
PAWS, PILLS, PROGRESS: THE LATEST IN VETERINARY DRUG DEVELOPMENT &

Sick puppy?
Help us stop the source.
If your client purchased a sick puppy, they can report it through our Puppy Buyer Complaint form at humaneworld.org/puppycomplaint. Information gathered guides clients on next steps they can take, and patterns of irresponsible breeding operations are recorded.
Share our flyer in your clinic and include it in client packets. Email chorning@humaneworld.org to request printed copies. Together, we can protect people and their pets.
Scan the QR code to report sick puppies
HERE WE GROW AGAIN!


Please join us in welcoming the newest full-time member of the VDS® Chadds Ford clinical team: Becca Feuer, VMD
We’re excited to share that Dr. Becca Feuer has officially joined our Chadds Ford team as a full-time veterinarian!
Dr. Feuer recently completed her residency in Dentistry and Oral Surgery right here at VDS®, and we couldn’t be more thrilled to have her continue with us in this new role.
A graduate of the University of Pennsylvania School of Veterinary Medicine, Dr. Feuer is dedicated to enhancing patients’ quality of life through advanced oral health care.
Since opening our doors in 2019, we’ve continued to grow thanks to your ongoing trust in our team. We are deeply grateful for your support and honored to provide your clients and patients with exceptional specialty care.
VDS® is the only referral practice in the nation dedicated to advanced dentistry and oral surgery for pets where a full-time board-certified veterinary dentist and a board-certified veterinary anesthesiologist are on staff to ensure the safest and most comfortable experience… and the best possible outcome.




Subscriptions:
The Keystone Veterinarian is mailed to PVMA Members at no charge as a member benefit. Subscriptions are available to non-members for $30/year or $10 for a single issue. Please contact Membership@PaVMA.org if you’re interested in receiving the Keystone Veterinarian magazine.
Notice to Readers:
Neither this publication, Hoffmann Publishing, nor PVMA assumes responsibility for material contained in articles and advertisements published, nor does publication necessarily constitute endorsement or approval of the advertiser, product, service or author viewpoint by the Keystone Veterinarian, its editors and publishers or the Pennsylvania Veterinary Medical Association. In addition, neither this publication nor PVMA guarantees the accuracy, reliability or completeness of any facts, views, opinions, recommendations, information or statements contained within this publication.
Reproduction in whole or in part is prohibited without the permission of the Pennsylvania Veterinary Medical Association.
Feline Infectious Peritonitis (FIP): From Fatal to Fixable— A New Era in Feline Care 22 Redefining Spay/Neuter with HQHVSN
A Grain of Truth: Giant Face-Eating Rats!
Now What? Bringing the Power of Large Language Models to Your Daily Practice
29 It’s Time to Rethink Client Payment Options in Your Clinic
32 Legislative and Regulatory Affairs Committee Update
34 Why Your Business Liability Insurance Needs to Keep Up with Your Medicine
36 Classified Ads
Hoffmann Publishing Group 2669 Shillington Road, #438 Sinking Spring, PA 19608 www.Hoffpubs.com
For Advertising Information & Opportunities Contact: Tracy Hoffmann, Tracy@Hoffpubs.com.
The Pennsylvania Veterinary Medical Association is dedicated to ensuring the vitality of the veterinary profession by promoting excellence in veterinary medicine, advancing animal health and welfare, and protecting and enhancing human health. PO Box 468, Elizabethtown, PA 17022 717.220.1437 | Info@PaVMA.org | PaVMA.org
EXECUTIVE COMMITTEE
President: Rhett Proctor, DVM
President-Elect: Andrea Honigmann, DVM
Vice President: Jeffrey Dill, DVM
Past-President: Thomas Munkittrick, MS,
Secretary/Treasurer: William Croushore, DVM
BOARD OF TRUSTEES
Western Region Trustee: Erin Johnson, DVM
Metro Philadelphia Region Trustee: Jill Stetz, VMD
North Central Region Trustee: Andrea Carr, DVM
South Central Region Trustee: Gary Brummel, DVM
Equine Veterinarian At-Large: James Holt, VMD
Production Animal Veterinarian At-Large: Robert Cloninger, VMD
Academic Veterinarian At-Large: Alessandro Lamacchia, VMD
Certified Veterinary Technician At-Large: Ashley Mase, CVT
AVMA Delegate: Tina Dougherty, VMD
AVMA Alternate Delegate: Kate Boatright, VMD
Student At-Large: Christian Nase

Message from the President

Rhett Proctor, DVM President, Pennsylvania Veterinary Medical Association
Change is often thrust upon us. We can choose to accept it, or we can choose to fight it. Often, we end up somewhere in the middle—fighting and accepting simultaneously. Over the past few years, the PVMA has gone through a multitude of changes. We have changed our management team and sold the office building, among others. Sometimes the changes we face are our own choosing, and sometimes they are due to circumstances we cannot control.
Such is the case with the Keystone Veterinary Conference, returning in August. After years of holding our annual conference in Hershey, the PVMA was forced to find a new venue due to huge increases in conference expenses. Had we stayed in Hershey, we would have had to either sacrifice the quality of the event or charge attendees an outrageous fee to attend.
Instead, our management team and education committee worked hard to find a new venue and settled on Harrisburg for 2025. This will allow us to provide the quality education our members and attendees have come to expect while keeping costs reasonable.
The need for a new venue, combined with the decision to reduce the number of conferences annually, has created an exciting opportunity to move the Keystone Conference around the state in future years. The education committee is already hard at work planning a phenomenal line-up of speakers for our 2026 conference in family-friendly Kalahari Resort.
The one constant in life is that change is inevitable. How we choose to accept and deal with these changes is what defines us. Hopefully this will prove to be a worthwhile change for our members and for the PVMA. New things will always offer their share of challenges, but with the right attitude, they can offer big benefits. We at the PVMA hope that you will join us in August at the Keystone Veterinary Conference as we embark down a new path with the familiar faces and quality program you have come to expect.
Rhett Proctor, DVM PVMA President

PAWS, PILLS, PROGRESS: THE LATEST IN VETERINARY DRUG DEVELOPMENT &
By Lauren Forsythe, PharmD, MBA, DICVP


You’ve graduated vet school and learned about all of the drugs being used in your clinical rotations across a variety of disciplines. Your favorite (and not so favorite) teachers explained the nuances of drug selection and why they like certain medications over others. Now you are in practice, and new drugs keep coming out. Should you use these over the ones you learned about as a student? Are these new drugs the miracle cures described by the sales reps? Are new agents worth the higher cost, and are new generics going to work as well as the good old reliable brand name product you’ve always used? These questions and more are probably circling in your head with each new drug approval. So, what is a vet to do? This article will provide you with a brief overview of some of the newest medications for small animal practice as well as tips for how to evaluate new drugs on your own when the next new agent hits the market.
Terminology
When talking about drugs and their pros and cons, it’s important to understand some key terminology, including:
• Pioneer Drug: A brand name drug approved by the Food and Drug Administration’s Center for Veterinary Medicine (FDA CVM). (In human medicine this is known as an innovator drug.)
• Generic Drug: An FDA-approved copy of a pioneer drug that has the same quality, safety, and strength.
• Unapproved Animal Drug: A medication that has not been reviewed by the FDA CVM. There are several unapproved drugs that are marketed and commonly used, including lidocaine and human phenobarbital preparations. Older drugs fit into this category because

they were “grandfathered in” when FDA-approval became required. However, when new formulations are developed, they require FDA approval.
• Conditionally Approved Drug: A medication that has provided sufficient evidence to the FDA to prove safety and provide a reasonable expectation of efficacy. However, more efficacy data is needed for full FDA approval. Medications that are given conditional approval provide a new therapy option that isn’t currently available. While conditionally approved, the drug can be legally marketed and efficacy data continues to be collected. The drug company is given five years of conditional approval to meet the requirements for full approval. If full approval isn’t obtained after five years, the drug must be removed from the market. Conditionally approved medications include ‘CA1’ after their name to indicate this status. These drugs cannot be used in an extra-label manner.
• Indexed Drug: A medication that is intended for use in non-food producing minor species, which has had its safety and effectiveness verified through an alternative FDA review process. Indexed drugs cannot be used in an extra-label manner.
• Compound: Historically, compounded medications were patient-specific preparations that were made pursuant to a prescription to meet the needs of an individual patient. However, some compounds are commonly required and it’s necessary to have them on hand for when a patient needs the medication. These office-use compounds are still compounded medications because they are not FDA-approved or grandfathered in.

New Drugs of Note
When considering new drugs, it’s important to determine if the new drug is a new dosage form of a previously available drug, a veterinary formulation of a previously available human drug, a generic form of a previously available drug, or an entirely new active ingredient. Determining which category the drug falls into will give you a lot of insight into how to proceed.
New Dosage Forms of Previously Available Drugs
For this category, you can consider these newly available dosage forms as an asset to cases where you have already been considering other dosage forms with the active ingredient. For example, methimazole oral solution (Felanorm®) and pimobendan oral solution (Vetmedin®) have recently been approved, so these liquid options may make administration more feasible for some clients and help with obtaining an appropriate dose. For this category, it’s important to note that if the dosage form is now commercially available, you cannot continue having it compounded unless there is a clinical reason why the approved product won’t work for your patient.
Veterinary Formulations of Human Drugs
For this category, you may already have been using these active ingredients in their human formulation. You can continue to do that, but the veterinary products may provide additional advantages in flavor, strength, and potentially absorption. Since the veterinary formulations have been studied in the labeled species, you have more reliable safety
A Veterinary Pharmacist’s Recommendations for Information on New Drugs
1. Promotional Material and Sales Reps: This is often one of the easiest types of information to gather. Use this to inform your initial baseline, but keep in mind that the goal of this information is to cast the drug in a positive light.
2. Drug Package Insert: The package insert information is all approved by the FDA. This information is designed to provide the drug information necessary for safe and effective use in accordance with the label. There is also summary data from safety and efficacy studies used for approval. You can find package inserts for all human and animal drugs on https://dailymed.nlm.nih.gov/dailymed/.
3. Specialists and Key Opinion Leaders: These individuals are often providing webinars, conference presentations, and editorial articles on new drugs. This can be a great source of information, but consider whether the presentation is sponsored by the drug company. Sponsored specialists can still provide valuable insight, but keep in mind that they may be prone to limit any negative comments.
4. Research Manuscripts: Formal research manuscripts can provide valuable information on drugs and many journals are becoming more open access, making these articles available to anyone.
5. Freedom of Information (FOI) Summaries: These are documents summarizing the information used for drug approval. They can be found on the Animal Drugs @ FDA webpage as a link at the top of the summary for each approved drug.
6. Anecdotal Opinions: These can be found wherever you like to chat with veterinary colleagues. Find out if others are using new drugs and what their experience has been. If you ask enough people, you will often start to see a trend emerge on what is actually happening in the trenches and how it compares to the carefully crafted studies.
7. FDA Animal Drug Safety-Related Labeling Changes: You can find information on safety-related labeling changes to animal drugs at https://www.fda.gov/animal-veterinary/ drug-labels/animal-drug-safety-related-labeling-changes. Labeling changes often occur after the drug has been used enough that additional adverse effects or human safety concerns have come to light.
Paws, Pills, and Progress: The Latest in Veterinary Drug Development

and efficacy data for using these formulations. As with the previous category, you cannot continue having these drugs compounded unless there is a clinical reason why the approved product won’t work for your patient. Some recent approvals in this category include pregabalin oral solution (Bonqat®), torsemide oral solution (UpCard-CA1®), and sirolimus delayed release tablets (Felycin-CA1®).
Generic Form of a Previously Available Drug
When a new generic medication is available and labeled for veterinary patients, you have the FDA approval process backing the fact that the generic will work equivalent to the brand name product in the labeled species. In those cases, there might be a packaging advantage, but otherwise, reach for the least expensive option. One example in this category is a new generic option for enrofloxacin flavored tablets that was approved in March of this year. It’s important to note that safety and efficacy data is collected only for the labeled species, so there is no guarantee that the generic product will work the same as the brand name when used off-label for another species.
Entirely New Active Ingredient
These are the drugs that could be game changers in treating our patients, but they also come with some uncertainty. In these cases, you need to do your research and proceed with informed use. Before the drugs reach the market, they have gone through extensive safety and efficacy studies in line with the labeling to gain FDA approval. That provides some level of assurance when using in accordance with how they are labeled. However, some side effects only come to light after approval due to their low incidence. A recent example in this category is ilunocitinib (Zenrelia®) which is labeled for controlled itch associated with allergic dermatitis and atopic dermatitis. Ilunocitinib is a
Janus Kinase (JAK) inhibitor, putting it into the same class as oclacitinib (Apoquel®). One head-to-head study of these two drugs showed that Ilunocitinib was more effective at decreasing itching than oclacitinib.1 With drugs in the same classes, you can often make initial assumptions about similar efficacy and adverse effects and then adjust those as clinical experience (yours and that of colleagues) adds to the available data.
Conclusion
New drugs are frequently coming to market with labels for veterinary patients. Sorting them into the four categories described here can make them seem a bit less overwhelming and help focus your research time to determine if you will prescribe and/or stock new drugs in your hospital. See page 7 blue box for a list of resources to consider when collecting information on new drugs.
References
1. Forster S, Boegel A, Despa S, Trout C, King S. Comparative efficacy and safety of ilunocitinib and oclacitinib for the control of pruritus and associated skin lesions in dogs with atopic dermatitis. Vet Dermatol. 2025 Apr;36(2):165-176. doi: 10.1111/vde.13319. Epub 2025 Jan 6. PMID: 39757965; PMCID: PMC11885073.
About the Author: Dr. Lauren Forsythe is an Assistant Professor at the University of Findlay College of Pharmacy. She is also a diplomat of the International College of Veterinary Pharmacists. After spending eight years in veterinary teaching hospitals doing pharmacy tasks, she developed her consulting company Foresight Pharma Solutions, LLC to help veterinarians in non-academic practice settings with their pharmacy-related needs such as controlled substance security. continued from page 7

Improving Profitability and Sustainability in Large Animal Practice

By Jody A. Kull, DVM
Working in the rural mixed/large animal veterinary medicine sector is extremely meaningful and rewarding for many unique reasons. It can also be physically demanding and emotionally taxing at times, leading to retention challenges and rural veterinary shortages. So how do you balance the windshield time between farm stops, the physical challenges of large animals, work-life balance, and a profitable and sustainable business model?
It can be done successfully! It is possible to practice veterinary medicine with producers who value both your knowledge and skill. One way to thrive as a veterinarian in your rural community is to shift to a more consultative role by utilizing your education and critical thinking skills.
One of my veterinary mentors once asked me what role I wanted to be on the farm for the producer. When I step out of the vehicle, what does the producer see? If I want to be a reproduction vet, I grab my ultrasound first. If I want to be a herd health veterinarian, I take my castration and vaccine toolbox. But, if I want to be a consultative partner for the producer, I need my brain. If I want to
continued on next page >

Evaluating milking procedures improves milk quality and ensures producer and animal safety and welfare. Creating a small ruminant neonatal protocol with producer training can help reduce emergencies.

