Nabilah Mustafa | Onyinyechi G. Nwosu | Beatrice Odhiambo | Marvin Paguio | Manav Patel, BSA
Amani R. Patterson, MBS, BA | Aaron T. Phillips, BS | Dylan Pillivant | Jaela Rose | Prajna A. Sahadeo, BA
Nangah N. Tabukum, BS | Alexis Thompson | Jada C. Tyler | Tiffany Williams, PhD
INQUIRES publications@snma.org
DISTRIBUTION
The Journal of the Student National Medical Association is published biannually by the SNMA. It is available online, digitally, and in print. For subscription information, please visit our website, www.snma.org, or send an e-mail to publications@snma.org.
REPRINTING
No articles, illustrations, photographs, and any other editorial matter herein may be reproduced without written permission of the JSNMA. To reprint articles appearing in this issue, reference the article using the following text: “This article was re-printed from the 2023 Spring Issue of the Journal of the Student National Medical Association, first published May 2023 by [AUTHOR].
The Student National Medical Association (SNMA) is committed to supporting current and future underrepresented minority medical students, addressing the needs of underserved communities, and increasing the number of clinically excellent, culturally competent and socially conscious physicians.
JOURNAL OF THE STUDENT NATIONAL MEDICAL ASSOCIATION
Oluleke Falade currently serves as the publications committee co-chair for SNMA. Born in Port Harcourt, Nigeria, he was raised in Houston, TX. He earned a B.S. in Chemistry along with a minor in Sociology from the University of Pittsburgh. Presently, he is a third year of medical student at the University of Pittsburgh School of Medicine.
Mikayla Shields
Mikayla Shields currently serves as the publications committee co-chair for SNMA. She grew up in Orlando, FL and graduated in December 2019 from the University of South Carolina with a Bachelor of Science degree. After completing four years as a Division 1 student-athlete and professional athlete, she matriculated into medical school at the University of Pittsburgh School of Medicine where she is currently a third-year medical student. She plans to graduate in 2025 and apply to residency with interests in Women’s Health and Orthopedic Surgery.
Chinyere Onyeukwu
Chinyere “Chinma” Onyeukwu grew up in a town in Northwest Indiana called Munster, Indiana. She received her B.S. in Medical Laboratory Sciences from Purdue University In West Lafayette. She is currently a fourth-year medical student at Rush University Medical College in Chicago, IL. She plans to apply for residency in internal medicine with interests in hematology-oncology, research, and health equity.
Destiny Farmer
Destiny Farmer is the current MAPS National Publications Liaison. She is a proud graduate of Xavier University of Louisiana, where she earned a bachelor’s degree in biology. She went on to pursue a master’s degree in biology from Chatham University and an MBA in healthcare administration from Mercer University. Destiny is a passionate advocate for women’s health. She is currently working to become an OB/GYN to reduce disparities in healthcare access for women.
CHAIR’S LETTER
Greetings SNMA Family,
It is with pride and deep reflection that I welcome you to the Summer Edition of the Journal of the Student National Medical Association (JSNMA), themed “Medicine at the Margins: Advocacy for the Unseen.” In this issue, we confront the uncomfortable truth that many voices remain unheard, and many lives remain underserved within our healthcare system. Our contributors have courageously given space to stories and studies that challenge us to see what has long been hidden.
Through compelling narratives, sharp analysis, and powerful creative works, this edition highlights the structural and institutional forces that often leave entire communities on the outskirts of care. These contributions remind us that equity cannot exist without visibility, and visibility requires advocacy. As physicians in training, we are uniquely positioned to advocate for those who are left out of traditional systems, and to reimagine a healthcare model rooted in justice.
May this issue challenge us all to look closer, speak louder, and push harder for the patients who are too often pushed aside. I hope the perspectives you find here stir your empathy, strengthen your resolve, and remind you of the responsibility we carry as future leaders in medicine.
With gratitude to our authors, editors, and all who brought this edition to life, thank you for being part of this mission.
Yours in SNMA,
Mychael T. Spencer, M.Ed. Student National Medical Association
Chairperson of the Board of Directors 2025-2026
Indiana University School of Medicine, Doctor of Medicine Candidate Class of 2026
Editorial Board
Meet the Team
Chair’s Letter
Listening in Silence: A Medical Student’s Reflection in Labor and Delivery
A Viewpoint on Medical School
Electives: Post-USMLE Step 1 Changes
Improving Primary Care in Underserved Metro Detroit Through Medical Student- Led Health Fairs
Unspoken Permission
Will I ever see home? Excerpt from the NICU wards.
My Beloved
The Hands That Built My Dream, A Tribute to My Dad and Grandfather
A Rare Case of “Hell’s Itch” in a Puerto Rican Female
Assessment of sunscreen usage among adults in the metropolitan area of Puerto Rico: Implications for skin cancer prevention
Exploring Alternative Therapeutics for Vitiligo: A Systematic Review
Amber
Vaccine Hesitancy and Uptake in South Africa: Factors Influencing the Effectiveness of COVID-19 Vaccine Regional Rollout
History of Sterilization and Birth Control of African Americans
The Ripple of Roe’s Reversal: A Retrospective Analysis of Shifts in IUD Utilization Among Women Aged 15–49 Before and After the Dobbs Decision
Anatomy of a Tumor
The Role of Cognitive Behavioral Therapy in Managing Chronic Pain and Transforming Psychological Distress: A Case Report
Breaking Barriers for Women of Color in Medicine: A Journey of Resilience and Empowerment
Listening in Silence: A Medical Student’s Reflection in Labor and Delivery
Dana Alshekhlee
Assalamu Alaikum. I am Dana. My patient’s room is guarded by an older hijabi woman. I approach hesitantly, not sure if the laboring mother-to-be inside would be comfortable with my presence through her delivery. I greet the lady, introducing myself as an eager third-year medical student, hoping to take part in the patient’s journey and already feeling connected to someone I do not yet know.
Wa alaikum assalam. I am the translator! She explains that the patient is from Somalia, and knows limited English. She also wants to make sure that only females enter the room. She rushes me inside, her rapid Somali firing. The patient and her mother beam at me, wanting to know more about who I am and where I am from. She welcomes me into their journey of delivering her son. I catch myself understanding waqt (time) and daqeeqah (minute), vocabulary that our ancestors share. The family brightens when I repeat the words back to them. The patient’s brother enters, reciting verses of the Quran over his sister. The patient’s mother maintains order and calamity. After all, her baby is delivering a baby. She covers her hair with a hijab, a scarf that many Muslims wear to maintain modesty in front of males. Depending on their comfort, women who choose to wear the hijab may remove it in front of women. I joke that she can take her scarf off, that I would make sure no male providers enter the room. She laughs, but insists on keeping it on. I shrug: Maybe she is just very religious.
Her stubborn cervix maintains six centimeters for hours. Enthusiasm transforms into anxiety as the night stretches on. Meconium stains her amniotic fluid while her amniotic fluid stains our morale. This is a post-term pregnancy, her placenta became too weak for her baby. Fetal monitoring reveals the late decelerations that I studied to worry about. A cesarean section might be necessary, but she is uncomfortable with this idea.
I will wait until I am 10 centimeters.
Terbutaline temporarily stops her contractions, allowing the baby boy to inhale the breath that his mother is holding. One by one, the team leaves the room until it is bare. The translator and I are left staring at each other while the patient closes her eyes. A teardrop is liberated, falling until it is absorbed into her scarf.
I am overtaken by the vulnerability of her circumstances. She speaks few words. The room flinches each time the curtain is thrown back. Every hour, a new healthcare provider assumes entry. I pull the curtain back each time, shielding her exposure. We are still only females in the room, but she continues to secure her scarf around us. Her body language is not loud enough. She has other children at home. Is she thinking of them? How long has she been in America? What is she wondering?
When her contractions resume, so do the baby’s decelerations. The attending and residents rush back into the room, I follow them with my own distress. It is 2:00 AM and the translator has left to her solace, leaving the patient with an even deeper barrier of communication. For the rest of the night, we rely on virtual translators who cut in and out. The attending declares a final recommendation, announcing the risk of neonatal brain injury or death if they cannot proceed to a c-section. The patient pulls her hijab again, which becomes damp with her tears. And finally she utters one word:
“Ok”
I chase the nurses and residents with the translator iPad into the operating room. There is scrubbing and gowning and gloving and anxiety. Warm blankets are not enough to comfort the quivering patient. Amidst the commotion, her scarf reveals small strands of hair. A crash c-section introduces us to baby boy in under three minutes. The beautiful, ninepound wide-eyed baby adds to the ruckus, sharing his mother’s tears. The NICU team swaddles him. He is healthy.
The concept of wearing a hijab during abdominal surgery might have seemed counterintuitive to me, but perhaps it insulated her sanity. Maybe she wasn’t just “too religious”. After the surgery, we transferred her onto her patient bed. I tucked her hair into her scarf: This shield was her safe haven. Each time she was uncomfortable, she tightened this barrier—it carried her resilience.
As a medical student, new to the clinical field and even newer to such intimacy, I have come to understand that each patient has a right to feel seen and to be cared for. Patients deserve autonomy, privacy, and the benefit of the doubt while they process their own realities. Sharing culture, religion, or language is not always enough to understand. Patient’s deserve to be heard, even if we cannot understand their vocabulary. Language barriers can strip away our depth, but only if we choose to remain shallow. Unspoken words are communicated by a multitude of avenues: arm positioning, eye contact, emotion, annunciation, inflection, or even silence. A sigh of relief. Her breath of anticipation. The tightening of her scarf was more than a gesture; I was humbled to witness this dialect of strength, autonomy, and courage.
A Viewpoint on Medical School Electives: Post-USMLE Step 1 Changes
Authors: Michael Denning, M.B.A., M.P.H.,1 Adrianne Mitchell, B.S.,1 Aaron T. Phillips, B.S.,1
Medical Education is an everevolving field with recent focuses on student wellness and exposure. Academic changes, such as the transition of USMLE Step 1 to pass-fail, institutional grading systems to pass/ fail, and Electronic Residency Application Systems (ERAS) limiting the number of experiences for learners to differentiate themselves. However, clinical experiences, extracurricular activities, residency personal statements, and letters of recommendation are becoming more critical, with no academic distinctions in standardized exams and grading1. Therefore, clinical and non-clinical electives are ample opportunities to fill this gap. Electives allow medical learners to explore their future career
interests, practice clinical care in low-stake environments, and build connections with mentors while engaging in extracurricular activities, such as research and service projects2.
Electives can be either clinicalbased or non-clinical-based. Clinical-based electives are immersive exposures in which learners serve as medical or surgical treatment team members3. The experiences can expose learners to the minutia of specialty-specific residencies and careers. Non-clinical electives operate either in in-person or online formats and provide exposure to pillars of medicine that produce holistic physicians, such as
qualities of leadership, sociology, research, or medical education. The curriculums with which these experiences occur vary3. Traditionally, clinical electives are offered during the clinical years of medical school, in the third and fourth years. This variation in curriculum is present within North Carolina’s Five medical schools. At rural MD-granting instructions, two designated twoweek electives are scheduled within the third academic year after the six-week core rotations4. Conversely, a research-tailored academic institution with a fouryear curriculum, where clinicals begin in year two rather than year three, offers two one-week “selective.” Both institutions offer
1. Brody School of Medicine, Department of Medical Education
more than 14 weeks of electives during the fourth year5. These electives are more tailored to the learner’s chosen field of practice.
Due to the limited opportunities for electives during the initial clinical years, it is pertinent that medical students are well-informed about the availability of electives, the process of placement, and the analysis of any external factors that may promote or deter participation in specific electives. Consequently, the shift from a numerical grading structure has placed greater emphasis on more holistic portions of the residency application. There is now a greater need for students to seek meaningful clinical experiences and mentorship for a successful residency match. In order for medical students to have successful electives, they should think about their elective experiences as early as possible so that they can begin to connect with physicians, hospitals, and coordinators. Many students have had little guidance in this matter; therefore, change is needed for the undergraduate medical professionals coming into future generations. Medical school leadership must think of the type of guidance students may need to make these experiences obtainable. Electives can be a crucial way to distinguish an applicant from another. Students should be encouraged to talk to upper-level students, meet with advisors, and enhance their physician network6. Let us always think about the four Cs: career exploration, career solidification, career advancement, and career longevity.
