
Continuing Professional Development MCQ Booklet
Provided to you by the Australasian College of Pharmacy
Official Education Sponsor of Pharmacy Connect 2025

ACCREDITATION DETAILS AND MCQs FOR WEDNESDAY 3 SEPTEMBER 2025 SESSIONS
Harm Minimisation Pre-Conference Workshop 2 consisting of: ‘Alcohol: old drug, new treatments’; ‘Advances in testing and treatment for Hepatitis C infection’; ‘Crazy little thing called addiction’, and ‘Panel Discussion’
Session Time: 9:30am – 1:00pm
Day: Wednesday
Venue: Wharf Room 3
Speakers: Dr Paul MacCartney, Professor Jason Grebely, Dr Reece Lancaster
Dr Hester Wilson
Duration: 3.25 hours
Accreditation code: A2509PC10
1.2,1.5, 2.1, 2.2, 2.3, 3.1, 3.2, 3.5, 3.6
After completing this activity, pharmacists should be able to:
• Describe the prevalence of Alcohol Use Disorder in Australia
• Outline the best practice treatment for Alcohol Use Disorder.
• Describe the pharmacist’s role in identifying need and supporting appropriate treatment.
• Identify the correct tests used for the diagnosis of hepatitis C virus infection.
• Describe testing strategies that facilitate the simplification of testing with an application to pharmacies.
• List key properties of currently available treatments for hepatitis C virus infection.
• Explain the concept of craving in opioid use disorder (OUD) and its implications for relapse, treatment engagement, and harm reduction.
• Describe the role of buprenorphine, including long-acting injectable formulations, in the management of OUD within community pharmacy practice.
• Apply principles of tailoring long-acting injectable buprenorphine (LAIB) dosing to individual patient needs, particularly in relation to craving and patientreported outcomes.
• Understand concepts of drug use, addiction, its history and changing understandings
• Describe the criteria for diagnosis and management options
• Elucidate the role pharmacists can play in supporting the people they see experiencing problems with substances
Presentation attendance only
Please self-record Group 1 Credits using the Self-Record CPD function on your account.
6.25 Group 2 CPD Credits
Presentation attendance and submission of MCQ responses.
Course Link Group 2
3.25 Group 1 CPD Credits
Harm Minimisation Pre-Conference Workshop 2 consisting of: ‘Alcohol: old drug, new treatments’; ‘Advances in testing and treatment for Hepatitis C infection’; ‘Crazy little thing called addiction’, and ‘Panel Discussion’
MCQs
1. How many people in Australia are estimated to have Alcohol Use Disorder (AUD)?
a. <100,000
b. 100,000 -500,000
c. 500,001- 1million
d. 1-2 million
e. >2 million
2. What percentage of people with Alcohol Use Disorder (AUD) currently receive the first line pharmacotherapies as per the Guidelines?
a. <5%
b. 5-10%
c. 11-15%
d. 15-20%
e. >20%
3. Which of the following medications have been found to be of benefit in AUD?
a. Naltrexone
b. Topiramate
c. Baclofen
d. Prazosin
e. All of the above
4. Which of the following are contraindications to prescription of Naltrexone?
a. Obesity
b. Abnormal Liver Function Tests
c. Cirrhosis
d. Intercurrent opioid use
e. Diazepam
5. Which of the following are appropriate roles for pharmacists in helping people with AUD?
a. Identifying people at risk
b. Asking brief screening questions
c. Giving accurate information about treatment options
d. Reassuring prescribers about medication safety
e. All of the above
Turn page for questions 6 to 10 (20 questions total)
Harm Minimisation Pre-Conference Workshop 2 consisting of: ‘Alcohol: old drug, new treatments’; ‘Advances in testing and treatment for Hepatitis C infection’; ‘Crazy little thing called addiction’, and ‘Panel Discussion’
MCQs | CONTINUED
6. What does it mean if you have a positive HCV antibody test?
a. The hepatitis C virus is present in your blood
b. You have not been exposed to HCV
c. You have been exposed to HCV at some time in your life but don't know if you have HCV now
