vaccination eligibility criteria, and Afluria Quad Junior for children aged 6–35 months who meet the eligibility criteria. These vaccines provide protection against the following four influenza strains and are fully funded for eligible adults and children from 1st April 2023 until 31st December 2023:
➤ A/Sydney/5/2021 (H1N1) pdm09-like virus
➤ A/Darwin/9/2021 (H3N2)-like virus
➤ B/Austria/1359417/2021-like virus
➤ B/Phuket/3073/2013-like virus (B/Yamagata lineage).
• Pharmacist vaccinators and provisional pharmacist vaccinators can administer influenza vaccines to adults and children from 3 years and over.
• Afluria Quad, Afluria Quad Junior, and Fluad Quad (not funded) can be given to people with a known history of egg anaphylaxis because residual ovalbumin in the vaccines is less than the one microgram necessary to trigger anaphylaxis.
• Those eligible for free influenza vaccination in 2023 include:
five days after they become sick. Flu season in New Zealand is usually from May to September, although can start earlier or last longer. Each year, the majority of influenza cases are caused by three to four major viruses. Symptoms of a flu (see under Your Customer) usually come on suddenly compared to cold symptoms that take several days to develop. Secondary bacterial infections such as bronchitis or pneumonia are common, especially in people with other health conditions such as asthma, COPD, diabetes, or who smoke.
➤ over 65s and Māori or Pasifika aged 55+
➤ children aged three to twelve years of age
➤ pregnant women (any trimester)
➤ anyone aged 6 months to 65 years with:
» cardiovascular disease (includes congenital, ischaemic, or rheumatic heart disease; congestive heart failure; or cerebrovascular disease)
» chronic respiratory disease (asthma, if on regular preventive therapy; conditions characterised by impaired lung function)
» diabetes or chronic renal disease
» cancer except non-invasive basal or squamous skin cancers
» certain mental health conditions (such as bipolar or schizophrenia) or accessing mental health or addiction services
» other eligible conditions (see www.influenza.org.nz/ eligibility/eligibity-criteria for the full eligibility criteria).
• Annual flu vaccination is recommended because, most years, the major prevailing viruses change (see text box Influenza Immunisation).
• If you contract the flu, rest in a quiet, darkened room, increase fluid intake and consider symptom control using paracetamol or other treatments (see Treatment options, over page). Keep contact with other people to a minimum. Do not go to work while you have the flu and avoid public places where possible for up to five days.
• See your doctor if symptoms worsen or persist for longer than a week.
• Many cold and flu remedies contain paracetamol, a decongestant and/or a cough suppressant. Watch for double-dosing with these products.
Category
Analgesic/antipyretics
Cough suppressants (antitussives)
Combination products
Examples
[GENERAL SALE]
eg, paracetamol (Lemsip range, Panadol), ibuprofen up to 25s (Advil range, Nurofen range)
[PHARMACY ONLY MEDICINE]
eg, ibuprofen >25s (Advil range, Nurofen range), ibuprofen suspension (Fenpaed, Nurofen for Children), paracetamol suspension (Pamol, Panadol suspension)
[PHARMACIST ONLY]
eg, dextromethorphan (Robitussin Dry Cough Forte, Strepsils Dry Cough Lozenges) Pholcodine (Durotuss Dry Cough Regular/Forte)
[GENERAL SALE]
eg, phenylephrine + paracetamol (Codral Relief Max Strength Cold & Flu + Decongestant hot drink)
eg, phenylephrine + paracetamol + expectorant (Codral Relief Max Strength 6 Signs Cold & Flu, Lemsip Max All In One Hot Drink)
[PHARMACY ONLY MEDICINE]
eg, phenylephrine + paracetamol (Codral Cold & Flu, Maxiclear Cold & Flu Relief Sinus & Pain Relief)
eg, phenylephrine + paracetamol + antihistamine (Codral Nightime Cold & Flu, Sudafed PE Sinus Day & Night Relief)
eg, phenylephrine + paracetamol (Codral Cold and Flu)
eg, phenylephrine + paracetamol + antihistamine (Codral Day & Night)
eg, paracetamol + phenylephrine + caffeine (Lemsip Max Cold & Flu Day & Night Capsules)
[PHARMACIST ONLY]
eg, dextromethorphan + phenylephrine (Benadryl PE Dry Cough & Nasal Congestion)
eg, dextromethorphan + phenylephrine + brompheniramine (Pharmacy Health Congested Cold & Cough)
eg, dextromethorphan + phenylephrine + paracetamol + chlorpheniramine (at night) (Codral Cold & Flu + Cough, Coldrex PE Cold & Flu Day & Night)
eg, dextromethorphan + guaiphenesin (Robitussin Cough & Chest)
Antiviral [PRESCRIPTION MEDICINE] [PHARMACIST ONLY under certain conditions (see comments)] eg, oseltamivir (Tamiflu capsules)
Influenza vaccinations [PRESCRIPTION MEDICINE] – except when administered by a registered pharmacist vaccinator to adults and children aged over 3 eg, Afluria Quad, Fluad Quad (65 and over, unfunded), FluQuadri (unfunded)
Natural / herbal products / supplements Comvita range, honey, Bifidobacterium, Lactobacillus, ginseng (American), elderberry, echinacea, N-acetyl cysteine, olive leaf, vitamin D eg, Kiwiherb range, Harker Herbals
Comments
Analgesics can make a person feel more comfortable. Paracetamol is effective for most people. However, remind the customer not to exceed the recommended dose. Ibuprofen can provide longer symptom relief and is the NSAID least likely to cause stomach irritation. NSAIDs may be unsuitable for people on certain other medications or with some conditions (eg, asthma, kidney disease – see Refer to pharmacist). Aspirin is not recommended for adolescents or children under 16 years old because of the risk of Reye’s syndrome.
Cough suppressants (eg, pholcodine, dextromethorphan) control or suppress the cough reflex and can provide relief from a dry, unproductive cough. Be aware that dextromethorphan can interact with other medicines that also have serotonergic activity (eg, antidepressants, tramadol, lithium, St John’s wort) (see also Coughs: Dry).
Refer to the packet for ingredients which may include a decongestant to unblock a congested nose (eg, phenylephrine), an analgesic (eg, ibuprofen or paracetamol), an antihistamine to dry up runny noses (eg, loratadine, chlorpheniramine), a cough suppressant to stop a dry cough (eg, pholcodine, dextromethorphan), an expectorant to help expel mucus from the lungs (eg, guaiphenesin), or a mucolytic (eg, bromhexine) to liquefy mucus and phlegm. Analgesics (eg, paracetamol and ibuprofen) can help make a person feel more comfortable if they are in pain. Watch for double-ups with other analgesic medicines. Some antihistamines may cause drowsiness and affect a person’s ability to drive or operate machinery. Avoid alcohol.
Cough suppressants (eg, pholcodine, dextromethorphan) control or suppress the cough reflex and can provide relief from a dry, unproductive cough. Dextromethorphan can interact with other medicines that also have serotonergic activity (eg, antidepressants, tramadol, lithium, St John’s wort). Products containing dextromethorphan and pholcodine are [PHARMACIST ONLY]. Cough expectorants (eg, guaiphenesin) loosen mucus and phlegm, allowing it to be coughed up more easily and can help a chesty cough. Mucolytics (eg, bromhexine) are often included with cough expectorants as these help to liquefy mucus and phlegm, aiding its passage from the lungs to the mouth.
Coughs associated with colds are more likely to be productive.
People who take other medicines or have other medical conditions may be unable to take cold and flu tablets – check with your pharmacist. Products containing guaiphenesin, bromhexine, ipecacuanha, dextromethorphan, pholcodine, phenylephrine, pseudoephedrine [PRESCRIPTION], doxylamine, brompheniramine, promethazine, chlorpheniramine, triprolidine or diphenhydramine should NOT be given to children aged less than six years and pharmacist advice should be sought before using them in children aged less than 12 years.
Shorten the duration and reduce the risk of complications of flu. Best when started within 48 hours of symptom onset. Can be sold by a pharmacist year round to adults and children aged 13 or older who have been exposed to the influenza virus. Available on prescription for younger children or for the prevention of influenza. Tamiflu is unfunded (customers pay full cost).
For customers unable to swallow, Tamiflu capsules may be given by opening the capsule up over a small bowl and mixing the contents with a teaspoonful of sweetened food product (regular or sugar free), eg, honey, condensed milk, apple sauce, yoghurt to mask the taste.
Privately purchased and funded influenza immunisations may be given by pharmacists who are approved vaccinators.
Honey soothes the throat and stops cough. Do not give honey to children under one due the increased risk of botulism due to their immature digestive systems.
Bifidobacterium, Lactobacillus, ginseng and vitamin D appear to protect against flu. Elderberry and echinacea root extracts and N-acetyl cysteine may reduce flu symptoms. Olive leaf contains five times the antioxidant capacity of vitamin C and helps boost immunity.
It’s the button that helps you keep up to date, CAPTURE a record of what you read, watch, listen to, delve into and explore on pharmacytoday.co.nz
• Iron supplements may be taken in certain circumstances to prevent iron deficiency from developing, or to treat irondeficiency anaemia (IDA).
• Anybody with symptoms of IDA without a formal diagnosis should be referred to a doctor for further investigation and monitoring.
• Gastrointestinal side effects from iron are common.
• Iron may interfere with the absorption of calcium, magnesium, and zinc.
Most people self-select iron supplements so the point of sale may be the first time that you are able to offer some advice to your customer. There should be a clear reason for them to take the supplements. If they are taking them because they have been told to take them by their doctor or midwife, then check they are tolerating the iron and that their haemoglobin levels are being monitored periodically. Run through the Refer to a Pharmacist checklist and refer any customers with concerns to a pharmacist.
If they are taking supplements because they feel tired all the time or feel they might be iron deficient, then encourage them to see a doctor for a formal diagnosis. Iron-deficiency anaemia (IDA) is not the only reason for chronic tiredness, and if a person does actually have IDA, then further investigations should be done to determine what is causing it.
Iron-rich foods are better absorbed than supplements and for customers with low, but not yet deficient levels, this is the preferred way to increase blood levels (see Advice for customers).
• Any person who has not had a formal diagnosis of IDA (ie, with blood tests) should be referred to a doctor.
• For other people buying iron supplements, who state that they have been told to do so by a doctor or their midwife, refer those:
➤ who have forgotten what dose they need
➤ who still feel tired or run down despite regular iron tablets
➤ with other symptoms, such as joint pain or unexplained weight loss
➤ with bright red blood in their stools (note that iron tablets will make the stools look dark or like tar)
➤ with unacceptable side effects (such as constant diarrhoea or severe constipation).
Iron supplements contain iron in one of three forms: ferric salts or carbonyl iron. Ferrous forms (Fe2+) are more soluble and absorbable than ferric forms (Fe3+). Ferrous forms of iron include ferrous sulphate, ferrous gluconate, and ferrous fumarate. No significant differences in absorption rates between the three ferrous salts have been found; with studies showing between 10% and 15% of a dose is absorbed.
Carbonyl iron requires gastric acid to make it soluble, and has a slower rate of absorption which may be associated with fewer side effects.
Some research has found that a morning dose of iron stimulates an increase in hepcidin, a substance that regulates systemic iron balance and interferes with iron absorption for up to 48 hours. Taking iron every second day may actually increase blood levels of iron more than a two to three times daily regimen.
Iron is an essential trace element (which means it is only needed in
Category Examples Comments
Iron supplements [GENERAL SALE]
eg, Douglas Carbonyl Iron (=elemental iron 18mg), Natures Own Liquid iron (=elemental iron 7.5mg), Sanderson Superior Organic Iron (=elemental iron 24mg), Spatone 100% Natural Liquid Iron Supplement (=elemental iron 5mg), [PHARMACY ONLY MEDICINE]
eg, Ferrograd (=105mg elemental iron)
Iron supplements in combination with other minerals or vitamins
[GENERAL SALE] eg, Ferro-Lipo Sachets* (with vitamin C, B12, and folic acid), Floradix Floravital Liquid Iron and Vitamin Formula, Incremin Iron Mixture, Iron Melts, [PHARMACY ONLY MEDICINE]
eg, Elevit with Iodine, FabFol Plus with Iodine (=elemental iron 60mg)
eg, Ferrograd C (=105mg elemental iron + vitamin C 500mg)
eg, Ferrograd F (=105mg elemental iron + folic acid 0.35g)
small amounts) that we must obtain from our diet. It is a component of many proteins, enzymes, is important for proper immune function and is found in every cell of the body. Iron is vital for normal child growth and intellectual development. It is also used to make haemoglobin, which is the substance in red blood cells responsible for transporting oxygen around the body.
Iron is stored in the liver, spleen, and bone marrow. Iron requirements are higher during periods of rapid growth and development – such as during early childhood, adolescence, and pregnancy, and low levels of iron are commonly seen during these times. Low body iron levels can also be caused by:
• clotting disorders or frequent blood donation
• kidney failure
• malabsorption syndromes (Crohn’s or coeliac disease)
• medical conditions that cause blood loss (eg, heavy periods, haemorrhoids, stomach ulcers)
• poor dietary intake of iron
• surgery.
Iron supplements contain either ferrous, ferric, or carbonyl forms of iron. Base iron dosages on the amount of elemental iron contained within the product (this is the amount of available iron), not the amount of iron salt present.
Ferrous sulphate: 325mg is equivalent to 105mg elemental iron.
Ferrous gluconate: 170mg is equivalent to 20mg elemental iron
Ferrous fumarate: 200mg is equivalent to 65mg elemental iron
LIPOFER iron (water dispersible/microencapsulated): 166.67mg is equivalent to 14mg elemental iron.
Recommended daily intakes (RDIs) vary according to age and gender and can be found at www.nutritionfoundation.org.nz
Iron supplements prescribed for anaemia may need to be taken for up to six months, or for three months after haemoglobin concentration is normal, to build up iron stores.
Iron supplements may cause nausea, constipation and/or diarrhoea, and make the stools a dark colour. Taking iron tablets with food may help settle gastrointestinal problems.
Iron is dangerous in overdose and keep all iron products out of reach of children. Sip iron liquid through a straw to avoid tooth discolouration. Combination formulations may contain vitamin C, folic acid, B vitamins (ie, B1, B6, or B12) and other vitamins. Many act as co-factors to facilitate absorption.
Ferro-Lipo Sachets contain iron microencapsulated in liposomal form to enhance absorption and reduce side effects.
• IBS is a group of symptoms, namely bloating, abdominal pain, constipation, and diarrhoea, that occur together but are not due to any other condition.
• Treatment aims to manage the most common symptom: usually constipation and/or diarrhoea.
If you have a customer that complains of persistent constipation, diarrhoea, or bloating, it is important to refer them to a pharmacist or doctor. Symptoms of IBS are similar to many other conditions, and it is important to refer anybody with obvious RED FLAGS (see Text box, opposite page) or with undiagnosed, persistent symptoms to a doctor. If your customer has already been diagnosed with IBS, they cannot be cured, but you can give them good advice about what products you sell that could help manage their symptoms.
Treatments for IBS include:
• laxatives to relieve constipation
• anti-diarrhoeals to relieve diarrhoea
• peppermint oil
• probiotics to improve the gut microbiota
• dietary changes (such as the FODMAP diet)
• hypnotherapy and relaxation techniques
• prescription medicines from a doctor.
Laxatives
Approximately 28% of people with IBS have IBS-C which is diagnosed when more than a quarter of stools are hard or lumpy and less than a quarter are loose or watery.
Category
• Refer anybody with symptoms suggestive of IBS, who has not had a formal diagnosis, to a pharmacist.
➤ Pharmacists should refer these people to a doctor.
• Pharmacists should also refer people with “Red Flags” to a doctor – these are symptoms that suggest a serious underlying cause (see Text box: Red Flags, opposite page).
Management includes increasing fluid intake, exercise, and avoiding caffeinated beverages. Fibre is a double-edged sword for people with IBS, because although fibre relieves constipation, certain types of fibre, such as wheat bran, increase gas production and bloating. The team at Monash University advise increasing fibre intake gradually, with low FODMAP, high-fibre foods, or supplements such as linseeds, oats, oat or rice bran, methylcellulose, sterculia, or psyllium.
Laxatives available over the counter include macrogol 3350, bisacodyl, docusate, senna, psyllium, and lactulose. Only macrogol 3350 has been evaluated in clinical trials in people with IBS-C and shown to improve stool texture and frequency; however, like many laxatives,it may increase abdominal cramping, bloating, or nausea. Advise your customer they may have to try several before finding one that suits them best.
Fibre supplements are often the first treatment
Antispasmodics [GENERAL SALE] eg, peppermint oil (Colpermin, Mintec)
Smooth muscle relaxants [PHARMACIST ONLY MEDICINE] eg, hyoscine (Gastro-Soothe)
Probiotics and prebiotics [SUPPLEMENT] eg, IB Guard, IBS Support, MultiFlora Digest, Gut Guard
Food supplements eg, gluten-free wheat dextrin (Benefiber) eg, inulin fibre
Laxatives [GENERAL SALE] eg, docusate (Coloxyl), lactulose (Laevolac), psyllium husk (Metamucil), sterculia (Normacol)
Anti-diarrhoea products [PHARMACY ONLY MEDICINE] eg, loperamide (Diamide, Imodium Zapid)
Natural / herbal products / supplements eg, guar gum, kiwifruit extract (Phloe Bowel), peppermint, slippery elm, turmeric
For people who have already had a formal diagnosis of IBS, refer anybody with the following to a pharmacist:
• constipation that is severe or has persisted for longer than a week
• other, atypical symptoms, such as fever, nausea or vomiting
• stools that float or are foul-smelling (may indicate malabsorption or an infection)
• symptoms that have become worse over time or changed recently.
recommended for people with IBS-D (diarrhoea-predominant IBS) which affects around 26% of IBS sufferers. Fibre can add form to stools and make them less loose or watery. Loperamide, which works by slowing down the motility of the gut, can also be used to decrease diarrhoea.
Peppermint oil has been found to be effective at relieving symptoms of IBS such as abdominal bloating or pain, diarrhoea, constipation, or gas in at least two good-quality randomised trials. One trial reports 75% of people having at least a 50% improvement in symptoms after 4 weeks when two enteric-coated capsules were taken twice a day.
There is not one probiotic that will treat all symptoms of IBS, but some evidence of an effect has been found for the following probiotics when taken regularly:
• S. boulardii: loose stools
Peppermint oil provides natural relief of abdominal bloating, distension and cramping.
May be helpful for abdominal pain or cramping.
May help to regulate the digestive system, reduce abdominal pain and bloating, and encourage more uniform stools. Studies have indicated a benefit for probiotics species such as Bifidobacterium, Lactobacillus, and Propionibacterium
Fine powder with minimum taste. Can be sprinkled on foods and in cooking without premixing to increase fibre content of the diet, encouraging more uniform stools.
Most laxatives only treat constipation; however, bulk-forming laxatives (containing psyllium or sterculia) can also be used to bulk up watery unformed stools. When used to regulate stool consistency, less water can be drunk as the fibre absorbs fluid from the bowel. See Constipation for more information about constipation.
Slow down bowel movements, allowing reabsorption of fluid by body. Can help reduce cramping, abdominal pain and the frequency of bowel motions. May be used regularly in people with IBS to regulate ongoing diarrhoea.
Many natural ingredients (including probiotics, guar gum, peppermint, turmeric) have been shown to be effective in IBS. Kiwifruit extract contains prebiotics, enzymes and dietary fibre to optimise bowel health.
• B.infantis 35624: abdominal discomfort, gas, bloating, straining
• B. lactis BB-12: straining, poor gut motility, bowel regularity
• B. lactis DN-173 010: bloating, gastrointestinal transit, constipation
• B. bifidum MIMBb75: abdominal pain and/or discomfort, bloating
• L. plantarum Lp299v: abdominal discomfort, gas, bloating, bowel regularity.
Food can trigger or exacerbate IBS symptoms and low FODMAP diets are recommended for IBS treatment. FODMAPs are various types of short-chain carbohydrates or sugar alcohols that rapidly ferment in the gut during digestion or encourage the growth of gas-producing bacteria, leading to uncomfortable side effects that mimic or magnify IBS symptoms.
FODMAP stands for Fermentable Oligo-, Di-, Mono-saccharides, And Polyols, and FODMAPs are present in fruit and vegetables, grains, and cereals, nuts, legumes, lentils, dairy foods, and manufactured foods. It is not possible to look at a food and tell if it is a low or high FODMAP, as it depends on serving size, an individual’s threshold level, and in some cases, the part of the food that you are eating. For example, ¾ cup of broccoli florets are low FODMAP but broccoli stalk grated into a coleslaw is high FODMAP (high in fructose). Research has shown three-quarters of trial participants experience IBS symptom improvement with low FODMAP diets (see www. monashfodmap.com).
Hypersensitive nerves in the gut or a
miscommunication between the gut and the brain are one suggested cause of IBS.
Hypnotherapy for IBS aims to influence and control the sensitivity of gut nerves and involves relaxation techniques and guided imagery to improve IBS symptoms. A systematic review of randomised controlled trials found it effective at improving abdominal pain, gastrointestinal symptoms, and quality of life.
Nerva is an App developed by the team at Monash University that delivers clinically proven hypnotherapy techniques via a subscription and takes 15 minutes a day. Research has found it to be just as effective as the Low FODMAP diet for people with IBS without the dietary hassle, with most people experiencing an improvement within six weeks, although it may take up to six months for the full effects to be seen.
Irritable bowel syndrome (IBS) is not technically a disease, rather it is a group of symptoms, namely bloating, abdominal pain, constipation, and diarrhoea, that occur together but are not due to any other conditions such as inflammatory bowel disease, diverticulitis, or bowel cancer.
IBS is estimated to affect around 7% of New Zealanders, although this may be an underestimation because it can be difficult to diagnose, and few people see a doctor about their symptoms. Most people are diagnosed while they are in their twenties or middle-aged (before age 45 years), but many people can trace the onset of their symptoms back to early childhood.
• Refer anybody with the following to a doctor:
➤ a lump or mass in their stomach or near their bottom
➤ a family history of gastrointestinal cancer, IBD or coeliac disease
➤ bleeding from the bottom that is not due to haemorrhoids
➤ new symptoms and aged over 50
➤ with night-time symptoms (eg, waking from sleep with pain or needing to defecate)
➤ with symptoms of iron-deficiency anaemia
➤ unintentional or unexplained weight loss.
IBS may be due to hypersensitive nerves in the gut, a miscommunication between the gut and the brain, infection, hormone imbalances, changes in the gut microbiota, stress, or food intolerances.
IBS is classified into:
• IBS-D: diarrhoea-predominant IBS
• IBS-C: constipation-predominant IBS
• IBS-M: mixed IBS. Alternating diarrhoea and constipation
In some people, particularly women, bloating may be the only symptom of IBS. This is caused by the muscles contracting or spasming suddenly and strongly, causing painful abdominal cramps and gas to become trapped in the intestine.
• Menopause is the permanent cessation of periods.
• Symptoms vary significantly between women, so treatment is not always needed. Lifestyle changes can help relieve mild symptoms.
• Menopause hormonal therapy (MHT) may be considered in some women, particularly those aged less than 60, whose quality of life is affected.
Not all women have significant symptoms around the time of menopause. Many who seek advice may just require information about possible symptoms and the expected duration of the transition.
Talk in a quiet part of the pharmacy and run through the Refer to a Pharmacist checklist and refer any women with concerns. Advise all women to talk to their doctor about their symptoms at their next visit as other medical conditions can cause heavier periods or an absence of periods (amenorrhoea). Bleeding that occurs after periods have been absent for a year warrants further medical investigation.
Offer some lifestyle advice and information about different products available for symptom relief (such as hot flushes and vaginal dryness) if requested.
Treatment for perimenopausal symptoms is not routinely offered or needed because individual symptoms vary markedly.
Several herbs may help with menopausal symptoms such as hot flushes, mood changes, or poor sleep. Some evidence of an effect has been found for black cohosh, Red clover, flaxseed, pycnogenol, soy, and St John’s wort at relieving some of the symptoms of perimenopause such as hot flushes, mood disturbances, excessive sweating, and vaginal dryness.
Many other complementary therapies such as dong quai, Chaste tree, evening primrose oil, panax ginseng, or wild yam have less convincing
• Women aged less than 40 experiencing menopausal-like symptoms.
• Women taking MHT who are experiencing unusual uterine bleeding.
• Women with irregular periods but without other typical menopausal symptoms.
• Women with particularly severe symptoms that are affecting their quality of life.

evidence, although some women may obtain benefits.
Refer any women with medical conditions or those taking medications to a pharmacist, because some medications can interact with herbal remedies (for example, chaste tree with hormonal treatments; dong quai with warfarin; red clover with tamoxifen). See the Herbal Supplements Interactions chapter, in this Handbook for common herb/drug interactions.
Prescription medicines, including menopause hormonal therapy (MHT) and non-hormonal prescription medicines (eg, SSRIs, venlafaxine, clonidine, gabapentin) may be considered for women who would benefit from these treatments, after a thorough discussion of the pros and cons.
Almost 50% of women develop symptoms such as vaginal dryness, irritation, or pain during sexual
Category Examples Comments
Vaginal dryness [GENERAL SALE]
eg, Aci-Jel Restore*, Anime Lubricant, Replens
Vaginal Moisturiser, Vagisil Prohydrate
Supplements [SUPPLEMENT]
eg, Harmony Menopause, Clinicians Menopause Balance, Nutralife Meno-life, Promensil, Remifemin, Premeno Duo eg, black cohosh, Chaste tree, DHEA, Dong quai, evening primrose oil, flaxseed, pycnogenol, red clover, soy, St John’s wort, wild yam
intercourse within a few years of menopause – caused by a thinning and drying out of the vaginal tissue (called vaginal atrophy) in response to reduced circulating levels of oestrogen.
Vaginal moisturisers reduce vaginal dryness by adhering to the surface of the vagina, creating a moist film over vaginal tissue and restoring vaginal pH. Some products will last up to three days. Vaginal lubricants are clear, thin, odourless liquids with a slippery feel that resemble natural vaginal secretions and can make sexual intercourse more comfortable.
Topical oestrogen creams and rings may also be prescribed by a doctor for vaginal atrophy.
Menopause is defined as the permanent cessation of periods and it is a fact of life for all women who were born with a uterus (womb). However, how easily they go through the transition varies significantly, with
Contain various ingredients including angelica polymorpha (Dong Quai), cimicifuga racemosa (black cohosh), peony, shatavari, trifolium pretense (red clover extract), vitex agnus-castus (Chaste tree) to help relieve symptoms of menopause such as night sweats and hot flushes. There is some evidence for the effectiveness of other supplements (ie, EPA, flaxseed, soy, St John’s wort) for relieving menopausal symptoms.
some women experiencing only mild, if any symptoms, whereas others experience significant effects that can interfere with their daily lives for several years.
The purpose of a woman’s menstrual cycle is to prepare her body for pregnancy, and usually, a single egg is released each month during her fertile years. Menopause occurs naturally when a woman’s ovaries run out of functioning eggs.
Menopause is a retrospective diagnosis. This means that a woman’s periods must have been absent for a year before she has technically gone through menopause. However, many people use the term to describe all the years a woman has symptoms associated with menopause. This is more correctly called “perimenopause”. For most women, complete cessation of periods occurs between the age of 45 and 55, with an average age of 52. Menopause that occurs in a woman before the age of 40 is called early menopause.
Menopause can also be brought on artificially, for example, in women who have their ovaries removed or if their ovaries are destroyed by cancer or radiation treatments. Symptoms tend to start abruptly in these women and are usually more severe than if they had had to go through the change naturally.
The five most common symptoms that women may ask about are:
• period changes
• hot flushes
• mood changes
• sleep disturbances
• vaginal dryness.
In addition, a woman’s risk of osteoporosis (bone thinning) and cardiovascular disease (heart disease, heart attack, or stroke) increases once menopause has occurred.
Often the first sign that a woman is going through perimenopause is a gradual or abrupt change in her menstrual cycle. Her periods may increase or decrease in frequency, and bleeding may be lighter or heavier than normal.
But not all menstruation-related changes are due to impending menopause and women with excessively heavy or abnormal bleeding should be referred to a doctor. All postmenopausal women who experience vaginal bleeding should be referred to a doctor.
Hot flushes (also called hot flashes in some countries) are experienced by more than 60% of women. A hot flush is a momentary sensation of heat that may be accompanied by a red, flushed face and sweating. Night sweats are also
• Dress in light clothing and in layers to help with hot flushes.
• Eat a balanced, healthy diet.
• Be conscious of your weight and be aware that some women are prone to weight gain after menopause. Begin weight control (see Weight Loss) before it becomes a problem.
• Falling oestrogen levels shift fat storage from your hips to your waist (truncal obesity) which increases your risk of cardiovascular disease.
• Eating frequent, smaller meals throughout the day may satisfy appetite better than eating three large meals.
• Partake in regular, weight-bearing exercise (ie, walking, dancing, tennis, aerobics, golf) on most days of the week. Exercise is also beneficial for reducing the
common and may interfere with sleep. Other physical and psychological symptoms include:
• aching legs/cramps, joint and bone pain
• body hair growth or itchy skin
• breast tenderness and low sex drive
• fluid retention (eg, swollen ankles, weight gain, bloating)
• forgetfulness, increased anxiety and stress, irritability and mood swings
• migraines/headaches or vertigo
• more noticeable skin ageing (ie, wrinkles)
• vaginal dryness (can result in painful intercourse).
Urinary tract infections (see Cystitis) and incontinence (see Urinary Incontinence) are also more common due to thinning of the vaginal and bladder walls.
risk of cardiovascular disease, preventing osteoporosis, and aiding sleep.
• Avoid foods which exacerbate menopausal symptoms or decrease sleep (eg, caffeine, fatty or spicy foods and alcohol).
• Practise pelvic floor strengthening exercises (Kegel exercises) to help with urinary incontinence.
• Use vaginal lubricants or moisturisers to help with vaginal dryness.
• Some women find yoga, massage, acupuncture or meditation beneficial.
• Stop smoking (see Smoking Cessation).
• Women going through premature menopause may like to consider joining a local support group (see www. earlymenopause.org.nz).
• Provide easily accessible information about conditions common to men.
• Sildenafil may be sold for erectile dysfunction by appropriately trained pharmacists to men aged 35 to 70 meeting strict criteria.
• Heart disease is the number one killer of men.
Men, on average, visit a pharmacy four times a year, compared with 18 for women. A man’s long working hours may be a factor in this statistic, but only a minor hindrance since most pharmacies in New Zealand have long opening hours and are open at least one day in the weekend. More likely, it’s a combination of an innate reluctance by many men to trouble anybody (doctor or pharmacist) unless they have a serious problem. Which means that pharmacies should be proactive in promoting men’s health and take every opportunity they can to enquire after a man’s health whenever appropriate. Ensuring there is a large “Men’s section” in your pharmacy is a good start. This section should include all the usual men’s facial and body products, but also other items such as bowel cancer screening kits, condoms, herbal supplements for increased libido, minoxidil for hair loss, weight loss products, and information about the procedure for obtaining sildenafil from a pharmacist.
Research has shown men like information they can take away and read, and your “Men’s section” could include well-written
Category Examples
Male condoms (latex) eg, Durex range, Gold Knight range, Lifestyle range
• Men wanting information about erectile dysfunction treatments.
• Men who have had unprotected sex and are worried about exposure to sexually transmittable infections.
• Men who identify they have a problem with alcohol or drugs and request further help.
• Men with symptoms that require further investigations (such as a chest pain, a lump in the testes, problems urinating, or shortness of breath).
• Men with obvious risk factors for cardiovascular disease who are not under the care of a doctor.
• Men worried about their mood or who identify aggressive tendencies.
brochures that discuss cardiovascular disease, depression and anxiety, diabetes, erectile dysfunction, high cholesterol, and common cancers in men (such as colorectal, prostate, and testicular). Information about screening for testicular cancer and lifestyle advice, such as how to stop smoking, lose weight, or reduce alcohol intake, can also be provided here.
Consider actively promoting your pharmacy by sponsoring a local rugby or soccer team or hosting a bloke’s night during Men’s Health month in June. For more information on men’s health see menshealthnz.org.nz
It’s no secret that men, in general, are less likely than women to go to the doctor or talk about their health in general. They are also three times more likely to attempt intentional suicide, with rates in Māori men almost twice those of non-Māori men.
In equality studies, men are at a disadvantage compared to women with regards to health and education, even though they are overrepresented
Male condoms (nonlatex) eg, polyisoprene (Durex Real Feel, Ansell Lifestyles Skyn Non-latex) eg, polyurethane (Trojan Supra)
Lubricants eg, Anime Lubricant, Sylk Natural, KY Jelly
Fertility testing eg, SwimCount Sperm Quality Test
Comments
in areas such as leadership roles and earnings.
Most cancers in men are slow growing, so symptoms may slowly worsen over time and be dismissed as something that is usual for them or attributable to another illness (for example, “I’ve always had a crook gut”, “I’ve had piles for the last two years”).
Lung cancer is the leading cause of cancerrelated death in men, mostly because it is found at a late stage. It is more common in people with a history of smoking but can still occur in nonsmokers. Symptoms include a long-standing, persistent cough, shortness of breath, hoarseness, and weight loss.
Bowel cancer can cause bleeding from the rectum or blood mixed into the stool, changes in bowel habits (constipation for a period followed by diarrhoea), or unexplained weight changes, and is more likely to affect people over the age of 50. In New Zealand, free bowel cancer screening is available for people aged 60 to 74 years.
Prostate cancer affects one in seven men, but
Home-made lubricants, such as vaseline or cooking oils, may damage latex condoms. Condoms routinely no longer contain spermicide. Some vaginal antifungal creams can damage condoms and diaphragms –refer to the pharmacist if the customer or their partner is using this type of product. Some brands are fully subsidised on a prescription (144 condoms per script).
Non-latex condoms are suitable for people with latex allergies and are safe to use with both water and oil-based lubricants.
Reduce friction during sexual intercourse enhancing pleasure and reducing the risk of condom damage. Use only water or silicone-based lubricants with latex condoms.
Measures sperm quality within 30 minutes. Abnormal results need to be further analysed by a professional. Erectile dysfunction treatments [Prescription medicine except when supplied by a pharmacist who has successfully completed an approved training programme in the treatment of ED in males aged 35–70]
eg, sildenafil (Silvasta, Vedafil)
Natural products eg, dehydroepiandrosterone (DHEA), Chaste tree, ginkgo, Maca, omega-3 and -6 fatty acids, Panax ginseng, Saw palmetto,
Pharmacists must follow privacy requirements, use the approved assessment form, provide approved written information and conduct a full screening each year. Sildenafil requires sexual stimulation to be effective and should be taken 60 minutes before intercourse. Tablets should not be taken with food or excessive amounts of alcohol.
May help improve blood flow and sexual function but evidence is limited. Note: Yohimbe (yohimbine) is a prescription medicine in New Zealand because of its potentially lethal side effects.
most cases are slow growing. Symptoms are similar to benign prostatic hyperplasia (BPH), which is an age-related prostate enlargement, and include difficulty starting and stopping urination, urine leakage and increased frequency of urination. Prostate cancer screening is not routinely offered in NZ unless a man has symptoms or requests a screening. This is because an elevated PSA (prostate specific antigen) test does not necessarily mean a man has prostate cancer, and even if he does, many prostate cancers do not initially require treatment.
Symptoms of testicular cancer include a peasized lump or area of hardness in the testicles which may or may not be accompanied by swelling or a change in shape. It is the most common type of cancer in men aged 15 to 39. Testicular cancer is very treatable if caught early.
Cardiovascular disease is a term referring to a range of different heart and blood vesselrelated conditions such as coronary artery disease (a narrowing and hardening of the arteries), high blood pressure, heart failure, and stroke.
A heart attack occurs when blood flow to a region of the heart muscle is blocked or significantly slowed. Symptoms may come on suddenly or slowly and may be mistaken for indigestion. Men usually describe chest pain or a feeling of heaviness or pressure in the upper part of their torso, neck or arms.
A cardiac arrest is more sudden, and a person will usually collapse and be unresponsive because the heart has stopped beating or is beating abnormally. A defibrillator is needed to shock the heart back into rhythm.
There is an association between cardiovascular
disease and erectile dysfunction which is why pharmacists selling sildenafil must ensure that a man’s blood pressure is within the required range before approving supply. All Māori men should have a heart health check starting at age 30, or from age 45 if non-Māori. See Heart Health for more information.
Condoms protect against pregnancy and sexually transmitted infections. Three different types are available: latex, polyurethane, and polyisoprene. See Sexual Health for more information.
Erectile dysfunction (ED) refers to an inability to get or maintain an erection firm enough to have sexual intercourse. ED affects more than 50% of men aged 40 to 70 and there is a clear association between ED and cardiovascular disease. Pharmacists who have completed accredited training in ED can sell sildenafil to men aged 35 to 70 who meet certain criteria. These are quite strict, so not every man is eligible. This is to ensure that men needing further
investigations or screening, such as that for heart disease or diabetes, are seen by their doctor.
Other prescription ED treatments, such as tadalafil, vardenafil, or injectable preparations may be more appropriate. Herbal preparations such as horny goat weed, Panax ginseng, or Rhodiola Rosea may help ED; however, there is little evidence supporting their use.
Depression and anxiety are considered just as common among men as women; men are just less likely to ask for help. Men with depression are more likely to talk about their physical symptoms, rather than their emotional ones. They might complain about constant headaches or pain, appetite or weight changes, digestive disorders, sleeping difficulties or a lack of interest in sex.
They may turn to drugs or alcohol as a way of coping or socially isolate themselves from others. Let them know that sleep/digestive issues/constant pain can be related to mood and prompt them to see their doctor.
• Condoms should always be used to protect against unintended pregnancies and sexually transmitted infections.
• Condoms should be stored away from heat and sunlight (ie, not in a car glove box), and should not be used after their expiry date.
• Latex condoms should only be used with water-based lubricants to decrease the risk of breakage.
• Men should check their testicles every month for pea-shaped areas of hardness (and see a doctor if any are found).
• Men should see a doctor for a cardiovascular risk assessment at the recommended age.
• Migraines are a type of severe headache.
• Refer any customers with RED FLAGS to a doctor.
• Pharmacists can sell 5-HT agonists and antiemetics to certain customers with migraines.
Ask your customer to describe their headache and listen to their response.
A headache is more likely to be a migraine if nausea and/or vomiting are present in combination with two of the following three symptoms:
• sensitivity to light
• sensitivity to loud sounds
• sensitivity to smells.
If you are not clear about what type of headache they have, the Table: Common Types of Headache (see Headache) may help. Some people may also suffer from combination headaches (such as tension headaches in addition to migraines).
If they have any RED FLAGS (see Text box, opposite page) or if their symptoms are typical of migraine, but they have never had a formal diagnosis, refer them to a doctor. Run through the Refer to a Pharmacist checklist and refer other customers with concerns to a pharmacist.
Category Examples
• Anybody who has not had the diagnosis of migraine confirmed by a doctor.
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People who take medicines, including herbal/complementary medications.
• Children or adolescents aged less than 18 or the elderly.
• Customers wishing to purchase a serotonin receptor agonist or whose symptoms have persisted despite taking over-the-counter analgesics.
• Customers reporting frequent migraines (more than two a month) or who request bulk packets of analgesics.
• Customers complaining of pain near an eye.
• People with allergies to medicines.
Research has shown that less than 50% of people who suffer from migraine are happy with their current treatment. This means that many could be self-medicating with overthe-counter pain relievers and may benefit from further advice. This advice could include information about available alternative treatments, non-pharmacological treatments, and the risk of regular analgesic use.
Always refer customers with Red Flags (see text box opposite page) or those with concerns identified by the Refer to a Pharmacist checklist. Migraine treatments can be divided into those that relieve the pain of migraine
Simple analgesics [GENERAL SALE] eg, paracetamol (Panadol range, Paracare)
Non-steroidal anti-inflammatory drugs (NSAIDs)
[GENERAL SALE] eg, aspirin (Aspro, Disprin range), ibuprofen up to 25s (Advil liquid capsules, Nurofen Migraine Pain, Nurofen Zavance)
[PHARMACY ONLY MEDICINE] eg, diclofenac (Voltaren Rapid 12.5), ibuprofen >25s (Advil liquid capsules, Nurofen range), naproxen (Sonaflam) [PHARMACIST ONLY] eg, diclofenac (Voltaren Rapid 25)
Combination analgesics [GENERAL SALE] eg, ibuprofen + paracetamol (Maxigesic*[16], Nuromol [12], Nuromol Dual Action Pain Relief* [<20])
[PHARMACY ONLY MEDICINE] eg, ibuprofen + paracetamol (Maxigesic* [50, 100], Nuromol [24])
[PRESCRIPTION] eg, paracetamol + codeine (Panadeine, Panadeine Extra), ibuprofen + codeine (Ibucode Plus, Nurofen Plus), paracetamol + doxylamine + codeine (Mersyndol)
Antiemetics
Serotonin (5-HT) receptor agonists
[PHARMACIST ONLY MEDICINE] eg, prochlorperazine (Antinaus)
[PRESCRIPTION MEDICINE]– except when sold in an approved pack of 2 oral dosage forms by a pharmacist eg, sumatriptan 50mg (Sumagran Active)
Natural / herbal products / supplements 5-HTP, caffeine, butterbur, coenzyme Q10, feverfew, magnesium, riboflavin (Clinicians MigraDol)
Comments
(treatment medicines) and those that aim to reduce the frequency or severity of migraine attacks (preventive medicines).
OTC pain relievers, such as paracetamol, aspirin, ibuprofen, or diclofenac can reduce the intensity of migraine pain, but are not usually enough to totally relieve the pain of severe migraine in most people. Because absorption from the stomach is reduced in people with migraine, quickly dissolving or dispersible preparations are preferred.
Triptans (eg, sumatriptan or rizatriptan) reduce pain severity in over 60% of people with migraine and totally relieve symptoms in 32%. They are prescription medicines, but
Generally effective at relieving mild-type pain. May not be strong enough as the sole analgesic for migraine. Few adverse effects.
Ibuprofen is the NSAID least likely to cause stomach irritation, aspirin is the most. NSAIDs may not be suitable for people on certain other medications or with some medical conditions (eg, asthma, kidney disease). Advise customers to stop taking if stomach upsets, increased bruising or prolonged bleeding occur. Aspirin is not recommended for adolescents or children under 16 years old because of the risk of Reye’s syndrome. See also Reference Section, OTC Medicines – Precautions
Try paracetamol or NSAIDs first.
Codeine-containing preparations were reclassified in November 2020 to PRESCRIPTION ONLY.
Mersyndol contains doxylamine which can cause drowsiness. See also Headache
Can be sold by a pharmacist in quantities of 10 or fewer tablets for nausea associated with migraine.
Proven effectiveness in migraine. Small packs may be sold by a pharmacist for adults with a stable, well-established pattern of migraine symptoms for relief of acute attacks. Follow packet instructions strictly.
Caffeine in combination with analgesics is effective at treating migraine. Other supplements may be more effective for preventing migraines when taken daily for at least three months.
pharmacists can sell two oral dosage forms to customers with a stable, well-established pattern of migraines. Prochlorperazine may also be sold by a pharmacist to treat nausea.
Stronger analgesics and preventive medications are available from the doctor and customers with frequent migraines should be encouraged to talk with their doctor further.
Migraine is a complex condition that causes extremely incapacitating symptoms. For most people, the main symptom is severe, throbbing, recurring pain that usually occurs on one side of the head, although
Refer anybody with the following to a doctor:
• a first episode of migraine in a person aged over 50
• a headache that develops after a head injury or major trauma
• any headache that is severe right from the start (rather than gradually develops)
• concurrent body-wide symptoms such as a fever, high blood pressure, muscle aches, weight loss or scalp tenderness
• describing the migraine as “The worst headache of my life” (urgent referral)
• headaches brought on by lying down, coughing, sneezing, bending or exertion
• headaches that have worsened over several months
• seizures, confusion, changes in consciousness or difficulty waking.
sometimes both sides of the head will be affected. The pain is usually accompanied by one or more of the following:
• extreme sensitivity to sound, light, touch, or smell
• nausea which may to progress to vomiting in one-third
• sleepiness, yawning, or a lack of energy
• visual disturbances, such as blurred vision, flashes of light, zigzag lines or blind spots
• weakness, tingling or numbness in the limbs or the face.
Approximately 25% of people with migraine experience an aura – which is a sensory disturbance that may be described as a funny smell, taste, feeling or visual effect that occurs about an hour before the pain of the migraine sets in.
Migraine affects one in 10 New Zealanders and three times as many women as men. It tends to run in families with 90% of sufferers having a family member with migraine.
The cause of migraine is not fully understood but experts suggest changes in the brainstem, an
• Rest in a quiet, darkened room. Reusable heat pads may provide relief.
• Keep a diary of when the migraines occur, paying particular attention to occurrence with food, stress or other events (eg, menstrual cycle).
• Analgesics or serotonin agonists, with or without antiemetics, should be taken at the first sign of an attack (once the attack
overreaction of the trigeminal nerve, or chemical imbalances in the brain might be involved.
Genetics and environmental factors play a major role as well.
Triggers are any external factor that tends to bring on a migraine within the preceding 6 or 8 hours. These are often unique to each individual and encourage your customer to keep a diary that records daily events, including food intake, to help identify triggers.
Common triggers include:
• caffeine, either too much or suddenly stopping
• changes in daily routines
• dehydration
• environmental changes, such as changes in altitude, weather, artificial lighting, loud noises
• food (such as bananas, beans, chocolate, citrus, corn, yoghurt, soft cheeses), red wine, or food additives (such as monosodium glutamate)
• hormonal changes (eg, menstruation or menopause)
• long periods in front of the computer
• missing meals
• sleep, too much or too little
• stress.
has started gastric motility is slowed, which decreases absorption of the medicine).
• Be careful not to overuse analgesics since medication overuse headache can coexist with migraine (see Headache).
• Drink plenty of water, maintain regular exercise and a healthy diet.
• Consider acupuncture, hypnosis and relaxation training.
• Look out for symptoms, such as swelling, restricted movement, or severe pain that suggest a more serious injury.
• Generalised muscle pain suggests a wholebody illness such as the flu or fibromyalgia.
• Typical treatment options for muscle pain associated with unaccustomed or overuse include rest, oral analgesics, topical rubs, and gentle stretching.
Try to establish the cause and ask about the severity of your customer’s muscle pain or tightness to help decide whether further investigation is necessary or to refer them to the pharmacist.
Symptoms of muscle pain caused by unaccustomed or overuse of a muscle are typically confined to specific groups of muscles, or a matching pair of muscles. The pain usually
• People with other health conditions or who are immunosuppressed, pregnant or breastfeeding.
• People who take medicines, including herbal/complementary medications (particularly medicines for high cholesterol).
• Children aged less than 12 or the elderly.
• People who have experienced a serious loss of movement or mobility.
• People with an excessive or abnormal range of movement in any joint (this may suggest major ligament disruption).
• With injuries that swelled almost immediately or that are severely painful.
• People who are unable to weight bear, or if a fracture is suspected.
• With pain that has persisted for longer than three to four days.
• With muscular pain with no identifiable cause.
• With allergies to medicines.
peaks within 72 hours before subsiding.
More severe muscle pain accompanied by swelling and restricted movement may indicate muscle, tendon, or ligament damage. Refer to a pharmacist (see also Strains and Sprains).
Oral analgesics or topical rubs are useful
Category Examples Comments
Topical non-steroidal antiinflammatory agents (NSAIDs) [GENERAL SALE] eg, ibuprofen (Nurofen Duralast patch*, Nurofen Gel), diclofenac (Voltaren Emulgel)
Oral non-steroidal antiinflammatory agents (NSAIDs) [GENERAL SALE] eg, ibuprofen (<25s) (Advil liquid capsules, Advil tablets, Nurofen, Nurofen Quickzorb*, Nurofen Zavance Tablets and Caplets*, Nurofen Zavance Liquid Capsules*), ibuprofen + paracetamol (Maxigesic [16], Nuromol Dual Action Pain Relief [<20]*) [PHARMACY ONLY MEDICINE] eg, diclofenac 12.5mg (Voltaren Rapid 12.5), ibuprofen >25s (Advil capsules/tablets, Nurofen, Nurofen Zavance Tablets and Caplets*, Nurofen Zavance Liquid Capsules*), naproxen (Sonaflam), ibuprofen + paracetamol (Maxigesic [50, 100], Nuromol Dual Action Pain Relief [>20]*) [PHARMACIST ONLY MEDICINE] eg, diclofenac 25mg (Voltaren Rapid 25), [PRESCRIPTION] eg, ibuprofen + codeine (Nurofen Plus) paracetamol + codeine (Panadeine)
Rubefacients (“heat” rubs) [GENERAL SALE] eg, Metsal Cream, Tiger Balm Oil, Tiger Balm Red Strength ointment, Tiger Balm White Regular Strength ointment
Agents that reduce bruising [GENERAL SALE] eg, Arnica cream eg, heparinoids (eg, Hirudoid)
Simple analgesics eg, paracetamol (Panadol range, Panadol Extra, Paracare)
Other topical products [GENERAL SALE] eg, Anti-Flamme range, Badger Sore Muscle Rub, Dencorub, Flexagil, Percutane, Rehab Fix, Zo-Rub
Muscle cramps [GENERAL SALE] eg, Crampeze Night Cramps, Muscle Magnesium
Natural / herbal products / supplements Capsaicin, camphor, comfrey, willow bark, acupuncture, chiropractic manipulation, yoga, magnesium, zinc
Reduce inflammation and pain. Apply to the skin overlying the affected area but do not apply to broken skin or near the eyes or mucous membranes. Wash hands after applying. Do not use under sealed dressings. Patches should not be used on children <16. May, rarely, cause the same adverse effects as oral NSAIDs.
These treat the body’s inflammatory reaction to injury and reduce pain, but may delay tissue healing if used for longer than three days after the injury. Consult a doctor for further advice. Ibuprofen is the NSAID least likely to cause stomach irritation.
Advise customers to stop taking if stomach upsets, increased bruising or prolonged bleeding occur.
Codeine-containing preparations were reclassified in November 2020 to PRESCRIPTION ONLY.
Opens blood vessels and creates a sense of warmth, which masks the sensation of pain. Good at relieving localised muscle aches or pains. Do not apply to broken skin or near the eyes or mucous membranes. Wash hands after applying. Do not use under sealed dressings.
Arnica cream contains a mixture of arnica flower and root and several essential oils to help relieve bruising. Hirudoid contains enzymes that help disperse excess fluid in swollen areas. Both creams also reduce swelling. Arnica also helps relieve pain.
May be beneficial as a first-line treatment for muscle pain. Suitable for people with contraindications to NSAIDs.
Rubbing these preparations onto the skin helps stimulate blood flow and create a feeling of warmth. Products contain ingredients such as arnica, cayenne pepper, chilli extracts, comfrey, ginger, menthol, and peppermint oil to relieve bruising and soothe sore muscles and stretched ligaments.
Magnesium may help relieve cramps and with tired, aching and restless legs.
Capsicum, camphor, comfrey, and willow bark have pain-relieving properties. Oral magnesium may be effective at relieving restless leg syndrome in some people. Oral zinc may help relieve muscle cramps in zinc-deficient people.
Products with an asterisk have a detailed listing in the Muscular Aches, Pains, and Tightness section of OTC Products.

• All plaque should be removed from teeth every day.
• Children should begin flossing as soon as two teeth touch.
Inspect the mouth if possible and safe
Category
Mouth ulcer treatments
• People taking medications that may cause mouth problems (such as inhaled/oral corticosteroids), who are immunosuppressed, or with health conditions such as diabetes.
• Children aged less than 10 years.
• Mouth conditions that have been present for longer than seven days or persisted despite treatment.
to do so, or ask the customer for a detailed description of the problem. Most oral health conditions require further input from a pharmacist or dentist (as detailed in each subsection below) and will need to be referred.
Treatment varies depending on the oral health condition (see under each individual subtopic).
Oral health conditions include bad breath, baby teething problems (see Baby Care), dry mouth, fungal infections (such as oral thrush), gingivitis, periodontal disease, mouth ulcers, sore throat (see Sore Throat), and tooth decay (see Dental Pain).
Bad breath – also called halitosis – can occur with abscesses, gingivitis, indigestion or reflux,
• Mouth sores or lumps that are large, bleed, painful, or swollen.
• Mouth ulcers that are reasonably large, irregularly shaped, or not painful.
• People who smoke.
• People with oral thrush.
• People with other symptoms (eg, fever).
• People with allergies to topical products.
tooth decay, after eating spicy foods or garlic, and when saliva production is low.
Check your customer’s teeth-cleaning regimen and consider chlorhexidine mouthwashes. Refer to a dentist or doctor if dental decay, gum disease, or a more serious underlying problem is suspected.
Dry mouth (xerostomia) is due to a lack of saliva. Medications, radiation therapy, dehydration and poorly controlled diabetes are some of the more common causes. If the cause cannot be corrected, saliva substitutes may provide some relief.
This usually presents as creamy-white, soft, elevated patches on the tongue or oral palate that can be removed to reveal inflamed mucosa underneath. Pain and soreness are also often present. Commonly seen in babies, oral thrush is usually caused by the yeast Candida albicans Although it is unusual for adults to get oral
Oral thrush
Examples
Topical analgesics/anaesthetics
[GENERAL SALE] eg, Bonjela Mouth Ulcer Gel, Orased Jel [PHARMACY ONLY MEDICINE] eg, Difflam Mouth Gel, Difflam-C Anti-Inflammatory Antiseptic, Frador, Medijel
Topical corticosteroids for oral use
[PHARMACIST ONLY MEDICINE] eg, Kenalog in Orabase, Oracort Dental Paste
Chemical cauteriser
[GENERAL SALE] eg, Hybenx (Oralmedic)
[PHARMACIST ONLY MEDICINE] eg, miconazole (Daktarin Oral Gel, Decozol Oral Gel), Nystatin (Nilstat Oral Drops)
Mouthwashes for gingivitis eg, Cepacol, Cepacaine, Chlorhexidine 0.2%, Kiwiherb Manuka, Savacol
Dry mouth [GENERAL SALE] eg, Aquae Dry Mouth Spray, Biotene range, Oralube Saliva Substitute, Oral Seven range, Xerostom Range
Products for maintaining or restoring good oral and throat health
[GENERAL SALE] eg, Air-Lift
[SUPPLEMENT] eg, BLIS K12 range, BLIS M18 range, Comvita Oral Spray, Radiance ManukaGuard Honey Lozenges
Oral hygiene eg, CareDent range, Interdental brushes, MouthWatchers Anti-bacterial Toothbrushes, Piksters Interdental brushes, TePe Interdental brushes, Waterpik range
Comments
Contain a topical oral pain reliever or anaesthetic (such as choline salicylate, lignocaine, aminacrine, or benzydamine) to relieve the localised pain associated with mouth ulcers.
Chlorbutol is a weak local anaesthetic with antibacterial and antifungal properties.
Forms a protective paste over the ulcer to speed healing. Apply after food. Dab onto ulcer and smooth over with saliva. Do not rub in.
Single-use treatment that extracts water from the damaged tissue and forms a seal over it, quickly eliminating mouth ulcer pain and aiding healing.
Hold dose in the mouth for as long as possible before swallowing. Avoid food and drink for half an hour before and one hour after taking a dose. Do not use oral gels in babies under six months or in people with poor swallowing.
Products containing chlorhexidine appear the most effective at reducing plaque and gingivitis, but prolonged use may stain teeth and gums brown.
Help to relieve dry mouth (xerostomia) and increase unstimulated salivary flow. Use as often as needed.
Air Lift uses oils to eliminate bad breath caused by foods or tobacco. BLIS products restore the balance of naturally occurring bacteria. Natural lozenges containing honey may help to maintain good throat health.
Brush teeth twice a day to remove plaque and keep gums healthy. Water jet systems remove food debris and bacteria from where brushing and flossing can’t reach. Interdental brushes help remove plaque and food from between teeth and are an alternative to dental floss. Daily attention to oral hygiene can help reduce tooth decay.
thrush, it may occur in people with asthma who fail to rinse their mouths after using steroid inhalers. Immunosuppressed people or people who have a dry mouth, ill-fitting dentures, or who have had recent antibiotic therapy, are also more at risk. Anybody presenting with oral thrush should be referred to the pharmacist. Treatment is with oral antifungal mouth gels or liquids.
Gum disease (also called periodontal disease) is an infection of the gums that hold teeth in place. It is usually caused by poor brushing or flossing habits that allow plaque to build up on teeth and harden into tartar. Healthy gums should be pink and firm and shouldn’t bleed when brushed.
Red, swollen, or bleeding gums; bad breath that won’t go away; or pain when chewing are common signs of early gum disease, called gingivitis. Receding gums, longer appearing or loose teeth, or gum abscesses can occur if gingivitis progresses to periodontitis and bone anchoring the teeth in the jaw can be lost. Gum disease has also been linked with cardiovascular disease, poor pregnancy outcomes, and even dementia.
People who smoke are at the highest risk for gum disease because smoking encourages plaque production and poorer oxygen supply to the gums which makes them less likely to heal. Other risk factors include diabetes, hormonal changes in women (such as puberty, menstruation, pregnancy, or menopause), medications that reduce saliva flow, medical conditions such as cancer or HIV, and genetic susceptibility.
If plaque has been allowed to build up on teeth and it has hardened to tartar, then no amount
of brushing or flossing will remove it; and you should refer these people for professional cleaning by a dentist or dental hygienist.
Providing good oral health information is important if you notice anybody in your pharmacy with early signs of gum disease or who complains of bleeding gums. Gum disease is very common, and most people experience it, but with good oral care, it can be slowed to a rate that most people keep their teeth for life (see Advice for Customers: Good Oral Hygiene)
Mouth ulcers are painful sores that appear inside the mouth. They are usually red, grey, white, or yellow and are different from cold sores which appear on the outside of the lips.
Mouth ulcers can be caused by trauma to the area, such as by biting the cheek or tongue, sharp braces, or poorly fitting dentures. Traumatic ulcers usually go away once the problem is removed, but mouth ulcer treatments help relieve pain.
Mouth ulcers that keep on coming back are called recurrent aphthous stomatitis. These are common and may exist as a cluster of four or six small ulcers inside the cheeks, on the inside of the lips, on the tongue or gums, or rarely, on the roof of the mouth. Sometimes they will appear as one large painful ulcer. They have been linked to stress, nutritional deficiencies, hormonal changes, and certain medications. Other less common causes include infections, such as herpes simplex, anaemia, or Bechet’s disease.
Cancer of the mouth can first appear as a mouth ulcer and symptoms usually include a single ulcer located on or under the tongue, often in a person who smokes or drinks heavily.
Modify or change any contributing cause,
• Use a soft toothbrush or preferably an electric toothbrush and brush teeth for two minutes twice a day.
• Brush gently around the back and front of the teeth, including where the teeth meet the gums.
• Change your toothbrush every three months.
• Spit out after toothbrushing, and don’t rinse. A small amount of fluoride left around the teeth protects them.
• Floss or use an interdental brush daily (minimum three times/week).
• Fluoride mouth rinses may be used in people older than six at high risk of dental caries.
• Eat a healthy diet and limit sugar intake.
• Avoid sipping sweet drinks for prolonged periods and discourage snacking and grazing
• Visit your dentist regularly (every six to 12 months) for check-ups.
• Talk to your dentist about taking fluoride supplements if your water supply is not fluoridated.
such as resizing poorly fitting dentures or using wax on protruding braces. Apply a topical product to reduce pain and aid healing.
Before applying any product, the mouth ulcer area should be dried as best as possible using a cotton bud.
• Osteoarthritis occurs when the cartilage that covers the end of each bone in a joint starts to break down and wear away, leaving the ends of the bones unprotected.
• It affects almost 50% of people over 60 and almost 100% of those over 80.
• Symptoms usually start in middle age and include morning stiffness in a joint.
When a customer says they have “arthritis”, try to confirm that they are talking about osteoarthritis rather than rheumatoid arthritis or another form of arthritis. Osteoarthritis is common, and covered in this chapter. Rheumatoid arthritis is a chronic, inflammatory autoimmune condition that affects multiple joints and organs and is treated by a doctor, and is not covered here.
If pain is the main complaint, then paracetamol is preferred and should be tried first. Heat rubs and other topical applications may also help. Refer anybody wishing to take a non-steroidal anti-inflammatory drug (NSAID) long-term to a pharmacist, or who answers “yes” to any of the Refer to a Pharmacist questions.
Category Examples
Simple analgesics (pain relievers)
Oral non-steroidal anti-inflammatory agents (NSAIDs)
• People with other health conditions (eg, heart or lung problems, diabetes) or who are pregnant or breastfeeding.
• People who take medicines, including herbal/complementary medications.
• If there is any creaking or a cracking sensation with movement.
• Joint pain that was caused by trauma or which started suddenly.
• Joint pain associated with back pain.
• Pain that is severe, burning or interfering with movement.
• People under 40 or older than 80.
• With joints that feel unstable or like they are about to give way.
• With joints that look red or swollen or if the person also feels unwell.
• People with allergies to medicines.
Treatment aims to control pain, maintain physical activity and mobility, and limit further injury. Although it cannot reverse the changes that have already taken place in the joints, analgesics can help relieve pain and make it easier for people to mobilise.
Always encourage customers with new-onset osteoarthritis to seek medical advice early.
Osteoarthritis is the most common form of arthritis, affecting almost 50% of all
[GENERAL SALE] eg, paracetamol (Panadol, Paracare) [PHARMACIST ONLY] eg, sustained-release paracetamol (Panadol Osteo)
[GENERAL SALE] eg, ibuprofen <25s (Advil, Nurofen) [PHARMACY ONLY MEDICINE] eg, diclofenac 12.5mg (Voltaren Rapid 12.5), ibuprofen > 25s (Advil, Nurofen), naproxen (Sonaflam) [PHARMACIST ONLY MEDICINE] eg, diclofenac 25mg (Voltaren Rapid 25)
Combination analgesics [GENERAL SALE] eg, ibuprofen + paracetamol (Maxigesic*[16], Nuromol Dual Action Pain Relief [20]*) [PHARMACY ONLY MEDICINE] eg, ibuprofen + paracetamol (Maxigesic* [50, 100], Nuromol Dual Action Pain Relief [>20]*) [PRESCRIPTION] eg, ibuprofen + codeine (Ibucode Plus, Nurofen Plus) paracetamol + codeine (Panadeine, Panadeine Extra)
Topical non-steroidal anti-inflammatory agents (NSAIDs)
[GENERAL SALE] eg, ibuprofen (Nurofen Duralast patch, Nurofen Gel), diclofenac (Voltaren Emulgel, Voltaren Osteo Gel 12 Hourly)
Rubefacients (‘heat’ rubs) [GENERAL SALE] eg, Deep Heat range, Ice Gel, Tiger Balm range
Other topical applications [GENERAL SALE] eg, capsaicin (Zostrix HP), Anti-Flamme, Zostrix
Natural / herbal products / supplements Avocado-soybean unsaponifiables (ASU), boswellia, bromelain, chondroitin, fish oil, folic acid, glucosamine, green lipped mussel, turmeric
Comments
people over 60 and almost everybody over the age of 80. It is sometimes called “wear and tear” or degenerative arthritis.
Osteoarthritis occurs when the cartilage that covers the end of each bone in a joint starts to break down and wear away, leaving the ends of the bones unprotected.
This affects the gliding surface of the bones in the joint and as a result they become painful and difficult to move. After a while, the joint can lose its shape and the bone underneath thickens and grows out the sides, further reducing movement.
The large weight-bearing joints (knees, hips
Regular paracetamol, two tablets (1g) three or four times daily, is the first choice of treatment for mild-to-moderate osteoarthritis. The maximum recommended dosage of 4g/day may need to be reduced in the elderly.
Osteoarthritis is initially not normally an inflammatory condition but occasionally when there is inflammation an NSAID may provide added benefit to simple analgesia. Ibuprofen is the NSAID least likely to cause stomach irritation. NSAIDs may not be suitable for people on certain other medications or with some medical conditions (eg, asthma, kidney disease – see Refer to Pharmacist). Advise customer to stop taking if stomach upsets, increased bruising or prolonged bleeding occur. Stronger NSAIDs are available on prescription. See Reference Section, OTC Medicines – Precautions
Simple analgesics (eg, paracetamol) should be tried first.
Codeine-containing preparations were reclassified in November 2020 to PRESCRIPTION ONLY. NSAIDs may have gastric side effects, particularly when used long-term. See Reference Section, OTC Medicines – Precautions
These treat the body’s inflammatory reaction to injury and reduce pain. These are usually effective at relieving localised muscle aches or pains. Do not apply to broken skin or near the eyes or mucous membranes. Wash hands after applying. Do not use under sealed dressings. May, rarely, cause the same adverse effects as oral NSAIDs. Similar care and consideration before use is recommended.
Cause blood vessels in the treated area to open and create a sense of warmth, which masks the sensation of pain.
Capsaicin reduces levels of a chemical called substance P, which helps transmit pain impulses to the brain. May take up to four weeks for an effect. Burning or tingling may occur on application. Anti-Flamme helps to stimulate blood flow and has an anti-inflammatory and analgesic action.
ASUs help with pain and stiffness of osteoarthritis and may delay progression. Glucosamine appears effective. Evidence for chondroitin has not been consistent. Turmeric is reported to have a natural anti-inflammatory effect.

