Just a few weeks after learning bystander CPR, high school senior Adrian used it to save a
— his father’s.
MANAGING
Erin Wegner
STAFF
Madison Loethen
CONTRIBUTING WRITERS
Christian Basi, Colton Downing, Jesse Godec, Andrea Primus, Jenny L. Workman
CONTRIBUTING
Lana Eklund
Please submit comments or feedback to erin.wegner@boone.health or call 573.815.3217
1600 East Broadway Columbia, MO 65201 573.815.8000
For a FREE subscription, scan the QR code, visit boone.pub/subscribe, or call 573.815.3392.
Board of Directors
Jerry Kennett, MD
Randy Morrow
Mary Beck, DNP, RN, FAONL
Judy Starr
Stacye Smith
Charles P. Bondurant, MD, FABNS, FACS
Jeffery Lashley, Ph.D.
EMERGENCY ROOM TOOL KIT
Emergencies are unexpected, and no one plans on spending a part of their day in the Emergency Room. If you find yourself or a loved one needing emergency room care, here’s a list of items to help make your visit more comfortable:
Standard Medical
Appointment Information
• Photo ID
• Health Insurance
• Emergency contact information
• Name of primary care provider
• Pharmacy preference
• List of medications, vitamins and dosage
• Allergies to medications, food, latex and other substances
• Payment method for your ER copay – this amount varies, depending on your health insurance plan
Personal Items
• Comfortable clothes
• Shoes that are easy to take on and off
• Phone, charger and headphones
• Reading materials – book or magazine
• Eyeglasses, hearing aids or other personal assistive devices you may need
• Water bottle
• Non-perishable snacks
What to Leave at Home
• Anything valuable
• Cash
• Jewelry
Protecting What Matters
When emergencies strike, every second matters—and Mid-Missouri residents can count on Boone Health's Emergency Department to deliver expert, compassionate care when it’s needed most.
Serving more than 36,000 people each year, our emergency department is equipped to handle significant injuries and medical events. The expanded and remodeled ER now has 16 patient rooms, a larger triage area and an additional treatment area to decrease wait times while still providing excellent care.
Our emergency team is dedicated to providing outstanding, individualized care to everyone who comes through the door.
“Every patient complaint is taken very seriously,” according to Dr. H. Orlando Heredia, director of Emergency Medicine. “We find that most people do not have a serious problem, but the only way to make sure is by having a thorough evaluation by one of our providers.”
As a designated Level I Stroke and STEMI Center, we offer the highest level of emergency response for lifethreatening conditions, including heart attacks and strokes. This distinction means faster diagnoses, immediate treatment, and better outcomes, all delivered by a team trained to act swiftly and treat patients with dignity. Our commitment to excellence is what drives us. It’s this commitment to excellence that led to our recognition by U.S. News & World Report ranking us as the No. 1 hospital in mid-Missouri.
In this issue of My Boone Health, you’ll read about what brings most people to the ER, the flow of a typical visit, and how the ER determines the order to treat patients. You’ll also read about ways our emergency department is advancing patient care. Our cover story is the account of one man’s health emergency and how he is alive today because his son took a proactive stance and was educated in Basic Life Support (BLS), including CPR.
From my own experience, I was first introduced to CPR when I was in high school. My football coach required the entire team to take the class. I maintained my certification over the years that I worked as a therapist. While I never had to use this training during high school or through my early career, many years later, I had to use the techniques I had learned to help dislodge a hotdog from my daughter’s airway when she began to choke on her lunch. There are few things as scary as a loved one needing immediate assistance. I will always be thankful for the training that helped ensure a good outcome.
I was taught CPR in high school, but children as young as nine can begin learning those skills even if they don’t have the strength to perform chest compressions on an adult. And ask yourself—if your family faces a life-threatening emergency, could they call on you to help save them, especially if a medical professional is several minutes away?
Learning Bystander CPR addresses one type of emergency in our community. From house fires and carbon monoxide poisoning to natural disasters, a variety of emergencies occur every day, so it’s important to take steps (even if they are small ones) toward being prepared now. We’re fortunate to have several resources in mid-Missouri that teach these critical skills.
To learn CPR through Boone Health Community Wellness, visit boone.pub/boonecpr
To schedule a free Red Cross home fire safety appointment, visit boone.pub/RedCrossSmokeAlarm
When we all work together to be prepared, we create a safer community for everyone.
Sincerely,
Brady Dubois CEO, Boone Health
Boone Health Nationally Recognized for Its Commitment to Quality Care for Heart Attacks In Mid-Missouri
Boone Health has received multiple quality achievement awards from the American Heart Association (AHA) recognizing its commitment to high standards of patient care for stroke, NSTEMI and STEMI heart attacks.
The American Heart Association’s Get With The Guidelines® - Stroke Gold Plus quality achievement award recognizes our commitment to ensuring stroke patients receive the most appropriate treatment according to nationally recognized, research-based guidelines, leading to more lives saved and reduced disability.
Program participants qualify annually for the award by demonstrating how their organization provides quality care for stroke patients, follows treatment guidelines, and educates patients to help them manage their health and recovery at home.
The American Heart Association’s Get With The Guidelines® – Coronary Artery Disease NSTEMI Gold award recognizes Boone Health for its commitment to offering rapid, research-based care to people experiencing a specific type of heart attack known as a non-ST elevation myocardial infarction, or NSTEMI.
Each year, more than 546,000 people in the U.S. experience this type of dangerous heart attack, caused by a partial blockage of blood flow to the heart. Like all heart attacks, this requires timely treatment to restore blood flow as quickly as possible.
Boone Health also received the American Heart Association’s Get With The Guidelines® – Coronary Artery Disease STEMI Silver recognition for its commitment to offering rapid, research-based care to people experiencing an ST elevation myocardial infarction, or STEMI, a type of heart attack known to be more severe and dangerous than other types of heart attacks. This type of heart attack requires immediate treatment.
Each year, more that 250,000 people in the U.S. experience a STEMI heart attack, which is considered a severe heart attack because it is caused by a total blockage of blood flow to the heart.
These designations are given to hospitals that demonstrate a commitment to treating patients following the most up-to-date, research-based guidelines for Stroke, NSTEMI and STEMI care as outlined by the American Heart Association.
The American Heart Association’s Get With The Guidelines programs help hospitals across the nation ensure their standards for patient care are consistently aligned with the latest research- and evidence-based guidelines for better patient outcomes.
Boone Health Named No. 1 Hospital in Mid-Missouri by U.S. News
U.S. News & World Report released its hospital rankings, naming Boone Health as the No. 1 hospital in Mid-Missouri and the No. 7 hospital in the state. In the past 12 months, five independent organizations have given top marks to Boone Health, emphasizing patient care, quality of care delivered, employee environment and culture, and nursing quality. And Forbes recently announced that Boone Health is the No. 1 employer in mid-Missouri.
“Once again, Boone Health has been independently verified as the best hospital and overall health organization in mid-Missouri,” said Brady Dubois, president and CEO of Boone Health. “We continue to give the nation’s very best care in mid-Missouri’s own backyard due to our dedication to excellence throughout our organization, from when you first check-in to when you are discharged. Boone Health is fortunate to have an incredibly talented and compassionate medical staff and care team who focus on each individual patient, and we are always looking for ways to improve above and beyond the stellar care that Boone Health is known for throughout the region.”
