The health of our planet and people are intertwined As the world warms, wellbeing wanes But this doesn't have to be the case
The Young Geographer Magazine provides a platform for young people to share issues that compel us Our team has chosen to address climate and health, not only because health is the basic necessity for a better world, but because we have the opportunity to protect it
This edition aims to inform, explore and inspire change to protect health in a changing climate. It features voices curated by our youth staff, including Scotland’s Chief Medical Officer, Professor Sir Gregor Smith, and many others from around the globe.
My request is that the impact of this edition is not contained between its covers. As you read, I encourage you to reflect. We all have influence, now it is the time to use it. For ideas of ways to take action, please see the back cover
I hope you enjoy reading and reflecting with the Young Geographers
Take care, take action.
RSGS would like to thank the Gannochy Trust for their support of this project
The views expressed in this magazine are not necessarily those of the RSGS
Royal Scottish Geographical Society
Lord John Murray House 15-19 North Port Perth, PH1 5LU Scotland
UK enquiries@rsgs org 01738 455050
Scottish Charity No SC015599
Front Cover Image Credit: Bill Metcalfe at Nelson Star, BC Canada
Picturing: Dr Kennedy, member of Doctors and Nurses for Planetary Health
o work with the Young hem in the creation of this in a great deal of hard e process, both to secure content but also to represent different and diverse perspectives, to help illustrate the depth of issues and concerns around climate and health
focused
Being a very future focused charity, RSGS is determined not only to stand up for concerns that young people have, and to work towards encouraging better long term decision making in society for their benefit, but also to give young people a platform of their own, and challenge them to learn new skills.
Once the have generations. sometimes is seen approach how that
Once again, the Young Geographer team have picked a climate topic because this still remains one of the most critical issues of our generations. Climate change is already impacting all over the world, sometimes in very subtle ways, and in the health arena it can be seen to be driving further inequalities, not just internationally, but domestically too As a result the climate emergency is increasingly being seen as a health emergency It is doubly worrying therefore that the US has not just withdrawn from the Paris climate agreement but also from the World Health Organisation It is as if it has chosen to shove a finger in each of its ears, to block out the roar of scientific opinion, and it does not bode well for us taking an informed and considered approach to the future
I have been impressed by how much the Young Geographer editorial team have embraced this challenge in the way they have, and I hope, like them, that it will continue to have an impact well beyond the pages of the magazine.
Mike Robinson Chief Executive Royal Scottish Geographical Society
Photo: Sharwar Apo
Photo: Sharwar Apo
Photo: Sharwar Apo
MEET THE YOUNG GEOGRAPHERS
Margaret Chingos Editor-in-Chief
Margaret Chingos Editor-in-Chief
Akshay Joshi
Associate Editor-in-Chief
Akshay Joshi Associate Editor-in-Chief
Ellie Kirkland
Ellie Kirkland
Interviews and Launch
Interviews and Launch
Marg y g p y and Sustainable Development student at the University of St Andrews She is interested in exploring the intersection of journalism and community resilience, with specific interest in coastal communities.
Margaret is a 3rd year Geography and Sustainable Development student at the University of St Andrews. She is interested in exploring the intersection of journalism and community resilience, with specific interest in coastal communities.
Grace
Holling Editor
Aksha nd Sustainable Development student at the University of St Andrews. Growing up in the oil and gas hub of Baku sparked his early interest in sustainability, inspiring engagement with academic research, conservation projects, and an internship with the RSGS.
Ellie is a G ng in health policy. She is passionate about the intersection of climate change and disability. As well as sourcing articles and coordinating the magazine’s launch, a particular highlight was interviewing the Chief Medical Officer for Scotland.
Grace Holling Editor
Grace is onmental Policy a hieved a Master o hy at the University of St Andrews Her research centres on conservation strategies and landuse conflicts, with a geographic focus on Kaieteur National Park in Guyana.
Grace is a master’s student in Environmental Policy at Sciences Po, Paris. She achieved aMaster of Arts (Honours) in Geography at the University of St Andrews. Her research centres on conservation strategies and landuse conflicts, with a geographic focus on Kaieteur National Park in Guyana.
Alice Main
Formatting
Alice Main Formatting
Akshay is a 4th year Geography and Sustainable Development student at the University of St Andrews. Growing up in the oil and gas hub of Baku sparked his early interest in sustainability, inspiring engagement with academic research, conservation projects, and an internship with the RSGS.
Ellie is a Geography graduate working in health policy. She is passionate about the intersection of climate change and disability. As well as sourcing articles and coordinatingthe magazine’s launch, a particular highlight was interviewing the Chief Medical Officer for Scotland.
Lara Diamond
Editor
Lara Diamond Editor
Lara is a from the Un ow begin tal consultancy on Orkney She is particularly interested in creating holistic data by colouring quantitative data with human stories and experiences.
Lara is a recent Geography graduate from the University of Glasgow and is now beginning a career in environmental consultancy on Orkney. She is particularly interested in creating holistic data by colouring quantitative data with human stories and experiences.
Niamh Hickey Launch Team
Followi ntal Science a sity of Dundee, rture Practitio e she enjoys eng doors
Niamh Hickey Launch Team
Niamh
tal Geography ng and is curre e is interested green industry an e links between climate and health.
Hannah Clark
Formatting
Hannah Clark Formatting
Hannah is
ent at the Univers ista at a local-sus h. Her research interests are in the intersection of climate change and mental health in climate vulnerable nations, specifically the impacts of PTSD and depression.
Dylan
Hannah is a 2nd year Geography student at the University of St Andrews, and a barista at a local-sustainable bakery in Edinburgh. Her research interests are in the intersection of climate change and mental health in climate vulnerable nations, specifically the impacts of PTSD and depression.
Dylan Hamilton Outreach
Hamilton Outreach 3
Following her studies in Environmental Science and Geography at the University of Dundee, Alice works as a Nature Nurture Practitioner in Aberdeenshire where she enjoys engaging children with the outdoors.
Niamh is a graduate in Environmental Geography from the University of Stirling and is currently working in Glasgow. She is interested in learning more about the green industry and finding out more about the links between climate and health.
Dylan is a c began his journ 14. Since th licy coord nGovern RY) attending U g , ngside organising grassroots mobilisations across the UK
Dylan is a climate justice activist who began his journey as a school striker at age 14. Since then, he has worked as the policy coordinator for the Alliance of Non-Governmental Radical Youth (ANGRY) attending UN climate negotiations, alongside organising grassroots mobilisations across the UK.
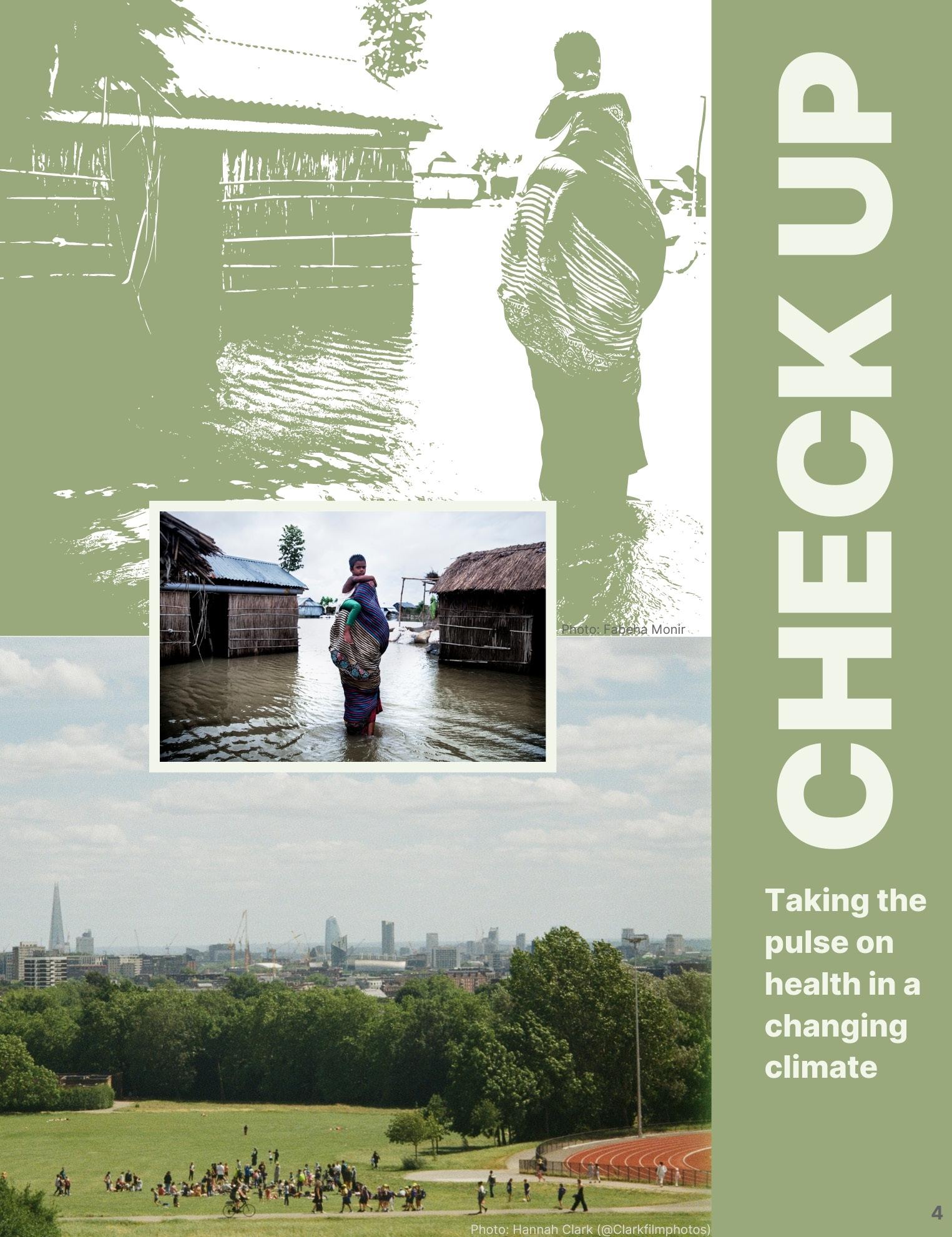
Photo: Hannah Clark (@Clarkfilmphotos)
An interview with Prof Sir Gregor Smith
Professor Sir Gregor Smith has been Scotland’s Chief Medical Officer since 2020 advising ministers and advocating person-centred care. A former NHS leader, he shaped Scotland’s GP contract and quality framework and is passionate about outdoor activity for health. He was knighted in 2022 and is an Honorary Professor at Glasgow University.
Planetary Health and Person-Centred Care: A Vision for Scotland’s Future
Sir Gregor Smith, interviewed by Young Geographer Ellie Kirkland
We know the NHS is under immense pressure and budgets are squeezed. Why does climate change need to remain a priority?
