science


Vaccines
The impact of ethnicity on health and diagnosis in the UK
The Multiverse: Are we living in one of many universes?
Theory of Relativity
What's on at The Abbey?
Why is Nuclear Chemistry important in Medicine?
Your next cardiologist won't be a robot - here's why
“Pizza Express" - The Journey of a Pizza
Eureka Competition Entry: Quarks, Cakes and Space!
Bird Poop 101: Why it's white and what that means
Get to know: Arminas Ragauskas
Change Competition: Why history's deadliest flu can't kill you anymore
Change Competition: Evolution of Calculators
Hana , Upper VI
Vaccines were invented to protect the world from preventable diseases - we all went through the Covid-19 pandemic and currently we are aware of the M-Pox epidemic.
The term ‘vaccination’ comes from ‘Vaccinia’, the first ever vaccine which was developed against Smallpox in 1796 by Edward Jenner.
Depending on the pathogen that is being targeted, there are different types of vaccines but ultimately all work on the same principle Vaccines provide our immune system with a memory of the pathogen, so that it can eliminate it if it encounters it in the future They do this by presenting a harmless version of the pathogen, or part of it, to our immune system
Vaccines come in different forms - needle injections, nasal sprays or oral doses
There are different vaccine methods/technologies The most conventional types are listed below:
These vaccines are made from a piece of a pathogen - one or more proteins found in the pathogen which are synthetically produced Subunit vaccines can be made from the original pathogen or recombinantly Recombinant vaccines use another organism to make the vaccine antigen (the part of the pathogen against which we want to make an immune response) The first vaccine of this type that was licensed is the hepatitis B vaccine It consists of a single viral protein which is produced in yeast cells and assembled into small particles that resemble a virus
As a subunit vaccine does not contain the whole organism, it cannot make you sick or cause infection, making it suitable for older people, young children, and immunocompromised people.
These types of vaccine are often used with an adjuvant - something that is added to a vaccine to increase the immune response. The most widely used adjuvant is alum, which is present in the hepatitis A and B vaccines.
This type of vaccine contains a live pathogen (virus or bacteria) which has been weakened so that it does not cause the disease when it spreads through the body after vaccination, but still produces a strong immune response Because these vaccines contain a live pathogen, the immune system reacts strongly to them and it will typically remember the pathogen for a very long time. Therefore boosters, or additional doses are not always needed. However due to such a strong immune response, these vaccines are not recommended to people with very weak immune systems. Examples currently in use are: MMR (Measles, mumps, and rubella) vaccine, chickenpox vaccine, BCG vaccine against tuberculosis, FluMist nasal vaccine against Influenza and the recent M-pox vaccine (JYNNEOS)
These vaccines use an inactivated (killed) pathogen, incapable of causing disease, but strong enough to create an immune response that can then act against the live pathogen The immune response is not as strong as from the live attenuated vaccine and therefore multiple doses are often needed in order to build up immunity and offer full protection Inactivated vaccines are cheaper and are easier to mass-produce Examples currently in use are: The polio vaccine, rabies vaccine, and most of the Influenza vaccines used across the world
Some bacterial pathogens produce toxins (poisonous proteins) which then cause disease Toxoid vaccines stimulate an immune response against the toxin rather than against the pathogen itself Toxoids are inactivated toxins, modified to resemble the toxin without causing illness Examples currently in use are the diphtheria, and tetanus vaccines Booster shots are typically recommended every 10 years.
Viral vector vaccines use an adenovirus virus (normally causing a mild respiratory or gastrointestinal illness) to deliver the genetic code of the pathogen’s antigen to the host’s cells The antigen is then produced inside the body after vaccination and triggers a very strong immune response Typically, only one dose of the shot is needed to develop immunity
At least one of the adenovirus genes has been removed, so that the vaccine cannot replicate and spread through the body, hence replication-deficient. Current examples are the COVID-19 vaccines by AstraZeneca and Johnson & Johnson.
There are many different adenoviruses that infect humans. For people who have been previously infected and made an immune response, the vaccine would not work well. To avoid this, either a rare human adenovirus or an adenovirus that does not normally infect humans can be used. For example, the Covid-19 AstraZeneca vaccine (ChAdOx1 nCoV-19) is based on an adenovirus found in chimpanzees.
One of the main differences between mRNA vaccines and other types of vaccines is the method by which our immune systems are presented with an antigen Some vaccines contain the whole virus or bacterium, and some contain selected parts of the virus or bacterium. mRNA vaccines are different as they provide the instructions for our bodies to produce the parts of the virus within our own cells.
When an mRNA vaccine is delivered, the RNA material teaches our body how to make a specific type of protein that is unique to the virus, and triggers an immune response. That way, if a person is ever exposed to that virus in the future, the body would have the antibodies to fight against it. Current examples are the Pfizer and Moderna COVID-19 vaccines.
The replication-deficient adenoviral vector and mRNA vaccines are both examples of platform technologies This means, a technology that can be used to make vaccines against many different diseases. Once the platform (carrier) is well understood, the development of a new vaccine can proceed rapidly, because much of the work (and trials) has already been done. The original pathogen is not used in the production of these vaccines. Synthetic DNA is produced that provides the instructions to make the antigen, which is added to the carrier to make the specific vaccine.

Ethnic disparities in diagnosis and treatment have been a long term issue, influencing both the physical health and mental well-being of communities around the UK, with differences shaped by a combination of genetics, culture, socioeconomic and healthcare factors. Whilst belonging to an ethnic minority group doesn't necessarily correlate with a higher risk of developing certain conditions or a lower rate of treatment, it is crucial to recognize, and address, the barriers that lead to some disparities in health outcomes. This reflects the importance of creating an equitable healthcare system that ensures accurate and timely care for all populations.
Ethnicity is defined as the “quality or fact of belonging to a population group or subgroup made up of people who share a common cultural background or descent” and, according to to 2021 census data, 18% of usual residents in England and Wales belong to a Black, Asian, Mixed or Other ethnic group In England, there is evidence of health inequality between ethnic minority and white groups, and between different ethnic minority groups, however this is a complex picture and patterns differ greatly depending on the condition
For example, latest ONS data shows that the highest mortality rates present in the White British group This is often considered to be the result of the ‘Healthy Migrant Effect’, which refers to observations that migrants have been found to be at a better health status at immigration compared to the rest of the population of that country, as they often constitute a selection of strong and healthy individuals who can handle the physiological, social and mental hardships of uprooting, travel and resettlement However, this conceals significant differences between conditions and between different ethnic groups - studies have found a consistently higher incidence, prevalence and mortality from Cardiovascular Disease (CVD) in South Asian groups compared to White groups, yet Black groups have a significantly lower risk compared to the rest of the population
CVD is the second most common cause of death nationally, causing 27% of all deaths in the UK in 2022. It has been found that there is a higher clustering of risk factors in South Asians, as while they typically show lower BMI levels, they have higher rates of excess abdominal fat and insulin resistance. This is largely due to intrinsic genetic differences and physical features restricting fat accumulation in certain areas and promoting it in others, however environmental factors would have modified these - people from Asian groups are less likely to report being active. On the other hand, despite the fact that there is a higher prevalence of hypertension and diabetes in Black groups which are other risk factors for CVD, their typical diets which are high in pasta, rice, vegetables and fruit but low in meat, lead to lower cholesterol levels. This could lead to lower rates of CVD within this population.
While the risk of CVD varies significantly across different ethnic groups, cancer rates also show distinct patterns based on demographic factors Interestingly, it has been found that Asian, Chinese and Mixed groups have a notably lower, around 20-60%, risk of getting cancer than White groups This can be due to a number of lifestyle factors - prevalence of smoking is lower in most ethnic minority groups than the white group, and, for cultural or religious reasons, adults from ethnic minorities may be less likely to drink alcohol at a hazardous, harmful or dependent level Despite this, cancer screening rates for some cancers such as breast and cervical cancer are lower among women from ethnic minority groups, and South Asians show lower rates of bowel cancer screenings This pattern is similar in stages of diagnosis, with Black and Asian women showing higher rates of late-stage diagnosis for breast, uterine and colon cancers compared with White British women This disparity can be credited to poor symptom awareness and language barriers, but many believe it to be the result of issues rooted deeply within the healthcare system - racism
Systemic racism is a form of institutional racism i.e. discriminatory treatment of an individual or group of individuals by an institution based on race or ethnic group. Within the NHS, this does not commonly manifest in overt acts of racism, which are condemned, but more frequently as cultural bias which operates in more covert ways This is more challenging to identify and address It can lead to biased decision-making processes within healthcare settings, and perpetuate stereotypes against patients from minority ethnic backgrounds A recent case exhibiting this problem was of a 31 year old pregnant black woman who died at Liverpool Women’s Hospital in March 2023, two days after a scan had found her baby had died and her condition critical The medical cause of death was recorded as acute intestinal ischaemia, a medical emergency caused by restriction of blood flow to the bowel An investigation by Maternity and Newborn Safety Investigations (MNSI) concluded that “ethnicity and health inequalities impacted on the care provided to the patient, suggesting that an unconscious cultural bias delayed the timing of diagnosis and response to her clinical deterioration In addition to this, an investigation in the maternal death of another black woman from sepsis in August 2023 is still ongoing, and a report by Mother and Babies: Reducing Risk Through Audits and Confidential Enquiries UK (MBRRACE-UK) found that between 2019 and 2021, women from black ethnic minority backgrounds were 4 times more likely to die during pregnancy or immediately after than white women
Evidence of these biases extends beyond patient care Minority ethnic healthcare professionals, which make up 24 2% of the NHS workforce, face barriers to career progression, unequal opportunities for training and development and workplace harassment and discrimination. In a BMA racism survey, 23% of respondents considered leaving their job due to racial discrimination, while 9% actually left. A multifaceted approach that acknowledges the existence of these issues, confronts implicit biases and promotes cultural competence among healthcare providers must be carried out to combat this problem. Furthermore, it is essential to implement policies that promote diversity and inclusion in recruitment including that of leadership positions, and to foster a culture of accountability and zero tolerance for discrimination, e.g., by establishing clear protocols for reporting and addressing instances of racism.
Overall, the disparities in health outcomes among different ethnic groups in the UK are complex, multifaceted, and deeply intertwined with systemic factors, including cultural bias and institutional racism within the healthcare system. While there is no simple explanation for these differences, it is clear that both biological and socio-economic factors play significant roles in shaping the health of various communities More importantly, the covert biases and inequalities that exist within healthcare settings must be addressed in order to ensure fair and equal treatment for all A healthcare system that recognizes these disparities and actively works to eliminate them will not only improve health outcomes but also foster a more inclusive and equitable society for all To move forward, we must prioritize lt l t f t i bi d t k d