For 2025-2026, Boone Health is ranked “High Performing” in 14 out of 22 categories. This is an increase from last year where Boone Health was ranked “High Performing” in 9 out of 21 categories. Those high performing areas are: abdominal aortic aneurysm repair; aortic valve surgery; colon cancer surgery; heart attack; heart bypass surgery; hip replacement; knee replacement; back surgery (spinal fusions); heart arrhythmia; hip fracture; leukemia, lymphoma and myeloma; pacemaker implantation; pneumonia; and prostate cancer surgery.
Boone Health Increasing Primary Care Capacity To Address Dire Need
The award-winning organization has hired 8 new doctors, each of which can see 1,800 patients, with more coming by the end of 2025.
Throughout the country, health care continues to experience shortages of providers in key areas, especially primary care. Here in mid-Missouri, Boone Health has been diligently working to address those shortages. Over the past 12 months, Boone Health has hired 25 medical providers, eight of whom are primary care providers while the others are offering health care in key areas, including general surgery, endocrinology and metabolism, gynecologic oncology, radiology, rheumatology and palliative care.
“Across the nation, there has been a strong need for primary care providers, and the mid-Missouri community is no different,” said Drew Wilkinson, Boone Health vice president of provider and ambulatory operations. “We’ve been working hard to address the issue here locally, and we’ve attracted several wonderful and experienced providers to join the best health care organization in mid-Missouri. We have more work to do, but we expect that these new providers will help us address the need for health care in both Columbia and many of our rural areas in the 26 counties that we serve.”
Each new provider can accept approximately 1,800 new patients. Individuals wanting to establish primary care with a Boone Health provider can call 573.815.3000 or visit boone.health/services/primary-care
Additionally, Boone Health is expecting at least four more primary care providers to join the organization by the end of 2025.
“My fiancé and I were looking for that next chapter in our lives and a community to call our own,” said Dr. Louis Gerges, a physician who recently joined the Boone Health Nifong Primary Care Clinic. “When care is rooted in community it becomes more than practicing medicine—it becomes belonging. I feel as though we found that community in Boone Health.”
Recently ranked as the No. 1 hospital in mid-Missouri and in the top 100 hospitals for overall service in the nation and for patient experience, over the past several months, Boone Health has announced several expansion efforts, including a standalone breast care clinic that also offers the only prosthetic bra shop in mid-Missouri, an expansion of the primary care clinic in Glasgow, and expanded hours at the Boone Health Convenient Care clinic.
“We’ve been growing, and we have plans to continue the expansion and improvement of health care in mid-Missouri,” Boone Health CEO and President Brady Dubois said. “Yet, even with all of our plans for expansion, we will never let go of the caring environment that we’ve built for more than 100 years. That focus on each, individual patient is what makes Boone Health stand out, whether you’ve come in for an annual physical or you’re at the hospital for a procedure. Every nurse, every doctor, every therapist, every employee is going to ensure that the focus remains on you, the patient, and that we get you back doing what you love as fast as possible.”
Dr. Sara Crowder’s 3,000th Surgery
Sara Crowder, MD hit a milestone when she performed her 3,000th surgery using the da Vinci robot machine. This places her in the top 5% of surgeons in the United States, and No. 1 in the state of Missouri, as it relates to experience with the surgical robotic machine. Dr. Crowder specializes in gynecological oncology and has been using the surgical robot since 2011. The da Vinci robot machine, with cutting edge technology only available here at Boone Health, allows Dr. Crowder to use minimally invasive techniques for many of her patients.
Boone CT Accredited for Cardiac Imaging
The Computed Tomography (CT) scanners at Boone Hospital received renewal from the American College of Radiology (ACR) for Head, Neck, Chest and Abdomen imaging. In addition, this is the first year that Boone Health CT has been Accredited for Cardiac Imaging in CT. Towards the end of summer, construction began for the placement of an additional CT scanner at the hospital. The new scanner is a dual-source, 256-splice Siemens Drive. Boone Hospital now has four CT scanners, with three located at the hospital and one located at the Nifong medical building.
What Brings Most People to the ER
— And What Happens Next
Chest pain. Abdominal pain. Back pain. Weakness.
These are the most common reasons people visit the Emergency Department at Boone Health, according to Dr. H. Orlando Heredia, MD, MPH, Chief and Facility Medical Director of Emergency Medicine. While these symptoms can sometimes point to serious conditions, they are often treatable — and even manageable with early evaluation.
“Every patient complaint is taken very seriously,” Dr. Heredia said. “We find that most people do not have a serious problem, but the only way to make sure is by having a thorough evaluation by one of our providers.”
That thoroughness is part of what defines emergency medicine. Because the same symptom can range from something minor to something life-threatening, emergency physicians are trained to evaluate quickly, effectively and with the full range of possibilities in mind.
“We frequently see both sides of the spectrum,” Dr. Heredia said. “Severe pain that ends up being something benign, and also mild symptoms that end up being a life-threatening illness. Some emergencies are obvious and others are not.”
1st Step: Triage
When patients arrive at the Emergency Department, the first step is triage — a system designed to ensure that everyone receives the right care at the right time.
In triage, a registered nurse will take your vital signs — things like blood pressure, heart rate, temperature and oxygen saturation — and ask brief questions about your symptoms. This initial screening helps the team determine the appropriate next steps for your evaluation.
“If they determine that you have an imminent threat to life or limb, you will be taken back to the main ED and will be evaluated promptly,” Dr. Heredia explained. “If not, they may draw blood
and get additional tests while you wait to be assigned a location to be seen by one of our providers.”
The space where you’re treated can vary depending on your needs. If you require a stretcher or cardiac monitoring, you’ll be assigned a room. Otherwise, you may be seen in a treatment chair or recliner.
This flexible setup helps maximize the department’s capacity and ensures that all patients receive timely care from trained emergency providers.
Treating the Most Common Complaints
While emergency departments are equipped to handle life threatening emergencies, many visits stem from everyday health concerns that are causing pain, discomfort or uncertainty. Among the most frequent are:
• Chest pain, which can range from muscle strain to heart-related concerns.
• Abdominal pain, which might be caused by digestive issues, infections, or other conditions.
• Back pain, often due to musculoskeletal strain but sometimes related to kidney or nerve issues.
• Generalized weakness, which can result from dehydration, infections, or other underlying causes.
Each of these concerns can be symptoms of something more serious — or may turn out to be mild — which is why prompt evaluation is key.
“If you are worried enough about how you feel, then we encourage you to be seen promptly,” Dr. Heredia said.
Care You Can Count On
The Emergency Department is a place designed not just for fast action, but for thoughtful, thorough care. From the moment a patient walks in the door to the time they leave with a treatment plan, the goal is the same: answers, relief and support.
“We care about you and we want to help you,” Dr. Heredia said. “Every patient will receive an evaluation to ensure there is nothing serious, and you will leave with a clear plan for next steps.”
So whether you’re experiencing sudden pain, unusual fatigue or symptoms that just don’t feel right, the emergency department at Boone Health is ready — with the expertise, compassion and responsiveness to guide you toward answers and recovery.
By Madison Loethen
Flow of a Typical Visit to the
Making a better emergency department visit: Boone Health is making important changes to how patients are evaluated when they come to the Emergency Department (ED). e changes include the establishment of a “Rapid Care Path,” where we are evaluating patients who are in stable condition when they arrive and do not need to be in a hospital bed. is allows us to make sure we have the availability for patients who do need a bed when they come to the ED. Here’s a look at the new process:
1
Arrival and Check-In
When a patient enters the Emergency Department (ED), you will be met by a member of Boone Health’s Care Team. You’ll be asked for your name, date of birth, and chief complaint for the visit. e team member will give you a wristband with your identifying information on it. (Occasionally, the ER sta is asked to assist the patient out of a car if they are unable to walk thru the entrance.)
