HEALTH, LIFE & HIV


Actor and advocate Jason Veasey shares his HIV journey
If you're living with viral load to
U=U means undetectable=untransmittable. It helps destigmatize living with HIV, raises awareness that medications can be e ective, and reminds people importance of continuing to take treatment as prescribed. Stay empowered to live a longer and healthier life.
little virus in the blood it. Current research prescribed and getting prevents the transmission also known as U=U It's important to be healthcare provider and your routine. No meet with them.
U=U means undetectable=untransmittable. It helps destigmatize living with HIV, raises awareness that medications can be e ective, and reminds people importance of continuing to take treatment as prescribed. Stay empowered to live a longer and healthier life.
Brett Klein is ready to ride for HIV awareness.
#ADVOCACY

Fighting against HIV and AIDS has always been a struggle. Much work remains to end the epidemic. POZ encourages you to get involved in advocacy. Go to poz.com/ advocacy to find the latest news and learn how you can make a difference in the fight. D
#CRIMINALIZATION

Advocates around the world are working to change laws that criminalize HIV, which harm people living with the virus. For more information and to learn how to get involved in reform efforts to make such laws reflect current science, go to poz.com/criminalization
D
#UNDETECTABLE

The science is clear: People who have an undetectable viral load don’t transmit HIV sexually. In addition to keeping people healthy, effective HIV treatment also means HIV prevention. Go to poz.com/undetectable for more. D

Scan the QR code (left) with your smartphone camera or go to poz.com/digital to view the current and past issues online.

22 UP CLOSE AND PERSONAL Actor and advocate Jason Veasey shares his HIV journey. BY MATHEW
RODRIGUEZ
28 WHAT DOESN’T KILL YOU MAKES YOU STRONGER Tony Valenzuela remains a proud activist. BY
TIM MURPHY
3 FROM THE EDITOR The Way It Is
4 POZ Q&A
Michael G. Lee, PhD, the author of When the Band Played On, shares his perspectives on the late journalist Randy Shilts.
6 POZ PLANET
As HIV cases rise in Arizona, a mural to increase awareness of the virus is unveiled in Phoenix • Tamar Braxton takes PrEP • first home test for three different STIs now available only for women • AI tool boosts clinical trials • the psychedelic mushroom experiment • POZ Stories: Bryan Fleury • Everyday: milestones in the epidemic
12 VOICES
Brandon Ogbunu, PhD, a computational biologist, argues that defending science today requires dealing with uncomfortable truths.
14 SPOTLIGHT
Advocates at Tesla protests and AIDSWatch
16 NUTRITION & FITNESS
Rainbow fried rice • managing your weight
17 BASICS
Trans people and HIV
18 CARE & TREATMENT
Federal health cuts threaten people with HIV • CMV treatment may improve immune function • bnAbs for HIV treatment and cure • benefits of weight-loss drugs
20 RESEARCH NOTES
Once-yearly PrEP trials advance • new antiretrovirals for HIV treatment • two more stem cell cures • people with both HIV and hepatitis C not getting treated
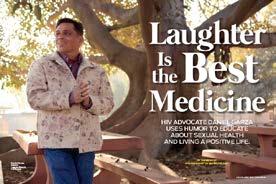
32 HEROES
HIV advocate Brett Klein
BY MATHEW
A new biography of the late Randy Shilts offers lessons for the current HIV fight.
THE LATE JOURNALIST RANDY SHILTS IS PROBABLY BEST
known for his 1987 masterpiece, And the Band Played On: Politics, People, and the AIDS Epidemic, a staggering piece of reportage that unearthed the particular ways that neglect, apathy and incompetence combined to cause the AIDS epidemic as much as HIV itself.
While many people know Band as a book or the 1993 TV movie that followed, fewer know about the life of the man who produced the work and who died of AIDS-related illness in 1994 at age 42.
In a new biography titled When the Band Played On: The Life of Randy Shilts, America’s Trailblazing Gay Journalist by writer, researcher and educator Michael G. Lee, PhD, Shilts himself becomes the story.
Here, Lee discusses not only the rich past he mined to write When the Band Played On but also how Shilts’s work as well as Lee’s own can help people navigate the newest unfolding chapter in the AIDS crisis.
How did you first encounter Randy Shilts?
Being a child of the ’80s, And the Band Played On was ubiquitous. I was 10 years old when that book came out. From that time forward, I was aware of the book as it’s related to the AIDS epidemic because that was a frightening part of the coming-out experience for people in my generation.
In terms of Randy himself, by the time I got to my PhD program, I’d read And the Band Played On a couple of times. I’d also read The Mayor of Castro Street [a 1982 biography of Harvey Milk by Shilts]. The impetus for the project really came from the research I was doing as a doctoral student at the University of Minnesota,
where I had the opportunity to do historical research. I wanted to look at the history of gay and lesbian community services before the AIDS epidemic in 1981 because I’d worked in AIDS organizations for several years.
People at those groups had talked about And the Band Played On and how much it helped to explain the political nature of human services and outreach and education. But there wasn’t a lot documented about how the gay activist tradition had informed the creation of AIDS groups in the ’80s. I wanted to look at what was happening between Stonewall [in 1969] and the advent of AIDS that would have informed their creation.
I was looking at back issues of The Advocate from the 1970s. They were producing some of the most in-depth and well-sourced articles on pandemic-level conditions in urban gay communities, especially around alcoholism, drug abuse, sexually transmitted diseases,




Like a belated valentine delivering radiance and joy to downtown Phoenix, a bright new mural spells out “LOVE” in predominant shades of red and pink while spotlighting several people of color, the phrase “U=U,” numerous hearts and plus signs, and more. Unveiled April 2 on a facade of the Parsons Center for Health and Wellness, the mural aims to raise HIV awareness, educate about prevention and treatment and honor those lost to the epidemic. Parsons is home to Prisma Community Care, which provides HIV and sexual health services to Arizonans, notably to underserved and minority populations, such as Latinos, LGBTQ and African Americans of all ages and genders.
The mural was created by local artists Quinn Murphy and Jake Early. Inspired by interviews with individuals affected by HIV, the artists wanted their work to convey an upbeat message showing happy and healthy people enjoying their lives.
“It’s not a death sentence anymore,” Early told KJZZ 91.5 news. “There’s joy.” He describes the folks depicted in the mural as regular people. “They may or may not be positive,” he added. “We don’t know, because they’re living a normal life.”
What’s more, according to KJZZ, the mural made its debut as Arizona reports a 20%
increase in new HIV cases. AIDSVu.org, an interactive site that maps and visualizes HIV data on communities across the nation, offers more detailed statistics. In 2022, about 18,700 people were living with HIV in Arizona, nearly 86% of whom were men. Among the newly diagnosed, 45% were Latino, 30% were white, 17% were Black and 5% were Native American, according to AIDSVu.org data.
The mural came together via the collaborative efforts of the City of Phoenix, Mayor Kate Gallego and the Phoenix Office of Arts and Culture in partnership with Artlink and with support from Prisma Community Care, one•n•ten, Valleywise and Aunt Rita’s Foundation.
Mayor Gallego spoke at the mural’s unveiling. “We are so proud to celebrate this incredible mural,” she said. “It’s a significant day in illustrating our values for those we lost, those who are thriving and the science that helped lead to longer lives for residents diagnosed with AIDS or HIV. You can see the beautiful message of love that this mural strongly communicates—and it’s a message that is very timely.” (Watch Gallego and other leaders speak at the unveiling in a video on the city of Phoenix’s YouTube channel.)

