Genetic engineering is a transformative capability that has invigorated the hope of a cure for several diseases while also opening the door for research to better understand the complexities of many more. St. Jude scientists are capitalizing on the power of CRISPR to make discoveries about the fundamental characteristics of cancer, identify novel targets for drug development, and even manipulate the genome itself therapeutically. This feature reflects the powerful combination that DNA and CRISPR can have on
treatment landscape.
INSPIRING VISIONARIES LEAD THE WAY
When Danny Thomas opened the doors of St. Jude Children’s Research Hospital in 1962, he believed St. Jude would one day make the impossible possible — that our discoveries would lead to a day when no child dies in the dawn of life from a catastrophic disease. In our 62-year history, we have made tremendous progress in curing the incurable, treating the untreatable, decreasing the side effects of therapy, and accelerating the adoption of diagnostic and therapeutic approaches globally to improve cure rates.
Despite this progress, there remains much more to accomplish. In developed countries, 15-20 percent of children with cancer die from their disease.
catastrophic diseases, progress has been even slower. To change these sobering facts, all of us at St. Jude remain committed to our mission to advance cures and means of preventing pediatric catastrophic diseases through research and treatment.
our extensive clinical experience, allows us to generate knowledge in the lab that can be implemented in the clinic. Our goal is to generate new knowledge that will forever change how medicine is practiced, not only in the United States but worldwide.
Please join me in celebrating the significant scientific progress described in this report.
Moreover, overall cure rates in low- and middle-income countries hover around 30 percent globally. For other childhood
Over the past year, we have made substantial progress in achieving our mission. This Scientific Report highlights some of the more notable advancements St. Jude faculty and staff made in 2023. The work described in this report underscores the unique scientific culture at St. Jude and illustrates how it drives our faculty and staff to tackle the most challenging problems and answer the most complex questions. Our commitment to understanding fundamental biological principles, coupled with
James R. Downing, MD President and Chief Executive Officer
St. Jude Children’s Research Hospital PRESIDENT’S LETTER
The ability to manipulate genetic material to introduce a specific change or edit has already proven transformative in biomedical science — with even more groundbreaking possibilities on the horizon.
Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR) technology has emerged as a gamechanger in research. It is a powerful tool for studying the genetic underpinnings of various diseases and consequently paves the way for developing novel therapeutic interventions.
The technology’s impact was exemplified in 2020, when the Nobel Prize in Chemistry was awarded to Emmanuelle Charpentier, PhD, a former St. Jude postdoctoral fellow, and Jennifer Doudna, PhD, for their roles in its development. CRISPR has made it possible to edit genes in living organisms with unprecedented precision and efficiency, significantly accelerating the pace of scientific discovery.
The system has two main components: a guide RNA and a DNA-cutting enzyme
called Cas protein. The guide RNA mirrors the gene’s DNA sequence to be edited (the target). Working together, the guide RNA and Cas protein locate the target gene. Once the guide RNA aligns with the target gene’s DNA, the Cas protein precisely cuts the DNA at the target site.
At St. Jude, CRISPR has propelled cutting-edge research in cancer, immunity, and the fundamental mechanisms of transcription and gene regulation. Transcription is an essential biological process in which DNA is copied into RNA. This process is the first required step a cell takes to access the code housed in DNA and ultimately translate that code into the amino acid or polypeptide building blocks that become active proteins.
Dysregulated transcription plays a role in many types of pediatric cancer.
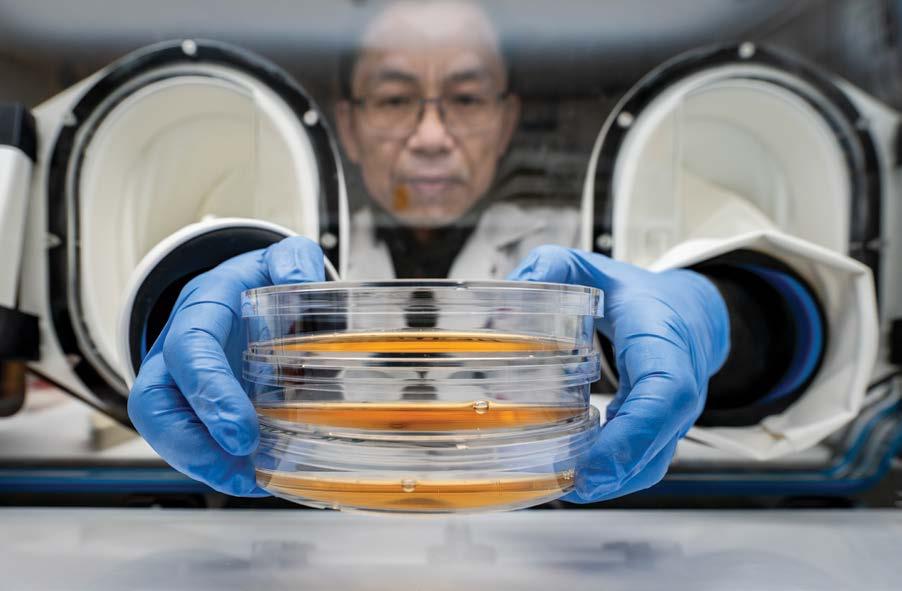
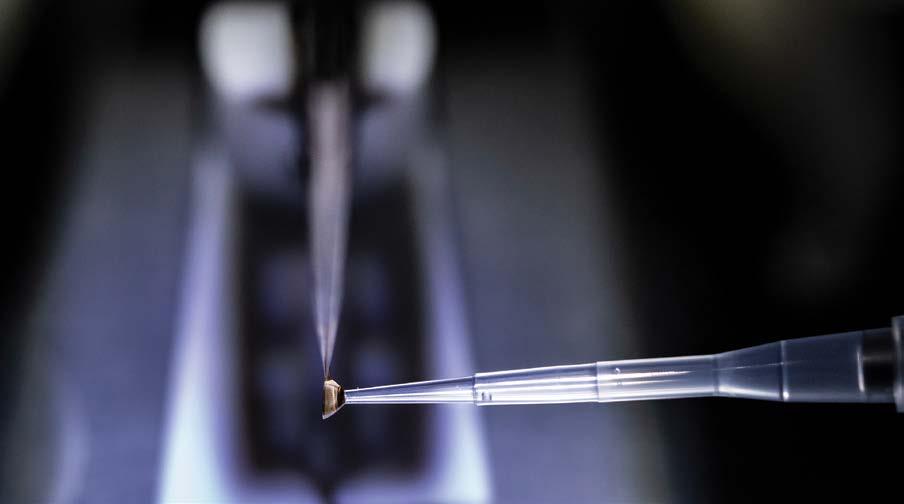
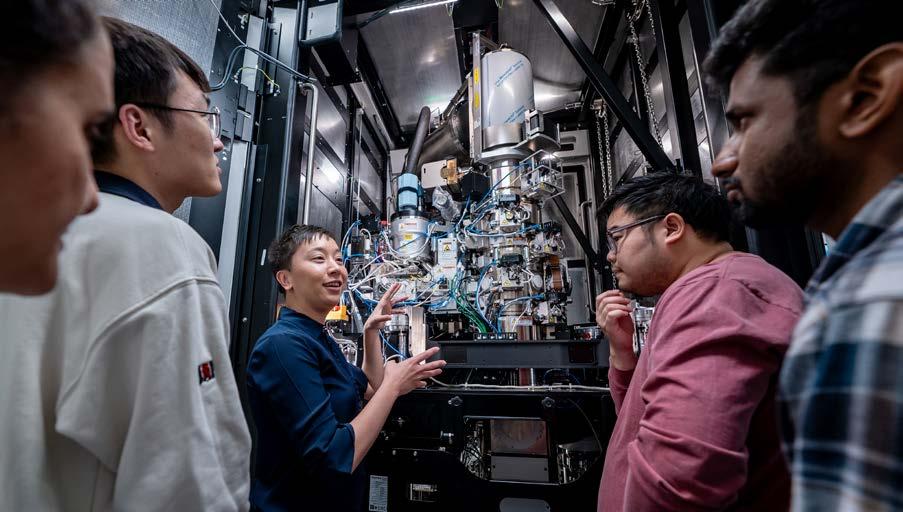
The liquid handler in the Center for Advanced Genome Engineering (CAGE) facilitates high throughput experimentation.
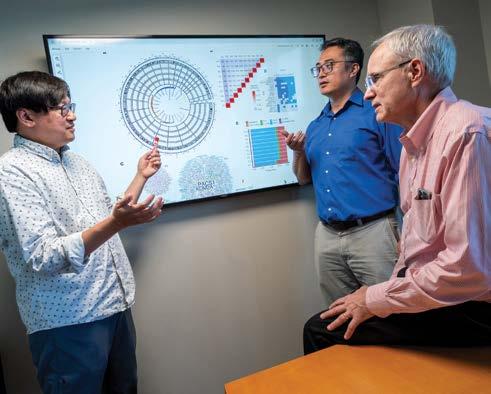
Instead of testing each of the hundreds of thousands of unique drug–drug combinations, we’re using CRISPR gene editing to knock out genes that we already know to be druggable, then giving those neuroblastoma cells a known chemotherapeutic to look for synergistic effects.
Paul Geeleher, PhD
Computational Biology
The interaction between departments and Shared Resources has been instrumental in driving these advancements. In the Center for Advanced Genome Engineering, a shared resource led by Shondra Pruett-Miller, PhD, a team of CRISPR
experts provides their guidance and technological capabilities to the entire research enterprise. Combining this powerful technology with the biological questions posed in St. Jude research labs is advancing our understanding of human health and disease.
CRISPR reveals new strategies to treat cancer
Cancer cells change and adapt, which makes the disease insidious and challenging to treat. Neuroblastoma, a childhood solid tumor that affects multiple tissues, is prone to relapse and resistance; 40% to 50% of affected children experience a return of their cancer after treatment is completed. Single chemotherapy agents are often insufficient for treating cancer due to drug resistance. However, combination therapy, which uses multiple drugs with different mechanisms of action, decreases the likelihood of cancer cells developing resistance, thus maximizing treatment efficacy.
Employing CRISPR technology, St. Jude researchers developed a new roadmap for the use of combination chemotherapy in patients with highrisk neuroblastoma. With thousands of available drugs and compounds, screening for combinations to enhance the standard of care in a particular disease setting is challenging. In Nature Communications, St. Jude researchers reported using largescale targeted CRISPR knockout screens to study various combinations of drugs in cancer cell lines.
“Instead of testing each of the hundreds of thousands of unique drug–drug combinations, we’re using CRISPR
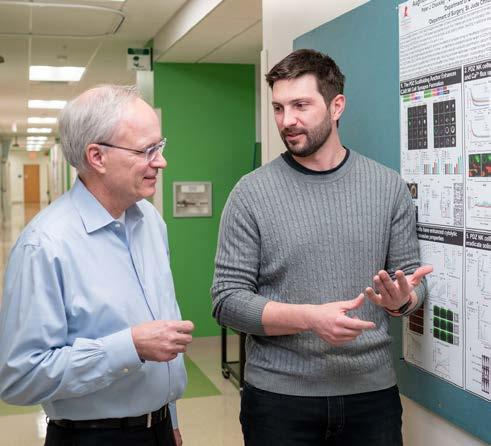
gene editing to knock out genes that we already know to be druggable, then giving those neuroblastoma cells a known chemotherapeutic to look for synergistic effects,” said Paul Geeleher, PhD, Department of Computational Biology.
The investigators found that blocking PRKDC expression in isolated neuroblastoma cells made them vulnerable to doxorubicin, a chemotherapy. They then demonstrated that using both doxorubicin and a PRKDC inhibitor in mouse models of neuroblastoma had a synergistic effect, which means that the combination of the two drugs controlled tumor growth more effectively than either drug alone.
“The goal, ultimately, is to find better treatments that are more targeted with less toxicity,” said Adam Durbin, MD, PhD, Department of Oncology. “Plus, we want to find effective treatments for children with relapsed disease so that kids can grow up without problems related to highintensity neuroblastoma therapy.”
With so many potential drug combinations largely untapped, screening for novel multidrug approaches could be transformative for neuroblastoma and other difficult-to-treat cancers.
CRISPR–Cas9 screening has also been instrumental in creating disease models suitable for studying and developing potential therapeutic targets in humans. Although liver cancers are rare among children, hepatoblastoma is becoming more common. A steady rise in prevalence has been observed globally among children younger than 5 years, including a notable increase of over 4.3%
annually in U.S. patients with high-risk hepatoblastoma, which is commonly treated with chemotherapy. Thus, novel treatment options are needed. It is crucial to establish a reliable and easily accessible research model to advance cancer treatment strategies.
In Nature Communications, St. Jude investigators used a newly developed mouse model to identify the genetic mutations underlying hepatoblastoma driven by the MYC family of proteins. The model enabled the team to perform a genome-wide CRISPR–Cas9 screen to identify the genes required for tumor cell survival. They identified over 1,500 genes as potential targets, with 100 preexisting inhibitors of these genes available.
“This means we can find many targets to test. Any researchers with a shared interest can use our detailed screening information to verify their hypotheses and develop new therapies,” said Jun Yang, PhD, Department of Surgery.
The CRISPR screen yielded potential targets that may enhance treatment efficacy when targeted in combination with conventional chemotherapy, such as doxorubicin, including PRKDC inhibition and increased DNA damage within tumor cells. This study sheds light on improving treatment outcomes for patients with hepatoblastoma and offers promising avenues for future therapies.
CRISPR and the immune system
In addition to helping researchers determine which therapies are most likely to succeed against different cancer types, CRISPR technology is a powerful tool that helps scientists better understand the immune response — the body’s natural defense mechanism that can react to cancer cells and promote their killing. Hongbo Chi, PhD, Department of Immunology, conducts research on the immune system by exploring how T-cells function to kill cancer cells.
A scientist returns flasks of cell lines to an incubator in CAGE.
In Nature, Chi and his team reported using single-cell CRISPR screens to map gene regulatory networks involved in anti-tumor immunity. This approach enabled the researchers to conduct a comprehensive examination of transcription factors, which mediate gene regulation, linked to the T-cell’s anticancer response. They sought to understand mechanisms underlying T-cell exhaustion, which reduces the T cell’s effectiveness against cancer cells.
The researchers also used this approach to study the gene regulatory networks involved in T-cell differentiation, a process that regulates T-cell function. They found that precisely perturbing the differentiation process could enhance anti-tumor efficacy. Specifically, they could increase the number of cancer-killing T cells by promoting differentiation to an intermediate T-cell state and blocking terminal differentiation.
“We’ve provided new potential strategies to enhance immunotherapy,” said Peipei Zhou, PhD, a postdoctoral fellow in Chi’s lab. “We increased the amount of functionally competent
cancer-killing T cells by differentiating them from upstream precursors or blocking their terminal differentiation.”
We showed this new technology, single-cell CRISPR screening in vivo, can drive novel biological discovery. I think we’re at the advent of something truly exciting.
Hongbo Chi, PhD Immunology
Hao Shi, PhD, a senior bioinformatics research scientist in the Department of Immunology, said, “The study generated a comprehensive T-cell differentiation map, which will be a valuable resource for future research, guiding scientists in enhancing T-cell–based immunotherapies.”
“Such a causal transcriptional network provides new insights into lineage differentiation, a fundamental process in biology,” Chi said. “The same approach may be more broadly applicable to increase our knowledge in many biological contexts beyond T cells and immunology. We showed this new technology, single-cell CRISPR screening in vivo, can drive novel biological discovery. I think we’re at the advent of something truly exciting.”
This comprehensive approach offers new strategies to improve T-cell–based immunotherapies that target cancer and other diseases and to guide future research. The study also underscores the potential of in vivo single-cell CRISPR screening in driving novel biological discoveries.
CRISPR sheds light on cellular mechanisms
As Chi and his team use CRISPR to understand the factors important in regulating immune response, Chunliang Li, PhD, Department of Tumor Cell Biology, and colleagues are employing CRISPR technology to address key questions in the transcriptional regulation of cancer cells.
KMT2A-rearranged leukemia is a high-risk subtype of the disease that comprises about 10% of all acute leukemia cases and is found in over 80% of infant acute leukemias. The HOXA9 protein is a key dependency in these high-risk leukemias, but directly targeting HOXA9 is challenging. Published in Nature Communications, a report from Li’s group meticulously unraveled the transcriptional regulation network orchestrated by HOXA9.
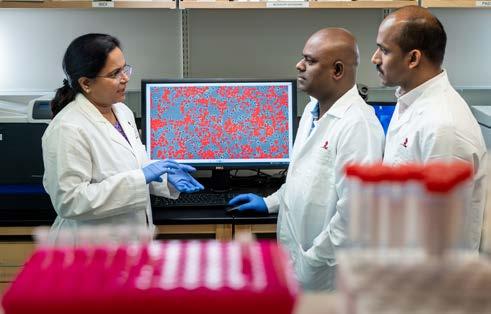
The researchers used dropout CRISPR screens to focus on how HOXA9 binds to
Shilpa Narina, lead researcher in CAGE, uses a state-of-the-art liquid handling robot to conduct highthroughput CRISPR screens.
Our expertise in combinatorial CRISPR screens allowed us to identify resistance mechanisms, but by also doing reverse screens, we identified the targetable options that will allow us to overcome resistance.
Chunliang Li, PhD Tumor Cell Biology
noncoding regulatory sequences of DNA and subsequently controls downstream genes crucial for cell survival. They found that HOXA9-associated regulatory programs influence leukemia cell dependency and provided new insights into regulation mechanisms.
“We confirmed two major known targets, FLT3 and CDK6,” said Li.
“Both genes can be therapeutically targeted by drugs, which shows good outcomes in preclinical models with HOXA9 overexpression. Our results provided direct evidence to support the enhancer regulation of FLT3 and CDK6 through HOXA9.”
Li’s lab also uses CRISPR technology to identify novel treatment strategies for KMT2A-rearranged leukemia. Patients with KMT2A-rearranged leukemia have few treatment options.
Bromo- and extra-terminal domain inhibitors (BETi) have shown promise but are prone to resistance.
In a paper published in the Proceedings of the National Academy of Sciences USA, Li’s team used genome-wide CRISPR screens to investigate how leukemia cells with KMT2A rearrangements respond to BETi. They found that a lack of the protein SPOP is the main reason for resistance to BETi.
“Our expertise in combinatorial CRISPR screens allowed us to identify resistance mechanisms, but by also
doing reverse screens, we identified the targetable options that will allow us to overcome resistance,” said Li.
Further CRISPR analysis suggested that inhibiting another protein called GSK3 could make the cancer cells sensitive to BETi again. Combining drugs that target both BET and GSK3 slowed the progression of leukemia and caused minimal toxicity in mice.
Digging deeper into the fundamental mechanisms of transcription and gene regulation, Li and his team used CRISPR and other cutting-edge technologies to better understand CTCF’s role in those processes. Although the biology of CTCF has been studied extensively, it was unclear how the different domains (parts) of CTCF function in relation to transcription regulation.
Microscopy equipment enables scientists to examine cell populations in vitro.
One of the most valuable ways to study a protein is to degrade, or remove, it from a model system and then study the functional changes that occur in its absence, providing insight into how the protein influences a cell. One system for degrading proteins is the auxin-inducible degron 1 (AID1) system. However, this system has limitations. Li’s work, published in Genome Biology, used the second-generation system, AID2, and a CRISPR single-guide RNA library screen to gain insight into the functional domains of CTCF.
The researchers found that depleting CTCF led to small changes, particularly in regions that play essential roles in controlling gene activity. The findings further show that the CTCF protein not only relies on binding to the DNA through the recognition of the CTCF DNA-binding motif but also relies on
certain domains to bind to specific sequences flanking the motif. For a subset of genes, transcription is regulated only when CTCF binds to these specific sequences.
“When the CTCF protein is gone, we and others have observed that very few genes transcriptionally change,” Li said. “We know when we remove most of the CTCF protein in cells, the impact on transcription is minimal. So, the disconnect between the depletion of protein and transcription must follow a mechanism. We identified part of the mechanism.”
