3 minute read
CLINICIAN’S CORNER

from April 2023 PULSE
by PTSMC

The Cyriax Approach to the Examination of Non-Surgical Soft Tissue Injuries at the Elbow
By: Russell Woodman, PT, MS, DPT, OCS, FSOM, MCTA Physical Therapist at PTSMC New Haven

Sam Zhu, PT, DPT
Physical Therapist at PTSMC Groton
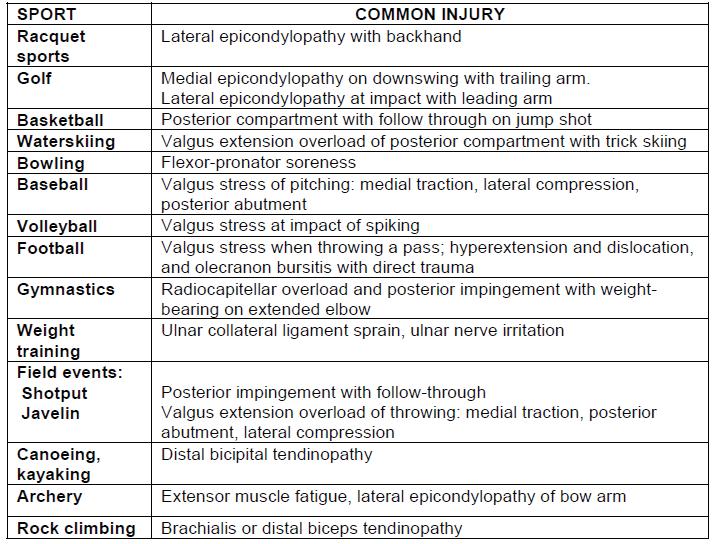
Non-surgical pathologies at the elbow include sprained ligaments, tendinopathies, bursitis, nerve compression or stretching, and capsulitis. This table presents the epidemiology of elbow injuries in sports.
Based on these results, clinicians should feel con dent prescribing early aerobic exercise when treating adolescents with sports-related concussions. Early aerobic exercise when non-symptomatic can be the key to returning athletes to the eld and preventing persistent post-concussive symptoms longer than 28 days. This study does not suggest that aerobic exercise should be the only treatment in concussion rehabilitation.