Imagine right now, in a parallel universe, another version of you is reading this same article - but maybe they’re wearing different coloured socks, or maybe they’re reading this on a different planet The idea of alternate realities and the vastness of possibilities within these realities has fascinated many scientists and philosophers alike.
What is the Multiverse?
By definition the Multiverse is, ‘A hypothetical space or realm consisting of a number of universes, of which our own universe is only one.’ These universes could have different physical laws, a different history or even different versions of ourselves. While this may sound like no more than a Sci-fi film, several scientific theories suggest that our universe may be one of many.
Different theories of the Multiverse:
The Many-Worlds Interpretation (MWI), Proposed by Hugh Everett III
The Many-Worlds Interpretation is a theory which suggests that every time a quantum event occurs with multiple possible outcomes, the universe splits and branches out into other realities, each reality with a different possible outcome taking place. Let’s say you flip a coin and it lands heads, in a parallel universe at that same moment that same coin will land tails. Therefore, according to MWI there are infinite versions of you living out every possibility of every decision you have ever made.
Currently there is no circumstantial evidence of MWI taking place or any way to detect these alternate universes, however MWI is mathematically consistent in providing an explanation behind many quantum mechanics phenomena including Superposition Superposition states that a quantum system, e g an electron or a photon, can exist in multiple states at the same time until it is measured To understand this concept we can think of superposition as a mathematical equation with two answers When we solve �� ² = 4, �� can either be 2 or -2 Both answers are correct Superposed wave functions are a little harder to solve but they can be approached with a similar mindset To learn more and understand these concepts better, you could research about Schrӧdinger’s Cat Experiment and the Double-Slit Experiment.
Imagine an object, what is it made up of? Molecules What are molecules made up of? Atoms What are atoms made up of? Electrons and a nucleus What are nuclei made up of? Protons and neutrons What are neutrons made up of? Quarks Conventionally we stop at quarks and scientists say that quarks are the smallest particles to ever exist. However, the String Theory suggests otherwise and that inside these quarks are tiny string-like filaments of energy. These strings vibrate at different speeds, which creates all the different types of particles making up everything around us. This would mean that Physics is nothing but the harmonies of the vibrating strings, Chemistry is the melodies that you can play when these strings interact with each other, and the universe is a symphony of strings. Essentially, the String Theory suggests that everything in the universe is made up of tiny vibrating strings and contains 10 dimensions - 3 for space, 1 for time and 6 other spatial dimensions curled up in a way the human mind can’t comprehend or observe
String Theory provides a plausible framework for the idea of a multiverse by suggesting that our universe is one “brane” or “membrane” existing in a multidimensional area of space, which scientists refer to as the “bulk ” Other branes or membranes could exist in the bulk each with its own universe This suggests an infinite number of parallel universes each with their own physical laws and constants
Again, currently there is no experimental evidence to prove the String Theory, especially since String Theory operates at extremely small scales (the Planck Length, 10 ³⁵ meters). However, with the help of quantum computers we may be able to explore aspects of String Theory mathematically and computationally.

