IPPOL03 Infection Prevention & Control Hand Hygiene Policy v9
Infection Prevention & Control Hand Hygiene Policy
Version: V9
Ratified by:
Infection Prevention and Control Group
Date ratified: 01/04/2025
Job Title of author: Head of Infection Prevention and Control
Reviewed by Committee or Expert Group
Infection Prevention and Control Group
Equality Impact Assessed by: Head of Infection Prevention and Control
Related procedural documents
IPPOL21- Standard Precautions for Infection Prevention and Control including TBPs and Isolation precautions.
IPPOL02 - Policy and Procedure for the Prevention and Management of Clostridium difficile Associated Disease (CDAD) in Community Hospital Wards
IPPOL16 – Management and control of an Outbreak of infection.
IPPOL01 - Policy and Protocol for the Management of MRSA in Provide Community Hospital Wards
HRPOL45 - Uniform Dress Code
LDPOL03 - Mandatory Training Policy
Review date: 01/04/2028
It is the responsibility of users to ensure that you are using the most up to date document template – i.e. obtained via the intranet.
In developing/reviewing this policy Provide Community has had regard to the principles of the NHS Constitution.
Version Control Sheet
Version Date Author Status Comment
V1 – V7 2006 – 2018 IPC Archived
V8 April2022 Specialist Infection Prevention and ControlNurse RatifiedatIPG 3yearreview Updated new policy template and added appendix2
V9 March2025 Head of Infection Prevention and Control Virtual Ratification Revised intro and narrative throughout on updated policy template
1. Introduction
There are many different forms of hand hygiene WHO (2009), however, within this policy, hand hygiene refers to the decontamination of hands by methods including routine hand washing and the use of alcohol hand sanitisers.
Direction is given on:
• Indications for hand hygiene
• Types of cleansing agents and indications for use
• Hand hygiene technique
• Promoting hand hygiene
• Healthcare workers with patient contact
• Bare Below the Elbows
• Failure in regard to formally assessed hand hygiene
Hand Hygiene is considered the single most important factor in the control of infection (Weston, 2013). It is an essential practice for patient safety, and should be carried out by all staff, visitors, and patients. Healthcare associated infections (HAI) are the most frequent adverse event during care delivery and continues to be a global problem for patient safety. The prevention and management of the risk of HAI's is an essential part of maintaining patient safety and is fundamental in any healthcare setting (WHO 2011). The transfer of organisms between humans can occur directly via hand, or indirectly via an environment source (e.g., clinical equipment, furniture, toys, or sinks)
2. Purpose
The purpose of this policy is to provide all staff employed by Provide with a clear and robust process for hand hygiene. This policy applies to all working within Provide including medical staff and any member of staff working on bank, agency, or honorary contracts. All health professionals should ensure that they work within the scope of their professional code of conduct. Hand hygiene is one of the simplest, most costefficient ways of reducing healthcare acquired infections and reducing the risk of cross infection from person to person. It is a mandatory requirement that all staff are aware of the hand hygiene policy and always adhere to the correct management of hand hygiene. Hand hygiene forms part of the mandatory training requirements for all clinical staff and should be updated every two years and this policy helps to supports that training.
3. Duties
Role Responsibility
Board of Directors
The Provide Group Board is accountable for ensuring that suitable arrangements are in place for managing infection prevention and control including hand hygiene. This includes an overview of performance, significant issues and development plans. These duties are conducted through the work of the Quality and Safety Governance Committee.
Chief Executive
Director of Infection Prevention and Control
The Chief Executive has ultimate responsibility to ensure the infection prevention and control is addressed according to Department of Health directives.
The Director of Infection Prevention and Control has overall responsibility for the organisational IPC standards and compliance toreduce infection risks. This includes working through the Infection Prevention and Control Group and formally reporting to the Organisational Board of Provide Group.
Infection Prevention and Control Team
The Infection Prevention and Control team (IPCT) is responsible for providing expert advice on Hand Hygiene.
The IPCT is responsible for ensuring resources are available on hand hygiene, and provide regular updates for Infection Control Link practitioners.
The IPCT is responsible for ensuring hand hygiene resources are available to support local programmes of education, including regular updates for Infection Control Link Practitioners
The IPCT will also periodically run Hand Hygiene campaign alongside continuing to promote the concept of ‘cleanyourhands’ Champions.
