Get the peace of mind and support it takes to self-fund your healthcare.
Self-insuring your healthcare benefits can open up new possibilities for your business — affording greater flexibility in how you manage your healthcare spend. Trust the expert team at QBE to tailor a solution that meets your unique needs.
We offer a range of products for protecting your assets, your employees and their dependents:
• Medical Stop Loss
• Captive Medical Stop Loss
• Organ Transplant
We’ll find the right answers together so no matter what happens, your business is prepared.
By Laura Carabello
Written By Kendall Jackson
Written By Lara Carabello
By Bruce Shutan
(ISSN
Written By Alston & Bird Health Benefits Practice
Biosimilars Offer Potential for Significant Savings for Health Plans
TheTWritten By Laura Carabello
buzz around biosimilars and their potential for health plan savings has been building since these drugs entered the market in 2015.
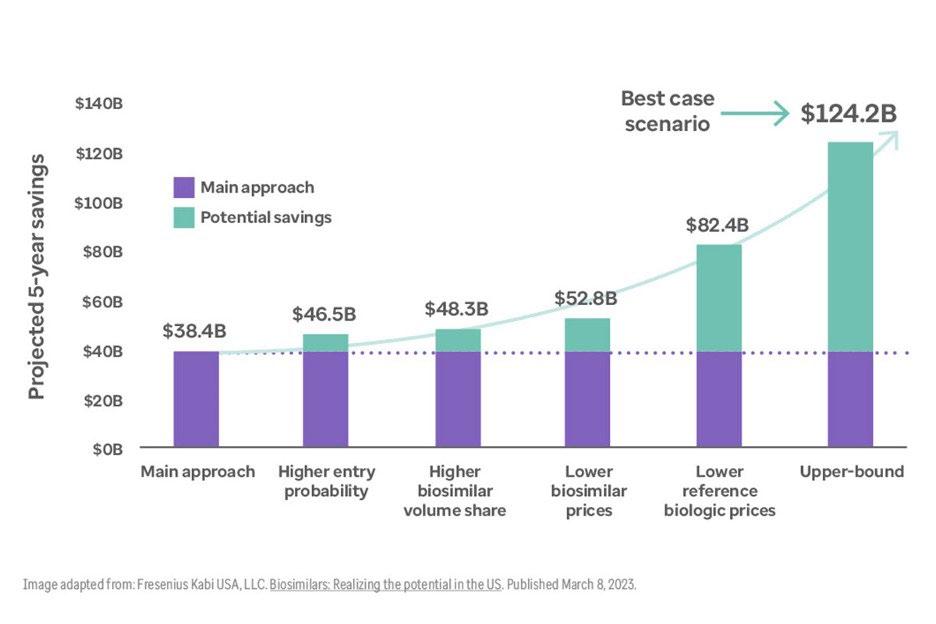
Fast forward to April 2025, when the US House Ways and Means Health subcommittee on the health of the biosimilar market reported that biosimilars had saved the entire US healthcare system over $23.6 billion. Committee members anticipate that biosimilars are poised to save the health care system up to $181 billion over five years if they are able to be adopted – although projected savings differ, depending upon the source, as shown to the right.
Witnesses testified that biosimilars lead to a 53 percent reduction in the average sales price for both the name brand and biosimilar medication and have added 344 million more days of therapeutic care than patients would have otherwise received. They reported that biosimilars launched at prices up to 35 percent lower than branded drugs and can drive further savings when they compete with drugs already on the marketplace. Biosimilars, say the legislators, will provide safe and effective treatment options for patients.
WHAT IS A BIOSIMILAR?
The Food and Drug Administration (FDA) defines a biosimilar as a biological product used in the prevention or treatment of disease and highly similar to an FDA-approved biologic (known as a brand reference product).
Biosimilars are medications with complex manufacturing compared to traditionally developed medications. They are intricately designed molecules that must demonstrate clinical similarity to their brand reference product. Biosimilars increase competition within a therapy class and will often drive down costs over time.
The biosimilar has no clinically meaningful difference from a reference product and is FDA-approved for use after rigorous evaluation and testing is demonstrated by the manufacturer applicant.
Source: Epiphany Rx
Lawmakers also contend that biosimilars help to increase drug supply and availability and have been used in nearly 700 million days of patient therapy. The committee calls for significant efforts going forward to ensure access -- from making drug reimbursement systems work correctly to incentivizing market competition to improve education and awareness among patients and providers.
As prescription medications represent the most influential part of the health plan spend, Glenn Fisher, CEO, NavMD, believes that biosimilars present a high-value, clinically equivalent alternative to costly biologics—especially in managing autoimmune conditions.
Glenn Fisher
Better outcomes. Long-term cost savings.
Mayo Clinic Complex Care Program
experienced a change in diagnosis 52% avoided a locally recommended surgery 23% 85% experienced a change in treatment plan
Discover how a customizable center of excellence program can help minimize healthcare costs while o ering high-cost, high-risk members exactly the care they need.
The Mayo Clinic Complex Care Program is for a small subset of a population with serious, complex or rare conditions who need subspecialized expertise that may not be available locally.
Learn more by calling 507-422-6103 or visit us online at mayoclinic.org/complex-care-program
“To maximize their impact, data analytics is key,” says Fisher. “By analyzing claims data, organizations can identify high-cost biologic utilization, model cost-savings scenarios, and track biosimilar adoption trends. Integrating clinical outcomes data ensures biosimilars are delivering comparable results.”
He observes that some employers are realizing 15–30% savings with no drop in care quality, noting, “PBMs are leveraging data to redesign formularies, align incentives, and drive education campaigns. Biosimilars do drive value without compromising outcomes. With data in hand, the question isn’t can you take advantage—it’s, will you?”
As more manufacturers continue to enter the biosimilar market, plan sponsors have unprecedented opportunities to control costs while maintaining access to the therapies members need most.
Beckie Fenrick, Pharm D, MBA, chief pharmacy officer, Navion, affirms, “Biosimilars deliver substantial market value—and at Navion, we strongly recommend that plan sponsors embrace proactive strategies to promote biosimilar adoption. By driving utilization toward clinically equivalent, lowercost options, organizations can enhance both affordability and access across their populations.”
She says biologics are a cornerstone in treating many autoimmune conditions—yet their high costs are often a barrier to care, adding, “The introduction of biosimilars has the power to reshape this landscape, injecting meaningful price competition and driving down treatment costs for patients and plan sponsors alike. Biosimilars make advanced therapies more accessible, ensuring that cost does not stand in the way of care.”
WHAT’S THE DIFFERENCE? BIOSIMILARS VS. GENERICS
Both biosimilar and generic drugs are unbranded versions of existing medications offered at lower costs. Biosimilars and generics are each approved through different abbreviated pathways that avoid duplicating costly clinical trials. However, biosimilars are not generics, and there are important differences between biosimilars and generic drugs.
Biosimilar drugs describe large-molecule medications that are extracted from living organisms and are often overly complex medications such as vaccines. Generic drugs involve small-molecule medicines, such as aspirin or ibuprofen, which use synthetic chemicals and are much simpler to reproduce.
Generics and biosimilars account for 90% of prescriptions dispensed in the US but only 13% of total drug spending, and their widespread adoption over the last decade has saved the healthcare system an astounding $3.1 trillion, reports the Association for Accessible Medicines.
Sources: 2025 Amneal Biosciences; Medical Packaging.
Beckie Fenrick
WHY BIOSIMILARS ARE FALLING BEHIND
Despite their proven value, biosimilar adoption has been slow, and there is a lot of finger-pointing to account for this trend. An AMA Journal of Ethics cites one strategy originator manufacturers have employed to limit biosimilar uptake: negotiating formulary exclusivity with payers. In one lawsuit, the originator manufacturer entered into contracts with commercial payers to exclude biosimilars from drug formularies or include “fail first” provisions, which would require a patient to have failed on the original product before a biosimilar could be reimbursed.
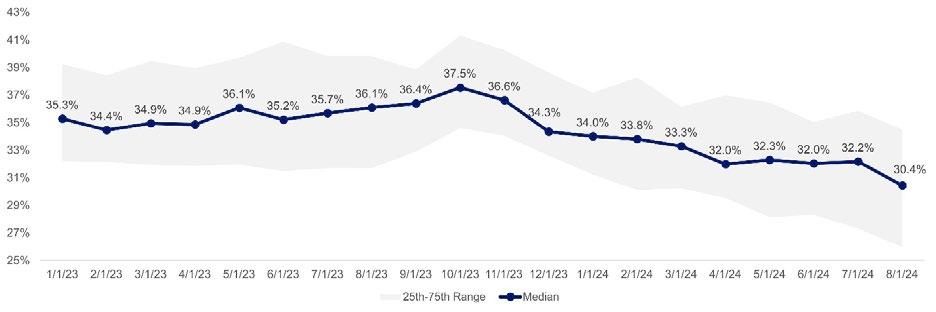
According to the Segal 2025 Trends Report on Biosimilars, for medications with available biosimilars, generally, less than 10 percent of prescriptions have been for a biosimilar. However, the percentage increased significantly in Q2 2024, resulting from changes in pharmacy benefit manager (PBM) practices.
Consequently, they say, rebates create a perverse incentive where physicians are able to make money on the higher-cost drug because of the rebate, while biosimilars are "underwater" because the physician's reimbursement is less than their cost. Relatedly, insurance plans with a PBM frequently limit the number of biosimilars covered by their formulary, which further restricts patient and physician choice.
Biosimilars as a Percentage of Monthly Biologic Prescriptions
Source: 2024 Segal’s SHAPE data warehouse, https://www.segalco.com/consulting-insights/q1-2025-trends-focus-biosimilars
Advisors at Segal say that manufacturers often use stalling tactics to delay the launch of competing biosimilar drugs, utilizing various tactics that include patent litigation and settlement agreements that effectively extend the monopoly period of the originator biologic. These tactics, often referred to as "stalling tactics," can include exploiting patent loopholes, engaging in "pay-for-delay" schemes or utilizing complex “patent thickets” to create an overlapping of patents that makes it difficult for others to develop or commercialize competing products without infringing on those patent rights.
Segal also says the way biosimilars are positioned within the formulary and represented in the PBM contract may discourage their use. To maximize rebates, PBMs and insurers may favor more expensive brand-originator products over lower-cost biosimilars.
As a result, the rebates create a contrary incentive where physicians are able to realize profits on the higher-cost drug because of the rebate, while biosimilars are marginalized because the physician’s reimbursement is less than their cost. Health plans with a PBM frequently limit the number of biosimilars covered by their formulary, which further restricts patient and physician choice.
Additionally, Segal advisors voice concerns that prescribing providers may be hesitant to convert to biosimilars due to efficacy concerns and often find inconsistency in insurers’ policies. Some physicians may not want to disrupt a prescription for a patient whose condition is stable, while patients may be reluctant to switch because they don’t understand biosimilars, including their safety, efficacy, and potential cost savings. Plan sponsors may also wish to avoid disrupting participants’ treatments.
WHAT IS AN INTERCHANGEABLE?
A manufacturer developing an interchangeable product must demonstrate that its product is expected to produce the same clinical result as the reference product in any given patient. Evaluation is required to determine the risk of administering a product to a patient more than once. This assessment is critical in terms of the safety and reduced efficacy of switching back and forth between an interchangeable product and a reference product.
While pharmacy laws and practices vary from state to state, interchangeable products may be substituted at the pharmacy level without the intervention of the healthcare provider who prescribed the reference product. A healthcare provider can also prescribe an interchangeable product just like they would prescribe a biosimilar or a reference product.
Source: 2025 Drugs.com
The Biosimilars Council cites two additional barriers to biosimilar adoption:
• Regulatory Burdens: The FDA’s approval process for biosimilars is still plagued by redundant and costly requirements, including unnecessary clinical efficacy studies and confusion about biosimilars vs interchangeable biologics. This slows down development and drives up costs, deterring investment in biosimilar pipelines.
• The Inflation Reduction Act’s Unintended Consequences: Instead of fostering biosimilar adoption, the IRA’s drug pricing policies have actually discouraged development by making it less financially viable for manufacturers to enter the market.
The new IQVIA report identifies yet another challenge with respect to sites of care (SOC). Hospital outpatient departments–which typically receive higher overall payments than physician offices–are less likely to adopt biosimilars, in part driven by higher relative reimbursement ratios for reference products. Furthermore, a Bernstein Research report finds that hospitals increase the charges for reference products with biosimilar competition more than for biosimilars. This creates a financial incentive for hospitals to stock reference products.
The highly anticipated Stealth State of the Market Report
Leveraging exclusive thought leadership and insights derived from our $2.3B+ portfolio of stop-loss business, along with data from leading stop-loss carriers and industry surveys, our report offers timely intelligence on market trends and actionable insights to help you stay at the forefront of meeting your clients’ needs.
This years report explores:
Economic Conditions
High Level Market Outlook
Strategic Stop Loss Procurement & Renewals
High Cost Claim Conditions
Cell, Gene and CAR-T Therapies
Carrier Insights
Exclusive Benchmarking Data from Stealth’s Book of Business
Recommended Best Practices and much more!
Sabine Enright, PharmD, VP of Integration, Payer Business Unit, AscellaHealth, shares, “The adoption of biosimilars and the optimization of SOC strategies are both highly effective in reducing costs individually. When combined, their impact on cost reduction is significantly greater.”
