Growth of Value-Based Purchasing and Contracting for Cell & Gene Therapies
Get the peace of mind and support it takes to self-fund your healthcare.
Self-insuring your healthcare benefits can open up new possibilities for your business — affording greater flexibility in how you manage your healthcare spend. Trust the expert team at QBE to tailor a solution that meets your unique needs.
We offer a range of products for protecting your assets, your employees and their dependents:
• Medical Stop Loss
• Captive Medical Stop Loss
• Organ Transplant
We'll find the right answers together so no matter what happens, your business is prepared.
By Laura Carabello
Written By Laura Carabello
By Bruce Shutan
Written By Bruce Shutan
(SIPC).
(ISSN 10913815)
Growth of Value-Based Purchasing and Contracting for Cell & Gene Therapies
Editor’s Note: This is the second of a two-part article. Part one appeared in the March edition of the Self-Insurer. Also, for information on this subject, please consider attending SIIA's Cell & Gene Therapy Stakeholder Forum, scheduled for May 27-28 in Minneapolis. Details can be accessed at www.siia.org.
IIMPROVING
ACCESS AND AFFORDABILITY
WITHOUT BANKRUPTING THE HEALTH PLAN
As research and development of these cutting-edge therapies rapidly progress, employers have an opportunity to explore and implement cost-effective approaches for making these therapies available to employees and covered dependents who need them. Strategies include paying over time, negotiating rebates based on the therapy’s effectiveness and buying stop-loss insurance.
Value-based contracts (VBCs), also referred to as risk-sharing or outcome-based agreements, are newer, evolving payment models used by pharmaceutical manufacturers and payers to connect reimbursement, coverage, or payment to a therapy’s actual outcome in a real-world setting. VBCs are performance-based reimbursement agreements between payers/plan sponsors and pharmaceutical manufacturers in which the price, quantity and nature of reimbursement are tied to agreed-upon clinical, intermediate, or economic measurable objective endpoints.
"VBCs can help provide earlier access to therapies for patients while allowing employers, health plans and payers to reduce their uncertainty regarding clinical value and help manage the risk with the therapy and overall financial impact if the therapy was not successful," explains Bob Gilkin, Senior VP, Trade and Specialty Strategy, AscellaHealth. “Additionally, pharmaceutical manufacturers can utilize VBCs to demonstrate the effectiveness of their product while sharing risk for the therapy outcome. VBCs provide a potential solution to address escalating costs and uncertain real-world effectiveness of medications.”
The chart below demonstrates a sample of Value-Based Arrangements.
Value-Based Arrangements
Lenmeldy
$4.25m
Casgevy:
$2.2m
Lyfgenia:
$3.1m
Hemgenix:
$3.5m
Zolgensma
Source: 2024 AscellaHealth
$2.32m
The world’s most expensive drug, a one-time gene treatment for metachromatic leukodystrophy (MLD), that adds a missing gene to the bone marrow cells of children, reversing the condition’s root cause in the brain. Manufacturer offers innovative outcomesand value-based agreements to both private and government insurers to ensure broad, expedient and sustainable reimbursed access.
First cell-based gene therapy employing CRISPR-based gene-editing technology for treating sickle cell disease (SCD) in patients ages 12 and older who have recurrent vaso-occlusive crises (VOCs). Approved first in the UK, followed by the US.
Another cell-based gene therapy for SCD patients aged 12 and older with a history of vaso-occlusive events.
CMS oversees the Medicaid program and introduced a pilot “access model” for expensive CGTs designating sickle cell as its initial focus CMS will negotiate an “outcomes-based agreement” that links payment for a drug to the health benefit it delivers. In sickle cell, for example, the targeted outcomes could be continued elimination of pain crises over time.
First gene therapy, one-time treatment for adults with moderate to severe bleeding disorder hemophilia B.
Manufacturer anticipates discounts, including value-based agreements with commercial payers. Manufacturer and UK's National Institute for Health and Care Excellence (NICE) have agreed the English government will pay for the treatment under an outcomes-based model.
A one-time gene therapy treatment for spinal muscular atrophy (SMA) in children under the age of two
Manufacturer will allow payments over five years, at $425,000 per year, and will give partial rebates if the treatment doesn’t work.
Gilkin advises that VBCs may potentially increase drug costs because the drug therapy costs are typically separated from overall healthcare costs and do not take into consideration the impact of the potentially greater benefits of more expensive therapies on overall patient outcomes and healthcare costs.
“Since payers are responsible for their patients' total cost of care, they need to consider the impact that CGTs may potentially reduce downstream medical utilization costs, longer-term complications and additional healthcare costs that can impact premiums for employers and patients,” he adds. “VBCs may provide an avenue where payer and pharmaceutical manufacturers are aligned and can demonstrate the positive impact of these therapies from health and economic perspectives.”
With the low volume of patients currently impacted by VBCs, Gilkin says it is unlikely that these agreements will directly impact premiums in the near future, noting, “But they hold the potential that if they prove to demonstrate positive health outcomes and show overall healthcare savings, they could positively reduce premiums in the future.”
Jakki Lynch, CCM, CMAS, CCFA, director of Cost Containment, Carbon Stop-Loss Solutions, further explains that in an effort to address the upfront high cost of care and uncertainty of the clinical outcomes, the market has seen an emergence of a broad range of innovative proposed payment models in the form of therapy product carve-outs, pay-over-time methodologies, clinical warranty templates based on retrospective payment adjustments and cost rebates tied to patient outcomes with new market intermediary solution providers that facilitate these services on behalf of all payer types.
“Outcomes-based contracts are the preference but come with ambiguity secondary to challenges on establishing transparent and verifiable outcomes criteria," she continues. "They require substantial resources for tracking outcomes and do not address the total cost of care with provider markup, administration charges and additional costs for potential complications. Certain manufacturers are accepting innovative payments for their therapies, including Luxturna, Zolgensma, Zynteglo, Hemgenix and Roctavian.”
Based on the significant cost and the complexities of the therapies, Lynch says plans need a comprehensive approach that spans the full spectrum of management strategies with specialized financial and clinical resources to manage and mitigate this emerging complex and novel risk.
“Strategic focus and risk assessment should include treatment plan validation supporting optimal member outcomes and covered plan benefits as well as optimal all-inclusive contract rates with favorable terms inclusive of value risk-based rebates,” she advises. “Claim payment integrity microanalysis with comprehensive medical record reviews ensure correct health plan or third-party administrator payments and contract terms compliance.”
Bob Gilkin
Jakki Lynch
Lynch offers the following Branch Contract Optimization + Claim Payment Integrity Review (CPIR) that demonstrates the effectiveness of bespoke specialty financial and clinical solutions to address this complex risk.
Jesse Roderick
Jesse Roderick, senior vice president of Accident & Health Claims, QBE North America. thinks that depending on the plan sponsors’ risk appetite and financial strategy, they may decide to pursue VBCs that align payment with the outcomes achieved by the therapy, making this an effective strategy to manage the high costs associated with treatments while ensuring patients receive effective care.
“These contracts can mitigate some financial risks by tying payments to the therapy's success, making it more feasible for health plans to cover therapies and thereby increasing patient access to potentially lifesaving treatments,” he imparts. “There are several value-based purchasing models in the current market that meet payer requirements. These include outcomes-based agreements, where reimbursement is linked to clinical outcomes, performance-based contracts that require meeting predefined metrics, and installment payment plans which spread the cost over time.”
OTHER NOVEL SOLUTIONS
New programs are being developed to help finance the risk of gene therapy treatments. Many pharmacy benefit managers (PBMs) and carriers offer coverage of gene therapies for a fixed per member per month (PMPM) fee. Some insurance companies are selling Netflix-like subscriptions where companies pay a monthly fee — often less than $2 a month per employee — for access to gene therapy. One large PBM covers 10 gene therapies through a subscription-type model, requiring employers to pay $1.25 PMPM, and the PBM assumes any additional financial risk.
In some instances, a subscription model can also be structured to exclude patients with pre-existing conditions. While state and federal laws prevent insurance companies from denying coverage for preexisting conditions, like the inherited diseases that gene therapies target, organizations that self-insure aren't required to cover all treatments and may reject some as a way to save money.
Years of Powering What’s Next
There are also outcomes-based agreements that offer pricing flexibility through rebates tied to the therapy’s results or a series of payments that can be made over time. These arrangements are typically negotiated with payers or PBMs that offer employers supplemental coverage. Outcomes-based contracting with pharmaceutical manufacturers typically offers milestone-based and performance-based arrangements.
Jeff Auten, director of Clinical Consulting (PharmD) at Leaf Health, concurs that multi-year performance-based contracts will be the mainstay of reimbursement models for gene therapies. “…allowing self-funded plan sponsors to spread therapy cost over several years and annual payments based on defined clinical metrics.”
Lockton, the world’s largest insurance broker, says these solutions will be challenging for employers, especially those with high employee turnover, since the member may leave the plan before the multi-year contract ends. For these payers, milestone-based or warranty-based arrangements may be appropriate, although these solutions may be challenging to operationalize since they require ongoing patient monitoring and a system that connects the provider, payer, and manufacturer to track outcomes and reconcile with the payment contract.
At Custom Design Benefits, Terri Martin and Alberta Manga, Medical & Risk Management, also observe this trend: “Our clients have demonstrated their commitment to value-based contracts during this plan year’s renewals. Employers and health plans are increasingly adopting valuebased contracts to enhance member access to treatment, anticipating that these arrangements will help manage the overall cost and access to quality facilities for their members.”
They do not point to any specific payment model and say there have not been any guarantees associated with the contracts.
“To establish guarantees, members who receive treatment must be monitored by Case Management for at least a year,” they caution. “This ensures that their progress and outcomes can be accurately tracked and evaluated. If a member changes employers, they can no longer be followed. Even monitoring for a year is not enough time to evaluate if the treatment is a cure.”
ROLE OF STOP-LOSS INSURANCE
Lockton maintains that the main payment option to pay for these therapies for a self-funded plan sponsor is their stop-loss policy, which should be evaluated on a year-to-year basis to reflect a material change in experience or price adjustments. They say that none of the carriers are denying coverage outright for CGTs or requiring the plan to transfer the liability to
Jeff Auten
Terri Martin
Alberta Manga
Zero in on catastrophic claims risks.
Curv® can isolate risk above a specified individual stop-loss threshold, giving finely tuned insight into potential high-cost claims. Depend on Curv’s predictive analytics for more accurate pricing across your spectrum of underwritten groups.
rxhistories.com/curv/group-health
another entity, such as a carve-out program. They also say it is critical to align the terms of the underlying health plan and the stop-loss coverage to ensure stop-loss reimbursement of claims related to these expensive treatments.
Stop-loss policies can protect the underlying health plan, at least temporarily, by transferring the risk of high-cost claimants. In some cases, stop-loss insurers can “laser” a specific enrollee or drug to set higher coverage thresholds, effectively removing financial protection for the employer. Consulting actuaries at Milliman observe a slowdown in demand for CGTs and believe the surge will emanate only from patients who tend to have the most severe cases or conditions with no other treatment options. For the foreseeable future, they recommend coverage under traditional means like stop-loss.
Jamie L. Holowka, B.S., Pharm.D., director of Clinical Strategy, Complete Captive Management Services, says that through her experience in medical stop-loss and re-insurance, she has participated in the payment and contracting process of more than two dozen gene therapies and hundreds of cellular therapies.
"I have observed the facts fall out through the medical data showing that some recipients had no response, but serious consequences, other recipients had a temporary response, also with serious consequences, and some had a response for a limited durability (limited amount of time) and supportive therapy, and treatment is still ultimately necessary," she explains. "Because of these lesser discussed outcomes to promote science, manufacturers contract with providers and carriers to authorize the therapies.”
HIGH-COST MEDICAL CLAIMS REQUIRE HIGH-POWERED NEGOTIATIONS
Lower your expenses on in- and out-of-network claims with savings as high as 90%
Our expert attorney negotiating team helps you avoid overpayment and achieve exceptional savings on your claims—even the highest cost treatments.
H.H.C. Group is your trusted partner to verify costs and ensure billing accuracy – more savings on more claims.
Jamie L. Holowka
Between these entities, she says there could be 340b contracts or traditional rebates and outcomesbased contracting. Since carriers may front the payment (at best) but stop-loss (and re-insurance) is the actual payer, she maintains that it is unacceptable that current contract participation does not extend to the stop-loss and re-insurance carriers.
“For all the CGTs, the manufacturer is not able to bill IF they are unable to produce enough product to meet FDA approved specifications (doses),” she continues. “For CGTs, IF a recipient passes away after a pre-determined amount of time, a 100% refund is returned to the carrier. If a recipient dies or the disease progresses, depending on onset and time, the carrier will receive a 75%-100% refund for the therapy.”
Although gene therapies are still limited to a one-in-alifetime dose, regardless of effectiveness, she believes that many providers still maintain or start their competitor therapies before or after the gene or cellular therapy, including bone marrow transplantation and other specialty therapies.
She contends that although we are living in an amazing medical science space, the risk is completely on the employer covering the products while the network retains all the incentives, adding, “For most of these diseases, the only potential
cure remains known to be stem cell transplants, like a bone marrow transplant. Potentially eligible recipients would be so much better served with a donor match campaign.”
