of the Department of Medicine at Mount Sinai Health System
Welcome to the 2023–24 annual report of the Mount Sinai Health System Department of Medicine. Inside you will find a collection of articles that reflect some of the research, clinical, and academic excellence of our programs across the Department’s 14 divisions and seven hospital sites over the past year. Additionally, there are stories that highlight our current initiatives in areas including education, faculty affairs, quality improvement, and more.
About the Department of Medicine at Mount Sinai Health System
The Department of Medicine at Mount Sinai Health System is one of the largest and most prestigious academic training grounds in the United States. We continue to create a dynamic department that upholds groundbreaking translational research and exceptional clinical outcomes.
The Health System’s largest department, the Department of Medicine comprises more than 1,800 full-time faculty members and voluntary physicians, all of whom are affiliated with at least one of our hospitals. With robust grant funding of more than $147 million from the National Institutes of Health, the Department of Medicine is ranked among the top 15 medical school departments of its kind in the United States, according to the Blue Ridge Institute for Medical Research.
Mount Sinai’s Department of Medicine attracts some of the world’s most talented medical students and trainees who seek to be taught by leading experts, many of whom have pioneered landmark therapies and treatments that are routinely used by their peers around the globe. Throughout its rich history of serving New Yorkers from all socioeconomic and ethnic backgrounds for more than 170 years, Mount Sinai’s Department of Medicine is committed to scientific research and clinical breakthroughs so that each and every one of our patients has the best possible outcomes, while teaching and exposing our students, residents, and fellows to the most advanced medical techniques, state-ofthe-art technology, and vigorous academic and training curricula.
Whether you are a current or prospective patient, physician, researcher, resident, fellow, graduate student, or supporter, this report will allow you to discover and gain a taste of some of the most prominent clinical and research advances in the Department of Medicine.
Happy reading!
Department of Medicine System Chair
Monica Kraft, MD
Murray M. Rosenberg Professor of Medicine
Click here to support the Mount Sinai Department of Medicine's clinical, education, and research goals.
About the Division of Cardiology
For more than a century, Mount Sinai has been the home of a premier Division of Cardiology. The Mount Sinai Hospital is ranked No. 4 in the nation for Cardiology, Heart and Vascular Surgery by U.S. News & World Report® for 202324, and Mount Sinai Fuster Heart Hospital is celebrated internationally as a world leader in all facets of cardiology.
The Division of Cardiology’s mission is to improve the heart health of patients locally and globally with dedication to the prevention, management, and eradication of cardiovascular diseases. It continues to pursue excellence in patient care, offering innovative prevention and treatments, pioneering research and clinical trials, and training future leading cardiologists by its world-renowned experts.
System Chief
Deepak L. Bhatt, MD, MPH
Dr. Valentin Fuster Professor of Cardiovascular Medicine and Director, Mount Sinai Fuster Heart Hospital
Non-Hispanic Black Adults Found Twice as Likely to Have Atherosclerosis as Hispanics in Study of Young Adults in Harlem
A unique Mount Sinai study focused on a multiethnic, underserved community in Harlem found that young non-Hispanic Black adult participants were twice as likely to have atherosclerosis as young Hispanic adults.
The research, published in the Journal of the American College of Cardiology in July 2022, is part of the FAMILIA Project at Mount Sinai Heart, a pioneering trial created by Valentin Fuster, MD, PhD, President of Mount Sinai Heart and Physician-in-Chief of The Mount Sinai Hospital.
The new study is one of the first to evaluate atherosclerosis the plaque build-up in the arteries that can lead to a heart attack or stroke in asymptomatic young populations. Its findings emphasize the importance of early screening and lifestyle interventions in high-risk minority groups to improve their cardiovascular (CV) health.
“What’s interesting about this study is that Black individuals appear to be more vulnerable to atherosclerosis early in life than people of Hispanic origin, even when adjusting for known cardiovascular and lifestyle risk factors such as smoking, unhealthy diet, lack of exercise, high blood pressure, and cholesterol,” Dr. Fuster says. “This can then put them at increased risk of cardiovascular disease, suggesting the existence of emerging or undiscovered cardiovascular risk factors in this population.”
The study is part of a multinational effort to intervene early in the lives of children, their caretakers, and teachers so they can form a lifetime of heart-healthy habits. These new results come after highly successful interventions involving more than 500 preschoolers, caretakers, and educators at 15 Head Start schools in the Harlem section of Manhattan, an urban area that is socioeconomically disadvantaged a situation commonly linked to higher rates of obesity, heart disease, and other health issues.
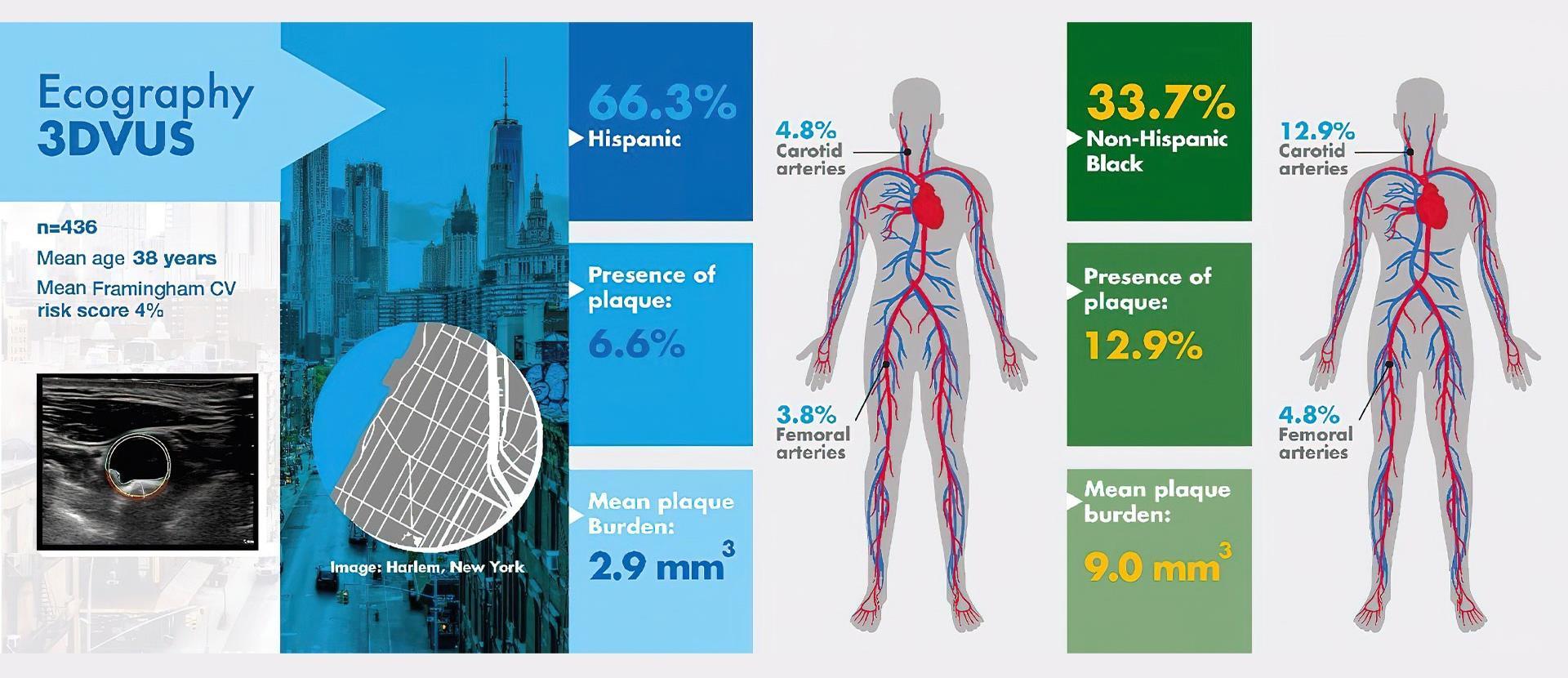
The FAMILIA team focused on 436 adults, including preschoolers’ family members, caretakers, teachers, and school staff. Of that group, 147 participants were non-Hispanic Black and 289 were Hispanic, with an average age of 38; 80 percent were women. Non-Hispanic white, Asian, and Native American groups each formed a small proportion of participants (2.3 percent, 2.3 percent, and 0.3 percent, respectively) and people in those groups were excluded from the analysis.
Each participant answered a comprehensive questionnaire at the start of the study, addressing their nutrition, physical activity, tobacco use, and
Virtual abstract of the article "Subclinical Atherosclerosis in Young, Socioeconomically Vulnerable Hispanic and Non-Hispanic Black Adults"
alcohol consumption, and whether they had conditions such as heart disease, hypertension, diabetes, or a family history of health problems. They also had their weight recorded, and blood pressure and cholesterol checked.
Overall cardiovascular risk factors were prevalent for both ethnic groups at baseline. Thirty percent of non-Hispanic Black participants had hypertension, almost triple the rate of the Hispanic group, 11 percent. Conversely, non-Hispanic Black participants had lower rates of dyslipidemia unhealthy levels of lipids/fat in the blood (18 percent) compared to the Hispanic group at 27 percent, and better eating habits, consuming more fruits and vegetables.
Researchers used these data to calculate a predicted cardiovascular risk score for each group. They found the overall risk of having a cardiovascular event in 10 years was low for both Black and Hispanic participants around four percent for both groups.
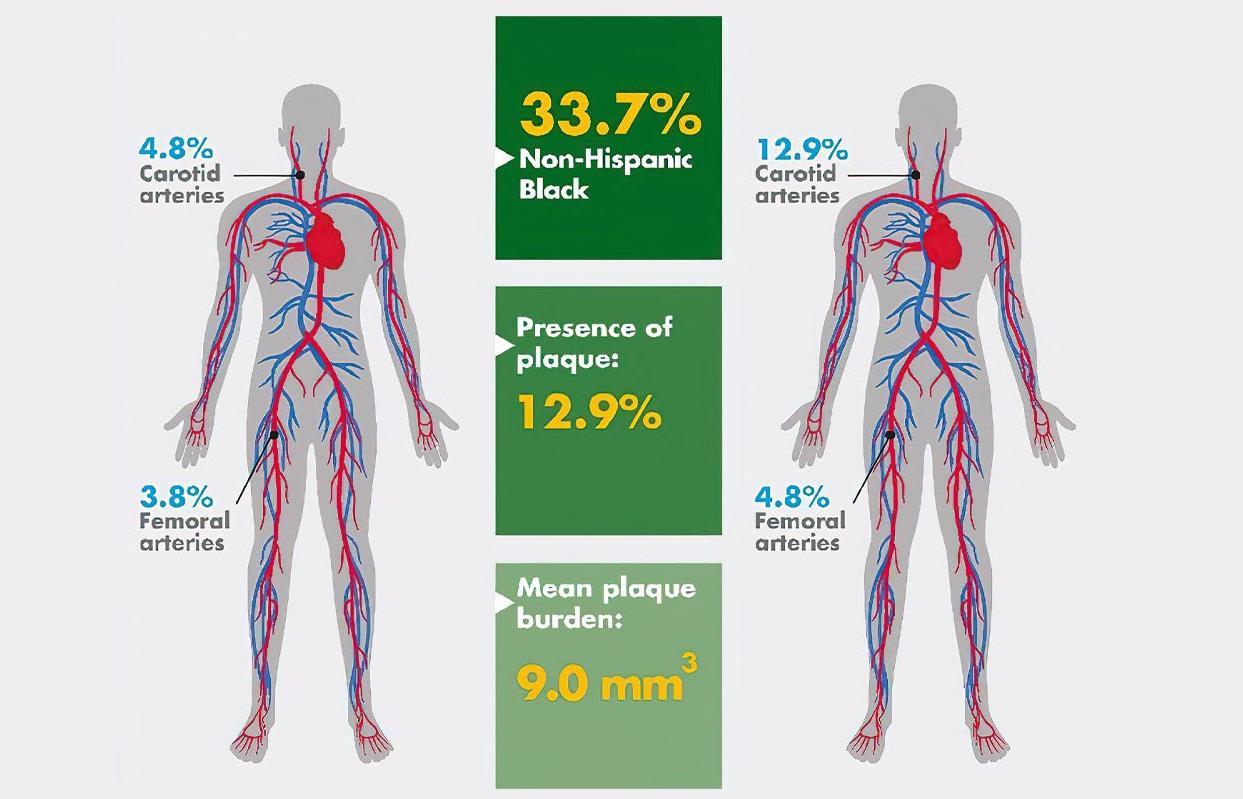
Participants also had 3D vascular ultrasounds to determine if they had atherosclerosis in their carotid (neck) and femoral (leg) arteries. These vascular ultrasounds pointed to a significant discrepancy between the groups. Overall, nine percent of participants had subclinical atherosclerosis (nearly one in ten participants showed at least one artery with plaque). Also, the rate of plaque build-up in the arteries was two times higher among non-Hispanic Black than Hispanic participants. The results were consistent even after adjusting for classic cardiovascular risk factors including age, sex, body mass index, hypertension, diabetes, and cholesterol; lifestyle factors including diet, physical activity, and tobacco use; and socioeconomic factors such as employment status.
The study noted some limitations and areas for further investigation. “The population included in the study was from a specic area, Harlem, with known intrinsic health disparities compared with
other areas in New York City,” the study says. “This could, to some extent, limit our results’ generalizability.” In addition, “Given the heterogeneity among racial and ethnic groups, assessing associations between self-reported racial or ethnic identity and disease is complex and is vulnerable to confounding due to the effects of socioeconomic inequality, environmental disparity, unequal access to care, and other possible emerging or unknown CV risk factors.”
However, the study is one of the first to assess the presence of subclinical atherosclerosis by 3D vascular ultrasounds in an underrepresented younger population, the research team says, and it contributes to the understanding of higher rates of CV disease observed at an early age in disadvantaged communities.
“These findings may in part help to explain the observed differences in cardiovascular disease prevalence between racial and ethnic groups,” Dr. Fuster says. “Until underlying biological factors and other undiscovered cardiovascular risk factors are better understood and can be addressed by precision medicine, affordable noninvasive imaging techniques such as the portable 3D vascular ultrasounds used in this study, which are easily used and affordable, can be an important form of early detection in underserved communities, and provide valuable information about population disparities and increase the precision of health promotion and prevention programs.”
Dr. Fuster and his team plan to expand the FAMILIA program to schools across the five boroughs of New York City in the next few years. This project will also evaluate how family socioeconomic status and teachers’ characteristics may affect the implementation and efficacy of school-based health promotion programs.
The FAMILIA project was funded by a grant from the American Heart Association.
Featured Faculty
Valentin Fuster, MD, PhD President of Mount Sinai Fuster Heart Hospital, and Physician-in-Chief of The Mount Sinai Hospital
Mount Sinai is Enhancing its Focus on Women’s
Cardiovascular Health
Mount Sinai Heart is launching a multispecialty Women's Heart and Vascular Center, with clinics specifically designed to screen, assess, and educate women about their level of individual risk through a team of cardiologists, subspecialists, and researchers with expertise in heart health issues specific to women.
The founding director of the Center is Roxana Mehran, MD, Professor of Medicine (Cardiology), and Population Health Science and Policy, and Director of Interventional Cardiovascular Research and Clinical Trials at the Icahn School of Medicine at Mount Sinai.
“Women need to be more knowledgeable about their health, and our new Women's Heart and Vascular Center is designed to give them access to the very best specialists at Mount Sinai who can inform them of their risk for heart disease by
cardiomyopathy, and fibromuscular dysplasia, which can lead to heart attack and stroke if untreated. Instead, symptoms such as angina and chest pain triggered by these diseases may be diagnosed as anxiety or other psychosomatic disorders.
“Women tend to be stereotyped into certain categories of health problems that miss the fact that what they really have is heart disease,” asserts Dr. Mehran, head of the Lancet Women and Cardiovascular Disease Commission, whose members from 11 countries have prepared the
making sure they have a full understanding of numbers such as cholesterol, blood pressure, and hemoglobin A1C, which are critical to assessing their heart health,” says Dr. Mehran. “The truth is, cardiovascular disease is underrecognized, underdiagnosed, and undertreated in this country, making it the No. 1 killer of women.”
Physicians are often not fully trained to recognize women-specific conditions such as spontaneous coronary artery dissection (SCAD), coronary microvascular dysfunction, Takotsubo
first-ever global report and recommendations for decreasing the burden of cardiovascular disease in women. A lead author of the report was Birgit Vogel, MD, a clinical researcher in Cardiovascular Imaging and Clinical Trials at Mount Sinai.
The clinics of the Heart and Vascular Center for Women are reaching out to women at high risk due to pregnancy-related complications and to cancer treatment. According to Dr. Mehran, every woman who has experienced pregnancy-related issues such as premature delivery, gestational
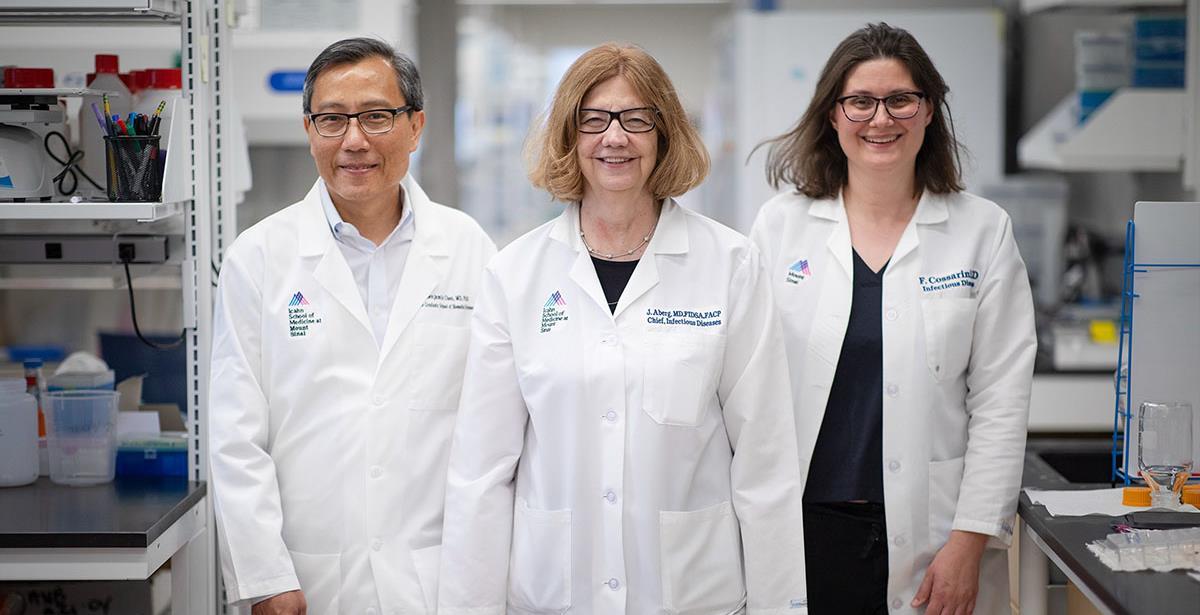
Roxana Mehran, MD, left, founding Director of the Women's Heart and Vascular Center, with Birgit Vogel, MD.
diabetes, preeclampsia, or low birth weight of a child should have a cardiovascular risk assessment. Female cancer patients should also be evaluated, she adds, as chemotherapeutic agents and radiation can adversely impact the heart and vascular tissue. Future clinics will be geared to detecting SCAD, ischemia, or myocardial infarction with nonobstructive coronary arteries, and peripheral arterial disease, which often affect women at a relatively young age.
The new Center is particularly committed to providing women from all socioeconomic groups with access to top-tier cardiovascular care. Explains Dr. Mehran: “We know that women of color and minorities have the highest risk of cardiovascular events, and one of our priorities is to bring them into our program so we can screen and educate them about preventive measures they can take to avoid a heart attack or stroke.” To that end, the Center hopes to eventually expand its clinics from their initial outpatient hospital setting to locations within the community.
“We want women to know that they truly matter,” Dr. Mehran says, “and that Mount Sinai is concerned enough about their cardiovascular health to bring together under one roof an extraordinary team of specialists who fully understand and are ready to provide the primary and secondary preventive care they need and deserve.”
Dr. Mehran, a renowned clinician and researcher, is also devoted to helping women advance in the field of medicine. In November 2022, the American Heart Association’s Council on Clinical Cardiology honored her with the “Women in Cardiology Mentoring Award,” recognizing her outstanding record of mentoring women cardiologists.
Featured Faculty
Roxana Mehran, MD
Professor of Medicine (Cardiology), and Population Health Science and Policy
About the Division of Clinical Immunology
The Division of Clinical Immunology at Mount Sinai provides cutting-edge patient care, research, and education in the fields of Allergy and Clinical Immunology. It leads the nation in the research of immune deficiency diseases and translating these findings to the design of pioneering treatments. Patients come to Mount Sinai’s Division of Clinical Immunology from across the country for the diagnosis and treatment of these immune disorders. The expert physicians in the Division provide comprehensive outpatient and inpatient consultations, and offer the latest advances in diagnostic procedures that may include examination of antibodies and cell functions and genetic analysis.
The Division launched the Biologics And Clinical Immunology Cohort at Sinai (BACICS) registry of patients with chronic immune-mediated diseases who are receiving biologics. The registry allows
state-of-the- art approaches to be applied to assess immunological and clinical responses that transcend previous single-disease and static paradigms. BACICS is designed to determine shared signals in risk-associated regulatory pathways relevant to multiple immune disorders and the efficacy of their treatments across time. Unlike other registries which focus on one-organ diseases, this novel registry is most suited to help fill research gaps that are wider in scope and may generalize to molecular mechanisms of multiple chronic diseases.
The Division of Clinical Immunology is the largest provider of allergy care in New York City. In addition to providing comprehensive evaluations for allergic disorders, its providers are recognized nationally for their expertise in the evaluation and treatment of asthma, atopic dermatitis, hereditary angioedema, and urticaria (hives).
The faculty is devoted to the training of the next generation of leaders in Clinical Immunology, including physicians and scientists, through fellowship and mentoring programs.
System Chief
Rachel Miller, MD
The Dr. David and Dorothy Merksamer Professor of Medicine (Allergy and Immunology)
Inhibition of BTK Could Be Used to Shut Down Inflammation Pathway
Mount Sinai researchers have discovered that an inhibitor of Bruton’s tyrosine kinase (BTK), an important mediator of B-cell receptor signaling, could be used to shut off inflammation in cells of patients with primary immunodeficiency diseases in which B cells are either failing to make antibodies or making incorrect ones.
Mount Sinai researcher Charlotte CunninghamRundles, MD, PhD, and her team have discovered that an inhibitor of Bruton’s tyrosine kinase (BTK), an important mediator of B-cell receptor signaling, could be used to shut off inflammation in cells of patients with primary immunodeficiency diseases.
There are more than 450 of these diseases, and unraveling their puzzles involves confronting surprises and innovating responses. Part of the puzzle is the heterogeneity of immunodeficiency diseases: All components of the immune system can experience defects.
Among these defects are failures in lymphocytes called B cells, which mature into plasma cells that last for years in bone marrow. B cells are responsible for making proteins called antibodies. The most common immunodeficiency is when a patient’s B cells don’t make an antibody they need, which can lead to infections.
“The other side of the coin, however, is that the B cells may do something other than make a needed antibody—for example, make an
antibody against platelets, or red blood cells, or the GI tract, or maybe the skin,” Dr. CunninghamRundles explains. “So patients come through my door with autoimmunity almost as often as they do with infections.”
But Dr. Cunningham-Rundles, who is the Director of the Immunodeficiency Clinic, is undaunted by the complexity of the research. Rather, she finds it invigorating.
The Complicated Genetics
Genetics clearly influences the pathophysiology of immune deficiency diseases. Dr. CunninghamRundles, who is the David S. Gottesman Professor of Immunology at the Icahn School of Medicine at Mount Sinai and heads an eponymous research lab, authored a 2020 report in Blood that identified a number of genes affecting the process of generating antibodies.
“For the first 20 to 30 years that I worked on B cell issues, people thought there must be something
Charlotte Cunningham-Rundles, MD, PhD, is Director of Mount Sinai's Immunodeficiency Clinic
wrong with the B cell,” she says. “So, perhaps that antibody-making cell has a malformation in the plasma cell or antibody recognition from a lymphocyte but that turns out not to be true in most cases. It turns out there are a great number of additional genes that are not unique to B cells that, when they don’t work, gives that person what looks like a B-cell problem.”
With colleagues in Stockholm, Sweden, and Tehran, Iran, the researchers studied the genetics of more than 500 patients with common variable immunodeficiency (CVID), a primary immunodeficiency disease. The 65 genes in the patients from the United States were predominantly autosomal dominant, whereas at the other two locations the result was an approximately equal mix of dominant and recessive genes further proof of the complexity of B cell research.
Dr. Cunningham-Rundles is quick to point out that this finding is far from the final word. She found culprit genes in only about 30 percent of the patients tested, meaning another 70 percent or so are out there waiting to be discovered. “There are many more to unpack, which is why we have been doing a lot of whole exome sequencing, with colleagues at Rockefeller University, and we may need to move on to whole-genome sequencing.”
Inflammatory Pathway Identified
For Dr. Cunningham-Rundles, the endeavor to unravel the mystery is both “confounding” and inspiring, and the ultimate beneficiaries of her work her patients are never far from her mind.
“I have patients who don’t make antibodies and I give them gamma globulin, so no problem. About 50 percent of those patients do fantastically. Some of them I’ve seen for decades,” she says. “But the other 50 percent develop interstitial lung disease, liver fibrosis, rampant autoimmune disease, granulomatous disease, and inflammatory diseases. So that’s the conundrum.”
Dr. Cunningham-Rundles and her team found there are about 120 genetic indicators that show markers of inflammation. Using a novel assay developed in her lab, she found that those patients with an extreme inflammatory phenotype have larger amounts of bacterial DNA from gastrointestinal organisms in their blood. This DNA activated a number of inflammatory pathways that could incite the conditions found in these patients. “We were pretty floored by this finding, but it is associated with a lack of isotypeswitched B cells, which make immunoglobulin A [IgA]. What we found suggests these patients have a mucosal-barrier defect.”
Unable to replace the IgA, Dr. CunninghamRundles and team found that an inhibitor of BTK could shut down inflammation in cells of patients with immunodeficiency disorders. The primary immunodeficiency disease known as X-linked agammaglobulinemia is caused by mutations in the BTK gene, and patients with this disorder do not commonly have the inflammatory pathway disorders that are seen in CVID patients
“It is counterintuitive to take someone who is immune deficient and say, OK, I will make you even more immune deficient. But we have been using rituximab with some CVID patients for years, and we’ve known that wiping out B cells helps for some conditions in these patients. This is not permanent, since the cells then come back in some months it’s like mowing a lawn,”
Dr. Cunningham-Rundles explains. “But BTK is in a lot of cells that lead to inflammation in humans and a BTK inhibitor could actually shut down the inflammation pathway.”
Dr. Cunningham-Rundles maintains an inventive approach to research and clinical care. For example, the mucosal-barrier defect mentioned above might be mitigated with the use of a small amino acid compound used in patients with celiac disease. She is looking into it. “We are very enthusiastic about what we do,” she explains. “One door opens up to another all the time.”
Featured Faculty
Charlotte CunninghamRundles, MD, PhD
David S. Gottesman Professor of Immunology
For Patients With Hereditary Angioedema, the Fight is on
Very few physicians specialize in treating hereditary angioedema (HAE), a rare and challenging genetic disease whose symptoms include swelling in the abdomen, extremities, face, and airway, the latter of which can be lifethreatening if not properly treated. Mount Sinai's Paula J. Busse, MD, not only treats these patients, but has helped develop the guidelines for managing this disease.
Paula J. Busse, MD, is a leader in the clinical care of patients with hereditary angioedema (HAE). And when it comes to fighting for her patients, Dr. Busse, Professor of Medicine (Clinical Immunology and Allergy) at the Icahn School of Medicine at Mount Sinai, is all in.
HAE is a rare and challenging genetic disease whose symptoms include swelling in the abdomen, extremities, face, and airway, the latter of which can be life-threatening if not properly treated. The number of those affected by the disorder is just a few thousand in the United States, and as a result there are very few physicians who specialize in treating the condition.
As explained in a 2020 review article in The New England Journal of Medicine co-authored by Dr. Busse, HAE causes vasodilation, which leads to fluid accumulation in tissues, producing angioedema. Angioedema of the gastrointestinal tract can cause severe abdominal pain and potential intestinal obstruction. Airway swelling can lead to death by asphyxiation. Swelling in the
hands or feet can be painful and significantly limit activities of daily living.
HAE is an autosomal-dominant genetic disorder. In around 80 percent of patients, a plasma protein known as C1-inhibitor (C1-INH) is both dysfunctional and present in deficient levels; this is known as HAE type 1. In those with HAE type 2, C1-INH is dysfunctional but at appropriate levels. A very rare third type of HAE is found in those with normal C1-INH and functional levels, secondary to defects in other genes (some of which have been identified), causing HAE-like symptoms.
Allergic reactions can cause angioedema, but those reactions are induced by histamine. In HAE, the angioedema is induced by bradykinin, a peptide that promotes vascular dilation with subsequent fluid extravasation to tissues. Bradykinin-mediated HAE is distinct from histamine-mediated angioedema and does not respond to antihistamines or corticosteroids, which are used for allergies. If not differentiated by the clinician, the result can be treatment that is ineffective a perilous prospect if the airway is involved.
Paula J. Busse, MD, is a leader in the clinical care of patients with hereditary angioedema
Evolving Guidelines
There are two major sets of guidelines for the clinical care of the patient with HAE, and Dr. Busse has helped develop both. One stems from work by the United States Hereditary Angioedema Association, a U.S.-based patient organization on whose medical advisory board Dr. Busse sits. Working together, the advisory board created guidelines for treatment of HAE in 2013 that were updated in 2020. Dr. Busse, who was the first author of this report, notes that the revised guidelines reflect advancements in the understanding of HAE and significant changes in its clinical management.
The other set of guidelines, for which Dr. Busse was a co-author, is an international effort from the World Allergy Organization and European Academy of Allergy and Clinical Immunology. Published in 2022, the guidelines addressed slight differences in treatment philosophies and access to therapies between U.S. and European clinicians. “At this point there are two guidelines, the U.S. and the international,” Dr. Busse explains, “but the gap between them on treatment recommendations has narrowed with the latest publication.”
The cost of HAE medications can be expensive and prohibitive. One dose of a C-1 inhibitor is several thousand dollars. “Many emergency rooms are not going to carry these drugs, although we have it on formulary here at Mount Sinai,” Dr. Busse notes. Because of the high cost, she often needs to fight for her patients, spending hours on the phone debating the merits of health care coverage with reluctant insurers.
“I spend quite a bit of time working to get patients assistance, for example through the Hereditary Angioedema Association. There is an emotional hardship for some of these patients and their families because they can’t get medications or appropriate care,” she says. “Some of these patients don’t have the insurance to see a specialist like myself, so they go to other physicians, who perhaps have mismanaged them because they don’t have the expertise, and that can lead to morbidity and even mortality. That is pretty upsetting to me.”