The mural also serves as an educational tool, the mayor explained. It features a QR code for people to use their phones to connect to informa-
tion about the Phoenix Fast-Track initiative to end the HIV epidemic.
Launched in 2014, the global Fast-Track Cities initiative was spearheaded by the International Association of Providers of AIDS Care, the Joint United Nations Programme on HIV/ AIDS, the United Nations Human Settlements Programme and the City of Paris. Fast-Track Cities is a partnership encompassing over 500 cities around the world as well as global HIV organizations with the goal of ending HIV in urban settings by 2030.
To accomplish this, they aim to get:
• 95% of people living with HIV to know their status;
• 95% of those people on HIV meds (antiretrovirals);
• 95% of people on meds to achieve viral suppression;
• Zero HIV stigma.
The phrase “U=U” that appears in the mural stands for “Undetectable Equals Untransmittable.” It refers to the fact that people with an undetectable viral load don’t transmit HIV to others through sex.
What’s more, people with HIV who achieve and maintain viral suppression experience slower disease progression, enjoy better overall health and are less likely to develop opportunistic illnesses. —Trent Straube
The celebrity is increasing awareness of HIV
After a year of not dating, R&B and reality TV star Tamar Braxton is ready for action. “I’m on PrEP,” the outspoken personality says in a video she posted on social media in March. “I would tell everyone to get on PrEP…because prepare yourself.” That’s pre-exposure prophylaxis (PrEP) to prevent HIV, available as daily pills or a shot given every two months.


Tamar Braxton
Tamar captioned her Instagram video with: “I’m on PrEP….. outside is CRAZY.” Before dropping the fact that she’s taking the prevention med, she spoke with her signature kooky candor about the challenges of hitting the dating scene, especially in Atlanta, with men wanting women to sign nondisclosure agreements and women willingly seeing the same man. “I ain’t sharing my man with the streets,” she declares.
The youngest of the six Braxton siblings—including Toni “Un-Break My Heart” Braxton—Tamar isn’t exactly tight-lipped about her intimate thoughts. But at least her sharing about HIV prevention helps educate and inspire her fans.
“I don’t think I’ve seen a hetero cis woman openly admit to being on PrEP,” @jared_tahj commented. “Kudos to you for sharing and letting people know women also have different options to protect themselves!”
Then there was this mini discussion among commenters:
“Do women take PrEP? Or am I thinking of something else?”
“Women absolutely take PrEP. Anyone can get HIV, therefore PrEP is for anyone who wants to protect themselves.”
And when some posters recommended Tamar remain celibate or leave the Atlanta scene, @jay_whin added: “You’re the first celebrity black woman I’ve heard mention PrEP, and I am so amazed. Don’t let the uneducated people get to you, I support you queen.”
In March, Tamar and her mom, Evelyn, debuted their new show, Cooking Sessions with Tamar & Ms. E, on CLEO TV. In April, Tamar dropped a new album and embarked on the October Nights Tour: Calling All Lovers, with October London and Ro James.
A new season of The Braxtons is scheduled for August. —TS

The Food and Drug Administration (FDA) granted marketing authorization in March to Visby Medical for the Visby Medical Women’s Sexual Health Test. This is the first diagnostic test for chlamydia, gonorrhea and trichomoniasis that can be purchased without a prescription and performed entirely at home. The test is intended for females with or without symptoms and delivers results in approximately 30 minutes.
According to the Centers for Disease Control and Prevention’s (CDC) Sexually Transmitted Infections (STI) Surveillance Report, more than 2.2 million cases of chlamydia and gonorrhea were diagnosed and reported in the United States in 2023.
Additionally, it is estimated that trichomoniasis is the most prevalent nonviral STI worldwide, affecting about 2.6 million people in the United States, according to the CDC’s treatment guidelines. Typically, all three infections can be treated with antibiotics, but if left untreated, they can cause serious health complications, including infertility.
The Visby Medical Women’s Sexual Health Test is a single-use at-home test that includes a self-collection kit (vaginal swab) and a powered testing device, which communicates securely to the Visby Medical App, which displays results when the test is complete.
The FDA reviewed this test under the FDA’s De Novo premarket review pathway, a regulatory pathway for low- to moderate-risk devices of a new type. Along with this De Novo authorization, the FDA is establishing special controls that define the requirements related to labeling and performance testing. When met, the special controls, in combination with general controls, provide a reasonable assurance of safety and effectiveness for tests of this type.
This action creates a new regulatory classification, which means that subsequent devices of the same type with the same intended use may go through FDA’s 510(k) premarket notification process, whereby devices can obtain marketing authorization by demonstrating substantial equivalence to a predicate device, which may save a developer time and expense compared to other review pathways.
This announcement follows last year’s authorization of the first at-home syphilis test as well as the authorization of the first diagnostic test for chlamydia and gonorrhea with at-home sample collection in 2023, which was the first FDA-authorized test with at-home sample collection for any sexually transmitted infection other than HIV. —FDA







































Recruiting and screening individuals for clinical trials is time-consuming and can account for up to one third of trial costs. But researchers have found that artificial intelligence (AI) could improve the process, resulting in enhanced screening methods and speedier enrollment, according to a research letter published in JAMA.
In recent years, AI has revolutionized health care. AI can help health care

professionals analyze colonoscopies, match individuals with appropriate cancer treatments, identify missed cases of liver disease and more.
While AI can support health care professionals and improve efficiency in several areas, many tasks still require a manual review of data. Indeed, traditional clinical trial screening requires health care professionals to manually sift through a pool of potentially eligible individuals and manually review charts to verify eligibility.
To speed up the process, Alexander Blood, MD, MSc, associate director of the accelerator for clinical transformation at Mass General Brigham, and colleagues developed a language model (a type of AI) that uses a Retrieval-Augmented Generation system called RAG-Enabled Clinical Trial Infrastructure for Inclusion Exclusion Review (RECTIFIER).
The AI-assisted screening tool yielded a much more rapid and comprehensive prereview of a person’s chart, according to the study. It also significantly reduced the time needed to determine eligibility and boosted enrollment rates.
“Implementing AI-assisted screening
tools like RECTIFIER enhances clinical trial efficiency and expedites the screening and recruitment process,” the study authors wrote, “which may lead to faster trial completion and earlier access to novel therapies for patients.”
RECTIFIER is considered a prescreening tool because patients were also screened by people before being deemed eligible for the trial.
Although the study focused on recruiting individuals for an ongoing heart failure clinical trial, Blood told JAMA that there are “no specifications, fine-tuning or special tuning to the model that made this a heart failure study–specific tool.”
When asked whether RECTIFIER could be used immediately for clinical trial recruitment, Blood said: “[We’re] starting to beta test this to additional researchers and research groups across our institution with the hope and intent that this will scale broadly across our enterprise. We’re excited to talk to friends, colleagues and partners and to also externally validate this research.”
—Laura Schmidt
Colorado regulators are issuing licenses for providing psychedelic mushrooms and are planning to authorize the state’s first “healing centers,” where the mushrooms can be ingested under supervision, in late spring or early summer.
The dawn of stateregulated psychedelic mushrooms has arrived in Colorado, nearly two years since Oregon began offering them. The mushrooms are a Schedule I drug and illegal under federal law except for clinical research. But more than a dozen cities nationwide have deprioritized or decriminalized them in the past five years, and many eyes are turned toward Oregon’s and Colorado’s
state-regulated programs.
“In Oregon and Colorado, we’re going to learn a lot about administration of psychedelics outside of clinical, religious and underground settings because they’re the first to try this in the U.S.,” says William R. Smith, MD, PhD, an assistant professor of psychiatry at the University of North Carolina School of Medicine.
Psychedelic mushrooms and their psychoactive compound, psilocybin, have the potential to treat people with depression and anxiety, including those unresponsive to other medications or therapy. The National Institute on Drug Abuse, part of the National Institutes of Health, says the risk of
mental health problems caused by ingesting mushrooms in a supervised clinical setting is low but may be higher outside of a clinical setting. Robert F. Kennedy Jr. said in a social media post in 2024, before his nomination as U.S. health secretary, that his “mind is open to the idea of psychedelics for treatment.”
Medical experts say more research is needed, particularly in people with a diagnosis or family history of psychotic or bipolar disorder. Adverse effects of psilocybin, including headache and nausea, typically resolve within one to two days. How-
ever, extended difficulties from using psychedelics can last weeks, months or years; anxiety and fear, existential struggle, social disconnection and feeling detached from oneself and one’s surroundings are most common. After the decriminalization and legalization in Oregon and Colorado, psychedelic mushroom exposures reported to poison control centers ticked up in these states and nationally.
—KFF Health News

