



YOUR COMMUNITY RESOURCE FOR WHAT’S HAPPENING IN HEALTH CARE SPRING 2024 Published by Pennsylvania’s First Medical Society Before Your Next Colonoscopy, Ask Your Doctor if They’re Using AI Insulation is So Last Year Lead Poisoning Prevention p 6 p 8 p 16 p 22 sandra Malamed
































Meet Our Healthcare Banking Expert Andre Jones, Senior Relationship Manager Healthcare Banking 484.947.6309 | CitadelBanking.com/Healthcare WELCOME TO BETTER Built for Your Practice BUSINESS BANKING We understand that starting, running, and expanding a practice is no small feat. Our team of Relationship Managers offers years of experience partnering with healthcare professionals to develop custom strategies that address your distinct needs and challenges. Citadel is recognized as a Forbes 2022 Best-in-State Credit Union. Federally Insured by NCUA

President
David E. Bobman, MD
President Elect
Mahmoud K. Effat, MD Vice President
Richard O. Oyelewu, MD Treasurer
Winslow W. Murdoch, MD Secretary
Christina J. VandePol, MD
Editor & Immediate Past President
Bruce A. Colley, DO
Board Members
Norman M. Callahan, III, DO
Asare Christian, MD
Heidar K. Jahromi, MD
Mian A. Jan, MD
John P. Maher, MD
Manjula K. Naik, MD
Sean V. Ryan, MD
Francis X. Speidel, MD
Lynne A. Stilley, MBA Executive Director
Chester County Medical Society 1050 Airport Road PO Box 5344
West Chester, PA 19380-5344
Website – www.CCMS.org
Email – OurCCMS@gmail.com Telephone –
Chester County Medicine is a publication of the Chester County Medical Society (CCMS). The Chester County Medical Society’s mission has evolved to represent and serve all physicians of Chester County and their patients in order to preserve the doctorpatient relationship, maintain safe and quality care, advance the practice of medicine and enhance the role of medicine and health care within the community, Chester County and Pennsylvania.
The opinions expressed in these pages are those of the individual authors and not necessarily those of the Chester County Medical Society. The ad material is for the information and consideration of the reader. It does not necessarily represent an endorsement or recommendation by the Chester County Medical Society. OFFICERS 2023
PUBLISHER: Hoffmann Publishing Group, Inc. 2669 Shillington Rd, Box #438, Reading, PA 19608 For Advertising Information & Opportunities Contact: Tracy Hoffmann 610.685.0914 x201 tracy@hoffpubs.com www.Hoffpubs.com Contents SPRING 2024 Letters to the Editor: If you would like to respond to an item you read in Chester County Medicine, or suggest additional content, please submit a message to OurCCMS@gmail.com with “Letter to the Editor” as the subject. Your message will be read and considered by the editor, and may appear in a future issue of the magazine. Cover: The Art of Chester County features the work of Sandra Malamed. Read more in The Art of Chester County on page 22. In Every Issue 4 President’s Message 22 The Art of Chester County 6 Before Your Next Colonoscopy, Ask Your Doctor if They’re Using AI 8 Lead Poisoning Prevention 14 Primary CNS Lymphoma: Who is at Risk, What to Look For, and What’s New in Therapy 16 Insulin is So Last Year 26 Chester County Offers Many Great Options for Senior Living 28 Negotiating Key Employment Contract Terms 30 Mindfulness in Medicine and Healthcare Features
(610) 425-9190

PRESIDENT’S MESSAGE
Spring 2024
 David E. Bobman, MD, MD, FACP, AGAF President, Chester County Medical Society
David E. Bobman, MD, MD, FACP, AGAF President, Chester County Medical Society
What’s on your mind?
Help us to learn more about emergent trends affecting your work!
Write to us at: OurCCMS@gmail.com
BY DAVID E. BOBMAN, MD PRESIDENT OF CHESTER COUNTY MEDICAL SOCIETY
Winter is through, the groundhog did not see his shadow and an early Spring is predicted. Despite the cold and dark of Winter, the Chester County Medical Society has not been hibernating.
There has been a lot to do, and we have had to divide into working committees to keep the ball rolling. An advocacy committee has been formed and is led by Dr. Christina VandePol. This committee will interact with our governmental policy makers with such topics as malpractice venue reform, physician reimbursements, etc. There are several important upcoming political races and her group will be arranging forums to allow us to assess their stances on issues relevant to the practice and delivery of health care.
A thorough review of the response to the Covid pandemic was undertaken by another committee chaired by Dr. Frank Speidel. Several observations were made and presentations have been underway, including at the Health Department. One issue which was mentioned included a relative paucity of input from our local physicians. Working with the Chester County Health Department, this has resulted in a closer future working relationship between us. We will also have a couple of our members participating with the Southeast Pennsylvania Health Care Coalition (SEPA), looking into future emergency preparedness.
Additional committees are working on topics such as increasing membership, providing social activities for our members and their families, updating our bylaws, and increasing our social media presence, among others. I strongly encourage participation by any Chester County Medical Society members who are interested in any of these topics or who have other topics which they feel should be addressed. I would also encourage non-members to join the Chester County Medical Society and hopefully also participate in our endeavors.
Fond Regards, David
www. CCMS .org
4 CHESTER COUNTY Medicine | SPRING 2024






2 | LANCASTER Thriving! hriving! | Spring 2024 DOWNTOWN COMMERCIAL PLAZA 50 NORTH 5TH STREET |READING, PENNSYLVANIA (ITERSECTION OF 5TH & WASHINGTON STREETS) CLASS Reading A L A N S H U M A N P RESIDENT , B ROKER OF R ECORD SDG @I NVEST I N R EADING COM | 610.736.3033 FOR LEASE CLASS “A” OFFICE SPACE Reading Central Business District! 50 North 5th Street | Reading, PA 19601 610.736.9393 | InvestInReading.com A L A N S H U M A N RESIDENT , B ROKER OF R ECORD SDG @I NVEST I N R EADING . COM | 610.736.3033 50 North 5th Street | Reading, PA 19601 610.736.9393 | InvestInReading.com
Before Your Next Colonoscopy, Ask Your Doctor if They’re Using AI
BY DAVID R. NEIBLUM, M.D., F.A.C.G, A.G.A.F., US DIGESTIVE HEALTH

Much has appeared in the press recently regarding the risks and dangers of artificial intelligence (AI). College students use ChatGPT to draft term papers instead of writing it themselves; lawyers rely on AI to write briefs – sometimes very inaccurately and with fictitious case examples, leading to sanctions. Even global destruction has been discussed as a possible threat of AI (link: https://www.safe.ai/statementon-ai-risk#open-letter).
However, some applications of AI are not only improving medical care, but in some cases may well save lives. In gastroenterology, we’re using it to find polyps during colonoscopy. The traditional method involves the doctor watching a TV screen as the scope is advanced through the colon, and then removed, relying on eyesight and experience to find the small growths which, over time, could turn into colorectal cancer (CRC). Since the National Polyp Study in the early 1990s, and in many studies since, it’s been proven conclusively that removal of adenomatous colon polyps significantly lowers the incidence of CRC. There have been many quality improvements in endoscopic technology over
the years, including using high-definition monitors, more maneuverable and variably rigid scopes, as well as new ancillary tools to remove polyps, stop bleeding, and even close defects in the colon, avoiding surgery.
We have quality measures we closely track during these procedures, such as the percentage of asymptomatic patients in whom we find polyps (Adenoma Detection Rate, ADR), how many minutes we spend on the inspection part of each colonoscopy (“withdrawal time”) and how often we get to the end of the colon – these reflect how skillful the doctor is in finding polyps. Finding more polyps generally means we prevent more cancers. Not all doctors and GI groups track these measures, but ideally should. Studies have also suggested that up to 25% of polyps can be missed on colonoscopy, even by experienced doctors. I’ve done many thousands of such procedures in my career, and at this point, I thought I was pretty good at it.
However, about 18 months ago, my group started using a new AI-powered device which uses computer-aided detection algorithms to find polyps – sort of like having another doctor
6 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org