Dr. Busse’s approach to the clinical care of patients with HAE is to be a leading expert on the disease and to keep fighting for them. “I have been able to get some companies to donate their medications and I spend a lot of time getting prior authorizations for these patients’ medications,” Dr. Busse recalls.
Her weapon of choice for these battles? The phone.
Featured Faculty
Paula J. Busse, MD
Professor of Medicine (Clinical Immunology)
About the Division of DataDriven and Digital Medicine
At a time when every medical decision, diagnosis, and treatment is underpinned by data, the Division of Data-Driven and Digital Medicine (D3M) is a leap toward a future where artificial intelligence (AI) and digital tools are not simply integrated into, but become intrinsic to, clinical practice.
The Division is committed to bringing data-driven and digital innovation to research, education, and clinical care, thereby empowering each to reach its maximum potential. Modern medicine’s transformative new era is fueled by data science, AI, and digital health. The Division aims to be the epicenter of that transformation, catalyzing groundbreaking research, training the next generation of physicians, and ensuring a seamless translation of digital innovation into clinical practice.
Mount Sinai recognizes that through education, it can ensure that its future biomedical leaders are
pioneers in this new era of medicine, rather than just participants. The Division is committed to training medical students, residents, and fellows by introducing them to the possibilities of AI, data science, and digital health innovation.
System Chief
Girish N. Nadkarni, MD
Irene and Dr. Arthur M. Fishberg Professor of Medicine
Data Science and AI Leave Their Mark on Medical School Education
As data science and artificial intelligence become more central to the practice of medicine, Mount Sinai is building out its efforts to educate budding physicians and scientists in these areas. It has also begun using these tools to enhance its own admissions process.
Data science and artificial intelligence (AI) are not only being meticulously woven into patient care across the Mount Sinai Health System, but also
“Much of today’s research uses machine learning, natural language processing, and other data science methods and tools, making it difficult for
being deployed in innovative ways to advance both the selection and ongoing education of medical school students. One way is helping clinical fellows master the language of data analysis and science at the start of their careers; another is streamlining the medical school applications process to make it less labor-intensive for screeners and more equitable for applicants.
Mastering a New Language
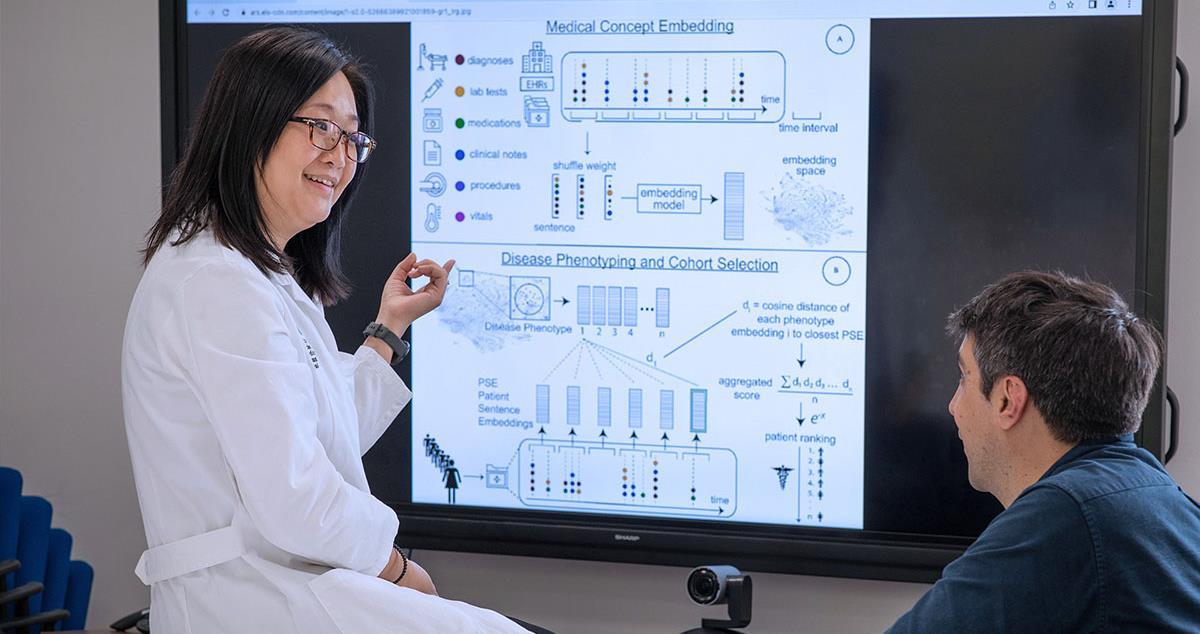
The rapidly growing use of data science in everyday clinical care has underscored the need for physicians to be fluent in the often arcane medium. To that end, Lili Chan, MD, Associate Professor of Medicine (Nephrology, and Data Driven and Digital Medicine) at the Icahn School of Medicine at Mount Sinai, is developing a comprehensive Data Analysis and Data Science course.
students who have no training in these disciplines,” says Dr. Chan, an expert in clinical research and data science. “We’re addressing this gap through a curriculum that’s focused on teaching trainees the digital skills necessary to conduct clinical research, or to simply digest the results of studies they read in leading journals that employ real-world health care data.”
Among topics to be covered in the lecture phase are databases, followed by the building of datasets that will be deployed through the remainder of the course. Machine learning (ML) will also be introduced, with a focus on decision trees, which form the basis for many advanced ML techniques.
“We believe this curriculum has the potential to transform trainee education,” emphasizes Dr. Chan, “by providing protected time for students to learn the data analytics and data science skills they’ll need to actively pursue research pathways.”
Lili Chan, MD, is developing a comprehensive Data Analysis and Data Science course.
Streamlining Med School Admissions
No less enticing are the opportunities to leverage data science to benefit the thousands of applicants each year to Mount Sinai’s highly competitive medical school program, as well as the faculty members who voluntarily take on the task of deciding which ones get selected. Aware of the challenges, Valerie Parkas, MD, Senior Associate Dean of Admissions and Recruitment for Icahn Mount Sinai, and Talia Swartz, MD, PhD, Director of the MD-PhD program, began looking for ways that ML could help streamline the complex process.
“Every application gets read by screeners who must sort through personal statements, letters of recommendation, and related materials, which is extremely time-consuming,” explains Dr. Chan, who collaborated with Drs. Parkas and Swartz, and Justin Kauffman, a student in the Master in Data Science program, to brainstorm how ML might streamline the process. “Our goal is to reduce the number of human hours required to make sure each application is thoroughly reviewed, and to continue to ensure the process is as objective as possible.”
The team came to recognize the power and potential of a computational solution. In the same way a machine learning algorithm can be trained on reams of electronic health records to phenotype patients, so a machine learning program might be built around medical school applications to facilitate the review of candidates. “We’re still in the early data-gathering stage,” explains Dr. Chan, “but are focused on developing an algorithm through natural language processing that could identify and highlight from each application consistent themes, such as leadership or resourcefulness, which are so important within the applicant pool.”
She concludes, “We can’t remove the human element from the selection process. But we can seek to create through digital technology an equitable system for selecting students for our medical school program one that also helps our screeners who, after all, are very busy physicians and researchers.”
Featured Faculty
Lili Chan, MD
Associate Professor of Medicine (Nephrology)
Valerie Parkas, MD
Professor of Medical Education
Talia Swartz, MD, PhD
Associate Professor of Medicine (Infectious Diseases), and Medical Education
Data Scientists Uncover Molecular Processes
Linking
Acute to Long-Term Stages
of
COVID-19
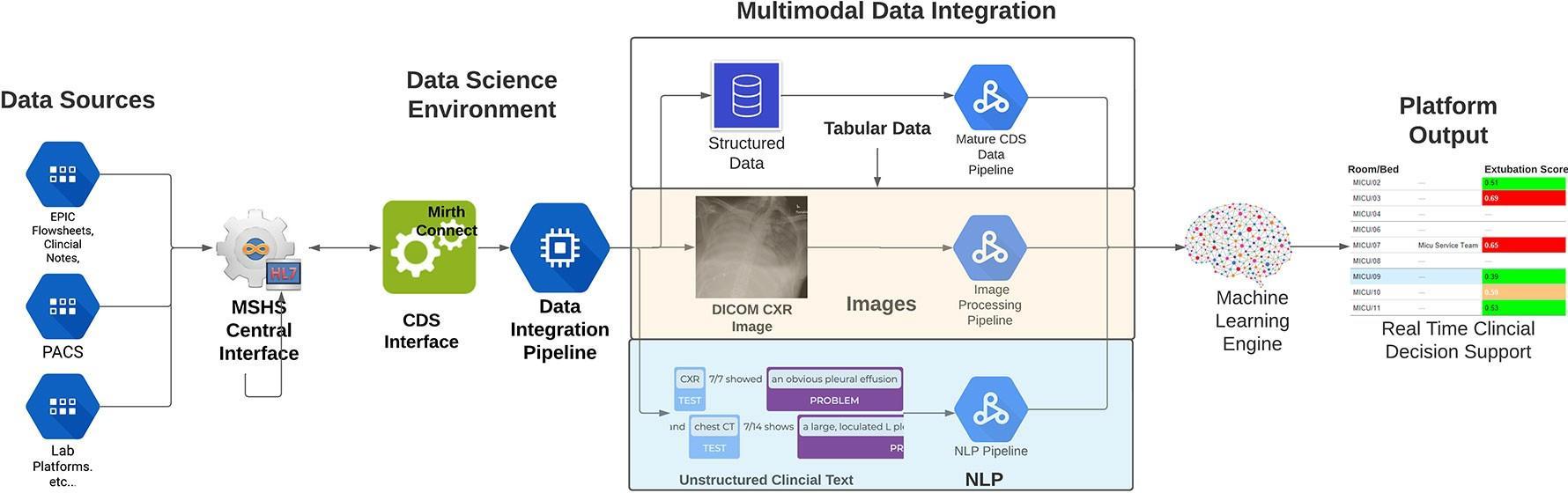
A study by Mount Sinai's Division of Data-Driven and Digital Medicine provides evidence for the first time that molecular signatures associated with “long COVID” are detectable in the acute stage of infection of SARS-CoV-2.
A Mount Sinai study provides evidence for the first time that molecular signatures associated with “long COVID” are detectable in the acute stage of infection of SARS-CoV-2. The finding underscores the enormous potential of computation and data science to statistically model and ultimately resolve some of the biggest clinical challenges of our time.
At the center of that effort is the Department of Medicine’s two-year-old Division of Data-Driven and Digital Medicine (D3M), which led the longCOVID investigation and views it as emblematic of the expanding effort at Mount Sinai to integrate data science and digital tools into translational research and clinical care.
“Data science is enabling us to understand disease on a much deeper molecular scale than ever before, and it’s clear that knowledge will play a transformative role in how we conduct research and practice medicine,” says Girish Nadkarni, MD, Irene and Dr. Arthur M. Fishberg Professor of
Medicine at the Icahn School of Medicine at Mount Sinai and Chief of the new Division. “Our team is already making a difference by integrating its work into the clinical side of the Mount Sinai Health System and acting as a powerful data resource for health care professionals who often find access to that information challenging.”
Indeed, the data-driven computational study of post-acute sequelae of SARS-CoV-2 infection (commonly referred to as long COVID), published in Nature Medicine, was a collaborative effort with The Charles Bronfman Institute of Personalized Medicine at Icahn Mount Sinai and the clinical data science team.
“We believe this study exemplifies the type of meaningful partnerships that will evolve between D3M as a data science and precision medicine hub, and clinicians across Mount Sinai who manage the patient populations,” notes senior author Noam Beckmann, PhD, Assistant Professor of Medicine (Data Driven and Digital
Medicine). “Together, we can create rich, patientcentric data sets that allow us to investigate the big medical problems of our time.”
Tapping into the vast resources of the Mount Sinai COVID-19 Biobank, researchers examined gene expression data in blood samples from more than 500 patients hospitalized with COVID-19 between April and June 2020. More than 160 provided selfreported assessments of a broad range of symptoms still present six months or more after hospitalization, including fatigue, dyspnea, sleep disruptions, and smell and taste problems. The team tested each gene expressed in the blood for association with each long COVID symptom, and then for associations specific to each of 13 different types of immune cells, including plasma cells. Finally, these associations were categorized by whether they matched up with changes in patients’ levels of antibodies specific to the virus.
Among the team’s breakthrough findings was the presence of two molecularly distinct subsets of long COVID symptoms with opposing gene expression patterns, often observed in the same plasma cells (the immune system’s antibodyproducing cells). In patients who progressed to pulmonary problems, for example, antibodyproduction genes were less abundant, while in patients with non-respiratory issues, such as loss of smell and taste or sleep problems, the same antibody-producing genes were more abundant.
“These opposing patterns point to the existence of multiple independent molecular processes leading to different long COVID phenotypes,” explains Dr.
Beckmann, whose omics skills include genomics, proteomics, and transcriptomics. “Just as importantly, our data revealed that these processes are already present during the acute infection stage of COVID-19. This finding has tremendous implications for the design of research studies as well as for the development of potential biomarkers, prevention strategies, and treatment options for individuals who develop long COVID.”
Featured Faculty
Noam Beckmann, PhD
Assistant Professor of Medicine (Data-Driven and Digital Medicine)
Girish Nadkarni, MD, MPH
Irene and Dr. Arthur M. Fishberg Professor of Medicine; Chief, Division of DataDriven and Digital Medicine
About the Division of Endocrinology, Diabetes and Bone Disease
The Hilda and J. Lester Gabrilove Division of Endocrinology, Diabetes and Bone Disease provides care for patients with endocrine diseases, including diabetes, throughout New York City by unifying protocols, programs, and treatments through outreach, education, and innovative community-based programs.
The Division is at the forefront of cutting-edge research on endocrine diseases and diabetes. It trains future leaders and innovators in the field of endocrinology through a world-renowned fellowship program, and is developing innovative quality improvement programs to achieve the highest quality standards in diabetes and endocrine patient care.
The Mount Sinai Diabetes, Obesity, and Metabolism Institute at the Icahn School of Medicine at Mount Sinai was created to find a cure and to develop better therapeutic and prevention strategies for those who experience diabetes, obesity, and
metabolic syndromes. Physician-scientists from various specialties across the Mount Sinai Health System, including endocrinology, surgery, genetics and genomics, and pharmacology and systems therapeutics, are conducting groundbreaking research to revolutionize the approach to all metabolic disorders.
System Chief
Andrea Dunaif, MD
Lillian and Henry M. Stratton Professor of Molecular Medicine
Researcher Awarded NIH Grant to Study Association Between Triglycerides and Triple Negative Breast Cancer
Emily Gallagher, MD, PhD, received a Method to Extend Research in Time (MERIT) Award from the National Cancer Institute to study the role of high triglyceride levels in driving triple negative breast cancer growth and metastasis.
A Mount Sinai researcher in 2022 received a $2.5 million, five-year grant from the National Institutes of Health (NIH) to conduct a novel study into the mechanisms linking elevated triglyceride levels and triple negative breast cancer.
Emily Gallagher, MD, PhD, Associate Professor of Medicine (Endocrinology, Diabetes and Bone Disease) at the Icahn School of Medicine at Mount Sinai, received the Method to Extend Research in Time (MERIT) Award from the National Cancer Institute (NCI), part of the NIH, to study the role of high triglyceride levels in driving triple negative breast cancer growth and metastasis. Dr. Gallagher is a physician-scientist with a clinical practice in the field of onco-endocrinology, the management of endocrine and metabolic complications of cancer.
More than 50 percent of women with triple negative breast cancer have elevated circulating triglycerides and these elevated levels are associated with reduced breast cancer survival. Further, a number of factors, including obesity, diabetes, high carbohydrate diets, and excess alcohol consumption can contribute to high circulating triglyceride levels. The link between hypertriglyceridemia (HTG) and triple negative breast cancer has been described in epidemiology studies, but checking and treating triglyceride levels in women with triple negative breast cancers is not part of standard oncology care.
Ultimately, my goal is to improve outcomes for women living with triple negative breast cancer and metabolic conditions.
Emily Gallagher, MD, PhD
“This grant from the NIH/NCI will give us a better understanding of how elevated triglycerides contribute to triple negative breast cancer growth and metastasis—something that, mechanistically,
hasn’t been previously studied,” says Dr. Gallagher, who is also Director of the Research Pathway, and Associate Program Director of the Internal Medicine Residency Program, both at Icahn Mount Sinai.
The grant will allow Dr. Gallagher and her team to explore how human breast cancers take up triglycerides from circulation in the form of verylow-density lipoproteins. To understand the biological links between HTG and the progression of triple negative breast cancer, the team is employing preclinical models of hypertriglyceridemia in isolation from other metabolic abnormalities. In preliminary studies, the team found that the mice with HTG develop more rapid growth and metastasis of triple negative breast cancers.
The HTG mice demonstrated lipid profiles with elevated very-low-density lipoprotein (VLDL) and high circulating of phospholipids associated with elevated VLDL. The team hypothesized that HTG promotes the growth and progression of triple negative breast cancer by increased VLDL uptake through the VLDL receptor, which contributes to lipid peroxidation products in hypoxic tumors. They hypothesized that lipid peroxidation affects cell signaling pathways, which enhance tumor cell survival and metastasis.
The team is also exploring the importance of tumor VLDL receptor expression in HTG-driven cancer growth and metastasis using xenografts derived from human triple negative breast cancers. Additionally, the researchers will examine therapeutic strategies to lower triglycerides, which, if successful, could be translated into clinical care to improve outcomes for women with high triglyceride levels and triple-negative breast cancer.
“In my oncoendocrinology clinical practice, I see many women who have high triglycerides and breast cancer, sometimes as a result of their breast cancer treatment,” Dr. Gallagher says. “My hope is that through this funding, we will be able to determine in preclinical models if starving triple negative cancer cells of these lipids can be exploited as a novel therapeutic strategy.
Ultimately, my goal is to improve outcomes for women living with triple negative breast cancer and metabolic conditions."
Featured Faculty
Emily Gallagher, MD, PhD
Associate Professor of Medicine (Endocrinology, Diabetes and Bone Disease)
Calls for Further Study to Fill Knowledge Gaps on Cardiometabolic
Risk in PCOS
Women with PCOS have increased prevalence rates of type 2 diabetes and metabolic syndrome, important risk factors for cardiovascular disease. However, there have been no definitive studies demonstrating that women with PCOS have increased cardiovascular events, such as myocardial infarction and stroke.
Polycystic ovary syndrome (PCOS) is one of the most common disorders of women of reproductive age, affecting up to 20 percent of this population worldwide, depending on the diagnostic criteria applied. It was originally described in the 1930s as a reproductive disorder characterized by irregular menstrual cycles, infertility, and hirsutism. Beginning in the 1980s, it was discovered that PCOS was a major metabolic disorder. Women with PCOS were found to have increased prevalence rates of type 2 diabetes and metabolic syndrome, important risk factors for cardiovascular disease. However, there have been no definitive studies demonstrating that women with PCOS have increased cardiovascular events, such as myocardial infarction and stroke.
The question of whether PCOS actually confers increased cardiovascular disease risk is of considerable public health importance, given its high prevalence rates. To begin to address this question, a two-day virtual workshop, “Cardiovascular (CV) Risk Across the Lifespan for Polycystic Ovary Syndrome,” was convened in October 2021 by the National Institutes of Health’s National Heart Lung and Blood Institute, Eunice Kennedy Shriver National Institute of Child Health
and Human Development, National Cancer Institute, National Institute of Diabetes and Digestive and Kidney Diseases, and Office of Disease Prevention. The objective of this workshop was to identify critical research needs and knowledge gaps regarding cardiovascular disease risk in PCOS. Andrea Dunaif, MD, Chief of the Hilda and J. Lester Gabrilove Division of Endocrinology, Diabetes and Bone Disease at the Icahn School of Medicine at Mount Sinai, and a global authority on PCOS, was one of the three workshop co-chairs who developed the workshop's scientific agenda.
A unique feature of this workshop was that it brought together preeminent experts in cardiology and epidemiology with leading investigators in PCOS. “Although there is a vast literature demonstrating that reproductive-age women with PCOS have surrogate markers for cardiovascular disease, the only way we’re going to conclusively determine whether PCOS increases cardiovascular disease is through long-term prospective studies that follow affected women to an age when they start to experience cardiovascular events, which is approximately 10 years after menopause, in their 60s and onward,” says Dr. Dunaif. To be successful in this
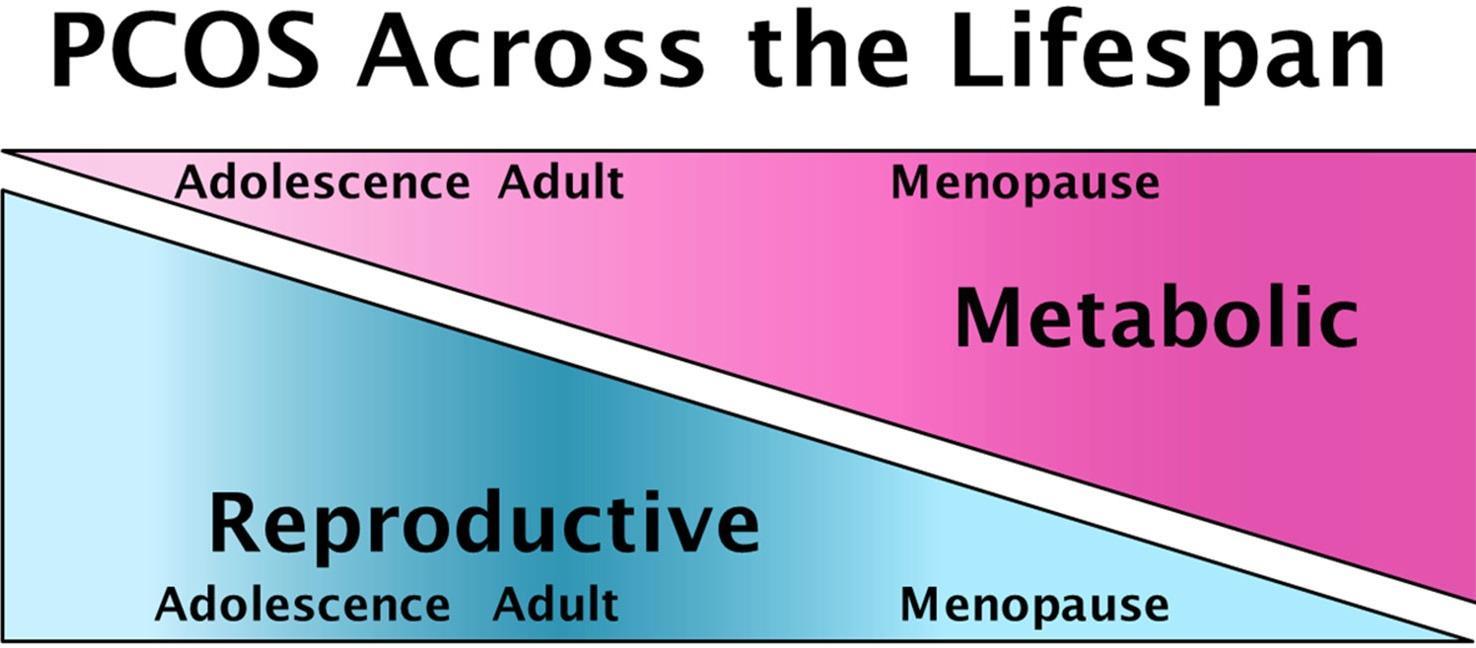
PCOS affects women across the lifespan, with reproductive features that begin in adolescence and resolve with age, and metabolic features that worsen in adulthood and persist after menopause.
endeavor, it is essential that scientists engaged in cardiovascular science are attracted to the field to address the numerous unanswered questions regarding disease risk.
One particularly intriguing possibility is whether PCOS itself might confer protection against cardiovascular disease. “Given the substantially increased risk for type 2 diabetes in young women with PCOS, we would expect to see a similar increase in cardiovascular disease risk, since diabetes abolishes the protective effect of premenopausal status on this risk,” notes Dr. Dunaif. However, some studies suggest that there is delayed ovarian aging and menopause in PCOS. Genetic analyses support this observation by finding a relationship between PCOS and genetic variants associated with later age at menopause. “Whether later menopause itself or ‘anti-aging’ actions in other organ systems reduce cardiovascular disease risk in PCOS is a critical unanswered question,” Dr. Dunaif says.
PCOS presents a unique opportunity for cardiometabolic risk reduction. “Since we are able to diagnose PCOS in girls within a couple of years of the start of their menstrual cycle, we could begin modifying risk factors for cardiovascular disease at a very young age,” she says. “These preventive measures could include, for example, carefully monitoring and controlling weight gain, lipid abnormalities, and blood pressure. Currently, there is no attempt to diagnose PCOS at an early age and no counseling about the risk for diabetes, which is really sad because women who are vulnerable to PCOS aren’t getting the care they need.”
Indeed, women with PCOS are highly dissatisfied with the health care they receive. It usually takes more than two years and visits to three or more health care providers before PCOS is diagnosed. “There is clearly a tremendous need for health care provider education regarding the diagnosis, multisystem manifestations, and management of PCOS. A major impediment to educational initiatives is the name ‘PCOS’ itself. It is a misnomer in that there are no cysts in the ovary. Further, the name focuses on the ovary when PCOS is actually much more than a reproductive disorder,” says Dr. Dunaif.
The expert panel from the last major NIH meeting on PCOS, the Evidence-Based Methodology Workshop, held in 2012, recommended that the name be changed to one that reflects the fact that it is a complex endocrine and metabolic disorder affecting women across the lifespan. Efforts to change the name to one that meets the requirements of all stakeholders, including patients, are ongoing.
Featured Faculty
Andrea Dunaif, MD
Lillian and Henry M. Stratton Professor of Molecular Medicine; Chief of the Hilda and J. Lester Gabrilove Division of Endocrinology, Diabetes and Bone Disease
Automated Insulin Delivery Shows Promise in Type 2 Diabetes
Use of an automated insulin delivery system improved glucose control among people with type 2 diabetes, representing a potential option for those who are struggling to keep their glucose levels in range.
Use of an automated insulin delivery system improved glucose control among people with type 2 diabetes, a study conducted by Mount Sinai endocrinologist Carol J. Levy, MD, CDCES, has shown.
The system tested, from Tandem Diabetes Care, comprises a t:slim X2 insulin pump and a continuous glucose monitor (CGM), both worn on the body. Incorporated within the insulin pump is software called “Control-IQ” that uses the glucose numbers and trends from the CGM to direct semi-automated insulin delivery. This system was approved in early 2020 based on research performed by a consortium of expert investigators (including Dr. Levy’s team) from a pivotal trial sponsored by the National Institutes of Health.
This “closed loop,” or “artificial pancreas” technology is recommended for people with type 1 diabetes, and its use is growing in that population. The 2022 study by Dr. Levy and colleagues indicated that the technology may also benefit people with type 2 diabetes who require insulin, regardless of how they were taking insulin at baseline and whether they were also using other oral or injectable glucose-lowering medications.
“It’s not for everyone with type 2 diabetes but rather those already requiring insulin with or without other medications for type 2 diabetes. But I think this could represent an option for those who are struggling to keep their glucose levels in range,” says Dr. Levy, Professor of Medicine (Endocrinology, Diabetes and Bone Disease), and Director of the Mount Sinai Diabetes Center
She presented data from the prospective, singlearm trial of 30 adults with type 2 diabetes in November 2022, during the virtual meeting of the Diabetes Technology Society. The study was sponsored by Tandem Diabetes Care, Inc., maker of the t:slim X2 insulin pump.
It’s not for everyone with type 2 diabetes but rather those already requiring insulin with or without other medications for type 2 diabetes
Carol J. Levy, MD, CDCES
The participants had a mean age of 54 years, median diabetes duration of 14 years, and a mean hemoglobin A1C of 8.6 percent, considerably higher than the recommended target of less than 7 percent. They were a diverse group; with an enrollment consistent with what would be seen in people with type 2 diabetes based on race and ethnicity.
At baseline, just over half were using CGMs, 13 were using only basal insulin, and 17 were using both basal and pre-meal insulin. Among those 17 participants, 15 were using multiple daily injections, and two were using insulin pumps.
Most participants were also taking other medications, including sodium-glucose cotransporter-2 (SGLT2) inhibitors, glucagon-like peptide 1 (GLP-1) agonistsdipeptidyl peptidase 4 (DPP-4) inhibitors or a combination of more than one medication in addition to insulin as is typical for people with type 2 diabetes. They continued taking these adjunctive medications throughout the trial.
After six weeks, the mean time spent in the glucose range of 70-180 mg/dL (the target recommended range for blood sugars) was 71 percent, the mean time spent with levels greater than 180 mg/dL was 29 percent, and time spent above 250 mg/dL was just 2.9 percent. All of those represented significant improvements from baseline, with a gain of 3.6 hours per day in range and one fewer hour per day above 250 mg/dL.
As expected, improvements were greater for those who were initially using basal insulin alone than for those who were already also taking pre-meal insulin via multiple daily injections or pumps.
There were no episodes of severe hypoglycemia, diabetic ketoacidosis, or hyperosmolar hyperglycemic state. Time spent with glucose levels below 70 mg/dL dropped by 0.03 percent, a significant improvement, while time below 54 mg/dL, rare to begin with, remained the same.
There was some weight gain, from 81.9 kg to 83.2 kg, a common occurrence with improved glycemic control. Total daily insulin dose rose from 0.53U/kg to 64U/kg, also often seen with improvement in blood sugar control.
Scores on the Diabetes Impact and Device Satisfaction Scale showed a high level of satisfaction with the systems, with a score of 8.8 on a scale of 1 to 10.
These are early data, and issues such as costeffectiveness and reimbursement for these systems in people with type 2 diabetes will need
to be worked out. But, Dr. Levy believes even the protection from hypoglycemia alone argues in favor of their use.
“The risk of negative outcomes with hypoglycemia can be pronounced in people with longer duration of diabetes. Most of the study participants were in their 50s, with another 20 to 30 years to live, so we believe that improvement in glycemia at least for this younger population will lead to a more robust outcome and potentially better quality of life.”
Featured Faculty
Carol J. Levy, MD
Clinical Director of the Mount Sinai Diabetes Center, and Associate Professor of Medicine (Endocrinology, Diabetes and Bone Disease)
About the Division of Gastroenterology
The mission of the Dr. Henry D. Janowitz Division of Gastroenterology at Mount Sinai is excellence in the delivery of patient care, research, and education in diseases of the GI tract. For more than a century, Mount Sinai gastroenterologists, surgeons, pathologists, and experts in related clinical and research areas have been at the forefront of innovation, shaping the future of GI medicine and clinical practice. Our pioneering work has led to advances in the diagnosis, treatment, and management of inflammatory bowel disease, peptic ulcer disease, esophageal disorders, gastrointestinal cancers, and pancreatic and biliary diseases.