Improving Profitability and Sustainability in Large Animal Practice
continued from page 9


be utilized for my veterinary knowledge, I have to put on my thinking cap when I arrive at the farm and tactfully look for ways the farmer can improve. I can always go back and grab the castration equipment if that is what I was called to the farm to do by the producer.
Making the transition to a more consultative role is not a departure from clinical work but rather an extension of it. It challenges you to become a strategic partner with the producer and their business. This can be achieved with producers of all sizes and species whether it is one pet, a menagerie of critters, or 1000 cows. Your collective goals should be to mitigate disease risks and avoid after-hours emergencies, both of which would ensure the long-term business success of both parties.
This model of veterinary practice allows you to offer tailored guidance to producers on disease surveillance, herd health planning, nutritional management, reproductive efficiency, and long-term animal health and welfare to allow them to make better, more informed decisions. It requires time, thought, and trust. These are things you already bring to the table, but too often give away without compensation. Clients do value your service and your knowledge! When you begin to recognize and charge for this “intellectual labor,” you create a practice model that is not only more sustainable for you, but more valuable for your clients.
Practical Examples
At a dairy farm, this could be walking into the office first to look at the herd records on the computer or paper, asking about somatic cell count, or challenges in the field planting this season. Alternatively, you could ask a farmer or employee what they recently read in trade magazines to open a new discussion topic. Strive to be their educational resource. And, yes, it is okay to bill for the conversations as a consultative line item in the invoice. Document the conversation, including notes about how to utilize the ideas on the farm in the future to encourage the dialogue to continue. Utilize the network of experts in the industry including the PSU veterinary extension group, pharmaceutical technical services veterinarians, or PA Center for Dairy Excellence (CDE) for additional consultative help.
For example, CDE rolled out a grant program this spring for veterinarians to help write biosecurity plans on dairy farms—a billable service for veterinarians. The grant provided a comparable hourly billable rate to veterinarians to save farmers the cost and showcase the relationship of veterinarians and biosecurity. What a great way to step into consulting! Writing a biosecurity plan provides you with the key topics to focus on and discuss on farms and add to the service in the future. Bill for the service and offset the charge through the grant program.
Another example can be seen in the growing small ruminant community. Small ruminant management provides ample opportunity for consultation services including hoof health and trimming education, nutritional management, neonatal health, and biosecurity protocols with neighboring goat farms that share breeding bucks. Parasite management is always an opportunity for education on farms—fecal egg count reduction samples, customized deworming protocols, FAMACHA score training, and integrated pest management.
Consultative veterinary medicine also creates opportunities to provide on-farm training—another often-overlooked service that clients value when presented clearly. For the beef farmer, Beef Quality Assurance (BQA) training allows you to guide producers through best practices in animal welfare and handling, recordkeeping, and improving carcass quality. At the Keystone Veterinary Conference in August, the PA Beef Council will be providing CE lectures on how to add BQA to your consultative toolbox as a veterinarian to mitigate disease risk for producers.
These are not hypothetical services. They are practical billable services utilizing your critical thinking skills as a veterinarian. Producers do see the value of these services! You build longerlasting, more collaborative relationships with clients that allow you to thrive long-term in rural veterinary medicine. Allow producers to see you as a strategic partner in their herd’s
Beef Quality Assurance training and handling facility assessment improves animal welfare and meat quality.


Utilize time in the dairy farm office to analyze computer records to improve animal health. Be sure to bill for this consulting service to show the value of your knowledge.
success and not just the emergency physical labor on the other end of the phone when they need it.
Creating Sustainable Practices
Adding consultative services to your veterinary toolbox in practice allows you to open the door to diversifying your practice offerings. Start small with a couple of clients and allow the services to grow organically within your practice. These additions will help you stay competitive in the industry, create value that goes beyond the transactional model of “call, treat, bill,” and make you indispensable in the community as a partner in the success of the farm. As a bonus, by focusing on prevention, planning, and mitigating risk, you reduce the number of unpredictable emergency calls. This practice model is ultimately more sustainable by alleviating the physical strain and long hours by shifting towards maximizing your problemsolving skills and education.
So, my question to you is What veterinary role do you want to have on the farm when YOU step out of the vehicle?
About the Author: Dr. Kull owned Valley Mobile Veterinary Service, a mobile food animal veterinary business serving Montour and surrounding counties She focused on producer, student, and community education. In 2023, after 19 years in clinical practice, Dr. Kull joined the Department of Veterinary & Biomedical Sciences at Penn State University as an Assistant Teaching Professor. She enjoys teaching and advising pre-veterinary students. She has been a Veterinary Ambassador for the Farm Journal Foundation since 2022.

Helping veterinary practices succeed

Ripples inthe Pond:
The Evolution of Veterinary Palliative Care

By Lynn Hendrix, DVM, CHPV

Veterinary medicine is constantly evolving, with an increasing focus on specialized care that mirrors advancements in human healthcare. Veterinary palliative care, a discipline committed to enhancing the quality of life for chronically and terminally ill animal patients, is an area experiencing substantial growth and recognition. Like other areas of veterinary medicine, palliative care encompasses a spectrum of services and is now expanding into a more specialized form of care.
Much like in human medicine, veterinary palliative care is most frequently administered within the familiar environment of a pet’s home—prioritizing comfort, pain, and symptom management for patients while offering emotional and physical support to the dedicated family. Advanced communication proficiencies are crucial for palliative care as the focus shifts from curing to comfort. Evidence-based medicine is utilized,
often translating from human palliative medicine due to a lack of veterinary evidence.
General practitioners and specialists can support clients and patients facing end-of-life decisions by offering additional support from hospice and palliative care practitioners, who possess advanced training in end-of-life care.
Olivia’s Story: A Case Study in Compassionate Care
Consider the case of Olivia, a beloved 12-year-old female spayed Golden Retriever. Her diagnosis of osteosarcoma brought a wave of fear and uncertainty to her family. As a palliative veterinarian, my role was to provide in-home care, offering a lifeline of comfort and support during this challenging time.

a retire so both the practice and real estate are for sale. (PA311)
PA: Eastern - Established companion animal practice in the Bethlehem-Allentown area It is a growing 2 doctor practice with revenues approaching $2 million The practice is housed in a free-standing building that is well-equipped and conveniently located within the community The owner is retiring so both the practice and real estate are for sale (PA324)
PA: Western - Solo small animal practice located only a couple of miles from the PAOH border This is an established practice with over 60 years history of providing veterinary care throughout the area It is housed in an attractive 2,200 sq ft facility with all the usual amenities and room for future growth Both the practice and real estate are for sale (PA410)
PA: Central - Small animal practice located in the vibrant and growing area of Carlisle The practice is housed in a 4,800 sq ft facility that is well-equipped and has room for growth Both the practice and real estate are for sale (PA520)

Current practices for sale in the Pennsylvania Area
PA: Central - New!!! Established, small animal hospital closely located to I-99 which makes it an easy commute to Altoona, State College, Hollidaysburg and on to Pittsburgh and DC-Baltimore The practice is housed in a 2,000 sq ft facility that has been well-maintained and is well-equipped The owner is ready to retire so both the practice and real estate are for sale (PA435)
PA: Southeast - New!!! Small animal practice located in the Route 30 corridor west of Philadelphia It is a fully equipped practice that provides full diagnostic medical/surgical and wellness care to pets in the region It is profitable with very nice cash flow to the owner The practice is housed in a large facility with plenty of parking for staff and clients It has 4 exam rooms and plenty of space for future growth Both the practice and real estate are for sale and the owner is open to staying post-closing on a part-time schedule to help with the transition (PA438)
PA: Eastern - Established, small animal hospital located in eastern, PA near the PA-MD border You could live in either state! The practice is housed in an attractive free-standing, leased facility that has a very good location with easy access for all current and future clients The owner is ready to retire so the practice is for sale The owner will help with the transition (PA437)
PA: Western - Small animal hospital east of Pittsburgh PA The practice is located on the periphery of Indiana, PA It is housed in a large 7,500 sq ft facility with 4 exam rooms - great opportunity for growth! It is well-equipped and utilizes the Avimark practice management system A long term lease will be provided for the real estate with a right of first refusal (PA503)
PA: Southeast - Do you own a practice in southeast, PA and want to add holistic, herbal and acupuncture services for your clients? This is a great opportunity This practice has an established client base with excellent cash flow (PA515)
When I first met Olivia, her pain was evident. Her once-robust appetite had diminished, and while she still yearned for her walks and the thrill of chasing squirrels, her endurance and speed were significantly reduced. Her family sought guidance on additional treatment options—desperate to alleviate her suffering but not yet ready to make an end-of-life decision. Olivia was receiving standard pain medications from her primary veterinarian, including carprofen and gabapentin, and had recently started subcutaneous, subanesthetic ketamine, all of which we continued.
We discussed the family’s current worries and fears for the future. We discussed their goals of care for Olivia. I educated them on the anticipated trajectory for her specific disease, chronic pain signs, and how to monitor both physical and emotional quality of life. We talked about quality of life for the family and how caregiving for a terminal patient can be challenging. In addition, we added tools, including apps like Vetpain and Cardalis. We talked about anticipatory grief, and how that affects decision making. Our team provided grief support and other client education handouts. Then we shifted to creating a daily plan that they felt comfortable with—a plan for crisis management.
Since pain is difficult to manage with osteosarcoma and recognizing that Olivia’s current regimen wasn’t providing adequate relief, I opted for a more aggressive, evidencebased approach, drawing inspiration from advancements in human palliative medicine. I incorporated a bisphosphonate, zoledronate, and LibrelaTM, an anti-Nerve Growth Factor monoclonal antibody, into her treatment plan.1-3
Bisphosphonates have a strong research foundation in both human and canine osteosarcoma, demonstrating their efficacy in managing pain and improving bone health. In human medicine, there is some indication zoledronate may also slow the progression of metastasis.2 LibrelaTM, a newer therapeutic, targets nerve growth factor, a key mediator of pain, offering another avenue for relief.4
This more tailored approach, based on the latest scientific understanding, aimed to significantly improve Olivia’s comfort and quality of life. And it worked. Dogs who just have the standard pain management often limp or become non-weight bearing. For Olivia, while it didn’t slow metastasis, this protocol allowed her to remain more active and weight-bearing on the limb. In addition to the daily medicine plan, we created a crisis plan, and gave the clients a significant amount of education, continued on next page >
**Photo by Dr David King, DVM, CVA
Ripples in the Pond: The Evolution of Veterinary
Palliative Care
continued from page 13


including an advanced directive, when to call, what distress would likely look like, disease trajectories and more.
Incorporating Palliative Care in Practice
Appointments like Olivia’s take a significant amount of time. Some clinicians are spending 2-3 hours to provide this advanced care, which is understandably beyond the capabilities of a standard general practice appointment. Veterinarians who want to provide this option should consider the amount of time this care takes and consider providing a referral option early in the course of disease. Palliative care can operate alongside curative medicine, prioritizing comfort. Later in the course of the disease, care can shift more towards comfort than cure.
Dr. Stephanie Freed of Golden Years Veterinary Services wants colleagues to know that palliative medicine is not meant to allow pets to suffer or only helpful for clients who aren’t ready to “let go.” On the contrary, palliative care is actually the antidote to unnecessary suffering at the end of life.
Freed believes that, “If we took an honest look as a profession at the patients that present for euthanasia, we’d see a majority come in grossly under-treated. Palliative medicine

100% Manufactured following FDA enforced regulations
Longer dating in comparison to other Buprenorphine alternatives
Tested for potency and sterility following FDA regulations
Less expensive per mg than other products on the market

provides our clients with the tools and education to know what signs and symptoms to monitor for, which can and should be addressed, and how to proactively track quality of life.”
With the addition of palliative and hospice care, “Clients are often able to process and feel supported in their pet’s transition, allowing them to feel more at peace with making the decision for humane euthanasia before it’s a crisis moment,” continues Freed.
If you are looking to add palliative care to your practice, remember that it is more than multi-modal pain and symptom management to improve patient comfort. It includes extensive client support as well, as Caregiving for terminal pets is a challenging endeavor that can be physically and emotionally taxing. Veterinary teams should focus on improving serious disease communication skills, adding resources to support clients such as advanced directives and crisis management plans, and gaining counseling skills.
Instead of trying to do this all yourself, consider adding or partnering with a colleague who has done post-grad study in either human palliative care or is IAAHPC-certified.
References
1. Lopes MG, Tosi G, McNaught KA, et al. Retrospective assessment of tolerability and efficacy of zoledronate in the palliative treatment



of cancer-bearing dogs. Aust Vet J. 2023;101(1-2):58-64. doi:10.1111/ avj.13218
2. Lorange JP, Ramirez Garcia Luna J, Grou-Boileau F, et al. Management of bone metastasis with zoledronic acid: A systematic review and Bayesian network meta-analysis. J Bone Oncol. 2023;39:100470. Published 2023 Feb 9. doi:10.1016/j.jbo.2023.100470
3. Williams K, MacDonald-Dickinson V. Progress in palliation: Managing pain caused by cancer in veterinary medicine. Can Vet J. 2023 Aug;64(8):789-791.
4. Enomoto M, Mantyh PW, Murrell J, et al. Anti-nerve growth factor monoclonal antibodies for the control of pain in dogs and cats. Vet Rec. 2019;184(1):23. doi:10.1136/vr.104590
About the Author: Dr. Lynn Hendrix is a passionate leader on the cutting edge of the animal hospice and veterinary palliative medicine field. She developed her own palliative practice and is certified in Hospice and Palliative Care though the IAAHPC. She began volunteering for the IAAHPC in 2012, and was a co-author on the 2013 IAAHPC guidelines for best practices in animal hospice and palliative care. She is the founder of the Facebook group, the Veterinarian Palliative Medicine group, with 6000 veterinarians from around the world. She is the founding consultant for the Hospice and Palliative medicine folder on VIN. Dr. Hendrix also wrote a textbook, Animal Hospice and Palliative Medicine for the House Call Veterinarian, and has 3 more textbooks in development. She also has an upcoming chapter in the Small Animal Veterinary Nerdbook, 4th edition.

