OPTIMIZING SEXUAL AND REPRODUCTIVE HEALTH FOR OUR ADOLESCENTS AND YOUNG PEOPLE

 Prof Cathy Ward, Dr Hlengiwe Sacolo, Chelsea Coakley, Consolata Nsanzimpaka Nsanzubuhoro, A/ Prof Elona Toska
Prof Cathy Ward, Dr Hlengiwe Sacolo, Chelsea Coakley, Consolata Nsanzimpaka Nsanzubuhoro, A/ Prof Elona Toska
DIGITAL HEALTH WEEK 10 October 2022
OUTLINE


PRESENTATION
• Potential of mobile phones in improving adolescents SRH • Research goal • Research team • Approaches & Considerations • Way forward • Discussion
AFRICA YOUTH’S CHALLENGES!
Africa has the youngest population in the world and will count
100 millions more youth by 2030 (UN DESA, 2019)
4,500

New HIV infections among adults (aged 15 years and older) every day


Among young men (aged 15-24 years)
Among young women (aged 15-24 years)
Among young people (aged 15-24 years)
Africa has the highest number of HIV infections and highest number of new infections among among youth (UNAID, 2020)
37%
15% 22%
Ages 15 19 Ages 20 -29 Ages 30 -39
WHY AN APP FOR SRH?

• Urgent need for good, accurate, engaging SRH education • App - based interventions • Easy, low-cost way to go to scale • Supports fidelity to the intervention • Engages the target audience • Cuts out the “cringe” factor for adultadolescent models
MOBILE PHONE USE & ADOLESCENTS’ SRH?
Access to internet: 69% of youth worldwide (40% only in Africa)
Public health experts and policymakers suggest that the use mobile phone for health will improve ASRHR
With the increasing internet coverage, mHealth presents opportunities to increase adolescent’s SRH knowledge
Future mHealth programme implementations can benefit from ongoing research on the topic
SEX DIFFERENCES
11 5 8 22 34 31 13 3 11 39 54 45 60 40 20 0 20 40 60 Health information Sex information HIV information For Facebook For SMS For WhatsApp Percent Mobile phone use Adolescents use mobile phone more for social media than for health-related information (MW study) 43 56 Girls Boys Access to mobile phone Higher proportion of access among girls than boys Boys Girls MOBILE PHONES: ACCESS, USE –
SOUTH AFRICA
Findings – only health use combined with social media makes a difference!
• No significant association between phone access and sexual risk behaviours
• Health content use is associated with reduced risks of sex after substance use (in general and mainly for boys) and infrequent condom use (in general and for both boys and girls)
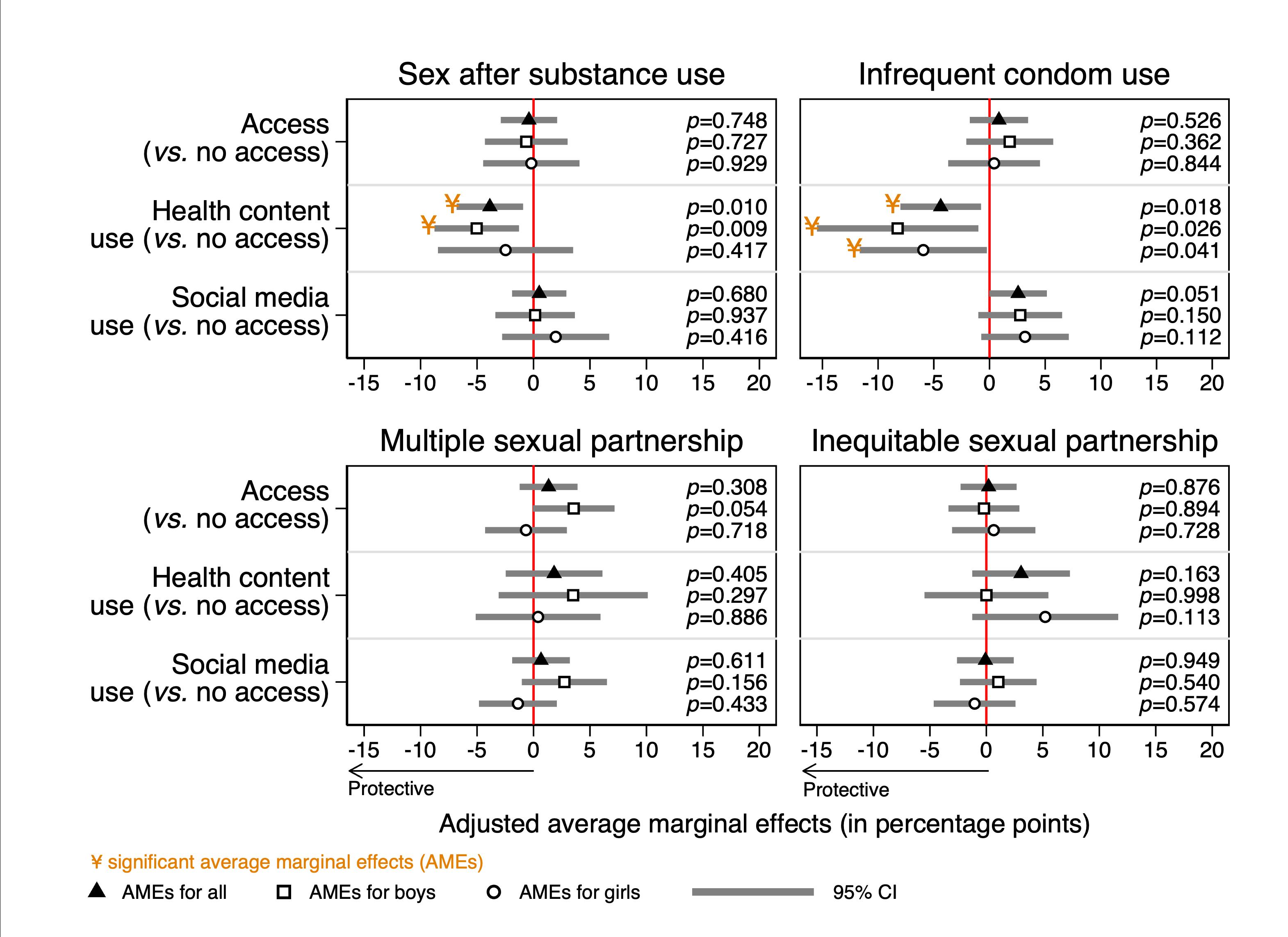
Banougnin, Toska, et al. analyses in progress.

