May 20, 2025
Presented by
Porzio, Bromberg & Newman, P.C.

May 20, 2025
The views expressed by the speakers in this program represent their personal thoughts and opinions and do not necessarily reflect the views of our current or past employers or clients.
Nothing presented as part of this program should be considered legal advice or as creating an attorney-client relationship.
QOL Medical (Nov. 2024)
• Company and its CEO agreed to pay $47 million; state suits followed
• Allegations of Anti-kickback and False Claims Act violations regarding provision of free Carbon-13 breath testing services, to induce claims for QOL’s drug Sucraid.
• QOL shared lab results with field force that contained the names of the health care provider who ordered the test, and the patient’s age, gender, symptoms and test result
• Allegedly made claims that test could definitely diagnose Congenital Sucrase-Isomaltase Deficiency
• Allegations brought in part by qui tam filed by Medical employees.
Pfizer/BioHaven (Jan, 2025)
• Almost $60 million settlement for alleged Anti-kickback and False Claims Act violations related to HCP activities regarding Nurtec
• Allegations involved inappropriate speaker honoraria, meals at high end restaurants, and HCP repeat attendees at programs
• Qui tam brought by former sales representative.
The Prometheus Group (March 2025)
• Company and president/owner agreed to pay $550,000
• Allegedly violated False Claims Act by causing health care providers to bill Medicare for re-use of single-user rectal sensors and single-use catheters on multiple patients.
Assertio Therapeutics (formerly DepoMed) (May 2025)
• Company agreed to pay $3.6 million for alleged violations of False Claims Act related to its product Lazanda, a fentanyl nasal spray, approved for break-through cancer pain
• Company allegedly targeted prescribers who prescribed immediate-relief fentanyl, including those flagged for diversion
• Used those same prescribers for its Speaker’s Bureau and Advisory Boards
• Qui tam brought by two sales representatives
• Discusses the agency’s evolving enforcement policy regarding how scientific information on unapproved uses (“SIUU”) of approved/cleared medical products can be communicated to HCPs engaged in prescribing or administering medical products to individual patients.
Interesting Development: Vanda Pharmaceuticals, Inc. v. FDA
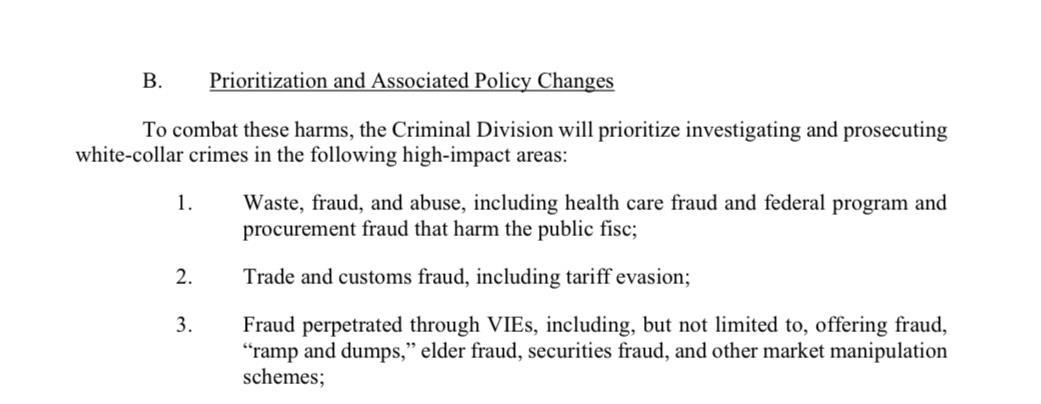
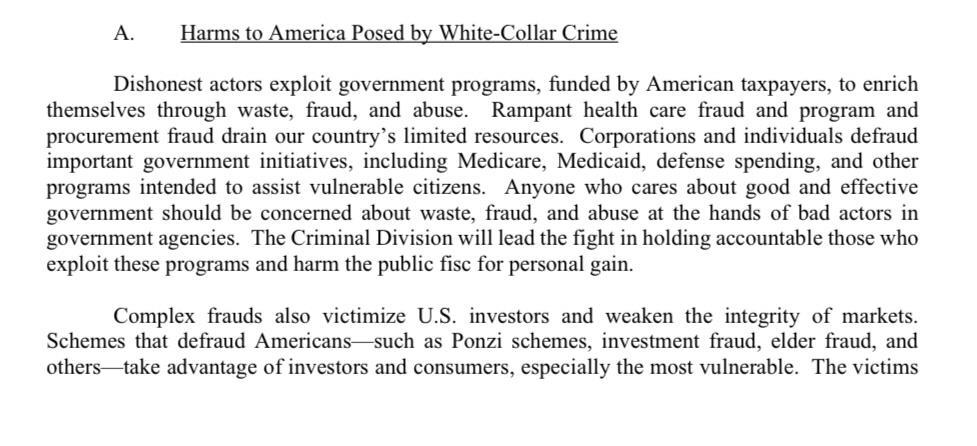
EXAMPLE: DOJ CRIMINAL MEMORANDUM, May 12, 2025
Focus, Fairness and Efficiency in the Fight Against White-Collar Crime
Sara R. Simon, Esq. Counsel, Porzio, Bromberg & Newman, P.C Grant Ostlund
Sr. Director, Strategy & Operations, US Operations, Ethics & Compliance
Novo Nordisk .