I wrote the poem “Saving Private Bryan” in 1998. I used it to introduce myself in a support group while on board an HIV cruise. Since then, I’ve shared it and my story with countless high school students throughout Massachusetts and Connecticut and at World AIDS Day events.
I started doing HIV advocacy with a group of seven speakers called Positive Perspectives, and it just took off from there. Every time I share my story, I read my poem. I began asking the teachers to have their students write a letter of reflection after hearing my story. I wondered about the effect it had on them and if they were hearing my prevention messages.
The high school kids started writing me letters and sent their own poems about my story and what they took away from the class. Today, I have 8,000 letters and 1,100 poems in my collection.
My partner, Millie Malave, and I were featured on the January/February 2006 cover of POZ; this past Valentine’s Day was our 22nd anniversary. I was also featured in the 2018 POZ 100, which celebrated HIV advocates over 50.
I continue to be an HIV advocate and share my story. It’s been cool to read the impact it’s had on so many high school kids.
2


SAVING PRIVATE BRYAN
Knowing that the shoe fits, I’m the guy from Massachusetts. I’ve come here seeking friendship and to sail the Seven Seas and maybe find some comfort in my [34-year] disease. Finally feeling fortunate, my smile now sincere, my struggles left behind me, speaking with no fear. Yet I fear my limbs on strings and skin that feels like paper, and all my other assets that soon began to taper. Temples of doom, eye sockets that bloom and a concave face that resembles the moon.
Veins on my body that look like a map, never directions for a normal crap. Blind to the mirror afraid of what I see, what lipoatrophy has done to me. Fearing old friends in public, avoiding eye to eye, the double take I get makes me want to cry. Crying doesn’t help, the tears begin to race quickly down the grooves of my tired sunken face. Unprotected heterosexual sex was my crime of passion, now I’m doing time living in puppet fashion. Isolation by choice has kept me apart, avoiding the stress that once stopped my heart. But now I’m Saving Private Bryan from all these years of lying. Too much pride to admit, too much love to submit to a disease that could mean dying. I’ve come back to my safe haven where I know I’m accepted, to gather more strength from people affected. I’m so happy to be here with my infection, and I hope and pray we made a connection.
Visit poz.com/aidsiseveryday

The debut episode of POZ AT HOME, a live online series that brings together community members to discuss HIV-related topics, features a conversation with Mark S. King, Venita Ray and Charles Sanchez about how they are coping during the coronavirus pandemic while living with HIV. (2020)
5
HIV LONG-TERM SURVIVORS AWARENESS DAY

19
PRESIDENT GEORGE W. BUSH promotes a $500 million initiative to prevent mother-to-child transmission of HIV. (2002)
24 16
Six members of the PRESIDENTIAL ADVISORY COUNCIL ON HIV/AIDS, three of whom are living with HIV, resign, citing concerns about how the Trump administration is failing to address the epidemic. (2017)

PRESIDENT RONALD REAGAN
issues an executive order to establish a presidential commission on the HIV epidemic to “recommend measures that Federal, State, and local officials can take to (1) protect the public from contracting HIV; (2) assist in finding a cure for AIDS; and (3) care for those who already have the disease.” (1987)
27

NATIONAL HIV TESTING DAY

In an opinion piece originally published by Undark.org and republished on POZ.com titled “The End of Science’s Peacetime,” C. Brandon Ogbunu, PhD, a computational biologist, argues that defending science today requires dealing with uncomfortable truths. Below is an edited excerpt.
INITIALLY, IT WAS HARD TO separate truth from rumor, but enough has happened that the worry cannot be branded as paranoia. A string of events affecting federal agencies and programs, set in motion since the presidential inauguration, has sent the nation into a frenzy of uncertainty. The consternation is justified. Although science is hardly the only or most consequential sector affected, it was an early target for a reason: Science is a battleground in the modern war against ideas.
Science and politics have a long history of conflict. But before 2020, science had—in my lifetime, at least—operated mostly in peacetime, as measured by public support and
abundant resources. But with this long peace has come naiveté and an unwillingness to fix flaws that have plagued American science for many decades, attitudes that have left it vulnerable to nefarious political agendas.
While some might say that now is not the time for self-reflection, I argue that we must recognize that current events serve as a social stress test for science, revealing its many fragilities. Today, harm reduction is the only route to mitigate the damage to vulnerable scientists and the stifling of scientific progress. And I believe that out of the ashes will come something new, but it cannot look like the science of today and yesterday. Diversity, equity and inclusion (DEI)
efforts appear to be a main justification for many of the new administration’s actions. This does not come as a surprise. Diversity initiatives have been a political target for several years, as have certain academic subjects that teach about inequality around race and gender.
The goal is to make racism and sexism go away—not by fighting them but by erasing evidence of them and marginalizing efforts to ameliorate their impact. By scapegoating DEI, the architects are executing a plain old divide-and-conquer strategy. People may appreciate efforts to diversify science—but not more than they like their jobs. So if removing Martin Luther King Jr. Day programming is what it
takes to keep the lights on, then so be it. Better that the bad things happen to “them,” the thinking goes, than to “us.”
Next to DEI, how research is funded might be the one area under the most scrutiny in recent times. On December 1, 2024, entrepreneur and politician Vivek Ramaswamy authored a social media post that criticized the National Institutes of Health’s university funding model, in which universities can use 70% of the money awarded via federal government grants to pay for overhead [costs not directly related to research]. (Actual figures vary and are usually lower.)
Ramaswamy contrasted that with funds awarded by private foundations, for which universities charge far less, quoting a 10% figure. He cast these figures in light of taxpayer funds going to university DEI initiatives. The caricature is one of hardworking Americans thinking they are funding cures for diseases while instead subsidizing gender identity workshops.
sity hallways. It is undeniable that creative and impactful science happens and should be applauded. But one can just as readily argue that these people have succeeded despite the modern practice of science and not because of it.
If we fear eliminating something that we love because it is flawed, we can invoke the idiom “Don’t throw out the baby with the bathwater.” It teaches that, yes, science has flaws. But we cannot discard it, as the alternative is to risk descending into a new Dark
“CURRENT
carefully thought-out science with transparent methods and cleaner data. Note that this does not mean that the science itself need be less radical or transformative. One can just as easily argue the opposite: that large-scale factory science (especially conducted in academia) encourages a herd mentality that stifles innovation as much as encourages it.
And what makes Ramaswamy’s message especially craven? It’s that his anti-DEI rant is linked to a valid criticism of the interaction between federal funding and higher education, an opinion he shares with some progressive scientists, including me. His post makes effective use of a disinformation tactic: deceptively fuse bad or misleading ideas to notions that everyone can understand or empathize with. The truth is that the funding model in science has been hopelessly broken for decades. And it feeds other problematic practices affecting the manner and sort of science conducted in laboratories around the world.
Sadly, science is full of other practices—college and graduate admissions, the science publishing cartel, hiring and promotion, professional hierarchy, institutional prestige and classroom education—dictated by weird religion. All are riddled with cultural baggage that, I might add, has nothing to do with DEI. The baggage undermines merit and stifles scientific progress. And many of its rules are unwritten and informal, which has made it challenging to tackle head-on.
One retort would highlight the impressive pace of discovery, authored by the brilliant minds who walk univer-
FRAGILITIES.”
Ages. But what if we remix the idiom?
In another version, the innocent baby isn’t science but responsible reimaginations of it. In that case, the saying still applies: We shouldn’t discard the need to improve science because we fear the vile intentions from authoritarians. Sure, we must be clear about where we stand: Holding science hostage will have catastrophic effects on our progress. But now is also the time to consider new possibilities.
Because the government has gone so far as to delete Centers for Disease Control and Prevention websites, remove data and order the withdrawal of manuscripts, the scientific community needs to rapidly reconsider how it shares information and data. For example, the importance of preprint servers and the relevance of data democracy are no longer intellectual debates. We need more instruments to communicate and evaluate scientific findings in a manner that is transparent and encourages us to do our work with replicability in mind (rather than for clicks or citations).
This last point is key: Scientific findings will be under more scrutiny than ever before. This might mean that we need to conduct more small-scale,
This suggestion is compatible with the need for new funding models. In some university jobs, scientists’ basic livelihood is tied to their ability to secure government money (so-called soft money jobs), with their associated institution receiving a share of the bread. Smart scientists sign up to study the natural world and end up professional fundraisers for higher education. To call it a scam might not be accurate, but it looks, walks and quacks like one. Many scholars have studied and criticized the funding model of biomedical research. The system is indefensible as it stands, yet hardly a dent has been made in its core components.
The model has persisted because of an academic system that has, in many settings, tied professional progress to the accumulation of federal funds. With this system no longer guaranteed, laboratories may have to build research programs that are more agile and that address specific questions rather than chasing the undercooked, often vacuous mysteries tied to large federal cash prizes and their associated professional spoils.
Conversations around publishing, data democracy and funding are but a handful of the areas in need of healing. Changing the practice of science doesn’t require black magic. But it does call for something that feels almost as supernatural: We must stand in support of science in the face of attacks and simultaneously admit that we’ve been doing it wrong.
One thing is certain: The changes we make ourselves will be healthier than the ones our adversaries demand. For what might be coming, we’ll need the best version of our army to defend a science that has given us so much. But as we reflect on its practice in an age of conflict, we must admit that we can do much better. ■
In response to extreme budget cuts at federal health institutions, such as the Centers for Disease Control and Prevention and the National Institutes of Health—not to mention the threat of cuts to Medicare, Medicaid and the Ryan White HIV/AIDS Program—health advocates continue to do what they’ve been doing since the start of President Trump’s second term: fighting back!
Under the direction of Trump adviser Elon Musk, the billionaire founder of automaker Tesla, and his Department of Government Efficiency (DOGE), public health is under attack in ways that directly affect the most vulnerable among us, namely low-income people, individuals living with HIV and other chronic diseases, and folks over 65.
On March 29, the movement known as Tesla Takedown organized national protests targeting Tesla showrooms and service shops to protest Musk and encourage folks to trade in their Tesla cars and stocks. And from March 31 to April 2, the annual AIDSWatch, the largest constituent-led HIV federal advocacy event, gathered together hundreds of advocates on Capitol Hill to urge lawmakers to protect HIV and other health programs. As these actions demonstrate, creative, long-haul activism must be the order of the day.