7. What does it mean if you have a positive HCV RNA test?
a. The hepatitis C virus is present in your blood
b. You have not been exposed to HCV
c. You have been exposed to HCV at some time in your life but don't know if you have HCV now
8. Which of the following testing strategies have improved the simplification of HCV testing and linkage to care?
a. Dried blood spot sample collection
b. Point-of-care HCV antibody testing
c. Venepuncture-based sample collection
d. Point-of-care HCV RNA testing
e. All of the above
f. a, b, and d
g. a, b, and c
9. What are some effective pharmacy-led HCV testing strategies?
a. Point-of-care HCV antibody test with dried blood spot sample collection for HCV testing
b. Point-of-care HCV antibody test with point-of-care HCV RNA testing
c. Venepuncture-based sample collection
d. All of the above
e. a and b
10. What is not one of the current properties of existing HCV treatments?
a. >95% proportion with viral cure
b. Once daily
c. 24-48 weeks treatment duration
d. Oral dosing
e. Minimal toxicity
Turn page for questions 11 to 15 (20 questions total)
Harm Minimisation Pre-Conference Workshop 2 consisting of: ‘Alcohol: old drug, new treatments’; ‘Advances in testing and treatment for Hepatitis C infection’; ‘Crazy little thing called addiction’, and ‘Panel Discussion’
MCQs | CONTINUED
11. Craving in opioid use disorder (OUD) is best described as:
a. A purely physical withdrawal symptom that resolves within 72 hours
b. A psychological urge that can persist and contribute to relapse even during maintenance treatment
c. A behavioural choice to use opioids despite awareness of harm
d. An adverse effect caused by long-acting injectable buprenorphine (LAIB)
12. Why is craving considered an important treatment target in OUD?
a. It is only relevant during opioid withdrawal, not during maintenance therapy
b. It predicts treatment adherence but has little relationship with relapse
c. It is strongly associated with relapse risk and impacts harm reduction outcomes
d. It is less important than addressing sedation and constipation as treatment side-effects
13. Which of the following best describes buprenorphine’s mechanism of action in OUD treatment?
a. Full agonist at the mu-opioid receptor with high abuse potential
b. Partial agonist at the mu-opioid receptor with a ceiling effect on respiratory depression
c. Dopamine antagonist reducing euphoria from opioids
d. Pure antagonist at opioid receptors similar to naloxone
14. In community pharmacy practice, which of the following is a key harm-reduction benefit of long-acting injectable buprenorphine (LAIB) compared with daily sublingual formulations?
a. Reduced need for pharmacist counselling
b. Elimination of opioid-induced constipation
c. Improved adherence by removing the burden of daily supervised dosing
d. Increased flexibility to adjust doses on a daily basis
15. When considering LAIB dose adjustments for a patient reporting breakthrough craving, which principle should guide pharmacist discussions with the prescriber?
a. Craving is not clinically relevant once a patient is on maintenance therapy
b. Dose tailoring should be guided by patient-reported outcomes, including intensity and timing of craving
c. LAIB dosing is fixed and cannot be altered once treatment is initiated
d. Pharmacists should independently adjust the dose without prescriber input
Turn page for questions 16 to 20 (20 questions total)
Harm Minimisation Pre-Conference Workshop 2 consisting of: ‘Alcohol: old drug, new treatments’; ‘Advances in testing and treatment for Hepatitis C infection’; ‘Crazy little thing called addiction’, and ‘Panel Discussion’
