AsChair-Electlastyear,Iwastaskedwithchoosingathemefor2024.Ichose“Time”asourtheme.Time affectseachofourlives,anditmanifestsinmanyissuesthatweaddresswithourclients.Andso,I began Foravarietyofreasons,IsuddenlyfeltthefocusandenergyIusedtofeelwhenIlivedintheD C , areawhereIhadatheatrecompanyandproducedand/ordirectedavarietyofplays.Iwaseagerto begintoplanandshapethe“season”forNPI.Whatwilltheplaysbe,andwhowillbethedirectors?Iam sogratefultothewonderfulpeoplewhoacceptedmyrequestforthemtopresentatourluncheons.I wanttothankandacknowledgethemhere:
DavidSacks,Ph D “Wow,ThatWentFast!TimeDilationandFlowinTherapy” LJRatliff,L.C.S.W.“GenerationalHealingandFamilyConstellationsWork:The BodyasTimeTraveler”
More than 20 million people in the US have a substance use disorder. Whether you work with individuals, couples, or groups, there is a VERY good chance your clients (or you) are impacted by this topic.
This workshop has something for almost everyone NOT JUST THOSE WHO WORK SPECIFICALLY IN THE SUD FIELD.
We have tried various locations and are always open to tweaking the format, even switching the night of the week every so often It does take much work (mostly volunteer), time, and energy to keep this treasured organization running! We are always excited to suggest to membership that serving on a committee or applying to serve on the Board are exciting ways to network with other members, contribute to the functioning of the organization, give back to a group that perhaps has benefited you in the past or present, and apply some of your talents.
We have eight standing committees - Communications, Development, Finance, Membership, Nominating, Programming, and Social Justice. These committees, along with an Ad-Hoc Committee focused on implementation of the 2023 Reset and Revision statement, serve as the backbone of the functioning of NPI.
We are excited to be at this particular juncture: to be able to look back on the formation and sustenance of NPI and at the same time to look forward to the possibilities of what the future holds for this organization. We are grateful to the founders who had the vision to support and connect psychotherapists and thrilled to have new and established members join us in this ongoing journey.
Promotion on Social Media
Logo/Link on NPI Website
“NPI Community Partner Spotlight” distributed to over 1,000 individuals
Networking & Promotional Opportunities at CE Meetings
Approved for 3.00 contact hours for Ethics and 2.00 contact hours for Suicide Prevention
Attend BOTH Sessions and SAVE BIG!
ATTENDEES CAN CHOOSE TO REGISTER FOR ONE OR BOTH THE ETHICS OR SUICIDE PREVENTION PORTIONS OF THIS WORKSHOP. THERE IS A DISCOUNTED REGISTRATION FOR ATTENDING BOTH SESSIONS.
Session I: “Prejudice and Suicidal Clients"
Time: 9:00 - 11:00 am
Presenter: Dr. Erin Carney, PhD
Session II: "The Ethical Frontier: AI Integration in Counseling"
Imagine a place you could go, arriving just as you are shook-up, broke-down, hurt, mad, lonely or filled with joy, love, elation and be received, supported, listened-to. No judgment, advice, comparisons. No self-improvement goals. No money involved. Just the warmth and support of kind fellow travelers. For the past 12 years, maybe more, for one night each month, I have been favored to have just such a place. I think we started out calling it a Wisdom Circle, but the good news was that I didn’t have to be wise to participate just open and curious.
I’m not a joiner. I’m shy and introverted. But the devotion to the heart that I have witnessed in this group of friends these colleagues, psychotherapists, NPI members has kept me coming back month after month, year after year. They know me; they accept me; they even seem fond of me. I am very fond of them.
Given the longevity of the group, we have, of course, been together through many changes We’ve lost two precious souls to the grave. (Though they do from time to time make appearances.) I feel an ache and a tenderness recalling the many gifts that have come my way by being a part of this circle.
Of course there’s no way of knowing how another group with different characters and circumstances would fair But our simple recipe honest sharing, mutual respect, no cross-talk (OK, some cross-talk) seems to have made for some pretty good cake. I encourage you to try the experiment with others in our healing community.
