Graves’ Hyperthyroidism: Treatment with Antithyroid Drugs, Surgery, or Radioiodine-A Prospective, Randomized Study*
OVE TijRRING, LEIF TALLSTEDT, G&AN WALLIN, G&AN LUNDELL, JAN-GUSTAF LJUNGGREN, ADAM TAUBE, MARIA SAAF, BERTIL HAMBERGER, AND THE THYROID STUDY GROUP?Departments of Endocrinology (O.T., M.S.), Surgery (G.W., B.H.), and General Oncology, Radiumhemmet (G.L.), Karolinska Hospital; the Department of Ophthalmology, Huddinge University Hospital (L.T.); and the Department of Medicine, St. G&an’s Hospital (J.-G.L.), Stockholm; and the Department of Statistics, University of Uppsala (A.T.), Uppsala, Sweden
ABSTRACT
To analyze the benefits and risks of three common treatments, we randomly assigned 179 patients with Graves’ hyperthyroidism as follows: 60 patients, 2034 yr of age (young adults), received antithyroid drugs for 18 months (medical) or subtotal thyroidectomy (surgical), and 119 patients, 35-55 yr of age (old adults), received medical, surgical, or radioiodine (iodine-131) treatment. The follow-up time was at least 48 months.
Antithyroid drugs, surgery, or iodine-131 treatment normalized the mean serum hormone levels within 6 weeks. The risk of relapse was highest in the medically treated young and old adults (42% us. 34%), followed by that in those treated with iodine-131 (21%) and that in the surgically treated young and old adults (3% vs. 8%), respec-
THREE DIFFERENT forms of treatment are commonly used for Graves’ hyperthyroidism: antithyroid drugs, surgery, and radioiodine (iodine-131). The treatment policy of Graves’ hyperthyroidism varies considerably within and between different countries (l- 5). Among thyroidologists in the USA, the first choice of treatment for a43-yr-old woman with moderate hyperthyroidism and diffuse goiter is antithyroid drugs in 30%,surgery in l%, and iodine-131 in 69%; the corresponding figures among colleagues in Europe are 77%(antithyroid drugs), 1%(surgery), and 22%(iodine-131), respectively (1,2). Thefigures for patients with typical, moderate, and uncomplicated Graves’ diseasein Japan are 88% (antithyroid drugs), 1% (surgery), and 11%(iodine-131), respectively (5). Thesedifferences arisebecausethere are large epidemiological differences in various geographical areas, and the physician needs to take a number of factors into consideration when choosing the treatment. Such factors in-
Received June 1, 1995. Revision received November 8, 1995. Rerevision received March 14, 1996. Accepted March 20, 1996.
Address all correspondence and requests for reprints to: Dr. Ove Tarring, Department of Endocrinology and Diabetology, Karolinska Hospital, S-171 76 Stockholm, Sweden.
*This work was supported by grants from the Swedish Medical Research Council (no. 5992 and 02330), the Gustav V Jubilee Foundation, the Swedish Society against Cancer and Traffic Injuries, the Nordic Insulin Foundation, the L. 0. Ostermans Foundation, and the Foundations of the Karolinska Institute.
t Members of the Thyroid Study Group are listed in the Appendix.
tively. Elevated TSH receptor antibodies at the end of medical therapy or increasing TSH receptor antibodies values after medical or surgical treatment increased the probability of relapse. Development or worsening of ophthalmopathy was not associated with relapse per se. Ninety percent of the subjects in all groups were satisfied with the treatment they received. No significant difference in sick-leave due to Graves’ or other diseases was seen during the first 2 yr after initiation of therapy.
The increased risk of ophthalmopathy in patients with high serum T, levels, especially when treated with iodine-131, and the relatively high frequency of relapse after treatment with antithyroid drugs are important factors to consider when selecting therapy for Graves’ disease. (J Clin Endocrinol Metab 81: 2986-2993, 1996)
elude the patient’s age and preferences, severity of disease, glandular size, local traditions, and resources.
The benefits and risks of each treatment are important becausethe prevalence of hyperthyroidism isin the range of 2% in women (6, 7). As a controlled study comparing the three treatment modalities with respectto overall results and complications had not previously beenpublished, we carried out a prospective study between 1983and 1990,recruiting 179 randomized patients. We previously reported an increasedrisk for development or worsening of Graves’ eye diseasein patients with high pretreatment serum total T, levels who received iodine-131 treatment during a 2-yr follow-up period (8). We have now observed each patient for at least 4 yr and present here the results for the three treatment forms, including quality of life measurements,based upon the patients’ own assessmentsof the therapies they received.
Subjects and Methods
Subjects and study design
All patients between the ages of 2055 yr who were referred to our units between November 1983 and June 1990 with hyperthyroidism caused by Graves’ disease and without a history of previous thyroid disease were evaluated for inclusion in the study.
Young adults. Patients, 20-34 yr old, were assigned to treatment with antithyroid drugs plus T, (medical therapy) or subtotal thyroidectomy followed by T, (surgery).
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023
Old adults. Patients, 35-55 yr old, were given iodine-131 therapy as a third alternative (iodine-131). We do not treat patients under 35 yr of age routinely with iodine-131.
The patients were randomized as follows. Each patient was assigned a treatment group consecutively using two lists, one for each age group, on which the treatment group occurred in random order but balanced to equalize the size of the treatment groups. The lists were unavailable to the clinicians throughout the study, and randomization was performed over the phone. Through May 1994, the 179 randomized patients who agreed to participate in the study have been followed for at least 48 months after the therapy begun (range, 48-121 months).
