

Beth Raucher, MD, SM
System Vice Chair, Quality & Clinical Affairs Department of Medicine, Mount Sinai Health System
Vinh-Tung Nguyen, MD Chair, Quality Improvement Committee Department of Medicine, The Mount Sinai Hospital
Jing Wang, MD Chair, Quality Improvement Committee Department of Medicine, The Mount Sinai Hospital
Patricia Dharapak, MD Chief Quality Officer Department of Medicine, Mount Sinai Beth Israel and Mount Sinai-Union Square
Amy Rosenberg, MD
Associate Chair, Administrative Affairs Department of Medicine, Mount Sinai Morningside and Mount Sinai West
Julie Pearson, MPH, RN Director, Performance Improvement & Analytics Department of Medicine, Mount Sinai Health System
Umar Jalloh, MPA, CPHQ, CPPS Manager, Performance Improvement & Research Department of Medicine, Mount Sinai Health System
Benjamin Dempsey, MHA Quality Analyst Department of Medicine, Mount Sinai Health System
Orie Wittek, MD Quality and Regulatory Affairs Specialist, Department of Medicine Liaison The Mount Sinai Hospital
Cynara Maceda, MD, CCRP Project Manager Department of Medicine, Icahn School of Medicine at Mount Sinai
Mount Sinai Beth Israel and Mount Sinai-Union Square Division Quality Champions
Clinical Immunology: Songhui Ma, MD
Endocrinology: Daniel Donovan, MD; Olga Kozachenko, NP-C
Gastroenterology: Custon Tafadzwa Nyabanga, MD
General Internal Medicine: Desiree Chow, MD
Hospital Medicine: Dahlia Rizk, DO, MPH
Quality Improvement Peer Review Committee: Patricia Dharapak, MD
Infectious Diseases: Tessa Gomez, MD, Sarah Humphreys, MD
Nephrology: Elliot Charen, MD
Pulmonary, Critical Care and Sleep Medicine: David Steiger, MD; Boram Kim, DO;*
Boris Gilyadov, MD*
Rheumatology: Latoya Freeman-Beman, MD
The Mount Sinai Hospital Division Quality Champions
Clinical Immunology: Eugene Choo, MD
Endocrinology: David Lam, MD; Nirali Shah, MD
Gastroenterology: Christopher Cao, MD; David Greenwald, MD
General Internal Medicine: Nikita Barai, MD; Kelsey Bryant, MD
Hospital Medicine: Anne Linker, MD
Quality Improvement Peer Review Committee: Aveena Kochar, MD
Infectious Diseases: Rachel Chasan, MD
Liver Diseases: Douglas Dieterich, MD; Anna Mageras, MPH
Nephrology: Joji Tokita, MD; Niraj Kothari, MD
Pulmonary, Critical Care and Sleep Medicine: Jing Wang, MD; Timothy Harkin, MD
Rheumatology: Wendy Weiwei Chi, MD
Mount Sinai Morningside and Mount Sinai West Division Quality Champions
Endocrinology: Ilana Ramer Bass, MD
Gastroenterology: Tina Park, MD
General Internal Medicine: Heather Viola, DO; Christopher Gold, DO
Hospital Medicine (MSM): Brian Markoff, MD; Faye Reiff-Pasarew, MD
Quality Improvement Peer Review Committee: Lindsey Fox, MD
Hospital Medicine (MSW): Shantheri Shenoy, MD
Quality Improvement Peer Review Committee: Irina Zaretsky, MD
Infectious Diseases: Rahul Gaikwad, MD
Nephrology: Ruchika Batwara, MD; Claire Schretlen, MD*
Pulmonary, Critical Care and Sleep Medicine (MSW): David Steiger, MD
Pulmonary and Critical Care (MSM): Avinash Singh, MD
Rheumatology: Kristaq Koci, MD; Saloni Mitchell, MD*
* New Department of Medicine Quality Champions beginning in 2025.
Dear Colleagues,
I’m pleased to share highlights from the Department of Medicine’s (DOM) quality and patient safety initiatives. This past year was marked by meaningful progress, collaboration across our department consistent with One Mount Sinai, and a shared commitment to delivering highvalue care.
Thanks to your continued dedication. We saw measurable improvement and growing engagement throughout the Department:
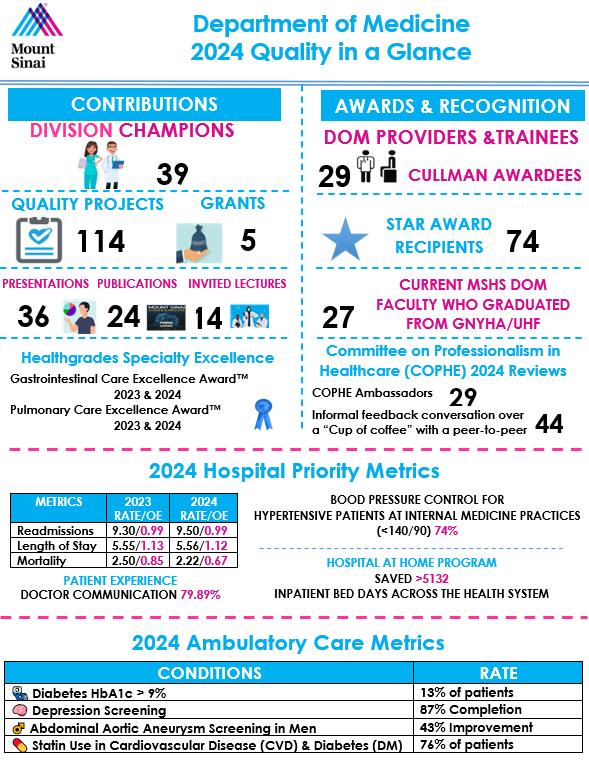
• Project Momentum: Under the guidance of our 39 Division Quality Champions and other leaders, we launched 114 quality-related projects in 2024, a reflection of our continued commitment to improving care delivery and patient outcomes. Many of these impactful initiatives are highlighted in the pages that follow.
• Recognition and Achievement: Our teams received 5 quality-related grants, delivered 14 invited lectures, and published 24 peer-reviewed articles. Seventy-four of our faculty and trainees were honored with STAR Awards, and 29 received the prestigious Cullman Award.
• Professionalism and Peer Support: Through the Committee on Professionalism in Healthcare (COPHE), DOM faculty and senior residents served as ambassadors, fostering a respectful and collegial environment. They facilitated 44 peer-to-peer “Cup of Coffee” conversations as part of our ongoing commitment to professional growth and support.
• Leadership Development: Many of our faculty have trained through the Greater New York Hospital Association and the United Hospital Fund (GNYHA/UHF) Clinical Quality Fellowship, with 27 active fellows currently on faculty. Their contributions as role models, mentors, and advisors continue to strengthen our department’s quality mission. Many have been appointed to leadership roles in the hospitals across the Mount Sinai Health System (MSHS)
We also saw important gains in clinical performance and patient outcomes:
• Mortality in the Division of Hospital Medicine dropped from 2.50 to 2.22, with the Observedto-Expected ratio improving from 0.85 to 0.67.
• Blood pressure control (<140/90) at internal medicine practices reached 74%.
• Depression screening rose to 87%.
• Doctor communication a key patient experience measure reached 79.9%.
• The Hospital at Home program saved more than 5,132 inpatient bed days across the Health System.
I want to thank our faculty and trainees for their contributions to this important work. Special thanks to our Quality Champions, the site-based quality leads, and to my outstanding team of quality and data experts who support our champions, committees, and the spread of best practices throughout MSHS.
I look forward to continuing this work together.
Respectfully,
Beth Raucher, MD, SM System Vice Chair, Quality & Clinical Affairs Professor Department of Medicine Mount Sinai Health System
The DOM congratulates the outstanding faculty, advanced practice providers, and residents across Mount Sinai Brooklyn, Mount Sinai Beth Israel, Mount Sinai-Union Square, The Mount Sinai Hospital, Mount Sinai Morningside and Mount Sinai West, and Mount Sinai Queens whose work was recognized by peers in 2024
Eric Ballecer (Gastroenterology)
Stacey V Cedeno* (Gastroenterology)
Nina S Fallick (Primary Care)
Alice C Furman (Primary Care)
Carolyn F Iocolano* (Primary Care)
Tonia K Kim* (Nephrology)
Aimee L Lucas (Gastroenterology)
Patrick R Parsell (Internal Medicine)
Maria Shtessel (Allergy & Immunology)
Aida C Vega (Primary Care)
Emily Carroll (Rheumatology) Kelly Cassano* (Primary Care)
Charlotte Cunningham-Rundles (Allergy & Immunology)
Kenneth M Fifer* (Internal Medicine)
Emily J Gallagher* (Endocrine, Diabetes & Bone Disease)
Jennifer A Kent* (Primary Care)
Alice C Levine* (Endocrine, Diabetes & Bone Disease)
Janette R Marcelo* (Primary Care)
Elliott C Rosch* (Primary Care)
Mark A Singer* (Primary Care)
Heather S Viola* (Primary Care)
Larry Di Fabrizio (Pulmonary, Critical Care & Sleep Medicine)
Thomas C Fiorentino* (Hospital Medicine/Primary Care)
Robert P Hirten (Gastroenterology)
Boram Kim (Pulmonary, Critical Care & Sleep Medicine)
Carol J Levy* (Endocrine, Diabetes & Bone Disease)
Jeffrey Mechanick (Endocrine, Diabetes & Bone Disease)
George M Schmitz* (Primary Care)
Kevin L Tack* (Gastroenterology)
* These providers have been recipients of the Cullman Family Award more than once
Adair, Regina Pereira, Ivonne Adih, Gifty Lott, Briana Rahman, Nimra Aguila, Annette Luciano, Marilou Reid, Damian Arias, Yesenia Marquez, Jose Reid, Evadne Baek, Seunghyup Mendez, Edyth
Renaud, Lisa Barnes, Tia Molina, Melba Reyes, Wascar Bido, Yael Monaghan, Michael Rodriguez, Jean Bonlarron, Leanna Murray, Lucinda Sanchez, Norelia Cadet, Sherry-Ann Nguyen, Vinh-tung
Sapeg, Eime Charles, Rodney Nieves, Maria Serrone, Elizabeth Eastwood, Emily Nurnberger, Alissa Solinsky, Lauren Eberhardt, Stacey Olaya, Johanna Stidham, Katherine Fyffe, Kaila Olivet, Dina Suarez, Vanessa Garcia, Jayleen Omeally-Soto, Shanique Tillett, Naima Hernandez, Xequiel Ortiz, Melissa Torres, Rosa Hernandez, Yaritza Palmieri, Joshua Turcios, Jennifer Hosang, Clive Pannell, Tashana Vargas, Ivan Im, Hyun Gyeong Parrilla, Wismelda Walker, Mary Ann Jimenez, Argendy Patel, Bindu Weinreb, Yocheved Kapadia, Sapina Pena, Evelyn Xu, Ruimin Laloo, Veena Yuson, Vida
Division Quality Champion: Songhui Ma, MD

In 2024, the Division of Clinical Immunology at Mount Sinai Beth Israel continued its quality improvement projects on penicillin delabeling.
Penicillin allergy is reported in up to 25 percent of the population. However, greater than 95 percent of patients with a history of penicillin allergy can tolerate it This discrepancy is due to the waning of the allergy over time and initial misdiagnosis. A penicillin allergy label carries multiple personal and public health implications, including broad-spectrum antibiotic use with potentially decreased effectiveness and increased adverse effects, higher rates of antibiotic resistance, and increased morbidity and mortality. For these reasons, a proactive effort to delabel patients (when appropriate) is a core focus of the Division.
Two quality improvement projects were developed to address this focus. The first project aims to risk stratify all patients seen in the allergy outpatient practice who are allergic to penicillin. The second project seeks to evaluate appropriate patients by penicillin skin testing and challenge, and to delabel when possible.
In 2023, a procedure room staffed by nursing and supervised by the allergy physician was created. A team of nurses was trained in penicillin testing and challenge as well as recognizing and managing anaphylaxis. To minimize scheduling errors, procedure visits were built into Epic, office administrative staff performed appointment confirmations, and written pre-visit instructions were provided to patients.
Overall, 76 percent of patients labeled penicillin allergic who presented to the clinic were risk stratified by history and 37 percent were delabeled. Analysis of gender, race, and ethnicity suggested that men were more likely to complete the evaluation than women, Hispanics more likely than non-Hispanics, and Blacks less likely than Whites.
Building on this success, a dedicated nurse practitioner for allergy testing joined the team in early 2024. Penicillin allergy information posters were displayed and tri-fold brochures placed in the exam rooms to increase patient awareness. In accordance with evolving best practice guidelines, the use of direct challenges in low-risk patients to streamline evaluation was introduced in September. Results for the first three quarters of 2024 were comparable to 2023. Race, ethnicity, and gender differences will continue to be monitored in 2025
Project team members and resident physicians Erika Tsutsui, MD, and Christian Gomez, MD, presented the below results at the Mount Sinai Department of Medicine Resident Research Day in May 2024.
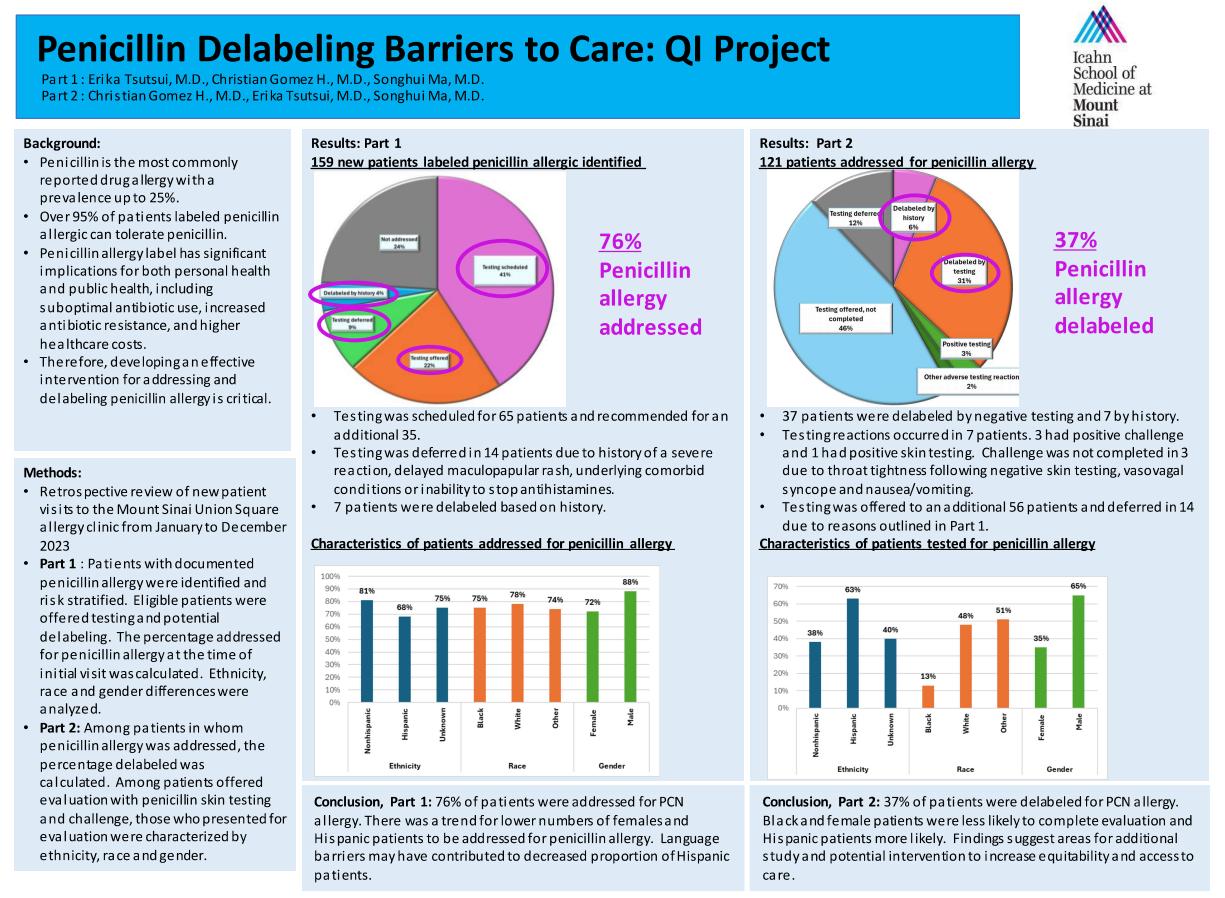
The penicillin allergy label was addressed in 79 percent of patients seen in the Allergy Clinic in 2024. Of these, 35 percent were evaluated with penicillin testing and challenge and 34 percent were delabeled (see graph below)
The graphs below show that analysis of gender, race, and ethnicity suggested that men were more likely to complete the evaluation than women, Hispanics more likely than non-Hispanics, and Blacks less likely than Whites. There were no significant differences regarding when the penicillin allergy was addressed.
PCN testing/challenge completed 2023-2024
PCN allergy addressed 2023-2024
Next steps for 2025 include collaborative projects with the primary care practices at 10 Union Square East and 281 First Avenue, led by General Internal Medicine QI Champion Desiree
Chow, MD, and resident physician Sneha Bupathi, DO, respectively. Patients labeled with a penicillin allergy and scheduled for a visit with their primary care provider will be identified prior to the visit. At the Union Square clinic, referrals to the Division for penicillin allergy evaluation will be pended to their visit note. Patients of the 281 First Avenue resident clinic will be sent an Epic bulk message inviting them to discuss their penicillin allergy with the provider. These outreach initiatives should continue to increase awareness and support further delabeling.
Division Quality Champion:
Eugene Choo, MD

In 2024, the Division of Clinical Immunology at The Mount Sinai Hospital continued its QI project to increase both patient and physician awareness regarding drug allergy and, in particular, penicillin allergy delabeling. Furthermore, the Division sought to improve institutional guidelines regarding alternative antibiotic choice for penicillin-allergic patients when possible, based on the updated National Drug Allergy practice parameters that were released in 2022.
To address physician education, the Division conducted several lectures regarding drug and penicillin allergies. This was preliminarily presented to The Mount Sinai Hospital QI committee, followed by a discussion at the adult Allergy/Immunology faculty meeting to promote a more universal approach to penicillin allergy delabeling. A grand rounds lecture was delivered, covering updates to the beta-lactam allergy guidelines with a focus on penicillin delabeling best practices. Additionally, a comprehensive drug allergy lecture was incorporated into the MSH infectious disease fellows’ didactics, featuring current guidelines and a focus on penicillin allergy and delabeling practices.
A pre/post-questionnaire was given to attendings and fellows in attendance:
How Comfortable Are You Risk-Stratifying the Likelihood of Penicillin Allergy Based on History?
Likely As Compared to Before, How Likely Are You to Utilize PENFAST Scoring to RiskStratify Penicillin Reaction Hx in Your Patients?
How Often Do You Refer Patients to Allergy Clinic Who Report Penicillin Allergy?
As Compared to Before, How Likely Are You to Refer Patients to Allergy Clinic for Penicillin Allergy Eval and/or Delabeling?
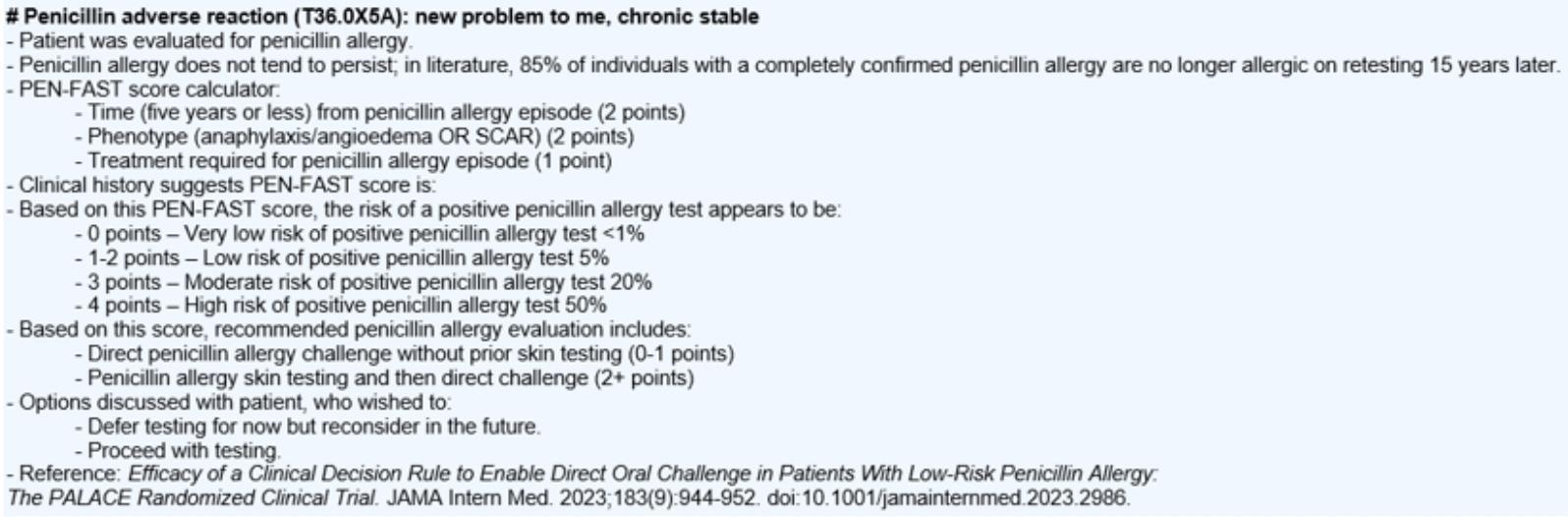
A related initiative sought to streamline clinical practice by creating an Epic dot phrase for use by the entire Clinical Immunology Division to standardize documentation regarding penicillin allergy and delabeling (shown below):
To promote patient awareness, the Division is planning to incorporate posters (shown below) in both allergy and non-allergy clinics in the coming months. These posters seek to alert patients that penicillin allergy is a label that can and should be evaluated by an allergy specialist and encourages patients to be proactive about pursuing this.
The Division worked with members of the infectious disease team to rewrite the clinical guidelines at Mount Sinai for antibiotic prophylaxis in penicillin-allergic patients undergoing gynecologic or liver transplant surgery. The new liver transplant guidelines have already been presented, accepted, and implemented. The gynecologic surgery guidelines are also nearing acceptance. After this, the Division intends to tackle the same type of surgical prophylaxis guidelines for all other pertinent procedures done at Mount Sinai.
The 2022 drug allergy practice parameters introduced notable updates from the 2010 guidelines, particularly regarding beta-lactam allergy. The revised guidelines placed less emphasis on skin testing and favored drug challenges in many cases It highlighted riskstratification of reaction based on time since the event (more than five years as lower risk) and reaction severity (non-anaphylactic reactions considered lower risk).
As a pertinent example, for cephalosporin administration to a penicillin allergic patient, the 2010 parameters specified three options:
1. Skin testing for the cephalosporin in question
2. Direct challenge with cephalosporin “only in absence of severe and/or recent penicillin allergy history ”
3. Penicillin skin testing, followed by routine cephalosporin administration if negative.
The 2022 update simplifies this to two options:
1. If the penicillin reaction was anaphylaxis, a non-cross-reactive cephalosporin may be administered
2. If the penicillin reaction was non-anaphylactic, any cephalosporin may routinely be given.
As such, the Division assisted the infectious disease team in integrating these updated guidelines into the creation of institutional protocols for perioperative antibiotic administration in penicillin-allergic patients.
Division Quality Champions:
Daniel Donovan, MD
Olga Kozachenko, NP-C


In 2024, the Division of Endocrinology at Mount Sinai Beth Israel began focusing on three new quality improvement goals.
The first quality initiative was to improve the number of patients with diabetes receiving statin therapy. The American Diabetes Association (ADA) recommends statin therapy for most patients with diabetes based upon their age and cardiovascular risk factors with the goal to reduce atherosclerotic cardiovascular disease (ASCVD) risk. As the baseline rate was determined to be 57 percent in 2023, the Division’s initial goal was 80 percent.
To drive improvement, a best practice alert (BPA) was implemented in Epic, prompting providers to initiate moderate- or high-intensity statin therapy in patients with diabetes aged 50 to 70 who were not already on treatment. During clinic visits, these patients were also counseled on the importance of statins, even with “normal” cholesterol levels, and common concerns about statin hesitancy were addressed. Clinicians received updated guidelines that aligned with ADA and AHA/ACC recommendations, including statin intensity criteria. As a result, the average rate of statin therapy reached 86 percent for Q2 and Q3 2024 although a slight drop was observed in October and November 2024.
Stratifying the data by race, the Division observed differences in the rates of statin therapy, with Unknown race and American Indian and Alaskan having the lowest average rates of statin therapy, followed by Blacks and then Asians. The division will continue to monitor variances by race, ethnicity, language, insurance status, and clinic location. They will also intervene with tailored outreach or decision-making tools for underrepresented groups
Percentage of Patients on Statin Therapy by Race
In 2024, the Division also focused on improving the number of patients with diabetes receiving ACEI/ARB therapy for hypertension. In accordance with ADA guidelines, antihypertensive therapy should include drug classes demonstrated to reduce cardiovascular events in people with diabetes. ACE inhibitors (ACEI) or angiotensin receptor blockers (ARBs) are recommended first-line therapy for hypertension in people with diabetes and coronary artery disease.
From an initial baseline of 70 percent in 2023, the Division aimed to increase the proportion of its patients with hypertension and diabetes receiving
to at least 83 percent
Despite several interventions, including Clinical Decision Support (CDS), provider education,
flagging patients with: diabetes and BP >140/90, and/or micro/macroalbuminuria, patient education on the benefits of ACEI/ARBs for kidney and heart protection, and managing medication side effects (e.g., cough with ACE inhibitors), the rate declined to 65 percent by November 2024.
In 2025, the Division will continue its efforts to address this gap by implementing comprehensive risk factor modification strategies to reduce residual cardiovascular risks. These interventions will focus on optimizing glycemic control, blood pressure management, and lifestyle modifications such as weight loss and smoking cessation.
With additional stratification by race, the division again observed some differences, notably the lower rate of ACEI/ARB use in Blacks. Like the statin initiative, additional review of the data capture and further investigation is planned to confirm the observations and identify potential driving factors. The Division will also intensify its efforts to improve the overall rate of ACEI/ARB use as clinically relevant in their patients with diabetes and hypertension.
Finally, the Division continued its goal to improve the number of patients with diabetes who receive a urine microalbumin/creatinine examination. In accordance with ADA guidelines, urinary albumin (e.g., spot urinary albumin-to-creatinine ratio [UACR]) and estimated glomerular filtration rate [eGFR] should be assessed at least annually in patients with type 1 diabetes with duration of ≥5 years and in all those with type 2 diabetes regardless of treatment.
Starting with a baseline rate of 83 percent in 2023, the Division aimed to achieve an improvement to 90 percent compliance with this metric. To achieve this, several interventions were implemented, including the use of a best practice advisory (BPA) for diabetic patients without a UACR test in the past year. Reminders were sent via patient portal and phone calls, and medical assistants and nurses were empowered to order the UACR test during rooming and to include it in standing orders. As a result, the Division observed an improvement in rates exceeding the goal in January and May 2024, with an overall average improvement to 88 percent in the first two quarters of 2024. The Division will continue to monitor compliance with this metric and reinforce adherence in 2025.
David Lam, MD
Nirali Shah, MD


In 2024, the Division launched a new quality improvement initiative aimed at increasing the adoption of diabetes technology among patients and continued its initiative to improve the rate of back-up insulin prescriptions for insulin pump users These initiatives were led by Dr. Grenye O’Malley and our team, including Suma Gondi, MD, Camilla Levister, NP, Carol Levy, MD, Madeleine Rouviere, RD, CDN, CDCES, and Selassie Ogyaadu, MD, MPH.
Diabetes technology refers to hardware, devices, and software designed to aid individuals with diabetes in managing their condition. According to the 2024 American Diabetes Association Standards of Care, diabetes devices should be offered to all individuals with diabetes (Grade A recommendation). Continuous glucose monitors (CGMs) are recommended for adults on multiple daily insulin injections (MDI) or insulin pump therapy (Grade A) due to their proven efficacy in reducing HbA1c levels in patients with type 1 diabetes (T1D) on insulin pumps and type 2 diabetes patients on basal insulin. Automated insulin delivery (AID) systems should also be offered to individuals with T1D (Grade A) and those with type 2 diabetes on MDI (Grade A).
Traditional diabetes care often involves the use of blood glucose meters, which require patients to prick their fingers to measure blood glucose levels. In contrast, CGMs provide near real-time glucose readings based on interstitial glucose levels, enhancing convenience and accuracy. Insulin delivery methods include MDI regimens and insulin pump therapy, the latter utilizing preprogrammed hourly insulin delivery rates and bolus settings for meals or hyperglycemia corrections. Innovations in insulin delivery also include smart pens, which record injections and
connect to apps for dosage recommendations, and AID systems, which adjust insulin delivery automatically based on CGM readings.
Despite these professional society recommendations and potential benefits of diabetes technology, there persists variable coverage and patient out-of-pocket costs across health insurances. To assess current adoption rates and potential impact of health insurance type, the Division compared data from Endocrinology practices at Mount Sinai-Union Square (MSUS) and The Mount Sinai Hospital (MSH). At the MSUS Endocrine practice, both commercial and Medicare/Medicaid patients are seen. At MSH, commercial and Medicare patients are treated at the 5 E 98th Street practice, while Medicaid patients are seen at the hospital-based practice at 17 E 102nd Street.
The data revealed the following usage rates of diabetes technology among patients with T1D:
Further analysis by insurance type and device usage highlighted disparities:
The most significant discrepancies were observed within the Medicaid population, particularly in CGM and pump usage. Key barriers contributing to these disparities were identified at three levels: patient, provider, and system/environment.
• Provider Level: Clinician inertia and lack of familiarity with technology and ordering process, time limitations during visit, lack of continuity of care
• Patient Level: Insufficient training on device use, lack of continuity of care/lost to follow-up, changes in insurance coverage.
• System/Environmental Level: Absence of standardized training programs, insurance restrictions and prior authorization process, limited support from device manufacturers, inefficient communication between team members and patients.
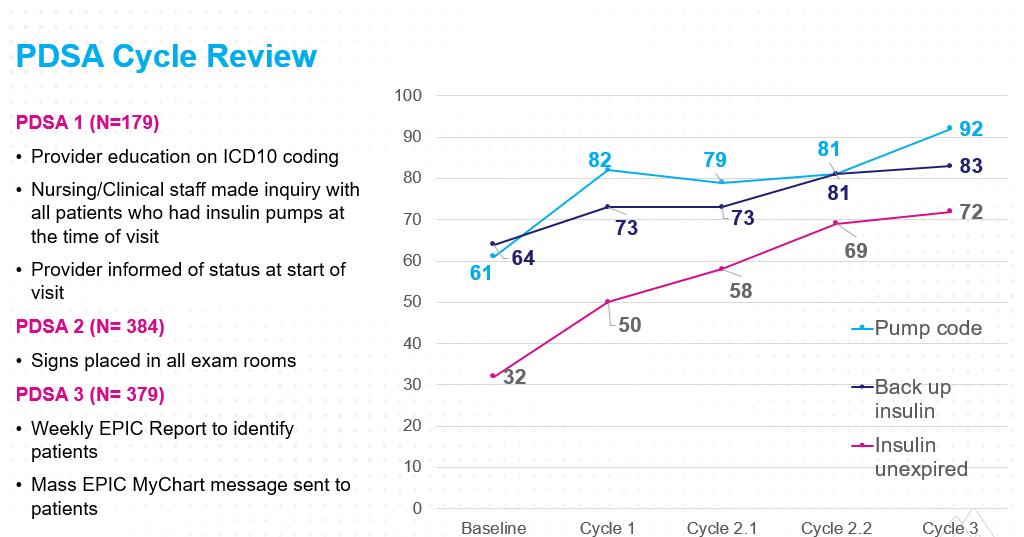
The Division has completed three PDSA cycles targeting these barriers:
PDSA Cycle 1: Provider Interventions
• Introduced an Epic dot phrase with prescribing instructions.
• Created a shared resource document with durable medical equipment (DME) and representative contact information.
• Conducted a noon conference on diabetes technology.
– Evaluated using a pre- and post-survey among fellows demonstrated improved comfort with prescribing CGMs and increased pump prescriptions, though smart pen prescribing patterns remained unchanged.
PDSA Cycle 2: Certified Diabetes Care and Education Specialists (CDCES) Interventions
• Increased referrals to CDCES for structured interventions.
• At MSH, patient appointments were scheduled, with follow-up pending.
• At MSUS, 15 T1D patients were evaluated; of these, five were already using CGM and pumps. Five additional patients were referred to the CDCES: three for pump initiation, one for CGM addition, and one for CGM initiation. Two of the three pump referrals resulted in successful starts.
PDSA Cycle 3: Patient Interventions
• Distributed technology handouts in clinics for patients and preceptors.
• Sent MyChart messages to T1D patients without pumps before their appointments, providing user-friendly information.
– Sent October 10, 2024: 25 patients at MSBI, 16 at MSH.
– Sent November 7, 2024: 25 patients at MSBI, 16 at MSH.
• Conducted a follow-up fellows survey on October 18, 2024, which indicated no patients had inquired about the intervention.
• A re-survey was conducted in January 2025. The results showed that over four weeks, 80 MyChart messages were sent to patients, but none mentioned these messages during their visits. The fellows reported that most patients instead referred to the technology-friendly handouts provided during the clinic visits. Therefore, the MyChart messages will no longer be sent to patients but will continue to provide handouts during their office visits.
In 2024, the Division also prioritized ensuring that T1D patients using insulin pumps had active back-up prescriptions for long-acting insulin. Continuous insulin delivery is critical for maintaining glucose levels and preventing diabetic ketoacidosis (DKA), a life-threatening condition. However, in the event of pump malfunction, the absence of back-up insulin can increase patient anxiety and lead to emergency provider consultations.
Barriers identified included:
• Patient-Level: Lack of awareness regarding back-up insulin and frequent changes in insurance formularies.
• Provider-Level: Forgetting to address back-up insulin needs and lacking tools to identify atrisk patients.
• System-Level: Difficulty identifying insulin pump users at the practice level due to documentation challenges in the electronic health record (EHR).
Quality Improvement Interventions and PDSA Cycles
PDSA Cycle 1:
• Integrated back-up insulin assessment into medical assistant (MA) pre-visit planning.
• Added specific ICD-10 codes for pump users to problem lists.
• MAs alerted providers about patients lacking back-up insulin.
PDSA Cycle 2:
• Posted signs in exam rooms prompting discussions about back-up insulin to reduce reliance on MAs.
PDSA Cycle 3:
• Identified patients with ICD-10 codes via Epic reporting.
• Sent MyChart messages reminding patients to check their back-up insulin supply before appointments.
These interventions increased back-up insulin prescriptions from a baseline of 32 percent to 72 percent by the end of the third cycle.
Division Quality Champion:
Ilana Ramer Bass, MD

The Division of Endocrinology at Mount Sinai Morningside and Mount Sinai West continued the ongoing quality improvement project to improve glycemic control using a supplemental virtual diabetes self-management and support group. The target population for the support group is English-speaking patients with type 2 diabetes mellitus (T2DM), with no cognitive impairment. Patients must also have access to MyChart and be agreeable to a group setting. The benefits of using telehealth to conduct the support group include the elimination of transport barriers and lower cost, which ultimately improve the no-show rate. The aim of this project was to utilize diabetes group education and support classes to improve HbA1c by 0.5 percent and to promote healthful lifestyle changes that result in at least one measurable behavior change (e.g., increase physical activity, eat balanced diet).
The diabetes self-management group meets bi-monthly, and prior to the class, the patient’s HbA1c and behavior goals are reviewed. During the group session, the patient creates at least one SMART (Specific, Measurable, Achievable, Relevant, and Time-bound) goal. At the next session, the patient reviews their SMART goal and discusses whether the goal was met, and as a group, any barriers are discussed, or new goals are created. After six months, each patient receives a phone call to assess progress on their behavioral goal and to collect a final HbA1c.
In 2024, three different sessions were offered that focused on an overview of diabetes management, monitoring, and nutrition. Demographic information for the participants is presented below.
Demographics (Q1-Q4, Year 2024)
Ten patients were referred but only eight participated in the group. On average, they attended two sessions each. Seven of the eight participants created a SMART goal (one did not as the spouse attended the class instead of the patient), and two were unavailable for follow up. Therefore, 62 percent met the behavioral goal with continued maintenance for more than three months.
The average HbA1c prior to the start of the self-management group was 7.8 percent compared to 8.1 percent after the group session. However, only six patients had HbA1c post-class available to record, and the data may be skewed by one patient whose HbA1c increased significantly from 11.5 percent to 14 percent and was later diagnosed as having type 1 diabetes.
In order to improve participation in 2025, we plan to remind providers in ACC-6 and in the primary care offices about the virtual diabetes classes and post signs/flyers in the waiting rooms.
The Division also sought to improve preoperative diabetes control in patients undergoing elective surgery who see a primary care provider (PCP) at Mount Sinai. Uncontrolled diabetes poses several peri-/postoperative complications including infections, ileus, acute renal failure, and prolonged length of stay. The target patient population for this intervention is patients who have a PCP at the Faculty Practice Associates with T2DM who are scheduled for non-emergent surgery. The initiative utilizes visits with a certified diabetes educator to improve diabetes control as measured by serum fructosamine (reflects glycemic control over 2 to 3 weeks). The goal of this project is to increase the number of patients who achieve a fructosamine of less than 325 (~HbA1c 8.0 percent).
Outpatient PCPs and surgeons were informed about the initiative and encouraged to make early referrals to the Certified Diabetes Educator (CDE) for patients needing improved glycemic control prior to surgery. The CDE then schedules rapid appointments within one to two weeks of referral, where baseline data is collected, and the patient’s antidiabetic regimen is optimized according to a standardized template. Follow-up fructosamine levels are monitored every three weeks until optimized for surgery. The original procedure date is tracked, and if postponed, the reason for delay is assessed, specifically whether glycemic control was a contributing factor.
Progress Update as of November 17, 2024
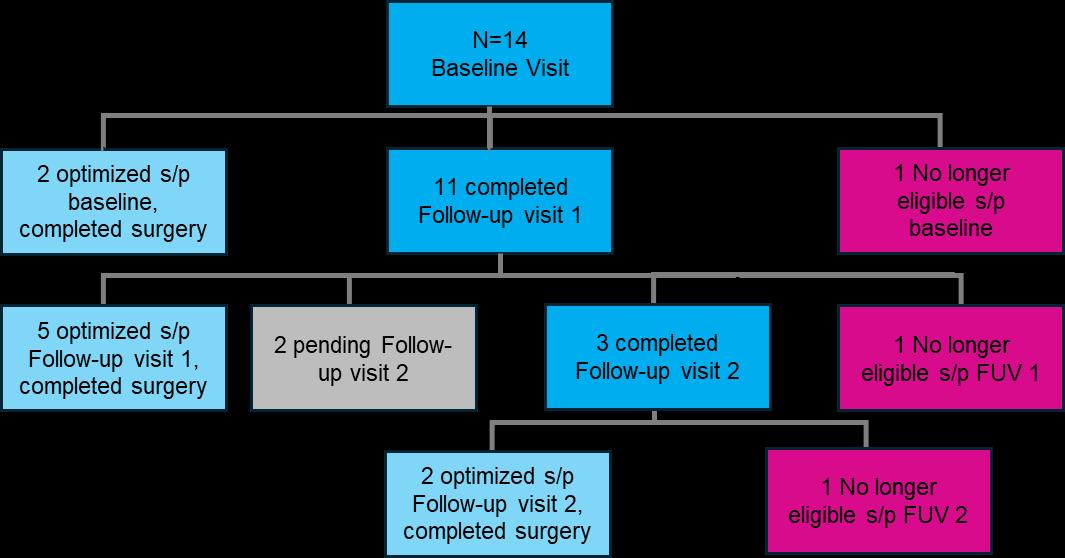
The project has been ongoing since December 2023, with a total of 14 patients identified from December 2023 to present, as depicted in the figure above. Of the 14 patients, nine have achieved successful optimization and completed their surgical procedures. Optimization was achieved for two patients after just the baseline CDE visit, five after one additional follow-up visit, and two after two follow-up visits. Three patients became ineligible at different points in the project due to their surgical procedure becoming indefinitely cancelled.
Patient demographics for preop glycemic control patients (N=14)
The average time from referral to CDE appointment (n=13) was 19.6 days (minimum 0, maximum 98) The average HbA1c at the time of presentation (n=14) was 10.5 percent (minimum 8.0, maximum 15.1). The average fructosamine at baseline (n=9) was 347 (minimum 237, maximum 473) The Division looks forward to continuing to follow current patients and enrolling more patients throughout 2025.
Connecting Patients with Supplemental Weight Management Resources