The CRISPR era is now
The innovative use of CRISPR technology at St. Jude is revolutionizing biomedical research. From identifying combination treatment approaches
to learning how the immune system responds to cancer or gaining novel insights into fundamental mechanisms of gene regulation that can be exploited therapeutically — CRISPR is opening new options for treating disease. At St. Jude, CRISPR expertise is available to all researchers through the Center for Advanced Genome Engineering and has quickly become the backbone of discovery in many laboratories. The boundaries of CRISPR’s potential have not yet been realized. With expertise, technical capability, and laboratory resources at their disposal, St. Jude scientists are charting the future of disease treatment using CRISPR.
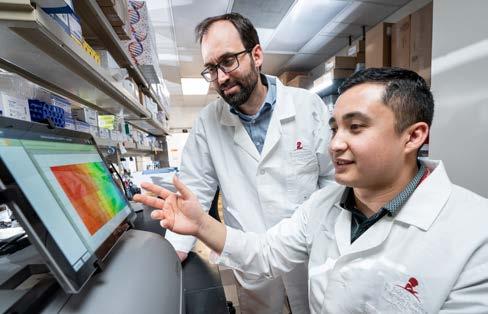
Jie Fang, PhD, scientist in CAGE, prepares samples for CRISPR screens.
Next-generation gene editing for sickle cell disease
Since its founding in 1962, St. Jude has been unwavering in its commitment to researching, understanding, and improving standards of care for people with sickle cell disease.
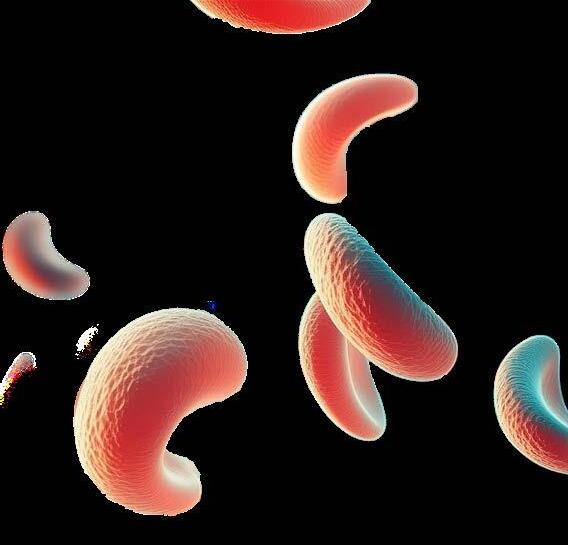
Sickle cell disease is a set of inherited blood disorders caused by mutations affecting red blood cells. Red blood cells contain hemoglobin, a protein that carries oxygen. Unlike healthy, roundshaped cells, the red blood cells of individuals with sickle cell disease have abnormal hemoglobin, which causes the cells to be rigid, sticky, and sickle- or crescent-shaped and die sooner than healthy red blood cells.
The premature death of sickle-shaped red blood cells leads to complications caused by dead cells sticking and obstructing blood flow in small vessels. This blockage can trigger severe pain and give rise to other health issues, including infection and stroke. For a patient with sickle cell disease, acute pain is a predominant factor in their life. These pain crises vary in intensity and duration and can arise suddenly, affecting any body part. Sickle cell disease affects approximately 100,000 individuals in the United States alone,
most prevalently African Americans and Hispanics. About 1 in 365 African Americans have the disorder.
The impact of sickle cell disease on patients’ lives underscores the urgent need for comprehensive research efforts to understand its intricacies and develop effective treatments. In recent years, groundbreaking advances in gene editing have opened new avenues for treating sickle cell disease.
For 40 years, the only potential cure for sickle cell disease has been bone marrow transplantation. This option has its roots at St. Jude because, in 1982, a St. Jude patient with acute myeloid leukemia (AML) and sickle cell disease underwent bone marrow transplantation to treat her cancer — and it cured her sickle cell disease. The results, published in 1984 in the New England Journal of Medicine, marked a turning point in treating patients with sickle cell disease. Since then, clinicians have refined transplantation
methods, yet challenges persist due to a lack of donor availability and potential side effects. Today, a new scientific era that applies leading-edge gene-editing technologies to human health and disease can potentially improve and expand treatment options for sickle cell disease.
Until recently, the primary method for editing human cells relied on nucleases like CRISPR–Cas9, which induce doublestranded breaks in DNA to disrupt target gene sequences. To improve standard gene-editing approaches, researchers continuously work to identify new strategies and techniques. For example, St. Jude scientists are investigating
Ultimately, we showed that not all genetic approaches are equal. Base editors may be able to create more potent and precise edits than other technologies. But we must do more safety testing and optimization.
Jonathan Yen, PhD Hematology
two new advanced techniques: base editing, a highly efficient method for directly altering single DNA bases, and prime editing, a more versatile technology capable of both base and gene edits. These innovations significantly broaden the possibilities and effectiveness of genome editing. Using these advanced approaches, scientists can directly convert the mutation underlying sickle cell disease by reverting the DNA to its healthy sequence. This work was conducted through the St. Jude Collaborative Research Consortium for Sickle Cell Disease, a multidisciplinary group of scientists from across the U.S. working together to develop new and effective treatments for this devastating disease.
St. Jude scientists Mitchell Weiss, MD, PhD, Department of Hematology chair, Jonathan Yen, PhD, Department of Hematology, and their collaborator David Liu, PhD, of the Broad Institute, explored adenine base editing to treat sickle cell disease and the blood disorder beta thalassemia. During fetal development, gamma-globin pairs with alpha-globin to create fetal hemoglobin. However, after birth, gamma-globin production decreases, allowing betaglobin to take over and form adult hemoglobin. Sickle cell disease and beta thalassemia arise from Hemoglobin subunit beta (HBB) mutations, which affect beta-globin. These conditions typically appear after birth when the body switches from relying on the fetal gamma-globin genes to the mutated genes that encode adult beta-globin. The study, published in Nature Genetics, used adenine base editing to induce fetal hemoglobin in red blood cells.
Through their research, Weiss and his colleagues discovered that one change made by adenine base editing was particularly potent for restoring fetal hemoglobin expression in red blood cells after birth. “The gamma-globin, or fetal hemoglobin, gene is a good target for base editing because there are very precise mutations that can reactivate
We have identified what might be the next wave of therapies for genetic anemias,” said Weiss. “We took the newest cutting-edge geneticengineering technology and showed that we could make meaningful gene edits for future therapies.
Mitchell Weiss, MD, PhD Hematology
its expression to induce expression after birth, which may provide a powerful ‘one-size-fits-all’ treatment for all mutations that cause sickle cell disease and beta thalassemia,” said Weiss.
The researchers found that, of the methods they tested to boost fetal hemoglobin levels in red blood cells, the adenine base editing generation of the gamma-globin –175A>G variant produced the most potent induction of fetal hemoglobin. “We used a base editor to create a new TAL1 transcription factor–binding site that causes powerful induction of fetal hemoglobin,” said Yen. “Creating a new transcription factor–binding site requires a precise base pair change — something that can’t be done using CRISPR–Cas9 without generating unwanted byproducts and other potential consequences from double-stranded breaks.”
Using adenine base editing at the most potent site in the gamma-globin promoter showed consistent and
clinically relevant levels of editing in the DNA of human stem cells. In contrast, Cas9-generated genetic alterations resulted in variable fetal hemoglobin levels, suggesting that adenine base editing may be better suited for treating sickle cell disease because it creates more predictable and potent genetic changes.
Besides adenine base editing, Weiss, Yen, and their colleagues are exploring a technique called prime editing that may be even more versatile. Prime editing allows modifications, including targeted small insertions, deletions, and base swapping without doublestranded DNA breaks. Prime editing expands the scope of base editing abilities to all 12 possible nucleotide combination swaps, making it a highly adaptable genetic modification tool. In a paper published in Nature Biomedical Engineering, Weiss, Yen, and Liu’s teams showed that prime editing can convert the defective adult hemoglobin gene to the healthy DNA sequence, successfully modifying as much as 41% of the DNA in blood stem cells from patients with sickle cell disease.
“Prime editing is a promising approach because, in theory, we can directly correct disease mutations to specific healthy DNA sequences of our choosing,” said Yen.
As advancements in sickle cell disease research unfold, the urgency for more effective treatments — and even cures — heightens. St. Jude researchers are at the forefront of genome-editing ability with base and prime editing.
Pediatric Cancer Dependencies Accelerator: Collaboration propels progress in the search for novel treatments
Uniting the world-class strengths of different institutions to tackle the same problems can result in greater progress than any single institution could achieve. The Pediatric Cancer Dependencies Accelerator is doing this by leveraging the expertise and capabilities of the Broad Institute of MIT and Harvard, Dana-Farber Cancer Institute, and St. Jude Children’s Research Hospital.
The project is accelerating the identification of vulnerabilities in pediatric cancers and translating them into better treatments by marrying innovation in mapping cancer dependencies to pediatric cancer expertise. This vision of transformative progress is supported by joint funding of more than $60 million from all three institutions over five years. The investment supports infrastructure development and scientific work by a team of more than 100 investigators, data scientists, trainees, and research staff.
The project is co-led by Charles W. M. Roberts, MD, PhD, St. Jude Executive Vice President and Comprehensive Cancer Center director, Kimberly Stegmaier, MD, vice chair for Pediatric Oncology Research, Dana-Farber/ Boston Children’s Cancer and Blood Disorders Center and institute member at the Broad Institute, and Francisca Vazquez, PhD, Broad Institute Cancer Dependency Map director.
leapfrog barriers to rapidly identify therapeutic vulnerabilities in childhood cancer and translate those into targeted therapies in the clinic much faster.”
Through this project, we believe we can now leapfrog barriers to
rapidly identify therapeutic vulnerabilities in childhood cancer.
Charles W. M. Roberts, MD, PhD
Comprehensive Cancer Center
and two cross-cutting interest areas (pan-cancer and data science). These working groups accelerate progress by combining unique strengths, resources, and technologies.
The project is advancing diverse scientific aims, which include:
• developing and deploying genomeediting approaches to identify hidden dependencies in a range of high-risk childhood cancers
• leveraging emerging technologies to characterize pediatric cancers’ genetic and epigenetic landscape
• developing model systems where none currently exist for high-risk childhood cancers that have poor outcomes
• identifying effective combination therapies and mechanisms of drug resistance and shortening the timeline for developing new therapies
• developing computational approaches to mine and integrate data and building innovative software tools for data sharing
This collaboration builds on groundbreaking research initiatives. The St. Jude–Washington University
Pediatric Cancer Genome Project yielded rich insights into the genomic landscape of pediatric cancers, including the discovery that most disease-driving genetic mutations are not druggable. The Cancer Dependency Map (DepMap) Initiative from the Broad Institute, in collaboration with Dana-Farber investigators, developed extensive, world-class datasets and computational infrastructure that impacted research and target discovery programs worldwide. Launched in 2015, the Pediatric Cancer Dependency Map Project served as a proof of concept for applying the DepMap approach to childhood cancers. That effort created infrastructure and expertise that is being leveraged and expanded through the Pediatric Cancer Dependencies Accelerator.
The Pediatric Cancer Dependencies Accelerator is a testament to collaboratively uniting diverse expertise to pursue opportunities with transformative potential.
Cutting-edge research at the St. Jude Center for Advanced Genome Engineering accelerates precision treatments, introducing novel therapies for childhood cancers.
STAYING ONE STEP
AHEAD OF
Why are you studying influenza at St. Jude?”
is a question that 91-year-old Robert Webster, PhD, Department of Infectious Diseases emeritus member, was asked repeatedly throughout his career. Webster created and grew a globespanning influenza research program at St. Jude. The researchers he trained and inspired continue his legacy, staying one step ahead of pathogens for the children of St. Jude — and the world at large.
As for the skepticism about why he chose to do his work at St. Jude, Webster has a clear logic to support that decision. “Immunosuppression, leading to infections such as influenza, mumps, measles, and the common cold, was the real threat to our kids at the time,” he said.
When Webster joined the St. Jude faculty in 1969, cure rates for pediatric cancers were improving drastically. One supportive care factor that improved those successful treatments even further was a better understanding of how to counter infectious disease threats to patients.
When it came to understanding the flu, one of the first steps was figuring out where new flu strains in humans came from. Over 50 years ago, no one knew where the annual seasonal flu viruses originated. Several animal reservoirs were being considered then, and Webster published an article describing the potential relationship between bird flu and human flu in Nature in 1967. Webster and his colleague Graeme Laver, PhD, noticed a pattern of birds in Australia succumbing to mysterious illnesses, prompting them to test seabirds at the Great Barrier Reef. Initial findings were positive for influenza virus and published in the Bulletin of the World Health Organization in 1972, along with another article describing how human pandemic flu may have arisen from an avian virus.
Zeroing in on wild birds by expanding specimen collections to the United States and Canada was a stroke of collaborative brilliance that prompted
Webster’s biggest breakthrough in identifying the reservoir of seasonal flu viruses. A visiting Russian scientist found that the influenza virus replicates in ducks’ intestines.
“It was one of those ‘eureka’ moments,” Webster explained. “The virus was not in the respiratory tract — we’d been looking in the wrong end of the bird for years.” The landmark result was published in 1976 in the Journal of General Virology with a follow-up article in Virology
Partially due to these findings, in 1975, St. Jude was designated the third (of now seven) World Health Organization (WHO) Collaborating Center for Influenza. With that came the WHO Global Influenza Surveillance and Response System (GISRS), enabling researchers to actively contribute to global surveillance and control of the virus.
Following the flu in fowl
“Dr. Webster’s projects are probably the longest-running animal flu surveillance programs in the world,” said Richard Webby, PhD, Department of HostMicrobe Interactions, who now oversees several of these programs himself. “We have partners worldwide that we work
(Left) A St. Jude scientist pipettes in the lab. (Top Middle) A researcher examines eggs before influenza inoculation. (Bottom Middle) Karlie Woodard, Host Microbe Interactions, inoculates an egg with influenza. (Right) Jeri Carol Crumpton and Jasmine Turner, Host-Microbe Interactions, prepare eggs for influenza inoculation in a Biosafety Level 2+ lab.
The pandemic H5N1 is better adapted to wild birds than any other highly pathogenic flu viruses we’ve ever seen.
Richard Webby, PhD Host-Microbe Interactions
with to collect samples in decadeslong collaborations he established.”
Webby, a former postdoctoral fellow in the Webster lab, follows in his mentor’s footsteps as a principal investigator at St. Jude, studying avian and human flu and expanding the globe-spanning research program and its collaborations. Recently, one of these collaborations identified the ancestors of the current H5N1 influenza strain killing birds in the Americas — and why it is spreading so fast.
“The pandemic H5N1 is better adapted to wild birds than any other highly pathogenic flu viruses we’ve ever seen,” explained Webby, corresponding author of a Nature Communications article reporting the findings from this study.
The transmissibility appears to be helped by access to a different assortment of virus genes in North American wild birds. This has produced a more transmissible and virulent strain that can enter the brains of infected animals.
Another collaboration, led by Webby and published in Emerging Microbes and Infection, showed the connection between wild birds, domesticated freerange ducks, and live poultry markets in Bangladesh and the emergence of a novel avian influenza virus.
“This is more evidence that these viruses are continually evolving,” Webby said. “The real drivers of that evolution occur at the interface of wild and domestic birds, then domestic birds move into urban areas, such as live poultry markets, and that’s where they interface with humans.”
Jumping from birds to mammals
Before proving bird flu could jump into humans, Webster first showed avian and mammalian influenza viruses could mix. Influenza virus genomes comprise eight independent segments. When multiple influenza viruses with different segments infect the same cell, they can hybridize by mixing those segments in their progeny. Webster showed that these hybrids can occur naturally in birds and swine in a study published in Virology in 1971.
The true proof of avian-to-human transmission was uncovered when a child succumbed to an influenza virus in May 1997 in Hong Kong. Seventeen more cases followed.
“When Dr. Webster and his collaborators went to Hong Kong and identified the virus,” explained Webby, “it was the first time anyone realized people could be directly infected with these bird flu viruses. It changed the world of influenza virology.” It was a result that was fittingly published in The Lancet later that year. Webster received a National Institutes of Health (NIH) grant to uncover how these viruses were maintained and evolved.
Jasmine Turner and Jeri Carol Crumpton, Host-Microbe Interactions, prepare eggs for influenza inoculation in a Biosafety Level 2+ lab behind a high-security door with a red circadian-rhythm preserving window.
In November and December 1997, Hong Kong experienced another outbreak of avian-to-human flu. Webster was quickly able to find infected birds in the live poultry market again. The findings were published in Nature, further cementing St. Jude as a world leader in influenza research.
Stacey Schultz-Cherry, PhD, Department of Host-Microbe Interactions, another expert in influenza and other pathogens, explained how Webster’s work in Hong Kong set the stage for the future. “For many years, people always thought that a bird flu strain had to get into a pig and mix with another mammalian virus for it to gain the ability to infect people,” Schultz-Cherry said. “That appears to be true in most cases, but Dr. Webster’s later work showed humans can get these viruses from birds directly.”
Getting ahead of influenza
“That first NIH grant was so tremendously successful that when seven years were up, NIH created the Centers of Excellence for Influenza Research and Surveillance (CEIRS), funding six centers, including St. Jude,” Webster said. “It grew out of St. Jude — we were responsible for these programs starting, and they’re still ongoing today.”
In 2021, the NIH again designated St. Jude a CEIRS through the third iteration of the original CEIRS program. The focus was on developing tools to control epidemic or pandemic influenza while finding ways to minimize the threat of an influenza pandemic.
“Having the Center for Excellence gives us the resources to do those high-risk, high-reward experiments that, if they work, will move the field forward and change textbooks,” said Schultz-Cherry, who co-directs CEIRS with Webby. “We can try novel, untested approaches and ideas, and if these projects work, we can move them forward to develop new basic understanding, technology, assays, or therapies.”
Schultz-Cherry’s work focuses on how the metabolic health of a host explains and may be able to minimize poor infection outcomes.
“Having a high body mass index (BMI) can impact anything from influenza disease severity to susceptibility to infection,” Schultz-Cherry said. Previous research from her lab characterized the difference in response between healthy and obese mice. In a paper published in mBio in 2023, her lab also showed that modern antivirals are less effective in obese mouse models than in fit mice.
Studying the host to understand how a virus will behave can be highly informative for scientists. Webby teamed up with a large collaborative group, including Paul Thomas, PhD, Department of HostMicrobe Interactions, an expert on how the immune system responds to pathogens. Together, they recently published results in Nature Immunology showing that having specific types of innate and adaptive immune cells present up to six months before infection correlates with increased protection from flu symptoms.
The researchers found that having a more functionally diverse set of immune cells was correlated with increased protection from flu symptoms. The group identified these cells by comparing the immune cells in the blood of patients who had symptoms of flu infection to those who were asymptomatic or uninfected. Those without symptoms not only had a more functionally diverse set of immune cells but those cells were also associated with an influenza-specific long-term response, sometimes called the memory response. Patients with symptoms tended to have a more similar set of inflammatory immune cells, which are more likely to be involved in a nonspecific, functionally narrow and short-term response. The work helps answer the age-old question of why some people get sick with infections and others do not.
“By understanding which immune cells are best for fighting the flu, we can start designing vaccines to push for those populations that are most protective,” said Thomas.
Having the Center of Excellence gives us the resources to do those highrisk, high-reward experiments that, if they work, will move the field forward and change textbooks.
The most powerful protection for influenza remains vaccination, especially in vulnerable groups. The world-leading expert in respiratory syncytial virus and the early immune system, Octavio Ramilo, MD, Department of Infectious Diseases chair, is taking a systems-level approach to explore immune response over time in infants, a group considered at high risk of severe infectious diseases.
“Infants die from many infections that adults don’t die from. The best thing we can do for this is vaccinate,” said Ramilo. “We know this strategy works, but we still don’t understand how the vaccines work very well.”
Published in Nature Communications, Ramilo’s team looked at responses to a routine vaccination series given
to infants at 2 months of age. They found substantial heterogeneity in the babies’ antibody responses to the different components of the initial vaccination, in contrast to what has been observed in older children. The researchers took a systems-level approach to explore the immune response over time, using bulk and single-cell transcriptomics. This allowed the researchers to explore the response with the benefit of a true baseline.