1., 2. Takedown protests aimed to surround all 277 of Tesla’s showrooms and service centers in the U.S. In San Francisco, takedowners partnered with the youth-led Planet Over Profit (POP), which advocates for a livable future by fighting against the fossil fuel industry and the hoarding of wealth. 3., 4., 5. In NYC, Tesla takedowners joined ACT UP, Housing Works and Rise and Resist to march from the AIDS Memorial in the West Village to the Tesla showroom in the Meatpacking District, where participants staged a die-in to protest the funding cuts that threaten some folks lives.


Add
THIS TAKEOUT CLASSIC IS AN EASY and adaptable one-pan dish. Green peas are high in fiber and have a high concentration of the phytonutrients lutein and zeaxanthin, which help promote eye health. They are also a powerhouse of vitamins and minerals, especially vitamins K and B, which help support healthy immune function. And of course, you can add any other vegetables you have lying around.
SERVINGS: 4 / INGREDIENTS: 16 / PREP: 25 MINUTES
INGREDIENTS
2 tablespoons low-sodium soy sauce or oyster sauce
1 teaspoon rice vinegar
1 teaspoon sesame oil
1 tablespoon canola or vegetable oil
1 large carrot, ¼-inch diced
1 small onion, ½-inch diced
8 ounces extra-firm tofu, drained, ½-inch diced
DIRECTIONS
3 eggs, whisked
4 cups cooked brown rice (day-old recommended)
3 garlic cloves, peeled, minced
1 1-inch piece of fresh gingerroot, minced or finely grated
4 green onions, thinly sliced
1 cup frozen peas, thawed
1 cup toasted and unsalted cashews, coarsely chopped
1 tablespoon fresh mint, roughly chopped
1 tablespoon fresh basil, roughly chopped
1. Mix together the soy sauce, vinegar and sesame oil in a small bowl and set aside.
2. Add canola oil to a large pan or well-seasoned wok over medium-high heat. When the oil is rippling, add carrot and onion and cook until tender, about 4 minutes.
3. Add tofu and cook until golden, about 3 minutes. Pour in whisked eggs from sides and let cook undisturbed for a few seconds before mixing up with cooked vegetables. Add rice, garlic, ginger, green onion, peas, cashews and soy sauce mixture, and cook for 1 to 2 minutes to heat through.
4. Serve immediately and top with fresh mint and basil.
CHEF TIPS
Use day-old rice (or other grain, like quinoa) to make this dish. Not only will you save time, but rice that’s a little dried out will absorb the sauce and flavors better. You can easily substitute two tablespoons of chopped cilantro for the mint and basil in this recipe.
NUTRITION FACTS (per serving)
Calories: 632; fat: 30 g; saturated fat: 5 g; polyunsaturated fat: 8 g; monounsaturated fat: 30 g; carbohydrates: 69 g; sugar: 5 g; fiber: 9 g; protein: 27 g; sodium: 355 mg

©2025 Fred Hutchinson Cancer Research Center, a 501(c)(3) nonprofit organization. Used by permission.
Both eating patterns and physical activity routines play critical roles in weight management. You can gain weight when you consume more calories than the number of calories you burn.
To maintain your weight. If you are not physically active, work your way up to 150 minutes a week of moderate-intensity physical activity. This could include dancing or doing yard work. You could meet the goal of 150 minutes a week with 30 minutes a day 5 days a week, 22 minutes every day or whatever other breakdown works best for you. When it comes to managing weight, people’s need for phy sical activity varies greatly. You may need to be more active than others to reach or maintain a healthy weight.
To lose weight and keep it off. You will need a high amount of physical activity unless you also adjust your eating patterns and reduce the number of calories you’re eating and drinking. Healthy eating combined with regular physical activity help you get to—and stay at—a healthy weight.
Adapted from: Physical Activity Basics, CDC.gov MANAGE YOUR WEIGHT

