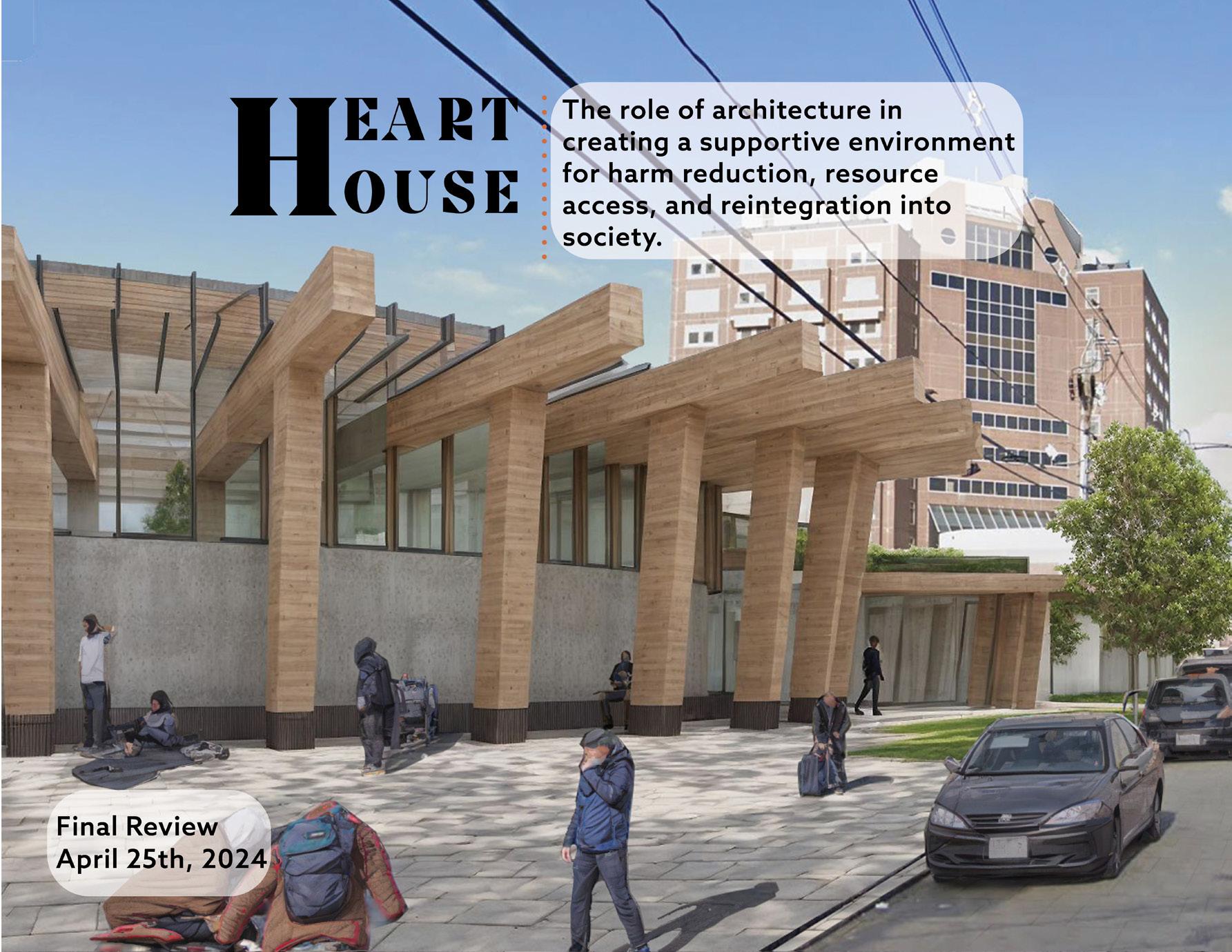
H EART OUSE
The role of architecture in creating a supportive environment for harm reduction, resource access, and reintegration into society
Thesis | Spring 2024
Master of Architecture Candidate
Boston Architectural College
GRAZIELLA PILKINGTON

3
DEDICATED TO
Dr. Paul Farmer, M.D., Ph.D., (1959-2022) whose life mission was to cure injustice through pioneering novel, community- based treatment strategies that demonstrated the delivery of high-quality healthcare in resource-poor settings.
“For me, an area of moral clarity is: you’re in front of someone who’s suffering and you have the tools at your disposal to alleviate that suffering or even eradicate it, and you act.”
— Dr. Paul Farmer
4
ACKNOWLEDGMENTS
Thank you Russ Feldman, AIA, Ian Taberner, AIA, and the review panel for continuously giving incredibly thoughtful feedback throughout.
Thank you to my Family for emotionally and financially supporting me through my educational career.
Thank you to my friends and studio colleagues for the enthusiastic encouragement.
And thank you to Matt for absolutely everything.
5
Introduction
Biographical Note
Abstract
Thesis Statement
Methods of Inquiry & Terms of Criticism
Part I Research & Exploration
Project Context
Precedents
Context | History
Context | Site Program
Part II Schematic Design
User Profiles
Massing | Exploration
Part III Design Development
Final Design Narratives
Part IV Next Steps & Conclusion
Part V Appendices
Appendix A - Thesis
Appendix
Appendix
6 TABLE OF CONTENTS
09 - 14 15 - 25
..................
Reviews
.................
B - Thesis Proposal
....................... 27 - 32 35 - 57 59 - 61 62 - 141 63-102 103-135 137-141
C - Bibliography
 Art by Grace Pilkington
Art by Grace Pilkington
“... I wish I could be with [these people] before they injected, that I had more chances to really know them before I’m hovering over them on the grimy bathroom floor, sliding an oral airway into their throat.
... We must be able to create cleaner, safer spaces for people to consume drugs and be connected to help. Supervised consumption sites would not only play an important part in stemming the tide of the opioid overdose deaths for people downstream in this epidemic, but they would also reduce the trauma associated with injection drug overdoses -- for both people who use drugs and the people who care about them.”
Dr. Jessie M. Gaeta, M.D., Chief Medical Officer at Boston Healthcare for the Homeless from 2015 - 2022.
8
Introduction
Biographical Note
Abstract
Thesis Statement
Methods of Inquiry & Terms of Criticism
9
Graziella (Grace) Pilkington is a Master of Architecture candidate at the Boston Architectural College. She completed her Bachelor of Arts in Architecture at Miami University of Ohio, graduating in 2020 during the COVID-19 Pandemic.
Grace’s passion lies at the intersection of architecture and global public health. Inspired by the work of Dr. Paul Farmer and Partners in Health, Grace decided to pursue a career in architecture in search of a way to explore the intersection of the built environment and public health. During her time at Miami, she created a customized concentration with this interdisciplinary focus. The courses included immersive experiences such as two study-abroad programs and an independent study dedicated to designing emergency shelters in response to the pandemic.
The first study-abroad opportunity was a comparison of the Public Health Systems in The UK and The Netherlands. In 2017, in Amsterdam, Grace got the chance to visit a drug consumption center, where she unknowingly sparked the idea for her Master of Architecture Thesis. She was shocked by the cultural differences of how healthcare systems treat folks with substance abuse issues between the Netherlands and the United States. The stark contrasts in healthcare approaches between cultures sparked her vision for innovative solutions at home.
The second study-abroad immersion led Grace to Cape Coast, Ghana, where she participated in a designbuild studio constructing a maternity ward alongside local artisans. This hands-on experience deepened her understanding of healthcare disparities and cultural nuances in architectural
design. The simple hand-made mud bricks transformed into a vital resource for rural women’s health was both gratifying and inspirational.
Lastly, in December 2019, Grace and the entire world had their eyes on what was unfolding in Wuhan, China - where the yet-unnamed SARS-CoV-2 virus was just starting to spread. Grace saw news images of massive temporary hospitals being built in just 10 days, and recognized a serious problem, spreading internationally, that needed a practical architectural response, fast. Grace envisioned the idea for her independent study - an Emergency Response for College Campuses if and when the Virus reached the United States. Grace used her Campus at Miami Ohio as a prototype for her Isolation Units, that could be set up on any campus quad, in a number of different formations. The units included two beds, a bathroom, and a reverse-air mechanical system. Other units were for nurses and doctors to don, doff, and scrub before entering the isolation rooms. Covered walkways connected the units. When the use for the units was no longer needed, they could be folded up and shipped on a truck to the next campus or stored for later emergency response needs.
Throughout her academic journey, Grace has consistently prioritized public health considerations in her designs. Whether conceptualizing healthcare facilities or other structures, her overarching goal remains to foster environments that nurture healing, both physically and emotionally. Guided by empathy and a commitment to social justice, Grace aspires to imbue her architectural practice with a profound sense of dignity, particularly for marginalized communities.
10
NOTE
BIOGRAPHICAL
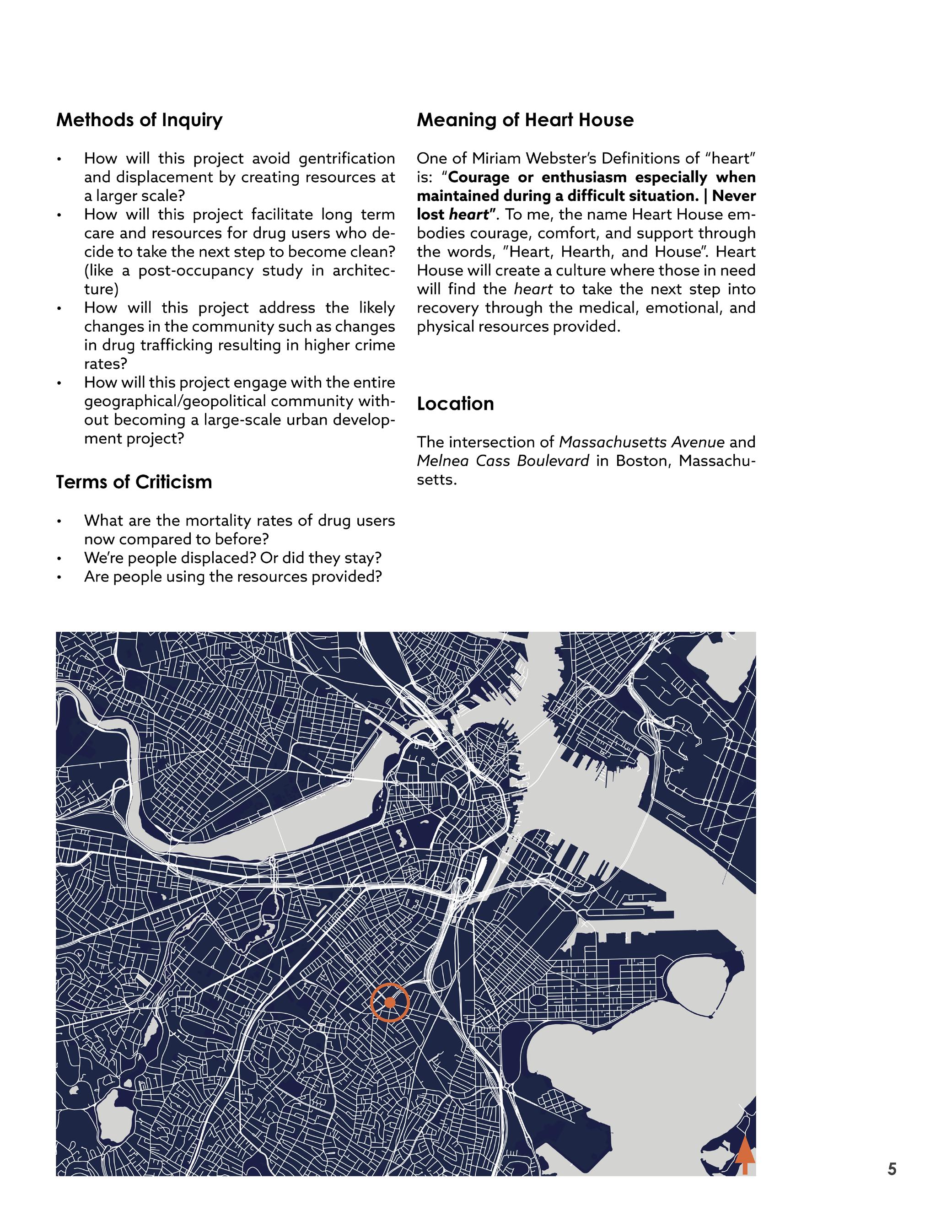
Meaning of Heart House
One of Merriam Webster’s Definitions of “heart” is: “Courage or enthusiasm especially when maintained during a difficult situation. | Never lost heart” . To me, the name Heart House embodies courage, comfort, and support through the words, ”Heart, Hearth, and House”. Heart House will create a culture where those in need will find the heart to take the next step into recovery through the medical, emotional, and physical resources provided.
— Graziella Pilkington 2024
11
1 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), “Perspectives on Drugs Drug consumption rooms: an overview of provision and evidence”, (2018)
ABSTRACT
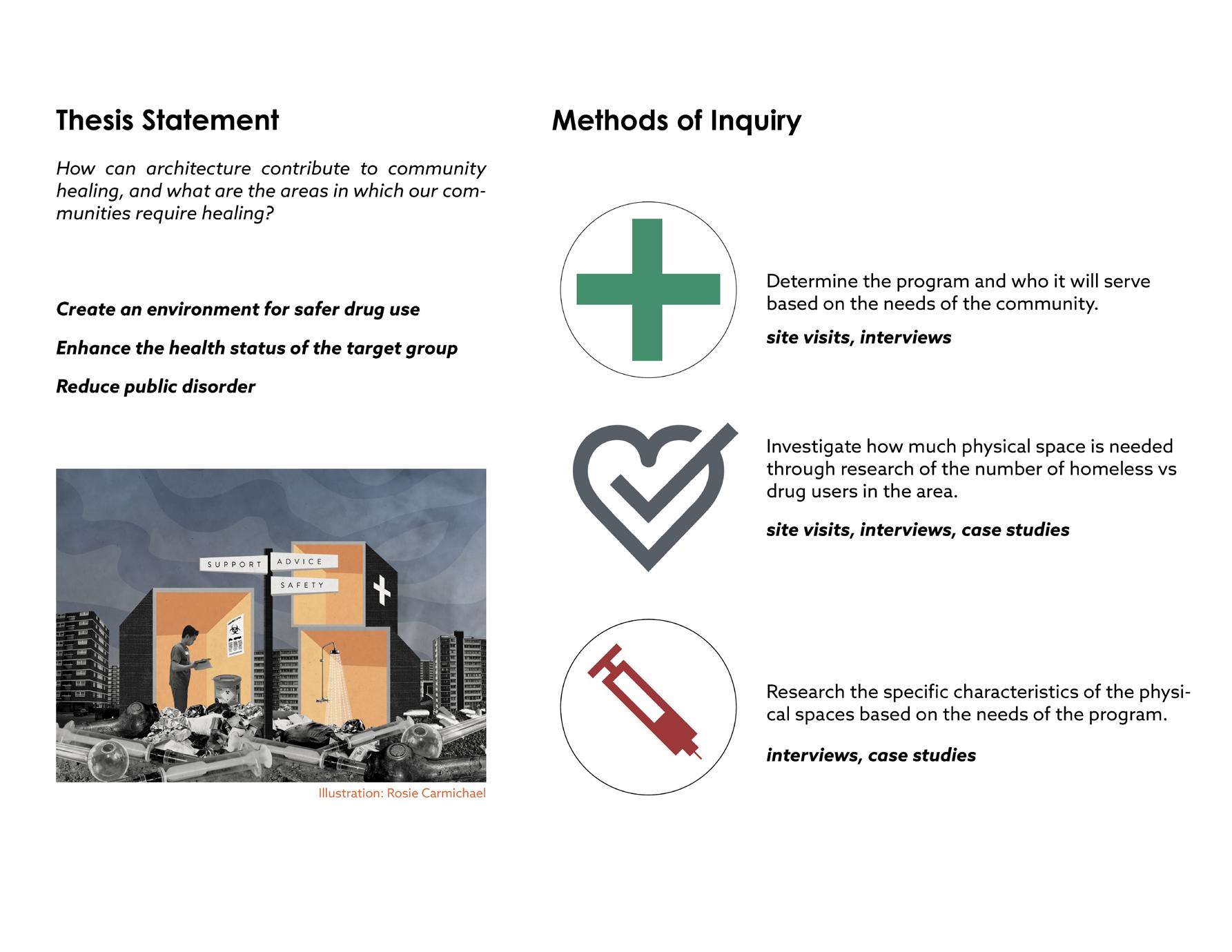
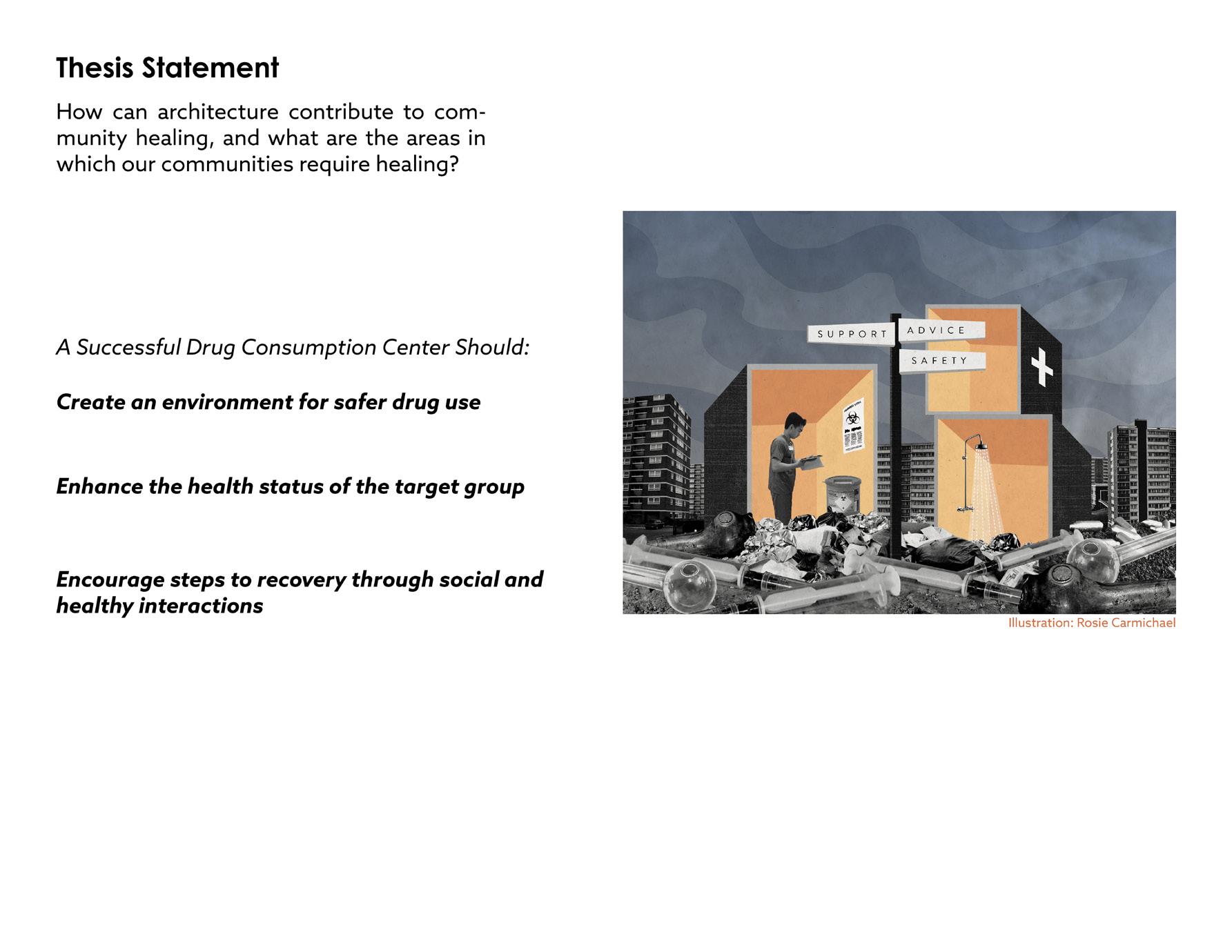
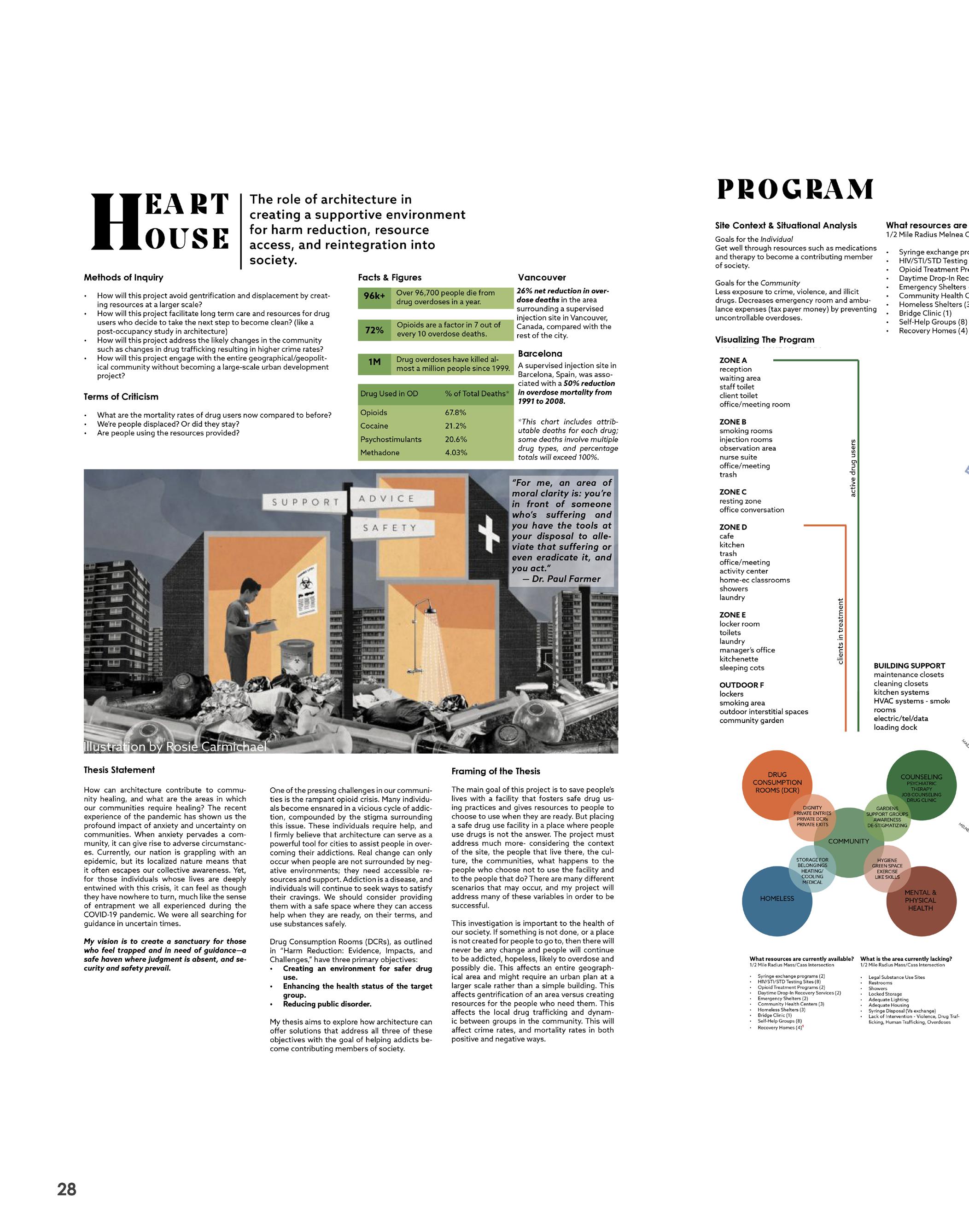
How can architecture contribute to community healing, and what are the areas in which our communities require healing?
The recent experience of the 2019 SARS-CoV-2 pandemic has shown us the profound impact of anxiety and uncertainty on communities. When anxiety pervades a community, it can give rise to adverse circumstances.
Currently, our nation is grappling with a different but familiar epidemic-- opioid abuse. This epidemic is very localized, and it often escapes our collective awareness. Yet, for those individuals whose lives are deeply entwined with this crisis, it can feel as though they have nowhere to turn, much like the sense of entrapment we all experienced during the COVID-19 pandemic. We were all searching for guidance in uncertain times.
Among the pressing challenges communities face in the rampant opioid crisis, is how individuals become ensnared in a vicious cycle of addiction, compounded by stigma.
These individuals require help, and I firmly believe that architecture can serve as a powerful tool for cities to assist people in overcoming their addictions. Real change can only occur when people are not surrounded by negative environments; they need accessible resources and support.
Addiction is a disease, and individuals will continue to seek ways to satisfy their cravings. We should consider providing them with a safe space where they can access help when they are ready, on their terms, and use substances safely.
Drug Consumption Rooms (DCRs), as outlined in “Harm Reduction: Evidence, Impacts, and Challenges,” have three primary objectives:
• Creating an environment for safer drug use.
• Enhancing the health status of the target group.
• Reducing public disorder.1
My vision is to create a sanctuary for those who feel trapped and in need of guidance— a safe haven where judgment is absent, and security and safety prevail.
12
THESIS STATEMENT
The thesis explores the role of architecture in fostering healing within an inner-city population affected by opioid addiction and homelessness, investigating how design interventions can alleviate social and health disparities, promote rehabilitation, and cultivate a sense of belonging and support among affected individuals.

METHODS OF INQUIRY
• Determine the program and who it will serve based on the needs of the community.
• Who exactly is the user group?
• Investigate how much physical space is needed through research of the number of homeless vs drug users in the area.
• Research the specific characteristics of the physical spaces based on the needs of the program.
• Create a low-threshold, no-barrier space that makes people feel dignified and welcomed.
TERMS OF CRITICISM
• Does the program meet the physical space requirements, requests, and needs of all the users?
• Is the space designed effectively for people to use dangerous illegal drugs in a safe and secure environment?
• Is the space designed effectively for people who are in recovery?
• Do the staff and clients experiencing homelessness feel safe and secure?
• Does the project integrate with the surrounding site context and community needs?
13
2
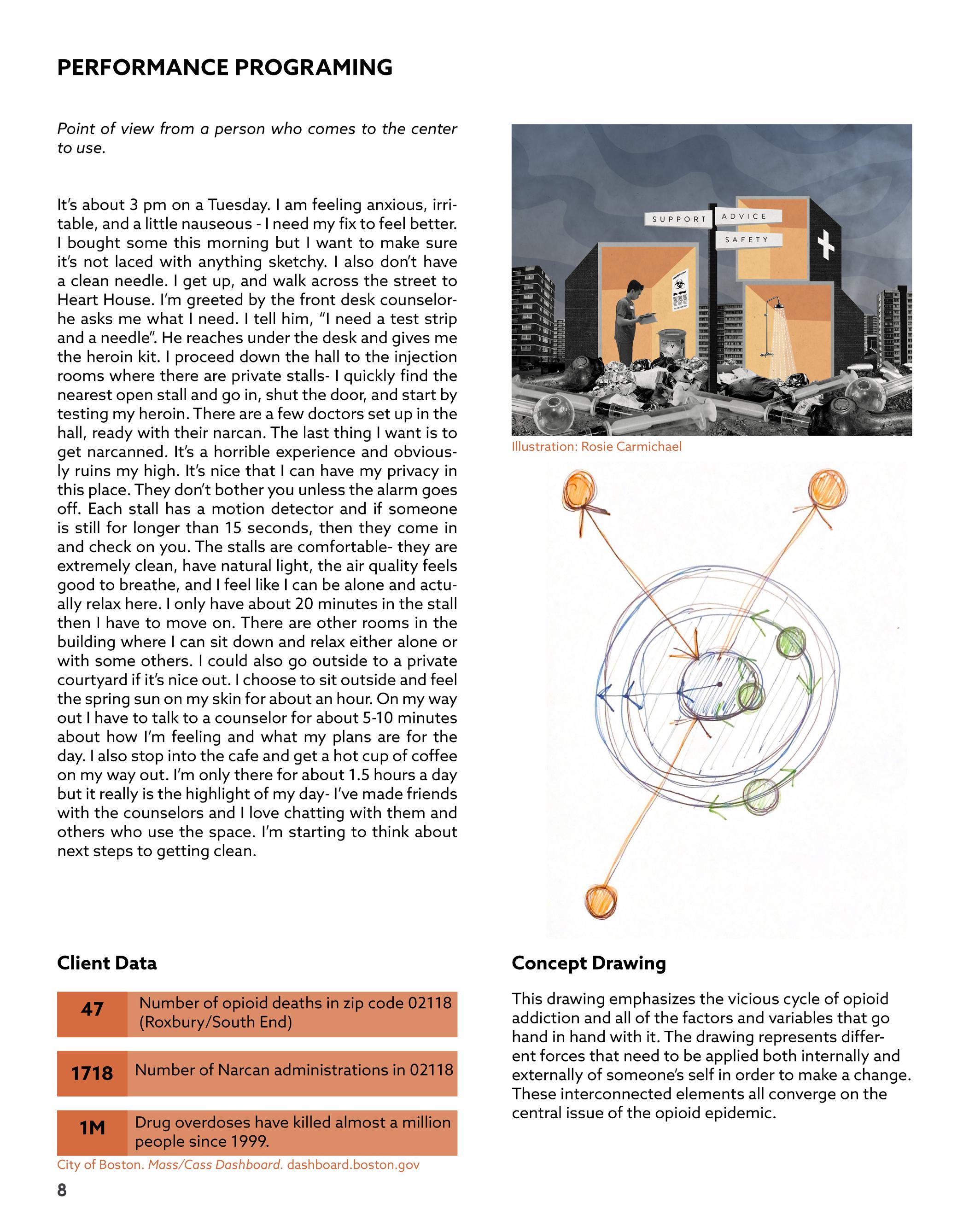
2 Illustration by Rosie Carmichael
What is Harm Reduction?
Harm reduction is a compassionate and evidence-based approach aimed at reducing the negative consequences associated with substance use disorder. The philosophy recognizes that individuals are at different stages of their journey and meets them where they are, without judgment or stigma. Central to harm reduction is the belief in treating all individuals with dignity, compassion, and respect, while opposing the stigmatization of substance use disorder. This approach acknowledges behavior change as an incremental process. Rather than focusing solely on abstinence, harm reduction prioritizes quality of life improvements for individuals in active addiction, in recovery, and within the community. It upholds universal human rights and empowers individuals as the primary agents responsible for reducing the harms related to their substance use.
Graziella Pilkington 2024
14
PART I
Research & Exploration
Project Context
Precedents
Context | History
Context | Site
15
Andrew Thurston, The Brink, a Boston University Publication August 3rd, 2023
“A Notorious Boston Intersection,
Mass and Cass,
Faces an Opioid Overdose Crisis. BU Researchers Are Turning to Survivors for Answers...
New study concludes it’s time to rethink sobriety requirements for housing and offer more harm-reduction options” 1
Mike Deehan, August 10, 2023
Boston
Amelia Caramadre, legal fellow for the Action Lab at Northeastern University School of Law and a member of the Massachusetts Rights Coalition for Health. August 9th, 2023
Boston Globe
“The tent city there has become the heart of the opioid epidemic and a public safety nightmare.” 2
Kristina Rex, August 2, 2023
CBS Boston
“It is not the time to diverge from methods with proven success. We need commitment to evidence-based public health approaches that center community treatment and housing.” 3
“Mass and Cass becoming increasingly dangerous as Boston eyes long term solutions” 4
Tori Bedford, March 6th, 2024
“After
Mass. and Cass crackdown, homeless community cast out into the shadows of Boston” 5
16 PROJECT CONTEXT
AXIOS
GBH,
4 2 5 1 3
Boston
COMMUTER TRAIN