The Theory of Relativity consists of two theories of general relativity and special relativity General relativity explains the laws of gravitation in relation to the forces of nature which deviates from Newtonian physics, encompassing the concept of spacetime. Whereas Special relativity focuses on physical phenomena in the absence of gravity, with main concepts of the structure of spacetime and regarding the principle of relativity, including time dilation and the speed of light
In Newtonian Physics, space and time are absolute and fixed, regardless of the events occurring in the universe, space is not affected, and time goes on, and of course gravity has no effect on both quantities General relativity challenges that by stating time and space are dynamic quantities that are relative and contingent, and can be affected by all events occurring in the universe
General relativity states that other than having the 3 space dimensions of length, width and height, there is a 4th time dimension in which merges with the 3 space dimensions to form spacetime, in which space and time are relative, as a flat fabric surrounding us and shaped and curved by the presence of celestial bodies. Spacetime basically influences the motion of matter and matter influences of the curvature of spacetime
For instance, imagine the sun as a bowling ball placed in the middle of a trampoline with elasticity which forms a curvature that we feel as gravity, a dip on the fabric of spacetime So planets do not follow a curved orbit around stars due to gravity of the attraction forces between two celestial bodies, but it is due to the sun’s heavy mass and the curvature of the fabric of 4D spacetime, so instead they follow the nearest thing to a straight line in a curved space, called a geodesic.
In other words, gravity is the effect of the spacetime curvature by heavy celestial bodies on other bodies, and it is not a force between massive objects, but rather something that emerges from the interaction of space and massive objects, explaining the orbits of planets
Imagine a window cleaner falls without the presence of air resistance, gravity would be the only force acting on the falling man So he would be accelerating towards the ground, however the ground would not be pushing up against his body during the fall (until he hits the ground), so he would feel no weight and would be in a state of Free Fall, equivalent to being weightless in space. The gravitational field strength of the Earth, 9.81N/kg, is basically the equivalent of acceleration at 9.81ms-2, they are different ways to describe the same event. If one’s mass is 40kg, one would roughly weigh 400N on Earth, and would still roughly be 400N on a spaceship accelerating upwards at 9 81ms-2
This thought experiment highlighting the principle of equivalence is extremely important to inspiring Einstein to come up with the Theory of Relativity If one aforementioned on a spaceship pointed a flashlight horizontally from one side of the room to the other, the height of the light on the other side of the room would be lower than the height of the light from the source (flashlight),
as the acceleration of the spaceship upwards would curve the light downwards as the light travels across the room of the spaceship
The same applies on Earth, where the height of the light on the other side of the room would also be slightly lower than the source as the gravitational force is curving it downwards So light must bend in the presence of a gravitational field as it is equivalent to acceleration, which is odd, as light always travels in the shortest path from one point to another. But a straight line isn’t always necessarily the shortest path, especially in the context of Relativity, where spacetime is curved. For example the great circle of the Earth is a geodesic as aforementioned, the shortest path between two points, and although it might seem curved in the 3D perspective, it is a straight line in the 2D sense This curved path is indeed the shortest path on the surface of the Earth So gravity causes the curvature of space due to the presence of the mass and energy of celestial bodies, forming the dips in the fabric of spacetime So in space, the shortest path is not a straight line, but a curved path
Light rays follow geodesics in spacetime, as space is curved, so light no longer travels in straight lines in space, as it is bent by gravitational fields, as aforementioned.
Light cones of points near the sun would be slightly bent inwards due to the mass of the sun hence the gravitational bend, so light from a distant star that happened to pass near the sun would be bent by the curvature of space due to gravity, and would be deflected through a small angle, causing the star to appear in a different position to an observer on the Earth. It would certainly be difficult to tell if that was the apparent position of the star deflected by the sun’s mass, or the actual position of the star in which is not near the sun hence its light is not deflected However, as the Earth orbits around the sun, different stars appear to pass behind the sun and have their light deflected, which would change their apparent position relative to other stars Normally it is very hard to see this effect as the light from the sun makes it impossible to observe stars that appear near to the sun in the sky However, on rare occasions of a solar eclipse, where the sun’s light is blocked out by the moon, it is possible to do so.
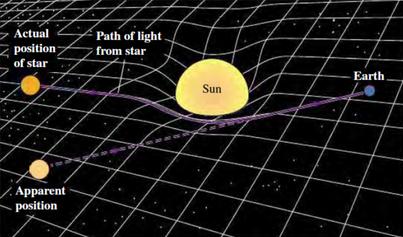
So the theory of general relativity that light can travel in a curved path as spacetime is bended by massive celestial bodies can be proved by an observation made in 1919, where an astronomer photographed stars near the sun during a total solar eclipse, and light was indeed deflected by the sun, just as predicted by the theory If the theory is correct, the position of the stars near the sun would appear different from their predicted location based on their actual position relative to other stars.
The mass of the sun curves spacetime in a way that although the Earth follows a straight path in 4D spacetime, it is moving
The orbits of the planets predicted by general relativity are almost identical as those predicted by Newtonian Physics, except for the mystery of Mercury. Mercury’s orbit, the planet closest to the sun, was unusual, as it feels the strongest gravitational effects so has an elongated orbit. Although its orbit was in an ellipse like all other planets, it had a precession, where its ellipse never closes, in which the point of the orbit farthest from the sun slightly advances every orbital period, as if the ellipse itself is orbiting the sun The equations in Newtonian physics have failed to predict precisely the precession of Mercury, whilst when the curved space theory was applied to this orbit, it predicted exactly the precession of Mercury more accurately than ever, matching the observations, confirming the theory The theory predicts that the long axis of the ellipse should rotate about the sun at the rate of about 1 degree in 10,000 years
Massive objects distort spacetime because they are so heavy, to a point where the mass makes spacetime curve. There are also regions of space where spacetime can become so distorted that nothing escapes it including light, and this is called a black hole, forming after the death of a star. Depending on the size of the predeath star, other than a black hole, stars after death can turn into bodies such as white dwarfs, brown dwarfs, neutron stars, gravastars and more Within the event horizon of a black hole, there is a singularity in the centre, where mass is concentrated to an infinitely small point with an infinite density, and information is deleted General relativity’s equations do not work at these extreme circumstances of infinities, and even Shrodinger’s equation from Quantum Mechanics do not work in cases involving singularities
General Relativity doesn’t only concern the distortion of space, but also time. Time dilation is the difference in elapsed time as measured by two clocks, which are two
different observers, the relative difference of time of the two observers are caused by a difference in gravitational potential between their locations in terms of general relativity. This is usually an effect caused by the contingent presence of the observer’s location of different astronomical bodies with different masses.
The theory of relativity eliminates absolute time, as time should appear to run slower near more massive celestial bodies, and this is due to a relation between the energy of light and its frequency (of the light waves), the greater the energy of light, the higher its frequency Take the Earth for example, as light travels upwards in the Earth’s gravitational field, it loses energy, so the frequency decreases, and the wavelength increases
Light always travels at the same speed regardless of the different perspectives of different observers or different frames of reference, indicating that light would have the same speed in an accelerating frame of reference or a stationary frame of reference. This means that the speed of light in a gravitational field in a curved path will be the same as its speed in empty space in a straight path. However if you consider v=d/t, since the distance of the curved path travelled by the light in a gravitational field is longer due to the curvature of space than the light traveling in a straight line in empty space, in order for the speed of light to remain constant, time itself must pass slower in the gravitational field relative to time in empty space
This is why, as aforementioned, time appears to run slower near more massive celestial bodies, due to a stronger gravitational field and a more distorted curvature and longer distance hence more time needed to achieve a constant speed of light.
So time increases proportionally with curvature of space near a gravitational
field compared to empty space, to keep the speed of light constant in both frames of reference, and this is why time is distorted by gravity along with space, as it is part of the same spacetime fabric, relative to each other. This implies that an observer in the absence of gravity sees the clock in a gravitational field running slower, for instance, the international space station or other GPS satellites orbiting around Earth, which this time difference is taken into account in order to keep the clocks there in sync with the clocks on Earth, otherwise GPS apps like google maps would provide inaccurate locations
Special relativity is a theory of the structures and phenomena caused by spacetime and the finite maximum speed of light. It states that the laws of physics are the same for all observers in any inertial frame of reference relative to one another. Two events, which are simultaneous for one observer, may not be simultaneous for another observer if the observers are in relative motion
An example of relativity of simultaneity is that two lightning bolts striking two trees is at the same time for a person standing in between the trees, but not simultaneous for a train travelling near the speed of light
The speed of light in vacuum is the same for all observers, regardless of relative motion That’s because if you consider the equation of Mass-energy equivalence E = mc2, energy and mass are equivalent and transmutable in relation to the speed of light, as energy equals mass times the square of the speed of light.
If you want to move an object you have to apply energy, when you accelerate an object the object possesses more energy and thus gets heavier, and its mass increases As an object approaches the
the speed of light, the ball becomes infinitely heavy, because the energy is transferred into mass. So nothing can travel faster than the speed of light in vacuum, as travelling faster than the speed of light requires more than an infinite amount of energy, so the maximum speed is finite
In general relativity, time dilation is caused by a difference in gravitational potential between the locations of two observers with motions relative to each other However in special relativity, time dilation can also be caused by the relative velocity between them The faster you travel through space, the slower you travel through time
Consider the twin paradox, where one twin stayed on Earth, and another rode a spaceship at nearly the speed of light, and time would occur much faster to the second twin with a much quicker velocity hence higher energy, and hence a higher
frequency and shorter wavelength, so time occurs much quicker to the twin on the spaceship, and everything happening on Earth seems to be occurring in slow motion as time is slower on Earth. In terms of absolute time, and more absolute time on Earth is equivalent to less absolute time on the spaceship. So the twin on Earth would be much older than the twin on the spaceship when they reunite.
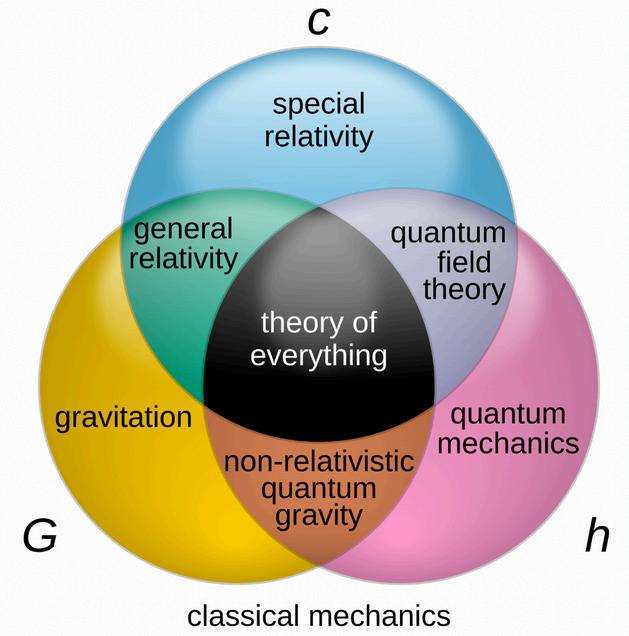
Quantum gravity tries to describe gravity in the principle of quantum mechanics, essentially combining theories from general relativity and quantum mechanics, to gain a full understanding of what gravity truly is. It is believed that if we somehow combine three extremely incompatible fields of theoretical physics together, Theory of Special Relativity and Gravity and Quantum Mechanics, we would get the theory of everything
Enrichment Lecture: Professor Dame
Ijeoma Uchegbu, President of Wolfson College, Cambridge
Professor Uchegbu gave an inspiring talk on science and her career in pharmaceutical nanotechnology on Friday 31 January at the Senior School
She outlined the process for testing medicines before they receive permission for use in the UK, expertly explaining the different stages and the high failure rates for new medicines. She discussed the moment of insight, and showed us the page of the notebook on which she first recorded, when she discovered the structure of a new molecule which is currently being tested. She described the advantages to delivering medicines to the areas where they would be most effective, improving outcomes and minimising side effects
She also spoke about her own career and the challenges of researching in Nigeria and the UK She spoke about the levels of time, dedication and belief her work has required, and the difficulties in maintaining these Her love of science and determination to improve people’s lives was evident to everyone who attended the talk
After the talk, Professor Uchegbu stayed to speak to students and their families A large number of the audience stayed too There was much discussion of how inspirational the talk was, and the consensus was that none of us had come across such a cool academic before We are very grateful to Professor Uchegbu for sharing her research, intellect and immaculate sense of cool with us
On Tuesday 24 June, we visited Amersham Field Studies Centre to carry out some ecology field work as part of our A Level Biology studies From counting woodlice to measuring soil pH, it was a brilliant opportunity to link our classroom learning of populations and ecosystems with real life applications It also taught us valuable skills about data analysis and evaluation, which without a doubt will be extremely helpful to us in our exams Overall it was an amazing day out in which we could fully immerse ourselves in biology!!
Jasmin, Lower VI