Roderick concurs, “The availability of stop-loss coverage can encourage plan sponsors to provide benefits for CGTs. Knowing there is a mechanism to manage the financial risk associated with these treatments makes it more feasible for plan sponsors to include them in their coverage options.”
When plan sponsors partner with the right medical stop-loss insurance providers, he feels it supports the implementation of VBCs by covering the financial risk of high-cost claims.
“This enables plan sponsors to confidently enter into value-based agreements, aligning financial protection with value-based care models to help ensure that members receive the best possible outcomes while managing costs effectively,” he comments.
MANAGEMENT SOLUTIONS
A debate continues on whether to cover gene therapy under the medical or pharmacy component of the plan. Some argue that the pharmacy component enables plan sponsors to better manage the cost, although this option requires a full understanding of the programs that the administrator has in place. For instance, if
outcomes-based contracting is under consideration to cover gene therapy, the medical component of the plan may be preferred since the member’s outcomes will likely be tracked through the medical claims experience.
Lockton cites other management solutions, including providing access to specific, high-value network providers, limiting out-of-network facility coverage, and adding a travel benefit to enable ease of access to high-value providers. Coverage for cancer gene therapy should be accompanied by robust programs for cancer care navigation, expert medical opinion, cancer decision-support services and identification of gene therapy clinical trials for members.
Lockton advisors say it may also be possible for some self-funded employers to cap the amount their plan will pay for specific gene therapy treatments. They explain that the Affordable Care Act’s ban on dollar limits applies only to “essential health benefits” (EHBs), as defined by the plan’s relevant “benchmark state,” and self-funded plan sponsors may choose which state’s benchmark plan they’ll use to determine their plans’ EHBs. Some state benchmark plans, for example, require that merely some, but not all, drugs in a specific therapeutic class be treated as EHBs.
Holowka characterizes CGTs as “interesting progressions and treatment options in the medical arsenal” but cautions, “We are still "scraping the mold off the petri dish; we have not formulated penicillin yet. They are great motivation for the development of other treatments for these rare diseases.
She advises that carrier formularies should be applied as standard to CGTs as they are with any other treatment policy and protocol in healthcare: “Clients should understand that other therapies are not inferior to CGTs and clients should not feel obligated to cover for ALL options of treatments available, when they are all considered equivalent. We need to consider that a handful of recipients does not provide solid evidence of safety or efficacy and that CGT options are being directed at our most vulnerable and most desperate populations.”
COVERAGE: A WEIGHTY LIFE OR DEATH DECISION
Denying CGT coverage triggers many consequences, primarily compliance and public relations risks. Some disabilities-based discrimination claims are surfacing, even if the exclusion is targeted at a member’s dependent. By amending a plan mid-year to exclude coverage because of an existing claim or impending claim, there is a risk of a HIPAA violation. Furthermore, if a self-funded employer chooses to exclude gene therapy but then determines an exception and offers coverage as a result of extenuating circumstances -negative publicity, the child of an executive needing the treatment, etc.-- the claim will not be eligible for stop-loss reimbursement because the service is not listed as covered in the underlying health plan.
Public relations nightmares are becoming all too common since these treatments are now viewed as essential, and many are for children. Imagine the headlines for not covering an FDA-approved gene therapy for a baby with a life-threatening condition with limited, if any, treatment options. When workers think they have coverage and are then denied access to a CGT, there are life or death implications.
OTHER OBSTACLES
Self-insured plans encounter multiple obstacles to providing access to these potentially lifesaving therapies. However, the extended treatment journey for most CGTs is one barrier to utilization since
medical appointments for the individual or their loved ones could interfere with work schedules and requirements.
For example, the infrastructure required to deliver sickle cell therapy is extremely specialized and currently only available at very few centers, typically bone marrow treatment facilities with sickle cell expertise. Younger patients have also been reluctant to embark on the demanding treatment process that lasts more than one year and requires periodic hospitalization – disrupting school schedules and apprehension about adding additional medical burdens to their routines. Furthermore, many sickle cell patients are so advanced in their disease that gene therapy is not clinically warranted.
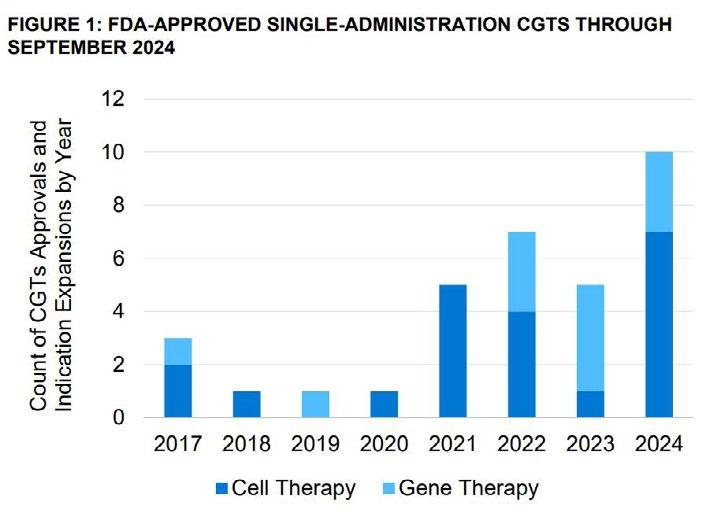
The advent of single-administration (CGTs) has the potential to change the landscape of treatment. A Milliman study reported that the FDA has approved 23 single-administration cell and gene therapies since 2017, totaling 35 approvals with additional expansions. Most approvals have come in the past two years, and roughly 60 more could hit the market in the next three years.
Milliman points out that these gene therapies are typically infused in one session, holding the promise of a cure that would avoid a lifetime of treatment. However, some employers, particularly retailers, hospitality, or trucking companies, where there is a large employee turnover, may hesitate to shoulder the hefty cost of a one-time treatment. Drug manufacturers argue the prices are justified because they offset a lifetime of medical costs patients would otherwise face.
Of the 17 one-time therapies approved by the FDA at the end of 2023, only eight had been used by more than 10 patients, according to Milliman’s analysis of 60 million commercially insured enrollees. Kite Pharma Inc.’s $425,000 lymphoma CAR T-cell therapy Yescarta had the most claims, at just 413 since its 2017 approval.
Source: Milliman DNA Gene and Cell Therapy Forecasting; v3.3.0, September 2024 release.
THE PRICE TAG FOR A CURE
CGTs potentially offer a cure for many diseases for which traditional approaches, medicines and surgery have simply halted disease progression or modulated the course of the disease. For diseases caused by mutations in single genes that a person is born with, it is estimated that there are more than 6,000 such diseases affecting over 350 million people worldwide.
Braving the gene therapy headwinds, attendees at the recent JP Morgan investor conference heard from the Alliance for Regenerative Medicine president Tim Hunt who offered a rosy outlook for CGTs, predicting 10 such treatments will become blockbusters by 2030. Peter Marks, director of the FDA’s Center for Biological Evaluation and Research, commented that 2024 was also a “good year” for gene therapy approvals, emphasizing that the agency is focused on boosting accelerated approvals with the launch of two pilots to aid gene therapies and treatments for rare diseases.
“The industry needs to think differently about CGTs,” says Keri Schoenbrun, Chief Engagement Officer, Actum Pharma, a company founded by a consortium of biopharma leaders that is committed to enabling the development and market introduction of novel therapies that effectively address patient suffering from debilitating and life-threatening conditions. “Because CGTS are in a completely pioneering space, virtually all of these therapies will be unfamiliar, on some level, to the entire ecosystem. CGT companies need to
Leading National TPA
Our decades of experience have taught us how to elevate member health and drive down costs.
How we do it:
• Specialized, in-house teams— implementation through renewal
• Tailored point solutions and a la carte programs
• Custom-built, scalable plans and network options
See what sets us apart from other
Not
Keri Schoenbrun
Better outcomes.
Long-term cost savings.
Mayo Clinic Complex Care Program
experienced a change in diagnosis 52% avoided a locally recommended surgery 23% 85% experienced a change in treatment plan
Discover how a customizable center of excellence program can help minimize healthcare costs while o ering high-cost, high-risk members exactly the care they need.
The Mayo Clinic Complex Care Program is for a small subset of a population with serious, complex or rare conditions who need subspecialized expertise that may not be available locally.
Learn more by calling 507-422-6103 or visit us online at mayoclinic.org/complex-care-program
think differently about many aspects of commercialization, but particularly stakeholder education, which will need to be conducted early and often.”
She says that even companies with deep experience launching products, like small molecule therapies, will need to think very differently about some fundamental work streams, especially payer education.
“Education will be about much more than articulating outcomes,” explains Schoenbrun. “Drug manufacturers need to be prepared to explain diseases that may be treatable for the first time, unique methods of administration and a broader view of benefits to both patients and payers.”
She advises the conversations between CGT’s and payers should begin with a single premise: all options are on the table and none of the parties can be constrained by previous models.
“Start by effectively painting a picture of the overall cost of care,” she continues. “Robust health economics and outcomes research studies may be needed to quantify the full burden of current treatment options relative to the emerging CGT. It starts with data but will likely require working with patient advocacy groups to understand the details and nuance of living with a given condition.”
She cites recent work focused on a rare skin condition where, for example, the cost of bandages alone could reach $25,000 per patient.
Schoenbrun also points to the role of genetic testing, adding, “Expect the role of genetic testing to also evolve. Historically, payers were reluctant to reimburse for genetic testing. But as CGTs evolve, smart payers will increasingly embrace genetic testing as a way to identify patients who are likely to benefit from a given therapy. This becomes an important way for payers to manage the risk associated with high-cost interventions. Drug manufacturers will need to do their part by ensuring related genetic tests are reliable and meet increasingly stringent standards set out by the industry."
A prediction for the future from Schoenbrun: “It is important to remember we are standing at the frontier of a whole new way to treat patients. While some of the costs might seem outrageous now, these are growing pains for the industry. We will soon see improvements in process, automation and testing begin to lower costs for patients and payers.”
Expounding on this topic, Dan Winkelman, Director, Offering Design Suite, IQVIA, says the decision to cover these therapies must be made on a plan-by-plan level and by disease state due to different levels of cost, efficacy, and alternative therapies.
“In some cases, the unprecedented efficacy results in positive economic models due to the likelihood of a reduction of hospital stays and/or reduced need for ongoing chronic care therapy,” he advises. “For example, the economics are seemingly clear for CAR T-Cell therapy for DLBCL because it can replace Stem Cell therapy which involves longer hospitalization (3 months vs. 1 month) and has curative potential, which we call “one and done”.” Another example is Luxturna for RPE65-mediated inherited retinal dystrophies. If patients have the biomarker, then this treatment can cure their blindness, resulting in a significant impact on their lives and their support system.”
Dan Winkelman
STOP LOSS INSURANCE
MANAGE THE RISK.
Prudential’s Stop Loss insurance helps reduce unpredictable risks from self-funded medical plans. This way you can focus on giving your employees the coverage they deserve, while helping to reduce your worries about the increased frequency of catastrophic claims.
Get Stop Loss insurance from a partner you can rely on:
• A highly rated, experienced carrier recognized for 150 years for strength, stability, and innovation
• Efficient, responsive service with streamlined processes across quoting, onboarding, and reimbursements
• A dedicated distribution team that works hand-in-hand with your existing relationships
• Flexible policy options so we can build a coverage plan that meets the unique needs of your organization
Did you know, medical and prescription drug costs are expected to rise 8.5% annually?* See how Prudential can help you manage the risk from your self-funded medical plan.
For more information, contact us at stoploss@prudential.com or visit our website: www.prudential.com/stoploss
In contrast, in other disease areas and therapies, he says the same efficacy could be achieved with lower cost therapies, noting, “One unique factor about these therapies is that they tend to target smaller patient populations which can buffer the budget impact despite the individual high cost of the treatment. Innovative models are required to understand the true value of treatment and must be updated regularly.”
Laura Carabello holds a degree in Journalism from the Newhouse School of Communications at Syracuse University, is a recognized expert in medical travel and is a widely published writer on healthcare issues. She is a Principal at CPR Strategic Marketing Communications. www.cpronline.com Get the most out of your healthcare plan and finding cost-saving opportunities with PAI Analytics.® Visit paisc.com to learn more.
Brad Hansen VP of Provider Relations
Questioning Authority
High court ruling that limits grip of federal agencies could affect regulatory landscape for self-insured employers
BBefore
Written By Bruce Shutan
Donald Trump won a second term as president and vowed to continue disrupting politics, the U.S. Supreme Court seeded a major disruption limiting the authority of federal regulators that continues to reverberate across the self-insurance industry.
In late June 2024, the justices overturned a 40-year-old judicial precedent known as Chevron deference – named after the American multinational energy corporation. In Chevron U.S.A. v. Natural Resources Defense Council, courts were directed to defer to federal agencies' interpretations of ambiguous laws. That practice ended with a 6-3 decision led by Chief Justice John Roberts in Loper Bright Enterprises v. Raimondo. Although widely applauded, it also has stirred questions about compliance with both old and new employee benefit laws.