Navigating Employment Laws in a Veterinary Practice

By Jeremy Farrell, Esq.
Veterinary practices can be as different as the animals they care for. They range from solo and small practices to large, multistate enterprises, with employees of varying skillsets, job responsibilities, and compensation levels. Understanding and complying with the many employment laws that regulate the modern workplace can be especially difficult in such a setting, whether it is a family practice with limited resources or a large employer managing hundreds of employees across state lines.
Highlighted below are some issues that veterinary practices operating in the Commonwealth of Pennsylvania must keep top-of-mind.
Onboarding and Hiring Considerations
Veterinary practices often experience staffing shortages, which can lead to a rushed onboarding process that creates unnecessary risks. Consider the following:
• Restrictive Covenants of Incoming Employees: Be mindful that those you hire may owe obligations to their former employers to not solicit their customers or to compete at all within a particular market location and that you can be liable if you knowingly interfere with those contractual commitments. Including language in offer letters compelling the disclosure of such obligations helps you identify potential problems at the outset, before they snowball into potentially costly legal disputes with your competitor. Reinforcing your new hire’s obligation to comply with any preexisting restrictive covenants in an employment agreement offers an additional layer of protection.
• Employment Agreements: Employment agreements should include provisions addressing standard employment terms as well as industry-specific concerns:
ο Create clearly defined compensation requirements and triggers, including setting objective parameters for production-based compensation.
ο Assess and implement reasonable restrictive covenants, if appropriate. Since veterinarians are not within the scope of Pennsylvania’s Fair Contracting for Health Care Practitioners Act, veterinary practices are free to include non-compete, non-solicit, and non-disclosure protections in their employment agreements for higher level employees, those with access to sensitive information, or those who manage particularly important customer relationships— so long as those provisions are reasonable under the circumstances and tailored to address the company’s legitimate business interests.
ο Address liability and malpractice coverage matters, including tail coverage for claims-made policies.
• Expanding Marijuana Laws: For almost a decade, Pennsylvania law has made one’s status as a certified medical marijuana cardholder a legally protected category. Since then, local laws in Pittsburgh and Philadelphia have placed restrictions on an employer’s ability to conduct pre-employment tests for marijuana.
Employee Accommodations
Veterinary practices, like other employers, must provide reasonable accommodations under federal laws (assuming they have more than 15 employees), including the Americans with Disabilities Act (ADA), Title VII of the Civil Rights Act of 1964, and the Pregnant Workers Fairness Act (PWFA). Smaller companies with more than four employees may also have to provide accommodations under the Pennsylvania Human Relations Act.


Under the ADA, accommodations must be explored with qualified employees with physical or mental impairments that limit the ability to do certain major life activities. Title VII may require accommodations for religious beliefs, such as scheduling adjustments. The PWFA mandates accommodations be provided to employees with known limitations related to pregnancy, childbirth, or related medical conditions, even if those limitations do not rise to the level of a disability.
Beyond that, employers need to understand that accommodation laws are inherently process-oriented, meaning that employers must generally work with employees cooperatively and to try to find an accommodation that helps the employee navigate his or her specific limitation.
Wage and Hour Practices
Veterinary practices can face significant wage and hour compliance risks, particularly related to employee classification and overtime. Misclassifying vet techs or assistants as exempt from overtime when they do not meet the specific requirements of the Fair Labor Standards Act (FLSA) could lead to private lawsuits or an investigation by the Department of Labor.
Veterinary practices must also ensure that all hours worked are accurately recorded, including time spent after hours completing charts, handling emergencies, or cleaning. This risk is particularly heightened in Pennsylvania, which has a broad obligation to pay employees for all “hours worked,” which is defined as follows:
Hours worked: The term includes time during which an employee is required by the employer to be on the premises of the employer, to be on duty, or to be at the prescribed work place, time spent in traveling as part of the duties of the employee during normal working hours, and time during which an employee is employed or permitted to work; provided, however, that time allowed for meals shall be excluded unless the employee is required or permitted to work during that time, and provided further, that time spent on the premises of the employer for the convenience of the employee shall be excluded (34 Pa. Code 231.1).
Employee Handbooks
Though often overlooked or left outdated, employee handbooks remain an effective way for veterinary practices, like all other businesses, to define the rules of the workplace, outline employee expectations, and potentially establish legal defenses that may be of use if litigation arises. Important policies to consider including in an employee handbook include:
• A procedure for handling investigations into employee complaints of discrimination, harassment, retaliation, or other matters, such as pay-related complaints.
• A policy for responding to reasonable accommodation requests.
• A substance abuse policy.
• Timekeeping policies for non-exempt employees that require accurate recording of all hours worked and prohibit off-the-clock work and unauthorized overtime.
• A policy prohibiting improper deductions from pay and providing employees with an effective way to raise concerns about potentially improper deductions or other issues affecting their paycheck.
• Company policy for animal care and safety, including handling and restraint protocols, use of PPE, reporting animal bites or injuries, and medication handling and storage.
About the Author: Jeremy Farrell, Esq., is an experienced management-side employment and litigation attorney who helps businesses resolve legal issues both inside and outside the courtroom. As Deputy Chair of Tucker Arensberg’s Litigation Department, Jeremy represents employers in a wide range of employment law matters, including discrimination, retaliation, wage and hour compliance, and restrictive covenants, and regularly advises clients on workplace policies, risk management, and compliance. Contact Jeremy at jfarrell@tuckerlaw.com or (412) 594-3938.




August 14 – 17 | Harrisburg, PA
Registration Now Open!
November 8 – 9 | Mars, PA
Details Available online
PVMA is thrilled to welcome Dr. Temple Grandin as this year’s keynote presenter.
Scan this code to access the PVMA calendar of events and online registration.
If her name sounds familiar, it could be because an HBO movie titled Temple Grandin was made about her life. In addition, Temple has been inducted into The National Women’s Hall of Fame and The Academy of Arts and Sciences. While many people know her from her work in the field of autism research, she has also made significant contributions to the world of animal care as well. Facilities she has designed handle more half the cattle in the United States. She has stated that caring for and riding horses helped her manage difficult teenage years when she was bullied and teased.
At the conference, Temple will present a session titled Animals Make Us Human. As Temple puts it, “To understand animals, you have to get away from words. The animal world is a sensory based world. Their memories are detailed pictures, sounds, smell, and other sensory impressions. This talk will help you understand animals but it will also give you insights into solving problems.”
Speaker Spotlight: Dr.GrandinTemple
August 14 – 17 | Harrisburg, PA
Registration Now Open!
About Temple Grandin
November 8 – 9 | Mars, PA
Details Available online
Temple Grandin is a professor of animal science at Colorado State University. When she was two and a half years old, she had no speech and all the symptoms of severe autism. Early intensive speech therapy enabled her to speak by age four. Her mother always encouraged her interest in art and urged her to draw many different things. Good teachers and mentors were essential for Temple’s success. Her high school science teacher challenged her with interesting projects where she had to figure out how to make things work. When studying in school became a pathway to becoming a scientist, she was motivated to study. Some of her most important books are New York Times Bestseller “Animals in Translation,” “Thinking in Pictures,” “The Autistic Brain,” and “The Way I See It.”

Scan this code to access the PVMA calendar of events and online registration.
A ticket for this keynote presentation is included with every full conference registration. Guest tickets can be purchased separately.
Scan to register
FELINE INFECTIOUS PERITONITIS (FIP): From Fatal to Fixable— A New Era in Feline Care

By Carrie Goldkamp, VMD, DACVIM, Small Animal Internal Medicine
Feline infectious peritonitis (FIP) is a fatal infectious disease in cats and has historically been a cause of feline death worldwide. Although diagnosis remains challenging, recent advances in antiviral therapy have significantly improved the prognosis.

Pathogenesis
FIP is caused by feline coronavirus (FCoV), an enveloped, positive-stranded RNA virus with a high mutation rate due to its error-prone RNA polymerase.
FCoV exists in two biotypes: feline enteric coronavirus (FECV), which causes mild gastrointestinal symptoms, and feline infectious peritonitis virus (FIPV), the mutated, virulent form that leads to FIP.1,2 FECV is widespread in multi-cat settings, transmitted via the fecaloral route, and shed in feces for several weeks (and in about 13% of cats, for life).3,4 Kittens less than one year of age are 2.5 times more likely to shed than adults and will shed higher loads.5
Only a small percentage (<10%) of FECV-infected cats develop FIP.6,7 due to mutation that enables viral replication in monocytes/macrophages rather than enterocytes.8-10 This shift causes an immune-mediated pyogranulomatous vasculitis,8 leading to protein-rich effusions. FIP is classified as effusive ("wet") or noneffusive ("dry"), though noneffusive cases can become effusive as the disease progresses.11,12
Diagnosis
FIP diagnosis is challenging and often presumptive, based on history, clinical signs, laboratory data, and FIP-specific testing. Definitive diagnosis requires immunohistochemistry to detect virus within macrophages, typically via invasive tissue sampling.13,14
FIP is more common in cats <2 years old, purebreds, and those from multi-cat environments.6, 15-19 Recent stressors (e.g., adoption, surgery, infection) and retroviral co-infections increase risk.16, 20,21 Males may be slightly predisposed.16-19
Nonspecific clinical signs include lethargy, anorexia, weight loss, and fever.16,20,22 Common findings are effusions (abdominal, thoracic) and signs of pyogranulomatous inflammation (e.g., uveitis, neurologic signs, abdominal masses or organ enlargement, skin nodules).16, 20, 22-26
A CBC may have nonspecific findings such as mild nonregenerative anemia, intermittent neutrophilia, or thrombocytopenia.16
continued on next page >
Feline Infectious Peritonitis (FIP): From Fatal to Fixable— A
New Era in Feline Care
continued from page 19