Grant Ostlund Sr. Director – Strategy & Operations
Novo Nordisk

Sara
Esq. Counsel

➢ Drug Price Transparency Laws ➢ Including PDABs
➢ HCP Spend Transparency laws
➢ Sales Rep Registration and Reporting ➢ Marketing Laws

➢ Annual or Quarterly WAC Reporting
➢ Quarterly- Louisiana*
➢ Annual- Texas and West Virginia
➢ New High Cost Drug Reporting/Notification
➢ California, Maine, Minnesota, New Hampshire**, New Jersey, New Mexico, Oregon, Vermont, Washington
➢ Price Increase Reporting/Notification
➢ California, Florida, Connecticut, Louisiana, Maine, Minnesota, Nevada, New Hampshire**, New Jersey, New Mexico, New York, Oregon***, Texas, Utah, Virginia, Washington, West Virginia
➢ Varying price increase thresholds, from 10%-50% starting at $40 (CA) WAC to $400 (NM)
➢ Varying deadlines for notices/reports
➢ Some states only require reporting if identified on state list(s) (Connecticut, Maine, Nevada, Vermont)
* ND just repealed its law at end of April so now LA only state that requires quarterly reports
** NH-New Drug and Price Increase reporting to NH PDAB paused until 6/30/25; DOI new drug report still required
*** OR- annual price increase report declared unconstitutional 2/24; 60 day notice and new drug notice still required
➢ PDAB laws in 11 states
➢ CO, MD, & OR most active
➢ Ability to set Upper Payment Limits (“UPLs”) in 4 states- Colorado, Maryland, Minnesota, and Washington
➢ Tracking all of the state price reporting laws to take into account all of the different triggers and filing requirements/who/when/how?
➢ Dealing with PDABs
➢ Challenges
➢ States/jurisdictions with compliance program requirements and/or limits include:
➢ California- “declaration” of compliance program/annual per HCP meal/gift limit
➢ Connecticut- adoption and implementation of a code that aligns at a minimum with AdvaMed/PhRMA Code and OIG CPG
➢ Maine- gift “prohibition” and limits on honoraria
➢ Massachusetts- adoption and implementation of a Marketing Code of Conduct (MA’s regs), which follows PhRMA and AdvaMed Codes/ annual compliance certification
➢ Minnesota- gift prohibition, including meals, in excess of $50 in aggregate per HCP, limited exceptions
➢ Nevada- adoption and implementation of a Marketing Code of Conduct, annual compliance certification
➢ New Jersey- meal limitation(s)/ fee (“bona fide” service fee) limitations
➢ Vermont- gift/meal ban, unless the HCP has a bona fide services arrangement with the company
Company/Operational Considerations:
➢ Keeping track of various requirements, including deadlines among states/jurisdictions
➢ Annual audit required for compliance certification in a few states
➢ Challenges
➢ States/jurisdictions with spend/payments/transfers of value disclosure requirements*:
➢ Chicago, IL- annual disclosure of rep’s TOVs, samples and interactions with HCPs (upon request)
➢ Connecticut- independent APRN disclosure/annual disclosure of reps’ TOVs, samples, and interactions- due by 7/1
➢ Massachusetts- annual disclosure of “sales and marketing activities” TOVs of $50+/ quarterly meal disclosure (not currently enforced) – due by 7/1
➢ Minnesota- annual disclosure of $100+ payments to speaker/faculty and consultants- due by 5/1
➢ Nevada- annual disclosure of (registered) reps’ TOVs of $10+ and samples- due by 3/1
➢ Oregon- annual disclosure of (registered) reps’ TOVs, samples, and interactions with HCPs- due by 4/1
➢ Vermont- annual disclosure of (allowable)TOVs, samples- due by 4/1
➢ Washington, DC- annual disclosure of TOVs of $25+ employee compensation, and marketing/advertising costs –due by 7/1
* Preempted by the Sunshine law
➢ States/Jurisdictions with registration requirements that apply to sales reps and other field-facing personnel include:
➢ Chicago, IL- registration required if “within city limits” for at least 15 days/CY
➢ Connecticut- no minimum time
➢ Nevada- registration required if in the state for at least 5 days/CY
➢ Oregon- must register if conducting business in the state for at least 15 days/CY
➢ Washington, DC- registration required if detailing in the District for at least 30 days/CY
➢ Should consider if “virtual” interactions count toward minimum # of days
➢ Nevada
➢ Oregon
Company/Operational Considerations:
➢ Keeping track of state limitations/prohibitions
➢ Violations
➢ How to cure
➢ Tracking(spend)beyond Sunshine
➢ Reporting
➢ Challenges
➢ States with marketing disclosure requirements (for HCPs):
➢ Colorado- drug reps must provide HCPs, in writing, the WAC and the names of at least three generic prescription drugs from the same therapeutic class (includes in-person meetings, mail, telephone calls, video conferencing, emails, texting, etc.)
➢ Connecticut- “pharmaceutical reps” must provide HCPs, in writing, the “list price” and any variation efficacy data in different racial and ethnic groups, if available (includes in-person meetings, telephone calls emails, texting, etc.)
➢ Vermont-drug reps must provide HCPs, in writing, the AWP per pill and the price relationship between the marketed drug and other drugs within the same therapeutic class and information must be posted on a public website (includes in-person meetings, mail, telephone calls, emails, texting, sampling, etc.)
➢ Format of disclosure, hard copy vs. electronic
➢ Who is responsible for drafting
➢ Training
➢ (Basically) the same for all 3 states?
➢ MLR/PRC approval required?
THANK YOU!
Alfred R. Brunetti. Esq., CIPP/US, CIPM Principal Porzio, Bromberg & Newman, P.C.