MCQs | CONTINUED
16. What of the following are the categories used to diagnose opioid dependence for ICD11? (select 3 correct answers)
a. Salience
b. Impaired control despite harm
c. Craving
d. Tolerance, withdrawal
17. TRUE/FALSE? Does a person need to have withdrawal or tolerance to have substance dependence?
18. Which of the following statements is CORRECT?
a. Addiction is a 20th century concept
b. Addiction is an inherent characteristic of an individual and part of their personality
c. Addiction is sometimes a symptom of underlying mental health issues or history of interpersonal trauma
d. Addiction is easily cured
19. What are the impacts of addiction? (Choose 3 correct answers)
a. Morbidity and mortality
b. Economic cost
c. Family breakdown and family violence
d. It makes people criminals
20. Which of the following are CORRECT? (select 3 correct answers)
a. Pharmacists are Important members of the treatment team
b. Pharmacists have expertise in medication management and are able to use that skill to support safe high risk medicine prescribing
c. Pharmacists should only check safe script if the person is clearly undertaking hazardous harmful or dependent use
d. Pharmacists should report all problematic and non-medical use
-- Questions complete
ACCREDITATION DETAILS AND MCQs FOR THURSDAY 4 SEPTEMBER 2025 SESSIONS
Australian Best Practice Guidelines on Acute Wound Care in Pharmacy
Session Time: 11.25am – 12:10pm
Day: Thursday
Venue: Grand Ballroom
Speaker: Assoc Prof John Smithson
Duration: 45 mins
Accreditation code: A2509PC7
After completing this activity, pharmacists should be able to:
• Identify the key components and purpose of the Australian Best Practice Guidelines for Acute Wound Care in Pharmacy.
• Explain how the guidelines support evidence-informed decision-making in dressing selection, patient education, and continuity of care in the pharmacy setting.
• Use the guidelines to identify appropriate interventions for common acute wound presentations in community pharmacy practice.
• Differentiate between standard and suboptimal wound care approaches, using the guidelines to critique real or hypothetical case scenarios.
Presentation attendance and submit MCQ responses
Link Group 2 MCQs
1. What is the primary purpose of the Australian Best Practice Guidelines for Acute Wound Care in Pharmacy?
a. To outline hospital-based wound closure procedures
b. To provide pharmacists with evidence-informed approaches to wound management
c. To replace GP consultations for all wounds
d. To regulate supply of all wound dressings in community settings
2. Which of the following wound dressings is transparent, waterproof, and allows oxygen and moisture vapor to pass?
a. Foam dressing
b. Film dressing
c. Hydrogel dressing
d. Alginate dressing
-- Turn page for questions 3 to 5 (5 questions total)
Australian Best Practice Guidelines on Acute Wound Care in Pharmacy
3. What phase of wound healing involves fibroblasts producing collagen and new blood vessel formation?
a. Hemostasis
b. Inflammation
c. Proliferation
d. Maturation
4. Which of the following statements about alginate dressings is CORRECT?
a. They are used for dry wounds to donate moisture
b. They can be used without a secondary dressing
c. They are made from seaweed-derived fibres and are highly absorbent
d. They are best used on superficial wounds with minimal exudate
5. A patient presents to your pharmacy with a superficial minor burn on the forearm. The area is painful, red, and weeping lightly. Which of the following dressing regimens is most appropriate according to best practice guidelines?
a. Apply a hydrocolloid dressing to occlude and protect the wound for 5–7 days
b. Use a hydrogel to donate moisture and rehydrate the burn
c. Use a foam dressing to absorb heavy exudate and provide compression
d. Use a low-adherent absorbent dressing with secondary fixation to absorb exudate and protect fragile skin
-- Questions complete
Empowering Women’s Health: Preventative care & innovations
Session Time: 12:15pm – 1:00pm
Day: Thursday
Venue: Grand Ballroom
Speakers: Belinda Duffy
Duration: 45 mins
Accreditation code: A2509PC1
After completing this activity, pharmacists should be able to:
• Describe the interplay of key nutrients to support women’s hormone balance
• Recognise the role of postbiotics and hyaluronic acid in preventative skincare
• Discuss the role of key nutrients in supporting muscle health with ageing.
MCQs
1. Which nutrients that are commonly depleted by oral contraceptive use are also known to impact oestrogen metabolism via COMT?
a. Iodine, folate, and vitamin B6
b. Magnesium, vitamin B6 and vitamin B12
c. Folate, Vitamin B12, and chromium
d. Iodine, HMB, and magnesium
2. Hormonal imbalances can cause PMS symptoms. Which nutrients specifically assist with dysmenorrhea?
a. Iodine and vitamin B6
b. Magnesium and chromium
c. Magnesium and vitamin B6
d. Iodine and magnesium
Turn page for questions 3 to 5 (5 questions total)
Empowering Women’s Health: Preventative care & innovations
MCQs | CONTINUED
3. Postbiotic L92™ helps to regulate which immune cell type to reduce skin irritation?
a. TH2
b. TH1
c. Mast cells
d. Eosinophils
4. What is the daily dose of HMB that research suggests can support the retention of muscle mass?
a. 1 gram with resistance exercise
b. 1 gram with cardiovascular exercise
c. 3 grams with resistance exercise
d. 3 grams with cardiovascular exercise
5. Low levels have body magnesium have been associated with decreases in grip strength, power in the lower limbs, and optimal joint extension. These effects began to accelerate in intensity after what age?
