2022 | 026 CLINICAL RESEARCHERS AND THE HEALTHCARE SYSTEM CELEBRATING CLINICAL RESEARCH EXCELLENCE 2022 HEALTH & MEDICAL RESEARCH AWARDS


And we are here ….. the end of another tumultuous year in health and medical research systems everywhere.
It is no wonder we continue to hear about the fatigue across our hospital networks. There are increasing delays in emergency departments, and waiting lists to see GPs and specialists alike are getting longer. We heard recently about a hospital in Geelong that is planning to close its maternity ward because of staff shortages. Many regional areas have struggled to fill healthcare positions for years, and now this same issue is affecting the suburbs of our big cities. We realise now more than ever before, our healthcare workforce is essential, and we are encouraging an even stronger policy and funding focus on ensuring we attract and retain this crucial cohort.
This issue of INSPIRE celebrates those healthcare professionals who straddle the two worlds of healthcare and research- individuals from all the healthcare disciplines who combine their healthcare practice with the conduct of research. Just like their
healthcare colleagues they too are facing increased work pressures, and yet they continue to undertake research, to translate research findings into their workplaces and identify new areas where research is required to improve health outcomes and make our health system safer and more effective.
From demonstrating the viability of community screening for TB in developing countries to providing earlier diagnosis and treatment for ear disease and new approaches to gestational diabetes, this issue is filled with inspiring stories from amazing individuals.
Equally inspiring are our Research Australia Award winners. Announced at the Annual Research Australia Awards dinner in Melbourne on 8 December, the Awards celebrate contributions by individuals and groups across the spectrum of health and medical research, from researchers just starting in their career to the sectors leaders in research, philanthropy and advocacy. These awards now in their 19th year are always special and the people
they honour are those incredible people who make a difference in all of our lives. It was a wonderful night, and it was a privilege to be joined by so many Research Australia members, politicians, and senior government officials.

Research Australia was also delighted to announce the appointment of Emeritus Professor Christine Bennett AO, as our new patron, and to present a life membership to Professor Alexandra McManus. These exciting announcements recognise the longstanding association that these two amazing women have both had with Research Australia.
In closing, I wish you all the best for the festive season and for the year ahead. I look forward to continuing to work with each of you to advance our shared vision of Health and Prosperity through Australian Research and Innovation.
Best wishes Nadia and the Research Australia Teama safe and happy festive season from the Team at Research Australia.






















The
advocates
Research Australia’s 19th Health and Medical Research Awards, celebrating the extraordinary researchers, philanthropists, and community champions



recognised
sector.
Researchers who discovered unique immune cells within breast ducts to help fight breast cancer and scientists who developed a breakthrough 3D bioprinter were among those honoured, as well as passionate advocates and philanthropists who help drive Australian health and medical research further.
Research Australia CEO Nadia Levin said the Awards were an opportunity to honour our dedicated researchers for taking risks, innovating and translating discoveries to improve the health of millions of Australians.
“Australians should be proud of the achievements within our world-class health and medical research, but we cannot take this progress for granted,” she said.
“If Australian health and medical research is to fulfill its potential as a cornerstone of our post-carbon economy, we must have the necessary manufacturing capacity as
nation’s brightest scientific minds and
have been
in
who are leading work with transformational impact for patients and the health
well as greater commitment to nurturing and rewarding the critical skills of this sector.
“With the right support, we have the talent we need to bring Australian discoveries to life on Australian soil. We need a cohesive national approach with pillars of support for early and mid-career researchers, bringing government and the sector together to ensure we achieve the greatest impact and exploit areas where we have a competitive advantage.”
Assistant Minister for Health and Aged Care Ged Kearney delivered the keynote address at the event, announcing a National Women’s Health Advisory Council to address stark differences in the health outcomes for women and girls.
The Shadow Minister for Health & Aged Care, Senator the Hon Anne Ruston (representing the Leader of the Opposition the Hon Peter Dutton MP) presented the Great Australian Philanthropy Award. Dr Monique Ryan MP (Member for Kooyong) presented the Advocacy Award sponsored by AbbVie.
Professor Ian Alexander received Research Australia’s flagship award, the prestigious Peter Wills Medal , recognising his leadership as a clinicianscientist bringing novel therapies to infants and children with devastating genetic diseases. Professor Alexander is Professor in Paediatrics and Molecular Medicine at the University of Sydney, Senior Staff Specialist in Genetic Medicine at the Children’s Hospital at Westmead, and Head of the Sydney Children’s Hospitals Network and Children’s Medical Research Institute Gene Therapy Research Unit.
As a clinician-scientist he has dedicated his career to the development of novel therapies for infants and children with devastating genetic disease and is internationally renowned for his leadership in pioneering the gene therapy field in Australia over 27 years.
Scientia Professor Justin Gooding received the Frontiers Research Award on behalf of Inventia Life Sciences, the Australian Centre for NanoMedicine, UNSW School of Chemistry and the Children’s Cancer Institute in recognition of the ‘Rastrum’ 3D bioprinter which enables cancer researchers to rapidly produce 3D cell cultures/assays and build more complex in vitro cancer models. The Award was sponsored by Australian National University.
Dr Caleb Dawson (Walter and Eliza Hall Institute) won the Griffith University Discovery Award for his discovery of unique cancer-aiding immune cells within the ducts of the healthy breast.
My Twitter : @chriskere
Professor Johanna Westbrook University) won the sponsored by the Victorian Government, recognising her achievements in evaluating the effects of information and communication technology in health care.
The Data Innovation Award AusVaxSafety Team at the National Centre for Immunisation Research for their work which enabled nationally consistent vaccine safety surveillance to be delivered in near-real time from the first day of the COVID-19 vaccine rollout, the largest and most complex immunisation program ever delivered in Australia.
Roy and Nola Thompson won the Great Australian Philanthropy Award, recognising their extraordinary generosity in supporting a neuroscience research institute at the University of the Sunshine Coast and developing this further to create the National PTSD Research Centre.
ghd received the Advocacy Award - sponsored by AbbVie - for their commitment to breast cancer research and raising awareness of the disease, particularly among younger women.
The GSK Award for Research Excellence was awarded to Professor Georgia Chenevix-Trench, a Distinguished Scientist at the QIMR Berghofer Medical Research Institute. Professor Chenevix-Trench is a world-renowned scientist who, with her collaborators, discovered over 240 regions of a genome that are likely to affect a person’s risk of developing breast cancer.
Ms Levin said the scope of talent among nominees had been exceptional, with commendable achievements across all categories.
“On behalf of Research Australia, I would like to thank all our nominees, nominators and members for helping us celebrate the world-class ability and dedication within this sector,” she said.
I would also like to thank the organisations who have supported the awards, including our premium event partner the University of Melbourne, Griffith University, Australian National University, AbbVie, the Victorian Government (DJPR), Digital Health CRC and GSK. Supporting research is as important as the research itself, and our gratitude goes to all those who help drive these achievements.”
Named in honour of Research Australia’s Director, Peter Wills AC, a great leader whose work led to the inception of Research Australia. The Peter Wills Medal is the flagship award and recognises someone who has made an outstanding, long-term contribution to building Australia’s international reputation in areas of health and medical research and fostering collaboration for better health.
Winner: Professor Ian Alexander (Sydney Children's Hospital Network)

Sponsored by Australian National University, this Award recognises the success of innovative health and medical research that extends existing knowledge, boundaries and/or understandings within health and medical research.
Winner: Scientia Professor Justin Gooding (Australian Centre for NanoMedicine, UNSW)

This Award recognises an early career researcher (anytime from qualification but no more than 5 years past PhD) whose paper/ patent/discovery has already demonstrated its importance or impact.
Winner: Dr Caleb Dawson (Walter and Eliza Hall Institute)



This Award profiles personal philanthropy that is outstanding in its generosity, effectiveness, vision, high impact and transformative quality. The Award recognises and encourages personal philanthropic donations over a period of time by an individual(s) or family to Australian health and medical research.

Winner: Roy and Nola Thompson
Sponsored by AbbVie, this Award recognises and congratulates exceptional contributions made by research champions who help raise community awareness and understanding about the importance of health and medical research.
Winner: ghd Ludovic Dellazzeri

This Award is for an individual or team who has provided leadership and made an outstanding contribution to health services research; driven research that has led to a significant improvement in healthcare; and/or has championed the development of the health services research field. Sponsored by the Victorian Government.
Winner: Professor Johanna Westbrook (Macquarie University)






This Award recognises an individual or team whose innovation is considered to represent one of the most impactful new data innovations in the health and medical research sector within the past five years.
Winner: the AusVaxSafety team (National Centre for Immunisation Research)
One of the most prestigious awards available to Australian researchers, this prize has been awarded since 1980 to recognise outstanding achievements in medical research with potential importance to human health. This year’s Award is accompanied by a grant of $80,000 to further the winner’s research.
Winner: Professor Georgia Chenevix-Trench (QIMR Berghofer Medical Research Institute).


Research Australia has been working with its members to develop reports on specific topics. Research Australia, together with Novo Nordisk, launched Australian Obesity Research: Global leadership and local change at two Parliamentary Events, in November at NSW Parliament with the Hon Brad Hazzard MP, NSW Minister for Health and the Hon Tara Moriarty MLC, NSW Shadow Minister for Medical Research; and at Federal Parliament alongside the Hon Ged Kearney MP, Assistant Minister for Health and Aged Care, and Mr Gavin Pearce MP, Shadow Assistant Minister for Health.
The Report identifies five key research themes Australia must prioritise to accelerate progress for the millions of Australians living with overweight and obesity:
• Healthy living programs and interventions.
• Developing a clearer picture of the social, economic, and personal impacts of obesity so that Australia can invest where it matters most.
• Obesity research focused on high priority populations, disproportionately impacted by the condition.
• Equipping our health care system with the evidence to prevent obesity.
• Equipping our health care system with the evidence to manage obesity.
Research Australia provides unique insight and expertise into the health and medical research ecosystem. These Reports and events are examples of the bespoke advice Research Australia can provide on health and medical research investment, discipline-specific planning, and policy. Drawing on the significant expertise of our team and deep expertise of our broader membership, Research Australia’s consulting service delivers strategic advice that is sensitive to the needs of research, the health system, and the political environments in which we operate.
To find out more about our advisory work, please contact us
Arthritis Australia recently hosted a Parliamentary launch of the Impactful Arthritis Research Report, prepared on their behalf by Research Australia. Research Australia worked directly with over 100 Australians, of all ages, living with some form of arthritis to identify what consumers prioritised from existing research and where they thought more research is needed. The consumer driven research priorities identified are:
• Research to support the delivery of better arthritis care.
• Fundamental research into the causes, symptoms, and prevention of arthritis, driven by consumer involvement and co-design.
• Ensuring arthritis research meets the needs of all Australians.