Many students come into medical school with a specialty in mind, but this is likely to change over the years. The opportunity to participate in specialized electives that are not a core clerkship to increase exposure to more specialties can be a pivotal moment for one’s career. Students can not properly
determine their medical interests without exposure and career exploration. In that same notion, students can think they want a particular career but have never seen the full extent of its pros and cons. Through these experiences, learners leaning strongly towards a specific specialty will have further career solidification via these hands-on exposures. The power of networking is often underscored in life, and even more so in medicine7. Think of the student applying for a competitive specialty like dermatology or radiology, with no home program, no financial capability for a research year, and no mentors8. Networking will be their best asset for career advancement, provide opportunities to work on projects, and assist in research paper writing. An elective can allow a student to meet professionals with whom they might have never been able to meet otherwise. Lastly, there is no secret about how significant burnout can be in medicine, especially for medical students and physicians9. An elective chosen by the student
can provide autonomy for them during a point when adjusting to the diversity of medical practice by various professionals can be mentally exhausting. Also, The Brody School of Medicine offers a wellness elective for students who need a mental health break4. These electives allow students to gain introspective skills, develop appropriate coping mechanisms, and partake in opportunities to recharge and return refreshed, thus promoting career longevity. Electives in medical school provide various benefits for students. Students can change their career trajectory with proper guidance, networking, and tenacity while maintaining proper mental health.
Though most American medical schools’ core six specialties students rotate through offer guidance into related specialties and subspecialties, students should have more opportunities to increase career decision comfortability. Experiences in competitive fields earlier in a student’s medical education can allow them to take the appropriate
pathways to maximize their potential to match into that specialty10. This includes considering time to engage in a research year, identifying potential mentors, and scheduling away rotations. Research years are becoming more common as they are looked upon favorably due to the increasing competitiveness of specific specialties, and not all medical schools have research requirements11. Hosting expanded elective time can assist in research productivity, as these periods can be dedicated to research endeavors12. As such, electives may provide exposure and proper guidance for maximal potential to match into a desired specialty. This increase would benefit both the students and the match results of their home institution, which could benefit the institution’s reputation and recruit more prospective students.
Professionals within student affairs are unlike general academic counselors, who receive training to provide budding medical professionals with professional development, career counseling, and academic support10. Consequently, they are the ideal faculty to propagate this enlightenment through participation in electives. These professionals should also be well-versed in specialty trends, including match trends, application requirements, and competitiveness of the application pool. With this skill set, they can schedule electives for students to complement core rotations, deepen their understanding of specialties, and refine their clinical skills10. With this involvement, they can synthesize individualized learning plans that beneficially utilize electives for students and give them an edge during residency applications. Student affairs can use electives to address news of students in the short term to fill knowledge gaps, strengthen their residency application, and cope with the pressures of medical school by offering exposure to careers with a generally more favorable work-life balance. In the long term, they help students make informed decisions before choosing a medical specialty, develop professional growth, and map out long-term goals to optimize students’ chances of matching.
Medical education is a multifaceted field with ever-changing requirements, policies, and assessments. Therefore, learners must have the utmost opportunities to excel academically, prepare, explore, and exemplify clinically. Electives are a mainstay method of completing these actions. Electives vary among institutions in length, quantity, structure, and offerings. However, it is pertinent that medical school students are engaged in these clinical and non-clinical spaces and are being appropriately advised to ensure maximum success with career exploration, advancement, and longevity.
REFERENCES
1. Cohn, Matthew R. MD; Bigach, Stephen D. MD; Bernstein, David N. MD, MBA, MA; Arguello, Alexandra M. BS; Patt, Joshua C. MD, MPH, FAOA; Ponce, Brent A. MD; Beal, Matthew D. MD; Kogan, Monica MD; Dyer, George S. M. MD. Resident Selection in the Wake of United States Medical Licensing Examination Step 1 Transition to Pass/Fail Scoring. Journal of the American Academy of Orthopaedic Surgeons 28(21):p 865-873, November 1, 2020. | DOI: 10.5435/JAAOS-D-20-00359
2. Sheu, L., Goglin, S., Collins, S., Cornett, P., Clemons, S., & O’Sullivan, P. S. (2021). How Do Clinical Electives during the Clerkship Year Influence Career Exploration? A Qualitative Study. Teaching and Learning in Medicine, 34(2), 187–197. https://doi.org/10.1080/10401334.2021.1891545
3. Ramalho, A.R., Vieira-Marques, P.M., Magalhães-Alves, C. et al. Electives in the medical curriculum – an opportunity to achieve students’ satisfaction?. BMC Med Educ 20, 449 (2020). https://doi.org/10.1186/s12909-020-02269-0
4. Office of Student Affairs. (n.d.). M3 elective information. ECU Brody School of Medicine. https://medicine.ecu.edu/studentaffairs/m3-elective-information/
5. Duke University School of Medicine. (n.d.). Second Year | Longitudinal Small Group Sessions. Doctor of Medicine (M.D.) Program. https://medschool.duke.edu/education/health-professions-education-programs/doctor-medicine-md-program/curriculum/second-year
6. Cree-Green M, Carreau A-M, Davis SM, et al. Peer Mentoring for Professional and Personal Growth in Academic Medicine. Journal of Investigative Medicine. 2020;68(6):1128-1134. doi:10.1136/jim-2020-001391\
7. Asuka, E. S., Halari, C. D., & Halari, M. M. (2016). Mentoring in medicine: a retrospective study. ASRJETS, 19(1), 4252.
8. Chen, J. Y., & Heller, M. T. (2014). How competitive is the match for radiology residency? Present view and historical perspective. Journal of the American College of Radiology, 11(5), 501-506.
9. IsHak, W., Nikravesh, R., Lederer, S., Perry, R., Ogunyemi, D., & Bernstein, C. (2013). Burnout in medical students: a systematic review. The clinical teacher, 10(4), 242-245.
10. Sawani, J. (2022, November 9). Pursuing passion-based electives during medical school. Health Lab. https://www michiganmedicine.org/health-lab/pursuing-passion-based-electives-during-medical-school
11. Pathipati AS, Taleghani N. Research in Medical School: A Survey Evaluating Why Medical Students Take Research Years. Cureus. 2016 Aug 18;8(8):e741. doi: 10.7759/cureus.741. PMID: 27672532; PMCID: PMC5026499.
12. Sateesh Babu Arja, Sireesha Bala Arja, Kumar Ponnusamy et al. Can medical education electives promote teaching and research interests among medical students?, 17 October 2023, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-3258921/v1]
Improving Primary Care in Underserved Metro Detroit Through Medical StudentLed Health Fairs
Abstract
Community health fairs serve as valuable interventions to address disparities in healthcare access and representation, particularly in underserved areas. The Annual Martin Luther King Jr. (MLK) Community Health Fair, organized by the Student National Medical Association (SNMA) at Oakland University William Beaumont School of Medicine (OUWB), has partnered with Chandler Park Academy (CPA) since 2012 to provide health screenings and education to a predominantly Black/African American community in metro Detroit. In January 2024, the 12th Annual MLK Community Health Fair hosted 128 attendees, offering blood pressure, blood sugar, and vision screenings alongside educational activities such as microbiology and
lifestyle medicine workshops. Survey results highlighted systemic barriers to healthcare access, including cost, lack of good providers, and transportation. The fair fostered connections between students and diverse medical professionals while addressing gaps in primary and preventive care. Continued efforts to expand outreach and inclusion could further reduce healthcare disparities and improve health literacy in underserved communities.
Introduction
Primary care plays a critical role in improving health outcomes, managing chronic diseases, and reducing overall healthcare costs. By emphasizing early detection and preventive measures, primary care fosters longterm patient engagement, mitigates
disease progression, and reduces hospitalizations for conditions that could otherwise be managed in outpatient settings.1 However, access to primary care remains uneven, with underserved communities—often composed of racial and ethnic minorities—facing disproportionately high barriers. These challenges include financial obstacles, limited transportation, and shortages of culturally competent providers.2,3
Black/African American communities bear a disproportionate burden of health disparities, including higher rates of hypertension, diabetes, and maternal mortality.4 These disparities are compounded by limited access to preventive care and systemic inequities such as poverty and underfunded healthcare infrastructure. Furthermore,
1. Oakland University, Rochester, MI, United States
2. Oakland University William Beaumont School of Medicine, Rochester, MI, United States
underrepresentation within the healthcare workforce negatively impacts trust, communication, and patient outcomes, as patients often feel more comfortable with providers who share similar cultural or racial backgrounds.5,6
Community health fairs have emerged as effective interventions to bridge gaps in healthcare access. By bringing essential services directly to underserved populations, health fairs address critical social determinants of health such as health literacy, preventive care access, and representation within healthcare professions.7,8 These events not only improve immediate health outcomes but also foster mentorship opportunities for individuals considering careers in healthcare. This paper evaluates the 12th Annual MLK Community Health
Fair, held in January 2024, with a focus on its role in improving access to primary care, addressing healthcare disparities, and fostering community engagement. Chandler Park Academy is located within Harper Woods, Michigan. According to Data USA, Black/African American, White/Non-Hispanic, and Multiracial/ Non-Hispanic are the three largest ethnic groups in Harper Woods. Of the total population within this city, 20% of Harper Woods community members live below the poverty line in 2022, compared to the national average of 12.5%. In terms of healthcare coverage, 6.63% are uninsured, 28.5% qualify for Medicaid, and 9.87% Medicare. Through a primary care lens, the patient to physician ratio in Harper Woods is 1,308 to 1in the year 2020. Due to the continued interest of Chandler Park Academy in hosting the Annual MLK Health Fair with OUWB, primary care services continue to improve the number of patients served at this event with new and established attendees every year. 9
Methods
The 12th Annual MLK Community Health Fair was held on January 19, 2024, at Chandler Park Academy (CPA) in Harper Woods, Michigan. CPA is a high school serving predominantly Black/African American students from economically disadvantaged households. Organized by SNMA in collaboration with OUWB’s Diversity, Equity & Inclusion department, the fair coincided with Martin Luther King Jr. Day and emphasized themes of equity and community engagement.
Health screenings were provided for blood pressure, blood sugar, vision, and flu vaccinations. Educational activities covered topics such as microbiology, CPR, ultrasound demonstrations, lifestyle medicine, wilderness medicine, alcohol safety, and balance and reflex assessments. Each station was coordinated and staffed by OUWB medical students, with faculty members present to provide guidance and oversight. Medical students and physicians were able to educate attendees on their health screening results and provide recommendations to maintain their health.
The event was open to CPA students, their families, and the surrounding community. 41 OUWB staff and medical student volunteers participated, representing
various student organizations. Attendees completed a pre-registration form that collected demographic information, reasons for attendance, and healthcare utilization patterns.
The fair was supported by partnerships with local vendors, including Eastern Market, CNS Healthcare, and Aetna Better Health of Michigan to further provide medical resources and educate attendees about available programs for mental health and primary care. Faculty members from OUWB were present to support medical student volunteers and facilitate community engagement.
Survey data were analyzed using descriptive statistics to identify trends in participant demographics, reasons for attendance, and perceived barriers to accessing healthcare. Qualitative feedback was reviewed to contextualize results within broader public health challenges.
Results
The fair attracted 128 attendees, with 63 survey respondents providing demographic data.
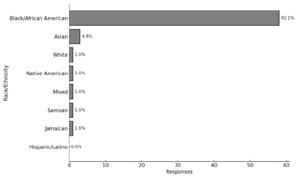
Of these identified: 92.1% as Black/African American 4.8% as Asian 1.6% as White 1.6% as Native American
1.6% as mixed race
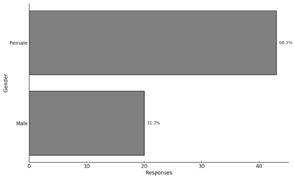
Female attendees comprised 68.3% of respondents, while 31.7% identified as male.
Discussion
Preventive care is the cornerstone of a healthy society, playing a pivotal role in reducing disease burden, improving quality of life, and lowering healthcare costs(10). The 12th Annual MLK Community Health Fair exemplified the importance of preventive care by providing free screenings and educational resources to a predominantly Black/African American community. These services targeted conditions such as hypertension, diabetes, and vision impairments, which disproportionately
This bar chart illustrates the racial and ethnic composition of the MLK Community Health Fair attendees who responded to the survey (n = 63). The majority of respondents identified as Black/ African American, with smaller proportions identifying as Asian, White, Native American, or mixed-race. No respondents identified as Hispanic/Latino. This demographic reflects the fair’s target population at Chandler Park Academy, a predominantly Black/ African American school.
Figure 2. Participant gender distribution.
This bar chart shows the gender distribution of the survey respondents (n = 63). Female attendees accounted for 68.3% of participants, while males represented 31.7%.
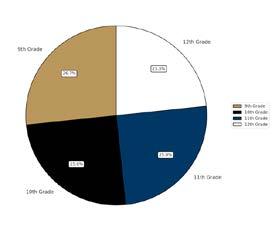
Figure 4. Grade-level distribution of student participants.
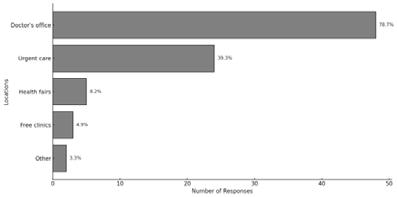
This pie chart highlights the grade levels of student participants at the health fair (n = 60). Attendance was relatively evenly distributed among ninth through twelfth grade, with the highest representation from tenth grade (26.7%). This even distribution reflects the fair’s accessibility to students across multiple age groups. Most respondents reported using doctor’s offices as their primary source of care (78.7%), followed by urgent care facilities (39.3%). Reliance on free clinics (4.9%) and health fairs (8.2%) was minimal, reflecting a preference for traditional care settings despite known barriers.
