
3 3 www.yourexpertwitness.co.uk


7 Opening Statement
8 Post Office Inquiry told of ‘instruction’ to expert witness by lawyer 9 Scotland strengthens hate crime legislation
9 PI lawyers call for an end to ‘inequality of arms’ in inquests 10 Consultation: CPR amendment on access to expert reports 10 Law Society warns of crisis in duty solicitor schemes TREE
11 Tree Preservation Orders: fact and fiction LEGAL
13 Construction company prosecuted following death of worker hit by excavator 13 Construction law essay prize-winners announced
15 CDM explained: HSE courses focus on the client and the designer
17 What does your construction contract say about insolvency? (Part 2)
FIRE INVESTIGATION
18 Council to commit further £1/2m to clean up after skip depot fire
19 Developers ordered to fund cladding remediation costs
THE OIL & GAS INDUSTRY
21 Law firm pinpoints main areas of oil and gas disputes
21 Govt announces expansion in gas plant provision
VIEWPOINT
23 Mediation: have the floodgates finally opened?
FORENSIC ACCOUNTANCY
25 Insurance contract disputes: what’s different about them?
27 Crime and cryptocurrency: a partnership of its time?
27 Law Society reports on changes to money laundering regime
29 What does the financial future hold?
31 Former MOD official convicted of receiving secret kickbacks
31 Taskforce advises City firms on cyber attacks
33 Fraud alert issued ahead of holiday season
COMPUTER FORENSICS
35 Cyber Security Centre issues update on Russian threat
35 Look to yourself! Cyber threat may be an inside job
TRANSLATING & INTERPRETING
37 English and Welsh translation bodies join forces
37 White paper outlines pluses and minuses of AI
38 Our new section for experts wishing to offer their expertise to the



4 4 www.yourexpertwitness.co.uk 35 17 10 CONTENTS IN THIS ISSUE 2YWY Copyright Your Expert Witness. All rights reserved. No part of this publication may be copied, reproduced or transmitted in any form without prior permission of Your Expert Witness. Views expressed in this magazine are not necessarily those of the publisher. Printed in the UK by The Magazine Printing Company Plc www.magprint.co.uk Your Expert Witness Suite 2, 61 Lower Hillgate, Stockport SK1 3AW Advertising: 0161 710 3880 Editorial: 0161 710 3881 Subscriptions: 0161 710 2240 E-mail: ian@dmmonline.co.uk A to Z WEBSITE GUIDE 39 Our A to Z guide to the websites of some of the country’s leading expert witnesses. EXPERT CLASSIFIED 102 Expert Witness classified listings 107 Medico-legal classified listings EXPERTS FOR MEDIA
range
print
vast
of
and broadcast media
NEWS
CARE
CONSTRUCTION
ISSUES IN
MEDICAL ISSUES
43 Medical Notes
NEWS
44 BMA lays down the law on MAPs
44 Research throws light on remote consultations
47 Study highlights economic effect on frailty
47 Brain charity laments Budget funding miss for ABI
49 Former care manager fined after resident sexually assaulted
49 Whooping cough on the rise in infants
51 GMC apologises for past homophobic censures
51 Podiatry institute clarifies position on injectables
CARDIOLOGY
53 What are the medicolegal challenges of coronary artery bypass grafts?
55 Cardiology has become a complex specialty
REHABILITATION
57 Rehabilitation: a cornerstone of compensation claims
59 Brain injury rehab can benefit from SLT
59 Film telling rehab story following amputation wins industry award
60 New arts therapy expert witness service launches
61 What are the considerations for costing rehabilitation requirements?
EMERGENCY MEDICINE
63 Infection control lapses threaten A&E patients and staff
63 Paramedics’ college gains chartered status
NEUROLOGY
65 Post-traumatic headache following head injury or whiplash
DENTISTRY & MAXILLOFACIAL SURGERY
67 New guidance clarifies position on indemnity for dentists
67 Dentists attack government’s Recovery Plan
RADIOGRAPHY & RADIOLOGY
70 Radiographer or radiologist: which is most appropriate for your negligence case?
OBSTETRICS & GYNAECOLOGY
73 Some medico-legal advice on consent for minor procedures
PLASTIC, RECONSTRUCTIVE & HAND SURGERY
75 Hand surgeons raise concerns over sterile implants
77 Hair transplant guidelines published by cross-national surgery bodies
VASCULAR SURGERY
78 What problems arise from ablation treatments for varicose veins?
PAIN MEDICINE
81 Medical student’s invention will help reduce chemo pain
81 Safety Alert issued re universal cannula connector for pain relief administration
PSYCHIATRIC & PSYCHOLOGICAL ISSUES
83 Ambulance leaders voice concerns over Right Care, Right Person
85 Expert in Mind unveils game-changing sister venture
86 Is there an expert in the house?
87 Violence and abuse are main drivers of mental ill-health in women and girls
87 Psychologists criticise closure of NHS mental health hubs
ORTHOPAEDICS
89 New course covers legal issues for orthopaedic surgeons
91 Collaboration moves nanotechnology closer to surgical reality
93 Robotic overreach vs the precision promise
95 Ortho-surgeons named in New Year’s Honours list
95 Widow awarded damages for husband’s death following surgery
OPHTHALMOLOGY & OPTOMETRY
97 College updates guideline for ophthalmologists to detect child abuse
97 There’s strength in unity in ophthalmic medicolegal practice
99 Royal colleges reiterate common ground
HEARING LOSS
100 RNID research
101 Implant or hearing aid? Trial looks to determine which is most




5 5 www.yourexpertwitness.co.uk
57 www.yourexpertwitness.co.uk
highlights audiology failings
suitable 75 101
Opening Statement
[IT’S TRADITIONAL with the first issue of a new year (yes, the last issue of Your Expert Witness was last year) to look forward to the next few months while casting a glance back to the previous year. In some respects we can, indeed, do both at the same time.
A month or so ago Lancaster City Council announced further funding to deal with the aftermath of a fire that burned for three weeks last December. Half of the funds used in the effort to date have been swallowed up in landfill tax – honest! HMRC says there is ‘no mechanism to waive’ the tax. Sometimes the law is ‘a ass’.
• Another issue that has spanned the years from the last issue, at least as far as this magazine is concerned, is that of provision for insolvency in a construction contract. Our correspondents from Womble Bond Dickinson round off their commentary on the subject.
• Turning our back on last year and looking ahead to 2024, Fiona Hotston Moore gazes into her crystal ball and predicts further expansion of mediation and arbitration, together with greater volatility caused by external events. She also predicts an increasing involvement of new technologies.
• The role of new technologies accounts for a sizeable proportion of this issue. A taskforce of financial institutions has convened to help businesses deal with the risks of cyber crime during financial transactions. The move comes against a backdrop of heightened awareness of security threats. While the government has redefined the definition of a ‘high risk’ country when it comes to money laundering, it has added more countries to its list of jurisdictions. Meanwhile, cyber attacks attributed to a number of Russian actors have become more sophisticated.
As if looking to more places abroad weren’t enough, a UK govt agency has counselled looking closer to home for breaches. Insider threats are often overlooked, the Cyber Security Council has pointed out.
• Even going abroad is fraught with cyber threats. Action Fraud, the police’s fraud reporting platform, has issued an alert to people booking holidays online as the holiday season looms. What seems to be an unbelievably good deal almost certainly is.
• The most publicly visible catastrophe involving a computer system is, of course, the Post Office Horizon scandal. There is little new light this publication can shed on the affair, other than to be aghast at the actions of those who came close to bringing the legal sector into disrepute.
• The increased use of artificial intelligence has also been exercising translators and interpreters in the public sector – including the courts. The Chartered Institute of Linguists has published a white paper on the subject, highlighting some of the advantages in terms of creating and improving content and also the technology’s tendency towards bias and mistakes.
As a reader of my local newspaper for the Talking Newspaper I can attest to the latter, as can any sub editor tired of removing rogue ‘z’s from what purports to be English.
• More seriously, a breakdown in communication and understanding between and inside communities can lead to the development of hate crimes. When misunderstanding degenerates into raw hate of a person for what they are, believe and represent there has to be some kind of sanction. In Scotland that has taken the form of the Hate Crime and Public Order (Scotland) Act, due to come into force on 1 April. This year that date is Easter Monday, traditionally a time for reconciliation: you never know. q
Ian Wild
Ian Wild, Director of Business Development Your Expert Witness

7 7 www.yourexpertwitness.co.uk
POST OFFICE INQUIRY TOLD OF ‘INSTRUCTION’ TO EXPERT WITNESS BY LAWYER
[
THE ON-GOING Post Office Horizon IT Inquiry has recently revealed how a senior Post Office lawyer told an engineer working on their defective IT system to provide a court with evidence that would help with ‘preserving’ it. That led to the jailing of a wrongly convicted and pregnant sub-postmaster, Mrs Misra, in 2010.
Warwick Tatford, the prosecuting barrister in the 2010 case, told the Inquiry that the advice sent by the Post Office lawyer was ‘disastrous’. He added: “As far as I’m concerned, I was prosecution counsel in the case…and I have obviously failed to ensure that there’s an atmosphere where an expert can be properly instructed.”
While giving evidence in the Inquiry, Mr Tatford was shown the email from Mr Singh, the Post Office lawyer, to Mr Jenkins, the ‘expert’, which read: “As you are our Horizon expert you need to telephone Charles McLachlan [ the defence expert ]…to arrange a meeting where you can discuss all his reports and his concerns about the Horizon so you can deal with it and rebut it.”
The email continued: “…and then write a detailed report which would go to some way of progressing and concluding this matter and importantly preserving the Horizon system. Maybe the simplest and practical way of dealing with this whole question is to find a shortest span of logs, analyse it, disprove or rebut what the defence expert is saying in his reports.
“Just a reminder you are an expert for Fujitsu, you will be giving evidence in court, the judge and jury will be listening to you very carefully and a lot will hang on the evidence.”
Commenting on the revelation, a commentator from Bond Solon wrote: “Expert witnesses are independent parties who owe a duty

to the court and not the party who instructed them.
“This Inquiry highlights how important it is for an expert witness to be independent from any of the parties in a case, and the dangerous consequences of an improper instruction. As emphasised above, the onus isn’t just on experts to ensure that they are aware of their legal duties, but also on the legal teams as well.
“Giving evidence in the Inquiry, Mr Tatford, the prosecuting barrister in the 2010 case, held back tears, saying he was ‘ashamed that I was part of this’, before apologising to Mrs Misra who sat in the public gallery.” q
8 8 www.yourexpertwitness.co.uk
SCOTLAND STRENGTHENS HATE CRIME LEGISLATION


[THE Hate Crime and Public Order (Scotland) Act will come into force in Scotland from 1 April. It creates new stirring up of hatred offences for protected characteristics including age, disability, religion, sexual orientation and transgender identity.
These extra provisions will add to the longstanding stirring up racial hatred offences which have been in place since 1986.
Recent statistics show that 5,738 charges of hate crime were reported in Scotland in 2022-23.
A new Scottish Government public awareness raising campaign supported by Police Scotland has been running throughout March. The Hate Hurts campaign shows the

impact of hate crime and encourages those who have witnessed or experienced a hate crime to come forward.
Minister for Victims and Community Safety Siobhian Brown said: “For those impacted by hatred and prejudice, the results can be traumatic and life changing. While we respect everyone’s right to freedom of expression, nobody in our society should live in fear or be made to feel like they don’t belong, and the Scottish Government is committed to building safer communities that live free from hatred and prejudice.
“Hate crime is behaviour that is both criminal and rooted in prejudice. It can be verbal, physical, online or face-to-face. The

new law will give greater protections to those who need it and helps to form the basis of understanding about the type of behaviour that is not acceptable in our society.”
Chief Superintendent Faroque Hussain, hate crime prevention lead at Police Scotland, commented: “Hate crime is vile and wrong. To target a person, a group or a community because of who they are, how they look or how they choose to live their lives undermines freedoms and rights we are entitled to enjoy as human beings.
“We know it can be hard for people to report a hate crime, and in some cases to even recognise or acknowledge that they have been a victim.” q
PI LAWYERS CALL FOR AN END TO ‘INEQUALITY OF ARMS’ IN INQUESTS
[BEREAVED FAMILIES are being forced to navigate inquests without legal help because the majority cannot obtain legal aid, the Association of Personal Injury Lawyers (APIL) has stated in its submission to the MoJ’s consultation on civil legal aid. APIL is calling for an end to the current one-sided situation, in which bereaved relatives cannot secure funding so they can be represented at inquests involving public bodies.
“Public bodies, such as hospitals and local authorities, will have legal support as a matter of course at inquests, and to boot it will be paid for out of the public purse,” said APIL vice president Kim Harrison. “Yet the grieving families are hardly ever granted the same publicly-funded legal aid. This disparity can make a fundamental difference to the coroner’s conclusion.
“Most grieving relatives will have little understanding of the inquest process and what questions they should ask, or which witnesses to call, to get the answers they need about how their loved one died. They may also have to handle reams of complicated and distressing evidence, without any experience or help,” she explained. “The lack of provision of legal aid for ordinary families simply does not provide access to justice.”
APIL also says that the application process is too complicated and needs simplifying. “While we welcomed the removal of financial means testing for some applications, this does not go far enough,” said Kim Harrison. “Families are still required to prove their case is in the wider public interest, or relates to a breach of Article 2 of the European Convention of Human Rights, which is complicated and challenging to prove.
“They are expected to deal with all this alone while the public body involved has access to legal representation. It’s a total inequality of arms.
“It is of benefit to society as a whole for inquests to find the truth and establish how someone came by their death, to ensure that any mistakes are not repeated,“ she added. “Take, for example, the case where a hospital patient has died due to negligent treatment. The right questions need to be asked and conclusions made so that lessons can be learned.” q
9 9 www.yourexpertwitness.co.uk
CONSULTATION: CPR AMENDMENT ON ACCESS TO EXPERT REPORTS
[ THE Civil Procedure Rule Committee (CPRC) is consulting on a proposed draft amendment to the Civil Procedure Rules (CPR) rule 5.4C (supply of documents to a non-party from court records).
The proposed amendment would permit a non-party to obtain specified documents in relation to the proceedings, including expert reports (except for medical reports or where a rule or practice direction provides otherwise), without the permission of the court.
A non-party will be able to obtain the documents (subject to certain restrictions) where the defendant has filed an acknowledgement of service or a defence, the claim has been listed for a hearing, or a judgment has been listed in the claim.
In its Explanatory Note the CPR Committee said: “This consultation was commissioned at the CPRC meeting on 1st December 2023 (the minutes of which can be read online) following careful consideration by a multi-jurisdictional working group, chaired by a Lord Justice of Appeal.
“The origins of the work flow from the UK Supreme Court judgment in Cape Intermediate Holdings Ltd v Dring [2019] UKSC 38 (see specifically, paragraphs 41-51 inclusive) and the consultation is also set in the context of the Lady Chief Justice’s broader agenda of looking at transparency issues.
“The 1st December 2023 CPRC meeting also noted the possibility of an amendment, in due course, to CPR 32.13 (availability of witness statements for inspection) to provide express provision in relation to the inspection of expert reports.”
The Expert Witness Institute (EWI) has indicated that it will be providing a response to the consultation and would welcome the views of EWI members on the proposed amendments to rule 5.4C to help inform the response. q
LAW SOCIETY WARNS OF CRISIS IN DUTY SOLICITOR SCHEMES
[
URGENT INVESTMENT IS NEEDED to halt the declining number of duty solicitors and avoid miscarriages of justice, the Law Society of England and Wales has warned. The Law Society sounded the alarm bell ahead of a Westminster Hall debate on 13 March.
“Duty solicitors work tirelessly around the clock providing essential legal advice to suspects at police stations,” said Law Society president Nick Emmerson. “Their presence allows investigations to move forward quickly and they are critical to ensuring victims and defendants alike get justice.
“However, across England and Wales, duty solicitor schemes are in crisis because governments continue to undervalue their work. Some schemes have fewer than seven members, making providing 24/7 access to a duty solicitor challenging.
“Without investment, more solicitors will be forced out of the criminal defence profession, representation will become difficult to provide and there is a serious risk of miscarriages of justice.”
Since 2017 more than 1,400 duty solicitors have left the sector. Those that remain are ageing. Fewer than 4% of duty solicitors are under 35 years old: the average age in 2021 was 49 and is higher in many regions. Across England and Wales, 32 duty solicitor schemes have fewer than seven members.
“Following our successful judicial review, the government should without any further delay implement the 15% increase recommended, in real terms, across all criminal legal aid rates,” added Nick Emmerson. “In the long term, wider reform of criminal legal aid and a longer-term approach to its sustainability is needed, too.
“As the High Court judges made clear, without a significant injection of funding the criminal defence system, which is already ‘coming apart at the seams’, will collapse, endangering justice for all.” q
10 10 www.yourexpertwitness.co.uk
TREE PRESERVATION ORDERS: FACT AND FICTION
By Mark Chester of Cedarwood Tree Consultants
[TREE PRESERVATION ORDERS (TPOs) have been part of the planning and legal scenes since the Town and Country Planning Act of 1947. Part of my work as an expert witness involves appraising cases with protected trees and guiding clients seeking to navigate the minefield presented.
The starting point is that the presence of a TPO on a site does not necessarily mean that all of the trees at that site are protected: it may even be that none are. The extent of protection depends on what was included in the order when it was made and what is present now. One type of order often used is the Area Designation. That covers everything present when the order was made; however, it doesn’t include any trees which grow naturally or are planted thereafter.
I helped one client recently whose property had a lime tree. An order was listed to the property and consents for pruning works had been granted in the past. The tree officer, the client and the arborist all assumed that the tree was protected. I was called in to help when an application to prune was rejected by the local authority. The TPO dated from the 1970s, and contained an Area Designation. When visiting the site it was evident that the tree was too young to have been present when the TPO was made, but had been planted as part of landscaping.
Those who had made the order had appreciated that the site would soon benefit from new trees being planted, and referred to that in the document. However, they couldn’t provide information on species and addresses. The intention to protect was evident, but intention is not sufficient to enforce. Without that capacity the order could not be said to apply to the specific tree. I was able to brief both the client and the arborist on the situation and they were able to progress.
The issue of protecting future planting on sites with development potential is one that planning officers often consider: it can be easy to lose trees planted in a development on completion. However, to be effective, the protection needs to be detailed.
For another client, the desire to construct a single-storey dwelling in their rear garden, which had many trees, was proportionate. Unfortunately, the desire to protect trees in neighbouring gardens from wider development, and also to protect future generations of trees, had led to a rather too inclusive order being made. Woodlands are an important feature of our landscapes and they can be protected in perpetuity. An order used for them protects all future natural regeneration. It recognises that they provide a tree nursery facility, which can be very effective.
For this client the Woodland Order had been used. It changed their garden, with lawn and shrub beds, into a woodland. Fortunately, by guiding the parties to a more suitable way forward – with an order that listed each tree to be protected – a more sustainable outcome was achieved.
Part of my role as a specialist is to guide either the tree owner or the local authority on the merits of enforcement action, and how to proceed. I also guide when an application to prune or fell is refused. Sometimes, a tree is making a contribution to the setting but is not widely visible, or is in need of pruning which would reduce its contribution so significantly as to make it not worthwhile. That argument has been successful with several appeals.
Part of the tree protection landscape involves dealing with trees in Conservation Areas. These are a bit of an anomaly because the designation is primarily due to the architectural merits of the setting, not the trees, and trees may be included regardless of their own merits. The process of consent is different for trees in a Conservation Area than for those subject to a TPO, but the consequences of breaching the process are the same. With correct guidance, a good outcome – for the client, even if not for the tree – may be achieved.
Sadly, for one client their eagerness to proceed without guidance resulted in a very different outcome. The client chose to contact the officer to see when they would be getting approval for their application
to fell a poor-quality specimen in the rear garden of their home, where they wanted to build a garden office. The officer promptly visited, decided they did not support felling and arranged for a TPO to be served as soon as it could be arranged. That also thwarted the plans for the garden office.

For one case where I was expert for the defendant, I received the portfolio of evidence presented by the local authority. The officers were convinced of the merits of their case and considered that the defendant had unlawfully felled protected trees. The defendant’s defence was that each tree was in decline, and therefore exempt. When I visited the site, the presence of dead and dying trees was evident.
The one disappointment I had professionally was that, in their summing up, the magistrates did not comment on my own contribution, but merely observed that ‘the two experts disagreed’. They listened to the defendant and concluded that they couldn’t see why he would intentionally damage the trees on the site if they were not exempt. The case was dismissed.
TPOs are not always used appropriately and sometimes the trees protected do not merit it. A key part of my role is guiding the parties so that they proceed on an informed basis. They can generate considerable emotion and need to be applied with care.
Last summer I worked with a client with a tree too close to their new home. The tree was planted after development and was not subject to a TPO, nor was it in a Conservation Area. It was subject to a local covenant which was strictly applied.
The client was applying to extend their new home and the local authority wished to retain the tree. My professional opinion was that it was too close to the property and did not have a long-term future. However, we needed to ensure that the tree officer did not consider it under threat and arrange for a TPO to be served. By working with all parties and remaining calm and diplomatic, we were able to obtain consent for the extension and avoid the TPO.
Another client wished to fell a tree for which pruning would not be appropriate. A covenant for that site permitted pruning but not felling. My technical statement explained that, and that the work permitted would be damaging. The client was able to proceed to fell.
There are myths about TPOs, such as that they can stop work to a tree or stop a development, and that they need to be removed from a tree for it to be felled. I guide clients around that, and ensure that they are able to proceed in an informed manner. q
11 11 www.yourexpertwitness.co.uk

CONSTRUCTION COMPANY PROSECUTED FOLLOWING DEATH OF WORKER HIT BY EXCAVATOR
[A NORTH YORKSHIRE construction company has been fined after a worker was struck on the head and killed by a 16-ton excavator.
On 13 January 2021, Dean Myers, an employee of HACS Construction Ltd, was undertaking groundwork activities in a partially excavated trench at a site in Ripon, North Yorkshire. During the works, the 56-year-old was struck on the head by the moving bucket of the excavator, suffering catastrophic injuries to his face and head. He was pronounced dead at the scene by the ambulance service.

The groundworks team had been preparing the trench for the laying of new drainage. Mr Myers had moved to the foot of an existing manhole directly adjacent to the trench when the excavator was reported to have met resistance whilst digging.
With nothing in place to prevent his entry into the danger zone of the excavator, Mr Myers exited the manhole via a makeshift opening to investigate. However, the excavator driver and other workers were not in a position to see that he had entered the danger zone. The excavator bucket then swung into him with fatal consequences.
CONSTRUCTION LAW ESSAY PRIZE-WINNERS ANNOUNCED
[ON 15 FEBRUARY the Judging Panel of the Society of Construction Law’s (SCL) Hudson Prize announced its results for the 2023 competition.
First Prize went to The lesser of two evils? A comparative analysis of how common law jurisdictions approach accrual of causes of action in negligence post-Pirelli by William Haslam, a pupil barrister at Atkin Chambers.
Second Prize was awarded to Shou Yu Chong of King’s College London for Enforcing Mediation and ADR Agreements in International Construction Contracts: Transnational Principles and Comparative Perspectives
Mariya Rankin of Eversheds-Sutherland was Highly Commended for What if construction can change?
Lauren Adams, chair of the SCL Hudson Prize Judging Panel, commented: The Judging Panel offers their congratulations to all recipients of awards and thanks all who entered the 2023 SCL Hudson Prize.”
The SCL Hudson Prize was launched in 1996 as a successor to the Alfred Hudson Prize – Hudson has been described as ‘virtually the founding father’ of construction law. It is awarded for an essay on a topic which is ‘part of, or closely related to, construction law’. The award currently stands at £2,500 for First Prize and £1,250 for Second Prize. Entrants can also be Highly Commended or Commended. All who are awarded prizes or commendations receive a year’s free membership of the Society of Construction Law. Founded in 1983, the SCL comprises over 3,000 members from all sections of the construction industry and associated legal practices. Lord Justice Coulson is its president and Hamish Lal is the current chair. Its mission is to ‘promote and encourage the study of construction law and the exchange of information and ideas concerning it’. q
HSE’s investigation found that HACS Construction Ltd had failed to identify or assess the risk arising from using the existing manhole chamber as an improvised refuge. That meant the company failed to implement a system whereby workers were prevented from entering the dangerous working zone of the excavator while the machine was being operated by a driver with limited sight. There was also inadequate supervision on site, alongside a failure to carry out monitoring visits which would have identified crucial safety failings.
At Leeds Magistrates’ Court on 24 January HACS Construction Ltd pleaded guilty to breaching Section 2 (1) of the Health & Safety at Work etc Act 1974. The company was fined £330,500 and ordered to pay £9,141 costs.
After the hearing, HSE inspector Ben Caines said: “This tragic incident could so easily have been avoided had HACS Construction Limited simply ensured that adequate control measures and safe working practices were identified and followed.
“The company should have put in place measures including the use of trained plant marshals for high-risk activities, such as the work Mr Myers was undertaking. Such measures are widely recognised and used across the construction industry as well as being advised within HSE and industry guidance.”
The HSE prosecution was brought by HSE enforcement lawyer Gemma Zakrzewski. q
13 13 www.yourexpertwitness.co.uk