Professor Uchegbu with her granddaughter, Ameerah, Lower V, who helped to arrange the talk.

- Dr Detina Zalli
For this year’s Jo Trott Memorial lecture, guest speaker Dr Detina Zalli gave an engaging talk on precision medicine and AI Her talk introduced us to exciting new ideas such as how the use of space can revolutionise medicine and 3D bioprinting in space, as well as expanding our knowledge on topics such as DNA, personalised medicine and how the human genome can be used to optimise our health.
On the 20th February we arrived in Geneva, Switzerland and began our trip by riding a double decker train, followed by an evening walk around Lake Geneva, enjoying the scenic view and the city’s calm atmosphere.
On the second day, we explored Geneva by taking a boat across the lake to the Old Town We visited the St Pierre cathedral, climbed to its top for a breathtaking panoramic view of the city, and even had time for some shopping A highlight of the day was trying Swiss fondue, a delicious local specialty In the afternoon, we boarded a tram to the United Nations headquarters, gaining insights into history and impact on world affairs
We began day four with a visit to the International Museum of the Red Cross The permanent exhibition was a moving and inspiring opportunity to learn more of humanitarian action and its challenges This was alongside a temporary exhibition ‘Tuning in –Acoustique de L’émotion’, an interactive collection linking humanitarian action to heritage and voices After a fascinating morning, we headed for food Some of us took the opportunity to try the traditional Swiss dish of raclette, which was delicious (but very filling!) In the afternoon, we walked down to Geneva’s History of Science Museum, full of not only engaging experiments, but also a rare collection of old scientific instruments To finish the day off, we all went to a lovely Italian restaurant and enjoyed an array of flavourful cuisine.
On our final day, we headed to Geneva Airport early, and after a fairly smooth flight we all arrived back safely and made our way home. This trip was a great opportunity to broaden our knowledge in Physics as well as parts of History and Politics, and we are so grateful to our teachers for making this amazing week happen!
Emily and Anika, Lower VI