• Coordinating research that cuts across multiple types of arthritis or broader musculoskeletal conditions.
The Research Australia University Roundtable provides a forum for Research Australia’s university members to discuss issues relating to health and medical research which are particular to universities. Membership of the Roundtable consists of individuals nominated by their university. The Roundtable meets three to four times each year.
The Roundtable on 16 November continued the theme of researcher development with a presentation from Professor Susan Hillier and Ms Claire Jackson on work at the University of South Australia to design a curriculum for developing researcher skills and knowledge that considers the needs of industry. The University has consulted with Industry Partners to identify areas of greatest need for skills and capabilities and is offering training and skills development in these areas as part of the broader researcher development curriculum.
The NHMRC released its revised policy on Open Access in October, and this inspired two other presentations to the Roundtable. The first was by Liz Allen, Director of Partnerships at F1000Research, a new Research Australia member. F1000Research is an Open Research publishing platform for scientists, scholars and clinicians offering rapid publication of articles and other research
outputs without editorial bias. Liz’s presentation provided an overview of the development of the movement towards Open Access, emphasising that it had different priorities internationally, including between the developed and developing world.
The second presentation on this topic was by Professor Virginia Barbour, Co-Lead, Office for Scholarly Communication, Queensland University of Technology (QUT) and Director of Open Access Australasia. Virginia a identified the recent moves by research funders to mandate open publishing as a key driver behind the current activity in this area. Virginia outlined the UNESCO Open Science initiative and the profound impact COVID-19 has had on research publishing and dissemination.
Virginia referred to policy developments in Australia and New Zealand, including the focus of Australia’s Chief Scientist on open publishing and trying to find a national solution. Virginia warned against trying to find one single solution, instead suggesting that the future lay in a range of different publishing options, formats and approaches, but with a common thread in the UNESCO Open Science Principles and a commitment to peer review (rather than the prestige of the journal) as a measure of quality.
This Report was launched at Australian Parliament House alongside Hon Ged Kearney MP, Assistant Minister for Health and Aged Care and Senator the Hon Anne Ruston MP, Shadow Minister for Health and Aged Care.
register, was established in 2020 to address key challenges to conducting clinical research in Australia, including the timely recruitment of participants, and streamlined access to linked data.
A key barrier to conducting clinical research in Australia is the ability to recruit participants on time and within budget, with many studies failing to meet recruitment targets. The national research sector has become less competitive than emerging markets on metrics of “cost, timeliness of trial start-up, and the capacity to recruit trial participants.”1 While there is data to show that around two-thirds of people would be willing to participate in research, in practice only about one percent will ever be involved in a clinical trial.
Another key challenge for clinical research is timely access to routinely collected health data that allow follow-up of participant outcomes. Access to routinely collected health data, particularly cross-jurisdictional data, requires multiples approvals, resulting in significant duplication of effort across studies.
Disease-specific registers are widespread and can be highly effective for engaging patients in research efforts. Internationally, several countries are now investing in infrastructure to support research recruitment across multiple disease and study types; the United States, Scotland, and Wales each have high-quality not-for-profit, disease-agnostic research registers supporting medical research recruitment.
Join Us was established, with initial funding from The George Institute and UNSW Sydney, as a shared piece of national infrastructure designed to connect the community to research opportunities relevant to them, while also increasing and streamlining access to routinely collected health data.
Join Us has been fully piloted and has 55 Partner Organisations across Australia spanning universities, medical research institutes, healthcare providers and community groups.
Australians aged 18 years and older can sign-up online to Join Us, consenting to be contacted about research opportunities and optionally providing consent for
1 2020 Australian Commission on Safety and Quality in Healthcare report

researchers to use their linked health data. Participants are matched to research projects using sociodemographic and health questionnaire data provided upon registration. The digital technology underpinning Join Us keeps participant data safe, securely storing identifiable personal data separately to de-identified health information.
Research projects with ethical approval can use Join Us for study planning or recruitment and, in the future, conduct research using de-identified routinely collected data of consenting participants.
To date, 1,270 participants have registered with Join Us, with plans to recruit hundreds of thousands more through healthcare and community settings over the coming years. Although still at an early stage, Join Us has helped recruit participants for 27 research studies, including 8 clinical trials.
The Join Us cohort contains highly engaged participants eager to learn more about the studies with which they are matched. Participants receive personalised email invitations with study details and can then contact the researcher for more information, or sign-up for the study if they are eligible.
Dr Christine Jenkins, a clinician researcher who has led several clinical trials of airways disease has found it increasingly difficult to recruit to clinical trials especially for well-established and chronic conditions like asthma. Working with Dr Anthony Sunjaya on the BREATHE study – a research study designed to develop a clinical pathway for the assessment and management of breathlessness in primary care – Join Us was employed as part of the participant recruitment strategy.
Overall, 238 Join Us participants were matched and invited to participate in BREATHE, with 5% of those invited reaching out to researchers, and 4% of the total matched ultimately participating. While this translates to a small number of participants, it demonstrates the power of Join Us to assist with recruitment as the register grows. If Join Us had 200,000 people registered, it could be expected that around 1,500 people would have been recruited for
this same study over just a few weeks with little effort, making it a very efficient recruitment approach.
Join Us is ultimately aiming to sign-up 1 million Australians who are interested in supporting clinical and health research. We are actively recruiting participants, with NSW Health providing funding to support recruitment of thousands of people to Join Us from NSW over the coming months.

We are calling for all those aged 18 years or older who are interested in helping support clinical and health research in Australia to sign up now at https://www.joinus.org.au/.
Registration takes only 15 minutes but is an important first step in supporting research to help discover new ways to prevent, diagnose and treat disease and improve the health of all Australians.
Researchers who are interested in using Join Us to plan or recruit for their study can contact the Join Us team on info@joinus.org.au or visit our website: www.joinus.org.au/ researchers for more information.

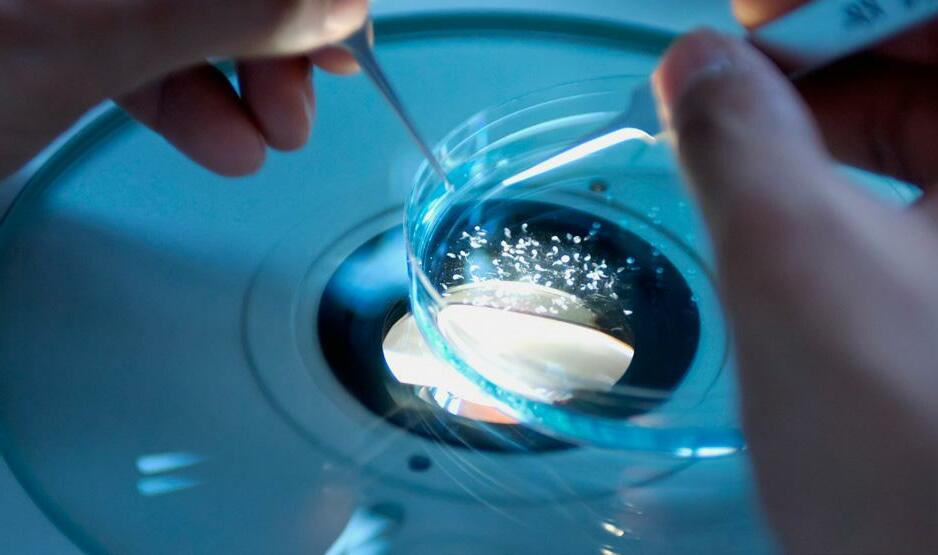
A year on from Australia’s first ever successful clinical gene therapy for an inherited blinding eye condition, clinician-scientist Professor Robyn Jamieson is excited by the progress.

Sydney is now seen by pharmaceutical companies worldwide as a leading centre for testing new treatments for these conditions. But with more interest, comes more challenge – especially when it comes to diagnosing and developing specific treatments for these diseases.
Since leading the team for delivery of the ocular gene therapy, LUXTURNA (Novartis), Professor Jamieson of Children’s Medical Research Institute at Westmead, Sydney Children’s Hospitals Network and Save Sight Institute, University of Sydney, has been contacted by patients, clinicians, and researchers around the world. She is now involved in three clinical trials and is leading development of novel therapies in house for conditions where treatments don’t exist, but a current challenge still lies in diagnosis.
“I’m working on several options for therapies, but we have to have the genetic diagnosis first, and for too many
of these conditions genomic testing returns a result of ‘variant of uncertain significance’. This means clinicians are unsure if the genetic change detected causes the disease. We each have thousands of genetic variations in our DNA, so we have to be sure the variant detected is responsible for the condition, else we won’t be developing or providing the correct treatment. This is where basic research comes in.
“People can’t be eligible for genetic therapy clinical trials unless they have a genetic diagnosis.’’
Professor Jamieson’s team recently presented to the American Academy of Ophthalmologists about a therapy for Stargardt Disease and an Usher Syndrome therapy. She is also developing genetic therapies for other conditions.
In addition, as a clinical geneticist, Professor Jamieson plays a key role in the diagnosis of patients.
They have to meet certain criteria to qualify for trial therapies, so we need to make it easier to give people a genetic diagnosis.’’
Around 1:1000 people are affected by inherited blinding eye diseases and around 60% get a genetic diagnosis, but it can take between two months and two years. Sometimes the result is still unknown.

“We work with disease specific specialists to figure out – well does this genetic diagnosis make sense with what we’re seeing? We need to know how to relate that genetic variant to the disease, and you’ve got to be really sure if you are going to give a patient a genetic therapy.
“When things are stuck, that’s our role as scientists. We perform functional genomics research to demonstrate that a variant of uncertain significance does in fact cause the disease. This also helps in developing the correct genetic
therapy. Without this research, 30-40% of patients can’t get a genetic diagnosis. We get them over the line so they can benefit from our new therapy developments and access to clinical trials and therapies.’’
This is an extraordinary and exciting time, with the future looking really bright with tremendous prospects for a genetic diagnosis for all patients and pathways forward for new therapies for all patients
eye conditions.
with inherited blinding

 Dr Peter Diamond Leukaemia Foundation
Dr Peter Diamond Leukaemia Foundation
Leukaemia Foundation’s Head of Research, Dr Peter Diamond said the organisation is committed to funding research innovations that drive advancements in new diagnostics, treatments, care options and novel therapies, supporting the careers of scientists and clinicians and giving Australians access to global clinical trials.
“Every significant improvement in treatment for people living with blood cancer has come from an investment in research. We have developed strong collaborative partnerships to co-fund research enabling more opportunities for investment in the best and brightest scientists and haematologists in Australia,” Dr Diamond said.
“The Leukaemia Foundation’s investment into research over the last 20 years, has supported most of the senior haematologists and blood cancer researchers in Australia at some stage in their career. It’s further contributed to a better understanding of blood cancers, better diagnostics, and the development of many new techniques and therapies which are now either undergoing clinical trials or are being used in clinics as part of everyday therapy. This includes treatments like Venetoclax, bortezomib, CAR T-cell therapy and liquid biopsies for blood cancers – a world first.”
Continuing to support the next generation of researchers, this year the Leukaemia Foundation in conjunction with the Haematology Society of Australia and New Zealand, have co-funded three clinician scientists to undertake innovative PhD scholarships, aimed at improving the lives and outcomes of Australians living with blood cancer.
The current round of PhD Scholarships will investigate home based management for blood cancer patients, understanding how acute myeloid leukaemia (AML) cells evade the immune system after stem cell transplant, and optimising treatments for cutaneous T-cell lymphoma.
One of the innovative projects being funded is an Australian first study that will see patients receive blood transfusions at home. They will be monitored during and after receiving their transfusion wearable devices that have been clinically validated.
The study is led by Dr Briony Shaw, a medical doctor and PhD candidate at Monash University, involves designing and conducting Australia’s first pilot clinical study where patients are transfused at home and monitored during and after receiving their transfusion.
While blood transfusions in the home are almost routine in some parts of the world including Sweden, USA, UK, Spain, Italy and some East Asian countries, there has been a barrier in Australia up until now. The aim of this research is to assess the feasibility of home transfusions with a pilot program.
The study will initially focus on elderly patients who have difficulty with transport as well as needing a caregiver to take them to hospital and attend appointments, but eventually aims to expand the study to include patients with blood cancer in general. Dr Shaw sees real benefits for patients, their carers and the health system. “For people with blood cancer, blood transfusions are a mainstay of their supportive care, and this new research will focus on providing those transfusions and other types of care in the home meaning earlier hospital discharge for patients, a more comfortable experience, and reducing the burden of caregivers and the overall cost to the healthcare system.”
Many patients face barriers to due to geographical restrictions, age and frailty meaning frequent trips to hospital could have a profound impact on their treatment outcomes. The study has the potential to revolutionise care for these patients.”
As part of this research, the wearable devices will be further developed to enable heart rate, blood pressure, oxygen saturation, temperature, and blood counts to be checked, to make sure patients stay safe and clinically stable while at home and to assess for early signs of deterioration or a change in their clinical state.
Accelerating research in blood cancer treatments is a key priority of the Leukaemia Foundation. The PhD scholarship recipients research projects will further help to pave the way towards the Leukaemia Foundations bold goal of zero lives lost to blood cancer by 2035.
Dr Diamond added, “The harsh reality is that with our ageing population, the number of people being diagnosed with blood cancer will continue to increase. By 2035, twice as many people will be diagnosed with blood cancer each day. We need better, more targeted treatments and care solutions and the only way we can achieve that is by investing in research and clinical trials.”
The Leukaemia Foundation has been supporting Australian blood cancer research for over 20 years, committing over $57million to research since 2000.