The following criteria were used for the diagnosis of Graves’ disease: presence of symptoms and signs of hyperthyroidism, nonnodular thyroid gland, and elevated total and free serum T, and/or total Ta levels. If the serum T, level was between 150-180 nmol/L or T, was between 2.5-3.5 nmol/L, the diagnosis was supported by a TRH test. Furthermore, all patients should have a thyroid uptake of iodine-131 that was not suppressed, a diffuse pattern of isotope uptake on the radionuclide scan, and a goiter size that should enable a single dose of iodine-131 to render the patient euthyroid or hypothyroid.
All patients underwent clinical examination and laboratory testing before randomization. The ophthalmological examination was performed in all patients by the same ophthalmologist throughout the entire observation period.
Therapy and follow-up
Medical tkempy. Ten milligrams of methimazole were given four times daily. Three to five weeks after the start of the antithyroid drug, T, was added in doses between 0.1-0.3 mg/day (mean, 0.17 mg/day). The antithyroid drug and T, were discontinued simultaneously after 18 months. If not contraindicated, propranolol in a dose of 20-60 mg three to four times daily or 50-300 mg metoprololl day in divided doses was given initially until the patients became euthyroid. In cases of adverse reactions to methimazole, the drug was exchanged with propylthiouracil(lO0 mg four times daily). After initiation of therapy, the patients were examined monthly for 2 months and then every 3 months during the first year. After discontinuation of treatment, the patients were followed twice during the first year and then at least once yearly.
Surgery. The patients were given at least 40 mg propranolol three to four times daily or an equivalent dose of metoprolol before operation. The patients were admitted to the hospital the day before surgery.
The standard procedure was subtotal thyroidectomy in general anesthesia, leaving approximately 1 g or less of thyroid tissue in each lobe. The recurrent laryngeal nerves were identified in all cases, and the area of the external branch of the superior laryngeal nerve was not dissected. The parathyroid glands were noted, but not searched for. The dissection was always close to the thyroid gland. At histopathological examination, none of the thyroid specimens was classified as thyroiditis, and there were no signs of malignancy in the resected thyroid specimens.
The oral /3-adrenergic blocking treatment was continued after the operation. If the pulse rate exceeded 100 beats/min, 1 mg propranolol was given iv. To prevent the development of postoperative hypothyroidism, all patients were started on 0.1-0.2 mg T, before being discharged on the fourth day postoperatively (median, 5% vs. 95% are 1 OS. 8 days, respectively). The patients were followed at the out-patient clinic at 5 weeks and 3, 6, 9, and 12 months postoperatively and then at least once a year.
TABLE 1. Clinical characteristics of the 179 patients at randomization
Treatment group
No. and sex of patients Age (M/F’) (VT) BW (kc) Y
Y medical 30 (3127) 29 k 4 59 k 9
Y surgery 30 (8/22) 29 + 4 58 5 11
0 medical 41 (9/32) 45 + 6 61 _f 11
0 surgery 37 (5/32j 45 k 6 65 k 14
0 iodine-131 41 (5/36) 45 2 5 63 ? 10
Reference range
Y, Young adults; 0, old adults. Values are the mean ? SD. a Specimens were not available in five of the patients.
Iodine-131. A single oral activity of iodine-131 was administered, based on thyroid size, 24-h iodine-131 uptake, and the measured effective half-life of the isotope in the thyroid (9). The activity was calculated to deliver 120 Gray units to the thyroid. Propranolol or metoprolol in doses equal to those in the medically treated patients were also given to all patients. The patients were examined 6 and 10 weeks after therapy, and 24-h iodine-131 uptake by the thyroid was measured at 10 weeks. The patients were considered to have hypothyroidism as soon as TSH was elevated and/or free T,, T, or T, was below the lower limit of the reference range. L-T~ therapy was then started. If euthyroid at 10 weeks, the patient was followed every 3 months the first year, twice yearly the second year, and then once yearly.
Follow-up. Examinations were performed at the department in which therapy was given and included clinical evaluation and laboratory tests. At each visit, body weight, degree of ocular proptosis, and patient’s report of eye complaints were recorded. In addition, the serum concentrations of T,, T4, free T,, TSH, and TSH receptor antibodies (TRab) were measured, and peripheral blood leukocyte counts in the medically and surgically treated patients as well as hemoglobulin and serum calcium measurements in the surgically treated patients were made.
Laboratory methods
The laboratory parameters were made as previously described (8). The reference ranges are as follows: serum T,, 1.1-2.5 nmol/L; T, 75-150 nmol/L; free T, 9-21 pmol/L; TSH, 0.1-4.5 mu/L; and TRab, less than lo%, respectively.
Patients’ assessment of the treatment
The patients’ views of the disease and treatment periods were recorded on the basis of a questionnaire that was sent to each patient at the time of follow-up at least 3 yr after the initiation of treatment. Sick-leave statistics for all patients from the day of initiation of treatment and the following 2 yr were obtained from the Social Insurance Office of Sweden by whom all sick-leaves, including absence of l-2 days or longer, as well as sickness allowances are registered.
Statistical analysis
The data analysis for Table 1 was based on the intention to treat principle and comprised all 179 randomized patients. The rest of the data analyses comprised only subjects who underwent the actual treatment unless otherwise stated in the text. The analyses used were 2 analysis, Fisher’s exact test, logistic, and proportional hazard regression analysis.