4
Continued Care
If you are getting an X-ray taken or having blood drawn for testing and you are in our Rapid Care Path, you might be asked to sit in our “Results Pending” area while your images are being reviewed or the blood tests are conducted. Even though it might not seem like actions are being taken, Boone Health ED sta are working hard to process the tests. Depending on what tests have been asked for, it might take some time for the results to come back.
5
Moved to a Room /Treatment Chair
If your condition changes, you may be moved to a bed inside the ED or into a treatment chair in an exam room (Rapid Care Path). During this time, you will continue to be monitored for any changes to your vital signs.
Emergency Department
2
Triage
A quick evaluation of your condition will be performed by one of our triage nurses. Depending on your condition, the triage assessment, and availability of an exam room or bed, you will be asked to wait in the ED Lobby, be sent to an exam room (part of our new Rapid Care Path), or be escorted to a bed in the Emergency Department. It’s important to note that you won’t be seen on a rst-come, rst-served basis. As part of the quick evaluation, we prioritize patients who are the sickest among those in the room at that time. However, with the establishment of our Rapid Care Path, we are able to see non-urgent patients much faster than before.
3
Screening Exam
Once you are in an exam room or ED bed, a physician, physician’s assistant, or nurse practitioner will complete an exam to determine what actions should be taken next. at could include getting an X-ray or other image (MRI, CT scan, etc.), drawing blood for testing, or giving medications. At any point, you may be moved to a di erent part of the ED depending on changes in your condition.
6
Visit with a Provider
After you have been placed in an ED bed, assigned to an exam room or when your blood tests/imaging results come back, a medical provider will either give you a thorough evaluation or discuss the results of your tests/images. A recommended treatment plan will be reviewed, including whether you might need additional services or require a specialist.
7
Final Steps
Once a decision about a treatment plan has been discussed with you, you’ll either be discharged to go home with some speci c instructions or be admitted to the hospital. In rare cases, we might suggest transferring you to a di erent facility if your situation warrants care with a particular specialist.
By Andrea Primus, Emergency Room Nurse
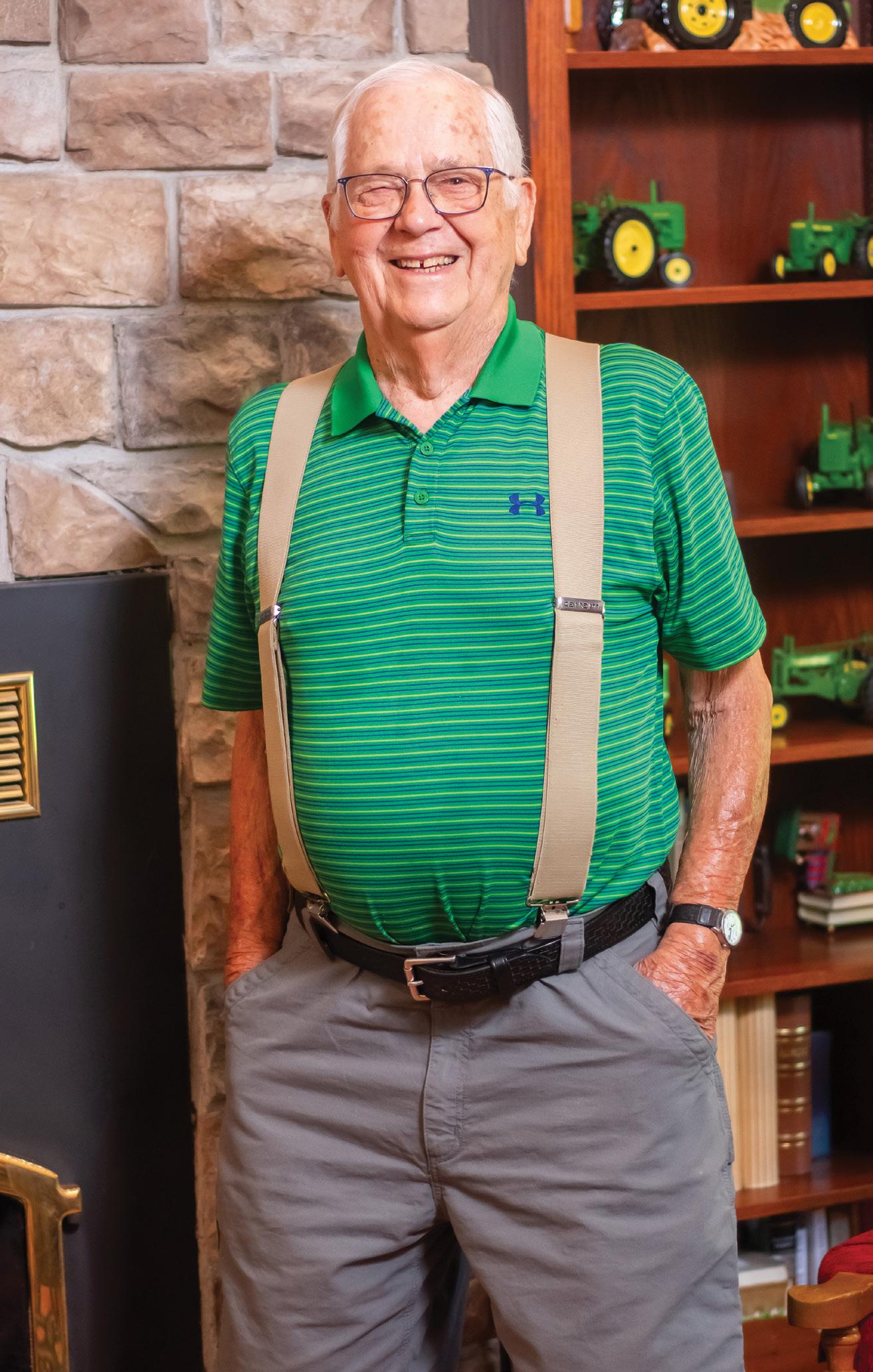
A Life-Saving
MOMENT
Adrian learned the effectiveness of bystander CPR and how important it can be when he had to use it to save his father’s life.
The morning of April 27, 2025, seemed to be just a run-of-the-mill, ordinary day in Adrian Tovar-Yampara’s house.
e Rock Bridge High School Senior was talking to his mother, Helen, about his hair. Adrian’s father, Alejandro, was in the bathroom just across the hall.
“I was getting ready for the shower,” Alejandro said, “ e last thing I remember was looking at my cell phone and getting it ready to start playing music.”
Just a few feet away, Adrian and Helen heard a thud and immediately rushed over to the bathroom where they found Alejandro on the oor unconscious.
“He was not responsive at all,” Adrian said. He quickly checked to see if his father was breathing and had a pulse. Not nding either, the emergency medical training that he had been learning in a current class took over.
“I told my mom to call 911 and immediately started CPR,” Adrian said. When his mother got the emergency dispatcher on the phone, Adrian provided key information so the responding crews would know exactly what to expect when they arrived.
While he was performing CPR, Adrian said that he was thinking about all the activities he hadn’t had a chance to do with his father, and questioned if he would ever have those precious opportunities.
Seven minutes later, an ambulance crew from Boone Health arrived at the house.
“As we were en route to the scene, we were informed that an adult male had collapsed, and that CPR was in progress by an EMT (Emergency Medical Technician) student who was there,” described Katie Gilmer, a paramedic for Boone Health. “ is was very uncommon to hear. When I got to the scene, I quickly realized that the student was his son.