The study found substantial heterogeneity in the antibody responses among the infants in the study. Singlecell transcriptomics offered the chance to identify the cause, which turned out to be the interferon response. Interferon functions as the cell’s alarm, recognizing invading pathogens and mobilizing the immune system. Given the centrality of interferon to both the innate and adaptive immune response, investigating these differences further may offer novel insights.
“We have begun to uncover these mechanisms and can think about how to design more effective vaccines for infants,” Ramilo concluded.
Once children reach a year old, vaccines are more consistently effective, though they can still be improved. Scientists at St. Jude are also investigating how to improve vaccines, especially the seasonal influenza vaccine, for older children and adults.
Scientists from St. Jude, including Schultz-Cherry, are part of the National Institute of Allergy and Infectious Diseases Collaborative Influenza Vaccine Innovation Centers (CIVIC) program. Published in Pathogens, a team from CIVIC showed that a computational method could design a vaccine with subtle mutations in viral proteins that then protected mice from influenza H5 viruses with different paired neuraminidase proteins. That increased efficacy and broad action are promising for the future improvement of the seasonal vaccine.
“Through our work CIVIC, we found that with some adjustments to the live-
attenuated vaccine, including changing flu proteins such as hemagglutinin, adding the neuraminidase, or modifying the vaccine platform,” Schultz-Cherry said, “we can protect models of highrisk populations from getting infected.”
A world of other pathogens beyond influenza
In addition to being a giant in influenza research, Webster worked with Elaine Tuomanen, MD, former Infectious Diseases chair and current member of Host-Microbe Interactions, to build the extensive infrastructure and expertise in infection biology at St. Jude. Over the decades, their efforts have sparked a wealth of research projects exploring other pathogens that threaten human health. In parallel, St. Jude has developed cuttingedge clinical diagnostic laboratories to protect patients directly.
“In the last few years, we have developed whole-pathogen sequencing to track potential organism spread in the institution, even preemptively trying to look before there is an outbreak situation,” said Randall Hayden, MD, Clinical and Molecular Microbiology director. He also serves as the Global Pathology and Laboratory Medicine Transversal program director, giving him unique insights into microbes that could be risky to patients.
Hayden and Hana Hakim, MD, Department of Infectious Diseases, Infection Prevention and Control medical director and a clinical investigator studying ways to prevent infections in St. Jude patients, collaborated on a genesequencing study reported in Clinical Infectious Diseases. They used genetic sequencing to track the spread of Clostridioides difficile, a bacterium that causes diarrhea and colitis, in pediatric oncology and bone marrow transplantation patients.
“We found that C. difficile transmission among St. Jude patients is very rare,” said Hakim. “And that the vast majority
of recurrent C. difficile infections in the same patient are caused by the same strain of a previous infection that the patient had rather than the acquisition of a new strain.”
“What we are doing from an infection prevention standpoint is working,” Hayden added. “Other institutions could use our results as a benchmark.”
In addition to bacteria and viruses, fungal infections are a major concern. Candida is a genus of yeast that includes several species that infect humans and is a common cause of life-threatening health care–associated bloodstream infections in the United States. “Candida parapsilosis is among the most common causes of Candida infections in pediatric and neonatal patients and is responsible for an increasing number of invasive Candida infections in many parts of the world,” said P. David Rogers, PharmD, PhD, Department of Pharmacy and Pharmaceutical Sciences chair, whose lab focuses on understanding the root cause of antifungal resistance. “In the last five to 10 years, we have seen an uptick globally in resistance to the common antifungal fluconazole among clinical isolates of C. parapsilosis."
As C. parapsilosis becomes resistant to antifungals, therapeutic options become limited. Published in Clinical Microbiology and Infection, a report from Rogers’s lab described their efforts to elucidate the underlying mechanisms driving antifungal
resistance of C. parapsilosis and learn how to predict, prevent, or overcome it. Led by the efforts of University of Tennessee Health Science Center College of Graduate Health Sciences student Laura Doorley, PhD, Rogers’s team found that mutations in TAC1, in addition to a well-known mutation in ERG11, drive high-level resistance, shifting conventional wisdom about fluconazole resistance in this species.
One common antifungal, fluconazole, targets a protein involved in sterol synthesis, encoded by the gene ERG11 A mutation in ERG11 can increase its expression, which will then increase the expression of other proteins known as drug transporters. These transporters will nonselectively pump antifungals out of fungi cells. In the study, mutated TAC1 increased the expression of several drug transporters to higher levels than mutated ERG11 alone, though both in combination drove the highest levels of antifungal resistance.
A legacy leading the future in pathogen research
From Webster’s initial work collecting influenza samples from wild waterfowl, the path paved by such infectious disease luminaries has been widening and expanding into what can today be considered a globe-spanning program based at St. Jude. By investing in understanding the viruses, bacteria,
and fungi that pose a risk to patients, St. Jude is leading an entirely new generation of researchers to stay one step ahead of pathogens.
“I have to admit that I’ve been very spoiled by St. Jude,” Webster concluded. “The facilities here are top-class, letting us lead the international infectious disease research community. That’s only possible through the full support of WHO, NIAID, and St. Jude donors. I hope that support continues so my trainees can continue the fight against the flu and other pathogens.”
Karlie Woodard, Host-Microbe Interactions, inoculates, candles and drills chicken eggs in a Biosafety Level 2 fume hood as part of her influenza research project.
Two new department chairs bring a bold vision to pathogen research
Scientists at St. Jude have been studying pathogens that cause severe infections in children for as long as the hospital has existed.
This is because children undergoing cancer treatment have weakened immune systems and are more vulnerable to infection than their peers are. From bacteria to viruses to fungi, combatting the pathogens that bombard patients’ immune systems requires a dedicated effort. As the COVID-19 pandemic demonstrated, there are many ways to go about studying pathogens, examining both the infectious agent itself and how the host immune system responds.
To take St. Jude into the next era of infectious diseases research, two new department chairs have been recruited to tackle microbial pathogens and their associated diseases through the Department of Infectious Diseases and the newly created Department of Host-Microbe Interactions. St. Jude investigators from across the research enterprise have been appointed to these two departments, forming an all-star workforce that takes bold steps toward meeting the pathogen threat.
Each department will conduct their own research, but then feed their learnings into the other discipline, creating a virtuous cycle that will lead to better methods of discovering
novel and effective strategies for treating and preventing infectious diseases in vulnerable patients at St. Jude and around the world.
Focus on the fundamentals in the Department of HostMicrobe Interactions
“St. Jude has a rich history of fundamental infection biology science,” said Victor Torres, PhD, Department of Host-Microbe Interactions chair. Torres brings decades of fundamental microbiology experience to St. Jude, giving him a unique vantage point to shepherd the new department’s aim. “The goal is to build on that history and perform fundamental research in infection biology to understand how microbes cause disease.”
Host-Microbe Interactions focuses on what happens at the molecular and cellular level when a pathogen challenges the immune system. With scientists from the St. Jude lineup of infectious disease and immunology experts, the department is now actively recruiting additional faculty.
“We want to bring people who are going to push the boundaries of discovery,” Torres said. “We will move the needle toward learning how microbes cause disease, how infection can be prevented, and explain disease prevalence.
“I aim to create a premier department and recruit researchers interested in infection biology and hostmicrobe interactions. We will create a diverse scientific portfolio that encompasses an understanding of the most important infectious diseases locally, nationally, and worldwide.”
Each scientist will help push diverse areas of research on hosts, microbes, and how they interact, all with an eye toward expanding knowledge to improve patient care.
“We want to bring precision medicine to infectious diseases,” Torres said. “To do that, we need to deploy cutting-edge tools while combining bench science with clinical samples and sophisticated
multi-omics so we can unearth the secret of that delicate dance, the interaction between a microbe and its host, to unravel new vulnerabilities.”
Pathogens, patients, and prevention with the Department of Infectious Diseases
“Collectively, infectious diseases are the number one cause of death in children across the globe,” said Octavio Ramilo, MD, Department of Infectious Diseases chair. “Vaccines and clean water access have improved infection survival over the last century, but we still have much to do.”
Victor Torres, PhD, Chair of the Department of Host-Microbe Interactions, looks at a culture plate in his new St. Jude lab.
About 60% of pediatric cancer-related deaths around the world are related to infection,” Ramilo continued. “For anything involved with cancer-related infections, we need to be the top institution bringing together cutting-edge care with clinical research.
Ramilo’s expertise in respiratory syncytial virus (RSV), a major pathogen that can be dangerous for children during the first two years of life, informs the department’s direction as Infectious Diseases focuses on understanding biology to optimize treatment strategies.
“We need to do fundamental discovery in the clinical context,” said Ramilo, “We know that early infections in life, such as RSV, shape your longterm health outcomes, but we don’t understand how.”
Octavio Ramilo, MD, new Department of Infectious Diseases chair, looks at a sample being kept cool by dry ice in his lab.
For Ramilo, understanding how to best treat infection goes back to understanding early immunity, examining immune function in healthy newborns and infants, and observing changes over time as children encounter pathogens or vaccination.
“We know that vaccines or infections can shape the infant immune response,” Ramilo said. “We could learn fundamental lessons key to developing new and more effective vaccines — preventing illness — and because the immune system is involved in everything, it could have a wide impact: how we make vaccines, immunotherapy, and even gene therapy. This work will help us design better therapies for children with cancer, as well as for previously healthy children.”
Ramilo and the Department of Infectious Diseases will leverage the long-standing reputation of St. Jude as a world leader in infectious diseases to embark on new collaborations and facilitate the launch of scientifically ambitious and logistically complex research.
Ramilo has his eye fixed on translational research, providing novel insights into the pathogenic threats patients face and how these diseases present clinically to inform the next generation of treatment approaches. Such work will also build a repertoire of knowledge on how the host immune system interacts with these pathogens, feeding back into the laboratories of Host-Microbe Interactions.
Two
departments,
one strategy
“We have an opportunity to leverage the fundamental research strength and expertise of St. Jude in Infectious Diseases, Host-Microbe Interactions, and even other departments to learn how to save more children,” Ramilo said.
Though each department will focus on different subfields, both are dedicated to improving survival and preventing suffering due to pathogens — and working together to do so. Together, Torres and Ramilo are leading their respective departments toward a future where the threat of pathogens can be met head-on.
“We like to tackle difficult things here at St. Jude, and we are good at making progress on issues others have deemed impossible,” Torres concluded. “That’s the challenge, and that’s why I came here. We want to transform the world by tackling one microbe at a time.”
ORGANIC
Unfolding the mysteries of biomolecular structure, dynamics, and function
The fundamental principles of origami, the Japanese art of paper folding, have endured for generations.
Rooted in symmetry and precision, origami involves basic folds that contribute to a larger, more complex vision. In biology, underlying almost every cellular process is a protein that must fold with precision into an intricate three-dimensional structure to carry out its function.
At St. Jude, researchers strive to understand the processes that govern biological function by teasing apart the organic origami of biomolecular activity like never before.
Capturing transporter structures paves the way for drug development
Transporters are proteins that move essential substances such as ions, neurotransmitters, and nutrients across membranes. Modulating these molecular gatekeepers can be a potent therapeutic route; thus, gaining a fundamental understanding of their intrinsic structure is paramount to accomplishing this task.
Chia-Hsueh Lee, PhD, Department of Structural Biology, studies the structures and dynamics of membrane transporters to better understand their function and links to disease.
Sphingosine-1-phosphate (S1P) is an important signaling molecule that regulates the immune system, blood vessel formation, auditory function, and the integrity of epithelial and endothelial membranes. Spinster homolog 2 (Spns2) is an S1P transporter that sits on the cell membrane and moves S1P across it to be released into the extracellular space.
We hope our structural information will pave the way for the development of improved, more specific small molecules with higher potency against Spns2 in the future.
Chia-Hsueh Lee, PhD Structural Biology
transport cycle and how a potential Spns2-targeted therapeutic binds. They found that the Spns2 inhibitor 16d blocks transport activity by locking Spns2 in its inward-facing state.
“We hope our structural information will pave the way for the development of improved, more specific small molecules with higher potency against Spns2 in the future,” said Lee.
In addition to Spns2, Lee also studies neuronal communication, which relies on releasing neurotransmitters from within the cell to the synaptic space between neurons. To transport neurotransmitters to the cell membrane for their release, the cell packages them into “cargo ships” called vesicles. Vesicular monoamine transporters (VMATs) are proteins located on the membranes of these vesicles and act as loading cranes to move specific neurotransmitters called monoamines from the cytoplasm into the space within the vesicle.
In work published in Nature, Lee used cryo-EM to capture multiple structures of VMAT2. “This transporter is a target for pharmacologically relevant drugs used in the treatment of hyperkinetic disorders such as chorea and Tourette syndrome,” Lee said.
Lee’s group captured this dynamic protein in multiple states and demonstrated two distinct binding
In their work published in Cell Research, Ji Sun, PhD, Department of Structural Biology, and colleagues presented the structure of the IFT-A complex and its assembled train form. The structure revealed previously unknown zincbinding sites in IFT-A. Zinc-binding sites are important to a protein domain called zinc fingers, which are critical for certain protein−protein interactions.
In a paper published in colleagues reported the six structures of Spns2 that they obtained using cryo-electron microscopy (cryo-EM), including two functionally relevant intermediate conformations (shapes) that tie together the Spns2 inward- and outward-facing states, illuminating how Spns2 functions. The findings reveal the structural basis of the S1P
Structures offer a framework for understanding how proteins work together
Proteins are not static. They move, bend, fold, and flex, offering multiple dynamic structural forms capable of different functions. Visualizing different forms of proteins during their activity cycle gives us a more complete understanding of their dynamics and how their structures relate to their function or dysfunction.
state. Here, the missing piece was Rab29, a member of the Rab GTPase family that regulates cellular trafficking and modulates the activity of LRRK2.
a follow-up study to previous work on
“In that first paper, we got the structure of LRRK2, but that structure showed an inactive conformation,” Sun explained.
Sometimes, it takes binding to another
Using cryo-EM, the researchers determined the first structures of the Rab29–LRRK2 2 complex. The structures included an unexpected tetramer comprising four pairs of Rab29–LRRK2 that has been shown to assemble only at the membrane surface in cells. This tetramer finally revealed the active form of LRRK2, informing the researchers on the biological path toward protein activation and function.
“We proposed a transition from monomer to tetramer upon membrane recruitment, wherein LRRK2 becomes active,” Sun explained. “These structures provide much-needed insights for medicinal chemists to design novel inhibitors against LRRK2 for Parkinson’s disease treatment.”
LRRK2’s complex with Rab29 is an example of a protein−protein interaction. Such interactions often drive protein function, occur universally
[SPOP
mutations in prostate cancer] are well understood. However, mutations found in patients with other forms of cancer, especially endometrial cancer, were puzzling [because] the mutated sites did not seem important for SPOP function.
Tanja Mittag, PhD Structural Biology
Protein structure studies in the St. Jude Cryo-Electron Microscopy Center begin with a single drop of protein in solution placed on a copper or gold grid.
throughout all organisms, and can occur between different proteins or multiple copies of the same protein.
In research published in Molecular Cell, Tanja Mittag, PhD, Department of Structural Biology, revealed structures of speckle-type POZ protein (SPOP). SPOP is involved in identifying and breaking down other proteins the cell no longer needs and is the most frequently mutated protein in prostate cancer. When SPOP is dysregulated, it can dramatically affect protein levels, triggering disruption of cellular processes and altered signaling pathways, ultimately leading to diseases like cancer.
“The prostate cancer–associated mutations are well understood,” said Mittag. “They are in the substratebinding site and prevent SPOP from recognizing its substrates. However, mutations found in patients with other forms of cancer, especially endometrial cancer, were puzzling. The mutated sites did not seem important for SPOP function, at least looking at previous structures of individual parts of the protein.”
Determining SPOP’s three-dimensional structure enabled the researchers to see how multiple copies of the
protein assemble to form long chains and to identify key interactions between the assembled proteins that had not been seen before. The SPOP interaction interfaces contain many endometrial cancer–linked mutations, which may further explain how SPOP contributes to disease.
Single-molecule imaging gives a new view of critical cellular structures
As Mittag’s research shows, defects in protein assembly can have disastrous results. Multiple approaches are required to reveal the mechanisms underlying protein assembly and the relation of those mechanisms to disease.
Led by Scott Blanchard, PhD, Department of Structural Biology, scientists at St. Jude and Rockefeller University combined their expertise to better understand the structural relations between the function and dysfunction of the cystic fibrosis transmembrane conductance regulator (CFTR) protein. CFTR is an anion channel, and mutations in CFTR cause cystic fibrosis, a fatal disease with no cure.
There are very few proteins that are more relevant for treating disease than CFTR because treatments for cystic fibrosis aim at ameliorating the defects in the mutant forms of this protein.
Scott Blanchard, PhD Structural Biology
Previous CFTR studies enabled the researchers to see the channel when it is either open or closed, but the transition between those two states has been incompletely understood. By deploying single-molecule fluorescence
Studying protein dynamics at single-molecule resolution requires the resources and expertise of the St. Jude Single-Molecule Imaging Center.
resonance energy transfer (smFRET), combined with channel conductance measurements, the team was able to provide pivotal insights into the moving pieces of the CFTR machinery and how disease mutations and small-molecule therapies affect the protein’s function.
In Nature, Blanchard’s team reported that two nucleotide-binding domains of CFTR dimerize (combine), and this conformational change drives the channel opening. Drugs used to treat cystic fibrosis enhance channel activity by increasing dimerized channelopening probabilities. Mutations that cause cystic fibrosis can reduce the efficiency of dimerization.
“There are very few proteins that are more relevant for treating disease than CFTR because treatments for cystic fibrosis aim at ameliorating the defects in the mutant forms of this protein,” said Blanchard.
In addition to using smFRET to better understand CFTR, Blanchard’s laboratory used the approach to gain a new understanding of a key biomolecular workhorse: the ribosome. After transcription occurs, the resulting messenger RNA is transported to the ribosome, where it is translated into the protein encoded by the RNA sequence. In research published in Nature, Blanchard and his team examined the human ribosomedecoding mechanism for the first time.
The researchers explored how quickly human ribosomes undergo the various decoding steps compared to the speed of comparable decoding steps in bacterial ribosomes. This work revealed kinetic and structural distinctions between the two species that shed light on regulatory mechanisms that may help guide the treatment of human diseases.
“Bacterial ribosomes have been well studied for many decades, but careful mechanistic studies have been missing on human ribosomes,” said Blanchard. “We’re very interested in human ribosomes because this system has shown potential to be targeted for clinical treatments for cancer and viral
By grasping the underlying mechanisms, we are setting the stage for potential innovative therapeutic approaches against fusion oncoprotein–driven cancers.
Richard Kriwacki, PhD
Structural Biology
infections, and deeper knowledge of this complex molecular machine may inform new therapeutic strategies.”
How altered DNA structure causes cancer
Cancer-causing mutations often affect the structural stability and function of proteins. These mutations arise from altered genetic instructions encoded in DNA. Because DNA constantly shifts, rearranges, and replicates, errors can and do happen frequently — sometimes with disastrous consequences.
Many cancers are caused by fusion oncoproteins, biomolecules that aberrantly form when a DNA rearrangement results in two proteins combining. “Fusion proteins are known to be oncogenic drivers in upwards of 15% of human cancers,” said Richard Kriwacki, PhD, Department of Structural Biology.
Fusion oncoproteins can undergo a process called biomolecular condensation, wherein biomolecules separate from the surrounding environment to form their own compartments, akin to oil droplets in water. “We hypothesized that gaining the ability to form
condensates could be linked with the oncogenic properties of fusion oncoproteins,” Kriwacki explained.
In a paper published in Nature Communications, the researchers revealed that 58% of the almost 200 fusion oncoproteins they examined formed condensates. They further observed that the condensateforming fusion oncoproteins likely promote oncogenesis by altering gene regulation or cell-signaling pathways. To validate their observations, the researchers created a machinelearning algorithm using 25 recurring features of condensate-forming fusion oncoproteins. This predicted that more than 67% of the approximately 3,000 additional fusion oncoproteins tested likely form condensates, highlighting this property as a potential therapeutic vulnerability.