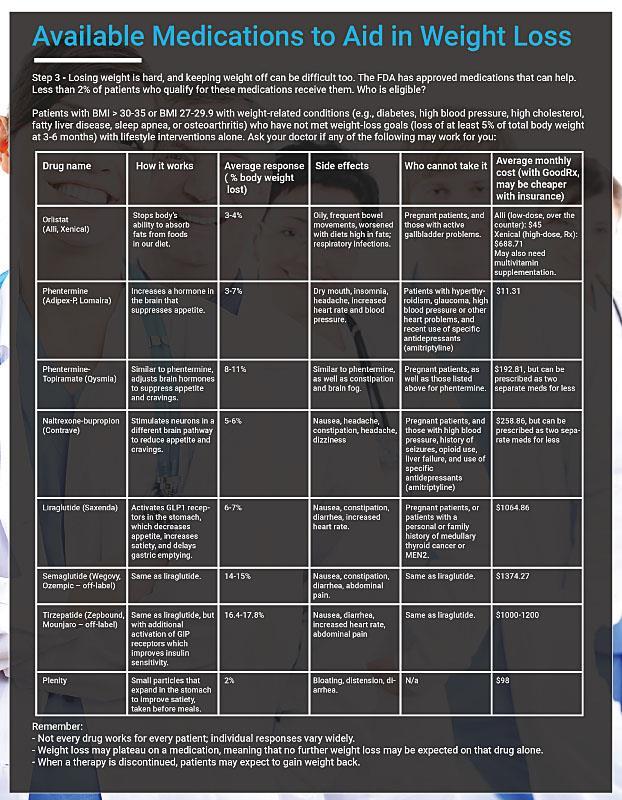
In 2024, a new guide was developed to connect patients with supplemental weight management resources linked with trackable QR codes to help integrate lifestyle with pharmacologic interventions explored in clinic.
Fourteen new weight management patients were provided with these resources. Of these 14, 11 had documented three-month follow-up visits, with four patients reporting engaging in lifestyle changes (mean=13.3 lb. weight loss, SD 5.1) and seven patients reporting no lifestyle changes (mean=7.9 lb. weight loss, SD 9.2). At least one QR code was scanned in 57 percent of cases, nearly matching the initial goal for engagement with resources and translation into action. Delivery of the weight management resource guides will be expanded and will continue in 2025.
Screening
for Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in Patients with Type 2 Diabetes at the Morningside Fellows’ Clinic
The Division’s newest initiative is a project focused on improving screening for MASLD in patients with T2DM. The American Academy of Clinical Endocrinology recommends screening high-risk groups, including patients with T2DM for MASLD with clinically significant fibrosis. Currently, this screening is not done as routinely in the fellows’ clinic as the other diabetic screenings (eye exams, urine microalbumin). The Division aims to increase screening rates by 10 percent over three months. First, a lecture was given to the Endocrinology fellows on MASLD in general and how to interpret a Fibrosis-4 index (FIB-4) score to guide management. Fellows are encouraged to calculate a FIB-4 score on all patients with T2DM seen in the Morningside clinic. This project uses an existing workflow in EPIC the FIB-4 dot phrase is available to all users and provides next steps based on the score. If a Fibroscan result indicates the patient should be seen by a Liver specialist, the referral is automatically placed by EPIC. FIB-4 screening rates are recorded and will be compared between the months prior to the initiation of this project, and the following three months. Additionally, the education component of this
project will be assessed with pre- and post-surveys of the fellows’ knowledge about MASLD and FIB-4 scoring.
Division Quality Champion:
Custon Tafadzwa (Taf) Nyabanga, MD

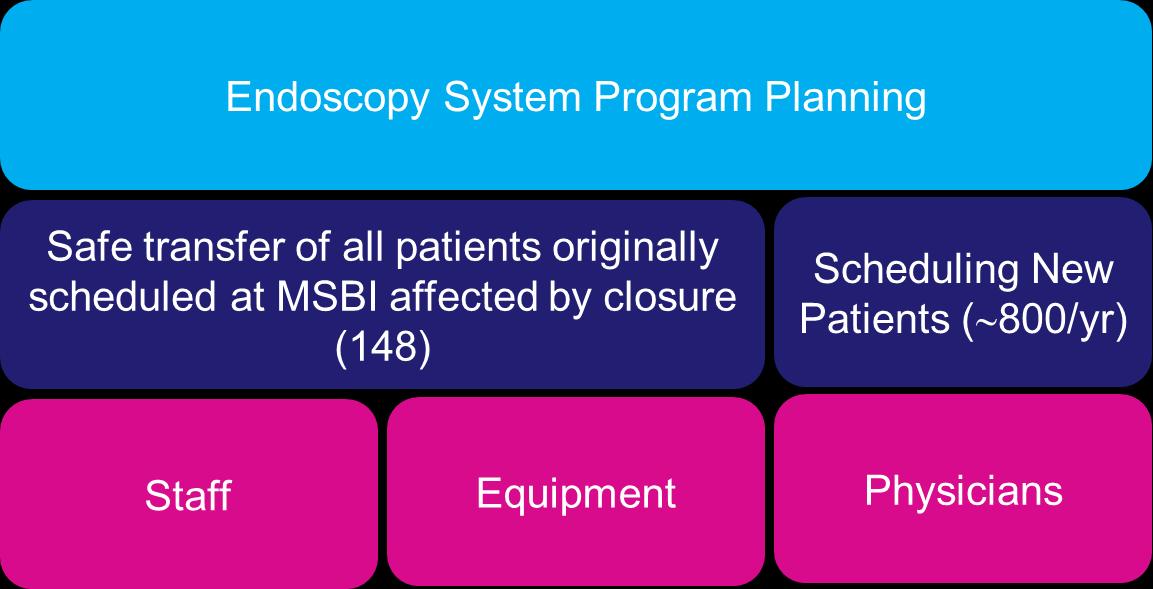
As part of the hospital closure plan, the endoscopy suite and inpatient GI services at Mount Sinai Beth Israel (MSBI) were scheduled to conclude operations in February 2024. The closure of existing endoscopic suites and relocation to a new facility presented unique challenges, including disruptions in patient flow, communication gaps, and increased risk of patient nonadherence to appointments due to confusion or logistical barriers. The Division sought to enhance patient outcomes, streamline clinical operations, and ensure the highest standards of care delivery during this critical transition period and beyond.
To ensure continuity of care and preserve patient satisfaction during this period, the Division set up an Endoscopy System Program Planning committee that met regularly to ensure safe transfer of procedures to other Mount Sinai sites with particular attention given to patient engagement, scheduling systems, and communication pathways
With the increase of volume at other sites, physicians, nurses, and technicians previously with MSBI were also transferred and/or credentialed to help with the transition. Currently, high-risk patients requiring in-hospital procedures are now being scheduled directly at Mount Sinai Morningside and Mount Sinai West, and The Mount Sinai Hospital The downtown patients are still experiencing longer wait times for their in-hospital procedures and efforts are underway to decrease the wait time.
Transition of Care: MSBI Closure
A second quality initiative was aimed at reducing no-show rates at the ambulatory endoscopy center (AEC). Last-minute cancellations negatively impacted the division’s productivity. AEC noshow rates have been hovering around 40 percent, and the aim is to achieve a no-show rate of less than 30 percent by the end of 2025. The division implemented a comprehensive patient navigation and reminder system to reduce patient no-shows. This initiative involved the deployment of a dedicated team responsible for:
• Educating patients about the new location, including travel directions, parking instructions, and what to expect at the new facility.
• Calling or texting patients 48-72 hours before appointments to confirm attendance and answer questions.
• Encouraging interested patients to join an email list to be notified of last-minute appointment openings due to cancellations.
• Performing a 10-day pre-procedure call for all scheduled patients, with any cancellations offered to an email list on a first-come, first-served basis.
• Gathering feedback on potential barriers and proactively addressing concerns in advance.
Future initiatives for the Division include evaluating use of AI in endoscopy with a focus on its potential to improve CRC screening quality measures and potentially introducing a protocol for Barrett’s esophagus screening and referrals as most patients meeting criteria are often missed particularly in the primary care setting.
Division Quality Champions: Christopher Cao, MD
David Greenwald, MD

In 2024, The Mount Sinai Hospital (MSH) Division of Gastroenterology engaged in several new quality initiatives.
The first of these involved compiling updated data to measure the quality metrics of endoscopy within the Division. Indicators of a thorough examination during a colonoscopy include cecal intubation rate (CIR), adenoma detection rate (ADR), scope withdrawal time (SWT), and percentage of colonoscopies with adequate bowel prep as measured by the Boston Bowel Prep Score (BBPS).
Cecal intubation rate (CIR) is defined as the percentage of colonoscopies in which the cecum was successfully intubated. The national benchmark has a goal rate of 90 percent of all colonoscopies, and 95 percent of all screening colonoscopies. In the most recent quarter, the Division’s mean CIR was 97 percent, exceeding the recommended national benchmark.
An additional indicator of thorough examination is adenoma detection rate. The goal is detection of adenoma in 25 percent of patients: 30 percent in males and 20 percent in females,
undergoing average risk colon cancer screening. The current ADR of the Division is 40 percent, which exceeds this goal.
Utilizing scope withdrawal time as an endoscopy quality metric ensures that adequate time is spent visualizing the colon and is defined by the time of colonoscope retraction after the cecum has been reached. National guidelines recommend a SWT of > 6 minutes. The Division has also exceeded this benchmark, with the most recent SWT among the Division averaging 8.2 minutes.
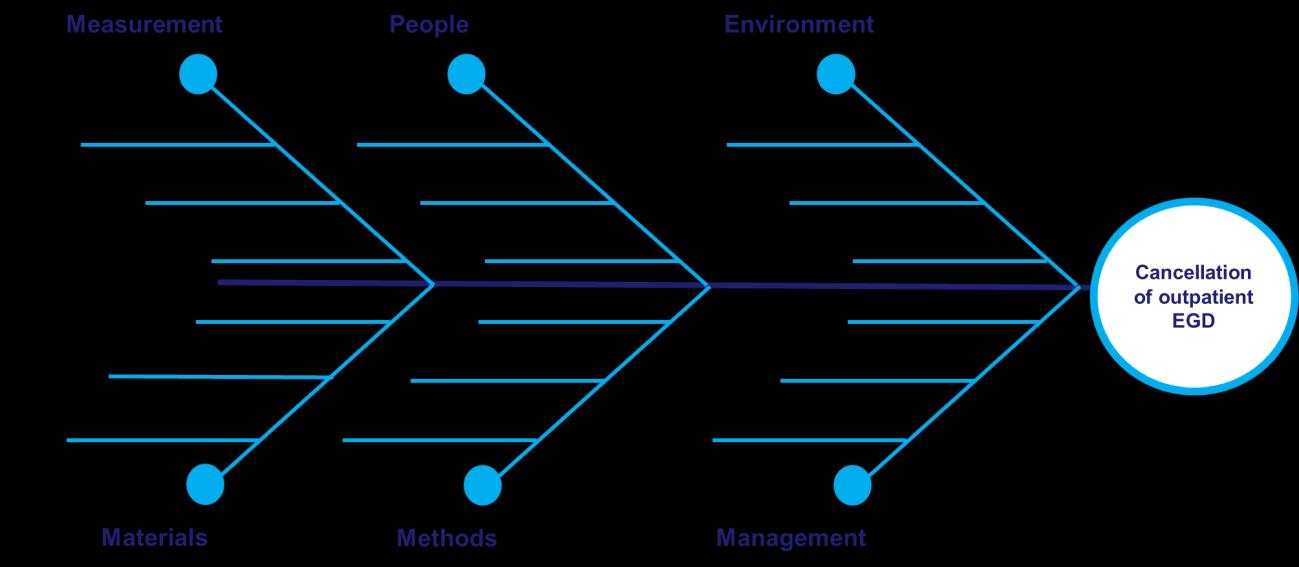
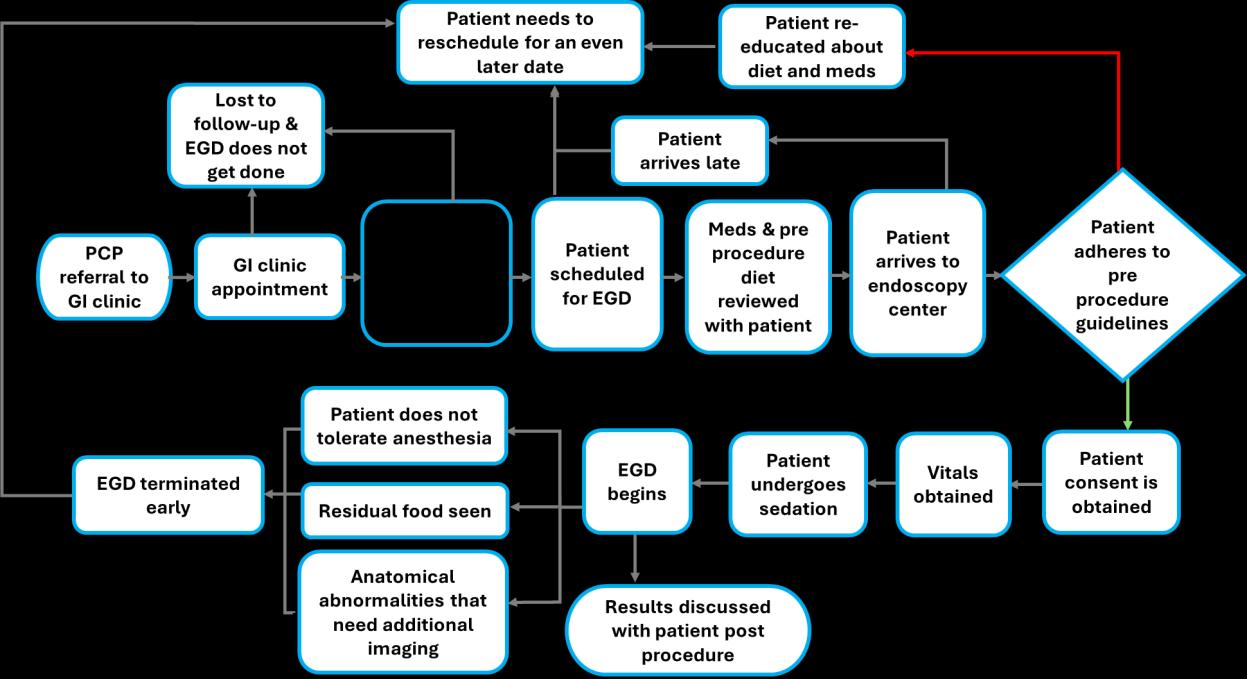
The Division has been working on improving rates of cancelled endoscopic procedures due to Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 RA). GLP-1 RA have risen in popularity given their weight loss properties through delaying gastric emptying and increasing satiety. The theoretical risk of GLP-1 RA includes that of gastric retention and aspiration during endoscopies. Anesthesia guidelines had recommended holding GLP-1 RA prior to endoscopic procedures. Consequently, procedures were cancelled if this medication had not been sufficiently withheld prior to the procedure. This guideline change resulted in an increased risk of endoscopy cancellations in the past year. In the second half of 2023, 24 percent of patients taking a GLP-1 RA experienced procedural cancellation. A fishbone and process map were created to identify reasons for cancellation of outpatient procedures due to GLP-1 RA.
The Division implemented several interventions to address this concern. The GI team performed a retrospective chart review, evaluating the percentage of aborted procedures due to food retention in patients on a GLP-1 RA. Data revealed a slight increase in aborted procedures in patients on a GLP-1 RA but the absolute number of aborted procedures remained low.
Liraglutide
Semaglutide
Tirzepatide
(0.8%)
(0.0%) 0/128 (0.0%) 4/467 (0.8%) 1/50 (2.0%)
Additionally, the Division created pre-procedural instructions for patients on a GLP-1 RA, giving detailed instructions about when their medication should be held, and what their diet should consist of prior to procedure (intervention 1). Later, a Mount Sinai system-wide change in policy advised that patients only need their GLP-1 RA to be held for one dose prior to endoscopy rather than the previously recommended two doses (intervention 2). Through these interventions, the Division noted a drastic decline in the rates of procedural cancellations in patients on a GLP-1 RA.
Another project in the Division was focused on improving Celiac disease (CeD) health maintenance. CeD is associated with higher rates of osteopenia/osteoporosis due to risk of malabsorption and pneumococcal infection. Patients with CeD are advised to undergo dual Xray absorptiometry (DEXA) one year after initiation of a gluten-free diet, and all CeD patients should be offered pneumococcal vaccine (PCV). In 2022, only 18 percent of CeD patients had undergone DEXA and 29 percent of patients had PCV at MSH. A process map for CeD health maintenance is presented below
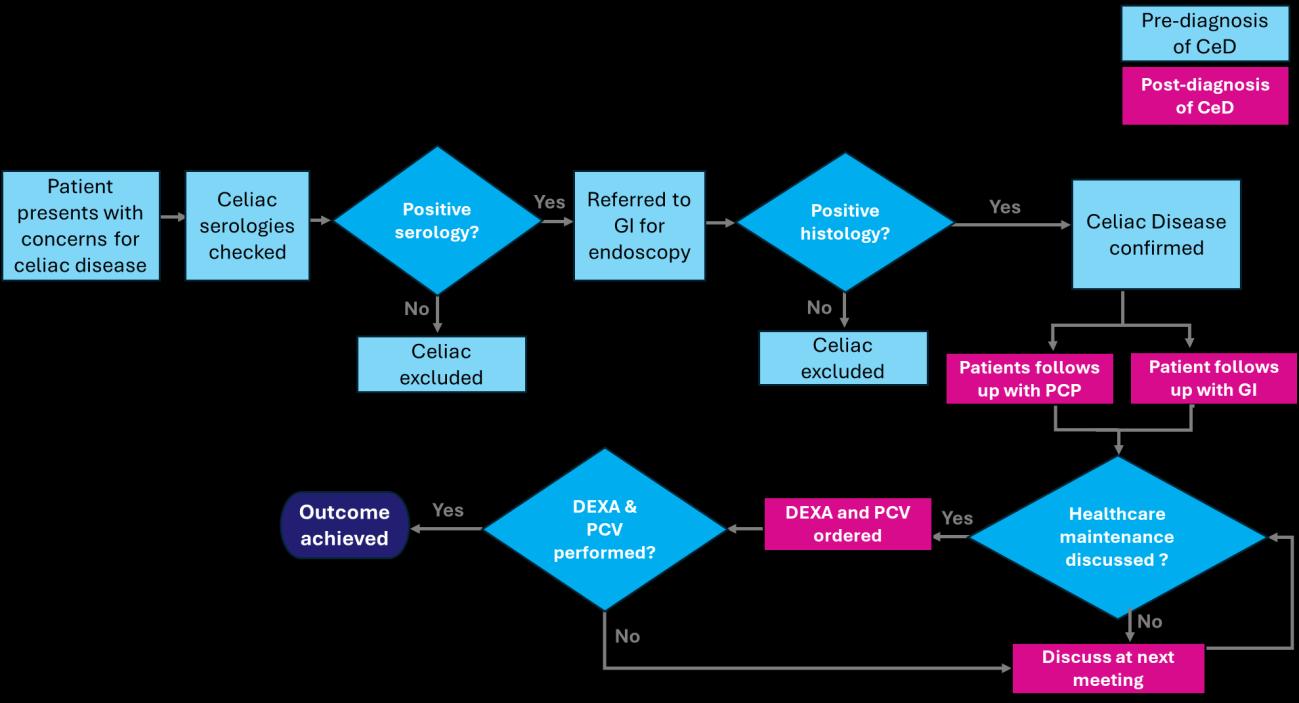
Over the past year, increased awareness of CeD health care maintenance was performed through CeD grand rounds lectures throughout the different Mount Sinai sites and establishment of the Mount Sinai Celiac Program. Through these efforts, the rates of DEXA in celiac patients
across MSH have increased. A future goal of the division is to create CeD order panel to improve rates of pneumococcal vaccine administration.
2022 2023-2024
The Division is excited to be working on new initiatives for this academic year that will continue into 2025
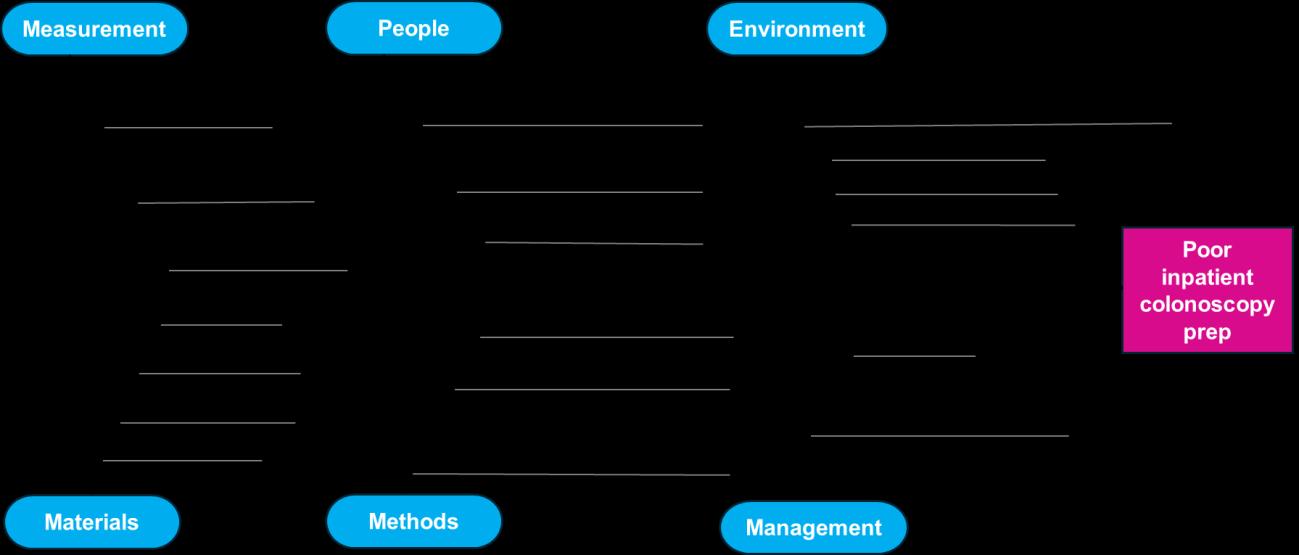
The Division continues to track and report the percentage of colonoscopies with adequate bowel prep by utilizing the Boston Bowel Preparation Scale (BBPS). BBPS is a standardized, validated scoring system used to determine the quality of bowel preparation. Providers document the cleanliness of three sections of the colon using an objective, zero to three scoring system. An adequate bowel prep is critical in allowing for optimal conditions to identify bowel pathology but has been an ongoing issue for the Division. This year, the Division is hoping to improve bowel prep in patients admitted to the hospital with three main goals: decrease patient delays for inpatient colonoscopy, streamline communication regarding bowel prep quality, and perform health equity analysis by age and preferred language. Preliminary data shows that 47 percent of colonoscopies in the inpatient setting at MSH were delayed due to inadequate bowel prep. The fishbone diagram below illustrates the processes involved in adequate bowel prep.
The Division hopes to develop an Epic order set for inpatient colonoscopy bowel preparation. A second ongoing project is to increase the rate of treat-to-target colonoscopies performed after starting a new biologic in patients with inflammatory bowel disease (IBD). All patients with IBD are recommended to undergo endoscopic evaluation of bowel mucosa after initiation of a biologic to confirm histologic healing and remission. Preliminary data at MSH revealed 558 IBD patients who were initiated on a biologic in 2023 of these, 30 percent underwent a colonoscopy or flexible sigmoidoscopy within six months of starting a biologic, and 47 percent underwent a colonoscopy or flexible sigmoidoscopy within 12 months of starting a biologic. A process map was developed.
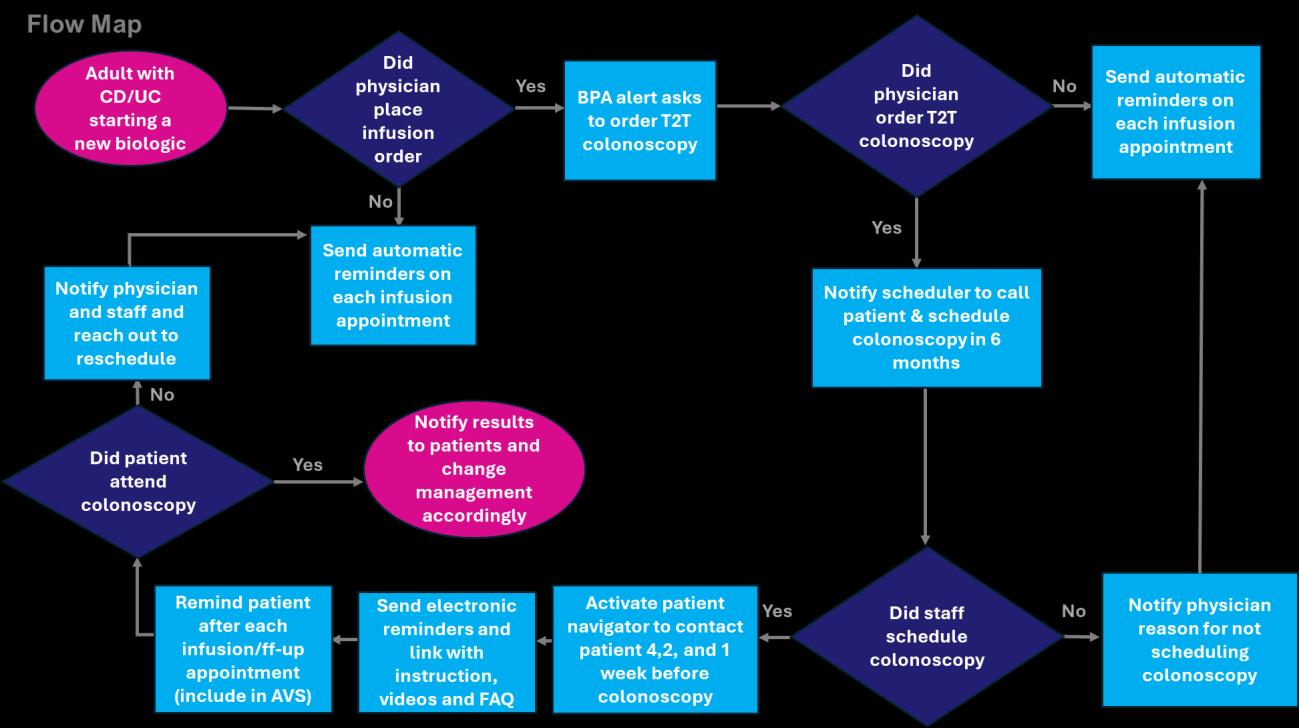
The Division hopes to incorporate a best practice advisory for clinicians that will alert for patients who were newly started on a biologic but had not yet undergone endoscopic surveillance.
Finally, the division has been working with the Department of Medicine to create a PEG checklist and order set at MSH. The aims of this checklist are to streamline referral processes, decrease time from consult to PEG placement, and allow for appropriate identification of patients eligible for PEG placement. The checklist and order set are now live in Epic, and the Division optimistically awaits the outcome of these efforts

In 2024, the Division of Gastroenterology at Mount Sinai Morningside and Mount Sinai West continued working on the quality improvement initiative of adequate bowel preparation quality for screening colonoscopies. Suboptimal bowel prep may hinder detection of polyps, thereby decreasing effectiveness of screening colonoscopy. The American Society for Gastrointestinal Endoscopy/American College of Gastroenterology (ASGE/ACG) task force recommends the rate of screening colonoscopies with inadequate bowel prep to be less than 15 percent. Therefore, target adequate bowel prep quality was set at ≥ 85 percent.
The baseline rate of adequate bowel prep in 2016 prior to intervention was 72 percent. With the standardization of bowel prep instructions across all sites, focus on patient education at each practice, and implementation of a split dosing prep, the rate of adequate bowel prep for screening colonoscopies improved to 80-88 percent from 2020 to 2022 (see graph below). The rate of adequate bowel prep decreased to 75 percent in 2023. With emphasis on patient education, dietary changes, and timely completion of bowel preparation, the rate improved to 84 percent in 2024.
Adequate Bowel Prep
Note: Data was not collected in 2019 or 2021.
In 2025, the Division plans to focus on patient education at the faculty practices and clinics. The Division will continue to improve the distribution of prep instructions to the patients. Instruction distribution will be via handout during the office visit or, for non-office patients, via email, mail, or MyChart message, as appropriate. Instructions are also available on the Mount Sinai website so they can be easily accessed by staff and patients. The Division will implement the use of a simplified graphic for prep instructions during patient education in the office to help improve patients’ understanding of the prep instructions. The graphic instruction presented below will be used as an adjunct to the standard bowel prep instructions. It contains a QR code for the Mount Sinai bowel prep website so that patients can access the detailed instructions electronically should they lose the paper copy.
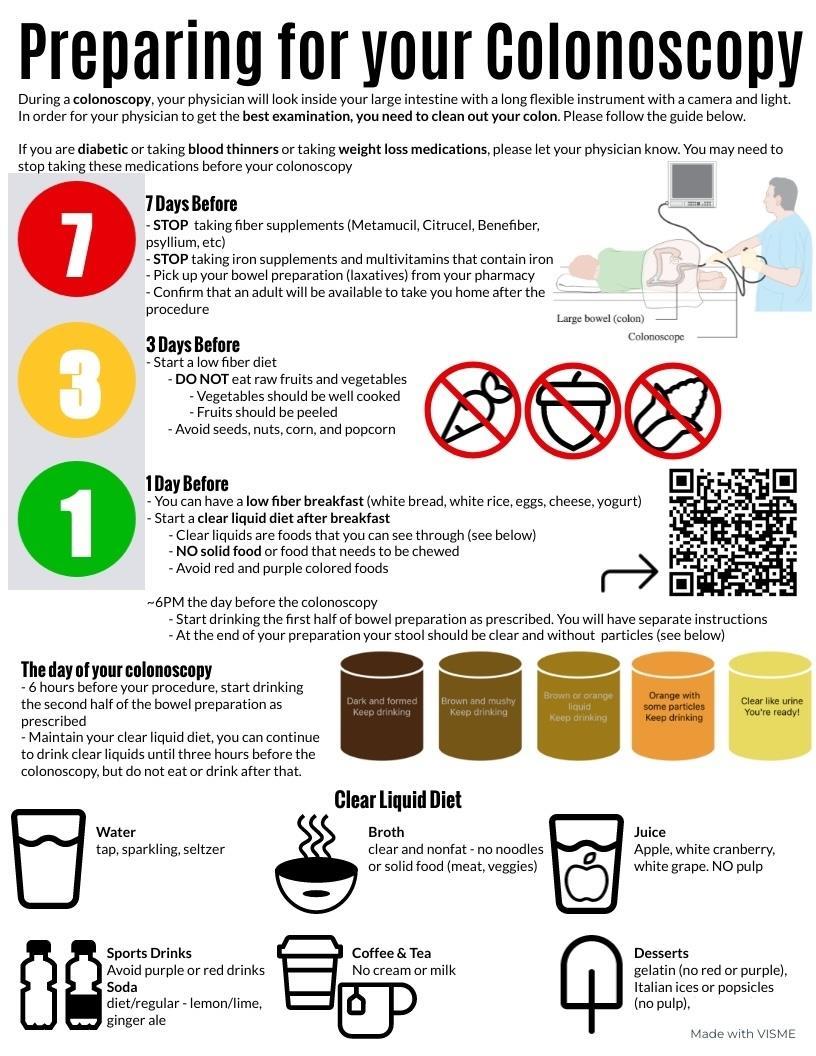
Note: Simplified bowel prep instructions with the QR code to the Mount Sinai website containing links to bowel prep instructions. Intended to be used as a visual tool during patient education and as an adjunct to the existing prep instructions.
The second quality improvement project sought to improve the rate of diagnostic paracentesis performed on patients being admitted with cirrhosis with ascites. The American Association for the Study of Liver Disease (AASLD) guidelines suggest all patients admitted with ascites receive a diagnostic paracentesis within 24 hours of presentation to rule out spontaneous bacterial peritonitis (SBP). Early identification of SBP helps prevent further
clinical decompensation. The goal of this study was to reduce the number of paracenteses not performed on admitted patients by 20 percent over a three-month period. A user-friendly workflow algorithm was created and contained information on specific labs to send on the ascites fluid, how to interpret data, and how to treat SBP. The algorithm was linked to a QR code and placed at multiple computer stations throughout both hospitals (below). It was made accessible to internal medicine and emergency medicine providers. Education sessions were provided to the Internal Medicine and Emergency Medicine house staff.
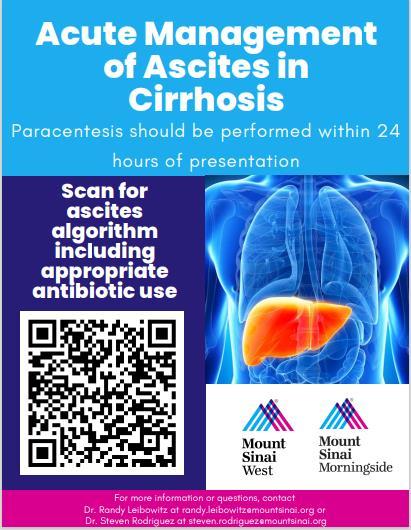
A random sample of 342 patients admitted with ascites over three years was analyzed. Diagnostic paracentesis was performed in 133 out of 342 patients (38.8 percent), with 37.6 percent of these patients undergoing a paracentesis after 24 hours of admission. The average time from admission to paracentesis was 1.44 days. Following the implementation of the QR code algorithm, there was a 16.3 percent reduction in patients with paracentesis not performed at the three-month point. This effect was sustained through three to six months post intervention (see graph below). The average time from admission to paracentesis over the six-month study period decreased from 1.44 days to 0.81 days. In an effort to ensure sustained improvement in the rate of diagnostic paracentesis, the team is working on imbedding this algorithm into an order set accessible through the electronic medical record system. This project was presented as a poster presentation at the Digestive Disease Week (DDW) annual meeting in May 2024.
3-Months Post
6-Months Post
Post-Intervention (total)
The third quality improvement project aimed to increase colorectal cancer (CRC) screening rates among patients at a single NYC federally qualified health center (FQHC). In 2022, the NYC FQHC’s CRC screening rate was 35.9 percent, below the 2020 national average of 69.7 percent and 40.1 percent among FQHC. The project aimed to improve CRC screening rates by implementing provider intervention (pre-intervention quiz, educational lectures with a follow-up knowledge assessment, daily pre-clinic reminders for internal medicine residents) and patient intervention (informational posters in patient rooms, two-minute educational videos on proper stool fecal immunochemical test collection/return, information on direct-access colonoscopy referral program). A retrospective chart review of patients ages 45 to 75 who were seen by internal medicine residents between August 14, 2022 and August 13, 2023 at a single NYC FQHC was performed to obtain a pre-intervention CRC screening rate at the FQHC. A similar chart review was performed post-intervention from August 14, 2023 to February 14, 2024. Postintervention, there was a 7 percent increase in CRC screening tests (see table below). For the stool fecal immunochemical test (FIT), the rate of this test being ordered increased from 17 to 22 percent in six months, and of those ordered, the rate of the stool test being returned increased from 50 to 76 percent. 100 percent of patients who had a positive stool FIT had a follow-up colonoscopy for further workup. The colonoscopy referral rate increased by 17 percent, but only 24 percent of these were completed by the end of the study period. The median time for test completion for the stool test was 14 days pre-intervention and 13 days post-intervention. The median time for test completion for colonoscopy was 56.5 days preintervention and 77 days post-intervention.
Comparison of CRC screening rates one year pre-intervention to six months post-intervention
Screening Test Characteristics - no. (%)
Non-White Race
Time from Test Order Date to Test Completion Date – median days (IQR)
Time from Positive Stool Test Result Date to Colonoscopy Procedure Date (n=2)
This project was presented at DDW in May 2024 and received the 2024 SCOPY Award by the American College of Gastroenterology (ACG). The team hopes to continue the project for ninemonth and 12-month data. Future directions of the project include utilizing the ACG screening flyers at the FQHC and working with the information technology team to create an automated system to send a MyChart message to patients due for CRC screening and to those with an unreturned stool FIT.
Desiree Chow, MD
In 2024, General Medical Associates (GMA) at Mount Sinai Beth Israel focused on enhancing quality measures set by the Mount Sinai Health Partners Clinically Integrated Network (MSHP) These measures encompass diabetes control, screening for diabetic retinopathy and nephropathy, hypertension control, colorectal cancer screening, and depression screening.
To enhance the retinopathy screening rate for diabetic patients, the Division continued its partnership with the ophthalmologists co-located in the same building. Additionally, the Division sent bulk MyChart messages encouraging patients to schedule an ophthalmology appointment if they were overdue, or to provide the practice with the details of their ophthalmologist if they had completed a visit in the past year. A total of 967 messages were sent. Tracking patient responses proved challenging, as patients either contacted their PCP directly or called the practice. To address this, the Division established a “GMA Team” account, allowing patients to respond directly and enable tracking of responses more effectively. In 2024, the rate of screening increased to 67 percent, just short of the 71 percent goal set by MSHP.
Similarly, to increase the nephropathy screening rate among diabetic patients, the Division implemented quarterly bulk MyChart messages advising patients who were due for screening. The Division placed bulk orders for screening and informed patients they were allowed to walk in during office hours. A small improvement was seen; however, other efforts will be needed in 2025 to reach the goal of 92 percent.
Achieved Target
To improve the percentage of patients with uncontrolled diabetes, the Division continued collaboration with an embedded clinical pharmacist and diabetes educator. During weekly team huddles with providers, patients with uncontrolled diabetes and upcoming appointments were discussed to review care plans and refer appropriate patients to remote patient monitoring for diabetes. Although the target goal was not met in 2024, there were fewer patients with uncontrolled diabetes.
Patients with diabetes aged 18-75 with HbA1c > 9%
Achieved Target
To increase the rate of colorectal cancer screening, GMA continued the previous quality project of having the medical office staff pend Cologuard orders for patients due for screening and having nurses make calls to patients with outstanding Cologuard orders. For patients interested in colonoscopy, the Division continued to utilize direct colonoscopy referrals.
Internal Medicine resident physician Mako Koseki, MD, along with GMA faculty mentor Rui Jiang, MD, led a focused project to increase Cologuard order and completion rates through education for both house staff and patients. This work was presented at the SGIM Annual Meeting and the ACG Annual Meeting in 2024. The second phase of the project involved sending blast portal messages to patients, explaining the importance of screening and the
available options. Patients were given the opportunity to respond directly to request a referral to gastroenterology for a colonoscopy or to receive a Cologuard kit. This approach resulted in more patients being screened in 2024 and surpassing the target rate of 72 percent.
Percent of Patients Ages 45-75 with Colonoscopy within 10 years, Sigmoidoscopy within 5 years, Cologuard within 3 years, or Fecal occult blood testing within 1 year
Achieved Target
The Division improved hypertension control through multiple interventions, including having providers repeat elevated readings and document home recordings, referring appropriate patients to the remote patient monitoring program, and conducting nursing outreach to patients with uncontrolled blood pressure to review medications and home blood pressure readings in between visits. In addition, GMA employed a nursing-led hypertension clinic to facilitate prompt follow-up of patients who had a change in their antihypertensive regimen or were newly started on an antihypertensive. While more patients achieved the goal blood pressure, the target of 75 percent was not met and efforts to reach more patients will continue in 2025.
Percent of Patients Ages 18-85 with a Diagnosis of Hypertension with Last Recorded Blood Pressure <140/90
Achieved Target
Using the MSHS PCI Measure performance report, stratified by race and ethnicity, the Division identified poorer blood pressure control in Black/African American patients compared to Asian, Hispanic, and White patients. To further investigate this difference, screening for social
determinants of health (SDoH) was started to identify specific factors to target for an intervention.
For the last metric of improving the rate of depression screening and follow-up, the medical office staff continued to perform Patient Health Questionnaire (PHQ)-2 screening on all patients during rooming and provided patients with a laminated PHQ-9 to complete if PHQ-2 screening was positive. Providers were reminded during huddles to ensure PHQ-9 questionnaires were completed and a plan documented. There was a significant improvement in PHQ-9 completion.
PHQ2 Screening PHQ9 Completed Follow up selected
In addition to the Primary Care metrics mentioned above, Internal Medicine resident physician Sneha Bupathi, DO, launched a collaborative project with the Allergy Division to increase referrals for patients with a documented penicillin allergy, with the goal of delabeling those without a true penicillin allergy. The intervention involves sending a portal message to all patients in the resident practice who have a recorded penicillin allergy. The message will offer brief education on penicillin allergies and invite patients to respond if they are interested in being referred for testing. This project will continue into 2025.
Division Quality Champions:
Nikita Barai, MD
Kelsey Bryant, MD