Common serum biochemical findings include hyperbilirubinemia, hyperglobulinemia, and hypoalbuminemia.16,29 An A:G ratio <0.4 supports FIP; >0.6 makes it unlikely.19,29,30 An acute phase protein, alpha-1-acid glycoprotein (AGP), >3 g/L is strongly associated with FIP.31,32
There is overlap between FCoV antibody levels in FIP and non-FIP cats, limiting the diagnostic use of serology.33 While a negative result makes FIP unlikely,34 some cats—especially those with neurologic involvement—may test negative.35 Similar to serum antibody testing, fecal testing for FCoV is not useful for FIP diagnosis.
FIP effusions are typically high in protein (>3.5 g/dL), have low A:G ratio (<0.4), and have a low cell count (<5,000/mL).16, 37 FIP is unlikely if protein <2.5 g/dL, A:G >0.8, or cell count >20,000/mL in an effusion. A negative Rivalta test makes FIP very unlikely.38 CSF analysis may show protein levels >2 g/dL and neutrophilic pleocytosis.39 RT-PCR or immunostaining for FCoV can support an FIP diagnosis.
RT-PCR detects viral RNA in fluids or tissues, but due to the virus’ frequent mutations, RT-PCR may not amplify all FCoVs.40,41,42 Quantitative PCR (RT-qPCR) detects the amount of virus in a sample. High viral loads are more consistent with FIP.42
An online FIP diagnostic tool is available at abcdcatsvets.org to assist clinical decision-making.
Treatment
First-line treatment involves nucleoside analogs that inhibit viral RNA replication. While no FDA-approved drugs exist, compounded formulations are widely used.
GS-441524, the active metabolite of remdesivir, is available orally and is the preferred treatment. Remdesivir (injectable) is an alternative. Both disrupt viral replication and achieve 80–100% survival rates for both effusive and noneffusive FIP.27,43,47 GS441524 is safer and better tolerated.37,43 Side effects include mild ALT elevations and urolithiasis (especially at high doses).37,46,49,50 Remdesivir injections can be painful and cause skin ulceration in up to 50% of cases.37,47 Remdesivir may be used if a cat does not respond to GS-441524, as there are anecdotal reports of rapid metabolism.
It is advised to start with once daily dosing of GS-441524. If there is not a response, divide the dose and give twice daily. Noneffusive FIP warrants a higher dose. Unlicensed formulations should not be used, as they have been found to contain much different amounts than advertised.51
Molnupiravir (EIDD-2801), another nucleoside analog, introduces copying errors during viral replication. It has been used in humans for treatment of COVID-19. Reports indicate that it is similarly effective but has a higher side-effect profile, including nausea, vomiting, transient liver enzyme elevation, leukopenia, tremors, and teratogenicity. 48,49 Caution is advised for pregnant owners due to reproductive risks. Its mutagenic mechanism also raises concerns about potential viral evolution.
Prognosis
FIP, once terminal, now has a favorable prognosis with nucleoside analogue treatment. Relapse risk is highest in the first three months post-treatment.52
References
1. Poland AM, Vennema H, Foley JE, Pedersen NC. Two related strains of feline infectious peritonitis virus isolated from immunocompromised cats infected with a feline enteric coronavirus. J Clin Microbiol. 1996;34(12):3180-3184.
2. Gao YY, Wang Q, Liang XY, et al. An updated review of feline coronavirus: Mind the two biotypes. Virus Res. 2023;326:199059.
3. Addie D. Feline coronavirus infections. In: Greene CE, ed. Infectious Diseases of the Dog and Cat. St Louis, MO: Elsevier; 2012:92-108.
4. Addie DD, Jarrett O. Use of a reverse-transcriptase polymerase chain reaction for monitoring the shedding of feline coronavirus by healthy cats. Vet Rec. 2001;148(19):649-653.
5. Klein-Richers U, Hartmann K, Hofmann-Lehmann R, et al. Prevalence of feline coronavirus shedding in German catteries and associated risk factors. Viruses. 2020;12(9):1000.
6. Addie DD, Toth S, Murray GD, Jarrett O. Risk of feline infectious peritonitis in cats naturally infected with feline coronavirus. Am J Vet Res. 1995;56(4):429434.
7. Foley JE, Poland A, Carlson J, Pedersen NC. Risk factors for feline infectious peritonitis among cats in multiple-cat environments with endemic feline enteric coronavirus. J Am Vet Med Assoc. 1997;210(9):1313-1318.
8. Kipar A, May H, Menger S, et al. Morphologic features and development of granulomatous vasculitis in feline infectious peritonitis. Vet Pathol. 2005;42(4):321-330.
9. Malbon AJ, Michalopoulou E, Meli ML, et al. Colony stimulating factors in early feline infectious peritonitis virus infection of monocytes and in end-stage feline infectious peritonitis; a combined in vivo and in vitro approach. Pathogens. 2020;9(11):893.
10. Dewerchin HL, Cornelissen E, Nauwynck HJ. Replication of feline coronaviruses in peripheral blood monocytes. Arch Virol. 2005;150(12):24832500.
11. Hartmann K. Feline infectious peritonitis. Vet Clin North Am Small Anim Pract. 2005;35(1):39-79.
12. Pedersen NC. An overview of feline enteric coronavirus and infectious peritonitis virus infections. Feline Pract. 1995;23(1):7-20.
13. Stranieri A, Scavone D, Paltrinieri S, et al. Concordance between histology, immunohistochemistry, and RT-PCR in the diagnosis of feline infectious peritonitis. Pathogens. 2020;9(9):852.
14. Giordano A, Paltrinieri S, Bertazzolo W, et al. Sensitivity of Tru-cut and fine needle aspiration biopsies of liver and kidney for diagnosis of feline infectious peritonitis. Vet Clin Pathol. 2005;34(4):368-374.
15. Pesteanu-Somogyi LD, Radzai C, Pressler BM. Prevalence of feline infectious peritonitis in specific cat breeds. J Feline Med Surg. 2006;8(1):1-5.
16. Riemer F, Kuehner KA, Ritz S, et al. Clinical and laboratory features of cats with feline infectious peritonitis—A retrospective study of 231 confirmed cases (2000–2010). J Feline Med Surg. 2016;18(4):348-356.
17. Rohrbach BW, Legendre AM, Baldwin CA, et al. Epidemiology of feline infectious peritonitis among cats examined at veterinary medical teaching hospitals. J Am Vet Med Assoc. 2001;218(7):1111-1115.
18. Worthing KA, Wigney DI, Dhand NK, et al. Risk factors for feline infectious peritonitis in Australian cats. J Feline Med Surg. 2012;14(6):405-412.
19. Norris JM, Bosward KL, White JD, et al. Clinicopathological findings associated with feline infectious peritonitis in Sydney, Australia: 42 cases (1990–2002). Aust Vet J. 2005;83(10):666-673.
20. Pedersen NC. A review of feline infectious peritonitis virus infection: 19632008. J Feline Med Surg. 2009;11(4):225-258.
21. Vennema H, Poland A, Foley J, et al. Feline infectious peritonitis viruses arise by mutation from endemic feline enteric coronaviruses. Virology. 1998;243(1):150-157.
22. Kipar A, Meli ML. Feline infectious peritonitis: still an enigma? Vet Pathol. 2024;51(5):505-526.
23. Stiles J. Ocular manifestation of feline viral diseases. Vet J. 2014;201(2):166173.
24. Foley JE, Leutenegger C. A review of coronavirus infection in the central nervous system of cats and mice. J Vet Intern Med. 2001;15(5):438-444.
25. Doenges SJ, Weber K, Dorsch R, et al. Detection of feline coronavirus in cerebrospinal fluid for diagnosis of feline infectious peritonitis in cats with and without neurologic signs. J Feline Med Surg. 2016;18(2):104-109.
26. Harvey CJ, Lopez JW, Hendrick MJ. An uncommon intestinal manifestation of feline infectious peritonitis: 26 cases (1986–1993). J Am Vet Med Assoc. 1996;209(7):1117-1120.
27. Yin Y, Li T, Wang C, et al. A retrospective study of clinical and laboratory features and treatment on cats highly suspected of feline infectious peritonitis in Wuhan, China. Sci Rep. 2021;11(1):5208.
28. Cannon MJ, Silkstone MA, Kipar AM. Cutaneous lesions associated with coronavirus-induced vasculitis in a cat with feline infectious peritonitis and concurrent feline immunodeficiency virus infection. J Feline Med Surg. 2005;7(5):233-236.
29. Tsai HY, Chueh LL, Lin CN, et al. Clinicopathological findings and disease staging of feline infectious peritonitis: 51 cases from 2003 to 2009 in Taiwan. J Feline Med Surg. 2011;13(1):74-80.
30. Sparkes AH, Gruffydd-Jones TJ, Harbour DA. Feline infectious peritonitis: a review of clinico-pathological changes in 65 cases, and a critical assessment of their diagnostic value. Vet Rec. 1991;129(7):209-212.
31. Paltrinieri S, Giordano A, Tranquillo V, et al. Critical assessment of the diagnostic value of feline alpha1-acid glycoprotein for feline infectious peritonitis using the likelihood ratios approach. J Vet Diagn Invest. 2007;19(3):266-272.
32. Hazuchova K, Held S, Neiger R. Usefulness of acute phase proteins in differentiating between feline infectious peritonitis and other diseases in cats with body cavity effusions. J Feline Med Surg. 2017;19(7):809-816.
33. Bell ET, Toribio JA, White JD, et al. Seroprevalence study of feline coronavirus in owned and feral cats in Sydney, Australia. Aust Vet J. 2006;84(2):74-81.
34. Meli ML, Burr P, Decaro N, et al. Samples with high virus load cause a trend toward lower signal in feline coronavirus antibody tests. J Feline Med Surg. 2013;15(4):295-299.
35. Addie D, Belak S, Boucraut-Baralon C, et al. Feline infectious peritonitis. ABCD guidelines on prevention and management. J Feline Med Surg. 2009;11(7):594-604.
36. Negrin A, Lamb CR, Cappello R, et al. Results of magnetic resonance imaging in 14 cats with meningoencephalitis. J Feline Med Surg. 2007;9(2): 109-116.
37. Green J, Syme H, Tayler S. Thirty-two cats with effusive or non-effusive feline infectious peritonitis treated with a combination of remdesivir and GS-441524. J Vet Intern Med. 2023;37(2):561-572.
38. Fischer Y, Sauter-Louis C, Hartmann K. Diagnostic accuracy of the Rivalta test for feline infectious peritonitis. Vet Clin Pathol. 2012;41(4):558-567.
39. Singh M, Foster DJ, Child G, et al. Inflammatory cerebrospinal fluid analysis in cats: clinical diagnosis and outcome. J Feline Med Surg. 2005;7(2):77-93.
40. Barker EN, Tasker S. Advances in molecular diagnostics and treatment of feline infectious peritonitis. Adv Small Anim Care. 2020;1(3):161-188.
41. Felten S, Leutenegger CM, Balzer HJ, et al. Sensitivity and specificity of a real-time reverse transcriptase polymerase chain reaction detecting feline coronavirus mutations in effusion and serum/plasma of cats to diagnose feline infectious peritonitis. BMC Vet Res. 2017;13(1):228.
42. Barker EN, Stranieri A, Helps CR, et al. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Vet Res. 2017;48(1):60.
43. Pedersen NC, Perron M, Bannasch M, et al. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J Feline Med Surg. 2019;21(3):271-281.
44. Murphy BG, Perron M, Murakami E, et al. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet Microbiol. 2018;219:226-233.
45. Dickinson PJ, Bannasch M, Thomasy SM, et al. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. J Vet Intern Med. 2020;34(5):15871593.
46. Krentz D, Zenger K, Alberer M, et al. Curing cats with feline infectious peritonitis with an oral multi-component drug containing GS-441524. Viruses. 2021;13(12):2228.
47. Coggins SJ, Norris JM, Malik R, et al. Outcomes of treatment of cats with feline infectious peritonitis using parenteral remdesivir, with or without transition to oral GS-441524. J Vet Intern Med. 2023;37(4):1036-1045.
48. Roy M, Jacque N, Novicoff W, et al. Unlicensed Molnupiravir is an effective rescue treatment following failure of unlicensed GS-441524-like therapy for cats with suspected feline infectious peritonitis. Pathogens. 2022;11(11):1209.
49. Clark TM, Coggins SJ, Korman R, et al. Treatment of feline infectious peritonitis in cats with molnupiravir: clinical observations and outcomes for 54 cases. Aust Vet J. 2025;103(6):339-353.
50. Allinder M, Tynan B, Martin et al. Uroliths composed of antiviral compound GS-441524 in 2 cats undergoing treatment for feline infectious peritonitis. J Vet Intern Med. 2023;38(1):370-374.
51. Kent AM, Guan S, Jacque N, et al. Unlicensed antiviral products used for the at-home treatment of feline infectious peritonitis contain GS-441524 at significantly different amounts than advertised. J Am Vet Med Assoc. 2024;262(4):489-497.
52. Taylor SS, Coggins S, Barker EN, et al. Retrospective study and outcome of 307 cats with feline infectious peritonitis treated with legally sourced veterinary compounded preparations of remdesivir and GS-441524 (2020–2022). J Feline Med Surg. 2023;25(9): 1098612X231194460.
About the Author: Dr. Goldkamp attended the University of Pennsylvania where she earned her Doctor of Veterinary Medicine degree. She completed a small animal medicine and surgery internship at Cornell University and a small animal internal medicine residency at the University of Florida. During her residency, she did research on feline retroviruses and is excited about the advancements that have been made in FIP treatment. She currently works at PETS in Lancaster, where she contributes her expertise in treating cats with infectious diseases, including FIP. Her role at PETS has given her hands-on experience with the latest advancements in FIP treatments, and she plays an active part in helping cat owners navigate the challenges of the disease.


Redefining Spay/Neuter with HQHVSN
By Becky Morrow, DVM, MS, CAWA
Chances are you have heard of High-Quality High Volume Spay/Neuter (HQHVSN), but how much do you know about HQHVSN in practice? The first time I heard of HQHVSN was not in veterinary school. I was taught all the “gold standard” techniques--making a large incision, using three hemostats on pedicles, double ligating everything, and closing the body wall with a simple interrupted suture pattern.
My Introduction to HQHVSN
After practicing for six years, my incisions were not as large, but I was still abiding by those tenets as if they were the ten commandments. I was not introduced to HQHVSN for a couple more years, ironically, after I had left general practice for academia and was trying to find my niche. My colleagues and I wanted to do a service-learning project revolving around community cats and were introduced to a local group that held monthly HQHVSN clinics to support Trap-Neuter-Return (TNR).
This was my first introduction to HQHVSN in action. I was amazed at how a group of people could come together and sterilize over one hundred cats in a single day. I also realized that many of my preconceptions were inaccurate. While I did not closely observe surgery that day, I could see that the system overall was well organized and efficient. No corners were cut, and no one was rushing. There was just an effective division of labor. I got drawn into the group as time went on and began understanding how the shelter veterinarians were more efficient. For cat spays, they made smaller incisions, used a spay hook, and altered the technique by using pedicle ties to ligate the ovarian pedicles and a single suture for the uterine body.
I was intrigued but still had doubts. I was never taught to use a spay hook. I worried, ‘What if I dropped a pedicle doing this technique?’ Placing one ligature rather than two and using fewer clamps in the limited space made sense, so I started
with that. I began practicing cord ties from a video that I found online on cat castrations and finally got brave enough to transfer that muscle memory to the pedicle ties.
Mindset Shift
What began as learning some techniques evolved into a fundamental shift in both my thinking and my philosophy of veterinary care. I began to question why we so often accept the status quo as the only “correct” way. As my experience with HQHVSN deepened, the so-called “gold standards” I had once held onto began to lose their shine. They no longer made sense in the context of the efficiency, safety, and impact I was seeing in the field.
And now, with the specialization of and training opportunities in shelter medicine, we have even more experience and data for our evidence-based practice of HQHVSN. There are shelter medicine programs in many veterinary schools, and boardcertified surgeons publishing articles on simple continuous closure of the body wall, single ligature placement on pedicles and the uterine body, scrotal castrations of dogs, and pedicle ties in cats.1,2
Benefits of HQHVSN for Patients and Beyond
These techniques not only benefit our patients through shorter surgery times and smaller incision sizes, but also our communities, and even our profession. It probably comes at no surprise that communities that have HQHVSN clinics have lower shelter intake numbers and higher live release rates due to the decreased need for euthanasia for over-population. One study even found that the decreased intake of cats led to a 99% decrease in euthanasia of the cats already in the shelter.3 This was because fewer cats entering the shelter kept
Learn More about HQHSVN Techniques and How to Improve Efficiency in Your Practice
Articles
High-quality, high-volume spay–neuter: Access to care and the challenge to private practitioners, by Dr. Philip Bushby https://pmc.ncbi.nlm.nih.gov/articles/PMC11132592/
The Association of Shelter Veterinarians’ 2016 Veterinary Medical Care Guidelines for Spay-Neuter Programs
https://www.aspcapro.org/sites/default/files/2023-04/asv_medical_ care_guidelines_for_spay-neuter_programs.pdf
High- Quality, High -Volume Spay and Neuter and Other Shelter Surgeries by Dr. Sara White (Wiley Blackwell)
Free Online Education or In-Person Workshops from Dr. Morrow at Frankie’s Friends Humane
Up Your Spay Game – 6.5 RACE-Approved Credits (online)
HQHVSN – It’s Not Just for Shelters - 12 RACE-Approved Credits (Pittsburgh Area Workshops) https://www.frankies-friends.org/hqhvsn-training
the numbers lower and reduced the stress levels, thereby decreasing the incidence of Upper Respiratory Infection (URI). It also freed up the staff to treat cats for URIs where they would not have previously had the resources to do so.
HQHVSN also has a positive impact on our profession. As a practitioner of HQHVSN, I not only have gained a high level of surgical proficiency in spay/neuter, but also in other life-saving surgical procedures that would have previously resulted in euthanasia of the animal. The skills and efficiency of HQHVSN are transferable and allow for increased access to care for underserved pet populations and an increase of revenue for the clinic providing the services. Even if a practice does not adopt the techniques themselves, HQHVSN clinics are always looking to partner with full-service clinics to provide life-long care for the pets after they are vaccinated and sterilized. This provides a constant source of new patients, and income, for general practitioners.
Final Thoughts

