Returning Home: Recommendations to the Arizona Health Care Cost Containment System
Returning Home
Recommendations to the Arizona Health Care Cost Containment System on the Implementation of its 1115 Reentry Waiver
January 2025
Authors: Md Rahmat Ali, Mustafa Ali-Smith, Laurel Cooke, Claire Fondrie-Teitler, Christopher Gliwa, Benjamin Harris, Julian Lutz, Tina Lee, Rachel Morrow, Daisha Roberts, Svyatoslav Karnasevych, and Keiana West.
Project Advisors: Heather Howard and Daniel Meuse.
Publication Date: January 27, 2025.
Photos from Unsplash and iStock.
Data Graphics by Laurel Cooke, Benjamin Harris, and Keiana West.
Geographic Data Visualization by Christopher Gliwa and Laurel Cooke. Layout by Laurel Cooke.
ACKNOWLEDGEMENTS
This report was written by Master in Public Affairs (MPA) students at the Princeton University School of Public and International Affairs (SPIA). It represents the culmination of extensive research, data analysis, and insights gathered from a series of interviews, most of which took place in Arizona from October 14 - 18, 2024.
This report fulfills Princeton SPIA’s graduation requirements, which stipulate that all students conduct research and produce a policy report for a client. We are deeply grateful to our professors, Heather Howard and Dan Meuse, who provided invaluable insights, guidance, and support throughout this project. Their expertise greatly enriched our learning experience and the quality of this report.
We want to extend our sincere thanks to Arizona’s Medicaid agency, AHCCCS, for providing us the opportunity to work on this project.
We also want to thank the following healthcare policy experts and stakeholders in Arizona who generously shared their perspectives, which were instrumental in shaping this report and our recommendations:
• Arizona Alliance for Community Health Centers
• Arizona Department of Corrections, Rehabilitation & Reentry
• Clarissa Nelson, Program Coordinator, Yavapai Reentry Project
• Corey Hemstreet, Legislative Specialist, Arizona Advisory Council on Indian Health Care
• Dr. John Molina, Director, Arizona Advisory Council on Indian Health Care
• Dr. William Ellert, Chief Medical Officer, Circle the City
• John McCarthy, Founding Partner, Speire Healthcare Strategies, LLC
• Kim Despres, Chief Executive Officer, Circle the City
• Maricopa County Sheriff’s Office
• McKayla Keams, Executive Project Coordinator, Arizona Advisory Council on Indian Health Care
• Michelle Cirocco, Chief Responsibility Officer, Televerde Foundation
• Steven Sheet, President and CEO, Southwest Behavioral & Health Services
• Tom Betlach, Partner, Speire Healthcare Strategies, LLC
Finally, we want to extend a special thank you to the women at Perryville Prison, who courageously shared their stories and experiences with us. Their insights provided a critical dimension to our understanding of how the healthcare system can better serve people returning.
ACRONYMS
ACC AHCCCS Complete Care MCO
ADCRR Arizona Department of Corrections, Rehabilitation & Reentry
AHCCCS Arizona Health Cost Containment System
CAA Consolidated Appropriations Act
CHW Community Health Worker
CLRS Closed Loop Referral System
CMS Centers for Medicare & Medicaid Services
FPL Federal Poverty Line
H2O Housing and Health Opportunities Demonstration
HRSN Health Related Social Need(s)
IEP Inmate Exclusion Policy
MAT Medication Assisted Treatment
MCO Managed Care Organization
MPA Master in Public Affairs
NEMT Non-Emergency Medical Transportation
RBHA Regional Behavioral Health Authority
SMI Serious Mental Illness
SPIA School of Public and International Affairs
SUD Substance Use Disorder
TI Targeted Investment
WPCI Whole Person Care Initiative
EXECUTIVE SUMMARY
Arizona is ready to be the national leader in keeping citizens healthy as they come home from incarceration. This report explains how, building on Arizona’s years of innovation in Medicaid services. In recent decades, Arizona’s Medicaid agency, the Arizona Health Care Cost Containment System (AHCCCS), has been a leader in expanding and improving care. Arizona has also led in addressing Health Related Social Needs (HRSNs), which are conditions in people’s lives that affect their health outcomes.
Yet AHCCCS is always seeking ways to expand, deepen, and improve its service to Arizonans. Now, Arizona seeks to make such an improvement by expanding services to AHCCCS members returning from incarceration. They will pursue this change through a Section 1115 waiver – a program through which the federal Center for Medicare and Medicaid Services (CMS) grants states permission to innovate and experiment in their Medicaid programs. Arizona is ready to innovate and learn from other states. We are writing to advise their efforts.
Our main recommendation is to lengthen pre-release services by offering 90 days of case management, covering some new clinical services, and ensuring
members connect with other clinical and social services providers in their communities before release. We also recommend integrating reentry case management with existing social services offered through AHCCCS – including transportation, housing, and food – to ensure members who are reentering receive all the support they need. And we offer implementation suggestions, such as addressing rural Arizona’s challenges and tribal populations’ needs, and we suggest evaluation best practices to ensure the waiver reaches its promise.
To achieve these goals and meet federal requirements regarding stakeholder collaboration, Arizona’s waiver should emphasize all relevant institutions throughout its design, implementation, and management –including managed care organizations (MCOs), carceral facilities, behavioral health advocates, law enforcement agencies, and community-based providers.1
With creativity and coordination, the reentry waiver will not only improve health outcomes for members leaving incarceration, but also honor AHCCCS’s values of “Passion, Community, Quality, Respect, Accountability, Innovation, Teamwork, Leadership, and Courage.”2
INTRODUCTION
AHCCCS, Arizona’s Medicaid agency, provides services to over 2.1 million members across Arizona. Arizona was one of the first states to expand Medicaid under the Affordable Care Act, effective January 1, 2014. While the Medicaid Inmate Exclusion Policy (IEP) prohibits Medicaid coverage for most incarcerated people, Arizona, like many states, addresses this by suspending, rather than terminating, Medicaid coverage, ensuring quicker reinstatement upon release. It has also innovated its delivery system and MCO contracts to create specific resources, including the establishment of Justice Clinics and Justice Liaisons, for members who are justice involved.
In 2018, the United States Congress passed the Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities (SUPPORT) Act, which allows CMS to waive certain IEP restrictions. In 2023, CMS provided guidance for states to create reentry service packages through 1115 demonstration waivers, as long as Medicaid coverage was suspended, not canceled. In May 2021, AHCCCS submitted a Section 1115 waiver for its Housing and Health Opportunities (H2O) program, but paused this request in 2023 – to align with opportunities under updated CMS guidance and to explore broader service designs. To inform this effort, AHCCCS collaborated with SPIA in Fall 2024 to research best practices and develop recommendations for improving reentry services.
To provide those recommendations, we are a group of thirteen MPA students from SPIA working under the guidance of two national healthcare policy experts – Heather Howard and Dan Meuse. Our project focuses on developing policies for AHCCCS to enhance reentry services for members transitioning from incarceration. We conducted 12 weeks of research, including fieldwork in Arizona from October 14-18, 2024. We conducted 14 interviews with key stakeholders in Arizona in October and November 2024, including staff at AHCCCS, women incarcerated at Perryville Prison, advocacy organizations, staff at the Arizona Department of Corrections, Rehabilitation, & Reentry (ADCRR), and Medicaid officials from other states. This report integrates insights from these interviews along with AHCCCS data, peer-reviewed research, and a diverse body of policy analyses.
Our analysis led to two sets of core recommendations. First, we propose a comprehensive package of services that should be provided 90 days prior to a person’s release from any carceral facility, including state prisons and county jails. These services include the mandatory services of case management, medication-assisted treatment (MAT), and pre-release prescription provisions, additional clinical services, and a set of social supports, such as housing and transportation, that address health related social needs (HRSNs). Second, we propose implementation recommendations. We also include recommendations on how best to evaluate the waiver’s efforts so that AHCCCS can ensure the fidelity of these services and learn from this latest round of policy and delivery system innovation.
BACKGROUND AND LANDSCAPE
About Arizona
Arizona has a population of 7.43 million. The state is 81.5% White, 5.7% Black, 5.2% Native American, and 4.1% Asian, while 31.6% of the state identifies as Hispanic or Latino.3 Arizona is also home to 22 Federally Recognized Tribes.4 There are 15 counties in Arizona, of which Maricopa County, which includes Phoenix, is the most populous.5
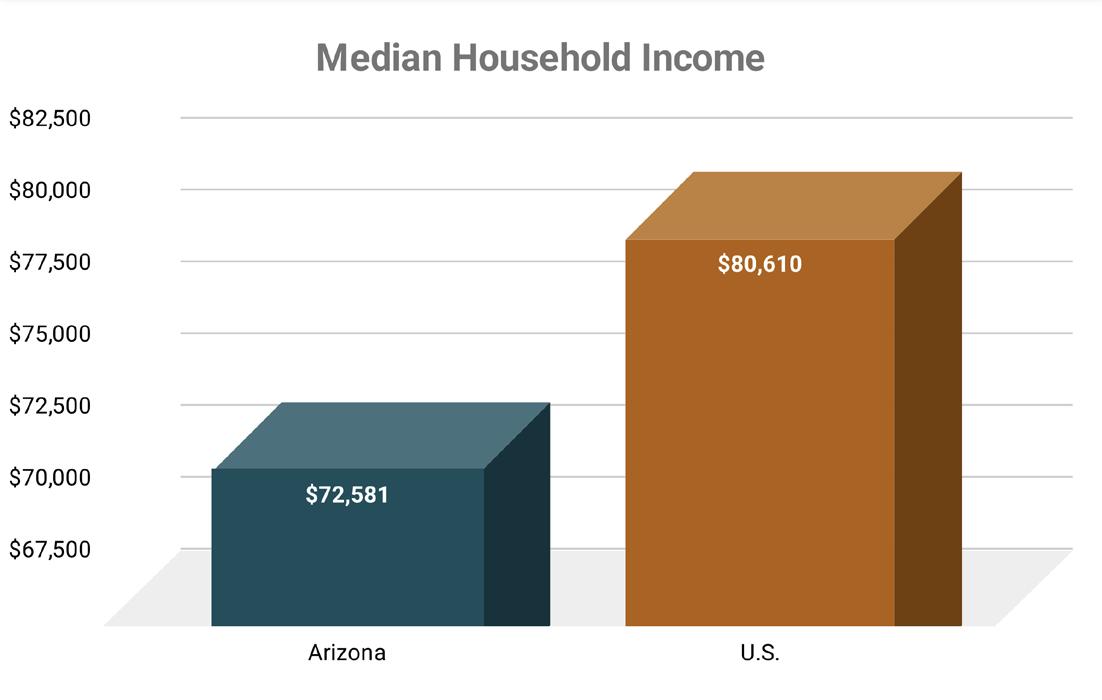
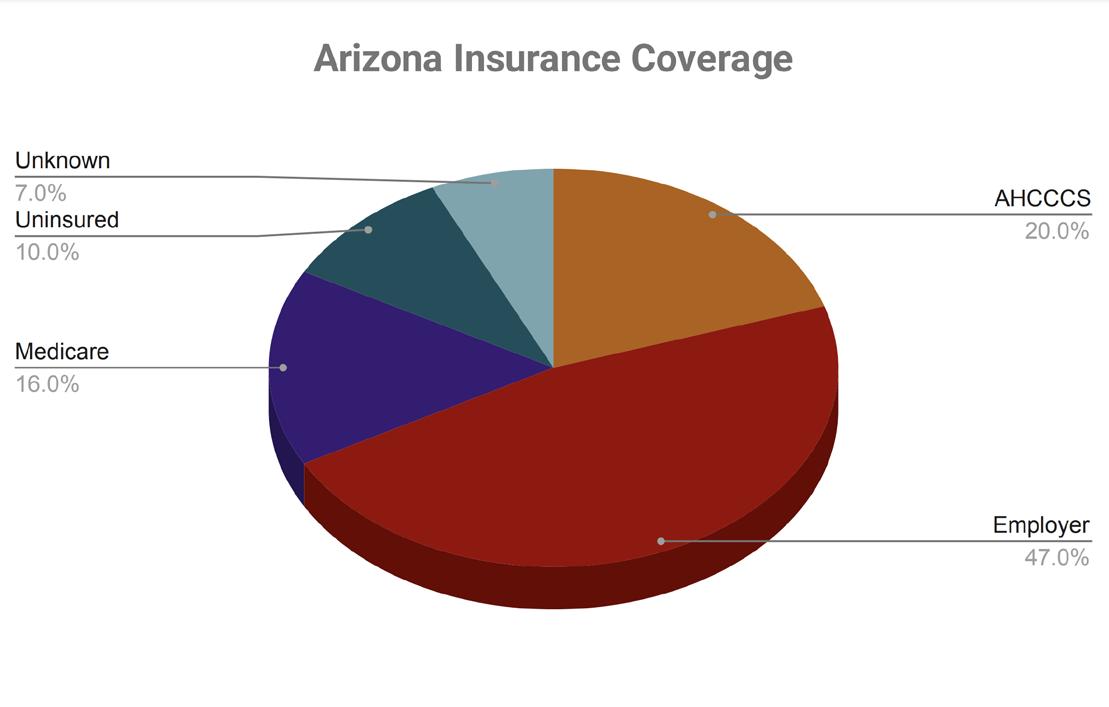
The median annual household income in Arizona is $72,581, compared to the national median of $80,610. 6Approximately 12% of people live in poverty within the state,7 and the unemployment rate is 3.6%.8 As of 2023, 9.8% of Arizonans were uninsured, which is slightly above the national uninsured rate of 8%.9 Approximately 20.4% of Arizonans are covered through AHCCCS, while 46.6% are on an employer-provided health plan, and 16.5% are on Medicare.10
Arizona’s Medicaid Population
AHCCCS serves over 2.1 million members across Arizona, including those who are fully eligible and those receiving only partial services.11 The membership includes more women (53.1%) than men (46.9%).
45.3% of members identify as white, 8.5% as Black, and 8.3% as Native American. 34.1% are categorized as of “Unknown” race. Approximately 3% of members have a recognized serious mental illness (SMI). Notably, Maricopa County has the highest number of AHCCCS members, with 59% of AHCCCS members residing there.12
Arizona was one of the first states to provide Medicaid coverage for childless adults making 0-100% of the federal poverty level (FPL) and working parents between 0-106% FPL. Coverage was implemented through a previous 1115 waiver13 and passage of Voter Proposition 204 in 2000.14 Today, these populations account for roughly 21.5% of AHCCCS’s caseload.15 In 2015, Arizona leveraged the coverage flexibilities of the Affordable Care Act (ACA) to extend coverage for these populations up to 138%. This extension brought in an additional 70,000 members. In total, these two expansions account for nearly 25% of AHCCCS’s membership.
The State of Incarceration in Arizona
Arizona has one of the highest incarceration rates in the nation, with 710 incarcerated people per 100,000 residents.16 It ranks seventh in the United States for having one of the highest incarceration rates.17 The state’s correctional facilities confine over 52,000 people, including approximately 34,000 in state prisons and 13,000 in local jails, with the remainder held in federal prisons, immigration detention centers, or juvenile facilities.18 Incarceration disproportionately affects communities of color, with Black Americans imprisoned at nearly five times the rate of White Americans nationwide.19
The Health and Social Impacts of Incarceration
Incarceration is not solely a criminal legal system issue. It represents a significant HRSN affecting the people directly involved, their families, their communities, and society at large.20 With close to two million people incarcerated in the United States, the health challenges faced by incarcerated people typically encompass three domains: physical health, mental health, and substance use.21
Figure 1: Median Household Income
Figure 2: Arizona Insurance Coverage
First, people who are incarcerated have significant physical health needs. Prisons are associated with a significant increase in the risk and spread of infectious diseases.22 For instance, the estimated prevalence of Hepatitis C among the incarcerated population is 17.4%, compared to about 1% in the general U.S. population.23 Since many prisons are densely populated with limited healthcare resources, containment and treatment are difficult to manage. The Covid-19 pandemic underscored these challenges, as correctional facilities became hotspots for rapid transmission.24 With limited access to testing, treatment, and preventative measures, incarcerated people faced additional layers of risks. Nutritional deficits are also prevalent. Prison meals often lack sufficient fruits and vegetables, leading to weight gain and an increased risk of chronic conditions like diabetes.25 Additionally, inadequate dental care exacerbates overall health deterioration, as oral health is closely linked to systemic health.26 People in prison also experience increased rates of chronic, non-communicable diseases compared to the general population, including hypertension, diabetes, asthma, and arthritis, as well as some cancers.27
Second, people who are incarcerated experience higher rates of mental health issues than the general population. Many people often enter the prison system with pre-existing mental health conditions, which can be exacerbated by prison’s isolation, stress, and harsh environments.28 Roughly 43% of people in state prisons are diagnosed with a mental health disorder.29 Despite these high mental health needs, access to necessary mental health counseling and support is limited. Only about 1 in 3 incarcerated people with mental health problems receive treatment while incarcerated.30
Finally, substance use is a common issue among the people who are incarcerated. Based on 2019 data from the National Survey on Drug Use and Health from the Substance Abuse and Mental Health Services Administration, 7.4% of people over the age of 12 met the criteria for substance use, but this figure rises dramatically with incarcerated populations.31 In the last year, 41% of people arrested in the last year noted substance use, and in 2016, 47% of people in state and federal prisons noted substance use in the 12 months prior to their incarceration.32 Despite this high prevalence, many do not receive adequate treatment for addiction while in prison.33 This lack of support not only affects their health during incarceration but also increases the risk of relapse and recidivism upon release.34
Incarceration’s effects are generational: its ripple effects extend deeply into families and neighborhoods.35 Families and children of incarcerated people experience trauma, economic hardship, and social stigmatization, which lead to adverse health outcomes and perpetuate cycles of incarceration.36 The absence of a family member – especially a primary caregiver – frequently results in emotional distress and economic hardship.37 Families bear considerable financial burdens from court and legal fees, exacerbating socioeconomic disparities. High incarceration rates can weaken community structures, reduce economic opportunities in impacted communities, and lead to limited access to essential services. This perpetuates cycles of poverty and poor health outcomes.
The Precarity of Reentry
While incarceration poses major health risks inside of prison, this reality extends into the lives of formerly incarcerated people reentering back into their communities. The lack of coordinated systems and immediate access to services, such as Medicaid, complicates reentry and successful transitions back into the community. As a result, the risk of death for formerly incarcerated people is especially high during the first two weeks, with a 40 times higher risk of fatal overdose compared to the general population.38 Over 15% of incarcerated people are homeless before their incarceration which increases post-release to to times higher than the general population.39 Unemployment post-release is also high, with 27% among formerly incarcerated people.40
Research indicates that incarceration and its subsequent impact on a person’s health and life expectancy.41 Each year spent in prison can reduce a person’s life expectancy by two years, contributing to a decrease in overall U.S. life expectancy given the large incarcerated population.42 Incarceration is associated with a 15.6% increase in the odds of death, and people who are formerly incarcerated have a mortality rate 3.5 times higher than the general population.43 Arizona also grapples with high recidivism rates: 36.4% of those released from incarceration become involved with the criminal legal system again within three years, highlighting systemic issues in reentry support and rehabilitation processes.44
The Medicaid IEP in the Social Security Act of 1965 bars state Medicaid agencies from delivering services to people who are incarcerated.45 A person who is incarcerated can only be covered by Medicaid if they receive inpatient services for 24 hours or longer in the community.46 As a result, county and state correctional budgets largely cover the cost of healthcare for people incarcerated in prisons and jails.
AHCCCS Strategies to Address the Needs of Members Who Are Incarcerated or Formerly Incarcerated
The passage of the ACA provided an unprecedented opportunity to bring people who are incarcerated or who have a history of incarceration into the public healthcare system. It extended life-saving healthcare coverage through health insurance exchanges and Medicaid expansion to people who historically experience higher rates of illness and death. In expansion states like Arizona, an estimated 80-90% of incarcerated people are eligible for Medicaid upon release.47
Following the expansion of Medicaid, many states began experimenting with their delivery systems to account for the additional social needs of vulnerable populations, including people who are or were incarcerated. Arizona was one of them. Over the past decade, AHCCCS has made the following changes to its delivery systems to better identify and serve people reentering who were eligible for Medicaid coverage.
Medicaid Suspension for People Who Are Incarcerated
First, Arizona’ implemented suspension capabilities in its eligibility systems. In 2004 and 2016, the Centers for Medicare and Medicaid Services (CMS) issued guidance to states encouraging them to merely suspend – rather than terminate – Medicaid coverage of people who are incarcerated, in an effort to remove administrative burdens for Medicaid agencies, carceral facilities, and Medicaid members, and to avoid gaps in coverage upon release.48 AHCCCS launched its initiative to switch from Medicaid termination to suspension in 2017.49 This policy allows AHCCCS to facilitate easier access to healthcare services once people who are incarcerated return to the community. Under this policy, a person can be screened for Medicaid eligibility upon being booked in a jail or prison, placed into a suspended status, and then redetermined for full Medicaid eligibility upon release.
