WHY LEARNING TO SURF CAN BE GREAT FOR YOUR MENTAL HEALTH, ACCORDING TO A PSYCHOLOGIST
‘IT’S ALMOST LIKE A SECOND HOME’: WHY STUDENTS WANT SCHOOLS TO DO MORE ABOUT MENTAL HEALTH
CAN CHEWING HELP MANAGE STRESS, PAIN AND APPETITE?
HERE’S WHAT THE SCIENCE SAYS
PIXELS ARE NOT PEOPLE: MENTAL HEALTH APPS ARE INCREASINGLY POPULAR BUT HUMAN CONNECTION IS STILL KEY
06 10 12
Pharmacists could help curb the mental health crisis – but they need more training
Jetlag hits differently depending on your travel direction. Here are 6 tips to help you get over it
Long COVID: a range of diets are said to help manage symptoms – here’s what the evidence tells us
Can chewing help manage stress, pain and appetite? Here’s what the science says
LEGAL DISCLAIMER
As publishers and owners of the Mental Health Awareness Magazine we are declaring that the information contained in this publication is for general information purposes only. While we endeavour to provide correct information, we make no representations or warranties and give no advice of any kind, express or implied, about the completenesss, accuracy, reliablity, suitability, effectiveness, correctness or availibilty of any information, text, data, chart, image, contact details, articles, announcements, advertisements, products, claims, services, qualifications or related graphics contained in the publication for any purposes. Any action by you, or failure to act by you or reliance you place on any information in the publication or any of the content of the publication is therfore strictly at your own risk and we take no responsibility and accept no liability for any consequences direct or indirect. The inclusion in this publication of any advertisement, article, advertorial, announcement, information, contact details, listing, image, design, chart, data, mark or representation does not constitute and does not imply advice, recommendation or endorsement by us of the associated practitioners, service providers, product providers, services, products, claims, opinions or views.
Articles sourced from the .
Pharmacists could help curb the mental health crisis – but they need more training
Authors: Joseph A Carpini- Lecturer, Organizational Behaviour and Human Resource Management, The University of Western Australia
Deena Ashoorian - Senior Lecturer, Pharmacy Discipline, The University of Western Australia
Rhonda Clifford - Professor, Allied Health, The University of Western Australia
Originally published on .
Chances are you live within 2.5 kilometres of a community pharmacy and visit one about every three weeks.
You don’t need an appointment. The wait time is usually short. These factors make pharmacists highly accessible healthcare professionals.
Pharmacists are regularly sought after for advice, including about mental health. In fact, pharmacists may be among the first health professional contacted about a health concern. They are also in regular contact with patients experiencing mental health issues or crises.
Despite the fact most pharmacists believe it is part of their role to provide mental healthrelated help, they may lack the confidence to respond to, raise or manage mental health issues with patients. In our recent study, pharmacists report not intervening about 25% of the time when they believe a patient is experiencing a problem or crisis.
Providing pharmacists with early intervention skills could help them address these challenges.
The pandemic has seen mental health decline
The COVID pandemic has seen anxiety and depression increase by 25% globally, signalling a broader mental health decline.
Poor mental health affects around 20% of the Australian population each year, and 44% of
advice about their health, including their mental health.
Generally, pharmacists in Australia have high levels of mental health-related literacy and evidence-based treatments.
Despite this, pharmacists report a lack of confidence which prevents them from raising mental
Your role is not to clinically diagnose a patient; however, it is valuable to assess the patient’s risk and level of urgency.
Australians over their lifetime. In a recent survey of 11,000 people, 24% of them said their mental health had declined over the previous six months.
Most concerning is that about 60% of people experiencing a mental health issue won’t seek help. This means people are more likely to remain undiagnosed and disconnected from support.
Pharmacists’ many hats
While dispensing and consulting are critical activities for pharmacists, they also help patients with questions and
health issues with patients. This is possibly because only 29% of pharmacists in Australia have mental health crisis training.
A lack of confidence in raising and addressing mental healthrelated issues means patients are likely to remain undiagnosed, untreated, and unsupported.
4 key elements of mental health first aid
Many of us are familiar with first aid as immediate help offered to an injured or sick person. But what if the issue is not physical, but mental? Many people don’t
know what immediate help they can offer.
As with physical injury or illness, timely and high-quality immediate help is critical.
There are a variety of not-forprofit and commercial mental health first aid training programs. A recent literature review of programs for mental health professionals suggests they can minimise stigma and increase knowledge. They can also bolster confidence and intentions to help.
Across the programs, there are four common elements to providing high-quality mental health first aid.