It’s really important that we see health as being linked to climate change. I see us facing four great health challenges in Scotland. First of all, the continuing threat of infectious diseases. Allied to that is the continuing presence of antimicrobial resistance and the rise of vaccine hesitancy and misinformation. The second is stalling life expectancies, particularly healthy life expectancies, that we see across many countries in Western society - and the deepening health inequalities that we experience. Thirdly, how we sustain health and care services in the face of a growing burden of disease. Health inflation and demographic changes challenge us every single year to keep up with the demands in the system.
But, the fourth challenge is the challenge of planetary health; that includes not just greenhouse emissions but also the loss of biodiversity and the risks associated with air pollution. This triple planetary crisis is absolutely interlinked with those first three challenges. We cannot separate them because if we don’t address the health challenges that will arise from the climate crisis, then we will see more, and different,
infectious diseases. Those impacts are going to be felt mostly or disproportionately by people who experience health inequalities already, and this will challenge our health and care services even more.
So for me, the climate crisis is a public health problem that we have to face. We cannot separate the challenges that health and care services in Scotland face just now from the challenges that our own planet faces, because if we do, then we’ll not be prepared. We need a carbon neutral, climate resilient, sustainable and equitable health system for the future.
You became CMO in the midst of the COVID pandemic. Are there any lessons from that period that can be applied to how we tackle the health risks posed by climate change?
One of the strongest pieces of learning for me out of the pandemic response is that actually by improving the background health of our
population, by reducing the health inequalities as much as we possibly can, when the inevitable next pandemic arrives on these shores then the population will be much more resilient to its effects. We need to get much better at preventing disease than perhaps we have in the past. By reducing the burdens caused by diseases and by reducing health inequalities we’re able to be more resilient to the threats that climate change poses.
Something else I learned was the importance of communication, and the right type of communication. People come together and act for the good of broader society, and I think the threat posed by climate change on the planetary health crisis is such a threat that we need that collective action again. Communicating science is often difficult. We had a number of people during the pandemic response who are very, very good at it. If we can establish trust - and if we can communicate both the steps people can take and why investments are needed in certain areas rather than others - that, for me, feels like a crucial way to apply the lessons learned from the pandemic to other threats to human health.
Above: Elmar Gubish Gulshan Kahn / Climate Visuals
Left: Ivan Camilo Ospina / Climate Visuals
An interview with Prof Sir Gregor Smith
Continued
Could you give us some examples of actions that are win-wins for the environment and healthcare?
If you look at some of the medicines that we use within the NHS, we know that some of those are potentially harmful to the environment. Asthma is a very common disease across Scotland, but sometimes it is not treated as well as it could be, unfortunately. Many of the inhalers that are used contain CFCs (Chlorofluorocarbons). We find that too many people are using their reliever inhaler too often and not using the preventer inhaler enough. If we can begin to rationalise how they’re using their inhalers and change the type of device so that it’s more environmentally friendly, then we’ve got a net benefit. First, and most importantly, improving the health of people with asthma by rationalising the approach to their care, but also leaving less of a footprint on the environment as well. There’s been some wonderful work started in Glasgow that’s now leading to a huge change in the way that we treat asthma in Scotland.
Another example is Green Health Partnerships. For me, the most important thing about this is that there are other ways of approaching disease states rather than just reaching for a prescription pad. The ‘green prescriptions’ that people have been issuing within these partnerships include taking part in groups where people spend more time in nature. We know the evidence suggests that the more time people spend in green space – or blue space for that matter – the better it is for their health, both physical and mental. We see community gardens beginning to be used across the NHS estate where people are spending more time in green space, participating in groups, very often reducing social isolation, helping to promote and empower people and develop their own agency in that space.
The net benefits are again less utilisation of potentially harmful pharmaceutical resources, more impact with people actually being out there in the environment and all the benefits that that has on them. We can’t get away from the fact that the costs associated with that are much less and lead to a more sustainable financial model for the NHS, but still creating that net health benefit for people at the same time.
Photo: Hannah Clark
We’re now four years into NHS Scotland’s Sustainability Strategy, could you reflect onthe progress and remaining challenges? How do we get to a net zero health service?
I think when we launched the strategy, Scotland showed that we had huge ambition in this space and we were riding very high on the crest of COP26. Across Scotland, there are teams who’ve been amazing in delivering various aspects of that plan under really difficult circumstances. During that time we’ve faced a number of challenges, not least the fiscal challenges that we continue to face across Scotland. But it’s the enthusiasm of our workforce across the NHS which I think has led us to where we are now.
So, I think that we’ve made really good progress. For me, it’s time to ramp up activity and inject a little bit more urgency and resource around this so that we can face the threats of the future. Let’s use innovation as our friend in all of this. There is no one part of science, there is no one part of society who can do this alone. The only way that we are going to reduce the impacts of climate change in the future is finding intersections where we can work together. The best of science happens when we get different disciplines and different thoughts coming together in a big melting pot. I think that’s possibly the most exciting aspect for me as a public health clinician is how we harness all that brainpower that’s out there to reduce the impacts on our population’s health in the future.
“...My message is that this is important and the threats from climate change, and the planetary health crisis that falls from that, are possibly the biggest existential threat we face to human health over the decades to come.Therefore, I think there’s a responsibility for healthcare professionals to
make sure that we are leading the discussion.
It’s reallyimportant that we frame this as a public health emergency as well as a climate emergency...”
I’m going to stay optimistic because I believe that people really want to make a difference in this space. I believe that society is coming to the point where it realises that it can no longer take the same approaches that it did in the past, that it has to change in order that we face some of these threats and reduce the impacts of them. I still firmly believe that we can make the changes necessary.
Alastair Johnstone / Climate Visuals
Source: European Center for Environment and Human Health/ University of Exeter
Missing Link: The Silent Struggle of Youth Living the Biodiversity Crisis
Ronja Fischer, Michael Ruggeri (GYBN Europe cocoordinators), and Roberto Muheto (Health focal point with GYBN Policy team), with additional inputs by Bine Liem and Ida Simonsen (Dutch Youth Delegates)
GYBN Europe: The Global Youth Biodiversity Network (GYBN) is the youth constituency of the Convention on Biological Diversity (CBD). It is a regional group aiming to bring the voice of the European youth to the negotiation table.
What are the links between Biodiversity and Health?
Within the CBD (Convention on Biological Diversity), biodiversity is defined as the variability among living organisms from terrestrial ecosystems to marine and other aquatic ecosystems. This variability encompasses diversity within species, between species, and of ecosystems. Health, as defined by the WHO, is not merely the absence of disease or infirmity but a state of complete physical, mental, and social well-being. Both are closely interlinked.
Healthy ecosystems play a crucial role in providing essential services such as clean air, fresh water, medicines, nutritional diversity, food security and mental welfare; all of which are fundamental to well-being. The drivers of change, such as habitat destruction, pollution, climate change, and over exploitation of natural resources, pose significant threats to biodiversity and, consequently, to human health. Ecosystem services are vital in regulating climate and controlling the spread of diseases. The loss of biodiversity can lead to an increased incidence of infectious diseases by disrupting ecosystem stability and allowing pathogens to thrive.
Agreement on COP16: The Global Action Plan on biodiversity and health
At the 16th meeting of the CBD parties (COP16), parties aimed and succeeded in finally adopting a Global Action Plan on Biodiversity and Health.
Despite the long history of negotiations, parties had a hard time agreeing on the Action Plan at COP16. A final agreement was reached only by adopting the Action Plan as a voluntary measure to support the Global Biodiversity Framework (GBF). The plan, which contains action areas related to GBF Targets and their relevance to health, welcomes targeted messages for integrating biodiversity into the health sector and encourages parties to designate national focal points and integrate interlinkages into policies and programs as appropriate. It recognizes the right to health, the right to a clean, healthy, and sustainable environment for present and future generations, and that inequity for children, youth, and vulnerable communities is increased by environmental degradation.
GYBN has been actively engaged in the negotiation from the beginning. We are happy that the plan finally got adopted, however, this plan could have been much stronger. Many issues are reflected weakly. Some are completely missing.
We have/ GYBN has been advocating to get the specific health burden and vulnerability of children and youth recognized and to provide a space for us/them to be part of the national implementation. While children are not considered for certain paragraphs on decision-making, youth participation is now required for the development and implementation of Biodiversity and Health Plans and should be invited for regional capacitybuilding activities.
Regarding weak aspects, language on humanmediated factors driving the emergence of
zoonotic diseases was watered down significantly, with some countries flat-out refuting scientific consensus and UNEP and IPBES reports. Those demonstrate that increasing human demand for animal protein, unsustainable agricultural intensification, and extractive industries increase the emergence of zoonotic diseases. Beyond the fact that the role of food systems and livestock is not adequately reflected in the decision, the fact that scientific consensus as portrayed through IPBES is rejected is worrisome - to say it mildly. Other issues covered too weakly are antimicrobial resistance, use of pesticides, and noise and light pollution. Regarding weak aspects, language on human-mediated factors driving the emergence of zoonotic diseases was watered down significantly, with some countries flat-out refuting scientific consensus and UNEP and IPBES reports. Those demonstrate that increasing human demand for animal protein, unsustainable agricultural intensification, and extractive industries increase the emergence of zoonotic diseases. Beyond the fact that the role of food systems and livestock is not adequately reflected in the decision, the fact that scientific consensus as portrayed through IPBES is rejected is worrisome - to say it mildly. Other issues covered too weakly are antimicrobial resistance, use of pesticides, and noise and light pollution.
The missing pieces: Mental health and ecoanxiety?
Despite the efforts of us and our allies, any reference to mental health and eco-anxiety was deleted again from the draft.
New generations are born within the climate and biodiversity emergency. Not only do we understand the emergencies we are in, but many of us already feel the consequences. At the same time, we are exposed to call to action - or call to action ourselves - but those calls do not find correspondence in practice to really address the emergency. For many of us, this creates frustration and a general sense of anxiety and powerlessness. This sense of “the ecological foundations of existence are in the process of collapse” is more and more being recognized as eco anxiety.
The missing change and action do not only cause mental health issues for youth, of course. This applies to Indigenous Peoples and local communities who see their customary surroundings dwindling, farmers who might be willing to act but are hindered by bureaucratic demands, or health workers who see the consequences for the population firsthand. It is often assumed that youth are more affected by eco-anxiety due to the longer exposure to emergencies, but so far scientific research on this is scarce.
The missing reference to anything on mental health and eco-anxiety is a missed opportunity by the countries sitting at the negotiation tables discussing our future. At the same time, evidence suggests that self-efficacy is one of the best answers to eco-anxiety. Therefore, let’s seize the opportunity of youth participation during the Global Plan of Action for Health.of youth participation during the Global Plan of Action for Health.