Diagnoses, Treatments, Medical History

Health data is typically any info related to a person’s physical or mental health, healthcare services, status or condition
Exercise routines, calories logging, etc (think fitness apps or trackers)
Biological, physiological or behavioral characteristic, patterns, rhythms, scans
Information
Info revealing health status or history (think geolocation)
Biometrics




Health Data


deceptively sharing consumer health data and Health Breach Notification Rule violation by failing to report unauthorized disclosure to advertising companies
deceptively sharing consumer sensitive data with 3Ps (email, IP, health questionnaire info with Facebook & others)



disclosure of website data to 3P advertising platforms, e.g. Meta and Google


❖ CONSENT requirements to collect (other than strictly necessary to deliver requested product / service)
Consumer Health Data
Health Data
❖ TRANPARENCY obligations, e.g. listing of 3P recipients or affiliates
❖ Affirmative and distinct NOTICE requirements
❖ Strong privacy RIGHTS and exercise instructions


Consumer Health Data
Health Data
Consumer Health Data
➢ Specifically created to gap fill between reality and consumer expectations about health data
➢ Fully effective since June 2024
➢ Broad Scope & Range
➢ Heighten, specific additional obligations & rights beyond traditional consent and notice
➢ Inferences are key
➢ PRIVATE RIGHT OF ACTION
“Regulated Entity”
Conducts business in WA state
OR Produces or provides products or services targeted to WA consumer
AND Alone or jointly “determines the purpose and means of collecting, processing, sharing or selling of consumer health data”
personal information that is linked or reasonably linkable to a consumer and that identifies the consumer's past, present, or future physical or mental health status.
(i) Individual health conditions, treatment, diseases, or diagnosis;
(ii) Social, psychological, behavioral, and medical interventions;
(iii) Health-related surgeries or procedures;
(iv) Use or purchase of prescribed medication;
(v) Bodily functions, vital signs, symptoms, or measurements of the info described in this subsection
(vi) Diagnoses or diagnostic testing, treatment, or medication;
(vii) Gender-affirming care info;
(viii) Reproductive or sexual health info;
(ix) Biometric data;
(x) Genetic data;
(xi) Precise location info that could reasonably indicate a consumer's attempt to acquire or receive health services or supplies;
(xii) Data that identifies a consumer seeking health care services; or
(xiii) Any info processed to associate or identify a consumer with the data described in this subsection that is derived or extrapolated from nonhealth information (by any means, including algorithms or machine learning)
or personal information that is used to engage in public or peer-reviewed scientific, historical, or statistical research in the public interest
But, the research must
✓ adhere to all other applicable ethics and privacy laws and ✓ be approved, monitored, and governed by an institutional review board (or similar) that determines business has implemented reasonable safeguards to mitigate privacy risks associated with research, including any risks associated with reidentification