As such, Loper Bright presents both challenges and opportunities for self-insured health plans, as observed by Kristy Wrigley-Durer, senior counsel at Crowell & Moring. She suggests working closely with corporate counsel or government affairs experts to closely monitor what's happening in the courts in terms of the impact on existing regulation and being nimble in responding to any changes. She's also sanguine about a new pathway to challenge any issued guidance that is considered less favorable and work toward getting out in front of issues by influencing new legislation.
One such opportunity involves reforming pharmacy benefit management practices, which she describes as a hot topic with bipartisan support in Congress. “We’re going to see something on that and probably not just PBMs, but all service providers to ERISA plans,” she surmises.
Fred Karlinsky, shareholder and chair of global insurance regulatory and transactions with Greenberg Traurig, describes the post-Chevron deference climate as a positive development that will help level the playing field when it comes to challenging agencies since courts will view cases from a more de novo perspective, which removes any reliance on previous case law. He adds that it doesn’t mean courts won’t take into account an agency's position; it just removes the practice of deferring to an agency's interpretation of a statute or regulation.
“I think that keeps true the notion that there are three separate but co-equal branches of government” wherein each one will stay in its lane to work in the best possible way, Karlinsky says. In effect, he believes it will help protect innovation and be good for consumers of products and services in the self-insurance space.
His experience with this issue actually dates back to 2017 and 2018 when serving on Florida’s Constitution Revision Commission during which time voters
overwhelmingly supported a ballot measure overturning Chevron deference in Florida.
FOCUSING ON NEW REGS
What the Loper Bright case essentially means is it will be easier to argue that newer issued regs are arbitrary and capricious than those that have been in place for at least three years or more and were subject to Chevron deference, explains SIIA Washington Counsel, Chris Condeluci. One example is that the provider community has filed a lawsuit over surprise-billing rules in the No Surprises Act and could challenge other parts of the law now that Chevron deference has been overturned. The other involves mental health parity.
“We thought that the administration exceeded its authority and rewrote the statute through the reg – irrespective of Chevron deference,” he says. “We would have argued that anyway but feel that much more confident in our legal arguments in trying to get the reg set aside based on Chevron deference and a recent lawsuit spearheaded by the ERISA Industry Committee [ERIC].”
Advocacy in Action
Legal services and innovative technology combined to defend health plans, plan sponsors and member participants nationwide aequum advocacy programs & services successfully resolve surprise billing and unreasonable out-of-network and balance billings
On average, aequum resolves claims within just 244 days of placement. Unmatched Savings aequum has achieved a remarkable 95.6% savings off disputed charges for self-funded plans. National Expertise aequum has successfully handled claims in all 50 states.
ERIC filed a lawsuit in January that seeks to invalidate the final rule issued under the Mental Health Parity and Addiction Equity Act of 2008 and the Consolidated Appropriations Act of 2021, known as the CAA. The lawsuit argues that the rule exceeds the Department of Health and Human Services authority, violates the due-process clause in the Fifth Amendment, is "arbitrary and capricious," and violates the Administrative Procedure Act.
Tom Christina, executive director of the ERISA Industry Committee’s Legal Center, hopes there’s a rethinking of these regulations, which self-insured health plans consider highly draconian. “They were drafted in the hopes of impeding non-quantifiable treatment limitations,” he says. Noting that the process of dialoguing with these agencies about these limitations is very prolonged, he says it suddenly picks up speed “almost before the employer knows that they find themselves staring at a determination that they’re in violation, which is a very big deal under the regulations.” That’s because employers are required to inform plan participants within just 10 days of receiving notice that they have violated the statute.
“None of this has any basis in the statutory language, in particular the remedy of notifying your employees,” Christina says. “You could read the act 100 times and won’t find anything that even suggests that the regulatory agencies have that power.”
Mental health parity is the one area where industry practitioners expected some of the first Loper Bright challenges as they would apply to ERISA plans, Wrigley-Durer observes. “It’s interesting to note that the DOL finalized those rules after the Loper Bright decision, and Loper Bright doesn’t seem to have particularly tempered their approach,” she explains. That case didn’t necessarily remove the authority of
agencies, she says, adding that they’re still issuing guidance. “It simply noted that they don’t get to interpret law, which is the role of the courts.”
Overturning Chevron deference has thus far not “opened the floodgates” to ERISA litigation of any kind, including litigation involving self-insured health plans, Christina notes. Loper Bright, however, has quite a few escape hatches, he adds. He's not surprised that a few district courts upheld the application of claims procedures regulations after the Loper Bright case was decided.
There have also been other ERISA cases in which he says enunciate principles that, if applied to self-insured health plan cases, would dampen the effects of Loper Bright. As one example, he cites a recent court decision upholding some Pension Benefit Guaranty Corporation (PBGC) regulations that faithfully follow Loper Bright – stressing “the longevity of those regulations as a reason for upholding them.”
While that case involved PBGC regulations pertaining to withdrawal liability in multiemployer pension plans, he explains that it illustrates how courts have limited the effect of Loper Bright on any area within ERISA, which would include selfinsured health plans.
Christina suggests the chief implication would be to expect
that long-standing regulations, including claims procedures, will be upheld, while fairly recent regulations are more vulnerable to being challenged in court. The best example he can think of involves analyses of non-quantitative treatment limitations for the purpose of achieving mental health parity.
When the Department of Labor issued regulations under ERISA 408(b)(2) in 2012 setting out disclosure obligations for retirement plan service providers, it noted that special guidance would be forthcoming to address the uniqueness of health plans. Part of the challenge is that the DOL may be thinking post-Loper Bright about whether it still has the authority to issue guidance, according to Wrigley-Durer. If Congress passes legislation on PBM reform or service provider disclosures, she expects clarity on what the DOL needs to do in terms of issuing guidance about those disclosures, their level of authority and even how aggressive they want the DOL to be.
In addressing concerns about recent ERISA preemption battles in various states, Wrigley-Durer says it's a statutory issue and is not likely to be implicated by regulations. Noting how ERISA has been around for 50 years, she doesn't expect that there will be huge swings in preemption challenges other than "it's interesting to watch what's happening in the PBM space because that's the first real place we're seeing it being chipped away at a bit."
MORE RIGOROUS REVIEW
Since the Loper Bright ruling is still relatively new, Wrigley-Durer believes it remains to be seen whether it could have a chilling effect on the development of products and services to contain group health plan costs. But she adds that there could be some hesitation to take potentially risky positions based on existing guidance if there’s any concern that it could later be challenged.
It’s worth noting that the Supreme Court itself hadn’t actually cited Chevron in nearly a decade before the Loper Bright decision. “So, there are a good number of practitioners in the space who don’t really view it as that big of a deal,” she says. “I think we’ll need a few court cases under our belt to see if it really starts shaking out that way.”
Christina also believes that, at least during the Trump administration, federal agencies are going to be much more rigorous about ensuring that their regulations conform to statutory language or at least have a basis in the statute before they even issue net by notice of proposed rulemaking.
"It's going to have an effect on the executive branch's thinking about how to go about regulating, and that'll be across the board, particularly because there will be a lot of OMB and DOGE supervision," he opines. "Loper Bright is going to be foremost in the minds of regulators."
The first step he'd recommend for self-insured health plans is to continue to assume the validity of all existing regulations, then give any proposed regulations much more than a cursory glance by having outside counsel review the proposal.
Field
Choose speed and savings with Stealth Advance! We fund claims up to $5 million within 72 hours of loss notification— no complex forms needed. Enjoy cash flow stability without being tied to any specific carrier, TPA, or PBM.
Get the rapid reimbursements of bundled stop-loss combined with the flexibility of direct writers. As your program manager, Stealth Partner Group simplifies the process with one transparent PEPM fee—no hidden costs.
Experience the Stealth Advance difference: fast reimbursements, competitive rates, and complete vendor freedom!
“In the future,” Condeluci predicts, “people are going to be very quick to file a lawsuit against a reg even if it’s pretty crystal clear that the department got it right.” As for whether Loper Bright complicates compliance with older regs, he says employers are still expected to comply, even if there’s a lawsuit filed against a particular regulation.
"You must comply until a court says that you don't have to comply anymore," he says, noting that it applies to ERIC's mental health parity litigation. "It doesn't matter if there's a lawsuit filed. It's still business as usual." It's also important to understand that litigation takes a long time, and regs still apply until an appeals court invalidates them, he adds.
CHANGING OF THE GUARD
Condeluci doesn’t think significant reductions in the federal workforce will have much of an impact on compliance. Instead, the background, experience and policy priorities of agency personnel moving into senior roles will have a much greater influence over what happens next inside the beltway.
At the top of that list is Lori Chavez-DeRemer, a former Republican U.S. Rep. from Oregon, who now serves as labor secretary and is a big proponent of requiring provider network owners to share health claims data with self-insured plans and their business associates. Another key player is Daniel Aronowitz, who was nominated to serve as assistant secretary of labor for the Employee Benefits Security Administration, which has jurisdiction over rules and compliance relating to self-insured health plans. He has expertise in stop-loss insurance and fiduciary liability and has been a critic of the plaintiffs' bar going after plan sponsors over fiduciary breach issues.
His view of Robert F. Kennedy Jr., who heads the Department of Health and Human Services, is that he probably will wield more influence over public health programs than the commercial insurance market. What will be more impactful is those in senior roles who report to him, he adds.
Years before any type of judicial deference was in effect, Karlinsky notes that there was more cooperation in Congress, which ran more efficiently. "Hopefully, we'll get back to that type of an era where some of these interpretations frankly aren't even necessary moving forward," he adds.
Bruce Shutan is a Portland, Oregon-based freelance writer who has closely covered the employee benefits industry for more than 35 years.
Do you aspire to be a published author?
We would like to invite you to share your insight and submit an article to The Self-Insurer! SIIA’s official magazine is distributed in a digital and print format to reach 10,000 readers all over the world.
The Self-Insurer has been delivering information to top-level executives in the self-insurance industry since 1984.
Articles or guideline inquires can be submitted to Editor at Editor@sipconline.net
The Self-Insurer also has advertising opportunties available. Please contact Shane Byars at sbyars@ sipconline.net for advertising information.
Not Afraid To Spill Some Milk
When your culture drives you to get comfortable being uncomfortable, you’re going to spill some milk to deliver innovation. ‘Yes, and…’ we embrace spilled milk to enable smarter, better, faster healthcare.
Learn more about how we’re delivering innovative solutions to simplify healthcare.
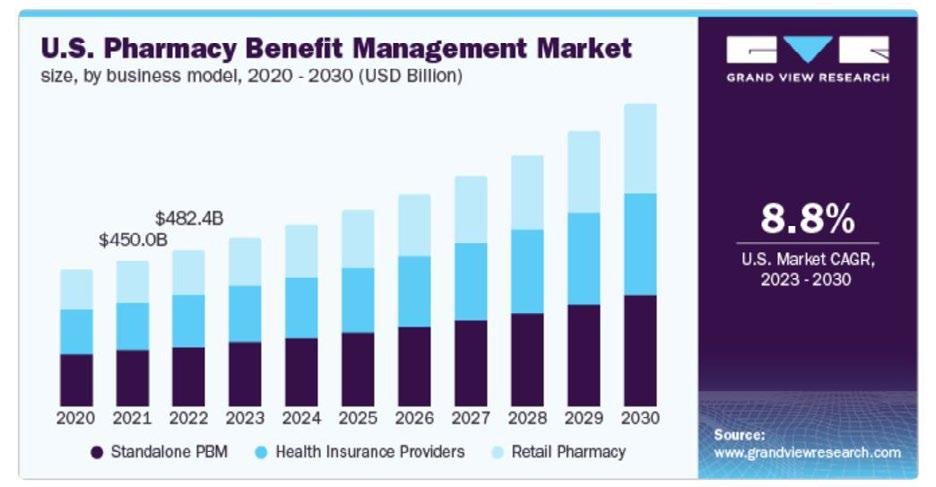
PBM QUAGMIRES TROUBLE EMPLOYERS
Editor’s Note: For more information about this topic, please plan to attend SIIA's High-Cost Drug Stakeholder Forum, scheduled for May 28-29 in Minneapolis. Event details can be accessed at www.siia.org
Written By Laura Carabello
AmidAa barrage of high-profile lawsuits, legislative challenges and widespread employer/payer dissatisfaction with escalating drug prices, the Pharmacy Benefit Management (PBM) industry is awash in negative publicity and uncertainty. In the wake of these complaints, the Pharmaceutical Care Management Association, a trade group representing the six-largest PBMs and others, said in a statement that the industry welcomes competition from newer entrants.
Now in the crosshairs of Congress, as well as State legislators such as Illinois, PBMs face a host of pending regulations to address criticisms such as steering patients toward their own pharmacies, requiring patients to use an in-network pharmacy or paying a pharmacy an amount less than the national average drug acquisition cost for the drug dispensed. Congress is tackling these issues, with proposals under consideration that include:
Requiring PBMs to charge flat fees that are not linked to drug prices
Creating standard pharmacy performance metrics on which fees are based
Requiring PBMs to disclose negotiated drug rebates and discounts -- and requiring those rebates and fees to be passed through to employers
Prohibiting spread-pricing
Employers lay blame on PBMs, generally described as “behind-the-scenes middlemen” that negotiate discounts with drug manufacturers and reimbursement rates with insurers to determine which medications qualify for coverage. Accusations include demanding discounts and rebates from drugmakers, which leads the manufacturers to charge higher list prices, which can drive up the price patients pay at the pharmacy. Concurrently, retail pharmacies say PBMs are literally driving them out of business by paying them less than what the PBMs charge health plans — a practice known as spread-pricing, where PBMs charge more to health plans than they pay pharmacies for prescription drugs.