In 2024, Internal Medicine Associates (IMA) prioritized enhancing team-based care processes to improve chronic disease management, ensure adherence to age-appropriate cancer screening guidelines, improve naloxone prescribing in patients at high risk of overdose, improve transitions of care workflow, and optimize clinician documentation in Epic
In 2024, the Ambulatory Care Quality Dashboard became an integral tool for improving quality metrics across IMA. Throughout the year, the Division leveraged data from the dashboard to drive improvements in all quality measures, supporting the commitment to excellence in patient care. Residents are now trained to use the dashboard during their scheduled education sessions, ensuring they are equipped to incorporate data-driven approaches into their practice.
Building on the foundation laid in 2023, the dashboard originally piloted by early adopters is now fully integrated into quality improvement workflows. This comprehensive tool provides realtime data at the system, department, clinic, and provider levels and includes population outreach features, such as batch messaging for patients with open care gaps and batch ordering for cancer screenings. These innovations continue to enhance efficiency and effectiveness in addressing care gaps across the population.
Hypertension
The Division remains steadfast in its commitment to achieving optimal blood pressure (BP) control. Key initiatives include standardizing workflows for both in-office and at-home BP monitoring, complemented by an innovative remote patient monitoring program. The interdisciplinary, team-based approach driving these efforts is illustrated in the workflow diagram below.
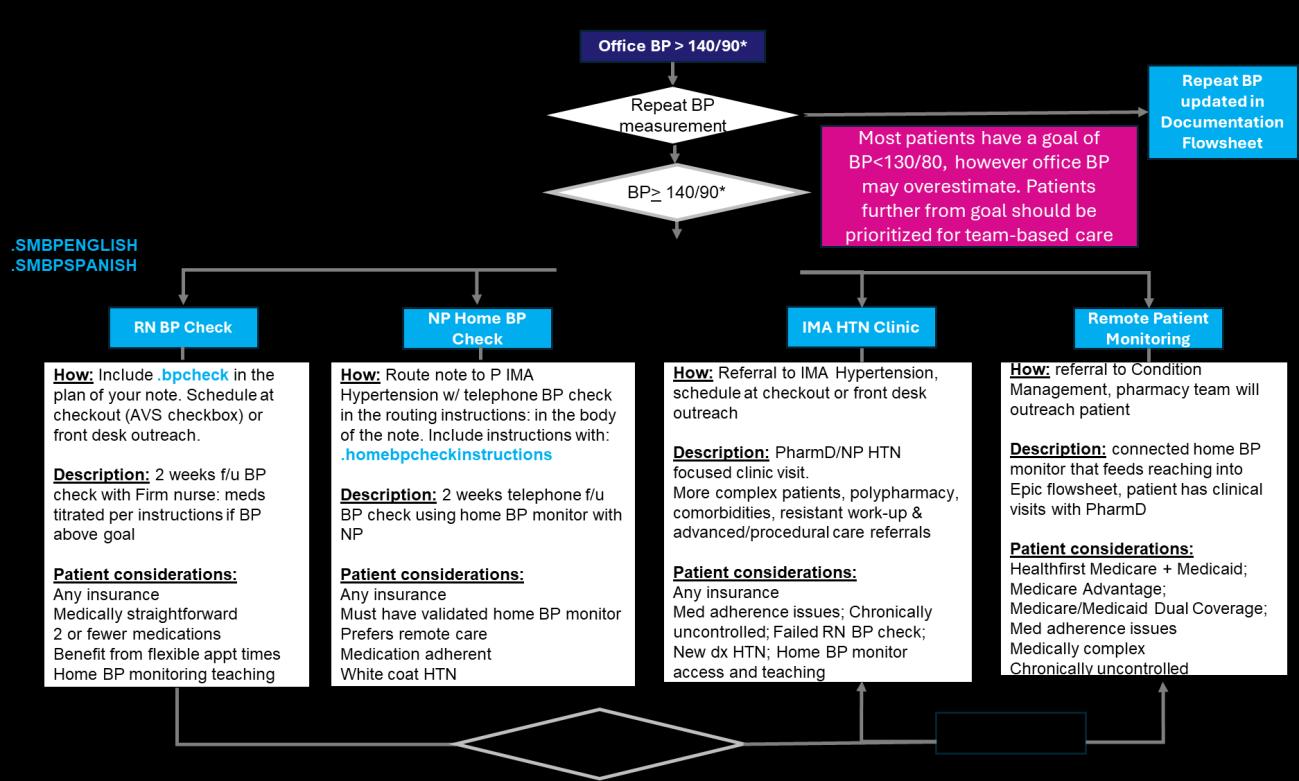
In 2024, efforts to improve hypertension control at the system level have expanded under the leadership of Drs. Barai and Bryant, who are conducting a comprehensive analysis of systemwide data. This work focuses on understanding the use of the last recorded blood pressure as a proxy for control, given the dynamic nature of BP measurements. Unlike static quality metrics such as diabetic nephropathy or retinopathy screening, hypertension control fluctuates as it is calculated based on the most recent ambulatory BP recorded in the system. Real-time insights into patients’ changing control status remain critical for effective population-level management.
Building on the foundational launch of the hypertension dashboard in Epic during the summer of 2023, efforts in 2024 have emphasized training attending and resident providers at IMA to leverage population health tools within the dashboard. These tools enable more proactive patient management and streamline referrals to established care pathways. Additionally, the Epic SmartSet, developed through a working group led by Dr. Barai, continues to support standardized and efficient hypertension management workflows.
The hypertension dashboard, accessible to all team members, remains central to these efforts. Ongoing workflow refinements aim to maximize its utility. Currently, front desk staff play a key role by identifying patients whose last recorded ambulatory BP is elevated (>140/90 mmHg) and whose average ambulatory BP exceeds 150/90 mmHg. For these patients who lack an upcoming primary care provider (PCP) appointment and are not enrolled in the remote patient monitoring program, the staff initiates outreach to facilitate their return to care, either with their PCP or the hypertension specialty clinic.
In 2024, one abstract related to hypertension control was presented at the American Heart Association Hypertension Sessions in September 2024 in Chicago, IL
Office BP measurements were analyzed for 89,130 patients. Of these, 71.2 percent had controlled hypertension based on the National Committee for Quality Assurance criteria of last measured BP <140/90 versus 68.9 percent using the average BP <140/90. Using the lower <130/80 threshold, 34.5 percent patients had controlled hypertension by the last measured BP versus 32.7 percent using the average BP. When the last systolic BP >140 or diastolic BP >90 was used, there was a greater likelihood that the patient had uncontrolled hypertension based on average BP (OR 2.00, 95% CI [1.88-2.12] and 7.43, 95% CI [6.96-7.93], respectively). A similar pattern was observed when the last recorded systolic BP was >130 or diastolic BP >80, (OR: 2.02, 95% CI [1.95-2.08] and 3.99, 95% CI [3.87-4.12], respectively).
An additional abstract was submitted to the American College of Cardiology by PGY-1 Dr. Shahrin Islam and is expected to be presented at their national meeting in March 2025 in Chicago, IL.
Additional academic activity related to hypertension included a clinical case presented by PGY2 Dr. Thomas Hanlon and Dr. Bryant at the International Society of Hypertension in Cartegena, Colombia, and an invited lecture on health equity and community-based BP screening by Dr. Bryant at the American Heart Association Scientific Sessions in November 2024 in Chicago, IL. Dr. Bryant also joined the steering committee of the National Hypertension Roundtable to
represent Mount Sinai. Three more abstracts and manuscripts are in progress and are expected to be published in 2025.
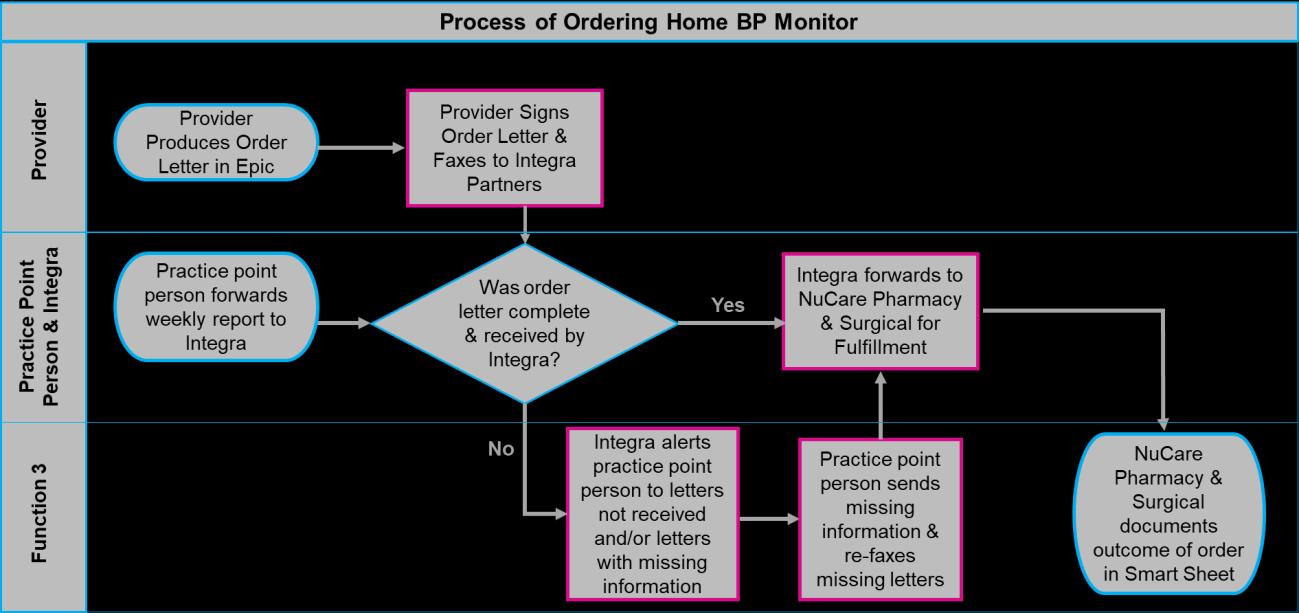
Home BP monitor access continues through a partnership with Integra (a benefits manager) by creating a closed-loop feedback process to track orders. In 2024, the Division was able to ensure devices dispensed had passed a validation process for accuracy and were nationally recognized on validatebp.org.
Through targeted outreach using the hypertension control dashboard and ongoing education on best practices, including the prescribing and use of single-pill combinations, the hypertension control rate has remained consistently above 70 percent since May 2024 and surpassed 73 percent as of July 2024. Looking ahead, the Division aims to refine these strategies further to achieve a control rate of 75 percent and beyond in 2025.
In 2024, IMA advanced its team-based model of care for diabetes management, incorporating certified diabetes educators and maintaining the dedicated high A1C clinic staffed by internal medicine interns. These efforts have further supported patients in achieving improved glycemic control through comprehensive, multidisciplinary care.
In May 2022, the proportion of patients with uncontrolled HbA1c (>9 percent) achieved the target goal of less than 15 percent. Since then, the Division has consistently remained below this threshold and, in 2024, set an ambitious new internal goal of reducing uncontrolled HbA1c rates to less than 10 percent, reflecting the continued commitment to delivering the highest quality of care.
IMA continues to provide on-site diabetic eye exams using a retinal camera, significantly enhancing access to same-day screening during primary care visits. This resource has led to a substantial increase in screening completion rates since its introduction in 2021. In 2024, the Division further strengthened its partnership with the ophthalmology department, which now proactively contacts patients with abnormal retinal scans to schedule dilated eye exams and initiate treatment for diagnosed conditions, ensuring timely and comprehensive eye care.
DM Eye Exam: HM Goal
In 2024, the Division maintained its focus on nephropathy screening for patients with diabetes, building on the progress made in 2023. A workflow piloted in late 2023 empowering medical assistants to identify patients with open care gaps, provide urine collection supplies, and pend the appropriate orders has been successfully implemented. This initiative is expected to drive further improvements in screening completion rates, reinforcing the commitment to early detection and prevention of diabetic nephropathy.
IMA continues to improve colorectal cancer screening (CRCS) rates. Colonoscopy access has improved after the addition of Medicaid-certified sites in MSHS, improving adherence to this test type. A novel patient navigation program for multitarget stool DNA (mt-sDNA) testing was launched in January 2023 and has resulted in marked improvement in test adherence rates (39 percent to 51 percent, 2022 vs. 2023) at IMA. In December 2023, the program was expanded to Victory Internal Medicine in Staten Island, with similar improvements (47 percent vs. 57 percent, pre- vs. post-intervention). In November 2024, Mount Sinai Doctors East 85th Street went live as a third site. The goal is to continue streamlining the workflow to maximize the reach of the navigator and to attain financial sustainability through downstream colonoscopies.
IMA Victory
This work has led to a new body of literature and significant academic growth for team members. Dr. Kyle Koster, an Assistant Professor in the Division and team, with former chief resident and current gastroenterology fellow Dr. Edward Cytryn as first author, submitted the IMA pilot for publication in Journal of General Internal Medicine, and it was accepted in October 2024. Program manager Kayla Jaeckel submitted an abstract on the expansion to Staten Island to the Institute for Healthcare Improvement Forum, and it was accepted in October 2024 for presentation in December 2024. The team intends to submit additional abstracts, manuscripts, and funding applications to continue expanding this work.
There is much room for improvement in stool-based test completion. Dr. Koster, Dr. Barai, Ms. Jaeckel, and colleagues in gastroenterology are planning to pilot MyChart-based reminders to improve test completion for patients not served by the navigation program. This program is under development and will continue into 2025.
Dr. Koster also submitted a grant to fund a randomized controlled trial of opt-in vs. opt-out interventions for CRC screening.
Breast cancer screening remained a challenge for IMA in 2024. The discontinuation of walk-in mammography has impacted accessibility; however, the Division is leveraging bulk orders through the dashboard and plans to utilize the new radiology self-scheduling feature in MyChart to streamline the process. Despite these challenges, IMA remains committed to improving screening rates and continue actively engaging patients in value-based contracts to schedule mammograms.
Cervical cancer screening rates have significantly improved in 2024, driven by enhancements in reporting processes to align with current guidelines and expanded access to scheduling. These efforts have streamlined the identification of patients due for screening and made it easier for them to complete testing, reinforcing the commitment to preventive care.
40%
Cervical Cancer Screening Goal
To increase the presence of naloxone in patients at risk of overdose, Dr. Eric Kutscher, an IMA and REACH faculty, and Gary Gravesandy, a third-year medical student, implemented a Best Practice Alert (BPA) in July 2024 The BPA is visible to all ambulatory practices to recommend prescribing an emergency naloxone kit to patients at high risk of opioid overdose, defined as history of opioid overdose, prior administration of naloxone during a visit or admission, diagnosis of opioid use disorder (not in remission), a recent prescription for an opioid medication, or a recent urine toxicology test positive for opiates or stimulants. The BPA was developed using addiction medicine best practices and accompanying educational materials about the alert have thus far been distributed to the Ambulatory Quality Workgroup, with additional education planned in 2025. Since the launch of the BPA, naloxone prescriptions have increased to 3,355 prescriptions in the past month compared to 2,889 in January 2024, a 16 percent increase in prescriptions.
IMA has a complex patient population with a high chronic disease burden and many psychosocial barriers to cost-effective care. Continuous efforts are underway to improve transitions of care for patients to steer utilization toward more cost-effective and lower-risk sites of care. The following initiatives are aimed at improving transitions of care.
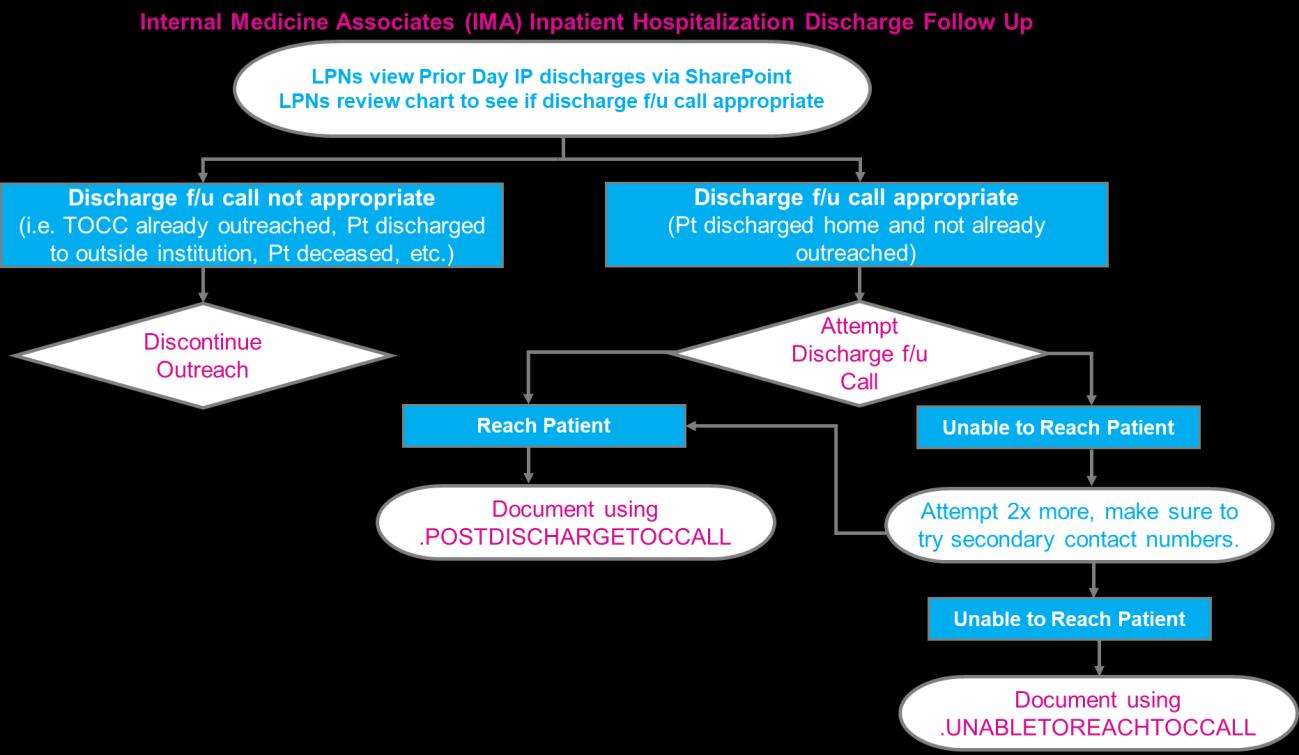
To prevent recurrent emergency department (ED) visits and hospital admissions prior to 2022, Licensed Practical Nurses (LPNs) called patients following discharge to review medications and schedule follow-up. In 2022, this process was enhanced with standardized documentation via Epic dot phrases and training from the Transitions of Care Center (TOCC). In 2023, reporting was developed to better monitor reach and, in 2024, reach and follow-up appointment rates improved, but remained limited by staffing shortages. In 2025, the Division will continue to monitor and evaluate the program to assess the impact on follow-up appointment rates and on 30-day post-discharge readmissions and ED visits.
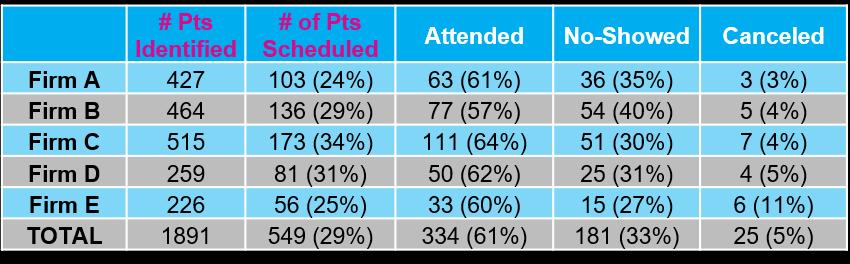
PTs w/ One IMA Appt scheduled w/in 14 Days PostDischarge
% of PTs Scheduled for an IMA Appt w/in 14 Days of Discharge Date but Cancelled or No Showed
PTs Who Had One IMA Appt scheduled w/in 30 Days Post Discharge Date % of PTs Scheduled for an IMA Appt w/in 30 Days of Discharge Date but Cancelled or No Showed
% of PTs Scheduled for an Ambulatory (IMA or Specialty) Appt w/in 30 Days of Discharge Date
(58/137) 61.89% (190/307) 34.21% (65/190) 67.43% (207/307)
Sep-24 44.53% (110/247) 32.73% (36/110) 59.92% (148/247) 38.51% (57/148)
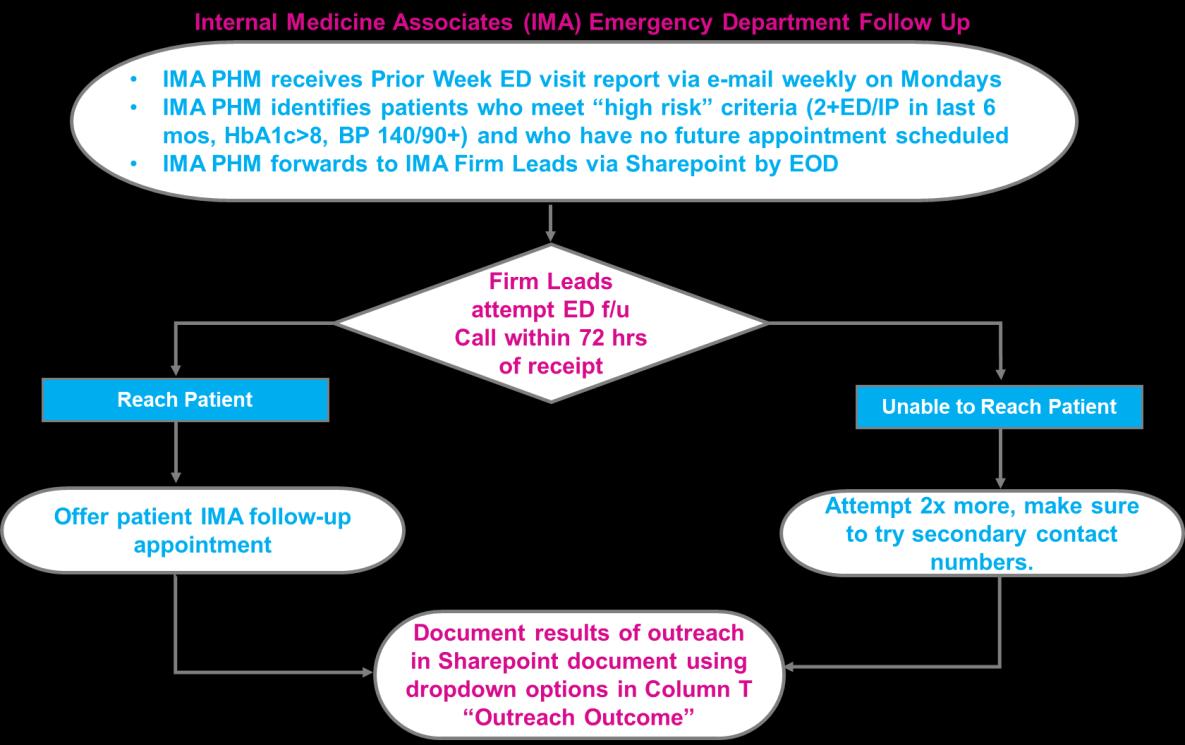
In 2022, IMA began a new process in which value-based care patients who are high-risk (defined as having either a last HbA1c > 8 percent and/or a last BP > 140/90 and/or 2 or more ED visits in the last six months and/or two or more hospital admissions in the last six months) with no future IMA appointment were contacted by front desk staff to schedule follow-up. In 2024, this work was transferred from the Front Desk to IMA’s Patient Encounter Associates. Reach rate has remained acceptable and the show rate is on par with the IMA average.
Data represents 5/2/22 – 9/27/24.
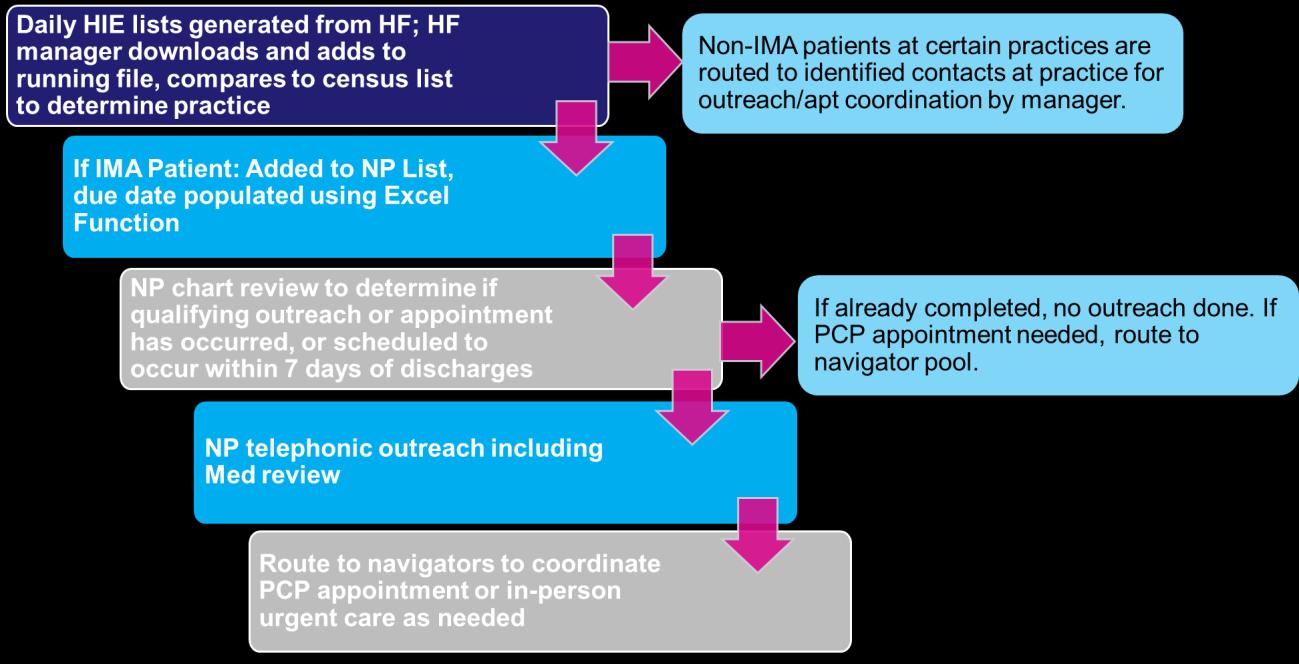
Nurse Practitioner Outreach for Discharge and ED Follow-up
Called/Reached
Unable to reach VM left
Reviewed-PT w/ Qualifying Outreach/appt
Not Outreached
Other
In addition, IMA piloted NP-based outreach in response to a Q3-4 initiative with Healthfirst to follow-up all patients within seven days of hospital discharge and to follow-up patients with multiple chronic medical conditions within seven days of an ED encounter (these quality measures are known as MRP and FMC, respectively). The reach rate was excellent, and the 2023 approach will be adjusted pending review of impact, cost-effectiveness, and available NP time in 2024. The goal is to scale successful work to all IMA patients as resources allow.
In January 2024, the IMA faculty, Drs. Eric Kutscher, Doug Halket, Cary Blum, Alison Koransky, and Mary Fishman and ambulatory chief resident, Dr. Fiona Desland, received a $50,000 grant from the Office of Well-Being and Resilience focused on improving clinic documentation and efficiency. In the spring of 2024, seven unique focus groups were conducted to assess areas for improvement among faculty, nurse practitioners, residents, interns, social workers, nurses, and administrative assistants. Using the result of these focus groups, a new standardized note template based on “problem-based charting” was developed. Faculty and residents received extensive training on the new charting methodology and importance of standardization Residents were also given the opportunity to receive payment for reviewing and updating patient charts to ensure accurate problem lists. In July 2024, all 160+ residents transitioned to problem-based charting and use of the standardized note template and orders preference list. A pre-intervention wellness and satisfaction survey was conducted in July 2024 and a postintervention survey will be administered in June 2025.
Preliminary review of the impact of transitions to problem-based charting has shown an increase in the documented complexity of patients measured by risk adjustment scores and a decrease in the number of characters in clinic notes. Six-month focus groups are currently underway to assess changes in satisfaction and wellness among all stakeholders at IMA. Data on user time in chart and time on documentation is being pulled from Epic with the help of DTP.
In addition to receiving training on standardized note templates and best practices for documentation, residents also received training on the importance of avoiding language that could be considered stigmatizing or offensive. This training was provided to PGY-1s during orientation and to PGY-2 and 3 residents as part of their required communication didactics. Residents were offered the chance to update charts in the medical record to ensure accuracy and include proper diagnostic information and remove inappropriate language or “never” words, with more than 1,200 charts manually reviewed and updated by forty-two residents. Since July 1, 2024, all 160+ residents at IMA have adopted use of this standardized note template that prevents copy-forward of previous information, which ensures that inappropriate text is not inadvertently carried forward, and that requires problem-based charting, which ensures the use of accurate medical diagnoses rather than subjective terms more subject to bias. IMA will continue assessing changes in the presence of “never” words since implementation of this intervention. IMA’s efforts to improve the quality of clinical documentation are part of the FAIR (Factual, Affirming, Informative, Respectful) Initiative.
Rate of notes with problematic language at IMA from faculty, residents, and NPs before vs after July 1 launch of problembased charting
Christopher Gold, DO
Heather Viola, DO


In 2024, the Division of General Internal Medicine at Mount Sinai Morningside and Mount Sinai West continued efforts to improve chronic disease management. Improving hypertension (HTN) control continued to be a focus for the Division. Efforts also continued regarding depression screening rates. Two recent projects in the last couple of years focusing on improving abdominal aortic aneurysm (AAA) screening among male patients with a history of tobacco use and liver fibrosis screening in diabetic patients continued to show growth as well. Statin use in cardiovascular disease (CVD) and/or diabetes was a new metric for the Division, which continues to be a top focus.
Additionally, with the utilization of the Ambulatory Quality Dashboard in Epic, providers can now, in real time, review their own metrics for all ambulatory quality measures and redirect performance efforts as indicated.
The Division continued efforts for controlling hypertension, with a target of 75 percent of patients having a last blood pressure (BP) on file of <140/90. The target metric has increased from 70 to 75 percent over the last few years. BP control has continued to increase since the initiation of the project, from 63 percent in January 2022 to 74 percent as of the end of 2024. All three practice sites realized improvement throughout the past two years, and as efforts continue, the Division is on the trajectory to reach the target of 75 percent.
The Division developed new strategies and workflows that were implemented in 2022. This fourphase approach was continued into 2024 with some additional updates.
The first phase was on provider education. Practice site champions were tasked with reminding providers during staff meetings of the available tools to improve BP management. If in-office BP readings were elevated, providers were reminded to repeat this measurement at the end of the visit and ensure this is documented in Epic. Providers were educated to inquire about home BP readings as well and, if taken the same day as the appointment, can be entered into Epic for both in-person and telehealth visits. These home BP readings do count towards the metric and can be helpful in populations such as those with white coat HTN. Providers were also encouraged to utilize telehealth for home BP review and medication adjustments. In addition to the above, BP visits were scheduled with on-site clinical pharmacists and nurses in between provider visits to ensure closer monitoring.
Recently added in 2024 is the new Hypertension Control Dashboard in Epic, where providers can review their patient panel HTN statistics in real time. This dashboard shows the percentage of controlled HTN patients for a particular provider. Additionally, for those that are uncontrolled, it tracks whether repeat BP readings were documented on the same day, and whether follow-up appointments were scheduled.
An additional tool that has been utilized for 2024 is the Primary Care Hypertension SmartSet. This SmartSet is an all-encompassing HTN panel for providers, including commonly prescribed medications, patient education materials such as BP machine recommendations and tips on accurate measurement, and a quick click option to place the “MyChart BP Flowsheet” order for patients to electronically record their home BP readings in Epic themselves.
Providers were also encouraged to refer qualifying patients to the remote BP monitoring program. The goal of this management program is to coordinate care with clinical pharmacists and patient care liaisons to help bridge the gap between provider office visits. The overarching goal is to improve HTN control to reduce future cardiovascular events and improve patient outcomes. This program allows patients to monitor their BP from the comfort of their own home with the coordination of a care team. In this four-part program, the physician first identifies qualifying patients and places a referral. Next, patients are enrolled, introduced to their care team, and provided with and oriented to their BP machines. The third component is the clinical management phase, where pharmacists reach out via telehealth to monitor and manage BP. Frequency of televisits vary by patient risk level, and all updates are shared with referring providers. The fourth part is the clinical maintenance phase, where patients who have reached their goal continue to be monitored monthly.
The second phase of the HTN strategy focused on medical assistant (MA) education. Practice site champions and clinical supervisors were tasked to educate staff on proper measurement techniques and to standardize the patient triaging process. Periodic check-ins with MAs were performed thereafter to ensure practices were implemented correctly.
The third phase included a shared HTN workflow that centered on MA engagement and presession huddles. Providers were encouraged to add a “last BP” column to their Epic schedule headers that would appear on their daily patient schedule. With this shared information, MAs and providers can then review those with uncontrolled readings during pre-session huddles or upon triage. This not only facilitates shared information for the entire care team but also adds an additional reminder to focus efforts accordingly for those with uncontrolled readings.
The fourth and final phase of the HTN initiative included increasing direct outreach to uncontrolled HTN patients. The goal of this program is to facilitate and ensure that follow-up appointments are made with either a provider, nurse, or clinical pharmacist. Generating outreach lists was facilitated with the addition of the HTN Control Dashboard in Epic, which can recall uncontrolled HTN patients who do not have an upcoming appointment scheduled. Care teams consisting of nurses and population health representatives conducted telephone outreach to patients to schedule appointments, remind patients to check BP at home, and ensure medication adherence. If patients were unable to be reached via phone, templated messages were sent to patients via MyChart.
With the success of these efforts, the Division saw a great improvement in HTN control, increasing from 70 percent in the beginning of the year to 74 percent at the end of 2024, nearing the target metric heading into 2025.
Upper West Side (UWS) Performance Target
Depression screening continued to be a focus for the division, which has proven to be a successful endeavor since initiation in 2022. Patient Health Questionnaire-2 (PHQ-2) screening and documentation of a follow-up plan for those with a positive result are tracked, with a target compliance of 70 percent. The Division continues to show tremendous success and remains well above this target.
A multidisciplinary workflow was recently implemented and continues to be utilized. This multidisciplinary care team includes MAs, providers, and social workers, who are all involved in the effort to improve depression screening. Clinical supervisors were tasked with MA education, reminding MAs to complete the PHQ-2 depression screen at all visits during rooming to standardize the triage process If the PHQ-2 is positive, MAs were instructed to notify providers, who can then complete the PHQ-9 during the visit and discuss with patients. Providers were also reminded to document the follow-up action taken (e.g., medication prescribed, therapy referral made, etc.) in the Epic flowsheet along with the PHQ-9 If providers determine that a referral to a behavioral health (BH) specialist is indicated, the recently improved BH referral pathway facilitates this with social worker (SW) engagement.
Evidence has shown that mental health follow-up is improved with personalized care coordination; patients are more likely to attend appointments and continue to follow up with a psychiatrist if linkage to care occurs through their primary care provider (PCP). In light of this, the Division recently initiated a new BH referral pathway to utilize SW and care management (CM) teams to directly link patients with BH specialists. The objectives were: to increase timely access to BH care for those referred from their PCP, to provide patients with a liaison who can ensure adherence and engagement with BH providers, and to track successful referral connections and recommend areas where additional capacity is needed.
The BH pathway starts with the PCP referring to SW or CM via telephone encounter or Epic referral. SW/CM then reviews options for therapy/psychiatry within Mount Sinai and reaches out to partner coordinators to help link patients to a BH provider. They will also check in periodically with patients to ensure continued engagement with the BH provider. SmartPhrase forms for SW documentation were developed to allow the population health team to track BH referrals and follow-up care. With the success of these workflows and pathways, the Division has continued to excel and, as of the end of 2024, is at 87 percent compliance
UWS Performance Target
The Division also continued to focus on completion rates of AAA screening in men aged 65-75 with a history of tobacco use. This has been a division-wide effort. With the help of the population health team, an opportunity for improvement was identified. In 2022, prior to the initiation of the intervention, only about 4 percent of eligible patients had AAA screening completed throughout the division.
The Division had a two-part approach to this initiative. The first part focused on provider education. Providers were reminded to discuss AAA screening alongside other screening tests at annual physicals, and instructions on how to order the test in Epic were reviewed. If eligible patients have already received an imaging test such as ultrasound, CT scan, or MRI scan during the recommended age range, and the report fully comments on the abdominal aorta, providers were reminded that this imaging fulfills the screening requirement Additionally, in 2024, the AAA screening was added to the “care gap” and “health maintenance” tab in Epic for eligible patients, further increasing provider engagement. The second part focused on direct patient outreach by nurses for those with incomplete screening. Outreach started in 2023 and has been ongoing since. Nurses at each site are periodically given a list of eligible patients requiring outreach. Telephone and MyChart message scripts were created for convenience and standardization. Nurses can call patients to discuss AAA screening and, if the patient is agreeable, orders can then be pended for the provider to sign. If patients do not answer after two attempts, nurses can then send templated MyChart messages via Epic
The percentage of AAA screening ultrasounds ordered has increased to 42 percent as of September 2024. In addition to screening rates, the Division is also tracking outcomes of these tests and whether proper referral/evaluation with Vascular Surgery is done. These numbers are expected to continue to increase into 2025 with implementation of the efforts described
The Division also continued to focus on improving liver fibrosis screening among diabetic patients Metabolic dysfunction-associated fatty liver disease (MAFLD) affects 25 percent of the population, and the incidence is higher in the diabetic population. Liver fibrosis is the most important predictor of clinical outcomes. The aim of this project is to increase fibrosis-4 (FIB-4) score utilization to 10 percent of patients with type 2 diabetes. Of those with elevated FIB-4 scores, the goal is for 50 percent of patients to receive appropriate referrals for a fibroscan, also known as vibration-controlled transient elastography (VCTE), or a liver specialist consultation based on the score.
The FIB-4 Index for liver fibrosis is a noninvasive scoring system based on age and several laboratory tests, specifically liver enzymes, and platelet count, which help to estimate the amount of scarring in the liver and the potential need for further investigation. A fibroscan is a quick and noninvasive diagnostic device using sound waves to assess liver stiffness and fibrosis. The stiffer the liver tissue is, the more severe fibrosis there is likely to be.
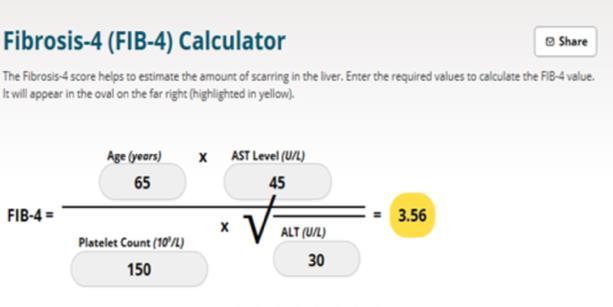
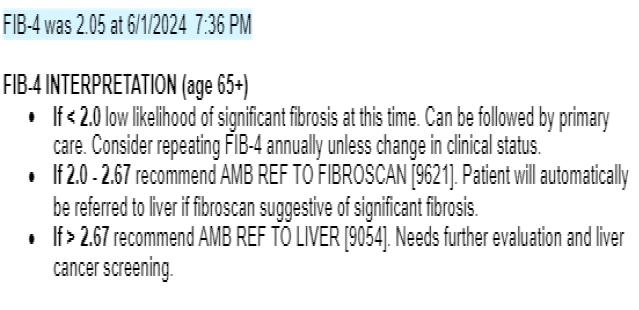
To increase engagement, providers were regularly reminded of the workflow. In patients with type 2 diabetes, FIB-4 scores should be calculated on an annual basis. During the visit, when diabetic patients are identified, the PCP can calculate the FIB-4 score utilizing the Epic SmartPhrase provided. This SmartPhrase automatically calculates the FIB-4 score and provides written recommendations based on the result. Providers then can place an Epic referral order for a fibroscan or to a liver specialist based on the score, as shown above To increase accuracy and avoid unnecessary referrals, the SmartPhrase was updated in 2024 to reflect a score adjustment for patients aged 65 and older.
The graph below illustrates the percentage of eligible patients screened utilizing the FIB-4 SmartPhrase From 2023 into 2024, the Division has met and continues to exceed the primary target of 10 percent.
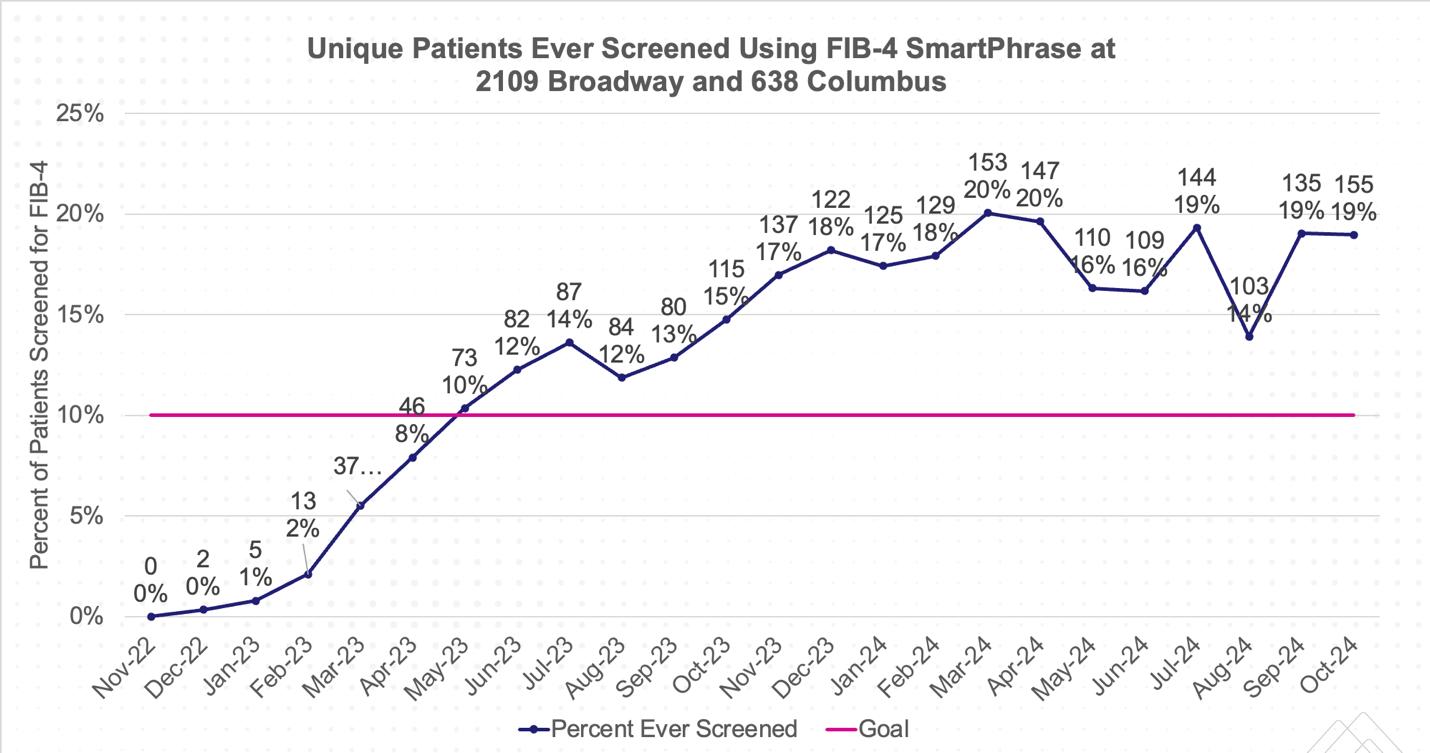
For those with elevated FIB-4 scores, the percentage of patients who received a referral for further investigation was 43 percent. This is slightly under the goal of 50 percent, and efforts will be focused on improving this outcome in 2025. Lists of patients who are indicated for a referral for a fibroscan or to a liver specialist based on their FIB-4 score will be generated, and coordinators will assist in patient outreach. This will be done both by phone call and arranging follow-up appointments with providers. Templated messages have also been created and distributed to both coordinators and providers, which can be sent to eligible patients via MyChart to increase engagement and awareness.
When looking at the results of the fibroscans completed, about 19 percent of patients were diagnosed with some level of fibrosis. Without use of the FIB-4 score, the fibrosis may not have otherwise been diagnosed or may have been found at a more advanced stage. This not only helps to identify liver fibrosis earlier and potentially minimize progression but also allows providers to connect patients to a liver specialist in a timely manner.
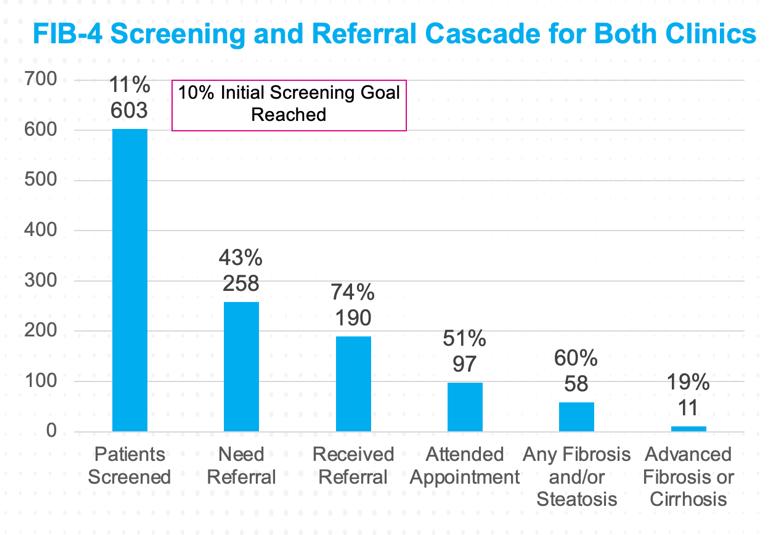
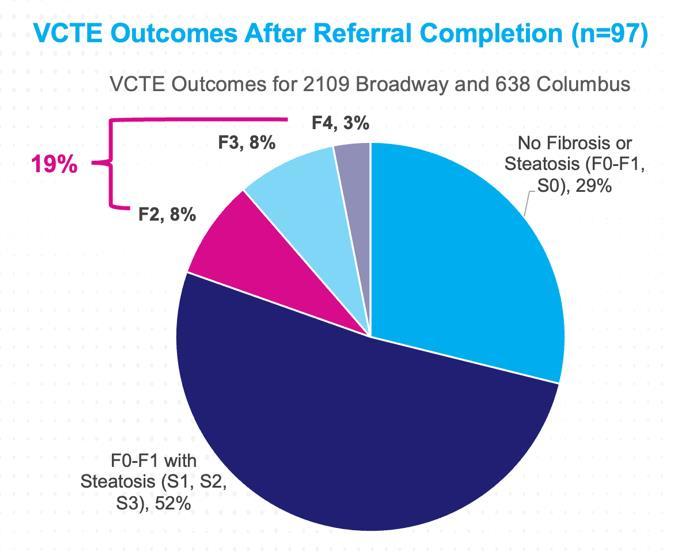
To highlight the importance and utility of FIB-4 scoring and fibrosis screening in diabetic patients, these findings were presented at the 2024 American Association for the Study of Liver Diseases (AASLD) conference. This was a collaborative effort between the departments of Gastroenterology and General Internal Medicine.