Results
During treatment and follow-up, no significant differences between the serum levels of TJ, T, free T, and TRab were found between medically treated young and old adults or between surgically treated young and old adults. The T, values for the medically treated young and old adults are, therefore, combined in Fig. 1 as are the data for surgically treated young and old adults. The individual serum T, valuesvaried somewhat more in the iodine-131-treated group
Serum T3 (rim&L) 6.3 t 2.0 5.6 2 1.8 5.4 k 1.7 5.4 _f 1.9 5.3 t 1.7 1.1-2.5
Serum total T, (nmoVL) 239 -+ 72 221 + 46 224 2 55 217 2 57 221 L 57 75-150
Serum free T, (pmoC 59 +- 26 60 + 24 57 k 17 57 -+ 25 55 t 19 9-21
Serum TRab (%Io)= 38 i 26 35 2 23 31 k 23 26 +- 20 34 2 21 <lo
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023
0 2 4 6 8 10 12 14
8060 -
0 2 4 6 6 10 12 14
Iodine-131
0 2 4 6 8 10 12 14
Months
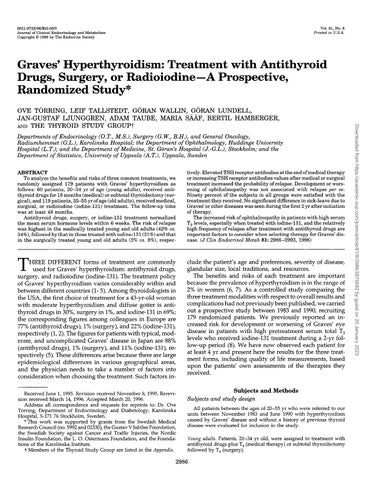
FIG. 1. The individual (open circles) and mean (solid line) values of serum T, during the first 14 months after initiation of therapy, i.e. the first day of antithyroid drug treatment, the day of operation, or the day of iodine-131 administration. The values for the patients who needed a treatment other than the randomized are omitted beyond the time the change occurred.
during the first year, but the mean values were within the reference range after 6 weeks (aswere the serum T, levels) and throughout the 4 yr of follow-up in all three treatment groups (Fig. 1).
The serum T, levels were significantly lower (P < O.OOl), but still within the reference range, after 10 weeks in the iodine-131-treated group compared with those in the other two groups (Fig. 1). The mean free T, serum levels were slightly above the normal reference range in all three groups from the time of T, administration and throughout the study.
The mean serum levels of TRab showed a steady decline in the medical groups after initiation of therapy and were around the normal reference range when the drugs were discontinued after 18 months. The TRab values from the medically treated young and old adults aswells as for the surgically treated young and old adults, respectively, arealso combined in Fig. 2.A similar TRabpattern was found in the surgery groups, However, in the iodine-131-treated group, a significant increase was found, with a peak 2 months after therapy, and the mean levels remained above the normal reference range throughout the follow-up period.
Surgery 8ob T Iodine-131 1 2 60 2 I- 40 3, 20 0 I, I II, I, I, I. I 0 6 12 18 24 30 36 42 48 Months FIG. 2. The serum concentration of TRab during the first 4 yr in the different treatment groups. See also Fig. 1.
80 t
levels of T, free T, TRab, and calcium between the five treatment groups atthe time of randomization. However, the meanT, value was somewhat higher in the younger groups than in the older groups. The data are presented in Table 1.
In the present follow-up, two additional patients had developed ophthalmopathy 7and 42months after treatment in the iodine-131-treated group, but none had done so in the other groups. In the iodine-131-treated patients, there was no association between the development or worsening of endocrine ophthalmopathy and biochemical evidence of hypothyroidism. Thus, the patients without endocrine ophthalmopathy had mean and range values that were higher for TSH and lower for free T, and T, than the patients with endocrine ophthalmopathy (Table 2).
Thenumber of smokersUS.the number of nonsmokerswas not significant different between the groups (smokers/nonsmokers/no information: medically treated young adults, 14/ 14/2; surgically treated young adults, 18/ 12/0; medically treated old adults, 18/22/l; surgically treated old adults, 19/18/O; iodine-131 treatment group, 23/ 17/ 1).
Patient assessment of the treatment
As shown in Table 3,almostall patients were satisfiedwith the randomized treatment they received. More patients in the iodine-131-treated group were likely to recommend the same treatment to a friend than the patients in the other groups. The relapse of the diseasewas considered a major disap-
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023
TABLE 2. The relation between the development or worsening of endocrine ophthalmopathy in the iodine-131-treated patients and the biochemical indexes of hypothyroidism at the time L-T* treatment was started
No ophthalmopathy (n = 26) Ophthalmopathy (n = 15) P
Values are the mean and range.
a By Mann Whitney U test.
Serum TSH (mu/L) Serum T, (nmoL’L) Serum free T, (pm&L) Serum T, (nmol/L) 16.2 (0.1-78) 41(24-66) 9.3 (1.4-59) 0.9 (0.5-1.7) 3.8 (0.1-42) 62 (25-113) 11.6 (3.2-20) 1.4 (0.9-2.2) 0.01 0.003 0.06 0.002
TABLE 3. The patients’ own view of their treatment according to the questionnaire The percentage of the number of replies, the percentage who did not remember (?) and the number (#) of replies are shown. The medical treated age-groups (young and old adults) are combined (n = 71) as are the surgical treated age-groups (young and old adults) (n = 67). I-131 denotes the iodine I-131-treated group (n = 41).