14 14 www.yourexpertwitness.co.uk
CDM EXPLAINED: HSE COURSES FOCUS ON THE CLIENT AND THE DESIGNER
[HSE HAS ANNOUNCED DATES and venues for two training courses on CDM. The Construction (Design and Management) Regulations 2015 (CDM 2015) set out legal requirements for those involved in construction projects, from concept to completion.
HSE’s two CDM training courses focus on the role of the principal designer and the client (as defined by CDM 2015). They cover what dutyholders must or should do to comply with the law to ensure projects are carried out in a way that secures health and safety.
CDM: The Role of the Client will help delegates understand the responsibilities of a client under CDM 2015 in ensuring that health and safety performance is an integral component of effective project management and delivery.
In its introduction to the course, HSE states: “Regardless of the size of the project, the client has contractual control, appoints designers and contractors and determines the money, time and other resources available. They set the project's culture and standards of performance through their commitment, behaviour and relationships with the project team.”
Delegates on the course will be provided with information that will help them to:
• Have an overview of CDM 2015 and where the client role fits within it
• Understand who the client is on different projects, including where there may be more than one
• Know about the health and safety considerations, expectations and management arrangements a client has to make for a project and how these can be communicated through things like a client’s brief
• Ensure the provision of adequate welfare facilities
• Understand the requirements for pre-construction information, the construction phase plan and health and safety file together with suitable arrangements for their delivery
• Know what is involved in assembling the project team including the appointments of a Principal Designer and Principal Contractor
• Know which projects are notifiable and the arrangements for that
• Understand the general CDM duties applicable to everyone on the project regarding appointments, cooperation, reporting and the provision of information
The following dates are available at £560 per person:
15 May – HSE Science and Research Centre, Buxton
10 September – Etc Venues, Manchester
19 November – HSE Science and Research Centre, Buxton
CDM: The Role of the Principal Designer will help delegates understand the role of the principal designer and the duties they are required to fulfil. It utilises the findings from recently published (2023) independent research commissioned by HSE, which give a comprehensive and up-to-date insight into how the principal designer role is working in practice.
“The Principal Designer (PD),” says HSE in its introduction, “is a key role in CDM 2015. They must plan, manage and monitor health and safety in the pre-construction (design) phase of a project. They must also co-ordinate the work of all the design functions and disciplines in the project team, ensuring that designers take proper account of the principles of prevention and any pre-construction information when preparing or modifying a design. Decisions taken at this point can significantly influence whether a project is delivered in a way that secures health and safety and meets the client’s brief.”
Delegates on this course will be provided with information that will help them to:
• Have an overview of CDM 2015 and where the PD role fits within it
• Understand pre-construction information requirements and the PD’s role regarding it
• Ensure design work in the pre-construction phase contributes to positive outcomes though knowledge and application of the

principles of prevention to foreseeable health and safety risks
• Understand the arrangements required by the PD to plan, manage, monitor and co-ordinate the pre-construction phase with a focus on the flow of health and safety information
• Prepare and handover the health and safety file
• Understand the general CDM duties applicable to everyone on the project regarding appointments, co-operation, reporting and the provision of information
• Understand the associated skills, knowledge, experience and organisational capabilities required to deliver the PD role and the challenges different contracts/project types may bring
The following dates are available at £560 per person:
16 May – HSE Science and Research Centre, Buxton
11 September – Etc Venues, Manchester
20 November – HSE Science and Research Centre, Buxton
To find out more about these and other HSE courses, visit the website at solutions.hse.gov.uk/health-and-safety-training-courses q
15 15 www.yourexpertwitness.co.uk



16 16 www.yourexpertwitness.co.uk
WHAT DOES YOUR CONSTRUCTION CONTRACT SAY ABOUT INSOLVENCY? (PART 2)

In this second part of their discussion on the provision for insolvency in a contract, Fintan Wolohan, Frances Antoniak and Nicola Deedes of Womble Bond Dickinson discuss what happens after the insolvency.
[ RECOGNISING THAT THE PROJECT cannot be left unfinished, the JCT, NEC4 and FIDIC all provide that, upon termination of the contractor’s employment for insolvency, the employer may employ others to carry out and complete the works, using the plant and machinery on site (JCT 8.7(1), NEC4 92.1 and FIDIC 15.2.4).
The contractor must also remove all goods from the site, provide copies of design documents and, at the request of the employer, the benefit of any supply agreements for the execution of any work shall be assigned (JCT 8.7, NEC4 92.2 and FIDIC 15.2.3).
It is worth checking the applicable contract for the employer’s rights in relation to assignment, for example the JCT acknowledges that such an assignment may be restricted to the extent that the contractor may lawfully be required to do so, while the FIDIC limits this right as the contractor only needs to comply with the employer’s ‘reasonable instructions’. Assignment could be helpful in facilitating the completion of the works by sub-contractors already engaged on site, as they are already mobilised and familiar with the project.
The employer should, however, keep in mind that the insolvency of a contractor will, practically speaking, lead to a significant amount of upheaval, making a smooth transition – including access to documents and the site – difficult. The administrator or liquidator is unlikely to have had any prior involvement with the insolvent contractor and will therefore spend the first few weeks simply getting up to speed. In an administration and other insolvency processes, there is also a moratorium on legal proceedings against insolvent company.
What to do about money due after an insolvency?
After a party becomes insolvent, it is only to be expected that the other parties check what monies they can recover, to protect themselves; and the contracts recognise that.
Under the JCT there is a separate final account procedure to determine the balance of the account between the employer and the insolvent contractor following completion of the works (8.7.4).
Continued good record keeping is therefore essential when administering a JCT contract after a contractor’s insolvency, because
depending on when the contractor became insolvent it can be some time before the final tallying takes place.
The NEC4 assesses the amount due at the time of termination. The contractor is paid for work that it has done and costs it has reasonably incurred in the expectation of completing the works up to the point of termination, less any amounts due from it and subject to any rights of set-off the client may have (A1). Under A3, a further deduction can be made of the forecasted amount of additional costs the client will incur in completing the works due to the termination. Such an assessment must be made within 13 weeks of the termination certificate and, as the name suggests, is a forecast rather than being based on actual costs. You should also check the main option used (for example Option C: target cost) as this may also impact on sums due following termination.
Under FIDIC, a valuation exercise is undertaken at the point of termination (15.3), after which the employer may withhold payment from the contractor and shall be entitled to payment of the additional costs of execution of the works (15.4).
From an insolvency law perspective, the relevant legislation includes its own regime for arriving at a ‘final account’ of what is owed and which way. This may have an impact on the application of the contractual mechanism. Seek advice before embarking on the process, or in the event you run into difficulties dealing with the administrator or liquidator of an insolvent company.
Other considerations
It is essential, in the first instance, that the parties understand what their contract says about insolvency, both in terms of the definition used and the consequences laid out. If these do not say or cover what you want them to, they should be amended before the contract is entered into.
There may be other options available to the parties outside of the ones that we've mentioned above, but understanding your core legal rights under the contract are key to understanding your position and your options. With clarity on the contractual position, it’s important that the parties factor in the impact of relevant insolvency law. q
17 17 www.yourexpertwitness.co.uk
COUNCIL TO COMMIT FURTHER £1/2M TO CLEAN UP AFTER SKIP DEPOT FIRE
Landfill
Tax swallows up half of previous funds
[ LANCASTER CITY COUNCIL has committed up to £500,000 from its reserves to remove waste from a former skip-hire depot, which caught fire in December and burned for three weeks.
A1 Supa Skips Ltd previously operated the site, but had its waste permit withdrawn by the Environment Agency in November 2022 after collapsing into administration. The Environment Agency is currently conducting a criminal investigation into operations on the site.
Previous funding provided by the city council from its reserve totalled £912,000. Almost half of the previous funding had to be paid to HMRC as Landfill Tax. Mark Cassidy, the council’s planning and climate change officer, told local press: “We’ve been raising this with government for some considerable time.
“We made a request to waive that Landfill Tax and HMRC said that there is no mechanism for waiving the tax. That’s really disappointing.”
While the blaze is contained for now, it is likely that pockets of fire will continue to be found and these have the potential to escalate further. And with spring and warmer weather just around the corner, the smell from the rotting piles of rubbish is also likely to increase.
Council leader Phillip Black explained: “We are in an unenviable position and while I fundamentally believe that it is not our responsibility to pay for the clean-up of the site, if we don’t do it then who will?

“With the site continuing to pose a risk through further fires, not to mention the environmental impact of 3,000 tonnes of rotting rubbish, this is the responsible course of action despite the financial burden it places on the council.
“We will, however, continue to press Government and other agencies to contribute their fair share of the costs, and I have been in discussion with the political leadership of Lancashire County Council and together we have been exploring what support they might be able to offer.
“I’m also very sympathetic to those people who said that the owners or their insurers should pay, and the council will continue to pursue every avenue it can to get the money back, but this process could take many years.” q

18 18 www.yourexpertwitness.co.uk
Image courtesy of Lancahire Fire & Rescue Service
DEVELOPERS ORDERED TO FUND CLADDING REMEDIATION COSTS
[ A FIRST-TIER TRIBUNAL has ordered a rental housing operator to pay up to £18m to remediate cladding defects at Stratford’s former Olympic Park development, the Fire Protection Association has reported.
East Village Management Ltd (EVML), responsible for the repair and maintenance of the retrofit development now known as East Village, undertook an investigation following the Grenfell fire that uncovered the use of combustible aluminium composite material (ACM) cladding on some plots. Plans to remove the Grenfell-style cladding were put into place.
In November 2020, further issues were found, with the court documents stating that, among others: “Serious fire safety defects were discovered, relating both to the design and the construction of the various non-ACM cladding systems adopted for the external facades.”
Remediation work at some of the affected blocks began in April 2023, with completion of works expected by August 2025. It is understood that, while EVML had been able to acquire some funding from the government’s Building Safety Fund, the total cost of works was expected to be more than £24.5m.
The owners of the private housing are Stratford Village Development Partnership (SVDP) and its parent company Get Living. The property management company on the sites is Triathlon Homes.
At the end of 2022, Triathlon made five applications – one for each block – against SVDP and Get Living to recover costs of remediation works. It included reimbursement of £1.058m that the company had already incurred for ‘services charges paid to EVML in respect of interim fire safety measures and investigative and preparatory works’.
“Of more significance the orders sought would also require SVDP and Get Living to reimburse expenditure of £16.03m incurred or to be incurred by EVML in remedying the defects, representing Triathlon’s share of the total remediation costs,” the document stated.
On 19 January this year, the First-Tier Tribunal (Property Chamber) found the developers liable to cover the costs of remediation, which also included the costs of waking watch patrols and fire evacuation officers.
The managing director of Triathlon Homes, Kath King, commented: "Our priority remains the safety of all Triathlon residents. We are therefore delighted by the tribunal’s decision and the certainty that all the required remediation in these five buildings will be funded.
"The decision recognises the state of terrible uncertainty into which leaseholders throughout East Village have been plunged by the discovery of building defects and creates a clear precedent.
“We hope Get Living will now fund the remediation needed in the other East Village buildings and we can bring an end to the delays that have caused such misery for our residents.”
A Get Living spokesperson said: “We are, of course, disappointed that the Tribunal has deemed it 'just and equitable' that we be held responsible for remediation costs, given that Get Living did not build the development and was not responsible for the retrofit of the athletes’ accommodation into homes after the 2012 Olympic Games.
“We continue to work hard to fix this problem we did not create, given the overriding importance of getting the works done.
“The implications of this judgment are profound, not just for Get
Living, but for the wider industry. We are reviewing our next steps, while pursuing claims against the responsible contractors and pushing ahead with our programme of remediation works in East Village.” q
19 19 www.yourexpertwitness.co.uk
LAW FIRM PINPOINTS MAIN AREAS OF OIL AND GAS DISPUTES

[
ACCORDING TO Lexis Nexis, global providers of legal and regulatory intelligence: “A significant proportion of international arbitration cases are energy disputes. It is expected that the energy sector will continue to generate a significant number of disputes in the years to come.”
International legal firm CMS publishes an annual Oil and Gas Disputes Survey that tracks trends. The latest survey, for 2023, has highlighted that regulator activity, environmental issues and global economic and political challenges are seen by those in the oil and gas industry to be driving the industry’s approach to disputes.
The survey canvassed the views of over 80 industry professionals covering most regions of the world. According to CMS’s release on the survey: “Project management, joint ventures, disputes with host states
GOVT ANNOUNCES EXPANSION IN GAS PLANT PROVISION
[THE GOVERNMENT has announced a commitment to support the building of new gas power stations in what it says is a move ‘to maintain a safe and reliable energy source for days when the weather forecast doesn’t power up renewables’.
It is the latest step in efforts to reach net zero in ‘a sustainable, pragmatic way that rids the UK of the need to rely on foreign dictators like Putin’.
The need for continued unabated gas generation into the 2030s as a back-up to ensure energy security and reduce costs has been recognised by the Climate Change Committee, the Department for Energy Security and Net Zero said in the announcement on 12 March.
Prime Minister, Rishi Sunak, said: “Our record on net zero speaks for itself – the latest stats show that we’re already halfway there, with greenhouse gas emissions 50% lower than in 1990. But we need to reach our 2035 goals in a sustainable way that doesn’t leave people without energy on a cloudy, windless day.
“I will not gamble with our energy security. I will make the tough decisions so that no matter what scenario we face, we can always power Britain from Britain.”
The plans announced form part of the second consultation on the Review of Electricity Market Arrangements, in which the Energy Secretary has set out a plan to boost gas power capacity.
Firstly, by broadening existing laws requiring new gas plants to be built net zero ready and able to convert to low carbon alternatives in the future such as carbon capture and hydrogen to power. Secondly, those gas power plants will run less frequently as the UK continues to roll out other low carbon technologies. Finally, it is in line with wider government plans to deliver net zero while keeping costs down for billpayers. q
and regulators and supply chain activities are the areas identified by respondents as being those where disputes are most likely to arise.
“Supply chain activity is now seen as the activity with the greatest risk of disputes arising. This perhaps reflects the facts that suppliers are under increased pressure and there are skills and materials shortages in the manufacturing sector (particularly in renewable energy). Project management, joint ventures and host state and regulator activities are also seen as key risk activities when it comes to disputes arising.”
Other areas seen as carrying high risk are energy transition activities – where the UK Continental Shelf and Europe are the areas seen as having the greatest risk of disputes – and decommissioning projects, alongside hydrocarbon exploration and production.
“Critically,” the release says, “more than two thirds of respondents believe that these risks can be better managed. Record keeping, close project management and early engagement with counterparties are seen as key tools in mitigating the risk of disputes arising.” q
21 21 www.yourexpertwitness.co.uk

22 22 www.yourexpertwitness.co.uk
MEDIATION: HAVE THE FLOODGATES FINALLY OPENED?
By CHRIS MAKIN chartered accountant, accredited civil mediator and accredited expert determiner
[ON 29 NOVEMBER the Court of Appeal gave its judgment in the long-anticipated case of Churchill v Merthyr Tydfil County Borough Council [2023] EWCA Civ 1416. It started life as a simple dispute between an individual and a council over Japanese knotweed, but assumed such importance that there were no fewer than seven bodies admitted as interveners: the Law Society, the Bar Council, CMC, CEDR, CIArb and two housing associations.
So what was the case really about, and does it change the way civil and commercial mediation disputes are to be handled in future?
The basic case
This was ever so simple. There was an outbreak of the horrible Japanese knotweed on some spare land owned by the council and it encroached onto the garden of a Mr James Churchill. As we know, this knotweed is extremely invasive and very expensive to remove.
The council, like many more, had a Council Complaints Procedure, and when Mr Churchill’s lawyers sent a letter of claim, they were asked why they had not used this procedure. Churchill’s lawyers persisted and issued proceedings. The council applied to the court for a stay, and for costs, to allow the procedure to be followed.
The district judge decided he could not order such a stay, being bound by the decision in the well-known case of Halsey v Milton Keynes General NHS Trust [2004] EWCA Civ 576 where Dyson LJ said: “…to oblige truly unwilling parties to refer their disputes to mediation would be to impose an unacceptable obstruction to their right of access to the court” and that this would offend Article 6 of the European Convention on Human Rights, which establishes the right to a fair trial.
Why does this matter to mediation?
Dyson LJ’s words have long been interpreted as saying that for the court to order a stay for mediation to take place, and especially if a party was unwilling, would offend a citizen’s right to a fair trial. The courts have tried to encourage mediation as much as possible, mainly by threatening costs orders against those who refused to mediate, and even Halsey itself had a checklist of situations where a party was at risk on costs if they declined an invitation to mediate. But no such forms of ‘persuasion’ have been entirely effective.
Churchill was a curious case to provoke so much interest about mediation, because it didn’t concern mediation as we know it. This Council Complaints Procedure was arguably not even independent, since it was conducted by a council employee, and all mediators know how important it is to be, and be seen to be, independent. But in the judgment there was talk of this procedure, early neutral evaluation, negotiation etc and especially mediation, so the procedure was seen to be near enough to a form of alternative dispute resolution (ADR) for it to be taken as an example.
Back to main principles
The main judgment was give by Sir Geoffrey Vos, Master of the Rolls. Also on the bench was Susan Carr, the new (and first ever) Lady Carr of Walton-on-the-Hill, Lady Chief Justice. So this was an impressive bench. The judgment was unanimous.
Turning back to Dyson LJ’s words above, one would have thought that they were unambiguous: imposing ‘an unacceptable obstruction to their right of access to the court’, and therefore contrary to Article 6.
This court thought different. There was lengthy discussion – the court avoiding the Latin where possible, though it surely still has its uses – of

the difference between ratio decidendi and ratio obiter. As lawyers well know, ratio decidendi is an argument which is central to the issue and determinative of the court’s decision, whereas ratio obiter is merely a superfluous comment which is not central to the case.
The court decided that Dyson LJ’s words were obiter : not central, just a side comment, and therefore this court was not bound by them. The court did indeed have the power to order a stay for mediation to take place. It follows that all inferior courts will be bound by the precedent that parties may be ordered, willing or otherwise, to follow a method of ADR before they can have a trial.
So now what?
At 74i) Vos MR said that “[9]-[10] of Halsey was not part of the essential reasoning in that case and did not bind the judge to dismiss the Council’s application for the stay of those proceedings.” At 74iii) he said he would not “…lay down any fixed principles as to what will be relevant to determining the question of a stay of proceedings…” so the trial judge could decide what he may order.
74ii) is worth quoting in full: “The court can lawfully stay proceedings for, or order, the parties to engage in a non-court-based dispute resolution process provided that the order made does not impair the very essence of the claimant’s right to proceed to a judicial hearing, and is proportionate to achieving the legitimate aim of settling disputes fairly, quickly and at reasonable cost.” One will recognise that the last few words come straight from CPR Part 1.
By this time, Japanese knotweed had lost its relevance. The important issue is that all the interveners had won, because litigators are no longer bound by Halsey : the court can indeed order a stay for ADR to take place. Mediators at last are going to be busy. The barrier of Halsey has gone and we get back to what Lord Woolf intended with his Civil Procedure Rules launched on 1 April 1999. Plus ça change, plus c’est la même chose q
About Chris Makin
[CHRIS MAKIN was one of the first 30 or so chartered accountants to become an Accredited Forensic Accountant and Expert Witness –see www.icaew.com/about-icaew/find-a-chartered-accountant/find-anaccredited-forensic-expert
He is also an accredited civil and commercial mediator and an accredited expert determiner. Over the last 30 years he has given expert evidence at least 100 times and worked on a vast range of cases. For CV, war stories and much more go to the website at www.chrismakin.co.uk – now with videos! q

23 23 www.yourexpertwitness.co.uk
24 24 www.yourexpertwitness.co.uk
INSURANCE CONTRACT DISPUTES: WHAT’S DIFFERENT ABOUT THEM?
By Roger Flaxman
[ ON THE FACE OF IT, a contract of insurance is subject to the same legal principles as any other commercial contract: but behind that face there lies a complex and often ambiguous array of jargon, insurance conventions, market practices and longheld, if not entirely well-founded, beliefs and opinions by insurance practitioners, from the very old to the modernly young.
Those beliefs and opinions are not written into the insurance policy, but in practice they can serve to confound the claimant and their legal team when they come up against them. A good, and public, example is the 2020/21 COVID Business Interruption insurance litigation. It was brought by the Financial Conduct Authority (FCA) as a test case against a representative selection of eight major UK insurers.
The overarching outcome of the FCA initiative’s test case is an unprecedented dissection of the ‘meaning’ of the chosen 21 policies, which were estimated to have an impact on over 700 types of policies sold among some 60 insurers, affecting some 350,000 policyholders.
For almost 50 years Business Interruption policies had included, without cost to the insured, cover for business interruption loss by reason of Notifiable Disease and by Denial of Access to the insured premises. In practice, the cover was rarely claimed upon and the clauses would not form part of a typical renewal negotiation because they were regarded by the industry as standard ‘free extensions’ to a typical commercial insurance policy.
The insurance industry thought they knew what the clauses meant, although they were all expressed in slightly different words and phrases, according to the whim of the person drafting the policy in their respective, ordinary vernacular. To the layman they all expressed the same intention and gave the same cover. Even the insurance practitioners arranging the policies believed they all gave the same protection, albeit expressed in a variety of similar, but not identical, language.
Too complex to comprehend?
The FCA test case proved their trust to be unfounded. The legal teams for the eight leading defendant insurance companies each advanced their own interpretation of what cover the clauses provided, how they
had to be ‘triggered’ and what the policy was liable to pay. There was very little common agreement between them. It was a startling revelation to the industry as well its some 350,000 affected policyholders.
Insurance is seen by the public as being a commodity. It is typically selected by price alone, it being too difficult to understand the policy wordings and make a comparison. The semantics and nuances of ‘policy language’ do not even occur to the mind of the ordinary policyholder. Reading one policy will convey much the same message to the layman as any other, because the true contractual obligations are obscured by the unwritten, but always practised, conventions of insurance industry claims practices that ultimately determine the insurer’s liability in contract.
The main reasons for the lack of consistency among competing insurers in the industry is the insurers’ desire to protect themselves by using their own preferred words, to convey their intention and limit their exposure to a loss. They are also conscious of potentially breaching competition law by all offering identically-worded policies.
The net result is that there are hundreds of directly competing insurance policies which appear, to the ordinary reader/policyholder, to be providing similar cover but which express that cover in indistinctly nuanced ways. The differences in the wording are further exacerbated by the differences in the unwritten insurance claims management and loss adjusting protocols that come into play when a claim arises. These, too, are not expressed in the policy and only come to light when there is a claim or a dispute about a claim.
Claims adjustment practices vary between insurers and loss adjusters, and the combination of nuanced policy wordings, individual interpretation of the contractual obligations and how the claim should be adjusted requires a profound understanding of market practices when trying to unravel a complex insurance claim dispute.
Brokers and intermediaries
Insurance claims are not, of course, confined to a dispute with the insurer. The causative issue can also be an error of a broker or intermediary. Typically, allegations of failure to advise the policyholder on matters of underinsurance, implications of

conditions or warranties, breach of specific onerous terms and conditions not brought to the insured’s attention – and many other errors – are not uncommon.
It is important to identify early in the insurance dispute resolution process if there is a combination of an issue concerning the insurer and an issue concerning the broker intermediary. It is equally important to consider the merits of the claim against the insurer before attempting to claim against a broker or intermediary.
Early expert evaluation
An early evaluation by an insurance expert will often reveal crucial factors about the merits of a successful insurance claim. Typically, insurance experts in the courts have many years practical experience of what the industry will do, or tolerate, in any given situation and what it will not agree to and will vehemently resist if put to the test. In insurance practice the precedent of what an insurer or group of insurers did in a particular situation will be used by insurance advocates, consultants and broker intermediaries to try to influence their present situation. Unlike precedents in law they are not legally binding, but they can still carry considerable weight in a negotiation with insurers. However, they are not written down and they are rarely, if ever, evident from the policy wording alone; and so the discovery of ‘how this works in practice’ at an early stage in the conduct of an insurance litigation can deliver a priceless advantage to the litigating party. q
• Roger Flaxman is a practitioner of some 50 years insurance and claims resolution practice and an experienced expert in the courts.
25 25 www.yourexpertwitness.co.uk

26 26 www.yourexpertwitness.co.uk
CRIME AND CRYPTOCURRENCY: A PARTNERSHIP OF ITS TIME?
By Shaun Walbridge FCCA FAE of Matrix Forensic
[ NOW IS THE TIME: cryptocurrency has seen a dramatic rise in its value over the past year, and it’s potentially going to rise even further with the upcoming quadrennial ‘halving’ event, threatening to push it beyond its all-time high of $69K!
Criminals are all over crypto and have been for some years. The police and other law enforcement agencies are not far behind; but they don't have the budget to thoroughly investigate all cases.
Money laundering in all forms is a major problem in the UK and around the world. The increase in the value of crypto has been a significant driver; and as a result of that, the number of those types of cases coming to court has risen exponentially.
Forensic accountants familiar with criminal cases are few and far between. The need for quality advice and experience in dealing with crypto cases is paramount, particularly where there are allegations of large crypto hidden assets or tainted gifts. The risk of significant default sentences if a thorough investigation is not carried out cannot be understated!
At Matrix Forensic we have both the experience and track record to deal with a wide range of complex fraud and financial cases, including cryptocurrency. These are just some of the areas in which we can assist:
• Pre-trial investigations
• Fraud and money laundering investigations
• HMRC criminal investigations
• Proceeds of crime and confiscation
• Giving expert evidence in court
LAW SOCIETY REPORTS ON CHANGES TO MONEY LAUNDERING REGIME
[FROM 22 JANUARY, HM Treasury has amended the definition of 'high-risk’ third countries in relation to money laundering. It removed Schedule 3ZA, which contained the list in the Money Laundering Regulations 2017. The Law Society reported the changes in an update to members.
Instead of referring to a separate schedule, regulation 33(3)(a) now defines a high-risk third country as ‘a country named on either of the following lists published by the Financial Action Task Force as they have effect from time to time, high-risk jurisdictions subject to a call for action or jurisdictions under increased monitoring’.
The FATF lists are updated three times a year, on the final day of each FATF plenary meeting, held every February, June and October.
HM Treasury also published an updated advisory notice on high-risk third countries. The next update to the list is expected on 28 June.
The Law Society explained: “Under the UK’s AML regime (regulation 33(1)(b)), any business relationship with a person established in a high-risk third country must be subject to enhanced due diligence. Until the end of the Brexit transition period, the list of high-risk countries was determined by the European Union (EU).
“From 1 January 2021, the UK has had its own standalone list. Since then, any amendments to the EU list do not have effect in the UK. The UK is entitled to amend its own list of high-risk countries under section 49 of the Sanctions and Anti Money Laundering Act 2018.
“The aim remains tackling strategic deficiencies in the identified countries with regards to their national AML and counter-financing of terrorism regimes.” q

If you require assistance with any financial aspect of a criminal or civil case, contact Matrix Forensic on 020 3463 1910; mob 07775 712961; or email enquiries@matrixforensic.co.uk q
• Shaun Walbridge FCCA FAE is a leading independent forensic accountant with extensive experience in criminal and civil cases. He is a Fellow of the Association of Chartered Certified Accountants (FCCA), a Registered Auditor and a practising Fellow of The Academy of Experts (FAE). He is also a TAE-accredited mediator and an expert determiner, and is one of the relatively few (less than 100) who hold the Institute of Chartered Accountants’ Accredited Forensic Accountant & Expert Witness designation.
27 27 www.yourexpertwitness.co.uk
WHAT DOES THE FINANCIAL FUTURE HOLD?
Expert forensic accountant Fiona Hotston Moore, of FRP Advisory, offers up some predictions for the coming year in litigation support and dispute resolution.