References
1. Shivley JM, Bushby PA, Brookshire WC, Woodruff K. Update on ovariohysterectomy. J Am Vet Med Assoc. 2020;257(6):595-600.
2. Shivley JM, Woodruff KA, Shealy AP, Bushby PA, Brookshire WC. Update on orchiectomy. J Am Vet Med Assoc. 2022;260(10):1166-1171.
3. Johnson KL, Cicirelli J. Study of the effect on shelter cat intakes and euthanasia from a shelter-neuter-return project of 10,080 cats from March 2010 to June 2014. PeerJ. 2017;5:e3739. doi:10.7717/peerj.3739
I have come full circle in my personal journey, from learning about HQHVSN and overcoming doubt in the techniques and lack of confidence in my skills, to paying it forward and teaching others – veterinary students, veterinarians, and the indispensable team members that support us. I have found my niche and now see HQHVSN not just as a surgical technique, but as a transformative approach to veterinary practice. It is a mindset shift that challenges convention and embraces progress. It empowers us to work smarter, serve more animals, and make a measurable difference in our communities.
As we move forward in this series of articles, I invite you to join me in exploring the many dimensions of HQHVSN and the impact it has on the lives of animals and those who care for them.
About the Author:Dr. Becky Morrow is a graduate of The Ohio State University College of Veterinary Medicine. She transitioned into academia after six years of small animal practice and was introduced to shelter medicine through a service-learning project with a local HQHVSN organization. She became fully immersed in shelter medicine while assisting with a large-scale animal cruelty case - managing the veterinary care of hundreds of cats for over a year and providing forensic documentation and testimony for the court. She earned a master’s degree and two graduate certificates (veterinary forensics and shelter medicine) from the University of Florida and became a Certified Animal Welfare Administrator (CAWA). Dr. Morrow has since performed tens of thousands of spay/neuters, taught HQHVSN to veterinary students and veterinarians, and worked on dozens of forensic cases. She has served on the boards and as the medical director of multiple nonprofit organizations and a veterinary molecular diagnostic laboratory. Dr. Morrow is an Adjunct Professor at the University of Florida College of Veterinary Medicine, an Assistant Professor at Penn State University, and is the President and Medical Director of Frankie’s Friends Humane.
Email Address for Correspondence: gervinsmith@blend.vet
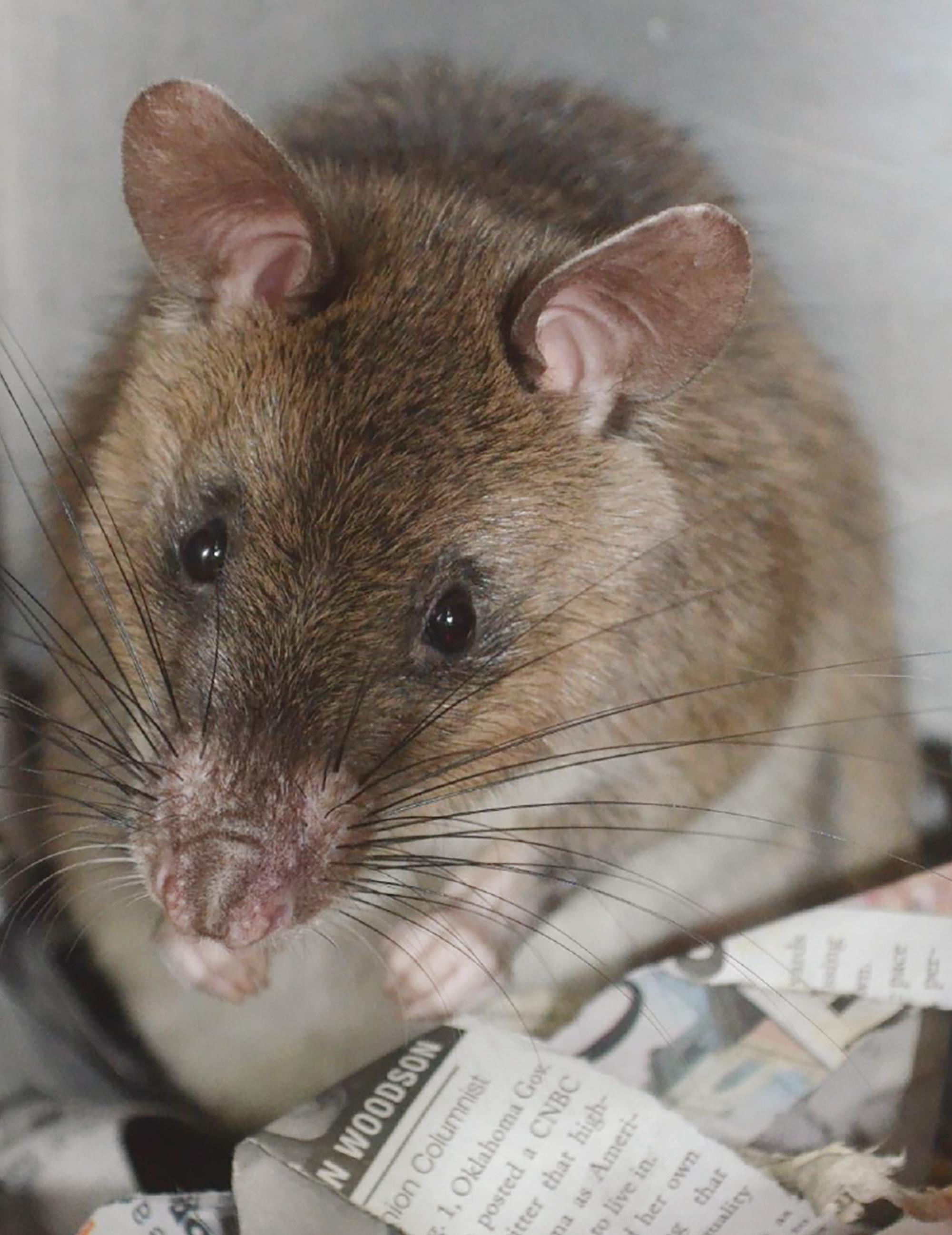
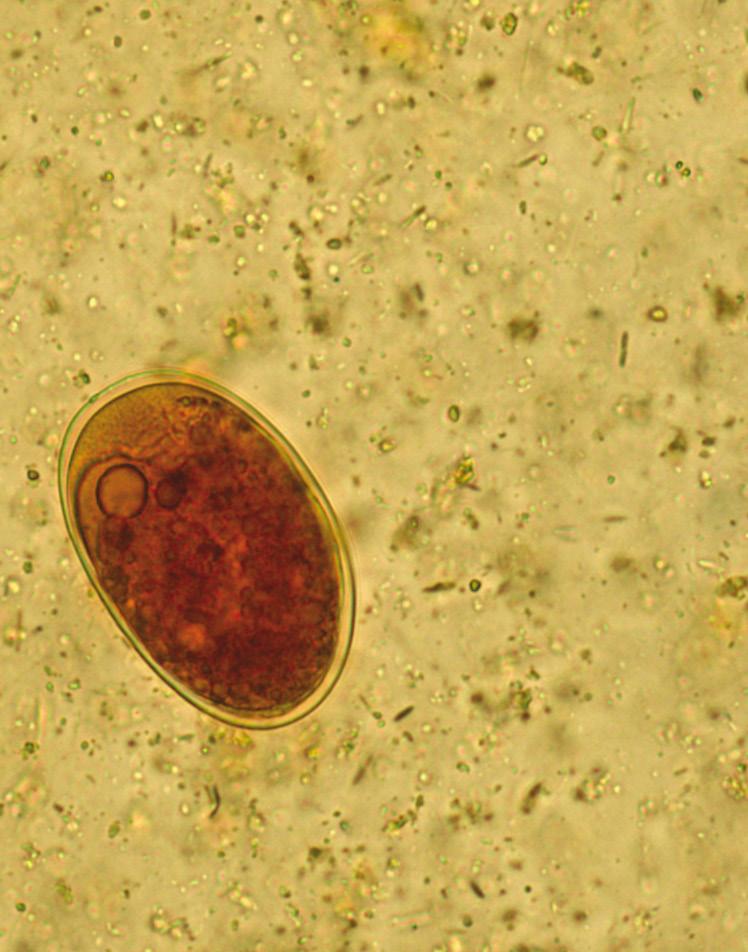
A Grain of Truth: Giant Face-Eating Rats!

By Todd A. Jackson, DVM, DACLAM
This series of articles depicts funny, tragic, terrifying, or otherwise memorable anecdotes from veterinary careers. Some of them might be mine, and some might belong to other people. I’m not telling. In all cases, the names have been changed to protect the innocent and the comically guilty.
Some are completely true, but at minimum, every story has a grain of truth. For those who haven’t been in veterinary medicine long enough to remember when the best available drug to treat arthritis in dogs was aspirin (available in 5 grain tablets), a grain is an obsolete unit based on the mass of an ideal seed. In the Apothecaries' system, it is equal to 64.79891 milligrams… so, maybe not much, but there is some truth in there.
Giant Face-Eating Rats!
One of the joys of being a former mixed animal practitioner and current laboratory animal specialist has been the variety of animals I get to work with. Other veterinarians are happier limiting their practice to just dogs or cats, but I enjoy the challenge of species variety… at least most of the time.
Some of the craziest critters ever in my care have been Cricetomys sp. They are cute, African rodents the size of a cat. If you add-on tail length, they can be a meter long. [Fans of The Princess Bride, yes- “R.O.U.S.’s” are real!]
People work with them because they have an excellent sense of smell; they’re able to detect buried landmines yet lightweight enough not to make the mines go “boom.” They can also detect tuberculosis in human sputum, faster than culture and cheaper than PCR. Just ask a big rat where the buried bomb is hiding or who has TB. If you don’t believe me, check out the information on “Hero Rats” at https://apopo.org.
Because little was known about Cricetomys sp. other than their amazing olfactory ability, we got the pleasure of studying their basic biology--what best to feed them, how long is their estrous cycle and gestation period, what is their average litter size, etc. Collaborators trapped 80 of them from the wilds of Tanzania, loaded them onto a plane, and had them delivered to the veterinary school where I worked. They arrived jetlagged and NOT people-friendly. It took months to tame them enough to be handled.
Cricetomys sp. were associated with an outbreak of Mpox (formerly monkeypox) in the U.S. in 2003. Hence, CDC required us to keep them strictly quarantined until we could collect saliva, serum, and dried blood from each rat for 3
separate Mpox tests. I tried to collect blood from the usual locations used in domestic rats to no avail. Their tails felt similar to cattle (just a little smaller), so I tried tail vein bleeding, which worked. That earned us our first publication: how to draw blood from Cricetomys sp. (It’s academia, so publish or perish.)

Our parasitology department was giddy about the variety of worm eggs seen on fecal flotation. There were at least 5 different types along with massive numbers of tapeworm proglottids. My brilliant idea was to give topical Cydectin® because a pour-on dewormer would be easier to administer to the feral furballs. It gave them bald spots, and their parasites lapped it up, laughing at us. After several trials using multiple dewormers, we found that either pyrantel pamoate or piperazine together with high dose praziquantel (3X that used for dogs or cats) eventually cleared the infections. (Cha-ching-second publication!) To get the anthelmintics into them, we mixed liquid dewormer with powdered peanut butter. They snarfed it down like candy.
One of their anatomical oddities is that they have cheek pouches like hamsters and rhesus monkeys. In the wild, they use these pouches to carry seeds, grains, or other food down into their burrows for storage. One particularly large male would take pieces of laboratory rodent chow from us through the bars of his cage and stuff them into his cheek pouches. A veterinary student helping me with the project asked how many blocks of chow he could fit into his pouches. I had no idea, but said she could keep giving the rat more to find out. “Cujo” the rat managed to get 6 pieces stuffed into each side of his face and hold a 13th piece in the front of his mouth. When continued on next page >
A Grain of Truth: Giant Face-Eating Rats!
continued from page 25