“By grasping the underlying mechanisms, we are setting the stage for potential innovative therapeutic approaches against fusion oncoprotein–driven cancers,” Kriwacki stated.
Biomolecular structure regulates gene expression
Protein folding is not the only biomolecular structure facet governing cellular processes. DNA also has structure regulated at multiple levels, from the chemical bonds between nucleotides that form the double helix to gene-regulating transcription factors that control access to and expression of DNA.
Myriam Labelle, PhD, Department of Oncology, has linked gene accessibility to the process of metastasis, exploring the driving forces of the movement and spread of cancerous cells through the body.
In a work published in Science Advances, Labelle reported that overexpression of the transcription factor ZBTB18 limits chromatin accessibility at gene locations important for metastasis, thereby decreasing the tumor cells’ ability to metastasize.
Building on prior work to understand the dynamic behavior of nucleosomes, we wanted to understand how other factors might utilize those dynamics to access chromatin.
Mario Halic, PhD Structural Biology
“Since it’s restricting chromatin accessibility, by overexpressing ZBTB18, we are essentially blocking the cells from being able to see the metastatic cues that they would normally respond to if the chromatin were more open,” explained Labelle.
These cues are tied to the cell’s plasticity, or adaptability, based on different environments. Considering that approximately 90% of cancerrelated deaths stem from metastasis, Labelle’s work has the potential to motivate future therapeutic advances.
While DNA accessibility can be limited by modulating the expression of proteins like ZBTB18, proteins called pioneer transcription factors control their target DNA’s expression even within compacted chromatin. This feature is vital to kickstarting gene expression during various cellular processes.
To better understand how pioneer transcription factors access tightly
wound DNA, Mario Halic, PhD, Department of Structural Biology, investigated how the pioneer transcription factor Oct4 cooperatively interacts with nucleosomes, the basic subunits of chromatin that consist of DNA tightly wound around a core of eight histone proteins, like thread on a spool. This structure not only packages DNA to fit inside the nucleus but also protects the genome from DNAdamaging perturbations. This structure is designed to safeguard the genetic material, and disruption to the factors that regulate it can lead to disease.
“Building on prior work to understand the dynamic behavior of nucleosomes, we wanted to understand how other factors might utilize those dynamics to access chromatin,” said Halic, corresponding author of the findings published in Nature
The researchers observed that the initial binding of an Oct4 molecule “fixes” the nucleosome in a position that increases the exposure of other binding sites, thus
The installation of a new Krios G4 microscope allows for the investigation of biomolecules in their native environment through cryo-electron tomography.
promoting the binding of additional transcription factors and explaining transcription factor cooperativity. They found that Oct4 contacts histones to promote chromatin decompaction. Cooperativity is further facilitated by post-translational modification of the histones, primarily the addition of acetyl groups to the histone. These findings explain how the epigenetic landscape, changes in gene expression such as post-translational modification that don’t involve alterations to DNA sequence, can regulate Oct4 activity to ensure proper cell programming.
From fundamental biology to therapeutic insights
While our understanding of biomolecular structure is the first foothold in designing new compounds for therapy, understanding how these compounds subsequently interact within the complex physiology of
of two specific amino acids in the protein’s active site, a threonine and an asparagine, the distinguishing feature of which is that they are polar and, therefore, hydrophilic. Mutating these to a featureless alanine demonstrated that the amino acids were crucial for binding hydrophilic chemicals.
ABCG2 inhibitors are often combined with chemotherapeutics, but preventing ABCG2 function can result in off-target detrimental effects. “The goal now is to design ABCG2 inhibitors that have minimal effect on normal tissues but target the tumor,” Schuetz said. This mechanistic insight can inform efforts to design more effective, less detrimental inhibitors that target the binding site threonine in ABCG2 and pair it with hydrophilic chemotherapies used in cancer treatment.
As technologies develop, understanding biomolecular structure at an atomic level has never been more critical to
From conformation to chemistry
Drug design has classically been represented as creating a key, a drug, that fits perfectly into a lock, the targeted protein. However, as our understanding of proteins’ dynamic nature has grown, scientists have gained insight into options for targeting them — new ways to try opening the lock.
At St. Jude, researchers explore in detail how small molecules, like natural ligands and drugs, bind their targets. However, these interactions do not happen in a vacuum. Drug–protein binding creates a chain reaction, starting at the first amino acid contact and carrying through an entire cellular pathway. Understanding the nuanced conformational changes that occur within drug targets is vital to the design of next-generation therapeutics.
Molecular origins of GPCR function
M. Madan Babu, PhD, FRS, Center of Excellence for Data-Driven Discovery director, and Department of Structural Biology member, leveraged data science, pharmacology, and structural information to study how each amino acid in the receptor that binds adrenaline contributes to receptor activity. Published in Science, the study revealed which amino acids control key pharmacological properties of the ligand.
The adrenaline receptor studied here is a member of the G-protein–coupled receptor (GPCR) family. One-third of all U.S. Food and Drug Administration (FDA)–approved drugs target receptors in this family. Thus, understanding how GPCRs respond to natural or therapeutic ligands is critical for developing new therapies with precise effects on receptor activity.
A key implication of this discovery is that if we want to make a more potent or efficacious drug, we now know there are specific residues that the new ligand needs to influence.
M. Madan Babu, PhD, FRS Center of Excellence for Data-Driven Discovery
“Through evolution, every amino acid in the receptor has been sculpted in some way or another to ensure that it binds the natural ligand and elicits the appropriate physiological response,” said Babu. “It was exciting to discover the allosteric network governing GPCR function and to reveal that some amino acids control efficacy, some control potency, and others affect both.
The researchers developed a data science framework to integrate pharmacological and structural data systematically and revealed
the first comprehensive picture of GPCR signaling. “When we mapped the pharmacological data onto the structure, they formed a beautiful network,” said Babu.
“It provided new insights into the allosteric network linking the ligand binding pocket to the G protein binding site that governs efficacy and potency,” added Brian Kobilka, MD, co-corresponding author and the 2012 Nobel Prize winner in Chemistry from Stanford University School of Medicine.
By understanding GPCR signaling at the atomic level, the researchers are optimistic that they can more closely observe the transient sub-states between the active and inactive conformations and thoroughly explore the proteins’ greater conformational landscape.
Unlocking the potential of nuclear receptors as drug targets
While GPCRs have long been a focus of drug discovery due to their welldefined binding sites and broad function, nuclear receptors have recently gained attention as potential therapeutic intervention routes.
Nuclear receptors are a family of 48 human proteins that regulate gene activation in response to signaling molecules. Their myriad versions (isoforms) comprise two distinct binding sites: a ligand-binding domain and a DNA-binding domain. Ligand binding acts as a signal for the receptor to move inside the cell’s nucleus. The DNA-binding site is naturally designed to then bind and activate a particular set of genes.
Although some noticeable trends exist, the range of genomic sites where nuclear receptors bind is confounding. Despite containing the same genome, a given nuclear receptor can bind at different genomic locations in different cells.
Local microstructure does matter. It can help distinguish between receptors expected to bind the same DNA sequence in principle.
Aseem Ansari Chemical Biology & Therapeutics
These factors contributed to defining the different binding patterns observed across different cells.
“Local microstructure does matter,” Ansari said. “It can help distinguish between receptors expected to bind the same DNA sequence in principle.”
Solving the riddle of drug metabolism
“One of our hypotheses is that maybe PXR is degraded by a certain E3 and that certain E3 might be downregulated in specific tissues like the liver, where PXR is highly expressed,” Chen explained. “There is potential to modulate selective PXR–E3 interactions to temporarily remove PXR from the equation.”
“Same genome, same binding sites. So, why are these receptors binding in different places?” questioned Aseem Ansari, Department of Chemical Biology & Therapeutics chair.
In a paper published in Nature Communications, Ansari and his team explored the underlying DNA-sequence patterns that enable nuclear receptor binding. To do so, they collaborated with Parameswaran Ramanathan, PhD, an electrical and computer engineer at the University of WisconsinMadison who uses a pattern-finding approach to design electrical circuits.
This process involves finding the shortest route with the minimum input necessary to perform a function. This collaboration resulted in the development of MinSeq Find, a search algorithm designed to solve, at the single-nucleotide level, the masked DNA-sequence features necessary for nuclear receptors to bind DNA.
They found a finely tuned process driven by not only the DNA sequence but also the initial ligand-binding restrictions. Such restrictions included whether one or two receptors are needed, the importance of communication between receptor-binding domains, and the structure of the DNA itself.
The ligand-binding domains of nuclear receptors have unique therapeutic potential and pitfalls. Pregnane X receptor (PXR) functions in detoxification by activating genes that encode drug-metabolizing enzymes, utilizing its remarkably malleable ligand-binding site to detect a diverse panel of foreign chemicals, including chemotherapeutics. In a report published in Proceedings of the National Academy of Sciences (USA), Taosheng Chen, PhD, Department of Chemical Biology & Therapeutics, explored the rules governing the promiscuous nature of PXR and how to break those rules.
The researchers changed a drug that normally binds well to PXR into one that stretches the protein’s binding region, making binding energetically unfavorable. The modified drug lowered the levels of PXR-induced enzymes — indicating this approach could be used in drug development to evade the detoxification network. The potential implications of this research are vast; many drugs interact with PXR, and over half of all FDA-approved drugs in the U.S. are metabolized by PXR-induced enzymes.
In addition to identifying routes to reduce a drug’s potential to activate PXR, Chen is exploring targeting PXR directly for degradation. The degradation pathway involves proteins called E3 ubiquitin ligases; these enzymes label proteins for removal. A “hijacked” E3 can be used to degrade PXR.
An example of such a PXR–E3 pair was published in Acta Pharmaceutica Sinica B, where researchers identified the F-box-only protein 44 assigned for PXR. The ability to target pathways such as this one would provide another avenue to block PXR-mediated drug metabolism.
The insight gained from a full conformational interrogation of drug targets has yet to be fully realized. Researchers no longer view these proteins as locks for which the correct key must be designed. Instead, St. Jude researchers continue to show that drug targets are complex networks for which our complete understanding is the key to unlocking their full therapeutic potential.
This is a significant change for the field, showing that it is, indeed, possible to study a structure/ activity relationship for such a promiscuous detoxification receptor.
Taosheng Chen, PhD Chemical Biology & Therapeutics
Shared Resources help Elizabeth Kellogg, PhD, take fundamental research to the next level
When Elizabeth Kellogg, PhD, Department of Structural Biology, came to Memphis in 2023, she was driven
more through a symposium and saw how different it was, how things that wouldn’t be possible
achievement. Her team built on this work and published in Molecular Cell in 2023, bringing to light fine details about the protein TniQ, which facilitates the transposition process. The shared resources at St. Jude are well positioned to enable Kellogg to expand upon her protein engineering background and take her insights to the cellular level.
“We are using many shared resources — the Cryo-EM Center, but also the Cell and Tissue Imaging Center. We’re pursuing a correlated light electron microscopy project, which was exceedingly difficult before we came to St. Jude because we had to learn how to do much of it ourselves,” Kellogg explains. “The data we’re now getting back is beautiful because the experts are the ones doing it.”
The Single Molecule Imaging Center, the Hartwell Center for Biotechnology, the Protein Technologies Center, and the Center for Advanced Genome Editing will also help advance Kellogg’s research. She highlights the unique ability to collaborate and
learn from the experts who operate these facilities as an added value.
“The setup of these resources means we can participate in the whole process. The experts are there to guide us in designing the experiments, to shepherd us through the whole process, and to help analyze the data. But we are ultimately the ones responsible for driving the project,” said Kellogg.
At St. Jude, Kellogg firmly believes she can receive the support she needs to pursue groundbreaking research; possibilities are now becoming realities. “We’ve been doing things that we’ve only ever dreamed of, and now that we’re here, we’ve been able to accomplish more in less time; it’s a dream come true.”
Elizabeth Kellogg, PhD, aims to combine her cryo-electron microscopy expertise with the abundant shared resources at her disposal to accelerate discovery at St. Jude.
Brain tumors in children are among the most challenging cancers to treat for an array of reasons.
The cancer’s location, the therapy’s impact on developing minds, and the molecular differences driving these malignancies are just a few factors that influence treatment outcomes. With a focus on translational research that grounds new clinical developments in the latest laboratory science, St. Jude is advancing the care and treatment of pediatric patients with brain tumors by learning more about the molecular underpinnings of those diseases.
Over the past several decades, molecular analyses, such as DNAmethylation profiling and nextgeneration genomic sequencing, have revealed molecular subgroups across various tumor types. By combining information about these molecular characteristics with findings from other diagnostic methods, such as medical imaging and histopathology, physicians can make an integrated diagnosis and select the best treatment
plan. With each discovery, scientists add elements to this molecular mosaic, creating a clearer picture of the brain tumor landscape.
Integrated diagnoses present new options
St. Jude is at the forefront of using integrated diagnoses to guide targeted treatment. In results published from the clinical trial SJYC07, led by principal investigator Amar Gajjar, MD, Department of Pediatric Medicine chair, researchers demonstrated how a more nuanced molecular understanding can influence patient care.
Younger children with high-grade glioma (HGG) tend to have more favorable outcomes than older children do, and this difference was historically thought to be age-related. However, according to corresponding author Giles Robinson, MD, Department of
A St. Jude patient, currently enrolled in clinical trial SJ901, walks from the Brain Tumor Clinic to Kay Kafe during her recent visit to St. Jude.
had an average age of less than one year and often suffered severe tumorand treatment-related morbidities.
Identifying gene fusions provides specific targets for the development of molecular therapies to noninvasively shrink tumors. These targeted therapies also offer new ways to decrease the adverse effects associated with traditional treatments, such as high-risk surgery, radiation, and chemotherapy.
“We’re breaking these diseases down into more descriptive categories, which open doors to more and better treatment options for these children,” said Robinson.
Identifying new molecular targets
When a brain tumor progresses despite therapy, understanding the biological factors that help the cancer advance becomes critical. Those factors can then become targets for therapy.
and the MAPK pathways to promote cell proliferation and processes that drive tumor progression. These results reinforce the new strategy employed by the Division of Neuro-Oncology to target the MAPK pathway with a brain-penetrant MEK inhibitor as firstline therapy on the clinical trial SJ901. SJ901 is for children with LGG and aims to highlight potential new targets for future combination therapies.
Oncology, Division of Neuro-Oncology director, this difference in outcomes instead has a molecular basis.
In a study published in Neuro-Oncology, a team of St. Jude researchers from oncology, pathology, computational biology, radiation oncology, diagnostic imaging, and neuropsychology conducted a comprehensive analysis of 56 children with HGG who were treated on SJYC07. By using advanced pathologic and molecular techniques, the researchers showed the tumors from these children could be separated into four diagnostic categories: HGG, low-grade glioma (LGG), infanttype hemispheric glioma (IHG), and other central nervous system tumors. IHG was the most prevalent tumor category, and most IHGs harbored highly specific receptor tyrosine kinase gene fusions involving ALK, ROS1, NTRK1/2/3, and MET. Although survival was favorable, the children with IHG
In a paper published in Neuro-Oncology, St. Jude scientists led by Jason Chiang, MD, PhD, Department of Pathology, identified potential targets for treating progressive hypothalamic/ optic pathway pilocytic astrocytoma.
The study retrospectively analyzed the clinical and molecular characteristics of 72 samples of pilocytic astrocytoma from patients treated at St. Jude between 1987 and 2020. The researchers identified an aggressive disease subtype with a high incidence of KIAA1549–BRAF fusion and overexpression of transcription factor TBX3 and protein kinase PIM1. This subtype was also resistant to conventional therapies like radiation and standard chemotherapy regimens. Overexpression of TBX3 and PIM1 is linked to many other cancers, activates the PI3K/mTOR pathways, and acts in concert with the cancer driver MYC.
Based on the relations among PIM1, MYC, and the tumor suppressor p53, the researchers validated a model in which the P53-PIM1-MYC axis and TBX3 act alongside the PI3K/AKT/mTOR
We’re breaking these diseases down into more descriptive categories, which open doors to more and better treatment options for these children.
Giles Robinson, MD Oncology
Using novel targets to improve and develop therapies
As researchers continue to discover molecular markers that serve as therapeutic targets, St. Jude uses that information to improve existing therapies and develop new ones. Radiation is a standard therapy for many pediatric brain tumors, but researchers are adapting this approach to fit new molecular information.
A St. Jude patient and her parents arrive for a check-up with neuro-oncologist Ibrahim Qaddoumi, MD. After her appointment, she spent the afternoon playing piano in the Family Commons.
embryonal tumors occurring in children younger than 3 years of age. These tumors are treated with chemotherapy and radiation, but prognoses are dismal. While the molecular understanding of AT/RT has expanded over the years, targeted treatments have not progressed in tandem. To fill this knowledge gap, St. Jude researchers examined existing treatments and their clinical impact on molecular subgroups of AT/RT to help determine how therapy should improve.
Led by Brent Orr, MD, PhD, Department of Pathology, the researchers analyzed clinical features and outcome data of patients with AT/RT belonging to the SHH subgroups (ATRT-SHH-1A, ATRTSHH-1B, and ATRT-SHH-2) treated in one of three St. Jude clinical trials or in a consortium trial. The team assigned consensus labels to 41 cases and noted observations of subgroup-specific differences related to tumor location and age at diagnosis. Published in Acta Neuropathologica, the results show that ATRT-SHH subgroups are not currently meaningful for guiding therapy but
should be considered for use in the future as ATRT-SHH research continues.
Continuing AT/RT research includes testing novel therapeutics, aligning with the St. Jude mission to keep searching for successful treatments for even the most challenging diagnoses. Published in Neuro-Oncology, the clinical trial SJATRT was the largest study to date to report the tolerability and efficacy of a molecularly targeted therapy in children with progressive or recurrent AT/RT. Co-authored by Gajjar, the study analyzed the therapeutic effectiveness of alisertib, a small-molecular inhibitor that targets Aurora kinase A, which is encoded by AURKA. The inhibitor was used to treat 30 patients representing three molecular subgroups of AT/RT: ATRT-MYC, ATRT-SHH, and ATRT-TYR.
The findings demonstrate that no molecular subgroup or germline alteration dependencies influenced outcomes, but alisertib may prolong survival in some children with progressive or recurrent disease and/ or serve as a bridge to other therapies.
The effectiveness of alisertib in combination with chemotherapy and radiation for newly diagnosed cases of AT/RT will be evaluated by ongoing portions of the SJATRT trial.
Exploring environmental influence on cognitive outcomes
A patient’s cancer experience is composed of more than just the biology of the disease and the clinical care that is administered. To understand the influence of a patient’s surroundings, St. Jude researchers examined lived environments to determine the impact homes and neighborhoods have on patient outcomes.
In a study published in NeuroOncology, led by Heather Conklin, PhD, Department of Psychology and Biobehavioral Sciences, Division of Neuropsychology chief, the researchers observed cognitive outcomes by conducting serial cognitive assessments over 10 years of 241 children who received conformal radiation therapy
for brain tumors. Neighborhood-level social and economic conditions were evaluated using the Economic Hardship Index (EHI). The EHI score measures unemployment, dependency, education, income, crowded housing, and poverty; socioeconomic status was also derived. The researchers correlated results from the cognitive assessments with EHI variables accounting for sex, age at treatment, and tumor location.
The results demonstrated that EHI variables predict cognitive performance at baseline and a change in intelligence quotient and math reasoning over time. EHI and poverty were the most consistent predictors, and patients with a high EHI (lower socioeconomic status) had worse cognitive outcomes. The findings suggest that providing additional resources to patients and families with a high EHI could protect against cognitive decline.
“At the simplest level, we found that a patient’s environment matters,” said
Conklin. “It’s not just the diagnosis or treatment the patient receives. It’s the family, neighborhood, and support they can access that predicts cognitive outcomes.”
With these results in mind, the latest St. Jude investigator-initiated brain tumor clinical trials, such as SJiMB21, which treats infants and young children with newly diagnosed medulloblastoma, are incorporating interventions to improve cognitive outcomes by increasing resources and access to interactive neurodevelopmental tools for patients and families.