“He looked up at me and said, ‘Am I doing this right?’”
In that moment, Katie said she was struck by Adrian’s calm and collected manner. She assured him that he was, indeed, “doing it right,” but that it was time for her and her team to take over.
Katie and her team continued CPR and put pads on Alejandro’s chest to de brillate him once. Katie thought she would need to de brillate him a second time, but after two more hand compressions, Alejandro reached up, grabbed Katie by the hand and said “Ow.”
“I immediately told everyone to stop as he opened his eyes and was able to communicate and talk to us,” Katie explained. e Emergency Services (EMS) team then moved Alejandro to the ambulance where an IV was started.
“Without that prompt response of Adrian engaging with CPR, there is no way that the single de brillation would have worked,” Katie said.
In her 12 years as a paramedic, the team responds to approximately 40-45 similar calls each year.
“We’ve saved a lot of people over the years, but I’ve only ever had three people who were conscious and able to talk with us before we reached the hospital,” Katie said.
Katie explained that what Adrian was able to do was a perfect example of the e ectiveness of bystander CPR and how important it can be. Adrian’s actions made sure that blood continued circulating throughout his father’s body, including vital areas such as the brain, while the Boone EMS team was headed to the house. at ability was due to an educational opportunity that Adrian had been taking advantage of while in high school.
For the past two years, Adrian had been enrolled in the Emergency Services Program o ered through the Columbia Area Career Center in partnership with Columbia Public Schools. e program requires a two-year commitment from students.
During their rst year, students take the Emergency Medical Responder course, which introduces them to key aspects of the life-saving career. e second year, students enroll in the o cial EMT course. Completion of the course allows students to qualify for the EMT certi cation test.
Adrian’s teacher, Michael Holz, has more than 25 years of experience as an
EMT and has seen a lot in his time responding to calls.
“One of the toughest things to teach is the emotional toll and how to deal with it when there is a need to put these skills into action,” Michael said. “Many students don’t understand that impact until they see or hear stories like this.”
After Adrian saved his dad’s life, he came in to talk to Michael about the experience.
“He was pretty shaken up when we talked just a couple of days after the event with his father,” Michael said. “I wasn’t surprised in the least that he was able to do this.”
Michael said that Adrian’s ability to work through scenario-based questions, taking all the information provided and making sound medical choices was a huge factor in how he handled himself in a lifesaving moment.
“ at can be a tough thing for students this young, and especially to have to perform CPR on your father!” Michael said. “Teaching young students not just the skills of an EMT, but how to handle their emotions in the moment can be challenging, especially because they are still maturing. But Adrian has a drive about him that makes his special.”
Back from the hospital after a small procedure, Alejandro is very grateful for his son and his dedication to helping others.
“My wife said that he was talking to the dispatcher on the 911 call and was very focused,” Alejandro said. “I could not be prouder.”
Adrian, who recently passed the National Registry of Emergency Medical Technicians exam is working on a
bachelor's degree, and then expects to apply for medical school. In the meantime, he has joined the Boone Health EMS department as a part-time EMT. Alejandro returned to his work at the University of Missouri, where he is part of a team surveilling environmental viruses for early detection aimed to protect public health. A job that he can continue due in large part to the lifesaving e orts of his son.
For his actions, Adrian was awarded a “challenge coin” from the Boone Health EMS department. ese coins are extremely rare and only provided to those who go above and beyond to help others in emergency situations. is is the rst time such a coin has been presented to an EMT student. Adrian was presented with the coin in front of his classmates at a surprise celebration that included both his mother and his father. By Christian Basi
Boone Health’s Community Wellness team regularly offers “hands-only” CPR classes. More information about the classes, which cost $50, can be found by scanning the QR code.
Ultrasound Guided IVs
Advancing patient care in the emergency department.
Historically, placing a peripheral IV involved using a tourniquet, identifying veins by touch and doing a blind stick. While many of our emergency department nurses are highly skilled at this, certain patient populations present signi cant challenges.
In cases where patients have been sick for extended periods of time, are on steroids, have low blood pressure, are obese, have been treated with dialysis or chemotherapy, or were recently transferred to Boone Hospital, additional needles can create signi cant discomfort, leading to delays in treatment.
To address this issue, the Emergency Department implemented a program to train nurses in ultrasound guided IV placement. Using the SonoSite X-Porte portable ultrasound machine, nurses are trained before using the machine to place IVs.
is program was implemented 7 years ago and bene ts the patient with fewer needle sticks, better patient comfort and getting medications delivered earlier. In many cases, a patient who must stay in the hospital is able to use the ultrasound guided IV for their entire stay.
If you’re a patient needing an ultrasound guided IV, you will rst be placed lying down or in a reclined seat for comfort and access to your arm. A tourniquet will be applied and then your arm will be cleaned thoroughly. A sterile ultrasound gel will be applied, and the nurse will start using the ultrasound to evaluate the di erent vessels. While the nurse is looking, they will be pressing around on the arm and sliding the gel around as they look for the right place to stick the needle. If numbing medication is used, that allows the nurse more time to manipulate the needle without causing a lot of pain.
If numbing medicine is not used, after a vessel has been selected, a longer needle will be used. Although the needle itself may look scary, it’s not a bigger needle, it’s just longer. After the skin has been punctured, they’ll guide the needle, watching it on the ultrasound machine the entire way, until it’s in the vessel. en they’ll slide the catheter in, clean up the arm, connect it to the IV, and do whatever else they need to, like draw blood or administer medicine.
e biggest di erence between a regular IV and an ultrasound guided IV is pressing around with the probe and the gel on the arm. But those things have to be cleaned up before they can put tape or stickers on to hold it in place.
For most patients, this process can take 10 minutes, compared to 1-2 minutes with a traditional IV. For patients who are on dialysis, receiving cancer therapies or on long term steroids, they become more challenging, and in some cases, it can take closer to 15 minutes.
Under ultrasound guidance, nurses can tell the di erence between veins and arteries. If they’re sticking in a sensitive area, they know exactly where they’re at, which makes it very easy.
Nurses report that they can see exactly where the needle is going. It’s kind of like x-ray vision, without the x-ray.
Ultrasound is a safe and e ective way to see what’s going on under the skin. Ultrasound doesn’t use any radiation, it uses sound waves, so it’s completely safe.
is is a huge bene t to patients who are very nervous about needles and those patients who have a long history of medical complications. When they come to the hospital, they may get stuck repeatedly, and no one wants that. Using the machine, nurses can have medicine into patients quicker and more e ciently without having to stick them multiple times.
Having enough sta to do this means patients don’t have to worry. It’s less painful and their treatment happens quicker versus having to wait for a specialist to come in and do it.
e machine in the emergency department is a multifaceted machine. It can look at abdominal organs like gallbladders, and kidneys, perform basic cardiac evaluations and assess heart function, and see and hear fetal imaging and precise heart tones for babies. e funding for this machine was provided by the Boone Health Foundation.
It's mobile, on wheels, so it's able to move around. With the number of people increasing who are needing ultrasound guided IVs, it's in use a lot. Our ICU and Infusion and Treatment Center also have these ultrasound machines.
As a sta educator, whenever high school students come through here for a tour, I tell them, this is the future. As you go to nursing school, this is what you need to learn, because it gives us more information quicker than sending someone over to CT or X-ray. Sometimes, those are appropriate, but this gives us instant information at the bedside. By Jesse Godec, Sta Educator, Emergency Department
HEART ATTACK HEADACHE TO
An emergency room employees’ headache took a scary turn, and the Boone Health team was there to help.