of the incident was very much like the scene from Monty Python and the Holy Grail where they used the Holy Hand Grenade of Antioch to vanquish a killer bunny. (Google it!)
she handed him the 14th piece, he had to drop the 13th piece to fit in number 14. Proving that they could hold 13 blocks of chow in their cheeks at the same time did not result in a third publication.
I wondered out loud why the rat so greedily hoarded the food, literally stuffing his face with as many pieces as he could carry. He had a full feeder, whichnever went empty. The veterinary student got a funny look on her face and asked if I had seen myself in the mirror recently. She remarked that many animals take in extra food because just because it’s there, whether they need it or not. (I am a V.O.U.S… a Veterinarian of Unusual Size.) I really wanted to give her an F (as in “Fat”) on her lab animal rotation, but you can’t flunk students for being right.
The most surprising fact we discovered about Cricetomys sp. was learned the hard way. A week or so after arrival, our animal caretaker, Steve, was moving the rats to clean cages so that we could wash their used cages. At the same time our veterinary assistant, Chuck, was helping me with examinations and treatments next door. Suddenly, Steve burst into the room with abject terror in his eyes!
“The big one, Cujo, got loose, and he looks really mean!”, Steve said quivering and pale.
Chuck gave Steve a pathetic glance and said “I’ll go put him back into the cage for you,” adding “you wimp” under his breath.
Chuck was an old farm hand who worked at the school’s research ranch for years before getting older and figuring out that working lab animals for a year or two before retirement might be less strenuous than working horses and cattle. He was still tough as nails and gave plenty of flack without ever taking any. I kept working and let Chuck handle the loose rat while Steve watched through the window from a safe distance. Just moments later, Chuck staggered back into the room, swearing up a storm, holding a hand to his forehead, and dripping blood everywhere. Cujo bit him in the face. Surprise!! Cricetomys sp. can jump 6 feet high! Chuck’s later description
I applied pressure with gauze to stop the bleeding and sent Chuck to the hospital for stitches. It wasn’t a large wound, but human foreheads are highly vascularized and bleed profusely when lacerated. As Steve helped me clean Chuck’s blood off the floor, two thing dawned on me: First, Someone still had to recapture Cujo. Second, I was the only someone left.
Gathering up my courage, I picked up a see-through plastic cage used to transport the rats while anesthetized and looked through the window into their housing room. Cujo was on the far side, searching for a way out. I opened the door, jumped through, and pulled it closed behind me as quickly as possible to keep Cujo from getting past me. I held up the plastic cage in front of me like a shield, and Cujo reared up on his hind legs, glaring with an evil grin. Suddenly, he made 2 hops directly towards me. On the 3rd hop, he leapt straight up in the air to bite me in the face, not understanding that he was seeing me through a clear, plastic cage. As Cujo hit the plastic with a cartoonish “SPLAT!”, I slammed the transport cage lid closed. Neither Cujo nor I were injured, except maybe for Cujo’s pride as a slayer of humans.
Steve came back into the room and remarked how impressed he was with my recapture skills, much faster and smarter than Chuck--obviously why I was a veterinarian and Chuck was just an assistant. I should have just let the comment stand, but I felt too guilty. I said, “It’s not that I’m smarter or faster than Chuck. It’s just that I got to go second. When you see bad stuff happen to the first guy, you know to try something different.”
After that horrifying event, our staff never referred to them as “Hero Rats” and called them “Giant Face-Eating Rats”. Sadly, journal editors would never let us publish using our name for them even though I suspect it would have lured in more readers.
About the Author: Dr. Jackson is a board-certified specialist in l aboratory animal medicine and serves as the Director of the Animal Resource Program at Penn State’s University Park campus. He is a Research Professor in the Office of the Senior Vice President for Research and the Department of Veterinary and Biomedical Sciences. He can be reached via e-mail at taj5330@psu.edu. https://vbs.psu.edu/directory/taj5330
Now What? Bringing the Power of Large Language Models to Your Daily Practice
By William Tancredi, DVM
You've heard the AI evangelists. You've read the implementation papers. You've probably rolled your eyes at another "revolutionary" and “innovative” technology announcement as recently as the last few days. Fair enough (also a bit of a “mea culpa” there). But here's the thing: while everyone's debating the future of artificial intelligence in veterinary medicine, the present is sitting right there, waiting for you to use it.
The conversation has shifted from whether AI will impact veterinary practice to how quickly you'll learn to use it effectively.
Noted AI expert and University of Pennsylvania professor Ethan Mollick recently shared his framework for deciding which model to use and how to use them. While I’m a fan of sharing use cases for the veterinary hospital, I liked Dr. Mollick’s broader approach. Unlike the specialized veterinary AI tools that promise the moon but have some deficiencies, the powerful general-purpose AI systems available today can supercharge your practice immediately. If you know how to use them properly.
Pick Your Tool and Pay the Price
Let's start with the easy part: which AI to use? For serious work, you have three excellent options: Claude from Anthropic, ChatGPT from OpenAI, and Google's Gemini. All three offer voice modes, document analysis, code execution, and research capabilities. The free versions are essentially demos, which may be useful for testing but not for real work. You'll need to invest about $20 each month for the full capabilities that will actually save you time and improve your practice.
(Veterinarians can be notoriously cheap, and I’m personally doing my best to uphold that stereotype, but this is worthwhile.)
This isn't merely a technology expense; it's a productivity investment. Think of it this way: if AI saves you just 30 minutes per day (a conservative estimate), that's 125 hours annually, and equivalent to three weeks of work time (or two, if you’re the type to overwork yourself). At veterinary hourly rates, the return on investment is immediate and substantial.
Understanding the Models: Sports Car vs. Tugboat
Here's where it gets interesting. Each AI system offers multiple models, and choosing the right one matters more than ever. Think of it like choosing between a sports car and a tugboat. Both are vehicles and useful in their own right, but you'd use them for different tasks.
For quick questions or casual brainstorming, the fast models work fine: Claude Sonnet, GPT-4o, or Gemini Flash. But for anything high-stakes or requiring complex analysis, such as detailed client communications, research synthesis, or treatment planning, you’ll want to switch to the powerful models: Claude Opus, OpenAI’s o3, or Gemini Pro. Most systems default to the fast model to save computing power, so you'll need to manually select the advanced option.
(Author’s note: This is my advice as of the time of this writing; given the astonishing rate of advancement in the field of Large Language Models (LLMs), it’s reasonable to assume that this advice may expire.)
Real-world example: My emails are often direct and straightforward, occasionally bordering on terse, even rude. The use of Claude’s Sonnet 4 makes my communications much gentler.
What Not to Do: Your car is not a boat. Just as if I were to drive my car into a lake and lament that it doesn’t float, so too is complaining that a poorly-selected model doesn’t do a job very well.
The Deep Research Revolution
Here's a capability that genuinely impresses most veterinary professionals: Deep Research reports. These AI-generated reports often rival the quality of work from consultants or researchers, with proper citations and comprehensive analysis. For veterinary applications, try Deep Research for:
• Comparative treatment protocols: "Compare current approaches to managing canine dilated cardiomyopathy, including recent research on genetic testing and novel therapeutic options"
• Client education materials: "Create a comprehensive guide for puppy owners on vaccination schedules, socialization windows, and early training, with current veterinary guidelines"
• Continuing education prep: "Analyze recent advances in feline chronic kidney disease management, focusing on therapeutic diets, phosphate binders, and emerging treatments"
continued on next page >
Now What? Bringing the Power of Large Language Models to Your Daily Practice
continued from page 27
The reports aren't perfect, but they're far more accurate than simple AI queries, and the citations actually work. This isn't just convenient; it's a potential game-changer for staying current in our rapidly evolving field.
Real-world example: Try this prompt, “Do deep research evaluating my hospital’s overall social media presence and its demographic area; create a report that suggests strategies to improve client engagement and community impact.”
What Not to Do: Do not fall asleep at the wheel. Internet research, whether performed by a person or an LLM, should not be treated as gospel without thorough professional review. Just as you would not drive into a lake because your GPS told you to turn right, you should retain your judgment and wisdom in evaluating the output of LLMs.
Voice Mode: Your AI Assistant in Action
Voice mode transforms AI from a typing exercise into a natural conversation tool.
I've used voice mode to:
• Talk through complex cases after uploading records and relevant files.
• Brush up on the latest research, having a Q&A on research publications.
• Make the most of drive time, using it as an interactive learning tool.
• Help process the complex dynamics, good and bad, of running a veterinary hospital; it’s essentially a neutral-butsupportive third party.
Most people use voice mode like an upgraded Siri. There’s a visual integration to it that some folks love, but I’ve found it less helpful for photographic analysis in our line of work.
Practical Implementation:
Start with Real Work
Your next hour should include three experiments with actual veterinary work:
First: Switch to the powerful model and give it a complex challenge from your practice (just pick one and go). Upload a
difficult case file, heavy or boring emails, or responding to a client review. Have an interactive discussion with the LLM: push back, poke and prod, ask for alternatives, request specific formats. Don't just ask for an answer; engage in the back-and-forth that reveals the AI's true capabilities.
Second: Try Deep Research on a professional question where you need comprehensive information. Maybe it's exploring new treatment options for a chronic case, researching equipment purchases, penning higher quality communications, or developing protocols for your practice. See how the quality compares to your usual research methods. And note how much faster it is when you use an LLM.
Third: Experiment with voice mode during routine activities. Use it while reviewing cases, preparing for client conversations, or brainstorming practice improvements. The goal isn't replacement, but rather augmentation of your thinking process.
Context Is Everything
The most important lesson about AI use: these systems only know what you tell them. They don't remember previous conversations or learn about your practice patterns. Every interaction starts fresh, so provide context liberally.
Upload relevant files: lab results, medical records, practice protocols, client communications. Describe your practice type, your patient population, and your specific concerns. The more context you provide, the more useful the responses become.
Instead of: "Write a client education handout about diabetes," try: "I'm a small animal practitioner treating a 9-year-old Golden Retriever newly diagnosed with diabetes mellitus. The owners are overwhelmed and need a clear, reassuring handout covering insulin administration, dietary management, monitoring requirements, and when to call for emergencies. They're educated professionals but have no medical background."
A general rule: if you’re getting bad outputs, try asking better questions.
The Reality Check
AI won't solve every problem in veterinary medicine. It can't replace clinical judgment, hands-on examination skills, or the intuitive pattern recognition that comes with experience. What it can do is handle the cognitive and emotional heavy lifting that drains your mental energy. It’s great at assisting with things like research compilation, document creation, protocol development, and crafting client communications.
Most practitioners use AI like Google: quick questions, no context, default settings. You now know better. The difference between casual users and power users isn't just prompting skill (which develops with practice), but also knowing these features exist and applying them to real veterinary work. You can be the best driver in the world, but an amateur in an F1 car will almost certainly get around the track faster than the expert in the tugboat.
The technology is here. The capabilities are proven. The only question remaining is how quickly you'll integrate them into your daily practice. While others debate the future of AI in veterinary medicine, you can start using it today to practice better medicine, reduce administrative burden, and focus more time on what you trained to do: care for animals and their people.
Those adopters won't just have a competitive advantage, they'll have more time, less stress, and better outcomes. In a profession already stretched thin, that's not just an opportunity; it's a necessity.
About the Author:William Tancredi, DVM, is a veterinarian and the owner of Old Ridge Veterinary Hospital in Chadds Ford, Pennsylvania. He is an experienced small animal clinician and entrepreneur with an interest in generative artificial intelligence (AI). He has lectured on AI and its use in veterinary medicine to the Independent Veterinary Practitioners Association, the Veterinary Hospital Managers Association, and private veterinary organizations; he has also published a number of articles in various publications.
It’s Time to Rethink Client Payment Options in Your Clinic


It shouldn’t surprise anyone working in a veterinary hospital that concerns around the affordability of veterinary care are growing rapidly. In 2018, the Access to Veterinary Care Coalition found that 28% of pet owners were unable to receive veterinary care in the preceding two years.1 Financial barriers were the most common for all levels of care, from preventive care to emergencies.1
Unfortunately, seven years later, these barriers have only grown.
The recent PetSmart Charities-Gallup Poll found that 52% of U.S. pet owners now report foregoing needed veterinary care—with 15% not visiting the vet even when care was needed and 37% visiting the vet but declining care while there.2 For 71% of these pet owners, finances were the reason for their decision.2
The growing number of pet owners impacted by financial limitations is due to rapidly rising costs of care combined with increasing economic uncertainty, both of which are beyond the scope of this article. But the need for change is undeniable. Now is the time for veterinary practices to rethink payment policies, increase options for pet owners to finance care, and focus on educating clients on preventing and preparing for illnesses and emergencies.
Financial Limitations are Ubiquitous
Veterinary practices should be aware that financial limitations affect pet owners of all ages, races, and income levels.2 While some demographics are at higher risk of financial barriers, even in the highest income bracket (>$90,000 annual income in the PetSmart Charities survey), 33% of pet owners stated they were unable to afford recommended care.2
By Kate Boatright, VMD
More concerningly, for 65% of pet owners, the maximum amount they could pay for an unexpected emergency is less than $1,000.2 For 26% of dog and cat owners, an unexpected expense of only $250 causes concern.3
Some people respond to these concerns by saying that individuals or families who can’t afford pets shouldn’t have them. But the reality is that many pet owners try to prepare, but costs have increased since they initially got their pet.3
Currently, Millenials and GenZ represent almost half of U.S. pet owners.4 But individuals in these two generations are more likely than any other to live paycheck-to-paycheck,5 meaning an unexpected expense like an illness, injury, or emergency can cause financial hardship.
How long can we continue to ask the majority of our pet owners—most of whom consider their pets to be family members—to choose between paying their basic living expenses like rent, groceries, and utilities and providing veterinary care for their pet?
Creating Change at the Local Level
Access to veterinary care is a sweeping challenge for our profession and addressing the challenge will require change at the professional level. But you can make changes at your individual practice level to support pet families and the patients they love. And you don’t have to cut costs or provide discounted care to do it.
First, offer a range of diagnostic and treatment options for each patient, taking into consideration the individual client’s continued on next page >
It’s Time to Rethink Client Payment Options in Your Clinic
continued from page 29
Access to Care Resources
Veterinary Innovation Council’s Access to Care Hub:
Database for veterinary professionals to find financial resources from credit-based solutions to payment plans and more. This is a great starting place to explore options, but remember that there may be companies not yet listed in the hub.
https://www.vetaccesshub.com/
Pet Help Finder:
Database for pet owners to find financially friendly pet health resources including veterinary care, pet food and supplies, and boarding.
https://www.pethelpfinder.org/m/phf
AVMF REACH:
Grant program available to all AVMA member veterinarians.
https://www.avmf.org/grants-andscholarships/reach-animal-care-program/
economic limitations as well as other client and patient factors, such as ability to attend rechecks, access to transportation, and patient stress levels. In recent years, this type of practice has been termed spectrum of care.6 While many veterinarians say they already do this, 73% of pet owners who declined care due to cost say they weren’t offered a lower cost alternative.2 This discrepancy in veterinarian and owner perceptions should be explored further.
Another way to support pet owners is by remaining aware of alternative avenues for veterinary and pet care resources in your community. These may include charitable grants, pet food resources, low-cost community clinics, or high quality high volume spay neuter (HQHVSN) clinics. See above for a list of Access to Care Resources you can use and refer clients to. Finally, consider expanding options for clients in how they can pay for care and train your team on financial triage, which is the process of identifying a client’s individual financial situation and determining an option that fits their needs. Historically, payment options have included pay at the time of service or apply for credit-based financing. But this doesn’t provide a solution for all clients.
Proactive clinics provide a variety of payment options, with at least one option in each of the following categories (please

note, this list is not meant to be exhaustive of all available companies):
• Pay at the time of service with cash, check, or existing credit card.
• Credit-based financing options (i.e. Care Credit, ScratchPay, All Pet Card). Most of these services require a hard credit check. Some may offer a promotional period with deferred interest, but be sure your clients are aware of the difference between no interest and deferred interest to avoid unpleasant surprises down the road.
• Payment plans (i.e. VetBilling, Varidi, Cherry). There are a growing number of payment plans available to veterinary clinics. While you can always offer a payment plan to clients directly from your practice, a growing number of companies can help you manage these payment plans, including collecting payments. Each company operates differently, and you’ll want to consider several factors, including if a credit check is required (and whether it is a hard or soft check), interest rates for clients, cost to your clinic to manage the plan, and who carries the risk if the client doesn’t pay. While payment plans may feel risky, there is strong evidence of repayment.7
• Charitable Funding (i.e. MyBalto, AVMF REACH program).
For clients who are unable to pay using any of the previous strategies, having access to a charitable fund within your clinic can be helpful. There are now companies that can help you set up and manage a charitable fund in your clinic. Be sure that your clinic team is aware of when these funds can be accessed and if there are specific limits for a given case. Additionally, stay aware of grants that may be available to help cover costs of veterinary care, such as the AVMF’s REACH program, which is available to all AVMA members.
Can We Prevent Financial Barriers?
Educating clients about veterinary costs before an illness or emergency arises is also an important factor to consider. Train your team to educate clients on preventive care—including the costs to treat versus prevent common diseases, such as Parvovirus, Lyme disease, pyometra, and Leptospirosis.
Additionally, be sure that your team is providing education on pet insurance to clients. Insurance won’t be the solution for every pet family, but all clients deserve to know that it is an option. This is especially important to discuss with owners of young, healthy pets, since pre-existing conditions won’t be a concern. Consider including information about pet insurance in puppy and kitten information kits.
When discussing pet insurance, focus on making pet owners aware of the variety of available plans and refer them to an insurance provider or broker to discuss plan specifics. You aren’t a licensed insurance agent, so focus on providing information, not selling a product. You can also remind clients that a growing number of companies are offering pet insurance plans as an employee benefit, so this may be a good starting place for clients
The Future of Veterinary Care
As costs continue to rise, many projections of future costs of care are concerning—from both the eyes of a pet owner and a veterinary professional. Let’s start to make changes now to support our clients and patients through education, diversifying payment options, and offering a wider range of care options. It’s time to stop ignoring the problem and making change at the local level—your clients and patients will thank you.
References
1. Access to Veterinary Care Coalition. Access to Veterinary Care: Barriers, Current Practices, and Public Policy. AVCC Website Httpavccutkedu. Published online December 17, 2018. https://trace.tennessee.edu/utk_ smalpubs/17
2. Hrynowski Z, Lall J. 52% of U.S. Pet Owners Skipped or Declined Veterinary Care. Gallup.com. April 16, 2025. Accessed May 25, 2025. https://news.gallup.com/poll/659057/pet-owners-skipped-declinedveterinary-care.aspx
3. New Synchrony Study Finds Nearly 8 out of 10 Pet Owners Underestimate the Cost of Care, Reaching Up to $61,000 During a Pet’s Lifetime. Accessed June 29, 2025. https://www.synchrony.com/contenthub/newsroom/newsynchrony-study-finds-nearly-8-out-of-10-pet-owners.html
One-Stop Shop for Legal Services for Veterinarians, Veterinary Clinics, and Animal Hospitals