She says that focusing on both strategies is essential for lowering expenses while ensuring the continued delivery of high-quality patient care and effective disease management: “While both strategies may encounter resistance from members or providers on different fronts, this can be overcome through education and increased awareness in the marketplace.”
Finally, regulatory burdens in the form of the FDA approval process for biosimilars are still plagued by redundant and costly requirements. This includes unnecessary clinical efficacy studies and confusion about biosimilars vs interchangeable biologics, slowing down development, driving up costs and deterring investment in biosimilar pipelines.
AVOIDING THE “BIOSIMILAR VOID”
While biosimilars have delivered billions in savings for patients, employers, and taxpayers, a new analysis from the IQVIA Institute has revealed a massive ‘biosimilar void’: a staggering 90% of biologic drugs losing patent exclusivity over the next ten years have no biosimilar competition in the pipeline.
This year, 25 high-revenue drugs, including Ozempic, Keytruda, and Eliquis, are set to lose patent protection, paving the way for biosimilar manufacturers to expand their portfolios and cater to a growing demand for affordable treatments. Moreover, the Biosimilars Council discloses that 118 biologics will lose patent protection between 2025 and 2034, but currently, only 12 of these medicines have biosimilars in development.
If action is not taken quickly, analysts at these organizations warn that millions of patients will be locked out of potential savings and forced to pay higher prices for essential medications.
THREAT OF PRIVATE LABEL BIOSIMILARS
Concerns have emerged around the growing use of these PBM-driven private-label biosimilars as being detrimental to future biosimilar development. By selling their own private-label products, the PBMs are incentivized to market (and cover) their own products over others, raising issues of transparency and conflict of interest. The biosimilar makers who do not reach private-label agreements with these PBMs may be blocked from sales to a large portion of the covered population, which can jeopardize biosimilar competition and, thus, biosimilar savings for all. Limiting the growth in biosimilars available or closing off a manufacturer’s pathway to future revenue can stunt interest by manufacturers to pursue new biosimilars. Commentary from Dr. F. Randy Vogenberg, Principal, Institute for Integrated Healthcare, and board leader, Employer Provider Council, reveals, “In this scenario, PBMs can sell private-label, low-wholesale acquisition cost (WAC) versions to their employer clients, thereby offering a "savings" opportunity. However, PBMs and manufacturing firms share the remaining revenues with contracted distributors,
Sabine Enright
creating additional income back to the PBM. For example, a product sold at an 80% WAC discount leaves 20% left for revenue sharing with the PBM's distributor and biosimilar manufacturer. This new income to the PBM's parent can offset potential losses to rebate revenue or audit efforts by employer plans.”
Recently, the BR&R Biosimilar Report published an update that demonstrates the impact of PBMdriven private-label biosimilars. Optum Rx will exclude Humira and prefer FDA-approved adalimumab biosimilars effective January 1, 2025, for patients new to therapy. Amjevita®, the unbranded version of this biosimilar, will be the primary biosimilar covered on its commercial formularies and will also be offered as a private-label product through Nuvaila, a subsidiary of UnitedHealth Group. All other adalimumab biosimilars (and Humira) will be excluded from its Premium and Select formularies.
Vogenberg says the promotion of PBMs’ private-label biosimilars may offer some savings today for plan sponsors, but it may also be threatening future savings opportunities, adding, “In the US, employer plan sponsors and their vendors have more than $100 billion in potential savings with a competitive, fully open, and transparent biosimilars marketplace. That opportunity derives from growing biologic patent expirations, increasing access to biosimilars across populations, and eliminating unnecessary middlemen pricing policies that can hinder long-term savings associated with biosimilars.”
IN DEFENSE OF PBMS
“Leading PBMs are deploying a variety of innovative tactics to accelerate biosimilar adoption and drive down drug spend,” says Fenrick, offering the following strategies that not only lower costs but also increase access to life-changing therapies for members:
• Formulary Strategy: Preferring or exclusively covering biosimilars over higher-cost originators.
• Utilization Management: Requiring step therapy or trials of biosimilars before allowing access to reference products.
• Prescriber Engagement: Providing academic detailing and outreach to support evidence-based transitions to biosimilars.
• Specialty Pharmacy Support: Facilitating member transitions with dedicated outreach and copay assistance for eligible members.
• Concierge & Digital Tools: Offering member support services and digital resources to spotlight costsaving opportunities with biosimilars.
• Expanded Pharmacy Access: Including disruptors like Mark Cuban’s Cost-Plus Drug Company to broaden access to affordable medications, including biosimilars.
Jay Gulley, PharmD, President, LeadwayRx, a 20-year-old transparent PBM that utilizes RxLogic claims processing, characterizes the challenge: "The original biologic product has name recognition with the
doctors plus the TV ads and commercials during the Super Bowl that attract consumers. When the drug loses its patent, and depending upon the manufacturer, a biosimilar can be introduced. Initially, there may not be significant adoption, but when employers start to calculate the savings of adding a biosimilar to the formulary, they are readily convinced."
He says PBMs typically support the employer in evaluating the opportunity. Some self-insured companies may not want to make any of their members switch to a biosimilar, while others say they need all the savings they can get and want the least expensive option – although the least expensive option is still costly.
STELARA
Everyone working or observing the biosimilar industry is watching the seven FDA-approved Stelara biosimilars, with two others under FDA review and a third in late-phase clinical development.
Some analysts say the experience that payers have had with Humira biosimilars may make for earlier and broader coverage of the Stelara biosimilars. The catch: No payer has announced plans to remove the brand name Stelara from 2025 formularies.
The uptake of Stelara biosimilars will largely depend on how quickly brand-name Stelara is removed from formularies — not when biosimilars are added — and that may not happen until 2026.
Source: IPD Analytics LLC
A key point of discussion is transparency regarding rebates.
Gulley continues, "Historically, there has been very, very little transparency in that space, but I think it has grown over the last couple of years as the drug spend has continued to climb and become such an issue for employers. People are starting to look a lot closer at these expenditures and wondering why it is so high. It is probably above their medical and hospital spend.”
With so many factors impacting a high drug spend, employers and brokers are really starting to hammer down and look a lot more closely at transparency for rebates.
“There's a big role for PBMs to work with pharmacies -- not against them -- to help lower drug costs for the employers, not just to pull in as much money as they can,” he quips. “PBMs are well-positioned to take on the complex challenges of advancing adoption of biosimilars. There may even be some manufacturers who say if you exclude a certain drug, you're not going to get rebates on any of our other ones. It's a big game. But when you start to see much lower prices, there is no argument. “
When it comes to interchangeability with biologics, he maintains that doctors will prescribe whatever biosimilar the insurance will pay for. Some states will even allow the pharmacist to make that change without a new prescription, while other states still require a new prescription for that particular biosimilar.
“I think there is great potential for biosimilars, especially with the newer pricing models that you're starting to see that carry some very significant discounts as opposed to the original branded product,” says Gulley.
“With more discounts resulting in lower costs, the more utilization there's going to be – and much of that has to do with transparency.”
SCALING THE REBATE WALLS
Rebate “traps” occur when a drug manufacturer pays list price discounts to health plans or pharmacy benefit managers (PBMs) based on meeting market share targets. Health policy analysts at Duke University explain that while such practices appear to lower net costs in the short term for a particular drug or biologic, they also have the effect of blocking patient use of competing, lower-priced products – like biosimilars.
Duke analysts maintain that rebate walls are particularly challenging in the context of biosimilar competition: "While biosimilars are as safe and effective as the originator biologic and offered at a reduced list price, demand for products has been slow to shift from incumbents, especially if clinicians and patients do not regard the products as clinically equivalent. The result can be harmful to patients and the healthcare system through reduced access to drugs that are just as safe and effective but cost less. Furthermore, growth in rebates has been linked to a growth in list prices, and highly rebated products are often accompanied by higher out-of-pocket costs for patients."
Fenrick concurs, “While rebate structures can complicate formulary decisions, the net cost advantage of biosimilars is clear. Many biosimilars are priced 85% to 90% below the originator brands, often yielding deeper savings even after rebates are applied to the innovator. Navion advises clients to carefully analyze net costs, not just rebates when evaluating formulary options. In nearly every case, biosimilars deliver superior value—helping plans achieve both clinical and financial objectives."
Employers should be aware that CVS/Caremark, Express Scripts and OptumRx have all formed joint ventures to manufacture private-label biosimilar drugs. It may be prudent to confirm that the PBM contract specifies that the formulary includes low-cost biosimilars from companies unaffiliated with the PBM.
PLAN SPONSORS CAN ENCOURAGE BIOSIMILAR ADOPTION
Despite this myriad of challenges, biosimilars are projected to generate substantial cost savings as adoption increases. Segal suggests several strategies that plan sponsors can use to encourage their utilization:
• Education and awareness campaign. Educate stakeholders, including providers, pharmacies, and participants, about the safety and increased availability of biosimilars. Interchangeable biosimilars may be automatically substituted by a pharmacist for the original biologic or reference product, like a generic substitution for brand-name medications, while non-interchangeable biosimilars require prescriber approval. Note that applicable laws vary by state.
• Plan design and utilization management. Revise the plan design to include incentives that encourage adoption. Consider the use of utilization management, such as step therapy, to require patients to try lower-cost options first or prior authorization for expensive biologics and include biosimilars as preferred alternatives.
• Financial incentives. Introduce provider incentives, either through a direct contracting arrangement or by working with the insurer or third-party administrator (TPA) to ensure that the contracted
providers are aware of and are considering biosimilars as a treatment option.
• Formulary management. Place biosimilars in preferred tiers with lower copayments to incentivize their use or remove the originator product from the formulary. Regularly update the formulary to include newly approved biosimilars and remove (or deprioritize) more expensive reference biologics.
• Real-time benefit programs. Consider implementing real-time benefit programs that integrate with prescribers’ electronic health record systems and provide comparative pricing for originators and biosimilars when providers e-prescribe.
• Monitoring and reporting. Ask the medical administrator and PBM for a current utilization report showing biosimilar vs. reference product utilization under both the medical and pharmacy benefits. This will help identify opportunities to encourage more biosimilar use.
Barbora P. Howell, Co-founder & CEO, True Claim, offers this guidance, “Biosimilars offer meaningful savings, but realizing their value depends on making the switch easy for members and financially aligned for all stakeholders. In an ideal world, that means no new prior authorizations, no changes in how the medication is administered, and no revenue compromised by any vendor involved.”
She also thinks that plans should "walk the talk" and offer financial incentives to members, such as lower copays.
“Finally, PBMs must support biosimilar adoption through formulary design and aligned contracting...so selecting the right PBM partner is key,” continues Howell. “When switching to a biosimilar is simple, transparent, and cost-effective, companies and members can save money without disrupting care.”
CHALLENGES AND OPPORTUNITIES
While biosimilars offer significant potential for cost savings, there are also challenges to consider, such as the need to address potential interchangeability issues and the potential for brand-name manufacturers to offer discounts to counter biosimilar competition. The role of members – as healthcare consumers – is equally important.
“Drug costs have increased every year, forcing consumers to evaluate their options,” observes Joe Dore, President, USBenefits Insurance Services. "This would include generic brands and other options, such as biosimilars. Unfortunately, due to financial considerations, some consumers drop the needed medication.”
Today, the cost of prescriptions represents about 20% of the healthcare expenditures on average, as Dore predicts, “This is expected to worsen, especially with increased usage of high-cost drugs, which will only increase the pressure on the employer groups to seek out alternative risk management strategies. It will also force the insurance industry to manage
Barbora P. Howell
Joe Dore
Systems That Don’t Sweat
towards premium adequacy for the additional exposure.”
He invites this topic for discussion on pharmaceutical company earnings, drug distribution channels, PBM models and potential conflicts of interest that affect the cost to the consumer.
The role of providers cannot be discounted. Physicians and hospitals play a critical role in biosimilar adoption, highlighting the importance of examining ways to remove obstacles that may discourage providers from utilizing lower cost biosimilars with their patients.
Source: 2025 Innovative Rx Strategies
Case in point: In a survey of US rheumatologists' beliefs and knowledge about biosimilars, nearly all respondents were familiar with the FDA definition of a biosimilar product. They were aware that an infliximab biosimilar -- an unbranded version of Remicade indicated for the treatment of adults living with moderately to severely active rheumatoid arthritis (RA) -- was FDA-approved.
Most respondents (84%) understood that an approved biosimilar was not automatically deemed interchangeable by the FDA. Researchers concluded that rheumatologists were more likely to initiate biosimilar treatment for a biologic treatment-naïve patient with RA (73%) than they were to switch to the biosimilar for a patient with RA doing well on the reference product (35%).
Other similar surveys have found that patients are satisfied with the outcomes achieved with biosimilar products, including those patients who had begun treatment on a reference product. The only major concerns reported for switching included not knowing enough about the medication (38%), potential side effects (35%), and loss of disease activity control (35%). Patients still have concerns regarding safety and efficacy, and their involvement in the switching decision-making process may allay concerns and enhance biosimilar uptake.
WHAT TO DO NOW
Kathy Oubre, MS, chief executive officer of Pontchartrain Cancer Center, Louisiana, suggests that the current landscape presents an opportunity for employers to revisit the inclusion of biosimilars in their formularies and to develop strategies that will allow their increased use and/or help manage ongoing utilization.