Satisfied with the treatment alternative 95 0
Questions % Medical Surgical I-131 ? # % ? # % % ?# 60 98 0 62 95 0 38
Afraid of adverse effect of treatment 8 7
Satisfied with the treatment procedure 93 0 Will recommend the treatment to a friend
Without reservation 68
No opinion 12
The relapse a major disappointment 57
Duration until you felt recovered
<3 months 24
3-12 months 15 >12 months 20 Not yet 10 Difficult to remember 31
a Answers were obtained from all patients who relapsed.
pointment in the young surgical patients, whereas the least disappointment of relapse was seen in the iodine-131treated group. Among the patients who remembered, significantly more patients (n = 30) who were treated by surgery than medically (n = 14) or with iodine-131 (n = 9) felt recovered within 3 months after treatment than after 3 months (n = 23 for surgery ‘us. 27 for medical and 21 for iodine-131; P = 0.025, by 2 test). A surprisingly high percentage in all three group did not feel recovered within 1 yr after treatment, and many still do not feel recovered even after 3 yr or more. The number of patients who did not remember the time at which they felt recovered was not different among the three groups.
Sick-leave
Data on the number of days the patients stayed at home from work due toGraves’ or other diseaseswere obtained for 95% of all participating patients and were not significantly different among the five groups. The values (mean ? SE) for the first 18 months after initiation of treatment VS.the following 6 months were asfollows: medically treated young adults, 71 ? 21 days VS.12 ?C4; surgically treated young adults, 65 + 15VS.10? 3;medically treated old adults, 62 ? 10 VS.10 + 4; surgically treated old adults, 75 t 12US.10 2 3; and radioiodine-treated group, 74 ? 12 VS.9 2 3 days, respectively.
Specific results from the three treatment
modalities
Medical groups.Seventy-one patients (30 young and 41 old adults) were randomized to antithyroid drugs plus T4ther-
60 11 5 63 8 3 38 60 89 0 62 89 0 38 59 63 37 74 84 14 11 22” 75 4” 40 8” 59 62 38 48 24 13 24 19 16 5 16 15 21
apy (Fig. 3). Two patients did not comply with the treatment, and 1waserroneously randomized. Among the remaining 68 patients, total reversible adverse effects, most likely induced by methimazole, were observed in 11 patients (16%). Of these,8 had skin rash, 2 had arthralgia, and 1had fever and convulsions. All patients were, therefore, switched over to propylthiouracil. Four of the 11patients showed similar adverse effects to propylthiouracil, and the medical treatment wasdiscontinued (Fig. 3). Oneof the 4 patients wasoperated upon, 2 received iodine-131 treatment, and 1 remained euthyroid without further treatment after 8 months.
Four ofthe 68patients (6%),2from eachagegroup, did not become euthyroid despite increase in dosesup to 60 mg methimazole or 600 mg propylthiouracil daily (Fig. 3). All four patients subsequently underwent subtotal thyroidectomy. Thus, 59 patients (83%) completed the 18 months of drug therapy (Fig. 3).
After discontinuation of the drugs, hyperthyroidism relapsed in 10 of 24 (42%) patients among medically treated young adults within a mean duration of 15 months (range, 2 weeks to 57months) and in 12of 35 (34%)patients among medically treated old adults within a mean duration of 13 months (range, l-33 months). Seven of the patients were operated upon, and 3 received iodine-131 among medically treated young adults. Among the medically treated old adults, 2patients were operated upon, 8received iodine-131, and 2 preferred a new course of drug therapy.
The likelihood of relapse after discontinuation of therapy could not be shown to be associatedwith high pretreatment values of TRab in either of the two agegroups, according to
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023
FIG. 3. Clinical outcome in the five treatment groups. Of the total number of randomized patients in each group (shown at the bottom), the open bars represent patients who fulfilled the randomized treatment without a change in the primary therapy. Other treatment, Patients who rejected the randomized treatment or did not comply; Adverse effects, a change in therapy because of adverse effects; Persistent disease, patients who underwent other therapy due to lack of therapeutic response to the randomized treatment; Relapse, patients who relapsed with Graves’hyperthyroidism after the randomized treatment was completed. Y and 0 denote young and old adults, respectively.
aproportional hazard regression analysis (P = 0.26for medically treated young adults; P = 0.73for medically treated old adults; P = 0.21 when the two agegroups were combined).
The 59 patients in whom hyperthyroidism relapsed had higher TRab levels at the end of medical therapy (Table 4). Furthermore, TRablevels in the combined medically treated young and old adults showed an increaseafter discontinued treatment before relapse in 12 of 22 cases(55%) compared with an increasein TRab levels in only 4 of 37 (9%) among patients who did not relapse (P < 0.001).
The likelihood of relapsewas positively correlated to the pretreatment serumlevels ofT, (P = 0.021)and T4(P = 0.007) and to the male gender (P = 0.038),but not to free T, (P = O.l), when the two agegroups were combined (proportional hazard regression analyses). Age, T,/T, ratio, presence of ophthalmopathy atrandomization, smoking habits, or presence or absenceof lymphocytes in the fine needle aspiration biopsy could not be shown to have any predictive value for the relapse of hyperthyroidism. Moreover, the relapse and pretreatment serum T3,T, or free T, in the different groups did not correlate. A deterioration or development of ophthalmopathy was not seenin any patient after the relapseto hyperthyroidism.
1Brandomized treatment DBrelapse Bpersistent disease madverse effects mother treatment
SurgicaZ groups. Thirty young adults were randomized to surgery, but two of thesestarted treatment with antithyroid drugs and were not operated upon. Thirty-seven of the old adults were randomized to surgery, and all were operated upon (Fig. 3). Relapsein hyperthyroidism was found in four patients (6%) after 12-84 months. Of these, one patient was from the surgically treated young adults, and three patients were from the surgically treated older age group (Fig. 3). They were treated with antithyroid drugs plus T, (one patient) or with iodine-131 treatment (three patients). One patient had persistently elevated TRabpostoperatively, and in two other patients, increased TRab preceded the relapse of thyrotoxicosis. No other patients had increasing TRablevels.