Before collecting, you must:
➢ get consent with specified purpose
OR
➢ Do so only to extent “necessary” to provide product or service consumer “has requested from [you]”

Before sharing, you must:
➢ Get consent that is “separate and distinct” from the collection consent
OR
➢ Do so only to extent “necessary” to provide product or service “has requested from [you]”
Consent must include categories, purpose and specifics on uses, recipients & how to withdraw consent

Tracking of bodily functions (like, e.g. digestion, perspiration or sleep) by an app, device or otherwise
info that is derived or extrapolated from nonhealth data to associate or identify a consumer with consumer health data (so, even potential inferences drawn from purchases of toiletries or other activities)

Make sure your business contracts and DPAs are detailed and specific because infractions could turn your processor into a directly regulated entity


• Categories of collected & shared
• Purpose of collection and how used
• Categories of sources
• Categoreis of 3P and affiliate share recipients
• How to exercise rights

✓PROPER POLICY LANGUAGE
✓FUNCTIONAL AND TESTED

✓ACCESS - DELETE* – WITHDRAW
✓45 DAY RESPONSE (+45 DAYS**)
✓DOWNSTREAM OBLIGATIONS IMPOSED ON VENDORS
✓ CLEAR, AFFIRMATIVE, VOLUNTARY PURPOSE-SPECIFIC OPT IN CONSENT TO COLLECT / SELL
✓ STAND ALONE CONSENT TO SELL
✓ REVOCABLE & TRACKABLE
✓ KEEP THE AUTHORIZATION TO SELL FOR 6 YEARS
General terms in unrelated info / closing a piece of content / dark patterns (i.e. deceptive designs)
THOUGHTFUL HEALTH DATA GOVERNANCE CAN
PROTECT PRIVACY, INCREASE SECURITY AND REDUCE RISK AND LIABILITY
✓ PRIVACY BY DESIGN, EARLY & OFTEN IN PRODUCT DEVELOPMENT & IMPLEMENTATION
✓ KNOW WHEN/HOW TO CONDUCT DATA PROTECTION IMPACT ASSESSMENTS
✓ TRAIN CROSS-FUNCTIONALLY
✓ MONITOR AND AUDIT VENDORS AND AFFILIATES
❑ Leverage existing compliance infrastructure to adopt a proactive approach to health data governance
❑ Is Health Data being processed for legitimate and lawful business purposes in accordance with policies, SOPs and applicable law?
❑ Policy creation / revisions to address collection, use and sharing/sale
❑ Accuracy and propriety of Notices and Consents / documented and preserve via Consent Management platform?
❑ Timely and functional opportunities to opt-out of certain processing activities
❑ Vendor Assessment & Contracts – Audit & Monitor
❑ TRAINING!! (at a regular cadence)