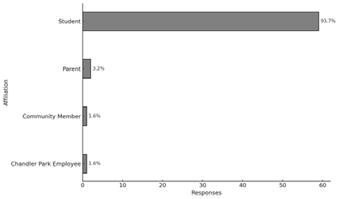
Figure 3. Participant affiliation.
This bar chart indicates the affiliation of attendees at the MLK Community Health Fair (n = 63). The vast majority (93.7%) identified as students, with smaller proportions identifying as parents (3.2%), community members (1.6%), or Chandler Park Academy employees (1.6%). This demonstrates the fair’s focus on engaging students in health-related activities.
affect this population due to systemic inequities and limited access to healthcare.1,2 By emphasizing prevention, the fair empowered individuals to identify health risks early and take proactive steps toward better health outcomes.
Chronic conditions like hypertension and diabetes often develop silently, and without regular screenings, many individuals remain unaware of their risks until complications arise. 11 The screenings offered at the fair addressed this gap by creating an accessible, judgment-free environment for participants to learn about their health status. Preventive care reduces the need for more expensive, invasive treatments later on and promotes long-term health equity. 10 Events like this demonstrate how community-led initiatives can bring critical healthcare services to underserved populations while fostering trust and engagement.
Figure 5. Usual sources of medical care.
This bar chart displays the usual sources of medical care reported by survey respondents (n = 61, multiple responses allowed). The majority reported obtaining care from a doctor’s office, followed by urgent care facilities. Few respondents indicated reliance on health fairs or free clinics as regular sources of care.
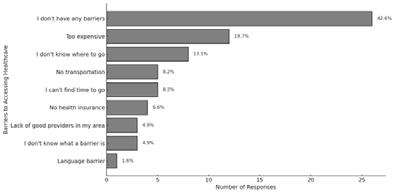
Cost was the most frequently cited barrier (19.7%), followed by not knowing where to go (13.1%) and transportation issues(8.2%). Fewer participants reported language barriers (1.6%) or health insurance gaps (6.6%). Notably, 42.6% reported no perceived barriers.
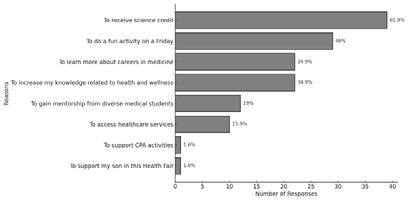
Figure 7. Bar chart displaying the reasons for attending the fair as reported by participants
(n = 63, multiple responses allowed).
The chart shows that “To receive science credit” was the most frequently selected reason, followed by “To do a fun activity on a Friday.” Other motivations included learning about careers in medicine, gaining health and wellness knowledge, mentorship, and healthcare access. Less common responses included supporting CPA activities and supporting a family member.
Figure 6. Barriers to accessing healthcare.
This bar chart illustrates the barriers to healthcare access reported by survey respondents (n = 61, multiple responses allowed). The most commonly cited barrier was cost, followed by being unsure of where to go, transportation challenges, and lack of time. Notably, 42.6% of respondents reported no perceived barriers to accessing healthcare.
Primary motivations for attending the fair included receiving science credit (61.9%), participating in a fun activity (46%), and learning about careers in medicine (34.9%). Additionally, 19% of attendees sought mentorship from medical students, while 15.9% attended to access healthcare services.
Health literacy—the ability to access, understand, and use health information to make informed decisions—is essential for adopting and maintaining healthy behaviors. At the MLK Community Health Fair, educational activities provided attendees with practical knowledge about nutrition, exercise, and chronic disease prevention. These efforts aimed to address gaps in health literacy that often contribute to poor health outcomes in underserved communities.4
Low health literacy is a significant barrier to preventive care. Individuals with limited health literacy are less likely to understand the importance of routine screenings, adhere to prescribed treatments, or navigate complex healthcare systems.12 By tailoring educational resources to the community’s needs, the fair enabled participants to build confidence in managing their health. Research shows that improving health literacy is associated with better health outcomes, including reduced hospitalizations, lower rates of chronic disease progression, and increased engagement with preventive care services.6,7
Preventive care is most effective when it is comprehensive, patient-centered, and culturally competent. The MLK Community Health Fair demonstrated a commitment to these principles by integrating screenings with educational programming and mentorship opportunities. Quality care extends beyond clinical services to include personalized support that addresses the social determinants of health, such as education, housing, and income.8 By acknowledging these broader influences, the fair fostered a holistic approach to health.
Mentorship opportunities at the fair were particularly impactful in empowering attendees to consider careers in healthcare. Representation within the healthcare workforce is critical for improving the quality of care and building trust between providers and patients. Attendees had the opportunity to engage with diverse healthcare professionals, who served as role models and provided guidance on navigating educational pathways. Expanding these mentorship initiatives could help address workforce disparities while inspiring the next generation of healthcare providers 13
The fair’s focus on fostering community trust is crucial for improving the quality of preventive care. Mistrust in the healthcare system, rooted in historical injustices and ongoing inequities, often deters individuals from seeking care.
By creating a welcoming and supportive environment, the fair helped bridge this gap and encouraged participants to prioritize their health. Establishing ongoing partnerships with local clinics and telehealth providers could further enhance the continuity of care and build long-term trust.14
Promoting a healthy lifestyle is integral to the success of preventive care initiatives. The MLK Community Health Fair emphasized the importance of nutrition, physical activity, and stress management as key components of a healthy lifestyle. These behaviors not only prevent chronic diseases but also improve overall well-being and quality of life. However, adopting healthier habits requires both knowledge and access to supportive resources. Participants at the fair were equipped with tools to make healthier choices, such as strategies for incorporating exercise into busy schedules or tips for managing stress through mindfulness practices. These interventions were designed to be practical and sustainable, recognizing that many attendees face significant barriers to maintaining a healthy lifestyle, including limited access to fresh food and safe spaces for physical activity 15
The absence of Hispanic/Latino attendees at the fair highlights the need for culturally tailored approaches to preventive care. Language barriers and cultural differences often limit access to
REFERENCES
1. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q. 2005;83(3):457-502. doi:10.1111/j.14680009.2005.00409.x
2. Murray K, Liang A, Barnack-Tavlaris J, Navarro AM. The reach and rationale for community health fairs. J Cancer Educ. 2014;29(1):19-24. doi:10.1007/ s13187-013-0528-3
3. Johnson JL, Spivey CA, Chisholm-Burns M. Comparison of Black student enrollment in US schools and colleges of pharmacy, medicine, and dentistry. Am J Pharm Educ. 2021;85(9):8493. doi:10.5688/ajpe8493
4. Barnes J, Abdul-Aziz T, Ramirez C. Addressing barriers to health equity for African Americans. Public Health Rep. 2020;135(1):85-90. doi:10.1177/0033354920923518
5. Lett LA, Orji WU, Sebro R. Declining racial and ethnic representation in clinical academic medicine: a review of the literature. J Gen Intern Med. 2018;33(5):851-857. doi:10.1007/s11606-018-4328-7
6. Carnethon MR, Pu J, Howard G, et al. Cardiovascular health in African Americans: A scientific statement from the American Heart Association. Circulation. 2017;136(21):e393-e423. doi:10.1161/ CIR.0000000000000534
7. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: An updated systematic review. Ann Intern Med. 2011;155(2):97-107. doi:10.7326/0003-4819-155-2-20110719000005
8. DeWalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and health outcomes: A systematic review of the literature. J Gen Intern Med. 2004;19(12):1228-1239. doi:10.1111/j.1525-1497.2004.40153.x
9. Data USA. Harper Woods, MI. Accessed November 21, 2024. https://
healthcare services, even when they are available. To ensure inclusivity, future fairs should prioritize bilingual materials, culturally relevant programming, and outreach efforts in collaboration with community leaders 16. Research shows that culturally competent care improves patient satisfaction, adherence to treatment, and overall health outcomes 17 .
Conducting longitudinal studies to evaluate the fair’s impact on health outcomes would provide valuable insights for refining future events. Collaborations with other academic institutions could enhance the rigor of these evaluations while creating opportunities for student involvement. Scaling up the fair to include multiple events throughout the year and across different locations would extend its reach and benefit more communities.
Conclusion
The MLK Community Health Fair exemplifies how student-led initiatives can address healthcare disparities while fostering community trust and engagement. By combining immediate healthcare services with education and mentorship, the fair empowered attendees to take charge of their health. Moving forward, expanding outreach efforts, integrating long-term care solutions, and addressing structural barriers will be essential to amplifying community health fairs’ impact.
datausa.io/profile/geo/harper-woods-mi
10. Maciosek MV, Coffield AB, Edwards NM, Flottemesch TJ, Goodman MJ, Solberg LI. Priorities among effective clinical preventive services: Results of a systematic review and analysis. Am J Prev Med. 2006;31(1):52-61. doi:10.1016/j.amepre.2006.03.012
11. Oni T, McGrath N, BeLue R, Roderick P, Colagiuri S, May CR, Levitt NS. Integrated models of care for diabetes and hypertension in low- and middle-income countries: a systematic review. Syst Rev. 2019;8(1):115. doi:10.1186/s13643-018-0865-8.
12. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15(3):259-267. doi:10.1093/ heapro/15.3.259
13. Bodenheimer T, Bauer L. Rethinking the primary care workforce—an expanded role for nurses. N Engl J Med. 2016;375(11):1015-1017. doi:10.1056/NEJMp1606869
14. Kvedar J, Coye MJ, Everett W. Connected health: a review of technologies and strategies to improve patient care with telemedicine and telehealth. Health Aff. 2014;33(2):194-199. doi:10.1377/hlthaff.2013.0992
15. Kegler MC, Swan DW, Alcantara I, Feldman L, Glanz K. The influence of rural home and neighborhood environments on healthy eating, physical activity, and weight. J Community Health. 2020;45(6):1226-1234. doi:10.1007/s10900-020-00901-0
16. Marmot M. Social determinants of health inequalities. Lancet. 2005;365(9464):1099-1104. doi:10.1016/S0140-6736(05)74234-3
17. Whitehead M. The concepts and principles of equity and health. Health Promot Int. 1991;6(3):217-228. doi:10.1093/heapro/6.3.217
Unspoken Permission
I grant you permission—
To breathe without fear, To believe in your own worth, To take the unconventional route, To wander, to wonder, to explore.
To follow the whispers of your dreams. To laugh freely, To live boldly, To embrace the fullness of your own life.
If no one has said it, hear it from me now: I give you permission—to simply be.
by Chika G
Will I ever see home? Excerpt from the NICU wards.
I am out of the womb and out into this new world prematurely. I am welcomed by warm hands and hearts trying to resuscitate me. Yet, I am still attached to the inside (physically). I am prodded and examined meticulously.
Am I pink?
Do I cry vigorously?
Is my heart beating fast enough?
Do I respond to stimuli?
Am I moving?
At this point, my mother hasn’t held me yet. Later, there’s even more fuss.
Am I stooling?
Am I urinating?
Am I breathing independently?
It is determined that I am not healthy enough to go home yet. Weeks will turn into a month…and one month will turn into three months. Will I ever see my home?
By Gift Ben-Bernard
MY BELOVED
Those eyes that twinkled like nickels in the half glowing moon. A lover, an enchanting mind that made one ponder, kindled I hoped, knowing tomorrow’s arrival would be soon.
We laughed, dreamed, cried but never knew, the coals within that made the flame flare will dwindle when warmth was needed anew. My bosom greys as the withering gravestone, in despair
I lay, still in silence as shadows mock, scarring my flesh with piercing wounds. I stay, gasping with lips etched, drunk as a quivering clock, onto sorrow’s grail as pain taunts with jeering sounds.
Fixed in the earth where you lay Hyacinths and irises sway mourning to dirges of ravens as I await to be ferried away.
Natan-EL A. Mensah Sowah Morehouse School of Medicine MD1 (Class of 2028)
The Hands That Built My Dream, A Tribute to My Dad and Grandfather
A Rare Case of “Hell’s Itch” in a Puerto Rican Female
Author: Shakira Bou Rolón, BS San Juan Bautista School of Medicine
Introduction:
Sunburns are caused by exposure to UV light. When a person is too exposed to sunlight, the body responds by increasing blood flow to the affected areas, causing erythema of the skin1. Repeated sunburns increase the risk of skin cancer and premature aging. One complication of sunburn is a rare
dermatologic reaction known as “Hell’s Itch”. This phenomenon is characterized by intense pruritus, muscle weakness, paresthesia, and severe anxiety, appearing several hours after extreme sun exposure. The literature is minimal with only a few reports describing this manifestation2,3,4. Here, we present a case of “Hell’s Itch”
in a female from Puerto Rico, a tropical Caribbean Island, to raise awareness and provide insight on this underreported consequence of sunburn.