Nuclear chemistry in medicine is the use of radioactive substances in order to diagnose and treat diseases. It includes imaging techniques like PET and SPECT scans to detect conditions early and targeted radiation therapies for treating cancers and other health issues.
Nuclear medicine plays a vital role in the treatment of select cancers, including prostate cancer and lymphoma, as well as hyperthyroidism (an overactive thyroid), and since it started being used in this way in the 1940s, thousands of patients have benefited from it Nuclear medicine therapy involves using radiopharmaceuticals which can detect the specific protein on cancer cells, and then bind specifically to the detected cells and either prevent them from growing or kill them due to the bombardment of radiation This type of cancer treatment is a targeted therapy, meaning that only cancer cells are attacked, with as little effect on healthy tissue as possible, creating fewer side effects such as hair loss and nausea than other treatments such as chemotherapy. However, it is often used alongside other therapies such as chemotherapy or radiation, as when used alone, it is unlikely to lead to a complete cure. Having said that, it is also used as the sole therapy in some palliative cancer cases, or in cases where the cancer has been resistant to all other treatments, with the aim of reducing symptoms and slowing down the progression of the disease.
One of the most well-known nuclear therapies is radioactive iodine (I-131) therapy, which is used to treat hyperthyroidism and thyroid cancer. Since the thyroid naturally absorbs iodine, I-131 selectively targets thyroid tissue, either shrinking overactive thyroid glands or destroying cancerous thyroid cells. Another example is lutetium-177 (Lu-177) PSMA therapy which is used in advanced prostate cancer, as it binds to prostate-specific membrane antigens (PSMA) on cancer cells, delivering radiation directly to tumors while not damaging normal tissues
However, nuclear medicine therapy is not recommended for every patient, as some radioactive drugs may temporarily affect bone marrow function or require special precautions to limit radiation exposure to others; which may not be possible for some people However, this field is exciting with a lot of new research taking place and new radiopharmaceuticals are being developed to improve success and make it more available for a wider range of people, making nuclear medicine an increasingly vital part of modern cancer care
As well as being used for medical treatment, nuclear chemistry is also used in a diagnostic manner by using radioactive tracers in diagnostic scanning By doing this, doctors can better assess the functioning of different structures within the body Each organ in our bodies functions differently so doctors and chemists have discovered various chemicals that are absorbed by particular organs, allowing for diagnostics that are more personalised to each patient For example, reiterating what was said previously, the thyroid absorbs iodine so radioactive iodine is used in scans of the thyroid By absorbing the chemicals the structures of the organs become more clearly defined, allowing for tumours to be detected/monitored more accurately while also providing better insights into how the specific organ is functioning Diagnostic radiopharmaceuticals are used in many different ways: to evaluate blood flow to the brain, to monitor the functioning of organs such as the liver, lungs, heart, and kidneys, to assess bone growth, and to verify various diagnostic procedures As well as that, they are also used to assess the success of a surgery, such as to see if all of a tumour has successfully been removed
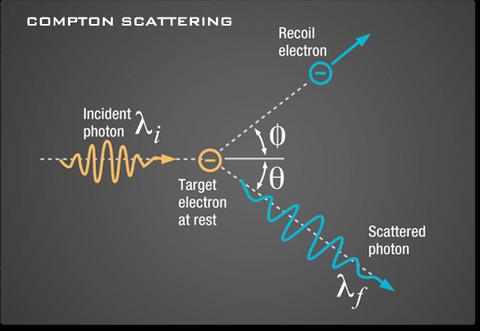
Single Photon Emission Computerised Tomography is the current most major piece of scanning technology used to diagnose a wide variety of medical conditions, based on the earliest technique of detecting single photons using a gamma camera SPECT scans use high energy gamma photons (electromagnetic particles) which are emitted from a radiopharmaceutical These meet a detector known as a “scintillation crystal” where the photons are amplified into light and processed by a camera
These scanners are often combined with CT Computerized Tomography, which enhances image quality and accuracy in order to better observe the uptake and spread of the radiopharmaceutical, overall giving doctors more accurate results to help diagnose patients and can provide an accurate 3D representation of the structure of large tissues and organs
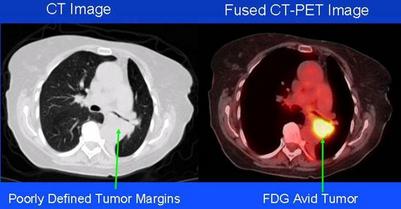
An even more modern technique is known as Positron Emission Tomography (PET scans). According to the National Cancer Institute, a radionuclide is “An unstable form of a chemical element that releases radiation as it breaks down and becomes more stable.” These are usually introduced to the body via an injection and build up in the targeted area. As these isotopes decay, they release a positron (a positive electron). When a positron and electron come together, they annihilate, consequently producing 2 identifiable gamma rays which travel in opposite directions. These are detected by a PET camera and so doctors are able to locate exactly where the particles annihilated.
PET scans are often used in oncology a study primarily focused on cancer treatment Fluorine-18 is often used as the tracer, and using radioactive tracers has proven to be the most accurate and non-invasive technique of treating, evaluating and diagnosing cancers Another use is to diagnose cardiovascular diseases and monitoring and diagnosing different types of dementia
These scanners can also be combined with CT scanners to provide better imaging According to The World Nuclear Association, combining PET with CT enables for 30% better diagnoses compared to using a traditional gamma camera alone PET can also be combined with MRI Magnetic Resonance Imaging, specifically for brain imaging which allows better imaging of soft tissue with more contrast using magnetic resonance spectroscopy
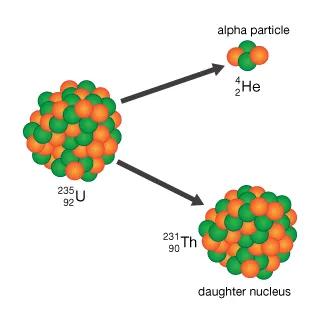
According to the International Atomic Energy Agency, a radioactive tracer is “ a chemical compound in which one or more atoms have been replaced by a radioisotope.” This means that when they decay, they release detectable particles or gamma rays which are often absorbed by tissue and so can be used to produce 3D imaging of 3D bodily structures such as the brain, heart, stomach and colon with sufficient contrast. They can also be used to track movement and flow of specific substances throughout the body An important aspect of Nuclear Medicine is deciding on what particles and isotopes to use, and this is decided fully by the radiation they emit and the particles’ half life Alpha decay is where an atom decays into a new atom, emitting an alpha particle which consists of one proton and two neutrons (the nucleus of a helium atom) This type of radioactive decay produces highly ionising radiation, meaning it has a very good ability of knocking electrons from atoms it penetrates This makes alpha decay dangerous, however, it has very little penetrating ability and can barely get through a piece of paper or the outer layers of skin Its high ionising ability means it can be used to selectively destroy cancer cells
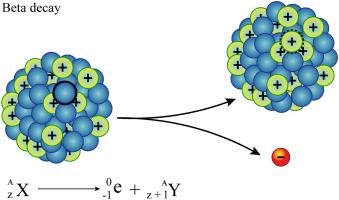
Beta decay is where an atom decays into a new atom by changing a neutron into a proton and fast moving electron (a beta particle)
Beta radiation is less ionising than alpha and can travel through centimeters or metres of air and millimeters through skin or tissue It is moderately ionising Beta-emitting radiopharmaceuticals have a wide range of uses in cancer treatment such as radioimmunotherapy
Beta radioisotopes are also used in brachytherapy and more specifically used to treat eye and bone conditions
Gamma decay (rays) are high energy electromagnetic waves, also known as a packet of photons, which are less ionising than alpha particles but very highly penetrating and can only be stopped by thick sheets of lead. This means they can easily pass through medical equipment and so are often used for sterilisation to kill viruses and bacteria which could contaminate penetrative equipment such as syringes. This decay often happens after alpha or beta decay and the atom isn’t changed while undergoing this decay
Gamma rays can also be used to target and kill cancer cells in radiosurgery However their high penetrating ability also puts healthy cells at risk and can even kill them or cause them to multiply themselves This often is what makes
radiotherapy so debilitating for patients, as it isn’t only their cancer cells which are being killed in the process Additionally, their ability to pass through the body is why they can be detected by SPECT and SPECT-CT scans This has revolutionized imaging, providing doctors with even more accurate results
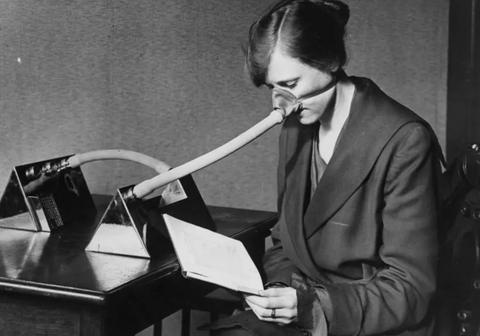
When using radioactive tracers in medicine, it is imperative to ensure that the patient spends as little time as possible with radioactive substances in their body. This means that doctors must choose radiopharmaceuticals with a relatively short half life the amount of time it takes for ½ of the atoms present to decay. Common radioactive isotopes used, for this reason are: Fluorine-18 (PET scans), Technetium-99m (generally used in nuclear medicine), Xenon-133 (introduced by inhalation for pulmonary function testing), and Rubidium-82 (introduced by IV for myocardial (heart muscle) imaging, Iodine-131 (thyroid cancers) and Radium-223 (treating bone tumors from metastasizing prostate cancer)
Through the use of radioactive tracers and advancing imaging technology, the field of radiology has massively benefited with earlier and more accurate diagnoses becoming more achievable Nuclear medicine therapy in cancer treatment has also extended the life of many people, and massively improved even more people's quality of life, and will continue to help thousands, especially thanks to exciting new scientific advances which will come in the future Using nuclear medicine is also minimally invasive, making trips to the doctor much less stressful for patients Despite this, radiation exposure always carries a risk, especially with repeated exposure Overall, nuclear medicine plays an incredibly important and significant role in diagnostic medicine and the field of cancer treatment and research