Julie A. Wohlstein, M.A.S., CSFS ®, President and CEO, Centrix Benefit Administrators, Inc., specifies the challenge, “PBMs often present self-funded employers with a double-edged sword. While they play a critical role in managing prescription drug plans and negotiating discounts, their opaque practices often lead to hidden costs and misaligned incentives.”
She says PBMs typically steer members toward higher-cost drugs as way to maximize rebates, a practice which inflates the overall costs.
“Employers are burdened by complex contractual terms that obscure true drug prices and make it difficult to identify cost-saving opportunities,” she continues. “Furthermore, the adoption of narrow pharmacy networks may limit employee access, which creates dissatisfaction among the workforces.”
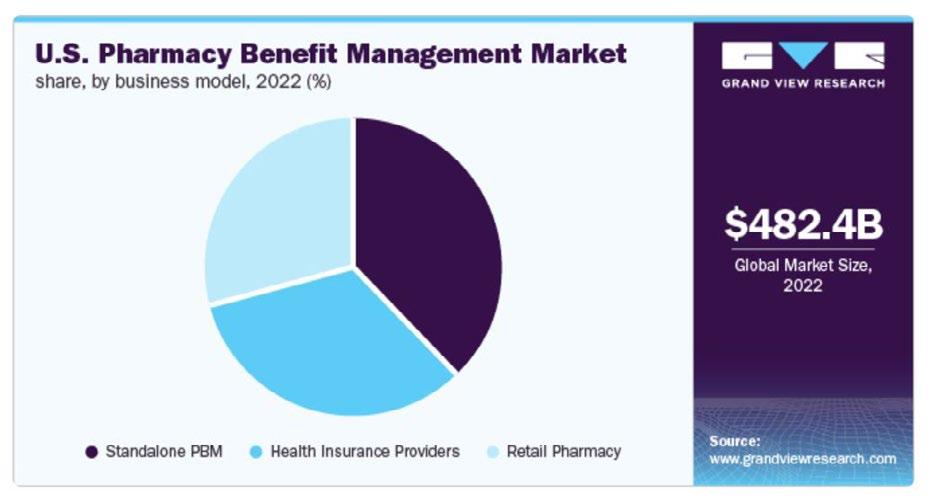
Across the board, plan sponsors say they have no idea what a drug will cost because many PBM contracts contain nondisclosure clauses. There are varying reports regarding the stranglehold on the industry. According to the American Medical Association, together, the big three -- CVS Caremark, Cigna’s Express Scripts and United Health’s OptumRx -- hold nearly 60% of the pharmacy benefits market based on their control over rebate negotiations, retail network management, and claims adjudication.
Furthermore, a recently released report from the Federal Trade Commission (FTC) shows that these three PBMs processed almost 80% of the 6.6 billion prescriptions filled nationwide last year, and the top six players control more than 90% of the market. The FTC found that those companies use tactics to point patients toward drugs that are more costly.
Wohlstein maintains that a major challenge lies in the lack of transparency in rebate structures, adding, “PBMs frequently retain a significant portion of manufacturer rebates rather than passing on the savings to the employer or employees, creating an environment where profitability outweighs patient outcomes. To navigate these challenges, self-funded employers must prioritize transparency and explore innovative solutions such as pass-through PBMs or carving out pharmacy benefits for direct negotiation. By adopting proactive measures, employers can better align PBM practices with their financial goals and the health needs of their workforce.”
In this current environment, employers are certainly scrutinizing PBM policies and capabilities more closely.
Lori Daugherty, CEO, RxLogic observes, “Employers select PBMs based upon transparency, cost savings, service quality, and alternative solutions. A transparent PBM ensures clear pricing, eliminates hidden fees, and passes through negotiated savings. While rebates may seem attractive, employers should assess total cost impact rather than just rebate amounts.”
She says that superior service and clinical support help optimize medication access while controlling expenses, noting, “Additionally, PBMs offering alternative pricing models, such as direct manufacturer savings and pass-through pricing, providing additional cost-cutting opportunities. Our model powers PBMs with the technology and services needed to meet these employer demands, enabling PBMs to deliver transparency, cost-efficiency, and advanced analytics, ensuring a superior service model for their clients.”
Re-cap of Some Issues to Date:
Last year, the FTC sued the three jumbo PBMS for anti-competitive practices, alleging that their practices artificially raised the price of insulin drugs. While the PBMs asked a Missouri district court to block the agency’s suit, as of mid-February, the lawsuit was slated to move forward after a federal judge declined to halt the case. Later in the month, the Big Three elevated their suit and asked the Missouri district judge to halt the FTC's administrative case against them. Stay tuned to the see-saw battle.
In 2024, The House Oversight Committee kept pressure on PBMs during hearings that criticized industry practices to steer patients to PBM-owned pharmacies while underpaying competing pharmacies. There is increased scrutiny on the way PBMs treat independent pharmacists, who say
they’re being drummed out of business by PBMs.
PBM executives were also summoned before Congress and reproved for creating corporate entities in Switzerland and Ireland to centralize the negotiation of rebates and fees. They were grilled with accusations of creating entities in Ireland and the Cayman Islands to manufacture and market certain highly profitable generics and biosimilars -- locations purportedly lacking in financial transparency and movement of operations that would be subject to impending regulations.
A group of legislators called upon the Department of Justice to investigate whether PBMs played a role in the opioid epidemic, pointing to reports that suggest the three largest PBMs worked together to steer patients to OxyContin prescriptions in exchange for $400 million in rebates and fees from Purdue Pharma across a yearlong period ending in late 2017.
Tangentially, in welcome news for the employer community, the Groom Law Group reported that the US District Court for the District of New Jersey dismissed in January 2025 a putative ERISA class action lawsuit in a much-followed case involving Johnson & Johnson (J&J). The plaintiff alleged that the plan fiduciaries for J&J’s group health plan violated ERISA by mismanaging its self-funded health plan’s prescription drug benefit. The Court found that the plaintiff's allegations that she paid too much in premiums, copays, and coinsurance and that her wages were adversely impacted by prescription drug costs were speculative "at best," and that her allegations regarding higher out-of-pocket costs for prescription drugs were not redressable.
At year-end 2024, while Congressional lawmakers reached a deal to put guardrails around these socalled “middlemen,” the agreement fell apart because it was tacked onto a larger spending package that
crumbled during a final vote. The employer PBM provision would have created new reporting requirements for employers' PBMs and required employers' PBMs to pass all rebates on to the employers' plans rather than keeping a percentage of the discounts they negotiated. When the spending package stripped out this provision, PBMs got a temporary reprieve -- but it’s likely to be a short honeymoon for them in Washington.
The issues are bubbling up in 2025 with bipartisan efforts that press the FTC to be tough on PBMs. The FTC’s ongoing campaign, which most recently focused on charges for high-cost specialty drugs, accused the three biggest PBM pharmacies of collecting $5.9 Billion in specialty drug mark-ups.
Chairman of the House Energy and Commerce Committee recently declared that he and his colleagues hope to pass new versions of the bipartisan health bills, many that have lingered for more than a year without final action. One measure that could be included is a bill that would regulate how PBMs serve employersponsored health plans.
The latest salvo came in February when A broad coalition of healthcare companies, employers, labor unions and trade associations called upon the White House and Congress to enact legislation to curb PNMs: Blue Shield of California, employers represented by the ERISA Industry Committee, pharmacies represented by the National Association of Chain Drug Stores and the National Community Pharmacists Association, and an umbrella group called America’s Agenda that includes the insurers Elevance Health, Centene and Kaiser Permanente along with unions and drugmakers, made their plea.
There’s even proposed legislation in Texas that could stop health insurers or other coverage issuers in the Lone Star State from requiring patients to use the carriers' own pharmacy benefit managers.
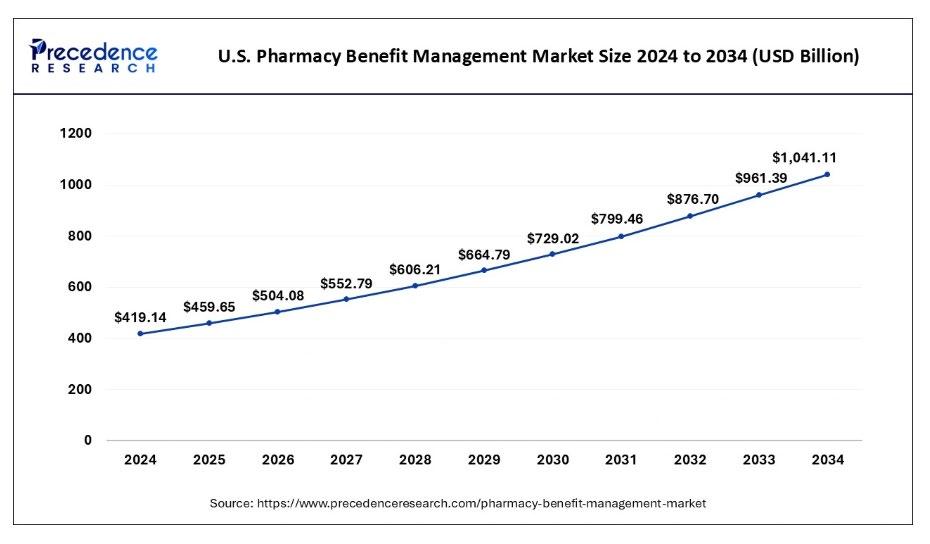
Amid all this market uncertainty, pharmacy spend is expected to rise 3.8%, with specialty pharmaceutical costs as the main driver and price increases to classic specialty drugs that treat oncology conditions and autoimmune disorders. A Vizient study showed that Humira, Stelara and Skyrizi, which all can treat Crohn’s disease, are projected to have the largest price increases.
GAUGING EMPLOYER DISSATISFACTION
Faced with projected healthcare cost pressures, employers are trying to hold their PBMs accountable –especially for pharmacy costs. According to the Business Group on Health, pharmacy costs accounted for more than a quarter of healthcare costs in 2023, with rising drug costs largely driven by expensive specialty medications, cell and gene therapies (CGTs) and GLP-1s.
A survey by the National Alliance of Healthcare Purchaser Coalitions, an advocacy organization for employers and purchasers, substantiates these perceptions: about 99% of respondents listed drug prices as a significant threat to affordability. Purchasers cite PBM vertical integration and opaque practices as the culprits.
Every size employer-sponsored health plan is facing increasing healthcare costs, but the impact on small employers and their employees is more acute and likely to continue. Many believe their PBM isn’t always looking out for their needs.
The National Alliance of Healthcare Purchaser Coalitions survey also documented employer dissatisfaction with their PBMs: 52% are considering changing their PBM in the next one to three years. According to their leadership, PBMs use “opaque business practices” that allow them to change the status of a drug from generic to specialty to name brand without the employer’s consent. They also point the finger at the big three PBMs that all own their own specialty, retail, and mail-order pharmacies and "strategically price drugs to maximize revenue to their internal pharmacy chains.”
EMPLOYERS MAKING A SWITCH
A growing number of employers would rather ‘switch than fight’ with their PBM partners, opting for a vendor that is more agile and offers alternative network models with greater price and quality transparency. Status quo PBM contracts may go by the wayside in favor of dropping the “Big Three” PBMs to “transparent PBMs,” which don’t camouflage their pricing and drug choice decisions.
In the Business Group on Health's annual survey published in late January, respondents indicated concerns about a lack of transparency in contracts with PBMs. While 6% of employers plan to change PBMs next year, nearly one-third said they will reassess their partnerships next year. Switching drug benefit policies at larger companies takes time since PBM contracts with the big three typically last three to five years. PBMs pay benefit plan consultants and brokers handsomely to steer business their way.
A few big employers are already changing their drug plans. Back in 2019, the State of Connecticut became CVS’ first PBM customer to negotiate a transparent fee structure. Its contract required 100% of drug rebates to be passed along to the state and eliminated spread pricing.
Other payers may be following this lead and learning from the Connecticut experience. The CT State Comptroller's office reported a further step in the new contract for its 214,000 employees. Instead of discounts and rebates, it demanded the lowest net cost per employee, with projected savings of up to $70 million a year. Of the three big PBMs, only CVS bid on the contract, edging out a few “transparent PBMs” and signaling that CVS wants to stay in the game.
Other examples include:
Highlighting the growing demand for change, Blue Shield of California made headlines by dropping CVS Caremark as its PBM in favor of a more transparent and innovative strategy. Partnering with companies like Amazon Pharmacy and Mark Cuban’s Cost Plus Drugs, Blue Shield aims to bypass traditional PBM structures, focusing on value-based pricing and direct relationships with pharmaceutical partners.