Because people have been willing to support and mentor me, my research endeavors have been fulfilling and constructive. This has reaffirmed my belief that nurses, and other allied health professionals are in a unique position to make an incredible difference to the day-to-day care patients in all realms of care.
I am in a unique position because when I was studying for my PhD, I was lucky enough to work with a great university team looking at and developing programs to support women’s health. I gained a greater understanding about conducting safe, appropriate research trials, and managing data. Through this collaboration, I co-wrote the materials for this and other interventions, as well as
developing the health professional training for delivery of the interventions.
Working at The Wesley Hospital Choices Cancer Support Centre (Choices) has enabled me to help incorporate supportive care and side effect management into programs such as The EMERALD Study a Younger Women’s Wellness after Cancer Program which will examine the potential for delivery of a lifestyle intervention addressing wellness and health issues in younger women after treatment for cancer.
The issues include fear of recurrence, increased stress and anxiety, sleep issues, early menopause, obesity, body image concerns, sexual dysfunction, and a risk of other chronic health issues such as heart disease and type 2
When I started my career as a nurse, I didn’t imagine I would be so involved in research.
diabetes as well as other cancers. Once treatment of their cancer is completed women often find themselves without the information and supports to manage these issues.
There are currently few holistic interventions aimed at helping young women overcome these late effects and ongoing chronic health risks and it is anticipated that this program can help address this gap whilst developing a bridge between hospitals and GPs.
Nurses and allied health researchers are engaged in multiple roles. One key aspect is being open to new research ideas and appraising the quality of the evidence to embed the research into practice.
Another is identifying where there may be knowledge gaps in practice and formulating questions to address these.
Importantly, seeking support from their organisation and collaborating with others who may also be actively involved in the patient’s care is highly significant.
This should not just be within the hospital or community setting but also in partnership with university experts and very importantly, in collaboration with advocates with lived experience, who provide a significant dimension to patient focused research.
In my experience, nurses and allied health practitioners are concerned about the research process, how to conduct research, understanding quantitative or qualitative data, managing statistics, writing research questions and so on.
Most of the research originates from scientists and medical doctors so nurses and allied health professionals may not readily think of research coming from their medical specialty.
Or they may doubt they have the skills to conduct research. However, there are great courses within the Universities that teach all these elements. Working as a research assistant on a clinical trial is another way of learning and understanding these tools and the research process.
It should be a responsibility of those within the hospital, research, and community setting already engaged in research translation, to educate and mentor others by actively supporting and demonstrating how to integrate evidence-based, cost-effective research into practice.
There is also the big issue of getting funding to undertake research. Writing grants is an extremely competitive
process which makes it even more important to collaborate effectively with teams who are experts in the area you might want to examine, improve, or change. We have been extremely fortunate to receive two recent grants through Wesley Research Institute.

Nurses bring their own unique perspective to research. A lot of their expertise focuses on the whole person, in the management of numerous illnesses and conditions, managing wound care, preventative work, delivering positive lifestyle interventions, improving patient comfort. Integrating research and clinical practice brings many benefits for all involved not only where it is being undertaken, but also nationally and internationally.
It positively increases the hospital’s reputation, provides the professional satisfaction that comes with improving patient care, and ultimately enhances outcomes for patients.
Author: Dr Janine Porter-Steele is The Clinical Nurse Manager of The Wesley Hospital Choices Cancer Support Centre in Brisbane. The centre offers support, sharing and information for women, men and their families affected by a diagnosis of cancer. For many years Janine has also been actively involved with the Women’s Wellness Research Programs as manager, delivering the programs, supporting the development of resources, and co-writing several journals.
This is the story of how allied health started building clinician-research leaders at Townsville Hospital and Health Service (HHS).

Townsville HHS, in collaboration with two other northern Queensland HHSs, obtained funds to employ Research Fellows to build research capacity. The funds were negotiated under a Queensland Health Industrial enterprise bargaining agreement (EBA) in 2008 with the first Fellow commencing in 2010. Altogether, the three Health Services employed three Research Fellows and a Professor of Allied Health. The funds were re-negotiated as permanent positions two years into the 3-year agreement resulting in fulltime Research Fellows in Cairns and Mackay, a part-time Research Fellow in Townsville and loss of the Professor. The remit of the Fellows was to build research capacity, publish and present their own research, and supervise higher degree research students.
In 2010, research activity in allied health at Townsville HHS was predominantly journal clubs and data collection with little or no allied health-led research. Results from a staff survey conducted in 2011 indicated low levels of experience but high levels of interest in research among allied health.
Therefore, initial efforts were raising awareness, presenting introductory research education sessions, attending staff in-services, and meeting individuals with a potential project. We explored why some allied health staff flourished as researchers despite the full-time clinical
load and low levels of research infrastructure and support processes.
Our study found flourishing researchers followed a research trajectory of 4 phases: debut; building momentum; developing a track record; and becoming an established researcher. We subsequently planned research support around these four phases.
For the debut phase, research education provided by the HHS (and online) or the Doctoral Cohort program at James Cook University (JCU) was the primary intervention.
Next, emphasis moved to providing support and mentoring of staff and upskilling in skills needed by researchers but not specifically supported by research education.
For example, scientific writing, data visualisation and design to improve allied health research presentations and most importantly upskilling in a variety of research methods. This latter support was facilitated through collaborations with experts in health economics, discrete choice experiments, systematic reviews, qualitative and mixed methods from JCU and other partner universities.
Since 2010, we have measured indicators of research activity including publications, grants and higher degree students.
The evolution of regional allied health clinicianresearch leaders.
The early years are marked by few publications and grant success with an upturn when allied health started enrolling in higher degrees (first candidates enrolled in 2014) with increasing publications starting in 2016 suggesting a lag time of 2-3 years for students to become productive (Diagram 1).
A steady increase has occurred over time such that in 2021 there were:
• 50% of allied health disciplines or multidisciplinary teams were research active
• 19 peer reviewed publications across eight disciplines as diverse as pharmacy, radiation therapy, physiotherapy, occupational therapy and medical imaging.
• more than $1.2 million (our highest to date) in grant funding,
• four staff members received research awards,
• 1 PhD candidature confirmed and 12 staff members enrolled in PhD.
Latter stages of the research trajectory are now being supported and implemented as staff progress as early career researchers. Examples include PhD graduates developing their track records by supervising honours or PhD students, applying for Category 1 grants, and encouraging others by establishing communities of research practice within their own disciplines.

Several staff members are building expertise in specific methods (e.g. health economics, DCE, qual methods, systematic review and translation and implementation science). Support directed to assisting staff to develop a
Garde (psychologist and PhD candidate), Alex Ryan (pharmacist and PhD candidate), Stephen Perks (pharmacist and PhD graduate),
to R back:
An important aspect of our efforts is taking time out to recognise achievements of allied health researchers. Celebrations mostly centre around publications, especially for first time publishers but also as a networking event to stimulate interdisciplinary research.
The aim of allied health research at THHS is, as yet, aspirational. Within 10 years we aim to establish a centre of research excellence for allied health research focusing on research methods rather than a discipline or disease, with the intention of increasing interdisciplinary collaboration.
The mechanism to fund the centre is via Category 1 grants and will develop over time as the current research leaders establish themselves as researchers. Progressively, we aim to increase human resources by employing research coordinators and fractional allied health clinicianresearcher positions. These aims are currently being planned as part of our research strategy to guide future allied health researchers at THHS.
Author: Dr Tilley Pain is the Health Practitioner (HP) Research Fellow at Townsville HHS and Adjunct Associate Professor at James Cook University. She commenced in the position in 2010.
 research track record aims to build local research leaders. The regional location of our health service increases the difficulty of recruiting to both clinical and research positions, necessitating growth of local researchers.
L
Vidula
Kelvin Robertson (pharmacist and PhD graduate), Amy Brown (radiation therapist and PhD candidate)
research track record aims to build local research leaders. The regional location of our health service increases the difficulty of recruiting to both clinical and research positions, necessitating growth of local researchers.
L
Vidula
Kelvin Robertson (pharmacist and PhD graduate), Amy Brown (radiation therapist and PhD candidate)
When your research skills need brushing up along the way, the challenge becomes even greater. So, when I found a research question that intrigued, inspired and smouldered within me, I knew I was finally ready to embark on some serious research.


As a clinical dietitian in a tertiary hospital, I was often confronted with clinical problems that I knew required more research to ensure that our dietary interventions were delivering the best possible outcomes for our patients. Although we consult the scientific literature regularly to confirm our interventions are in line with current best-practice guidelines, there are many gaps in the research that are waiting to be filled. It seems obvious that these questions are best identified and answered by practising clinicians, however there are many barriers to Allied Health clinicians embarking on research.

Even answering a simple research question takes a significant investment of time and resources.
Unlike many professions, Allied Health Professionals such as Dietitians rarely have protected time allocated to research in their contracts. Inevitably, the clinical caseloads become overwhelming and time for reflection on practice and formulating research questions evaporates. Sometimes our research training is no longer current, or not at the level needed to commence research independently. Additionally, we have few clinicianresearchers in our profession as mentors. So, there is a sense of not quite knowing where to start, who to ask and whether research will fit into a busy life. These all applied to me, and I needed a spark to ignite the will to overcome these barriers.
Working as a Diabetes Dietitian brought with it frustration that, despite good adherence to evidence-based dietary recommendations, many women I saw with gestational diabetes (GDM) still required insulin therapy to achieve optimal blood glucose levels.