a. 50
b. 30
c. 70
d. 40
-- Questions complete
From microbiome to mind: Empowering pharmacists with evidence-based natural solutions for managing IBS, mood & sleep
Session Time: 2:00pm – 2:45pm
Day: Thursday
Venue: Grand Ballroom 1
Speaker: Mick Alexander
Duration: 45 mins
Accreditation code: A2509PC2
After completing this activity, pharmacists should be able to:
• Explain the drivers of irritable bowel disease (IBS) and the interplay with mood disturbance and poor sleep through a disrupted gut-brain axis
• Discuss the importance of treating a disrupted gut-brain axis and how this improves IBS, mood disturbance and poor sleep.
• Recommend probiotic supplements, lifestyle advice and herbs for a disrupted gut-brain axis to improve the symptoms of IBS, poor mental health and disrupted sleep.
MCQs
1. Which of the following best describes the drivers of irritable bowel syndrome (IBS) and its connection to mood disturbance and poor sleep through a disrupted gut-brain axis?
a. IBS is caused solely by dietary factors and does not affect mood or sleep patterns.
b. A disrupted gut-brain axis can contribute to IBS by affecting gut motility and immune signalling, but it has no influence on mood or sleep.
c. The interplay between a disrupted gut-brain axis, poor sleep quality, and mood disturbances can exacerbate IBS symptoms due to changes in the gut microbiota and stress responses.
d. IBS is typically transient, resolving on its own without impacting the brain-gut connection, mood, or sleep.
2. What is the primary role of the gut-brain axis (GBA) in managing IBS, mood disorders, and sleep disturbances?
a. The GBA only affects the digestive system and does not influence mood or sleep patterns.
b. The GBA enables direct hormonal communication between the gut and brain, which solely regulates the immune response.
c. The GBA facilitates bidirectional communication between the gut and brain, helping regulate stress, inflammation, and neurotransmitters to impact IBS, mood, and sleep.
d. The GBA primarily controls dietary nutrient absorption and has minimal effect on the brain.
Turn page for questions 3 to 5 (5 questions total)
From microbiome to mind: Empowering pharmacists with evidence-based natural solutions for managing IBS, mood & sleep MCQs | CONTINUEDs
3. Why is treating a disrupted gut-brain axis important for improving IBS, mood disturbance, and poor sleep?
a. It directly cures IBS by eliminating all symptoms permanently.
b. Addressing the gut-brain axis improves communication between the gut and brain, helping regulate stress responses, reduce inflammation, and restore a healthy microbiome balance.
c. Treating the gut-brain axis only reduces sleep disturbances without affecting IBS or mood.
d. Probiotic treatments completely replace the need for medical or lifestyle interventions.
4. Which of the following approaches is most effective in managing a disrupted gut-brain axis to alleviate symptoms of IBS, mood disturbances, and poor sleep?
a. Relying exclusively on antidepressants to address mood and sleep issues while ignoring the gut.
b. Recommending multi-strain probiotics, alongside lifestyle modifications such as stress reduction and sleep hygiene, while considering selective herbal remedies like saffron.
c. Suggesting strict dietary restrictions and avoiding all supplements or lifestyle advice.
d. Using over-the-counter sleep aids without addressing gut health or mood balance.
5. How do probiotics help in repairing a disrupted gut-brain axis (GBA)?
a. Probiotics act solely as laxatives, improving bowel movement frequency without influencing the gut-brain connection.
b. They strengthen the intestinal barrier, reduce gut permeability, modulate the immune response, and support neurotransmitter balance, improving GBA function.
c. Probiotics replace the need for other treatments like lifestyle changes or medications in managing GBA dysfunction.
d. They provide temporary symptom relief without addressing the underlying mechanisms of GBA dysfunction.