Occupational Health
The Occupational Health Team (OHT) can offer expert advice to inform the choice of products for hand hygiene and also to staff who experience skin problems with the hand washing/ disinfectants provided by the Trust.
Clinical Directors and Corporate Heads of Department Clinical Directors and Corporate Heads of Department are responsible for infection prevention and control in their own sphere of control. This role includes ensuring suitable and sufficient systems are in place to comply with Trust policy on Hand Hygiene
Divisional Leads Governance
Divisional Leads (or equivalent) are responsible for ensuring that infection prevention and control (including hand hygiene) is monitored in their own directorate, action plans are implemented to address any significant issues and learning is shared. This includes participating in the Healthcare Governance Risk Management Audit Programme. The groups should keep appropriate governance records, reports and minutes.
Line Managers/ designated Supervisors
Line managers/designated supervisors must ensure that their staff, and any temporary staff students or volunteers working in their area, are compliant with the requirements within this policy that apply to them. Line managers/designated supervisors must ensure their staff have access to and receive mandatory training in infection prevention and control including hand hygiene training.
Staff members
All staff are responsible for their own actions and staff must be constantly vigilant to ensure that something as basic as hand hygiene is practised correctly.
Staff are to ensure that they receive training on effective hand hygiene specified by their line manager/designated supervisor.
4. Consultation and Communication
Review of this policy has been undertaken with consultation of the national guidance and best practice reference material available, as supported and recommended by the expertise of Infection prevention and control advisors, authors and working groups. This policy has been circulated to the members of the infection prevention and control group for comment and approval
5. Monitoring
Provide will monitor the operation of this policy in order to:
• Measure its effectiveness
• Comply with Provides’ legal obligations
• Highlight practical issues and seek solutions
6. Hand decontamination
Hand decontamination and technique is the most effective way to protect both the patient and the healthcare worker (HCW) from acquiring micro-organisms which may cause harm.
HCWs have the greatest potential to spread micro-organisms that cause infection by:
• transfer from one patient to another/staff to patient/patient to staff
• transfer from the environment to patient
• transfer from equipment to patient
Hands must be decontaminated at critical points to prevent transmission of microorganisms. Opportunities for hand hygiene have been described as 5 Key Moments by the World Health Organisation (WHO, 2009A).
To prevent the transfer of micro-organisms it is essential to decontaminate hands:
1. Before patient contact
2. Before an aseptic task
3. After body fluid exposure risk
4. After patient contact
5. After contact with patient surroundings.
To ensure hands are free from contamination hand hygiene must be performed when:
• Having used the toilet
• Having sneezed, blown your nose
• Before and after handling food and drink
• Before and after entering clinical area
• After handling patient notes
• After cleaning equipment and / or the environment
It is important:
• To risk assess and determine whether to use alcohol-based hand rub / gels (ABHRs) or soap, water and paper towels
• When completing one procedure on a patient use the ABHRs before commencing another procedure
7. Hand washing
Handwashing is widely acknowledged to be the single most important activity for reducing the spread of infection. The aim of handwashing is to remove transient microorganisms that accumulate on the skin as a result of activities undertaken by the individual. Transient micro-organisms do not form part of the skin flora and are easily removed by mechanical methods using soap and water (or hand-wipes). Transient micro-organisms include those found in body fluids that may contaminate hands if soiled or visibly dirty.
Hands must be washed using soap and water and an evidence-based technique (WHO) for 15-30 seconds, and then rinsed and dried thoroughly. Single use patient hand wipes should also be available for patients who are unable to access liquid soap and water for hand washing e.g. before meals or after using the toilet etc.
Facilities for staff hand hygiene i.e. hand wipes, bottle of liquid soap, bottles of alcoholbased hand rubs must be available for community staff if environmental risk assessment identifies working conditions where liquid soap and water are not always available.
8. Surgical Hand washing
Surgical hand washing uses chemicals to reduce or eliminate transient organisms as well as reducing the number of micro-organisms that live on the skin and are known as skin flora. It is only necessary to undertake this procedure before surgical procedures and some invasive procedures. If sterile gloves are required, then surgical handwashing is recommended.
Products used for surgical handwashing contain an aqueous antiseptic solution applied for a standard time (usually 2 minutes). Preparations currently available are 4% Chlorhexidine gluconate in a surfactant solution and 7.5% in Povidone - iodine in aqueous solution.