Purdue University, which sought control over the drug formulary to provide more lower-cost options for its 25,000 employees and dependents. They recently switched from CVS Caremark to AffirmedRx.
Capital District Physicians' Health Plan dropped CVS Caremark two years ago to partner with CapitalRx to administer pharmacy benefits for its 400,000 members. The non-profit health experienced a 9% drop in costs for commercial members under the contract, noting that at times, CVS Caremark would recommend excluding a generic medication over a brand drug in favor of a higher rebate.
The non-profit, 600,000-member health plan UCare ended its 13-year relationship with Express Scripts and in January began a multi-year contract with Navitus Health Solutions, a pass-through PBM owned by St. Louis-based SSM Health and Costco Wholesale Corporation. Citing another motivation for the switch, UCare sought to support local pharmacies, which have called out the major PBMs for forcing unfair contract terms that deliver lower reimbursements than those delivered to PBM-affiliated pharmacies.
Geisinger Health Plan has 600,000 members, and while they never contracted with one of the major PBMs, it doesn’t dismiss them when re-evaluating contracts. One of Geisinger's biggest challenges is persuading employers to adopt the transparent approach, saying it has lost employer
clients to health plans operated by the major players pitching large rebates.
Investment company Voya Financial, with 7,200 U.S.-based employees, was rethinking its relationship with CVS Caremark and began a multi-year contract with retailer Costco Wholesale Corporation's PBM Costco Health Solutions. Voya anticipates 10% savings for both its employees and the company.
Throughout the industry, many groups are dealing with this issue. Wohlstein explains that as a TPA, her organization was faced with this conundrum and made the decision to look for another PBM.
Transparency was a top priority in their decision to make a change.
“Hidden fees, spread-pricing and unclear rebate structures were having a significant impact on our plan costs,” she continues. “Ensuring rebates are passed directly to the plan and eliminating unnecessary administrative charges are crucial in managing overall drug expenses and maintaining trust. Pharmacy spend was the highest claims increase trend for our Plans,” she continues.
While large PBMs bring scale, broad networks, and deeper manufacturer relationships, Wohlstein found this is often at the cost of transparency and member customization.
“Boutique PBMs, on the other hand, excel in personalized service, flexible solutions, and often better alignment with employers' goals,” she insists. “The trade-off depends on the employer's specific priorities, such as cost control or member satisfaction. As a TPA, we must align the PBM vendor with the employer’s benefit strategy to determine the best critical path forward for their plans.”
She further contends that because their current large national PBM was not meeting their clients’ needs, as stated above, “…we selected a boutique vendor who was more innovative, and their offerings could be more tailored to the needs of our clients. I think PBMs will face heightened scrutiny for their opaque practices, and therefore, government intervention seems increasingly likely.”
The power to get it done.
AmeriHealth Administrators is one of the largest national third-party administrators. We provide innovative, value-based health benefits programs and outsourcing services for self-funded health plans and other organizations.
Whether locally focused or on a national level, our scalable capabilities allow us to service many unique customers, including self-funded employers, Tribal nations, international travelers, and labor organizations.
Learn how we can help you successfully navigate and thrive in today’s complex health care environment. Visit amerihealthtpa.com.
As with any regulatory mandate, Wohlstein cautions that while such intervention might improve transparency and curb unethical practices, “This could also lead to unintended consequences, such as reduced flexibility or increased administrative burdens. The outcome will depend on how well regulations address the root causes of misaligned incentives without stifling innovation, and that is what is truly important to the self-funded community.”
On a related front, Walgreens outlined its corporate turnaround strategy to include renegotiating contracts with PBMs and reports having renegotiated all contracts up for renewal in 2025, about a third of its total contracts. Walgreens says it is working with PBMs to balance brand-name drugs and generics, carve out new categories for high-cost drugs such as GLP-1s and implement alternative payment models.
INTEREST SPIKES IN SMALLER PBMS
Many smaller PBMs are seeing an uptick in interest, but the newer entrants will continue to face stiff competition and significant obstacles as they seek more business in the employer marketplace ---- from massive employers to small-to-midsize groups. These smaller PBMs usually offer more restricted drug formularies that can become a frustration point for members, while larger vendors typically feature attractive rebates and greater access to branded drugs resulting from their buying power to obtain medications at lower prices.
On the plus side, smaller PBMs are looking to attract customers by giving them more control over formularies and providing access to data. Many tout potential savings for employers between 30-50% on their pharmacy spend. These smaller companies are passing along drug rebates, disclosing cost negotiations with drugmakers, reimbursing pharmacies at higher rates and rejecting spread pricing.
Questioning the value of large PBMs, Rachel Strauss, VP of Strategic Development at Employee Health Insurance Management, Inc., says, “The big PBMs operate like monopolies, with complex systems that obscure true costs and limit choice for the employer. Their contracts often read like mortgages and have even harder-to-understand terms. However, when the correct contract is executed, they can offer the buying power the boutiques do. But this is often without guardrails. Would you rather get a bigger discount on a more expensive item, to begin with, or less of a percentage, but on a lower net cost product?”
Conversely, she thinks boutique PBMs are "…refreshingly straightforward, prioritizing transparency and a tailored approach to optimize costs and care for their clients. Employers often find they get far more value from the smaller, hands-on players with the creativity and flexibility they offer.”
Strauss believes the government and new administration will step in during 2025 to implement regulations aimed at reining in the PBM industry, adding, “This will be a positive shift for the self-insured community which can hopefully transfer to the patient itself. Increased oversight and transparency will help eliminate hidden fees and conflicts of interest that have long driven up costs without adding value.”
She thinks these regulations could empower employers to make better-informed decisions, negotiate more effectively, and ultimately provide their members with more affordable, high-quality care.
“While change can be hard, these reforms are a necessary step to level the playing field and prioritize the needs of patients and employers over PBM profits – finally,” concludes Strauss.
Staying the course, Nick Soman, CEO of Decent, reports that they proudly partner with DisclosedRx, a PBM committed to transparency through full rebate pass-through and no hidden fees.
corporatesolutions.swissre.com/esl
“Their exceptional member services team and Prescription Navigators provide 24/7 support, expert advice, and consistent follow-through, ensuring a seamless experience for members," says Soman. “DisclosedRx aligns with our mission of delivering affordable, transparent healthcare by prioritizing the well-being of employers and their members.”
With tailored solutions, flexibility, and an innovative approach, Soman says DisclosedRx stands out as a trusted partner.
“Their commitment to clear, predictable pricing drives cost savings and satisfaction across the community,” he states.
For John Wiklund, FSA, MAAA, Vice President and Actuary, Small Business Benefits, a preferred PBM is offered to clients so they can access the financial benefits and programs.
“Important considerations are the pharmacy network, formulary disruption, administrative capabilities, customer service, adaptability to legislative actions, access to mobile apps and cost comparison tools,” expands Wiklund. "Transparency is important for a great user experience, though its true impact on pharmacy spend is unknown. We currently utilize rebates to offset admin costs, keeping coverage affordable. Regulatory changes could potentially jeopardize the cost offset structure we implement today.”
Wiklund and his colleagues continually evaluate their choice of PBM, emphasizing, “Prescription drugs are the largest category of health plan spend and represent a high volume of members’ interactions with the plan. We need to be vigilant with our plans’ funds, offer stateof-the-art coverage options, and feel confident in the value of our pharmacy services.”
He observes that despite partisanship, “The government’s strong focus on PBMs will likely lead to regulation. State and federal proposals could increase transparency but may also result in higher costs for plans and members.”
Employers often require guidance when choosing a PBM and establishing benchmarks to support a decision.
Paige Zimmer. EVP of Business Development, RxLogic, explains, “We empower employers with data-driven solutions to optimize pharmacy benefits while reducing costs. Employers should prioritize transparency, flexibility, and analytics-driven decision-making when selecting a PBM.”
The organization provides a PBM claim adjudication platform that is tailored for self-funded employers, allowing for customized, cost-effective pharmacy benefit management. Through rebate
Depend on Sun Life to help you manage risk and help your employees live healthier lives
By supporting people in the moments that matter, we can improve health outcomes and help employers manage costs.
For over 40 years, self-funded employers have trusted Sun Life to help them manage financial risk. But we know that behind every claim is a person facing a health challenge and we are ready to do more to help people navigate complicated healthcare decisions and achieve better health outcomes. Sun Life now offers care navigation and health advocacy services through Health Navigator, to help your employees and their families get the right care at the right time – and help you save money. Let us support you with innovative health and risk solutions for your business. It is time to rethink what you expect from your stop-loss partner.
Ask your Sun Life Stop-Loss Specialist about what is new at Sun Life.
For current financial ratings of underwriting companies by independent rating agencies, visit our corporate website at www.sunlife.com. For more information about Sun Life products, visit www.sunlife.com/us. Group stop-loss insurance policies are underwritten by Sun Life Assurance Company of Canada (Wellesley Hills, MA) in all states, except New York, under Policy Form Series 07-SL REV 7-12 and 22-SL. In New York, Group stop-loss insurance policies are underwritten by Sun Life and Health Insurance Company (U.S.) (Lansing, MI) under Policy Form Series 07-NYSL REV 7-12 and 22-NYSL. Policy offerings may not be available in all states and may vary due to state laws and regulations. Not approved for use in New Mexico.
administration services, a copay program, eVoucher programs, discount card network and commercial network partners, employers can provide solutions that can be essential to lowering their costs, as well as their employees.
“Employers also seek advanced analytics and reporting tools that provide insights into medication usage, cost trends and opportunities to optimize their plans,” says Zimmer. “Employers need ways that deliver transparency, efficiency, and innovative solutions. By equipping employers with these capabilities, we help employers access the best financial and healthcare outcomes."
JUMBO PBM RESPONSE
One large PBM is taking the rebate criticism off the table. Optum Rx announced that it will soon pass all rebates it gets from prescription drug manufacturers on to employer health plan sponsors and other clients. Leaders maintain that the PBM already passes 98% of the rebates it negotiates on to the customers, but customers that account for about 2% of the rebates have voluntarily chosen compensation arrangements that let UnitedHealth keep about 2% of the rebates.
UnitedHealth does not post details about the cash flow related to drug debates, but it reported in its annual financial statement for 2023 that it accumulated $11 billion in prescription rebate receivables on its consolidated balance sheets as of the end of 2023, up from $8.2 billion at the end of 2022.
Signaling change, CVS Health continues to undergo significant leadership shuffling as it navigates challenges in its insurance and PBM segments. Its Caremark PBM ushered in a new president as part of the executive shifts as the company grapples with increased medical costs and heightened regulatory scrutiny.
Laura Carabello holds a degree in Journalism from the Newhouse School of Communications at Syracuse University, is a recognized expert in medical travel and is a widely published writer on healthcare issues. She is a Principal at CPR Strategic Marketing Communications. www.cpronline.com
M&A MANIA INFUSING SELF-INSURANCE WITH POWER PLAYS
Private equity investment leads the way as partnerships scale their presence
Editors Note: For additional M&A-related content, please consider attending SIIA's Corporate Growth Forum, scheduled for June 9-10 in Charleston. Details can be accessed at www.siia.org
Written By Bruce Shutan
TheTself-insurance sector is rapidly approaching a $40 billion premium market – nearly three times what it was valued in the late 1990s, observes Dan Bolgar, CEO of Carbon Stop Loss Solutions. That makes it palatable for investors seeking a solid return on their investment. In turn, all the money pouring into this space is expected to help self-insured employers level up their efforts to contain costs and improve clinical outcomes.
He says major players include the BUCAs (Blue Cross Blue Shield UnitedHealthcare Cigna Aetna), Tokio Marine HCC, Voya, and Sun Life, while about 80% of reinsurance premium is written by the top 20 market players and roughly 50 MGUs have invested in this space.
“PE [private equity] firms and investors love a business that’s organically growing at 12% or 13% a year, and I don’t see that stopping anytime soon,” Bolgar explains. Another big driver is the massive need for efficiency in healthcare. "It's much easier for them to go after it as an independent MGU [managing general underwriter] than it is to pick up a carrier,” he says, noting how carriers that take on risk associated with massive balance sheets can become a volatile investment, whereas MGUs are fueled by fee income. MGUs are also significantly smaller and easier to invest in than a large carrier, and they can flip the investment after five to seven years of growth, he adds.
There’s no doubt that M&A activity is heating up in the reinsurance space, whose total stop-loss market is currently valued at $37 billion and posting annual double-digit growth as more employers self-fund their group health plans, according to Bob Black, executive managing director for Aon, which last year acquired NFP, the owner of four stop-loss MGS.
VERTICAL INTEGRATION
The most interesting and innovative M&As in the selfinsurance space centers around vertical integration that pairs cost-containment, clinical capabilities and additional products on top of an administrative platform, says Trey Marinello, managing director for Houlihan Lokey. “Companies in the lower middle market, especially cases or groups of 50 to 200 lives, tend to have pronounced profitability relative to those focused up market,” he explains. “The next phase will be the introduction of risk-taking to round out a closed-loop system.”