Case Presentation:
A 27 y/o Puerto Rican female with no prior medical history presented to the ED with a first-degree sun burn on her
chest and extremities after spending two hours at the beach, approximately from 12 pm to 2 pm, without using sun protection. That evening, she reported experiencing muscle weakness and paresthesia in her hands and forearms, for which she took one tablet of ibuprofen 500 mg with mild relief. These symptoms persisted for the next two days despite continued ibuprofen use. Three days after the patient had developed the sunburn, the patient reported that her wounds took on a more roseous appearance and concurrently, she began to experience pruritus throughout her body. In order to alleviate this discomfort, the patient reported trialing hydrocortisone cream, aloe vera, three tablets of diphenhydramine 25 mg aerosolized lidocaine with minimal improvement. The patient’s symptoms became so severe that it prevented her from talking, walking, and sleeping appropriately. She also began to experience some anxiety.
Patient ultimately presented to the ED where she was treated with IV saline, IV diphenhydramine, and IV Pepcid which improved her symptoms greatly. At this point, she rated her pruritus a 4/10 from 10/10. She was discharged on the morning of the
fourth day of the sunburn with the diagnosis of “Hell’s itch”, due to excruciating pain, itching and paresthesia, and was prescribed the antihistamine hydroxyzine 25 mg every 6 hours for pruritus. At home, the itching continued but with less intensity; it now decreased 3/10. Throughout the fourth day, the pruritus intensified again to 7/10 with no relief over medication. After taking a cold shower to diminish the itching, the symptoms worsened, becoming unbearable and 10/10 on intensity. Now she felt like “fire was traveling through my body” with paresthesia even on the skin of her legs that was not sunburned, as well as at the palms of her hands, and extreme weakness on the legs. Due to the intolerable pain and discomfort, she went to the ER again and was given IM diphenhydramine which lessened the itching to 5/10. She was discharged and prescribed methylprednisolone tablets for six days. As the days followed, the pruritus continued but with less intensity until it disappeared completely.
Discussion:
“Hell’s Itch” is a rare complication of sunburn characterized mainly by intense pruritus, pain, difficulty sleeping, and paresthesia or tingling, according to a survey performed in 100 self-diagnosed
people with this condition4 These symptoms were rated with an average severity from 7.61 to 9.17, respectively4. Even though “Hell’s Itch” symptoms can be extremely severe, sometimes requiring emergency medical assistance, the literature is scarce, and the treatment options remain unclear.
Sunburn’s pathophysiology has been linked to oxidative DNA damage by UVA and UVB rays⁵. The body responds by releasing inflammatory markers and chemokines that ultimately cause red skin, activate its pain receptors, and promote tissue destruction⁵. Specifically, a previous study found that UVB triggers TRPV4 channel activation in the presence of histamine and endothelin 1, which leads to calcium influx into keratinocytes, generating sunburn pain and inflammation by converting them into pain generator cells that send signals to peripheral sensory neurons6,8 Another study established the role of vitamin D in the recovery of sunburns, as it promotes tissue repair by inhibiting inflammatory cytokines, arresting wound progression, delaying skin inflammation, and enhancing the autophagic activity of antiinflammatory macrophages in the dermis7,8
Figure 1. Sunburned skin of patient after tepid water 3 hours after the last sun exposure.
Sunburn’s risks are higher due to specific environmental and behavioral factors. In terms of time of the day, from 10 AM to 4 PM⁵, the sun’s radiation is stronger than at other times, such as early in the morning or late in the afternoon. Another factor is the location, as certain countries located near the equator receive more UV exposure⁵. The patient described here is from Puerto Rico, an island located just above the equator and spent from 12 PM to 2 PM in the sun; in the middle of the day when the intensity of the sunlight is the greatest.
Recommendations to avoid sunburns and its complications include wearing sun-protective clothing, seeking shade, using broadprotection sunscreen of at least a SPF of 30 and reapplying it every 2 hours, avoiding tanning beds, and limit sun exposure from 10 AM to 4 PM⁹. When sunburns do occur despite recommendations, they should be treated with cool baths, aloe vera moisturizer, drink water, and use ibuprofen or aspirin to relieve discomfort⁹. However, at the first sign of “Hell’s itch,” as described in this case, such as worsening of symptoms with a cool shower or after applying aloe vera or other topical agent, patients should seek medical treatment as soon as possible. Pharmacological treatments for “Hell’s itch” are still uncertain, although one previous report showed diminishing symptoms after the use of benzos, NSAIDs, and oral antihistamines². Due to the inflammatory reaction and immune system response involved in sunburns, we can speculate that is why antihistamines and oral steroids, immunological modulators, have shown some improvement in relieving “Hell’s itch” symptomatology, as seen in this case.
Conclusion:
“Hell’s Itch” remains a rare yet severe complication of sunburn, characterized by intense itching and discomfort. This case highlights the importance of recognizing and addressing this phenomenon promptly. While treatment options are limited, early medical intervention and preventive measures, such as sun protection, are crucial in reducing its incidence and severity. Continued research is needed to better understand and manage this challenging condition.
REFERENCES:
1. Sunburn - Symptoms and causes. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/sunburn/symptoms-causes/syc20355922#:~:text=Sunburn%20is%20inflamed%2C%20painful%20skin
2. Wilder-Smith AJ. Hell’s itch due to sunburn. Journal of Travel Medicine. 2018;26(1). doi:https://doi.org/10.1093/jtm/tay124
3. Toljan K. Another report of Hell’s itch due to sunburn. Journal of Travel Medicine. 2020;27(7). doi:https://doi.org/10.1093/jtm/taaa182
5. Guerra KC, Crane JS. Sunburn. PubMed. Published 2020. https://www.ncbi.nlm.nih.gov/books/NBK534837/
6. Moore C, Cevikbas F, Pasolli HA, et al. UVB radiation generates sunburn pain and affects skin by activating epidermal TRPV4 ion channels and triggering endothelin-1 signaling. Proceedings of the National Academy of Sciences. 2013;110(34):E3225-E3234. doi:https://doi.org/10.1073/ pnas.1312933110
7. Das LM, Binko AM, Traylor ZP, Peng H, Lu KQ. Vitamin D improves sunburns by increasing autophagy in M2 macrophages. Autophagy. 2019;15(5):813-826. doi:https://doi.org/10.1080/15548627.2019.1569298
8. Wyckmans MM. Hell’s itch could be caused by neurogenic inflammation: proposed pathophysiology and treatment options. Journal of Travel Medicine. 2020;28(1). doi:https://doi.org/10.1093/jtm/taaa204
9. How to treat sunburn. American Academy of Dermatology. https://www.aad.org/public/everyday-care/injured-skin/burns/treat-sunburn#:~:text=Apply%20 a%20moisturizer%20that%20contains
Assessment of sunscreen usage among adults in the metropolitan area of Puerto Rico: Implications for skin cancer prevention
Báez-Cruz, A., MS4; Pastrana, I. MS4, BS; De la Torre, E., MD
Hypothesis
Understanding of sunscreen terminology, application methods, and sun exposure risks is significantly associated with sunscreen usage habits among adults in Puerto Rico’s metropolitan area.
Background
Skin cancer incidence is increasing in the U.S., including Puerto Rico, according to “El Registro Central de Cáncer de Puerto Rico.” While some studies have examined sunscreen usage habits, limited data exist on the public’s understanding of sunscreen and its role in reducing skin cancer risk.
Methods
This cross-sectional study surveyed 205 adults in Puerto Rico’s metropolitan area about their sunscreen habits. Participants completed a 31-question survey, accessible online via QR codes or flyers at a dermatology clinic. Data analysis included descriptive statistics, Chi-square tests, and t-tests to evaluate behaviors, knowledge, and demographic factors.
REFERENCES:
Results
Sunscreen use was reported by 53.66% of participants, with 57.58% applying it only during sun exposure. Only 32.19% reported daily reapplication, while 20.88% did not reapply at all. The face (94.18%) and neck (69.63%) were the most common application sites. While 81.95% recognized sunscreen’s role in preventing skin cancer, 66.93% understood its role in reducing skin aging. Younger participants (21–34) experienced significantly more sunburns (84.62%) compared to those aged 35+ (50.88%; p<0.001). Family members were the primary source of education for 53.91% of participants, while only 29.82% cited healthcare professionals. Education level significantly influenced sunscreen usage and knowledge (p<0.05).
Conclusion
Despite moderate awareness of sunscreen benefits, gaps in proper usage and reapplication persist, particularly among younger adults. Targeted educational initiatives emphasizing sunscreen use and the risks of inadequate protection are critical to improving adherence and reducing the rising incidence of skin cancer in Puerto Rico.
1. 1- Charles, J., Soto-Torres, B., Sutton, S. K., Doyle, S. H., Kim, Y., Roetzheim, R. G., Vadaparampil, S. T., & Kanetsky, P. A. (2023). Skin cancer prevention behaviors, beliefs, distress, and worry among hispanics in Florida and Puerto Rico. BMC Public Health, 23(1). https://doi.org/10.1186/s12889-023-17039-y
2- De La Torre-Lugo, E. M., Figueroa, L. D., Sánchez, J. L., Morales-Burgos, A., & Conde, D. (2010). Skin cancer in Puerto Rico: a multiannual incidence comparative study. Puerto Rico health sciences journal, 29(3), 312–316.
3- Green, A. C., & Williams, G. M. (2007). Point: Sunscreen Use Is a Safe and Effective Approach to Skin Cancer Prevention. Cancer Epidemiology Biomarkers & Prevention, 16(10), 1921–1922. https://doi.org/10.1158/1055-9965.epi-07-0477
4- Moloney, F. J., Collins, S., & Murphy, G. M. (2002). Sunscreens. American Journal of Clinical Dermatology, 3(3), 185–191. https://doi.org/10.2165/00128071-200203030-00005
5- Skin Cancer Foundation. (2023, January). Skin Cancer Facts & Statistics - The Skin Cancer Foundation. The Skin Cancer Foundation; The Skin Cancer Foundation. https://www. skincancer.org/skin-cancer-information/skin-cancer-facts/
6- Vasicek, B., Szpunar, S., & Manz-Dulac, L. (2019). Patient knowledge of FDA-mandated sunscreen labeling terminology: A cross-sectional survey. Journal of the American Academy of Dermatology, 81(4), AB100. https://doi.org/10.1016/j.jaad.2019.06.384
7- Wang, S. Q., & Dusza, S. W. (2009). Assessment of sunscreen knowledge: a pilot survey. The British journal of dermatology, 161 Suppl 3, 28–32. https://doi.org/10.1111/j.13652133.2009.09446.x
Exploring Alternative Therapeutics for Vitiligo: A Systematic Review
Prajna A. Sahadeo, B.A.¹
Raveena Khanna, M.D.²
Cheri Frey, M.D.²
Affiliations: ¹Howard University College of Medicine, ² Department of Dermatology, Howard University College of Medicine
Abstract
Background
Vitiligo is a chronic autoimmune dermatological condition caused by the destruction of melanocytes and subsequent loss of skin pigment. The most common treatments for vitiligo include topical medications, phototherapy and surgery, all with the prevailing goal of restoring lost skin color and evening out skin tone. While such methods have been mostly successful, their efficacy is limited and their respective side effects prompt further investigation into alternative methods.
Methods
A systematic review was conducted using PRISMA guidelines. We used a keyword search on the PubMed database with “vitiligo” as our core word and incorporated phrases such as “herbal treatments,” “natural remedies,” and “alternative treatments.” The studies we included provide relevant and significant clinical trial data and observations. The inclusion
References:
criteria included patient efficacy and minimal side effects.
Results
Of the 28 studies reviewed, 14 met the inclusion criteria and showed significant positive patient efficacy when treated with alternative therapeutics. The treatments that this review focuses on include picrorhiza kurroa of Ayurvedic medicine, ginkgo biloba, L-Phenylalanine, aloe vera, Chinese herbal medicine, green tea extract and quercetin. Repigmentation was noted in patients who utilized these treatments either alone or in conjunction to conventional topical medications and light therapy with little to no side effects.
Conclusion
Overall, our findings suggest that these alternative therapeutics offer great potential benefits in the treatment and management of vitiligo and encourage further clinical trials to confirm their efficacy.
Limitations
Large scale clinical trials are needed to further evaluate the safety and efficacy of these treatments.
Conflict of Interest Statement
The authors declare that there are no conflicts of interest regarding the publication of this review.
Antoniou, C., Schulpis, H., Michas, T., Katsambas, A., Frajis, N., Tsagaraki, S., & Stratigos, J. (1989). Vitiligo therapy with oral and topical phenylalanine with UVA exposure. International journal of dermatology, 28(8), 545-547. Chen, Y. J., Chen, Y. Y., Wu, C. Y., & Chi, C. C. (2016). Oral Chinese herbal medicine in combination with phototherapy for vitiligo: a systematic review and meta-analysis of randomized controlled trials. Complementary Therapies in Medicine, 26, 21-27.