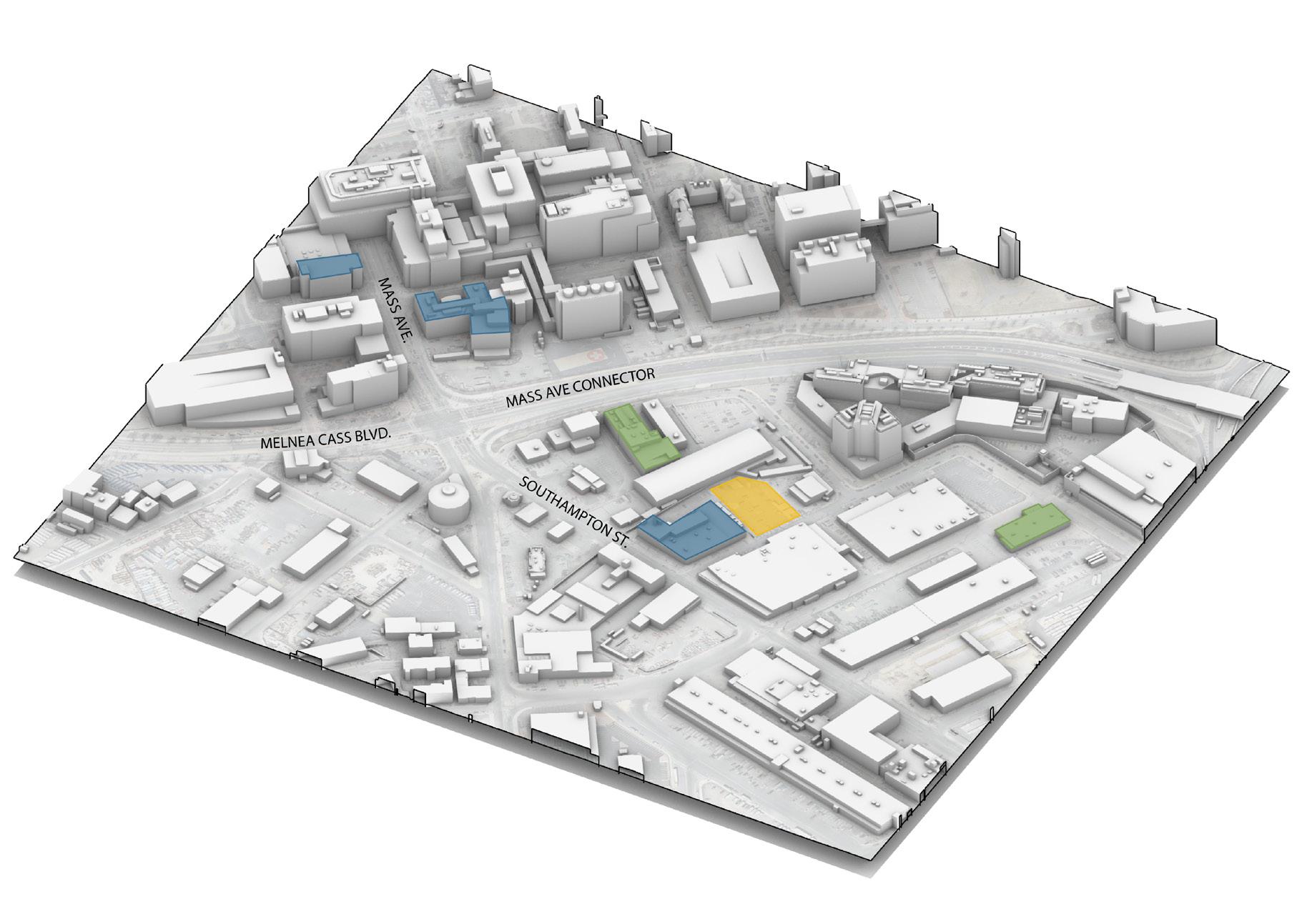
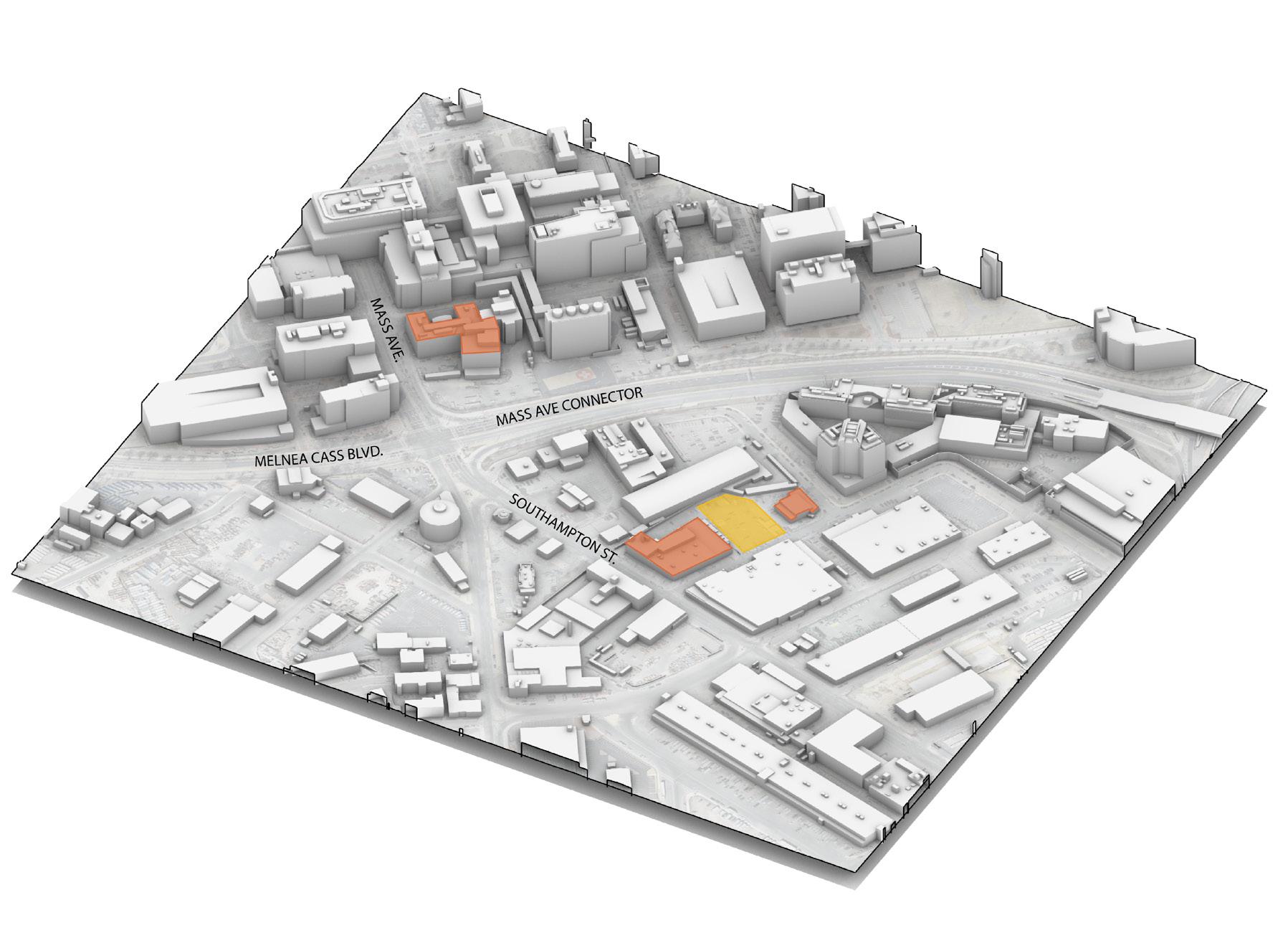
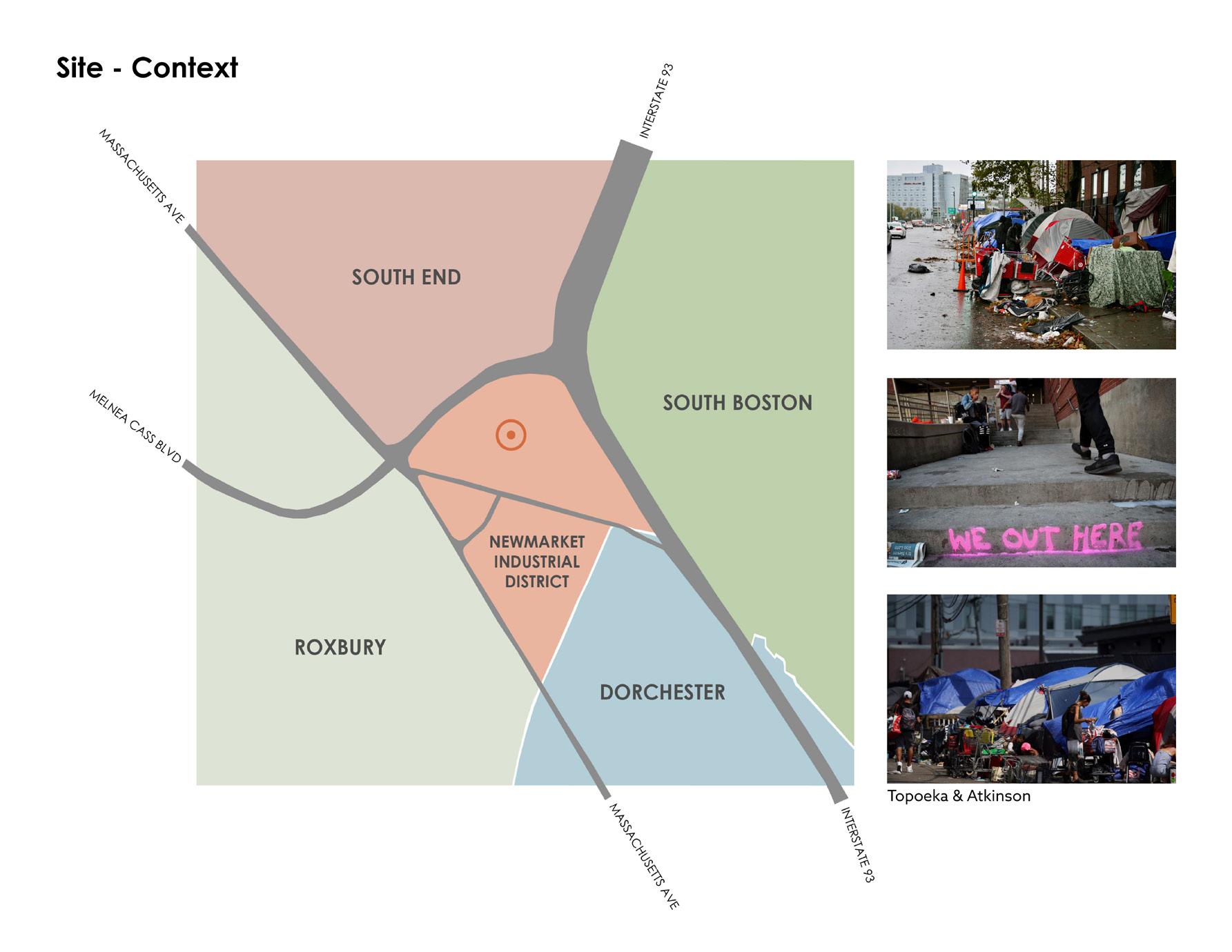
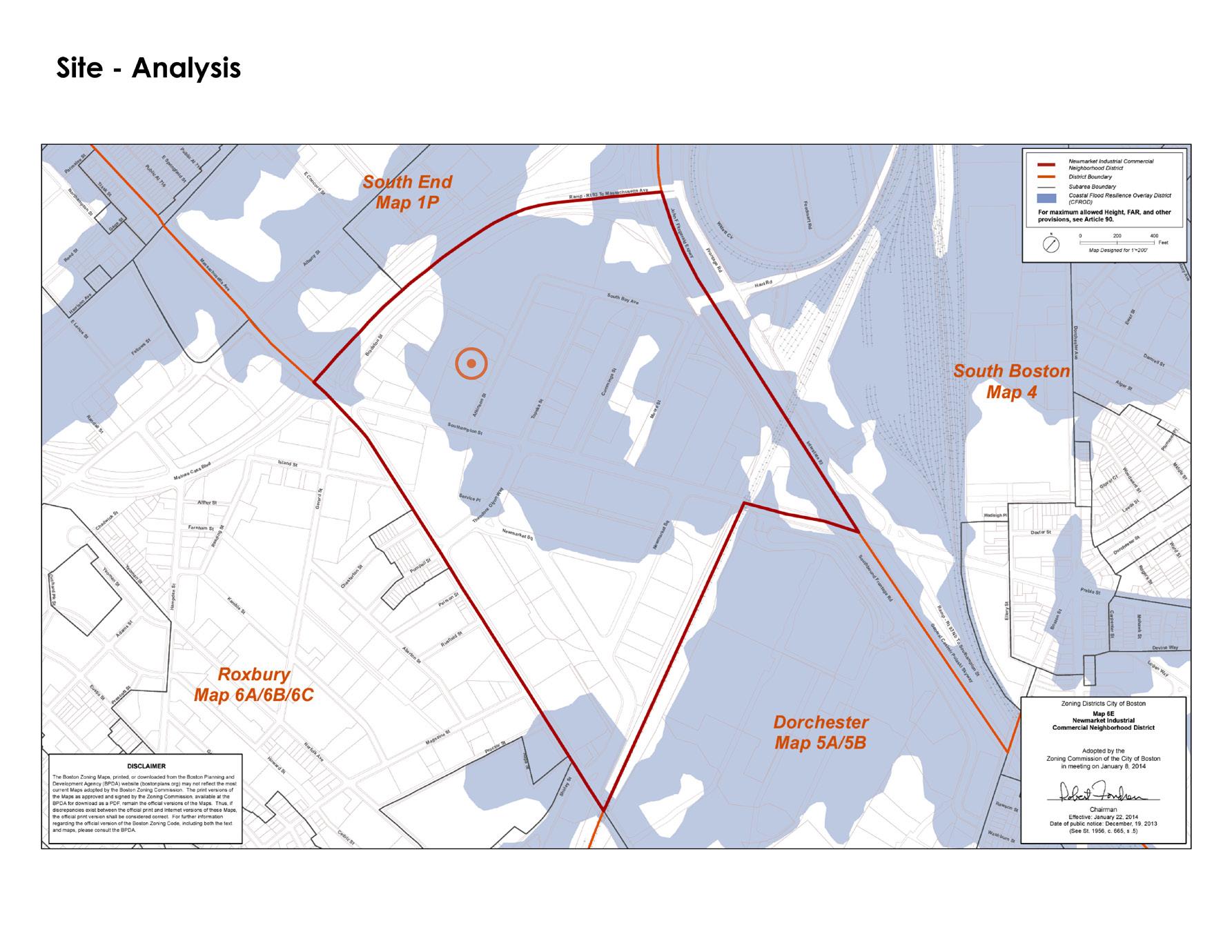
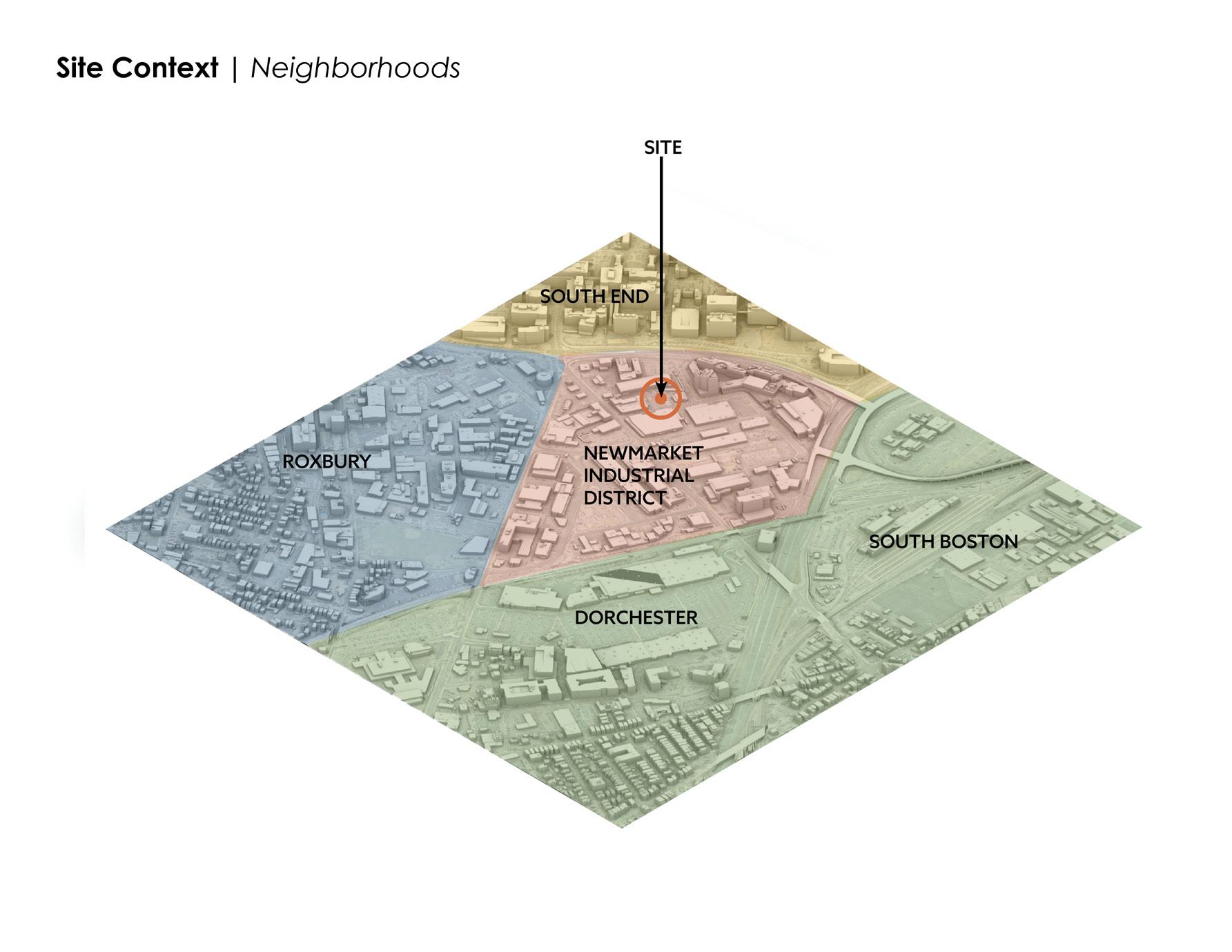
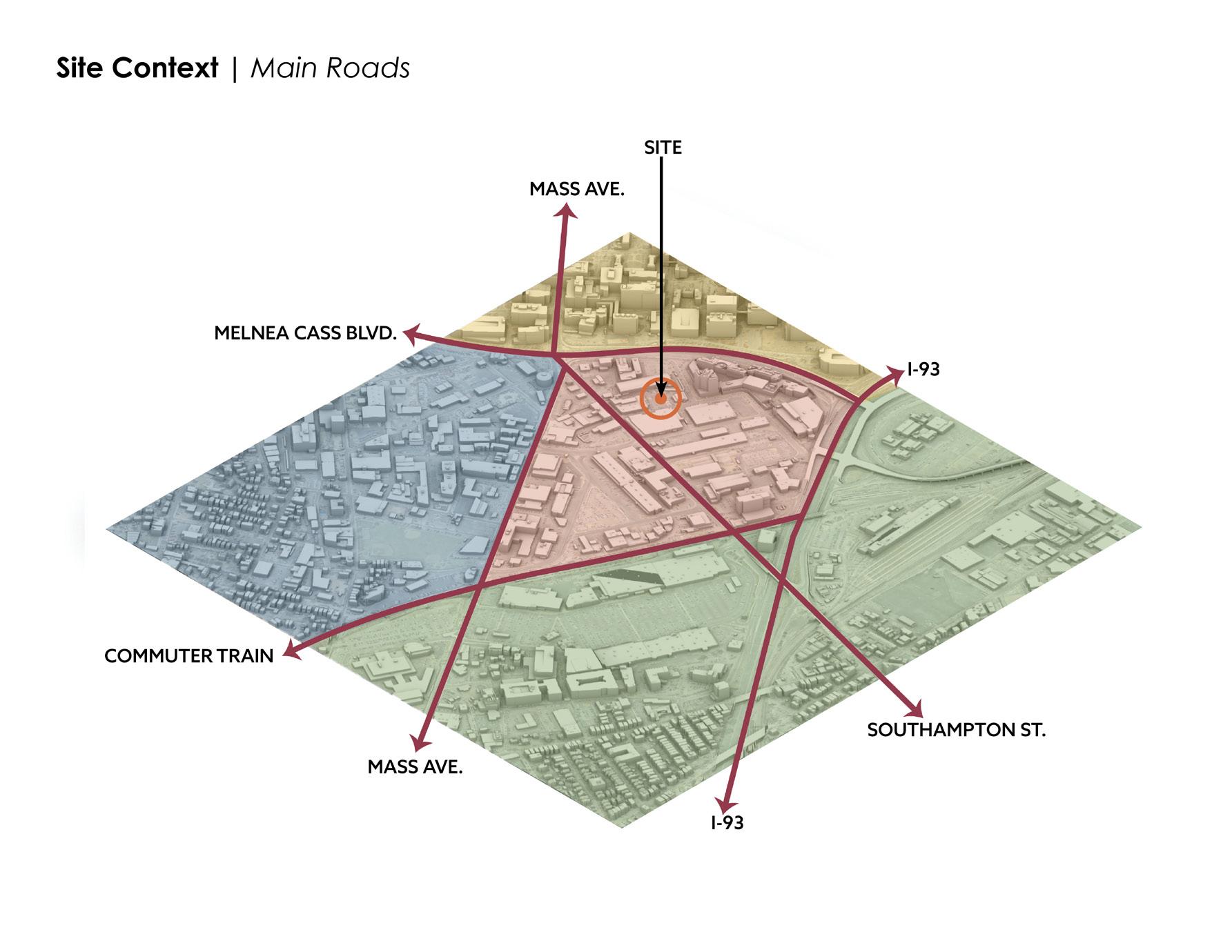
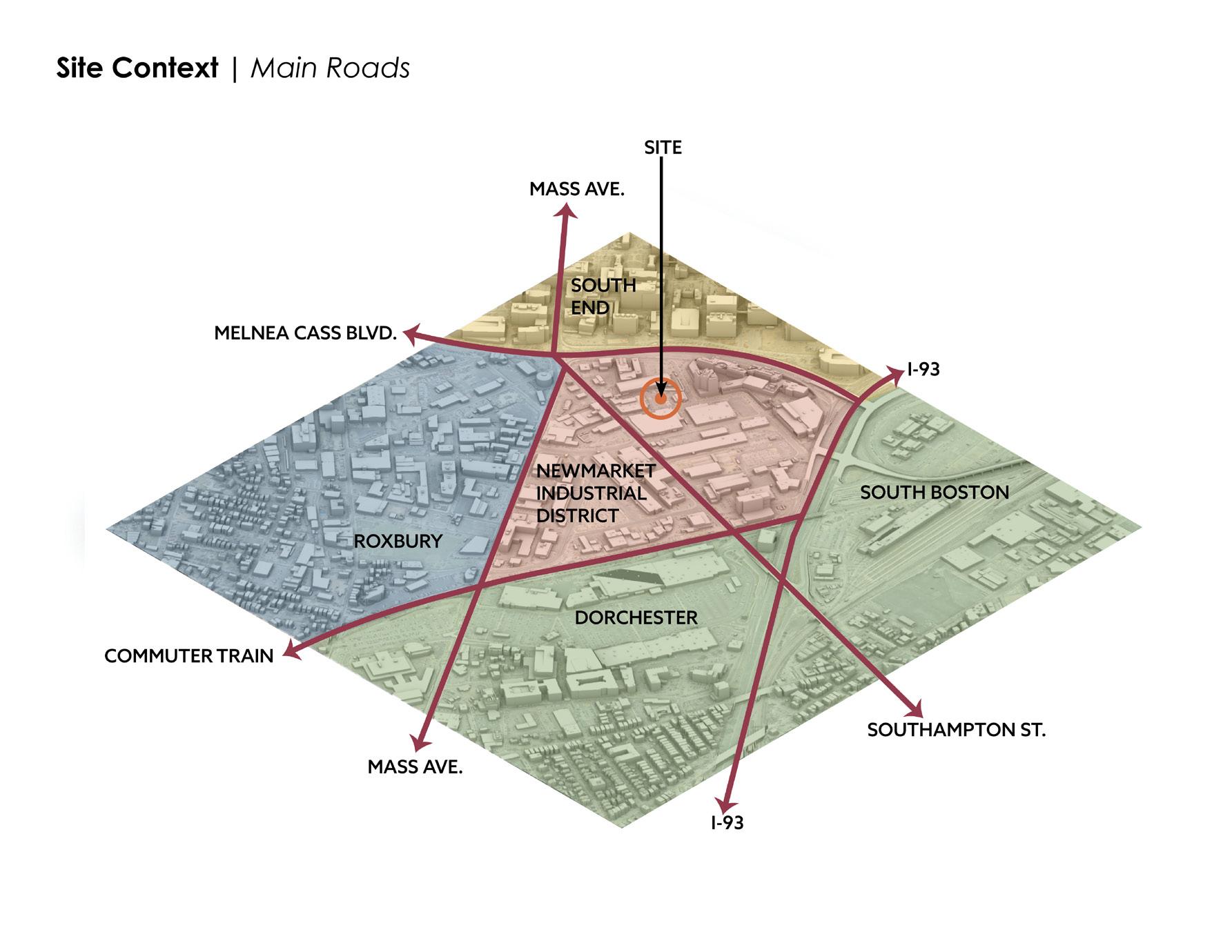
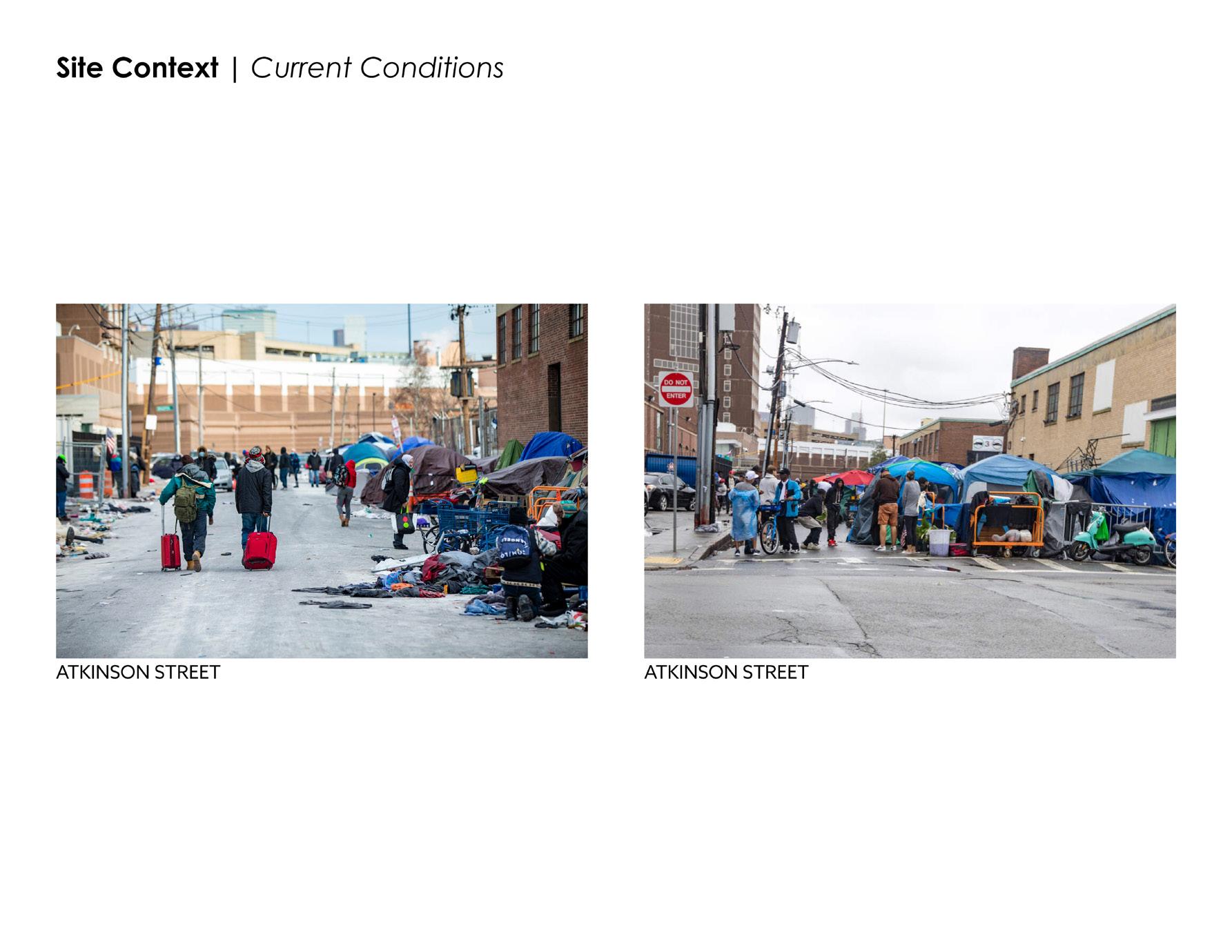
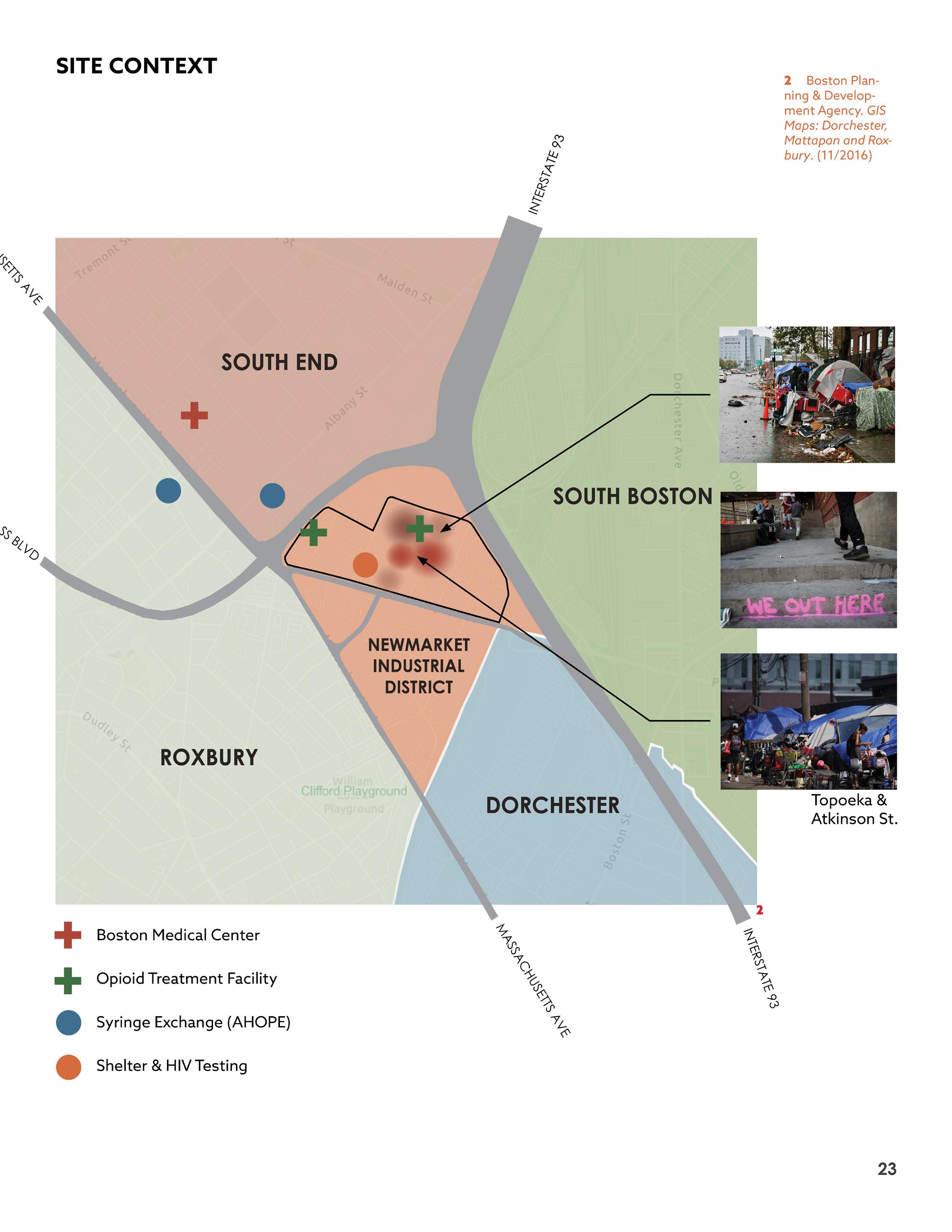
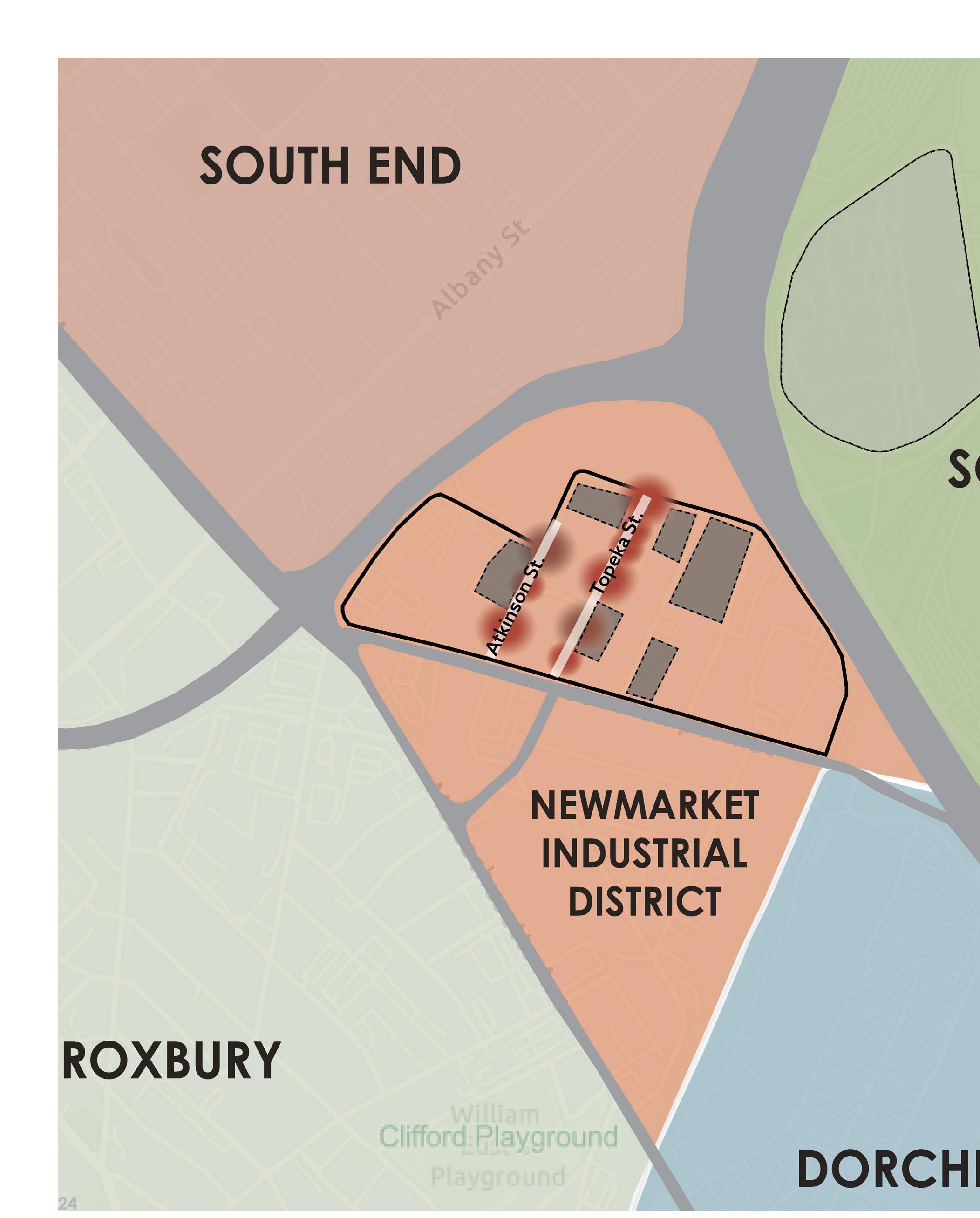
The site is located on Atkinson Street as shown above and in the photos to the left. The area, known as “Methadone Mile” or favorably, “Recovery Road” is mainly on Atkinson and Southampton Streets, South-East of the Intersection at Massachusetts Avenue & Melnea Cass Boulevard, locally known as “Mass and Cass”.
The area is notoriously ridden with drug use, violence, crime, sex-trafficking, and unsanitary conditions including undisposed feces and used syringes covering the streets and sidewalks.
For the last 10 years this area has fluctuated with drug use and homelessness as successive mayors and their administrations have tried to clean it up, but unfortunately no measures have stuck.
17
MELNEA CASS BLVD.
MASS AVE.
MASS AVE.
I-93 I-93
SOUTHAMPTON ST.
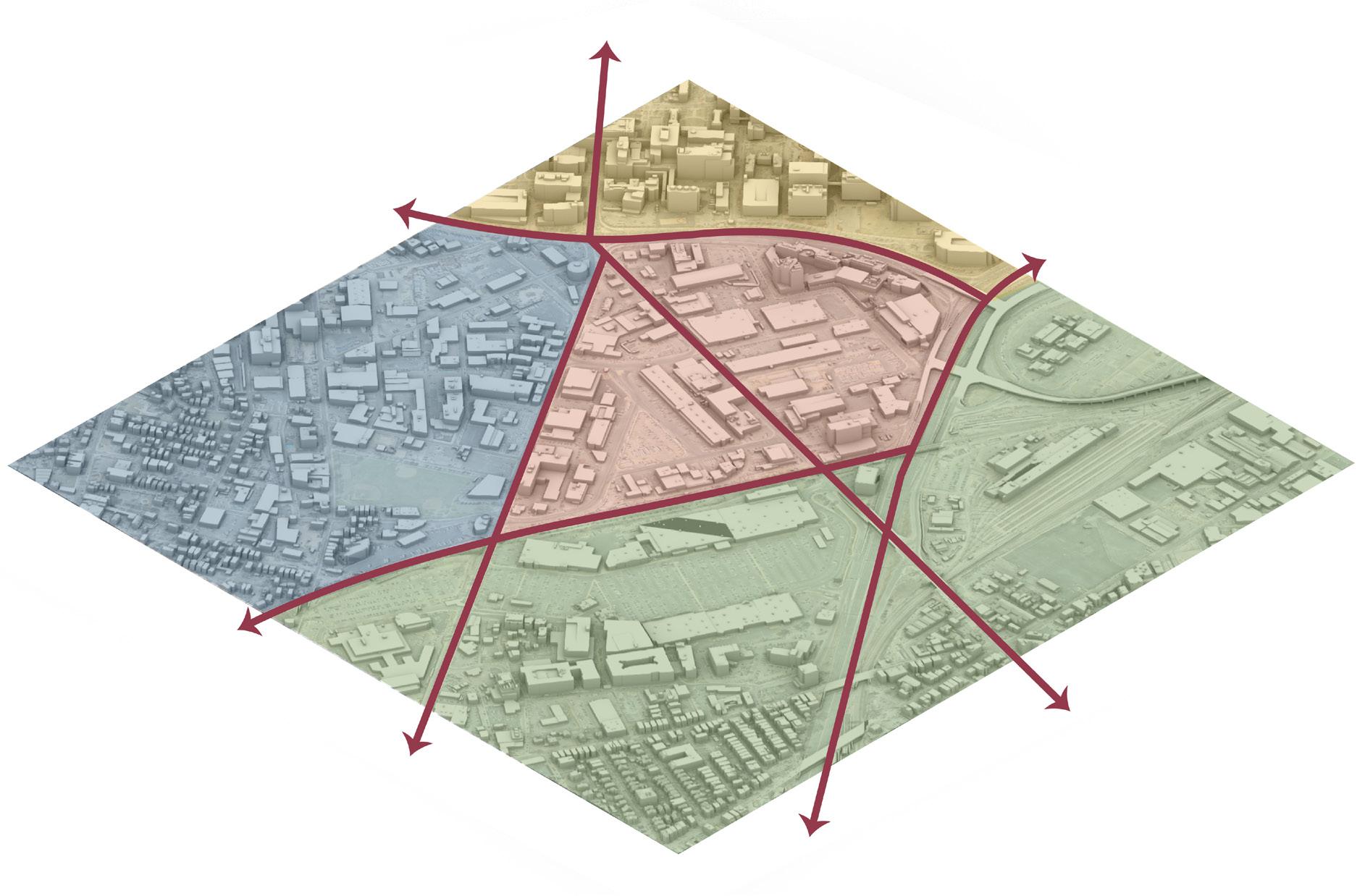
SITE NEWMARKET INDUSTRIAL DISTRICT SOUTH BOSTON SOUTH END ROXBURY DORCHESTER 6 6 Jesse Costa, WBUR 6
1 As Boston police prepare to remove ‘Mass. and Cass’ encampment, some wonder what comes next Deborah Becker, WBUR October 31st, 2023
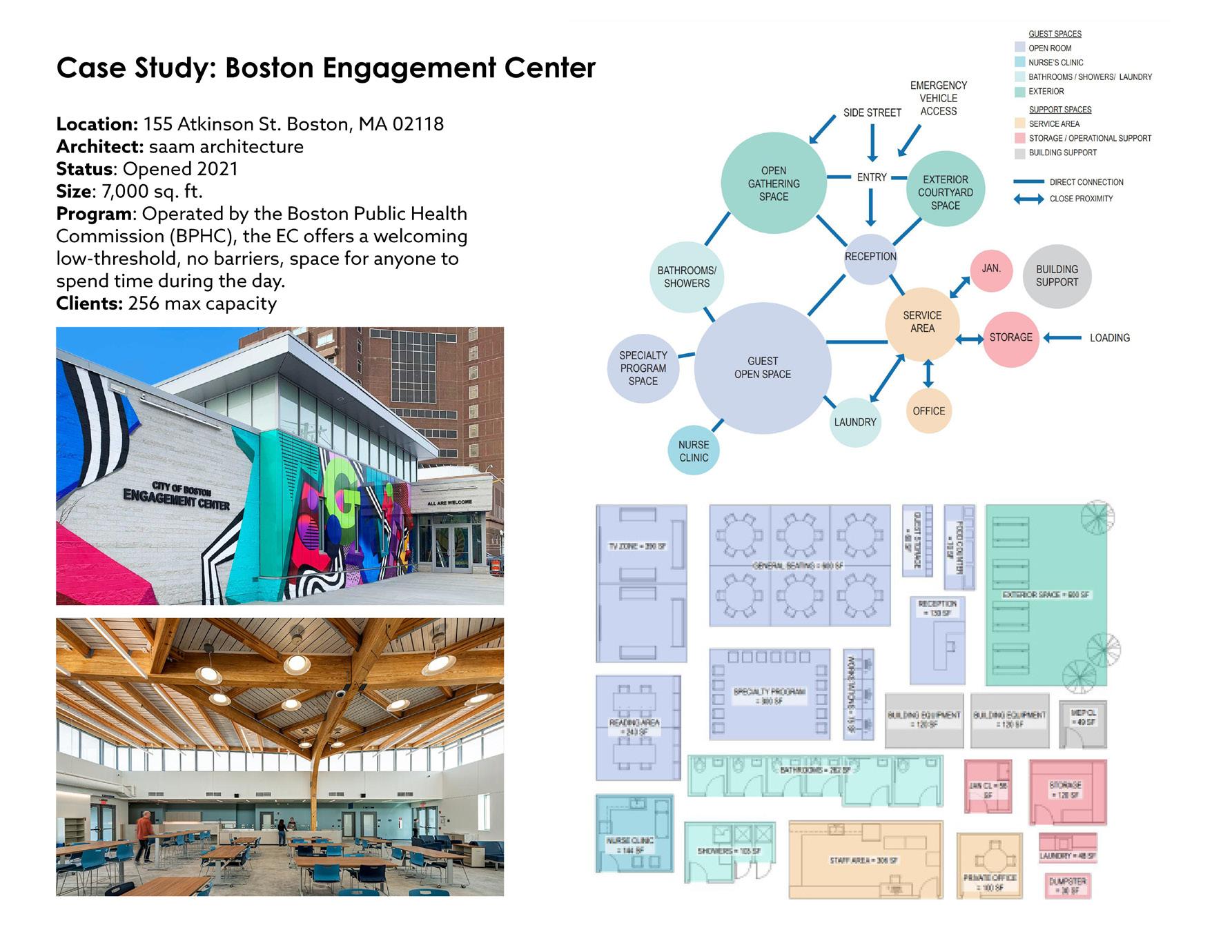
PRECEDENT | BOSTON ENGAGEMENT CENTER
Location: 155 Atkinson St. Boston, MA 02118
Architect: saam architecture
Status: Opened 2021
Size: 7,000 sq. ft.
Program: Operated by the Boston Public Health Commission (BPHC), the EC offers a welcoming low-threshold, no barriers, space for anyone to spend time during the day.
Clients: 256 max capacity

Note: The Engagement Center is located directly adjacent to the proposed project site. Due to unsafe conditions for outreach workers, the Engagement Center closed in November 2023 and is currently being used as a temporary overflow shelter for migrants. For the purpose of this Thesis, it is assumed that the EC will be reopened to complement the proposed program.1

and photos by saam architecture
18
Diagrams
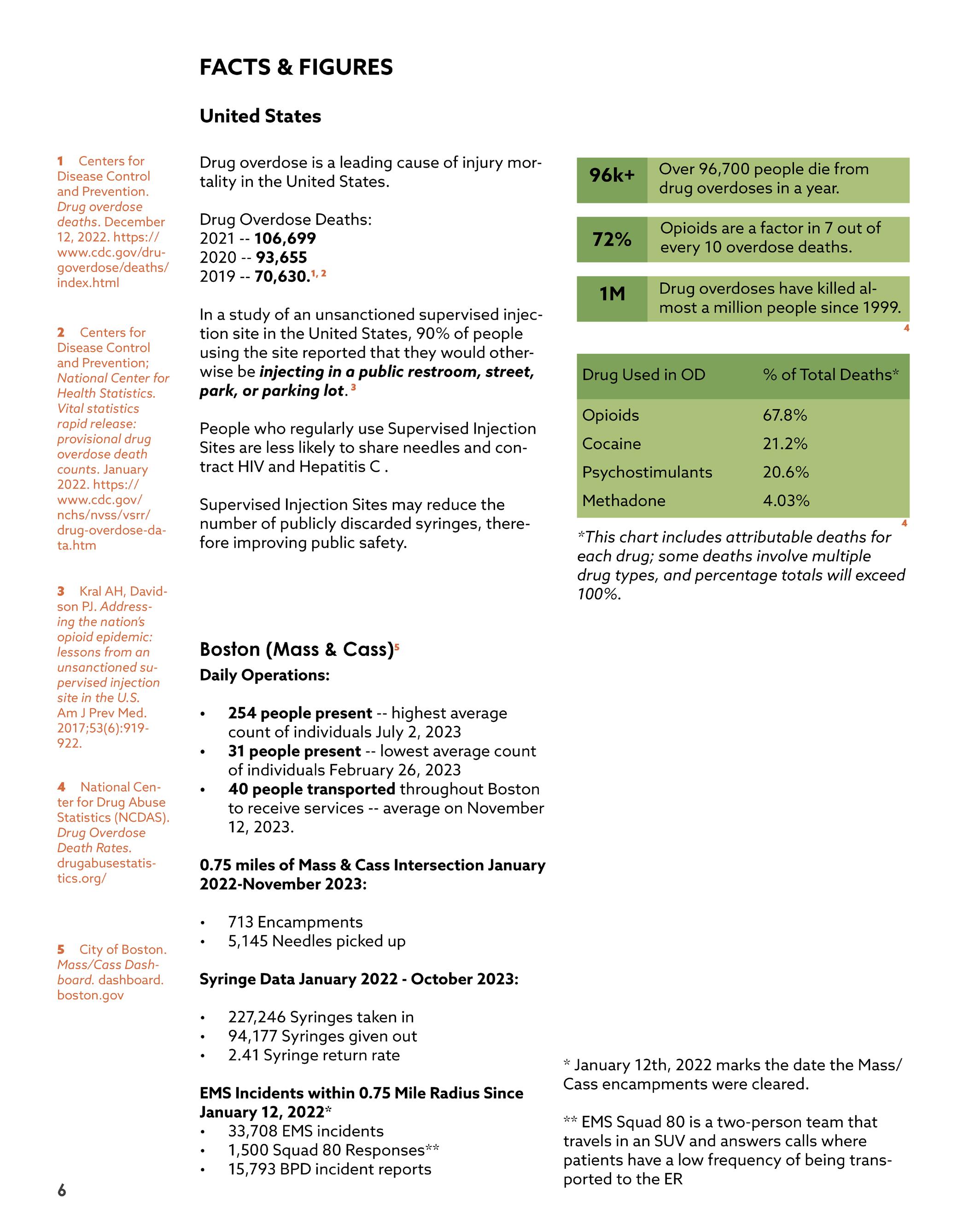
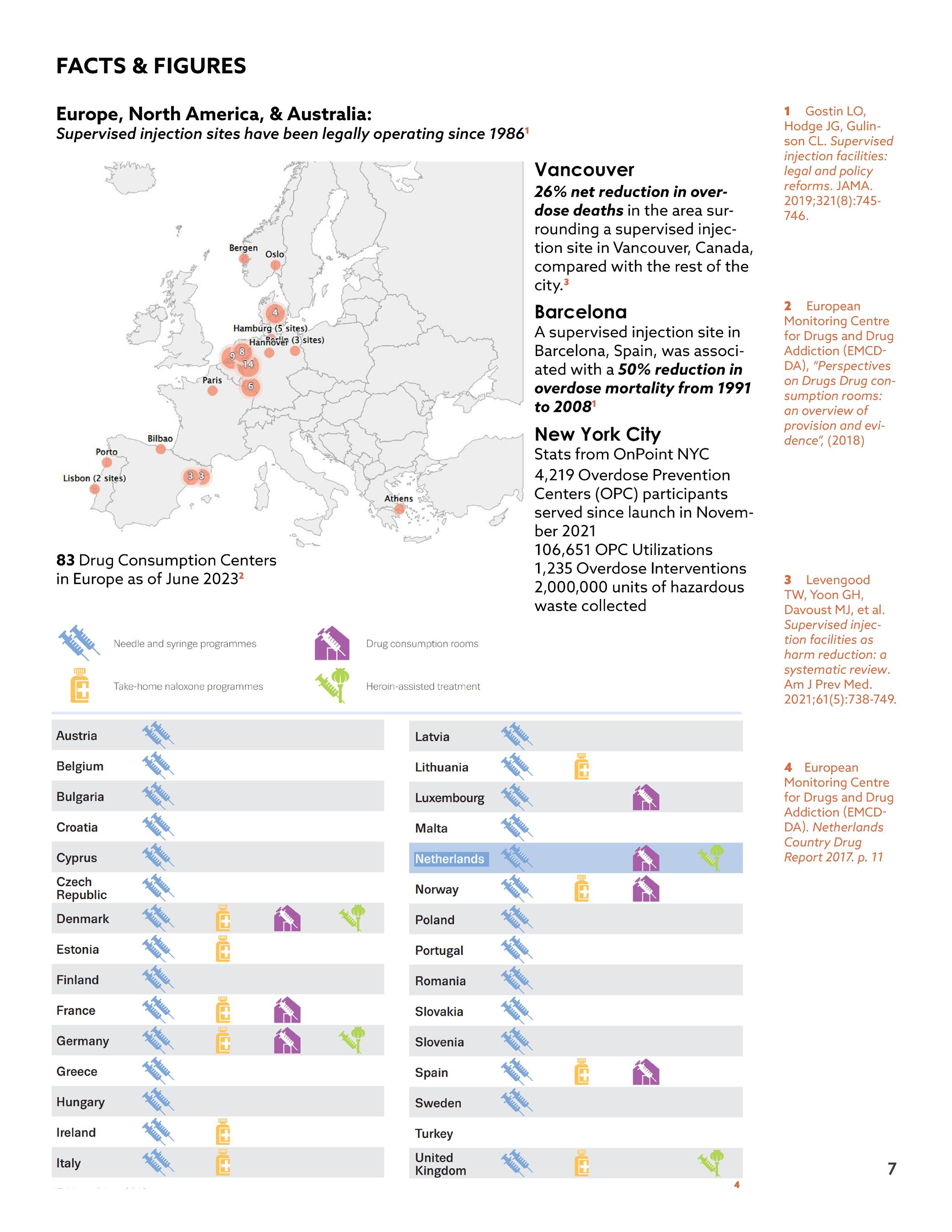
Europe, North America, & Australia:
Supervised injection sites have been legally operating since 19861
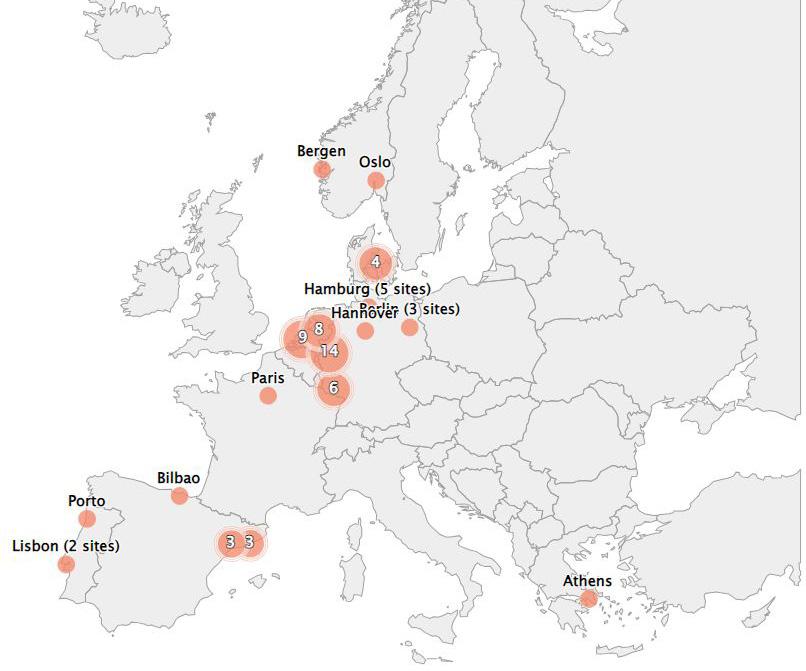
83 Drug Consumption Centers in Europe as of June 20232
Vancouver
26% net reduction in overdose deaths in the area surrounding a supervised injection site in Vancouver, Canada, compared with the rest of the city.3
Barcelona
A supervised injection site in Barcelona, Spain, was associated with a 50% reduction in overdose mortality from 1991 to 20081
New York City
Stats from OnPoint NYC
4,219 Overdose Prevention Centers (OPC) participants served since launch in November 2021
106,651 OPC Utilizations
1,235 Overdose Interventions
2,000,000 units of hazardous waste collected5
1 Gostin LO, Hodge JG, Gulinson CL. Supervised injection facilities: legal and policy reforms. JAMA. 2019;321(8):745746.
2 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), “Perspectives on Drugs Drug consumption rooms: an overview of provision and evidence”, (2018)
3 Levengood TW, Yoon GH, Davoust MJ, et al. Supervised injection facilities as harm reduction: a systematic review. Am J Prev Med. 2021;61(5):738-749.
4 European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Netherlands Country Drug Report 2017. p. 11
5 OnPoint, NYC nonpofit, operates two privately run safe injection sites in East Harlem and Washington Heights
19
4
| BEYOND BOSTON
PRECEDENT
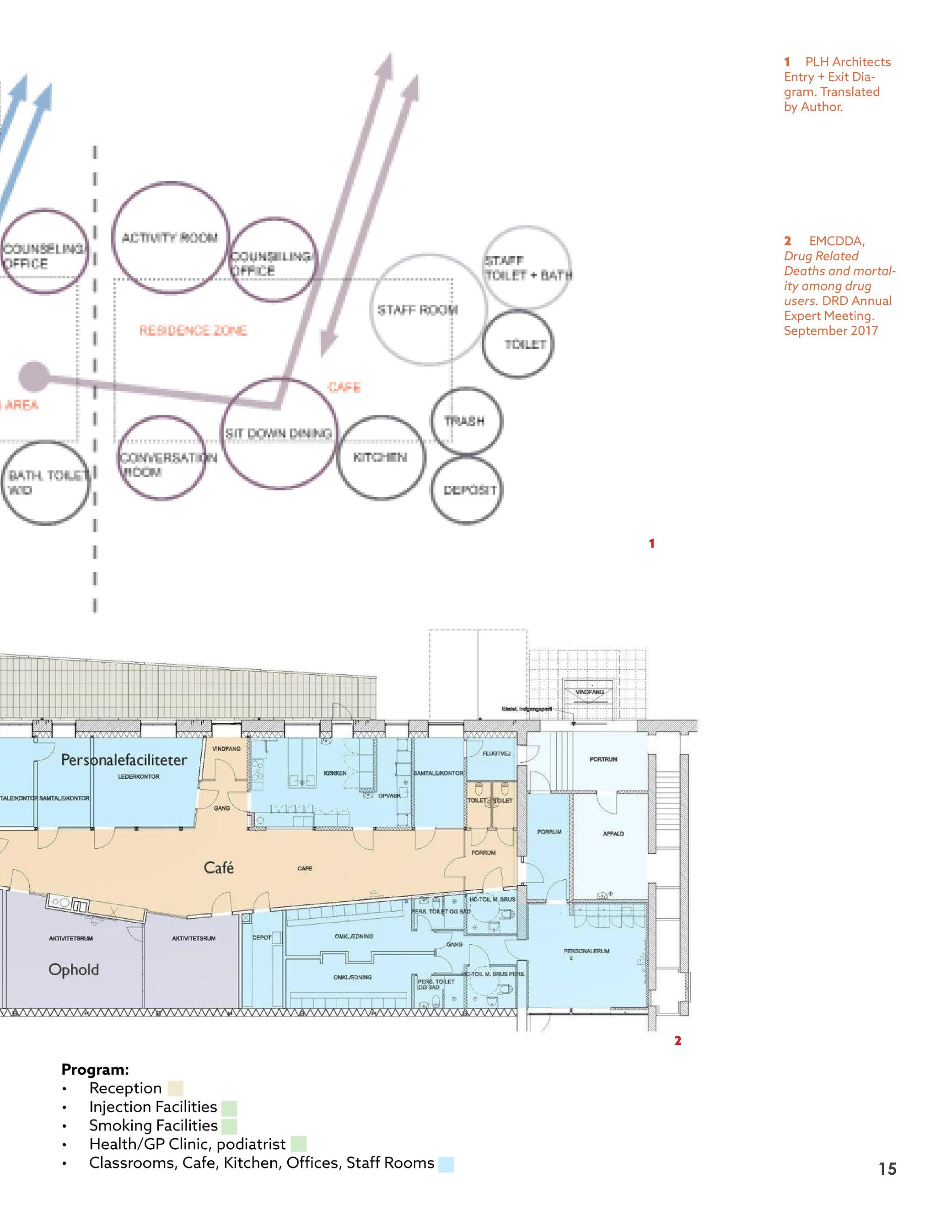
1 PLH Architects Entry + Exit Diagram. Translated from Danish by Grace Pilkington, using Google Translate
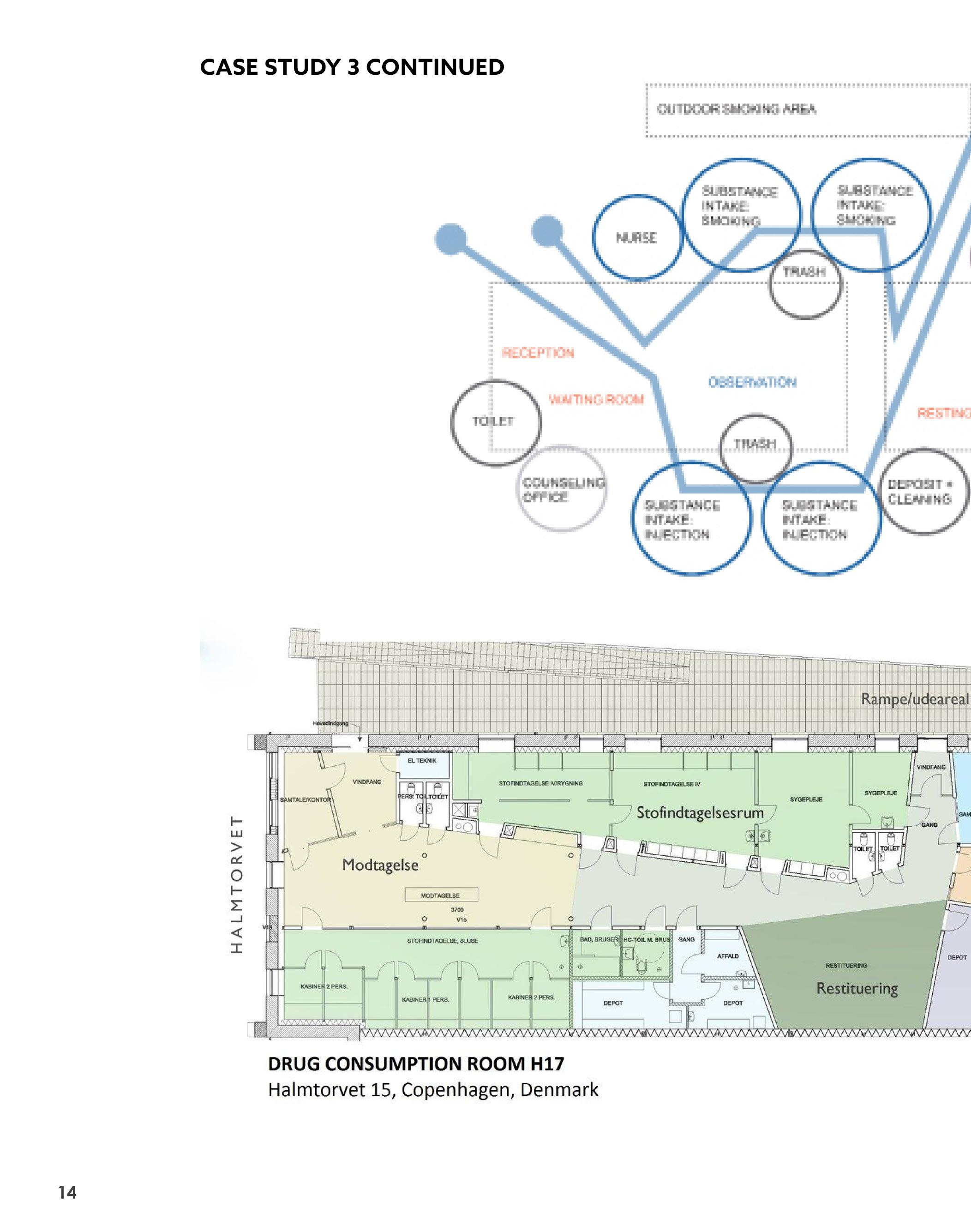
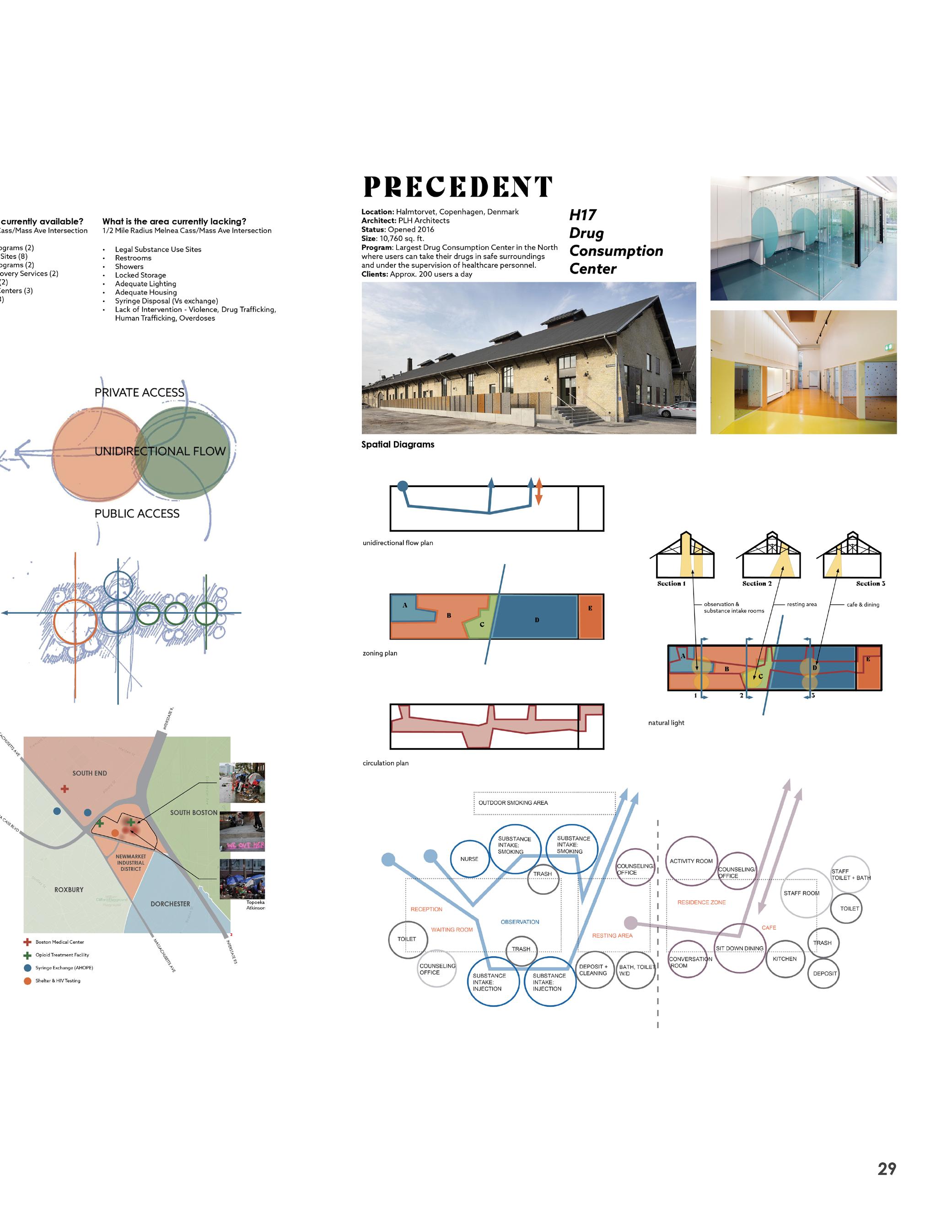
PRECEDENT | H17
Location: Vesterbro, Copenhagen, DK
Architect: PLH Architects
Status: Opened 2016
Size: 10,760 sq. ft.
Program: Largest Drug Consumption Center in the North where users can take their drugs in safe surroundings and under the supervision of healthcare personnel.
Clients: Approx. 200 users a day