-- Questions complete
The business of sleep: Building a high-performing sleep study and CPAP clinic in Pharmacy
Session Time: 2:00pm – 2:45pm
Day: Thursday
Venue: Grand Ballroom 2
Speaker: Justin Chan
Duration: 45 mins
Accreditation code: A2509PC11
After completing this activity, pharmacists should be able to:
• Describe the incidence and health impacts of sleep disorders including Obstructive Sleep Apnoea (OSA)
• List the key components of a sleep service
• Describe important considerations when choosing a sleep provider
1.
2. Which of the following are key components of a sleep service?
a. Bulk billed home sleep studies
b. Respiratory & Sleep physician telehealth
c. CPAP services
d. All of the above Turn page for questions 3 to 5 (5 questions total)
The business of sleep: Building a high-performing sleep study and CPAP clinic in Pharmacy
3. Which of the following is an important consideration when choosing the right sleep provider?
a. Comprehensive clinical support
b. Extended appointment times regardless of clinical need
c. Complimentary luxury bedding for patient comfort
d. Flexible decor themes to enhance relaxation
4. What are some health impacts of untreated OSA?
a. Only mild daytime fatigue without long-term health impacts
b. Increased risk of hypertension, heart disease, stroke, and type 2 diabetes
c. Increased resilience to stress and stronger immune function
d. Improved sleep quality over time as the body adapts to disrupted breathing
5. Which of the following are benefits of the HST device?
a. Fast hookup of 5 minutes
b. Whole pharmacy team can be trained to use it
c. Disposable electrodes, reducing staff time cleaning and better signal quality
d. All of the above
-- Questions complete
Full Scope: Making the dream a reality
Session Time: 2:50pm – 3:35pm
Day: Thursday
Venue: Grand Ballroom 2
Speaker: Felicity Crimston & Jessica Burrey
Duration: 45 mins Accreditation
After completing this activity, pharmacists should be able to:
• Describe the impact of full scope of practice in rural settings
• Recognise the concept of clinical return on investment in pharmacy practice
• Recognise workflow innovations that enhance efficacy and improve patient experience
• Identify the relationship between consultation length and patient sales outcomes.
• Identify operational challenges in implementing full scope of practice in solepharmacist settings
1. What is a key benefit of full scope pharmacy in rural areas?
a. Reduced cost of medications
b. Increased retail sales
c. Improved patient access to healthcare
d. Elimination of GP services
2. Which of the following best describes ‘clinical ROI’ in the context of pharmacy?
a. Increased retail margins from front-of-shop sales
b. Measurable improvements in patient outcomes from pharmacist-led interventions
c. Reduction in staff wages through automation
d. Higher consultation fees for long appointments
Turn page for questions 3 to 5 (5 questions total)
Scope: Making the dream a reality
3. What workflow innovation was highlighted as improving both team efficiency and patient experience?
a. Eliminating intern involvement
b. Pharmacist-led intake for all consults
c. Delegation of intake tasks to triage assistants and interns
d. Removing structured consult templates
4. Why do longer consultations tend to result in higher average sales per patient?
a. They include mandatory product bundles
b. Patients are charged more for prescriptions
c. They allow for deeper engagement and tailored recommendations
d. They are subsidised by PBS
5. What challenges remain in implementing full scope practice in single-pharmacist communities?
a. Lack of interest from patients
b. Over-reliance on PBS funding
c. Inadequate booking and clinical systems
d. Excessive product recommendations
-- Questions complete
Pain, pain grow away: Shaping a positive experience of pain management throughout childhood
Session Time: 4:05pm – 4:50pm
Day: Thursday
Venue: Grand Ballroom 2
Speaker: Dr Jacinta Johnson
Duration: 45 mins
Accreditation code: A2509PC3
After completing this activity, pharmacists should be able to:
• Describe guideline recommendations for over-the-counter (OTC) pharmacological management of common acute inflammatory pains experienced by children under 12 years of age.