Employers can play a significant role in promoting biosimilars as an alternative to more expensive biologic drugs, where medically appropriate, by 1) Increasing understanding of biosimilars by health plan
participants and health care providers through education and incentives, 2) Adopting clinical management programs, 3) Designing the payment feature of prescription drug benefits to account for biosimilars 4) Addressing biosimilar drugs when negotiating PBM contracts.
There is widespread consensus throughout the industry that employers can maximize savings from biosimilars. Oubre and others suggest starting with these questions when developing and implementing strategies to promote their utilization and then initiating communications with the PBM to encourage biosimilar use:
• What is my PBM's strategy, and how flexible is it in adopting biosimilars?
• Should biosimilars be added as a preferred or non-preferred formulary option?
• Does a brand or generic copayment apply?
• If the plan offers copayment assistance, how will that impact costs?
• Should it be added only for new patients?
EDUCATE MEMBERS -- ENCOURAGE BIOSIMILAR USE
Bruce D. Roffé, President and CEO, H.H.C. Group, a cost containment company using claim negotiation, repricing, and independent review solutions, suggests that employers can provide meaningful education to plan participants regarding biosimilar adoption, highlighting biosimilar use and potential cost savings as well as real-time benefit lookup tools and cost calculators.
Proactively explain to members who started taking a brand-name version before a biosimilar was available that there should be no adverse impact from switching to the biosimilar.
“With a robust pipeline and steady stream of newly launched biosimilars, plan sponsors may find it appropriate to provide updated biosimilar education and demonstrate how biosimilars fit into their plan benefit design,” says Roffé. "This type of education can also be communicated to healthcare providers as an opportunity to promote awareness and consideration of biosimilars as a preferred treatment option. The FDA is a great resource for these materials, which can be readily accessed at www.FDA.gov/biosimilars.”
REFINE FORMULARY STRATEGY
Ensure PBM formulary includes available biosimilars, will adopt new ones as they are introduced and base their selection on which product offers the lowest net cost to the member and plan. Formularies may exclude coverage for name-brand versions or create a tier that includes them but with significantly higher copays.
Clarify how your plan will handle biosimilars not designated by the FDA as “interchangeable,” meaning
Bruce Roffé
that pharmacists (in most states) can substitute them for brand-name biologics. Confirm that your PBM has procedures to encourage doctors to prescribe biosimilars that haven’t yet been classified as interchangeable. This issue also impacts “rebate credit” since PBMs may use these provisions to reduce your rebate payments if members switch from high-rebate biologics to no-rebate biosimilars.
Require PBMs to be fully transparent about the rebates they receive and return back to the plan. If the PBM is handling Prior Authorizations, confirm that biosimilars are included in the process as a high-quality, less costly alternative to more expensive biologic drugs.
PLAN DESIGN
Plan design can be used to help mitigate growing prescription drug costs with the goal of balancing quality and cost savings. “Tiering” places equally effective drugs in different tiers to incentivize the use of the least costly tiers and is designed to further drive consumerism around the price of a medication. As the number of biosimilars in the market grows, there may be increased use of multi-tier plan designs, especially for specialty drugs.
During PBM negotiations, there may be consideration of inflation-protection caps, which are intended to shield plans from the full impact of year-over-year price increases. This is a good opportunity for employers to understand how their plan’s inflation cap is calculated by the PBM and confirm the PBM delivers these protections to all specialty drugs, including biosimilars.
When it comes to manufacturer rebates associated with biosimilar inclusion, plan sponsors should use this opportunity to ensure that biosimilars are included in rebate payment calculations, review their PBM contract provisions with their benefit advisors and legal counsel and confirm inflation-protection caps and manufacturer rebates.
Finally, employers should confirm that biosimilars are included in the payment provisions of their prescription drug benefit, either through plan design or formulary strategy.
INTRODUCE CLINICAL MANAGEMENT PROGRAMS
By including biosimilars in their utilization management strategies, employers can help safeguard the appropriate use of selected drugs. Prior authorization, one of the most common UM strategies used by employers and payers to contain cost, can advance the adoption of these high-quality, less costly alternatives to more expensive biologic drugs.
Advocacy in Action
Legal services and innovative technology combined to defend health plans, plan sponsors and member participants nationwide aequum advocacy programs & services successfully resolve surprise billing and unreasonable out-of-network and balance billings
Efficient Claim Resolution
On average, aequum resolves claims within just 244 days of placement.
Unmatched Savings
aequum has achieved a remarkable 95.6% savings off disputed charges for self-funded plans.
National Expertise
aequum has successfully handled claims in all 50 states.
| www.aequumhealth.com
No Guarantee of Results - Outcomes depend upon many factors and no attorney can guarantee a particular outcome or similar positive result in any particular case.
As noted earlier, Site of Care (SOC) management is also a viable clinical management program, enabling employers to evaluate the cost differences among hospitals and community-based practices that dispense the same drug. Several studies show that the outpatient hospital setting incurs higher charges than community-based physicians or home-based administration for the same treatment. This cost differential could lead to potential savings for employers through site-of-care analysis, plan design, and contracting strategies, which avoid high-cost settings.
EMPLOYERS FOLLOW MARKET TRENDS
As of April 30, there have been 74 biosimilars approved by the US Food and Drug Administration (FDA), including at least 15 that are designated by the FDA as interchangeable products. So far this year, 10 biosimilars have already received FDA approval, a robust start on the heels of a record-breaking 19 approvals in 2024.
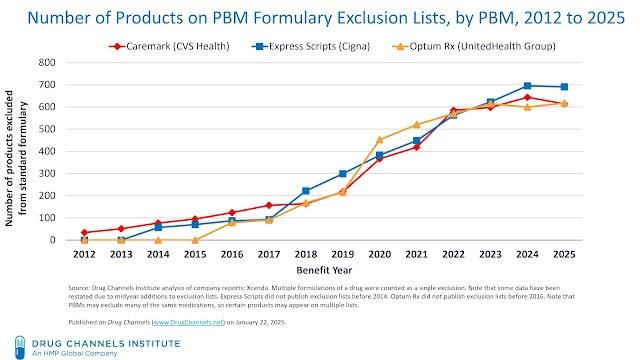
If the three largest PBMs are any bell weather of what’s in store for biosimilars, they have again each excluded hundreds of drugs from their standard formularies. This blocks access to specific products on a PBM’s recommended national formulary and emerges as a powerful tool for PBMs to gain additional negotiating leverage against manufacturers.
In turn, manufacturers offer deeper rebates to avoid having their products cut from the formulary. A drug’s appearance on an exclusion list does not guarantee that all patients will lose access. Plan sponsors— the PBM’s clients— can choose not to adopt their PBM’s standard formulary but would then face reduced rebates and/or higher plan costs. It is anticipated that each PBM’s formulary will give plan sponsors the option of a high-list-price biosimilar, a lower-priced private label product and a low-list-price unbranded biosimilar. The combination of formulary exclusion and private labels is creating an increasingly puzzling and crowded
biosimilar marketplace. Whether employers agree or disagree, the financial benefits from these private-label products align with the benefits to plan sponsors and patients. The complexity of the drug pipeline and market dynamics means progress for biosimilar adoption is gradual.
Laura Carabello holds a degree in Journalism from the Newhouse School of Communications at Syracuse University, is a recognized expert in medical travel and is a widely published writer on healthcare issues. She is a Principal at CPR Strategic Marketing Communications. www.cpronline.com
Capturing savings from biosimilars: What to do now. | Alliant https://waysandmeans.house.gov/event/health-subcommittee-hearing-on-lowering-costs-for-patients-the-health-of-the-biosimilar-market/
US rheumatologists' beliefs and knowledge about biosimilars: a survey - PubMed Patient Perspectives on Switching from Infliximab to Infliximab-dyyb in Patients with Rheumatologic Diseases in the United States - PubMed https://biopharmaapac.com/analysis/60/5727/25-high-value-drugs-losing-patent-protection-in-2025-what-it-means-for-healthcare.html
The Biosimilar Void: A Crisis in Patient Access and a Call to Action — Biosimilars Council https://medpak.com/biosimilar-vs-generic-drugs/
Why Are Biosimilars Not Living Up to Their Promise in the US? | Journal of Ethics | American Medical Association https://biosimilarscouncil.org/resource/the-biosimilar-void-a-crisis-in-patient-access-and-a-call-to-action/
PBM Private Labeling: A Boon or Bane to Biosimilar Drug Makers? | BR&R https://natlawreview.com/article/sick-healthcare-healthcare-benefit-update-employers-what-watch-2025
Isaac Leanos Member Advocate
Leveraging the Power of Group Purchasing Association
health plans and multiple employer welfare arrangements gaining traction for small and midsize employers seeking to pool risk
WhileWWritten By Bruce Shutan
self-insurance is built on wresting control of an organization’s medical claims from third parties that muddle the supply chain with added layers of cost, some vehicles gain strength in numbers. Small and midsize employers in the 100 to 500-employee range, for instance, may want to pool their risk through a homogeneous or heterogeneous group captive arrangement with like-minded employers and reap dividends from wise investments.
But there also are other self-insured avenues leveraging the power of group purchasing that are better suited to small or midsize groups so they can manage their risks as effectively as large employers.
Two such solutions that allow groups to share resources and have earned renewed attention include association health plans (AHPs), which were developed in the late 1990s and promoted during President Donald Trump’s first term, and multiple employer welfare arrangements (MEWAs), which have survived periodic headwinds dating back to their 1983 creation.
AHPs also may be classified as MEWAs, depending on how they're structured and are considered a type of group health plan that allows small businesses or self-employed individuals to band together (often by industry or geography) through a bona fide association to purchase insurance. They're typically governed under ERISA and can sometimes avoid some Affordable Care Act requirements if classified as a large group plan.
MEWAs, on the other hand, involve two or more unrelated employers that provide health or welfare benefits to their employees under a single plan that can be fully insured or self-insured. They’re also governed by ERISA but subject to both federal and state regulation, often more heavily than AHPs.
These vehicles offer a large enough risk pool wherein healthy enrollees theoretically counterbalance the claims experience involving unhealthy members of the group. Actuaries will develop premiums based on the blend of individuals and their health claims experience that will sufficiently handle each risk pool.
PARSING OUT SIMILARITIES AND DIFFERENCES
While the differences between AHPs and MEWAs are slight from both a regulatory and risk standpoint, deciding whether to adopt one or the other approach comes down to risk pooling, according to David Wilson, president and senior actuary of Windsor Strategy Partners, Inc. He believes groups with fewer than 100 lives “may have some financial benefits from working at a well-run MEWA or AHP vs. staying in a larger insurance pool.”
SIIA Washington Counsel Chris Condeluci estimates that there are at least hundreds of self-insured MEWAs operating today, while Department of Labor (DOL) M-1 reporting forms MEWAs must file suggest that about three million employees and family members are covered by both fully insured and self-insured arrangements. Estimating the number of AHPs is another story. “It’s not easy to get the data or accurate enrollment number,” he explains.
While AHPs and MEWAs are essentially one and the same, he says many MEWAs that could be characterized as AHPs offer a comprehensive range of major medical health coverages that mirror a large employer's benefits offering.
While some arrangements offer a series of limited benefit plans with indemnity, disability, short-term or so-called “skinny plan” coverage that a broker ties into an association, he doesn’t consider them an AHP. That distinction is important because opponents of self-insured MEWAs and AHPs, which include insurance regulators and health insurance companies tied to the fully insured market, argue that they don’t provide good coverage.
EASING PLAN RESTRICTIONS
When Rene Alexander Acosta served as labor secretary in Trump’s first administration, the hope among MEWA advocates at that time was to allow these arrangements to easily cross state lines. That meant breaking free of the patchwork of 50 state regulatory requirements – an aspiration that never was realized.
Bill Dyer, co-founder and VP of member relations for the MEWA Association of America and co-founder and VP of HCP National, who is sometimes known as “Mr. MEWA,” notes that risk-retention groups through which associations acquire liability insurance have been crossing state lines for 40 years.
“I don’t understand why this particular class of business could be any different if they’re meeting the reserving requirements of the state that is also regulating them?” he wonders about MEWAs, adding that it has stunted the industry’s growth.
Asked when it would make sense to adopt a single-employer AHP, Condeluci notes that the DOL treats employers in the same industry that have pooled their purchasing power as a single plan, whereas that’s not the case for non-industry-based employers sponsoring a health plan. However, he adds that actuaries still pool everybody together, irrespective of this distinction.
The first Trump administration sought to treat non-industry-based plans like industry-based ones as part of a single risk pool – a streamlined definition currently being worked on that hope will find its way into congressional legislation. "That would, in theory, increase adoption by providing more legal certainty and less ambiguity for employer members of associations and chambers of commerce and for insurance regulators," he adds.
AHP bills recently introduced in the House and Senate seek to help employers work around federal rules that restrict employers and individuals teaming up to buy health coverage. Sen. Rand Paul’s (R-Ky.) proposal, similar to a health marketplace pool bill he introduced last November, is nearly identical to a version from Rep. Tim Walberg (R-Mich.), who chairs the House Education and the Workforce Committee.
THREAT OF INSOLVENCY
While there are merits to pooling risk, the fact is that it can be a risky business. In groups of about 500 lives, Dyer explains that a few significant catastrophic claims could knock a MEWA upside down, whereas one with 20,000 to 30,000 lives would involve a bigger spread of risk and more predictability. If a MEWA is well run, he says rates will decrease, stay the same or increase only slightly.