Veterinary practice involves a wide variety of legal issues. Tucker Arensberg attorneys have experience working with veterinarians in all of the legal aspects of their practice.
We offer full-service legal representation and consulting services throughout the entire lifecycle of your business from startup to transfer of ownership, including:
• Employment matters
• Business entity formation and governance
• Contract drafting and negotiation
• Real estate
• Purchase or sale of a business
• Succession planning
• Financing transactions, debt, or equity
To learn more visit www.tuckerlaw.com, follow us on LinkedIn , or call 412-566-1212.






4. Megna M. Pet Ownership Statistics 2025. Forbes Advisor. April 10, 2023. Accessed June 29, 2025. https://www.forbes.com/advisor/pet-insurance/ pet-ownership-statistics/
5. Paycheck-to-Paycheck Statistics 2025. MarketWatch - Guides. Accessed June 29, 2025. https://www.marketwatch.com/financial-guides/banking/ paycheck-to-paycheck-statistics/
6. Stull JW, Shelby JA, Bonnett BN, et al. Barriers and next steps to providing a spectrum of effective health care to companion animals. J Am Vet Med Assoc. 2018;253(11):1386-1389. doi:10.2460/ javma.253.11.1386
7. Cammisa HJ, Hill S. Payment options: An analysis of 6 years of payment plan data and potential implications for for-profit clinics, non-profit veterinary providers, and funders to access to care initiatives. Front Vet Sci. 2022;9:895532. doi:10.3389/fvets.2022.895532
About the Author: Dr. Kate Boatright has been in rural small animal practice since graduating from the University of Pennsylvania in 2013. After nearly 8 years of full-time practice in both general practice and emergency clinics, she moved to part-time clinical work to pursue her passion for educating veterinary professionals as a freelance speaker, author, and consultant. Dr. Boatright enjoys discussing topics that promote connection with colleagues and clients, especially mentorship and the spectrum of care. She currently serves on the PVMA Board of Trustees, AVMA House of Delegates, and the dvm360 Advisory Board. If you’re looking to have a conversation about access to care or mentorship, please reach out at hello@writetheboat.com.


Legislative and Regulatory Affairs Committee Update
By William Crousore, DVM and Alessandro Lamacchia, VMD
The Legislative and Regulatory Affairs Committee of the PVMA are busy engaging the PA state government. We currently have several legislative and regulatory priorities. Among them are seeking passage of an amendment to the “The Controlled Substance, Drug, Device and Cosmetic Act” that would schedule medetomidine with an exemption for licit veterinary use, expanding enumerated duties and title protection for Certified Veterinary Technicians, especially in rural large animal practice, and supporting the veterinarians interfacing with research animals in Pennsylvania.
Controlled Substance, Drug, Device and Cosmetic Act amendment
The Amendment scheduling medetomidine with a veterinary exemption is similar to what was passed last year, shepherded by PVMA LRAC, in which xylazine was legally made a Schedule III controlled substance by the Commonwealth of Pennsylvania. There is, however, an exemption for veterinary formulations used under the supervision of a veterinarian for legal purposes. Veterinary xylazine formulations are not considered a controlled substance when prescribed by a veterinarian.
The impetus for such legislation last year was the fact that xylazine had been found in a large percentage of illicit fentanyl and heroin used by drug abusers in the Commonwealth. It is believed that opioids cut with xylazine increases the potential for overdose, and there is no reversal agent for xylazine as there is for opioids. In addition, perivascular xylazine causes vasoconstriction leading to tissue necrosis and ulcers. Law enforcement wanted penalties to prosecute possession, but more importantly the ability to prosecute dealers for homicide in the event that an abuser died of an overdose. This would only be possible if the drug is a controlled substance.
The veterinary exemption in both the governor’s executive action and the legislation (that the PVMA was instrumental in inserting) is critical since it was likely that if all forms of xylazine
were scheduled as a Class III, the manufacturer’s regulatory burden would have been such that it would not be available to veterinarians in the Commonwealth anymore. A coalition from PennVet, PVMA, AABP, and AAEP lobbied the Shapiro Administration and then the legislature to ensure that veterinary xylazine was exempt from scheduling.
Fast forward to today. Now medetomidine is being used in the same way as xylazine to cut opioids but is not currently a controlled substance. The effects of medetomidine, however, are similar, and law enforcement wants medetomidine classified the same as xylazine. The beautiful thing is now that the precedent is set with xylazine, the bill proposing to classify medetomidine as a schedule III controlled substance mirrors the xylazine legislation that the PVMA and its coalition worked so hard to shepherd two years ago.
This is the result of many hours of work and connections with the legislature and Shapiro administration. Without this work by LRAC, both compounds may well have become schedule III controlled substance and likely unavailable to veterinarians in Pennsylvania.
Veterinary Technician Enumerated Duties
Rural veterinary practice is under unprecedented challenges with recruiting and retaining veterinarians willing to practice on farm animals. To compound the problem, Certified Veterinary Technician (CVT) utilization in this segment of practice is not well developed. This is a multifactorial problem, but we believe that CVT revenue generation is difficult in this practice setting because of Practice Act and regulatory constraints. The lack of revenue generation contributes to underutilization of CVTs in this segment.
PVMA LRAC has been working on a solution to expand the enumerated duties of the CVT on farm animal practice, similar to what is the case in companion animal practice, while protecting the vital functions of the veterinarian to diagnose, prescribe,
prognose, and perform surgery. Current enumerated duties for CVTs in farm animal practice settings are either very few or ambiguous. Enumeration of duties will protect veterinarians who utilize CVTs under indirect supervision from legal jeopardy. We are currently engaging multiple stakeholders, including the Pennsylvania legislature, to find an answer to this problem. This complex situation has the very real potential to progress toward a mid-level practitioner initiative, which the PVMA vehemently opposes, if we do not proactively address it.
CVTs play a crucial role in companion animal practice, generating revenue for the practices. This same model can be applied in farm animal practice, allowing rural practices to continue to serve their farm animal clients while allowing the veterinarian to be more efficient with his or her time, but we need clarity this in both the Practice Act and regulations. At the same time, our other primary goal is to ensure that the crucial tasks that veterinarians perform on farms remain under the umbrella of the veterinarian. A mid-level practitioner model would not do that and would be devastating for rural practice and the farms they serve.
Senate Bill 381
“Beagle Bill”
The bill bars any Commonwealth funding for studies classified by USDA as pain-category D or E, even when animals are anesthetized or receive analgesia. Many peer-reviewed veterinary studies (e.g., orthopedic implant trials, oncologic surgical investigations etc.) fall in category D precisely because they involve post-operative observation. The blanket ban would force investigators to either abandon studies or move them out of Pennsylvania. This will ultimately decrease the long-term knowledge base of all practicing veterinarians as we will no longer have an avenue to conduct clinical trials in client-owned animals.

Finally, the proposed requirements for adoption of a former research animal are in some ways counter-productive to what institutions are already doing. Research institutions typically have adoption policies, and they make every effort to adopt out all animals deemed eligible by veterinarians. Rescue organizations frequently ask to remain anonymous when adopting animals as they do not want to be targets of publicity, but this bill will force them to be public. Additionally, institutions trying to adopt to individuals already do their due diligence to ensure the new owner(s) can support the animal transitioning out of a research setting and are set-up to support a new pet financially through its lifetime. The increased burden and transparency will only make this more difficult. Blanket adopting to rescues will ultimately increase shelter populations, which are already brimming, which is why institutions try to adopt directly to new homes.
Unfortunately, at the time of the writing of this article, the Beagle Bill has cleared the Senate Judiciary Committee and appears to be fast tracked in the legislature. We are actively working on voicing our concerns in the hope that we can bring some common sense to this emotionally charged issue.



The main lynch pin of this bill is the devocalization of research dogs, and to be clear, this practice is obsolete. This is not taught in veterinary schools in the US nor is it a part of private practice. The only modern use is to treat specific laryngeal disease in individual pets. Much like declaw bans, this is legislating veterinary medical decision making and should be opposed, especially since the AVMA already has a position statement on the topic.
One of the provisions of this bill requires posting the full IACUC (Institutional Animal Care and Use Committee) roster publicly. This would expose named veterinarians—which IACUCs are required by law to have—to harassment campaigns that have targeted colleagues in other states. The veterinarians working in research settings are tasked with caring for the animals and maintaining their welfare. To allow them to be targets feels counter-productive to ensuring animal well-being.




WHY YOUR BUSINESS LIABILITY INSURANCE NEEDS TO KEEP UP WITH YOUR MEDICINE

If you’re staying current, you know veterinary medicine is not what it used to be — and that’s a good thing. We’re healing dogs with stem cells, managing feline arthritis with laser therapy, and easing chronic pain with acupuncture and CBD oil. The frontiers of veterinary care are expanding, and so is your toolkit for helping animals live longer, healthier lives.
But there’s a catch: while your medical techniques may be cutting-edge, your insurance policy might still be stuck in 2010. And that mismatch can leave your practice exposed. What if something goes wrong? What if the client sues? What if the treatment isn’t approved by the FDA or Pennsylvania?
Let’s talk about risk—the other side of innovation—and how the right insurance (and a knowledgeable broker) can make sure your practice doesn’t just push boundaries, but protects them, too.
Where Insurance Gets Tricky
The problem with many standard veterinary liability policies is that they’re built around traditional care models. So when you start offering therapies considered "experimental," "alternative," or "off-label," you could unintentionally find yourself outside your coverage boundaries.
For example:
• Your policy might exclude experimental treatments — meaning anything not broadly accepted by the mainstream veterinary community or approved by regulatory bodies.
• Off-label drug use may not be covered if it leads to an adverse outcome and you didn’t document that the client was educated of potential risks properly .
• Procedures like acupuncture or chiropractic care might not be covered at all unless you’ve added coverage for them within your policy — and have the appropriate certifications.
What this boils down to is a simple truth: you can be doing great medicine and still be at great risk.
Potential Scenarios
Let’s say you treat a senior golden retriever with arthritis using stem cell therapy. The owner is hopeful. But the dog doesn’t improve—in fact, it develops an unrelated infection. The owner sues, claiming your experimental treatment caused harm. You call your insurance carrier... only to find out the procedure wasn’t covered.
Or maybe you’ve been using CBD products to help manage feline anxiety. One cat experiences an adverse reaction. Again, the insurance company denies the claim—because CBD use wasn’t disclosed, and it’s not FDA-approved.
Those may just be hypothetical scenarios, but the point is as real as can be. As procedures evolve, so do liability risks. And with legal gray areas, even the most cautious vets can find themselves at risk for expensive, stressful, and time-consuming legal action.
Your Insurance Broker: Your Practice’s Best Friend
This is where having the right insurance broker makes all the difference. A good broker doesn’t just sell you a policy. They:
• Understand your practice—what you do, what services and treatments you offer, and what makes your care unique.
• Help you disclose high-risk or non-traditional procedures to the insurer so you’re not blindsided later.
• Identify coverage gaps and offer solutions like endorsements or specialty policies.
• Stay up-to-date on veterinary trends and regulatory changes.

Think of your broker as your translator, advocate, and safety net all rolled into one. If you're trying a new therapy or bringing in an integrative medicine vet, they should be one of the first calls you make. You won’t want to purchase that new piece of equipment or make that new hire before knowing whether you have the coverage to make use of them safely!
How to Protect Your Practice
Here’s how to make sure your insurance evolves with your medicine:
1. Keep your broker in the loop, especially when adding new treatments or services.
2. Ask about exclusions. Don’t assume a procedure is covered just because it’s common in your field.
3. Get proper documentation. Use detailed client consent forms and document outcomes thoroughly.
4. Seek endorsements. Many insurers offer add-ons for alternative treatments, telemedicine, or those using AI tools.
5. Review your policy annually. A lot can change in a year. Your coverage should reflect that.
Final Thoughts
Veterinary medicine is on the move, and that’s a beautiful thing. But as you innovate and expand, your insurance needs to keep up. Otherwise, all that progress could come with unintended consequences.
Talk to a broker who understands your world. Review your policy like you’d review a treatment plan. And stay curious—not just about medicine, but about the legal and financial side of care, too.
Because at the end of the day, your job is to care for animals. Let your insurance do the job of caring for you.
Here’s where PVMA partner Alera Group can help. Our team has been helping members since 2018, so we’re familiar with your needs and are aware of changes and innovations taking place within your industry. With the personal, local service that your practice deserves, as well as a national scope of carriers and coverage options for business insurances (and employee benefits), it’s worth a call or a message to our team to learn how we can help you.
Visit cloud-aia.aleragroup.com/pvma to get in touch with our team!