Students of Class III pose in front of their Boat School in Faridpur, Bangladesh (Abir Abdulla/Climate Visuals Countdown)
Photo: Hannah Clark(@clarkfilmphotos)
Abir Abdullah / Climate Visuals
Gulshan Khan / Climate Visuals
Visuals
Photo: Dibakar Roy
Photo: Dudubangbang Travel
Stormy minds and Rising Seas: Why
We Must Attend to Mental Health in a
Warming
World
Hertzog Young
Charlie Hertzog Young is a writer and researcher. He first became involved in climate activism in the mid-2000s. As a teenager he spoke at Davos and the UN, before suffering mental health crises. He has since worked for many organisations fighting for economic transformation and political change.
Climate chaos drove me mad. Clinically mad. We tend to think of mental health issues as isolated phenomena, to be treated in an isolated manner. Few understand the reality: most mental health issues are driven by social forces. They are also, increasingly, seeded by ecological calamity. This assault on our internal worlds is spreading like wildfire, except that there is no smoke, no light, no sound nor smell to warn us.
When people hear ‘climate change and mental health’ they usually think of eco-anxiety. But what’s happening goes much deeper. After interviewing over a hundred people on every habitable continent for my book Spinning Out, I outlined two broad categories. The first is Climate Despair: psychological distress brought on by relating to climate change at a distance. The second is Climate Trauma: mental health issues triggered by direct
experience of climate impacts.
Both are a huge global burden. Already mental health issues are the leading cause of disability worldwide, responsible for 15% of deaths. The WHO and the UN agree that climate change is ramping up the epidemic. It’s also threatening our collective ability to respond.
In the UK, the US and Australia, between a quarter and a third of young people report being worried about climate change (i.e. Climate Despair) to the extent that many struggle to sleep, eat, or work. Another survey found that 4% of young people in the UK were so affected that they were dissociating and struggling to connect with loved ones. The authors described some cases as ‘disabling’. Some 20% of British children have climate nightmares. Meanwhile in the Philippines, 74% say that thinking about climate change makes day-to-day functioning
Charlie
A member of the Guajajara forest guard in a moment of sad silence at the sight of a toppled tree cut down by illegal loggers. Photo: Tommaso Protti
difficult. In Brazil, half are struggling to function because of eco-anxiety. In Nigeria, it’s two-thirds. In India, three-quarters. 2 in 5 young people worldwide now say they don’t intend to have children – because of climate change.
Climate Despair is driving up rates of depression, fear, dread, feelings of unreality, anxiety, psychosis and many other difficulties that fall anywhere on the spectrum from negative emotions to serious mentalhealth issues. The realisation of the enormity of the crisis, coupled with a generalised apathy in society can also cause people to fundamentally reanalyse what they want out of life, question who they are, and the nature of the system we live in. This can be destabilising, and it is incredibly difficult to deal with alone, especially when we feel powerless.
Climate Trauma, by overhauling material circumstances, can lead to depression, generalised anxiety, PTSD, psychosis, prolonged grief, dissociation, crippling phobias, eating disorders, schizophrenia, bipolar disorder and suicide. It is already happening. The tendrils spread menacingly. Climate change will increase poverty, which will impact people’s mental health. It will increase inequality, within and between countries. It will create food shortages, which tipped people over the edge during the pandemic and has done throughout history. Climate-induced conflict and natural disasters could mean over a billion climate migrants by 2050. Migrants are some of the most likely people to develop mental-health issues. They are also the least likely to receive support.
Flooding decimates and depresses, often knocking out medical infrastructure. So do PTSD-fuelling wildfires. Heatwaves trigger domestic abuse, alcoholism and gun violence, as well as psychiatric episodes in their own right. Meta-analyses of social media posts have found spikes in depressive language in hot temperatures. They also prime people for manic, neurotic and psychotic episodes – especially in hot countries during Ramadan. In the US and Mexico, just the temperature increase caused by climate change could mean up to 40,000 additional deaths by suicide by 2050. This is comparable to the estimated impact of economic recessions, the absence of suicide-prevention programmes, or gun-restriction laws.
More resilient communities are far less likely to suffer Climate Despair and Climate Trauma. On the latter, community cohesion is one of the biggest predictors of whether people develop a mental health issue post-disaster. Engaging meaningfully in community-based mitigation and adaptation, then, is potent medicine.
Psychological buckling in the face of climate chaos is an appropriate response to an unravelling world. We must make sure we listen to these signs, band together, care for one another and use our experiences to build a better world.
Photo by Hannah Clark (@clarkfilmphotos)
Photo: Tommaso Protti
SPINNING OUT
Taking collective action in the outside world has documented and incredible power for working through psychological issues. This is especially true when it is bolstered by reaching out for support and building networks of meaningful relationships. This empowers us and gives us genuine agency, both of which are hard to find in an age when dependency and precarity are sold to us via the medium of calculated lies about freedom and material affluence.
There is a spectacular and fortuitous set of feedback loops that turn engaged action into a powerful therapeutic method. This is not a utilitarian transaction, where helping others or doing good just makes us feel better. It’s a reciprocal arrangement, like the management of a commons, and it is about finding purpose and meaning by joining communities of care. It’s also about creativity, the opportunity to align our talents with our ethics and creating enclaves in which we can more fully explore who it is we want to be. Together, we try to build the relationships we have always wanted, out of new practices and priorities. This leads to meaningful, impactful action: it is fertile territory for the birth of new worlds.
Even the most effective trauma therapies known to modern medicine all attempt to close the loop. Climate change, and all the despair and trauma it visits upon us, is impossible to confront in its entirety. It is a total planetary disequilibrium. It’s pervasive, mysterious and refracting. But against the backdrop of a burning world, taking charge of opportunities to tackle the crisis hands-on is a powerful way of meaningfully addressing its psychological impacts. Facing up to what is happening helps us to retain and reproduce collective resilience, building platforms in shared realities that are healthier than the dismal, frenetic and constrained imaginaries of the present.
This kind of systemic visioning and reworking requires a touch of madness: lunacy of the best kind. In 1913, Theodore Roosevelt wrote: ‘There is apt to be a lunatic fringe amongst the votaries of any forward movement.’ He obviously meant it derisively but it’s time for us to take the idea as a compliment and utilise the power and creativity of different ways of being in the fight for a better world.
The prospect of dealing with the combined climate and mental health crises is daunting and immense.
Book Excerpt
Charlie Hertzog Young
But the resulting fear is something we can digest, helping us to find the joy on the other side of action. The fear itself can motivate us when it is channelled into a passionate anger, navigated by love. Posttraumatic growth can happen on a personal level, and on a collective level. Relationship-building and collective effort will help us form new elements of our identities, more densely woven communities, along with enriching, exciting and unexpected experiences. These will act as dependable mental flood barriers against the rising tide. They will only become more useful, even necessary, as the state of the crisis intensifies, threatening to tear apart whatever bonds we already have. Disconnection and domination got us here. Connection and equity will set us free.
The people I’ve talked to for this book have had diverse, but for the most part mutually reinforcing, views about the socio-psychological effects of activism. Some initially struggled to pinpoint and communicate helpful psychological benefits to the work they do. I personally think this emerges, at least in part, from a progressive culture of duty and sacrifice comingling with the lived experience of disempowerment under oppression. When I asked Professor Noam Chomsky whether he felt there were positive mental-health outcomes from activism, for the activist themselves, he said that his own experience of addressing injustice ‘means
living in a constant state of simmering fury for almost all my life back to childhood, a background that is always there.’ Later, he told me that he thought building healthier, regenerative models for movements was nonetheless ‘important’. ‘You’re right,’ he said, ‘groups of mutual support make a great difference to many people in hard times.’
A better life needs to be an intrinsic part of the fight. Ideologically, I can’t relegate it to the end result of an otherwise thankless struggle. The good news is that it doesn’t have to be.
Photo: Alden Arnold
Photo: Tommaso Protti
Climate Change and the Brain:
Why It Matters
Professor Sanjay Sisodiya
Sanjay Sisodiya is Professor of Neurology at UCL Institute of Neurology and Honorary Consultant Neurologist at the National Hospital for Neurology and Neurosurgery and the Epilepsy Society.
His main interests are in epilepsy, genomics, imaging and multimodal analyses. He was chair of the Association of British Neurologist Epilepsy Advisory Group from 2015-2021. In 2021, he was appointed to the posts of Deputy Director for Sustainability and Climate Change at the UCL Queen Square Institute of Neurology, and Chair of the International League Against Epilepsy Climate Change Commission.
nervous system – people with existing neurological diseases.
Why is this important? We need our brains to be working well. This is obvious on a day-to-day basis but becomes especially clear when we face serious global challenges. However imperfect in retrospect our responses may have been, we needed our brains through the COVID-19 pandemic: to devise strategies to attempt to contain viral spread; to observe those measures at population-level; to invent and implement treatments and vaccines – and now to review our actions and, hopefully, plan better for future. However, when the brain is not working as it should, responses to challenges may be impaired - for example, at the level of the individual with a chronic neurological disease. One in six people have a neurological condition; such conditions feature prominently amongst causes of death from heatwaves. About a quarter of excess deaths in France during the 2003 heatwave had neurological disorders/causes of death; a similar estimate for the 2022 UK heatwaves is 18.7%. ‘Brain health’ is considered key to all 17 Sustainable Development Goals by the United Nations. It is important.
There are many reasons that people with neurological diseases may be vulnerable to impacts of climate change. The brain coordinates thermoregulation. Acting on sensory (e.g. increased afferent activity of peripheral heat sensors in the body) and cognitive (e.g. daily weather forecasts,
Climate change has been identified as the major challenge to human health by authoritative reports spanning decades, and growing in urgency and stridency. The challenges are here now – just like climate change. Concerns have focused on measures that can be robustly determined and followed, and necessarily these are around the health of the general population, rather than specifically groups of people with health conditions. But those with chronic diseases have been identified as amongst those particularly vulnerable to impacts of climate change, alongside the very young and older groups, outdoor workers, those sleeping rough, and pregnant women. Amongst those with chronic conditions, some recent work has focused on those with conditions affecting the
Photo by Hannah Clark
heat-health alerts) inputs, it generates adaptive responses. Some responses are automatic, not under voluntary control – dilatation of blood vessels in the skin and increased sweating; other responses are behavioural - drinking water, seeking shade, and removing items of clothing. All of these responses require activity of the nervous system. If that nervous system is compromised, thermoregulatory responses may be blunted, impossible, or even counterproductive (for example, wandering about in the heat). Moreover, some diseases may themselves be vulnerable to the impacts of climate change, for example, some conditions become worse directly as a result of rising ambient temperature – some forms of multiple sclerosis, epilepsy, and stroke as important examples. Some neurological conditions may become more common, for example, those generated by infectious agents spread by vectors, such as mosquitoes and ticks, whose geographical ranges are extending because of climate change. There are further complicating factors – for example, some treatments used in neurological diseases can themselves compromise thermoregulation, affecting the central coordinating mechanisms, or
reducing sweat production. The direct and indirect impacts of climate change may affect any number of the multilayered complexities of neurological conditions - some may not yet even be apparent. Finally, the adverse psychological and psychiatric outcomes of climate change have to be considered: climate anxiety is prevalent, especially amongst the young.