I came across research suggesting that a higher dietary intake of a kind of fibre called resistant starch could enhance the gut microbiome of people with diabetes and lower blood glucose levels. This had not been tested in GDM women, but I thought it might work. Here was my spark, which became a burning desire to find out if my hunch was right.
I read as much as I could to determine whether my theory seemed plausible. I identified what kind of research I wanted to do to answer my question but knew that I needed structured guidance from experienced researchers. I finally contacted Professor Amanda Devine and Associate Professsor Claus Christophersen at Edith Cowan University who had substantial track records in dietary interventions to modify the gut microbiome. They outlined how a PhD program worked and how they could support me as PhD Supervisors. It was a daunting thought to commit to so many years of study on top of my job. Yet, I enrolled knowing clearly that this was what I needed to do to answer my burning question.
With my supervisors’ guidance, grants from the Spinnaker Health Research Foundation and the WA Chief Allied Health Officer, and utilising the many resources available to me at South Metropolitan Health Service, I am now conducting a hospital-based randomised control trial. It is investigating if a higher dietary intake of resistant starch can alter the gut microbiome of women with GDM and improve their blood glucose levels. In turn, we hope to optimize health outcomes for both the mother and
child. These include reducing the requirement for insulin therapy, reducing neonatal admissions to intensive care and passing a healthier gut microbiome on to the child. This simple dietary strategy has the potential to be a costeffective solution to a real-world problem. It continues to inspire me to carry on the research and I am learning many research skills along the way.
I trust that I can use the knowledge and experience I am gaining to help other Clinical Dietitians take the first steps to develop more research-oriented clinical career paths. I share the practical aspects of my research journey and accomplishments with my colleagues. I hope to clarify the research processes and encourage more Dietitians to undertake a Higher Degree by Research. Their research contributions will directly improve clinical care, improve job satisfaction and provide an alternative pathway to building a satisfying career.
As the research capacities and participation of Clinical Dietitians and other Allied Health Professions increase, it will be important for existing career structures to be redesigned to recognise and reward clinicians with significant research output. The risk is losing their discoveries and expertise to academia, whereas, maintaining researchers within the clinical setting allows them to apply their knowledge to patient care routinely, continue to embed it into the practice of their teams and fuel the enthusiasm of the next wave of clinicianresearchers. As I share my research journey with my colleagues, I hope that I will be the spark that ignites the possibility of a research pathway for others.
Author: Cathy Latino, AdvAPD, CDE, is a practising Clinical Dietitian and a PhD candidate at Edith Cowan University
Central to accelerating healthcare innovation and leading research impact, clinician-researchers are ideally positioned to drive healthcare transformation.
Nationally, the lack of a consistent career pathway and strategy for clinician-researchers is recognised as a significant barrier to realising the healthcare, research, community, experience and global benefit.
Sandra was a dedicated senior physiotherapist with 14 years of clinical expertise in adult neurology, leading an evidence-based approach to practice with a keen interest in research. Motivated to further her career, she gained a PhD scholarship in her clinical specialty area whilst working part time.
At the conclusion of her PhD, after successfully balancing research and clinical commitments, she reverted to her substantive clinical role with no quarantined time for research nor acknowledgement of her specialised postgraduate qualifications. Models to continue her clinicalresearcher career pathway were explored, however, no such roles existed and the health organisation was not able to create such a position.
Disillusioned, Sandra resigned from her clinical role to become a full time academic. This loss represents a key barrier to achieving a dynamic, self-improving health system. Clinician-researchers are central to accelerating healthcare innovation and implementing evidence into practice.
Research-intensive health services have lower patient mortality rates, increased staff retention, increased patient and staff satisfaction, and greater organisational efficiency. Clinicians working in the health system at the ‘front line’ have capacity for leading both clinically relevant research and research translation.
Research led by, or involving, clinician-researchers addresses issues encountered in clinical practice,
A call to action for a national strategic framework for clinicianresearcher career pathways.CHRISTOPHE KEREBEL CHRISTOPHE KEREBEL CHRISTOPHE KEREBEL My Twitter : @chriskere
improves timeliness and effectiveness of translation of research and ultimately improves patient care and outcomes.
This is best illustrated through the exemplar of medical clinical-academic career pathways. These are jointly funded academic and clinical roles which incorporate research as a requisite of formal training and demonstrate how an articulated pathway of embedded research can drive and shape research-informed care.
Among newer professions such as allied health, and diversified nursing professionals in highly specialised and extended scope roles, the appetite for clinician-researcher career pathways is increasing.
Despite fulfilling an essential role as key pillars underpinning the health workforce, clinician-researchers in allied health and nursing disciplines working in the health system are underrepresented in the clinician-research workforce.
The reasons for this are multifactorial, including both cultural and capacity priorities. It is time to re-think career pathways where clinical work and research activity are no longer considered mutually exclusive but rather cohesive, complementary and integrated.
By applying a strategic vision to development of a national career pathways framework, we can create a nextgeneration health workforce that is actively engaged in and leading research. This will benefit patients and the healthcare system alike.
A key challenge in sustainable integration of research into clinical care is the lack of articulated career pathways in which allied health and nursing professionals can progress as a clinician-researcher. There is a need for implementation of a system-level and organisation-wide approach to improving research capacity and culture for allied health and nursing professionals.
Evidence-based implementation interventions to improve research capacity at an organisation level include: embedding research in role descriptions and KPI’s; including research activities in strategic and operational plans; and implementing research leadership in the form of conjoint academic roles.
At a team level we can embed mentors and colleagues who are research active, instilling a culture of research excellence and research that is close to practice; and build on existing networks to grow partnerships. At an individual level we need tacit knowledge transfer; including how to use evidence in practice and write grants; provide protected time for research; and identify and resource emergent clinician-researchers.
Health professionals, by nature and definition, are high academic performers. As such, there is a demand for career growth and development that nurtures and sustains our very best performers in a long and productive career in healthcare.
The imperative now is to retain research-active allied health and nursing clinicians, to avoid them leaving front line health care positions to migrate to academia or other industry. Despite well-described interventions to improve capacity and culture, there is no established model for embedding the well-recognised interventions to improve talent retention.
Relationships and creation of mutually beneficial pathways with universities and government bodies will enable sustainable integration of research culture and capacity within the healthcare sector.
These partnerships can create the capacity to nurture current and potential allied health and nursing clinicianresearchers and facilitate a cultural shift that allows every clinician to regard research as part of routine healthcare. Focusing on those professions where these pathways do not exist will afford new opportunities for research, career growth and better healthcare for all.
Author: Dr Paula Bray is Director of Research for the Sydney Children’s Hospitals Network. Clinical Associate Professor Merran Findlay is a Sydney Health Partners Research Translation Fellow; Maridulu Budyari Gumal (SPHERE)
Cancer Clinical Academic Group Senior Research Fellow; and Advanced Accredited Practising Dietitian. The authors wish to thank Professors Jennifer Allison and Andrew Bailey for their passion, stewardship and partnership in this work.
Humans are social beings. The importance of social connection for our health and longevity is well documented. Being part of a social group provides us with important psychological resources to support our health – giving us a sense of belonging, purpose, self-esteem and support.
Being social also protects us against declines in mental and physical health, including lowering blood pressure, increasing cognitive function and reducing depression, to name just a few. Research shows this to be the case with healthy adults within the general community population and with adults who are experiencing clinical levels of mental ill-health.
Interventions for loneliness have, traditionally, been individualist in focus – either training the individual in social skills, or organising opportunities to create friendships. For example, pairing a lonely person in aged care with a young person.
However, the effectiveness of these interventions was described as “disappointing” in a 2010 meta-analysis by Masi and colleagues, achieving “at best, modest improvement but not recovery”.
The Groups 4 Health Program (G4H) is different because it builds on the social psychological science of how social connection works, and focuses on building group-based belonging rather than individual cognitive change or oneon-one friendships. It has the best supporting evidence of any loneliness intervention in the world.
Created in 2014, led by researchers Cath Haslam and Tegan Cruwys at the University of Queensland (UQ), the intervention is a group-based psychotherapeutic program, accompanied by a facilitator manual and participant workbook providing guidance on the topics and skills to
be covered in each session, that focuses on empowering people to build meaningful social group connections.
It is suitable for use by any practitioner with training in supportive counselling skills including social workers, teachers, allied health professionals, and of course, psychologists.
Clinical trials undertaken by the Australian National University (ANU) and UQ show that it outperforms standard care for loneliness, and is comparably effective for depression as other ‘Treatment As Usual’ that people may have been accessing, including the gold standard of Cognitive Behavioural Therapy (CBT).
The most recent clinical trial found that participants in the G4H program maintained their lowered levels of depression at a similar rate to CBT, 12-months post program. Perhaps more importantly, G4H outperformed CBT in its effectiveness in reducing loneliness in a postprogram follow-up.
G4H is potentially suitable for any population experiencing or at risk of loneliness, including those going through a life transition. For example, we know that loneliness predicts the health of a person in retirement four times more strongly than their financial status. Retirees routinely receive support for financial planning; why not social planning?
Multiple adaptations of the program are currently in use within Australia and internationally, including adaptions that target substance use (Groups 4 Belonging), long-term hospital stays (Groups 4 Health: Going Home), retirement (Groups 4 Health: Retirement), and integration into new educational settings (Groups 4 Education). There are also plans for a version for people with chronic disease to be combined with a lifestyle management program (Groups 4 Diabetes) pending funding.
The Groups 4 Health program was recently accepted for publication in the Treatments that Work Oxford University series, an honour reserved for those behavioural interventions with only the strongest evidence of efficacy, and will soon be available for purchase globally.
Clinical and social psychology researchers have created a group-based program that addresses social isolation and loneliness, decreasing the burden on the healthcare system.

The five-year DAP+ program, worth $12.4m, will see the creation of a ‘medibus’ that is equipped to be a clinic on wheels delivering diabetes care to vulnerable communities.
This builds on the existing work of the Diabetes Alliance Program (DAP) developed by Hunter Medical Research Institute (HMRI) researcher, Associate Professor Shamasunder Acharya, Clinical Director of Endocrinology at Hunter New England Local Health District (HNELHD) and his team.
Associate Professor Acharya says, “DAP was first established in 2015 because specialists and GP practices were working in isolation. We saw a need to integrate them. Our key vision has been to enable GP practices to deliver high quality clinical care to the majority of patients with diabetes, while at the same time providing timely access to those who need specialist referral to a tertiary referral centre.”
The DAP program proved so successful that the team started to look for ways to expand its reach in rural and regional areas, boost its specialist workforce and build on the existing research into the impacts of nutrition, exercise and healthy ageing.
A medibus model of care was identified as the most effective way to meet these goals, while also enabling specialists to visit indigenous community members in their towns or even in their homes.
Michael DiRienzo, Chief Executive of HNELHD, explains, The bus will allow us to take specialist multidisciplinary teams including endocrinologists, diabetes nurses, dietitians, Aboriginal health workers and podiatrists to rural and remote towns that may not have access to these services locally.
“These clinical teams will provide training to local providers, and directly care for patients in a way that empowers them to better manage their own condition,” said DiRienzo.
One in 10 people - around 1,000 000 - in the Hunter New England region have been diagnosed with diabetes. People living in disadvantaged areas are more likely to develop the disease and are less likely to receive timely treatment. It is one of the health system’s biggest challenges, costing an estimated $14.6 billion each year – and its unmanaged progression leads to higher rates of heart attack, amputations, strokes, kidney failure, blindness and even premature death.
“DAP+ is specifically designed to improve evidence-based diabetes care in rural and remote areas, so it’s fitting that we will be able to drive our specialists to where they’re needed most and deliver the program on the ground,” said DiRienzo.
The model of care can also easily be customised for rapid application to other chronic and complex health conditions, which could have a big impact on health outcomes for rural and remote communities.
The Diabetes Alliance Program is a joint initiative delivered by HMRI, HNELHD, the Hunter New England Central Coast Primary Health Network (HNECCPHN) and the University of Newcastle.
For more information about the Diabetes Alliance Program, click here: Diabetes Alliance - Primary Health Network (thephn.com.au)
Author: Associate Professor Acharya is the Clinical Director and Senior Staff Specialist in Endocrinology and Diabetes at John Hunter Hospital, Hunter New England Health District. His goal is to build the Diabetes Alliance across the Hunter New England health district, focusing on rural and remote regions. He is also developing online Post Graduate Learning courses in Diabetes and Endocrinology, including a Master’s program with University of Newcastle, aimed at Australasian and Indian subcontinent health care workers.
Thanks to a record-breaking donation from the Colonial Foundation, the next phase of the Diabetes Alliance Program (DAP), dubbed DAP+, will bring much-needed support to regional and remote areas.
Nurses, midwifes and academics unite to build clinical research capacity in regional NSW

ANSW Regional Health Partners initiative between the University of Newcastle, and the Hunter New England, Central Coast and Mid North Coast Local Health Districts is building nursing and midwife research capacity, engagement, impact and leadership.