Chris Duncan started his medical career as an EMT- paramedic in Kansas City in 1985. He then joined the U.S. Navy and served for four years as a hospital corpsman during peacetime. After the Navy, he attended nursing school and was a hospice nurse for 23 years.
Before joining Boone Health, Chris worked in Kansas City, Northern Arizona and Arkansas before moving to Columbia two years ago. He worked as a hospice nurse for a local agency for a while before switching roles to a case manager for the emergency room.
Chris’ role helps with improving throughput of patients from the emergency room that get admitted to the hospital. He interviews patients so when they get in a hospital room, the case management staff has a better idea of who they are, what their needs are and what their barriers to discharge may be. This helps the discharge process flow much easier which is better for the patient and better for the families.
On April 2, 2025, Chris woke up and went to work. It was a normal day. He had a pretty bad headache, mainly in the back of his head, but besides that, he felt fine. About an hour after he got to work, his headache intensified. He took some ibuprofen, but after 20 minutes, the headache hadn’t gotten better and Chris was also feeling slightly short of breath, something that he had never experienced before.
Chris went to Gerrad Bard, PA-C and asked, “Hey, can you listen to my lungs?” Bard had recently purchased an electronic stethoscope that not only allows one to hear better, but it shows heart rhythms as well. He listened to Chris’ heart first and was able to identify the arrhythmia immediately. He said, “We should get an EKG.”
Chris tried to brush it off, saying he’d get one later, but the provider insisted, “No, we need to do it now.” Clearly, he heard something that alarmed him.
By the time, Chris had walked into Emergency Room #2, the provider had alerted several nurses who hooked him to an EKG - EKG’s have 12 leads. Each lead represents a different direction of cardiac activity. Right away the first few leads showed what’s known as a “tombstone” pattern—classic for a heart attack known as the “widow maker.”
The STEMI team was called. Within minutes, it seemed like 17 people were in the room: one nurse was stripping off Chris’ clothes, another was asking for his phone to contact a family member, and another was asking if he had advance directives (a living will). It was chaos, but Chris could tell they were acting fast for a reason.
“It was pretty scary,” Chris said. “I was having the headache and didn’t associate
anything with my heart. If I was having chest pains, I would have said, ‘oh my gosh I’m having a heart attack.’”
If a patient is having a heart attack in the hospital, a STEMI team is called. The STEMI team at Boone Health includes physicians, nurses and other staff from the emergency department and cardiology. They got Chris prepped for surgery and he was in the Cath lab in under 15 minutes.
They found that Chris had a 100% blockage in his left anterior descending (LAD) artery—a “widow maker.” They went in through his right wrist with a long probe and cleared the blockage. Then two stents were inserted to keep the artery open.
After leaving the hospital and taking some time off from work, Chris started outpatient cardiac rehab and attends three times a week. Chris admits he had to tailor the program to him because he has developed bad knees and a bad back.
“That’s one of the reasons I changed jobs,” Chris said.
The damage to Chris’ heart was significant. A healthy ejection fraction— how much blood the heart pumps with each beat—is normally 60-70%. Chris’ ejection fraction was 20-30%. An ejection fraction below 40% is a sign of heart failure. Cardiac rehab is helping Chris slowly build his heart muscle back up with the goal of improving his ejection fraction.
Looking back, Chris says, “I don’t know why I took a job here in the emergency room and left my industry after 23 years, but there must have been a reason. Due to the severity of blockage I had and because the heart attack was a widow maker, I might not be alive today.” He truly believes being at work—just steps from the EKG machine—saved his life. The Emergency Room staff, STEMI team, Cardiology, ICU and telemetry floors— everyone did exactly what they were supposed to do. By Erin Wegner
Boone Health is a Designated Level 1 STEMI Center
Heart Disease, which includes heart attacks, is the leading cause of death in the United States.
What is a STEMI Heart Attack?
A STEMI (ST-Elevation Myocardioal Infarction) is a type of heart attack that can be identi ed on an EKG. It is caused by a prolonged blockage of blood supply to the heart and requires immediate medical intervention.
A STEMI is visible on an EKG and generally more severe. A non-STEMI, although still a heart attack, is not detectable on an EKG and may have subtler symptoms. Both require prompt medical attention, but STEMIs typically involve more immediate and aggressive intervention.
What happens in the hospital when the STEMI team is needed?
When a patient presents with chest pain, the emergency department preforms an EKG to detect ST elevation. If STEMI is diagnosed, an emergency protocol is activated. Noti cations go out to the cardiac catheterization lab, ICU and to our interventional
cardiologist. e emergency room doctor evaluates the need for immediate interventions like intubation. e patient is quickly moved to the cardiac catheterization lab to unblock the coronary artery and then will be transferred to the ICU. Recovery times vary from next-day discharge to a few days, depending on the individual case.
Why is it important to patients that Boone Health is a Level 1 STEMI center?
Having a specialized STEMI team is critical because these types of heart attacks are life-threatening. A trained team ensures swift diagnosis and treatment, which improves patient outcomes. E ective STEMI care involves coordination between several departments and having the trained sta is essential to quickly diagnosing and treating the heart attack.
Do not delay if you experience chest pain. Delays in treatment can lead to irreversible heart damage. TIME IS HEART!
Boone Health is a Certified Level 1 Stroke Center
Stroke is the 5th cause of death and the leading cause of disability in the United States.
What is a stroke?
A stroke occurs when a blood vessel carrying oxygen and nutrients to the brain is impaired, causing brain cells to die. A stroke can be caused by a blood clot (thrombosis), a blockage (embolism), or bleeding (hemorrhage).
Strokes can be classified into two main categories:
• Ischemic Stroke: An ischemic stroke occurs when a blood vessel that supplies the brain becomes blocked, and blood is unable to ow to part of the brain. e brain cells and tissues begin to die within minutes from lack of oxygen and nutrients. 87 % of strokes are ischemic strokes
• Hemorrhagic Stroke: Hemorrhagic strokes occur when a blood vessel that supplies the brain ruptures and bleeds. When an artery bleeds into the brain, blood compresses the surrounding brain tissue and brain cells do not receive oxygen and nutrients. 13% of strokes are hemorrhagic strokes
Treatment
Immediate treatment is key to limiting the extent of brain injury resulting from stroke. Boone Health o ers a full spectrum of services to treat those who have su ered from a stroke, including neurology, neurosurgery, neuroradiology, an echo vascular lab, and both inpatient and outpatient rehabilitation.
Why is it important to patients that Boone Health is a Level 1 Stroke Center?
Boone Health understands the importance of rapid, accurate treatment to prevent death and preserve brain function. Patients arriving here are treated by specially trained neurology specialists who are on the forefront of new and specialized stroke treatments, giving more patients a better chance against this debilitating condition. By Colton Downing
Do not delay if you are experiencing stroke symptoms. Delays in treatment can lead to irreversible brain damage. TIME IS BRAIN!
Mental Health-Related EMERGENCY ROOM VISITS
“ T here’s a wide variety of mental health issues that arise in the emergency room,” said Melissa Rapp, Boone Health Social Worker. “It is such an integral part of our lives and when you have good mental health, you tend to take it for granted.”