[ WITH THE BACKLOG in the courts and the substantial costs associated with legal proceedings, I anticipate we will see an increase in mediations, arbitrations, round table discussions and expert determinations. In my opinion experts can play a significant part in ensuring the success of alternative dispute resolution.
The expert can assist the parties, legal advisers and a mediator or arbitrator to understand the key issues in a financial dispute and the potential outcomes. In my experience the expert can ensure there is equity in the knowledge and understanding of the parties, which will facilitate open discussion.
A meeting of experts ahead of mediation allows the key points of disagreement to be identified and the impact on any financial settlement to be quantified.
In drafting my reports – whether court compliant or a preliminary opinion – I seek to ensure my opinion is as clear as possible, with the objective of facilitating a good understanding of the issues which will assist in a negotiated settlement. It is great to hear that a case has settled without a court hearing.
A volatile political and economic landscape
The current complex economic and political landscapes lead to greater volatility in business valuations. Company valuations are inherently subjective and the expert valuer will need to draw on their own experience as well as the considerable market data that can be accessed. The past year has seen a range of challenges, with inflationary pressures – particularly in energy and labour costs – as well as consumer uncertainty, interest rate rises and the uncertainties surrounding Ukraine and the Middle East. All of these result in additional complexity for business valuations and the need for real expertise.
In matrimonial cases we are often asked to produce updated valuations to reflect changes in the business and the impact on valuations between two dates across two or three years can, at present, be significant.
independent investigations in areas such as suspected failings in financial reporting and misappropriation of company assets by officers or employees. Charities have been badly hit by the pandemic and we are seeking an uptick in financial failures in the sector. Trustees may require an independent view of the cause of the financial pressures and any apparent ‘black holes’.
Forensic technology
I anticipate technology will play an increasing part in dispute resolution. My own experience is that disclosure of the content of messaging platforms such as Teams can be key in reviewing the roles of individuals in a dispute. However, it can be time consuming to extract and review such material. I anticipate forensic technology experts will improve the efficiency and reliability of such disclosures.
In the past few years the cost of analysing bank statements has reduced significantly and I expect we will see similar savings in other areas due to forensic technology becoming more readily available and adopted by legal teams.
Professional negligence claims
In the past decade we have seen an increase in clients seeking to make claims against their professional advisers. In my experience claims in respect of auditor negligence tends to be complex, due to the inherent subjectivity of both financial reporting standards and auditing standards. Claims in respect of negligence by tax advisers tend to be more clear cut in terms of the negligence, albeit calculating the quantum of loss can be tricky.

I am also seeing an uptick in engagements as ‘shadow adviser’, where a party in a dispute requires an independent review of the report produced by the single joint expert. A shadow adviser can assist the party in deciding if they should challenge the valuation prepared by the single joint expert. As shadow adviser I will identify the key assumptions in the valuation and assist in drafting questions to be asked of the single joint expert.
Financial pressure also tends to increase the motivation for financial fraud and I anticipate we will receive instructions to conduct
I expect to continue to receive instructions on professional negligence matters and that they will typically be at an early stage in the dispute, to allow the insurer to reach a view on the strength of the case and a negotiated settlement.
Regulatory investigations
The conduct and defence of investigations by regulatory bodies is key in ensuring an equitable outcome in what can be a very stressful time for the professional, and can endanger their professional reputation and career. As forensic accountants we can be instructed to give a view on the conduct of accountants in practice and those employed in industry. We will work with the instructing counsel to focus on the key issues and to provide an objective and informed view.
In conclusion, I predict that, as forensic accountants and financial experts, we will continue to be busy throughout 2024, but perhaps with a greater focus on alternative dispute resolution. q
29 29 www.yourexpertwitness.co.uk

30 www.yourexpertwitness.co.uk
FORMER MOD OFFICIAL CONVICTED OF RECEIVING SECRET KICKBACKS
[ON 6 MARCH the Serious Fraud Office (SFO) secured the conviction of former Ministry of Defence (MoD) official Jeffrey Cook for misconduct in public office, by taking secret payments in exchange for commissioning work from offshore consultants for the MoD. Cook was convicted at Southwark Crown Court, where he will be sentenced on 12 April.
SFO investigators uncovered that Cook concealed payments and gifts totalling more than £70,000 while he was employed at the MoD and seconded to a defence contractor, called Paradigm, which was owned by Airbus.
Between 2004 and 2008 Cook used his position as a civil servant to commission five reports for the MoD on its SANGCOM project to provide military communications equipment and services to the Saudi Arabian National Guard. The reports examined topics including ‘SANGCOM project activities’, ‘strategic considerations’ and ‘business strategy’. ME Consultants Ltd, registered in the Cayman Islands and where
Cook held personal contacts, were paid £700,000 for the work, with at least 10% of the fee going back to Cook directly. Cook received over £44,000 in cash and two cars worth over £30,000, arranged via a Chelmsford car dealership belonging to Peter Austin, the principal shareholder at the consultancy.
Following his secondment, Cook left the MoD to join the UK defence firm GPT Special Project Management Ltd – which was bought by Paradigm in 2007 – as its managing director. The SFO successfully prosecuted GPT as part of the case in 2021, when the company pleaded guilty to corruption and paid a penalty totalling almost £30m for its actions.
Director of the Serious Fraud Office, Nick Ephgrave QPM, said: “This was an exceptionally complex investigation and prosecution which no other public body could have delivered.
“Jeffrey Cook betrayed public confidence and, thanks to our tenacity on this case, has rightly been held accountable today.” q
TASKFORCE ADVISES CITY FIRMS ON CYBER ATTACKS
[A CITY-WIDE TASKFORCE charged with helping businesses understand and manage cyber security risks during corporate finance transactions was unveiled in London on 31 January.
The initiative is being led by ICAEW in collaboration with the National Cyber Security Centre (NCSC) and 12 other organisations involved in deal making, investment and cyber security. Guidance for businesses on the threats posed by cyber-crime were also launched at an event hosted by the institute’s Corporate Finance Faculty.
The guidance, entitled Cyber Security in Corporate Finance, will advise companies on how to mitigate against cyber attacks during corporate finance transactions and protect commercially sensitive data exchanged during the deal process; and provide information on types of cyber risks and how to respond to cyber breaches.
Alongside ICAEW and the NCSC, the taskforce comprises representatives from Association of Corporate Treasurers, BDO, British Private Equity and Venture Capital Association, Deloitte, EY, Grant Thornton, KPMG, the Law Society, London Stock Exchange, PwC, the Takeover Panel and UK Finance.
Commenting at the launch event, Michael Izza, ICAEW chief executive, said: “Corporate finance transactions are a critical part of the economy, but the flow of sensitive information and data during a deal can leave a business vulnerable to cyber security breaches. This new guidance and taskforce will be key in helping to raise awareness and minimise the risks posed by cyber criminals.
“A cyber attack could have a potentially disastrous impact on the dealmaking process, and so it is crucial that boardrooms across the country treat threats very seriously and take preventative action.
“We must do all that we can to ensure London remains a pre-eminent

place to do deals, raise investment and generate growth.”
Sarah Lyons, NCSC’s deputy director for economy and society, added: “We know the sensitive information that the accounting sector often manages, whether it is financial records, risk analysis or external audits, can make chartered accountants attractive targets for cyber criminals.
“A breach in this sector can not only jeopardise organisations and their customers, but can also undermine trust, confidence and reputation.
“I’d encourage everyone from across the industry to engage with this report and the NCSC’s range of practical guidance, to help increase their cyber resilience.” q
31 31 www.yourexpertwitness.co.uk

FRAUD ALERT ISSUED AHEAD OF HOLIDAY SEASON
[ ACTION FRAUD, the national fraud and cyber crime reporting service, has launched a holiday fraud campaign ahead of the summer months, urging holiday goers to play it safe online and do their research before booking their trip.
Last year, 6,640 reports of holiday fraud were made to Action Fraud. Data shows that July and August saw the highest number of reports made, at 804 and 781 respectively. Holiday makers lost a combined total of £12.3m, meaning there was an average loss of £1,851 per victim.
Pauline Smith, Head of Action Fraud, commented: “As people think ahead to book their holidays, understandably everyone is increasingly on the lookout for the best deals. With the cost-of-living crisis squeezing our finances, it's easy to forget to stay vigilant against fraudsters offering cheaper deals and great prices that are too good to be true.

“We want to avoid people losing their hard-earned money and help raise awareness of the signs of holiday fraud. Before booking any trips or signing up to any deals, do your research and check for ABTA and ATOL logos before clicking the confirmation button. Remember: stay alert online and be wise to fraudsters.”
ABTA chief executive Mark Tanzer added: “Fraudsters are using increasingly sophisticated methods to target consumers, with a particular focus on destinations and times of year when demand is high and availability limited, as they know people will be looking for good deals. Victims will often only find out they have been defrauded just before they are due to travel, or even in a resort, when it can be very difficult to find a legitimate replacement leading to yet more cost and potential disappointment.
“One of the simplest ways to protect yourself when booking is to look for a company that is a member of ABTA when booking your holiday.”
Anna Bowles, Head of Consumers and Enforcement at the UK Civil Aviation Authority, which runs the ATOL financial protection scheme, said: “Our research shows almost three in five of us are planning to go overseas this summer and expect to spend thousands of pounds on these trips. Before booking your trip abroad make sure you are doing everything you can to thwart fraudsters.
“Some protective measures include visiting the atol.org website to check your package trip is financially protected by ATOL, pay by credit card if you can, and take out travel insurance as soon as you book.”
Action Fraud has compiled a checklist of tips to help prevent falling victim to holiday fraud. q
33 33 www.yourexpertwitness.co.uk

34 34 www.yourexpertwitness.co.uk
[MALICIOUS CYBER ACTORS linked to Russia’s Foreign Intelligence Service (SVR) are adapting their techniques in response to the increasing shift to cloud-based infrastructure, UK and international security officials have revealed.
In a new joint advisory, the National Cyber Security Centre (NCSC) –which is a part of GCHQ – and agencies in the United States, Australia, Canada and New Zealand have detailed how the threat group, which is known as APT29, has adapted its techniques for intelligence gain to target organisations that have moved to cloud-hosted environments.
Many of the sectors targeted by the SVR, including think tanks, healthcare and education, have moved to cloud-based infrastructure, which means that traditional means of access – such as through the exploitation of software vulnerabilities – are more limited.
Instead, SVR actors have over the past 12 months been observed stealing system-issued access tokens to compromise victim accounts, enrolling new devices to the victim’s cloud environment via credential reuse from personal accounts, and targeted system accounts with password spraying and brute forcing, which is successfully enabled by weak passwords and the absence of two-step verification.
Once initial access has been gained, the actor is then capable of deploying highly sophisticated capabilities.
Along with updated threat information, the advisory also provides mitigation advice on how to counter the evolving tactics of APT29. The NCSC assesses that APT29 – also known as Midnight Blizzard, the Dukes or Cozy Bear – is a cyber espionage group which almost certainly operates as part of Russia’s Foreign Intelligence Service.
NCSC Director of Operations, Paul Chichester, said: “We are resolute in our commitment to exposing malicious cyber activity, which includes
CYBER THREAT MAY BE AN
INSIDE JOB
[IN THE CYBER SECURITY SPACE, most people think of a group of cyber professionals forming a line of defence against external threats like hackers. While it’s true that malicious hackers present an increasing problem for UK businesses, that isn’t the only concern for an organisation’s cyber team. Sometimes, the threats come from somewhere a little closer to home.
Insider threats, referring to a cyber security risk that comes from within an organisation, are an often overlooked aspect of an organisation’s cyber resilience. However, according to US cyber security site Security Intelligence, 60% of data breaches are primarily caused by insider threats. With cyber attacks rising it’s even more important for businesses to be vigilant against the most common form of cyber attack.
Unlike other forms of cyber attack, insider threats can be difficult to identify against normal activity, because the offender will likely have security authorisation. Insider attackers also have an advantage over outside threats because of their knowledge of systems and users, making it easier for them to manipulate procedures.
The UK Cyber Security Council has published guidance on countering the threat. Visit www.ukcybersecuritycouncil.org.uk q

raising awareness of changes in the behaviour of groups which persistently target the UK. The NCSC urges organisations to familiarise themselves with the intelligence and mitigation advice within the advisory to help defend their networks.”
The NCSC has previously detailed how SVR actors have targeted governmental, think tank, healthcare and energy targets for intelligence gain, and has more recently observed how their targeting has expanded to include aviation, education, law enforcement, local and state councils, government financial departments and military organisations.
SVR cyber actors are most commonly known for the supply chain compromise of SolarWinds software in 2020 and the targeting of organisations involved in the development of the COVID-19 vaccine, also in 2020.
The advisory has been published jointly by the National Cyber Security Centre, the US Cyber National Mission Force, the US Cybersecurity and Infrastructure Security Agency, the Federal Bureau of Investigation, the Australian Signals Directorate, the Canadian Centre for Cyber Security and the New Zealand National Cyber Security Centre. q
CYBER SECURITY CENTRE ISSUES UPDATE ON RUSSIAN THREAT LOOK TO YOURSELF!
35 35 www.yourexpertwitness.co.uk

ENGLISH AND WELSH TRANSLATION BODIES JOIN FORCES
[TWO BODIES at the heart of the translation and interpreting sector in the UK have agreed to work together to both raise the profile of translation and interpreting and to promote standards and best practices within the language services industry.
The Association of Translation Companies (ATC) and Cymdeithas Cyfieithwyr Cymru (CCC) have signed a Memorandum of Understanding that commits both bodies to work together for the mutual benefit of the respective associations.
WHITE PAPER OUTLINES PLUSES AND MINUSES OF AI

[THE CHARTERED INSTITUTE OF LINGUISTS (CIOL) has published a white paper which explores the risks, opportunities and challenges of artificial intelligence (AI) for linguists – especially professional translators. The white paper, CIOL AI Voices, provides expert voices and initial reflections, as well as major concerns from the CIOL Council on AI's use in translation and language services.
The white paper comes at a time when AI is transforming the context for translation and language services, with the emergence of new tools and technologies that can both create and improve content – but which also contain biases and can make significant and serious mistakes. CIOL highlights the need to adapt to these changes, seize the opportunities and support CIOL members and stakeholders in navigating this complex, emerging landscape.
The white paper flags some of the recent initiatives and frameworks for the responsible development and use of AI –such as the EU AI Act, the US Executive Order on the Safe Use of AI, and the UK AI Safety Summit – and the significance and importance of these developments for CIOL and its position on AI.
CIOL chair of council Steve Doswell said: “As a Royal Chartered body CIOL is here to represent and act in the best interests of the entire translation profession and industry, and indeed the wider profession of linguists. It is clear that transparency, safety and ethical considerations should be at the forefront of our approach.
“We will advocate for these principles in our thinking and advise on the use of AI in translation and language services, and we will encourage our members and language professionals to do the same.” q
The Association of Translation Companies is a trade association representing the interests of language service companies in the UK and internationally. It is the leading voice for companies operating in the UK’s language services industry.
Cymdeithas Cyfieithwyr Cymru is the only professional association that exclusively represents translators and interpreters working in English and Welsh and leads, develops and promotes the profession in Wales.
Ruth Partington, chair of the ATC, commented “This Memorandum of Understanding between the ATC and Cymdeithas Cyfieithwyr Cymru opens up possibilities for collaboration across a variety of language services industry topics, activities and initiatives. Wales has a thriving translation and interpreting sector, both commercial and institutional, and we are delighted to be working with CCC on future joint projects.”
Manon Cadwaladr, chair of CCC, said “I’m very pleased to see Cymdeithas Cyfieithwyr Cymru and the ATC agreeing to work closer. Both associations are important to the sector generally and to me personally, as I am member of both. This agreement joins up two important elements of the language services industry and I look forward to a productive and developing relationship over the coming years.”
Both associations were party to the recent Working Together white paper on the issues facing procurement and provision of language services in the public sector. Further collaboration between the parties could result in joint policy development, events, PR and marketing, and submissions to governments. q
37 37 www.yourexpertwitness.co.uk
EXPERTS FOR MEDIA
The following experts offer their expertise to the media
EXPERTS FOR MEDIA is a new section in Your Expert Witness for experts who wish to offer their views and the benefit of their experience to the vast range of print and broadcast media.
Ever wondered how news teams find the experts they consult to explain the ramifications of breaking news stories, seemingly at the drop of a hat? Or how the producers of TV drama series ensure their stories are accurate and reflect the realities of the professions they portray?
The fact is that researchers consult registers of experts and expert periodicals just as lawyers do. In fact, Your Expert Witness is receiving an increasing number of enquiries from media researchers and public relations agencies looking to locate appropriate experts to inform their clients.

Experts for Media is therefore an ideal space to attract their attention. For prices and to book your space, contact Ian on 0161 710 3880 or via ian@dmmonline.co.uk
Professor Charles Davis MBBS FRCS Consultant Neurosurgeon
Professor Charles Davis acts as an expert witness with very extensive experience in cases relating to neurosurgery, including the preparation of medico-legal reports and appearing in court. Speedy reporting, free advice and screening.

Contact: Marlene Scruton T: 01772 761150 F: 01772 761150 E: marlene.scruton@talktalk.net
Dr Emma Ferriman MBChB MRCOG FRCOG Consultant Obstetrician and Fetal Medicine Specialist
Medical negligence cases involving:
• multiple pregnancy and high
• risk obstetrics including intra
• partum complications and
• birth asphyxia
• prenatal diagnosis
• obstetric ultrasound
• first trimester screening
T: 07812 353820 E: emmaferriman@doctors.org.uk W: www.emmaferriman.co.uk

Mr Robert Hensher
FRCS FDSRCS
Consultant Oral and Maxillofacial Surgeon
Mr Hensher’s subspeciality interests include dental implantology, facial injury and temporomandibular joint replacement. He prepares over 50 reports yearly including negligence and criminal cases.
E: jackiesorrell0101@gmail.com M: 07947445414
E: roberthensher@gmail.com M: 07836540457


Mr Luke Meleagros BSc MBBS MD FRCS Consultant Surgeon
Mr Meleagros completes around 6-10 expert reports per month, the majority in medical negligence cases and a smaller number of personal injury cases. He has reported extensively on cases involving abdominal laparoscopy surgery and hernia surgery.
T: 0208 527 0977 E: L.Meleagros@btinternet.com
Sec: jawdobson@gmail.com
Professor Panayiotis Kyzas
FRCS(OMFS) PhD MBBS BDS FST GDL Consultant OMFS Head & Neck Surgeon


Professor Panayiotis Kyzas is a Consultant OMFS Head and Neck Surgeon who specialises in major oncological head and neck cancer surgery. Professor Kyzas accepts cases relating to facial trauma, oral surgery, facial cosmetic surgery, TMJ disorder and facial skin cancer surgery. He can take instructions on behalf of either claimant or defendant or as a Single Joint Expert. T: 07505 402640 E: kyzasp@icloud.com
Dr Ian C Perry
MBBS MFOM DAvMED(Lond) CFIOSH FCIM MAE Consultant in Occupational Medicine
Clinical negligence and personal injury cases on behalf of claimant, defendant or as a Single Joint Expert. Specialist areas of expertise include work related accidents and injuries – most notably in the aviation industry – and those due to long term exposure to chemicals, noise and vibration.

T: 07836 664670 E: ian@ianperry.com W: www.ianperry.com

Mr Thomas Wood MSc MPhil CUBS Data Science Consultant
Mr Thomas Wood is a CUBS-accredited Expert Witness, certified for civil litigation. He also offers due diligence services for acquisitions of technology companies using AI. • Natural language processing (NLP) • Machine learning • Data science • Artificial intelligence (AI)
T: 020 3488 5740 E: thomas@fastdatascience.com W: fastdatascience.com

38 38 www.yourexpertwitness.co.uk
Welcome to our A to Z guide of the websites of some of the Expert Witness field’s leading players.
If you are one of our many online readers simply click on any of the web addresses listed below and you will be automatically directed to that particular website.

To get your website listed on this page just give us a call on 0161 710 3880 or email ian@dmmonline.co.uk
Clarke Gammon
Translations and Interpreting for the Legal Profession since 1997. Specialists in Personal Injury and Clinical Negligence. www.abc-translations.co.uk
Andrew F Acquier BA FRICS
Chartered Art & Antiques Surveyor
Expert witness reports and representation at court for matters involving: • Divorce settlements • Insurance valuation disputes
• Arts litigation • Contentious Probate
www.andrewacquier.co.uk
Salam Alaswad LLM PGDip BSc
• Financial derivatives • Contracts for Difference (CFD)
• Forex fraud • Financial crimes • Pre-action assessment
• Charts and diagrams for complex cases www.fxandcfd.com/expert-witness
Dr Paul Baskerville MA DM FRCS
Expert witness instructions in cases relating to all aspects of vascular disease. Can act on behalf of claimant, defendant or as Single Joint Expert. www.baskervilleclinic.com
David Berry PhD FRC Path MFSSoc MRSC



Independent Toxicology Consultant Specialist in Clinical and Forensic Toxicology with particular emphasis on drugs (both illicit and therapeutic) and alcohol. www.toxicologyservices.co.uk
Mr Timothy Burge MBChB FRCS FRCS(Plast) DMCC MSc
Consultant Burns & Plastic Surgeon
• Cosmetic and aesthetic surgery of the breast and trunk • Burns • Trauma • Scars www.clifton-plastic-surgery.co.uk
Professor Frank Chinegwundoh MBE
Consultant Urological Surgeon specialising in Personal Injury and Medical Negligence cases on behalf of either claimant or defendant or as a Single Joint Expert. www.urologyconsultant.co.uk



Professor Paul J Ciclitira MB PhD FRCP MRCS FRCP AGAF
Professor of Gastroenterology with particular interest in food allergy, including Coeliac disease, peptic ulcer, inflammatory bowel disorder and hepatology. www.profpaulciclitira.co.uk
Mr Jeremy P Crew MA MD BChir FRCS
Consultant Urological Surgeon Medical reports on all legal aspects of urology. Reports in some cases based on hospital notes only. www.oxfordurology.co.uk


Chartered Surveyors with experience in All Aspects of Property • Residential property values
• Asset valuations • Land values and more www.clarkegammon.co.uk
D & HB Associates Ltd
Experts in Road Traffic Offences


• Accident investigation and reconstruction • Tachograph analysis • Stolen vehicle examination and identification • Statement Taking www.dandhb.com
Dr Lars Davidsson MRCPsych MEWI
Consultant Psychiatrist and Accredited Mediator
Reports within most areas of general adult psychiatry. Specialist in PTSD, anxiety disorders & mood disorders. www.angloeuropeanclinic.co.uk
Chris Dawson MS FRCS LLDip

Consultant Urologist with 20 years experience of medico legal report writing and expert witness work and has completed over 1,850 reports. He also regularly completes Fitness to Practice reports for the General Medical Council.
www.chrisdawson.org.uk
DRC Forensics Limited


DRC Forensics Limited offers the complete range of forensic accounting & litigation support: • Fraud • Money laundering
• Partnership disputes • Loss of profit • Professional negligence www.drcforensics.co.uk
Mr Mark Duxbury MA (Oxon) DM FRCSEd (Gen Surg)
Consultant Hepatobiliary, Pancreatic & General Surgeon • General & emergency surgery • Hernia surgery • Liver & pancreatic surgery • Gallbladder & biliary surgery • Laparoscopic

Mr Roger Emmott CEng BSc(Hons) MSc/MBA MA FCMI FIC
Steel and iron ore expert with international arbitration and cross-examination experience in complex disputes
• Industry • Pricing • Contractual • Valuations T: 07974 351704 E: roger@rogeremmottassociates.com www.rogeremmottassociates.com www.equip2speak.co.uk
Instruction




39 39 www.yourexpertwitness.co.uk
Equip2Speak Specialists in Brain and Spinal Injury. SLT & AT Consultants • CUBS Certified Experts since 2012/2013 • Accident, Negligence and Criminal Cases • Experienced in High Value Claims • Claimant/Defendant/Joint
surgery • Hepatobiliary surgery
Face Restoration • Complications of cosmetic eyelid surgery • Brow lift surgery • Ptosis • Non-surgical aesthetics • Orbital diseases • Watery eyes • Thyroid eye disease www.facerestoration.com
www.markduxbury.info/medicolegal
FHDI - Kathryn Thorndycraft-Pope
Examining documents & handwriting • to determine authenticity • to expose forgery • to reveal aspects of origin. Electro Static Detection Apparatus and Mi-Scope used. www.forensichandwriting.co.uk

Forensic Collision Investigation & Reconstruction Ltd
Specialists in the analysis of road traffic collisions
• Collision Reconstruction • Expert Witness
• Vehicle Examinations
www.FCIR.co.uk
Formedecon Ltd

Forensic & Investigative Services to the Legal Profession
• All Aspects of Forensic Work Undertaken
• LAA and Privately Funded • Free Estimates www.Formedecon.com

Professor Parviz Habibi MB ChB PhD FRCP FRCPCH
Consultant in Paediatric Intensive Care & Respiratory Medicine. Specialist in treating respiratory conditions and sleep disorders as well as paediatric intensive care.
www.childrensrespiratorydoctor.co.uk
Fiona Hotston Moore (FRP Advisory)


Fiona is a partner of FRP’s Forensic Services practice specialising in share and business valuation cases, commercial and tax disputes and professional negligence. www.frpadvisory.com/people/people-profiles/fiona-hotston-moore/
Griffin Forensics eForensics and Data Recovery Experts
• CCTV Recovery and Analysis • Computer Media
Investigations
• Mobile Phone Extraction and Analysis • Forensic Data Recoveries
www.griffinforensics.com
Mr Kim Hakin FRCS FRCOphth
Consultant Ophthalmic Surgeon and Expert Witness on ophthalmological matters
www.kimhakin.com
Haydn Jones MEng DipLaw FIET
Data Technologist & Digital Regulation Expert
• Injunctive relief • Money laundering


• Digital currency theft • Counter funding of terrorism E: Haydn.Jones@kroll.com
Atul Khanna FRCS (Plast)
Consultant Plastic, Reconstructive and Hand Surgeon
• Hand surgery • Soft tissue injury • Burns management
• Medical negligence in cosmetic surgery www.atulkhanna.co.uk/expert-witness/
Dr Raj Kumar – Dental Expert


Causation and Liability and Condition and Prognosis Reports
• General dentistry • Cosmetic dentistry • Patient consent
• Dental implantology • Orthodontics • Facial aesthetics
07802 456 804 | info@dentalexpert.me | www.dentalexpert.me
Laird Assessors


The UK’s leading independent automotive expert witness firm supporting claimant, defendant and criminal solicitors. From instruction to court. www.laird-assessors.com
Kulvinder Lall Consultant Cardiothoracic Surgeon
Instructions taken in cases relating to cardiac and thoracic surgery, including aspects relating to surgical care and those following trauma to the structures of the chest.
www.kulvinderlall.com
Mr Chris Makin

• Chartered Accountant • Accredited Civil Mediator
• Accredited Expert Determiner www.chrismakin.co.uk
Martyn Slyper Consultancy
Expert Witness in Assistive Technology
• Personal Injury • Clinical Negligence • Industrial Injury E: ms@martynslyperconsultancy.co.uk www.martynslyperconsultancy.co.uk
Matrix Forensic Accounting & Investigations
Matrix Forensics are an independent niche practice of Chartered Certified Accountants providing expert witness and alternative dispute resolution services. matrixforensic.co.uk
Mr Fredrik P Nath FRCS MBChB
Consultant Neurosurgeon • Head injury • Spinal injury
• Acoustic neuroma • Lumbar and cervical degenerative disease • Musculo-skeletal injury including whiplash www.neurosurg.co.uk
Mr Abraham Odumala
MBBS M.MedSci FWACS FRCS FRCS(Tr & Orth)
Consultant Orthopaedic Surgeon – Upper Limb Specialist. Expertise in all upper limb conditions and treatment. Shoulder, elbow, wristand hand injuries. www.yorkshire-upperlimb.co.uk
Mr Faz Page Bsc(Hons) Dip Registered Osteopath
Personal injury claims involving back, neck and joint pain as a result of road traffic accidents, work related injuries, occupational injuries and sports injuries. www.pageosteo.co.uk
Dr Shanthi Paramothayan
BSc PhD MBBS LLM MScMedEd FHEA FCCP FRCP






Consultant Respiratory Physician specialising in negligence cases relating to all aspects of respiratory medicine. www.paramothayan.com
Dr Stuart Porter Chartered Physiotherapist
PhD MCSP HCPC BSc Hons Grad Dip Phys MLACP PgCAP Cert.MHS SFHEA Specialist areas of expertise include: • Clinical negligence • Breach of duty • Allegations of inappropriate contact • Assessment of adults and children. stuartbporter@aol.com
Simon Quinton Smith BSc FRICS MI Hort Expert Witness to the Garden Centre & Horticultural Industry • Rent Reviews • Lease Renewals • Valuation • Planning • Compensation • Tax Issues
www.quintonedwards.co.uk
Professor Christopher Raine MBE
Specialist in paediatric and adult otology
• Medical negligence • Personal injury cases involving noise induced hearing loss. www.profchrisraine.co.uk




40 40 www.yourexpertwitness.co.uk
Mr Sameer Singh MBBS BSc FRCS Orth
Consultant Orthopaedic Surgeon • All aspects of trauma – soft tissue and bone injuries • Upper and lower limb disorders and injuries
• Whiplash injuries • Expert Witness for defence and claimant Clinic locations – London, Milton Keynes and Bedford
www.orthopaedicexpertwitness.net
Andrew Smith FPC III CeMAP
Financial Conduct Authority Compliance & Risk Consultant Cases relating to FCA compliance in consumer credit and mortgage lending.
• Mediation • Arbitration • Adjudication • Expert Determination
www.paxen.co.uk


Prof. Elizabeth J. Soilleux MA MB BChir PhD FRCPath PGDipMedEd
Expert Witness Pathologist with a particular interest in haematopathology. Short reports on specimens, full court compliant reports and expert biopsy reporting. www.expertwitnesspathologist.co.uk

Mr Bernard Speculand MDS FDS FFD FRACDS (OMS) Consultant Oral and Maxillofacial Surgeon. Personal injury and clinical negligence cases for claimant, defendant and as Single Joint Expert. Special interest is TMJ Surgery.