and spine) are most often affected, although osteoarthritis can also affect the ankles, neck, hands, lower back, base of the toes, and, as a result of injury or stress, the wrist, elbow, shoulder or jaw.
Osteoarthritis is caused by a combination of factors, such as ageing, genetic defects in joint cartilage, joint injury, joint stress, overuse through sports or certain occupations, and carrying excessive weight. There is no one specific cause.
Osteoarthritis is often very mild and some people may not realise they have it until an x-ray reveals joint changes. Symptoms tend to start in middle age and morning stiffness in a joint (lasting less than 30 minutes), or a deep ache in a joint which is hard to localise, may be the only initial sign.
Twinges of pain may be experienced in older people which tend to be relieved with rest and warmth. People with more pronounced
osteoarthritis are likely to have a more persistent pain that increases with use and decreases with rest. Other symptoms include:
• joint stiffness after resting the joint
• joint swelling caused by an increase in synovial fluid production
• bony growths (Heberden’s nodes) in finger joints
– these are more common in women over 40.
Symptoms become more severe as osteoarthritis progresses. Inflammation is more common in advanced disease and the joint may feel hot and inflamed. Osteoarthritis may come and go, and some people identify particular times when the pain is worse, eg, in damp, cold, or humid weather.
A properly designed exercise programme is considered the most effective nonpharmacological treatment for osteoarthritis. Exercise helps to keep joints moving and reduce overall pain, improve flexibility and increase fitness. Evidence also supports
acupuncture as a treatment for osteoarthritis of the knee. Many communities offer exercise programmes just for people with arthritis such as:
• gentle movement to music classes or t’ai chi
• walking groups
• water aerobics, hydrotherapy, or swimming classes.
The ultimate treatment for osteoarthritis is joint replacement. However, hip and knee replacements have a limited life – about 15 years – before another replacement is required. Replacement is considered only when joint destruction and pain is severe. The improved mobility and quality of life after these operations is often dramatic.
Several complementary products, such as glucosamine, chondroitin, or turmeric, claim to help with the symptoms of osteoarthritis. Controversy exists regarding the effectiveness of many of these products; however, they may benefit some individuals and are often worth a trial.
• If pain worsens or continues longer than two to three days, see a doctor.
• Supportive footwear will help protect joints. See an orthotics expert.
• A walking stick for osteoarthritis of the knee and hip helps reduce stress on these joints.
• Weight control reduces the load on joints (see Weight Loss).
• Heat may be useful before exercise and ice packs after exercise.
• Special aids to help with everyday life, eg, opening jars, turning on taps, putting on stockings and picking up objects, are available from some pharmacies and Arthritis New Zealand, see Support Groups, page 223
• Arthritis New Zealand also delivers regular exercise and information sessions in some main centres (see www.arthritis.org.nz for more details).
• Medicines and their dosage should be reviewed every two to three months because pain severity can increase or diminish.
• Osteoporosis (which means “porous bones” ) is a common bone disease that increases the risk of fracture.
• Bone is a living tissue that is constantly being broken down and renewed. Osteoporosis occurs when bone breaks down faster than it rebuilds.
• Encourage customers to eat a diet high in calcium and to expose their arms and face briefly to the sun each day to maintain adequate vitamin D levels.
Customers who look thin or frail, postmenopausal women, those on longterm oral corticosteroids (such as prednisone), and older adults with a bone fracture are more likely to have osteoporosis.
All customers should be encouraged to eat a diet that includes the recommended amount of calcium per day (500–1300mg). Dietary sources of calcium (see Table: Calcium Content of Some Foods opposite page) are preferred over supplements; however, supplements of calcium (no more than 500–600 mg/day) and vitamin D may be beneficial for elderly people or those living in residential or nursing homes. Encourage children to consume foods high in calcium while they are young to ensure they continue building bone mass until their early twenties. Growing teenagers need calcium every day to maximise the strength of their skeleton. Continued calcium intake is also important to maintain established bone mass once people are over the age of 25.
Suggest ways to reduce falls in those with a high risk of fracture (see Advice for customers) and encourage safe weight-bearing exercises to help with muscle tone and balance. Motivate smokers to stop smoking (see also Smoking Cessation) and those who drink, to limit their alcohol intake.
Calcium is an important component of bone, so adequate dietary calcium is needed in order to maintain good bone health.
Category Examples
• People with other health conditions (eg, heart or lung problems, diabetes) or who are pregnant or breastfeeding.
• People taking medicines (such as benzodiazepines, blood pressure-lowering agents) that might cause dizziness or drowsiness and increase the risk of falls.
• Anybody without osteoporosis taking calcium supplements, unless recommended by a doctor.
• People having frequent falls.
• People with a history of fractures.
• People under 40 or over 80.
• People with allergies to medicines.
Calcium from dietary sources is preferred over supplemental calcium. Research suggests there is no added benefit in taking more calcium (in the form of supplements) than needed, and in fact, too much calcium can be detrimental.
Vitamin D is made in the skin as a result of sunlight exposure. Supplements may be beneficial in people who never go outside (eg, frail elderly), or with reduced exposure to the sun (eg, veiled women, dark-skinned individuals). There is no evidence that vitamin D supplements improve bone health in people who are not deficient.
People with established osteoporosis are usually prescribed medicines that slow or stop bone loss, or increase bone density. Examples of medicines used for the treatment and prevention of osteoporosis include cholecalciferol (vitamin D3), calcitriol (active vitamin D), bisphosphonates (eg, alendronate, etidronate, pamidronate, risedronate, zoledronic acid), oestrogen modulators (eg, raloxifene), and hormones (eg, hormone replacement therapy, teriparatide).
Osteoporosis (which means “porous bones”) is a common bone disease that leads to an increased risk of fracture. One in three women and one in five men over the age of 50 are affected by osteoporosis.
Bone is a living tissue made up of proteins and minerals, such as calcium and phosphorus. Throughout life, bone is constantly being broken down and renewed. Bone density – the amount of
Calcium +/- vitamin D [GENERAL SALE] eg, calcium (Nutralife) calcium + vitamin D (Ostelin) calcium + vitamins (Clinicians Bone Care)
Vitamin D preparations [SUPPLEMENTS] eg, vitamin D3 (Puria Vitamin D drops, Nutralife) eg, vitamin D3 + other vitamins (Mvite, Vitabdeck)
bone tissue in a certain volume of bone – reaches a peak between 18 and 25 years of age. Higher peak bone masses are associated with a lower risk of fracture or osteoporosis later in life. Women lose bone density more quickly after menopause due to a decrease in oestrogen levels. Regular weight-bearing exercise and an adequate dietary intake of calcium and other minerals is also needed to maintain good bone density in addition to oestrogen in women and testosterone in men.
Osteoporosis occurs when bone breaks down faster than it rebuilds. Although bones remain the same size, they become thinner and more brittle. Osteoporosis can cause significant disability and affect quality of life.
Risk factors for osteoporosis include:
• age (older than 50 years)
• being underweight
• coeliac disease, Crohn’s disease or rheumatoid arthritis
• early menopause or low testosterone levels
• excessive alcohol intake (more than 2 glasses wine/day)
• family history of osteoporosis and fractures
• female gender
• low dietary intakes of calcium
• physical inactivity (particularly lack of weight-bearing exercise)
• previous fracture as a result of a minor fall or bump
• smoking
• some medicines (eg, antiandrogens, aromatase inhibitors, corticosteroids)
• vitamin D deficiency.
Comments
Milk and dairy products are the most readily available sources of dietary calcium and have the added advantage of being high in protein and other micronutrients important for bone health. Dietary calcium is preferred over supplements. Customers should seek medical advice before taking calcium supplements.
The D3 form of vitamin D is most effective at maintaining body stores of vitamin D. This form is available as supplements and also manufactured in specialised cells in the skin on exposure to sunlight. Vitamin D2 found in foods and some supplements is not as well utilised. Certain groups of people (eg, elderly, dark-skinned) may require supplements (see also Vitamins and Dietary Supplements). There is no evidence that vitamin D improves bone health in people who are not deficient. Usual supplemental dosage is 400–800IU/day.
The condition is usually asymptomatic – it is not painful until there is a fracture. Fractures usually occur in the spine (vertebral compression fractures), wrist, or hip.
Fractures can have a dramatic effect on a person’s quality of life, with up to 50% of people unable to return to a fully independent lifestyle after a hip fracture and requiring long-term ongoing care.
BMD is a measure of the amount of bone in a particular part of the body and can be calculated using a special type of x-ray, called DEXA. The World Health Organization (WHO) defines osteoporosis in women as
Helpful websites
• www.osteoporosis.org.nz
• www.nutritionfoundation.org.nz
a BMD 2.5 standard deviations below peak bone mass (20-year-old healthy female average) as measured by DEXA.
• Discuss with a pharmacist any medicines you take that may increase your risk of falling and therefore fracture; there may be alternatives available.
• Reduce the risk of falls around your home by improving furniture placement and removing rugs (see www.acc.co.nz).
• Consider t’ai chi, which research shows can improve balance and prevent falls.
• See an optometrist regularly. Good eyesight is needed to avoid tripping over or bumping into objects.
• Wear shoes with non-slip soles and avoid high heels.
• Make regular weight-bearing exercise part of your daily routine, to improve muscle strength and balance.
• Consider a walking stick to help improve balance if falling remains a problem.
• Consider an alarm/alert system, worn around the neck or wrist, which could be easily activated if you fall and cannot move.
• Expose your face and arms to the sun without sunscreen in the early morning or late afternoon every day in order to maintain adequate vitamin D levels. Just five minutes of exposure in summer is considered sufficient. Supplements may be required by some people (such as resthome residents).
*RDI: Recommended Daily Intake Reference: www.nutritionfoundation.org.nz
• Age has the most influence on a woman’s fertility and chance of having a baby.
• To conceive naturally, intercourse needs to occur during the “fertile window”.
• Women planning to conceive should be taking folic acid supplements. Iodine is also necessary once a pregnancy has been confirmed (see Pregnancy and Pregnancy Supplements).
Deciding to have a baby is a major life decision. While there is no obligation for any woman to have a baby, the chances of conceiving decline significantly from age 30 onwards.
Women may come into your pharmacy requesting ovulation kits, pregnancy tests, or both. Ensure you know what kits and tests your pharmacy stocks and can confidently describe how each one works and their effectiveness.
Remind women who are planning to conceive to refrain from alcohol, drugs, and smoking; to minimise caffeine intake; and to avoid foods at high risk of being contaminated with listeria (see Listeria at www.health.govt.nz)
If a woman has not been previously vaccinated against rubella (German measles; see Childhood Diseases and Immunisations), she should talk to her doctor about vaccination before conception. Women who are pregnant should also receive a whooping cough (pertussis) booster and a flu vaccination.
Advise pregnant women to organise a lead maternity carer (LMC) as soon as possible if they have not already done so – this can be a midwife or a specialist doctor. See www. findyourmidwife.co.nz or women can ask their doctor for a local list of LMCs.
Home ovulation tests can be used to
• Women with irregular periods or taking fertility medicines.
• Women who seem like they may become distressed by news that they are pregnant.
• Women who have missed a period but the pregnancy test was negative.
• Women who found out they are pregnant some time ago but who have not yet organised an LMC or seen a doctor.
• Women with abdominal pain or period problems.
identify a woman’s “fertile window” (see Need to Know below) and may be useful for women planning a pregnancy. They are not reliable enough to be used to prevent a pregnancy. See the subtopic Ovulation kits for an explanation of the different kits available.
Home pregnancy tests detect the presence of human chorionic gonadotrophin (HCG) in a woman’s urine. See the subtopic Pregnancy testing for more information.
Women are most fertile between the ages of 16 and 25. By age 30, the chance of conceiving each month is about 20%. This declines to about 5% by age 40.
The best time to try and conceive is during the five days before ovulation (ovulation is when an ovum [egg] is released from an ovary), up until the day of ovulation. This is called the “fertile window” and reflects the lifespan of sperm (five to seven days) and the lifespan of the ovum (24 hours).
The likelihood of pregnancy increases dramatically the closer sex happens to ovulation. Women under 30, without fertility issues and not using contraception who have sex in the three days leading up to ovulation have a 27%–33% chance of becoming pregnant.
For women with regular 28-day cycles, ovulation typically occurs on day 14 (day one is the first day of the menstrual period), so days 12, 13
Category Examples Comments
Pregnancy testing [GENERAL SALE] eg, Clearblue range, EasyCheck Pregnancy Test, First Response range, Pregnosis In Stream, Prima Pregnancy HCG Test
Ovulation testing [GENERAL SALE] eg, ClearBlue Ovulation Test, EasyCheck Ovulation Kit, MaybeBaby Easy Ovulation Tester, Prima Ovulation LH Test
Male fertility testing eg, SwimCount Sperm Quality Test
Natural / herbal products / supplements [GENERAL SALE] Black haw, burdock, crampbark, ginger, Lady's Mantle, Red Raspberry, Slippery Elm
and 14 will be their most fertile. On days 11 and 15 there is still a slight chance of pregnancy. However, most women do not have consistently regular cycles. But it is possible to work out the day of ovulation by either looking for changes in the consistency of cervical mucus, measuring the basal (baseline) body temperature, or by using an ovulation kit.
Cervical mucus is a substance that is secreted by the cervix and regulated by oestrogen. Immediately following a period, cervical mucus production is low. As oestrogen levels build up during a cycle, production of cervical mucus increases and it takes on a creamy appearance. Once ovulation is imminent, oestrogen surges and the cervical mucus becomes slippery and stretchy, resembling egg whites. This consistency enhances sperm transport through the cervix to the fallopian tube.
A woman’s basal body temperature (BBT) is her body temperature while resting. It is best measured immediately on waking, at the same time every day, and before getting out of bed.
For most of a woman’s cycle, her BBT will be roughly the same each day. Once ovulation has occurred, an increase in the hormone progesterone causes a subtle shift in the BBT of about 0.5°C. A woman can track her BBT by
Follow the manufacturer’s instructions exactly as stated on the packet. Some test sticks are held in midstream urine, while others need a urine sample collected in a clean container, which is tested with a dipand-read stick. Test urine samples immediately after collection. Some fertility drugs may give false-positive results. Traces of the HCG hormone may be found in urine for up to eight weeks after a miscarriage or termination, and for up to four weeks after the birth of a child.
Luteinizing hormone (LH) controls egg release. LH levels noticeably rise about 24–36 hours before ovulation. Home ovulation tests usually either measure LH in the urine, or oestrogen levels in saliva, and help to pinpoint the most fertile days in a woman’s cycle.
Measures sperm quality within 30 minutes. Abnormal results need to be further analysed by a professional.
Creams or oils applied twice daily from the first trimester of pregnancy may reduce the development of stretch marks. Ginger has been shown to alleviate nausea in pregnancy. Other herbs may help settle morning sickness and tone the uterus but futher information should be sought before use during pregnancy. Many other herbs are not considered safe during pregnancy.
using an accurate digital or glass thermometer and a piece of graph paper. Fertility charting websites and apps are also popular.
Preconception health checks
Women looking to start a family should consider seeing their doctor before conceiving to ensure their body is ready for pregnancy.
Conception is more likely in women close to their ideal body weight, who don’t smoke or drink alcohol, who exercise enough – not too little or too much, and who are under the age of 30.
A doctor can also check for the presence of sexually transmitted infections (STIs), medical or anatomical conditions that may affect fertility or pregnancy, and check all vaccinations are up to date. The risks versus benefits of taking any regular medications throughout pregnancy can also be discussed, as well as recommended supplements such folic acid and iodine (see Pregnancy and Pregnancy Supplements).
Ovulation kits
For women who find it unappealing or impractical to track their basal body temperature and cervical mucus daily, ovulation kits can help pinpoint the time of ovulation to help maximise their chance of successfully conceiving.
Tests sold in New Zealand detect elevations in luteinising hormone (LH), oestrogen, or an oestrogen metabolite, estrone-3-glucuronide (E3G). Sometimes, women have a surge in these hormones, but an egg is not released. The accuracy of ovulation kits is approximately 90% for predicting the fertile window.
LH is a hormone produced continuously by the pituitary gland and 24 to 36 hours before ovulation there is a surge in LH. Ovulation kits
that measure LH detect this surge in urine, but testing must begin at the correct time of the cycle or the tests may be unreliable.
Oestrogen also surges just before ovulation. This increases the levels of salt in saliva, and ovulation tests are available that use a microscope to look for “saliva-ferning” or the appearance of fern-shaped patterns caused by salt crystals in dried samples of saliva. In some women, accuracy can be very good; however, saliva-ferning can be unpredictable in other women and eating, drinking, smoking, or teeth brushing can all affect test results.
E3G is a breakdown product of oestrogen, and an increase in E3G levels also occurs around the time of ovulation which can be measured in urine. E3G is responsible for causing cervical mucus to become thin and slippery. Some tests measure both LH and E3G.
Doctors can also arrange blood tests to test for LH, oestradiol, or follicle stimulating hormone (FSH). Several ovulation testing kits also include a pregnancy test.
HCG is a hormone secreted by developing placental tissue shortly after a fertilised egg
• Women without regular menstrual cycles should test for pregnancy first thing in the morning when the HCG concentration is at its highest. Use a mid-stream urine sample.
• Retesting in a few days is recommended if a women gets a negative result after using an early pregnancy test seven days
implants itself in the wall of the uterus. Levels of HCG increase rapidly after implantation, doubling every one to two days until they peak at around 10 to 12 weeks.
High sensitivity (early result) pregnancy tests can detect HCG at the 20 mIU/HCG threshold and testing can begin seven to 10 days after conception. However, a negative result does not rule out a pregnancy.
The rate of development of HCG varies among women, and for some women it develops slowly. First morning urine samples yield the highest concentrations of HCG, and women with a negative result who still suspect they are pregnant should conduct follow-up testing every 24 to 48 hours. Women with a positive result should be referred to a doctor for follow-up testing and advice.
A disadvantage of high-sensitivity tests is that they may detect a “chemical pregnancy”. This is essentially a miscarriage that takes place soon after implantation. These are reasonably common and before the advent of highsensitivity testing, usually went unnoticed. When instructions are followed correctly, home pregnancy tests are 99% accurate.
post ovulation.
➤ Alternatively, blood tests (from a doctor) are sensitive at detecting HCG six to eight days after ovulation.
• For more information on medications that can be safely taken during pregnancy see Drugs in Pregnancy, page 221
• Females with period pain that causes distress or prevents them from going to school or work should be investigated for endometriosis.
• NSAIDs are usually more effective for period pain than paracetamol.
Although many girls and women experience period pain, many do not seek medical advice or are undertreated.
Pharmacy staff are in an ideal position to offer advice about regular dosing of non-steroidal anti-inflammatory drugs (NSAIDs) to manage period pain, and to advise women to seek further medical investigation for pain that causes distress or does not respond to over-the-counter treatment.
Be alert for any girls or women who describe their period pain as “really bad”. Tell them about the possibility it could be endometriosis and direct them to the Endometriosis NZ website (www.nzendo.org.nz) or to a doctor who specialises in women’s health.
Most experts recommend a threemonth trial of a non-steroidal antiinflammatory drug (NSAID), such as ibuprofen or naproxen, and/or paracetamol for endometriosis-related pain, and as a pharmacy team member you can suggest your customer tries this initially or while waiting to see a doctor. NSAIDs are generally preferred because they reduce prostaglandin production and prostaglandins are thought to be responsible for period cramping. If pain relief is inadequate,
• Women with other health conditions (eg, heart or lung problems, diabetes) or who are breastfeeding.
• Women who take medicines, including herbal/complementary medications.
• A woman older than 30 experiencing period pains for the first time.
• If fever or vomiting are also present.
• Pain that seems to worsen with each period.
• Pain that persists beyond the first two days of a woman’s period.
• When NSAIDs are ineffective or only partially effective.
• With an abnormal discharge or bleeding that occurs between periods.
• With pain that occurs during sexual intercourse or unrelated to menstruation.
• With very heavy menstrual bleeding (having to change a pad or tampon every one to two hours).
• Women who are pregnant or postmenopausal and experiencing vaginal bleeding.
• Woman whose moods are significantly affecting her quality of life.
• Women with lower abdominal pain that is described as severe or distressing.
• Women with an intrauterine device (IUD).
• Women with allergies to medicines.
then she should be referred to a doctor for further assessment and other treatments. Doctors can prescribe a much wider range of treatment options and hormonal treatment with a progestogen-only oral contraceptive, intra-uterine system, or an implant can be used. Desogestrel may be the preferred progestogenonly contraceptive because it consistently inhibits ovulation and this seems to be the key to inhibiting endometriosis-related pain. Higher doses of intramuscular medroxyprogesterone acetate or oral progestogens may be tried to control breakthrough bleeding or symptoms. Other prescribed treatments include combined oral contraceptives containing cyproterone acetate [unapproved indication], gonadotrophin-releasing hormone (GnRH)
Category Examples Comments
Oral non-steroidal anti-inflammatory agents (NSAIDs)
[GENERAL SALE] eg, ibuprofen <25s (Advil, Nurofen range)
[PHARMACY ONLY MEDICINE] eg, ibuprofen >25s (Advil, Nurofen range), mefenamic acid (Ponstan), naproxen (Naprogesic, Sonaflam) [PHARMACIST ONLY MEDICINE] eg, diclofenac 25mg (Voltaren Rapid 25)
Combination analgesics [GENERAL SALE] eg, ibuprofen + paracetamol (Maxigesic* [16], Nuromol [12]) [PHARMACY ONLY MEDICINE] eg, ibuprofen + paracetamol (Maxigesic* [50/100], Nuromol [24/48]) [PRESCRIPTION] ibuprofen + codeine (Nurofen Plus), paracetamol + codeine (Panadeine range), paracetamol + codeine + doxylamine (Mersyndol)
Natural / herbal products / supplements Ashwagandha, ginger, evening primrose oil, magnesium, omega-3 fatty acids, pyridoxine (vitamin B6), saffron, turmeric, vitamin C, D or E, Vitex chastetree
analogues, amitriptyline or gabapentin (both unapproved indications) or surgery. Surgery is the preferred treatment when fertility is a priority.
Period pain and other menstruationrelated symptoms are collectively called dysmenorrhoea. In addition to lower abdominal cramping, many women also suffer from other symptoms around the time of their period, these may include:
• breast tenderness or pain
• depression, irritability, anxiety, or sleeplessness
• facial blemishes and flushing
• headaches, backaches, or aching legs
• loss of appetite, weakness, or dizziness
NSAIDs reduce prostaglandin production, reducing uterine contractions and pain. Start NSAID treatment at the first sign of pain or one to two days before the period is due. Continue taking regularly for about two days after bleeding starts. Ibuprofen is the NSAID least likely to cause stomach irritation. NSAIDs may not be suitable for people on certain other medications or with some medical conditions (eg, asthma, kidney disease – see Refer to Pharmacist). Advise customer to stop taking if stomach upsets, increased bruising or prolonged bleeding occur. See Reference Section, OTC Medicines – Precautions
Combination products may help women who experience strong period pain. Some women may get relief from a simple analgesic (eg, paracetamol), but as prostaglandins are considered a primary cause of period pain, NSAIDs are usually preferred, providing these are not contraindicated.
Codeine-containing preparations were reclassified in November 2020 to PRESCRIPTION ONLY.
Several natural ingredients such as pyridoxine (vitamin B6), St. John’s wort, or Vitex chastetree may help relieve symptoms of PMS. Magnesium may be effective at relieving premenstrual migraine, fluid retention, and mood in magnesium-deficient women.
• Remind all customers to store their medicines and household chemicals out of reach of children.
• If you suspect a poisoning, call 111 if the person has severe symptoms, otherwise call 0800 POISON (0800 764 766) for advice from the Poisons Centre (open 24/7).
• New Zealand has the highest youth suicide rate in the developed world.
Remind all customers when they collect their medicines to store them up high, out of reach of children. This applies even to people without children, as unintentional poisonings are more likely to happen in homes of people not used to having children around. Suicide by poisoning is unfortunately reasonably common. Most people who commit suicide give some warning of their intentions to a friend, family member, or someone they trust. Show concern if you feel that somebody is having difficulty coping or is saying things that make you think they may be planning to take their own life. Offer to source professional help for them and reassure them that depression can be treated and problems can be solved. Suggest they call or text the Need toTalk helpline on 1737, the SuicideCrisisHelpline on 0508 828 865 (0508 TAUTOKO), or Lifeline on 0800 543 354 or text HELP to 4357.
If you suspect a person has ingested something poisonous call 111 if they are having difficulty breathing or are unconscious. For other poisonings, call 0800 POISON (0800 764 766) for professional advice BEFORE administering
Type of poisoning First aid
Poisons that have been swallowed
Poisons that have been inhaled or breathed in
Poisons that have been splashed in the eye
Poisons that have been splashed onto the skin
any first aid. Calls to the Poisons Centre take only a couple of minutes, and provide the appropriate course of action, saving time and anxious moments overall (see Advice For Customers: In an Emergency for more information.
See Advice For Customers: In an Emergency and the Treatment options table below.
Any substance that has the potential to cause injury, illness, or death if it enters the body is considered a poison. This means that almost anything can be poisonous if taken in a large enough quantity. Children and older adults and people with coexisting medical conditions are at a much higher risk of dying from poisoning.
New Zealand has a relatively high rate of suicide – more than 600 people each year take their own lives, with many more attempting to but not succeeding.
Our youth suicide rate (teenagers aged 15 to 19) remains the highest in the developed world despite fewer suicides reported during 2021. Māori men are also disproportionately represented, with a rate of 20.24 per 100,000 reported in 2020 (rates for 2021 were not available at the time of going to print).
Promote the fact that your pharmacy provides easily accessible, free health advice for everyone in your community. Always be willing to listen to people or take the initiative to ask what is troubling them and direct them to further services if need be.
Fortunately, fatalities in New Zealand from eating poisonous plants are extremely rare. Most plants are not tempting for children to eat and usually a child does not eat enough of a poisonous plant to cause serious illness.
However, it is important to be aware of what poisonous plants may be present near where young children play and to educate young children about the dangers of eating new plants, particularly ones with fruits or berries, without the supervision of an adult. Examples of plants commonly found in New Zealand gardens, parks and recreation areas that may not be safe for children if they eat or come into contact with them include arum lillies, black nightshade, daffodils, foxglove, jonquils, snowflakes, snowdrops, swanplants, poinsettias, and rhododendrons.
For more information see poisons.co.nz, under Articles & Info: Common Poisons Around the Graden.
More than 300 children are admitted to hospital in New Zealand each year as a result of unintentional poisoning; 81% of these poisonings occur in the home or the home of a family friend or relative.
Chemical or cleaner poisonings account for most cases among children aged less than two, and prescription and over-the-counter medicines (notably anti-inflammatories,
Do NOT make the person vomit unless told to do so by a doctor or the Poisons Centre: 0800 POISON (0800 764 766)
Remain calm. Protect yourself from poisoning and seek first-aid advice from the Poisons Centre or call 111 if the person is displaying serious symptoms of poisoning. If the person is unconscious, place in the recovery position and call 111. Bring the product container to the phone if you can. Do not give fluids unless instructed to do so by the Poisons Centre. Fluids may cause a person to vomit. For some toxic substances this can help the substance to be absorbed into the body and cause poisoning or may increase risk of burns to the throat. Do NOT rely on first-aid advice on labels (this is sometimes incorrect or out of date). Wipe the mouth out to clear away any remaining substance.
Protect yourself from harm. Ventilate the area and quickly move the person away from the gas or fumes to fresh air if it is safe for you to do so. Check skin and eyes for chemical burns. Flush with water if necessary. Call the Poisons Centre for advice. If the person becomes unconscious, place in the recovery position and call 111. Do not attempt to remove an unconscious person from an area where highly toxic or unknown gas is without proper safety equipment including breathing apparatus. Keep yourself safe at all times.
Flush immediately with clean room-temperature water poured from a jug, bottle, or low-pressure tap for at least 15 minutes. Pour water continuously across the eye. Ask a bystander to contact the Poisons Centre for further advice while flushing if possible. Do not use eye baths or solutions since these may react with the chemical. Take to a medical centre or hospital for an eye examination as soon as possible.
Immediately flush the exposed area with lots of water for 15–20 minutes to remove all traces of the spilled poison. Seek medical attention if the skin is damaged or the person is showing other worrying signs.
Poisons that are bites or stings Treatment varies depending on type of bite or sting (see Bites and Stings for more detailed information), but generally the area should be washed with mild soap and water. See a doctor if there are signs of infection (redness, swelling, blistering, pain) and seek immediate medical attention if the person develops an allergic reaction (eg, rash, temperature, difficulty in breathing, swelling of the face and neck). DO NOT take an analgesic for pain without advice from a doctor unless the sting is from a common non-venomous creature.
antidepressants, multivitamins, opioids, oral contraceptives, and paracetamol) are responsible for most incidents in children under five.
Children aged one to four years are the most likely age group to be poisoned, but, fortunately, death from poisoning in children is relatively rare.
The majority of adult poisonings are intentional. Most fatal, intentional, self-poisoning events involved carbon monoxide, while most poisoning admissions involved prescription and over-the-counter medicines.
Construction workers and people who are exposed on a regular basis to chemicals or harmful dusts in the course of their work are also at high risk of chronic poisoning.
The NZ National Poisons Centre is New Zealand’s only poisons and hazardous information centre and runs a 24-hour, sevenday-a-week hotline – 0800 POISON (0800 764 766) or 03 479 7227 if non-urgent.
Every year the centre receives over 30,000 telephone enquiries. Most people are able to be treated at home, but approximately 20% will require active treatment or hospitalisation.
The centre maintains TOXINZ (www.toxinz.com), which details over 200,000 chemical and medicinal products, plants and hazardous creatures and gives clear recommendations on patient management. Full access requires an annual subscription.
The National Poisons Centre website (poisons. co.nz) section Articles & Info: Preventing
• If a child or adult is unconscious or having difficulty breathing, call 111 for an ambulance.
• For other suspected poisonings, call 0800 POISON (0800 764 766) – the National Poisons Centre Urgent Phoneline, open 24-hours a day, seven-days a week.
• Do NOT assume that first-aid information on the label is correct.
• Do NOT induce vomiting unless told to do so by the Poisons Centre.
• Bring the product container or plant to the phone if you can, and remain calm. The poisons information officer will need to ask you some questions.
• Save any vomit, containers and labels in case they are needed later to help identify the poison.
• Always protect yourself from the poison.
Poisoning/ Child Resistant Closures contains information on medicines that should be dispensed with child safety caps. It is a requirement for Pharmacy Contractors to place child safety caps on the so-called “dirty dozen” which are anticonvulsants, antidepressants, benzodiazepines, beta-2-agonists, digoxin, iron salts, narcotics, paracetamol, phenothiazines, salicylates/NSAIDs, theophylline, and thyroxine. Ensure you also tell customers:
• that child-resistant packaging is not completely childproof, although “thirdgeneration caps” allow an increased level of protection while providing easier access for adults
• to store medicines and toxic substances out of reach and sight of children and to keep them in their original container away from food and drink
• to return unwanted medicines to the pharmacy.
Check that customers are able to open and close safety caps correctly. Tell them to also be mindful of any substance that is potentially toxic
(eg, antifoul for boats, antifreeze) and take all recommended precautions, including storing chemicals and pesticides up high in the garage or garden shed.
Children may also be curious about a dishwasher and there are numerous cases of children eating the powder, tablets, or residual detergent before or after the wash cycle, causing serious burns to their throat. Dishwasher detergents should be stored up high and the dishwasher turned on immediately after detergent is put in it.
When giving out medicines, check that the customer understands the instructions and not to exceed the recommended dosage.
• Ensure the customer has an appropriate measure to use for liquid medicines.
• Warn the customer of other products that may contain the same ingredient to avoid potential “double-ups” of the same medicine.
See poisons.co.nz for leaflets on childresistant packaging, disposal of hazardous substances, medicines, and chemicals, and more.
• All women who are pregnant should be under the care of a midwife or doctor.
• Women who are pregnant should continue taking folic acid for the first three months after conception and iodine for the whole pregnancy and duration of breastfeeding.
• Other supplements (such as calcium, iron, and vitamin D) may be required under the advice of a midwife or doctor.
Pregnancy can be both an exciting and daunting time in a woman’s life, especially if she is expecting her first child.
Women who are already pregnant should have been taking folic acid for at least one month before conception. If they haven’t been, then it is still considered beneficial to start folic acid and continue taking it up until week 12 of pregnancy.
Iodine supplementation is beneficial throughout pregnancy and during breastfeeding. Ask the woman what supplements she is already taking and check if any contain iodine at the recommended dosage. You may need to suggest a different supplement if she is not getting the required 150 micrograms per day, but talk with your pharmacist about this.
During pregnancy women should refrain from alcohol, drugs and smoking; minimise caffeine intake; and avoid foods at high risk of being contaminated with listeria (search Listeria at www.health.govt.nz). If a lead maternity carer (LMC) – this can be a midwife or specialist doctor – has not already been organised, suggest women look at www. findyourmidwife.co.nz or ask their doctor for a local list of LMCs.
Category Examples
• Women who are pregnant and who also have other health concerns, such as epilepsy, or thyroid problems.
• Women who take medicines, including herbal/complementary medications.
• Women who seem distressed or worried about being pregnant.
• Women who have not have their pregnancy confirmed by a doctor.
• Women who say they are pregnant but are experiencing abdominal pain or bleeding.
• Women with allergies to excipients in medicines.
Folic acid and iodine are two supplements that have been recommended by the Ministry of Health for women around the time of pregnancy.
Folic acid supplementation
Folic acid is a synthetic form of folate, which is a B-vitamin (B-9) found naturally in some foods such as asparagus, citrus, leafy green vegetables, legumes, liver, wholemeal bread and yeast.
Folate is involved in DNA and RNA replication, and together with vitamin B12 and iron, the synthesis of red blood cells. Folate is especially important during periods of rapid growth.
During pregnancy, folate requirements increase two to three-fold, making it difficult for women to fulfil folate requirements from their diet alone.
This is why our experts recommend supplementation with 800 micrograms (0.8mg) of folic acid for at least one month before a woman becomes pregnant until at least 12 weeks after conception. Supplementation has been shown to reduce the risk of neural tube defects (NTD) in the developing baby. NTDs arise when the embryonic neural tube fails to close by the fourth week after conception (28 days). This can result in malformations of the brain and spine, such as anencephaly and spina bifida.
Folic acid supplements [PHARMACY ONLY MEDICINE] eg, folic acid (Apo-Folic 0.8, Blackmores Folic Acid), folic acid with iodine, iron + other (Elevit, Blackmore’s Conceive Well), folic acid with iron (Ferrograd F)
Iodine [PHARMACY ONLY MEDICINE] eg, NeuroTabs (contains equivalent iodine 150mcg), Elevit with iodine (contains potassium iodine 250mcg)
Relieve leg cramps
Crampeze Pregnancy Leg Cramps
Natural / herbal products / supplements [GENERAL SALE] eg, Mumomega Pregnancy 30 Capsules, Bio-Oil, Mustela Stretch Mark Double Action, ginger, horsetail, Lady's Mantle eg, Sea-Band Mama
Comments
Women at high risk of an NTD-affected pregnancy (including spina bifida) may require a 5mg folic acid supplement and should ask their doctor for advice. This includes those who have previously had an NTD-affected pregnancy, have a family or personal history of NTD (or whose partner has a family or personal history), who are on insulin treatment for diabetes, or women taking medications known to affect folate metabolism, such as carbamazepine, clomiphene, valproate, or retinoids.
Iodine should be supplemented from the day pregnancy is confirmed until the day breastfeeding stops. Iodine is important for normal brain growth and development, and, because our soils are naturally deficient in iodine, and use of iodised-salt in cooking has decreased, iodine-deficiency is common in New Zealand. The recommended dose is 150 micrograms per day and iodine tablets are available over-thecounter or for a lesser charge on prescription.
Pregnant women should be encouraged to eat plenty of iodine-rich foods in addition to supplementation, such as store-bought bread (has iodine added to it); properly cooked, pregnancy-safe seafood; milk and eggs.
Like folic acid, it is difficult to achieve an
A daily 150mcg iodine-only tablet should be taken from the confirmation of pregnancy until the discontinuation of breastfeeding in addition to eating iodine-containing foods. Women with pre-existing thyroid disease or with currently high iodine intakes should be referred for further medical advice.
Contains magnesium, vitamin B6 and D, and viburnum opulus to assist with the relief of leg cramps during pregnancy and while breastfeeding.
Mumomega capsules contain DHA-rich marine fish oils and evening primrose oil. Creams or oils applied twice daily from the first trimester of pregnancy may reduce the development of stretch marks. Ginger has been shown to alleviate nausea in pregnancy. Horsetail may help tone the uterus and Lady's Mantle may help prevent spot bleeding. Pressure applied to the Nei-Kuan acupressure point may help relieve morning sickness.
adequate iodine intake during pregnancy and breastfeeding from diet alone.
Although calcium requirements increase during pregnancy, calcium absorption also increases, so supplements are not deemed necessary if a woman is getting from 1000–1300 mg/day from nutritional sources.
All dairy products are high in calcium and foods such as legumes, canned fish, spinach, and broccoli contain varying amounts. Calcium supplementation in the form of calcium tablets is not without its risks, and pregnant women suspected to have a low dietary intake of calcium should be referred to a doctor.
Routine iron supplementation during pregnancy is not encouraged; however, blood iron levels should be monitored throughout pregnancy by a woman’s LMC and supplementation started if necessary.
Vitamin D is vital for proper immune functioning, healthy cell division, and bone health. The best way to get vitamin D is by exposure to sunlight, although sun protection guidelines should also be adhered to. Low vitamin D levels during pregnancy may be associated with hypertension, pre-eclampsia, and increased caesarean section rates; however, it is not known whether vitamin D supplementation lowers these. Although some countries recommend widespread routine supplementation of pregnant women, New Zealand currently does not, although women at high risk of vitamin D deficiency such as those with pigmented skin, who wear veils for religious reasons, or who are immobile are best referred to a doctor to discuss their requirements.
Despite a lack of evidence regarding any benefits, many pregnant women choose to take a general multivitamin tablet throughout pregnancy. Ensure any tablet chosen meets the Ministry of Health’s recommendations for iodine or folic acid, and does not contain high doses of vitamin A (more than 10, 000 IU/day) as vitamin A toxicity can increase the risk of birth defects.
On average, a pregnancy lasts 266 days, or 38 weeks. Because it is difficult to work out the exact day of conception, most health professionals calculate the date a woman’s baby is due as 280 days from the first day of her last menstrual period (LMP).
This means that at conception, a woman would be considered two weeks pregnant. For example, if a woman’s LMP was the 1st of May, her due date would be around the 8th of February. A woman’s first ultrasound scan will give a more accurate due date. It is important to remember that due dates are only an estimate. Only 4% of babies are born on their due date.
Pregnancy is divided into three trimesters. The first trimester is from the first day of the LMP up to and including week 13; the second from week 14 up to and including week 27; and the third from week 28 until the birth of the baby.
A missed period is generally the first sign of pregnancy; however, because menstrual irregularities are common, missing a period does not always mean a woman is pregnant. Up to 25% of women experience slight bleeding or spotting that tends to be lighter in colour than normal
menstrual blood around the time of implantation and during the first 12 weeks of pregnancy.
Other common pregnancy signs include tender or swollen breasts, tiredness, constipation, food aversions or cravings, headaches, lightheadedness, nausea or vomiting. These signs are caused by profound changes in the cardiovascular system, anatomy and function of the renal system (the kidneys), an increase in plasma volume, increased hormone levels, and an increased demand for oxygen.
Experts are unsure why nausea and vomiting affects 50%–90% of pregnancies, but the most likely reason is increased levels of hormones such as human chorionic gonadotrophin (hCG), oestrogen, progesterone, or thyroid-related hormones. In most women, nausea resolves by week 20; however, 10%–20% experience symptoms beyond this time. Hyperemesis gravidum, a severe form of nausea and vomiting often requiring hospitalisation for intravenous fluids and vitamin and mineral supplementation, affects 0.5%–3% of pregnant women.
• A probiotic is a live bacteria or yeast that is beneficial to our health.
• A prebiotic is a non-digestible food ingredient that can provide food for bacteria. A symbiotic is a prebiotic and probiotic together.
• Over 70% of our immune system is located in our gut, as gut-associated lymphoid tissue (GALT).
Ask your customer what they need the probiotic for to help select the most appropriate species and strain. Refer any customers with concerns identified through the Refer to a Pharmacist checklist.
Probiotics should be taken with food because food makes the stomach more alkaline which helps the probiotic to survive. If the person is also taking antibiotics they should separate the administration of the probiotic and antibiotic by at least two hours. Store products as per their label and throw away once past their expiry date.
The most studied probiotic species are:
• Lactobacillus: gram-positive rods that produce lactic acid. Over 200 different strains
• Bifidobacteria: gram-positive, non-motile, anaerobic, rods that colonise the colon. Over 60 different strains
• Saccharomyces boulardii: a yeast that is believed to be a strain of S. cerevisiae (baker’s yeast)
• Streptococcus salivarius: gram-positive, spherical bacteria that are found mainly in the mouth
• S. thermophiles: anaerobic bacteria that rapidly convert lactose to lactic acid and are used to ferment dairy products, such as yoghurt
• Eschericia coli: Most E. coli strains are harmless and play an essential role in keeping the digestive system healthy, helping to digest food, and producing Vitamin K, but some can be harmful.
See Table 1: Possible Uses For Probiotics on page 132 for an overview of common conditions that may be treated with probiotics and the
• People who are immunosuppressed, with cancer, or women who are pregnant or breastfeeding.
• People who take medicines, including herbal and other complementary products.
• If probiotics have been tried before without success.
• Probiotics requested for children who are
preferred strain.
Dietary sources of probiotics include probiotic yoghurt, fermented drinks such as Yakult or kombucha, or fermented foods such as kefir and sauerkraut. If consumed daily, these may help maintain a healthy gut, although the quantities of probiotics contained in them are significantly less than most supplements.
The study of gut ecology and its impact on human health and disease is one of the most active and exciting areas of research today. But the concept that our gut health is central to our overall health is not a new one. Early medicine relied on fasting, diets, spring waters, laxatives, and the use of excrements from various species of animals as remedies for various conditions, and the discovery of living organisms in our gut dates back to the 1840s. One by one, names were given to these different types of bacteria, but it took until the 1890s for Henry Tissier to discover a rod-shaped bacterium in the stools of healthy infants which he named Bacillus bifidus communis. This species of bacteria, Bifidobacterium, is still one of the most widely used probiotics today.
The term gut microbiota is preferred instead of gut microflora because it represents the many non-bacterial elements, such as viruses, eukaryotes (organisms with a nucleus), and archea (methane-producing organisms that stimulate food fermentation) that are also present, and play an important role, in our gut.
Immune Health L. rhamnosus and/or B. lactis (eg, ProNordic Fastmelt)
Digestive health eg, L. acidophilus and/or B. lactis +/- others (eg, Bioglan Restore, Clinicians, Go Healthy, Inner Health Plus, LifeSpace, Nutralife, Rawbiotics) eg, L. reuteri (Blackmores Digestive Bio Balance) eg, kiwifruit extract (Phloe Capsules/Chewable Tablets)
Oral health eg, S. salivarius K12 (eg, BLISS K12 range), S. salivarius M18 (BLIS M18 Probiotic for Teeth and Gums)
very young.
• People who have recently travelled to a developing country.
• People with symptoms of concern (eg, blood in the faeces, unexplained weight loss, inconsistent bowel movements).
• People with allergies to milk or lactose.
Colonisation of our gut happens at birth and studies have shown reduced microbial numbers in the gut of one-month-old infants delivered via caesarean section compared to those delivered vaginally, although these differences largely disappear by six months. The composition of the gut microbiota in infants under the age of one largely reflects their mother’s but can fluctuate depending on feeding modes such as breast- or formula-feeding to weaning and the introduction of solid food. This initial colonisation appears instrumental in shaping later gut composition as an adult.
In addition to digesting food and excreting waste, our gut also acts as a boundary to the outside world, and 70% of our immune system is in our gut, as gut-associated lymphoid tissue (GALT). Every day, our GALT works together with our microbiota to decide what antigens we eat or ingest are harmful and which are not. An immune system that reacts to every foreign antigen causes the digestive tract to be in a state of constant inflammation, which can occur with some chronic inflammatory diseases, food allergies, or intolerances. Small changes in our microbiota or GALT have also been associated with mood disorders, obesity, irritable bowel syndrome, type 2 diabetes, and memory loss.
The idea of giving probiotics to improve our gut microbiota and to influence our immune response, and ultimately, improve our health, sounds promising, but to date, only a few good quality clinical trials support that idea. Many other trials have shown inconclusive results or no
Contain probiotic bacteria to aid digestive health and other conditions resulting from an imbalance of bacteria within the gut. Helps restore the balance between beneficial and harmful bacteria.
Kiwfruit extract contains a combination or prebiotics, enzymes and fibre to aid good digestive health and help relieve constipation.
Use in conjunction with regular oral hygiene to establish a healthy balance of bacteria in the mouth.
effect. Tellingly, large expert organisations such as the American Gastrointestinal Association, do not support the use or probiotics unless they are given as part of a clinical trial.
Probiotics are intended to modify the microbiota favorably (the term probiotics comes from pro-biota) and are defined as live bacteria or yeasts that are good for you when administered in adequate amounts. Pharmacies stock a wide range of probiotics, but not all have the same effect or even have evidence that they work, so let your customer know which type is more likely to be beneficial for their condition. Reassuringly, most side effects of probiotics are mild and may include bloating, flatulence, or nausea, and many customers are happy to give probiotics a go to see if one works for them. Tell your customers that it is important that the right probiotic is taken daily, in an adequate amount. Probiotics are considered safe for infants, children, adults, and older adults but are not recommended for those who may be immunosuppressed.
The potency of a probiotic is measured in colony-forming units (CFU) which is the usual number of colonies expected per dose. Because probiotics degrade with time, a product that states the CFUs at the end of shelf life (EOSL) may be preferred over a product that states CFUs at the time of product release.
Unfortunately, the label can be unclear about which point in time the CFUs refer to, and you may wish to clarify this from the manufacturer if a product is near its expiry date.
A Cochrane review found a dosage of 5 billion CFUs or greater per day was significantly more effective than a lower dosage. Individual
strains should be at least 3 billion CFUs each (EOSL) when in combination.
Prebiotics are essentially food for bacteria and taking prebiotics either with probiotics or by themselves can help reduce gastrointestinal symptoms such as bloating, constipation, or diarrhea. They are usually non-digestible foods, and most are obtained from carbohydrate fibres called oligosaccharides. Most prebiotics commercially marketed in New Zealand contain
either inulin or oligofructose and they can be found naturally in whole grains, bananas, onions, garlic, honey, and artichokes. Prebiotics can increase the number of beneficial bacteria in the intestine by stimulating their growth and they should be taken daily.
A prebiotic combined with a probiotic is called a symbiotic and represents a substance that contains both live bacteria and the fuel it needs to survive.
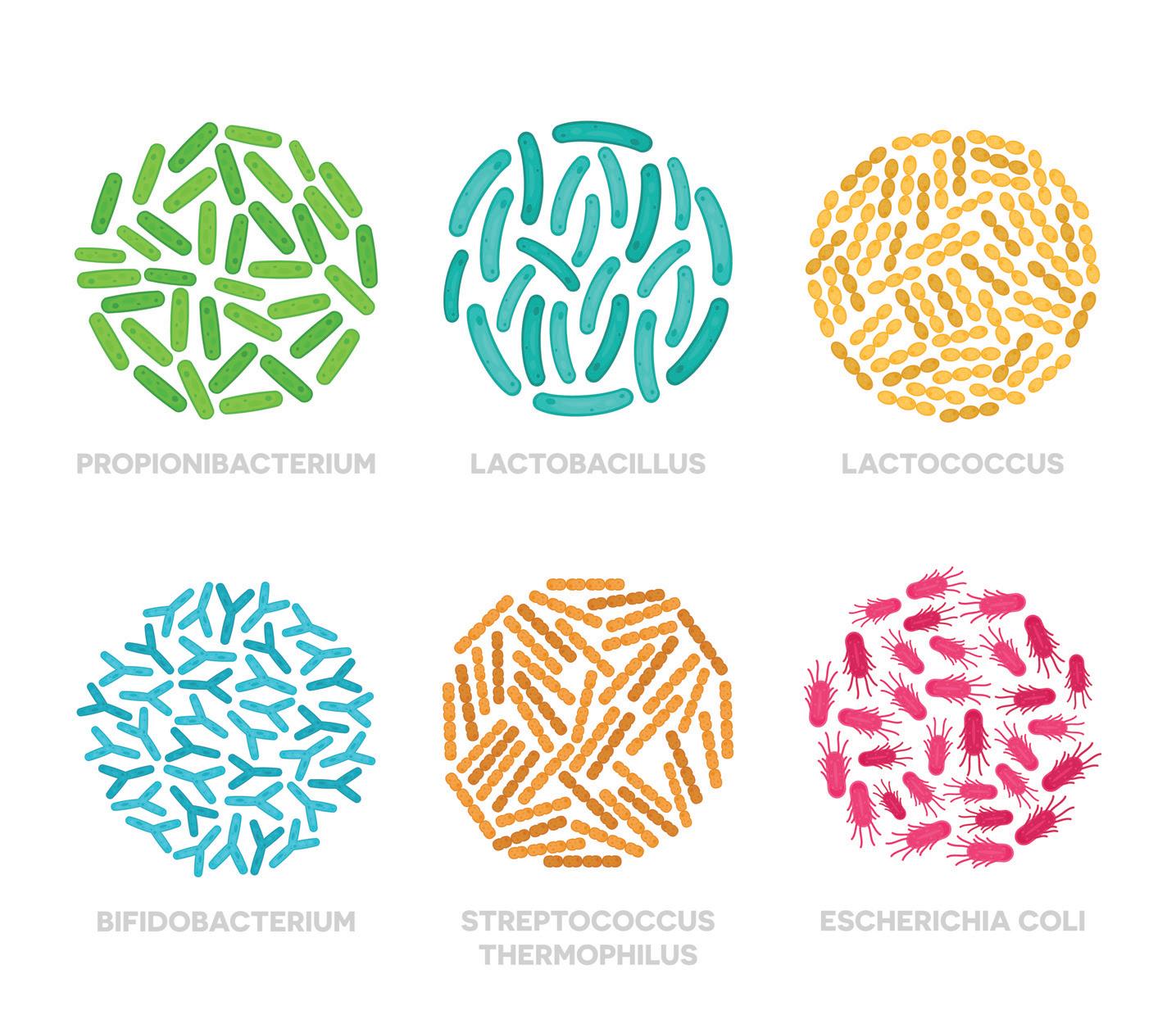
Acute infectious diarrhoea
Antibiotic-associated diarrhoea
Atopic eczema
Bacterial vaginosis
Clostridium difficileassociated diarrhoea (CDD)
Colic
Constipation
Crohn’s disease
Hepatic encephalopathy
Irritable bowel syndrome
Lactose intolerance
Necrotising enterocolitis (NE)
Oral health
Pancreatitis (acute)
Ulcerative colitis
• Lactobacillus reuteri, L. rhamnosus GG
• Saccharomyces boulardii
• Bifidobacterium animalis, lactis, bifidum, breve, longum, infantis
• L. acidophilus, casei, rhamnosus, reuteri, + others
• S. boulardii
• Streptococcus thermophilus
• L. rhamnosus GG, reuteri, sakei
• L. acidophilus, rhamnosus, fermentum RC-14
• B. animalis, lactis, bifidum, breve, longum, infantis
• L. acidophilus, casei
• L. reuteri
• Bifidobacterium spec
• S. boulardii
• B. breve, longum, infantis
• Escherichia coli
• L. acidophilus, casei, + others
• S. thermophilus
• B. animalis, breve, lactis, longum, infantis
• Escherichia coli
• L. acidophilus, rhamnosus, + others
• S. cerevisiae
• L. bulgaricus
• S. thermophiles
• B. animalis, breve, lactis, longum, infantis
• Bacillus cereus, subtilis
• L. acidophilus, rhamnosus, + others
• S. boulardii
• S. thermophilus
• S. salivarius K12, M18
• None
• B. animalis, breve, lactis, longum, infantis
• Escherichia coli
• L. acidophilus, rhamnosus, + others
• S. thermophilus
KEY
• Reduction in the number of days with diarrhoea, vomiting, and in hospital stay
• Continue for one to two weeks following symptom resolution
• May prevent traveller’s diarrhoea; start two days before travel
• 50 to 40 billion CFUs/day
• Start on first day of antibiotic Rx and continue for one to two weeks following completion of Rx
• Mixed results
• Improvement seen mostly in IgE-sensitised infants
• Most studies favour probiotics for recurrence
• 10 billion CFU daily for 2 months
• Administration of probiotics close to initiation of antibiotic reduces the incidence of CDD by 50%
• Inconsistent results
• Reduced risk of crying time at days 14 and 21
• Start at onset of symptoms and continue as needed
• Increases number of stools per week
• Weak evidence
• Mixed results: may improve the development of, or the recovery from, hepatic encephalopathy
• Weak evidence
• Reduces abdominal pain, bloating, and flatulence
• Start at onset of symptoms, continue as needed
• Improves lactose digestion
• Reduces the symptoms of lactose intolerance
• Reduced risk of NE and death
• Start in those at risk of the condition and continue as needed
• Combination Bifidobacterium species products most beneficial
• 3 billion CFUs each organism for first seven days
• Prevents immune activation induced by periodontal disease pathogens
• Reduces dental caries-producing bacteria
• Not shown to be effective
• May improve remission rates but not maintenance of remission
• Start at onset of UC exacerbation and continue for one to two weeks after
• Psoriasis can be hard to live with and 60% say it impacts on their daily lives.
• There are several different types of psoriasis but plaque psoriasis is the most common.
• Emollients may be all that are needed for mild psoriasis and are useful in addition to other treatments for more severe psoriasis.
Living with psoriasis can be challenging, and 60% of people with psoriasis say it impacts on their daily lives. Even when a flare-up of psoriasis has resolved, the itch caused by the condition may linger which may cause sleep disturbances and daytime fatigue.
Finding the right non-irritating moisturiser, shampoo or body wash takes time, and if you can, offer samples for them to take home to try. Refer any customers with concerns identified through the Refer to a Pharmacist checklist.
There is no cure for psoriasis and it can be difficult to manage, although most people can keep it under control for long periods of time with continued treatments. Topical treatments for psoriasis aim to slow down or normalise increased skin cell turnover. Some customers may have to try several different products before finding one that works for them.
Emollients (products that contain a fat or oil such as lanolin or white soft parraffin) may help decrease skin cell turnover in addition to their skinsoftening and skin-hydrating properties. They may be all that is necessary to treat mild psoriasis and can be used in combination with other treatments.
Coal tar and vitamin D analogues (eg,
• People with other health conditions (eg, heart or lung problems, diabetes) or who are pregnant or breastfeeding.
• People who take medicines, including herbal and other complementary products.
• With extensive or severe lesions, or if the lesions look infected.
• If itching is severe.
• If the diagnosis of psoriasis is in doubt.
• If the psoriasis is affecting a person’s mood or quality of life.
• If this is the first presentation of psoriasis in a person.
• People with psoriasis that involves the nails.
• When products have been tried before without success.
• People with allergies to topical medicines.
calcipotriol) may be used for plaque psoriasis. Products containing crude coal tar (1%–10%) are more effective than more refined extracts of coal tar; however, the smell may put a few people off and they can be messy. Coal tar products increase the sensitivity of skin to the sun, and although there have been concerns about an association with cancer, studies have failed to show an increased risk when people use coal tar products for psoriasis.
Calcipotriol may cause skin reactions, and in people with calcium metabolism disorders or very inflammed (red) psoriasis, there is an enhanced risk of high blood calcium levels. Salicylic acid and UV light may also inactivate calcipotriol. Calcipotriol by itself or in combination with betamethasone (a steroid) is fully funded on prescription.
Topical corticosteroids may be used to treat small areas of psoriasis, although they should only be used short-term because there is a risk of precipitating an unstable form of psoriasis when they are stopped.
Category Examples Comments
Moisturisers [GENERAL SALE] eg, Derma E, Dermal therapy Psoriasis cream, Lipobase, Lucas Papaw ointment, NeoStrata Ultra Moisturising Cream, QV Skin Lotion
Products containing coal tar [GENERAL SALE] eg, Pinetarsol, Egoderm, Egopsoryl TA Gel, eg, shampoos (Neutrogena T Gel, Sebitar, Scytera Foam, Polytar)
Combination coal tar products [GENERAL SALE] eg, Coco-Scalp*
Topical corticosteroids [PHARMACY ONLY MEDICINE 0.5%] [PHARMACIST ONLY MEDICINE 1.0%] eg, hydrocortisone (Dermaid, Skincalm)
Natural / herbal products / supplements Aloe, honey, Milk thistle, Neem oil, Vitamin D eg, Hopes Relief, Native Neem, Skybright Chickweed, Sven’s Island Miracle
Keratolytics such as salicylic acid help to slough off dead skin cells and may be useful when combined with other ingredients such as coal tar.
Stronger topical preparations, oral medicines, and injectable biologics are available through a GP or specialist. Phototherapy (ultraviolet B radiation) and photochemotherapy (ultraviolet A radiation combined with a psoralen) may also be prescribed.
Psoriasis is a long-term skin condition that can occur on any part of the body. It affects 2%–4% of New Zealanders and is more common in those with European ancestry.
Psoriasis can occur at any age, but usually begins in the late teens or around the age of 50. Psoriasis affects males and females equally, and approximately one-third of people have a family history of the condition.
There are several different types of psoriasis. Plaque psoriasis is the most prevalent form and symptoms include rough, inflamed, thick raised areas of skin (called plaques), covered
Frequently used to help soften and soothe skin, reducing cracking and dryness. Useful for mild psoriasis. It is best to patch-test products to ensure no skin sensitivity reactions occur.
Coal tar and coal tar-related products (eg, pine tar, oil of cade or ichthammol) are old but effective treatments, although it is not known how they work. Tar is most useful for scalp psoriasis and chronic plaque psoriasis. Can be messy and some people may dislike the smell.
Contains coal tar, sulphur and salicylic acid in a coconut-oil base. Apply to the scalp and wash off after an hour, usually with a tar-containing shampoo.
Restrict use to small areas to reduce risk of absorption. Use for longer than seven days only on medical advice. May be used in combination with an antifungal agent to combat candida.
Some natural extracts may help decrease symptom severity. Topical vitamin D is effective at treating plaque psoriasis in some patients.
by a silvery scale. These are usually found on the elbows, knees, lower back or scalp but can occur anywhere. Plaque psoriasis that occurs on the scalp can be easily mistaken for dandruff; however, it tends to have a silvery sheen and the scales are larger and dryer than dandruff scales.
Guttate psoriasis consists of smaller plaques (around 5–10mm in diameter) on the trunk or limbs, and more commonly occurs in people under the age of 30; respiratory illnesses or viral infections are common triggers.
The lesions seen with flexural psoriasis tend to be smooth and shiny and confined to the skin folds, armpit, under the breasts, or in the groin area.
Generalised pustular psoriasis is a severe acute illness that may be triggered by systemic or potent topical corticosteroids, infections, overexposure to UV light, or stress. It is characterised by painful red skin and pustules.
Palmoplantar pustulosis – where pustules are confined to the palms and soles – is strongly associated with smoking.
Nearly half of all people with psoriasis also have psoriasis that affects the nails with symptoms such as pitting, separation of the nail from the nail bed, distortion, and flaking of the distal portion of the nail.
About 25% of people find their psoriasis is itchy and others may have a burning feeling on the skin. Approximately 5% of people with psoriasis will also have psoriatic arthritis, which causes pain, stiffness, and swelling of the joints and can be very debilitating.
Psoriasis severity
Mild psoriasis is defined as that which affects less than 5% of the body surface area (BSA); moderate psoriasis affects 5% to 10% of the
BSA, and severe psoriasis, >10%. Psoriasis tends to come and go over time and most people experience acute episodes of psoriasis (called flares) interspersed with periods of relative skin normality. Some 80% of people have a mild form of the disease. Rarely, hospitalisation is necessary if the disease is severe.
Psoriasis cause
The cause of psoriasis is not fully understood but it may result from genetics, an abnormal activation of cell death pathways (apoptosis), or an overactive immune system that causes inflammation, proliferation of extra blood vessels and increased skin cell turnover.
Psoriasis may be confused with seborrhoeic dermatitis and other types of dermatitis (see Dermatitis/Eczema), candida and dermatophyte fungal infections (see Fungal Infections: Skin and Scalp), as well as other skin conditions.
• Stress is one of the main triggers of psoriasis.
➤ Find ways to relax, such as yoga or meditation.
➤ Build a good support network. Contact a local psoriasis support group (see page 223 for contact details of support groups).
• Follow a healthy diet, maintain an optimal weight, and limit intake of alcohol, fried or processed foods. Do not smoke.
• Try not to scratch or pick psoriatic lesions
Psoriasis triggers
Certain triggers seem to precipitate psoriasis or make it worse, such as:
• alcohol
• certain medicines (eg, angiotensin converting enzyme [ACE] inhibitors, beta-blockers, hydroxychloroquine, lithium, non-steroidal anti-inflammatory drugs [NSAIDs], oral/ topical corticosteroid withdrawal)
• high-glycaemic diets
• hormonal changes (common post-puberty)
• infections (eg, streptococcal throat infections, candida, Malassezia yeasts)
• injury to the skin, including sunburn
• obesity (severity of psoriasis correlates with insulin resistance)
• smoking
• stress, both physical and psychological.
(it may make them more resistant to treatment and trigger new lesions).
• Keep skin cool and moisturised to help reduce itching and scratching. Apply emollients frequently and regularly for relief.
• Bathing with oils or coal tar solutions can help soften the psoriasis and lift the scale.
• Warn patients to be careful when getting out of the bath or when using bath additives that may make the bath slippery.
• While some sun exposure is beneficial, avoid overexposure or getting burnt.
• Scabies is a highly contagious skin condition caused by a tiny mite, Sarcoptes scabiei.
• Symptoms typically include a mild rash accompanied by intensely itchy skin.
• Treatment is with a scabicide containing permethrin.
If a customer complains of a widespread itch or asks you to look at their skin, take them to a private area of your pharmacy where they can sit down.
Put on some gloves, and have a good look at their arms, hands and face. If you notice they have a mild rash, but the customer is saying they are really itchy, search carefully for burrows between the fingers or on the wrists or palms. These look like a 5–10mm zigzag line and are most commonly found in these areas although may also be present in the armpits, buttocks, on the genitalia, insteps of the feet or backs of the heels. In some people, the burrows may be obscured by scratching, eczema or an infection. Normally the mite is too small to see with the naked eye (a full-grown mite is about the size of a pinpoint). Refer any customers with concerns identified through the Refer to a Pharmacist checklist. Treat all other customers with a scabicide.
Treatment is with a scabicide, usually permethrin. In severe cases, ivermectin prescribed by a doctor (a single dose of 200 micrograms/kg) may be used when other treatments have proven ineffective.
According to the NewZealandFormulary (NZF), treatment should be applied to the whole body including the scalp, neck, face and ears. Advise customers to use a nailbrush to get the product under their nails and to pay particular attention to the finger and toe webs. The product will need to be reapplied to the hands every time they are washed during the treatment period.
Most people will require help to get to hardto-reach areas, such as their back. Permethrin
• People with other skin conditions (eg, dermatitis, psoriasis) or who are pregnant or breastfeeding.
• People who take medicines, including herbal/complementary products.
• Children under the age of two.
• If the itch is localised to one specific area.
• If you are not sure the person has scabies.
• With a very severe rash or evidence of infection (crusting or pus visible).
• With symptoms such as a fever, swelling, or intensely red skin.
• With symptoms that have persisted or recurred despite treatment (note that a scabies itch can persist for several weeks after successful treatment).
• People with allergies to topical medicines.
products need to be left on for eight to 12 hours before washing off. Experts now recommend products are applied twice, one week apart.
Products are best applied to the body after a bath or shower once the skin has cooled down (do not apply to hot skin). All household members, and anybody with recent direct and prolonged contact with a person with scabies, should be treated at the same time, even if they are not itchy.
It is important to tell people they may still remain itchy for up to four weeks after they have treated their scabies, due to the ongoing allergic reaction to the mite’s byproducts until they are cast off by the skin.
A persistent itch can also indicate a persistent infection (if the treatment was not applied correctly) or reinfestation. Anybody worried about a persistent itch despite already treating themselves for scabies should be re-examined by a doctor or pharmacist. Further treatment may be needed or an alternative diagnosis considered.
Crotamiton cream, oral antihistamines, 0.5% hydrocortisone cream, or emollients can help relieve an ongoing itch when there is no evidence of a current infestation.
Scabies is a very contagious skin condition caused by the barely visible

Category Examples Comments
Treatment products [GENERAL SALE] eg, permethrin 5% (A-Scabies Lotion, Lyderm cream)
[GENERAL SALE] eg, crotamiton (Eurax Cream, Itch Soothe Cream)
Effective against scabies. Pregnant women and children aged between two months and two years should be treated under medical supervision. Needs to stay on the body for at least 8 hours (up to 12 hours). Although manufacturer states to exclude head and neck, NZF recommend to include scalp, neck, face, and ears, but to avoid contact with the eyes.
Not as effective as permethrin for the treatment of scabies. Mainly used to treat the itch that persists after scabies treatment (just apply to the affected areas).
• Try not to let your own attitude towards sex influence the way you treat customers with sexual health queries.
• Place your condom and lubricant display in an easy to find, logical area, and consider having smaller, satellite displays near the sunglasses stand or a till.
• Male condoms are made of latex, polyurethane, or polyisoprene. There are pros and cons for each.
Being able to educate and offer professional advice about sexual health is what sets pharmacies apart from supermarkets and other stores that also sell condoms and lubricants.
When approached by a customer, offer to talk with them in a private area of the pharmacy and keep things factual. Many people like take-home brochures and these should contain relevant information in an easy to understand format. Ensure you stock a good variety of condoms and lubricants and that they are in an easy to find area of the pharmacy. Have some information panels nearby that explain the different condom types. Let people buying condoms know they can also obtain up to 12 boxes on a script through a doctor or a family planning clinic nurse. Family planning visits are free for anyone under 22. Refer anybody with a suspected sexually transmitted infection (STI) to a doctor.
Male condoms are made of either latex rubber, polyurethane, or polyisoprene. (see Table, opposite page). They are put on over a man’s erect penis before intercourse to greatly reduce the risk of pregnancy or sexually transmitted infections (STIs).
Their theoretical effectiveness rate against pregnancy is high (98%); however, their real-life
Category Examples
• Customers who have had unprotected sex and are worried about exposure to STIs or who want information about the emergency contraceptive pill (ECP) (see Contraception).
• People who have had sex against their will and are wanting further advice.
• Customers wanting to buy oral contraceptives over-the-counter (see Contraception).
• Customers wanting information about erectile dysfunction treatments (see Men’s Health).
effectiveness rate, which considers less than perfect use, is around 85%.
For protection against STIs, their effectiveness varies. They are highly effective at preventing STIs that are transferred through bodily fluids, such as HIV, gonorrhoea and chlamydia, when used consistently and correctly. However, they are less effective at protecting against STIs spread via skin-to-skin contact, for example, genital herpes, human papillomavirus (genital warts), and syphilis. Male condom use should always be encouraged to reduce the risk of transmission of STIs, even for men having sex with women taking hormonal contraceptives or who are postmenopausal.
Female condoms are made of nitrile polymer which is latex-free. A flexible ring at each end
keeps it in place. They are available online and through some pharmacies and from family planning clinics.
Reduced natural lubrication during sexual intercourse is common and can be caused by hormonal changes in a woman’s body (such as breastfeeding or menopause), medications (such as hormonal contraceptives, antihistamines or antidepressants), diabetes, stress, dehydration or lack of arousal. Lubricants are usually either water-based and contain glycerine, silicone, are glycerine-free or oil-based. They are usually applied prior to sex to enhance sexual activity or ease any discomfort during sex. Water-based lubricants that contain glycerine

Comments
Male condoms (latex) eg, Durex range, Ansell range, Marquis Condoms
Male condoms (non-latex) eg, polyisoprene (Durex Real Feel) eg, polyurethane (Trojan Supra)
Female condoms eg, nitrile polymer (eg, FC2)
Lubricants eg, Anime Lubricant, Astroglide, Durex range, Lubrigel, Sylk
Natural products eg, DHEA, Chaste tree, ginkgo, Maca, omega-3 and -6, Panax ginseng, Saw palmetto, vitamin C
Home-made lubricants, such as vaseline or cooking oil, may damage latex condoms. Condoms do not contain spermicide but most are pre-lubricated. Some vaginal antifungal creams can damage condoms – refer to the pharmacist. Only latex condoms are fully subsidised (144 condoms per script). Additional lubrication is not routinely required but may help reduce the risk of condom breakage or irritation.
Non-latex condoms are suitable for people with latex allergies and are safe to use with both water and oil-based lubricants.
Inserted just prior to sexual intercourse. Available from www.fc2.co.nz
Reduce friction during sexual intercourse enhancing pleasure and reducing the risk of condom damage. Use only water or silicone-based lubricants with latex condoms.
May help improve blood flow and sexual function but evidence is limited.
are the most common, and are safe to use with latex condoms and will not stain fabric. However, they may dry out quickly, trigger yeast infections, and cause irritation.
Glycerine-free, water-based lubricants usually last longer and are less likely to trigger yeast infections.
Silicone lubricants last three times as long as water-based lubricants but tend to be more expensive and may deteriorate silicone sex toys.
Oil-based lubricants usually contain synthetic or vegetable-derived oils and are long-lasting but incompatible with latex condoms and will stain fabric.
Vaginal moisturisers are different from lubricants and are used to restore a loss of natural vaginal moisture caused by low oestrogen levels (see Women’s Health).
Sex is an important part of being human, and also one of the biggest influences on our physical, mental and emotional health. When sex is part of a mutual, loving relationship, it improves cardiovascular function, boosts the immune system, and relieves stress. However, sex also carries a risk of infection, mixed emotions, and unintended consequences that can all negatively impact on a person’s quality of life.
Sexually transmitted infections (STIs) are most prevalent in young people under the age of 25; however, rates have dramatically increased in the past decade among 40 to 50-year-olds, possibly due to a lack of safe sex practices including poor condom use when starting a new relationship.
Chlamydia is the most frequently diagnosed
STI in New Zealand; however, genital herpes, genital warts, and gonorrhoea are also common.
Testing for STIs is free for those under the age of 22 from many providers throughout New Zealand. Encourage anyone not in a monogamous relationship to use condoms and to consider regular STI testing.
Barrier contraceptives are the name given to products that prevent pregnancy by a physical means (ie, they prevent sperm from entering the
Latex
Strong.
Easy to use.
The least expensive.
Helpful website
Justthefacts.co.nz
vagina or the uterus). Condoms are currently the only type of barrier contraceptive available in New Zealand. Diaphragms (silicone domes which cover the cervix) are no longer sold here.
Perish easily. Use only with water or silicone-based lubricants.
Keep away from heat and sunlight.
Polyisoprene Have a soft, natural feel.
Conform to the skin easily.
Suitable for people with latex allergies.
Easier to use than polyurethane condoms.
Can be used with water or oil-based lubricants.
Keep away from heat and sunlight.
Polyurethane Thin, so may offer better sensitivity.
Not as flexible or stretchy as latex condoms; possibly more prone to ripping.
More expensive than latex condoms.
Latex-free and may be used with water, silicone, or oil-based lubricants.
Have a longer shelf-life than latex condoms.
Keep away from heat and sunlight.
• If unprotected sex occurs, or if a condom breaks, women should see a doctor as soon as possible.
➤ The ECP is available from accredited pharmacists and accredited nurses without prescription, but must be taken within 72 hours of unprotected sexual intercourse (see Contraception: Oral and Emergency).
• Remind customers to store condoms away from heat and sunlight (ie, not in a car glove box), and to only use condoms that have not passed their expiry date.
• Only use water-based lubricants with latex condoms to decrease the risk of breakage.
• Shingles occurs as a result of reactivation of the chickenpox virus.
• A painful rash of blister-like sores on one side of the body (usually the face or torso) is the most common presenting symptom.
• Refer all customers with suspected shingles to a pharmacist.
Shingles causes a distinctive rash of blister-like sores that usually affects only one side of the body, and this typically prompts people to seek treatment. If you suspect somebody has shingles, refer them to the pharmacist who should refer them to a doctor because prompt treatment with an antiviral medicine can help reduce symptoms and complications.
Make sure you avoid close contact with anybody with shingles if you have never had chickenpox, or if you have not been vaccinated against chickenpox or shingles.
Antiviral drug treatment (such as oral aciclovir or valaciclovir) prescribed by a doctor can reduce the severity of the attack and incidence of post-herpetic neuralgia if started within 72 hours of the rash appearing. The Treatment options table below lists OTC and topical agents that may also be considered.
Shingles (herpes zoster) occurs as a result of a reactivation of the varicella zoster virus, the same virus that causes
Category Examples
Oral analgesics [GENERAL SALE]
• Anybody with suspected shingles.
• People with diagnosed shingles that has persisted despite treatment.
• People whose rash appears to be getting worse, not better, despite ongoing treatment.
• People in severe pain.
• People whose mood appears to be affected or who are having trouble sleeping.
• People with severe post-herpatic neuralgia (post-shingles nerve pain).
chickenpox (see Childhood diseases and immunisation).
Shingles occurs only in people who have had chickenpox. Although chickenpox generally occurs in children and young people, the virus is not eliminated from the body once the episode of chickenpox has resolved. Instead it lies dormant in nerve cells close to the spinal cord. Many years later it can reactivate to cause shingles, an infection that has vastly different symptoms from the original chickenpox infection.
Exactly how the virus remains latent in the body, and reactivates, is not understood. However, people whose immune systems are impaired due to medications or diseases that lower immunity (eg, cancer, HIV) are most at risk.
Occasionally, trauma (eg, a surgical scar) may trigger shingles at the site of the injury. Contact with somebody who currently has varicella zoster (chickenpox) may also cause reactivation. Shingles can occur at any age but is more common in adults aged over 60.
Rarely, shingles may occur in young children who were either born with chickenpox or had it soon after birth. Most people get shingles only once in their lifetime.
eg, paracetamol (Panadol, Paracare), ibuprofen up to 25s (Advil, Nurofen) [PHARMACY ONLY MEDICINE] eg, paracetamol – greater than 20 tablets, suspension (Pamol All Ages, Paracare, Panadol), ibuprofen >25s (Advil, Nurofen), ibuprofen + paracetamol (Maxigesic, Nuromol)
Topical pain relievers
[GENERAL SALE]
eg, capsaicin cream (Zostrix HP), lignocaine preparations (Soov cream/spray) [PHARMACY ONLY MEDICINE] eg, lignocaine/prilocaine (Emla)
Shingles vaccine [PRESCRIPTION MEDICINE] – except when administered by a registered pharmacist vaccinator to an adult over 50 for herpes zoster prevention eg, Shingrix
Natural / herbal products / supplements Papain, DMSO (dimethylsulfoxide), calendula ointment, zinc cream, Harker Herbals Chronic Itch
Comments
Early symptoms may include non-specific complaints, such as headache, fever and malaise, which may be easily misdiagnosed. After a couple of days, itching, tingling, numbness or burning, and/or a stabbing pain may develop in the affected dermatome (an area of skin supplied by one spinal nerve). Usually, after one or two days (but sometimes as long as three weeks), the initial phase is followed by the appearance of the characteristic skin rash.
The pain and rash most commonly appear on the areas of skin supplied by the lumbar (torso), thoracic (chest), cervical (neck), or ophthalmic (forehead) nerves. The rash usually starts as a crop of red papules and may look like hives but, since the virus spreads along certain nerves located off the spinal cord, it typically has a stripe-like presentation affecting just one side of the body, unlike hives which are usually widespread. Within a few days, the papules form small, painful, exudate-filled blisters, which may persist for up to seven to 10 days before they crust over and heal.
Once the blisters have appeared, and until the rash has developed crusts, a person is extremely
Paracetamol should be used first-line for pain relief, but NSAIDs should only be used on a doctor’s advice. This is because NSAIDs have been associated with an increased risk of severe skin complications (including necrotising fasciitis) in people with varicella zoster virus. Mechanism is thought to be by impairment of the immune response or by masking of the symptoms of secondary infection. See Reference Section, OTC Medicines –Precautions.
Capsaicin cream (made from chilli seeds) may provide relief from post-herpetic neuralgia for some patients. It reduces levels of a chemical called substance P, which helps transmit pain impulses to the brain. Pain relief may take up to four weeks to be noticed. Burning or tingling may occur briefly when applied to the skin, but this resolves with continued use. Products containing lignocaine provide pain relief by anaesthetising the skin.
Pharmacists must have successfully completed a vaccinator training course. Used for the prevention of herpes zoster (shingles) and related pain, and postherpetic neuralgia.
Both papain and DMSO can help improve the symptoms of shingles. Calendula or zinc cream may help skin healing. Chronic Itch contains natural ingredients in an olive oil base to moisturise and relieve the itch of shingles.
contagious and transmission of the virus can occur to people without immunity to the virus. These people may develop chickenpox, but will not develop shingles, unless they have already had chickenpox.
Shingles may be associated with serious complications including post-herpetic neuralgia, bacterial superinfection, infection of internal organs, visual impairment, hearing loss, and death. Sometimes after severe blistering, scarring and discoloured skin may remain.
Post-herpetic neuralgia
This is defined as pain that persists or recurs more than a month after the onset of shingles. It is more common in people older than 40 and is more likely in people with facial shingles infections.
The pain may be burning and continuous, or spasmodic and shooting; or, rarely, an itchy, crawling variety. The overlying skin may feel numb or extremely sensitive to touch. Topical pain relievers including capsaicin cream may help, but some people may require further referral for ongoing assessment and management with prescription medicines, acupuncture or transcutaneous electrical nerve stimulation (TENS) therapy.
Prevention
Vaccination against the herpes zoster virus with Shingrix may be considered in people older than 50 because they are more at risk of severe complications from shingles. These vaccines can be given regardless of an individual’s history of either chickenpox or shingles and will help prevent against herpes zoster (shingles) and
post-herpetic neuralgia and reduce acute and chronic zoster-associated pain.
Shingrix is the only shingles vaccine funded in New Zealand for people aged 65 years only (two doses needed). Shingrix is 97% effective at preventing shingles in adults aged 50 to 69 years. Unfunded Shingrix may be administered
to people aged over 50 years by registered pharmacists who have successfully completed an approved vaccinator training course. People who were given Zostavax in the past should be advised to consider a course of Shingrix (this would be unfunded).