Whatever the circumstances might be, he says there are five key ingredients to a successful MEWA. First, an association must have at least $1 million for actuarial and legal expenses, as well as paying for stop loss and having adequate reserves. Secondly, the group has to be fully integrated to a point where it can drive volume very quickly by having at least 1,000 lives but, ideally, 5,000 in order for a greater spread of risk that will help sustain success over the long run. Thirdly, it helps to be located in a state that allows underwriting so that a higher premium can be charged to insure risky health conditions. Finally, it’s important to have adequate stop-loss and liability coverages, as well as hire the right management company to handle compliance.
"That's a huge issue, and there's no clear guidance as to what entity is required to disclose both direct and non-direct fees under the CAA [Consolidated Appropriations Act of 2022)." But it also could be extremely difficult for self-insured plan sponsors to attest what they're paying in fees that are bundled and understand how they're calculated, he explains. Moreover, problems could arise when there's a potential conflict between delegating fiduciary obligation and not periodically assessing plan data.
Apart from the CAA’s impact, COVID also has been a significant factor in that it caused some plans to shut down. For example, Wilson notes that while many MEWAs had enough capital to absorb random fluctuations in their business, they fell short of the mark when it came to the larger impact of the pandemic.
“Nobody anticipated a pandemic, and then the government’s response where maybe they were doing the right thing from a population health standpoint, but plans were asked to cover expenses that were never part of their mandate,” he explains.
Since that time, he says rates have stabilized, and his firm has done several feasibility studies suggesting a desire to expand these plans to more states or start new ones altogether.
Another issue that arose soon after MEWAs were introduced and continues to be a concern involves intentional misrepresentation or fraud. If the fees being paid are nearly 100% opaque, Flores can’t imagine how a group of plans would ever be able to properly identify and reconcile what they’re paying in fees –and, therefore, be caught up in malfeasance.
Steadfast protection for the unpredictable
Our Stop Loss Insurance mitigates the impact of costly medical claims through flexible contracts, customizable plans and a consultative, client-focused approach. Our experience and service in the Stop Loss market has provided a guiding hand for 50 years - while maintaining a pulse on new trends. We work with self-funded groups down to 100* lives and individual deductibles down to $25,000. Our Stop Loss Edge program offers an innovative way to take advantage of self-funded health plan coverage for employers with 100*-500 employees. Whether you’re carving out Stop Loss for the first time or an experienced client looking for cost containment solutions, we can help. We’ll be by your side every step of the way.
Visit voya.com/workplace-solutions/stop-loss-insurance for more information
* 150 enrolled employee minimum for policies issued in CA, CO, CT, NY, or VT.
When Healthcare Works as ONE, Patients, Payers, Providers,
Plans
and
“I think there’s ample legal evidence over the past few years that this is actually happening,” he observes, noting that many employers are suing carrier TPAs that are refusing to provide them any clarity with respect to their own plan data. “Ultimately, they may be suing them because they know that they’re probably going to get sued themselves by their own members if they don’t go after this money.”
Other issues beneath the surface that must be addressed include whether a group or trustees will be tasked with hearing and deciding on an appeal that complies with ERISA and who is liable if that process is not followed. “It just creates a Pandora’s box of issues as to who’s accountable,” he says.
Where captives would be more useful than AHPs or MEWAs is when small employers actually purchase medical stop-loss insurance through the captive – a growing part of the market – and the price tag makes more sense to them.
"The reason why it's not a MEWA is because stop loss is not major medical coverage, and therefore, it doesn't meet the definition about distinguishing major medical vs. limited benefit plans," Condeluci explains. Those small employers that worry about plan administration, want to be hands off or feel it’s important to support their trade association will want to choose an AHP or MEWA, he adds.
STATE OBSTACLES TO PLAN CREATION
Dyer, meanwhile, laments the sad state of affairs in some states where insurance companies with tremendous political power create barriers to even starting a MEWA. In California, where he's based, it costs $5 million just to launch a MEWA. "Who has that kind of money?" he asks.
He admits "there was a lot of shenanigans going on" in the salad days of MEWA when brokers would naively start them, not realizing they had to go through their state department of insurance and the federal government. Some nefarious brokers, along with other individuals, would even charge steep commissions, keep premiums, and not pay claims. "Most of the stop-loss insurers told us to get lost because they thought MEWAs were prone to fraud and abuse," Dyer reports.
But today, he says the majority of MEWAs are legitimate, and many have been around for a very long time. They're subject not only to state regulatory requirements but also filing with the DOL, which he says does its share of audits to catch illegal activities.
One caveat to consider along the way to starting a MEWA is the importance of vetting stop-loss carriers. “We have seen three clients that had claims denied because the insurer used language in their policy that is oriented toward a self-insured single employer, not a MEWA,” he says. Employers, therefore, need to know what a MEWA is, how to find the right stop-loss insurance and how to get an insurer to rewrite their policy.
Being in a self-insured MEWA can be a costly proposition for employer members relative to a fully insured MEWA arrangement because they’re the ones that hold all the liability as fiduciaries, even though another service provider is being paid to adjudicate claims and fill in some of these roles, Flores cautions.
Without clear guidance from the federal government on who’s responsible for what in a MEWA, he believes it opens the door to chaos. However, he doesn’t expect any clear guidance from the Trump administration because it’s not a simple issue, nor is it a priority relative to the dozens of other new policy initiatives that have been seeded.
“The best people in the country disagree about the best ways to do this – even those with the best intentions,” Flores opines. "We need a sophisticated advocate on the government side who understands this and, at minimum, could provide accountability."
Bruce Shutan is a Portland, Oregon-based freelance writer who has closely covered the employee benefits industry for more than 35 years.
You know the name — let’s talk numbers. Here’s what sets us apart as a true plan administration partner:
Some firms are just now introducing themselves to TPAs. The Phia Group has been building partnerships for years and our results speak for themselves.
3x More cases identified (1 per 150 EEs)
5x More dollars recovered ($25 PEPM)
of services designed for TPAs
We don’t just identify opportunities — we deliver outcomes.
BUSINESS ASSOCIATE AGREEMENTS -A CASE EXAMINING OBLIGATIONS
IWritten By Kendall Jackson
In the self-funded industry, the prevalence of business associate agreements (“BAAs”) is undisputed, as covered entities and business associates regularly execute them. The Health Insurance Portability and Accountability Act (“HIPAA”) generally requires covered entities and business associates to enter into contracts with their business associates. The BAA is integral to the relationship between a covered entity and business associate, as it defines the contractual obligations for the use and disclosure of protected health information (“PHI”).
Elements of a BAA are quite standard, although the parties do have some flexibility when drafting other contractual provisions, such as indemnification or audits language. As for the standard elements, HIPAA lists ten mandated provisions that must be included and also generally requires that the contractual language adequately establish the permitted and required uses and disclosures of PHI. These provisions are not only essential for compliance with HIPAA but are also important when considering the liability of the business associate. Deviating from the uses and disclosures permitted in the BAA or those required by law can have significant repercussions and may result in civil or criminal liability.
Through a complaint filed on April 11, 2025, in the United States District Court, Western District of Texas, Austin Division, a business associate recently experienced this situation. In CareNexa, LLC v. Ntirety, Inc., CareNexa, LLC, dba Molecular Testing Labs (“MTL”), alleged that its business associate, Ntirety, Inc., failed to safeguard the PHI of its patients and satisfy the indemnification provision within their BAA. Within the complaint, MTL asserted its identity as a “covered entity,” as defined by HIPAA, by virtue of being a healthcare provider that collects, manages, and stores PHI. The complaint notes that Ntirety, a data hosting and security provider, is a business associate of MTL. As such, the parties entered into a BAA on September 28, 2018.
MTL’s complaint discusses Ntirety’s alleged failure to use appropriate safeguards to prevent the unauthorized use or disclosure of PHI, a provision that is required to be within the BAA. As noted above, of the ten mandated provisions, HIPAA requires that the BAA state that the business associate will “use appropriate safeguards and comply, where applicable, with [the HIPAA Security Rule] with respect to electronic protected health information, to prevent use or disclosure of the information other than as provided for by its contract.” Guidance from the United States Department of Health and Human Services (“HHS”) indicates that the phrase “appropriate safeguards” includes reasonable and appropriate administrative, physical, and technical safeguards for securing electronic PHI. Rather than dictating specific safeguards, HHS provides that, when establishing such safeguards, regulated entities should consider several factors, such as the entity’s size, capabilities, technical infrastructure, hardware and software security capabilities, security costs, and the probability of potential risks to electronic PHI.
MTL alleges that Ntirety failed to implement these administrative, physical, and technical safeguards, resulting in a violation of the BAA and the HIPAA Security Rule. MTL’s allegation is based on information it received notifying it of a material breach of data that was required to be secured by Ntirety per the BAA. The forensic investigation performed at the request of MTL indicated that electronic PHI under Ntirety’s management, control, and protection was obtained by unknown threat actors.
As a result of this breach, the threat actors demanded a ransom payment from MTL. Failure to pay the ransom would result in public disclosure of the electronic PHI. MTL insists that the investigation confirms that the threat actors took advantage of the deficiencies in Ntirety’s safeguards, allowing them to access PHI from both Ntirety’s and MTL’s computer systems. Consequently,
MTL argues that the investigation’s findings are evidence of Ntirety’s violation of the BAA and the HIPAA Security Rule.
MTL’s complaint also asserts that Ntirety breached its obligations under the BAA by failing to indemnify MTL. As noted above, the indemnification provisions within a BAA are separate from HIPAA's required provisions, and the parties may draft the language in a mutually agreed-upon manner. The complaint offers a glimpse into the BAA by describing the relevant portions of the indemnification provision for purposes of Ntirety’s alleged breach. MTL asserts that the relevant contractual provisions require Ntirety to indemnify and hold MTL harmless from any losses, expenses, damage, or injuries sustained as a result of Ntirety’s breach of the BAA, including any unauthorized use, disclosure, or breach of PHI, as well as Ntirety’s negligence or failure to perform its obligations as a business associate under the BAA and HIPAA. MTL outlined a series of damages it has or will incur and seeks indemnification from Ntirety.
This case is in its infancy, as it was only filed last month. It is important to note that with only the complaint and no response yet filed on behalf of Ntirety, the situation is only represented through the point of view of one party, and Ntirety’s position remains unknown. Despite being in its early stages, the themes within this complaint function as key reminders for both covered entities and business associates.
The complaint emphasizes the importance of a BAA as a means of protecting the covered entity when PHI may be mishandled by the other party. It also creates awareness for business associates to confirm they are utilizing processes that are thorough and adequate for the safeguarding of PHI under HIPAA and their BAAs. Fundamentally, implementing appropriate safeguards is necessary for compliance with HIPAA, but this case serves as a reminder that adequate and appropriate safeguards can insulate the business associate from what could otherwise be a source of contractual liability for the business associate under the BAA.
Kendall Jackson is a Health Benefits Consulting Attorney with the Phia Group.
Do you aspire to be a published author?
We would like to invite you to share your insight and submit an article to The Self-Insurer! SIIA’s official magazine is distributed in a digital and print format to reach 10,000 readers all over the world.
The Self-Insurer has been delivering information to top-level executives in the self-insurance industry since 1984.
Articles or guideline inquires can be submitted to Editor at Editor@sipconline.net
The Self-Insurer also has advertising opportunties available. Please contact Shane Byars at sbyars@ sipconline.net for advertising information.
Proceed With Confidence Mind Over Risk
We study it, research it, speak on it, share insights on it and pioneer new ways to manage it. With underwriters who have many years of experience as well as deep specialty and technical expertise, we’re proud to be known as experts in understanding risk. We continually search for fresh approaches, respond proactively to market changes, and bring new flexibility to our products. Our clients have been benefiting from our expertise for over 50 years. To be prepared for what tomorrow brings, contact us for all your medical stop loss and organ transplant needs.
Tokio Marine HCC – A&H Group
HCC Life Insurance Company operating as Tokio Marine HCC – A&H Group
PREVIEWING THE FUTURE OF HEALTH SCREENINGS
NWritten By Lara Carabello
No-cost-share coverage for preventive care and health screenings may have narrowly escaped the chopping block as the Supreme Court of the United States (SCOTUS) seems likely to uphold a key Affordable Care Act (ACA) mandate.
But the jury is still out.
Hearings held in mid-April and then again in May -- Kennedy v. Braidwood Management— focused upon the statutory relationship between the HHS secretary and the members of the US Preventive Services Task Force (USPSTF) – not the value of screenings. The question centers on the issue of whether Congress has 'by law' vested the secretary of the HHS with the authority to appoint members of the USPSTF. The outcome of the case is expected to impact various federal advisory panels rather than on employers' preventive services benefits.
A ruling expected by the end of June will determine the fate of these benefits, affecting employers with 50 or more full-time employees. ACA provisions cover medications and screenings recommended by several sources:
USPSTF: a volunteer panel of experts that works to improve the health of people nationwide by making evidence-based recommendations about clinical preventive services.
Health Resources and Services Administration (HRSA): recommends a variety of screenings for women, including HIV, syphilis, and anxiety and for newborns, encompassing a wide range of heritable disorders; supports screenings for conditions like urinary incontinence and breast cancer, alongside contraceptive care, and domestic violence screening.