To achieve its mission, the Division of Gastroenterology has developed continually expanding, world-leading digestive disease centers of excellence that include the Susan and Leonard Feinstein Inflammatory Bowel Disease Clinical Center and the GI Motility Center. Each center, with its distinct subspecialty and focus area, allows us to further the science of gastroenterology on several fronts and keeps us
at the cutting edge of delivering the highest quality of patient care. Other programs of excellence include advanced colonoscopy and therapeutic endoscopy services and pancreatic cancer.
The Division of Gastroenterology at The Mount Sinai Hospital was recently ranked No. 1 in New York by Newsweek for 2024 and No. 6 in the United States by U.S. News & World Report® for 2023-24.
System Chief
Bruce E.
Dr. Burrill
Sands,
MD, MS
B. Crohn Professor of Medicine
Targeting Disease Prediction and Prevention: The New Frontier in IBD
Mount Sinai researchers have found strong evidence that before the first symptoms of Crohn’s disease and ulcerative colitis occur, there’s a preclinical phase in which immune and inflammatory pathways are already altered. By targeting and treating the early pathogenic events that promote IBD development, they believe, disease onset could be prevented or impeded.
While a torrent of new drugs and therapeutic targets has brought relief to patients with inflammatory bowel disease (IBD), disease modification and cure remain critically needed but elusive endpoints.
Jean-Frederic Colombel, MD, Professor of Medicine (Gastroenterology) at the Icahn School of Medicine at Mount Sinai, believes those holy grails are achievable through the pursuit of a bold new target that has proven successful in other medical fields: disease prediction and prevention. In other words, by targeting and treating the early pathogenic events that promote IBD development, disease onset could be prevented or impeded, and a true opportunity to change its course revealed.
“We now have strong evidence that before the first symptoms of Crohn’s disease and ulcerative colitis ever occur, there’s a preclinical phase in which immune and inflammatory pathways are already altered,” says Dr. Colombel, who is Director of Mount Sinai's Susan and Leonard Feinstein Inflammatory Bowel Disease Clinical Center and its research counterpart, The Helmsley Inflammatory
Bowel Disease Center. “Being able to identify in the blood or stool those dysregulated pathways through biomarkers, such as proteomics, metabolomics, gut microbiome, and antimicrobial antibodies, will lead to the development of prediction models and prevention strategies.”
Dr. Colombel has made measurable progress toward that goal through several new investigations. One study, in Gastroenterology, reported the presence of anti-granulocyte macrophage-stimulating factor autoantibodies (aGMAbs) in the sera of patients with Crohn’s disease up to six years before diagnosis, suggesting they could contribute to the pathophysiology of the disorder. “Our study demonstrated IgG2- and IgA-skewed isotopes of aGMAbs in patients with Crohn’s disease, indicating an origin within the intestinal mucosa,” explains Dr. Colombel. “We also found that aGMAbs not only predict the diagnosis of Crohn’s disease well in advance, but, in a subset of patients, they are associated with ileal involvement, disease severity, high relapse rates, and complications at disease onset.”
The research team included, from left: Manasi Agrawal, MD, MS; Jean-Frederic Colombel, MD; Saurabh Mehandru, MD; Alexandra Livanos, MD, PhD
We now have strong evidence that before the first symptoms of Crohn’s disease and ulcerative colitis ever occur, there’s a preclinical phase in which immune and inflammatory pathways are already altered
Jean-Frederic
Colombel, MD
To make new inroads into IBD prediction and prevention, Dr. Colombel’s team has reached beyond traditional epidemiological research platforms and pressed into service “multiomics,” an advanced methodology designed to leverage unbiased high-throughput data relevant to IBD. As outlined in a recent Mount Sinai study in Nature Reviews Gastroenterology and Hepatology, multiomics is uniquely equipped to find the critical links between the genome, microbiome, proteome, and exposome on the road to developing a model to characterize IBD risk factors and molecular pathways.
Nothing is more critical to IBD research, however, than Mount Sinai’s collaboration with a consortium of academic, industry, and government organizations. This partnership is drawing on a powerful resource: the U.S.
Department of Defense’s (DOD) serum repository. Its millions of blood samples were taken from soldiers when they enlisted, and every two years of service thereafter, from 1998 through 2013 as part of the United States Defense Medical Surveillance System. “Some of these soldiers go on to develop IBD, and we’re able to link these samples to their medical records and track the development of markers preceding the clinical diagnosis,” Dr. Colombel says.
“If we’re going to find a way to prevent Crohn’s disease and ulcerative colitis, it will require the global GI community actively embracing this new paradigm of prediction and prevention,” declares Dr. Colombel. “We are making great progress, but so much work remains.”
Featured Faculty
Jean-Frederic Colombel, MD
Professor of Medicine (Gastroenterology)
Stem Cell Transplants Prove
Effective for Patients With Severe Crohn’s Disease
A clinical study of autologous stem cell transplantation for severe Crohn's disease is offering the sickest of patients a transformative therapy that is achieving remarkable early results in this group for whom nothing in the past has worked.
For people with severe Crohn’s disease, life often becomes a grueling carousel of narcotics and surgery, with no way off. Mount Sinai is starting to change that paradigm with a clinical study that is offering the sickest of patients a transformative therapy autologous stem cell transplantation that is achieving remarkable early results in this group for whom nothing in the past has worked.
“We’re finding that autologous stem cell transplants benefit about 90 percent of Crohn’s disease patients who fit very specific criteria, compared to maybe 15 percent who benefit from new drugs when they’re introduced,” says Louis Cohen, MD, Assistant Professor of Medicine (Gastroenterology) at the Icahn School of Medicine at Mount Sinai, who is heading up the trial. “Even when the disease returns, it seems to be in a different form, and patients suddenly become responsive to medication. We’re conducting rigorous research to try and understand why.”
Autologous stem cell transplants for Crohn’s disease are offered by only a handful of medical centers in the world. Liz Palen is one of the
beneficiaries. Diagnosed with Crohn’s in 2012, the 36-year-old registered nurse began a 10-year regimen of biologic injectables, steroids, surgical bowel resection, and a colostomy to try and control recurring symptoms. “I had joint pain, skin rashes, fatigue, nausea, and no appetite,” she recalls. “I was on all the medications, and nothing seemed to improve my quality of life for more than a brief time.”
Desperate for a solution, she heard about the nascent field of stem cell transplants. With a referral from her local gastroenterologist, she wound up in Dr. Cohen’s office in November 2019. After determining that she met the entry criteria, Dr. Cohen carefully explained the procedure, which required nearly six weeks of hospitalization. After undergoing a baseline endoscopy, colonoscopy, and MRI to document mucosal disease activity, patients are tapered off all medications in preparation for stem cell mobilization. That process involves low-dose chemotherapy; administration of growth factors; and harvesting healthy red blood cells, immune cells, and platelets from the patient’s hematopoietic system.
Patient Liz Palen in 2020, just after receiving an autologous stem cell
Ms. Palen in 2022: "It was a life-changing experience for me," she says transplant for Crohn's disease
“We believe that in patients predisposed to Crohn’s disease, there are certain triggers that cause the immune system to essentially go wild,” explains Dr. Cohen. “Through stem cell transplants, we’re in essence resetting, or turning back, the immune system to a time when it functioned normally.”
Ms. Palen opted to divide the procedure into two in-hospital segments, allowing her some time in between to rest. For the stem cell mobilization phase, she entered The Mount Sinai Hospital in Manhattan in December 2019, and returned three weeks later to have the harvested stem cells returned to her bloodstream. Throughout her hospitalization, she was able to access as part of the clinical trial program a panoply of support services designed to relieve the inpatient burden. These included a team of nutritionists, palliative care specialists, a social worker, a psychologist, and even a massage therapist.
Within six weeks of discharge, Ms. Palen began noticing an improvement in her Crohn’s disease symptoms. At six months, she was in full remission. “I did a 180-degree turnabout in symptoms and energy level, and was able to get back to activities such as camping and golfing, which I couldn’t do before. I also got married and bought a new home. There’s no question it was a life-changing experience for me.”
As for medications, right after transplantation, Ms. Palen began taking vedolizumab an antiintegrin agent that’s a critical part of the Mount
Sinai clinical trial regimen. “Our overriding goal is complete remission for our patients,” emphasizes Dr. Cohen, “and we think that vedolizumab is an outstanding way to achieve that by keeping the immune system in check and helping to turn back the clock on the disease.” Indeed, Ms. Palen reports she is now able to take medications that were previously off the table because of antibodies her body had developed against them.
Adds Dr. Cohen, “No one has ever attempted this type of surgical and therapeutic approach before, but we believe it can open the door to stem cell transplants for growing numbers of people with Crohn’s disease before they spend years of their lives suffering.”
Featured Faculty
Louis Cohen, MD
Assistant Professor of Medicine (Gastroenterology)
Aggressive Surveillance Paves the Way for Early Detection of Pancreatic Cancer
Recent studies underscore the benefit of highrisk pancreatic surveillance programs that have helped push three-year survival rates as high as 85 percent in some cases, in large part by catching a higher proportion of malignant lesions while they are still resectable.
Pancreatic cancer the third leading cause of cancer death in the United States is typically thought of as a terminal diagnosis, even by professionals in the field. The five-year survival rate for pancreatic adenocarcinoma remains around 9 percent.
But the tide could well be turning thanks to advanced new treatments and aggressive surveillance. Indeed, recent studies have underscored the benefit of high-risk
genetic counselors. Tethered to this program is a robust research initiative driven by a registry of more than 800 high-risk patients who, in many cases, have undergone surveillance and agreed to participate in clinical trials.
“In our program, patients are offered a full risk assessment based on a very detailed threegeneration family history focused on pancreatic cancer, as well as other neoplasms such as breast, ovarian, skin, and colon cancers,” says
pancreatic surveillance programs that have helped push the three-year survival rates as high as 85 percent in some cases, in large part by catching a higher proportion of malignant lesions while they are still resectable.
From the opening of its specialized pancreatic cancer surveillance program 10 years ago, Mount Sinai has been in the vanguard of the field. The focus is on early detection through active risk assessment particularly in families where two or more immediate members have a history of the disease led by a team of clinicians experienced in gastrointestinal cancers, working closely with
Aimee Lucas, MD, MS, Professor of Medicine (Gastroenterology) at the Icahn School of Medicine at Mount Sinai, who launched the surveillance clinic in 2012. “After seeing our genetic counselors, patients typically meet with me to plan a personalized clinical surveillance program, which may include endoscopic ultrasound or MRI. At the end of the visit, we draw blood for genetic testing and any clinical or research labs that might be indicated.”
About a third of patients screened at the Upper East Side clinic in Manhattan show small, subcentimeter pancreatic cysts on imaging. “The
Aimee Lucas, MD, MS, has launched a pancreatic screening program for high-risk patients like Martin Abrams.
majority of cysts do nothing over time, so we simply watch them,” Dr. Lucas says. Some features, however, can serve as markers for neoplastic progression to high-grade dysplasia or pancreatic cancer, including the presence of multifocal cysts, cyst growth, or solid nodules.
In fact, telltale biomarkers are at the heart of Dr. Lucas’s growing body of research for detecting early pancreatic cancer. One study in which she was senior author found, for example, that highrisk patients with elevated hemoglobin A1c (HbA1c) were more likely to have pancreatic cysts compared to patients with lower levels observable through screening findings that could be helpful in tailoring surveillance protocols for individuals at increased risk of developing pancreatic adenocarcinoma. Past research in the field has established new-onset diabetes mellitus as a precursor to pancreatic cancer, with approximately 85 percent of patients diagnosed with the malignancy also having impaired fasting blood glucose or diabetes.
In another study, Dr. Lucas significantly expanded the boundaries of that knowledge with the discovery that metabolic changes such as worsening glycemic control and weight loss may be harbingers of underlying pancreatic cancer. More specifically, she and her research team
learned that glycemic elevations may occur up to three years before diagnosis, and weight loss up to two years prior to diagnosis. For that reason, they recommended including markers of glucose intolerance and body mass index trends in predictive models of pancreatic cancer.
“One of the major reasons pancreatic cancer remains so deadly is because of late detection,” Dr. Lucas points out. “That’s why we’re so focused on investigating genetic predisposition and biomarkers for early detection, and pairing that information with an aggressive surveillance program that could lead to improved outcomes.”
Featured Faculty
Aimee Lucas, MD, MS
Professor of Medicine (Gastroenterology) Chief, Division of Gastroenterology at Mount Sinai Morningside and Mount Sinai West
About the Division of General Internal Medicine
The Mount Sinai Division of General Internal Medicine encompasses much more than outstanding clinical care. Continuous qualityimprovement efforts, innovative care models, dynamic educational programs, and health services research characterize the Division. A personal and interdisciplinary approach involving colleagues and services in nursing, social work, medical and surgical subspecialties, psychiatry, and rehabilitation is often used to diagnose, treat, manage, and heal the whole patient. The Division of General Internal Medicine is able to make referrals and coordinate care with a vast array of outstanding specialty services, and collaborate with them to create new models of care.
Faculty members are consistently championing population health initiatives, an important step in the evolution of health care delivery. The Division is using information technology and data systems to tailor entire clinical programs that better manage chronic illnesses and preventive care
efforts, thereby improving patients’ overall health and decreasing health care costs.
Over the last year, Internal Medicine Associates (IMA) has continued to focus on refining teambased care processes for chronic disease management, as well as improving medication adherence rates, adherence to age-appropriate cancer screening, and transitions of care.
For diabetes, IMA continues to use a teambased model of care involving Certified Diabetes Educators and a dedicated high-A1c clinic staffed by our internal medicine interns with faculty oversight. In August 2022, our A1c >9% control rate reached 13.5 percent, which is below the goal of less than 15 percent. We have continued to meet or exceed that goal since then.
Among patients with hypertension, the IMA is increasing the control rate from 60 percent to 70 percent with a goal of 75 percent. A robust
management guideline includes home blood pressure monitoring. The Division improved its home blood pressure monitor access via a partnership with Integra (a benefits manager that is responsible for providing home cuffs for patients) by creating a closed-loop feedback process to track orders. In 2021, fulfillment was 50-60 percent and it is now at 80-90 percent. IMA continues to work with its population health teams on outreach efforts to connect value-based contract patients to these programs.
System Chief
Juan Wisnivesky, MD, DrPH
Drs. Richard and Mortimer Bader
Professor of Medicine
Multidisciplinary CrossPollination Is Key Component of Research Training Program
Mount Sinai houses several National Institutes of Health (NIH)-funded T32 fellowships to train researchers. Among them are a program focusing on cancer prevention and control for clinical and non-clinical scientists, and a program focusing on disparities in aging and dementia.
Mount Sinai is not only a renowned center of medical research, but also a center for research training, housing several National Institutes of Health (NIH)-funded T32 fellowships. Diversity of background, training, and thought are important components of these fellowships, creating crosspollination that can significantly advance the field.
Two T32 programs stand out. The two-year Cancer Prevention and Control (CPC) in Priority Populations T32 fellowship program, established in 2018, focuses on training clinical and nonclinical scientists whose aim is to advance CPC in specific populations that are disproportionately vulnerable to cancer.
“CPC is a way of thinking about doing research that either looks at ways to prevent cancer or control it, usually in the realm of cancer survivorship,” explains Jenny J. Lin, MD, MPH, the system director for mentoring and Professor of Medicine (General Internal Medicine) at the Icahn School of Medicine at Mount Sinai. Dr. Lin is also the Associate Director of the CPC program
“The research can be about cancer treatment, but it is often about survivorship for example, how cancer survivors manage comorbid illnesses or palliative care. This research is broad, tending to be about health services or epidemiology. There is also behavioral research, and quite a bit of work done on cancer prevention that focuses on patient education, patient outreach, and comparative effectiveness,” Dr. Lin says.
Alex Federman, MD, MPH, a mentor for the program, Professor of Medicine (General Internal Medicine), and Geriatrics and Palliative Medicine, and the Division’s Director of Research, adds, “One thing that characterizes this program and others is that we support multiple disciplines and methodologies.”
Indeed, one of the great strengths of the CPC fellowship is the diverse backgrounds from which the fellows come, allowing for crosspollination of ideas and expertise from divergent areas. One fellow is a nurse scientist, another an endocrinologist, a third a behavioral health scientist, the fourth a gastroenterologist.
From left: Jenny J. Lin, MD, PhD, Professor of Medicine (General Internal Medicine); Alex Federman, MD, MPH, Professor of Medicine (General Internal Medicine); and Juan Wisnivesky, MD, DrPH, the Drs. Richard and Mortimer Bader Professor of Medicine (General Internal Medicine)
All have strong research interests in so-called priority populations, which is a broad term designed to be inclusive of groups that are in some way vulnerable, and thus at risk for worse health outcomes. “So, priority populations might include minorities, the elderly, individuals with certain comorbidities, those with different sexual orientations or low socioeconomic status, and those living in a rural population,” explains Program Director Juan Wisnivesky, MD, DrPH, the Drs. Richard and Mortimer Bader Professor of Medicine and Chief of the Division of General Internal Medicine. “We also include individuals exposed to the World Trade Center site because it is a specific population that is served by Mount Sinai and has experienced worse cancer outcomes.”
The DiAD Program
The second notable two-year T32 training program is the Research on Disparities in Aging and Dementia fellowship hence its acronym, DiAD whose directors are Drs. Lin and Federman, as well as Albert L. Siu, MD, Chair Emeritus of the Brookdale Department of Geriatrics and Palliative Medicine
The program, now in its third year, focuses on people with Alzheimer’s disease and other dementias, as well as older adults experiencing inequities in health outcomes. “The program has to do with cognitive impairment, but it doesn’t necessarily have to be in older adults,” Dr. Lin notes.
As with the CPC program, the DiAD program benefits greatly from the many disciplines of its fellows, which currently include a hospice and
palliative care physician-scientist, an internist, a nurse scientist, and a clinical neuropsychologist. “I think the uniqueness of these two programs is because we have so many different people from different departments from different fields,” Dr. Lin says. “They are not all physicians, and that really promotes a lot of cross-disciplinary collaboration as well as thinking.”
Both the CPC and DiAD programs include interdisciplinary curricula and are especially strong in mentorship, with as many as 20 faculty researchers supporting the fellows in each program. “There are multiple levels of mentorship,” Dr. Federman explains. “The most important is the trainee’s primary mentor, who is the person they are working with on their main project. That is often the closest working relationship that the fellows will have.
“But for both programs we strive to create a mentorship team for the trainees, which we aim to be a multidisciplinary experience. We look at the individual needs of the trainee. Those needs may be content-specific, or methodological, or general career direction. We link up the appropriate mentors with each trainee.”
One of the goals of both the CPC and DiAD programs is to launch the careers of its fellows. By that measure the programs have been highly successful, with trainees continuing on to rewarding academic research careers at Mount Sinai and elsewhere and receiving career development awards and research grants from the NIH, American Society of Clinical Oncology, the American Cancer Society, and others.
Featured Faculty
Alex Federman, MD, MPH
Professor of Medicine (General Internal Medicine), and Geriatrics and Palliative Medicine
Jenny J. Lin, MD, MPH
Professor of Medicine (General Internal Medicine)
Albert L. Siu, MD
Professor and Chair
Emeritus of Geriatrics and Palliative Medicine; Professor of Medicine, and Population Health Science and Policy
Juan Wisnivesky, MD, DrPH
Drs. Richard and Mortimer Bader
Professor of Medicine; Chief of the Division of General Internal Medicine
Breaking the Mold of Standard Health Care Delivery
The Mount Sinai Division of General Internal Medicine has developed several innovative models that provide for highly coordinated and multidisciplinary care to patient populations that often find themselves outside the mainstream.
Constantly looking for ways to improve the traditional delivery of health care, the Mount Sinai Division of General Internal Medicine has developed several innovative models that provide for highly coordinated and multidisciplinary care to patient populations that often find themselves outside the mainstream.
A case in point is the creation of a comprehensive obesity management program directed at individuals from disadvantaged groups that disproportionately struggle with weight issues, who often find it difficult to access appropriate clinical services. Aware of that void, the Division of General Internal Medicine at Mount Sinai Morningside and Mount Sinai West opened a clinic in the fall of 2023 under the direction of Rebecca Shafer, MD, a certified obesity management physician. Known as the Center for Healthy Weight Management, it is believed to be the first of its kind in the New York metropolitan region and is being run in partnership with Ryan Health, which has been providing a wide
range of medical services for the past 50 years to underserved communities in Manhattan.
“We’ve developed a unique way to integrate an obesity management program into the primary care setting in order to give patients access to a specialized program they wouldn’t normally find at the community level,” said Fernando Carnavali, MD, Associate Professor of Medicine (General Internal Medicine) at the Icahn School of Medicine at Mount Sinai, and Chief of General Internal Medicine at Mount Sinai Morningside and Mount Sinai West. “We’re focused on medication management, nutrition support, education, and mental health, all of which are closely aligned with the broad-based model of care the Ryan network has so successfully brought to the community.”
The framework for this newest program began taking shape more than a year ago when Mount Sinai hired a physician with fellowship training in obesity management. The Division of Internal
Fernando Carnavali, MD, and Juan Wisnivesky, MD, DrPH, are leading the development of innovative models that provide for highly coordinated and multidisciplinary care.
Medicine is now grooming a number of residents pursuing primary care tracks to also become certified in that field. At the same time, points out Dr. Carnavali, these clinical trainees are gaining valuable exposure to underserved populations and public health services by working alongside specialists at the Ryan sites, which include clinics and community outreach centers offering adult medicine, women’s health, mental health, pediatrics, and other specialized forms of care.
The concept of a seamless health care environment for the community also figures heavily in the key role General Internal Medicine is playing in the recently opened Mount SinaiBehavioral Health Center in Lower Manhattan. Specifically, the $140 million facility co-locates on its second-floor outpatient psychiatry services with a primary care practice equipped to manage a full range of patient morbidities an unusual and novel partnership by traditional health care standards.
“Our goal was to bring primary care to a community on the Lower East Side of Manhattan where access to such quality services is sparse,” notes Leonard Amoruso, DO, Assistant Professor of Medicine (General Internal Medicine) at Icahn Mount Sinai, and Chief of General Internal Medicine at Mount Sinai Beth Israel. “Now, while patients are visiting the psychiatry clinic, they could walk down the hallway and have a sameday appointment with a primary care doctor for health care screening, routine labs, or many other services they wouldn’t normally get, given the fact that mental illness often stands as a barrier to general medical care.”
In addition to creating innovative new approaches to health care delivery, the Division of General Internal Medicine takes pride in its ability to recruit in a post-pandemic world a rich crop of professsional talent for its faculty and trainee ranks. “Amid all the competition, we’ve been
capturing people from all over the country, as well as from our own hospitals,” says Juan Wisnivesky, MD, DrPH, Drs. Richard and Mortimer Bader Professor of Medicine and System Chief of the Division of Internal Medicine. “We’re securing the future of our entire department by drawing people with fresh ideas and strategies on how to make health care work for growing populations of patients.”
Featured Faculty
Fernando Carnavali, MD
Associate Professor of Medicine (General Internal Medicine)
Leonard Amoruso, DO
Assistant Professor of Medicine (General Internal Medicine)
Juan Wisnivesky, MD, DrPH
Drs. Richard and Mortimer Bader Professor of Medicine; Chief of the Division of General Internal Medicine
About the Division of Genomic Medicine
Around the world, researchers, clinicians, and the general public are recognizing the integral role of genomics within numerous areas of health and medicine. To position the Department of Medicine at the forefront of this rapidly expanding landscape in the era of precision medicine, Mount Sinai established the Division of Genomic Medicine. Its mission is to advance, implement, and scale genomic approaches to improve the diagnosis, treatment, and prevention of disease.
The scarcity of genetics experts in health care, including medical geneticists and genetic counselors, limits the widespread use of meaningful genomic information. The need for delivery and interpretation of genomic results adds to growing demands on physicians in primary and specialty care, who are increasingly expected to interpret genomic findings, recognize genomic risk, and assimilate genomics into the care of their patients.
Through patient-centered clinical applications, collaborative research, and innovative outreach and training programs, the Division of Genomic Medicine is dedicated to creating an individualized health care experience in which genomic data are a routine part of patient care. The Division supports physicians and scientists across the Mount Sinai Health System to bring genomics into all aspects of medicine.
System Chief
Michael Murray, MD Professor of Medicine
Making Genomics a Routine Part of Clinical Care
Mount Sinai's Division of Genomic Medicine has a goal as ambitious as it is sweeping: to make genomic medicine a routine part of patient care for the diagnosis, treatment, and prevention of all types of disease.
The Icahn School of Medicine at Mount Sinai has long been a pioneer in genetics, starting with the establishment of BioMe, one of the country’s first medical record-linked biobanking programs in 2006, and continuing with the recently announced Mount Sinai Million Health Discoveries Program to genetically sequence 1 million Mount Sinai patients within the next five years.
The Department of Medicine’s newest entity, the Division of Genomic Medicine, builds on that work with a goal as ambitious as it is sweeping: to make genomic medicine a routine part of patient care for the diagnosis, treatment, and prevention of all types of disease.
“Genomics provides extremely rich data about an individual’s risk for disease over the course of their entire life, and we want to deliver on its enormous promise by integrating it into health care decisions that result in the most effective management of our patients,” says Eimear Kenny, PhD, Mount Sinai Professor of Genomic Medicine. “That involves working closely with our primary and specialty care physicians to empower them with the knowledge and tools they need to interpret genetic findings, recognize genomic risk, and use those insights to respond to each patient’s unique health care needs.”
That effort is well underway through patientcentered clinical applications, collaborative research, and innovative education and training programs. The Division’s Genomic Health Clinic, for example, is among the first of its type to engage directly with individuals seeking one-onone genomic risk evaluation and testing from an experienced medical geneticist-genetic counseling team (see our accompanying article on the Genomic Health Clinic).
In the field of research, the Division of Genomic Medicine partners with Mount Sinai's Institute for Genomic Health to conduct cutting-edge work “to bring genomic information into the clinic for everyday health care, and not just for some of the specialty areas where it currently fits,”
according to Dr. Kenny, who is Founding Director of the Institute.
A current clinical trial, for example, is investigating the use of polygenic risk scores which aggregate information spanning the entire genome to provide individuals from diverse populations with precision reports on their risk exposure to common diseases. For this study and others, the computation-driven Institute relies heavily on artificial intelligence and machine learning to scale up its research.
We are building programs to turn genomic results from the Discoveries Program when they are medically actionable into follow-up care designed to benefit our patients.
Eimear
Kenny, PhD
In education and training, the Division is one of the first to create a Genomic Medicine Training Track for residents, fellows, and interns interested in gaining a deeper knowledge of genomics and its applications within clinical care, especially ordering and interpreting genetic tests. The online curriculum, now in its third year with six participants, will receive National Institutes of Health support to carry out the next phase of its growth.
The Division’s influence is already being felt across Mount Sinai through its screening programs for a variety of hereditary diseases. It has teamed up with Amy Kontorovich, MD, PhD, Director of the Center for Inherited Cardiovascular Disease, for instance, to test individuals for amyloidosis, a multisystemic disorder caused by a mutation in the transthyretin (TTR) gene. Amyloidosis manifests as cardiovascularneurological-musculoskeletal symptoms, and African American and African populations are
at higher risk for it. “We’ve successfully tested for this condition in patients enrolled in the Mount Sinai BioMe Biobank and referred those who may have a predisposition to our High-Risk Amyloidosis Clinic for professional care,” notes Dr. Kenny.
Similarly, the Division is leveraging the Health System’s massive bio repository to identify mutations in the breast and ovarian cancer susceptibility genes BRCA1 and BRCA2 As a result of this growing screening initiative, numerous patients have been referred for follow-up care to oncologists and other health specialists at Mount Sinai.
No project promises more profound results, however, than the Mount Sinai Million Health Discoveries Program, which will sequence and analyze the DNA of a million participating patients, the largest effort of its type ever undertaken by a health system. This trove of data will enable researchers to assess the true potential of genetics-based precision medicine approaches to guide everyday patient care. The Division of Genomic Medicine is an important partner in this endeavor.
“We are building programs to turn genomic results from the Discoveries Program when they are medically actionable into follow-up care designed
to benefit our patients,” says Dr. Kenny. “We are committed to being a leader in the creative use of this data, and that takes on added significance given the fact Mount Sinai treats one of the most diverse patient populations, with ties to more than 160 countries around the world.”
Featured Faculty
Eimear Kenny, PhD
Mount Sinai Professor of Genomic Health
Amy Kontorovich, MD, PhD
Associate Professor of Medicine (Cardiology, and Medical Genomics)
Genomic Health Clinic Gives People a Window
On Early Disease Detection and Prevention
Mount Sinai's Genomic Health Clinic the only advanced service of its type in New York City and one of a handful in the country—is emerging as a vital ally to people who hope to understand the risks to themselves and family members from information embedded in their genomes.
As genetic testing moves beyond the realm of rare disease to mainstream disorders such as cardiovascular disease and cancer, the Division of Genomic Medicine’s Genomic Health Clinic is emerging as a vital ally to people who hope to understand the risks to themselves and family members from information embedded in their genome.
The only advanced service of its type in New York City and one of a handful in the country, the Clinic connects patients with a highly skilled medical geneticist-genetic counselor team to identify potential health hazards. If a genetic risk is found, the team refers the individual to appropriate physicians within the Mount Sinai Health System for monitoring or treatment before it becomes a serious issue.
Patients have traditionally been referred for a genetic evaluation when they have a strong personal or family history of certain diseases. But with genetic testing now widely accessible through direct-to-consumer products such as 23andMe and others, more people can potentially benefit from a thoughtful analysis of their screening results or consideration of proactive genetic testing by genetic experts.
“We’re trying to help people recognize there may be subtle clues in their family history that help explain many common diseases from a hereditary standpoint,” says Emily Soper, MS, Instructor in Medicine at the Icahn School of Medicine at Mount Sinai and a genetic counselor at the Genomic Health Clinic. “That level of information can truly empower them to be much more proactive about their health and not wait for problems to develop before they take action.”
Launched in 2020, the Clinic currently sees four to six new patients a week, though that number is poised to grow exponentially as genetic screening becomes more deeply woven into the fabric of routine health care. As the Clinic’s medical geneticist, Ayuko Iverson, MD, points out, the opportunities to address potentially troublesome conditions are as unlimited as the human genome itself.
“We often get referrals for people with a family history of thrombophilia; various cancers such as breast, pancreatic, and colon; and Alzheimer’s disease or dementia,” says Dr. Iverson, Assistant Professor of Medicine, and Genetics and Genomic Sciences, at Icahn Mount Sinai. “But there are genes that play a role in developing common
Emily Soper, MS, and Ayuko Iverson, MD, explain how genes could play a role in a patient’s family history of disease at the Genomic Health Clinic.
diseases that we know are treatable or even preventable if caught early enough.”
The U.S. Centers for Disease Control and Prevention, for example, has identified three Tier 1 conditions associated with high genomic risk in 1 of every 75 people, though as many as 90 percent are unaware of the potential threat.
Those conditions are hereditary breast and ovarian cancer, Lynch syndrome, and familial hypercholesterolemia. “Each of these conditions is actionable,” notes Dr. Iverson, “and if we detect any of them through genetic screening there are specific care management and surveillance guidelines that can be implemented.”