Reasons that people need emergency room care when having a mentalhealth crisis can include patients who are having thoughts of harming themselves or others, patients who are struggling to take care of themselves, severe depression, anxiety, and thought disorders such as Schizophrenia or Bipolar Disorder. ere are also elderly patients who might be experiencing dementia, and patients who are struggling with addiction and possibly a whole host of other social issues that may be a symptom of mental health problems. Substance abuse and addiction presents in all ages and demographics.
e emergency department’s social workers consult patients who come with mental health issues who are on a spectrum – mental health conditions can vary in severity and are not all equal. “Some are in more serious situations than others,” Melissa said.
“Often times, what comes with mental health issues are physical health issues, so our emergency department may also have to assist in addressing those physical conditions as well,” Melissa said.
Physical health conditions can include diabetes, dental infections, cardiovascular issues or even substance withdrawal. “It’s a very wide range of issues that a person could present with to our emergency department. It may be that they have those conditions because they are unable to attend to their own self-care or what they are doing to themselves may be
damaging to them physically,” Melissa said.
Patients who have mental health issues who end up unhoused will come to the emergency room. ey may not be eating regularly, may not be getting adequate sleep, and struggle with getting medications or even being able to connect with a provider. e social workers in the emergency department can help with those things before the patient leaves. e social workers also assist patients getting connected with outpatient resources in the community or help get them referred if they require inpatient hospitalization.
“It’s common place for us to call all over the state of Missouri looking for facilities that might have beds open for psychiatric inpatient,” Melissa said. “ e resources in the state of Missouri are really limited for that. It can be quite time-consuming to locate and facilitate the transfer of a patient to a psychiatric unit.”
Depending on the needs of the patient, there are several options in midMissouri for substance use as well as for mental illness. Services like therapy and medication management are o ered. Burrell Behavioral Health, Compass Health and New Horizons are examples of where they might refer a patient who is limited nancially and can’t go through a private provider.
“We provide information on mental health and substance abuse daily in the emergency department,” Melissa said. Boone Health’s Emergency Department has three social workers:
“It’s my hope that someday, our society will regard mental health’s importance equal to other physical health conditions.”
– MELISSA RAPP
Melissa Rapp, Kim Oliver and Trish Gonzales. Kim and Melissa are Licensed Clinical Social Workers (LCSW) and Trish is a Licensed Master Social Worker (LMSW) with over 400 hours of supervised training in their eld.
“It’s a profession even more rigid than others,” Kim said. “We have a code of ethics that guides our practice. is document outlines core values, ethical principles and standards for practice. It helps us navigate ethical dilemmas and make sound decisions in our practice.”
“Mental health is an area that, as a society, we have really neglected. Period,” Melissa said. “ e system is far from perfect. It’s my hope that someday, our society will regard mental health’s importance equal to other physical health conditions.”
By Erin Wegner
A More Emergency Room Efficient
David experienced a very long ER wait time with his late wife.
When he returned years later, he was pleasantly surprised with how quick his ER visit was.
Boone Hospital has been part of David Strodtman’s family’s life for decades. His son was born here in 1961. Although they moved to Colorado for 40 years, they returned 20 years ago and went straight back to Boone Hospital. “I’ve always considered it to be the best hospital in the area,” David said.
In late 2022, David arrived at Boone Hospital’s emergency room early in the morning due to a severe nosebleed his wife, Ruth, was experiencing. At the time, she was battling multiple serious health issues and nose bleeds were one of several ongoing problems. e admittance process was long. After some time, Ruth was taken to triage and then moved to the general waiting area with a warm blanket. She remained very ill, and her family was concerned about the urgency of her care. Her nose continued to bleed while they waited, and her family members were anxious.
Eventually, the lead nurse was able to get her into treatment. However, Boone’s ER did not have the necessary resources to fully address the issue — speci cally, an Ear Nose and roat specialist was needed. ey were able to stop the bleeding temporarily, but it was only a stop-gap measure. For the next occurrence, David and his wife had to go to an ENT specialist outside of Boone Hospital to be treated.
While the sta at Boone were courteous and kind, the procedures in place at that time did not allow for prompt treatment. “We were in the ER for six to eight
hours.” David said. “It’s hard sitting in the waiting room when your wife is sick like that. It took us a long time to get treatment. at experience left us feeling helpless and anxious. When your wife is terminally ill, you want someone to respond to her immediately, and seeing patients who appeared less critical being seen ahead of her was hard. It felt like with such a serious nosebleed, she could have been prioritized.”
Sadly, Ruth passed away on January 5, 2023 due to multiple complications, primarily heart failure.
David’s own emergency room visit happened in May 2025, and it was very di erent. David had fallen and hit the back of his head. He’s taking Plavix, a blood thinner, so he rst called his primary care physician, Dr. Scoles, and was advised to go to the ER.
is time, David was taken to triage immediately and received a CT scan almost right away. After a brief wait,
a nurse informed him his scan was clear and led him to a small, curtained cubicle where a doctor came in promptly, con rmed the scan results, and told him he could go home once paperwork was done. e whole visit took just under two hours.
" is was much more streamlined and e cient," David said. David's family was very appreciative of him being treated and released without the prolonged ER wait time.
It wasn’t an unpleasant experience at all. Of course, ERs have their share of chaos, but this time they avoided much of that. It was methodical and smooth. Knowing that Ruth was terminally ill, David wanted her to receive urgent attention, which isn’t always possible. After returning to the ER, he’s grateful to see improvements in the system. “We were very thankful for the change in procedures,” David said.
By Erin Wegner
Rapid Care Path
Before the initiation of our Rapid Care Path, the emergency room only had its 16 beds to treat patients. When the ER was busy, those beds filled up quickly.
In Spring 2025, Rapid Care Path was initiated, allowing the ER to utilize a space in their department that had previously been underutilized.
5 chairs – kind of like big recliners – were set up and sectioned off with curtains to provide as much privacy as possible. This space allowed for 5 additional treatment areas.
These treatment areas were designed to see patients who come to the ER with non-urgent needs who require less resources: a prescription refill, a laceration or cut that is easy to treat, an adult with dental pain who needs pain meds and antibiotics.
The Rapid Care Path is open from 9 AM – 9 PM, 7 days a week and is staffed by an emergency department nurse, an emergency department provider and a patient care technician.
They can do all of the same things that can be done in a treatment room, this just helps the ER expedite the care of these patients if they can be seen in this area.
On a busy day, the ER has seen over 30 patients in the Rapid Care Path in a 12-hour window. That’s 30 less patients waiting for one of those 16 treatment beds.
It's been a huge success with helping the ER maximize its efficiency while also minimizing patient wait times. By Nick Woods, Emergency Department Manager
Andrea Primus, BSN, RN, PNDP-5
Emergency Department
Iwas born and raised in Columbia, Mo. I attended the University of Missouri and graduated with a Bachelor of Science in Nursing. For the first several years of my nursing career, I worked in Kansas City, Mo., in large Level 1 Trauma Centers. Following that, I worked as a flight nurse for Staff for Life Helicopter Service and had the opportunity to train and learn under Frank Mitchell, MD who our local Trauma Center was named after. I would have to say this role was the highlight of my nursing career! I stayed home for a couple of years with my children and then returned to Boone Hospital in the Emergency Department.
Why did you get into the health care field? I knew during high school that I wanted to be a nurse. Science was always my favorite subject, so a degree in health care was a natural choice. During my first year of college, I worked at a local nursing home as a Certified Nursing Assistant (CNA) and at a Veterans Administration Hospital as a phlebotomist; this solidified my desire to become a nurse. I thoroughly enjoyed the patient interaction and belonging to a team of caregivers.