Themean duration from randomization to surgery was 26 days (range, 8-79 days, except 127days in one patient) for young and old adults combined. The patients were discharged, on the average, 4 days postoperatively. The mean preoperative dose of propranolol was 180mg daily (range, 120-320).
In 13patients, the preoperative /3-adrenergicblockage was insufficient. Eight of those were identified preoperatively and received additional treatment with Lugol’s solution.
Sevensurgeonsparticipated; all were experienced in thytreated young adults and 86% of the medically treated old roid operations, and the mean operating time for both age adults patients expressed no problems with taking the an- groups combined was 133 min (75-190 min). No serious tithyroid drugs four times a day. Furthermore, 78% of the complications, including paresis of the recurrent laryngeal medically treated young adults and 94% of the medically nerves, persistent hypoparathyroidism, wound infection treated old adults declared that they had no major problem preoperative or postoperative death, were observed. All pawith the l&month treatment. tients received T, postoperatively; the mean dose for both
According to the questionnaire, 80% of the medically
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023
groups was 0.16 mg (0.1-0.2 mg). The mean dose at the latest visit was 0.17 mg (0.1-0.3 mg).
Fourteen patients, who had initially been randomized to and received medical treatment were later operated upon by subtotal thyroidectomy, as explained above. Altogether 82 of the I79 patients were treated by bilateral subtotal thyroidectomy.
Radioiodine groups. Two patients rejected the assigned treatment (Fig. 3). In 8 of the 39 patients who received iodine-131 (21%), hyperthyroidism relapsed 4.5-16 months after iodine131 treatment. Seven patients had persistent hyperthyroidism 10 weeks after the initial iodine-131 treatment. Three patients with ophthalmopathy were given more than 1 iodine-131 treatment for the purpose of ablating an autonomous thyroid. Thus, 18 patients received more than 1 iodine131 treatment. All patients, however, developed hypothyroidism after the initial or additional treatments and were given T,. The mean time from the initial treatment until T, was prescribed was 3.7 months (range, 7 weeks to 12 months). The mean dose of T, at the last visit was 0.175 mg (range, 0.1-0.25 mg). The mean iodine-131 activity administered was 250 megabecquerels or 6.8 mCi (mean value of the first treatment; n = 39). Fifteen patients experienced worsened ophthalmopathy. Thirteen of these received more than 1 iodine-131 treatment.
According to the questionnaire, 14% of the patients were concerned about receiving a radioactive isotope.
Discussion
Many questions related to the outcome of treatment remain to be answered, such asthe development of Graves’ ophthalmopathy and the overall outcome and complications aswell asa comparison of the patients’ own assessmentsof the three treatments.
Essentially all 3 therapy forms accomplished an almost similar decline in thyroid hormone levels; the iodine-131 therapy was a few weeks slower due to the later supplementation of T, to the patients in this group. T, supplementation alsoexplains the similar T, and T, levels achieved with the 3 treatment modalities after 1 yr and during the 4-yr follow-up period. The side-effects were few for all treatment forms. In the medically treated groups, no serious side-effects occurred. Moreover, the medical therapy was either changed in 6% (4 of 68) of patients due to adverse reactions to the antithyroid drugs or it was insufficient in 6% (4 of 68) due to insufficient effect or perhaps poor compliance. Moreover, relapse of the diseaseafter the end of medical therapy occurred in 42% of the young patients and 34% of the older agegroup. Thus, in 30of 68patients (44%),the treatment was a failure if the goal was to achieve permanent euthyroidism after 1courseof antithyroid drugs. High serumT,, T,, or free T, levels also implied increased risk for relapse in subjects over 35 yr of age. As has been shown in other studies, increasedTRab levels at end of therapy and increasing levels after therapy were associatedwith increased relapse incidence (10-14). On an individual basis,however, the clinical value of TRab is a relatively weak marker for relapse, asin 23% of those with normal levels at the end of therapy, hyperthyroidism relapsed. This frequency, however, is less
than the 34-42% in this study without considering the TRab values. Therefore, if elevated TRablevels arefound, we prolong medical therapy, particularly in patients with endocrine ophthalmopathy and alsobecauseof the possibleimmunomodulatory role proposed for methimazole (15).
The main drawback of antithyroid drug treatment is the high relapse rate, which varies between 20-75% in other studies (16). The relatively low rate in our study may be explained partly by 18-month duration of the medical treatment and the 4-yr follow-up, partly by the relatively high doseof antithyroid drugs we used, and perhaps by the rarenessof large diffuse goiters in our region of Sweden and the exclusion of thesefrom the study. In two prospective studies, 58% and 70% relapse rates were observed among patients treated for 6 months, compared to 38% and 25% of the patients treated for 18months, respectively (17,18). In addition, in a controlled study, significantly lower recurrence rates were found using high doseofmethimazole (average,60mg) than those found when a lower dose (average, 14 mg) was used (19). On the other hand, this could not be confirmed in two other studies (20). An additional explanation for the lower recurrence rate might be the addition of T, to prevent hypothyroidism. This regimen is used by 45% of the members of the European Thyroid Association and 20% of the members of the American Thyroid Association (1, 2). The relapse rate approaches the results of two other Swedish studiesthat reported about 50%cumulative incidence during afollow-up period ofup to108months (21,22). Therelatively high methimazole dose, however, implied a somewhat higher frequency of adverse effects (6%) than that reported using lower doses. The mechanism behind the persistent hyperthyroidism in four of the patients is not known, but poor compliance could be the causeof some,but not all, of this. The level of T, substitution (-0.17 mg/day) that we used in all three treatment forms may seemhigh, but canbe explained in two ways. First, although someinvestigators do accept measurable serum TSH levels during treatment of Graves’ disease,we favor the concept of “letting the thyroid rest,” asTSH may induce the expression of thyroid antigens that could beinvolved in the immune processbehind relapse and/or endocrine ophthalmopathy. Second, the level of T, substitution generally has been decreasing during the last decades.