Another focus for the Division was a recently added metric: statin use in CVD and/or diabetes
The target goal for this metric is for 83 percent of eligible patients to be marked as actively taking or having received a prescription for statin therapy during the measurement period. This metric includes all patients between the ages of 21 and 75 who either have a diagnosis of atherosclerotic cardiovascular disease (ASCVD), familial hypercholesterolemia, or a low-density lipoprotein cholesterol (LDL-C) level at or above 190. It also includes patients aged 40 to 75 with a diagnosis of diabetes.
For this initiative, the Division focused on provider awareness and engagement. Providers were routinely reminded of evidence-based recommendation criteria for statin therapy as listed above. In addition, providers were updated on how the metric is met and certain exclusion criteria. These exclusion criteria include any patients who are ordered for a PCSK-9 inhibitor, have a diagnosis of end-stage renal disease or rhabdomyolysis during the measurement period, are receiving hospice/palliative care, or are pregnant or breastfeeding. Additionally, any diagnosis of statin-associated muscle symptoms or any patients with a listed statin allergy are excluded. To further engage and remind providers, the statin metric was added to the “care gap” and “health maintenance” tab in Epic in 2024 for eligible patients.
Throughout 2024, the accuracy of the data provided for this metric improved. One example of how this was done was by updating exclusion diagnosis codes. This allows for a more accurate identification of statin intolerance and removes ineligible patients from the metric. The Division saw a large improvement in achieving this metric, increasing from 70 percent at the end of 2023 to 76 percent at the end of 2024. The Division expects continued improvements in 2025.
The Division also continued initiatives to improve the rate of diabetic eye exams This metric includes patients aged 18 to 75 with a diagnosis of diabetes. The eye exam should be done every two years if there is no diagnosis of retinopathy, and annually if a diagnosis of retinopathy is documented in the last three years. This differs from the data recording in 2023, where the lookback period for retinopathy diagnosis was one year. Additionally, external visit codes through Epic have been narrowed to reflect accuracy. These changes may explain the decrease in performance from end of 2023 to beginning of 2024, though improving up to 61 percent at the end of this year. The continued efforts for this metric were multidisciplinary: MAs pending referrals to ophthalmology during triaging, providers placing referrals during both in-person and telehealth visits, and nurses completing direct outreach to patients. If a patient reported an
ophthalmology visit outside of the system, the provider/MA can obtain the visit date and enter this into the Epic “health maintenance” tab to fulfill the gap
UWS Performance Target
The Division continued to focus on breast cancer screening for women aged 50 to 74 Starting in 2025, this metric is scheduled to be updated to include women aged 40 to 74, reflecting new recommendations from the United States Preventative Services Task Force The reporting of this metric was shifted to the Epic dashboard in 2024, which improved data accuracy. It was noted in the prior year that some credit was given for mammogram orders even if screening was not completed. This is reflected in the dip in performance at the end of 2023 and start of 2024, though this improved throughout the year, ending above the target goal at year end. Several interventions were continued to help the Division reach the target. MAs routinely asked about mammograms during triage if the care gap was noted to be open Providers asked during visits as well. An order can then be pended by the MA or placed by the provider for the patient to complete. If the mammogram was done externally, MAs were asked to call outside radiology centers to obtain the report and record the completion date into the “health maintenance” tab. Epic also automatically and routinely captures mammograms completed at Mount Sinai and by outside claims in the “health maintenance” section.
In addition, the existing mammogram van initiative continued at all practice sites. The van sets up outside each of the three practice sites once or twice a month. Providers have the capability to directly schedule their patients for an appointment at the mammogram van. This allows for easier and faster access for patients to complete the mammogram, and an alternative option for those with physical or social barriers preventing a visit to the radiology center.
UWS Performance Target
Colorectal cancer screening was another initiative for the Division that continued in 2024 Completion rates continued to increase, from 71 percent in the beginning of 2023 to 78 percent as of the end of 2024, surpassing the goal of 72 percent. The Division continued to collaborate with the Gastroenterology department to facilitate direct colonoscopy referrals Colonoscopy referrals can be directly placed by PCPs, bypassing the need for Gastroenterology consultation. After a direct referral is placed, the Gastroenterology scheduling coordinator will directly reach out to the patient to discuss and schedule the procedure. If a patient reports a colonoscopy performed at an outside facility, MAs were tasked with calling to retrieve the report, placing the completion in the “health maintenance” tab, and modifying the screening interval to reflect this testing For patients who were hesitant or had barriers to colonoscopy, providers were encouraged to offer alternative screening options for average-risk patients including Cologuard and fecal occult blood testing (FOBT).
UWS Performance Target
Continued efforts were also focused on decreasing the percentage of diabetic patients with hemoglobin A1C (HbA1c) level >9, indicating uncontrolled diabetes. New to 2024, in addition to diabetic patients with a HbA1c >9, diabetic patients with no HbA1c on file in the last 12 months are also considered uncontrolled. This change partially explains the rise in patients considered uncontrolled from the end of 2023 to the beginning of 2024.
The Division continued efforts including coordinated care with certified diabetes educators (CDEs) and clinical pharmacists on site to follow poorly controlled patients more closely, scheduling regular office visits in between provider visits. For patients who qualify, providers were reminded to consider the remote patient monitoring program for diabetes. To qualify, patients must have a diagnosis of type 2 diabetes and have two HbA1c values >8 in the last 12 months, or a new diagnosis of diabetes in the last three to six months with a HbA1c >8. They cannot be on a continuous glucose monitor. Like the remote BP monitoring program, a multidisciplinary care team helps bridge the gap between provider office visits. Patients are given a glucometer and test strips. The enrollment, education, and monitoring processes are like those of the BP monitoring program.
With the above efforts, as of the end of 2024, the Division has met the goal of <18 percent of uncontrolled diabetic patients with a last HbA1c of >9.
UWS Performance Target
Finally, the Division continued to focus on patient reduction of inpatient (IP)/Emergency Department (ED) utilization and overall reduction of total cost of care (TCoC). The goals were to identify high-utilizer patients at each practice site (defined as two or more preventable ED or IP admissions), reduce unnecessary utilization and overall total cost of care, and identify interventions that can be implemented to aid in these goals
This project was coordinated by a multidisciplinary outreach team that included population health members, schedulers, referral coordinators, SWs, and nurses. Interventions included CM and specialist referrals, increased scheduling of follow-up appointments with PCPs, patient education regarding escalation of care (e.g., office visits, urgent care, ED), and education regarding community resources (e.g., community paramedicine, Meals on Wheels). Outreach was focused on patients with diabetes, congestive heart failure, or chronic obstructive pulmonary disease, as these populations tend to have higher complexity and utilization rates
From 2022 to 2024, both IP and ED utilization have substantially decreased, down 76 percent and 68 percent, respectively. This decrease was noted at all three practice sites. As a result, the total cost of care has also decreased, and the observed-to-expected ratio (O:E) improved. This is illustrated in the two graphs below.
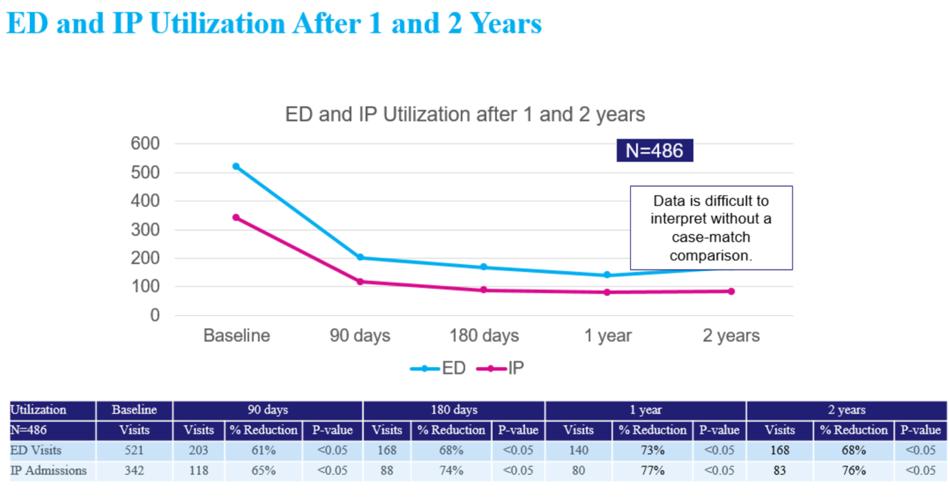
2021 FY 2022 FY 2023 FY 2024 (thru June 2024) Target (0.89)
As the Division continues to ensure a reduction in observed utilization for IP/ED visits, efforts will now also be focused on improving the expected component of the ratio. One way this can be done is by improving accurate documentation of complex diagnoses. Annual Hierarchical Condition Categories (HCCs) recapture rates have decreased slightly in the last years, illustrating room for improvement for the Division. Similarly, the best practice advisory (BPA) completion rates on Epic were recently noted to be lower among newer providers. These BPA
alerts remind providers to consider using diagnosis codes that can document the increased complexity of patient care. With the click of a button, providers can decide whether to agree and add the code or disagree. To improve BPA touch rates, the Division held brief, small-group education sessions to increase understanding and importance with new providers. These sessions proved to be successful, and BPA touch rates increased across all three sites. As the Division continues to focus on this into 2025, these practices will continue to be implemented and expanded.
BPA Touch Rate for Providers Who Received Small-Group Education
May 2024 Pre-intervention 5 Months Posts
Division Quality Champions:
Dahlia Rizk, DO, MPH
Kristine Favila, DO
Svetlana Chernyavsky, DO



In late 2023, the health system implemented a 10-month closure plan for Mount Sinai Beth Israel (MSBI) with a final date of operations target of July 2024. The 230-bed academic institution underwent careful coordination of floor closures and diversion of specialty lines and ancillary services. On July 1, 2024, all trainees (residents and fellows) departed the campus. However, due to complexities of the closure process and external complications, the hospital remained open and continued to operate with an average of 55 occupied hospital medicine/critical care beds. The Division transitioned from an academic care delivery model that once included 120 internal medicine residents to one that combined direct care and locum tenens advanced practice practitioner (APP)-paired shifts. A robust transfer process within the Health System for ED, floor, or ICU patients in need of specialty or care escalation was also employed. After July, the hospitalist group remained largely intact while the ED, ICU, and nursing departments were mostly staffed with locum tenens, per diem, and moonlighting providers.
While MSBI did not join the Health System in transitioning to the Vizient platform for riskadjusted performance data, raw data for length of stay (LOS), mortality, and discharge before noon (DBN) remained available to review high-level trends. Comparing hospital medicine metrics from pre- and post-July 2024 (when the most significant changes to hospital staffing and workflow occurred), the risk-unadjusted average LOS improved from 4.98 to 4.21, average DBN improved from 11 percent to 9.48 percent, and average mortality rate remained relatively stable (1.17 percent vs. 1.22 percent). Hospital-acquired infection (CAUTI, CLABSI, CDI) rates also improved. While a decline in average case mix index of 0.2 compared to 2023 and reduction in census contributed to these improved metrics, a protective factor was likely the intact division of experienced hospitalists who were already adept at navigating care within the Health System under dynamic conditions.
Source: tableau.mountsinai.org Accessed: 1/2025
Regarding patient experience, top box scores for the HCAHPS domain of “doctor communication” also remained favorable since Q1 2023 despite the changes. The Division postulates that the lower census and care delivery model changes facilitated bedside time with patients and families and streamlined communication.
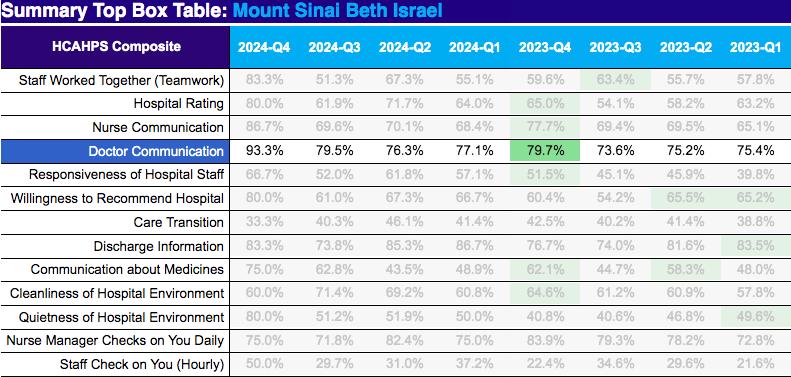
Source: tableau.mountsinai.org Accessed: 01/2025
The observations that an institution can potentially undergo a drastic transformation to staffing and care delivery without sacrificing quality, efficiency, or patient experience will be shared as an invited poster presentation at the Society of Hospital Medicine (SHM) annual meeting “SHM Converge 2025” in Las Vegas, Nevada.
Division Quality Champion: Anne Linker, MD
The Division of Hospital Medicine (DHM) at The Mount Sinai Hospital (MSH) is active in many distinct aspects of quality improvement and patient safety, including improving length of stay, reducing readmissions, safety in transitions of care, reducing hospital-acquired infections, and working to improve equity in care. MSH DHM is also part of the system-wide effort to expand
the Mount Sinai at Home program and is proud to be a strong contributor to the enrollments in Hospitalization at Home and Rehabilitation at Home. The faculty are also active in multiple hospital-wide committees, including the MSH Root Cause Analysis Committee, MSH Clinical Review Committee, MSH Department of Medicine (DOM) Quality Improvement Committee, MSH Length of Stay/Readmissions Committee, MSHS Sepsis Committee, and the MSHS Pneumonia Committee.
In 2024, DHM worked on several projects to improve length of stay (LOS). The Division has worked to balance the rising census with efficient care coordination. Ongoing initiatives to target reduced LOS included: the Discharge Acceleration at Sinai Hospital (DASH) program (which has been previously reported in the Annual Report); the “Phone-A-Friend” Program, through which experienced hospitalists provide real-time guidance and mentorship to faculty caring for complex patients; and ongoing work to optimize electronic handoffs to improve transitions of care when new attendings come on service.
In 2024, the Division focused on addressing several drivers of prolonged LOS. These initiatives included efforts to improve interhospital transfers, foster better collaboration with the Emergency Department for admitted patients experiencing extended stays in the Emergency Room, understand barriers to discharge for patients undergoing tracheostomy during hospitalization, and streamline the coordination of bedside procedures for hospitalized patients through the Hospital Medicine Procedural Service.
The Division has seen a trend towards improvement in the overall LOS over the past three years with a combination of these interventions.
(Source: Tableau Excess Days Dashboard, Medicine Service MSH 1/1/2021-12/31/2024). Blue line is ALOS. Q2 2021
A multidisciplinary workgroup was created in collaboration with the ED to better understand the impact of extended boarding times for patients admitted to the Department of Medicine but boarding in the emergency room. The workgroup was formed after anecdotal evidence suggested an opportunity to discharge more patients directly from the ED, as some were being discharged shortly after transferring to an inpatient unit. This scenario results in unnecessary duplication of work for nursing and social work teams, as well as bed management and environmental cleaning. A process map was developed (below) to identify the following opportunities for improvement: communication (e.g., unclear plans from frontline providers, varying approaches to pace discharge planning, and delays in placing IDP/discharge orders), care delays (e.g. need to expedite imaging/testing and team assignments), inefficient workflows (e.g., duplication of efforts by case management and social work), and patient dissatisfaction.
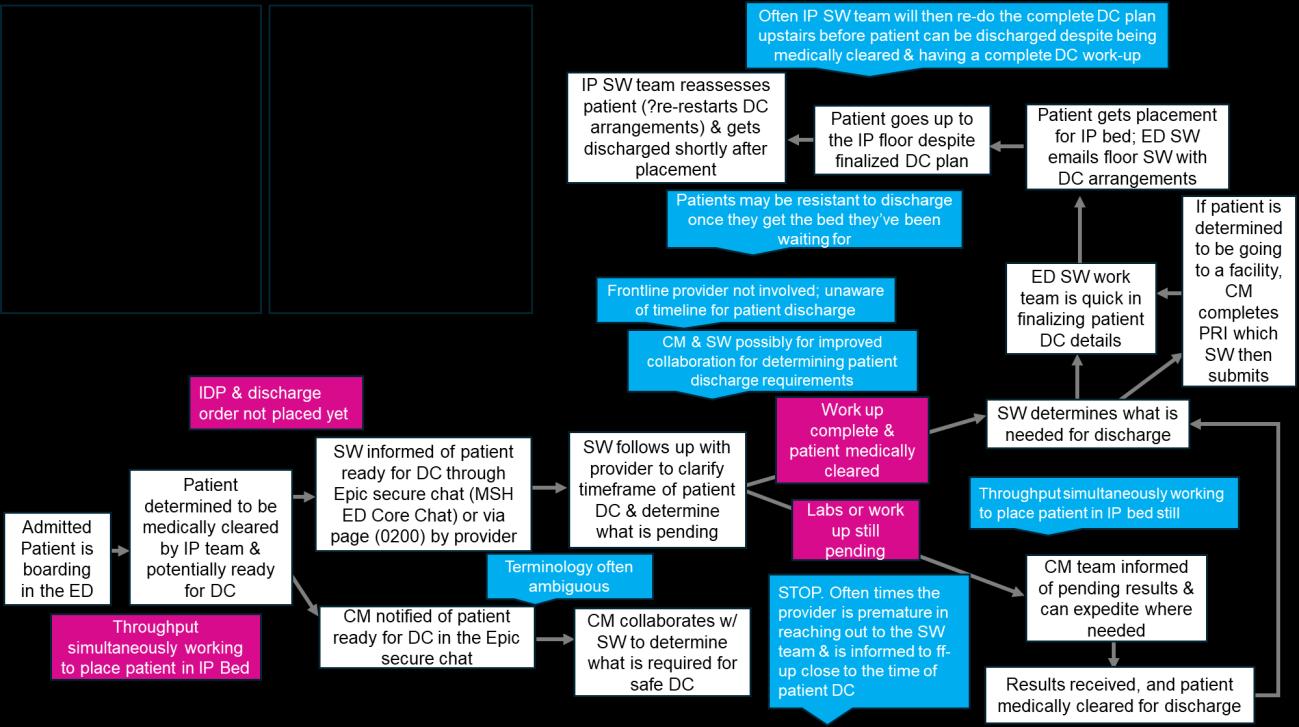
Baseline data on the percentage of patients who are discharged within 12 or 24 hours of arriving on the unit from 2023 is presented below.
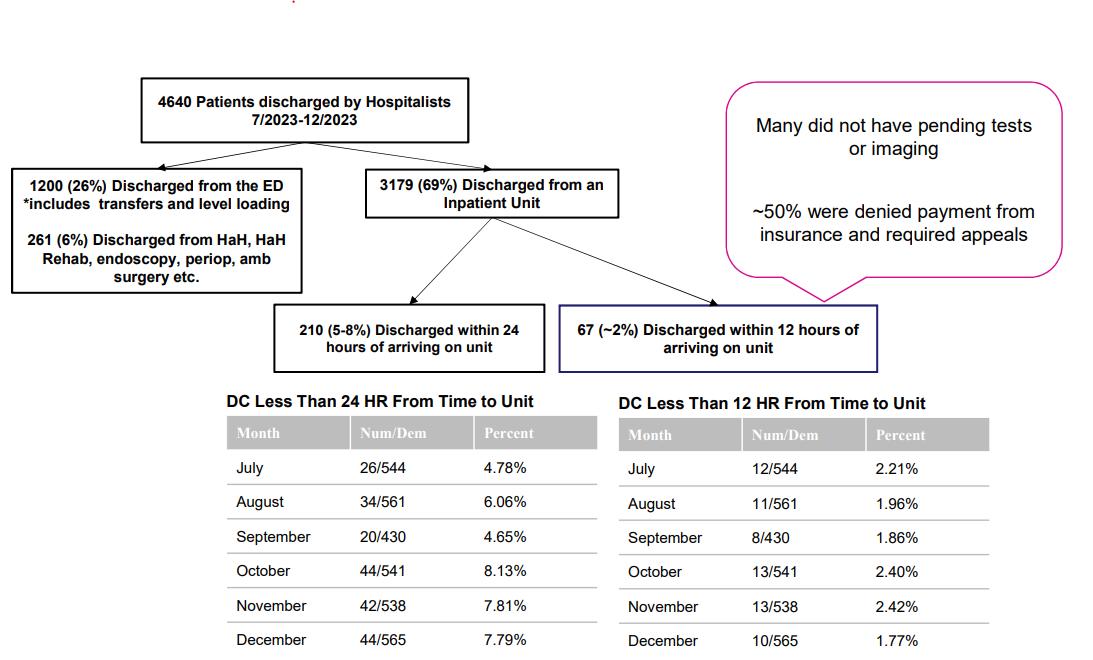
Several initiatives emerged from the current state evaluation to improve workflows, efficiency, and communication for admitted patients in the ED. These include ensuring that ED nurses can easily print the After Visit Summary from the inpatient context, streamlining workflows to connect Social Work and Case Management with primary teams for patients nearing discharge through an Epic chat workflow, improving access to contact information for key ED staff (e.g., the nurse manager), devising an escalation pathway for patients requiring a location change for procedures or interventions, and reviewing and working on nursing workflows to avoid redundant tasks during admission evaluations.
Updated data from 2024 is presented below. Overall, there was an increase in the percentage of patients being discharged from the ED by hospitalists.
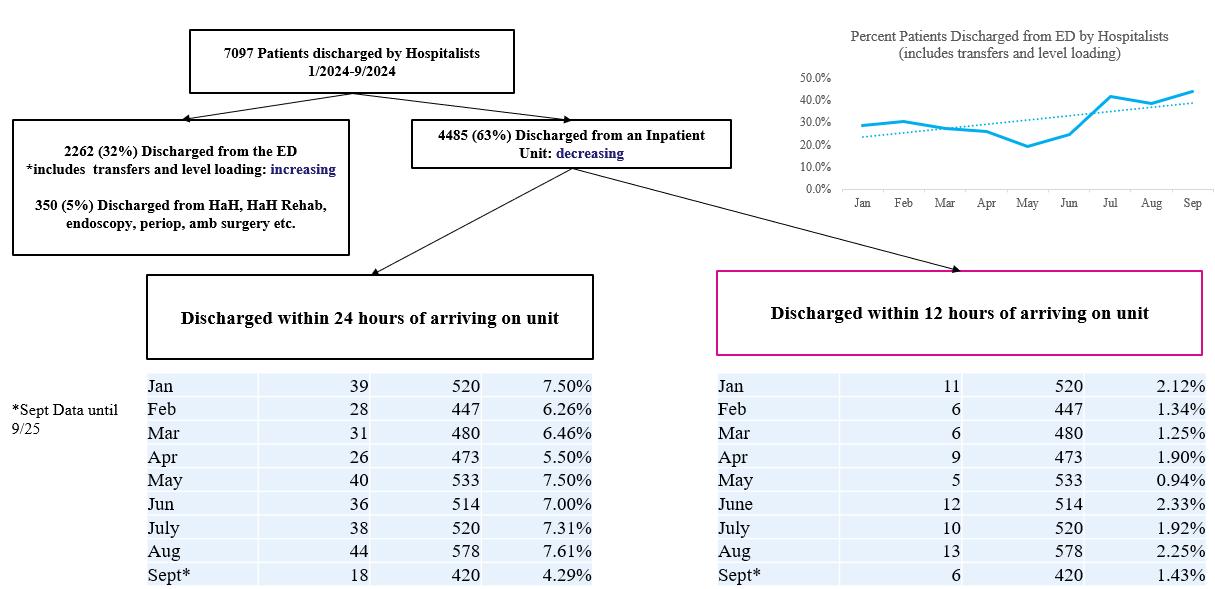
The work group also examined the relationship between the LOS of hospital boarding time and hospital length of stay (presented below). In 2025, the team will review cases of patients who had a hospital length of stay of seven to ten days who spent three or more days in the ED.
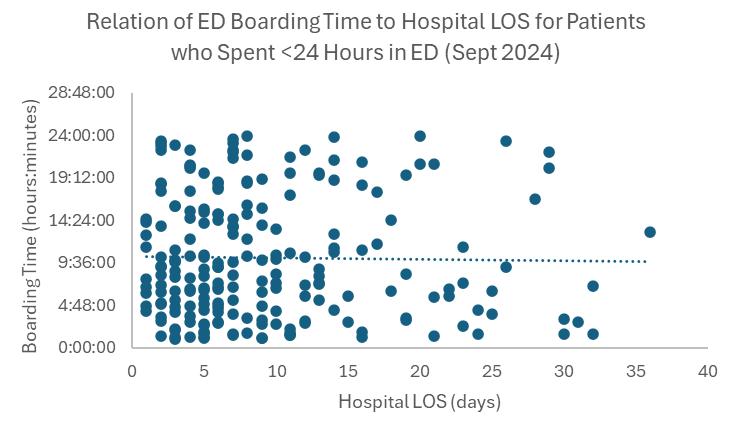
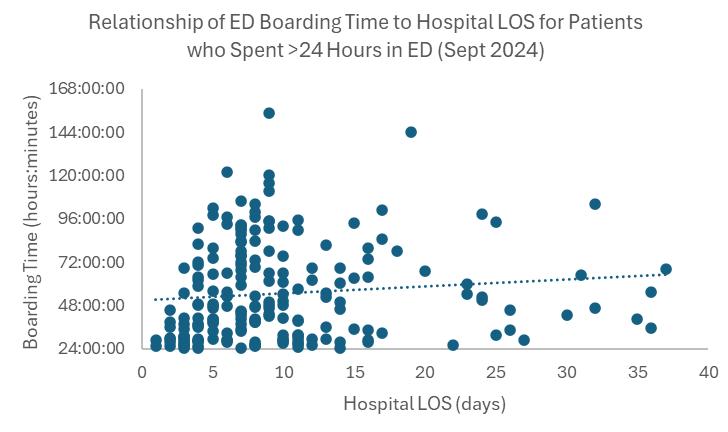
In addition to the initiatives set forth by the workgroup, the DOM quality team is investigating the impact of boarding in the ED after hospital admission among older patients (i.e., patients older than 65 years, admitted to the DOM at MSH, who spend more than 12 hours in the ED while waiting for an inpatient bed). The primary outcome variable is in-hospital mortality within 30 days of admission. Secondary outcomes include in-hospital complications such as falls, infection, bleeding, myocardial infarction, stroke, thrombosis, and pressure ulcers. Hospital
LOS, type of admission, and discharge disposition will also be collected in addition to basic demographic information (age, sex) and relevant comorbidities. Race, ethnicity, and language data will be collected as measures of diversity, equity, and inclusion. This IRB-approved study is ongoing and will continue in 2025.
Members of the quality team completed a retrospective review of interhospital transfers accepted to MSH from March 27-June 30, 2023. The review aimed to identify indications for transfer, patient outcomes during this period, and potential opportunities for improvement in the transfer process. The results of this review were described in the 2023 DOM Annual Report. Based on this work, DHM members collaborated with the Central Hospitalist group to create a checklist to standardize the information collected by the accepting hospitalist for patients transferred from other sites or outside the Mount Sinai Hospital System. In 2025, an evaluation is planned to assess the impact of this checklist on acceptance rates compared to the rate at which procedures are performed for these patients. The goal is to reduce transfers to MSH that do not undergo the planned procedure, thereby improving care efficiency for the hospital and enhancing patient-centered care by avoiding facility transfers without changes in management.
This collaboration between the Institute for Critical Care Medicine (ICCM) and DHM aimed to describe the clinical characteristics of patients who undergo tracheostomy during their admission. The goal was to better understand and address barriers to discharge and improve patient-centered outcomes including rates of decannulation. A workgroup was formed, and data from patients who underwent tracheostomy from December 2022 until September 2024 were collected, focusing on the 26 patients who graduated from the Rapid Weaning Program (RWP) during that period. The mean LOS was 87.5 days, with a median LOS of 64 days. The mean LOS after graduation from the RWP was 47 days, with a median of 31 days.
Significant challenges that arose for these patients included agitation, the need for restraints after tracheostomy placement, and difficulty communicating. Patients who underwent decannulation had a median LOS that was 12 days shorter compared to those who did not undergo decannulation. There was variable follow-up by procedural teams, and opportunity for standardization of trach size, advancing to speaking valve, and decannulation. The plan for 2025 is to create a post-tracheostomy standardized pathway and checklist, with the hope of promoting increased decannulation for patients successfully weaned from the ventilator.
Historically at MSH, DHM has been responsible for completing certain bedside procedures, including paracenteses and lumbar punctures (LPs). However, due to the low volume of these procedures, many faculty members have had little opportunity to perform them, resulting in insufficient procedural skill to supervise or maintain clinical privileges.
In a needs assessment survey among hospitalists, of 26 respondents, only 26 percent reported feeling comfortable performing an LP and 58 percent reported comfort with paracentesis. Among those with more than four years of experience, 0 percent felt comfortable performing an
unsupervised LP. Additionally, delays in procedures like LP caused by the need for assistance from other teams (e.g., neurology) have contributed to delays in patient care and longer LOS for some patients. As such, DHM established an On-Call Procedure Team (OPT) comprising five full-time hospitalists to perform LPs and paracenteses.
The OPT was implemented in April 2023. Before the launch of the hospitalist-run OPT, LPs for patients on hospitalist services were performed by neurology (27.2 percent), neuroradiology (23.5 percent), ED (16.0 percent), medicine primary team (13.6 percent), surgical services (9.9 percent), oncology (7.5 percent), and critical care (2.5 percent). After the team was instituted, most LP requests by hospitalist services were completed by the procedure team (73.6 percent). The unsuccessful procedures were eventually completed by neuroradiology (14.9 percent), with the remaining completed by neurology (2.3 percent), and critical care (2.3 percent).
The initial analysis of the OPT’s work was reported in the 2023 Annual Report. A further analysis was conducted looking at data from April 2022 to April 2024 to determine if there was improvement in time from request to the time of the procedure after establishment of the OPT. Eighty-one cases were completed during the pre-OPT period and 84 cases were completed during the OPT period. The median LOS were 19.0 and 21 days, respectively (p=0.16). Of the cases completed during the OPT period, 63 cases were successful (75 percent) on the initial attempt. The median LOS for successful vs. unsuccessful LPs were 21.0 vs. 23.0 days (p=0.95).
The mean request-procedure time before and after the procedure team was instituted were 2.8 and 2.1 days, respectively (t=1.38, p=0.17). The mean time to procedure was significantly lower for successful compared to unsuccessful LPs (1.5 vs. 4.1 days, respectively; t=5.57, p<0.05). This analysis suggests that, in 2024, the OPT improved LOS for patients who required lumbar puncture.
In 2023, MSH DHM created a new program called “Phone-A-Friend,” which served as a peer resource for hospitalists to discuss challenging or complex patients, and to promote clinical development for less experienced hospitalists. A peer mentoring model was developed in which three senior hospitalists (SHs) with at least 10 years of clinical and administrative leadership experience were available to discuss complex cases. SH were available daily and as needed, and the program was promoted regularly to DHM staff. In 2025, the plan is to focus on how to target the use of the Phone-A-Friend program with proactive triggers to identify patients earlier in the hospital stay who could benefit from advanced care coordination.
DHM is proud to continue ongoing work in transitions of care, with the goal of improving readmissions. The readmissions rate was 14.8 percent from January to December 2024. There has been active work with several divisions, including Pulmonology and Cardiology, to improve the readmissions rates related to chronic obstructive pulmonary disease and congestive heart failure. DHM also provides a lecture series to the internal medicine categorical interns during ambulatory blocks focused on improving communication and coordination of care during the transition that occurs at discharge from the hospital.
To improve readmissions, in 2024, the Division embarked on a project with the Internal Medicine Associates (IMA) clinic to improve timely discharge follow-up for patients either already followed by the IMA clinic or without an established primary care provider, and who were hospitalized under the Hospital Medicine service. Initial data from April 2023-April 2024 suggested improvement compared to prior years in follow-up rates by 7- and 14-days postdischarge. However, rates remained low at 14.2 percent for one-week follow-up and 29.02 percent for two-week follow-up. Approximately 50 percent of patients completed an ambulatory appointment (primary care or specialty care) within 14 days of discharge. The DHM and IMA teams met with case management and utilization management specialist (UMS) teams to identify opportunities for improvement, and the plan is to implement interventions to improve registration into IMA post-discharge clinic visits for patients hospitalized on the Hospital Medicine service.
Medication reconciliation (MR) is foundational to patient safety during and after a hospital admission. Though MRs are consistently obtained at the point of admission, they may be incomplete due to missing information or not being documented in the appropriate electronic hospital record (EHR) tab. A QI intervention was conducted from July 31 to November 3, 2023, to increase the number of MR completed in the EHR tab. An online guide showing the workflow was created and distributed to all residents. Each week, a “Med Rec Monday” email was sent out to resident teaching teams with their current MR completion rates, along with a reminder of how to correctly complete and verify MRs. At the end of each two-week block, cookies were rewarded to the team with the highest percentage of MR completion. The names of the winning team were publicized to the entire residency program. In the three months leading up to the project, the average completion rate of MRs among admissions to General Medicine Teaching Service (GMTS) was 39.5 percent. Over the entire course of the project, the MR completion rate was 62.4 percent on average.
A third PDSA cycle was completed from July 29, 2024, to November 3, 2024. Three new interventions were introduced to ensure sustainability: first, a dedicated time for MR completion, branded “Med Rec O’clock,” added to the resident daily schedule; second, MR worksheets were created and distributed to patients or caregivers to aid in MR completion; and third, attending physicians were engaged by sending weekly MR dashboards to hospitalists on service. In the baseline period prior to the intervention, the average MR completion rate was 41.0 percent, which was slightly higher than the baseline of 38.8 percent in 2023 (χ2=1.1, p>0.25), and a large absolute increase from the pre-PDSA baseline of 22.9 percent. Over the three-month course of PDSA cycle 3, the MR completion rate increased to an average of 67.8 percent, a statistically significant improvement from baseline (χ2=170.0, p<0.01), and from the 62.4 percent rate observed after PDSA cycle 2 (χ2=6.23, p<0.05). The highest completion rate of 77.4 percent occurred during the last block of the cycle. In total, 112 dashboards were distributed to 36 GMTS attendings. Survey data showed that only 20 percent of residents used the MR worksheets. (See graph below.)