20
1
Diagrams by Grace Pilkington
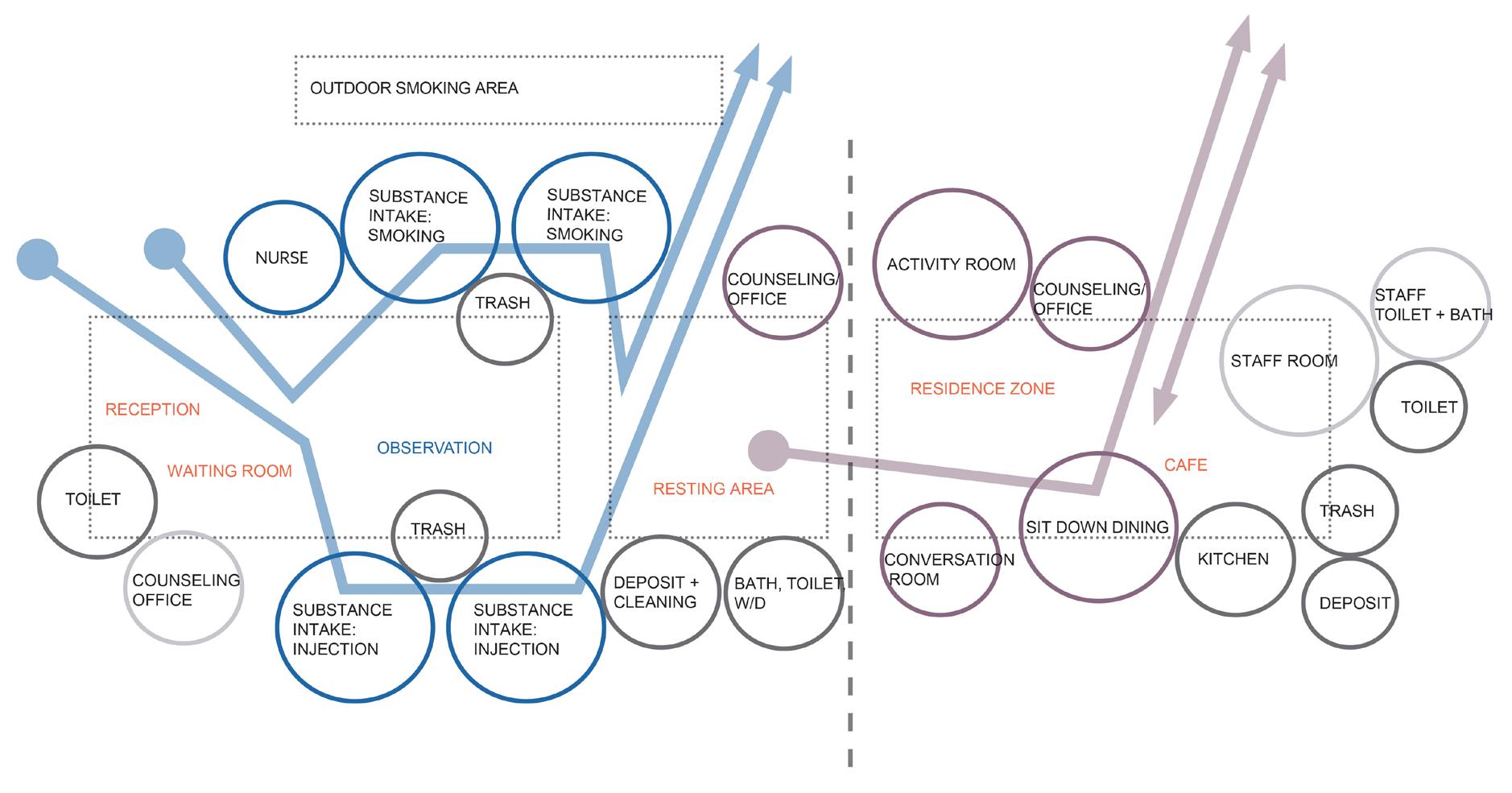
PROGRAM | H17
GENERAL REQUIREMENTS
ARRIVAL
• Clear wayfinding on interior and exteriorvisible from the street
• Adequate lighting to prevent dark areas
• Spacious indoor conditions to prevent conflict
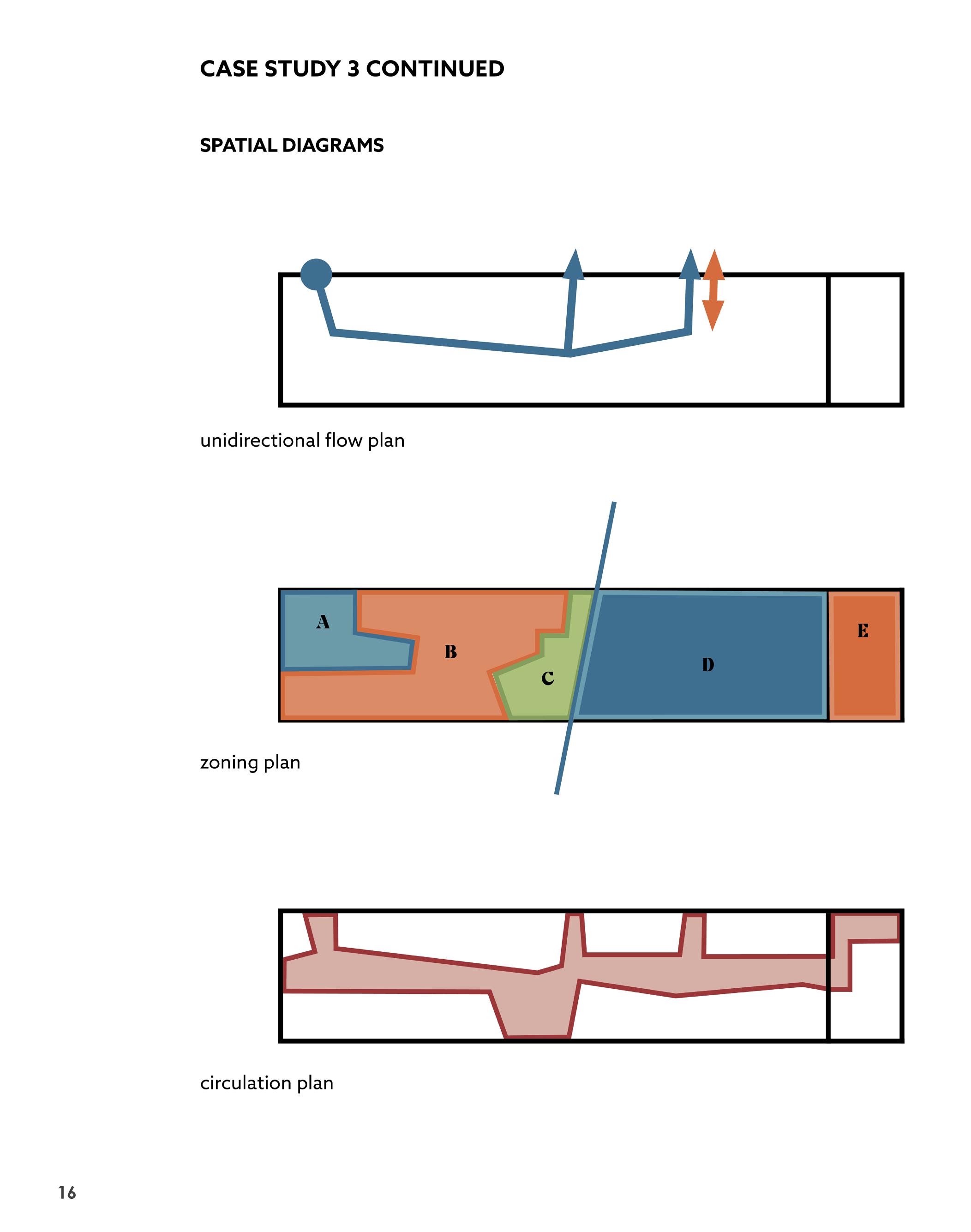
• Unidirectional flow
DRUG RECOVERY ROOMS
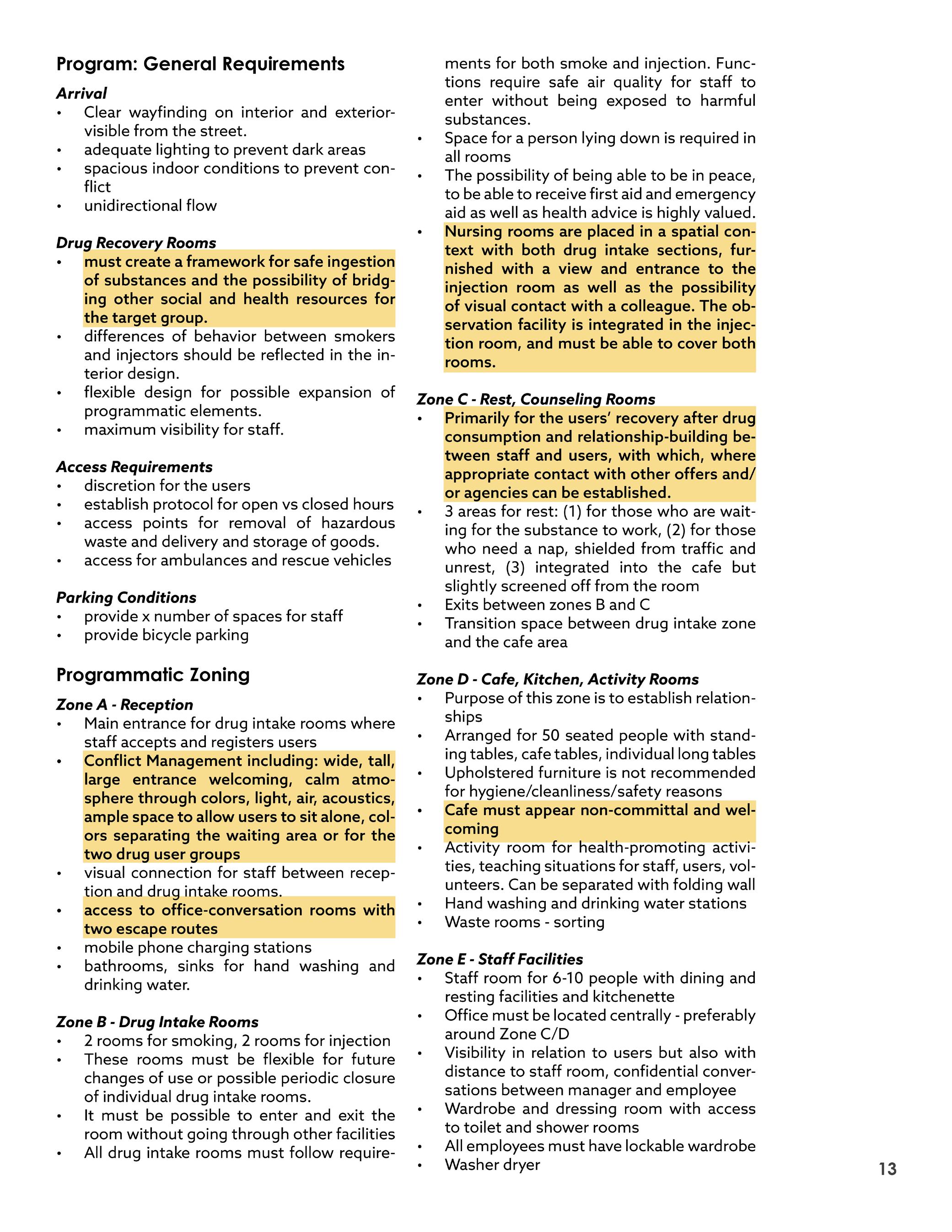
• Must create a framework for safe ingestion of substances and the possibility of bridging other social and health resources for the target group
• Differences of behavior between smokers and injectors should be reflected in the interior design
• Flexible design for possible expansion of programmatic elements
• Maximum visibility for staff
ACCESS REQUIREMENTS
• Discretion for the users
• Establish protocol for open vs closed hours
• Access points for removal of hazardous waste and delivery and storage of goods
• Access for ambulances and rescue vehicles
PARKING CONDITIONS
• Provide x number of spaces for staff
• Provide bicycle parking
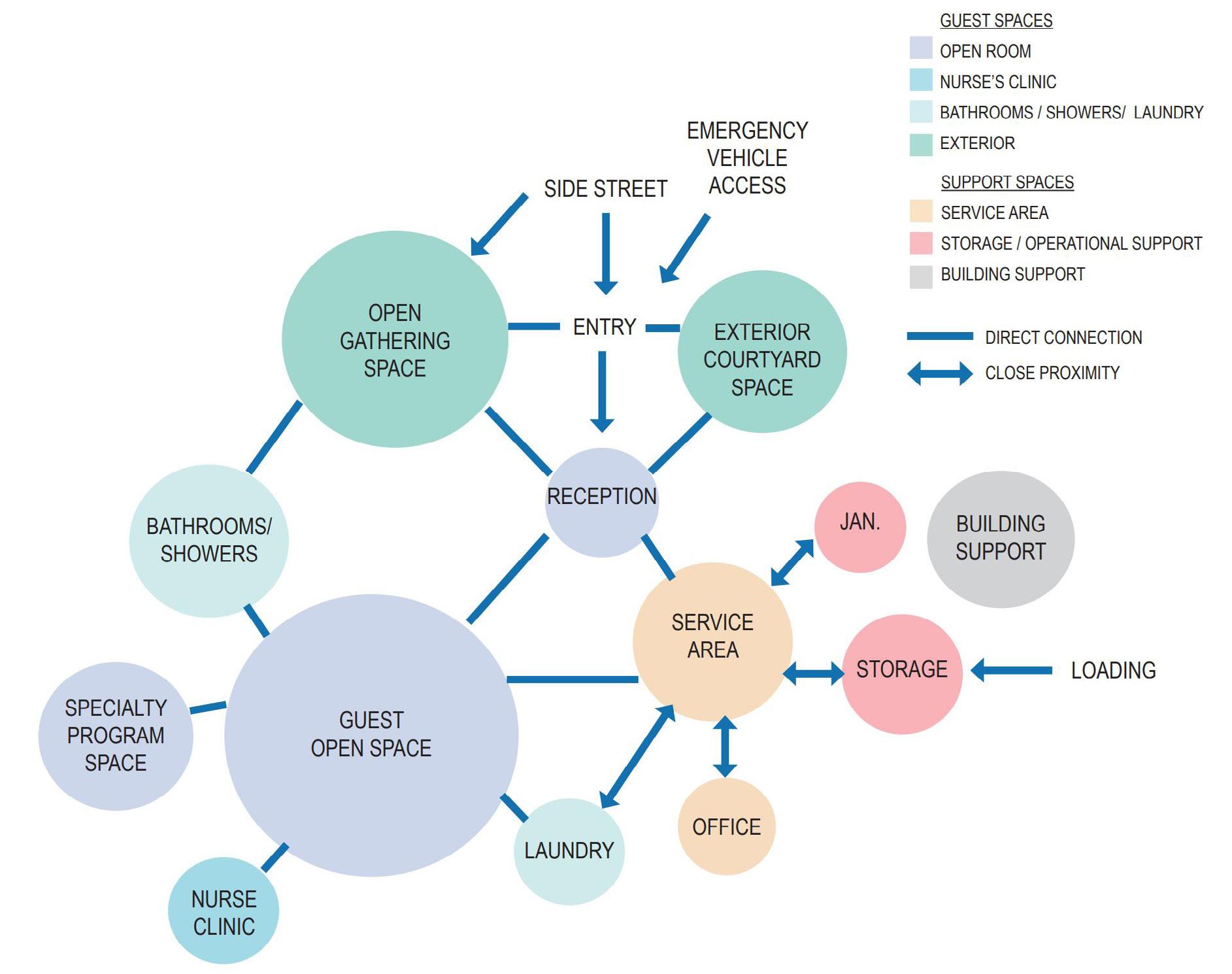
ZONE A - RECEPTION
• Main entrance for drug intake rooms where staff accepts and registers users
• Conflict Management including: wide, tall, large entrance welcoming, calm atmosphere through colors, light, air, acoustics, ample space to allow users to sit alone, colors separating the waiting area or for the two drug user groups
• Visual connection for staff between reception and drug intake rooms
• Access to office-conversation rooms with two escape routes
• Mobile phone charging stations
• Bathrooms, sinks for hand washing and drinking water
ZONE B - DRUG INTAKE ROOMS
• 2 rooms for smoking, 2 rooms for injection
• These rooms must be flexible for future changes of use or possible periodic closure of individual drug intake rooms
• It must be possible to enter and exit the room without going through other facilities
• All drug intake rooms must follow require-
ments for both smoke and injection. Functions require safe air quality for staff to enter without being exposed to harmful substances.
• Space for a person lying down is required in all rooms
• The possibility of being able to be in peace, to be able to receive first aid and emergency aid as well as health advice is highly valued.
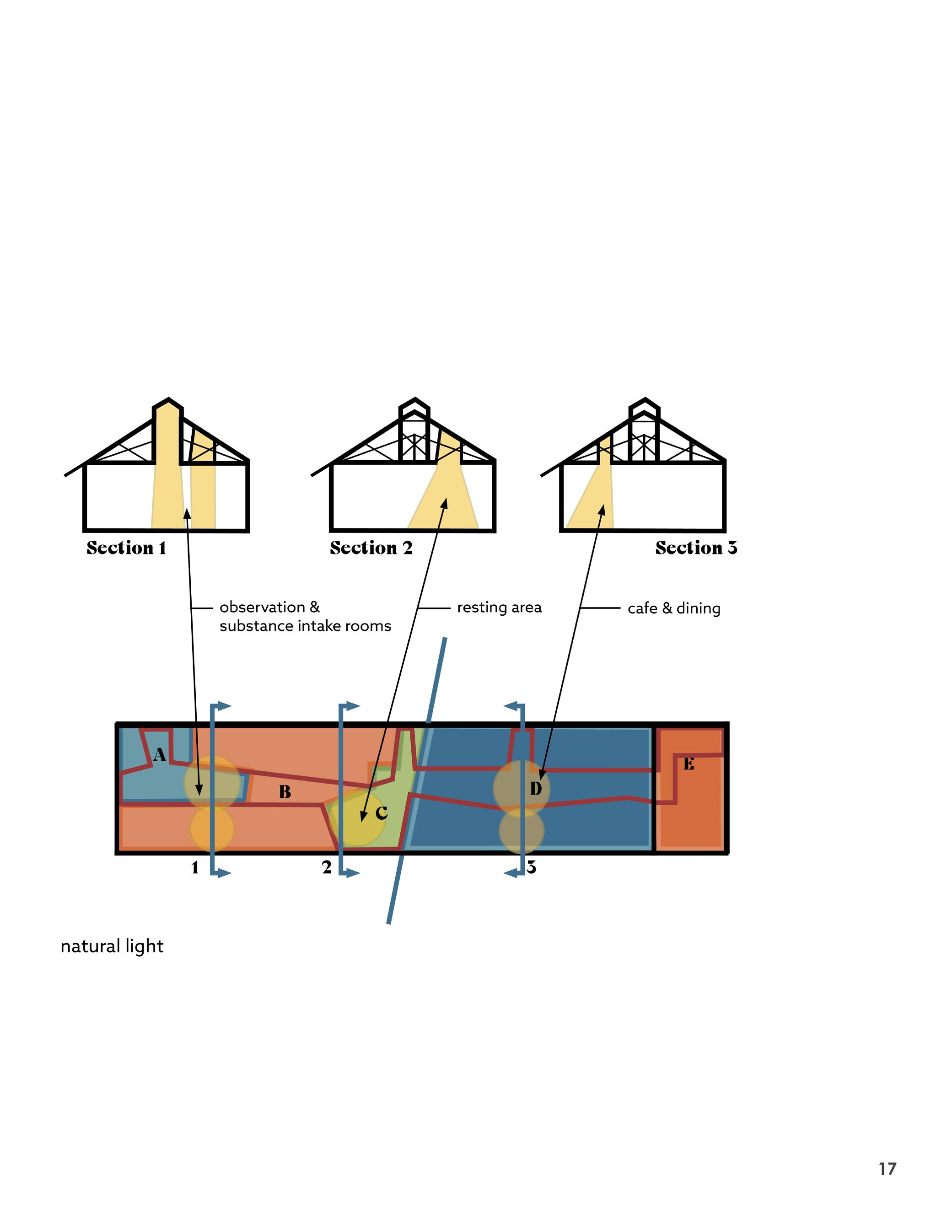
• Nursing rooms are placed in a spatial context with both drug intake sections, furnished with a view and entrance to the injection room as well as the possibility of visual contact with a colleague. The observation facility is integrated in the injection room, and must be able to cover both rooms.
ZONE C - REST, COUNSELING ROOMS
• Primarily for the users’ recovery after drug consumption and relationship-building between staff and users, with which, where appropriate contact with other offers and/ or agencies can be established.
• 3 areas for rest: (1) for those who are waiting for the substance to work, (2) for those who need a nap, shielded from traffic and unrest, (3) integrated into the cafe but slightly screened off from the room
• Exits between zones B and C
• Transition space between drug intake zone and the cafe area
ZONE D - CAFE, KITCHEN, ACTIVITY ROOMS
• Purpose of this zone is to establish relationships
• Arranged for 50 seated people with standing tables, cafe tables, individual long tables
• Upholstered furniture is not recommended for hygiene/cleanliness/safety reasons
• Cafe must appear non-committal and welcoming
• Activity room for health-promoting activities, teaching situations for staff, users, volunteers. Can be separated with folding wall
• Hand washing and drinking water stations
• Waste rooms - sorting
ZONE E - STAFF FACILITIES
• Staff room for 6-10 people with dining and resting facilities and kitchenette
• Office must be located centrally - preferably around Zone C/D
• Visibility in relation to users but also with distance to staff room, confidential conversations between manager and employee
• Wardrobe and dressing room with access to toilet and shower rooms
• All employees must have lockable wardrobe
• Washer dryer
PLH Architects Drug Consumption Center, Halmtorvet plh.dk/
Notes translated from Danish by Grace Pilkington, using Google Translate
21
1
Abrupt closing of Long Island Bridge was slow to arrive.
Meghan, E. Irons, Nicole Dungca, Boston Globe, December 14, 2014
2
Homeless Displaced By Long Island Bridge Closure Remain In Flux. Deborah Becker, Lynn Jolicoeur WBUR, December 18, 2014
CONTEXT |
Why here?
Why did Mass & Cass become the epicenter of New England’s opioid addiction crisis?
On October 8th, 2014, The City of Boston condemned the Long Island Bridge, deeming it unsafe. This was the only bridge connecting Boston to Long Island, an island located in Boston harbor that had numerous recovery services and shelters. 1 57% of the city’s substance use treatment beds were housed on Long Island. 2 The 12+ buildings were abruptly abandoned and now sit dilapidated on the island.
In the summer of 2023 there was a major increase in crime and violence. “According to BPD [Boston Police Department] statistics, July and August were the busiest two months in the area this year for overall “part 1” crime — violent crime and property crime — with July’s 99 incidents almost double the previous July’s 53. Other tragedies are hidden. When the encampment was temporarily cleared in January of last year, two bodies were found inside the tents.” 5
Boston Opens Expanded Southampton Street Homeless Shelter.
Benjamin Swasey WBUR June 25, 2015
3 ‘It’s never ever been this bad’: 100+ tents set up along Methadone Mile concern community leaders.
Drew Karedes, Boston 25 News September 3rd, 2021
4 Mass. and Cass shows the failure of progressive drug policies Left-leaning officials insist that police crackdowns on open-air drug encampments backfire. But the hands-off approach has sown violence and misery.
Carine Hajjar, Boston Globe October 8th, 2023 5
The bridge closure displaced around 700 people. Many women were placed in the Barbara McInnis House, located on the Boston Medical Center Campus and men were placed nearby in the South End Fitness Center. The shelters were overflowing with people and living conditions were atrocious. 2
Due to the need for shelters, in January 2015, Mayor Walsh had nearby buildings in the Newmarket area converted into shelters and increased the capacity of existing shelters. 3
With the increase of folks experiencing addiction, homelessness, and mental illness, opioid treatment facilities started popping up, such as the methadone clinic on Topeka Street.
The migration of homeless and addicts to the area caused businesses to start reporting more and more incidents of vandalism and camping. The encampments kept growing and the number of tents grew from a dozen in Sept 2021 to 140 by July 2023. 4
By October 2023 there had been 220 overdoses reversed, with a weekly average of 345 medical emergencies. 5
It is thought that there are about 8090 people truly living in the area, while the majority of people come only during the day to buy or sell drugs.
Since mayor Wu assumed office in November 2021, she has had numerous efforts to “sweep” the area, specifically Atkinson Street. During these sweeps, folks are only notified to remove their belongings one day before- only to move to another site further away from medical resources.
Mayor Wu has made it illegal to camp in the area - with the threat of being arrested.
Many folks are placed in short-term substance use treatment facilities and some are sheltered in low-threshold sites. But for those who fall between the cracks or are not offered one of these housing options - they have nowhere to go.
22
HISTORY
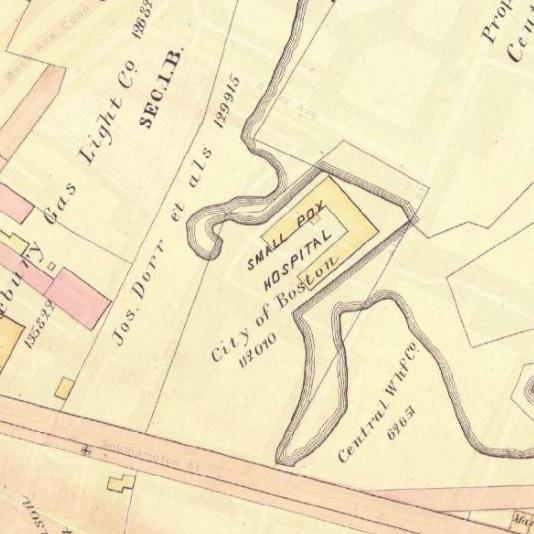
1900
Building on site is a Small Pox Hospital

MassAve.Connector
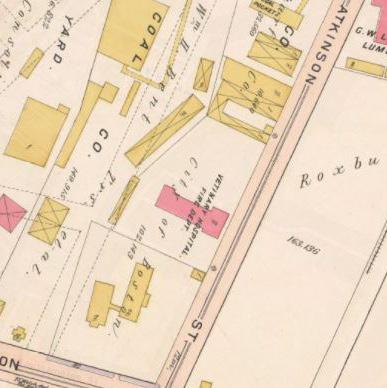
1906
Building on site is a Veterinary Hospital + Fire Dept.
1969
Mass Ave. Connector is built. Creates a divide between the South End and Newmarket Industrial Area.
MelneaCassBlvd.