These are hard times
byTerrenceReal
ByPhilip Chanin, Ed.D., ABPP, CGP BoardCertifiedClinical Psychologist/Assistant Clinical Professor, Department of Psychiatry VanderbiltUniversity MedicalCenter philchanin@gmail.com
Real continues, “The repair process is unilateral, not mutual. One partner asks for and receives help from the other in order to move out of a state of acute discontent (disharmony) back into the experience of closeness and connection (harmony) The listener must put his or her own needs aside someone experiencing distress, even if he’s intent on making things right, isn’t really interested in your thoughts, your feelings, or your reasons or explanations. In those first raw moments of reconnection, the upset partner doesn’t care all that much about you one way or the other What he needs to know if whether or not you care about him ” (p 207)
Real adds, “Once you have demonstrated your care and sincerity, once you have addressed his concerns, then he might have an interest in you. But before that occurs, a distressed partner will inevitably perceive any bid on your part to focus on your experience as a deflection And though you may have nothing but the best of intentions, he will see your behaviors as defensive, ungiving, selfish, or evasive And, by the way, he’d be right!” (pp. 207-208)
Real elaborates on this point: “The truth is that when most of us engage in so-called listening, we have a hot nanosecond’s worth of attention span before we’re off and running. And just what are we off and running to? Rebuttal. ‘Geez, that’s not right,’ we might say, or ‘Hey, I never said that. That is such an exaggeration.’ Or, if you’re a psychologically sophisticated couple, you might sound something like this: ‘Honey, that’s your projection ’ ‘No, dear, it’syour denial ’” (p 212)
Real addresses the most profound question for troubled couples: “What’s best for your children?” He writes, “We are living in very conservative times, and a lot of emphasis has been put on preserving families at all cost. That’s simply unreasonable Yes, children are damaged by divorce There’s no question about that The real question is, how damaged are they by staying in miserable homes?...As bad as divorce is, a child would be better off without the exposure to yelling and fighting and a blatantly disturbed environment. Few people argue that point So now the question ratchets down to this: How damaged do children get in homes with a miserable marriage that is more contained? Many would argue that children are better off in such environments than with divorced parents. As a family therapist, I must say that I’m skeptical…It’s not at all clear to me that the so-called contained or hidden misery in nonexplosive marriages is really as hidden as we might like to think ” (pp 268-269)
Real continues, “Even if you were to convince me that children in such homes were less damaged in general, I will nevertheless guarantee you that they will sustain considerable damage when it comes to having healthy relationships of their own in the future Almost every troubled relationship I have ever worked with was a replay of some aspect of the troubled relationship each partner grew up with…Even if it were proven somehow that children are more damaged through divorce than through remaining in homes with unhappy marriages, it is not at all clear to me that the moral imperative is for adults to sacrifice living healthy lives for the sake of their children I have helped unhappy couples break up; I also have helped them stay together precisely for the sake of the children.” (pp. 269-270)
Real concludes, “In extreme circumstances, the choice seems clear In less blatant situations I mistrust anyone, frankly, who claims to be able to tell you what’s best for your children, or for either of you for that matter. You must decide. Think long and hard; talk it out with those you trust, and listen to what you feel. In the end, most people I’ve encountered over the years who have been through this decision rarely speak about what they should have done, one way or the other They speak about what they felt they had to do ” (p 270)
Next Real asks, “When should you pull the plug?” He writes, “It serves no one’s interests to preserve endlessly toxic interactions. Addicts and abusive partners can be helped, and the first step should always be an ultimatum: Get treatment or else! But if someone simply refuses, or if he won’t allow his treatment to be effective, I don’t think there’s much choice I firmly believe that any two partners who love each other and who are willing to do the work can transform even a terrible relationship into a good one, and even into a great one over time. Once both partners are at the table in good faith, anything can be worked out.