What can we do? There are important signals that there are already impacts related to climate change on people with neurological diseases, including the occurrence of new cases of such diseases. But there are many gaps in our understanding, especially for regions of the world with little data, but already sizeable and growing environmental and health impacts from climate change. These are topics vital to research further, with important opportunities for collaboration across disciplines.
Most importantly, we need to take action within our spheres of influence, and together in promoting reduction of emissions. It may turn out that what is happening now to people with neurological diseases is a foretaste of what happens to brain-function in otherwise healthy people as climate change progresses. It is in all our interests to work together to understand and address climate change’s impacts on the health of the brain.
Elina Araja (Pexels)
The Linkage between Climate Change and Transmission of Vector-borne Diseases in Nonendemic Areas
Professor Shlomit Paz
Shlomit Paz is professor at the School of Environmental Sciences and the head of the Climate and Environmental Sustainability Center at University of Haifa. Her research is focused on the human health impacts of climate change, with special attention to the transmission of vectorborne diseases in Europe and the Mediterranean.
Climate change is impacting human health in a variety of ways. The health impacts are mediated by complex ecological, environmental and social processes. While the effects vary in their scale and duration, as a function of their local environment or human vulnerability, the impacts can be direct, through exposure to extreme heat, cold, drought and storms, or indirect by changes in water availability, food provision and quality, or changes in ecosystems.
Vector-borne diseases (VBDs, transmitted mainly by mosquitoes and ticks) such as malaria and dengue are highly sensitive to climatic change since a warmer climate and changing rainfall patterns may create hospitable environments for both vectors (insects) and pathogens (virus and bacteria) that are necessary for their emergence
and persistence. Although climate is one of several factors that influence the distribution of these diseases (as socio-demographic conditions, healthcare quality and globalisation), it is well known that climate and weather factors are major environmental drivers influencing their emergence, re-emergence, and spread to new geographical areas, including non-endemic regions. Weather conditions (in particular, temperature, precipitation and humidity) affect the survival and reproduction rates of the vectors, their habitat suitability, distribution and abundance. Additionally, climatic factors affect the rates of development, reproduction and survival of pathogens within the vectors.
Resulted by the changing climate, tropical species are currently spreading towards the poles, and species everywhere are tracking their thermal niche along elevational gradients. These processes include the spreading of disease vectors to new, including non-endemic areas due to a better (warmer) habitat suitability.
Pathogens may be dispersed into non-endemic regions through travel, trade or migration while autochthonous transmission (i.e. cases with no travel history, two weeks before the disease onset) can then occur in areas where the vector is established and where climatic conditions are favorable for transmission. For example, due to increasing urbanisation and globalisation, the risk of local outbreaks of dengue and chikungunya across Europe is increasing and, furthermore, global warming increases climatic suitability for Aedes albopictus, an invasive mosquito species acting as a vector for the dengue and chikungunya viruses.
In parts of southern and eastern Europe, A. albopictus had not been endemic earlier, but climate change made conditions more suitable both for mosquito and virus transmission and now it is established in the region. Local (autochthonous) outbreaks of dengue and chikungunya have occurred over the last years in southern Europe when infected travelers passed the pathogen to the mosquito vector, which in turn caused secondary cases of human infection. In France, following high temperatures during the spring and summer of 2022, the number of autochthonous cases of dengue achieved the highest record and the maximum number among
the EU countries. That geographical spread of autochthonous cases from the Mediterranean areas both westward and northward reflects the colonisation of new territories by A. albopictus, raising a public health concern.
Malaria is a life-threatening disease mostly spread to people through the bites of some infected female Anopheles mosquitoes. It is mostly found in tropical countries. In Africa, warming temperatures have caused malaria to spread both to higher elevations and higher latitudes. The geographic distribution of the Ixodes Ricinus tick that transmits bacteria from the genus Borrelia (causing Lyme disease) is related to various climatic factors such as humidity and air temperature. As a result of temperature increase I. ricinus has shifted its seasonal activity and geographical range on both latitudinal and elevation limits. Indeed, warmer and shorter winters have been pointed out as one of the factors driving the colonisation of the tick at northern latitudes in Europe. In Canada, a geographic range expansion of the Ixodes scapularis tick, associated with elevated temperatures, has been detected as well.
As predictions show an increasing potential of VBDs spreading to new areas, actions are needed to prevent outbreaks and their establishment in the future. Alongside data collection and improved surveillance by health agencies, it is essential to strengthen public awareness through the media and social networks. This will help inform people about infection risks, disease symptoms, and recommended preventive measures, such as eliminating small breeding sites. Parallel with greenhouse gas mitigation, effective surveillance, targeted interventions and measures to avoid mosquito bites are vital to prevent VBDs- protecting lives and securing public health.
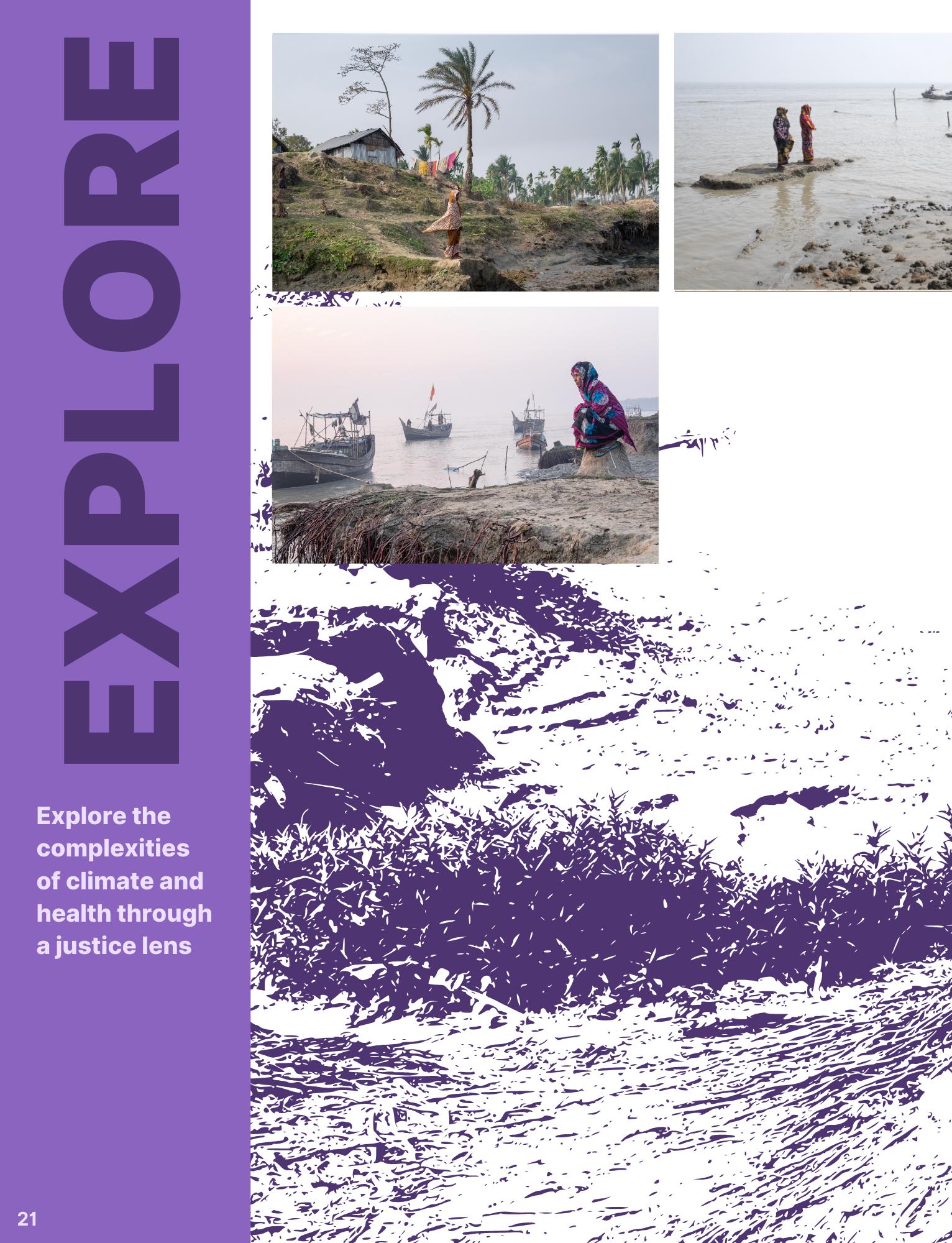
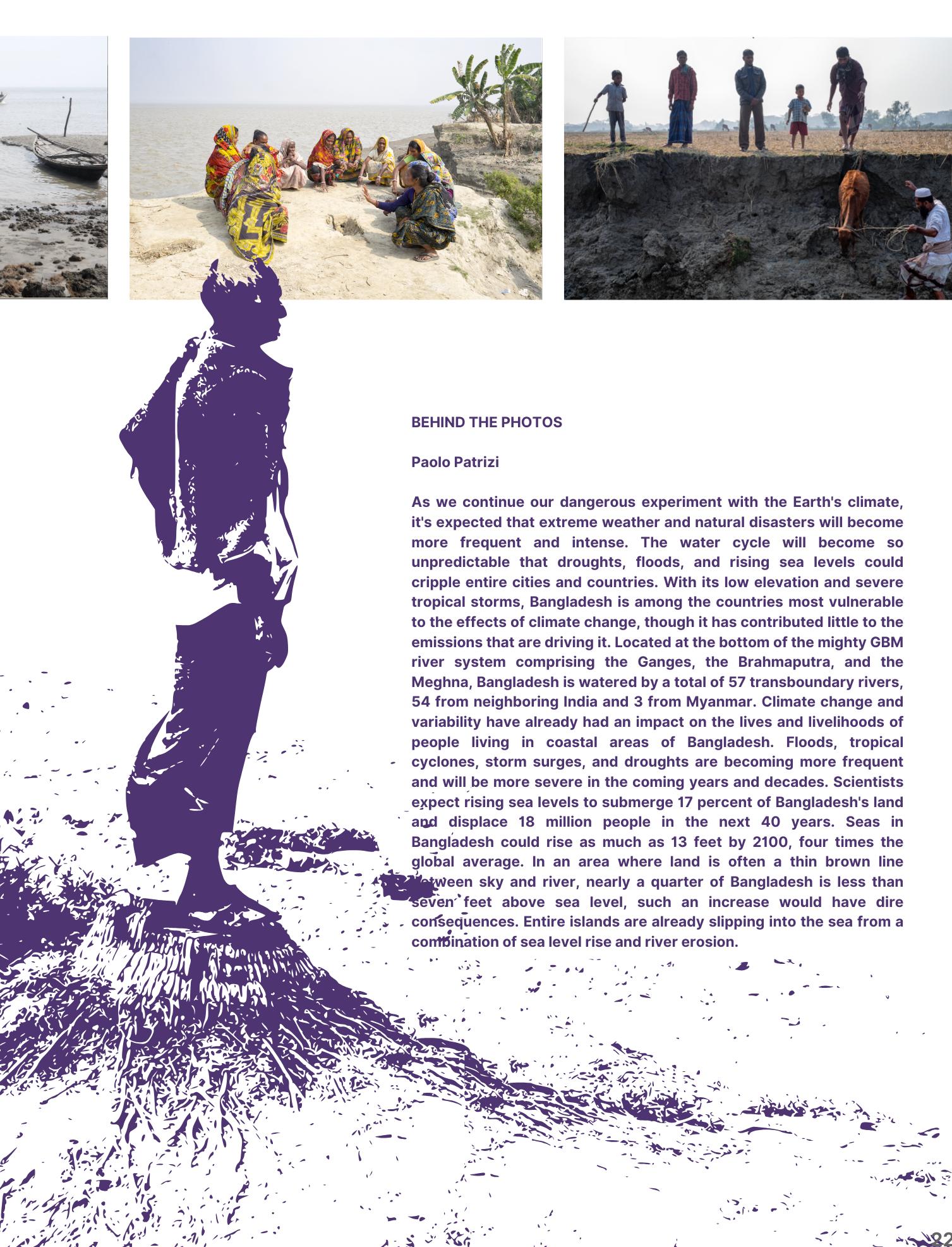
Explore the complexities of climate and health through a justice lens
The Physiological and the Psychological: Intersectional Gendered Impacts of Climate Change
Melania is a dedicated feminist leader and the director of the Shine Collab, bringing a wealth of expertise in advancing women’s human rights within the context of the global climate crisis. Holding a PhD in Development Studies, Melania has led transformative programs that centre feminist solutions to climate challenges.