All of Arizona’s work predated federal policy mandating that states implement suspension. In 2018, the SUPPORT Act required that states begin suspending Medicaid for all incarcerated juveniles who are eligible and that they redetermine eligibility for certain incarcerated youth pre-release.50 The CAA of 2024 went further and required that states implement this functionality by January 1, 2025.51 That Arizona had implemented this functionality well before federal legislation speaks to the state’s commitment to serve for this critical population.
Integration of Information and Data Systems
In addition to implementing the suspension functionality, AHCCCS worked with its peer agencies, including ADCRR, to develop an interagency data sharing feed. This feed passes information regarding Medicaid members incarcerated in an ADCRR facility, such as their Medicaid identification number, facility, and release date, to AHCCCS. AHCCCS merges this feed with additional information from its own eligibility system to create a master roster of members who are incarcerated. This master roster is then transmitted to AHCCCS MCOs, which are responsible for administering Arizona’s Medicaid program.
Targeted Investments, Justice Clinics, and Justice Liaisons
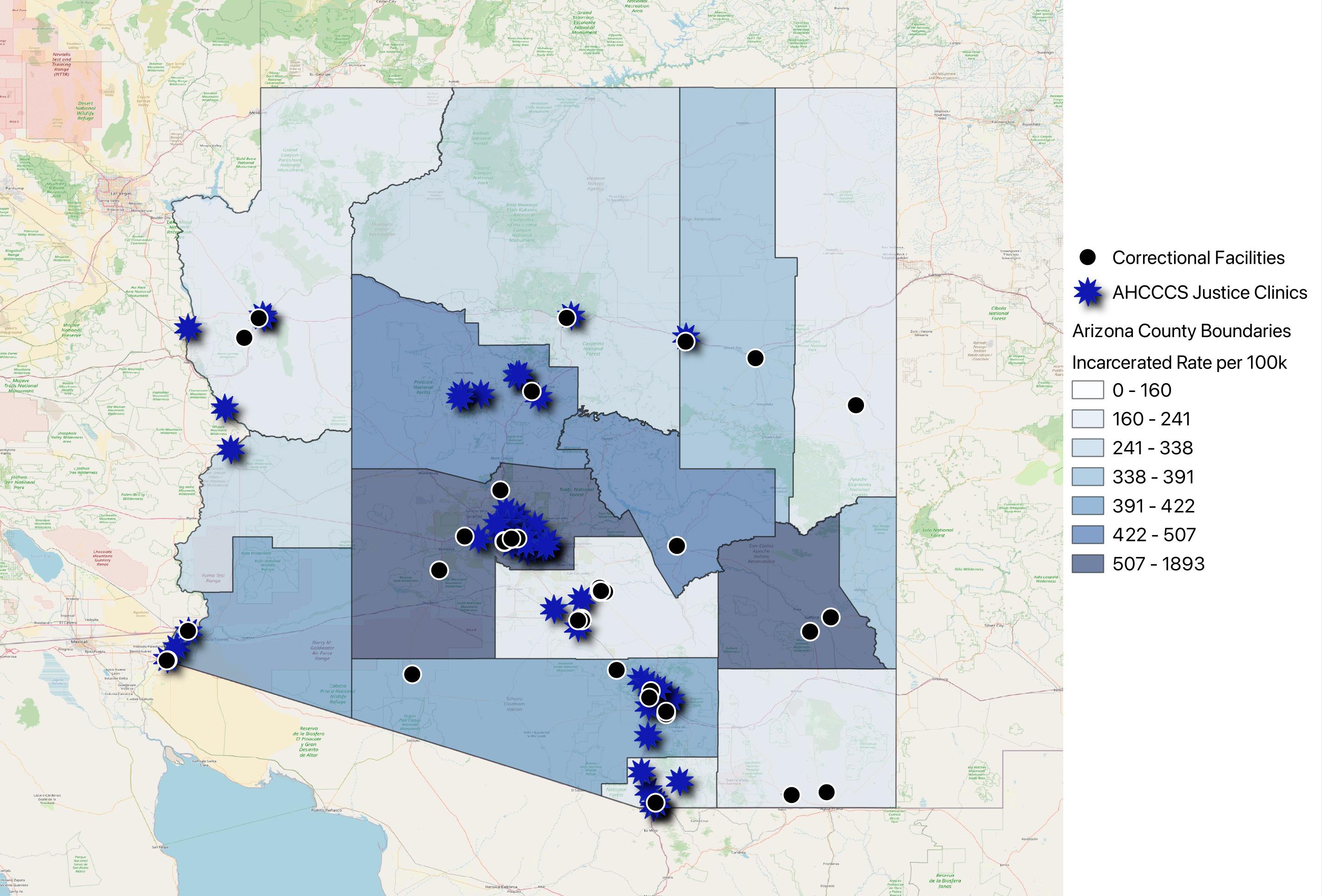
In 2017, AHCCCS began to improve its delivery system’s capacity to deliver more integrated care through its Targeted Investment (TI) Program. The TI program incentivizes Medicaid providers to effectively address social determinants of health. If a provider meets certain benchmarks, they will receive financial benefits through managed care plans to address members’ health related social needs and improve their health outcomes.52 As part of the TI Program, AHCCCS supported the establishment of 13 clinics that are co-located or adjacent to probation or parole offices.53 These are known as Justice Clinics. These clinics ensure that formerly incarcerated people are able to receive a sameday appointment upon release and during any visits to a probation or parole office.54 They also offer nonemergency medical transportation.55
We analyzed the location of the Justice Clinics and their proximity to ADCRR facilities. The map on the following page provides a spatial analysis of incarceration rates across Arizona counties, visualized using a graduated color ramp, with darker colors indicating higher rates of incarceration. Overlaid on this map are the locations of AHCCCS Justice Clinics (stars) and correctional facilities (points) offering a comprehensive view of how these resources align with areas of greatest need.
The program’s Justice Clinics are not equally distributed across the state, with notable gaps in access to these clinics across the East and Southeast portion of the state. Six counties do not have AHCCCS Justice Clinics, five of which have one or more correctional facilities. Graham County, a predominantly rural county, has a high incarceration rate and does not have an AHCCCS Justice Clinic within the county. Having both an interested justice partner and healthcare provider is necessary for a county to apply for an AHCCCS Justice Clinic, meaning there are some institutional barriers. While AHCCCS has made extensive strides at bolstering network capacity to provide culturally competent care for individuals reentering the community, continued engagement with potential healthcare providers and carceral partners is still needed to achieve full network adequacy.
AHCCCS also modified its contracts with its MCOs to create specific staff at the MCO, called Justice Liaisons, that delivered care coordination to people returning from incarceration. All MCOs are now required to appoint a Justice Liaison to support their members. These Liaisons are principally responsible for transitioning the care of Medicaid members who are incarcerated at ADCRR facilities, county jails, and juvenile detention centers back into their communities upon release. This includes developing and maintaining partnerships
with critical reentry staff at carceral facilities and with community providers, processing rosters from the shared data between AHCCCS and ADCRR, and, most importantly, conducting “reach-in” activities to ensure that AHCCCS has contact with eligible members prior to release. These reach-in activities have evolved over time, and now consist of meeting in-person or virtually with members who are enrolled in a plan with the MCO, screening them for needed clinical and social services within the community, and developing a coordination plan that outlines the steps within the reentry process for that specific member, including accessing a clinical appointment within seven days of release.
AHCCCS has steadily expanded and professionalized these delivery system reform strategies by including more carceral facilities in the interagency data feed and developing a formal policy and contract to govern and oversee the Justice Liaisons’ work. These strategies have helped make AHCCCS’s delivery system more accountable for, and responsive to, the needs of Medicaid members approaching reentry.
AHCCCS has also steadily integrated resources that address their membership’s HRSNs into the broader delivery system. These initiatives recognize that factors such as housing, mental health, and substance use are deeply interconnected with overall well-being, particularly for populations that have historically faced systemic barriers to accessing comprehensive care.
The first key reform is AHCCCS’s Whole Person Care Initiative (WPCI). The WPCI is focused on improving the essential HRSN of enrolled members including socioeconomic factors, physical environment and health behaviors. One of WPCI’s main ways of supporting those goals is through the CommunityCares statewide closedloop referral system (CLRS), which is used to screen and refer members enrolled in care management.
The second key reform is the H2O program. The H2O program aims to provide housing-related services and support to AHCCCS members experiencing homelessness or housing instability, including those leaving incarceration. By connecting eligible members with transitional housing, rental assistance, and case management, H2O seeks to reduce recidivism, avoidable hospitalizations, and emergency room visits while improving health outcomes. This program was approved in October 2022.
Together, these eligibility system and delivery system reforms have provided a solid foundation that AHCCCS can build upon for an 1115 reentry waiver.
The Opportunity of the 1115 Reentry Waiver
Until 2018, Arizona and other states that expanded Medicaid still faced significant limitations to overcome the barriers of the IEP and the subsequent health challenges related to reentry. However, federal policy changed significantly with the SUPPORT Act’s passage in 2018.56 The SUPPORT Act authorized CMS to develop strategies for state Medicaid agencies to waive certain aspects of the IEP. After conducting a mandatory stakeholder feedback process and producing a report to Congress,57 CMS issued formal guidance to states on developing a package of services that could be provided during the reentry period through 1115 demonstration waivers.58
CMS established three requirements for states to include in their 1115 demonstration waivers. First, all Medicaid-eligible members must maintain their eligibility in a suspended state, rather than having their eligibility terminated. As noted previously, Arizona already initiated this policy in 2017. Second, CMS outlined a minimum standard for pre-release health care services, which must be provided at least 30 days before release. Such services must include case management, medication assisted treatment (MAT), and a 30-day supply of all prescription medications. CMS also allows states to cover additional services of their choosing. Finally, CMS specifies that states must cover all proposed services for a minimum of 30 days pre-release but can extend that timeframe for up to 90 days pre-release.
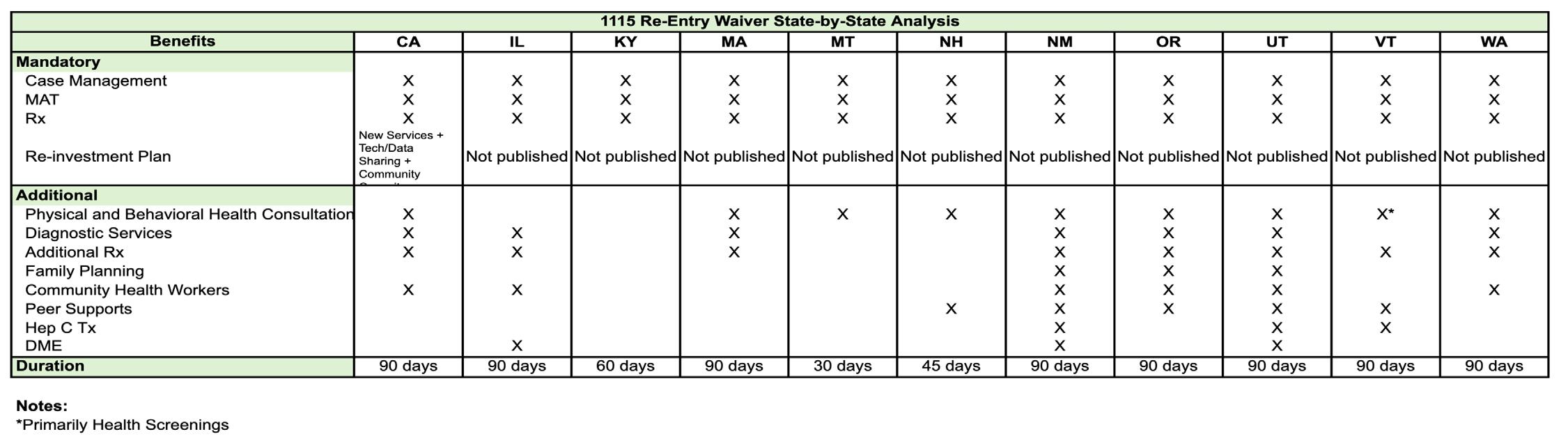
Eleven states have already received approval from CMS for 1115 demonstration waivers. We present a highlevel overview of those states, their service packages, and the coverage window in Table 1. Throughout our recommendations, we reference many of these states and their approach to services that overlap with our suggestions for AHCCCS. Frequently, we highlight three states, California, Washington, and Montana: California, because it has helped shape federal policy and as the first state to implement will inform other states’ efforts, and Washington and Montana because they are geographic analogs to Arizona with urban and rural regions and significant tribal populations.
In May 2021, AHCCCS submitted a Section 1115 demonstration waiver for its H2O program, which included provisions for a limited scope of reentry services. However, this proposal preceded CMS approval of several state demonstration waivers and CMS’s comprehensive guidance on reentry services. In 2023, AHCCCS requested that consideration of the reentry services within the H2O waiver be paused to allow the state to craft a new proposal considering newly approved state demonstration waivers and new guidance on reentry services. In mid 2024, faculty at SPIA developed an agreement with AHCCCS under which our graduate policy workshop would research best practices for reentry services and care to inform a renewed effort to obtain 1115 waiver authority. In late 2024, AHCCCS received approval for a reentry waiver and initiated the development of an implementation plan and strategy, leveraging the ongoing work of the policy workshop included in this report.
Research Team and Process
Thirteen Master in Public Affairs candidates at SPIA, under the guidance of co-instructors Heather Howard and Dan Meuse, conducted research – including field research in Arizona – over 12 weeks to build this report and its respective recommendations. The team conducted 14 interviews with Arizona subject matter experts and stakeholders in October and November 2024. The team met with AHCCCS staff, and women who were incarcerated at Perryville Prison, employees of local advocacy groups focused on homelessness and incarceration, ADCRR staff, and Medicaid officials from peer states.
This report synthesizes feedback from those meetings, analysis of AHCCCS data, conversations with other states, publicly available policy analysis, and peerreviewed research in order to provide AHCCCS with recommendations for a Section 1115 waiver request to extend coverage for a package of services 90 days prior to a person’s release from incarceration.
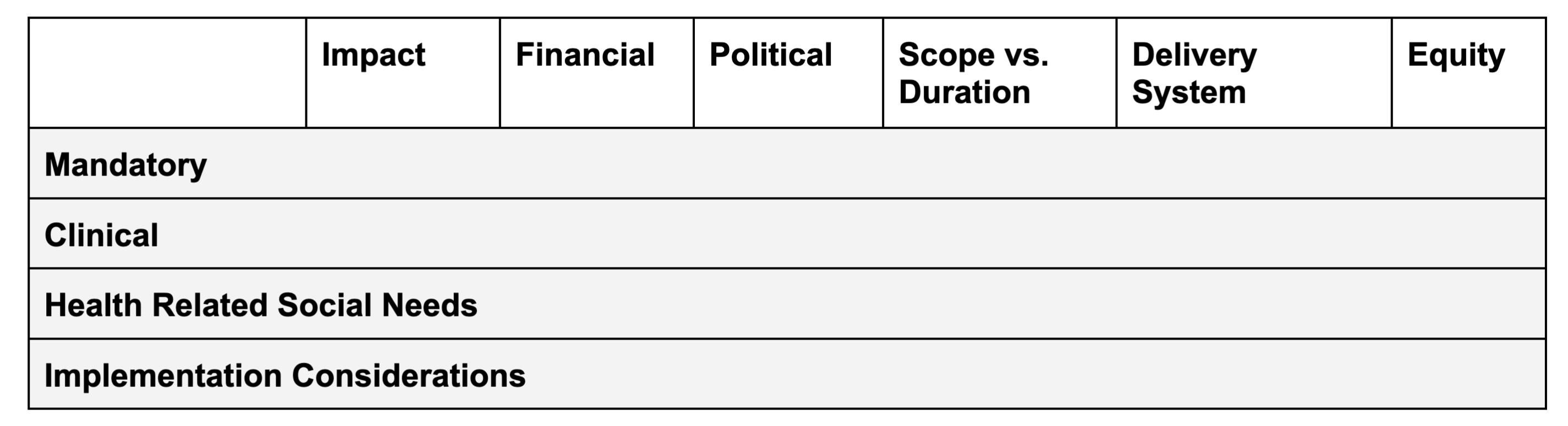
DECISION CRITERIA
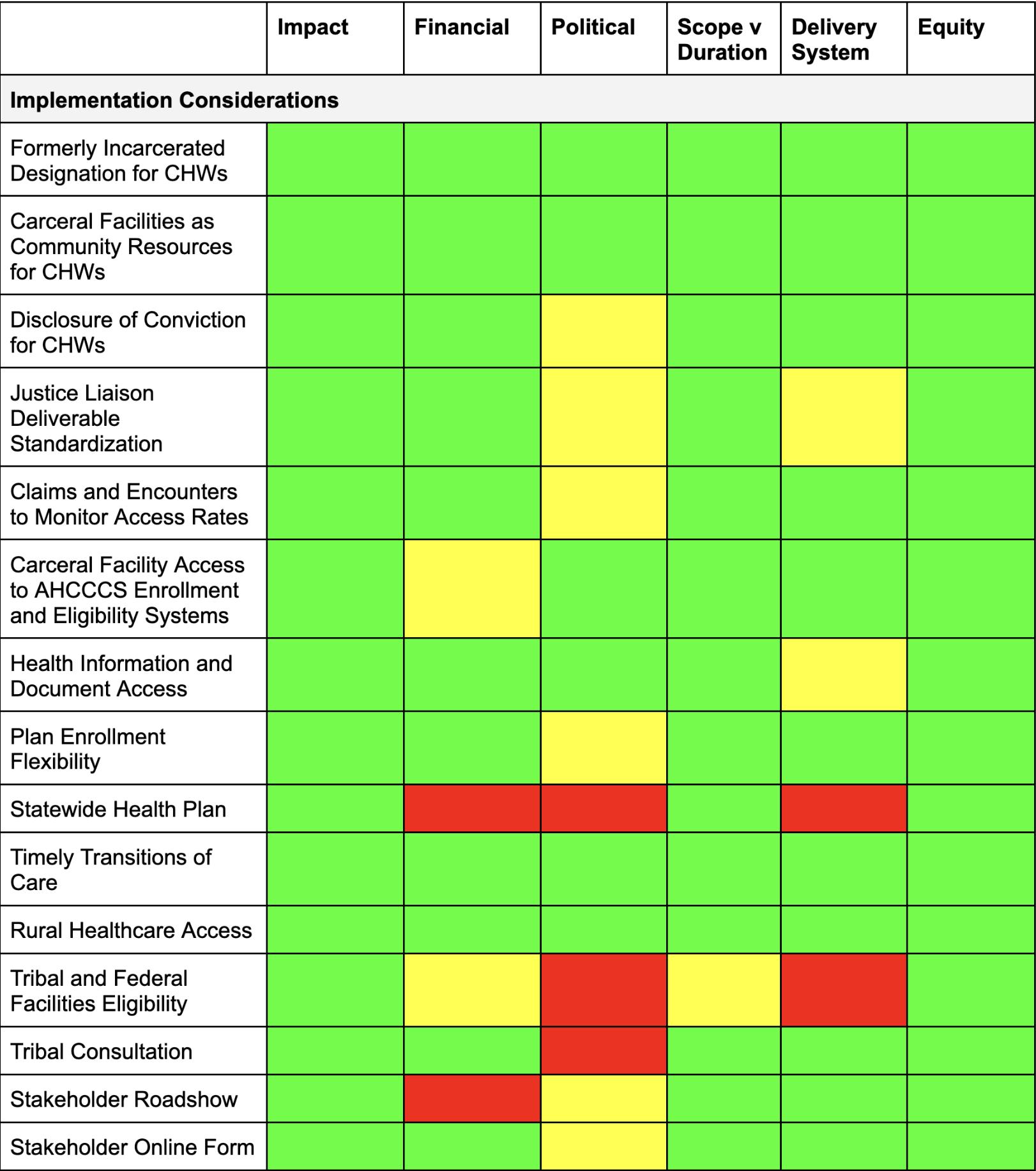
We created the following decision criteria to help AHCCCS analyze and prioritize our recommendations for adoption and implementation. Each recommendation is screened through all decision criteria and ranked based on a “stoplight” ranking system, where green represents easier implementation, yellow represents moderate implementation, and red represents difficult implementation.