• Explain the role of inflammation in the development of childhood acute pain and fever, and how this may affect treatment choice
• Illustrate individualised counselling to parents/caregivers on appropriate management of children’s acute inflammatory pain after consideration of life stage and children’s needs
1. Ibuprofen and paracetamol are first-line treatment options for acute headaches in children, but parents/caregivers should limit the use of analgesics for headache to no more than 14 days per month. Which of the below is the primary reason for this recommendation?
a. To avoid dependence on ibuprofen
b. To reduce the risk of gastrointestinal complications
c. To reduce the risk of developing medication overuse headache
d. There are no limits on number of days per month to use analgesics
2. Which of the following is the most appropriate advice to give a parent/caregiver asking about pain relief for their two-month-old child with a fever?
a. A precise weight measurement is needed to determine dosing
b. Ibuprofen is preferred over paracetamol as an antipyretic
c. Be sure the child is properly hydrated and wearing climate-appropriate clothing
d. Children under 3 months of age with a fever should always see a doctor
Turn page for questions 3 to 5 (5 questions total)
Pain, pain grow away: Shaping a positive experience of pain management throughout childhood MCQs | CONTINUEDs
3. According to recommendations in the Australian Immunisation Handbook, when can infants and children be given ibuprofen or paracetamol after receiving an immunisation?
a. When they have a fever higher than 38.5°C or pain at the injection site
b. Only when they have pain at the injection site one hour after their immunisation
c. Neither ibuprofen nor paracetamol are recommended to be used in children post-immunisation
d. Only if they are experiencing irritability or fever higher than 40°C
4. You are discussing the correct administration of ibuprofen with a first-time parent when they mention their concern it may upset their baby’s stomach. Which of the following is the most appropriate response?
a. Explain that ibuprofen must always be taken with food or milk to prevent gastrointestinal side effects
b. Reassure them that when taken as directed, ibuprofen has a low risk of causing gastrointestinal side effects even in young children
c. List all the potential adverse effects that may occur when giving ibuprofen or paracetamol to children
d. Explain that ibuprofen is far less dangerous than paracetamol
5. Which of the following statements is false?
a. Ibuprofen is the only over-the-counter non-steroidal anti-inflammatory drug recommended for children <12 years of age in Australia
b. Paracetamol is an appropriate first-line treatment option for children’s acute pain
c. Fever is triggered by the action of prostaglandins in the hypothalamus
d. Post-immunisation fever is due to inflammation, but post-immunisation pain is not
e. Toothache may be caused by inflammation resulting from dental treatment
-- Questions complete
ACCREDITATION DETAILS AND MCQs FOR FRIDAY 5 SEPTEMBER 2025 SESSIONS
Driving momentum in adult vaccination against shingles and RSV: How can pharmacists continue to be leaders?
Session Time: 11:30am – 12:15pm
Day: Friday
Venue: Grand Ballroom 1
Speakers: Christine Kelly
Duration: 45 mins
Accreditation code: A2509PC6
After completing this activity, pharmacists should be able to:
• Discuss age-related decline in immunity and the role of vaccines in healthy aging
• Outline the risk and impact of shingles and RSV in the older adult populations.
• Describe the role of pharmacists to support vaccination uptake to reduce the rates of shingles and RSV in older adults.
Presentation attendance only
Please self-record Group 1 Credits using the Self-Record CPD function on your account.
(Presentation attendance and submission of MCQ responses)
1. Adjuvants may enhance immune responses in older adults by:
a. Stimulating immune responses in impaired immune systems.
b. Extending immune responses and improving memory.
c. Activating innate immunity.
d. All of the above.
2. What proportion of overall burden due to vaccine-preventable diseases in Australia occurs among people aged 65 years and older?
a. Less than 10%.
b. Approximately one third.
c. Approximately half.
d. More than 90%.
-- Turn page for questions 3 to 5 (5 questions total)
Driving momentum in adult vaccination against shingles and RSV: How can pharmacists continue to be leaders?
MCQs | CONTINUED
3. Which of the following actions is NOT a strategy for pharmacists to increase vaccine uptake in older adults?
a. Educating patients on immunisation as a safe and effective health intervention.
b. Explaining why it is important to help prevent shingles and RSV.
c. Scheduling all immunisations on behalf of a patient as soon as they turn 65 years old.
d. Minimising missed vaccination opportunities in community pharmacy.
4. Which of the following statements regarding immunisation against shingles is INCORRECT?
a. The efficacy of SHINGRIX is only confirmed when patients complete the 2-dose series.
b. SHINGRIX is a 2-dose series, spaced 12 months apart.
c. SHINGRIX is designed with an adjuvant system to enhance the immune response to the vaccine antigens.