Surgery, with the technique used at our hospital and with only P-adrenergic blocking treatment preoperatively was also safe and without complications, but in 20% of the patients, preoperative treatment with p-blocking agents only wasnot sufficient. Three subjectsalsohad high or increasing TRablevels before the relapse,which supports our findings using the medical treatment.
Surgery is a feasible therapeutic alternative and can be considered the treatment of choice in many patients, e.g. thosewith alarge goiter, especially those with symptoms of compression, and patients who prefer surgical treatment to other alternatives. Also, in patients with aggressive hyperthyroidism and moderate to severe ophthalmopathy, surgery may have a definite role after initial antithyroid drug treatment. Four patients (6%)relapsedup to48months postoperatively. The risk of relapseof hyperthyroidism hasbeen reported tobe l-28% after surgery (23-25). Most relapsesare
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023
the patients for many years.
The mean weight of the resected tissue was 29 g, and we estimated the weight of that left in situ to be 2 g, which is less than that in most previous reports (23,25,27,28). At present, one patient relapsed as much as 8 yr postoperatively. In the future, it may be possible to use different tests to select the patients with Graves’ disease who are likely to relapse or develop hypothyroidism, indicating the amount of glandular tissue that should remain after surgery.
Forty-five percent (18 of 40) of the patients needed more than one iodine-131 treatment, of which 38% were due to failure to cure the disease. This is a relatively high failure rate, as other studies found figures between O-41%, and the rate is inversely related to the dose given (16). A relatively high absorbed dose was the goal, and the high failure rate may also be due to the fact that patients with relatively large goiters were randomized to iodine-131 therapy. In addition, the iodine-131-treated patients in this study had more severe hyperthyroidism. This is illustrated by the fact that the mean serum Ta level of 5.3 nmol/L in the present study is higher than the 4.3 nmol/L level for a representative sample of iodine-131-treated patients in another study, in which 82% were cured with one dose of iodine-131 (29).
All patients eventually developed hypothyroidism, and at 12 months, all had T, substitution therapy. The majority of iodine-131-treated patients develop hypothyroidism (21,3033), and the proportion does not seem to depend on the dose given. Low dose iodine-131 therapy has been effective in preventing hypothyroidism only over the short term, but the cumulative incidence of hypothyroidism is about the same as that with high dose therapy (34, 35).
Iodine-131 treatment is generally followed by a transitory increase in the serum concentration of TRab (36-39). This was also found in our study, in which only five patients did not show such an increase. None of these five patients needed more than one iodine-131 treatment.
As we previously reported in the 2-yr follow-up of these patients, the risk for developing or worsening of ophthalmopathy was 22% for a patient with serum T, levels above 5 nmol/L compared to a 2% risk if T, levels were below 5 nmol/L (8). Iodine-131 treatment further increased the risk from lo-58% for corresponding T, levels. Greater risk for development of ophthalmopathy has been proposed to be associated with posttreatment development of hypothyroidism (40-42). However, we found no association between the biochemical indexes for hypothyroidism and development or worsening of endocrine ophthalmopathy. Similarly, smoking is unlikely to be the cause of the observed association between iodine-131 treatment and ophthalmopathy, because the properties of smokers in the groups did not differ very much. We found that the common denominator for the development of ophthalmopathy was a more severe and unstable disease, i.e. higher serum T, levels or varying T3 or free T4 levels after treatment rather than posttreatment hypothyroidism with TSH elevation. The presence of residual functioning tissue after radioiodine treatment, therefore, could be involved in the process. On the other hand, in a subsequent study, early administration of T, could reduce
therapy be started early after iodine-131 treatment of Graves’ disease to stabilize the course of the disease after 131-iodine treatment.
No major difference among the three treatments exists according to the questionnaire. There was a surprisingly high number of patients who did not feel recovered even 1 yr or more after treatment. However, it must be kept in mind that we lacked an untreated control group. The numbers of days the patients stayed home after work were similar with all three treatments and, therefore, most likely reflect the character and severity of the disease and its impact on the general health of the patient rather than the differences due to treatment mode. In addition, the relatively long period of sickleave for all groups also reflects the Swedish relatively high reimbursement (-90% of the salary) for staying at home due to disease. Finally, relatively more patients in the iodine131-treated group would recommend the same treatment to another person, an observation that may favor this choice of treatment for a patient.
Treatment of Graves’ hyperthyroidism can be stratified according to the severity of the disease, the presence of ophthalmopathy, the patients’s age, and personal preference of treatment. For a patient with moderate disease activity, i.e. serum T3 levels less than 5-7 nmol/L and without pretreatment ophthalmopathy, any of the three treatment modalities can be used with little risk of complications and posttreatment ophthalmopathy. Moreover, the time lapse until the patient becomes euthyroid is, on the average, similar with all three therapy forms. Patients in this category above 35 yr of age are most often treated by us with iodine-131.