PentaHealth is an independent, physician-led group of dedicated providers located throughout Southeastern Pennsylvania who proactively deliver seamless, high quality, and accessible care to all, one person at a time.









www.pentahealth.com New




























(or three) looking over one’s shoulder when doing the procedure. The program is loaded with over 13 million images of polyps, in all shapes and sizes, including the very flat sessile ones that we sometimes struggle to find. In studies, doctors using the system increased their ADR up to 14% higher than previously. That may not sound so impressive, until one realizes that each 1% increase suggests a 3% drop in colon cancer risk. That’s a whopping 42%. When the system detects what it considers a polyp, a bright green box flashes around that site, alerting us to the spot to examine more closely; and it’s been measured that the system finds these lesions over 80% faster than the doctor’s eye can find them.
The device is the first of its kind for this application, but others are in the works. There are also other related devices becoming available, to detect lesions and bleeding sites in the small intestine, where our scopes have a difficult time reaching. For over 15 years, we and other groups have used a “capsule endoscope,” a swallowed pill-sized camera that tumbles through the small bowel to visualize this area, with images being downloaded wirelessly to a cellphone-sized device over about 6 hours as the patient goes about his business at home. We then view the 70,000 images taken as sort of an old fashioned “card flip” motion picture, looking for abnormal images. The film takes precious time to watch, however, and is fairly tedious. The new AI-powered systems will preview the images for us and




















7 days a week
direct us quickly to anything abnormal – freeing up time to see more patients.
When I first tried the colonoscopy AI system, I was annoyed and distracted by the green flashing box popping up – it seemed to think some normal colon folds were polyps, so these were “false positives.” But the miraculous thing about this technology is that it learns – so now it almost never flashes unless a polyp is really there – including some I’d likely have missed. It’s over 99% sensitive for polyps, and has less than 1% false positives in its latest iteration. I and my colleagues now love it.
Welcome to the future; in this case, a potentially lifesaving one.
David R. Neiblum, M.D., F.A.C.G, A.G.A.F.
US Digestive Health, West Chester
915 Old Fern Hill Rd., Suite 300 West Chester, PA 19380
Penn Medicine Chester County Hospital West Chester, PA 19380
References:
https://pubmed.ncbi.nlm.nih.gov/32371116/
SPRING 2024 | CHESTER COUNTY Medicine 7 www. CCMS .org
patients
Appointments
Our
Call us first, we are always available 610-423-8181
always welcome
available
family caring for your family

www. CCMS .org 8 CHESTER COUNTY Medicine | SPRING 2024
Lead Poisoning PREVENTION
SUBMITTED BY WILLIAM F. KRAMER, D.O.
Lead poisoning prevention, and in particular, childhood lead poisoning prevention, has become a hot public health issue recently with the much-publicized lead poisoning outbreak linked to cinnamon applesauce pouches. The active investigation has involved a recall of WanaBana, Schnucks, or Weis’s brand fruit puree products. There have been over 400 cases in 44 U.S. states, including Pennsylvania. The recalled apple cinnamon puree pouches should not be eaten and can be thrown away or returned to place of purchase. Parents should contact their healthcare provider and ask about getting a blood test for lead if they or their children have consumed the recalled products.
Lead is a naturally occurring metal found in the Earth’s crust that negatively impacts the health of children and adults. Its widespread use has resulted in massive environmental contamination, human exposure, and significant public health problems worldwide.
Lead and Children
Children under six years of age are at an increased risk of lead poisoning. Their rapidly developing bodies absorb more lead, and they also exhibit more hand-to-mouth behavior and are at risk for ingesting more. Young children absorb 4-5 times as much ingested lead as adults from the same source (WHO, Lead Poisoning, 2023). Immigrant and refugee children from less developed countries that may not have strict lead regulations are at even higher risk. Malnourished children are more susceptible to lead absorption when nutrients such as calcium or iron are lacking.
Lead poisoning can cause serious health issues for children. High levels of exposure can damage the brain and central nervous system causing coma, convulsions, and death. In addition to severe neurological symptoms, children may present with weakness and fatigue, anemia, abdominal pain, constipation, and nausea. Children surviving severe lead poisoning may have permanent intellectual disability and behavioral issues. Lower levels of exposure may cause no obvious symptoms, but result
continued on next page >
www. CCMS .org
SPRING 2024 | CHESTER COUNTY Medicine 9
Lead Poisoning Prevention continued from page 9

in reduced IQ, behavioral changes, anemia, hypertension, renal disease, immunotoxicity, and reproductive damage.
Lead and Adults
Pregnant women acutely exposed to high levels of lead may experience miscarriage, stillbirth, premature birth, and low birth weight. Lead, from a prior exposure, is stored in the bones, and is released during pregnancy and passed to the developing fetus. Breast feeding also transfers lead to a baby.
Lead can also cause long-term health problems for adults. Once lead is ingested, lead is distributed to multiple organs, including the brain, kidneys, liver, bones, and teeth. Lead can accumulate in the bones and teeth for long periods of time. Hypertension, cardiovascular disease, and kidney damage are common.
Sources of Lead Poisoning
Children can be exposed to lead not only where they live, but where they learn, or play. Any place that a child spends time can provide a source, including relatives, and babysitters. Lead sources include chipping or peeling paint in homes built before 1978, water from lead pipes or pipes joined with lead solder, and soil near airports, highways, smelters, battery recycling plants or other lead releasing factories. Imported jewelry, toys, stained glass, lead crystal glassware, ceramic glazes, ammunition, traditional cosmetics, or medicines may contain lead. Much of the lead in global commerce is now obtained from recycling (WHO, Lead Poisoning, 2023).
While any child may be exposed to lead, some groups of children are at a higher risk. Children who are in households with incomes below the federal poverty level, members of racial-ethnic minorities that have been economically and socially marginalized, and recent immigrants from countries with lead in the environment are at higher risk. Additional risks include siblings, housemates, or playmates with known lead exposure, and having parents or housemates who are exposed to lead at work or through a hobby.
www. CCMS .org
10 CHESTER COUNTY Medicine | SPRING 2024
Another Membership Request, Right?
 David E. Bobman, MD, President, Chester County Medical Society Chester County Medical Society
David E. Bobman, MD, President, Chester County Medical Society Chester County Medical Society

1050 Airport Road PO Box 5344
West Chester, PA 19380-5344
Lynne Stilley Executive Director
680-389-4222 lastilley@gmail.com
As physicians, I know we are all pressed for time. Between prepping for patient visits, staying abreast of the latest science and medical advances, learning more about new treatments that may impact our patients, understanding the constantly changing insurance, HIPPA, and medical education requirements, and finding time for our spouses, children, friends and community, where do we find the time to participate in professional associations. I get it!
But fellowship through a common association of like-minded physicians really does have its benefits. As members of the Chester County Medical Society, we continue to bring value to the merits of joining a membership association. We provide benefits that coincide with many of your licensing requirements, educational programming, practice management services, advocacy and more. We also bring value to the Chester County community through many additional programs and scholarships to keep our community at the forefront of excellence in community healthcare. And there is no substitute for the peer dialog that is available within disciplines or general medical practice ideas.