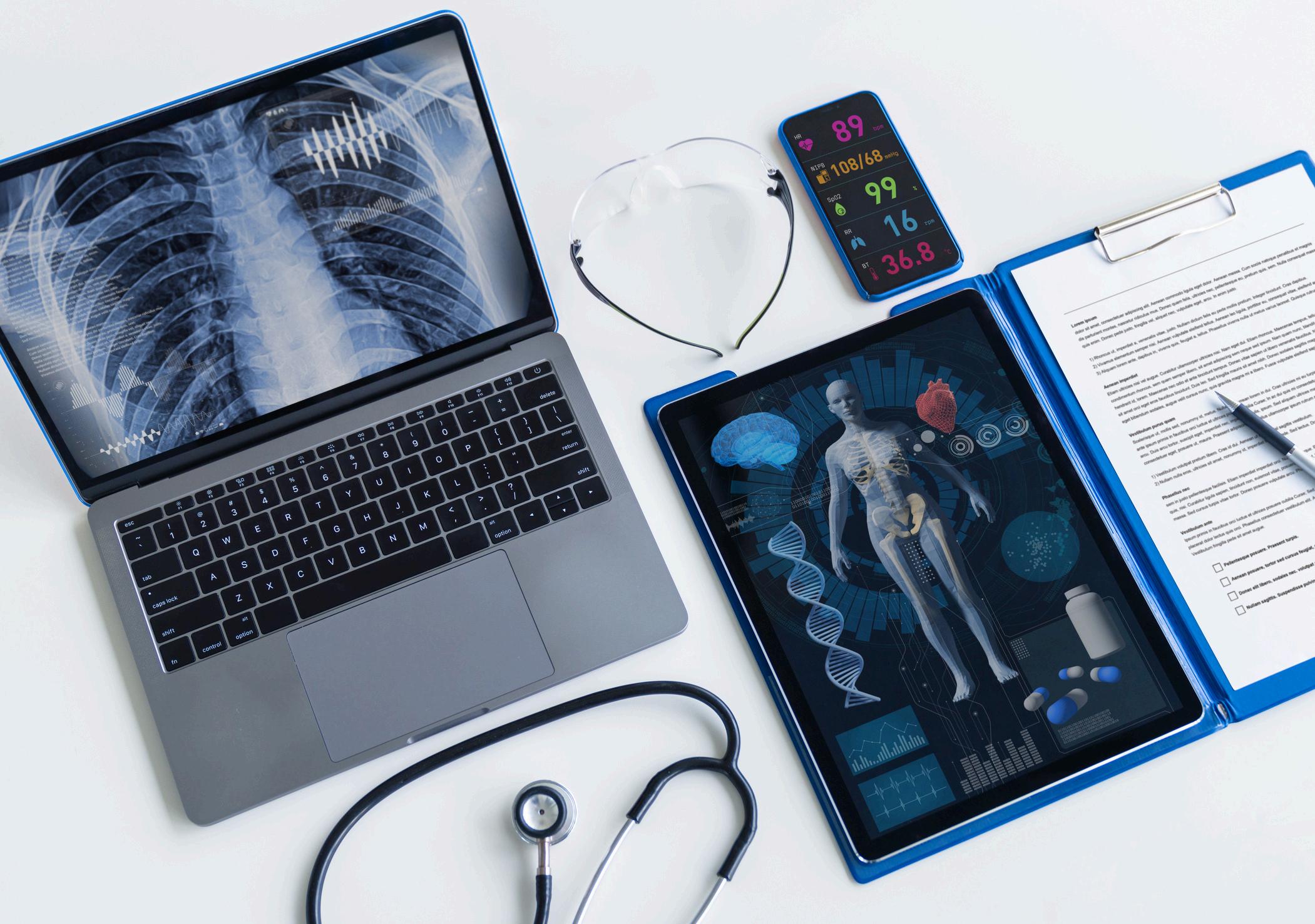
Medicine and technology both fields that are everexpanding, ever-changing, and ever-improving. With gene editing becoming more apparent, telemedicine taking over the industry and AI towering over the world, it’s evident now more than ever that the bridge between these two vast worlds is slowly narrowing. In fact, 500 million people all around the world are undeniable proof of this, as they wear smartwatches every day. This number has increased since the creation of the smartwatch in 1998, and likely will only increase further as technology improves and becomes more widely accessible And this is only one example of how technology has helped millions around the world manage and track their health and it’s wonderful, it really is In fact, imagine a world where everyone wears an advanced smartwatch; a world where everyone has access to high-tech medical instruments; a world where everyone’s doctor is a highly technical, highly trained, highly efficient robot However, this begs a question would this world be the utopia everyone’s dreaming of or would you end up at an appointment with the next M3GAN?
Well, what better way to understand how technology is improving or perhaps infiltrating the medical field, than to speak to someone who has been involved in it for over 30 years? So, I hopped onto a Zoom call with Doctor Govindan Unni, the Professor and Head of Department in Jubilee Mission and Medical College Research Institute in Thrissur, Kerala better known to me as my great-uncle, and attempted to answer the question everything boils down to will your next doctor be a robot?
However, before directly diving into the future of medicine, I first wanted to understand the past, and look into Dr Unni’s journey into cardiology In fact, he never grew up dreaming of white coats, stethoscopes, or saving lives in dramatic, movie-worthy moments His decision to pursue medicine wasn’t fueled by passion at all

“To be frank, I didn’t join because of passion,” he confessed. Instead, he was simply caught in the great academic tidal wave of his time where the brightest students were expected to become doctors, whether they liked it or not. “If you didn’t get into medicine, then you had to figure something else out,” he said to me with a chuckle It wasn’t so much about following a calling as it was about avoiding the dreaded fate of being labeled an academic underachiever by society at the time But despite not entering the field out of some burning childhood dream, Dr Unni has no regrets Over time, medicine grew on him, and today, he enjoys his work His specific choice of cardiology, however, was more deliberate Surgery was off the table “I didn’t have the best motor skills, so that was out of the question” however, after studying general medicine and looking into specialisations, cardiology, in particular, stood out. “Two things drew me in,” he explained. “One, I had a great cardiology teacher at the time, who made it very interesting. Two, I was always interested in Physics and Mathematics. And well, the heart is basically just a pump, which is heavily related to Physics and Maths.” In a way, it was the perfect blend of logic and life-saving work, and that was enough to win him over.
And so began a career spanning over thirty years, long enough to witness just how dramatically cardiology has changed.
“How has
“When I first started, we had no fancy machines just a stethoscope and our brains,” he quipped. He also said that diagnosing a patient back then was part science, part detective work, and wholly satisfying. “It was challenging, but that was the fun of it,” he recalled. “You had to rely on your own knowledge, instincts, and a little bit of trial and error.” Then came the era of machines.
First, the electrocardiogram (ECG) a device to help track heart rates and rhythms easier than ever before and then the angiogram a device to track blood flow through arteries and they were exciting “ a new toy,” as he put it But over time, technology kept advancing, leading to today’s reality, where most of the diagnostic work is done by technicians operating hightech equipment “Now, I just oversee everything,” he says “The machine does most of the work, and I step in if something looks off The challenge the fun has decreased ” That’s not to say it’s a bad thing In fact, Dr Unni was quick to clarify that he fully embraces these advancements “For the patient, it’s great You get a fast, accurate diagnosis, and there’s little room for error But for the physician, the thrill of solving a medical mystery has definitely faded a bit ” It’s a trade-off more precision, less detective work He is also quick to point out that this is a positive trade-off, however
“With AI rapidly making its way into the medical field, the question arises—will doctors one day be replaced by machines?”
As I asked him, Dr. Unni didn’t seem convinced. “We’ve been hearing about AI revolutionizing medicine for at least ten years now, and honestly, not much has really changed.” While AI is making exponential strides in areas like radiology and diagnostics, it’s clear he doesn’t see it completely taking over. “In general medicine, AI hasn’t reached a point where we can rely on it too much,” he explained. “Right now, it’s great for looking up information. Instead of going through hundreds of research papers, you can just ask ChatGPT. And most of the time, it’s surprisingly accurate.” He also added that if he had doubts, then he dug deeper. AI’s real power, he noted, lies in its ability to process vast amounts of data something the human brain simply can’t match “Take something like high blood pressure,” he says “There are general guidelines for which medicine to prescribe, but every patient is different AI has the potential to analyze thousands of factors at once and make more precise recommendations Maybe one day, it’ll tell us the perfect treatment for each individual ”
But there’s a catch He asked a thought-provoking question “If AI makes a mistake, who’s responsible? The doctor or the machine? At the end of the day, medicine isn’t just about the numbers It’s about human judgment, experience, and the ability to adapt when things don’t go as expected ”
“So,
“No,” he confirmed firmly “But it will definitely change how we work ” The future of medicine isn’t doctors versus AI it’s doctors and AI working together It’s evident that AI can analyze data, spot patterns, and help doctors make better decisions But a machine can’t replace human intuition, empathy, or the ability to think outside the box ” In short, don’t worry your next doctor won’t be a robot yet But they might have one helping them out And as far as Dr Govindan Unni is concerned, that’s a future worth embracing
Jess, Lower IV

Welcome aboard the pizza express, Don’t forget to clear up after your mess.
Our first stop, eating, ingestion, Please do shout if you have a question.
Mechanical digestion, chomping with your pearly whites, Breaking down the food with every single bite.
From large to small, insoluble to soluble, Enzymes breaking down nutrients into little molecules.
Chemical digestion is what this process is known as.
Occurring in the mouth, stomach, small intestine and all that jazz.
The journey continues, nutrients absorbed into the bloodstream.
Your circulatory system passing them to parts of the body, what a dream team!
The final stop is egestion, removal of the waste, Squeezed out as faeces, like a tube of toothpaste.
The pizza express is never late Isn’t our digestive system simply just great?
(P.S. I hope there wasn’t too much pizza on your plate?!)