There are a number of alternative / additional methods for preparing the hands, nails and forearms prior to undertaking a surgical procedure which will be determined by local theatre protocols
9.
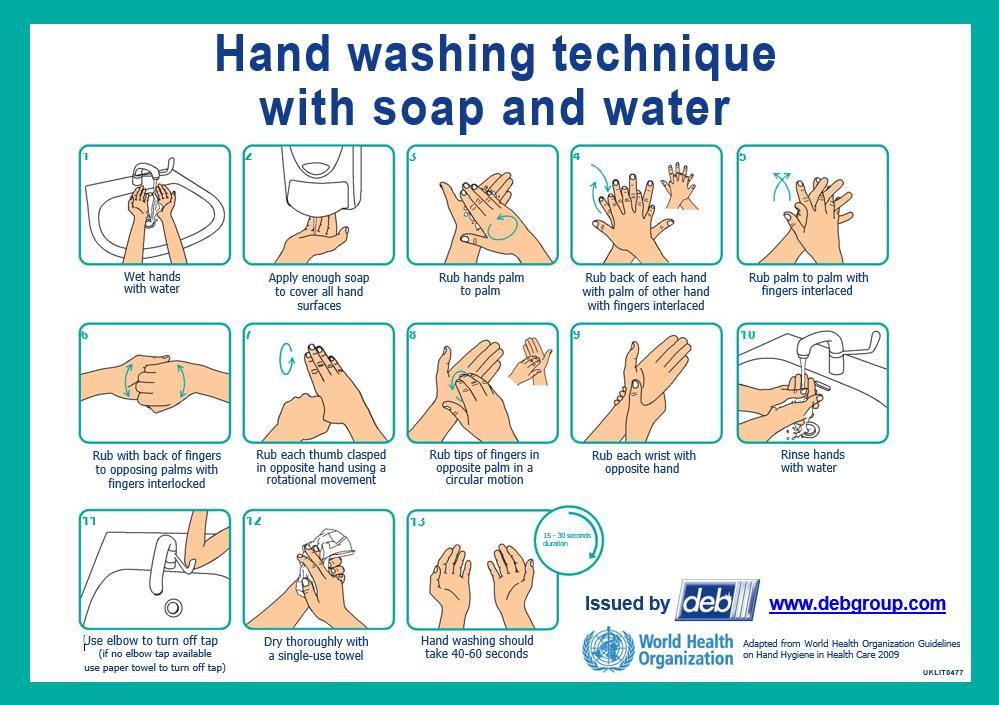
Hand washing techniques
A. Preparation
Before washing hands, all wrist and hand jewellery should be removed. Cuts and abrasions must be covered with waterproof dressings.
Arms must be bare below the elbows to facilitate lathering with soap or the application of alcohol based hand rubs over the base of the hands and wrists (and lower arms as required for a surgical handwash).
Hands should be wet under tepid running water before applying liquid soap or an antimicrobial preparation.
B. Washing and Rinsing
When washing hands apply enough soap to cover all hand surfaces to ensure that the hands are well lathered.
The hands must be rubbed together thoroughly for a minimum of 10-15 seconds, paying particular attention to the tips of the fingers, the thumbs and the areas between the fingers. Hands must be rinsed thoroughly under running water.
C. Hand Drying
This is an essential part of hand hygiene. Microbes can transmit with greater success to wet hands therefore hands must be dried thoroughly using good quality paper towels. In clinical settings disposable paper towels must be used, as communal towels are a source of cross-contamination.
Hot air dryers are not recommended in clinical settings. However, if they are used in other areas, they must be regularly serviced and users must dry hands completely before moving away.
10.Using Alcohol-based hand rubs (ABHRs)
Alcohol-based hand rubs/gels/sanitisers are recognised (by WHO) as the gold standard method for hand decontamination at the point of care. ABHRs can be used when handwash facilities (basins, water and hand towels) are not readily available.
However, ABHRs are not effective against all micro-organisms (for example viruses such as Norovirus and spore forming micro-organisms such as Clostridium difficile) I these circumstances e.g. when caring for patients with infectious diarrhoea then hands should be washing using soap and water. ABHRs will not remove dirt or body fluids when hands should be washed using soap and water.
A risk assessment must be undertaken when the easy availability of ABHRs is considered unsafe e.g. paediatrics, mental health and special learning needs environment. These products are toxic if ingested.