Advisory Committee on Immunization Practices (ACIP): a federal advisory committee that develops recommendations on the use of vaccines in the US civilian population.
BACKGROUND ON THE “BRAIDWOOD” CASE
The lawsuit challenged the ACA’s process for determining which services must be covered by health insurance, arguing whether a volunteer expert panel can dictate insurer coverage mandates without presidential or congressional approval. Plaintiffs argued that because USPSTF task force members aren’t appointed by the president and confirmed by Congress, it’s unconstitutional for this body to have the authority to dictate what health insurers must cover.
Instead, they claimed only “principal officers” who go through that process, like the secretary of Health and Human Services (HHS) and those under these officers' command, should have that power. A ruling against the ACA provision could shift power to the HHS secretary, enabling future administrations to approve or veto preventive care coverage, depending upon political priorities.
The lawsuit reached the Supreme Court after the Fifth Circuit Court of Appeals sided with employers, who had argued they should not be required to provide certain services. These employers also challenged the mandate on religious grounds, arguing that the ACA’s requirement that plans cover medication for HIV prevention violated the Religious Freedom Restoration Act (RFRA).
Proponents of the mandate argue that covering these benefits at no cost-share leads to earlier detection of serious medical conditions, earlier medical intervention, and more positive patient outcomes, which can decrease the number of high-cost claims in the population and deter costs. Critics oppose the increased costs to employers/plan sponsors and may also oppose certain preventive services on religious grounds, such as the requirement to cover pre-exposure prophylaxis for HIV (PrEP) or birth control.
While some expect that SCOTUS will uphold the mandate, legal and medical experts say that either way the court decides, the ruling could have profound ramifications for the future of preventive health care in the United States. If SCOTUS sides with the Justice Department, the mandate will remain in force.
But affirming the authority of the Secretary of HHS to overrule the expert panels may empower this cabinet-level executive branch department of the federal government to deviate from
how this policy is implemented. The outcome could give the administration broader latitude to shape the recommendations issued by the entities that were originally established with the goal of providing independent analysis and review.
FATE OF SCREENINGS
Kevin Conroy, the chief executive officer of screening test firm Exact Sciences, thinks that quality rating programs and market forces will cause employers and other payers to continue to cover common cancer screening tests -- even if the SCOTUS kills the mandate.
"Payers are highly motivated to get patients screened," Conroy told analysts during a recent meeting. Screenings are considered a subset of preventive care services and interventions that also include routine check-ups, vaccinations, health counseling and lab tests, all designed to help people stay healthy, detect health problems early, determine the most effective treatments and prevent certain diseases. They also include programs for health monitoring, along with counseling and education to help individuals take care of their own health.
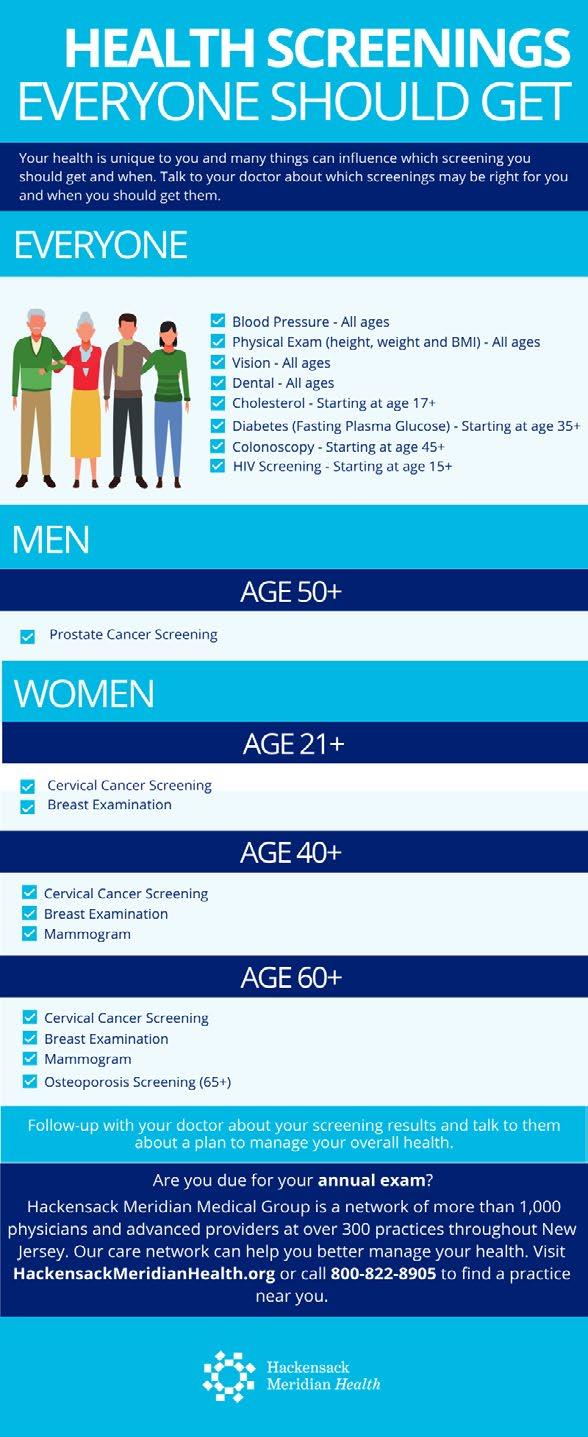
Most health plans extend coverage to a wide range of screenings, including those for cancer, diabetes, cholesterol, and other conditions, at no cost to the employee – no deductible, co-payment, or coinsurance.
The ACA also mandates coverage for women's preventive care, including screenings for cervical cancer and prenatal care. The USPSTF now advises that women should have the option of taking their own test samples for cervical cancer screening, and US regulators recently approved the first cervical cancer testing kit from Teal Health. This test allows women to collect their own samples at home before shipping them to a laboratory to detect the HPV virus that causes cervical cancer. Women in their 20s should get a Pap test every three years, but from age 30 to 65, they can get an HPV test every five years.
On a positive note and further endorsement of the value of screening, a new study presented at the American Association for Cancer Research Annual Meeting 2025 found that mortality from breast cancer decreased in women ages 20 to 49, from 9.70 per 100,000 in 2010 to 1.47 per 100,000 in 2020, even though the incidence has increased. The research attributed the mortality decline to advances in treatment and detection.
Furthermore, USPSTF now recommends physicians screen pregnant and postpartum women for domestic or intimate partner violence, pointing to the value of behavioral interventions to effectively reduce domestic violence in postpartum and pregnant women and women of reproductive age. In a sign of the times, syphilis cases are at a 3-year high despite widespread adoption of screening guidelines as the USPSTF just renewed its recommendation for early and universal screening for syphilis during pregnancy.
At Northwell Direct, a wholly owned subsidiary of Northwell Health, the largest health care system in NY as well as the largest private employer in New York State, Sandy Balwan, MD, chief medical officer, says, “Screening and prevention are foundational and are critical components of our population health strategy. The USPSTF guidelines are built into the foundation of our initiatives, especially those with level A and B recommendations such as breast cancer, colorectal and hypertension screening.”
She insists that screening costs are affordable for most, as many plans are required to cover these tests under the ACA. Common screenings like mammograms, colonoscopies, Pap smears and others are often free of charge to the members if performed in the plan's network.
“By definition, good screening tests should be cost-effective, accurate (low false positive results and false negative results), safe to administer, able to detect a high number of cases or preclinical diseases that are common, have high morbidity and mortality and lead to demonstrated improved health outcomes,” continues Dr. Balwan. “Therefore, if a screening test is implemented, diseases that burden a significant portion of the population would be detected early, lead to improved health outcomes, and lower total cost of care for patients over time.”
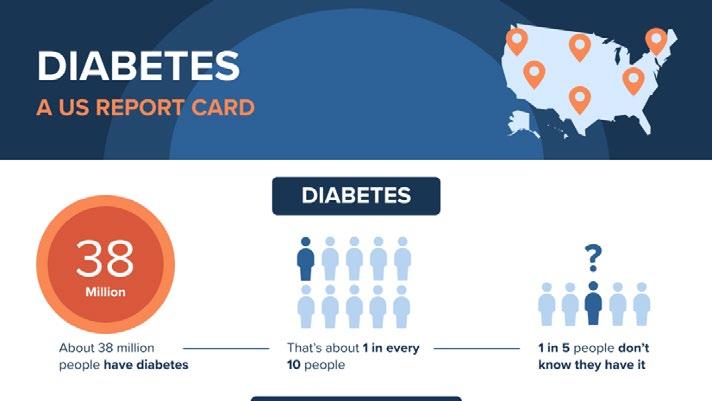
She points to one study in which the annual screening of employees and spouses found that for every 10,000 participants screened, 287 (2.9%) had previously unrecognized hyperglycemia (laboratory evidence of diabetes; A1C >6.4% or FG >125 mg/dL), and estimated that within 1 year, for every 1000 patients with confirmed diabetes, about 105 would experience complications. Within 5 years, about 489 would experience complications, including 50 patients with CVD, 68 patients with retinopathy, 168 patients with neuropathy, and 203 patients with nephropathy. The average annual cost of diabetes with complications is about $30K.
SOCIAL MEDIA MISINFORMATION
In a cross-sectional study of social media posts on Instagram and TikTok, most posts about five popular medical tests were misleading or failed to mention important harm, including overdiagnosis or overuse. As reported in JAMA, the tests included full-body magnetic resonance imaging, the multicancer early detection test and tests for Anti-Mullerian hormone (produced by the ovaries in females and the testes in males}, gut microbiome, and testosterone.
WHAT’S AT STAKE?
Self-insured employers have a vested interest in keeping employees healthy since the price tag that accompanies extensive and pricey medical care can impact their health plans with significantly higher financial burdens than preventing medical emergencies or diseases with a routine check-up or screening.
Joe Dore, President, USBenefits Insurance Services, emphasizes, “It’s likely that everyone agrees that any preventative healthcare measure is a positive to ensure illness is discovered in the earliest possible stages. Simple coughs, aches, and unexplained illness can be signs of serious concerns, such as autoimmune issues, heart disease, diabetes, cancer, and mental health.”
He says health screenings should be a part of an annual check-up, noting, “However, for most people, this isn't the case and is often unaffordable. Healthcare screenings should become a part of an employer's wellness program, possibly with some form of financial assistance and/or incentives to encourage this practice. This is especially true for self-funded groups, who can have more control of their risk management and financial objectives.”
Reinstating cost-sharing or declining coverage for screening services would discourage preventive care and increase costs for those who receive them, according to a report from the Employee Benefit Research Institute (EBRI). As a leading nonpartisan, tax-exempt organization dedicated to research and education on employee benefits, EBRI expressed concern that reintroducing cost-sharing could deter care on the individual beneficiary level and likely worsen health inequities, with little impact on employers’ overall spending.
Joe Dore
A CLOSER LOOK AT SCREENINGS
“The most valuable screenings are those that target conditions that can lead to chronic diseases, such as diabetes, hypertension, and high cholesterol,” offers Dr. Balwan. “Early detection through screenings like blood pressure checks, cholesterol panels and glucose tests can help prevent the progression of these conditions, which are often costly to manage long-term.”
She adds that cancer screenings, such as breast cancer and colorectal cancer, are crucial for early detection and can save lives by identifying cancers before symptoms appear or in early stages, where treatment can be curative. The value of these screenings lies in their ability to catch potentially serious conditions early, leading to better outcomes and lower treatment costs in the long run.
Source: Hackensack Meridian Health
CANCER
The American Cancer Society stresses that early detection of breast and cervical cancer through screening can improve survival and reduce mortality by finding cancer at an early stage when treatment is more effective and less expensive.
One study of the patient population of Kaiser Permanente of Northern California affirmed that when free cancer screenings became available, the incidence rate of colorectal cancer declined by 17%, and outcomes have improved. Moreover, the CDC said that modern mammography programs can lower breast cancer mortality by more than 40%, and Pap smears have helped to decrease more than 50% in cervical cancer incidence and mortality over the past 30 years.
What’s especially relevant and sometimes troubling for employers is that cancer is occurring in more adults at younger ages— before they turn 40 or 50 and sometimes even earlier. Researchers at Yale Medicine
characterize this trend as “early-onset” cancers, which are diagnosed in adults between the ages of 18 and 49. Because advancing age is the top risk factor for cancer in general, they view the recent rise in early onset as worrisome.
A new government study conducted by scientists from the National Cancer Institute provides the most complete picture yet of early-onset cancers in people 15 to 49 years old. Findings show the largest increases are in breast, colorectal, kidney and uterine cancers. Of 33 cancer types, 14 cancers had increasing rates in at least one younger age group and about 63% of the early-onset cancers were among women.
When it comes to determining the right age for screening, experts say to be aware of family history. For example, women who are at average risk for breast cancer may start biennial mammography screening at age 40, according to the newest USPSTF recommendations. However, women with a family history of breast cancer are generally advised to start when they are 10 years younger than the first-degree relative (a mother and/or sister) was at their time of diagnosis.
Unfortunately, more women are hearing the words ‘late-stage, invasive breast cancer’ when they’re initially diagnosed. A new study from the Radiological Society of North America finds that late-stage breast cancer, which has metastasized or spread to other parts of the body, is much harder to treat. The results showed women 20-39 years of age experienced the largest annual increase in late-stage breast cancer diagnosis at initial presentation (2.9%).