Yvette Young (Secretary) T: 0121 605 1884 E: info@medsecadmin.co.uk www.birminghamtmj.co.uk
Dr Ian Starke MSc MD FRCP
Stroke Medicine and Medicine for the Elderly Reports and examinations for clinical negligence and fitness to practise cases in stroke medicine and geriatric medicine www.expertwitnessinstrokes.co.uk
Mr David Anthony Sykes (Tony Sykes)
BSc CEng CITP MBCS MIET FAE MEWI
Specialist in IT and Telecommunications. Expert witness and consultancy services to lawyers, insurers and loss adjusters. Experience in international arbitrations and the High Court TCC.

Vincent Theobald-Vega
Health and Safety expert • Asbestos management & removal
• Construction design and management • Laboratories
• Biological & chemical safety and much more. www.safety4hed.co.uk www.rocksideconsultants.co.uk
Target Psychology Ltd
• Public & Private Law Proceedings • Pre-Proceedings
• Immigration Proceedings • Criminal Proceedings • Court of Protection Proceedings
• Personal Injury and Clinical Negligence www.targetpsychology.co.uk
Myles J O Taylor BA(Oxon) PhD FRCOG


Expert witness specialising in: • General obstetrics & gynaecology • Fetal Medicine • Multiple pregnancy – including twin to twin transfusion syndrome, intrapartum care and general gynaecology. www.mylestaylor.co.uk

Mr. William E G Thomas Bsc, MBBS, FRCS, MS
Consultant Surgeon specialising in general surgery, hernia surgery, gastrointestinal surgery, hepatobiliary-pancreatic surgery, laparoscopic surgery and endocrine surgery
T: 0114 262 0852 E: wegthomas@btinternet.com
W: www.wegthomas.com



UK Ophthalmology Experts
UK Ophthalmology Experts are a team of leading, independent ophthalmology experts covering all aspects of ophthalmology. www.ukophthalmologyexperts.co.uk
Dr David Usher BSc DPhil FCIEHF

DR S V MEDICALS (Mr Sen Venkat)

MSc Ortho (London) FRCS Consultant Orthopaedic Surgeon
• Whiplash injuries • General trauma • Sports injuries
• Clinical negligence work • Joint replacement surgery of hip and knee • Hand, shoulder, elbow and wrist injury www.drsvmedicals.co.uk
WOODEXPERTS
Specialist Timber Consultancy and Training since 1991
• Site visits & investigations • Structural surveys
• Desktop analysis & review of documents
• Specialist reports • Species identification
Identification of ergonomic and biomechanical issues underlying injuries. Assessment of tasks, equipment, forces and postures. Civil & Criminal cases undertaken. www.interactionofbath.com www.woodexperts.com
Ms Leyla Ziyal MPhil AFBPsS CPsychol
HCPC Registered clinical Neuropsychologist
• Neuropsychological assessment and rehabilitation
• Depression • Occupational stress • PTSD • Anxiety www.accentpsychology.co.uk





41 41 www.yourexpertwitness.co.uk

MEDICAL NOTES
[A NUMBER OF MEDICAL ORGANISATIONS have marked the first part of the year by reminding physicians within their orbit of their responsibilities under the law to avoid claims for misconduct or negligence.
The General Dental Council has issued new guidance on the steps dental professionals should take to protect themselves from claims and the consequences thereof. Indemnity insurance is a legal requirement for practising dental professionals and the new guidance offers help on the questions they should ask of their insurers.
At the same time the BOA, which represents orthopaedic surgeons, is offering a comprehensive course on the legal issues their members may need to be aware of.
• For the general public, knowing which medical professional is which can be a bewildering experience: as it can also for lawyers who are not themselves experts in the field.
To help clear up confusion in a number of fields, we offer explanations on the difference between radiologists and radiographers, and the broad range of specialisms who practise under the umbrella of cardiology.
• To add to the confusion for patients, in recent years there has been the introduction – and rapid expansion – of the roles of medical associate professionals: physician associates and anaesthesia associates. The BMA has for some time been concerned about the potential for patients confusing the roles of MAPs with trained medical professionals. Now, following the death of a patient and other serious incidents, the BMA has published a guide to MAPs’ roles.
• Alongside the introduction of associates, in particular in general practice, primary care consultations have moved online with the scourge of COVID. Again, there is scope for a lack of clarity or even confusion on the part of both the consulting physician and the patient.
The increased risk of litigation has prompted NHS Resolution – the body tasked with settling claims against NHS trusts – to assist researchers from Nottingham University with an analysis of claims arising from online consultations.
• No amount of research or learning from experiences can account for the fact that some negligence cases arise from a lack of professionalism or care, or even outright bad behaviour.
Ophthalmologists can sometimes be the professionals that alert the authorities to the latter, specifically when it comes to the abuse of children. Again, new guidance has been issued to ophthalmologists regarding the detection of child mistreatment from the presence of head trauma, particularly ocular injury.
A disturbing example of the former has been reported by the Care Quality Commission. A former care manager has been fined after a female resident of a care home was sexually assaulted by another, male, resident. Apart from shock that such an event should take place in a place of safety –particularly as a repeat offence took place after the manager had been alerted to the first – the case illustrates the precarious state of care in recent years, in light of rising costs, staff shortages and soaring numbers of frail elderly people.
• Fortunately, the scales are rebalanced by stories of individuals being inspired to help others, either through guiding victims of adversity through their own journey or being instrumental in the creation of life-enhancing products. We are pleased to be able to highlight examples of both: the creation of an award-winning film on gaining redress following an amputation and an invention to alleviate pain following chemotherapy. We salute all those who deserve our admiration in that way. q

43 43 www.yourexpertwitness.co.uk
BMA LAYS DOWN THE LAW ON MAPS
[ THE BRITISH MEDICAL ASSOCIATION has published a guide setting out the scope of responsibilities for medical associate professionals (MAPs), including physician associates (PAs) and anaesthesia associates (AAs). The BMA believes this is the first time such clear recommendations have been made: laying out what MAPs should and should not do for patients under the careful supervision of a doctor.
After the death of Emily Chesterton and other serious patient safety incidents involving PAs, together with mounting concern from the medical profession about the risk to patients across the NHS posed by employing individuals with only a twoyear qualification, the BMA has drawn on doctors’ expertise and experiences to draft this crucial guide for safe practice.
Using a simple ‘traffic lights’ system, the report clearly identifies what MAPs might be expected to do on their own (green), what they might do under supervision (orange) and what they must not do (red). This
covers both the general field of medicine and specialties from anaesthetics to psychiatry.
It follows a call from the BMA for a pause in the recruitment of MAPs, as reported in the last issue of Your Expert Witness
Four years ago, the BMA published a report which looked at how to improve the ways that doctors and MAPs work together and identified possible solutions to some of the common problems that had arisen with the introduction of MAPs. Since then, due to the expansion of PAs and AAs, the experience of doctors has become more negative and patient safety concerns have dramatically increased.
The BMA believes, in writing and publishing this report, it is addressing the crux of the problem, filling a void that has lasted for over 20 years: that of defining the scope and responsibility of MAPs.
Professor Phil Banfield, BMA chair of council, said: “The need for guidance, implemented at a national level, about what
a physician or anaesthesia associate can do safely and to be a valued member of a medical team, is paramount. Our guide has been written by doctors, for doctors, to explain to the medical profession what MAPs should and should not do alongside their doctor colleagues. But it is also to help patients, to improve patient safety.
“With the government’s clear intent to expand the numbers of MAPs in the medical workforce, but without the clarity on the scope of their skills and responsibilities, it is even more important that patients must know who is treating them and the skills and abilities that clinician has.
“We know that MAPs are working in roles that increasingly cross the line into situations more appropriately requiring the expertise of a doctor, so our report sets out what the association considers a safe scope of practice that will keep patients protected and allow the NHS to effectively employ MAPs to assist medical teams – which was their original purpose.” q
RESEARCH THROWS LIGHT ON REMOTE CONSULTATIONS
[ NHS RESOLUTION recently assisted research teams from the Universities of Oxford and Plymouth and the Nuffield Trust to identify learnings and effective approaches from primary care remote consultations undertaken in general practice, by analysis of claims data.
The research identified three areas to focus on in order to improve safety in remote consulting:
• Effective communication: That can be more challenging during telephone calls, but establishing rapport quickly, listening to and probing the patient’s story and understanding the patient’s concerns are mission-critical. Best practice includes ensuring that the patient understands what will happen next and getting the patient to repeat back instructions. This can minimise confusion and the risk of patients getting ‘lost in the system’.
• Robust processes and support for staff: Practices should review their processes, as the rapid adoption of remote consulting during the pandemic may mean processes designed for a face-to-face world may still be in use and not optimised for reviewing patients remotely.
• Tailoring to patient needs: Teams should be aware that some clinical conditions such as acute abdominal or chest pain, breathing difficulties, an unusual lump, on-going provision for palliative care, new psychosis and diabetic foot checks can be difficult to diagnose and treat remotely. In such cases, considering face-to-face assessments is recommended. In-person assessment should also be considered at the extremes of age when communication is difficult, when patients are not improving as expected, or when an acute condition is overlaid onto pre-existing complex illness.
NHS Resolution acknowledge the real benefit of partnering with academic organisations in potential areas of quality improvement within the NHS.
Dr Alex Crowe, deputy director of safety and learning at NHS Resolution, commented: “This is a great example of collaboration, drawing on expertise from each organisation to enhance the quality of research and improve patient safety and experience. NHS Resolution acknowledge the real benefit of partnering with academic organisations in potential areas of quality improvement within the NHS.” q

44 44 www.yourexpertwitness.co.uk


46 46 www.yourexpertwitness.co.uk
STUDY HIGHLIGHTS ECONOMIC EFFECT ON FRAILTY
[ A STUDY LOOKING INTO rates of frailty among older people has been welcomed by the British Geriatrics Society (BGS). The study, published in the journal PLOS ONE , found that more older people developed frailty during the years of government austerity policies in the 2010s, with those from lower socioeconomic groups more likely to develop frailty.
Frailty refers to the decline in an individual’s ability to recover from a period of ill health, the BGS explains, meaning that illnesses which are usually minor are more likely to have a more serious effect on health and wellbeing.
Frailty affects around one in 10 people over 65 years of age and up to 50% of those aged 85 and over. Over half of adults in hospitals or care home settings at any one time experience frailty, with the condition costing health systems in the UK £5.8bn a year.
Inequalities contribute to worse health outcomes across the life course, resulting in increased levels of frailty experienced by people from lower socioeconomic groups, often at younger ages. The recent research shows the impact of poverty on developing the condition.
Professor Adam Gordon, president
of the British Geriatrics Society, said: “BGS members are frontline healthcare professionals and every day we see how social isolation, the inability to get out, to exercise and to eat well can impact upon the health and wellbeing of our older patients.
“Older people with frailty use health and social care services more than any other population group. Despite this, services are not designed around the needs of this user group. Older people are more likely than other age groups to face long waits in emergency departments and are more likely to get stuck in hospital because of a lack of care available in the community.
“This has a knock-on effect on the whole system; if older people cannot be discharged, new patients cannot be admitted. This contributes to overcrowding in emergency departments, longer waits for ambulances to attend emergencies and a massive backlog for elective care. In addition to the suffering experienced, these examples illustrate the longer term costs of austerity.
“Frailty is not an inevitable part of ageing – we know that it can be prevented and, if identified early enough, may be reversed with the right interventions. As we approach an election, it is essential that all
BRAIN CHARITY LAMENTS BUDGET FUNDING MISS FOR ABI
[ BRAIN INJURY CHARITY HEADWAY expressed its ‘frustration’ that the Chancellor once again missed an opportunity to allocate funding for those living with acquired brain injury (ABI) in his Spring Budget.
Headway chief executive Luke Griggs wrote to Mr Hunt, highlighting the significant financial challenges being faced by ABI charities across the country. Too many of these charities, which support thousands of families, are at risk of collapse. Should they close, the effect on these families will be devastating.
Speaking after the Budget, Headway’s senior policy and public affairs manager Sarah Russell said: “We are frustrated that the Chancellor once again missed an opportunity to provide funding for the high-quality community-based rehabilitation and reablement services that survivors rely on.”
While the Chancellor chose not to announce funding during the Budget, there is a growing consensus that funding should be allocated to support those living with ABI: not only to fund the essential community services, but also to ensure the governmentled ABI Strategy can really transform the lives of survivors.
Sarah Russell added: “We are very grateful to parliamentarians like Sir Chris Bryant MP for keeping the pressure on the government to provide essential funding needed to support the implementation of the ABI Strategy.” q
major political parties have clear strategies for investing in prevention, care and support services, not just for older people who already live with frailty, but for those at risk of developing it in the future.” q
47 47 www.yourexpertwitness.co.uk
48 48 www.yourexpertwitness.co.uk
FORMER CARE MANAGER FINED AFTER RESIDENT SEXUALLY ASSAULTED
[ A FORMER REGISTERED MANAGER at Cherry Tree Lodge, a Warwickshire care home, has been ordered to pay £10,000 by Birmingham Magistrates’ Court, following a prosecution brought by the Care Quality Commission (CQC) for failing to protect a resident from exposure to a significant risk of avoidable harm.
Denise Mary Clark pleaded guilty to an offence of failing to provide safe care and treatment, and one offence of failing to safeguard a resident from abuse and improper treatment, thereby exposing them to avoidable harm.
She was fined £1,600 in court on 15 February. She was also ordered to pay £8,240 costs to CQC which brought the prosecution, and a victim surcharge of £160.
A female resident of Cherry Tree Lodge had a diagnosis of Alzheimer’s disease and lacked capacity to consent to sexual relations. On 21 October 2021 a male resident at Cherry Tree Lodge was found by members of staff in her bedroom, leaning over her and kissing her, with his trousers lowered and engaging in an indecent act.
Members of staff told Ms Clark what they had witnessed and suggested that the male resident should be moved to another room to prevent a re-occurrence. Ms Clark advised action would
be taken, but gave no advice or guidance to staff, and did not take action in line with the service’s safeguarding policy or make referrals to other agencies.
On 2 November 2021, a member of staff found the same male resident on top of the same female resident engaging in sexual activity with her. As a result of this incident police were called and the man was arrested on suspicion of rape on the basis that she did not have capacity and was unable to consent. The man was interviewed by Warwickshire Police and released under investigation. No further action was subsequently taken by the police on this matter.
An investigation by the CQC found that Ms Clark failed to adequately assess and mitigate the risks posed by this man and protect the female resident living at Cherry Tree Lodge from abuse and improper treatment, leading to the incident.
Amanda Lyndon, CQC’s deputy director of operations in the midlands, said: “The registered manager’s failure to protect a vulnerable woman in its care from a resident who was known to present a threat is appalling. What makes it much worse is the harm she was subjected to was potentially avoidable if Denise Mary Clark had done what was required of her under CQC regulations and the safeguarding policy.” q
WHOOPING COUGH ON THE RISE IN INFANTS
[ NEW DATA published on 11 March by the UK Health Security Agency (UKHSA) shows there has been a continued increase in pertussis (whooping cough) cases at the start of this year, with 553 confirmed in England in January, compared with 858 cases for the whole of 2023.
The increase in whooping cough across England is occurring after a prolonged period of low case numbers due to restrictions and reduced social mixing patterns during the COVID-19 pandemic. Cases of whooping cough rise cyclically every few years, with the last peak year, 2016, recording 5,949 cases. The current increase is coming at a time when there has been a steady decline in uptake of the vaccine in pregnant women and in children.
In response to increasing case numbers, the UKHSA is reminding mums-to-be to get protected against whooping cough so that their young baby has protection from birth against this serious disease and to ask their midwife if they are unsure. UKHSA is also urging parents to check that their children are vaccinated against whooping cough, which is offered to all infants at eight, 12 and 16 weeks of age (as part of the 6-in-1 combination vaccine) with an additional dose included in the pre-school booster vaccine.
Data for January show that there were 22 infants aged under three months diagnosed with whooping cough. Those infants, who are too young to be fully vaccinated, are at greater risk of severe disease, including death. UKHSA is strongly encouraging expectant mothers to take up the maternal vaccine. Vaccination of pregnant women is 97% effective at preventing death in young infants from whooping cough.
As a result of the rising cases in 2024, the UKHSA has also moved to a monthly reporting cycle for whooping cough infections to provide timely information on disease rates across the country, to help local public health teams respond to outbreaks and to support the health professionals delivering the routine NHS Childhood Vaccination Programme. q

49 49 www.yourexpertwitness.co.uk

50 50 www.yourexpertwitness.co.uk
GMC APOLOGISES FOR PAST HOMOPHOBIC CENSURES
[ THE GENERAL MEDICAL COUNCIL (GMC) has issued a formal apology for taking regulatory action against doctors who, in historic cases, had convictions under now-repealed homophobic laws. Its chair, Professor Dame Carrie MacEwen, said the regulator was ‘truly sorry’ for compounding the harm already faced by doctors who had convictions that would now be considered unjust.
The GMC has been the independent regulator of UK doctors for more than 160 years. During that time it considered cases against at least 40 practitioners for engaging, or attempting to engage, in consensual sexual activity and intimacy with other men.
In the formal apology, Dame Carrie said: “Homophobic laws and attitudes, that were in place into the 1890s and beyond, caused personal and professional harm. We compounded that harm when we also took additional regulatory action against those who were on the medical register. In some cases that meant the end of a
PODIATRY INSTITUTE CLARIFIES POSITION ON INJECTABLES
[THE Institute of Chiropodists and Podiatrists has issued a position statement on the injection of medicines – including intra and peri-articular injection therapies – by HCPC-registered podiatrists.
The statement says that qualified podiatrists who are awarded licences in POM-A (prescription only medicine- administration), as either part of their undergraduate degree or as stand-alone qualifications, are given statutory permission to administer medicines by injection that they may lawfully access.
“The POM-A licence also contains a specific permission to obtain (without the usually required prescription) a range of injectables which include various local anaesthetics, adrenaline (epinephrine) and the anti-inflammatory synthetic steroid methylprednisolone,” the statement says. “That permission continues while said podiatrist remains on the statutory register of the Health and Care Professions Council, and ceases should they leave, or be removed from, the stated register.”
However, it is a requirement of safe and responsible practice that podiatrists with POM-A must ensure that they:
• Have a full and detailed understanding of the pharmacology
• of said medicines including their pharmacokinetics and
• pharmacodynamics – essentially how the body affects the drugs
• and the drugs affect the body
• They have suitable medical indemnity insurance for use of the
• items above.
The training course leading to granting of POM-A covers the requirement for local anaesthetic, however: “In respect of the licensed steroid, the institute requires the completion of an approved course which explains, in substantial detail, the action of when to use and, perhaps even more importantly, when not to use the permitted steroid.
“By virtue of the holding of a POM-A licence it is clear that the holders are already trained and safe injectors and the simple techniques of safe administration will already be known; but nonetheless, these are specifically restated (with some practical tips and information pearls) during the course and delegates to the course will readily grasp the analogy between local anaesthetics and steroids.” q
practitioner’s career. For this we are truly sorry.”
The GMC’s archivist, working with members of the regulator’s LGBTQ+ staff network, has searched records for cases of doctors who were subject to fitness to practise proceedings because they had criminal convictions based on sexuality. At least 40 individuals were found, dating back to the 1890s. At least eight doctors were struck off the medical register as a result. The last confirmed erasure was in 1966, although other doctors were issued with warnings.
Dame Carrie continued: “We cannot be sure of the true number of doctors we took historic action against based on convictions that would now be considered unjust. But the impact on every one of them, and on those close to them, will have been considerable. Laws and attitudes have changed in the years since, as has the GMC. These are historic cases, but it is right that we apologise for them.”
Dr Duncan McGregor of GLADD, the Association of LGBTQ+ Doctors and Dentists, said: “GLADD welcomes this apology by the GMC for the historic injustices of regulatory action taken against doctors due to homophobic laws. The profound impact of these actions on their lives cannot be overstated. This apology is an important step in righting the wrongs of the past and, while the hurt and damage that has been caused to those doctors cannot be undone, it is important to acknowledge past injustices.
“Although the threat of erasure from the medical register due to a doctor's sexuality no longer looms, prejudice against LGBTQ+ healthcare staff persists to this day. This apology represents progress towards justice for those impacted by these historic homophobic laws, and progress for the LGBTQ+ community. We hope this gesture brings some measure of solace to those affected doctors and their loved ones.” q
51 51 www.yourexpertwitness.co.uk

52 52 www.yourexpertwitness.co.uk
WHAT ARE THE MEDICOLEGAL CHALLENGES OF CORONARY ARTERY BYPASS GRAFTS?
By Mr George Asimakopoulos, Consultant Cardiac Surgeon
[
CORONARY ARTERY BYPASS GRAFTING (CABG) – also known as heart bypass surgery – involves taking a blood vessel from another part of the body, usually the chest, leg or arm, and attaching it above and below the damaged area of the coronary artery.
Although percutaneous coronary intervention is viewed as a less invasive treatment, CABG is now accepted as a highly-effective solution to obstructive disease of the coronary arteries.
Improvements in the procedure mean that long-term patency of the graft can be expected, which compares favourably with the higher requirement for reintervention after percutaneous treatments. Following the operation, cardiac function is improved and the incidence of angina pectoris is reduced. Patient life expectancy is also increased.
However, the use of grafts is not without its challenges and there are some important considerations which must be taken into account before the procedure is undertaken. When it comes to the choice of graft material, several options are available. As the quality and application of the bypass graft are major predictors of both survival and the development of significant complications, appropriate selection is vital.
Other issues that may lead to graft failure include poor graft preparation, inappropriate or poor operative technique and patient factors. Most graft failures arise due to events that occur early in the procedure. Graft ischemia can be prevented through careful harvesting, vasodilatation and storage prior to implantation.
Vasodilatation is necessary to minimise the risk of potentially lethal graft spasm, but care should be taken to protect the endothelial function of the graft. The long-term patency of vein grafts can be improved by a daily dose of aspirin, assuming there are no contraindications, which should commence within 24 hours of the procedure. However, there is no evidence that aspirin improves the patency of arterial grafts.
the recipient coronary artery.
The secretion of NO helps to prevent platelet aggregation, thrombosis, intimal hyperplasia and inflammatory cell migration, all of which can lead to coronary obstruction. Not surprisingly, ITA grafts are currently considered the preferred option in most patients.
Historically, saphenous vein grafts (SVG) were considered better than internal thoracic artery (ITA) grafts, and were used more commonly. That is because the SVG has a low physiological resistance to coronary blood flow, which leads to higher coronary flow as measured during surgery. However, it has since been demonstrated that ITA grafts can adapt to higher flow demands by increasing in diameter. Those changes, which are usually apparent a few weeks after surgery, can result in coronary flow up to 2.4 times higher than in the resting state.
Another potential issue with SVGs is that physical damage of the endothelial layer of the vessel often occurs during preparation of the graft if high-pressure dilatation of the vein takes place. That loss of function can result in degenerative and atherosclerotic processes being initiated when the graft is implanted into the arterial circulatory system. Local narrowing with intimal hyperplasia and degenerative dilation often occurs and can ultimately lead to atherosclerosis.
Conversely, ITA grafts differ in their tissue structure from both the coronary artery and the saphenous vein. A thin smooth muscle layer, abundant elastic fibres and tight lamina interna mean that ITA grafts are inherently resistant to atherosclerosis. Furthermore, the superior secretion of nitrous oxide (NO) by ITA grafts means that beneficial metabolic effects are not only maintained in the graft itself, but also in

A number of patient factors influence the success of coronary artery bypass grafts. Patients with diabetes mellitus pose particular problems. Disease of the coronary arteries tends to be more diffuse in these patients than in those without diabetes, and often affects several blood vessels. Furthermore, the saphenous vein is often more calcified and changes are seen in all layers of the vessel wall. Therefore, ITA grafts should be strongly considered.
However, there is an increased risk of sternal infection following ITA harvesting, which is more than doubled in diabetic patients. Other complications include increased rates of stroke, myocardial infarction, recurrent angina and mortality, as well as an increased need for reintervention.
As the population ages CABG will be carried out more frequently in older patients, who have more comorbid conditions. Those factors may influence the choice of graft material. Arterial grafts may not be seen as the best option, due to the presumed limited life expectancy of older patients.
Other vessels are likely to undergo medial calcification over time, although this may not always be clinically relevant and can be prevented by the appropriate use of adjuvant cholesterol-lowering agents or similar medications. Patients with renal disease suffer from an increased risk of early complications, such as further loss of kidney function, infections and progressive loss of graft function. Thus, the use of bilateral ITA grafts may not be justified.
Improvements in technique mean that CABG is now suitable for most patients with coronary artery disease, even when extensive grafting is required. With careful selection of graft material and good preparation, long-term graft patency can be achieved. Secondary prevention of coronary disease, encompassing smoking cessation, the use of cholesterol-lowering drugs and the control of hypertension and diabetes, should ensure even better patient outcomes. q
• Mr Asimakopoulos has been a consultant cardiac surgeon at the Royal Brompton Hospital in London since 2014 and has performed over 3,000 cardiac surgical procedures.
His main areas of interest include coronary artery bypass grafting using the off-pump technique, aortic valve replacement including less invasive surgery with sutureless valves, and aortic surgery. He has extensive experience in treating aneurysms of the aortic root, the ascending aorta and aortic arch, infections of the heart valves (endocarditis) and aortic dissections. He regularly performs re-operations on patients who have had previous heart surgery.
Read Mr Asimakopoulos’s full biography and download his CV at www.medicolegal-partners.com/our-experts/mr-george-asimakopoulos
53 53 www.yourexpertwitness.co.uk

CARDIOLOGY HAS BECOME A COMPLEX SPECIALTY
 By Mr Neil Roberts MB ChB MRC MD FRCS (C-Th) Consultant Cardiothoracic Surgeon
By Mr Neil Roberts MB ChB MRC MD FRCS (C-Th) Consultant Cardiothoracic Surgeon
[THE WORLD OF CARDIOLOGY has moved on dramatically in the past 20-30 years, such that many areas are now very specialist and niche. Whereas in the past a cardiologist was one general and generic specialty, it is now much more sub-specialised, with areas of expertise between each subset of cardiology.
That contrasts with the field of cardiothoracic surgery. While the fields of cardiac and thoracic surgery have split into distinct specialties, the cardiac surgeon has now become more of a generalist, treating arrhythmias, valve lesions and coronary artery disease, whereas the cardiologist has become much more subspecialised in their own fields.