1981
Melnea Cass Blvd. is built. Creates a divide between the South End and Roxbury.
1991
Suffolk County House of Correction is built. Many folks experiencing homelessness spend their time between the Correctional Facility and the adjacent Atkinson Street.
Maps are from the Boston Planning & Development Agency (BPDA).
3D Data & Maps. Map Library
The site has a history of being a healthcare facility, as it was once a Veterinary Hospital, and once a Small Pox Hospital
23 CONTEXT | HISTORY
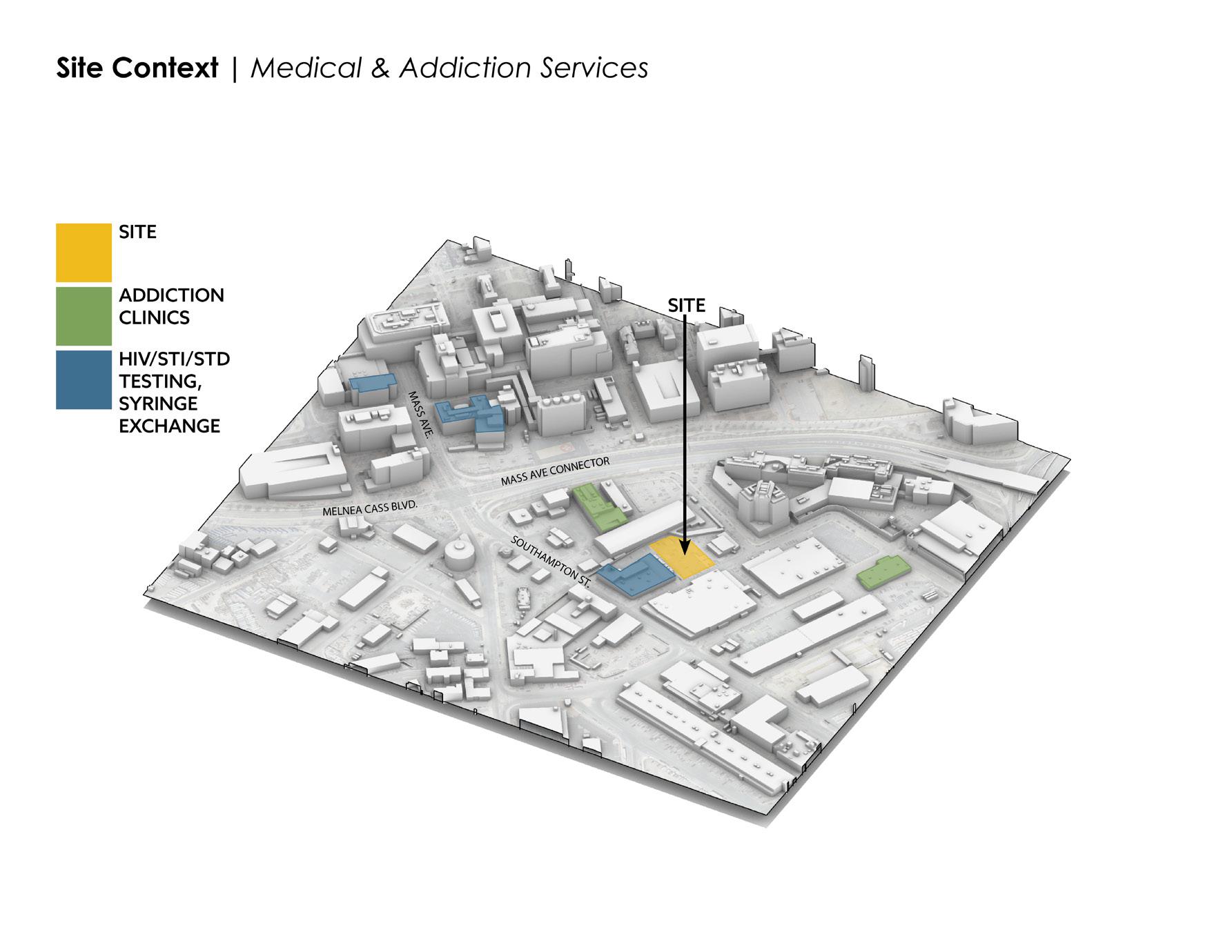
SITE
ADDICTION CLINICS
HIV/STI/STD TESTING, SYRINGE EXCHANGE
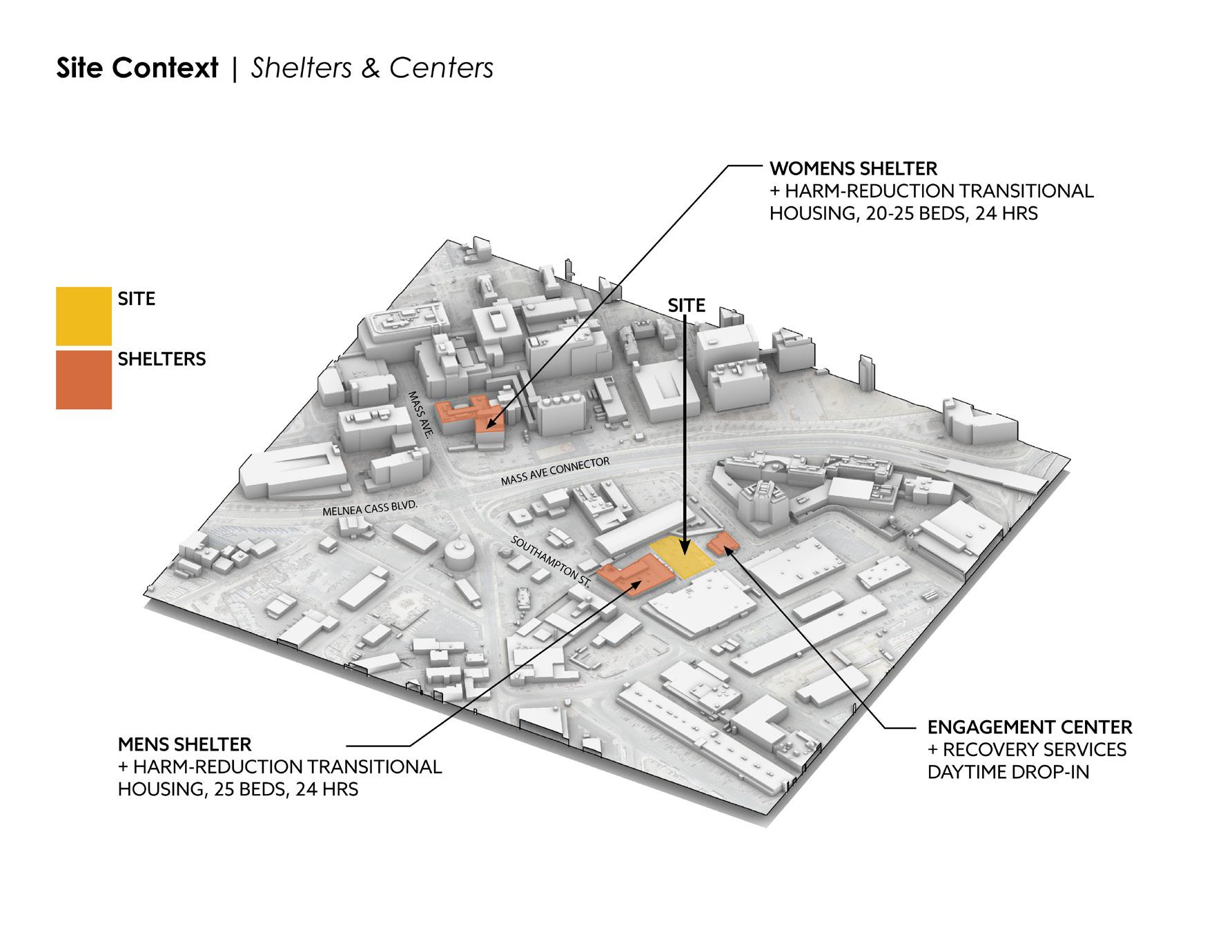
SITE
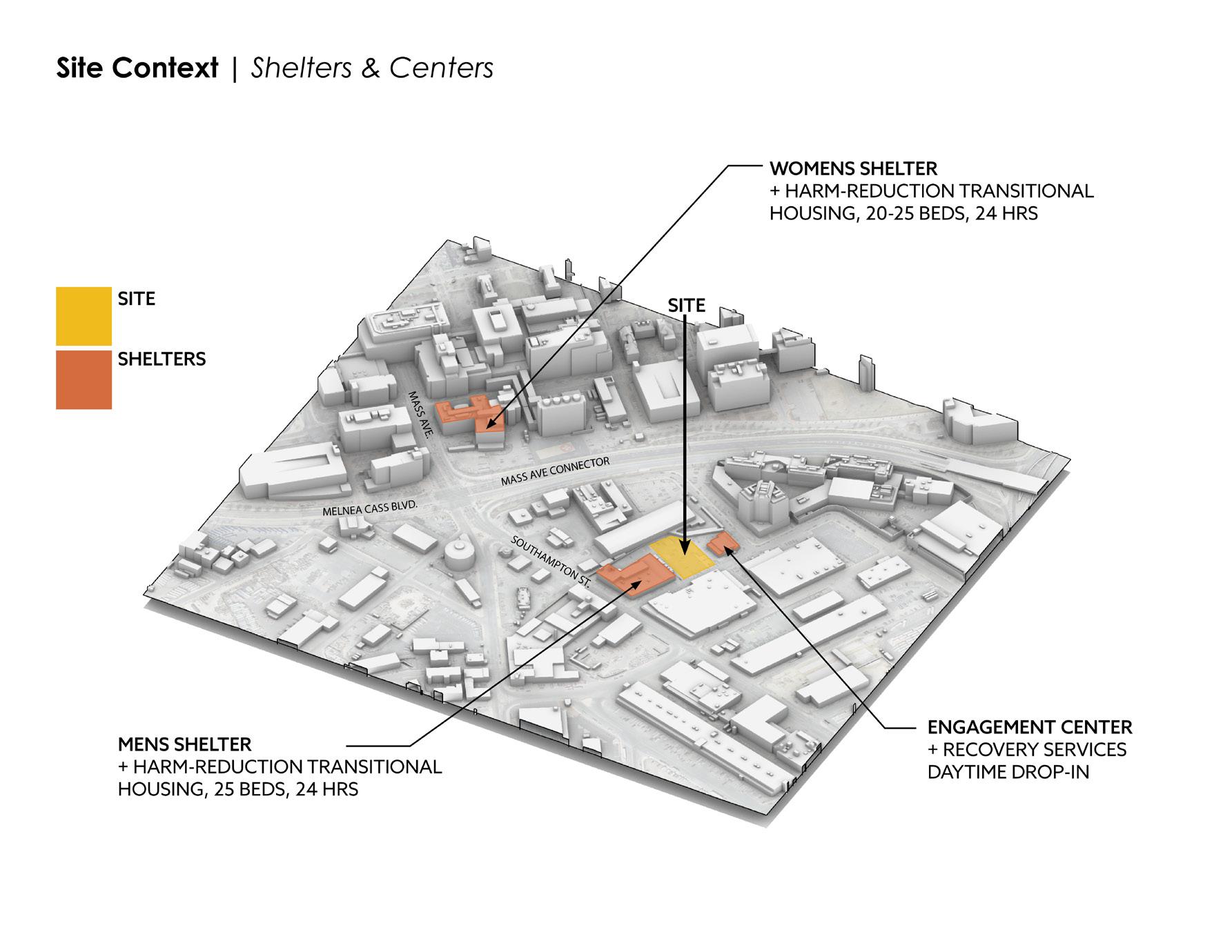
SITE SHELTERS
WOMENS SHELTER + HARM-REDUCTION TRANSITIONAL HOUSING, 20-25 BEDS, 24 HRS
SITE
MENS SHELTER + HARM-REDUCTION TRANSITIONAL HOUSING, 25 BEDS, 24 HRS
ENGAGEMENT CENTER + RECOVERY SERVICES DAYTIME DROP-IN
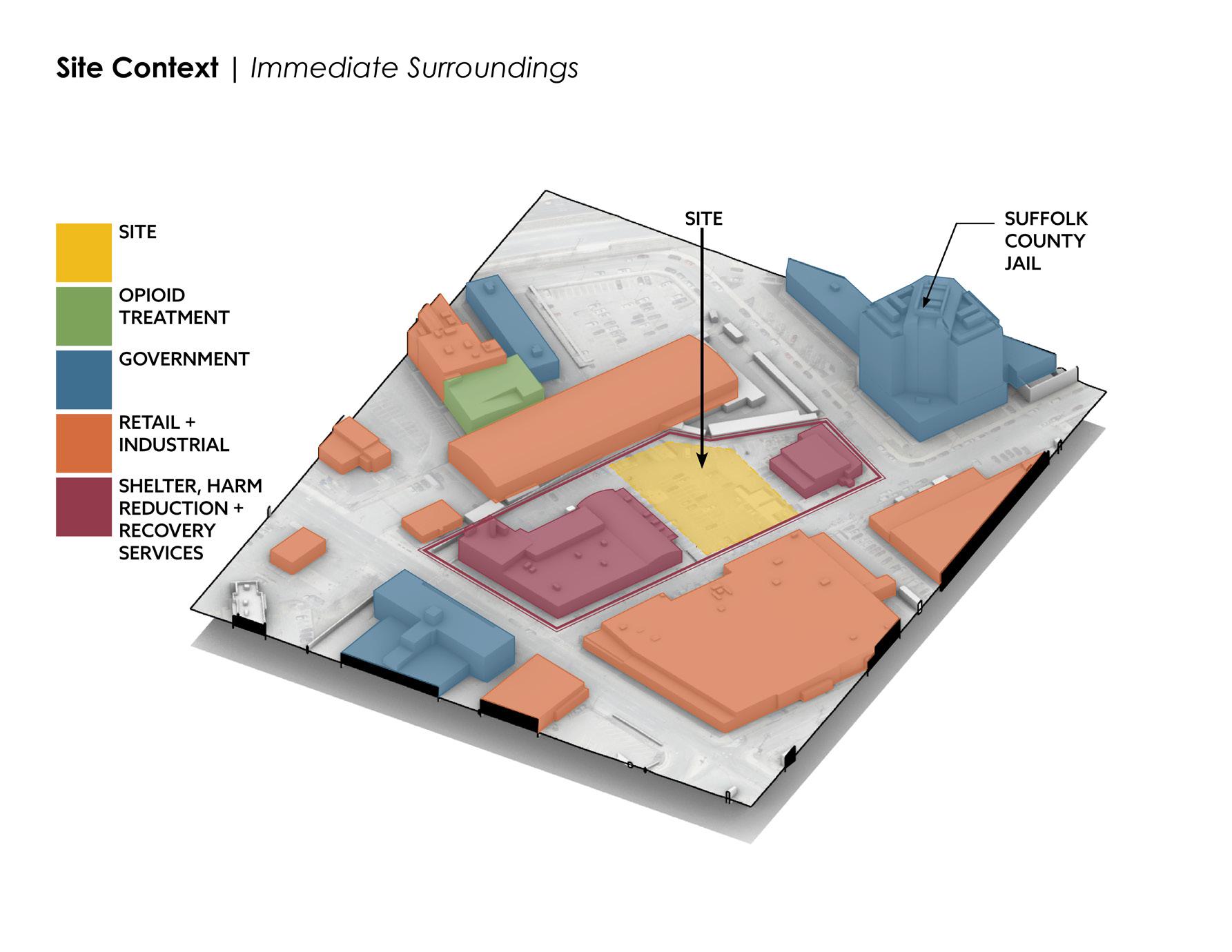
24 CONTEXT | SITE
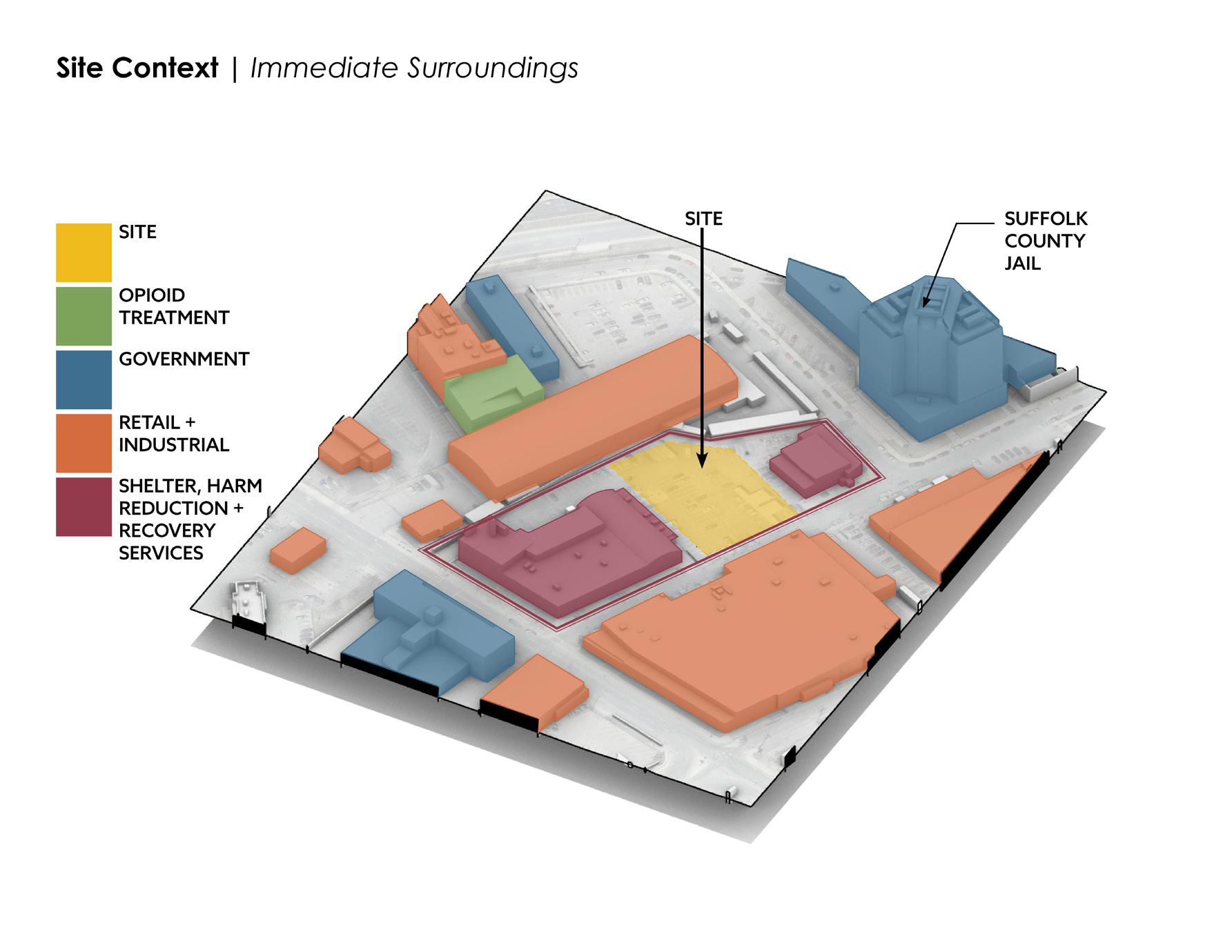
SITE
OPIOID TREATMENT
GOVERNMENT
RETAIL + INDUSTRIAL
SHELTER, HARM REDUCTION + RECOVERY SERVICES
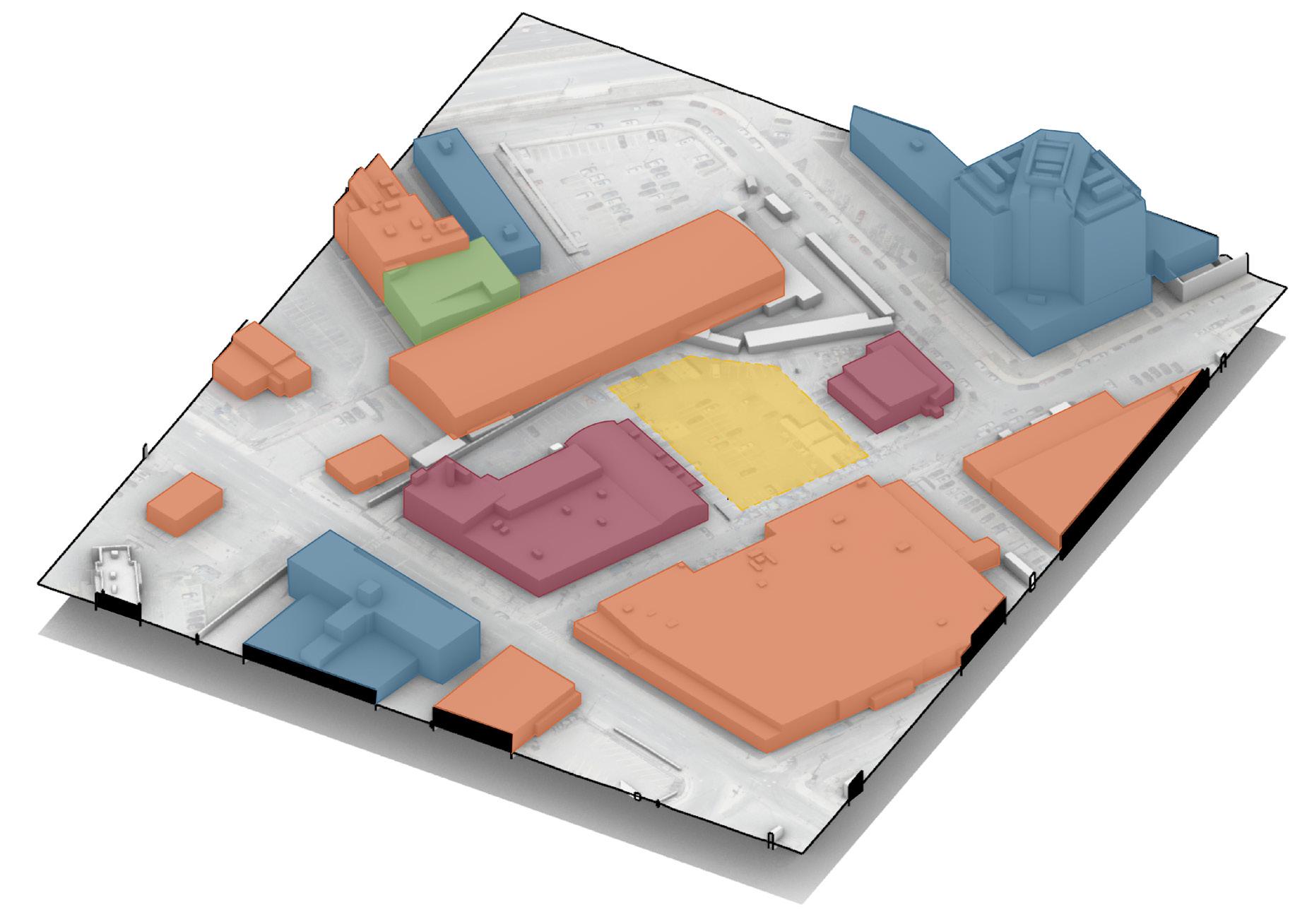
The many recovery services in the area are what lends the moniker “Methadone Mile” or “Recovery Road”.
SITE
SUFFOLK COUNTY JAIL
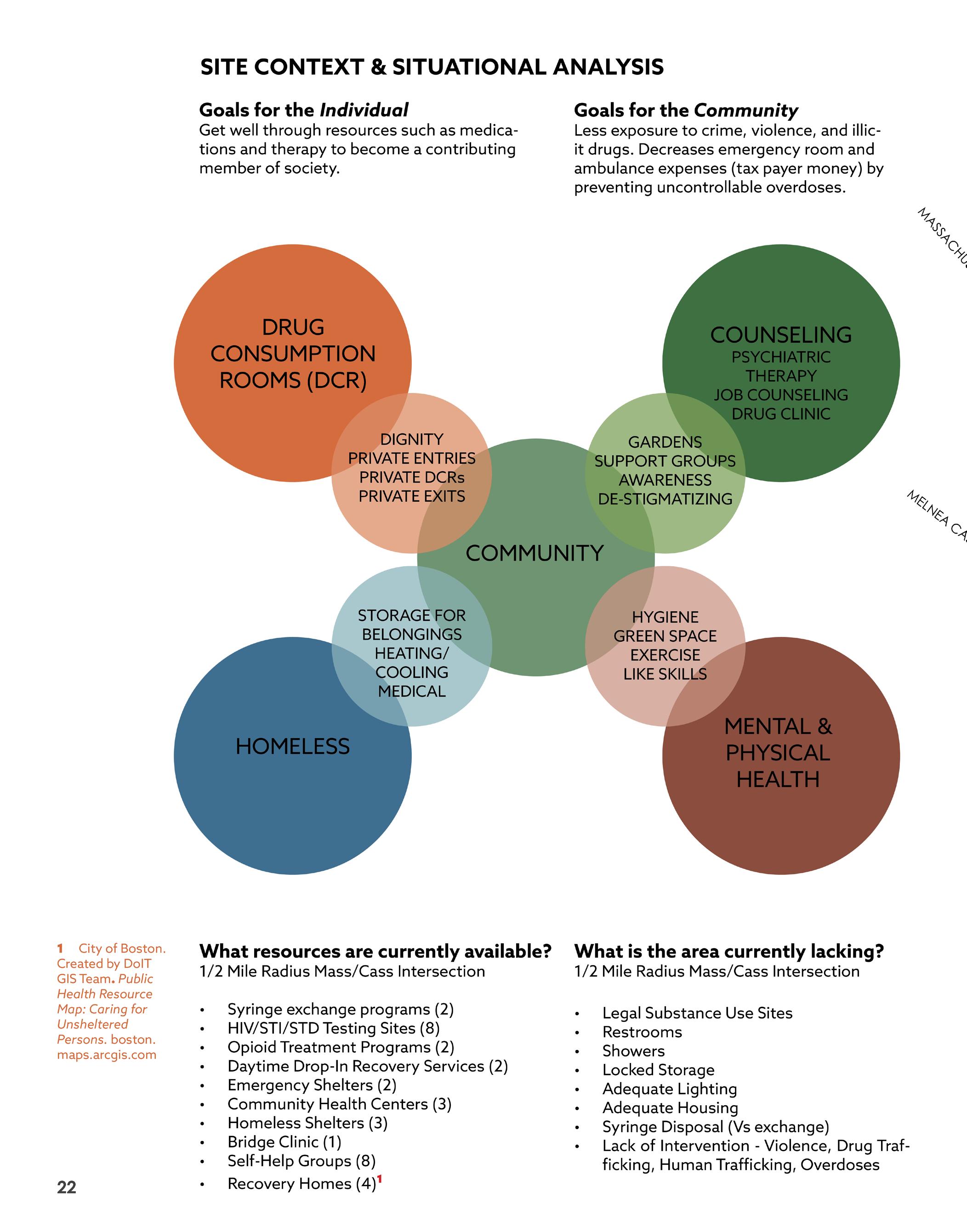
What resources are currently available?1
1/2 Mile Radius Mass/Cass Intersection
• Syringe exchange programs (2)
• HIV/STI/STD Testing Sites (8)
• Opioid Treatment Programs (2)
• Daytime Drop-In Recovery Services (2)
• Emergency Shelters (2)
• Community Health Centers (3)
• Homeless Shelters (3)
• Bridge Clinic (1)
• Self-Help Groups (8)
• Recovery Homes (4)
One of my main goals is to activate the entire block as a harm reduction, resource access campus for the Mass and Cass Area.
What is the area currently lacking?
1/2 Mile Radius Mass/Cass Intersection
• Legal Substance Use Sites
• Restrooms
• Showers
• Locked Storage
• Adequate Lighting
• Adequate Housing
• Syringe Disposal (Vs exchange)
• Lack of Intervention - Violence, Drug Trafficking, Human Trafficking, Overdoses
1
of Boston. Created by DoIT GIS Team. Public Health Resource Map: Caring for Unsheltered Persons. boston.maps. arcgis.com
25
CONTEXT | SITE
City
26
PART II
Schematic Design Program
User Profiles
Massing | Exploration
27
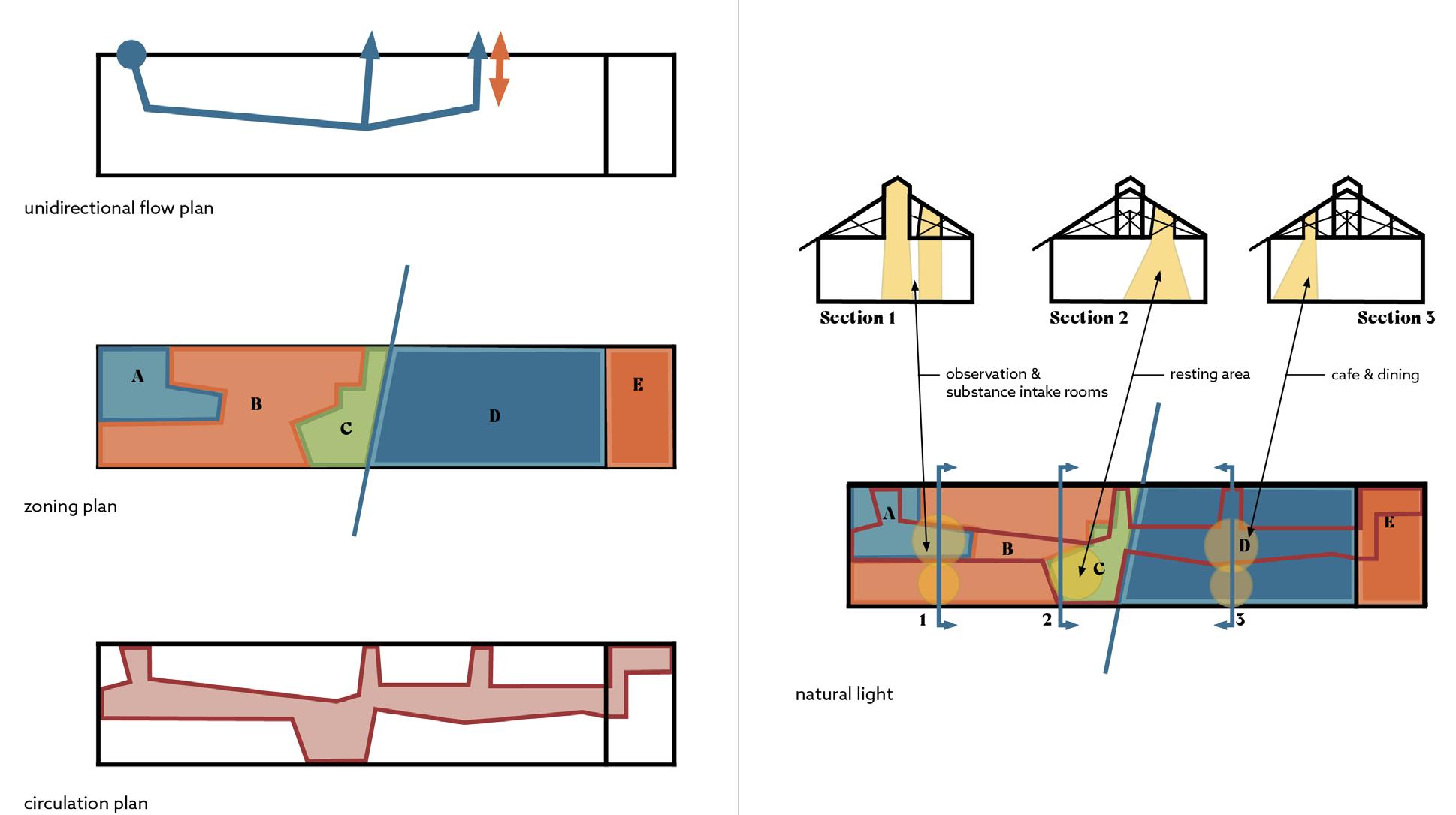
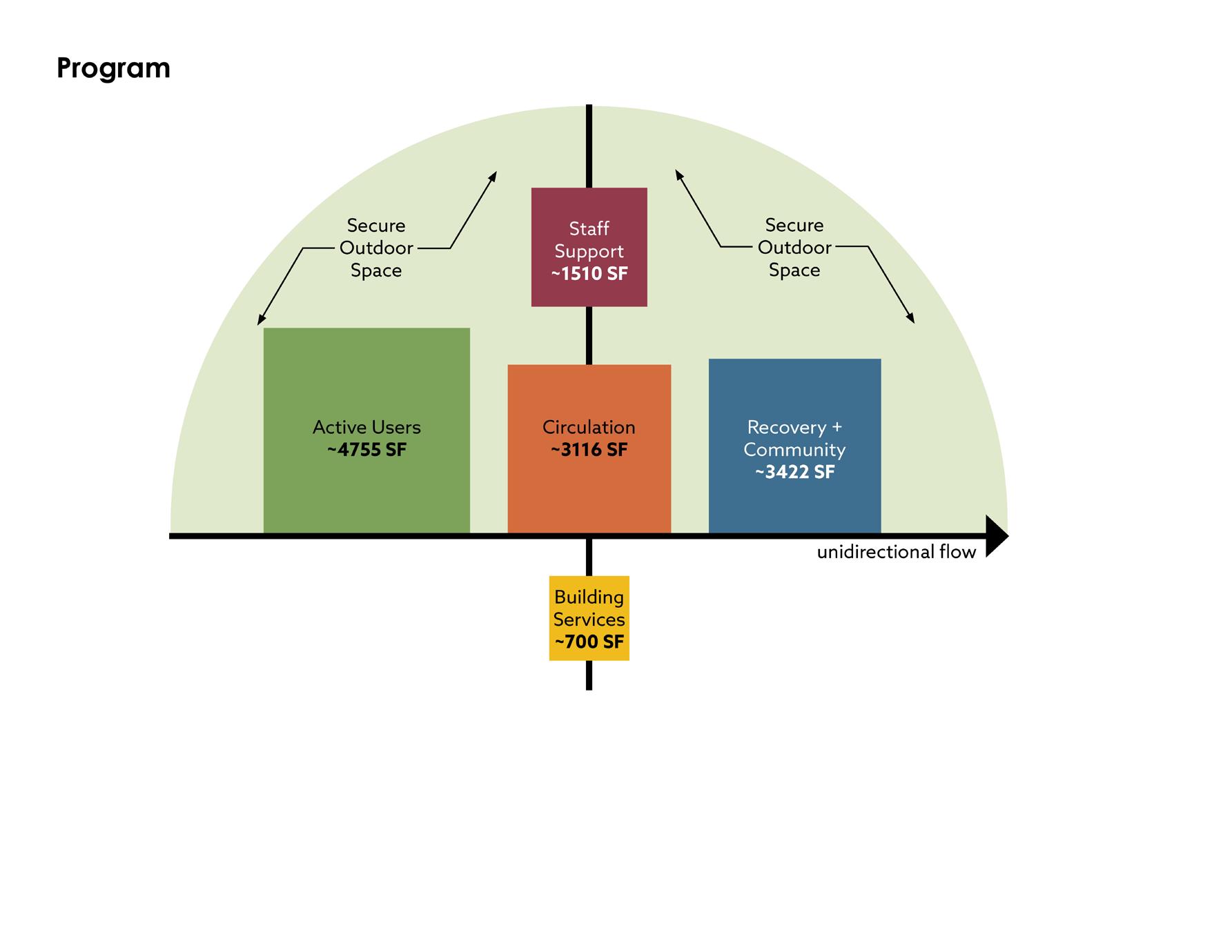
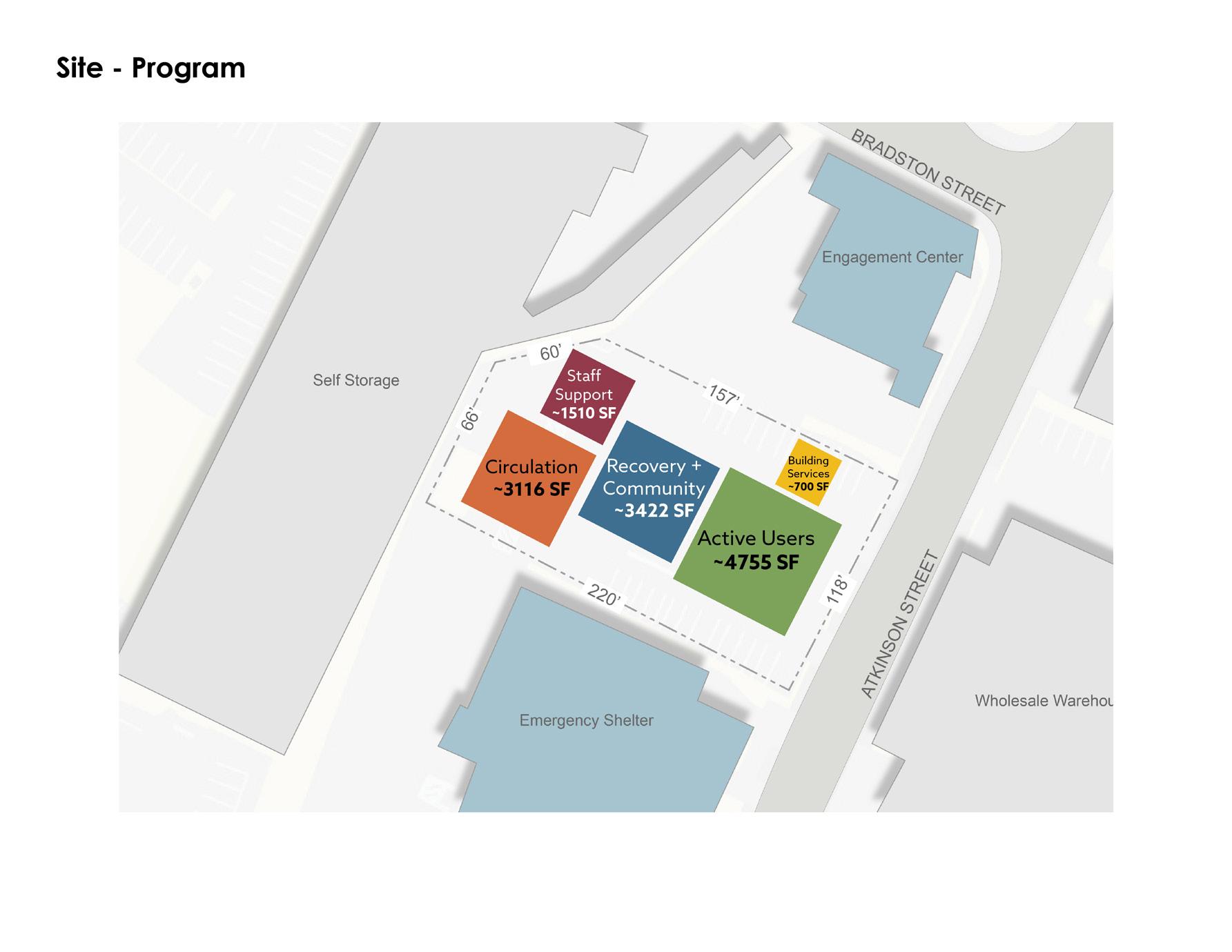
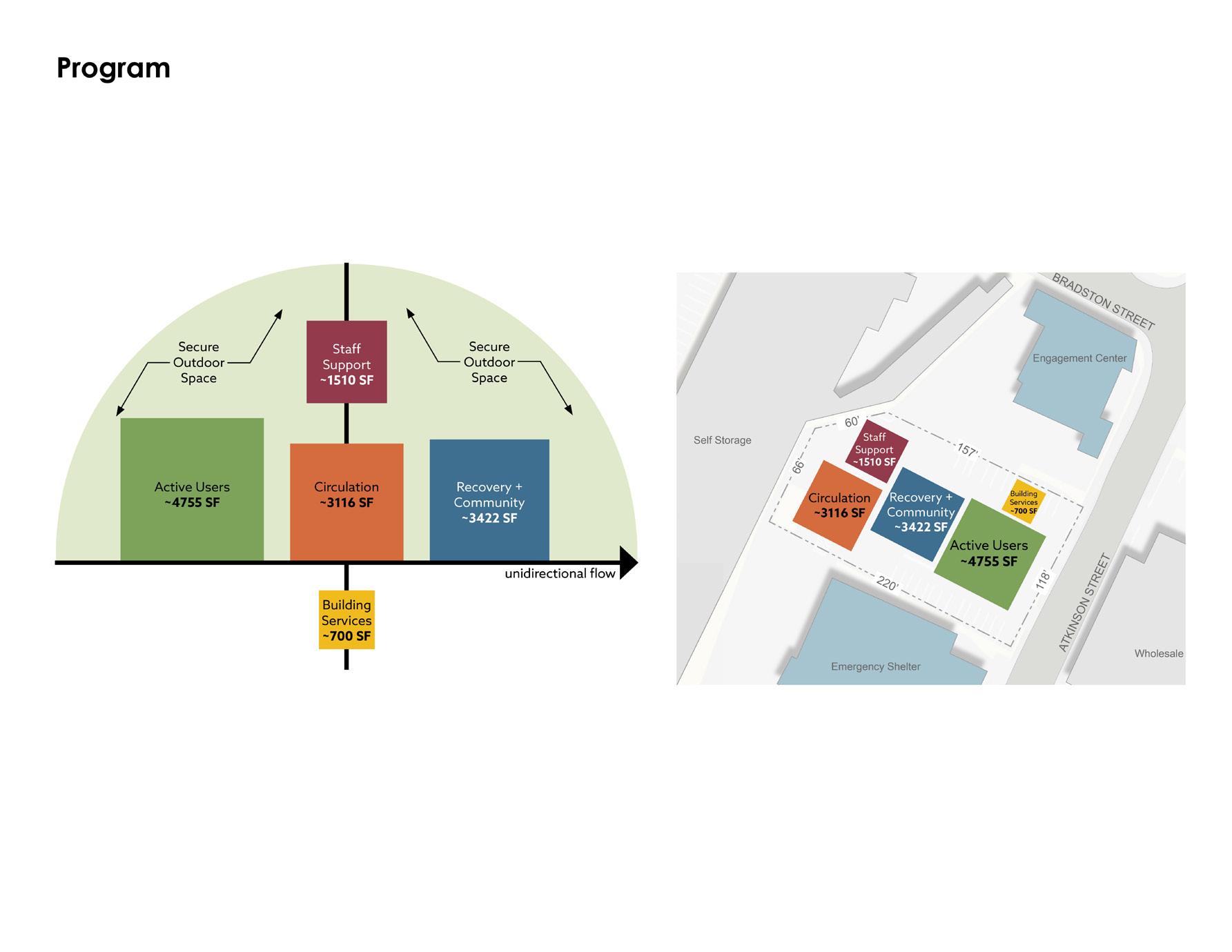
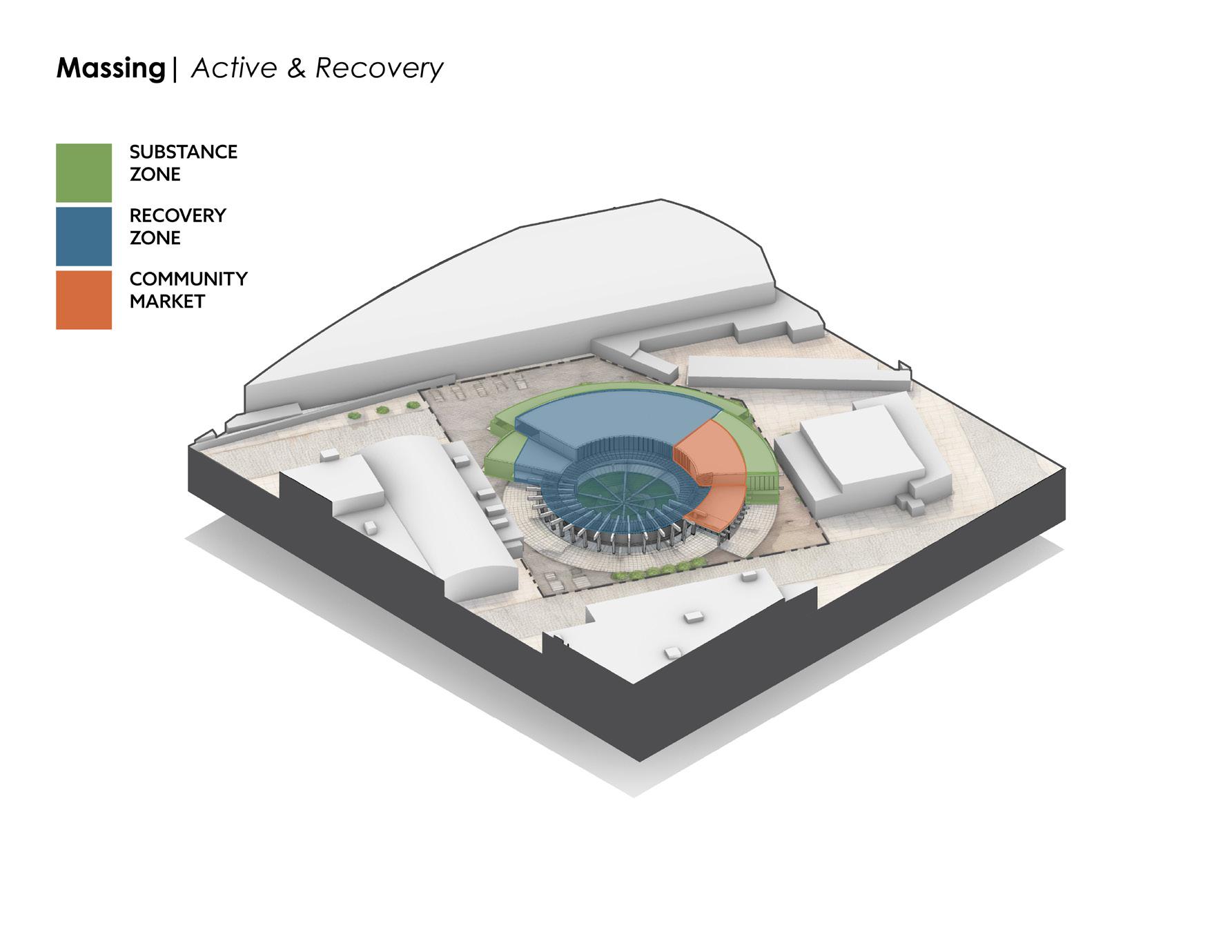
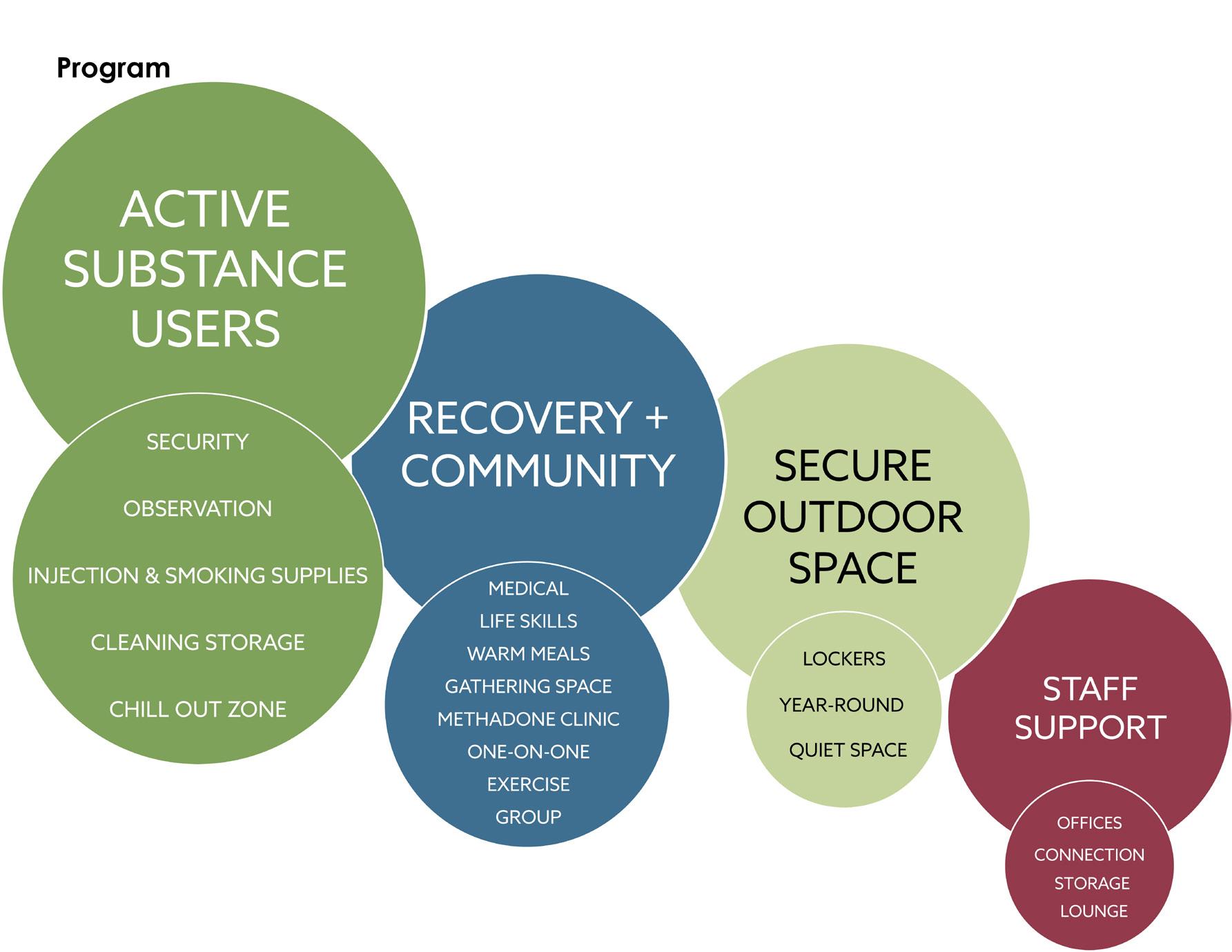
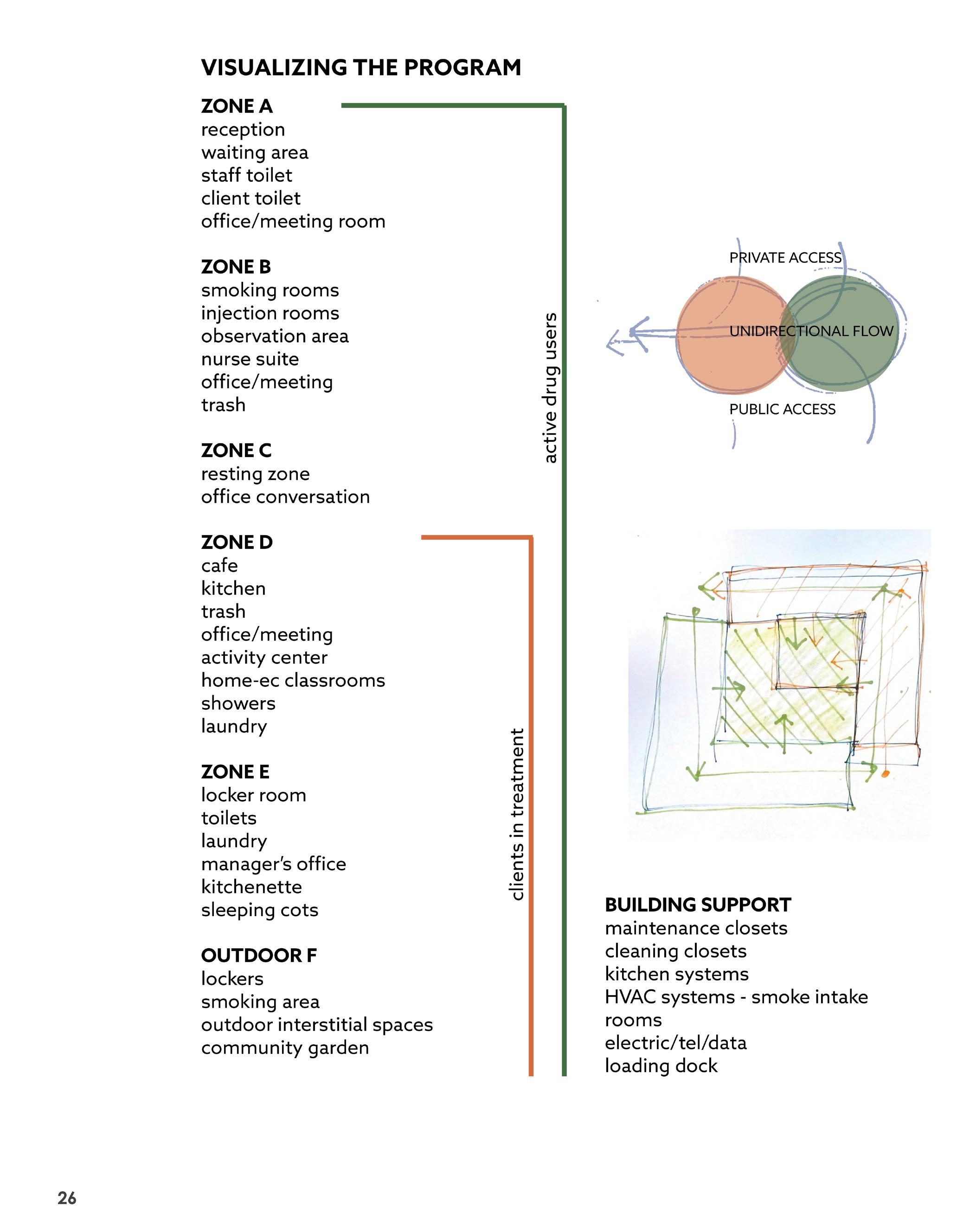
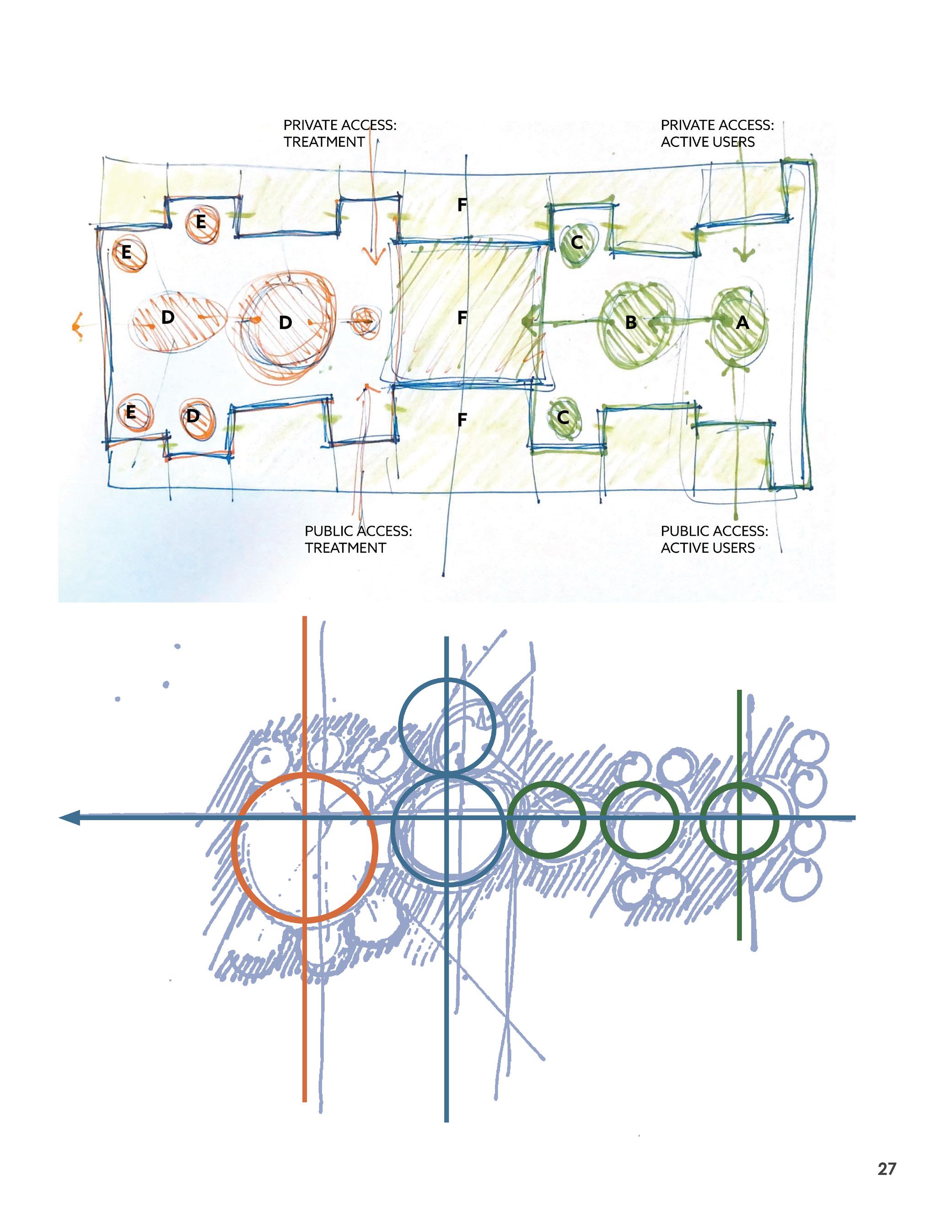
The main programmatic zones are the substance zone and the recovery zone.
The two zones never intersect to avoid folks in recovery being triggered by active drug use.
Ample circulation helps to prevent conflict between clients.
Staff support spaces are spread out throughout the building, allowing only staff to intersect between the substance and recovery zones.
Secure outdoor space , which is lacking in the area, separates guests from the noise and distraction of the street, while providing a sense of nature in the city.
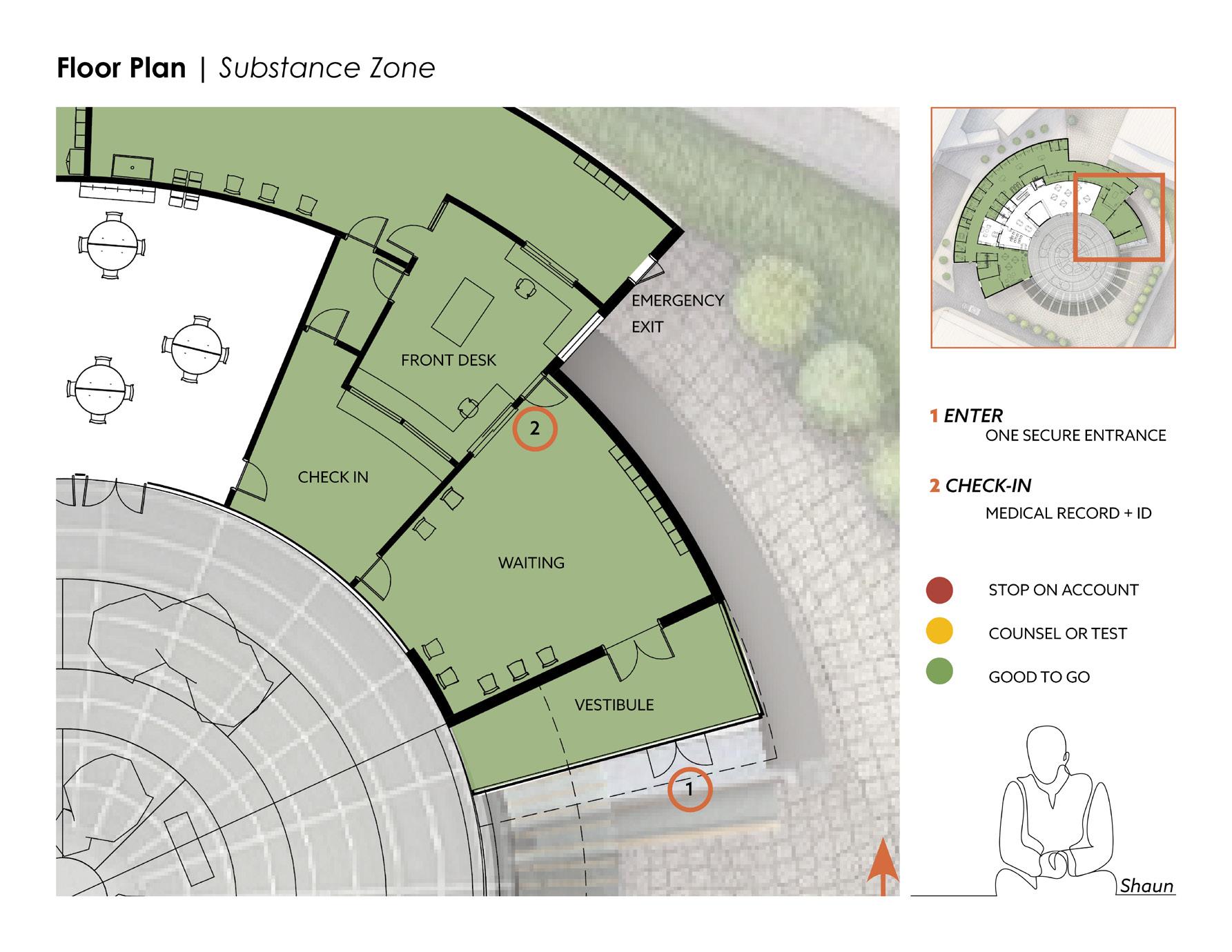
Unidirectional flow is a concept used to prevent conflict. For the active substance zone, there is one secure entrance and one exit on opposite sides of the building. This helps folks with wayfinding by not needing to go back and forth through the floor plan.
28 Recovery + Community ~3422 SF Building Services ~700 SF Circulation ~3116 SF Staff Support ~1510 SF Active Users ~4755 SF Secure Outdoor Space Secure Outdoor Space unidirectional flow
PROGRAM
ACTIVE SUBSTANCE USERS
SECURITY
OBSERVATION
INJECTION & SMOKING SUPPLIES
RECOVERY + COMMUNITY
CLEANING STORAGE
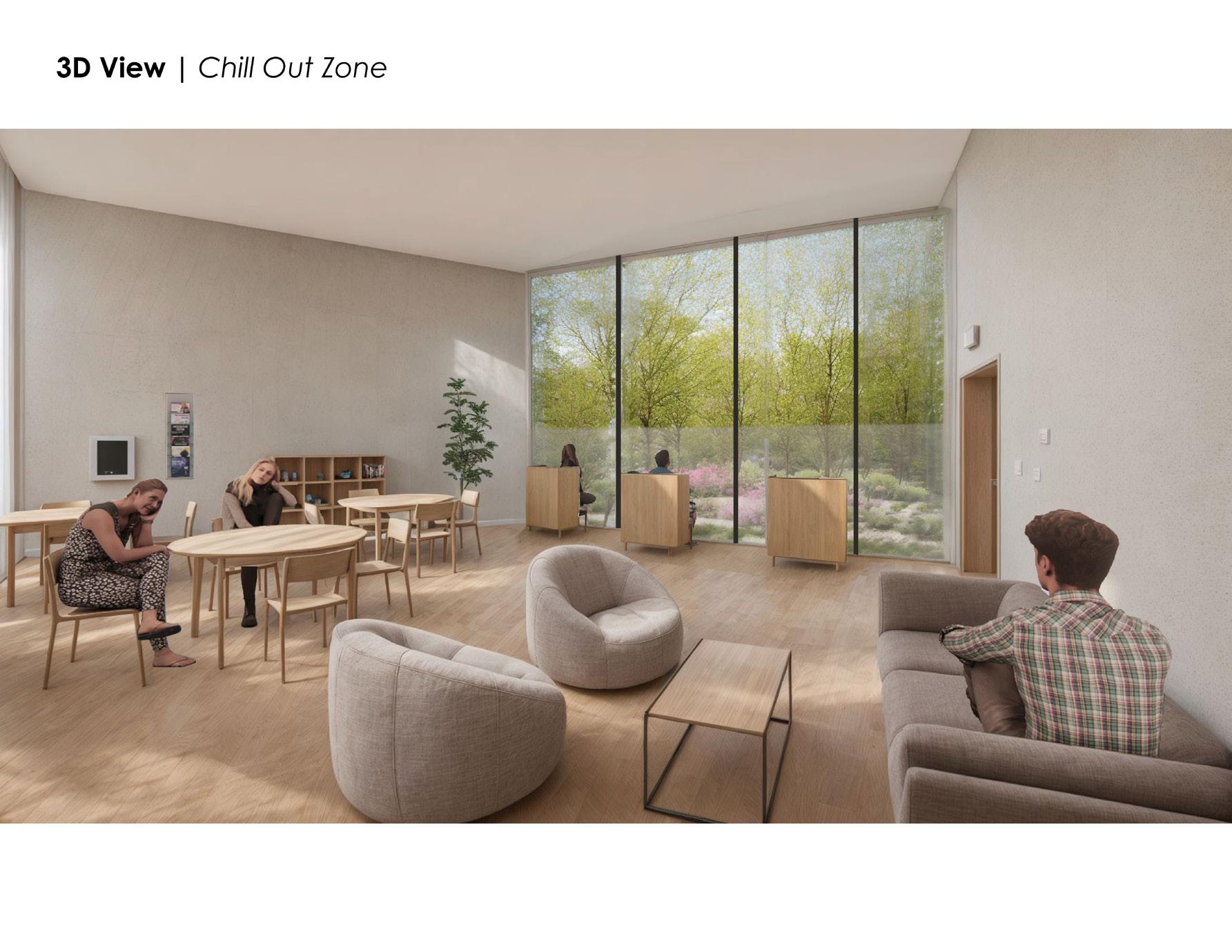
CHILL OUT ZONE MEDICAL
GATHERING SPACE
SECURE OUTDOOR SPACE
LOCKERS
YEAR-ROUND
QUIET SPACE
29
STAFF SUPPORT
OFFICES LOUNGE STORAGE CONNECTION
LIFE SKILLS
WARM MEALS
GROUP
METHADONE CLINIC ONE-ON-ONE EXERCISE
THE FIGHTER
“I love heroin. I live it. The first time I ever did it I fell in love with it. But you hate it. You want to kill it. But you can’t. It always wins. It’s the biggest lie.”
STATUS: LIFE, HEALTH, HOUSING
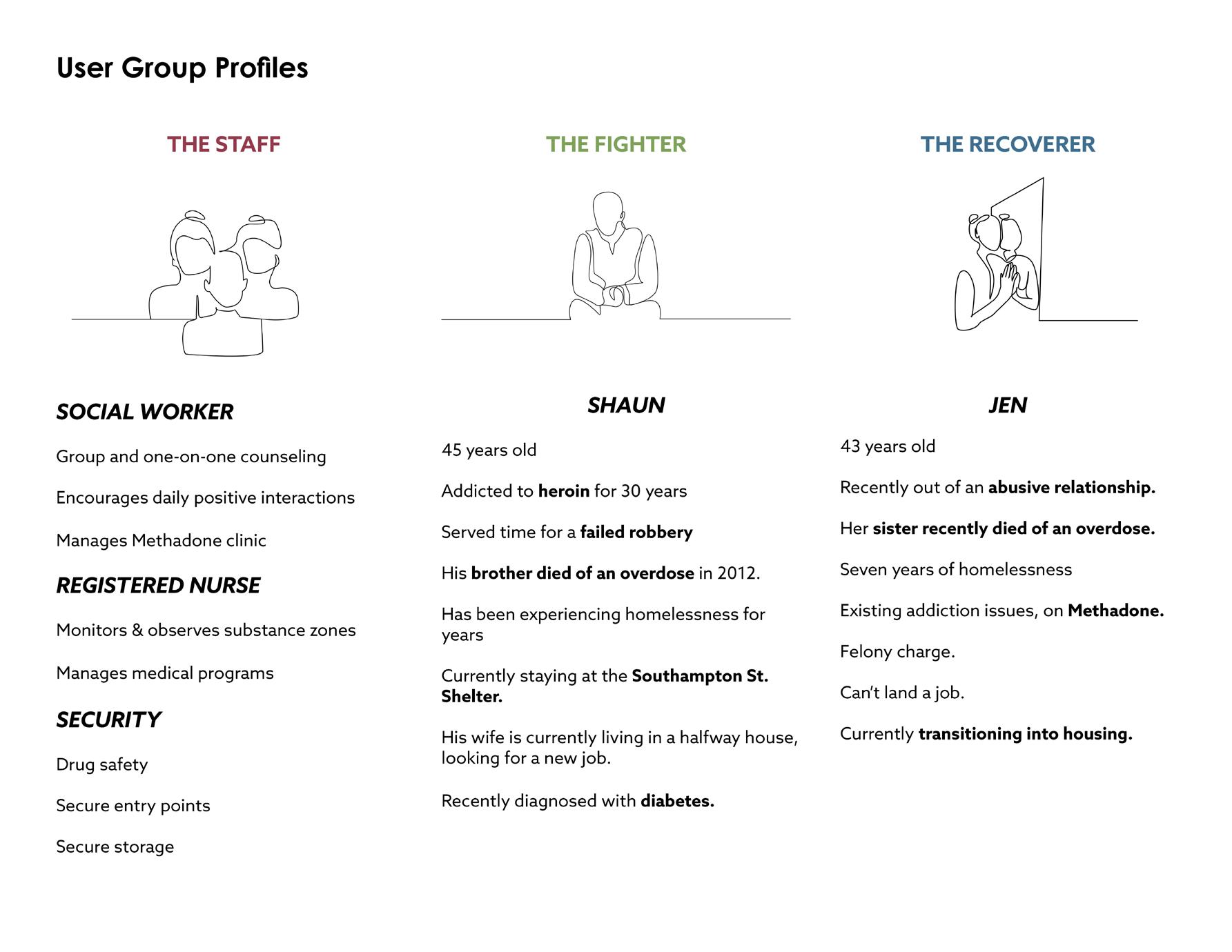
45 years old
From Lynn, MA
He started drinking at 8, by 13 he was smoking angel dust, snorting cocaine, and using LSD; he started using Oxycontin in the late ’90s, before switching to heroin
He served time for a failed robbery at a McDonald’s
His brother died of an overdose in 2012
He has been experiencing homelessness for years and is currently staying at the Southampton St. Shelter
His wife is currently living in a halfway house, looking for a new job
Recently diagnosed with diabetes
RESOURCES USED
Social workers helped him enroll in Mass Health, the Commonwealth’s Medicaid program
He mainly uses the facilities to use heroin
His goal is to get clean so he can start methadone treatment
Foot clinics, massage days, counseling, group, vaccine clinics, HIV and HEP C testing days
Garden for relaxation
Storage for his belongings
RELATIONSHIPS
He has a great rapport with the nurses and social workers
He knows almost everyone in the building-both guests and staff
He’s met some friends who have been successfully clean for their longest record and they are encouraging him to stop using for long enough to get into treatment
GOALS
To become a father and provide for his family
To be valued as a human being
CHALLENGES
Feeling heard by shelter staff & physicians
Regular access to diabetes medication and medical appointments
Finding a safe place to inject, where addiction and recovery services are combined
30 USER GROUP PROFILES | ACTIVE USER, SHAUN
THE RECOVERER
“This place is a Godsend. My God, to not have something like this? ... It’s a place to come and not have to be out there, in the mix of all that. Cuz you get out, and the next thing you know, you relapse and you get high.”
RESOURCES USED
Regular methadone clinic visits
Reading in quiet spaces
Hot meals
Socialization with friends
Private rooms for phone calls and computer use
Counseling
Life skills to learn how to live in an apartment
RELATIONSHIPS
Jen has made many friends at Heart House
She finds strength in surrounding herself around others in recovery
She enjoys spending time with the staff
STATUS: LIFE, HEALTH, HOUSING
43 years old
Recently out of an abusive relationship
Her sister recently died of an overdose
Seven years of homelessness, existing addiction issues, felony charge
Can’t land a job
She has been clean for eighty-five days and credits Heart House for helping her get to this point.
Currently transitioning into housing
She has made connections and networks for potential work in the future
GOALS
To find a job and an apartment in about 1-3 years
To stay occupied in a drug-free environment
CHALLENGES
Being around people who are high
Concerned about the well-being of her partner
Finding a job
Shaun and Jen’s profiles are based on real people. Information on these persons comes from:
“The Boston Engagement Center Research Report by Ethnographers Felice Ling and Cecilia Ackerman”. May 4th, 2018 & Nestor Ramos, Evan Allen, “Life and loss on Methadone Mile”. The Boston Globe, April - July 2016
31
USER GROUP PROFILES | IN RECOVERY, JEN
THE STAFF
SOCIAL WORKER
One-on-one and Group counseling sessions with both active substance users and folks in recovery.
Socializes with folks in the community spaces.
Checks people in, helps them get their medical records set up and insured with Mass Health.
Manages the mental health activity groups such as meditation and yoga programs.
REGISTERED NURSE
Manages the weekly medical program clinics such as massages, podiatry, dentistry, vaccines, HIV and HEP C testing.
Helps folks with choosing which supplies they need to inject or smoke.
Monitors and assists people who are using substances.
Will administer Narcan if needed.
Accompanies people into private rooms to inject if necessary.
Observes people in the chill-out zone after they are done using.
SECURITY
Security is performed discreetly.
Low-threshold, no barriers
No metal detectors
No bag search
ID and medical history are required for guest’s safety in case they need to be transported to the hospital or jail.
Cameras on site
Staff has line of sight to monitor guests unobtrusively.
Visible lockers
Exterior storage units for carts, chairs, belongings
CONNECTION
Each guest has a go-to staff member. Relationships are built over time and guests tend to form connections with staff members based on personality, gender, race, language, or the staff member’s personal experience with homelessness and/or addiction.
32
GROUP PROFILES | STAFF
USER
33
34
PART III
Design Development
Final Design
Narratives
35
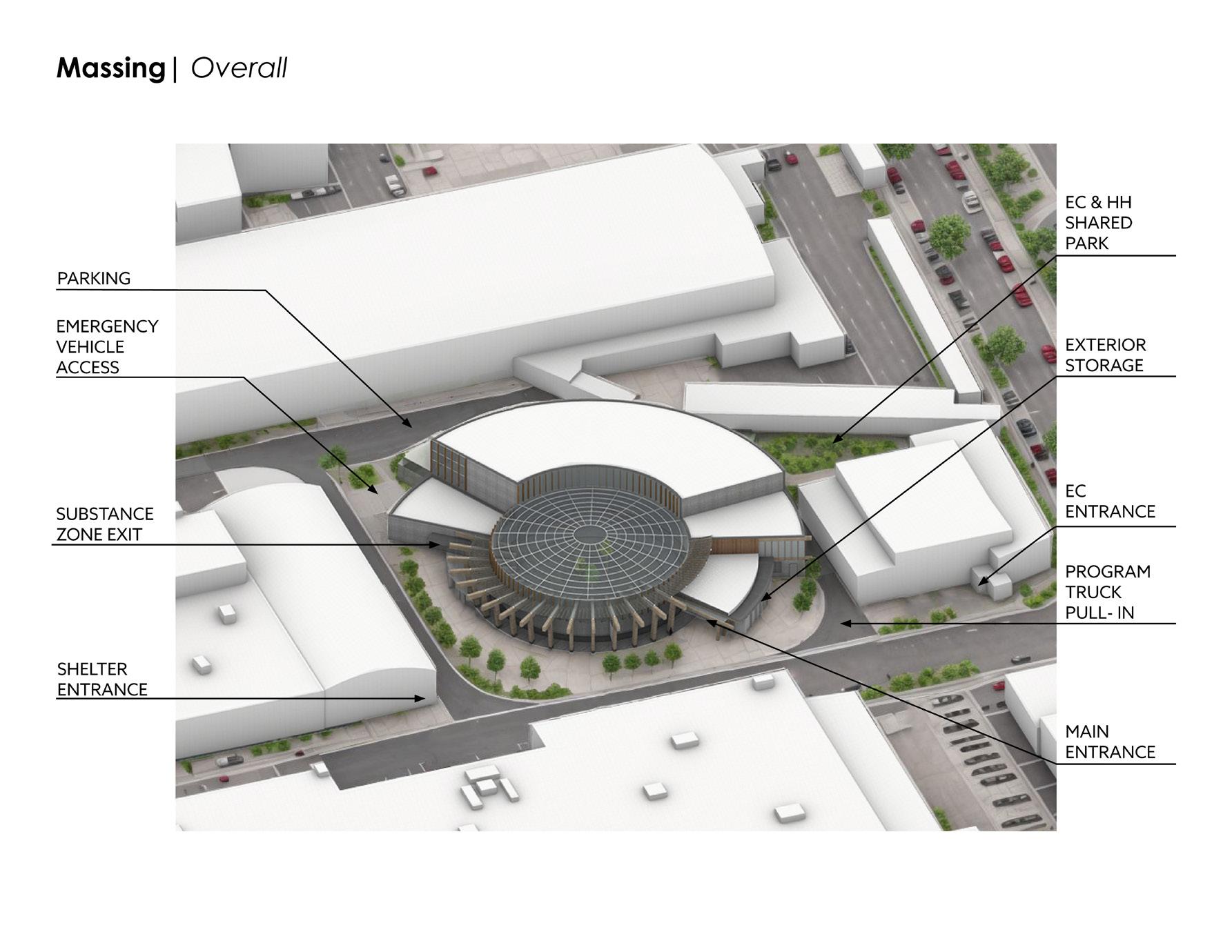
36 FINAL DESIGN | MASSING MAIN ENTRANCE ATKINSON STREET MEN’S SHELTER ENTRANCE SUBSTANCE ZONE EXIT PARKING LOT ENGAGEMENT CENTER & HEART HOUSE SHARED PARK PROGRAM TRUCK PULL-IN ENGAGEMENT CENTER ENTRANCE EXTERIOR STORAGE LOCKERS 1 3 4 2 1 8 7 5 4 2 3 6 8 7 6 5 Men’s Shelter Engagement Center
To fully leverage the available resources and optimize the tight site, the design integrates the entire block, fostering a unified space geared towards harm reduction. This is achieved through the development of the spaces between the buildings within the block, ensuring integration of space and resources.
In between the Men’s Shelter (#2) and Heart House, an access road was added with a pull off at the emergency exit of the substance zone (#3).The pull off is necessary to allow other vehicles to pass. The access road also serves the Men’s Shelter which has as exit in the back of the building, with direct access to the new road. The road also allows access to parking behind these two buildings (#4).
The space between the Engagement Center (EC) and Heart House (HH) is a sidewalk, leading to a park shared by both buildings. The EC has an existing patio in this location, which is expanded to incorporate the HH site.
#6 is a program truck pull-in. This location is off of Atkinson street so that people on the street as well as clients in all three buildings can access the truck. Programs that might use this area could be a shower truck, a food truck, or a syringe pick-up vehicle.
37
ACCESSROAD
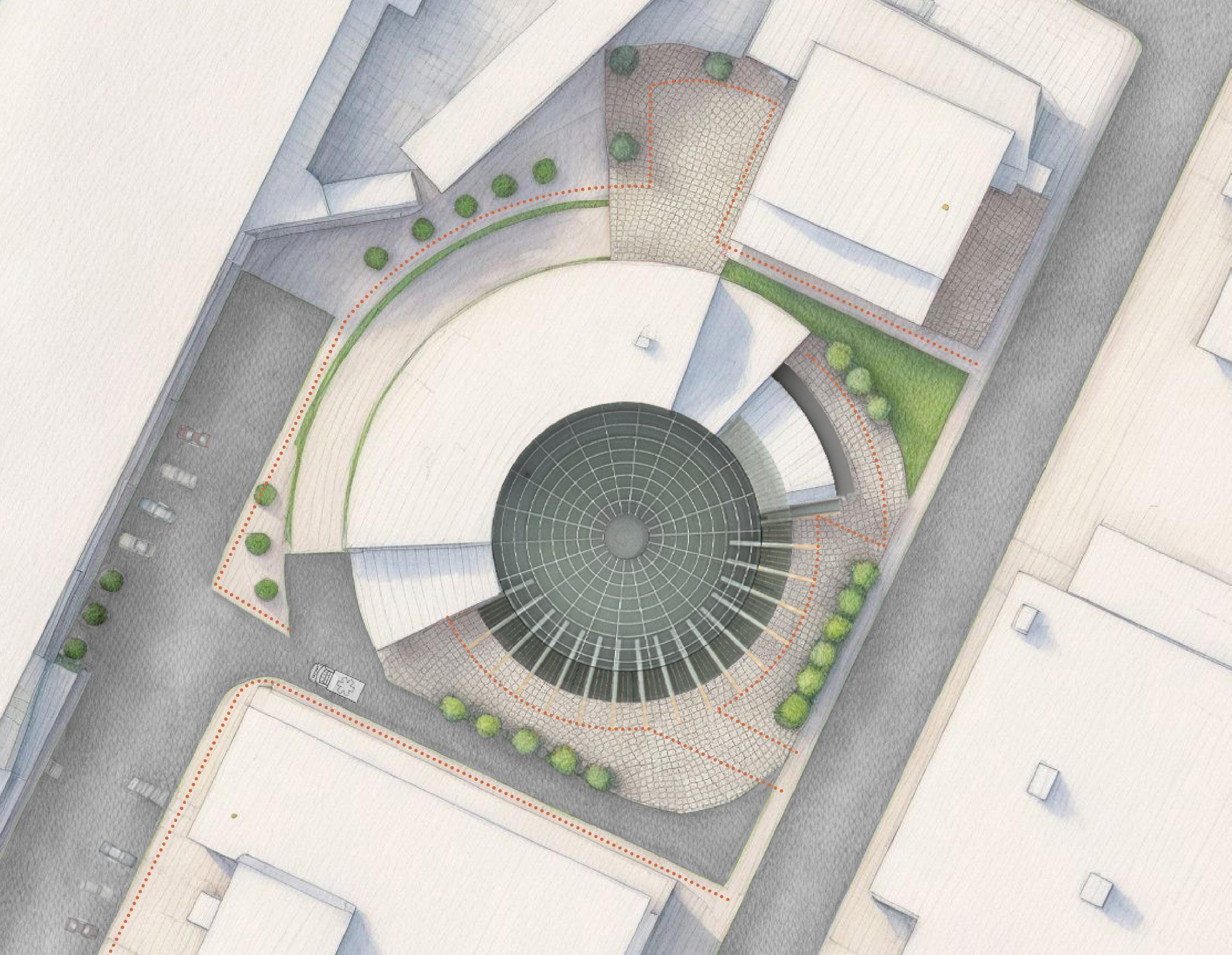
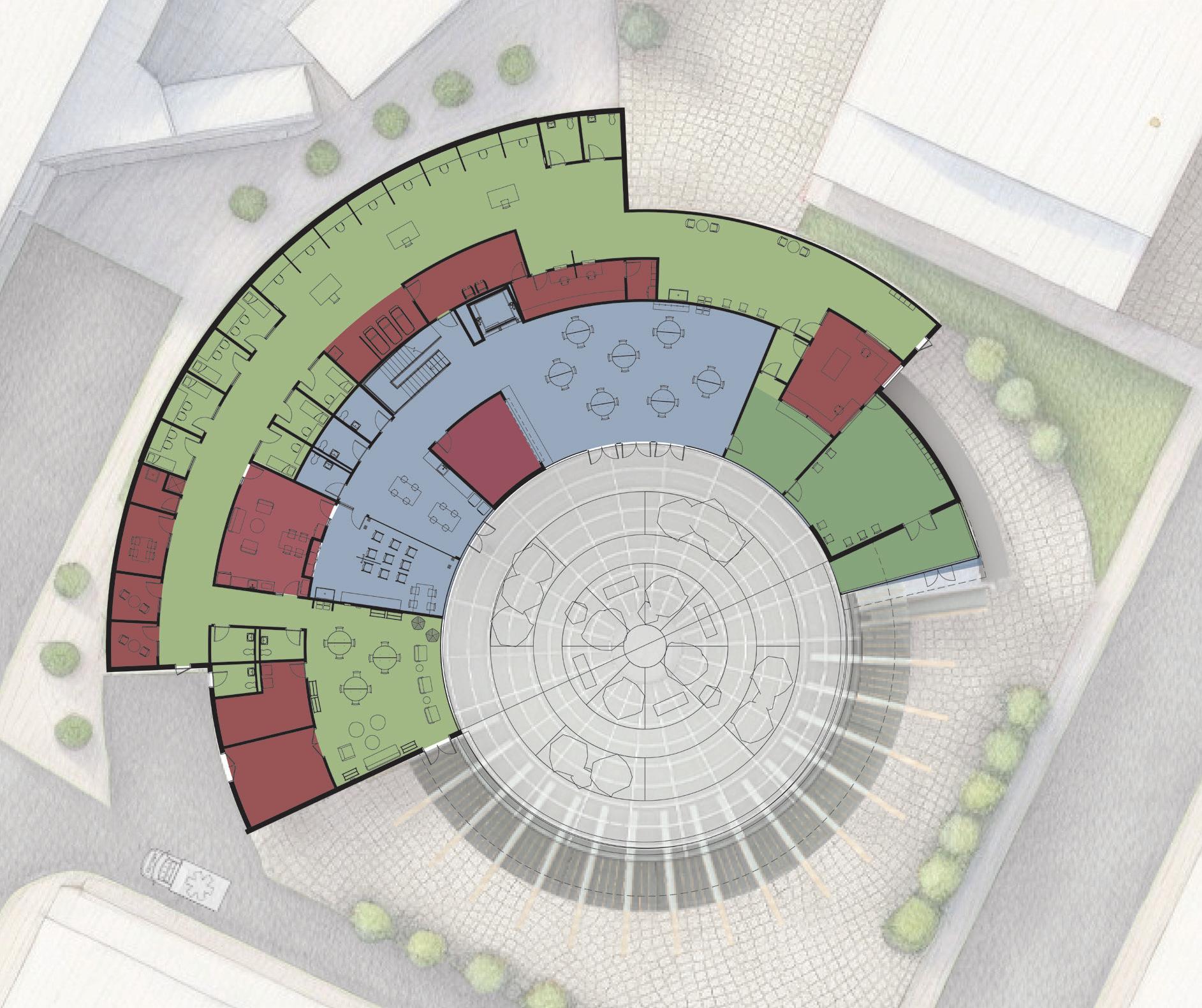
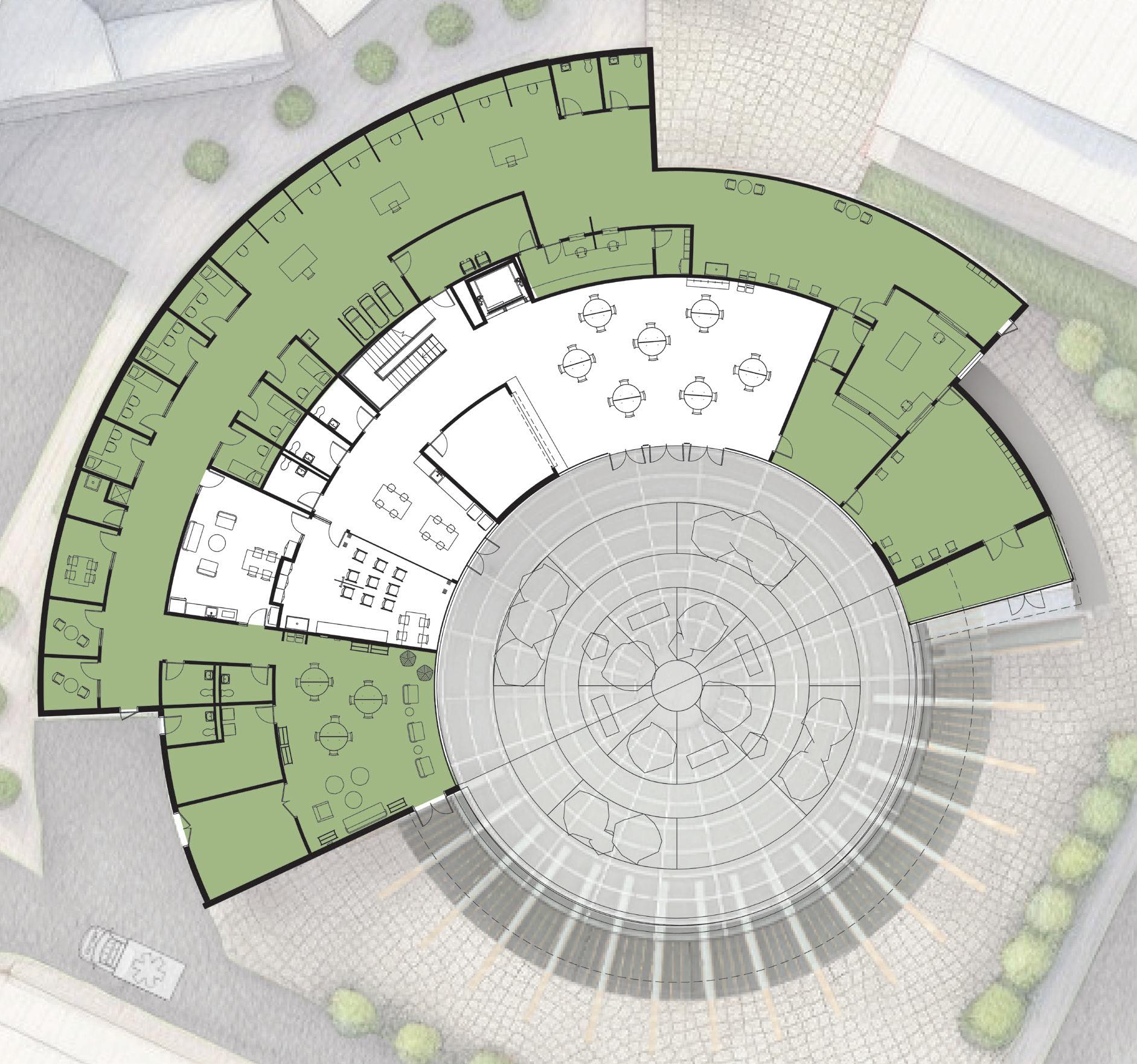
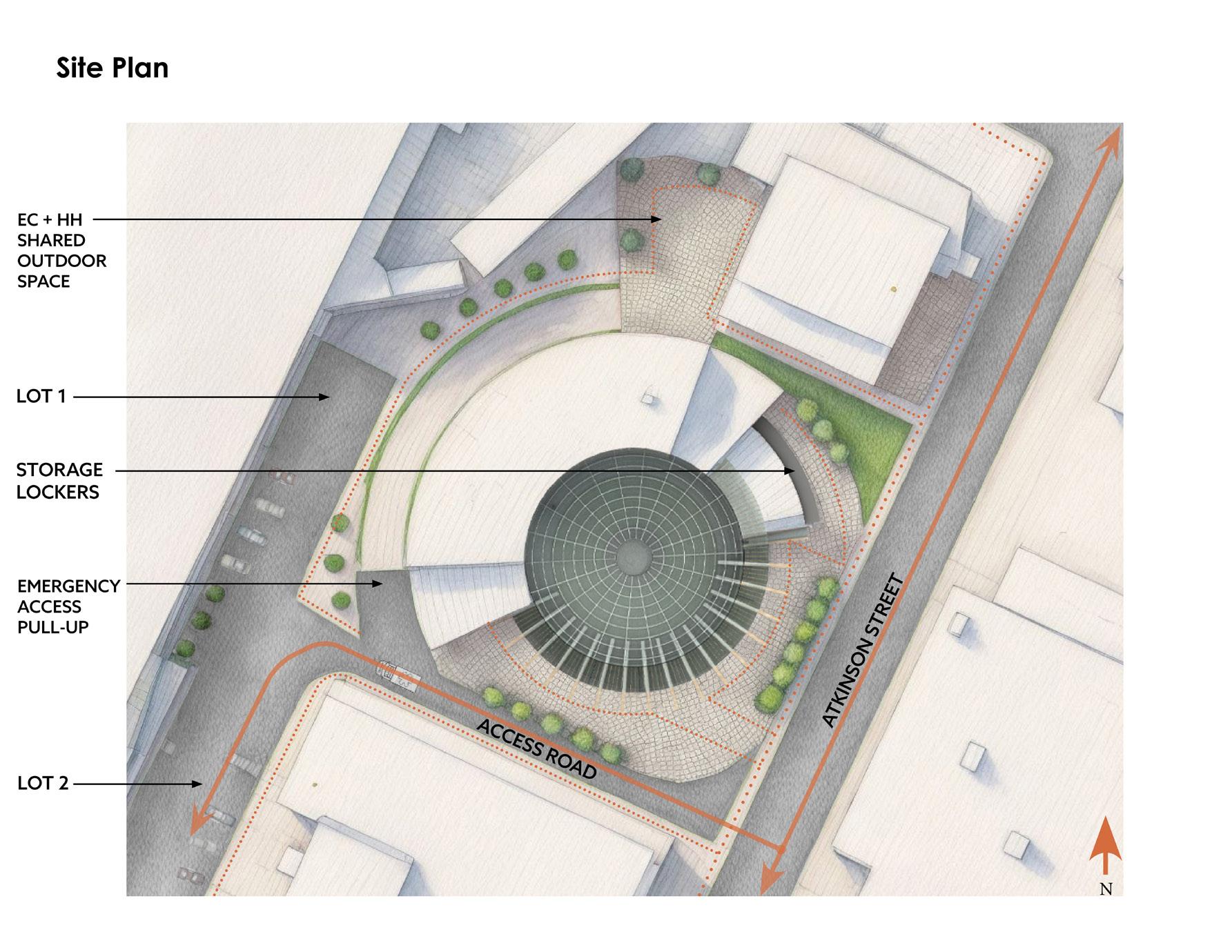
38 FINAL DESIGN | SITE PLAN N
ATKINSON STREET
50’ 100’ 0’
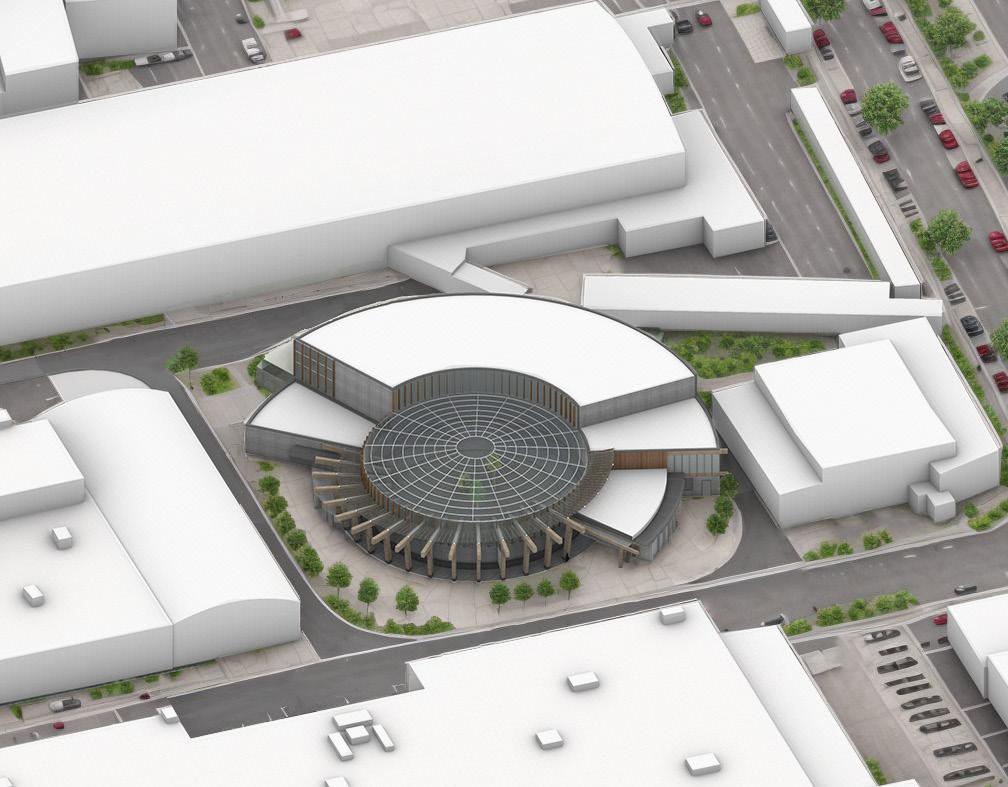
The building’s orientation toward Atkinson Street is intentional, with its curvilinear geometry softening the edge condition, inviting pedestrians from both the street and sidewalk. The main entrance, strategically set back, acts as a buffer zone, mitigating the impact of the busy street on the building’s ambiance.
An access road serves both the building and the adjacent men’s shelter, facilitating smooth traffic flow. Featuring a pull-off area, it ensures emergency vehicles can reach the exit of the Substance Zone swiftly without obstructing other vehicles. This road loops behind the men’s shelter, connecting to Southampton Street where Boston Medical Center is a block away. The road also provides access to two parking lots designated for staff and clients.
The design prioritizes pedestrian accessibility, with concrete and pervious pavers facilitating easy movement throughout the site. Thoughtfully distributed plantings, create greenery , which is lacking in the area. The plantings also provide some privacy, shade, and directional guidance for people as they move through the site.
39
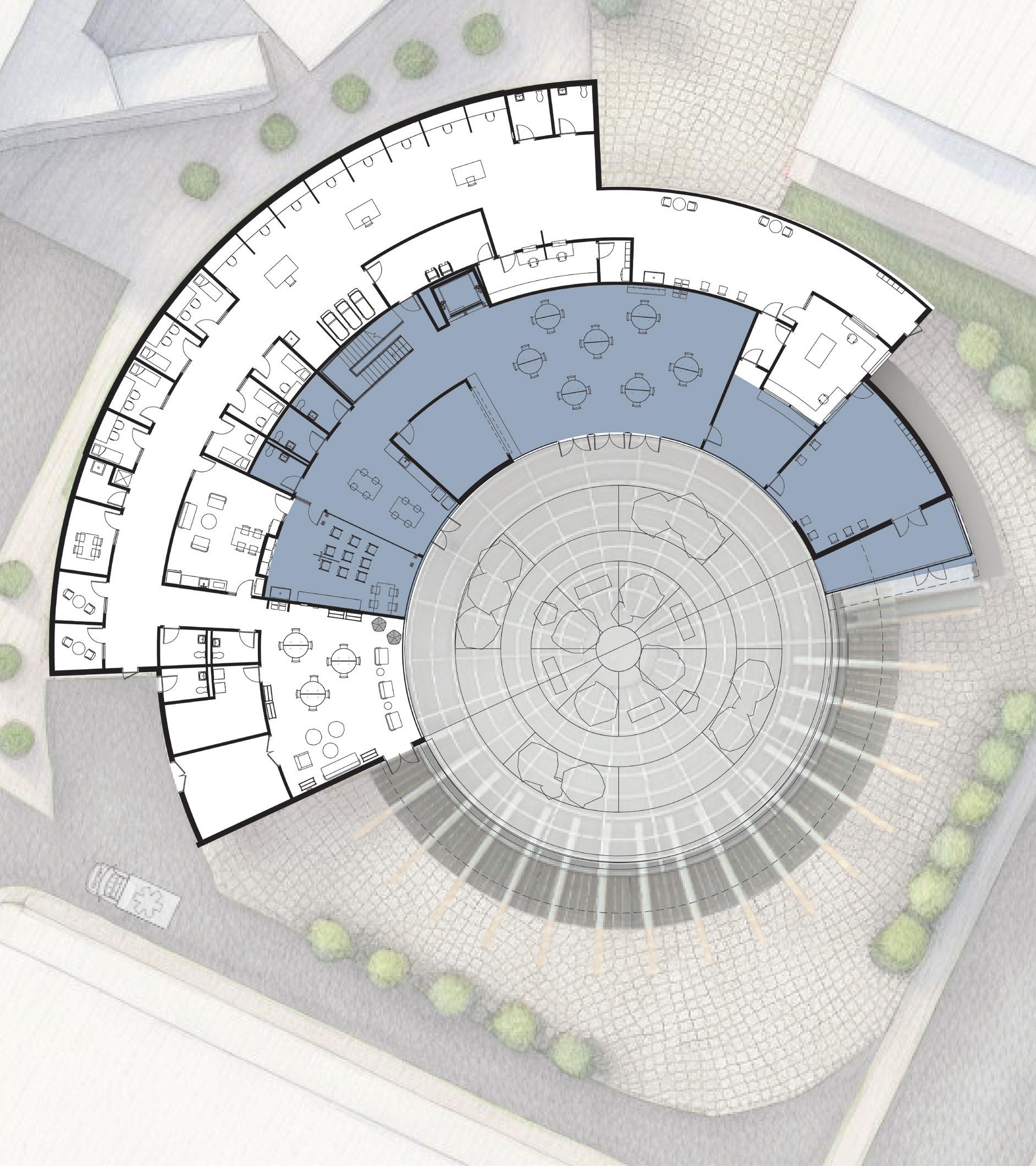
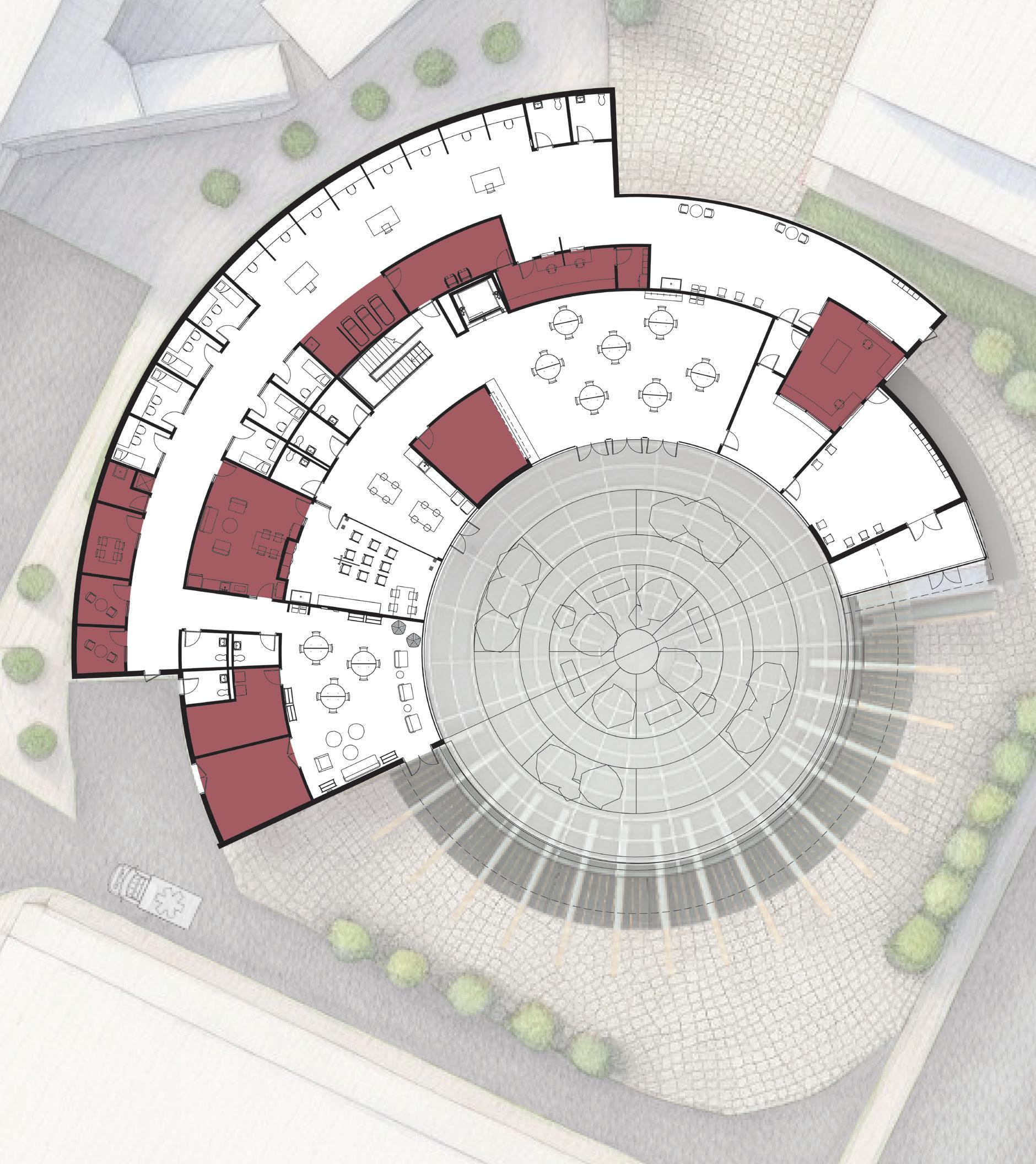
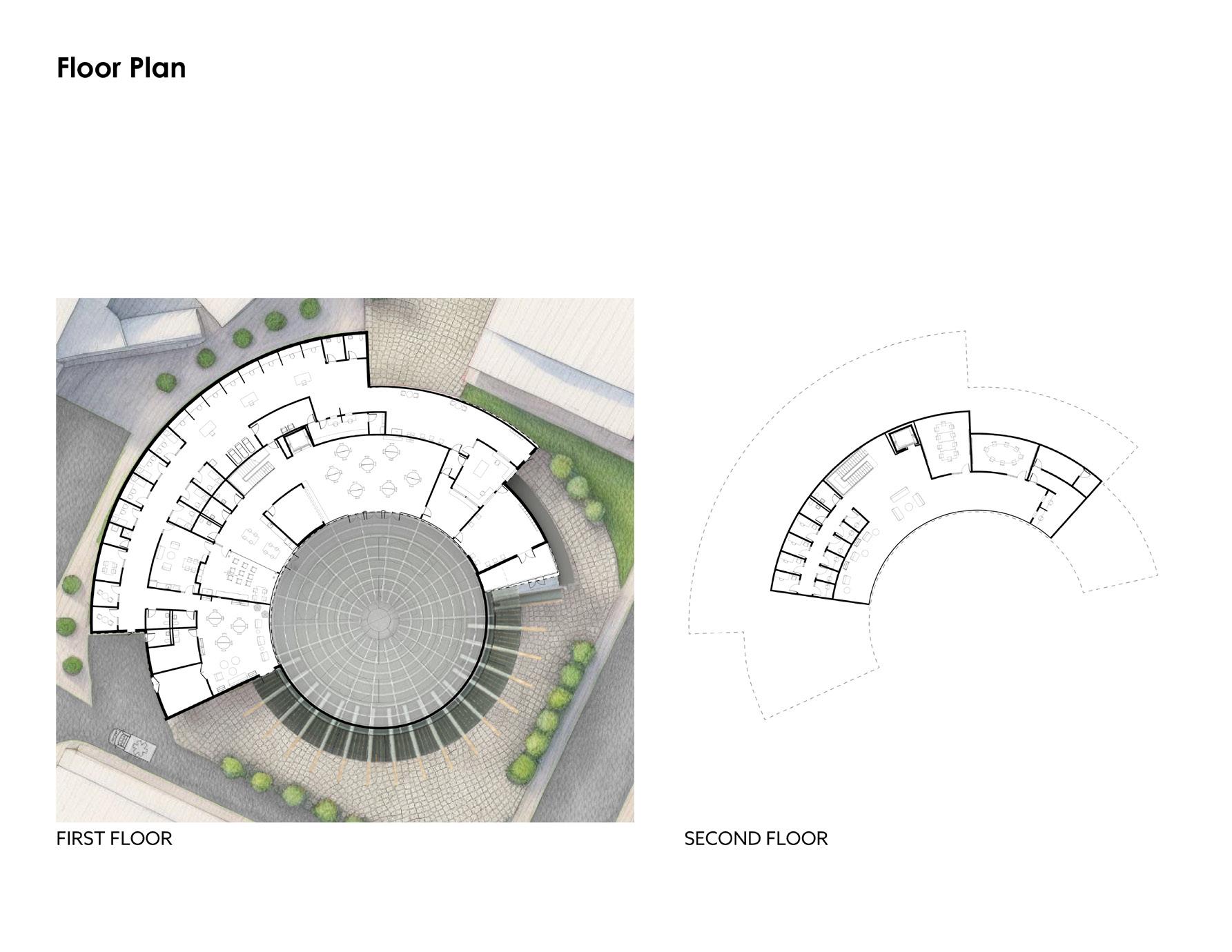
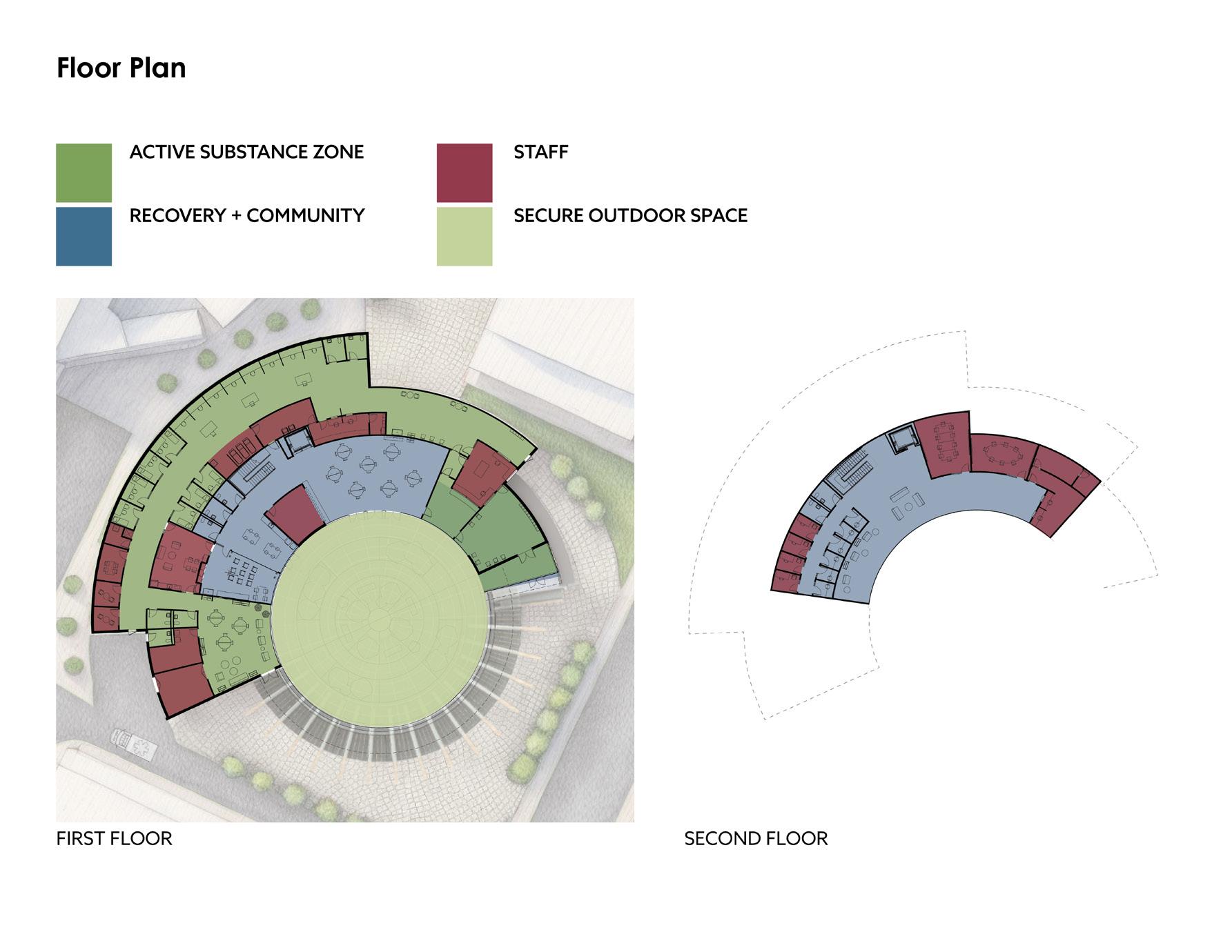
FINAL DESIGN | FLOOR PLANS
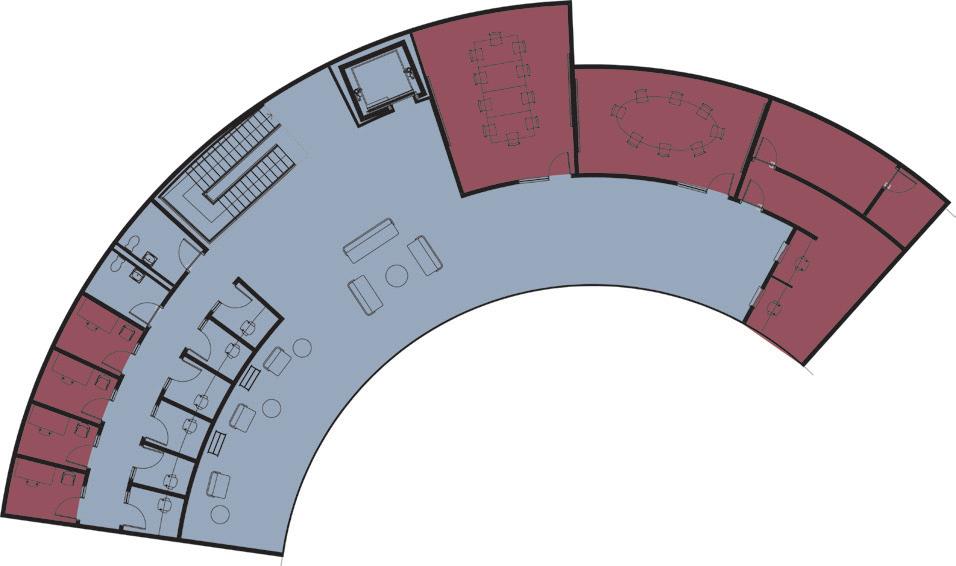
SECOND FLOOR
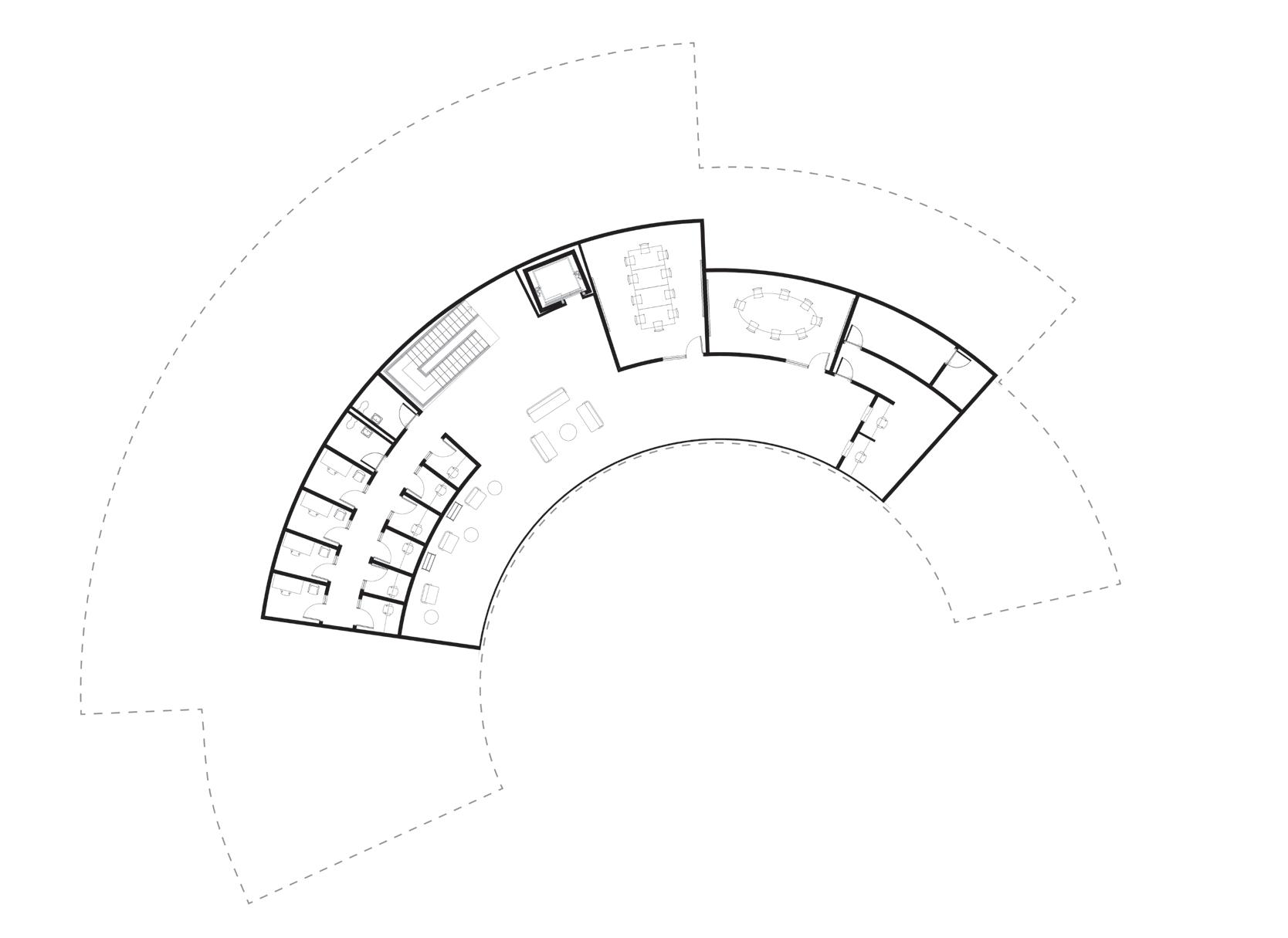
FIRST FLOOR
40
50’ 100’ 0’
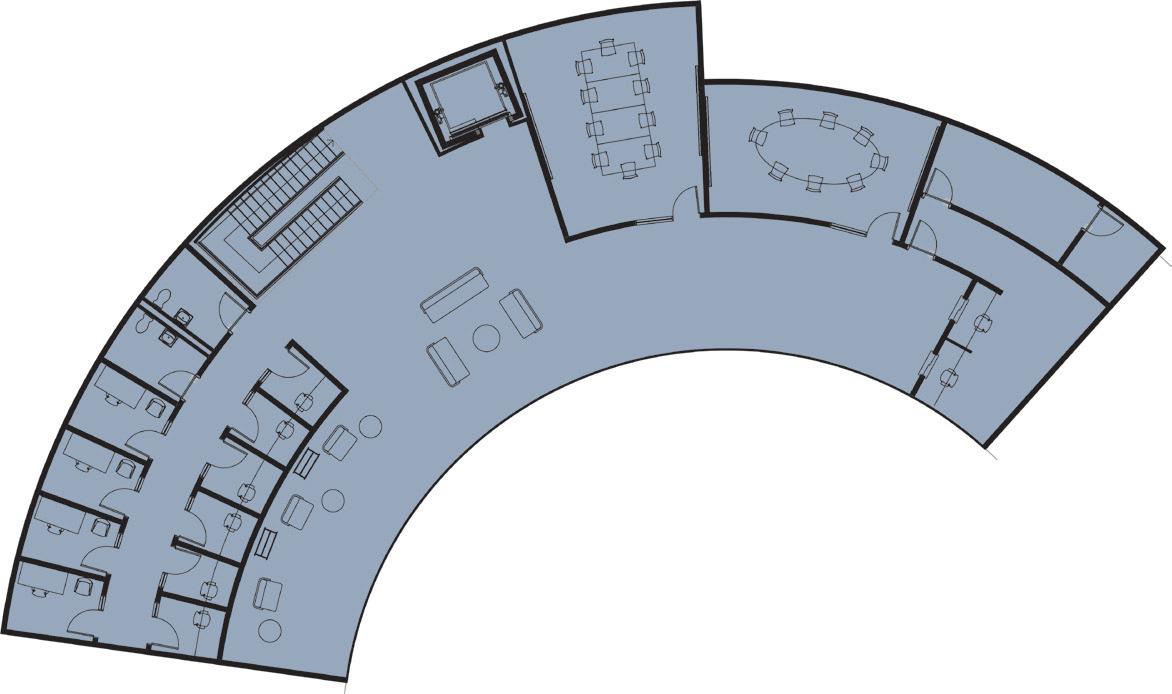
ACTIVE SUBSTANCE ZONE
RECOVERY + COMMUNITY
SECURE OUTDOOR SPACE STAFF
ENTRANCE & EXIT
The floor plan is arranged in a circular geometric form, which is further detailed on subsequent pages. Primarily, the plan is designed to separate the active substance zone from the recovery zone while creating distinct spaces for staff to interchange between the two zones.
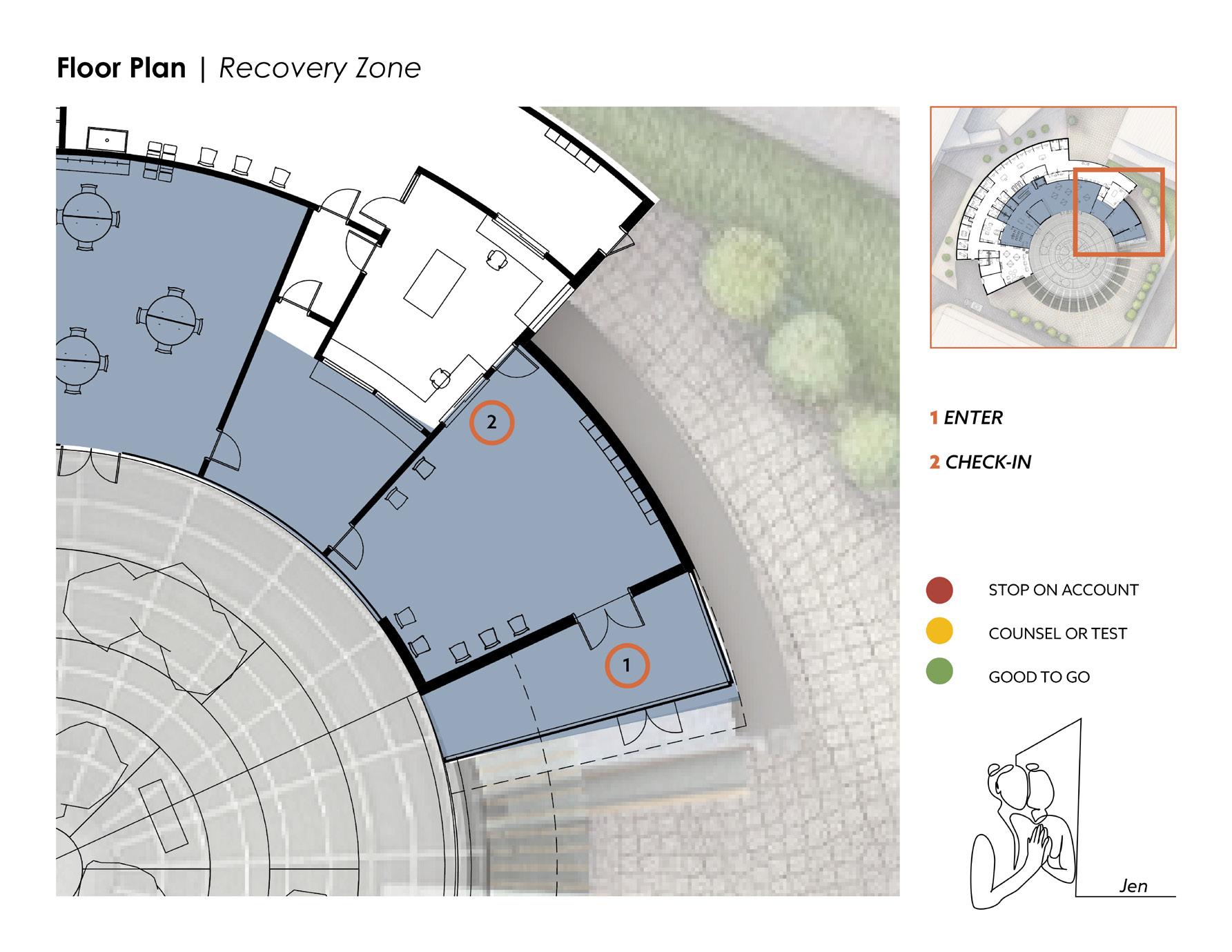
The entry sequence is crafted to safeguard clients’ privacy. A single secure entrance alleviates the stigma associated with having two separate doors—one for recovery and one for drug use. In the designed scenario, a client checks in with the front desk, confirms their medical information and identification, then waits in the waiting room until called. The waiting room sequence establishes a secure boundary between the service areas and the waiting clients, ensuring that waiting individuals remain unaware of the destination of any particular client. Should a client require extra time or space for paperwork or health insurance setup, a secondary room adjacent to the waiting area is available, featuring a service window for assistance from front desk staff.
Despite the “no barrier” ethos of the building’s concept, security measures are necessary. The entrance layout is designed to instill clients with confidence, ensuring their comfort and freedom from feeling surveilled. The presence of double doors to access the drug zone serves security purposes due to the presence of controlled substances within the building.
The substance zone features one main entry, two emergency exits, and one primary exit, facilitating a unidirectional flow from one end of the building to the other to minimize client movement.
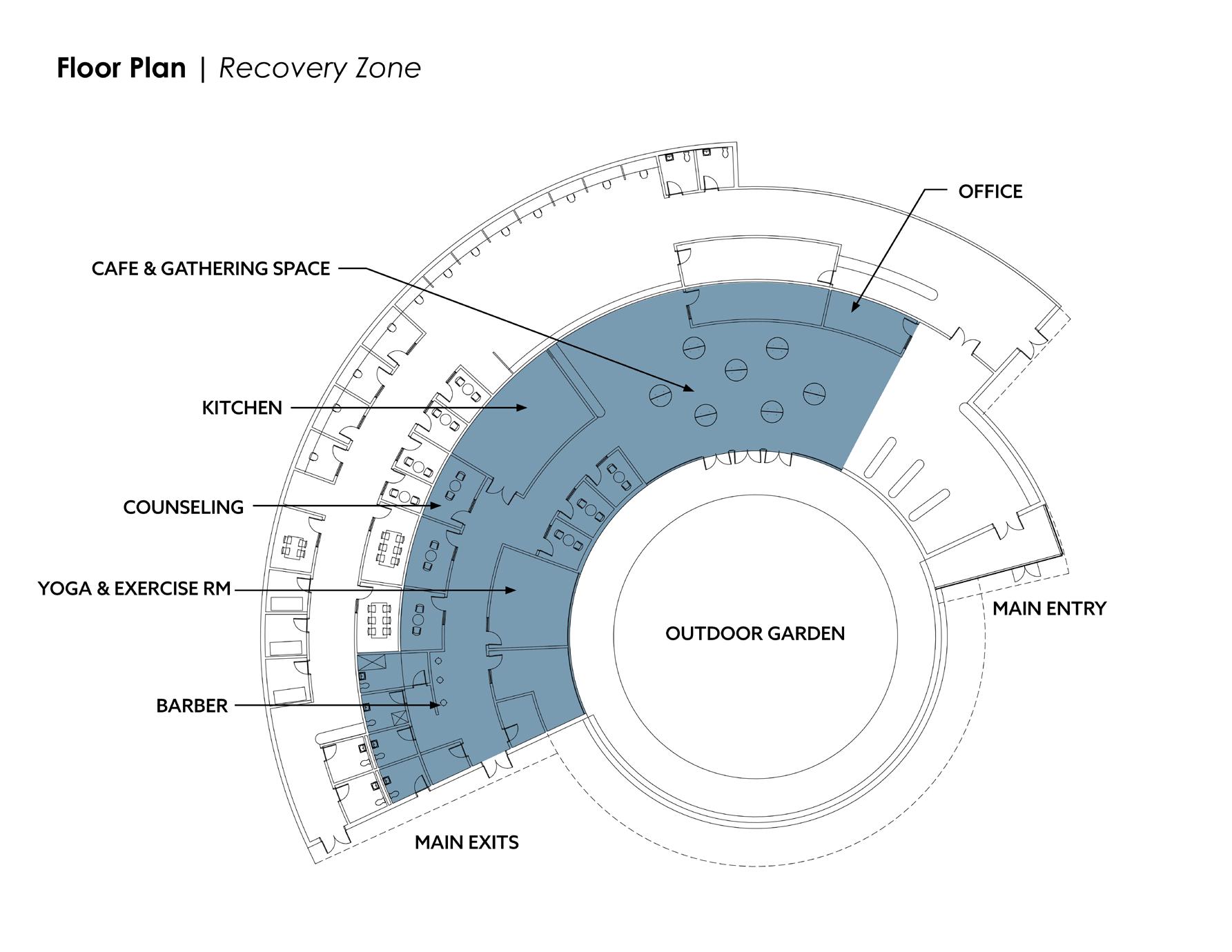
The recovery zone is nestled at the heart of the building and alongside of the private garden, fostering the development and nurturing of community. The entry and exit are congruent, encouraging fluid movement within the space.
41