Jeong, Y. M., Choi, Y. G., Kim, D. S., Park, S. H., Yoon, J. A., Kwon, S. B., ... & Park, K. C. (2005). Cytoprotective effect of green tea extract and quercetin against hydrogen peroxide-induced oxidative stress. Archives of pharmacal research, 28, 1251-1256.
Padmakar, S., Kumar, G. A., Khurana, N., Kumari, S., & Pal, B. (2023). Efficacy and safety of natural Aloe Vera gel in the treatment of stable vitiligo. Clinical Epidemiology and Global Health, 22, 101332-. https://doi.org/10.1016/j.cegh.2023.101332
Parsad, D., Pandhi, R., & Juneja, A. (2003). Effectiveness of oral Ginkgo biloba in treating limited, slowly spreading vitiligo: Effectiveness of Ginkgo biloba in treating vitiligo. Clinical and Experimental Dermatology, 28(3), 285–287. https://doi.org/10.1046/j.1365-2230.2003.01207.x
thrown and turned white clay ceramic vase coated with tenmoku gold glaze and oxidation fired.
Vaccine Hesitancy and Uptake in South Africa: Factors Influencing the Effectiveness of COVID-19 Vaccine Regional Rollout
Mustafa Oluchukwu Dele-Oni
Kimberly Deering Jada C. Tyler
Introduction
Since the emergence of the COVID-19 pandemic, vaccine acceptance has become pivotal in controlling viral transmission. Yet, various factors, such as sociocultural factors, misinformation, and regional disparities, have influenced vaccine uptake, particularly in South Africa (SA). While national surveys in August 2020 indicated a hypothetical vaccine acceptability of 75%, less than 33% of the population completed the vaccination series as of January 2023. This research explores factors influencing COVID-19 vaccine acceptance and uptake among South African adults and assesses the impact of regional vaccine rollout strategies.
Methods
The review was conducted using sourced from two search engines: Google Scholar and PubMed. Research published on socio-demographic, cultural, and healthcare system factors in SA that affect vaccine acceptance, alongside an analysis of vaccine rollout strategies, was included.
Results
The South African government outlined a three-phase COVID-19 vaccine rollout approach to vaccinate 67% of the population by the end of 2021. Community-driven efforts, such as mobile clinics and partnerships with trusted leaders, proved particularly effective in increasing vaccine uptake in rural and underserved areas. People aged 55–78 years were 7.39 times more likely to accept vaccination than those aged 18–24 years. Key motivators for vaccination included strong belief in its efficacy for preventing COVID-19, knowing a vaccinated neighbor, and cohabitating with vaccinated individuals. Conversely, major barriers included inaccessibility to vaccines and vaccination sites, low confidence in vaccine safety and efficacy, and mistrust and misinformation.
Conclusion
Preliminary findings suggest that trust in health institutions, cultural beliefs, and access to healthcare services shape vaccine acceptance. Culturally sensitive communication and community engagement have proven effective in building trust and improving access, influencing the success of rollout strategies. These insights can inform future public health policies and campaigns on reducing COVID-19 vaccine hesitancy, enhancing coverage, and strengthening pandemic response efforts across South Africa.
Nabilah
History of Sterilization and Birth Control of African Americans
Contributors: Kaitlynn Esemaya, Alexis Thompson, Beatrice Odhiambo, and Onyinyechi G. Nwosu
Edited by: Annique McLune and Anamaria Ancheta
Unfortunately, the United States has a long and unknown history of compulsory sterilizations. Over 60,000 people have been forcibly sterilized in the United States and these sterilizations often disproportionately affect Native American, Hispanic, Black, incarcerated, migrant, and disabled people. In the 1960s it was discovered that in the south, Black women were often sterilized without having a medical reason or giving consent. It was common for medical students to be allowed to perform these unnecessary procedures on these women as a form of practice. These acts were so common that they were known as the “Mississippi Appendectomy”. Many believe that these sterilizations occurred years ago, but forced sterilizations have been happening within the United States from the 20th to the 21st century.
The belief in eugenics, the social control of human reproduction to improve desired traits in the human population, was supported by many government officials and even Margaret Sanger, a founder of Planned Parenthood. Planned Parenthood has released a statement acknowledging this fact about their founder, but strongly denounces that this belief is currently being upheld within the organization and emphasizes their support of all people.
Due to the 1927 Supreme Court Case Buck v Bell, which ruled that individuals can be deemed unfit to reproduce, forced sterilizations are still legal today. As of today, 31 states and Washington D.C. still legally allow forced sterilizations to be conducted on individuals and 17 states allow sterilizations on disabled children.
From the 1920s to the 1980s, a disturbing practice nicknamed the “Mississippi Appendectomy” caused poor Black women to be subjected to forced sterilization. Hospitals, particularly in the south, performed unnecessary hysterectomies on these women for medical training purposes, exploiting their poverty and race.
Fannie Lou Hamer, a prominent activist, experienced this injustice firsthand in 1961 when she went in for a fibroid removal but was given a hysterectomy without her consent, while under anesthesia.
Shockingly, 3 out of 5 Black women in her Sunflower County community endured similar unwanted sterilizations. Hamer’s unwavering commitment to amplifying the voices of marginalized communities included fighting against forced sterilization and advocating for access to comprehensive reproductive healthcare services, highlighting the intersectionality of race, gender, and bodily autonomy in the struggle for equity. Across states like North Carolina and Mississippi, nearly 8,000 individuals, predominantly women and 40% African American, underwent forced sterilization during this era.
The Negro Project was started by Margaret Sanger, a founder of Planned Parenthood in 1939. Sanger was an avid believer in eugenics and sterilizing people against their knowledge and will. According to her original funding proposals, she described the project as geared towards helping African Americans living in the southern states aiming to gain control over their reproductive decisions. To help institute the
projects, Sanger convinced African American leaders and Pastors to help convince their communities that participating in this project was safe and a way to reduce poverty and unplanned pregnancies.
However, the project veered significantly from its original proposed ideas by refusing to cooperate with Black physicians and failing to follow up with patients. Additionally, women were also often sterilized against their knowledge when they presented at birth control clinics. Due to these events, the African American community began to suspect that there were two different pills: one for Caucasian women, which allowed family planning, and the other for African American women, which caused sterility, thus further promoting distrust of health care providers.
The Mississippi Appendectomy represented a gross violation of human rights and reproductive autonomy, perpetuating systemic racism and eugenics.
Similarly, Planned Parenthood initially promoted sterilization as a form of birth control in the mid20th century, particularly targeting marginalized communities. However, it later faced criticism for coercive practices, such as targeting low-income and
minority women. This history reflects complex intersections of reproductive rights, social justice, and medical ethics.
Efforts to raise awareness have led to increased scrutiny of medical practices and calls for accountability and reparations for victims. However, there is still much work to be done to ensure that such atrocities are not repeated in the future.
Future physicians can play a crucial role in preventing similar injustices by advocating for ethical medical practices and actively confronting biases within the healthcare system. Institutionally, integrating a curriculum focused on cultural humility and the historical context of medical racism into medical training can help medical professionals recognize and deconstruct personal biases. On an individual level, physicians must educate their patients and empower them with the knowledge to make autonomous decisions that align with their health goals. Through this approach, physicians foster an environment that promotes shared decision-making and honors the values of their patients. Through these steps, future physicians can build an equitable and empathetic healthcare system that prioritizes patient autonomy.
Reflection Questions
If you were a physician at a facility that was conducting these forced sterilizations, would you advocate for these patients? Why or why not?
How could you advocate for patients who wrongfully receive procedures they did not consent to?
How can you recognize medical practices aimed at marginalizing certain groups of people? After seeing these practices, what actions can you take to stop these practices from spreading?
Consider the responsibility of healthcare institutions and professionals in acknowledging and addressing past wrongs, such as the forced sterilization of marginalized communities. What steps can be taken to promote healing, reconciliation, and trust- building within affected communities?
Fannie Lou Hamer’s experience is a poignant example of violating patient autonomy and consent. How can healthcare professionals ensure that patients are fully informed and empowered to make decisions about their care, especially in marginalized communities where trust in the medical system may be compromised?
Helpful Links
• National Human Genome Research Institute: Eugenics and Scientific Racism
• The Long Shadow of Eugenics in America
• Belly of the Beast
• PBS American Experience: Fannie Lou Hamer
• Planned Parenthood: Opposition Claims About Margaret Sanger
References:
1. Averbach, S., Ha, D., Meadows, A., Brubaker, L., & Gyamfi-Bannerman, C. (2023). Failure to progress: structural racism in women’s healthcare. EClinicalMedicine, 57, 101861. https:// doi.org/10.1016/j.eclinm.2023.101861
3. Black History Month, Week 2: Fannie Lou Hamer. (2022, February 7). Washington University School of Medicine. Retrieved February 4, 2024
4. Fayyad, Abdallah. “America’s Shameful History of Sterilizing Women - The Boston Globe.” The Boston Globe, The Boston Globe, 18 Sept. 2020, www.bostonglobe.com/2020/09/17/ opinion/americas-shameful-ongoing- history-sterilizing-women/.
6. Ko, Lisa. “UNWANTED STERILIZATION AND EUGENICS PROGRAMS IN THE
7. UNITED STATES.” PBS, Public Broadcasting Service, 29 Jan. 2016, www.pbs.org/independentlens/blog/unwanted-sterilization-and-eugenics- programs-in-the-united-states/.
8. Kugler, Sara. “Day 17: Mississippi Appendectomies and Reproductive Justice.” MSNBC, NBCUniversal News Group, 27 Mar. 2014, www.msnbc.com/msnbc/day-17-mississippiappendectomies-msna293361.
9. Latson, Jennifer. “Margaret Sanger, Race and Eugenics: A Complicated History.” Time, Time, 14 Oct. 2016, time.com/4081760/margaret-sanger- history-eugenics/.
10. MANJESHWAR, SANJANA. “America’s Forgotten History of Forced Sterilization.” Berkeley Political Review, 4 Nov. 2020, bpr.berkeley.edu/2020/11/04/americas-forgotten-history-offorced- sterilization/.
11. “New NWLC Report Finds over 30 States Legally Allow Forced Sterilization.” National Women’s Law Center, 25 Jan. 2022, nwlc.org/press-release/new- nwlc-report-finds-over-30-stateslegally-allow-forced-sterilization/.
12. “Opposition Claims About Margaret Sanger.” Planned Parenthood, www.plannedparenthood.org/uploads/filer_public/cc/2e/cc2e84f2-126f- 41a5-a24b-43e093c47b2c/210414-sangeropposition-claims-p01.pdf.
13. Accessed 9 Feb. 2024.
14. Parenthood, Planned. “The History & Impact of Planned Parenthood.” Planned Parenthood, 2024, www.plannedparenthood.org/about-us/who- we-are/our-history.
15. Robinson, Simone. “Black History Month: Why It’s So Important That We Celebrate It.” Lappthebrand, 9 Oct. 2020, www.lappthebrand.com/a/blog/black-history-month-why-its-soimportant-that-we-celebrate-it.
16. What the ‘Mississippi Appendectomy’ says about the regard of the state towards the agency of black women’s bodies. (2019, May 1). Black Women in the Black Freedom Struggle. Retrieved February 4, 2024
The Ripple of Roe’s Reversal:
A Retrospective Analysis of Shifts in IUD Utilization Among Women Aged 15–49 Before and After the Dobbs Decision
RAVEN C. HARDING, BS, BA1; AMANI R. PATTERSON, MBS, BA1; JOSHUA LEWIS, BS1; MAAME A. EFFIRIM, BS2; OYETOJUNBO IBIDAPO-OBE, MD3
1 John Sealy School of Medicine, University of Texas Medical Branch, 301 University Boulevard, Galveston, Texas 77555-1317
2John P. and Kathrine G. McGovern Medical School, University of Texas Health Houston, 6431 Fannin St. Houston, Texas 77030
3Department of Family Medicine, University of Texas Medical Branch, 301 University Boulevard, Galveston, TX 77555-1317
Abstract
Intrauterine devices (IUDs) are highly effective forms of contraceptives, making them a popular option for family planning in the United States. In 2022, the Supreme Court’s Dobbs decision overturned Roe v. Wade, restricting abortion access. Studies have now shown an increased demand for contraceptives as individuals seek alternatives to maintain reproductive autonomy. Given this issue’s urgency and public health implications, examining long-
term shifts in contraceptive utilization in a post-Roe landscape is crucial. This study investigates trends in IUD utilization among United States patients aged 15–49 years, two years before and after the Dobbs ruling, to explore how these legal changes influence reproductive health choices.