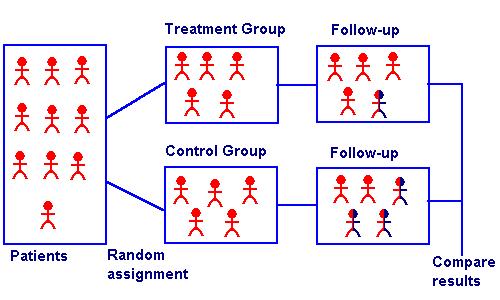
1. No unintended, nor any harmful effects 2. Investigate if the app works to achieve desired outcomes (effectiveness) WHY RESEARCH? 3. Explore how the app is taken up, used by young people (acceptability & feasibility) 4. Cost the intervention to support prioritization & scale-up
DESIGNING PUBLIC HEALTH INTERVENTIONS COMPLEX ISSUES, COMPLEX SOLUTIONS
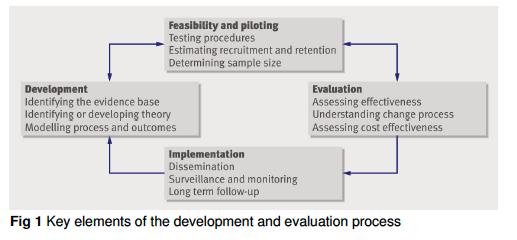

Phase 3. Refine, adapt Acceptability Feasibility Phase 1. Formative research STUDY PHASES Phase 2. Effectiveness Phase 4. Costing & Scale-Up
STUDY TEAM
Prof Cathy Ward



Investigator
Investigator

Principal
A/ Prof Elona Toska Co-Principal
Dr
Hlengiwe Sacolo Lead Investigator Dr Bolade Banougnin Lead quantitative investigator Chelsea Coakley Co-Investigator Consolata Nsanzimpaka Nsanzubuhoro Early Career Researcher
PHASE 1. FORMATIVE RESEARCH
1.
To understand initial impressions of the look and feel, usability and content of the App including the acceptability of survey questions.
To explore potential barriers and facilitators to initial engagement.
To explore experiences and lessons learnt (what worked well and what didn’t)
2.
3.
PHASE 2. RESEARCH OBJECTIVES
1. To use the inbuilt data collection system, pre- and postintervention surveys, and qualitative interviews to investigate initial evidence of effectiveness on target outcomes by evaluating the effect of the programme on primary and secondary outcomes