So, I invite you to call or email us today to discuss how you may benefit more directly with membership in the Chester County Medical Society.
David E. Bobman, MD, President, Chester County Medical Society

CDC’s Blood Lead Reference Level
Beginning in 2012, the CDC introduced a blood lead “reference level” (BLRV) to identify children with higher levels of lead in their blood. The level is based on the 97.5th percentile of the lead values among U.S. children ages 1-5. Children with blood lead levels at or above the BLRV, set at 5ug/dL, represented those at the top 2.5% with the highest blood lead levels. These levels were calculated with the aid of the National Health and Nutrition Examination Survey cycles and are updated regularly. In May 2021, the CDC updated the BLRV from 5ug/dL to 3.5ug/ dL. The PA DOH adopted the new lower BLRV on 1/1/2022.
The CDC’s BLRV is a screening tool to identify children who have higher levels of lead in their blood compared with most children. This value is not health-based and is not a regulatory standard. States independently determine action thresholds based on state laws and are encouraged to follow the CDC guidance. No safe blood lead level in children has been identified.
continued on next page >
www. CCMS .org
SPRING 2024 | CHESTER COUNTY Medicine 11
Lead Poisoning Prevention continued from page 11

Primary Lead Poisoning Prevention
Primary prevention is the removal of lead hazards from the environment before a child is exposed to lead. A home inspection by a licensed inspector to check for lead-based paints in homes built before 1978, asking the local water authority to test water for lead, and fixing surfaces that have peeling or chipped lead-based paint are steps that renters can ask landlords to perform before habitation. Cleaning floors, windowsills, and other surfaces using wet methods will remove lead dust. Removing shoes before entering the home, and washing children’s hands, bottles, pacifiers, and toys are helpful. Feeding children nutritious meals rich in iron and calcium prevents absorption of lead as well.
Secondary Lead Poisoning Prevention
Secondary prevention includes blood lead testing, follow-up care, and referral and is essential for children who have been exposed to lead. The first step in testing is a finger or heel prick capillary test. A blood lead level above 3.5ug/dL is followed by the more accurate venous blood draw. Health care providers can test for blood lead, and many private insurance plans cover the cost of testing. The cost of blood lead testing for children enrolled in Medicaid is covered, and testing is required at ages 12 and 24 months. Universal screening is the best practice for all children, regardless of insurance status. At present, only two jurisdictions in Pennsylvania have local regulations for universal lead testing – Philadelphia and Allegheny.
All blood lead levels drawn on children under age 16 are reported to the PA Department of Health via the PA-NEDSS system. The CDC provides a summary of Recommended Actions based on Blood Lead Level. If a child has lead in their blood, actions may be recommended such as finding and removing lead from the home, feeding the child a diet rich in iron and calcium, connecting the child to early educational services, and follow-up blood lead testing. Early intervention is key to reducing long-term effects. Additional testing and treatments, such as chelation therapy, may be recommended if a child has high levels of lead in their blood. In addition to the
12 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org
COLONOSCOPY CANCER
It could be the choice of
your patient’s life.

CDC, the PA Department of Health and the Chester County Health Department are sources of information and guidance.
Summary
There is no cure for lead poisoning. Lead poisoning is preventable. Proactive steps before exposure is the best course to prevent lead poisoning, especially in young children, who are the most vulnerable to lead exposure. Universal testing is strongly advised for all children.
Information found in this report is available online at the CDC website, the PADOH website and the Chester County Health Department website.
IT’S YOUR #1 DEFENSE AGAINST ONE OF THE MOST LETHAL CANCERS.
It’s fast. It’s painless. Most insurance will cover it for patients 45 or older. And it could save their lives.
Colon cancer can be deadly when it’s not caught early. But it can be completely eradicated through early detection by colonoscopy. Now, thanks to a GI Genius™-enabled colonoscopy, technology aided by artificial intelligence, doctors at Main Line Gastroenterology Associates can diagnose colon cancer with unprecedented accuracy.
DON’T PUT IT OFF. REFER YOUR PATIENTS FOR A COLONOSCOPY TODAY.
Main Line Gastroenterology Associates
Main Line Gastroenterology Associates
Call USDH at 610-644-6755 or schedule online at usdigestivehealth.com.
SPRING 2024 | CHESTER COUNTY Medicine 13 www. CCMS .org
PRIMARY CNS LYMPHOMA: WHO IS AT RISK, WHAT TO LOOK FOR, AND WHAT’S NEW IN THERAPY
 BY MICHAEL B. DABROW, DO, MS, FACOI, FACP, MEDICAL DIRECTOR, PAOLI CANCER CENTER
BY MICHAEL B. DABROW, DO, MS, FACOI, FACP, MEDICAL DIRECTOR, PAOLI CANCER CENTER
Primary central nervous system lymphoma (PCNSL) is a rare but often aggressive lymphoma that occurs in the brain, spinal cord, CSF or the eye. Only 2% of brain tumors are PCNSL and this entity represents about 4% of all Non-Hodgkin Lymphomas. An incidence rate of .45/100,000 translates into about 1700 new cases per year in the US. During the early days of the AIDS pandemic, before adequate retroviral therapies, the incidence of PCNSL rose and the average age of onset diminished. Now, with highly effective anti-retroviral therapy (HAART), the highest risk group is those between 70-79 years of age.
Immunosuppression is by far the most significant risk factor along with age. Where HAART is lacking, PCNSL remains an issue. In the US, those patients on immunosuppressive medication for organ transplant remain at higher risk for this disease. In addition, those with autoimmune syndromes, especially if they are treated with agents causing immunosuppression, are at increased risk. These groups include those receiving azathioprine, Mycophenolate and methotrexate.
The vast majority of these cancers are B cell malignancies –diffuse large B cells predominate, expressing B cell antigens CD19, CD20 and CD79a. They tend to have a high proliferation rate with a Ki-67 of around 80%. Most PCNSLs are activated B cell subclass.
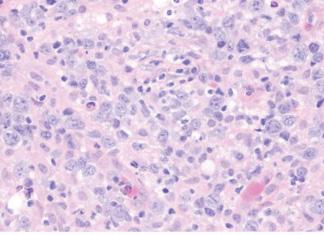
Figure 1. Lymphoma cells in PCNSL are round to oval and contain irregular, vesicular nuclei with prominent nucleoli.
As these lymphomas are aggressive, symptoms are usually acute. Interestingly, the common B symptoms of fever, night sweats and weight loss are not usually expressed. Most present with focal neurologic findings – motor weakness and language deficits. Gait disturbance and confusion with behavioral changes can be seen. As most lesions are deep in the brain, parenchyma seizures are relatively rare (10-15%)
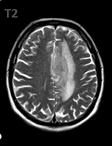
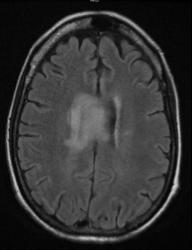
Radiographically, MRI of the brain gives the most information about this lymphoma. Lesions are iso- or hypointense on T1 weighted images and hyperintense on T2 weighted images. In HIV associated PCNSL multiple ring enhancing and necrotic lesions can be seen.
14 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org
The diagnosis is made by stereotactic biopsy or if deemed necessary by neurosurgery, open biopsy. Surgical debulking is not recommended due to the diffuse nature of this disease unless removal of a mass effect will improve performance status and the ability to deliver systemic chemotherapy.
The prognosis can be aided by using the International Extranodal Lymphoma Study Group score which uses age >60, ECOG performance status > 1, elevated LDH, increased CSF protein and deep brain involvement as poor prognostic factors. For example, those with 0-1 risk factor are considered low risk and have a 2-year overall survival rate of 80% while those with 4 or 5 of these poor risk factors have a 2-year overall survival rate of only 15%.
For those patients with adequate performance status and renal function, systemic chemotherapy that includes high dose methotrexate (MTX) is the standard of care. Typical doses of MTX are from 3g/m2 to 8 g/m2 – these high doses allow better penetration into the CNS but they come with toxicity and require close monitoring during treatment. MTX is combined with rituximab (an anti-CD20 antibody) in addition to other cytotoxic drugs such as temozolomide, procarbazine, vincristine, etoposide or cytarabine. Most regimens give a progression-free survival rate at 2 years of about 55% with a 4-year survival rate of 65%. High dose chemotherapy with autologous stem cell transplantation can be considered for the fit patient as consolidation treatment.