Improving patient outcomes, from molecules to milestone
Much work remains to bring forward new treatments for pediatric brain tumors, as the survival probabilities of these diseases lag behind those of cancers like pediatric acute
lymphoblastic leukemia. However, progress is being made every day in the laboratory and the clinic. As research and clinical experience continue to expand and a more defined molecular mosaic of pediatric brain tumors emerges, care and research efforts at St. Jude remain steadfast on not only finding cures but also improving the lives of patients with brain tumors.
“When the brain tumor program began in 1985, we knew very little about these devastating tumors,” said Gajjar. “Treatments were intense, and less than
A St. Jude patient and her dad pause to share a hug and a little bit of hope during an afternoon walk around the St. Jude campus.
Neuro-oncology leaders continue a legacy of excellence
Over the past six decades, through seminal contributions to research and care for pediatric brain tumors, St. Jude has built a legacy of excellence in neuro-oncology.
Now, as the institution works to advance that legacy, new leadership takes the reigns to continue innovative research and care for children and young adults with brain tumors.
Giles Robinson, MD, Department of Oncology, understands that legacy of excellence. In 2023, Robinson was appointed the Director of the Division of Neuro-Oncology within the Department of Oncology. Robinson takes on this role after Amar Gajjar, MD, Department of Pediatric Medicine chair, who led the division for two decades.
Over the past 16 years, Robinson has led research and clinical efforts that have increased the survival of children with brain tumors, making him an internationally recognized expert in pediatric neuro-oncology. At the core of his work is a belief that therapy can be improved through an increased understanding of genomics. This approach shapes his clinical research, including the clinical trials he leads.
Under Robinson’s leadership, clinical research for pediatric brain tumors takes a targeted, molecular approach. SJiMB21 is the first clinical trial to tailor molecular therapies for infants with medulloblastoma by using a tumor’s molecular makeup as a therapeutic guide, and clinical trial SJ901 assesses targeted treatments for children with low-grade gliomas.
Robinson’s simultaneous appointment as co-leader of the Neurobiology and
known as Centers of Excellence. These Centers are designed to advance science in each focus area by facilitating cross-laboratory collaborations via shared physical space and ease of access to technology and expertise.
To further advance the basic science foundation of neuro-oncology research, St. Jude recently launched the Center of Excellence in Neuro-Oncology Sciences (CENOS). Led by Paul Northcott, PhD, Department of Developmental Neurobiology, CENOS will apply bold, innovative strategies to advance
Brain Tumor Program within the St. Jude Comprehensive Cancer Center, a title he shares with Suzanne Baker, PhD, Department of Developmental Neurobiology, ensures that he steers both clinical and research efforts in neuro-oncology across major initiatives and departments at St. Jude.
“Our team will continue its mission of improving survival and reducing treatment-related toxicities for children with brain tumors by developing effective therapies through a better understanding of the disease,” said Robinson. Situated at the helm of these two units, he now leads one of the largest clinical brain tumor programs in North America.
To unite major initiatives among research programs and departments across St. Jude, the institution has recently established resource hubs
disease understanding, enhance treatment, and improve outcomes for children with malignant brain tumors.
Northcott has contributed significant, impactful discoveries, including the original description of molecularly and clinically distinct subgroups of medulloblastoma and their developmental origins. He is prepared to lead a bold research program to address fundamental questions shaping the field of pediatric neuro-oncology
“This Center of Excellence is living up to the spirit of excellence across the St. Jude campus,” said Northcott. “We are doing transformative research that further solidifies our presence in the pediatric neurooncology community for making discoveries and driving change to ultimately impact patient care.”
Paul Northcott, PhD; Giles Robinson, MD; and Amar Gajjar, MD, discuss how intersections between science and clinical care can advance treatment opportunities for rare pediatric brain tumors.
HIGHLIGHTS
Every year, the breadth and depth of the research enterprise at St. Jude expands. The Scientific Highlights capture a snapshot of the diversity of fields, departments, and researchers charting new discoveries at St. Jude. These high-impact publications provide a window into the scientific accomplishments of St. Jude investigators in 2023.
X-linked severe combined immunodeficiency disorder (SCID-X1), commonly called “bubble boy disease,” is a disorder in which patients are born with a defective gene that prevents them from producing immune cells. In a study published in the New England Journal of Medicine in 2019, St. Jude scientists used lentiviral gene therapy to restore multiple infants’ immune systems by supplying copies of the corrected gene.
Through ongoing monitoring efforts, the researchers have now documented where the corrected gene copies integrate into patient DNA and why the vector integrates at that site. Published in Science Advances, their findings provide a foundation for understanding the biology and safety of using lentiviral vectors in the clinical setting.
“We now have a robust pipeline to monitor the safety of lentiviral gene therapies,” said senior co-corresponding author Jiyang Yu, PhD, Department of Computational Biology interim chair. “This gives hope to patients with genetic diseases that can be cured by lentiviral gene therapy.”
Several years posttreatment, the St. Jude lentiviral gene therapy for SCID-X1 appears effective and safe. Previous research indicated that lentiviral gene therapies integrated into areas of DNA that seemed safer than the sites, such as oncogenes, affected by earlier technologies, but until recently, researchers could not explain why. The team identified where the gene was added to the participants’ DNA and why the vector integrated at that location.
The new, corrected gene had been inserted into certain genomic hotspots within the study participants’ DNA. The reason was deceptively simple: From a three-dimensional structural perspective, the hotspots are regions the lentiviral vector first encounters after entering the cell’s nucleus through a channel called the nuclear pore.
“It’s like someone coming into a room and taking the first available seat near the door,” said co-corresponding author Stephen Gottschalk, MD, Department of Bone Marrow Transplantation and Cellular Therapy chair. “The room is the nucleus; the seats are these DNA elements right near the door of the nuclear pore.”
This integration-site pattern of the gene therapy into patient cells illuminates the safety and efficacy of the approach.
The group used single-cell multiomics analysis to understand whether a functional copy of the corrected gene was in patient cells, to what extent it was expressed, and the chromatin organization. The lentiviral vector used in the current study does not disrupt oncogenes, which improves treatment safety.
The same integration pattern was observed with a lentiviral vector used to create chimeric antigen receptor (CAR) T cells, suggesting that the phenomenon is a general mechanism that is not restricted to the SCID-X1 vector.
“The integration-pattern data could serve as a map of potentially safe integration sites,” Gottschalk explained. “The single-cell analysis is like deep cartography — a map with a near pixelperfect resolution. The many integration sites could be used as a safety reference for future lentiviral gene therapies.”
First author Koon-Kiu Yan, PhD; senior co-corresponding author Jiyang Yu, PhD; and co-corresponding Stephen Gottschalk, MD, documented where corrected gene copies integrate into patient DNA, improving our understanding of lentiviral vector safety when used in clinical settings.
Pediatric rhabdomyosarcoma is a cancerous tumor that arises in soft tissue, such as muscles, and consists of multiple disease subtypes. The origin of one of the most aggressive subtypes, fusion-positive rhabdomyosarcoma, has been a long-standing mystery.
Fusion-positive rhabdomyosarcoma cells express a hybrid protein (or oncoprotein) that results from the fusion of two genes, PAX3 and FOXO1. Pediatric fusion-positive rhabdomyosarcoma has a poor prognosis and is challenging to treat. Rhabdomyosarcoma cells appear muscle-like; however, fusionpositive tumors can form in areas without skeletal muscle. They also occur as diffuse tumors that resemble metastatic disease.
Scientists at St. Jude have shown in proof-of-concept models that expressing the fusion oncoprotein
in either muscle or blood vessel (endothelial) cells produces aggressive tumors, which are molecularly identical to fusion-positive rhabdomyosarcoma. The researchers generated models to find where and how these fusionpositive tumors arise. Their findings, published in Nature Communications, have implications for treating aggressive rhabdomyosarcoma.
“When we compared the tumors that develop from muscle or endothelial cells, they were nearly indistinguishable,” said corresponding author Mark Hatley, MD, PhD, Department of Oncology. “We performed detailed analyses, including looking at gene expression, chromatin architecture, and enhancer accessibility. Despite how hard we looked, we could not find a single distinguishing feature that told us that the tumor from the endothelial cells came from endothelial progenitors and not muscle cells.”
Hatley’s lab generated a mouse model expressing the PAX3–FOXO1 fusion oncoprotein in blood vessel cells. The researchers compared this new model to a previously established mouse model of fusion-positive rhabdomyosarcoma that arises from muscle cells. The study indicates that it may not be possible to find the cellular origin of these cancerous cells using standard methods. Instead, focusing on the fusion oncoprotein’s effects may be a better way to identify potential therapeutic interventions.
To explore this alternative approach, the Hatley lab developed a model to examine the genetic and epigenetic effects of the fusion oncoprotein in human cells more closely. They exploited the oncoprotein’s strength as a cancer driver in human induced pluripotent stem cells (hiPSCs), which can differentiate into any cell type. The scientists first differentiated the hiPSCs into endothelial cells and then added the fusion oncoprotein. This in vitro system enabled the team to look even closer at what happens when the cells undergo malignant transformation.
The fusion oncoprotein still acted as a potent activator of muscle cell fate in the system. The aberrant protein bound to DNA regions that enhance the expression of genes well known to be major regulators of muscle cell development, such as MYOD1. These findings serve as a proof of concept that this hiPSC system can be used to find downstream targets of the PAX3–FOXO1 oncoprotein and increase confidence in any targets found in future studies.
Co-first author Randolph Larsen IV, corresponding author Mark Hatley, MD, PhD, both of the Department of Oncology, and co-author Brian Abraham, PhD, Department of Computational Biology, discuss their paper.
scientific highlights
Computational tool targets oncofusions’ weakness
When mutations that combine two genes occur, the resulting fusion may act as an oncogene to encode a fusion oncoprotein, which drives tumorigenesis. Although fusion oncoproteins are demonstrated drivers in various cancer types, designing therapies that target them can be complex. Therapeutically targeting fusions has much potential because cancer cells depend on the fusion oncoproteins to thrive. However, the seemingly random manner in which these fusions form and work has hampered drug-development efforts.
To address this knowledge gap, St. Jude computational biologists have developed a tool that comprehensively categorizes and identifies the mechanism underlying the formation of oncogenic fusions in pediatric cancer cells.
“We’ve made something similar to the periodic table for understanding oncogenic fusions,” said Xiaotu Ma, PhD, Department of Computational Biology. “By cataloging the underlying mechanisms, we’ve enabled other scientists to study fusions in better detail.”
In a paper published in Nature Communications, the researchers illustrated that targeting oncogenic fusions with genome-editing tools, such as CRISPR–Cas9, could potentially cure disease. Most oncogenic fusions are currently considered undruggable (with a few exceptions, such as those involving ABL1, ALK, and NTRK).
Genome editing presents an exciting curative option for fusions that cannot currently be targeted therapeutically.
The mutations that produce fusion oncoproteins are present only in cancer cells. A precise genetic-editing tool, such as the CRISPR–Cas9 system, could selectively remove the fusion gene from cancer cells, eliminating their ability to produce the hybrid protein needed to thrive, thus leading to a cure.
“The fusion gene–specific sequence only exists in cancer cells; it wouldn’t target any normal cells,” explained first author Yanling Liu, PhD, Department of Computational Biology. “We used CRISPR–Cas9 to perturb the fusion-specific alleles in two cancer cell lines and killed them.”
This work provides proof of principle for a genome-editing cure for cancers; however, it also highlights the difficulties of developing such cures. The cell lines were derived from pediatric cancers with currently poor prognoses, even with treatment. Although genome editing effectively killed one cell line, the other unexpectedly compensated by using multiple splice variants, which are different RNA sequences derived from the same DNA region.
Using CRISPR–Cas9, the scientists disrupted the splice variants of the oncogenic fusion in the second cell line, successfully killing the cancer cells. However, preemptively identifying splice variants is technically challenging, and current genome-editing technologies are not yet efficient enough to bring the approach into a clinical setting for these diseases.
Despite the challenges facing its use in therapy, the computational tool holds exciting potential for identifying the underlying cause of fusion oncoprotein–driven pediatric acute myeloid leukemia. The study serves as proof of principle, offering a new resource in the toolbox of options for developing new interventions for fusion-driven pediatric cancers.
First author Yanling Liu, PhD (left), and senior and co-corresponding author Xiaotu Ma, PhD (right), focused their efforts on developing a tool to categorize and identify the underlying mechanisms of oncogenic fusion formation.
A new drug target for inflammation
Many infectious and inflammatory diseases, including malaria, COVID-19, and sickle cell disease, cause red blood cells to rupture, releasing the oxygen-binding molecule hemoglobin in a process called hemolysis. The hemoglobin then breaks down in the bloodstream, releasing a substance called heme. Circulating heme can cause significant inflammation and organ damage, leading to morbidity and mortality.
In a paper published in Cell, St. Jude researchers reported their discovery that the NLRP12 protein, an innate immune pattern recognition receptor, is the key molecule driving hemeinduced inflammatory cell death. However, heme alone is insufficient to induce NLRP12 expression and the subsequent cell death process.
“After a two-decades-long search for the trigger of NLRP12 and the specific signaling pathway it activated, we found that heme, combined with specific components of infection or cellular
damage, can activate NLRP12 to drive inflammatory cell death and pathology in disease,” said corresponding author Thirumala-Devi Kanneganti, PhD, Department of Immunology vice chair and Center of Excellence for Innate Immunity and Inflammation director.
The researchers showed that cell death can occur when heme combines with certain pathogen-associated molecular patterns (PAMPs) or cytokines. These combinations are common during infections and disease. When present, they signal the cell, causing NLRP12 to interact with other proteins. These interactions enable NLRP12 to form a PANoptosome, a complex comprising several cell death–inducing molecules, including the NLRP3 inflammasome, caspase-8, and RIPK3. These components are central to inducing PANoptosis, a form of innate immune inflammatory cell death, and inflammation downstream of NLRP12 activation.
Overactivation of PANoptosis leads to inflammatory disease. Therefore, NLRP12 is a direct bridge from hemolysis to inflammatory disease.
The team found that NLRP12 is expressed highly in patients with various diseases, including diseases with a prominent hemolytic component, such as sickle cell disease and malaria, and infections, such as COVID-19, influenza, and bacterial pneumonia. When the researchers knocked out Nlrp12 in a mouse model of hemolytic disease, the mice no longer succumbed. This work demonstrated that NLRP12-mediated PANoptosis is a key driver of morbidity and mortality. The results also identified NLRP12 as a potential drug target to block tissue damage, pathology, and mortality during hemolysis.
“Beyond the fundamental contribution to the innate immunity and cell death fields, this study identifies a druggable target to directly reduce the organ-damaging inflammation caused by infection and hemolytic diseases,” said Kanneganti.
The results’ implications are important in hemolytic disease and extend to infections and other conditions in which hemolysis occurs. Research has linked genetic mutations in NLRP12 to several diseases. Now that NLRP12’s regulation and function in inflammatory cell death have been identified, scientists can develop potential therapies to prevent cell death and inflammation in diseases. Additionally, these findings lay the foundation for new research on PANoptosomes and PANoptosis in health and disease.
Corresponding author Thirumala-Devi Kanneganti, PhD, and co-first authors Balamurugan Sundaram, PhD, and Nagakannan Pandian, PhD, showed how NLRP12 connects hemolysis to inflammatory disease.
scientific highlights
Pediatric Early Warning Systems save lives in Latin American hospitals
Children who are hospitalized can experience clinical deterioration, defined as a change in a patient’s status that requires a transfer to the intensive care unit (ICU) or an ICUlevel intervention, such as mechanical ventilation or cardiopulmonary resuscitation outside the ICU. Pediatric Early Warning Systems (PEWS) are tools that help identify clinical deterioration in hospitalized children. Through a multicenter collaborative called Proyecto EVAT, investigators from St. Jude worked with partners across Latin America to bring PEWS into hospitals in the region.
PEWS starts at the patient’s bedside with an assessment that includes a scoring tool to evaluate a patient’s
neurologic, cardiovascular, and respiratory status alongside staff and family concerns. It considers vital signs, physical examination findings, and treatment requirements. An action algorithm interprets the score and guides the team through the next steps, which are adapted to the local context and health care systems.
“When children with cancer are in the hospital, they may develop clinical changes that, if not recognized early, can become significantly worse, leading to death,” said first and corresponding author Asya Agulnik, MD, MPH, St. Jude Global Critical Care Program director.
“Most hospitals in high-resource settings use some form of PEWS to help identify
deterioration, but they are underutilized in resource-limited settings.”
Through the work of St. Jude Global, Agulnik collaborates with doctors and nurses in hospitals in Latin America to implement PEWS. An analysis of this program, published in The Lancet Oncology, looked at the impact of PEWS in 32 hospitals in 11 countries, demonstrating that PEWS saves lives — often in the hospitals with the greatest need.
“We see this as a real call for the need to scale up PEWS globally,” Agulnik added. “This intervention should be used in the care of every single hospitalized child with cancer.”
The global burden of pediatric cancer is greatest in low- and middle-income countries, where approximately 90% of children at risk of cancer live and where the probability of survival is as low as 20%. Hospitals in low-resource settings frequently lack adequate infrastructure and staff to provide supportive care, resulting in the late identification of clinical deterioration and high rates of preventable deaths. Proyecto EVAT was created to address this gap.
In hospitals that implemented PEWS through Proyecto EVAT, the researchers found an 18% reduction in the rate of clinical deterioration event–related mortality and a reduction in the percentage of events that resulted in mortality. They found fewer cardiac arrests outside of the ICU, and patients with deterioration were identified earlier and transferred to a higher level of care at a lower severity of illness. Notably, ICU resource use remained the same after PEWS implementation. The results also showed that PEWS are most likely to be present in hospitals of higher resource levels but are most effective in settings with higher mortality rates, making them valuable interventions to address global disparities in childhood cancer outcomes.
Asya Agulnik, MD, MPH, St. Jude Global Critical Care Program Director, and colleagues in Latin America led research to show that Pediatric Early Warning Systems save lives.
Gain-of-function mutation reveals new target in pediatric acute myeloid leukemia
Pediatric acute myeloid leukemia (AML) accounts for 20% of all pediatric leukemia cases and is associated with poor outcomes, especially if the disease relapses. Part of the struggle with treating pediatric AML is that the current understanding and interventions stem primarily from knowledge of adult AML, which differs from pediatric disease. However, St. Jude scientists are working to change this.
Jeffery Klco, MD, PhD, Department of Pathology, and his team aim to narrow the knowledge gap and improve treatment for pediatric AML through a better mechanistic understanding of the disease.
The researchers had previously categorized pediatric AML into 23 molecular subtypes, including 12 unrecognized by the World Health Organization’s classification system
for AML. One such subtype associated with poor outcomes involves the gene UBTF, which encodes a critical protein for transcription. In this AML subtype, UBTF mutates by undergoing a DNA replication error called tandem duplication. These genetic duplications vary in size and lead to functional yet mutated proteins.
In earlier work examining UBTF and its role in pediatric AML, the team detected mechanistic clues that helped them uncover the role of UBTF tandem duplications.
Disease-linked proteins may be affected by loss-of-function mutations, meaning that the protein no longer works, or by gain-of-function mutations, meaning that the protein still works but in a way that differs from normal. In pediatric AML linked to UBTF tandem duplications, the researchers observed a functional UBTF protein,
which indicated that a gain-offunction mechanism contributes to this subtype of pediatric AML.
The team’s research led them to HOX genes, which are dysregulated in many cancers, including UBTF–tandem duplication pediatric AML and other pediatric AML subtypes. Their findings, published in Blood, illustrate the role HOXA and HOXB gene clusters play in UBTF-linked pediatric AML.
“The models elegantly show that this mutant protein will directly bind to the HOXA and HOXB loci — the gene location on a chromosome — whereas the wild type doesn’t,” said corresponding author Klco.
The findings also uncovered two other proteins, KMT2A and menin, alongside mutated UBTF at these loci, which was unsurprising to the researchers. KMT2A, a protein involved in hematopoiesis, and menin, a protein linked to gene regulation, are often implicated in HOX-related leukemias.