GENETIC CANCER SCREENINGS
Genetic testing for cancer without requiring a co-payment is a mandated benefit under the ACA for individuals who meet specific criteria outlined by the USPSTF. This includes genetic counseling and BRCA testing to assess the risks of developing breast and ovarian cancer for individuals with relevant personal or family cancer histories.
Up to 10% of cancers are thought to be related to inherited genetic factors and can be readily identified by commercially available multigene tests; as Dr. Balwan points out, “Primary care practices are often a point of contact for patients. As such, they are well-suited to risk-stratify and offer genetic cancer screenings to individuals. Patients with a strong family history of cancer, certain early-onset cancers, or specific genetic syndromes should be prioritized for risk assessment and testing. By preventing more advanced and costly cancer treatment, integrated genetic cancer screenings can be cost-effective in the long run. “
She cautions that it is important for primary care practices to balance this with cost-effectiveness and ensure that genetic screenings are used in the right populations to avoid unnecessary testing. It should be part of a broader personalized care strategy alongside other screenings and preventive measures.
DECLINING CANCER SCREENINGS
Among the reasons cited for patients missing their cancer screening are lack of awareness that they need to be screened for a certain type of cancer, don’t have any symptoms of disease or lack family history of illness. People also express fear of bad news, personal embarrassment, inconvenience, logistical barriers -- difficulty finding a babysitter, taking time off from work, or finding transportation -- and distrust/dislike of doctors or skepticism of the healthcare system, especially among younger adults.
2025 Prevent Cancer Foundation Survey: Only half of Americans are getting regular cancer screenings and routine medical care, a significant 10 percentage-point downswing from last year’s survey. Only 65% of women over age 40 had a routine mammogram; just 32% of men are up to date on their
testicular cancer screenings; only 36% of adults said they are up to date on skin cancer checks.
Aflac’s third annual 2025 “Wellness Matters Survey”: Most Americans (94%) put off getting a health check-up or screening. There is also widespread confusion regarding what insurance does and doesn't cover. Previous Aflac surveys show that millennials are most lax about health or wellness screenings, and millennials avoided tests such as pap smears, STD screenings, full body skin cancer exams and blood tests at much higher rates than other generations.
“A UNION ON A MISSION”
Preventative cancer care is not always convenient, especially for employees with unique schedules outside the traditional nine-to-five. Blue-collar workers in industries such as trucking and warehouse and supply can find it challenging to make time for cancer screenings and other types of care because of the amount of time they spend on the road or the timing of their shifts.
But the need for diligence in overall preventative care is especially important for this population: Studies show truck drivers are at higher risk for certain cancers, such as lung and prostate, the latter being the cause of death for an estimated 35,000 men in 2024, according to the American Cancer Society.
At Teamsters Health & Welfare Fund of Philadelphia and Vicinity, a partnership with Color Health is helping its 6,300 union members prioritize their health and practice early intervention. Since 2020, Teamsters has worked with Color to offer genetic testing, preventative cancer screenings and 24/7 cancer support.
One employee received an early-stage diagnosis for a cancer that may otherwise have been deadly. The cost savings of later-stage treatments for this one member covered the genetic testing program for the year.
Source: Employee Benefit News, February 2025
COST OF CANCER SCREENINGS
Despite multiple reports of the value of cancer screening to save lives, a study published in The Annals of Internal Medicine and based on data for the year 2021 shows that it comes at a high cost. The US spent $43 billion annually on screening to prevent five cancers: breast, cervical, colorectal, lung and prostate cancers, and the study concluded that the total was less than the reported cost of cancer treatment within the first 12 months after diagnosis. More than 88% of screening was paid for by private insurance, and the rest mostly by government programs.
Cancer screening makes up a substantial proportion of what is spent every year on cancer in the United States, which most likely exceeds $250 billion. For Karen E. Knudsen, chief executive of the American Cancer Society, the value of screening for cancers is clear, as early detection allows a better chance of survival. She says the cost is small compared to the cost of being diagnosed with late-stage disease.
However, other researchers contend that screening is overused, arguing that there is a weak link between early detection and cancer survival and that the money invested in cancer testing is not being well spent. A dermatology researcher at the University of Texas at Austin who studies screening maintains that some
studies repeatedly fail to show that people live longer if they are screened -- screening barely lowers the death rate from the cancer being screened since some cancers are deadly from the start and detecting them may not help.
BOOSTING CANCER SCREENING RATES
Public education campaigns are among the most important steps for improving cancer screening rates, advises Prevent Cancer Foundation. Their survey data indicates patients are 73% more likely to get a routine screening when they learn the benefits. Additional findings point to these opportunities for early detection:
Offering more screening modalities could make cancer screening more convenient. Around 42% of respondents said they'd complete a routine cancer screening if an at-home test was made available to them.
32% of patients said they'd get a cancer screening if they were more affordable. While the ACA mandates free preventive screenings for most cancers, follow-up diagnostic testing is not part of that mandate, and these costs are proven to deter patients from getting a cancer screening in the first place.
61% of respondents said they'd like a text, phone call or email reminder message to help them prioritize cancer screening, and 51% said it'd be helpful to connect with a patient navigator to answer questions or connect them to care.
73% of adults worry about cancer screenings, with a third specifically worrying about the possibility of finding out they actually have the illness.
Cancer screening might indicate how likely people are to beat the disease. Research reported in JAMA compared cancer-detection trends in states that have banned short-term health insurance policies, which tend to provide few, or no cancer screening benefits, with cancer-detection trends in states that allow easy access to short-term health insurance. The team found that in the states that allowed easy access to shortterm health insurance, cancer-detection improvement trends were about 2.3% worse than in the states that banned the use of short-term health insurance.
Dr. Balwan emphasizes that Northwell encourages employees to participate in health screenings by offering incentives such as wellness credits that result in decreased premiums for employees and dependents.
” These incentives help increase engagement and emphasize the importance of proactive health management," she continues. "Throughout the year, we deploy ongoing campaigns to encourage our members to obtain their annual preventive visit exams and to obtain age-appropriate cancer screenings, with the ability to schedule appointments with one click.”
Northwell also conducts onsite screenings at various client workplaces to make it easier for employees to access these services. As Balwan explains, 'We partner with top Northwell Health providers who specialize in occupational health services to ensure that screenings are delivered efficiently and with the highest quality. This approach eliminates barriers like time constraints and makes it convenient for employees to prioritize their health.”
The power
AmeriHealth Administrators is one of the largest national third-party administrators. We provide innovative, value-based health benefits programs and outsourcing services for self-funded health plans and other organizations.
Whether locally focused or on a national level, our scalable capabilities allow us to service many unique customers, including self-funded employers, Tribal nations, international travelers, and labor organizations.
environment. Visit amerihealthtpa.com.
MENTAL HEALTH
As the modern workplace evolves and with expectations around employee well-being, discussions about mental health become more prominent. Gallup research shows that organizations prioritizing mental well-being see higher engagement, lower turnover, and improved productivity.
Mental health screenings allow for early identification and treatment intervention that leads to better outcomes. The National Alliance on Mental Illness advises that early treatment may also lessen long-term disability and prevent years of suffering.
Dani Kimlinger, CEO, MINES and Associates, reflects on her market experience, “Several of our client organizations do encourage or incentivize employees to participate in mental health screenings, and in some cases, they integrate these check-ins into their broader wellness programs. We partner with employers to offer both online screening tools and direct assessments.”
An example of an organization that Kimlinger works with is a public entity that does this well.
“Employees receive half a day of PTO for completing twice-yearly “mental health check-ups,” she explains. "This is like scheduling a routine dentist appointment: a proactive approach that helps identify potential needs and supports ongoing well-being. While not every employer engages in these, we do screen for every client who requests counseling services. We provide the clinical support and guide individuals toward the right resources.”
a Leading National TPA
Creating solutions for better healthcare outcomes is at the heart of everything we do.
In-house client support from implementation through renewal
Tailored point solutions and a la carte programs
The latest in navigation tools and concierge services
Member advocacy solutions
Innovative
hpiTPA.com
Dani Kimlinger
Depend on Sun Life to help you manage risk and help your employees live healthier lives
By supporting people in the moments that matter, we can improve health outcomes and help employers manage costs.
For over 40 years, self-funded employers have trusted Sun Life to help them manage financial risk. But we know that behind every claim is a person facing a health challenge and we are ready to do more to help people navigate complicated healthcare decisions and achieve better health outcomes. Sun Life now offers care navigation and health advocacy services through Health Navigator, to help your employees and their families get the right care at the right time – and help you save money. Let us support you with innovative health and risk solutions for your business. It is time to rethink what you expect from your stop-loss partner.
Ask your Sun Life Stop-Loss Specialist about what is new at Sun Life.
For current financial ratings of underwriting companies by independent rating agencies, visit our corporate website at www.sunlife.com. For more information about Sun Life products, visit www.sunlife.com/us. Group stop-loss insurance policies are underwritten by Sun Life Assurance Company of Canada (Wellesley Hills, MA) in all states, except New York, under Policy Form Series 07-SL REV 7-12 and 22-SL. In New York, Group stop-loss insurance policies are underwritten by Sun Life and Health Insurance Company (U.S.) (Lansing, MI) under Policy Form Series 07-NYSL REV 7-12 and 22-NYSL. Policy offerings may not be available in all states and may vary due to state laws and regulations. Not approved for use in New Mexico.
Kimlinger believes mental health and emotional well-being assessments such as integration of Screening, Brief Intervention and Referral to Treatment (SBIRT) and Patient Health Questionnaire (PHQ) are particularly valuable.
“These screenings identify conditions such as depression, anxiety, or substance use concerns,” she continues. “These screenings help us determine if someone is engaging in substance abuse, is depressed, or may be at risk for harm to self or others, which allows us to intervene promptly and connect them with the most appropriate care.”
Although “physical health” screenings such as getting blood work done are most often thought of as important screenings, she cautions that mental health check-ins can often be overlooked, yet they play a critical role in an employee’s overall health and productivity.
Kimlinger reports hearing concerns from clients and addresses any anxiety or misinformation about screening by emphasizing confidentiality and highlighting how these screenings can lead to personalized support.
“By offering education and open conversations about what screenings involve, such as a brief questionnaire to gauge risk factors, we help normalize the process,” she explains. “In addition, we remind employees that the goal is to provide proactive support and assistance. Through confidential counseling services, coaching, peer support, mindfulness, and other resources, our team supports clients at every step, ensuring they feel safe and informed throughout the process.”
DIABETES
The number of undiscovered cases of diabetes is astounding. More than 38 million people have diabetes, but fewer than 30 million of them know it. Nearly nine million adults with diabetes are undiagnosed, according to the National Diabetes Statistics Report.
The CDC reports that medical costs for people with diabetes are double the costs for those without. In fact, diabetes is the most expensive chronic condition, with health care costs and lost work and wages totaling $413 billion a year.
Diabetes is often described as a “silent killer” because it can inflict damage long before any outward signs appear. In the absence of a diagnosis, people do not get the care they need to prevent damage to their blood vessels and nerves that could lead to serious complications, like heart and kidney damage and diabetic retinopathy.
There is an urgent call for intensive screening for diabetes in the primary care setting to ensure that anyone who meets the criteria of being at risk gets screened. Intensive screening also allows providers to detect prediabetes in their patients. According to the National Diabetes Statistic Report, there are 97.6 million people aged 18 years or older -- 38% of the adult US population -- who have prediabetes.
Screening primarily relies upon blood tests. The American Diabetes Association's Standards of Care 2025 guidelines emphasize the use of antibody-based screening for pre-symptomatic type 1 diabetes in high-risk individuals. For type 2 diabetes and prediabetes, the focus remains on A1C, fasting plasma glucose, and oral glucose tolerance tests.
The ADA and USPSTF recently expanded their criteria for who should be screened, with the goal of identifying more patients with type 2 diabetes and prediabetes. For example, in addition to screening patients with risk factors such as obesity, a family history of diabetes, a sedentary lifestyle, and a history of gestational
diabetes, guidelines now recommend that screening for type 2 diabetes and diabetes begin at age 35 years, regardless of whether a patient has any other risk factors.
Source: 2025 Centers for Disease Control and Prevention (CDC)
OVERCOMING BARRIERS TO SCREENING
Attorneys writing for the National Law Review advise that until SCOTUS renders an opinion, employers subject to the ACA should continue to cover the preventive services recommended by the USPSTF at no cost-share to their employees. They say that if the challenge is successful, employers may be able to impose cost-sharing on certain preventive services and/or benefits, which may initially reduce healthcare costs.
Babst, Calland, Clements & Zomnir, P.C. counsel, “However, it is important to remember that federal law sets the floor, and not the ceiling for required covered benefits – and that while imposing cost-sharing on employees may have an immediate financial gain in the short-term, shifting costs to employees can cause delays in care, which can lead to later medical interventions, higher cost claims, and ultimately, a sicker workforce.”
Employers should also be aware of the resources available from the
CDC’s National Breast and Cervical Cancer Early Detection Program (NBCCEDP), providing breast and cervical cancer screenings, diagnostic tests, and treatment referral services to US communities that are limited income, underserved, underinsured, or uninsured.