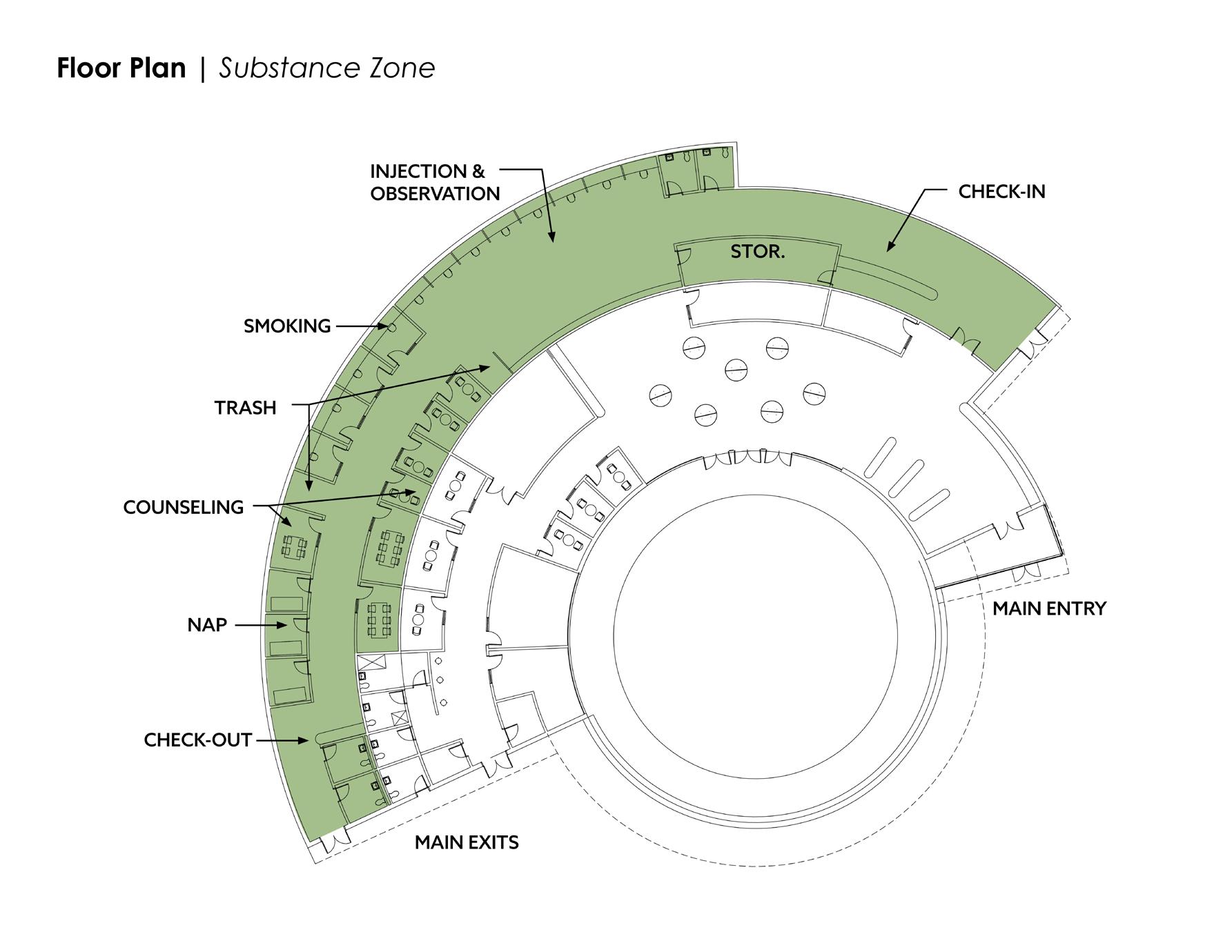
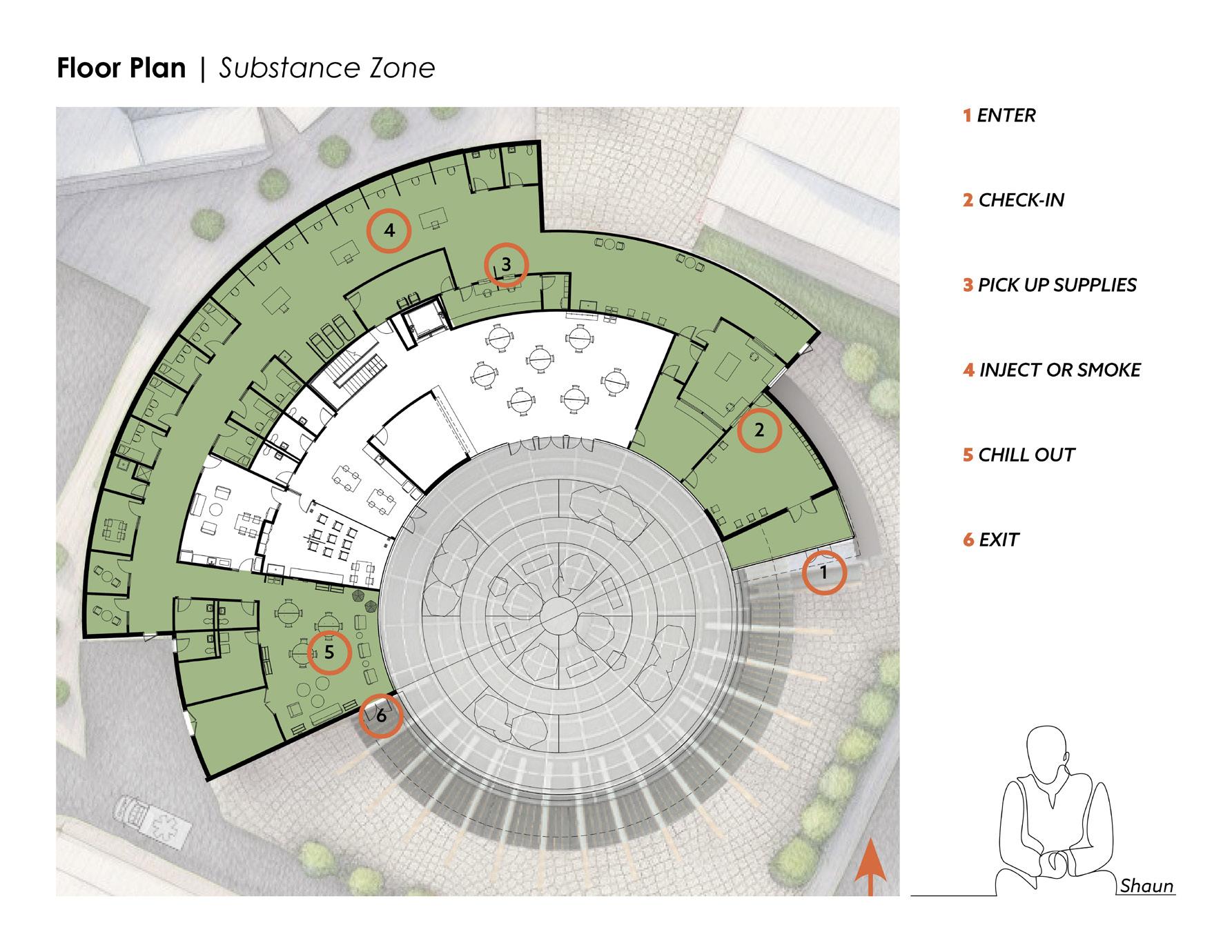
42 2 CHECK-IN 4 SUPPLY PICK UP 1 ENTRANCE 6 OBSERVATION 3 WASH HANDS 5 INJECTION 1 2 3 4 5 6 FINAL DESIGN | SUBSTANCE ZONE CHILL OUT ZONE 9 COUNSELING PRIVATE DRUG INTAKE ROOMS 7 SMOKING 11 EXIT EMERGENCY EXIT 7 8 10 12 11 12 10 8 9 1 8 7 5 4 2 3 6 9 10 11 12 Injection & Observation Areas