1. Recognise someone may be experiencing a mental health issue or crisis
Recognising a mental health issue or crisis involves taking notice of verbal, physical, emotional and behavioural
indicators. Given pharmacists interact with patients about every three weeks, they may be in a good position to notice changes.
They may express sadness, anger, frustration, hopelessness, shame or guilt. Patients might say: “There’s no hope” or “I can’t go on like this”.
Physical indicators include fatigue, sleeping difficulties, restlessness, muscle tension, upset stomach, sweating, difficulty breathing, changes in appetite or weight.
Emotional indicators reflect how a person is feeling and include significant mood changes, teariness, agitation, anger, desperation or anxiety.
Symptom guides for anxiety, depression, bipolar disorder, and suicidal ideation are available.
2. Approach and assesses the person
Opening the dialogue can be as simple as, “How are you? I have noticed [symptoms] and am concerned.”
Your role is not to clinically diagnose a patient; however, it is valuable to assess the patient’s risk and level of urgency. Risk and urgency will help inform whether the person is in immediate danger or can use other non-urgent support services.
The TED acronym can guide first discussions in the following way:
- Tell me …
- Explain how that has been impacting you …
- Describe what is happening …
3. Listen in an active way and communicate without judgement
Active listening involves confirming you are hearing and understanding the other person. Ways of doing this include: nodding,
appropriate eye contact, and summarising what has been shared. Communicating without judgement involves demonstrating genuine concern for the other person and talking about their experience.
Open-ended questions usually use “how” and “what” queries. You could say something like: “I’ve noticed some changes recently, what’s happening for you?” or “I see you are filling a prescription for sleep tablets. How are you sleeping?”
4. Refer the person to supports People who are struggling with their mental health can benefit from sharing details with professionals, like general practitioners, or family and friends – but they might need encouragement to seek this support out.
The support system recommended should match the level of urgency. Urgent services include Lifeline for free 24-hour phone, chat, and text message support. The Suicide Call Back Service is also a free 24/7 counselling service.
If in doubt or in an emergency, dial 000.
Non-urgent and free online support is available from Head to Health, the Black Dog Institute and Beyond Blue.
Could training community pharmacists help?
Studies in Australia, New Zealand, Canada and abroad all point to pharmacists’ believing they need more training in mental health first aid.
Research suggests almost 70% of patients believe all pharmacists should have mental health first aid
training. Patients report feeling significantly more comfortable speaking about mental illness with a pharmacist with this training.
And emerging evidence shows mental health first aid training can increase the quality of help provided by pharmacists.
In our study, we found Australian pharmacists with mental health first aid training were more likely to intervene than untrained pharmacists.
While the overall quality of the first aid provided by both mental health first aid trained and untrained pharmacists was high, some key differences existed. Trained pharmacists assessed patients and encouraged other supports (such as from friends and family) more. They also felt more confident discussing suicide risk.
JET LAG HITS DIFFERENTLY DEPENDING ON YOUR TRAVEL DIRECTION.
Here are 6 tips to help you get over it
After a few difficult years of lockdowns and travel restrictions, people are finally winging their way across the globe again; families are being reunited and sights are being seen.
Yet the joys of international travel often come with a side of jetlag, which can make it hard to initially enjoy a holiday, and to settle in once you return home. Why do people experience jet lag? And is there anything you can do to lessen its effects?
What causes jet lag?
The term “jet lag” describes the physical and cognitive symptoms people experience when travelling quickly across several timezones.
Before you leave for a trip, you’re synchronised to your local time. Once you enter a new timezone,
Authors: Sally Ferguson
Director, Appleton Institute, CQUniversity Australia
Dean J. Miller
Senior Postdoctoral Fellow, CQUniversity Australia
Originally published on
your body’s rhythms are no longer lined up with the clock on the wall. That’s when jetlag symptoms hit. You’re sleepy when you want to be awake, and wide awake when you want to be asleep. You’re hungry in the middle of the night, and might feel bloated or nauseous if you eat during the day.
Until your body clock and all the rhythms it controls line up with the new local time, you are physiologically and mentally discombobulated. Not a happy holiday vibe!
Jet lag isn’t the same for everyone Interestingly, the experience of jetlag varies between people. That’s because we all tick along to our own internal rhythm.
Most of us have a natural daily cycle of about 24.2 hours. So if we lived in a cave and didn’t see any light, our sleep/wake cycle and other daily rhythms would tick along at about 24.2 hours. Researchers think this is
an evolutionary adaptation that allows us to adjust to different day lengths across the year.
But some people have slightly longer cycles than others, and this may play a role in how a person experiences jetlag.
