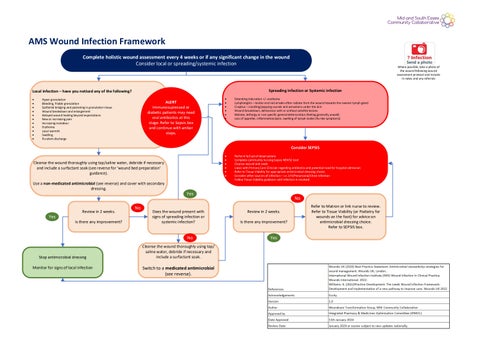
AMS Wound Infection Framework Complete holistic wound assessment every 4 weeks or if any significant change in the wound Consider local or spreading/systemic infection
Spreading infection or Systemic infection
Local infection – have you noticed any of the following? • • • • • • • • • • •
Where possible, take a photo of the wound following wound assessment protocol and include in notes and any referrals
Hyper granulation Bleeding, friable granulation Epithelial bridging and pocketing in granulation tissue Wound breakdown and enlargement Delayed wound healing beyond expectations New or increasing pain Increasing malodour Erythema Local warmth Swelling Purulent discharge
ALERT Immunosupressed or diabetic patients may need oral antibiotics at this stage. Refer to Sepsis box and continue with amber steps.
• • • • • •
Extending induration +/- erythema Lymphangitis – tender and red streaks often radiate from the wound towards the nearest lymph gland Crepitus – crackling/popping sounds and sensations under the skin Wound breakdown, dehiscence with or without satellite lesions Malaise, lethargy or non specific general deterioration (feeling generally unwell) Loss of appetite, inflammation/pain, swelling of lymph nodes (flu-like symptoms)
• • • • • • •
Perform full set of observations Complete community nursing Sepsis NEWS2 tool Cleanse wound and swab Liaise with Primary Care Clinician regarding antibiotics and potential need for hospital admission Refer to Tissue Viability for appropriate antimicrobial dressing choice Consider other sources of infection – i.e. UTI/Pneumonia/Chest Infection Follow Tissue Viability guidance until infection is resolved
Consider SEPSIS Cleanse the wound thoroughly using tap/saline water, debride if necessary and include a surfactant soak (see reverse for ‘wound bed preparation’ guidance). Use a non-medicated antimicrobial (see reverse) and cover with secondary dressing.
Yes
Review in 2 weeks. Is there any improvement?
No
Yes
Does the wound present with signs of spreading infection or systemic infection?
No
Stop antimicrobial dressing Monitor for signs of local infection
Cleanse the wound thoroughly using tap/ saline water, debride if necessary and include a surfactant soak.
Switch to a medicated antimicrobial (see reverse).
No Review in 2 weeks. Is there any improvement?
Yes
Refer to Matron or link nurse to review. Refer to Tissue Viability (or Podiatry for wounds on the foot) for advice on antimicrobial dressing choice. Refer to SEPSIS box.