• 45 years old
SHAUN
• Addicted to heroin for 30 years
• Served time for a failed robbery
• His brother died of an overdose in 2012
• Has been experiencing homelessness for years
• Currently staying at the Southampton St. Shelter.
• His wife is currently living in a halfway house, looking for a new job
• Recently diagnosed with diabetes Shaun comes to Heart House today to inject the heroin he picked up yesterday. He stored his drugs in the safe yesterday within the substance zone so that he wouldn’t get them stolen off of him last night when he was sleeping at the Southampton Shelter. He also didn’t want to get caught with drugs on him at the shelter as it would cost him being kicked out for 30 days.
He enters the building and checks in at the front desk. He confirms his identification and medical record. He tells the staff that he is here to inject. When the staff pulls up his account, they see he has a green dot. This means he is all set and clear. If Shaun had a red dot on his account, it would mean there is something wrong, like a warrant out for his arrest. If Shaun had a yellow dot it would mean he either is due for a counseling session or a urine sample.* Shaun waits in the waiting room un-
til his name is called by his favorite nurse, Jim. Jim escorts Shaun through the double doors, Shaun immediately catches eye-contact with one of his long time buddies who is sitting with a counselor chit-chatting. They have a quick handshake and Shaun moves on to wash his hands as directed by Jim.
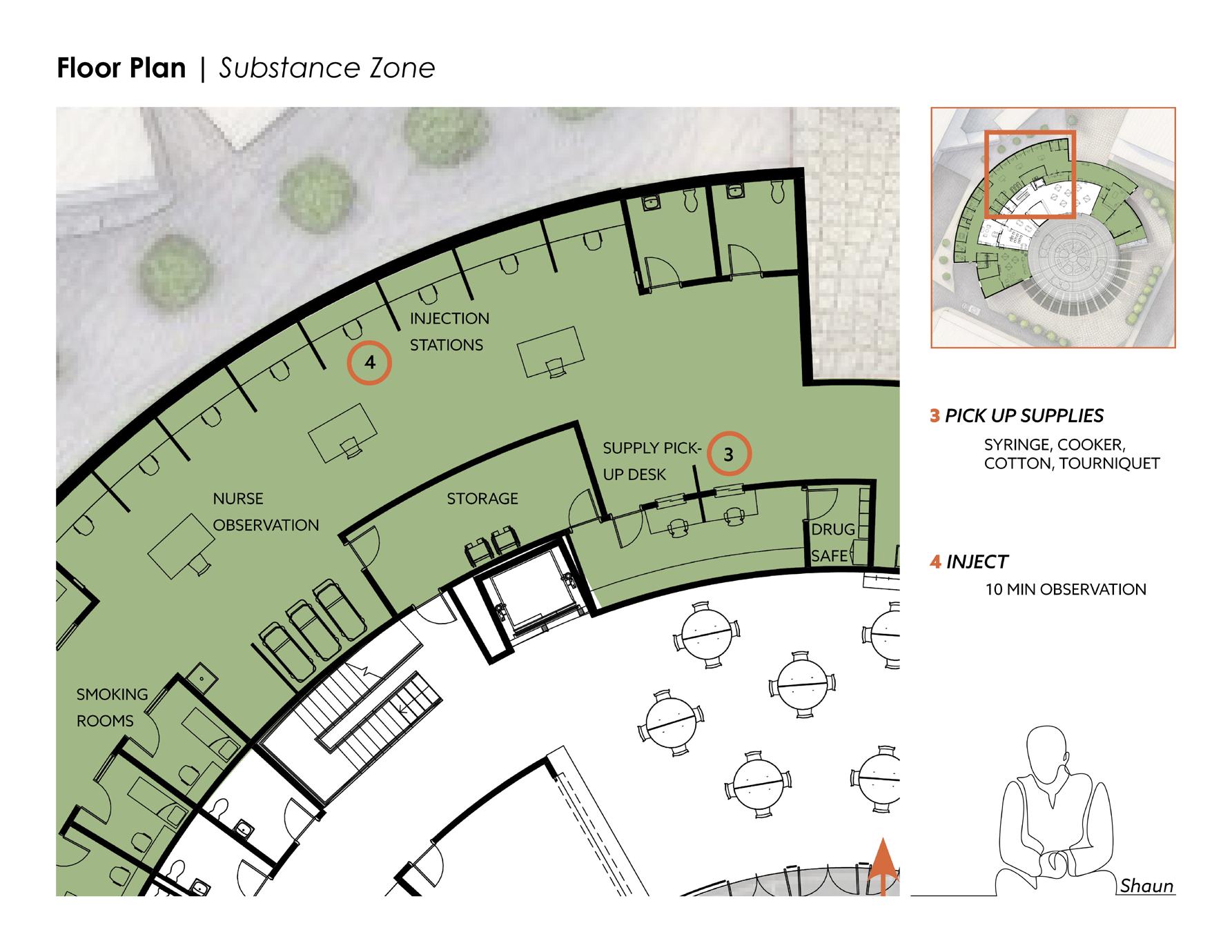
Next, Shaun goes to the window where he picks up his supplies. He lets the nurse know what he’s taking today and they give him a tray with his drugs from the safe, a tourniquet, syringe, cooker, cotton, and a fentanyl test strip
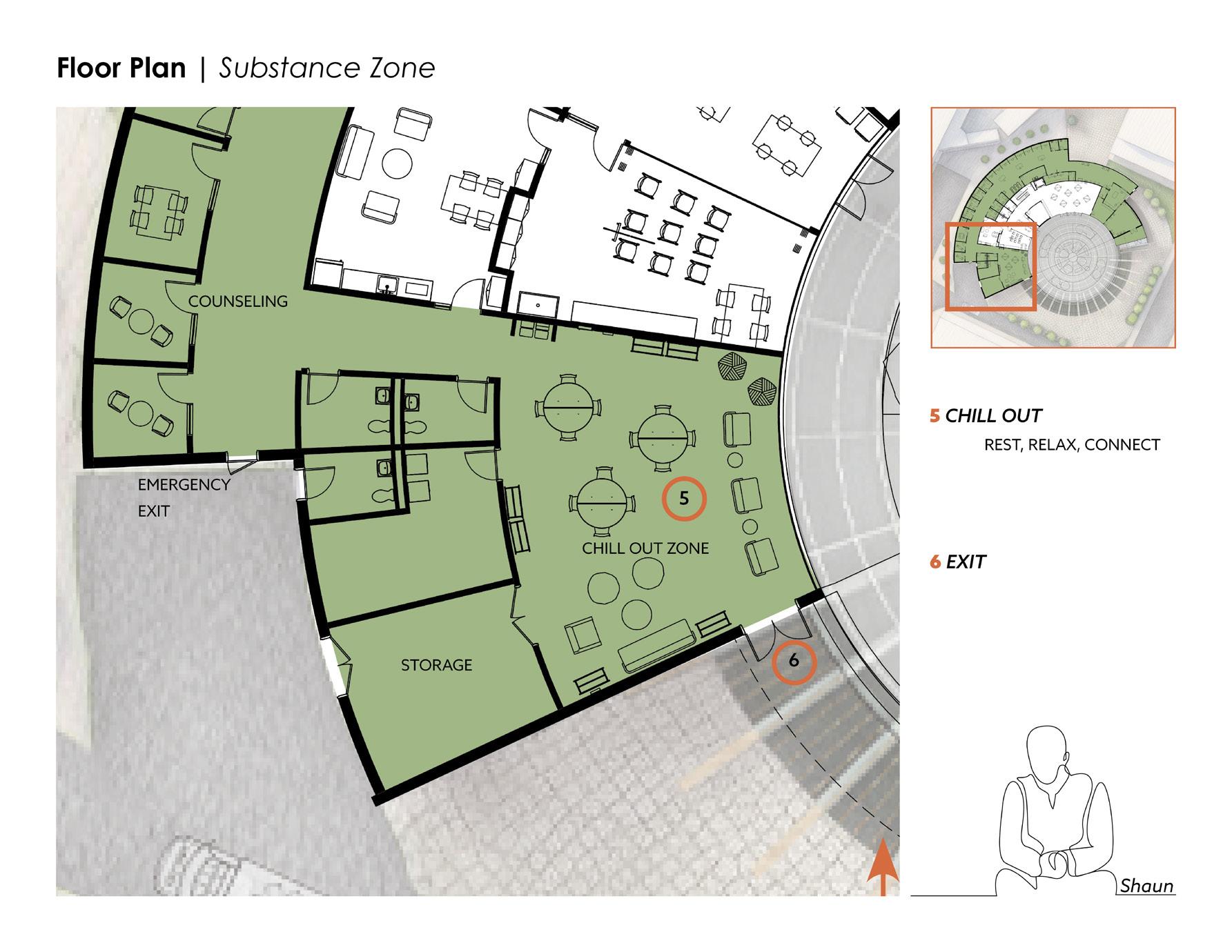
Jim then escorts Shaun to his assigned station, where he sits down and starts his injection routine.** Jim asks him if he needs anything or any help, and Shaun declines. Jim says he will be right over there if he needs him. Jim then sits at one of the tables behind the injection stations and observes Shaun. After the ten minute observation time is up*** , Jim escorts Shaun to the chill out room, where he can relax, read a book, chat with friends, or take a nap. Shaun is welcome to stay as long as he would like. He eventually leaves after about 2 hours of hanging out. He exits through the primary exit and carries on with his day.
By using Heart House today, Shaun prevented himself from using a dirty syringe which saved him from potentially contracting infections such as HIV, HEP C, MRSA, or Necrotizing Fasciitis. If he had overdosed, his life would have been saved by Jim through the administration of Narcan. Shaun also made positive connections through interactions with Jim and his long time buddy who is beginning his journey of getting clean. Shaun felt worthy, respected, and part of a community.
* Restrooms are available before the smoking and injection phases for urine samples, as well as near the chill-out zone.
** There are 8 injection stations, 4 private rooms for injecting (with the company of a staff member) and 3 rooms for smoking, each with a negative pressure mechanical system.
*** The first ten minutes after injecting or smoking is the most crucial time for an overdose. If someone does not overdose in those first 10 minutes, they will most likely not overdose from this drug-taking session and are free to move on to the next area.
43 | NARRATIVE