By identifying UBTF–tandem duplications as a previously unrecognized target, this work can guide the development of novel treatment strategies. The researchers also demonstrated that leukemia with UBTF–tandem duplications is sensitive to menin inhibitors. Disrupting KMT2A and menin interactions affected UBTF binding to the genome, thus presenting a potential new strategy for treating UBTF–tandem duplication pediatric AML.
“This collective work offers mechanistic insights that nominate and validate a new therapeutic option,” said Klco. “It’s well known that kids with these alterations have a dismal outcome. This has an opportunity to be somewhat transformative in how these kids are treated.”
Jeffery Klco, MD, PhD (left), and Juan Barajas, PhD (right), explored genes uniquely linked to pAML and tracked a gain-of-function mutation in one protein with therapeutic potential.
scientific highlights
Co-corresponding
author J. Paul Taylor, MD, PhD, Executive Vice President and Scientific Director, discusses research with first author Ane Korff, PhD, and co-corresponding author Hong Joo Kim, PhD, both of the Department of Cell & Molecular Biology.
Preventing neurodevelopmental disorders through genetic compensation
The body has checks and balances. A misaligned system can often be rescued by a related protein or the up- or down-regulation of alternative pathways. To find the chain of events that causes disease, the layers of effect must be peeled back, piece by piece.
HNRNPH2 mutations have been found in over 30 individuals with traits of neurodevelopmental disorders, such as intellectual disability, developmental delay, and autism spectrum disorder. The gene encodes a specific protein within a group called the heterogenous nuclear ribonucleoprotein (hnRNP) family. These hnRNPs are pivotal to many processes tied to RNA handling, including transcription and translation.
In a study published in the Journal of Clinical Investigation, cocorresponding authors Hong Joo Kim, PhD, Department of Cell & Molecular Biology, and J. Paul Taylor, MD, PhD,
Executive Vice President, Scientific Director, and Department of Cell & Molecular Biology chair, uncovered the role that the protein hnRNPH2 (H2) plays in neurodevelopmental disorders, shedding light on the mechanisms underlying its pathogenicity. The work provides critical insight into the biology of this poorly understood disorder, with the potential to develop future therapeutics that target this and related mechanisms.
“The findings from this study represent crucial documentation on the path to introducing a therapy for children with mutations in HNRNPH2,” Taylor said. “It’s an essential pre-clinical step.”
Most HNRNPH2 mutations are found within or adjacent to H2’s nuclear localization signal, which acts as the protein’s security clearance to enter and exit the nucleus. Considering that H2’s function is vital to RNA
processing, mutations affecting its nuclear localization signal are significant because they can cause the protein to become stranded outside the nucleus. However, detailed mechanistic insight has been elusive due to a lack of robust disease models.
When the researchers evaluated the pathogenic form of H2 containing a mutated nuclear localization signal, they saw that access to the nucleus had been reduced. The team dug deeper using mouse models and human cell lines either completely lacking HNRNPH2 or containing the disease-causing mutation. Mice with mutated H2 showed signs of the disorder, demonstrating that the researchers successfully created a faithful disease model.
Surprisingly, mice lacking the murine homolog Hnrnph2 showed no detectable phenotypes, indicating that this was not a simple case of loss of function. The team examined the expression patterns of other hnRNP family members to identify any correlations. One stood out: hnRNPH1 (H1), a protein functionally related to H2. The researchers found elevated H1 levels in mice and human cells lacking H2, suggesting that H1 can compensate for the complete loss of H2 and act as a fail-safe to rescue the affected cells. However, while the loss of H2 can trigger compensation by H1, the diseasecausing mutated form of H2 does not.
These fundamental genetic insights identified a strategy for therapeutic intervention using antisense oligonucleotides (ASOs), synthetic RNA molecules designed to bind to naturally occurring messenger RNA. ASOs have been used to successfully treat spinal muscular atrophy and hnRNPH2related disorders. The compensatory relation between H1 and H2 suggests that one could design an ASO aimed at reducing the levels of H2, thereby inducing an upregulation of H1 to compensate for the loss of H2 function.
SWI/SNF complexes ‘bookmark’ cell identity during division
When a stem cell divides, it retains information about how to grow, including instructions about what type of cell to become. Scientists at St. Jude gained a new understanding of how these processes can work. They revealed that subunits of the SWI/SNF chromatin-remodeling complex, which is mutated in 20% of all cancers, help cells remember their differentiation state during mitosis.
During differentiation, stem cells transform into a different cell type. Typically, the new cell type has a more specialized function, such as a skin or muscle cell. As cells divide, they must retain the “memory” of their differentiation state to transfer the proper identity to their daughter cells.
Chromatin is a complex of DNA and proteins tightly compacted inside cells. Chromatin must unwind to turn
genes on and off in closely regulated epigenetic processes. SWI/SNF complexes facilitate the control of a cell’s identity during differentiation by recognizing histone marks to change chromatin architecture and regulate gene expression. These changes in chromatin architecture are maintained across cell divisions, but how this occurs has been uncertain.
Cancers often carry mutations that affect the SWI/SNF chromatinremodeling complex. One example is the loss of the SWI/SNF subunit SMARCB1. Mutations in SWI/SNF subunits are also the basis of several neurodevelopmental disorders.
In the current study, scientists at St. Jude discovered how subunits of SWI/SNF act as “bookmarks” during mitosis to preserve chromatin architecture and safeguard cell identity
during division. The study, published in Nature, points to the importance of SWI/SNF core subunits SMARCE1 and SMARCB1 and their roles in the process.
“This work provides an understanding of a new component of mitotic memory clues to why a mutation of this SWI/SNF complex subunit would disrupt memory of what a cell should normally be doing and allow it to go into a cancerous state,” said senior author Charles W. M. Roberts, MD, PhD, Executive Vice President and St. Jude Comprehensive Cancer Center director.
Previously, researchers knew the enzymatically active subunit of the SWI/SNF complex was not bound to DNA during mitosis, so they assumed that SWI/SNF complexes had no role in that process. Surprisingly, Roberts’s team found that two individual SWI/ SNF complex subunits, but not the rest of the complex, bind to mitotic DNA. They then showed that mitotic binding of SMARCE1 and SMARCB1 is required for the appropriate reactivation of bound genes after mitosis.
Experiments that removed SMARCE1 during mitosis showed that the loss of SMARCE1 impairs the ability of some other bookmarks to bind to their targets, disrupts gene expression, and causes abnormal neural differentiation. These findings demonstrate that SMARCE1 functions as a mitotic bookmark and is essential for retaining appropriate differentiation programming during mitosis.
“In adult cancers, where many genes are mutated, it is often challenging to figure out what any single mutation contributes. In rhabdoid tumor, we have a pediatric cancer apparently driven by just this one mutation,” Roberts added.
“It’s a beautiful model to understand how these processes work and then begin to leverage that understanding for the myriad adult cancers that also have SWI/SNF mutations.”
Research led by Charles W. M. Roberts, MD, PhD, Executive Vice President and St. Jude Comprehensive Cancer Center director, found a new role for the SWI/SNF chromatin remodeling complex.
scientific highlights
Pharmacotyping provides a precision medicine blueprint for acute lymphoblastic leukemia treatment
Acute lymphoblastic leukemia (ALL), a cancer of white blood cells called lymphocytes, is the most common pediatric cancer. Approximately 98% of children with ALL experience remission within weeks of starting treatment, and about 90% of those children are eventually cured. These levels of success are due to advances in ALL treatment. Chemotherapy is tailored based on clinical features, leukemia genomics, and the degree of minimal residual disease (the presence of microscopic levels of cancer cells remaining after the initial treatment).
In a report published in Nature Medicine, St. Jude scientists examined how ALL cells respond to different therapeutics in the context of their genomic features.
This is the most comprehensive study to date describing variations in drug response across genetic ALL subtypes.
“Compared to traditional cancer genomics research, our work starts with defining the drug-response phenotype of each patient,” explained corresponding author Jun J. Yang, PhD, Department of Pharmacy and Pharmaceutical Sciences. “We then look into genomics to search for the biological basis for the inter-patient variability in leukemia drug sensitivity.”
The team determined the sensitivity of leukemia cells to 18 different chemotherapy drugs in patients whose ALL cells represented 23 molecular subtypes defined by leukemia
genomics. The results revealed wide variability and distinct patterns of drug sensitivity across ALL subtypes.
The disease subtypes with the most favorable prognoses were particularly sensitive to the chemotherapeutic drugs asparaginase and glucocorticoids. Surprisingly, some ALL subtypes share genomic similarities but show different patterns of drug sensitivities. The team also found that patients could be grouped based on their distinct drug-sensitivity profiles, which were associated with prognosis, even after accounting for known risk factors.
Pharmacogenomics is the study of how genetic attributes affect drug response; pharmacotyping is defining a patient’s drug response phenotype (characteristics resulting from the interaction of genomics and environment). The study’s findings highlight the importance of understanding ALL pharmacotypes for survival outcomes.
ALL is a heterogeneous disease; there are many phenotypic differences between genomic subtypes, such as clinical features and prognoses. This work demonstrates that drug sensitivity can also vary between subtypes.
“This work is a big step in the right direction to individualize ALL therapy to spare children the side effects of drugs that will not work against their cancer, as well as to steer them to novel therapies to which their cancer will likely respond,” Yang said. “It is functional precision medicine; it’s not just about sequencing leukemia mutations but also about knowing what drug to use for which mutations.”
Wenjian Yang, Shawn Lee, MBBS, and Jun J. Yang, PhD, published a comprehensive study describing drug response variations across genetic ALL subtypes.
Proton therapy improves neurocognitive outcomes of childhood craniopharyngioma
Craniopharyngioma is a rare brain tumor that forms in the central region of the brain, making it difficult to treat without exposing surrounding healthy brain tissue to radiation. Conventional radiation therapy, called photon therapy, increases the probability of five-year survival of pediatric patients with craniopharyngioma to 90%; however, patients may experience treatmentrelated neurocognitive late effects.
In a recent phase 2 clinical trial for children with craniopharyngioma, researchers at St. Jude found that photon therapy and the more targeted proton therapy resulted in similar survival, but patients who received proton therapy had a better neurocognitive outcome than those who received photon therapy. This clinical trial may set the new “gold standard” for pediatric craniopharyngioma treatment.
Photons pass through the tumor, whereas protons can be directed to
stop within the tumor. Thus, proton therapy spares normal brain tissue and reduces collateral effects. This St. Jude trial highlights the therapeutic advantage of proton therapy for children and adolescents with craniopharyngioma for the first time.
“The trial is an unprecedented study comparing proton and photon therapy for craniopharyngioma,” said principal investigator Thomas Merchant, DO, PhD, Department of Radiation Oncology chair. “We found a benefit for cognitive outcomes in patients treated with proton therapy while maintaining a high survival rate.”
The study, published in the Lancet Oncology, showed that overall survival, progression-free survival, and cognitive outcomes five years after treatment were improved with proton therapy when compared with other treatment approaches.
“We have long recognized a theoretical benefit of this approach but now have
proof that proton therapy causes fewer cognitive side effects than photons,” said co-author Frederick Boop, MD, Department of Surgery.
Although proton therapy was developed to decrease radiation exposure to the brain, no previous clinical trials for children with brain tumors had prospectively shown its functional benefit compared to photon therapy in a single tumor type. A unique feature of craniopharyngioma is that it is consistently located in the central part of the brain and intimately associated with the central blood supply, optic nerves and chiasm, hypothalamicpituitary axis, and other critical areas associated with cognitive function.
The researchers compared proton therapy results over five years to a historical control group treated with photon therapy at St. Jude. Patients treated with photon therapy experienced an average loss of 1.09 more intelligence quotient points every year than those treated with proton therapy for the five years of the study. Similarly, patients exposed to photon therapy lost 1.48 more adaptive behavior points, a parental report of self-care skills, per year than those treated with proton therapy. The cognitive and adaptive behavior deficits of those treated with proton therapy were stable by the end of the study.
“These results could be practicechanging if they convince caregivers to recommend proton beam therapy over radical surgery or referral of patients using proton beam therapy instead of radiotherapy using photons,” Merchant said. “The results of this trial are important for pediatric radiation oncology because they realize a goal to show the benefit of proton therapy over photon therapy. We’ve been waiting years for these results.”
Thomas Merchant, DO, PhD, Department of Radiation Oncology chair, led research into the treatment of craniopharyngioma.
scientific highlights
Anchoring domain in chimeric antigen receptors improves immunotherapies
Scientists can reprogram immune cells to target cancer cells by adding engineered chimeric antigen receptor (CAR) proteins to their surface. Researchers at St. Jude have found a way to “anchor” the CAR molecule within immune cells by adding four specific amino acids to the end of the conventional CAR. The molecular anchor concept was designed to improve CAR-based immunotherapies, which have demonstrated success in certain cancers, such as relapsed leukemia, but have yet to deliver that same success in solid tumors.
The addition of a molecular anchor enabled the immune cells to be
more easily activated and kill cancer cells more effectively than their conventional counterparts. In a paper published in Nature Biotechnology, the team demonstrated that the anchored CARs increased the survival of multiple solid tumor models, including lung, bone, and brain cancers.
“The anchor domain discovery is easily translatable into early phase clinical testing; it doesn’t require any other new technology,” said senior author Stephen Gottschalk, MD, Department of Bone Marrow Transplantation and Cellular Therapy chair. “We strongly believe this approach needs testing in the clinic because no one
has tried it before, and it looks very promising from our preclinical work.”
CARs are a key molecule in the cancerkilling process. The outside of the molecule recognizes a protein on the cancer cell and forms a complex of molecules and proteins between the two cells, called an immune synapse. As the immune synapse forms, signals from the CAR trigger the immune cell to activate and kill the cancer cell.
However, these communications can be muddled, making it challenging for conventional CAR T cells and natural killer cells to interpret.
“Our approach is different because it focuses on organization,” explained first and corresponding author Peter Chockley, PhD, postdoctoral fellow in the Department of Bone Marrow Transplantation and Cellular Therapy. “CAR immune cells form synapses that are very disorganized. The anchoring domain we added organizes internal scaffolding proteins, making a better synapse, and then brings in other extant signaling proteins. The simple addition of organization improves CARs dramatically.”
By adding the four amino acids to the CAR sequence, the group tuned the signals within the immune synapse. The amino acids specifically bind the protein Scribble, which is involved in creating an ordered scaffolding system of other proteins. This scaffolding system enables efficient communication and an effective immune response to tumors.
“The most attractive thing about this approach,” said Gottschalk, “is that you can add the anchor domain to any CAR or other antigen-specific receptor you like. The engineering is simple and easily translatable to a broad range of cellular immunotherapies that are currently being developed.”
Senior author Stephen Gottschalk, MD (left), and corresponding author Peter Chockley, PhD (right), demonstrated that anchored CARs increased the survival of multiple solid tumor models.
Unraveling predisposition to bilateral Wilms tumor
Children with bilateral Wilms tumor have a tumor in each of their kidneys — a condition that strongly suggests an underlying genetic or epigenetic predisposition driving the disease. Treating bilateral Wilms tumor is complicated. When Wilms tumor occurs in just one kidney, surgeons can remove the entire organ, but when the disease is bilateral, removing both kidneys is not the optimal approach, as it would eliminate renal function. Instead, patients with bilateral Wilms tumor first receive chemotherapy to shrink the tumors as much as possible and then undergo organsparing surgery to remove the tumors without removing the kidneys.
“We see a lot of patients with bilateral Wilms tumor here at St. Jude, offering these organ-sparing surgeries so that patients do not become dependent on
dialysis and require kidney transplants,” said co-corresponding author Andrew Murphy, MD, Department of Surgery. “This means we were also uniquely privileged to have access to patient tissue samples, which enables us to do this research to establish the relative frequencies of different modes of predisposition.”
The researchers gathered the largest cohort reported for bilateral Wilms tumor and conducted whole-exome, whole-genome, RNA-sequencing, and DNA-methylation analyses to unravel the factors involved in predisposition to this type of cancer. Published in Nature Communications, their study revealed the predominant genomic events predisposing patients to bilateral Wilms tumor. These include prezygotic (before fertilization) germline (inherited) variants detectable in
blood samples, such as WT1, NYNRIN, TRIM28, and BRCA-related genes.
The researchers also identified an epigenetic mechanism, post-zygotic (in the early embryo) hypermethylation at the gene location coordinates 11p15.5 H19/ICR1, that predisposes patients to bilateral Wilms tumor. DNA methylation is a fundamental biologic process in which methyl groups are added to the cytosine residues of DNA. The process guides the instructions for how gene expression is regulated. In this case, abnormal hypermethylation at chromosome 11p15.5 inherited from the mother leads to increases in gene expression. In bilateral Wilms tumor, this phenomenon, also called loss of imprinting at 11p15.5, leads to the increased expression of IGF2, one of the major genes previously implicated in cancer predisposition.
The researchers also found evidence of hypermethylation at 11p15.5 on chromosomes in cells within the blood of patients with Wilms tumor, not just in the tumor or the non-diseased kidney. The hypermethylation signature in the bilateral disease was a higher level than that in unilateral Wilms tumor or in healthy individuals.
“Realizing that a pair of bilateral tumors from the same patient shared almost no somatic mutations, we suspected there were several ways genomes predisposed patients to develop bilateral Wilms tumor, but it is essential to drive the research forward to holistically determine their frequency and interplay across a large cohort,” said co-corresponding author Xiang Chen, PhD, Department of Computational Biology. “We needed to study germline and post-zygotic factors by integrating analyses, and we have now thoroughly characterized the landscape of predisposing events.”
The work has implications for counseling patient families, guiding treatment decisions, and informing the design of future clinical trials.
Xiang Chen, PhD, Department of Computational Biology and Andrew Murphy, MD, Department of Surgery, are co-corresponding authors of a study that sheds light on predisposition to bilateral Wilms tumor.
scientific highlights
A healthy lifestyle may reduce mortality risk in adult survivors
An analysis of childhood cancer survivors by St. Jude scientists shows that while adult survivors of childhood cancer experience four times the risk of death as compared to that of the general population, steps can be taken to reduce that risk. Published in The Lancet, the St. Jude analysis showed that survivors have a 20% lower mortality risk when they practice a healthy lifestyle. Mitigating factors included maintaining a healthy weight through diet and exercise, eschewing smoking, and minimal alcohol consumption.
Survivors with hypertension or diabetes had a significantly higher mortality rate than survivors without those conditions. However, these conditions are also modifiable through healthy
lifestyle changes and effective treatments from physicians.
Treatments for pediatric cancers have improved, vastly increasing survival and reducing toxicity. More than 85% of U.S. patients are effectively cured of their primary tumor after treatment. This increased success has led to a growing survivor population reaching adulthood.
This study used data from the Childhood Cancer Survivor Study (CCSS), a national collaborative housed at St. Jude. By comparing the data from thousands of CCSS participants to that from the public, the investigators found that even decades after anticancer treatment, survivors experience four times the expected mortality risk of the general population.
“We identified that long-term survivors of childhood cancer are experiencing a rate of death above what would be expected for the general aging population,” explained first and corresponding author Stephanie Dixon, MD, MPH, Department of Oncology. “We were the first to find that these excess deaths are predominantly due to the same leading causes of death as in the general population, including second cancers, heart disease, cerebrovascular disease or stroke, chronic liver and kidney disease, and infectious causes of death, experienced at a younger age and higher rate in childhood cancer survivors.”
The CCSS is the largest cohort of childhood cancer survivors in North America, representing an estimated 20% of survivors in that region. The researchers used this cohort’s vast data to isolate variables affecting survivor mortality statistically. Their work demonstrated that even when common confounders, such as sociodemographic features, were controlled for, the gap between survivors and the public persisted — but so did the protective effects of a healthy lifestyle.
“Independent of prior treatment and sociodemographic factors, a healthy lifestyle and absence of cardiovascular risk factors, such as hypertension and diabetes, were associated with reduced health-related mortality risk,” said Dixon. “This suggests that while continued efforts to reduce treatment intensity and improve five-year survival are needed, future research should also focus on tailoring interventions for modifiable lifestyle and cardiovascular risk factors to survivors to reduce chronic disease development and extend their lifespans.”
Co-author Yutaka Yasui, PhD, senior author Greg Armstrong, MD, MSCE, and first and corresponding author Stephanie Dixon, MD, MPH, showed that a healthy lifestyle can reduce mortality in survivors.