➢ Clear Rules of the Road
➢ Ownership/Leadership
▪ Tone from the Top
➢ Knowledge / Training
➢ Transparency /Candidness
➢ Consistency & Accountability
➢ Challenge & Test
➢ Continual Improvement
➢ Is the compliance program well designed?
➢ Is the program being applied earnestly and in good faith?
➢ Is it adequately resourced and empowered to function effectively ?
➢ Does the company’s compliance program work in practice?
“Even a well-designed compliance program may be unsuccessful in practice if implementation is lax, under-resourced, or otherwise ineffective.”
“Prosecutors are instructed to probe specifically whether a compliance program is a ‘paper program’ or one implemented, resourced, reviewed, and revised, as appropriate, in an effective manner.”
(SEPTEMBER 2024)
➢ Are Emerging Technologies (Including AI) Properly Deployed, Integrated, Monitored and Used?
➢ Are Whistleblowers Properly Protected and Incentivized?
➢ Does The Compliance Program Have Appropriate Access To Data - and the Technological Tools Needed To Assess Such Data?
“Now is the time to make the necessary compliance investments [inAI and other technology] to help prevent, detect, and remediate misconduct.”
Participation: Speak-Up Culture? Process: Well –Designed?
Protection: Triage & Privilege? Prevention: Causation & Remediation?
➢ Sets The “Proper Tone” / Foundation
➢ Encourages Business “Buy-In”
➢ Bolsters Participation Across Enterprise
➢ Fosters Open Communication and Trust
➢ Values Transparency, Consistency and Accountability
➢ Energizes Itself, Leads To Continuous Process Improvements
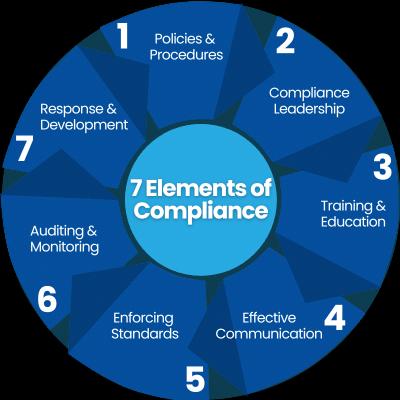
➢ Establish Clear Policies and Procedures
➢ Have a Formal Investigation Plan
➢ Use and Rely On Technology/Data Analytics
➢ Preserve Confidentiality & Prevent Retaliation
➢ Conduct Root-Cause Assessments
➢ Implement/Confirm Remedial Measures
➢ Continuously Improve Process
➢ Understand Your Resources / Know Your Data
➢ Utilize Analytics and AI To Enhance Anomaly Detection
➢ Leverage AI To Keep Up With Industry Trends and Developments
➢ Establish Real Time Compliance Monitoring
➢ Automate Data Collection and Integration
➢ Evaluate Predictive Compliance Analytics
➢ Monitor Industry to Seek Out New Tools
➢ Should Be Integrated Into Broader Corporate Enterprise Risk Management (ERM) Processes
➢ Should Be Used to Enhance Accuracy and Efficiency of Compliance Program (Including Investigations)
➢ Should Be Available To, and Utilized By, Compliance Team in Similar Manner to Its Use Elsewhere In Company
➢ ESTABLISH WRITTEN POLICIES AND PROCEDURES
➢ EDUCATE EMPLOYEES (INVESTIGATORS)
➢ CONDUCT EARLY ASSESSMENT
➢ INVOLVE COUNSEL
➢ IDENTIFY PRIVILEGED MATTERS
➢ CONTINUALLY MONITOR OPEN MATTERS

➢ ATTORNEY CLIENT PRIVILEGE
▪ Protects confidential communications between a lawyer and a client for the purpose of seeking or obtaining legal advice
➢ WORK PRODUCT PRIVILEGE
▪ Protects certain materials prepared in anticipation of litigation and/or at the direction of counsel.


➢ ENSURE COUNSEL DIRECTS INVESTIGATION
➢ LIMIT DISTRIBUTION OF PRIVILEGED COMMUNICATIONS
➢ SEPARATE LEGAL ADVICE FROM STANDARD BUSINESS
➢ MARK DOCUMENTS AS “PRIVILEGED AND CONFIDENTIAL”
➢ EDUCATE EMPLOYEES ON PRIVILEGE PROTECTIONS
➢ ENGAGE OUTSIDE COUNSEL – AS APPROPRIATE

Conduct Post-Mortem & Identify Lessons Learned
Analyze Root-Cause & Identify Corrective Measures
Ensure Enforcement of Remedial Action & Document/Close Case
Implement Necessary Systemic Changes To Mitigate Future Risk
Validate Effectiveness of Corrective Measures (Using Tech/Data)
Jeff Kawalek, MBA Chief ComplianceZambonOfficer US Gil Rodriguera Sr. Director, Compliance Business Partner Mallinckrodt
Jennifer A. Romanski, Esq. Principal Porzio, Bromberg & Newman, P.C.
Daniel Spicehandler VP, Compliance, Commercial Divisions Stryker

Jeffrey Kawalek, MBA Chief Compliance Officer Zambon USA

Gil Rodriguera
Sr. Director, Compliance Business Partner Mallinckrodt

Jennifer A. Romanski, Esq. Principal Porzio, Bromberg & Newman, P.C. JARomanski@pbnlaw.com

Daniel Spicehandler VP, Compliance, Commercial Divisions Stryker
For additional resources and to complete the CLE survey, please scan the QR code below.