“CHILL-OUT
ZONE” LOOKING OUT ON THE PRIVATE COURTYARD
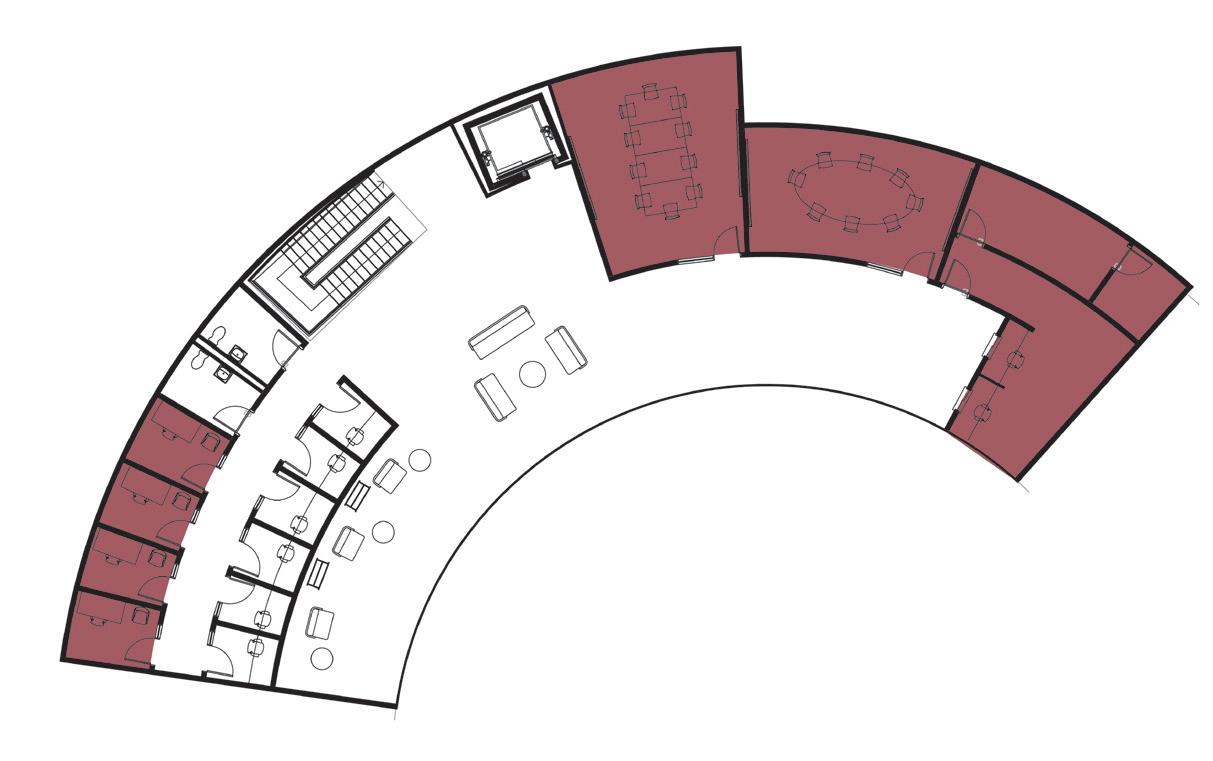
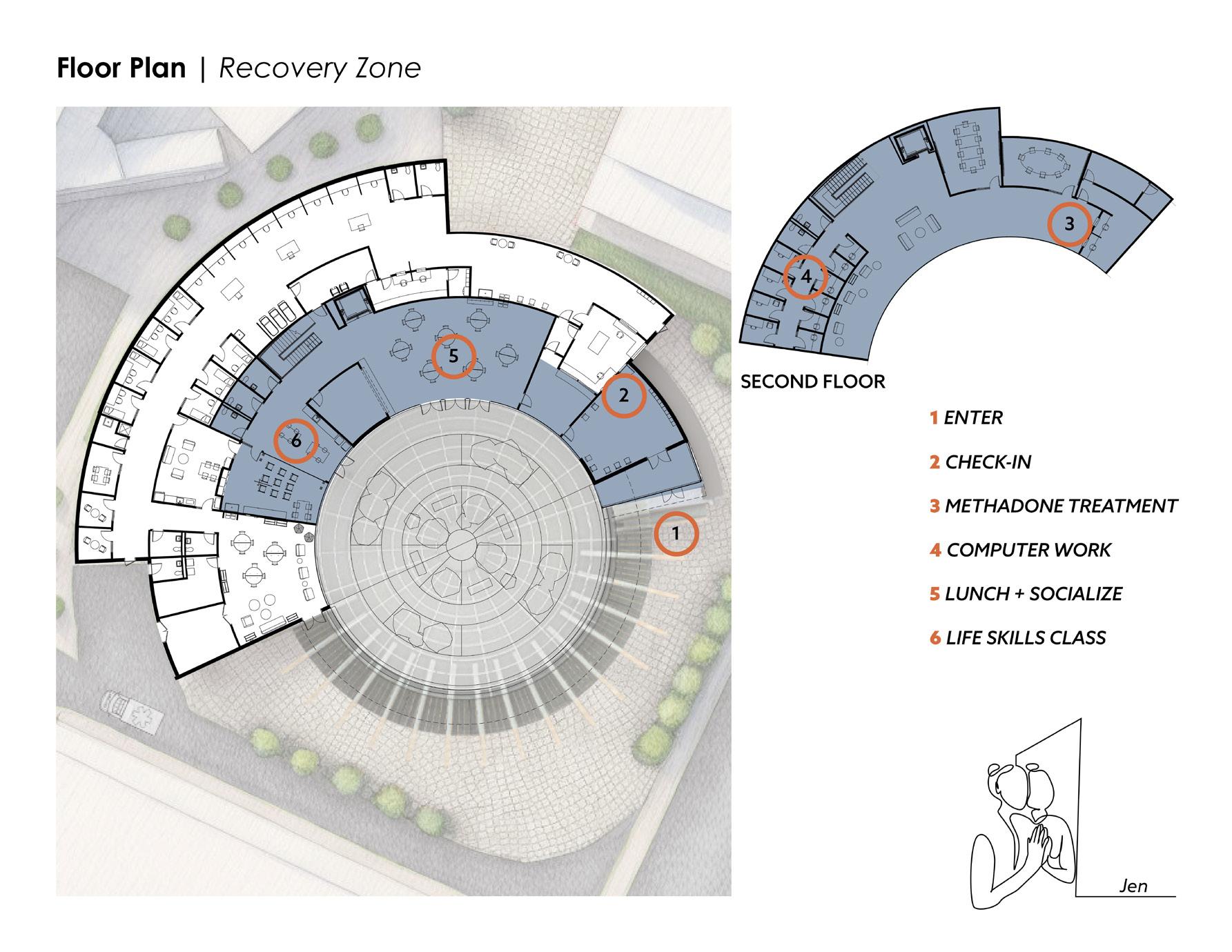
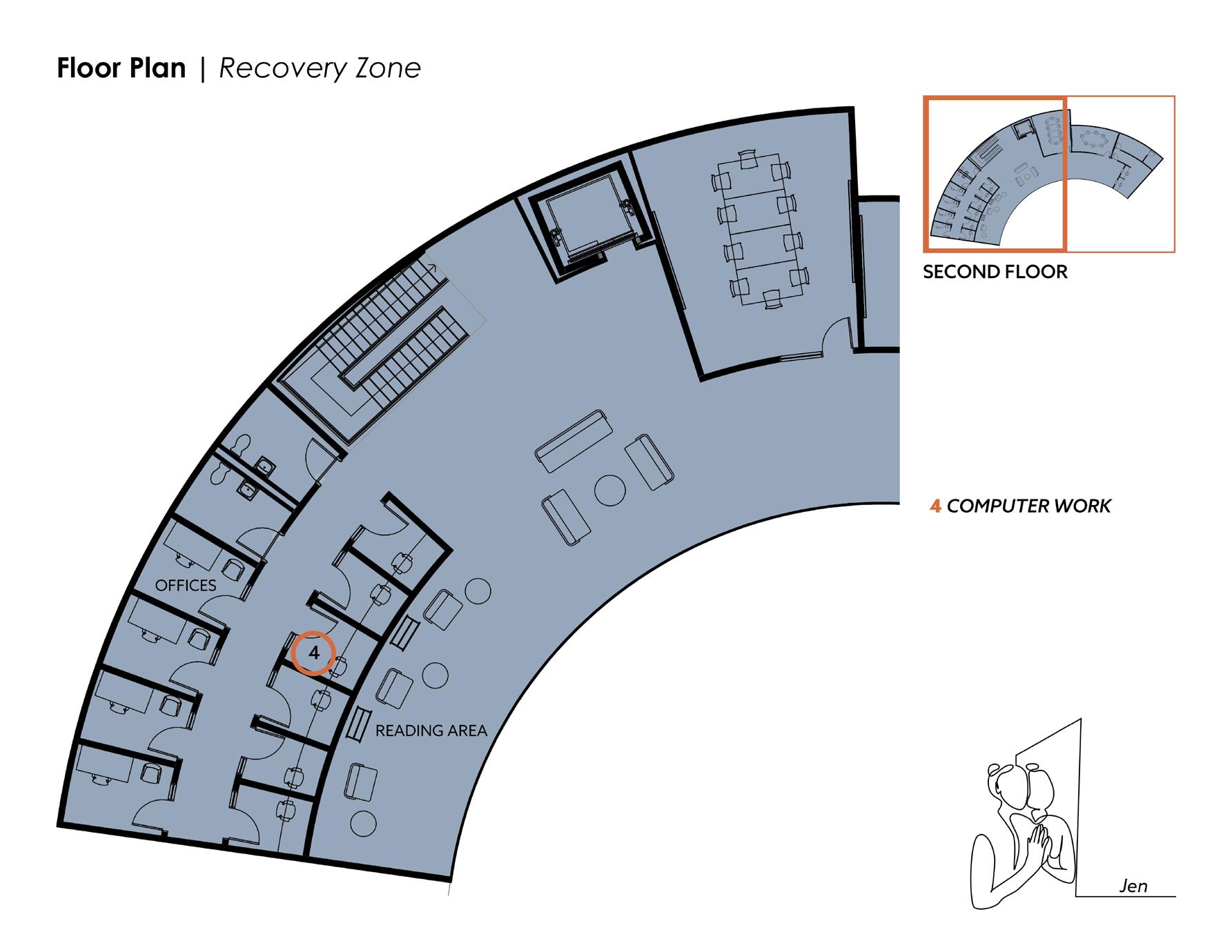
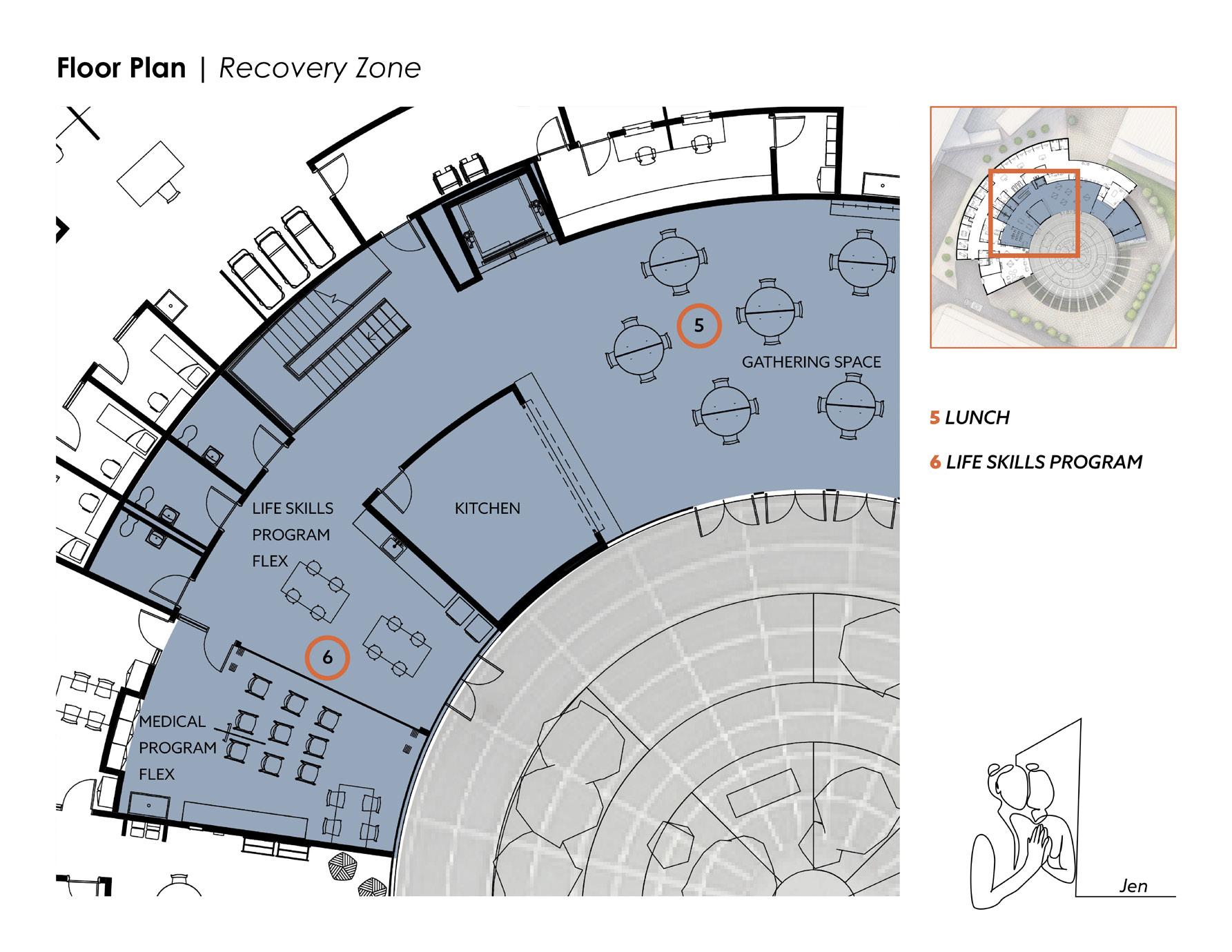
46 2 CHECK-IN COMPUTER ROOMS 1 ENTER 5 LIFE SKILLS FLEX METHADONE TREATMENT 3 CAFE SECOND FLOOR 1 2 3 5 6 FINAL DESIGN | RECOVERY ZONE 5 5 5 5 5 1 8 7 5 4 2 3 6 9 10 11 7 4 KITCHEN 6 MEDICAL FLEX GROUP COUNSELING 8 9 READING AREA 10 11 OFFICES 12 COVERED MEDITATION GARDEN 12
JEN
• 43 years old
• Recently out of an abusive relationship
• Her sister recently died of an overdose
• Seven years of homelessness
• Existing addiction issues, on Methadone
• Felony charge
• Can’t land a job
• Currently transitioning into housing
It’s 10am, Jen usually arrives at Heart House around this time everyday. She’s getting used to taking methadone and finds it’s best to take it in the morning so that she doesn’t experience withdrawal symptoms throughout the day.
Jen is currently in and out of nearby shelters. She likes to keep her belongings on her at all times because theft is rampant in the shelters and when “rough sleeping”, so when she arrives at Heart House, she locks up her cart of belongings in one of the lockers near the building entrance. She’s not worried about her things getting stolen because they are secure, and security has a window with direct sight of the lockers.
She checks in at the front desk and says she’s here for the methadone clinic. The person at the front desk checks her medical record and says she is all set to head upstairs.
Jen proceeds through the waiting room doors and enters the cafe, where she
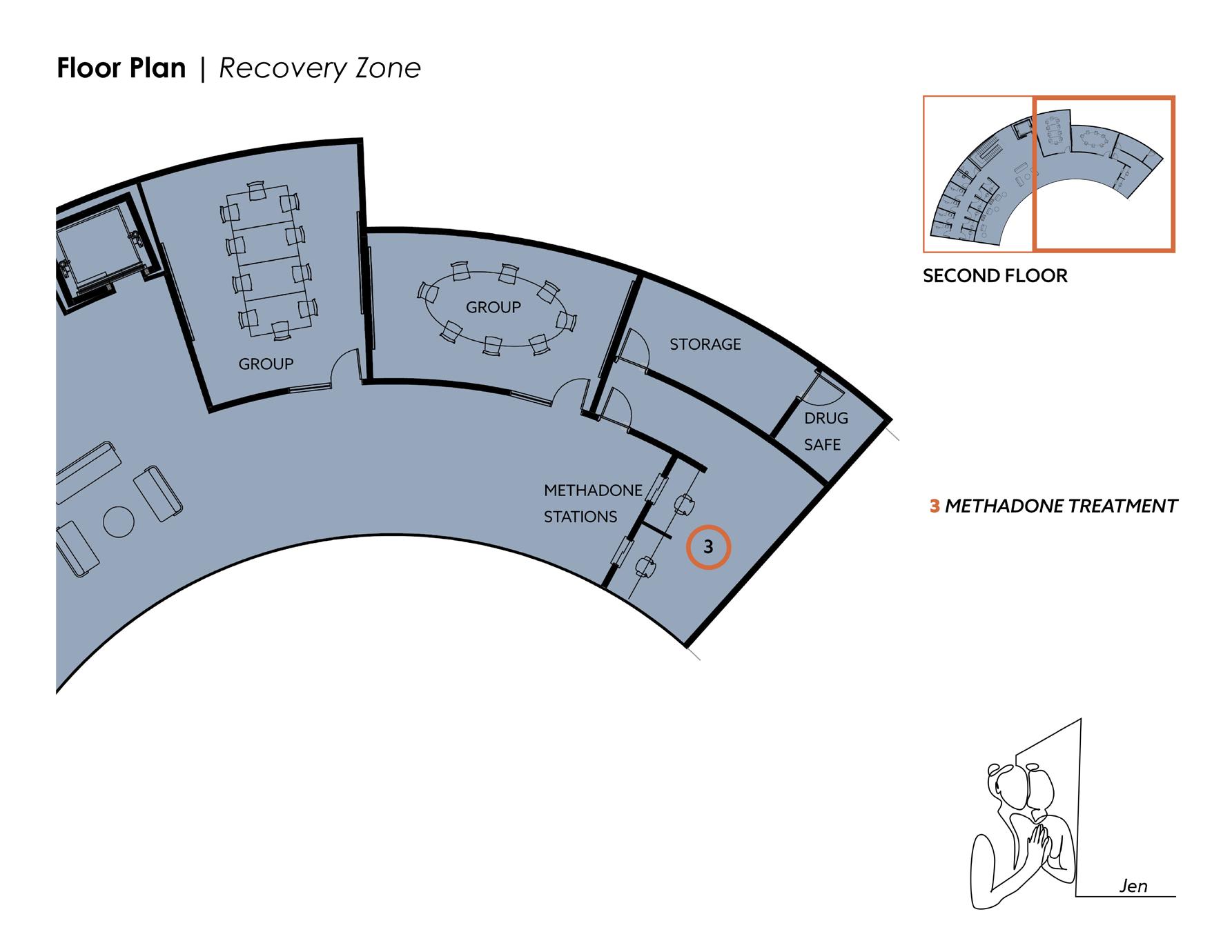
says hi to a couple of her friends who are having coffees and croissants. She heads upstairs to the Methadone Clinic window, where she checks in with the nurse. The nurse confirms her prescription and gets the methadone from the drug safe. Jen is handed her prescribed amount of Methadone, takes it and washes out her mouth with a cup of water.
Jen is planning to spend the rest of her day at Heart House. Right after she takes her dose, she heads over to the private computer rooms, where she charges her phone, fills out a few job applications and responds to some emails. When she’s done, she goes back downstairs for a hot lunch with a few friends.
Jen has never lived on her own, and next week she’s moving into an apartment. This will be the first time in seven years that Jen will be living indoors, and for the first time in her life, she will have her own space.
This is a huge step for Jen and it feels quite overwhelming. Thankfully, there’s a life skills class this afternoon that will help her learn the skills that come with indoor living.
Jen takes the cooking class this afternoon. A group of instructors and volunteers come in with hot plates, cooking utensils, and fresh ingredients. They set up in the Life Skills Flex Room, where there are high and low-top tables with a retractable power cord over each one for the hot plates to plug into. There’s also a large sink to wash hands and produce. Jen learns how to find ingredients in the grocery store, how to properly use a knife and how to cook a simple meal with a protein, grain, and vegetable. She eats her freshly cooked meal as an early dinner, and feels incredibly proud of herself for what she’s created. She feels confident that she can do this on her own when she moves into her new apartment next week.
47
| NARRATIVE
Arrows
Dots represent
circulation
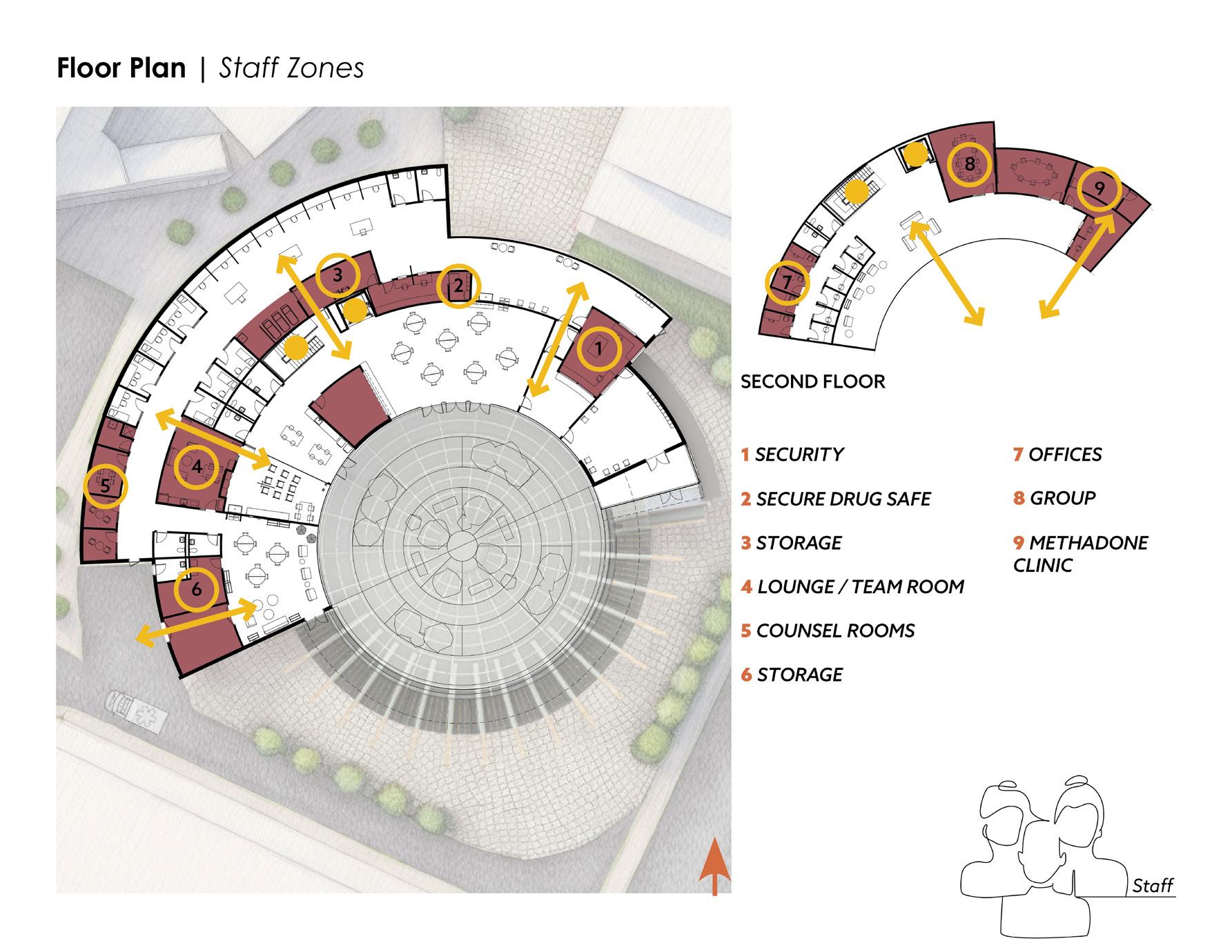
48 SECOND FLOOR 1 2 3 4 5 6 7 8 9 FINAL DESIGN | STAFF ZONES 2 DRUG SAFE 1 SECURITY 5 COUNSELING OFFICES 3 STORAGE 7 4 TEAM ROOM 6 STORAGE GROUP COUNSELING 8 METHADONE CLINIC 9 1 8 7 5 4 2 3 6 9
represent the access points and view corridors between zones
the vertical
Security’s role is to watch who comes in and out of the main entrance from their post at the front desk (#1 in graphic, page 48). They should not interrupt the flow of the client’s journey through the space unless absolutely necessary. Security’s role is important because, although all drugs are kept in safes, there are many different kinds of legally prescribed and controlled substances on site, making the building susceptible to break-ins. The active substance user group could also be volatile at times, so it is important to have security on site for the safety of staff and clients. Security also keeps an eye on both interior and exterior lockers, and is aware of whose belongings are placed in which locker, to reduce the chance of theft.
The Nurse Staff and the Social Worker Staff roles are very interchangeable. The likelihood of this facility’s programs being short staffed are high, so the layout is designed for staff to easily move in between zones, at equally spaced points throughout the plan. Nurses will primarily be in the active substance zone. Although anyone can administer Narcan, it is best to have nurses on hand, as they have more medical knowledge, and can help clients with a variety of medical needs. Nurses will also be very involved in the medical flex zone area, where they can help with medical programs that use the space for programs such as a foot clinic, dentistry, vaccines, or blood work.
Social Workers will primarily work in the recovery zone, where they will lead group counseling, have one-onone counseling, and make meaningful connections with clients. Either social workers or nurses may work in the methadone clinic. After a client establishes their prescription with a doctor, their information is on their chart, so any staff member working in the clinic can give them their dose. However, it is important that staff roles stay consistent so that clients build relationships with the same person, and don’t feel blindsided when “their person” is not in their regular location.
Team rooms are for staff to collaborate or take a break. It is important for staff to build a rapport with each other, as their dynamic will directly affect the clients.
Plenty of storage is necessary for flexible spaces. Storage is also needed for medical supplies - large and small, as well as large cleaning devices. There is also laundry, outdoor storage, and private locker storage for staff.
49 | NARRATIVE

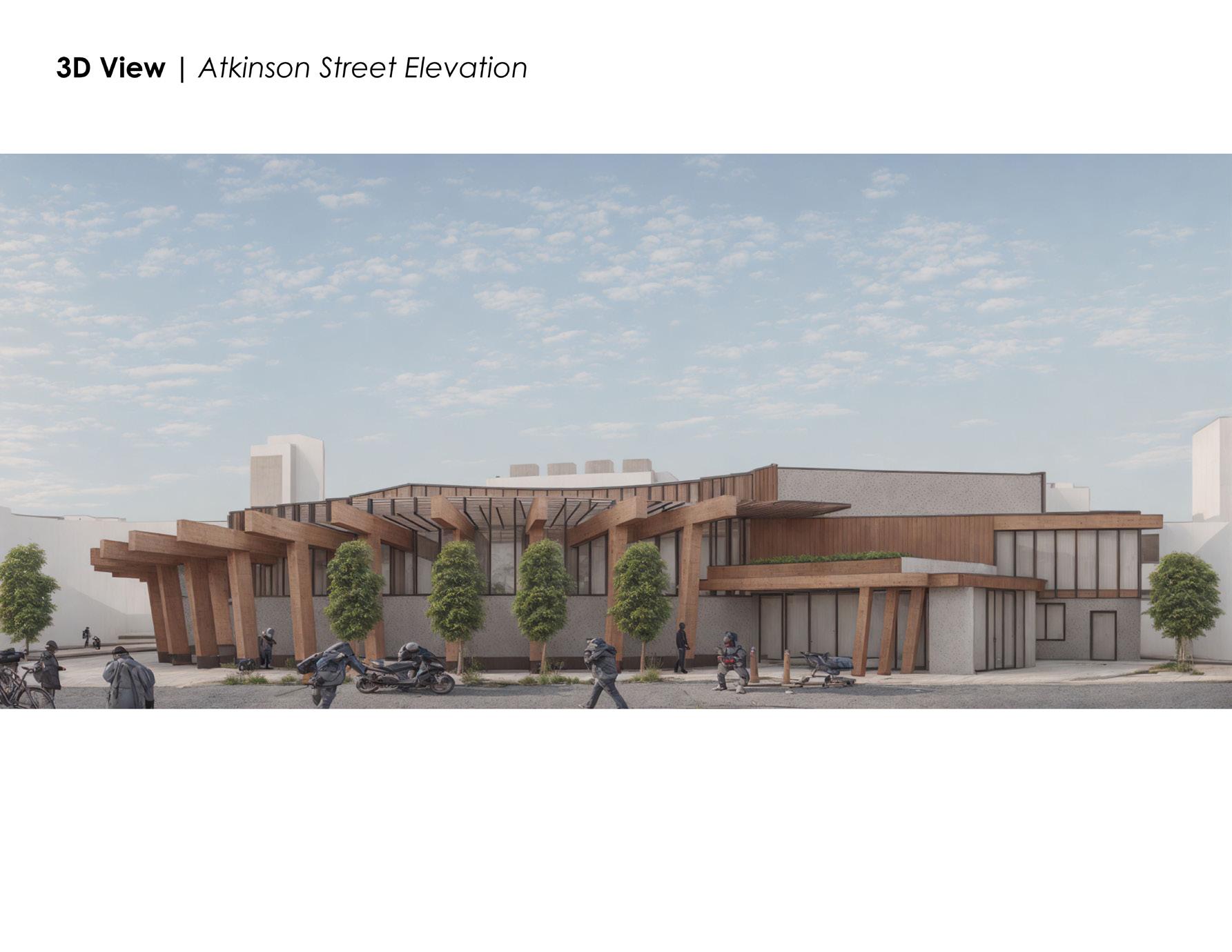
 ATKINSON STREET ELEVATION
ATKINSON STREET ELEVATION

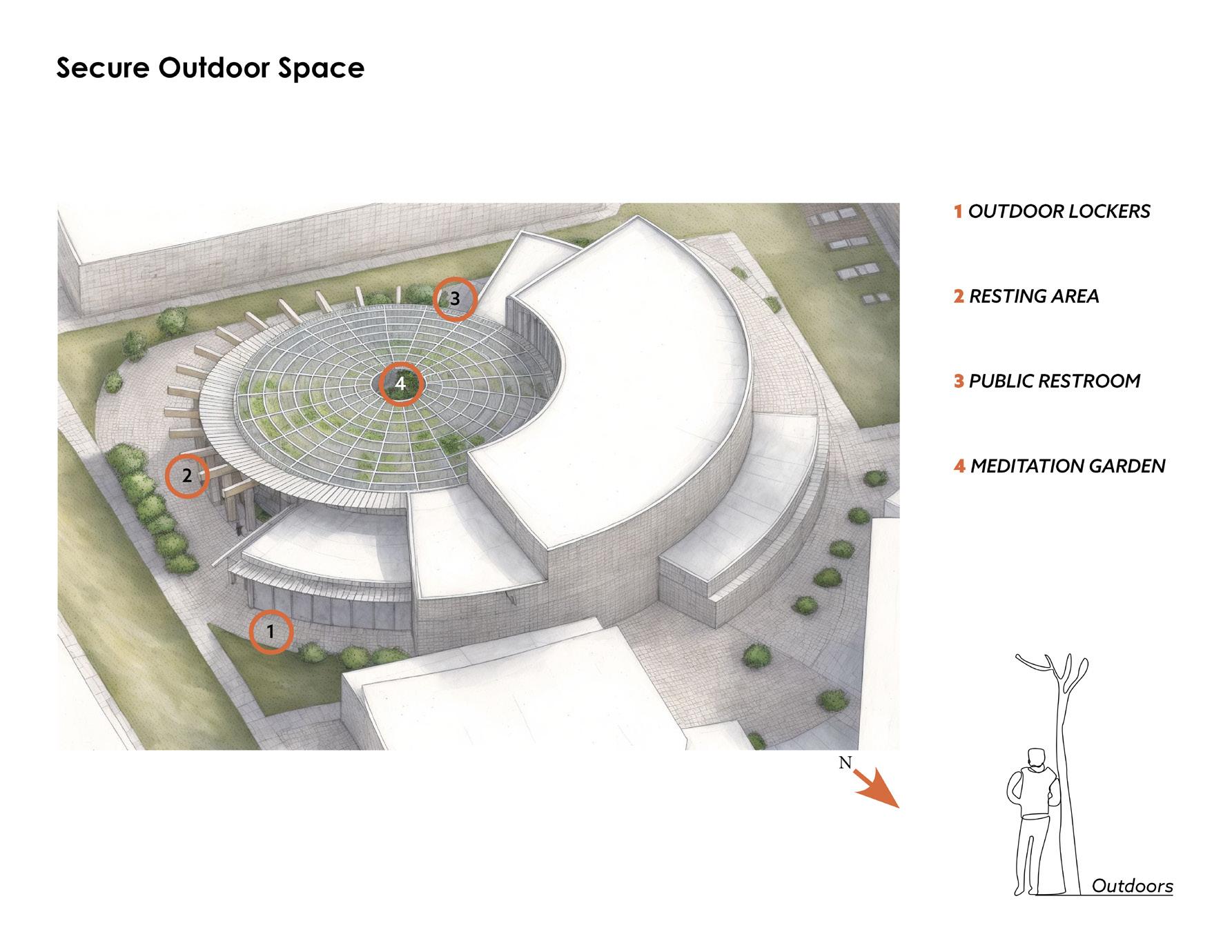
One of the outdoor features is the colonnade on the front elevation of the building, facing Atkinson Street. The timber columns create a colonnade effect on both the exterior of the building, and on the interior courtyard side of the building. Along both sides of the wall- interior courtyard and exterior wall- there is a granite bench. On the exterior of the building, in between the column and the wall, there is radiant heat that runs underground (#1). This heats the pavers in the winter, serving as a warm place for folks experiencing homelessness to camp.
Another feature is a restroom for public use (#2 on page 53). The restroom is monitored by staff and uses the same alarm system as the interior private rooms. The alarm alerts staff of a possible overdose if there is no movement sensed after 90 seconds once the room is occupied, and the restroom door unlocks. The restroom is located right outside of the substance zone emergency exit, and opens onto the emergency vehicle pull-off area.
Exterior storage lockers are also available for public use (#3 page 53). Anyone who needs to store their larger belongings such as shopping carts or wheelchairs, can use these storage units. All they need is a padlock and a key. The front desk can hold the key for anyone if they would like. There is also a window from the security office with visuals of the lockers for extra protection.
52 FINAL DESIGN | SECURE OUTDOOR SPACE
Illustrative section through colonnade
1 1
ATKINSON STREET
RADIANT HEAT
SUBSTANCE ZONE EMERGENCY EXIT
EMERGENCY
VEHICLE PULL-OFF
Enlarged Plan - First Floor at Emergency Vehicle Pull-Off

53
2
1 3
Illustrative view from Atkinson Street


CENTRAL COURTYARD VIEW FROM CAFE
Dignity
What does dignity mean as it relates to architecture?
Dignity is a sense of pride in oneself; self-respect. How can architecture make someone feel this pride in themselves?
Heart House is made FOR those who have never felt worthy enough to walk into a building because they have only ever been pushed out - by hostile architecture and by a hostile society.
This building gives people the opportunity to feel worthy-- worthy to walk into a beautiful building that is FOR them.
Self-worth is the first step in recovery.
Graziella Pilkington 2024
56