The difficult problems arise when patients have severe disease and ophthalmopathy. For example, in patients with high serum concentration of T, (>5-7 nmol/L), iodine-131 therapy with late administration of T4may carry a higher risk for developing ophthalmopathy based on our previous experience (8). Such patients may benefit from primary treatment with antithyroid drugs. Because of the high relapse rate in this type of patient, either surgery or radioiodine is often planned as definite treatment if the patient agrees. The conclusions from this study do not give us an adequate answer of how to manage these patients. Therefore, there is a need for further randomized studies to find the optimal treatment for this category of patients.
Acknowledgments
We are indebted to the staff of the Departments of Endocrinology, Oncology, and Surgery and the Oncology Center at Karolinska Hospital, and the staff of the Department of Immunology, National Laboratory of Microbiology, who performed the TRab analyses, and to Ulrika Sjijstedt and Karin Winberg for technical help.
Appendix
The Thyroid Study Group also included the following institutions and investigators: Department of Endocrinology, Karolinska Hospital: H. E. Sjijberg and M. Thoren; Department of Internal Medicine, Sabbatsberg’s Hospital: I. Blinder; Department of Surgery, Karolinska Hospital: L.-O. Farnebo; Department of General Oncology, Radiumhemmet,
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023
RANDOMIZED TREATMENT OF GRAVES’ DISEASE
Karolinska Hospital: H. Blomgren and I’. Hall; St. Erik’s Eye Hospital: B. Tengroth; Department of Pathology, Karolinska Hospital: T. Lowhagen; Department of Immunology, National Laboratory of Bacteriology: R. Norberg; and Department of Chemistry, Karolinska Hospital: T. Curstedt.
References
1. Glinoer D, Hesch D, Lagasse R, Laurberg P. 1987 The management of hyperthyroidism due to Graves’ disease in Europe 1986. Results of an international survey. Acta Endocrinol (Copenh). 285(Suppl):5-23.
2. Solomon B, Glinoer D, Lagasse R, Wartofsky L. 1990 Current trends in the management of Graves’ disease. J Clin Endocrinol Metab. 70:1518-1524.
3. Wartofsky L, Glinoer D, Solomon B, Lagasse R. 1991 Differences and similarities in the treatment of diffuse goiter in Europe and the United States. Exp Clin Endocrinol 97243-251.
4. Ford HC, Delahunt JW, Feek CM. 1991 The management of Graves’ disease in New Zealand: results of a national survey. NZ Med J. 104:251-252.
5. Nagayama Y, Izumi M, Nagataki S. 1989 The management of hyperthyroidism due to Graves’ disease in Japan in 1988. The Japan Thyroid Association. Endocrinol Jpn. 36:299-314.
6. Tunbridge WMG, Evered DC, Hall R, et al. 1977 The spectrum of thyroid disease in a community: the Whickham survey. Clin Endocrinol (Oxf). 7481-493.
7. Petersen K, Lindstedt G, Lundberg P-A, Bengtsson C, Lapidus L, Nystrom E. 1991 Thyroid disease in middle-aged and elderly Swedish women: thyroid related hormones, thyroid dysfunction and goitre in relation to age and smoking. J Intern Med. 229:407-414.
8. Tallstedt L, Lundell G, Tijrring 0, et al. 1991 Occurrence of ophthalmopathy after treatment for Graves’ hyperthyroidism. N Engl J Med. 326:1733-1738.
9. Larsson L-G. 1955 Studies on radioiodine treatment of thyrotoxicosis: with special reference to the behavior of the radioiodine tracer tests. Acta Radiol. 126(Suppl):l-164.
10. Davies TF, Yeo PPB, Evered DC, Clark F, Rees Smith 8, Hall R. 1977 Value of thyroid-stimulating-antibody determinations in predicting short-term thyrotoxic relapse in Graves’ disease. Lancet. 1:1181-1182.
11. McGregor AM, Rees Smith 8, Hall R, Petersen MM, Miller M, Dewar PJ. 1980 Prediction of relapse in hyperthyroid Graves’ disease. Lancet. l:llOl-1103.
12. Teng CS, Yeung RTT. 1980 Changes in thyroid-stimulating antibody activity in Graves’ disease treated with antithyroid drug and its relationship to relapse: a prospective study. J Clin Endocrinol Metab. 50:144-147.
13. Hardisty CA, Hanford L, Munro DS. 1981 The prediction of relapse after drug treatment of Graves’ disease by assay of long acting thyroid stimulator-protector (LATS-I’). Clin Endocrinol (Oxf). 14:509-517.
14. Madec AM, Laurent MC, Lorcy Y, et al. 1984 Thyroid stimulating antibodies: an aid to the strategy of treatment of Graves’ disease? Clin Endocrinol (Oxf). 211247-255.
15. TGtterman TH, Karlsson FA, Bengtsson M, Mendel-Hartvig I. 1987 Induction of circulating activated suppressor-like T cells by methimazole therapy for Graves’s disease. N Engl J Med. 316:15-22.
16. Orgiazzi J. 1987 Management of Graves’ hyperthyroidism. Endocrinol Metab Clin North Am. 16:365388.
17. Allannic H, Fauchet R, Orgiazzi J, et al. 1990 Antithyroid drugs and Graves’ disease: a prospective randomized evaluation of the efficacy of treatment duration. J Clin Endocrinol Metab. 70:675-69.
18. Tamai H, Nakagawa T, Fukino 0, et al. 1980 Thionamide therapy in Graves’ disease: relation of relapse to duration of therapy. Ann Intern Med. 92:488-490.