DHM plans to continue building on this work to improve patient safety, with the overall goal of improving both HCAHPS scores related to medication teaching and hospital readmissions.
In 2024, the Division worked closely with the Mount Sinai at Home team to improve the coordination of care during transitions between the inpatient and home setting and to increase referrals and admissions to the program. There is strong representation from MSH DHM among the hospitalists who serve as Hospitalization at Home attendings. The Hospital at Home and Rehabilitation at Home programs are described in a dedicated section of the DOM Annual Report.
DHM has taken an active role in interdisciplinary work to improve rates of central lineassociated bloodstream infection (CLABSI) at MSH. Previous work has included unit dyad (unit medical director and unit nurse manager) weekly rounding on our medicine units, partnership with hybrid units to ensure weekly rounding on patients who have central lines on non-medicine units, dedicated monitoring of CHG bathing on medicine units, and review of CLABSI efforts at monthly dyad meeting with Quality leadership. Huddles also occur for frontline staff when a CLABSI occurs, in cooperation with Infection Prevention. In addition, there have been dedicated efforts to improve awareness of which patients have central lines, the need for intravenous to PO conversion of common medications when possible, and documentation of central line duration as well as peripheral IV duration in daily progress notes.
This year, DHM undertook a more in-depth evaluation of patients who experienced CLABSI to better understand unaddressed drivers of CLABSI rates. Data was collected from all CLABSI cases attributed to the Department of Medicine from January 1 to August 2, 2024. Data collected included types of central line, line indication, and adherence to best practices for
CLABSI prevention, including consistent chlorhexidine gluconate (CHG) bathing and conversion of IV medications to enteral formulation when possible. The analysis also included a collection of relevant patient characteristics to elucidate potential risk factors for CLABSI: admission from nursing facility, LOS, overall mortality, pressure injury, and use of total parenteral nutrition (TPN).
Infections were most common in tunneled dialysis catheters, followed by peripherally inserted central catheter, non-tunneled catheter, and tunneled non-dialysis catheter, with a lower proportion of infections in patients with ports. 100 percent of patients received CHG bathing in the prior seven days, and there was little opportunity for intravenous to oral conversion of medications. 42 percent of cases were in patients who were previously in a long-term care facility. Median LOS was 62 days (IQR 32.75-120.25), with median LOS prior to CLABSI event of 27.5 days (IQR 10.5-57.75). Half of patients received TPN, and 71 percent of patients had an infection at the same encounter prior to the CLABSI. Fifty-eight percent of patients had a wound/pressure injury, and hospice or comfort care had been recommended in ~40 percent of cases, with patient mortality of 25 percent for the hospital stay.
This analysis demonstrates that patients experiencing CLABSI at MSH are often chronically ill and experiencing acute decompensation, have been hospitalized for an extended time, and have other risk factors, including use of TPN and pressure injuries. These results will hopefully allow identification of patients at higher risk of CLABSI in 2025 and create more targeted interventions to prevent CLABSI in the patient population.
The Student High-Value Care Curriculum is an active part of the DHM Quality Improvement efforts. In the past years, the curriculum was expanded to create partnerships with several other divisions and departments. This curriculum mobilizes and empowers groups of medical students, master’s students, and nursing students to work together to solve real-world challenges and to decrease overuse of materials and services in the hospital.
In the 2023-2024 academic year, the curriculum sponsored three projects. The first was a project targeting improved sleep for patients on the medicine service at MSH. The project is continuing into the 2024-2025 academic year. The second was a collaboration with Mount Sinai at Home geared towards improving the recruitment materials and process for patients approached for Hospital at Home admission. The third was a collaboration with Obstetrics and Gynecology to reduce readmissions for patients who experience pre-eclampsia. Data monitoring is ongoing for the third project.
A multi-modal quality improvement (QI) initiative to improve safety in interhospital transport was undertaken to address concerns of prior events that occurred in patients on the Step-Down Unit at MSH. The initiative included the adoption of a universal protocol requiring clinical personnel to accompany step-down patients during transport, as well as clear criteria for nurses, frontline providers, and respiratory therapists to ensure appropriate staffing. Additionally, the use of a “Ticket-to-Ride,” a written assessment and handoff tool, was implemented to promote safe patient transports.
The patient transport tickets were designed collaboratively by unit staff, including frontline nurses, the nurse manager, and physician leadership. Input was also gathered from Radiology nurses and physician leadership, given that most transports from the unit were for radiologic studies. To ensure familiarity and ease of use, a handoff format based on the Situation Background Assessment Recommendation (SBAR) framework was adopted. Patient demographics including identifiers and procedure location were included in “S,” patient characteristics including visual/hearing impairment and language were included in “B,” safety considerations including oxygen device evaluation and mental status were identified in the “A,” and personnel accompaniment requirements were listed in “R ” Nurses completed the tickets, which were placed in the physical charts that accompanied patients during transport to radiology studies. Upon return to the unit, tickets were removed from these charts and stored securely. The project consisted of 1) training nursing staff on how to complete the patient tickets, 2) measuring the rate of ticket completion for patients requiring transport on the Step-Down Unit from December 2023-September 2024, and 3) recording the number of reportable adverse events that occurred during patient transport on this unit over the same time span.
Data from the patient transport department showed that 1,146 transport events occurred during our intervention period. A total of 457 patient tickets were completed (39.9 percent). There was significant month-to-month variability in completion rates, ranging from 27.5 percent to 55.5 percent. Safety data, based on a review of safety reports, demonstrated that no adverse events occurred during patient transport during the period of interest.
Standardized patient handoffs are critical to patient safety during transport. Close patient monitoring through delineating requirements for the accompaniment of patients with clinical personnel successfully eliminated patient safety events during transport. While the Ticket-toRide process did not achieve optimal completion rates, it still helped in reducing events. Next steps include conducting a post-intervention survey to gather feedback from nursing staff and identify barriers to more successful implementation. By addressing these challenges and improving ticket completion rates, the aim is to enhance the effectiveness of the intervention and make it more adaptable for implementation in other health care settings seeking to standardize patient handoffs.
Division Quality Champions:
Brian Markoff, MD
Faye Reiff-Pasarew, MD
Laboratory Stewardship


Excessive laboratory testing can be painful, disturb sleep, decrease satisfaction, increase length of stay, increase transfusions, lead to venipuncture complications, and is labor intensive. Physician trainees often order extraneous labs due to a lack of understanding of what is necessary and fear of supervisor criticism. Electronic medical systems have simplified the ordering of lab tests, which can lead to recurrent ordering without much consideration.
In the past year, we continued our collaboration across MSM and MSW to improve laboratory stewardship. The Division’s interventions included education sessions with faculty and house staff, posters in the team rooms, contests, and audits with feedback to the teams. While the Division met the initial goal of decreasing recurrent lab orders significantly, this did not lead to an overall reduction in lab draws. The current focus is to discuss thoughtful and judicious lab ordering, as opposed to focusing entirely on recurrent lab orders.
This project was presented at the Society of Hospital Medicine (SHM) conference in April 2024.
The Division of Hospital Medicine continued its work with the Pulmonary Division to improve smoking cessation rates in COPD patients by initiating varenicline prior to discharge. The American Thoracic Society strongly recommends initiation of varenicline for smoking cessation, even in patients who are not ready to quit. Hospitalist initiation of varenicline takes advantage of the hospitalized patient’s forced abstinence from tobacco use, provides an opportunity for counseling on varenicline’s safety and efficacy, and decreases the barriers to initiation.
This project is a collaboration between the Pulmonary Division and the Division of Hospital Medicine at MSM/MSW/MSBI. The Pulmonary Division generates a daily Epic list of patients admitted with COPD with active tobacco use and notifies the hospitalist teams. Hospitalists lead physician trainees and advanced practice practitioners in conducting varenicline counseling and initiation via an opt-out approach with the messaging “I’m going to give you a medicine that will change your relationship with nicotine.” Patients are discharged on varenicline and referred to a smoking-cessation clinic. After discharge, data is collected on smoking reduction and quit rates via chart review and phone calls.
Future expansion of this project will be to include additional hospitals within the Health System as well as non-COPD patients who could most benefit from smoking cessation, such as cardiac patients.
This project was presented at the Society of Hospital Medicine (SHM) conference in April 2024.
The Division has prioritized providing comprehensive evidence-based care to inpatients with opiate use disorder to address the enormous health burden incurred by our patients and the lack of systematic approaches. Hospitalists at MSM and MSW have collaborated with the Department of Medicine QI team to gather data on this population to determine baseline metrics and outcomes, which will be used to identify patients appropriate for the initiatives below. This project is progressing in two directions. At the System level, the Division is working with Linda Wang, MD, in her initiative to develop addiction consultation at MSH and MSM along with an Epic dashboard for patients with addiction, exploring the use of the Clinical Opiate Withdrawal Scale (COWS) by nursing across sites, and developing a System guideline on medication-assisted therapy. At the local level, the Division arranged faculty development sessions to address relevant issues in opiate use disorder management, such as medicationassisted therapy, transitions of care, pain management, and stigma. The team is developing an Epic order set to provide evidence-based guidance (as developed in the System group) in a practical format for primary providers to use in managing opiate withdrawal and medication-
assisted therapy. The order set would also include associated care such as infectious disease screening, harm reduction resources such as drug test strips, naloxone kits, needle exchange, and drug testing community resources, as well as options for ambulatory follow-up after discharge. The Division is monitoring quality outcomes, which include 30-day readmissions, length of stay, workplace violence incidence, and equity.
Throughput is a top priority for the Health System and discharging patients before noon is an important metric for ensuring timely and appropriate discharge planning. Faced with the additional challenge of the loss of geography at MSM and MSW with the new residency structure in July 2024, the Division sought to redesign its interdisciplinary discharge communication. The “Discharge Today” tool (DCT) was embedded in Epic and already used by case managers as well as some of the faculty from MSBI. The current workflow begins with communication between the primary team and the unit interdisciplinary staff during interdisciplinary rounds at 10:30 am Monday through Friday. The Case Managers update the DCT with the expected discharge timing and barriers. Before 3:00 pm, the primary teams are responsible for updating the DCT for anyone who will be discharged the following day with the expected time. Based on this information, the unit case managers begin an Epic chat for any next-day discharges based on DCT with the unit interdisciplinary group and the primary team to confirm coordination of the discharge. Ultimately, the attendings are responsible for making sure the process is followed, though they do include the house staff in this work. The case managers have been collecting data to create a Pareto Chart to better understand the reason for identified discharges not leaving before noon as well as actual discharges that did not have prior conversations. The team meets regularly across both sites to discuss this data.
Division Quality Champion: Shantheri Shenoy, MD

The Joint Commission recognizes medication reconciliation as a critical National Patient Safety Goal, emphasizing its vital role in health care. This process enhances patient safety by identifying and addressing medication discrepancies, significantly reducing the risk of adverse drug events. The Division sought to improve medication reconciliation completion within 24 hours of admission by 10 percent between August 1, 2023 and April 1, 2024 through a project led by Loren Barhold, Chief Physician Assistant in Hospital Medicine. The interventions included implementation of electronic medical record tools, step-by-step visual guides in documentation rooms, educational “bootcamp” sessions to reinforce best practices, and team-based rewards for the highest completion rates. Admission medication reconciliation completion rates within 24 hours of admission improved remarkably from 23 percent in August 2023 to 62 percent in October 2024.
This project was selected for a poster presentation at the Society of General Internal Medicine Meeting.
% Med Rec
The aim of this project was to improve compliance with utilization of the pneumonia pathway in the electronic medical record and was led by Dr. Fatma Abdel-Qader. Care standardization has been shown to reduce length of stay and readmissions. The interventions included education for housestaff, advanced providers, and hospitalists in addition to periodic emails, reminders during interdisciplinary rounds, and the distribution of a pneumonia pathway tip sheet to providers. The team, in conjunction with the MSHS pneumonia workgroup, developed a pneumonia recovery guide to be distributed to patients. The rate of pathway utilization increased from 2.6 percent in 2022 to 6.5 percent in 2023 and 12.8 percent in 2024.
Naloxone Kit Dispensing on the Inpatient Medicine Service
The opioid crisis continues to be a significant threat to public health nationwide. In New York City, there were 3,046 drug overdose deaths in 2023, a decrease of only 1 percent from 2022, with fentanyl involved in 80 percent of these fatalities. The Division initiated take-home naloxone kit dispensing on the inpatient medicine service in October 2023, with the goal of achieving a 20 percent dispense rate by March 2024. Naloxone kits are supplied through the Opiate Overdose Prevention Program (OOPP), sponsored by the New York City Department of Health
(DOH). The Department of Medicine hospitalists, advanced practice providers, and house staff became certified naloxone dispensers after completing a 30-minute training session led by our OOPP Director. A kit dispensing algorithm was developed (see figure below) and a SmartPhrase was created in Epic for standardized documentation of naloxone dispensing by providers. Several Plan-Do-Study-Act (PDSA) cycles were implemented from October 2023 to March 2024, including: 1) manual chart audits and secure chat reminders sent to primary teams, 2) nursing education on naloxone dispensing, 3) provider education paired with a raffle incentive, and 4) secure chat reminders sent only to those providers with eligible patients who were within 24 hours of discharge.
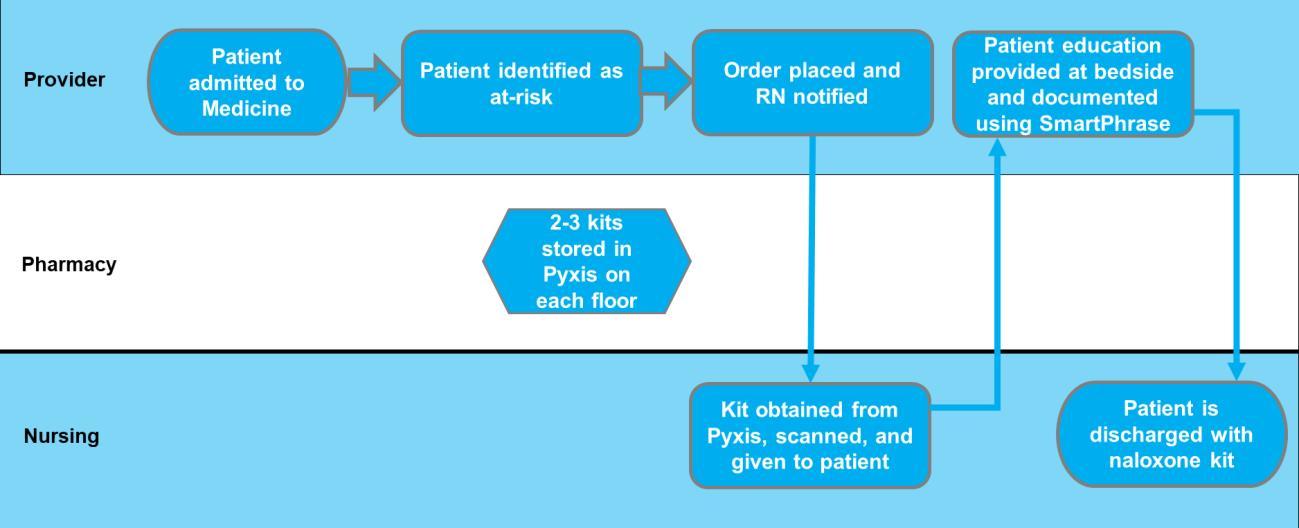
Baseline data was obtained using ICD-10 codes and prescription reports from January through March 2023, indicating an average of 71 at-risk patients discharged from the medicine service per month. A database was updated every two weeks to include information about patients, their take-home naloxone orders, and records of when those orders were placed. Manual chart reviews of unadministered orders were conducted to determine any documentation of kit dispensing outside of the medication administration record (MAR). A separate report was generated using the provider dispensing SmartPhrase to determine the number of patients who declined a kit. Monthly naloxone orders were analyzed and categorized into four groups: 1) orders confirmed as dispensed via a checkmark in the MAR, 2) orders confirmed as dispensed via documentation in the chart (other than the MAR), 3) orders that were declined by patients, and 4) orders that could not be confirmed as dispensed or declined after chart review, thus labeled as “lost. ”
Data collected from October 2023 to March 2024 showed a marked increase in the number of take-home naloxone kit orders placed, increasing from eight in October 2023 to 45 in March 2024 (see graph below). The number of naloxone kit orders placed reached 63 percent of the expected monthly target in March 2024, exceeding the goal of 20 percent. The most effective strategy proved to be manual chart audits and secure chat reminders for eligible patients within 24 hours of discharge. However, this intervention was labor-intensive and was not sustainable in the long term as evidenced by the decline in orders placed from July 2024 onward. Next steps include continued educational sessions for providers and an effort to develop a best practice advisory alert for naloxone dispensing in Epic.
Post-acute care includes services used to help patients recover after hospitalization and includes skilled nursing facilities, inpatient rehabs, long-term care hospitals (LTACH), and home health agencies. Discharges to home are associated with shorter length of stay, improved patient outcomes, and patient satisfaction. The discharge to home rate in 2023 for Mount Sinai Morningside was 82 percent and 81 percent at Mount Sinai West. This project was launched in the fall of 2024 with the goal of increasing the discharge to home rate for both hospitals by 2.5 percent.
The interdisciplinary team led by Dr. Shantheri Shenoy and Carol DeJesus, VP, Transitions of Care at MSMW, implemented several key initiatives to improve patient discharge outcomes. These efforts include daily review of patients with high Activity Measure for Post-Acute Care (AMPAC) scores who have non-functional barriers to home discharges during interdisciplinary rounds and connecting them with appropriate community resources. The team is also educating frontline staff and creating awareness about alternate discharge options to enhance patient flow, collaborating with nursing teams to improve mobility on the units. Additionally, the Division is collaborating with the Centralized Skilled Nursing Facility (SNF) transfer team to review individual cases and identify those with potential for home discharges. The team is also collaborating with the Rehab at Home team to identify eligible patients for home discharge early in their hospital admission.
The Division has several other projects that will continue in 2025, which include creating a paracentesis work group to improve rates of diagnostic paracentesis in patients admitted with ascites and reduce time to procedure. The group is led by Dr. Lance Maresky and includes certified house staff and attendings who can be reached by an Epic chat to “MSMW paracentesis team” group. Once contacted, the team will review patient details and identify providers available at the site to expedite the procedure. This project is in the process of collecting preliminary data.
Dr. Foram Parikh was awarded the Office of Well-Being and Resilience’s Faculty ReDUCE grant for her project titled “Enhancing Provider Well-Being: A Collaborative Interdisciplinary Approach to Medication Reconciliation ” This collaborative project aims to decrease provider burnout by shifting the medication reconciliation workload to a pharmacy technician. The project plans to pilot a Continued Education Medication History Taking Certification Program for pharmacy technicians as an extension to the existing MSHS Pharmacy Technician Training Program. The group plans to measure the project’s effect on well-being by administering a postintervention survey of physicians and advanced practice providers
Quality Champions:
Kristine Favila, DO
Dahlia Rizk, DO, MPH
As health systems consolidate, the appropriate use of bed resources becomes increasingly crucial to meet the needs of the community. The Central Hospitalist (CH) role was piloted in July of 2022 to support the throughput, quality, and efficiency of inter-institutional transfers within the Mount Sinai Health System and from outside organizations.
Functioning between the hours of 8:30 am and 10:00 pm daily, the CH role comprises a small group of senior hospitalists specially trained to assist with:
• Level-loading transfers within the Health System to efficiently offload the busiest emergency rooms and improve patient satisfaction and quality of care
• Triaging transfer requests from outside of the Health System to adjudicate appropriateness for transfer into the Health System
• Triaging patients in our emergency rooms and wards for appropriateness and eligibility for our Hospital at Home (HaH) program, thereby improving inpatient bed access
• Reviewing emergency room and ward patients in one of the system’s hospitals to ensure proper placement on EMR pathways for sepsis with the goal of optimizing outcomes
In 2022, a data support tool was implemented, and the CH cohort has since collaborated on several algorithms using this tool to streamline workflows to adjudicate and triage patients to appropriate beds within the Health System to support quality and throughput initiatives.
Since the inception of the role in 2022, more than 5,000 patient cases have been reviewed by the Central Hospitalist and transferred within or into the Health System. Level-loading cases accounted for most of these transfers. By Q4 (November 2024), ED boarding time was reduced by 15.93 hours, average length of stay was reduced by 1.8 days, excess days were reduced by 2,072 days, and additional bed capacity for 261 inpatient admissions was created through the CH pilot program. The average CH decision time, defined as time from initial contact by Clinical Command Center to disposition decision, was 32 minutes, with a median time of 17 minutes. While this nearly met the pilot goal of less than 30 minutes, the average CH decision time significantly improved from 100 minutes prior to the pilot start, with a reduction of more than 90 minutes per case.
Transfer Performance Metrics:
Additionally, the CH has been instrumental in increasing referrals to our HaH program, which has exceeded their prior admission volumes largely due to enhanced referrals. The growth of appropriate referrals and accepted cases continues to be monitored by the HaH program. 2024 data from Palantir, which tracked patients identified as eligible for HaH by the CH and their subsequent admission status, shows that almost one-third of HaH admissions came from CH referrals, with the number increasing toward the end of the year (see graphs below). This highlights the CH’s role in contributing to HaH’s growing volume and saved hospital bed days.
Percentage of HaH Admissions from CHReviewed Eligible
Monthly HaH Admission from CH Referrals
CH-Reviewed Eligible HaH Admission
Monthly Percentage HaH Admission from CH Referrals
2024 Total HaH Admission Based on CH Referral
CH-Reviewed Eligible CH-Reviewed Ineligible Not Reviewed by CH
The effectiveness of this novel virtual Central Hospitalist program will be shared as a poster presentation at the Society of Hospital Medicine (SHM) annual meeting “SHM Converge 2025” in April 2025.
In 2025, the CH program will continue working on increasing level-loading transfers within the Health System, expanding the CH role coverage to 24 hours a day, expanding sepsis reviews to include additional hospitals in the Health System, and maximizing HAH referrals.
Quality Champion: Tuyet-Trinh (Trini) Truong, MD

The Mount Sinai at Home program offers inpatient-level medical services to patients in their own homes. The spectrum of services provided is constantly expanding and now includes intravenous treatment (e.g., antibiotics, fluids, resuscitation, Lasix), daily labs, wound care, supplemental oxygen and weaning, nebulizer treatments, X-rays, ultrasounds, and EKGs (with advanced imaging possible with round trips to the hospital). The Hospital at Home (HaH) program coordinates care with daily physician televisits, twice daily in-person nursing visits, televisits with consulting subspecialists when needed, and 24/7 access to the clinical team. Ancillary services include physical and occupational therapy, social work, home health aides, as well as screening and assistance with food insecurities, internet support during the care, and robust post-discharge services. Patients are eligible for HaH if they require acute hospitalization, live in New York City (except Staten Island), insurance agnostic, and have a safe home, defined as having running water, electricity, and refrigeration. The referral pathway and top diagnoses for HaH are presented below.
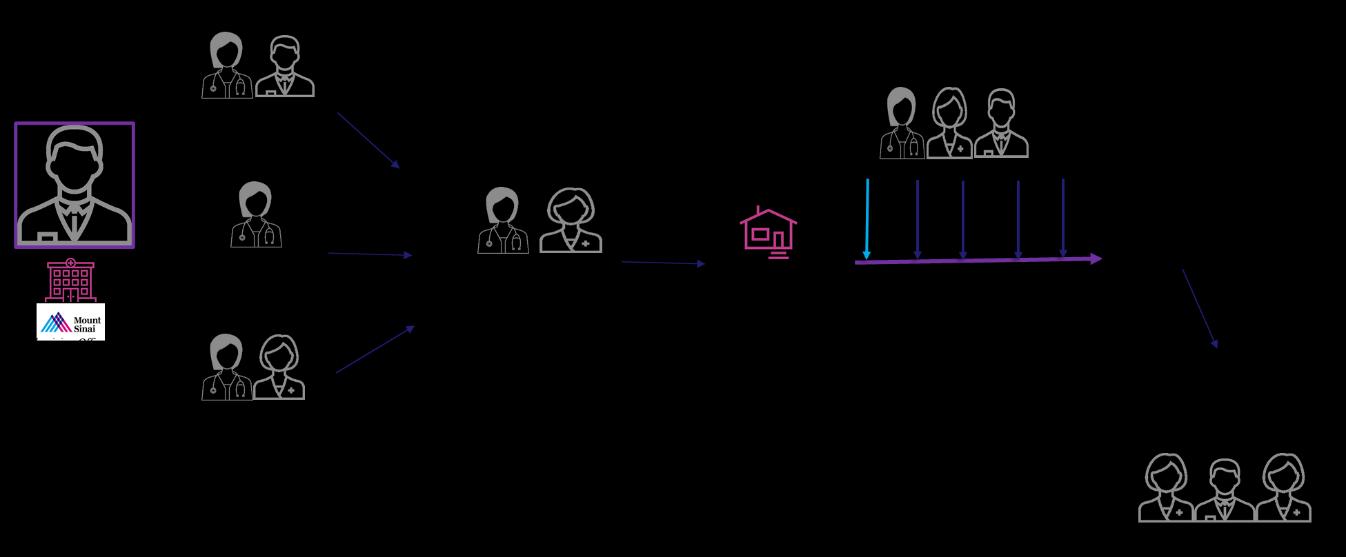
HaH admission rates and bed-days saved has significantly increased over the last year Compared to 2023, when the HaH service saved 2,500 direct bed-days for the Health System, it saved 4,500 bed-days year-to-date in 2024 and is projected to save up to 5,500 bed-days by end of year.
2023: Saved 2,500
2024: YTD 4,500 bed-days saved and projected to save 5,500 direct bed-days
Admissions
Bed Days Saved
In 2024, the Division of Hospital Medicine worked closely with the Mount Sinai at Home team to improve the coordination of care during transitions between the inpatient and home setting and to increase referrals and admissions to the program. Admission by locations is shown below.
Mount Sinai HaH has treated more than 2,000 patients and maintained a less than 10 percent escalation rate (i.e., a patient enrolled in HaH requiring a higher level of care, such as needing to go to the emergency room or be admitted to a hospital). The rates of hospital complications such as falls, delirium, and hospital-acquired infections are low (see table below). There were two unanticipated mortalities: one patient died two days after hospital escalation and one died 10 days after hospital escalation. Both cases were reviewed by the Department of Medicine Quality Improvement Peer Review Committee and no concerns were found. However, earlier goals of care discussions were recommended. More than 90 percent of patients and/or caregivers “recommend Hospital at Home to friends and family” in patient satisfaction surveys.
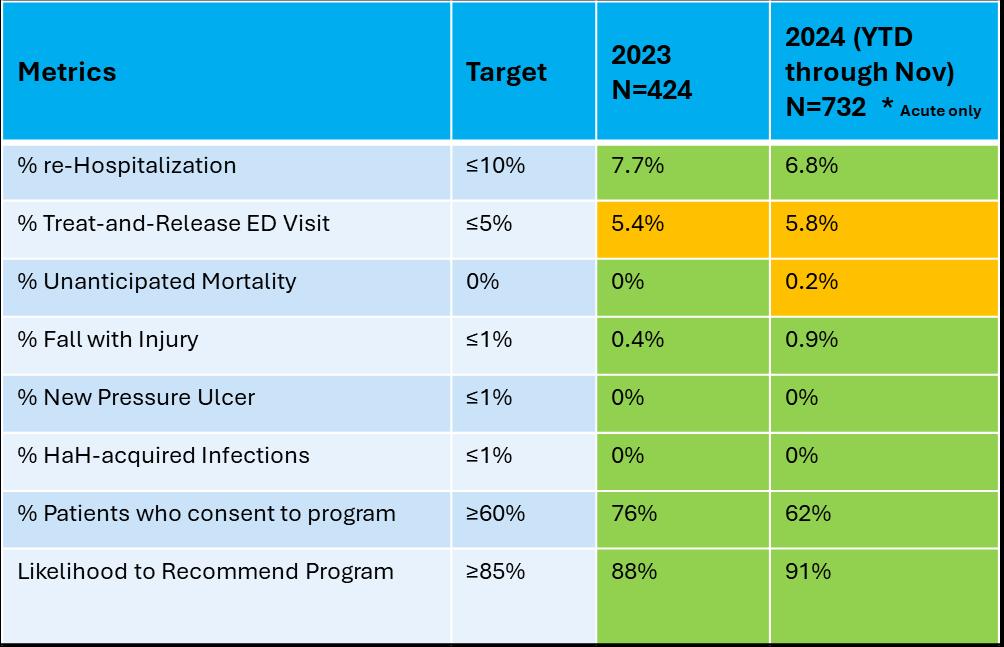
In 2024, the HaH team sought to reduce falls with injuries and reviewed all falls to find areas of opportunity. Five of the patients who fell remained at home and had minor injuries, such as pain and discomfort. One patient who fell outside the home during admission transport was returned to the emergency department (ED) for evaluation but was found to have minor injuries. To improve the overall fall rate, RNs completed a fall prevention course, and patient-facing placards were distributed to patients (see picture). The fall assessment on admission was also moved to the start of care in the home and physical therapists or durable medical equipment (e.g., cane, walker) were used to fill safety gaps identified. A fall prevention course was added to the team’s online learning and will continue to be part of onboarding in 2025.
A second quality initiative the HaH team worked on in 2024 was to reduce and prevent ED escalations, including ED treat-and-release visits. In 2023, 25 patient visits were reviewed: six
patients returned for blood transfusion, four returned for catheter placement/replacement, three had neuro-symptoms (e.g., altered mental status), and two had uncontrolled pain. In the first two quarters of 2024, there were 26 treat-and-release visits to the ED. The reasons for return included: nine patients for midline placement and or intravenous (IV) access, two patients for blood transfusion, two patients for uncontrolled pain, and two patients with shortness of breath or respiratory decompensation. To reduce the rates of return to the ED, the HaH team negotiated a new vendor contract in the third quarter of 2024 to provide additional IV access in the home and leveraged an existing relationship with the oncology clinic for transfusions in oncology patients.
In August 2024, the Centers for Medicare and Medicaid Services (CMS) published data comparing HaH programs with originating traditional inpatient hospitals. The CMS study included more than 300 hospitals/health systems with more than 11,000 Medicare fee-forservice patients from November 2021 to March 2023. The CMS population had a 7.4 percent rate of escalations back to hospitals and a less than 0.5 percent mortality rate. The CMS comparison analysis with the Mount Sinai HaH program is below and notes that Mount Sinai HaH performed better in several areas.
With regards to demographic data, Mount Sinai HaH patients are more likely to be minorities and have lower socioeconomic status than the MSHS patient population. HaH provides a holistic approach to care and is a key to equity. Examples of services provided to patients in addition to health care include: Uber eats, setting up Meals on Wheels, home health aides, PT and OT to assess the home environment, bringing additional lighting into the home, and calling services for plumbing. For all other quality metrics, the Mount Sinai HaH program performed similarly to the national data.
Quality Metrics
Demographics More likely to be white and live in an urban location and less likely to receive Medicaid or low-income subsidies
30-day readmission
• HaH had higher rates for two DRGs (*higher HCC scores)
• HaH had lower rates for three DRGs
HaH’s rates were better: CAUTIs, pressure ulcers, poor glycemic control, CABSIs, falls, iatrogenic pneumothorax Cost and Utilization
• LOS: on average, HaH had slightly longer (<1 day)
• 30-day post DC resource utilization: HaH less ($1,640.43/b less) Patient Experience
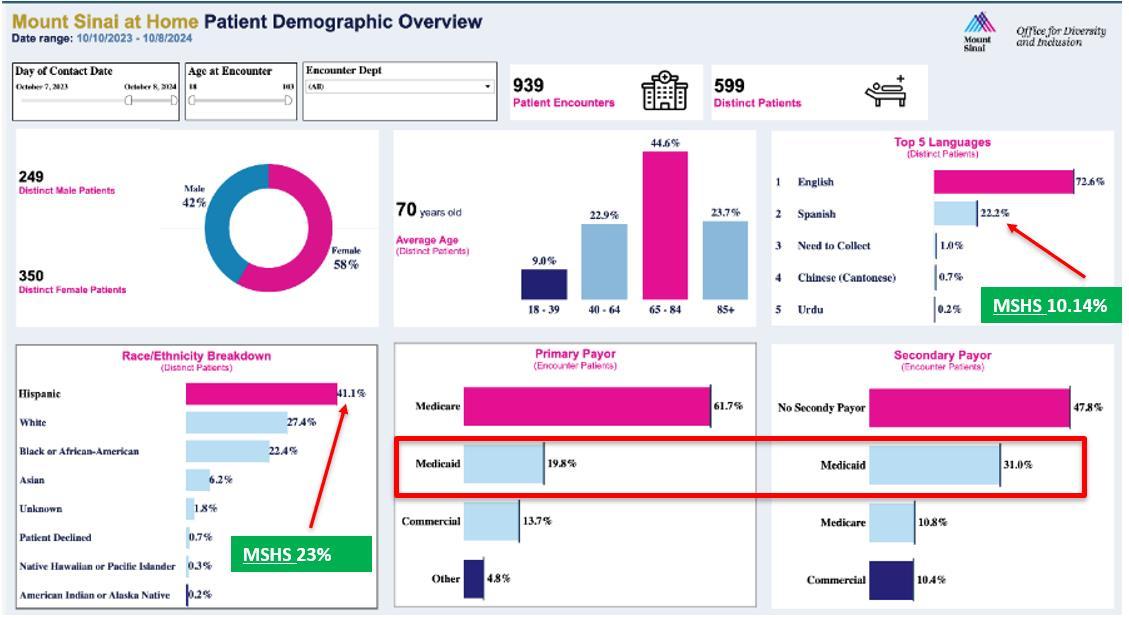
In 2025, the HaH team will seek to increase the program acceptance rate by improving scripting and increasing inpatient team engagement in identifying patients and timely referral. The service also plans to expand to include oncology, end-stage renal disease, and surgical patients.
Mount Sinai Beth Israel
Division Quality Champion: Patricia Dharapak, MD

The MSBI Quality Improvement Peer Review Committee (QIPRC) meets monthly to discuss the cases of patients who expired on the medicine service with the goal of improving care by identifying contributing circumstances and opportunities for improvement. Mortality cases are derived from the Quality Improvement Peer Review Trigger Tool (QIPRTT) and electronically assigned to reviewing faculty by the committee chair prior to each meeting. Each case is presented to the committee for discussion, after which the members determine whether the standard of care (SOC) was met through general consensus. If the SOC is met, the case will be closed. When the SOC is not met or met with room for improvement,
corrective actions aligned with the identified contributing factors are implemented with the goal of preventing future occurrences.
There were 46 deaths on the medicine service through December 2024. To date, the committee has reviewed 42 mortality cases. Thirty-one percent of the mortalities reviewed were admitted to the ICU during their stay, palliative care was consulted in 69 percent of cases, and 93 percent were DNR and receiving comfort-based care at the time of expiration.
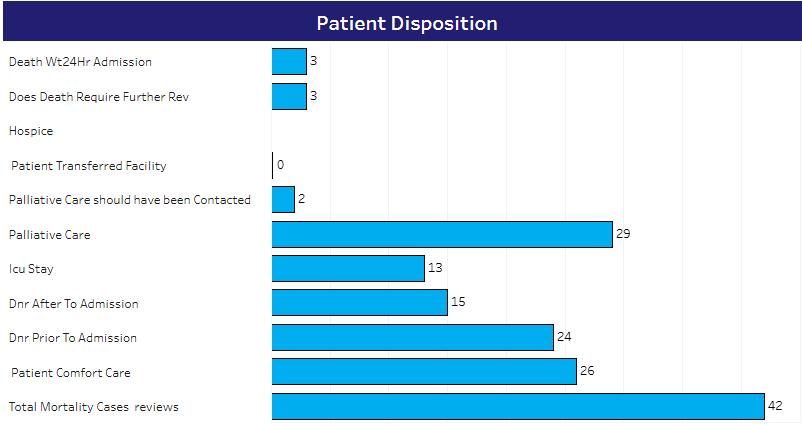
Compared to 2023, the committee’s mortality SOC attributions improved slightly. The committee consensus was that SOC was met in 35 (83 percent) cases and met with room for improvement in 7 cases (17 percent). No cases were determined to have SOC not met.
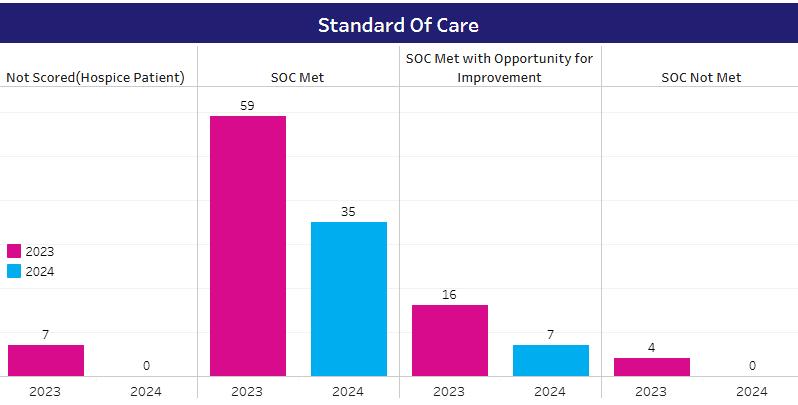
For cases in which SOC was not met or met with opportunity for improvement, contributing factors were assigned. The most common contributing factors included delay in diagnosis (n=1), poor documentation (n=1), and goals of care not documented (n=1).
For cases where the contributing factors were related to treatment, management, and diagnosis, efforts to improve quality of care were addressed through multidisciplinary peer learning case conferences and individual provider debrief.
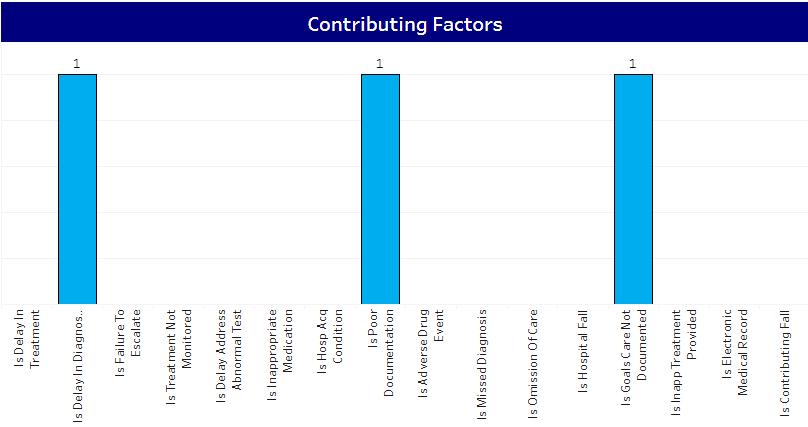
In 2018, a resident Quality Improvement Peer Review curriculum was developed where trainees are invited to participate in peer reviews alongside the faculty committee. Prior to reviewing a case, residents attend a didactic session, which includes introduction to a framework for peer review and attribution of standards of care, and a review of different failure types and error subtypes. Paired with a faculty mentor, participating residents present their peer review findings at the meeting. In 2022, the curriculum became a required experience for all Internal Medicine PGY-3s as it augments core skills required for internal medicine training (e.g., practice and systems-based learning and improvement) and provides an opportunity for individual reflection on providing care within a complex system. Since inception, the curriculum and committee received consistent positive feedback from trainees who have participated in peer reviews and committee discussions. In May 2024, the curriculum concluded as all trainees were permanently transitioned from the MSBI campus.