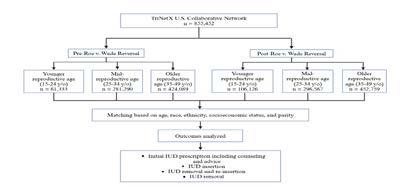
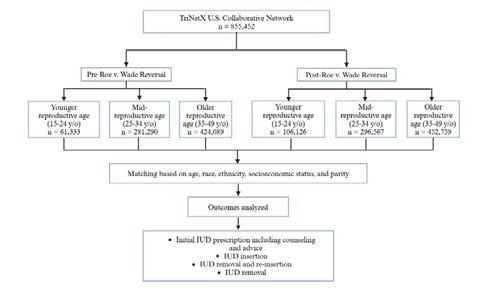
Aretrospective analysis was conducted using the TriNetX database. Six cohorts were formed based on age: younger reproductive-aged (15-24 years), mid-reproductive-aged (25-34
years), and older reproductive-aged (35-49 years) in the setting of the study’s Dobbs timeframe. Patients were matched by age, race, ethnicity, socioeconomic status, and parity to adjust for confounding factors. Outcomes analyzed included IUDseeking behavior (counseling and advice), IUD insertion, IUD removal, and IUD removal with reinsertion.
A total of 855,452 patients were analyzed. Results showed nuanced changes in IUD-seeking behavior
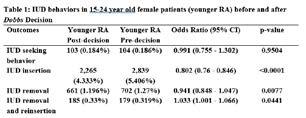
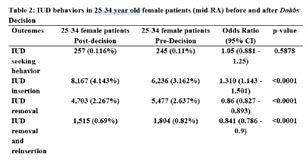
for younger reproductive-aged patients, with significantly declined IUD insertion rates post-Roe reversal (OR= 0.802, p <0.0001). In the mid-reproductive age group, IUD insertions significantly increased (OR=1.310, p<0.0001), while IUD removals (OR=0.86, p<0.0001) and removal with reinsertion (OR=0.841, p<0.0001) significantly decreased. Similarly, among older reproductiveaged patients, there were significant increases in IUD insertion and decreases with removal and removal with reinsertion.
This study demonstrates significant shifts in IUD-seeking behavior following the Dobbs decision. These findings echo how contraceptive choices evolve in the context of abortion restrictions. Future research should examine these trends locally, particularly in abortion-restrictive states.
Intrauterine devices (IUDs) are among some of the most effective forms of contraception currently available, with a 99% efficacy rate in preventing pregnancy¹. IUDs are categorized as long-acting reversible contraception (LARC) and have reduced the number of unplanned pregnancies in the United States1,2. Due to their effectiveness, patients highly regard these devices as a safe, accessible, and reliable form of birth control for their personal and family planning needs¹.
The topic of family planning has played a central role in legislative debates concerning reproductive rights in the United States. The use of contraceptives was made legal for married couples in 1965 through the Griswold v. Connecticut Supreme Court ruling and extended to unmarried individuals in 1972 with the Eisenstadt v. Baird decision. This was followed by the landmark 1973 Roe v. Wade Supreme Court ruling, which provided the constitutional right to have an
abortion in the United States based on the right to privacy³. However, in 2022, the United States Supreme Court overturned Roe v. Wade in the Dobbs v. Jackson Women’s Health Organization decision, significantly restricting abortion access in many states⁴. As a result of the Dobbs decision, women’s reproductive rights regarding access to abortions are no longer guaranteed under federal law. This ruling has reshaped reproductive healthcare in the United States, leading to more deliberate family planning and increases in contraceptive interest, access, and demands, including long-term options like IUDs⁵.
In the aftermath of a post-Roe world, examining how contraceptiveseeking behaviors have evolved is imperative. The implementation of stringent reproductive laws nationwide may influence women to urgently seek highly effective contraception options at increased rates as a means of maintaining bodily autonomy or circumventing unplanned pregnancies. Studies have begun to show an uptick in demand for contraceptive options, including LARCs, since the Dobbs ruling5,6. While beneficial to many, this heightened demand could disproportionately
they relate to the impact of abortion restrictions across many states. Given the current political climate surrounding reproductive rights and the high efficacy of intrauterine devices (IUDs) in preventing pregnancy longterm, we hypothesize that there is likely an increase in IUD utilization since the implementation of Dobbs in 2022. To further explore this hypothesis, we will assess trends in IUD utilization among patients aged 15-49 years in the United States before and after the Dobbs decision, using a database search of electronic medical records. Through this study, we aim to better understand the impact of current reproductive policies on nationwide patient contraceptive needs and help clinicians anticipate potential shifts in contraceptive-seeking behaviors and demands.
Methods
Data Source:
To conduct this retrospective analysis, data was collected utilizing the TriNetX health research database (live.trinetx. com). All patient data included in this study has been de-identified. To define study cohorts, specific International Classification of Diseases (ICD) codes were applied. On November 29, 2024, the United States (U.S.)
impact women from marginalized backgrounds, potentially leading to consequences such as limited access to contraception, supply shortages, and the further exacerbation of existing health disparities in the United States5,6
It is crucial to understand patient reproductive health behaviors as
Collaborative Network within TriNetX was utilized to form cohorts from 855,452 patients and 64 healthcare organizations (HCOs). This study is not categorized as humansubject research and, therefore, has been granted exemption from our Institutional Review Board (IRB). Figure 1 delineates the data collection
Figure 1: Flow diagram of data collection process utilizing TriNetX Inclusion criteria
process for this analysis.
Inclusion Criteria:
Six cohorts were formed for this study: pre and post-Dobbs decision for younger reproductive-aged (15-24 years), pre and post-Dobbs decision mid-reproductive aged (25-34 years), and pre and post-Dobbs decision older reproductive aged (35-49 years) patients. All individuals included in this study were patients between the ages of 15 and 49 years with or without abnormal findings on gynecological exams (Z01.411, Z01.419). These individuals also had IUD-seeking behaviors, as indicated by an ICD10 code for initial prescription which includes counseling and advice (Z30.014), an IUD insertion (Z30.430), undergoing IUD removal and reinsertion (Z30.433), or those who had an IUD removed (Z30.432) between June 24, 2020 and June 24, 2024.
Variables:
This investigation’s aim was to assess intrauterine device-seeking behaviors and utilization among 15-49-year-old patients in the United States before and after the Dobbs decision (2022). To execute this, cohorts were stratified by age group: younger reproductive age (15-24 years), mid-reproductive age (25-34 years), and older reproductive age (35-49 years old), and by time frame, before or after the reversal of Roe v. Wade. Additional covariables included specific IUD behaviors (prescription, insertion, removal, or both) and relevant clinical factors, including parity.
Propensity Score Matching:
Propensity score matching was implemented to adjust for potentially confounding factors. This ensures comparability between cohorts. Patients in each age group were matched by age, race, ethnicity, socioeconomic status, and parity (ICD10 Z3A.00, O09.4, O09.40, O09.41, O09.42, and O09.43). The propensitymatching process minimizes bias, reduces or eliminates confounding variables, and increases the power of the data set. This produces precise and accurate data on IUD behaviors of patients in the United States two years pre- and post-Dobbs decision.
Statistical Analysis:
The TriNetX health research database employs JAVA, Python, and R programming softwares for data analysis. These software programs use measures of association, including risk ratios, risk differences, odds ratios analyzed with t-tests, and 95% confidence intervals (CIs) to determine significant versus insignificant data. A p-value of <0.05 was deemed statistically significant for our dataset. Ensuring a comprehensive dataset, supplementary information has been delineated and included in tables formed with Microsoft Excel.
Results
Table 1 presents an analysis of IUDrelated behaviors among younger reproductive-aged (RA) female patients aged 15–24 years before and after the Dobbs decision. The findings reveal nuanced trends in IUD seeking, insertion, removal, and removal with reinsertion behaviors during these
periods. Post-decision, IUD-seeking behavior remained consistent with pre-decision rates, showing no significant difference (Odds Ratio [OR] = 0.991, p = 0.9504). However, IUD insertion rates experienced a significant decline after the decision (OR = 0.802, p < 0.0001), indicating a notable decrease in this behavior. Additionally, IUD removal showed a significant reduction post-decision (OR = 0.941, p = 0.0077). Interestingly, the rate of IUD removal followed by reinsertion showed a significant increase in the post-decision period (OR = 1.033, p = 0.0441).
Table 2 presents an analysis of IUD-related behaviors among midreproductive aged (RA) female patients aged 25–34 before and after the Dobbs decision. Post-decision, IUD-seeking behavior showed no significant change compared to predecision rates (Odds Ratio [OR] = 1.05, p = 0.5878). However, IUD insertion rates significantly increased in the post-decision period (OR = 1.310, p < 0.0001), indicating a notable rise in this behavior among this age group. In contrast, IUD removal rates decreased significantly after the decision (OR = 0.86, p < 0.0001), reflecting a reduction in removal practices. Additionally, the rate of IUD removal followed by reinsertion also declined significantly post-decision (OR = 0.841, p < 0.0001), suggesting a shift away from this combined behavior during the observed period.
49 before and after the Dobbs decision. IUD-seeking behavior showed an increased odds of IUD-seeking behavior, however, with no significance (Odds Ratio [OR] = 1.006, p = 0.9402). However, IUD insertion rates significantly increased post-decision (OR = 1.333, p < 0.0001), indicating a rise in this behavior among patients in this age group. Conversely, IUD removal rates experienced a marked decline post-decision period (OR = 0.691, p < 0.0001), reflecting a significant reduction in removal practices. Similarly, the rate of IUD removal followed by reinsertion showed a significant decrease post-decision (OR = 0.706, p < 0.0001), suggesting a shift away from this combined behavior during the observed time frame.
Discussion and Conclusion
Our study reveals significant and persistent changes in IUD-seeking behavior and utilization across different age groups following the Dobbs decision. These findings highlight the need for policies that ensure equitable access to effective contraception, particularly for marginalized populations who face additional barriers in receiving health care. Future policies must address these disparities and support reproductive autonomy by prioritizing access to long-acting reversible contraceptives like IUDs. Continued research is essential in understanding the long-term impact of these legislative changes on contraceptive choices and public health. It is imperative to examine state-level variations in IUDtrends, especially as it pertains to abortion-restrictive states. These analyses can help identify if other state-specific strategies may be necessary to ensure IUD accessibility to individuals from all paths seeking quality contraceptive healthcare.
References
1. Lanzola EL, Ketvertis K. Intrauterine Device. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557403/#
2. Stark, E. L., Gariepy, A. M., & Son, M. (2022). What Is Long-Acting Reversible Contraception?. JAMA, 328(13), 1362. https://doi.org/10.1001/ jama.2022.14239
3. Solinger, R. (2017, November 20). Politics of Reproductive Rights in 20th-Century America. Oxford Research Encyclopedia of American History.
4. Dobbs v. Jackson Women’s Health Organization. (n.d.). Oyez. Retrieved November 30, 2024, from https://www.oyez.org/cases/2021/19-1392
5. Zhu, D. T., Zhao, L., Alzoubi, T., Shenin, N., Baskaran, T., Tikhonov, J., & Wang, C. (2024). Public health and clinical implications of Dobbs v. Jackson for patients and healthcare providers: A scoping review. PloS one, 19(3), e0288947. https://doi.org/10.1371/journal.pone.0288947
6. Beshar, I., Corn, M., & Blumenthal, P. D. (2024). Two years in a post- Dobbs world: clinical, social and professional consequences. Current opinion in obstetrics & gynecology, 36(6), 426–432. https://doi.org/10.1097/GCO.0000000000000975
Anatomy of a Tumor
The Role of Cognitive Behavioral Therapy in Managing Chronic Pain and Transforming Psychological Distress: A Case Report
1Texas Tech University Health Sciences Center School of Medicine, 3601 4th Street, Lubbock, Texas 79430-0002
2John Sealy School of Medicine, University of Texas Medical Branch, 301 University Boulevard, Galveston, Texas 77555-1317
3Department of Family Medicine, University of Texas Medical Branch, 301 University Boulevard, Galveston, Texas 77555-1123
4Department of Anesthesiology, University of Texas Medical Branch, 301 University Boulevard, Galveston, Texas 77555-0877
Acknowledgments
The authors thank Norma A Pérez Raifaisen, MD, DrPH, CPC-ELI-MP, Director of the UTMB Center of Excellence for Professional Advancement and Re-search (COEPAR), for assistance with manuscript preparation.