A visit to the Genomic Health Clinic typically begins with a review of the individual’s personal and family health history going back three or four generations, and a physical examination. Based on this evaluation, the genomics team then discusses genetic testing options with the patient including any medically indicated tests as well as proactive screening—and what potential implications of testing should be considered. For patients seeking a better understanding of their response to certain medications, a pharmacist also reviews the patient's medication history and discusses pharmacogenetic testing to evaluate how their genes affect the body’s metabolism of medications. If the patient opts to proceed, a blood or saliva sample is taken and sent to a clinical testing laboratory for analysis. A second visit is then scheduled at which the patient receives the results along with counseling and, when appropriate, referrals to specialists such as a hematologist, cardiologist, endocrinologist, or oncologist. Other times, the genomic specialists may simply suggest that the patient confer with their primary care doctor.
Indeed, the Genomic Health Clinic is looking to expand its relationship with primary care practices within Mount Sinai, knowing they represent a major channel for preventive care and referrals. Other patients find their way to the Clinic through web searches.
“People often come in after having done a directto-consumer or commercial self-driven genomic test and want to know what it means for their health care,” explains Ms. Soper. “We’re able to interpret the data for them in terms of risk to not just themselves but their family. Many times, the greatest benefit we provide patients is just being able to walk them through the results and reassure them that something found in their test is not as worrisome as they had thought.”
Featured Faculty
Ayuko Iverson, MD
Assistant Professor of Genetics and Genomic Sciences, and Medicine (General Internal Medicine, and Medical Genomics)
Emily Soper, MS
Instructor of Medicine (Medical Genomics))
About the Division of Hematology and Medical Oncology
The Division of Hematology and Medical Oncology has experienced tremendous growth over the past several years, while also staying true to its dual mission of delivering the best, most compassionate care to patients and pursuing excellence in research and training.
The Division, as an integral component of The Tisch Cancer Institute at Mount Sinai, builds on a long history of excellence in hematology and hematological malignancies, as well as solid tumor oncology.
Through clinical and research collaborations, the Division is committed to providing patients with the most advanced therapies, including access to revolutionary clinical trials.
System Chief
Joseph A. Sparano, MD
Ezra M. Greenspan,
M.D.
Professor in Clinical Cancer Therapeutics
Mount Sinai Renews Efforts to Seek
Innovative Approaches to Blood Cancers
The National Cancer Institute has again renewed its support for the Mount Sinai-led Myeloproliferative Neoplasm Research Consortium, which is making progress on treatments for adult leukemias and myeloproliferative neoplasms.
Through its work advancing bold therapeutic solutions to a complex range of adult leukemias and myeloproliferative neoplasms (MPNs) that compromise the lives of millions of patients, a 15member team of investigators from Mount Sinai’s Department of Medicine continues to burnish its international credentials.
Reinforcing that reputation was the recent renewal for the fourth time of a National Cancer Institute (NCI)-funded grant supporting the Mount Sinai-led Myeloproliferative Neoplasm Research Consortium (MPN-RC), a unique group of translational researchers from 13 institutions across North America that has driven innovative clinical trials for such breakthroughs as Janus kinase 2 (JAK2) inhibitors for treating myelofibrosis, and restoring the tumor suppression activity of the TP53 gene, which encodes the p53 protein, through smallmolecule inhibitors of the MDM2 protein.
The focus of the renewed NCI grant, which originated in 2006, is to improve the median sixyear survival rate of individuals with myelofibrosis, a chronic leukemia characterized by excessive production of inflammatory cytokines. Under the leadership of Principal Investigator Ronald Hoffman, MD, Albert A. and Vera G. List Professor of Medicine (Hematology) and Director of the Myeloproliferative Disorders Research Program at the Icahn School of Medicine at Mount Sinai, scientists are attempting to deplete the pool of cancer stem cells by targeting malignant hematopoietic stem cells and reversing their tumor-promoting microenvironment.
“Our combination laboratory-clinical team is trying to effectively eliminate the malignant stem cell from which the disease is derived and, ultimately, change the natural course of lethal blood cancers,” says John Mascarenhas, MD, Professor of Medicine (Hematology and Medical Oncology) at Icahn Mount Sinai, and Director of the Adult Leukemia Program and of the Center of Excellence for Blood Cancers and Myeloid Disorders. As evidence of that dogged scientific pursuit he points to the team’s rational approaches
to silence such cytokines as IL-1 and IL-8, which are pathologically overexpressed in myelofibrosis, with canakinumab and reparixin, respectively.
If we’re going to change the trajectory of acute leukemia and myeloid disease, we need to train and promote the next generation of clinical and laboratory scholars.
John Mascarenhas, MD
Just as importantly, MPN researchers have built on Dr. Hoffman’s considerable body of work over the years by activating the p53 pathway. These prior studies led to the observation that MDM2, a negative regulator of p53, is highly expressed in the CD34+ cells of patients with myeloproliferative neoplasms, and that it could be targeted by small-molecule antagonists known as nutlins, which occupy the p53 binding pocket of MDM2. From this seminal work has emerged a number of phase 3 registration trials for similar class compounds, as well as the development of cutting-edge combination approaches with BET protein inhibitors designed to dampen the myelofibrosis environment, which are poised to move from laboratory to the clinic.
Another way Mount Sinai researchers are taking combination therapy to new levels is through the development of targeted protein degraders, which have become one of the hottest fields of cancer drug discovery in recent years. Partnering with Jian Jin, PhD, Mount Sinai Professor in Therapeutics Discovery and Director of the Mount Sinai Center for Therapeutics Discovery, myeloid researchers have developed MDM2 and PPM1D protein degraders that are part of a new therapeutic class known as proteolysis-targeting chimeras (PROTACs). Dr. Jin’s pioneering work with PROTACs has created numerous degraders of a wide range of oncogenic proteins, including some considered undruggable for decades. The hope is
that ongoing laboratory evaluation and agent optimization will soon lead to clinical testing in patients with blood cancers.
Among the most recent pivotal trials from the MPN/leukemia research program were those leading to approval of the JAK2 inhibitor pacritinib for patients with myelofibrosis and thrombocytopenia. “Previously these patients had an extremely poor prognosis,” explains Dr. Mascarenhas, who was lead investigator for the agent’s phase 3 registration trial. “The results of our PERSIST-2 study provided for the first time a promising therapeutic option for patients who are ineligible due to low platelets, or have failed therapy with the JAK1-JAK2 inhibitor ruxolitinib.”
Amid its flurry of past and current clinical work to arrest deadly blood cancers, Mount Sinai is also eagerly looking to the future.
“If we’re going to change the trajectory of acute leukemia and myeloid disease, we need to train and promote the next generation of clinical and laboratory scholars,” Dr. Mascarenhas says. “For that reason, we’re particularly proud of our talented team of junior faculty and fellows who have been awarded grants by the American Society of Hematology and Leukemia and Lymphoma Society to push the research envelope, and to hopefully develop curative approaches in our lifetime.”
Featured Faculty
Ronald Hoffman, MD
Albert A. and Vera G. List Professor of Medicine (Hematology)
John Mascarenhas, MD Professor of Medicine (Hematology and Medical Oncology)
Jian Jin, PhD
Mount Sinai Professor in Therapeutics Discovery
Seeking Biomarkers and Therapies to Harness Immunotherapy Against Bladder Cancer
Standard treatment for muscle-invasive bladder cancer involves surgical removal of the bladder. Through a multitude of first-ever clinical trials, Mount Sinai scientists are deploying cutting-edge immunotherapeutic approaches to help patients avoid this life-changing operation and improve the length and quality of their lives.
Few research centers have done more over the past decade to dissect the biology and mechanisms of bladder cancer, along with their response and resistance to modern-day therapies, than the Icahn School of Medicine at Mount Sinai. Through a multitude of first-ever clinical trials, scientists are deploying cuttingedge immunotherapeutic approaches to not just improve the length and quality of life for patients but potentially cure a disease that accounts for more than 70,000 new cases and approximately 15,000 deaths each year in the United States.
Here are three major areas of investigation that encapsulate that targeted effort:
Combination Therapy to Prevent Bladder Removal
Standard treatment for muscle-invasive bladder cancer involves surgical removal of the bladder, a life-changing operation. At the same time, when chemotherapy is given to these patients prior to bladder removal, about 30 percent show no residual traces of the tumor. This has created a dilemma for doctors since there is no way of knowing which patients have achieved a complete pathological response until after the bladder has been removed and analyzed under the microscope.
“We realized what a game changer it could be if we were able to combine immunotherapy with chemotherapy and identify through a battery of tests if a complete response had occurred without removal of the bladder,” says Matthew Galsky, MD, Professor of Medicine (Hematology and Medical Oncology), and Urology, at Icahn Mount Sinai, and Co-Director of the Center of Excellence for Bladder Cancer at The Tisch Cancer Institute. “We could potentially treat patients curatively with chemotherapy plus immunotherapy and prevent them from losing their bladders.”
From that manifest need emerged the country’s first clinical trial, led by Dr. Galsky, to integrate chemotherapy and immunotherapy to advance a
bold new personalized medicine approach to bladder-sparing. After four cycles of chemotherapy, participants underwent a thorough assessment, and if their biopsy showed the cancer had been eradicated, they were offered immunotherapy alone and spared bladder removal.
“The results were very encouraging for patients,” Dr. Galsky reports, noting that they showed a complete clinical response in 43 percent of patients, and that among patients who did not have surgery to remove their bladders, approximately two-thirds showed no signs of recurrence two or more years later. “We’re now analyzing blood and tumor samples to develop biomarkers that could be used to identify patients who could benefit most from this bladder-sparing approach, and have hopes it could eventually become part of our standard treatment.”
We could potentially treat patients curatively with chemotherapy plus immunotherapy and prevent them from losing their bladders
Matthew Galsky, MD
Overcoming Treatment Resistance
While immune checkpoint inhibitors have transformed the treatment landscape for bladder cancer, only a subset of patients respond well to this approach. Earlier research by Dr. Galsky and Nina Bhardwaj, MD, PhD, Ward-Coleman Chair in Cancer Research at Icahn Mount Sinai and a renowned immunology expert, revealed that macrophages play a pivotal role in the resistance of bladder cancer patients to immunotherapy, suppressing the body’s natural defenses. Moreover, they believed that a specific protein was the source of the problem and that blocking it
with an existing immunotherapeutic agent could potentially overcome resistance.
The two scientists are now testing that hypothesis through a unique clinical trial combining drugs to target these macrophages in combination with immunotherapy. “This project will reveal important information about how immunotherapy interfaces with bladder cancer, and why the disease in certain patients might resist treatment,” says Dr. Galsky. “This knowledge could then inform new treatment combinations that could render immune checkpoint inhibitors effective for greater numbers of patients.”
A New Biomarker for Personalized Cancer Treatment
Having already established through groundbreaking research the benefits of immunotherapy after bladder cancer surgery, Dr. Galsky is now investigating the use of a biomarker known as circulating tumor DNA (ctDNA) to determine which patients are likely to realize the greatest gains. ctDNA refers to small fragments of DNA that cancer cells release into the bloodstream, and can be detected through blood tests that are useful for diagnosis, monitoring, and treatment.
Dr. Galsky and his team are launching a phase 3 clinical trial, supported by the National Cancer Institute, that will enroll 1,200 patients nationally to undergo ctDNA testing after cystectomy. Those with detectable ctDNA will be randomized to receive a single immunotherapeutic drug or a combination of drugs.
“In the absence of any tests to detect micrometastatic cancer, we’ve treated all patients after surgery with systemic (also known as adjuvant) therapy despite the fact that only a subset harbor the disease,” Dr. Galsky explains. “Findings from our study have the potential to establish a ctDNA-based approach that could remove the guesswork from that process. And that would be a major step forward for patients with muscle-invasive bladder cancer.”
Featured Faculty
Matthew Galsky, MD
Professor of Medicine (Hematology and Medical Oncology), and Urology
Nina Bhardwaj, MD, PhD
Ward Coleman Chair in Cancer Research
About the Division of Hospital Medicine
The Division of Hospital Medicine at the Icahn School of Medicine at Mount Sinai is a dynamic, innovative, and patient-centered team dedicated to delivering exceptional care, advancing medical education, and driving groundbreaking research. Our hospitalists are at the forefront of transforming health care delivery and providing comprehensive inpatient care across a wide range of specialized services. As leaders in medical education, we are passionate about nurturing the next generation of health care professionals. Our faculty hold key leadership positions throughout the medical school and are actively involved in shaping the curriculum at every level. We offer unparalleled mentorship and career development opportunities, equipping our trainees and faculty with the skills and knowledge needed to become tomorrow's health care leaders.
Our commitment to continuous improvement is evident in our robust quality and patient safety initiatives, which have garnered national recognition and prestigious awards. Through our multidisciplinary approach and innovative programs, we are constantly pushing the
boundaries to enhance patient outcomes and experiences. The Division of Hospital Medicine is also at the forefront of research. Our research spans a wide range of areas, from clinical care and health care delivery models to high-value care; humanism; and medical education.
As we continue to expand our innovative care models, strengthen our educational programs, and deepen our research endeavors, we remain dedicated to advancing the field of hospital medicine.
System Chief
Andrew S. Dunn, MD Professor of Medicine (Hospital Medicine)
First-Year Med Students Are Championing Creative Ways to Improve Patient Care
The Department of Medicine’s Student High Value Care Initiative enables around 20 medical, master’s, and nursing students to team up each year with a junior faculty member to create, implement, and monitor projects designed to improve patient care. Students learn the fundamentals of high-value care and design an improvement project during a sixmonth curriculum.
As if the first year of medical school isn’t hectic enough, a small group of students is further enriching its learning experience through a unique program that’s improving the quality and cost of health care, at Mount Sinai and even beyond.
They are part of the Department of Medicine’s Student High Value Care Initiative, which enables around 20 trainees, including master’s and nursing students as well as those in the MD program, to team up each year with a junior faculty member to create, implement, and monitor projects designed to improve patient care. Some of these efforts gain national exposure through well-attended conferences and publication in academic journals.
“Educating trainees to practice high-value care is now recognized as critical to systemwide change,” says Anne Linker, MD, Assistant Professor of Medicine (Hospital Medicine) at the Icahn School of Medicine at Mount Sinai, and Co-Director of the Student High Value Care Initiative. “Our program gives students the chance to see the health system as something that is changeable and open to improvement, and our hope is they’ll carry that
valuable lesson to the remainder of their training and, eventually, into their clinical careers.”
As part of the eight-year-old program, students learn the fundamentals of high-value care (HVC) and design an improvement project during a sixmonth curriculum led by Dr. Linker and Co-Director Reem Aoun, MD, Assistant Professor of Medicine (Hospital Medicine) at Icahn Mount Sinai. This introduction is followed by six months of implementation in which students are divided into teams and collaborate with a faculty member, who may also serve as a mentor, as they jointly pursue an HVC project. Past and future initiatives have included interventions to reduce unnecessary diagnostic tests, mobilize patients in ways that reduce falls and injury, and decrease overuse of continuous intravenous fluids.
The success of these efforts is reflected in the steady growth of the Student High Value Care Initiative. “It’s an interesting program that has grown organically over time, driven in large part by the realization that we could be effective in areas outside just hospital medicine,” explains Dr. Linker, who has led a variety of projects to improve the value and quality of patient care at The Mount Sinai
Reem Aoun, MD, second from left, and Andrew Dunn, MD, second from right, debrief with new residents as part of the Student High Value Care Initiative.
Hospital. “That mindset has led us to create partnerships with other groups, including Emergency Medicine, Obstetrics and Gynecology, Infectious Disease, and Primary Care.”
One way the program gets a chance to truly shine is through its annual “Pitch Day.” This event, held in early December, allows each team to present its project in a “Shark Tank”-like setting to fellow medical students, residents, faculty, and hospital leaders. In the audience are four judges who provide valuable feedback on project planning and implementation strategy.
“It’s really exciting to see the enthusiasm and positivity this course generates,” notes Dr. Aoun, who was a project mentor before becoming Co-Director last year. She underscores how the initiative has grown in influence and visibility by citing Andrew Dunn, MD, Chief of the Division of Hospital Medicine, who has called it “one of the most important programs in our division.”
One example of the high-value care projects that have won critical praise is a sleep hygiene intervention to improve sleep quality for hospitalized patients. Aware of how poor sleep can contribute to adverse health outcomes, first-year medical students developed a nonpharmacologic hygiene protocol that included options such as turning lights off, eye masks, earplugs, lavenderscented pads, and relaxing music, all explained to the patient using a structured script. Front-line champions were also identified to aid with implementation. As described in The Joint Commission Journal on Quality and Patient Safety, the team’s study of 931 patients reported improved sleep depth, decreased awakenings after sleep onset, and enhanced quiet at night.
Another study in the same journal outlined a program initiated by first-year students to improve physician adherence to prescribing guidelines for patients discharged on opioids. During biweekly sessions held in resident lounges over donuts and coffee, the students opened a dialogue with physicians around best-practice recommendations
from the Society of Hospital Medicine and the Centers for Disease Control and Prevention. Favorable outcomes from the program included a reduction in opioid prescriptions longer than seven days, increases in post-discharge appointments, and documentation of opioid prescription histories.
“We’re proud of how students have repeatedly used their creativity and innovation to benefit the quality of care for our patients,” emphasizes Dr. Linker. “We typically launch three new projects a year, and the fact so many have achieved statistically significant results speaks volumes about the ongoing success of the Student High Value Care Initiative.”
Featured Faculty
Anne Linker, MD
Assistant Professor of Medicine (Hospital Medicine)
Reem Aoun, MD
Assistant Professor of Medicine (Hospital Medicine)
Andrew Dunn, MD
Professor of Medicine (Hospital Medicine); Chief, Division of Hospital Medicine
A Pioneering At-Home Care Model Continues
to Advance
Many hospital at home programs now sprouting across the country have drawn from the model Mount Sinai established in 2014. Mount Sinai, meanwhile, continues to differentiate itself through its high standard of care and the breadth and depth of its at-home services.
For a growing number of Mount Sinai patients, acute hospital care has taken on all the comforts of home. That’s because many of the staples of inpatient care from imaging and intravenous medications to regular bedside monitoring by nurses and daily management by physicians have been forwarded to their homes through the Mount Sinai Hospital at Home program.
While hospitalization at home has lately become a national movement, Mount Sinai can trace its roots to a Centers for Medicare and Medicaid Services (CMS) Innovation grant in 2014 to study the effectiveness of providing acute hospital care
Medicine (Hospital Medicine) at the Icahn School of Medicine at Mount Sinai. “At the same time, we’re creating a continuum of home care by recently launching Rehabilitation at Home, in addition to offering Palliative Care at Home. We’ve also built into that platform Community Paramedicine, Home Infusion, and Home Health to afford patients seamless transitions along their medical journey.”
Mount Sinai Hospital at Home, the largest of those complementary initiatives, plans to begin admitting between 50 and 60 new patients a month this year, roughly doubling its current monthly census
in the home. Based on that seminal work, Mount Sinai established itself as the pioneer in the field; many programs now sprouting across the country have drawn from the Mount Sinai model, which continues to differentiate itself through its high standard of care and the breadth and depth of its at-home services.
“We’re committed to delivering quality services where patients most want to receive them, and that often means right in their homes,” says Tuyet-Trinh Truong, MD, Chief Medical Officer of Mount Sinai at Home and Associate Professor of
of about 30 patients. Referrals from the case managers, social workers, physicians, nurses, and other providers in the hospital setting are helping to drive that growth, as well as the satisfaction of patients and families who have experienced its level of care first-hand.
To be eligible, participants must demonstrate an inpatient-level need, live in New York City (except for Staten Island), and have an insurance plan with Healthfirst, Aetna, Empire, or Fee-forService Medicare if they wish to be admitted to Hospital at Home directly from an emergency
Andrew Dunn, MD, and his team have built a robust Hospital at Home program that has kept patients out of the hospital while still achieving exceptional health outcomes.
room. If the patient has been in the hospital for more than 48 hours, all insurance plans are accepted by the program.
“We have a team of acute-care nurses who visit the patient in their home twice a day and, depending on the illness, are able to draw blood; give diuretics, antibiotics, or other IV medications; administer respiratory treatment, and much more,” explains Joanna Mecca, MD, Medical Director of Hospital at Home and Assistant Professor of Medicine (Hospital Medicine) at Icahn Mount Sinai. “Patients can also access our team of physicians and nurse practitioners around the clock through our virtual care command center.” One of the features of that telemedicine capability, she points out, is an audioenhanced stethoscope that allows clinicians to remotely hear heart and lung sounds as recorded by nurses at the patient’s bedside.
For one elderly patient who experienced a stroke and was doing poorly in the hospital, Mount Sinai’s home-based program translated into rapid results. Surrounded now by family, home-cooked meals, and 24/7 professional care, the patient’s appetite and alertness returned and previous discussions about the use of a feeding tube or even hospice care were no longer needed. Hospital at Home also proved a blessing to a 40-year-old woman who entered the emergency room with a severe kidney infection. Because she had a school-age son and no family or friends to care for him, she requested the intervention of Hospital at Home and was able to receive the intense care, including intravenous fluid and antibiotics, she required.
“There are many drivers of Hospital at Home, but the one we’re proudest of is keeping patients out of the hospital while achieving health outcomes that are as good if not better than those possible with an inpatient stay,” emphasizes Andrew Dunn, MD, System Chief of Hospital Medicine and Professor of Medicine at Icahn Mount Sinai. Indeed, a recent study in Journal of the American Geriatric Society showed that Medicaid patients enrolled in Hospital at Home experienced better outcomes than those
in the traditional hospital setting, with hospital readmissions down by half and return visits to the emergency room lower by two-thirds.
Satisfaction levels are as high among the program’s nurses and clinicians as they are for patients and their families.
“The pandemic forced a lot of people in our field to reassess their careers,” says Dr. Truong, “and they have since gravitated to home hospitalization because it allows them to deliver the highest level of one-on-one patient care without feeling rushed or burned out.”
Featured Faculty
Tuyet-Trinh Truong, MD
Associate Professor of Medicine (Hospital Medicine)
Joanna Mecca, MD
Assistant Professor of Medicine (Hospital Medicine)
Andrew Dunn, MD
Professor of Medicine (Hospital Medicine);
Chief, Division of Hospital Medicine
About the Division of Infectious Diseases
The Division of Infectious Diseases within the Department of Medicine at the Icahn School of Medicine at Mount Sinai is a hub of innovation and expertise in combating infectious threats. We blend research, education, and patient care to address the complex challenges posed by various pathogens. Our Division specializes in preventing and treating infections, with particular emphasis on healthcare-associated infections, antimicrobial stewardship, and care for immunocompromised patients. By integrating diverse disciplines, we've cultivated a unique environment that fosters pioneering research and comprehensive care, positioning us to tackle both current and emerging infectious disease challenges.
Our team leads the charge in implementing evidence-based interventions to prevent healthcare-associated infections across the Mount Sinai Health System. We conduct surveillance of infections and multidrug-resistant organisms, create policies to prevent healthcareassociated infections, investigate outbreaks, and spearhead interventions to reduce the use of invasive devices. We also maintain educational
programs for healthcare workers and advise on regulatory requirements, all while upholding health equity in our analyses and interventions.
Our strengths are further exemplified by our Antimicrobial Stewardship Program, established in 2004 and recognized as a Center of Excellence by the Infectious Diseases Society of America. This program co-led by the Division’s physicians and clinical pharmacists offers clinical consultations, leads research to advance the field, and provides specialized training opportunities for fellows interested in this subspecialty. Additionally, faculty in our Transplant Infectious Diseases Program provide specialized care for immunocompromised patients, including solid organ transplant recipients and patients with hematologic malignancies. Lastly, ID fellows interested in further training in the immunocompromised host can complete a transplant ID track in their second year of fellowship.
System Chief
Judith A. Aberg, MD
Dr. George Baehr Professor of Clinical Medicine
Transplant ID Expands Clinical Services and Revamps Fellowship
Liver, kidney, heart, lung, intestinal, pancreas, and bone marrow transplantation are all available at Mount Sinai, and the Transplant Infectious Diseases Program is an integral part of each. The program includes three inpatient consult services, an expanding ambulatory footprint, and a streamlined fellowship program.
The Mount Sinai Hospital’s Transplant Infectious Diseases (ID) Program, already one of the nation’s largest with eight clinical faculty members, is building on its success with a streamlined fellowship track as well as a significant expansion in transplant ID clinical teams and services.
“What we do is prevent, manage, and treat infections in the immunocompromised host we have special expertise in taking care of that particular patient population,” says Meenakshi M. Rana, MD, the Program’s Director and an Associate Professor of Medicine (Infectious Diseases) at the Icahn School of Medicine at Mount Sinai
awaiting abdominal organ transplants at the Recanati/Miller Transplantation Institute
The importance of transplant ID in the pre-evaluation and clearance of potential transplant patients is vital, as is the care they provide should infectious complications ensue following transplantation.
"Prevention of infection is a particular focus of ours,” Dr. Rana says. “We recommend vaccines, and any history of infections the patient may have had prior to transplant is reviewed. The most common viral infection we see after transplant is cytomegalovirus, so patients are on prophylaxis for several months after transplant to prevent this.”
Liver, kidney, heart, lung, intestinal, pancreas, and bone marrow transplantation are all available at Mount Sinai. Dr. Rana and colleagues work as an integral part of the multidisciplinary team involved with any such transplant, seeing patients awaiting lung transplantation at the Mount Sinai – National Jewish Health Respiratory Institute and those
The growing service now includes three inpatient consult services dedicated to transplant ID. The transplant ID team also has expanded its outpatient ambulatory care, Dr. Rana says: “We provide ambulatory care, co-located with their underlying condition, and we see patients in the general ID clinic.”
Top row, left to right: Dhruv Patel, MD; Dallas Dunn, MD; Meenakshi M. Rana, MD; Tim Sullivan, MD. Bottom row, left to right: Samantha Jacobs, MD; Risa Fuller, MD; Sarah Taimur, MD; Emily Baneman, MD
For HIV Transplant Patients, HOPE
Mount Sinai is one of a select group of transplant centers approved for HOPE Act participation. The HIV Organ Policy Equity Act, enacted in 2013, approved research on organ transplantation between donors and recipients with HIV. The HOPE Act answered a need within the transplant community.
“Patients with HIV are vulnerable to long-term complications of kidney disease and liver disease,” Dr. Rana explains. “For patients with HIV, who generally had longer wait times for transplant, they now had the opportunity to be on two lists: the one with everyone else waiting for a transplant, and a second list for those getting a transplant from a donor with HIV and that helps shorten their wait time for transplant.” For example, the wait time in New York City might be halved for a kidney from a donor with HIV.
“The HOPE Act allowed us to start doing HIV-toHIV transplantation in this country, and we have been doing that here as part of clinical research since 2016,” Dr. Rana says. “We have done 126 of these transplants at Mount Sinai, making us one of the largest HIV-to-HIV transplant centers in the country.”
Generally, the donor with HIV is deceased, though living donors with HIV are possible in HIV-to-HIV kidney transplantation. The research program at Mount Sinai also includes deceased-donor HIV-toHIV liver transplantation. All recipients are on retroviral therapy and have well-controlled HIV with a suppressed viral load. “We have had good outcomes in this patient population,” Dr. Rana says. “Even though these patients have received a kidney or liver from a donor with HIV, their HIV still stays under good control as long as they continue to take their antiretroviral therapy.”
Innovation in Fellowship Training
With the large and growing transplant ID program coupled with the research stemming from the HOPE Act, there is an outstanding opportunity to educate ID fellows at Mount Sinai. The transplant ID team has created an innovative program with a curriculum that folds transplant ID training into its second year, rather than requiring a third year, which is often the case elsewhere.
“Fellows who complete the first year of fellowship who have a special interest in pursuing additional training in care of the immunocompromised host can go on to do extra training during their second year of fellowship, and this involves a few components,” Dr. Rana says. “There’s about four months of extra clinical time on the inpatient side, and then there is also an ambulatory component where they take care of patients in the outpatient transplant ID setting.
“They conduct a research project on infectious disease under the mentorship of a transplant ID faculty member as part of the track,” she says, adding, “Many of our fellows who have completed the track have been able to go on and obtain transplant ID faculty positions at other institutions.”
The explicit purpose of the ID fellowship program is to “educate future academic leaders in our field,” and all evidence points to continued success with this goal.
Featured Faculty
Meenakshi
M. Rana, MD
Associate Professor of Medicine (Infectious Diseases)
HIV Cellular Research Uncovers Promising
Vaccine
Strategies
Mount Sinai scientists are pursuing two related lines of research into the fundamental physiology of HIV: trying to understand how the major protein on the surface of the virus enables it to spread from cell to cell, and whether the human immune system can be stimulated to create antibodies against it.
Approximately 40 million people in the world are HIV-positive, and though antiretroviral medications suppress viral replication and are clinically effective, not everyone can get or afford them. So long as the virus is out there unchecked, HIV remains a threat.
To address that threat, researchers at the Icahn School of Medicine at Mount Sinai are exploring everything from HIV cellular physiology to translational clinical strategies.
by engineering either fluorescent viruses or viruses that turn on genetic switches.”
Bioengineered viruses that carry fluorescent proteins can be used to visualize cell-cell interactions that support HIV infection. This live imaging technique has revealed that when HIVinfected cells are co-cultured with uninfected cells, durable cell-cell interactions form adhesive contacts, called virological synapses, which in turn promote immune evasion. Dr. Chen and
The laboratory of Benjamin K. Chen, MD, PhD, Irene and Dr. Arthur M. Fishberg Professor of Medicine and Vice Chair for Research in the Department of Medicine at Icahn Mount Sinai, has been focused on the pathogenesis of human immunodeficiency virus type 1 (HIV-1) infection, including a deep dive into cell-cell interactions.
“Cell-cell interactions are very important in how they allow HIV to spread efficiently,” explains Dr. Chen, who is also a Professor of Microbiology, and Pharmacological Sciences. “We have been developing models to observe and accurately measure different steps in the lifecycle of the virus
co-authors have explained how the dynamic movements of the HIV Env protein support virological synapse formation in a study published in Viruses, and an emerging view of how these cell-cell infections affect the Env on the surface of cells and allow the virus to evade immune responses, published in mBio
“This approach has helped us understand how the virus spreads and how it evades immune responses,” Dr. Chen notes. “We have been focused on trying to understand how the major protein on the surface of the virus, the envelope glycoprotein which is also the main target of vaccines enables it to spread from cell to cell,
Benjamin Chen, MD, PhD; Judith A. Aberg, MD and Francesca Cossarini, MD, are leading groundbreaking HIV cellular research at Icahn Mount Sinai.
and how it is different on the surface of cells than it is on the surface of viruses.”
An active area of HIV research has focused on stimulating a patient’s own immune system to recognize and eliminate cells that are infected with the virus. This line of inquiry was prompted by the identification of individual antibodies isolated from patients that can neutralize a variety of different HIV strains, so-called broadly neutralizing antibodies (bNAbs). These bNAbs are being tested clinically as a new immune-modulating therapeutic strategy. Thus far, however, this strategy by itself has not been shown to be capable of suppressing the virus in the long term. In addition, which patients with HIV should be given which bNAb or bNAb combinations has yet to be elucidated.