The Mount Sinai Hospital Quality Improvement Peer Review Committee evaluates all mortalities and morbidities and meets monthly to identify quality issues. Prior to the meeting, cases are reviewed by faculty or house staff under faculty supervision. Cases raising quality concerns are then escalated for in-depth committee review. Cases for review are also acquired through referrals from faculty, Safety Net, or The Mount Sinai Hospital’s serious adverse event (SAE) process. Even in cases where hospital-level review determines that the standard of care (SOC) has been met, improvement areas are frequently identified in the departmental review. This interdisciplinary committee includes a wide range of health care professionals who, after discussing a case, vote on the SOC provided. If the SOC is deemed not to be met or met with room for improvement, strategies for patient safety and risk reduction are adopted to prevent recurrence. When provider errors are identified, the providers involved are counseled.
For cases with significant safety concerns or requiring interdepartmental involvement, the committee forwards them to the hospital leadership’s SAE process for a comprehensive review to identify root causes and develop corrective actions, aiming to mitigate patient risks and prevent future incidents. Cases are often referred to various divisions for additional, indepth review.
In 2024, the department reviewed 161 cases of mortality, representing an increase from 151 in 2023. Eighty-four patients had a Do Not Resuscitate (DNR) status after admission, slightly down from 85 in 2023, and 50 had DNR status prior to admission, an increase from 35 in 2023, with 46 ICU stays (see graph below). The patient would have benefitted from Palliative Care consultation during the admission in 11 mortality cases in the past year, a decrease from the previous year of 15 cases.
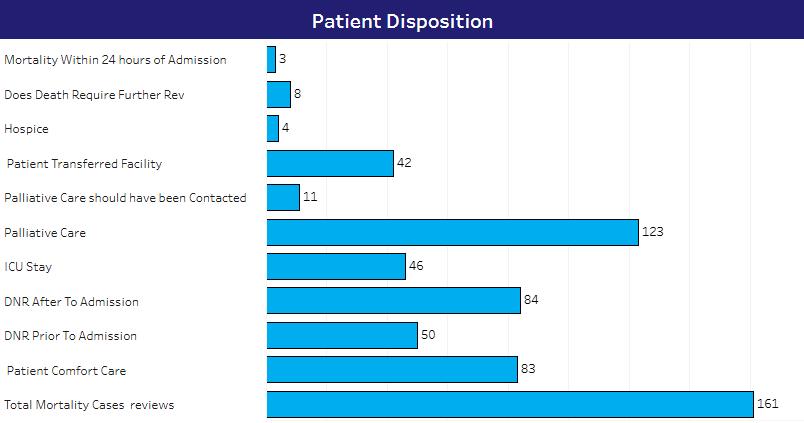
Of the 161 cases reviewed in 2024, 139 (86 percent) met the standard of care, compared to 141 (89 percent) in 2023. In 2024, 17 cases (11 percent) met the SOC with an opportunity for improvement, while 15 (10 percent) did so in 2023. There was one patient case that did not meet SOC. Six patients expired within 48 hours of transfer to the ICU from a medicine unit where SOC was not met, and these cases were also reviewed. The SOC was not scored in four deaths in 2024, as these patients expired while in hospice care and did not necessitate further review.
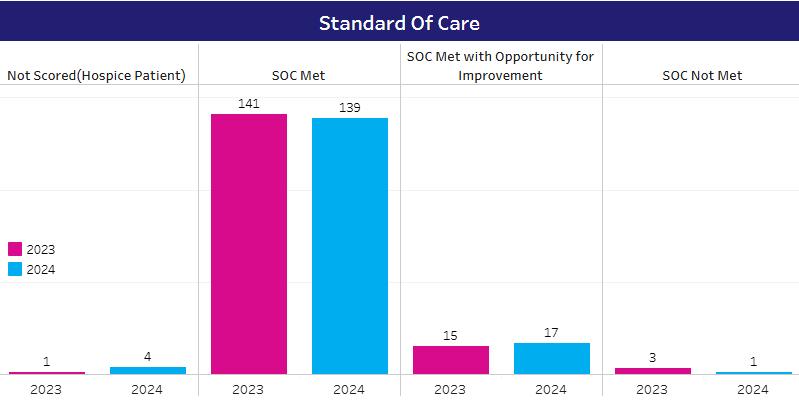
*Six additional mortalities that occurred within 24-48 hours of transfer to an ICU where SOC was not met were also reviewed
Most common factors attributed to mortalities and adverse events were treatment delays (n=7), delay in diagnosis (n=3), hospital-acquired condition (n=3), delay in addressing an abnormal test (n=3), and hospital fall (n=3). Other factors included poor documentation and goals of care not documented.
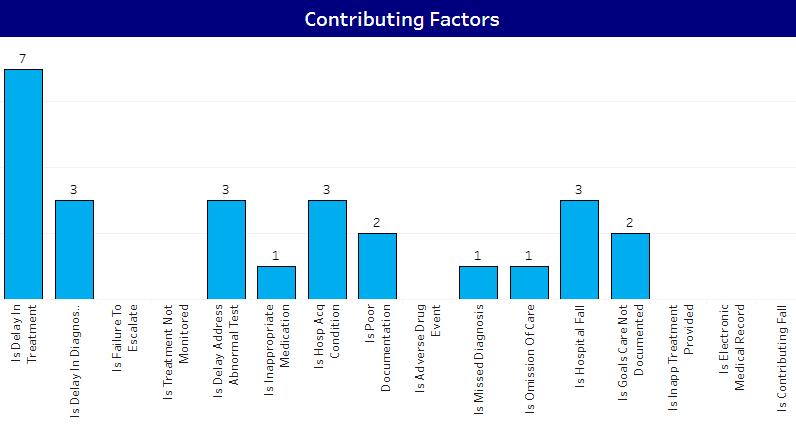
From 2022 to 2024, mortality trends among racial and ethnic groups remained relatively stable, generally aligning with inpatient discharges. The Mortality committee will continue to monitor this data in 2025 to identify any variances should they develop.
Percent of Deceased Patients by Race/Ethnicity: Hospital Medicine Service (2022-2024)
Percent of Discharges by Race/Ethnicity: Hospital Medicine Service (2022-2024) 2022 (n=8064)
In 2024, various patient safety solutions were implemented. The solutions addressed improvements in clinical care as well as improvements in workflow. Many of the cases were referred back to divisions for further review and the creation of safety solutions. In 2024, referrals were made to the following departments: Pulmonary, Rapid Response Team (RRT), Nursing, Emergency Department, Infectious Disease, and many others.
In addition, many of the cases where room for clinical improvement was identified were presented at the Resident Quality Improvement conference as well as the Division of Hospital Medicine (DHM) QIPRC conference for further discussion and education to providers. During these case review presentations, opportunities for earlier diagnosis and strategies for improving a multidisciplinary approach to patient care with consultant involvement and coordination of care were discussed. In 2024, the cases discussed in the DOM QIPRC meeting uncovered three main areas of focus: (1) Improve communication and collaboration, (2) identify opportunities for education, and (3) create guidelines.
In 2024, a significant improvement in communication and collaboration involved the availability of phone numbers for frontline providers on Epic. A mortality case was reviewed and identified a challenge with nursing being able to find the contact information for the intern or resident covering the pager and the additional workflow step of logging into Amion. In collaboration with Epic, members of the DOM QIPRC team created a new workflow of residents and interns signing in with their phone numbers so that the number is visible on Epic for the nurses. This change in workflow has improved nursing’s ability to identify the frontline provider
In 2024, a mortality case brought to light an education gap among residents on interpreting EKGs. A group of members of the DOM QIPRC committee collaborated to develop a curriculum for the residents on learning and improving their skills on EKG interpretation.
Several guidelines were also created through cases discussed in the DOM QIPRC in 2024. A case identified that during a code, there was confusion on the roles of individual members of the team, specifically the residents and rapid response team (RRT) and attending. Through
collaboration with the RRT and residency, role guidelines were updated and implemented. Additionally, through another case, it was discovered that there were challenges in identifying when to utilize RRT versus a MICU consult for patients who needed escalation of care. Clear guidelines to direct this escalation step were created and disseminated.
In addition to the above interventions, several other improvements, interventions, and discussions were initiated, including and not limited to gaining a deeper understanding of the Hospital at Home review process, the tracking of multiple cases through the hospital incident review process, and various related quality improvement measures.
Division Quality Champion: Lindsey Fox, MD

The QIPR Committee at Mount Sinai Morningside meets every month to discuss cases of patients who died in the hospital or experienced a serious adverse event. Cases are assigned to attendings through the QIPR Trigger Tool (QIPRTT) for review prior to each meeting. If a reviewer determines there are quality and safety concerns with opportunities for improvement for a particular case, the reviewer will refer to the QIPR Committee for further discussions.
Committee members identify opportunities for improvement attributions after case presentation and discussion. If an opportunity for improvement is identified, a corrective action plan will be developed and implemented. Peer-reviewed cases with quality concerns deemed beyond the scope of the department are referred to the hospital quality review team for further discussion.
When reviewing the 2024 cases by language, the Division found that the primary language listed for most mortalities was English (56 percent), followed by Spanish (25 percent). In terms of race, many patients identified as Other (40 percent), followed by White (20 percent), and Black or African American (22 percent). Fifty-nine percent identified as non-Hispanic, followed by 14 percent as Dominican, and 11 percent as Puerto Rican.
From 2022 to 2024, mortality trends generally aligned with inpatient discharges across most racial groups, except for Hispanic patients, whose mortality increased in 2024 (34.1 percent vs. 27.1 percent in 2023) while inpatient discharges remained consistent. It is difficult to explain this variance given the small sample sizes and lack of adjustments for factors such as age and severity of illness. Further analysis will be performed in 2025 to explore potential variances and contributing factors if the trend continues.
Percent of Deceased Patients by Race/Ethnicity: Hospital Medicine Service (2022-2024)
White Black or African American Hispanic Other Asian Unknown
White Black or African American Hispanic Other Asian Unknown
Percent of Discharges by Race/Ethnicity: Hospital Medicine Service (2022-2024) 2022 (n=6658)
Data from the QIPR show that the team reviewed a total of 102 cases. Seventy-six of the cases had palliative care consultation during their admission and 61 were made comfort care. Fifty-five cases had a Do Not Resuscitate (DNR) status after admission due to worsening clinical status, while 27 were DNR upon admission to the hospital. Thirteen deaths required further review.
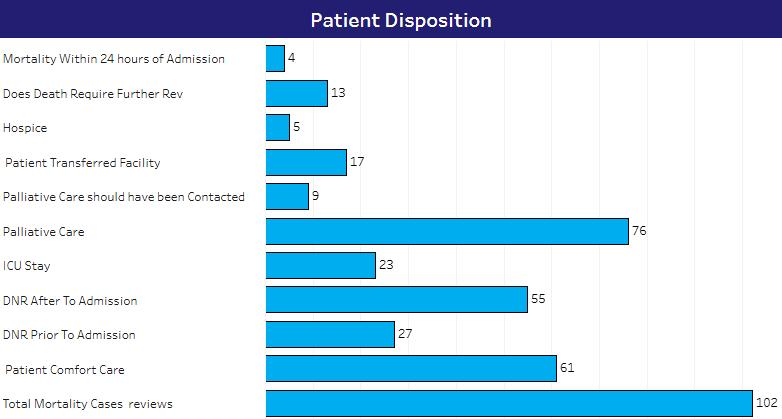
After reviewing a case, the committee votes to determine whether standard of care (SOC) was met, met with opportunity for improvement, or not met. In 2024, as the graph depicts below, the committee determined that SOC was met in 77 cases, met with opportunity for improvement in 18 cases, and not met for two cases. There were five cases not scored because the patients died while under hospice care and, therefore, did not require further review.
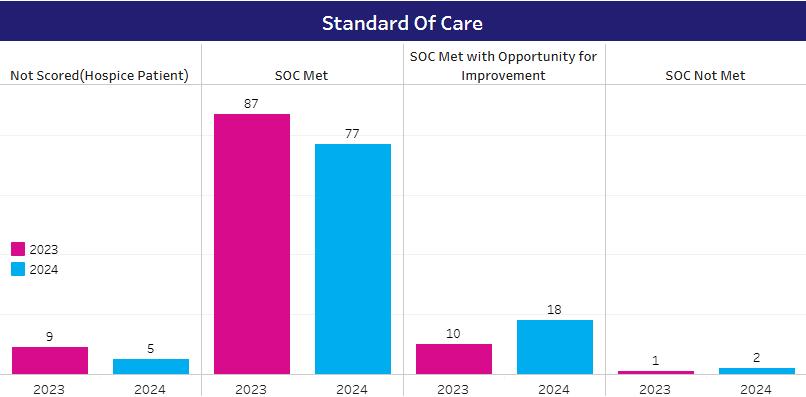
In cases where SOC was not met or met with opportunity for improvement, corrective action plans were developed and implemented when appropriate. Cases with quality concerns not appropriate for the committee were referred to the hospital quality department for further review and discussion.
The graph below shows that the most common contributing factors in 2024 were delay in treatment (n=9 cases), delay in addressing abnormal test (n=2), inappropriate medication given (n=2), and then delay in diagnosis (n=1), poor documentation (n=1), omission of care (n=1), and inappropriate treatment provided (n=1).
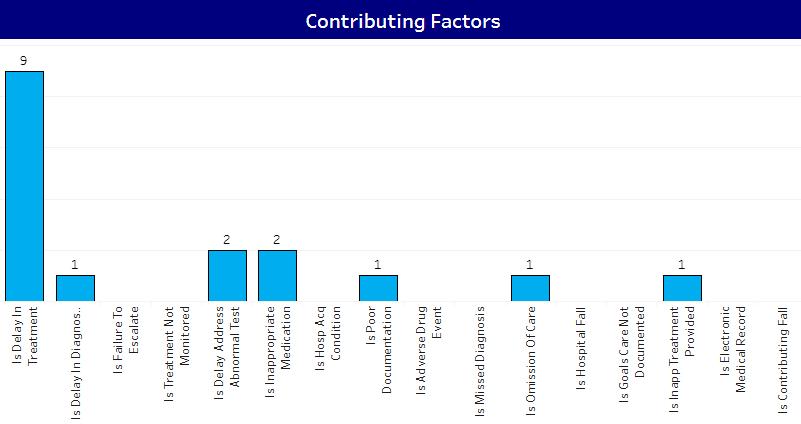
There were several areas identified as opportunities for improvement. Medication reconciliation in general continues to be an area of focus, both on admission and on discharge. A focus this past year was on discharge medication reconciliation to ensure proper and timely review of medications prescribed on discharge. The Division aimed to increase the detection of medication errors prescribed on discharge by the medicine teams by December 2024. The process measure was utilization of a dot phrase that drew in all discharge medications for review. Once reviewed, the medications were to be deleted, with the remaining phrase in bold: “I have reviewed the discharge medication list.” This phrase was tracked via chart audit. The outcome measure was a survey completed by medicine attendings with a subjective report of how many errors were caught using the tool. About ~45 percent of attendings, on average, are utilizing the dot phrase. Eleven out of 25 hospitalists have responded to the survey thus far, with 10 out of 11 finding it helpful. Fifty-four percent have utilized the dot phrase more than 10 times. Six providers found between one and five errors, two providers found zero errors, and two providers found 5-10 errors.
Errors Caught Using the Dot Phrase Among Hospitalists Who Found It Helpful
# of Hospitalists
Next steps include collaboration with MSW to increase hospitalist participation and presentation of the project again to the DHM with a follow-up survey.
The escalation pilot stemmed from review of several cases where there was a delay in escalating to the attending or consulting critical care. The framework was based on practices already in place at Mount Sinai Beth Israel, whereby the day attending would check in with the senior in the evening to briefly discuss new admissions. The goal of this project was to pilot evening check-in with a subset of residents to explore the effect on resident management plans, sense of autonomy, and willingness to reach out to attendings in the future. The eventual goal is to normalize and standardize evening check-in with the senior resident and hospitalist of record. Of 13 residents surveyed, six responded. One found the check-in extremely useful, three found the check-in particularly useful, and two found it somewhat useful. Five indicated they were more likely to reach out to the attendings in the future, one replied other. The average length of check-in time was 15 minutes. Residents found that discussing admissions with the attending assisted with their management plans: 1 to 24 percent of the time (n=1), 25 to 50 percent of the time (n=2), 51 to 74 percent of the time (n=1), and 75 to 99 percent of the time (n=2). Next steps include presenting the data to the MSM/W hospitalist division and gauging interest in standardizing this practice.
Irina Zaretsky, MD

The Mount Sinai West (MSW) Quality Improvement Peer Review (QIPR) Committee convenes monthly to deliberate on morbidity and mortality cases leading to death and/or significant adverse events. Each month, faculty members are tasked with reviewing cases beforehand. Cases identified with quality concerns and necessitating deeper examination are presented to the entire committee during the meeting for discussion. Opportunities for improvement are identified with corrective action plans developed and implemented as required by participants.
In 2024, the faculty reviewed 149 cases. Of the deceased patients, 70 percent (104) received comfort care. Forty-six percent (68) had a “Do Not Resuscitate” (DNR) status prior to admission, while 37 percent (55) acquired DNR status after admission to the hospital. Twenty-six percent (39) of these patients had an ICU stay before passing away. Eighty percent (120) had interactions with palliative care, and it was suggested that an additional five percent (8) could have benefited from palliative care intervention. Nineteen percent (28) of the deceased patients were transfers from other facilities, five percent (8) were on hospice at the time of death, and six percent (9) passed away within 24 hours of admission. Eleven of the patient deaths were deemed to necessitate further review.
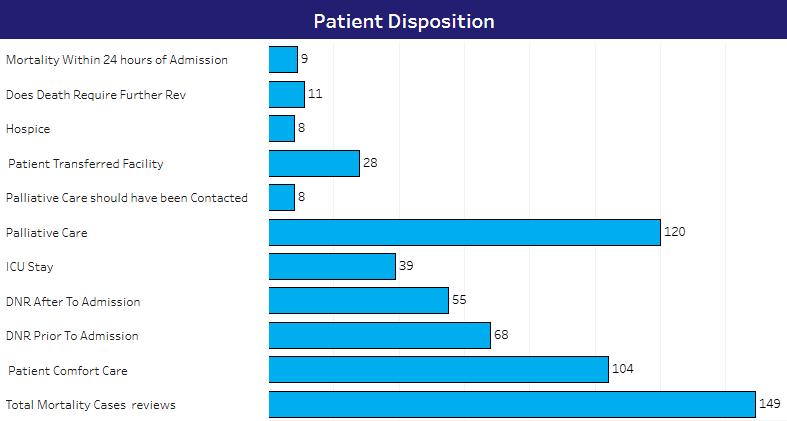
Of the mortalities reviewed, 76 percent (88) were English speakers, nine percent (11) were Spanish speakers, and two percent (2) were Cantonese speakers. Data for 13 percent (15) were not collected.
In terms of race, 43 percent (52) of patients were white, 23 percent (28) identified as other, 18 percent (21) were Black or African American, and three percent (4) were Chinese. Data was not collected in eight percent (10) of cases and one percent (1) declined to disclose their race. The remaining four percent comprised patients of Asian, Grenadian, Japanese, and Korean descent.
Seventy one percent (85) were non-Hispanic, 12 percent (14) were Puerto Rican, three percent (3) were Latin American, and three percent (4) were Dominican. The remaining three percent identified as Colombian, Cuban, and Panamanian. Data was not collected in nine percent (11) of the cases.
The graphs below present inpatient mortality trends by race/ethnicity from 2022 to 2024 within the Hospital Medicine Service, alongside relatively stable discharge volumes. Among Black patients, mortality declined from 28.9 percent in 2022 to 18.2 percent in 2024. Hispanic patient mortality decreased from 16.5 percent in 2022 to 11.6 percent in 2023, then rose to 22 percent in 2024. Asian patient mortality varied, with rates of 8.3 percent in 2022, 10.1 percent in 2023, and 6.1 percent in 2024, while discharge proportions remained steady at approximately 5 percent. These observations reflect changes over time but are not adjusted for age, comorbidities, or other clinical and demographic factors. Without observed-to-expected (O:E) ratios or risk adjustment, no inferences should be drawn at this stage. The trends, however, highlight areas for further review and may inform future analysis in 2025.
Percent of Deceased Patients by Race/Ethnicity: Hospital Medicine Service (2022-2024)
Percent of Discharges by Race/Ethnicity: Hospital Medicine Service (2022-2024) 2022 (n=5788)
All cases are thoroughly discussed and voted on electronically to determine if the standard of care (SOC) was met, met with opportunity for improvement (OFI), or not met at the monthly QIPR meetings by the multidisciplinary team of clinicians.
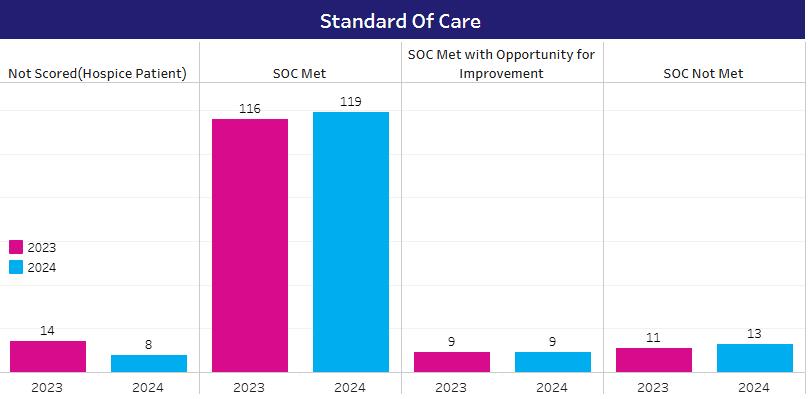
As the graph above depicts, 80 percent of cases were deemed to have met SOC in 2024 compared to 78 percent in 2023. Standard of care was not met in nine percent of cases in 2024 compared to six percent in 2023. Six percent of cases were scored as standard of care met with opportunity for improvement by the committee in 2024, the same as compared to 2023 Five
percent of cases were not scored in 2024, compared to three percent of cases in 2023 because these patients had a designation of hospice and therefore do not require further review
Contributing factors to cases not meeting the standard of care included treatment delays (n=3), delays in diagnosis (n=1), poor documentation (n=1), in-hospital falls (n=1), and undocumented goals of care (n=1).
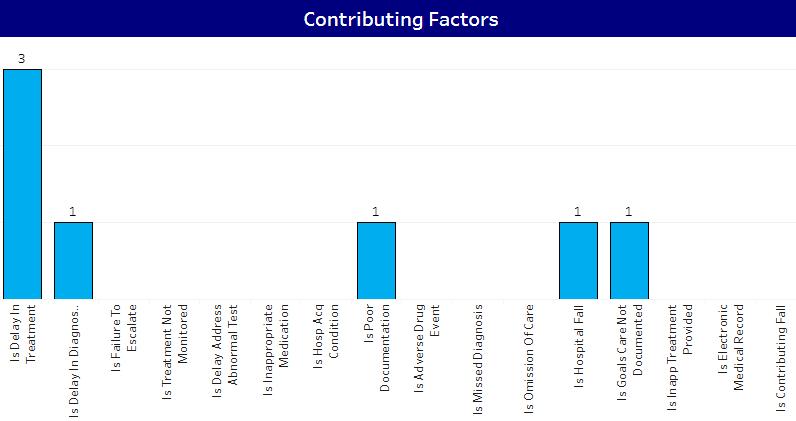
Following the identification of cases where the standard of care was not met, key areas for improvement were identified and addressed through specific actions:
Clostridium Difficile (C. Diff) Testing: The C. diff order process at MSW previously required an ID attending name for all specimens collected after 72 hours of admission. However, a significant number of orders were submitted with this field left blank, preventing the lab from processing the specimens. As a result, providers had to be notified, ID approval obtained, and a new order placed requiring a fresh sample to be collected and sent to the lab for evaluation. This system caused delays in stool sample processing and, ultimately in C. diff diagnosis. In one case, a four-day delay in diagnosis resulted in severe sepsis and the patient’s death. To address this, the team collaborated with IT to modify the order system, implementing a hard stop that prevents providers from signing an order without entering the ID attending’s name. This change has streamlined the process, ensuring timely specimen processing.
Morphine Best Practice Advisory: Morphine is commonly used in the ED and on the medicine floors for acute pain management. However, because it is renally cleared, its use in patients with renal impairment has led to adverse outcomes As a corrective action, a best practice advisory was implemented to instruct providers against prescribing morphine for patients with acute kidney injury or chronic kidney disease, defined as an eGFR of less than 30 mL/min/1.73m2 .
Do Not Resuscitate (DNR) Wristbands: Quick identification of patients who have a DNR order is important to prevent unintended resuscitation during emergencies. Currently, MSW lacks a
system for easily recognizing these patients. To address this, the Division will begin implementing purple DNR wristbands to provide a clear, immediate visual cue Nursing and provider education on this initiative is currently underway.
Elopement Policy: The safety of patients lacking medical decision-making capacity poses a challenge for both providers and nursing staff. Without proper supervision, these patients are at risk of eloping from the hospital. The current elopement policy lacks specific criteria for supervision and places the burden of decision making on nursing, much of which is subjective. The plan is to re-evaluate the elopement policy to determine how to better stratify patients at the highest risk of elopement and identify those who would benefit from increased observation.
Division Quality Champions:
Tessa Gomez, MD
Sarah Humphreys, MD


In 2024, the Division of Infectious Diseases at Mount Sinai Beth Israel remained committed to increasing viral load suppression rates at the Peter Krueger Clinic (PKC). The ultimate goal of HIV treatment is viral load suppression, or the reduction of HIV viral load to an undetectable level. Key interventions by the Division were designed to increase patient adherence to treatment regimens and follow-up appointments while educating patients on living with HIV/AIDS.
Through weekly care gap reports, the care team identified unsuppressed patients with and without an upcoming appointment. Care coordinators then implemented outreach to schedule follow-up or provide appointment reminders, and to confirm if patients are taking their antiretroviral medications as prescribed. Nurses and social workers provided education, community support, and assistance with obstacles to care as needed
Standardized guidelines were utilized to manage patients with treatment failure, defined as having two consecutive unsuppressed viral loads or intermittent viremia. The following checklist guided the process for unsuppressed patients:
• Ensure a resistance test is performed to exclude resistance as a cause of non-suppression
• Assess for factors associated with treatment failure (e.g., resistance, substance misuse, unstable housing, mental health, side effects, insufficient insurance, treatment complexity, diversion)
• Connect patients to social services, mental health, and substance abuse treatment as clinically indicated
• Recommend and (if accepted) enroll patients in care coordination
• Arrange monthly follow-up appointments for six months to assess response
• Avoid providing more than one-month refills for those with detectable viral loads to emphasize and facilitate the importance of medication coordination and adherence
• Discuss patients who fail to appropriately manage their treatment at monthly multidisciplinary meetings
• Submit a list of patients lost to follow-up to the NYC DOH Care Status Report to determine care status
To reduce the number of unsuppressed patients at PKC, the Division compared patient and provider adherence to the treatment failure checklist, reinforcing the ongoing interventions to mitigate patient non-adherence.
The PKC care coordinators were also crucial in increasing the identification of patients with mental health and/or substance use disorders. These patients were ultimately linked to care and those who were not linked were aggressively targeted. The presence of on-site psychiatry and psychotherapy was associated with a steady, albeit gradual, increase in patient appointments. These additions to the team facilitated linkage to mental health care and further augmented the Division’s efforts to achieve and maintain viral load suppression at PKC.
Provider identifies patients from the weekly care gap list provided by IAM Quality Data Team
During visit, the Provider educates importance of viral load suppression and schedules nurse visit in four weeks
Four weeks later, the Nurse sees the patient and smart phrases are utilized to document education, counseling, and barriers
Care Coordinator sends reminder call to all patients for all scheduled appointments, including rescheduling Overall impact on rates of viral load suppression
In 2024, the Division aimed to reduce the number of unsuppressed patients at PKC by at least 50 percent over the time period of January-December. Data was collected monthly from January 2024 and tracked a new group of unsuppressed patients identified outside of the original cohort of 76 patients from 2023 While the total number of patients each month increased as more unsuppressed patients were identified and added to the study, the number of patients who achieved viral load suppression monthly continued to increase. By Q3 2024, the viral load suppression rate reached 44 percent, inclusive of the new rolling cohort of patients in addition to the original cohort. The Division will continue to enhance its workflows and methods to reach its goal of at least 50 percent.
In 2024, the Division also focused on improving cervical cancer screening rates. Cervical cancer screening is of particular importance for patients with HIV infection. The incidence of cervical intraepithelial neoplasia (CIN) is four-to-five times higher in HIV patients than in nonHIV patients.
From 2021 to mid-2023, an on-site Gynecology (GYN) provider was available at PKC for four screening sessions per month. The baseline cervical cancer screening rate at the end of Q4 2021 was 67.5 percent, below the benchmark of 76 percent. The clinic worked to improve cervical cancer screenings by implementing new workflows designed to increase utilization of the co-located GYN provider. By Q1 2023 and Q2 2023, the average cervical cancer screening rate for eligible patients showed improvement at 70.3 percent and 69.3 percent, respectively.
Provider refers to weekly care list to identify patients who are overdue for cervical cancer screening
Provider refers patient to gynecological provider inhouse and coordinates with front desk staff to schedule appointment during medical visit
Care Coordinator sends reminder calls to patient about upcoming appointment
For no show patients, nurses reach out to patient to re-schedule appt. Nurses also identify patients who receive gynecological care outside Mount Sinai and relay provider to document in health maintenance
Nurses educate patients on the importance of cervical cancer screening through outreach
Unfortunately, PKC’s on-site GYN services ended in August 2023, which hampered the improvement effort. Additional challenges and limitations that were identified include patient non-adherence to screening appointments despite reminder phone calls, patient discomfort with screening by a male gynecology provider, some insurances not covering services, and overstretched referrals to female gynecology providers. By October 2024, the YTD average cervical cancer screening completion rate dropped to 47.6 percent.
Data for the PKC patients due for cervical cancer screening was analyzed by age and race for the review period. Ninety-two patients were due for cervical cancer screening at the end of Q3 2024. The majority identified as Black compared to white and about 33 percent identified as other. Approximately 25 percent were between 50 to 60 years of age and 30 percent were over 60 years of age.
Next steps in 2025 include enhancing interdisciplinary workflows and intensifying nursing and care coordination outreach. Future steps will potentially include monthly provider meetings to address clinical care gaps, incentives for patients (possibly using care coordination funds), nurse counseling for no-show patients regarding the importance of cervical cancer screening in the HIV population, outreach to overdue patients to schedule a new appointment, and focus groups among women who are due for cervical cancer screening to identify perceived individual or systemic barriers to screening.
In 2024, the Division continued work on another quality project aimed at increasing health care proxy (HCP) completion for HIV-positive established PKC patients aged 65 years and older The goal is to reach out to HIV-positive established patients who are 65 years and older to complete HCP forms. Ultimately, the goal will be to reach out to the rest of the HIV-positive population at PKC
IAM Quality team sends weekly health proxy care gap list for patients with an upcoming appointment with provider to relevant RN and provider
Designated
RN/Provider discuss health care proxy (HCP) form during the visit
Patient completed HCP form
HCP form is uploaded in Epic under Ambulatory Advance Directives by front desk staff
RN/Provider countersigns the HCP form as a witness
At project inception in August 2023, baseline data provided by the Institute for Advanced Medicine’s (IAM) quality improvement data team found that of 222 established patients, 150 lacked health care proxy documentation while 72 did, resulting in a proxy ratio of 32.4 percent Alternatively, 68 percent of established patients seen at PKC aged 65 years and older did not have health care proxy documentation at baseline. The goal was to decrease the number of individuals who do not have an HCP by at least 50 percent in the next six months
Implementing a similar workflow of reviewing weekly HCP care gap lists from the IAM Quality team of patients with an upcoming appointment, the relevant nurse and/or provider is prompted to discuss the HCP during the visit. Once the physical HCP documentation is completed, it is uploaded to the EHR by the front desk staff.
As of September 2024, from the initial cohort of 222 established PKC patients aged 65 years and above, 131 patients had a proxy form completed while 91 did not. The proxy ratio significantly increased to 59 percent, suggesting an improvement in documenting and/or assigning proxies over the past year. When analyzing HCP completion rates for the 81 new patients to the practice between August 2023 and September 2024, 44 had a proxy while 37 did not, resulting in a proxy ratio of 54.3 percent. While the HCP completion rate is slightly lower for this cohort, more than half of the new patients have proxies, suggesting adoption of the HCP documentation workflow by the office. Combining established and new patients, the proxy ratio is 57.75 percent.
Barriers encountered to HCP completion included the patient remaining undecided about whom to assign as HCP and lack of living relatives or friends with whom the patient felt sufficient intimacy to assign the HCP role. The Division will continue to review HCP completion data to reassess their progress and support ongoing outreach to patients by utilizing the HCP care gap list. Future steps will include expansion of project scope to all patients seen at PKC. 22
Chasan, MD

In 2024, The Mount Sinai Hospital’s Division of Infectious Diseases (ID) continued work on several important quality initiatives, with a focus on antimicrobial stewardship efforts, key ambulatory goals, and cultivating the fellows’ quality improvement skills.
The Division continued work on two ongoing quality metrics in 2024, which remain highly clinically relevant: improving the rate of HIV virologic suppression and improving the rate of COVID-19 vaccination. In addition, the Division recently developed a new initiative related to an antimicrobial stewardship app, Firstline, which was launched in January 2024. The Division devoted significant efforts throughout the year to educating providers on the app and continued to optimize the tool through the development of additional content. Finally, the second-year ID fellows each worked on a quality initiative during their fellowship. The projects cover a broad range of ambulatory and inpatient ID issues.
HIV virologic suppression remains a major focus in ambulatory ID care at MSH. In late 2023, the Jack Martin Fund Clinic (JMFC) relocated to the new Harlem Health Center, consolidating services with Mount Sinai Morningside to continue providing HIV ambulatory services. A working group, established a year before the move, ensured clear communication with patients and facilitated ongoing retention and virologic suppression efforts. Since the relocation, the Division has monitored these outcomes. Importantly, the HIV virologic suppression rate among patients at the JMFC reached a goal of 90 percent by September 2023, prior to the move, and this remained stable at 91 percent in October 2024 at the Harlem Health Center. This is in large part due to the efforts put towards linkage and continuity of care in the time before and after the relocation, as well as the support of the Department of Health-funded (DOH) care coordination program that continues to work on assisting patients in need of additional adherence support.
Additionally, the Harlem Health Center team, along with clinic leadership from across the Institute for Advanced Medicine (IAM), continued to work on expanding the injectable antiretroviral treatment (ART) program, particularly to include patients with HIV viremia who are struggling to become undetectable on conventional oral ART. A multidisciplinary working group was formed with clinical leadership from all IAM sites, care coordination/patient navigation, nursing, pharmacy, and a dedicated program manager, to optimize and expand this program. This working group has developed a long-acting injectable (LAI) workflow, including order sets, templates for streamlined documentation, and education to guide patient selection. Most recently, the group collaborated on formal guidance for the use of LAI in viremic patients who meet criteria as outlined by the IAS-USA (International Antiviral Society-USA) guidelines, namely those who are unable to take oral ART despite extensive efforts and are at high risk for disease progression. The workgroup developed a process to review patients carefully for eligibility and ensure close monitoring, starting with a monthly regimen and with the support of
intensive case management. This has been highly successful in the group of viremic patients who have started on LAI thus far, and the group plans to expand on this important tool moving forward in 2025 to continue to achieve HIV virologic suppression in patients for whom this has been a challenge.
The Division has devoted significant efforts toward COVID-19 vaccination since the vaccines became available widely in early 2021. Throughout 2021 and 2022, these multidisciplinary efforts involved active outreach by nursing, providers, social work, and the care coordination team. All team members encouraged vaccination, and patients were frequently sent from their appointments at the JMFC to the vaccine pod directly for vaccination. A report was created in April 2021 to track vaccination metrics, and this was distributed to providers to review their panels, target unvaccinated patients to facilitate vaccination, and reconcile vaccine data in the EMR. These multidisciplinary efforts led to the program reaching a goal of 80 percent vaccination with the primary COVID-19 vaccination series. In 2022, the Division continued to focus on both ensuring patients had received their primary vaccine series and encouraging booster doses, and approximately 76 percent ultimately received a booster dose.
However, uptake of subsequent doses of COVID-19 vaccination in more recent seasons has been more challenging. In the fall of 2023, the monovalent XBB-containing mRNA COVID-19 vaccines were recommended for all persons 6 months and older, and the Division began work to address barriers to vaccination and increase uptake. This was the first year that distribution occurred outside the US government, and there were issues with access to the vaccine and uptake nationwide. At the Harlem Health Center (HHC), 29.8 percent of patients received an updated vaccine; this was similar to rates nationwide, and higher than the vaccination rate noted at IAM sites that did not offer the vaccine on site.
In mid-2024, the Advisory Committee on Immunization Practices (ACIP) recommended an updated 2024-2025 COVID-19 vaccination for all persons aged six months and older. This recommendation was made because SARS-CoV-2 continues to evolve and updated vaccines have been developed to match the strains that are widely circulating, as well as to address the fact that COVID-19 vaccine effectiveness is known to wane. Additionally, COVID-19 continues to account for a significant number of hospitalizations and deaths in the US, and a universal recommendation can help to simplify messaging and ensure equitable access. The Division is focused on increasing COVID-19 vaccination rates to a goal of 40 percent at HHC this season, through ensuring timely access to the vaccine on site. The Division is also actively engaged in educating providers outside of ID on the role for updated COVID-19 vaccination, and the benefits of access to the vaccine at the site of care.
The Division of Infectious Diseases began to focus on developing an app to support antimicrobial stewardship efforts in 2023, through a collaboration with Firstline and the New York City Department of Health and Mental Hygiene (DOHMH), and this app went live in January 2024. The app provides easy access to institution-specific ID guidance, including treatment guidelines and detailed information on pathogens and antimicrobials, and is available both as a mobile app as well as through the desktop launcher. Beginning with the launch in
January and throughout 2024, the Division provided education on the app to numerous groups of providers, including those in internal medicine, family medicine, critical care, general surgery, vascular surgery, and emergency medicine. This education and campaign to raise awareness of the app was done through email blasts, targeted educational sessions, orientation at the start of the academic year, as well as screen savers and dissemination of the QR code in email signatures. In November 2024, the antimicrobial stewardship team also promoted the app at a tabling event held to recognize Antibiotic Awareness Week.
The Division has measured app uptake and usage as an initial metric of success, with more than 2,000 users per month accessing the app by October 2024 and more than 30,000 clinical decisions supported.
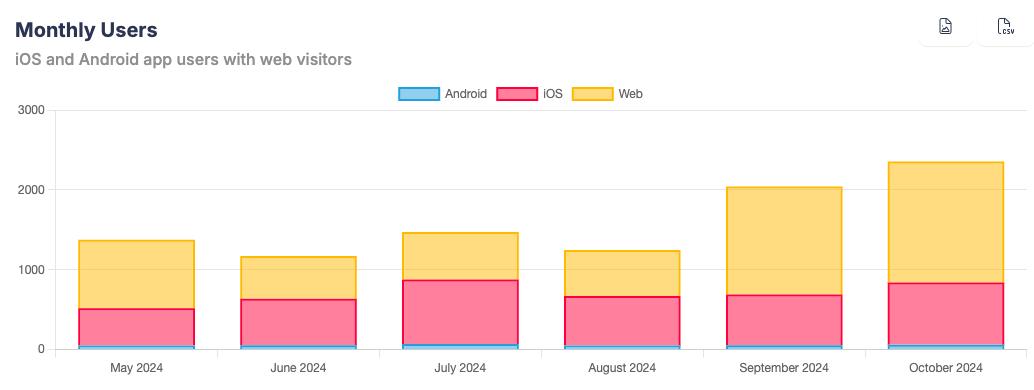
Source: Firstline app
Additionally, the Division has been able to view which guidance has been most frequently utilized, with the urinary tract infection algorithm and community-acquired pneumonia guidance in the lead.
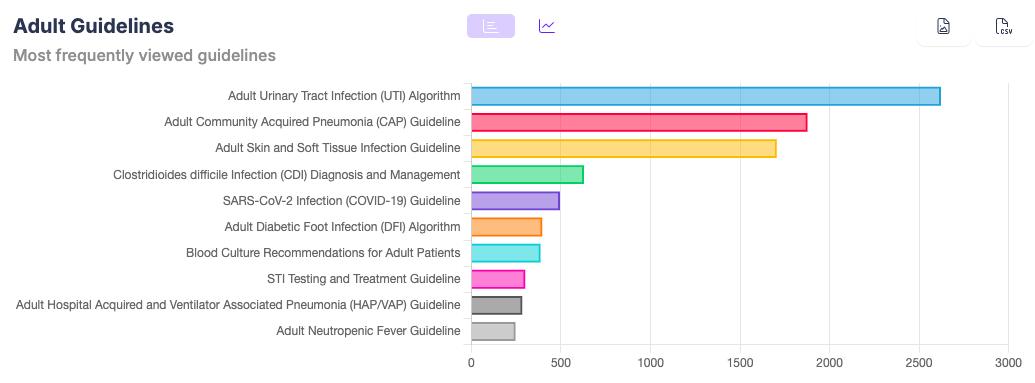
Source: Firstline app
Ultimately, the Division plans to measure guideline concordant care to determine to what extent clinical care has been optimized to match our guidance through access to this educational tool
Every ID fellow works on a quality-improvement project in the second year of ID fellowship at The Mount Sinai Hospital. One project was developed by a former second-year ID fellow to optimize the transition to two-drug ART regimens in the ambulatory setting and prevent complications related to co-morbid hepatitis B. This is increasingly relevant with the growing number of two-drug ART options, including injectable cabotegravir and rilpivirine. These regimens are effective for HIV control and are well tolerated, but do not provide coverage for chronic hepatitis B, with which a significant number of patients with HIV are co-infected. A recently graduated second-year ID fellow developed guidance on this transition by obtaining consensus from stakeholders across the system, including IAM and hepatology. This facilitated the implementation of an Epic-based intervention to alert providers placing medication orders for two-drug ART regimens, reminding them to check hepatitis B serologies. A current third-year internal medicine resident has continued work on this project and found that the quality improvement initiative led to an increase in screening with complete hepatitis B serologies (30 percent pre-QI to 71 percent post-QI, p < 0.0001) as well as a decrease in switch to two-drug regimens in patients at increased risk for hepatitis B-related events (9 percent pre-QI to <1 percent post-QI, p < 0.01). This work was presented with an oral abstract at ID week 2024
Recently graduated second-year ID fellows completed quality projects in June 2024, including: a successful educational initiative to improve understanding of syphilis diagnosis and management among house staff and other frontline providers; the implementation of a protocol to optimize toxoplasmosis prophylaxis for patients post-bone marrow transplant; and the development of tools to support the rollout of Doxy-PEP (doxycycline as post exposure prophylaxis to prevent sexually transmitted infections), including guidance in the Firstline app.
Current second-year ID fellows are working on several important quality projects, including: a diagnostic stewardship project to optimize the use of serum (1-3)-beta-D-glucan testing; a collaboration with allergy/immunology to update the peri-operative prophylaxis for liver transplant and obstetric procedures in patients with penicillin allergy; an ambulatory project to educate providers and increase uptake of the RSV vaccine; and development of an educational initiative to increase use of the MRSA PCR and decrease inappropriate vancomycin use in patients admitted with pneumonia.
Quality
Champion:
Rahul Gaikwad, MD

The Division of Infectious Diseases at Mount Sinai Morningside and West continues its initiative to improve HIV viral load suppression among ambulatory HIV patients through a focus on patient retention. The COVID-19 pandemic impacted retention, but through renewed nursing and social work efforts, retention rates have returned to near pre-pandemic levels. In late 2023, the Morningside Clinic and the Jack Martin Clinic (eastside campus) closed, and their patients were transitioned to the Harlem Health Center. Retention rates for the new Harlem clinic were slightly lower than other Institute for Advanced Medicine (IAM) clinics through 2024, likely related to difficulties transitioning patients to the new site. The Samuels clinic continues to see improvement in both retention and suppression rates driven by ongoing efforts by its nursing and social work teams to actively engage patients in care.
The Division also began a new project, led by ID fellow Maria Haider Baig, MD, aimed at improving rates of ordering respiratory cultures and subsequently de-escalating anti-pseudomonal antibiotics for patients with pneumonia in the intensive care units at MSM and MSW. Professional societal guidelines recommend collecting respiratory cultures for all patients with severe respiratory disease who have risk factors for nosocomial pathogens such as pseudomonas or MRSA and then using this culture data to change unnecessary broad-spectrum antibiotics if no drug-resistant pathogens are isolated. Pre-interventional data analysis revealed 121 patients who met criteria for severe pneumonia in the ICU between January and March 2024. Seventy-nine of these patients had respiratory cultures collected, and 56 patients were not appropriately deescalated. The study team’s planned intervention is to present this data to the Critical Care Committee and give biweekly talks in the MSMW ICUs to providers and nurses regarding the importance of collecting respiratory cultures and de-escalating antibiotics appropriately. The intervention is currently ongoing.
Another project, led by ID fellow, Elmarie Alexander, MD, started in 2024, was aimed at improving oral care hygiene in non-ventilated patients who are unable to care for themselves at MSMW. It has been shown that functionally dependent patients are at risk for poor oral hygiene, which is a
risk factor for dental infections and hospital-acquired pneumonia. There currently is no standard practice in place to deliver oral care to non-ventilated patients in the Mount Sinai Health System Therefore, the objective of this project is to develop an oral care bundle and then to assess its implementation and ultimately the impact on downstream complications such as new pneumonia diagnoses. A written policy was developed with guidelines for nursing staff and patient care associates for assessing functional capacity to provide independent oral care and to help as appropriate. The trial pilot will start in early 2025, with the subsequent incorporation of feedback from registered nurses and patient care associates, and then the potential system-wide rollout by the second quarter of 2025.
Division Quality Champions:
Douglas Dieterich, MD
Anna Mageras, MPH