It is also the case that there is more overlap between cardiologists and cardiac surgeons, and that many procedures and operations are performed jointly with both a cardiologist and cardiac surgeon present. In addition, many more cases now have their management discussed in multidisciplinary team meetings. Whereas 20-30 years ago a cardiologist would write to a cardiac surgeon and ask for a specific operation to be performed, now the cardiac surgeon and different specialties of cardiologist will sit together and discuss the prognosis and treatment options across the different techniques available to treat certain pathologies.
The lines blur even further, in that many cardiological procedures taking place in the cardiology catheterisation laboratory – the ‘cath lab’ – also involve minor surgery. Those procedures are often undertaken by subspecialty cardiologists rather than cardiac surgeons and patients often refer to operations, when they have actually undergone what a surgeon would describe as a procedure. I will now go on to describe each of the subspecialties and what their specific areas of expertise are.
Non-invasive cardiologist
A non-invasive cardiologist is a doctor specialising in the treatment of the heart who does not undertake invasive procedures. That would include cardiologists with a special interest in imaging technology such as echo or MRI scans, doctors who specialise in the medical treatment of heart failure and endocarditis (infections of the heart), and those involved in the longerterm follow up of patients who have previously undergone either invasive cardiology intervention or cardiac surgery.
The non-invasive cardiologist will be involved in treating a range of cardiac pathology, including seeing patients initially for their presentation of arrhythmias, blood pressure problems, chest pain, heart failure and valvular lesions, as well as infections of the heart. Such cardiologists would often either manage a patient medically themselves or refer to an interventional cardiologist, cardiac surgeon or electrophysiologist for more subspecialty interventions.
Interventional or invasive cardiologist
The interventional or invasive cardiologist would be a cardiologist involved in interventional procedures – for instance, performing invasive coronary angiograms such as stent placements to the coronary arteries, either for stable chronic angina or for the emergency treatment of heart attacks.
The emergency treatment of heart attacks (primary PCI) is a treatment that has emerged over the past 15 years or so. Whereas prior to then patients having an acute heart attack may have been given clot busting drugs in their district general hospital, they are now transported by ambulance to the nearest primary PCI cardiac catheter lab hospital to have the occluded heart artery opened up as an emergency procedure.
It is often the case, however, that such primary acute heart attacks are to what is called the culprit heart artery: the heart artery that has blocked and
caused the acute heart attack. There is often then discussion between the invasive cardiologist and non-invasive cardiologist and cardiac surgeon as part of an MDT meeting to decide on how to treat other heart artery narrowings that were not the cause of the acute heart attack, but could have a prognostic or symptomatic problem in the future. Therefore, the treatment of the on-going bystander coronary artery disease and decisions on future prognosis and treatment options would all fall within the expertise of the non-invasive cardiologist, the invasive cardiologist and the cardiac surgeon.
There is also a subsection within invasive cardiology called structural interventional cardiology, which is involved in the treatment of non-heart artery or coronary interventional techniques. Structural interventional cardiologists would perform percutaneous valve interventions, percutaneous closure of holes in the heart such as PFO or ASD, the percutaneous treatment of valves such as aortic stenosis with Tavi, or mitral regurgitation with mitraclip techniques. Such procedures are often done in conjunction with a cardiac surgeon and, therefore, the structural interventional aspects of cardiology would be considered within the expertise of structural interventional cardiologists and cardiac surgeons.
Electrophysiology
The treatment of rhythm disturbances of the heart has developed into a specific subspeciality of cardiology called electrophysiology. Such cardiologists are involved in the medical treatment and interventional treatment for heart rhythm disturbances. Therefore, they would treat patients with atrial fibrillation, heart block, ventricular tachy-cardia and inherited rhythm disturbances. They are the cardiologists who would insert pacemakers, internal cardiac defibrillators or combinations of pacing and defibrillating lead and wires attached to pacemaker box devices.
They are also the cardiologists who would be involved in the ablation of cardiac arrhythmia pathways such as the interventional ablation of atrial fibrillation, which is a procedure performed within the cardiology cath lab via the groin. A wire is passed into the right side of the heart, a puncture made into the septum and an ablation catheter or cryoablation balloon passed into the left atrium to try and ablate the pathway thought to be causing the cardiac rhythm disturbance.
Such AF ablation can take place percutaneously as a technique done in the cardiac catheterisation laboratory, but AF ablation can also be undertaken from the outside of the heart at the time of cardiac surgery and that aspect would fall within the realm of a cardiac surgeon. There is, therefore, significant overlap between the medicolegal aspects of AF ablation procedures and surgery as, if there is a complication such as a perforation of the heart from the inside, a cardiac surgeon is then often required to assist.
It is also the case that combined procedures by electrophysiology cardiologists and cardiac surgeons are often undertaken to explant infected pacing systems or pacing systems that have been placed by an electrophysiologist many years before.
Cardiac surgeon
A cardiac surgeon is a surgeon who undertakes open heart surgery, often requiring the use of a full open chest incision and using a cardiopulmonary bypass machine to allow the heart to be stopped and opened to allow valve replacements or bypass operations to take place to treat a variety of pathologies. Cardiac surgeons are therefore involved in the MDT meetings to discuss the treatment of ischaemic heart disease (coronary artery problems) and valve disease such as aortic stenosis, Tavi, valve replacement, mitral regurgitation etc.
55 55 www.yourexpertwitness.co.uk
They are also involved in MDT discussions about the treatment of endocarditis (infections of the heart valves) and also AF ablation, removal of infected pacing systems and any complications that occur within the cardiology catheterisation laboratory that could involve perforations or bleeding within the cath lab requiring open surgery to help correct.
It is not unusual, therefore, for a cardiac surgeon to be involved in leading the care of someone with complex valve, coronary and rhythm problems and liaising with electrophysiologists, imaging cardiologists and interventional cardiologists to come up with treatment plans that are collaborative. Therefore, there is a huge amount of overlap between the subspecialty of cardiology and the cardiac surgeon.
Cardiothoracic trauma
While the specialties of cardiology, cardiac surgery and thoracic surgery have split over the past 10-15 years, the primary qualification for all cardiac or thoracic surgeons is being a cardiothoracic surgeon. All cardiothoracic surgeons are trained in both specialties and are involved in the treatment of blunt and penetrating chest trauma.
Blunt or penetrating chest trauma can affect the heart, lungs, sternum, ribs, the pleural spaces and large blood vessels within the chest such as the aorta or pulmonary vessels; and therefore it would be considered within the realm of most cardiac or thoracic surgeons – given their global qualification of cardiothoracic surgery – to treat, examine and opine on aspects of cardiothoracic trauma which often are complicated and do not conform to the specialty divisions.
Thoracic surgeons use sternal incisions and minimal access incisions between the ribs, as do cardiac surgeons, and therefore incisions or problems with the ribs or sternum would be considered within the expertise of the global cardiothoracic qualification, as both specialties are involved in accessing the chest through the front or the side.
Medical negligence: cardiac and thoracic surgeons
When we are talking about medical negligence and not blunt chest trauma and personal injury, which is more a global topic, a cardiac surgeon would confine themselves to treatment of the heart, whereas a thoracic surgeon would confine their expertise to treatment of the lungs. It is therefore likely that, even though all cardiothoracic surgeons have the global cardiothoracic qualification and would call themselves cardiothoracic surgeons, surgeons that specialise in the heart predominantly would not comment on mesothelioma, lung cancer or infections or operations on the lungs themselves; and a thoracic surgeon would not provide expert opinion on open heart surgery cases, infections of the heart such as endocarditis or heart attacks or treatment of coronary disease.
Paediatrics
Under the age of 18 years, all patients are treated by paediatric specialists, and it is fair to say that all the subspecialisations of cardiology also exist with varying degrees of overlap in the paediatric population. What complicates matters is that paediatric patients with congenital heart disease are now living to a greater age; therefore, there is a transition point at the age of 18 years when the hospitals treating children would transition treatment to adult or ‘grown-up’ congenital heart disease (GUCH). Different solutions exist for each region depending on the surgical services and cardiology provisions within that region.
There is obviously significant overlap between the two specialties between the two age groups and there are paediatric cardiac surgeons that have a special interest in GUCH and operate not only on children, but also on adult patients that have had a long history of interventions on their heart as paediatric patients and then as they grow into adulthood.
Summary
I hope I have made it clear to instructing solicitors that there are a number of sub-specialties within cardiology and many experts who, like myself, will have collected a team of collaborators so that when instructed, if a case falls slightly more within the expertise of an electrophysiology cardiology expert, an interventional cardiology expert or a cardiothoracic surgeon with more of a thoracic specialist interest, the instructions are often passed on within our group to try and ensure the instructing solicitor is furnished with the correct expert for the case. q

56 56 www.yourexpertwitness.co.uk
REHABILITATION: A CORNERSTONE OF COMPENSATION CLAIMS
[FOR MOST PEOPLE involved in a personal injury or clinical negligence claim, the main objective is to return as far as is possible to their previous state of health and wellbeing. To that end, personal injury lawyers and insurers alike have a great deal invested in the concept of rehabilitation.
Rehabilitation is recognised by the courts as a primary aim of any process, enshrined in the Rehabilitation Code. First established in 1999 and updated in 2007 and 2015, the aim of the code is to ‘promote the use of rehabilitation and early intervention in the compensation process so that the injured person makes the best and quickest possible medical, social and psychological recovery’.
According to the Association of Personal Injury Lawyers (APIL): “Research has shown that in many cases rehabilitation can help injured people recover more quickly, have a better quality of life and return to work sooner. Thus rehabilitation can be the key to returning the injured client to the same position that they would have been in were it not for the negligence of the defendant.”
Following the publication of the latest revision of the Rehabilitation Code in 2015, APIL produced its own guide for its members. The guide is ‘intended to have practical application, and includes case studies and process maps. It anticipates a new era in which personal injury lawyers will take the lead in a proactive manner to instigate rehabilitation wherever this is possible’.
Insurers, too, are signatories to the code, and also promote rehabilitation as a cost-effective measure in employer health insurance, getting claimants back to work quickly and effectively.
Research from the Association of British Insurers found that 86% of

people who accessed insurer-provided vocational rehabilitation were successfully supported to stay in work or return to work following an absence. More than half of customers received support for a mental health condition, approximately one in four remained well enough to work and two in three (64%) were supported to return to work.
While rehabilitation can be provided by the NHS, in many cases private providers are engaged. APIL explains: “The only remedy in court cases involving personal injury is money, but in most instances rehabilitation must be paid for, and so the cost of this can be recoverable as a head of special damage. As with all other special damages, the court will allow the cost of rehabilitation to be recovered as long as it can be shown to be reasonable.”
Assessing what the costs of that provision is likely to be – whether it be for vehicle or home adaptations, lifetime cost analysis or equipment costs – is the role of a range of experts, as the following pages show. q

57 57 www.yourexpertwitness.co.uk

58 58 www.yourexpertwitness.co.uk
BRAIN INJURY REHAB CAN BENEFIT FROM SLT
[ONE OF THE THERAPIES often recommended to help rehabilitation following traumatic brain injury is speech and language therapy.
The National Institute for Health and Care Excellence (NICE) defines acquired brain injury as ‘any trauma to the head which disrupts the function of the brain’. According to the Royal College of Speech and Language Therapists: “It may involve the scalp, the skull, the brain or its protective membranes. The injury can result in speech, language, communication and swallowing difficulties.”
It further refines the definition of traumatic brain injuries as:
“Traumatic brain injury, also referred to as ‘head injury’, results from an outside force and subsequent complications which can follow and further damage the brain. These include a lack of oxygen, rising pressure and swelling within the brain.
“Speech and language therapists support people who have a brain injury with communication and eating, drinking and swallowing difficulties that can arise from it.”
In adults, speech and language therapists work with adults who have acquired a brain injury. They:
• Assess the speech, language, communication, social interaction
FILM TELLING REHAB STORY FOLLOWING AMPUTATION WINS INDUSTRY AWARD
[A MOVING SHORT FILM about how the law on personal injury is vital in helping victims to piece their lives back together has won a major industry award for the Association of Personal Injury Lawyers (APIL).
The film, called Victoria’s Story, was produced for APIL’s Rebuilding Shattered Lives campaign, which has the long-term aim of putting injured victims of negligence at the heart of policymaking.
The film won Gold in the Best Blog, Podcast or Video category at the Association Excellence Awards 2023. It tells the true story of Victoria Lebrec (pictured), who had to have her leg amputated after a horrific road crash that was not her fault.

“Rebuilding Shattered Lives is about ensuring the needs of people who are injured due to someone else’s negligence are held paramount when the government devises policies,” explained APIL chief executive Mike Benner.
“The law can be a fragile thing, subject to erosion by lawmakers who are all too often influenced by false myths and ignorance about the needs and motivations of injured people. Victoria’s Story demonstrates how critical personal injury law is to victims of negligence. She explains first-hand how the law helped her to get her life back on track.
“In Victoria’s case, the law meant she could secure the compensation she is entitled to so she could get a prosthetic leg that fitted correctly. The one she was initially given by the NHS left her falling over, bruised and in pain. She also explains with eloquence how her life changed forever in an instant.”
The award was announced at a ceremony in London, with the judges saying the film portrayed a ‘very powerful story’ and was ‘sensitively made’.
“A win like this for Rebuilding Shattered Lives is a significant step forward,” added Mike Benner. “This campaign is for the whole sector and the injured people it serves. If you are a victim of negligence, you should be able to rely on the law for the help you need.”
To view Victoria’s Story visit rebuilding-shattered-lives.org.uk
and eating, drinking and swallowing abilities
• Contribute to diagnosis
• Provide individualised treatment interventions
• Plan appropriate therapeutic interventions to address the speech, language, communication and swallowing difficulties
• Advise on devices that can make communication for the person easier
• Train individuals and their families and/or carers in methods of promoting communication and where necessary using assistive or alternative communication aid devices
• Work jointly with other members of the inter-professional team (medical, social and voluntary bodies)
• Provide well-planned and goal-oriented rehabilitation in a specialist setting by expert professionals working in a co-ordinated inter disciplinary team
• Educate and work with family members, carers and relevant staff to provide an understanding of the nature of the difficulties and strategies to optimise function and independence
• Train relevant people to work with the individual and provide support to them over a long period of time
• Advise, demonstrate, practise and provide strategies on the most effective way to engage the individual in verbally and communication mediated interventions and to minimise the effects of the communication difficulties where possible
• Reduce the barriers to interaction to individuals and their social environment
Leading service provider SLT UK explains: “Speech and language therapy input will depend upon the severity of the injury and the area of the brain affected. The level of speech and language therapy intervention will be determined by each individual case and discussed accordingly.” q
59 59 www.yourexpertwitness.co.uk
NEW ARTS THERAPY EXPERT WITNESS SERVICE LAUNCHES
[A NEW EXPERT WITNESS SERVICE
from arts therapy specialists Chroma has been hailed a success by personal injury lawyers and case managers.
Chroma, the UK’s leading provider of arts therapies, launched the first creative arts therapies (CATs) expert witness service in the UK in February, and many PI lawyers are already looking forward to sending instructions to use the service.
The service aims to help secure the best rehabilitation package for clients. It enables legal teams to access independent expert witness testimony to help put forward a compelling case for the benefits of CATs within rehabilitation programmes and make clear how such therapies will improve victims’ quality of life.
CATs encompass music, art and dramatherapy. Either one – or more – can be used within a rehabilitation programme, depending on goals, to gain the best outcome for a client. When implemented alongside physiotherapy, occupational therapy and speech and language therapy, they positively affect rehabilitation outcomes, supporting
improvements in clients’ functional and cognitive abilities as well as their psychological wellbeing. Consequently, the use of CATs has become commonplace in rehabilitation programmes, bringing about the need for expert witness evidence in cases where they may form a significant head of cost.
The keynote speaker on the evening was Dr Corene P Hurt-Thaut PhD MT-BC. Dr HurtThaut is program director at the Academy for Neurologic Music Therapy and also assistant professor at the Faculty of Music and program head, Applied Music and Health at the University of Toronto.
Corene’s presentation on neurologic music therapy was well-received by those attending and brought home the importance of such therapy for their clients.
The evening also saw Richard Williams-Lees LLB (Hons) PgDip (Law), chief executive of McCollum Consultants and co-founder/director of ALLDOQ, introduce the platform which Chroma will adopt.
ALLDOQ is a specialist medico-legal workspace that allows users to securely


store, organise and complete medico-legal work in the cloud, avoiding the hassle of disorganised files and duplication with a single, easy-to-use workspace built for medico-legal expert witnesses.
Solicitors attending the launch included representatives from Irwin Mitchell, Higgs LLP, CL Medilaw and Slater & Gordon.
Chroma MD Daniel Thomas commented: “Our expert witness launch was a great success, with attendees wanting to know more about how to improve the quality of life for their clients. Having Corene speak was invaluable and helped illustrate just how effective neurologic music therapy can be in rehabilitation. Several firms commented on looking forward to sending us instructions.
“Attendees also expressed their appreciation that ALLDOQ would be the platform of choice for Chroma, as it keeps client data safe and provides a time and cost-effective expert witness service.” q
60 60 www.yourexpertwitness.co.uk
WHAT ARE THE CONSIDERATIONS FOR COSTING REHABILITATION REQUIREMENTS?
By Barbara Franks, deputy quality assurance and training lead and occupational therapy expert witness at Somek & Associates
[WHEN CONSIDERING home adaptations and equipment costs for a clinical negligence or personal injury claim, it is essential as a care expert to fully understand the claimant’s preinjury position. It is only in that way that reasonable restitution can be achieved.
The pre-injury position has to consider not only any health issues that pre-dated the index event, but also the claimant’s previous lifestyle. For example, a claimant who was independent in all aspects of their life and did not have any health problems will have very different recommendations compared to a claimant who had a number of co-morbidities and required assistance for some activities of daily living in any event.
What is also essential is an understanding of the expert medical evidence in terms of causation and prognosis. Without that, the future-proofing of recommendations is difficult. An example of that would be a claimant who had pre-existing health conditions and in later life was going to need mobility equipment. In terms of costing for any equipment that is required as a result of the index event, those later needs have to be considered to inform when such equipment should be costed to.
It is also imperative to consider what impact any future treatment may have on a claimant’s level of function, and whether it is likely to affect care and/or equipment needs. That may require the provision of more than one scenario, depending on the medical opinion of the experts instructed.
The care expert has to be careful about not ‘double costing’ when care and equipment is recommended. That is not to say the two cannot be recommended together, but there has to be careful analysis of the reasons and that has to be clearly articulated in the report.
Clinical rationale is the most important aspect of any care report, as it is not enough to say what a claimant needs but the reasons why, so the reader can understand how the care expert came to their conclusions.
This case study concerning a claimant who sustained a soft tissue injury to their lower limb highlights some of the points raised.
The injury did not heal as expected and they were subsequently diagnosed with complex regional pain syndrome (CRPS). Their participation in domestic activities of daily living, such as gardening, DIY and leisure, was affected as a result of pain and reduced mobility. Psychologically, they were

also affected with low mood and anxiety, and they had been unable to return to work. Prior to the index event they were fully independent and working in a full-time capacity.
The medical opinion on the case was divided, with the claimant’s experts considering the diagnosis of CRPS to be an appropriate one, and that from a prognostic point of view they were likely to make some improvements with the recommended rehabilitation but would remain restricted in the longer term. They were supportive of some adaptive equipment, including an adapted vehicle, to assist the claimant to return to improved participation in daily activities which, in turn, would have psychological benefit.
Conversely, the defendant’s experts offered different opinions, ranging from a diagnosis of CRPS to a localised nerve injury with neuropathic pain, malingering or a somatic symptom disorder.