Clinical Nurse Consultants (CNCs) and Clinical Midwife Consultants (CMCs) are pivotal to delivery of high quality and safe healthcare, through provision of clinical leadership and delivery of evidence-informed practice. Research is an embedded domain of practice for CNCs and CMCs, recognising the essential role research plays in driving quality care and practice improvements and to respond to clinical practice gaps. Research skills and access to research support varies greatly, particularly for those working in regional centres. For CNCs and CMCs to conduct research, a need exists to build research skills, foster collaboration and provide access to research expertise and mentorship.
The School of Nursing and Midwifery (University of Newcastle) partnered with the Mid North Coast, Central Coast and Hunter New England Local Health Districts to establish an innovative program of CNC and CMC research capacity building. Funded and supported by NSW Regional Health Partners, a NHMRC accredited Research Translation Centre (Regional, Rural and Remote), the ClinicalRCB project was born.
Led by Professor Leigh Kinsman and with project management from Adam Quirk, ClinicalRCB aims to build CNC and CMC research capacity, engagement, impact and leadership, through a collaborative program. The program supports the 420 CNCs and CMCs employed by the three health districts, who work across diverse geographies and disciplines, and with varying levels of research experience.
Central to establishing this program was the development of a virtual meeting space with embedded access to digital resources. The digital platform (www.clinicalrcb. com) is an online community that provides CNCs and CMCs access to colleagues, communities of practice, resources, research expertise, peer support, discussion forums and news of upcoming events. This platform was developed through a co-design process with academic and health service staff, and web design experts.
A governance structure, developed to ensure ClinicalRCB operated in line with its purpose, includes a Leadership Team, comprising Clinical Directors of Nursing and Midwifery and senior nurse researchers from each local health district, Head of School for Nursing and Midwifery, University of Newcastle, and professoriate from two
Attendees – ClinicalRCB Conference 2022, Crowne Plaza Hunter Valley
regional universities (University of Newcastle and Charles Sturt University). The Leadership Team meets monthly to direct activities and monitor progress and is supported by an expert Advisory Committee that meet quarterly to provide strategic advice and leadership.
Implementing the program of research capacity building initiatives involves five main areas:
• Broad consultation: University and local health district staff participated in co-design workshops to identify facilitators of engagement, resource requirements and local research priorities.
• Online Community of Practice: A Learning Development Team developed a framework and resources to embed the Community of Practice into the digital platform.
• Establishing Teams and Themes: Through member-wide consultation, initial priority research themes were identified and grown into Communities of Practice, supporting collaborative research efforts and partnerships.
• Annual conference: Given the geographical spread of ClinicalRCB participants, an annual two-day conference fosters face to face network building, and provides hands-on training in research skills through developing research projects within Teams and Themes.
• Mentorship: The platform includes a mentorship program, with academics, CNCs and CMCs able to request a mentor or mentee to grow their research and leadership skills.
With more than 150 participants now engaged in the project, ClinicalRCB has surpassed its initial goal of supporting 15% of the local CNC and CMC workforce. Contributing to the success is the level and strength of engagement of CNCs and CMCs – as participants in consultation, co-design workshops, the Communities of Practice, and the conference.
This speaks to the need and demand for this program, as well as the appropriate methods used to support engagement. This however could not have been achieved without the support of nursing and midwifery managers within the local health districts, who provided release from work, back-filled positions and supported attendance at the ClinicalRCB conference. Further, support from the University of Newcastle allowed three School of Nursing and Midwifery early career researchers to contribute to the

annual conference, participate in workshops, and join the advisory team to inform future programs.
The immediate benefit of this project is its success in supporting and guiding CNCs and CMCs to fulfil the research domains matched to their appointment grade. This enhanced capacity increases the ability of CNCs and CMCs to positively influence practice through research. Approximately one third of all CNCs and CMCs have engaged in the project and more than 40 CNCs, CMCs and their academic partners have developed new research proposals.
The impact of this project will be realised in the longer term, with improved service delivery and patient outcomes achieved through research.
From the university perspective, the project provides recognition for industry partnerships, work integrated learning and engagement and impact. Strong clinicalacademic partnerships and new cross-health district collaborations fostered through ClinicalRCB form the bedrock for ongoing research that can respond to recognised local health service needs. The framework and
resources built for ClinicalRCB can be adapted for other professional groups across broad geographical distances.

All nursing and midwife researchers in our regions are encouraged to join ClinicalRCB. With continued engagement from CNCs, CMCs, and academic partners, together with support from the Local Health Districts, Universities and NSW Regional Health Partners, ClinicalRCB can continue to support CNC and CMC active engagement in research to improve care and health outcomes for our communities.
Authors: Chief Investigator and current project lead Professor Kerry Inder, project manager Adam Quirk, the School of Nursing & Midwifery, University of Newcastle and Associate Professor Nicolette Hodyl, Director, NSW Regional Health Partners. The authors acknowledge the project funding support from NSW Regional Health Partners and contributions from the research team and advisory committee. Special thanks to Professor Leigh Kinsman for leading this initiative, Lisa McFayden for ongoing support, and the research team and advisory committee.


Rehabilitation clinicians provide vital services to people who have been injured or are disabled through traumatic brain, spinal or musculoskeletal injury or amputations. They are thirsty for knowledge about how to improve those services and through a unique long-term partnership with Griffith University, they are building evidence into their daily practice.
Clinicians are critical to solving the challenges faced by people with disability, so the best solutions are likely to be those developed in partnership with clinicians and consumers. This idea has underpinned the Clinical Fellowship Academy at the Hopkins Centre, the result of a long-term partnership between Metro South Health Division of Rehabilitation, Griffith University, the Motor Accident Insurance Commission, and consumer organisations such as Spinal Life Australia and Synapse.
Co-Director of the Hopkins Centre, Professor Elizabeth Kendall, said the centre cultivates a unique culture defined by knowledge mobilisation and deep collaboration between rehabilitation clinicians, academic researchers, community practitioners, policymakers, citizens, and service-users with disability.
“The Hopkins Centre Clinical Fellowship Academy was established to harness the leadership, expertise and knowledge of clinicians, partnering them with academic researchers and citizen scientists where needed and supporting them to solve the challenges they face in their own daily practice”, she said.

Clinical Fellowships vary, but could extend up to two years, during which time clinicians’ existing roles are backfilled. They enter the Academy where they are mentored and supported to design research. Their research directly responds to challenges they have identified in their practice, which allows healthcare organisations to convert those findings into new ways of working.
Eight Clinical Fellows have been supported by the Academy, producing new knowledge, resources and approaches that are now embedded in practice. They have also advanced the research skills and capacity of other rehabilitation staff and have contributed to a research culture within the rehabilitation units. The projects covered by clinician-researchers have been diverse, covering a wide spectrum of ideas. Physiotherapist, Brooke Wadsworth designed and implemented new ventilator procedures in critical care in response to challenges she observed in practice. In another project, Kylie Bower, an Occupational Therapist, explored the clinician-researcher role, with the view to build capacity, confidence, resources and understanding in research for rehabilitation clinicians.

Working in a busy clinical setting, she developed a research capacity building model that highlights the need to keep research close to practice, sustained in practice and champion research into clinical service delivery.
Occupational Therapist, Soo Oh developed and evaluated a service to improve therapist confidence in prescribing life changing technology. Her work has resulted in an ongoing service known as HabITec which is driven by people with disability and engages engineers, software design students and practitioners from all disciplines.
Senior Speech Pathologist, Kate Cameron explored changes in the ability to communicate following an acquired brain injury, developing much needed supports, resources and tools to better support people with cognitive communication issues returning to work. Using the Knowledge-to-Action process framework, key clinical tools for assessing cognitive communication skills were developed and integrated in to existing vocational rehabilitation services.
Another Speech Pathologist, Clare Morgan trained community members to be supportive conversation partners for people with brain injury who were returning to their community after rehabilitation. Physiotherapist Delena Amsters developed a model for consumer engagement in the design of services and systems that continues to drive the Hopkins Centre and it’s partners.
Physiotherapist Glen Verner-Wren is one of the most recent recipients of a clinical fellowship. He has been exploring solutions to optimise processes for the management of people with spinal cord injury.
People with spinal cord injury are individuals with unique issues and perspectives and our embedded Researcher-Clinician mechanism allows us to implement the best possible care,” said Glen.
Glen’s fellowship was a clinical redesign project aiming to optimise the care management of people with a newly acquired spinal cord injury (SCI). It aimed to improve seamless clinical processes and expertise across acute and rehabilitation for the benefit of quality care for patients with a SCI where there are known transition delays. He found that there is some variability in rehabilitation transition waiting times and that there are areas where processes of care might be improved to manage these patients. His fellowship has led to direct improvements in the way care is delivered to people with SCI including:
• Introduction of a joint ward round (orthopaedics and SIU)
• New equipment for the orthopaedics team to care for SCI
• A formal education program for nursing staff
• A care pathway report for the management of people with SCI
By improving the interface between acute and rehabilitation services, it is anticipated that people with SCI and orthopaedic injuries will receive better and more rapid support, leading to better outcomes, improved staff satisfaction and hospital wide efficiencies.

Dr Verner-Wren says, ‘This research is really important because it has involved working with the clinicians, stakeholders and people with a SCI to come up with tailored solutions to improve how we provide care to people who have just had a SCI.

Feedback from staff and patients highlight how these initiatives have led to better clinical care for people with an acute SCI, improved education for clinicians managing acute SCI and more effective communication and collaboration between acute and rehabilitation work areas.
Clinical fellow and Nurse Dr Letty Burridge is another example of the success of The Hopkins Centre clinical fellowship program. Dr Burridge’s research built on a successful mentorship program for rehabilitation clinicians, developing a research masterclass for nurses and physicians to build research capacity and close links between best practice and rehabilitation research. The fellowship project identified key research skills, engagement, experience, priorities and training needs of medical officers in rehabilitation. Her work has enabled medical officers to apply for grants, fellowships and to be more involved in research.
She developed practical research training modules for busy medical offers using small steps in a self-paced form to fit around clinical work. The modules were pilot-tested and interactive worksheets were established. Dr Burridge helps coordinate a stream of research to enable people to be meaningfully engaged with research that is relevant and seeks to design and deliver care that is personcentred. She developed learning materials and events to support clinicians in the practicalities of building their research capacity and an interactive 2 hour workshop.
Her fellowship has been an important part of engaging medical officers in growing their research capacity, developing a research knowledgeable workforce, generating interdisciplinary priority driven research, and building collaborative research partnerships for practice implementation.
“These clinical fellowships have allowed us to translate bold ideas into better solutions where and when we need them” said Prof Tim Geraghty, Director of Division of Rehabilitation at Metro South Health and co-Director of the Hopkins Centre. “They have expanded our ability and stretched the boundaries of our current knowledge so we can really focus on the needs of the people we serve”.
Clinicians have enjoyed having the opportunity to learn research skills and improve their performance, but there are also significant benefit to academic researchers who are linked with clinical researchers and embedded into the clinical or community setting. Prof Geraghty said, “Our academic researchers aren’t simply providing knowledge from an ivory tower, they are heavily invested in the clinical setting and engaged in delivering practical rehabilitation services, so they have a strong connection to the translation of their research into sustainable solutions so they value their partnership with clinicians and consumers.” As time has passed, the boundaries that divide clinicians, researchers and consumers have disappeared, making collaboration even easier.
For people living with rare diseases, expert clinicians can also be rare. Researchers, rarer still.
Too often these critical roles remain unconnected. So the rare disease clinicianresearcher is a precious thing. Dr Nicholas Smith, a paediatric neurologist at the Women’s And Children’s Hospital, Adelaide, has been a focal point and driving force for the Sanfilippo research community in Australia.
Clinician researchers serve an important role integrating efforts to improve patient outcomes. They provide a common touch-point for all stakeholders - patients, families, researchers and industry. They can gather these common threads, help focus attention where it is needed, and catalyse the sharing of information and resources.
For Sanfilippo syndrome these needs are great. It is a rare lysosomal storage disease that robs children of their ability to communicate, think, play and move, and takes their lives before adulthood. No treatments are yet available, only supportive care and symptom management.