• Early treatment from a doctor will reduce the severity and duration of shingles.
• Rest and take pain relief, such as paracetamol.
• Apply a bland, protective cream such as white soft paraffin to the rash, cover with a
dressing, and wear loose clothing.
• If the pain persists following treatment, return to your doctor.
• Warn customers that they are highly contagious until the rash crusts over.
• Inflammation that occurs in the nose all year round is called perennial allergic rhinitis. Symptoms are similar to hay fever.
• Bacterial infections can sometimes make viral sinus and nasal problems worse.
The time of the year combined with a person’s description of their symptoms should help you work out what condition they have. Run through the Refer to a Pharmacist checklist and refer any customers with concerns. For other customers, base product selection on your customer’s most troublesome symptom, for example:
• blocked nose – an oral or nasal decongestant (three days only) or saline nose drops/spray
• runny nose or sneezing – an oral or nasal antihistamine
Category Examples
Oral antihistamines Non-sedating
[PHARMACY ONLY MEDICINE]
• itchy eyes – an antihistamine eye drop
• sinus pain – an oral analgesic and possible referral to a doctor.
Not being able to breathe properly through your nose can be distressing. Reasons include allergies, viral or bacterial infections, strong-smelling substances, structural problems (such as a deviated septum), and nasal polyps.Treatment varies depending on the condition (see under each subtopic).
There are several different nose and sinus disorders.
Allergic rhinitis is inflammation in the lining of the nose that occurs because of an over-reaction
eg, bilastine (Labixten), cetirizine (Razene), desloratadine (Aerius), fexofenadine (Fexofast), levocetirizine (Levrix), loratadine (Loraclear)
Sedating [PHARMACIST ONLY MEDICINE] eg, dexchlorpheniramine (Polaramine), promethazine (Phenergan)
Topical (nasal and ocular) antihistamines, nasal corticosteroids
[PHARMACY ONLY MEDICINE] eg, levocabastine (Livostin Eye Drops/Nasal Spray), naphazoline + pheniramine (Naphcon-A, Visine Allergy), naphazoline + zinc (Clear eyes-A), naphazoline + antazoline (Albalon A Allergy), ketotifen (Zaditen)
Nasal corticosteroids [PHARMACY ONLY MEDICINE] eg, beclomethasone (Alanase, Beconase Allergy & Hayfever), budesonide (Butacort), fluticasone (Flixonase), triamcinolone acetonide (Telnase)
Decongestants Topical (nasal)
[PHARMACY ONLY MEDICINE] eg, oxymetazoline (Sudafed Nasal Spray), xylometazoline (Otrivin range)
Oral
[GENERAL SALE] eg, phenylephrine (Sudafed PE Nasal Decongestant)
Combination products (contain analgesics)
[GENERAL SALE] eg, ibuprofen + phenylephrine (Nurofen Cold & Flu) eg, ibuprofen + paracetamol + phenylephrine (Maxigesic PE)
eg, paracetamol + phenylephrine (Sudafed PE Sinus + Pain Relief) [PHARMACY ONLY MEDICINE]
eg, paracetamol + phenylephrine + chlorpheniramine (Sudafed PE Sinus Day + Night Relief)
Other nasal products [GENERAL SALE]
eg, cellulose and peppermint powder (Nasaleze)
eg, saline (Otrivin Clear Saline Plus, Fess Original Nasal Spray*)
eg, Neil Med Range
Natural / herbal products / supplements Cowslip, elderflower, sorrel, verbena, bromelain, quercetin, Sanderson Sinus & Allergy
to an allergen. When it ocurs all year round it is called perennial allergic rhinitis (also called persistent allergic rhinitis). When it occurs seasonally, such as during spring or summer, it is called seasonal allergic rhinitis (see Hay Fever), although symptoms of perennial allergic rhinitis may worsen during pollen season.
Nasal congestion and sneezing are the most common symptoms of perennial allergic rhinitis, although sneezing is usually less than that experienced with hay fever. The eyes are not commonly involved, but the risk of developing sinusitis is higher. Some people may lose their sense of smell or develop nasal polyps (see subtopic, Nasal polyps, opposite page).
Allergens, such as house dust mites, moulds and animal dander that exist year round are the most likely cause, and people with perennial allergic rhinitis should take steps to limit their ongoing exposure to these. Skin-prick
Comments
Useful for symptoms that persist during the day. Although drowsiness with these products is rare, it may still occasionally occur in some people. Always caution about driving or operating machinery if feeling drowsy.
May be useful to aid sleep when symptoms are more problematic at night. Warn about drowsiness and the risk of driving or operating machinery. Avoid alcohol. These are [PRESCRIPTION ONLY MEDICINES] for children under two years old.
Have a localised effect and a rapid onset of action. Use eye drops combining antihistamines with decongestants short term only (ie, less than three days). Throw drops away one month after opening. Stinging and a bitter taste after application have been reported.
Useful for treatment and prevention and as a first-line therapy for moderate-to-severe allergic rhinitis. A decongestant or antihistamine may also be required initially on starting a nasal corticosteroid as relief may be delayed two to three days.
Best reserved for when nasal congestion needs to be treated quickly. Useful for symptom relief while waiting for nasal corticosteroids to take effect. Rebound congestion can occur with extended use. Topical decongestants should not be used longer than three days. Do not use in children aged under two years unless on medical advice.
Decongestants dry up a runny nose. Some products are also not recommended for children under six, see Colds. Watch for double-dosing if taking more than one product.
May be useful for periods where symptoms are particularly bad. Watch for double-dosing of decongestant ingredients if taking more than one product. Some products are not recommended for children under six, see Colds
Cellulose powder is delivered as a fine mist into the nasal passages where it forms an impermeable barrier to allergens. Fess contains saline which thins nasal mucus and moisturises dry nasal passages. It allows mucus to break down faster and washes away pollen, animal dander and dust.
Nasal-oral aspirators allow nasal mucus to be removed efficiently. Automatic irrigators can help with postnasal drip and nasal dryness.
A combination of cowslip, elderflower, sorrel and verbena reduces symptoms of acute and chronic sinusitis. Other natural products (eg, bromelain, quercetin) may also help.
testing can help identify which one is to blame. Wooden flooring should replace carpets, protective covers should be used on mattresses and pillows, and bed linen should be washed regularly. Pets should be kept outside.
Nasal corticosteroids are the first-line treatment for perennial allergic rhinitis. These reduce the inflammatory response which helps relieve congestion and nasal itching or watering. For optimal control they may be used with oral antihistamines. Decongestants should only be used intermittently for less than three days at a time.
There is a strong association between allergic rhinitis and asthma, and people should be encouraged to talk to their doctor about being evaluated for asthma at their next visit.
Infective rhinitis is an inflammation of the nasal mucous mebranes due to a viral infection and the common name for it is a cold (see Colds).
Vasomotor rhinitis is another name for nonallergic rhinitis. Symptoms are similar to those of allergic rhinitis but are not due to an allergy, and may be triggered by alcohol; certain odours, such as perfume, cigarette smoke and paint fumes; environmental factors (eg, barometric pressure, bright lights, temperature); or spicy foods.
Our sinuses (more correctly called paranasal sinuses because they surround the nose) are four pairs of air-filled cavities located in the low part of our forehead, behind our cheeks, between our
• People with other health conditions (eg, heart or lung problems, diabetes) or who are pregnant or breastfeeding.
• People who take medicines, including herbal/complementary products.
• Children aged under 12.
• If other symptoms are present, such as a fever, swollen glands or a persistent headache.
• If only one side of the nose is affected, or if a foreign object appears to be lodged up the person’s nose.
• People who are short of breath or with a cough or wheeze.
• With a coloured or yellow discharge from the nose.
• With nasal symptoms that have developed soon after beginning a new medication.
• People complaining of severe pain or whose symptoms have persisted despite treatment.
• People with allergies to medicines.
eyes, and behind the bridge of our nose.
All our sinuses are connected via tiny openings, some only millimetres wide, called ostia, and all drain into the nasopharynx (back of the nose). Sinuses produce mucus, which protects the nose and sinuses from dirt, pollutants, and microorganisms, such as bacteria and viruses.
When our sinuses are functioning normally, mucus is swept slowly out of each sinus into the nose via the ostia and drained into the nasopharynx before being swallowed.
Sinusitis occurs when the sinuses become inflamed or infected, and the swelling that results interferes with drainage and causes mucus to build up. This makes it difficult for people to breathe through their nose, and causes facial pain (which may be misinterpreted as a toothache) or a headache. A thick yellow or greenish discharge from the nose or down the back of the throat (a postnasal drip) may also occur.
Acute sinusitis is most often associated with
a cold (see Colds), and usually resolves within seven to 10 days. Saline nasal sprays, nasal corticosteroids, decongestants, or analgesics may be given to help relieve the symptoms. Sometimes a viral sinusitis can be complicated by bacteria and antibiotics prescribed by a doctor may be needed, but not always.
Persistent or chronic sinusitis is that which occurs for longer than 12 weeks despite medical treatment. Refer customers back to their doctor.
Nasal polyps are smooth, round, projections that hang down like teardrops into the nasal cavity and are attached to the lining of the nose. They are associated with conditions that cause inflammation such as asthma, allergic rhinitis, aspirin sensitivity, recurrent infections and certain immune disorders, and are more common in adults. Surgery is sometimes needed to remove them if they start to severely interfere with breathing or nasal fluid drainage.
• Sleep can usually be improved by establishing regular bedtime routines and addressing adverse lifestyle factors.
• On average we experience about four or five 90-minute sleep cycles a night.
• Sleep apnoea is a risk factor for cardiovascular disease.
Persistent lack of sleep can take a toll on somebody’s health, and you may notice your customer looks tired or admits to not sleeping well.
Our bodies like predictability, which is why many people find themselves waking up just minutes before their alarm goes off. Creating a regular bedtime schedule; avoiding stimulants and blue/green light from devices two hours before bed; and calming the mind throughout the day will all help improve sleep (see Text box: How to Improve Sleep). Remind your customers that it can take several weeks and sometimes months to undo bad sleep habits. Refer anyone with concerns identified by the Refer to a Pharmacist checklist.
Refer all customers seeking help with sleep to a pharmacist, as all products (apart from herbal supplements), are Pharmacist Only, and it represents an opportunity for pharmacists to identify any underlying conditions that may warrant referral to a doctor.
Self-medication with alcohol for sleep is also common and addressing this may be more
• People with other health conditions (eg, heart or lung problems, diabetes) or who are pregnant or breastfeeding.
• People who take medicines, including herbal/complementary products that may be contributing to their lack of sleep.
• Children and adolescents aged under 18.
• If self-help remedies, over-the-counter medicines, or devices for snoring have been tried without success.
• Insomnia that has lasted for more than three weeks.
• People who appear anxious or depressed.
• People whose sleep is disrupted by frequent night-time urination.
• People whose symptoms are suggestive of obstructive sleep apnoea (OSA).
• People with other symptoms that may suggest a previously undiagnosed medical condition.
• People with pain that prevents them from getting a full night’s sleep.
• People with allergies to medicines.
beneficial than just suggesting an oral sleep remedy.
A recent overseas survey of pharmacists showed 86% recommended a sedating antihistamine to customers to improve sleep, after just 0.2 to 4 minutes consultation. But pharmacological treatment for sleep is not always the best option, although it may represent an easy one.
Non-pharmacological advice on lifestyle and sleep hygiene, although it takes time, remains the best long-term measure.
Doxylamine and promethazine are two sedating antihistamines that can be used for sleep in adults. Few studies support their use, and suggest they are only minimally effective at inducing sleep and may reduce sleep quality. They are also linked with residual drowsiness
Category Examples Comments
Sedating antihistamines [PHARMACIST ONLY MEDICINE] eg, doxylamine 25mg (Dozile)
Melatonin [PRESCRIPTION MEDICINE] – except when sold in MOH approved packs and dosages by a registered pharmacist for the treatment of primary insomnia in adults aged at least 55, for up to 13 weeks eg, melatonin 2mg (Circadin)
Anti-snoring treatments eg, Aveo TSD Anti-Snoring Aid (device holds the tongue forward to keep airway open during sleep), Breathe Right nasal strips (adhesive nasal strips to reduce nasal congestion), Silence AntiSnoring Spray, Snorel, Snoreeze, Snorestrap (supports the lower jaw during sleep), SnoreRx (a mouth guard that moves the lower jaw forward to open the airways)
Restless legs/muscle cramps [GENERAL SALE] eg, magnesium + other ingredients (Crampeze Night Cramps)
Natural / herbal products / supplements Valerian, lemon balm, hops, lavender oil, magnesium, kava, passionflower, skullcap, tart cherry, tyrosine eg, Artemis Sleep Tea, Clinicians Sleep, Remifemin Sleep, Sleep drops, Swisse Ultiboost Relax & Sleep
(the hangover effect) and tolerance to them can develop within as little as three days. Side effects include dry mouth, constipation, and confusion. Older individuals are particularly sensitive to these effects.
Melatonin 2mg prolonged-release tablets have been reclassified to allow approved pharmacists to supply them to customers aged 55 years and older who satisfy the criteria after completing the 20-question sleep screening tool.
This is based on research that shows the production of natural melatonin is generally decreased in older adults and supplemental melatonin can improve sleep and morning alertness in 17% to 47% of participants. Research also shows melatonin to be beneficial in delayed sleep phase disorder (often affects teenagers), for shift work, or jet lag.
Use only for temporary insomnia due to an identifiable cause (eg, jet lag) and restrict use to five days. Take 20 minutes before going to bed. Tolerance may develop and side effects include dry mouth, constipation or blurred vision. Avoid drinking alcohol and driving or operating machinery within eight hours of taking doxylamine. Has the potential to be abused so refer suspicious requests to a pharmacist. See OTC Reference section, Precautions
Melatonin is a hormone produced by the pineal gland which is thought to play a role in maintaining the body’s circadian rhythm (body clock) as it is stimulated by darkness and suppressed by light. May cause daytime drowsiness and impaired concentration. Melatonin for oral use containing 3mg or less (immediate-release) or 2mg or less (modifiedrelease) may be sold by pharmacists who can competently identify primary insomnia.
These products will only help snoring, not sleep apnoea. Can be effective for mild snoring. If snoring persists and/or becomes severe despite using these strategies, refer the snorer to their doctor.
Magnesium products may provide relief from, and help reduce, muscle cramps and spasms, tired, aching and restless legs.
Evidence supports the use of valerian and lemon balm to improve quality and quantity of sleep. Many other ingredients (eg, tart cherry – a natural source of melatonin), lavender, passionflower) are reported to help sleep; however, evidence is often limited.
Despite years of research, there is still a lot about sleep that we don’t understand. A self-analysis of sleep is difficult – half the time we don’t know that we are sleeping when we are asleep. And although sleep studies can record brain waves and other physiological changes characteristic of sleep, experts are still not sure why these occur and how they benefit our bodies. Sleep used to be considered a period of inactivity during which our brain shut down. However, it is now clear that our brain and body stay remarkably active during sleep; in fact, during some sleep stages, our brain is more active than when we are awake.
A hypnogram provides a graphical representation of sleep and progression through the various sleep stages. Most people cycle through four or five sleep cycles per night and each sleep cycle may consist of up to three non-rapid eye movement (NREM) stages, N1, N2, and N3 (called quiet sleep) and one rapid eye movement (REM) stage (dreaming sleep). Between each cycle, we may briefly wake up, although most of us won’t remember doing so.
Snoring is a sign that a person’s breathing is being affected by sleep and the risk is higher in people who are overweight or with a thick/ wide neck, who drink too much alcohol, have a blocked nose, have certain medical conditions (such as Parkinson’s disease), smoke, or take medicines that make them sleepy.
Obstructive sleep apnoea (OSA) is a form of snoring where breathing pauses or is markedly
• Valerian: Appears to get its sedative effect by affecting the transmission of GABA. Trial results are inconclusive, and it has been associated with side effects such as headache, diarrhoea, daytime sedation/dullness, and withdrawal symptoms on discontinuation.
• Kava: Appears to act on both GABA and benzodiazepine binding sites and has anxiolytic properties but there is a lack of trials investigating its use for chronic insomnia. Side effects include nausea, diarrhoea, and liver toxicity.
• Passionflower: Animal studies indicate passionflower may help with sleep but there is a lack of human studies. Side effects include drowsiness and confusion.
• Hops: Some studies do report an effect on sleep, particularly when combined with Valerian.
• Avoid stimulants, such as caffeine, from the afternoon onwards, and do not eat a large meal, spicy food, or drink alcohol within two hours of bed.
• Stop using devices two hours before bed. They emit blue/green light which can neutralise the effect of melatonin. Amber glasses may be used with devices to protect against the light.
• Exercise during the day but not too late at night. Consider yoga, mindfulness, or meditation. The mind during sleep is a continuation of the mind during the day and these three practices teach people how to let go of stressors and transfer their focus to the breath or other calming actions.
• Have a routine before you go to bed and do it every night. It might be to take a bath, meditate for 15 minutes, or to listen to soothing music with the lights down low.
• Your bedroom should be quiet, dark, and tidy. The optimum temperature for sleep is around 18°C to 20°C.
• As soon as you get out of bed in the morning, expose your face to bright light, either sunlight or artificial.
reduced for short periods of time during sleep. People with OSA have a higher risk of heart attack and stroke, high blood pressure, heart arrhythmias, and driving accidents.
People with OSA usually snore very loudly, snort or grunt, or gasp for air when their
breathing pauses during sleep, and complain of daytime fatigue. Refer anybody with suspected OSA to a doctor or a sleep apnoea clinic.
• Nearly 85% of New Zealanders are smokefree; however, Māori are overrepresented in smoking statistics.
• Some smokers can make up to 14 quit attempts before they permanently stop smoking.
• Nicotine replacement therapy (NRT) increases the rate of quitting by 50% to 60%.
• Smoking cessation products are available free for most people.
If you suspect a customer smokes, tactfully enquire as to their smoking status. Pharmacy staff are in an ideal position to deliver personalised, empathic smoking cessation advice, since there is good evidence that even brief advice from health professionals has a significant effect on smoking cessation rates. Pharmacists can also provide funded NRT. Success is increased when repeated interventions are delivered from several different sources over a long period of time. This may be as little as saying the words “If you ever want to stop smoking, we can help” to a customer who you know smokes. Smokers cycle through the stages of contemplation, quitting and relapse an average of 14 times before achieving permanent success. A free online smoking cessation training course for health professionals, Helping People to Stop Smoking is available at learnonline.health.nz. The most important variable determining how smokers will respond to any intervention is their readiness to change (ie, they have to want to stop).
Smoking cessation advice is based around the mnemonic ABC:
• Ask customers about their smoking status.
• give specific Brief advice about stopping smoking to all smokers
• strongly encourage every person who smokes to use Cessation support and offer to help them
Category Examples
Nicotine replacement therapy (NRT) [GENERAL SALE]
• Women who are pregnant or breastfeeding, elderly people, or people with diabetes, heart disease, or who are underweight.
• People who don’t want to totally abstain from smoking.
• People who have sensitive skin and request nicotine patches.
• People who smoke irregularly.
• People who have had a reaction to nicotine products in the past.
access it.
Enquire about a customer’s progress or problems when they buy or collect their smoking cessation products and encourage continued abstinence.
There are many effective treatments (some prescription only) that can produce long-term abstinence, but evidence has shown the success rate is improved when treatment is combined with personalised counselling and behaviour modification.
Quitline Me Mutu (www.quit.org.nz or 0800 778 778) offers free smoking cessation advice and nicotine replacement therapy (NRT). NRT is also subsidised on a prescription and may be free in some districts through smoking cessation coaches and pharmacists.
QuitStrong NZ (quitstrong.nz) is another platform connected with Quitline that will help a person locate a free Quit Coach in their area, who can deliver free NRT and provide full support and kaupapa Māori services.
Research has indicated that few people stop smoking by going “cold turkey” alone.
NRT is available as a gum, lozenge, patch, and inhalator. Heavy smokers experience better rates of success if high dosages of a long-acting form of NRT (such as a patch) is combined with a short-acting form (such as nicotine gum), that is able to quickly relieve cravings. Hypnosis,
eg, Habitrol Gum, Habitrol Patches, Habitrol Lozenges, Nicorette CoolDrops Lozenge, Nicorette Gum, Nicorette 16hr InvisiPatch Patch, Nicorette QuickMist [PHARMACY ONLY MEDICINE] Nicorette Inhalator
Comments
acupuncture, and prescription medicines (eg, bupropion, nortriptyline, varenicline) are also options for smoking cessation.
Electronic cigarettes mimic the look and feel of conventional cigarettes and although they do not contain all the carcinogens present in tobacco products, they are not completely risk free. Some evidence does support their use as an aid to stopping smoking in adults; however, they are also associated as a gateway to smoking in teenagers.
Almost 5000 New Zealanders die annually from smoking-related illnesses, such as heart disease, lung cancer, and stroke. The lifespan of people who smoke is shortened, on average, by about 15 years, and children exposed to passive cigarette smoke (secondhand smoke) have a higher incidence of asthma, bronchiolitis, croup, and pneumonia. Smoking also contributes to socioeconomic and ethnic inequalities in health.
Māori are over-represented in smoking statistics. Research has shown over 22% of Māori adults smoke cigarettes, compared with just 8% of New Zealanders of European ethnicity. The New Zealand Government is committed to the goal that fewer than 5% of New Zealanders will be smokers by 2025. Promotion of the auahi kore (smokefree) message (www.smokefree.org.nz) throughout
NRT offers relief against nicotine withdrawal symptoms, including cravings, irritability, excitability, anxiety, headaches, nausea, dizziness, lethargy, loss of concentration, insomnia, gastric disturbance and respiratory problems. NRT is the preferred method for smoking cessation, as recommended by the New Zealand Ministry of Health.
Ensure correct strength. Under-dosing leads to nicotine craving and loss of confidence. Guidelines recommend staying on the same starting dose for at least eight weeks to allow time to create new habits and routines. Do not exceed stated doses.
Keep out of reach of children and pets; poisoning has occurred from improperly discarded patches. Fold sticky ends of the patch together, wrap and place in bin.
Patches may cause skin reactions. Always reapply on a new part of the skin. Use surgical tape over the patch to hold in place if the patch does not stick well. Patches may be worn while showering, exercising, or swimming. Remove patches overnight if they disturb sleep.
Natural / herbal products / supplements L-tryptophan, Naturo Pharm Quit Smoke May help with smoking cessation.
• Most sore throats are caused by cold or flu viruses and treatments just temporarily relieve symptoms.
• Strep throat infections are more prevalent among Māori and Pasifika children and those living in crowded homes.
• Untreated strep throats may lead to rheumatic fever which can affect the heart or kidneys.
Ask your customer for a description of their symptoms, or if appropriate, don a face mask and gloves and take them to a private area to look at their throat, especially if they are reluctant to go to a doctor.
Try to assess the degree of redness (ie, mild, moderate or severe) and look for any unusual features (such as white patches on the back of the throat or pus). Refer any customers with
Category Examples
concerns identified by the Refer to a Pharmacist checklist.
Products such as oral and topical analgesics, numbing sprays, and lozenges temporarily relieve the pain associated with viral sore throats. Even sucking non-medicated lozenges can provide some relief as the action of sucking produces saliva, which lubricates and soothes inflamed tissue.
People with a suspected strep sore throat should be referred to a doctor because some may require antibiotics.
Sore throats are common and symptoms can vary from a mild scratchiness at the back of the throat to severe pain.
Visually, the throat may look dry and red and
Soothing products eg, Radiance ManukaGuard Honey Lozenges eg, Weleda Throat Relief Oral Spray
Antiseptic/antibacterial agents
Comments
[GENERAL SALE]
eg, Codral Sore Throat Lozenges Antibacterial Honey & Lemon, Codral Sore Throat Lozenges Antibacterial Menthol, Strepsils Lozenges*, Strepsils Plus Sore Throat & Blocked Nose
[PHARMACY ONLY MEDICINE]
eg, Difflam-C Solution Sugar-Free (+ anti-inflammatory), Difflam Lozenges Sugar Free (+ anti-inflammatory)
Antiviral agents [PHARMACY ONLY MEDICINE] eg, Betadine Sore Throat Gargle
Anti-inflammatories (locally acting)
Locally acting anaesthetics
Oral non-steroidal anti-inflammatory agents (NSAIDs)
[PHARMACY ONLY MEDICINE] eg, benzydamine (Difflam range)
[GENERAL SALE]
eg, Codral Sore Throat Lozenges Antibacterial and Anaesthetic Lime & Lemon, Difflam Lozenges Plus Anaesthetic, Strepsils Anaesthetic Lozenges*, Strepsils Plus Anesthetic Throat Spray*
[GENERAL SALE]
eg, aspirin (Aspro range, Disprin) eg, ibuprofen <25s (Advil, Nurofen) eg, ibuprofen + paracetamol (Maxigesic [16], Nuromol [12])
[PHARMACY ONLY MEDICINE]
eg, diclofenac 12.5mg (Voltaren Rapid 12.5), ibuprofen >25s (Nurofen range), ibuprofen suspension (Nurofen for Children, Fenpaed), ibuprofen + paracetamol (Maxigesic [50, 100], Nuromol [24, 48])
Locally acting non-steroidal antiinflammatory agents (NSAIDs)
[PHARMACY ONLY MEDICINE]
eg, flurbiprofen (Strepfen Intensive Lozenges*, Strepfen Intensive Throat Spray*)
Simple analgesics [GENERAL SALE]
Treatment and prevention using natural bacteria
eg, paracetamol (Children’s Panadol, Pamol, Panadol, Paracare range)
[SUPPLEMENT]
eg, Streptococcus salivarius K12 (BLIS K12 Throat Guard Boost, Blis K12 Throat Guard Daily)
Natural / herbal products / supplements eg, honey, echinacea, eucalyptus, liquorice, slippery elm eg, Bosistos range, Comvita Fortacold Lozenges with Propolis, Kiwiherb Herbal Throat Formula
the tonsils inflamed and swollen. Often, lymph nodes in the neck become enlarged and tender and can be easily felt from the outside of the neck. It may be hard for the person to swallow and their voice may sound husky or hoarse.
Sore throats caused by viral infections may also be accompanied by a cough, conjunctivitis, or a runny nose.
Viruses account for almost 90% of all infections, with a cold virus the most common cause. The Epstein-Barr virus, which is responsible for glandular fever, and the measles virus can also cause sore throat.
Bacterial sore throats caused by Streptococcus pyogenes, also called group A streptococcus [GAS] or a “Strep throat”, are more likely to occur in children aged between three and 14 years, during winter, and in people living in
Soothe a sore throat. Most also contain an antiseptic agent. Do not exceed the maximum recommended dose. Many contain an artificial sweetening agent that may have a laxative effect in some people.
May kill viruses and bacteria associated with sore throats but offers little symptom relief.
Effective at relieving pain associated with sore throats. If solution stings, it may be diluted with water. Benzydamine is not recommended for children aged under six years.
These contain lignocaine or benzocaine and are effective at soothing and numbing sore throats.
Warn customer to be careful when eating or drinking hot foods or drinks due to altered perception of heat.
Not recommended for children aged under six years.
Effective at reducing inflammation, which will help ease sore throat pain. Ibuprofen is the NSAID least likely to cause stomach irritation.
NSAIDs may not be suitable for people on certain other medications or with some medical conditions (eg, asthma, kidney disease – see Refer to Pharmacist). Advise customer to stop taking if stomach upsets, increased bruising or prolonged bleeding occur.
Soluble aspirin may be used as a gargle to treat a sore throat. Avoid aspirin in children aged under 12 years.
See Reference Section, OTC Medicine Interactions, Precautions
Effective and well tolerated for the relief of sore throats.
Not recommended for children aged less than 12. Usual precautions for NSAIDs apply.
Effective at relieving pain but these are not anti-inflammatory, so will not relieve swelling or inflammation in the area. Suitable for people with contraindications to NSAIDs.
Streptococcus salivarius helps replenish naturally occurring beneficial throat bacteria, providing one month’s protection.
Several natural ingredients have soothing effects on the throat.
• People with other health conditions (eg, heart or lung problems, diabetes) or who are pregnant or breastfeeding.
• People who take medicines, including herbal/complementary products.
• Children and adolescents complaining of a particularly sore throat, especially those from deprived families.
• If swallowing is extremely difficult and preventing the person from drinking any fluids or is the person showing signs of dehydration.
crowded circumstances. S.pyogenes accounts for up to 30% of all cases of sore throat in children and 5%-10% of adults.
Sore throats may also be caused by dry air, excessive yelling, smoking, trauma, or regurgitation of stomach acid. The throat is usually only slightly red and the cause obvious with a bit of questioning. Suggest the customer eliminate the cause (if possible) or treat it if it is appropriate (for example, antacids or proton pump inhibitors for stomach acid).
Streptococcal (strep) sore throats
Strep throats are more likely to persist for longer than viral causes and be associated with
• People complaining of very severe sore throats; with signs of pus, ulceration or white patches on their tonsils.
• Sore throats that do not appear to be caused by a cold.
• With a sore throat that has persisted for several weeks or recurs often.
• With other symptoms, such as a rash, fever, vomiting, ear pain, breathlessness or general fatigue.
• People with allergies to medicines.
a high fever and severe symptoms. Pus on the tonsils is common in children over three but not in infants, who are more likely to have a thickened or bloody nasal discharge as their main symptom. Headache, nausea, vomiting and abdominal pain are also common in children. Occasionally the person may develop a rash that feels rough to the touch. It may start on the neck and chest and eventually spread to the whole body. A strep throat infection accompanied by this distinctive rash is known as scarlet fever. The rash is caused by toxins produced by the streptococcal bacteria. Rheumatic fever can develop from an
• Eat cool, soft food such as smoothies and drink cool or warm liquids such as chicken soup. Avoid crunchy or spicy foods with severe sore throats. Increase water and fluid intake to offset dehydration.
• Rest as much as you can. Talk to a doctor if your sore throat does not get better within a few days.
• Regular sucking of lozenges or pastilles stimulates saliva, which will lubricate and soothe sore throats. Do not exceed the recommended dosage.
untreated sore throat or scarlet fever. It is an inflammatory disease that can lead to heart or kidney damage. An algorithm authorised by the Heart Foundation of New Zealand helps identify who is at high risk for rheumatic fever (see heartfoundation.org.nz) and recommends an appropriate course of action. Refer those with concerns to a doctor or a free community sore throat clinic (see hpa.org.nz for locations). Treatment is not always necessary in those with a low rheumatic fever risk.
• Avoid smoking – it can make a sore throat feel worse.
• Strep throats are highly infectious and all members of a household should be tested for the presence of bacteria. Cough into the crook of your elbow or cover your mouth with a tissue when you sneeze or cough. Wash your hands or use a sanitising hand gel immediately if you cough on your hands.
• Wash hands thoroughly before preparing food, and before and after tending to small children.
• Sprains and strains are types of soft tissue injury. Sprains are usually more serious than strains.
• Sprains occur when a ligament has been stretched or torn and strains occur when a muscle or a tendon has been stretched too far.
• Although the PRICED regimen is still recommended, the evidence supporting some of the steps in it is limited.
Sometimes it is not immediately obvious whether the injury is a strain or a sprain and how severe it is. Asking your customer to describe the events leading up to the injury as well as the symptoms at the time of the injury may help, but you should be alert for key features that warrant an immediate referral to a doctor or physiotherapist, such as:
• changes in skin colour atypical of normal bruising or numbness around the site of injury
• deformities (the joint or muscle looks out of shape compared with the unaffected side)
• large amounts of swelling around the injury site
• severe pain or bruising
• complete loss of movement or severe instability. Some athletes benefit from prompt surgery, but the only way to definitely tell if a ligament has ruptured is with an MRI scan.
You should always err on the side of caution and refer customers with seemingly significant injuries or concerns identified by the Refer to a Pharmacist checklist.
• People with other health conditions (eg, heart or lung problems, diabetes) or who are pregnant or breastfeeding.
• People who take medicines, including herbal/complementary products.
• Children under the age of 16 years.
• If the injured area looks crooked, there is numbness, or the person is unable to weightbear at all.
• If this is a repeat injury of an area that has been injured before.
• People who have symptoms of an infection near the injury site such as significant redness or red streaks spreading out from the injury.
• People with severe pain or severe swelling.
• With pain that has persisted for more than five days or worsened.
• People with allergies to medicines.
The PRICED regimen (see text box PRICED regimen opposite page) is still the most advocated approach, although some experts are concerned that using ice may have a negative effect on tissue healing.
According to a 2020 Cochrane review, compared to paracetamol, NSAIDs make no difference to pain caused by a soft tissue injury at one to two hours, two to three days, or at day seven or beyond. Use of NSAIDs may result in a small increase in gastrointestinal events but it is unclear if they are detrimental or beneficial for soft tissue healing and more trials are needed.
Some experts suggest soft tissue injuries should be managed by PEACE:
• Protect the area by unloading or restricting movement for one to three days.
Category Examples Comments
Topical antiinflammatory agent
Topical non-steroidal anti-inflammatory agents (NSAIDs)
Oral non-steroidal anti-inflammatory agents (NSAIDs)
[GENERAL SALE] eg, mucopolysaccharides (eg, Hirudoid)
[GENERAL SALE] eg, ibuprofen (Nurofen Duralast, Nurofen Gel), diclofenac (Voltaren Emulgel)
[GENERAL SALE] eg, ibuprofen up to 25s (Advil, Nurofen)
[PHARMACY ONLY MEDICINE] eg, diclofenac 12.5mg (Voltaren Rapid 12.5), ibuprofen >25s (Advil, Nurofen), ibuprofen + paracetamol (Maxigesic, Nuromol) [PHARMACIST ONLY MEDICINE] eg, diclofenac 25mg (Voltaren Rapid 25)
Simple analgesics [GENERAL SALE] eg, paracetamol (Panadol, Paracare)
Sports taping and mouthguards eg, Elastoplast sport, Kinesio Tex Tape, Leuko tape, USL sports tape and mouthguards
Sports supports eg, elastic supports, neoprene supports (Elastastrap, Thermastrap Supports)
Natural / herbal products / supplements eg, arnica, comfrey, menthol eg, Anti-Flamme Creme, Anti-Flamme Extra, Tiger balm, Zorub
• Elevate the limb higher than the heart
• Avoid anti-inflammatories because these may be potentially detrimental to tissue healing.
• Compress the area by taping or bandaging
• Educate people that they should take an active approach to recovery and set realistic expectations about recovery times.
After the first few days have passed, soft tissue injuries need gentle exercises that do not exacerbate pain but promote blood flow to the injured area. This promotes tissue repair and rebuilding and helps restore mobility, strength, and proprioception.
Refer people with moderate or severe sprains or strains to a doctor or physiotherapist for a precise diagnosis and ongoing treatment and monitoring.
Use for contusions, sprains, haematomas, bruises and swelling.
These treat the body’s inflammatory reaction to injury and reduce pain, but evidence suggests they may delay tissue healing if used after an injury. Consult a doctor for advice. Patches should not be used on children <16. May, rarely, cause the same adverse effects as oral NSAIDs. Similar care and consideration before use is recommended. Avoid massaging for the first 48 hours after injury – rub in gently.
These treat the body’s inflammatory reaction to injury and reduce pain, but evidence suggests they may delay tissue healing after a soft tissue injury.
Ibuprofen is the NSAID least likely to cause stomach irritation.
Advise customers to stop taking if stomach upsets, increased bruising or prolonged bleeding occur see Reference Section, OTC Medicine Interactions, Precautions
May be beneficial as a first-line treatment for sprains and strains. Effective at relieving pain. Suitable for people with contraindications to NSAIDs.
Strapping tape helps stabilise joints during exercise and should be removed immediately after exercise. Kinesio tapes have specific stretch, recoil and adhesive properties and can be worn for three to five days. Mouthguards should always be worn during contact sport.
Elastic supports provide compression and support for wrists, ankles, knees and elbows.
Comfrey and arnica have some pain-relieving properties. Menthol has a cooling effect. Heat rubs and other topical applications can also relieve pain and swelling (see also Muscular Aches and Pains: Treatment options).
Sprains and strains are common injuries, especially in children and those who play sport.
A sprain can be a serious injury and occurs when a ligament is stretched and/or torn. Ligaments are fibrous bands of connective tissue that join one end of a bone to another. Ligaments stabilise and support the body’s joints. Sprains happen immediately causing sudden pain and/or the injured person may report a pop, tear, or sudden loss of power.
Signs of a sprain include pain, swelling, bruising, instability, and loss of the ability to move and use the joint (called functional ability). Signs and symptoms can vary in intensity and with a mild sprain, minimal pain and swelling and little or no loss of functional ability is experienced. Swelling with sprains is usually greater than that seen with strains and it can be difficult to move or walk on the injured part.
Sprains typically occur through direct or indirect trauma such as a fall, awkward landing or blow to the body. It knocks the joint out of position, overstretching and, in severe cases, rupturing the supporting ligaments. Ankles, wrists and knees sprain easily.
The 2018 British Journal of Sports Medicine guidelines on ankle sprains state that ankle ligament ruptures benefit best from support using tape or a brace in combination with an exercise programme, rather than long periods of immobilisation.
A strain is when a muscle or tendon (fibrous cord of tissue that attaches the muscle to the bone) has been stretched too far.
Strains often happen when too much pressure is exerted on a muscle or the muscle is pushed too far (eg, when lifting a heavy object). Strains can happen suddenly or the pain may not begin until a few hours after the event that caused the strain.
People with strains typically experience pain, limited motion, muscle spasms and, sometimes, muscle weakness. There may also be bruising or swelling around the affected area, cramping, or inflammation and some loss of muscle function. Severe strains are often very painful and disabling.
Back, necks and legs can commonly be strained, especially if no proper warm-up has been done, or when somebody returns to a sport after a period of absence. Bad work habits (including bad posture and incorrect lifting techniques) can also lead to strains
• Protect from further injury – Use splints, pads or crutches.
• Rest – Restrict activity for 48–72 hours.
• Ice – Apply ice for 20 minutes every one to two hours for the first 48 hours while awake.
• Compression – Apply light compression (do not restrict blood flow).
• Elevation – Raise the injury above the heart.
• Diagnosis – Consult a doctor or physiotherapist if needed.
• Avoid HARMS for the next 48–72 hours (Heat,Alcohol,Running,Massage, Stretching ).
• Supports such as shoes with good ankle support, tape for ankle strapping, knee braces, etc, are important once activity is resumed.
• Organise work areas to make them more comfortable and avoid awkward working postures.
• Practise correct lifting techniques and use two-person lifts.
• Incorporate stretching and strengthening exercises into your exercise programme.
• Warm up, stretch and take regular breaks from intensive activities.
• Sunscreens that do not provide the protection promised on their label can now be fined under the Fair Trading Act.
• Many sunscreen ingredients are toxic to aquatic life.
Despite New Zealand having high levels of UV radiation, we are not generally very good at applying sunscreen. For customers buying sunscreen, take note of their skin type and stress the importance of never getting sunburnt, especially to those with fair skin. Help them to choose a more environmentally friendly product.
Sunscreen should not be used as a way of staying in the sun for longer, but as a way of reducing a person’s risk of UV exposure.Encourage proper and regular application (see Sun Protection Advice). Educate customers about the dangers of our sun and to keep their skin protected from 9.30am until 5.30pm during summer.
Mild sunburn can be treated with topical cooling preparations (such as aloe vera), topical anaesthetics, or moisturisers. Refer anybody with severe sunburn or other concerns identified by the Refer to a Pharmacist checklist.
Sunburn occurs from overexposure to ultraviolet (UV) radiation, most commonly from the sun but also from sunbeds. Symptoms of mild sunburn include reddened skin that is painful and hot to touch, and tiredness and a headache from dehydration caused by prolonged exposure to the sun.
Severe sunburn causes skin blisters and often a
• People who are immunosuppressed or with cancer.
• People taking medicines that may increase their sensitivity to the sun.
• People with severe sunburn and a headache, in extreme pain, or nauseous.
• People who burn easily with minimal sun exposure.
• Young children with moderate sunburn.
• People with suspicious-looking moles or blemishes on their skin.
• People with allergies to topical ingredients.
fever; although the person may complain of feeling cold (chills). It may also cause dehydration which, if left untreated, can lead to electrolyte imbalances, shock, or even death. Four to seven days after exposure, sunburnt skin starts to peel and flake off.
Sunburn causes microscopic changes in the skin, and weakens the skin’s immune defence system. Premature ageing (wrinkling, skin sagging, age spots), brown spots and freckles, premalignant lesions (such as solar keratoses) and eye damage (see Sun Care: Eye protection) also occur with long-term sun exposure, not necessarily just with sunburn.
The Sunscreen Product Safety Standard Act passed in March, 2022 means that products labelled as sunscreens must meet certain standards or be fined under the Fair Trading Act.
Sunburn and skin cancer
Basal cell carcinoma and squamous cell carcinoma are the most common types of skin cancer, but melanoma is the deadliest form, killing more than 350 New Zealanders each year.
Adults of fair complexion with excessive previous sun exposure or repeated sunburn, especially during their childhood years, are more at risk. One blistering sunburn is thought to double the chance of a person developing skin cancer in their lifetime.
Category Examples Comments
Sunscreens (contain chemical with or without physical agents)
[GENERAL SALE] eg, Cancer society, Neutragena Ultra Sheer, Reef, Skinnies range, UV Guard
Physical sunscreens [GENERAL SALE] eg, zinc oxide (Invisible zinc, Sunsense Sensitive)
Lip balms [GENERAL SALE] eg, Badger range, Sunsense Lip Balm SPF 50+, Blistex Medicated Relief
Sunburn treatment products [GENERAL SALE] eg, moisturisers (Cancer Society After Sun Gel, Lucas Papaw) eg, cooling gel + vitamins (Sunsense After Sun) eg, MEBO Burn Repair eg, local anaesthetics (Soov Cream/Spray)
Natural / herbal products / supplements Aloe vera gel, vitamin C with vitamin E, vitamin D (see the Vitamins and Dietary Supplements chapter)
UV index and the Sun Protection Alert
UV radiation is not something that can be seen or felt. The UV index (UVI) is a standardised way of measuring the intensity of UV radiation on a particular day in a particular place. It takes into account the sun elevation angle, ozone amount, cloud cover, sun-earth separation, altitude, pollution and surface reflections (eg, snow). A UVI greater than 10 is considered extreme and a UVI of less than 3, low. Daily UV indices are available at www.niwa.co.nz
The Sun Protection Alert (SPA) is a simpler tool that indicates the period during the day when sun protection is required. A daily SPA is published in many New Zealand newspapers during summer and can be found with town-specific predictions on several websites (eg, sunsmart.org.nz, www. metservice.com) and the MetService App.
In New Zealand, sun protection is generally required daily, even on cloudy and cooler days, from September through to April. Sun protection may also be required during winter, especially at high altitude and in snow.
Sun protection involves the use of protective clothing, sunglasses, avoidance of the sun around the hottest period of the day (solar noon: NZ 1pm) and use of sunscreen on exposed skin.
Deflect UV radiation from the skin rather than absorbing it. Both zinc oxide and titanium dioxide provide UVA and UVB protection and are formulated as ultra-fine particles so as not to leave a sheen on the skin. Less likely to cause allergies.
Protect lips with special lip sunscreens – lips burn easily and sunburn can reactivate a cold sore on the lips. Reapply lip balm frequently as it gets “licked off”.
A moisturiser will not prevent peeling or damage but will help relieve irritation of dry, flaky skin. Cooling gels can be kept in the fridge and applied when the skin is hot.
MEBO Burn Repair promotes faster healing after sunburn by encouraging stem cell regeneration. Also helps cool the skin and relieves discomfort.
Local anaesthetics (eg, lignocaine) offer pain relief after sunburn. Avoid broken skin.
Aloe vera has a soothing, cooling action on skin that has been exposed to the sun. Combinations of vitamin C and E taken orally or applied topically prior to sun exposure can reduce risk of sunburn. They can also help heal sunburn when applied afterwards.
Many sunscreen ingredients have detrimental effects on aquatic life. Several countries, such as Palau, Mexico, Hawaii, Key West, Bonaire, and Aruba, have bans on certain sunscreen ingredients, although none are as comprehensive as Palau’s.
Research has found sunscreen chemicals and their metabolites present in aquatic wildlife and in sediment. Some also cause coral bleaching at lower-than-normal temperatures. Coral has a symbiotic relationship with microscopic algae called zooxanthellae that are the coral’s primary food source and give them their colour. If their relationship becomes stressed due to changes in temperatures, light, or pollution, the algae leave the coral, which turns white or pale, and usually dies.
The Haereticus Environmental Laboratory (HEL) publishes a list of sunscreen ingredients that are of concern, and they are:
• oxybenzone
• octinoxate
• octocrylene (naturally degrades into the chemical, benzophenone; a known carcinogen
Slip, Slop, Slap and Wrap!
• Slip on sun-protective clothing and seek shade from 10am–4pm.
• Slop on an approved SPF 50+ broadspectrum sunscreen 15–20 minutes before going outside
➤ Reapply every two hours as well as after swimming or sweating.
• Slap on a wide-brimmed hat.
• Wrap on a pair of sunglasses.
and endocrine disrupter)
• homosalate
• 4-methylbenzylidene camphor
• para-aminobenzoic acid (PABA)
• parabens (eg, methyl paraben, ethyl paraben, propyl paraben, butyl paraben, benzyl paraben)
• zinc or titanium nanoparticles.
• microplastics, such as exfoliating beads (most skincare products containing microbeads were banned in New Zealand in 2018)
• triclosan (an antibacterial/antifungal agent).
Oxybenzone is considered the most worrisome ingredient, because it can cause allergic reactions, and laboratory tests have shown it has weak oestrogenic and antiandrogenic effects. Oxybenzone can also be detected in the blood of people who use sunscreens containing it. Further investigations into other sunscreen ingredients are ongoing.
Avobenzone is another ingredient that is popular in sunscreens, but while this ingredient hasn’t been found to cause reef damage or hormone disruption like some others, it can be irritating and is not sun-stable which means
that it has to be mixed with other UV blocking ingredients. The FDA restricts the concentration amount to 3% in sunscreens.
Zinc-based sunscreens that contain particles larger than 100 nanometers (often referred to as non-nano) are considered reef and environmentally friendly.
There is little evidence that sunscreen use affects vitamin D production in the skin, and most experts recommend that concerns about vitamin D should not stop people from following skin cancer protection advice. Research has also shown vitamin D is still made by the skin in the shade with sunscreen on.
Sunsmart NZ suggest 30 seconds to 3 minutes of sun exposure, near the middle of the day, to make Vitamin D. Foods such as egg yolks, liver, milk, and oily fish also contain vitamin D. It is also added to some foods or can be taken as supplements.
• Sunscreen can wash off in the sea and waterways and damage aquatic life. Consider using rash shirts or swim clothes that cover the body, rather than sunscreen when going in the water.
• Avoid misting or spray sunscreens. These create a chemical cloud that can be inhaled or settle on sand and wash off into the ocean.
• Stay undercover and avoid the hottest part of the day. Cover up with a T-shirt or hat but there is no need to apply sunscreen under clothing.
• Avoid sunscreens with retinyl palmitate (can trigger skin lesions) or insect repellent (decreases sunscreen effectiveness and increases DEET absorption, especially in children).
• Protecting eyes from UV radiation is just as important as protecting skin.
• Your pharmacy should only stock sunglasses that meet AS/NZS1067.1/2:2016 or an equivalent recognised standard.
• Know enough to be able to explain to a customer the pros and cons of different frames, tints, lens types, and lens effects.
Help customers select sunglasses that best suit the main activity for which they will be worn. For example, polarised sunglasses are best for fishing and driving; nylon blended frames are resistant to hot and cold, and easily moulded into wrap-around styles so are ideal for high-intensity sports; and purple or rose tints offer the best contrast of objects against a green or blue background so are perfect for hunting or water-skiing. Importantly, the customer needs to like and feel comfortable wearing the sunglasses, which makes them more likely to be worn.
People who wear corrective glasses may consider having a UV protective coating added to their everyday glasses, investing in a pair of prescription sunglasses, or buying protective shades that can be worn over their visioncorrecting glasses.
Protecting your eyes against the sun is just as important as protecting your skin. While most people are aware of the link between ultraviolet (UV) radiation and skin cancer (see also Sun Care), few appreciate the connection between UV radiation (UVR) exposure and eye damage.
Particles in the atmosphere scatter UVR so even staying out of direct sunlight does not eliminate this hazard. UV damage to the surface tissues and internal structures of the eye (such as the cornea and lens) can occur from either natural sunlight or artificial UV rays.
In the short term, excessive exposure to UV radiation from daily activities can burn the surface of the eye, similar to a sunburn on the skin. Exposure is exacerbated by reflections off snow, concrete, water, or other shiny or white surfaces.
Acute effects of UV radiation on the eye include inflammation of the cornea and the iris,
Category Examples
photoconjunctivitis (an inflammation of the conjunctiva; the membrane that lines the inside of the eyelids), and photokeratitis (also called snow blindness – a temporary painful burn to the cornea).
Long-term exposure to UV radiation can lead to, or increase the risk of:
• age-related macular degeneration (AMD): a deterioration in macular tissue (light-sensitive tissue at the back of the eye) that causes loss of central vision
• cataracts: a clouding of the eye’s lens that can blur vision
• pterygiums: a white or creamy opaque growth attached to the cornea (white of the eye). These are usually non-cancerous, but may grow over the cornea, partially blocking vision, and may require surgery to be removed
• skin cancer around the eyelids; basal cell carcinoma is the most common.
In order to reduce the risk of eye damage, sunglasses should always be worn outside, particularly when it’s sunny, at the beach or near water, when driving or outside at high elevations or participating in snow sports. Anybody with an eye disease, who has had cataract surgery, or is taking photosensitising medicines (see Suncare: Common heat/sun sensitising medicines) should always wear sunglasses outside.
While more expensive sunglasses may use slightly dearer materials for both the frame and the lens, sunglasses cost has more to do with the brand name than a reflection of UVR protection.
Pharmacies should choose to only stock sunglasses that comply with the Australian/NZ standard (AS/NZS)1067.1/2:2016, or another internationally recognised standard. Note that this standard is voluntary in New Zealand, but a
version of this standard is mandatory in Australia.
AS/NZS: 1067.1:2016 sets limits on the allowed transmittances of fashion spectacles and sunglasses for adults and children. Sunglasses that are allowed to be worn while driving must comply with the colouration limits of this standard. Colours, in particular traffic signals, must still be recognisable when viewed through the lenses. The standard defines five categories of lenses – see below.
Several other markings may be found on sunglasses including the Eye Protection Factor (EPF) rating. This takes into account the frame coverage, UV protection, blue light and infrared protection (ability to shield the eyes from heat). Sunglasses labelled EPF 9 or 10 provide excellent protection, blocking almost all UV radiation.
Sunglasses may also be labelled UV400. These block all wavelengths up to 400 nanometers (which covers all UVA and UVB rays).
• Keep a good selection of each brand on display and ensure the eyewear and display cabinet is thoroughly dusted, clean, and tidy.
• Keep the best-selling styles at eye level.
• Know your product and be aware of different features and benefits. Ask your supplier for more information if you need it.
• Ask customers what they need their sunglasses for and what style they prefer (ie, large, rimless, metal, plastic).
➤ Allow them to try on several pairs and listen to their feedback.
• Choose styles based on their face shape:
➤ oval: oversized frames
➤ diamond: oval, cat-eye, or round frames
➤ square: round or oval
➤ round: rectangular, geometric, or cat-eye.
0 Fashion spectacles with very low sunglare reduction. Some UVR protection None
1 Fashion spectacles – not sunglasses. Limited sunglare reduction. Some UVR protection Not suitable for driving at night
2 Sunglasses – medium sunglare reduction and good UV protection None
3 Sunglasses – high sunglare reduction and good UV protection None
4 Special purpose sunglasses – very high sun-glare reduction. Good UV protection Must not be used when driving
Comments
Sunglasses eg, Bill Bass, Oakley, Ray Ban, Smith Sunglass suppliers offer
Common sunglasses components
COMPONENT MATERIALS INFORMATION
Frame Moulded plastic polymer
Cellulose acetate
Nylon
Metal (eg, titanium, beryllium, stainless steel, aluminium)/monel
Lens Polycarbonate
CR39
Plastic injected into a desired mould. Cost-effective but frames cannot be reheated or generally take a prescription lens.
Frames are cut from solid sheets of acetate. Retain their shape and do not shrink. Hypoallergenic and easily coloured.
Nylon blends make superior sports and performance frames and are resistant to hot and cold, flexible and readily moulded.
Lighter than plastic and easy to adjust. Less obtrusive to the field of vision. More expensive and less durable than other types and not for high-impact activities. Can get hot.
Titanium is a hypoallergenic metal that is lightweight, strong, durable and corrosion resistant. Produced in a variety of colours.
Beryllium is less expensive than titanium. Resists corrosion and tarnish – good for people with high skin acidity or around salt water.
Stainless steel is light weight and strong and provides excellent resistance to corrosion, abrasion and heat. Usually hypoallergenic.
Aluminium is lightweight and corrosion resistant and usually combined with silicon and iron to increase strength.
Monel is a rust-proof metal alloy, composed of nickel and copper with some traces of iron. Good malleability.
Expensive, virtually unbreakable thermoplastic that is 1/3rd the weight of acrylic and 1/6th as heavy as glass. Usually made from bis-phenol
A. Excellent transparency, durability, and high refractive index. Can be made thinner than glass or conventional plastic. Polarising filters can be incorporated. High impact resistance. Easily shaped but more likely to scratch. Can discolour over time.
Patented plastic polymer. Reasonably cheap. Same optical qualities and visual acuity as glass but more lightweight and impact resistant. Optically superior to polycarbonate. High glossy surface finish.
Plastic Light and impact resistant. Naturally UVR resistant.
Acrylic Synthetic cast lens. Same optical qualities and visual acuity as glass but more lightweight and 20 times more impact resistant. Can crack when exposed to extreme temperatures. More easily scratched than other lenses since softer. Good optical qualities at a low price.
Glass Excellent optical quality and scratch resistant. Heavy. Can shatter on impact. No UVR protection unless coated.
Lens effects Mirrored Reduce glare by reflecting light off the lens surface. Scratch easily as coating applied last.
Photochromatic/ photochromic
Polarised
Tinted
Other
Become darker when exposed to UV radiation. Can take up to two minutes for adjustment to happen, and may not darken inside vehicles with glass that blocks UV light.
Block polarised light reflected off horizontal surfaces and reduce light intensity. Enhance visual acuity. Recommended for water sports and driving but not as effective against snow glare as snow reflects light equally in all directions, rather than just horizontally.Test if truly polarised by holding lens up to a reflective surface (eg, car bonnet) and slowly rotating 90 degrees. Polarised sunglasses will show a significant diminishing of glare. Cost and optical quality depends on polarising method used and includes external film coating (cheapest), sandwiching polarising filter between layers of the lens (more durable and expensive), combining the polarising filter with the lens material while in liquid form (best optical quality).
Tint reduces visible light but does not provide protection from UVR. May affect ability to drive at night. Various tints are available: –grey, grey-green, smoke: good all-purpose tint. Reduces brightness while preserving 100% colour recognition. SPORTS: all outdoor sports –blue: reduces glare and helps define contours. Enhances colour perception. SPORTS: skiing, golf, fishing, watersports. –green: heightens contrast (mildly) while preserving colour balance. SPORTS: tennis, golf, baseball. –dark amber, copper, brown: good for blocking blue light (ie, on a cloudy day). Contains a red element to enhance depth perception. Useful to improve contrast on grass and against blue skies. SPORTS: fishing, cycling, golf, hunting, skiing, watersports.
–yellow, orange: less glare protection but perfect for moderate-to-low level light conditions. Excellent depth perception and contrast enhancement in flat-light conditions. SPORTS: skiing, snowboarding, hunting, indoor sports. –amber, rose, red: heightens contrast in partly cloudy and sunny conditions but causes significant colour imbalances. Reportedly more soothing to the eyes and reduce eyestrain. SPORTS: cycling, fishing, hunting, skiing, snowboarding, water sports.
See bit.ly/2TPifss for a visual sunglasses lens colour guide according to weather, activity, and features and benefits.
Hydrophobic coatings repel water. Anti-scratch coatings improve durability. Anti-fog coatings good for high-energy activities.
Other Reduce fogging “Air dams” direct the flow of air over the inside of the lenses. Small ventilator holes can also reduce fogging.
Hinges Metal are more durable than plastic.
Grips Rubber nose or ear pieces help keep sunglasses from sliding down nose.
Side protection Wide plastic temples and wraparound lenses give more protection from dust, snow, wind, rain and glare that may come in from the side.
• Hyperhidrosis (excessive sweating) is a common condition that can cause embarrassment and impact on work, school, or social relationships.
• Antiperspirants containing at least 20% aluminium salts may be tried initially.
• If antiperspirants are ineffective, refer your customer to a doctor or skin clinic for other types of treatment.
Be mindful of your customers’ privacy when talking with them about products for hyperhidrosis.
Explain the difference between an antiperspirant and a deodorant if they are not aware, and describe how higher concentrations of aluminium salts cause a more long-lasting closure of the sweat gland, but should be used only as directed.
Offer them some practical advice (see Advice for customers) and warn customers that aluminium antiperspirants can stain clothing.
Reassure people who experience hyperhidrosis that there are effective treatments available through skin or cosmetic clinics if antiperspirants do not effectively control the condition.
Products available in a pharmacy for sweating include deodorants, natural deodorant crystals, and antiperspirants.
Deodorants only contain a fragrance to mask unpleasant smells, they do not reduce perspiration, and are not appropriate for hyperhidrosis.
Deodorant crystals have natural antibacterial or antifungal properties to limit odour-causing bacteria and may be considered as a “natural” alternative to chemical products; however, they will not decrease sweating.
Antiperspirants reduce sweat release and usually contain an aluminium salt, such as aluminium chloride, aluminium chlorohydrate, aluminium hexahydrate, or aluminium zirconium, at a concentration of 10% to 25%.
• Women who are pregnant or breastfeeding.
• People who take medicines or supplements that may contribute to hyperhidrosis or body odour.
• Newly experienced hyperhidrosis in an adult.
• Sweating accompanied by other symptoms such as fever, weight loss, chest pain, shortness of breath, or a rapid heartbeat.
• Sweating in a child independent of heat or exercise.
• Sweating that occurs during sleep.
• People with allergies to topical ingredients.
Aluminium zirconium tends to be better tolerated by the skin and less likely to cause irritation or aggravation after razor use.
In low concentrations, aluminium ions cause a temporary closure of the sweat glands, reducing the amount of sweat produced, but reapplication is often needed.
An antiperspirant containing at least 20% aluminium chloride hexahydrate or aluminium zirconium is the preferred initial treatment for both primary hyperhidrosis and secondary hyperhidrosis. This high concentration of aluminium results in a more long-lasting closure of the sweat glands and regular use will ultimately shrink the gland, decreasing the amount of sweat it can produce.
Products marketed for hyperhidrosis are usually applied at night then washed off in the morning. Several weeks of nightly use are usually needed to control the sweating before switching to a two to three times weekly maintenance schedule. Before recommending an antiperspirant, run through the Refer to a Pharmacist checklist and refer any customers with concerns. Sometimes aluminium salts are combined with salicyclic acid to enhance penetration, or with natural plant extracts such as clove, sage, or Usnea barbata (Old Man’s beard) which can prevent skin irritations.
If your customer has limited relief from overthe-counter antiperspirants, then refer them to a doctor for other types of therapy such as:
• anticholinergics (eg, oxybutynin) – help prevent sweat gland stimulation but can cause side effects such as dry mouth, dry skin, flushing, urinary retention, and cardiac arrhythmias
• botulinum toxin type A – decreases the release
Category Examples Comments
Aluminium-containing antiperspirants for hyperhidrosis
[PHARMACY ONLY] eg, contains aluminium chloride (Perspi-Guard), aluminium zirconium (Rexona Clinical Protection)
Other products [GENERAL SALE] eg, aluminium chlorohydrate (Neat 3B Action Cream/ Body powder)
of acetylcholine from nerves supplying eccrine glands, inhibiting sweating for about five to nine months. Can be injected into armpits, palms, or the forehead
• iontophoresis – uses a gentle current of electricity to turn off sweat glands but is a lengthy process and only effective for the hands or feet
• MiraDry – uses heat from a microwavetype device to break down sweat glands in the armpits. Expensive but claims to offer a permanent solution to excessive sweating.
Beta-blockers have also been used for stressinduced sweating, and surgery that involves excision of sweat glands in troublesome areas may be considered as a last resort if all other treatments fail.
Although everybody sweats to a certain extent, some people have a problem with excessive or uncontrollable sweating, known medically as hyperhidrosis. The condition mainly affects the underarms, but may also affect the palms or the feet.
Although hyperhidrosis is not life-threatening, it can cause significant embarrassment and discomfort to the person involved and impact on work, school, or social relationships. The excessive sweating can stain clothing, skin chafing can occur leading to dermatitis and infections, and damp feet can begin to smell or damage footwear.
There are two types of glands located in the skin that contribute to sweat production. These are the apocrine and eccrine glands.
Do not shave 24 hours before applying product. Use pH neutral soap. Apply at night to clean, dry underarms and wash off the next morning. Use normal deodorants during the day. Reduce frequency of application once sweating has stopped. May damage clothing.
Reduces the amount of sweat on the area it is applied to, preventing friction and chafing. Can be applied to any affected body part (eg, hands, amputated stumps, between the toes, under the breasts, on the groin area, skin folds).
• People travelling overseas should talk to their doctor eight to 12 weeks before departure about any required vaccines (including a COVID-19 vaccination) or malaria prophylaxis if appropriate.
• Regular medicines should be taken in their original packet accompanied by a note from a doctor.
If your customer is intending to travel either locally or internationally, ask if they have a first-aid kit that includes travel-related essentials such as antihistamines, anti-nausea medication, pain-relief, plasters, sunscreen, and insect repellent.
For customers travelling overseas, advise them to see their dentist before they travel and to talk to their doctor or a travel clinic about which vaccines they may need, including the COVID-19 vaccination.
Encourage travellers going to less developed parts of the world to use self-purified or properly sealed bottled water for drinking and cleaning teeth, and to avoid ice. Remind them to wash their hands thoroughly before eating and after toileting or use hand sanitiser if washing facilities are unavailable or not adequate. They should only eat foods that are cooked thoroughly and served piping hot and avoid vegetables or fruits that cannot be peeled, as well as raw seafood and shellfish.
Customers should also be directed to the New Zealand Government’s official source of advice for New Zealanders travelling or living overseas (www.safetravel.govt.nz) which contains information on everything from passports and visas to weather warnings and recommendations about what countries NOT to visit. Travellers can also register their travel plans on the site. Information about the association between venous thromboembolism (blood clots) and air travel can be found in the Varicose Veins and Support Stockings chapter.
Advise customers to see their doctor or travel vaccination clinic ideally eight
to 12 weeks before departure to discuss what vaccines they will need and to allow time to begin the course prior to their departure.
Whether vaccinations are required or not depends on the customer’s age and:
• duration of visit and planned activities (eg, cycling, caving, trekking)
• how the person plans to travel (eg, car, bus, safari truck, on foot)
• if women are pregnant or breastfeeding
• long-term health conditions (eg, asthma, diabetes) or regular medicines
• likely contact with animals and type of accommodation
• previous vaccinations (including completion of childhood immunisations).
Most travel vaccinations are not free and can cost from $20 to over $250 per dose. Yellow fever vaccinations can only be given by an approved vaccination centre which will issue an International Certificate of Vaccination, which certain countries require before entry is granted. Commonly encountered diseases for which vaccinations are available are summarised in the table. Because no vaccine guarantees complete immunity, good hygiene and selfprotection measures (eg, applying insect repellent, safe-sex, social distancing, washing hands) should still be practised.
With some forward planning and sensible precautions, New Zealanders can reduce their risk of getting sick while overseas.
Medicines should only be taken overseas if they are for a customer’s personal use, or the personal use of someone travelling with them. All medicines should be left in their original packaging, and a note from the prescriber explaining what the medicine is for, together with a copy of the prescription (if applicable) should be carried.
Since some medicines may not be legal in certain countries, customers should check with the Embassy or High Commission of that country before departing. Customers should also be wary of purchasing prescription medicines over the counter overseas since counterfeit or substandard products are rife.
Category Examples Comments
Vaccines [PRESCRIPTION MEDICINE] – except in the form of an oral liquid when sold in a pharmacy by a registered pharmacist eg, Dukoral
Other products eg, MicroCleanz, Purell eg, 1Above, No Jet Lag eg, Blis K12 Travel, Inner Health Travel Bug
Diarrhoea affects over half of all travellers. Causes are numerous including changes in food or drinking water, bacteria, viruses, or other microbes (eg, Escherichia coli, rotavirus, Giardia). Treat with electrolyte solutions to replace fluids lost through diarrhoea and vomiting, with antidiarrhoeal medicines (eg, loperamide), and if necessary, antibiotics (but only under medical supervision). See Diarrhoea for OTC product information.
Several life-threatening illnesses are transmitted by mosquitoes and travellers need to be aware of which ones they may be at risk from during their trip.
Malaria is more common in Central and South America, Africa, Asia, Indonesia, and Eastern Europe. Symptoms occur anywhere from seven days to one year after infection and include fever and flu-like illness, chills, headache, muscle aches, and tiredness.
Customers should consult with a doctor familiar with current anti-malarial recommendations, as these are always changing. If malaria prophylaxis is prescribed, it should be taken exactly as directed, and precautions also taken to avoid getting bitten (see also Bites and Stings).
Dengue fever is a mosquito-borne viral illness that has dramatically increased in prevalence in tropical and subtropical parts of the world. The largest number of dengue cases ever was reported in 2019, with 3.1 million cases in the American region alone. High case numbers were also reported in Bangladesh, Malaysia, the Philippines, and Vietnam.
Symptoms of dengue fever are usually mild and flu-like and include a high fever, headache, pain behind the eyes, joint pain, muscle and bone pain, rash, and mild bleeding such as nose bleeds. Some people are at risk of developing severe dengue which can be fatal without immediate medical attention. Symptoms of severe dengue include a decrease in temperature (this does not mean the person is recovering), severe abdominal pain and persistent vomiting, rapid breathing, bleeding gums, blood in their vomit, fatigue, and restlessness. Dengue fever
Oral vaccine. Provides approximately 85% protection against Vibrio cholerae and at least 50% protection against enterotoxigenic E. coli. Follow recommended algorithm to assess customer suitability.
Hand sanitisers may be used if hygienic hand washing facilities are unavailable. Products are available that may help alleviate the symptoms associated with jet lag. Other products may help support our body's natural immune defence system.
Chickenpox (varicella)a Virus transmitted through airborne droplets
COUNTRIES WHERE PREVALENT (NOT ALL INCLUSIVE)
Generally mild, with a rash. Serious complications rare 10–20+ years Common in countries with low vaccination rates
Cholera Bacteria transmitted through contaminated water and food Acute, profuse, watery diarrhoea and dehydration 6 months–2 years Endemic in much of the developing world
Dengueb
Mosquito-borne virus
Generally mild and flu-like but severe dengue can be fatal
Unknown (2+ years) Common throughout tropical and subtropical countries
Influenza Virus transmitted through infectious airborne droplets Flu symptoms which can be fatal in certain groups of people 1 year (since virus changes) Worldwide
Hepatitis A Exposure to sewerage-contaminated water, ice, shellfish, or uncooked, unpeelable fruits, vegetables or other foods
Hepatitis Ba Contact with blood or blood-derived fluids, contaminated needles, unprotected sex
Japanese B encephalitis
Measles, Mumps, Rubellaa
Meningococcal disease (various)
Poliomyelitisa
Mosquito-borne virus
Direct contact with infectious droplets, sometimes airborne
Direct contact
Viral infection of the liver – fever, anorexia, abdominal discomfort, jaundice. Not associated with chronic or long-term infection
Viral infection of the liver – fever, anorexia, abdominal discomfort, jaundice. Can become chronic
Only 1:250 infected people develop encephalitis symptoms
Measles: Rash, fever, cough, sometimes severe complications
Mumps: Swelling of salivary glands, sometimes severe complications and infertility
Rubella: Can cause birth defects in pregnant women
Fever, headache, nausea, vomiting. Can be fatal
Virus transmitted by faecal–oral or oral route Most infections asymptomatic, but in some people acute paralysis, respiratory failure, and rarely death can result
Rabies Animal bite that inoculates virus into wound
Tetanus/Diphtheria/ Pertussisa Tetanus: Bacteria transmitted usually through contaminated wounds though has occurred during clean surgical procedures
Diphtheria: Raw milk or dairy products
Pertussis: Contact with respiratory droplets
Tuberculosis (BCG) Usually airborne spread of bacilli through coughing or prolonged sharing of same air space. Can be transmitted through unpasteurised milk from infected cattle
Traveller’s diarrhoea Can be due to changes in food or water or microbes (eg, bacteria, virus, protozoa)
Typhoid Bacteria transmitted through unboiled water, or uncooked or poorly reheated foods
Incubation period of 1–3 months after which no treatment is effective. Delirium and convulsions followed by coma and death
Tetanus: Muscle rigidity and painful spasms, sometimes fatal Diphtheria: Bacteria causes membrane to form over mucous membranes. Can be fatal
Pertussis: Severe cough, sometimes serious complications
Latent TB is asymptomatic. Active pulmonary TB causes cough, fever and weight loss
Dehydration caused by excessive diarrhoea and vomiting can be very debilitating and even fatal
Persistent very high fever, sometimes rash, can be fatal
Yellow feverc Virus transmitted through mosquito bites Can cause severe hepatitis and haemorrhagic fever
Vaccine: 20+ years Common throughout the developing world
Lifelong
South-East Asia, Africa, Carribean
2–3 years Most of Asia especially rural agricultural regions where flooding irrigation is used
15+ years Common in countries with low vaccination rates
2–3 years
Sub-Saharan Africa, Haj pilgrims Epidemic in New Zealand 1991–2004
10+ years Low incidence worldwide due to vaccination
1–10+ years Found in many parts of the world. Risk highest with unprotected outdoor exposure
10–20+ years Common in countries with low vaccination rates
Long for miliary and meningeal forms. Variable for pulmonary disease
3+ months
Vaccination unreliable in adults. Not generally recommended since treatment is usually effective
Although traveller’s diarrhoea is common, routine vaccination is not considered necessary unless under the advice of a health professional
2–3 years South-Asia, Central America
10 years Parts of Sub-Saharan Africa (eg, Guinea, Kenya) and South America (eg, Columbia, Brazil). Some countries require International Certificate of Vaccination for entry
Protective effect of vaccination varies according to information source. a. Included in NZ immunisation schedule; b. Limited availability internationally (not currently New Zealand) and vaccination may put people at risk of severe dengue, and is usually only recommended for people who have had Dengue before; c. Must be given at an authorised yellow fever vaccination centre.
vaccine is not available in New Zealand.
In 2018, Zika, another mosquito-borne viral illness, was prevalent in over 80 countries. As of May 2023, there were no areas with a current
Zika outbreak.
Zika is usually mild; four out of five people experience no symptoms. The remainder develop a low-grade fever, headache, a rash, joint pain, and
conjunctivitis. Hospitalisation is uncommon and symptoms usually resolve within a week. Other mosquito-borne illnesses include chikungunya and Japanese encephalitis.
• Travel sickness remedies are usually more effective if taken before the motion starts.
• Most oral medicines for motion sickness cause drowsiness, although some less than others.
Most people buy products in anticipation of future motion sickness, having had a bad experience before.
Try to establish what their symptoms are while travelling and what mode of transport it relates to (ie, boat, plane, or vehicle). Run through the Refer to a Pharmacist checklist and refer anybody with concerns to a pharmacist.
Most medicines effective for the treatment of motion sickness are more successful at alleviating symptoms if taken before the motion starts, rather than waiting until it has happened.
Sedating antihistamines (eg, cyclizine, meclozine, and promethazine) and anticholinergics (eg, scopolamine) are most commonly used before travel. Antiemetics (anti-nausea medicines) may be used to control nausea or vomiting that occurs as a result of motion. Most of these medicines cause drowsiness, although cyclizine and meclozine are the least likely to do so.
Natural remedies, such as ginger or peppermint, and pressure bracelets that act on the Nei-Kuan pressure point on the front of the wrist may also be effective.
Category Examples
• People with other medical conditions or who are pregnant or breastfeeding.
• People who take medicines, including herbal/complementary products.
• Children aged less than 12 or the elderly.
• If travel sickness symptoms have worsened with time.
• People who act suspiciously and may be drug seeking.
• People who suffer from prolonged vomiting while travelling.
• People with severe anxiety associated with travelling.
• People with allergies to medicines.