5. Which of the following statements regarding immunisation against RSV is INCORRECT?
a. RSV vaccines cannot be co-administered with any other vaccines.
b. ABRYSVO and AREXVY are for single dose, intramuscular injection only.
c. Immunisation against RSV is recommended for adults aged ≥60 years who have medical risk factors for severe RSV disease.
Questions complete
What’s new in risk management? A PDL perspective
Session Time: 11:30 – 12:15pm
Day: Friday
Venue: Grand Ballroom 2
Speaker: Gary West
Duration: 45 mins
Accreditation code: A2509PC8
After completing this activity, pharmacists should be able to:
• Identify the areas of pharmacy practice that generate the most incident reports to PDL
• Describe the common causes of wrong patient incidents
• Undertake a risk assessment using common contributing factors and risk categories in pharmacy practice.
the Self-Record
MCQs
1. Select the option which lists the top five PDL Dispensing and DAA incident report types in order from more common to less common.
a. Drug, strength, directions, quantity, person
b. Strength, directions, drug, person, quantity
c. Directions, drug, strength, quantity, person
d. Strength, drug, directions, person, quantity
2. Select the option which lists the top five PDL Vaccination incident report types in order from more common to less common.
a. Injection incident, age-related, selection error, post-admin event, incorrect interval
b. Selection error, injection incident, incorrect interval, age-related, post-admin event
c. Selection error, age-related, injection incident, post-admin event, incorrect interval
d. Injection incident, selection error, age-related, post-admin event, incorrect interval
e. Selection error, incorrect interval, age-related, injection incident, post-admin event
Turn page for questions 3 to 5 (5 questions total)
What’s new in risk management? A PDL perspective
3. Select the option that is NOT a common contributing factor in wrong patient supply incidents as identified by PDL.
a. Age of the person collecting the medicine
b. Culturally and linguistically diverse people
c. Electronic prescriptions
d. Closed questions used to confirm identity
e. Limited forms of patient identification
4. Which one of the following options does NOT align with PDL’s advice for provision of high quality professional and clinical practice?
a. Services can be provided if pharmacists are authorised and suitable facilities are available
b. Documentation for a service should be clinically appropriate, secure, contemporaneous, retrievable
c. Informed consent should be sought for professional, financial and clinical aspects of the service
d. Referral options are understood by the pharmacist and patient, and occur when a service is inappropriate or outside of regulatory or professional limits
e. Follow up with patients is to occur after each service as a pharmacist’s duty of care
5. PDL suggests DAA patients are at higher risk of incident and impact. Which one of the following points is NOT considered by PDL to be a contributing factor to DAA incidents and impact?
a. The involvement of carers collecting and administering DAA medicines
b. DAA patients are accustomed and accepting of generic changes
c. Multiple medicines supplied in a DAA increase the chance of error and negative impact
d. Patients receiving DAAs are generally older with more health conditions
e. DAA patients often have complex dosing regimes
Questions complete
Medicinal cannabis in women’s health: Emerging applications and the pharmacist’s role
Session Time: 12:20pm – 1:05pm
Day: Friday
Venue: Grand Ballroom 1
Speakers: Laila Moola
Duration: 45 mins
Accreditation code: A2509PC4
After completing this activity, pharmacists should be able to:
• Describe the historical context and current role of medicinal cannabis in the management of women's health conditions.
• Assess the appropriateness of medicinal cannabis treatments for a range of conditions affecting women, using evidence-based criteria.
• Integrate medicinal cannabis knowledge into pharmacy practice to improve patient care and therapeutic outcomes in women's health
1. Which of the following best describes the historical use of cannabis in women's health?
a. It was primarily used for recreational purposes in ancient societies
b. It was commonly prescribed for menstrual and childbirth-related issues
c. It was banned globally due to its ineffectiveness in treating women's conditions
d. It was only introduced into women's health in the 21st century
2. What is a key reason for the renewed interest in medicinal cannabis for women’s health today?
a. Increased recreational use among women
b. Lack of other treatment options for all chronic condition
c. Emerging evidence supporting its efficacy in managing specific women’s health conditions
d. Government mandates requiring its use in pharmacies
Turn page for questions 3 to 5 (5 questions total)
Medicinal cannabis in women’s health: Emerging applications and the pharmacist’s role MCQs | CONTINUED
3. Which of the following conditions has shown the MOST promising evidence for treatment with medicinal cannabis in women?