These children have a form of dementia and I see first-hand the toll it takes on families and their many unmet needs in terms of managing the disease and of course the pursuit of a cure,” says Dr Smith. “This is what drives me into the laboratory and fuels my own research to develop therapies for Sanfilippo and similar diseases.”
Beyond his own research, however, Dr Smith has acted as a seed around which a small but growing army of Sanfilippo researchers have crystallised. Not least of these is his close partnership with Professor Kim Hemsley of Flinders University who heads the Childhood Dementia Research Group. She has been studying Sanfilippo pathology and developing experimental treatments for the condition for over 20 years. This powerful combination of clinical and laboratory expertise has allowed them to form productive research partnerships with industry and drawn in numerous collaborators from the fields of adult dementias, neurodegenerative diseases and neuroinflammation.
The pair co-lead the MRFF-funded flagship research project of the Sanfilippo Children’s Foundation, known as Brain in a Dish. They teamed up with adult neurodegenerative disease and iPSC expert, Associate Professor Cedric Bardy from the South Australian Health and Medical Research Institute, and neuropharmacologist Professor Mark Hutchinson from the University of Adelaide. Together they have developed a panel of patient-derived iPSC neuronal cells to screen for repurposed drugs that might alter the disease course. Dr Smith’s role in this fruitful collaboration is crucial - his strong rapport with families supports patient recruitment, his coordination of medical teams ensures the seamless collection of samples from children with complex medical needs, and his contributions to the ongoing guidance of the project means it always remains focussed on the needs of families.
He brings these same qualities to numerous projects ongoing around Australia and globally, many of them funded by the Sanfilippo Children’s Foundation and their partner patient organisations around the world. The projects include fundamental studies to identify the pathological pathways at play and projects aiming to identify biomarkers for disease progression, tools vital for clinical trials. “As a clinician my eye is always on the translational pipeline, the feasibility of therapeutic targets and creating change for families,” says Dr Smith.
Clinical trials, of course, would be nearly impossible without a well-connected, pro-active and driven clinician-researcher, particularly for a rare disease in a


geographically distant, population-challenged country. Dr Smith played a vital role in establishing the first ever Australian arm of a gene therapy clinical trial for Sanfilippo syndrome. The excitement and hope that this brought for Australian families cannot be underestimated. Even those whose children could not participate could see that this meant change was on the horizon for families in the future.
Dr Smith is clear on what he feels to be his responsibilities. “For a rare disease like Sanfilippo syndrome, many challenges remain in bringing these hopes to fruition. But I feel that as both a clinician and a researcher I can really contribute by connecting the dots and sharing resources. These challenges are not insurmountable.”
Dr Smith is indeed a rare gem, and although he rallies a network of clinical colleagues around Australia to the cause, he still needs to squeeze more working hours into a week than would seem humanly possible or desirable! Greater support is needed for these rare and vital conduits for translational research who increase the flow of knowledge between patients and laboratories and back to patients again.
Sanfilippo Children’s Foundation is enormously grateful for the work of Dr Smith and his colleagues around the world who fight tirelessly for children and families with these devastating conditions.
Author: Dr Lisa Melton is Head of Research at the Sanfilippo Children’s Foundation, a not-forprofit organisation that funds medical research into Sanfilippo syndrome, a form of childhood dementia.
As a young audiologist, Associate Professor Chris Brennan-Jones experienced constant frustration and sadness from seeing a child’s ear health made significantly worse by the long wait for treatment.

Entirely preventable when treated early, otitis media (OM) can cause permanent hearing loss and lead to serious, lifelong complications impacting language development, education and employment prospects.
Affecting 650,000 Australian children each year, the treatment of ear disease comes at an annual cost of $400 million for Australia’s public health system. Unfortunately, the conventional hospital service model is unable to accommodate the demand for OM-related services, and children are forced to wait more than two years for a specialist appointment and treatment.
For A/Prof Brennan-Jones, this delay was far too long, so the highly skilled clinician-scientist from the Wesfarmers Centre of Vaccines and Infectious Diseases at Telethon Kids Institute, Curtin University and Perth Children’s Hospital has spent nine years dedicated to researching the prevalence of ear disease, optimal treatment and barriers to equitable service provision.
“If you can’t hear, you can’t learn, meaning kids fall behind their peers in the crucial years leading up to starting school. Unfortunately, Aboriginal children are disproportionately affected by this – 50 per cent of Aboriginal kids living in metropolitan Perth experience persistent OM and hearing loss by six to eight months of age,” A/Prof Brennan-Jones said.
“Our research has demonstrated that by their first birthday, 69 per cent of Aboriginal children were experiencing significant hearing loss. The average hearing level of children in our study was just over 40 dB, meaning it would be difficult for them to hear voices clearly, and delays in treatment only exacerbate this.”
Collaborating closely with clinicians, health services and Aboriginal Community Advisory Group members, A/Prof Brennan-Jones and his team explored opportunities to fast-track the diagnosis and treatment of ear disease in young children.
In 2018, they developed a new diagnostic approach called the Ear Portal program, utilising cutting-edge telehealth technology and support from local health workers to obtain high-quality images that would enable remote diagnosis and management by ear specialists.
Designed to improve efficiency without compromising accuracy, the results of the Ear Portal speak for themselves – slashing wait times down from two years to just four weeks and substantially reducing costs to the healthcare system.
Four years down the track, the multi-award-winning program has now been implemented across multiple health regions in Western Australia. “It’s an absolute privilege to work alongside so many dedicated Aboriginal Community Advisory Group members and collaborators to achieve such a fantastic result for the kids, including Austal, Cockburn Integrated Health, Perth Children’s Hospital ENT and Audiology Departments, Child and Adolescent Health Service, Moorditj Koort Aboriginal Corporation, South Coastal Babbingur Mia, East Metropolitan and South Metropolitan Health Services, Dr Francis Lannigan, Dr George Sim, Hearing Australia, Telethon Speech and Hearing and St John of God Murdoch Hospital,” A/Prof Brennan-Jones said.
The new service also proved invaluable throughout the COVID-19 pandemic, with Perth Children’s Hospital using Ear Portal to establish a diagnosis for children with ear disease when access to the hospital was limited. And while A/Prof Brennan-Jones’ research in this field has generated breakthrough knowledge and policy change around the treatment of OM, the true measure of the success of the Ear Portal is the life-changing outcomes for families.
For many parents, it’s the sheer relief they feel when they have access to diagnostic services and treatment in their own community, with one saying “I think I would have lost my sanity without this service. Without it I would have lost my job. My child needed check-ups so often, I just couldn’t get enough time off work to travel to Perth.”
And for A/Prof Brennan-Jones, there is no better validation than the joy and relief on parents’ faces when their child gets the care they need, and the smiles on kids’ faces when they can hear their loved one’s voices again.
“For me, the power of the program can be measured the fact that these kids will be able to hear what their teacher is saying when they are ready to start school,” A/Prof Brennan-Jones said.
It means they can look forward to a bright educational future with dreams of potential career opportunities, rather than sitting bored in a classroom because they can’t hear what’s going on, falling behind, and eventually giving up on further studies.”
There are more than 25,000 Australians living with multiple sclerosis (MS), a disease of the central nervous system that affects motor, sensory and cognitive functions.

Although the cause and cure of MS is yet to be found, the last decade has seen significant advances in our understanding of the factors that contribute to its onset, and in the development of potential treatments. One of the people leading the charge is neurologist and clinician researcher Professor Bruce Taylor.
Since his 2007 appointment as a professorial research fellow at the University of Tasmania’s Menzies Institute for Medical Research Professor Taylor has been the recipient of more
Professor Bruce Taylor’s mission is to transform our understanding of the personal, environmental and genetic factors that contribute to the onset of multiple sclerosis, and translate research discoveries into effective interventions and treatments.
than 60 grants, including a prestigious NHMRC Investigator Grant for improving outcomes for people with MS.
As the recipient of an MS Australia incubator grant earlier this year, Professor Taylor and his team will update estimates of the prevalence (number of existing cases) and incidence (number of new cases) of MS at different latitudes in Australia.
MS has been consistently more common at higher latitudes (further away from the equator), including in Australia where occurrence in Hobart, Tasmania has been two- to seven-fold greater than sites in mainland Australia. This latitudinal gradient has been one of the strongest pieces of indirect evidence for the role of sun exposure and vitamin D in the development of MS.
Professor Taylor and his team recently found that rates of MS recorded in Hobart, while continuing to increase over time, are reducing in magnitude compared to those recorded at similar times in Newcastle, NSW from roughly two-fold to now almost equivalent. The reasons for this change, and to what extent this reduction in the latitudinal gradient may be nationwide, are unknown.
Through the incubator grant the team is setting up a multicentre study and building on these findings, measuring and comparing the prevalence and incidence of MS in three sites in mainland Australia in addition to Hobart, (which is at latitude 42.9): Geelong, VIC (latitude 38.1; Newcastle, NSW (latitude 32.5); and Townsville, QLD (latitude 19.3).
This study will provide a comprehensive survey of the epidemiology of MS across the latitudinal range of Australia. It will also help inform whether further study of modifiable lifestyle factors, such as sun exposure and supplement use, is required.
Professor Taylor is also the clinical lead of a groundbreaking clinical trial assessing the effects of magnetic brain stimulation (MBS) on MS.
The phase two trial known as TAURUS.2, which recently opened its doors to participants at the Menzies in Hobart, will eventually be rolled out across six sites nationally. It follows on from a phase one trial which found that MBS was safe and has significant potential to sustain brain insulation in MS. This in turn was based on laboratory work carried out at the Menzies led by Professor Kaylene Young, lead neuroscientist and co-lead investigator of TAURUS.2.
Many MS symptoms directly or indirectly result from the death of brain cells called oligodendrocytes. Oligodendrocytes protect nerve cells by producing an insulating substance called myelin and providing metabolic support. The death of oligodendrocytes leads to the loss of myelin (demyelination), formation of brain lesions and increasing disability.
There’s no treatment that addresses this issue directly, however in laboratory studies of mice MBS was found to increase the number of new oligodendrocytes producing myelin. MBS —delivered to patients by placing a magnetic coil over the head — non-invasively activates nerve cells in the brain to subtly change their activity, and it’s proposed that this will protect brain insulation in people with MS.
The TAURUS.2 team will measure the effect of MBS on trial participants’ MS symptoms including upper and lower limb function, cognition, fatigue, anxiety, depression, sleep and quality of life. They will also use advanced brain imaging techniques such as MRI to assess whether MBS effectively increases brain myelin levels in people with MS.
In October Professor Taylor was awarded a prestigious fellowship with the Australian Academy of Health and Medical Sciences. He was specifically recognised for how his research has transformed our understanding of the personal, environmental and genetic factors that contribute to the onset of MS, and why its progression is highly variable.
Note: Funding for the TAURUS.2 trial has been received from the Australian government (Medical Research Future Fund and Emerging Priorities Consumer Driven Research), the Irene Phelps Charitable Trust, the National Health and Medical Research Council and Multiple Sclerosis Australia
 Professor Bruce Taylor, Menzies Institute for Medical Research, Tasmania Author: Rachel Clemons, Communications Officer - MS Research and Translation, MS Research Flagship, Menzies Institute for Medical Research, University of Tasmania.
Professor Bruce Taylor, Menzies Institute for Medical Research, Tasmania Author: Rachel Clemons, Communications Officer - MS Research and Translation, MS Research Flagship, Menzies Institute for Medical Research, University of Tasmania.