Comments
Antihistamines [PHARMACY ONLY MEDICINE] eg, meclozine (Sea-Legs), promethazine (Avomine) [PHARMACIST ONLY MEDICINE]
eg, cyclizine (Nausicalm), promethazine (Allersoothe, Phenergan Tablet/Elixir)
Hyoscine (scopolamine) [PHARMACY ONLY MEDICINE] eg, hyoscine/scopolamine (Scopoderm TTS Patches)
Other products eg, @-ease, 1-Above, No Jet Lag, Trip Ease eg, Nei-Kuan pressure point bands (eg, Sea Band Nausea Relief Adult/Child, Travacalm Travel Band) eg, Blis K12 Travel Protect, Inner Health Travel Bug
Sea-Legs are not for children under six years. Avomine is not for children under 10 years. Ensure packet instructions are followed for the correct dose according to age. Meclozine and cyclizine are generally less sedating than promethazine (although sedation may be an advantage for some people). Warn about the risk of drowsiness and to avoid driving or operating machinery if affected. Refer people on medications, with certain health conditions, or wanting to purchase Pharmacist only products (see Reference section, OTC Medicines – Precautions). Avoid alcohol. Be wary of the potential for these medicines to be abused and refer any suspicious requests to the pharmacist. Non-sedating antihistamines are ineffective for motion sickness.
Not for children under 10 years. Apply to the hairless area behind the ear at least four hours before travel (eight hours is best for maximal effect). Remove or replace with a new patch after 72 hours. Do not cut patch in half (although a half patch can be obtained by covering half the patch with an occlusive dressing).
Dispose of the patch carefully after use and wash hands after applying to prevent inadvertent transfer to the eye. Warn about the risk of drowsiness and to avoid driving or operating machinery if affected. Avoid alcohol.
Homeopathic remedies may help alleviate symptoms associated with travel. Bands that apply constant pressure to the Nei-Kuan pressure points in the wrists may help reduce feelings of nausea. Apply in the middle of the inner wrist, about three finger widths from the crease where the wrist joins the hand.
Other products support the body’s natural immune defence system.
Ginger may help relieve symptoms such as nausea associated with travel sickness. Pycnogenol may help reduce both the severity and duration of jet lag. Probiotics may help to reduce the risk of traveller’s diarrhoea.
Travel sickness (more correctly called motion sickness) is a common problem, especially in young and elderly people. Research has shown that every individual has a threshold for nausea, one that changes minute by minute depending on their anxiety levels, anticipation, expectation, and adaption to whatever has the potential to make them sick.
Although the exact cause is not fully understood, most experts believe that motion sickness arises from conflicts occurring between the various sensory inputs to the brain, or an overstimulation of balance mechanisms located within the inner ear. Sensory systems involved in monitoring balance include the:
• inner ears – semicircular canals within the inner ears contain a fluid which can tell the brain the direction of motion (up, down, side to side, round and round, forward, backward)
• eyes – these also help let the brain know if a person is moving and in what direction
• skin receptors – these let the brain know what parts of the body are touching the ground
• muscles and joint sensors – these tell the brain if a person’s muscles are moving and what position their body is in.
When a person is moving, either under their own steam or with the aid of a vehicle, boat or plane, the brain receives a report from these sensory systems and attempts to make sense of what the person is doing.
Of the four systems mentioned above, the sensory apparatus in the inner ear seems to be most critical in the development of motion sickness. If this becomes overstimulated or if any of the other sensory reports do not fit together, the brain gets confused and people start to feel sick or dizzy.
For example, if a person is travelling in a car, reading a book with their head down, the inner ears and skin receptors tell their brain that their body is moving forward. However, their eyes are looking at a book that isn’t moving and the muscle and joint sensors are telling their brain that they are sitting still.
During the early stages of motion sickness, most people start to feel a little tired and dizzy,
• Keep food light and avoid heavy, fatty or spicy meals and alcohol before travelling. Peppermint or ginger taken before travel may help.
• Take the recommended medicine at least one to two hours before travelling (or even the night before).
• Reduce symptoms by choosing seats with the smoothest ride (eg, front seat of a car, front carriages of a train, seats between the wheels of a bus, centre of a boat and seats over the aircraft wing).
• Focus on distant objects or the horizon, do something distracting (eg, listen to music) or keep eyes closed.
a bit nauseous, and may begin to salivate. Many people never progress to vomiting, while others are more severely incapacitated and require medical intervention (such as an anti-emetic injection). Other symptoms include yawning, hyperventilation (rapid, deep breathing), sweating, and looking pale.
Women who are pregnant or menstruating, people who are feeling scared or anxious, or those who suffer from migraines or conditions that interfere with sensory input, are more at risk of motion sickness.
In some people, smells, such as those of food or petrol, coupled with the anticipation of travel can also bring it on.
People who are subjected to repeated exposure of the same motion develop a tolerance for it after a period of time – often referred to as “gaining your sea legs” if on a boat. Once the motion stops, the feeling of still moving persists for several hours until the body readapts to the lack of movement.
• Avoid activities, such as reading, that encourage looking down and require close visual concentration.
• Minimise head movement with a head support, or try lying down.
• Get plenty of fresh air (open personal air vents on planes).
• If a person is feeling car sick, stop in a safe spot and allow them to get out and walk around a bit.
➤ Keep a plastic bag in the car just in case!
• Incontinence pads or briefs provide temporary protection from urinary leakage; however, bladder retraining or surgery may provide better long-term control.
• Overactive bladder (also called urge incontinence) is the sudden, strong urge to urinate during the day or night.
• In children, wetting is common and not considered incontinence unless it doesn’t resolve by age seven.
There is a wide range of incontinence pads and pants available, and it can be confusing for a customer to try and determine which one best suits their need. Research shows that most people waste around $150 before finding a dependable product that fits well.
If you notice a customer buying incontinence pads or pants, discreetly and politely ask if the product suits their needs. Run through the Refer to a Pharmacist checklist and refer any customers with concerns.
Skin irritation can also be a problem for people with incontinence and barrier creams should be kept alongside incontinence products so customers can buy them at the same time.
Direct customers seeking more information and support to the NZ Continence Association’s website at continence.org.nz A related site, pelvicfloor.co.nz, provides detailed information and advice about maintaining a strong pelvic floor.
In most cases, people with incontinence that has recently started should be referred to a doctor to establish a cause.
Products available in a pharmacy for incontinence include absorbent pads and underwear, and these may be used as a temporary measure before people see a doctor, or for when the cause of the incontinence has been established, but cannot be resolved. Bladder training, surgery, and other
If the person suddenly CANNOT pass urine, then they should see their doctor immediately.
• People who have not seen a health professional before about their urinary incontinence.
• If urine leakage is stopping them from doing everyday activities (such as leaving the house, going to the supermarket).
• People with signs of a bladder infection (eg, pain when passing urine, see Cystitis).
• People with blood in their urine.
procedures may provide better long-term control of urinary incontinence so suggest customers have a look online (continence.org. nz) or talk with their doctor at their next visit if they are not managing well with the products that you have available.
Urinary incontinence, or loss of bladder control, is when urine accidentally leaks from the bladder. In some people, just laughing, coughing, or sneezing can cause leakage. The amount that leaks can range from just a few drops up to the entire contents of the bladder.
More than one million New Zealanders experience bladder or bowel control problems. Urinary incontinence has been identified by the World Health Organization as a major health issue in developed and developing nations.
Stress incontinence
This is when the bladder leaks due to physical pressure, usually from lifting, exercising, coughing, sneezing, or laughing. It happens when a person has weak pelvic floor muscles or a weak urethral sphincter.
Pelvic floor muscles hold all the pelvic organs in their correct positions, and also help keep the urethra closed, preventing leakage. The urethral sphincter is a band of muscles around the urethra that, for the majority of the day, remain tightly squeezed, keeping urine in the bladder.
Nerve endings in the bladder send a message to the spinal cord and brain for urination to occur once a certain amount of urine has accumulated in the bladder. This results in
Incontinence pads/pants eg, Advance Breathable, Comforts Pads, Confitex, D-Brief range, Depend range, Molicare range, MoliMed, Oi Under Control Naturally, Poise Pad Rrange, Tena range
liners eg, Brolly
DryLife Absorbent Bedliner,
relaxation of both the sphincter and pelvic floor muscles. In people with stress incontinence, these muscles are not strong enough to withstand the extra pressure lifting, exercising, coughing, or sneezing places on them. They involuntarily relax, allowing urine to escape.
Causes of stress incontinence include pregnancy and childbirth, menopause, constant coughing, lots of heavy lifting, being overweight, straining to empty the bladder or bowel, ageing, a lack of fitness, or extreme exercise.
Urge incontinence is when there is a sudden, strong urge to pass urine and the person is unable to hold on until they reach the toilet. People with urge incontinence may also feel the need to urinate more often, including at night, even though their bladder is not full.
Urge incontinence occurs as a result of an inappropriate contraction of the urethral sphincter muscle, or the detrusor muscle of the bladder wall. Often these contractions occur regardless of the amount of urine that is in the bladder.
Causes include urinary tract infections, stroke, Alzheimer’s disease, Parkinson’s disease, diabetes, certain medications and prostate problems. A “Can’t Wait” toilet card is available free from continence.org.nz for people with a medical condition to enable them to discreetly let strangers know that they need a toilet in a hurry.
Some people (mostly women) can experience stress incontinence and urge incontinence at the same time.
contact between urine and skin. May be reusable or disposable. Useful for temporary incontinence, before seeing a doctor, or if medical options have been unsuccessful or are not appropriate. Most provide high absorbent capacity with little bulk. Menstrual pads are not suitable for urinary incontinence since their absorption capacity is limited and they become lumpy and leak when sodden. Consider the customer’s needs (light, moderate or heavy) and whether assistance is needed to use and change the product.
Seatliner, Oi range Draws in and traps moisture, protecting bedding or furniture and minimising wetness. Absorbs 2.5L over eight hours. Machine washable.
Barrier products eg, dimethicone (Silic 15), zinc (Sudocrem), zinc and castor oil, vitamin A and calamine (Ungvita Cream)
Silicone or zinc-containing barrier creams protect the skin from the irritating effects of urine. Wash urine off the skin with a mild cleanser and water before applying.
Overflow incontinence
This happens when the bladder is unable to fully empty itself. It becomes too full, causing it to overflow and regularly leak or dribble small amounts of urine. Causes include prostate problems, diabetes, and certain medications.
Incontinence due to physical/ neurologic abnormalities
Anatomic or neurologic abnormalities may affect the urinary system and cause incontinence, such as fistulas (abnormal openings between the bladder and other structures).
Damage to the nervous system that regulates bladder control can also occur due to trauma, disease, or injury. This may cause the bladder to be underactive (unable to contract and empty completely) or overactive (contracting too quickly or frequently).
Surgical procedures, such as prostate, rectal, or caesarean surgery, can cause incontinence.
It can also occur in people who are unable physically to get to a toilet in time.
Overactive bladder (OAB) syndrome is a general term used to describe the symptoms of urinary urgency with or without urge incontinence, including the frequent need to go to the toilet, and having to urinate more than once at night. Urinary incontinence is a symptom of OAB.
The age at which children achieve dryness varies. Wetting in very young children is common and is not considered incontinence. The term enuresis is often used to describe the inability to control urination in those old enough to exercise such control.
Daytime enuresis affects around 3%–4% of children between the ages of four and 12 with girls being more commonly affected than boys. Children older than four experiencing daytime enuresis should initially be assessed by a doctor
• Ensure the customer has discussed an incontinence management plan with their doctor which usually consists of several of the following options:
➤ ensuring an adequate, but moderate, fluid intake (eg, 1000 –1500ml/day)
➤ a pelvic floor muscle exercise programme
➤ a bladder retraining and toileting programme
➤ medicines for incontinence
➤ incontinence aids (eg, pads, condom drainage, catheters)
➤ advice about toileting outside of the home situation.
• Some exercise regimens are not pelvic floor friendly. See the website pelvicfloor.co.nz for safe exercises.
to rule out a urinary tract infection and also constipation, which can also adversely affect bladder function. Some children may also need an ultrasound if structural abnormalities are suspected. In most cases a cause is not identified.
Nocturnal enuresis (wetting the bed at night) is not usually diagnosed until age seven and typically resolves with age, with only 1%–2% of 18-year-olds still being affected. It occurs slightly more in boys than girls and tends to run in families with most children having at least one relative who also wet the bed.
Information about toilet training and the management of both daytime and nocturnal enuresis for parents and caregivers can be found at continence.org.nz Daytime enuresis may resolve once fluid intake is increased because this makes it easier for a child to recognise that their bladder is full and allows bladder retraining techniques to be put in place. Alarm systems that wake a child at night have proven to be a good long-term treatment for nocturnal enuresis with a 70% success rate.
• Customers with incontinence of recent onset should keep a bladder diary before seeing their doctor.
➤ Record when and how much leakage occurs, how strong the urge is to urinate, what activity was being done when the urge to urinate occurred, medicines taken (prescription, over the counter) and daily fluid intake.
• Avoid foods and drinks that can irritate the bladder, eg, spicy foods, caffeine, alcohol, fizzy drinks, chocolate, citrus fruits and juices.
• Weight loss may help in people who are overweight.
• Community incontinence nurse educators are available to provide education and advice.
• Urticaria is a skin rash characterised by raised red or skin-coloured itchy bumps that may occur with swelling (angioedema).
• Most cases of urticaria are not caused by allergy, but by non-allergic causes of histamine release.
• Oral antihistamines may help relieve the itch, although higher than normal dosages may be needed.
If the urticaria is in a place that is easy to see, and your customer is happy for you to take a look at it, take them to a private area, sit them down, and put on a pair of gloves. Have a good look at their skin. Does the rash look typical of urticaria, and do the hives blanch (turn white) when pressed. Ask about the extent of spread, if they have recently started any new medicines, and run through the Refer to a Pharmacist checklist and refer any customers with concerns.
The best treatment for urticaria is to identify and eliminate the cause if possible. Oral non-sedating antihistamines are usually effective at relieving the itch and work best if taken on a regular schedule (see Allergies for an overview of common antihistamines). Higher than normal dosages given on the advice of a doctor may be needed.
If non-sedating antihistamines do not work, then sedating oral antihistamines can be tried and/ or H2 receptor antagonists, such as famotidine. H2 receptor antagonists may be of benefit because 15% of histamine receptors in the skin are H2 type. Tricyclic antidepressants, oral corticosteroids and other medicines such as leukotriene
Seek urgent medical help if the person has any signs of facial swelling, or difficulty swallowing or breathing.
• People who are immunosuppressed, with diabetes, have other skin conditions, or women who are pregnant or breastfeeding.
• Children aged less than 12.
• If blisters, crusting or pus is associated with the urticaria.
• If the urticaria is covering a large area of the body.
receptor antagonists (eg,montelukast) or omalizumab can be prescribed by a doctor if necessary.
The term urticaria is derived from the Latin word for stinging nettle, Urtica dioica. Urticaria describes a group of skin disorders characterised by weals (also called hives) and/or angiodema (swelling under the skin).
Weals (also spelt wheal) may last a few minutes to several hours and are red or skin-coloured superficial swellings, usually surrounded by erythema (redness). When pressed, the centre of a red weal will usually blanch (turn white). Weals are generally itchy, 1–2cm in width, and may merge together to form a map-like pattern or one giant patch.
Occasionally, the surface weals may be accompanied by angioedema – which is a swelling beneath the skin that usually occurs around the facial area (ie, eyes and lips) but may also be present on the hands, feet, throat, or just under the skin. Angiodema may progress to
Category Examples Comments
Oral antihistamines Non-sedating [PHARMACY ONLY MEDICINE] eg, bilastine (Labixten), cetirizine (Razene), desloratadine (Aerius), fexofenadine (Fexofast), levocetirizine (Levrix), loratadine (Loraclear)
Sedating [PHARMACIST ONLY MEDICINE] eg, dexchlorpheniramine (Polaramine), promethazine (Phenergan)
Topical anti-itch products [PHARMACY ONLY MEDICINE] eg, Anthisan Cream
Natural / herbal products / supplements Vitamin C Aloe vera gel
• People with a fever or who feel unwell.
• People who take regular medicines, or who have recently started a new medicine, either prescribed by a doctor or bought from a shop.
• People with urticaria that has lasted longer than 24–48 hours.
• Urticaria that recurs frequently.
• If oral antihistamines been tried but have not been effective.
• People with allergies to medicines.
anaphylaxis; symptoms include breathing and swallowing difficulty and shock (see Allergies). Urgent medical advice must be sought. Angioedema may also occur without weals. Urticaria can occur anywhere on the body but is mainly found on the trunk, arms, and legs. Sometimes the rash can change shape and disappear from one place, only to reappear a few hours later somewhere else. The underlying chemical responsible for urticaria is histamine. Most cases of urticaria resolve within a few days although, occasionally, a person will have hives for many months or years.
Acute urticaria refers to a rash that lasts for less than six weeks. The rash may be triggered by an allergic or a non-allergic cause. Mast cells and white blood cells in the skin release histamine, which causes small blood vessels to leak fluid which pools to form weals.
In acute urticaria due to an allergic cause, the substance responsible is usually ingested, inoculated, or inhaled, though in some people skin contact with the allergen may be enough
These help to control total body itch and wheals. Try and eliminate the underlying cause (eg, food, medication). Oral antihistamines are more convenient than topical antihistamines when itch affects the whole body area.
Generally, non-sedating medicines do not cause drowsiness; however, some people may be more sensitive than others. Warn about the risks of driving or operating machinery if they do get drowsy.
Similar to non-sedating antihistamines (above); however, these medicines can be quite sedating. May be useful when taken at night to improve sleep quality if itching is severe. Warn about the sedating effects and risks of driving or operating machinery while taking these medicines and to avoid alcohol (see Reference Section, OTC Medicine Precautions). Sedating antihistamines are [PRESCRIPTION ONLY MEDICINES] for children under two.
Relieves localised itch and inflammation. Good for short-term use (two to three days) on small localised areas. Some people with sensitive skin may react to excipients in the cream and develop a contact dermatitis.
Higher doses of vitamin C (ie, 1000mg) may help reduce histamine levels. Aloe vera has a cooling, soothing action.
to set off the urticaria (eg, latex). The most common allergic causes of urticaria are:
• bee or wasp stings
• foods – particularly nuts, fish or shellfish, eggs, tomatoes, milk, strawberries or kiwifruit
• contact allergens, eg, latex or cosmetics
• medicines – antibiotics although most types of medicine can be implicated.
Most cases of urticaria are NOT due to allergy, and can occur without previous exposure. Non-allergic causes of acute urticaria include:
• contact with irritating plants (eg, thistles, stinging nettle) or stinging jellyfish
• infections – such as viral upper respiratory tract infections (eg, colds, sinusitis), Candida infections, dental abscesses, Helicobacter pylori, or viral hepatitis
• non-allergic food reactions – common examples include salicylates in fruits, azo-dye food-colouring agents, benzoate preservatives, and histamine due to bacterial decomposition in fish (eg, scombroid fish poisoning)
• non-allergic release of mast-cell granules, which can occur with opiates (eg, morphine, codeine) and radio-contrast agents
• serum sickness – as a result of a blood transfusion, viral infection, or medicines.
Acute urticaria can also be caused by sunlight, heat, cold, water, pressure, vibration, or exercise. The trigger is not known or identified in about half of all cases.
Chronic urticaria lasts more than six weeks and may be due to autoinflammatory diseases such as systemic lupus erythematosus. Refer the customer to a doctor.

• Avoid triggers for urticaria if known and if possible.
• Dietary changes may help. Some urticaria is aggravated by salicyclates in certain fruits, or additives including amines, tartrazine (102), benzoates (210-220) and other food chemicals.
• Seek medical advice if certain medications appear to precipitate urticaria. Similar classes of medications may do the same thing.
• Customers with urticaria should:
➤ avoid alcohol (it causes the surface blood vessels to dilate)
➤ avoid tight clothes as sweating and pressure may worsen symptoms
➤ cool the affected area with a fan, cold flannel, ice pack, or cream containing menthol; alternatively a tepid or cold shower may be soothing
➤ treat any pain with paracetamol
➤ see a doctor if the urticaria does not respond to an antihistamine, or persists more than a few days.
• Only compression stockings with a pressure rating of less than 20 mmHg can be sold over the counter.
• Anybody travelling by car, bus, or plane for more than four hours is at risk of traveller’s thrombosis.
If a customer asks you to recommend something for varicose veins, ask if they have ever seen a doctor about them. Varicose veins may be a sign of a circulatory disorder or harbour blood clots and are best diagnosed by a doctor. A doctor will conduct a physical exam and use other tests, such as an ultrasound, to determine valve functioning.
For customers wanting flight socks, check they do not have any circulatory problems (such as diabetes), and that they have the physical capability to pull on the socks. Run through the Refer to a Pharmacist checklist and refer any customers with concerns.
There is no way to completely prevent varicose veins from developing in people at high risk for them. However, exercise, maintaining a healthy body weight, elevating legs, and avoiding high heels or prolonged standing can improve muscle tone and circulation and help reduce their occurrence.
Treatment is considered optional in people with simple varicose veins that have not caused serious complications; however, many people request treatment in an effort to improve the appearance or slow progression of the veins.
Graduated compression stockings/socks may be all that is required if aching and swelling
Category Examples
Graduated compression hosiery
• Any person who has not been formally diagnosed with varicose veins.
• People complaining of swelling, redness, or tenderness in one leg or a cramping, aching, persistent pain with no identifiable cause (ie, not due to recent exercise).
• People who take medicines that may cause fluid retention or affect blood clotting.
• People with cardiovascular disease, diabetes, at high risk of stroke or heart attack, obesity, or women who are pregnant or breastfeeding.
• People with chest pain or breathlessness.
• People with other skin conditions such as eczema or dermatitis.
• With broken or discoloured skin or signs of infection near their veins.
• With large varicose veins.
are the main problems. It is essential that the correct grade of stocking is used after proper fitting. Many patients find these very effective for symptoms although they may be inconvenient, particularly in warm weather.
Graduated compression stockings/socks apply pressure to the legs in a sequential way, being tighter at the ankle and slightly looser higher up the leg. They help veins and leg muscles to return blood back towards the heart, and relieve the heavy, aching feeling commonly associated with varicose veins as well as reducing the risk of developing a deep vein thrombosis (DVT).
With every step a person takes, the stockings/ socks act as a layer of muscle, squeezing the stretched walls of the vein together and allowing the valves to close. This forces blood up the vein, reducing distension, restoring blood flow, and aiding overall circulation.
Stockings are available in different compression ratings based on how much pressure they provide and should be sized according to calf and upper leg size, rather than shoe size. It is essential that the correct grade is used and in New Zealand, a prescription is needed for stronger
eg, Encircle Merino, Jobst range, Mediven range, Scholl Flight Socks, TGX Socks, Venosan
Comments
levels of compression (Class 2 and above) because of the importance of fitting them correctly.
Unfortunately, there is no unanimously agreed upon compression standard, despite worldwide efforts to create one, so you may encounter variations in pressure ratings depending on the product. The RAL-GZ standard, developed in Germany and preferred by Pharmac is:
• Class I: Low compression, 18-21 mmHg
• Class II: Moderate compression, 23-32 mmHg
• Class III: High compression, 34-46 mmHg
• Class IV: Very high, 49+ mmHg.
Compression is guaranteed for six months. Surgery, vein glue (Venaseal), radiofrequency ablation (RFA), endovenous laser ablation (EVLA), and ultrasound guided sclerotherapy (UGS) are other types of treatment that may be considered. No treatment can erase every visible varicose vein, and people still retain the tendency to develop varicose veins, so there is always the possibility that they will return.
Our circulatory system consists of our heart and an extremely long and complex
Support hosiery is classified into four different grades of compression: Class 1 may be sold in pharmacies and without a doctor’s recommendation. Classes 2 to 4 may be sold only on the recommendation of a doctor.
Grade/class 1 compression is recommended for people with tired, aching legs, mild varicose veins, mild ankle swelling and to prevent ankles and feet swelling during long flights, eg, Scholl Flight Socks.
Grade/class 2 compression is used for people with moderate-to-severe varicose veins, pronounced ankle swelling after vein surgery, and to prevent recurrence of venous leg ulcers.
Grade/classes 3 and 4 compression hosiery is used for people with severe varicose veins or ankle swelling, active leg ulcers and to prevent leg ulcers recurring. These would probably be recommended by a specialist.
Full-length hosiery – stockings or pantyhose – are usually preferred for people with varicose veins in the thigh, and for pregnant women.
Knee-high support stockings provide enough support for people with lower leg problems, eg, varicose veins, swollen ankles and ulcers.
It is important to fit people with the correct size, according to the properly taken measurement.
Other products [GENERAL SALE] eg, mucopolysaccharide polysulfate (eg, Hirudoid) Contains enzymes that help disperse excess fluid in swollen areas. They reduce swelling and bruising. Can also be used as a treatment following sclerotherapy.
Natural / herbal products / supplements Butcher’s broom, horse chestnut (Venotrex), gotu
There is some evidence for the benefits of horse chestnut, butcher’s broom, grape, pycnogenol, and sweet clover in chronic venous insufficiency and for the improvement in symptoms of varcose veins. Gotu kola, nattokinase or pycnogenol may decrease the risk of DVT related to long-distance travel.
• Supplements should not take the place of a healthy, well-balanced diet, but may be needed by some people for various reasons.
• Children should do at least 60 minutes of physical activity daily, and adults at least 150 minutes of moderate-intensity exercise per week.
Supplements shouldn’t take the place of a well-balanced diet, so encourage people looking for supplements to try to obtain the recommended nutrients from food (see the information provided under the subtopic, Eating and Activity Guidelines).
Always refer people currently taking medications, with chronic illnesses, or who are pregnant or breastfeeding to the pharmacist. Also refer if your knowledge of supplements is limited, because you may be doing your customer harm by recommending supplements they don’t need.
Vitamins and dietary supplements are intended to provide essential nutrients,
Calcium [GENERAL SALE] eg, calcium (Caltrate, GO Calcium)
such as vitamins, minerals, fatty acids or amino acids, which are missing or not consumed in sufficient quantities in a person’s diet.
Dietary intake of these nutrients may be reduced due to certain diets or medications, poor dietary intake, food costs, pregnancy or lactation, or chronic medical, psychological, or physical reasons. Being aware of the recommended dietary intakes (RDI) or upper intake limits of different types of nutrients, according to age and energy expenditure, helps determine what (if any) supplement a person needs to take.
NRVs refer to the levels of recommended intakes of essential nutrients, such as vitamins and minerals.
In 2006, New Zealand and Australia developed joint recommendations for nutrient intakes necessary to keep people healthy and to reduce their risk of chronic disease. In 2016 these recommendations were updated for fluoride and in 2017, for sodium. NRVs are also used by the Food Safety Authority of New
Vitamin C eg, Vitamin C Lipo-Sachets*, Blackmores Bio C, GO Extra-C/Vita-C, Thompson’s Vitamin C
Omega-3/omega-6 fatty acid supplements eg, Bioglan range, Goodhealth range, GO Healthy range
Probiotics eg, Bliss range, Clinicians range, Inner Health range, Lifestream range
Folic acid supplements [GENERAL SALE]
eg, folic acid (Apo-Folic 0.8) eg, folic acid with iodine, iron and other vitamins and minerals (FabFol Plus) eg, folic acid with iron (Ferrograd F)
Iron supplements eg, Ferro-Sachets*, Fab Iron Liquid Iron (10mL =10mg elemental iron + B vitamins) [PHARMACY ONLY MEDICINE]
eg, Ferrograd (=105mg elemental iron) eg, Ferrograd C (=105mg elemental iron + vitamin C 500mg)
Vitamin D with or without other supplements
eg, vitamin D (Go Healthy D3, Sanderson Premium D3, Vitamin D Lipo-Sachets*) eg, vitamin D + other vitamins (Mvite, Vitabdeck, Vitadol C
Vitamins for Age-Related Macular Degeneration eg, Macu-Vision (contains ascorbic acid, cupric oxide, zinc oxide, vitamin E)
Iodine [PHARMACY ONLY MEDICINE] eg, NeuroTabs (potassium iodate 268mcg [= iodine 150mcg]), Elevit + iodine (potassium iodine 250mcg)
Foods/Drink eg, Go Superfood, Whole Live Nutrients, Biogenic Aloe Vera Tonic

Zealand for guidance on food labelling requirements. A link to the recommendations – known as the Nutrient Reference Values for Australia and New Zealand – is available from the Ministry of Health website at: health.govt.nz. The NZ Nutrition Foundation (nutritionfoundation.org.nz) also provides summaries about
Actual RDI is controversial (ranges from 500–1000mg). Calcium from dietary sources is preferred over supplemental calcium (see Osteoporosis). Supplements may cause kidney stones or affect the heart.
May help reduce the severity and duration of a cold and reducing the incidence of pneumonia in people who are vitamin C deficient. Lipo-sachets contain vitamin C encapsulated in Liposhell liposomes to enhance absorption.
Omega-3 and omega-6 fatty acids are essential for optimum growth and development, including brain development.
Probiotic bacteria aid digestive health and can restore imbalances between beneficial and harmful bacteria, especially following antibiotic therapy (see Probiotics and Prebiotics)
Folate is an essential B vitamin and is found naturally in leafy vegetables, citrus fruits, wholemeal bread, yeast, liver and legumes, and is important for cell growth and reproduction. Folic acid is the synthetic form of folate. For more information about use of folic acid during pregnancy see Pregnancy and Pregnancy Supplements
For more information about iron supplements see Iron Deficiency
Be aware that iron is dangerous in overdose and tablets must be taken as directed for the recommended course. Keep all iron products out of reach of children.
Ferro-sachets contain iron microencapsulated in liposomal form to enhance absorption and reduce side effects.
Fortification of milk and margarine products with vitamin D is voluntary in New Zealand. Vitamin D helps maintain bone strength by regulating the amount of calcium in the blood, and is obtained from the action of sunlight on skin (produces D3 or cholecalciferol) or from a limited range of foods (contain D2 or ergocalciferol), although it is hard to obtain sufficient vitamin D from the diet alone. Since too much vitamin D is toxic, people at risk of vitamin D deficiency should talk to their doctor before taking supplements.
The types and quantities of antioxidants included in Macu-Vision are based on the AREDS (Age-Related Eye Disease Study) research. May help protect the macular region of the eye and protect against Age-Related Macular Degeneration (see Eye Conditions).
The Ministry of Health recommends healthy pregnant and breastfeeding women take a 150mcg iodine tablet daily from the confirmation of pregnancy until the discontinuation of breastfeeding in addition to eating iodine-containing foods such as low-fat milk products, eggs, seafood, and commercially prepared bread. Refer women with pre-existing thyroid disease or with currently high iodine intakes to a doctor.
Several whole-food supplements and drinks are now available that can be used to boost diets that are deficient in certain nutrients.
nutrients, vitamins, and minerals.
The Nutrient Reference Values document also outlines suggested dietary targets to reduce chronic disease risk. Some of these include:
• reducing sodium intake to less than 2 grams/ day (equivalent to less than 5 grams of salt per day) in adults
• a dietary fibre intake of 38g/day (men) and 28g/day (women) to reduce cardiovascular disease risk
• increasing dietary intake of omega-3 fatty acids (DHA/EPA/DPA) to 610mg/day (men) and 430mg/day (women).
Research has shown it is possible to achieve recommended daily intakes (RDIs) of all nutrients by consuming commonly eaten foods, although in Australia and New Zealand, intake of folate (folic acid), calcium, and iron for women, as well as iodine and selenium in all people, are generally borderline.
Thirteen vitamins are recognised:
• fat-soluble vitamins: A, D, E, and K
• water-soluble vitamins: B1 (thiamine), B2 (riboflavin), B3 (niacin), B5 (pantothenic acid), B6 (pyridoxine), B7 (biotin), B9 (folate), and B12 (cobalamin), and vitamin C.
Fat-soluble vitamins are soluble in lipids (fats) and stored in our body. Our body can make vitamin D and K itself. Supplements of fat-soluble vitamins can cause side effects or be toxic at certain dosages.
Water-soluble vitamins dissolve in water and are not stored in our body, so are generally required from our diet on a regular basis.
Evidence for the benefit of vitamins is often
conflicting, except when an actual deficiency exists. However, during times of infection, illness, and stress, demands for certain vitamins increase and supplementation may be considered. Other groups of people that may benefit from supplementation include:
• anybody who does not eat fruit or vegetables on most days of the week
• elderly people, babies of vitamin D-deficient mothers, housebound or institutionalised people, people with darker skin, or those who cover their skin for religious or cultural reasons (vitamin D)
• individuals with eating disorders
• older adults with poor nutritional intake, such as those with dementia, or living alone (vitamin C, protein-rich supplement drinks or meal replacement powders)
• people with conditions such as Crohn’s disease or ulcerative colitis that affect their absorption of nutrients
• people with food allergies
• pregnant and lactating women (folic acid required during early pregnancy, iodine supplementation recommended throughout; iron and calcium supplementation may also be needed; see Pregnancy Tests and Supplements)
• strict vegetarians who consume no animal foods (supplements of vitamin B12 , omega-3 fatty acids, iron, or zinc).
Probiotics may also be considered to restore the balance of natural bacteria in the gut and help relieve common digestive complaints or maintain good oral health (see Probiotics and Prebiotics).
People with chronic diseases, or premature infants, require specialist advice about supplements.
and when to refer
Some nutrients can interact with other nutrients or medicines in either a good or a bad way.
Examples include:
• vitamin C can help iron absorption if consumed at the same time
• high intakes of iron may interfere with the absorption of zinc (both use the same absorption pathway)
• vitamin K contained in some supplements may interact with warfarin.
If an interaction is not desirable, taking the nutrient or medicine two or three hours apart may be advised (although this would not stop the vitamin K/warfarin interaction).
The Eating and Activity Guidelines (updated 2020) recommend adults:
• eat a variety of nutritious foods everyday including plenty of vegetables and fruit; grain foods (wholegrain or high fibre); some milk and milk products (low or reduced fat); some legumes, nuts, and seeds; fish and other seafood; poultry and some red meat with the fat removed
• choose foods that contain unsaturated fat (not saturated or trans fat), are low in sodium, with little or no added sugar, and mostly unprocessed. Salt should be iodised and used sparingly
• make water their preferred drink
• keep alcohol intake low; avoid alcohol if pregnant or when trying to conceive
• partake in at least 150 minutes of moderate or 75 minutes of vigorous intensity physical activity spread throughout the week. Do muscle strengthening exercises on at least two days per week. Break up long periods of sitting with regular activity.
• Warts are caused by the human papillomavirus (HPV).
• Most warts are benign (this means they are not cancerous) and usually disappear by themselves within two years; however, treatment makes them go away faster.
Ask your customer if the wart is on an exposed part of their body and if they are happy for you to look at it. Take them to a private area and put on gloves before you start. If there are multiple warts, determine if they are in a defined area or widespread.
Run through the Refer to a Pharmacist checklist and refer any customers with concerns.
Although most warts disappear by themselves within two years, many people seek treatment for cosmetic reasons if the wart is unsightly, or because the wart is painful.
OTC treatment options include home cryotherapy products (use extreme cold to freeze the wart off), salicylic acid-containing paints or gels, or salicylic-impregnated plasters.
Cryotherapy products contain mixtures of propellants such as dimethyl ether, propane and/ or isobutane to freeze warts at negative 50°C. Stubborn warts may require more than one application. These products should only be used on common, flat or plantar warts not located in sensitive areas (ie, not on the face, neck, or armpits).
Wart remover solutions use a mixture of salicylic and lactic acid, both of which break down keratin, allowing skin cells in the wart to shed more easily.
Medicated plasters contain higher concentrations of salicylic acid (up to 40%) and slowly remove skin layers over several weeks. The effectiveness of salicylic acid-containing
• If you are not sure that the lesion is actually a wart.
• People with circulatory disorders or diabetes, or who are immunosuppressed, pregnant or breastfeeding.
• People aged over 50 years or very young children with a first episode of warts.
• Anybody with multiple or widespread warts, or warts resistant to OTC treatments.
• If the wart has an irregular border, pigmentation or a reddish colour, or if it has changed colour.
• If there is itching or bleeding associated with the wart.
• People with warts that are located on the feet, face, genital region, or inside the mouth.
• With warts larger than 7mm in diameter or warts that have grown recently.
• With warts that look smooth or have a central dimple.
• People with allergies to ingredients in topical medicines.

treatments is enhanced by soaking the wart in warm water before applying treatment. Treatment may need to be suspended for several days if the wart becomes painful.
Homeopathic Thuja promotes healthy skin and helps stimulate the body’s immune system. Both oral and topical treatments are available and good adherence to dosage schedules for several months is required before an improvement is seen. Consultation with a qualified homeopath
Category Examples Comments
Salicyclic/lactic acid [PHARMACY ONLY]
eg, Duofilm Wart Remover, Scholl Wart Remover system (fabric/washproof)
Volatile hydrocarbons (home cryotherapy)
[GENERAL SALE] eg, Excilor Warts, Wartie Freeze Wart Remover, Warteze, Wartner Wart Remover, Wart-Off Freeze Spray/Paint/Stick/Pen, Scholl Freeze Verruca & Wart Remover
Other products [GENERAL SALE] eg, Wartfree Wart Remover Pen
Natural / herbal products / supplements Homeopathic Thuja wart paint, Naturo Pharm Wartoff Paint/Tablets/Spray Garlic, green tea extract
is recommended before embarking on treatment; however, anecdotally, success has been reported.
Covering the wart with duct tape has also been found to be effective.
Warts are caused by human papillomaviruses (HPV). This group of viruses has a high prevalence in communities
Soak affected area in warm water and towel dry before applying product. Effectiveness may be improved by rubbing the surface with pumice stone or emery board to remove any hard skin. Daily treatment is necessary except for fabric-based systems which are changed every 48 hours.
Contain ingredients that freeze the wart, such as dimethyl ether and propane. Usually just a one-off application of 20 seconds is needed; however, it may be repeated after 15 days. May be uncomfortable for a few minutes and may result in blistering. May take several repeat attempts over several months to completely get rid of the wart. There is no evidence to suggest this treatment is any more beneficial than other wart treatments; however, it may be more convenient.
Typically contain corrosive ingredients that induce peeling of the surface of the wart.
Homeopathic remedies aim to stimulate the immune system to attack the virus responsible for warts. Topical garlic has some effectiveness for warts. Effectiveness for a green tea extract ointment against genital and perianal warts has been reported.
and is easily acquired through small breaks and tears in skin.
More than 150 different types of HPV are capable of causing infection; at least 14 of these are high-risk types linked to cancer. Two strains, HPV types 6 and 11, cause 90% of warts but these strains are considered low-risk and very unlikely to cause cancer. Many people harbour the HPV virus with no visible signs of warts or other infections at all.
HPV infection can also cause cervical and other genital and oropharyngeal cancers. HPV types 16 and 18 are responsible for about 70% of cervical cancers.
Wart viruses aren’t considered very contagious but they can spread through close skin-to-skin contact, or by contact with skin shed from the wart, or via something that has touched the wart, such as a towel. It may take several months for the wart to grow large enough to see, making it difficult to pinpoint the exact source or time of transmission.
Warts are generally benign (meaning not harmful); however some skin cancers (eg, basal, squamous cell carcinomas, or melanomas) may look like a wart so refer the customer to a doctor or skin specialist if there is any doubt.
Warts can grow anywhere on the body, but for treatment purposes, are best separated into those on the body (excluding the feet), the feet, or the genitals.
Common warts and flat warts are the most likely type of wart you will see in a pharmacy. Common warts are usually either skin-coloured, brown or grey-black, and feel rough and spongy. Some contain black dots that look like seeds.
Flat warts are small and smooth, and tend to grow in clusters of 20-100 at a time. Both types occur more frequently in children because their immune systems are less developed. Common warts occur more on knees, on the backs of the hands, on fingers, or around nails – especially in children who bite or pick their nails. Flat warts are more common on the face, along scratch marks, and in areas prone to shaving such as the beard area in men or legs in women.
Plantar warts (also known as plantar verrucae or verrucas) are most commonly seen on the bottom of the foot, but can also appear on the top. They often grow in clusters and tend to be
• Do not pick or scratch warts. Warts are easily spread to other parts of the body this way. Never share razors.
➤ Avoid going barefoot in public places like showers, gyms, and changing rooms. Wear jandals or pool shoes in public showers, locker rooms, and pool areas
➤ Avoid touching another person’s wart
flat and inward-growing rather than outward like common warts. Small dots or lines are usually visible inside the lesion which can help differentiate them from corns or calluses.
Conservative management (ie, no treatment, cushioning the wart) is a reasonable option since most disappear by themselves within a couple of years and many are resistant to multiple treatments. Treatment options include cryotherapy and topical therapy with salicylic acid, and may be suggested to customers who find walking painful.
Genital warts are growths or bumps that appear on or around the genitals (ie, in or around the vagina, vulva, cervix, anus, penis, scrotum, groin, or thigh). They may occur singly or cluster together to form a cauliflower-like shape, be raised or flat, small or large. Contact with warts on other parts of the body does not seem to cause genital warts.
Most genital wart infections clear up spontaneously; however, treatment is often sought as warts may be unsightly or uncomfortable. Refer to a doctor for treatments which include imiquimod, cryotherapy, or laser therapy.
➤ Change shoes and socks daily and keep foot warts dry, as moisture tends to allow the warts to spread
➤ Stop treatment for a few days if the skin becomes sore, then recommence, paying particular attention to not getting the paint on unaffected areas of skin.
• Some weight loss is easy initially but keeping weight off long-term can be challenging.
• Excessive weight is associated with infertility, cardiovascular disease, gallstones, sleep apnoea, type 2 diabetes, and several cancers.
Recognising the barriers to losing weight is just as important as selling your customers meal replacement products or herbal supplements. One of the biggest is knowing how hard it is to keep the weight off – up to 95% of people who have lost weight, regain some of it within one year, and most of it within five years. Tell your customer that losing just 5% to 10% of their body weight can improve their health. They should aim to lose a small amount of weight, and to keep that off for a year or more, rather than try to reach their ideal body weight.
Three factors are key to maintaining weight loss: good support and mentorship, good lifestyle changes, and keeping the weight loss process practical and simple.
Meal replacement programmes/ products, pharmacological treatments, and herbal supplements are all available for weight loss through pharmacies in New Zealand, but there are pros and cons for each of these strategies.
Meal replacement products
Many meal replacement products have the abbreviation VLCD after them. This stands for Very Low-Calorie Diet and even though these originated as a form of obesity treatment, they can be a challenging and potentially harmful
• People wanting information about weight-loss products or regimens that you have not been specifically trained in.
• Anybody requesting large quantities of laxatives.
• Anyone on a weight-loss regimen complaining of persistent dizziness.
• Children who are overweight.
• People who appear to be losing weight exceptionally fast or who appear to have lost too much weight.
• People who you suspect may have an eating disorder.
• People with signs of obesity who also have other medical conditions (such as heart disease).
diet to maintain because of their low-calorie count and the general lack of nutrition they provide. Side effects include persistent hunger and tiredness, dry mouth, constipation or diarrhoea, headaches, hair thinning, cramps, and dizziness. Meal replacement products are attractive for those wanting to lose weight because weight loss occurs quickly due to the low-calorie count; however, long-term weight loss is not guaranteed.
Orlistat is a pharmacist only medicine that reduces fat absorption by inhibiting pancreatic lipase, an enzyme that digests and absorbs fats. It may cause gastrointestinal side effects such as flatulence, bloating, and cramps if not taken with a low-fat diet, and reduce the absorption of fat-soluble vitamins, such as A, D, E and K. Weight losses of 2.5 to 3.4kg have been reported in studies where participants took Orlistat for 12 months.
Prescription medicines, such as phentermine and liraglutide (Saxenda), are also available and bariatric surgery may be considered.
Many different supplements and herbs are
Meal replacements eg, Optifast VLCD (Very Low Calorie Diet), Optislim VLCD and LCD (low calorie diet)
eg, Kate Morgan Weight Management Programme
eg, Medical Vita Diet (MVD) Weightloss Programme
Oral medication for weight loss [PHARMACIST ONLY MEDICINE] eg, orlistat 120mg (Xenical)
touted for weight loss. Research into their effectiveness is generally limited or mixed, and many have side effects.
Chitosan is a type of sugar that comes from the shells of crustaceans such as lobsters or crabs. It binds to fat and cholesterol in the digestive tract, preventing their absorption, but there is not enough evidence to say if it is effective for weight loss. People who are allergic to shellfish should not take chitosan and it may cause an upset stomach or constipation.
Chromium is a mineral that enhances the effects of insulin and supplements claim to reduce appetite, burn calories, cut body fat, and boost muscle mass. A review of 24 studies found no significant benefits for chromium 200 – 1000 micrograms/day and large dosages may cause insomnia, irritability, headache, or kidney damage.
Conjugated Linoleic acids (CLA) contain chemicals found in linoleic acid, an omega-6 polyunsaturated fatty acid. Some research suggests 1.8 to 6.8 grams of CLA per day may curb body fat and build muscle mass, but other research suggests it doesn’t help with weight loss. It may also increase insulin resistance, lower HDL cholesterol, cause nausea, diarrhoea, and tiredness.
Glucomannan is a soluble fibre extracted
VLCDs provide 800 calories or less per day. Weekly weight losses average 1-2.5kg per week. Optifast has online help see optifast.com.au There is no online support for Optislim and extra protein may be required for VLCDs.
Offers four different weight-loss programmes, using shakes (VLCD programme) or meal replacements. Guidance on low GI foods, low fat meals and physical activity provided. See katemorgan.co.nz
Medically proven diet that combines two MVD shakes a day with water, multivitamins and exercise. A daily main meal is prepared from an allowed list of foods. See vitadiet.com.au
Only for people with an initial BMI of 30 or more or 27 with additional risk factors (eg, high BP, raised cholesterol, diabetes). Blocks the absorption of up to 30% of dietary fat.
Other products eg, Horley’s Slim, Radiance Smoothies May contain ingredients that bind fat or create a feeling of fullness.
Natural / herbal products / supplements Artemis Slim & Trim tea, whey protein powder, Caralluma fimbriata, chromium, carnitine, Cissus quadrangularis, dandelion, garcinia cambogia, green coffee bean, green tea, hoodia, nettle eg, GO Healthy Apple Cider Vinegar with Capsi-Slim
Whey protein may help reduce body weight and increase insulin sensitivity. Hoodia is used by Kalahari bushmen to prevent hunger during long journeys. Growing and extracting the active ingredient out of the plant is difficult and evidence of a benefit for weight loss is limited. Evidence for a benefit for caralluma fimbriata or garcinia is also limited. Small studies have been favourable towards green coffee bean extract. Apple cider vinegar can support digestion and healthy blood sugar balance.

from the Konjac plant that may promote weight loss by binding to fat in the intestine, preventing its absorption; however, there is not enough evidence to say that it works. There have been some reports of tablet formulations of glucomannan becoming stuck in the throat or causing a blockage in the oesophagus or intestine and powdered or capsulated forms are considered safer.
Many other supplements are touted for weight loss, such as green tea extract, green coffee extract, guar gum, Hoodia, 7-Keto-DHEA, Ephedra, and bitter orange. Natural Medicines, the most authoritative resource available on dietary supplements, says all of these are either ineffective or there is not enough evidence to say they are effective. Ephedra and bitter orange are considered possibly unsafe.
The Keto diet
The Keto diet is a medical diet that was promoted in the 1920s and 30s as a way to treat epilepsy
and has gained popularity in recent years as a way to lose weight. Anecdotally it is effective, at least in the short-term, but this low-carbohydrate, high-fat diet is not without its risks.
The Keto diet forces your body to use ketones for energy – these are a type of fuel the liver produces from stored fat. Even though burning fat seems like an ideal way to lose weight, getting your liver to make ketones requires that you deprive your body of carbohydrates and consume fewer than 20 to 50 grams of carbohydrates per day. This typically takes a few days and requires your diet to include mostly saturated fats, such as coconut or palm oil, butter, or lard; although some healthy unsaturated fats, such as nuts, tofu, avocado, and olive oil are allowed. Because fruits and vegetables are high in carbohydrates, these are usually restricted to small amounts of berries, leafy greens, and a few other options, such as broccoli and asparagus.
The Keto diet is high in saturated fat and has been associated with an increase in LDL cholesterol and heart disease. It is also low in certain nutrients, such as selenium, magnesium, phosphorus, and vitamins B and C; may not
be suitable for people with existing liver problems, due to the amount of fat needing to be metabolised; and may overload the kidneys with protein. Constipation from a lack of fibre is common and it may cause mood swings and irritability from a lack of carbohydrates. People should seek advice from a nutritionist or dietician before attempting this diet.
With one in three adults over the age of 15 classified as obese in New Zealand, including up to 66.5% of Pasifika and 48.2% of Māori, pharmacy staff are in an ideal position to help and tactfully encourage obese patients to lose weight. Weight loss in those who are overweight reduces the risk of heart disease, indigestion or heartburn, gallstones, sleep apnoea (see Sleep Problems), type 2 diabetes and a number of cancers (including breast, colorectal, endometrial, and liver cancers). Reducing weight may also benefit customers with osteoarthritis or those having issues with reproductive health.
• Have a realistic weight-loss target. A weekly weight loss of 0.5–1kg is healthy and achievable.
• Weigh yourself daily.
• Waist measurement is also important for measuring fat loss.
• Targeting weight loss from just one spot, does not work, aim for overall weight loss.
• A change in lifestyle is usually necessary to maintain weight loss.
• Choose healthier foods and make use of wristband activity monitors. Download the FoodSwitch app to identify what’s in packaged foods and switch to healthier options.
• A woman’s health needs can change dramatically throughout her life.
• Pharmacists can sell women oral or topical treatments for vaginal thrush, contraceptives, antibiotics for a urinary tract infection, and give advice about supplements needed during pregnancy, breastfeeding, and at menopause.
Healthcare needs for women can change dramatically with age and pregnancy. Women are more likely to visit a pharmacy than men, and your pharmacy should actively promote various women’s health topics, such as breast cancer awareness, cervical cancer screening, heart disease in women, and menopause relief, regularly throughout the year.
Discussions on vaginal health are best conducted in a private area by a pharmacist since most conditions either require a pharmacist to sell the treatment (such as vaginal thrush) or refer the customer to a doctor. The exception is vaginal dryness, common in women going through menopause, for which a vaginal lubricant or gel can be sold by a pharmacy assistant.
Thrush treatments: Topical versus oral
• Breastfeeding
• Cost
• Customer preference
• Interacting medicines
• Liver disease
• Pregnancy*
• Younger customers ( >16 but <18)
• Condom use
• Convenience
• Customer preference
• Discreet
• Intolerance to topical products
• Menstruation
• Travel
* Limit applicator insertion to halfway
• Any woman requesting treatment for vaginal thrush, or oral or emergency contraceptives.
• Any woman with an abnormal vaginal discharge.
• Any woman who appears overly anxious, distressed or depressed.
• Women with allergies to ingredients in topical products.
Please refer to the individual topics listed under treatment for other instances where women need to be referred to a pharmacist.
Several other chapters in this handbook discuss the management of conditions pertinent to women such as Contraception: Oral and Emergency; Cystitis (Bladder Infection); Menopause; Ovulation and Pregnancy Testing; Period Pain and Endometriosis; and Pregnancy and Pregnancy Supplements and you should refer to these topics for further information.
In addition, women should be educated about Heart Health, and that signs of a heart attack may be more subtle in women than in men. Keep your pharmacy child-friendly so that new mothers can shop freely and educate yourself so that you can provide accurate advice about Baby Care and Childhood Immunisations
Both oral and vaginal antifungal preparations are available from a pharmacist for the treatment of vaginal thrush. These inhibit the growth of Candida yeast without affecting the “helpful” bacteria in the vagina.
Vaginal dryness is also common among women, particularly after menopause. There are several non-hormonal creams and gels available that help replenish moisture within the vagina and restore the pH to normal. Hormonal treatments are also available from a doctor.
Category Examples Comments
Imidazole antifungal vaginal products [PHARMACIST ONLY MEDICINE] eg, clotrimazole (Canesten range), miconazole (Micreme Vaginal Cream)
Triazole antifungal vaginal products [PHARMACIST ONLY MEDICINE] eg, fluconazole (Canesoral, Diflucan One, Flucazole 150)
Combination antifungal vaginal products
Vaginal lubricants and gels
[PHARMACIST ONLY MEDICINE] eg, clotrimazole cream + oral fluconazole capsule (Canesten Duo)
[GENERAL SALE] eg, Aci-Jel Balance, Anime lubricant, Kolorex, Lactigel, Premeno duo vaginal ovules, Replens, Vagisil Prohydrate Plus eg, astodrimer sodium 1% (Fleurstat BV gel)
Natural / herbal products / supplements Horopito extract (eg, Kolorex Candida Care), Lactobacillus acidophilus, L. casei GG, Bifidobacteria, echinacea, Naturopharm Thrushmed Relief Gel
The vagina is a closed muscular canal that is naturally acidic and contains rich quantities of beneficial bacteria and yeasts.
Changes to the natural environment or structure of the vagina, as a result of endometriosis, hormonal contraceptives, feminine hygiene products, infection, menopause, pregnancy and childbirth, psychological distress, or trauma can upset its proper functioning, leading to abnormal discharge, genital sores, infertility, sexual discomfort, urinary incontinence, or vaginitis.
Good vaginal health is an important contributor to a woman’s overall state of health.
A healthy vagina secretes a small amount of discharge to keep itself clean, and a change in this discharge (colour, smell or consistency) is often the first sign that something is wrong.
Other symptoms of concern include abdominal pain; a noticeable lump or bulge inside the vagina; bleeding between periods, after sex, or after menopause; and vaginal redness, itching or irritation.
Pharmacists should also not assume any
Vaginal antifungal products are available as creams, pessaries or ovules for intravaginal use in single-dose, three and six-day treatments. Single-dose treatments are more convenient; however, longer therapy may be required in some circumstances (eg, if the woman is still on antibiotics). Disposable applicators are supplied in the packet and treatment is best used at night.
Only one capsule needs to be taken, once. Similar in efficacy to imidazole vaginal antifungals. Avoid use if the patient has previously had liver disease with fluconazole (rare). Note possible drug interactions (see OTC Medicines Interactions). Pharmacist is not able to sell OTC in females aged under 18 or in pregnancy or breastfeeding.
A combination pack, see above for selling notes related to individual products.
Vaginal gels, creams, and ovules restore moisture levels in the vagina helping to maintain a healthy vaginal pH which reduces the risk of vaginal infections. Some may help suppress bacterial vaginosis-associated bacteria. Most are usually safe to use with condoms but check manufacturers’ recommendations.
Horopito is an effective antifungal agent. Several probiotics are effective at returning gut yeast populations back to normal. Echinacea stimulates the immune system and the body’s ability to overcome Candida overgrowth.
abnormal discharge is vaginal thrush as many other conditions (such as bacterial vaginosis and trichomoniasis) present in a similar way.
Vaginal dryness is usually caused by a reduction in oestrogen levels, and is common following menopause. However it can also be caused by childbirth, oral contraceptives, stress, vaginal deodorants or perfumed bubble baths.
If left untreated, atrophy (a thinning) of the vaginal tissues may occur causing a loss in elasticity. In addition, the environment inside the vagina can become less acidic, increasing the risk of infections. Damage can more easily occur leading to pain during sex, itchiness, or blood spotting.
Vaginal thrush (vaginal candidiasis) is a common fungal infection caused by overgrowth of the yeast, Candida albicans. Vaginal thrush is uncommon in girls before their first menstrual cycle and in women after menopause.
Although not considered a sexually transmitted infection, occasionally the yeast can be transferred to a male partner causing redness, itching, and soreness around head of the penis. Treat males with symptoms with an antifungal cream.
Symptoms of vaginal thrush in women include itching, irritation, soreness, or a burning sensation in the vaginal area. There is often a thick, white, or creamy vaginal discharge.
If itching is the main symptom and there is no thick discharge, consider other reasons for the symptoms such as cystitis (bladder infection), vaginal dryness, or an allergy to toiletries or synthetic underwear. If a “fishy” or malodorous smell is present, consider bacterial
vaginosis (refer to a doctor).
Occasional episodes of vaginal thrush may be treated with over-the-counter vaginal antifungal agents sold by a pharmacist. Vaginal creams and pessaries come in one, three, and six-day courses. Usually one-day treatments will cure most bouts of thrush but consider longer courses for women still taking antibiotics or prone to recurrent thrush. A single, oral dose of fluconazole 150mg provides rapid relief and may be more convenient. Refer customers who have not responded to pharmacist-only treatments to a doctor. Some medical conditions, such as diabetes or autoimmune conditions make women prone to recurrent thrush. Sometimes thrush can be caused by other yeasts (eg, Candida glabrata) or is actually bacterial vaginosis, a sexually transmitted infection, or rarely, cancer.
Many things can affect the delicate pH balance of the vagina, triggering an overgrowth of C. albicans and an episode of thrush. The most common triggers include:
• a course of broad-spectrum antibiotics (eg, tetracycline, amoxicillin with clavulanic acid)
• higher-dose combined oral contraceptive pills or oestrogen-based menopausal replacement therapy
• immunodeficiency (eg, HIV)
• iron-deficiency anaemia
• hot and humid weather
• emotional or physical stress
• poorly controlled diabetes
• pregnancy.
• Be sexually responsible. Always use condoms unless you are in a mutually monogamous relationship with a partner who is free from sexually transmitted infections (STIs).
• Keep up-to-date with vaccinations. The human papillomavirus (HPV) vaccine is available free to all females and males aged nine to 27 (see Childhood Diseases and Immunisations). The hepatitis B vaccine also helps to prevent sexual transmission of hepatitis B.
• Keep pelvic floor muscles toned and limit exercises that are likely to place strain on pelvic floor muscles.
• Wear loose cotton underwear and avoid tight-fitting synthetic clothing. Avoid perfumed soap, vaginal deodorants, douches, or bath salts or foam.
• After urinating, wipe from front (vagina) to back (anus).
• Women prone to recurring episodes of thrush should consider using a water-based lubricant during intercourse and when inserting tampons if the vagina is dry, using a vaginal gel to regulate vaginal pH which can alter during the menstrual cycle, and showering straight after exercise.
• Oral probiotics may be useful to recolonise bacterial flora within the vagina.
• Pinworms may also be referred to as threadworms in New Zealand.
• Pinworms are common, especially in children at daycare, kindergarten, or primary school.
• Mebendazole and pyrantel are available over the counter to treat worms.
• Children should be reminded to always wash their hands before eating and after toileting.
In a quiet area of the pharmacy, talk with the person who suspects they have worms (or a caregiver if it is a child). Ask about their symptoms but even if they haven’t actually sighted a worm (they can be really hard to see), still offer a worm treatment if there is a possibility they might have worms.
Reassure your customer that pinworms are easily transferred, and anybody can get them. Children are more likely to be exposed to worms because they play outside and often forget to wash their hands. Some families regularly treat their children for worms every six months.
Run through the Refer to a Pharmacist checklist and refer anybody with concerns to a pharmacist. For all other customers, show them the treatment products available, discuss the dosage, and suggest ways to prevent reinfection.
Anti-worm products (called anthelmintics) that are sold in New Zealand contain either mebendazole or pyrantel (see Treatment options below). Both are effective at treating pinworm, roundworm, and hookworm infections.
People with a suspected tapeworm infection or whose symptoms persist despite treatment should be referred to a doctor.
Pinworms (Enterobius vermicularis) are small worms that live in the lower digestive tract. Pinworms may also be called threadworms, enterobiasis, or oxyuriasis. They
• People who are immunosuppressed, pregnant or breastfeeding.
• Children aged less than two years.
• If the person complains that the skin around the anal area is broken due to scratching.
• People reporting blood in their faeces or significant weight loss.
• People who have recently visited a developing or remote country.
• People with symptoms suggestive of worms who also have diarrhoea.
• When previous treatment has not been successful.
• With recurrent worm infestations.
• People with allergies to medicines.
are white and thin and look like a cotton thread and are about the size of a staple (2–13mm).
Occasionally they can be spotted in the stool (poo) or around the anus, but are usually difficult to see. A “sticky tape” test involves sticking and then quickly removing a piece of sticky tape to the anus in an attempt to catch any pinworm eggs. This is best done late at night or early morning as the female pinworm deposits her eggs outside the anus during the night. The tape is then viewed under a microscope for the presence of eggs. Generally, it is not considered necessary to find or see a worm or an egg and treatment is usually just given because people “think they might have worms”.
Humans are considered the only hosts of pinworms, so this type of worm cannot be caught from pets. Pets carry other sorts of worms, such as roundworm, tapeworm, and hookworm
which can be transmitted very occasionally to people. Children and people who are immunocompromised are more vulnerable to infection with animal worms than adults.
Pinworm is the most common worm infection occurring in New Zealand and it is estimated that every child is infected with worms at least once before reaching high school.
Many people infested with worms have no symptoms at all. Some people, particularly children, are more likely to complain of:
• itching around the bottom, typically at night – this is caused by a reaction to the glue used by the pinworm to attach its eggs to the skin
• sleep disturbance from scratching, which may result in daytime tiredness or irritability
• teeth grinding or bed-wetting
Category Examples Comments
Mebendazole [PHARMACY ONLY MEDICINE] eg, Mebendazole 100mg (Combantrin-1, De-Worm, Vermox) eg, mebendazole 500mg (DeWorm Extra Strength)
Pyrantel [PHARMACY ONLY MEDICINE] eg, Combantrin
When treating pinworms, the dose of mebendazole 100mg is suitable for everybody aged over two years. Repeat dose in two to four weeks. Chewable tablets, squares or suspension are available. The tablet can also be crushed and given to children mixed with honey, food, or fruit juice. Extra strength tablets (500mg) may be considered when other types of worms (such as hookworm, whipworm, or roundworm) are suspected, particularly for people who have travelled or immigrated from Asia, Africa, or the Pacific Islands.
The dose is 10mg/kg (consult guide on back of packet). Recommended for children aged one year or older. Treatment of children aged less than one year should be under medical advice. Repeat in two to four weeks. Chewable squares, suspension and tablets are available.
• Refer any deep, dirty, or profusely bleeding wounds to a doctor immediately.
• Low-toxicity, topical antiseptics applied before dressings help to reduce the risk of infection.
If a customer comes into your pharmacy with a wound that has recently occurred, put on gloves and stem any bleeding with a gauze pad, and quickly assess the wound to determine if it is appropriate to deal with in a pharmacy setting.
If it is appropriate, run through the Refer to a Pharmacist checklist as well. Some wounds are best referred straight away to the nearest accident and emergency or medical centre.
If the wound is relatively minor and you are comfortable treating it, carry on with first aid.
Category Examples
Sanitising products
Saline for cleansing
Antiseptic wound care applications
If there is copious bleeding call for an ambulance immediately.
• People with circulatory disorders or diabetes, or who are immunosuppressed, pregnant or breastfeeding.
• People who are elderly or frail, or who have a chronic wound, such as a leg ulcer, varicose ulcer or bleeding mole, that is not being managed by a doctor.
• Wounds that are extensive, deep, very dirty, or contain pus.
• Wounds that contain foreign objects which are embedded or unable to be easily removed.
• If the skin surrounding the wound is very red or painful.
• People who also have a fever or flu-like symptoms.
• If it has been more than five years since the person’s last tetanus vaccination.
• People with allergies to topical antiseptics or plasters. Products with an asterisk have a detailed listing in the Wound Care section of OTC Products.
Proper wound care aims to minimise the risk of infection and scarring, see Table, page 180, for treatment advice about different types of wounds.
Generally, any bleeding should be stopped by
eg, Dettol hand sanitiser, MicroCleanz
[GENERAL SALE]
eg, saline 0.9% (Crystawash Wound Wash)
[GENERAL SALE]
benzalkonium chloride (eg, Bepanthen)
bufexamac + chlorhexidine + lignocaine (eg, Ethics 4 Way Antiseptic Soothing Cream)
chlorhexidine ± cetrimide (eg, Medipulv Antiseptic Powder (with allantoin), Savlon, Soov Cream [with lignocaine]) chloroxylenol (eg, Dettol Antiseptic)
honey, medical grade topical (eg, Manuka Health Wound Gel, Medihoney Antibacterial Wound Gel) polyhexanide with betaine (eg, Prontosan) povidone iodine (eg, Betadine Antiseptic liquid/ointment/ spray)
silver (eg, Skybright Colloidal Silver, Silvergel) stabilised hydrogen peroxide (eg, Crystaderm cream*) super-oxidising solutions (eg, Microdacyn Wound Care solution/hydrogel)
[PHARMACY ONLY]
eg, chlorhexidine, cetrimide, lignocaine (eg, Medicreme Antiseptic cream)
Products to stop bleeding eg, Celox Nose Bleed dressings, Celox Granules, Celox Gauze Pad
Wound healing products [GENERAL SALE] eg, Mebo Wound repair
Dressings eg, Manuka Health Wound Dressings, Nexcare Sensitive Skin range, Nexcare Waterproof Bandages
Topical anaesthetics [PHARMACY ONLY MEDICINE] eg, lignocaine/prilocaine (Emla cream)
Natural / herbal products / supplements Honey, calendula ointment, magnesium sulphate, St John’s wort, tea tree oil, trypsin, vitamin A ointment, zinc
Comments
using a clean bandage to apply pressure to the area for 10 minutes. If bleeding is brisk and does not stop or spurts out with each heartbeat, seek urgent medical attention.
The wound should be cleaned with water, saline, or a low-toxicity antiseptic solution.
Eliminates most common harmful germs and bacteria. Convenient alternative to hand washing.
Normal saline (saline 0.9%) or tap water have similar outcomes when used to clean wounds.
Topical antiseptic agents may help reduce the risk of future infection when applied to an acute wound. They are preferred over topical antibiotic agents because they are broader in their spectrum of activity, less likely to cause allergic reactions, and rarely associated with bacterial resistance. Ensure correct dilutions are used.
Super-oxidising solutions, polyhexanide, diluted bleach, chlorhexidine, silver and cadexomer iodine cause less rejuvenating tissue damage than unstabilised hydrogen peroxide and povidone iodine.
Super-oxidising solutions and solutions that contain betaine also possess antibiofilm activity.
No clinically important resistance has been noted to super-oxidising solutions, polyhexanide, diluted bleach, silver, iodine, hydrogen peroxide and honey. Gram negative bacilli resistance has been reported with chlorhexidine and benzalkonium. Some strains of Staphylococcus aureus (including methicillin-resistant S. aureus [MRSA]) are resistant to chlorhexidine, cetrimide or benzalkonium. Honey has antibacterial properties and provides a moist environment for healing minor wounds. Diabetics may need to monitor blood sugars (refer to pharmacist).
Hydrogels donate moisture to a dry wound, improving healing.
Contain chitosan obtained from shrimp shells that clots blood within 30 seconds. Effective even for people who take anticoagulants such as warfarin. Does not affect long-term wound healing. No adverse reactions reported even in patients with a known hypersensitivity to shrimp or crab.
Supports the body’s immune response to fight infection, and promotes natural skin healing, minimising scarring.
Wound dressings containing medical-grade manuka honey have natural antibacterial properties and help maintain a moist wound surface. For more information about other dressings see Treatment options in Cuts, Abrasions and Blisters
Lignocaine/prilocaine creams can be used before cleaning painful wounds, such as leg ulcers. Apply to the skin 45–60 minutes before the procedure.
Topical honey-impregnated dressings or creams appear to improve wound healing, reduce odours, help clean the wound and decrease risk of infection. Topical St John’s wort, trypsin, calendula, vitamin A and zinc also have skin-healing properties.