AndrewKrichels,DirectorofCreativeActionSeminars;JackieWelch-Schlicher, OwnerofVisionsManifestCoachingandWildhairPottery– “Techniques forLiving a Grounded, Centered and CreativeLifeinanAging Body”
EboniWebb,Psy.D. “The TimelessWound: Understanding Trauma’s Hold on Past,PresentandFuture”
Ihopemostofyouwerethereforthesewonderfulpresentations.Theywereagreatexperienceandwellworth thetimeandattention.Andthankyou,speakers,foryourgenerosityandforsharingyourgiftsof expertise,knowledge,perspective–andtime. (AndI’dliketo givea special thank you to John Nichols, LPC, for preparingapresentation as backup in the event of a last-minute cancellation).
Reflections on the FDA Denial of MDMA-Assisted Psychotherapy for PTSD
By Tom Neilson, Psy.D.
In August, the Food and Drug Administration (FDA) declined to approve MDMA-Assisted Psychotherapy for Post-Traumatic Stress Disorder (PTSD). This decision was based largely on the conclusions of the FDA Advisory Committee, which voted overwhelmingly against approval. The negative Advisory Committee vote, and the subsequent FDA decision came as something of a surprise to the mental health community The FDA had previously designated MDMA as a “breakthrough therapy,” and the FDA helped design the Phase III studies that showed MDMA-Assisted Psychotherapy to be effective in treating PTSD In two Phase III studies (Mitchell, et al , 2021; Mitchell, et al , 2023), more than two thirds of those who were treated with MDMAAssisted Psychotherapy no longer qualified for a PTSD diagnosis by the end of treatment, and changes in CAPS-5 scores before and after treatment were significant at the P<0.0001 (in the 2021 study) and the P<0.001 level (in the 2023 study). These results are remarkable and frankly unheard of in psychotherapy research. They are even more remarkable given the low success rate therapists typically have treating moderate to severe PTSD.
Functional Unblinding
The Advisory Committee’s main concern was functional unblinding The Phase III studies were double-blind studies, meaning that neither the subjects nor the investigators were told whether the subjects received MDMA or a placebo Despite the double-blind procedures, almost all the subjects and researchers could tell who received MDMA and who received placebo. This functional unblinding should not be surprising; the acute effects of MDMA are not subtle, and almost anyone would be able to tell who did and did not receive MDMA.
While functional unblinding is a valid concern, it appears that a double standard is being applied here. In antidepressant research, the side effects of antidepressants can tip off subjects and researchers about who received the medication and who received the placebo For example, in one study of bupropion for smoking cessation, participants who guessed that they were assigned to the bupropion group were more than twice as likely to have been given bupropion, and participants who guessed placebo were more than twice as likely to have been assigned to the placebo group. (Schnoll, et al, 2008). In these subjects, the double blind clearly failed. One review of blinding, primarily in antidepressants, found that blinding is largely unsuccessful in both subjects and investigators. In addition, it found that few randomized clinical trials in a range of fields, including chronic pain and general medicine, report information about the success of blinding.
Furthermore,itseemsunlikely thattheseextremely significantresultswereduetoaplaceboeffect;wehave neverseenaplaceboeffectevenclosetothissizeinpsychological research
Inclusionof Psychotherapy.A secondconcernof theAdvisory Committeewastheinclusionof psychotherapy inthedrug approval process TheFDA hasneverapproved,norbeenaskedtoapprove,adrug incombination withpsychotherapy Traditional psychiatricmedicationsaredesignedtowork ontheirown,althoughmany patientsreceivemedicationcombinedwithpsychotherapy.
TheAdvisory Committee’sobjectiontotheinclusionof psychotherapy reflectsalack of understanding of this newandrevolutionary treatmentmodel Therapistswithexperiencetreating moderateandseverePTSD know thattherapy oftenfailsbecausethepatientcannottoleratetheintensepainof working withvividandoften horrifictraumamemories.Therapy oftentriggersflashbacks,nightmares,andintrusivethoughtsof thetrauma; thelimbicsystem becomesoverwhelmedinthetreatmentprocess.Therapy grindstoahalt,andmany patientsquittherapy becauseof thepainof theprocess
AbusePotential. TheAdvisory Committeewasalsoconcernedthatdatawasnotcollectedontheabuse potential of MDMA AnMDMA experienceisoverwhelmingly pleasurableformostpeople,andconcernabout abuseandaddictionmakessomesense However,tolerancedevelopsquickly withMDMA use Frequentuseof MDMA rapidly becomesunsatisfying,making chronicMDMA abuseandaddictionanunlikely phenomenon.