a. Osteoporosis
b. Endometriosis
c. Polycystic Ovary Syndrome (PCOS)
d. Urinary tract infections
4. When assessing a patient for medicinal cannabis suitability, which factor is MOST critical?
a. The patient’s age
b. The patient’s preference for natural therapies
c. The presence of contraindications and current medications
d. The cost of the product
5. How can pharmacists best support patients using medicinal cannabis for women’s health?
a. By recommending over-the-counter hemp products
b. By providing evidence-based counselling and monitoring for side effects
c. By discouraging its use due to limited evidence
d. By referring all patients to a specialist without discussion
Questions complete
FREQUENTLY ASKED QUESTIONS
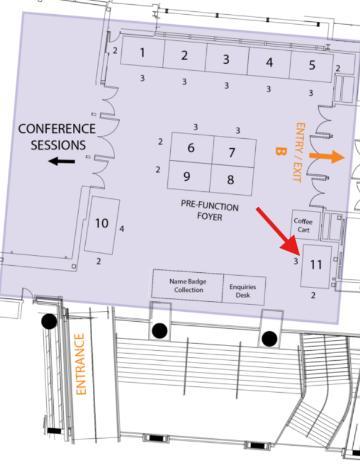
Q: Where can I find the College trade stand?
A: You can find us at Trade Stand 11, next to the Name Badge Collection and Enquiries Desk!
Visit us to discover how our range of full scope courses and membership options can elevate your practice! As the home of expanded scope of practice training, the College is committed to providing flexible, accessible, and affordable options to support your professional development, and we’d love to help you find the perfect courses tailored to your needs.
We also offer QCPP refresher courses on essential topics like iron deficiency, allergic rhinitis, and the treatment of headaches, and opioid dependence! Come and chat to us to learn more!
Q: Where can I log my CPD points?
A: To log your CPD points, you need to enrol in and complete the courses associated with each session via the College CPD Library (the rebranded GuildEd platform).
Each session page in this booklet provides a link to the Group 2 CPD course. Make sure you follow these links to ensure your points are properly recorded. If you are wishing to record Group 1 CPD credits (if you are not completing the assessment, or if you have not passed the assessment), you can record these credits by using the Self-Record CPD function on your College CPD Library account. Click Here to log in to the portal or visit www.acp.edu.au/cpd-library.
Q: I can’t log in – what should I do?
A: If you are having trouble logging, please follow these steps:
1. Verify the Website
Ensure you’re using the correct website by clicking on the course links provided in each session in this booklet.
2. Check Your Email
Confirm that you are attempting to log in with the email address you used to register for Pharmacy Connect 2025, or the email you normally use to access GuildEd. This is the email associated with your access to the conference CPD courses.
3. Reset Your Password
If you still can’t log in, try resetting your password by using the ‘Forgot Password’ option on the login page of the College CPD Library You should receive a password reset email within 30 minutes. Be sure to check your Junk/Spam or Social/Promotions folders.
4. Contact Support
If you don’t receive the password reset email within 30 minutes, please contact our helpdesk by sending a support request. Please ensure you include your full name, and the email address you are using to try to login in the body of your email. Alternatively, come see our team at Trade Stand 11!
Turn page for more FAQs
Q: I am logged in, but I cannot access the courses
A: If you're logged in but unable to access the courses, it may be because you do not have the correct permissions assigned to your account. Please reach out to our helpdesk by sending a support ticket by clicking here. Be sure to include your full name and the email address you use to log in. Our team will review your access settings and make any necessary adjustments or provide further instructions. Alternatively, come see our team at Trade Stand 11!
Q: I failed the Group 2 assessment, can you please reset my attempts so I can claim Group 2 credits?
A: Unfortunately, CPD activities cannot be reset if you do not pass within two attempts. If you are unable to pass the assessment, you can still claim Group 1 CPD credits for the session by self-recording using the Self-Record CPD function in your account.