• Impact: AHCCCS endeavors to be responsive to its members’ needs and stakeholders’ input. For example, patients may visit pharmacies frequently post-release because they need medication, but may experience major transportation barriers. Therefore, covering both pharmacy and transportation services would respond to a high need and generate a deep impact. We assess our recommendations based on impact by asking the following questions:
• What was elevated frequently in our stakeholder interviews?
• When analyzing data, what services are used most consistently?
• What services address the mortality risk this population faces?
• Financial: Like all state Medicaid agencies, AHCCCS faces significant funding constraints and must evaluate the operational and financial trade offs of covering services. For example, AHCCCS may be able to provide low-cost behavioral health therapy, but care provided by a physical health specialist, like a radiologist, may need to be reserved for the members with the highest needs. This criterion assesses recommendations based on the cost AHCCCS would likely bear in covering and implementing them, by asking the following questions:
• What are the cost and utilization estimates for a particular benefit?
• How much would it cost to ensure the delivery system’s capacity to administer a particular benefit?
• Political: Successful implementation of this initiative will require suppor t from a broad range of stakeholders, including but not limited to clinical providers, community-based organizations, advocates, carceral agencies and facilities, and elected officials. In many cases, these stakeholders’ preferences may not be perfectly aligned. For example, carceral agencies may want AHCCCS to cover specialty services, whereas behavioral health providers may prefer an expanded scope of substance use services. This criterion assesses recommendations based on expected support or opposition from various stakeholders, by asking the following questions:
• Who would support or oppose the recommendation?
• What is the basis for their position?
• What leverage do they have in the policy-making process?
• Scope vs. Duration: AHCCCS explicitly noted the trade off between the scope of services covered and the amount of time that each service could be covered pre-release. For example, AHCCCS may prefer to cover benefits for the longest time possible to ensure a person establishes a relationship with a provider, or it may prefer to cover more benefits to address as many clinical needs as possible. This criterion assesses recommendations based on whether increased time or benefits would have a greater impact by asking the following questions:
• How does this benefit build trust between an enrolled member and a clinical provider?
• How does this benefit align with historic mortality risk data for this population?
• What do providers and community advocates say they value more?
• Delivery System: AHCCCS and community partners have limited capacity to administer and deliver proposed services. For example, AHCCCS may not have enough substance use providers to deliver quality and timely MAT. This criterion assesses recommendations based on whether AHCCCS’s existing delivery system has the capacity to realistically administer proposed services by asking the following questions:
• Do Medicaid provider networks historically include providers who deliver these services?
• Do alternative partners who could be involved in implementing this recommendation, such as community-based organizations, carceral facilities, or local governments, have the capacity to implement this recommendation?
• Would this recommendation require additional resources and capacity-building to execute?
• Equity: Meeting the specific needs of formerly incarcerated people may require benefits that are not offered in the same capacity to AHCCCS’s general membership. Thus, equity, or tailoring to the unique needs of a population, may need to be weighed against equality, in which all AHCCCS members would receive the same benefits. Additionally, even within the incarcerated population, members of some subgroups face additional socioeconomic barriers and may require additional support to achieve similar outcomes to the rest of the incarcerated population. For example, women may need access to reproductive health in the pre-release period to effectively establish care in the community post-release. Tribal members may require alternative coordination services because most are not enrolled in a MCO. This criterion assesses recommendations based on how well they respond to a distinct need of incarcerated members, and how they may differentially impact subgroups of the reentry population by asking the following questions:
• Is this service effective in responding to the unique needs of the incarcerated population?
• Does a subpopulation face particular barriers around this service?
• Is there an additional social stigma for a group or population once they are released from incarceration – beyond the stigma associated with being formerly incarcerated?
• Do any subpopulations require additional services to achieve successful reentry?
RECOMMENDATIONS FOR AHCCCS’S 1115 REENTRY WAIVER APPLICATION
Below, we present two sets of core recommendations.
In our first set of recommendations, we propose a comprehensive package of services that should be provided 90 days prior to a member’s release from any carceral facility, including state prisons and county jails. We divided the services package into three categories: 1) mandatory services required by CMS, 2) additional clinical services, and 3) non-clinical services that address HRSNs.
These services were recommended based on the following goal and principle: to build a meaningful relationship between an individual returning to the community and a community provider to address needs and establish trust. While some – if not all – services proposed are in some cases duplicative of services provided by carceral facilities, there is a demonstrated need for more and better services, a sentiment shared by stakeholders and members alike. AHCCCS has an opportunity to both meet this demonstrated need, create psychological safety and build trust for individuals who are reentering society and experiencing a scarcity mindset. This safety and trust is a crucial foundation for successful reentry over the long-term.
We propose providing the following services 90 days pre-release:
• Mandatory Services
• Case management
• Medication Assisted Therapy (MAT)
• 30 day supply of medication
• Reinvestment Plan
• Clinical Services
• General consultation for physical and behavioral health
• Family planning services
• Dental care
• Dermatology
• Lab and radiology services
• HRSN Services
• Housing navigation services
• Transportation services
• Food and nutrition support
In our second set of recommendations, we outline recommendations for administrative policies that will ensure effective implementation. These include recommendations related to improving capacity within AHCCCS’s delivery system, bolstering workforce capacity specifically for community health workers, improving the flow of and access to health information, providing flexibility in the health plan enrollment process, addressing access challenges in rural parts of the state, and addressing the specific needs of Tribal members. We also include recommendations on how best to evaluate the waiver’s efforts.
Reentry Service Package
Duration of Services
AHCCCS expressed strong interest in exploring whether to create a more expansive package of services or a longer duration of a smaller set of services. This tradeoff reflects the financial and administrative constraints of any Medicaid program. Throughout our interviews and analysis of other states’ waivers, stakeholders stated that the duration of services mattered more than the scope. One provider told us, “Time, by far, outweighs anything else.” Much of their rationale reflects what is already documented in the Report to Congress59: a longer time period affords clinicians, a Justice Liaison, and other community members greater opportunity to build a relationship with a person who is reentering. This trust is foundational for engagement in critical services and, ultimately, successful reentry.
Recommendations:
1. AHCCCS should pursue the full 90-day coverage opportunity afforded by CMS. This should be the foundational cornerstone of AHCCCS’s waiver design. Eight of the 11 states that have received authority for their 1115 reentry waivers will provide services for 90 days pre-release: California, Illinois, Massachusetts, New Mexico, Oregon, Utah, Vermont, and Washington. We recommend a suite of potential services in the section below. However, AHCCCS should ultimately select services for the 90 day service provision window based on the other decision criteria that we identified.
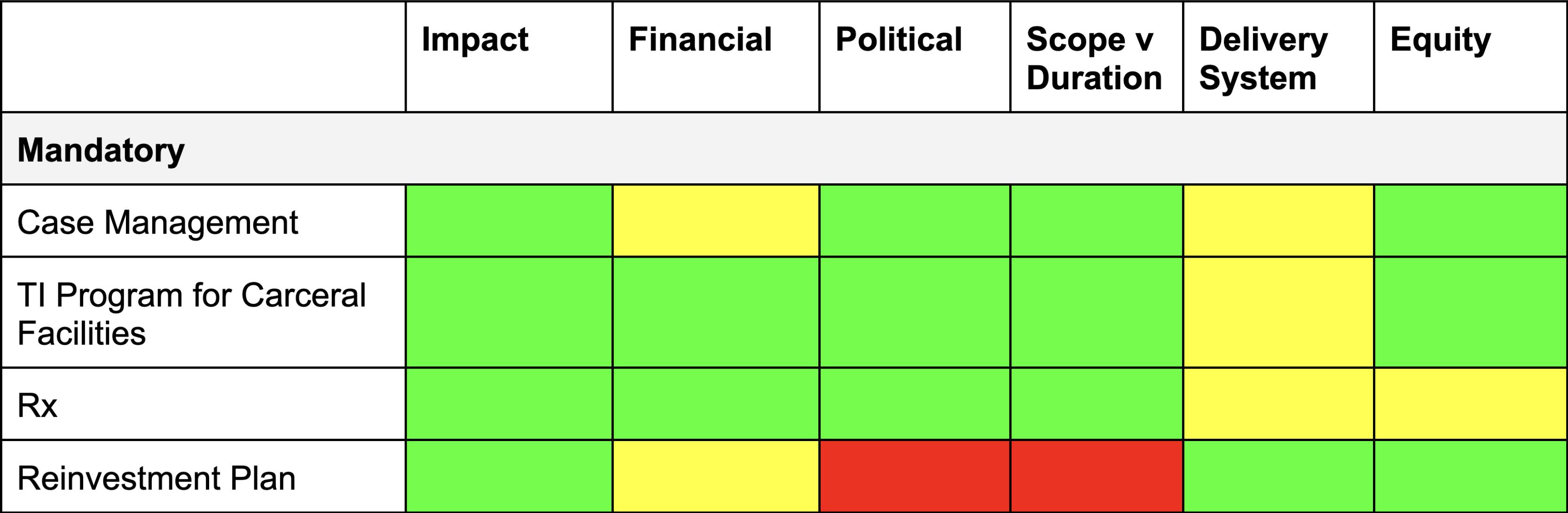
Mandatory Services
CMS’s 2023 guidance letter outlined four mandatory services which any state applying for an 1115 reentry waiver should include: case management, MAT, prescription drug provision prior to release, and reinvestment of profits into the communities each care provider serves. We recommend using these mandatory services to maximize the impact of other services AHCCCS decides to provide, as the mandatory services address core health challenges during the reentry window.
Service 1: Case Management
CMS requires states to include case management services to “assess and address physical and behavioral health needs and [health-related social needs]” for all covered beneficiaries.”60 Case management includes any service “furnished to assist individuals, eligible under the State plan who reside in a community setting or are transitioning to a community setting, in gaining access to needed medical, social, educational, and other services.”61 Specifically, CMS has encouraged states to include the following activities in its case management services under the reentry waiver: 1) conducting comprehensive assessments and periodic reassessments of an individuals’ needs, 2) developing and periodically revising of a specific care plan based on the information collected through the assessment, 3) making referrals and scheduling appointment for individuals, and 4) following up with contacts to ensure the care plan is effectively implemented.62
Case management is the vital administrative link between benefits promised by Medicaid and benefits needed and, ultimately, received by Medicaid members. For members leaving incarceration, case managers can develop a specific care plan based on their goals and needs, which can then serve as a checklist during postincarceration check-ins.63 To borrow a famous analogy, case management turns providers and administrators from “cowboys,” working without coordination on the respective areas, into “pit crews” who work in concert on a member’s overlapping and complex health needs.64 Case management is especially important because, as Medicaid expands to offer more services, each member and case manager has more services to keep track of and manage.
Other states have used the case management requirement as a chance to connect members to services that address their HRSNs. California puts responsibility for case management in a “lead care manager” who is expected to proactively identify programs, including HRSN offerings, for which members
may qualify.65 To ensure effective resource allocation based on the acuity of a member, California maintains three levels of case management tiered by frequency of monitoring: basic case management, complex case management, which applies to members with acute or complex conditions, and enhanced case management, which requires frequent, face-to-face visits to members with serious medical needs who are part of an atrisk population – including those returning from incarceration.66
Recommendations:
2. AHCCCS should create a tier approach to case management based on the acuity of a member’s needs. For members with higher needs, AHCCCS should prioritize case management that entails higher frequency and in-person contacts. They should also designate case managers as the authoritative and consistent contact persons for enrolled members.
3. AHCCCS should develop a comprehensive checklist for case managers to quickly screen a member for a range of benefits they may be eligible for and need. AHCCCS should build this checklist from existing intake and care planning forms to that it has used in other initiatives, including the Whole Person Care Initiative and H2O.
4. AHCCCS should require a base standard of in-person meetings for each level of case management. Case managers should also be required to identify and establish with the member the desired and primary mode of contact as the pair navigates the member’s care plan.
5. AHCCCS should require case managers to schedule at least one post-release health care appointment for all members, regardless of acuity. AHCCCS should track and publish these appointment rates as a key performance indicator.
6. AHCCCS should use some of its Reinvestment Plan money to build workforce programs that improve the supply of case managers and to ensure consistent access to case management services. These programs can be developed and executed with local universities and community colleges.67
7. AHCCCS should convene a working group with its MCOs and other justice partners to determine how case management services align with the current programming. There is a high degree of overlap between the Justice Liaisons and the opportunity afforded under case management. AHCCCS will need to determine an appropriate division of labor between Justice Liaisons, case managers, TI Justice Clinics, Parole Officers, and pre-release reentry coordinators at carceral facilities in order to reduce duplication in its delivery system.
Service 2: Medication Assisted Treatment
CMS requires states to provide MAT services as part of their demonstration benefits package. MAT services must include medication coupled with counseling and other behavioral therapies. Services must be clinically appropriate and individually determined so as to meet the core components of a State’s and CMS’s definition of medical necessity. They must also be available for all types of substance use disorders (SUD), including alcohol and opioid use disorder. States are encouraged to cover as many FDA-approved medications as possible to ensure treatment flexibility. These medications can include buprenorphine, methadone, naltrexone, and acamprosate.
This benefit recognizes that people who are incarcerated experience higher rates of SUD than the general population.68 Poor access to post-release treatment and lack of continuity of care increase mortality rates from overdose for this population during the reentry window.69 MAT services have been shown to effectively address these health needs and risks, both in carceral settings70 and the broader community.71 Earlier engagement in MAT offers community-based providers the opportunity to build trust with this population72 – trust that can have positive spillover effects on the use of complementary therapies and services.
All states that have submitted reentry waivers have pursued MAT services. Where states vary is in their approach to assisting carceral agencies with delivering these services. Not all carceral settings have the capacity to deliver the full range of SUD treatment and services offered by their respective Medicaid programs, creating a potentially dangerous discontinuity in treatment and service provision. Washington has developed a capacity building program using their demonstration’s $303M of technical assistance money to address this dilemma.73 The program offers funding on a per-capita basis for carceral facilities to adopt and implement an electronic health record that can communicate with community providers and bill Medicaid, as well as to develop care management
policies and protocols that help the facilities effectively deliver the demonstration’s services.
Recommendations:
8. AHCCCS should use part of its waiver budget for capacity building for MAT service delivery in carceral facilities. Funds should be devoted to the adoption of electronic health records that can communicate with community providers, the development of SUD care initiation and management protocols, and the administrative capacity to screen for and enroll people in Medicaid at booking.
Service 3: 30-Day Supply of Prescription Medications
CMS requires states to provide incarcerated members with a 30-day supply of prescribed medications upon their release. This mandate addresses the critical need for continuity of care and aims to close gaps in access to essential medications during the challenging transition back into the community.
A 30-day supply of prescription medications is vital for improving health outcomes and reducing recidivism among formerly incarcerated members. Evidence from Medicaid demonstration projects highlights the benefits of this approach, including smoother care transitions, reductions in emergency department visits and hospitalizations, and overall enhancement of health and well-being for this vulnerable population.74 By mitigating barriers to access, the mandate decreases the risk of health crises, relapse, self-harm, and mortality during the high-risk post-release period.75
Several states have effectively implemented this policy, including California, Illinois, Kentucky, Massachusetts, Montana, New Hampshire, New Mexico, Oregon, Utah, Vermont, and Washington. For example:
• California has leveraged its Section 1115 Medicaid waiver to support continuity of care during reentry, ensuring members who are released receive the medications and support necessary for a successful transition.
• North Dakota supplements the 30-day supply with follow-up care and support, demonstrating improved health outcomes and reduced recidivism.
• Washington employs a comprehensive strategy through its Reentry Initiative, which incorporates a phased approach to medication management. This initiative prioritizes providing members who are released with essential medications while offering additional support services to stabilize health conditions and mitigate adverse events.
Washington’s phased medication management approach exemplifies how tailored strategies can address the unique healthcare needs of formerly incarcerated members. By focusing on continuity of care and resource allocation, this initiative helps to improve health outcomes, promote successful reintegration, and reduce recidivism.76
Recommendations:
9. AHCCCS should work with ADCRR and other carceral systems to ensure consistency of medication formularies and awareness of current treatment as permitted by 42 CFR Part 2 across carceral facilities and community providers.
Service 4: Reinvestment Plan
CMS requires states to submit a Reinvestment Plan as part of their demonstration application. The plan must outline the state’s strategy to reinvest the total amount of new federal matching funds in services or structures that complement the demonstration’s approved services. These additional services must be aimed at improving at least one of the following areas: 1) access and quality of care for people who are currently incarcerated or formerly incarcerated and 2) health-related social needs that may decrease a person’s likelihood of criminal justice involvement.
CMS has given the following topics as potential areas for reinvestment: improved 1) access to communitybased physical and behavioral health services, 2) access to and quality of demonstration services offered in carceral settings, 3) information technology and data sharing capacity, and 4) capacity for communityproviders to holistically meet the needs of this population, including their HRSNs. These categories are not meant to be exhaustive. However, CMS prohibits the use of any reinvestment funds to build new carceral settings or expand overall operating capabilities other than improving the ability to deliver improved health care services.
The requirements of the Reinvestment Plan are consistent with CMS’s previous policy approach for other delivery system adaptations, specifically the Delivery System Reform Incentive Program (DSRIP) initiative. This policy approach affords states the ability to make targeted investments in their delivery systems in order to better adapt them for value-based payments and the holistic needs of their members. The extension of this approach to this particular population is also in response to feedback77 from stakeholders about the need to make additional investments that improve reentry and diversion from the justice system to the health and social services system.
Currently, only California has developed and received approval for its Reinvestment Plan.78 The plan has three focus areas: improved 1) access and quality of demonstration services in carceral settings, 2) information technology and data sharing capacity, and 3) capacity for community providers to holistically meet the needs of this population, including their healthrelated social needs. All other approved states are due to submit their Reinvestment Plans in Winter 2025.
Recommendations:
10. AHCCCS should consider developing a Reinvestment Plan that builds additional capacity for demonstration services that extend into the community, community-based HRSN services, and community-based behavioral health services. Specifically, AHCCCS should create enterprise loans for community clinics to hire and sustain community health workers, create a permanent supportive housing finance fund that helps build affordable housing, and bolster pre-school and other school-based behavioral health and social and emotional development programs and services that deter future criminal activity and involvement. The funds allocated under the Reinvestment Plan are wholly distinct from any funds devoted to capacity building under AHCCCS general waiver budget.
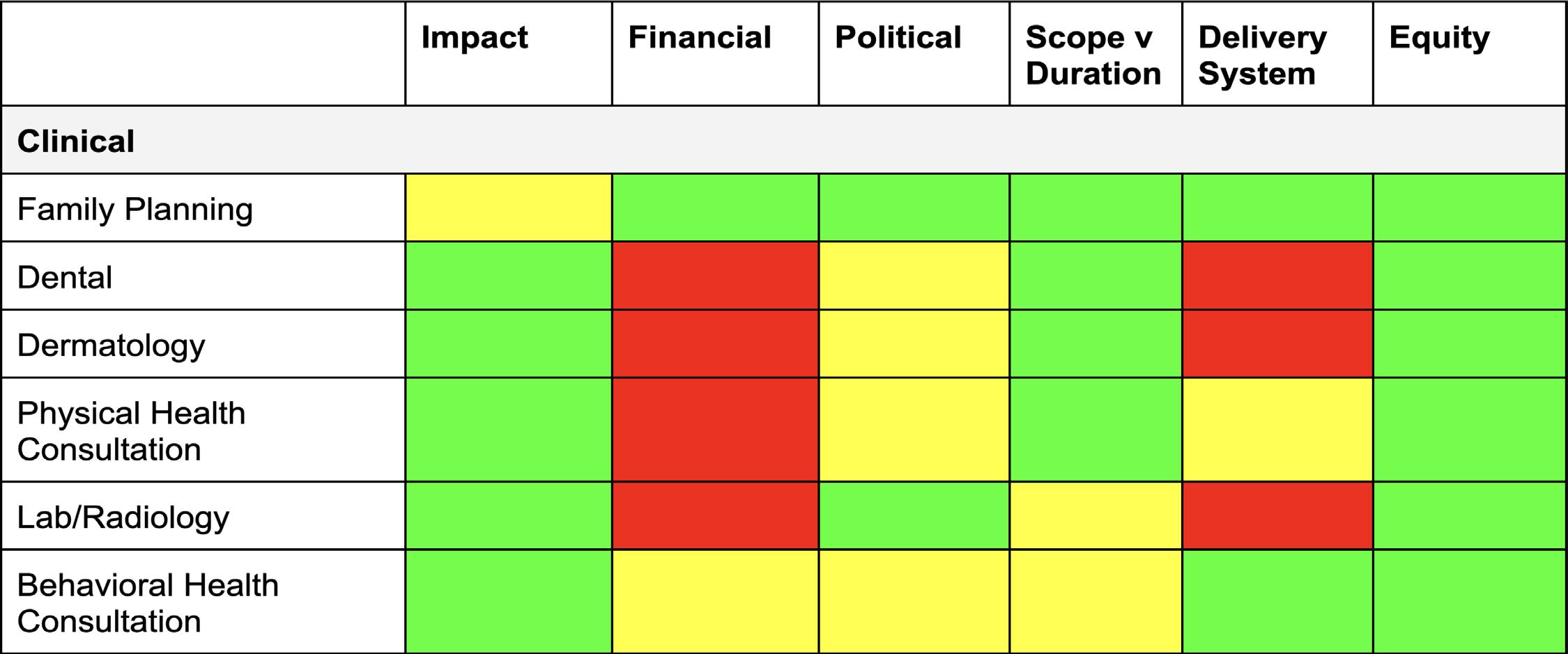
Clinical Services
In addition to mandatory services AHCCCS must incorporate, we recommend a few additional clinical services. These services are intended to address additional healthcare needs of people who are returning from incarceration and improve the likelihood that a person establishes a relationship with a trusted clinician prior to release to improve outcomes once released
Physical Health Consultation
People who are incarcerated experience worse physical health on average than the general population. The women at Perryville Prison saw a physical health consultation as a way to begin addressing these poor health outcomes, particularly diabetes and other chronic health conditions, and as an opportunity to establish care with an outside clinician before being released. Pre-release consultations would allow a member and clinician to build a relationship, and more crucially, trust, which will increase the odds that a member will receive follow-up care once they return. Currently, nine states are providing physical health consultations as part of their waivers.