In response to the high prevalence of chronic hepatitis C virus (HCV), hepatitis B virus (HBV), and hepatitis delta virus (HDV) infections in New York City (NYC), Mount Sinai’s Division of Liver Diseases aims to enhance screening rates and subsequent linkage to care and treatment for patients who test positive for these viral diseases.
Hepatitis C
In May 2024, a New York State law took effect, making a one-time offer of HCV screening mandatory for all adults in health care settings. The law further mandates completion of HCV RNA PCR testing after a positive HCV antibody (Ab) result, as well as linkage to care for those with positive HCV RNA. The law also mandates risk-factor-based screening for persons under 18 years of age.
Given previous efforts by the Mount Sinai Division of Liver Diseases to expand HCV screening and linkage to care, Mount Sinai Health System (MSHS) outpatient clinics already had the infrastructure to be compliant with this new law. The Division has also partnered with the emergency department (ED) to ensure that universal HCV screening is offered
To further improve screening rates, several initiatives were implemented. The Division updated the ambulatory provider-facing language in the HCV screening silent best practice alert (BPA) in Epic to reference the new law and link to the New York State Department of Health’s website with the official language. The team also met with ambulatory nursing to provide guidance on how to institute nursing-driven screening. Nursing leadership is working with Epic IT to institute a nursing-facing prompt. The Division also provided guidance to pediatrics leadership for addressing their new screening requirements.
The Division’s LEAP (Liver Education & Action Program) outreach team tries to further improve HCV screening rates with a three-pronged approach: by sending individual providers lists of screening-eligible patients before upcoming appointments, by engaging patients through MyMountSinai messages ahead of their visits, and by collaborating with the marketing department to promote HCV screening on social media platforms and monitors across the Mount Sinai Health System.
In 2024, HCV screening rates of screening-naïve patients in primary care continued to exceed the Division’s goal of screening at least 20 percent of patients in 2024. IMA’s screening rate increased from 25 percent to more than 30 percent between 2022 Q4 and 2023 and remained more than 30 percent in 2024. HCV RNA PCR order rates for Ab+ adults remained at 100 percent, meeting the Division’s goal for 2024.
2021 Q42022 Q12022 Q22022 Q32022 Q42023 Q12023 Q22023 Q32023 Q42024 Q12024 Q22024 Q3
IMA Goal
The number of HCV RNA-positive patients identified at MSHS in 2024 was lower than in 2022 and 2023. This reflects a general trend in the region, as the New York City Department of Health and Mental Hygiene (DOHMH) recently reported a decrease in HCV prevalence between 2014 and 2023, and half as many newly reported cases in 2023 compared to 2019.
Nevertheless, rates of linkage to care in the MSHS remained consistent. In 2024, 66 percent (234) of eligible HCV RNA-positive patients at MSHS were linked to care, defined as attending at least one appointment with an HCV provider, many assisted by LEAP patient navigators. LEAP navigators continue to engage an additional 7 percent (n=25), putting the department on track to meet the 70 percent linkage goal for the year. The LEAP team’s patient navigators utilize a weekly Epic report to identify HCV-positive patients, conducting chart reviews and outreach to engage patients not already in HCV care. Navigators employ a comprehensive approach, making multiple phone attempts, sending physical letters or MyMountSinai messages, and reopening cases when patients re-engage. Once a patient is engaged, the navigators provide health education, schedule HCV evaluation appointments, offer reminders, and assist with insurance, transportation, and referrals. The Division also collaborates with the ED’s health education program to engage HCV-positive patients seen in the ED
Linked to Care In Progress
The Division remains committed to improving HCV treatment rates in Liver Medicine. For patients enrolled in LEAP care coordination at the Mount Sinai Institute for Liver Medicine in 2024, 74 percent (n=80) of eligible patients initiated HCV treatment, just short of the 76 percent target, though the goal is expected to be reached as the team continues to work with patients in 2025. The following graph shows treatment initiation and completion rates over the past three years.
Treatment Continuum for Patients in LEAP HCV Care Coordination
In March 2023, the Centers for Disease Control and Prevention revised the guidelines for HBV screening, transitioning from risk-factor-based assessments to recommending universal onetime screening for adults. Mount Sinai’s Division of Liver Diseases proactively implemented universal one-time HBV screening for adults in primary care clinics in October 2022, becoming the first major health system in the United States to do so. The initiative was motivated by a high prevalence of chronic HBV prevalence in New York City, estimated at 2.9 percent in 2019 by the DOHMH. In their 2023 report, the DOHMH saw an increase in newly reported cases of HBV from 5,518 in 2022 to 6,947 in 2023, and updated their prevalence estimate to 3.1 percent. Causes for this increase are unknown, but the expansion of testing, especially in the MSHS, may at least partially explain this trend.
To promote HBV screening, a health maintenance care gap in the Epic electronic medical record (EMR) was created. This prompts providers to test patients who have never been screened for HBV at MSHS. This mirrors the HCV screening alert. The care gap links to a triplepanel (HBsAg, HBsAb, and HBcAb) order set that can be placed with one click to satisfy the screening. To complement the EMR alert, in 2024, outreach to PCPs across Manhattan and in Nassau County was continued via presentations in faculty meetings and offers of patient navigation support.
Since implementation of the EMR alert, the HBV screening rate in MSH primary care has increased from six percent at baseline in September 2022 to 32 percent by October 2024, exceeding the initial target of 15 percent.
LEAP patient navigators conducted patient outreach and navigation via phone, MyMountSinai messages, and PCP engagement for patients who tested HBsAg-positive, with the goal of connecting them to liver care. From September 2022 to November 2024, the team identified 419 HBsAg-positive patients who were screened or had an encounter at one of the pilot clinics and were not receiving AASLD (American Association for the Study of Liver Diseases)-guidelineconcordant care. LEAP linked 65 percent (n=271) of these patients to their first appointment, and 20 percent (n=84) are currently being followed by the patient navigators.
HBV Navigation Outcomes September 2022 to November 2024 (n=419)
Deceased/Moved
/Too Ill, 9, 2%
LTFU, 30, 7%
Declined, 25, 6%
In Progress, 84, 20%
Linked to Care, 271, 65%
In mid-2024, the Division secured a new grant from the Center for Disease Analysis Foundation to support strategies aimed at re-engaging diagnosed but untreated patients living with HCV or HBV. Through this project, the Division is offering $20 cash incentives to HCV patients who attend their first liver appointment. The plan is to evaluate the impact of this monetary incentive on rates of linkage to care. Another initiative to improve linkage to care involves HBV navigators sending MyMountSinai messages as a first outreach attempt instead of phone calls. Results from these initiatives will be presented in 2025.
Hepatitis Delta
Hepatitis delta virus (HDV) is the most severe form of viral hepatitis. According to one study, 25 percent of HDV cases in the U.S. are in the NYC metro area. At baseline in the MSHS, only 54 percent of HBsAg-positive patients had ever received HDV Ab testing. With new treatments on the horizon and several patients already on treatment via compassionate use at the Institute for Liver Medicine, improved screening is more urgent than ever.
To improve the screening rate in the MSHS, the Division successfully implemented HBsAgpositive to hepatitis delta virus antibody (HDV Ab) reflex testing for Article 28 sites, with
excellent help from Mount Sinai’s laboratory leadership. The reflex test was also integrated into the existing HBV screening care gap in Epic. The logic of the reflex test flow is illustrated here:
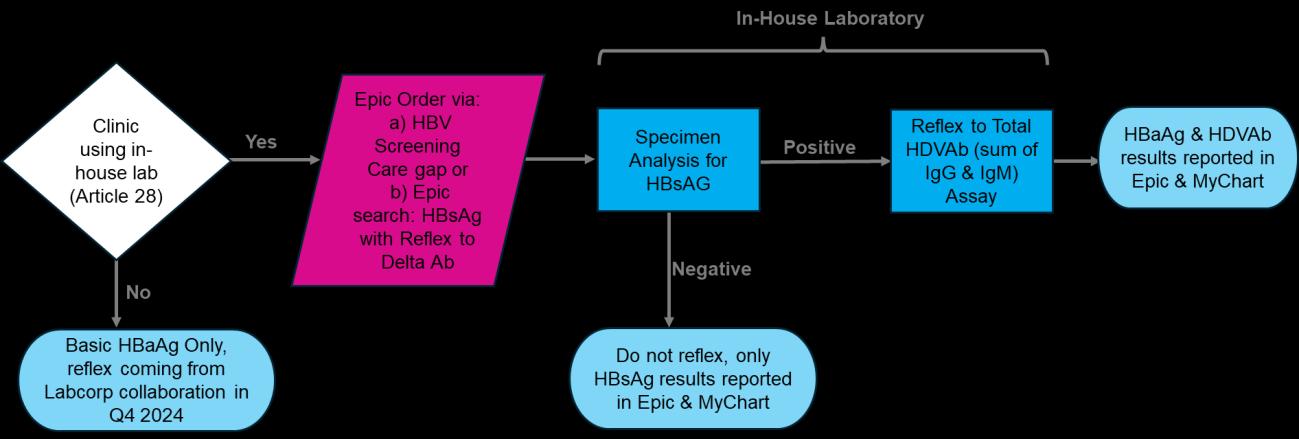
Results from implementation in March 2024 through October 2024 are promising. The HDV Ab testing rate among HBsAg-positive patients who received a standalone HBsAg test was 48 percent compared to 100 percent among HBsAg-positive patients who received the reflex test. The median time to HDV Ab test result was also shorter for those receiving the reflex test (2.5 days versus 13.5). The reflex test identified 35 HBsAg-positive patients, all of whom successfully reflexed to HDV Ab. Seventy-six percent of reflex tests were ordered in primary care, indicating that integration with the HBV care gap drove most of these orders. The Division is now working with the ED team to integrate the reflex test into their existing STI panel. The Division is also collaborating with LabCorp to make reflex testing available to FPA sites, pending New York State or FDA approval of their assay. The implementation process and initial results were presented in an oral presentation at AASLD’s The Liver Meeting in November 2024.
Regarding linkage to care, one HDV Ab-positive patient was identified through reflex testing and promptly linked to hepatology.
HDV Ab Screening Rate (Ever Screened) after Reflex Implementation March - October 2024 (n = 939 HBsAg+)

In 2025, the Division will continue its efforts to improve screening, linkage to care, and treatment rates for patients with chronic HBV, HCV, and HDV. It will continue expanding navigation for patients with HBV and HDV to capture patients system-wide. Additionally, the Division will continue to engage primary care providers around screening and to facilitate referrals. A short manuscript is also in progress to summarize implementation and initial results of HDV reflex testing.
Future projects may include screening, case-finding, and navigation enhancements for patients at risk for metabolic dysfunction-associated steatotic liver disease, metabolic dysfunctionassociated steatohepatitis, and primary biliary cholangitis.
Division Quality Champion: Elliot Charen, MD

The Division of Nephrology at Mount Sinai Beth Israel focused its efforts on reducing anemia by increasing the percentage of patients who achieve their target hemoglobin levels Patients with chronic kidney disease (CKD) experience abnormal red blood cell production and are at an increased risk for anemia. Anemia in patients with CKD is typically addressed with an erythropoietin stimulating agent (ESA) and treated to a goal hemoglobin no higher than 11.5 g/dL. The Division increased the percentage of patients who met their anemia goal by an
Percent of patients with chronic kidney disease meeting anemia goals
average of 11 percentage points over the course of the year (graph below). The team accomplished this by reviewing weekly hemoglobin results and improving the timely dosing of ESA. The team also educated providers on adjusting the hemoglobin lab orders if a treatment was missed and ensuring that anemia and iron algorithms were ordered on admission.
Another Division goal was to improve bone and mineral metabolism in alignment with the Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines. With kidney disease comes abnormal bone health given that calcium, phosphorus, parathyroid hormone, and vitamin D regulation are disturbed. In addition, the rate of turnover and mineralization changes. To improve bone health, efforts were made to drive patient adherence to phosphate binders, vitamin D analogs, and calcimimetics. Abnormal levels of these quality markers may not cause physical symptoms, which makes education and behavior change difficult. To improve these metrics, the Division increased the use of phosphate binders, vitamin D, and calcimimetic use and increased patient education on the impact of diet. These efforts led to an average four percent improvement in indicators involving calcium, phosphorus, and parathyroid hormone (graph below).
Percent of patients with chronic kidney disease meeting bone and mineral metabolism indicators
In 2024, the Division renewed the focus on increasing serum albumin levels. KDOQI guidelines warn that serum albumin is a reliable predictor of mortality and hospitalization, thus increased efforts were placed on education, nutrition, and fluid removal. With these interventions, the percentage of chronic hemodialysis patients with serum albumin greater than 4 g/dL increased over the course of the year (graph below).
In 2024, the Division published a resident-led quality initiative in collaboration with the critical care team in the Point of Care Ultrasound (POCUS) Journal A novel renal POCUS curriculum was integrated into a two-week nephrology rotation for internal medicine residents to improve knowledge of the use of POCUS as a screening tool and confidence in using it to screen for obstructive acute kidney injury. The project aimed to assess the accuracy of resident-performed renal POCUS and its impact on the management of acute kidney injury. After the curriculum, residents demonstrated improved knowledge and confidence in using POCUS.
Division Quality Champions:
Niraj Kothari, MD
Joji Tokita, MD


In 2024, the Mount Sinai Chronic Kidney Disease (CKD) Program continued to expand its reach across the Health System. The program utilizes registry data to identify patients with CKD, stratify them by glomerular filtration rate (GFR) and albuminuria levels, and facilitate guideline-based care.
Of particular interest are individuals at increased risk of progressive decline in kidney function such as those with diabetes and/or hypertension. The program supports advanced risk stratification for early diabetic nephropathy with KidneyIntelX, used within an IRB-approved study to evaluate the impact of test results on subsequent clinical decision making. This includes changes in prescribing key medication classes (ACE/ARB, SGLT2 inhibitors, GLP-1 receptor agonists, and MRAs). By late 2024, approximately 8,500 patients had undergone testing with a target enrollment of 10,000 expected by late 2025. The 12-month data was previously described in the 2023 DOM Annual Report. Key findings included:
• Increased post-test action in high- and intermediate-risk groups compared to low-risk
• A reduction in median HbA1c in patients with high-risk test results
Two-year follow-up data will be available by 2025 and will be reported upon release
Program growth has been noteworthy, but challenges persist. Early-stage diabetic nephropathy is often asymptomatic, making clinician and patient engagement difficult. Some clinicians hesitate to classify patients with normal or near normal GFR as having CKD. Additionally, conversations about kidney disease can be stressful, time-consuming, and often delayed due to the perceived remoteness of its consequences. Efforts to address these barriers include:
• Enhancing communication strategies for early-stage CKD
• Streamlining access to medications despite cost and insurance challenges
CIO Disclosure: KidneyIntelX is an FDA-approved predictive test that combines patient information and biomarker results. KidneyIntelX is based on technology developed by Mount Sinai faculty and licensed to Renalytix, Inc. Mount Sinai faculty and Mount Sinai have equity ownership in Renalytix, Inc.
In 2024, The Mount Sinai Hospital (MSH) and Mount Sinai Queens (MSQ) successfully completed the triennial Joint Commission (JC) recertification. The dialysis programs performed very well. The MSH dialysis program received no citations; MSQ had one citation related to staff training, which was promptly corrected. Overall, the surveyors commended the institution for substantial compliance with JC standards and ongoing commitment to quality and patient safety.
Mount Sinai Kidney Center at 117th Street and East River Plaza (117th Street)
In late spring 2024, the clinical leadership team at 117th Street worked closely with a nearby Manhattan facility that was forced to close on short notice, accommodating more than 20 dialysis patients on various shifts 117th Street played an instrumental role in ensuring timely and seamless access to high-quality dialysis. The facility concluded the year with the highest total census over seven years, including the re-opening of a fourth shift.
Despite the significant increase in patient census, in November 2024, 117th Street received its first-ever five-star quality of patient care rating from Centers for Medicare and Medicaid Services (CMS). The B1 Renal Treatment Center (B1) dialysis improved to three stars. The dialysis facility quality of patient care website shows how a specific unit compares to others on measurements of clinical performance. The rating, between 1 to 5 stars, is an aggregate score calculated from several clinically relevant metrics, including: preventing hospitalization and death, avoiding unnecessary transfusion, fistula rate, meeting clearance targets, metabolic bone disease control, and fraction of patients on the transplant waitlist. These scores are publicly available and can be an important factor that referring entities and new patients consider when looking for a destination for maintenance hemodialysis. 117th Street outperformed state and national averages in several of these parameters, and transplant rates remain a strength of the facility, with most patients choosing Mount Sinai for their kidney transplant care. Bloodstream infections remain a rare occurrence, with the Standardized Infection Ratio (SIR) averaging below 1.0 for most of 2024. Dialysis adequacy as measured by monthly Kt/V >1.2 exceeded 98 percent compliance and remains close to the 10 percent nationwide.
While B1 did not achieve five stars, the clinical practice, policies, and procedures are maintained on par with 117th Street. B1, however, has several important differences, which make achieving the same rating more difficult. These include a much smaller census and multiple modalities, including a pediatric population with a higher frequency of new starts who are more likely to have central venous catheter (CVC) access as they await transplant.
Encompassing the peritoneal dialysis (PD) and home hemodialysis (HHD) programs, the home dialysis programs are listed under the B1 identifier, so they contributed to and benefited from the improvement in quality star rating. In addition to hosting the nationally recognized 10th annual Advances in Peritoneal Dialysis Symposium in September, the home programs remain a key part of the Mount Sinai Kidney Center, ensuring patients have access to all dialysis modalities. Despite hurricane Helene impacting Baxter’s production facility in North Carolina, the home dialysis program has implemented creative solutions to mitigate supply constraints and ensure patients continue to receive adequate therapy.
Despite ongoing multidisciplinary efforts to reduce the total number of inpatient CLABSI across 2024, the incidence remains elevated. A subset of these catheters include large-bore CVC used for extracorporeal therapies such as kidney replacement therapy, mechanical ultrafiltration, and apheresis. These catheters may be tunneled or non-tunneled depending on the expected duration of use and other clinical factors.
Nephrology and dialysis nursing participate in all dialysis CLABSI huddles and continue to work with Infection Prevention and key stakeholders to identify factors that may increase risk for infection as well as interventions that aim to provide a sustainable, long-term reduction in events. Reducing inpatient catheter days remains a key objective. Patients only have dialysis if it is in active use (no idle catheters). The outpatient dialysis facilities and CKD clinics aim to ensure arteriovenous (AV) access is in place as this reflects best practice but will also reduce line days if patients are admitted to the hospital. As noted in the ESKD section above, the census at 117th Street has increased substantially over the year, including admission of several new patients dialyzing via tunneled catheters. The facility is actively working with the patients and its partners in vascular surgery to ensure that patients have non-catheter access in place in a timely fashion.
A review of inpatient CLABSI events demonstrated a non-uniform distribution with respect to location. A majority of cases occur in patients dialyzed off-center rather than in those who are transported to B1. This does not necessarily mean that locations with higher CLABSI numbers are not delivering good catheter care; rather, these locations may have patient clusters at higher risk such as chronically ill patients on the ventilator or patients who are immuno-compromised (oncology and/or transplant). Regardless of the underlying cause, dialysis is working closely with those locations to address the opportunity to reduce events across the hospital.
Ruchika Batwara, MD
Claire Schretlen, MD


In 2024, Mount Sinai Morningside (MSM) and Mount Sinai West’s (MSW) Division of Nephrology continued its efforts to simplify the complex referral process for incident dialysis patients at MSM who are transitioning from inpatient (excluding ICU) to outpatient dialysis units The goal was to reduce the length of stay (LOS) by 15 percent, decreasing the median from 20 days to 17 days. The Division identified several causes contributing to delays, including issues within the outpatient unit, patient decision-making, expired lab tests, access problems, and patients not being medically ready for discharge To address these challenges, two key interventions were implemented: first, a standardized lab order set was created for the labs required for referrals, and second, a smart phrase was developed for social workers to facilitate targeted referrals, with its usage being tracked as a performance metric. Since the implementation of the designated lab order set, the median LOS has been reduced from 20 days to 19 days. The team worked on improving the use of the dialysis referral smart phrase; however, the project had to be terminated prematurely due to significant logistical challenges in gaining buy-in from the unit social workers.
The second major initiative in 2024 was focused on enhancing standardized blood pressure measurement in an outpatient office setting at the ACC-6 multispecialty practice. Identified barriers included workflow constraints, a lack of regulatory oversight, and insufficient staff training. To address these issues, the Division implemented staff training, periodic re-training sessions, and daily random checks conducted by the practice manager. The evaluation included 3,254 patients (March to May 2023), pre-intervention, and 3,443 patients, post-intervention (June to August 2024), revealing a decrease in the percentage of patients with a systolic blood pressure (SBP) greater than 140mmHg from 29.2 percent to 22.6 percent The Division plans to continue improving staff training and to collaborate with other groups working on similar hypertension projects.
In 2025, the Division identified two new initiatives, both focused on improving referral logistics. The first initiative will work to increase transplant evaluation referrals for renal clinic patients with an estimated glomerular filtration rate (eGFR) below 20 mL/min/1.73m2. The second initiative aims to improve the scheduling of nephrology follow-up appointments for inpatients at MSM and MSW before discharge, ensuring a standardized workflow that integrates referral scheduling into discharge planning.
Mount Sinai West, Mount
Sinai Beth Israel, Mount Sinai-Union Square
Division Quality Champions:
David Steiger, MD; Boram Kim, DO
Sleep: Boris Gilyadov, DO


In 2024, the Division of Pulmonary, Critical Care and Sleep Medicine at Mount Sinai West (MSW) and Mount Sinai Beth Israel (MSBI) and the Respiratory Institute at Mount Sinai-Union Square (MSUS) continued collaborative efforts on various quality projects that encompassed both inpatient and outpatient practices.
Chronic obstructive pulmonary disease (COPD) is the third leading cause of 30-day readmissions among Medicare patients. Approximately 20 percent of patients admitted for an acute exacerbation of COPD will be readmitted within 30 days. The Division is actively involved in a systemwide standardization of COPD care initiative, which has introduced several protocols and templates based on best practices and evidence-based data. The goal of the initiative is to optimize COPD management and improve the quality of care and safety of patients admitted with COPD. Identifying patients admitted with an acute exacerbation of COPD (AECOPD) in real time facilitates the necessary multidisciplinary care of these patients to optimize their inpatient management and reduce the risk of a potential readmission.
The Division, in collaboration with Clinical Integration at Mount Sinai Health System, follows a COPD Care Bundle designed to optimize the management of admitted patients with an AECOPD and reduce avoidable readmissions. COPD admissions appear on an Epic COPD list if the admitting providers use an admitting COPD order set, or if the admitting diagnosis, based on the Diagnosis-Related Group (DRG), is an AECOPD. Patients on the COPD list may receive multidisciplinary care from Respiratory Therapy, Pharmacy, Social Work, and the Pulmonary Consult team. Following discharge, the patient receives a phone call from the Transitions of Care team within 72 hours, and there is an attempt to provide a pulmonary outpatient clinic appointment within 7-14 days post-discharge. The patient may also be referred for Pulmonary Rehabilitation, smoking cessation counseling, palliative or hospice care, or to the Remote Monitoring Program (described in detail below).
The COPD readmission rate at MSW to date for 2024 was 16.4 percent compared to 18.9 percent for 2023, and 24.7 percent for 2022.
A steady decrease in both the in-patient and 30-day COPD mortality rates since 2022 was observed. Specifically, the 2024 30-day mortality rate to date was 2.1 percent, compared to 3.1 percent in 2023 and 5.2 percent in 2022. Similarly, the 2024 in-patient COPD mortality rate to date was 2.1 percent, improved from 2.3 percent in 2023 and 4.1 percent in 2022.
In 2024, 42.7 percent of patients admitted with AECOPD were on the COPD pathway, compared to 23.1 percent in 2023, and 4.1 percent in 2022. Efforts to reduce the wait time for discharged patients to be seen in the outpatient Pulmonary Clinic are ongoing. Patients admitted for COPD can now be prescribed varenicline during their admission to minimize nicotine withdrawal and facilitate smoking cessation. Varenicline is prescribed at the time of discharge to enable the patient to continue use as an outpatient.
In 2024, further goals of the COPD readmission reduction program include analyzing dashboard process metrics and outcomes as well as understanding health disparities. In this regard, there has been an improvement in the precision of the data available for race and ethnicity in the COPD Tableau dashboard. Patients characterized as high risk for readmission for AECOPD are referred to a Remote Monitoring Program based at MSH that aims to detect early deterioration in the health status of enrolled high-risk COPD patients and can result in early intervention to optimize patient health and potentially prevent an in-hospital admission. As part of the “My Next Steps” initiative, educational material available for patients with COPD after an outpatient visit may help to reduce COPD readmissions by empowering patients to take further responsibility for “self-management,” including a focus on nutrition, exercise, and compliance with prescribed pharmacotherapy.
The Division also sought to improve outcomes for patients with pulmonary embolism (PE) through the use of the Pulmonary Embolism Response Team (PERT). PERT is a multidisciplinary team of pulmonologists, cardiologists, cardiothoracic surgeons, and interventional radiologists who co-manage patients with acute massive and sub massive PE. The program provides an infrastructure to deliver rapid input from these experts to optimize and streamline treatment.
The PERT at MSBI and MSW and Mount Sinai Morningside (MSM) work collaboratively, and patients who require specific advanced therapies for treatment of intermediate or high-risk PE may be transferred to MSM or Mount Sinai Hospital (MSH). PERT was activated at MSBI, MSW, and MSM and managed 78 patients in 2019, 88 patients in 2020, 47 patients in 2021, 82 patients in 2022, 95 patients in 2023, and 77 in 2024. For each PERT activation, there was full and prompt engagement of all members of the PERT. The multidisciplinary team reached a consensus regarding acute PE management for each patient managed. With respect to 2024 data, using the European Society of Cardiology (ESC) classification, 5.19 percent, 2.6 percent, 66.2 percent, and 26 percent were low risk, intermediate-low risk, intermediate-high risk, and high risk, respectively, for PE mortality. Advanced therapies for the PERT-managed patients in 2024 included catheter-directed thrombolysis (1.3 percent), catheter-directed embolectomy (10.4 percent), systemic thrombolytics (3.9 percent), and inferior vena cava filter placement (6.5 percent).
Outcomes of Acute PE Patients Managed by PERT (n=77) 2024
IM/Pulmonary Follow-Up at Discharge
Causes of 30-day mortality in 9.09 percent of patients (n=7) included: high-risk PE (n=3), concurrent severe sepsis (n=1), malignancy (n=1), and concurrent Acute Respiratory Distress Syndrome (ARDS) (n=2). Major bleeding occurred in 6.49 percent of patients (n=5) with causes including lower GI bleed (n=2), and hematuria (n=2). The readmission rate at 30 days was 5.19 percent (n=4), secondary to recurrent PE (n=2), sepsis (n=1), and pneumonia (n=1). Sixty-four (83.12 percent) patients with acute PE and managed by PERT followed up at either Mount Sinai Internal Medicine or Pulmonary outpatient clinic.
Aims for 2025 include establishing a multidisciplinary Venous thromboembolism (VTE) clinic at MSM, evaluating drivers of hospital length of stay for patients admitted with acute PE, creating management protocols for patients who follow up in the VTE clinic, and continuing the systemwide PERT conferences where the team reviews PERT outcomes data, discusses new literature pertaining to acute PE management, and shares ongoing PErelated research projects.
Inter-Hospital Transfer Acute PE Patients, Association of Transfer Time, and Delays with Outcomes
Management options for acute PE have evolved in recent years with wider availability of advanced treatment modalities. Most institutions are not equipped or staffed for advanced PE care and patients often require transfer to centers with more comprehensive resources. An organized approach to the process of inter-hospital transfer (IHT) of critically ill PE patients to loco-regional expert PERT centers is still an unmet need. IHT has been previously studied for patients with acute trauma, ST-elevation MI, and acute CVA. There is a paucity of data relating to the outcomes of patients with acute PE who receive IHT.
The Division performed a retrospective review of consecutive patients diagnosed with acute PE from September 2021-June 2023 who received IHT as recommended by the system-wide PERT. The patients were referred by hospitals in the MSHS and from local non-affiliated hospitals. Data from a total of 139 patients who received IHT were analyzed, including data from “out-of-system hospitals.”
Sixty patients who received IHT were excluded due to incomplete data or the IHT occurred for non-PE diagnoses.
Almost all IHT acute PE patients were classified as intermediate or high risk, and only 0.72 percent of patients transferred were at low risk. The survival rate was 94.2 percent. No patients died during IHT. The “door to diagnosis,” “diagnosis to PERT” consultation, IHT, “arrival to procedure,” and “procedure to discharge” times were the designated process metrics. A propensity score was calculated from six variables (i.e., age, sex, BMI, PESI score, ESC risk group, and presence of saddle PE) and matching on the propensity score was performed. A minority (33.8 percent) of IHT patients received advanced intervention at the hospital where they were transferred. Of the 139 patients who received IHT, 66.25 percent received standard-of-care therapeutic anticoagulation, and the remainder received advanced therapies that included catheter-directed embolectomy (19.4 percent), systemic thrombolysis (7.9 percent), surgical embolectomy (3.6 percent), and catheter-directed thrombolysis (2.9 percent). All patients who received advanced therapies were at intermediate or high risk for mortality from acute pulmonary embolism.
The median “door to diagnosis” time was 4.1 (IQR: 3.0‒6.4) hours. The median “diagnosis to PERT” time was 50 (IQR: 10‒166) minutes and the median IHT time was 4.1 (IQR: 2.3‒8.3) hours. For patients who received advanced therapies (i.e., catheter-directed thrombolysis, catheter-directed embolectomy, or surgical embolectomy), the “arrival to procedure” time was 10.9 (IQR: 5.1‒16.2) hours. The time taken to achieve IHT and the day of the week or time of day when IHT occurred were not associated with either the receipt of advanced therapies or mortality. The rates of 30-day mortality, 30-day major bleeding, and 30-day re-admission were 7.2 percent, 2.2 percent, and 11.5 percent, respectively.
The team concluded that IHTs for acute PE were safe, the time from evaluation in the ED to intervention was variable, and the timing of IHT did not impact overall outcomes or the decision to pursue advanced therapies.
The Division performed a retrospective review from January 2023 to July 2024 to determine the compliance rate of Pulmonary attendings ordering low-dose chest CT (LDCT) scans in patients eligible for lung cancer screening who were evaluated at the Respiratory Institute at Mount Sinai-Union Square (MSUS) and in the Pulmonary Faculty Practice at MSW. A total of 701 patients were seen, 186 at MSW and 515 at MSUS. The median age of patients was 67 years, 40.5 percent of patients were white, 16.4 percent Black, and 31.8 percent had Hispanic ethnicity. Follow-up patients represented 79.9 percent of patients and 15.8 percent were new patients.
Lung cancer screening using LDCT occurred in 74.6 percent and 78.4 percent of eligible patients seen at MSW Pulmonary Faculty Practice and MSUS, respectively. It is possible that the calculated lung cancer screening rate is an underestimation as it does not include patients who received an order for a LDCT and were screened at a facility not connected with the Mount Sinai Health System. The team is performing a review of all patients who did not receive a LDCT but met screening eligibility to determine if the patient had a LDCT elsewhere that was either not captured in Epic or the results were scanned into the “media” section of Epic, resulting in lack of data capture during the initial retrospective review, or the patient is still due for LDCT screening.
A retrospective review from January 2023 to July 2024 was conducted to determine the compliance rate of Pulmonary attendings ordering pneumococcal vaccines for patients who met eligibility criteria for pneumococcal vaccination who were evaluated in the Respiratory Institute at MSUS and in the Pulmonary Faculty Practice at MSW. Vaccination occurred in 77 percent of patients at MSW and in 83.7 percent of patients at MSUS. It is possible that the vaccination rate is underestimated due to the inability to access records of pneumococcal vaccination performed outside of the Mount Sinai Health System, and when patients are unable to recall receiving the vaccination.
A retrospective study led by resident physician Priyanka Sridhar, MBBS, pulmonary faculty Paru Patrawalla, MD, and Boram Kim, DO, to evaluate the use of POCUS in an outpatient pulmonary clinic demonstrated its feasibility and diagnostic utility. Among the 100 consecutive patients (mean age 57 +/- 17 years, 64 percent females), POCUS was performed mostly by residents (70 percent) and the median exam time was 5 minutes. Results showed normal lung use with a predominant bilateral A-line pattern (71 percent) was most commonly associated with obstructive airway disease (31 percent). A bilateral B-line pattern (13 percent) was associated with either interstitial lung disease (7 percent) or heart failure (8 percent) and focal dense Blines (10 percent) were seen with atelectasis (3 percent) or other abnormal CT findings (3 percent). Pleural effusions were evaluated in 18 percent of cases. No additional imaging was ordered in 51 percent of cases and for the 49 percent of cases who had additional imaging ordered, there was 100 percent concordance between POCUS findings and follow-up imaging. POCUS was most useful in evaluation of pleural effusions and pneumothorax. The project demonstrated the potential role of lung POCUS in replacing traditional diagnostic imaging
modalities including chest X-ray. Seamless integration of POCUS use into a daily outpatient pulmonary workflow is an area for future study
In late 2024, the Division began a quality initiative on Indwelling Pleural Catheter (PleurX)
Multidisciplinary Care at MSW, spearheaded by MSWM Pulmonary and Critical Care Medicine fellow Patrick Tobin-Schnittger, MD, and faculty mentor Boram Kim, DO. Inpatient indwelling pleural catheters (IPC) are typically inserted in outpatients, where a protocol is in place for interventional pulmonology to arrange supplies for home, follow-up, and VNS as needed. At MSW, inpatient IPCs are less frequently placed and miscommunication and misunderstanding of IPC aftercare responsibilities and expectations between inpatient medicine, pulmonary, social work, and interventional pulmonology has led to discharge delays and care team frustration. The project aims to reduce delays to discharge after inpatient IPC placement by streamlining the discharge workflow and communication through a post-procedure templated note or dot phrase and multidisciplinary education on IPC aftercare expectations. This project will continue in 2025.
The Division at Mount Sinai-Union Square (MSUS) is advancing quality improvement initiatives in the sleep medicine program by evaluating current barriers to home sleep apnea test (HST) completion rates at MSUS and planning a prospective intervention study to address disparities. Supporting project team members include resident physicians Toshiro Goto, MD, and William He, MD. Among 1,796 patients included in a retrospective analysis of the first six months of HST orders in 2024, HST completion rates were highest for orders from sleep medicine (76.4 percent), pulmonary medicine (61.7 percent), and otolaryngology (73.0 percent) and lowest for primary care orders, with significantly reduced odds of completion for internal medicine (OR 0.20) and family medicine (OR 0.25). Patients with commercial insurance, which often allows the same day dispensing of HST devices, had much higher completion rates compared to those with Medicaid plans, highlighting disparities in access to care. Some patients had HST orders placed for Metroplus Medicaid and Empire BC/BS Medicaid, but those plans do not cover the WatchPAT and had completion rates of zero percent
The Division’s planned interventions, targeted for implementation in early 2025, will focus on streamlining workflows and addressing these gaps. Key strategies include integrating WatchPAT scheduling into Epic MyChart, automating patient notifications, improving patient education, and enhancing clinician outreach. Additional strategies will also be implemented, such as closer collaboration with the weight loss clinic to address comorbidities that may affect outcomes, including sleep disordered breathing. With HST completion as the primary outcome, these initiatives aim to reduce barriers, address disparities, and improve access to diagnostic care for patients referred for sleep apnea evaluation.
Sleep Medicine had the highest HST completion rates, while primary care specialties including Internal Medicine and Family Medicine had notably lower rates.
Division Quality Champions:
Timothy Harkin, MD
Jing Wang, MD

In 2024, the division of Pulmonary, Critical Care and Sleep Medicine continued to work on quality initiatives spanning the outpatient and inpatient arenas.
Chronic Obstructive Pulmonary Disease (COPD) Program
The COPD program, led by Kathryn Dubowski, MD, actively identifies patients admitted with COPD exacerbation and tracks utilization of COPD resources with the goal of improving the care of hospitalized COPD patients and reducing COPD readmissions by building and optimizing MSHS COPD resources:
• COPD dashboard, centralized Epic patient list, and COPD order set to help identify patients admitted with COPD exacerbation and guide treatment recommendations for inpatient providers
• Standardized COPD consult note template for effectively communicating to teams about the severity of disease, the need for adjustment of home medications, the establishment of a follow-up plan that includes likely triggers and barriers to care, smoking cessation recommendations, and discharge planning to ensure a safe transition to outpatient follow-up
• Pulmonary function testing, including inpatient spirometry
• Dedicated respiratory therapist to provide bedside education, review inhaler technique, perform bedside spirometry, and work to ensure close pulmonary follow-up and referral to Pulmonary Rehab
• COPD discharge bundle to optimize care transitions
• Registry of outpatients with COPD
• Focus on racial disparities in care utilization and outcomes
As of September 2024, the COPD readmission rate (defined as encounters coded in the COPD diagnostic-related group) at MSH was 12 percent (improved compared with 2023) with an average length of stay of three days (stable compared with 2023). There was continued growth in the utilization of the COPD pathway and respiratory therapy consult services.
The COPD discharge bundle, which launched at MSH in the fall of 2023, focuses on improving the discharge planning process for patients admitted with COPD, reducing avoidable readmissions, and ensuring patients have access to post-acute services. Key interventions include comprehensive patient education during the hospital stay about diagnosis, inhaler regimen and use, and the COPD action plan; smoking cessation counseling; spirometry testing; and establishing a pulmonary follow-up appointment within one to two weeks post-discharge. Discharge medication reconciliation, along with post-discharge phone follow-up, also helps facilitate care transition. When comparing the six months pre- and post-implementation of the COPD discharge bundle, the readmission rate fell from a baseline of 17 percent to five percent
To further complement the above, the remote patient monitoring (RPM) program, led by Jaclyn Hess, PharmD, continued to follow COPD patients in 2024. Technology interventions can enhance self-management of COPD, increase smoking cessation, improve inhaler technique, and aid early recognition of exacerbations. Through this program, the remote monitoring team checks in regularly with patients and reaches out if patients exhibit out of range readings in vitals and symptoms. The RPM clinical pharmacist initiates pharmacomanagement of outpatient COPD exacerbations, adjusts outpatient COPD medications, refines Red/Yellow/Green Action plans for patients, and works with primary care providers to optimize pharmacologic management of depression, anxiety, and/or insomnia for patients. General education is provided to patients on self-management strategies, in addition to nutritional support.
As of October 2024, 13 patients were enrolled for at least 12 months in the COPD-RPM. In this group, there was a 17 percent reduction in pulmonary-related hospitalizations and 67 percent reduction in pulmonary-related 30-day readmissions. Interestingly, there was also an 11 percent increase in pulmonary office visits, a pattern consistent with current literature and likely reflecting redirection of patients to office evaluations instead of emergency room/urgent care visits. There was a 75 percent increase in pulmonary-related ED visits, though analysis showed that most of these visits occurred early in the program and that there has been a decline in ED visits over time. In the coming year, the Division hopes to continue expanding utilization of remote patient monitoring, onboarding additional providers, and optimizing how to proactively identify potential patients who may benefit from the RPM program.
The demand for sleep testing in the community and within the Mount Sinai Health System (MSHS) remains high. Top referral indications include sleep disordered breathing such as obstructive sleep apnea (OSA), respiratory failure/hypoventilation, central sleep apnea (CSA), as well as non-respiratory sleep disorders such as hypersomnia, insomnia, and sleep-related movement disorders. In 2024, the sleep program, led by Jing Wang, MD, Zachary Roberts, RPSGT, Nathan Ramey, RPSGT, Billy Taylor, MSHA, aimed to continue efforts to improve access to sleep testing.
The sleep lab, located at the New York Eye and Ear Infirmary at Mount Sinai with a total capacity of 11 polysomnography studies per night, was successfully reaccredited by the American Academy of Sleep Medicine (AASM) last year and serves as the largest sleep testing center in the system. Collaborative efforts with the in-lab facility at Mount Sinai South Nassau have also begun to further standardize and expand the sleep testing network for patients. In addition, the sleep program continued to work in collaboration with the Department of Pediatrics
to operate the pediatrics sleep lab in Kravis Children’s Hospital. Together, these sleep testing sites allow the program to provide specialized and full-age spectrum sleep testing and care.
Since 2019, the Division has utilized the patient data and lab management system Compumedics Nexus360 for in-lab testing. The software is cloud-based, allowing for remote access and review of study results. The process of reviewing studies and completing reports within seven days is now standardized.
Additional sites have also been added to the home sleep testing (HST) program across the Health System, further expanding capacity to provide this faster and more convenient diagnostic tool in clinically appropriate patients. Through education and outreach, the referring network has expanded to include additional Mount Sinai practice sites in primary care, cardiology, ENT, and bariatric surgery. The sleep team continued to work with referral bases to develop more streamlined pathways for expedited testing and follow-up in patients undergoing surgery and procedures such as arrhythmia ablation. The program continues to use primarily disposable home sleep testing (HST) units and offers a direct shipping option to patients’ homes when needed. A centralized SharePoint site is utilized for communication, aiding in referral tracking and quality assurance. Each home testing location has a full-time technician to administer HSTs. The chief technician reeducates technicians in response to failed studies, and the team continues to work on improving education and training for patients on the use of home sleep testing devices. With these efforts, home study failure rates have remained consistently low. Similar to in-lab studies, the process to review and finalize reports for home sleep studies within seven days of study return also remains standardized.
Some challenges to meet the high demand for sleep testing have included ongoing faculty, technician, and support staff shortages, due to departures and illness. In an effort to counteract and overcome these challenges, the following interventions were continued: streamlining scheduler workflow through Epic referral work queues, optimizing third-party vendor workflow to assist with prior authorization, centralizing the scheduling team, expanding scheduling staff and sleep lab staffing to ensure a seven-day operation, ongoing tech education, ongoing recruitment of sleep technologists and clinical faculty, and optimizing centralized tracking of home sleep studies while dispensing from multiple sites.
With the above, the Division saw continued growth in overall sleep study volume and an overall downward trend in sleep study order to completion time.
Average Wait Times for Sleep Study (Order to Study Completion)
In-lab HST
Of the nearly 6,000 home sleep studies completed in 2024, a diagnosis of obstructive sleep apnea (OSA) was confirmed in a majority of cases. Most patients without an existing sleep provider are referred for follow-up with MSHS pulmonary/sleep consultants. Patients with “negative” home testing in whom clinical suspicion of OSA remains high typically go on to complete in-lab sleep testing, as recommended by diagnostic guidelines.
In addition, in-lab testing can be utilized for evaluation of other sleep disorders, including complex sleep-related breathing disorders (central sleep apnea, hypoventilation/respiratory failure), parasomnias, hypersomnias, and sleep-related movement disorders, which again represented approximately 50 percent of testing indications in our lab in the past year. A new
initiative undertaken in 2024 was an effort to improve study quality in patients with suspected REM-behavior disorder (RBD), a rare sleep disorder characterized by dream enactment behavior that relies on detection of abnormal EMG tone during REM sleep for diagnosis. The sleep lab team carried out a series of training exercises for technologists to review sensor placement and signal quality verification in these specialized sleep studies. Working closely with our neuro-sleep specialist, several interventions were implemented, including an updated protocol for study acquisition, a real-time feedback system to track study EMG impedances, and standardized study scoring and review procedures. In 2024, there were consistent improvements in signal and study quality observed.
To better capture patient satisfaction with the sleep testing process, the Division continued to administer patient surveys via Q-reviews following in-lab and home sleep study appointments. Patient experience with our sleep technicians and staff remained consistently positive. Wait time scores aligned with ongoing efforts at access improvement. Individual patient concerns were addressed through individual outreach, and the sleep team incorporated issues identified via feedback into regular safety and process improvement efforts.
In the coming year, the Division will continue to work on further improving wait times for scheduling a sleep study and access to sleep medicine consultation. To do so, the team will focus on systems optimization, staffing, and standardizing and streamlining workflows and protocols as the sleep program grows. There will be further efforts to improve durable medical equipment (DME) management and facilitate better patient follow-up and treatment compliance monitoring, along with continued integration of sleep patient care via a multidisciplinary approach that now includes pulmonary/sleep, neurology, ear, nose, and throat specialists, and dental specialists in the MSHS. Education for sleep lab technicians on complex sleep studies and titrations will also continue.
On the inpatient side, the Medical Intensive Care Unit (MICU), led by Samuel Acquah, MD, and Camille Davis, BSN, RN, continued to maintain tidal volume compliance in mechanically ventilated patients Ventilator set tidal volume at </= 8 cc/kg (ideal body weight) was more than 90 percent in the MICU (average 97 percent compliance).
The MICU continued to meet goals for performing tracheostomy by day 12 when indicated (achieved in 95 percent of cases, with goal of more than 90 percent) and documentation of health care proxy and/or surrogate for admitted patients prior to discharge from unit.
Hand hygiene compliance, completion of daily goal documentation on rounds, and utilization of respiratory pathway for intubated/vented patients remained consistently high. In recognition for maintaining the highest nursing standards for patient outcomes, evidence-based practice, patient and staff satisfaction, and collaboration among health professionals, the MICU received the prestigious Beacon Gold Award in 2024.
In 2025, the MICU will continue its culture of multidisciplinary quality improvement efforts. New initiatives include projects to improve nutritional support of critically ill patients (initiation of feeding, achievement of goal tube feeding rate, and meeting target caloric requirements), improve glycemic control in MICU patients with severe sepsis to a target between 140 and 180
within 24 hours of admission, optimize fluid balance via a nursing-driven protocol, and optimize ventilator liberation through an integrated decision support tool.
The Division continued efforts to improve outcomes in patients undergoing bronchoscopy, especially in American Society of Anesthesiologists (ASA) physical status classification system (ASA)s 3 & 4 level patients. This initiative was led by Timothy Harkin, MD.
Bronchoscopy volume continued to grow with 2024 volume at a procedure’s total of 1,345. The proportion of ASA 3- and 4-level patients represented 96 percent of all bronchoscopy cases performed, which was similar to the prior year. There was again the addition of two ASA 5- and 6-level cases. The number of complications associated with 2024 bronchoscopies was 18 (1.3 percent), a sustained low rate compared with prior years. All cases with complications are reviewed and corrective actions implemented where appropriate.
The booking process for inpatient bronchoscopy cases remains standardized with reinforcement of clinical information documentation and pre-procedure IP/pulmonary team assessment, as well as automated team-wide communication between Endoscopy and IP. A pre-procedure history and physical examination smart phrase contains the procedure planned, patient respiratory or other clinical concerns, transfusion requirements before procedures, and medications. The Division also continued to utilize a QR code for inpatient scheduling that links to a menu-driven questionnaire that generates an automated email upon submission to the inpatient team, pulmonary administrative assistant, endoscopy front desk, and endoscopy nursing leaders. This further helps to ensure that patients are scheduled properly and transported safely.
Division Quality Champion:
Avinash Singh, MD