Research suggests if you have a longer cycle you might adjust quicker to westward travel, such as when travelling from Australia to South Africa, but we don’t know if a shorter cycle helps going the other way.
We also get a little less resilient as we age, so the older among us might have worse jetlag symptoms.
Does direction of travel matter?
More generally, many people find westward travel, where you “gain” time, a bit easier.
Say Jasmine and Sarah depart Adelaide at the same time.
Jasmine lands in Perth in the afternoon, where it’s about 2.5 hours earlier in the day. She sees some sights and easily falls asleep at about 8.30pm local time. She
then wakes up very early and starts her day.
Because Jasmine’s body clock naturally delays – shifting a little later relative to the local time each day – after a few days she is fully synchronised.
Sarah, meanwhile, lands in Auckland which is about 2.5 hours later in the day. She takes advantage of the balmy evening and some of the night, and is wide awake until 2am. She then struggles out of bed when the alarm goes off at 7am, because it’s still 4.30am on her body clock.
Sarah will likely feel the effects of jetlag more severely than Jasmine, and for longer.
Is jet lag just ‘psychological’?
Some people might wonder if jet lag is just in your head. Well, in a way it is, because it’s a mismatch between your body’s internal time (which is determined in your brain) and your local time.
But that doesn’t mean you can talk yourself out of jetlag.
It’s better thought of as a physiological condition, rather than a psychological one.
Luckily, there are a few simple ways to alleviate jetlag symptoms and help your body clock adjust. This is particularly important for elite athletes who travel to compete.
1. First, decide whether it’s worth trying to adapt to the new time or not. If it’s only a short trip, it might make more sense to stay on your home time. If it’s longer than three days, start consciously moving your own rhythms – such as when you sleep, eat, exercise and get sunlight – towards the new timezone.
2. If you’re trying to shift your body clock, it’s a good idea to start on the plane. Set your watch to your destination’s timezone and line up your activities accordingly.
3. Keep caffeine and alcohol intake low on the journey. This will be better for sleep and hydration, and
will help with adjusting your body clock to the new timezone.
4. When adjusting to a new timezone, try to sleep during the local night time and just rest when you need to at other times. Short naps can give you a boost to get through the day and evening activities. Aim for about 30 minutes and avoid naps later in the day as you near your actual planned bedtime.
5. Gastrointestinal discomfort is a symptom of jet lag. If you’re prone to or experience tummy trouble while travelling, stick to small meals and eat when you’re hungry. Your body will tell you when it’s ready for food. Tip 3 about caffeine and alcohol applies here too.
6. Get outside. Sunlight is key to adjusting to a new timezone. Depending on your timezone change, appropriately-timed outside activities will help.
Lockdowns doubled your risk of mental health symptoms
Author: Gery Karantzas Associate professor in Social Psychology / Relationship
Deakin University
During the almost two years of on-again off-again COVID lockdowns, we heard lots of concern from many different corners about the mental health effects of forcing people to stay home and keep away from friends and family.
Many research projects were undertaken to attempt to measure the scale of the impacts on mental health.
However, the speed with which research was generated meant in some cases, research quality was sacrificed, and some research found evidence of an effect on mental health, and some didn’t. To make sense of the very mixed findings, my colleagues and I conducted a review of all of the studies on mental health conducted during the first year of the pandemic.
We included 33 published papers which studied a total of nearly 132,000 people across various world regions.
We found that overall, social restrictions doubled people’s odds of experiencing mental health symptoms. This means, of those who participated in these studies, those who experienced lockdowns were twice as likely to experience mental ill health than those who didn’t.
This finding can be broken down further by different mental health symptoms. Social restrictions saw the odds people would experience symptoms of depression increase by over 4.5 times, the odds of experiencing stress increased by nearly 1.5 times, and the odds of experiencing loneliness almost doubled.
When we drilled down further into these results, we found the length and strictness of lockdowns affected mental health symptoms differently. For example, strict lockdowns increased depression, whereas the onset of social restrictions increased stress. Low
social restrictions, where there were some restrictions in place but not total lockdown, were associated with increases in anxiety.
Also, mental health outcomes differed by age, with young and middle-aged adults reporting greater negative mental health symptoms than older adults.
What lessons can we take away from these findings?
The findings give us a good idea
of what public health outreach should look like in the event of future pandemics. Anxiety was most prevalent when low restrictions were introduced. This could be due to the fact people were nervous about the precarity of the situation and where the virus could be circulating. The introduction of such measures should be accompanied by public health messaging and interventions that focus on alleviating chronic fear and worry.