Recommendation:
11. AHCCCS should cover a general physical consultation to identify and address chronic conditions, including making referrals to appropriate specialists, in the pre-release window.
Behavioral Health Consultation
Behavioral health, including pre-release therapy services, will allow incarcerated members to plan coping mechanisms for stressors they may encounter postrelease. In the post release-period, suicide and overdose rates are significantly higher than in the general population.79 The incarcerated women at Perryville repeatedly mentioned lack of behavioral health care as a concern, especially those diagnosed with SUD or SMI. They also noted that under the current system, they do not see the same provider each visit in prison, which prevents them from developing the level of trust required for effective therapy. Access to a behavioral health consultation with a clinician to perform screenings or initiate treatment during the pre-release window would help mitigate these challenges and help establish a more stable relationship with a provider in the community.
Currently, nine states have included behavioral health consultations in their waivers. Washington’s waiver includes behavioral consultation pre-release, and Montana’s includes a provision for a warm hand-off to behavioral health providers post-release.
Recommendations:
12. AHCCCS should cover a behavioral health consultation, including screenings and initiation treatment.
13. AHCCCS should leverage telemedicine to better connect members with behavioral health clinicians who are located in the communities where the members will be returning.
Family Planning Services
Approximately 77,000 women are incarcerated in state prisons nationwide.80 A 2006 survey of incarcerated women in the U.S. found that 85% planned to be sexually active upon release, but only 9% reported wanting to be pregnant.81 Affordable and reliable contraception and education are important in preventing unintended pregnancies in an already difficult period of transition. Oral contraceptives, when taken properly, can take up to 7 days to prevent pregnancy. If people are not able to access contraception while in prison, they risk a minimum of a 7 day window after release when they are at higher risk of unwanted pregnancy. A onemonth supply of medicine or a long-acting reversible contraceptive would allow the reentering person to connect with a provider outside the walls with enough time to avoid a lapse in coverage. Currently, New Mexico, Utah, and Oregon’s waivers cover “family planning services and supplies”.
Recommendation:
14. AHCCCS should cover reproductive health education and contraceptive access, including oral contraception and long-acting reversible contraceptives (LARCs), and STI testing, treatment, and prevention education prior to release.
15. AHCCCS should work with ADCRR and its carceral partners to align its coverage with any family planning policies at the carceral facility. For example, the current policy at Perryville Prison, ADCRR’S sole women’s facility, is to offer oral contraception to incarcerated people 30 days before their release. This policy will need to be revised based on AHCCCS decision.
Dental
Incarcerated members often face significant barriers to oral health care, resulting in a high prevalence of untreated dental issues such as decay and periodontal disease.82 Limited access to preventive and routine dental care is compounded by factors such as inadequate resources, insufficient staffing, and a general lack of prioritization within carceral healthcare systems (see Appendix). Many prisons are designated as Dental Health Professional Shortage Areas, with inmate-to-dentist ratios often exceeding 1,500:1.83 Poor oral health among incarcerated members is linked to broader systemic health issues, including diabetes, cardiovascular disease, preterm delivery, and osteoarthritis.84
Comprehensive dental care during the pre-release period can help address these poor health outcomes. These services can include screenings to identify urgent dental issues, treatment options like fillings, extractions, or denture fittings, as well as the distribution of oral hygiene kits and education on proper oral care.85 Such preventive care, combined with health education, counseling, and links to community providers, can encourage better oral hygiene habits and reduce reliance on emergency services after release. Pre-release healthcare services also involve preventive measures such as fluoride varnishes and screenings for conditions like diabetes and cardiovascular disease.86 Establishing links with community providers and preparing individualized transition plans are crucial for ensuring that continuity of care is upheld post-release, thereby aiding members in their successful reintegration into society.87
Currently, no states have included dental care as part of their waivers. Including this service offers AHCCCS to be a leader in addressing this critical need for people who are returning from incarceration. AHCCCS’s current dental coverage focuses on comprehensive services for members under 21 and limited emergency and preventive care for members 21 and older, including a $1,000 annual benefit for ALTCS members. While this aligns with addressing urgent dental needs, it does not fully encompass the targeted pre-release services we propose, such as screenings, oral hygiene education, and preventive measures like fluoride varnishes, which could reduce emergency care reliance and improve continuity of care post-release.88
Recommendations:
16. AHCCCS should offer cost-effective, targeted dental care during the pre-release period to address urgent oral health issues and promote preventive care, reducing reliance on expensive emergency services post-release. Services should include basic screenings, necessary extractions, and oral hygiene education with distribution of hygiene kits, minimizing costs while addressing critical needs. Incorporating low-cost preventive measures like fluoride varnishes and brief health education can improve long-term health outcomes and reduce future healthcare expenditures.
Dermatology
Members in Arizona who are incarcerated face significant dermatological challenges. Prolonged incarceration in Arizona’s intense sun and low humidity raises the cumulative risk of actinic keratosis and skin cancer, especially among aging inmates who are more prone to age-related dermatological issues.89 Carceral settings can contribute to outbreaks of scabies, fungal infections, and athlete’s foot, worsened by inadequate ventilation.90 These settings and the stress they create can aggravate conditions like psoriasis, eczema, and alopecia.91 Pre-release dermatology care can improve these poor health outcomes and prevent complications from more severe conditions like skin cancers or infections.92 Pre-release care also reduces the risk of transmission of scabies or fungal infections across the community.93 Furthermore, early treatment is more costeffective than emergency care post-release, alleviating financial strain on public health systems.94 Currently, Arizona would be the only state proposing to cover dermatology.
Recommendations:
17. AHCCCS should leverage tele-medicine strategies to address potential access issues for dermatology. Tele-dermatology services, such as those implemented by the Federal Bureau of Prisons, allow inmates to consult remotely with specialists. This programming has reduced costs and logistical challenges associated with transportation.95
Lab Services and Radiology
Lab and radiology services include imaging and diagnostic services such as X-rays. These services would enhance disease diagnosis and allow people to seek and begin treatment plans upon release. Access to these diagnostic services is important for managing chronic conditions, detecting latent health issues, and addressing injuries or illnesses that may have gone untreated during incarceration. For example, one woman we spoke with discovered she had cancer after repeatedly being told by the doctor she just needed exercise. This case, described in the Appendix, illustrates how improper diagnosis harms incarcerated people.96
Currently, four states have included lab and radiology services in their waivers including Washington State. In Washington, lab and radiology services aligned with the state plan are provided in the pre-release period.
Recommendation:
18. AHCCCS should cover lab and radiology services.
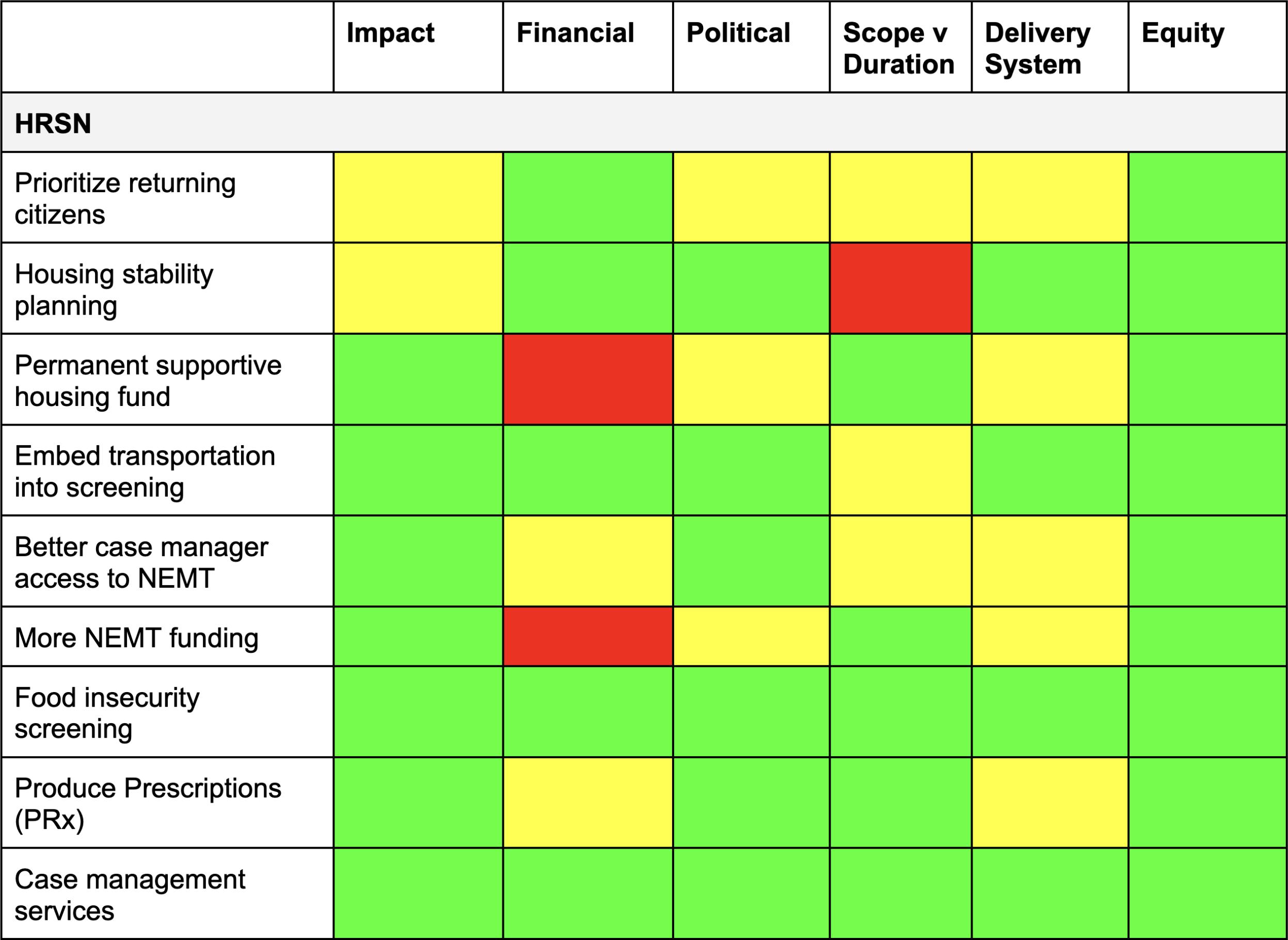
Finally, we recommend three non-clinical services that address key HRSNs of the people who are leaving incarceration. These services are intended to meet the holistic needs of this population and are consistent with AHCCCS’s goal of building new programming and reforming existing programming that delivers whole person care.
Housing
Housing instability and homelessness are closely linked with various poor health outcomes. People experiencing homelessness and housing instability face a heightened risk of chronic diseases like cardiovascular disease, hypertension, and diabetes, as well as infectious diseases due to limited access to healthcare, unstable living conditions, and social isolation.97 The stress of housing instability and homelessness worsens mental health challenges and contributes to substance use, creating additional barriers to achieving stable housing.98 Without a stable environment to support routine care and medication management, people experiencing homelessness often face a cycle of poor health that is difficult to escape. Programs that provide permanent supportive housing and other housing supports, like the AHP and H2O, have shown promising results in reducing emergency department visits, supporting chronic disease management, and lowering healthcare costs by addressing the foundational role of housing in health.99
The intersection of housing instability, homelessness, and incarceration is strong. People experiencing homelessness are disproportionately likely to be incarcerated, often due to criminalization of povertyrelated behaviors like loitering or sleeping outdoors.100 Incarceration can perpetuate homelessness by disrupting social ties, limiting job opportunities, and imposing restrictions on accessing public or subsidized housing upon reentry.101 Formerly incarcerated people, especially those with mental health challenges and SUD, face significant barriers to securing stable housing and are often funneled back into the criminal legal system due to insufficient support and housing options.102 The cycle between homelessness and incarceration underlines the need for integrated housing and social services to break this pattern and improve outcomes for a particularly vulnerable population.
AHCCCS should build on its H2O waiver and align its reentry waiver with that work. The H2O waiver already covers housing transition navigation services, one-time transition and moving costs, medically necessary home modifications and remediation services, and temporary rent/housing for up to 6 months for people at high risk of experiencing homelessness upon release from a correctional facility.
Currently, no other state has sought to include housing as an explicit service in its reentry waiver program. This could largely be because many states, like Arizona, are pursuing authority to cover housing supports through concurrent yet separate waivers. Still, we believe there is opportunity for Arizona to go further and to leverage the flexibility of its reentry waiver and the high housing needs of this population to cover additional supports. In conversations with the women in Perryville and officials with Circle the City, we heard about the unmet need for long term housing stability among the reentry population.
To avoid duplication with H2O, the reentry waiver should focus on longer term housing stability through better planning and a housing financing fund in the Reinvestment Plan that helps support the building of more supportive housing. In doing so AHCCCS can both support a vulnerable population and unlock significant cost savings. In New York, the Medicaid Redesign Supportive Housing Initiative led to a 40% reduction in patient days, 26%reduction in emergency department visits, 15% reduction in overall Medicaid health expenditures among members experiencing homelessness.103
Recommendations:
19. AHCCCS should prioritize people who are leaving incarceration or who are formerly incarcerated as critical populations for permanent supportive housing and housing supports under its H2O program.
20. AHCCCS should provide long-term housing stability planning for members through case management or its Justice Liaisons. Alongside other housing transition navigation services, justice liaisons should provide consultation on housing plans beyond the interim. When applicable, they should refer people who are incarcerated with services that offer long term housing.
21. AHCCCS should create a permanent supportive housing fund in its Reinvestment Plan to address the lack of long-term housing for people who are leaving incarceration or who are formerly incarcerated.
Transportation
Transportation plays a critical role in reentry. It enables access to healthcare, employment, social services, and social connections. Addressing transit barriers can reduce health disparities, improve reentry outcomes, and lower recidivism risks.104 105 AHCCCS provides non-emergency medical transportation (NEMT) for medically necessary ground and air travel to and from medical services, excluding Federal Emergency Services. Prior authorization is required for roundtrip ground transportation over 100 miles but not for shorter trips.106
People who are formerly incarcerated also need transportation support for other facets of their lives, including job interviews, training programs, court hearings, probation appointments, accessing social services, and reuniting with family members. Transportation barriers can have very significant consequences, such as a missed healthcare appointment.107 A variety of stakeholders we interviewed confirmed these challenges. They indicated that without reliable access to transportation immediately following release, it can be difficult to re-acclimate and to fulfill obligations that are needed to successfully reenter.
Currently, no state is pursuing additional coverage or changes to its NEMT benefit under its reentry waiver. We believe there is an opportunity to go further and to specifically address the challenges associated with prior authorization and transportation to and from other HRSN activities.
Recommendations:
22. AHCCCS should embed transportation as an issue that is screened for and planned around during the initial case management visit.
23. AHCCCS should ensure case managers have smooth and easy access to the prior authorization process for NEMT while executing a member’s care plan. Since many carceral facilities are significantly far away from healthcare providers, NEMT may be required to be set up well in advance and, thus, go through the prior authorization process. By giving a care manager improved access to this process, the care manager can proactively set up transportation appointments the day a member is released.
24. AHCCCS should augment and devote new funding to its NEMT benefit to include and cover additional service destinations that are specific to the needs of people who are formerly incarcerated. These service destinations could include: job interviews, training programs, court hearings, probation appointments, food banks, homeless shelters, and family visitations.
Food and Nutritional Supports
Higher rates of chronic illness among people who are incarcerated – such as diabetes and heart disease – can be facilitated or exacerbated by lack of access to nutritional food in prisons.108 In fact, only weeks of poor nutrition and limited physical activity can have longer term health implications.109 Additionally, 20% of formerly incarcerated people suffer from food insecurity,110 and people who are formerly incarcerated are more likely to live in areas with low access to nutritional food.111
In alignment with the U.S. Department of Health and Services’ Food is Medicine initiative, CMS joined other federal agencies in releasing guidance encouraging states to develop plans to incorporate nutrition services in their Medicaid programs.112 Additionally, the National Produce Prescription Collaborative is working with states to include Produce Prescriptions (PRx) as a covered benefit in Medicaid programs.113 As of July 2024, 21 states have either approved or pending Section 1115 waivers that would allow for coverage of nutrition services.114 Such programs have been shown to reduce food insecurity, improve financial wellbeing, and improve health outcomes.115 Currently, no state has included food and nutritional supports in its reentry waiver, most likely due many of them already pursuing a Food is Medicine waiver.
In lieu of an additional waiver, we believe AHCCCS can leverage its existing food services, the expansive case management definition, and the 30-day prescription requirement to ensure quality food access as a way to improve health outcomes for members reentering the community.
Recommendations
25. AHCCCS should require case managers to screen all pre-release members for eligibility for food insecurity services in the initial case management visit and care plan development.
26. AHCCCS should test and cover Produce Prescriptions (PRx) to pre-release members with certain chronic health conditions for up to six months as part of its covered medications requirement.
27. AHCCCS should require case managers to partner with and make referrals to nutrition service providers, including SNAP and WIC offices.
IMPLEMENTATION RECOMMENDATIONS
In our second set of recommendations, we outline recommendations for administrative policies that will ensure effective implementation of our recommended services.
Workforce Development and Capacity
Community Health Workers (CHW) are an emerging and promising innovation in the healthcare system. CHWs often serve in a boundary-spanning capacity, help connect the various pieces of the healthcare system and the community together, and more importantly, educate members on the healthcare system in a culturally competent way. There is a growing evidence base that shows that CHWs have positive impacts on a member’s health.116117
Currently, Arizona covers CHWs as a service. However, there is an opportunity to adjust current state rules to tailor services to people who are returning from incarceration’s needs and, ultimately, to maximize the state’s impact. People who are incarcerated experience limited access to health education, which prevents people who are incarcerated from understanding their medical conditions, treatments, and preventative care, and it impedes quality continuity of care post-release.118 Additionally, the criminal justice system - facility staff, management, and healthcare providers - may have limited understanding of Medicaid and the benefits it provides to people during and after their incarceration. Finally, CHWs have potential to become a tool for economic and workforce development by providing jobs to people within the communities that utilize and benefit from CHWs’ services.119 Adapting AHCCCS’s rules on CHWs in light of these opportunities will help extend existing delivery system capacity to this critical population.
Recommendations:
28. AHCCCS should include a history of incarceration as a documented barrier in its administrative rules, state plan, or programmatic guidance regarding CHWs. This will help call attention to this population and direct CHWs to more intentionally work with this population. Additionally, any subsequent changes and policy direction should include guidance on how CHWs should collaborate with case managers who are serving this population.
29. AHCCCS should encourage CHWs to conduct health education trainings and fairs at carceral facilities. These trainings can cover the basics of Medicaid and communitybased healthcare with facility staff, and the fairs can provide health education and promotion materials, including information on Medicaid benefits, to people who are currently incarcerated. Increasing the awareness of Medicaid benefits among carceral staff will help improve cross-training between carceral staff and community providers. Improving health literacy among people who are incarcerated prior to release would promote independent and confident living by educating members on their health needs, treatment options for chronic conditions, and how and when to seek care.