increase the spread of vector-borne diseases, like malaria and Zika virus, which lead to adverse pregnancy outcomes, including birth defects and complications during childbirth. Often not spoken about enough, but critical, is how climate change affects women’s sexual and reproductive health. For instance, in Zimbabwe and Mozambique in 2019, during Cyclone Idai healthcare services were disrupted. Women’s reproductive healthcare needs were pushed to the periphery as governments focused on ‘more pressing’ issues. Women affected by the Cyclone encountered barriers to accessing contraception, prenatal care, and safe delivery services. In Malawi in February 2023, Cyclone Freddy hit; pregnant women faced challenges accessing medical care, leading to increased maternal and infant mortality. Across Africa, climate change-induced displacements have resulted in sexual violence and exploitation, as women become more vulnerable during crises. Forced migration and resettlement can uproot communities, leading to a breakdown in social structures that usually provide protection and support for women. This precarious situation often results in increased rates of sexually transmitted infections and unintended pregnancies, compounding the health risks women face.
The psychological implications of climate change are profound, particularly for women. The mental health consequences of environmental degradation, climate-induced disasters, and climate-related displacements can lead to
The burning of fossil fuels, industrial processes, and an extractivist development model have resulted in excessive emissions of greenhouse gases into the atmosphere, resulting in climate change. Though climate change affects everyone, the impacts are not evenly distributed, with women, indigenous groups, and marginalized groups carrying the severe burden of the crisis. Heat stress and extreme weather conditions have resulted in significant health challenges that disproportionately affect women due to their gender roles and biology. Women and communities in Africa, and small island countries face unique vulnerabilities due to their social, economic, and biological circumstances.
The shifting climate exacerbates existing health conditions and creates new health risks. Temperatures rise and changing rainfall patterns
Dr. Melania Chiponda
increased anxiety, depression, and posttraumatic stress disorder. Women endure most of the caregiving responsibilities in their families and communities, and as climate-related stressors intensify, their mental health suffers.
The anxiety associated with climate change is, too, worsened by societal pressures. Women often feel a heightened sense of responsibility for the family’s well-being amidst uncertainty, which can exacerbate feelings of helplessness and despair. Loss of homes and livelihoods may lead to the erosion of community ties, leaving women isolated and unable to cope with the accompanying psychological burdens.
It is essential to recognise that the impacts of climate change on women’s health are interconnected and influenced by various factors, including socioeconomic status, and location. Women from marginalized communities often face the greatest challenges due to systemic inequalities. Initiatives that promote women’s leadership in climate action not only contribute to better health outcomes, but also strengthen community resilience. By prioritizing women’s voices and experiences, we can develop more effective strategies to mitigate the health impacts of climate change and promote gender equity in the face of this global crisis. A concerted effort towards building women’s power is essential for building resilient communities capable of facing the challenges posed by climate change.
Vidura Jang Bahadur / UN Women Asia and the Pacific Top Image: Women brings fresh drinking water to her make-shift shelter, following the 2010 floods in Sindh Province, Pakistan. Photo by Vicki Francis/Department for International Development24Vidura
Women in Sundarbans, India queuing to plant mangrove saplings along the Matla river, to protect villages from increasing floods and cyclones.Photo by Avijit Ghosh/Climate Visuals
the Anthropocene - an era defined by a state of perma-crisis, pandemics, changing climates, and growing inequalities, causing increasingly scary and dystopic visions of the future.
AMR is already estimated to be directly responsible for the deaths of over 1 million people each year; come 2050, it’s thought it will be responsible for 2 million deaths each year. Antimicrobials are essential not only to human health but also to the health of animals and plants, and so are a vital tool in ensuring food security. However, with a changing climate driving increased disease transmission amongst humans, animals, and plants, there are implications for the antimicrobial drugs developed to fight disease.
geography at the School of Geographical and Earth Sciences at the University of Glasgow. Her research pays particular attention to the real-life experiences of individuals dealing with illness and the challenges faced by healthcare providers working in complex health systems.
With just a brief glimpse of the bright yellow bottle of penicillin, I am transported back in time, tasting the artificial banana flavour of my childhood medicine. As a child who had undergone heart surgery, I was prescribed it more often than most, a precaution by doctors wary of infections reaching the scar tissue on my heart. It ensured that dental work was safe for me and that standard childhood infections didn’t escalate into something more dangerous. My ready use of antibiotics represents what has been dubbed the golden era of medicine.
What does that sticky yellow medicine have to do with climate change? The medication so many of us have enjoyed to fight infection and disease is becoming increasingly ineffective as the microorganisms - such as bacteria, viruses, fungi, and parasites - build resistance to them. This is known as antimicrobial resistance (AMR). And, as I will explain, AMR is interwoven with
There is now significant research detailing the ways that climate change is, and will, impact health. And, with AMR a growing global health issue, many now consider climate change and AMR a dual threat. Climate change affects health in direct and indirect ways. For example, infectious diseases are set to rise on a warming planet with increased temperatures creating the conditions for a series of disease vectors to survive. There are also concerns that new diseases will emerge and new pandemics fueled, especially diseases that spread between animals and humans (known as zoonotic diseases). Indirectly, climate disaster events often impact safe water supplies and damage vital health infrastructure, leading to disease outbreaks and limiting the capacity for adequate drug diagnosis. These issues, plus many more, place increased strain on antimicrobial medicines and create new opportunities for microorganisms to develop their resistance to the drugs we have relied upon.
Like so many aspects of climate change, the consequences of AMR will not be felt evenly.
Emma Laurie is a senior lecturer in human
Emma Laurie
Haley Lawrence on Unsplash
Currently, the majority of global infectious diseases are shouldered by the world’s economically poorest, living in Low—and Middle-Income Countries, and so this burden is set to become heavier still. More worrying still, instead of global efforts seeking to address these inequalities, I fear they will only exacerbate global health inequalities due to the fear-mongering and blame circulating about AMR.
Apocalyptic imagery is often used to frame the future of climate change—worlds ravaged by disasters, heatwaves, floods, and (problematically assumed) unrest. The apocalyptic narrative is similarly being used to imagine AMR. Sally Davies, the UK special envoy for AMR, often draws upon the idea of a ‘post-antibiotic apocalypse’, urging the public and policymakers to imagine a world where simple infections, childbirth, and surgical procedures become life-threatening. This narrative often blames AMR on drug “misuse” in LMICs,
overlooking the reality that, while I benefited from easy access to banana-flavoured medicine, many do not. For many of the world’s economically poor, a lack of access to life-saving drugs and fatal outcomes from minor infections are presentday realities rather than future worlds to fear. Health decisions like purchasing medication without prescriptions often stem from poverty and inadequate healthcare, not behaviour to be demonised. History shows that fear rarely produces equitable health policies, as seen in responses to AIDS, Ebola, H1N1, and COVID-19, which prioritised the wealthy at the expense of the world’s poorest.
Antimicrobial resistance is a problem that requires careful global responses that advocate for the rights of all, rather than blame and limit access to vital medications for those who will carry its burden.
Photo: Tina Leahy
Water Scarcity and the Hidden Crisis of Sextortion
Simavi is a Dutch development organisation that works with partners in Africa and Asia on water and sanitation for all, more equality for women and local climate solutions. Our vision is a climate-just world in which all women and girls can enjoy their human rights to water and sanitation.
Karin Bojorge-Alvarez, Manager of Communications, Simavi,
Amsterdam
The climate crisis is more than just an environmental issue—it is a health crisis that affects the most vulnerable in society. Water scarcity, one of the most visible consequences of climate change, has a particularly severe impact on women and girls. As droughts, floods, and extreme weather events intensify and access to safe drinking water diminishes, women and girls face increased risks of sexual violence and exploitation, especially when fetching water or accessing sanitation facilities.
It has long been acknowledged that Water, Sanitation, and Hygiene (WASH) services are highly gendered. Women and girls, often responsible for collecting water, are particularly vulnerable when these services are inadequate. In many regions, they walk long distances or queue for hours to secure water for their families. In these situations, sextortion can become a grim reality.
Sextortion occurs when those in control of water services demand sexual favours in exchange for access. This can happen in various forms: it may be an overt demand by individuals in positions of
power, or it may occur subtly, where women initiate sexual activity out of fear that they will be denied access to water. The power imbalance in these exchanges leads to what researchers call “coerced consent”—a situation where women feel forced to comply, knowing that their families’ survival is at stake. This is not an act of free will, but rather an exploitative abuse of power, with devastating social, economic, and health consequences.