During the periods of strict social restrictions, the predominant mental health issue was depression, meaning mental health responses should focus on combating depressive-related symptoms such as hopelessness and loss of purpose.
The findings for stress suggest symptoms are likely to intensify during the early stages of social restriction enforcement. This is probably because the onset of restrictions communicates to people an increase in the seriousness of the pandemic threat, and people have to work very hard to re-organise their lives if restrictions involve the need to work from home and home-school.
During these times, providing messaging and interventions that help people manage their stress, such as dealing with work stress or the stress of home-schooling children, may be especially important. For parents,
making them feel capable in the home classroom and promoting strategies that foster positive family functioning (such as more constructive communication and problem-solving) could reduce parental and family stress.
Given social restrictions were found to be associated with increases in loneliness, promotion of digital technologies to keep people feeling connected is also important.
Across all these mental health issues, messages that communicate these symptoms are to be expected are likely to help individuals normalise and acknowledge the nature and
people’s mental health symptoms on the day social restrictions were first enforced. Most people are likely to experience heightened but temporary spikes in mental health symptoms that may naturally reduce after the initial lockdown announcements. This means it’s difficult to get a handle on the “true” mental health effects of social restrictions on the first day restrictions are activated.
However, the effects of social restrictions on mental health symptoms were similar across studies where people were surveyed at one time point and where they were surveyed on more than one occasion during restrictions. This
severity of their symptoms. This, in turn, may prompt people to seek help for their mental health symptoms.
Research quality was poor
Another important point to highlight from our review is the research conducted during the first year of the pandemic was generally of poor quality.
This is because good measures of social restrictions were hard to come by in studies. Some studies didn’t detail the specific restrictions in place in various cities, or did not ask study participants to what extent they complied with restrictions.
Also, some studies surveyed
suggests the estimated effects seem robust, despite many studies not having the best assessments of social restrictions.
The findings of our review show that although we have a way to go in the way we conduct research into the mental health effects of COVID-19 social restrictions, the initial research highlights these restrictions indeed negatively impacted the mental well-being of citizens.
Although such restrictions may be an effective public health response to mitigate the spread of viruses such as COVID-19, there needs to be a co-ordinated response to safeguard people’s physical and mental health.
Can chewing help manage stress, pain and appetite? Here’s what the science says
Ever feel a bit stressed or need a concentration boost? Research suggests one remedy may be right under your nose. Chewing has benefits for brain function, stress, anxiety, exam performance, pain perception, as well as hunger and food intake.
Here’s what the research about chewing more says, in experiments that used either food or chewing gum.
What do teeth have to do with your brain?
Being able to chew efficiently is related to how many teeth you have. While adults usually have 32 teeth, you need 20 teeth, with at least nine or ten pairs making contact, in order to chew properly.
The hippocampus area of the brain assists with information transfer from short-term to longterm memory. It also processes spatial memory, which helps you remember practical things, like where you’ve put your phone or how to get to the shops.
Research shows not being able to chew properly, whether due to tooth loss or gum disease, affects the hippocampus through stimulating the production of stress hormones, called glucocorticoids. These impair your ability to acquire and process information.
A review of research on chewing and cognitive decline in adults found people with fewer teeth didn’t get the same amount of brain activation. The more strongly people could chew, the more blood flowed to their brains, leading to more oxygen and activity in regions of the brain linked to learning and memory.
Another review found poorer chewing was associated with faster cognitive decline and the risk of developing dementia.
This adds to the evidence that chewing ability and oral health are central to healthy ageing.
Anxiety reliever and attention booster
Chewing gum can be an inexpensive and effective way to help relieve anxiety and boost attention.
Results across eight research trials that included more than 400 adults found chewing gum more often, compared to never chewing gum, resulted in a significant reduction in anxiety.
Clare Collins Laureate Professor in Nutrition and Dietetics AO, University of Newcastle Originally published on .
Although the exact mechanism in not currently known, research in animal models suggests not being able to chew properly leads to the stimulation of neurons involved in emotional regulation.
Another meta-analysis of eight intervention studies that tested the effect of chewing gum found there was a small improvement in levels of sustained attention, with improved ability to maintain alertness during mentally demanding tasks in the group given gum to chew.
To reduce the amount of dental plaque and risk of tooth decay, opt for sugar-free chewing gum.
Stock up on gum when preparing for exams
A 2019 intervention study tested the effect of regularly chewing gum or not, on stress, anxiety, depression, attention and exam success.
They randomised 100 final year nursing students to either chew sugarless gum for at least 30 minutes a day for 19 days, a group who chewed gum for seven days only, or a control group who did not chew gum at all.