30. AHCCCS should partner with Arizona Department of Health Services (ADHS) to revise the requirements to disclose a felony or misdemeanor conviction in the employment application of CHWs.120 CHWs often reflect the communities that they serve. In doing so, they can build greater trust with members and increase the likelihood that members will engage in life saving services.121 Moreover, this approach can be an economic and workforce development tool for many marginalized communities.122 People with a history of incarceration should be no different. We engaged with a community representative in a rural county in Arizona who was formerly incarcerated and functioned like a CHW but did not have the official title. The impact of their work was profound, both in terms of engaging with people who were formerly incarcerated and building quality relationships with carceral facilities to improve the reentry processes. A simple policy change could tap into a missing market of critical workers.
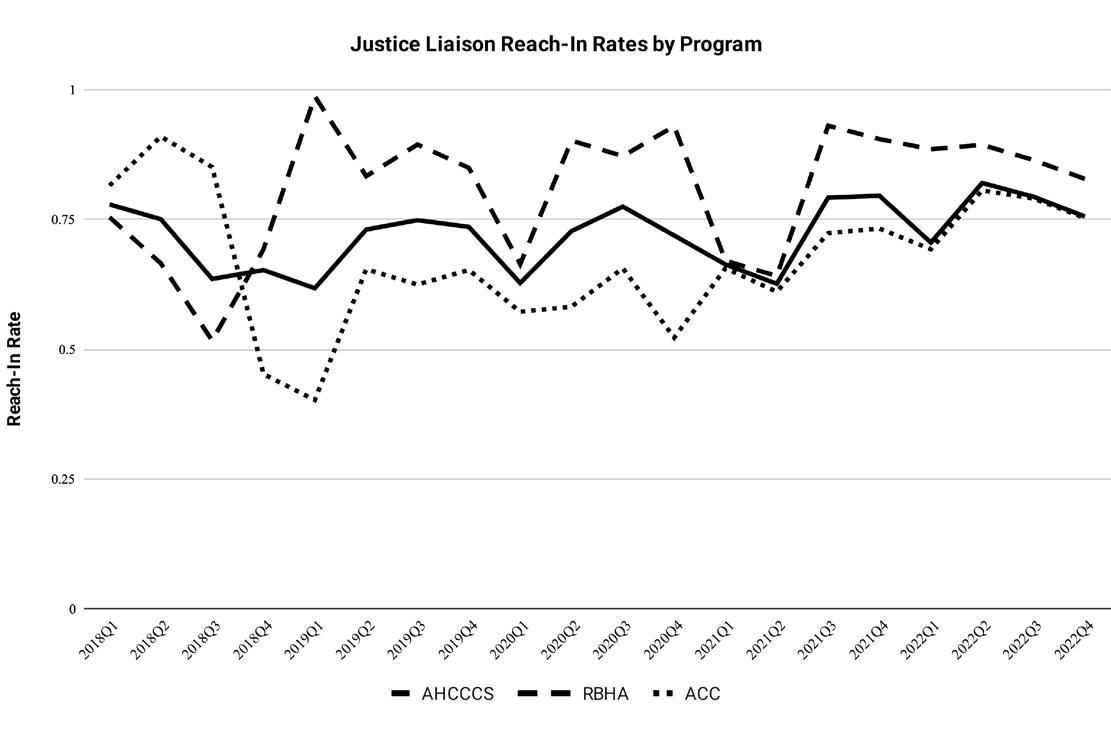
Growing evidence indicates that the Justice Liaisons have a positive effect on outcomes for people who are incarcerated. Data extracted from all Justice Liaison deliverables indicate that the Justice Liaisons are consistently delivering reach-in services123 to nearly 70% of eligible members (see Figure 3). However, performance varies across MCOs. Regional Behavioral Health Authorities (RBHAs) have a reach-in rate of 83% while AHCCCS Complete Care MCOs (ACCs) have a rate around 75%. The disparity may arise because RBHA Justice Liaisons are responsible for a smaller population than the ACC Justice Liaisons and, thus, can devote relatively more resources and time to conduct reach-in services for their members. AHCCCS should consult with its Justice Liaisons to understand why reach-in rates vary by program.
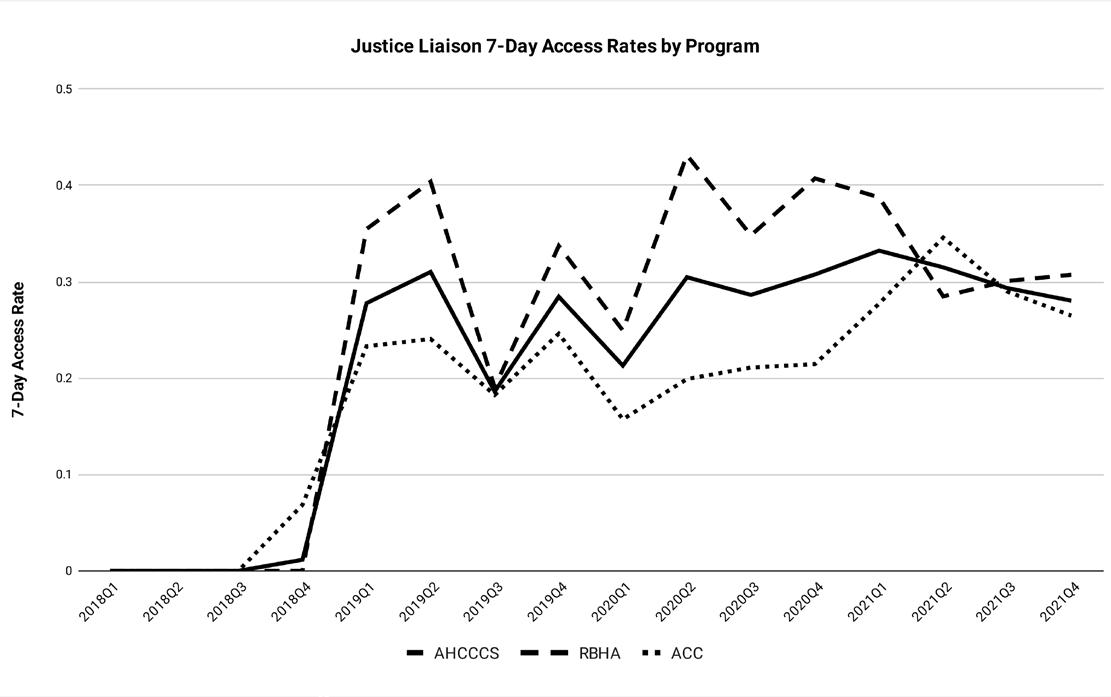
AHCCCS policy specifies that Justice Liaisons should coordinate a clinical appointment within seven business days of release. While data on appointment access is much less consistent than reach-in activities, the available data indicate a positive trend. Overall, 28% of members released on Medicaid into the community received access to clinical services within seven days of release (see Figure 4). The RBHAs’ most recent access rate was 31%, whereas the ACCs’ rate was 27%. Declines in access rates for RBHAs could indicate increasing barriers to accessing behavioral health services such as smaller networks and workforce.
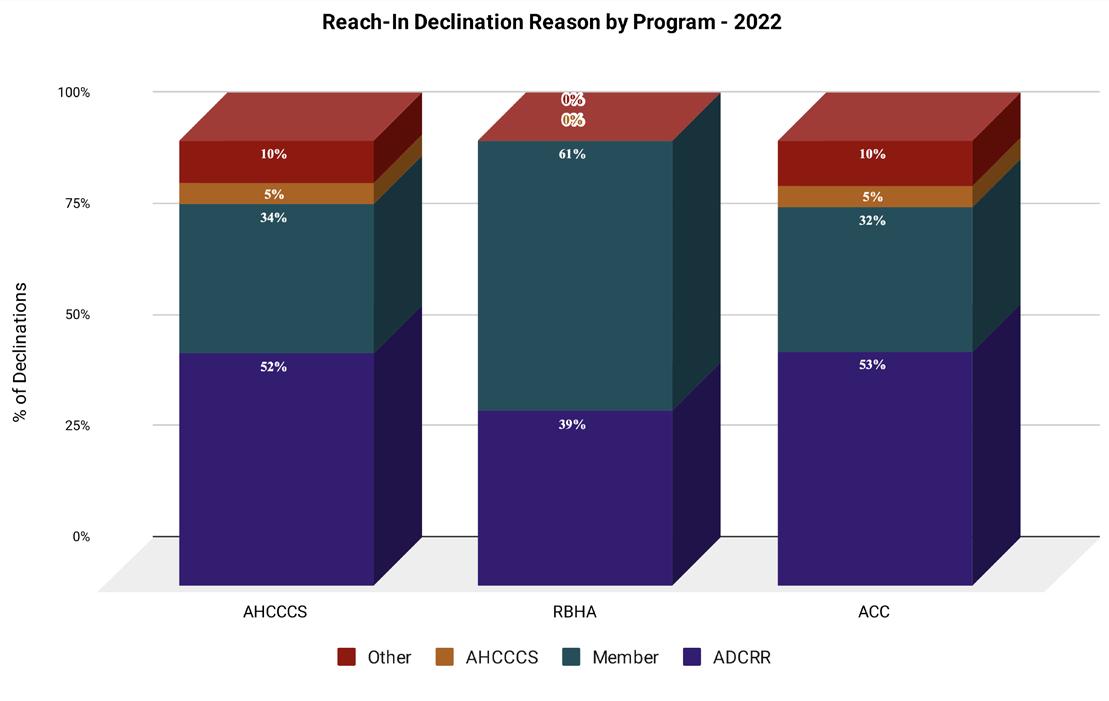
However, not all enrolled Medicaid members who are incarcerated choose to accept reach-in services. In 2022, AHCCCS began requiring that MCOs consistently report the reasons a member declined Justice Liaison services within the deliverable. Analysis of these reasons provides insight into how AHCCCS can improve its delivery system reforms. Overall, ADCRR errors and member refusal account for 85% of all declinations (see Figure 5). RBHAs have similar reasons but their proportions differ: 61% are due to member refusal and 39% are due to ADCRR error. Declinations for ACCs match AHCCCS’s overall rates: ADCRR error (52%), member refusal (32%), an assortment of other reasons, which constitute no more than 2% individually (10%), and AHCCCS error (5%).
This data provides a window into how the current programming is working and, more importantly, how the delivery system could get better as AHCCCS expands reentry services.
Figure 3: Justice Liaison Reach-in-Rates by Program
Figure 4: Justice Liaison 7-Day Access Rates by Program
Figure 5: Reach-In Declination Reason by Program (2022)
Recommendations:
31. AHCCCS should standardize deliverable reporting for declination of reach-in services. MCOs self-reported the reasons a member declined reach-in services, making it challenging to appropriately categorize and analyze the data. AHCCCS should coordinate with MCOs to standardize these reasons to ensure ease of analysis and oversight.
32. AHCCCS should begin using Medicaid claims to measure access rates to communitybased services for members who receive reachin services. Currently, MCOs are self-reporting whether an individual who received reach-in services ultimately accessed care during the reentry period. AHCCCS should collect the Medicaid identification numbers of individuals who received reach-in services from MCOs in the Justice Liaison deliverable and then match it any subsequent claims in its claims database. While this may prolong the time window to monitor access rates, it will greatly improve the independence and reliability of the performance measure.
33. AHCCCS should grant ADCRR and other carceral facility staff minimal access to AHCCCS eligibility systems to update release dates. Over 50% of member declinations for reach-in services were due to errors in a member’s release date or Medicaid eligibility. Granting carceral facility staff minimal access (to ensure data integrity) to AHCCCS’s eligibility systems would allow them to update critical information and to engage with Justice Liaisons in a timelier manner.
Health Information and Documentation Access
Effective care coordination and continuity requires that case managers and providers know critical information about a member’s current and past health needs. However, timely and reliable transfer of medical records may not always be available, and may not be available in a medium compatible with providers’ digital recordkeeping software.
Case managers and providers face a four step process to gather and coordinate all medical information for easy access by providers. First, they need to retrieve all existing medical records from the carceral facility. These records may exist in electronic or paper form, the latter of which increase the amount of time required to obtain it. Second, case managers and providers must include questions about health history and current health needs
in intake sessions with incarcerated members. Third, all gathered information should go into an electronic format that can be shared with other members of the care team. Finally, subsequent case managers should continue to augment records through post-enrollment follow-up meetings and interviews.
AHCCCS will need to address any challenge that may impede the effective and timely transfer for critical health information.
Recommendations:
34. AHCCCS should coordinate with ADCRR and jails to ensure case managers and community providers have the ability to access and retrieve all relevant medical records of a member who is returning from incarceration. All case managers’ intake questionnaires should include questions about whether members have any new health problems or health problems for which they have not received treatment while incarcerated.
35. AHCCCS should help enroll all case managers and community providers in Arizona’s Health Information Exchange and CommunityCares to upload and share a member’s care plan with other members of the care team. If financial barriers exist to enrolling in and obtaining licenses for these platforms, AHCCCS should provide financial assistance to these providers.
Plan Enrollment Flexibility
Many stakeholders, including people who are incarcerated, we spoke with expressed concern about the access challenges that arise when members return to a part of Arizona where the MCO they are initially enrolled does not provide coverage. This can happen for a variety of reasons, including automatic assignment to a plan if one was not chosen at the time of enrollment or a member changing their relocation plans between the time of enrollment124 and the time of release from incarceration. During our meetings in Arizona, multiple stakeholders shared that it is not uncommon for prerelease members’ housing situations to shift in the weeks prior to reentry.
Because AHCCCS health plans are regional, and because there is currently a 90 day post-enrollment limit on switching plans,125 members can get stuck in a plan that does not cover their area and experience difficulty accessing the care they need. There may be no innetwork providers in their area, and transportation to the area of coverage may be unobtainable.
AHCCCS will need to provide additional flexibility within its enrollment procedures to account for the sudden changes that may occur within a member’s reentry and relocation plans.
Recommendations:
36. AHCCCS should require its Justice Liaisons, CHWs, TI Justice Clinics, and case managers to provide education to individuals during the reentry period on how to change their MCO based on their residence, preferred provider, and needs.
37. AHCCCS should create a statewide MCO and enroll all people reentering into it. Because formerly incarcerated people face unique challenges in finding stable housing,126 they may find themselves stuck in a plan that does not cover their area if they switch residences. A plan with coverage across Arizona would prevent gaps in coverage for populations who struggle to find long-term housing, including formerly incarcerated members.
38. AHCCCS should use collective performance measures to incentivize timely and coordinated transitions of care across MCOs when a member switches MCOs. AHCCCS should use financial performance incentives for this population that measure and pay for performance based on the entire system - not individual MCO performance. In combination with the established transitions of care contractual requirements, these performance incentives will encourage MCOs to collectively manage this population, proactively coordinate the transitions from one MCO to another, and ensure effective treatment access and continuity.
Rural Healthcare Access
Geography can play a significant role in health outcomes, and AHCCCS’s implementation of the 1115 reentry waiver should consider the specific needs of incarcerated people returning to rural areas. Rural Americans are more likely to have heart disease, a stroke, cancer, chronic lung disease, suicide risk, and have higher death rates from COVID-19 in comparison to urban Americans.127 Residents in rural areas tend to be older, poorer, and sicker than urban residents, and a higher proportion of rural Americans report limited physical activity due to chronic conditions, and some social circumstances and behaviors in rural communities can impact mortality rates.128
Geography not only shapes health risks, but also affects access to medical providers. According to CMS, only 12% of physicians are in rural communities, and 61% of the areas that are deemed “health professional shortage areas” are located in rural communities.129 In Arizona, every county has a partial shortage of primary care physicians, but this is more pronounced in rural areas, where 10.7% of the population lives according to the 2020 Census.130 The rate of primary care physicians per every 100,000 people ranges from 72-105 in some of Arizona’s urban counties, in comparison to ten rural counties in which the rate is under 55 physicians.131 Additionally, multiple predominantly rural counties like Navajo, Apache, and Graham have correctional facilities but don’t have AHCCCS Justice Clinics. These counties do have Rural Health Clinics and FQHC sites.132
Many stakeholders who came from rural communities described how there were fewer providers, physical and behavioral health, and longer travel times to appointments. They also mentioned that these access challenges were only compounded by a lack of transportation access.
Recommendation:
39. AHCCCS should conduct stakeholder engagement in rural communities to understand the particular challenges for serving this population and develop community-based solutions. Due to time constraints and the scope of this project, we were not able to interview many rural AHCCCS providers or formerly incarcerated members in rural areas. Rural members often face unique healthcare challenges, including provider shortages and transportation barriers. In order to make targeted recommendations about how AHCCCS can better support rural residents, further in-depth research and interviews would be needed.
Arizona has the third largest American Indian population of any state in the country, with 22 Federally Recognized Tribes.133 The nation-to-nation relationship between the Tribal governments and the Federal government presents a unique challenge of balancing federalism concerns with providing access to benefits to incarcerated American Indians.
Eligibility of Tribal and Federal Facilities
As of May 2023, there are 700 AHCCCS members incarcerated on Tribal lands in Arizona.134 If a crime is committed by a Tribal member on Tribal lands, Tribal members may be tried by the federal government and incarcerated in a facility administered by the Federal Bureau of Prisons (BOP) or a facility administered by the Bureau of Indian Affairs (BIA), which oversees carceral settings on Tribal lands.135
The 2023 CMS guidance states that CMS “expects states to refrain from including federal prisons as a setting in which demonstration-covered pre-release services are provided under the demonstration.”136 The guidance, however, only explicitly addresses facilities administered by BOP, which provides health care services for its incarcerated population. The guidance does not address facilities administered by BIA, which lack on-site healthcare services, or the inability of Indian Health Service (IHS) facilities to receive reimbursement for outpatient services to incarcerated Tribal members.137
The absence of on-site healthcare services at Tribal and BIA facilities presents a significant challenge in offering pre-release healthcare services. Before expanding the waiver to these facilities, it is essential to ensure that proper healthcare infrastructure is either already in place or adequately funded to support these services. Otherwise, the goal of providing comprehensive prerelease healthcare services will not be met.
IHS facilities currently cannot receive reimbursement for outpatient services provided to incarcerated Tribal members. The inability of IHS to receive reimbursement for these services could create a gap in care, particularly for incarcerated individuals who need medical services upon release. Without addressing this gap, the waiver risks failing to meet the health needs of this population.
The complex Federal-Tribal jurisdictional relationship must be considered when determining how pre-release services are implemented in these facilities. Given the unique legal structure of Tribal lands, the process for coordinating pre-release services between BIA facilities and Tribal governments will require more detailed planning and consultation.
Managed Care Exemption
AHCCCS’ existing mandatory managed care model exempts American Indians from mandatory enrollment. As a result, American Indians primarily access health care with a fee-for-service (FFS) delivery system with the option to enroll in managed care. While CMS allows the use of FFS for the demonstration waiver, FFS may not provide enrollees with the same quality of coordinated care available through the managed care system.138
An advantage of the managed care system is the availability of Justice Liaisons positioned within the MCOs to facilitate reentry, a service that may be unavailable depending on the case management services contracted to serve the enrollees. MCOs also provide care coordination and case management services, as mandated in the demonstration waiver, that would be prohibitively expensive to implement using a fee-for-service model.139
States may obtain approval from CMS to require American Indians to enroll in managed care through the demonstration waiver, though CMS has historically not approved waivers that mandate American Indians to enroll in managed care.140 While there is benefit in pairing incarcerated people with Justice Liaisons prior to release, we ultimately cannot provide a recommendation on whether AHCCCS should exempt incarcerated American Indians and instead encourage AHCCCS to conduct a meaningful and thorough Tribal Consultation.
Tribal Consultation Process
CMS requires states with Federally Recognized Tribes to conduct Tribal Consultations on issues that affect American Indians and Alaska Natives.141 While AHCCCS has conducted its Tribal Consultations in a manner compliant with federal guidelines, Tribal stakeholders have noted that AHCCCS conducts its consultations too late into the policy development process for Tribes to provide meaningful input.
Recommendations:
40. AHCCCS should work with CMS to clarify how reimbursement for incarcerated Tribal members can be handled under this waiver, particularly for outpatient care provided by the IHS and Tribal 638 Facilities.
41. AHCCCS should strengthen coordination with the Arizona Advisory Council on Indian Health Care (AACIHC) and consult Tribal leadership on the reentry waiver’s coverage of Tribal members in federal facilities, whether to exempt incarcerated Tribal members from managed care enrollment, and the potential adaptations to the managed care model that would make it more inclusive and effective for Tribal members.
Stakeholder Engagement
Throughout our 14 different interviews, we heard different responses to the awareness around the waiver. Some stakeholders knew about the waiver and its implications, including large behavioral health providers, Maricopa County Jail, and ADCRR. Other stakeholders did not, including FQHCs and AACIHC.