ONSITE HEALTH SCREENINGS
Onsite workplace health screenings are becoming increasingly popular, with the latest Reward and Employee Benefits Association (REBA) and Axa Employee Well-being Research finding that screening or health assessments are now offered by 59% of employers. Maximizing the value of health screening is now recognized as an opportunity to extend health benefits across the entire workforce, as REBA offers these suggestions:
1. Effective launch/introduction
Set aside time, resources, and budget to properly launch and promote screenings.
2. Regular reminders
Repeat. Repeat. Repeat the message with regular communications, newsletters and reminder invitations that go directly to employee inboxes.
3. Remove barriers to testing
Make it as easy as possible for employees to attend an appointment and potentially introduce an onsite health assessment day. Dispel the "fear factor" among employees who may be worried about test results or the actual screening procedure. Provide education and communication about the value of screening.
4. Leadership support
Train line managers to encourage the adoption of a screening benefit and provide top-down support from leadership. When senior managers set an example and share their experience with screening via the intranet or team meetings, employees have an example to follow.
5. Sharing stories
Real-life experiences and sharing stories are powerful ways to spread the message about the value of health assessments. If an employee has learned something new about his/her health and has been able to tackle it – and, most importantly, is willing to talk about it – others will be motivated.
6. Effective integration
Create clear paths for employees to take their health assessment results through to providers. Make health assessments part of ongoing communications, campaigns, or charity fundraising activities – October is Breast Cancer Awareness Month, and November is Diabetes Month as well as Ovarian Cancer Awareness Month.
7. Actionable insight
Aggregate screening data and use it to create change. This will enable a better understanding of underlying health issues affecting the workplace and overall business performance, facilitating decision-making and informationsharing to create health initiatives. The goal is to help motivate individuals to make lifestyle changes, lower sickness absenteeism, boost engagement and improve productivity.
8. Repeat testing
Repeat testing annually or every 24 months and track patterns and trends.
PLOTTING THE FUTURE
The Forbes Business Council reports that more than 150 million people, including 37 million children, with private health insurance receive preventive health services at no cost to them under the ACA.
If the mandate is struck down or any ambiguity is left surrounding its validity, coverage and access are at risk, warns Richard Hughes IV, partner, Epstein Becker Green.
He maintains that while this is less likely to manifest in the form of overnight coverage rescissions for major services, like mammograms or colonoscopies, degradation of coverage is more likely to occur gradually through increased utilization management. This might include prior authorization, stricter adherence to or narrowing of recommended age ranges or cohorts, formulary management of products like PrEP for HIV, or the imposition of cost-sharing.
The consequences of this decision have health experts worried, as a Morning Consult survey found that at least 2 in 5 US adults said they are not willing to pay for 11 of the 12 preventive services currently covered by the ACA. Some observers predict that even $20 copays can reduce adherence substantially to cancer screenings, which could ultimately lead to more cancers being diagnosed at advanced stages.
This eventuality would be alarming for employers struggling to avoid high healthcare expenses. If employees choose to forgo preventive care and screening because of associated costs, companies will carry a heavier burden from more expensive and time-consuming care related to later-stage diseases. Screenings can be recognized as incredibly cost-effective. Preventing disease progression, like advanced cancer, tends to be a lot less expensive than treating it.
Dr. Balwan asserts that education is a critical part of the Northwell approach to health screenings, adding, “Many employees may feel anxious or reluctant to participate in screenings due to fear, misinformation, or lack of understanding. To address this, we provide educational materials, monthly educational bulletins, and email reminders that explain the importance of screenings and how early detection can save lives. By fostering an environment of trust and open communication, we aim to alleviate concerns and encourage employees to take an active role in their health.’
For employers with significant workforce turnover, there is another consideration. As people move to different jobs and states or get older, and as the insurance provider changes, there may be a time gap between the first screening and when the individual is actually diagnosed with the disease. It is conceivable that some employers may decide it’s not worth it to keep paying fully for all members to undergo screenings if they are not forced to do so.
As employers await a decision from the highest court that could impact access to free health screenings, they need to weigh the advantages of preventive care vs. “sick care.” Some industry observers regard this as “pay now or pay more later,” as the evidence supporting health screenings is compelling.
Laura Carabello holds a degree in Journalism from the Newhouse School of Communications at Syracuse University, is a recognized expert in medical travel and is a widely published writer on healthcare issues. She is a Principal at CPR Strategic Marketing Communications. www.cpronline.com
PREVENTIVE CARE MANDATE FACES SUPREME COURT SCRUTINY
Written By Alston & Bird Health Benefits Practice
UUnder the ACA, non-grandfathered group health plans must cover certain preventive care services innetwork without imposing any cost-sharing requirements.1 The preventive services that plans must cover are based on recommendations from three entities:
• U.S. Preventive Services Task Force (USPSTF) – plans must cover evidence-based items or services with an A or B recommendation from the USPSTF
• Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention – plans must cover immunizations for routine use for children, adolescents or adults recommended by ACIP
• Health Resources and Services Administration (HRSA) – plans must cover other evidence-informed preventive care and screenings provided for in HRSA’s comprehensive guidelines for infants, children, adolescents, and women
In Braidwood Management v. Becerra, plaintiffs challenged the ACA’s preventive services mandate, arguing, among other things, that the structures of the USPSTF, ACIP, and HRSA violate the Appointments Clause of the U.S. Constitution. They also contended that requiring coverage of pre-exposure prophylaxis (PrEP) for HIV prevention infringes upon their religious freedoms under the Religious Freedom Restoration Act (RFRA).
On March 30, 2023, the U.S. District Court for the Northern District of Texas ruled in favor of the plaintiffs, holding that:
• The USPSTF’s authority to mandate coverage of preventive services with an “A” or “B” recommendation after March 23, 2010, is unconstitutional.
• Mandating coverage of PrEP medications violates the plaintiffs’ rights under RFRA.
The district court’s decision effectively blocked the federal government from enforcing these preventive care requirements nationwide. However, on appeal, the 5th Circuit affirmed the district court’s judgment to the extent that it enjoined the Agencies from enforcing the USPSTF’s recommendations with respect to the named plaintiffs; reversed the district court’s judgment to the extent it imposed a nationwide injunction; and remanded to the district court for further proceedings.2
The court did not address the constitutionality of ACIP and HRSA’s roles, leaving those questions unresolved and remanding the question back to the district court for further consideration. On August 28, 2024, the district court entered a stay pending proceedings in the Supreme Court. The case, now titled Kennedy v. Braidwood Management, reached the Supreme Court, which heard oral arguments on April 21, 2025. Afterward, the court directed the parties to file supplemental letter briefs addressing the question of whether Congress "by Law" vested the Secretary of the Department of Health and Human Services with the authority to appoint members of the USPSTF.
The central issue before the Supreme Court is whether the structure of the USPSTF violates the Appointments Clause of Article II of the U.S. Constitution and whether the 5th Circuit erred in declining to sever the ACA provision to insulate the USPSTF from the Secretary’s supervision. HHS filed a brief defending the ACA requirements and arguing that USPSTF members are inferior officers because the Secretary of HHS, a quintessential principal officer, remains responsible for final decisions about whether the USPSTF's recommendations will be legally binding and can remove USPSTF members at will, for any reason.3
HHS recommends that, at a minimum, the Supreme Court reverse the severability holding to allow the USPSTF to make recommendations that will have legal effect only under appropriate supervision by the Secretary. However, if the district court’s holding is upheld, the following ACA preventive services mandates would be unenforceable: screenings for breast, cervical, colorectal, lung and skin cancer; screenings for diabetes, depression, hepatitis and vision problems in children; screening and treatment for HIV, including PrEP; and care for those who are pregnant and breastfeeding and care for their young children.4
WHAT’S NOT BEFORE THE SUPREME COURT
As noted, the plaintiffs also asserted Appointments Clause challenges to ACIP and HRSA. Although the district court rejected those challenges, the Fifth Circuit reversed and remanded the question to the district court to consider the argument that the Administrative Procedures Act required public notice and comment to ratify the recommendations and guidelines of ACIP and HRSA. The Supreme Court is not considering the arguments involving ACIP and HRSA, but only USPSTF.
As a result, the Supreme Court’s decision will only impact the mandate to cover evidence-based items or services with an A or B recommendation from the USPSTF. The ACIP and HRSA-based preventive care mandates will remain in effect until the district court considers the arguments and issues a ruling, which might apply nationwide or only to the litigants. From there, the district court’s ruling on ACIP and HRSA
might be appealed to the Fifth Circuit and maybe even the Supreme Court. In other words, rinse, wash, and repeat the process for the USPSTF preventive mandate challenge for the ACIP and HRSA preventive mandates. It could be years before there is clarity.
Until the Supreme Court issues its decision, the preventive services mandate remains in effect for most health plans. Employers should continue to comply with existing requirements based on USPSTF, ACIP, and HRSA recommendations and prepare for 2026 updates. For example, the Supreme Court’s ruling will not impact the HRSA updated recommendations for 2026, which, among other updates and new guidelines, state that "Women may require additional imaging to complete the screening process or to address findings on the initial screening mammography. If additional imaging (e.g., magnetic resonance imaging (MRI), ultrasound, mammography) and pathology evaluation are indicated, these services also are recommended to complete the screening process for malignancies.”5 Employers should work with their advisors, including legal counsel, to ensure their plans comply with preventive care mandates and understand the scope of the Supreme Court’s decision once it is issued.
Attorneys John Hickman, Ashley Gillihan, Steven Mindy, Amy Heppner, Laurie Kirkwood, and Bria Smith provide the answers in this column. John is partner in charge of the Health Benefits Practice with Alston & Bird, LLP, an Atlanta, New York, Los Angeles, Charlotte, Dallas and Washington, D.C. law firm. Ashley and Steven are partners in the practice; Amy and Laurie are senior members in the Health Benefits Practice; Bria Smith is an associate in the Employee Benefits Practice. Answers are provided as general guidance on the subjects covered in the question and are not provided as legal advice to the questioner's situation. Any legal issues should be reviewed by your legal counsel to apply the law to the particular facts of your situation. Readers are encouraged to send questions by E-MAIL to John at john.hickman@alston.com .
References
1. 42 U.S.C. § 300gg-13(a)(1).
2. See 104 F.4th 930 (5th Cir. 2024), petition for cert. filed, (U.S. September 19, 2024) (No. 24-316).
3. https://www.supremecourt.gov/DocketPDF/24/24-316/343079/20250218171629934_24-316tsUnited States.pdf (last visited May 20, 2025).
4. See https://www.dol.gov/agencies/ebsa/about-ebsa/our-activities/resource-center/faqs/aca-part-59 and https://www.dol.gov/agencies/ebsa/about-ebsa/our-activities/resource-center/faqs/aca-part-68 (last visited May 20, 2025).
At Pinnacle Claims Management, we empower Benefits Consultants to achieve lasting success through smarter health management solutions.
Our integrated approach—combining clinical expertise, seamless technology, and hands-on support—delivers real, measurable results. From early intervention to chronic condition management, we help members manage ongoing illnesses like diabetes and heart disease, while helping you build stronger, longer-lasting client relationships.
We’re more than a TPA—we’re your trusted partner delivering proven health management solutions.
www.pinnacletpa.com/excellence
NEWS FROM SIIA MEMBERS
JULY 2025 MEMBER NEWS
SIIA boasts a very active and dynamic membership. Here are some of the latest developments from the companies powering the self-insurance industry.
Companies Combine Under Beyond Health Brand
Beyond Risk Topco Holdings, LP announced the strategic consolidation and rebranding of its three premier employee healthcare benefits insurance businesses under the unified "Beyond Health" brand.
This strategic initiative combines:
• Beyond Health - A premier employee health benefits group captive program with multiple cells operated within HatterasRe Ltd. and managed by Bev Cap Management, LLC (“BevCap”)
• SL Management Partners, LLC –(SLMP) A leading full-service medical stop loss managing general underwriter (MGU) providing innovative stop loss and claims solutions
• BeyondRe Stop Loss Insurance Services - A fast-growing underwriter of stop-loss captive programs and a business unit within BevCap
This strategic integration creates a comprehensive platform that streamlines the client experience while maintaining specialized expertise in both captive and traditional stop-loss solutions. The executive leadership team brings together industry veterans with more than 120 years of combined employee benefits and underwriting experience:
• SLMP founders Steve Solomon and Robert (Bob) Lang, who joined Beyond Risk in 2024
• John Kirke, President of BevCap's Healthcare Captives business
• Steve McFarland, Chief Underwriter, Managing Director of BeyondRe
• Lance Abbott, CEO of BevCap and Beyond Risk Board Member
"This rebrand and collaboration perfectly aligns with our vision for Beyond Health, BevCap, and the Beyond Risk suite of medical stop loss services," said Lance Abbott, CEO of BevCap and Beyond Risk Board Member. "By uniting our teams and leveraging our collective expertise, we're creating a more efficient, scalable platform that can better address the evolving needs of our carrier partners and clients."
H.H.C. Group Maintains IRO Accreditation
H.H.C. Group (H.H.C.) announced that it has been re-approved by multiple states in which it currently conducts Independent Medical Reviews (IMRs), typically for disputes regarding coverage by payors based on medical treatment necessity or appropriateness. These state designations reinforce H.H.C.'s position as a URAC-accredited Independent Review Organization (IRO) and highlight the company's vital role in helping payors resolve claim disputes efficiently, compliantly and with clinical precision.