57
PART IV
Next Steps & Conclusion
59
NEXT STEPS
The next steps in developing this project would be as follows:
Building Sections
• Show the relationship between the central courtyard and the two levels of space in the building.
Details including:
• Glulam structural connections
• Connection at the bottom of the glulam column - reinforced with steel and set on a granite slab
• The connection where the glulam intersects the glass clerestory
• The phenolic wood fins connection to the glass facade and clerestory
• The granite bench along the exterior front and the interior courtyard
• The mullions and structure for the glass canopy covering the central courtyard
Design Aspects that I would like to explore further include:
• The central courtyard landscape. I would like to develop this space to have smaller, more intimate areas where clients can peacefully reflect, or make meaningful connections with others.
• I would like to further explore the types of plants that would be suitable for this space.
Exterior Materials
• What could be a more welcoming/ less stark material than concrete?
• What kinds of glass should be used for the clerestories vs the curtain walls?
Interior Materials
• What might be best for these varying spaces? Gypsum walls and wall tile?
• What materials are best for maintenance and hygiene?
60
The thesis explores the role of architecture in fostering healing within an inner-city population affected by opioid addiction and homelessness, investigating how design interventions can alleviate social and health disparities, promote rehabilitation, and cultivate a sense of belonging and support among affected individuals.
My goal in being an architect are to approach every design with empathy. I like to ask myself how is this work contributing in a meaningful way to society?
Architecture has the essential and tangible capability to empower individuals and communities by providing spaces for social interaction, education, recreation, respite, nourishment, and self-expression. When people feel agency and ownership over their built environment, they are more likely to experience a sense of dignity and pride. When people feel this pride, they develop an urge to give back - to themselves, to their families, and to their communities. This is how Heart House gives back to the community.
Ultimately, architecture can play a profound role in shaping the way people perceive themselves and their place in the world. By creating environments that prioritize dignity, architects have the opportunity to contribute positively to the well-being and self-esteem of individuals and communities.
61 CONCLUSION
PART V
Appendices
A - Thesis Reviews
B - Thesis Proposal
C - Bibliography
62
Thesis Reviews Appendix A
63
February 8th, 2024
This first review introduced the project to the panel of thesis critics. It explained the focus of the inquiry, reviewed the most relevant precedents from my research, and introduced the site and program.
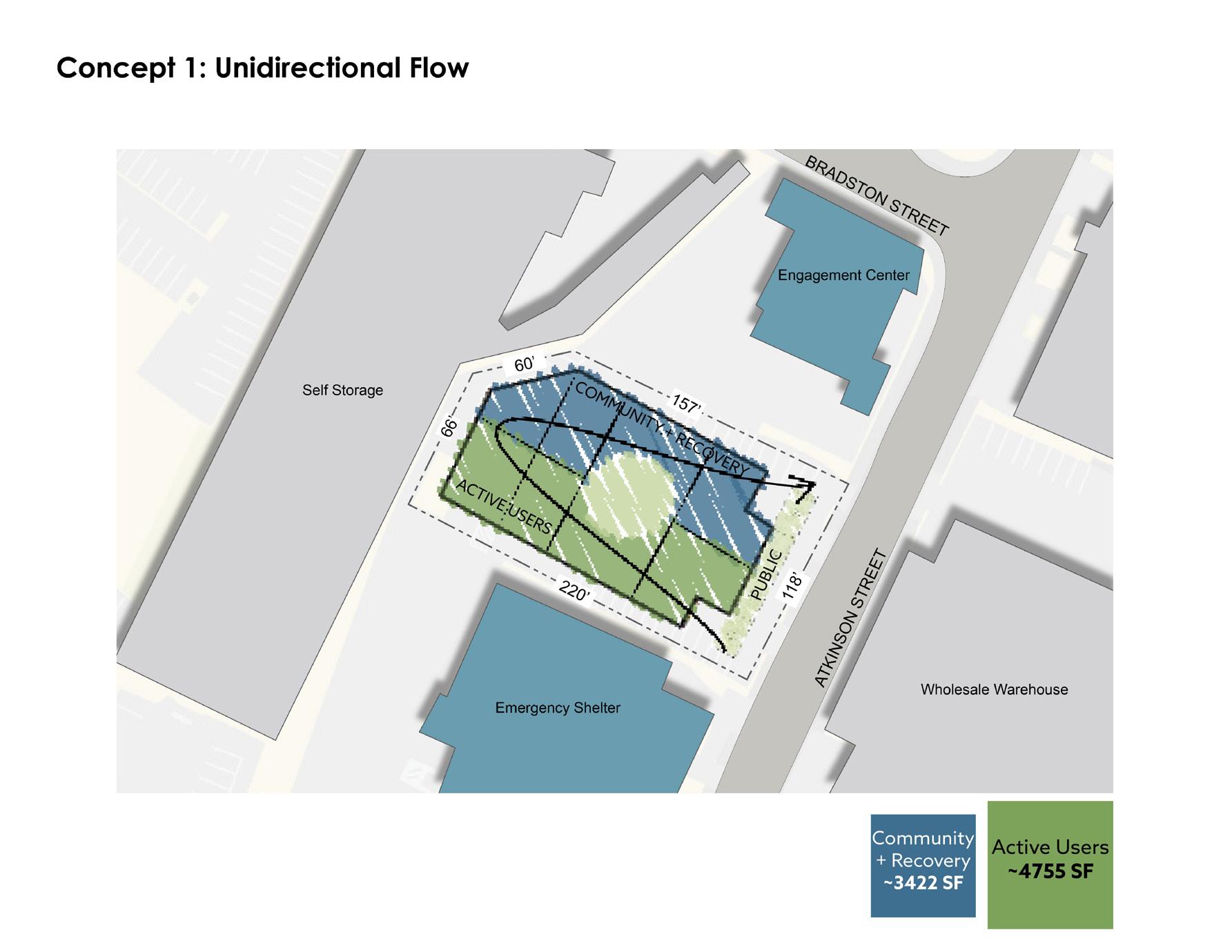
Four concepts were developed for this initial review.
ConCept 1 explores unidirectional flow. This layout requires the active substance users to exit through the recovery space, exposing them to the available recovery resources. The central green space is accessible through the building. This concept was not further developed because it was decided that the active users should not be forced to go through the recovery spaces for two reasons: (a) because they will not be in the right state of mind after using, and (b) folks in recovery shouldn’t have to see someone on drugs in their safe sober spaces.
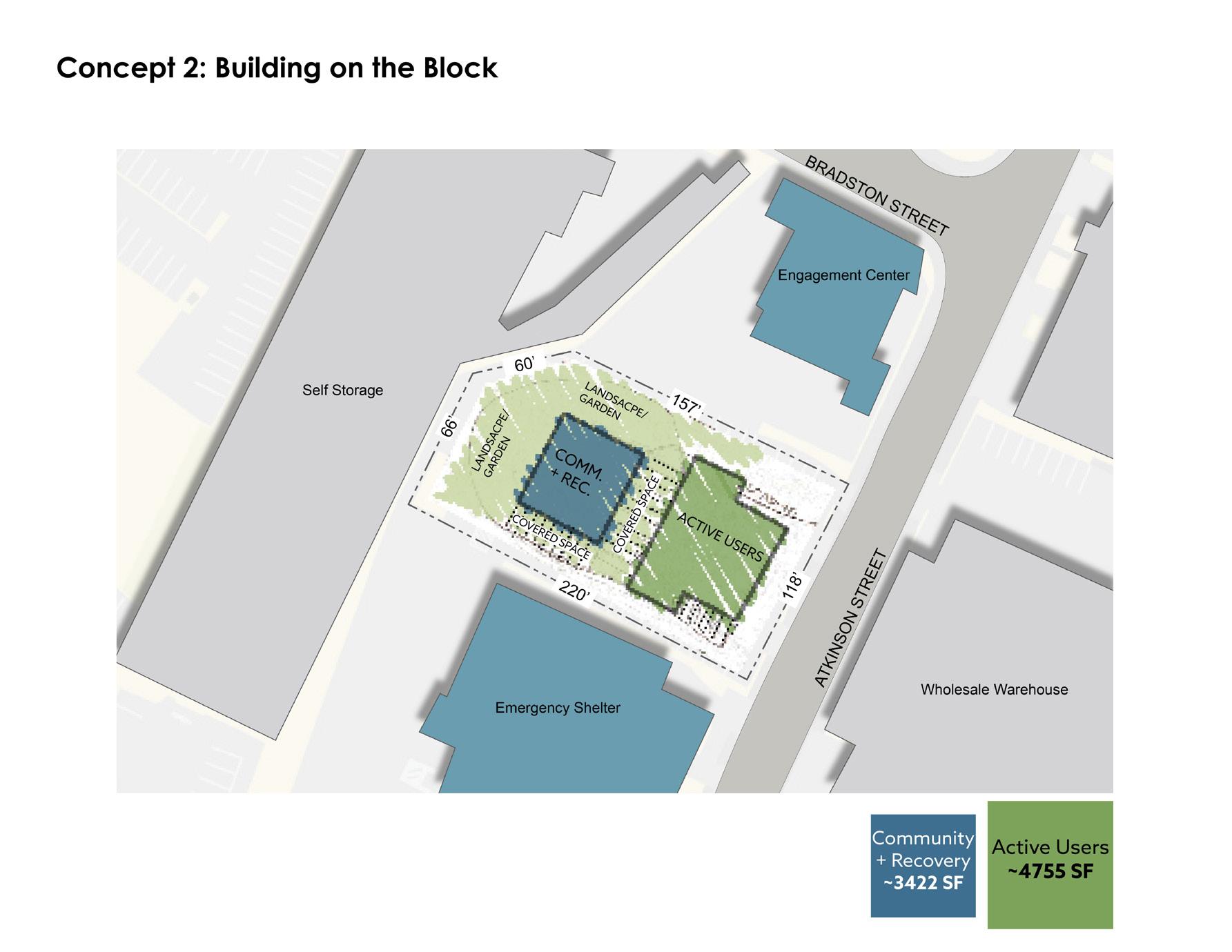
ConCept 2 is a campus-like layout with multiple buildings. The buildings are joined together by a covered outdoor space. Many people who experience homelessness are more comfortable outside than indoors so it will be important to have some of the programming outside for those folks who are not comfortable being indoors.
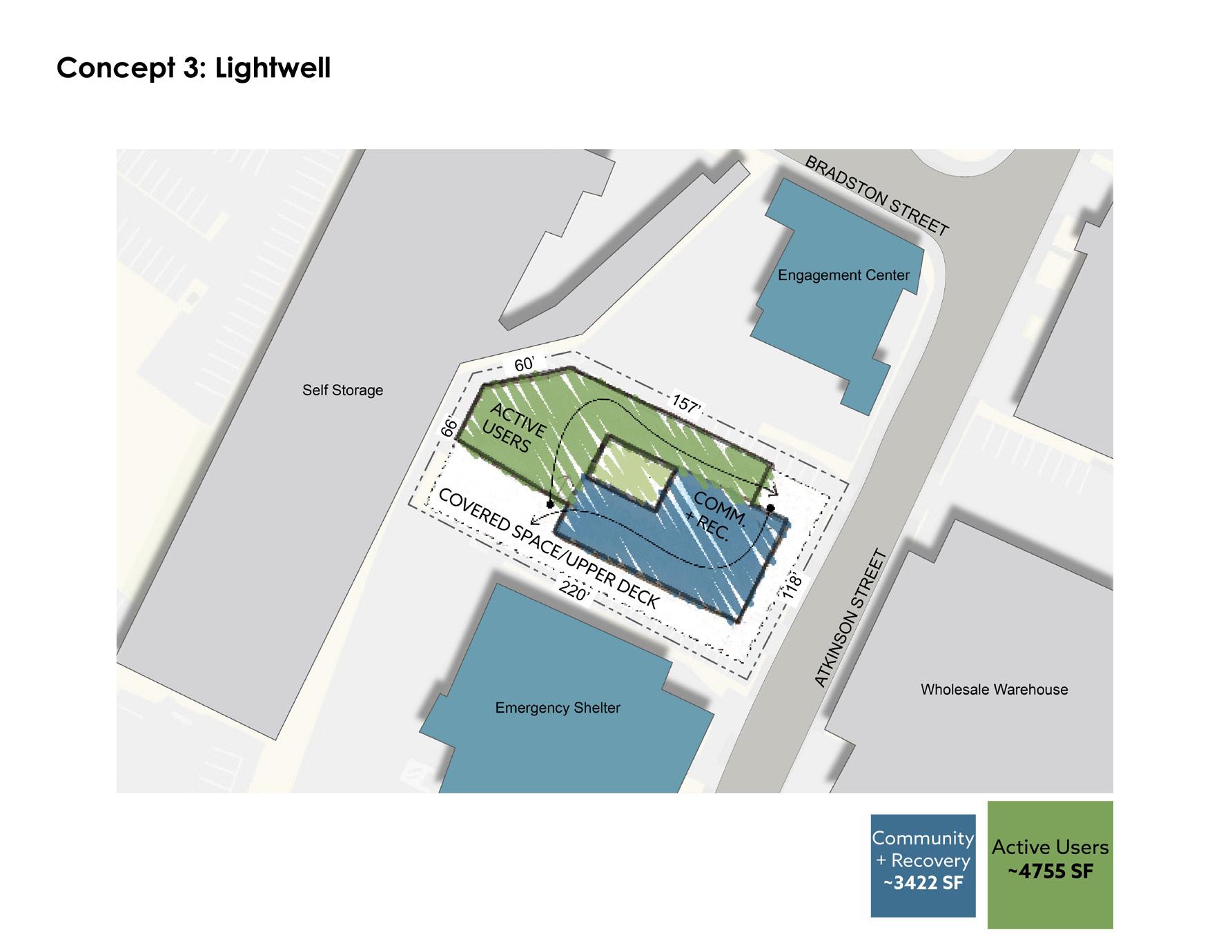
ConCept 3 separates the active users and recovery spaces by providing separate entries and exits. The central green space in this concept is not to be occupied, and its main purpose is to provide natural light and a nature-view with little to no maintenance required. This concept was not favorable due to the separate entrances which would cause a stigma for the clients and would require more security measures.
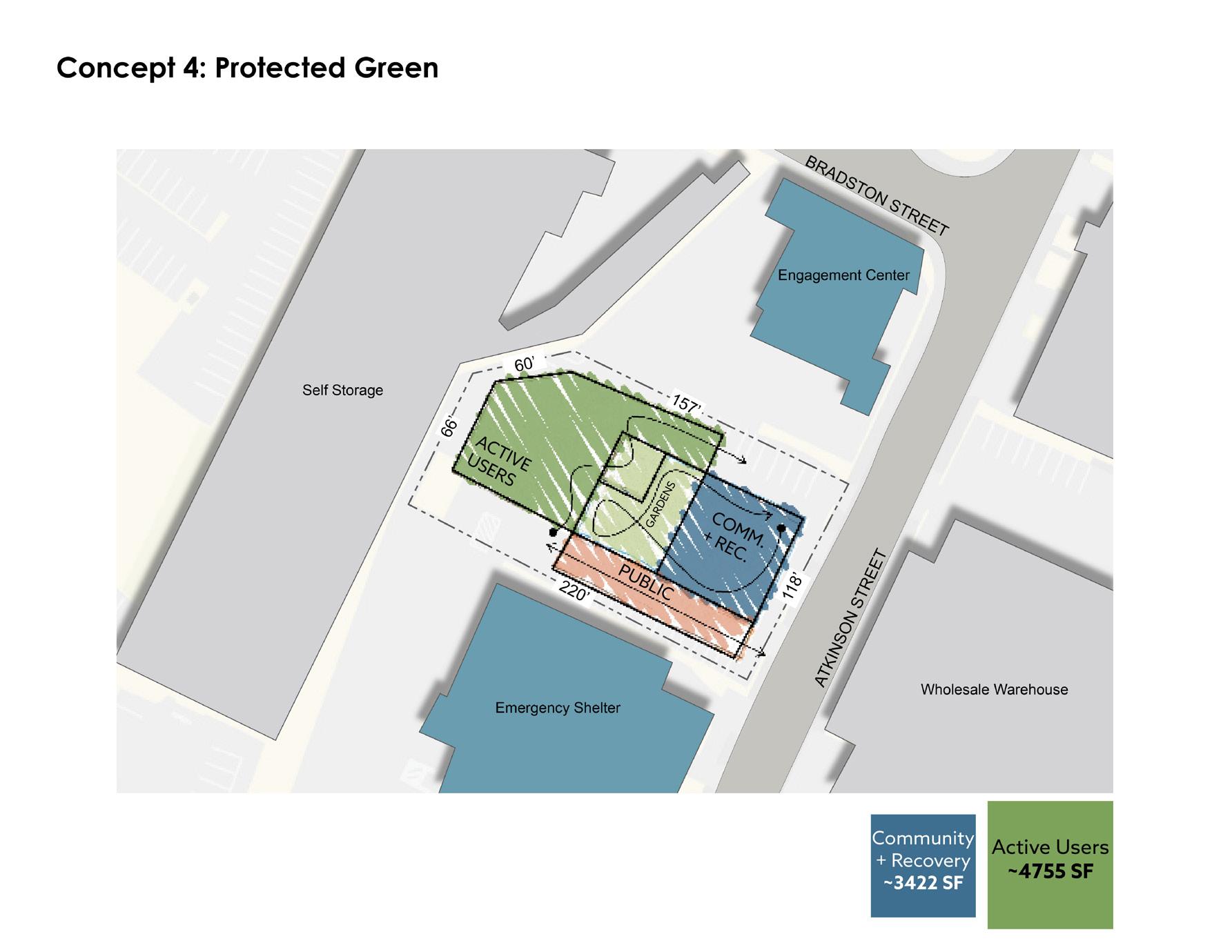
ConCept 4 is very similar to the previous, but the central outdoor space is occupied. The central outdoor space is sectioned off between the active users and recovery zone- which I decided against designing any further due to the segregated-feel and the potential of drug dealing between the clients when they are outdoors. As the program and plans were further developed, it was quickly realized that much more square footage was necessary to fit the program. The circular interior garden space of Concept 1, along with the tight site restrictions, are what inspired the circular geometry of the building which will be shown in the second review.
64 REVIEW 1 | CONCEPTUAL REVIEW
65 APPENDIX A - THESIS REVIEWS

66 APPENDIX A - THESIS REVIEWS
67 APPENDIX A - THESIS REVIEWS


68 APPENDIX A - THESIS REVIEWS
69 APPENDIX A - THESIS REVIEWS
70 APPENDIX A - THESIS REVIEWS
71 APPENDIX A - THESIS REVIEWS
• Institutional Context - Chuck: will this be open 24 hours? [theoretically yes] (you might have mentioned the issue of available resources and the closed community center building) Is there a residential component? [no] (I added here about the shelter next door. Further explaining the institutional context would be a good response to Chuck’s two questions, showing that they are well considered. It also shows that you had clear answers that explain your choice to complement adjacent uses, not duplicate them.)
• Why Recovery and Active on same site - Dan: is this for people trying to quit? [yes] It seems like having this here is reinforcing what you’re trying to get away from. [yes, it’s a challenge] (You could also argue that it enables outreach to the user population. It would also be good to cite research about where these facilities are usually located, if you have this.)
• More Research - Sarah: You speak of reaching out to people who provide shelter services to this population. They could assist you to know more about available resources and clarify your positions on a topic like this. It’s a difficult topic and not a lot of facilities to examine. She suggests that you bring more research into this. Specifically you should answer the question about combining a facility for active drug use and recovery populations. The Boston public health department might be a source of information.
• Site Plan - On another topic: she suggests that it would be helpful to have a more detailed site plan that includes the two adjacent properties so the entire block’s program is considered as a whole.
• Stigma & Dignity - Hyacinth: Is this only for homeless people fighting addiction? (Not clear on your answer, do you intend it to be largely for the homeless? The police might have info on the area’s population, how many homeless, how many coming from elsewhere to find drugs). Hyacinth’s student Lukas had a solution that was opened up to the larger population. (Lukas Machaj’s book is in the sample book file.) A user’s family support could lead to success. Think about the edges, the transitions from the sidewalk into the building. Would there be a stigma about entering this facility? How do you encourage them to do that and still save face? The entrance will be an important design feature. It’s important to help preserve their dignity. Perhaps there can be one or several uses at the edge that allows for some ambiguity about what you’re doing when you enter.
• Amenity Space - Chuck: is there any amenity space included? [barber, hairdresser, telephone charging, job application, video call] (This was a good response – nicely considered)
• Landscape - Sarah: it’s not just the building that’s important, it could be landscaping that helps with the transition. Also, ambulance and police access will be important to consider. Other projects she’s seen on homelessness includes space to safely store their shopping carts or backpacks. [The engagement center allows for shopping cart storage.]
• Transitions & Edge ConditionsChuck: think about the edges of the program, and edges to the building. Transition areas need to be comfortable, welcoming, providing needs.
72 DISCUSSION | REVIEW 1: CONCEPTUAL REVIEW
APPENDIX A - THESIS REVIEWS
March 28th, 2024
The second review presented the proposed design at a schematic level. This included building massing, site plan, floor plans, building circulation, and program organization.
Addressed comments from review 1:
• Added more institutional contextimproved graphics for what other resources are in the area.
• Improved argument on why Recovery and Active should be on the same site.
• Revised site plan to show relevant buildings adjacent to proposed building.
• Focused on stigma regarding the entrance of the building.
• Further developed landscape to address the edge conditions, access for emergency vehicles, trash, and delivery
APPENDIX A - THESIS REVIEWS
73
PRESENTATION
REVIEW 2 | DESIGN
74 APPENDIX A - THESIS REVIEWS

75 APPENDIX A - THESIS REVIEWS
76 APPENDIX A - THESIS REVIEWS
77 APPENDIX A - THESIS REVIEWS
78 APPENDIX A - THESIS REVIEWS

79 APPENDIX A - THESIS REVIEWS

80 APPENDIX A - THESIS REVIEWS
81 APPENDIX A - THESIS REVIEWS

DISCUSSION | REVIEW 2: DESIGN
Who are the users? What is their state of mind when they’re finished using drugs? [users are mostly homeless, existing clinic provide support but creates no community.] What about storage of their stuff? [considered outdoor storage.] What’s your goal for Mass/Cass? [not used by everyone but they are used by most] Safe needles aren’t available in MA but this could be a pilot. (I mention that this needs legislation but is being considered.) Who are the people who use this: as part of your narrative, create personas and move them through the building. (this would help avoid the confusion and restatement of user behavior that you had earlier.) Mahesh suggests that you develop a narrative way to describe things before you jump back into design. Create a diary of a user. Also, work with sections more than just plans.
How does your front door not become an encampment? (defend this with planned spaces for safe encampments and safe storage)
Sequence from the street to injection to recovery? How do the outside users, drug users and recovery users relate to each other?
Circulation and program, injection and observation: how does the activity happen here? How do people actually seek out a private place to inject? Is this space protecting the users? [you explain] (a diagram illustrating the process would help here; also you could mention the movement detectors) Could you have larger private rooms where a staff member could participate. (hard to know if this would be helpful – can you contact someone with experience? It’s hard for you personally to argue for what’s
82 APPENDIX A - THESIS REVIEWS
needed without reference to research or interviews with experienced social workers/care givers) Requires balancing privacy and protection/observation.
Multiple stories This seems like an underutilized urban space. (this may be true but are either of the adjacent buildings multiple stories?) One story isn’t cost effective, consider more space for administration, (staff, storage, recovery,) counseling? Consider enclosing all or part of the garden for year-round use. It might help people survive the winter. What about garden security, damages by users? Thinks staff and counseling could work on a second floor.
Value of quiet space
Transition from public spaces to the interior – you can make simple moves to bring people in such as paving patterns extending to street. Likes the perspective of the entrance, seems to bring them in slowly. Push this further, make it feel less closed as you get to the street. Break down the transition from outside to inside.
Entering through the market place to get to injection/counseling spaces seems like the wrong thing to do. Market is too small, busy for mixing traffic. A separate entrance to the injection spaces, might be the preferred approach.
Missing staff break spaces, need for supplies, equipment to maintain cleanliness, storage. Consider separating the circulation areas for visitors and support staff. (difficult but not impossible – would this be beneficial?) Two programs probably share staff – they’ll need to move between programs. Is there a laundry facility? Can the user observation area include sleeping spaces?
Some injection user spaces might be intermingled.
Building security doesn’t seem to have an area. (not sure it needs it as long as they’re at the entrance, but should there be some sort of check-in?)
It seems like the project needs to clarify what it wants to be: is this a community center, a transformational space, how does it work with other facilities?
The circular configuration is a difficult choice. The purest geometries are for the most rigid and stable programs. The traffic flow seems rigid, like an assembly line. Explore a less rigid geometry to allow for responsiveness to other site conditions. Alignment with and connections with other uses could be important. (you never described the two neighbors) (Mahesh’s critique of rigorous geometry is pertinent. Can you start with the geometry and intersect it with another system overlaid on the circular form, or employ your radius cuts to intersect circular the movement between spaces?)
Consider how the garden might become better integrated, some inside, some outside. This would allow people to meet each other. (is this an important goal?)
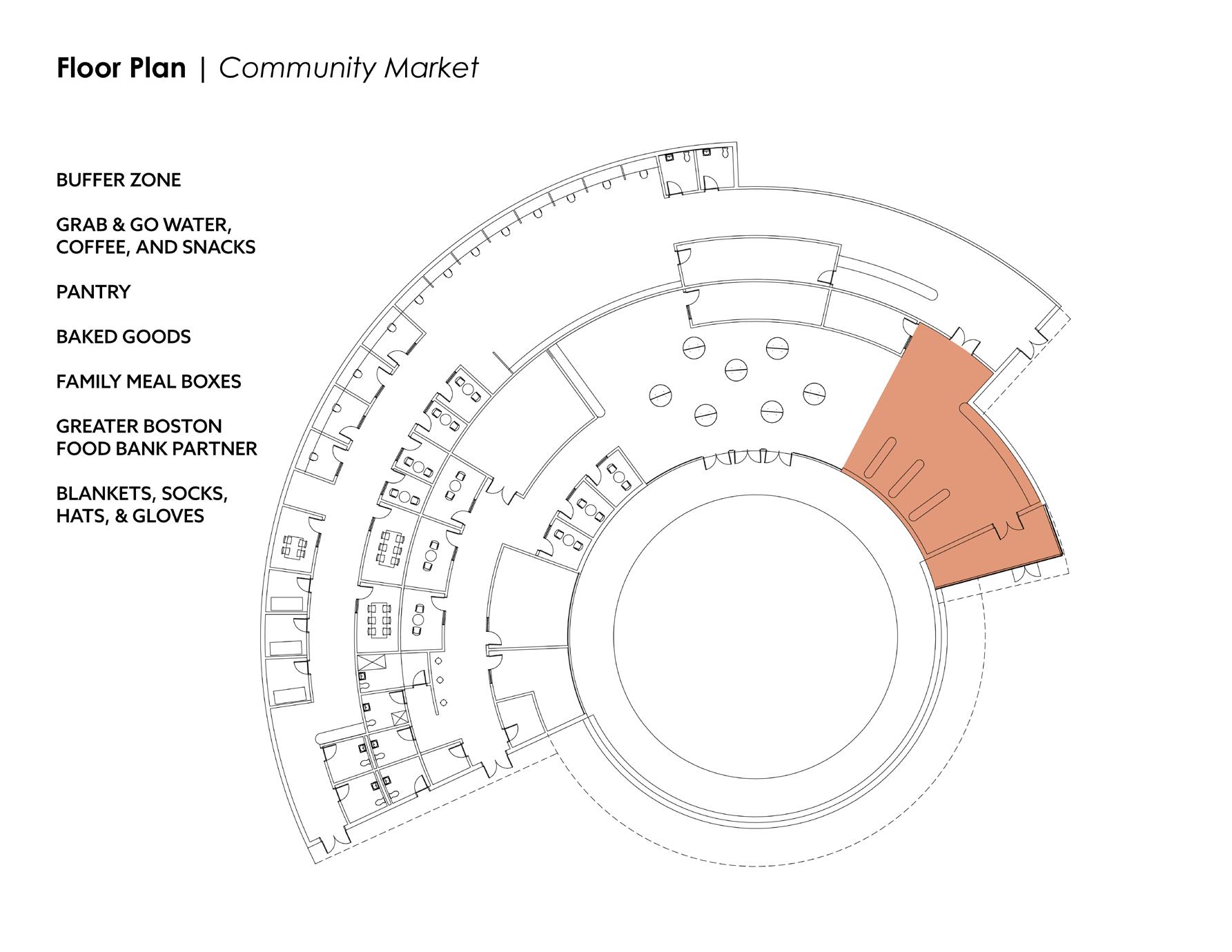
Important to provide dignity for the user. There’s a mobile shower clinic that provides services to this population– trailers with showers for people to clean up. Consider building that in. The community market seems tacked on, should either have more of its own identity, or pull it out. It seems improbable in this facility. Consider your haircut facility could be more multi-use. Allow some flexibility. Uses will be messy, programs in support will be quick to change.
83 DISCUSSION | REVIEW 2: DESIGN APPENDIX A - THESIS REVIEWS
April 25th, 2024
The third and last review reflects the work of the entire semester. The overall designs remain at a schematic level, given that the project scope and topics are too large to complete in a single semester.
Addressed comments from review 2:
• Who are the users? This was addressed by creating user group profiles, and explaining how each user moves through the space.
• Front door as an encampment - This question is defended by graphically showing and verbally explaining that the front of the building actually allows for camping. When people are caught having substances on them at shelters, they are turned away for 30 days. If it is the middle of the winter, and someone has nowhere to go, Heart House allows camping within the colonnade at the front of the building. Radiant heat warms the ground and lighting helps prevent overnight theft and crime.
• Privacy when injecting - Unfortunately, privacy is not really an option due to safety concerns, as clients must be observed while injecting and for 10 minutes after. After speaking with Noble Powell, a counselor in a methadone clinic at the Mass. and Cass area, he suggested that providing private rooms for couples to help each other inject is a major safety hazard - especially for women’s health and safety. The response to this critic is that private rooms for injecting will be provided, but a staff member must be present in the rooms with the client or clients. All private rooms including smoking, injecting, and restrooms will have a motion sensor - which will alarm if no motion is detected after 90 seconds. The alarm will alert staff that there is a possible overdose situation.
• Sequence from the street to injection to recovery? How do the outside users, drug users and recovery users relate to each other? - The entry sequence addresses this comment. The stigma around two separate entrances is avoided by having one secure entrance, where clients privacy is protected. The waiting room is larger than necessary, and is monitored by the front desk to prevent conflict between clients. No client knows where another client is headed once they pass through the waiting room doors.
• Multiple stories - as suggested by the critics, another story was added to expand program space. The second floor also has views into the courtyard, so staff can keep an unintrusive eye on clients in that space.
• Market space - One of the critics suggested that this space was not necessary and would not be utilized. Instead of having a market space, more flexible program space was created to allow different programs in the area to use the spaces. This created a much more flexible design to accommodate and adapt to clients’ and the community’s needs.
• Staff break spaces, need for supplies, equipment to maintain cleanliness, storage - more staff support spaces were added including ample storage for a range of medical supplies. Also added were offices, more counseling rooms, and a mini methadone clinic to support the other two clinics in the area.
84 REVIEW 3 | FINAL PRESENTATION
85 APPENDIX A - THESIS REVIEWS

86 APPENDIX A - THESIS REVIEWS
87 APPENDIX A - THESIS REVIEWS
88 APPENDIX A - THESIS REVIEWS
89 APPENDIX A - THESIS REVIEWS
90 APPENDIX A - THESIS REVIEWS
91 APPENDIX A - THESIS REVIEWS
92 APPENDIX A - THESIS REVIEWS
93 APPENDIX A - THESIS REVIEWS

94 APPENDIX A - THESIS REVIEWS
95 APPENDIX A - THESIS REVIEWS
96 APPENDIX A - THESIS REVIEWS
97 APPENDIX A - THESIS REVIEWS
98 APPENDIX A - THESIS REVIEWS

99 APPENDIX A - THESIS REVIEWS


100 APPENDIX A - THESIS REVIEWS

DISCUSSION | REVIEW 3: FINAL
David: materials? [timber from garden to entry, benches; simple interior, wall tile]
Chuck: this seems foreboding, not welcoming. The biggest space is closed off – not welcoming. How did you develop the shape? [Grace farms, curvilinear but tight site led to oval, then circle] It will stand out in the neighborhood [bold architecture=dignity, respect for user groups]
David: the personas are nice to see, a good presentation overall. Your addition of a second floor is good. Thinks the neighborhood won’t always be so difficult and this building could be reused in other ways of the need for drug treatment changes.
Chuck: he likes 2nd floor, you can look out into the garden. He thinks it would be good to look outside to the neighborhood as well. (Not sure if the building form would allow this, looking down through the garden clerestory to the street – a section would tell this.)
David: section of outside is confusing, doesn’t understand the relative grades. (Creating a well against the building might be a problem for drainage, your bench against the wall as it was originally would avoid this.) Thinks columns and seating brakes things up
101
APPENDIX A - THESIS REVIEWS
Mahesh: You’ve provided good response to the feedback you received in the second review. It’s a very clear presentation and he appreciates the personas to take you though. The geometry and circulation is clear throughout the building. You needed to work with many constraints – a tight site, many program requirements, security etc. Thinks he’s learned a lot listening to your presentation. You goal is very elevated, offering architecture to this user group is important. (He implies that he’d design this differently, but “you’re the designer” and he respects that.)
Your solution is comprehensive and complete.
He thinks the use of heavy timber isn’t fully resolved, wonders whether juxtaposing wood with concrete as you have is the right move. Would users know what this building does? What might a passer-by think of this? How will this work at night? Does this building engage the neighborhood? He thinks the section of the garden and outside bench space is unclear. There are several reasons for a building section: it can be technical or illustrate the relationships between spaces. Reconsider the section - it doesn’t show the nature of the spaces. Why cut through glulam, not the wall and clerestory? This might not be what you intend. Keep in mind what you want to do with your image. He accepts your case for smooth movement, flow, through your geometry. This provides momentum through spaces, and circle has a center = garden. Why is this so important?
Chuck: you need a section through the whole project.
Mahesh: The section should present the relationship between spaces – pay attention to the center. It has meaning, so what is it? You should think more about this, how do you program it? You need to consider what activities occur here? You want people to feel dignified by being here. It’s a place where they are transformed. Consider opportunities for reflection – might drug users be inspired by seeing some recovery activities?
David: he deeply applauds how you illustrate the homeless in front of building. (tears! Congratulationsthat’s literally never happened in a review.) This reflects a deep empathy for your users – this will serve you well in practice.
102
DISCUSSION | REVIEW 3: FINAL APPENDIX A - THESIS REVIEWS
Appendix B
Thesis Proposal
103
105 APPENDIX B - THESIS PROPOSAL
106 APPENDIX B - THESIS PROPOSAL
107 APPENDIX B - THESIS PROPOSAL

108 APPENDIX B - THESIS PROPOSAL
109 APPENDIX B - THESIS PROPOSAL
110 APPENDIX B - THESIS PROPOSAL
111 APPENDIX B - THESIS PROPOSAL
112 APPENDIX B - THESIS PROPOSAL
113 APPENDIX B - THESIS PROPOSAL
114 APPENDIX B - THESIS PROPOSAL
115 APPENDIX B - THESIS PROPOSAL
116 APPENDIX B - THESIS PROPOSAL
117 APPENDIX B - THESIS PROPOSAL
118 APPENDIX B - THESIS PROPOSAL
119 APPENDIX B - THESIS PROPOSAL
120 APPENDIX B - THESIS PROPOSAL
121 APPENDIX B - THESIS PROPOSAL
122 APPENDIX B - THESIS PROPOSAL
123 APPENDIX B - THESIS PROPOSAL
124 APPENDIX B - THESIS PROPOSAL
125 APPENDIX B - THESIS PROPOSAL
126 APPENDIX B - THESIS PROPOSAL
127 APPENDIX B - THESIS PROPOSAL
128 APPENDIX B - THESIS PROPOSAL
129 APPENDIX B - THESIS PROPOSAL
130 APPENDIX B - THESIS PROPOSAL
131 APPENDIX B - THESIS PROPOSAL
132 APPENDIX B - THESIS PROPOSAL
133 APPENDIX B - THESIS PROPOSAL
134 APPENDIX B - THESIS PROPOSAL
135 APPENDIX B - THESIS PROPOSAL
Bibliography
Appendix C
ANNOTATED BIBLIOGRAPHY
Kidder, Tracy. “Rough Sleepers | Dr. Jim O’Connell’s urgent mission to bring healing to homeless people.” Thorndike Press, a Part of Gale, a Cengage Company, 2023.
Over the span of five years, the author of Rough Sleepers follows Doctor Jim O’Connell, “a gifted man who invented a community of care for [Boston’s] unhoused population, including those who sleep on the streets -- the ‘rough sleepers’”. Experiencing first hand the encounters he has with this community, Kidder tells Jim’s story from going to Harvard Medical school to running the night truck and the relationships he develops with the homeless along the way. Almost all of the medical and cultural information shared in this book are only obtainable through real life experience.
Murphy, Michael P., and Jeffrey Mansfield and MASS Design Group. “The Architecture of Health: Hospital Design and the Construction of Dignity”. Cooper-Hewitt Museum, 2021.
The Architecture of Health explores the history of hospital design through diagrams and typologies. The book identifies how to make today’s hospitals safe, dignified, and beautiful by explaining what succeeded and what failed throughout historical case studies across the globe.
Tran, Vincent, et al. “Assessing drug consumption rooms and longer term (5 year) impacts on community and clients”. Risk Management and Healthcare Policy, Volume 14, 15 Nov. 2021, pp. 4639–4647, https:// doi.org/10.2147/rmhp.s244720.
This document assesses the long-term impacts of Drug Consumption Rooms/Safe Injection Facilities through a systematic approach, literature review of published peer-reviewed literature.
Finke J, Chan J. “The Case for Supervised Injection Sites in the United States”. Am Fam Physician. 2022 May 1;105(5):454-455. PMID: 35559640.
A recent (2022) editorial supporting why Supervised Injection Sites are a viable option in the United States. The author backs up their argument with examples of successful injection sites in Europe and North America.
Marshall, Brandon DL et al. “Reduction in overdose mortality after the opening of North America’s first medically supervised safer injecting facility: a retrospective population-based study” The Lancet, Volume 377, Issue 9775, 1429 - 1437.
A study based in Vancouver, BC, Canada to determine whether the opening of an Supervised Injection Facility was associated with a reduction in overdose mortality.
Ng, Jennifer et al. “Does evidence support supervised injection sites?.” Canadian family physician Medecin de famille canadien vol. 63,11 (2017): 866. https://www. ncbi.nlm.nih.gov/pmc/articles/PMC5685449/ “Evidence from cohort and modeling studies suggests that SISs are associated with lower overdose mortality (88 fewer overdose deaths per 100 000 person-years [PYs]), 67% fewer ambulance calls for treating overdoses, and a decrease in HIV infections. Effects on hospitalizations are unknown.”
Spencer MR, Miniño AM, Warner M. “Drug Overdose Deaths in the United States, 2001–2021. NCHS Data Brief, no 457. Hyattsville, MD: National Center for Health Statistics 2022. DOI: https://dx.doi.org/10.15620/ cdc:122556
Data, charts, and graphics on drug overdose deaths in the United States from 2001-2021. Evidence of the epidemics growth in the last 20 years.
Esben Houborg, Marie Jauffret-Roustide, “Drug Consumption Rooms: Welfare State and Diversity in Social Acceptance in Denmark and in France”, American Journal of Public Health 112, no. S2 (April 1, 2022): pp. S159-S165. https://doi.org/10.2105/ AJPH.2022.306808. PMID: 35349316
Two case studies based in Copenhagen, Denmark and Paris, France. Study includes discussion on political challenges and stigmatization.
Kappel, N., Toth, E., Tegner, J. et al. “A qualitative study of how Danish drug consumption rooms influence health and well-being among people who use drugs.” Harm Reduct J 13, 20 (2016). https://doi.org/10.1186/ s12954-016-0109-y
A very comprehensive study including social acceptance, health and wellbeing, and bridge building between DCRs and other sectors.
Interview with Noble Powell, 19 Oct. 2023. Noble is a Clinical Supervisor at Boston Comprehensive Treatment Center, an Acadia Healthcare facility located on Topeka St. near the Mass & Cass intersection in Boston. Noble is also a counselor for those in the treatment process. We discussed topics including the different medications to help with treatment and overdose, what kinds of street drugs the patients are using and their effects, and the culture at the Mass & Cass Intersection. Major problems that Noble noted in the area are: Needles, feces everywhere; Women’s safety/ sex crime; lack of bathrooms, showers, & security; lost belongings in everyday shuffle, lack of shelter capacity; theft of property in sleep at shelters.
138 APPENDIX C - BIBLIOGRAPHY
On Point, NYC onpointnyc.org/
First organization in the United States to launch two Overdose Prevention Centers (Supervised Consumption Centers). Dedicated to improving the health, safety, and well-being of marginalized people who use drugs or engage in sex work.
Interlandi, Jeneen. “One Year Inside a Radical New Approach to America’s Overdose Crisis”. New York Times Opinion Article. 22 Feb. 2023. nytimes.com/2023/02/22/opinion/drug-crisis-addiction-harm-reduction.html
From the point of view of someone who works at OnPoint, NYC.
Snyder, Jason. “A whole new breed of architecture can help fight drug addiction and save thousands of lives every year”. The Architect’s Newspaper. 13 Jun. 2017. archpaper.com/2017/06/architecture-drug-addiction-feature/
European Monitoring Centre for Drugs and Drug Addiction (EMCDDA).
“An overview of provision and evidence.” “Netherlands Country Drug Report 2017”. p. 11 “Infographic. Location and number of drug consumption facilities throughout Europe.” June 2023
Glaser, Susan. “Dutch cut overdose deaths by dispensing pure heroin”. Cleveland Metro. 15 Jul. 2018 cleveland.com/metro/2018/07/in_amsterdam_the_ government_pr.html
Edwards, Matty. “A Safe Fix for Bristol’s Drug users and the city”. The Bristol Cable. 25 Jan. 2019
Illustration: Rosie Carmichael https://thebristolcable.org/2019/01/a-safe-fix-forbristols-users-drug-consumption-rooms-needles/
National Institute on Drug Abuse (NIDA). “Overdose Prevention Centers.” National Institute on Drug Abuse, 28 Aug. 2023, https://nida.nih.gov/research-topics/ overdose-prevention-centers Accessed 29 Nov. 2023.
Governor’s Opiod Addiction Working Group
mass.gov/lists/governors-opioid-addiction-working-group
City of Boston
boston.gov/government/cabinets/boston-public-health-commission/mass-and-cass-showingwhats-possible
Includes the City’s Long Term Strategic Outlook, Data Dashboard, Transitional Housing Initiative, The City’s encampment Protocol, Advocacy priorities and efforts.
City of Boston’s Coordinated Response Team
“Working to better serve unsheltered neighbors experiencing substance use disorder centered in the intersection of Massachusetts Avenue and Melnea Cass Boulevard, also known as ‘Mass and Cass’.”
Includes:
1. The City’s Long Term Strategic Outlook Plan
2. Regularly updated Data Dashboard
3. Low Threshold Transitional Housing Initiative
4. The City’s Unlawful Camping Ordinance
5. The City’s Advocacy Priorities and Efforts
Long-Term Public Health Strategic Outlook boston.gov/sites/default/files/file/2022/05/Strategic%20Outlook.pdf
“Serving the Mass & Cass area and unsheltered individuals in Boston”.
Includes resources on Outreach, Service Navigation, Low-Threshold Shelter + Housing, Permanent Housing, Harm Reduction + Treatment, Recovery Supports, Behavioral Health Workforce, and Contextual Data.
Mass/Cass Dashboard dashboard.boston.gov/t/Guest_Access_Enabled/ views/MassCassDashboardv2/MonthlySyringeTab?%3Aembed=y&%3Aiid=4&%3AisGuestRedirectFromVizportal=y
Includes data on Daily Operations, 311, Syringe Return Rates, Public Safety, Treatment, and Housing.
City of Boston: Public Health Resource Map: Caring for Unsheltered Persons https://boston.maps.arcgis.com/apps/webappviewer/index.html?id=67e786fa06c045f7a736f220166889c7
Includes Public Health Resources within Boston. Also includes visual “buffer zone” of 3/4 and 1/2 Mile Radius from the Mass Ave/Melnea Cass Intersection.
139 APPENDIX C - BIBLIOGRAPHY
Interview with Chin Chin Yao, saam architecture, Architect for the Engagement Center. 6 Feb. 2024
Discussed EC programming, research, definition of “no barriers” and “low threshold”
Quote pg. 8 by Dr. Jessie M. Gaeta, M.D., Chief Medical Officer at Boston Healthcare for the Homeless from 2015 - 2022.
Over the past two decades, she has spearheaded numerous innovative initiatives to rethink how we approach care for individuals with substance use disorder and complex health conditions, particularly when these conditions are exacerbated by severe poverty, racism, trauma, and social stigma.
Headlines, pg. 16:
Kristina Rex, “Mass and Cass becoming increasingly dangerous as Boston eyes long term solutions”, CBS Boston, August 2, 2023
Mike Deehan, “The tent city there has become the heart of the opioid epidemic and a public safety nightmare.” AXIOS Boston, August 10, 2023
Amelia Caramadre, “It is not the time to diverge from methods with proven success. We need commitment to evidence-based public health approaches that center community treatment and housing.” Boston Globe, August 9th, 2023
Caramadre is a legal fellow for the Action Lab at Northeastern University School of Law and a member of the Massachusetts Rights Coalition for Health.
Andrew Thurston, “A Notorious Boston Intersection, Mass and Cass, Faces an Opioid Overdose Crisis. BU Researchers Are Turning to Survivors for Answers...
New study concludes it’s time to rethink sobriety requirements for housing and offer more harmreduction options” The Brink, a Boston University Publication, August 3rd, 2023
Tori Bedford, “After Mass. and Cass crackdown, homeless community cast out into the shadows of Boston” GBH, Boston, March 6th, 2024
Images pg. 17
Jesse Costa, WBUR
Deborah Becker, “As Boston police prepare to remove ‘Mass. and Cass’ encampment, some wonder what comes next”, WBUR, 31 Oct, 2023
Gostin LO, Hodge JG, Gulinson CL. “Supervised injection facilities: legal and policy reforms.” JAMA. 2019;321(8):745-746.
Levengood TW, Yoon GH, Davoust MJ, et al. “Supervised injection facilities as harm reduction: a systematic review”. Am J Prev Med. 2021;61(5):738-749
PLH Architects
Drug Consumption Center, Halmtorvet
plh.dk/
Notes translated from Danish by Grace Pilkington, using Google Translate
Meghan, E. Irons, Nicole Dungca, “Abrupt closing of Long Island Bridge was slow to arrive.” Boston Globe, 14 Dec. 2014
Deborah Becker, Lynn Jolicoeur, “Homeless Displaced By Long Island Bridge Closure Remain In Flux.” WBUR, 18 Dec. 2014
Benjamin Swasey, “Boston Opens Expanded Southampton Street Homeless Shelter.” WBUR, 25 Jun. 2015
Drew Karedes, ‘It’s never ever been this bad’: 100+ tents set up along Methadone Mile concern community leaders.” Boston 25 News. 3 Sept. 2021
Carine Hajjar, “Mass. and Cass shows the failure of progressive drug policies... Left-leaning officials insist that police crackdowns on open-air drug encampments backfire. But the handsoff approach has sown violence and misery.” Boston Globe, 8 Oct. 2023
Maps pg. 23
Boston Planning & Development Agency (BPDA). 3D Data & Maps. Map Library
City of Boston. Created by DoIT GIS Team. Public Health Resource Map: Caring for Unsheltered Persons boston.maps.arcgis.com
Walter Wuthmann, “Boston prepares to remove tents from ‘Mass. and Cass’ area”. WBUR, 26 Oct. 2023
Harold Cox, “Lessons of the Kitchen: Harold Cox shares what he has learned about the power of compassion and listening while volunteering at a local shelter.” Boston University School of Public Health. 21 Sept. 2023
140 APPENDIX C - BIBLIOGRAPHY
Nik DeCosta-Klipa, “Where did the people living at Mass. and Cass go? Here’s what we know”. WBUR, 02 Nov. 2023
Deborah Becker, “Boston officials look to revive Long Island as hub for addiction services, homeless care”. WBUR, 24 Aug. 2023
Helen Redmond, “Boston’s ‘Methadone Mile’ and the Wars on Drug Users, Unhoused People”. Filter Magazine, 9 Feb. 2021
Nestor Ramos, Evan Allen, “Life and loss on Methadone Mile”. The Boston Globe, April - July 2016
Ling, Felice and Ackerman, Cecilia “The Boston Engagement Center Research Report by Ethnographers Felice Ling and Cecilia Ackerman”. 4 May 2018.
The Gubbio Project. Co-founded in 2004 by community activists Shelly Roder and Father Louis Vitale as a nondenominational project of St. Boniface Neighborhood Center located in San Francisco’s Tenderloin neighborhood in response to the increasing numbers of homeless men and women in need of refuge from the streets.
141 APPENDIX C - BIBLIOGRAPHY
Art by Grace Pilkington