Concerns about abuse seem even more overblown when we consider that drugs with enormous addiction potential, including opioids and Adderall, have been approved by the FDA Again, there seems to be a double standard here
Finally, I would like to point out that the Advisory Committee included only one expert on psychedelics, who was the only member who voted to approve MDMA-Assisted Psychotherapy.
Conclusions. In my opinion, the Advisory Committee neither understood nor appreciated the MDMA-Assisted Psychotherapy model. They also applied egregious double standards in their decision. It may be that MDMAAssisted Psychotherapy is too much of a quantum leap for many traditional mental health experts to understand and appreciate at this time. The model may be threatening to experts who have ties to Big Pharma or who are invested in older and, to be frank, less effective approaches to treating PTSD.
The FDA has asked for a third Phase III study, and that study will happen. The FDA decision is also being appealed, but I am not optimistic that the appeal will find sympathetic ears. I am confident that MDMAAssisted Psychotherapy will be approved by the FDA at some point in the future, but the recent FDA decision set the process back two to five years In the meantime, veterans, victims of sexual assault, and other trauma victims will needlessly suffer, and we clinicians will continue working with our current and less than adequate treatment resources
References
Hysek, C M , Brugger, R , Simmler, L D , Bruggisser, M , Donzelli, M , Grouzmann, E , Hoener, M C , & Liechti, M E. (2012). Effects of the α₂-adrenergic agonist clonidine on the pharmacodynamics and pharmacokinetics of 3,4-methylenedioxymethamphetamine in healthy volunteers. The Journal of pharmacology and experimental therapeutics, 340(2), 286–294. https://doi.org/10.1124/jpet.111.188425
Mitchell, J. M., Bogenschutz, M., Lilienstein, A., Harrison, C., Kleiman, S., Parker-Guilbert, K., Ot'alora G, M., Garas, W., Paleos, C., Gorman, I., Nicholas, C., Mithoefer, M., Carlin, S., Poulter, B., Mithoefer, A., Quevedo, S., Wells, G., Klaire, S. S., van der Kolk, B., Tzarfaty, K., … Doblin, R. (2021). MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nature medicine, 27(6), 1025–1033. https://doi.org/10.1038/s41591-021-01336-3
Mitchell, J M , Ot'alora G, M , van der Kolk, B , Shannon, S , Bogenschutz, M , Gelfand, Y , Paleos, C , Nicholas, C R , Quevedo, S , Balliett, B , Hamilton, S , Mithoefer, M , Kleiman, S , Parker-Guilbert, K , Tzarfaty, K , Harrison, C , de Boer, A , Doblin, R , Yazar-Klosinski, B , & MAPP2 Study Collaborator Group (2023) MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial Nature medicine, 29(10), 2473–2480 https://doi org/10 1038/s41591-023-02565-4
Scott, A. J., Sharpe, L., & Colagiuri, B. (2022). A systematic review and meta-analysis of the success of blinding in antidepressant RCTs. Psychiatry research, 307, 114297. https://doi.org/10.1016/j.psychres.2021.114297
Schnoll, R. A., Epstein, L., Audrain, J., Niaura, R., Hawk, L., Shields, P. G., Lerman, C., & Wileyto, E. P. (2008). Can the blind see? Participant guess about treatment arm assignment may influence outcome in a clinical trial of bupropion for smoking cessation. Journal of substance abuse treatment, 34(2), 234–241. https://doi.org/10.1016/j.jsat.2007.04.004
This fall, NPI members will see changes to our publication previously known as NPI Reflects that is distributed to over 1000 therapists, counselors, and students in the Nashville area and posted online. We are excited to rebrand this publication NPI Endeavors as we believe the new name more clearly states the purpose of this publication and eliminates some of the confusion between it and our weekly email blast.