New restrictions on research and services threaten to reverse recent progress.
TRANSGENDER, GENDERnonconforming and nonbinary people are at greater risk for HIV and are more likely to be living with the virus than the population at large. Targeted studies and tailored services have helped close this gap, but recent political shifts put this progress in jeopardy.
About 1.6 million adults in the United States identify as transgender, but accurate data about how many are living with HIV have been hard to come by. Trans women used to be classified as “men who have sex with men,” while trans men were generally excluded from research. Recent studies have done a better job, but the Trump administration has changed how trans people are counted, removed data from federal health agencies and reduced funding for targeted research and services.
According to the latest available data from the Centers for Disease Control and Prevention (CDC), transgender people accounted for 2% of new HIV
diagnoses in 2019. Of these, 625 were trans women and 46 were trans men. Based on data from seven U.S. cities, 42% of transgender women were living with HIV (62%, 35% and 17% of Black, Latina and white trans women, respectively).
Increased focus on transgender people has led to more tailored services.
According to the 2019 CDC estimates, 96% of trans women have been tested for HIV, 92% are aware of pre-exposure prophylaxis (PrEP) and 32% have used it—figures that compare favorably with those for gay and bisexual men.
The daily PrEP pill tenofovir disoproxil fumarate/emtricitabine (Truvada) is highly effective for trans women, but it has not been studied in trans men. Tenofovir alafenamide/emtricitabine (Descovy) is also effective for trans women, but due to inadequate research, it is not approved for people exposed to HIV through vaginal sex .
Long-acting injectable cabotegravir PrEP (Apretude), which is administered every other month, is even more effective
than daily pills for transgender women, but again, studies have not included trans men. Long-acting lenacapavir PrEP, administered every six months, was highly effective in a trial that included trans women, trans men and nonbinary people.
Some older research found that trans people are less likely to receive ongoing HIV care and treatment, but things have improved thanks to targeted education and services. According to the 2019 CDC data, 84% of trans women received some HIV care, and 67% achieved viral suppression on antiretroviral therapy; for trans men, the rates were 85% and 68%.
Studies have shown that transgender women respond as well as cisgender (non-trans) men and women to antiretroviral medications, and those who remain in care are as likely to maintain viral suppression. There has been little research on trans men with HIV, but there’s no reason to think they would not also respond well to treatment.
Many trans people are concerned that the medications used for PrEP or HIV treatment could interfere with gender-affirming hormones. But research to date has found that commonly used antiretrovirals do not have clinically significant interactions with feminizing hormones, nor does hormone therapy alter the effectiveness of antiretrovirals.
Trans and gender-nonconforming people often face stigma and discrimination, which contributes to higher levels of poverty, unemployment, homelessness, sex work, mental health problems and substance use—all of which are linked to higher rates of HIV acquisition and worse treatment adherence. What’s more, many trans people have had negative experiences with the health care system, which can discourage them from seeking care.
Yet gender-affirming care can improve outcomes: One recent study found that trans people who received hormone therapy were 37% less likely to acquire HIV and 44% more likely to achieve viral suppression.
Recent improvements in HIV prevention, care and treatment for transgender and gender-diverse people are welcome, but new restrictions on research and services threaten to reverse this progress. Finding providers who are knowledgeable about and sensitive to trans people can be a challenge, but LGBTQ advocacy groups or local AIDS service organizations may be able to point you in the right direction. ■
The Trump administration continues to make cuts that threaten the lives and health of people living with or at risk for HIV. While the earliest funding reductions affected international aid programs, like PEPFAR (the President’s Emergency Plan for AIDS Relief), more recent moves imperil the domestic HIV response.
In late March, Health Secretary Robert F. Kennedy Jr. announced a “dramatic restructuring” of the Department of Health and Human Services, reducing staff at federal health agencies, including the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH), by some 20,000 people. Highlevel staff cuts included Jonathan Mermin, MD, MPH, director of the CDC’s National Center for HIV, Viral Hepatitis, STD, and Tuberculosis Prevention, and Jeanne Marrazzo, MD, MPH, head of the National Institute for Allergy and Infectious Diseases.

The administration also canceled hundreds of NIH grants for HIV research; for example, it eliminated funding for the Adolescent Medicine Trials Network for HIV/AIDS Interventions. Grants for the AIDS Clinical Trials Group, the HIV Prevention Trials Network and the HIV Vaccine Trials Network were delayed, and their fate remains uncertain.
Many of the cuts are part of the administration’s push to eliminate “gender ideology” and diversity, equity and inclusion. HIV disproportionately affects gay and bisexual men, transgender people and Black and Latino people; as a result, much HIV research focuses on these populations. The grant termination “threatens to halt decades of progress,” says HIV Medicine Association chair Colleen Kelley, MD, MPH. “The return on investment in HIV research goes well beyond HIV, with the discoveries laying the foundation for curative therapies for hepatitis C and treatments for cancer.”
Letermovir (Prevymis), an antiviral drug used to treat cytomegalovirus (CMV), was associated with reduced inflammation, improved immune function and better physical function in people with HIV on antiretroviral treatment, according to research presented at the Conference on Retroviruses and Opportunistic Infections. CMV infection is usually asymptomatic in people with a healthy immune system. The virus goes dormant after acute infection, but it remains in the body and can reactivate if immunity wanes, potentially leading to severe illness. The new research suggests that even latent virus can have more subtle detrimental effects.
In the ACTG A5383 trial, people with HIV on suppressive antiretroviral therapy who tested positive for CMV were randomly assigned to add letermovir or continue their antiretrovirals alone for 48 weeks. CMV treatment led to declines in various biomarkers of inflammation and pro-inflammatory cytokines linked to comorbidities such as cardiovascular disease and cancer.
People in the letermovir group also experienced a greater increase in their CD4 T-cell count, which was especially pronounced among those who started with a count below 350 at baseline. Letermovir recipients also saw a significantly larger increase in their CD4/CD8 ratio (an indicator of better immune function), particularly among women. What’s more, those who took letermovir scored better on tests of physical function, including leg strength.
Letermovir “is probably the most exciting intervention that has been done in people with HIV for inflammation and aging over the last 20 years,” says lead investigator Sara Gianelle Weibel, MD, of the University of California San Diego.

As twice-yearly lenacapavir for pre-exposure prophylaxis (PrEP) nears approval, researchers at Gilead Sciences are now working on onceyearly HIV prevention shots. Twice-yearly lenacapavir PrEP was 100% effective for young cisgender women in the PURPOSE 1 trial, while PURPOSE 2 showed that lenacapavir injections every six months reduced the risk of HIV acquisition by 96% for gay and bisexual men and gender-diverse people. At the Conference on Retroviruses and Opportunistic Infections, researchers presented the first data from a Phase I trial of two once-yearly lenacapavir formulations administered via intramuscular injection. The study enrolled 40 healthy adults at low risk for HIV acquisition. Lenacapavir levels were even higher than those seen with twice-yearly injections, remaining above the 95% effective concentration for at least 56 weeks. The most common side effect was mild injection site pain. Gilead plans to start a Phase III trial of once-yearly lenacapavir PrEP later this year, bypassing intermediate Phase II trials. Data could be ready for Food and Drug Administration review in 2027.

Two new antiretrovirals from ViiV Healthcare look promising for HIV treatment based on early studies. Researchers evaluated oral versions of the third-generation integrase inhibitor VH184 and the HIV capsid inhibitor VH499 in small Phase IIa proof-of-concept trials that enrolled previously untreated people with HIV. Both drugs demonstrated potent antiviral activity when used alone for 10 days. The mean maximum changes in HIV RNA were −2.31 and −2.17 log copies using the highest tested doses of VH184 and VH499, respectively—comparable to viral load reductions seen in early studies of the second-generation integrase inhibitor dolutegravir. No one in the VH184 study developed drug resistance, but one person taking the lowest dose of VH499 had a mutation associated with reduced sensitivity to capsid inhibitors. Both novel drugs were safe and well tolerated with no serious adverse events. These results set the stage for ongoing trials of long-acting injectable formulations of VH184 and VH499. Ultimately, the goal is complete regimens that can be administered every six months or less.

Two more people appear to be free of HIV after stem cell transplants for cancer treatment. If they remain in remission, they will be the ninth and tenth cases. The Chicago Patient, a 67-year-old man, received a stem cell transplant from a donor with two copies of a rare mutation called CCR5-delta32 that blocks HIV from entering cells. This case is notable because he stopped antiretroviral treatment 15 months after the transplant, experienced viral rebound, restarted antiretrovirals, tried a second treatment interruption two years later and has now been in HIV remission for 10 months. The Oslo Patient, a 58-year-old man, received a stem cell transplant from a brother with the double mutation. He developed severe graft-versus-host disease and received the immunosuppressive drug ruxolitinib. He stopped antiretrovirals two years after the transplant, and his viral load remains undetectable two years later. Stem cell transplants are too risky for people without cancer, but each new case offers clues that could help scientists develop a more widely accessible functional cure.