Pay particular attention to removing any small pieces of foreign material (such as wood, soil and clay) or damaged tissue.
A piece of moist gauze or tweezers may aid removal. If the wound is difficult to clean or cannot be cleaned thoroughly, refer the customer to a doctor.
Apply a topical antiseptic agent to reduce the risk of infection. Super-oxidising solutions, polyhexanide, diluted bleach, chlorhexidine, silver and cadexomer iodine cause less rejuvenating tissue damage than unstabilised hydrogen peroxide and povidone iodine. If the product requires dilution, ensure your customer knows how to do it correctly. Apply a dressing to protect against further trauma. The dressing should keep the wound moist, but not wet; have the capacity to absorb discharging fluid or blood; and be shower-proof. Change the dressing regularly depending on the type.
Consider referring your customer to a doctor
• Watch for signs of infection (eg, redness spreading out from the wound or yellow drainage from the area) and seek medical advice if this occurs.
• Topical antibiotics are usually not necessary. Overuse of these medicines can lead to bacterial resistance and oral antibiotics are usually more effective if antibiotics are deemed necessary.
• Do not pick scabs off as the wound heals – this can cause scarring.
• Correct any nutritional deficiencies. Deficiencies of vitamins A, C, and zinc and poor dietary protein intake impair normal wound-healing mechanisms.
• People with diabetes should seek medical advice with any wound, especially wounds on the lower extremities (ie, feet, lower leg). This is because people with diabetes have a reduced blood flow to their extremities (which delays healing) and commonly have peripheral neuropathy, a reduced sensation in the hands and feet, which means an injury may not be noticed straight away.
• For elderly people at risk of skin tears:
➤ keep skin moisturised and use sheepskin boots and elbow pads to reduce friction
➤ self-adhesive bandages are less likely to damage the skin than adhesive tapes and dressings
➤ assist those at risk of falling, and pad furniture and equipment to prevent bruising from collisions.
for a booster tetanus shot if it has been more than five years since the person’s last tetanus vaccination.
Our skin acts as a barrier to the outside world, protecting us from allergens, infection, temperature extremes and UV radiation. It also protects our internal organs and other structures from damage.
A wound is a break in the skin which may be caused by burns, cancer, cuts or abrasions (see also Cuts, Abrasions and Blisters), infection, penetrating objects, pressure, surgery, trauma, and many other things. Some people are more
prone to wounds, such as elderly people, people with diabetes or circulatory problems, and people taking corticosteroids or other medicines that thin the skin.
Most wounds heal faster and with less scaring if the wound is kept moist. Modern dressings contain hydrogels and other substances to prevent wounds from drying out while absorbing excess fluid (exudate) from discharging wounds.
Serious wounds often need long-term management and people with these wounds should be monitored by a nurse or doctor. However, patients may wish to buy their dressings from a pharmacy.
Surgical wounds
Puncture wounds eg, splinters or nail puncture
• For surgical wounds, keep wound edges together and follow surgeon's instructions for wound care.
• For small puncture wounds clean the wound with saline, tap water, or a lowtoxicity antiseptic cleansing solution, and apply an antiseptic. Refer to a doctor more serious puncture wounds, or if it has been more than five years since a person's last tetanus shot.
• If a protective dressing is needed, use an island adhesive dressing and change daily.
• Wound closure strips eg, Elastoplast, Steristrip, Nexcare Butterfly/ Steri-strip Closures
• Wound pad non-stick dressings eg, Elastoplast, Melolin, Telfa
• Film dressing eg, Elastoplast, Opsite, Tegaderm
• Dressings impregnated with honey eg, Manuka Health Wound Dressings, ApiNate dressing
• Island dressings eg, Elastoplast, Opsite Post-Op, Nexcare, Telfa, Tegaderm with pad.
• Silver dressings eg, Acticoat, Allevyn Ag
• Wound closure strips hold wound edges together, are flexible, help reduce scarring and have hypoallergenic adhesive.
• Non-stick wound pad dressings absorb fluid but won’t stick to the wound.
• Film dressings are water and bacteria-proof moist dressings, which do not absorb exudate.
• Self-adhesive island dressings have two types: – non-waterproof, with non-adherent wound pad, which absorbs wound exudate without sticking to the wound.
– waterproof and bacteria-proof dressings which are covered by a special film. This waterproofs and protects the wound against bacteria. The transparent film allows the wound to be monitored.
Household burns
Skin tears
Skin ulcers
• Remove heat source from the patient.
• Immediately cool the area for up to 20 minutes with cool running water from a tap or shower. In the absence of water, any cool clean fluid can be used.
• Remove any affected clothing if it is wet with hot liquid or affected by a chemical splash. Remove tight rings or jewellery from the injured area before swelling occurs. Do not try to remove fabric stuck to skin.
• Call 111 for patients with serious burns or refer them to their doctor.
• After cooling the area for 20 minutes, remove any non-viable tissue and apply an antiseptic if the burn has compromised the skin integrity. Apply a sterile dressing. Improved outcome results have been reported for sustained-release silver dressings and honey dressings.
• Skin tears often occur in fragile skin of the elderly. Salvage the skin flap if possible. Keep the flap moist and stop any bleeding by using impregnated gauze. Realign the skin using wound closure strips.
• Cover skin tear with a moist, healing wound dressing.
• Skin ulcers should be correctly diagnosed by a doctor before commencing treatment.
• Provide a moist healing environment.
• Use dressings which absorb exudate from the wound.
• Dressings keep the wound at body temperature – optimum for new skin growth.
• Dressings impregnated with honey eg, Manuka Health Wound Dressings, ApiNate dressing
• Hydrocolloid dressings eg, Elastoplast, Nexcare Waterproof
• Island dressings eg, Elastoplast, Opsite Post-Op, Nexcare, Telfa, Tegaderm with pad.
• Silver dressings eg, Acticoat, Allevyn Ag
• Island dressings – see above.
• Hydrocolloid dressings are highly absorbent, binding exudate and preventing skin maceration and breakdown.
• Dressings impregnated with honey help absorb fluid exudate, keep the wound moist, will not stick to the wound and have antibacterial properties. Cover with waterproof dressing, or if moderate to heavy exudate use a dry dressing with tape and bandage. Caution: Diabetics may need to monitor blood sugars (refer to pharmacist).
• Impregnated gauze eg, Jelonet
• Wound closure strips eg, Elastoplast, Steristrip, Nexcare Butterfly/ Steri-strip Closures
• Film dressing eg, Elastoplast, Opsite, Tegaderm
• Follow doctor's advice regarding choice of wound dressing. Dressings are usually occlusive as ulcers heal better in a moist environment. Honey dressings may be helpful.
• Hydrocolloid/Hydroactive dressings eg, Elastoplast, Allevyn and Duoderm
• Dressings impregnated with honey eg, Manuka Health Wound Dressings, ApiNate dressing
• Impregnated gauze keeps the area moist.
• Wound closure strips hold wound edges together, are flexible, help reduce scarring and have hypoallergenic adhesive.
• Film dressings are water and bacteria-proof moist dressings, which do not absorb exudate.
• Hydrocolloid dressings are highly absorbent, binding exudate and preventing skin maceration and breakdown
• Dressings impregnated with honey help absorb fluid exudate, keep the wound moist, will not stick to the wound and have antibacterial properties. Cover with waterproof dressing, or if moderate to heavy exudate use a dry dressing with tape and bandage.
It’s the button that helps you keep up to date, CAPTURE a record of what you read, watch, listen to, delve into and explore on pharmacytoday.co.nz
Acute New, immediate, sudden
Absorption Transfer of a substance into another area, eg, into the body through skin or mouth
ACE inhibitor Medicine used to treat heart and blood pressure problems
Adsorption The accumulation of gases, liquids, or solutes on the surface of a solid or liquid
Analgesic Pain-relieving medicine
Angioedema Rapid swelling of the dermis, subcutaneous, mucosa and submucosal tissues. Airway obstruction and suffocation may result
Antipyretic Medicine which reduces fever
Antitussive Medicine which helps stop coughing
Candidiasis Fungal infection commonly called thrush
Cardiac Relating to the heart
Chronic Long-term medical condition
Congenital anomalies Disease or disorder that is present at birth
Congestion Nose, sinuses or chest blocked with mucus; swollen tissue
Contraindicated Treatment is inadvisable
Emetic A medicine which causes vomiting
Expectorant A medicine which loosens chest congestion
Diabetes mellitus Chronic high blood glucose, now referred to as type 2 diabetes
First-line therapy First choice of medicine for treatment
Gastro-oesophageal reflux Acid stomach contents rising up to cause heartburn
Haematuria Presence of blood in the urine
Heart failure Heart disease
Hepatic Relating to the liver
Humectant Adds moisture or dampness
Hypertension High blood pressure
Hyperthyroidism Overactive thyroid gland causing weight loss and nervousness
Immunosuppression Loss of the normal immune protection
Keratolytic Skin-peeling agent
Malaise Feeling of being unwell or not healthy
Nocturia Frequent need to arise during the night in order to urinate
NSAID Non-steroidal anti-inflammatory drug, used for relief of pain, fever and inflammation
Occlusive Sealed, eg, an occlusive dressing
Opiate/Opioid Originating from or similar to morphine
Papules Red bumps on skin
Pharynx Throat area containing openings to both the trachea and the oesophagus
Pustules Red bumps with pus, on skin
Renal Relating to the kidneys
Rhinitis Inflamed, swollen lining of the nose, common when you have a cold
Secondary infection Infection which develops from an earlier condition
Stools Bowel motion, faeces
Subarachnoid haemorrhage Bleeding into the space between the two membranes that surround the brain
Topical agent Product applied to the skin
Urinary retention Unable to pass urine properly
Vesicles Little pimples with clear fluid
Welt Raised, pink, itchy patch on skin
Acne
Elsaie M. Hormonal treatment of acne vulgaris: an update. Clin Cosmet Investig Dermatol. 2016;9:241-248 https://doi.org/10.2147/CCID.S114830 https://www.dovepress.com/ hormonal-treatment-of-acne-vulgaris-an-update-peer-reviewed-fulltext-article-CCID
Kucharska A, Szmurlo A, Sinska B. Significance of diet in treated and untreated acne vulgaris. Advances in Dermatology and Allergology 2016;33(2):81-86. doi:10.5114. ada.2016.59146.
Bergler-Czop B, Brzezińska-Wcisło L. Dermatological problems of the puberty. Postepy Dermatol Alergol. 2013;30(3):178 187. doi:10.5114/pdia.2013.35621
Palmer A. Treating Acne in Teenage Boys Very Well health Jan 13, 2023 https://www.verywellhealth.com/treating-teen-acne-in-boys-15939
Oakley A. Acne management. Dermnet. http://www.dermnetnz.org/topics acne-management/
Tan J. Current Measures for the Evaluation of Acne Severity. Expert review of Dermatology 2008;3(5):595-603. Medscape http://www.medscape.com/viewarticle/582896
Alikhan A, Maibach H. Keratolytic Treatments for Acne: A Review https://www.cosmeticsandtoiletries.com/formulating/category/skincare/premiumKeratolytic-Treatments-for-Acne-A-Review-208733901.html
Milani M, Bigardi A, Zavattarelli M. Efficacy and safety of stabilised hydrogen peroxide cream (Crystacide) in mild-to-moderate acne vulgaris: a randomised, controlled trial versus benzoyl peroxide gel. Curr Med Res Opin. 2003;19(2):135 138. doi:10.1185/030079902125001523
Tirado-Sánchez A, Ponce-Olivera RM. Efficacy and tolerance of superoxidized solution in the treatment of mild to moderate inflammatory acne. A double-blinded, placebo-controlled, parallel-group, randomized, clinical trial. J Dermatolog Treat. 2009;20(5):289 292. doi:10.1080/0954663090297399
Allergies
Allergy and anaphylaxis guidelines for early childhood services and schools. Allergy NZ. www.allergy.org.nz/
Diagnosing Allergic Diseases. Auckland Allergy and Eczema Clinic. 2023. http://www.allergyclinic. co.nz/diagnosing-allergic-diseases
Anaphylaxis. Allergy New Zealand. http://www.allergy.org.nz/A-Z+Allergies/Anaphylaxis.html
Church MK, Church DS. Pharmacology of Antihistamines. IndianJournalofDermatology 2013;58(3):219-224. doi:10.4103/0019-5154.110832.
The Australasian Society of Clinical Immunology and Allergy (ASCIA). 2023 www.allergy.org.au Asthma and COPD
Asthma. Health Quality and Safety Commission New Zealand. https://www.hqsc.govt.nz/ our-programmes/health-quality-evaluation/projects/atlas-of-healthcare-variation/asthma/ COPD. Mayo Clinic. http://www.mayoclinic.org/diseases-conditions/copd/basics/treatment/con Living with Asthma. Asthma and Respiratory Foundation of New Zealand 2023. https://www.asthmafoundation.org.nz/your-health/living-with-asthma What is COPD. COPD Foundation 2023 http://www.copdfoundation.org/What-is-COPD/ Understanding-COPD/What-is-COPD.aspx
Baby Care
Johnson JD, Cocker K, Chang E. Infantile Colic: Recognition and Treatment. Am Fam Physician. 2015 Oct 1;92(7):577-82. PMID: 26447441. Colic Mayo clinic. 2023. https://www.mayoclinic.org/diseases-conditions/colic/symptomscauses/syc-20371074
Springen K, Bilich K, Reece T. How to Soothe a Colicky Baby. Parents.com. https://www.parents.com/baby/care/colic/how-to-soothe-a-colicky-baby/ Colic Relief Tips for Parents. American Academy of Pediatrics. 2023 https://www.healthychildren.org/English/ages-stages/baby/crying-colic/Pages/Colic.aspx Diaper rash. E-Medicine. www.emedicinehealth.com/diaper_rash/page2_em.htm Napkin dermatitis. DermNet. http://dermnetnz.org/dermatitis/napkin-dermatitis.html Nappies and nappy rash. Plunket. Whanua awhina https://www.plunket.org.nz/ caring-for-your-child/hygiene-and-daily-care/poos-nappies-and-toilet/nappies-and-nappy-rash/ Nappy rash. The Royal Children’s Hospital Melbourne. www.rch.org.au/clinicalguide/ guideline_index/Nappy_Rash/ Baby Feeding
Breastfeeding is perfect for you and your baby. Ministry of Health. https://www.health.govt. nz/your-health/pregnancy-and-kids/first-year/ Feeding your baby infant formula. How to prepare infant formula safely. Ministry of Health. https://www.healthed.govt.nz/resource/feeding-your-baby-infant-formula Infant formulas – overview. Medline Plus. https://medlineplus.gov/ency/article/002447.htm Low Milk Supply. Baby Center.com http://www.babycenter.com/0_low-milk-supply_8487.bc Martin V. Infant formulas - a parent’s guide. Family Doctor NZ. http://www.familydoctor. co.nz/categories/childrens-health/infant-formulas-a-parents-guide/ Pregnancy Nutrition and Baby Feeding Advice. ForBaby http://www.forbaby.co.nz/ Thrush when breastfeeding. Ministry of Health. http://www.health.govt.nz/your-health/ conditions-and-treatments/diseases-and-illnesses/thrush-when-breastfeeding Bites and Stings
Story: Sandflies and mosquitoes Te Ara NZ. https://teara.govt.nz/en/ sandflies-and-mosquitoes/
Mosquito Information for New Zealand. Southern Monitoring Services. https://www.smsl. co.nz/Pests/Commonly+Asked+Questions+about+Mosquitoes.html
All About Bedbugs! SMS Southern Monitoring Services. https://www.smsl.co.nz/Pests/ All+About+Bedbugs.html
stopping-bed-bugs-in-their-tracks-at-southland-huts/ Jellyfish stings NZ MOH http://www.health.govt.nz/your-health/conditions-and-treatments/ accidents-and-injuries/bites-and-stings/jellyfish-stings Spider bites. Dermnet NZ. http://www.dermnetnz.org/arthropods/spider-bites.html Rademaker M. Swimmer’s itch DermNet NZ https://www.dermnetnz.org/topics/ swimmers-itch/
Bruises, Scars, Spider Veins
Goedemans, A, Liang, K, Cottell, B et al. Topical Arnica and mucopolysaccharide polysulfate (Hirudoid) to decrease bruising and pain associated with haemodialysis cannulation-related infiltration: A pilot study. Renal Society of Australasia Journal 2014. 10(2):62-65
Keloids & hypertrophic scars. DermNet NZ. https://www.dermnetnz.org/topics/ keloids-and-hypertrophic-scar/ Sclerotherapy. DermNet NZ. http://dermnetnz.org/procedures/sclerotherapy.html
Varicose veins and spider veins. Medscape. http://emedicine.medscape.com/ article/1085530-overview
What are bruises? NHS. https://www.nhs.uk/common-health-questions/ accidents-first-aid-and-treatments/what-are-bruises/
Childhood Diseases and Immunisations
Chickenpox (varicella). DermNet NZ. www.dermnetnz.org/viral/varicella.html
Immunisation Advisory Centre. Arainga mate. University of Auckland. www.immune.org.nz
Genital HPV Infection - Fact Sheet. CDC. www.cdc.gov/std/hpv/stdfact-hpv.htm
The Core Health Checks. Well Child provider visit. Well Child. http://www.wellchild.org.nz/ wcto-programme/well-child-provider-visit
Vaccines for Meningococcal Disease. The Meningitis Foundation. http://www.meningitis. org.nz/vaccines_for_meningococcal_disease
Varicella (Chickenpox). Immunisation Advisory Centre 2023 https://www.immune.org.nz/ diseases/varicella-chickenpox
New Zealand Immunisation Schedule. 1 March 2023. Manatu Hauora. Ministry of Health. https://www.health.govt.nz/our-work/preventative-health-wellness/immunisation/ new-zealand-immunisation-schedule
Covid 19 Vaccines April 2023. Unite against Covid https://covid19.govt.nz/covid-19-vaccines/ Derqui N, Koycheva A, Zhou J, et al. Risk factors and vectors for SARS-CoV-2 household transmission: a prospective, longitudinal cohort study. The Lancet Microbe April 6, 2023 https://www.thelancet.com/journals/lanmic/article/PIIS2666-5247(23)00069-1/fulltext Gardasil 9. Immunisation Advisory Centre. Accessed 14 April 2023. https://www.immune.org. nz/vaccine/gardasil-9
Deadly meningococcal disease cases rising among our most vulnerable, prompting expert’s warning. 12 Dec 2022. NZ Herald. https://www.nzherald.co.nz/kahu/deadly-meningococcaldisease-cases-rising-among-our-most-vulnerable-prompting-experts-warning/ JHVXLVAU6JH4NDM6EO3Y6XQP64/
Childhood Pain
Kanabar DJ. A clinical and safety review of paracetamol and ibuprofen in children. Inflammopharmacology. 2017;25(1):1-9. doi:10.1007/s10787-016-0302-3.
Managing pain in children aged under 12 years. BPAC NZ 2014 (59). https://bpac.org.nz/ bpj/2014/march/pain.aspx
Mathews L. Pain in children: neglected, unaddressed and mismanaged. Indian J Palliat Care 2011;17(Suppl):S70-3.
Pain in Childhood Special Interest Group The Australian Pain Society. https://www.apsoc.org. au/pain-in-childhood
Pierce CA, Voss B. Efficacy and safety of ibuprofen and acetaminophen in children and adults: a meta-analysis and qualitative review. Ann Pharmacother. 2010;44:489–506. doi:10.1345/aph.1M332.
Cold Sores
Famvir once. New Zealand Datasheet. Novartis Consumer Health Australasia Pty Ltd. http://www.medsafe.govt.nz/profs/Datasheet/f/famvironcetab.pdf
Herpes Simplex. DermNetNZ. http://dermnetnz.org/viral/herpes-simplex.html
Colds and COVID-19
Colds. Ministry of Health. Manatu Hauora. http://www.health.govt.nz/your-health/ conditions-and-treatments/diseases-and-illnesses/colds
How COVID-19 vaccines work. Ministry of Health. 5 September 2022. https://www.health.govt.nz/ covid-19-novel-coronavirus/covid-19-vaccines/how-covid-19-vaccines-work
Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis Sze, Shirley et al. EClinical Medicine, Volume 29, 100630
Constipation
Constipation. Ministry of Health. Manatu Hauora. http://www.health.govt.nz/your-health/ conditions-and-treatments/diseases-and-illnesses/constipation
Stewart M. Macrogols for constipation or bowel cleansing. Sep 2020. https://patient.info/ medicine/macrogols-for-constipation-or-bowel-cleansing
Contraception, Emergency and Oral
Combined oral contraceptive pill. New Zealand Family Planning. http://www.familyplanning. org.nz/advice/contraception/combined-oral-contraceptive-pill
Emergency Contraception accreditation training. College Education and Training. PSNZ. https://www.psnz.org.nz/
Practice Guidelines. Pharmacist Supply of the Emergency Contraceptive Pill. Pharmaceutical Society. https://www.psnz.org.nz/ What should I do if I miss a pill (progestogen-only pill)? Your contraception guide. NHS. https://www.nhs.uk/conditions/contraception/miss-progestogen-only-pill/
Coughs: Dry
Canning BJ, Chang AB, Bolser DC, et al. Anatomy and Neurophysiology of Cough: CHEST Guideline and Expert Panel Report. Chest. 2014;146(6):1633-1648. doi:10.1378/ chest.14-1481.
Cough-symptoms. NHS choices. www.nhs.uk/Conditions/Cough/Pages/Symptoms.aspx
Lamas A, Ruiz de Valbuena M, Máiz L3. Cough in children. ArchBronconeumol2014 Jul;50(7):294-300. doi: 10.1016/j.arbres.2013.09.011. Epub 2014 Feb 5.
Mahashur A. Chronic dry cough: Diagnostic and management approaches. Lung India 2015;32(1):44-9.
Goldman RD. Honey for treatment of cough in children. Canadian Family Physician 2014;60(12):1107-1110.
Solo-Josephson P. Coughing. Kidshealth. https://kidshealth.org/en/parents/childs-cough. html
Coughs: Productive
Canning BJ, Chang AB, Bolser DC, et al. Anatomy and neurophysiology of cough: CHEST Guideline and Expert Panel report. Chest. 2014;146(6):1633-1648.
Causes of chronic productive cough: An approach to management. Respiratory Medicine 2015;109 (9):1105-13 http://www.resmedjournal.com/article/S0954-6111(15)30001-9/fulltext
Cough in Children. BPAC NZ 2010 BPJ 29. https://bpac.org.nz/bpj/2010/july/cough.aspx
Goldman RD. Honey for treatment of cough in children. Canadian Family Physician 2014;60(12):1107-1110.
That nagging cough. Common causes, cures for a persistent cough. Harvard Health Medical School. 2022. https://www.health.harvard.edu/staying-healthy/that-nagging-cough Cuts, Abrasions and Blisters
Abrasions, Cuts, Lacerations. World of Sports Science. www.faqs.org/sports-science/A-Ba-and-timeline/Abrasions-Cuts-Lacerations.html
Collins S, White J, Ramsay M, Amirthalingam G. The importance of tetanus risk assessment during wound management. IDCases. 2014;2(1):3-5. Published 2014 Dec 10. doi:10.1016/j.idcr.2014.11.003
Wound care. Family Health Diary. https://www.familyhealthdiary.co.nz/conditions/ wound-care-cuts-and-grazes/ Cystitis [Bladder Infection]
Barclay Jonathan, Veeratterapillay Rajan, Harding Chris. Non-antibiotic options for recurent urinary tract infections in women. BMJ 2017; 359 :j5193
Juthani-Mehta M, Van Ness PH, Bianco L, et al. Effect of Cranberry Capsules on Bacteriuria Plus Pyuria Among Older Women in Nursing Homes. A Randomized Clinical Trial. JAMA 2016;316(18):1879-1887. doi:10.1001/jama.2016.16141
Kranjec B1, Papeš D, Altarac S. D-mannose powder for prophylaxis of recurrent urinary tract infections in women: a randomized clinical trial. World J Urol 2014 Feb;32(1):79-84. doi: 10.1007/s00345-013-1091-6.
Lee BSB, Bhuta T, Simpson JM,Craig JC. Methenamine hippurate for preventing urinary tract infections. Cochrane Database of Systematic Reviews 2012, Issue 10. Art. No.: CD003265. DOI: 10.1002/14651858.CD003265.pub3.
O’Kane DB, Dave SK, Gore N, et al. Urinary alkalisation for symptomatic uncomplicated urinary tract infection in women. Cochrane Database of Systematic Reviews 2016, Issue 4. Art. No.: CD010745. DOI: 10.1002/14651858.CD010745.pub2
Urinary-tract infection New Zealand Formulary v.131 1 May 2023. https://nzf.org.nz/ nzf_71068?searchterm=cystitis
Urinary tract infections (UTIs) – an overview of lower UTI management in adults 10 December 2021. BPAC NZ. https://bpac.org.nz/2021/uti.aspx
Nitrofurantoin for UTI Algorithm. Pharmaceutical Society. https://learn.psnz.org.nz/ pluginfile.php/40765/mod_resource/content/3/Nitro%20algorithm%20final%20 December%202022.pdf
Dandruff
Dandruff. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/dandruff/ symptoms-causes/syc-20353850
Dandruff: How to treat. American Academy of Dermatology. https://www.aad.org/public/ diseases/hair-and-scalp-problems/dandruff-how-to-treat
DE Angelis YM, Gemmer CM, Kaczvinsky JR, et al. Three etiologic facets of dandruff and seborrheic dermatitis: Malassezia fungi, sebaceous lipids, and individual sensitivity. Journal of Investigative Dermatology. Symposium Proceedings. 2005. 10(3):295–57. Ranganathan S, Mukhopadhyay T. Dandruff: The most commercially exploited skin disease. Indian Journal of Dermatology. 2010;55(2):130-134. doi:10.4103/0019-5154.62734. Seborrhoeic dermatitis and eczema. DermNetNZ. http://dermnetnz.org/dermatitis/ seborrhoeic-dermatitis.html
Dental Pain
Fluoride. Ministry of Health. https://www.health.govt.nz/your-health/healthy-living/ teeth-and-gums/fluoride
Healthy Smiles. www.healthysmiles.org.nz
Gum disease information. American Academy of Periodontology. http://www.perio.org/ consumer/gum-disease.htm
Classification of codeine. Information paper for the Medicines Classification Committee. June 2019 https://www.medsafe.govt.nz/profs/class/Agendas/Agen63/MCC63_53a_Reclassificationofcodeine.pdf
Dermatitis/Eczema
Allergic Contact Dermatitis. DermNet NZ. http://www.dermnetnz.org/dermatitis/contact-allergy.html Atopic dermatitis. DermNet NZ. http://dermnetnz.org/dermatitis/atopic.html
Cradle cap (infantile seborrhoeic dermatitis) DermNet NZ. http://dermnetnz.mobify.me/ dermatitis/cradle-cap.html
Dermatitis (Eczema). DermNet NZ. www.dermnetnz.org/dermatitis/dermatitis.html
Dry skin. DermNet NZ. http://dermnetnz.org/dermatitis/dry-skin.html
Seborrhoeic dermatitis and eczema. DermNet NZ. http://dermnetnz.org/dermatitis/ seborrhoeic-dermatitis.html
The causes of atopic eczema. DermNet NZ. http://dermnetnz.org/dermatitis/atopic-causes.html
Diabetes
Diabetes NZ. https://www.diabetes.org.nz Diabetes. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/diabetes/ symptoms-causes/syc-20371444
Diarrhoea and Vomiting Diarrhoea. Ministry of Health. http://www.health.govt.nz/your-health/ conditions-and-treatments/diseases-and-illnesses/diarrhoea Viral gastroenteritis. KidsHealth http://www.kidshealth.org.nz/gastroenteritis
Dry Skin
Dry skin. Dermnet NZ. http://www.dermnetnz.org/dermatitis/dry-skin.html
Dry Skin. Mayo Skin Clinic. www.mayoclinic.com/health/dry-skin/DS00560/DSECTION=causes Icthyosis. Dermnet NZ. http://dermnetnz.org/scaly/ichthyosis.html
Lawton S (2019) Skin 1: the structure and functions of the skin. Nursing Times [online]; 115, 12, 30-33.
Kang BC, Kim YE, Kim YJ, et al. Optimizing EEMCO guidance for the assessment of dry skin (xerosis) for pharmacies. Skin Res Technol. 2014 Feb;20(1):87-91. doi: 10.1111/srt.12089. Epub 2013 Jul 2.
Dermatologists top tips for relieving dry skin. 2023 American Academy of Dermatology. https://www.aad.org/public/everyday-care/skin-care-basics/ drydermatologists-tips-relieve-dry-skin
De Pessemier B, Grine L, Debaere M, Maes A, Paetzold B, Callewaert C. Gut-Skin Axis: Current Knowledge of the Interrelationship between Microbial Dysbiosis and Skin Conditions. Microorganisms. 2021;9(2):353. doi:10.3390/microorganisms9020353
Ellis SR, Nguyen M, Vaughn AR, et al. The Skin and Gut Microbiome and Its Role in Common Dermatologic Conditions. Microorganisms. 2019;7(11):550. Published 2019 Nov 11. doi:10.3390/microorganisms7110550
Ear Conditions
Hearing problems in children. Kids Health NZ www.kidshealth.org.nz/ hearing-problems-children#block_2205
Swimmer’s Ear. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/swimmers-ear/ symptoms-causes/syc-20351682
Eye Conditions
Eye Problems and Diseases. www.allaboutvision.com/conditions/ Garrity J. Structure and Function of the Eyes. http://www.merckmanuals.com/home/ eye-disorders/biology-of-the-eyes/structure-and-function-of-the-eyes
Eyes: Contact Lenses
Consumer guide to contact lenses www.allaboutvision.com/contacts/ Rogers Cameren. LASIK: Know the Rewards and the Risks. WebMD Health News. https://www.webmd. com/eye-health/news/20180727/lasik-know-the-rewards-and-the-risks#:~:text=Around%20 700%2C000%20LASIK%20surgeries%20are,the%20procedure%20is%20remarkably%20high Segre L. Contact lens basics. All About Vision 2023. http://www.allaboutvision.com/contacts/ contact_lenses.htm
Refractive Lens Exchange. Eye Institute 2023 https://eyeinstitute.co.nz/ refractive-lens-exchange/ Fever
Febrile seizures. Epilepsy Foundation. http://www.epilepsy.com/learn/types-seizures/ febrile-seizures
Febrile seizures. Paediatric Society NZ. https://www.kidshealth.org.nz/febrile-seizures Fever. Paediatric Society NZ. https://www.kidshealth.org.nz/fever Foot Care
Athlete’s Foot. DermNet NZ. http://dermnetnz.org/fungal/athletes-foot.html
Cracked Heels. DermNet NZ. http://dermnetnz.org/scaly/cracked-heels.html Foot corns and callus. DermNet NZ. www.epodiatry.com/corns-callus.htm
Fungal nail infections. DermNet NZ http://dermnetnz.org/fungal/onychomycosis.html
How to treat corns and calluses. American Academy of Dermatology. https://www.aad.org/ public/skin-hair-nails/skin-care/corns-and-calluses
Paronychia. DermNet NZ. http://dermnetnz.org/fungal/paronychia.html
Viral warts. DermNet NZ. http://dermnetnz.org/viral/viral-warts.html
Fungal Infections: Skin and Scalp
El‐Gohary M, van Zuuren EJ, Fedorowicz Z, Burgess H, Doney L, Stuart B, Moore M, Little P. Ely J, Rosenfeld S, Seabury M. Diagnosis and Management of Tinea Infections. Am Fam Physician. 2014 Nov 15;90(10):702-711. https://www.aafp.org/afp/2014/1115/p702.html#:~:text=For%20tinea%20 capitis%2C%20adjunctive%20topical,Instead%20use%20griseofulvin
Topical antifungal treatments for tinea cruris and tinea corporis. Cochrane Database of Systematic Reviews 2014, Issue 8. Art. No.: CD009992. DOI: 10.1002/14651858.CD009992. pub2.
Fungal infections. Dermnet NZ. www.dermnetnz.org/fungal/ Mycology of dermatophyte infections. Dermnet NZ. www.dermnetnz.org/fungal/mycology.html Nappy Rash. DermNet NZ. https://www.dermnetnz.org/topics/napkin-dermatitis/
Paronychia. DermNet NZ http://dermnetnz.org/fungal/paronychia.html
Pityriasis versicolour. DermNet NZ http://www.dermnetnz.org/fungal/pityriasis-versicolor.html
Tinea Corporis. DermNet NZ. https://www.dermnetnz.org/topics/tinea-corporis/ Tinea capitis. DermNet NZ. http://dermnetnz.org/fungal/tinea-capitis.html
Tinea corporis. DermNet NZ. www.dermnetnz.org/fungal/tinea-corporis.html Tinea cruris. DermNet NZ. www.dermnetnz.org/fungal/tinea-cruris.html
Fungal Nail Infections (Onychomycosis)
Ameen M, Lear JT, Madan V et al. British Association of Dermatologists’ guidelines for the management of onychomycosis 2014. British Journal of Dermatology 2014;171:937-958 DOI 10.1111/bjd.13358
Ghannoum M, Isham N (2014) Fungal Nail Infections (Onychomycosis): A Never-Ending Story? PLoS Pathog 10(6): e1004105. https://doi.org/10.1371/journal.ppat.1004105
Gupta AK, Daigle D, Foley KA. Topical therapy for toenail onychomycosis: an evidence-based review. Am J Clin Dermatol 2014;15(6):489-502. doi: 10.1007/s40257-014-0096-2. Gupta AK, Simpson FC New pharmacotherapy for the treatment of onychomycosis: an update. Expert Opin Pharmacother. 2015 Feb;16(2):227-36. doi: 10.1517/14656566.2015.993380. Epub 2014 Dec 19.
Lauharanta J. Comparative efficacy and safety of amorolfine nail lacquer 2% versus 5% once weekly. Clin Exp Dermatol 1992;17: 41–3. doi: 10.1111/j.1365-2230.1992.tb00277.x
Tietz HJ, Hay R, Querner S, et al. Efficacy of 4 weeks topical bifonazole treatment for onychomycosis after nail ablation with 40% urea: a double-blind, randomized, placebocontrolled multicenter study. Mycoses 2013;56(4):414-21. doi: 10.1111/myc.12037
Gout
Batt C Phipps-Green A, Black M. Sugar-sweetened beverage consumption: a risk factor for prevalent gout with SLC2A9 genotype-specific effects on serum urate and risk of gout http://ard.bmj.com/content/early/2013/09/10/annrheumdis-2013-203600.full.pdf
Dalbeth N, House ME, Horne A, et al. The experience and impact of gout in M ori and Pacific people: a prospective observational study. Clin Rheumatol 2013;32(2):247-51. doi: 10.1007/ s10067-012-2110-5. Epub 2012 Nov 1.
Gout. Health, Safety and Quality Commission New Zealand, 6 July 2022. https://www.hqsc. govt.nz/our-programmes/health-quality-evaluation/projects/atlas-of-healthcare-variation/ gout/
Hyperuricemia (High Uric Acid). Chemocare https://chemocare.com/chemotherapy/sideeffects/hyperuricemia-high-uric-acid.aspx
Long term Control Of Gout. NZ Formulary. V. 131 1 May 2023 https://nzf.org.nz/ nzf_5676?searchterm=gout
Neogi T et al. 2015 Gout Classification Criteria. An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. JArthritisandRheumatology; 67(10):2557-68. DOI 10.1002/art.39254 http://www.rheumatology.org/Portals/0/Files/2015%20Gout%20 Classification%20criteria.pdf
Singh JA, Reddy SG, Kundukulam J. Risk factors for gout and prevention: a systematic review of the literature. Curr Opin Rheumatology 2011;23(2):192–202. doi:10.1097/ BOR.0b013e3283438e13
Haemorrhoids
Hemorrhoids and what to do about them. Updated Nov, 2021 Harvard Health Publications. http://www.health.harvard.edu/diseases-and-conditions/ hemorrhoids_and_what_to_do_about_them Haemorrhoids (piles) - symptoms and treatment. Southern Cross. https://www.southerncross. co.nz/group/medical-library/haemorrhoids-piles-symptoms-treatment Hair Loss
Dyall-Smith D. Alopecia from Drugs. DermNet NZ 2009. https://www.dermnetnz.org/topics/ alopecia-from-drugs/ Finasteride. Dermnet NZ http://dermnetnz.org/treatments/finasteride.html Gupta AK, Foley KA. 5% Minoxidil: treatment for female pattern hair loss. Skin Therapy Lett 2014 Nov-Dec;19(6):5-7. Hair Loss. Dermnet NZ. http://dermnetnz.org/hair-nails-sweat/hair-loss.html Telogen effluvium. Dermnet NZ http://dermnetnz.org/hair-nails-sweat/telogen-effluvium.html
Hay Fever
Mahmoodi NS, Reza Okhovat SA, Reza Abtahi SH, Moslehi A. The Comparison of Nasaleze and Mometasone Nasal Spray to Control the Symptoms of Allergic Rhinitis. AdvBiomedRes 2018;7:27. Published 2018 Feb 16. doi:10.4103/2277-9175.225590
12.2.1 Drugs used in nasal allergy New Zealand Formulary v131 1 May 2023. https://nzf.org.nz/ nzf_6109?searchterm=nasal%20allergy
Head Lice
Abdel-Ghaffar F et al. Efficacy of a single treatment of head lice with a neem seed extract: an in vivo and in vitro study on nits and motile stages. Parasitol Res 2012 Jan;110(1):277-80. doi: 10.1007/s00436-011-2484-3
Greive KA, Barnes TM. In vitro comparison of four treatments which discourage infestation by head lice. ParisitolRes.2012;110(5):1695-1699. doi:10.1007/s00436-011-2687-7
Head lice. Dermnet NZ. http://dermnetnz.org/arthropods/headlice.html
Head lice. Education.govt.nz. https://parents.education.govt.nz/primary-school/wellbeing/head-lice/ Headache
Hodman H. Have a headache? The top 7 triggers. Harvard Health. March 30, 2020. https://www. health.harvard.edu/blog/have-a-headache-the-top-7-triggers-2020033019330#:~:text=Diet.,%2C%20 dairy%20products%2C%20and%20onions
Headaches. Ministry of Health. www.health.govt.nz/your-health/conditions-and-treatments/ diseases-and-illnesses/headache
Headaches. Danger signs. Medline Plus. US National Library of Medicine. https://www.nlm. nih.gov/medlineplus/ency/patientinstructions/000424.htm
Resources. Headache Disease Tools. National Headache Foundation. https://headaches.org/ resources/#headache-tools Pray WS. Patients With Headaches: The Pharmacist’s Role https://www.uspharmacist.com/ article/patients-with-headaches-the-pharmacists-role Puledda F, Shields K. Non-Pharmacological Approaches for Migraine. Neurotherapeutics 2018;15(2):336-345.
Heart Health
Eating and Activity Guidelines. NZ Ministry of Health. Dec, 2020. http://www.health.govt.nz/ our-work/eating-and-activity-guidelines Heart attack. Health A-Z 2023. https://www.healthnavigator.org.nz/health-topics/ heart-disease/
Managing high blood pressure Heart Foundation. 2023 https://www.heartfoundation.org. nz/wellbeing/managing-risk/managing-high-blood-pressure Statistics. General heart statistics in New Zealand. Heart Foundation NZ. http://www.heartfoundation.org.nz/statistics/
Indigestion, Heartburn, Gastritis
Katz P, Gerson L, Vela M. Diagnosis and Management of Gastroesophageal Reflux Disease. Am J Gastroenterol 2013; 108:308–328; doi: 10.1038/ajg.2012.444
Managing dyspepsia and heartburn in general practice-an update. BPAC NZ www.bpac.org. nz/magazine/2011/february/dyspepsia.asp Influenza
Dobson J et al. Oseltamivir treatment for influenza in adults: a meta-analysis of randomised controlled trials. The Lancet 2015;385(9979):1729-37 http://www.thelancet.com/journals/ lancet/article/PIIS0140-6736(14)62449-1/
Immunisation Advisory Centre. Arainga mate. The University of Auckland. www.immune.org.nz
Influenza (flu). Centers for Disease Control and Prevention http://www.cdc.gov/flu/ Influenza information for health professionals The Immunisation Advisory Centre 2023. https://www.influenza.org.nz/ Iron Deficiency
Oral Iron Supplementation. Cleveland Clinic https://my.clevelandclinic.org/health/ articles/14568-oral-iron-supplementation
Fei C. Iron Deficiency Anemia: A Guide to Oral Iron Supplements. Clinical Correlations March 26 2015 https://www.clinicalcorrelations.org/?p=8405
Hemoglobin and Functions of Iron. UCSF Health. 2023 https://www.ucsfhealth.org/education/hemoglobin-and-functions-of-iron#:~:text=Iron%20is %20an%20essential%20element,the%20lungs%20to%20the%20tissues
Iron. NZ Nutrition Foundation. www.nutritionfoundation.org.nz/nutrition-facts/minerals/ iron
Iron in the vegan diet. The Vegetarian Resource Group. www.vrg.org/nutrition/iron.php
Santiago P. Ferrous versus Ferric Oral Iron Formulations for the Treatment of Iron Deficiency: A Clinical Overview. The Scientific World Journal. 2012;2012:846824. doi:10.1100/2012/846824.
Irritable Bowel Syndrome
Lembo A. Probiotics — even inactive ones — may relieve IBS symptoms Harvard Health. June 22, 2020. https://www.health.harvard.edu/blog/probiotics-even-inactive-ones-may-relieveibs-symptoms-2020062220303
Diagnostic Criteria. June, 2017. Irritable Bowel Syndrome https://irritablebowelsyndrome. net/testing-and-diagnosis/criteria
Endo Y, Shoji T, Fukudo S. Epidemiology of irritable bowel syndrome. Ann Gastroenterol 2015;28(2):158-159.
Fraser A. Irritable Bowel. Gastro-info http://www.gastro-info.co.nz/gastro-information. aspx?pid=5
Irritable bowel syndrome. Mayo Clinic 2022. https://www.mayoclinic.org/ diseases-conditions/irritable-bowel-syndrome/diagnosis-treatment/drc-20360064
New Rome IV Criteria for Diagnosing Irritable Bowel Syndrome GI Society. 2016. https:// badgut.org/information-centre/a-z-digestive-topics/rome-iv/ Leuven KU. Scientists reveal mechanism that causes irritable bowel syndrome. January 17, 2021 https://www.sciencedaily.com/releases/2021/01/210117132238.htm
Irritable Bowel Syndrome (IBS) and Diet: The Foods You Can Eat GI Society. Canadian Society of Intestinal Research. 2022. https://badgut.org/information-centre/health-nutrition/ ibs-the-foods-you-can-eat/
Hypnosis for IBS. About IBS. 2022. https://aboutibs.org/treatment/complimentary-oralternative-treatments/hypnosis-for-ibs/ Menopause
Managing postmenopausal vaginal atrophy. Harvard Health Publishing. June 2019 https://www.health.harvard.edu/womens-health/ managing-postmenopausal-vaginal-atrophy
Davis SR, Castelo-Branco C, Chedraui P et al. Understanding weight gain at menopause. Climacteric 2012, doi: 10.3109/13697137.2012.707385
Menopause and hot flashes. WebMD. www.webmd.com/menopause/guide/hot-flashes Menopause - signs, symptoms, treatment. Southern Cross. https://www.southerncross.co.nz/ group/medical-library/menopause-signs-symptoms-treatment
Johnson A, Roberts L, Elkins G. Complementary and Alternative Medicine for Menopause. J Evid
Based Integr Med. 2019;24:2515690X19829380. doi:10.1177/2515690X19829380
Franco OH, Chowdhury R, Troup J, et al. Use of plant-based therapies and menopausal symptoms: a systematic review and meta-analysis. JAMA 2016;315:2554-63.
ACOG Practice Bulletin No. 141: management of menopausal symptoms. Obstet Gynecol 2014;123:202-16.
The North American Menopause Society. Nonhormonal management of menopause-associated vasomotor symptoms: 2015 position statement of The North American Menopause Society. Menopause 2015;22:1155-72.
Men’s Health
Erectile Dysfunction. Mayo Clinic. 2023 http://www.mayoclinic.org/diseases-conditions/ erectile-dysfunction/basics/definition/con-20034244
Heart Risk Assessment. Health Navigator New Zealand. https://www.healthnavigator.org. nz/health-a-z/h/heart-risk-assessment/
Erectile dysfunction. University of Maryland Medical Center 2023 https://www.umms.org/ ummc/health-services/urology/conditions-treatments/erectile-dysfunction
Prostate Cancer. Prostate Cancer Foundation of New Zealand. 2023 https://prostate.org.nz/ prostate-cancer
Migraine
Migraine. Neurological Foundation of New Zealand. www.neurological.org.nz/disorders/ migraine
Carter J Dr, Cearns C DR. Migraine headache. A Patients guide. Family doctor. www. familydoctor.co.nz/index.asp?U=conditions&A=29530
Migraine - What is it? The Migraine Trust. https://www.migrainetrust.org/about-migraine/ migraine-what-is-it/ 4.7.4.1. Treatment of acute migraine. New Zealand Formulary V. 131 1 May 2023 https:// nzf.org.nz/nzf_2557
Muscular Aches, Pains and Tightness
Ghosh N, Kolade OO, Shontz E, Rosenthal Y, Zuckerman JD, Bosco JA 3rd, Virk MS. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) and Their Effect on Musculoskeletal Soft-Tissue Healing: A Scoping Review. JBJSRev. 2019 Dec;7(12):e4. doi: 10.2106/JBJS. RVW.19.00055. PMID: 31851037.
Jones P, Lamdin R, Dalziel SR. Oral non‐steroidal anti‐inflammatory drugs versus other oral analgesic agents for acute soft tissue injury. Cochrane Database of Systematic Reviews 2020, Issue 8. Art. No.: CD007789. DOI: 10.1002/14651858.CD007789.pub3. Muscle Pain Cleveland Clinic. https://my.clevelandclinic.org/health/ symptoms/17669-muscle-pain
Muscle Aches. Medline Plus. https://medlineplus.gov/ency/article/003178.htm
Muscle Pain. Mayo Clinic. http://www.mayoclinic.org/symptoms/muscle-pain/basics/causes/ sym-20050866
Oral Health
Teeth and gums. NZ MOH http://www.health.govt.nz/your-health/healthy-living/ teeth-and-gums
Gum disease Information. American Academy of Periodontology. http://www.perio.org/ consumer/gum-disease.htm
Mouth ulcers. Oral Health Foundation. 2023. https://www.dentalhealth.org/mouth-ulcers Periodontal (Gum) Disease. 2023. https://www.nidcr.nih.gov/health-info/gum-disease/moreinfo
Osteoarthritis
Osteoarthritis. Mayo Clinic. www.mayoclinic.org/diseases-conditions/osteoarthritis/basics/ definition/CON-20014749
Osteoarthritis. Arthritis New Zealand. https://www.arthritis.org.nz/osteoarthritis/ Osteoporosis
Prevention Calcium. International Osteoporosis Foundation. 2023 https://www. osteoporosis.foundation/patients/prevention/calcium
What is osteoporosis? Kidspot. https://osteoporosis.org.nz/osteoporosis-fractures/ what-is-osteoporosis/ Calcium. Nutrition Foundation. www.nutritionfoundation.org.nz/nutrition-facts/minerals/ calcium
Osteoporosis - Symptoms, Prevention, Treatment. Southern Cross. https://www. southerncross.co.nz/group/medical-library/osteoporosis-symptoms-treatment-prevention Ovulation and Pregnancy Testing
Immunisations for mums-to-be Plunket https://www.plunket.org.nz/being-a-parent/ preparing-for-your-baby/health-and-care-during-pregnancy/immunisations/ Ovulation Prediction Kits. Kidspot. https://kidspot.co.nz/pregnancy/ ovulation-prediction-kits/
Whooping cough vaccine for pregnant women Health info. https://www.healthinfo.org.nz/ patientinfo/45079.pdf
Period Pain and Endometriosis
Endometriosis NZ. www.nzendo.co.nz
Period Pain. Medline Plus. https://medlineplus.gov/periodpain.html Endometriosis.org https://endometriosis.org/resources/articles/myths/
Premenstrual syndrome - a patients guide. Family Doctor NZ. www.familydoctor.co.nz/ index.asp?U=conditions&A=32701 7.5.
Endometriosis. New Zealand Formulary. NZF Vol 131. 01 May 2023. https://nzf.org.nz/ nzf_71113?searchterm=endometriosis
Foods that fight inflammation Harvard Health. Nov 16, 2021.
https://www.health.harvard.edu/staying-healthy/foods-that-fight-inflammation Poisonings
Articles and Info. National Poisons Centre https://poisons.co.nz/ articles-and-info/?f=22&c=23
Peiris-John, R., Kool, B. and Ameratunga, S. (2014), Fatalities and hospitalisations due to acute poisoning among New Zealand adults. Intern Med J, 44: 273-281. doi:10.1111/ imj.12364
Poisonous plants. Landcare research. http://www.landcareresearch.co.nz/publications/ factsheets/poisonous-plants
Poisoning. Safe Kids Aotearoa http://www.safekids.nz/Safety-Topics/Details/Type/View/ ID/10/Poisoning
Understanding suicide in New Zealand. Ministry of Health. http://www.health. govt.nz/our-work/mental-health-and-addictions/working-prevent-suicide/ understanding-suicide-new-zealand
Pregnancy and Pregnancy Supplements
Brown L. Nutrition requirements during Pregnancy. Chapter 1. http://samples.jbpub. com/9780763777920/77920_CH01_001_024.pdf
Choosing Your Midwife. Find Your Midwife https://www.findyourmidwife.co.nz/ howichoose
Due date calculator. Baby Centre UK. www.babycentre.co.uk/ pregnancy-due-date-calculator
Folic acid and Spina Bifida/iodine and Iodine deficiency. HealthEd. www.healthed.govt.nz/ resource/folic-acid-and-spina-bifidaiodine-and-iodine-deficiency
How long it takes to conceive. Baby Center.com http://www.babycenter.com/ how-long-does-it-take-to-get-pregnant
Eating safely and well during pregnancy. Ministry of Health. https://www.health.govt. nz/your-health/pregnancy-and-kids/pregnancy/helpful-advice-during-pregnancy/ eating-safely-and-well-during-pregnancy
Understanding your fertility. Fertility Associates. www.fertilityassociates.co.nz/ Understanding-your-fertility.aspx
Soma-Pillay P, Catherine N-P, Tolppanen H, et al. Physiological changes in pregnancy. Cardiovascular Journal of Africa. 2016;27(2):89-94. doi:10.5830/CVJA-2016-021. Pregnancy calculator. Health Navigator NZ https://www.healthnavigator.org.nz/tools/p/pregnancy-calculator/ Folic acid, iodine, and vitamin D. HealthEd. https://www.health.govt.nz/yourhealth/pregnancy-and-kids/pregnancy/helpful-advice-during-pregnancy/ folic-acid-iodine-and-vitamin-d
Shinde P, Patil P, and Bairagi V. Herbs in pregnancy and lactation: A review appraisal. International Journal of Pharmaceutical Sciences and Research IJPSR, 2012; Vol. 3(9): 3001-06
Probiotics and Prebiotics
Bifidobacteria. Medline Plus. https://medlineplus.gov/druginfo/natural/891.html
Farré-Maduell E, Casals-Pascual C. The origins of gut microbiome research in Europe: From Escherich to Nissle. Human Microbiome Journal 2019 (14) 100065. https://doi.org/10.1016/j. humic.2019.100065
Probiotics: What you need to know. National Center for Complementary and Integrative health. Us Department of Health and Human Services. 2023. https://www.nccih.nih.gov/ health/probiotics-what-you-need-to-know
Cayzeele-Decherf A, Perin F, Leuillet S, et al. Saccharomyces cerevisiae CNCM I-3856 in irritable bowel syndrome: An individual subject meta-analysis. World J Gastroenterol. 2017 Jan 14;23(2):336-344. doi: 10.3748/wjg.v23.i2.336.
Fakruddin M, Hossain MN, Ahmed MM, et al. Antimicrobial and antioxidant activities of Saccharomyces cerevisiae IFST062013, a potential probiotic. BMC Complement Altern Med 2017 Jan 21;17(1):64. doi: 10.1186/s12906-017-1591-9.
Jäger, R., Mohr, A.E., Carpenter, K.C. et al. International Society of Sports Nutrition Position Stand: Probiotics. J Int Soc Sports Nutr 16, 62 (2019). https://doi.org/10.1186/ s12970-019-0329-0
Jabr F. Do Probiotics Really Work? Scientific American July 1 2017. https://www. scientificamerican.com/article/do-probiotics-really-work/
Su G, Ko C, , Bercik P, et al. AGA Clinical Practice Guidelines on the Role of Probiotics in the Management of Gastrointestinal Disorders. Gastroenterology 2020;159:697–705. https://www.gastrojournal.org/action/showPdf?pii=S0016-5085%2820%2934729-6
Kelesidis, T. Efficacy and safety of the probiotic Saccharomyces boulardii for the prevention and therapy of gastrointestinal disorders. David Geffen School of Medicine, UCLA, Los Angeles, CA. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3296087/ Lactobacillus. Medline Plus. https://medlineplus.gov/druginfo/natural/790.html
Mouton G. The uses of prebiotics www.optibacprobiotics.co.uk/about-probiotics/the-usesof-prebiotics.html
Probiotics: elixir or empty promise? Editorial. The Lancet Gastroenterology & Hepatology Volume 4, Issue 2, 81
Probiotics: In Depth. National Center for Complementary and Integrative Health https:// nccih.nih.gov/health/probiotics/introduction.htm
O’Callaghan A, van Sinderen D. Bifidobacteria and Their Role as Members of the Human Gut Microbiota. Front Microbiol. 2016;7:925. Published 2016 Jun 15. doi:10.3389/ fmicb.2016.00925
Jäger R, Mohr AE, Carpenter KC, et al. International Society of Sports Nutrition Position Stand: Probiotics. J Int Soc Sports Nutr. 2019;16(1):62. Published 2019 Dec 21. doi:10.1186/ s12970-019-0329-0
Vighi G, Marcucci F, Sensi L, Di Cara G, Frati F. Allergy and the gastrointestinal system. Clin
Exp Immunol. 2008;153 Suppl 1(Suppl 1):3–6. doi:10.1111/j.1365-2249.2008.03713.x
Psoriasis
Psoriasis. DermNet NZ. https://www.dermnetnz.org/topics/psoriasis/
Psoriasis - a patient’s guide. Skin problems. Family Doctor. http://www.familydoctor.co.nz/ categories/skin-problems/psoriasis-a-patients-guide/ The treatment of psoriasis in primary care. Best Practice Journal 2009;23 https://bpac.org. nz/bpj/2009/september/psoriasis.aspx
Scabies
Oakley A. Scabies. Dermet NZ. http://www.dermnetnz.org/topics/scabies/ Scabies. Diagnosis and management. BPAC NZ. www.bpac.org.nz/magazine/2009/february/ docs/bpj19_scabies_pages_12-16.pdf
Scabies. Ministry of Health. www.health.govt.nz/your-health/conditions-and-treatments/ diseases-and-illnesses/scabies
Sexual Health
Condoms. Advising on the options. BPAC New Zealand. 7 March 2019. https://bpac.org. nz/2019/contraception/condoms.aspx
Just The Facts on STIs. Just The Facts. https://www.justthefacts.co.nz/ sexually-transmitted-infections-stis/facts-about-stis-sexually-transmitted-infections-stds/
Relative effectiveness of birth control methods. Options for Sexual Health. https://www. optionsforsexualhealth.org/birth-control-pregnancy/birth-control-options/effectiveness
Shingles
Herpes Zoster. Dermnet NZ. http://www.dermnetnz.org/topics/herpes-zoster/ Mikaeloff Y, Kezouh A, Suissa S. Nonsteroidal anti-inflammatory drug use and the risk of severe skin and soft tissue complications in patients with varicella or zoster disease. www. ncbi.nlm.nih.gov/pubmed/18251759
Post-herpetic neuralgia - Treatment. NHS. www.nhs.uk/Conditions/postherpetic-neuralgia/ Pages/Treatment.aspx
Shingles. DermNet NZ http://dermnetnz.org/viral/herpes-zoster.html
Sinus and Nasal Problems
Acute sinusitis. Mayo Clinic. 2023. https://www.mayoclinic.org/diseases-conditions/ acute-sinusitis/diagnosis-treatment/drc-20351677
Nasal polyps. Mayo Clinic. 2023. https://www.mayoclinic.org/diseases-conditions/ nasal-polyps/symptoms-causes/syc-20351888
Sinusitis and Allergy. ASCIA. https://www.allergy.org.au/patients/ allergic-rhinitis-hay-fever-and-sinusitis/sinusitis-and-allergy
Sinus infection (sinusitis) definition and facts. MedicineNet.com www.medicinenet.com/ sinusitis/article.htm
Sleep Problems and Snoring Guideline for Pharmacist-supply of Melatonin. www.psnz.org.nz Sleep hygiene. National Sleep Foundation. sleepfoundation.org
Namni Goel PhD, Hyungsoo Kim & Raymund P. Lao (2005) An Olfactory Stimulus Modifies Nighttime Sleep in Young Men and Women, Chronobiology International, 22:5, 889-904, DOI: 10.1080/07420520500263276
De Baaij J, Hoenderop J, Bindels R. Magnesium in man: Implications for health and disease. Physiol Rev 95: 1–46, 2015 doi:10.1152/physrev.00012.2014
Bent S, Padula A, Moore D, Patterson M, Mehling W. Valerian for sleep: a systematic review and meta-analysis. Am J Med 2006;119(12):1005–1012. doi:10.1016/j.amjmed.2006.02.026
The Science of Sleep: Stages and Cycles Circadian Rhythms, Sleep Stages, and Sleep Architecture. Help Guide. Harvard. https://www.helpguide.org/harvard/biology-of-sleepcircadian-rhythms-sleep-stages.htm
Smoking Cessation
Beat the addiction and become smokefree Community and Public Health. Te Mana Ora. 15/04/2021. https://www.cph.co.nz/your-health/smoking-cessation/ Blaha M. Will Vaping Lead Teens to Smoking Cigarettes? John Hopkins Medicine. https:// www.hopkinsmedicine.org/health/wellness-and-prevention/does-vaping-lead-to-smoking Klemperer EM, Fagerstrom KO, Hughes JR. Abrupt versus gradual smoking cessation with pre-cessation nicotine replacement therapy for cigarette smokers motivated to quit. Annals of Translational Medicine. 2016;4(19):384. doi:10.21037/atm.2016.08.16. Quitline Me Mutu https://quit.org.nz/en Smokefree Aotearoa NZ 2025 http://smokefree.org.nz/ Hartmann-Boyce J, Chepkin SC, Ye W, Bullen C, Lancaster T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database of Systematic Reviews 2018, Issue 5. Art. No.: CD000146. DOI: 10.1002/14651858.CD000146.pub5 Facts and Figures. Smoke Free NZ. https://www.smokefree.org.nz/smoking-its-effects/ facts-figures
Sore Throat
Sore Throat in Adults. Health Navigator New Zealand http://www.healthnavigator.org.nz/ health-a-z/s/sore-throat/
Sore throat. Medicine Net https://www.medicinenet.com/sore_throat_pharyngitis/article. htm
Sore throat. Ministry of Health www.health.govt.nz/your-health/ conditions-and-treatments/diseases-and-illnesses/sore-throat Rheumatic fever. Ministry of Health. https://www.health.govt.nz/your-health/ conditions-and-treatments/diseases-and-illnesses/rheumatic-fever#listofclinics
Strains and Sprains
Knee Ligament Injuries. www.patient.co.uk/health/knee-ligament-injuries-leaflet
Sprains and Strains. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/ sprains-and-strains/diagnosis-treatment/drc-20377943
Tripp A. The P.R.I.C.E. protocol principles. Sports-Health. https://www.sports-health.com/ treatment/price-protocol-principles
Vuurberg G, Hoorntje A, Wink LM, et al Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline Br J Sports Med 2018;52:956. Newsham, Katherine. The Ubiquitous Lateral Ankle Sprain: Time to Reconsider Our Management? The Journal for Nurse Practitioners, Volume 15, Issue 5, 343 - 346.e3
Dubois B, Esculier J-F. Soft tissue injuries simply need PEACE & LOVE. Br J Sports Med https://blogs.bmj.com/bjsm/2019/04/26/soft-tissue-injuries-simply-need-peace-love/ Sun Care
12 Medications That Can Make You More Sensitive to the Sun. The Good Rx. Jan 27. 2023. https://www.goodrx.com/health-topic/dermatology/avoid-the-sun-if-you-take-these-drugs Sunprotection. Cancer Society of NZ https://otago-southland.cancernz.org.nz/ reducing-cancer-risk/what-you-can-do/sunsmart/sun-protection/ Melanoma. DermNet NZ. www.dermnetnz.org/lesions/melanoma.html Sunburn. DermNet NZ. https://www.dermnetnz.org/topics/sunburn/ Sunsmart NZ www.sunsmart.org.nz
Palau bans toxic sunscreens. 3 January 2020. RNZ. https://www.rnz.co.nz/international/ pacific-news/406565/palau-bans-toxic-sunscreens#:~:text=Palau%20became%20the%20 first%20nation,also%20home%20to%20healthy%20reefs
How Does Sunscreen Harm Coral Reefs? Oct 24, 2019. Sustainable Travel. https:// sustainabletravel.org/safe-sunscreen-coral-reefs/#:~:text=How%20Does%20Sunscreen%20 Harm%20Coral%20Reefs%3F&text=One%20of%20the%20main%20culprits,increase%20 abnormal%20growth%20and%20deformities.
What is coral bleaching? National Ocean Service. https://oceanservice.noaa.gov/facts/ coral_bleach.html
Protect Land + Sea Certification. Haereticus Environmental Laboratory (HEL) https://haereticus-lab.org/protect-land-sea-certification-3/ Reef Safe Sunscreen Guide. https://savethereef.org/about-reef-save-sunscreen.html What Sunscreen Ingredients to Look for — and Which Banned Ones to Avoid. Healthline. https://www.healthline.com/health/beauty-skin-care/ best-sunscreen-ingredients#avobenzone
Dale J. Eco-friendly Sunscreens - what you need to know. Oct 5, 2021. https://www. thegreatecojourney.co.nz/post/eco-friendly-sunscreens-what-you-need-to-know Sun Care: Eye Protection
A Guide to Sports & Activity Tints. VSP. www.vsp.com/lens-tints.html
How to chose sunglasses. REI CO-OP. www.rei.com/expertadvice/articles/sunglasses.html Sun safety. EPA. www.epa.gov/sunwise/doc/eyedamage.pdf
Macular Degeneration and Low Vision: Making the Most of Low Vision. American Academy of Opthamology. https://www.aao.org/eye-health/diseases/amd-low-vision Your Guide to Sport Sunglass Lens Tints www.allaboutvision.com/sportsvision/lens-tintschart.htm
Vitamin D. (2023). Sunsmart.org.nzhttps://www.sunsmart.org.nz/sunsmart-facts/vitamin-d/ Sweating: Excessive (Hyperhidrosis)
Excessive sweating. Palm clinic. https://www.palmclinic.co.nz/aesthetic/cosmetic-medicine/ areas-of-concern/excessive-sweating
Hyperhidrosis DermNet NZ www.dermnetnz.org/hair-nails-sweat/hyperhidrosis.html
Hyperhidrosis Medline Plus www.nlm.nih.gov/medlineplus/ency/article/007259.htm
Excessive sweating – hyperhidrosis www.patient.co.uk/health/Excessive-Sweating.htm Hyperhidrosis DermNet NZ www.dermnetnz.org/hair-nails-sweat/hyperhidrosis.html
Stashak AB, Brewer JD. Management of hyperhidrosis. Clin Cosmet Investig Dermatol 2014;7:285-99. Published 2014 Oct 29. doi:10.2147/CCID.S53119
Travel Health
Dengue and severe dengue. World Health Organization https://www.who.int/news-room/ fact-sheets/detail/dengue-and-severe-dengue
Dengue Vaccination: What Everyone Should Know. (2023) Centers for Disease Control and Prevention. https://www.cdc.gov/vaccines/vpd/dengue/public/index.html
Zika Travel Information. (2023) Centers for Disease Control and Prevention. https://wwwnc. cdc.gov/travel/page/zika-information
Immunization Advisory Centre (NZ Childhood Immunization Schedule) www.immune.org.nz Safe Travel NZ www.safetravel.govt.nz
WHO – World Health Organization International Travel and Travel Health Advice www. who.int/ith/ Zika virus. CDC. http://www.cdc.gov/zika/ Travel Sickness (Motion)
Motion sickness - causes. NHS. www.nhs.uk/Conditions/Motion-sickness/Pages/Causes.aspx
Urinary Incontinence
Nocturnal Enuresis in Children. Patient www.patient.co.uk/doctor/ nocturnal-enuresis-in-children
NZ Continence Association www.continence.org.nz/
Urinary incontinence Mayo clinic www.mayoclinic.org/urinary-incontinence/types.html
Urinary incontinence in children. National Kidney and Urologic Diseases Information Clearinghouse (NKUDIC) http://kidney.niddk.nih.gov/kudiseases/pubs/uichildren/ Urticaria
Acute urticaria. Patient. www.patient.co.uk/health/acute-urticaria-hives Urticaria. DermNet NZ http://dermnetnz.org/reactions/urticaria.html
Varicose Veins and Support Stockings
Sclerotherapy. DermNet NZ http://dermnetnz.org/procedures/sclerotherapy.html Travellers’ Thrombosis. Medsafe. www.medsafe.govt.nz/profs/PUarticles/travthromb.htm
Vein Treatments and Symptoms. Skin Institute. http://www.skininstitute.co.nz/ Vitamins and Dietary Supplements
Kamangar F, Emadi A. Vitamin and Mineral Supplements: Do We Really Need Them?
International Journal of Preventive Medicine. 2012;3(3):221-226.
Folic acid, Iodine, and Vitamin D. Ministry of Health. https://www.health.govt.nz/ your-health/pregnancy-and-kids/pregnancy/helpful-advice-during-pregnancy/ folic-acid-iodine-and-vitamin-d
Mursu J, Robien K, Harnack LJ, et al. Dietary supplements and mortality rate in older women: the Iowa Women’s Health Study. Arch Intern Med 2011 Oct 10;171(18):1625-33. doi: 10.1001/archinternmed.2011.445.
Nutrients. The Nutrients Reviewed. Nutrient Reference Values for Australia and New Zealand. https://www.nrv.gov.au/nutrients
Listing of vitamins Harvard Health Publishing. Harvard medical school. https://www.health. harvard.edu/staying-healthy/listing_of_vitamins
Warts
Warts. KidsHealth. https://www.kidshealth.org.nz/warts
What is HPV. Web MD. 2022. https://www.webmd.com/sexual-conditions/hpv-genital-warts/ hpv-virus-information-about-human-papillomavirus#1
Weight Loss
Eating and Activity Guidelines for New Zealand Adults. Updated Dec 2020. https://www. health.govt.nz/system/files/documents/publications/eating-activity-guidelines-newzealand-adults-dec20.pdf
Why do I need to be a healthy weight. Health Ed. MOH NZ https://www.healthed.govt.nz/ resource/why-do-i-need-be-healthy-weight
Onakpoya I, Hung S, Perry R, et al. The use of garcinia extract (hydroxycitric acid) as a weight loss supplement: a systematic review and meta-analysis of randomised clinical trials. Journal of Obesity 2011: 509038
Women’s Health
Vulvovaginal candidiasis DermNet NZ http://dermnetnz.org/fungal/vaginal-candidiasis.html Women’s Health. Mayo Clinic. http://www.mayoclinic.org/healthy-lifestyle/womens-health/ in-depth/vagina/art-20046562?p=1 Worms
All You Need To Know About Parasitic Worms. KidSpot Health. https://kidspot.co.nz/health/ kids-health-threadworm-pinworm-ringworm-hookworm/ Parasites – Enterobiasis (also known as pinworm infection) CDC www.cdc.gov/parasites/ pinworm/gen_info/faqs.html
Pinworms. DermNet NZ www.dermnetnz.org/arthropods/pinworm.html
Pinworms. Medline Plus. www.nlm.nih.gov/medlineplus/ency/article/001152.htm
Parasites. Soil transmitted helminths. CDC. https://www.cdc.gov/parasites/sth/ Wound Care
Leg ulcers. DermNet NZ www.dermnetnz.org/site-age-specific/leg-ulcers.html Burns. St John. www.stjohn.org.nz/First-Aid/First-Aid-Library/Burns/
*The only combination pain relief that provides the maximum recommended daily OTC dose of paracetamol and ibuprofen, if required^