"Acceptance by 32 states positions us as a trusted partner from coast to coast," says Bruce D. Roffé, president and CEO of H.H.C. Group. "In most states, once a coverage denial occurs, insurers must refer the case to the state, which assigns it to an approved IRO. In others, insurers can contract directly with an IRO like H.H.C.-and we are fully equipped to support both pathways. Additionally, numerous insurers have H.H.C. help them determine if they should cover a treatment requested by a plan enrollee."
Tony Minnich Promoted at Tokio Marine HCC – A&H Group
Tokio Marine HCC – A&H Group announced the promotion of Tony Minnich to Senior Vice President of Captives. We extend our congratulations to Tony on this significant achievement.
"I am very excited and honored to continue to lead the TMHCC Stop Loss Captive. In this new role, I look forward to helping our captive members and partners continue to grow and thrive, as we have done for 13 years," said Tony Minnich.
Centivo Names New Chief Financial Officer
Centivo announced the appointment of Sarah Fraser as Chief Financial Officer. This key leadership hire comes as Centivo enters a new phase of growth, expanding the reach of its primary care-focused health plan for self-funded employers.
In her role, Fraser will lead Centivo’s capital markets strategy, overseeing banking, debt, and equity relationships in addition to applying a strategic, data-driven approach to financial performance across customer segments, product lines and markets to fuel the company’s expansion.
"To support our mission of fixing healthcare for the working American family, we need world-class financial leadership—and Sarah brings just that," said Centivo co-founder and CEO Ashok Subramanian. “Her depth of experience across high-growth healthcare and tech companies, combined with a keen strategic mind and a collaborative approach, will be instrumental as we scale our impact and continue to deliver on our promise of radically affordable healthcare.”
Dallas Scrip Joins Marpai as President & COO
Marpai, Inc. announced a significant addition to its leadership team with the appointment of Dallas Scrip as President and Chief Operating Officer. This strategic hire underscores Marpai's commitment to accelerating profitable growth and enhancing operational excellence within the dynamic healthcare landscape.
Prior to joining Marpai, Mr. Scrip demonstrated significant success in startup, early-stage, and growth situations, scaling private equity and venture capital-owned companies. His expertise spans servicing healthcare consumers, employers, providers, and payor markets, with a strong foundation in sales and
Sarah Fraser
Tony Minnich
business development. Scrip is known for his process-oriented approach, identifying market needs, and strategically transforming companies through organic growth initiatives.
"We believe that the addition of Dallas to our leadership team is a pivotal step in Marpai's journey towards sustainable and profitable high growth," stated Damien Lamendola, Chief Executive Officer of Marpai Inc. "His extensive experience and proven ability to deliver results in complex healthcare environments will be invaluable as we continue to scale our operations and enhance our service offerings. Dallas' deep understanding of the TPA landscape and his commitment to building high-performance teams align perfectly with Marpai's vision for the future."
QBE Reorganizes Geographic Operations
QBE North America announced that it has reorganized the East region of its Accident & Health business into two distinct territories: the Northeast and the Southeast. Bruce Shaver, based in Atlanta, GA, has joined the company to lead the newly established Southeast region. With nearly two decades of insurance experience, Shaver brings a strong foundation in both risk assessment and client engagement. Zach Sullivan will continue to lead the Northeast region from Marblehead, MA.
At UME, we offer flexible, data-driven products to help brokers and employers:
Reduce claim costs with Reference-Based Pricing
Stabilize spend through customizable StopLoss coverage
Transition confidently to self-funding with the Maximum Advantage Program
Maintain compliance with MEC plans
Let’s create smarter, sustainable benefit strategies — together. l
Dallas Scrip
"As our Accident & Health business continues to grow, we've made a strategic investment to deepen our understanding of — and responsiveness to — our partners," said Tara Krauss, President of Accident & Health. “With Bruce aboard, we aim to deliver more localized support and enhance our connections with partners across the Southeast.”
Alliant Insurance Services Taps Dan Powers to Help Lead ValueBased Health Care Practice
Dan Powers has joined Alliant Insurance Services as Senior Vice President with the Value-Based Healthcare and Risk Management Solutions practice of Alliant’s Employee Benefits Group. With more than two decades of experience in business development, partner strategy, and reinsurance, Powers will lead the practice’s reinsurance strategy and alternative risk initiatives.
"Dan's leadership and deep expertise will be instrumental in advancing the ongoing expansion of our Value-Based Healthcare and Risk Management Solutions practice," said Kevin Overbey, President of Alliant Employee Benefits. "He brings a forward-thinking approach and a strong grasp of the complexities shaping today's healthcare landscape".
Based in Boston, Powers will work closely with healthcare providers, systems, and payers to design customized financial protection strategies. His leadership and expertise in risk transfer solutions, alternative risk arrangements, captive insurance programs, and population health risk analytics will further the team's ability to improve care and reduce costs for clients in valuebased contracts.
PBA to Acquire JP Farley
Professional Benefit Administrators Inc. (PBA), based in Oakbrook, Illinois, announced it would be acquiring JP Farley (JPF), headquartered in Westlake, Ohio, and merging operations, creating a unified entity poised to offer enhanced benefits and administrative services to clients nationwide.
This strategic acquisition brings together two organizations with a rich history of providing exceptional service with over 80 years of combined experience in self-funded health plan administration.
The combined expertise and resources of PBA and JPF will enable PBA to deliver innovative solutions, improved efficiencies, and an expanded suite of services to meet the evolving needs of brokers and employers in our market.
Jeff Walter, President of Professional Benefit Administrators Inc., is enthusiastic about the acquisition: "We are thrilled to work with Jim and his team to take our long-term association to the next level with this merger. Adding JPF's innovative benefit design portfolio to PBA's suite of products, management, and
Bruce Shaver
Dan Powers
processes will allow us to offer a strong alternative for succession and growth in the independent TPA market. This merger represents a significant milestone in our commitment to providing exceptional benefit administration services. Together, we will create a stronger, more dynamic organization that is wellequipped to meet the challenges and opportunities in our industry.”
Jim Farley, President and CEO of JP Farley, echoed these sentiments: "PBA is a great fit for JP FarleyCorp. I've been determined to execute a succession arrangement within an independent TPA structure so that JP Farley Corp can maintain its sole focus on serving the employer plan sponsors and their employees we are privileged to work with. It was important for me to avoid the inevitable conflicts of interest in ownership that hospitals, insurers, or private equity organizations have historically created for independent TPAs. I am looking forward to working together for another 10 or 15 years!"
The transaction is expected to be finalized early in the fall of 2025, subject to all administrative tasks and customary closing conditions. Both organizations are dedicated to ensuring a smooth transition for their clients and employees.
Skyward Recognized as One of the Best Companies for Employees
Skyward Specialty Insurance Group, Inc.TM has been named one of 2025-2026 Best Companies to Work For by US News & World Report for the second consecutive year. The company earned recognition in three categories, including Overall, Industry: Finance & Insurance, and Region: South. US News & World Report selects recipients of this honor based on an independent analysis of publicly available data, not applications or corporate submissions.
“What makes this recognition so meaningful is that it is grounded in the real experiences of our employees,” said Skyward Specialty Chairman & CEO Andrew Robinson. “In the five years since our rebrand as Skyward Specialty, we’ve built an incredibly engaged and compassionate culture that is only possible because of the people building it. This honor reinforces the strength of our culture and the depth of our commitment to every team member.”
Hamilton, NJ – Berkley Accident and Health, a Berkley Company, is pleased to announce the appointment of David Braxton as Regional Sales Manager in the Southeast. In this role, David will be responsible for driving growth and developing new Stop Loss relationships and Captive
David Braxton
Insurance programs, primarily in North Carolina and South Carolina.
"We are excited to have David join our team," said Brad Nieland, President and CEO of Berkley Accident and Health. “David brings more than 20 years of insurance experience to our organization. He has held sales and leadership roles in a number of large national insurance carriers. David's deep understanding of stop loss and health insurance will be an asset to our policyholders and broker partners.”
Jeff Miller Returns to Lockton to Lead Stop-Loss and Pharmacy Practices
Lockton announced the appointment of a new national practice leader to help drive the continued growth of its People Solutions business.
Jeff returns to Lockton as National Practice Leader for the Stop Loss and Pharmacy practices, bringing more than three decades of industry leadership and a wealth of experience developing and deploying innovative solutions to meet changing client needs across a range of capabilities.
He previously served as President of Point6 Healthcare and Office President at Ryan Specialty Benefits, where he oversaw organizational growth while aligning operations across several acquisitions.
"It's a pleasure to welcome Jeff back home to Lockton," said Tim Meacham, President, People Solutions. "His leadership and experience across several critical areas of employee benefits is just what we need, at the right moment, to continue to provide the best possible value to our clients.”
Jeff Miller
In his previous Lockton tenure, Miller was EVP and Practice Leader, directing senior leadership across practice areas like actuarial, integrated absence, precision health and wellbeing, compliance, global benefits, and voluntary benefits. He also played a key role in the acquisition and integration of Excelsior Solutions, a pharmacy consulting practice, and the alignment of offices in both Houston and San Antonio.
Take Command Taps Jamie Potecha to Run Operations
Take Command announced that Jamie Potecha has been appointed the company's Chief Operating Officer. Potecha will lead efforts to strengthen the systems and teams that make it easier for employees to navigate and maximize their health benefits.
Potecha brings more than 15 years of experience leading healthcare companies, and he most recently served as Head of Operations, Product Strategy, & Compliance at Granular Insurance. He was an early leader for the health risk management company and built scalable processes that helped transform Granular into one of the largest stop-loss insurers.
"Jamie is a natural leader who will bring extensive expertise in operations, strategy, and product management to Take Command," said Take Command CEO Jack Hooper. "He will build upon his track record of scaling systems and assembling high-performing teams to support our growth and innovation. Jamie's arrival reinforces our commitment to providing our customers and partners with the infrastructure and resources they need to deliver an exceptional employee health insurance experience on a reliable, predictable budget.”
Jamie Potecha
SIIA NEW MEMBERS
JUNE
2025
NEW CORPORATE MEMBERS
Amanda Beach Senior Sales Executive BASELoad and W-9 Corrections Rock Hill, SC
Shannon Jensen Founder/Consultant
Clover Consulting Group Billings, MT
Austin Browning CEO Faros Health Dallas, TX
Hadley Waterbury Marketing Coordinator Navion Williamsville, NY
Elle Fair Associate, People & Culture RxSense Boston, MA
Sarah Zoccolante VP Client Services
Triton Healthcare Partners Boston, MA
Charlie Hildebrand President, Payer Solutions Unity Preferred Network Oklahoma City, OK
Robert Williams Chairman Vengroff Williams Inc. Sarasota, FL
Jacob Brody Co-Founder & CEO ZorroRX Patterson, NY
2025 SELF-INSURANCE
INSTITUTE OF AMERICA
BOARD OF DIRECTORS
CHAIRMAN OF THE BOARD*
Matt Kirk
President
The Benecon Group
CHAIRPERSON ELECT, TREASURER AND CORPORATE
SECRETARY*
Amy Gasbarro
President
ELMCRx Solutions
DIRECTOR
Mark Combs
CEO/President
Self-Insured Reporting
DIRECTOR
Orlo “Spike” Dietrich Operating Partner
Ansley Capital Group
DIRECTOR
Jeffrey L. Fitzgerald
Managing Director
SRS Benefit Partners
Strategic Risk Solutions, Inc.
DIRECTOR
Mark Lawrence
President
HM Insurance Group
DIRECTOR
Matthew Smith
Managing Director
Risk Strategies
DIRECTOR
Beth Turbitt
Managing Director
Aon Re, Inc.
VOLUNTEER COMMITTEE CHAIRS
Captive Insurance Committee
George M. Belokas, FCAS, MAAA
President Beyond Risk
Future Leaders Committee
Erin Duffy
Director of Business Development
Imagine360
Price Transparency Committee
Christine Cooper CEO aequum LLC
Cell and Gene Task Force
Ashley Hume President
Emerging Therapy Solutions®
* Also serves as Director
2025 BOARD OF DIRECTORS
SIEF CHAIRMAN
Nigel Wallbank President New Horizons Insurance Solutions Wellington, FL
Les Boughner Chairman Advantage Insurance Management (USA) LLC Charleston, SC
Matt Hayward Office President Ryan Specialty Benefits Greenwood Village, CO
FEBRUARY 2025
Elizabeth Midtlien Vice President, Emerging Markets AmeriHealth Administrators, Inc. Bloomington, MN
Jonathan Socko President
East Coast Underwriters, LLC Spartanburg, SC
See the Zelis difference:
Focus on leading, not firefighting.
Managing claims, networks, and payment systems doesn’t have to feel like an uphill battle.
Supercharge Your TPA Operations with Zelis. Call us today at (888) 311-3505 or scan the QR code to get started.
Efficient workflows that save time.
Lower costs with seamless systems.
Happier clients who see the difference.
José faced more setbacks after receiving his new liver. Stop Loss helps protect his self-funded employer.
Catastrophic claims can arise unexpectedly. Medical claims could reach $1.5 million if a liver transplant is complicated by sepsis and renal failure.* When the self-funded employer has the right Stop Loss protection in place, focus can remain on achieving business goals and supporting José through his recovery.
When you work with the experts at HM Insurance Group, you can be confident that claims will be paid. We process 99% of Stop Loss claims within six business days, with more than 99% technical and financial accuracy. Find more at hmig.com.