Dr. Chen and his lab have recently received a National Institutes of Health grant to develop assays to test the sensitivity of HIV to bNAbs. “We have found that bNAbs are really potent blockers of HIV infection,” Dr. Chen says. “These are much better at blocking cell-free virus infections than they are at blocking at the virological synapse. We are trying to better define this and use it as a clue to identify antigens or vaccines that would block cell-cell infections and cell-free virus infections.”
The Quest for a Therapeutic Vaccine
The work on virological synapses and bNAbs by Dr. Chen and his lab colleagues has informed the fight for new drugs and vaccines against HIV infection.
That fight has been taken up by, among others, Francesca Cossarini, MD, an Assistant Professor of Medicine (Infectious Diseases) at Icahn Mount Sinai and an Infectious Diseases attending physician at The Mount Sinai Hospital. As Dr. Chen explains, “Our research relates to Dr. Cossarini’s clinical trials, because these same bNAbs are being tested as drugs to help recruit
the immune system to clean up infected cells in ways that the normal immune response cannot.”
Dr. Cossarini notes that in the controlled phase of HIV infection, even as patients take antiretroviral therapy, the virus hides, persisting in long-lived immune cell subsets called the viral reservoir. “I have focused on the gastrointestinal (GI) tract, which is the major lymphoid tissue in the body,” Dr. Cossarini explains. “I started off by working on how to better define the responses to the interaction of the GI immune cells with HIV and some of the environmental factors in the intestinal mucosa, specifically the intestinal microbiome.”
Dr. Cossarini has begun a clinical trial that will focus on the effects of proposed treatments for HIV on the gastrointestinal immune system one of the sites of the lymphoid viral reservoir. The study will track a small group of patients as they are treated with experimental HIV treatments. Via colonoscopy, GI tissue will be collected and the effect of the treatments on the GI tract’s viral reservoir will be ascertained. The findings should help gauge the therapeutic efficacy of different approaches.
Both Drs. Chen and Cossarini note that the hunt for an HIV-preventive vaccine has failed after more than 40 years of effort. The problem, as Dr. Chen explains, is that “all the vaccines are targeting the glycoprotein, which is on the surface of virus particles. But glycoprotein is also on the surface of cells mediating spread, where we think it assumes very different conformational states.” The diversity of HIV, which mutates readily, is a challenge for creating a preventive vaccine.
More promising, in their view, is to use bNAbs or other molecules as HIV therapies to recruit the immune system to clear the latent viral reservoir. “I would venture to guess that we might obtain a therapeutic strategy that is able to eliminate most of the residual virus before we have an effective preventive vaccine,” Dr. Cossarini says.
Featured Faculty
Benjamin K. Chen, MD, PhD
Irene and Dr. Arthur M. Fishberg Professor of Medicine
Francesca Cossarini, MD
Assistant Professor of Medicine (Infectious Diseases)
Judith Aberg, MD
Dr. George Baehr Professor of Clinical Medicine; Chief, Division of Infectious Diseases
Institute for Advanced Medicine at the Forefront of Comprehensive HIV Care
Mount Sinai's Institute for Advanced Medicine is growing and moving. The Institute is a New York State Designated AIDS Center, whose core mission is to provide comprehensive care to people who have or are at risk for HIV.
Among several recent accomplishments of note for Mount Sinai’s Institute for Advanced Medicine is one in bricks and mortar: the opening of a new space on West 124th Street off Adam Clayton Powell Boulevard in central Harlem.
The Institute decided to merge its Morningside and Jack Martin clinics, which had been situated on Mount Sinai Health System hospital campuses in neighborhoods adjacent to Harlem and move them to this new address in order to bring its services directly to a population that needs them.
The Institute is a New York State Designated AIDS Center (DAC), whose core mission is to provide comprehensive care to people who have or are at risk for HIV. The Institute’s broader focus is on providing for the needs of the HIV/AIDS community, the LGBTQ+ community, those who were recently incarcerated and have been released, and people experiencing domestic violence, among others. The goal: “Quality care; every patient; every time.”
The location of the new clinic is recognition that Black and Latino populations constitute a considerable portion about two-thirds of the Institute’s patient demographics.
“Moving the whole operation to Harlem will really assist us in our efforts to help more people from those populations get primary care and testing, treatment, and prevention,” explains Michael Mullen, MD, Executive Director of the Institute and a Professor of Medicine (Infectious Diseases) at the Icahn School of Medicine at Mount Sinai.
“The two programs, Morningside and Jack Martin, were both based within the hospitals,” adds Matt Baney, the senior administrative director of the Institute. “By combining these two programs, we are taking co-located services and bringing them out to where the people live. It is about increasing access to care. It’s an important shift for us to bring services into people’s neighborhoods rather than have them come to us.”
We are taking co-located services and bringing them out to where the people live. It is about increasing access to care. It’s an important shift for us to bring services into people’s neighborhoods rather than have them come to us
Matt Baney
Grants Fuel Growth
Innovating how and to whom care is delivered is a hallmark of the Institute. Other major medical centers in the New York area have DACs, but the size of the Institute’s programs and number of services offered are extraordinary. For that, a lot of credit must go to the Institute’s program development and grant-writing capabilities.
“Mount Sinai’s DAC has become a very, very large program,” Dr. Mullen says. “We have been very successful in getting grants for special populations. When we see a need, we go and write a grant for it, and get it.”
“Some of our services have become more expansive than similar services elsewhere,” Mr. Baney says. “Part of the credit goes to the support from our institution, Mount Sinai, which has really made a commitment to this population.”
Unusually, nearly 70 percent of the Institute’s 350 employees are funded through grants. “We realize our services are expensive,” Mr. Baney adds. “So we go out and get other funding.”
The Institute has received many grants. Recent programs funded by grants include:
• The VIP (Voices in Partnership) program, which supports transgender, intersex, gendernon-conforming, and non-binary people with HIV/AIDS. The program works to identify these individuals and offers enhanced HIV and psychosocial case management.
• The Food and Nutrition program, which helps HIV-positive individuals with food insecurity and chronic health conditions. The program offers food vouchers and medical nutrition therapy.
• The Coming Home program, which provides services to those who have recently been released from prison or jail or who have a history of incarceration.
Another unique program is the result of a partnership between the Institute and Mount Sinai’s Brookdale Department of Geriatrics and Palliative Medicine, with support from the Keith Haring Foundation. “The majority of our patients are older than 50,” Dr. Mullen notes. “We know there are many needs in the HIV-positive geriatric population that should be addressed; for example, comorbidities associated with HIV. Some of these patients have been on medications for 40 years, and that takes a toll on the body.”
The program embraces a new care model that includes comprehensive assessment and treatment of both the physical and psychological challenges of older patients with HIV. The grant also has enabled the creation of a fellowship-like training program that will help replicate similar programs for the future.
The Institute’s programs also inform patients about additional help available in the community. “We know we can’t do everything, so to expand the continuum of care for our patients we have links to complementary services out in the community,” Mr. Baney says. “We have about 60 links with other groups within New York City, and others link with us. We are definitely a community-based program.”
As part of an academic medical center, the Institute is also involved in research and educating the next generation of caregivers. Whether involved in clinical care, research, or education, the Institute’s staff display exceptional dedication, which is highlighted by a remarkable film that focuses on the Peter Krueger Clinic (see related article).
As new challenges come their way, new innovations respond. An example is Tele-PrEP, an extension of the Institute’s Pre-Exposure Prophylaxis (PrEP) program that is delivered using telemedicine technology, which was first implemented in response to the COVID-19 pandemic. The program is web-based; patients interact with staff through video visits. With the exception of occasional lab tests, everything else is done on the internet. Recently introduced, the service like the Institute itself continues to grow.
From Darkness to Light: A Film About AIDS Care
The film From Darkness to Light captures the voices of patients and caregivers at the forefront of the HIV/AIDS crisis, highlighting the groundbreaking care provided by the Peter Krueger Clinic
The Clinic, one of the first HIV/AIDS clinics in the United States, was established at Beth Israel Medical Center, now Mount Sinai Beth Israel, in
1989. Started during the height of the epidemic in New York City, the Peter Krueger Clinic boldly stood against the stigma of the disease and served as a beacon of hope and a model of care for those New Yorkers diagnosed with HIV/AIDS. This film tracks the clinic’s origins and its impact over the last three decades, as told by the patients and staff that have called it home.
The work of the clinic continues today as a part of the Institute for Advanced Medicine at Mount Sinai
Featured Faculty
Michael Mullen, MD
Professor of Medicine (Infectious Diseases); Director, Institute for Advanced Medicine
About the Division of Liver Diseases
Originally led by Hans Popper, MD, “The Father of Modern Hepatology,” The Division of Liver Diseases has played a pivotal role in the advancement of hepatology both within and beyond the United States. Today we continue this legacy within the Department of Medicine at the Icahn School of Medicine at Mount Sinai, where we provide outstanding clinical care, breakthrough research, and comprehensive training programs for the future pioneers of our field.
The Division’s commitment to research has driven several key advances in hepatology. In partnership with the Recanati-Miller Transplantation Institute in 1988, we were the first to perform a liver transplantation in New York State. Additionally, we developed the first effective oral therapy for liver cancer. We continue to test new therapies every day, striving to rapidly
translate discoveries into more effective treatments for a diverse range of liver diseases. Our multidisciplinary approach to clinical care has made Icahn Mount Sinai a magnet for those seeking personalized treatment for Hepatitis B and C virus infections, autoimmune and druginduced liver disease, hepatic fibrosis, steatotic liver disease (previously known as fatty liver disease), cirrhosis, and liver cancer. By closely collaborating with specialists in transplantation, pathology, radiology, and oncology, we deliver integrative plans that are tailored to each patient's needs. Within the Mount Sinai Health System, we offer advanced treatment at three sites: The Mount Sinai Hospital, Mount Sinai West, and Mount Sinai Morningside. We remain equally dedicated to training the next generation of premier hepatologists. The
Division’s Transplant Hepatology Fellowship at The Mount Sinai Hospital offers advanced clinical training to applicants who have also completed a gastroenterology fellowship. This program was the first of its kind to be approved by the Accreditation Council for Graduate Medical Education (ACGME) in the Northeast and remains one of the largest such fellowships in the United States.
System Chief
Meena Bansal, MD Professor of Medicine (Liver Diseases); System Chief, Division of Liver Diseases
Obesity Drugs Among Those Being Examined for Efficacy Against MASH/NASH
Newly popular obesity drugs like Ozempic® and Wegovy® are among several undergoing clinical trials at Mount Sinai for metabolic dysfunctionassociated steatohepatitis (MASH), formerly known as nonalcoholic steatohepatitis (NASH). If the trials are successful, they would fill an important gap, as no medications are currently approved by the FDA for the growing population with this disease.
No drugs are currently approved by the Food and Drug Administration (FDA) for the treatment of metabolic dysfunction-associated steatohepatitis (MASH), formerly known as nonalcoholic steatohepatitis (NASH). But that may be about to change, thanks to work by Mount Sinai researchers who are conducting trials on a number of medications with different mechanisms of action against the growing threat.
Among the medications in trials for MASH are new drugs for treating diabetes and obesity that have been recently in the spotlight, says Meena Bansal, MD, Director of the MASLD/MASH Center of Excellence and Professor of Medicine (Liver Diseases) at the Icahn School of Medicine at Mount Sinai, and Chief of the Division of Liver Diseases for the Mount Sinai Health System.
“Both of those comorbidities are present in many people with MASH, and we know that if you lose 10 percent of your body weight, you can see improvement in MASH-related fibrosis,” Dr. Bansal says.
We know that if you lose 10 percent of your body weight, you can see improvement in MASHrelated fibrosis.
Meena Bansal, MD
Among the trials she and her team are running is a phase 3 trial involving semaglutide (sold under brand names that include Ozempic® and Wegovy®). A previous study published in 2021 in The New England Journal of Medicine found that patients treated with semaglutide experienced significantly more MASH resolution than those on placebo. But the secondary endpoint improvement in fibrosis stage with no worsening of MASH produced inconclusive results because of unusually high rates of response in the placebo group and overall small numbers.
Meena Bansal, MD, with Elizabeth Peck, Clinical Research Coordinator for the semaglutide trial
The Mount Sinai trial, begun in 2022 and sponsored by the drug’s maker, Novo Nordisk, seeks to examine whether a weekly subcutaneous dose of 2.4 mg of semaglutide the standard dose used for treating obesity can improve either MASH or the degree of fibrosis, versus placebo, in patients with MASH and fibrosis stages 2 and 3 (F2 and F3).
The trial’s primary endpoint will be either MASH resolution without worsening of fibrosis, or at least a one-stage regression of fibrosis without worsening MASH. Patients will be assessed via biopsy at 72 weeks and will continue to be followed for a total of 240 weeks and assessed for clinical outcomes ranging from esophageal bleeding to liver transplant.
1. Dr. Bansal and Greidy M. Diaz Almonte, Clinical Research Coordinator on the resmetirom
2 Resmetirom, unlike some other drugs under investigation for efficacy against MASH, is an oral medication.
The trial is one of eight at the MASH Center of Excellence that are currently seeking to enroll patients. Three of those trials involve resmetirom, a thyroid hormone receptor-²agonist; other drugs under investigation include lisinopril, an angiotensin-converting enzyme inhibitor, and lanifibranor, a pan-peroxisome proliferator–activated receptor agonist.
The resmetirom trials, for which Dr. Bansal is also the Principal Investigator, are exploring the hypothesis that metabolic dysfunctionassociated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD), is a result of relative intrahepatic hypothyroidism, and that increasing thyroid hormone signaling in the liver can lead to MASH resolution with no worsening of fibrosis, or at least a one-stage improvement in fibrosis with no worsening of MASH.
The initial phase 2 trial found that daily oral resmetirom resulted in a significant reduction in liver fat content at 12 and 36 weeks compared with placebo. Resmetirom responders with >30 percent magnetic resonance imaging proton density fat fraction (MRI-PDFF) reduction at week 12 had higher rates of MASH resolution (37 percent) on week 36 liver biopsy compared with nonresponders (4 percent), suggesting that early MRI-PDFF response could predict future histologic improvement. Resmetirom also positively affected patients’ lipid profiles by reducing blood levels of atherogenic lipids. Thus, it may reduce the incidence of cardiovascular disease, which is the leading cause of mortality in patients with MASH.
Recent topline data from the phase 3 trial looking at liver biopsies after 52 weeks of treatment suggests that resmetirom can cause both improvement of at least one stage in fibrosis and MASH resolution in a subset of patients. Based on these data, the sponsor, Madrigal Pharmaceuticals, received accelerated approval from the FDA for the drug in March 2024.
The ongoing studies at Mount Sinai are looking to see if continued therapy will ultimately improve liver-related outcomes.
A third drug, obeticholic acid (OCA), was furthest along in trials; however, an FDA advisory panel voted in May 2023 against accelerated approval of it to treat MASH and the FDA followed with a rejection of accelerated approval in June 2023, citing safety concerns. The decision came despite a trial, known as REGENERATE and led by Dr. Bansal as PI, that met its primary endpoint of an improvement in fibrosis by one stage without worsening of MASH. Based on this disappointing news, the drug's maker, Intercept Pharmaceuticals Inc., has decided to halt further development of this compound for MASH.
The wave of medications progressing through clinical trials marks a sea change for the treatment of MASH, Dr. Bansal says.
“It has been very challenging to get MASH therapeutics to market,” she says. “Early optimism was dashed by the failure of numerous trials. However, the promising data for these newer medications should make us optimistic that we will finally have effective treatments for this growing condition.”
Featured Faculty
Meena Bansal, MD
Professor of Medicine (Liver Diseases); System Chief, Division of Liver Diseases
Targeting New York’s Vast Hepatitis B Population With
Universal Testing and Vaccination
In the face of hepatitis B virus (HBV) levels in New York City significantly above the World Health Organization’s acceptable standard, Mount Sinai has launched a system of digital alerts that appear on the screens of primary care physicians when a patient in their offices is a candidate for testing, vaccination, or treatment for hepatitis B.
In the face of hepatitis B virus (HBV) levels in New York City significantly above the World Health Organization’s acceptable standard, Mount Sinai has responded with an initiative aimed at universal surveillance and vaccination of adults. As part of that effort, in August 2022 it launched a system of digital alerts that appear on the screens of primary care physicians when a patient in their offices is a candidate for testing, vaccination, or treatment for hepatitis B.
“If our laboratory records show no hep B or C serology results for a patient, then the primary care providers can simply click on their screens to order the right tests and learn how to interpret them,” says Douglas Dieterich, MD, Director of the Institute for Liver Medicine, which has responsibility for liver care across the Mount Sinai Health System
“If the results are negative, vaccination would be the appropriate next step to help the patient acquire lifelong immunity,” Dr. Dieterich, Professor of Medicine (Liver Diseases) at the Icahn School of
Medicine at Mount Sinai, adds. “If the surface antigen is positive, however, we want to encourage the patient to seek treatment through our Institute for Liver Medicine and, if appropriate, offer them a clinical trial that’s focused on a cure.” A team of navigators is available to help patients with care coordination, Dr. Dieterich adds.
In New York City, public health authorities have estimated there are 241,000 individuals with chronic hepatitis B, of whom 46 percent are undiagnosed. Many children were vaccinated by pediatricians starting in 1991 as part of a nationwide effort, but because older teenagers were often missed, a sizable number of adults today never received protection.
Adding urgency to the vaccination and surveillance movement is the upsurge in New York City and the country of the highly contagious hepatitis Delta virus (HDV), a small RNA virus that uses the same receptor as hepatitis B to enter the liver cell and requires infection with hepatitis B to replicate.
Douglas Dieterich, MD, is leading an effort to test all Mount Sinai primary care patients for hepatitis B and the related hepatitis Delta virus.
“We want to test for Delta in everyone who tests positive for hepatitis B,” notes Dr. Dieterich. “Delta is the most severe form of viral hepatitis, and we know there are many people in New York who are carrying the virus. It can progress to cirrhosis within five years and to hepatocellular carcinoma within 10 years and has an extraordinarily high mortality rate.” The good news, he adds, is that several drugs could soon be approved for treating the Delta virus, including one that has worked very well in Europe for the past three years.
Against that backdrop, Mount Sinai is doubling down on its goal of eliminating both hepatitis B and hepatitis C. A program of universal screening and treatment for hepatitis C, rolled out by Mount Sinai in 2015, is now returning to its prepandemic volumes. Moreover, it has been broadened to include hepatitis B and Delta. Also returning to full strength is Mount Sinai’s Hepatitis Outreach Network (HONE), which goes into the community to conduct hepatitis B and C screening events, then link individuals who test positive to specialized care. According to Dr. Dieterich, HONE is being expanded beyond the African immigrant community to include Chinese, Russian, and Latinx populations in New York City.
Significantly, a cure already exists for hepatitis C infection thanks to several U.S. Food and Drug Administration (FDA)-approved direct-acting antivirals that work in different ways to prevent the virus from making copies of itself. For hepatitis B, Mount Sinai is part of several clinical trials that are making progress toward finding a “functional cure,” defined by the FDA as undetectable
hepatitis B virus surface antigens (HBsAg) of less than 0.05 international units per milliliter.
Among those studies is a phase 1b trial of a core inhibitor of hepatitis B (from Assembly Biosciences) that has shown increased potency against covalently closed circular DNA (cccDNA) formation, thus blocking delivery of the genetic code needed to build new viruses. Another clinical study involves a monoclonal antibody (from Vir Biotechnology) that neutralizes hepatitis B virus and has been engineered to also potentially act as a therapeutic vaccine. This investigational drug is designed to block entry of all 10 genotypes of HBV into hepatocytes, while reducing the levels of virions and subviral particles in the blood.
“We’re certainly encouraged by the many new drug candidates on the horizon,” emphasizes Dr. Dieterich, “and the role they could potentially play along with aggressive surveillance and treatment of hepatitis B and C to bring these viruses under control, if not prevent them from ever occurring.”
Featured Faculty
Douglas Dieterich, MD
Professor of Medicine (Liver Diseases); Director, Institute for Liver Medicine
NASH Center of Excellence Wins Grants for Two Initiatives
Two new grants from Pfizer will help Mount Sinai educate primary care providers on how to identify at-risk patients and address inequities in diagnosis and care of nonalcoholic steatohepatitis.
Two new grants from Pfizer will help the Mount Sinai NASH Center of Excellence deliver on its dual mission: to provide exemplary care to all patients with metabolic dysfunction-associated steatotic liver disease (MASLD) and metabolic dysfunction-associated steatohepatitis (MASH), and to increase scientific knowledge about the causes of these conditions. The grants will enable the Center to educate primary care providers on how to identify at-risk patients and address inequities in diagnosis and care.
A $250,000 educational grant awarded to the Center’s Director, Meena Bansal, MD, will support efforts to raise awareness about electronic health record system tools such as FIB-4, a noninvasive test that estimates a patient's degree of liver
fibrosis and is integrated into Mount Sinai’s Epic system. These tools can assist primary care and other front-line providers in screening patients who are at risk of developing MASH with significant fibrosis and in making appropriate referrals for evaluation and treatment based on the American Gastroenterological Association’s Clinical Care Pathway.
Dr. Bansal says providers will receive customized reports that demonstrate both the value of screening patients for advanced fibrosis and the impact of adhering to the established care pathway, such as referring patients with intermediate MASLD fibrosis scores for a FibroScan®
Meena Bansal, MD, is working to encourage primary care providers to screen their patients for liver diseases like MASLD and MASH.
“Primary care providers are the first line of defense, and they need to have appropriate tools to identify patients who should undergo further evaluation,” says Dr. Bansal, Professor of Medicine (Liver Diseases) at the Icahn School of Medicine at Mount Sinai. “By introducing them to these tools, showing them how they work, and then providing feedback on the impact of using the care pathway, we believe we can promote continuous learning and quality development among primary care providers. Equally important, we believe our efforts will lead to increased screening and identification of at-risk patients.”
A second Pfizer grant, valued at $140,000, is enabling Andrea D. Branch, PhD, and her colleagues to use the National Health and Nutrition Examination Survey datasets to identify MASLD and fibrosis risk factors that differ among non-Hispanic Black, Mexican American, and nonHispanic white populations. The goal is to build a more comprehensive understanding of the unique risk factors among these populations.
For example, in previous studies supported by the Centers for Disease Control and Prevention and the National Institute for Occupational Safety and Health, Dr. Branch found that advanced liver scarring among non-Hispanic Black populations is not only associated with cadmium exposure which is associated with scarring in all populations but also with lead exposure and poverty. These findings suggest that toxic and environmental exposures play a larger role in liver scarring among non-Hispanic Black than among non-Hispanic white populations.
“We have assumptions about disease presentation and risk factors that are not appropriate for all demographic groups and that
can result in care policies that are not equitable,” says Dr. Branch, Professor of Medicine (Liver Diseases) at Icahn Mount Sinai. “I want to ensure that policies are equitable. My hope is that, through this grant, we will identify distinct factors that enable us to catch disease at an earlier stage among these populations. We plan to use these findings to develop an algorithm that will flag people at risk in our electronic health record system, enabling their early diagnosis and linkage to care.”
These grants complement several undertakings launched by the Center since its formation in January 2022 that seek to better understand disease drivers and thus achieve improved patient prognosis and treatment. Among the most notable is a longitudinal registry that will enroll 5,000 Mount Sinai patients across the whole spectrum of the disease and Mount Sinai’s diverse patient population to explore why inflammation and fibrosis are stimulated in some individuals but not others. The goal, given the heterogeneity of MASH, Dr. Bansal says, is to develop a rigorous algorithm that enables phenotyping and risk stratification of patients for likelihood of rapid fibrosis progression based on biological and social factors. This will facilitate earlier interventions that can be tailored to the drivers of disease in individual patients.
“We want to be the leader in MASH in all aspects from basic science to clinical,” Dr. Bansal says. “Through our combined expertise, work, and our diverse patient population, I think we are uniquely positioned to make valuable contributions to understanding and treating this disease.”
Featured Faculty
Meena Bansal, MD
Professor of Medicine (Liver Diseases); System Chief, Division of Liver Diseases
Andrea D. Branch, PhD
Professor of Medicine (Liver Diseases)
About the Division of Nephrology
The Dr. Barbara T. Murphy Division of Nephrology at Mount Sinai is dedicated to advancing the knowledge and understanding of renal disease and its development, progression, treatment, and prevention. The Division offers a broad array of opportunities for training in clinical nephrology and research. The faculty is nationally and internationally renowned for their research and clinical expertise; many are leading experts in renal development, polycystic kidney disease, HIV- associated nephropathy, diabetic renal disease, hypertensive renal disease, gene therapy, transplantation, peritoneal dialysis, and hemodialysis.
With more than 21 National Institutes of Health (NIH)-funded Principal Investigators, the Division is among the best NIH-funded divisions of its kind in the United States. Additionally, the Division has one of the largest and most well-recognized nephrology fellowship programs in the country and has developed several innovative subspecialty tracks, including general nephrology, critical care nephrology, transplant nephrology, palliative care
nephrology, and home dialysis. Regardless of the national challenges in nephrology fellowship recruitment, Mount Sinai has been able to successfully match top candidates each year.
Within the Mount Sinai Health System, there are now more than 20 outpatient dialysis centers, covering more territory and expanding into many parts of Manhattan, Brooklyn, and the Bronx, making dialysis more accessible to patients.
System Chief
John Cijiang He, MD, PhD
Irene and Dr. Arthur M. Fishberg
Professor of Medicine
A Persistent Researcher Develops a Potential New Anti-Fibrosis Agent
More than a decade of work on kidney fibrosis has yielded a promising new anti-fibrosis agent that can target fibrotic pathways without risking the development of cancer. Clinical trials are expected later in 2023.
Clinical trials are beginning on a new drug to treat kidney fibrosis the culmination of more than a decade of work by John Cijiang He, MD, PhD, Chief of Nephrology at Mount Sinai Health System, and his team.
The journey began with the discovery by Dr. He’s laboratory of a specific regulator of kidney fibrosis called homeodomain interacting protein kinase 2 (HIPK2). Researching further, they recently identified an allosteric small molecule of HIPK2 which several animal models of kidney disease have shown is an effective anti-fibrosis drug. Preclinical testing has yielded encouraging results.
It is a classic example of dogged scientific determination, in which an interesting finding leads eventually to a significant advance, but not without a side trip or two along the way.
Dr. He, Irene and Dr. Arthur M. Fishberg Professor of Medicine at the Icahn School of Medicine at Mount Sinai, is an advocate of a systems biology
approach to research, focusing on computational biology and bioinformatics to elucidate a fuller picture of interactions within an organism. By doing this, he strives to identify key drivers of disease processes, which could be potential drug targets for kidney disease therapy.
One focus of his research has been kidney fibrosis, a key element of the progression of chronic kidney disease. In a paper published in 2012 in Nature Medicine, Dr. He and colleagues, performing transcriptomic and proteomic studies of glomerular cells, found protein kinases that regulate gene expression in the kidneys of animal models with kidney fibrosis. The research team was able to identify HIPK2, the regulator of kidney fibrosis, and found that HIPK2 was upregulated in human kidneys with various types of kidney disease.
These findings were promising, since HIPK2 had never been identified as being important in the pathogenesis of kidney fibrosis. Clearly, this
Cijiang He, MD, PhD, and Kyung Lee, PhD, are among the researchers working to develop and bring to market anti-fibrotic therapies.
protein kinase had become a possible target for therapeutic intervention in kidney disease.
But there was a problem. Inhibiting all HIPK2regulated pathways posed unwanted side effects. One downstream molecule, known as p53, could incite tumor growth if dysregulated by HIPK2. “If you inhibit HIPK2 you also inhibit p53,” Dr. He explains. “And because of that, there is a chance of developing cancer. That fact explains why several companies that were very interested in an anti-fibrosis drug walked away, their enthusiasm greatly reduced.”
An Important New Compound
Five years after their original study was published, Dr. He and his research team announced in the Journal of the American Society of Nephrology that they had identified BT173, which can specifically inhibit the TGF-²1S/ mad3 pathway an important pro-fibrotic channel without also significantly inhibiting HIPK2 kinase activity or p53 activation. That finding made it possible to attenuate the renal fibrosis of chronic kidney disease (CKD) without employing the broad approach of inhibiting all HIPK2 pathways.
“This is a new compound,” Dr. He says. “It has a high potency and can be given as a PO dose daily instead of by IV injection.” TGF-²1is thought to be the most important profibrotic element in kidney disease, and knockout of Smad3, a downstream target of HIPK2, has been found to reduce kidney fibrosis in animal models. Thus, blocking this pathway should be an effective approach to treating kidney fibrosis. “Our inhibitor blocks specifically the Smad3 activation,” Dr. He says.
A 2020 study in JCI Insight continued this work, further elucidating the novel mechanisms behind the anti-fibrosis role of HIPK2 in kidney disease. “This study will help develop better HIPK2 inhibitors for kidney disease,” Dr. He says.
Now, Dr. He and others, including Kyung Lee, PhD, Associate Professor of Medicine (Nephrology) at Icahn Mount Sinai, in collaboration with ShangPharma Innovation, Inc., have founded Rila Therapeutics, whose goal is to develop and bring to market antifibrotic therapies. Their focus will be on a small molecule developed from BT173. “Preclinical data have been very positive,” Dr. He says, adding they have so far seen no toxicity.
Clinical trials are expected to start in the spring of 2024. “This has been a really big journey, a 10year story, but I think in the end a successful one,” says Dr. He.
The Division Is a Center for Research
Although Dr. He’s research is exciting, he is also quick to point out the impressive research being undertaken by his colleagues in the Division of Nephrology. The division has 20 National Institutes of Health (NIH)-funded Principal Investigators and receives about $15 million in NIH funding yearly “one of the best-funded nephrology divisions in the country,” Dr. He notes.
The Mount Sinai division maintains both a registry of patients with CKD that numbers more than 150,000 and the BioMe Biobank with more than 10,000 specimens from patients with CKD all vital elements of nephrology research. There is also a kidney tissue biobank that adds another 100 samples annually.
Mount Sinai’s nephrology research generates more than 100 high-impact papers in any given year, and investigators regularly engage in pharmaceutical company-sponsored randomized controlled trials. Licensing agreements with pharma companies and the generation of patents are ongoing.
Mount Sinai and Mount Sinai faculty members (Dr. He and Dr. Lee) have equity in Rila Therapeutics.
Featured Faculty
Kyung Lee, PhD
Associate Professor of Medicine (Nephrology)
John Cijiang He, MD, PhD
Irene and Dr. Arthur M. Fishberg Professor of Medicine; Chief, Division of Nephrology
Research Initiatives in the Division of Nephrology
Division of Nephrology Turns Pandemic Challenge Into a Success
The COVID-19 pandemic presented special challenges for dialysis patients and the providers serving them, but Mount Sinai Health System's Division of Nephrology rose to the test.