What interested you in your particular specialty? I was interested in emergency nursing because of the fast pace and unique environment that it brings. Working very closely with physicians and learning a great deal about all specialties and variations of patient populations. Every day is different, and I enjoy the challenge of adapting to an ever-changing environment. There’s also opportunity for professional growth and development with unlimited opportunities to engage with topics that fuel your passion, whether that’s teaching new nurses or working on process improvement projects to make the ED more efficient.
What is the most rewarding part of your job? I find nursing very rewarding because you know you can make a direct impact on your community, patients and families. I also appreciate the flexibility that a nursing career provides. As you move through different stages of life – whether you’re focused on building your career or transitioning into motherhood – nursing offers adaptable schedules and hour commitments that support a healthy work-life balance.
What is the most challenging aspect of your job? One of the more challenging aspects of nursing is constantly having competing priorities to juggle. You have to find a balance that maximizes the benefits to patients. In the emergency department, things can go from calm to chaotic very quickly. You have to learn
to adjust and pivot to meet the needs of your patients as well as your coworkers.
What has changed in your field since you started practicing? I have seen lots of changes in the field of nursing over the last 32 years. One large change was the conversion to electronic health records from paper. Another ever-changing part of nursing is evidence-based practice. This impacts change in everything we do: CPR, Advanced Cardiovascular Life Support (ACLS), how to care for burns, trauma, sepsis and strokes. Nursing practice changes constantly as we gain more technology and knowledge with regards to illness and injury.
What do you see changing in the next 5 to 10 years? In the next 5 to 10 years, it will be interesting to watch how Artificial Intelligence will advance and change the healthcare field. I anticipate a lot of what we do as healthcare professionals will be delivered remotely using technology.
What do you enjoy doing outside of work? Outside of work, I enjoy spending time with my two daughters, friends and family. I enjoy cooking, baking, walking with our dogs and being outside in the sunshine.
What advice would you give someone looking to become a nurse? A career in nursing is a wonderful choice for anyone who enjoys connecting with people, often in time of challenge. Nursing offers great flexibility in geographic choices, schedules, as well as vast areas of interest. My best advice for someone looking to join our profession is to be committed to becoming a lifelong learner. Lifelong learning is necessary for nurses because of the ever-evolving changes in healthcare.
Kevin Oliver, DO Emergency Medicine
Iwas born in Enid, Ok. I did my undergraduate and graduate school here at Mizzou in chemistry and physical chemistry then back to Oklahoma State University for Medical School. I practiced full-time family practice and full-time emergency medicine in St. Charles County for 15 years then moved to Central Illinois where my wife’s family is. We spent 15 years there. Three years ago, we had two kids in school at Mizzou, and my wife decided that she wanted to move to Columbia; we’ve been here since, and we’ve loved it. I have three kids: one’s in art school in London, one’s in med school in Wichita, Kansas and one’s in pre-med here at Mizzou.
Why did you get into the health care field? I was interested in health care because my father was a physician, but I also really enjoyed chemistry. I did great with chemistry, but I realized at the time that the people I was working with had worked with the same three people for 30 years, and I decided I liked people better than that. So I decided to pursue medicine, and I’m really glad that I did.
What interested you in your particular specialty? I did family practice and emergency medicine full time for 15 years. They both have their benefits. Family practice is wonderful as far as relationships and consistency, but emergency medicine is contiguous — a one-flow process. I see a patient, order a test, get a result and discuss it with the patient. That just seems to work better for me. Also, the lifestyle is nice because in family practice, I was on call 24/7 365 days a year. In emergency medicine, I’m off when I’m off.
What is the most rewarding part of your job? Helping people that really need help when they need help. It’s wonderful when someone comes in, I can actually do something to help them. It’s extremely rewarding.
What is the most challenging aspect of your job? The electronic medical record. Documenting in the computer, dealing with the computer. I really like people more than computers. So, that’s obviously my biggest challenge, spending time away from my patients, having to do computer work.
What do you see changing in health care in the next 5 to 10 years? That’s a much more difficult question. I see a greater shortage of physicians. Advanced practice providers are going to fill
the gaps. I see a lot more involvement of AI. What I hope to see is people being empowered and encouraged to really start taking responsibility for their own health and their own wellbeing.
What advice would you give someone looking to become a doctor? Do it because you’re passionate about it. When I started, being a physician was a calling. It’s a career, and it’s not just a job. It’s rewarding from many standpoints, but if you don’t like what you’re doing, it’s never going to be rewarding.
What do you enjoy doing outside of work? Spending time with my wife and my kids. I absolutely love spending time with them. One of the nice things about emergency medicine is you work hard, and you play hard. I enjoy water skiing, snow skiing, and wood working. I love projects. My wife says I’m a project person. If I have a project, I’m happy. I don’t do idle well.
What advice would you give to someone who is going to be a patient in a hospital for a period of time? Be patient. The process does not go quickly. Be understanding. The people that are taking care of you want to be here because they like taking care of people. They might be overwhelmed, but understand that they’re doing the best they can. It also helps to have someone with you as much as possible. It’s nice to have another set of ears to hear what everybody has to say and to keep things organized. Write down your questions so when you see the provider, you’ll have all your questions ready.
Staying Safe
DURING RESPIRATORY SEASON
What do we mean by “respiratory season”?
Respiratory season covers a range of illnesses, most notable in uenza ( u), COVID-19 and Respiratory Syncytial Virus (RSV). Boone Health’s Infection Prevention Department monitors case numbers for these illnesses closely. is helps determine if visitor restrictions are needed to protect Boone Health’s patients.
When is respiratory season?
Respiratory season varies from year to year and doesn’t follow a xed calendar date range. It begins when illness rates rise above the normal level, and usually peaks between October and March – although some years it can start earlier or end later.
In uenza is the most commonly reported infectious disease during this season and is often used as the marker to signal its start. Hospitals rely on local trends and state-level data to decide when to o cially announce the beginning of respiratory season and when to encourage vaccination for employees and patients.
Will this be a bad flu year?
e only thing you can predict about the u is that it’s unpredictable. Flu viruses can mutate rapidly in ways that can make it easier for them to spread. One notable example was H1N1, which emerged in Spring 2009 and caused a pandemic that lasted through August 2010. What we do know, is that each year, in uenza causes between 120,000-710,000 hospitalizations and 6,300-52,000 deaths in the United States. Hospitals prepare each year to meet the increased need for inpatient care during respiratory season in the communities we serve.
Who should take precautions during respiratory season?
While everyone can take steps to prevent the spread of respiratory illness, there are several groups who are the most vulnerable during respiratory season.
Infants and young children are vulnerable due to their underdeveloped immune systems. While newborns are too young for most vaccines, parents and adult caregivers can get vaccines to reduce their risk of bringing a respiratory illness home.
Older adults, especially those 65 and over, are at an increased risk for severe illness due to their decreased immune response. For these individuals, a highdose u vaccine is available. Additional respiratory illness vaccines may be recommended depending on a patient’s medical history.
Immunocompromised individuals, including people on medications that suppress immune function are also at an increased risk for severe outcomes. Additional respiratory illness vaccines may be recommended depending on a patient’s medical history.
Everyone should have a conversation with their healthcare provider about what vaccines are recommended to help protect them during respiratory season.
While vaccines may not always prevent infection, they reduce the risk of severe illness, helping to lower the risk of hospitalization and death.
How can you keep yourself and your family safe during flu season?
• Get vaccinated – Influenza, RSV, COVID-19, pertussis and pneumococcal vaccines are available. Talk with your provider about vaccine recommendations for your specific medical history.