When cleaning hands, 1 pump from the dispenser of ABHR will provide a 3ml dose, which is sufficient for covering all surfaces of the hands and wrists.
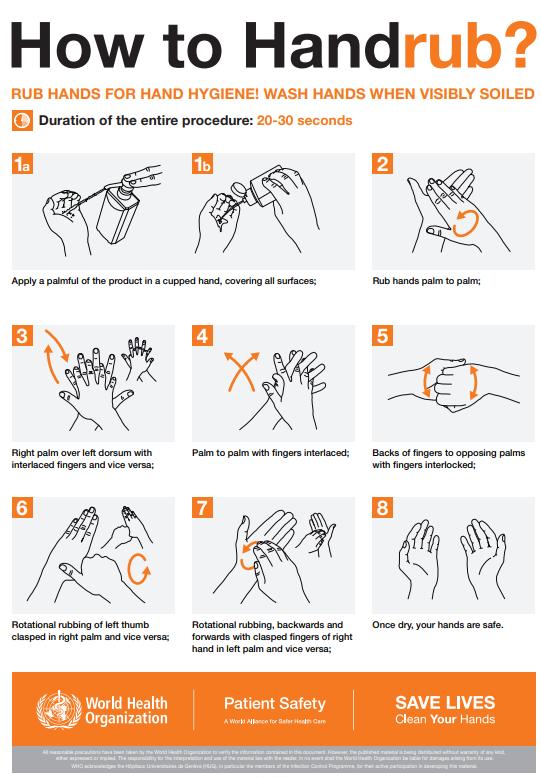
ABHRs must come into contact with all the surfaces of the hand. The hands must be rubbed together thoroughly, paying particular attention to the tips of the fingers, the thumbs and the areas between the fingers, until the solution has evaporated, and the hands are dry.
Individually carried single-use dispensers (bottles) should be available for staff that don’t have easy access to dispensers e.g. community staff, domiciliary visits by GPs and podiatrists etc.
All hand hygiene products must be of medical grade and purchased via an approved supplier.
11.Risk Assessment for Hand wash / decontamination
1. Hand washing Liquid soap
2. Hand decontamination
3. Surgical scrub –hand disinfection
Alcohol-based hand rub (ABHR) e.g. Purell, Deb Cutan
For all routine tasks (please refer to 8.3 in this Policy)
Rapid decontamination for hands not visibly soiled
Please refer to manufacturer’s instructions
Prior to surgical and other invasive procedures
Please refer to manufacturer’s instructions
Intact skin is a natural barrier to infection, consequently all staff need to be aware of the potential damaging effect of increased hand hygiene. Staff should protect and maintain skin integrity through regular use of moisturisers, which should be perfume free, preferably water-based and contain an effective preservative and provided by the organisation. Staff should not provide their own moisturisers. Moisturisers should only be dispensed from sealed units and should not be re-filled. If hand moisturiser is supplied via occupational health for a particular member of staff and therefore is not dispensed from a sealed unit it should be clearly identified for individual staff use. Any member of staff who is unable to use the available hand hygiene products due to the development of, or existing skin condition / allergy, must seek advice from Occupational Health and/or their general practitioner and report to their line manager. Staff can be referred to Occupational Health by their manager or can self-refer.
13.Hand hygiene facilities
Adequate facilities should be provided in a healthcare environment complying to HTM 64 (2014) to encourage staff to clean their hands appropriately when indicated, this includes:
• Dedicated hand wash basins that are clean and accessible
• Liquid soap in wall mounted easy to sue and easy to clean holder systems that contain single use disposable cartridge sets
• Wall mounted disposable paper towel dispensers containing soft absorbent disposable paper towels
• Hand wash basins must not be equipped with overflow or plug
• Nail brushes must not be used
• All hand wash basins in healthcare settings, wherever possible, should be fitted with elbow operated or hands-free mixer taps
• Foot operated lidded pedal bins must also be positioned near the wash basin. In areas where facilities are either unavailable or do not meet Provide standards? (Such as patients own home) then alternative provisions should be made/sought. Healthcare professionals working within the primary care environment should be provided by the organisation with a personal supply of liquid soap, alcohol hand sanitiser, and hand cream. A supply of disposable paper towels/kitchen towels for hand drying will also need to be provided.