It was ultimately a matter for the court, as was the claimant’s veracity; but to reflect the range of opinion a number of different future care, equipment and therapy scenarios were provided.
The future care scenarios ranged from provision of a support worker to assist the claimant to re-engage with previously enjoyed leisure activities and domestic support, to a reducing support package leading to no on-going care if it were accepted that the claimant’s condition was psychologically mediated and a significant recovery was accepted as being the most likely outcome.
Similarly with equipment: a number of pieces of equipment were recommended if the court preferred the evidence of the claimant’s experts. They ranged from items to assist with mobility and personal care, to equipment to enable improved participation in meal preparation. Consideration was given to items that were a need in any event, such as an oven, and credit given for that.
In the event of the court accepting that the claimant would make a significant recovery, no equipment recommendations were made. This pattern followed through the entire report, with heads of claim being costed depending on which viewpoint was preferred.
Thorough examination of the differing expert viewpoints enabled recommendations to be well reasoned and backed up by medical opinion – regardless of which viewpoint was preferred – and ensured a balanced approach was provided, avoiding ‘cherry picking’ of evidence.
Care reports vary hugely depending on many factors, but the above scenario gives a snapshot of the types of issues that have to be considered when costing future needs. q

61 61 www.yourexpertwitness.co.uk
62 62 www.yourexpertwitness.co.uk
INFECTION CONTROL LAPSES THREATEN A&E PATIENTS AND STAFF
[INFECTION CONTROL STANDARDS
in A&E departments – vital for containing the spread of infectious diseases – have fallen significantly since the pandemic, according to new research published by the Royal College of Emergency Medicine (RCEM). The findings are contained in the final report of RCEM’s three-year Quality Improvement Programme (QIP) on Infection Control and Prevention (IPC), published on 26 February.
The QIP collated and analysed data and captured patient experiences from 127 Emergency Departments across all four nations. It found that the number of EDs achieving the standards seen in 2020 at the height of the pandemic had fallen, but concluded that the increasing pressure and crowding in EDs will have impacted clinicians’ ability to attain the previous levels.
The infection control and prevention measures included things such as screening patients on arrival for COVID-19, isolating vulnerable patients in side rooms and moving those with infections to isolation areas.
The report also highlighted the drop in the number of staff obtaining and maintaining their own vaccinations.
The QIP team, led by Dr Fiona Burton, EM consultant, IPC topic team lead and co-
PARAMEDICS’
chair of the RCEM Quality Assurance and Improvement committee, made the following recommendations:
• Awareness that COVID-19 is present and a real risk to both patients and staff should be maintained.
• Screening and documentation of IPC measures by healthcare staff must be routinely completed.
• Staff vaccinations must be promoted and actively encouraged.
• IPC teams must use their local intelligence to work with each ED to guide PPE and departmental configuration to try and ensure appropriate areas are available to maximise staff and patient safety.
Dr Burton said: “The drop in the standards we observed is worrying, but it has to be considered in the highly unusual context of a global pandemic, combined with the escalating demands being heaped on our overstretched and over capacity emergency departments.
“As COVID emerged there was naturally strong messaging about the importance of escalating infection control measures, including the focus on identifying the people who were most vulnerable. However, with the successful vaccination programme the
messaging has lessened and assessing people’s vulnerability as soon as they enter the ED is perhaps no longer as prominent a consideration as it was – especially as other system pressures mount.
“But we have to remember that COVID has not gone away and it, and other infectious diseases, still pose a serious threat to patients and to staff; and that not being able to provide adequate IPC measures can put people’s lives at risk. It must remain a priority.
“We will now be sharing this important piece of work with healthcare leaders in the four nations and also their governments to ensure the lessons and good practice that were commonplace during the pandemic do not slip as time passes.”
President of the Royal College of Emergency Medicine Dr Adrian Boyle said: “I’m grateful to Dr Burton and the Quality Improvement team for doing this important work. It is unconscionable that, directly after a terrible pandemic, the system is not providing the standards that staff and patients need.
“We must ensure that an environment where staff and patients are protected properly against infectious diseases is the norm.
“Everyone has a part to play in this.” q
COLLEGE GAINS CHARTERED STATUS
[THE COLLEGE OF PARAMEDICS has been granted the Charter of Incorporation by HM King Charles III. The Royal Charter was granted to the college in recognition of its objectives to inspire and enable all paramedics to participate in the profession within an environment based on safety, collegiality, inclusiveness, mental and physical wellbeing and innovation.
The issue of the Royal Charter represents an important milestone in the development of the College of Paramedics. It provides recognition for the profession, gives strength to its professional voice and leadership and offers members a moment of immense pride. It also cements the college in perpetuity, meaning that there will always be a College of Paramedics for the future, supporting and guiding the profession forevermore.
The college’s chief executive Tracy Nicholls commented: “I am delighted we have been able to achieve this on behalf of our members, and to strengthen the college for the future. Gaining the Royal Charter is the first step towards being granted the title ‘Royal’, but our journey to increase leadership and development across our profession has a solid foundation for future chartered titles and more scope for development of paramedics.”
The College of Paramedics began life as the British Paramedic Association on 14 December 2001, when it was established as the professional body for paramedics in the UK. Three years later the organisation rebranded itself the College of Paramedics and, within 15 years of its inception, the college had 10,000 members. That figure has continued to grow over the years and today stands at more than 20,000 members.
Since its early days, the college has been instrumental in developing the paramedic profession and was responsible for writing the first
standards of proficiency for paramedics in 2004, introducing the British Paramedic Journal, presenting the first paramedic curriculum framework in 2006, raising the threshold for entry to the Health and Care Professions Council’s register to degree status and achieving independent prescribing for paramedics.
More recently, thanks to the college’s work with Public Health England and NHS England Public Health Commissioning and Operations, it was announced in September 2023 that primary care paramedics would be able to undertake the training required to become sample takers in the NHS Cervical Screening Programme. q
63 63 www.yourexpertwitness.co.uk

64 64 www.yourexpertwitness.co.uk
POST-TRAUMATIC HEADACHE FOLLOWING
HEAD INJURY OR WHIPLASH: HOW COMMON IS IT AND HOW DO WE TREAT IT?
By Dr Anke Hensiek Dr med PhD FRCP, Consultant Neurologist and Affiliate Assistant Professor at the University of Cambridge.
[ POST-TRAUMATIC HEADACHE is the most common symptom in individuals who suffer mild traumatic brain injury (mTBI) or whiplash injuries. According to the ICHD-II diagnostic criteria, post-traumatic headache is a secondary headache that is caused by head or neck trauma. It is defined as the occurrence of either a new headache or significant worsening of pre-existing headaches within seven days of mild traumatic brain injury or whiplash injury and can be categorised as acute, if present for less than three months, or persistent if it persists beyond that time.
The reported prevalence of post-traumatic headache varies markedly among studies, with reported figures ranging between 30-90%. That variation highlights the complexities of defining post-traumatic headache: in some situations, post-traumatic headaches may be misdiagnosed as migraine or other primary headache syndromes, particularly in those with a history of headaches. Furthermore, there are differences in study design. The type of assessed population is likely to play a role: for example, post-traumatic headache frequencies may differ in populations of young men with sports injuries, compared to individuals of varying ages who had accidents and are still involved in litigation.

structures and cranial or spinal nerves. Stretching, dilatation, constriction or any nociceptor stimulation within those structures can result in the perception of headache.
The mechanism of how that happens is complex and influenced by numerous factors which are often unique to an individual. An activation of trigemino-vascular pathways is causative in certain primary headache disorders and probably relevant for some posttraumatic headaches. That pathway is more likely to be activated in genetically predisposed individuals, for example those with a preexisting predisposition to migraine, but can also be triggered as a result of lifestyle changes, mood or sleep disturbance.
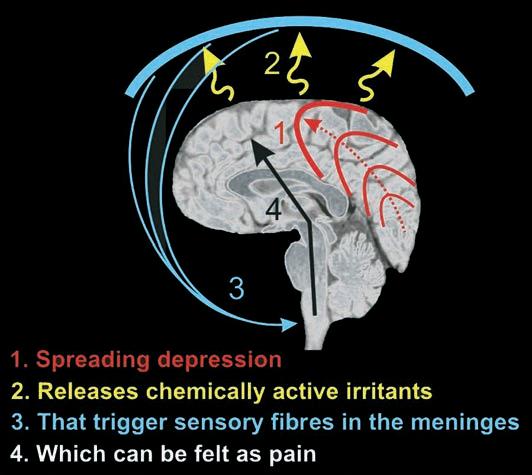
A recent study of 1,800 individuals with mild traumatic brain injury found that 60% experienced headaches fulfilling the diagnostic criteria for acute post-traumatic headache. Half of them went on to have a persistent post-traumatic headache and around 15% were still symptomatic after one year.
It is evident that not everyone with a mild traumatic head injury or whiplash injury will develop a post-traumatic headache. Consistently identified risk factors that predispose to headache development include pre-existing history of migraines or headaches, female gender, younger age, greater severity of the head injury and co-occurring psychological symptoms such as anxiety and depression.
The pathophysiology of why a post-traumatic headache occurs in the first place is complex and an understanding of it is important in order to clearly diagnose and holistically manage individuals with the condition. First, it is important to note that the brain parenchyma is not a pain-sensitive structure and injury to the brain itself does not therefore result in pain. The pain that manifests as a headache is instead the result of pain originating in surrounding structures, such as blood vessels, meninges, muscle fibres, facial
While most individuals with post-traumatic headache improve spontaneously and have a good prognosis, an understanding of the underlying pathophysiology and risk factors is important in order to provide comprehensive and holistic management strategies for the small proportion who have prolonged and disabling symptoms. In that regard, management with pharmacological therapies does not only consist of treatment with analgesics, but may also include painmodulating medications such as tricyclic antidepressants or antiepileptic medication. Furthermore, there is an important role for nonmedication approaches, including cognitive behavioural therapy, relaxation techniques, acupuncture or physical therapy.
It is important to treat and recognise analgesia overuse, which can lead to persistent and worsening chronic headaches. The presence of mood or sleep disturbances can exacerbate the severity and duration of post-traumatic headache and that needs to be recognised and treated. Finally, lawyers and doctors should recognise the potential psychological impact of on-going litigation and perceived injustice, which adds several stressors and could contribute to prolonged recovery.
In summary, while most post-traumatic headaches are short-lived and associated with a good prognosis, a proportion have prolonged and disabling symptoms. An understanding of the complex pathophysiology of post-traumatic headaches and recognition of individual risk factors in those individuals are crucial in order to provide an individualised holistic patient-centred management approach, which may not only include pharmacotherapies, but also interventions such as psychological support, physical therapies or lifestyle changes. q
65 65 www.yourexpertwitness.co.uk
Pathogenesis of primary and post-traumatic headaches
66 66 www.yourexpertwitness.co.uk
NEW GUIDANCE CLARIFIES POSITION ON INDEMNITY FOR DENTISTS
[REVISED GUIDANCE from the General Dental Council (GDC) for dental professionals on the issue of indemnity and insurance came into effect on 12 February.
The new guidance came out of a consultation carried out last year to ensure it is up-to-date and better supports dental professionals to understand and meet their legal and regulatory obligations, in the interest of patients and maintaining public confidence in the profession.
The GDC explained: “Although the updated guidance does not introduce any new requirements for dental professionals, it clarifies the requirements around holding cover that will compensate patients who have suffered harm, in the event of a successful claim. The updated guidance also encourages dental professionals to consider the level of cover they require across their scope of practice.
“The guidance includes a checklist and series of questions for dental professionals to consider when choosing an indemnity or insurance cover – all of which is there to make it easier for dental professionals to decide on the type and level of cover they’ll
need to protect themselves and their patients. The guidance also explains the additional benefits that dental professionals should consider when arranging their indemnity, such as including advice and support for their wellbeing during a claim.
“Updates to our guidance reflect our wider ambition to promote professional behaviours, skills and attributes across dentistry. With the Guidance on Indemnity and Insurance, we aim to encourage professionalism and decision-making about the choice of cover that is in the best interests of patients.”
Dental professionals are required by law to have appropriate indemnity or insurance in place before they practise. That is to ensure any patient who suffers harm during treatment can seek appropriate compensation. The GDC is encouraging dental professionals to familiarise themselves with the updated guidance as it now provides more information to better support them to meet their responsibilities towards patients.
The GDC added: “We received a good number of responses to our consultation from a range of stakeholders, including dental professionals and providers of indemnity and

insurance, with most welcoming the proposed changes to the guidance. We also received much valuable feedback and suggestions for improvements, all of which has helped shape the finalised revised guidance that we publish today.” q
DENTISTS ATTACK GOVERNMENT’S RECOVERY PLAN
[ THE BRITISH DENTAL ASSOCIATION (BDA) has described the recent Recovery Plan for NHS dentistry as ‘unworthy of the title’, given its ‘failure to break with the discredited contract fuelling the exodus from the NHS workforce’.
According to the BDA, there are currently a record number of dentists registered to practise with the General Dental Council, but the number of dentists undertaking NHS activity in England has fallen to levels not seen since 2016/17.
“There is no evidence that overseas dentists are any more willing to maintain a long-term commitment to the failed system of tick boxes and targets than their UK counterparts,” the BDA said.
BDA chair Eddie Crouch commented: “A broken contract is forcing dentists out of the NHS with every day it remains in force. Overseas dentists are no more likely to stick with a failed system than their UK colleagues. Ministers need to stop trying to fill a leaky bucket and actually fix it.”
“The claims made by government on the ‘millions’ of new appointments created by the Recovery Plan are ‘not recognised’ by the BDA, and the Department of Health and Social Care has still not published any of the modelling underpinning the numbers.
“There are no measures in the plan that increase capacity in the struggling service, or that are likely to bring dentists back to the NHS.” q
67 67 www.yourexpertwitness.co.uk

RADIOGRAPHER OR RADIOLOGIST: WHICH IS MOST APPROPRIATE FOR

YOUR NEGLIGENCE CASE?



 By Kathy Priday, Clinical Diagnostic Radiographer and Mammographer, Expert Witness
By Kathy Priday, Clinical Diagnostic Radiographer and Mammographer, Expert Witness
[IN CASES OF NEGLIGENCE, misdiagnosis, verification of correct diagnosis or breach of duty and causation, it can be quite complicated to discern which type of expert is most suitable.
It is helpful to understand the difference in skills and roles of both radiologists and radiographers and their specialist branches. I offer consultation prior to writing a report, to establish that it is my specific specialism that is required – and am always happy to recommend otherwise as appropriate.
Radiologists
Radiologists are medical doctors who work with the images acquired by the radiographer via a variety of medical imaging techniques such as X-rays, MRIs, CT etc, to support the diagnosis and treatment of certain conditions and injuries. There are various types of radiologist: general diagnostic radiologists, interventional radiologists, paediatric radiologists, radiation oncologists and more.
There are several different specialties of radiology, each of which plays a different role in medicine. For example, a diagnostic radiologist helps support diagnosis and treatment, while an interventional radiologist uses imaging to guide and perform interventional procedures.
Radiologists are primarily responsible for image interpretation, supported by a typed, signed report, and working with other doctors/specialists to diagnose and offer guidance to advise on treatment and management of a wide range of conditions and injuries.
Radiographers
Radiographers are highly-qualified medical professionals and fall into two distinct categories:
Therapy radiographers operate a range of specialised equipment to deliver accurate doses of radiation to tumours, to destroy diseased tissue. They are extensively involved at all stages of the patient’s radiotherapy journey, from pre-diagnosis to treatment options.
Diagnostic radiographers operate various imaging systems to capture images of a patient's internal organs, muscles, joints and other parts of their body, using many different types of specific imaging systems.
The types of images obtained include general X-ray, ultrasound, MRI, CT (including a specific specialty of post-mortem CT) and mammography. Those images are then used to assist doctors in diagnosing diseases and injuries to determine the future management of a patient’s condition. Some radiographers have further specialised in image reporting and interpretation.
Radiographers are primarily responsible for:
• Producing quality images, which include all the necessary ‘pictorial’
• information to assist the radiologist or reader to make an accurate and
• correct diagnosis
• Having the knowledge to operate a wide range of imaging devices
• Ensuring that all health and safety protocols are adhered to
• Verifying that the request is appropriate in accordance with the clinical
• request
• Verifying that all patient details are correct
• Obtaining patient’s permission to carry out the examination and obtaining
• their signature in cases of possible pregnancy
• Managing patient confidentiality and always preserving dignity
• Appropriately preparing patients in accordance with the type of imaging
• requested and giving a full explanation of the procedure
• Ensuring that the radiation dose is as low as reasonably possible to
• produce an image of diagnostic quality
When a radiologist is required and not a radiographer
Dear Ms K Priday,
We may have a potential instruction in relation to the above case reference. Please note case details:
The claimant suffered sprains to their left neck, lower back and their left ankle as well as abrasions to their left elbow. The claimant has seen an emergency medical expert who completed a report recommending the claimant’s radiology images of their L3 vertebrae be reviewed to conclude whether they sustained a fracture or not.
[We] require a radiology expert to review the claimant’s radiology images of their L3 vertebrae and compile a report concluding whether the claimant did or did not sustain a fracture.
Please advise if you’re able to assist. If so, please confirm fees and availability.
In the above situation I was not able to accept the case as I am not qualified to report on clinical images.
When a radiographer, qualified as a mammographer, would be specifically required and not a radiologist
The following instruction was received and an expert witness report was requested, based on breach of duty and causation. The claimant had stated that the cardiac loop recorder (CLR) inserted in her breast was crushed during the mammogram.
Please consider whether the force used to perform the mammogram would amount to a breach of duty and negligence.
The key word to consider here is ‘perform’. That is an indication that the expert witness would be required to comment on the imaging procedure itself and not to determine a clinical diagnosis based on the resultant images. To write such a report would necessitate a written explanation to be given of how to perform a mammogram, according to guidelines from the Society of Radiographers’ Statements for Professional Conduct (SoR, 2002).
An explanation needs to be written for the report as to how a mammogram is performed and according to what criteria. That can only be given by a radiographer qualified as a mammographer. A radiologist would not be able to do so as it is not in their skill set.
A mammogram is an X-ray of the breast(s) and successful mammography is dependent on the performance of the equipment, the expertise of the mammographer and the co-operation of the participant. The skills of the mammographer and other factors associated with the
70 70 www.yourexpertwitness.co.uk
person undergoing the examination affect the quality of the mammogram.
The expert response was: “According to the information presented to me and having reviewed the pre-examination mammography questionnaire, the procedure was followed in accordance with that of any other qualified mammographer. The presence of the CLR [cardiac loop recorder] was documented, the number of years that it had been in situ was stated as three years and, as with any other type of medically implanted device, its presence does not contraindicate the performance of a mammogram. The procedure remains as standard for any mammogram.
Based on the documented evidence provided to me it is my opinion that xxxx did not fall short of the expected standard of care. I cannot comment on the expected standard of care provided by any other clinicians involved.”
When a radiographer would be required and not a radiologist
This is an extract from an inquiry letter that I received requesting an expert witness report to be prepared on the standard of care received.
Dear Ms Priday,
I act on behalf of xxxx, who lives in xxxx and who sustained burns to her right lower leg in May 2022 during an MRI scan at an MRI unit owned and operated by xxxx.
We are instructed that, before the scan started, our client was not advised to remove her leggings and whilst she was undergoing the scan she felt a burning sensation and informed the radiographer, who replied that there was nothing wrong.
I would be very grateful if you could please let me know if you are in a position to act on behalf of our client and prepare an expert report on the procedure, and standard of care, provided by the radiographer in respect of the MRI scan, particularly around the necessity for the removal of leggings
In the request, the reference is specifically made to the procedure itself. This report requires the skill set of a radiographer who has
specialist knowledge of how an MRI scan should be performed, and the health and safety rules that must be adhered to.
A radiologist would not be able to write the report as it is not in their skill set. Their knowledge would be required if the report was related to a possibility of a missed or incorrect diagnosis based upon the images presented to them.
When a radiographer may be required as well as a radiologist
The case study below also serves to illuminate to solicitors how to determine when to instruct a radiographer not a radiologist.
Dear Ms Priday,
I hope you are well. I am instructed by xxxx to obtain independent expert evidence on breach of duty and causation from a radiographer to inform the decision on liability in this case.
Briefly, it is alleged that the machine used for the claimant’s MRI scan was too small, causing pain and burns in my claimant’s shoulders, arms, crashed nerves and whiplash.
I write to see if you would be able to accept instructions to prepare a short-form screening report commenting on the allegations of breach of duty
This report can only be written by a radiographer, as it is specifically referring to the positioning of the claimant within the MRI scanner.
A radiologist would be unable to write such a report as they are not themselves positioning the claimant and would not have the requisite knowledge. Had the request been solely based upon the part of the sentence ‘causing pain and burns in his shoulders, arms, crashed nerves and whiplash’ then a radiologist would be required to write a clinical report based upon the information from the images provided following the procedure.
There is a caveat with this request and that is there are radiographers who are further qualified in MRI image interpretation, and they could then write the report based on the entire request. q
71 71 www.yourexpertwitness.co.uk

72 72 www.yourexpertwitness.co.uk
SOME MEDICO-LEGAL ADVICE ON CONSENT FOR MINOR PROCEDURES
By Professor Rotimi A K Jaiyesimi Consultant Obstetrician and Gynaecologist
[CONSENT IS REQUIRED before any type of medical treatment or examination is undertaken and it is required regardless of the procedure. The principle of consent is an important part of medical ethics and human rights law. Minor medical procedures refer to surgeries or interventions performed on superficial tissues, usually without anaesthesia or, when necessary, under local anaesthesia and with minimal invasive equipment. Such procedures are safe and often have few complications.
An example is outpatient hysteroscopy, a minor gynaecological procedure which involves examining the uterine cavity with the hysteroscope. The procedure is done in the outpatient clinic, usually without general anaesthesia or sedation and is used to investigate abnormal uterine bleeding. Though it is safe, quick, and with relatively few complications, complications can occur and these risks must be discussed with the patient. They include infection, bleeding, perforation of the uterus, damage to abdominal viscera and, rarely, death.
Current practice with regard to consent
The British Society for Gynaecological Endoscopy (BSGE) has a procedure-specific Outpatient Hysteroscopy Consent Form that details the risks associated with the procedure. It is common for clinicians not to document the risks of minor procedures in the clinical notes or complete the consent form prior to the patient attending for the procedure. The patient information developed by the Royal College of Obstetricians and Gynaecologists (RCOG) in 2018 states that ‘on arrival you will meet your healthcare professional, who will discuss the procedure and ask for your consent’.
The dilemma occurs when patients arrive in the outpatient procedural clinic and state that the risks of the procedure were not discussed with them in the general clinic prior to being referred. The practitioner in the procedural clinic has the option of carrying out the procedure without further counselling and consenting, or discussing the risks and benefits at that stage. However, the time required to undertake the latter is not factored into the time allocated for patients.
I proffer that the RCOG/BSGE patient information published six years ago may no longer satisfy the legal requirement for informed and valid consent and needs to be revisited. It is also noteworthy that the RCOG Obtaining Valid Consent, Clinical Governance Advice No 6, published in January 2015, states that ‘in the modern NHS, efficiencies such as placing patients directly onto waiting lists and admitting patients to hospital on the day of operation require careful attention to the organisation of consent. These initiatives have the potential to shorten or even eliminate the cooling-off period during which a woman can reflect on her condition and the proposed treatment options. Deferral must be retained as an option in the best interests of patient care even if it means that their procedure is postponed’.
Paradoxically, the RCOG makes a disclaimer that the ultimate implementation of a treatment plan must be made by the doctor after the valid consent. Effectively, the ball lies in the court of the clinician to obtain informed and valid consent prior to the day of the operation.
What is medical consent in the eyes of the legal system?
Failure to obtain consent can be construed as ‘battery’, which in law refers to an intentional and unlawful act that causes harmful or offensive physical contact with another person. Respect for patient autonomy and ethical consent are essential in medical practice, ensuring trust between patients and healthcare providers.

Hospitals have administrative practices where patients are pooled and the surgeon who carries out the procedure may not be the practitioner who took the decision to offer the patient the surgical procedure. In situations where the counselling and consenting process did not take place in the clinic, some patients arrive in the procedural clinic for the surgical intervention stating that they are not aware of all the risks as these were not discussed at the initial consultation. As those procedures are not emergencies, it raises the question as to whether it is appropriate to undertake the counselling prior to the procedure.
Going forward
Clinicians have a choice to make a compelling case for added clinical times per patient to allow for the consenting process. Failure to do so exposes them to potential negligence claims. The GMC does not accept time constraint as an excuse for inadequate consent.
As a clinician and expert medical witness, I advise that clinicians err on the side of caution in the face of the ambiguity that surrounds obtaining consent for outpatient procedures. It will be good practice to ensure informed and valid consent has been obtained for minor outpatient procedures by ensuring that the process is initiated and conducted when the decision to perform the procedure is taken in the clinic. The legal implication is that failure to obtain valid consent can result in criminal assault or civil claims.
The medico-legal advice on consent for minor procedures needs further discussions between clinicians, specialty organisations and the legal practitioners. If the changes required are not drawn up by clinicians, there may come a time when the practice will be changed by case law, as is in Montgomery v Lanarkshire Health Board [2015] UKSC 11. q
• Professor Rotimi Jaiyesimi is the Group Associate Medical Director and Consultant Obstetrician and Gynaecologist at Mid and South Essex University Hospitals.
He is a GMC medical expert witness, CQC maternity assessor and an NHS National Patient Safety Specialist. He is Visiting Professor of Law at the University of Ibadan, Nigeria and is an experienced expert witness providing expert opinion in obstetrics and gynaecology.
73 73 www.yourexpertwitness.co.uk

74 74 www.yourexpertwitness.co.uk
HAND SURGEONS RAISE CONCERNS OVER STERILE IMPLANTS
[ ON 28 NOVEMBER the British Society for Surgery of the Hand (BSSH) issued a statement concerning sterile implants in hand and wrist surgery, which forms the current expert opinion of the BSSH.
In the statement the BSSH says: “We recognise concerns exist around the re-processing of so-called single-use items and the difficulties in implant traceability that non-sterile implants on an implant tray may cause. However, it is the clinical opinion of the BSSH that a move to sterile packed implants in hand and wrist trauma surgery will unavoidably compromise surgery and the clinical outcome.
“There has been a recent push towards sterile packed implants on orthopaedic implant trays. The driver for this is recent legislative changes around medical device regulation and concerns regarding infection as well as theoretical risks of corrosion and the secondary concerns around increased infection risk. These have not been proven clinically.”
The BSSH identified ‘significant and unacceptable clinical risks’ surrounding the use of pre-packed sterile implants in hand and wrist surgery, all leading to an increased risk of patient harm.
They include:
• Increased operative time with the associated added risks of infection and ischaemic tourniquet damage
• Increased difficulty in operative fracture reduction
• Increased difficulty for scrub staff
• Impossibility of optimal implant selection
• Increased risk of appropriate implant unavailability
• Requirement for additional stock management and supply
• Massive increase in plastic waste and reduced sustainability
• No demonstrable or proven benefit for hand surgery patients
The statement continued: “As a specialist society representing the views of hand and wrist surgery experts across the UK, we have made huge improvements along the principles of Getting It Right First Time (GIRFT). The move to sterile packed screws goes against these principles, making hand surgery considerably more difficult to get it right first time. Furthermore, we do not acknowledge the theoretical risks of infection secondary to resterilised implants – this has not been a recognised clinical problem in the history of fracture surgery. However, we have vast experience of the difficulties this directive will cause for the safe and effective treatment of hand and wrist trauma patients.
“The BSSH recommends that any plans to move to sterile packed implants are only made with the full agreement of the relevant stakeholders after an appropriate consultation process. It is imperative
that theoretical risks of harm are not attributed a greater importance than the demonstrable risks described above.”
The BSSH is to commission a full review of the issues surrounding sterile packed implants, with particular reference to hand and wrist trauma surgery. The full report of the working group will be available later this year. q
75 75 www.yourexpertwitness.co.uk

76 76 www.yourexpertwitness.co.uk
HAIR TRANSPLANT GUIDELINES
BY CROSS-NATIONAL SURGERY BODIES

[ THE British Association of Hair Restoration Surgery (BAHRS), the British Association of Aesthetic Plastic Surgeons (BAAPS), the British Association of Plastic, Reconstructive and Aesthetic Plastic Surgeons (BAPRAS) and the Turkish Society of Plastic, Reconstructive and Aesthetic Surgeons (TSPRAS) have issued a joint statement on patients travelling abroad for hair loss surgery.
There has been a significant increase in the number of people travelling abroad for hair transplant surgery, the statement says.
BAAPS and BAPRAS support the BAHRS position that hair transplant surgery for male and female pattern hair loss is a treatment for a diagnosable genetically caused and hormonally mediated medical condition, and in the majority of cases should not be considered ‘cosmetic surgery’.
It is, however, important that members of the public understand that hair transplant surgery is not without risk. While the chances of lifethreatening complications are less than with general plastic surgery procedures, they still occur. Appearance related complications are more common and can have a significant psychological impact on patients.
The BAHRS, BAAPS, BAPRAS and TSPRAS have issued the joint statement to promote patient welfare and safety.
The statement continues: “The BAHRS, BAAPS, BAPRAS and TSPRAS understand and recognise that there will always be patients from different countries who will seek medical and surgical treatments abroad. There are a variety of reasons for this, but multiple reports have highlighted concerns that our four national societies share regarding minimum standards of patient care.
“Undergoing any form of surgery risks experiencing a complication; however, when having hair transplant surgery, these can be minimised if the surgery is agreed and planned ahead of time by the doctor who will be doing it and if the surgical steps of the procedure are performed by a doctor rather than a technician.”
The four organisations strongly urge anyone from the UK
considering travelling to Turkey for hair transplant surgery to consider the following points:
• Patients should have a consultation with the doctor who will be performing the surgery and who will make the recommendation on donor hair harvesting method, number of follicular units/hairs required, and hairline/transplant design.
• Patients should be given two weeks to consider the doctor’s recommendation and the proposed consent form before making any form of payment for surgery.
• Patients should be explicitly informed at the initial consultation if it will not be a doctor operating on them by making skin incisions to harvest the donor hair or implant it, including whether this will be a technician.
• The interim progress and final result of the hair transplant should be assessed by the doctor who performed the surgery and patients should have the opportunity to voice any grievances they have as well as a clear process for complaints.
• Systems should be in place for complications to be dealt with by the clinic during and outside of working hours, such as assessing skin necrosis, infection, cysts or dysaesthesia, and supplying antibiotics.
President of the BAHRS, Chris D’Souza, said: “Whilst in the United Kingdom patients can report suboptimal care by doctors (including inappropriate delegation of surgery) to the General Medical Council and unregistered clinics to the CQC (or the equivalent regulatory bodies in the devolved nations), this is not always the case in other countries.
“The BAHRS, BAAPS, BAPRAS and TSPRAS have come together to offer advice and guidance for patients seeking hair transplant surgery in Türkiye (Turkey), which has a large hair transplant surgery tourism industry. The aim of this guidance is to help to protect patients from harm and ensure that they are aware of the standards of care (both before and after surgery) that they should expect as a minimum.” q
77 77 www.yourexpertwitness.co.uk
PUBLISHED
WHAT PROBLEMS ARISE FROM ABLATION TREATMENTS FOR VARICOSE VEINS?
By Philip Coleridge Smith DM MA BCh FRCS Consultant Vascular Surgeon, Medical Director of the British Vein Institute and Emeritus Reader in Surgery at UCL Medical School
[ A RANGE OF TREATMENTS are in use for the management of varicose veins in the UK and throughout the world. In the UK most varicose veins are currently treated by ‘thermal ablation’ treatments, in which heat is applied to the troublesome veins in order to destroy them. Another commonly used treatment is foam sclerotherapy: a modern enhancement of injection treatment for varicose veins. Surgical treatment in the form of ‘stripping’ varicose veins has largely been abandoned, since it leads to significant pain, bruising and discomfort following treatment.
How does thermal ablation work?
In thermal ablation techniques heat is applied directly to the varicose veins via a catheter passed along the vein. The heat source is either radiofrequency electrical energy (RF ablation) or a laser (laser ablation). The saphenous veins, in which varicose veins develop, run longitudinally along the leg and visible varicose veins arise directly from those.
The heating catheter is introduced into the great saphenous vein over the inside of the knee, where the vein runs reasonably close to the skin. It is then passed upward towards the conclusion of the saphenous vein where it joins the main, femoral vein in the groin.