PROGRAMS
Comprising five research programs and nine shared resources, the Comprehensive Cancer Center is designed to foster interdisciplinary basic and translational research, clinical trials, and population science focused on childhood cancer and survivorship.
The National Cancer Institute (NCI) supports 72 Cancer Centers in the United States. The St. Jude Comprehensive Cancer Center, under the direction of Charles W. M. Roberts, MD, PhD, is the first and only NCI-designated Comprehensive Cancer Center solely focused on pediatric cancer. Charles G. Mullighan, MBBS(Hons), MSc, MD, serves as deputy director.
Shared resources include Bioinformatics and Biotechnology, Biostatistics, Cell and Tissue Imaging, Center for In Vivo Imaging and Therapeutics, Cytogenetics, Flow Cytometry and Cell Sorting, Pharmacokinetics, Protein Production, and Transgenic/Gene Knockout.
CANCER BIOLOGY PROGRAM
Co-leaders:
Douglas Green, PhD
Richard Kriwacki, PhD
The diverse nature of pediatric cancers, coupled with the complex molecular, genetic, and developmental contexts in which they form, necessitates a broad spectrum of basic research to build a strong foundation for translational studies. This program aims to explore and understand the fundamental biology of cancer. In working toward this goal, program members lead integrated and transdisciplinary efforts to define pathways related to cancer, identify driver mutations and genetic anomalies as new targets for translation into clinical trials, and advance understanding of the cancer microenvironment as a route to therapy.
CANCER CONTROL & SURVIVORSHIP PROGRAM
Co-leaders:
Gregory Armstrong, MD, MSCE
Kirsten Ness, PT, PhD, FAPTA
As treatments for childhood cancers improve, the number of long-term survivors of childhood cancer increases. This multidisciplinary program strives to improve the quality of life of individuals surviving childhood cancer by identifying and reducing treatment sequelae and promoting health-protective behaviors through conducting innovative clinical, genetic, and observational research. Leading two of the world’s largest pediatric survivorship research studies, the St. Jude Lifetime Cohort Study and the Childhood Cancer Survivor Study, program members are researching a wide range of health-related and quality-of-life outcomes.
Senior Leadership
Charles W. M. Roberts, MD, PhD Director
Charles Mullighan, MBBS(Hons), MSc, MD Deputy Director
Elizabeth Fox, MD, MS Associate Director, Clinical Research
Melissa Hudson, MD Associate Director, Population Sciences
DEVELOPMENTAL BIOLOGY & SOLID TUMOR PROGRAM
Co-leaders:
Michael Dyer, PhD
Alberto Pappo, MD
HEMATOLOGICAL MALIGNANCIES PROGRAM
Co-leaders:
Charles Mullighan, MBBS(Hons), MSc, MD
Ching-Hon Pui, MD
NEUROBIOLOGY & BRAIN TUMOR PROGRAM
Co-leaders:
Suzanne Baker, PhD
Giles Robinson, MD
Some of the most devastating and poorly understood cancers that affect children arise in the peripheral nervous system, muscles, and bones. Members of this program are working to understand how the normal development of these tissues goes awry, resulting in malignant diseases such as neuroblastoma, sarcomas, and retinoblastoma. Research in this program extends from basic mechanistic development studies to therapeutic studies in preclinical models and, ultimately, to testing new anti-cancer agents in clinical trials.
The program’s overall goal is to improve the cure rates for childhood leukemias and lymphomas while minimizing treatment-related adverse effects. This established, highly interactive, transdisciplinary program has a long track record of significant discoveries in cancer biology. Translation of these findings into new diagnostic and treatment approaches has changed the standard of care for children with hematological malignancies. The members of this program have used whole-genome approaches to identify novel leukemia subgroups and the mutations that drive these diseases and translate these findings into innovative precision-medicine studies worldwide. The same genetic tools are being used to uncover genetic variations that dictate susceptibility to childhood cancers, as well as the response of patients to essential chemotherapies.
Brain tumors are the leading cause of cancer-related death in children. The goal of the Neurobiology & Brain Tumor Program is to improve survival and reduce morbidity for children with brain tumors by developing effective, relatively nontoxic therapies through a better understanding of pathogenesis. By integrating the latest genomic and genetic technologies into studies of the developing nervous system, members of this program are efficiently translating laboratory findings into opportunities for new treatments. Key advances include identifying the cells of origin of important pediatric brain tumors and modeling some of the most aggressive forms of these tumors, including highgrade gliomas. Close collaboration among the laboratory and clinical members of the program enables the rapid translation of high-throughput drug screens of mouse models to clinical trials.
Julie Park, MD
Associate Director, Translational Research
Shondra PruettMiller, PhD
Associate Director, Shared Resources
Carlos RodriguezGalindo, MD
Co-Associate Director, Outreach
Dana Wallace, MS
Associate Director, Administration
Carolyn Russo, MD
Associate Director, Diversity, Equity & Inclusion
Gerald Zambetti, PhD
Associate Director, Education & Training
The affiliate clinics support participant recruitment for clinical trials and the geographic extension of St. Jude clinical care. The St. Jude Affiliate Program has a two-fold mission:
The eight affiliate clinics in the Southeast and Midwest regions of the United States expand the catchment area for St. Jude–led clinical trials.
TO EXTEND ST. JUDE CARE CLOSER TO A CHILD’S HOME COMMUNITY
TO ENCOURAGE ENROLLMENT IN ST. JUDE CLINICAL RESEARCH TRIALS
Delivering specialized pediatric oncology care between multiple sites requires effective communication and coordination of care. In the past fiscal year, the Affiliate Program expanded our navigation program to include nurse navigators in addition to the existing patient navigator. This program has improved communication and fostered a culture of understanding for families transitioning between multiple health care facilities in our pediatric oncology network.
ST. JUDE AFFILIATE SITES
Baton Rouge, LA
Our Lady of the Lake Children’s Hospital – Our Lady of the Lake Regional Medical Center
Medical Director • Jeffrey Deyo, MD, PhD
Kacie Sims, MD
Sakshi Bami, MD
Katherine Helo, NP
Jessica Templet, PA-C
Joseph Kent, PA
Charlotte, NC
Novant Health Hemby Children’s Hospital
Medical Director • Christine Bolen, MD
Jessica Bell, MD
Jenny McDaniel, MD
Joanne McManaman, MD
Felipe Bautista, MD
Holly Edington, MD
Courtney Saine, NP
Jennifer Weisner, NP
Andria Kokoszka, NP
Courtney Carr, NP
Administration
Carolyn Russo, MD
Medical Director
Jennifer Morgan, MSN Nursing Director
Nica Graunke, MPH Clinical Operations Director
Linda Stout, MD Rotating Physician
Huntsville, AL
Huntsville Hospital for Women & Children – Huntsville Hospital
Medical Director • Marla Daves, MD
Sana Mohiuddin, MD
Jamie Musick, MD
Heidi Simpson, NP
Megan Vann, NP
Emily Clawson, NP
Ameila Jantz, NP
Johnson City, TN
Niswonger Children’s Hospital – Ballad Health
East Tennessee State University
Medical Director • Marcela Popescu, MD
Myesa Emberesh, MD
Meghan Srinivas, MD
Angela Willocks, RN, MSN, CFNP
Lauren Wyatt, NP
Amy Shaw, NP
Peoria, IL
OSF HealthCare Children’s Hospital of Illinois
University of Illinois College of Medicine at Peoria
Medical Director • Brinda Mehta, MD
Pedro de Alarcon, MD
Prerna Kumar, MD
Mary Beth Ross, MD, PhD
Jennifer Light, MD
Kay Saving, MD
Beth Speckhart, NP
Sue Gaitros, NP
Diana Simmons, NP
Dana Stephens, NP
Shreveport, LA
Ochsner LSU Health – Shreveport
Medical Director • Ayo Olanrewaju, MD
Elizabeth Wadhwa, MD
Diana Townsend, NP
Amanda Saunders, NP
Springfield, MO
Mercy Children’s Hospital – Springfield
Mercy Health System
Medical Director • Francisca Fasipe, MD
Batool El-Atoum, MD
Carolyn Sullivan, NP
Danielle Lee, NP
Tulsa, OK
The Children’s Hospital at Saint Francis
Medical Director • Greg Kirkpatrick, MD
Martina Hum, MD
Shilpa Shukla, MD
Jill Salo, MD
Sara Mednansky, MD
Cori Ryan, NP
Allison Taylor, NP
In 2023, the St. Jude Global initiative created many growth opportunities and strengthened engagement through the St. Jude Global Alliance.
As many of the models and projects of the regional and transversal programs reached maturity, a new focus was initiated in India, with institutions in the country serving as crucial mentors and facilitators for both the Eastern Mediterranean and Asia Pacific regional programs. Additionally, St. Jude Global identified rehabilitation services, surgery, radiation oncology, and cellular therapy as growing areas for cross-regional work and partnerships within the institution have enabled those new programs to progress. Last year, the initiative also saw the revitalization of the Global Hematology Program under new leadership, which has increased partnerships in sickle cell disease in Africa, Brazil, and India as part of our effort to expand access to quality care for children with catastrophic diseases.
St. Jude Global and the St. Jude Global Alliance celebrated their milestone five-year anniversaries in 2023. The theme of the annual Alliance Convening was “Alliance Now: World of Knowledge,” and it encouraged and enabled attendees to build, share, and generate knowledge in more than 40 general and interactive breakout sessions hosted by St. Jude Global programs. As participation in the Alliance has grown to more than 300 medical institutions and foundations in over 80 countries, it is critical to analyze how the innovative collaboration style of the Alliance is creating a new model of trust and empowerment in global child health, which in turn is enabling the practice of new methodologies and advancing knowledge at all levels of health systems.
RESEARCH
The St. Jude Global research core developed 77 projects in 13 categories in 2023. These projects include clinical trials; adapted treatment guidelines; and quality improvement, implementation, and observational studies. More than 100 countries are participating in these research projects and incorporating a growing portfolio of research methods at their institutions. Qualitative research has been a significant expansion area as more programs and Alliance members seek to engage and build understanding.
Examples of global research collaboration efforts include the DIVIA Program implemented through the St. Jude Blue Sky mechanism, which aims to develop innovative and transformative diagnostic methods using novel sequencing technologies and cloud-based computing in resource-limited settings; the implementation of Pediatric Early Warning Scores and early administration of antibiotics for children at risk of clinical deterioration in resource-limited centers; the development and implementation of sustainable programs for newborn screening and care for children with sickle cell disease; the development of novel therapies and adapted guidelines; policy research; studies on financial toxicity, patient communication, and implementation of palliative care; and pain reduction models in low- and middle-income countries (LMICs) and diverse cultures, among others.
St. Jude Global continues to collaborate with the St. Jude Comprehensive Cancer Center Clinical Trials Administration, in particular in launching GLOBOTRK, a phase 2 study of entrectinib as a single-agent frontline therapy for young children with NTRK or ROS1 fusion–positive brain malignancies, which will open at St. Jude and
member sites in Brazil, Egypt, India, Jordan, and Peru, thereby creating a model for global collaborations in drug development and facilitating access to novel therapies for children in countries with limited resources.
EDUCATION AND DEVELOPMENT
One essential factor in achieving the St. Jude Global mission is creating educational and professional development opportunities for the global health care workforce. Developing and facilitating training materials, coursework, and assessments has also generated substantial data and motivated numerous collaborative projects based on the experiences and mentorship. The St. Jude Global Academy offers online learning through Cure4Kids and Academy seminars, hybrid educational initiatives combining online and presential experiences. In 2023, the St. Jude Global Academy worked with St. Jude Global program teams to offer in-person courses in palliative care, neuro-oncology, critical care, nursing, and infectious diseases. Advanced clinical education is provided by regional fellowship programs in pediatric hematology and oncology in Latin America, Eastern Mediterranean, and China; fellowship training programs in pediatric palliative care, neuro-oncology,
and critical care are also offered in those regions. At the end of 2023, nearly 800 individuals had been trained through the St. Jude Global Academy seminars, and 51 fellows had participated in those programs.
The fifth cohort of the Global Scholars Program, which includes 10 new scholars, began their coursework in the summer of 2023. This year, the program launched the Global Scholars Projects; the projects are designed to affect system changes that will enhance the treatment and care of children worldwide and involve continued mentorship from multiple St. Jude departments and St. Jude Global programs.
CAPACITY BUILDING
St. Jude Global continues to expand program offerings to Alliance members in areas identified as significant gaps in patient care in their regions. The SJCARES implementation platform is a suite of tools to improve capacity and quality of care. As of the end of 2023, the SJCARES Registry is active in 146 institutions, contributing data on approximately 7,000 patients. The Registry is a viable solution for measuring and tracking the impact of interventions and is considered one of the most reliable ways for the global health community to begin comprehending the breadth of disease burden in LMICs. Worldwide implementation of PrOFILE (Pediatric Oncology Facility Integrated Local Evaluation), a comprehensive selfevaluation tool for health services, has grown to include 171 assessments; institutional and national workshops are facilitating the data review and strategic planning. The ARIA Guide, a platform with adapted pediatric cancer treatment guidelines, is expected to launch in 2024 with the first set of consensus guides. Global Packages,
which are quality improvement and implementation science packages of interventions, continue to deliver specific supportive-care interventions. To strengthen health systems and create paths for national capacity, the Systems and Policies tools, including C5, the Policy Monitor, and the NCCP Digest, provide governments and nongovernmental actors the resources for national cancer control planning. The National Cancer Control Planning integrating Children, Adolescents, and Young Adults is a policy science–driven workshop series delivered in four languages to help ministries develop national cancer control plans that include childhood cancer. During 2023, 17 ministry-led country teams participated in the first workshop series.
WHO COLLABORATIONS
St. Jude Global and the World Health Organization (WHO) continued to strengthen their partnerships and develop St. Jude’s role as the first and only Collaborating Centre for Childhood Cancer.
September marked the five-year anniversary of the Global Initiative for Childhood Cancer (GICC) launch, which is now active in more than 70 countries and has provided 165 deliverables through the CureAll technical package. The anniversary was recognized at the United Nations (UN) Second High Level Meeting on
Universal Health Coverage in which St. Jude and the WHO joined the Permanent Mission of Slovakia to the UN to host the “CureAll Implementation Advancing Toward UHC Realization and Bridging the Survival Gap in Childhood Cancer” side event to further generate political support to elevate awareness for, and action on, childhood cancer through actions such as promoting more equitable cancer policies and accelerating implementation of the GICC by activating stakeholders and nongovernment actors.
Development of the Global Platform for Access to Childhood Cancer Medicines continues with the initiative entering the pilot phase. Six countries (Ecuador, Jordan, Mongolia, Nepal, Uzbekistan, and Zambia) have been identified to co-design the pilot phase of the project. In April 2023, St. Jude hosted a meeting of representatives of the ministries of health and Alliance members from each of the pilot countries, as well as staff from the WHO, UNICEF (United Nations International Children’s Emergency Fund), Pan American Health Organization Strategic Fund, International Society of Pediatric Oncology, and Childhood Cancer International to facilitate the exchange of best practices and to discuss strategies to address end-to-end needs relevant for access to childhood cancer medicines. The first-of-its-kind meeting represented an opportunity for all stakeholders to work together to co-design the platform process and address challenges for implementation. By the end of 2023, the Platform had completed the tender process for the prioritized essential medicines through UNICEF. The Platform is expected to launch in 2024, creating transformational opportunities for learning and innovation and paving the way to scale to more countries and serve more children.
The St. Jude Children’s Research Hospital Graduate School of Biomedical Sciences (Graduate School) comprises three degree-granting programs:
01
DOCTORATE OF PHILOSOPHY IN BIOMEDICAL SCIENCES (PHD-BMS)
Training young scientists to advance our understanding of the molecular basis of disease and therapy
02
MASTER OF SCIENCE IN GLOBAL CHILD HEALTH (MS-GCH)
Developing a global community of agents of change and leaders dedicated to improving children’s health worldwide
03
MASTER OF SCIENCE IN CLINICAL INVESTIGATIONS (MS-CL)
Training clinicians and medical professionals to perform clinical research and conduct clinical trials.
Approximately 210 faculty members and staff at St. Jude are now formal Graduate School faculty members involved in teaching, mentoring, serving on committees, and continuing to enhance the school’s future. In 2023, 90 PhD-BMS students, 31 MS-GCH students, and 21 MS-Cl students were actively enrolled.
In January 2023, Steven Varga, PhD, began his tenure as Dean of the Graduate School. Varga is also a member of the Department of Infectious Diseases. Before coming to St. Jude, he served as the Associate Dean of Academic Affairs and Graduate Student Development and as a professor in the Departments of Microbiology and Immunology and Pathology at the University of Iowa. Varga has over 10 years of leadership experience in graduate education.
Drawing on the deep expertise of a leading biomedical research faculty focused on the eradication of catastrophic childhood diseases and state-of-the-art infrastructure and technological support available at St. Jude, the PhD-BMS Program has now graduated 15 doctoral awardees, who have begun to contribute to diverse fields, including professional and industry research, scientific policy, academic postdoctoral studies, scientific writing and communications, and faculty at St. Jude. In the spring of 2023, in response to the growth and maturation of the program, Wilson Clements, PhD, associate member in the Department of Hematology, was appointed Associate Dean of the PhDBMS Program; Cassandra VanDunk, PhD, was recruited as Assistant Dean from Northwestern University; and Alex Frawley was hired as a Program Specialist. In the fall of 2023, the PhD-BMS Program welcomed its largest class yet of 21 matriculants
and accepted its first two transfer students under the guidance of newly recruited faculty members.
Led by Associate Dean Shaloo Puri, MBBS, DTCD, MPH, MPA, and Assistant Dean Julie Laveglia, the MS-GCH Program has a mission to provide transformative education, facilitate collaborative opportunities, build capacities, and cultivate a diverse community of agents of change with the overall aim of enhancing equity, access, and quality of health care for children globally. The program completed its fourth academic year in 2023 and admitted another cohort of 10 health care professionals. The Winter Intersession returned to an in-person format in January 2023, with 20 students attending leadership, management, and communication workshops on campus. In May, the third cohort participated in the Commencement ceremony to receive their diplomas. During the summer, five cohorts (students and alumni) came to Memphis to participate in Orientation, Summer Intersession, Professional Development, Convocation, and Commencement for two weeks. The MS-GCH Program has 29 alumni living in 21 countries and has identified a Program Specialist to join the staff in 2024.
Co-led by Associate Deans Patricia Flynn, MD, and Victor Santana, MD, and Assistant Dean Sally Utech, PhD, the MS-CI Program provides students with a transformative education that will create a cadre of health care professionals who are adept at designing, conducting, and reporting clinical investigations that promote human health. The program creates a unique opportunity to understand these concepts in a pediatric and young adult research setting, leveraging the expertise of St. Jude faculty and staff
in undertaking clinical research. The MS-CI Program graduated its first class of four students in 2023, all remaining active in clinical research and patient care. The program also matriculated its third class of nine students in the fall of 2023, composed of postdoctoral fellows, St. Jude faculty, and research and medical staff members. The growth of the program necessitated an expansion of the program’s staffing. At the end of 2023, Jimmi Lampley joined the staff as the Program Specialist.
Renovation of the Graduate School space in the Marlo Thomas Center began in the winter of 2023, as
additional administrative offices and cubicles are needed to accommodate the Graduate School’s growing staff. The Graduate School has leased new space for student use in the Inspiration4 Advanced Research Center, doubling the previous study capacity. A new student activity center space is also being leased on the plaza level of the Danny Thomas Research Tower.
The Graduate School spent much of 2023 preparing for its initial application for membership to the Southern Association of Colleges and Schools Commission on Colleges (SACSCOC) in early 2024. This crucial step will
begin the accreditation process, which ensures a school maintains the highest educational standards, as judged by external evaluators.
Finally, none of these activities and accomplishments would have been possible without the support of our Board of Trustees. The Graduate School relies heavily on the advice and insight this group of dedicated volunteers provides. In 2023, Sarah Larsen, PhD, vice provost and dean of the Graduate School at the University of Houston, joined the Board of Trustees and will contribute her extensive knowledge of graduate education.