As a result, it will be critical for AHCCCS to not only consult with but widely publicize this waiver, its implications, its development, and, ultimately, its implementation to its provider networks and broader stakeholder networks.
Recommendations:
42. AHCCCS should conduct a roadshow tour of the waiver in all counties across the state and solicit feedback on it during community engagement events. In advance of the roadshow, AHCCCS should develop and publish a white paper that describes the reentry waiver and its proposed services at a high level. AHCCCS should use this white paper to facilitate constructive feedback sessions.
43. AHCCCS should create an online feedback form to solicit comments from stakeholders who are unable to attend in person roadshow meetings.
PROGRAM AND IMPLEMENTATION EVALUATIONS
CMS requires that states create an evaluation plan as part of their waiver. AHCCCS has the opportunity not only to evaluate the effectiveness of its approach to reentry services but also to inform future policy development in other contexts. Below, we recommend an evaluation strategy AHCCCS can use to assess the impact of the waiver. We also recommend that AHCCCS develop a data collection strategy, including critical partnerships, to measure and track key outcomes. We recommend that AHCCCS contract with a third-party evaluator to conduct this evaluation.
In the program evaluation, AHCCCS should consider short-term outcomes like healthcare utilization and homelessness. We include homelessness as a key short-term outcome because many of our recommendations aim to reduce homelessness, and unhoused people face significant health risks as a result of their housing situation. AHCCCS should consider long-term outcomes like healthcare utilization, recidivism, and mortality rates.
The determination of these short-term and long-term outcomes are based on a hypothesis that improved continuity of care and decreased incidence of homelessness will result in improved health outcomes, reduced recidivism rates, and a lower incidence of behavioral health crises and emergency care usage. We can also examine the mortality rates for people returning from incarceration before and after the waiver.
Short-term Outcomes: Healthcare Utilization and Homelessness
AHCCCS is best equipped to track healthcare utilization using claims data. This provides insight into the continuity of care, as claims data can be used to determine whether someone was able to get an appointment with a provider outside prison within a critical period (e.g., 2 to 4 weeks post-release) to refill their prescriptions, access behavioral healthcare or MAT, or address other non-emergency medical issues.
While the rate of homelessness for formerly incarcerated people is challenging to measure, AHCCCS can effectively proxy for homelessness using claims data from homeless shelters and healthcare providers who serve unhoused populations. AHCCCS can also encourage or require providers to submit social needs assessments and provide data on housing situation, food, security, access to transportation, and utilities.
Long-term Outcomes: Healthcare Utilization, Recidivism, and Mortality
AHCCCS can also use claims data for the second stage of the evaluation by tracking hospitalizations, emergency room visits, and mental health crises. In partnership with the Arizona Judicial Branch, AHCCCS can track recidivism
rates to determine whether improved access to care while incarcerated and after release affects someone’s likelihood of committing a crime in the future. AHCCCS should also pursue a collaboration with the Arizona Department of Health Services to track mortality rates and causes for formerly incarcerated people.
Program Evaluation Design
AHCCCS can employ a retrospective interrupted time series with control, staggered roll-out, or a difference-in-difference design. The retrospective interrupted time series with control allows the evaluator to observe any changes in outcome directly attributable to the intervention (i.e., enrollment and access to pre-release services) while using a control group of individuals who have already entered and left the justice system prior to implementation as a counterfactual. In the staggered roll-out design, the evaluator can exploit differences in the timing of when AHCCCS expanded services to different prisons. The difference-in-difference approach can compare outcomes in Arizona with a similar state such as New Mexico that does not have robust pre-release services to isolate the effect of increased access to pre-release care rather than political or other changes.
Implementation Evaluation
The implementation evaluation should triangulate on three main factors: content, contrast, and challenges. The evaluation should aim to record what was actually provided to enrollees (content), how this differed from what non-enrollees received (service contrast), and the factors that facilitated or inhibited implementation (challenges). To conduct this implementation evaluation, AHCCCS or an independent third-party evaluator should conduct interviews with a variety of stakeholders including, but not limited to: carceral staff, health staff like justice liaisons and community health workers, and enrollees. The evaluator may choose to randomly select individuals to be interviewed but should consider a judgement selection process instead to ensure a diversity of experiences is represented, particularly amongst people experiencing SMI, SUD, other diagnoses requiring regular care such as diabetes, and homelessness.
Data sources
• Social needs assessments
• Arizona Department of Health Services
• AHCCCS claims data
• Arizona Judicial Branch (Arizona Courts)
• Interviews with carceral staff, health staff, and enrollees
CONCLUSION
This report calls on Arizona to lead the nation in reentry services. In it, we found impactful ways for Arizona to do more of what works well, adjust its current practices, and better tailor the reentry healthcare experience to the lived needs of AHCCCS members approaching their release from incarceration. To make this report, we analyzed Arizona’s health policy landscape and the opportunities surrounding the healthcare needs of the justice-involved population from every angle we could find. Our work draws on extensive field research, interviews with stakeholders, data analysis, and evaluation of comparable programs in other states. The resulting recommendations largely urge Arizona to build on its existing Medicaid program to better serve the clinical and social needs of an incarcerated population at high risk.
We identify that health and social needs for incarcerated and formerly incarcerated members are complex and interwoven with barriers to healthcare access and the systemic inequities. Our recommendations focus on expanding the services during 90 days prior to release, fostering greater continuity of care, addressing the HRSNs of this population, and strengthening AHCCCS’ existing delivery systems.
We propose a service package that includes the four mandatory services outlined by CMS - case management, MAT, 30-day of prescription medications, and a Reinvestment Plan - as well as additional clinical services and non-clinical services that address the HRSNs of this population. Specifically, we propose adding a general physical and behavioral health consultation, family planning services, dental care, dermatology, lab and radiology services, housing supports, transportation, and food and nutritional services. Implementing these recommendations requires some adjustments as well. We propose expanding the use of CHWs, improving the coordination and communication with carceral systems, improving access to critical health information of people returning from incarceration, increasing the flexibility of health enrollment, engaging with critical stakeholders, specifically rural communities and Tribes, to develop strategies that address their specific needs.
Finally, we provided recommendations on an evaluation and monitoring framework to assess the effectiveness of the waiver, ensuring that immediate and long-term impacts, such as continuity of care, healthcare utilization, recidivism, and mortality, are adequately captured.
For many recommendations, Arizona would be joining several other states in implementing improved care; however, for several benefits, Arizona would be the first in the nation to provide them. We believe AHCCCS will become the national role model as it implements these recommendations. Most importantly, Arizona will improve the health and wellbeing of a population that has been forgotten about and marginalized for too long.
APPENDIX
Insights from Breakout Groups with Incarcerated Women at Perryville Prison
During our visit to Perryville Prison, we met with incarcerated women in breakout groups where they courageously shared the challenges they faced within the prison system. One of the most striking issues was the state of healthcare. Many women spoke of an over-reliance on antipsychotic medications, prescribed as a one-size-fits-all solution to mental health concerns, without addressing the underlying issues. They described reproductive healthcare as invasive and inadequate. Women reported difficulties accessing oral contraceptives and shared many stories of being advised to undergo hysterectomies for relatively minor problems, with little exploration of less extreme alternatives.
The lack of follow-up care compounded their struggles. One woman described her battle with chronic joint pain that went untreated because she couldn’t secure necessary follow-up appointments. Another recounted visiting the prison clinic for persistent symptoms, only to be told to “exercise more.” She later discovered she had cancer. Dental care was similarly inadequate, with tooth extractions often presented as the only solution for dental problems. One woman shared that she had four teeth pulled within a year and a half, leading her to avoid dental care out of fear of losing more. Recovery after these procedures was difficult for many women as well due to lack of sterile environments. Women managing chronic conditions like diabetes described feeling abandoned in their care, left to research their conditions on their own because they received little to no guidance. The system’s failures were amplified by the high cost of medications, which put even necessary treatments out of reach, and the difficulty of obtaining medical records to advocate for themselves.
Beyond healthcare, multiple women spoke emotionally about their roles as mothers and the difficulty of maintaining connections with their children and families. Many expressed an overwhelming sense of helplessness, describing how the prison system erected barriers to regular communication and family unification efforts. They emphasized how the trauma of separation not only harmed them but also deeply affected their children, creating cycles of pain and trauma that could last generations.
Mental health services, especially trauma counseling, were another area of concern. Some women were unsure whether Federally Qualified Health Centers (FQHCs) would provide the trauma-informed care they needed after release. Others described the lack of consistent therapeutic support within the prison. The absence of comprehensive mental health care left many to manage their trauma alone, adding to the emotional toll of incarceration.
The transition out of prison also emerged as a significant pain point. Women described being unprepared to navigate life after incarceration due to gaps in education and reentry planning. Many were unaware of what health services they would qualify for upon release, particularly those who relied on programs like MAT for substance use recovery. The lack of clear, accessible guidance left them feeling ill-equipped to successfully reenter their communities.
FULL RECOMMENDATION LIST
1. AHCCCS should pursue the full 90-day coverage opportunity afforded by CMS. This should be the foundational cornerstone of AHCCCS’s waiver design. Eight of the 11 states that have received authority for their 1115 reentry waivers will provide services for 90 days pre-release: California, Illinois, Massachusetts, New Mexico, Oregon, Utah, Vermont, and Washington. We recommend a suite of potential services in the section below. However, AHCCCS should ultimately select services for the 90 day service provision window based on the other decision criteria that we identified.
2. AHCCCS should create a tier approach to case management based on the acuity of a member’s needs. For members with higher needs, AHCCCS should prioritize case management that entails higher frequency and in-person contacts. They should also designate case managers as the authoritative and consistent contact persons for enrolled members.
3. AHCCCS should develop a comprehensive checklist for case managers to quickly screen a member for a range of benefits they may be eligible for and need. AHCCCS should build this checklist from existing intake and care planning forms to that it has used in other initiatives, including the Whole Person Care Initiative and H2O.
4. AHCCCS should require a base standard of in-person meetings for each level of case management. Case managers should also be required to identify and establish with the member the desired and primary mode of contact as the pair navigates the member’s care plan.
5. AHCCCS should require case managers to schedule at least one post-release health care appointment for all members, regardless of acuity. AHCCCS should track and publish these appointment rates as a key performance indicator.
6. AHCCCS should use some of its Reinvestment Plan money to build workforce programs that improve the supply of case managers and to ensure consistent access to case management services. These programs can be developed and executed with local universities and community colleges.
7. AHCCCS should convene a working group with its MCOs to determine how case management services align with the current Justice Liaison programming. There is a high degree of overlap between the Justice Liaisons and the opportunity afforded under case management. AHCCCS will need to determine an appropriate division of labor between Justice Liaisons and case managers in order to reduce duplication in its delivery system.
8. AHCCCS should use part of its waiver budget for capacity building for MAT service delivery in carceral facilities. Funds should be devoted to the adoption of electronic health records that can communicate with community providers, the development of SUD care initiation and management protocols, and the administrative capacity to screen for and enroll people in Medicaid at booking.
9. AHCCCS should work with ADCRR and other carceral systems to ensure consistency of medication formulatories across carceral facilities and community providers.
10. AHCCCS should consider developing a Reinvestment Plan that builds additional capacity for demonstration services that extend into the community, community-based HRSN services, and community-based behavioral health services. Specifically, AHCCCS should create enterprise loans for community clinics to hire and sustain community health workers, create a permanent supportive housing finance fund that helps build affordable housing, and bolster pre-school and other school-based behavioral health and social and emotional development programs and services that deter future criminal activity and involvement. The funds allocated under the Reinvestment Plan are wholly distinct from any funds devoted to capacity building under AHCCCS general waiver budget.
11. AHCCCS should cover a general physical consultation to identify and address chronic conditions, including making referrals to appropriate specialists, in the pre-release window.
12. AHCCCS should cover a behavioral health consultation, including screenings and initiation treatment.
13. AHCCCS should leverage telemedicine to better connect members with behavioral health clinicians who are located in the communities where the members will be returning.
14. AHCCCS should cover reproductive health education and contraceptive access, including oral contraception and long-acting reversible contraceptives (LARCs), and STI testing, treatment, and prevention education prior to release.
15. AHCCCS should work with ADCRR and its carceral partners to align its coverage with any family planning policies at the carceral facility. For example, the current policy at Perryville Prison, ADCRR’S sole women’s facility, is to offer oral contraception to incarcerated people 30 days before their release. This policy will need to be revised based on AHCCCS decision.
16. AHCCCS should offer cost-effective, targeted dental care during the pre-release period to address urgent oral health issues and promote preventive care, reducing reliance on expensive emergency services post-release. Services should include basic screenings, necessary extractions, and oral hygiene education with distribution of hygiene kits, minimizing costs while addressing critical needs. Incorporating low-cost preventive measures like fluoride varnishes and brief health education can improve long-term health outcomes and reduce future healthcare expenditures.
17. AHCCCS should leverage tele-medicine strategies to address potential access issues for dermatology. Teledermatology services, such as those implemented by the Federal Bureau of Prisons, allow inmates to consult remotely with specialists. This programming has reduced costs and logistical challenges associated with transportation.
18. AHCCCS should cover lab and radiology services.
19. AHCCCS should prioritize people who are leaving incarceration or who are formerly incarcerated as critical populations for permanent supportive housing and housing supports under its H2O program.
20. AHCCCS should provide long-term housing stability planning for members through case management or its Justice Liaisons. Alongside other housing transition navigation services, justice liaisons should provide consultation on housing plans beyond the interim. When applicable, they should refer people who are incarcerated with services that offer long term housing.
21. AHCCCS should create a permanent supportive housing fund in its Reinvestment Plan to address the lack of long-term housing for people who are leaving incarceration or who are formerly incarcerated.
22. AHCCCS should embed transportation as an issue that is screened for and planned around during the initial case management visit.
23. AHCCCS should ensure case managers have smooth and easy access to the prior authorization process for NEMT while executing a member’s care plan. Since many carceral facilities are significantly far away from healthcare providers, NEMT may be required to be set up well in advance and, thus, go through the prior authorization process. By giving a care manager improved access to this process, the care manager can proactively set up transportation appointments the day a member is released.
24. AHCCCS should augment and devote new funding to its NEMT benefit to include and cover additional service destinations that are specific to the needs of people who are formerly incarcerated. These service destinations could include: job interviews, training programs, court hearings, probation appointments, food banks, homeless shelters, and family visitations
25. AHCCCS should require case managers to screen all pre-release members for eligibility for food insecurity services in the initial case management visit and care plan development.
26. AHCCCS should test and cover Produce Prescriptions (PRx) to pre-release members with certain chronic health conditions for up to six months as part of its covered medications requirement.
27. AHCCCS should require case managers to partner with and make referrals to nutrition service providers, including SNAP and WIC offices.
28. AHCCCS should include a history of incarceration as a documented barrier in its administrative rules, state plan, or programmatic guidance regarding CHWs. This will help call attention to this population and direct CHWs to more intentionally work with this population. Additionally, any subsequent changes and policy direction should include guidance on how CHWs should collaborate with case managers who are serving this population.
29. AHCCCS should encourage CHWs to conduct health education trainings and fairs at carceral facilities. These trainings can cover the basics of Medicaid and community-based healthcare with facility staff, and the fairs can provide health education and promotion materials, including information on Medicaid benefits, to people who are currently incarcerated. Increasing the awareness of Medicaid benefits among carceral staff will help improve cross-training between carceral staff and community providers. Improving health literacy among people who are incarcerated prior to release would promote independent and confident living by educating members on their health needs, treatment options for chronic conditions, and how and when to seek care.
30. AHCCCS should partner with Arizona Department of Health Services (ADHS) to revise the requirements to disclose a felony or misdemeanor conviction in the employment application of CHWs. CHWs often reflect the communities that they serve. In doing so, they can build greater trust with members and increase the likelihood that members will engage in life saving services.142 Moreover, this approach can be an economic and workforce development tool for many marginalized communities.143 People with a history of incarceration should be no different. We engaged with a community representative in a rural county in Arizona who was formerly incarcerated and functioned like a CHW but did not have the official title. The impact of their work was profound, both in terms of engaging with people who were formerly incarcerated and building quality relationships with carceral facilities to improve the reentry processes. A simple policy change could tap into a missing market of critical workers.
31. AHCCCS should standardize deliverable reporting for declination of reach-in services. MCOs self-reported the reasons a member declined reach-in services, making it challenging to appropriately categorize and analyze the data. AHCCCS should coordinate with MCOs to standardize these reasons to ensure ease of analysis and oversight.
32. AHCCCS should begin using Medicaid claims to measure access rates to community-based services for members who receive reach-in services. Currently, MCOs are self-reporting whether an individual who received reach-in services ultimately accessed care during the reentry period. AHCCCS should collect the Medicaid identification numbers of individuals who received reach-in services from MCOs in the Justice Liaison deliverable and then match it any subsequent claims in its claims database. While this may prolong the time window to monitor access rates, it will greatly improve the independence and reliability of the performance measure.
33. AHCCCS should grant ADCRR and other carceral facility staff minimal access to AHCCCS eligibility systems to update release dates. Over 50% of member declinations for reach-in services were due to errors in a member’s release date or Medicaid eligibility. Granting carceral facility staff minimal access (to ensure data integrity) to AHCCCS’s eligibility systems would allow them to update critical information and to engage with Justice Liaisons in a timelier manner.
34. AHCCCS should coordinate with ADCRR and jails to ensure case managers and community providers have the ability to access and retrieve all relevant medical records of a member who is returning from incarceration. All case managers’ intake questionnaires should include questions about whether members have any new health problems or health problems for which they have not received treatment while incarcerated.
35. AHCCCS should help enroll all case managers and community providers in Arizona’s Health Information Exchange and CommunityCares to upload and share a member’s care plan with other members of the care team. If financial barriers exist to enrolling in and obtaining licenses for these platforms, AHCCCS should provide financial assistance to these providers.
36. AHCCCS should require its Justice Liaisons, CHWs, TI Justice Clinics, and case managers to provide education to individuals during the reentry period on how to change their MCO based on their residence, preferred provider, and needs.
37. AHCCCS should create a statewide MCO and enroll all people reentering into it. Because formerly incarcerated people face unique challenges in finding stable housing, they may find themselves stuck in a plan that does not cover their area if they switch residences. A plan with coverage across Arizona would prevent gaps in coverage for populations who struggle to find long-term housing, including formerly incarcerated members.
38. AHCCCS should use collective performance measures to incentivize timely and coordinated transitions of care across MCOs when a member switches MCOs. AHCCCS should use financial performance incentives for this population that measure and pay for performance based on the entire system - not individual MCO performance. In combination with the established transitions of care contractual requirements, these performance incentives will encourage MCOs to collectively manage this population, proactively coordinate the transitions from one MCO to another, and ensure effective treatment access and continuity.
39. AHCCCS should conduct stakeholder engagement in rural communities to understand the particular challenges for serving this population and develop community-based solutions. Due to time constraints and the scope of this project, we were not able to interview many rural AHCCCS providers or formerly incarcerated members in rural areas. Rural members often face unique healthcare challenges, including provider shortages and transportation barriers. In order to make targeted recommendations about how AHCCCS can better support rural residents, further in-depth research and interviews would be needed.
40. AHCCCS should work with CMS to clarify how reimbursement for incarcerated Tribal members can be handled under this waiver, particularly for outpatient care provided by the IHS and Tribal 638 Facilities.
41. AHCCCS should strengthen coordination with the Arizona Advisory Council on Indian Health Care (AACIHC) and consult Tribal leadership on the reentry waiver’s coverage of Tribal members in federal facilities, whether to exempt incarcerated Tribal members from managed care enrollment, and the potential adaptations to the managed care model that would make it more inclusive and effective for Tribal members.
42. AHCCCS should conduct a roadshow tour of the waiver in all counties across the state and solicit feedback on it during community engagement events. In advance of the roadshow, AHCCCS should develop and publish a white paper that describes the reentry waiver and its proposed services at a high level. AHCCCS should use this white paper to facilitate constructive feedback sessions.
43. AHCCCS should create an online feedback form to solicit comments from stakeholders who are unable to attend in person roadshow meetings.
BIOGRAPHIES
Rahmat is a Master in Public Affairs student at the Princeton School of Public & International Affairs concentrating in international development and health policy. He is a career diplomat and joined Bangladesh Foreign Service in April 2019. Rahmat has experience in bilateral and multilateral diplomacy and organized and participated in high-level meetings. He has received diplomatic trainings in Bangladesh, India, Turkiye, the Netherlands and Belgium. Before his diplomatic career, Rahmat worked for two years as a research assistant in Microbial Genetics and Bioinformatics Laboratory at the University of Dhaka, where he developed a trivalent vaccine against circulatory Foot-and-Mouth Disease viruses in Bangladesh and published multiple peer-reviewed research articles in international journals. Rahmat obtained his bachelor's and master's degrees in microbiology from the University of Dhaka, Bangladesh.