People living with both HIV and hepatitis C virus (HCV) can benefit from direct-acting antiviral (DAA) therapy, but many are not receiving treatment. This is a concern because people with HIV/HCV coinfection are more likely to experience severe liver disease than those with HCV alone. Researchers looked at disparities in DAA uptake among people with HIV in the United States and Canada. Among 6,300 treatmenteligible people with HIV/HCV coinfection, 58% initiated DAAs between 2014 and 2021. While the treatment gap narrowed over time, some groups are still falling through the cracks. Heterosexuals and people who inject drugs were less likely to start DAA treatment than gay or bisexual men. Black and Latino people also had lower rates of DAA initiation, as did those who reported heavy alcohol use, smoking, a detectable HIV viral load or a prior AIDS diagnosis. Conversely, those with worse liver fibrosis were more likely to start DAAs. The researchers highlighted the need to develop targeted approaches to increase equity in DAA initiation by addressing disparities to eliminate HCV among people with HIV.







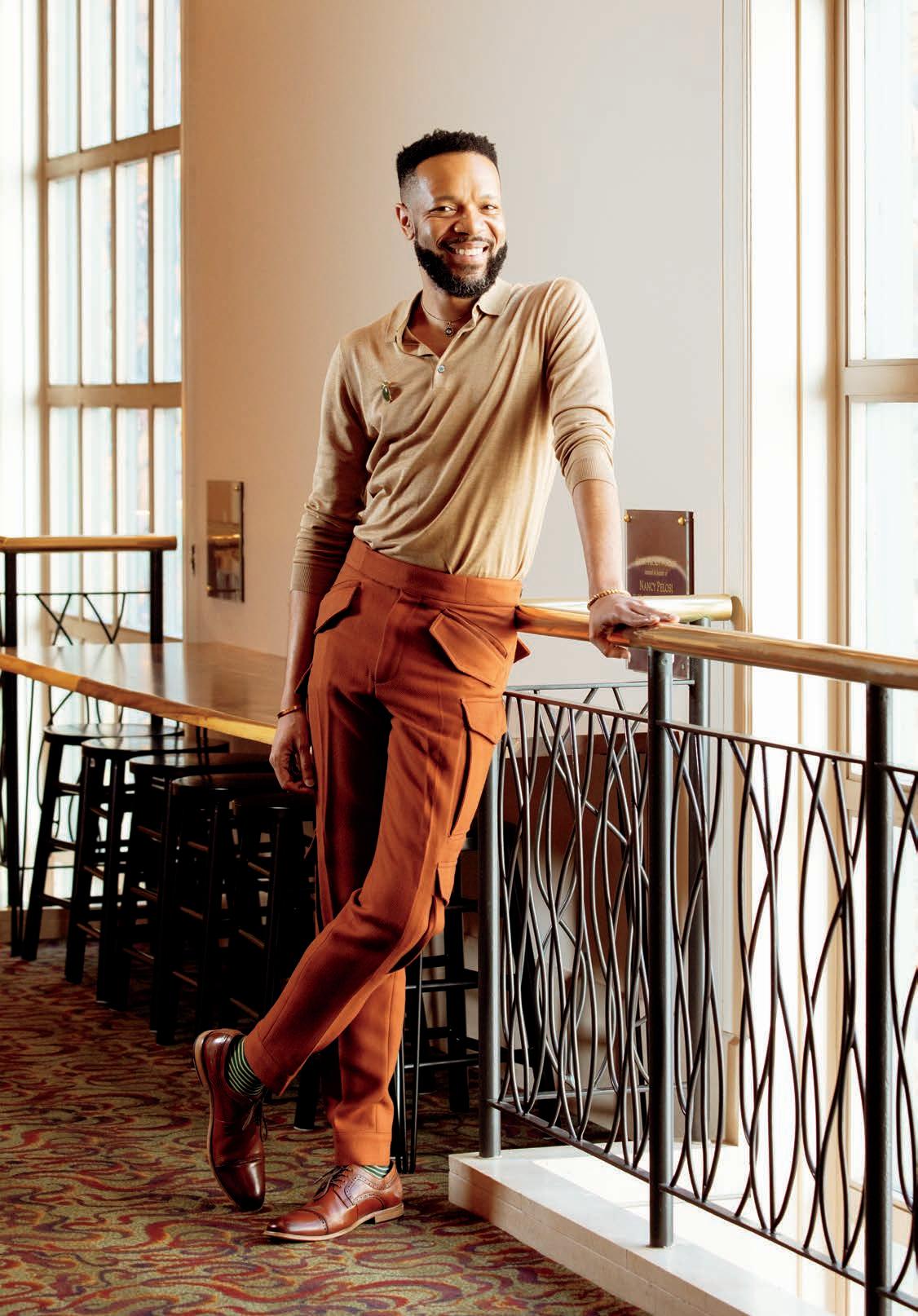
ACTOR AND ADVOCATE JASON VEASEY SHARES HIS HIV JOURNEY.

BY MATHEW RODRIGUEZ
AS AN ACTOR, JASON VEASEY DOESN’T usually go off script. But on a balmy, windy evening in November 2024, in front of a couple of dozen people—a mix of friends, colleagues and strangers— gathered at New York’s Michelangelo Hotel, Veasey lowered the barrier between him and the audience. In theater talk, he broke the fourth wall.
The occasion was an event sponsored by Playbill in observance of World AIDS Day honoring the hard work of Tom Viola, the outgoing director of Broadway Cares/Equity Fights AIDS. As part of Playbill’s Storytellers series, Veasey had previously recorded a scripted video in which he discussed the importance of continuing to tell stories about HIV. In the video, he wears a white lace shirt and black pants and sits on a chair in front of a red background.
“While we have a long way to go with releasing stigma and shame and finding a cure for HIV/AIDS, there has been an advancement,” he says in the video, which can be seen on YouTube. “And I find that I know—and you all out there know, or you don’t know that you know—that there are many people living positively with HIV.”
Before recording the video, Veasey had contemplated whether he would seize the opportunity to come out as living with HIV. Though he was not out publicly, many people who love him knew his status—he tested positive January 22, 2015. But when he sat down and began to deliver his monologue, he decided it wasn’t time. “I trusted my gut feeling,” he tells POZ.
When it came time to deliver the same speech to the audience gathered at the Michelangelo that November night, all Veasey had to do was what he had done hundreds, if not thousands, of times before: stick to the libretto. He wore two different earth tones, as if his outfit were a reminder to stay grounded. On his chest, he wore a red ribbon. As he stood up to recite his monologue, something—let’s call it the muse of improv—urged him to go a step further. This time, when he delivered the line about people living with HIV, he appended it with two life-changing words: “There are many people living positively with HIV, like me.”
“It just came out,” he says. After his talk, he returned to his seat in the audience, where people were waiting to embrace him. They knew that this was more than a performance—it was a deeply personal step into a new phase of his life. He says, “It felt like the training wheels came off.”
Veasey has been working on an acting career since he was a child. His mother recalls him trying to “get into the box” as a kid, that is, trying to enter the world of the TV. Even then,
he was sharply aware that the people on the screen were acting, creators of an artifice he hoped to help create someday.
“I remember thinking, It can’t just be fake—it has to be real,” he says. “I didn’t know what acting was, but I knew it was more than pretending.” Thus, he landed on acting as his dream profession, just as other kids might have picked careers that seemed just as surreal, like astronaut or president.
A self-identified military brat, Veasey moved around often in his youth. He never stayed at one school for long, and his upbringing included time spent living in Colorado, California, Texas, Germany and Alabama.
In the Yellowhammer State, his family resided in Montgomery, which houses both a military base and the Alabama Shakespeare Festival, the state’s official theater. When Veasey joined the local theater, he worked with some of the best in the business on such productions as A Midsummer Night’s Dream as well as non-Bard stage classics, like A Raisin in the Sun and, one of his favorites, Peter Pan
Veasey has since performed on Broadway and appears in Hulu’s acclaimed hit Only Murders in the Building. Recently, he was the breakout star of the trailer for the new A24 film Friendship. Though the movie centers on the budding friendship between characters played by Tim Robinson and Paul Rudd, Veasey’s velvety voice dominates the teaser. As the action unfolds, Veasey sings the beloved R&B classic “My Boo” by Ghost Town DJ’s. As the trailer went semi-viral, Veasey’s voice—the voice of a person living with HIV—took over the internet.
Internet fame has leaked into real life, he says. The day the trailer hit, his phone started to blow up, and he was even treated to a drive-by serenade while walking down the street in California. “This is about to be my life,” he says. “People are about to be singing that goddamn song to me nonstop. But I’m excited.”
Veasey made his mark on Broadway as an original cast member of the Tony- and Pulitzer Prize–winning musical A Strange Loop. He played one of the five Thoughts— Thought 5, to be exact—before the lauded musical even made it to the Great White Way. He started working on the play in 2012 and was there at one of its earliest live performances in 2015, the year he tested HIV positive, when a ticket to the show was a mere $12. He remained with the