Research conducted by the Dutch development
organisation Simavi in Bangladesh, Nepal, and Uganda highlights how women and girls experience harassment and violence when accessing public toilets or communal water sources. In Uganda, for example, women reported being coerced into sextortion at water holes by individuals abusing their authority. These incidents are widespread, and the climate crisis is only amplifying them.
In Colombia and South Africa, studies have shown that sextortion in access to water is a lived reality for many women. In Bogotá, women reported being asked for sexual favours in return for having water delivered or for having their water meters intentionally misread to avoid high charges. Similarly, in Johannesburg, women faced demands for sexual favours to prevent water disconnections. This form of exploitation disproportionately affects poor households in water-insecure areas.
As the planet warms, water resources become increasingly scarce. In Africa and Asia, many regions are experiencing prolonged droughts and
erratic rainfall, making it harder for communities to access clean drinking water. The increasing competition for water, combined with the unequal status of women in many societies, creates a dangerous environment where sexual violence can flourish.
Simavi has been working to raise awareness of these issues, drawing attention to the phenomenon of “sex for water” in regions where the consequences of climate change are felt, and water scarcity is most acute. In countries like Kenya, Uganda, Bangladesh, and Nepal, the daily struggle to access water has far-reaching consequences beyond health—women’s dignity and safety are at risk.
Women bear the brunt of water scarcity, yet they are rarely involved in the decisions about how water resources are managed. This lack of representation at decision-making tables only exacerbates their vulnerability. To address this, governments and international organisations must prioritize women’s participation in water governance. Their voices must be heard in policy discussions about water management and distribution, especially as the climate crisis intensifies.
In addition to ensuring representation, increased funding is needed for local, community-driven solutions to water scarcity. These initiatives can provide women with safer access to water, reducing their exposure to violence. Addressing this issue also requires a broader societal shift - one that
challenges cultural norms and power structures that perpetuate gender inequality and violence. The climate crisis is not just about melting glaciers and rising sea levels - it is about the lives of women and girls who are disproportionately affected by its consequences. Water scarcity is putting women at risk of sexual violence in ways that are often invisible to policymakers and the wider public. To truly tackle the climate crisis, we must recognize it as a water crisis. Ensuring water justice for women and climate-vulnerable communities is not just a moral imperative; it is essential for achieving gender equality and sustainable development in a changing world.
Photo: https://simavi.nl/en
Photo: https://simavi.nl/en
Photo: https://simavi.nl/en
The Cost of Inaction on Climate Change is Human Life
Dr Elaine Mulcahy
Dr Elaine Mulcahy, Director of the UK Health Alliance on Climate Changean alliance of 49 UK-based health organisations with a shared vision for a sustainable, just, healthy world. The Alliance brings together health professionals to advocate for just responses to the climate and ecological crisis, promote the health benefits that flow from those responses, and empowers members and health professionals to make changes in their professional and personal lives to respond to the crisis.
“The public health impact of climate change and the loss of biodiversity is now so severe, it is time for the World Health Organization to declare a global health emergency that requires a coordinated international response.”
So was the plea from 300 health editors, thousands of doctors, nurses, surgeons, paramedics, and a range of other health professionals before COP28 in October 2023.
A few months later, at the World Health Assembly in Geneva, the WHO passed a resolution on climate and health that recognised climate change as the greatest threat to health, and made action on climate change the number one priority for their programme of work.
The editorial and petition that had called for greater recognition of the severe health risks from the climate and nature crisis had been coordinated by the UK Health Alliance on Climate Change - an alliance of 49 UK-based health organisations advocating for faster, better, and fairer actions to protect us from the harms that climate change and loss of nature bring to our health, livelihoods, and precious health service.
Health professionals are already seeing firsthand the impacts of
climate change. In the UK, there are currently tens of thousands of excess deaths, cardiovascular and respiratory diseases, poorer birth outcomes and mental health impacts associated with heatwaves, extreme weather, and air pollution. At the same time, delivery of health services is increasingly at risk from overheating, flooding, and other infrastructure challenges.
The UK Health Alliance on Climate Change brings health organisations together as a collective voice to call for change in government policy and health service delivery. The message is focused on presenting the threats of our current way of life, which is highly dependent on fossil fuels for energy and excessive and wasteful in terms of consumption, and providing the vision for a future that is cleaner, greener, fairer and brings benefits for people and planet.
The reality is that the 29 years of UN Climate Change Conferences (COPs) are failing to deliver the
action needed. Greenhouse gas emissions have risen year on year since the landmark Paris Agreement in 2016, wherein countries agreed to limit global temperature increases to 1.5C above pre-industrial levels.
The existential threat, the harm to patients and communities, and the duties that health professionals have to prevent harm has led many to become involved in climate protests. For these professionals, it is a proportionate response to the threat and the degree of injustice they see, especially when other means have failed.
On the eve of the first-ever level 4 UK heatwave in July 2022, six health professionals went to JP Morgan Bank’s offices in London with a sign - in case of emergency, break glass - and cracked eight panes of glass with the intent of making the connections between the heatwave, the acute harm to health and the funding of fossil fuels - JP Morgan has invested $400 billion into fossil fuel projects since the 2016 Paris Agreement.
They were arrested and charged, but the jury refused to convict them after hearing the rationale behind their actions. Others who have been charged have not been allowed to explain their motivations, and were convicted. Some also lost their licence to practise and the UK Health Alliance on Climate Change has called on the GMC to explore ways in which it can avoid removing the livelihood of doctors involved in climate activism.
The Intergovernmental Panel on Climate Change has warned that every increment of warming results in rapidly increasing hazards that threaten human
health. In June 2024, it was reported that global average temperatures had remained above the 1.5C limit for a full year. The UN has said emissions need to be drastically reduced by 43% by 2030 if we are to have any chance of keeping within the 1.5C limit longer term - but still, greenhouse gas emissions continue to rise.
Health professionals around the world are calling on governments to put health at the forefront of discussion at COP29, recognising the catastrophic consequences of inaction and the significant cobenefits for health and the planet that can be achieved with positive and meaningful action.
Time for talk has run out. It’s time for global leaders to deliver.
Photo: Pietro Naj-Oleari
Growing Community-based Solutions for People in Nature
Rehema White
Rehema White is a sustainability scholar at the University of St Andrews. She is interested in human nature relationships and gathers academics, practitioners and policy makers to co-design sustainability solutions. She is also involved in local community action and likes to spend time in the woods.
The sun is baking hot, but it is cool in the forest. I stroll past slim white birches with their fluttering leaves; along the path, mighty beech trees hold ancient canopies aloft. I am walking through a Scottish community woodland, which is managed by local people for biodiversity, whilst providing a place of respite for adults, adventure for children and escape for village teenagers. Such greenspaces are havens from the unpredictable and extreme weather and are examples of community responses to climate change that support the wellbeing of people and nature. It is easy to feel despondent at international news on climate change. The recent 2024 report on climate change and health from the Lancet showed how global heating dangerously close to the planned limit of 1.5°C is causing significant issues. Older people are dying more from heat, and high temperatures adversely affect physical and mental health, including sleep and physical capacity. Extreme weather events cause fire, drought, flooding, infectious disease spread and water contamination. These effects are often felt most by the world’s most vulnerable populations. Despite this global context, our research reveals local success stories of projects that support wellbeing and enable nature based solutions to the climate crisis.
First, let us travel to Berlin, where PhD student Richard Marenbach is working with community food initiatives. Community gardens grow healthy food for those in need of nourishment. One project
involves daily visits to gather unsold bread from bakeries and nearly expired supermarket products and deliver this ‘food waste’ to foodbanks. A cooperative sells healthy, local produce and members volunteer work hours in return for food vouchers. Children are taught imaginative ways to eat more vegetables. In this way, a network of mostly young people are running projects that reduce carbon emissions, support environmentally friendly farming, provide healthy food and encourage people to have fun together.
Second, in Mexico, postdoctoral researcher Sofia Mardero studies how local communities use traditional and Indigenous knowledge to adapt farming methods to the changing climate.
Excessively high summer temperatures mean that smallholder farmers must rest in the shade for the heat of the day, and their crops are affected by drought. But people alter the timing of planting and harvesting, adopt traditional sustainable agriculture techniques, such as composting, and use ancient seed varieties to ensure genetic diversity for whatever the weather throws at them.
Next, in a raised peatbog in Scotland, a local community is working on peat restoration with the nature conservation agency. Together, participants block old drainage ditches and pull up invasive tree seedlings. They talk of how good this work makes them feel. We know that being in nature confers physical and mental wellbeing benefits; exercise in nature offers more health advantages than the same effort expended in a gym; volunteering makes people happier; and knowing the nature around you makes you more determined to save it. In this case, as the songs of bog living birds are heard again, people know they are enhancing carbon storage, conserving biodiversity and enhancing community wellbeing.
There are many more examples of such community based projects. You could explore the website for the St Andrews Prize for the Environment for more inspiration. If you want to get involved, you can join a local group, such as Transition, or a community garden. If you feel anxious at the state of the world, take a moment to sit in nature. You could start your
own initiative, and galvanise others.
Together, we can make a huge contribution in our local areas. However, we still need structural changes to help us achieve the magnitude of change we require. We need to grow hope and demonstrate change in our gardens and forests and bogs, but also advocate for political leadership and transformation at national and global scales. Finally, let us return to our community woodland. The trees there are deeply rooted in the history of the land and people. A few of the larger trees have lived since before the industrial revolution and subsequent anthropogenic climate change. The cool and the calm in this place help put concerns into perspective and to restore the ambition and energy to make a difference elsewhere.