More recently, a group from Japan has utilized tirabrutinib, a second generation oral Bruton tyrosine kinase (BTK) inhibitor, in PCNSL that has relapsed or was refractory to initial therapy. These BTK-inhibitors are already an important drug class for the treatment of chronic lymphocytic leukemia, small cell lymphoma and Waldentrom macroglobulinemia. In the study from Japan, 44 relapsed or refractory PCNSL patients were treated with tirabrutinib at either 320 mg or 480 mg once daily. Th response rate was 67% with complete remissions identified in 36% of subjects. Toxicity was consistent with other BTK-inhibitors.
Based on this data, in the US, the PROSPECT trial has begun. This clinical trial examines the use of tirabrutinib as a single agent in patients with relapsed or refractory PCNSL as well as looking at tirabrutinib together with a high dose MTX regimen (MTX/ temozolomide/rituximab or rituximab/procarbazine/vincristine) as first line therapy. This study is being conducted across the US with two centers in Pennsylvania (Pittsburgh and Hershey) actively recruiting and plans for opening the study at the University of Pennsylvania are in progress.
In conclusion, PCNSL is a rare type of Non-Hodgkin lymphoma that clinicians need to suspect in the appropriate at-risk population. New treatment options are being explored that hopefully will ease the burden of PCNSL in this group of lymphoma patients.
SPRING 2024 | CHESTER COUNTY Medicine 15 www. CCMS .org
T2 weighted MRI images of PCNSL
16 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org

Insulin Is So Last Year A free clinic’s take on the impact of Dulaglutide on glycemic control and quality of life
WRITTEN BY LUCY MERRILL ON BEHALF OF COMMUNITY VOLUNTEERS IN MEDICINE
Type 2 diabetes can be a difficult diagnosis for anyone, but it is particularly daunting for the uninsured. At Community Volunteers in Medicine, a non-profit free clinic for uninsured and low-income residents of Chester County, we have been fortunate enough to gain access to Dulaglutide as part of our medical arsenal to treat type 2 diabetes, a disease which impacts about 20% of our patient population. After noting anecdotally the positive impact it seemed to be having on our patients, we decided to take a closer look.

medication titrations, administrations, and finger sticks.
We first gained access to Dulaglutide in October of 2021 and have since been able to maintain a steady supply for our patients through Lilly, Direct Relief, and Dispensary of Hope. The injectable is considered a second-line agent after Metformin for patients with an A1C greater than 8%. In order to demonstrate how we use Dulaglutide here at CVIM, let’s look at a patient case.
Dulaglutide is a once-weekly, injectable GLP-1 medication designed to improve blood glucose in patients with type 2 diabetes mellitus by limiting the escape of sugar from the liver into the blood, delaying stomach emptying, and stimulating the pancreas to release insulin in response to high blood glucose levels after eating. For our patients, this means a reduction in blood sugar without risk of hypoglycemia, feeling full faster and longer when eating, and a lowered risk of cardiovascular disease and chronic kidney disease. The once-weekly dosing also makes adherence easier and improves patient experience by reducing frequency of
Patient JL, a 54-year-old Latino male, presented to our clinic in May of last year with type 2 diabetes and obesity. A widow and Ecuadorian immigrant in the US since 2003, JL lives with his nephew and works as a cook in a local restaurant. JL was diagnosed with type 2 diabetes in 2019 at a clinic in Norristown, where he received treatment until it closed down during the pandemic. He was then referred to a clinic in Philadelphia but was unable to maintain continuity of care due to transportation barriers. When he arrived at CVIM for the first time, JL reported that just the week prior he had run out of his one-year supply of insulin, obtained from Walmart with the financial support of a friend, which he had been injecting himself once per week, estimating the
continued on next page >
SPRING 2024 | CHESTER COUNTY Medicine 17
www. CCMS .org
Insulin is So Last Year continued from page 17
amount due to difficulties seeing the numbers on the syringe. The patient was also taking a pill every day but was unsure of the name of either medication, was not storing his insulin properly, and had not had access to nor been taught how to use a glucometer.
Medical Director Dr. Jacapraro initiated care by prescribing him 500 mg daily Metformin, sending him for routine labs and an A1c, and internally referring him to diabetes education. The patient’s A1c that week was 11.1. JL met with the diabetes educator, Carla Graves, four days after his initial visit, at which point she taught him how to use a glucometer and relayed basic dietary education. The team decided to initiate Dulaglutide and increase his dose of Metformin to twice daily. As is routine, Carla then taught the patient how to use the injectable, giving him the opportunity to self-administer for the first time here in the clinic, and explained to him the potential for early satiety and GI symptoms, particularly with high fat meals.
JL was then to follow up with diabetes education monthly and a medical provider after three months. When JL returned for his medical visit in August 2023, his A1c was 6.9. In just three months, we were able to get him from uncontrolled to within target range. The patient is now stable on Metformin XR 1000 mg in the morning and Dulaglutide 0.75mg once weekly. This patient case lays testament to the power of Dulaglutide; in addition to its biological benefits, the dosing and injection technique are simple and eliminate the need for dose measurement, reducing patient error and making the process more accessible to patients with low health literacy.
In our analysis of Dulaglutide here at CVIM, we then conducted a retroactive observational study to compare it to standard care. For the purposes of this study, we looked at patients with type 2 diabetes in our clinic from October 2021 to June 2023 who were over the age of 18, had not previously been on a GLP1, had an initial A1c over 8%, and for whom we had at least 3 months of consecutive data. This group totaled 265 patients, 223 of whom were prescribed Dulaglutide, and 42 of whom were not. After eliminating patients who were non-adherent or intolerant to the medication, we were left with 95 patients in our intervention group and 42 in our control. This was a much smaller group than we anticipated, having not considered how many of our patients are only with us for a short time or intermittently. Of note demographically, the patients in both groups were 90% Hispanic.
In the first component of this study, we took a look at a few things, namely, A1c reduction, weight loss, and impact of Dulaglutide on insulin usage. We saw no difference in A1c reduction between groups, with both experiencing an average A1c reduction of 2.5%. The control group on average gained 1.5 pounds, whereas the Dulaglutide group on average lost 2.5 pounds. Zooming in on the Dulaglutide group alone, we found the highest reduction in A1c among patients who were on Metformin as a first line agent and Dulaglutide as a second, the lowest reduction in A1c among those with a 6th grade education or less, and the highest reduction in A1c among those with the lowest income. Of those on insulin when they started Dulaglutide, 61% were able to lower their insulin dose and another 27%
18 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org
discontinued insulin altogether.
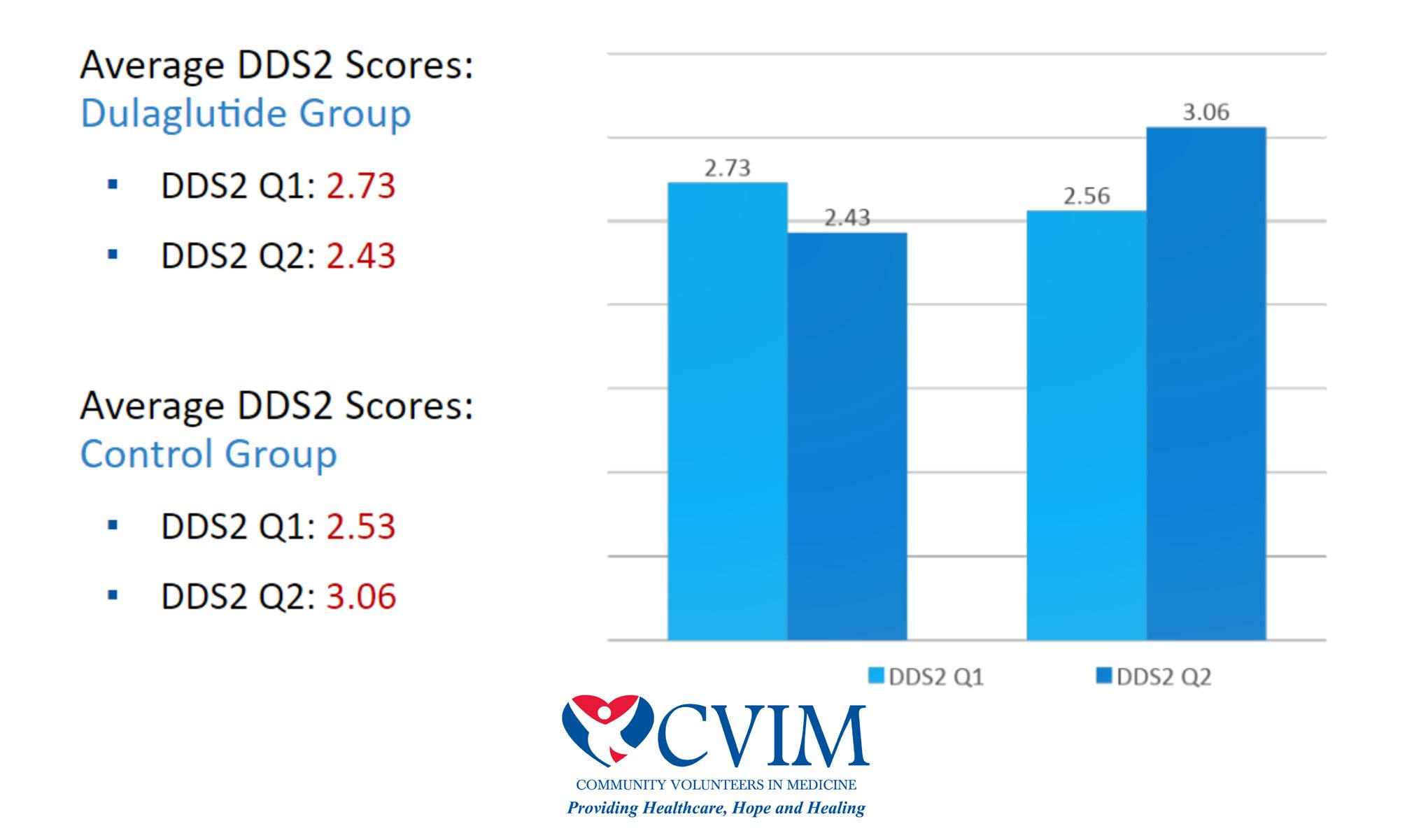
In the second component of this study, we sought to measure diabetes distress, or the emotional burden of living with diabetes and the self-care it requires. We did so by using a two-item distress scale, the DDS2, asking each participant to rate on a scale of one to six the following two statements: “Feeling overwhelmed by the demands of living with diabetes.” and “Feeling that I am often failing with my diabetes.” The score for item one was higher in our Dulaglutide group, while the score for item two was higher in the control group. This indicates that the Dulaglutide group is feeling just as overwhelmed as the control group, if not more, but that
they are less likely to think that they are failing. As perhaps may be expected, both groups saw an increase in diabetes distress as A1c increased. When asked how Dulaglutide has impacted their quality of life, many patients spoke to improved glycemic control, weight loss, and appetite control. Others mentioned the convenience of dosing and improvement of diabetes symptoms.
Our numbers are small, so these data may not be generalizable to other populations, but based on our findings it would seem that Dulaglutide is non-inferior to standard care for A1c reduction and modestly superior to standard care for weight loss and addressing of diabetes distress.
continued on next page >
SPRING 2024 | CHESTER COUNTY Medicine 1 9 www. CCMS .org
Insulin is So Last Year continued from page 19