These results of this study suggest that early aerobic exercise combined with traditional use of vestibular, balance and postural training may be bene cial in preventing post-concussive symptoms as well as returning athletes to sports. Clinicians should educate their patients on the e cacy of physical therapy intervention in the treatment of acute sports related concussions. It is important as clinicians that we feel con dent and can educate our patients on the ways to prevent a concussion as well as the proper way to recover from one.
overuse. Strong and painful muscle testing is consistent with tendinopathy. A severe tendinopathy will elicit a weak and painful response.
4. Muscle belly strains frequently have a sudden onset. A grade I strain will exhibit a strong and painful muscle test. A grade II or III strain will elicit a weak and painful response.
5. Muscle testing that reveals a weak and painless response is secondary to a nerve lesion or a total tear of the muscle.
II: INSPECTION
History documentation is followed by inspection. Severe muscle strains will cause localized subdermal bleeding. An olecranon bursitis is very visible on the posterior aspect of the elbow appearing as a “bubble”.
III: SELECTIVE TISSUE TENSION TESTING
A variety of tests are documented in the literature. Most soft tissue lesions at the elbow can be diagnosed by performing ten selective tissue tension tests. When performing passive motion tests the examiner is examining range of motion, end feel and potential reproduction of pain. At the elbow the normal end feels are tissue approximation for exion, boney for extension, and capsular for supination and pronation.
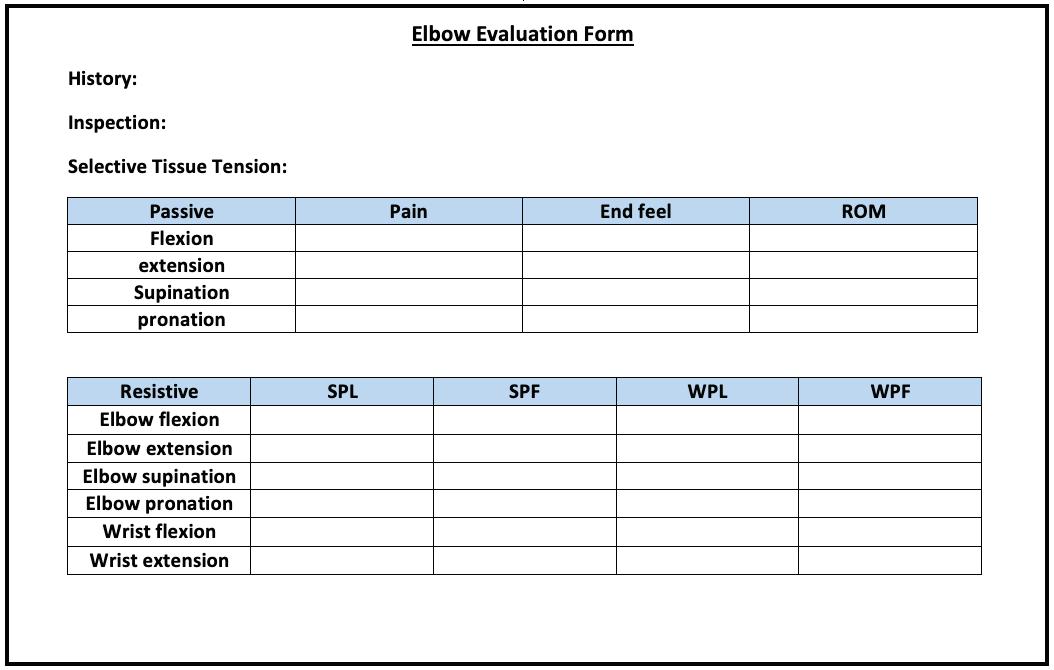
Interpretations of mid-range isometric muscle testing: a. Strong and Painless (SPL) =Muscle is normal b. Strong and Painful (SPF)=Minor tendinopathy or minor muscle strain c. Weak and Painless (WPL)=Peripheral nerve lesion or a total tear of the muscle d. Weak and Painful (WPF)=Severe tendinopathy or severe muscle strain, or fracture
The purpose of this article is to introduce the systematic approach of the elbow examination developed by Dr. James Cyriax.
CYRIAX EXAMINATION of the Elbow
First, the clinician must be aware that lesions at the cervical spine and/or shoulder can refer pain to the elbow. Therefore, at the clinician’s discretion it may be necessary to perform an examination of the cervical spine and shoulder before examining the elbow.
I: HISTORY
When taking a history for soft tissue lesions at the elbow, the following are examples of what may occur:
1. The capsular pattern at the elbow is LOSS OF FLEXION > LOSS OF EXTENSION. Indicating the presence of arthritis.
2. A loose body in the elbow will usually result in either a loss of exion or extension, sometimes a loss of pronation or supination. This loss of range of motion is in the non-capsular pattern.
3.Tendinopathies usually have a gradual onset of pain associated with muscle
Results Of The Examination
The following serves as an introduction on how to employ the Cyriax algorithm to reach a diagnosis.
The clinician must make a judgement as to which selective tissue tension test(s) are painful. If the passive tests are more painful than the resistive tests, the lesion lies in the non-contractile tissue. The clinician then decides if the loss of range of motion is in the capsular pattern. If yes, some form of arthritis might be present; The most common cause of non-capsular pattern loss of range of motion in the elbow is a loose body. A loose body at the elbow usually responses well to manipulation to move the fragment to a pain free location within the joint.
If the resisted motion is more painful, then the lesion “probably” lies in the contractile tissue. The lesion may be within the muscle belly (strain) or at its boney attachment (tendinopathy). Lesions can occur in any of the muscles that span the elbow joint. Since the wrist exors and extensors originate at the humerus, muscle testing of wrist exion and extension is also part of the elbow exam. Depending on the location of the contractile lesion, Graston (IASTM), Deep friction massage and/or a steroid injection are bene cial.
When the tissue lesion “probably” lies in the contractile, the clinician must be aware of TWO other possibilities.The rst is a fracture. When the muscle test is weak and painful, lesion could be a severe muscle strain, a severe tendinopathy, or a fracture. In this case, an MRI is a sensitive test for a soft tissue lesion and a radiography is a sensitive test for a fracture.