production throughout its permutations and has become close friends with the entire team, including creator Michael R. Jackson.
“It has been one of my greatest honors to be artistic collaborators and, more importantly, friends with Jason for over a decade,” Jackson tells POZ. Jackson added that Veasey shared his HIV status with him very early on in the process of developing A Strange Loop. “I have looked to Jason as a symbol of hope and as a beacon of light and strength. Jason will be a powerful advocate and role model for so many living with HIV. He is a true hero, and I love him.”
Loop depicts the story of Black queer aspiring musical theater writer Usher, who is an usher for Broadway’s The Lion King. The play includes several explicit mentions of the stigma and shame associated with HIV, including a storyline about a friend of Usher’s who died after refusing to take his HIV medication—that narrative culminates in an intense musical number titled “AIDS Is God’s Punishment,” in which the Thoughts sing the title phrase over and over, to an almost numbing effect.
During the number, Veasey perched atop an imposing two-story structure that looms large onstage. Behind him illuminated letters spelled out H-I-V. Friends who came to see the show were concerned that singing these lyrics on a daily basis might affect him personally. What was it like to have to repeat the idea that AIDS is a sign of God’s wrath night after night?
But he has never equated AIDS with God’s wrath. He was not raised in a religious household, and he realized early on in his life with HIV, at a support group for newly diagnosed people, that he didn’t have the same relationship with his status as those in the room who had grown up in the church.
“I couldn’t grasp why I was not having some of those intense feelings,” he says of his time in the group alongside people who had grown up religious. “I never once thought that this was a punishment for me existing as a gay person.” Thus, he never felt dread performing Loop ’s AIDS song. In fact, he feels he had the best seat in the house, watching Broadway-goers react to the confrontational number. Veasey says that because he started working on the show before testing
Veasey has been living with HIV since 2015.
positive for the virus, he never associated his HIV status with the work of mounting the production. Also, he considers his experience to be diametrically opposed to the one depicted in the show. “That number has always been about how silence and stigma can be killers for those of us living with HIV,” he says. By contrast, he considers his own story to be one about what happens when you come out and have the support of loved ones. “That’s how I was able to do the show without feeling emotionally charged.”
PRIOR TO HIS 2015 diagnosis, Veasey’s relationship with HIV was like that of many queer Black kids who had grown up with AIDS happening around them rather than as a member of the first generation of gay adults who experienced the AIDS crisis. Veasey, 45, was born just a year before the Centers for Disease Control and Prevention first announced the earliest cases. “I’m the safersex generation,” he says. “I was never taught about sex without someone saying, ‘Oh, this could kill you. Use a condom.’”
his health insurance coverage can be erratic, and he often relies on the AIDS Drug Assistance Program to pay for meds. During the last three years, between private health insurance and public assistance, he’s barely gone two months without some red tape coming between him and his medication.
“That’s the only time that I feel really overwhelmed with emotion by the reality that I’m HIV positive,” he says. “I’m kind of like, I can’t believe this is my life right now.”
“SILENCE AND STIGMA CAN BE KILLERS FOR THOSE OF US LIVING WITH HIV.”
While dealing with the behind-the-scenes work of living with HIV is sometimes marked by discord, Veasey’s colleagues commend him for his ability to bring harmony and collaboration to his acting work. Michael Cyril Creighton, who plays Veasey’s love interest on Only Murders, describes Veasey as “disarming, joyous, open, confident, funny and kind” and says he knows “he’ll always have my back.”
However, when he was diagnosed in 2015 at New York’s Callen-Lorde Community Health Center, where he continues to receive care, he didn’t feel shame. Instead, he went into fact-finding mode, hoping to learn as much as he could. He began to share his status with everyone who needed to know, including loved ones and friends.
The only people he waited to tell were his parents, whom he wanted to tell in person. About three months after his diagnosis, his parents could tell, even over the phone, that something was bothering their son—“They always know,” he says—and they scheduled a visit. He shared his status with his father outside a Jamaican restaurant in the Bronx; a few hours later, he told his mother in their hotel room. His mother excused herself to go to the bathroom and returned moments later. They hugged, and she asked a single question, “What are the next steps?”
“I can imagine the fear or concern that can wash over you when it’s your child,” he says. “But I remember this beautiful moment of a mother being loving and holding her child and wanting to know what to do moving forward.”
Afterward, his parents accompanied him to a doctor’s appointment, where his physician answered their questions about HIV. He explained to them how treatment works, what a viral load is and that their son was in good health.
Most days, Veasey says, his status does not come to his mind. Only when he is forced to deal with the bureaucracy of getting his HIV meds does he really start to feel the weight of his status. Because of the nature of acting work,
“He’s a remarkable scene partner,” Creighton says. He noted specifically that Veasey helped assuage his nerves about having to yodel during a scene in the show’s second season. “Jason immediately put me at ease. He made it so easy to fall in love with his character and was my biggest cheerleader.”
As a person with HIV working in media, Veasey is acutely aware of the usual stories about HIV that continue to permeate our collective understanding of the AIDS crisis. “While I love so many of the pieces that are cornerstone, like And the Band Played On or Angels in America, I think we’re good for a while with tragedy, drama and people dying,” he says.
Were he able to wave a magic wand and become the head of a major studio, he has a radical idea: a comedy about AIDS. Though he recognizes the need for dramas about the ongoing crisis, especially about people struggling to access good care or medication, Veasey would green-light a funny show about HIV set in a support group for newly diagnosed people. But he’d upend the idea of a group of people sharing while sitting in a circle.
In his imagination, the show would be a sort of Sex and the City focusing on a group of HIV-positive people for whom HIV is only a small part of their lives. The show would tackle them trying to have a baby, for example, or having relationship drama that’s not about their status. One character would be single and ready to mingle. While HIV would always be present, it would often be subtext.
“Not every episode is about someone taking a pill and crying,” Veasey says, envisioning storylines in which “HIV is just a fraction of someone’s life and not the wholeness of someone’s life—that’s what I would like to see.” ■