20 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org

Cheryl
3801 Kennett Pike, Suite C200 | Greenville, DE 19807
M: 302.379.9647 | O: 302.571.7210
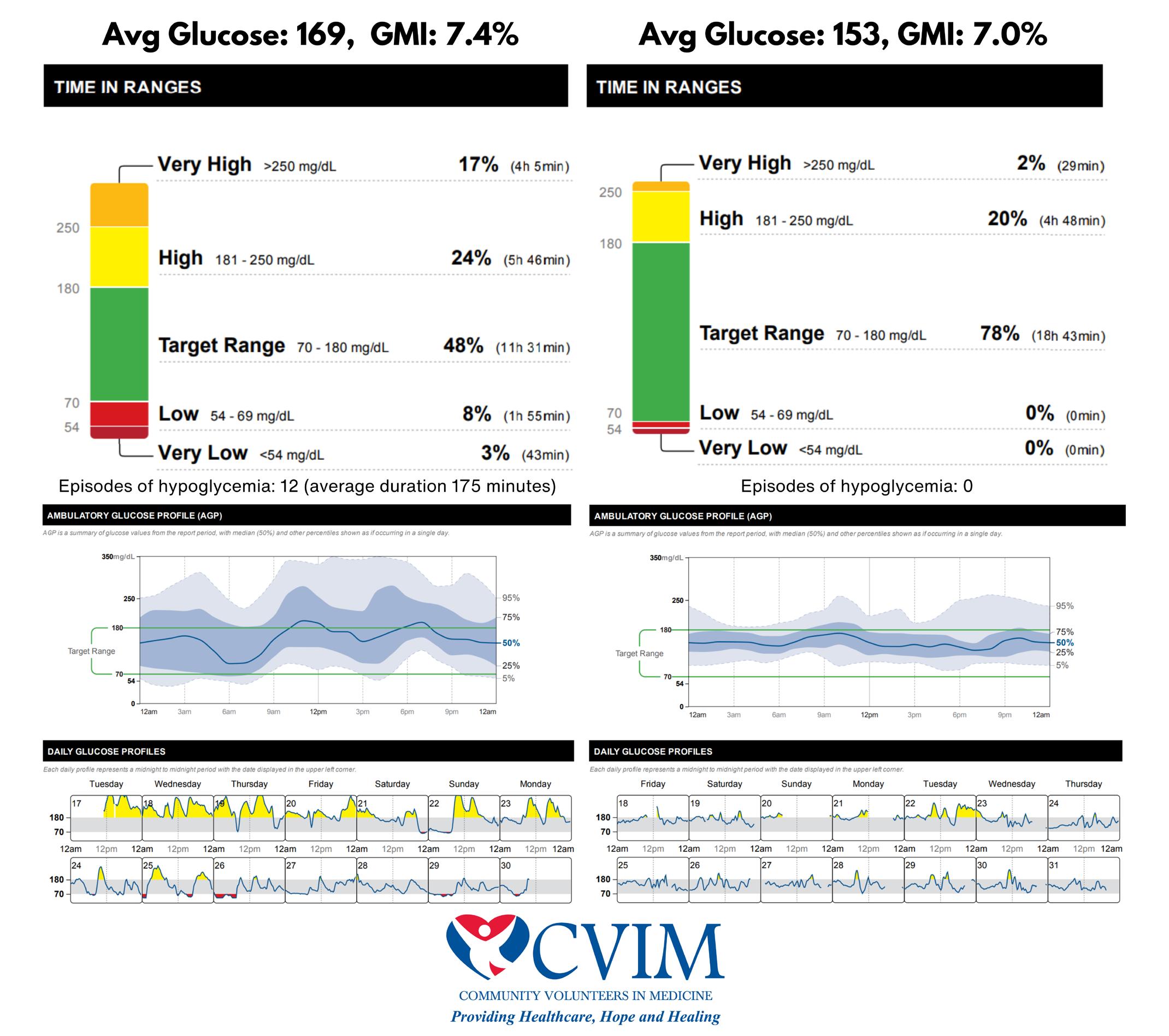
We hypothesize that another benefit of Dulaglutide may not be evidenced in these data but could be in the future through the use of continuous glucose monitors. In a particular patient, we saw a correlation between Dulaglutide initiation and an increase in time spent within blood glucose target range, a measure not well represented in A1c. One particular patient with an average glucose of 169 and GMI of 7.4% saw marginal improvement on Dulaglutide down to an average glucose of 153 and a GMI of 7.0%, but when we look closer, we find that the patient went from spending 48% of time in target range and experiencing 12 episodes of hypoglycemia per two-week period, with each episode lasting an average of over two hours, to spending 78% of time in target range and experiencing 0 episodes of hypoglycemia per twoweek period. This case shows us that just a 0.4% decrease in A1c on Dulaglutide can be concealing the full benefit of stable daily blood sugar and its associated improvement of symptoms.
Dulaglutide use comes with its challenges; the cost can be prohibitive, patient satisfaction may be a barrier considering objections to injections or intolerance to potential GI side effects, and it requires training of providers to feel comfortable prescribing these novel agents. Even so, Dulaglutide appears to be a drug of great benefit and promise, allowing our free health clinic to quickly and efficiently reduce blood sugar in our patients with uncontrolled type 2 diabetes.
About CVIM
Founded in 1998, Community Volunteers in Medicine (CVIM) delivers free, comprehensive, high-quality medical services, dental care, behavioral healthcare, and prescription medications to more than 4,000 individuals and families among the working uninsured in the region. Services are provided by 350 volunteers who donate their time and professional services. Area healthcare institutions contribute diagnostic services and advanced care that cannot be offered in a primary care setting. Virtually 100% of CVIM’s revenue comes from philanthropy. Beyond providing direct care that improves the health of the overall community, CVIM is an expression of our highest ideals as a society: compassion and equity for everyone.
SPRING 2024 | CHESTER COUNTY Medicine 21 www. CCMS .org The guidance and expertise you expect. The personal attention you deserve. Member FDIC | NMLS #417673 | wsfsbank.com/pb Wealth Management | Private Banking Lending and Deposit Solutions | Mortgages
M. Vaughan Senior Relationship Manager
WSFS Wealth Center
Sandra Malamed
BY BRUCE A. COLLEY, DO