The Eurekas is an annual physics competition for students aged 11-16 It is part of the Limit Less campaign, which has been conceived by the Institute of Physics to broaden and diversify the range of people doing physics after age 16 Click here to read Sophia’s entry

If you ' ve ever walked through a park or spent time outdoors, you’ve probably had an unexpected encounter with bird droppings While it’s not the most glamorous part of nature, bird poop is pretty fascinating, especially when you wonder why it’s white To figure this out, I had to dive into the science behind a bird’s digestive and excretory system - and trust me, it’s more interesting than you might think!
Birds have a highly specialized digestive system that’s made for efficiency. Their bodies are designed to maximize nutrient absorption while minimizing energy loss. When food enters a bird’s beak, it gets picked up and broken down, but no chewing happens. The food travels down the oesophagus and into the crop, where it’s softened and temporarily stored. From there, it moves to the proventriculus, which secretes digestive enzymes and acids Afterward, the food enters the gizzard, where it’s ground up, sometimes with the help of grit or stones Once partially digested, the food moves into the small intestine for nutrient absorption, and any undigested material continues to the ceca, where fermentation occurs Finally, the large intestine absorbs water and salts before the waste heads toward the cloaca for expulsion
But here's where it gets really interesting: birds don’t just expel waste like mammals. Instead of releasing nitrogenous waste as
urea (a liquid), birds excrete it as uric acid - a solid paste. This method is incredibly water-efficient, which is essential for birds that often live in arid environments. Birds have two kidneys that filter waste from their blood and produce concentrated urine. But instead of excreting it as liquid, this waste is turned into a solid and passed through the ureters to the cloaca, where both urine and solid waste are expelled Birds don’t have a urinary bladder, so they don’t need to store liquid waste This helps conserve water, which is crucial for survival in dry environments
The white color of bird poop comes from the high concentration of uric acid, the nitrogenous waste that birds excrete This crystalline compound is what gives bird droppings their distinctive white appearance Uric acid’s molecular structure is made up of carbon and nitrogen atoms, and it’s a solid that doesn’t require much water to excrete. This makes it perfect for birds that need to conserve water. In addition to uric acid, bird poop may contain minerals like calcium, sodium, potassium, magnesium, and phosphorus, depending on their diet. Birds that eat calcium-rich foods, such as seeds or bones, are more likely to excrete calcium, though uric acid is the dominant component responsible for the white colour
In some species, another nitrogenous compound alled guanine may also
appear in droppings Guanine is a purine derivative like uric acid, but it’s much less common It typically forms in birds that eat fish or invertebrates Guanine contributes to the white crystalline appearance of bird poop, though it’s usually in smaller amounts than uric acid.
The way birds excrete uric acid instead of urea is an evolutionary advantage. By excreting solid nitrogenous waste, birds conserve water more effectively than mammals, making them better suited to survive in hot, dry climates. Whether they’re soaring through the sky or perched on a fence, their white droppings are a sign of their efficient, water-saving adaptations
So, next time you find yourself beneath a bird, remember that the white droppings aren’t just a mess - they’re a great piece of evolutionary design They’re the result of a highly efficient system that conserves water, maximizes nutrient absorption, and supports the high metabolism required for flight While bird poop might not be the most glamorous thing in nature, it’s a fascinating testament to how birds have adapted to their environments.
Ellanya, Upper IV
Dhanya, Upper IV
Born in Kaunas, Lithuania, Arminas Ragauskas invented the very first non invasive, ultrasound head gear device that detects the early stages of brain pressure in both zero gravity and here on earth In his early years, he had a real interest in science and therefore he studied in one of the best universities in Lithuania (Kaunas Technology University) To further his scientific research, he opened the Telematics Science Laboratory at the Kaunas University of Technology Because of his incredible STEM related discoveries he won the European inventor award in 2016 Ragauskas’ main motivation was due to his mother’s diagnosis of a stroke Driven by his passion he decided that if there were no cures on the market he would invent it himself
Well, his non-invasive headgear device is the safest way to measure brain pressure, perhaps after TBI (traumatic brain injury) or to check brain tumours, strokes, blood clots and infections (all of these forms of trauma can increase pressure in the skull rapidly) But how does it work? Ragauskas’ invention is similar to a blood pressure monitor, where an artery is temporarily blocked by inflating the cuff The pressure in the cuff is gradually reduced, and as the external pressure resembles the blood pressure in the body, blood can flow freely through the artery again. The doctor will then hear the patient’s pulse, however this does not work with the brain as the rigid skull is in the way. Ragauskas decided to apply his knowledge of this and replace it with a similar scenario. Checking pressure in the brain by sending ultrasonic waves through the eyes. He invented a special pair of glasses that are airtight with an ultrasonic probe integrated with an air hose, so air pressure in the eye can be controlled. The ultrasound targets the eye but specifically the ophthalmic artery. This vessel has a very special feature as the inner half of it lies in the brain and the outer part sits directly behind the eye which is important for the monitor to work. If there is a dangerous increase of pressure within the skull the ophthalmic artery is compressed, causing blood flow in the inner part of the artery to increase more rapidly than the outer half. An easier way to find the inner pressure is to make the blood flow equivalent to the outer part and so it must be increased until both arteries flow at the same speed and time. This will happen if the pressure on both sides of the ophthalmic arteries are the same He says, ‘We are slightly changing the diameter of the ophthalmic artery’s shape in order to find the balance between them ’ and ‘This procedure is completely safe as the pressure exerted by the device on the eye is as minimal as being in a depth of 70 centimeters of water, you will actually feel more pressure on a plane than with this device ’
Currently Ragauskas’ invention is being tested in zero gravity because of a space phenomenon that had scientists puzzled for years The consequences leave 60% of astronauts, who spend one to two weeks in weightless space, blind or with impaired vision Scientists have found that the reason is still somewhat unknown however they know it has something to do with intracranial pressure (inner brain pressure) which results in brain swelling Fortunately, for NASA and their astronauts, Ragauskas’ eye gear will make it possible for them to stay in space for a longer period of time in the near future

This year the theme of British Science week was ‘Change and Adapt’. The students were invited to write an article on this theme and submit it to the annual Science competition We had many excellent entries, but two standout ones were from Emily in LVI and Nikita in UIV.
Imagine it’s 1918, and in a small rural village in Italy, a young boy of seven lies in a small cot, his body burning with fever, his face a grotesque shade of indigo His mother, who is weary and frail, sits beside him, gently wiping his forehead with a cloth The room is stifling, filled with a scent of sickness that has been marinating in the village for weeks He’s likely got days, hours even, before he succumbs to the illness, as many of his friends and family have in the previous few months.
This was the harsh reality for 1 in 5 people worldwide during the “Purple Death” (promptly named after the colour it turned people’s skin when infected) pandemic that swept across the globe. In fact, by 1919, the disease had cruelly claimed the lives of 50 million people around the world adults and children alike
However, as of today, we’re all likely to have contracted an extremely similar strain of influenza to the Purple Death (or Spanish flu1) and healed from it without any complications or purpling skin for that matter In fact, scientists associate strains of it with type A influenza, which is the most common of the three types, and often circulates as the “winter flu” So how is it that history’s deadliest flu, that killed more people in mere months than any other virus in recorded history, no longer affects us any more than a seasonal cold? How is it that such a monstrosity of a virus can now be cured with a packet of tissues, an orange a day, and history’s greatest cure time?
In short, it’s thanks to change in medicine, in human immunity and in the way we handle the virus itself