14.Signage
• Handwash posters demonstrating the correct technique should be available and positioned close to handwash basins in all areas accessed by staff. Posters should be laminated for protection
• Signage explaining the importance of hand hygiene compliance must be visible on entry to all inpatient health care facilities
• There must be clearly signposted hand hygiene facilities on entry and exit from inpatient/clinical areas
• Visitors and patients need to be encouraged to comply with requests for hand hygiene through the use of easily visible and clear signage and information leaflets
15.Audit
Hand hygiene compliance is audited monthly using an observational audit tool. Audits are undertaken by the Link Practitioner or Associate Practitioner for the department/service.
The audit results are reported to each Divisional Lead and form part of the quality assurance process with results presented at the IPC Group as a standing agenda item. The continuous audit cycle supports improvement in hand hygiene and reviews compliance to the hand hygiene policy.
The infection prevention team also undertakes a schedule of verification audits.
Observational Hand Hygiene Audit Tool
The hand hygiene audit has a clear escalation standard ensuring that an immediate response occurs at a local level when compliance drops below the agreed set
performance target, and a rapid improvement cycle is started until compliance is met (Please refer to the HII: Observational hand hygiene audit tool on the staff intranet).
16.References
1. "Infection Prevention and Control" by Debbie Weston – Discusses best practices for minimizing cross-contamination in healthcare settings, including linen handling.
2. Department of Health (2008, 2015) Health and Social Care Act: Code of Practice for the prevention and control of healthcare associated infections. DOH, London.
3. World Health Organisation (2009a) Hand Hygiene Technical Reference Manual: To be used by health-care workers, trainers and observers of hand hygiene practices. WHO, Geneva.
4. Loveday HP, Wilson JA, Pratt RJ et al. (2014) Epic3: National evidencebased guidelines for preventing healthcare-associated infections in NHS hospitals in England, recommendation SP6.
5. National Institute for Health and Clinical Excellence (2012) Infection: Prevention and Control of healthcare associated infections in primary and community care. NICE Clinical guidance 139. Accessed at: www.nice.org.uk/cg139
6. NHS England & Improvement (2019) Standard Infection Control Precautions: national hand hygiene and Personal Protective Equipment (PPE) Policy DOH, London.
Appendix 1: Hand washing technique with soap and water
Appendix 2: How to Handrub?
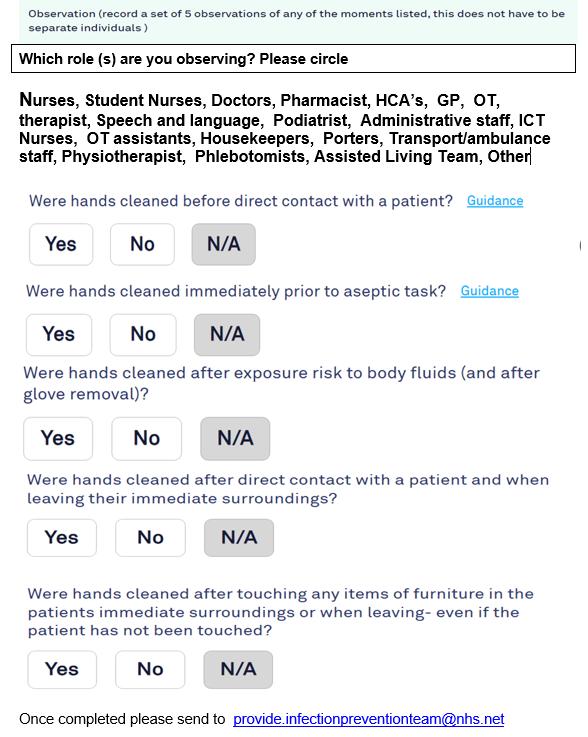
Appendix 3: Hand hygiene WHO 5 moments observation tool
Name of project/policy/strategy (hereafter referred to as “initiative”):
Infection prevention and Control Hand Hygiene Policy
Provide a brief summary (bullet points) of the aims of the initiative and main activities:
Provide the aims of when and how to perform hand hygiene.
Project/Policy Manager: Head of Infection Prevention and Control Date: 12.03.2025
This stage establishes whether a proposed initiative will have an impact from an equality perspective on any particular group of people or community – i.e. on the grounds of race (incl. religion/faith), gender (incl. sexual orientation), age, disability, or whether it is “equality neutral” (i.e. have no effect either positive or negative). In the case of gender, consider whether men and women are affected differently.