Sometimes the small saphenous vein on the back of the calf is affected by varicose veins and it too can be managed by thermal ablation. The treatment is usually done under local anaesthetic by infiltrating along the track of the vein with an anaesthetic solution. That avoids the need for general anaesthesia.
Varicose veins arising in tributaries of the saphenous vein can be managed by injection treatment or by ‘phlebectomies’ – a small operation to remove the troublesome veins. The outcome is that patients can leave the treatment room soon after conclusion of the operation and can go home.
Post-operative discomfort is modest and can be managed by simple analgesics. Rapid recovery and return to normal activities is usually the outcome. It has been shown that these treatments lead to enduring freedom from varicose veins in most patients.
Problems with thermal ablation
In general, the outcome from the treatments is very satisfactory and few problems arise. However, I have advised in a number of cases where adverse outcomes have been encountered – in some cases leading to lifelong problems with pain in the leg.
RF ablation requires a catheter which treats the vein at a temperature of about 120oC. In laser ablation, it is estimated that the temperature in the region of treatment reaches as high as 800oC. Human tissues are readily destroyed by temperatures of that magnitude, accounting for the efficacy of thermal ablation methods. The heated tissues are usually irreversibly destroyed. Veins treated in that manner are reabsorbed over a period of a few weeks without the need to remove them. However, unintentional heating of nearby structures may lead to adverse events.
Two types of tissue lie in the region of varicose veins: the skin overlying the veins and the cutaneous nerves supplying sensation
to the leg. Caution has to be taken to ensure that neither tissue is damaged during varicose vein treatments. The tissues are protected during thermal ablation surgery by using local anaesthetic in a form known as ‘tumescent anaesthesia’.
The anaesthetic is diluted in a larger volume of saline, which is infiltrated around the vein to be treated. The anaesthetic is effective in removing any sensation from the vein and the volume of solution provides thermal insulation around the vein. That prevents heat applied to the vein reaching the skin or nearby nerves. In general, this strategy is very effective in providing anaesthesia and thermal insulation.
Complications of treatment leading to litigation
All varicose vein operations may give rise to post-operative bruising and discomfort, as well as to deep vein thrombosis on rare occasions. Pre-operative counselling of patients should include those features of treatment.
The risk of skin burns following thermal ablation is very small, assuming appropriate measures are taken. Sometimes varicose veins run very close to the skin, in which case thermal treatments are probably inadvisable. Alternative methods such as foam sclerotherapy can be used for veins running close to the skin.
Skilled practitioners will inject a substantial layer of local anaesthetic between the skin and nearby vein in order to prevent the heating effect reaching and damage the skin. In RF ablation treatments, the manufacturers recommend that the catheter inside the vein is compressed against the vein by local manual compression applied to the limb. That may obscure the fact that the skin has been heated excessively as the vein is heated.
These problems may give rise to skin burns overlying a section of successfully treated vein. Often the main purpose of treatment is cosmetic improvement, but that will be substantially impaired should regions of skin burn arise. The skin may need to be excised leading to a permanent scar in the limb.
78 78 www.yourexpertwitness.co.uk
Treatment of the great saphenous vein using a combination of laser ablation of the saphenous vein and foam sclerotherapy of the tributaries.
The cutaneous nerves to the limb run close to the saphenous veins which are the source of varicose veins. The saphenous nerve runs alongside the great saphenous vein in the calf; however, it is well separated from the vein in the thigh. In general, thermal ablation to the great saphenous vein is limited to the region of vein at the knee and in the thigh. Thermal ablation of the saphenous vein in the calf may result in thermal injury to the nerve, leading to severe and permanent neuropathic pain from this nerve, as well as loss of sensation in the calf.
Similar problems may be encountered where the small saphenous vein on the back of the calf is heated below the mid-calf level. These problems are well-documented in published literature and cautions have been issued in practice guidelines from a number of sources. Where such advice has been ignored and adverse outcomes have been experienced, claimants may assert that avoidable pain and suffering has been experienced which would have been prevented had published guidelines been heeded.
Patients should receive verbal and written advice concerning adverse outcomes in varicose veins surgery prior to treatment. If the problems of skin burns and neuropathic pain have been omitted from such advice, it may enhance the ability of claimants to show that substandard care has been provided.
Conclusion
Thermal ablation treatments for varicose veins remain safe and effective methods of achieving symptomatic and cosmetic improvements in patients with varicose veins. However, the cosmetic outcome of treatment may be adversely affected by unintended skin burns. Where thermal damage occurs to cutaneous nerves, permanent neuropathic pain may arise in the leg, leading to substantial loss in quality of life. Patients affected by those problems often seek redress through the civil courts. q

79 79 www.yourexpertwitness.co.uk
80 80 www.yourexpertwitness.co.uk
MEDICAL STUDENT’S INVENTION WILL HELP REDUCE CHEMO PAIN
[ A FIFTH-YEAR STUDENT DOCTOR at the University of Liverpool School of Medicine has embarked on a mission to alleviate discomfort and pain associated with chemotherapy, leading to the creation of innovative cooling gloves and boots for cancer patients.
Over the past year, Emily Kelly (pictured) has been the driving force behind the project at Clatterbridge Cancer Centre, which has sites in Liverpool and The Wirral. The cooling mittens and boots are aimed at patients undergoing certain types of chemotherapy in an attempt to reduce the associated complications. The inspiration for this project struck Emily during her fourth-year oncology placement when she discussed her own mother’s treatment with a doctor.
While observing oncology consultant Dr Rick Walshaw’s clinic last year, Emily mentioned that her mother was receiving chemotherapy and was concerned about the potential side effects, one of them being peripheral neuropathy.
Peripheral neuropathy, a common side effect of certain chemotherapy drugs, causes nerve damage to the fingers and toes and can be incredibly debilitating, with potential permanent pain. Emily’s research led her to discover that some patients in the US were using cold therapy during their chemotherapy infusions to alleviate the effect. It works by minimising blood flow to the extremities with the aim of lessening the amount of chemotherapy drug reaching those areas, therefore reducing the risk of neuropathy.
Emily realised this service wasn’t offered in the UK and there were no large-scale studies looking into its success. Driven by her desire to help cancer patients like her mother, Emily shared her idea with Dr Walshaw.
She recalled: “Little did I know I was speaking to a member of the hospital’s CREATE team, which is a peer support group for staff in the

trust who have an idea for a project but don’t have any background in research and don’t know where to start.
"So, Dr Walshaw took my idea and ran with it, taking it to the CREATE group where they jumped through all the necessary hoops to begin the first part of the research – a feasibility study, which has just finished.”
As the project is being trialled, positive outcomes have been reported in participants taking part and the feedback is promising, which certainly brings hope to patients.
Reflecting on her experience and thinking to the future, Emily said: “Prior to this journey I didn’t think my career path would involve much research. However, having now seen how one of my ideas has snowballed into a potentially very impactful project, I can definitely see myself getting involved in research and plenty of quality improvement projects in the future.” q
SAFETY ALERT ISSUED RE UNIVERSAL CANNULA CONNECTOR FOR PAIN RELIEF ADMINISTRATION
[ A NATIONAL PATIENT SAFETY ALERT has been issued by the NHS England National Patient Safety Team, co-badged by the Association of Anaesthetists, Royal College of Anaesthetists and the Safe Anaesthesia Liaison Group, instructing all relevant NHS-funded providers to transition to NRFit connectors for all intrathecal and epidural procedures and delivery of regional blocks.
The National Patient Safety Alert instructs all relevant NHSfunded organisations to complete the transition to using these safer connectors by 31 January 2025.
The NHS has long used a range of medical devices with the universal Luer connector to administer medicines via different routes of administration, including the intravenous, intrathecal and epidural routes.
That commonality of connector carries significant risk of accidental wrong route administration of medication. The potential for a fatal outcome from that is well known, especially if medication intended to be administered via a vein (intravenous administration) is wrongly injected into the spine (intrathecal or epidural administration). Previous patient safety alerts have been issued to support providers and staff to reduce that risk.
To overcome the issue NRFit, a dedicated standard connector for procedures and medicines administration involving the intrathecal and epidural route, was developed. A full portfolio of these NRFit devices is now available for use across the NHS.
NRFit devices are not compatible with Luer connectors, reducing the risk of medication being delivered by the wrong route. For example, medication prepared for intravenous administration in a syringe with a Luer connector cannot be accidentally connected to a device that will deliver the medicine via the intrathecal or epidural route, as the cannula in the patient will have a NRFit connector, preventing connection. q
81 81 www.yourexpertwitness.co.uk
82 82 www.yourexpertwitness.co.uk
AMBULANCE LEADERS VOICE CONCERNS OVER RIGHT CARE, RIGHT PERSON
[THE Association of Ambulance Chief Executives (AACE) has warned that both patients and paramedics are coming to harm following the roll out of the Right Care, Right Person (RCRP) initiative that sees police forces reducing, or in some instances altogether stopping, responding to mental health related calls.
According to a policy document published jointly by the Department for Health and Social Care and the Home Office: “Right Care, Right Person is an approach designed to ensure that people of all ages, who have health and/ or social care needs, are responded to by the right person, with the right skills, training and experience to best meet their needs.
“At the centre of the RCRP approach is a threshold to assist police in making decisions about when it is appropriate for them to respond to incidents, including those which relate to people with mental health needs.”
Figures analysed by the AACE reveal that London Ambulance Services are now receiving up to 250 calls daily which have been transferred from the police, and in some cases police have not attended incidents that have resulted in harm coming to the patient and/or clinician.

It said: “Nearly all of these people do legitimately have a healthcare need and the NHS is better placed to meet this than the police were, but most of the patients did not need an emergency ambulance.”
In a letter to Steve Brine, chair of the Commons Health Committee, the AACE, which represents all ambulance trust chiefs in the country, said: “To date this is the single biggest feedback theme we have heard from ambulance services, with some control room staff describing feeling like they’re in a ‘high stakes game of chicken’ where the police have refused to attend and told the caller to hang up, redial 999 and ask for an ambulance.”
AACE warned: “We are concerned by reports from ambulance services of occasions where the police have not attended incidents when requested to provide support that have subsequently resulted in patient harm or ambulance clinicians being assaulted.”
Addressing the speed of the roll-out, the letter continued: “We are surprised that such a significant system change – with such clear risks for some of the most vulnerable people in society – has gained so much momentum in the absence of a full understanding of the impact. But in this context, it becomes even more important for police forces to implement RCRP in line with the principles of the NPA, in a true spirit of partnership, in a way that enables health systems to build the capacity needed to ensure the continuity of public safety.”
Gemma Byrne, policy and campaigns manager at mental health charity Mind, said: “These reports from frontline ambulance staff are extremely troubling. When someone is experiencing a mental health crisis they need timely and effective care as soon as possible. We know the police are not always the most appropriate people to support someone in these situations, but keeping people safe is part of core police business and this can’t change: an emergency is an emergency.
“We are extremely worried about the pace at which Right Care, Right Person is being rolled out across the country and how the changes will play out in practice. We know that many agencies have faced decades of underfunding and are struggling to keep pace with the surge in demand for mental health support. But at the centre of this are people in a deeply distressing mental health crisis, and we cannot risk people falling through the gaps between agencies.
“The UK government needs to slow down the roll-out of Right Care, Right Person, and allow the time and funding necessary to ensure agencies can work together to put the needs of people with mental health problems first.” q
83 83 www.yourexpertwitness.co.uk

EXPERT IN MIND UNVEILS GAME-CHANGING SISTER VENTURE
[EXPERT IN MIND has introduced a new venture: The ADHD Clinic. Recognising the increasing demand for ADHD assessments and the prolonged waiting lists within the NHS, they are ‘thrilled’ to offer a solution.
With almost 16 years of experience in organising mental health assessments and providing ADHD assessments through the clinical division of its business, establishing a dedicated clinic was a logical step forward for the mental health expert witness agency. The endeavour reflects their commitment to addressing the growing need for accessible and timely ADHD assessments, ensuring individuals receive the care they require without unnecessary delays.

Dr Sajid Suleman (above), a dedicated consultant psychiatrist with a wealth of experience in diagnosing ADHD since 2008, stands as a passionate advocate for the subject. Driven by a commitment to delivering assessments of the highest quality in adherence to NICE guidelines, he will be at the helm of a distinguished team comprising 15 accomplished psychiatrists and psychologists. Together, they share a collective dedication to ensuring excellence in ADHD assessments and contributing to the well-being of those seeking their services.
For adults, the service offer two tiers of assessment. Tier 1 is a multi-disciplinary assessment: the client has an appointment with a psychologist and then an appointment with a psychiatrist. They will complete a joint report giving a comprehensive and nuanced perspective.
Neurodevelopmental difficulties are largely cognitive constructs diagnosed based on mainly observable behavioural symptoms. In simple terms, neurodevelopmental difficulties are problems with how our brain develops and experts figure that out mainly by looking at how people behave in certain situations.
A psychologist can carry out various psychometrics and can also complete cognitive assessments to look at impairments associated with ADHD. Their extensive training in behavioural and cognitive theory allows for a more in-depth evaluation, ensuring a holistic understanding of an individual’s challenges.
A psychiatrist, with their medical training, brings a unique viewpoint to the assessment, examining aspects from a clinical physiological standpoint. A psychiatrist is medically trained and will undertake a structured medical assessment of the client’s mental health and psychiatric history. It means that the doctor will look at other health conditions, especially mental health conditions, which may either exist alongside possible ADHD or instead of ADHD. For example, if people have depression and/or anxiety that is not responding to standard treatments, sometimes it is because ADHD is present and needs to be treated first to enable other conditions to be treated subsequently.
The collaboration between a psychologist and a psychiatrist, supplemented by input from a trusted, familiar person and the completion of targeted questionnaires, is exceptionally thorough. It offers patients a more detailed understanding of their presentation, diagnosis, behaviours and cognitions, enhancing the overall quality of care and paving the way for a tailored intervention plan.
That thorough approach facilitates personalised support for the patient’s journey: a psychologist making in-depth and specific recommendations for work and/or education focusing on the social, emotional and practical difficulties associated with ADHD; a psychiatrist recommending and prescribing medication based on an assessment of its potential benefits, diligently monitoring its effectiveness and observing progress and improvements to ensure optimal outcomes.
For those seeking a more expedited process and a concise report, The ADHD Clinic has introduced Tier 2 assessments. In this streamlined approach, assessments are conducted solely by a psychiatrist. While the medical expertise ensures a high standard, it may not delve as deeply as the Tier 1 assessments, where both a psychiatrist and psychologist collaborate to provide a more comprehensive perspective. Opting for a Tier 2 assessment offers a quicker route without compromising quality, catering for individuals who prioritise efficiency in their evaluation process.
When catering for children, the team boasts highly-experienced child and adolescent psychiatrists committed to delivering meticulous and comprehensive assessments. Beyond a structured interview, the approach involves a thorough examination of school records and medical histories, and in-depth discussions with parents. To ensure a comprehensive understanding, questionnaires will also need to
be completed. The ADHD Clinic’s dedication to the holistic evaluation of each child underscores their commitment to providing the highest standard of care in the assessment process.
The ADHD Clinic has also introduced the inclusion of QbTests in their services – a computer-based diagnostic screening tool that meticulously gauges the three core symptoms of ADHD: activity, attention and impulsivity.
Beyond initial assessments, QbTests prove to be exceptionally valuable in monitoring the impact of prescribed medications on an individual's ADHD symptoms. As a cuttingedge method, QbTests are spearheading the evolution of ADHD assessments, offering a precise evaluation of activity associated with ADHD and signalling a progressive approach for the future.

Company director Zofia Ludwig (above) commented: “At the core of our business we uphold values that embody professionalism, knowledge, clarity and respect. Recognising the financial considerations associated with ADHD assessments, we're pleased to introduce a convenient finance option, making the assessment process more accessible. To enhance transparency, we've outlined post-diagnosis costs on our website, detailing expenses related to follow-up appointments, the treatment process and review appointments for individuals seeking ADHD treatment.
“Throughout your journey, rest assured that our dedicated team will provide unwavering support, ensuring you're well-informed and cared for at every step. Your wellbeing is our priority and we're committed to making the entire process as clear and supportive as possible.” q
• To find out more, or to book an assessment, contact the team on office@theadhdclinic.co.uk or visit the website www.theadhdclinic.co.uk

85 85 www.yourexpertwitness.co.uk
IS THERE AN EXPERT IN THE HOUSE?
By Lisa Crowther, Quality Assurance Manager at Carter Brown
[FINDING THE RIGHT EXPERT can be a challenge all of its own. Without sounding like Liam Neeson, every expert comes with their own particular set of skills, built over a number of years within different settings. It can be difficult to make a like-for-like comparison; indeed, experts with very similar skill sets on paper can often take different routes to get to the same goal: a robust, evidence-based assessment.
In this article, I’ll explore how to go about finding an expert and navigating an expert’s CV, to maximise the chances of them being the right person for your client’s assessment.
Finding your expert
A good expert is hard to find. Many of Carter Brown’s clients choose to repeat instruct experts, because of greater certainty as to their abilities, and a capacity to engage with their clients and offer a quality service. That is certainly one way to screw down on some of the variables; however, it can sometimes lead to delays as popular experts can quickly become booked up.
Word of mouth
Experts rely heavily on building a good reputation to secure repeat instructions from solicitor clients. We actively encourage experts to engage in regular training and development activities, including training specific to different types of proceedings and the role of an expert, to ensure that they continue to meet with and exceed clients’ expectations.
While word of mouth recommendations come with the backing of a fellow professional, experts can often find themselves very popular and struggle to navigate the volume of requests from potential clients; and it is important that they have appropriate strategies in place to manage that.
Credentials and experience
Look for professionals with relevant credentials and extensive experience in handling cases similar to yours. Experts should have an understanding of the context in which they are instructed, for example public or private family law proceedings. That helps to enable them to make useful recommendations.
An initial call with an expert can sometimes help to gain a sense of them and their communication style and the approach they might take to an assessment.
Read client reviews and testimonials

to gain insights into the professional's track record and client satisfaction. Positive feedback can be a valuable indicator of a reliable and effective expert.
The expert’s CV
When commissioning an assessment, the CV will usually be most people’s starting point. It’s a reasonable expectation that it will be professionally presented, with a clear and logical flow. It is essentially the expert’s shop window and should be thought of as such. You should expect there to be clarity around:
• The expert’s title
• Their credentials
• Qualifications
• Areas of expertise
• Employment history
• Experience of acting as an expert
• Practical measures, such as insurance and DBS checks
Finding the right expert is a crucial step in case progression. Their expertise can make a significant difference in achieving a fair and satisfactory outcome, with recommendations tailored to a client’s individual circumstances. By conducting thorough research and considering credentials and experience, you can find yourself one step closer to sourcing the right expert.
At Carter Brown, we have over 20 years experience of matching experts to clients’ requirements. Our robust recruitment checks mean that when a client is referred to us for assessment, we’ll narrow down the field of experts for you – allowing you the freedom to choose the most suitable expert. q

86 86 www.yourexpertwitness.co.uk
VIOLENCE AND ABUSE ARE MAIN DRIVERS OF MENTAL
ILL-HEALTH IN WOMEN AND GIRLS
[IN A GROUNDBREAKING SURVEY of psychiatrists, the majority of respondents (59%) say violence and abuse are contributing to mental illness in their female patients. That was the most common cause identified, closely followed by relationship issues (49%) – often caused by coercive behaviour – and home and family pressures (48%) which are also causing significant harm.
The Royal College of Psychiatrists (RCPsych) is calling for government, the NHS and the general public to recognise that these factors are leading to women experiencing poor mental health, and to prioritise providing therapeutic support.
Dr Catherine Durkin, joint presidential lead for women and mental health at the Royal College of Psychiatrists, said: “We have long been aware of the serious harm violence and abuse can do to women and girl’s mental health. Tragically, it is not uncommon for female patients to experience
PSYCHOLOGISTS CRITICISE CLOSURE OF NHS MENTAL HEALTH HUBS
[THE BRITISH PSYCHOLOGICAL SOCIETY (BPS) is calling on the government to urgently fund mental health support for NHS and social care staff, as NHS Staff Mental Health and Wellbeing Hubs, which were set up in response to the pandemic to provide rapid help to traumatised staff, continue to close.
With many staff presenting to the remaining hubs with significant and complex mental health issues, the BPS is highlighting that, without dedicated services, staff will be added to lengthy waiting lists for mainstream mental health services. That could lead to staff taking more time off sick or delaying their return to work, at a time when staff shortages and retention issues are rife.
Most of the funding for the 40 NHS Staff Mental Health and Wellbeing Hubs in England was cut in March 2023, with just £2.3m provided to hubs in July: a fraction of the original £38.5m annual budget. Of the original 40 hubs, 18 have closed since March 2023, a further four are slated for closure at the end of March and a further eight hubs are yet to have confirmation of funding and are under threat of closure. Just eight hubs have confirmed some funding for the year ahead.
Of those hubs that have remained open this year, the majority have offered a reduced service, and snapshots of evidence demonstrate the severity of the issues staff are presenting with.
In the first two months of 2024, one hub has seen its highest number of referrals to date, with 65% presenting with complex PTSD: 67% were managers, leaders and senior clinical practitioners.
In another hub, of the 1,187 people registered for one-to-one support between April and Dec 2023, 78% presented with moderate to severe depression. 30% of users in one hub identified themselves as being senior leaders. In a different hub, in Q4 of 2023-2024, 19% of users were managers or leaders.
Dr Roman Raczka, president-elect of the BPS, said: “Staff at all levels, including senior management, are experiencing unacceptable levels of burnout and distress, presenting to hubs with significant and complex mental health issues that require intervention from experienced professionals. The hubs and equivalent services give all staff quick access to the right support, preventing them from being just another statistic on a waiting list. Instead of investing in these services, they are sadly being dismantled at the time they’re needed the most.” q
long-term abuse that causes serious symptoms, including suicidal ideation or symptoms of psychosis.
“I regularly see patients who are dependent on an abusive partner or family member due to emotional, family or financial reasons. Victims often feel unable to speak openly about such issues, meaning their problems go unnoticed, sometimes for years.
“Not all abuse is physical: psychological abuse also causes extreme harm and casts a long shadow over victims. We need to identify and respond to trauma if we are to reduce the likelihood of women and girls developing mental illness.”
RCPsych also wants ring-fenced funding for independent domestic violence advocates to be placed in every mental health trust, in line with best practice. That should sit alongside an expansion of the evidencebased, Identification and Referral to Improve Safety (IRIS) programme, to support the primary care response to domestic violence and abuse.
Dr Philippa Greenfield, who is also a joint presidential lead for women and mental health at the Royal College of Psychiatrists, explained: “Clinicians often do not realise that violence, abuse and coercive behaviour can have serious mental health implications. This lack of awareness can leave victims undetected and their mental health needs not appropriately addressed.
“As soon as the need arises, victims of domestic abuse should be offered the right support. Access to independent domestic violence advocates is an essential part of this.
“If we carry on waiting until victims reach crisis point, we won’t improve outcomes for women and girls’ mental health. Every victim should know that the NHS is there for them when they need to escape the harm of an abuser.” q
87 87 www.yourexpertwitness.co.uk

88 88 www.yourexpertwitness.co.uk
NEW COURSE COVERS LEGAL ISSUES FOR ORTHOPAEDIC SURGEONS
[THE British Orthopaedic Association
(BOA) is making available a course on the subject of Law for Orthopaedic Surgeons –Avoiding Jeopardy It is a course structured by pre-recorded lectures available six weeks before the delivery day, of case-based discussions and Q&A, which provides broad coverage of the interface between law and the practice of orthopaedic surgery.
The course is specifically designed to highlight potential pitfalls in practice from the medico-legal perspective and to help steer surgeons away from potential jeopardy.
The course is aimed at consultants, SAS doctors and orthopaedic trainees who wish to gain knowledge of the elements of law which underpin various aspects of contemporary surgical practice. It includes:
• Practical advice on how to approach giving evidence in legal proceedings such as coroner’s court
• Advice on practical measures to avoid jeopardy with employers, the courts and the regulator
• A full delivery day of case-based discussion talks with Q&A, including a mock coroner’s inquest