The change in medicine is likely the most prominent medicine being an everimproving and expanding field. We know today that the Purple Death was likely a subtype of influenza, deeming it a virus Because of this simple fact, we now know that a simple antiviral such as Oseltamivir would prove effective against the disease with modern scientists having tested common influenza vaccines on mice with the flu, and even those having provided some protection against it Despite today’s solution seeming simple and nothing short of ordinary, the fact that medical professionals at the time did not know it was a virus prevented them from providing successful medical solutions for patients Their collective understanding of infectious diseases was still in its early stages, and the concepts of viruses and how to cure them were not well-established. Doctors had little to no clear understanding of how the flu was spreading or how to treat it effectively, leading them to treat patients with ineffective remedies, such as quinine or the use of herbal treatments. However, doctors often administered treatments that were symptomatic, so painkillers like Aspirin were extremely common The lack of antiviral medication and vaccines meant that medical professionals had no means of directly targeting the virus, only helping with the pain and symptoms,
causing the pandemic spread unchecked.
In today’s world, we have vaccinations and cures built on decades of research and understanding, as well as tools and knowledge to help create new ones as we did during Covid majorly lessening the chance that frequent epidemics will occur, let alone a resurgence of a past one We also know that viruses such as Influenza pass through respiration and contact, so we would be able to put up valid security measures like social distancing and put in place guidelines such as wearing masks in public places to lessen the chances of rapid spread.
Additionally, to suffer from the virus, we must first catch it an incredibly hard thing to do today. The reason we don’t see the Purple Death anymore, and why it can’t kill us in the same way, is in part thanks to the evolution of human immunity. Human populations today have been exposed to similar viruses, particularly influenza A, which, as mentioned before, is very similar to the Purple Death variant, and people have developed immunity to it either through natural exposure or vaccination Also, as the virus spread over time, people (especially in Europe, which was most heavily affected),
gradually built up immunity to it the bodies of those who survived the virus itself naturally developing antibodies protecting them from getting ill again
How is it possible that a virus that killed over three times more people than World War I would barely affect us today if we were to be exposed to it? Well the answer is evidently change. The way that we as humans have learnt to adapt, to develop, to cure over time is nothing short of fascinating. All in all, I’m sure we’re all grateful for this change partially because we didn’t have to wear these outrageous flu masks during Covid-19
Calculators are our best friends, we use them in every Maths lesson, sometimes even in Science lessons before GCSE. After that, some of us may walk separate paths and not encounter calculators anymore. Nevertheless, calculators were one of the greatest innovations in human history; without them, countless science theories could not be proven; without them, innumerable businesses would run into bankruptcy. But have you ever wondered about the story behind calculators?
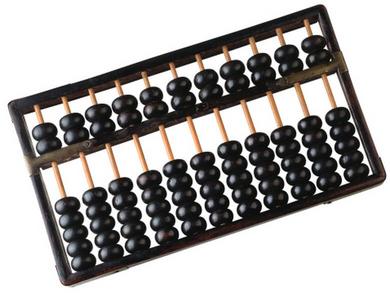
The first ‘calculator’ was the Abacus Introduced and created in the ancient time (about 2000 BC), it was popularly used among Ancient Civilizations like China, Rome and Egypt Though these civilisations were never proven to have communicated, they all happened to invent a similar tool to serve an equivalent cause: trade This tray-like tool assists humans in performing basic addition and subtraction for simple trading in markets The increase in human populations led to the increased numbers in trading, thus leading to the development of the Abacus. Each column was its unit; for example, the one far right is ones, and the one next to it is tens. Each bead in the bottom part accounts for one, and each bead on top accounts for five. Simply move the beads towards the middle rod for addition and away for subtraction. The number represented by the beads on the middle rod is the answer. Though this tool was useful, users still rely on counting; therefore, it could not be seen as an actual calculator.
Fast forward 3600 years, the world's first calculator recorded in history was created: the Pascal Calculator It was invented by French Physicist Blaise Pascal in 1642, initially for his father's job as he was a tax collector Unlike the manual Abacus, the Pascal Calculator was an actual machine, a fully functional automated mechanical calculator that ran by ‘counting integers’. The image on the right shows the brilliantly calibrated machine with six input wheels that correspond to six standings and two display bars. Like using old-school rotary telephones, digits are inputted by rotating the wheels (each digit corresponds to a spacing in the wheel), the gears inside the machine will rotate by its corresponding distance and thus display the answer in addition. But there is a problem with mechanical gears: they can’t rotate in both directions. So, how do they perform subtraction? To tackle such an issue on a mechanical calculator, Pascal came up with an idea

He used the 9’ complement. The 9’ complement of a digit is the difference between 9 and the digits, e.g. the 9’ complement of 5 is 4. Pascal figured out that the 9’ complement of the difference in any two numbers equals the sum of the 9’ complement of the minuend and the subtrahend. For instance, if the calculator has to calculate 8 minus 2, it would first find the 9’ complement of 8, which is 1. Then, do an addition between 1 and 2. The answer would be 3, which is the 9’ complement of 6: the answer of the initial subtraction. This way, subtraction can be easily turned into addition and be performed on a mechanical calculator.

From then on, mechanical calculators were the major machines that performed calculations automatically They played an important role in science and accounting in the next 300 years The Curta Mechanical calculator on the left was one of the newer models created in the 1950s As one can see, the size had shrunk to palm-sized, but surprisingly, the mechanisms and fundamental principles of mechanical calculators were unchanged The 9’ complement was still used in newer models, proving Pascal’s success and contribution to the development of mechanical calculators The change in development path was predictable; as war time approached, demand for portable mechanical calculators increased. Soldiers and officers needed to do simple calculations in war zones, but they couldn't carry a bulky machine with them, thus leading to rapid development in mechanical calculators. These calculators are much more durable than our electronic ones! Many Curta Calculators are still being kept in pristine condition and are still functioning, costing more than £1000 for collections!
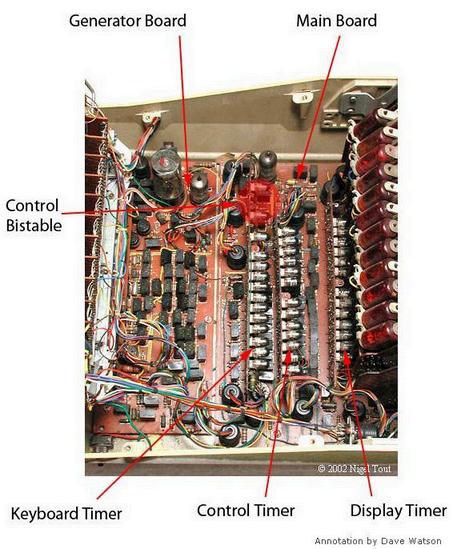
After the war, global economics had finally started to regrow. With more small businesses being set up and the rapid population boost after WWII, calculators were once again in high demand. However, mechanical calculators are too expensive as they are mostly made of metal gears and valves. It’s difficult to reduce their cost just by shrinking their sizes. Therefore, manufacturers started to focus on electronic calculators By 1962, Bell Co of Uxbridge, an English company, had invented the first all-electronic calculator Smaller businesses in British colonies like Jamaica and Hong Kong became the biggest customers for the new electronic calculator due to its lower price The image on the left is a picture of the motherboard Can you notice something special about it? Compared to modern digital calculators with silicon motherboards that run by codes, these calculators run in vacuum tubes! Pulses are sent to the motherboard when individual digits are entered in the standings For example, 5 pulses will be sent by the generator board if a digit 5 is entered The keyboard timer, control timer and display timer are made of small vacuum cathode-ray tubes, they are small electron guns that shoot a beam of electrons to the neon-filled light bulb in the far right of the image. This is how they display numbers! Shooting electrons through pigmented gas! More interestingly, these cathode tubes also store a small amount of data in calculations, this means that they will flash and flicker when being used!
Now, we have entered the era of digital calculators Our calculators can perform subtraction independently, without converting them into addition, and unfortunately, they do not flicker and flash anymore Nowadays, calculators are mostly used by students and scientists, they are still one of the most important tools in academia They can perform much more complex calculations and draw graphs Some calculators are even programmable and can be used to play games! Check out if yours is programmable! (But remember, don’t play them in lessons!)