This project focuses on enhancing the timely identification and referral of eligible patients with chronic and progressive lung diseases, such as COPD and ILD, to the hospital’s lung transplant team. A key component of this initiative was the targeted education provided to fellows, ensuring they were well versed in the criteria for lung transplant eligibility and the importance of early referrals. This educational effort aimed to equip fellows with the knowledge to identify patients who could benefit from transplant evaluation. Additionally, the QI project streamlined the referral process by fostering closer communication and collaboration with the transplant team, ensuring that referrals are made efficiently and without delays.
Pre-intervention data revealed a total of 156 patients who were seen by pulmonary fellows at Mount Sinai Morningside (MSM) and Mount Sinai-Union Square (MSUS), of whom eight patients met criteria for referrals. Only one patient received a transplant evaluation. Multiple educational sessions were conducted for the fellows over the course of the academic year. Analysis of post-intervention data is currently in process. The aim for 2025 is to streamline communication between the pulmonary and the transplant teams
With the introduction of the updated pneumococcal vaccine and simplified pneumococcal vaccination regimen, the Division’s goal is to identify patients seen in the pulmonary fellows’ clinic who are candidates for and receive pneumococcal vaccination. The goal is to increase pneumococcal vaccination rates to 80 percent, across all chronic lung disease patients Pneumococcal vaccine rates in the MSM Fellow’s Clinic for patients with COPD currently stand at 52 percent for the third quarter and 54 percent for the fourth quarter of 2024 (preintervention). The goal for 2025 is to improve this rate to above 80 percent. In addition, preliminary data demonstrates an unmet need in the adult pertussis vaccination measure, with the vaccination rate at 47 percent and 44 percent for Q3 and Q4, respectively.
Under the leadership of Dr Mary O’Sullivan, the Division was able to successfully introduce and incorporate Varenicline into the inpatient formulary. This medication can now be provided to patients who smoke while they are admitted to the hospital. This evidence-based smoking cessation strategy incorporates smoking cessation counselling and prescribing of pharmacotherapy to patients when they are most receptive to behavioral change and prevents nicotine withdrawal. The QI initiative focuses on inpatient COPD patients who currently smoke,
and do not have contraindications to varenicline. Between August 2022 to August 2024, 328 patients with a primary or secondary diagnosis of COPD at MSM, 150 at Mount Sinai West (MSW), and 198 at Mount Sinai Beth Israel (MSBI) were prescribed varenicline. The varenicline team continues to gather data on all patients who get this prescription, along with smoking cessation counseling, and referral to the Mount Sinai Morningside and Mount Sinai West (MSMW) Smoking Cessation Clinic.
The goal for 2025 is to streamline data gathering from the electronic health record (EHR), and to formally incorporate varenicline into the COPD readmission order set. The Division will continue to track the patients who receive smoking cessation counselling while admitted to the hospital and then follow them for referrals and show rates at the MSMW Smoking Cessation Clinic. The goal is to decrease no-show rates at this clinic and improve medication compliance rates as patients transition from inpatient to outpatient care
As part of our comprehensive COPD care practice, the Division tracks and reviews compliance rates for lung cancer screening via low-dose chest CT (LDCT) scans among its Pulmonary fellows. The comparator group is the pulmonary faculty practice at MSM. The goal is to sustain a compliance rate of more than 80 percent over all the quarters of the year In 2024, compliance rates distributed over the four quarters were 74 percent, 69 percent, 78 percent, and 81 percent, respectively, compared to the pulmonary practice (attendings), which were 72 percent, 70 percent, 66 percent, and 70 percent, respectively. This data likely underrepresents real LDCT rates as it does not incorporate tests that may be performed outside the health system. As part of the plan for 2025, the Division will continue to provide education to its members to enhance uptake of LDCT after appropriate shared decision making (SDM) with the patient.
The Division will be introducing a new QI initiative for 2025 that will examine efforts to increase sleep apnea testing with home sleep tests in patients identified to have an increased pretest probability of OSA. Identification of these patients can be made by EHR data if patients meet at least three criteria from the STOP-Bang questionnaire
STOP-Bang
Snoring
Tired, fatigued, sleepy during daytime
Observed stopping breathing
Treated for high blood pressure
BMI >35 kg/m2
Age >50
Neck circumference >16 in
Gender: Male?
YES [ ] NO [ ]
YES [ ] NO [ ]
YES [ ] NO [ ]
YES [ ] NO [ ]
YES [ ] NO [ ]
YES [ ] NO [ ]
YES [ ] NO [ ]
YES [ ] NO [ ]
Total Score
High risk OSA: 5-8
Intermediate risk OSA: 3-4
Low risk OSA: 0-2
Appropriate patients who meet at least three criteria above should be evaluated for OSA with either a home sleep test or an in-lab sleep test. The goal will be to identify current rates of sleep apnea testing, and to improve rates up to 50 percent for the first year and 60 percent for the second year of implementation.
Division Quality Champion:
Latoya Freeman-Beman, MD

In 2024, the Division continued its efforts to increase annual tuberculosis (TB) screening rates in patients with rheumatoid arthritis (RA) on therapeutic biologics who are seen at Mount Sinai-Union Square (MSUS) - Rheumatology. The addition of resident team members Melissa Akselrad, MD, and Evan Zyskowski, DO, invigorated the Division’s efforts. New initiatives included same-day huddle reminders and faculty meeting reminders. Adjustments were also made to the data retrieval parameters. Despite these efforts, TB screening rates for 2024 remained stable. New interventions for 2025 include mass mailing of patients with RA on biologics and development of a best practice alert for ordering clinicians.
The Division’s efforts to improve tuberculosis screening in RA patients on therapeutic biologics were presented at the 2024 Mount Sinai Department of Education Research Day and the New York State Rheumatology Society spring meeting in May 2024.
A new quality initiative for the Division in 2024 involved collaborating with nursing to achieve adequate pain management, as assessed by general pain screening and post-procedure pain follow-up. The aim for general pain screening is to have a pain plan documented in 100 percent of patients with a pain score >7/10. The pain score is taken in rooming vitals by the medical office staff. Clinicians were reminded quarterly of the pain score plan documentation initiative. To monitor compliance with this metric, the nurse manager conducted random manual chart audits monthly on patients with pain scores >7 for evidence of a pain plan documented by the treating physician. The results of the audit are compiled into a Pain Screening Score Card (see table). As of November 2024, the average compliance rate for a documented pain assessment was 97.18 percent and the average compliance rate for a pain management plan for scores >7/10 was 98.18 percent. Future directions involve working with IT to develop automated extractions of patients with a pain score >7/10.
The aim for post-procedure pain follow-up is for 100 percent of patients to be contacted within 48-72 hours of an in-office procedure to reassess their pain. To achieve this metric, the Division collaborated with nursing staff to ensure that a pain score callback is scheduled within 48-72 hours of a procedure. Epic smart phrases are planned for use by the clinician to document preand post-procedure pain scores within the procedure note, and by the nurse to document the outcome of the post-procedure callback with escalation to the clinician as appropriate (see below). Monthly random chart audits for documentation of post-procedure callbacks will be performed by the nurse manager. Both facets of the adequate pain management initiative will continue in 2025.
The Division also sought to improve vaccination rates for both influenza and pneumonia among patients with rheumatoid arthritis according to guidelines set by the Centers for Disease Control and Prevention. To improve vaccination rates, the Division collaborated with nursing to ensure that clinic nurses pre-screened eligible patients, provided alerts via same-day huddle, and pended appropriate orders for review. Thus far, more than 90 percent of vaccines ordered were administered. Efforts for 2025 will focus on reviewing opportunities that may have been missed, such as patients who may not have been ordered vaccines when eligible.
In 2024, the Division also began to focus on visit throughput as measured by the Press Ganey question section on “moving through the visit,” which reflects the degree to which the patient felt informed about delays and the patient’s experience with wait time at the office (time from arrival to leaving). The aim was to increase the score to above 90 percent from a baseline of 80-85 percent. At the end of 2024, a modest improvement in percentile rank from 7 to 10 percent was observed in this survey domain. Interventions for 2025 will include minimizing overbooking or self-scheduling of new patients into follow-up spots, increasing the medical assistant pool available to assist with rooming, and daily adjustments to room assignments. Previous efforts such as minimizing non-clinical exam room use and staff informing the patient of any delays will continue.
Lastly, a new quality project led by resident physicians Emily Cosentino, MD, and Priscilla Abate, MD, will begin in 2025. The project aims to increase the number of patients with systemic lupus erythematosus on hydroxychloroquine with a completed annual eye exam by at least 5-10 percent from baseline rates within a year. Planned interventions include
best practice care reminders for providers and bulk prompts to alert appropriate patients via patient portal messaging and/or emails.
Division Quality Champion: Wendy
Weiwei Chi, MD

In 2024, The Mount Sinai Hospital Division of Rheumatology sought to increase the rate of tuberculosis (TB) screening for patients on biologics, in accordance with a Centers for Disease Control and Prevention (CDC) recommendation to complete this screening before initiating biologics and annually while using biologic medications. The Division continued efforts to increase utilization of a health maintenance smart phrase that was added to Epic in late 2020 that made it easier to view and document TB screening status.
This intervention has been helpful, but improvement plateaued over the course of 2023 and into 2024. In 2025, the Division aims to continue improving TB screening rates to reach the goal of 90 percent for patients on biologics. The Division plans to increase rates by promoting the uptake of the smart phrase by newer members of the faculty, as well as among support staff such as medical scribes. The Division also plans to create reminders within Epic to prompt providers to order the appropriate screening tests when needed.
The Division also sought to increase the rate of annual ophthalmologic exams for patients taking hydroxychloroquine (Plaquenil) to 90 percent. This is a critical measure because Plaquenil may cause irreversible retinal damage, and early detection is the key to prevention. Unfortunately, the screening rate decreased to 52 percent in 2021 following the COVID-19 pandemic. In 2023, the Division continued to send individualized feedback to providers to reinvigorate efforts to improve this metric. A survey and flowsheet were also created and implemented to help with data gathering for this metric for patients who receive their ophthalmologic care at other institutions. The survey is automatically sent to patients via MyChart and allows the Division to more accurately collect data and identify patients who are overdue for their exams.
The Division was able to improve the ophthalmologic screening rates to 74 percent over the course of 2024 and plans to continue its efforts to achieve a goal rate of 90 percent in 2025. In
addition to continuing the above measures, new interventions will include implementing a more direct referral process for patients who need ophthalmologic screening.
Ophthalmologic Screening Rates
Q4 2022 – Q2 2024
Additionally, in 2024, the Division continued a project to increase rates of pneumococcal vaccination for patients on biologics. Baseline rates of pneumococcal vaccination in 2021 were low, with only 23 percent of patients on biologic medications receiving any pneumococcal vaccine. The Division implemented a multidisciplinary intervention that involved providers generating lists of patients scheduled to be seen each week who have not yet received the vaccine and registered nurses reminding providers, both in person and through Epic, about the vaccine for eligible patients at the time of the appointment.
Since these interventions were implemented in 2022, rates of pneumococcal vaccination have increased to 40 percent. The Division will continue these efforts in 2025 with the goal of increasing the rates to at least 50 percent by the end of the year. The Division also aims to evaluate some of the reasons behind patient vaccine hesitancy to better guide further interventions to improve these rates.
Kristaq Koci, MD
Saloni Mitchell, MD


The Division of Rheumatology has focused on ensuring thorough TB screening for patients on biologics, as it helps prevent serious infections and supports safer, more effective use of immunomodulatory therapies in this patient population. In collaboration with the Medication Access Program (MAP) nurse practitioners (NPs), this quality improvement initiative has led to a notable increase in the rate of TB screening among patients receiving biologics from 85 percent in 2022 to 93 percent in 2024, as illustrated in the accompanying graph. To achieve this improvement, the NPs from the medication access program notify the rheumatologist when they initially apply for new biologics or when the medication is due for prior authorization renewal. This prompts the rheumatologist to order QuantiFERON or have it repeated at the next clinic visit.
Percentage of QuantiFERON screening
The Division is leading a quality improvement project to address smoking cessation in the rheumatology clinic population, where smoking can significantly affect disease progression and treatment efficacy. Data analysis revealed that among 192 smokers, the majority are light smokers (n=124) versus heavy smokers (n=68), with a notable gender variance showing 82.1 percent were female. The Division is further investigating this apparent variance given that there are more females with connective tissue disease and osteoporosis. The racial distribution highlighted diversity in the patient population, with Black or African American patients comprising the largest group (33.2 percent), followed by white/Caucasians (24.1 percent), and Hispanic/Latinx (11.1 percent). Similar to the variance observed with female patients and smoking, the large percentage of Black patients who test positive could be a result of the
majority of the Division’s patients with lupus being Black. In addition, there are systemic health care differences in treatment resources as well as education that could be a factor. These findings will be further analyzed in 2025.
Using the Plan-Do-Study-Act methodology, the intervention plan includes: (1) utilizing Epic’s Slicer/Dicer tool to identify and categorize smokers, (2) implementing a multifaceted approach with varenicline guidance through provider education, (3) establishing a referral system to free smoking cessation clinics that accept all insurances, and (4) introducing a “blue sticky” flag system in patients charts to ensure consistent addressing of smoking cessation. The success metrics will include referral rates, documentation compliance, and, ultimately, smoking cessation rates among the patient population. This project will continue into 2025.
The Division of Rheumatology aims to enhance patient care by systematically incorporating Clinical Disease Activity Index (CDAI) scores into routine patient evaluations. This standardized approach will enable more precise assessment of inflammatory conditions, particularly rheumatoid arthritis, while helping identify patients at higher risk for disease progression or adverse outcomes. By implementing this data-driven strategy, the Division can ensure comprehensive patient monitoring and facilitate timely interventions with personalized follow-up care. Additionally, the systematic collection of CDAI scores and related patient data will create a valuable database for future projects, supporting efforts to optimize treatment strategies, enhance long-term patient outcomes, and advance rheumatology care.
Analysis using Epic’s Slicer/Dicer tool revealed that CDAI usage among rheumatology providers is currently below 50 percent, partly due to provider variation in disease activity measurements. To address this gap, the Division is collaborating with the Epic team to develop and implement smart list features that will streamline CDAI documentation. Once implemented, providers will receive quarterly performance feedback on their CDAI utilization rates. Given this structured approach and regular monitoring, the Division anticipates significant improvement in CDAI documentation compliance.
Mount Sinai Beth Israel & Mount Sinai-Union Square Publications
Peer Reviewed
Hospital Medicine
Gill A., Leiner D., Steinberg D. High Reliability Organization in Health Care. Medical Clinics of North America. (In Press)
Lim S, Megaris A, Miyakawa L, Filopei J, Dharapak P. Increasing health care proxy documentation in an intensive care unit: a quality improvement initiative. BMJ Open Quality 2024;13: e002854.doi: 10.1136/ bmjoq-2024-002854
Sweigart JR, Watson R, Burger A. The Accidental Teacher Direct-Care Physicians Increasingly Placed in Teaching Roles. JAMA. 2025;333(3):203–204. doi:10.1001/jama.2024.17626
Nephrology
Ishisaka Y, Wang HY, Mitaka H, Charen E, Patrawalla P. Implementation and Assessment of a Curriculum for Renal Point of Care Ultrasound (POCUS) Training. POCUS J. 2024 Nov 15;9(2):62-67. doi: 10.24908/pocus. v9i2.17479. PMID: 39634687; PMCID: PMC11614398.
Pulmonary, Critical Care and Sleep Medicine
Sridhar P, Wang HY, Velo A, Nguyen D, Singh A, Rehman A, Filopei J, Ehrlich M, Lookstein R, Steiger DJ. Outcomes of patients with acute pulmonary embolism managed in-house vs those transferred between hospitals: a retrospective observational study. Res Pract Thromb Haemost. 2024 Oct 29;8(8):102606. doi: 10.1016/j.rpth.2024.102606. PMID: 39687927; PMCID: PMC11647229.
Non-Peer Reviewed
Hospital Medicine
Miller T, Dharapak P, Smith K, Virapongse A. Demystifying Performance Measures for Hospitalists: HCAHPS - The Hospitalist. Published May 1, 2024. Accessed June 27, 2024. https://www.the-hospitalist.org/hospitalist/article/37005/business-of-medicine/demystifyingperformance-measures-for-hospitalists-hcahps/
Mount Sinai Beth Israel & Mount Sinai-Union Square Presentations
(Abstracts and Posters)
General Medicine
Koseki M, Fliehman R, Jiang R. Exploring Disparities in Colorectal Cancer Screening Completion Rate: A Retrospective Analysis by Age, Zip Code, and Clinic Variation in a Primary Care Setting. Society of General Internal Medicine Annual Meeting. May 2024, Boston, MA.
Koseki M, Bharati D, Debroff J, O’Ferrrall C, Fliehman R, Chow D, Jiang R. Enhancing the Colorectal Cancer Screening Rates Through Targeted Interventions: A Focus on Cologuard. May 2025, San Diego, CA.
Hospital Medicine
Burger A. Changing Your Environment; Hospitalists as Agents of Change, Managing and Leasing. SHM Converge 24. April 14, 2024, San Diego, CA.
Burger A. Change Management - Tools to Realize a Better Tomorrow. SGIM annual Meeting. May 16, 2024, Boston, MA.
Dharapak P, Steinberg D, Raucher B, Pearson J, McGreevy J. Closing an academic institution: a quality analysis from the inside. Accepted as a poster presentation to the Society of Hospital Medicine (SHM) national conference, SHM Converge 2025, April, Las Vegas, Nevada
Favila K, Rizk D. Optimizing Patient Flow: The Role of Hospitalists in the Clinical Command Center. To be presented at Society of Hospital Medicine Annual Meeting SHM Converge 25, April, Las Vegas, NV (poster).
Favila K, Rizk D, Tricarico C, Christophe K, Yu I, Goldberg J, Wallach W. Implementing a night float curriculum at a small academic medical center. Society of Hospital Medicine, SHM Converge 25, April 2025. Las Vegas, NV. (poster)
Gasper J, Burger A, Zheng A, Cruz C, Mitaka H, Loughney W, Aslanova M, Saeed Y, Raghavan S. Developing Discrepancy in Resident-Led Teaching Goals Resulted in Durable Cultural Change. Abstracts from the 2024 Annual Meeting of the Society of General Internal Medicine.
Pulmonary, Critical Care and Sleep Medicine
He W, Goto T, Roberts Z, Grbach VX, Gilyadov B. A Cross-Sectional Analysis of Home Sleep Apnea Testing in a New York City Ambulatory Population. Am J Respir Crit Care Med 2025; S10846.
He W, Goto T, Roberts Z, Grbach VX, Gilyadov B. A Retrospective Analysis of Patients With Obstructive Sleep Apnea, Asthma, and COPD by Home Sleep Testing Outcomes. Am J Respir Crit Care Med 2025; S10998.
Singh A, Sridhar P, Wang HY, Rehman A, Nguyen D, Agostina V, Ehrlich M, Shapiro JM, Acquah SO, Lookstein R, Steiger D. Interhospital Transfer for Acute Pulmonary Embolism: Investigation of Process Metrics, Including Transfer Times, and Outcomes (abstract). Am J Respir Crit Care Med 2024;209: A2177.
Sridhar P, Patrawalla P, Steiger D, Kim B. A Nationwide Survey on the Use of Point of Care Ultrasonography (Pocus) in Pulmonary Clinics. Chest. 2024 Oct 1;166(4): A4060. Boston, MA.
Peer Reviewed
General Medicine
Cytryn E, Stauber Z, Jaeckel K, Barai N, White P, Wang CP, Fishman M, Wisnivesky JP, Jandorf LH, Itzkowitz SH, Koster KM. Evaluation of a Tailored Patient Navigation Program for Improving Multitarget Stool DNA Test Adherence. J Gen Intern Med. 2024 Nov 18. doi: 10.1007/s11606-024-09201-y. Epub ahead of print. PMID: 39557750.
Hospital Medicine
Burden M, Astik G, Auerbach A, Bowling G, Kangelaris KN, Keniston A, Kochar A, Leykum LK, Linker AS, Sakumoto M, Rogers K, Schwatka N, Westergaard S. Identifying and Measuring Administrative Harms Experienced by Hospitalists and Administrative Leaders. JAMA Intern Med. 2024 Sep 1;184(9):1014-1023. Doi: 10.1001/jamainternmed.2024.1890. PMID: 38913371; PMCID: PMC11197021.
Callister C, Astik G, Atkins RM, Alday A, Dayton K, Keniston A, Linker A, McBeth L, Merriman J, Westergaard S, Yu A, Auerbach A, Burden M. Optimizing learners on direct care teaching services: A qualitative study of hospitalist clinicians at 26 sites. J Hosp Med. 2024 Dec 15. Doi: 10.1002/jhm.13561. Epub ahead of print. PMID: 39674907.
Crecelius T, Linker AS, Gottenborg E, Kwan B, Keniston A, McBeth L, Martin SK. A Qualitative Study of Internal Medicine Subspecialty Fellowship Program Directors’ Perspectives on ShortTerm Hospitalist Employment Prior to Fellowship. J Grad Med Educ. 2024 Apr;16(2):210-220. Doi: 10.4300/JGME-D-23-00550.1. Epub 2024 Apr 15. PMID: 38993320; PMCID: PMC11234311.
Fine M, Hirt Wilner L, Ormiston CK, Wang L, Lee TG, Herscher M. A Hospital-Based Intervention to Improve Access to Buprenorphine for Patients with Opioid Use Disorder. Subst Use Addctn J. 2024 Nov.
Fine M, Hirt Wilner L, Ormiston CK, Wang L, Lee TG, Herscher M. A Hospital-Based Intervention to Improve Access to Buprenorphine for Patients with Opioid Use Disorder. Subst Use Addctn J. 2024 Nov 18:29767342241292416. doi: 10.1177/29767342241292416. Epub ahead of print. PMID: 39552546.
Finkelstein J, Gabriel A, Schmer S, Truong T, Dunn AS. Identifying facilitators and barriers to implementation of AI-assisted clinical decision support in an electronic health record system. J Med Systems. 2024; 48:1-23.
Hundert S, McLlarky J, Dunn AS, Markle W. Fixed-dose phenobarbital versus as-needed benzodiazepines for the management of alcohol withdrawal in acute care general internal medicine. South Med J. 2024; 117:25-30.
Hundert S, Dunn AS. Inpatient management of alcohol withdrawal: A review. Can J Gen Intern Med.19:2024:52-62.
Linker AS, Astik GJ, Bowling G, Kangelaris KN, Kara A, Keniston A, Kulkarni SA, Sakumoto M, Schwatka N, Westergaard S, Leykum LK, Auerbach A, Burden M. Collaborative research: The power of multiorganizational affinity groups and adaptive research methods. J Hosp Med. 2024 Jun 11. Doi: 10.1002/jhm.13424. Epub ahead of print. PMID: 38862414.
Niehus H, Gunesch AN, Rodriguez N, Khoury J, Ma A, Gu N, Cao T, Muller M, Moriates C, Linker AS, Prochaska M, Fish D, Moulder G, Stephens M, Carney PA, Smeraglio A. Factors Associated with Medical Students’ Attitudes About Cost-Conscious Care: A Mixed-Methods Multi-School Study. J Gen Intern Med. 2024 May 6. Doi: 10.1007/s11606-024-08783-x. Epub ahead of print. PMID: 38710863.
Schwatka NV, Keniston A, Astik G, Linker A, Sakumoto M, Bowling G, Auerbach A, Burden M. Hospitalist Shared Leadership for Safety, Health, and Well-Being at Work: United States, 2022‒2023. Am J Public Health. 2024 Feb;114(S2):162-166. Doi: 10.2105/AJPH.2024.307573. PMID: 38354355; PMCID: PMC10916734.
Truong TT, Siu AL. The Evolving Practice of Hospital at Home in the United States. Annu Rev Med. 2024 Jan 29; 75:391-399.
Ushpol A, Parsons C, Golec S, Frousios R, Tsega S, Linker AS, Ronquillo M, Gidwani U. Promoting early goals of care conversations in the CICU with a surprise question-based EHR workflow. BMC Palliat Care. 2024 Dec 20;23(1):288. doi: 10.1186/s12904-024-01602-4. PMID: 39707263; PMCID: PMC11662718.
Ushpol A, Parsons C, Golec S, Frousios R, Tsega S, Linker AS, Ronquillo M, Gidwani U. Promoting early goals of care conversations in the CICU with a surprise question-based EHR workflow. BMC Palliat Care 23, 288 (2024).
Westergaard S, Bowden K, Astik GJ, Bowling G, Keniston A, Linker A, Sakumoto M, Schwatka N, Auerbach A, Burden M. Impact of billing reforms on academic hospitalist physician and advanced practice provider collaboration: A qualitative study. J Hosp Med. 2024 Jun;19(6):486494. Doi: 10.1002/jhm.13356. Epub 2024 Apr 10. PMID: 38598752.
The Mount Sinai Hospital Invited Presentations
Hospital Medicine
National CME courses
Dunn, Andrew. 19th Annual Mid-Atlantic Hospital Medicine Symposium, October 2024.
Herscher, Michael. “Opioid Use Disorder.” 19th Annual Mid-Atlantic Hospital Medicine Symposium, October 2024.
Jogendra, Dilan Mather R. “Periop – Key Updates from ACC/AHA.” 19th Annual Mid-Atlantic Hospital Medicine Symposium, October 2024.
International lectures
Dunn A. Clot Controversies. Sri Lanka College of Internal Medicine annual meeting. Colombo, Sri Lanka. Nov 2024. Oral Presentation.
Dunn A. Perioperative Management of Oral Anticoagulants. Sri Lanka College of Internal Medicine annual meeting. Colombo, Sri Lanka. Nov 2024. Oral Presentation.
Xu T. “Enabling Change Across a Whole System.” International Forum on Quality and Safety, London April 2024, hosted by BMJ and IHI.
Xu T. Panelist, “AI in Healthcare.” American Chamber of Commerce in Arab Health, Dubai, Jan 2024.
The Mount Sinai Hospital Media Resource and Educational Materials
Liver
Dieterich DT, Mageras A Universal Screening & Vaccination for Viral Hepatitis Elimination. Empire Liver Foundation, Webinar, May 2024. https://empireliverfoundation.org/webinararchive/
The Mount Sinai Hospital Presentations (Abstracts and Posters)
General Medicine
Bryant, K. Uneven Bars: Enhancing Equity Through Community-Based Screening. American Heart Heart Association Scientific Sessions. November 16, 2025, Chicago, IL.
Cotton J, Feinberg A, Cluett J, Singh N, Islam S, Fishman M, Yang E, Barai N, Bryant K. Average blood pressure predicted by last blood pressure by race/ethnicity. Society of General Internal Medicine
Hanlon T, Bryant K. When something doesn’t match up, a case of subclavian artery stenosis. International Society of Hypertension Meeting. September 2024, Cartagena, Colombia
Islam S, Feinberg A, Baria N, Cluett J, Bryant K. Suboptimal Hypertension Control in Young Patients Compared to Older Patients in a Large Health System American College of Cardiology. March 2025, Chicago, IL.
Islam S, Feinberg A, Cluett J, Barai N, Fishman M, Bryant K. Correlation of Last Recorded InOffice Blood Pressure Measurements with Hypertension Control in a Large Academic Medical Center Society of General Internal Medicine
Singh N, Feinberg A, Barai N, Cluett J, Fishman M, Bryant K. Last Recorded Blood Pressure Measurement as a Proxy for Average Blood Pressure Control American Heart Association, Hypertension Scientific Sessions. Sept 2024, Chicago, IL
Hospital Medicine
Aoun R, Liu D, Zhang E, Soong B, Park S, Nguyen VT. “Limiting Waste: Reducing Urine Culture Testing in Inpatients.” Society of Hospital Medicine National Meeting, San Diego, CA. April 13, 2024.
Baek M, Nguyen VT, Dunn A. “Fill in the Procedural Gap: An On-Call Hospitalist Procedure Team.” Society of Hospital Medicine National Meeting, San Diego, CA. April 13, 2024.
Burden M, Astik G, Auerbach A, Bowling G, Kangelaris K, Keniston A, Kochar A, Leykum L, Linker AS, Sakumoto M, Rogers K, Schwatka N, Westergaard S. “Administrative Harm: A Qualitative Study Across 32 Organizations.” Oral Presentation Society of Hospital Medicine National Meeting, San Diego, CA; 2024. (Presented by Burden M )
Dharapak P, Chokshi K, Nguyen VT, Sawant A, Raucher B, Dunn A, Linker AS. “Utilizing Voice Recognition to Improve Practice Efficiency and Reduce Burnout.” Society of Hospital Medicine National Meeting, San Diego, CA. April 13, 2024.
Dunn A, Canas A, Chokshi K, Kaatz S. “Solving Major Problems: Major Bleeding and Major Surgery for Patients on Anticoagulants.” Society of Hospital Medicine National Meeting, San Diego, CA; 2024.
Hack B, Epstein J, Nguyen VT. “Med Rec Mondays: Improving Medication Reconciliation Among Internal Medicine Residents.” Society of Hospital Medicine National Meeting, San Diego, CA. April 13, 2024.
Knees M, Yu A, Keniston A, Peterson R, Schwatka N, Sakumoto M, Kochar A, Westergaard S, Burden M. “Beyond Beepers: Navigating the Digital Shift in Hospital Communication.” Society of Hospital Medicine National Meeting, San Diego, CA. April 13, 2024.
Nguyen VT, Gabriel E, Reyna M, Gronowitz M. “Phone-A-Friend: A Clinical Mentorship Model to Discuss Complex Cases.” Society of Hospital Medicine National Meeting, San Diego, CA. April 13, 2024.
Plick N, Gabriel E, Nguyen VT. “Indications and Outcomes of Interhospital Transfers to an Academic Center.” Society of Hospital Medicine National Meeting, San Diego, CA. April 13, 2024.
Plick N, Nguyen VT. “No Acid-Fast? Not so Fast…” Society of Hospital Medicine National Meeting, San Diego, CA; 2024.
Rajda G, Dunn A, Varga A, Vincent R. “Impact of Dynamic Lighting on Hospitalized Patients.” Society of Hospital Medicine National Meeting, San Diego, CA; 2024.
Truong T, Schmer S, Dunn A. “Assessing an Artificial Intelligence-Assisted Discharge Prediction Tool.” Society of Hospital Medicine National Meeting, San Diego, CA; 2024.
Infectious Disease
Margolis M, Vasishta S, Aberg J, Urbina A, Dieterich D, Mullen M, Chasan R. A Quality Improvement Pilot to Increase Hepatitis B Screening and Optimize Patient Selection for Switch to Two-Drug Antiretroviral Regimen in Patients with HIV. ID week, October 2024, Los Angeles, CA.
Liver
Jeon J, Collado F, Mageras A, Blanco A, Bhuiyan T, Funes L, Hummel D, Leocadio D, PageCook DS, Paulino L, Dieterich DT. Reasons patients with hepatitis B and C declined linkage to care and strategies for re-engaging this reachable cohort Poster presentation, EASL International Liver Congress, June 2024, Milan, Italy.
Mageras A, Mendu DR, McGuire M, Alpert L, Wu J, Heiden K, Fisher M, Rodriguez N, Katzenstein C, Branch AD, Dieterich DT, Kushner T Implementation of System-Wide HBsAg to HDV Ab Reflex Testing in a New York City Health System. Parallel presentation, AASLD The Liver Meeting, November 2024, San Diego, CA.
5-Star CMS Quality Rating for 117th Street Dialysis
Hospital Medicine
Awards
Alan T. Hirsch Travel Award, Society of Vascular Medicine Scientific Sessions, 2024
Research Snapshot Presenter, Critical Care Congress, 2024
Grants
ISMMS student Nnamde Igwe received Society of Hospital Medicine Diversity, Equity and Inclusion Scholarship Fund ($25,000) under mentorship of Dr. Anne Linker and Dr. Vinh Nguyen.
Achieving Diagnostic Excellence through Prevention and Teamwork (ADEPT) - AHRQ
October 2022-September 2026: DHM MSH is a site for this multicenter federally funded project evaluating rapid response, ICU transfers, and deaths on general medicine services. The goal is to implement an enhanced case review infrastructure to identify diagnostic error and diagnostic processes among these patients, develop site-level and group-wide benchmarking reports of error rates, diagnostic processes, and diagnostic performance, and also identify and pilot Safety I and Safety II interventions at target sites
Mount Sinai Morningside and Mount Sinai West Publications
Peer Reviewed
Hospital Medicine
Pearson J, Keller K, Veldboom E, Waite H, Reiff-Pasarew, F (2025). Tackling Throughput with a Novel Care Team Rounding Model. PATIENT SAFETY. 2025 Apr 3;7(2).
Mount Sinai Morningside and Mount Sinai West Presentations
(Abstracts and Posters)
Gastroenterology
Leibowitz RM, Wilkoff M, Patel S, Markley A, Knorr IV, Rodriguez S, Nelson F. Using QR code technology to improve guideline-directed care for admitted patients with decompensated cirrhosis. Digestive Disease Week Annual Meeting, May 2024, Washington, DC.
Mehra S, Alpert L, Rios J, Jandorf L, Gottlieb Z, Kushner T, Luo Y The Gender Scope: Elevating Patient Comfort for Direct Access Procedures New York Society for Gastroenterology & Endoscopy Annual Course. Dec 2024, New York, NY. 1st place winner.
Miguez Arosemena P, Seltzer E, Olivo Freites C, Nurani S, Olivo Freites C, Andrilli J, Nelson F, “Anal Cancer Screening, Are We Doing Enough in Federally Qualified Health Centers?” Mount Sinai Morningside/West Internal Medicine Residency Annual Research Day, May 14, 2024, NY, NY, and also at Digestive Disease Week Annual Meeting, May 2024, Washington, DC.
Miguez Arosemena P, Seltzer E, Wang A, Andrilli J, Nelson F “Patient and Provider Perspective on Anal Cancer Screening in a Federally Qualified Health Center.” American College of Gastroenterology (ACG) Annual Meeting, October 29, 2024, Philadelphia, PA
Miguez Arosemena P, Kim D, Wang A, Andrilli J, Nelson F. “Enhancing Anal Cancer Screening Proficiency in Internal Medicine Residents: A Targeted Educational Initiative ” American College of Gastroenterology (ACG) Annual Meeting, October 29, 2024, Philadelphia, PA.
Wilkoff M, Wang A, Markley AR, Patel S, Hussein R, Piniella NR, Yan K, Simoes PK. Increasing colorectal cancer screening rates among patients at a federally qualified health center: a quality improvement project. Digestive Disease Week Annual Meeting, May 2024, Washington, DC
General Medicine
Nathani R, Mageras A, Villaroel C, Yarra S, Priven N, Viola H, Wang S, Mack T, Arron M, Carnavali F, Zhang W, Bansal M. AASLD/AGA MASLD Practice Guidance for Screening
Diabetics: Factor Associated with Advanced Fibrosis, Implication for Care Delivery, and CostReduction Using Aga-Adjusted FIB-4 Cut-offs. American Association for the Study of Liver Disease Annual Meeting, November 2024, San Diego, CA.
Hospital Medicine
Barhold L, Hernandez K, Johnson S, Huang K. “Complete for Treats”: Improving Medication Reconciliation Completion in the Inpatient Setting. Society of General Internal Medicine Annual Meeting; May 2024; Boston, MA.
Reiff-Pasarew F, Hernandez K, Shenoy S, Pearson J, Parikh F, Singh V, Chernyk A, Sadud S, Dempsey B, Chen P, Athari Anaraki N. (2024, April 12) Laboratory Stewardship Project [Poster Abstract]. Society of Hospital Medicine Annual Meeting. April 2024, San Diego, CA.
Reiff-Pasarew F, Keller K, Veldboom E, Pearson J, Waite H. (2024, April 12) Care Team Rounds: Development of Interdisciplinary Working Rounds [Poster Abstract]. Society of Hospital Medicine Annual Meeting. April 2024, San Diego, CA.
Reiff-Pasarew F, O’Sullivan M, Hurta J, Antretter J. (2024, April 12) Inpatient Varenicline for Smoking Cessation in COPD Patients [Poster Abstract]. Society of Hospital Medicine Annual Meeting. April 2024, San Diego, CA.