19. Romaldini JH, Bromberg N, Werner RS, et al. 1983 Comparison of effects of high and low dosage regimens of antithyroid drugs in the management of Graves’ hyperthyroidism. J Clin Endocrinol Metab. 57563-570.
20. Reinwein D, Benker G, Lazarus JH, Alexander WD, European Multicenter
Study Group on Antithyroid Drug Treatment. 1993 A prospective randomized trial of antithyroid drug dose in Graves’ disease therapy. JClin Endocrinol Metab. 76:1516.
21. Berglund J, Christensen SB, Dymling JF, Hallengren 8. 1991 The incidence of recurrence and hypothyroidism following treatment with antithyroid drugs, surgery or radioiodine in all patients with thyrotoxicosis in MalmG during the period 1970-1974. J Intern Med. 229:435-442.
22. Winsa 8, Dahlberg A, Jansson R, .&gren H, Karlsson FA. 1990 Factors influencing the outcome of thyrostatic drug therapy in Graves’ disease. Acta Endocrinol (Copenh). 122:722-728.
23. Mori Y, Matoba N, Miura S, Sakai S, Taira Y. 1992 Clinical course and thyroid stimulating hormone (TSH) receptor antibodies during surgical treatment of Graves’ disease. World J Surg. 161647-653.
24. Okamoto T, Fujimoto Y, Obara T, Ito Y, Aiba M. 1992 Retrospective analysis of prognostic factors affecting the thyroid function status after subtotal thyroidectomy for Graves’ disease. World J Surg. 16:690-696.
25. Menegaux F, Ruprecht T, Chigot J-P. 1993 The surgical treatment of Graves’ disease. Surg Gynecol Obstet. 176:277-282.
26. Sugme D, McEvoy M, Feely J, Drury MI. 1980 Hyperthyroidism in the land of Graves-results of treatment by surgery, radioiodinc and carbimazole in 837 cases. Q J Med. 4951-61.
27. Riiher H-D, Horster FA, Frilling A, Goretzki PE, Witte J. 1991 Surgery for immunogenic hyperthyroidism. Exp Clin Endocrinol. 97292-296.
28. Andaker L, Johansson K, Smeds S, Lennquist S. 1992 Surgery for hyperthyroidism: hemithyroidectomy plus contralateral resection or bilateral resection? A prospective randomized study of postoperative complications and longterm results. World J Surg. 16:765-769.
29. Tallstedt L, Lundell G, Blomgren H, Bring J. 1994 Does early administration of thyroxine reduce the development of Graves’ ophthalmopathy after radioiodine treatment? Eur J Endocrinol. 130:494-497.
30. Nofal MM, Beierwaltes WH, Patno ME. 1966 Treatment of hyperthyroidism with sodium iodide I-131. JAMA. 197:605-610.
31. Douglas JG. 1973 The Vanderbilt experience with I-131 treatment for Graves’ disease. South Med J. 6692-94.
32. Holm L-E, Lundell G, Israelsson A, Dahlqvist I. 1982 Incidence of hypothyroidism occurring long after iodine-131 therapy for hyperthyroidism. J Nucl Med. 23:103-107.
33. Holm L-E. 1982 Changing annual incidence of hypothyroidism after iodine131 therapy for hyperthyroidism, 1951-1975. J Nucl Med. 23:108-112.
34. Sridama V, McCormick M, Kaplan EL, Fauchet R, DeGroot LJ. 1984 Longterm follow-up study of compensated low-dose i3rI therapy for Graves’ disease. N Engl J Med. 311:426-432.
35. Glennon JA, Gordon ES, Sawin CT. 1972 Hypothyroidism after low-dose i3rI treatment of hyperthyroidism. Ann Intern Med. 76:721-723.
36. McGregor AM, Petersen MM, Capiferri R, Evered DC, Rees Smith B, Hall R. 1979 Effects of radioiodine on thyrotropin binding inhibiting immunoglobulins in Graves’ disease. Clin Endocrinol (Oxf). 11:437-444.
37. Hardisty CA, Fowles A, Munro DS. 1984 The effect of radioiodine and antithyroid drugs on serum long acting thyroid stimulator protector (LATS-I’). A three year prospective study. Clin Endocrinol (Oxf). 20:597-605.
38. Beth K, Nistrup Madsen S. 1980 Influence of treatment with radioiodine and propylthiouracil on thyroid stimulating immunoglobulins in Graves’ disease. Clin Endocrinol (Oxf). 13:417-424.
39. Gamstedt A, Wadman B, Karlsson A. 1986 Methimazole, but not betamethasane, prevents 13iI treatment-induced rises in thyrotropin receptor autoantibodies in hyperthyroid Graves’ disease. J Clin Endocrinol Metab. 62773-777.
40. Almqvist S, Algvere P. 1972 Hypothyroidism in progressive ophthalmopathy in Graves’ disease. Acta Ophthalmol (Copenh). 50:761-770.
41. Karlsson FA, Dahlberg PA, Jansson R, Westermark K, Enoksson P. 1989 Importance of TSH receptor activation in the development of severe endocrine ophthalmopathy. Acta Endocrinol (Copenh). 121(Suppl 2):132-141.
42. SjGberg HE, SfBf M, Bostriim L, Lundell G, Tallstedt L. 1989 Observations on progress periods in Graves’ ophthalmopathy. Acta Endocrinol (Copenh). 121(Suppl 2):179-181.
Downloaded from https://academic.oup.com/jcem/article/81/8/2986/2875682 by guest on 20 January 2023