Q1. Who will benefit from this initiative? Is there likely to be a positive impact on specific groups/communities (whether or not they are the intended beneficiaries), and if so, how? Or is it clear at this stage that it will be equality “neutral”? i.e. will have no particular effect on any group.
Neutral
Q2. Is there likely to be an adverse impact on one or more minority/under-represented or community groups as a result of this initiative? If so, who may be affected and why? Or is it clear at this stage that it will be equality “neutral”?
N/A
Q3. Is the impact of the initiative – whether positive or negative - significant enough to warrant a more detailed assessment (Stage 2 – see guidance)? If not, will there be monitoring and review to assess the impact over a period time? Briefly (bullet points) give reasons for your answer and any steps you are taking to address particular issues, including any consultation with staff or external groups/agencies.
N/A
Guidelines: Things to consider
Equality impact assessments at Provide take account of relevant equality legislation and include age, (i.e. young and old,); race and ethnicity, gender, disability, religion and faith, and sexual orientation.
The initiative may have a positive, negative or neutral impact, i.e. have no particular effect on the group/community.
Where a negative (i.e. adverse) impact is identified, it may be appropriate to make a more detailed EIA (see Stage 2), or, as important, take early action to redress this – e.g. by abandoning or modifying the initiative. NB: If the initiative contravenes equality legislation, it must be abandoned or modified.
Where an initiative has a positive impact on groups/community relations, the EIA should make this explicit, to enable the outcomes to be monitored over its lifespan.
Where there is a positive impact on particular groups does this mean there could be an adverse impact on others, and if so can this be justified? - e.g. are there other existing or planned initiatives which redress this?
It may not be possible to provide detailed answers to some of these questions at the start of the initiative. The EIA may identify a lack of relevant data, and that data-gathering is a specific action required to inform the initiative as it develops, and also to form part of a continuing evaluation and review process.
It is envisaged that it will be relatively rare for full impact assessments to be carried out at Provide. Usually, where there are particular problems identified in the screening stage, it is envisaged that the approach will be amended at this stage, and/or setting up a monitoring/evaluation system to review a policy’s impact over time.
EQUALITY IMPACT ASSESSMENT TEMPLATE: Stage 2:
(To be used where the ‘screening phase has identified a substantial problem/concern)
This stage examines the initiative in more detail in order to obtain further information where required about its potential adverse or positive impact from an equality perspective. It will help inform whether any action needs to be taken and may form part of a continuing assessment framework as the initiative develops.
Q1. What data/information is there on the target beneficiary groups/communities? Are any of these groups under- or over-represented? Do they have access to the same resources? What are your sources of data and are there any gaps?
N/A
Q2. Is there a potential for this initiative to have a positive impact, such as tackling discrimination, promoting equality of opportunity and good community relations? If yes, how? Which are the main groups it will have an impact on?
N/A
Q3. Will the initiative have an adverse impact on any particular group or community/community relations? If yes, in what way? Will the impact be different for different groups – e.g. men and women?
N/A
Q4. Has there been consultation/is consultation planned with stakeholders/ beneficiaries/ staff who will be affected by the initiative? Summarise (bullet points) any important issues arising from the consultation.
N/A
Q5. Given your answers to the previous questions, how will your plans be revised to reduce/eliminate negative impact or enhance positive impact? Are there specific factors which need to be taken into account?
N/A
Q6. How will the initiative continue to be monitored and evaluated, including its impact on particular groups/ improving community relations? Where appropriate, identify any additional data that will be required.
N/A
Guidelines: Things to consider
An initiative may have a positive impact on some sectors of the community but leave others excluded or feeling they are excluded. Consideration should be given to how this can be tackled or minimised.
It is important to ensure that relevant groups/communities are identified who should be consulted. This may require taking positive action to engage with those groups who are traditionally less likely to respond to consultations, and could form a specific part of the initiative.
The consultation process should form a meaningful part of the initiative as it develops, and help inform any future action.
If the EIA shows an adverse impact, is this because it contravenes any equality legislation? If so, the initiative must be modified or abandoned. There may be another way to meet the objective(s) of the initiative.
Further information:
Useful Websites www.equalityhumanrights.com Website for new Equality agency www.employers-forum.co.uk – Employers forum on disability www.efa.org.uk – Employers forum on age