The response to the COVID-19 pandemic by the Department of Medicine’s large Division of Nephrology was multifactorial, as Joji Tokita, MD, Associate Professor of Medicine (Nephrology) at the Icahn School of Medicine at Mount Sinai, explains.
“It was a multifaceted task that was extraordinarily complex,” he says. “But as far as our work during the pandemic is concerned, I think it was a great success.”
Part of the response to the challenge of the pandemic included regular consultations with other local academic health systems, major national dialysis providers, supply chain management, the New York ESRD [end-stage renal disease] network, and the New York State Department of Health. Home dialysis programs ramped up, and novel solutions were developed to allow patients to continue home therapy while still receiving all necessary monitoring and care. At the height of the pandemic, urgent-start peritoneal dialysis was extended to support inpatients with acute kidney injury requiring dialysis. Telemedicine played a key role in allowing nephrologists to keep track of their patients’ health remotely.
A Challenge and an Opportunity
The Division of Nephrology of the Mount Sinai Health System has nearly 100 nephrologists on staff and more than 25 clinical fellows. Central to the Division’s mission is its belief in health equity and access to care. As such, the Division has developed clinics in outer New York City boroughs and staffed nephrologists at more than 10 dialysis facilities across the city. Faculty members see patients in diverse locations throughout Manhattan and in Queens; Brooklyn; and Oceanside, Long Island.
During the pandemic, the size of the Health System was both a challenge and an opportunity, Dr. Tokita explains. “Large programs can generate a nexus of opportunity for thought and innovation.
However, they can be complex to manage, and integration and standardization across geographies often takes time.”
Ensuring continuation of clinical operations throughout the Health System was indeed challenging. “For example, most dialysis patients receive treatment at a nearby center three times per week and many have complex medical conditions,” Dr. Tokita says. “The need to travel to and from the center as well as share close quarters during several hours of treatment required us to think about how best to mitigate these increased risks.” Health care workers were also affected by the pandemic, presenting additional challenges in ensuring centers remained open.
“A major concern was that if those patients were unable to receive maintenance hemodialysis in their home facility, they would potentially flood hospital emergency rooms, which would threaten to collapse the health care system,” Dr. Tokita says. The Division needed to develop very clear plans right from the start to ensure that would not happen.
“Throughout the pandemic it was imperative that we ensure continuity of operations across all of our dialysis facilities,” Dr. Tokita says. That the Division was able to do just that proved to be a notable success of Mount Sinai’s pandemic health care.
Stratifying Risk for Chronic Kidney Disease
Chronic kidney disease (CKD) is a significant and growing public health problem. The Centers for Disease Control and Prevention notes that approximately 15 percent of U.S. adults, or 37 million people, are thought to have CKD. Diabetes and high blood pressure are leading causes of CKD, as are heart disease, obesity, and genetic predisposition. Significantly, of the patients with CKD, as many as 90 percent do not know they have it, and of those with severe CKD, almost 40
percent are unaware of the condition. About a quarter of adults with type 2 diabetes develop diabetic kidney disease, and every year about 50,000 patients progress to kidney failure, requiring dialysis or a kidney transplant.
addresses issues including intra-individual variability of eGFR, uACR, and hyper-filtration that masks early diabetic kidney disease. It provides risk stratification, to appropriately triage care and minimize patient burden and resource use.
For these reasons, accurate risk stratification of susceptibility to progressive kidney disease is a key clinical objective. Risk stratification historically has used the Kidney Disease Improving Global Options (KDIGO) approach, in which progression is defined as a sustained drop in glomerular filtration rate (GFR) category and/or a 25 percent decrease from GFR baseline, while rapid progression is a decline in GFR of >5 ml/min/1.73m2 per year.
A novel bioprognostic test, KidneyIntelX, developed by Mount Sinai faculty and licensed to Renalytix AI, is a lab test that defines the risk of CKD progression in patients with type 2 diabetes and CKD stages 1-3. The test combines estimated GFR (eGFR), novel serum biomarkers (sTNFR1, sTNFR2, KIM-1), urine albumin-creatinine ratio (uACR), and electronic health record data to provide a low, intermediate, or high-risk score of kidney function decline in the next five years. It
Mount Sinai is studying the impact of KidneyIntelX testing on clinical decision-making at its ambulatory practices in an IRB-approved Real World Evidence study. Interim results were published in 2022 in Journal of Primary Care & Community Health. These interim results from 1,686 patients with six months of data found:
• Type 2 diabetes care: a 10 percent improvement in hemoglobin A1c
• CKD care: a 15 percent improvement in albuminuria in low-intermediate risk groups
• Early-stage diabetic kidney disease: Patients with high-risk scores received more frequent clinical visits, guide-recommended care, and specialist referrals
• Fifty-three percent of high-risk patients followed up within one month of their test and 57 percent had some action taken (medication change or referral) within three months,
From left: Marsha Griffiths, RN, Shuchita Sharma, MD, Joji Tokita, MD, Jaime Uribarri, MD, and fellow Gilana Gomberg, MD, on the dialysis floor at The Mount Sinai Hospital
compared with 13 percent and 35 percent, respectively, in low-risk individuals
• Twenty-five percent of high-risk patients started SGLT2 inhibitors, medications that reduce progression of CKD, compared with 7 percent in the low-risk group.
Gaps remain in the continuum of care for patients with diabetic CKD. Based on these findings, KidneyIntelX testing should help. Dr. Tokita, the first author of the study, notes, “A key aspect of this work is improving patient and provider awareness of the condition and early use of evidence-based therapies currently available to treat it and reduce progression.”
KidneyIntelX is a commercially available, CLIAapproved predictive test that combines patient information and biomarker results. KidneyIntelX is based on innovative technology developed by Mount Sinai faculty and licensed to Renalytix AI. Mount Sinai faculty and Mount Sinai have equity ownership in Renalytix AI.
Featured Faculty
Joji Tokita, MD
Associate Professor of Medicine (Nephrology)
John Cijiang He, MD, PhD
Irene and Dr. Arthur M. Fishberg Professor of Medicine; Chief, Division of Nephrology
About the Division of Pulmonary, Critical Care and Sleep Medicine
The Catherine and Henry J. Gaisman Division of Pulmonary, Critical Care and Sleep Medicine provides state-of-the-art consultation, diagnostic testing, and clinical and multidisciplinary care to patients with simple and complex respiratory and respiratory-related diseases. The combined strengths of the site divisions at all hospitals within the Mount Sinai Health System have created a unique opportunity to significantly impact training and translational research.
Home of the Mount Sinai – National Jewish Health Respiratory Institute, the Division conducts research, offers educational opportunities, and provides multidisciplinary care to patients with all forms of lung diseases, including asthma, cystic fibrosis, pneumonia, emphysema, and chronic
obstructive pulmonary disease. Its comprehensive Asthma Program offers personalized treatment for adults, incorporating the latest research into the effective management of the condition. The Center for Sleep Medicine provides advanced diagnostic and treatment plans for patients with sleep-related disorders, and the Critical Care program uses sophisticated technology to provide specialized care for patients with various forms of lung disease. In addition, Mount Sinai houses one of 10 Centers of Excellence for sarcoidosis research in the nation and has one of the largest programs of its kind in the world.
The Division of Pulmonary, Critical Care and Sleep Medicine at The Mount Sinai Hospital was recently ranked No. 8 in the world, No. 7
in the United States, and No. 1 in New York by Newsweek for 2024 and No. 12 in the United States by U.S. News & World Report® for 2023-24.
System Chief
Charles A. Powell, MD, MBA
Florette and Ernst Rosenfeld and Joseph Solomon Professor of Medicine
Chief Executive Officer, Mount Sinai –National Jewish Health Respiratory Institute
New Understanding of Asthma Could Yield
More Precise Treatments
Mount Sinai is undertaking several initiatives to better understand the factors that contribute to severe asthma and identify different subtypes of the disease. The work is intended to bring a precision medicine approach to asthma.
Despite significant progress in therapeutic approaches over the past decade, an estimated 5 percent to 10 percent of patients with severe asthma are not well served by current therapies. Part of the problem, according to Linda Rogers, MD, is that researchers have traditionally approached asthma as a single disease.
Dr. Rogers is playing a key role in one of several initiatives at Mount Sinai to better understand the factors that contribute to severe asthma and identify new treatments. She is the site Principal Investigator for the Precision Interventions for Severe and/or Exacerbation-Prone Asthma (PrecISE) Network Study, funded by the National
“When we look at patients whose asthma is not controlled by existing therapies, we find that they are very heterogenous in terms of disease drivers,” says Dr. Rogers, Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine), Icahn School of Medicine at Mount Sinai; Clinical Director, Adult Asthma Program, Mount Sinai – National Jewish Health Respiratory Institute; and Clinical Director, Medicine Clinical Trials Office.
“Some of the therapies we administer do not necessarily treat the type of inflammation they have, or their inflammation might be better controlled by other treatments such as ones used to treat other diseases based on disease mechanisms research we have done. Thus, we are interested in the potential of a precision medicine approach to treating these patients.”
Heart, Lung, and Blood Institute. This study was designed with input from Monica Kraft, MD, while she was at the University of Arizona; Dr. Kraft is now the Murray M. Rosenberg Professor of Medicine, and Chair of the Department of Medicine, at Mount Sinai Health System and Icahn Mount Sinai.
Through this study, more than 30 centers nationwide are working on developing precision medicine approaches to the treatment of severe asthma. That includes investigating the possibility of using biomarkers and other patient factors to inform patient treatment.
“Although biomarkers such as blood eosinophil counts and exhaled nitric oxide levels have been used in the clinical setting to assess patient eligibility for certain advanced therapeutics, this
study is collecting samples such as sputum, nasal brushings, and exhaled breath condensate to better understand the disease and identify more biomarkers and targets for therapy,” Dr. Rogers says. “We are also collecting genetic data and using that to select novel targeted therapies that are not currently used in clinical practices.”
The study is unique in that it is using an adaptive protocol to assess the efficacy of five therapeutic agents imatinib mesylate, Broncho-Vaxom® , clazakizumab, medium chain triglycerides, and cavosonstat among 600 participants who have severe asthma with symptoms that are not well
“Adaptive platform studies have been used in both COVID-19 and cancer clinical trials but to our knowledge this is one of the first times this protocol has been used to develop precision medicine therapeutics for asthma,” Dr. Rogers says. “It will enable us to conduct a series of five parallel phase 2 studies to assess asthma treatments that are promising but that are not under commercial development for an asthma indication. If we determine one agent is unsuccessful based on statistical analysis, we can abandon it to explore the efficacy of another agent, which accelerates the drug development process.”
controlled through high-dose inhaled corticosteroids and other therapies. These therapeutic agents were proposed by participating centers based on preliminary data from mechanistic, animal, and other studies suggesting efficacy. Each participant will be administered one of these agents, or a placebo, for a period and, following a washout, will be eligible to receive up to four additional therapies over the course of the study.
As Dr. Rogers evaluates a precision medicine approach to treat severe asthma, Sonali Bose, MD, MPH, is investigating the impact of environmental and nutritional factors on asthma control among a cohort of 30 pregnant individuals. Her goal is to identify opportunities to improve health outcomes among pregnant patients and potentially reduce the intergenerational risk of respiratory disease in their children.
From left: Nicholas Brereton, Clinical Research Coordinator; Sonali Bose, MD, MPH; Rachel Meislin, MD, fellow; Zhi-Yuan Wang, MD, Clinical Research Coordinator
“Asthma is the most common respiratory disease in pregnancy and can have a significant impact on both the health of mom and baby. Poor asthma control during pregnancy has been associated with many complications of pregnancy and a higher risk of respiratory disease in the offspring. Since asthma control can be dynamic during pregnancy, it is important to capture asthma health throughout gestation in a way that will allow us to intervene in a timely manner,” says Dr. Bose, Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine), and Pediatrics, at Icahn Mount Sinai.
“We want to gain a better understanding of the determinants of asthma control during pregnancy, particularly among urban Black and Hispanic populations, who have a disproportionate risk for asthma morbidity and traditionally have the highest rates of pregnancy complications as well.”
Dr. Bose is conducting two pilot studies among this cohort. One, building on her prior work on the influence of indoor exposures on asthma in other populations, focuses on the impact of indoor air pollution, specifically indoor fine particulate matter exposure, on asthma during pregnancy among 20 participants. Each trimester, Dr. Bose and her research team are collecting one week of data from two air monitors a traditional model that captures particulate matter in real time and a PurpleAir sensor, a low-touch commercially available monitor. Simultaneously, her team is performing daily home spirometry tests and capturing home activities, asthma symptoms, and medication use. The one-week data collection duration was chosen to maximize resources for the study.
The second study assesses whether a higher omega-3 status is associated with improved asthma control during pregnancy among 30 participants 15 recruited from her cohort and 15 from Duke University. The team is rigorously collecting nutritional intake data as well as measuring blood omega levels repeatedly during
each trimester of pregnancy. Previous studies have demonstrated that omega-3 polyunsaturated fatty acids (PUFAs) have an anti-inflammatory influence, which could have therapeutic value among patients with asthma. The team is specifically interested in whether downstream metabolites of PUFAs called specialized proresolving mediators help combat the inflammation associated with asthma.
Dr. Bose is particularly interested in exploring that protective aspect at an individual level among pregnant people and is collaborating with the Mount Sinai Maternal Fetal Medicine division, as well as researchers at the University of Nebraska, University of Colorado, and Duke University, to complete this work.
In addition to a better understanding of risk factors that influence the asthma health of the mother and its likely implications for the fetus, data gleaned from these studies will enable Dr. Bose to design larger follow-up studies that assess the efficacy of interventions such as reduction of indoor air pollution or increased omega-3 intake.
“Poor asthma control during pregnancy has been linked to consequences such as spontaneous premature birth, gestational hypertension, and gestational diabetes,” Dr. Bose says. “Through our work, we can gain more knowledge about upstream factors that impact asthma control and thus help improve maternal and fetal health.”
Dr. Bose's research is supported by a Mount Sinai Transdisciplinary Center on Early Environmental Exposures Pilot Research (P30) grant (grant number P30ES023515) and the American Lung Association Airways Clinical Research Center (ALA-ACRC) pilot award.
Video resource visible at https://youtu.be/ZfSbpEb oaSA
Featured Faculty
Linda Rogers, MD
Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine)
Monica Kraft, MD
Murray M. Rosenberg Professor of Medicine; System Chair of the Department of Medicine
Sonali Bose, MD, MPH
Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine), and Pediatrics)
Charles A. Powell, MD, MBA
System Chief of Pulmonary, Critical Care and Sleep Medicine; Chief Executive Officer, Mount Sinai – National Jewish Health Respiratory Institute
Brief Withdrawal of Apnea Therapy Could Increase Alzheimer's Risk
A first-of-its-kind study led by a Mount Sinai researcher suggests that even a brief withdrawal of continuous positive airway pressure therapy for sleep apnea might increase one’s risk of developing Alzheimer’s disease.
Skipping a few nights of continuous positive airway pressure (PAP) therapy for sleep apnea might not seem like a big deal. But a first-of-itskind study led by Mount Sinai neuroscientist Andrew W. Varga, MD, PhD, suggests that even a brief withdrawal might increase one’s risk of developing Alzheimer’s disease (AD).
Dr. Varga found that withdrawal from PAP therapy among subjects with severe sleep apnea resulted in significant overnight changes in AD biomarkers and markers of neural injury measured in blood,
“For the first time we are showing that sleep apnea significantly induces some measure of neural injury,” says Dr. Varga, Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine) at the Icahn School of Medicine at Mount Sinai. “However, we do not know whether that injury is reversible, so the long-term implications remain to be seen. That said, our findings do imply that if an individual continues to skip therapeutic PAP, cumulative neural injury could occur.”
and that an observed change in neurofilament light (NfL), a marker of neural injury, was significantly associated with apnea-related increases in intermittent hypoxia and sleep fragmentation.
The study, published in the American Journal of Respiratory and Critical Care Medicine, is the first to show an acute effect of sleep apnea on AD biomarkers a field of exploration that is relatively nascent but Dr. Varga cautions that these findings necessitate further study.
The findings were based on analysis of blood collected in the evening (10:40 pm) and the next morning (6:40 am) across a night of polysomnographically recorded sleep among 30 participants with severe sleep apnea during conditions of therapeutic PAP or the third consecutive night of acute withdrawal from PAP in a counterbalanced fashion. The average age of the participants was 51.5; 27 percent of the participants were women and 67 percent were non-Hispanic white.
Andrew Varga, MD, PhD, and Korey Kam, PhD, use a centrifuge to process plasma for Alzheimer's disease biomarkers in sleep apnea patients who use continuous positive airway pressure therapy.
Dr. Varga and the research team looked at overnight changes in four plasma biomarkers associated with neural injury and AD total tau; brain amyloid-beta40 (Aβ40) and brain amyloidbeta42 (Aβ42),peptides that contribute to formation of amyloid plaques; and NfL, an axonal protein that is released in response to neural injury and is highly correlated with the progression of the disease between the two sleep conditions. Plasma samples were analyzed using a single molecular array (SIMOA) Neurology 3-Plex A assay kit, which enables detection of picomolar concentrations of amyloid and tau, and NF-Light™ kits. All samples were tested in duplicate and samples with a coefficient of variation e20 percent were excluded from the analysis.
Looking at the samples, the researchers observed a significant decrease in Aβ40 and a significant increase in NfL among participants after a third consecutive night without PAP therapy versus the therapeutic PAP sleep condition. “When we withdrew PAP therapy and induced sleep apnea acutely, the strongest signal we saw was the overnight increases in neurofilament light,” Dr. Varga says.
Although there was no significant difference observed in the other two AD biomarkers between the two sleep conditions, Dr. Varga says there appeared to be a signal for increased tau in the PAP withdrawal condition, and this warrants further study. There was no difference in all four AD biomarkers between the two sleep conditions at the start of the night within subjects.
Based on those findings, Dr. Varga and the research team subsequently investigated whether there are sleep physiology predictors of the biomarker changes that they observed. They looked at several sleep physiology biomarkers driven by PAP withdrawal and found that the number of sleep stage transitions a marker of sleep fragmentation and the amount of time below 90 percent O2 saturation were significantly associated with NfL. However, no identified sleep physiology biomarkers predicted the overnight change in Aβ40.
“There is considerable debate in the apnea field about what the apnea hypopnea index, or AHI, means,” Dr. Varga says. “There are those who believe it is bad to have a high AHI even if no
From left: Korey Kam, PhD, Assistant Professor of Medicine; Saranya Ravi, MS, Research Coordinator; Andrew Varga, MD, PhD, Associate Professor of Medicine; Daphne Valencia, MA, Research Coordinator; Ankit Parekh, PhD, Assistant Professor of Medicine; Indu Ayappa, PhD, Professor of Medicine
events are associated with significant dips in oxygen. In the cardiovascular field, the consensus is that only intermittent hypoxia matters. Our findings suggest that it is both the dips in oxygen and the sleep segmentation that seem to predict change in this neural injury marker.”
Dr. Varga is exploring the significance of these findings further through a new study that is recruiting individuals ages 55 and older who have been newly diagnosed with sleep apnea. He will collect baseline measurements of the participants’ AD and neural injury biomarkers, administer PAP therapy, and measure biomarkers over a threemonth treatment period to assess changes.
Additionally, Dr. Varga will conduct high-field brain magnetic resonance imaging of the participants using a 7-Tesla brain MRI. This will enable him to resolve sleep-wake regulating centers in the brain and explore changes in functional connectivity in the brain as a result of treatment. That could yield
more vital insights on the impact of PAP therapy on the biomarkers of AD and risk of developing the disease.
“Very few sleep scientists have really researched the impact of treatment with regard to sleep apnea,” Dr. Varga says. “Through our studies, we are filling that gap and our findings have the potential to improve long-term outcomes for patients with sleep apnea.”
Featured Faculty
Andrew W. Varga, MD, PhD
Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine)
Pleuroscopy Program Drives Growth and a Cultural Change
The Mount Sinai – National Jewish Health Respiratory Institute’s Pleural Service, launched in 2020, has used pleuroscopy to dramatically increase its reach and the number and acuity of patients it can serve.
Just three years ago, pleural disease diagnosis and management at Mount Sinai Health System involved invasive approaches such as pleural biopsies and pleurodesis performed using videoassisted thoracoscopic surgery. Patients required general anesthesia and hospital admission.
Realizing that many of the patients he sees are too ill to tolerate such procedures, interventional pulmonologist Udit S. Chaddha, MBBS, saw an opportunity to effect positive change.
“Nobody in our division was performing pleuroscopy at the time,” he says. “It is a minimally invasive procedure, and we are able to perform a biopsy or pleurodesis as a 20-minute outpatient procedure using moderate sedation and a single port. Once we introduced pleuroscopy, it resulted in a cultural change that led to Pulmonology being consulted on almost every patient with pleural disease. It also resulted in a dramatic increase in referrals, and that provided the impetus for us to start a formalized pleural disease program.”
Launched in 2020, the Mount Sinai – National Jewish Health Respiratory Institute’s Pleural Service has attracted considerable interest and referrals, resulting in a 100 percent growth in pleural procedures. Dr. Chaddha, the program’s director, attributes that accomplishment, in part, to state-of-the-art equipment, the implementation of patient management protocols, and the comprehensive array of services and expertise available through the program.
“Pleuroscopy is probably the main procedure we do,” says Dr. Chaddha, Assistant Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine), and Thoracic Surgery; Associate Program Director of Interventional Pulmonology; and Associate Director of Interventional Pulmonology with the Catherine and Henry J. Gaisman Division of Pulmonary, Critical Care and Sleep Medicine at the Icahn School of Medicine at Mount Sinai
“We also perform indwelling pleural catheter placement, large- and small-bore chest tubes,
Udit S. Chaddha, MBBS (center), along with assistants Christian Lo Cascio, MD (Interventional Pulmonology fellow; right) and Idayat Brimah, MD (Pulmonary Critical Care fellow; left), and endoscopy technician Bongick Jang (far left), performing a pleuroscopy in the Mount Sinai West endoscopy suite.
thoracentesis, closed pleural biopsies and biopsies of pleural-based or chest wall masses using ultrasound, and pleurodesis. Additionally, we participate in the management of empyema patients, such as decisions on when to administer tissue plasminogen activator and deoxyribonuclease, and in the management of pneumothorax patients, managing them in the acute setting and conducting follow-ups to ensure their care is appropriate.”
The goal of the program is to provide timely delivery of treatment within minutes for emergent situations and hours for all other cases. A dedicated weekly clinic staffed by Dr. Chaddha; a nurse, Lilibeth Simporios, RN; and a fellow has facilitated that effort, resulting in patients undergoing pleural procedures within one week of referral. Additionally, procedure time is reserved in endoscopy, so that all patients can be attended to without delay.
“It is a set system, which sounds simple, but it enables state-of-the-art care to be the norm here, which is not the case nationwide,” Dr. Chaddha says. “There are very few pleural programs nationwide, as there are only approximately 40 interventional pulmonology fellowship programs. And there are only 400 interventional pulmonologists who are fellowship-trained, which is a requirement for launching a program like this. This means that, for the next decade, it will not be possible for smaller hospitals to offer patients an allencompassing program.”
Dr. Chaddha anticipates the program will fill that gap through the services it offers and through a dedicated interventional pulmonology fellowship.
Led by Timothy Harkin, MD, Associate Professor of Medicine (Pulmonary, Critical Care and Sleep
Medicine), and Thoracic Surgery, and Director of Bronchoscopy at Icahn Mount Sinai, the fellowship is offered to one candidate each year. Dr. Chaddha sees other ways that the program can have an impact, such as increased research and clinical trial activity to gain more insights on the pathology of pleural disease and offer more therapeutic options to patients.
“Our goal is to have dedicated fellows and research coordinators in place so that we can increase that activity within the next two to three years,” he says. “That will enable our research efforts to be smoother and faster, and we will be able to recruit more patients and address the unmet need for treatment.”
Featured Faculty
Udit S. Chaddha, MBBS
Assistant Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine), and Thoracic Surgery
Timothy Harkin, MD
Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine), and Thoracic Surgery
When Can a Patient Come Off a Ventilator?
This AI Can Help Decide
A Mount Sinai physician has developed an algorithm that uses a range of electronic medical record data to identify patients who are ready to be liberated from ventilation. It's a goal that has long been elusive.
A simple tool that accurately calculates a patient’s readiness to be liberated from a mechanical ventilator has long been a holy grail for intensive care unit (ICU) clinicians. Pranai Tandon, MD, believes he may have found it.
Dr. Tandon is assessing the potential of applying artificial intelligence to clinical data to enable more accurate assessments of patient readiness. Working with Icahn School of Medicine at Mount Sinai colleagues in Pulmonology, Clinical Data Science, and Data-Driven and Digital Medicine, he has developed and is studying a predictive algorithm that uses a range of electronic medical record (EMR) data such as patient breath sounds and PaO2/FiO2 ratio to identify patients who are ready to be liberated from ventilation. If successful, Dr. Tandon believes that the algorithm could be impactful for both ICUs and patients.
“Patients who are left on a ventilator too long not only experience a wide variety of health problems but also contribute to a decrease in overall ICU throughput, which has ramifications for outcomes among other patients requiring ventilation,” says Dr. Tandon, Assistant Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine) at Icahn Mount Sinai.
“Liberating patients too early from a ventilator can also cause harm, whether that is from the stress of not being able to breathe easily or the need to reintubate. For these reasons, there is a strong desire among physicians for a simple tool or calculation to augment their expertise in making these determinations. Machine-learning algorithms are a potential solution, as they are not only able to synthesize the wide range of data necessary to make these complex decisions but also can provide customized predictions for each patient.”
The inspiration for Dr. Tandon’s algorithm originated with ReSCUE-ME (Realtime Streaming Clinical Use Engine for Medical Escalation), an innovative Mount Sinai clinical trial that assessed the potential to use machine-learning algorithms to predict clinical deterioration. A literature review revealed several successful studies involving
predictive algorithms, but Dr. Tandon notes that they were typically small, and the algorithms could not be applied in patient care. “We have a large patient cohort, we are streaming data from patients, and we have a clinically focused team. For those reasons, I saw that we could potentially develop an algorithm that we could weave into actual care,” Dr. Tandon says.
Liberating a patient from ventilation neither too early nor too late
Initially, Dr. Tandon developed a simple algorithm to collect data on intubation and extubation times from the EMRs of patients in The Mount Sinai Hospital ICU, which are updated every two minutes. He then partnered with the department’s respiratory therapists for a two-month study to validate his findings. He demonstrated that the algorithm captured more accurate intubation and extubation times than those recorded by hand. Dr. Tandon subsequently looked at other variables, such as average number of patients intubated at any given time in the ICU, time of day that extubation typically occurs, and percentage of patients who are reintubated. These variables demonstrated an opportunity for improvement of the predictive algorithm, which Dr. Tandon trained on a cohort of 2,615 Mount Sinai patients who underwent an extubation attempt at least once between 2011 and 2019. The cutoff was chosen to exclude COVID-19 patients, due in part to low rates of successful ventilator liberation, and to evolutions in best practices and patient populations that would render any model obsolete.
“We split them into testing, training, and validation training sets so we could decide which variables
should ultimately be included in the model,” Dr. Tandon says. “The process requires a considerable degree of experimentation in which you generate hundreds of different possible models and then pick the best-performing one for validation.”
The model that Dr. Tandon chose for validation included predictive factors such as level of consciousness, PaO2/FiO2 ratio, lactate production, and patient breath sounds. The latter, which was the most powerful predictor, are categorized as clear, rhonchi, wheeze, diminished, or null (i.e., absent data) based
predictive value of 11.8 percent. He found that his model achieved an area under the curve of 75 percent versus 54 percent for the index. “What we observed was that the algorithm was similar to the index in terms of patients who were ready for extubation, but the difference was that the algorithm was more intelligently selecting the patients in which the decision for extubation was no,” Dr. Tandon says.
But the question remains as to how well the algorithm is able to make predictions based on live data. Dr. Tandon is currently analyzing the results
upon twice-daily assessments and descriptions provided by a respiratory therapist or nurse. The model produces numeric probabilities from 0 to 1, but for the purposes of validation, Dr. Tandon used a false positive/true positive balance threshold of 0.45, resulting in a positive predictive value of 89.5 percent and a negative predictive value of 50.6 percent.
Using the historic cohort, Dr. Tandon compared the predictive potential of this model against the rapid shallow breathing index the most used index for determining patient liberation readiness at the traditional threshold of 105 breaths/minute/liter, which has a positive predictive value of 85.5 percent and a negative
of a three-month study in which the algorithm was fed live EMR data from the ICU each day at 5 am. The results, which he is reviewing with his respiratory therapy colleagues, could necessitate further tweaks to the model or a return to the drawing board. But success would enable him to proceed with a pilot study that demonstrates the potential impact of this tool.
“Our hope is that we achieve an algorithm that enables us to safely decrease the time patients spend on ventilators, enabling us to achieve improved outcomes for them,” Dr. Tandon says. “Even a decrease of 12 hours would greatly revolutionize the throughput of the ICU and enable us to achieve cost efficiencies in care.”
Flow chart of the algorithm
Featured Faculty
Pranai Tandon, MD
Assistant Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine)
About the Division of Rheumatology
The Division of Rheumatology at Mount Sinai Health System has a long tradition of clinical excellence, patient care, and education for medical students, medicine residents, and intraining rheumatology fellows. With Musculoskeletal ultrasound becoming a regular part of rheumatology practice, Mount Sinai established its own musculoskeletal ultrasound program, aiming to provide a monthly opportunity for fellows to become familiar with the use of ultrasound for the evaluation of rheumatic diseases.
Rheumatology fellows learn how to maneuver the ultrasound probe and adjust ultrasound settings for optimal image capture, as well as how to recognize effusions, synovitis, erosions, and signs of soft tissue injury. It also allows them to practice ultrasound-guided procedures, such as aspiration in patients with difficult anatomy, and guided injections of joints, tendon sheaths, and nerve tunnels.
Musculoskeletal ultrasound is also required for the guidance of synovial biopsies, performed as part of an institutional review board- approved study of patients with refractory inflammatory arthritis, and for selected clinical scenarios where indolent infections are suspected. In addition to the educational benefits for trainees, patients are receiving highly accurate diagnosis and intervention.
The establishment of the Inflammatory Bowel Disease-Arthritis (IBD- ART) Program led by Bahar Moghaddam, MD, and Abhik Bhattacharya, MD (Division of Gastroenterology), makes it possible for patients with Crohn’s disease or ulcerative colitis to be evaluated for rheumatic disease manifestations. Other new initiatives include the launch of the Lupus Program and the Osteoporosis Program, both housed at Mount Sinai Morningside.
System Chief (interim)
Rachel Miller, MD
The Dr. David and Dorothy Merksamer Professor of Medicine (Allergy and Immunology)
Program Addresses the Physical and Neuropsychiatric Challenges of Lupus
Lupus has a broad clinical presentation that means the disease can affect nearly all aspects of a person’s life. Mount Sinai's new Lupus Program takes a comprehensive approach to addressing the physical and neuropsychiatric challenges this complex condition poses.