BY TIM MURPHY
Anyone who has grown up never knowing a world before Undetectable Equals Untransmittable (U=U) the fact that people living with HIV on effective treatment cannot transmit the virus via sex—and the HIV prevention regimen pre-exposure prophylaxis (PrEP) might have a hard time understanding what happened in San Diego in November 1997 at the Creating Change conference, an annual gathering of LGBTQ advocates organized by the National Gay and Lesbian Task Force.
But what indeed happened speaks to both the immense grief over AIDS losses and the fear of HIV transmission that prevailed at the time. On a panel about HIV prevention, a handsome, brainy Mexican-American queer activist living with HIV named Tony Valenzuela, then 29, said before a jury of his peers: “The level of erotic charge and intimacy I feel when a man comes inside me is transformational, especially in a climate which so completely disregards its importance.” And then he went on: “I am a sex gourmet in a community serving sexual TV dinners.”
It didn’t matter that he added, “When I talk about having unprotected sex, I am speaking for myself and not as a proponent of condomless sex for all.” It also didn’t matter that he was talking about being a bottom (the one who receives, not gives, during anal sex) and that it was well established by that point that it was difficult for a top to get HIV from a bottom. Nor did it matter that, often, Valenzuela was having sex with other gay men living with HIV—a practice known at the time as serosorting (having sex with people of the same HIV status).
Despite all that, the room erupted in outrage, with one audience member after another denouncing Valenzuela. Said one lesbian activist, according to “They Shoot Barebackers, Don’t They?” a 1999 POZ article about the event: “Lesbians have been, in a way, the wife of the gay male
movement. You got sick, and we were there. I’m not saying, ‘We did this for you, and therefore you’ve got to be a good boy.’ But you wonder why we’re so upset. Because 15 years later, when we’re facing breast cancer [and other problems], we’re hearing ‘I want to do what I want.’ Well, do what you want. But I’m not going to be there to clean up after you this time. I have too much pain.” She was loudly applauded.
A torrent of anti-Valenzuela op-eds in LGBTQ papers followed. “Tony is responsible for speaking out to a room full of young students, parents and community members,” read one, written by a member of San Diego PFLAG, “with the words, ‘It is OK to have unprotected sex whether you or your partner is HIV-infected or not because it is the only way you can experience the spiritual aspect of sexuality.’”
To hear Valenzuela, now 56 and living happily in Los Angeles with his longtime husband, Rob, tell it today—that’s not what he meant at all. “What I was trying to say was that sex without condoms is not easily given up or disposable,” he says on a call from his office in Hollywood, where he helms One Institute (formerly the ONE Archives Foundation), which does public educational programming around its massive collection of LGBTQ documents and photos dating back to the 1930s, which are housed and viewable at the University of Southern California.


Valenzuela points to studies in the ’80s and ’90s that found that when asked, up to half of gay men said they either declined or failed to use a condom every single time during sex. “I felt like I was giving voice to that reality,” he says, “but I should’ve realized that many people there were going to be hearing that idea for the first time.”
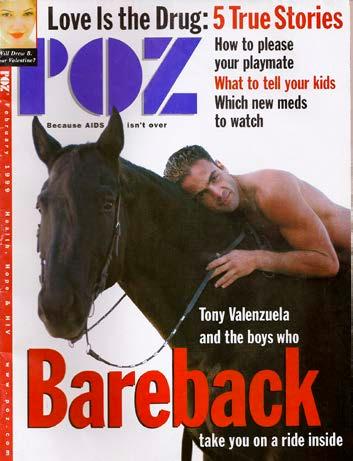
That may be understating it. “Because after I gave that speech, my life turned upside down,” he says. “There was so much vitriol directed toward me. I was reading about myself in gay newspapers nationwide, and, without fail, I was always written about in some deeply biased way.” He became so bitter that he agreed not only to talk to POZ about it in 1999 but also to appear naked, from the waist up, lying on a real live horse—bareback, of course. He was interviewed by POZ contributing editor Stephen Gendin, who agreed with
Valenzuela that practicing sexual harm reduction and being honest about one’s desires were not incompatible. Gendin died in 2000.
The spicy cover line read: “Tony Valenzuela and the Boys Who Bareback Take You on a Ride Inside.” Says Valenzuela now: “Me on that cover was my middle finger to the world.”
But beneath the anger lay deep hurt that a community he had given so much to had discarded him so easily. His career as a queer activist started in 1987, in college in Santa Barbara, when his roommate found his journal and told their entire dorm that Valenzuela was gay—and that he frequented the local bathhouse. After a female friend finally told Valenzuela about the gossip, he had his resident adviser call a surprise dorm meeting and came out to the entire dorm. “I stood up and said, ‘I’ve felt different my whole life. I’m gay—and I’m not ashamed of it.’”
He was met, to his surprise, with almost complete acceptance and hugs. (He cries when recounting this part of the story.) When the school asked Valenzuela whether he wanted to see his roommate expelled, he answered that probation would suffice. (“I wasn’t going to be responsible for ruining his life.”)
So it was ironic that he had been accepted by largely straight people in college, only to be rejected by his own LGBTQ peers after the Creating Change conference. He couldn’t get a job in queer activism to save his life after that, he says, so he started doing sex work to make a living as well as a little bit of porn as an openly HIV-positive actor, including a video with an HIV storyline titled Positively Yours. “That allowed me to buy a computer and go to conferences,” he says. “And I also decided that I was going to be open about escorting” to try to counter the stigma against it—a choice that earned him yet more disapproval from some corners of the queer world.
Meanwhile, he met Rob in 2004, went to grad school for creative writing and began quietly volunteering at the long-

As Brett Klein of Palm Springs, California, gears up for the California AIDS/LifeCycle taking place June 1 to 7 from San Francisco to Los Angeles, he’s eager to shatter a major fundraising milestone.
“When the ride happens, I will have raised over $100,000 during my eight years participating,” he tells POZ. “That includes three years as a roadie and five years as a rider. I’m very proud of that.”
Klein has personal and professional skin in the game. Currently the marketing and events specialist for Eisenhower Health, Klein was the president of the HIV+ Aging Research Project–Palm Springs (HARP-PS) and served on the board of Dining Out For Life International. He tested HIV positive in 1993.
Founded in 1994 as the California AIDS Ride and rebranded in 2002, the event has raised over $300 million for HIV treatment and prevention. By demonstrating their prowess as endurance athletes, the riders, many of whom live with HIV, have challenged the stigma associated with the virus.
“I did my first California AIDS Ride in 1999,” Klein says. “I was a roadie, which can be very long days. Those days were so hard that I decided it’s easier to ride.”
“It’s 545 miles on a bike over seven days,” Klein explains. “The first three days are by far the hardest, up to 110 miles per day, navigating hills and weather from San Francisco to Los Angeles. There’s no easy day per se, but you just grind it out. They have support stops every 20 miles. We’re heavily supported out there.”
For Klein, the annual bike ride is a chance to find fellowship with other riders and to challenge himself physically and mentally. Klein believes that living with HIV has given him an edge, especially on the days when he’s forced to dig deep on the road. “People living with HIV know how to adapt,” he says.
This year’s ride is slated to be the last, marking the end of an era. The deadly wildfires in Southern California were just the latest setback for organizers still working to bounce back from diminished ridership resulting from the COVID-19 pandemic and the changing HIV landscape.
“It’s an interesting time because of the LA fires,” Klein says. “Everything you see on TV, the damage to the Pacific Coast Highway—that’s usually the backdrop for our final day, entering Los Angeles. It’s a big question how this all will transpire.”
Klein is already looking ahead to continue his fundraising. “We are going to participate in some Northern California weekend rides, and Los Angeles folks may do the same,” he says. “And then we’re going to host something here in Palm Springs next year, possibly a two-day social ride, fun yet challenging, just to keep the AIDS Ride spirit alive and mostly to keep the message alive. The whole point of the AIDS Rides is to remind people— especially in the next four years—that HIV has not gone away. It’s still here, and people are still going undiagnosed.” ■