Iwas lucky to be introduced to our Winter edition’s featured artist, Sandra Malamed, by Rhoda Kahler, a previous Chester County artist we featured (see the Spring 2017 issue) who thought she would be an attractive fit for our Journal. As it turns out Sandra was in the medical mission field for ten years at the Graduate Hospital in Philadelphia in the AIDS/Oncology unit. So, it is with pride to present “one of our own.” Before coming to Philadelphia, Sandra grew up in Corning, New York, then attended Rochester University where she earned her BS and MS degree in nursing science. Though immersed in science during her formal education, art was a central part of her life since childhood. It was in kindergarten when she had an epiphany of realization that she was “way better” than her classmates at drawing, cutting, and making things. And from then on Sandra enjoyed her poly-artistic talents in a hobby mode. Especially, designing and making clothing.
It was when Sandra and her husband, a radiologist, moved to Chester County in 1993 and she retired from her nursing position that art became not only her passion but now her full-time vocation. Sandra quickly discovered the thriving and dynamic art community here in Chester County. By serendipity they moved from Philadelphia to Chester Springs (some consider it the epicenter of the Chester County art world, though those in the Wyeth part of the county may disagree).
I met Sandra at her studio in Chester Springs on a beautiful, bright sunny day in February. I was delighted to find the grounds peppered with ceramic and glass
www. CCMS .org 22 CHESTER COUNTY Medicine | SPRING 2024
Topsy turvy drinking buddies for wine or martinis
Victims of pandemic disinformation


www. CCMS .org SPRING 2024 | CHESTER COUNTY Medicine 23
Then She Just Took Off
And
8.5 x 16
Cessation of Hostilities 9.5 x 35
continued on next page >
The Art of Chester County continued from page 23

creations, along with concreate statuary. Entering her studio was like entering Merlin’s workshop. Ceramics of all forms and variety and themes, as well as oil paintings garments, and applique. Applique, a unique form of fabric art, was new to me. Enjoy Sandra’s talent and her many oeuvres shared on these pages. Sandra, thank you for sharing what you have described as your “ little world.” We will all be better for it. And do not we all live in our own little worlds. And really, all we dare to accomplish with this “little” Journal and Medical Society is to share our knowledge, experience, and concerns, striving to improve the health and safety of our fellow Chester Countians.

“Corona Crown”
The crown is made from porcelain. There is writing on every surface of the crown. The words are direct quotes from a politician about the pandemic during the very pinnacle of the death toll. This was when mass graves were being dug in NYC and most every hospital had a refrigerated semi serving as an auxiliary morgue.
The colored discs are the tops of corona virus vaccine vials.
Purple: Pfizer, Red: Moderna, Blue: J&J, and the pink ones are from the dilutant. I collected these during the months that I volunteered for the Chester County Medical Reserve Corp at vaccine clinics around the county. Tens of thousands of vaccines were administered by health department staff and volunteers during those clinics.
24 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org
Nerikomi Platter 16 x 16 colored procelain inlay
Fox table full length 42H x 36L x 24W porcelain and wood

SANDRA MALAMED
Artist Statement
My work centers around my love of creative play. I am driven by novelty and fun. I do what makes me happy and try a lot of things that have a pretty good chance of failing just to see what happens. When I find something that works, I continue to play and push the limits of what I can achieve. As a self-taught artist, I have learned to accept failure and embrace it as a teaching tool. This way of working may not be efficient, but it allows me to practice my art in a world with very few rules or limitations. I have experimented many times with inlaid colored clay techniques. My latest experimentation involves creating “fabric” of inlaid color clay, cutting it up into strips and piecing it back together as I might do in my second love, creating narrative fabric appliqué. Once I have created my “fabric,” I work without a formal plan to see where my imagination leads me. I find this process very pleasing, and I am happy with the results.
My work has been shown and sold across the country. It can be viewed in my studio by appointment and can always be found in The American Folk Art Museum Store in New York City.

www. CCMS .org SPRING 2024 | CHESTER COUNTY Medicine 25
Mosaic mural in progress May 2018
“BUTTERFLY GARDEN”

Recovering from knee or hip surgery can be painful and arduous, and most patients will tell you that they “just want to go home” after a night or two in the hospital.
But is home really the best place to heal and regain strength?
CHESTER COUNTY OFFERS MANY GREAT OPTIONS FOR SENIOR LIVING
BY KELLY ANDRESS, FOUNDER AND PRESIDENT, SAGELIFE