• Stay home if you’re sick – If you have respiratory symptoms – cough, sore throat, runny nose, fever.
• Practice good hand hygiene – Wash hands regularly and avoid touching your face.
• Cough and sneeze properly – Cover your nose and mouth with a tissue, then throw away the tissue and wash your hands. If you don’t have a tissue, cover your nose and mouth with your elbow, not your hands.
• Wear a mask when visiting the doctor or around vulnerable individuals if you’re experiencing symptoms.
• Limit contact with high-risk individuals if you’re sick or have been exposed to someone who is sick.
Not every cough or fever needs an ER visit, but some symptoms require emergency care: experiencing severe shortness of breath or di culty breathing, blue lips or face, a high fever that isn’t responding to fever-reducing medication, worsening of chronic conditions like COPD and asthma, and heart-related symptoms –chest pain, tightness when breathing, irregular heartbeat or feeling faint.
Boone Health’s Convenient Care is also an option for mild to moderate symptoms such as cough, sore throat, low-grade fever or u and COVID-19 symptoms without troubled breathing.
If you feel like something is seriously wrong, trust your instincts, especially with breathing or chest symptoms. It’s always better to be safe and get checked.
By Boone Health Infection Prevention
A Skill That Can SAVE LIVES
The vital importance of learning CPR.
In the realm of emergency response, few skills are as universally crucial as Cardiopulmonary Resuscitation, or CPR. CPR serves as a beacon of hope in dire situations when a person’s heart ceases to beat or their breathing stops. The ability to administer CPR can mean the difference between life and death and can empower individuals to act decisively during an emergency, making it a skill that everyone should prioritize learning. Need more reasons? Read on!
Immediate response to cardiac arrest
The primary purpose of CPR is to provide immediate assistance during cardiac arrest, a medical emergency where the heart suddenly stops beating. In these critical moments, every passing second is vital. The prompt initiation of CPR can maintain blood circulation and oxygen flow, preventing irreparable damage to vital organs.
Increased chances of survival
Studies consistently demonstrate that immediate bystander CPR significantly improves survival rates for people experiencing cardiac arrest. Swift administration of CPR serves as a bridge until professional medical help arrives, increasing the likelihood of a positive outcome.
Community resilience and preparedness
CPR training contributes to the overall resilience and preparedness of both individuals and communities. Bystanders with CPR skills become valuable assets during emergencies, capable of providing immediate assistance until emergency medical services arrive.
Protection of brain function
By sustaining blood circulation, CPR also protects the brain from potential damage. Brain cells can start to die within minutes of a cardiac arrest. The immediate application of CPR is critical to minimize the risk of long-term neurological consequences.
Accessible and empowering
Anyone, regardless of age or background, can learn CPR. This accessible knowledge can empower people to take an active role in emergency situations and foster confidence and community responsibility.
Legal protections and workplace requirements
In many jurisdictions, legal protections exist for individuals who provide CPR in good faith during emergencies. Certain professions and workplaces mandate CPR certification as a requirement for employees. Employees with CPR skills can contribute to a safer working environment.
Public health impact
A population well-versed in CPR builds a healthier and safer community. Widespread CPR knowledge increases potential for a quicker, more effective response to emergencies anytime and anywhere, ultimately reducing the overall impact of cardiac arrest.
Learning CPR is not just a skill; it’s a societal imperative. The ability to administer CPR embodies the essence of community care and preparedness, enabling individuals to be active participants in emergency response. Life is unpredictable but acquiring CPR skills gives all of us a tangible way to make a difference, provide hope, and save a life when it matters most. By embracing the importance of CPR, we collectively contribute to a safer, more resilient world where every individual has the power to be a life-saving hero. By Jenny L. Workman
Your Financial Future, Clear and Confident
UMB Private Wealth Management
UMB Private Wealth Management cuts through the noise to provide time-tested solutions and uncomplicated advice. We ask the right questions and use the best tools for a financial strategy that aligns with your needs for today and dreams for tomorrow.
Schedule an appointment at UMB.com/privatewealth
mob welltower com
Boone Hospital Foundation Helps Keep Our Community Safe
In the last year, the Boone Hospital Foundation has supported the Emergency Services (EMS) department at Boone Health with financial backing to help improve patient experience. Through the generosity of Drs. Gary and Roberta Minish, we were able to buy a medically equipped UTV with trailer that enables the EMS team to access patients easier in specific settings. Gary Minish grew up in a rural area and envisioned the UTV being sent out to help those injured or taken ill in rural settings to receive medical treatment more quickly, and accessing places where ambulances cannot reach. The vehicle is also able to get to patients during crowded events. We are grateful for their willingness to help the EMS team at Boone Health do their best for our community.
The Foundation approved the request to buy the HAAS Alert system for the Boone Health Ambulance Fleet. The system sends out alerts to certain factory infotainment equipment and cellular navigation applications in vehicles to help avoid traffic incidents, one of the biggest threats first responders face while responding to calls for help. It also connects with other emergency vehicles in the area. The HAAS system helps protect those on the road during emergencies.
The Foundation also supports ongoing training and certification for the Emergency Services team, sending Boone Health employees to an emergency vehicle drivers instruction course that would enable them to become instructors, ensuring that the Boone Health fleet is well-trained in the field. We also recently sent eleven EMS employees to the Bryant Gladney Foundation education conference in May 2025, for continuing education and best practice training. These efforts speak to the Foundation’s mission to improve the health of the people and the communities we serve.
In health and wellness,
Monica Collins, MPA Executive Director, Boone Hospital Foundation
2025 Boone Hospital Foundation Board of Directors
OFFICERS
Arlene Heins President
John Franken Vice President
Drew Wilkinson Treasurer
Valerie Ninichuck Secretary
Dr. James Roller Past President
BOONE REPRESENTATIVES
Jan Beckett
Boone Board of Trustees Representative
Stacye Smith
Boone Health CHAS
Board Representative
DIRECTORS
Dr. Mark Adams Director
Dawn Daly Director
Stephanie Goans Director
Pat Hostetler Director
Dr. Angela Hull Director
Erica Pefferman Director
John Pile Director
Jolene Schulz Director
573-815-8000
We know your life is busy, and injuries and illness don’t always happen at the most convenient times. Our compassionate and knowledgeable staff are dedicated to meeting your needs with extended hours 7-days-a-week. No appointment necessary.
COMMON ILLNESSES
• Colds, cough, congestion and flu
• Sore throats and strep throats
• Ear infections
• Sinus infections
• Urinary tract infections (UTIs)
• Bronchitis
• Asthma flare-ups
• Allergies and allergic reactions (minor)
• Fevers
• Skin rashes and infections
• Gastrointestinal issues
• Migraines and headaches MINOR INJURIES
• Sprains and strains
• Minor fractures
• Cuts, lacerations and minor wounds requiring stitches
• Minor burns
• Sports-related and work-related injuries
• Insect, spider bites and stings
• Animal bites
ADDITIONAL SERVICES
• X-rays for minor injuries
• Lab services as necessary per provider
• Physical examinations for school, sports or employment
• DOT exams
• Tdap, Hepatitis B, influenza vaccines available
• Testing for sexually transmitted diseases
• Pregnancy Testing
CONVENIENT CARE BUSINESS LOOP: 601 Business Loop 70 West Suite 275 Columbia, MO 65203
OFFICE HOURS: Everyday, 7 AM - 6:30 PM Hours may change due to holidays. Please call before arriving.