2. To examine the impact of the Love Land App in promoting positive behaviour change (including developing adolescents’ decision making, communication and negotiation skills in a safe virtual environment to prevent early sexual initiation, unwanted pregnancies, STIs and sexual violence).
WHAT DO WE NEED TO ESTABLISH EFFECTIVENESS
• POPULATION: age-group, location, platform (school, community), etc.
• INTERVENTION: design refined and tested with young people
• CONTROL: school-based study?
• OUTCOME(S): knowledge, beliefs, norms, self-reported practices, access to SRH services
• TIMELINE: how long do we expect change to take place in/ happen
How do we get what works to people with greater quality, speed, fidelity, efficiency, and relevant coverage?
PHASE 3. IMPLEMENTATION SCIENCE
IMPLEMENTATION SCIENCE: REQUIREMENTS FOR SUCCESS

WHAT HOW WHO + WHERE
Implementation Science
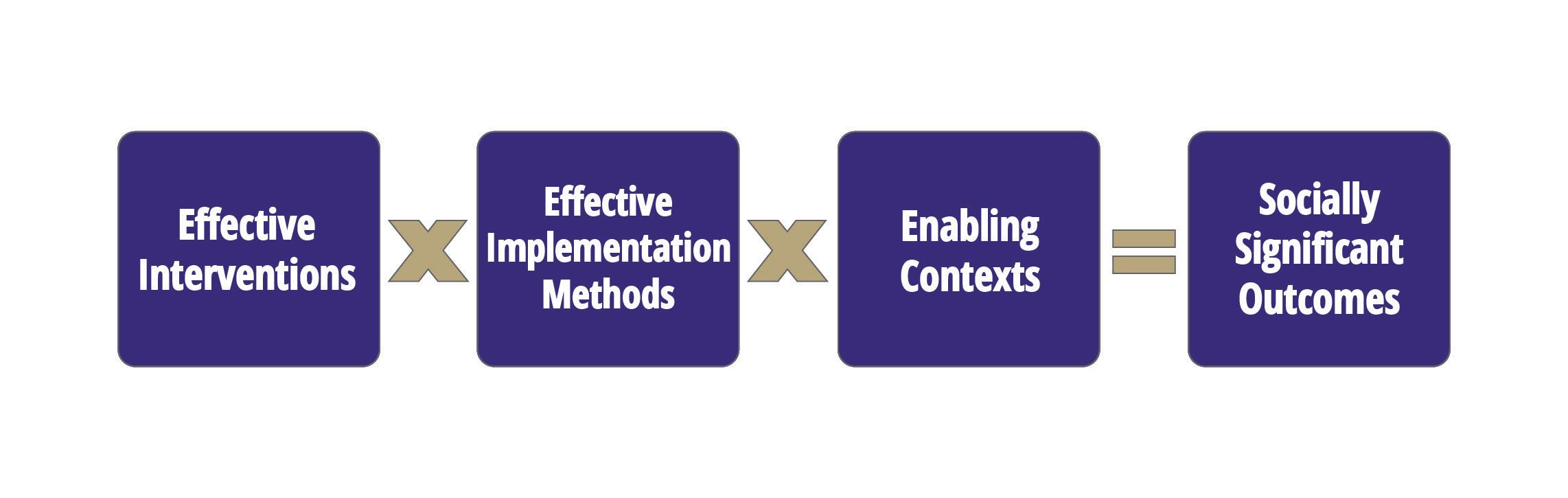
16
Adapted from the
National Implementation
Research Network
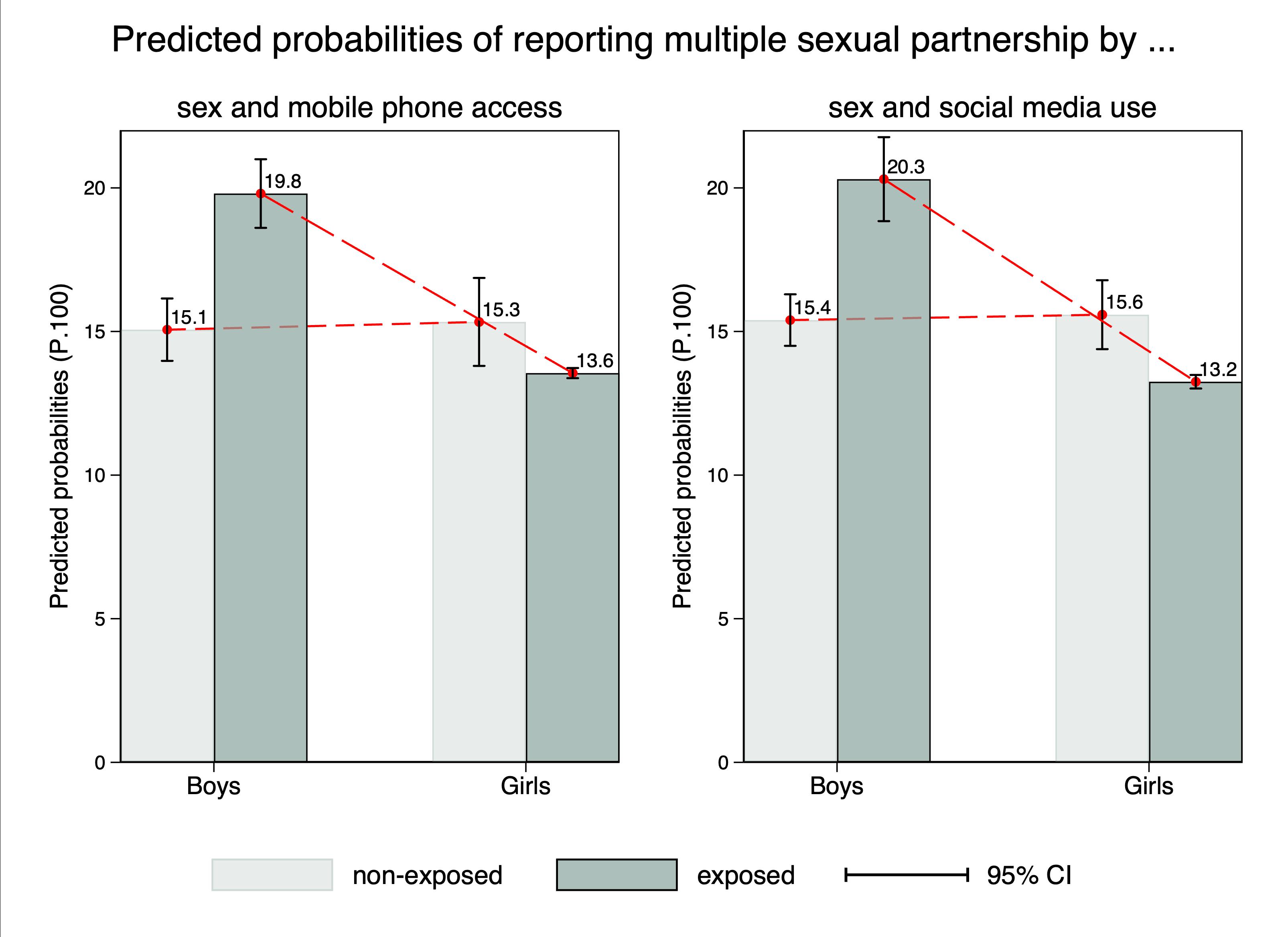
SEX DIFFERENCES
Mzantsi Wakho: access & social media use works differently for boys and girls!
Access and social media use were non-protective of multiple sexual partnership for boys but protective for girls
IMPLEMENTATION SCIENCE RESEARCH QUESTIONS (e.g.)
• Does it work the same for adolescent boys and girls?
• Does it work differently when delivered in schools or out-of-school clubs?
• Are facilitators (peers, teachers, etc.) needed?
• YOUR EXAMPLES?

STEPS
Partnerships and stakeholder engagement
development/ update
funding applications
NEXT
•
• Intervention
• Research

THANK YOU cathy.ward.sa@gmail.com Elona.Toska@uct.ac.za HNSacolo@gmail.com