• Pre-recorded material to be watched in advance, which will be available six weeks prior to the course delivery day
The course covers topics of surgical relevance, including consent, gross negligence manslaughter, the Medical Practitioners Tribunal Service and the GMC, blood transfusion refusal, introduction to coronial law and coroner’s court, confidentiality and data protection, clinical negligence and the pitfalls of social media.
Consent: The module will consider the legal background to consent and how surgeons can ensure they comply with it, particularly in the elective setting.
Clinical negligence: The session looks at the criteria to be fulfilled in order to prove clinical negligence with examples of case law.
Medical Practitioners Tribunal Service and the GMC: The module will consider the regulatory role of the MPTS and the GMC
Consent in trauma: The session will cover the McCulloch judgment case examples, an update on consent in trauma in light of the GMC guidance and an update on the most recent Supreme Court cases.
Introduction to coronial law and coroner’s court: This session will give participants an understanding of the coronial system and how this interacts with medicine. The aim is to reduce the mystique behind the coronial system and provide confidence when dealing with coroners and attending the inquest.
Confidentiality and Data Protection: The session deals with the importance of confidentiality in medical care and its ethical and legal basis.
Gross Negligence Manslaughter: An exploration of how the criminal law impacts on clinical practice
Safe social media for doctors: By the end of this session participants will understand the risks of engaging with social media as a doctor, GMC guidance and the ‘online disinhibition’ effect.
All sessions will include case studies. q
• For more information, including course dates and costs, visit the website at www.boa.ac.uk.
89 89 www.yourexpertwitness.co.uk
90 90 www.yourexpertwitness.co.uk
COLLABORATION MOVES NANOTECHNOLOGY CLOSER TO SURGICAL REALITY
[ THE ROYAL ORTHOPAEDIC HOSPITAL is collaborating with MICA Biosystems, a Birmingham-based biotechnology company, to bring its futuristic remote-controlled cell technology closer to clinical trials, to be used in orthopaedic medicine and beyond.
The research will investigate how revolutionary cell-augmenting nanotechnology can be used in regenerative medicine, to help patients with arthritis and osteoporosis after surgery and tendon repairs.
The research is being carried out at the hospital’s Dubrowksy Regenerative Medicine Laboratory in Birmingham, using donated samples from patients for laboratory work, prior to developing a clinical trial. The aim is to move to clinical trials with patients at the end of this year.
Professor Adrian Gardner, consultant spine surgeon and director of research and development at the Royal Orthopaedic Hospital, commented: “We’re thrilled to be working with MICA Biosystems on their pioneering research which has the potential to improve patient outcomes, in orthopaedics and beyond.
“We work closely with world-leading industry partners to ensure that our patients have access to the very latest innovations in orthopaedic care and it’s brilliant to be collaborating with MICA who are also based in Birmingham – it’s a testament to just how much innovation is taking place right here in the Midlands.”
MICA Biosystems’ groundbreaking technology is able to remotely give instructions to individual cells inside the body, by binding magnetic nanoparticles to the surface of the chosen cells and then controlling them with an external magnetic field, worn as a bandage by patients following their surgery.
The ‘instructions’ can be migration signals (telling the cell which direction to travel), which is useful, for example, for tendon repairs or tissue ‘messages’ which create specific tissue inside a patient – for example a higher density of bone cells where the patient has a lower density of bone, such as patients with scoliosis or other back issues.
Dr Michal Zurawski, chief executive officer at MICA Biosystems, commented: “Our strategic partnership with the Royal Orthopaedic Hospital cannot be overstated in its importance to the progress of our revolutionary nanotechnology. We plan to start our Phase 2a clinical trials within the year – a timeline made possible in large part thanks to the work we were able to complete at the Dubrowsky Laboratory.
“Our nanotech-augmented, remote-controlled cells have the possibility to change the face of medicine, improving the lives of millions of patients. The ability to collaborate with world-class, researchminded clinicians was an important factor in our decision to make Birmingham our home, and the centre of our strategy to bring medicine into the future.”
The current focus is on how MICA’s technology could be used in spinal fusion procedures, which is a key part of many spinal surgeries, including for scoliosis. The nanotechnology would be used to control a patient’s cells in situ in the body, to influence how the body heals. That is an alternative to using cultured cells – where the cells are grown in a lab – that are extracted during an initial surgery and then implanted back into the patient several weeks later in another surgery.
Instead, the approach can be done as part of spinal fusion surgery using the patient’s own cells, with the procedure taking about 15 minutes. During the operation, the surgeon would take out part of the patient’s bone marrow and bind the nanoparticles (the signalling technology) to the cells which are then placed back into the patient during the same surgery.
The Dubrowsky Laboratory was made possible by a legacy donation of £1.5m to the Royal Orthopaedic Hospital, and was officially opened in 2019. The laboratory focuses on research into rare bone cancers and other orthopaedic problems and their treatments. q

91 91 www.yourexpertwitness.co.uk
Dr Michal Zurawski (left) and Professor Adrian Gardner
ROBOTIC OVERREACH vs THE PRECISION PROMISE: THE LEGAL QUAGMIRE OF HIGH-TECH JOINT REPLACEMENTS
By orthopaedic consultant
and
expert witness Professor Paul Lee

[ THE MARCH OF INNOVATION in orthopaedic surgery has introduced robotic-assisted procedures as a hallmark of modern knee and hip replacements. Promising unmatched precision, these technological marvels, however, present a paradox: they bring forth novel complications and elongated surgery times without clear evidence of long-term advantages.
Insights from journals such as Knee Surgery, Sports Traumatology, Arthroscopy and Clinical Orthopaedics and Related Research cast a shadow of doubt, revealing increased risks without substantial improvements. That dichotomy ushers in a pivotal legal enquiry: when complications emerge, who bears responsibility?
Legal foundations: breach of duty and causation
The cornerstone of a medical negligence claim rests on proving a breach of duty and establishing causation. The complexity of applying those legal principles intensifies with robotic surgery. Does the adoption of a cutting-edge yet potentially riskier approach constitute a breach of duty, especially amid contested benefits?
Recent evaluations – notably the American Joint Replacement Registry’s 2017-2020 analysis, published in Clinical Orthopaedics and Related Research – scrutinise the effectiveness of roboticassisted total knee arthroplasty (TKA). Out of 142,550 TKAs, 14,216 employed robotics, revealing no discernible improvement in revision rates. That finding marks a critical juncture, indicating that technological precision does not necessarily correlate with better surgical outcomes.
The issue of pin-site complications in robotic-assisted TKA, with a reported rate of 4.1%, underlines a significant risk to patient well-being. Such a high incidence, highlighted in the Journal of Experimental Orthopaedics in 2023, raises a fundamental question: does introducing robotic technology – and its inherent risks –constitute a breach of healthcare providers’ duty?
Legal standards require demonstrating that this breach directly resulted in harm, blurring the lines in the context of robotic TKA. That scenario necessitates a thorough legal and ethical examination of the outcomes associated with robotic intervention.
Informed consent and ethical considerations
The crux of informed consent is ensuring that patients are fully apprised of the risks and benefits of their surgical options. The lack of substantial benefits from robotic-assisted TKA, juxtaposed with increased pin-site complications and increased surgical time risks, underlines the need for a transparent consent process. That approach should reflect an accurate understanding of robotic surgery’s implications, allowing patients to make decisions based on evidence rather than the allure of innovation.
Healthcare providers must carefully weigh the promotion of technological advances against the imperative to fully inform patients about potential new complications and the absence of proven long-term benefits.
Robotic precision: a legal dilemma
The exactitude promised by robotic assistance might inadvertently result in ‘precisely wrong’ outcomes, given its reliance on non-weightbearing scans for planning. That discrepancy poses significant legal questions about informed consent and the surgeon’s understanding of the robotic system’s planning, accentuated by the Montgomery ruling’s emphasis on material risks and alternatives.
Causation: disentangling technology from outcome
Determining causation in robotic surgery complications requires a meticulous analysis to discern whether adverse outcomes were directly attributable to robotic technology or other factors. That legal principle is entangled with medical complexities, necessitating a nuanced understanding of both technology and patient-specific considerations.
Looking ahead with caution
As we delve deeper into the era of medical innovation, the implications of adopting robotic-assisted surgery for joint replacements call for a reassessment of standard practices. The legal and medical fields must collaborate to ensure that the quest for precision does not compromise patient welfare and informed decision-making.
The question looms: are we ready to tackle the legal and ethical challenges that accompany technological advancements in surgery? q
93 93 www.yourexpertwitness.co.uk
94 94 www.yourexpertwitness.co.uk
ORTHO-SURGEONS NAMED IN NEW YEAR’S HONOURS LIST
[ A NUMBER OF ORTHOPAEDIC SURGEONS were honoured in the King’s 2024 New Year Honours and the British Orthopaedic Association offered its congratulations to the recipients. They were:
Professor Neil Mortensen, lately President of the Royal College of Surgeons of England, was awarded a Knighthood for services to surgery.
Professor Simon Kenny, National Clinical Director for Children and Young People at NHS England and consultant paediatric
surgeon at Alder Hey Children's Hospital, was awarded an OBE for services to paediatric surgery.
Professor Panagiotis Giannoudis, Professor of Trauma and Orthopaedics at the University of Leeds and founder of Day One Trauma Support, was awarded an MBE for services to trauma and orthopaedic surgery.
Professor Antony Johansen, consultant ortho-geriatrician at Cardiff and Vale University Health Board, was awarded an MBE for services to older people. q
WIDOW AWARDED DAMAGES FOR HUSBAND’S DEATH FOLLOWING SURGERY
[ LEIGH DAY have reported on a case where a woman whose husband died aged 71 following revision knee replacement surgery has settled her claim against an NHS hospitals trust for £150,000.
The widow argued that the surgery her husband underwent was negligent, as a tourniquet and mechanical calf compression were used despite guidance from a consultant vascular surgeon that they should not be. The NHS hospitals trust concerned denied liability for the man’s death, arguing that the surgery could not have taken place without the use of a tourniquet, but agreed to pay compensation.
The patient had suffered for several years with his right knee and had initial surgery in 2014. It was unsuccessful and left him unable to walk fully or straighten his right leg. He remained in a lot of pain. He saw various orthopaedic surgeons and eventually decided to have further surgery at the NHS hospitals trust.
Ahead of the revision knee surgery, he had to have tests from a consultant vascular surgeon due to some of his other health problems. The vascular surgeon advised that the knee surgery could proceed, but only on the basis that a tourniquet and mechanical calf compression were not used during the operation. He wrote a letter to the treating orthopaedic surgeons to inform them of that.
However, despite the trust having received the letter from the vascular surgeon, both a tourniquet and mechanical calf compression were used during the procedure.
Following surgery his right foot was seen to be cold and blue and he was transferred urgently to the vascular team at a different hospital, who found that his right femoral/popliteal artery was blocked.
His condition deteriorated and he suffered a heart attack. He never regained consciousness and died on 17 October 2016, after his family
made the difficult decision to turn off his life support machine.
His widow instructed Leigh Day medical negligence solicitor Stephen Clarkson to bring a claim against the NHS hospitals trust. Stephen argued that, had the failures not occurred, the deceased would not have had the surgery which required the tourniquet or mechanical calf compression, and his death would have been avoided. The settlement of £150,000 is intended to provide compensation for the trauma that he experienced before his death, as well as going some way to compensate the impact that his death has had on his family. q
95 95 www.yourexpertwitness.co.uk


96 96 www.yourexpertwitness.co.uk
COLLEGE UPDATES GUIDELINE FOR OPHTHALMOLOGISTS TO DETECT
CHILD ABUSE
[ AN UPDATED CLINICAL GUIDELINE, Abusive Head Trauma and the Eye in Infancy, is now available to ophthalmologists. It is an important evidence-based document that updates the previous guideline published in 2013.
Abusive head trauma (AHT) in infants and children is a form of child maltreatment. Infants and children suspected of being subjected to abusive head injury are often referred by paediatricians to the on-call ophthalmology team for examination of signs of overt external ocular injury or occult vitreoretinal trauma.
It is important for ophthalmologists to be familiar with the clinical features of AHT, how to examine an infant and document their findings.
The incidence of abusive head injury in children is highest in infancy and less frequently seen in children over three years of age. Retinal haemorrhages have a high positive predictive rate for abusive head injury. In the presence

of head injury without any plausible medical explanation, the description of the retinal findings help in distinguishing between abusive injury and other causes.
It is incumbent on the ophthalmologist to be familiar with clinical presentation, the differential diagnosis and controversies associated with attributing the presence or absence of retinal findings to abusive head injury in children.
The guideline aims to help ophthalmologists in this respect.
Incorporating up-to-date literature, the guideline includes reviews of newborn retinal haemorrhages, non-vitreoretinal ocular manifestations of physical injury and fabricated or induced injury.
This document is primarily aimed at ophthalmologists in practice but also provides an evidence-based resource for any doctor dealing with children and those practising in child protection. q
THERE’S STRENGTH IN UNITY IN OPHTHALMIC MEDICOLEGAL PRACTICE
By Mr Irfan Jeeva MBBS FRCOphth FEBO Cert LRS
[IN THE INTRICATE and demanding world of ophthalmic medicolegal practice, where every detail counts and our steadfast commitment to justice runs deep, the journey towards providing comprehensive expert witness statements invites us to consider new pathways and more collaborative models of practice.
Traditionally, the path has often been walked alone, but there's a growing recognition of the strength found in unity. The collaborative spirit of a group practice not only enriches our professional landscape but also offers a robust support system for solicitors, expert witnesses and, most importantly, the individuals relying on our expertise.
Within the embrace of a group practice we're not just a collection of individuals; we become part of a dynamic ecosystem called the Eye Law Chambers.
This model is not predicated on the involvement of several specialists in a single case, but rather on establishing a supportive infrastructure that ensures clients are matched with the most appropriate expert within the group. It fosters a culture of shared wisdom and resources, where the unique strengths of each specialist are harnessed to contribute to the collective success of the group and, by extension, to the outcomes for our clients.
In a collaborative setting like the Eye Law Chambers, the approach to case management is fundamentally transformed. The model does not operate based on assigning cases to any available expert; instead, it is built around a supportive infrastructure designed to ensure that clients

are connected with the most suitable specialist within our team.
That ensures that every case is approached with the utmost precision and care, tailored to the intricate details that define it. The result is a more efficient and effective service that maintains the high standards of meticulous attention required, while also respecting the timelines and pressures that often accompany legal proceedings.
Adopting a group practice in ophthalmology does more than just elevate the professional standards: it nurtures a supportive environment that benefits all stakeholders. For solicitors, it means having a reliable, cohesive team that's equipped to provide the highest quality assessments. For expert witnesses, it offers a collaborative network that supports professional growth and development. Finally, for our clients, it ensures they receive the bestsuited expertise to support their cases.
As we navigate the complex terrain of ophthalmic medicolegal opinions, the power of a collective approach becomes increasingly evident. It's about more than just advancing our professional practice; it's about creating a system that upholds the values of justice, care and excellence at every turn. In the unity of group practice, we find not only the future of our profession but also a deeper commitment to the individuals and communities we serve. q
• Mr Irfan Jeeva is a consultant ophthalmologist and director of Eye Law Chambers. For further information visit www.eyelawchambers.com
97 97 www.yourexpertwitness.co.uk

98 98 www.yourexpertwitness.co.uk
ROYAL COLLEGES REITERATE COMMON GROUND
[THE College of Optometrists and The Royal College of Ophthalmologists have published an updated joint vision for the continued collaboration of the two professions, to support the delivery of safe and sustainable eye care services in the UK.
The two professional bodies first developed a joint vision in 2020, as a tool to help drive the transformation of English eye care services and ensure safe care during the pandemic. In 2021 they published a UKwide joint vision.
The updated 2024 version re-emphasises their guidance for the integration of services. It will help commissioners and clinicians design eye care services that ensure patients are prioritised based on their clinical need and receive care that is appropriate and accessible. It champions multidisciplinary eye care professionals providing that care, working collaboratively in primary care, community, hospital and independent sector provider settings.
The publication sets out what care should look like for patients in different parts of the care pathway, and contains practical recommendations around long-term service frameworks, models of care, referrals and governance.
The 2024 update highlights and reflects the current scale of work increasingly being undertaken in primary eye care and emphasises the need for enhanced digital two-way communication and image sharing between all health professionals involved.
It is underpinned by four key principles:
• The provision of timely eye care in an equitable, appropriate and accessible way; to reduce the risk of visual loss caused by delay
• Multidisciplinary professionals working collaboratively in primary care, community and hospital settings (including the independent sector) to provide care that is facilitated by effective digital communication and connectivity
• Direct patient contact taking place with a clinician capable of making appropriate management decisions including, where required, support by a senior decision-maker – eg an optometrist with higher qualifications or independent prescribing status, or the hospital eye service
• All pathways being led by the highest standards of joint optometry and ophthalmology clinical governance, applied equitably to all who are providing care and underpinned by patient centred outcome measures
Speaking about the updated joint vision, the president of the College of Optometrists, Professor Leon Davies FCOptom, said: “With better integration of services, the knowledge, skills and expertise of optometrists and ophthalmologists – and their colleagues – can be most effectively used to provide safe and sustainable patient care. Not only should more services be commissioned within primary eye care, we also need much better digital integration, image sharing and twoway communication between all eye care providers.
“Working with the Royal College of Ophthalmologists to update this

joint vision for integration also supports The College of Optometrists’ workforce vision – to recognise and effectively utilise the skills of the whole eye care workforce and improve outcomes for patients and local communities. We are pleased to continue this important collaboration and will work with all partners to achieve this vision.”
Speaking on behalf of the Royal College of Ophthalmologists, its president Professor Ben Burton commented: “With patient need expanding, it is more crucial now than ever that ophthalmology and optometry are able to work together to provide timely and highquality care.
“Currently, just 17% of NHS ophthalmology departments report that their services are very well integrated with optometry, and a lack of shared electronic patient record systems and interoperable imaging standards are preventing more joined-up pathways.
“So we are pleased to launch our and the College of Optometrists’ updated joint vision for safe and sustainable eye care services fit for the future. We look forward to working with commissioners and clinicians to make this vision a reality.” q
99 99 www.yourexpertwitness.co.uk
RNID RESEARCH HIGHLIGHTS AUDIOLOGY FAILINGS
[ THE RNID has published its latest review of the state of UK audiology services, as experienced by people with hearing loss.
In Their Own Words is the result of a survey of 1,204 people, summarising the latest insights on people’s experiences and their ideas for service improvement.
Audiology services play a crucial role in providing support and treatments to improve people’s hearing health, the RNID points out. In recent years audiology services have had reduced capacity due to staff shortages and inadequate funding, which has been exacerbated by the impacts of the COVID-19 pandemic.
“Given the growing number of people with hearing loss, and the high level of unmet need with an estimated five million people that could benefit from hearing aids but do not have them, urgent action is needed to address both the current and future demand for adult hearing services,” the RNID says.
“Our ambition is to improve hearing outcomes for people experiencing hearing loss. We want as many people as possible to have access to high-quality hearing loss assessments, treatments and support.”
A staggering 12 million adults in the UK are deaf, have hearing loss or tinnitus. That is one in five. By 2035, RNID estimates there will be around 14.2 million adults with hearing loss across the UK.
Even so, the experiences of people with hearing loss suggests the need for urgent improvement within current audiology services and investment to meet future demand.
The service improvements identified by the In Their Own Words report include:
• New service models, such as remote online support options and flexible drop-in clinics
• Better service accessibility – by using accessible communication and waiting rooms, improving access to ear wax removal and local community support
• Encouraging new technology and patient empowerment – such as people trying hearing devices in a more natural environment, the ability of hearing devices to automatically tune themselves to users’ needs and greater control or involvement in hearing device settings
One issue highlighted was a lack of accessibility when booking and attending appointments, suggesting that their communication needs are not being met. Service users expressed frustration that telephone booking systems do not meet their communication needs and pose a significant barrier to people who are deaf or have hearing loss.
Among the comments quoted are:
“My audiology expects people to phone to get an appointment, this of course is ridiculous for people who cannot use a phone.”
“My NHS audiology department still call me. I have profound hearing loss and do not take voice calls, which has been stated many times on my notes.”
“Wish there was some way to make an appointment without asking someone else to do it for me.”
Those who shared their experiences have helped to highlight the key challenges and potential solutions for healthcare providers and decision-makers to consider. RNID will use those insights to guide its work in collaborating with others to rethink the future of audiology. q
• To download the report visit rnid.org.uk
100 100 www.yourexpertwitness.co.uk 100100
IMPLANT OR HEARING AID? TRIAL LOOKS TO DETERMINE WHICH IS MOST SUITABLE
[ THE WORLD’S FIRST STUDY into the best treatment options for adults living with severe hearing loss has launched in the UK.
Severe hearing loss affects over a million people in the UK and the World Health Organization estimates that by 2050 nearly 2.5 billion people worldwide will experience some degree of hearing loss, and at least 700 million will require hearing rehabilitation. If left untreated, hearing loss can negatively affect education, employment and quality of life, and increases the risk of dementia and cognitive decline.
Now, researchers at the NIHR Nottingham Biomedical Research Centre and the University of Nottingham have embarked on a new study, sponsored by the University of Nottingham, which will inform the most effective treatment for people with hearing loss greater than 65 dBHL. Working with hospitals in the UK, the COACH study, led by Dr Pádraig Kitterick and Professor Doug Hartley, will aim to find out what is better for that group of patients – hearing aids or a cochlear implant.

COACH is the first study world-wide set up to answer that question and could change the way patients are treated in the UK and around the world.
The group of patients included in the research are those with hearing test results and speech understanding scores that fall just outside the range where they would be eligible to receive a cochlear implant on the NHS.
Dr Pádraig Kitterick, Head of Audiological Science at the National Acoustic Laboratories in Sydney, Australia explained: “The COACH trial is a landmark research study in the field of hearing loss and it will address an important question about who can benefit from cochlear implants. We are delighted to have secured investment to enable the NHS to deliver this important clinical trial, which will be led by a world-leading team of academics, clinicians and scientists. But more importantly, it has been designed and developed with patients living with severe hearing loss.”
Professor Doug Hartley, Professor of Otology at the University of Nottingham and consultant ENT surgeon at Nottingham University Hospitals NHS Trust, added: “The trial will bring together the research expertise in the University of Nottingham and Nottingham University Hospitals NHS Trust, supported by the world-class research infrastructure of the NIHR Nottingham Biomedical Research Centre. This is a great example of the UK and our National Health Service being at the forefront of conducting clinical trials to improve the lives of people with hearing loss both here at home and around the world.”
The costs of the trial are being funded by Cochlear Ltd, a global manufacturer of implantable hearing devices. The company is not involved in delivering the trial, which will be run independently by NHS doctors and audiologists, as well as researchers from the Nottingham Biochemical Research Centre and the University of Nottingham.
Sarah Chapman, a member of the public with hearing loss who is working alongside the trial team for the COACH study, said: “The COACH trial is so important because we don’t know how hearing aids and cochlear implants compare for people with severe hearing loss just above the current eligibility criteria for implants. This trial, which is being shaped by people with severe hearing loss working alongside researchers, will provide evidence to fill this important gap in knowledge. Instead of best guesses, we’ll have best evidence to inform decisions about treating severe hearing loss.”
A patient research partners group will advise the researchers throughout the trial on aspects such as when and how to approach
people who might wish to take part and what kind of information people will need and want to hear before taking part.
Patients using the audiology services at Nottingham University Hospitals NHS Trust are among those who will be offered the chance to take part in the study. Nottingham is one of nine NHS Trusts in England and Wales taking part. q
101 101 www.yourexpertwitness.co.uk 101101







AGRICULTURAL & HORTICULTURAL CONSULTANTS

ARTS & ANTIQUES SURVEYORS


102 102 www.yourexpertwitness.co.uk 102102 ACCOUNTANCY








COLLISION INVESTIGATION & RECONSTRUCTION

103 103 www.yourexpertwitness.co.uk 103103 103 BUILDING, PROPERTY & CONSTRUCTION

COMPUTER & MOBILE FORENSICS


CRIMINOLOGY
DIAMOND & JEWELLERY VALUERS

DIGITAL TECHNOLOGY

ENERGY CONSULTANTS

ERGONOMICS

FINANCIAL SERVICES

FORENSIC SERVICES

104 104 www.yourexpertwitness.co.uk 104104 104 COMPLIANCE CONSULTANTS

GEOTECHNICAL CONSULTANTS

INSURANCE


MECHANICAL & PROCESS ENGINEERING



105 105 www.yourexpertwitness.co.uk 105105
POLICE CUSTODY
RISK MANAGEMENT
TRANSLATING & INTERPRETING


TREE


106 106 www.yourexpertwitness.co.uk STEEL & IRON ORE
WOOD & TIMBER
CONSULTANTS 106
MEDICO-LEGAL EXPERTS
ACCIDENT & EMERGENCY MEDICINE


ANAESTHESIA

CARDIOLOGISTS & CARDIOTHORACIC SURGEONS

DENTAL & ORTHODONTIC EXPERTS


ENDOCRINOLOGY
107 107 www.yourexpertwitness.co.uk
107


GASTROINTESTINAL & COLORECTAL SURGEONS

GENERAL SURGEONS

HAEMATOLOGY


108 108 www.yourexpertwitness.co.uk 108
ENT CONSULTANTS 108
LIVER SURGEONS & HEPATOLOGISTS

MEDICAL NEGLIGENCE

MICROPIGMENTATION
NEONATAL MEDICINE
NEUROLOGY

NEUROPSYCHOLOGISTS

NEUROSURGEONS


109 109 www.yourexpertwitness.co.uk 109 109 INTENSIVE CARE MEDICINE

NURSING, CARE & REHABILITATION CONSULTANTS



OBSTETRICS & GYNAECOLOGY

OCCUPATIONAL MEDICINE & THERAPY

ONCOLOGISTS
110 110 www.yourexpertwitness.co.uk
OPHTHALMIC SURGEONS
110



ORTHOPAEDIC SURGEONS


111 111 www.yourexpertwitness.co.uk
111
ORAL & MAXILLOFACIAL SURGEONS




ORTHOTICS


OSTEOPATHS

PATHOLOGY

PHARMACOLOGY


PHYSICIANS
112 112 www.yourexpertwitness.co.uk
PAIN MEDICINE
112
PLASTIC & HAND SURGEONS

PROSTHETICS

PSYCHIATRISTS

113 113 www.yourexpertwitness.co.uk
113


PSYCHOLOGISTS


RADIOLOGISTS
REHABILITATION


SOCIAL CARE

114 114 www.yourexpertwitness.co.uk
114
TOXICOLOGY



UROLOGICAL SURGEONS

VASCULAR SURGEONS

115 115 www.yourexpertwitness.co.uk
SPEECH & LANGUAGE THERAPY
115