effective pain relief in the first 6 hours vs paracetamol and ibuprofen alone1
Medsafe (New Zealand Medicines and Medical Devices Safety Authority) uses a variety of methods to monitor the safety of vaccines, medicines, medical devices, and related products in New Zealand. These activities are known as pharmacovigilance and include information from clinical and observational studies, published medical literature, pharmaceutical companies, and voluntary reporting of adverse events.
Suspected adverse reaction reports are collected and processed by Medsafe and non-routine reports are medically assessed by the physicians at the Centre for Adverse Reactions Monitoring (CARM). These include:
• spontaneous reports of adverse reactions to medicines, vaccines, herbal products and dietary supplements sent in by health professionals, patients and pharmaceutical companies throughout New Zealand
• reports relating to specific medicines, vaccinations or devices identified through the Medsafe safety communications.
Over 110,000 reports are currently held on the Medsafe/CARM database providing New Zealand-specific information that can help contribute to knowledge already known about the adverse reaction profiles of certain medicines or complementary therapies. This knowledge can help support clinical decision making.
An anonymised version of an adverse event report collected by Medsafe/CARM and other international monitoring centres is sent to the World Health Organization (WHO) and pharmaceutical companies responsible for each medicine to meet New Zealand’s international medicine and vaccine safety reporting obligations. Medsafe also publishes anonymised data on its Suspected Medicine Adverse Reaction Search (SMARS). Go to medsafe.govt.nz and search SMARS.
It is important to report any suspect reactions of clinical concern. This includes adverse reactions or interactions to all:
• medicines
• over-the-counter remedies or medicines
• vaccines
• herbal, traditional, and alternative remedies
• psychoactive and recreational substances, including vaping products.
All serious and medically significant reactions and interactions should always be reported; however, if you are unsure of its significance, report it!
It is also important to report ANY serious allergic reactions so that a danger warning can be entered against the patient’s name in the national health database, so re-exposure can be avoided for that individual.
Anybody can report an adverse event. An online reporting form is available via the Medsafe website medsafe.govt.nz; search safety reporting.
Psychoactive substances are regulated in New Zealand by the Psychoactive Substances Act 2013 which aims to minimise harm to and protect the health of individuals who use psychoactive substances. The Act is administered by Psychoactive Substances Regulatory Authority which is a dvision of Manatū Hauora Ministry of Health.
Health professionals and members of the public can report reactions to psychoactive and recreational substances in the same way as they report reactions to medicines and vaccines, through an online reporting form via the Medsafe website medsafe.govt.nz; search adverse reaction reporting.
Identifying the brand name of the product involved is crucial and helps the Ministry of Health make a decision around the particular safety of a product. For more information about substances and drug misuse, see www.drugfoundation.org.nz
Medsafe’s safety communications (www.medsafe.govt.nz/safety/ SafetyCommunications.asp) aims to provide information about newly identified safety concerns for medicines and medical devices. There are two parts to the early warning system: monitoring communications and alert communications.
Monitoring communications outline the newly identified potential safety concern and often request further information from users about the medicine or medical device, and are symbolised by M2. Consumers should continue to use the medicine or medical device as per the product’s instructions.
Alert communications contain information on the safety concern with specific advice on what to do, and are issued once the review of the safety concern is complete. Subscribe to Medsafe’s early warning communications at www.medsafe.govt.nz/profs/subscribe.asp.
The latest medicines or medical devices being monitored or with safety concerns issued up until 18 August 2024 include:
• Direct acting oral anticoagulants and mood changes
• Dipeptidyl peptidase-4 (DPP-4) inhibitors (eg, vildagliptin, saxagliptin) and intestinal obstruction including ileus
• Oral promethazine and children under 6 - do not use due to the risk of psychiatric and nervous system effects
• NaturaCoco Moisturising Cream or Dok Apo Moisturiser Soothing Cream - avoid use because these products contain fluocinonide, a potent steroid
• Calcium channel blockers and the possible risk of new-onset eczema
• Ayurvedic Medicines and recent cases of lead poisoning
• Sodium valproate use in people who can father children within the 3 months prior to conception and an increased risk of neurodevelopmental disorders in the child
• Interleukin inhibitors and the possible risk of pancreatitis.
Always ask customers buying medicines in your pharmacy if they are taking any other medicines or herbal/dietary supplements. If they are, check with your pharmacist that the product being sold will not interact with the medicine(s) they currently take.
Interactions in this table are generally clinically relevant in the community pharmacy environment. This table is NOT ALL INCLUSIVE, and does not include isolated reports of interactions, theoretical interactions, undocumented interactions, or interactions with uncommonly prescribed medications.
When considering a potential interaction, consider those medications that have a narrow therapeutic index (such as warfarin or digoxin), because even a single dose of an interacting medicine may affect blood
levels of these medicines, and therefore effectiveness or side effects. For other medicines, a one-off dose is likely to have no ill effects (eg, short-term infrequent dosing of a NSAID will usually have clinically irrelevant effects on blood pressure).
Always recommend antacids be taken at least two hours apart from other medications, since they can affect the absorption of many drugs.
Customers prescribed colestipol and cholestyramine should be reminded these medications can cause reduced or delayed absorption of most medicines and to administer separately, at least one hour before or 4–6 hours after cholestyramine or colestipol.
See the New Zealand Formulary (nzf.org.nz) or individual drug datasheets (medsafe.govt.nz) for more information.
DRUG/DRUG GROUP INTERACTING SUBSTANCE DETAILS
Analgesics – aspirin (moderate-high dose)
(Interactions are usually not clinically relevant with low dose aspirin eg, 75–100mg/day)
Analgesics – NSAIDs
ACE inhibitors and angiotensin II receptor blockers
Acetazolamide
Alcohol
Antacids and urinary alkalinisers
Anticoagulants (eg, dabigatran, heparin, warfarin)
Antidiabetic agents (oral hypoglycaemic agents and insulin)
Calcium
Increased risk of renal impairment
Reduced antihypertensive effect. Low dose aspirin combination acceptable
Both acetazolamide and salicylate toxicity possible with high dose aspirin
Risk higher in elderly or those with renal impairment
Risk of gastric bleeding and ulceration increases as alcohol consumption increases
Increased excretion of aspirin in alkaline urine
Bleeding time is prolonged and risk of major bleeding episode increased. Avoid combination (only use low dose aspirin only on medical advice)
Increased hypoglycaemic effect (excludes metformin). Monitor blood glucose and adjust dosage of oral hypoglycaemics if necessary (unlikely to apply to low dose aspirin)
Reduces renal tubular reabsorption of salicylates. May reduce analgesic effects
Calcium channel blockers (eg, amlodipine) Reduced antihypertensive effect. Low dose aspirin combination acceptable
Clopidogrel
Corticosteroids
Gold compounds
Loop diuretics (eg, furosemide)
Methotrexate
Metoclopramide
NSAIDs
Omeprazole, lansoprazole
Phenytoin
Sodium valproate
SSRI
Increased risk of bleeding (low dose aspirin only on medical advice)
Reduced plasma salicylate concentrations resulting in reduced aspirin effect. Increased risk of GI bleed and ulceration
Increased risk of hepatotoxicity
Analgesic doses may blunt diuretic and natriuretic response to loop diuretics. Monitor
Reduced renal clearance of methotrexate resulting in increased risk of toxicity. Less likely to occur with weekly low dose methotrexate therapy
Increased rate of aspirin absorption and higher peak plasma salicyclate levels. Combination may be beneficial for migraine attacks
Additive GI toxicity including increased risk of GI ulceration. Possible prolonged bleeding time. Possible reduction of cardioprotective effect of low dose aspirin
Possibly may decrease absorption of aspirin. May also cause premature dissolution of enteric coated formulations
Aspirin may increase pharmacologic and toxic effects of phenytoin. Monitor combination
Increased risk of toxicity. Monitor or avoid high dose aspirin combination
Higher incidence of upper GI bleeding reported (even with low dose aspirin)
Uricosurics (eg, benzbromarone, probenecid) Aspirin, at analgesic doses antagonises the effects of uricosuric drugs. Consider an alternative analgesic/anti-inflammatory.
Vaccinations
Warfarin
ACE inhibitors and angiotensin II receptor blockers (ARBs)
Alcohol
Alendronate
Avoid aspirin use for six weeks after immunisation due to Reye’s syndrome being reported after natural varicella and wild-type influenza infection. Risk is greater in children (avoid aspirin in children <16 years)
See anticoagulants above
Increased risk of renal impairment. Elderly people or people with, poor renal perfusion, dehydration, heart failure, or also on diuretics at higher risk. Reduced antihypertensive effect
Increased risk of gastric bleeding and ulceration proportional to amount of alcohol consumed
Possible increased risk of GI damage (controversial)
Anticoagulants (eg, heparin, warfarin) Bleeding time is prolonged and risk of major bleeding episode increased. Avoid combination
Antidiabetic agents (oral hypoglycaemic agents)
Antihypertensives
Aspirin (analgesic doses)
Aspirin (low dose)
Clopidogrel
Increased hypoglycaemic effect (excludes metformin). Monitor blood glucose and adjust dosage of oral hypoglycaemic agent if necessary
Possible reduced hypotensive effect. Monitor BP
Additive GI toxicity including increased risk of GI ulceration. Possible prolonged bleeding time. Avoid analgesic/anti-inflammatory doses of aspirin
Increased risk of GI bleed. Possible reduction of cardioprotective effect of low dose aspirin
Increased risk of bleeding (low dose aspirin only on medical advice)
DRUG/DRUG GROUP INTERACTING SUBSTANCE DETAILS
Analgesics – NSAIDs cont…
Analgesics – paracetamol
Corticosteroids
Cyclosporin
Digoxin
Lithium
Diuretics (eg, bendrofluazide, furosemide)
Methotrexate
Other NSAIDs
Potassium-sparing diuretics and aldosterone antagonists
Probenecid
Quinolones (eg, ciprofloxacin, norfloxacin)
Spironolactone
SSRI antidepressants
Warfarin
Alcohol
Anticonvulsants (eg, carbamazepine, phenytoin)
Metoclopramide
Warfarin
Antacids
Antidiarrhoeals – loperamide
Antifungals – clotrimazole vaginal cream
Acetazolamide
Digoxin
Enteric coated and delayed release medications
H2-antagonists (eg, famotidine)
Hexamine
Iron supplements
Isoniazid
Lithium
Tetracyclines
Other medications
Phenylephrine, pseudoephedrine
Quinolone antibiotics (eg, ciprofloxacin, norfloxacin)
Zinc supplements
Clozapine
Desmopressin
Ergotamine or related compounds
Latex condoms
Warfarin
Increased risk of GI bleed and ulceration
Increased risk of nephrotoxicity, increased diclofenac blood levels (reduce diclofenac dose by 50%).
Possible increased cyclosporin blood levels with some NSAIDs
Possible decrease in renal excretion of digoxin resulting in increased digoxin levels with some NSAIDs. Monitor digoxin level
Reduced renal excretion of lithium may result in increased lithium level and toxic effects. Avoid combination unless close monitoring possible
Reduced diuretic and antihypertensive effect, possibly due to salt and water retention. Congestive heart failure may be exacerbated. Increased risk of nephrotoxicity, especially with ACE inhibitor or angiotensin II receptor antagonist combination
Reduced renal clearance of methotrexate resulting in increased risk of toxicity. Less likely to occur with weekly low dose methotrexate therapy
Additive GI toxicity including increased risk of GI ulceration. Increased bleeding time. Avoid
Reduced diuretic and antihypertensive effect. Increased risk of nephrotoxicity and hyperkalaemia
Increased plasma levels of NSAIDs. Reduce dose of NSAID if using combination
Increased risk of CNS stimulation and convulsions. Monitor for CNS adverse effects (eg, seizures, tremors) and avoid combination in patients with epilepsy
May reduce diuretic and antihypertensive effect. May increase risk of hyperkalaemia and renal impairment. Risk increased further with ACE inhibitor or ARB, especially if elderly
Higher incidence of upper GI bleeding reported
See anticoagulants
Risk of severe and sometimes fatal liver damage in people who drink excessively and take even moderate doses of paracetamol. Reduce dose or avoid paracetamol
Efficacy of paracetamol may be reduced due to increased clearance. Increase in toxic metabolites of paracetamol may increase risk of hepatotoxicity. Avoid prolonged use
Increased rate of paracetamol absorption. Combination may be beneficial for migraine
Possible increased INR with sustained high dose administration of paracetamol. Monitor
Increased risk of renal calculi if administered with sodium bicarbonate. Avoid regular dosing
Bioavailability may be decreased. Mechanism unknown. Separate administration by 2–3 hours
Early dissolution of formulation may result in dose-dumping in stomach.
Separate administration by 2–3 hours
Reduced gastric absorption and bioavailability reported. Separate administration
Sodium bicarbonate alkalinises the urine. Hexamine requires a urinary pH of 5.5 or lower to be active so alkalinisation of urine reduces antibacterial effect. Avoid
Some studies show significant reductions in amount of iron absorbed. Separate administration by 2–3 hours
Aluminium salts may decrease absorption. Separate administration
Sodium-containing antacids increase lithium excretion (reduce plasma lithium concentrations). Avoid regular dosing
Antacids may decrease plasma tetracycline concentrations by chelation. Separate administration by 2–3 hours
Potential for decreased absorption. Separate administration by 2–3 hours
Sodium bicarbonate alkalinises the urine so renal excretion of phenylephrine or pseudoephedrine may be reduced, increasing risk of side effects (eg, tremors, anxiety, insomnia and/or tachycardia). Monitor for signs of toxicity and adjust dosage as necessary
May decrease the solubility of fluoroquinolones in the urine and increase the risk of crystalluria
Reduction in the amount of zinc absorbed with calcium containing antacids. Separate administration by 2–3 hours
One fatal report. Possible increased risk of toxic megacolon
Increased GI absorption of desmopressin caused by reduction in GI motility caused by loperamide. Monitor for increased adverse effects (eg, hyponatraemia)
Although systemic absorption is limited, azole antifungals may inhibit the metabolism of ergot derivatives resulting in increased adverse effects. Avoid if possible
Some intravaginal clotrimazole products may damage latex condoms causing contraceptive failure
Potential to interact (rare reports)
DRUG/DRUG GROUP INTERACTING SUBSTANCE DETAILS
Antifungals – fluconazole (Fluconazole inhibits CYP2C9 and 3A4 but to a lesser extent than ketoconazole)
Benzodiazepines (eg, midazolam, triazolam)
Carbamazepine
Celecoxib
Cyclosporin
Ergotamine or related compounds
Phenytoin
Quetiapine
QT-interval prolonging drugs (eg, amiodarone, erythromycin, sotalol)
SSRI antidepressants
Statins
Sulphonylureas and possibly thiazolidinediones
Warfarin
Zidovudine
Antifungals – miconazole oral gel
Antihistamines
– sedating
(eg, brompheniramine, chlorpheniramine, cyclizine, diphenhydramine, promethazine, triprolidine, meclozine)
Warfarin
Antihypertensive medicines
Inhibits metabolism of benzodiazepines metabolised by CYP3A4 (eg, midazolam, triazolam) resulting in increased risk of toxicity. Use lowest dose or change to benzodiazepine metabolised by glucuronidation (eg, temazepam, lorazepam)
Decreases carbamazepine metabolism causing a possible increase in carbamazepine levels. Monitor
Inhibits celecoxib metabolism and can increase celecoxib levels up to two-fold. Initiate celecoxib at lowest recommended dose
Inhibits cyclosporin metabolism, increasing cyclosporin levels and risk of toxicity. Avoid combination or closely monitor
Inhibits metabolism resulting in increased adverse effects of ergot alkaloids (risk of vasospasm and serious/life-threatening ischaemia increased). Avoid
Inhibits metabolism resulting in increased phenytoin levels and possible toxicity. Avoid combination or closely monitor
Possible increased levels quetiapine through inhibition of metabolism
Increased risk of QT prolongation although combination may often be used. Monitor
Fluconazole also inhibits CYP2C19 so may increase serum concentrations of citalopram and escitalopram. Increased risk of serotonin syndrome
Some reports of serious or life-threatening musculoskeletal toxicity associated with increased plasma levels of statins. Generally avoid with atorvastatin or simvastatin. Pravastatin may be safer as not metabolised by CYP450 3A4
Inhibits metabolism resulting in increased serum concentrations and possible hypoglycaemia. Monitor and reduce dosage of oral hypoglycaemic agent if necessary
Inhibits metabolism resulting in increased prothrombin time/INRs and increased risk of bleeding events. Single doses of fluconazole may also potentiate warfarin effects
Increased serum concentrations and half-life of zidovudine. Increased risk of adverse effects
Inhibits metabolism resulting in increased prothrombin time/INRs and increased risk of bleeding events
May potentiate hypotensive effect. Monitor closely CNS depressants (eg, anxiolytics, hypnotics, sedatives, alcohol, opiate analgesics, antipsychotics)
Other agents with anticholinergic/ antimuscarinic effects (eg, amantadine, benztropine, bromocriptine, disopyramide, levodopa, selegiline, pergolide, procyclidine, sedating antihistamines, phenothiazines, tricyclic antidepressants, orphenadrine)
Phenytoin
Antihistamines – non-sedating (eg, cetirizine, loratadine)
Antimuscarinics (eg, hyoscine [scopolamine])
Additive CNS depressant effects may occur (eg, sedation)
Additive cholinergic adverse effects (eg, dry mouth, urine retention, constipation, confusion in elderly)
Some reports of increased phenytoin levels. Monitor Topiramate
Amiodarone
Nefazodone
Alcohol, other CNS depressants
Metoclopramide
Nitrates
Other agents with antimuscarinic effects (eg, amantadine, benztropine, bromocriptine, disopyramide, levodopa, selegiline, pergolide, procyclidine, sedating antihistamines, phenothiazines, tricyclic antidepressants, orphenadrine)
Potassium salts (solid-dose formulations)
Chloramphenicol (ocular) Bone marrow depressant medications
Phenytoin
Warfarin
Diphtheria/ tetanus/ pertussis (Tdap)
Other injectable vaccines or immunoglobulin
May potentiate the risk of oligohydrosis and hyperthermia associated occasionally with topiramate, especially in pediatric patients or those exposed to hot weather
Possible increased risk of QT prolongation (rare)
Possible increased risk of QT prolongation with higher doses of loratadine (20mg/day)
Additive sedative effects
Possible reduction in prokinetic effect of metoclopramide
Possible reduced effect of sublingual nitrates (failure to dissolve under tongue due to dry mouth)
Increased adverse effects (eg, dry mouth, urine retention, constipation, confusion in elderly)
Antimuscarinic action may slow transit time. Severe GI injury reported due to high localised concentration of potassium salts. Avoid if possible
Although concerns around aplastic anaemia occurring with ocular chloramphenicol have been largely discounted, literature recommends avoiding concomittant use
Theoretically may increase plasma phenytoin levels. Avoid or monitor closely
Some case reports available which document an increased INR with concomitant warfarin and ocular chloramphenicol use. Monitor
Administer at different sites
DRUG/DRUG GROUP INTERACTING SUBSTANCE DETAILS
Dukoral Food/ drink
Typhoid vaccine (oral)
Famciclovir
Hormonal contraceptives (applies to the emergency and oral contraceptive pill)
Iodine supplements (oral)
Probenecid
Viral vaccines
Antibiotics or other medicines (eg, orlistat) that cause diarrhoea or vomiting
Enzyme inducers (eg, barbiturates, carbamazepine, primidone, phenytoin, topiramate, St John’s wort (Hypericum perforatum), rifampicin, ritonavir, griseofulvin)
Amiodarone
Anti-thyroid medicines (eg, propylthiouracil, iodide)
Lithium
Potassium-sparing medicines (eg, ACE inhibitors, angiotensin II receptor antagonists, spironolactone)
Warfarin
Iron supplements (oral) Antacids
Antibacterials – quinolones (eg, ciprofloxacin, norfloxacin)
Antibacterials – tetracyclines (eg, doxycycline, minocycline)
Bisphosphonates (eg, alendronate, etidronate)
Carbidopa and levodopa
Cholestyramine
Levothyroxine
Methyldopa
Penicillamine
Vitamin E
Zinc
Laxatives – bulk laxatives
Meningococcal vaccine
Digoxin
Lithium
Vaccine is acid labile so separate administration from food or drink by one hour as food and drink may increase acid production in stomach
Take at least eight hours apart
Probenecid may increase the serum concentrations of famciclovir and its active metabolite, penciclovir, through competitive inhibition of renal tubular secretion. Monitor
Famciclovir is an antiviral and may reduce the activity of viral vaccines. Administer 24 hours apart
May reduce the absorption of oral contraceptives. However, generally antibiotics that are not enzyme-inducing do not interact with oral contraceptives
Increased hepatic metabolism of ethinylestradiol and progestogens. Possible reduction in effectiveness. Consider higher dosages
Additive effect as amiodarone contains iodine. Avoid combination except on medical advice
Potentiation of hypothyroid effect. Avoid combination unless under medical advice
Combination can cause hypothyroidism
Most iodine supplements contain potassium.Some medicines reduce the excretion of potassium by the kidneys and the combination can increase potassium levels in the body. Avoid combination unless under medical advice
Anticoagulant effect of warfarin may be decreased
Some studies show significant reductions in amount of iron absorbed. Separate administration by 2–3 hours
Decreases absorption and may reduce plasma concentrations of quinolone antibiotics to subtherapeutic levels. Separate administration by at least 2–3 hours. Monitor response
Insoluble chelate formed which decreases absorption of tetracyclines. Separate administration by at least 2–3 hours. Monitor patient for reduced response
Reduced absorption of bisphosphonates. Separate administration by at least 30 minutes to 2 hours depending on biphosphonate used
Reduced absorption may be clinically significant in some patients. Separate administration by at least 2–3 hours. Monitor patient for reduced response
Reduced absorption of iron
Poorly soluble chelate formed which reduces absorption of levothyroxine
Separate administration by at least 2–3 hours. Monitor patient for reduced response
Reduced absorption of methyldopa may reduce antihypertensive effect. Separate administration by at least 2–3 hours
Reduced absorption of penicillamine. Separate administration by at least 2–3 hours
May reduce absorption of vitamin E. Separate administration by at least 2–3 hours
Reduced absorption of iron and zinc. Separate administration by at least 2–3 hours
May decrease digoxin absorption resulting in decreased digoxin levels
Reports of reduced lithium absorption resulting in reduced plasma levels. Monitor lithium levels, separate administration by at least 2 hours, or use alternative laxative
Immunosuppressive therapies May reduce the immune response to the vaccine
Metoclopramide Alcohol
Aspirin, paracetamol
Bromocriptine
Cyclosporin
Dantrolene
Digoxin
Additive CNS effects (eg, sedation)
Increased rate of aspirin and paracetamol absorption. Combination may be beneficial for migraine attacks
Antagonises hypoprolactinaemic effect of bromocriptine
Increased absorption of cyclosporin resulting in increased plasma levels. Monitor
Increased absorption of dantrolene resulting in increased plasma levels. Monitor for signs of dantrolene toxicity (eg, CNS disturbances, diarrhoea)
Absorption of digoxin decreased possibly by increased gut motility. Plasma levels of digoxin may be reduced. Monitor
DRUG/DRUG GROUP INTERACTING SUBSTANCE DETAILS
Metoclopramide cont…
Lithium
MAOIs (irreversible eg, phenelzine, tranylcypromine)
Medicines with antidopaminergic actions (eg, antipsychotics, tetrabenazine)
Parkinson’s drugs (eg, cabergoline, levodopa, lisuride)
Medications with antimuscarinic effects (eg, amantadine, benztropine, bromocriptine, levodopa, selegiline, pergolide, procyclidine, sedating antihistamines, phenothiazines, tricyclic antidepressants, orphenadrine)
Morphine
SSRIs
Methyl salicylate (topical) Warfarin
Risk of extrapyramidal adverse effects or severe neurotoxicity increased. Avoid combination if possible or carefully monitor for signs of neurotoxicity
Possible additive hypertensive effects. Avoid combination if possible, or monitor
Increased risk of extrapyramidal adverse effects
Metoclopramide is a dopamine antagonist and antagonises action of medications used to treat Parkinson’s disease. Avoid combination
Possible reduction in prokinetic effect of metoclopramide
Additive CNS effects (eg, sedation) possible. Increased rate of morphine absorption (faster onset of action)
Possible increase in metoclopramide absorption with increased risk of adverse effects (eg,extrapyramidal effects)
Topical use of methyl salicylate has been shown to increase INR/PT and result in bleeding and bruising. Present in many OTC analgesic liniments, creams or medicated oils. Use alternative topical analgesics if possible, or use with great caution and monitoring
Nasal corticosteroids Other corticosteroid use, eg, inhaled Additive systemic effects of corticosteroids
Nitrofurantoin
Omeprazole, lansoprazole
Orlistat
Phenylephrine, pseudoephedrine
Povidone iodine (see also iodine supplements [oral])
Prochlorperazine
Magnesium trisilicate May impair absorption of nitrofurantoin
Quinolone antibiotics (eg, ciprofloxacin, norfloxacin)
Urinary alkalisers
Antifungals
Antiretroviral medications (eg, atazanavir, nelfinavir, saquinavir)
Clopidogrel
Clozapine
Digoxin
Medications metabolised by CYP 2C19 (eg, citalopram, diazepam, phenytoin, warfarin, other vitamin K antagonists)
Other CYP 2C19 or CYP 3A4 inhibitors (eg, clarithromycin, voriconazole)
Amiodarone
Cyclosporin
Fat-soluble vitamins (eg, vitamin A, D, E, K)
Oral contraceptives
Warfarin
Cardiac glycosides, quinidine, tricyclic antidepressants
Ergotamine or related compounds
MAOIs – irreversible (eg, phenelzine, tranylcypromine)
MAOIs – reversible (eg, moclobemide)
Methyldopa
Other sympathomimetics
Selegiline
Tricyclic antidepressants
Other medications
Lithium
Antihypertensives
CNS depressants (including alcohol, opiods)
Drugs causing QT prolongation (eg, erythromycin, haloperidol, sotalol)
Nitrofurantoin may inhibit the antibacterial activity of quinolones
Antibacterial effect of nitrofurantoin is enhanced by acidic conditions
Reduces absorption of itraconazole and ketoconazole
Decreases serum levels of atazanavir, nelfinavir (avoid combination). Increases levels of saquinavir (contact prescriber)
Reduces efficacy of clopidogrel (approximately 30% less inhibition of platelet aggregation)
Three reports of elevated clozapine levels documented (two resulted in seizures). Monitor
Reduces absorption of digoxin. Monitor
Theoretically may inhibit the metabolism of these agents, but few clinical reports documented. Monitor
May increase serum levels of omeprazole or lansoprazole, although dosage adjustment not usually required
Decreased absorption of amiodarone. Plasma levels of amiodarone may be reduced. Monitor
Markedly decreased cyclosporin levels. Avoid combination
Decreased absorption of fat-soluble vitamins. Separate administration by at least 2 hours or take vitamins at bed time
Absorption of oral contraceptives may be compromised by any diarrhoea caused by orlistat. Possible failure of contraceptive action
Isolated report of INR increase, possibly due to reduction in vitamin K absorption. Monitor INR
Possible increased risk of arrhythmias (rare reports)
Additive vasopressor effects. Combination not recommended
Significant risk of hypertensive crisis (up to 2 weeks after stopping MAOI). Avoid combination (includes all oral, nasal and ocular products with phenylephrine or pseudoephedrine)
Possible increase risk of hypertension. Best avoided
Isolated report of hypertension. Monitor blood pressure
Additive effects, increased toxicity
Increased risk of hypertension with higher dosages
May enhance the pressor response causing hypertension, headache, or tremor
Pseudoephedrine especially may interact with beta blockers, prostate medications, St. John’s Wort, and many other medications. Always use an interactions database to check for interactions
Additive hypothyroid effect possible with long term topical povidone iodine administration
Possible additive hypotensive effect
Additive CNS depressant effects (eg, sedation)
Possible increased risk QT prolongation (rare reports)
DRUG/DRUG GROUP INTERACTING SUBSTANCE DETAILS
Prochlorperazine cont… Lithium
Other agents with anticholinergic/ antimuscarinic effects (eg, amantadine, benztropine, bromocriptine, disopyramide, levodopa, selegiline, pergolide, procyclidine, sedating antihistamines, phenothiazines, tricyclic antidepressants, orphenadrine)
Phenytoin
Parkinson’s drugs (eg, cabergoline, levodopa, lisuride)
SSRI and tricyclic antidepressants
Sildenafil Alcohol
Possible increased risk of neurological adverse effects
Additive cholinergic adverse effects (eg, dry mouth, urinary retention, constipation, confusion in the elderly)
Alteration in phenytoin metabolism. Plasma levels may be increased or decreased. Monitor. Phenothiazines may also reduce seizure threshold
Effects of Parkinson’s disease drugs may be antagonised since prochlorperazine has some dopamine antagonist activity
Metabolism may be inhibited increasing risk of adverse effects (eg, extrapyramidal reactions, sedation, possibly QT prolongation)
May reduce both standing and supine blood pressure. Dizziness reported
Alpha blockers (eg, doxazosin) May reduce both standing and supine blood pressure. Dizziness reported
Antacids
Sumatriptan, zolmitriptan
Trimethoprim
Urinary alkalisers
May reduce absorption of sildenafil if taken at the same time
CYP 3A4 (eg, erythromycin, saquinavir) Drugs that inhibit these enzymes may increase sildenafil concentrations
Nitrates (eg, glyceryl trinitrate, isosorbide dinitrate)
Several other medicines
Ergotamine or related compounds
MAOIs – irreversible (eg, phenelzine, tranylcypromine)
MAOIs – reversible (eg, moclobemide)
Medications that increase serotonin levels (eg, SSRIs, venlafaxine, tricyclic antidepressants sibutramine, St John’s wort)
Medications that lower the seizure threshold (eg, neuroleptics, antidepressants)
Cyclosporin
Digoxin
Diuretics - amiloride
Methotrexate
Phenytoin
Warfarin
Aspirin
Flecainide
Fluroquinolones (eg, ciprofloxacin, norfloxacin)
Hexamine
Laxatives
Lithium
Methadone
Methotrexate
Mexiletine
Nitrofurantoin
Contraindicated. Potentiates hypotensive effects
Refer to data sheet
Additive vasoconstriction may result in fatal reactions (eg, MI). Avoid combination
MAOIs can inhibit metabolism of sumatriptan increasing risk of serotonin syndrome. Avoid for 2 weeks after stopping MAOI
Moclobemide inhibits metabolism of sumatriptan. Increased risk of serotonin syndrome. Avoid
Increased risk of serotonin syndrome. Avoid combination or careful monitoring required
Sumatriptan can also lower seizure threshold so additive effects possible
Reversible deterioration of renal function observed if combination used following renal transplantation
May increase plasma levels of digoxin in elderly people
Excessively low serum sodium levels seen. May theorectically cause hyperkalaemia. Monitor electrolytes
Consider folate supplementation if combination used
May prolong half-life. Watch for phenytoin toxicity. Monitor
May potentiate anticoagulant activity of warfarin. Monitor
Increased clearance of salicyclates, possible reduced levels
Alkalinisation of the urine reduces the renal excretion of flecainide. Risk of flecainide toxicity increased. Monitor
May decrease the solubility of fluoroquinolones in the urine and increase the risk of crystalluria
Requires urinary pH of 5.5 or lower to be active so alkalinisation of urine reduces antibacterial effect. Avoid
Additive laxative effect possible
Often contain substantial amounts of sodium, which increases the urinary excretion of lithium, reducing plasma lithium levels. Avoid if possible or monitor
Alkalinisation of the urine reduces clearance of methadone. Increased risk of toxicity
Alkalinisation of the urine increases renal clearance of methotrexate. Therapeutic efficacy of methotrexate may be reduced
Possibly reduced clearance of mexiletine
Antibacterial effect of nitrofurantoin is enhanced by acidic conditions
REFERENCE SOURCES FOR TABLE: Medsafe data sheets www.medsafe.govt.nz
Please note this list is NOT ALL INCLUSIVE. Only the more commonly reported or important precautions and contraindications are included.
When selling any OTC medicine, consider the patient as a whole, including comorbid conditions and medicines, general health, age and
DRUG/DRUG GROUP CONDITION
Analgesics – aspirin
(usually less important with low-dose aspirin, eg, 75–100mg)
Allergy including rash, anaphylaxis, rhinitis or asthma from aspirin, other NSAIDs or food dyes
Asthma
Cardiovascular disease
Children/adolescents with viral illness
Dehydration
Elderly
Gastric irritation (indigestion, reflux, nausea, vomiting)
Gastric ulcer
Gout
G6PD deficiency
Haemorrhagic disorders
Hearing difficulties
Hepatic impairment
High blood pressure
History of asthma, rhinitis, atopy, nasal polyps
Infection
Renal impairment
Surgery or dental work (1 week prior, or just after)
frailty and weigh up risks versus benefits. Refer to a pharmacist if you are unsure. Always be cautious when selling medications to pregnant or breastfeeding women and refer them to a pharmacist so they can check the most recent literature sources for recommendations.
DETAILS
Allergic symptoms, cross-sensitivity with NSAIDs. Avoid
Asthma attack/worsening of asthma, rhinitis or sinusitis in asthmatics (occurs in 3-5% of population and up to 20% of asthmatics)
Sodium and water retention
Reye's syndrome risk. Do not use in children aged less than 16 years with a viral illness
Risk of renal failure
Increased risk of adverse effects
Aggravates pre-existing symptoms
Risk of bleed. Avoid in active gastric ulcer. Caution, preferably avoid, in history of gastric ulcer
Increases serum uric acid concentrations
High doses can precipitate haemolytic anaemia
Increased risk of bleeding
Analgesic/anti-inflammatory doses may aggravate and/or cause tinnitus
Avoid in severe hepatic impairment
Sodium and water retention
Increased risk of allergy to aspirin and exacerbation of existing asthma, rhinitis, atopy or nasal polyps
May mask fever and inflammation
Sodium and water retention, worsening of renal impairment
Prolongs bleeding
Analgesics – NSAIDs
Analgesics – paracetamol
Antacids
Allergy including rash, anaphylaxis, rhinitis or asthma from aspirin or NSAIDs
Asthma
Cardiovascular disease
Dehydration
Elderly
Gastric irritation
Gastric ulcer
Haemorrhagic disorders
Hepatic impairment
High blood pressure
History of asthma, rhinitis, atopy, nasal polyps
Infection
Renal impairment
Alcohol dependence
Renal or hepatic impairment
Calcium kidney stones (or history of)
Constipation
Low phosphate diets (aluminium hydroxide)
Low sodium diet, eg, heart failure, hypertension, renal failure, cirrhosis
Porphyria
Renal impairment
Allergic symptoms, cross-sensitivity with NSAIDs
Asthma attack/worsening of asthma, rhinitis or sinusitis in asthmatics (occurs in 3–5% of population and up to 20% of asthmatics)
Sodium and water retention, increased blood pressure
Risk of renal failure
Increased risk of adverse effects
Aggravates pre-existing symptoms
Risk of bleed. Avoid in active gastric ulcer. Caution, preferably avoid, in history of gastric ulcer
Increased risk of bleeding
Avoid in severe hepatic impairment
Sodium and water retention
Increased risk of allergy to aspirin and exacerbation of existing asthma, rhinitis, atopy or nasal polyps
May mask fever and inflammation
Sodium and water retention
Use with caution. Avoid high or prolonged dosing
Use with caution. Avoid high or prolonged dosing
Avoid calcium containing antacids
Aluminium hydroxide can exacerbate
Phosphate depletion, increased bone resorption, hypercalciuria, risk of osteomalacia
Consider sodium content (sodium bicarbonate, sodium alginate). Preferably avoid
sodium-containing antacids
Avoid aluminium hydroxide
Possible accumulation of some elements, eg, magnesium, aluminium, calcium
DRUG/DRUG GROUP CONDITION
Antidiarrhoeals
Abdominal distension
Acute inflammatory bowel disease, ileus development, when inhibition of peristalsis is to be avoided
Antibiotic-associated pseudomembranous colitis
Antifungals (eg, fluconazole)
Antihistamines – sedating (eg, promethazine, brompheniramine, azatadine, chlorpheniramine, diphenydramine, triprolidine, cyclizine, dimenhydrinate, meclozine)
Antihistamines – non-sedating
Antimuscarinics (eg, scopolamine/hyoscine)
Bromhexine
DETAILS
Avoid antidiarrhoeals
May cause intestinal obstruction or toxic megacolon
Avoid antidiarrhoeals
Diarrhoea associated with enterotoxin producing bacteria Avoid antidiarrhoeals
Dysentery
Hepatic disease
Infants, young children
Intestinal obstruction
Impaired renal function
Previous liver disease with fluconazole, existing liver disease/ dysfunction in hepatic impairment
Potentially proarrhythmic conditions
Broken skin
Epilepsy
Hepatic impairment
Narrow angle glaucoma, prostate problems, constipation, urinary retention
Porphyria
Productive cough
Renal impairment
Significant renal impairment
The very old, the very young
Hepatic or renal impairment
Children, elderly
Epilepsy
Impaired metabolism, liver or kidney function
Narrow angle glaucoma, prostate hypertrophy, constipation, urinary retention
Porphyria (hyoscine butylbromide)
Asthma
History of peptic ulcer disease
Severe hepatic or renal impairment
Chloramphenicol (ocular) Blurred vision, eye pain, or photophobia
Contact lens wearers
Unsure of diagnosis
Diphtheria/ tetanus/ pertussis (Tdap)
Dukoral
Ear wax softeners
Head lice products (pesticide-based)
Acute illness
Prior reaction to Tdap
Acute illness
Inflamed ear/perforated ear drum
Skin disease
Young children
Iodine supplements (oral) Excessive use
Thyroid disorders (eg, hypothyroidism, goitre, thyroid tumours)
Do not use antidiarrhoeals alone
Increased levels loperamide
Not generally recommended, have been associated with paralytic ileus
Avoid antidiarrhoeals
Caution
Liver disease may occur (fluconazole). Avoid miconazole oral gel
Rare cases of QT prolongation and torsade de pointes with fluconazole
Avoid topical antihistamines
Occasional reports of convulsions
Caution advised. Dose reduction may be necessary
Anticholinergic effects may aggravate these conditions
Possible acute attacks of porphyria with some antihistamines (eg, diphenhydramine, promethazine)
Thickens respiratory tract secretions
Dose reduction may be needed
Increased levocabastine blood levels likely after nasal usage
Increased risk of side effects, including paradoxical stimulation. Avoid in young children
Possible accumulation of drug, may need dose reduction
Increased risk of side effects
Seizures possible (rare)
Increased CNS effects (scopolamine)
Antimuscarinic effects aggravate these conditions
Association with acute attacks of porphyria
Care advised with bromhexine
May disrupt the gastric mucosal barrier
Reduced clearance bromhexine or metabolites
Refer to the doctor or TPA-endorsed optometrist
Refer to the doctor or TPA-endorsed optometrist
Refer to the doctor or TPA-endorsed optometrist
Postpone vaccination
Dependant on reaction. Refer to doctor
Postpone vaccination
Avoid use
Caution with some treatments
Caution with most chemical treatments
Higher intakes than recommended can cause adverse effects such as thyroid problems
Can worsen these conditions
Influenza vaccine
Acute illness
Iron Gastrointestinal diseases, eg, inflammatory bowel disease, diverticulae
Iron storage/iron absorption diseases, eg, haemochromatosis
Postpone vaccination
Use only under medical advice
Use only under medical advice
Repeated blood transfusions, anaemia without iron deficiency Do not give iron
DRUG/DRUG GROUP CONDITION
Laxatives
Levonorgestrel
Meningococcal vaccine
Methyl salicylate
Metoclopramide
Abusers
Acute abdominal conditions, undiagnosed abdominal pain (eg, possible appendicitis)
Colonic atony, immobile patients, insufficient fluid/ dehydration
Dehydration (severe)
Diabetes
Difficulty swallowing
Faecal impaction or obstruction
Galactose or lactose intolerance
Haemorrhoids, anal fissures, proctitis
Inflammatory bowel disease
Regular use
Breast cancer
Severe malabsorption syndrome, eg, Crohn's disease
Severe liver disease
Acute illness
Extensive topical application, exercise, heat occlusion
Children, young patients and elderly
Gastrointestinal conditions
Hepatic impairment
History of depression, epilepsy
Parkinson’s disease
Phaeochromocytoma
Porphyria
Renal impairment
Nasal corticosteroids
Broken skin, nose bleeds, untreated nasal infection
(including nasal cold sores), nasal surgery, tuberculosis
Nicotine replacement therapy Broken skin
Recent cerebrovascular accident, severe cardiovascular disease, severe arrhythmias, unstable angina pectoris
Peripheral vascular disease, endocrine disorders, peptic ulcer disease
Renal or hepatic impairment
Nitrofurantoin
Glucose 6-Phosphate deficiency
Peripheral neuropathy
Pregnancy at term (38 to 42 weeks)
Pyelonephritis
Renal impairment (CLCR <60 mL/min)
Urinary Alkalisers
Omeprazole, lansoprazole
Long-term gastric pain
Unexplained weight loss, persistent regurgitation of food or vomiting, difficulty swallowing or symptoms of
gastrointestinal bleeding
Worsening symptoms
Oral contraceptives
Abnormal vaginal bleeding
Cardiovascular disease
Clotting disorders
Diabetes
HIV
Hormone dependent cancer or liver tumor
Migraines, Smoking
Pregnancy and lactation (six months post-partum)
DETAILS
Electrolyte disturbances, especially potassium loss, diarrhoea. Excessive weight loss
Possible complications if laxatives used
Bulk-forming laxatives may cause intestinal obstruction or faecal impaction
Further dehydration and electrolyte imbalance with stimulant laxatives
Can affect blood sugars in poorly controlled diabetes
Avoid bulk-forming laxatives
Avoid oral laxatives, risk of colonic perforation
Lactulose contains galactose and lactose. Avoid
Avoid laxative suppositories
Increased adverse effects with stimulant laxatives
Avoid regular use of stimulant laxatives due to changes in rectal epithelium and risk of atonic colon
Relative contraindication (but levonorgestrel less risk than pregnancy)
Impaired efficacy of levonorgestrel; increased dose may be required
Interferes with metabolism of levonorgestrel
Postpone vaccination
Increased absorption of salicyclic acid into bloodstream (can be toxic)
Increased risk of extrapyramidal reactions. Use lower dosages especially if <60kg
Stimulates muscle contraction
Possible dose reduction required
Caution advised
Metoclopramide has central dopamine antagonistic effects and opposes action of drugs used to treat Parkinson’s disease
Possible hypertensive crisis
Possibly causes acute attacks porphyria
Significant accumulation of metoclopramide
Avoid nasal corticosteroids; may delay healing
Avoid patches
Avoid
Caution
Caution
May induced haemolytic anaemia
May be associated with prolonged use
Interferes with neonate’s red blood cell enzyme systems
Tissue distribution into the kidneys is poor
Increased risk of toxicity and decreased efficacy
Antibacterial activity of nitrofurantoin is enhanced by acidic conditions
Use only under medical advice
Use only under medical advice
Use only under medical advice
Seek medical advice
Relative contraindication. Use only under medical advice
Avoid
Use only under medical advice
Risk of viral transmission and potential interactions with HIV enzyme inducers. Use only under medical advice
Avoid
Progesterone only preferred. Refer to a doctor
Avoid in pregnancy. Progesterone only preferred in lactation
DRUG/DRUG GROUP CONDITION
Orlistat
Oseltamivir
Phenylephrine, pseudoephedrine
Povidone iodine (see also iodine supplements [oral])
Prochlorperazine
Sildenafil
Sumatriptan, zolmitriptan
Chronic malabsorption syndrome
Cholestasis (reduced/halted bile flow)
High fat intake
History of calcium oxalate kidney stones
Type 2 diabetes
Renal impairment
Cardiovascular disease, high blood pressure
Diabetes (poorly controlled)
Hyperthyroidism
Infants and young children
Narrow angle glaucoma
Renal impairment
Severe burns/extensive areas
Thyroid disorders
Dehydration
Elderly, debilitated
Impaired kidney, CV, CNS, respiratory function
Narrow angle glaucoma, parkinsonism, paralytic ileus, urinary retention, prostatic hypertrophy, epilepsy, blood dyscrasias, impaired liver, myasthenia gravis
Phaeochromocytoma
Diabetes, smokers, self-reported high cholesterol, previous coronary intervention, cardiovascular disease, unusually high or low blood pressure
Under 35 years and over 70 years
Heart disease or symptoms of heart disease, peripheral vascular disease, history of heart attack, stroke or TIA
Hemiplegic, basilar or ophthalmoplegic migraine
History of seizures or conditions predisposing to seizures
Hypertension, including controlled hypertension
Increased risk of heart disease
No previous history of migraine
Prinzmetal’s angina (pain at rest)
Renal or hepatic disease
Sulphonamide allergy
Unclear migraine diagnosis
Under 18 years or over 65 years
Trimethoprim
Antibiotic use (within 6 months)
Pregnancy
DETAILS
Avoid
Avoid
Increased risk of adverse GI effects
Caution
May need hypoglycaemic dose adjusted
Moderate renal impairment reduce dose, avoid in severe renal impairment
May increases heart rate and blood pressure
May alter blood glucose control
Possible additive tachycardia
Increased risk
Aggravated by sympathomimetics
Caution advised
Increased sytemic effects iodine – avoid
Regular or prolonged use may aggravate thyroid disorders
Hypotension
Increased risk of side effects
Increased risk of side effects, avoid
Contraindicated
Hypertensive crisis
Refer to doctor
Refer to dcotor
Do not use – sumatriptan causes vasoconstriction
Avoid
Seizures have occurred in some patients with history or predisposing factors
Transient increases in blood pressure may occur – do not use OTC
Refer to doctor
OTC sumatriptan not allowed
Avoid
Avoid OTC use
Possible cross-sensitivity (sumatriptan only)
Use only with a clear migraine diagnosis
OTC sumatriptan or zolmitriptan not indicated
Avoid
Avoid in first trimester of pregnancy (folate antagonist)
Renal impairment or abnormality, catheterisation, stones Refer to a doctor
Commonly reported adverse effects that do not require laboratory tests to detect are listed below. These tables are NOT ALL INCLUSIVE and do not
ADVERSE EFFECT CAUSED BY
Anorexia
Diphtheria/ tetanus/ pertussis (Tdap)
Anxiety Possibly phenylephrine, pseudoephedrine
Asthma (exacerbation of)
Black stools
Constipation
Dependence
Diarrhoea
Dizziness
Dry eyes
Dry mouth
Fever
Flushing
Gastric Irritation
Aspirin and salicylates
Benzoates, Sulphites (preservatives)
NSAIDs
Propolis, Royal jelly
Tartrazine (colouring agent)
Iron
Aluminium hydroxide (in antacids)
Antihistamines (sedating only)
Bulk-forming laxatives (if taken with too little fluid, or in people with dehydration)
Calcium (supplements or in antacids)
Iron salts
Laxatives (overuse, abuse)
Omeprazole, lansoprazole
Nicotine nasal spray, nicotine gum
Oxymetazoline, xylometazoline (overuse of nasal products)
Stimulant laxatives (eg, prolonged use of sennosides)
Aloes
Cascara
Fluconazole
H2 antagonists
Iron salts
Isphaghula
Laxatives (overuse or abuse)
Magnesium (supplements or in antacids)
NSAIDs
Omeprazole
Orlistat
Psyllium husk (bulk-forming laxative)
Senna
Oseltamivir
Sumatriptan
Antihistamines (sedating only)
Prochlorperazine
Scopolamine
Antihistamines (sedating)
Hyoscine
Prochlorperazine
Phenylephrine
Pseudoephedrine
Diphtheria/ tetanus/ pertussis (Tdap)
Influenza vaccine
Meningococcal vaccine
Sildenafil
Sumatriptan
Aspirin
Bromhexine
Bulk-forming laxatives (flatulence, bloating)
list medicines or supplements known to cause renal or hepatic impairment or blood dyscrasias.
ADVERSE EFFECT CAUSED BY
Gastric irritation
Cont…
Headache
Increased bleeding
Caffeine
Calcium (flatulence)
Diphtheria/ tetanus/ pertussis (Tdap)
Dukoral (GI upset and rarely cramping)
Eucalyptus
Fish oils
Fluconazole (abdominal pain, flatulence, nausea, vomiting)
Garlic
Iodine (oral)
Iron salts
Lactulose (cramps, flatulence)
Levonorgestrel (nausea)
Loperamide
Magnesium, Potassium, Zinc salts
Mebendazole
Meningococcal vaccine
NSAIDs
Omeprazole
Orlistat (flatulence, faecal urgency, fatty stools, discharge)
Oseltamivir (nausea, vomiting, abdominal pain)
Parsley
Pyrantel
Sildenafil
Sodium bicarbonate (stomach cramps)
Squill
Stimulant laxatives (colic, cramps)
Sumatriptan (nausea, vomiting)
Turmeric
Antihistamines (sedating)
Analgesics (overuse)
Black cohosh
Diptheria/ tetanus/ pertussis (Tdap)
Fluconazole
Influenza vaccine
Levocabastine eye drops and nose spray
Meningococcal vaccine
Nicotine replacement
NSAIDs (including overuse)
Omeprazole
Oseltamivir
Sildenafil
Aspirin
Bilberry
Bromelain
Clove
Coleus
Docosahexaenoic acid (DHA)
Dong quai
Feverfew
Fish oils
Garlic
Ginger
Ginkgo
ADVERSE EFFECT CAUSED BY
Increased bleeding cont...
Increased blood pressure
Increased risk of blood clots
Injection site reactions
(pain, redness, swelling)
Insomnia
Irritability/ fatigue
Local irritation
Menstrual bleeding changes
Metallic taste
Mouth ulcers/irritation
Nasal bleeds
Nasal stuffiness
Rebound acid secretion
Sedation
Ginseng
Guggul
Horse chestnut
NSAIDs
Turmeric
Aspirin (possibly)
Liquorice (large doses)
NSAIDs
Phenylephrine
Pseudoephedrine
Sumatriptan (transient)
Combined oral contraceptives (risk depends on dosage and specific hormone)
All injectable vaccinations
Caffeine
Ginseng, guarana
Nicotine
Oseltamivir
Phenylephrine (possibly)
Pseudoephedrine
All injectable vaccinations
Chloramphenicol
Nasal or ocular antihistamines
Nasal corticosteroids
Nasal decongestants
Nicotine, nasal spray, inhalation
Povidone iodine
Rectal bisacodyl
Tea-tree oil (Melaleuca alternifolia)
Oral contraceptives (amenorrhoea, breakthrough bleeding, short-cycles)
Iodine (oral)
Aspirin
Feverfew
Iodine (oral)
Nicotine lozenges, gum
Nasal corticosteroids
Nasal nicotine
Decongestant nasal drops and sprays (prolonged use)
Sildenafil
Calcium carbonate (after long-term use)
Antihistamines (sedating)
Azelastine nasal spray
Chamomile
Diphtheria/ tetanus/ pertussis (Tdap)
Hops
Hyoscine butylbromide
Kava
L-5-HTP
Levocabastine eye drops and nose spray
Loperamide
Metoclopramide
Passionflower
Prochlorperazine
Scopolamine
Skullcap
Sumatriptan
Valerian
ADVERSE EFFECT CAUSED BY
Skin reactions
Aciclovir, penciclovir (transient stinging, burning)
Aluminium chloride topical (irritation)
Aniseed (furanocoumarins, photosensitivity, contact allergy)
Antifungals (burning, irritation)
Antihistamines (topical)
Aspirin and salicylates (hypersensitivity reactions)
Benzyl benzoate (irritation)
Benzoyl peroxide (irritation)
Bergamot oil (photosensitivity)
Capsaicin (stinging, burning)
Celery (photosensitivity)
Chamomile (contact allergy)
Cinnamon (contact allergy)
Coal tar and derivatives (photosensitivity, irritant dermatitis)
Dandelion (contact allergy)
Dong quai (photosensitivity)
Feverfew (hypersensitivity reactions)
Garlic (sulphur allergy)
Gotu kola (contact dermatitis)
Head lice and scabies treatments
Idoxuridine (irritation, hypersensitivity)
Menthol (contact dermatitis)
Nicotine transdermal patches (irritation, allergy)
NSAIDs (hypersensitivity reactions)
Omeprazole
Paracetamol (rarely serious skin reactions)
Povidone iodine (hypersensitivity, irritation)
Promethazine (photosensitivity)
St John’s wort (sensory nerve hypersensitivity)
Salicylic acid (irritation)
Tea-tree oil (allergic dermatitis)
Trimethoprim (rash, pruritis, dermatitis)
Wood tars (irritation)
Stimulation
Tachycardia (fast heart beat) or palpitations
Teeth staining
Urinary retention
Sedating antihistamines (paradoxical)
Caffeine
Ginseng
Nicotine replacement therapy
Phenylephrine (possibly)
Prochlorperazine
Pseudoephedrine
Chlorhexidine
Liquid iron (dilute with water and use straw)
Povidone iodine gargle (rinse teeth with water)
Tannin-rich agents (eg, green tea)
Antihistamines (sedating only)
Hyoscine
Prochlorperazine
Phenylephrine
Scopolamine
NOTE: While the author has made every effort to ensure that the information given in this table is accurate and up to date, no responsibility can be held for the clinical safety of any of the above combinations or contraindications, or any future information that may become available on this constantly changing subject (August 2024).
In considering the likelihood of a potentially dangerous or desirable
GROUP
Aloe vera gel
American ginseng (Panax quinqefolium)
Andrographis (Andrographis paniculata)
Anthraquinone
Digoxin and other cardioactive glycosides
interaction between a Herbal Supplement and other Medicines in clinical practice, factors such as the patient situation, dosage and type of supplement, duration of treatment, and criticality of efficacy of other concomitant medicines, should also inform the clinician or pharmacist, as it should when proposing to alter any treatment regimen.
of
Reduced anti-cancer activity implicated by in vitro study involving aloe emodin
depletion (hypokalaemia) leading to increased risk
(eg, valerian, kava, passionflower, hops)
Anti-platelet agents (eg, ginger, garlic, clove, feverfew) Anticoagulants (eg, warfarin, heparin) Potentiation of anticoagulant effect and bleeding theoretically possible with large doses
Astragalus (Astragalus membranaceous)
(Scutellaria baicalensis)
bioavailability of metoprolol after IV astragaloside in rats; astrogalosides also reduce myocardial calcium overload
of anti-inflammatory effects & reduction in gastric ulcer side effects in rats
HERB/HERB GROUP
Barberry (Berberis vulgaris)
Berberine (also found in Coptis, Barberry, Golden Seal)
Antihypertensives
Antibiotics
Azithromycin
Berberis vulgaris Losartan
Betel nut (Areca catechu)
Bitter melon (Momordica charantia)
Blackseed (Nigella sativa)
Black
(Piper nigrum)
Bladderwrack (Fucus vesiculosus)
Boldo (Pneumus boldo)
Brassica rapa & Brassica napus (Turnip leaf)
Broom (Cytisus scoparius)
Buckthorn (Rhamnus frangula)
Bugleweed (Lycopus virginicus; Lycopus europaeus)
Bupleurum spp.
Butterbur (Petasites hybridus)
Capsicum / cayenne pepper
enhanced hypotensive effect, with large doses of fruit extract
oral bioavailability
overcome multidrug-resistance, through overcoming efflux pump inhibition
Enhanced in vitro activity against Pseudomonas aeruginosa & survival in a mice model of cystic fibrosis
oral bioavailability reported
Reduced adverse events reported in various rodent studies
Enhanced in vitro cytotoxicity in bladder cancer reported
increased Cmax and AUC of losartan in rats (inhibition of CYP3A4 proposed)
Antipsychotic drugs Increased parkinsonian side effects reported with flupenthixol and fluphenazine
potentiation of
Chaste tree (Vitex agnus castus)
Cinchona bark (contains quinine)
chlorpromazine, metoclopramide and other dopamine receptor antagonists
(Cuminum cyminum)
(Rheum tanguticum, Citrus aurantium)
HERB/HERB GROUP
Echinacea Immunosuppressive drugs (eg, cyclosporin, tacrolimus)
Ephedra sinica
Antihypertensive agents
CNS stimulants
Digoxin and cardioactive glycosides
Ergotamine and oxytocin
Halothane
Monoamine oxidase inhibitors (MAOIs)
SSRI antidepressants
Eurycoma longifolia (Tongkat ali; Pasak bumi)
Possible antagonism of antihypertensive effect
Sympathomimetic effects; hypertension
Arrhythmias possible
Hypertension possible
Arrhythmias possible
Life-threatening acute hypertensive response + hyperpyrexia and coma possible
Potentiation of serotonergic effects possible
(Linum
glauca (Thryallis)
Ginkgo (Ginkgo biloba)
Ginseng (Panax ginseng)
Anticoagulants and antiplatelet agents
oral drug bioavailability reported in rats
Theoretical potentiation of anticoagulant or antiplatelet effects, though no effect
healthy volunteers
effect
Pretreatment decreased Cmax and AUC of clopidogrel, but high dose ginko increased Cmax and AUC of the clopidogrel active metabolite
in cardiotoxicity in animal studies
of oral simvastatin
HERB/HERB
Hawthorn
Hemidesmus indicus Gentamicin
Hibiscus (Hibiscus sabdariffa)
Holy Basil (Ocimum sanctum)
Honey
Houttuynia cordata
Japanese honeysuckle (Lonicera japonica)
Jia-Wei-xiao-yao-san (Kami-shoyo-san;TJ-24)
Kaempferia parviflora
Karela (Momordica charantia)
Kava
Levo-dopa & other
(eg, hypnotics, benzodiazepines, opiates, some analgesics)
Kelp Antithyroid agents (carbimazole, propylthiouracil etc)
Kyushin (Japanese preparation)
Laxative herbs (containing anthraquinone)
(Chinese; Glycyrrhiza uralensis, European; Glycyrrhiza glabra)
HERB/HERB GROUP
Milk (St Mary’s)
Moringa oleifera (Drumstick tree) Amodiaquine
Navel Orange (Citrus sinensis)
Nishi Amalaki (formulation of Curcuma longa & Phyllanthus emblica)
Ocimum gratissimum (African Basil)
Oregon Grape (Mahonia aquifolium)
Paeony (Paeonia lactiflora)
Pepper Piper nigrum (black)
Piper longum (long)
Phellodendron (Phellodendron amurense var wilsonii)
Phellopterin
Pink Knotweed (Polygonum capitatum)
Pomegranate (Punica granatum)
(Citrus maxima)
and
A and silybin B may increase raloxifene systemic exposure by inhibiting intestinal raloxifene
HERB/HERB GROUP
Reishi mushroom (Ganoderma lucidum)
Resveratrol
Rhodiola rosea Losartan
Rhubarb (Rheum palmatum) (Rheum officinale)
Safflower flowers (Carthamus tinctorius)
Salboku-to (Asian herbal mixture; contains same herbs as Sho-saiko-to,plus xiao chai hu tang,poria cocos, Magnolia officinalis, Perillae frutescens)
Salvia miltiorrhiza (Dan Shen)
Schisandra (Schisandra chinensis and S. sphenanthera)
and other cardiac glycosides
Sedatives (eg, valerian, hops, kava, passionflower)
Self Heal (Prunella vulgaris) spikes or whole plant
Senna (Cassia spp)
Senega (Polygala senega)
Shankhapushpi (Ayurvedic preparation)
Sho-saiko-to (Minor bupleurum)
Siberian ginseng (Eleutherococcus senticosus)
Slippery elm
Sophora flavescens (Kushen)
Sorrel (Rumex acetosa)
Cytotoxics
A
drugs (eg, benzodiazepines, clonidine, opioid analgesics, phenobarbitone)
glycosides and antiarrhythmics (eg, quinidine)
hypolipidaemic effects
oral drug bioavailability at low but not high drug dosages in rats
Increased drug AUC and Cmax when administered with schisandrin A and schisantherin A
Possible enhanced cytotoxic effects by large doses due to reversal of multi-drug resistance by gomisin A and schisandrol A
Enhanced oral bioavailability of tacrolimus in healthy volunteers. Concomitant proton pump inhibitor use may also influence
of
St John’s wort cont...
(eg, ephedrine and pseudoephedrine from Ephedra spp.)
Cyclosporin, tacrolimus and other immunosuppressants
Indinavir, saquinavir, ritonavir and other protease inhibitor antivirals
transplant rejection
(eg, fluoxetine, sertraline, paroxetine)
Theoretical possibility of serious
Triptans (sumatriptan, naratriptan, rizatriptan, zolmitriptan) Theoretical possibility of
syndrome, though few case reports to
HERB/HERB GROUP
Tamarind (Tamarindus indica)
Tannin-rich agents
Tienchi ginseng (Panax notoginseng)
Many drugs
Theoretical reduction in absorption from GIT, although virtually no evidence to date
Protein-rich preparations Possible reduced protein absorption from GIT
Thai Black Ginger (Kaempferia parviflora)
Tinospora cordifolia Glibenclamide
Trikatu (Ayurvedic preparation containing ginger, black pepper, and Piper longum)
Tripterygium wilfordi
Turmeric (see also curcumin) Platelet inhibitors (eg, aspirin, dipyridamole)/ anticoagulants (warfarin)
Uzara root (Ayurvedic preparation)
Valerian Benzodiazepines, hypnotics, tricyclic antidepressants, opioid analgesics, anaesthetics
Vasoconstrictors (eg, broom)
Vasodilators (eg, hawthorn)
Vitamins
Wormwood (Artemisia absinthium)
Willow bark
Withania (Ashwagandha)
Wolfberry or Goji (Lycium barbarum)
Xanthine-rich remedies (eg, cola, guarana, mate)
Yohimbe (Pausinystalia yohimbe)
Sympathomimetics
Antihypertensives
Large doses increased glibenclamide bioavailability in rats
(SSRIs)
Note: While the author has made every effort to ensure that the information given in this table is accurate and up-to-date, no responsibility can be held for the clinical safety of any of the above combinations or contraindications, or any future information that may become available on this constantly changing subject. (August 2024). Entire contents of Herbal Supplements: Interactions Copyright, Phil Rasmussen, 2024.
TABLE REFERENCES
1. Vinson JA et al, Phytomedicine 12(10):760-5, Nov 2005. 2. Yuan CS et al, Ann Intern Med 141(1):23-7, Jul 6, 2004. 3. Moriarty KJ, Silk DB. Dig Dis 6(1):15-29, 1988. 4. Greenfeld D et al, Am J Psychiatry 152(1):60-3, Jan 1995. 5. Wheatley D. J Psychopharmacol 19(4):414-21, Jul 2005. 6. Carrasco MC et al, Phytother Res 23(12):1795-6, Dec 2009. 7. Vaes LP, Chyka PA. Ann Pharmacother 34(12):1478-82, Dec 2000. 8. Kar A et al, J Ethnopharmacol 81(2):281-5, Jul 2002. 9. Lai MY et al, Planta Med 70(2):132-7, Feb 2004. 10. Shao ZH et al, Am J Chin Med 32(1):89-95, 2004. 11. Fan L et al, Clin Pharmacol Ther 83(3):471-6, Mar 2008. 12. Fatehi M et al, J Ethnopharmacol 102(1):46-52, 2005. 13. Deahl M, Mov Disord 4(4):330-2, 1989. 14. Pulliero G et al, Fitoterapia 60:69-75, 1989. 15. Basch E et al, Am J Health Syst Pharm 60(4):356-9, Feb 15, 2003. 16. Nivitabishekam SN et al, Chem Biol Interact 177(3):247-53, Feb 12, 2009. 17. Limtrakul P et al, Cancer Chemother Pharmacol 54(6):525-30, Dec 2004. 18. Clark CD et al, Endocr Pract 9(5):363-9, Sept-Oct 2003. 19. Teas J et al, J Med Food 10(1):90-100, Mar 2007. 20. Hazard R, Mouille P. C R Seances Soc Biol Fil 160(10):1814-7, 1966 (French). 21. Winterhoff H et al, Arzneimittelforschung 44(1):41-5, Jan 1994. 22. Beer AM et al, Phytomedicine 15(1-2):1622, Jan 2008. 23. Nose M et al, Chem Pharm Bull 37(10):2736-40, Oct 1989. 24. Lee DK. Et al. Clin Exp Allergy. 34(1):110-4. 2004. 25. Thabrew MI et al, Drug Metabol Drug Interact 19(3):177-87, 2003. 26. Thabrew MI et al, Drug Metabol Drug Interact. 20(4):263-72, 2004. 27. Cruz L et al, Can J Physiol Pharmacol 77(6):441-6, 1999. 28. Bouraoui A et al, Drug Nutr Interact 5(4):345-50, 1988. 29. Kobayashi Y et al, J Ethnopharmacol In press. Available online 16 June 2005. 30. Meier B et al, Phytomedicine 7(5):373-81, 2000. 31. Milewicz A et al, Arzneimittelforschung 43(7):752-6, Jul 1993. 32. Munafo A et al, Eur J Clin Pharmacol 38(3):269-73, 1990. 33. Martin ES et al, Pacing Clin Electrophysiol 20(8 Pt 1):2024-5, Aug 1997. 34. Aronson JK, Carver JG. Lancet 1(8235):1418, Jun 27, 1981. 35. Wanwimolruk S et al, Br J Clin Pharmacol 22(3):346-50, Sept 1986. 36. Khan A et al, Diabetes Card, 26(12):3215-8, Dec 2003. 37. Xiao C et al, Clin Vaccine Immunol 14(12):1634-9, Dec 2007. 38. Rajput ZI et al, J Zhejiang Univ Sci B 8(5):331-7, May 2007. 39. De Souza NJ. J Ethnopharmacol 38(2-3):177-80, Mar 1993. 40. Stephenson PE. J Am Diet Assoc 71(3):240-7, Sept 1977. 41. Kondal A, Garg SK. Methods Find Exp Clin Pharmacol 25(10):823-5, 2003. 42. Li LS. Et al. Zhonggou Zhong Xi Yi Jie He Za Zhi. 16(12):733-7, 1996. 43. Suvarna R et al, BMJ 327(7429):1454, Dec 20, 2003. 44. Grant P. J Heart Valve Dis 13(1):25-6, Jan 2004. 45. Lilja JJ et al, Clin Pharmacol Ther 81(6): 833-9, Jun 2007. 46. Greenblatt DJ et al, Clin Pharmacol Ther 79(1):125-33, Jan 2006. 47. Griffiths AP et al, J R Soc Health 128(6):324-6, Nov 2008. 48. Mergenhagen KA, Sherman O. Am J Health Syst Pharm 65(22):2113-6, Nov 15, 2008. 49. Pham DQ, Pham AQ. Am J Health Syst Pharm 64(5):484-90, Mar 1, 2007. 50. Paeng CH et al, Clin Ther 29(8):1730-5, Aug 2007. 51. Li Z et al, J Am Diet Assoc 106(12):2057-61, Dec 2006. 52. Rindone JP, Murphy TW Am J Ther 13(3):283-4, May-Jun 2006. 53. Aston JL et al, Pharmacotherapy 26(9):1314-9, Sept 2009. 54. Mohammed Abdul MI et al, Br J Pharmacol 154(8):1691-700, Aug 2008. 55. Sachin BS et al, Phytother Res 21(2):157-63, Feb 2007. 56. Anuchapreeda S et al, Biochem Pharmacol 64(4):573-82, Aug 15, 2002. 57. Jagota A, Reddy MY. Cell Mol Neurobiol 27(8):997-1006, Dec 2007. 58. Tang WF et al, Biomed Chromatogr 22(8):851-6, Aug 2008. 59. Chan TY, Ann Pharmacother 35(4):501-4, Apr 2001. 60. Qiao BP et al, Zhongguo Zhong Xi Yi Jie He Za Zhi 21(8):611-4, 2001 (Chinese). 61. Widmer P et al, Eur J Clin Pharmacol 49(1-2):31-6, 1995. 62. Wang BH, Ou-Yang JP. Cardiovasc Drug Rev 23(2):161-72, Summer 2005. 63. Barnes J et al, J Pharm Pharmacol 57(8):929-54, Aug 2005. 64. Rasmussen PL, personal communication with patient, 2004. 65. Ueng YF et al, J Pharm Pharmacol 57(2):227-32, Feb 2005. 66. Jan W-C et al, J Ethnopharmacol 102(3):440-5, 1 Dec, 2005. 67. Saxena A, Vikram NZ. J Altern Complement Med 10(2):369-78, Apr 2004. 68. Thompson-Coon JS, Ernst E. J Fam Pract 52(6):468-78, Jun 2003. 69. Makheja AN, Bailey JM. Prostaglandins Leukot Med 8(6):653-60, Jun 1982. 70. Laitinen LA et al, Pharm Res 21(10):1904-16, Oct 2004. 71. Mukherjee S et al, BMC Pharmacol 3:16, Dec 20, 2003. 72. German K et al, Br J Urol 76(4):518, Oct 1995. 73. Burnham BE. Plast Reconstr Surg 95(1):213, Jan 1995. 74. Beckert BW et al, Plast Reconstr Surg 120(7):2044-50, Dec 2007. 75. Piscitelli SC et al, Clin Infect Dis 34(2):234-8, Jan 15, 2002. 76. Mukherjee S. et al. BMC Pharmacol. 3(1):16. 2003. 77. Jiang X et al, Br J Clin Pharmacol 59(4):425-32, Apr 2005. 78. Chiang HM et al, Am J Chin Med 34(5):845-55, 2006. 79. Lala LG et al, J Ethnopharmacol 91(2-3):277-80, 2004. 80. Rosenblatt M, Mindal J. N Engl J Med 336(15):1108, Apr 10, 1997. 81. Zhang XY, J Clin Psychiatry 62(11):878-83, Nov 2001. 82. Zhang XY, Chin Med J (Engl) 112(12):1093-6, Dec 1999. 83. Agha AM. Et al. J Exp. Cancer Res. 20(1):39-50; 2001. 84. Kudolo GB et al, Clin Nutr 25(4):606-16, Aug, 2006. 85. Blumenthal M. Clin Nutr 26(1):164-5, Feb 2007. 86. Uchida S et al, J Clin Pharmacol 46(11):1290-8, Nov 2006. 87. Jones BD, Runikis AM. J Clin Psychopharmacol 7(3):201-2, 1987. 88. Clauson KA et al, J Am Pharm Assoc 92003) 48(3):e55-63, May-Jun 2008. 89. Dasgupta A et al, Am J Clin Pathol 119(2):298-303, 2003. 90. Chow L et al, J Clin Lab Anal 17(1):22-7, 2003. 91. Liu TP et al. Horm Metab Res 37(3):146-51, Mar 2005. 92. Lam AY et al, Ann Pharmacother 35(10):1199-201, Oct 2001. 93. Leung H et al, Food Chem Toxicol, Jan 15, 2008. 94. Gurley BJ et al, Mol Nutr Food Res 52(7):755-63, Jul 2008. 95. Gnanapragasam A et al, K. Life Sci 76(5):585-97, Dec 17, 2004. 96. Honig PK et al, J Clin Pharmacol 36(4):345-51, Apr 1996. 97. Kiani J, Imam SZ. Nutr J 6:33, Oct 30, 2007. 98. Ali BH et al, Clin Exp Pharmacol Physiol 29(8):704-6, 2002. 99. Banfield C et al, Clin Pharmacokinet 41(4):311-8, 2002. 100. Greenblatt DJ et al, J Clin Psychopharmacol 21(4):357-9, 2001. 101. Ando H et al, Br J Clin Pharmacol 60(5):494-7, Nov 2005. 102. Golden EB et al, Blood 113(23):5927-37, Jun 4, 2009. 103. Huupponen R et al, Eur J Clin Pharmacol 26(2):279-81, 1984. 104. Leach MJ. J Altern Complement Med 13(9):977-83, Nov 2007. 105. Rigelsky JM, Sweet BV. Am J Health Syst Pharm 59(5):417-22, Mar 2002. 106. Kotnis MS et al. Nephrology 9(3):142-52. 2004. 107. Koumaravelou K et al, Indian J Exp Biol 40(5):560-3, May 2002. 108. Koumaravelou K et al, Indian J Exp Biol 40(10):1164-8, 2002. 109. Sukriti, Garg SK, Methods Find Exp Clin Pharmacol 25(5):36770, 2003. 110. Schiller H et al, Phytomedicine 13(8):535-41, Sept 2006. 111. Rasmussen PL, Phytonews 3, Phytomed Medicinal Herbs Ltd, April 1999. 112. Stoewsand GS. Food Chem Toxicol 33(6):537-43, Jun 1995. 113. Leung L et al, Br J Nutr 102(12):1703-8, Dec 2009. 114. Schelosky L et al, J Neurol Neurosurg Psychiatry 58(5):639-40, May 1995. 115. CDC,
Centers for Disease Control and Prevention, MMWR Morb Mortal Wkly Rep 51(47):1065-7, Nov 29, 2002. 116. Clough AR et al, Intern Med J 33(8):336-40, Aug 2003. 117. Wheatley D. Phytother Res 15(6):549-51, Sept 2001. 118. Mahmoud BM et al, J Antimicrob Chemother 33(5):1005-9, 1994. 119. Walker BR, Edwards CR. Endocrinol Metab Clin North Am 23(2):359-77, Jun 1994. 120. Wu YT et al, Phytother Res 20(8):640-5, Aug 2006. 121. Tang J et al, Phytother Res 23(5):603-7, May 2009. 122. Hukkanen J et al, Blood Press 26:1-4 (epub ahead of print), Jun 2009. 123. Rajnarayana K et al, Arzneimittelforschung 54(2):109-13, 2004. 124. Huseini HF et al, Phytother Res 20(12):1036-9, Dec 2006. 125. Stilinovic N, Raskovic A. Med Pregl 61(1-2):95-8, Jan-Feb 2008. 126. Al Faraj S. Ann Trop Med Parasitol 99(2):219-20, Mar 2005. 127. Nweze El, Eze Ee. BMC Complement Altern Med 28(9): 37, Sept 2009. 128. Lilja JJ et al, Eur J Clin Pharmacol 61:337-340, 2005. 129. Lilja JJ et al, Clin Pharmacol Ther 75(3):184-90, Mar 2004. 130. He JX et al, Phytomedicine 2006 (epub ahead of print). 131. He JX et al, Biol Pharm Bull 24(12): 1395-9, Dec 2001. 132. He JX et al, J Pharm Pharmacol 55(3):313-21, Mar 2003. 133. Hiwale AR. Indian J Exp Biol 40(3):277-81, Mar 2002. 134. Lala LG et al, J Ethnopharmacol 91(2-3):277-80, Apr 2004. 135. Grenier J et al, Clin Pharmacol Ther 79(3):255-62, Mar 2006. 136. Egashira K et al, Transplantation 75(7):1057. Apr 2003. 137. Rossander L, Scand J Gastroenterol Suppl 129:68-72, 1987. 138. Garcia JJ et al, Contraception 62(5):253-7, Nov 2000. 139. Bansal T et al, Life Sci 83(7-8):250-9, Aug 15, 2008. 140. Chu QP et al, Pharmacol Biochem Behav 86(4):693-8, Apr 2007. 141. Amin A, Hamza AA. Life Sci 77(3):266-78, Jun 3, 2005. 142. Plouzek CA et al, Eur J Cancer 35(10):1541-5, Oct 1999. 143. HommaM et al, J Pharm Pharmacol 47(8):687-92, Aug 1995. 144. Iwata H et al, Drug Metab Dispos, Sept 1, 2004. 145. Wan CK et al, Biochem Pharmacol 72(7):824-37, Sept 28, 2006. 146. Fong WF et al, Planta Medica Feb 22, 2007 (epub ahead of print). 147. Xin HW et al, Br J Clin Pharmacol 64(4):469-75, Oct 2007. 148. Kako M et al, Planta Med 62(5):440-3, Oct 1996. 149. Dandekar UP et al, J Ethnopharmacol 35(3):285-8, Jan 1992. 150. Ohnishi N et al, Biol Pharm Bull 25(11):1461-6, 2002. 151. Dasgupta A et al, Am J Clin Pathol 119(2):298-303, 2003. 152. Lee SS et al, Phytother Research 21(11):1096-9, Nov 2007. 153. Johne A et al, J Clin Psychopharmacol 22(1):46-54, Feb 2002. 154. Andren L et al, Eur J Clin Pharmacol 63(10):913-6, Oct 2007. 155. Burstein AH et al, Clin Pharmacol Ther 68(6):605-12, Dec 2000. 156. Shibayama Y et al, Life Sci 81(2):103-8, Jun 20, 2007. 157. Ruschitzka F et al. Lancet. 355(9203):548-9. 2000. 158. Wang LS et al, Clin Pharmacol Ther 75(3):191-7, Mar 2004. 159. Komoroski BJ et al, Clin Cancer Res 11(19 Pt 1):6972-9, Oct 2005. 160. Wang Z et al, Clin Pharmacol Ther 71(6):414-20, Jun 2002. 161. Xu H et al, Br J Pharmacol 153(7):1579-86, Apr 2008. 162. Smith PF et al, Blood 104(4):1229-30, 2004. 163. Piscitelli SC et al, Lancet 355(9203):547-8, 2000. 164. Mathijssen RH et al. J Natl Cancer Inst. 165. Hu Z et al, Pharm Res 22(6):902-14, Jun 2005. 166. Portoles A et al, J Clin Pharmacol 46(10):1188-94, Oct 2006. 167. Eich-Hochli D et al, Pharmacopsychiatry 36(1):35-7, 2003. 168. Wang Z et al, Clin Pharmacol Ther 70(4):317-26, Oct 2001. 169. Uchida S et al, Biol Pharm Bull 31(2):240-5, Feb 2008. 170. De Maat MM et al, AIDS 15(3):420-1, 2001. 171. Wang XD et al, J Chromatogr B Analyt Technol Biomed Life Sci 852(1-2):534-44, Jun 1, 2007. 172. Wang LS et al, Clin Pharmacol Ther 75(3):191-7, Mar 2004. 173. Hall SD et al, Clin Pharmacol Ther 74(6):525-35, 2003. 174. Pfrunder A et al, Br J Clin Pharmacol 56(6):683-90, Dec 2003. 175. Murphy PA, et al, Contraception 71(6):402-8, Jun 2005. 176. Zhou S et al, J Psychopharmacol 18(2):262-76, Jun 2004. 177. Spinella M. Epilepsy Behav 2(6):524-32, 2001. 178. Dasgupta A et al, Arch Pathol Lab Med 131(7):1094-8, Jul 2007. 179. Kawaguchi A et al, Br J Clin Pharmacol 58(4):403-10, Oct 2004. 180. Sugimoto K et al, Clin Pharmacol Ther 70(6):518-24, Dec 2001. 181. Schwarz UK et al, Clin Pharmacol Ther 81(5):669-78, May 2007. 182. Mai I et al, Nephron Dial Transplant 18(4):819-22, Apr 2003. 183. Hebert MF et al, J Clin Pharmacol 44(1):89-94, Jan 2004. 184. Tannergren C et al, Clin Pharmacol Ther 75(4):298-309, 2004. 185. Yue QY. et al. Lancet. 355(9203):2015-6. 2000. 186. Jiang X et al, Br J Pharmacol 57(5):592-9, May 2004. 187. Holstege CP et al, Med Clin North Am 89(6):1225-7, Nov 2005. 188. Gallo JA Jr, Contemp Anesth Pract 9:7-30, 1987. 189. Aviado DM. J Clin Pharmacol 15(10):641-55, Oct 1975. 190. Lippman SB, Nash K. Drug Saf 5(3):195-204, May-Jun 1990. 191. Aggarwal A, Ades PA. Coron Artery Dis 12(7):581-4, Nov 2001. 192. Drew CD et al, Br J Clin Pharmacol 6(3):221-5, Sept 1978. 193. Reeves RR, Pinkofsky HB. J Fam Pract 45(2):164-6, Aug 1997. 194. Garba M et al. Eur J Drug Metab Pharmacokinet. 28(3):179-84. 2003. 195. Mahmoud BM. J Antimicrob Chemother. 33(5):1005-9. 1994. 196. Bravo L, Nutr Rev 56(11):317-33, Nov 1998. 197. Fujita M et a, Microbiol Immunol 49(4):391-6, 2005. 198. Karan RS et al, J Ethnopharmacol 64(3): 259-64, Mar 1999. 199. Jantan I et al, Phytomedicine 15(4):306-9, Apr 2008. 200. Thurmann PA et al, Int JClin Pharmacol Ther 42(5):281-4, May 2004. 201. Chaplin RL et al, AANA J 75(6):431-5, Dec 2007. 202. Seligmann H et al Clin Neuropharmacol 22(5):268-72, 1999. 203. Drinka PJ, Nolten WE. J Am Geriatr Soc 32(5):405-7, 1984. 204. Mars H, Arch Neurol 30(6):444-7, 1974. 205. Dasgupta A et al, Arch Pathol Lab Med 131(8):1298-303, Aug 2007. 206. Lam et al. Ann Pharmacother. 35(10):1199-201. 2001. 207. Carrillo JA, Benitez J. Clin Pharmacokinet 39(2):127-53, Aug 2000. 208. Pirich C et al, Wien Klin Wochenschr 105(1):3-6, 1993. 209. Grossman E et al, J Cardiovasc Pharmacol 22:22-6, 1993. 210. Hojo Y et al, J Clin Pharm Ther 2010 Nov 8. Epub ahead of print. 211. Nieminen TH et al, Eur J Pain 2010 Sept:14(8):854-9. 212. Liu G et al, Evid Based Complement Altern Med 2011; 2011:207076. 213. Ming ZJ et al, Phytomedicine 17(8-9):575-80, Jul 2010. 214. Yang TH et al, J Nutr Biochem Dec 27, 2010 (epub ahead of print). 215. Salman SA et al, J Clin Pharm Ther 2010 Dec; 35(6):691-6. 216. Chien CF et al, Chem Biol Interact 2010 Mar 30;184(3):458-65. 217. Zhou J. Autophagy 2012 Mar 1; 8(3)(epub ahead of print). 218. Enomoto R et al, Cancer Chemother pharmacol 2011 May; 67(5):1063-72. 219. Wiegman D et al, AIDS 2009; 23(9):1181-5. Naccarato M et al, J Int Assoc Physicians AIDS Care (Chic) 2012 Feb 9 (epub ahead of print). 220. Van strater AC, Bogers JP. Int Clin Psychopharmacol 2012 Mar; 27(2):121-4. 221. Jin J et al, Phytother Res 25(8):1250, 2011. 222. Minocha M et al, Int J Pharm 2011 Jul 15;413(1-2):44-50. 223. Chatterjee M et al, Neurochem Res 2012 Apr;37(4):759-70. 224. Rodrigues M et al, Food Chem Toxicol 2013 Feb;52:121-8. 225. Ali B et al, Indian J Med Res 2012 Apr;135(4):555-9. 226. Jung IH et al, Exp Mol Med 2012 May 31;44(5):311-8. 227. Dai LL et al, Xenobiotica 2013 Mar 1 (epub ahead of print). 228. Rivera CA et al, Pharmacotherapy 2012 Jan 31. Doi:10.1002/PHAR.1018 (epub ahead of
print). 229. Rodrigues M et al, Evid Based Complement Alternat Med 2012;2012:428560. Doi:10.1155/2012/428560. 230. Lee KS et al, Xenobiotica 2013 Mar;43(3):303-10. 231. Spanakis M et al, Pharmacology 2013;91(1-2):112-6. 232. Xue XP et al, Phytother Res Sept 21. Doi:10.1002/ptr.4849 (epub ahead of print). 233. Li R et al, Can J Physiol Pharmacol 2012 Jul;90(7):941-5. Doi:10.1139/y2012-080 (epub 2012 Jun 12). 234. Arafa NM et al, Neurochem Res 2013;38(1):174-85. 235. Hussain A et al, Cancer Biother Radiopharm 2011;26(5):519-27. 236. Poonam T el al, Drug Metabol Drug Interact 2013;28(4):225-30. 237. Dias MC et al, BMO Complement Altern Med 2013 May 1;13:93. 238. Vardy J et al, Springerplus 2013;2(1):126. 239. Shia CS et al, Am J Chin Med 2013;41(6):1427-38. 240. Qin XL et al, Phytomedicine 2015 Jan 21. 241. Acikgoz SK, Acikgoz E. Drug Metabol Drug Interact 2013;28(3):187-9. 242. Mucalo I, 2013. J Evid Based Complement Alternat Med 2014; 2014:969168. 243. Chen EYH et al, Phytother Res 2012; 26:1166-1172. 244. Rodrigues M et al, J Pharm Pharm Sci 2014; 17(3):302-315. 245. Al-Jenoobi FI et al, Pharm Biol 2015; 53(2):296-300. 246. Bhatt C et al, Indian J Pharmacol 2013; 45(2):202-203. 247. Lau WC et al, J Cardiovasc Pharmacol 2011; 57(1): 86-93. 248. C Balap A et al, J Ethnopharmacol 2015, Nov 16. 249. Fong SY et al, J Ethnopharmacol 2015; 170: 106-116. 250. Wang R et al, Eur J Drug Metab Pharmacokinet 2015; Dec 9 (epub ahead of print). 251. Liao S et al, Phytother Res 2016; Jan 22 (epub ahead of print). 252. Kambie B et al, Chem Biol Interact 2016; 245:30-38. 253. Chiang MH et al, Evid Based Complement Alternat Med 2015; 2015:729679. 254. Mekjaraskul C, Sripanidkulchai B, J Nat Med 2015; 69(2):224-31. 255. Gufford BT et al, Drug Metab Dispos 2015; 43(9):1353-1359. 256. Liao S et al, 2016. 257. Balap A et al. Phytother Res 2017;31(1):75-80. 258. Balap A et al, J Ethnopharmacol 2017; 195:214-221. 259. Samojlik I et al, Phytother Res 2016; 30(2):253-259. 260. Yu CP et al, J Pharm Sci 2016; 105(1):343-9. 261. Li H et al, Pharm Biol 2016; 54(12):2886-2894. 262. Vatsavai LK, Kilari EK. J Exp Pharmacol 2016; 8:69-76. 263. Deng Y et al, Phytother Res 2016; 30(11):1886-1892. 264. Awad R et al, Neuro Endocrinol Lett 2016; 37(3):202-206. 265. Yu CP et al, Xenobiotica 2016; 46(8):677-82. 266. Bedada SK et al, Phytother Res 2016; 30(3):397-401. Sun S et al, Pharm Biol 2018; 56(1):104-108. 267. Hassanzadeh-Taheri M et al, J Tradit Complement Med 2017; 8(1):178-183. 268. Maher HM et al, J Chromatogr B Analyt Technol Biomed Life Sci 2017; Apr 1; 1049-1050. 269. Igbinoba SI et al, J Clin Pharmacol. 2015;55(3):348-54. 270. Vaghela M et al, Chem Biol Interact 2017; 278:141-151. 270. Sun S et al, Pharm Biol 2018; 56(1):104-108. 272. Zhou CH et al, Food Chem Toxicol 2018; Feb 26 (epub ahead of print). 273. You BH et al, Phytother Res 2018; Feb 26 (epub ahead of print). 274. Raish M et al, Biomed Pharmacother 2017; 90:694-698. 275. Sahu R et al, J Pharm Biomed Anal 2018; 151:310-316. 276. Zhang X et al, Pharm Biol 2018; 56(1):351-356. 277. Dogra A et al, Phytother Res 2018; 32(10):1967-1974. 278. Santillán-Urquiza MA et al, Biomed Pharmacother 2018; 103:879-888. 279. Rebol B et al, Br J Clin Pharmacol 2019; Jan 30. 280. Olawoye OS et al, J Clin Pharm Ther 2018; 43(5):626-632. 281. Shengule S et al, Biomed Pharmacother 2018; 101:591-598. 282. Zhao Q et al, Xenobiotica 2019; 49(5):563-568. 283. Ma S et al, Evid Based Complement Alternat Med 2018; Oct 18;2018:5651989. 284. Wang Z et al, Pharm Biol 2018; 56(1):269-274. 285. Bedada SK, Boga PK. Eur J Clin Pharmacol. 2017;73(3):343349. 286. Bedada SK, AppaniR, Boga PK. Drug Res (Stuttg). 2017;67(1):46-51. 287. Pattanaik S et al. Phytother Res. 2006;20(8):683-6. 288. Kondo A et al. Biopharm Drug Dispos 2019;40(8):302-306. 289. Kotwai P et al. J Agric Food Chem 2020;68(4):1257-1265. 290. Zhang H et al. Pharm Biol 2019;57(1):306-309. 291. Patel O et al. Front Pharmacol 2019;10:1243. 292. Kiss T et al. BMO Pharmacol Toxicol 2019;20(1);54. 293. Han SY et al. J Ethnopharmacol 2019;238:111892. 294. Fang Y et al. Biomed Res Int 2019;5953619. 295. Choudhary M, Kochhar A, Sangha J. Hypoglycemic and hypolipidemic effect of Aloe vera L. in non-insulin dependent diabetics. J Food Sci Technol. 2014;51(1):90-96. doi:10.1007/ s13197-011-0459-0. 296. Choi BY et al, BMC Complement Altern Med 2017; 17:277. 297. Wang W et al, Int J Nanomedicine 2015; 10:3737-3750. 298. Ahad A et al, Xenobiotica 2020; 50(7):847-857. 299. Kumar R et al, J Ethnopharmacol 2021; 270:113784. 300. Darweesh RS et al, BMC Pharmacol Toxicol. 2020 Nov 16;21(1):77. 301. Siu WS et al, Exp Ther Med 2021 Apr; 21(4):328. 302. Nurfaradilla SA et al, Evid Based Complement Alternat Med. 2020 Jun 17;2020:5013898. 303. Sarangi SC et al, J Ethnopharmacol 2020; 249:112389. 304. Yuan L et al, Evid Based Complement Alternat Med 2020; 2020:2178656. 304. Bhutani P et al, Xenobiotica. 2020 Dec;50(12):1483-1489. 305. Ahn JH et al, Pharmaceutics 2020; 12(6):547. 306. Mekjaruskul C et al, Drug Chem Toxicol 2020; 43(6):602-608. 307. Ye, L. et al. Frontiers in Pharmacology, 2021;12, 773126. 308. Shi Z et al, Current Drug Metabolism, 2022; 10.2174/1389200223666220128143133. 309. Meng D. Am J Chin Med, 2005;33(1), 11–20. 310. Lu Y, et al, BMC Pharmacol Toxicol. 2021;22(1):48. 311. Zhou X et al, Biomed Pharmacother 2021; 138, 111445. 312. Waisundara VY et al, Am J Chin Med 2008; 36:517-540. 313. Abushammala I. Die Pharmazie, 2021;76(10), 468–472. 314. Li, Y. et al, Cellular Physiology and Biochemistry: International J Exp Cell Physiol Biochem & Pharmacol. 2017 42(4), 1657–1669. 315. Xin, H. et al, Methods and Findings in Experimental & Clinical Pharmacology, 2006; 28(1), 25–29. 316. Wu, X. et al. Eur J Clinical Pharmacology, 2005; 61(8), 567–572. 317. Damjanović, A. et al, Molecules (Basel, Switzerland), 2020; 25(22), 5233. 318. Ibrahim Fouad G, et al. Neurochem Res. 2021;46(12):3247-3263. 319. Ibrahim Fouad G, et al, Tissue Cell. 2021;73:101612. 320. Wu YZ, et al. Oxid Med Cell Longev. 2019;2019:2150394. 321. Gao, X. et al, Oncology Reports, 2022; 47(2), 33. 322. Lyu, Y. et al, Life Sciences, 2019; 235, 116818. 323. Zheng F et al, J Cell Mol Med 2018; 22(1):600-612. 324. Hou Q et al, Eur J Clin Pharmacol 2013; 69:1861-1862. 325. Unsal, O. et al. J Oncology Pharmacy Practice: International Society of Oncology. 326. Wang, Z. et al, Chemico-Biological Interactions, 2022;353, 109801. 327. Yu CP et al, J Food Drug Anal 2018; 26(2S):S125-S132. 328. Li H, et al. Pharm Biol. 2016;54(12):2886-2894. 329. Zeng, W. et al, Frontiers in Nutrition, 2022; 9, 850318. 330. Thakkar, D. et al, Biomedical Chromatography : BMC, 2021; 35(11), e5201. 331. Zhai, K. et al, Biomolecules, 2021; 11(12), 1841. 332. More SJ, Tandulwadkar SS, Balap AR, Lohidasan S, Sinnathambi A, Mahadik KR. Effect of Andrographis paniculata extract and Andrographolide on the pharmacokinetics of Aceclofenac and Celecoxib in rats. Futur J Pharm Sci. 2023;9(1):1. 333. Li C, Kim M, Choi H, Choi J. Effects of baicalein on the pharmacokinetics of tamoxifen and
its main metabolite, 4-hydroxytamoxifen, in rats: possible role of cytochrome P450 3A4 and P-glycoprotein inhibition by baicalein. Arch Pharm Res. 2011;34(11):1965-1972. 334. Herman A, Herman AP. Herbal Products and Their Active Constituents Used Alone and in Combination with Antibiotics against Multidrug-Resistant Bacteria. Planta Med. 2023;89(2):168-182. 335. Leino AD, Emoto C, Fukuda T, Privitera M, Vinks AA, Alloway RR. Evidence of a clinically significant drug-drug interaction between cannabidiol and tacrolimus. Am J Transplant. 2019;19(10):2944-2948. 336. Paduch M, Thomason AR. Potential Drug Interactions Between Cannabinoids and Its Derivatives and Oral Anticoagulants. Hosp Pharm. 2022;57(1):188-192. 337. Greger J, Bates V, Mechtler L, Gengo F. A Review of Cannabis and Interactions With Anticoagulant and Antiplatelet Agents. J Clin Pharmacol. 2020;60(4):432-438. 338. He X, Zhang W, Cao Q, et al. Global Downregulation of Penicillin Resistance and Biofilm Formation by MRSA Is Associated with the Interaction between Kaempferol Rhamnosides and Quercetin. Microbiol Spectr. 2022;10(6):e0278222. 339. Liu JM, Li M, Luo W, Sun HB. Curcumin attenuates Adriamycinresistance of acute myeloid leukemia by inhibiting the lncRNA HOTAIR/miR-20a-5p/WT1 axis. Lab Invest. 2021;101(10):1308-1317.340. Yang L, Tsai TH. Neuroprotective effect and herbal-drug pharmacokinetic interaction of Gastrodia elata extract on valproic acid. Biomed Pharmacother. 2022;156:113938. 341. Leite PM, Miranda APN, Gomes I, et al. Antithrombotic potential of Lippia alba: A mechanistic approach. J Ethnopharmacol. 2023;301:115744. 342. Leite PM, Freitas A, Amorim J, et al. In vitro anticoagulant activity of selected medicinal plants: potential interactions with warfarin and development of new anticoagulants. J Basic Clin Physiol Pharmacol. 2021;33(4):499-510. 343. Mansoor K, Bardees R, Alkhawaja B, et al. Impact of Pomegranate Juice on the Pharmacokinetics of CYP3A4- and CYP2C9-Mediated Drugs Metabolism: A Preclinical and Clinical Review. Molecules. 2023;28(5):2117. 344. Hossain S, Yousaf M, Liu Y, Chang D, Zhou X. An Overview of the Evidence and Mechanism of Drug-Herb Interactions Between Propolis and Pharmaceutical Drugs. Front Pharmacol. 2022;13:876183. 345. Shin SC, Choi JS, Li X. Enhanced bioavailability of tamoxifen after oral administration of tamoxifen with quercetin in rats. Int J Pharm. 2006;313(1-2):144-149. 346. Shohan M, Nashibi R, Mahmoudian-Sani MR, et al. The therapeutic efficacy of quercetin in combination with antiviral drugs in hospitalized COVID-19 patients: A randomized controlled trial. Eur J Pharmacol. 2022;914:174615. 347. Chen L, Ji N, Zhang M, Chen W. The Influence of Wuzhi Capsule on the Pharmacokinetics of Cyclophosphamide. Recent Pat Anticancer Drug Discov. 2022;17(2):195-203.348. Wang W, Yang L, Song L, et al. Combination of Panax notoginseng saponins and aspirin potentiates platelet inhibition with alleviated gastric injury via modulating arachidonic acid metabolism. Biomed Pharmacother. 2021;134:111165. 349. Xie Y, Wang C. Herb-drug interactions between Panax notoginseng or its biologically active compounds and therapeutic drugs: A comprehensive pharmacodynamic and pharmacokinetic review. J Ethnopharmacol. 2023;307:116156. 351. Wang L, Huang Y, Yin G, et al. Antimicrobial activities of Asian ginseng, American ginseng, and notoginseng. Phytother Res. 2020;34(6):1226-1236. 352. Zhang Y, Chi X, Wang Z, et al. Protective effects of Panax notoginseng saponins on PME-Induced nephrotoxicity in mice. Biomed Pharmacother. 2019;116:108970. 353. Lopera V, Rodríguez A, Amariles P. Clinical Relevance of Drug Interactions with Cannabis: A Systematic Review. J Clin Med. 2022;11(5):1154. Published 2022 Feb 22. 354. Duan Y, Huang P, Sun L, et al. Dehydroandrographolide ameliorates doxorubicin-mediated cardiotoxicity by regulating autophagy through the mTOR-TFEB pathway. Chem Biol Interact. 2024 Aug 25;399:111132. 355. Lee WH, Kung YY, Sun CK, et al. The anti-COVID-19 drug nirmatrelvir crosses the blood-brain barrier and exhibits herb-drug pharmacokinetic interactions with Scutellaria baicalens formulations. Heliyon. 2024 Jul 20;10(15):e34820. 366 Sun CK, Kung YY, Lee WH, et al. Pharmacokinetic analysis of antiviral drug ritonavir across the blood-brain barrier and its interaction with Scutellaria baicalensis using multisite microdialysis in rats. J Pharm Biomed Anal. 2024 Aug 1;245:116162. 367. Lambert JP, Cormier J. Potential interaction between warfarin and boldo-fenugreek. Pharmacotherapy. 2001 Apr;21(4):509-12. 368. Nachnani R, Knehans A, Neighbors JD, et al. Systematic review of drug-drug interactions of delta-9-tetrahydrocannabinol, cannabidiol, and Cannabis. Front Pharmacol. 2024 May 22;15:1282831 369. Evans AA, Jesus CHA, Martins LL, et al. Pharmacological Interaction Between Cannabidiol and Tramadol on Experimental Diabetic Neuropathic Pain: An Isobolographic Analysis. Cannabis Cannabinoid Res. 2024 Jun;9(3):728-739. 370. Wu H, Xie S, Chen X, et al. Development of UPLC-MS/MS method for studying the pharmacokinetic interactions of fuzuloparib with curcumin in rats. J Pharm Biomed Anal. 2024 Oct 15;249:116383. 371. Thongpon P, Intuyod K, Chomwong S, et al. Curcumin synergistically enhances the efficacy of gemcitabine against gemcitabine-resistant cholangiocarcinoma via the targeting LAT2/glutamine pathway. Sci Rep. 2024 Jul 11;14(1):16059. 372. Dibaei M, Hosseini A, Lavasani H, et al. Assessment of metabolic interaction between curcumin and tramadol using the isolated perfused rat liver. Heliyon. 2024 Jul 23;10(15):e35070. 373. Lambert JP, Cormier J. Potential interaction between warfarin and boldo-fenugreek. Pharmacotherapy. 2001 Apr;21(4):509-12. 374. Ndu CC, Abotsi WKM, Mante PK. Investigation of Herb-Drug Interactions between Xylopia aethiopica, Its Principal Constituent Xylopic Acid, and Antidepressants. Adv Pharmacol Pharm Sci. 2024 May 25;2024:9923801. 375. Yu CP, Li PY, Chen SY, et al. An acute herb-drug interaction of Magnoliae Officinalis Cortex with methotrexate via inhibiting multidrug resistance-associated protein 2. J Food Drug Anal. 2024 Mar 15;32(1):103-111. 376. Chen HY, Wu TS, Su SF, et al. Marked decrease of cyclosporin absorption caused by phellamurin in rats. Planta Med. 2002 Feb;68(2):138-41. 377. Cheng Z, He Y, Chen Y, Zhao G, Liu Y, et al. MechanismBased Inactivation of CYP2D6 by Phellopterin and Related Drug-Drug Interaction with Metoprolol. J Agric Food Chem. 2024 Jan 24;72(3):1745-1755. 378. Patel R, Stine A, Zitko K. Enhanced Anticoagulant Effect of Warfarin When Co-administered With Quercetin. J Pharm Technol. 2022 Dec;38(6):374-375. 379. Ahmad E, Jahangir M, Ismail MA, et al. Influence of Quercetin Pretreatment on Pharmacokinetics of Warfarin in Rats. Curr Drug Saf. 2023;18(4):547-554. 380. Huang S, Song W, Jiang S, et al. Pharmacokinetic interactions between tacrolimus and Wuzhi capsule in liver transplant recipients: Genetic polymorphisms affect the drug interaction. Chem Biol Interact. 2024 Mar 1;391:110906.
The aviation environment is complex and demanding on human performance. Everyone who works in aviation needs “a clear head”, good mental alertness, unimpaired vision and balance, the ability to concentrate (often for long periods), the ability to respond quickly and appropriately to emergencies, and good coordination and motor skills. Medicines which interfere with these safety requirements must not be taken prior to, or while on, duty. These include products which cause:
• behaviour problems, including excitement or agitation
• sedation
• memory, concentration, vigilance impairment
• locomotor impairment, tremor
• disturbances of the special senses, particularly vision and balance. Some non-prescription medicine ingredients such as antihistamines, even some labelled as non-sedating, can have significant side effects which may compromise safety in the aviation workplace.
Many common products may not be safe to use. These include products used to treat:
• abdominal pain
• colds
• diarrhoea
• hay fever
• itchy eyes
• motion sickness
• pain or inflammation
• smoking addiction (ie, varenicline).
All over-the-counter medication or health preparations should be regarded with caution, including preparations used for body-building, which may contain anabolic steroids. Complementary remedies, including Chinese herbals and even homeopathic remedies may be unsafe as their content is not subject to the same stringent requirements as registered medicines, or they may cause side effects such as drowsiness,
or interfere with other medicines the person may be taking.
Medicine side effects can be further aggravated in the flight environment when combined with other environmental stressors such as hypoxia, reduced barometric pressure, accelerations, noise, and reduced humidity and temperature. There are other aggravating factors to consider, such as working at night, jet lag and fatigue. Interactions with prescription medicines should also be considered. An important factor is the condition being treated. A pilot requiring treatment may be unable to safely exercise the privileges of any licence held.
It is essential that anyone involved in prescribing or recommending medicines for aviation workers ensures patients/purchasers are cautioned about possible adverse side effects and safety implications in the workplace. This applies to products such as medicinal cannabis, which are generally not compatible with flying.
Individuals are ultimately responsible to establish the safety of the medicines they are taking. It is best to seek medical opinion, preferably from a medical examiner designated by the Civil Aviation Authority, and inform their operations manager. It may be necessary to declare that they are unfit for flying or Air Traffic Control duties. The safety of the individual, co-workers and passengers depends on responsible and informed users of non-prescription and medically prescribed drugs or complementary remedies.
Licence holders should be aware of their obligation under Section 27C of the Civil Aviation Act – see www.caa.govt.nz. In particular, licence holders are reminded of their duty to report any change of medical condition to the Director of Civil Aviation (preferably via their Medical Examiner), unless it is a temporary condition specifically exempted by the Director of Civil Aviation in a General Directions notice (GD).
Civil Aviation Authority of NZ central medical unit help desk: 04 560 9466 or med@caa.govt.nz
REVIEWED BY Dr Claude Preitner, Senior Medical Officer, Civil Aviation Authority of New Zealand, August 2024.