Mustafa is a Master in Public Affairs student at the Princeton School of Public & International Affairs concentrating in domestic policy. Prior to enrolling at Princeton, Mustafa worked for several years in the criminal justice space. He was appointed by the Mayor of Knoxville, TN to help build out a new Office of Community Safety that focused on violence prevention through alternatives to 911 calls and street outreach teams. He also previously worked at the Vera Institute of Justice, a national nonprofit working to end mass incarceration, where he provided technical assistance and urged prosecutors to take up diversion programs and alternatives to incarceration through community centered approaches. Mustafa graduated from the University of Tennessee, Knoxville with a Bachelor's degree in Public Administration and received a Master's degree at the University of Pennsylvania concentrating in criminal justice, education, and race.
Laurel is a Master in Public Affairs candidate at the Princeton School of Public and International Affairs, specializing in domestic policy with a focus on health policy. Before Princeton, she served as a Legislative and Regulatory Policy Analyst at AHIP, where she monitored healthcare legislation across multiple states, wrote policy comment letters, and collaborated with federal agencies on Medicaid and public health initiatives. Her commitment to advancing health equity has been demonstrated during her tenure as a Graduate Researcher with the Western Cape Government in South Africa, where she evaluated a public-private partnership aimed at improving healthcare access for rural farmworkers. Laurel’s professional experience spans diverse roles, including positions at Habitat for Humanity International, political campaigns, nonprofits, the U.S. Department of State, and Capitol Hill. She holds a Bachelor of Arts in International Studies with a concentration in Environmental Sustainability and Global Health from American University.
Claire is a Master in Public Affairs student at the Princeton School of Public and International Affairs, concentrating on Economics and Public Policy. Prior to SPIA, Claire worked as a Research Assistant at the Federal Reserve Bank of Philadelphia until their interest in criminal legal reform and prison industrial complex abolition led them to their most recent job as a Data Analyst for the Quattrone Center for the Fair Administration of Justice at Penn Carey Law School, where she conducted research on bail reform, police policy, and conviction review, among other topics. Claire interned this past summer at OneDay Health in Gulu, Uganda. Claire grew up in Philadelphia and New York City and graduated with a degree in Economics from Vassar College.
Christopher is a Master in Public Affairs student at the Princeton School of Public & International Affairs concentrating in domestic policy. He previously served as a policy fellow at the White House Office of Science and Technology Policy, U.S. Environmental Protection Agency, and U.S. Department of State, working to develop and implement federal environmental and scientific policy. Christopher graduated from Princeton University with a Bachelor's degree in Civil and Environmental Engineering and is a proud resident of New Jersey.
Ben is a Master in Public Affairs student at the Princeton School of Public and International Affairs concentrating on economics and public policy. Prior to enrolling at Princeton, he worked for the Colorado Department of Health Care Policy & Financing (HCPF), the executive agency that oversees Colorado’s Medicaid Program. There, he oversaw the performance of the Accountable Care Collaborative, the state’s primary delivery system. In that role, he managed the compliance of the state’s seven managed care contracts, created novel performance and financial incentives, developed and managed a team of seven, managed stakeholder relationships across the state, and served on statewide advisory committees on criminal justice reform and behavioral health. He also developed a novel partnership with the Department of Corrections that tripled behavioral health access rates for individuals re-entering from state prisons. Prior to his time at HCPF, Ben managed clinical quality and operations improvement in the run-up to the transition to value-based care at Erie Family Health Center in Chicago. During his time at Princeton, he established medical respite programs in homeless shelters across New Jersey as a Social Impact Fellow at Princeton. Ben earned his Masters in Business Administration from The University of Chicago Booth School of Business where he graduated with honors in Strategic Financial Management and Entrepreneurship and was Neubauer Family Civic Scholar and Obama Foundation Scholar. He earned his bachelor’s from Northwestern University.
Md Rahmat Ali
Mustafa Ali-Smith
Laurel Cooke
Benjamin Harris
Claire Fondrie-Teitler
Christopher Gliwa
Svyatoslav Karnasevych
Svyatoslav is a Master in Public Affairs candidate at the Princeton School of Public and International Affairs concentrating in economics and public policy. Prior to enrolling at Princeton, Svyatoslav worked as a research analyst at the Federal Reserve Bank of Philadelphia, studying housing, population, and location amenities. Svyatoslav graduated summa cum laude from the University of Pennsylvania with a degree in Political Science and Economics. He is interested in urban policy around housing affordability, transit access, and community development.
Julian Lutz
Julian is a Master in Public Affairs student at the Princeton School of Public & International Affairs, concentrating on domestic policy. Prior to enrolling at Princeton, Julian worked as a Peggy Browning Fellow at the Sheet Metal Workers' Local Union #19, and worked as a paralegal at Regional Housing Legal Services, a nonprofit legal services provider that fosters affordable housing in Pennsylvania. Julian is a joint degree JD/MPA student pursuing his law degree at the University of Pennsylvania Carey Law School, and does pro-bono work with the STAR post-carceral reentry program in the United States District Court for the Eastern District of Pennsylvania. He received a Bachelor's degree in Political Science from Saint Joseph's University.
Tina Lee
Tina is a Master in Public Affairs student at the Princeton School of Public & International affairs concentrating in domestic policy. Prior to enrolling at Princeton, Tina worked on the Housing and Community Development team at the National League of Cities, where she managed eviction prevention technical assistance programs for 40+ cities in partnership with Stanford Law School’s Legal Design Lab, and research projects on topics like short-term rentals and institutional investors. Tina works part time with a California-based housing consultancy firm on strategic planning, research, and policy. Tina graduated with a Bachelor’s degree in Economic and Environmental studies from the University of Toronto.
Rachel Morrow
Rachel is a Master in Public Affairs student at the Princeton School of Public and International Affairs concentrating in domestic policy. Prior to enrolling at Princeton, Rachel served as the Chief of Staff/Executive Officer for the NASA Heliophysics Division, working as the primary advisor to the Director for strategic actions, long-term planning and organizational efficiency while advising 50-plus staff members on division operations and best practices. Rachel graduated from Stanford University with honors and a Bachelor’s degree in International Relations before embarking on a career in federal government consulting at Booz Allen Hamilton. Rachel is a proud Arkansan and served as Director of Communications for the Young Democrats of Arkansas and on the Arkansas Democratic Party State Committee.
Daisha Roberts
Daisha Roberts is a Master in Public Affairs student at the Princeton School of Public and International Affairs concentrating on domestic policy. Prior to enrolling at Princeton, she interned with the Department of State in Casablanca, Morocco. Daisha graduated from Yale University with a B.A in East Asian Studies and the History of Science, Medicine, and Public Health. Daisha was selected as a 2023 Charles B. Rangel International Affairs Fellow, and last summer completed her overseas internship with the U.S. Department of State in Riyadh, Saudi Arabia.
Keiana West
Keiana West is a Master in Public Affairs student at the Princeton School of Public and International Affairs. Prior to enrolling at Princeton, Keiana worked at the Center for Policing Equity, a national non-profit where she engaged community members in local public safety redesign initiatives. Previously, at the Equal Justice Initiative, she helped advance anti-mass incarceration efforts in Alabama and advised community coalitions throughout the U.S. in developing responses to the impact of historical racial violence. She also worked as a Princeton in Africa Fellow in South Africa, where she helped implement monitoring and evaluation processes at a NGO supporting low-income students attending formerly segregated schools. Keiana graduated with a B.A. in Psychology and a concentration in Africana Studies from Williams College. She aspires to continue working with local and state governments to implement policies that prioritize community safety and well-being.
ENDNOTES
1. U.S. Office of Justice Programs, Bureau of Justice Assistance, Getting Ready: Key Elements for the Implementation of Section 5121 Youth Requirements in Adult Correctional Facilities, accessed December 10, 2024, https://bjatta.bja.ojp.gov/sites/default/files/Getting_Ready_Key_Elements_for_the_Implementation_of_Section_5121.pdf.
2. Arizona Health Care Cost Containment System (AHCCCS), About the Arizona Health Care Cost Containment System (AHCCCS), accessed December 12, 2024, https://www.azahcccs.gov/AHCCCS/AboutUs/
3. "QuickFacts: Arizona," U.S. Census Bureau, accessed November 19, 2024, https://www.census.gov/quickfacts/fact/table/AZ/PST045223.
4. "22 Federally Recognized Tribes in Arizona," Arizona Department of Education, accessed December 5, 2024, https://www.azed.gov/oie/22-federally-recognized-tribes-arizona.
5. "Profile of Arizona," U.S. Census Bureau, accessed December 5, 2024, https://data.census.gov/profile?q=arizona.
6. "QuickFacts: Arizona."
7. "QuickFacts: Arizona."
8. U.S. Census Bureau, Income and Poverty in the United States: 2023, P60-282 (Washington, DC: U.S. Government Publishing Office, 2024), https://www. census.gov/library/publications/2024/demo/p60-282.html.
9. "Health Care in Arizona," KFF, accessed November 10, 2024, https://www.kff.org/statedata/election-state-fact-sheets/arizona/.
10. "Health Care in Arizona."
11. AHCCCS, AHCCCS Population Highlights, October 2024, https://www.azahcccs.gov/Resources/Downloads/PopulationStatistics/2024/PopulationHighlights_10012024.pdf.
12. "Population by County," Arizona Health Care Cost Containment System (AHCCCS), accessed November 1, 2024, https://www.azahcccs.gov/Resources/Reports/population.html.
13. “Proposed Changes to Medicaid Expansion in Arizona, Kaiser Family Foundation (KFF), November 2015, https://files.kff.org/attachment/ fact-sheet-proposed-changes-to-medicaid-expansion-in-arizona#:~:text=1%20Prior%20to%20the%20ACA,result%20of%20Voter%20Proposition%20204.
14. State of Arizona, Proposition 204, 2000, Arizona Secretary of State, https://apps.azsos.gov/election/2000/Info/pubpamphlet/english/prop204. htm#:~:text=Proposition%20204%20would%20require%20Arizona,the%20Arizona%20Health%20Care%20Cost.
15. "Population by Category," AHCCCS, accessed December 9, 2024, https://www.azahcccs.gov/Resources/Downloads/PopulationStatistics/2024/PopulationbyCategory_12052024.pdf.
16. “The 10 States With the Highest Incarceration Rates,” US News & World Report, June 10, 2024, https://www.usnews.com/news/best-states/slideshows/10-states-with-the-highest-incarceration-rates. 17. Id.
18. Emily Widra, “States of Incarceration: The Global Context 2024,” Prison Policy Initiative, June 2024, https://www.prisonpolicy.org/global/2024.html 19. Ashley Nellis, “The Color of Justice: Racial and Ethnic Disparity in State Prisons,” The Sentencing Project, October 13, 2021, https://www.sentencingproject.org/reports/the-color-of-justice-racial-and-ethnic-disparity-in-state-prisons-the-sentencing-project/
20. Hedwig Lee, Lauren C. Porter, and Megan Comfort, "Consequences of Family Member Incarceration: Impacts on Civic Participation and Perceptions of the Legitimacy and Fairness of Government," The American Academy of Political and Social Science 651, no. 1 (January 1, 2014): 44–73, https://doi. org/10.1177/0002716213502920.
21. Wendy Sawyer and Peter Wagner, “Mass Incarceration: The Whole Pie 2024,” Prison Policy Initiative, March 2024, https://www.prisonpolicy.org/reports/pie2024.html.
22. Niyi Awofeso, "Prisons as Social Determinants of Hepatitis C Virus and Tuberculosis Infections," Public Health Reports 125, no. Suppl 4 (2010): 25–33, https://doi.org/10.1177/00333549101250S406.
23. Aiden K. Varan et al., "Hepatitis C Seroprevalence Among Prison Inmates Since 2001: Still High but Declining," Public Health Reports 129, no. 2 (2014): 187–95, https://doi.org/10.1177/003335491412900213.
24. Miltonette Olivia Craig, Mijin Kim, and Dawn Beichner-Thomas, “Incarcerated in a Pandemic: How COVID-19 Exacerbated the ‘Pains of Imprisonment,’” Criminal Justice Review 49, no. 2 (July 27, 2023): 244–66, https://doi.org/10.1177/07340168231190467.
25. Elizabeth Allen, "Cheap Jail and Prison Food Is Making People Sick. It Doesn’t Have To," Vera Institute of Justice, February 27, 2024, https://www. vera.org/news/cheap-jail-and-prison-food-is-making-people-sick-it-doesnt-have-to.
26. For a detailed write up of what women shared with us during our Perryville Prison visit, see appendix.
27. Thomas Hewson et al., “Interventions for the Detection, Monitoring, and Management of Chronic Non-Communicable Diseases in the Prison Population: An International Systematic Review,” BMC Public Health 24, no. 292 (January 24, 2024), https://doi.org/10.1186/s12889-024-17715-7.
28. Olga Cunha et al., "The Impact of Imprisonment on Individuals’ Mental Health and Society Reintegration: Study Protocol," BMC Psychology 11, no. 1 (July 25, 2023): 215, https://doi.org/10.1186/s40359-023-01252-w.
30. "Mental Health Treatment While Incarcerated," National Alliance on Mental Illness, accessed December 5, 2024, https://www.nami.org/advocacy/policy-priorities/improving-health/mental-health-treatment-while-incarcerated/.
31. Substance Abuse and Mental Health Services Administration (SAMHSA), 2019 National Survey on Drug Use and Health - Table 5.2B, 2019, https:// www.samhsa.gov/data/sites/default/files/reports/rpt29394/NSDUHDetailedTabs2019/NSDUHDetTabsSect5pe2019.htm.
32. Emily Widra, “Addicted to Punishment: Jails and Prisons Punish Drug Use Far More than They Treat It,” Prison Policy Initiative (with data compiled by SAMHSA and the Bureau of Prison Statistics), January 30, 2024, https://www.prisonpolicy.org/blog/2024/01/30/punishing-drug-use/.
33. Institute of Medicine (US) Committee for the Substance Abuse Coverage Study, Treating Drug Problems: Volume 2: Commissioned Papers on Historical, Institutional, and Economic Contexts of Drug Treatment, ed. Dean R. Gerstein and Henrick J. Harwood (Washington, DC: National Academies Press, 1992), http://www.ncbi.nlm.nih.gov/books/NBK234750/.
34. Institute of Medicine (US) Committee for the Substance Abuse Coverage Study, Treating Drug Problems, ed. Gerstein and Harwood, http://www.ncbi. nlm.nih.gov/books/NBK234750/.
35. Mark Halsey and Melissa de Vel-Palumbo, Generations Through Prison: Experiences of Intergenerational Incarceration, 1st ed., (London: Routledge, 2020), https://doi.org/10.4324/9781351240574.
36. Halsey and de Vel-Palumbo, Generations Through Prison.
37. Ofira Schwartz-Soicher, Amanda Geller, and Irwin Garfinkel, "The Effect of Paternal Incarceration on Material Hardship," The Social Service Review 85, no. 3 (September 2011): 447–73, https://doi.org/10.1086/661925.
38. Medicaid and CHIP Payment Access Commission (MACPAC), Access to Medicaid Coverage and Care for Adults Leaving Incarceration, June 15, 2023, https://www.macpac.gov/publication/access-to-medicaid-coverage-and-care-for-adults-leaving-incarceration-2/.
39. MACPAC, Access to Medicaid Coverage and Care.
40. MACPAC, Access to Medicaid Coverage and Care.
41. Evelyn J. Patterson, "The Dose–Response of Time Served in Prison on Mortality: New York State, 1989–2003," American Journal of Public Health 103, no. 3 (March 2013): 523–28, https://doi.org/10.2105/AJPH.2012.301148.
42. Emily Widra, “Incarceration Shortens Life Expectancy,” Prison Policy Initiative, June 26, 2017, https://www.prisonpolicy.org/blog/2017/06/26/life_expectancy/.
43. Ingrid A. Binswanger et al., "Release from Prison—a High Risk of Death for Former Inmates," The New England Journal of Medicine 356, no. 2 (January 11, 2007): 157–65, https://doi.org/10.1056/NEJMsa064115.
44. "Recidivism Rates by State," World Population Review, accessed December 5, 2024, https://worldpopulationreview.com/state-rankings/recidivism-rates-by-state.
45. Mira Edmonds, "The Reincorporation of Prisoners into the Body Politic: Eliminating the Medicaid Inmate Exclusion Policy," Georgetown Journal on Poverty Law and Policy 28, no. 3 (2021): 279–319.
46. Evelyne P. Baumrucker, "Medicaid and Incarcerated Individuals," IF11830 (Washington, DC: Congressional Research Service, 2024), https://crsreports. congress.gov/product/pdf/if/if11830.
47. Elaine Michelle Albertson et al., “Eliminating Gaps in Medicaid Coverage During reentry After Incarceration,” American Journal of Public Health 110, no. 3 (March 2020): 317, https://doi.org/10.2105/AJPH.2019.305400.
48. Centers for Medicare & Medicaid Services (CMS), Ending Chronic Homelessness, SMDL, U.S. Department of Health and Human Services (HHS), May 25, 2004, https://www.hhs.gov/guidance/sites/default/files/hhs-guidance-documents/2004.smdl.suspension%2520for%2520inmates%2520of%2520a%2520public%2520institution_4.pdf.; CMS, To Facilitate successful reentry for individuals transitioning from incarceration to their communities, SHO 16-007, U.S. HHS, April 28, 2016, https://www.hhs.gov/guidance/sites/default/files/hhs-guidance-documents/sho16007_41.pdf.; Baumrucker, "Medicaid and Incarcerated Individuals," https://crsreports.congress.gov/product/pdf/if/if11830.
49. "Support for AHCCCS Members Who Become Incarcerated: Enrollment Suspension/Reinstatement," AHCCCS, accessed December 5, 2024, https:// www.azahcccs.gov/AHCCCS/Initiatives/CareCoordination/Justice/enrollmentsuspense.html#:~:text=In%20an%20effort%20to%20reduce,detention%20 facilities%20to%20allow%20Medicaid.
50. "CMS Releases Guidance on New Required Services for Incarcerated Young People," National Association of Medicaid Directors, accessed December 5, 2024, https://medicaiddirectors.org/resource/cms-releases-guidance-on-new-required-services-for-incarcerated-young-people/.
51. Elizabeth Hinton, Akash Pillai, and Amaya Diana, "Section 1115 Waiver Watch: Medicaid Pre-Release Services for People Who Are Incarcerated," KFF, August 19, 2024, https://www.kff.org/other/issue-brief/section-1115-waiver-watch-medicaid-pre-release-services-for-people-who-are-incarcerated/.
52. “Integration of Health Care Service Delivery: Targeted Investments Program - Justice,” AHCCCS, accessed December 11, 2024, https://www.azahcccs.gov/AHCCCS/Initiatives/CareCoordination/Justice/targetedinvestments.html.
53. “Integration of Health Care Service Delivery: Targeted Investments Program - Justice,” AHCCCS.
54. “Integration of Health Care Service Delivery: Targeted Investments Program - Justice,” AHCCCS.
55. “Integration of Health Care Service Delivery: Targeted Investments Program - Justice,” AHCCCS.
56. SUPPORT for Patients and Communities Act, H.R. 6, 115th Congress, introduced June 18, 2018, Public Law 115-271, https://www.congress.gov/ bill/115th-congress/house-bill/6.
57. U.S. HHS, Health Care Transitions for Individuals Returning to the Community from a Public Institution: Promising Practices Identified by the Medicaid reentry Stakeholder Group, January 26, 2023, https://aspe.hhs.gov/sites/default/files/documents/d48e8a9fdd499029542f0a30aa78bfd1/ health-care-reentry-transitions.pdf.
58. CMS, Opportunities to Test Transition-Related Strategies to Support Community reentry and Improve Care Transitions for Individuals Who Are Incarcerated, SMD 23-003, U.S. HHS, April 17, 2023, https://www.medicaid.gov/federal-policy-guidance/downloads/smd23003.pdf.