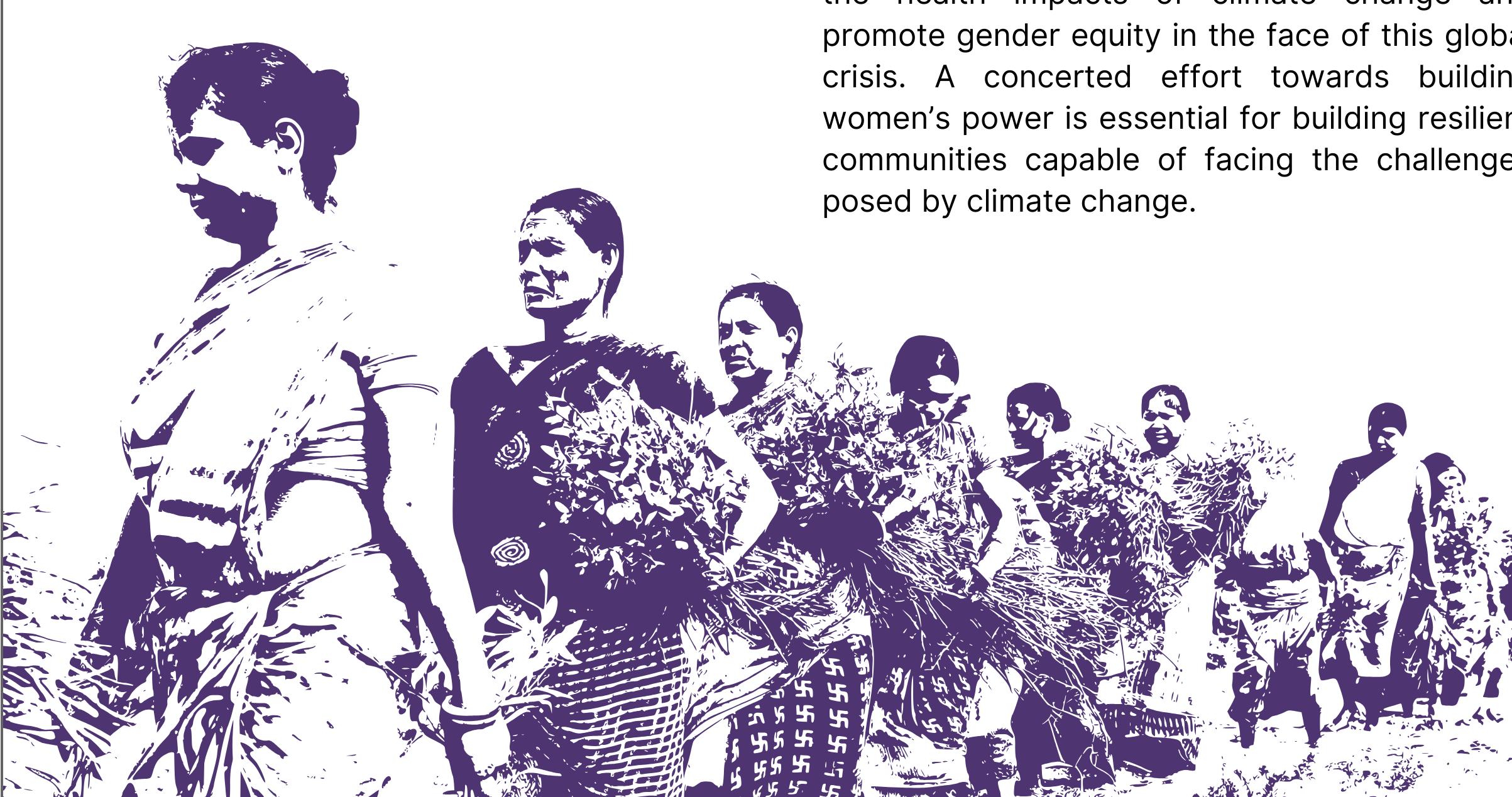
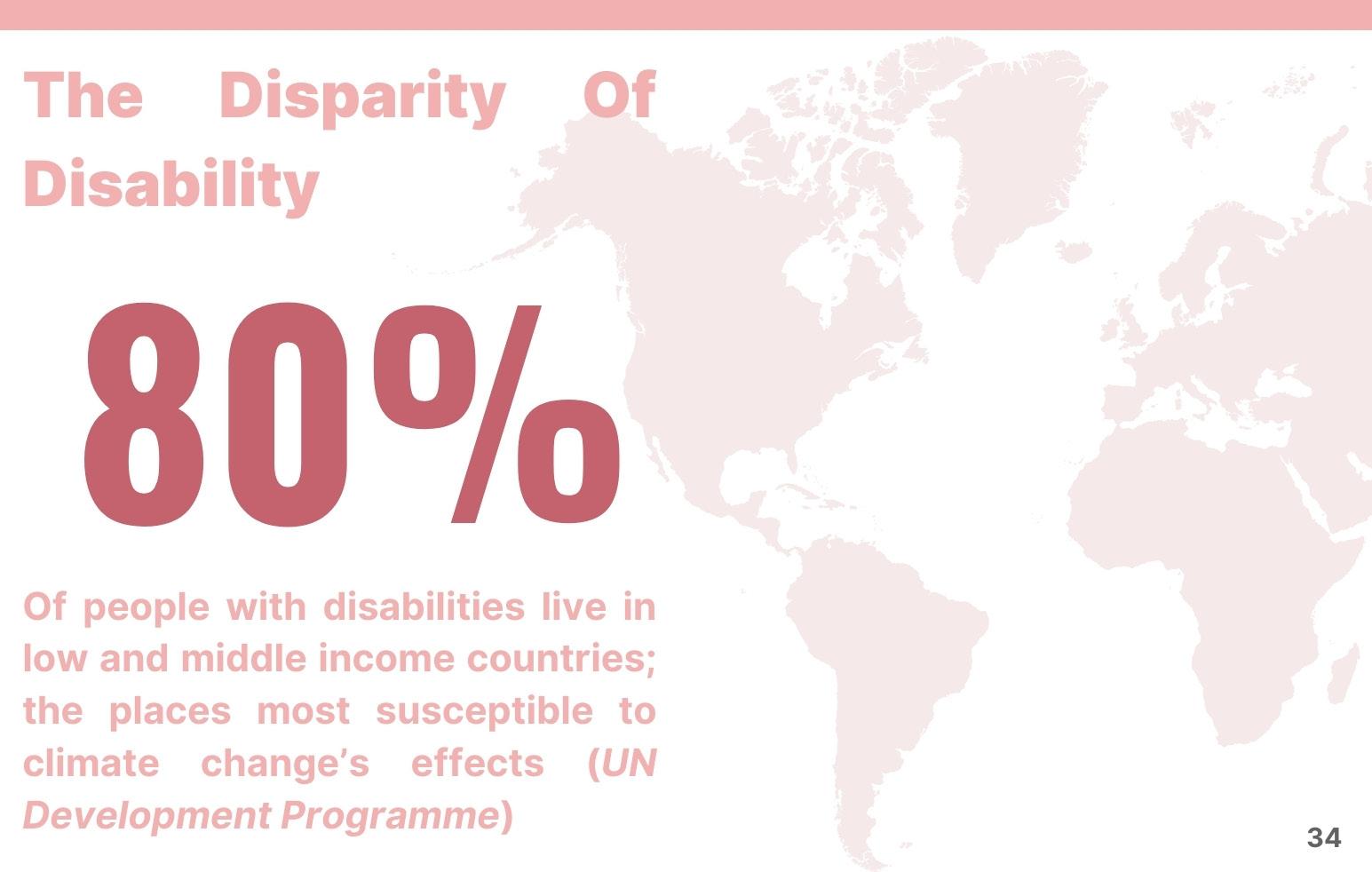
Climate Crisis Makes Us Recognize Our Limits. Disability Culture Can Show Us
How
Julia Watts Belser is a scholar, activist, and rabbi working at the intersections of disability studies, queer feminist Jewish ethics, and environmental justice. She is a professor at Georgetown University, a Senior Research Fellow at the Berkley Center for Religion, Peace, and World Affairs, and directs the Disability and Climate Change Public Archive Project.
This piece is extracted with permission from the full article published by TruthOut in July 2023.
For most of my life, the world has told me lies about limits. People take one look at my wheelchair, and they’re quick to tell me all the things I cannot do. Disabled people face intense pressure to diminish our dreams, to settle for less, to accept other people’s estimations of what’s possible. Like many disabled folks, I’ve built robust armor against ableism. In a world full of naysayers, watch me has long been my touchstone.
But there’s a second kind of lie people tell about limits, one that’s gotten deeper under my skin. It’s the lie that says, “You can do anything, if you work hard enough.” That promise is the siren song of the U.S.’s no limits culture, the ideology of a nation founded on the myth that grit and determination will allow us to triumph over adversity. For disabled people, that story fuels a vicious cultural pressure to “overcome” our disabilities — to prove that we aren’t held back by pain, that circumstance will never get us down. The ideology of overcoming veils an entire edifice of structural inequality, making it seem like all that stands between a person and their success is individual force of will. The rules of
the game are brutal: Never let them see your limits. Never falter. Never pull back.
Disability culture says no. It’s disability community that’s helped me realize that the measure of my life is more than a simple tally of accomplishment. My work is not my worth. Living with disability, as Rabbi Elliot Kukla observes, “is a long, slow detox from capitalist culture and its mandate that we never rest.”
In these times of increased climate disruption, this is disability wisdom that the world desperately needs. Climate change is a consequence of the collective human choice to push past our limits, to force this planet to carry more than it can bear. We live in a take-and-burn culture, one that pushes us to blaze bright without regard for the cost. I don’t just mean fossil fuels and fracking. I mean a broader set of cultural patterns that privilege growth and speed, that valorize profit over care, that fuel the fires of greed.
As a climate activist, I want us to recalibrate the way we think about limits. I want us to listen to disabled people, to let disability wisdom lead the way.
I want us to embrace the future in a way that centers Patty Berne’s clarion call for disability justice: “We move together, with no body left behind.” Let’s learn to press pause for migraines, brain fog, for exhaustion and grief. Let’s learn to work more slowly, move more deliberately. Let’s learn to listen, when
Julia Watts Belser
Raunaq Chopra / Climate Visuals Countdown
our bones say no. Let’s mandate breaks for anyone who works outside. Let’s require air purifiers, ventilation systems, safe work environments. Let’s make sure that all of us can breathe.
But to reckon well with limits, we have to grapple with power.
Limits are complicated, a tangled blend of private realities and public responsibilities. Beloved friends who live with chronic illness and Long COVID give voice to the raw frustration of fatigue, the hard ache of loss. These are limits imposed by the body. But they’re made harder and more isolating by the way our world sidelines those who live with longterm illness, the way our medical system is set up to deny persistent pain, the way our workplaces and social spaces aren’t set up to embrace bodies and minds that move at a different pace.
When I talk about honoring limits, these aren’t the realities I want us to embrace. Some limits are intertwined with inequality, shot through with structural injustice. Some limits are a consequence of pervasive public failures. Some limits hit hardest against those who are already marginalized. Some limits are trash.
But disability has also taught me that limits can be generative. Disabled people know precarity intimately. But we also know something about how to find beauty and claim pleasure, even when we
ache. Disability is a masterclass in adaptation, an invitation to work creatively within constraint. There’s a good life here, grounded by limits. In these days of intensifying climate disruption, that’s wisdom our world desperately needs.
Photo: Kathryn Hansen / NASA
Read stories of action towards health in a changing climate
Photo: Mark Linel Padecio/Climate Visuals
Photo: Kunal Gupta/Climate Visuals Countdown
Photo: Alastair Johnstone / Climate Visuals
Medical Community Recognises the Climate Crisis as a Threat to Health
Dr Matthew Lee and Dr Sarah Bartlett
Dr Matthew Lee works at the Royal College of Physicians in Edinburgh. He is the Deputy Special Adviser on healthcare, sustainability and climate change. He is a year three foundation doctor with a deep commitment to environmental conservation and restoring our natural world.