With the focus of this first issue to be Reflections on 2024 and Projections for 2025, we hope to highlight and celebrate our members, our presenters, and their vast experiences, as well as generate excitement around programming for next year.
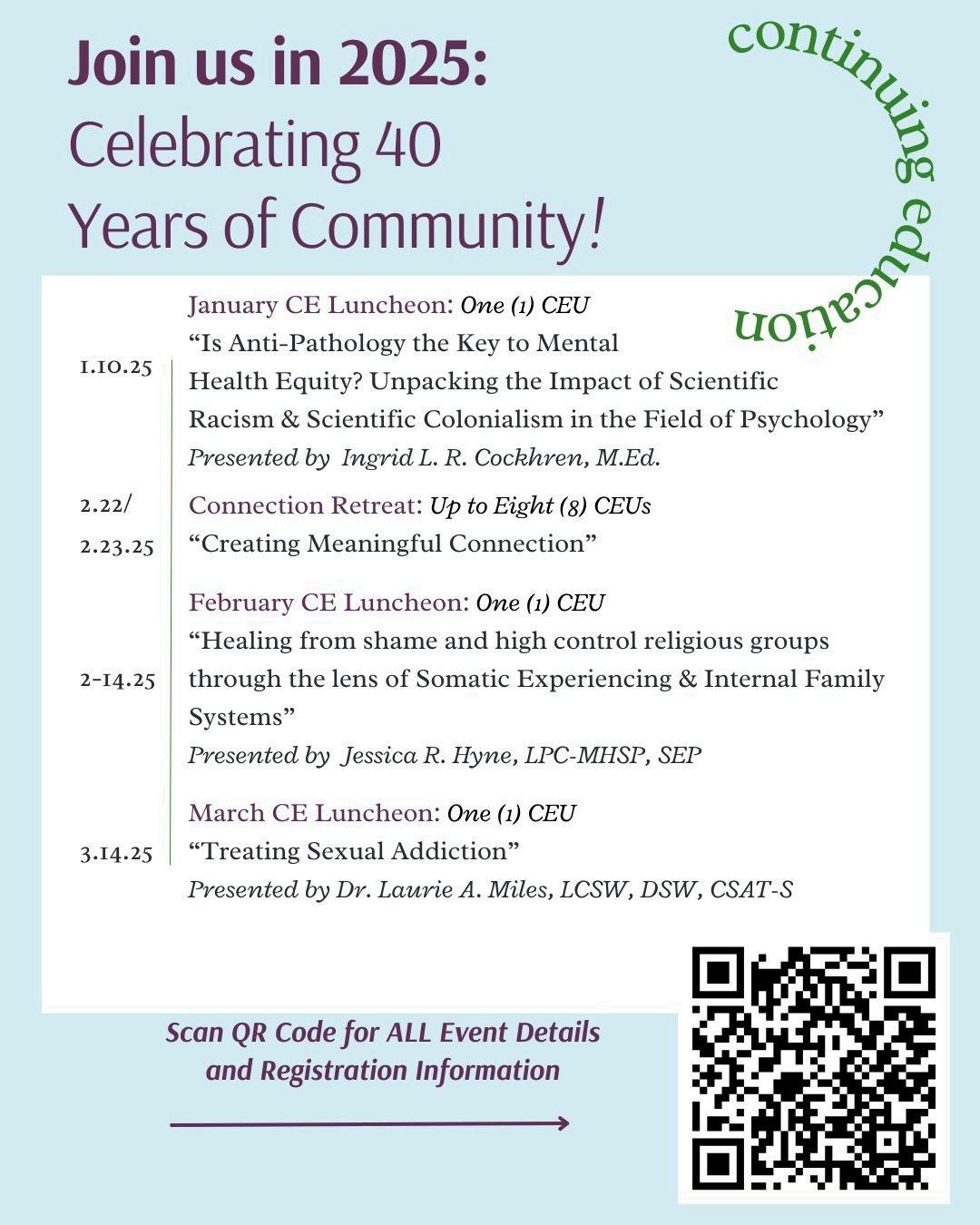
We hope that you have enjoyed this publication, and that you are making plans to join us in 2025 as we celebrate 40 years of connecting and community!