Graduate School Board of Trustees
Steven J. Bares, PhD, MBA (Chair)
Former President and Executive Director Memphis Bioworks Foundation
William E. Troutt, PhD (Vice Chair)
President Emeritus Rhodes College
Gabriel G. Haddad, MD
Chairman, Department of Pediatrics University of California San Diego
James E. K. Hildreth, PhD, MD
President and Chief Executive Officer Meharry Medical College
Sarah C. Larsen, PhD
Vice Provost and Dean of the Graduate School
Interim Dean, Graduate College of Social Work Professor of Chemistry University of Houston
James R. Downing, MD
President & CEO
St. Jude Children’s Research Hospital
J. Paul Taylor, MD, PhD
Executive Vice President and Scientific Director
St. Jude Children’s Research Hospital
Biostatistics
CHAIR
Motomi Mori, PhD, MBA1, Endowed Chair in Biostatistics
Design and analysis of early phase clinical trials, biomarker discovery and validation, risk prediction models
MEMBERS
Cheng Cheng, PhD1
Statistical methods in cancer biology, clinical & translational studies
Meenakshi Devidas, PhD, MBA1,2 Biostatistics, pediatric hematology and oncology
Guolian Kang, PhD1
Statistical genetics/genomics, modeling of complex data
Yimei Li, PhD1
Statistical analysis of complex imaging data, survival data analysis & clinical trial design
Metabolic imaging, MR spectroscopy, molecular MRI, & cancer metabolism
Kiel Neumann, PhD1
Translational Imaging and radiopharmaceutical development
Devendra Sawant
Molecular imaging, radionucleotide therapy, and cancer biology
INSTRUCTOR
Soniya Pinto, MD
Imaging of neurologic complications of CAR T–cells therapy
Epidemiology & Cancer Control
CHAIR
Gregory Armstrong, MD, MSCE1, Endowed Chair in Epidemiology & Cancer Control Cancer survivorship & long-term follow-up
MEMBERS
Heather Brandt, PhD1 HPV vaccination and cervical cancer screening
I-Chan Huang, PhD
Patient-reported outcomes measurement after pediatric cancer
Melissa Hudson, MD1,2, The Charles E. Williams Endowed Chair of Oncology – Cancer Survivorship Health outcomes after childhood cancer
Kirsten Ness, PT, PhD, FAPTA1, Endowed Chair in Cancer Survivorship
Physical health and accelerated aging in childhood cancer survivors
Leslie Robison, PhD4
Yutaka Yasui, PhD1 Genetics & risk of therapyrelated outcomes
ASSOCIATE MEMBERS
Nickhill Bhakta, MD, MPH1,2
Global health, survivorship, epidemiology, childhood leukemias
Tara Brinkman, PhD1,2
Psychosocial outcomes of pediatric cancer
Daniel Mulrooney, MD, MS1,2 Cardiovascular outcomes of cancer therapy
Zhaoming Wang, PhD1
Genetic epidemiology of pediatric cancer & survivorship
ASSISTANT MEMBERS
Angela Delaney Freedman, MD2 Hypothalamic/pituitary dysfunction in childhood cancer survivors
Yadav Sapkota, PhD
Genomic basis of pediatric cancer outcomes
Carmen Wilson, PhD1
Late effects of childhood cancer therapy
Genetics
MEMBERS
Alessandra d’Azzo, PhD1, Jewelers
Charity Fund Endowed Chair in Genetics and Gene Therapy Lysosomal/proteasomal function in health & disease
Gerard Grosveld, PhD4
Global Pediatric Medicine
CHAIR
Carlos Rodriguez-Galindo, MD1, Executive Vice President, Four Stars of Chicago Chair in International Pediatric Outreach Global medicine, pediatric solid tumors
MEMBERS
Miguela Caniza, MD, MPH1 Global health, infection care and control
Meenakshi Devidas, PhD, MBA1 Biostatistics, pediatric hematology and oncology
Jane Hankins, MD, MS1 Sickle cell disease, transition to adult care & health outcomes during adolescence & young adulthood
Sima Jeha, MD1
Global health, childhood leukemias, developmental therapeutics
Gaston Rivera, MD4
Victor Santana, MD1, Charles B. Pratt Chair in Solid Tumor Research Global health, novel therapeutics, neuroblastoma, research ethics
ASSOCIATE MEMBERS
Asya Agulnik, MD, MPH1 Global health, pediatric oncocritical care, quality improvement
Nickhill Bhakta, MD, MPH1 Global health, survivorship, epidemiology, childhood leukemias
Paola Friedrich, MD, MPH1 Global health, health disparities, health services, pediatric solid tumors
Catherine Lam, MD, MPH1 Global health, health systems, pediatric solid tumors
Ibrahim Qaddoumi, MD, MS1
Global health, brain tumors, telemedicine, retinoblastoma
Phillip Doerfler, PhD Improving the safety of gene and cell therapy
ADJUNCT MEMBERS
Kenneth Ataga, MD Sickle cell disease and related hemoglobinopathies, thalassemia and other red blood cell disorders
Francisca Fasipe, MD Leukemia, lymphoma, hemoglobinopathies, and solid tumors
Marcela Popescu, MD Clinical pediatric hematology
Host–Microbe Interactions
CHAIR
Victor J. Torres, PhD1, Albert and Rosemary Joseph Endowed Chair in Host-Microbe Interactions Interactions between antimicrobial-resistant bacteria and their mammalian host
MEMBERS
Elaine I. Tuomanen, MD1 Pathogenesis of pneumococcal infection
Charles O. Rock, PhD5
Jason W. Rosch, PhD1 Bacterial genomics & pathogenesis
Stacey L. Schultz-Cherry, PhD1 Pathogenesis of influenza & enteric virus infections
Paul G. Thomas, PhD1 Mechanisms of antiviral and antitumor immunity
Richard J. Webby, PhD1 Influenza virus pathogenicity
ASSOCIATE MEMBER
Charles J. Russell, PhD1 Respiratory viruses: disease, cures, and prevention
Immunology
INTERIM CHAIR
Terrence L. Geiger, MD, PhD1,2, Endowed Chair in Pediatrics
T-cell regulation, adoptive immunotherapy
VICE-CHAIR
Thirumala-Devi Kanneganti, PhD1, Rose Marie Thomas Endowed Chair Mechanisms of host defense & inflammation
MEMBERS
Hongbo Chi, PhD1, Robert G. Webster Endowed Chair in Immunology
Immune signaling and metabolism
Peter Doherty, PhD4, Nobel Laureate
Douglas Green, PhD1, Peter C. Doherty Endowed Chair in Immunology
Cell death, autophagy, and immune function
Benjamin Youngblood, PhD1
T-cell memory differentiation, exhaustion, and immunotherapy
ASSOCIATE MEMBERS
Yongqiang Feng, PhD1
Epigenetic & transcriptional basis of T-cell immunity
Maureen McGargill, PhD3
ASSISTANT MEMBER Bo Hu, PhD
Neuroimmunology and interrogations of neuroimmune interactions in health and disease
Infectious Diseases
CHAIR
Octavio Ramilo, MD1, Endowed Chair in Infectious Diseases Viral respiratory infections and early life immunity
MEMBERS
Miguela Caniza, MD, MPH1,2 Global health, infection care and control
Patricia Flynn, MD1, Arthur Ashe Endowed Chair in Pediatric AIDS Research HIV/AIDS in children & infections in children with cancer
Aditya Gaur, MD, MD, MBBS1 Clinical research in HIV prevention & treatment
Hana Hakim, MD Infection prevention and control
Julia Hurwitz, PhD1 Pathogen/vaccine-induced immunity, nuclear hormones
Steven Varga, PhD, Endowed Chair – Dean St. Jude Children’s Research Hospital Graduate School of Biomedical Sciences Immunopathogenesis of respiratory viruses
Robert Webster, PhD4
ASSOCIATE MEMBERS
Elisabeth Adderson, MD1 Epidemiology & treatment of infections
Katherine Knapp, MD Perinatal HIV exposure/ HIV clinical trials
Gabriela Marón Alfaro, MD1
Infectious complications in transplant patients
Nehali Patel, MD1 HIV clinical care
Megan Wilkins, PhD2
Clinical & research psychological services for youth with HIV/AIDS
Joshua Wolf, PhD, MBBS1 Prediction, prevention, & treatment of infections in immunocompromised children
ASSISTANT MEMBERS
Diego Hijano, MD, MSc1
Host–pathogen interactions of respiratory virus
Ellie Margolis, MD, PhD1
Microbiome dynamics in immunocompromised patients
Sheena Mukkada, MD, MPH1,2 Global health, infection care and control
INSTRUCTORS
Timothy Flerlage, MD3
Amanda Green, MD
Human immune responses to co-infection and chronic viruses, including HIV and CMV
RESEARCH ASSOCIATE Christopher Radka, PhD3
ADJUNCT MEMBERS
Nicholas Hysmith, MD, MS, FAAP
Emerging infections & hospital epidemiology
Jonathan A. McCullers, MD
Interactions between viruses & bacteria
Oncology
CHAIR
Julie Park, MD, Endowed Chair in Pediatric Oncology
Translational research to improve survival of children with cancer
MEMBERS
Gregory Armstrong, MD, MSCE1,2, Endowed Chair in Epidemiology & Cancer Control
Pediatric neuro-oncology & cancer survivorship
Justin Baker, MD3
Sara Federico, MD1
Drug development, pediatric soft-tissue sarcomas
Elizabeth Fox, MD1
Developmental therapeutics in pediatric oncology
Wayne Furman, MD4
Amar Gajjar, MD2, Scott and Tracie Hamilton Endowed Chair in the Brain Tumor Program Novel treatments for children with brain tumors
Daniel Green, MD1
Adverse hepatic, renal, and reproductive effects of therapy
Melissa Hudson, MD1, The Charles E. Williams Endowed Chair of Oncology – Cancer Survivorship Health outcomes after childhood cancer
Hiroto Inaba, MD, PhD1
New therapeutic strategies for leukemia
Sima Jeha, MD1,2
Global health, childhood leukemias, developmental therapeutics
New therapies for sarcomas & rare pediatric cancers
Ching-Hon Pui, MD1, Fahad Nassar Al-Rashid Endowed Chair in Leukemia Research
Biology & treatment of childhood leukemia
Raul C. Ribeiro, MD1
Hematological malignancies
Charles W. M. Roberts, MD, PhD1, Executive Vice President, Lillian R. Cannon Comprehensive Cancer Center Director Endowed Chair SWI/SNF (BAF) chromatin remodeling/tumor suppressor
Jeffrey E. Rubnitz, MD, PhD1 Treatment of acute myeloid leukemia
Jun J. Yang, PhD1,2, Endowed Chair in Pharmacogenomics Pharmacogenomics of anticancer agents & drug resistance
ASSOCIATE MEMBERS
Asya Agulnik, MD, MPH1,2
Global health, pediatric onco-critical care, quality improvement
Nickhill Bhakta, MD, MPH1,2 Global health, survivorship, epidemiology, childhood leukemias
These volunteers served on the Board of Governors of St. Jude Children’s Research Hospital during 2023. Officers are indicated by the titles under their names.
2023 Board of Governors
Joyce A. Aboussie
Steven J. Allen MD1
Joseph S. Ayoub Jr.
Paul J. Ayoub Chair2
Frederick M. Azar, MD
Martha Perine Beard
Robert A. Breit, MD
Terry L. Burman
Ann M. Danner2
Joseph M. DeVivo1
Lisa R. Diller, MD
James R. Downing, MD3, St. Jude President and CEO
Joseph E. Eid, MD
Fred P. Gattas III, PharmD
Judy A. Habib Vice Chair2 Chair4
Gabriel G. Haddad, MD Vice Chair4
Charles C. Hajjar
Fouad M. Hajjar, MD
Frederick R. Harris Jr., MD Secretary
J. David Karam II
Scott A. Kupor
Sharon L. McCollam
Michael D. McCoy2
Samia Melhem4
Robert T. Molinet
Neela M. Montgomery4
Ramzi N. Nuwayhid
Thomas J. Penn III
Christina M. Rashid
Kathryne G. Reeves4
Camille F. Sarrouf Jr.
Richard C. Shadyac Jr.3
Joseph C. Shaker
Joseph G. Shaker
George A. Simon II
Michael C. Simon
Tony Thomas
Richard M. Unes2
Paul H. Wein
Tama H. Zaydon
Emeritus Members
Thomas G. Abraham
Susan Mack Aguillard, MD
Mahir R. Awdeh
James B. Barkate
Jack A. Belz
Sheryl A. Bourisk
Stephen J. Camer, MD
Ann M. Danner4
George Elias Jr.
Hasan M. Elkhatib
Fred P. Gattas Jr.
Ruth C. Gaviria
Christopher B. George, MD
Paul K. Hajar
Sam F. Hamra
Frederick R. Harris
Bruce B. Hopkins
Richard J. Karam
Salli E. LeVan
Paul J. Marcus
Michael D. McCoy4
James O. Naifeh
Talat M. Othman5
Manal B. Saab
Frederick W. Smith5
Ronald A. Terry
Terre Thomas
Pat Kerr Tigrett
Richard M. Unes4
Thomas C. Wertz
Robert P. Younes, MD
Ramzi T. Younis, MD
Leah J. Domitrovic Chief Governance Officer/ Corporate Secretary
This panel of physicians and scientists, serving during 2023, fostered the institution’s development through discussion with faculty members, reports to the Board of Governors, and advice to the President and CEO on scientific and clinical research directions.
Kimberly Stegmaier, MD, Chair
Ted Williams Investigator, DanaFarber Cancer Institute
Vice Chair of Pediatric Oncology Research, Dana-Farber Institute
Co-Director, Pediatric Hematologic Malignancy Program, Boston Children’s Hospital and Dana-Farber Cancer Institute
Professor of Pediatrics, Harvard Medical School
Institute Member, Broad Institute
Dana-Farber/Boston Children’s Cancer and Blood Disorders Center
John M. Maris, MD, Vice Chair
Giulio D’Angio Professor of Pediatric Oncology
Perelman School of Medicine at the University of Pennsylvania Division of Oncology
Children’s Hospital of Philadelphia
Smita Bhatia, MD, MPH
Gay and Bew White Endowed Chair in Pediatric Oncology
Distinguished Professor, Pediatric Oncology
Vice Chair for Outcomes Research, Department of Pediatrics
Director, Institute for Cancer Outcomes and Survivorship
University of Alabama at Birmingham School of Medicine
University of Alabama at Birmingham
Carsten G. Bönnemann, MD
Senior Investigator and Chief, Neuromuscular and Neurogenetic Diseases of Childhood Section
Neurogenetics Branch, National Institute of Neurological Disorders and Stroke
National Institutes of Health
Michael J. Eck, MD, PhD
Professor of Biological Chemistry and Molecular Pharmacology
Harvard Medical School
Professor of Cancer Biology, DanaFarber Cancer Institute
David Ginsburg, MD
James V. Neel Distinguished University Professor
Departments of Internal Medicine, Human Genetics, and Pediatrics
University of Michigan Medical School
Member of the National Academy of Medicine
Member of the National Academy of Sciences
Mary K. Gospodarowicz, MD, FRCPC, FRCR (Hon)
University Professor, University of Toronto Consultant, Princess Margaret Cancer Centre
Nathanael S. Gray, PhD Member, ChEM-H
Program Leader, Small Molecule Drug Discovery for the Innovative Medicines Accelerator
Co-Director, Cancer Drug Discovery
Co-Leader, Cancer Therapeutics Research Program
Krishnan-Shah Family Professor, Chemical and Systems Biology
Stanford University
Sallie R. Permar, MD, PhD
Pediatrician-in-Chief, New YorkPresbyterian/Weill Cornell Medical Center
Nancy C. Paduano Professor and Chair, Department of Pediatrics
Professor of Immunology and Microbial Pathogenesis
Weill Cornell Medicine
Rob Pieters, MD, PhD, MSc
Board of Directors, Chief Medical Officer
Princess Maxima Center for Pediatric Oncology
Stanley R. Riddell, MD
Burke O’Reilly Family Endowed Chair in Immunotherapy
Professor, Department of Medicine
Fred Hutchinson Cancer Research Center
Joshua R. Sanes, PhD
Jeff C. Tarr Professor of Molecular and Cellular Biology
Founding Director, Center for Brain Science
Harvard University
Member of the National Academy of Sciences
Kevin M. Shannon, MD
American Cancer Society Research Professor
Roma and Marvin Auerback Distinguished Professorship in Pediatric Molecular Oncology
University of California, San Francisco
Helen Diller Family Comprehensive Cancer Center
Sarah A. Teichmann, FMedSci FRS
Head of Cellular Genetics and Senior Group Leader
Wellcome Sanger Institute
Richard M. Unes2
Paul H. Wein
Tama H. Zaydon
James R. Downing, MD, Chair President and Chief Executive Officer
Aseem Z. Ansari, PhD Chair, Chemical Biology & Therapeutics
Gregory T. Armstrong, MD, MSCE Chair, Epidemiology & Cancer Control, Oncology
M. Madan Babu, PhD, FRSC Director, Center of Excellence for Data Driven Discovery Structural Biology
Justin N. Baker, MD1 Chief, Division of Quality of Life & Palliative Care Oncology
Suzanne J. Baker, PhD Director, Division of Brain Tumor Research Developmental Neurobiology
Shari M. Capers, MBA, MHA Senior Vice President Strategic Planning & Decision Support
Catherine Corbin, AIA Senior Vice President Chief Business Innovation Officer
John D. Crispino, PhD, MBA Director, Division of Experimental Hematology
Sarah Currie, RNC, MSN, NEA-BC2 Senior Vice President Chief Nursing Executive
Andrew M. Davidoff, MD Chair, Surgery
Robyn Diaz, JD Senior Vice President Chief Legal Officer
Michael A. Dyer, PhD Chair, Developmental Neurobiology
David W. Ellison, MD, PhD Chair, Pathology
Richard S. Finkel, MD Director, Center for Experimental Neurotherapeutics Pediatric Medicine
Elizabeth Fox, MD, MS Senior Vice President, Clinical Trials Research Oncology
Amar J. Gajjar, MD Chair, Pediatric Medicine
Terrence L. Geiger, MD, PhD
Senior Vice President Deputy Director for Academic & Biomedical Operations Pathology Interim Chair, Immunology
Stephen M. Gottschalk, MD Chair, Bone Marrow Transplantation & Cellular Therapy
Douglas R. Green, PhD Immunology
Gerard C. Grosveld, PhD3 Chair, Genetics
James M. Hoffman, PharmD
Senior Vice President, Quality and Safety Chief Patient Safety Office
Melissa M. Hudson, MD Director, Division of Cancer Survivorship Oncology, Epidemiology & Cancer Control, Psychology and Biobehavioral Sciences
Charalampos G. Kalodimos, PhD Chair, Structural Biology
Pat Keel, MHA
Executive Vice President Chief Administrative & Financial Officer
Richard W. Kriwacki, PhD Structural Biology
Kevin R. Krull, PhD Chair, Psychology and Biobehavioral Sciences
1 Data represent the period from July 1, 2022, to June 30, 2023.
2 Average number of employees in 2023.
3 Data include original research articles only.
4 Data include 63 full-time St. Jude fellows and 231 rotating fellows and residents from the University of Tennessee Health Science Center or other medical schools.
5 Data represent the number of beds in use. St. Jude is licensed for 80 beds.
Translating Science into Survival Scientific Report 2024
Faculty Editorial Board
Terrence L. Geiger, MD, PhD
Tanja Mittag, PhD
Shondra Pruett-Miller, PhD
Richard J. Webby, PhD
Giles W. Robinson, MD
Editorial Direction
Erin Podolak
Jennifer L. Stripay, PhD
Photography
Justin Veneman
Creative Direction and Design
Ben Hampton
Rachel Byrd
Briana Williams
Leena Xaypanya
Contributing Writers
Emilia Asante, PhD
Josh Dodson, PhD
Alex Generous, PhD
Brian O’Flynn, PhD
Kathryn McCullough
Taylor Wewel
Editing Support
Angela J. McArthur, PhD, ELS
Prepared By Scientific Communication; Strategic Communication, Education and Outreach Department (SCEO)