59. U.S. HHS, Health Care Transitions for Individuals Returning to the Community from a Public Institution.
60. CMS, Opportunities to Test Transition-Related Strategies, 17.
62. CMS, Opportunities to Test Transition-Related Strategies, 28.
63. US HHS, Report to Congress: Health Care Transitions for Individuals Returning to the Community from a Public Institution: Promising Practices Identified by the Medicaid Reentry Stakeholder Group, January 2023, 17-18. https://aspe.hhs.gov/sites/default/files/documents/d48e8a9fdd499029542f0a3 0aa78bfd1/ health-care-reentry-transitions.pdf
64. Atul Gawande, "Cowboys and Pit Crews," The New Yorker, May 26, 2011, https://www.newyorker.com/news/news-desk/cowboys-and-pit-crews. 65. California Health and Human Services Agency (CHHS), California Advancing & Innovating Medi-Cal (CalAIM) Proposal, January 2021, 44-45, https:// www.dhcs.ca.gov/provgovpart/Documents/CalAIM-Proposal-03-23-2021.pdf.
66. CHHS, California Advancing & Innovating Medi-Cal (CalAIM) Proposal, 36-38.
67. Oregon and Nevada, for example, include workforce training under their community reinvestment guidelines. In Nevada, some MCOs have lent grants to providers to fund recruitment and training for staff. For general information, see Manatt. Oregon Health Authority, Supporting Health for All through REinvestment: the SHARE Initiative, January 22, 2024, https://www.oregon.gov/oha/HPA/dsi-tc/Documents/SHARE-Initiative-Guidance-Document.pdf.; “2024 Community Reinvestment Plan,” Molina Healthcare of Nevada, April 9, 2024, https://dhcfp.nv.gov/uploadedFiles/dhcfpnvgov/content/Public/AdminSupport/MeetingArchive/MRAC/2024/MRAC_04_09_24_MHC_111_Community_Reinvestment_Plan_2.26.2024.pdf.; Alison Shippy, Shelli Silver, and Sydney McClendon, “Community Reinvestment: Forging New Partnerships in Medicaid,” Manatt, September 17, 2024, https://www.manatt.com/insights/ newsletters/health-highlights/community-reinvestment-forging-new-partnerships-in.
68. Adam Chamberlain et al., "Illicit Substance Use After Release from Prison Among Formerly Incarcerated Primary Care Patients: A Cross-Sectional Study," Addiction Science & Clinical Practice 14, no. 7 (2019): https://doi.org/10.1186/s13722-019-0136-6.
69. Binswanger et al., “Release from Prison."
70. Kelly E. Moore et al., "Effectiveness of Medication-Assisted Treatment for Opioid Use in Prison and Jail Settings: A Meta-Analysis and Systematic Review," Journal of Substance Abuse Treatment 99 (April 2019): 32–43, https://doi.org/10.1016/j.jsat.2018.12.003.
71. National Academies of Sciences, Engineering, and Medicine et al., Medications for Opioid Use Disorder Save Lives (Washington, DC: The National Academies Press, 2019), https://doi.org/10.17226/25310.
72. U.S. HHS, Health Care Transitions for Individuals Returning to the Community from a Public Institution.
73. Washington State Health Care Authority (HCA), Washington’s reentry Initiative, May 2024, https://www.hca.wa.gov/assets/program/reentry-overview-facilities.pdf.
74. CMS, Opportunities to Test Transition-Related Strategies to Support Community reentry and Improve Care Transitions for Individuals Who Are Incarcerated, SMD 23-003, U.S. HHS, April 17, 2023, https://www.medicaid.gov/federal-policy-guidance/downloads/smd23003.pdf.
75. Kinda Serafi, Patricia Boozang, and Gini Morgan, “CMS Issues Guidance on Section 1115 Demonstration Opportunity to Support Reentry for Justice-Involved Populations,” State Health & Value Strategies, April 19, 2023, https://www.shvs.org/cms-issues-guidance-on-section-1115-demonstra-
76. Washington State Health Care Authority, “Washington’s Reentry Initiative: Overview and Call for Carceral Facility Participation, May 2024, https:// www.hca.wa.gov/assets/program/reentry-overview-facilities.pdf
77. U.S. HHS, Health Care Transitions for Individuals Returning to the Community from a Public Institution.
78. Angela Garner, Director, CMS Division of System Reform Demonstrations, letter to Tyler Sadwith, State Medicaid Director, California DHCS, approving California’s Advancing and Innovating Medi-Cal Section 1115(a) Demonstration Proposal Number 11-W-00193/9, October 2, 2024, https://www.medicaid. gov/medicaid/section-1115-demonstrations/downloads/ca-calaim-reentry-intve-impltn-pln-aprvl-10022024.pdf.
79. Binswanger et al., “Release from Prison.”
80. Aleks Kajstura and Wendy Sawyer, “Women’s Mass Incarceration: The Whole Pie 2024,” Prison Policy Initiative, March 5, 2024, https://www.prisonpolicy.org/reports/pie2024women.html.
81. Jennifer Clarke et al., “Reproductive Health Care and Family Planning Needs Among Incarcerated Women,” American Journal of Public Health 96, no. 5 (May 2006): 834-39, https://doi.org/10.2105/AJPH.2004.060236.
82. Nicholas S. Makrides and Jay D. Shulman, "The Oral Health Needs of the Incarcerated Population: Steps Toward Equal Access," American Journal of Public Health 107, no. S1 (June 2017): S46–47, https://doi.org/10.2105/AJPH.2016.303593.
83. Henrie M. Treadwell et al., "Implications for Improving Oral Health Care Among Female Prisoners in Georgia’s Correctional System," American Dental Hygienists’ Association 90, no. 5 (October 2016): 323–27, https://jdh.adha.org/content/90/5/323.
84. Treadwell et al., "Implications for Improving Oral Health Care," 323-27.
85. Makrides and Shulman, "Oral Health Needs," S46–47.
86. Horst, Jeremy A., et al. “Fluorides and Other Preventive Strategies for Tooth Decay.” Dental Clinics of North America, vol. 62, no. 2, Apr. 2018, pp. 207–34. DOI.org, https://doi.org/10.1016/j.cden.2017.11.003., CDC. “Promoting Oral Health.” Diabetes, 23 July 2024, https://www.cdc.gov/diabetes/ hcp/clinical-guidance/how-to-promote-oral-health-for-people-with-diabetes.html.
87. Esther Galletta et al., "Societal Reentry of Prison Inmates With Mental Illness: Obstacles, Programs, and Best Practices," Journal of Correctional Health Care 27, no. 1 (March 2021): 58–65, https://doi.org/10.1089/jchc.19.04.0032.
88. Arizona Health Care Cost Containment System (AHCCCS). (2021). Emergency Dental Benefit for Adults Age 21 Years and Older. https://www.azahcccs.gov/Resources/Downloads/DFSMTraining/2021/EmergencyDentalBenefitfor21.pdf
89. Fatiha El Ghissassi et al., "A Review of Human Carcinogens—Part D: Radiation," The Lancet Oncology 10, no. 8 (August 2009): 751–52, https:// doi.org/10.1016/S1470-2045(09)70213-X.; “Aging Changes in Skin,” MedlinePlus, accessed December 7, 2024, https://medlineplus.gov/ency/article/004014.htm.
90. Richard Armitage and Laura B. Nellums, "COVID-19 and the Consequences of Isolating the Elderly," The Lancet Public Health 5, no. 5 (May 2020): e256, https://doi.org/10.1016/S2468-2667(20)30061-X.; Olumayowa A. Oninla and Olaniyi Onayemi, "Skin Infections and Infestations in Prison Inmates," International Journal of Dermatology 51, no. 2 (February 2012): 178–81, https://doi.org/10.1111/j.1365-4632.2011.05016.x.; Madison Ferris et al., "An International Review of Skin Conditions in Incarcerated Persons," JAAD Reviews 2 (December 2024): 113–26, https://doi.org/10.1016/j.jdrv.2024.10.001.
91. Madhulika A. Gupta et al., "Psychologic Trauma, Posttraumatic Stress Disorder, and Dermatology," Dermatologic Clinics 23, no. 4 (October 2005): 649–56, https://doi.org/10.1016/j.det.2005.05.018.
92. “Standards,” National Commission on Correctional Health Care, accessed December 7, 2024, https://www.ncchc.org/standards/.
93. Ferris et al., "An International Review," 113-26.
94. Thomas Hewson et al., "Interventions for the Detection, Monitoring, and Management of Chronic Non-Communicable Diseases in the Prison Population: An International Systematic Review," BMC Public Health 24, no. 1 (January 2024): 292, https://doi.org/10.1186/s12889-024-17715-7.
95. Samir Kamat et al., "Teledermatology Within Correctional Settings in the United States: A Narrative Review of the Literature," JMIR Dermatology 6 (May 2023): e47115, https://doi.org/10.2196/47115.
96. Angela Garner, Director, CMS Division of System Reform Demonstrations, letter to Charissa Fotinos, State Medicaid Director, Washington HCA, issuing technical corrections to Washington’s Medicaid Transformation Project 2.0 (Project Numbers 11-W-00304/0 and 21-W-00071/0), December 8, 2023, https://www.medicaid.gov/medicaid/section-1115-demonstrations/downloads/wa-medicaid-transformation-ca-12082023.pdf.
97. Lydie A. Lebrun-Harris et al., “Health Status and Health Care Experiences among Homeless Patients in Federally Supported Health Centers: Findings from the 2009 Patient Survey,” Health Services Research 48, no. 3 (June 1, 2013): 992–1017, https://doi.org/10.1111/1475-6773.12009.; Sarah C. Oppenheimer, Paula S. Nurius, and Sara Green, “Homelessness History Impacts on Health Outcomes and Economic and Risk Behavior Intermediaries: New Insights from Population Data,” Families in Society 97, no. 3 (July 1, 2016): 230–42, https://doi.org/10.1606/1044-3894.2016.97.21.
98. Amanda Stafford and Lisa Wood, "Tackling Health Disparities for People Who Are Homeless? Start with Social Determinants," International Journal of Environmental Research and Public Health 14, no. 12 (December 2017): 1535, https://doi.org/10.3390/ijerph14121535.; Travis P. Baggett, Samantha S. Liauw, and Stephen W. Hwang, "Cardiovascular Disease and Homelessness," Journal of the American College of Cardiology 71, no. 22 (June 5, 2018): 2585–97, https://doi.org/10.1016/j.jacc.2018.02.077.
99. Jessica L. Mackelprang, Susan E. Collins, and Seema L. Clifasefi, "Housing First Is Associated with Reduced Use of Emergency Medical Services," Prehospital Emergency Care 18, no. 4 (October 2, 2014): 476–82, https://doi.org/10.3109/10903127.2014.916020.; Verughese Jacob et al., "Permanent Supportive Housing with Housing First: Findings from a Community Guide Systematic Economic Review," American Journal of Preventive Medicine 62, no. 3 (March 1, 2022): e188–201, https://doi.org/10.1016/j.amepre.2021.08.009.
100. Greg A. Greenberg and Robert A. Rosenheck, "Jail Incarceration, Homelessness, and Mental Health: A National Study," Psychiatric Services 59, no. 2 (February 2008): 170–77, https://doi.org/10.1176/ps.2008.59.2.170.
101. Stephen Metraux, Caterina G. Roman, and Richard S. Cho, Incarceration and Homelessness (paper developed for the National Symposium on Homelessness Research, 2007), https://aspe.hhs.gov/sites/default/files/migrated_legacy_files//139216/report.pdf.
102. Dale E. McNiel, Renée L. Binder, and Jo C. Robinson, "Incarceration Associated With Homelessness, Mental Disorder, and Co-Occurring Substance Abuse," Psychiatric Services 56, no. 7 (July 2005): 840–46, https://doi.org/10.1176/appi.ps.56.7.840.; Lucius Couloute, "Nowhere to Go: Homelessness among Formerly Incarcerated People," Prison Policy Initiative, August 2018, https://www.prisonpolicy.org/reports/housing.html.
103. “Governor Hochul Announces $500 Million for New Social Care Networks Program to Deliver Social Services and Improve Health Outcomes for Millions of Low-Income New Yorkers,” Office of the Governor of State of New York, August 7, 2024, https://www.governor.ny.gov/news/governor-hochul-announces-500-million-new-social-care-networks-program-deliver-social-services.
104. Sam McCann, "People Need Transportation Access After Release from Jail and Prison," Vera Institute of Justice, July 7, 2018, https://www.vera.org/ news/people-need-transportation-access-after-release-from-jail-and-prison.
105. Miriam Northcutt Bohmert, Access to Transportation and Outcomes for Women on Probation and Parole (East Lansing, MI: Michigan State University, 2014), https://www.ojp.gov/pdffiles1/nij/grants/248641.pdf.
106. “FAQs for Non-Emergency Transportation,” AHCCCS, accessed November 18, 2024, https://www.azahcccs.gov/PlansProviders/RatesAndBilling/ ProviderManuals/NEMT.html.
107. Meredith Moran, “Arizona County Works to End Homelessness, Reduce Recidivism for Formerly Incarcerated,” National Association of Counties,
October 7, 2024, https://www.naco.org/news/arizona-county-works-end-homelessness-reduce-recidivism-formerly-incarcerated.
108. Elizabeth Allen, “Cheap Jail and Prison Food Is Making People Sick. It Doesn’t Have To,” Vera Institute of Justice, February 27, 2024, https://www. vera.org/news/cheap-jail-and-prison-food-is-making-people-sick-it-doesnt-have-to
109. Åsa Ernersson, Fredrik H. Nystrom, and Torbjörn Lindström, “Long-term Increase of Fat Mass after a Four Week Intervention with Fast Food Based Hyper-alimentation and Limitation of Physical Activity,” Nutrition & Metabolism 7, no. 68 (August 25, 2010), https://doi.org/10.1186/1743-7075-7-68.
110. Alexander Testa and Dylan B. Jackson, “Food Insecurity Among Formerly Incarcerated Adults,” Criminal Justice and Behavior 46, no. 10 (June 2019): 1493–1511, https://doi.org/10.1177/0093854819856920.
111. Alexander Testa, “Access to Healthy Food Retailers Among Formerly Incarcerated Individuals,” Public Health Nutrition 22, no. 4 (October 2018): 672–680, https://doi.org/10.1017/S1368980018002720.
112. CMS, Coverage of Health-Related Social Needs (HRSN) Services in Medicaid and the Children’s Health Insurance Program (CHIP), November 2023, https://www.medicaid.gov/health-related-social-needs/downloads/hrsn-coverage-table.pdf.
113. “Improving Health by Embedding Produce Prescriptions (PRx) into Healthcare Practice,” National Produce Prescription Collaborative, accessed November 20, 2024, https://nppc.health/.
114. Erika Hanson et al., “Food is Medicine: A State Medicaid Policy Toolkit,” Harvard Law School Center for Health Law and Policy Innovation and Food is Medicine Coalition, July 2024, https://fimcoalition.org/wp-content/uploads/2024/07/Food-is-Medicine-A-State-Medicaid-Policy-Toolkit_Final-July-2024-1.pdf.
115. “Significant Cost Savings Realized as Healthy Opportunities Pilots Reach Two-Year Anniversary,” North Carolina Department of Health and Human Services, May 21, 2024, https://www.ncdhhs.gov/blog/2024/05/21/significant-cost-savings-realized-healthy-opportunities-pilots-reach-two-year-anniversary.
116. Jerilyn K. Allen et al., “Cost-effectiveness of Nurse Practitioner/Community Health Worker Care to Reduce Cardiovascular Health Disparities,” The Journal of Cardiovascular Nursing 29, no. 4 (July 2014): 308–314, https://doi.org/10.1097/JCN.0b013e3182945243.
117. Miya L. Barnett et al., “Mobilizing Community Health Workers to Address Mental Health Disparities for Underserved Populations: A Systematic Review,” Adm Policy Ment Health 45 (March 2018): 195–211, https://doi.org/10.1007/s10488-017-0815-0.
118. David Young and Clarann Weinert, "Improving Health Literacy With Inmates," Corrections Today 75, no. 5 (November / December 2013): 70–74, https://www.proquest.com/trade-journals/improving-health-literacy-with-inmates/docview/1464623815/se-2?accountid=13314.
119. Elaine Chhean, Elinor Higgins, Sandra Wilkniss, and Hemi Tewarson, “Lessons for Advancing and Sustaining State Community Health Worker Partnerships,” National Academy for State Health Policy, December 20, 2021, https://nashp.org/lessons-for-advancing-and-sustaining-state-community-health-worker-partnerships/.
120. Arizona Administrative Code, Title 9, Chapter 16, Article 8, accessed December 10, 2024, https://apps.azsos.gov/public_services/Title_09/9-16.pdf.
121. Sweta Haldar and Elizabeth Hinton, “State Policies for Expanding Medicaid Coverage of Community Health Worker (CHW) Services,” KFF, January 23, 2023, https://www.kff.org/medicaid/issue-brief/state-policies-for-expanding-medicaid-coverage-of-community-health-worker-chw-services/#endnote_link_576635-11.
122. Chhean, Higgins, Wilkniss, and Tewarson, “Lessons for Advancing and Sustaining State Community Health Worker Partnerships.”
123. Reach-in services are when a representative from the community, in this instance a Justice Liaison, contacts a member who is incarcerated while they are still in a facility. During these contacts, the community representative and the member who is incarcerated begin to develop a proactive plan to coordinate the healthcare and other social services in the community that will be needed to ensure treatment continuity and a successful reentry.
124. AHCCCS, Choosing a Health Plan, June 2023, https://www.azahcccs.gov/AHCCCS/Downloads/ChoosingaHealthPlan.pdf.
125. AHCCCS, Choosing a Health Plan.
126. Danya E. Keene, Amy B. Smoyer, and Kim M. Blankenship, “Stigma, Housing and Identity after Prison,” The Sociological Review 66, no. 4 (June 12, 2018): 799, https://doi.org/10.1177/0038026118777447.
127. Meena Seshamani et al., “Addressing Rural Health Inequities in Medicare,” CMS, February 10, 2023, https://www.cms.gov/blog/addressing-rural-health-inequities-medicare#:~:text=Approximately%2061%20million%20Americans%20live,effort%20to%20improve%20health%20equity.
128. Garcia et al., “Reducing Potentially Excess Deaths.”
129. Seshamani et al., “Addressing Rural Health Inequities in Medicare.”
130. U.S. Census Bureau, U.S. Census Updates: Arizona’s Rural Population, June 2023, https://crh.arizona.edu/sites/default/files/2023-06/2300601_ Census-RuralUpdate-Brief.pdf.; “Health Professional Shortage Areas: Primary Care, by County, October 2024 - Arizona,” Rural Health Information Hub, accessed December 11, 2024, https://www.ruralhealthinfo.org/charts/5?state=AZ.
131. Arizona Department of Health Services, Bureau of Women’s and Children’s Health, Arizona Medically Underserved Areas Biennial Report, October 2024, https://www.azdhs.gov/documents/prevention/health-systems-development/data-reports-maps/reports/azmua-biennial-report.pdf.
132. Selected Rural Healthcare Facilities in Arizona,” Rural Health Information Hub, accessed December 11, 2024, https://www.ruralhealthinfo.org/ states/images/arizona-rural-health-facilities.jpg?v=571.
133. “Tribal Health Initiatives,” The University of Arizona Center for Rural Health, accessed December 2, 2024, https://crh.arizona.edu/programs/tribal-health.
135. “Division of Corrections,” U.S. Department of the Interior Bureau of Indian Affairs, accessed December 2, 2024, https://www.bia.gov/bia/ojs/doc#.
136. CMS, Opportunities to Test Transition-Related Strategies, 12-13.
137. Arizona Tribal Correctional Healthcare Coalition, Locked Up and Forgotten The Federal Government’s Failure to Fund Tribal Correctional Healthcare, June 2016, 2, https://aacihc.az.gov/sites/default/files/2022-03/Locked-Up-Forgotten.pdf.
138. CMS, Opportunities to Test Transition-Related Strategies, 22.
139. Washington State HCA, Medicaid managed care and fee-for-service, November 1, 2016, 2, https://www.hca.wa.gov/sites/default/files/program/ managed-care-and-ffs.pdf.
140. CMS, Medicaid and Children’s Health Insurance Program (CHIP) Managed Care Final Rule Overview of the Indian Specific Provisions, October 2016, 17, https://www.cms.gov/files/document/all-tribes-call-october-2016pdf.
141. CMS, State Exchange Grantee Meeting, September 2011, 3, https://www.cms.gov/CCIIO/Resources/Presentations/Downloads/18_tribal_consultation.pdf.
142. Sweta Haldar and Elizabeth Hinton, “State Policies for Expanding Medicaid Coverage of Community Health Worker (CHW) Services,” KFF, January 23, 2023, https://www.kff.org/medicaid/issue-brief/state-policies-for-expanding-medicaid-coverage-of-community-health-worker-chw-services/#endnote_link_576635-11.
143. Chhean, Higgins, Wilkniss, and Tewarson, “Lessons for Advancing and Sustaining State Community Health Worker Partnerships.”