Employers are pursuing levelor self-funded strategies in partnership with forwardthinking insurance brokers and independent third-party administrators (TPAs) to help take ownership of their healthcare costs, Marinello notes. The goal is to make the company more profitable while at the same time elevating member benefits by improving the health of the member population preventively and reactively. “As time goes by,
claims data informs the TPA as to how to better control costs without sacrificing benefits,” he adds.
Regulatory changes and a new administration could serve as a catalyst for new opportunities within the healthcare market, notes Vinny Esposito, CEO at S&S Health who has a hedge fund background. “We see a ton of activity in the TPA and technology space,” he says. “You got companies like Valence that have been very acquisitive over the past few years. Companies with really solid execution operations are finding homes, whether it be through private equity, a PE-backed asset or BUCA.”
Esposito sees money flowing into telehealth mostly around behavioral health aspects, as well as on the captive side and TPA space. Two standout deals in his view include the merger of Virgin Pulse and HealthComp – rebranded Personify Health – and recapitalization of Allied Healthcare Products when it was acquired by Flexicare (Group) Limited. “There’s a lot of big money going into everything within the supply chain for product to service components,” he reports.
PE powerhouses such as Blackstone, KKR and Apollo Global Management have been actively investing in healthcare and insurance-related companies. Stop-loss now includes health plans, health systems, traditional health insurers, aggregators, reinsurers, wholesalers, venture capitalists and PE firms that have entered the market through entities that they own or brokers, Black explains.
The lines of demarcation are often blurred. For example, he says Unum sold its block to Amynta Group, which is an aggregator, and then Amynta hired Byron Way from Skyward Accident & Health to lead the firm and partner with Crum & Forster. Once they’ve established a stronghold, many of these entities then buy other blocks of business.
Prudential and Old Republic are new entrants into the stop-loss market over the past year, which Black says opens up quite a bit of opportunity. As companies become acquired, individuals who control portfolios from large writers like Sun, Symetra or Voya sometimes start their own entities, which he says happened with Evolution Risk Partners, an MGU formed by underwriters at a much larger organization. Some recent players in self-insurance have tried to develop almost like a health system, Black observes, citing as examples Gravie, Angle Health and Sana Benefits.
A COMMON THREAD
The common thread is an underwriting model featuring a TPA, some of whom are taking risk with an insurance entity or captive, as well as their own brokerage talking directly to employer groups or other agents to bring in business. Their objective is to control data, understand and correctly price risk and exposure, and then manage claims. “When companies develop all of that, they’re thinking that they can have a better impact on the business than if they just handle one component of that whole ecosystem,” he explains.
Among the noteworthy deals Bolgar has seen over the past two years: Crum & Forster’s acquisition of Partners Managing General Underwriters LLC, an MGU rolled into the carrier space, as well as his own firm, Sequoia Reinsurance Services, being acquired by Carlyle Group, the world’s third-largest PE firm, combined with two other MGUs and rebranded. Others include Ryan Specialty’s acquisition of an MGU called AccuRisk Holdings, which had previously been acquired
by another PE-backed firm, Ardonagh Group, Amynta Group’s acquisition of Unum Group’s medical stop-loss business and Core Specialty’s acquisition of the medical stop-loss unit of American National Group.
Aside from PE, Bolgar notes that other sources of capital may pour into the self-insurance space from publicly traded companies being pushed to grow, hedge funds (albeit a bit more removed) and pension funds looking for a nice return. But there are caveats to consider. “If the market looks like it’s returning to a lower interest rate environment, then we expect capital from all angles to probably come back in an even bigger way looking for a return on that growing market,” he says.
Houlihan Lokey closed six transactions in 2024 across the employer-sponsored healthcare space for more than $3 billion. That momentum in the category has translated into several new assignments for 2025. Among the 2024 employer-sponsored transactions were two TPAs, two clinical businesses and two health-engagement companies.
Of note, the firm represented a leading TPA called Allied Benefit Systems for the second time in a recapitalization transaction on behalf of Stone Point Capital and a new investor. The business had experienced outstanding organic growth over a 20-year period; now, the goal was to continue that growth trajectory alongside a new investor by bolting onto the TPA’s platform additional costcontainment solutions, clinical
capabilities, data analytics or specialty benefit management services for a more comprehensive service offering via M&A.
Another interesting emerging growth company worth keeping a close watch on is a digital mental health provider called CuraLinc. Houlihan Lokey, along with Alliant Insurance Services, advised Lightyear Capital on the platform acquisition in 2024. Since the platform investment by Michael Langer, CuraLinc has pursued an inorganic expansion strategy bolting on multiple complementary horizontal tuck-ins. The business is differentiated vs. traditional employee assistance programs in its ability to drive heightened engagement and utilization at a modest price point, thereby adding real value to members and plan sponsors as opposed to a check-the-box EAP.
Employer-sponsored healthcare has captured the attention of private-equity investors over the past five to seven years “partially because it’s about healthcare lite,” according to Marinello. “The reality is that many of the businesses in this category are business services sold into a healthcare end market. They can be more administrative than clinical, which sidesteps certain risks from which healthcare providers cannot so easily distance themselves. In addition, this ecosystem has a large and growing total addressable market, high-quality revenue streams and real switching costs, among other sought-after investment criteria."
The big payoff for PE is equipping a platform with multiple costcontainment solutions and possibly the ability to write reinsurance or retain risk. Together, these solutions provide exceptional visibility into forward earnings, he says. Once selfinsured companies are able to turn a corner controlling costs, especially when it comes to heading off chronic conditions with preventive medicine, Marinello says member sentiment improves, employer-TPA adhesion strengthens, and costs diminish as a percentage of revenue, which is the overarching goal.
With a growing need to take fiduciary responsibilities more seriously since passage of the Consolidated Appropriations
Act known as the CAA and avoid litigation, HR teams need to double down on their commitment to doing right by their employees, notes Trish Watson, senior vice president for Alliant Insurance Service. She says that includes everything from network and plan designs to Rx programs, which is why welcoming new investment opportunities in the self-insured space is so critically important.
RISE OF GROUP CAPTIVES
There seems to be a lot of interest in group captives from across the industry, Black reports. “Everybody looks at Pareto and how big they are and thinks they can duplicate that,” he says. “They’re the 800-pound gorilla on the market approaching $2 billion. I don’t know if that’s ever going to happen, but when you’re able to pull together a good number of smaller risks and aggregate that to be a more credible block, it starts to make sense when you’re supporting them.”
In the captive insurance space, however, Marinello cautions that the Pareto’s of the world are few and far between. The firm, owned by two prominent PE sponsors, Warburg Pincus and Great Hill Partners, continues to grow and serve the lower middle market. “It’s a great complement to a self-insured plan and a divergent strategy from just carrying reinsurance,” he opines.
The most recent player in this category that is capturing market share is ClearPoint Health, whose CEO Jeb Dunkelberger “has done a nice job putting the necessary pieces in place to capture market share,” he says. The Stone Point Capital-owned company has "all the elements necessary to be successful, and an ability to draw benefit from other investments across the parent company's portfolio is unique to the industry," he adds.
Some traditional insurance carriers are launching their own captive solution to compete against industry behemoths like Pareto and Roundstone, notes Chad Schulz, executive vice president and managing director of private equity, mergers, and acquisitions for Alliant Insurance Services.
"We've seen a growing interest in independent third-party administration," he says. "As a result, many of the BUCAs have purchased their own TPA, with UnitedHealthcare buying UMR, Aetna buying Meritain Health, and Cigna buying Allegiance. That’s a way for them to have an offering that looks like an independent TPA when it’s still owned by a BUCA.”
Other areas of interest are also emerging. Marinello is bullish on the direct primary care (DCP) category, whose leader is the OMERS Private Equity-owned Premise Health, which Marinello says will be looking for liquidity this year. Care ATC, Marathon, Proactive MD, and Next Level Healthcare are other noteworthy players that have caught his attention.
He predicts that the pharmacy category, which is a $650 to $700 billion market in the U.S. alone, will likely draw considerable attention in the coming years. While questions persist around future state regulation of PBMs, Esposito says the space is still drawing quite a bit of capital – especially those that are going to market with a direct message and disclosing transparent fees.
Another category that’s attracting considerable interest is concierge or advocacy services to help members navigate their health plan. Finally, he has noticed investment in several early and midsize companies that are “at an escape velocity point in the data and predictive analytics work where they’ve embraced the most level of AI.”
When assessing the extent to which all this investment pouring into the self-insured space will help bolster cost-containment strategies, Schulz cites several areas where it could really help move the needle. They include independent third-party administration, direct primary care in onsite and near-site clinics, the glucagon-like peptide-1 category (better known as GLP-1), steering covered lives to high-quality providers, transparent PBMs and independent coverage health reimbursement arrangements. With regard to ICHRAs, he believes the next two to three renewal cycles will be an indication of whether they’re here to stay.
SMALLER INDEPENDENT MEDICAL PRACTICES BANDING TOGETHER
A combination of inflation and labor shortages have prevented independent providers from being able to compete as aggressively in denser, more vibrant markets, explains Roger Hau, founder and CEO of PayerPrice, whose software identifies healthcare provider M&A targets.
“What we’ve seen is independent funders like private equity take a few smaller independent groups, combine them, consolidate back offices, reduce costs and at the same time provide a higher quality of care perhaps in an outpatient setting compared to the hospital," he says, noting that such steps are only enabled by scale. What motivates these providers is that it gives them superior negotiating power when there is strength in numbers.
Strategies to divert care from the most expensive side of inpatient to outpatient settings, while not guaranteed to deliver better patient results, drive material costs and quality improvements for patients and, ultimately, self-insured employers, according to Hau.
In helping physician practices stay independent, Hau cautions that over-consolidation of the healthcare space can lead to extreme cost overruns and some large hospital systems or providers monopolizing their markets, especially with the entry of private equity.
Since the Trump administration would like to see more competition between smaller and midsize groups, as well as larger hospital systems, he predicts that transaction activity will be markedly higher in the next three years.
“What we’re going to end up seeing is a convergence of supply and demand in this market where the payers are going to feel pressure to lower cost and improve the quality of care,” Hau says, “and they’re going to rejigger all their fee schedules to pay those outpatient providers more probably at the expense of some of these hospital systems.”
Bruce Shutan is a Portland, Oregon-based freelance writer who has closely covered the employee benefits industry for more than 35 years.
FINAL MENTAL HEALTH PARITY RULES: A PLAN SPONSOR’S IMPLEMENTATION GUIDE
PART II: COMPLYING WITH NQTL AND COMPARATIVE ANALYSIS REQUIREMENTS
InIEditor’s Note: This is the second article in a three-part series. Part one was published in the March edition of the Self-Insurer.
Written By Alston & Bird LLP Health Benefits Practice
September 2024, the U.S. departments of Labor, Treasury, and Health and Human Services (the “Departments”) issued a Final Rule under the Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA). The Final Rule, which codifies prior guidance, has a general effective date of the first day of the plan year beginning on or after January 1, 2025. Note that most of these requirements for completing the comparative analysis were first due as of February 10, 2021, under the Consolidated Appropriations Act, 2021 (CAA). Additional new requirements are effective within the first plan year starting on or after January 1, 2026.
This article is the second in a three-part series designed to inform plan sponsors of self-insured plans about the key components of the Final Rule and compliance steps for satisfying regulatory requirements. In Part I, we provided a high-level overview of the essential elements of the Final Rule, focusing on the two-part test for nonquantitative treatment limitations (NQTLs) and the requirement to perform an NQTL comparative analysis. In this Part II, we note the key differences from the proposed rule and provide an overview of compliance action steps, timeframes, and requirements for the Final Rule in further detail. First, though, we start with some highlights from the Department of Labor’s (DOL) 2024 Report to Congress, released in January 2025. For purposes of this article, "mental health/substance use disorder" is referred to as "MH/SUD," and "medical/surgical" is referred to as "Med/Surg."
2024 REPORT TO CONGRESS: MORE OF THE SAME
MHPAEA requires the Departments to submit a “Report to Congress” on MHPAEA compliance by group health plans every two years (previous reports are available here). In the 2024 Report to Congress (released in January 2025), the Departments repeated the concerns from prior reports that plans have either failed to prepare a comparative analysis altogether or have prepared a deficient comparative analysis. The Departments identified some of the most common compliance failures that they continue to see:
• failure to document a comparative analysis before designing and applying the NQTL;
• conclusory assertions lacking specific supporting evidence or detailed explanation;
• lack of meaningful comparison or analysis;
• nonresponsive comparative analysis;
• documents provided without adequate explanation;
• failure to identify the specific MH/SUD and Med/Surg benefits or MHPAEA benefit classifications affected by an NQTL; and
• focusing only on similarities—rather than explaining differences—to show parity.
The Departments attribute these deficiencies to inadequate preparation of the comparative analysis that attempts to justify practices that were adopted without taking MHPAEA into account at all. To assist plans and issuers in performing and documenting sufficiently, the Departments announced that they are developing “sample” comparative analyses that “will reflect a combination of the kinds of information” that investigators found helpful in investigations of similar NQTLs and will comply with the requirements of the 2024 Final Rules.