Lupus is an immense clinical challenge characterized by heterogeneous presentations that make diagnosis and treatment both difficult and delayed. Add to that neuropsychiatric, psychosocial, and cognitive threats to the health of patients with lupus, and the need for a center dedicated to the physical and behavioral care of these patients becomes clear.
Which is why the Lupus Program at Mount Sinai Morningside was recently created.
Lupus, or systemic lupus erythematosus, is an autoimmune disease in which the immune system misfires, attacking the skin, joints, kidneys, brain, lungs, heart, and other organs. It is fairly rare, afflicting 1 in 1,000 people. The vast majority of them are women, though the 10 percent or so of lupus patients who are male tend to have more severe disease. Lupus is often diagnosed in women between the ages of 20 and 40 and is an underappreciated leading cause of mortality in younger women, particularly Black women.
“There is often a very long lag time between the onset of symptoms and the time the patient presents to us in the rheumatology clinic,” explains Chrisanna Dobrowolski, MD, MS, Co-Director of the Lupus Program and Assistant Professor of Medicine (Rheumatology) at the Icahn School of Medicine at Mount Sinai. Dr. Dobrowolski is an attending physician at The Mount Sinai Hospital and Mount Sinai Morningside.
Symptoms of lupus might include fever, fatigue, rash, joint pain and swelling, swollen lymph nodes, mouth ulcers, and chest pain, all of which are also complaints of myriad other conditions one reason for the typically long time it takes patients with lupus to receive correct diagnoses.
In addition to the above symptoms, Dr. Dobrowolski says, “Patients with lupus often have debilitating fatigue, brain fog, and diffuse myofascial pain, which are not necessarily responsive to lupus-specific treatments but regardless, have significant impacts on patients’ quality of life.”
Chrisanna Dobrowolski, MD, MS, and Nicholas Kopple-Perry, DO, lead the Lupus Program at Mount Sinai Morningside.
Addressing Collateral Effects
The broad clinical presentation of lupus also means that the disease can affect nearly all aspects of a person’s life, explains Nicholas Kopple-Perry, DO, Associate Director of Psychiatry Education and Training at Mount Sinai Morningside and Director of the Consultation Liaison Psychiatry Service at Mount Sinai Morningside and Mount Sinai West. Dr. KopplePerry has specialized training working with individuals with comorbid medical illnesses that affect their psychiatric and psychological health expertise that explains his role as Co-Director of the Lupus Program.
The neuropsychiatric symptoms of the disease have been well documented, with studies finding that those with lupus suffer more lifetime mood or anxiety disorders, major depression, phobias, panic disorder, and obsessive-compulsive disorder than those in non-lupus comparative samples.
“People with lupus have twice the incidence of depression and higher levels of anxiety compared to the general population,” Dr. Kopple-Perry says. “Also, up to 80 percent of individuals living with lupus will have impaired working memory, impaired attention, and general cognitive slowing over the course of their lives, which has a huge impact on a person’s functioning. Financial issues and housing insecurity can become factors, as can registering and recalling treatment recommendations.”
The disease tends to first appear in early adulthood, typically during a woman’s reproductive years, and the advent of the disease can have an effect on one’s sense of self. Cutaneous manifestations also can disrupt one’s body image. “This disease really hits every domain of a person’s life and can be quite crippling,” Dr. Kopple-Perry says, “so in some ways treating lupus is more than just managing symptoms but also its collateral effects.”
Lupus is known to be more common among people who have high levels of stress and among those with a lower socioeconomic status. Dr. Dobrowolski notes that there is a significant lupus population in Morningside Heights and surrounding areas of Manhattan. “Having the clinic in the area where current patients live provides easier and better access and is really important for reducing barriers to treatment.”
The many presentations of lupus, and the wide disparity in disease acuity, means that most people do not have a good understanding of the challenge that patients face. “You have this illness that’s painful and debilitating and changes your body, affecting your emotions and your ability to think,” Dr. Kopple-Perry notes, “but the general population doesn’t always have a great understanding of the disease, which can make finding social support in one’s community a challenge.”
“These are patients with a high incidence of cognitive dysfunction, depression, and anxiety, for multiple reasons,” Dr. Dobrowolski says. “These issues present a huge barrier to proper lupus treatment, so addressing psychosocial aspects of the illness is really paramount to treating the patient.”
The unique spectrum of coverage of clinical and psychiatric manifestations of the disease makes the lupus clinic at Mount Sinai Morningside stand out. In addition, because the clinic is part of the Mount Sinai Health System, other specialists are readily available to augment patient care.
Although the lupus program is new, there are already discussions on how to grow it. One likely addition will be a patient support group, and both rheumatology and psychiatry fellows may soon help support the clinic as part of their educational experience.
Featured Faculty
Chrisanna Dobrowolski, MD, MS
Assistant Professor of Medicine (Rheumatology)
Nicholas KopplePerry, DO
Assistant Professor of Psychiatry
Key Initiatives in the Department of Medicine
Mount Sinai Center is World Leader in Transgender Health Care
Mount Sinai’s Center for Transgender Medicine and Surgery the most comprehensive such program of its kind in the world—offers a full menu of health care options, including primary care, hormonal therapy, endocrinology, gender-affirming plastic surgery, urology, gynecology, otolaryngology, social work, spiritual care, and mental health services.
Surveys suggest there may be millions of transgender and gender-diverse people in the United States.Mount Sinai’s Center for Transgender Medicine and Surgery the most comprehensive such program of its kind in the world is dedicated to supporting them with health care, research, and education.
An architect of the Center and a tireless engine of its success has been Joshua D. Safer, MD,FACP, theCenter’sfoundingExecutiveDirector,whoisa Professor of Medicine (Endocrinology, Diabetes and Bone Disease) at the Icahn School of Medicine at Mount Sinai.
Since the Center’s inception in 2016, its services have expanded to include a full menu of health care options, including primary care, hormonal therapy, endocrinology, gender-affirming plastic surgery, urology, gynecology, otolaryngology, social work, spiritual care, and mental health services.
“There are perhaps 30 places around the country that offer certain parts of what we do, but we are far and away the largest program of this sort in the country, and even the world,” explains Dr. Safer, who joined the Center in 2018.
The number of transgender people in the United States might seem insignificant, but that is not the case. “In anonymous surveys, somewhere between half a percent and a full percent of people say they are transgender,” Dr. Safer explains. “If you do the math, that could be up to 3 million or more people.”
At the Center, patient volumes, for both genderaffirming hormonal therapy and gender-affirming surgery, have steadily climbed.
Focus on Research and Education
The health care needs of this group of patients can be complex, which is why continued research, and education of the next generation of clinicians, are vital aspects of the Center’s mission.
For example, Dr. Safer is interested in exploring the relative risks of various treatment regimens, since there is concern that some hormone therapy might create risks.
“People were worried that it might be unsafe to maintain estrogen therapy while a patient is set for
Joshua D. Safer, MD, and Eleanore Elizabeth Egan, PA
surgery, and it was common practice for transgender women to stop estrogens during the several weeks around surgery,” Dr. Safer says. “But we don’t do that for postmenopausal women taking estrogens for hormone replacement therapy, and, in fact, we can see no difference and no benefit to having transgender people stop their hormones. I hope to disabuse people of some of these fears, and I think there are opportunities to look at what hormones do to various tissues at a more sophisticated level."
Dr. Safer was the inaugural president of the United States Professional Association for Transgender Health (USPATH) and oversaw Mount Sinai’s hosting in 2023, for the third time, of the live surgery conference of the World Professional Association for Transgender Health (WPATH). He serves on the board of directors of WPATH as well as on its Standards of Care revision committee. Dr. Safer co-wrote the Endocrine Society’s 2017 guidelines for the medical care of transgender patients, and is the chair of the Society’s current committee to revise those guidelines. He also co-wrote “Care of Transgender Persons,” a 2019 clinical practice review in The New England Journal of Medicine
Dr. Safer and colleagues at the Center work hard to disseminate the knowledge they have accumulated. Dr. Safer was a co-author of a 2023 Endocrine Society scientific statement concerning health care disparities and endocrine health, which, he explains, “reframes increased morbidity in transgender people to be more connected to social determinants of health than to hormone treatment.” He also co-wrote “Update in Adult Transgender Medicine” for the Annual Review of Medicine, among several other publications, and coauthored several presentations at the 2023 Endocrine Society meeting, including a case report of occult endometriosis in the prostate of a transgender woman.
The Center has been innovative in its role as educator, creating fellowship programs that are
unavailable elsewhere. “We at Mount Sinai established the first fellowship program for gender-affirming surgery, which sits with our plastic surgeons,” Dr. Safer says. “We also established the first fellowship program for gender-affirming psychiatry and we have a genitourinary fellowship program.”
“We were also asked by the State of New York to host a fellowship program for transgender medicine formedical providers, and we’ll train two people per year,”
Dr. Safer says. And the endocrinology fellowship includes a core rotation on gender-affirming hormones, which Dr. Safer notes is “significant. We compete with the most prestigious programs nationally for this reason, and it’s one of the reasons why fellows choose our program.” Mount Sinai also offers a free online course for primary care providers of transgender health care, which has amassed thousands of students worldwide.
Despite the political issues that have swirled around transgender health care, Dr. Safer and his colleagues plan to press on.
“I’m amazed that anyone thinks that it is okay to target a vulnerable group of people and try to take away their health care,” Dr. Safer says. “We are here at Mount Sinai, and we’re not political. We are just trying to deliver health care to our patients, that’s all.”
Featured Faculty
Joshua Safer, MD
Professor of Medicine (Endocrinology, Diabetes and Bone Disease); Director, Center for Transgender Medicine and Surgery
Mount Sinai Beth Israel
Finds New Ways to Deliver Front-Line Care to the Community
Even as Mount Sinai Beth Israel moves toward closure of its inpatient campus on 16th Street, its modern outpatient sites across a wide swath of downtown Manhattan are more vital than ever to the Mount Sinai Health System. They include a multispecialty ambulatory center with more than 30 medical practices in Union Square and a recently opened, state-of-the-art behavioral health center.
Even as Mount Sinai Beth Israel moves toward closure of its inpatient campus on 16th Street, its modern outpatient sites across a wide swath of downtown Manhattan are more vital than ever to the Mount Sinai Health System. They offer a vast range of primary and specialty care under one roof, with high-quality, innovative medicine informed by Mount Sinai’s backbone as an academic medical center.
“We’re expanding and improving our outpatient platform to make sure patients are getting the specialized care and social services they require,” says Matthew Weissman, MD, MBA, Chair of the Department of Medicine for Mount Sinai Beth Israel and Downtown. “And we’re constantly finding new ways to deliver that care where they need it, whether it’s at our renovated Union Square site, our newly opened Mount Sinai-Behavioral Health Center, or through a growing network of primary care practices across downtown.”
With more than 30 medical practices, imaging suites, a pharmacy, and an urgent care clinic,
Mount Sinai-Union Square has truly stepped up to meet the clinical demands of the diverse community it serves. Sometimes described as a “hospital without beds,” the huge facility has co-located primary care physicians and medical subspecialists on the same floor for the convenience of patients, as well as to promote collaborative care by its multidisciplinary teams. Patients who need a CT scan, for example, can simply walk up a floor, or down a floor, for physical therapy.
When the Union Square facility, just steps from one of the city’s subway hubs, took over Mount Sinai’s sleep disorders program in the summer of 2022, site leaders saw another opportunity to cater to patients. They actively promoted a new generation of mobile sleep-monitoring kits that individuals can take home to test for obstructive sleep apnea, instead of committing to an overnight stay in a sleep lab. Once the data are uploaded to the device, they are read and analyzed by a specialist at the sleep disorders center, with results relayed to the patient within weeks, down from months under
From left, Chief Resident Natasha Qureshi, MD; Matthew A. Weissman, MD, MBA; and residency program staff members Michelle Torres-Avelar and Denny Ayala Reyes review orientation materials for new residents.
the sleep lab regimen. Presented with this attractive alternative, patients in growing numbers have gravitated to the take-home kits, increasing the hospital’s diagnoses of a sleep disorder with potentially serious health consequences.
The $140 million Mount Sinai-Behavioral Health Center in Lower Manhattan takes the concept of patient-sensitive health care to a new level, serving as a “one-stop shop” for mental health care, substance use treatment, and primary care. Specifically, the new center representing the largest private investment in mental health in the history of New York State integrates general outpatient mental health and substance-use disorder treatment services with primary care services, providing seamless access and comprehensive care for its patient population.
“We’ve responded to the needs of a community that’s often underserved by primary care doctors by placing full-time hospitalists and internists at our Behavioral Health Center,” notes Dr. Weissman, who is a Professor of Medicine, and Pediatrics, at the Icahn School of Medicine at Mount Sinai. “And if patients there require consultation with an infectious disease, gastroenterology, endocrinology, or other specialist, we’ll use telemedicine to conveniently link them to Mount Sinai Beth Israel or Mount Sinai-Union Square. That’s how we’re effectively managing resources among different sites on behalf of a typically high-needs patient population.”
Sensitivity to patient needs is evident in other notable ways within Mount Sinai Beth Israel’s realm. For example, Danielle Loeb, MD, MPH, a primary care physician with experience in treating transgender patients, was recently hired and has begun training residents in providing culturally and medically appropriate care to this growing
population. In addition, several hospitalists serve as advocates for Chinese-speaking patients breaking down language and cultural barriers for them and making sure they are connected to the right doctors and social services within the hospital and the health care community.
“Even when these hospitalists aren’t directly treating Chinese-speaking patients, they’ve made it a point to go to the ICU to see them and family members to help broker, in some cases, end-oflife conversations, or to make sure there’s continuity of care with doctors in the community,” says Dr. Weissman. “It’s that kind of personalized care and commitment that strongly defines Mount Sinai Beth Israel and makes us feel very much a part of the community.”
That connection extends to individuals who are still experiencing symptoms that originated during COVID-19. Mount Sinai Beth Israel is home to the Center for Post-COVID Care, treating about 50 patients a week with such lingering health issues as shortness of breath, headaches, dizziness, and “brain fog,” which can include memory loss and difficulty focusing. The Center was the first in the country to treat so-called long COVID cases when it opened in mid-2020.
“Though the volume and intensity of COVIDrelated illness have since diminished, we’re still seeing patients in our clinic who have failed to get better,” notes Zijian Chen, MD, Associate Professor of Medicine (Endocrinology, Diabetes and Bone Disease) and Director of the Center for Post-COVID Care. “We use an array of imaging and clinical tools and the knowledge we’ve acquired to diagnose and treat their conditions, including referring many to our rehabilitation specialists who are often able to restore a normal quality of life.”
Featured Faculty and Site Leadership
Zijian Chen, MD
Associate Professor of Medicine (Endocrinology, Diabetes and Bone Disease)
Danielle Loeb, MD, MPH
Associate Professor of Medicine (General Internal Medicine)
Matthew Weissman, MD, MBA
Professor of Medicine (General Internal Medicine), and Pediatrics; Chair, Department of Medicine, Mount Sinai Beth Israel
Growing its Medical Services Under the Family Brand of Quality Care
Since becoming part of the Mount Sinai Health System a decade ago, Mount Sinai Brooklyn has worked diligently to build an enviable reputation within the community for quality service in cardiology, stroke, vascular surgery, bariatric surgery, gastroenterology, and robotic surgery.
For patients entering Mount Sinai Brooklyn with complex medical and surgical needs, the Mount Sinai logo adorning the 200-bed hospital in the Midwood section is a reassuring sight. That’s because this busy acute-care center, serving the ethnically and racially diverse neighborhoods of southern Brooklyn, has become a gateway for more than 1,200 patients annually who are transferred to Mount Sinai hospitals in Manhattan for specialized care and advanced procedures.
Mount Sinai Brooklyn has worked diligently over the past decade, since becoming part of the tertiary and quaternary Mount Sinai Health System, to develop and grow that linkage across an array of medical and surgical fields. At the same time, it has built an enviable reputation within the community for its own quality service in cardiology, stroke, vascular surgery, bariatric surgery, gastroenterology, and robotic surgery. Discussions are underway with the parent Health System to widen that range by bringing in specialists from Manhattan weekly to treat patients for liver, endocrine, pulmonary, and immunologic disorders.
“The greatest change we’ve made over the past decade is our ability to attract to our hospital Mount Sinai-caliber physicians to improve the quality and delivery of health care and the overall patient experience,” says Scott Lorin, MD, MBA, President and Chief Operating Officer of Mount Sinai Brooklyn, who took the helm in 2018. “That’s reflected in our quality metrics particularly the hospital-acquired infection rate that have improved dramatically from among the worst to the best within the Mount Sinai system, and the entire state.”
A major contributor has been a highly successful hospitalist program launched in the wake of COVID-19, when Radfan Gazali, MD, Assistant Professor of Medicine at the Icahn School of Medicine at Mount Sinai, was brought in from Mount Sinai Morningside to head up the fledgling effort as Chief of the Division of Hospital Medicine at Mount Sinai Brooklyn. Over the past two years, the program has grown to 10 full-time Mount Sinai physicians who are responsible for 30 percent of all hospital discharges. This team has also received special training in end-of-life care and
Scott Lorin, MD, and Radfan Gazali, MD, are among those who have led a dramatic quality improvement at Mount Sinai Brooklyn.
now admits all inpatient hospice patients who were previously managed by an independent group. Underscoring the magnitude of this change is the fact that 65 percent of Mount Sinai Brooklyn’s patients are older than 65, and 25 percent are older than 85, an unusually high ratio for any hospital.
Further enhancing care has been the hospital’s expanded use of Mount Sinai’s telehealth programs, effectively bringing subspecialists from across the river in Manhattan to the bedside of patients in Brooklyn.
“We’ve worked closely with Mount Sinai to set up telehealth services that can connect patients and doctors from the Emergency Department or from inpatient units to medical experts in fields that range from stroke to dermatology to psychiatry,” notes Peter Shearer, MD, Chief Medical Officer and Vice President of Medical Affairs at Mount Sinai Brooklyn, and Associate Professor of Emergency Medicine at Icahn Mount Sinai. “We’re now looking to add more subspecialties, such as rheumatology and endocrinology, for medical consults.”
Accompanying the many changes have been extensive physical renovations and upgrades in recent years. The hospital now has, for example, two advanced 128-slice computed tomography scanners, and in May 2023 dedicated a new stateof-the-art magnetic resonance imaging machine. Moreover, the hospital migrated to Epic in 2019, resulting in enhanced communication and care coordination around the transfer of patients among institutions. The transition to Epic included reconfiguring most inpatient floors to make them telemetry-capable, a move that has reduced intrahospital transfers of patients by 50 percent.
Housing much of this activity is a renovated ambulatory care building on the hospital grounds, which has become a thriving faculty practice. “We recently opened the Tisch Cancer Center with 15 infusion chairs and a brand-new mammography suite, and our oncologists are actively participating in clinical trials,” points out Dr. Lorin, who is
Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine) at Icahn Mount Sinai. “We also have a robust orthopedic practice, neurology, and stroke services in this building, and recently moved all outpatient surgical services to a renovated suite on the top floor with 12 exam and two minor procedure rooms.”
As a fast-growing member of the Mount Sinai family, the Brooklyn hospital has also realized significant gains in physician recruiting, which in years past was a challenge. The solution lay in enticing graduates from Mount Sinai’s medical training programs to work at the Midwood site.
“We put a lot of effort into recruiting these graduates, who sometimes split their time with the Manhattan hospitals,” acknowledges Dr. Lorin. “And their experience was so positive that they began telling colleagues, who were encouraged to come to Brooklyn. And that’s how we built our faculty practice, and how we continue to build a Mount Sinai level of quality care.”
Featured Faculty and Site Leadership
Scott Lorin, MD, MBA
President and Chief Operating
Officer,
Mount Sinai Brooklyn
Radfan Gazali, MD
Assistant Professor of Medicine (Hospital Medicine); Chief of the Division of Hospital Medicine, Mount Sinai Brooklyn
Connecting Manhattan’s West Side With Medicine’s
Top Clinicians and
Services
Mount Sinai Health System's hospitals on the West Side of Manhattan Mount Sinai Morningside and Mount Sinai West—offer expertise in areas ranging from lung cancer detection and screening to gastrointestinal disorders.
Aware of its essential role in meeting the medical needs of communities on Manhattan’s West Side, Mount Sinai Health System has worked diligently in recent years to ensure that residents have access to the city’s leading specialists and most advanced clinical services and programs, anchored by the health care hubs of Mount Sinai Morningside and Mount Sinai West
That effort has met with remarkable success, resulting in a 60 percent increase in Department of Medicine faculty since 2015 and the strengthening of such vitally needed services as primary care and lung cancer detection and screening. Also included are the development of centers of excellence for patients with pancreatic cancer and gastrointestinal physiology and motility disorders.
“Every medical specialty in our space has experienced significant growth in terms of faculty and the level of expertise the public can readily tap into,” says Samuel Seward Jr., MD, Former Chair of Medicine for Mount Sinai Morningside and Mount Sinai West. “In primary care alone, we’ve hired, over the past two years, 12 new fulltime physicians and have transformed this clinical program into one of the largest of its kind within the Mount Sinai Health System, and within the city. And over the last few months, we’ve added an urgent care center as a way of growing the breadth and depth of our primary care model to include just-in-time care for patients.”
No initiative better encapsulates Mount Sinai’s growing commitment to residents on the city’s West Side than the Incidental Lung Nodule Program. Launched recently at Mount Sinai Morningside, this unique and ambitious effort is harnessing the expertise of the hospital’s pulmonary specialists and primary care doctors in the Division of General Internal Medicine to establish the hospital as a screening hub for diagnosing and monitoring lung nodules identified in patients who have undergone CT scans for conditions such as coronary disease, chest pain, or pulmonary embolism.
“We want to be sure we’re finding lung cancers both when we’re specifically looking for them and when we’re not, through our Incidental Lung Nodule Program,” says Javier Zulueta, MD, Professor of Medicine and Chief of Pulmonary, Critical Care and Sleep Medicine at Mount Sinai Morningside, who has overseen and championed the program at the hospital. Once an incidental nodule is detected through a CT scan, he explains, specially designed software alerts the provider who ordered the image and the patient, urging follow-up with a hospitalbased pulmonologist.
Adds Dr. Seward: “Because patients are often asymptomatic in the early stages of lung cancer, this program has enormous potential to save many lives through quick intervention by our pulmonary specialists. In just a few months we’ve already captured hundreds of patients who are following up based on the findings of our radiologists.”
We’ve definitely upped our game to meet the needs of patients by putting in place the finest faculty and highest-quality medical care that’s accessible to them.
Samuel Seward, Jr., MD
Timely intervention is also critical in treating patients with pancreatic and biliary cancers. For this reason, the Department of Medicine’s decision to move its Center of Excellence for Pancreatic Cancer to Mount Sinai West has proven to be a huge asset to residents in surrounding communities. The program’s leadership team includes Edward Lung, MD, MPH, Professor of Medicine and Director of Endoscopy for the Division of Gastroenterology at Mount Sinai West and Mount Sinai Morningside. A widely known expert in advanced endoscopy, Dr. Lung ensures
that every patient who arrives at the Center is surrounded by a multidisciplinary team that’s able to offer a wide range of personalized treatment options and clinical trials.
Mount Sinai’s rapid growth on the West Side is further showcased in its Center for Gastrointestinal Physiology and Motility, a highly specialized unit that has added within the past two years six faculty members, including experts in motility disorders throughout the GI tract and in pelvic floor dysfunction in women. The Center’s new Director is a nationally recognized expert in the field, Daniela Jodorkovsky, MD, Associate Professor of Medicine (Gastroenterology). Thanks to her group’s extraordinary growth and cutting-edge platform for diagnosing and treating both upper and lower GI motility disorders, it is now poised to be an international leader in that space.
“Rounding out our many clinical initiatives is a large residency training program that serves as a robust pipeline for the talent and services we’re constantly adding to our West Side operations,” notes Dr. Seward. “We’ve definitely upped our game to meet the needs of patients by putting in place the finest faculty and highest-quality medical care that’s accessible to them, both as inpatients and, increasingly, at convenient sites within their communities.”
As a long-time physician at Mount Sinai Mount Sinai Morningside and Mount Sinai West, and as graduate of the internal medicine residency program, I am very excited to have been given the opportunity to serve as Interim Site Chair of the Department of Medicine. My goal is to increase access to the highest quality primary and subspecialty care available on the West Side of Manhattan while opening and establishing new, innovative programs to serve the needs of the community. An important strategic objective is the integration of more clinical research into our clinical care programs
Amy Rosenberg, MD
Featured Faculty and Site Leadership
Javier Zulueta, MD
Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine)
Daniela Jodorkovsky, MD
Associate Professor of Medicine (Gastroenterology)
Samuel Seward, MD*
Professor of Medicine (General Internal Medicine); Former Chair, Department of Medicine, Mount Sinai Morningside and Mount Sinai West
Amy Rosenberg, MD
Interim Site Chair, Mount Sinai Morningside and Mount Sinai West
* As of the publishing of this report, Dr. Seward has since left Mount Sinai
Breaking Down Barriers to Health Care in a
Highly Diverse Section of Queens
In western Queens, a third of the patients don’t speak English and face other barriers to health care. To help them, Mount Sinai Queens in recent years has added a state-of-the-art stroke program, a massive investment in cardiovascular care, and an expanded presence in oncology, endocrinology, gastroenterology, and outpatient services, all conveniently available at several new ambulatory care sites.
Located in one of the most polyethnic communities in the country, Mount Sinai Queens is an acutecare center keenly equipped to handle the population’s complex and diverse medical needs. In recent years it has added a state-of-the-art stroke program, a massive investment in cardiovascular care, and an expanded presence in oncology, endocrinology, gastroenterology, and outpatient services, all conveniently available at several new ambulatory care sites. Most recently, the hospital added a geriatrician to optimize its care of older adults.
“There’s a great interest nationally in disparities in health care, and nowhere are they on greater display than in western Queens, where a third of our patients don’t speak English,” says Kathy Navid, MD, Associate Professor of Medicine (Hospital Medicine) at the Icahn School of Medicine at Mount Sinai, and Chair of the Department of Medicine at Mount Sinai Queens. “That’s what we’re focused on: taking a population that faces so many barriers to health care and working our hardest to offer them the same kind of specialized services and quality health care they would enjoy if they lived in Manhattan.”
To that end, the 170-bed campus in the Astoria section of Queens is developing centers of excellence around cardiology, neurology, and oncology, drawing on the resources and expertise of The Mount Sinai Hospital, its parent across the East River. In launching a certified stroke program, for example, the hospital benefited from a highly skilled neurology subspecialty team that came over from The Mount Sinai Hospital and took up round-the-clock residence at the main Astoria site. That huge investment enabled the hospital to become a thrombectomy-capable stroke center featuring a state-of-the-art CT machine with X-ray fluoroscopy that could be deployed for interventional procedures as well as scanning. The stroke center the first of its kind in Queens performed its first cerebral thrombectomy in 2017.
The real turning point for Mount Sinai Queens occurred the prior year, however, with the opening of a spacious new ambulatory pavilion in Astoria, replete with outpatient operating rooms and a wide range of specialty and primary care offices. As part of the dramatic shift, the hospital also hired six physicians for its hospital medicine program
The Mount Sinai Queens Department of Medicine serves the complex and diverse medical needs of one of the most polyethnic communities in the country,
and started evolving into “more of a Mount Sinai presence,” as Dr. Navid puts it. Over the past two years, the expanding Department of Medicine footprint has included seven endocrinologists at five ambulatory care sites on and off the main hospital campus, and smaller but growing teams of gastroenterologists, nephrologists, infectious disease specialists, and renal doctors.
Nowhere has the growth been more impressive, however, than in cardiology, which now encompasses nine cardiologists and is tripling its physical size. “A cardiac catheterization unit was recently opened, the first one in the area, and all of our cardiovascular services are being consolidated in a new state-of-the-art building across the street from the hospital with a CT scanner, echocardiogram, and stress- and other advanced-testing modalities,” explains Stephen Sigworth, MD, Associate Professor of Medicine (General Internal Medicine) at Icahn Mount Sinai. Dr. Sigworth has been leading ambulatory care development for the past four years at Mount Sinai Queens and Mount Sinai Brooklyn
The Mount Sinai investment in Queens is also paying dividends for individuals waiting for a kidney or liver transplant. “These patients are pretty sick, and their ability to travel is limited,” notes Dr. Navid. “They’re now able to get subspecialty care from transplant teams based at Mount Sinai that come over to Queens once a week. They never had that option before.”
Given the sensitivity of Mount Sinai Queens to the diverse population it serves, it’s not surprising that community outreach continues to be an area of intense pride and robust activity.
“Our patients have tremendous needs, and because many of our staff are from the community, they’re equipped to recognize and address them,” acknowledges Dr. Navid, herself an internal medicine physician. “One area of focus, for example, is breast cancer screening in the Bangladeshi American community, as well as blood pressure testing, knowing the prevalence
of cardiovascular disease in this population. Our cardiologists look for opportunities to practice and advocate for disease detection and prevention in this community.”
That sensitivity is no less evident in the inpatient setting. In a hospital where several dozen languages are spoken on the floors, physicians and staff are equipped with a sophisticated video interpretation system on their monitors and phones for instant onsite translation. Palliative care teams consisting of physicians, nurse practitioners, and social workers are also attuned to the multiplicity of cultural needs, especially when having end-of-life discussions with patients and their families.
Sums up Dr. Navid: “It’s really gratifying to be able to bring this level of passionate and highly skilled care to the small, closely knit neighborhoods of Queens. Even better, with the support of our tertiary care partner we continue to up our game.”
Featured Faculty and Site Leadership
Kathy Navid, MD
Associate Professor of Medicine (Hospital Medicine); Chair, Department of Medicine, Mount Sinai Queens Stephen Sigworth, MD
Associate Professor of Medicine (General Internal Medicine)
Mount Sinai’s Flagship Hospital on Long Island
Is Growing its Clinical and Academic Footprint
The Department of Medicine at Mount Sinai South Nassau is bringing specialized medical services that were previously only available in Manhattan to the roughly 900,000 residents the hospital serves on Long Island’s South Shore.
Five years after becoming Mount Sinai’s flagship hospital on Long Island, Mount Sinai South Nassau is growing in a way that is impossible to miss. Initiatives range from the ongoing half-billion-dollar construction project that includes the sleek Feil Family Pavilion on its main campus in Oceanside, to an expanded internal medicine residency training program, to ambitious plans underway to become a regional center for cardiac surgery and thrombectomy-capable stroke treatment.
For the roughly 900,000 residents the hospital serves on the Island’s South Shore, that new footprint brings to their community the kind of specialized medical services they previously had to go to Manhattan to access.
“We were always a very successful community hospital, but since joining Mount Sinai we’ve become an even stronger and larger academic tertiary care center that still has a very unique and nice community hospital feel,” says Aaron Glatt, MD, MACP, Professor of Medicine (Infectious Diseases) at the Icahn School of Medicine at Mount Sinai and Chair of the Department of Medicine at Mount Sinai South Nassau. “We’ve enjoyed a very collegial relationship and exchange of services and doctors that are allowing our
patients to get the same great quality of Mount Sinai care right in their backyard.”