Unless a patient has a full-time cook, cleaning staff, caregiver, and driver to take them to and from their follow-up appointments, they’re facing household chores, inconvenience, and discomfort in addition to a long recuperation. A stay at a modern rehab community, complete with all the necessary care, support, and meals, can be the most comfortable — and safest option.
But even without surgery, where is the best place for your 80-plusyear-old loved ones and patients? What if they could live independently while enjoying a completely no-maintenance lifestyle and the peace of mind of knowing that care is available should they ever need it?
In the past few decades, senior living communities have evolved from illness-focused care and cookie-cutter activities to comprehensive
and holistic wellness programs to support resident needs, interests, and abilities — not disabilities, actual or perceived.
Chester County offers many great options for seniors who wish to live life to the fullest, making connections and building friendships as they enjoy their favorite pastimes and discover new pursuits. Building a supportive community in this way staves off the steep decline in health that social isolation and boredom so often bring.
Seniors are celebrated and supported as the individuals that they are, whether they are fitness buffs, music and art lovers, life-long learners, craftsmen and women, extroverts, introverts, and everyone in between.
On-campus health facilities offer routine healthcare, eliminating often unnecessary appointments in your offices. Many communities offer a continuum of care, and the peace of mind of knowing that additional support is available if needed!
26 CHESTER COUNTY Medicine | SPRING 2024
www. CCMS .org

Misconceptions about senior living often delay seniors and their loved ones from enjoying the benefits these communities have to offer. My colleagues and I repeatedly hear, “I wish I came here 3 – 5 – 7 years ago.”
I can’t tell you how many times we hear or speak to adult children who tell us that they are not afraid to answer the cell phone call from mom or dad for the first time in years because they know their parents are safe — and happy.
It is so often, in fact, that when people do tell me they or their loved ones prefer to age in place, with in-home meals and other types of care, I tell them without mincing words they are paying for a substandard product when they could be experiencing an environment rooted in creativity, independent thinking, and truly unique offerings with like-minded individuals. They could be thriving and growing, while enjoying support that helps them maximize their independence. Instead of aging in place, they could be aging successfully.
Resort-style amenities like golf simulators, bocce courts, pools, bars, gyms, libraries, and art studios keep residents engaged while calendars full of fun events, club meetings, games, classes, and parties foster interpersonal connections and cognitive health.
Plus Chester County’s senior living communities also offer some of the best, freshest, chef-prepared food in the region.
Thankfully, many local communities offer these amenities, services, and care at competitive price points — often not requiring large down payments (another misconception, by the way).
So next time you think about — or are asked about — senior living, please remember that your patients have amazing options that help residents feel their best, achieve their life and health goals, and pursue their interests.



SPRING 2024 | CHESTER COUNTY Medicine 27

NEGOTIATING KEY EMPLOYMENT CONTRACT TERMS
BY KAREN E. DAVIDSON, ESQ.

Physician employment contracts encompass relationships between doctors and savvy hospitals/health systems, academic medical centers and private practices. These contracts have evolved into sophisticated instruments drafted principally for the benefit of the employer. They specify the duties and obligations of the physician (from clinical hours to on-call duties), outline compensation, address professional liability insurance coverage, and delineate termination rights. This article seeks to raise awareness of four key contract areas and highlight some related negotiation tips.1
1. Compensation.
While physician compensation historically was a set amount with annual increases, changes in reimbursement and the health care marketplace have vastly increased compensation complexity, often shifting risk to physicians. What exists now are elaborate compensation models that typically provide guaranteed base compensation for one or two years, after which the base and/ or bonus is subject to incentives and productivity benchmarks. These include work relative value units (wRVUs: a measure of physician work effort) or collections, quality measures and others that serve as targets to determine if a physician will retain, lose or garner certain compensation. Anticipated compensation should be analyzed based on a specialty’s compensation survey data (available through subscription). Physicians should fully understand their compensation/incentive targets, ascertain if they are likely to achieve them and estimate the amount or range of compensation to which they ultimately will be entitled.
Negotiation Tip: Seek to negotiate compensation that is definitive for as long as possible through set compensation with specified bonus amounts including perhaps sign-on or retention bonuses, with set increases, whether established amounts or
percentages. For variable portions of compensation (such as floating base or productivity bonuses) seek lower target thresholds for wRVUs or collections, and greater wRVU dollar values based on compensation survey data.
2. Professional Liability Insurance.
Most physician contracts specify that the employer will purchase professional liability insurance covering the physician for services rendered during the period of employment. They should also address which party is responsible for purchasing a post-termination extended reporting endorsement (i.e., tail coverage) if the underlying policy was written on a “claims made” basis. Absent an express obligation by an employer to purchase tail coverage, physicians are generally liable for the cost. It is critical that the contract clearly specifies the party responsible for tail coverage cost and the circumstances under which such party will assume tail responsibility. It has become increasingly important to ascertain if there is any limit on the extent of tail coverage. This is because some employers limit tail coverage to the applicable statute of limitation period, leaving the physician open to potential future liability.
Tail coverage is expensive, ranging from 100% to 200% of a physician’s annual professional liability premium. The cost can be exorbitant for high risk specialties with costly annual premiums. For example, an OB/GYN physician’s tail coverage could cost upwards of $80,000 during the first year of medical practice. Regardless of the tail arrangement, the physician should fully understand the extent of tail coverage liability he/she could be obligated to assume.
Negotiation Tip: Negotiating tail contract provisions can be tricky because who pays the tail may depend on the type of termination. Ascertain if the employer will assume the full cost of unlimited tail coverage upon termination regardless of the termination reason. If that is not possible, consider seeking to
28 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org
have the employer assume the full tail coverage cost if it terminates the contract “without cause” or if the physician terminates “for cause.” Alternatively, it may make sense simply to seek a cap on the physician’s tail obligation amount or propose that the parties share the cost equally.
3. Term/Termination.
Physicians are often told by prospective employers that they are being offered a multi-year contract. Yet, the contracts often allow the parties to terminate for any reason (i.e., without cause) at any time upon relatively short notice (e.g., 60 or 90 days). Contracts also typically include “for cause” termination provisions allowing an employer to immediately terminate due to acute circumstances such as loss of licensure or professional liability coverage, or contract breach. These provisions can be based on subjective factors and drafted too broadly, so should be carefully reviewed.
When assessing the impact of termination provisions, physicians should ascertain what the fall-out will be under “without cause” and “for cause” circumstances. That is, under what termination circumstances might the physician be liable for tail coverage (discussed above), be obligated to repay a sign-on bonus, moving expenses, educational loan amounts or other items, or lose a productivity, quality or other bonus or compensation. Note that a physician may only be entitled to certain incentive compensation payments if he/she is employed at the time of payment, which is often many months after it is earned. Bottom line, physicians should try to limit such losses and repayments as much as possible.
Negotiation Tip: Ascertain if it makes sense to seek a “no cut” deal where neither party has the right to terminate the contract “without cause” for 1 or 2 years. Doing so may limit the need to repay certain items. Also, if a significant obligation (such as tail cost) is triggered by a “for cause” termination, try to negotiate objective, narrow “for cause” provisions. Physicians should also seek to reduce repayment obligations by negotiating burn-offs that gradually reduce repayment amounts over the course of one or two years.
4. Non-Compete Clauses.
Non-compete clauses typically limit physicians from practicing within certain geographic areas (often based on a mileage radius around a location or multiple sites) for a specified time-period following contract termination. Most states uphold non-compete restrictions that legitimately protect an employer from unfair competition and that are reasonable in geographic area and time. Time restrictions of one to two years are usually upheld as reasonable. Reasonableness of mileage restrictions may depend on whether the employer is in an urban, suburban or rural area. For example, a 10-mile non-compete may be reasonable in a suburban locale, but unreasonable in the heart of a city. Note that a Spring 2024 Federal Trade Commission vote is anticipated on its proposed rule banning non-competes; however, such a ban is not
expected to apply to non-profit entities/organizations.
In the meantime, physicians should carefully analyze noncompete restrictions and ascertain all locations from which a mileage restriction applies. Online distance calculator tools can facilitate examination of an anticipated restricted area. If a restricted area is extensive and applies to several of an employer’s sites or locations, the physician should ascertain if he/she will have to relocate upon termination of employment.
Physicians need to understand the extent of the non-compete restriction(s) and determine where they could work if subject to the non-compete. Some contracts contain remedies for noncompete violations including liquidated damages which can be a multiple of the physician’s annual compensation. For physicians leaving a position which is subject to a non-compete restriction, care must be taken to ensure that any new position will not be violative. Ultimately, physicians should not sign a non-compete with which they do not intend to comply.
Negotiation Tip: Seek to limit a non-compete to locations where the physician renders services for the employer. This may entail a further limitation if the physician covers multiple locations, perhaps limited to the location where the physician primarily renders services but delineated with as much specificity as possible. If there are realistic future employment opportunities within certain geographic areas, try to reduce the mileage or negotiate zip-code or institution carve-outs where the physician might seek employment after termination.
Summary
Physician employment contracts are sophisticated instruments with potential for significant adverse impact on physicians. They should be carefully analyzed and negotiated to limit physicians’ exposure to financial loss and other liability.
About the Author: Karen E. Davidson, Esq., managing member of Law Offices of Karen E. Davidson, LLC, is a veteran attorney focused on representing health care professionals. She has over 30 years’ experience serving the legal needs of her clients in business, regulatory and reimbursement matters. Ms. Davidson is a graduate of Temple University – James E. Beasley School of Law, licensed to practice law in the Commonwealth of Pennsylvania, State of Maine and the District of Columbia (inactive), and a member of the Bar Associations in those jurisdictions. She is also a member of the American Health Law Association and Board of Directors of Southeastern Pennsylvania Area Health Education Center. Ms. Davidson speaks regularly to professional groups, providing insight into legal issues in professional practice. She can be reached by telephone at (610) 940-4041 or email at karend@ kdavidsonlaw.com, or through www.kdavidsonlaw.com website.
1 This article is solely for informational purposes and does not constitute legal advice. The advice of a qualified attorney should be sought in connection with review, interpretation and negotiation of any employment contract.
SPRING 2024 | CHESTER COUNTY Medicine 29 www. CCMS .org
Mindfulness in Medicine and Healthcare
 BY DIANE REIBEL, PHD, & ALEEZE MOSS, PHD
BY DIANE REIBEL, PHD, & ALEEZE MOSS, PHD