Abstract
Chronic pain is a multifaceted condition that can severely affect one’s physical function and mental health, and is often resistant to standard medical treatments. This case report presents a unique example of a 47-year-old woman who developed chronic, debilitating pain after multiple toe amputations due to MethicillinResistant Staphylococcus Aureus (MRSA) infection, further complicated by severe depression, anxiety, and PTSD. Despite the complexity of her condition, significant progress was made through Cognitive Behavioral Therapy for Chronic Pain (CBTCP), a biopsychosocial intervention rarely emphasized in post-surgical amputation cases. Over six CBT-CP sessions focusing on pain education, activity pacing, relaxation techniques, and cognitive coping strategies, the patient experienced remarkable reductions in both pain and
psychological distress. Her Patient Health Questionnaire-9 (PHQ-9) depression score dropped from 23 to 5, her Generalized Anxiety Disorder-7 (GAD-7) anxiety score from 18 to 5, and her Pain, Enjoyment, and General Activity (PEGS) pain score from 8 to 6, reflecting both substantial emotional and physical improvements. This case underscores the importance of integrating psychological therapies in managing chronic pain, particularly in complex cases involving multiple mental health comorbidities. The striking reduction in both physical symptoms and psychological burden highlights the potential for CBT-CP to be a critical component in chronic pain management, contributing new insights to literature on pain treatment after severe infections and amputations.
Chronic pain remains a debilitating condition that affects approximately
20% of the adult population, often imposing profound physical and psychological burdens(Dydyk & Conermann, 2024). Despite advancements in medical treatments, including pharmacologic and surgical interventions, many patients continue to suffer due to the complex and multifaceted nature of chronic pain, which extends beyond physical discomfort.(Cao et al., 2024; Dydyk & Conermann, 2024; Roditi & Robinson, 2011).Mental health comorbidities, such as depression, anxiety, and posttraumatic stress disorder (PTSD), frequently exacerbate the severity of chronic pain, leading to significant disability and reduced quality of life (Institute of Medicine (US) Committee on Pain et al., 1987; Vadivelu et al., 2017). The growing recognition of this interrelationship highlights an urgent need for integrated treatment approaches that address both the physical and psychological dimensions of pain.
Cognitive Behavioral Therapy for Chronic Pain (CBT-CP) has gained attention as an innovative approach that targets the cognitive, emotional, and behavioral aspects of chronic pain.(Knoerl et al., 2016; Lim et
al., 2018; Murphy et al., 2022).By focusing on cognitive restructuring, behavioral modification, and coping mechanisms, CBT-CP offers a comprehensive, biopsychosocial framework for pain management. (Thorn, 2020a) While the efficacy of CBT-CP in improving both painrelated outcomes and psychological resilience is well-documented, its application in cases involving complex, post-surgical chronic pain remains underexplored in the literature. This case underscores the vital role that CBT-CP can play in managing chronic pain, particularly in cases where mental health conditions are closely intertwined with the pain experience. This report contributes valuable insights to the existing literature by illustrating how CBT-CP can be effectively utilized in complex chronic pain cases involving both physical trauma and mental health comorbidities.(Dydyk & Conermann, 2024; Institute of Medicine (US) Committee on Pain et al., 1987; Lim et al., 2018; Thorn, 2020b) By highlighting the patient’s significant clinical improvements and the underutilization of CBTCP in such multifaceted cases, this case advocates for broader adoption of biopsychosocial approaches in chronic pain management.
Case Introduction
The patient is a 47-year-old woman who experienced severe chronic pain following multiple toe amputations due to a Methicillin-resistant Staphylococcus aureus (MRSA) infection. Her primary concerns included generalized pain in her lower extremities, compounded by severe depression, anxiety, and posttraumatic stress disorder (PTSD).
Presenting Complaints
Upon presentation, the patient endorsed severe depression and anxiety, with a Patient Health Questionnaire-9 (PHQ-9) score of 23 and a Generalized Anxiety Disorder-7 (GAD-7) score of 18. She also reported chronic pain in her lower extremities, particularly following her toe amputations. Her symptoms had severely impaired her mobility and quality of life, prompting her to seek psychological intervention for pain management.
Patient History
She had a significant medical
history, including morbid obesity and a substantial weight loss of 300 pounds. Psychosocially, she had a history of trauma, difficulty sleeping, low energy, and low motivation, alongside a diagnosis of probable Bipolar 2 Disorder, which was later ruled out. Past interventions included pharmacologic treatment with vortioxetine and buspirone for her mental health conditions, but they did not sufficiently alleviate her chronic pain.
Timeline
The timeline outlines key events from the onset of chronic pain following multiple toe amputations due to MRSA infection in 2007, the progression of symptoms, and the initiation of Cognitive Behavioral Therapy for Chronic Pain (CBT-
Event
Toe amputations due to MRSA
Onset of chronic pain
required additional assessments, added to the complexity of the case.
Diagnosis:
The patient was diagnosed with chronic pain related to multiple toe amputations following a MRSA infection, compounded by severe depression, generalized anxiety disorder, and PTSD. Bipolar 2 Disorder was ruled out after further assessment.
Prognosis:
The patient’s prognosis was moderate, as her improvement would depend on her adherence to Cognitive Behavioral Therapy for Chronic Pain (CBT-CP) and her ability to manage both physical and psychological symptoms through cognitive and behavioral strategies.
Date
2007
Post-2007
Presentation to Pain Management 2023
CBT-CP initiation 2023
Final CBT-CP session
6 weeks later
Table 2: Timeline of the patient’s chronic pain development and therapeutic intervention
CP) in 2023. The patient underwent six weeks of CBT-CP, resulting in significant improvements in pain levels, depression, and anxiety. (Table 2).
Assessment
Diagnostic Methods:
At her initial visit, the patient underwent a clinical interview and completed selfreported questionnaires including the Patient Health Questionnaire-9 (PHQ9), Generalized Anxiety Disorder-7 (GAD-7), and the Pain, Enjoyment, and General Activity Scale (PEGS). Her PHQ-9 score was 23, indicating severe depression, while her GAD7 score was 18, indicating severe anxiety. These instruments were used to assess her mental health in relation to her chronic pain. Physical examination revealed generalized pain in her lower extremities.
Diagnostic Challenges:
Given the patient’s history of multiple mental health comorbidities (depression, generalized anxiety disorder, PTSD), it was difficult to assess the full extent of her chronic pain independent of her psychological conditions. Additionally, ruling out other conditions like Bipolar 2 Disorder
Case Conceptualization
In this case, the clinician’s conceptualization centered on understanding the interconnected nature of the patient’s chronic pain, post-amputation trauma, and significant psychological distress, including depression, anxiety, and PTSD. Recognizing that her chronic pain was not solely a physical experience but deeply entwined with her mental health, the clinician selected Cognitive Behavioral Therapy for Chronic Pain (CBT-CP) as a holistic approach that addressed both her physical and psychological needs. This biopsychosocial model allowed the clinician to tailor interventions that targeted maladaptive beliefs and behaviors sustaining her pain while building resilience through cognitive restructuring, relaxation techniques, and activity pacing. Each CBT-CP module was selected to address specific aspects of her distress—such as pain education to demystify her experience, pacing to improve physical engagement without overexertion, and cognitive coping strategies to manage anxiety and depressive symptoms. The clinician’s approach was driven by an understanding of the patient’s complex clinical profile, prioritizing
interventions that would empower her to manage pain autonomously while fostering psychological growth and improved quality of life.
Course of Treatment and Assessment of Progress
Types of Therapeutic Intervention:
The patient underwent six modules of CBT-CP over six weeks. Dr. Ryaja Johnson executed this therapy. This therapy targeted pain education, activity pacing, relaxation techniques, and cognitive coping strategies, aiming to improve her pain perception and psychological resilience. During this period of therapy, no other medications were taken in conjunction with CBT-CP.
Administration of Therapeutic Intervention
Module 1: Pain Education and Goal Setting: The patient was introduced to the difference between acute and chronic pain and how chronic pain is best managed using a biopsychosocial approach. She identified biological, psychological, and social factors negatively impacted by pain. The chronic pain cycle was explained, and the patient was introduced to SMART goals. SMART goals are specific, measurable, achievable, relevant, and time-bound objectives designed to improve focus and increase the likelihood of success. Her shortterm goal was to walk upstairs to eat dinner with friends at least once a week, while her long-term goal was to walk four times a week for 30 minutes without using a walker.
and progressive muscle relaxation techniques. Despite a pain flareup, the patient noted it “didn’t hurt as bad as usual,” reflecting early improvement in managing pain. She was tasked with practicing relaxation techniques daily to reduce pain intensity.
Module 4: Cognitive Coping (Part 1): The patient began identifying automatic negative thoughts (ANTs) related to pain and learned how unhelpful thoughts can exacerbate pain. She practiced challenging these thoughts using the Catching Automatic Negative Thoughts Worksheet.
Module 5: Cognitive Coping (Part 2): The patient practiced cognitive coping skills by countering her negative thoughts, particularly those related to her weight loss journey. She reviewed her progress in challenging ANTs and developed helpful coping statements for future pain flareups.
Module 6: The Pain Action Plan: In this final session, the patient reported significant improvement in both pain and mood. She was more active and had fewer automatic negative thoughts. A relapse prevention plan was created, focusing on long-term adherence to the CBT-CP strategies.
depressive mood but also a reduction in the negative cognitive patterns associated with chronic pain. Similarly, her GAD-7 score, initially reflecting severe anxiety (18), decreased to 5, indicating minimal anxiety symptoms. This reduction suggests improved emotional regulation and a better ability to manage anxiety-provoking situations, particularly those related to fear of pain flare-ups and movement. Her PEGS score, which assesses the impact of pain on her enjoyment of life and general activity, dropped from 8 to 6. Although this represents a more modest improvement compared to her psychological symptoms, it still indicates a meaningful reduction in pain interference. These outcomes collectively reflect a significant reduction in both her psychological distress and her perception of chronic pain, demonstrating the effectiveness of the CBT-CP intervention in addressing both aspects of her condition. Importantly, the patient reported subjective improvements in her daily functioning and quality of life. She regained the confidence to engage in activities she had previously avoided due to fear of exacerbating her pain, such as walking up stairs and socializing with friends. These self-reported outcomes suggest that the improvements observed through standardized measures were accompanied by tangible, real-world benefits. Summary of all of these values is indicated in Table 1.
Module 2: Activities and Pacing: The patient demonstrated improvements in mood and reported achieving her goal of walking up the stairs. A new goal was established: “not letting pain be my excuse.” The patient explored her fear of movement and learned about activity pacing to avoid overexertion. She composed a pacing schedule to balance activity and rest.
Module 3: Relaxation Training: During this session, the patient was introduced to diaphragmatic breathing
Follow-up and Outcomes
Clinician- and Patient-Assessed Outcomes: By the end of the six-week Cognitive Behavioral Therapy for Chronic Pain (CBT-CP) intervention, both the patient and the clinician, Dr. Ryaja Johnson, observed marked improvements across various measures of psychological distress and pain intensity. The patient’s PHQ9 score, which initially indicated severe depressive symptoms (23), dropped to 5, reflecting a shift to minimal depressive symptoms. This change suggests not only an alleviation of
Four weeks after completing the six-week intervention, the patient’s improvement was sustained, with no significant regression in her PHQ9, GAD-7, or PEGS scores. She reported continued engagement in activities and maintained gains in her quality of life, expressing confidence in her ability to manage pain and psychological symptoms independently. These outcomes collectively reflect a significant reduction in both her psychological distress and her perception of chronic pain, demonstrating the lasting effectiveness of the CBT-CP intervention. Importantly, the patient reported subjective improvements in her daily functioning and quality of life.
Intervention Adherence and Tolerability
The patient demonstrated excellent adherence to the CBT-CP modules, actively participating in each session and completing the associated
PEGS = Pain, Enjoyment, and General Activity Scale
GAD-7 = General Anxiety Disorder-7
PHQ-9 = Patient Health Questionnaire-9
exercises. Throughout the six weeks, she consistently engaged with the strategies taught, such as activity pacing, relaxation techniques, and cognitive coping exercises. Her commitment to practicing relaxation skills daily, as well as setting and working toward SMART goals, played a crucial role in her progress. Weekly feedback sessions allowed for adjustments to the intervention, and the patient’s self-reported progress indicated that she was highly motivated to apply the coping mechanisms outside of therapy sessions. The patient’s ability to manage her pain and psychological symptoms was systematically evaluated through weekly check-ins, where she shared her experiences using the learned techniques and discussed any challenges she encountered. Her active involvement in therapy was evident in her ability to track progress on her SMART goals, such as walking more frequently and engaging in social activities with minimal pain-related setbacks.
Moreover, she reported that the cognitive restructuring exercises, which focused on identifying and challenging automatic negative thoughts (ANTs), were particularly helpful in reshaping her pain-related thinking. The patient reported feeling more in control of her pain and mood, and she consistently completed the cognitive worksheets, further demonstrating her adherence to the intervention plan.