Cardiovascular care drives the point home. While the hospital has maintained for years a recognized Center for Cardiovascular Health it’s the only acute-care center on Long Island’s South Shore to perform emergency and elective angioplasty it has been limited by its lack of onsite cardiac surgery.
That will soon change upon completion of the Feil Family Pavilion, which includes new operating rooms, surgical beds, and an intensive care suite, setting the stage for a vastly expanded cardiac surgery and interventional cardiology program expected to begin in the summer of 2025. The program will include specialists from the Mount Sinai Health System (including Mount Sinai South Nassau) performing and training others in surgical procedures such as TAVR (transcatheter aortic valve replacement) for patients with severe aortic stenosis, and leftsided transseptal ablation for atrial fibrillation. Enhancing that capability will be the migration of Mount Sinai South Nassau to Mount Sinai’s Epic electronic health records system.
Haiwen Ma, MD; Clotaire Ariste, MD; Dmity Konsky, DO; Indra Daniels, MD; and Aaron Glatt, MD, are among the intrepid team of clinicians at Mount Sinai South Nassau who have established it as Long Island’s premier hospital for cardiovascular and cancer treatments with excellent outcomes.
Cancer treatment is another specialty benefiting significantly from the Mount Sinai connection. A Joint Comprehensive Cancer Center at Mount Sinai South Nassau gives patients access to cutting-edge clinical trials and treatment in conjunction with Mount Sinai’s oncology team at its main campus in Manhattan. An integral and robust part of that joint effort is infusion services offered locally and regionally for both oncology and non-oncology patients across the Mount Sinai Health System. The program also plans to expand academically. Elaborates Dr. Glatt: “The potential for our hospital to offer fellowships in cardiology, oncology, and other medical specialties, in addition to our current gastroenterological fellowships, is one of the most exciting prospects on our horizon.”
Under the banner of Icahn Mount Sinai, Mount Sinai South Nassau has already received approval from the Accreditation Council for Graduate School Education to enlarge its Internal Medicine Physician Residency Program from 30 to 39 slots next summer. The hospital also maintains residency training in surgery, obstetrics and gynecology, podiatry, and family medicine.
Clinically, Mount Sinai South Nassau is working toward having a Level III Neonatal Intensive Care Unit, building on its Level II status while enhancing high-risk obstetrical care for Long Island’s South Shore. The hospital currently delivers more than 2,000 babies a year. In terms of ambulatory care, Mount Sinai South Nassau has 37 sites outside its main facility where physicians practice primary and specialty medicine, and recently built an advanced 15,000-square-foot medical arts pavilion in Long Beach. That community is also the site of a freestanding, full-service Emergency Department (ED), one of only a handful in New York State, and the Feil Family Pavilion project will include a doubling in size of the hospital’s main ED.
True to its roots as a community hospital, Mount Sinai South Nassau takes particular pride in its extensive outreach program. That effort gained
high visibility during COVID-19, when its distinctly marked mobile vaccination bus (the “Vaxmobile”) traveled up to six days a week to hard-hit communities to administer vaccines and boosters to all eligible residents, as well as to provide treatments such as Paxlovid after they became available. The outreach now brings to the region’s towns and neighborhoods a multitude of health screening programs, including ones for breast cancer, cardiovascular/blood pressure, prostate cancer, and dermatological/melanoma. In addition, clinical professionals frequently appear before community groups to give lectures on proactive health care.
Given Mount Sinai South Nassau’s full range of clinical, ambulatory, and community services, it’s not surprising that the hospital is perennially ranked among the “Best Regional Hospitals” in the metropolitan area by U.S. News & World Report® with recognized expertise in 10 areas, plus recognition from the Infectious Diseases Society of America as a “Center of Excellence” in Antimicrobial Stewardship.
“Many of us live in the neighborhood,” acknowledges Dr. Glatt, himself a frequent community lecturer, “and we’ve all worked extremely hard to make Mount Sinai South Nassau a hospital where our own families and friends can get the finest-quality medical care around.”
Featured Faculty and Site Leadership
Aaron Glatt, MD, MACP
Chair of the Department of Medicine, Mount Sinai South Nassau
Ambulatory Care Works Overtime to Improve Patient Access to
its Services
Efforts to grow and improve the delivery of ambulatory care have led to an enormous increase in the volume of outpatient visits over the past few years. That has prompted a commensurate increase in the hiring of new physicians and their integration into Mount Sinai faculty practice offices, both at and beyond the eight hospitals of the Mount Sinai Health System.
As Mount Sinai Health System expands its ambulatory care footprint across New York City and beyond, it is working diligently to improve delivery of primary care and specialty services to patients in ways that address how, when, and where they need them.
Through video visits, for example, patients can speak directly to and coordinate their care among doctors in an extraordinary range of medical fields. Or they can make an outpatient appointment with a physician at a hospital-based office or standalone clinic or facility that’s close to their home.
“Ensuring that patients have timely access within seven days to just about any ambulatory service they need, from primary care to multispecialty, continues to be our top priority,” says Aida Vega, MD, Associate Professor of Medicine (General Internal Medicine) at the Icahn School of Medicine at Mount Sinai and Vice Chair for Ambulatory Care of the Department of Medicine “We’re also improving the patient experience in terms of how they get their care, which is helping us to reduce visits to emergency rooms along with hospital admissions.”
The success of these efforts is reflected in the enormous increase in the volume of outpatient visits over the past few years. That has prompted a commensurate increase in the hiring of new physicians and their integration into Mount Sinai faculty practice offices, both at and beyond the eight hospitals of the Mount Sinai Health System. The latter includes the newly renovated Mount Sinai-Union Square site, which houses 30 medical practices nearly a hospital in itself at a convenient downtown Manhattan location.
That co-location of services constitutes another important way ambulatory care is improving access for patients. At several sites, including Union Square, Mount Sinai is interweaving psychology and primary care offices to facilitate coordination between both specialties. Similarly, the new Mount Sinai-Behavioral Health Center in lower Manhattan includes primary care to complement its mental illness and substanceuse-disorder services.
“Around half, if not more, of the cases we see in primary care involve anxiety, depression, or other stress-related disorders,” says Dr. Vega. “So, we
Miranda Veeser, NP, and Aida Vega, MD, on their way to see a patient
see co-location as a great way to foster collaboration between psychologists and primary care doctors in terms of prescribing medications and behavioral treatments, such as short-term interventions with cognitive therapy, which psychologists can enact.”
Enhanced access to care also means new initiatives aimed at hypertension and diabetes control across entire populations of patients. On the hypertension side, ambulatory doctors are a crucial part of Mount Sinai’s aggressive drive to identify and manage patients with higher-thannormal blood pressure, treating them and bringing them back to the office for follow-up checks until they are within nationally accepted guidelines. They are also playing a prominent role in reducing hemoglobin A1c levels of diabetic patients to below 9 percent by collaborating with nutritionists, diabetes educators, and endocrinologists to reinforce best practices in patients for managing their conditions.
For Dr. Vega, the flipside of enhanced patient access to services such as these is improving workflow within the system itself, thereby enabling doctors to commit their full time and attention to what they were trained to do: be excellent doctors. Nationwide, physicians are overwhelmed with the daily paperwork from their jobs and, more recently, with responding to the onrush of queries from patients over electronic portals. The Health System has launched an effort to address this challenge through more robust support at the practice level.
“We’re strengthening our team-based model through a huge effort this year to add advanced practice providers, particularly nurse practitioners and physician assistants, and to make sure every staff member is working at the top of their license,” notes Dr. Vega. As part of this wideranging workflow redesign, she adds, nurses and medical assistants are helping to screen and review patient calls and prioritize those that need a more timely response. And they’re working to ensure that test results are returned more quickly to patients.
“We’ve made tremendous gains over the past year in terms of productivity of our physicians and clinical staff and their responsiveness to patients,” reports Dr. Vega. “But we also realize we’re only halfway to our goal, and that we need to keep pushing hard to streamline our workflow at the same time we’re improving patient access to care.”
Featured Faculty and Ambulatory Care Leadership
Aida Vega, MD
Associate Professor of Medicine (General Internal Medicine); System Vice Chair for Ambulatory Care, Department of Medicine
Residency and Fellowship Programs Put Trainees on the Cusp of Change
Mount Sinai's Department of Medicine has built one of the largest and most sought-after Internal Medicine residency programs in the country, with more than 400 trainees at three Manhattan-based hospitals, in addition to 30 fellowship programs across a wealth of specialties. It has added programs in advanced fields such as genomics and point-ofcare ultrasound (POCUS) while building skills and knowledge in disciplines, such as primary care, transgender medicine, and geriatrics, where physicians can have clinical as well as societal impact in the course of their careers.
Staying laser-focused on the future direction of medicine has enabled the Icahn School of Medicine at Mount Sinai to tailor its training to the evolving needs of Internal Medicine residents and fellows.
It has added programs in advanced fields such as genomics and point-of-care ultrasound (POCUS) while building skills and knowledge in disciplines, such as primary care, transgender medicine, and geriatrics, where physicians can have clinical as well as societal impact in the course of their careers. In the process, the Department of
programming we’re able to educate any medical student in the country by personalizing a plan geared to their clinical and academic needs and interests. That makes our agenda unique.”
POCUS is a fitting example. As ultrasonography has become an increasingly important diagnostic tool at the patient’s bedside, Mount Sinai has responded with a robust curriculum for trainees developed by a newly hired associate program director for POCUS. That initiative includes an expansion of elective courses residents can take
Medicine has built one of the largest and most sought-after Internal Medicine residency programs in the country, with more than 400 trainees at three Manhattan-based hospitals, in addition to 30 fellowship programs across a wealth of specialties.
“We’re constantly thinking about where medicine needs to be in 2030 and beyond, and what our residents will need to know when they become faculty,” says David C. Thomas, MD, MHPE, Professor of Medicine (General Internal Medicine) at Icahn Mount Sinai, Dean for Medical Education, and System Vice Chair for Education for the Department of Medicine. “Through innovative
to ensure both didactic and hands-on experience with the sophisticated machines during their clinical rotations. The program also acquired two hand-held ultrasound devices, giving them access to training opportunities in more ways than ever before.
Also launched in recent years were several primary care tracks that, in addition to providing broad-based clinical education, are helping to change the notion of what good doctoring looks like in communities.
“Our goal is to encourage more residents to pursue careers in primary care, which is always a challenge for medicine,” acknowledges
David C. Thomas, MD, MPHE, and Program Director Adrian Majid, MD, lead one of the most competitive internal medicine residency programs in the United States.
John Andrilli, MD, Associate Professor of Medicine (General Internal Medicine) at Icahn Mount Sinai and Director of the Internal Medicine Residency Program at Mount Sinai Morningside and Mount Sinai West. “Our residents not only spend more time in primary care offices than other residents, but actually go out into the community to spend a day or two at senior citizen centers or to work closely with other local partners to understand the type of care and services patients are receiving.”
According to Dr. Thomas, that type of outreach extends to residencies at The Mount Sinai Hospital as well as Mount Sinai Morningside and Mount Sinai West. “In addition to their medicine component, our programs have a strong emphasis on understanding a patient’s social determinants and sending trainees into the community to learn more,” he explains. With their feet on the ground, Mount Sinai residents have become actively involved in diabetes and hypertension screening and management programs, for example, as well as exploring the social barriers to health care that many community members face.
For students in search of a specialty that urgently needs more practitioners (such as primary care), geriatrics offers a four-year program that incorporates both residency and fellowship training.
Enhancing its appeal is the fact that Mount Sinai’s Brookdale Department of Geriatrics and Palliative Medicine is consistently ranked No. 1 in the country by U.S. News & World Report®. “We’re in our second year of recruiting residents who want to pursue careers in geriatrics,” says Dr. Andrilli, “and are extremely excited about the ways we’re growing this program.”
Transgender medicine is another discipline where residents and fellows can get highly specialized training at one of the nation’s leading sites, the Mount Sinai Center for Transgender Medicine and Surgery. Embedded in that curriculum is exposure to a wide range of disciplines that are integral to delivering care to transgender and nonbinary people.
“We added gender-affirming care to our ambulatory curriculum this past year and hired faculty to develop an educational program that integrates subspecialties such as endocrinology, urology, plastic surgery, behavioral health, and other supportive services,” says Sreekala Raghavan, MD, Associate Professor of Medicine (General Internal Medicine), and Medical Education, at Icahn Mount Sinai and Director of the Internal Medicine Residency Program at Mount Sinai Beth Israel
John Andrilli, MD, second from left, with the 2023-24 Mount Sinai Morningside and Mount Sinai West Chief Residents, Joseph Elias, MD; Jeeyune Bahk, MD; and Randy Leibowitz, DO
As a large academic institution, Mount Sinai is also able to offer its trainees vast research opportunities that combine scholarly projects in countless investigative fields with evidence-based medicine and the experience of publishing their work for a national audience. To guide their research and clinical education, residents benefit from a highly structured mentorship program tailored to their academic and clinical directions.
“Having a large faculty means we’re able to link them to mentors spanning traditional specialties such as cardiology and oncology, as well as to nontraditional fields such as addiction medicine and weight management,” observes Dr. Raghavan. Indeed, trainees could end up with five or six mentors, each with a different focus.
“Residents and fellows are able to avail themselves of so much within our health care system, including patients and pathologies that are among the most diverse in the country,” emphasizes Dr. Thomas, who helped found the East Harlem Health Outreach Partnership, a student-run, attending-directed free clinic for uninsured individuals. “As a result, we’ve seen amazing outcomes from our trainees who typically go on to rewarding roles as physicians serving patients and their communities.”
Helping to ensure the steady growth and success of The Mount Sinai Hospital’s Internal Medicine Residency Program is the recent appointment of its new Program Director, Adrian Majid, MD. His passion for teaching and commitment to the professional and personal development of his trainees over the years are seen as a perfect fit for Mount Sinai’s nationally recognized residency program.
* Starting in July 2024, the Mount Sinai Beth Israel internal medicine residency program will merge with that of Mount Sinai Morningside and Mount Sinai West becoming the largest program of its kind in the United States.
Featured Faculty and Residency Program Leadership
David C. Thomas, MD, MHPE
Professor of Medicine (General Internal Medicine); System Vice Chair for Education, Department of Medicine
Dean for Medical Education, Mount Sinai Health System
John Andrilli, MD
Associate Professor of Medicine (General Internal Medicine); Internal Medicine Residency Program Director, Mount Sinai Morningside and Mount Sinai West
Sreekala Raghavan, MD
Associate Professor of Medicine (General Internal Medicine), and Medical Education; Internal Medicine Residency Program Director, Mount Sinai Beth Israel
Adrian Majid, MD
Associate Professor of Medicine (Infectious Diseases); Internal Medicine Residency Program Director, The Mount Sinai Hospital
Paving the Pathway to Success for Junior Faculty Members
Mount Sinai’s Department of Medicine is working to ease the transition from fellow to faculty, through supportive programs and tailored pathways designed to give junior faculty members the traction, confidence, and resources they need to launch their professional careers.
The road from fellow to faculty is more challenging than ever for physician-scientists as they run the gantlet of applying for research funding, keeping up with ongoing training, and meeting the demands of the clinic, which compete with protected time in the research lab.
Mount Sinai’s Department of Medicine is working exceptionally hard to ease that burden through supportive programs and tailored pathways designed to give junior faculty members the traction, confidence, and resources they need to launch their professional careers.
“Our field is losing large numbers of physicianscientists at a time when we should be nurturing more of them,” says Benjamin K. Chen, MD, PhD, System Vice Chair for Research of the Department of Medicine, and Irene and Dr. Arthur M. Fishberg Professor of Medicine at the Icahn School of Medicine at Mount Sinai. “The Department of Medicine has invested heavily in developing and transitioning our junior faculty through mentoring, grant-writing, and other
creative ways to support them along the long road to becoming independent researchers.”
Among the most vital ways is the Junior Faculty Mentorship Program. Senior faculty mentors, most of whom are specially trained for these roles, serve as mentors and advisors. They help mentees put together a thoughtful Individual Development Plan (IDP), similar to what the National Institutes of Health (NIH) has incorporated into its degreegranting programs. “We try to tailor these IDPs to the more advanced research needs of junior faculty as they transition to their new role of independent investigator,” explains Dr. Chen.
To that end, the main goal of the program is to put junior faculty researchers on a track that makes them competitive for independent grant funding. Mount Sinai is paving the way through a range of constructive programs, including grant-writing workshops, which bring in outside experts to help junior faculty hone their grant-writing skills through both classroom and individual instruction. This training is especially geared to the NIH K series of
Francesca Cossarini, MD, and Benjamin Chen, MD, PhD
career development awards, which are typically awarded in the early stages of a scientist's career.
Reinforcing that effort is a unique Grants-Work-InProgress program, a biweekly series of seminars that allow grant applicants to air their ideas and get valuable feedback from junior faculty peers at the same level of training, as well as from their own mentors or, in many cases, team of mentors.
That training can again prove crucial once they have a career development (K-type) award in hand and are now making the “K to R” transition to independent researcher, vying for R01 grants. To further bolster the pipeline of new physicianscientists, the Department of Medicine is planning a new supportive program for medical residents through a program known as StARR (Stimulating Access to Research during Residency). Expected soon through this vehicle is funding for a National Heart, Lung, and Blood Institute grant that ensures protected research time during residency training.
The support network Dr. Chen and his team have put in place has yielded impressive results for all junior faculty. “We’ve enjoyed ongoing success by maintaining a robust pipeline of K awards, as well as a strong K-to-R transition rate,” he observes. “But we’re always trying to do better.”
Featured Faculty and Research Leadership
Benjamin K. Chen, MD, PhD
Irene and Dr. Arthur M. Fishberg Professor of Medicine; System Vice Chair for Research, Department of Medicine
Ensuring the Health of Our Faculty so They Can Focus on Healing Others
Burnout, as well as such issues as career development, work-life balance, promotions, and tenure, can affect not just the overall job satisfaction of faculty members at academic health centers, but their ability to care effectively for patients. At the Icahn School of Medicine at Mount Sinai’s Department of Medicine, the Office of Faculty Affairs is working to address these challenges.
All academic medical centers face a common challenge today: the grueling workloads and long hours spent in the lab, hospital, and clinic by faculty members can often lead to exhaustion and burnout.
In the Icahn School of Medicine at Mount Sinai’s Department of Medicine, the Office of Faculty Affairs is carefully attuned to drivers of burnout, as well as to such issues as career development, work-life balance, promotions, and tenure. These can affect not just the overall job satisfaction of faculty but their ability to care effectively for patients. Overlying these variables for Faculty Affairs are the imperatives of employee recruitment and retention, which the office is uniquely equipped to address for its approximately 2,000 faculty members.
“Much of my role is making the jobs of faculty easier so they’re excited about coming to work each day and making a difference in the lives of patients,” says Neomi Shah, MD, MPH, Professor of Medicine (Pulmonary, Critical Care and Sleep
Medicine) at Icahn Mount Sinai and System Vice Chair for Faculty Affairs in the Department of Medicine. “Retention, in particular, is an acrossthe-board problem in the field of health care now, and we’re working hard to solve it by improving the workplace culture for all of our faculty.”
Serving as the champions of this effort are the members of the Faculty Well-Being Committee, who have been named to represent their respective medical divisions, advocating for and expressing at the highest levels the needs, interests, and concerns of their colleagues.
“Well-Being Champions enable us to understand what the pressing issues are among our faculty with regard to workplace culture and efficiency, burnout, turnover, and much more,” explains Krishna Chokshi, MD, MS, Assistant Professor of Medicine (Hospital Medicine) at Icahn Mount Sinai and Faculty Well-being Director for the Department of Medicine.
Neomi Shah, MD, MPH, with Jenny J. Lin, MD, MPH, the Department of Medicine's Director of Mentoring
Dr. Chokshi is developing a significant expansion of the faculty well-being program, using data collected by each clinical department to drive new projects and strategies in such areas as enhancing work-life balance, improving faculty appreciation efforts, and increasing psychological safety among teams.
Mentoring is another critical touchpoint for the Office of Faculty Affairs. Already in place is a highly developed mentorship program that helps connect junior faculty to experienced clinical, educational, and/or research experts who can help them set career goals and support them at each step along the way.
“We put a lot of emphasis on helping junior faculty at the outset identify and then grow with the most appropriate mentors to show we’re as committed as they are to moving their careers forward,” says Jenny J. Lin, MD, MPH, Professor of Medicine (General Internal Medicine) at Icahn Mount Sinai and System Director for Mentoring in the Department of Medicine. To make an established program even stronger, Dr. Lin has been focused on building a formal mentor-training component through seminars that encourage mentors to thoughtfully assess and then hone the skills they’ll need to become more effective coaches and advocates for the faculty members under their wings.
Featured Faculty and Faculty Affairs Leadership
Neomi Shah, MD, MPH
Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine); System Vice Chair for Faculty Affairs, Department of Medicine
Krishna Chokshi, MD, MS
Assistant Professor of Medicine (Hospital Medicine)
Director for Faculty Wellbeing in the Department of Medicine
Jenny J. Lin, MD, MPH
Professor of Medicine (General Internal Medicine)
Director for Mentoring in the Department of Medicine
Translating Quality and Safety Into Outstanding Patient Outcomes
Mount Sinai's Department of Medicine has brought more than 100 post-pandemic projects to fruition that have achieved widespread improvements in the performance of services, systems, and processes that directly impact the quality of care provided to patients.
From chronic disease screening to mortality review to hypertension control, the Department of Medicine’s Office of Quality and Patient Safety at Mount Sinai Health System has been extraordinarily active, bringing more than 100 post-pandemic projects to fruition that have achieved widespread improvements in the performance of services, systems, and processes that directly impact the quality of care provided to patients.
“These projects were successfully managed by our 38 Quality Champions who work closely with faculty, fellows, and residents at our hospitals,” says Beth Raucher, MD, Professor of Medicine (Infectious Diseases) at the Icahn School of Medicine at Mount Sinai and System Vice Chair for Quality and Clinical Affairs. “In the case of screening, monitoring, and educating patients with chronic disease, for example, that commitment translated into outstanding results by building best practices and quality measures
into each program.” Dr. Raucher leads a team of quality and data specialists who support the projects at each of the hospitals.
Mortality review reflects the breadth and depth of these initiatives. Led by on-site Quality Champions, each hospital death triggers an intense review to determine whether all standards of care were met and where opportunities to improve systems of care may lie. At the center of this process are the Quality Improvement Peer Review Committees at each hospital, which meet monthly to review cases referred to them after an initial review by a faculty member in the Division of Hospital Medicine
“What makes our program unique is that residents, interns, nurses, and other hospital staff are brought into the review process in a collaborative, safe, and transparent learning environment,” observes Vinh-Tung Nguyen, MD, Co-Chair of the Quality Improvement Committee
From left: Vinh-Tung Nguyen, MD; Data Analyst Haley Waite; Jing Wang, MD, Co-Chair of the Quality Improvement Committee at The Mount Sinai Hospital; and Beth Raucher, MD, reviewing the quality priority metrics for the hospital's 10 West unit on the daily management board.
at The Mount Sinai Hospital. “We disseminate these lessons learned through improvement projects, didactics, or written policy changes based on our findings.”
The Office of Quality Improvement and Patient Safety also seeks to prevent future quality and performance missteps by daily monitoring of an internal website that reports safety concerns over the previous 24 hours events that range from the seemingly trivial (a patient’s broken TV) to the more concerning (a patient who falls, or is given wrong medication). “Oftentimes we’re on top of these events before the hospital is,” says Umar Jalloh, MPA, Manager of Performance Improvement and Research, and a member of Dr. Raucher’s team who conducts the surveillance and briefs site quality leaders in the early morning for potential follow-up.
In a more proactive vein, the department’s quality and safety teams work to improve chronic disease management through robust efforts to control hypertension, diabetes, and hepatitis at each Mount Sinai hospital.
In the case of hypertension, for example, Amy Rosenberg, MD, Associate Chair for Administrative Affairs, Department of Medicine at Mount Sinai Morningside and Mount Sinai West, observed that one of the quality projects focused on provider education by consistently reminding the professional staff about tools available to help them improve blood pressure management. These include remote home monitoring of patients with higher-than-normal blood pressure, as well as telehealth counseling to ensure they remain on their medications. Another tool is direct telephone outreach to uncontrolled hypertensive patients with the goal of bringing them back to the office for follow-up checks by either a provider, nurse, or clinical pharmacist. Mount Sinai Morningside and Mount Sinai West achieved tremendous success with their programs by bringing at least 70 percent of hypertensive patients under the goal of 140/90 in 2022. Other practice sites also reached comparable target compliance.
Decreasing hemoglobin A1C (HbA1c) levels of diabetic patients to less than 9 percent was a core goal of the quality team at Mount Sinai Beth Israel’s Division of General Internal Medicine. Certified Diabetes Educators were pivotal to this effort, instilling in patients best practices for managing their condition and preventing complications. Moreover, the diabetes care team employed continuous glucose monitoring to improve patient motivation and knowledge of how food affects blood sugar. Providers were also encouraged to schedule frequent appointments with patients to closely monitor their progress, while language interpreters were deployed to improve outreach and care to non-English speaking patients.
Identifying individuals with hepatitis B or C who are often unaware they have the disease was a priority for the quality team in the Division of Liver Diseases at The Mount Sinai Hospital. In a city where more than 91,000 people have chronic hepatitis C (HCV) infection, the Liver project team worked to increase the rate at which patients are screened and, consequently, treated for their infections. Part of this strategy involved alerting providers to new Centers for Disease Control and Prevention guidelines encouraging HCV testing for all adults over 18 at least once in their lifetime. Furthermore, providers were sent a list of screening-eligible patients with upcoming office appointments. HCV screening was also promoted to patients via social media and on monitors throughout the hospital campus. This project is now being rolled out to the other hospitals in the Health System.
The Division of Pulmonary, Critical Care and Sleep Medicine at The Mount Sinai Hospital helped decrease the amount of time patients need to wait for sleep testing by streamlining the scheduling workflow and optimizing Epic-referral work queues. Sleep studies are in high demand because they help to diagnose sleep disorders and can ultimately improve patients’ quality of life. Jing Wang, MD, Co-Chair of the Quality Improvement Committee at The Mount Sinai
Hospital, explained, “Sleep studies shed light on the underlying causes of sleep disorders to help us identify tailored interventions that lead to more restful and rejuvenating sleep for our patients. Giving patients the tools to reclaim their nights leads to improved overall well-being and a higher quality of life.”
The Department has also achieved major improvements around osteoporosis evaluation and education of patients admitted with hip fractures. At Mount Sinai Morningside and Mount Sinai West, the quality team in the Division of Endocrinology, Diabetes and Bone Disease informed patients of fall risk and fall prevention, and patients were given nutritional advice about calcium and vitamin D upon discharge. At the same time, providers were encouraged to add fragility fracture and osteoporosis as diagnoses in their discharge paperwork, and to refer the patient to endocrinology for further evaluation and treatment.
Particularly impressive in terms of quality care improvement was what the Peter Krueger Clinic part of the Institute for Advanced Medicine, which
specializes in infectious disease treatment and management achieved in viral load suppression for patients living with HIV. The clinic recorded a 67 percent reduction in the number of patients with unsuppressed viral loads through the third quarter of 2022, compared to all of 2021. Responsible for this dramatic shift were such interventions as active patient monitoring and outreach to patients to schedule appointments and to confirm they are taking their antiviral medications.
“The success of this program was shared by Peter Krueger with other sites within the Institute for Advanced Medicine and resulted in amazing across-the-board reductions in viral load,” says Patricia Dharapak, MD, Associate Professor of Medicine (General Internal Medicine, and Hospital Medicine), and Chief of Quality for the Department of Medicine at Mount Sinai Beth Israel. “It’s another great example of how our team of Quality Champions is significantly improving the wellbeing of patients across Mount Sinai through interventions that bring them up to the stringent standards our organization has set.”
Featured Faculty,
and Quality and Clinical Affairs Leadership
Beth Raucher, MD
Professor of Medicine (Infectious Diseases); Vice Chair for Quality and Clinical Affairs, Department of Medicine
Vinh-Tung Nguyen, MD
Associate Professor of Medicine (Hospital Medicine)
Amy Rosenberg, MD
Professor of Medicine (Infectious Diseases)
Jing Wang, MD
Associate Professor of Medicine (Pulmonary, Critical Care and Sleep Medicine)
Patricia Dharapak, MD
Associate Professor of Medicine (General Internal Medicine, and Hospital Medicine)
Mount Sinai's Specialized Skills
Are Making a Difference in Guyana
A 20-member contingent from Mount Sinai Health System is working to improve the public health system in Guyana, one of South America's poorest countries.
Zijian Chen, MD, is an extremely busy endocrinologist at Mount Sinai Beth Israel. He not only sees patients and serves as Site Director for Endocrinology and Rheumatology, but also heads up the Mount Sinai Health System’s Center for Post-COVID Care.
Why, then, is this much-in-demand professional 2,600 miles away in the remote nation of Guyana for several weeks each year?
In one way, it’s no different from what he does in New York advancing health care to promote a better quality of life for patients. Except in Guyana, the focus is on one of South America’s poorest populations within a resource-strapped environment. Dr. Chen is part of a 20-member contingent from Mount Sinai International, which seeks to improve local medical care around the globe, and Mount Sinai’s Arnhold Institute for Global Health
“Our entire team is committed to elevating Guyana’s health care system, whether it’s by improving its supply chain for acquiring
medications and equipment, or by helping its doctors take better care of patients through enhanced education and updated medical practice guidelines,” says Dr. Chen. “I’m a diabetes specialist, so my role as part of an eight-member workstream is to rewrite the guidelines for diabetes management and to train doctors so they can become trainers for other providers and health care workers on the front lines.”
That mission has brought Dr. Chen and his colleagues to Guyana, a nation of 741,800 in the northeastern corner of South America, three times over the past year for one-week visits, with at least two more planned for the remainder of this year. While on the ground, they collaborate with other physicians and administrators at Georgetown Public Hospital in the nation’s capital, while also traveling to local clinics and what are known as “health posts” further inland in the hinterlands or the rainforest.
Already, these journeys are having an impact, especially in the field of diabetes.
Mount Sinai Health System is helping to bolster the public health system in the South American nation of Guyana.
“We’ve completed the guidelines, which will change the way diabetes care is delivered in the country, now and down the road,” reports Dr. Chen. “And the training we’ve started will build knowledge and expertise within the medical community, allowing doctors to focus on early detection and treatment of diabetes, instead of end-stage complications involving dialysis and amputations. That’s an advantage the people of Guyana have never had before, and the thought of making that kind of difference in their lives is the most rewarding thing for all of us on the Mount Sinai team.”
Featured Faculty
Zijian Chen, MD
Assistant
Professor
of Medicine (Endocrinology, Diabetes, and Bone Disease);
Medical
Director, Center for Post-COVID Care
Click here to support the Mount Sinai Department of Medicine's clinical, education, and research goals.