The Departments also provide information on top enforcement priorities in the reports. The six priority areas the Departments first identified in the July 2023 Report to Congress continue to comprise the vast majority of NQTLs that are the subject of review in enforcement cases:
• Prior authorization requirements for in-network (INN) and out-of-network (OON) inpatient services
• Concurrent care review for INN and OON inpatient and outpatient services
• Standards for provider admission to participate in a network, including reimbursement rates
• OON reimbursement rates (methods for determining usual, customary, and reasonable charges)
• Adequacy standards for MH/SUD provider networks
• Impermissible exclusions of key MH/SUD treatments
The 2024 Report added that the DOL has deepened its focus on the last two NQTLS in the list, a focus that is also reflected in the 2024 Final Rule.
KEY DIFFERENCES BETWEEN THE PROPOSED RULE AND THE FINAL RULE
The Final Rule adopted much of the rule proposed on July 25, 2023, with two significant changes:
1. No substantially all/predominant test. Instead of adapting the substantially all/predominant mathematical test to NQTLs, the Final Rule provides that this statutory requirement is met if both (i) the design and application requirements and (ii) the relevant data acquisition requirements are met (see Part I for a thorough review of the two-part test used to determine whether NQTLs are more restrictive on MH/SUD benefits); and
2. No automatic violation of MHPAEA for material difference in network composition. Under the Proposed Rule, a material difference regarding network composition NQTLs would be a violation of the MHPAEA. In the Final Rule, the departments treat data collection and analysis for a network composition NQTL the same as any other NQTL under the “strong indicator” standard.
Other noteworthy changes include how independent professional medical or clinical standards and fraud and abuse measures factor into the analysis of an NQTL; modification to the fiduciary certification of the NQTL comparative analysis; and a determination, at this time, not to adopt a “relevant data requirement” safe harbor for network composition NQTLs that was suggested in the Technical Release that accompanied the Proposed Rule.
NQTL COMPARATIVE ANALYSIS CONTENT REQUIREMENTS
The CAA required each plan to have a written NQTL comparative analysis with five elements.
The Final Rule, like the Proposed Rule, reorganizes and expands on these requirements, incorporating a demonstration of the two requirements for NQTLs, as discussed in Part I (i.e., the design and application requirements and the relevant data evaluation requirements). The six broad requirements are:
1: Description of the NQTLs. There are three subparts here:
• Identifying NQTLs from plan documents, policies, guidelines, provider contracts, or other places they might appear;
Under the Proposed Rule, application of the substantially all/predominant test was also part of this requirement. With the removal of that requirement from the Final Rule, it has also been removed as a part of the comparative analysis.
2: Identification and definition of the factors used to design or apply the NQTL. This is part of the design and application requirements that, in large part, have been the basis of the required NQTL comparative analysis since February 10, 2021. Here, the plan will identify and give a detailed description of the factors relied upon to design and apply the NQTL, as well as the evidentiary standards supporting those factors. The Final Rule adds a provision prohibiting the use of “discriminatory” or biased information in design and application of NQTLs, unless a plan has taken steps necessary to correct, cure, or supplement any information, sources, or standards that would otherwise be biased or not objective. This prohibition against using discriminatory or biased information is effective for plan years beginning on or after January 1, 2026.
3: Description of how the factors are used in the design and application of the NQTL. This requirement codifies much of the prior 2021 FAQs Part 45 on the content of an NQTL comparative analysis. For this part, a plan must provide a detailed explanation of how each factor is used to determine which MH/SUD and Med/Surg benefits are subject to the NQTL, as well as an explanation for the evidentiary standards or other information or sources (if any) considered or relied on in designing or applying the factors or relied upon in designing and applying the NQTL, including in the determination of whether and how MH/SUD or Med/Surg benefits are subject to the NQTL. When specific decisions made in the administration of benefits affect the NQTL, the comparative analysis would be required to provide information on the nature and timing of the decisions, and on the professional designations and qualifications of each decision-maker. Also, this description would include any weighting and ordering of factors and the reasons for the weighting and ordering. Any deviations or variations from a factor would also have to be included in this part of the comparative analysis.
4: Determination of comparability and stringency as written. Here, the plan must look at each classification and evaluate whether, under the terms of the plan as written, any processes, strategies, evidentiary standards, or other factors used in designing and applying the NQTL to MH/ SUD benefits are comparable to, and are applied no more stringently than, these same evidentiary standards and factors for Med/Surg benefits. This includes a showing of why or why not an NQTL was applied to MH/SUD or Med/Surg benefits in the same classification, how the NQTL is applied, as written, to MH/SUD or Med/Surg benefits (including the use of any forms, checklists, procedure manuals, or other documentation in applying or designing the NQTL), and an explanation for deviations or variations.
5: Determination of comparability and stringency in operation. The “as written” and “in operation” stringency requirements are similar in that they both require discussion of the results of the relevant data evaluation requirements. The Final Rule includes provisions on stringency in operation requiring a detailed identification of the data collected, an evaluation of the outcomes of the data, a detailed description of any material differences found that are not attributable to access of MH/SUD benefits as compared to Med/Surg benefits, and actions taken to address any material differences.
The Final Rule adds or augments several provisions to this fifth requirement:
• For a new NQTL for which data is currently unavailable, there must be a detailed explanation of the lack of relevant data, the basis for the plan’s conclusion that there is a lack of relevant data, and when and how the data will become available and be collected and analyzed.
• Except in the case of a new NQTL, when a plan asserts no data exists, there must be a “reasoned justification” as to the basis for the conclusion that there is no data, an explanation of why the nature of the NQTL prevents the plan from reasonably measuring its impact, an explanation of what data was considered and rejected, and documentation of any additional safeguards or protocols used to ensure that the NQTL complies with all applicable requirements.
• The Final Rule requires more specifics on instances when material differences are not attributable to differences in the comparability or relative stringency of an NQTL as applied to MH/SUD benefits as compared to Med/Surg benefits. There must be a reasoned and detailed discussion of any considerations beyond a plan’s control that contribute to the existence of material differences, as well as a detailed explanation of the bases for concluding that material differences are not attributable to differences in the comparability or relative stringency of the NQTL. This explanation should be comprehensive and include evidence to support the conclusion that considerations beyond a plan’s control contribute to the existence of material differences in access to MH/SUD benefits.
• To the extent differences in access to MH/SUD benefits are attributable to generally recognized independent professional medical or clinical standards or fraud and abuse measures that comply with the Final Rule, there needs to be an explanation of how any such differences are attributable to those standards or measures.
• Finally, more detail is required on reasonable actions taken to address material differences and whether such differences persist after such action.
6: Findings and conclusions. The comparative analysis must address the findings and conclusions, including those that indicate that the plan “is or is not (or might or might not)” be in compliance, as well as explain any actions the plan is taking or intends to take to address areas of concern. This must be accompanied by a “reasoned and detailed discussion” of the findings and conclusions, complete with citations to any additional information not otherwise included in the comparative analysis. Basic formalities of date completed and title and credentials of all relevant persons who participated in the performance and documentation of the comparative analysis are also required, as well as an assessment of the qualifications of any participating reviewer or consultant considered by the plan to be an “expert,” and the extent to which the plan ultimately relied upon the expert’s evaluation. Significantly, the Final Rule modified the Proposed Rule on the fiduciary certification. As part of the findings and conclusions of the NQTL comparative analysis, the Proposed Rule required one or more named fiduciaries to certify the results for ERISA-covered plans. The Final Rule requires one or more named plan fiduciaries to confirm such fiduciary’s engagement in a prudent process to select one or more qualified service providers to perform and document a comparative analysis as well as satisfaction of the duty to monitor those service providers.
NQTL COMPARATIVE ANALYSIS PROCESS
The Final Rule provides further clarity on the NQTL comparative analysis process. All plans should at least have the initial comparative analysis that was due to be completed as of February 10, 2021 (under the CAA). The Employee Benefits Security Administration (“EBSA”) is the DOL agency responsible for enforcing MHPAEA. Its general process for reviewing NQTL comparative analyses is as follows:
• EBSA requests NQTL comparative analyses and supporting documentation from plans or issuers with potential NQTL violations or complaints.
Response time for requests from EBSA: at least 10 business days unless an additional period of time is specified.
• EBSA assesses the sufficiency of the NQTL comparative analysis and information provided. If insufficient, EBSA issues an insufficiency letter, and the plan or issuer is given an opportunity to provide additional information.
Response time for follow-up requests from EBSA: at least 10 business days unless an additional period of time is specified.
• EBSA determines the NQTL’s compliance with the law. If the NQTL is in violation of parity laws and/or documentation was insufficient, EBSA issues an initial determination letter.
Response time to provide EBSA with a corrective action plan and additional comparative analyses that address the violation: 45 calendar days.
• EBSA reviews the submitted documentation to determine the plan’s or issuer’s compliance. If EBSA determines the NQTL is still in violation of parity laws, a final determination letter is issued. The plan or issuer must notify all participants and beneficiaries that it was not in compliance with MHPAEA. The notice must also be provided to any service provider involved in the claims process and to any fiduciary responsible for deciding benefit claims. In addition, EBSA names the violator in the annual report to Congress.
Response time for notifying all participants and beneficiaries that it was not in compliance: 7 business days.
If the Departments determine that the comparative analysis for the NQTL is incomplete or contains insufficient information (i.e., noncompliant) based on a facts and circumstances test, the departments may direct the plan not to apply the NQTL to MH/SUD benefits. This failure is different from a finding that an NQTL itself is in violation of the MHPAEA after applying the design and application requirements and the relevant data evaluation requirements. There, the Departments have full authority to prevent the plan from applying the NQTL.
Lastly, we note that a February 2025 report from the Office of the Inspector General (OIG) identified several challenges that limit EBSA’s efforts to enforce MHPAEA, including NQTL requirements. Notably, EBSA has no ability to directly assess a civil monetary penalty on a plan or issuer for an MHPAEA failure, and the audit revealed that EBSA is not maximizing the use of tools that are available to it. Consequently, EBSA relies primarily on voluntary compliance in its investigations.
Plans Must Provide the Comparative Analysis to Participants Upon Written Request
EBSA is not the only entity that may request a copy of the comparative analysis from a plan. For ERISAcovered plans, the Final Rule provides that the comparative analysis is an instrument under which a plan is established or operated under Section §104(b)(4) of ERISA, which means the plan must provide it to participants and beneficiaries within 30 days of a written request or face up to a $110 per day penalty.
For Next Month….
In the third and final installment, we will cover practical action steps, particularly for service agreements, and cover any new compliance tools that the Departments may issue. We will also provide relevant updates, if any, related to the February 2025 report from the OIG.
Attorneys John Hickman, Ashley Gillihan, Steven Mindy, Amy Heppner, Laurie Kirkwood, and Bria Smith provide the answers in this column. John is partner in charge of the Health Benefits Practice with Alston & Bird, LLP, an Atlanta, New York, Los Angeles, Charlotte, Dallas, and Washington, D.C. law firm. Ashley and Steven are partners in the practice; Amy and Laurie are senior members in the Health Benefits Practice; Bria Smith is an associate in the Employee Benefits Practice. Answers are provided as general guidance on the subjects covered in the question and are not provided as legal advice to the questioner’s situation. Any legal issues should be reviewed by your legal counsel to apply the law to the particular facts of your situation. Readers are encouraged to send questions by E-MAIL to John at john.hickman@alston.com.
NEWS FROM SIIA MEMBERS
2025 APRIL MEMBER NEWS
Provided below are news highlights from these upgraded members. News items should be submitted to membernews@siia.org.
All submissions are subject to editing for brevity. Information about upgraded memberships can be accessed online at www.siia.org.
If you would like to learn more about the benefits of SIIA’s premium memberships, please contact Jennifer Ivy at jivy@siia.org.
SIIA boasts a very active and dynamic membership. Here are some of the latest developments from the companies powering the self-insurance industry.
ParetoHealth Names New CEO
ParetoHealth has appointed Maeve O'Meara as its new Chief Executive Officer. O'Meara, who has served as President since September 2023, will succeed Andrew Cavenagh, the company's co-founder, who will remain deeply engaged in the business in the role of Executive Chairman.
O'Meara brings 20 years of leadership in healthcare and technology, having previously served as CEO of Castlight Health, where she transformed the business into a market-leading navigation platform serving millions of Americans. "This is an exciting milestone for ParetoHealth and reflects that our best years are in front of us. Maeve lives our core values and brings a unique combination of leadership, vision, and operational rigor to lead us in this next chapter," said Andrew Cavenagh, Executive Chairman of ParetoHealth.
Since joining ParetoHealth, O'Meara has led initiatives to deepen consultant and member engagement, put in place the technology and infrastructure to operate at scale, and built out the leadership team. This work supports ParetoHealth's continued mission to eliminate volatility and lower health benefits costs for midsize employers. A savings study from 2024 shows that members of the community realize 16.5% annual savings compared to traditional insurance.
"I'm honored to lead a team that has truly challenged the status quo in enabling midsize employers to offer more affordable health benefits," said O'Meara. "It is a privilege to partner with our incredible consultant and employer community to continue to innovate and redefine what is possible."
Vālenz Expands Executive Team with New Chief Client Officer
Vālenz® Health announced that Anthony Naes has been named Chief Client Officer.