Recommendations to Clinicians and Students
This case underscores the power of Cognitive Behavioral Therapy for Chronic Pain (CBT-CP) in addressing
complex, multifaceted conditions involving both chronic physical pain and severe psychological comorbidities, such as depression, anxiety, and posttraumatic stress disorder (PTSD). (Dydyk & Conermann, 2024; Lim et al., 2018; Roditi & Robinson, 2011) The strength of this approach lies in its holistic integration of psychological and physical health interventions, which allowed the patient to regain control over both her mental state and physical functioning. By leveraging cognitive restructuring, relaxation techniques, and activity pacing, the treatment targeted the underlying cognitive distortions and maladaptive behaviors that perpetuated her pain experience. This biopsychosocial model of pain management exemplifies the importance of addressing not just the physical symptoms of chronic pain but also the emotional and psychological factors that exacerbate suffering.(Meints & Edwards, 2018)
The existing medical literature supports the efficacy of CBT-CP in managing chronic pain, particularly in cases where pain is exacerbated by mental health conditions such as depression and anxiety. (Driscoll et al., 2021; Mayhew et al., 2023; Murphy et al., 2022; Sanabria-Mazo et al., 2023; Taguchi et al., 2021) Studies have shown that CBTCP helps to reduce pain-related disability, improve psychological resilience, and challenge maladaptive cognitive patterns that sustain the pain experience.(Driscoll et al., 2021; Lim et al., 2018; Yang et al., 2022) In this case, the patient’s successful outcomes mirror these findings, further demonstrating that CBTCP can be a crucial component in the management of chronic pain, especially for patients with complex
mental health needs.
The rationale for concluding that CBTCP was highly effective in this case is based on the clear, quantifiable improvements in the patient’s emotional and physical well-being. The significant reductions in her PHQ9, GAD-7, and PEGS scores reflect improvements in both her mood and her ability to function despite chronic pain. Additionally, her reported ability to re-engage in social activities and physical exercise points to a broader enhancement of her quality of life. These outcomes align with the goals of CBT-CP, which seeks to empower patients to manage their pain through cognitive and behavioral changes rather than relying solely on medical or pharmacological interventions.
This case highlights the transformative potential of Cognitive Behavioral Therapy for Chronic Pain in treating patients with complex, chronic conditions involving both physical and psychological components. The patient’s significant improvement in mood, anxiety, and pain-related interference demonstrates the efficacy of a biopsychosocial approach, underscoring the importance of addressing both mind and body in chronic pain management. The primary takeaway from this case is that CBT-CP can be a powerful tool in reducing pain and psychological distress, enabling patients to regain control over their lives and engage more fully in daily activities. Clinicians should consider integrating psychological interventions like CBTCP into chronic pain management plans, especially when mental health comorbidities are present.
Table 1: Outcome scores at each visit
References:
1. Cao, B., Xu, Q., Shi, Y., Zhao, R., Li, H., Zheng, J., Liu, F., Wan, Y., & Wei, B. (2024). Pathology of pain and its implications for therapeutic interventions. Signal Transduction and Targeted Therapy, 9(1), 1–49. https://doi.org/10.1038/ s41392-024-01845-w
2. Driscoll, M. A., Edwards, R. R., Becker, W. C., Kaptchuk, T. J., & Kerns, R. D. (2021). Psychological Interventions for the Treatment of Chronic Pain in Adults. Psychological Science in the Public Interest. https://doi. org/10.1177/15291006211008157
3. Dydyk, A. M., & Conermann, T. (2024). Chronic Pain. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK553030/
4. Institute of Medicine (US) Committee on Pain, D., Osterweis, M., Kleinman, A., & Mechanic, D. (1987). Psychiatric Aspects of Chronic Pain. In Pain and Disability: Clinical, Behavioral, and Public Policy Perspectives. National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK219250/
5. Knoerl, R., Lavoie Smith, E. M., & Weisberg, J. (2016). Chronic Pain and Cognitive Behavioral Therapy: An Integrative Review. Western Journal of Nursing Research, 38(5), 596–628. https://doi.org/10.1177/0193945915615869
6. Lim, J.-A., Choi, S.-H., Lee, W. J., Jang, J. H., Moon, J. Y., Kim, Y. C., & Kang, D.-H. (2018). Cognitive-behavioral therapy for patients with chronic pain. Medicine, 97(23), e10867. https://doi.org/10.1097/MD.0000000000010867
7. Mayhew, M., Balderson, B. H., Cook, A. J., Dickerson, J. F., Elder, C. R., Firemark, A. J., Haller, I. V., Justice, M., Keefe, F. J., McMullen, C. K., O’KeeffeRosetti, M. C., Owen-Smith, A. A., Rini, C., Schneider, J. L., Von Korff, M., Wandner, L. D., & DeBar, L. L. (2023). Comparing the clinical and costeffectiveness of remote (telehealth and online) cognitive behavioral therapybased treatments for high-impact chronic pain relative to usual care: Study protocol for the RESOLVE multisite randomized control trial. Trials, 24, 196. https://doi.org/10.1186/s13063-023-07165-8
8. Meints, S. M., & Edwards, R. R. (2018). Evaluating Psychosocial Contributions to Chronic Pain Outcomes. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 87(Pt B), 168. https://doi.org/10.1016/j.pnpbp.2018.01.017
9. Murphy, J. L., Cordova, M. J., & Dedert, E. A. (2022). Cognitive Behavioral Therapy for Chronic Pain in Veterans: Evidence for Clinical Effectiveness in a Model Program. Psychological Services, 19(1), 95–102. https://doi. org/10.1037/ser0000506
10. Roditi, D., & Robinson, M. E. (2011). The role of psychological interventions in the management of patients with chronic pain. Psychology Research and Behavior Management, 4, 41–49. https://doi.org/10.2147/PRBM.S15375
11. Sanabria-Mazo, J. P., Colomer-Carbonell, A., Fernández-Vázquez, Ó., NoboaRocamora, G., Cardona-Ros, G., McCracken, L. M., Montes-Pérez, A., CastañoAsins, J. R., Edo, S., Borràs, X., Sanz, A., Feliu-Soler, A., & Luciano, J. V. (2023). A systematic review of cognitive behavioral therapy-based interventions for comorbid chronic pain and clinically relevant psychological distress. Frontiers in Psychology, 14. https://doi.org/10.3389/fpsyg.2023.1200685
12. Taguchi, K., Numata, N., Takanashi, R., Takemura, R., Yoshida, T., Kutsuzawa, K., Yoshimura, K., & Shimizu, E. (2021). Integrated cognitive behavioral therapy for chronic pain: An open-labeled prospective single-arm trial. Medicine, 100(6), e23859. https://doi.org/10.1097/MD.0000000000023859
13. Thorn, B. E. (2020a). Putting the brain to work in cognitive-behavioral therapy for chronic pain. Pain, 161(Suppl 1), S27–S35. https://doi.org/10.1097/j. pain.0000000000001839
14. Thorn, B. E. (2020b). Putting the brain to work in cognitive-behavioral therapy for chronic pain. Pain, 161(Suppl 1), S27. https://doi.org/10.1097/j. pain.0000000000001839
15. Vadivelu, N., Kai, A. M., Kodumudi, G., Babayan, K., Fontes, M., & Burg, M. M. (2017). Pain and Psychology—A Reciprocal Relationship. The Ochsner Journal, 17(2), 173.
16. Yang, J., Lo, W. L. A., Zheng, F., Cheng, X., Yu, Q., & Wang, C. (2022). Evaluation of Cognitive Behavioral Therapy on Improving Pain, Fear Avoidance, and SelfEfficacy in Patients with Chronic Low Back Pain: A Systematic Review and Meta-Analysis. Pain Research & Management, 2022, 4276175. https://doi. org/10.1155/2022/427617
Breaking Barriers for Women of Color in Medicine: A
Journey of Resilience and Empowerment
WINIFRED CHIJIOKE, OMS II
Entering the world of medicine as a woman of color often feels like stepping into a realm that wasn’t designed with you in mind. The well-trodden paths of medical schools, hospitals, and healthcare institutions have historically been paved by individuals who do not share our experiences, and too often, women of color find themselves navigating a system that overlooks our unique contributions and struggles. But, as I reflect on my journey as a medical student, I realize that each step I take is not just for me, it is for every young girl who grows up feeling small, unseen, and unworthy. It is for those who will come after me, who deserve to see themselves reflected in the faces of the doctors who care for them.
I did not always feel like I belonged in medicine. Growing up as a little black girl in rural Indiana, I was often isolated, carrying the weight of expectations while being treated as if I were invisible. The image of a doctor was not someone who looked
like me. But despite the obstacles, I found a way to break through. I pushed forward, inspired by a sense of purpose greater than myself, the desire to serve women of color and be the advocate I had needed.
Now, as a medical student, I can see how deeply the barriers persist. Women of color face not only the academic rigor of medical school but also the weight of microaggressions, implicit bias, and systemic inequities. These challenges can be isolating, leaving us with a sense of not truly belonging. But instead of feeling defeated, I see an opportunity for institutions to take bold steps to dismantle these barriers and create environments where women of color can thrive.
The Power of Mentorship
One of the most powerful ways to challenge these norms is through mentorship. I’ve been fortunate to find
mentors who understand my journey, who not only guide me academically but also nourish my spirit. For women of color, mentorship is more than career guidance, it is an affirmation of our worth and potential. Institutions need to recognize the value of mentorship programs that connect women of color with professionals who share their lived experiences. Mentorship programs that are intentional in pairing students with mentors of similar backgrounds can make a profound difference. Seeing someone who has walked your path and succeeded is incredibly empowering. Mentorship provides more than academic support; it builds confidence, offers a safe space for navigating the complexities of identity, and fosters resilience in an environment where we are often underrepresented.
Organizations like the American Medical Women’s Association (AMWA) and Student National Medical Association (SNMA) already
understand this need and have created spaces for mentorship to flourish. Yet, there is more work to be done. Medical schools and institutions must institutionalize mentorship programs specifically for women of color, ensuring that these relationships are not only encouraged but prioritized. By doing so, we cultivate a generation of women physicians who feel empowered, seen, and supported.
The Need for Policy Reforms
In addition to mentorship, policy reform is crucial for breaking down the systemic barriers that disproportionately affect women of color in medicine. We need policies that actively work to close the gap in representation and create environments that are inclusive by design.
For example, medical schools must go beyond lip service when addressing diversity and inclusion. Institutions should enact admissions policies that look beyond traditional metrics like MCAT scores, which often fail to capture the full potential of candidates from diverse backgrounds. Holistic admissions, which consider an applicant’s lived experiences, resilience, and commitment to underserved communities, can better identify the future leaders in medicine, those who are equipped not only with academic prowess but also the cultural competency needed to serve diverse populations.
Moreover, financial barriers remain a significant hurdle for many women of color pursuing medicine. Scholarships, financial aid programs, and debt relief initiatives tailored to underrepresented minorities can alleviate the immense burden of medical school expenses. Policy reforms that make medical education more affordable will open the doors wider, allowing more women of color to step into spaces traditionally reserved for the privileged few.
Community-Based Advocacy and Collective Change
Beyond institutional changes, community-based advocacy is a vital component of fostering inclusivity in medicine. Women of color in medicine
are not just physicians; we are advocates, deeply connected to the communities we serve. Our personal experiences often mirror those of our patients, and this connection gives us a unique ability to address health disparities and systemic injustices.
Organizations like Black Women in Medicine, Black Girl White Coat, and The Black Mama’s Matter Alliance are leading the way in advocating for reproductive justice, maternal health, and reducing healthcare disparities. As a medical student involved in advocacy efforts for maternal health and domestic violence survivors, I have witnessed firsthand the power of community-based initiatives. These movements not only uplift the voices of women of color in medicine but also empower the communities we serve to demand better care.
We must continue to build and support networks of women physicians, advocates, and community leaders who are working to dismantle the structures that perpetuate inequality in healthcare. Medical schools can partner with community organizations to provide service-learning opportunities that allow students to engage in meaningful advocacy work. By doing so, we cultivate a generation of physicians who are not only healers but also champions for justice.
The Future of Medicine
As I envision the future of medicine, I see a field where women of color are no longer an anomaly but a powerful force driving change. I see a future where medical institutions challenge the status quo and recognize that
diversity is not a box to be checked but a pillar upon which healthcare is built. I see a future where mentorship, policy reform, and community-based advocacy create a system that not only welcomes women of color but celebrates us.
Breaking barriers for women of color in medicine is not just about increasing numbers, it is about transforming the culture of medicine itself. It is about ensuring that the next generation of women physicians feels valued, respected, and empowered to lead. It is about creating a healthcare system that understands that our voices, experiences, and perspectives are not peripheral but central to the advancement of medicine.
For every woman of color who has ever questioned whether she belongs in this field: You do. Your journey is not defined by the barriers you face but by your courage to break through them. And as we continue to rise, we will leave a legacy of empowerment, resilience, and hope for those who will follow in our footsteps.
References
1. Smedley, B. D., Stith, A. Y., & Nelson, A. R. (2003). Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. National Academies Press.
2. American Medical Women’s Association. (n.d.). Programs and Advocacy. Retrieved from https://www.amwa-doc.org/advocacy
3. Student National Medical Association. (n.d.). Mission and History. Retrieved from https:// snma.org/
4. The Black Mama’s Matter Alliance. (n.d.). Our Work. Retrieved from https:// blackmamasmatter.org/