Mindfulness is a natural human capacity to be fully aware and present in the moment. However, we are often not present, lost in thoughts about the past, overwhelmed by worries and projections about the future. This tendency of our minds to think about what could or should have happened in the past, or worry about what might happen in the future, can contribute to feelings of stress and anxiety. One way to strengthen our ability to stay more present and aware is to practice mindfulness meditation.
Mindfulness-Based Stress Reduction (MBSR) is a program that has at its core intensive training in mindfulness meditation. It is an evidence-based educational program that was developed by Jon Kabat-Zinn and colleagues in 1979, as a way to teach patients with chronic medical conditions how to live fuller, healthier, and more adaptive lives. Kabat-Zinn defines mindfulness as the awareness that arises from paying attention in a particular way: on purpose, in the present moment and with an attitude of nonjudgement. Practicing mindfulness meditation cultivates moment to moment awareness, allowing us to reduce automatic reactivity and to respond more skillfully and wisely in our lives.
MBSR is currently offered in hundreds of medical centers in the United States and around the world. The evidence base for MBSR has helped to extend its use beyond patient populations, into education, corporate and community settings.
30 CHESTER COUNTY Medicine | SPRING 2024 www. CCMS .org

APRIL 5-14
Reading, PA




MBSR is a formalized and well structured group intervention that is participant-centered, experiential and educational. During the 8-week program participants learn a variety of different formal mindfulness practices, which they are asked to practice at home with guided recordings in between the weekly classes. There is also emphasis on bringing mindfulness into everyday life through informal practices. Through both the formal and informal practices participants not only strengthen their attentional skills and their ability to be present, but also cultivate attitudes that support their wellbeing. These attitudes of mindfulness include nonjudgment, curiosity, patience, and kindness.
Over forty years of research on MBSR in various clinical and non-clinical populations has shown reduced anxiety, depression, and chronic pain, as well as improved cognitive, brain, and immune function. Studies have also found that MBSR can reduce stress and burnout in healthcare providers, improve their wellbeing and enhance the provider-patient relationship. A very recent randomized controlled study, published in Journal of the American Medical Association, found that MBSR was equally as effective in reducing anxiety as a widely used anti-anxiety medication. There were also significantly less side effects in the MBSR group.
MARCUS MILLER & JONATHAN BUTLER
LEE RITENOUR & DAVE GRUSIN and KIRK WHALUM
WEST COAST JAM! RICK BRAUN, RICHARD ELLIOT, PETER WHITE and the WEST COAST HORNS
BRIAN CULBERTSON: THE TRILOGY TOUR
CELEBRATING WOMEN IN JAZZ III featuring MELBA MOORE, NICOLE HENRY, MAYSA and more JOEY ALEXANDER plus TUCK & PATTI
PAT METHENY: DREAM BOX TOUR
ERIC DARIUS & REBECCA JADE and many more must-see concerts!
PRESENTED BY
BERKS ARTS
The Myrna Brind Center for Mindfulness at the Marcus Institute of Integrative Health at Jefferson Health is one of the longest-standing mindfulness centers in the nation. The Center has been providing mindfulness training for over 25 years in healthcare, education, and corporate settings. Thousands of people have benefited from the mindfulness offerings of the Center, including patients and health care providers. In addition to teaching MBSR, we have been running mindfulness programs for medical students and residents, as well as providing mindfulness teacher training for professionals for decades. We also specialize in adapting mindfulness programs to meet the needs of specific populations. We have developed programs for chronic pain patients with opioid addictions, older adults in long-term retirement communities, people with vision impairment, and people with ALS. We also do community outreach to underserved populations and offer scholarships to those with financial need so that they can experience the multitude of benefits of mindfulness.
For more information about the programs at the Myrna Brind Center for Mindfulness, please visit jeffersonhealth.org/ mindfulness.
SPRING 2024 | CHESTER COUNTY Medicine 31 www. CCMS .org
Featuring ...
INSPIRE ENGAGE UNITE Tickets on sale NOW at berksjazzfest.com! 33RD ANNUAL
PROUD SPONSOR OF BOSCOV’S BERKS JAZZ FEST
When it comes to MRI providers, there is a difference.
MRI Group has a long tradition of excellence: Accurate image reading. Collaborative, highly trained physicians. Exceptional patient experience. Affordable rates.
• Images read by local radiologists
• Radiologists available 24 hours a day, year round, to read images and provide consultation
• All MRI Group locations are ACR accredited
• All radiologists are board certified by American Board of Radiology
• Experts in various radiology specialties including cardiovascular, interventional, neuroradiology, vascular, musculoskeletal, and pediatric imaging
• Evening appointments available
CHESTER COUNTY LOCATION:
950 S. Octorara Trail, Parkesburg (Intersection of Routes 30 and 10)
We are located at the Penn Medicine Lancaster General Health Parkesburg outpatient facility.
MRI scans performed at our Parkesburg location
• Abdomen
• Brain
• Chest
• Extremity
• Joint
• Magnetic Resonance Angiography (MRA)
• Pelvis
• Spine
Phone: 717-291-1016
Fax: 717-509-8642
MRIGroup.com
Several locations in Lancaster County and Chester County