Naes joined Valenz with the acquisition of Healthcare Bluebook™ in July 2024, bringing together the companies' complementary services as a one-of-a-kind member engagement and digital "front door" experience and payment integrity data platform. He served as Senior Vice President of Sales at Healthcare Bluebook, where he led go-to-market teams to help brokers, employers, and third-party administrators lower medical benefits spend and improve quality of care for health plan members.
"Anthony brings a wealth of market knowledge to his new role, along with demonstrated sales acumen, natural leadership skills and a passion for mentoring," said Nathan Nelson, Chief Growth Officer at Valenz. “Leading
Maeve O'Meara ParetoHealth
Anthony Naes Vālenz® Health
our client service function, Anthony will foster and grow our customer relationships while continuing to deliver on the unmet and underserved needs of our clients across the self-insurance industry.”
MultiPlan Changes Name to Claritev
Long-time self-insurance industry leader MultiPlan has announced it has changed its name to Clartev as part of a corporate re-brand.
"Claritev is proud of the clients that we serve and has come a long way since our founding while playing an important role in the healthcare industry. We will continue to do that,” said Travis Dalton, Chairman, CEO and President of Claritev. “However, today’s announcement opens a new chapter for Claritev as we accelerate the use of innovation and technology to better serve our core clients and the broader healthcare ecosystem. By embracing technology modernization, data infrastructure, cutting edge tools like AI and scale partners, we believe we will be best positioned against the competition, but most importantly, best equipped to bring value to our clients and those they serve.”
Boon-Chapman Strengthens Sales Team
Boon-Chapman announces the appointment of Marcus Kammrath as Regional Vice President.
Kammrath brings over a decade of industry experience, having held leadership roles in account management, business development, sales, and partner enablement in the health plan analytics space. A passionate employer advocate, he has a proven track record of driving growth and innovation with an analytics-driven approach.
"Employers rely on strong partnerships to navigate the complexities of the healthcare industry. Marcus's deep understanding of data-driven decision-making, coupled with his commitment to employer advocacy, will strengthen our relationships with consultants and employers alike— delivering the strategies and support they need to drive results," said Kari L. Niblack, President of BoonChapman.
Prior to joining Boon-Chapman, Marcus worked at Springbuk, where he supported consultants and employers in leveraging data to drive smarter benefits strategies. He understands that a lack of data comprehension can lead to ineffective plan decisions, and he is committed to bridging that gap. In his new role, Marcus will focus on strengthening partnerships, ensuring employer needs remain a top priority, and empowering consultants to showcase Boon-Chapman’s extensive suite of services. He believes in the power of a strong TPA partnership as the first line of defense in benefits strategy, ensuring employers receive the guidance and insights they need.
H.H.C. Group Receives ISO Certification
H.H.C. Group (H.H.C.) has achieved the globally recognized ISO 9001:2015 certification with the expert guidance of ISOP Solutions. This certification validates H.H.C. Group’s steadfast commitment to operational precision, compliance and delivering exceptional value to its clients.
Marcus Kammrath Boon-Chapman
We deliver best-in-class solutions that cover your clients and support you with experts in data analytics, underwriting, claim reimbursements, dedicated account management and CompanionCARE SM
With CompanionCARE, you have access to experts in large case management and emerging therapies.
Our stop loss contracts are backed with the strength reflected in our A+ AM Best company rating.
In addition to specific and aggregate stop loss insurance, Companion Life offers an array of innovative products:
"Attaining ISO 9001:2015 certification means that H.H.C.'s systems and processes align with rigorous international standards, allowing the Company to enhance customer satisfaction, streamline operations and ensure consistently high-quality service," says Bruce D. Roffé, President and CEO of H.H.C. "This milestone reinforces H.H.C.'s position as a trusted partner for self-insured employers, TPAs, stop-loss carriers and unions across the country."
ISO 9001:2015 certification is a globally respected framework for quality management systems designed to help organizations improve efficiency, enhance customer experiences, and demonstrate their capability to deliver reliable and consistent outcomes. Certification is recognized as a symbol of operational integrity and excellence in industries worldwide.
“You have become a key partner in our company’s attempt to fix what’s broken in our healthcare system.”
- CFO, Commercial Construction Company
“Our clients have grown accustomed to Berkley’s high level of customer service.”
- Broker
“The most significant advancement regarding true cost containment we’ve seen in years.”
- President, Group Captive Member Company
“EmCap has allowed us to take far more control of our health insurance costs than can be done in the fully insured market.”
- President, Group Captive Member Company
“With EmCap, our company has been able to control pricing volatility that we would have faced with traditional Stop Loss.”
- HR Executive, Group Captive Member Company
People are talking about Medical Stop Loss Group Captive solutions from Berkley Accident and Health.
Our innovative EmCap® program can help employers with self-funded employee health plans to enjoy greater transparency, control, and stability.
Let’s discuss how we can help your clients reach their goals.
This example is illustrative only and not indicative of actual past or future results. Stop Loss is underwritten by Berkley Life and Health Insurance Company, a member company of W. R. Berkley Corporation and rated A+ (Superior) by A.M. Best, and involves the formation of a group captive insurance program that involves other employers and requires other legal entities. Berkley and its affiliates do not provide tax, legal, or regulatory advice concerning EmCap. You should seek appropriate tax, legal, regulatory, or other counsel regarding the EmCap program, including, but not limited to, counsel in the areas of ERISA, multiple employer welfare arrangements (MEWAs), taxation, and captives. EmCap is not available to all employers or in all states.
Nova Administrators Named a Best Place to Work
Nova Healthcare Administrators, Inc. has once again been named one of the Best Companies to Work for in New York—marking its eighth consecutive year on this distinguished list.
The statewide awards program honors top workplaces that contribute positively to New York's economy, workforce, and business community. Winners will be recognized at an awards ceremony in Albany on April 10, where final rankings will be announced.
"Earning this recognition for eight years in a row is a tremendous achievement," said James Walleshauser, President of Nova Healthcare Administrators. “It’s a testament to the dedication and collaboration of our team. At Nova, we foster a culture that values creativity, inclusivity, and engagement—where every associate feels empowered and motivated to make a difference.”
John Weitzel Joins HM Insurance Group Sales Team
HM Insurance Group has named John Weitzel the Director of Houston Regional Sales. In this role, he will work to grow and maintain the HM Insurance Group (HM) Stop-Loss book of business in HM’s Houston Regional Sales territory, which serves southern Texas and Louisiana.
John came to HM from Voya, where he served as a senior sales representative since 2015. He also has held senior account executive roles at The Hartford and MetLife. With more than 30 years of sales experience in the Southern Texas and Louisiana group insurance markets, John brings a great deal of knowledge to HM.
Blackwell Promotes Scott Lydon
Blackwell Captive Solutions has announced the promotion of Scott Lydon to Senior Vice President, National Sales. As demand for alternative risk management solutions grows, Lydon will spearhead Blackwell's nationwide sales initiatives and oversee client management, driving the company’s continued growth and commitment to delivering tailored solutions that help employers control healthcare costs.
"I am honored to step into this new role at such a dynamic time for Blackwell Captive Solutions," said Lydon. "As demand for creative and cost-effective healthcare solutions rises, I am committed to leading
John Weitzel HM Insurance Group
Scott Lydon
Blackwell Captive Solutions
Give Your Clients The Power of True Independence
At Pinnacle Claims Management, we answer only to you and your clients, not investors.
As an independent TPA, we’re free from conflicts of interest and short-term pressures, giving you the flexibility to offer unmatched health benefits solutions that others can’t. With transparency and a focus on long-term service, we’re the partner who always puts your clients first.
Discover how PCMI’s independence can elevate your client relationships. Partner with us today. Discover
Kesler Prodigy Health Insurance Services
our sales efforts and fostering strong relationships that drive value for our clients."
David Kesler Joins Prodigy Health Insurance Services
Prodigy Health Insurance Services has welcomed David Kesler as Vice President of Underwriting. Kesler's arrival aligns with Prodigy's strategic growth and our mission to deliver innovative risk management solutions across the healthcare insurance landscape.
Kesler will be heavily involved in the recently launched IHS level-funded quoting tool for brokers and TPA. The system is currently available by invitation only, but Prodigy is looking forward to a full rollout in the months ahead.
"We are thrilled to welcome David to the team," said John Youngs, CEO of Prodigy Health Insurance Services. “His expertise and strategic insight bring tremendous value to our underwriting team, strengthening our capabilities and enhancing our initiatives with IHS.”
David
Proceed With Confidence Mind Over Risk
We study it, research it, speak on it, share insights on it and pioneer new ways to manage it. With underwriters who have many years of experience as well as deep specialty and technical expertise, we’re proud to be known as experts in understanding risk. We continually search for fresh approaches, respond proactively to market changes, and bring new flexibility to our products. Our clients have been benefiting from our expertise for over 50 years. To be prepared for what tomorrow brings, contact us for all your medical stop loss and organ transplant needs.
Tokio Marine HCC - Stop Loss Group
member of the Tokio Marine HCC Group of Companies
HCC Life Insurance Company operating as Tokio Marine HCC - Stop Los Group
UME Adds Three New
Philadelphia, PA – Underwriting Management Experts (UME), a leading Managing General Underwriter (MGU) specializing in self-funded employer stop-loss coverage and innovative insurance solutions, is proud to welcome three accomplished professionals to its growing team. These strategic hires bring a wealth of new knowledge, with decades of industry experience and a wide range of skills and strengths. Their addition to the team will reinforce UME’s commitment to innovation, operational excellence, and providing best-in-class self-funding solutions for our partners and clients.
Michael Famularo joins UME as Vice President of National Captive Sales, bringing over a decade of experience in alternative funding, employee benefits, and group captives. He has structured successful captive programs and developed self-funding solutions that maximize efficiency and mitigate risk.
Michael Famularo Vice President of National Captive Sales Underwriting Management Experts (UME)
In his new role, Michael will oversee the development and expansion of Sapient Health™, a trademarked, employer-owned division of Lass Re, a division of UME. Sapient Health™ is a fully integrated, transparent, self-funded healthcare insurance solution that prioritizes cost efficiency, financial control, and memberfocused care. With Michael leading the sales efforts, Sapient Health™ aims to provide a strong alternative to traditional insurance models.
Before joining UME, Michael served as Regional Vice President of Sales at ClearPoint Health, where he was instrumental in establishing national partnerships and generating significant top-line revenue. His background also includes various leadership and sales roles at Captive Resources LLC, The Difference Card, and Sun Life Financial, where he consistently surpassed sales targets and built successful captive and self-funded programs for employers of all sizes.
2025 SELF-INSURANCE
INSTITUTE OF AMERICA
BOARD OF DIRECTORS
CHAIRMAN OF THE BOARD*
Matt Kirk
President
The Benecon Group
CHAIRPERSON ELECT, TREASURER AND CORPORATE SECRETARY*
Amy Gasbarro President
ELMCRx Solutions
DIRECTOR
Mark Combs
CEO/President
Self-Insured Reporting
DIRECTOR
Orlo “Spike” Dietrich Operating Partner
Ansley Capital Group
DIRECTOR
Jeffrey L. Fitzgerald
Managing Director
SRS Benefit Partners
Strategic Risk Solutions, Inc.
DIRECTOR
Mark Lawrence
President
HM Insurance Group
DIRECTOR
Matthew Smith
Managing Director
Risk Strategies
DIRECTOR
Beth Turbitt
Managing Director
Aon Re, Inc.
VOLUNTEER COMMITTEE CHAIRS
Captive Insurance Committee
George M. Belokas, FCAS, MAAA
President Beyond Risk
Future Leaders Committee
Erin Duffy
Director of Business Development
Imagine360
Price Transparency Committee
Christine Cooper CEO aequum LLC
Cell and Gene Task Force
Ashley Hume President
Emerging Therapy Solutions®
* Also serves as Director
2025 BOARD OF DIRECTORS
SIEF CHAIRMAN
Nigel Wallbank President New Horizons Insurance Solutions Wellington, FL
Elizabeth Midtlien Vice President, Emerging Markets
AmeriHealth Administrators, Inc. Bloomington, MN
Jonathan Socko
Senior Vice President East Coast Underwriters, LLC Spartanburg, SC
SIIA NEW MEMBERS
APRIL 2025
NEW CORPORATE MEMBERS
Shannon Ganzer Senior Marketing Specialist Fabric
New York, NY
See the Zelis difference:
Focus on leading, not firefighting.
Managing claims, networks, and payment systems doesn’t have to feel like an uphill battle.
Supercharge Your TPA Operations with Zelis. Call us today at (888) 311-3505 or scan the QR code to get started.
Efficient workflows that save time.
Lower costs with seamless systems.
Happier clients who see the difference.
When you work with the experts at HM Insurance Group, you can be confident that claims will be paid. We process 99% of Stop Loss claims within six business days, with more than 99% technical and financial accuracy. Find more at hmig.com. After back-to-back heart surgeries,
Catastrophic claims can arise unexpectedly. The cost of a cardiac surgery with an additional corrective procedure can quickly reach $800,000.* When the self-funded employer has the right Stop Loss protection in place, focus can remain on achieving business goals and welcoming Leo back when he’s able to return.