Medical professionals need to exercise caution when treating athletes because many medications are not permitted for use in sport.
Athletes at any level may be subject to drug testing, and those whose samples test positive for banned substances may face a ban from all sport. Testing may be conducted at a competition or event or out-ofcompetition when an athlete is training, travelling, or at home. Athletes have a responsibility to inform every doctor or specialist treating them that they are subject to drug testing in sport.
The Sport Integrity Commission Te Kahu Raunui (the Commission) is responsible for New Zealand’s anti-doping programme. They provide information on medications, their status in sport, and related anti-doping processes.
The Prohibited List
Medications that are banned in sport are listed in the World Anti-Doping Agency’s Prohibited List which is published on January 1st each year. Read the Prohibited List at sportintegrity.nz/prohibited
Check the status of all medications before prescribing to an athlete. If unsure whether something is banned in sport, you can check by:
• searching for the medication on Global Drug Reference Online (Global DRO) at globaldro.com
• calling the Commission on 0800 378 437.
If a medicine is banned in sport, check if there is an appropriate permitted alternative. If not, check that the athlete is aware that they may require a Therapeutic Use Exemption (TUE). Check a medication at sportintegrity.nz/medications
If an athlete has one or more of the following conditions it is likely that prohibited substances will be part of the recommended treatment:
• ADHD
• asthma (maximum thresholds can apply)
• cardiovascular disease
• diabetes
• severe acne and other severe skin conditions
• severe hay fever or other allergic reactions.
Athletes who require anaesthesia, surgery or dental work are also likely to require medication which is prohibited in sport. Check the status of common medications at sportintegrity.nz/commonmeds
In-advance for certain athletes
Certain high-level athletes need to apply for a TUE before they take medication containing a prohibited substance. If an athlete meets any of the following criteria, they will need a TUE in advance of competing:
• selected in a New Zealand Olympic, Paralympic, or Commonwealth Games Team
• registered, qualified, selected, named, or contracted for any of the listed teams or events as per the Commission’s website.
The TUE application form and all supporting medical records must be submitted to the Commission (or the athlete’s International Federation if applicable).
The athlete must wait for TUE approval before using the medication unless the situation is an emergency whereby the athlete’s health is at great risk. In these circumstances, a TUE application should be submitted as soon as possible once the situation is resolved.
for others
Athletes who compete in sports or at levels not defined by the Commission can apply for a TUE retrospectively. They will require a full medical file supporting the diagnosis in the event of adverse analytical finding results from testing. Find TUE information at sportintegrity.nz/tue
The Commission advises athletes that they take supplements at their own risk. It warns athletes to be wary of supplements for the following reasons:
• supplements are not manufactured to the same rigorous standards as pharmaceuticals
• some supplements may be cross-contaminated with prohibited substances MEDICINE
Salbutamol by inhalation (eg, Asthalin, Respigen, Ventolin)**
Salmeterol by inhalation (eg, Meterol, Serevent)**
eFormoterol by inhalation (eg, Oxis, Foradil, Symbicort, Vannair)**
Glucocorticoids by inhalation (eg, Beclazone, Flixotide, Pulmicort) Permitted
Terbutaline (eg, Bricanyl)
required from IF
required from the Commission TUE required retrospectively if a positive test occurs
Systemic salbutamol (eg, Ventolin) TUE required from IF TUE required from the Commission TUE required retrospectively if a positive test occurs
Systemic glucocorticoids (eg, prednisone – oral, parenteral, intramuscular, rectal)*** TUE required from IF for in-competition use
Nasal/eye/ear/topical corticosteroids Permitted
required from the Commission TUE required retrospectively if a positive test occurs
Note: IF stands for the athletes’ International Federation – we advise International Level athletes to check their IF’s criteria online when a TUE is required.
** Thresholds exist. If used at standard prescription dosages, the threshold should not be exceeded.
*** Washout periods exist. Please be aware that administration around competition periods may mean some substances are still detectable. For further information please

• labelling laws are not the same in all countries meaning that some ingredients may not be listed
• manufacturing standards vary greatly around the world and some supplement manufacturers use phrases such as “pharmaceutical standards” or “approved by XXX sports league”. This does not mean they are safe for use in sports.
• The Commission has a Supplement Decision Making Guide available at sportintegrity.nz/supplement-guide
PERMITTED AND PROHIBITED
CONDITION PERMITTED
Cough, cold, flu, sore throat
Diarrhoea or vomiting
Hay fever
Pain/inflammation/ headache
Skin conditions
* Prescription medicines
If you have any questions about medications, TUE’s or other anti-doping matters, please contact the Commission.
Phone: 0800 378 437 | Email: admin@sportintegrity.nz
Website: sportintegrity.nz
Reviewed by The Sport Integrity Commission Te Kahu Raunui, August 2024.
Anaesthetic throat sprays/lozenges containing benzocaine or lignocaine
Antihistamines (see hay fever below)
Aspirin, benzydamine, or non-steroidal anti-inflammatories (see pain below)
Cough medicines containing bromhexine, dextromethorphan, guaiphenesin, or pholcodine and no prohibited medicines
Phenylephrine
Antinausea medications, such as hyoscine/scopolamine (Scopoderm TTS), prochlorperazine
Loperamide (eg, Diamide, Imodium)
All antihistamines (eg, cetirizine, dexchlorpheniramine, fexofenadine, levocetirizine, loratadine, promethazine)
Glucocorticoid nasal sprays (eg, beclomethasone, budesonide, fluticasone, triamcinolone)
Oxymetazoline, xylometazoline
All non-steroidal anti-inflammatories (eg, aspirin, ibuprofen, diclofenac, naproxen)
Combination analgesics that include codeine with other permitted medicines (eg, Mersyndol, Nurofen Plus, Panadeine)*
Paracetamol
Products containing caffeine (eg, Panadol Extra, Parafast Extra)
Topical hydrocortisone preparations (eg, Derm-Aid)
EXAMPLES OF PROHIBITED MEDICINES
All pseudoephedrine products are prohibited in competition. The Commission recommends athletes consider using products that contain phenylephrine as a permitted alternative
Products containing morphine
Alcohol is prohibited in-competition in certain sports
All pseudoephedrine products are prohibited in competition
Oral prednisone
In-competition, all medicines containing tramadol, morphine, pethidine, fentanyl, oxycodone, etc are prohibited
Glucocorticoids (eg, methylprednisolone, prednisone) administered by any oral, injectable, or rectal route are prohibited in-competition
Oral/systemic glucocorticoids (eg, methylprednisolone, prednisone) are prohibited in-competition
Note: The intravenous (IV) infusion and/or injection of more than 100mL per 12-hour period of any substance is a prohibited method, even if the substance itself is not prohibited, unless it is received while being treated in a hospital, during surgery, or during clinical diagnostic investigations.

Any drug which could influence the physiology or psychology of an individual may well impact on diving and diving safety. If a person has a condition which is a contraindication to diving, it is better not to dive than to take a medicine to ameliorate the symptoms.
The following classes of drugs may be unsafe to use while diving.
Analgesics
Analgesics may contain other ingredients, for example, sedating antihistamines such as doxylamine. These ingredients may cause drowsiness or contribute to the deterioration in mental function associated with nitrogen narcosis.
Bronchodilators
Theophylline may be associated with cardiac arrhythmias and central nervous system effects such as anxiety and restlessness. Salbutamol is short-acting and may stop working during diving. Diving should be avoided if a bronchodilator is considered necessary.
Decongestants (short acting)
Short-acting decongestants such as phenylephrine or pseudoephedrine may wear off during the dive, and cause a reverse block. Although their use by divers is widespread, decongestant use may encourage diving with underlying conditions that are contraindicated, for example, upper respiratory tract infections or allergies.
Decongestants can cause tachycardia, and vertigo or disorientation have also been reported during diving.
Earwax softening drops
Although the use of earwax softening drops is not contraindicated for diving, earwax should be removed before diving.
Nicotine/smoking
Nicotine increases production of carboxyhaemoglobin, which lowers the oxygen-carrying capacity of the blood, and causes an overall decrease in cardiovascular fitness. The acute effect of nicotine is to increase heart rate and blood pressure.
Smoking also increases mucus production and reduces the ability for the lungs to clear secretions, which could increase the risk of air trapping and pulmonary barotrauma.
Recreational drugs
All recreational drugs such as alcohol, marijuana, cocaine, opiates, etc., are strongly advised against when diving.
Sedating drugs
Antihistamines used for allergy or as an antiemetic could cause drowsiness or contribute to the deterioration in mental function associated with nitrogen narcosis.
Herbal remedies
Herbal remedies should be avoided in combination with diving, as many of these are inadequately labelled as to their contents. Some “herbal” remedies have been found to contain steroids, opiates and even Viagra. Anyone intending to dive after having taken ANY kind of medicine should first seek a medical opinion, preferably from a Dive Doctor.
REVIEWED BY Dr Chris Sames, Senior Medical Officer, Slark Hyperbaric Unit, Waitemata DHB, August 2024.

When talking to women of childbearing age, determine if it is appropriate to enquire about the possibility of pregnancy, because this can affect medicine choice. If a woman is pregnant, consider non-pharmacological interventions and lifestyle advice first. In general, OTC medicines should be avoided if possible, particularly during the first 12 weeks of pregnancy, although some may not be appropriate at any stage.
• The first 8 to 12 weeks are the most vulnerable for the foetus in terms of risk of malformations because this is the period during which the major organs including the brain, heart, and lungs; neural pathways; and limbs start to form. The embryo is connected to the mother’s blood supply and anything she ingests can be transferred to the growing baby.
• OTC medicines should only be considered if the benefit to the mother outweighs the potential risk to the foetus.
• Only consider medicines or products that have been widely used in pregnancy with a good safety record.
• Women with severe or persistent symptoms of any kind should be referred to their LMC or doctor.
• If any medicine needs to be given, give the lowest effective dose for the shortest possible time.
• Use topical preparations, if available, to minimise systemic exposure, but absorption may be significant if used on a large area, eg, methyl salicylate.
Non-pharmacological treatments for pain relief include rest, hot and cold compresses, massage, strapping, or neoprene support belts.
• One-off or intermittent doses of paracetamol may be given. A 2019 study* showed paracetamol use during pregnancy was not associated with a higher risk of asthma in children.
• NSAIDs are contraindicated from the 28th week of pregnancy, but there is controversy as to whether they can be used before then, with the New Zealand Formulary advising that there is a risk in the first and third trimesters.
Apply ointment, such as white soft paraffin or cellulose and peppermint
powder around the nose to trap dust and pollen. Saline nasal sprays or steam inhalation can help relieve congestion. Intranasal corticosteroids, such as fluticasone, may be considered for severe symptoms. Secondline options include non-sedating antihistamines such as cetirizine or loratadine, or cromoglycate. Avoid oral or nasal decongestants, eucalyptus oil, and menthol.
Coughs and colds
Use non-medicated lozenges, lemon and honey drinks, saline nasal sprays, intermittent paracetamol, and steam inhalations.
Head lice treatment
Wet combing using conditioner (see Head Lice chapter) can be effective if done every three days until no more lice are seen; otherwise, a dimethicone head lice treatment may be considered.
Conjunctivitis
Irritation and discomfort can be reduced by wiping the eyes with a clean flannel and cool water, using warm compresses, and instilling lubricating eye drops. Data are lacking about the use of chloramphenicol eye drops during pregnancy.
Insect bites and stings
Reduce swelling by applying a cool compress. Lignocaine or hydrocortisone creams (0.5% or 1%) may be used short-term to relieve itch and one-off paracetamol taken to relieve pain.
Useful websites:
• Prescribing medicines in pregnancy, online database, TGA Australia: tga.gov.au/prescribing-medicines-pregnancy-database
REVIEWED BY Carmen Pope Editorial Pharmacist August 2024
* Shaheen SO, Lundholm C, Brew BK,Almqvist C. Prescribed analgesics in pregnancy and risk of childhood asthma. Eur Respir J.2019;53(5):pii:1801090. doi: 10.1183/13993003.01090-2018.

Many medicines can affect driving, and it is an offence to drive a motor vehicle while impaired as a result of taking a prescription medicine or specified controlled drug.
On 11 March 2023, The Land Transport (Drug Driving) Amendment Act 2022 came into force, and this is part of the ‘Road to Zero’ strategy.
Key changes include a list of 25 qualifying drugs (4 illicit drugs and 21 prescription medicines) with specified high-risk blood concentration levels for drug-driving offences (see Schedule 5 of the Amendment Act, 2022, for the detailed list). These drugs have been identified as having the highest risk to road safety and include benzodiazepines, codeine, THC, and zopiclone.
Police can stop drivers at random for drug or alcohol testing. People will be required to take a blood test if they fail a Compulsory Impairment Test (this is a behavioural test that checks for impairment). This will measure blood concentration levels for Schedule 5 drugs.
The blood concentration determines the type of offence, which may be a fine, demerit points, licence disqualification, or a criminal conviction.
If a qualifying drug is identified, then a medical defence can be used for
prescription medicines if the following criteria are met:
• the driver can show that the medicine has been taken according to a current and valid prescription from a health practitioner, and
• they have followed the instructions from a health practitioner or manufacturer of the medicine.
Pharmacists should use the PSNZ Cautionary and Advisory Label number 1, rather than the shortened computer-generated message, on all medicines likely to cause sedation.
This written warning that “This medicine may make you sleepy and make it dangerous to drive or operate machinery” should also be supported by clear, verbal advice to ensure patients understand the significance of the information. If impaired, the person must not drive.
REVIEWED BY: Carmen Pope, Editorial Pharmacist, August 2024
References
New legislation about medicines that can impair driving. 2 March 2023. Medsafe. medsafe.govt.nz/safety/Alerts/driving-impairment.asp
Schedule 5. Land Transport (Drug Driving) Amendment Act 2022. legislation.govt.nz/act/public/2022/0005/latest/LMS378964.html
ADHD New Zealand
Phone: (09) 625 1754
Email: info@adhd.org.nz adhd.org.nz
Age Concern New Zealand
Freephone: 0800 652 105
Email: locations via website ageconcern.org.nz
Alcoholics Anonymous New Zealand
Freephone: 0800 229 6757
Email: help@aa.org.nz aa.org.nz
Allergy NZ
Freephone: 0800 34 0800
Phone: (09) 623 3912
Email: allergy@allergy.org.nz allergy.org.nz
Alzheimers NZ
Freephone: 0800 004 001
Email: admin@alzheimers.org.nz alzheimers.org.nz
Arthritis NZ
Freephone: 0800 663 463
Email: info@arthritis.org.nz arthritis.org.nz
Asthma New Zealand
Phone: (09) 623 0236
Email: anz@asthma.org.nz asthma.org.nz
Asthma & Respiratory Foundation NZ
Freephone: 0800 100 506
Phone: (04) 499 4592
Email: info@asthmaandrespiratory.org.nz asthmafoundation.org.nz
Autism NZ Inc
Freephone: 0800 288 476
Phone: (04) 803 3501
Email: info@autismnz.org.nz autismnz.org.nz
Barnardos NZ (National Office)
Phone: locations via website
Email: nationaloffice@barnardos.org.nz barnardos.org.nz
Blind Low Vision
Freephone: 0800 24 33 33
Email: info@blindlowvision.org.nz blindlowvision.org.nz
Bowel Cancer New Zealand
Freephone: 0800 226 901
Email: info@bowelcancernz.org.nz bowelcancernz.org.nz
Burnett Foundation Aoteoroa (HIV, MPOX)
Phone: (09) 303 3124
Email: contact@burnettfoundation.org.nz burnettfoundation.org.nz
Cancer Society of NZ
Freephone: 0800 226 237
Email: info@cancersoc.org.nz cancernz.org.nz
Continence NZ
Helpline: 0800 650 659
Email: info@continence.org.nz continence.org.nz
Crohn’s and Colitis New Zealand
Freephone: 0800 275 423 (0800 ASK IBD) Email: info@crohnsandcolitis.org.nz crohnsandcolitis.org.nz
Cystic Fibrosis NZ
Freephone: 0800 651 122 Email: info@cfnz.org.nz cfnz.org.nz
Cure Kids
Phone: (09) 370 0222 Email: admin@curekids.org.nz curekids.org.nz
Diabetes NZ
Freephone: 0800 342 238 (0800 DIABETES)
Email: via website diabetes.org.nz
Eating Disorders Association New Zealand (EDANZ)
Freephone: 0800 233 269 (0800 2 EDANZ)
Email: info@ed.org.nz ed.org.nz
Endometriosis New Zealand
Phone: (03) 379 7959
Email: info@nzendo.org.nz nzendo.org.nz
Epilepsy NZ
Freephone: 0800 37 45 37
Email: via website epilepsy.org.nz
Family Planning
Phone: via website (varies due to area) Email: national@familyplanning.org.nz familyplanning.org.nz
The Federation of Disability Information Centres
Phone: 0800 693 342 Email: admin@thefederation.nz thefederation.nz
Fertility NZ
Freephone: 0800 333 306 Email: support@fertilitynz.org.nz fertilitynz.org.nz
Healthline
Free 24-hour health advice (all ages) Freephone: 0800 611 116 health.govt.nz
Heart Foundation
Freephone: 0800 863 375 Phone: (09) 571 9191
Email: via website heartfoundation.org.nz
The Hepatitis Foundation of New Zealand
Freephone: 0800 33 20 10
Email: hepteam@hfnz.nz hepatitisfoundation.org.nz
KidsCan
Phone: (09) 478 1525 kidscan.org.nz
Kidney Health New Zealand
Freephone: 0800 543 639
Email: info@kidney.health.nz kidney.health.nz
La Leche League New Zealand
Phone: via website (varies due to area)
Email: help@lalecheleague.org.nz lalecheleague.org.nz
Leukaemia and Blood Cancer
New Zealand
Freephone: 0800 15 10 15
Phone: (09) 638 3556
Email: info@leukaemia.org.nz leukaemia.org.nz
Lifeline
Freephone 24/7: 0800 543 354
Text HELP to 4357
Suicide Crisis Helpline: 0508 828 865 lifeline.org.nz
Look Good Feel Better
Freephone: 0800 865 432
Email: info@lgfb.co.nz lgfb.co.nz
Myalgic encephalomyelitis (ME)/ Chronic Fatigue syndrome – ANZMES
Phone: (09) 269 6374 or (03) 471 6203
Email: info@anzmes.org.nz anzmes.org.nz
Mental Health Foundation of NZ
Phone: (09) 623 4810 (reception)
Email: mhfadmin@mentalhealth.org.nz
Text: 1737 mentalhealth.org.nz
Miscarriage Support
Phone: (0508) 72 63 72 miscarriagesupport.org.nz
Motor Neurone Disease Association
Phone: 0800 444 474
Email: via website mnd.org.nz
Multiple Sclerosis New Zealand
Freephone: 0800 675 463 (0800 MS LINE) Phone: (03) 366 2581
Email: via website www.msnz.org.nz
Muscular Dystrophy New Zealand
Freephone: 0800 800 337 Email: info@mda.org.nz www.mda.org.nz
National Foundation for the Deaf & Hard of Hearing
Freephone: 0800 867 446
Phone: (09) 307 2922
Email: enquiries@nfd.org.nz nfd.org.nz
Neurological Foundation
Freephone: 0508 272 467 (0508 BRAINS) Phone: (09) 309 7749
Email: info@neurological.org.nz neurological.org.nz
NZ Nutrition Foundation
Email: via website nutritionfoundation.org.nz
Osteoporosis New Zealand
Phone: (04) 499 4862
Email: info@osteoporosis.org.nz osteoporosis.org.nz
Parents Centre Aotearoa
Phone: (04) 233 2022
Email: info@parentscentre.org.nz www.parentscentre.org.nz
Parkinson’s New Zealand
Freephone: 0800 473 4636
Email: info@parkinsons.org.nz parkinsons.org.nz
Plunket
Freephone 24/7: 0800 933 922
Email: via website plunket.org.nz
Prostate Cancer Foundation NZ Freephone: 0800 660 800 Email: via website prostate.org.nz
Quitline Me Mutu
Freephone: 0800 778 778 Text QUIT to 4006 quit.org.nz
Stroke Foundation NZ
Freephone: 0800 78 76 53 (0800 STROKE)
Email: strokenz@stroke.org.nz stroke.org.nz
Suicide Crisis Helpline (Lifeline Aotearoa)
Freephone 24/7: 0800 543 354 Text HELP to 4357 lifeline.org.nz
Acne
Allergies
Baby Care
Childhood
Colds
LEMSIP
LEMSIP
Coughs
Cuts, Abrasions and Blisters
Diarrhoea
Eye Conditions
Eye Conditions
Haemorrhoids
AFT PHARMACEUTICALS LTD
Presentation: Cream. 10g, 15g tubes
Active Ingredients: Lipid stabilised hydrogen peroxide 1% w/w
Approved Indications: Treatment and prevention of minor skin infections such as acne, cuts, scrapes, burns or school sores.
Contraindications: Known hypersensitivity to any ingredient.
Precautions: Use under medical guidance in pregnancy and breastfeeding. Avoid contact with the eyes. Do not use in the presence of iodine, permanganate and any other strong oxidising agents.
Adverse Effects: Mild sensation of burning may be experienced for a short time after application.
Directions: After cleansing the area, apply cream 2-3 times daily on affected area. A dry film will appear on the skin after application, which can be washed off with water.
Price Band: $10 - $20. Available on Pharmaceutical Schedule.
Subsidy Conditions: Fully subsidised (10g only)
Medicine Classification: General Sale
AFT PHARMACEUTICALS LTD
Presentation: Tablet. 30s
Active Ingredients: Loratadine 2.5mg and phenylephrine hydrochloride 10mg
Indications: For the temporary relief of nasal and sinus congestion, hayfever, runny nose, watery and itchy eyes and sneezing.
Contraindications: Hypersensitivity to Phenylephrine, severe hypertension, coronary heart disease, narrow angle glaucoma, prostate hyperplasia, hypersensitivity to loratadine.
Precautions: Do not use in children under 12 years. Prolonged or excessive use may be harmful.
Adverse Effects: Phenylephrine may cause insomnia or sleeplessness in some people.
Directions: Adults and children over 12 years: One tablet four times daily. Do not exceed the recommended dosage.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: Pharmacy Only Medicine
CARE PHARMACEUTICALS PTY LTD
Presentation: Infant eye wipes.
Indications: Removes secretions, crusted matter and residue from around the eyes.
Precautions: Do not use if the sachet is open, damaged or marked.

Ingredients: Water, Polysorbate 20, Disodium Phosphate, Lauryl Glucoside, Sodium Chloride, Sodium Phosphate, PVP, Disodium EDTA, Chamomilla Recutita (Matricaria) Flower Extract, Caprylic/Capric Triglyceride, Glycerin.
Directions: Use a separate sterilised wipe for cleansing each eye and use a clean wipe for each application. Tear open sachet and unfold the Little Eyes wipe. Wipe from the inner corner of the eye (next to the nose) toward the outer corner. Use a clean area of the wipe so that drainage being cleaned away is not rubbed back across the eye. Take care to cleanse in between the lashes and sides of the eyelid. Do not wipe along inner eyelid. After use dispose of Little Eyes wipe in a suitable container and then wash your hands.
Price Band: RRP $21.15
Subsidy Conditions: Not subsidised
Classification: Cosmetics
RECKITT BENCKISER (NZ) LTD
Presentation: Suspension. Strawberry + Orange 200ml, Strawberry 100ml
Active Ingredients: Ibuprofen 100mg/5mL
Approved Indications: For reduction in temperature for up to 8 hours including fever caused by immunisation. For the temporary relief of pain associated with teething, toothache, earache, sore throats, headache, minor aches, sprains & strains, cold and flu symptoms.
Contraindications: Use in babies < 3 months of age, impaired kidney or liver function, stomach disorders or stomach ulcers, heart problems, allergy to aspirin ibuprofen or other anti-inflammatory medicines, last 3 months of pregnancy.
Precautions: Use in children <1 year of age, asthma, varicella, concomitant use of anti-inflammatories or regular medications, dehydration through diarrhoea and/or vomiting, in women trying to conceive or first 6 months of pregnancy, >65 years of age, use >3 days.
Directions: 3-4 mL (in those aged 3-6 months/6-8-kg), 4-5 mL (in those aged 6-12 months/8-10kg), 5-7mL (in those aged 1-3 years/10-14kg), 7-9 mL (in those aged 3-5 years/14-18-kg), 9-11 mL (in those aged 5-7 years/18-22kg), 11-14 mL (in those aged 7-9 years/22-28kg), 14-20 mL (in those aged 9-12 years/28-40kg). Repeat dose every 6 to 8 hours as necessary (max. 3 doses in 24 hours).
Price Band: $13 - $20 (Price varies with pack size)

Subsidy Conditions: Not subsidised Medicine Classification: Pharmacy Only Medicine TAPS DA2249CO Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Suspension Liquid 5-12 Years. Orange + Strawberry 200ml, Strawberry 100ml
Active Ingredients: Ibuprofen 200mg/5mL
Approved Indications: For reduction in temperature for up to 8 hours including fever caused by immunization. For the temporary relief of pain associated with teething, toothache, earache, sore throats, headache, minor aches, sprains and strains, cold and flu symptoms.
Contraindications: Use in babies < 3 months of age, impaired kidney or liver function, stomach disorders or stomach ulcers, heart problems, allergy to aspirin ibuprofen or other anti-inflammatory medicines, last 3 months of pregnancy.
Precautions: Use in children <1 year of age, asthma, varicella, concomitant use of anti-inflammatories or regular medications, dehydration, in women trying to conceive or first 6 months of pregnancy, >65 years of age, use >3 days.
Directions: 4.5-5.5mL (in those aged 5-7 years/18-22kg), 5.5-7mL (in those aged 7-9 years/22-28kg), 7-10mL (in those aged 9-12 years/2840kg). Repeat dose every 6 to 8 hours as necessary (max. 3 doses in 24 hours).
Price Band: $26 - $40 (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: Pharmacy Only Medicine TAPS DA2249CO Reckitt Benckiser, Auckland
Presentation: Soft Chewable Capsules. 12s & 24s Active Ingredients: Ibuprofen 100mg
Approved Indications: For the temporary relief of mild to moderate pain such as sore throat, dental pain, earache, headache, minor aches, sprains and strains and the pain of cold and flu. Reduces fever.
Contraindications: Stomach ulcer, impaired kidney or liver function or heart failure, allergy to ibuprofen or other antiinflammatory medicines, last 3 months of pregnancy.
Precautions: use > 3 days at a time, age < 7 years, children and adolescents suffering from dehydration through diarrhoea and/or vomiting, asthma, chickenpox (varicella), use with products containing ibuprofen, aspirin or other anti-inflammatory medicines taken regularly, age 65 years and over, if trying to become pregnant, during the first 6 months of pregnancy.