Elif Ekinci is Principal Research Fellow in Metabolic Medicine at the University of Melbourne and Director of Diabetes at Austin Health. Passionate about improving outcomes for people living with diabetes, Associate Professor Ekinci has, for many years, seen the impact that clinical research – in particular clinical trials and digital innovations – has had on improving outcomes for people living with diabetes.
“As a clinician researcher, I see first-hand the impact of diabetes-related kidney disease – including foot ulcers, painful neuropathy and amputations – and how lifethreatening diabetes emergencies affect people living with diabetes and their families,” says Associate Professor Ekinci.
As a young doctor, seeing the positive impact clinical trials and diabetes devices and digital technologies were having on people living with diabetes in different clinical settings, Elif decided that in addition to looking after and caring for patients, she would ease their burdens by pursuing the latest innovations through clinical research.

With her most recent appointment as Director of the Australian Centre for Accelerating Diabetes Innovations (ACADI), Associate Professor Ekinci now has her sights set on improving the quality of life for people living with diabetes in urban, rural and remote settings, as well as in Indigenous communities.
The future looks bright. Thanks to the Australian Government’s Targeted Translation Research Accelerator program, a MRFF initiative, delivered by MTPConnect, as well as over 65 partners and a formidable team of researchers across the country, ACADI will deliver 18 innovative projects aimed at preventing and treating these serious and life-threatening complications.
In the process, she hopes that, over time, the innovations progressed by ACADI will have a significant positive
Over 1.5 million Australians live with diabetes, as do almost 500 million globally. Alarmingly, an additional 51 per cent more are expected to be afflicted by the disease by 2045.CHRISTOPHE KEREBEL CHRISTOPHE KEREBEL CHRISTOPHE KEREBEL My Twitter : @chriskere
impact on the Australian economy, and believes that ACADI is well positioned to improve the lives of thousands of Australians and millions worldwide.
I am confident that the establishment of ACADI will position Australia as a global leader by progressing innovations to address complications arising from diabetes,” says Associate Professor Ekinci.
“It will do this using a model for accelerating diabetes innovations and responding to key barriers currently slowing such innovations, including therapeutics, devices, in-vitro diagnostics and digital health products.”
As well as the promise of new treatments and innovations, ACADI will train future leaders, providing critical skills in clinical evaluation, translation and commercialisation, and will be a place of new ideas intersecting with innovation in diabetes.
“My research through clinical trials and cohort studies is really about elevating suffering that diabetes complications can cause to my patients,” she says.
“Essentially it’s posing and answering a series of important questions: “What can we do to improve patients’ kidney function?” “How can we improve painful neuropathy?” “How can we prevent hospitalisations due to low or high glucose levels?” “What can we do to reduce the risk of blindness?” “What can we do to prevent future heart attacks?”
As a medical student, with the support of a John Flynn Scholarship, Associate Professor Ekinci spent time at Maningrida in Arnhem Land. She recalls with fondness “a wonderful place where I had an unforgettable experience working with wonderful members of the community.”
The experience alerted Associate Professor Ekinci to the health disparities in rural and remote Australia, especially in Indigenous communities.
“What I saw was an insidious disease that struck people down at the prime of their lives,” says Associate Professor Ekinci, “leading to devastating complications such as kidney failure requiring dialysis, foot ulcers, amputations, strokes and heart attacks, and ultimately forcing people to leave their communities in order to seek specialist treatment such as dialysis.”
“In some of the worst-affected communities in Australia, Indigenous Australians are experiencing a 10-fold increase in kidney failure for people aged between 35–44 and an alarming eight-fold mortality attributed to CVD,” says Associate Professor Ekinci.
She believes that for too long, Indigenous Australians living in remote communities have been experiencing an earlier onset of diabetes, and complications such as kidney disease, blindness, cardiovascular disease and amputations at an early age.
Newly developed medications for diabetes have shown to be effective in reducing blood glucose and consequently the complications of diabetes including cardio-vascular disease (CVD) and death.
“We know that the social determinants of health matter here and that these include significant cultural losses and dispossession, racial discrimination and food insecurity.
These historical, social and other issues, including the influence of genetic factors, contribute to Indigenous Australians developing early onset and rapidly progressive forms of diabetes,” she says.
She feels that Indigenous leadership and governance of research projects, significant community engagement, co-design with people living with diabetes are important elements of study design. She is hopeful that trials of newly developed medications for diabetes and new diabetes technologies such as flash glucose monitoring which have been shown to be effective in reducing blood glucose and consequently the complications of diabetes including kidney disease, cardio-vascular disease (CVD) and death will have a positive impact on health outcomes for both Indigenous communities and the wider community.
Associate Professor Ekinci wants to ensure a future where people don’t develop diabetes complications and is committed to keep working to see fewer and fewer of the severe complications that she has seen over the course of her career.
She is just getting started.



Every nine minutes a child in Australia is born who is at risk of developing a neurodevelopmental disorder (NDD), with one in five Australian children living with an NDD.
Early detection and evidence-based intervention – within the first 1,000 days of life – are vital in order to get children and families the support they need and significantly improve outcomes.
But because we are currently unable to reliably identify difficulties in very young babies, all too often children –particularly those in poorly served regional, rural and outer metropolitan areas, are not diagnosed with NDDs until well after this critical early window of neuroplasticity.
Early Moves co-leads Professor Jane Valentine (left) and Professor Catherine Elliott.Our clinician-researcher-led clinical trial, Early Moves, shifts the paradigm to very early risk diagnosis: finding the right child at the right time (early) and in the right place (locally), and getting them into the right service.
Led by Curtin University and Perth Children’s Hospital (PCH) in collaboration with The ORIGINS Project and research partners across Australia, the Early Moves project is recruiting families from Joondalup Health Campus and St John of God Public and Private Hospitals Midland. It is the biggest study in the world designed to reliably identify early biomarkers of neurodevelopmental disorders.
Under the study, specially trained clinicians closely assess and score parent-captured smartphone videos of babies’ General Movements (GMs) – a set of specific movements only present up to the age of five months.
These three-minute videos, taken at key points within the first weeks and months of life and uploaded to a research app, give us a window into the brain of these developing babies and reveal clues that could flag later difficulties with movement. Early Moves aims to determine whether these clues can, in turn, help us reliably predict a range of NDDs.
Since starting in 2019 our team has recruited more than 2,200 out of a projected 3,000 babies, and we are already identifying children at risk of a variety of NDDs and fasttracking them into local health services and supports.
But another important goal is to translate what is currently a labour-intensive process that can only be undertaken by highly trained specialists into an AI-driven screening tool that can extend the relevance and impact of this research to the broader health system and community.
With the help of AI and machine-learning specialists including Professor Svetha Venkatesh and her team at Deakin University, our dedicated team is working to develop algorithms that can automatically score the assessments with a high degree of accuracy.
Once ready, this could see the program built into mainstream care across Australia and beyond – including to rural and remote areas, where babies identified as at risk of NDDs could be referred to appropriate services much earlier than currently possible.
This approach would not only reach more babies, but help reduce unnecessary screening and waitlisting of those on the normal spectrum – freeing up resources and specialist clinicians to concentrate on providing high level care and support to those who need it.
The beauty of Early Moves is not only the way it embeds research into clinical care and paves the way for rapid translation to ensure better health outcomes for more
children, but the way it is enhancing the workforce by training clinicians in the latest tools and techniques.
The project has already trained more than 20 clinicians to conduct specialised General Movement and child development assessments, many of whom are able to apply these skills working in other roles and workplaces across the Child and Adolescent Health Services (CAHS), Child Development Service (CDS) and the private sector. This number will rise significantly, with knowledge translation a key aim of the project.
Another critical ingredient has been the level of consumer and community involvement. Parents want to know if there are any concerns with their child’s development early so they can help maximise their child’s potential.
We have relied heavily on the support of our two consumer groups – one from The ORIGINS Project, one of our two recruitment sites; and one from Kids Rehab WA, a state-wide, integrated clinical, research, education and training unit headquartered at Perth Children’s Hospital. In addition, one of our chief investigators is a consumer representative.
Early Moves is a multicentre trial led by Curtin University and Perth Children’s Hospital and recruiting at Joondalup Health Campus through The ORIGINS Project, and at the St John of God Public and Private Hospitals Midland. Other research partners include the Telethon Kids Institute, The University of Western Australia, Murdoch Children’s Research Institute, UNSW Sydney, Mater Research, Griffith University, the University of Melbourne, the University of Queensland, the University of Sydney, the Australasian Cerebral Palsy Clinical Trials Network, and the Applied Artificial Intelligence Institute at Deakin University.
Early Moves is funded by a National Health and Medical Research Council Clinical Trials and Cohort Study Grant combined with a project grant from the WA Child Health Research Fund, and philanthropic support from the Cerebral Palsy Alliance, the Perth Children’s Hospital Foundation, Channel 7 Telethon Trust, and Mineral Resources Limited.
Aphasia, a condition experienced by more than 140,000 Australians, affects a person’s ability to communicate and typically occurs after a stroke or head injury.

People with aphasia often experience depression and social isolation, which can lead to reduced quality of life.
The development of innovative treatments that maximise the use of technology and provide tailored support for individuals to prevent these negative outcomes is the focus for leading researchers and clinicians in aphasia rehabilitation at the Queensland Aphasia Research Centre (QARC).
The Centre was established thanks to a $1 million gift from the Bowness Family Foundation and $500,000 from an anonymous donor in partnership with The University of