Classified Ads
Veterinarians
North Versailles, Pennsylvania | Full-Time
We are seeking a Medical Director with a vision to help grow our hospital, North Versailles Veterinary Care, while advancing our quality of care. The Medical Director is responsible for providing medical leadership, managing associate veterinarians, and assuring regulatory compliance relating to the practice of veterinary medicine. The Managing Veterinarian is also responsible for creating an environment of teamwork in which quality medicine and exceptional client service are consistently delivered to our clients and their pets. Interest in surgery is great but not necessary. If you're someone who prefers wellness and sick appointments, we are open to that as well. Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.Dowhaniuk@nva.com.
Pittsburgh, Pennsylvania | Full-Time
Holiday Park Animal Hospital, located on the Golden Mile Highway, is a full-service animal hospital providing comprehensive healthcare services. Our facility includes in-house testing for accurate diagnosis, digital x-ray, ultrasound, surgical suite, dental suite, pharmacy, and more. We are looking for an enthusiastic and passionate Veterinarian to help us continue to grow. Our ideal candidate has strong communication skills, is team-oriented, and excited to help our vibrant practices excel in our community. If you want a place where your passion and skills are valued, where your feedback, input, and ideas are heard, then apply today! Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.Dowhaniuk@nva.com.
Edinboro, PA | Full-Time
Join Our Team at Camboro Veterinary Hospital! Located in Edinboro, PA, near scenic Lake Erie, Camboro Veterinary Hospital is seeking a Managing Veterinarian/Medical Director to lead our dedicated team. Joint ownership opportunities are available for interested candidates. In this role, you'll oversee medical practices, manage a team of veterinarians, ensure regulatory compliance, and contribute to the financial success of the hospital. You'll enjoy a competitive salary, management bonus, 4-day work weeks, health benefits, 401(K) matching, and more. Edinboro offers small-town charm with access to outdoor activities and nearby cities like Pittsburgh, Cleveland, and Buffalo. Join us for a rewarding career! Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.Dowhaniuk@nva.com.
Chambersburg, PA | Full-Time
Chambersburg Animal Hospital, a full-service pet hospital, is seeking a full-time Associate Veterinarian with an interest in dentistry, surgery or emergency. Join our 6-doctor team in our state-of-theart facility, offering in-house labs, digital X-ray, ultrasound, and laser surgery. We prioritize collaboration, mentorship, and continuing
education. Enjoy limited evening/weekend hours, no emergency shifts, and a competitive salary with excellent benefits including health insurance, 401(K), and paid time off. Licensure in PA required. Come be apart of our compassionate team! Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.Dowhaniuk@nva.com.
Chambersburg, PA | Full-Time
Join Our Team at Best Friends Animal Hospital! Are you a compassionate veterinarian looking to make a difference in the lives of pets? Best Friends Animal Hospital is seeking a dedicated vet to join our dynamic, three-doctor team. We offer state-of-theart facilities, including 5 exam rooms, digital x-rays, ultrasound, and more. Enjoy a supportive work environment focused on collaboration and care. Benefits include a competitive salary, health coverage, 401K, paid vacation, student loan assistance, and continuing education. If you're passionate about providing exceptional care and building relationships with pets and owners, we’d love to hear from you. Apply today! Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.Dowhaniuk@nva.com.
Dover, PA | Full-Time
Dover Area Animal Hospital in Dover, PA, is looking for a passionate Veterinarian to join our team. As a busy mixed animal practice, we cater to dogs, cats, exotics, and large animals, offering a diverse caseload from routine wellness to full diagnostic workups. Operating with a 6-Doctor team, we provide cutting-edge facilities and a supportive environment for all experience levels. If you are a new graduate, we offer mentorship at the hospital level as well as oneon-one training with our mentor veterinarian via a specialized 12-month formal mentorship program. 4-day work weeks available and no on call or afterhours. Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.Dowhaniuk@nva.com.
York, PA | Full or Part-Time
Petz R Us Express Care is an animal hospital in York, providing urgent care services for cats and dogs and some routine wellness services. Come join our team in providing quality care to our patients. We are looking for a dedicated and compassionate (part time or full time) veterinarian to join our team - new graduates are welcome! We have a supportive work environment with experienced staff. Enjoy a 3-3.5-day work week. Evenings and some weekend work required. No overnight work. Benefits include a competitive salary, health coverage, paid time off, and employee. Danielle at 717-400-5650 or petzrusmanager@gmail.com.
Butler, PA | Full-Time
Butler Veterinary Associates & Emergency Center is seeking an Emergency Veterinarian for swing shifts (2–10 PM, no overnights). Join our busy, multi-doctor practice offering both general and emergency care. We provide mentorship, a flexible 32-hour workweek, and no on-call responsibilities. While not a 24-hour
hospital, overnight patient care is supported by experienced technicians. Our modern facility includes an in-house lab, digital X-ray, ultrasound, and more. We offer competitive compensation with sign-on, retention, relocation, and student loan bonuses. Ideal candidates are passionate about ER medicine and teamwork. Must be licensed in PA or eligible through ECFVG or PAVE. Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.dowhaniuk@nva.com.
Pittsburgh, PA |
Full-Time
Cat Clinic and Hospital, Full-Time Veterinarian
Unique opportunity in the city of Pittsburgh for a veterinarian who has always wanted to work in a successful, feline only veterinary practice, and help develop and guide a path into the future with us. This is a privately owned, 46-year-old practice, and well-established in the area. We currently are staffed with one full-time (Dr. Robert Bebko), two long time, part-time veterinarians, and competent, seasoned support staff. Rather than list all of the equipment we own/use and our employment package, we invite you to:
1) Look us over on our website (www.catclinic.net)
2) Email us (catclinic@hotmail.com) and set up an appointment to talk and ask questions
3) Schedule a day to stop by and spend with us to see what our typical day looks like, and,
4) If you find you would like to work with us for a week, schedule as relief and really get to know the practice.
Don’t overlook pursuing your dream. An opportunity to learn from seasoned veterinarians who have spent their lifetimes in feline medicine and surgery, and an opportunity to help shape our path into the next decade and beyond.
Looking forward to meeting you!
State College, PA | Full-Time
Join Mt. Nittany Veterinary Hospital as our Managing Vet! We’re seeking a motivated leader to guide our collaborative team in State College, PA. Enjoy a positive culture, generous benefits, and no weekend/evening emergencies. Responsibilities include leading medical care, managing associates, and ensuring compliance. Must hold a DVM / VMD degree and state licensure (or ability to obtain one), leadership training available. Benefits include a sign-on bonus, relocation allowance, competitive salary, CE, 401(k), insurance, and more. MNVH is equipped with advanced technology and a skilled support staff. Enjoy outdoor adventures and community events in beautiful Centre County. Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.dowhaniuk@nva.com.
Williamsport, PA | Full-Time
The Animal Hospital on the Golden Strip in Williamsport, PA, is seeking a dynamic Managing Veterinarian/Medical Director to lead our team. This role offers joint ownership potential (optional).
Responsibilities include providing medical leadership, overseeing protocols, and managing financials alongside the Hospital Manager. You'll also drive community engagement and support team training, including mentorship for new grads. Our state-of-the-art facility offers six exam rooms, surgery suites, in-house lab, digital x-ray, ultrasound, and more. We offer competitive salary, benefits, and a supportive, growing team. Please call Kelli Dowhaniuk at 818-309-3709 and/or email Kelli.Dowhaniuk@nva.com.
practice for sale
Practice for Sale - Allentown-Bethlehem, PA
This is an established, companion animal practice in the BethlehemAllentown area in eastern PA. It is a growing 2 doctor practice with revenues approaching $2 million. It is well-equipped with inhouse lab equipment, digital x-ray, therapy laser and more. They have a solid staff that is committed to the practice. The practice is housed in a free-standing building that has a good location in the community, on the edge between mixed residential areas and a professional business area. The facility has 4 exam rooms, the surgical suite, lab/pharmacy and more. Both the practice and real estate are for sale. (PA324). Please call David McCormick at 814-466-7084 and/or email MidAtlantic@Simmonsinc.com.
Practices/Equipment For Sale – Bucks County, PA
Highly-profitable small animal practice generating over $800K in collections, with margins over 30%. Steady growth of 15 new patients monthly. Prime location 30 min from Philadelphia with efficient team in place. Hospital building is the newest and most modern in the area due to recent move in 2025. Strong history of quality care since the 1980s. Strong brand and reputation in Bucks County.
Contact Rohit Malhotra at 234-353-3268 or rohit@omnipg-vet.com for more information. (PAV101)
Practice for Sale- Southeast, PA
This is a small animal practice that is in the Route 30 corridor, west of Philadelphia. It is a fully equipped, small animal practice that provides full diagnostic, medical/surgical and wellness care to pets in the region – and it is profitable with very nice cashflow to the owner! The practice is housed in a large facility that has a great location in the community with easy access and plenty of parking for staff and clients. It has 4 exam rooms and plenty of space for future growth. Both the practice and the real estate are for sale. (PA438).
Please call David McCormick at 814-466-7084 and/or email MidAtlantic@Simmonsinc.com.
continued on next page >
classified ads continued from page 37

Practice for Sale, Central PA in the I99 Corridor
This is an established, small animal practice that is located in central PA. The owner and team have a good reputation and an easy, 4.5 day work schedule. You can have a nice life-work balance! The practice is housed in an attractive, free-standing, 2,000 square foot facility that has 3 exam rooms and all the usual amenities. It has been well-maintained and it is well-equipped. It has Neo for the practice management software. The owner is ready to retire so both the practice and the real estate are for sale. (PA435). Please call David McCormick at 814-466-7084 and/or email MidAtlantic@simmonsinc.com.
Northeast, PA Outside of Scranton
Well-established Small Animal Hospital for sale in Northeast PA. Can support 1-2 doctors. Ample modern equipment, great clientele, safe neighborhood. Building in good repair, on two commercial lots. 2024 gross was $912,000. Interested parties please contact me via email at savemevm47@gmail.com. No corporations or multipractice owners, please.
Lancaster Area, PA
This is a small animal practice that is located in the Lancaster area. This practice has a long history of serving clients and their pets – almost 30 years! It enjoys an excellent reputation for compassionate, quality care and service. It is housed in a 2,700 square foot, well-equipped facility that has all the expected amenities and room for growth – it can easily handle being a 2-3 doctor practice. The owner is ready to retire so both the practice and the real estate are for sale. (PA431). Please call David McCormick at 814-466-7084 and/or email MidAtlantic@Simmonsinc.com.
Centre County, PA
Thriving small animal hospital in an excellent location along a major east-west highway with over 13,000 vehicles passing daily! 2,600 square foot leasehold facility with 2 exam rooms and potential for a 3rd. Full X-ray suite, an isolated surgery suite, and advanced diagnostic, ultrasound, and dental capabilities. Steady year-over-year growth. 2024 gross revenue over $744K with a solo DVM and appointments offered only on weekdays. Room for multiple doctors. Negotiable post-sale employment available. With proximity to Penn State University, the surrounding region offers a stable, educated population, top-rated schools, abundant outdoor recreation, and a high quality of life. (Listing PA12)
Contact PS Broker at: 800-636-4740 | info@psbroker.com | https://go.psbroker.com/PA12
Western, PA -Near Ohio Border
This is a solo, small animal practice that is located in western PA, only a couple miles from the PA-OH border. This is an established practice with over 60 years history and a growing client base. It is housed in an attractive, 2,200 square foot facility that is located in a busy road in the community. It is a nice facility with the usual amenities – and room for future growth. The owner is ready to retire so both the practice and the real estate are for sale. (PA410). Please call David McCormick at 814-466-7084 and/or email MidAtlantic@Simmonsinc.com.
North of Scranton-Wilkes Barre- PA
This is an established, small animal practice that is located north of Scranton-Wilkes-Barre – in northern Luzerne County. The practice is an AAHA Accredited, small animal hospital that has an easy work schedule and NO after-hours calls. It is very well-equipped and organized for efficient work-flow. It has a good team that is committed to the practice and is expected to stay. It has an attractive, free-standing, 2,400 square foot facility that has two exam rooms and all of the usual amenities. The owner is ready to retire so both the practice and real estate are for sale. (PA311) Please call David McCormick at 814-466-7084 and/or email MidAtlantic@Simmonsinc.com.
Western PA,-East of Pittsburgh
This is small animal practice that has been serving clients since the early 1970s. The practice located on the periphery of Indiana, PA which is home to the Indiana University of Pennsylvania. It is housed in a large, 7,500 sq ft facility with 4 exam rooms – great opportunity for future growth without having to expand! It is well-equipped and utilizes the Avimark practice management system. The practice is for sale. A long term lease will be provided for the real estate with a right of first refusal. Everything is ready for an easy step into ownership! (PA503). Please call David McCormick at 814-466-7084 and/or email MidAtlantic@Simmonsinc.com.
Eastern PA, Near MD Border
This is an established, small animal veterinary hospital that is located in eastern PA, near the PA-MD border. You can live in either state! The practice provides complete medical, surgical, diagnostic and wellness care to clients throughout the region – and the team has an excellent reputation. It is housed in an attractive, free-standing, leased facility that has a very good location in the community for visibility and easy access by current and future clients. The practice enjoys a positive relationship with the landlord. The owner is ready to retire so the practice is for sale. (PA437). Please call David McCormick at 814-466-7084 and/or email MidAtlantic@Simmonsinc.com.







Hope. Healing. And Expert Cancer Care.
At Lancaster Veterinary Specialties, we deliver exactly that—close to home.
When a pet faces cancer, it’s not just about treatment—it’s about trust and teamwork.
Dr. Binstock and the Oncology Team at Lancaster Veterinary Specialties offer expert, personalized cancer care focused on comfort and quality of life. Each plan is tailored to the diagnosis and unique needs of the pet, whether through chemotherapy, targeted therapies, advanced diagnostics, or coordinated surgical care.
Specialties include lymphoma, relapse therapy, oral tumors, and advanced imaging. Dr. Binstock treats a wide range of cancers such as:
• Lymphoma & leukemia
• Mast cell tumors
• Osteosarcoma
• Melanoma & soft tissue sarcomas
• Liver, mammary & bladder cancers


OUR SERVICES INCLUDE:
• Cardiology
• Internal Medicine
• Oncology
• Ophthalmology
• Radiology
• Surgery

Our expert approach blends clinical expertise with compassion, supporting families and referring veterinarians through every step of the journey.
Give your pet every advantage with expert cancer care led by Dr. Binstock – call 717-347-0838 to consult or refer today.