Directions: Doses should be given as necessary every 6 to 8 hours (or with a minimum of 6 hours between each dose if required). For children aged between 7 and 10 years (average weight of 22-32 kg): 2 capsules (max. 8 in 24 hours). For children aged between 10 and 12 years (average weight 32-40kg): 3 capsules (max. 12 in 24 hours). Children should take plenty of fluids.
Price Band: $10 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: Pharmacy Only Medicine
RECKITT BENCKISER (NZ) LTD
Presentation: Capsules. 16s
Active Ingredients: Paracetamol 500mg, phenylephrine hydrochloride 6.1mg, guaifenesin 100mg
Indications: Temporary relief of colds and flu, chesty cough and chest congestion. Includes relief of blocked and runny nose, headache, sore throat, fever and body aches and pains.
Contraindications: Age < 12 years, Porphyria, breastfeeding, concomitant use with paracetamol-containing products.
Precautions: Concomitant use of medicines intended to treat symptoms of the common cold, Use > 48 hours (adolescents and children > 12 years), use > a few days (adults), pregnancy, hypertension, liver, kidney or heart problems, concomitant antidepressant use.
Directions: Adults and children over 12 years: 2 capsules. Dosage maybe repeated every 4-6 hours as necessary, Maximum 8 capsules in 24 hours
Price Band: Under $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale

RECKITT BENCKISER (NZ) LTD
Presentation: Satchet. 10s. Available in lemon and menthol lemon flavour.
Active Ingredients: Paracetamol 1000mg, phenylephrine hydrochloride 12.2 mg, guaifenesin 200mg
Indications: For temporary relief of colds and flu, chesty cough and chest congestion, includes the relief of blocked and runny nose, headache, sore throat, fever and body aches and pains.
Contraindications: Age 12 years and under, concomitant use with paracetamol-containing products, breastfeeding, porphyria.
Precautions: Concomitant use of medicines intended to treat symptoms of the common cold, concomitant paracetamol use, use > 48 hours (adolescents and children > 12 years), use > a few days (adults), pregnancy, hypertension, liver, kidney or heart problems, concomitant antidepressant use, phenylketonuria.
Directions: Adults and children over 12 years: 1 sachet every 4-6 hours. Maximum 4 sachets in 24 hours. Dissolve in a cup of hot but not boiling water. Do not take more than 1 sachet per dose.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT Reckitt Benckiser, Auckland
LTD
Presentation: Capsule. 16s
Active Ingredients: Each capsule contains paracetamol 500mg, phenylephrine hydrochloride 6.1mg
Indications: FFor the temporary relief of cold and flu, including blocked or runny nose, headache and fever, sore throat, body aches and pains, and is non-drowsy.
Contraindications: Use <12 years, breastfeeding, concomitant use with paracetamol-containing products.
Precautions: Concomitant use of medicines intended to treat the symptoms of the common cold; concomitant paracetamol use; use > 48 hrs (adolescents and children > 12 years); use > a few days (adults); pregnancy; hypertension; liver, kidney or heart problems; concomitant antidepressant use, phenylketonuria.
Directions: Swallow whole with water. Do not chew. Adults and children over 12 years: 2 day capsules up to 3 times a day, dosage may be repeated every 4-6 hours as necessary. 2 night capsules at night. Maximum 6 day capsules and 2 night capsules in 24 hours. Do not give to children 12 years and under.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT Reckitt Benckiser, Auckland
Presentation: Capsule. 16s
Active Ingredients: Paracetamol 500mg, phenylephrine hydrochloride 6.1mg, caffeine 25mg (day capsules); paracetamol 500mg, phenylephrine hydrochloride 6.1mg (night capsules).
Indications: For the temporary relief of colds and flu including daytime fatigue, blocked or runny nose, headache and fever, sore throat, body aches and pains.
Contraindications: Age <12 years, concomitant use with paracetamol-containing products, breastfeeding, concomitant use of other medicines for the relief of cold and flu or congestion.
Precautions: concomitant paracetamol use, Use > 48 hours (adolescents and children > 12 years), use > a few days (adults), pregnancy, hypertension; liver, kidney or heart problems, concomitant antidepressant use.
Directions: Adults and children over 12 years: 2 day capsules up to 3 times a day, dosage may be repeated every 4-6 hours as necessary. 2 night capsules at night. Maximum 6 day capsules and 2 night capsules in 24 hours.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale TAPS
RECKITT BENCKISER (NZ) LTD
Presentation: Hot drink sachet/oral powder. 10 sachets. Available in lemon flavour
Active Ingredients: Each sachet contains Paracetamol 1000mg
Indications: For the temporary relief of pain, including symptoms of colds and flu, body aches and pains, sore throat, headache. Reduces fever
Contraindications: Children 12 years and under, concomitant use with other paracetamol-containing products.
Precautions: Concomitant paracetamol use, use > 48 hours (adolescents and children > 12 years), use > a few days (adults), pregnancy, breastfeeding, phenylketonuria, liver or kidney problems.
Directions: Adults and children over 12 years: 1 sachet. Do not use more than one sachet per dose. Dosage may be repeated every 4-6 hours as necessary, maximum 4 sachets in 24 hours.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Hot drink sachet/oral powder. 10 sachets. Available in lemon, and blackcurrant flavour
Active Ingredients: Each sachet contains Paracetamol 1000mg, Phenylephrine Hydrochloride 12.2mg
Indications: For the temporary relief of symptoms of colds and flu, including body aches and pains, sore throat, headache and nasal congestion. Reduces fever.
Contraindications: Children 12 years and under, breastfeeding, concomitant use with other paracetamol-containing products.
Precautions: Concomitant use of medicines intended to treat the symptoms of the common cold, concomitant paracetamol use, use > 48 hrs (adolescents and children > 12 years), use > a few days (adults), pregnancy, hypertension, liver, kidney or heart problems, concomitant antidepressant use, phenylketonuria.
Adverse effects: This product may cause sleeplessness.
Directions: Adults and children over 12 years: 1 sachet. Do not use more than one sachet per dose. Dosage may be repeated every 4-6 hours as necessary, maximum 4 sachets/24 hrs.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
(NZ) LTD
AFT PHARMACEUTICALS LTD
Presentation: Tablet, 30s
Presentation: Hot drink sachet/oral powder. 10 sachets. Available in lemon, and blackcurrant flavour
Active Ingredients: Loratadine 2.5mg & phenylephrine hydrochloride 10mg.
Active Ingredients: Each sachet contains Paracetamol 1000mg, Phenylephrine Hydrochloride 12.2mg
Indications: For the temporary relief of nasal and sinus congestion, hayfever, runny nose, watery and itchy eyes and sneezing.
Indications: For the temporary relief of symptoms of colds and flu, including body aches and pains, sore throat, headache and nasal congestion. Reduces fever.
Contraindications: Children 12 years and under, breastfeeding, concomitant use with other paracetamol-containing products.
Contraindications: Hypersensitivity to Phenylephrine, severe hypertension, coronary heart disease, narrow angle glaucoma, prostate hyperplasia, hypersensitivity to loratadine.
Precautions: Do not use in children under 12 years. Prolonged or excessive use may be harmful.
Adverse Effects: Phenylephrine may cause insomnia or sleeplessness in some people.
Precautions: Concomitant use of medicines intended to treat the symptoms of the common cold, concomitant paracetamol use, use > 48 hrs (adolescents and children > 12 years), use > a few days (adults), pregnancy, hypertension, liver, kidney or heart problems, concomitant antidepressant use, phenylketonuria.
Adverse effects: This product may cause sleeplessness.
Directions: Adults and children over 12 years: One tablet four times daily. Do not exceed the recommended dosage.
Price Band: $10 - $20
Directions: Adults and children over 12 years: 1 sachet. Do not use more than one sachet per dose. Dosage may be repeated every 4-6 hours as necessary, maximum 4 sachets/24 hrs.
Subsidy Conditions: Not subsidised
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: Pharmacy Only Medicine
Medicine Classification: General Sale
AFT PHARMACEUTICALS LTD
Presentation: Film Coated Tablets, 20s, 30s
Active Ingredients: Paracetamol 500 mg + Ibuprofen 150 mg + Phenylephrine Hydrochloride 2.5 mg
Approved Indications: For the temporary relief of cold and flu symptoms including headache, fever, pain and nasal congestion.
Contraindications: Hypersensitivity to any ingredient. Existing peptic ulceration or other stomach disorders, asthma, impaired kidney function or heart failure, severe hypertension, ventricular tachycardia. Urticaria or rhinitis associated with aspirin or other NSAIDS, pregnancy except on doctor’s advice. Do not use in the last 3 months of pregnancy.
Precautions: Do not combine with any other paracetamol or ibuprofen containing medications. Do not exceed the recommended dose.
Adverse Effects: Nausea, dyspepsia, rash, constipation, dizziness, GI bleeding (rare at OTC dose). Hepatic dysfunction and papillary necrosis may occur. Phenylephrine may cause sleeplessness in some people.
Directions: Adults and children over 12 years: Take 2 tablets every 4 hours as required, up to a maximum of 8 tablets in 24 hours. Do not use in children under 12 years old.
Price Band: $10 - $20
Medicine Classification: General Sale Medicine (20s), Pharmacy Only Medicine (30s)
RECKITT BENCKISER (NZ) LTD
Presentation: Tablet. 12s, 24s, 48s
Active Ingredients: Ibuprofen 200mg, phenylephrine hydrochloride 5mg.
Approved Indications: Temporary relief of the symptoms associated with cold and flu without causing drowsiness, including headache, sore throat, sinus pain, body aches and pains, runny nose, blocked nose, fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy, age < 12 years.
Directions: Adults and children from 12 years: 2 tablets every 4 to 6 hours as necessary (max. 6 tablets in 24 hours).
Price Band: $10 - $40
Subsidy Conditions: Not subsidised
Medicine Classification: General sale, Pharmacy Only medicine


Precautions: Hypertension, use >3 days at a time, asthma, concomitant use of ibuprofen, aspirin or other antiinflammatory medicines, concomitant use of other medicine for cold and flu, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea or vomiting, concomitant regular medication use (in particular antidepressants), age 65 years or older.
RECKITT BENCKISER
Presentation: Tablet 24s.
LTD
Active Ingredients: Ibuprofen 200mg, Pseudoephedrine hydrochloride 30mg.
Approved Indications: For the temporary relief of the symptoms of colds and flu with associated congestion, including aches and pains, headaches, fever, sore throat, runny nose, blocked nose and sinuses.
Contraindications: Age < 12 years, stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to paracetamol, ibuprofen, aspirin or other anti-inflammatory medicines, last 3 months of pregnancy
Precautions: Hypertension, regular concomitant medications, particularly antidepressants, >3 days use at a time, asthma, taken other cold and flu medications, taking other medications containing ibuprofen, aspirin or other anti-inflammatory medicines, trying to conceive and during first 6 months pregnancy, children suffering from chicken pox or dehydration through diarrhoea and/or vomiting, age 65 years or over.

Directions: Adults and children 12 years and over: Initial dose of 2 tablets then, if necessary, 1 or 2 tablets every 4 hours. Not to be given to children under 12 years. Do not exceed 6 tablets in any 24 hour period. Do not use for a period of more than three days at a time except on medical advice.
Price Band: RRP $32.9 Subsidy Conditions: Not subsidised.
Medicine Classification: Controlled Drug C3 (Pharmacist Only Medicine).
TAPS
AFT PHARMACEUTICALS LTD
Presentation: Oral gel, 30 x 5g sachets. Available in Original flavour (Adults) and Blackcurrant flavour (Adults and Kids).
Active Ingredients: Each 5g sachet contains: Sodium Ascorbate 1000mg equivalent to 889mg Vitamin C (Adults); Sodium Ascorbate 500mg equivalent to 444.5mg Vitamin C (Kids).
Indications: High absorption liposomal supplement that supports immune system health, recovery from ills and chills, collagen formation and absorption of iron. Antioxidant. Reduces free radicals formed in the body and helps connective tissue formation.
Precautions: Consult a pharmacist or doctor before use if you are pregnant or likely to become pregnant, breastfeeding, or if you have a predisposition to kidney stones formation or iron disorders. Vitamins are supplementary to, and not a replacement for, a balanced diet.
Directions: 1 sachet once daily. Consume the contents of each sachet as is or add to a small amount of cold, still water or juice. Do not exceed the recommended daily dose.
Price Band: $30.00 - $50.00
Medicine Classification: Supplement
AFT PHARMACEUTICALS LTD
Presentation: Oral gel, 5g sachet. Melon Flavour
Active Ingredients: Each 5g sachet contains Cholecalciferol 25 micrograms equivalent to 1000IU vitamin D3
Indications: Promotes calcium absorption, supports healthy bone development, helps support immune system and nervous system function, helps promote healthy muscle function, supports healthy foetal development and helps enhance general health and wellbeing.
Precautions: Advise your doctor of any medicine you take during pregnancy, particularly in your first trimester. Vitamins are supplementary to, and not a replacement for, a balanced diet.
Directions: Adults only: 1 sachet once daily. Consume the content of one sachet as is or dissolve in a small amount of cold, still water. Do not exceed the daily recommended dose. Not to be used in children under 12 years of age without medical advice.
Price Band: $30.00 - $50.00
Medicine Classification: Supplement
RECKITT BENCKISER (NZ) LTD
Presentation: Tablets, 100s

Active Ingredients: Each tablet contains Senna Fruit Alexandrian Powder 154mg standardised to contain sennosides 7.5mg.
Approved Indications: Predictable relief from occasional or non-persistent constipation.
Contraindications: Existing abdominal pain, nausea or vomiting, or the development of diarrhoea.
Precautions: If symptoms persist seek medical advice. For short term use only. Do not use for longer than a week unless advised by your healthcare professional. Excessive use can be harmful. Keep out of reach of children. Not recommended for use by children under 12 years of age. Laxatives do not help with weight loss. Do not use if abdominal pain, nausea or vomiting are present or if you develop diarrhoea. Unless a doctor has told you, do not use. If you are pregnant or breastfeeding. In children 18 years and under. Contains lactose.
Directions: Adults and children over 12 years: take 2-4 tablets daily. Do not exceed 4 tablets daily except on doctor’s advice. Doses of more than 4 tablets are best divided and taken morning and night, or as prescribed by doctor. Drink plenty of water and increase the fibre in your diet.
Price Band: $10.00 - $20.00. Available on Pharmaceutical Schedule.
Medicine Classification: Pharmacy Only Medicine TAPS DA2306JT Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Linctus. 180mL
Active Ingredients: Each 5 mL oral liquid contains Glycerol Ph. Eur 0.25mL
Indications: For temporary relief for sore and tickly throats caused by dry coughs.
Precautions: Should not be used in children < 6 years age without medical advice. If symptoms persist consult with doctor. Do not exceed stated dose.
Directions: Adults and children 12 years and over: 20mL per dose, 3 or 4 times daily as required. Children 6-12 years: 10mL per dose, 3 or 4 times daily as required. Maximum 4 doses in 24 hours.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland

RECKITT BENCKISER (NZ) LTD
Presentation: 12-hour modified release tablet. 10s, 20s
Active Ingredients: Guaifenesin 600mg
Indications: Thins and loosens mucus to help relieve chest congestion.
Contraindications: Age < 12 years, concomitant cough suppressant use.
Precautions: Concomitant use of other products for the relief of colds, flu or cough, renal problems, asthma, bronchitis, COPD, emphysema, smokers cough, porphyria.
Directions: Swallow whole with water. Do not crush, chew or break tablet. Adults and children over 12 years: 1 or 2 tablets every 12 hours. Do not exceed 4 tablets in 24 hours. Do not give to children 12 years and under.
Price Band: $10 - $20
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: 12-hour modified release tablet. 14s
Active Ingredients: Guaifenesin 1200mg
Indications: Thins and loosens mucus to help relieve chest congestion.
Contraindications: Age < 12 years, concomitant cough suppressant use.
Precautions: Concomitant use of other products for the relief of colds, flu or cough, renal problems, asthma, bronchitis, COPD, emphysema, smokers cough, porphyria.
Directions: Adults and children 12 years and over: 1 tablet every 12 hours. Maximum 2 tablets in 24 hours. Do not crush, chew or break tablets.
Price Band: $30 - $40
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland
AFT PHARMACEUTICALS LTD
Presentation: Cream: 10g and 15g tubes
Active Ingredients: Lipid stabilised hydrogen peroxide 1% w/w
Approved Indications: Treatment and prevention of minor skin infections such as acne, cuts, scrapes, burns or school sores.
Contraindications: Known hypersensitivity to any ingredient.
Precautions: Use under medical guidance in pregnancy and breastfeeding. Avoid contact with the eyes. Do not use in the presence of iodine, permanganate and any other strong oxidising agents.
Adverse Effects: Mild sensation of burning may be experienced for a short time after application.
Directions: After cleansing the area, apply cream 2-3 times daily on affected area. A dry film will appear on the skin after application, which can be washed off with water.
Price Band: $10 - $20. Available on Pharmaceutical Schedule.
Subsidy Conditions: Fully subsidised (10g only)
Medicine Classification: General Sale
AFT PHARMACEUTICALS LTD
Presentation: Ointment, 40g tube
Active Ingredients: Coal tar solution 12% w/w, sulphur-precipitated for external use 4% w/w, salicylic acid 2% w/w.


Approved Indications: For treatment of dry scaly skin disorders of the scalp such as psoriasis, eczema, seborrhoeic dermatitis and dandruff.
Contraindications: Known sensitivity to any ingredients, in the presence of acute local infections or acute pustular psoriasis.
Precautions: Avoid contact with eyes - wash hands immediately after use. Stop use if irritation develops. If symptoms persist after 4 weeks, consult a doctor. Use during pregnancy/breastfeeding at physician’s discretion. Not recommended in children under 6 years. Children 6-12 years: Use under medical supervision only. Avoid contact with clothes and jewellery.
Adverse Effects: Skin irritation, folliculitis and rarely, photosensitivity.

Directions: Adults and children over 12 years: Mild dandruff - use intermittently as adjunctive treatment, about once a week. Psoriasis, eczema, seborrhoeic dermatitis and severe dandruff - use daily for 3-7 days until improvement is achieved. Intermittent repeated applications may be necessary to maintain improvement. Affected area should be treated and shampooed off, using warm water, approximately 1 hour later.
Price Band: $10 - $20. Available on Pharmaceutical Schedule.
Subsidy Conditions: Fully subsidised Medicine Classification: General Sale
AFT PHARMACEUTICALS LTD
Presentation: Tablets: 10s 20s 50s 100s
Active Ingredients: Paracetamol 500mg & ibuprofen 150mg.
Approved Indications: For relief of pain and reduction of fever and inflammation. For use in headache, toothache, arthritis, rheumatic pain, migraine headache, dental procedures, tennis elbow, aches and pains associated with cold and flu, tension headache, backache, period pain, sinus pain, sore throat, and muscular pain.
Contraindications: Hypersensitivity to any ingredient. Existing peptic ulceration or other stomach disorders, asthma, impaired kidney function or heart failure. Urticaria or rhinitis associated with aspirin or other NSAIDS, pregnancy except on doctor’s advice. Do not use in the last 3 months of pregnancy.
Precautions: Do not combine with any other paracetamol or ibuprofen containing medications. Do not exceed the recommended dose.

Adverse Effects: Nausea, dyspepsia, rash, constipation, dizziness, GI bleeding (rare at OTC dose). Hepatic dysfunction and papillary necrosis may occur.
Directions: Adults & children over 12 years: Take 1 or 2 tablets every 4 to 6 hours as required up to a maximum of 8 tablets in 24 hours. Not recommended for children under 12 years old.
Price Band: $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: General Sale (10s, 20s), Pharmacy Only (50s, 100s)
AFT PHARMACEUTICALS LTD
Presentation: Ointment, 40g tube
Active Ingredients: Coal tar solution 12% w/w, sulphur-precipitated for external use 4% w/w, salicylic acid 2% w/w.
Approved Indications: For treatment of dry scaly skin disorders of the scalp such as psoriasis, eczema, seborrhoeic dermatitis and dandruff.
Contraindications: Known sensitivity to any ingredients, in the presence of acute local infections or acute pustular psoriasis.
Precautions: Avoid contact with eyes - wash hands immediately after use. Stop use if irritation develops. If symptoms persist after 4 weeks, consult a doctor. Use during pregnancy/breastfeeding at physician’s discretion. Not recommended in children under 6 years. Children 6-12 years: Use under medical supervision only. Avoid contact with clothes and jewellery.
Adverse Effects: Skin irritation, folliculitis and rarely, photosensitivity.

Directions: Adults and children over 12 years: Mild dandruff - use intermittently as adjunctive treatment, about once a week. Psoriasis, eczema, seborrhoeic dermatitis and severe dandruff - use daily for 3-7 days until improvement is achieved. Intermittent repeated applications may be necessary to maintain improvement. Affected area should be treated and shampooed off, using warm water, approximately 1 hour later.
Price Band: $10 - $20. Available on Pharmaceutical Schedule.
Subsidy Conditions: Fully subsidised Medicine Classification: General Sale
AFT PHARMACEUTICALS LTD
Presentation: 3.25g sachet, powder
Active Ingredients: Diosmectite 3g
Indications: For the symptomatic relief of diarrhoea.
Contraindications: Hypersensitivity to any ingredient. Do not use in children under 1. Do not use if pregnant or breastfeeding.
Precautions: Don’t use for more than 3 consecutive days. Do not take when lying down. Should not be taken together with basic or amphoteric medicines, such as metronidazole or diazepam. Do not use DiaRelieve if suffering from: gastric or intestinal lesions (e.g. ulcers), chronic constipation, intestinal irritation, intestinal blockage.
Adverse Effects: There are no known side effects related to the long-term use. In case of overdose, constipation can occur.
Directions: Adults: 1 sachet 3 times per day, Children 6 - 18 years: 1 sachet 2 - 3 times per day. Add sachet contents to 100mL of water or other liquid, mix well and consume immediately. Children 1- 6 years: 1 sachet 1- 2 times per day. Sachet contents can be mixed with 50mL water or other liquid and divided into 2 - 3 doses throughout the day, as appropriate. Can be suspended in semi-solid food.
Price Band: $15.00 - $25.00
Medicine Classification: Medical Device
CARE PHARMACEUTICALS PTY LTD
Presentation: Effervescent tablets
Active Ingredients: Citric acid 672mg, Glucose 1620mg, Potassium chloride 149mg, Sodium bicarbonate 378mg, Sodium chloride 87.5mg
Approved Indications: Helps replace water and electrolytes lost due to vomiting, diarrhoea, heavy sweating, vigorous exercise and excess alcohol consumption.
Precautions: If diarrhoea persists for more than 6 hours in infants under 6 months, 12 hours in children under 3 years, 24 hours in children aged 3-6 years or 48 hours in adults and children over 6 years, seek medical advice. Contains 156mg of potassium per 200mL dose. If you have kidney disease or are taking heart or blood pressure medicines, consult your doctor or pharmacist before use. Keep out of reach of children. Contains 276mg of sodium per 200mL dose. Quantity of sodium per maximum daily dose is 5.52g. Contains: Sugars, sucralose, mannitol. Use only as directed. If symptoms persist consult your healthcare practitioner.
Directions: Remove 2 tablets from tube and replace the cap tightly. Dissolve in 200mL of fresh, cold drinking water. For babies under 6 months use freshly boiled and cooled water. Sip slowly and frequently while symptoms persist. Discard unused solution after 2 hours or 24 hours if refrigerated. Do not mix Hydralyte with cordial, fruit juice, soft or sports drinks. Always dissolve in water. Never place tablet directly into mouth.
Price Band: RRP: $20.50 Medicine Classification: General Sale
CARE PHARMACEUTICALS PTY LTD
Presentation: Eye drops
Active Ingredients: Polyvinyl Alcohol 5 mg/mL, Povidone 6 mg/mL
Indications: A gently buffered solution specially formulated to soothe and moisturise dry eyes.
Precautions: Do not touch dropper tip to any surface since this may contaminate the solution. If irritation persists, discontinue use, and consult a physician. Remove contact lenses before using. Discard contents 4 weeks after first opening the container.
Directions: Gently squeeze 2 or 3 drops into each eye as often as directed or needed. Replace cap after using.
Price Band: RRP $15.60
Medicine Classification: Medical Device

AFT PHARMACEUTICALS LTD
Presentation: Preservative-free, phosphate-free and sterile multi-dose lubricating eye drops 10mL.
Active Ingredients: Sodium hyaluronate 1mg/mL
Approved Indications: Ocular lubricant for the temporary relief of mild to moderate dry eye symptoms.
Contraindications: Hypersensitivity to any ingredient.
Precautions: For external use only. Discard 6 months after opening.
Adverse Effects: Hypersensitivity reactions may occur, eg. burning or excessive watering of the eye.
Directions: 1 drop per eye, 3 times daily, or more as needed or directed. Compatible with contact lenses. Can be used for 6 months after opening.
Price Band: $30 - $40. Available on Pharmaceutical Schedule.
Subsidy Conditions: Special Authority (SA1388) criteria apply. Confirmed diagnosis by slit lamp of severe secretory dry eye; and either: patient is using eye drops more than four times daily on a regular basis; or patient has had a confirmed allergic reaction to preservatives in eye drop.
Medicine Classification: General Sale
AFT PHARMACEUTICALS LTD
Presentation: Preservative-free, phosphate-free, aqueous-free, surfactant-free multi-dose lubricating eye drops 3mL.
Active Ingredients: Perfluorohexyloctane 100%, 3mL.
Indications: For lubrication of the eye surface, stabilisation of the tear film, to provide relief from dry and irritated eyes and to help reduce excessive tear evaporation.
Contraindications: Hypersensitivity to Perfluorohexyloctane.
Precautions: If using with any other eye medication allow at least 15 minutes between using the other product and NovaTears. Not suitable for use with contact lenses. Should not be used in children under 18 years. Should not be used while pregnant or breastfeeding.
Adverse Effects: Do not use if you are hypersensitive (allergic) to the ingredient perfluorohexyloctane.
Directions: Administer 1 drop in the lower eyelid up to 4 times daily. Can be used for 6 months after opening.
Price Band: $30 - $40
Medicine Classification: Medical Device


RECKITT BENCKISER (NZ) LTD
Presentation: Eye spray, 10mL
Active Ingredients: 1mL contains: 10mg lecithin, 8mg sodium chloride, 8mg ethanol, 0.25mg vitamin A palmitate, 0.02mg vitamin E, purified water.
Approved Indications: For the relief of dry eyes due to disturbed lipid layer of the tear film, approx. 80% of dry eye cases.
Contraindications: Hypersensitivity to any of the ingredients.
Precautions: Refer to product information leaflet.
Adverse Effects: Potential hypersensitivity reactions may appear, in very rare cases, in the form of a temporary skin irritation. The (skin) irritation (e.g. reddening and swelling) is confined to the application area and may be accompanied by a burning sensation or by itching. If a skin rash appears, it usually appears acutely, is mild in form and subsides rapidly, with no lasting effect once use of the spray has stopped.
Directions: When using for the first time, push down the nozzle 3-4 times. Hold 10cm from your closed eyelids. Spray 1 to 2 times onto closed eyelids, 3 to 4 times per day. Read leaflet for full instructions, warnings and precautions for use.
Price Band: $20.00 -$35.00

Medicine Classification: Medical Device TAPS DA2306JT Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Eye drop. 10mL
Active Ingredients: Naphazoline Hydrochloride 0.1mg/1mL
Approved Indications: For relief of minor eye irritations.
Contraindications: For external use only. Do not use in children under 12 years, if you have glaucoma or other serious eye conditions. May interact with other topically applied autonomic drugs e.g. those used in the treatment of glaucoma. Not suitable for use with hydrophilic (soft) contact lenses. Contains Benzalkonium Chloride and Borax as preservatives.
Precautions: Consult a doctor or pharmacist before use if you are using other eye products or have heart problems, if symptoms persist. Whilst using this medicine prolonged use may be harmful. Use of naphazonline in the eye may liberate pigment granules from the iris, especially when given in high doses to elderly patients. Discard contents four weeks after opening.
Directions: Please read enclosed leaflet carefully before use. Adults and Children over 12 years. Tilt head back, gently squeeze 1 or 2 drops into the corner of each eye. Take care not to touch the eye with the tip of the dropper. Repeat up to 3 times daily.
Price Band: $10.00 -$20.00 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: Pharmacy Only Medicine TAPS DA2306JT Reckitt
RECKITT BENCKISER (NZ) LTD
Presentation: Eye drop. 10mL.
Active Ingredients: Aqua, hamamelis virginia (witch hazel 13%v/v), alcohol, boric acid, glycerin, sodium borate, benzalkonium chloride.
Approved Indications: For relief for sore, irritated eyes.
Contraindications: Do not use whilst or just before wearing soft contact lenses. Contains preservative: Benzalkonium chloride BP 0.005%w/v.
Precautions: For serious eye problems or if irritation develops with use, speak to your doctor, pharmacist or optician.
Directions: Adults and children gently squeeze 1-2 drops into each eye.
Price Band: $10.00 - $20.00 (Price varies with pack size).
Subsidy Conditions: Not subsidised
Medicine Classification: Medical Device
TAPS DA2306JT
Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Eye Spray 10mL
Ingredients: 1mL contains 10mg soy lecithin, 8mg sodium chloride, 8mg ethanol, 5mg phenoxyethanol, 0.25mg vitamin A palmitate, 0.02mg vitamin E, purified water.
Approved Indications: For the relief of dry eyes due to disturbed lipid layer of the tear film, approx. 80% of dry eye cases.
Precautions: Refer to product information leaflet.
Contraindications: Hypersensitivity to any of the ingredients.
Adverse Effects: Potential hypersensitivity reactions may appear, in very rare cases, in the form of a temporary irritation. The (skin) irritation (e.g. reddening and swelling) is confined to the application area and may be accompanied by a burning sensation or by itching. It usually appears acutely, is mild in form and subsides rapidly, with no lasting effect once use of the spray has stopped.
Directions: When using for the first time, push down on the nozzle 3-4 times. Hold 10cm from your closed eyelid. Spray 1 to 2 times onto closed eyelids, 3 to 4 times per day. Refer to product information leaflet for full directions.
Price Band: $20.00 - $35.00


Classification: Medical Device TAPS DA2306JT Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Wash with eye bath, 110ml, 300ml.
Ingredients: Aqua, Hamamelis Virginia (Witch Hazel), Alcohol, Boric Acid, Glycerin, Sodium Borate, Benzalkonium Chloride.
Approved Indications: To cleanse and soothe tired, irritated and uncomfortable eyes.
Contraindications: Remove contact lenses before use, allow at least 15 minutes before replacing them after use.
Precautions: Do not return used eye wash to the bottle.
Directions: Please see product label for complete directions.
Price Band: $10.00 - $20.00 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: Medical Device
TAPS DA2306JT
Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Eye drops, 10mL.
Ingredients: Aqua 98.2%, Sodium Chloride, PEG 8000, Boric Acid, Sodium Hyaluronate 0.165%, Potassium Chloride, Sodium Chlorite, Calcium Chloride, Magnesium Chloride, Hydrogen Peroxide.
Approved Indications: Effective relief of dry eyes, instantly rehydrate & lubricate dry eyes, safe for use with contact lenses.
Contraindications: Do not use if you are allergic to any of the ingredients. This product contains boron. Consult a doctor before use of this product during pregnancy or breast feeding. Not suitable for use in children under the age of 12.
Precautions: Check tamper evident seal is intact before first use. Do not use if compromised. Avoid touching the dropper tip with your hands, the eyelid, eye or any other surface. Discard the product if the top of the dropper comes into contact with the eyelid or any other surface. Do not swallow the solution. Do not use with another eye drop unless directed by your doctor or eye practitioner. If you experience irritation or any other adverse effects, remove lenses and consult your eye care specialist. If symptoms persist, seek medical advise.
Directions: Wash hands thoroughly before use. Tilt head backwards and gently squeeze 1-2 drops into each eye, when required, up to 15 times per day. Blink a few times toensure the whole eye is covered. Replace the bottle top tightly after use.
Price Band: $10.00 - $20.00 (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine
HEALTHCARE LOGISTICS, AUCKLAND
Presentation: Ointment
Ingredients: Glyceryl Trinitrate 0.2% w/w

Indications: For the relief and treatment of anal fissures and relief of the symptoms associated with anal fissure. May assist in relief of pain and discomfort associated with haemorrhoids and haemorrhoidectomy
Contraindications: Severe anaemia, glaucoma, hypotension, increased intracranial pressure, pregnancy, lactation, idiosyncrasy to glyceryl trinitrate. Do not co-administer with medicines for high blood pressure or depression (tricyclic anti-depressants), acetylcysteine or alteplase, PDE5 Inhibitors used to treat erectile dysfunction e.g. Viagra (sildenafil citrate), Ciolis tadalafil, Levitra (vardenafil).
Precautions: Safety has not been established in pregnancy, lactation or in children. May cause dizziness, light headedness, blurred vision, headaches or tiredness in some patients. Caution with driving or operating machinery. Alcohol may enhance vascular effects. Caution in patients already using glyceryl trinitrate.
Directions: Apply a 1 - 1.5cm strip of ointment as directed three times daily
Price band: RRP $43.99 Subsidy conditions: Fully funded for patients with chronic anal fissures.
Medicine classification: Pharmacist only
AFT PHARMACEUTICALS LTD
Presentation: Tablets: 10s 20s 50s 100s
Active Ingredients: Paracetamol 500mg & ibuprofen 150mg.

Approved Indications: For relief of pain and reduction of fever and inflammation. For use in headache, toothache, arthritis, rheumatic pain, migraine headache, dental procedures, tennis elbow, aches and pains associated with cold and flu, tension headache, backache, period pain, sinus pain, sore throat, and muscular pain.
Contraindications: Hypersensitivity to any ingredient. Existing peptic ulceration or other stomach disorders, asthma, impaired kidney function or heart failure. Urticaria or rhinitis associated with aspirin or other NSAIDS, pregnancy except on doctor’s advice. Do not use in the last 3 months of pregnancy.
Precautions: Do not combine with any other paracetamol or ibuprofen containing medications. Do not exceed the recommended dose.
Adverse Effects: Nausea, dyspepsia, rash, constipation, dizziness, GI bleeding (rare at OTC dose). Hepatic dysfunction and papillary necrosis may occur.
Directions: Adults & children over 12 years: Take 1 or 2 tablets every 4 to 6 hours as required up to a maximum of 8 tablets in 24 hours. Not recommended for children under 12 years old.
Price Band: $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: General Sale (10s, 20s) Pharmacy Only (50s, 100s)
RECKITT BENCKISER (NZ) LTD
Presentation: Tablets: 12s, 24s, 48s, 96s (Bottle). Caplets: 12s, 24s.
Active Ingredients: Ibuprofen 200mg
Approved Indications: For the temporary relief of pain and/or inflammation associated with: headache, migraine headache, tension headache, back pain, muscular pain, cold and flu symptoms, period pain, dental pain, sinus pain, arthritic pain. Reduces fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy.
Precautions: Use > 3 days, asthma, concomitant use of ibuprofen, aspirin or other anti-inflammatory medicines, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea and/or vomiting, concomitant regular medication use, age 65 years or older, age <7 years.

Directions: Adults and children from 12 years: 2 tablets/caplets, then 1-2 tablets/caplets every 4-6 hours as required. Maximum 6 tablets/caplets in 24 hours. Children 7-12 years: 1 tablet every 6 to 8 hours as necessary (max. 4 tablets in 24 hours). Take with water.
Price Band: Under $10 - $20 and over (Price varies with pack size) Subsidy Conditions: Not subsidised TAPS DA2249CO
Medicine Classification: General Sale (packs up to 25), Pharmacy Only Medicine (packs more than 25) Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Caplets 12s & 24s
Active Ingredients: Ibuprofen lysine 342mg (equiv. ibuprofen 200mg)
Approved Indications: Temporary relief of pain and/or inflammation associated with headache, migraine headache, tension headache, backpain, muscular pain, cold and flu symptoms, period pain, dental pain, sinus pain, arthritic pain. Reduces fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy.Precautions: Pregnancy, breastfeeding, asthma, intolerance to some sugars.

Precautions: Use > 3 days, asthma, concomitant use of ibuprofen, aspirin or other anti-inflammatory medicines, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea and/or vomiting, concomitant regular medication use, age 65 years or older, age < 7 years.
Directions: Adults and children from 12 years: 2 caplets then 1 or 2 caplets every 4 to 6 hours as necessary (max. 6 caplets in 24 hours). Children 7-12 years: 1 caplet every 6 to 8 hours as necessary (max. 4 caplets in 24 hours). TAPS DA2249CO
Price Band: $10.00 - $20.00 Subsidy Conditions: Not subsidised Medicine Classification: General Sale Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Tablets: 12s, 24s, 48s, 96s. Caplets, 12s, 24s.
Active Ingredients: Solid dose tablets/capsules: ibuprofen sodium dihydrate 256mg (equiv. ibuprofen 200mg).
Approved Indications: For the temporary relief of pain and/or inflammation associated with: headache, migraine headache, tension headache, muscular pain, cold and flu symptoms, back pain, period pain, dental pain, sinus pain, arthritic pain. Reduces fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy.
Precautions: Use > 3 days, asthma, concomitant use of ibuprofen, aspirin or other anti-inflammatory medicines, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea and/or vomiting, concomitant regular medication use, age 65 years or older, age <12 years (liquid capsules), <7 years (tablets/caplets).

Directions: Adults and children from 12 years: 2 tablets/caplets or liquid capsules, then 1-2 tablets/caplets or liquid capsules every 4-6 hours as required. Maximum 6 tablets/caplets or liquid capsules in 24 hours. Children 7-12 years (for Ibuprofen sodium dihydrate tablets/caplets): 1 tablet/caplet every 6-8 hours as required, maximum 4 tablets/caplets in 24 hours. Take with water.
Price Band: Under $10 - $20 and over (Price varies with pack size) Subsidy Conditions: Not subsidised
Medicine Classification: General Sale (packs up to 25), Pharmacy Only Medicine (packs more than 25)
RECKITT BENCKISER (NZ) LTD
Presentation: Liquid Capsules. 10s, 20s, 40s, 80s
Active Ingredients: Ibuprofen 200mg
Approved Indications: For the temporary relief of pain and/or inflammation associated with: headache, migraine headache, tension headache, muscular pain, cold and flu symptoms, back pain, period pain, dental pain, sinus pain, arthritic pain. Reduces fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy.
Precautions: Use > 3 days, asthma, concomitant use of ibuprofen, aspirin or other anti-inflammatory medicines, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea and/or vomiting, concomitant regular medication use, age 65 years or older, age <12 years (liquid capsules).

Directions: Take with water. Adults and children from 12 years: 2 capsules, then 1 or 2 capsules every 4 to 6 hours as necessary (maximum 6 capsules in 24 hours).
Price Band: Under $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale (packs up to 25), Pharmacy Only Medicine (packs more than 25)
Presentation: Tablets: 12s, 20s, 24s, 48s, 72s.
Active Ingredients: Ibuprofen 200mg and Paracetamol 500mg
Approved Indications: For the temporary relief of pain and/or inflammation associated with: back pain, period pain, cold and flu symptoms, muscular pain, sore throat, rheumatic pain and non-serious arthritic pain, dental pain, migraine headache, tension headache, headache. Reduces fever.
Contraindications: Age < 12 years, stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to paracetamol, ibuprofen, aspirin or other anti-inflammatory medicines, last 3 months of pregnancy.
Precautions: Diabetes, concomitant use of other medicines containing ibuprofen, aspirin or other anti-inflammatory medicines, >3 days use, during the first 6 months of pregnancy, women trying to conceive.
Directions: Take with water. Adults and children from 12 years take 1 or 2 tablets every 6 to 8 hours as required. Maximum 6 tablets in 24 hours. Keep to the recommended dose.
Price Band: $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale (packs up to 20), Pharmacy Only Medicine (packs more than 20)

RECKITT BENCKISER (NZ) LTD
Presentation: Liquid, peppermint and mixed berry flavour, 300ml, 600ml.
Active Ingredients: Each 10mL contains 500mg sodium alginate, 213mg sodium bicarbonate and 325mg calcium carbonate.
Approved Indications: For the relief of the pain and discomfort Heartburn (gastric reflux) and indigestion
Precautions: Do not use in children under 6 years. Contains hydroxybenzoates, saccharin and sodium. If symptoms persist, see your doctor. The maximum total daily intake (80mL) for adults contains 1023mg sodium (take into account if on a low sodium diet).
Directions: Adults & children over 12 years: 2 sachets. Children 6-12 years: 1 sachet. Take as required after meals and before going to bed, up to 4 times a day or as directed. Ensure sachet seal is unbroken. Massage sachet well and tear across perforated line. Squeeze liquid from bottom of sachet either directly into mouth or onto a spoon.
Price Band: $10 - $30 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT

RECKITT BENCKISER (NZ) LTD
Presentation: Liquid sachets 12 x 10ml
Ingredients: Each sachet (10ml of oral liquid suspension) contains 500mg sodium alginate, 213mg sodium bicarbonate, 325 calcium carbonate.
Indications: For the relief of the pain and discomfort of Heartburn (gastric reflux) and indigestion.
Precautions: Do not use in children under 6 years. Contains hydroxybenzoates, saccharin and sodium. If symptoms persist, see your doctor. The maximum total daily intake (80mL) for adults contains 1023mg sodium (take into account if on a low sodium diet).
Directions: Adults & children over 12 years: 2 sachets. Children 6-12 years: 1 sachet. Take as required after meals and before going to bed, up to 4 times a day or as directed. Ensure sachet seal is unbroken. Massage sachet well and tear across perforated line. Squeeze liquid from bottom of sachet either directly into mouth or onto a spoon.
Price band: $10.00
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Available in peppermint 16s, 32s and 48s, mixed berry 16s and 48s.
Active Ingredients: Each tablet contains 250mg sodium alginate, 106.5mg sodium bicarbonate and 187.5mg calcium carbonate.
Approved Indications: For the relief of the pain and discomfort of Heartburn (gastric reflux) and indigestion.
Precautions: If symptoms persist, see your doctor. Keep out of reach of children. Not recommended for children under 6 years. The maximum total daily intake (16 tablets) for adults contains 894mg of sodium (take into account if on a low sodium diet) and 9.6g mannitol and 4.6g of xylitol. Products containing mannitol or xylitol may have a laxative effect or cause diarrhoea. Contains phenylalanine, mannitol, aspartame, sulphites and sodium.
Directions: Adults and children over 12 years: 4 tablets. Children 6-12 years: 2 tablets. Take as required after meals and before going to bed up to 4 times a day or as directed. Chew tablets throughly before swallowing and follow with water if desired.
Price Band: $10.00 - $20.00 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
RECKITT BENCKISER
Presentation: Liquid. Aniseed flavour, 300mL and peppermint 300mL

Active Ingredients: Each 10 mL dose contains: Sodium alginate 1000mg, Potassium bicarbonate 200 mg and Calcium carbonate 200mg
Approved Indications: For the relief of the pain and discomfort of Heartburn (gastric reflux) and indigestion.
Precautions: Not recommended for children under 12 years. The maximum total daily intake (40mL) for adults contains 424mg of sodium (take into account if on a low sodium diet). Contains hydroxybenzoates, saccharin and sodium. This medicine contains 78 mg of potassium per 10 mL, to be taken into consideration by patients with reduced kidney function or patients on a controlled potassium diet. Glass bottle - handle with care. Do not drink directly from the bottle. If symptoms persist see your doctor. Keep out of reach of children
Directions: Adults and children over 12 years: 5-10mL. Take as required after meals and before going to bed up to 4 times a day or as directed.
Price Band: $10.00 - $20.00 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland

RECKITT BENCKISER (NZ) LTD
Presentation: Tablets, peppermint flavour, 24s and 60s.
Active Ingredients: Sodium alginate 500mg, sodium bicarbonate 267mg, calcium carbonate 160mg.
Approved indications: For the relief of the pain and discomfort of Heartburn (gastric reflux) and indigestion.
Contraindications: Hypersensitivity to any ingredient.
Precautions: If symptoms persist, see your doctor. Keep out of reach of children. Not recommended for children under 12 years. The maximum total daily intake (8 tablets) for adults contains 984mg of sodium (take into account if on a low sodium diet) and 4.1g mannitol. Products containing mannitol may have a laxative effect or cause diarrhoea. Contains Phenylalanine, aspartame, mannitol, sulphites and sodium.
Directions: Adults and children over 12 years: 1-2 tablets as required after meals or before going to bed, up to 4 times a day or as directed. Chew tablets before swallowing and follow with water if desired.
Price Band: $10.00 - $30.00. Available on Pharmaceutical Schedule (60 tub only).
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland
Presentation: Sachets, 30s.
Active Ingredients: Sodium alginate 225mg, magnesium alginate 87.5mg per sachet.
Approved Indications: For the treatment of regurgitation and gastric reflux for infants and young children.
Contraindications: Use with feed thickeners or infant milk containing thickeners, allergy to any ingredient, vomiting, fever, diarrhoea, if on low salt diet, kidney damage, intestinal obstruction.
Precautions: Please read enclosed leaflet before use. Do not use Gaviscon Infant with other feed thickening agents or infant milk preparations containing a thickening agent. Do not use more than the stated amount. Keep out of reach and sight of children. Gaviscon infant is not to be used in infants under 1 year of age, except under medical supervision. Contains mannitol and sodium. Products containing mannitol may have a laxative effect or cause diarrhoea. Each sachet of Gaviscon Infant contains approximately 23.9mg of sodium. If your infant has been put on a low sodium (salt) diet as your doctor or other health professional before taking the product.


Directions: Prepare immediately before use, as directed: Breast fed infants aged 1-2 years under 4.5kg: 1 sachet; over 4.5kg, 2 sachets. Add 5mL of cooled, boiled water to the powder in a glass. Mix to a smooth paste and add another 10ml water to the mix. Give after each feed, using a spoon or feeding bottle. Bottle-fed infant aged 1-2 years under 4.5kg: 1 sachet. Mix into no less than 115mL of each feed in the bottle and shake well. Over 4.5kg: 2 sachets. Mix into no less than 225mL of each feed in the bottle and shake well. Maximum daily dose for infants over 4.5kg (10lb) equates to intake of 3.45g of mannitol E421. Do not give more than six times in 24 hours. TAPS DA2306JT
Price Band: $10 - $20. Available on Pharmaceutical Schedule. Subsidy Conditions: Fully subsidised Medicine Classification: General Sale Reckitt Benckiser, Auckland
AFT PHARMACEUTICALS LTD
Presentation: Oral gel, 5g sachet. Strawberry flavour
Active Ingredients: Each 5g sachet contains Ferric ammonium citrate 93.5 mg equivalent to 20 mg of elemental iron
Indications: May assist you if you are feeling tired, lacking in energy, looking to maintain healthy iron levels and is intended for adults with an increased demand for iron, such as in pregnant women, women in the perimenstrual period, in blood donors, vegetarians and vegans.
Precautions: Vitamins and minerals are supplementary to, and not a replacement for a balanced diet. If symptoms persist, talk to your health professional. Not for the treatment of iron deficiency conditions.
Directions: Adults only: 1 sachet once daily. Consume the contents of one sachet as is or dissolve in a small amount of cold, still water. It can be consumed with a meal. Do not exceed the daily recommended dose.
Price Band: $30.00 - $50.00
Medicine Classification: Supplement
HEALTHCARE LOGISTICS, AUCKLAND
Presentation: Vaginal mucosa suppository.

Ingredients (% m/m): Purified Water 78.82, Polycarbophil AA-1 2.00, Mineral Oil 4.20, Glycerine 12.90, Hydrogenated palm oil glycerides 1.00, Carbomer 974P 1.00, Sorbic acid 0.08.
Indications: A non-hormonal moisturising gel for long lasting symptomatic relief from vaginal atrophy, dryness, itching, irritation and discomfort.
Contraindications: For Adults only. It is not known whether Aci-Jel Restore can cause foetal harm when administered to a pregnant woman. Although there is no evidence that any of the components of this product are detrimental to the mother or foetus, the use during pregnancy should be carefully assessed and administered only if clearly indicated.
Precautions: For vaginal use only. Aci-Jel Restore should be avoided if you are trying to conceive due to concerns over sperm toxicity.
Directions: Apply Aci-Jel Restore directly into the vagina from the pre-filled applicator. Grip the applicator by the thick end. Shake down the contents to ensure they’re at the thin end of the applicator. Twist off the tab and discard. The applicator can be inserted into the vagina while you are lying down on your back with your knees bent or in a sitting position. Gently insert the thin end into your vagina as far as it will go comfortably. Squeeze the thick end of the applicator firmly to deposit gel. Remove the applicator and discard appropriately.
Price band: $34.55 Subsidy conditions: N/A
Medicine classification: Class IIb Medical Device
AFT PHARMACEUTICALS LTD
Presentation: Tablets: 10s 20s 50s 100s
Active Ingredients: Paracetamol 500mg & ibuprofen 150mg.
Approved Indications: For relief of pain and reduction of fever and inflammation. For use in headache, toothache, arthritis, rheumatic pain, migraine headache, dental procedures, tennis elbow, aches and pains associated with cold and flu, tension headache, backache, period pain, sinus pain, sore throat, and muscular pain.
Contraindications: Hypersensitivity to any ingredient. Existing peptic ulceration or other stomach disorders, asthma, impaired kidney function or heart failure. Urticaria or rhinitis associated with aspirin or other NSAIDS, pregnancy except on doctor’s advice. Do not use in the last 3 months of pregnancy.
Precautions: Do not combine with any other paracetamol or ibuprofen containing medications. Do not exceed the recommended dose.
Adverse Effects: Nausea, dyspepsia, rash, constipation, dizziness, GI bleeding (rare at OTC dose). Hepatic dysfunction and papillary necrosis may occur.
Directions: Adults & children over 12 years: Take 1 or 2 tablets every 4 to 6 hours as required up to a maximum of 8 tablets in 24 hours. Not recommended for children under 12 years old.
Price Band: $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: General Sale (10s, 20s) Pharmacy Only (50s, 100s)
Presentation: Liquid capsule Active Ingredients: Ibuprofen 200mg, Paracetamol 500mg
Approved Indications: Nuromol Dual Action Pain Relief contains two ingredients that together deliver temporary relief of (short term) pain and/ or inflammation associated with: back pain, period pain, cold & flu symptoms, muscular pain, sore throat, rheumatic pain & nonserious arthritic pain, dental pain, migraine headache, tension headache, headache
Contraindications: Asthma, concomitant use of other medicines containing ibuprofen, aspirin, or other anti-inflammatory medicines, age 65 years or over, use > 3 days, age < 12 years, you are pregnant or trying to become pregnant, stomach ulcer or other stomach disorders or if you have had these conditions or gastric bleeding in the past, impaired kidney or liver function, heart failure, allergic to ibuprofen, aspirin or other anti-inflammatory medicines.
Precautions: If you are taking other medicines, you suffer diabetes.
Adverse reactions: STOP USE AND SEE YOUR DOCTOR IMMEDIATELY IF: you have an allergic reaction.
Directions: Take with water. Adults under 65 and children from 12 years: Take 1 or 2 capsules every 6 to 8 hours as necessary, maximum 6 capsules in 24 hours. Keep to the recommended dose. Do not take for more than 3 days at a time (2 days for adolescents aged 12 to 17 years).
Price Band: Under $20 to $20 and over (price varies with pack size).
Subsidy Conditions: Not subsidised.
Medicine Classification: General sale (packs up to 20); Pharmacy Only Medicine (packs more than 20).
RECKITT BENCKISER (NZ) LTD
Presentation: Dermal Patch. 2s, 4s Active Ingredients: Ibuprofen 200mg per patch.
Approved Indications: Short-term symptomatic treatment of local pain in: muscular strains, sprains and localised inflammation due to injury of the joint such as osteoarthritis.
Contraindications: Allergy to ibuprofen, aspirin or other anti-inflammatory medicines, use during the last 3 months of pregnancy, use on the eyes, mouth, lips or genital area, use on broken or damaged skin, use if the patch is wet, using more than one patch at a time, age < 16 years, use > 5 days.
Precautions: Concomitant use of other anti-inflammatory medicines, concomitant regular medication use.


Directions: For use on the skin only and should only be used on healthy, unbroken skin. Adults, the elderly, and adolescents aged 16 years and over: Use one medicated patch every 24 hours. Do not use more of this medicine than the label tells you to. Do not cut the patch or cover with other plaster or non-breathable dressings/bandages. The patch can be applied at any time during the day or night, but should be removed and a new patch re-applied at the same time on the following day. Wash and dry the area to be treated before applying the patch. The patch is flexible and conformable, and if necessary, can be applied on or near a joint and will allow for normal movement.
Price Band: Under $15-$15 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: General Sale
RECKITT
Presentation: Caplets 12s & 24s
Active Ingredients: Ibuprofen lysine 342mg (equiv. ibuprofen 200mg)
Approved Indications: Temporary relief of pain and/or inflammation associated with headache, migraine headache, tension headache, backpain, muscular pain, cold and flu symptoms, period pain, dental pain, sinus pain, arthritic pain. Reduces fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy.Precautions: Pregnancy, breastfeeding, asthma, intolerance to some sugars.
Precautions: Use > 3 days, asthma, concomitant use of ibuprofen, aspirin or other anti-inflammatory medicines, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea and/or vomiting, concomitant regular medication use, age 65 years or older, age < 7 years.
Directions: Adults and children from 12 years: 2 caplets then 1 or 2 caplets every 4 to 6 hours as necessary (max. 6 caplets in 24 hours). Children 7-12 years: 1 caplet every 6 to 8 hours as necessary (max. 4 caplets in 24 hours).
Price Band: $10.00 - $20.00 Subsidy Conditions: Not subsidised Medicine Classification: General Sale
RECKITT BENCKISER (NZ) LTD
Presentation: Tablets: 12s, 24s, 48s, 96s. Caplets, 12s, 24s.
Active Ingredients: Solid dose tablets/capsules: ibuprofen sodium dihydrate 256mg (equiv. ibuprofen 200mg).
Approved Indications: For the temporary relief of pain and/or inflammation associated with: headache, migraine headache, tension headache, muscular pain, cold and flu symptoms, back pain, period pain, dental pain, sinus pain, arthritic pain. Reduces fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy.
Precautions: Use > 3 days, asthma, concomitant use of ibuprofen, aspirin or other anti-inflammatory medicines, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea and/or vomiting, concomitant regular medication use, age 65 years or older, age <12 years (liquid capsules), <7 years (tablets/caplets).

Directions: Adults and children from 12 years: 2 tablets/caplets or liquid capsules, then 1-2 tablets/caplets or liquid capsules every 4-6 hours as required. Maximum 6 tablets/caplets or liquid capsules in 24 hours. Children 7-12 years (for Ibuprofen sodium dihydrate tablets/caplets): 1 tablet/caplet every 6-8 hours as required, maximum 4 tablets/caplets in 24 hours. Take with water.
Price Band: Under $10 - $20 and over (Price varies with pack size) Subsidy Conditions: Not subsidised
Medicine Classification: General Sale (packs up to 25), Pharmacy Only Medicine (packs more than 25)
RECKITT BENCKISER (NZ) LTD
Presentation: Liquid Capsules. 10s, 20s, 40s, 80s
Active Ingredients: Ibuprofen 200mg
Approved Indications: For the temporary relief of pain and/or inflammation associated with: headache, migraine headache, tension headache, muscular pain, cold and flu symptoms, back pain, period pain, dental pain, sinus pain, arthritic pain. Reduces fever.
Contraindications: Stomach ulcer or other stomach disorders, kidney, liver or heart problems, allergy to ibuprofen, aspirin or other anti-inflammatory medicines, during the last 3 months of pregnancy.
Precautions: Use > 3 days, asthma, concomitant use of ibuprofen, aspirin or other anti-inflammatory medicines, women trying to conceive, during the first 6 months of pregnancy, children suffering from chicken pox (varicella), children suffering from dehydration through diarrhoea and/or vomiting, concomitant regular medication use, age 65 years or older, age <12 years (liquid capsules).
Directions: Take with water. Adults and children from 12 years: 2 capsules, then 1 or 2 capsules every 4 to 6 hours as necessary (maximum 6 capsules in 24 hours).
Price Band: Under $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised TAPS DA2249CO
Medicine Classification: General Sale (packs up to 25), Pharmacy Only Medicine (packs more than 25)
RECKITT BENCKISER
Presentation: Liquid capsule Active Ingredients: Ibuprofen 200mg, Paracetamol 500mg
Approved Indications: Nuromol Dual Action Pain Relief contains two ingredients that together deliver temporary relief of (short term) pain and/ or inflammation associated with: back pain, period pain, cold & flu symptoms, muscular pain, sore throat, rheumatic pain & nonserious arthritic pain, dental pain, migraine headache, tension headache, headache
Contraindications: Asthma, concomitant use of other medicines containing ibuprofen, aspirin, or other anti-inflammatory medicines, age 65 years or over, use > 3 days, age < 12 years, you are pregnant or trying to become pregnant, stomach ulcer or other stomach disorders or if you have had these conditions or gastric bleeding in the past, impaired kidney or liver function, heart failure, allergic to ibuprofen, aspirin or other anti-inflammatory medicines.
Precautions: If you are taking other medicines, you suffer diabetes.
Adverse reactions: STOP USE AND SEE YOUR DOCTOR IMMEDIATELY IF: you have an allergic reaction.
Directions: Take with water. Adults under 65 and children from 12 years: Take 1 or 2 capsules every 6 to 8 hours as necessary, maximum 6 capsules in 24 hours. Keep to the recommended dose. Do not take for more than 3 days at a time (2 days for adolescents aged 12 to 17 years).
Price Band: Under $20 to $20 and over (price varies with pack size).
Subsidy Conditions: Not subsidised.
Medicine Classification: General sale (packs up to 20); Pharmacy Only Medicine (packs more than 20).
AFT PHARMACEUTICALS LTD
Presentation: Tablets: 10s 20s 50s 100s
Active Ingredients: Paracetamol 500mg & ibuprofen 150mg.
Approved Indications: For relief of pain and reduction of fever and inflammation. For use in headache, toothache, arthritis, rheumatic pain, migraine headache, dental procedures, tennis elbow, aches and pains associated with cold and flu, tension headache, backache, period pain, sinus pain, sore throat, and muscular pain.
Contraindications: Hypersensitivity to any ingredient. Existing peptic ulceration or other stomach disorders, asthma, impaired kidney function or heart failure. Urticaria or rhinitis associated with aspirin or other NSAIDS, pregnancy except on doctor’s advice. Do not use in the last 3 months of pregnancy.
Precautions: Do not combine with any other paracetamol or ibuprofen containing medications. Do not exceed the recommended dose.
Adverse Effects: Nausea, dyspepsia, rash, constipation, dizziness, GI bleeding (rare at OTC dose). Hepatic dysfunction and papillary necrosis may occur.
Directions: Adults & children over 12 years: Take 1 or 2 tablets every 4 to 6 hours as required up to a maximum of 8 tablets in 24 hours. Not recommended for children under 12 years old.
Price Band: $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: General Sale (10s, 20s) Pharmacy Only (50s, 100s)
AFT PHARMACEUTICALS LTD
Presentation: Tablets: 10s 20s 50s 100s
Active Ingredients: Paracetamol 500mg & ibuprofen 150mg.
Approved Indications: For relief of pain and reduction of fever and inflammation. For use in headache, toothache, arthritis, rheumatic pain, migraine headache, dental procedures, tennis elbow, aches and pains associated with cold and flu, tension headache, backache, period pain, sinus pain, sore throat, and muscular pain.
Contraindications: Hypersensitivity to any ingredient. Existing peptic ulceration or other stomach disorders, asthma, impaired kidney function or heart failure. Urticaria or rhinitis associated with aspirin or other NSAIDS, pregnancy except on doctor’s advice. Do not use in the last 3 months of pregnancy.
Precautions: Do not combine with any other paracetamol or ibuprofen containing medications. Do not exceed the recommended dose.
Adverse Effects: Nausea, dyspepsia, rash, constipation, dizziness, GI bleeding (rare at OTC dose). Hepatic dysfunction and papillary necrosis may occur.
Directions: Adults & children over 12 years: Take 1 or 2 tablets every 4 to 6 hours as required up to a maximum of 8 tablets in 24 hours. Not recommended for children under 12 years old.
Price Band: $10 - $20 and over (Price varies with pack size)
Subsidy Conditions: Not subsidised Medicine Classification: General Sale (10s, 20s) Pharmacy Only (50s, 100s)
Presentation: Ointment, 40g tube
Active Ingredients: Coal tar solution 12% w/w, sulphur-precipitated for external use 4% w/w, salicylic acid 2% w/w.
Approved Indications: For treatment of dry scaly skin disorders of the scalp such as psoriasis, eczema, seborrhoeic dermatitis and dandruff.
Contraindications: Known sensitivity to any ingredients, in the presence of acute local infections or acute pustular psoriasis.
Precautions: Avoid contact with eyes - wash hands immediately after use. Stop use if irritation develops. If symptoms persist after 4 weeks, consult a doctor. Use during pregnancy/breastfeeding at physician’s discretion. Not recommended in children under 6 years. Children 6-12 years: Use under medical supervision only. Avoid contact with clothes and jewellery.
Adverse Effects: Skin irritation, folliculitis and rarely, photosensitivity.
Directions: Adults and children over 12 years: Mild dandruff - use intermittently as adjunctive treatment, about once a week. Psoriasis, eczema, seborrhoeic dermatitis and severe dandruff - use daily for 3-7 days until improvement is achieved. Intermittent repeated applications may be necessary to maintain improvement. Affected area should be treated and shampooed off, using warm water, approximately 1 hour later.
Price Band: $10 - $20. Available on Pharmaceutical Schedule.
Subsidy Conditions: Fully subsidised Medicine Classification: General Sale
CARE PHARMACEUTICALS PTY LTD
Presentation: Nasal spray
Active Ingredients: Sodium chloride 9 mg/mL
Indications: For the relief of nasal congestion due to sinusitis, hayfever & allergies, cold & flu.
Precautions: For use by one person only. Do not use if carton seals are missing or broken. If congestion persists, see your doctor. Store below 30°C.
Directions: 1. Direct the nozzle into your right nostril. 2. Aim slightly back and out towards the top of your right ear. 3. Fully depress the pump.
4. Repeat in the left nostril. Adults: 2 - 6 sprays per nostril. Children: 2 - 3 sprays per nostril or use FESS Children's. Babies: Use FESS Little Noses.
Price Band: RRP $14.05
Medicine Classification: Medical Device
RECKITT BENCKISER (NZ) LTD
Presentation: Lozenge in orange and honey lemon flavours 16s.
Active Ingredients: Flurbiprofen 8.75mg.
Approved Indications: For relief of pain, swelling and inflammation associated with severe sore throat.
Contraindications: Stomach ulcer, impaired kidney function, heart failure, allergy to flurbiprofen or other anti-inflammatory medicines, last 3 months of pregnancy, age < 12 years.
Precautions: Asthma, in women trying to conceive, first 6 months of pregnancy, use > few days at a time, concomitant use of other medicines containing flurbiprofen, aspirin or other anti-inflammatory medicines, concomitant use of regular medicines. Excessive use can be harmful and increase the risk of heart attack, stroke or liver damage.
Directions: Adults and children over 12 years: Suck one lozenge slowly every 3 to 6 hours as needed. Move lozenge around the mouth occasionally as you suck it. Max. 8 lozenges in 24 hours.
Price Band: $10.00 - $20.00
Subsidy Conditions: Not subsidised


Medicine Classification: Pharmacy Only Reckitt Benckiser,
RECKITT BENCKISER (NZ) LTD
Presentation: Throat spray 15mL
Active Ingredients: Flurbiprofen 2.91mg per spray (8.75mg per dose of 3 sprays)
Approved Indications: For relief of pain, swelling and inflammation associated with severe sore throat.
Contraindications: Use > 3 days, stomach ulcer, impaired kidney function, impaired liver function, heart failure, allergy to flurbiprofen or other anti-inflammatory medicines, last 3 months of pregnancy, age < 18 years.
Precautions: Asthma, in women trying to conceive, first 6 months of pregnancy, use > few days at a time, concomitant use of other medicines containing flurbiprofen, aspirin or other anti-inflammatory medicines, concomitant use of regular medicines. Excessive use can be harmful and increase the risk of heart attack, stroke or liver damage.
Directions: One dose (3 sprays) to the back of the throat every 3-6 hours as required, max. 5 doses (15 sprays) per 24 hours.
Price Band: $20.00
Subsidy Conditions: Not subsidised
Medicine Classification: Pharmacy Only
TAPS DA2306JT
Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Lozenge. 16s, 36s
Active Ingredients: Per lozenge: amylmetacresol 600mcg, dichlorobenzyl alcohol 1.2mg, lidocaine (lignocaine) hydrochloride monohydrate 10mg
Approved Indications: For relief from painful and inflamed sore throats.
Contraindications: Age < 6years, taking food or drink soon after using this product as it may burn the mouth.
Precautions: If symptoms persist >2 days accompanied by fever, headache or nausea consult your doctor.
Directions: Adults and children over 6 years: one lozenge every 2 hours as required. Max 8 per 24 hours.
Price Band: $10.00 - $20.00 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Lozenge. 16s, 36s.
Active Ingredients: Dichlorobenzyl alcohol 1.2mg, Amylmetacresol 600mg, menthol 8mg
Approved Indications: For relief from the discomfort of sore throats, minor mouth infections and helps clear the nose.
Contraindications: Age < 6 years.
Directions: Dissolve one lozenge slowly in the mouth every 2 to 3 hours as required.
Price Band: $10.00 - $20.00 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland
RECKITT BENCKISER (NZ) LTD
Presentation: Lozenge. 16s, 36s. Available in honey & lemon, orange, sugar free strawberry, and sugar free lemon.
Active Ingredients: Dichlorobenzyl alcohol 1.2mg, amylmetacresol 600mg
Approved Indications: For relief from the discomfort of sore throats, minor mouth infections.
Contraindications: Age < 6 years.
Precautions: If symptoms persist consult your doctor.
Directions: Adults and children over 6 years: 1 lozenge every 2-3 hours as required.
Price Band: $10 - $20 (Price varies with pack size)
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland


RECKITT BENCKISER (NZ) LTD
Presentation: Throat spray 20mL
Active Ingredients: Amylmetacresol 0.29mg/spray, 2,4-Dichlorobenzyl Alcohol 0.58mg/spray, Lidocaine 0.78mg/spray
Approved Indications: For effective and rapid relief from the symptoms of painful and inflamed sore throats, mouth and dental ulcers and the discomfort associated with tonsilitis and pharyngitis.
Contraindications: Allergy to any of the ingredients in this product, age < 12 years.
Precautions: Pregnancy, breastfeeding, asthma.
Directions: Adults and children over 12 years: For optimal use rotate the nozzle 90o. Spray twice directly onto the sore/ inflamed area and swallow gently. Repeat every 3 hours as necessary. Up to a maximum of 6 times in 24 hours.
Price Band: $10.00 - $20.00
Subsidy Conditions: Not subsidised
Medicine Classification: General Sale
TAPS DA2306JT
Reckitt Benckiser, Auckland
AFT PHARMACEUTICALS LTD
Presentation: Oral gel, 5g sachet. Strawberry flavour
Active Ingredients: Each 5g sachet contains Ferric ammonium citrate 93.5 mg equivalent to 20 mg of elemental iron.

Indications: May assist you if you are feeling tired, lacking in energy, looking to maintain healthy iron levels and is intended for adults with an increased demand for iron, such as in pregnant women, women in the perimenstrual period, in blood donors, vegetarians and vegans.
Precautions: Vitamins and minerals are supplementary to, and not a replacement for a balanced diet. If symptoms persist, talk to your health professional. Not for the treatment of iron deficiency conditions.
Directions: Adults only: 1 sachet once daily. Consume the contents of one sachet as is or dissolve in a small amount of cold, still water. It can be consumed with a meal. Do not exceed the daily recommended dose.
Price Band: $30.00 - $50.00
Medicine Classification: Supplement
AFT PHARMACEUTICALS LTD
Presentation: Oral gel, 30 x 5g sachets. Available in Original flavour (Adults) and Blackcurrant flavour (Adults and Kids).
Active Ingredients: Each 5g sachet contains: Sodium Ascorbate 1000mg equivalent to 889mg Vitamin C (Adults); Sodium Ascorbate 500mg equivalent to 444.5mg Vitamin C (Kids).
Indications: High absorption liposomal supplement that supports immune system health, recovery from ills and chills, collagen formation and absorption of iron. Antioxidant. Reduces free radicals formed in the body and helps connective tissue formation.
Precautions: Consult a pharmacist or doctor before use if you are pregnant or likely to become pregnant, breastfeeding, or if you have a predisposition to kidney stones formation or iron disorders. Vitamins are supplementary to, and not a replacement for, a balanced diet.
Directions: 1 sachet once daily. Consume the contents of each sachet as is or add to a small amount of cold, still water or juice. Do not exceed the recommended daily dose.
Price Band: $30.00 - $50.00
Medicine Classification: Supplement
AFT PHARMACEUTICALS LTD
Presentation: Oral gel, 5g sachet. Melon Flavour
Active Ingredients: Each 5g sachet contains Cholecalciferol 25 micrograms equivalent to 1000IU vitamin D3
Indications: Promotes calcium absorption, supports healthy bone development, helps support immune system and nervous system function, helps promote healthy muscle function, supports healthy foetal development and helps enhance general health and wellbeing.
Precautions: Advise your doctor of any medicine you take during pregnancy, particularly in your first trimester. Vitamins are supplementary to, and not a replacement for, a balanced diet.
Directions: Adults only: 1 sachet once daily. Consume the content of one sachet as is or dissolve in a small amount of cold, still water. Do not exceed the daily recommended dose. Not to be used in children under 12 years of age without medical advice.
Price Band: $30.00 - $50.00
Medicine Classification: Supplement
AFT PHARMACEUTICALS LTD
Presentation: Cream: 10g and 15g tubes
Active Ingredients: Lipid stabilised hydrogen peroxide 1% w/w
Approved Indications: Treatment and prevention of minor skin infections such as acne, cuts, scrapes, burns or school sores.
Contraindications: Known hypersensitivity to any ingredient.
Precautions: Use under medical guidance in pregnancy and breastfeeding. Avoid contact with the eyes. Do not use in the presence of iodine, permanganate and any other strong oxidising agents.
Adverse Effects: Mild sensation of burning may be experienced for a short time after application.
Directions: After cleansing the area, apply cream 2-3 times daily on affected area. A dry film will appear on the skin after application, which can be washed off with water.
Price Band: $10 - $20. Available on Pharmaceutical Schedule.
Subsidy Conditions: Fully subsidised (10g only).
Medicine Classification: General Sale
AFT Pharmaceuticals Ltd
Ph: 09-488 0232
Care Pharmaceuticals Pty Ltd
Ph: 0800 226 598
Distributed in New Zealand by: Healthcare Logistics, Auckland
Ph: 09-918 5100
Reckitt Benckiser (NZ) Ltd
Ph: 09-839 0200