Queensland (UQ) and Metro North Health as part of the Surgical, Treatment and Rehabilitation Services Education and Research Alliance (STARS).
The QARC Director Professor David Copland said the experiences and opinions of people living with aphasia are central to the vision of the Centre.
To ensure the programs developed are meaningful and relevant our team of over 40 clinicians, researchers and students with backgrounds in speech pathology, psychology, engineering, software design, allied health, and neuroscience work closely with people with aphasia. We also engage expert advisory groups to ensure outcomes have maximum impact.”
An example of a program developed and run in partnership with people with aphasia is the Aphasia Tech Hub. It was set up to improve access to technology for people with aphasia and their significant others, as well as speech pathologists and healthcare providers. Current support includes advice on which technology might help to meet communication and life goals, demonstrations on how to use smart phones, tablets, therapy programs and apps, and technology coaching.
A major achievement for QARC has been the implementation of CHAT (Comprehensive High-dose Aphasia Treatment) by the Queensland Health team at the STARS hospital. The program, developed by the CHAT team is an eight-week therapy program tailored to individuals.
To date, 48 people have completed the CHAT program with more than 2000 hours of evidence-based, goal directed aphasia therapy delivered. Results have shown significant improvements in communication, confidence and quality of life with high completion rates and high participant/patient satisfaction.
A NHMRC Partnership grant will enable the CHAT program to be rolled out across seven Hospital and Health services with the support of five professional organisations/ networks in Australia. Led by Professor Copland the project will evaluate the effectiveness of implementing the CHAT program across multiple health settings.
The team have also developed an online equivalent of the CHAT program (TeleCHAT), enabling the intervention to be delivered in a person’s home via telerehabilitation. Early results are promising, suggesting a new approach to aphasia therapy that significantly increases accessibility.
The team have strong clinical backgrounds working in hospitals and community centres locally, nationally, and internationally. This enhances the relevance and
applicability of research conducted. Strong collaborations and communication between the QARC research team and clinical teams from over 40 partner sites across Australia enable translation of research into practice, the development of new clinical research ideas and increased clinical research capacity at hospitals. Several QARC team members have clinical positions in addition to their research positions. Rachel Levine is part of the QARC team investigating the implementation of the CHAT program nationally. With almost seven years’ experience as a speech pathologist, Rachel is completing a PhD at UQ fulltime and has a part-time clinical role at STARS.
Through my PhD studies, I’m exploring the feasibility, acceptability, and potential effectiveness of implementing the structured, group-run model for conducting goal setting and clinical planning as part of the CHAT program. I’m also involved in establishing the Clinical Advisory Group, a new QARC initiative which forms a key part of the governance structure for the Centre. It will provide a platform for clinicians’ input into the research, operations, and future development of QARC.”
Clinician researchers who work in and with the QARC team enable wholistic management for people with aphasia. The team work with clinician researchers across healthcare settings and at various research institutions and organisations, industry, professional and not-for-profit organisations.
“The clinician researchers we work with bring together the best of both worlds- research and clinical, to ensure programs and services being developed and delivered to people with aphasia are relevant and evidence-based. They are integral to the future of QARC research as they identify problems or gaps in clinical practice that need to be researched and they are in an optimal position to identify facilitators and barriers to research projects and to recruit participants for research,” Professor Copland said.
50 international peer reviewed publications have been cowritten by QARC researchers and clinicians.
For more information on QARC visit shrs.uq.edu.au/qarc
Authors: QARC Director Professor David Copland; UQ PhD student and STARS clinician Rachel Levine; UQ QARC Senior Research Assistant Emma Caird; UQ Faculty of Health and Behavioural Sciences Principal Advisor, Media and Communication Kirsten O’Leary.
Tuberculosis is an ancient disease. However, contrary to common belief, it is not history.
Before COVID, tuberculosis (TB) caused more deaths (1.5 million every year) than any other infectious disease. Unfortunately, since COVID, the two decades of slow decline in the number of deaths due to TB has been reversed.
Although TB is a forgotten disease in Australia and other ‘developed’ countries, our victory over this disease was hard earned.
The Australian Tuberculosis Campaign, initiated during the Second World War period and continued until 1974, included many important initiatives, such as:
• regular and free x-ray screening of all adults (with fines for those who did not comply);
• a tuberculosis pension to support those unable to work due to the disease; and
• funding for research into the disease.
The campaign was so successful that by the mid-1970s there were few cases to find, and the campaign was abandoned.
While this was the correct decision for Australia, unfortunately, a similar decision was taken around this time by the World Health Organisation, on behalf of the whole world! It was decided that screening the general
population – which had been so successful in eliminating TB in rich countries – was not affordable for poor countries. Sadly, this has condemned people in those countries to continue to live, and die, with the disease.
TB is an infectious disease, like COVID, influenza, and measles. People who have untreated active TB affecting the lungs (the most common type of TB) expel infectious aerosols into the air. We now know that many people with active TB affecting the lungs do not have symptoms: or, if they do have symptoms, do not recognise it as a problem and do not get medical attention. In some countries, as many as 1 in 100 adults have this infectious type of TB. In these ‘high burden’ settings, it is reasonable to say that everyone is at risk of being infected with TB, all the time, everywhere.
To stop TB in high burden settings, it is necessary to interrupt the chain of transmission by finding and treating all people who are living in the community with undiagnosed and untreated active TB affecting the lungs.
The good news is that we have highly effective treatments, which both cure the disease and rapidly render people with active TB non-infectious to others. Since many of these people do not have recognised symptoms of illness, and
since everyone and anyone may have TB, in high burden settings it is necessary to test everyone for the disease.
Currently, testing requires either a chest x-ray (the same method that was used in the Australian Tuberculosis Campaign), a highly sensitive ‘molecular’ test on expectorated sputum, or some combination of these two tests.

Everyone who is found to have active TB then needs to be offered, and supported to complete, an effective course of treatment for the disease. A campaign to break the chain needs to be sustained for long enough to ‘eliminate’ the disease: probably 10 to 15 years, but maybe less.
Although TB elimination campaigns have been successfully implemented in many countries (including Australia, Europe, parts of North America, Japan, and Cuba), they have been regarded as not feasible in ‘developing’ countries.
However, our team at Woolcock Vietnam has shown that contrary to popular opinion, TB elimination may also be feasible in developing countries.
We recently conducted a proof-of-concept trial in a southern, rural province in Vietnam. In 60,000 people, screened annually for four years, we were able to reduce the proportion of the population with TB at the time of screening (the prevalence) by 44 percent compared to a similar population who were not screened. We also reduced the annual incidence of TB, that is, the number of people who did not have TB in one year but did have it the next year, by 58 percent.
These dramatic reductions are encouraging but need to be scaled up to larger and more diverse settings, to prove that it is feasible to eliminate TB. That is what we are working towards.
Many of the historical advances in TB control, over more than a century, have been made by clinicians and public health practitioners who have asked important questions and sought to answer them by research. Our work in Vietnam is one step in that process. There is much more to do. We are engaging and supporting our colleagues in countries with a high burden of TB in this process.
The team from Woolcock Vietnam has recently published a paper in the prestigious journal The Lancet, which reinforces the importance of active case-finding programs in countries with a high burden of TB, and sets out barriers and solutions for eliminating TB in those countries. Read Epidemiological approach to ending tuberculosis in highburden countries, The Lancet, August 2022.
Find out more about Woolcock Vietnam’s TB projects at the Woolcock Vietnam website.
Author: Professor Guy Marks AO FAHMS is a respiratory and public health physician and environmental epidemiologist. He is Scientia Professor in the School of Clinical Medicine, at UNSW Sydney and a physician in the Department of Respiratory Medicine at Liverpool Hospital. He is currently an NHMRC Senior Principal Research Fellow. He is head of the Respiratory and Environmental Epidemiology group at the Woolcock Institute of Medical Research, co-leader of Woolcock Vietnam, and an Honorary Professor at The University of Sydney (Sydney Medical School). His other major role is as President (and interim Executive Director) of the International Union Against Tuberculosis and Lung Disease (The Union).
In this issue of INSPIRE we introduce newest member, the F1000 fosters a culture of innovation in open research publishing, accelerating the reach of knowledge and putting it in the hands of those who will shape the future.
For more information on Research Australia and how you can join contact us at admin@researchaustralia.org
We partner with funders, institutions, societies, and associations around the world to create high quality and bespoke publishing venues that help their communities to achieve their open research ambitions. Our current partners include the European Commission, Wellcome, the Bill & Melinda Gates Foundation, University College London, the Association for Medical Education in Europe, the Institute of Materials, Minerals and Mining, Max Planck Society, University of Tsukuba, and many more. We also partner directly with researchers through our own publishing platform, F1000Research.
F1000’s publishing model combines the benefits of pre-printing, including the ability to publish rapidly, with functionality and processes that ensure the robustness, quality, reproducibility, and transparency of research through rigorous editorial checks, open data support and invited open peer review. Authors have autonomy throughout the entire publishing process.
The F1000.com website provides comprehensive information about our publishing model and range of services. You can also read and engage with debates forming open research policy through our Open Thinking pages.
We are excited to work with organisations across Australia and welcome inquiries from Research Australia members.

F1000 FOSTERS A CULTURE OF INNOVATION TO ACCELERATE THE REACH OF KNOWLEDGE AND PUT IT IN THE HANDS OF THOSE WHO WILL SHAPE THE FUTURE.
Ihad been a clinician in the allied health discipline of exercise physiology since 1986, assessing patients with predominantly chronic disease and prescribing exercise programs to alleviate the symptoms and ameliorate some of the side-effects of pharmaceutical treatments. But it was during three years teaching and researching at a university in the United States from 1999 to 2002 that I came to appreciate the power of exercise as a medicine not only to treat injury and disease but also to slow structural and functional decline in the ageing human.
It was also around this time that I was supporting my father at the end of his life following prostate cancer diagnosis and treatment. Dad suffered overwhelming fatigue and weakness as a result of surgery and radiation therapy and although all of my training and experience taught me that he should be exercising, the medical advice of the day was that patients with cancer

Twenty years ago I was recruited to Edith Cowan University as a research professor and my key “pitch” to the University was that I would develop exercise medicine as a major teaching, research, industry, and community engagement portfolio.
related fatigue should rest. Two years after his prostate cancer diagnosis he died of a stroke.
I thought, “there has to be a better way”, and so I completely changed my research direction from human high performance to the clinical application of exercise medicine, with predominant emphasis in the field of oncology. Here lies key point #1.
To vigorously pursue decades of research and clinical practice it is highly desirable to have a passion for the work and although my experience with my father continues to be a strong motivator, as a clinician researcher I also derive great satisfaction in seeing the work of our team and others being translated into medical practice and the resulting benefit to patients and their carers.

Before moving from the US to Western Australia I had never spent any time in Perth and had absolutely zero research or clinical contacts. I was very fortunate that the head of research for my Faculty, Professor Linda Kristjanson was the Chair in Cancer and Palliative Care and she introduced me to two radiation oncologists who were highly experienced and also had a keen interest in research.
Professors Nigel Spry and David Joseph also believed that supportive care for people with cancer needed to be greatly improved and that exercise medicine would have a significant role.
These oncologists highlighted what they observed as major health issues facing their patients and then we planned multiple research projects to trial exercise medicine interventions to test safety, feasibility, and efficacy of what was at this time a quite radical approach to cancer management.
Two decades ago, the clinical advice was that patients with cancer should rest and limit their physical activity. But Professors Spry and Joseph could see on a daily basis that this strategy was counter-productive, and their patients were suffering considerable treatment toxicities, decline in body composition, physical function and quality of life.
Our early investigations were to use exercise medicine to ameliorate the side-effects of androgen deprivation therapy in men with prostate cancer and we demonstrated
considerable benefits, with our findings now integrated into international guidelines.
Key point #2 is that clinicians are in an ideal position to identify gaps in healthcare and priority issues that are compromising patient health and it is this insight which is essential to drive research directions.
Around 10 years later I was presenting our research findings that exercise medicine could prevent progression of cardiovascular disease, fat gain and muscle loss in men with prostate cancer. After my talk, several men and their partners thanked me for the presentation but advised that I was not really working on solutions to the major problems that impacted their lives.
“Sexual health and incontinence! That is what you should be researching for us because this is having a major impact on our quality of life.”
We subsequently launched a program of research culminating in an NHMRC funded research project to trial the effects of targeted exercise to address sexual health in these men. Key point #3 is to listen to your patients and health consumers so that they drive and inform research priorities rather than what we as clinician researchers think is important.
In 2006 exercise physiology services were added to Medicare and patients could receive a rebate for consultation with accredited exercise physiologists in the management of their chronic disease. This was a watershed moment in chronic disease management for Australia as targeted exercise medicine was and is established as a major therapy for these patients.
This monumental change in Medicare was the result of researchers collaborating with clinicians to convince the then Minister for health, Tony Abbott, that such a change would be beneficial for health care and more financially viable management of chronic disease. Key point #4 is clinician researchers have considerable influence to improve health and medical care at all levels from local to national.
In my experience, clinicians who are also involved in research are far more effective in supporting their patients and driving beneficial change in healthcare. For those that wish to pursue such a path, encouragement and support should be embedded within our health care systems, universities, and funding organisations. Evidence of the benefits for patients is extensive and tangible.
Author: Professor Robert Newton is Professor of Exercise Medicine in the Exercise Medicine Research Institute that he established in 2004 at Edith Cowan University, Perth, Western Australia. He was the 2019 WA Premier’s Scientist of the Year and a Highly Commended Finalist for the Research Australia 2021 Frontiers Award.