Climate change is causing an increase in the frequency of heatwaves, wildfires, heavy rainfall and flooding in the UK, threatening the health of the population and adding more strain to the health service. In 2022, temperatures reached new all-time highs in the UK, over 40C, causing over 3,000 excess deaths. On the current trajectory of greenhouse gas emissions, this could rise to more than 10,000 excess heat-related deaths annually by 2050. Air pollution is also having an extreme impact on people’s health, with between 28,00036,000 deaths every year from outdoor air pollution. The impact of flooding on people’s mental health is also becoming more evident.
This dire situation is set to worsen. As global temperatures continue to rise, there will be a greater prevalence of antimicrobial resistance, vector-borne infectious diseases and healthrelated deaths; amongst many other environmental impacts. Global security will be threatened by flooding, conflict and famine, leading to climate migration that will create challenges for human health and the delivery of healthcare. Much of this is not only down to fossil fuel burning, but the intensive ways we use our land for our meat and dairy consumption. In 2023, land across the world failed to capture any net carbon, in part due to the amount of deforestation for animal agriculture.
To limit the impact of climate change, it is imperative that governments around the world enable a just
Dr Sarah Bartlett works at the Royal College of Physicians Edinburgh and is the chair of the College Advisory Forum on the Environment (CAFÉ). She is in her seventh year of speciality training at the Western General Hospital where she focuses on geriatric and stroke medicine.
transition away from fossil fuel use and take action to reach net zero. But our own health service has a role to play as well – NHS Scotland contributes about 5% of Scotland’s overall carbon footprint and NHS England accounts for 4% of England’s overall emissions. As the new UK government sets out its ambitions for the health sector over the next ten years, it must prioritise actions that enable the NHS in England and Scotland to reach its net zero ambitions.
With sufficient support, it will be NHS staff that are the key to driving forward system-wide changes to make healthcare more sustainable. As doctors, we
Ishan Tankha / Climate Visuals Countdown
are already seeing the effects of climate change present in our patients. When there’s a heatwave, we see greater exacerbation of underlying illnesses like cardiovascular disease or diabetes. In areas with greater rates of air pollution, our patients are more likely to develop asthma or respiratory diseases.
Doctors’ medical training equips them with the knowledge to decide what is clinically appropriate for each individual patient. But, there is a role for us as medical royal colleges to support our members to build their understanding about the links between health and climate change.
There is a common feeling among clinicians about wanting to practice healthcare in a more sustainable way but not knowing where to start. This is why the Royal College of Physicians Edinburgh has developed an open access e-learning resource outlining the ten things a doctor can do to combat climate change. This resource provides guidance in a range of areas, including practicing preventive medicine and reducing investigations.
This is also an area of focus for the Royal College of Physicians London, who in July 2024 launched the Green Physician Toolkit. The toolkit is aimed
at physicians starting their journey, suggesting actions all physicians can do to help slow the pace of climate change and adapt to its effects, such as prescribing carefully and having conversations with vulnerable patients about their health during a heatwave. Changes to the way we deliver care, whether large or small, will make an important contribution to the NHS’s response to the climate and nature crisis.
We must also end the burning of fossil fuels and take decisive action to restore nature through financial divestment and shifting our dietary habits. As doctors, we must speak out and keep raising awareness on the health implications of climate change and empower our colleagues, patients, friends and family to make the changes they can for a safe and livable future for us all.
Photo: Jörg Farys / Fridays for Future
Giving Healthcare a Shot in the Arm:
How Sustainability Can Improve the Quality of
Healthcare
The Eye Surgery Hastings is a specialised eye care facility in New Zealand. It is solar powered and carbon neutral, and led by Doctors Sophie and Alex Buller. In 2023 it was named the Health Care Climate Champion for the Pacific region by Health Care Without Harm due to an innovative approach which included getting their waste down to 1kg from 100 patients in the outpatient clinic.
You’re probably familiar with the story of the three little pigs; there’s a big bad wolf coming so they all build houses. The houses made out of straw and sticks don’t survive and the one made from bricks does. Superficially, the moral of the story is to build houses out of bricks, and the metaphor for doing things properly is well illustrated by a story timeless enough to become a classic. However, the crux of the story relies on the absolutely key piece of information that the little pigs know the wolf is coming.
Global warming is a wolf we can see coming. The early warning signals have been blaring for decades, and they’re close enough for everyone to see. The wolf you can see coming is the easiest to deal with, right? That’s the thing with wolves; different wolves need different types of bricks. This introduces the question - what properties does a carbon emission stopping “brick” have, and is it implementable in healthcare?
Enter healthcare; a very busy service industry with very high stakes. For a long time healthcare has been improving quality and reducing clinical problems with increasing reliance on single use instruments and other packaging and waste-heavy practices. It’s pushed this so far, that overall, healthcare is responsible for more emissions than the aviation industry.
Unfortunately, the dilemmas are not between right and wrong - it’s right versus right choices.
Healthcare has core values it won’t compromise on. Patients come first. Decrease the quality of care, and you’ll get resistance from staff and patients. Make something slower, and there’s absolutely zero leeway in the already overstretched system. Increase complexity, and whatever can possibly go wrong will, and people will soon revert to the simplest option.
So, that means the “bricks” needed for healthcare must be the same, or better, than current practices in quality, speed, complexity and ease of use. Now, multiply that by the total number of procedures done in medical practices and hospitals, including variation of practices or dealing with unusual circumstances, and you can imagine the challenge.
Dr. Alex Buller
Another wolf is at the door - energy prices. It was with this in mind that we put solar panels on our roof. The usual sweet spot for return on investment with solar panels is, fewer solar panels than you would need to produce all your electricity. The turning point, however, is that we put as many solar panels as could fit on the roof. We have a standalone eye clinic and operating theatre with a large, flat roof and our region is unusually sunny, even for New Zealand (Hawkes Bay has recently been named as the world’s newest Great Wine Capital - come visit sometime)! Additionally, our estimated electricity production became 150% of our annual usage!
This was great for all the obvious reasons, the electricity bills were tiny - completing New Zealand’s first ever solar-powered operationswe were exporting electricity, joined a peer to peer solar network, and we were very proud of the ecological ramifications. It took quite a while before we realised; there was more to what we had done- a lot more.
What do you do with excess electricity? With energy and pandemic wolves biting, our suppliers raised their prices. The price of bottled oxygen
and medical air inflated rapidly. With free and abundant electricity we could switch to an oxygen machine and air compressor, and make these on site. This hits the brief for our “bricks”: it reduces cost, increases the certainty of supply and frees us from a supply chain. We switched to reusable instruments being sterilised with free power, which also gave us better quality instruments. The laundry costs plunged and we switched to reusable surgical gowns and operating theatre covers. Our list goes on, and on, and on. It’s also a very comfortable place to work, with as much free heating in winter and cooling in summer as we feel fit.
The point is; power has a hidden power. To make the switch from current practices to a low emission version will take resources such as money, time and research. Renewable electricity can be the key resource crucial to finding the low-carbon solution which allows the bricks to withstand the wolves.
Photo of Eye Surgery Hastings’ solar array40
The Climate Crisis is a Health Crisis:
Avoid, Shift and Improve should be the principle; and Net zero, Liveable and Healthy Cities the Goal
Professor Mark J Nieuwenhuijsen
Professor Mark J Nieuwenhuijsen PhD is director of the Urban Planning, Environment and Health initiative and the Climate, Air pollution, Nature and Urban Health research program at ISGlobal Barcelona, Spain. He is a world leading expert in environmental exposure assessment, epidemiology, and health impact assessment with a strong focus and interest on healthy urban living.
The recent tragic events, on Tuesday the 29th September, in Valencia that left more than 200 people dead and billions of euros of damage show the severe impacts of climate change. Although this “gota fria” (cold drop) has occurred before, this time the severity was enhanced by the warmer-than-usual Mediterranean sea, which lead to enhanced evaporation followed by severe rain. Although there was a warning from the weather agency a few days before, it was not taken seriously, increasing the devastation. The slow response of the emergency services led to civil unrest and a mass demonstration on the 9th of November.
As is often the case with disasters, it was a coming together of different circumstances; climate change (more energy in the climate system), poor urban planning (too many impermeable surfaces), poor politics (political denialism and opportunism), and lack of appropriate warning and response mechanisms - to name a few.
It is obvious now that we need to take climate change more seriously, and that we need to have effective early warning and emergency systems in place. We need to recognise that the climate crisis is a health crisis, and it is therefore the World Health Organisation demands urgent integration of health in climate negotiations of the COP that are ongoing in Baku (COP29).
Recent years have been amongst the hottest on
record, and high temperatures claimed over 60,000 lives in Europe alone in 2022. Current climate projection shows that we are going towards a 2.7 degree celsius warming, with further devastation expected.
Cities are where most people live now and a recent, large-scale review of multiple city-based studies showed the clear relationship between urban and transport planning, and environmental quality, greenhouse gas emissions and health. Therefore, better urban planning could be a solution to reduce climate change impacts and improve health. The co-benefits of climate action are well recognized and documented, but the urgency to implement them is still missing.
Photo: Paolo Patrizi
Climate mitigation strategies targeting land use, transport, buildings, and waste management have demonstrated quantified multiple health co-benefits such as reduced premature mortality and rates of disease. Decarbonization, more sustainable transport and housing and greening of cities are urgently needed, as is a more sustainable and healthy diet to reduce our greenhouse gas emissions.
Principles such as Avoid, Shift and Improve (ASI) should be implemented. For example for mobility; reducing car use and flights by avoiding unnecessary trips, shifting from car use to public and active transportation, and improving the remaining car use by using electric vehicles.
Cities should be compact to reduce the need for long distance travel, and novel innovative urban models such as the Paris 15 Minute City, Barcelona Superblock, the London Low-Traffic Neighbourhoods and the Vaugban Freiburg CarFree Neighbourhood should be implemented to to make the shift from car-centric planning to peoplecentric planning.
A better, more health orientated narrative may help to address the climate crisis, but we need a more integrated and holistic vision of what
our society and cities should be and look like to capture the imagination of politicians, decision makers and citizens and change their behaviour. For example, a shift away from our car-centric planning and more greening are essential. Urban lifestyles, particularly in high-income countries are detrimental to the planet - and therefore our health - therefore, concepts such as degrowth need to be promoted.
By 2050, societies and cities that have embraced climate action will be cleaner, greener, more resilient, and more livable, with urban environments that prioritize sustainability and the health and well-being of their residents. Societies and cities that do not take decisive climate action by 2050 will likely be characterized by environmental degradation, social inequality, economic decline, and a lower quality of life for their residents. The contrast between societies and cities that act and those that do not will become increasingly stark, with inaction leading to potentially irreversible consequences.
2050 is tomorrow and therefore urgency in climate action is essential; we must stop looking for excuses not to act, and act now. Valencia is another warning.