They found levels of depression, anxiety and stress were significantly lower in both chewing gum groups, while academic success scores were higher in 19day gum chewers only compared to the other groups. There was no effect on self-focused attention.
So chewing gum before exams may help students overcome exam stress and enhance exam success, but might not help those who have difficulty focusing their attention.
Chewing may alter your perception of pain
Another study randomised 161 adults undergoing routine colorectal surgery to either chew gum four times a day postoperatively, or not chew gum.
People in the chewing gum
group reported lower perceived pain on days two to five post-surgery.
Interestingly, there was no difference between groups in how long it took to pass flatus (fart) or a bowel motion. These signal a return to normal gut function after surgery.
A trial in a children’s hospital in Turkey randomised 73 children having an IV cannula inserted to receive either a chewing gum intervention during the procedure or standard care only.
Both nurses and children reported significantly lower pain levels among the chewing gum group compared to the usual care.
While exact mechanisms are not confirmed, the analgesic effects of chewing gum appear to be mediated via neurons in the brain related to serotonin, a neurotransmitter that affects body functions including mood and anxiety.
Chewing your food well can reduce your appetite
A systematic review of studies using foods looked at the impact of people receiving advice to consciously slow down when eating and chew more, on aspects of appetite and food intake.
The study participants reported less hunger, desire to eat and ate significantly less food, compared to people eating as usual.
Putting all this research together, it appears that chewing gum may be an easy “go to” intervention with benefits for your brain. Take care though, as “sugar free” gum usually contains sorbitol, a common artificial sweetener and can trigger diarrhoea if consumed in excess.
Chewing gum can also lead to aerophagia, meaning too much air is swallowed, and trigger abdominal distention or discomfort
– although researchers found chewing gum does not make you burp more.
When it comes to food, the advice to “take time to chew your food properly” is wise.
Maintain good oral health by brushing your teeth, having regular dental check ups and, for those with tooth loss, good fitting dentures. And, if you grab some chewing gum, make sure it’s sugar-free.
Why learning to surf can be great for your mental health, according to a psychologist
Author: Lisa Olive - Senior Research Fellow & Clinical Psychologist, Deakin University
Nothing clears the mind like going for a surf. With the escapism and simplicity of riding waves, it’s no secret that surfing feels good.
Now our preliminary study in children and adolescents adds to growing evidence that surfing really is good for your mental health.
But you don’t have to have a mental illness to get the benefits. Here’s how you can use what we’re learning from our research to boost your own mental health.
How surfing is good for you
Evidence showing the mental health benefits of surfing ranges from improving self-esteem and reducing social isolation to treating depression and other mental disorders.
Such evidence mainly comes from specific surf therapy programs. These combine supportive surfing instruction with one-to-one or group activities that promote psychosocial wellbeing.
At their core, most of these programs provide participants with the challenge of learning to surf in an emotionally safe environment.
Any benefits to mental health are thought to arise through:
- an increased sense of social connection
- a sense of accomplishment that people can transfer to other activities
- respite from the day-today stressors due to the allencompassing focus required when surfing
- the physiological response when surfing, including the reduction of stress hormones and the release of mood-elevating neurotransmitters
- exercising in a natural environment, in particular “blue spaces” (on or near water).
What we did
Our pilot study aimed to see whether the Ocean Mind surf therapy program improved child and adolescent mental health.
We also wanted to see whether participants accepted surfing as a way to address their mental health concerns.
The study involved 36 young people, 8–18 years old, who were seeking help for a mental health concern, such as anxiety, or a neurodevelopmental disorder (attention deficit hyperactivity disorder or autism spectrum
Originally published on .
disorder). They were referred by their mental health provider, GP or school counsellor.
Participants were allocated at random to the Ocean Mind surf therapy program or were placed on a waitlist for it. Those allocated to surf therapy continued with their usual care, which included case management from a mental health provider. Those on the waitlist (the control group) also continued with their usual care.
The surf therapy program ran for two hours every weekend for six weeks. Young people were partnered one-to-one with a community mentor who received training in mental health literacy and surf instruction.
Each session included supportive surf instruction and group mental health support, all conducted at the beach. Sessions were run by the program coordinator who was also trained in mental health and surf instruction.
What we found
By the end of the sixweek program, those receiving surf therapy had reductions in depression, anxiety, hyperactivity and inattention symptoms, as well as fewer emotional and peer problems. This
was compared with those in the control group, who had increases in these symptoms.
However, any improvements were not sustained six weeks after the program finished.
Those receiving surf therapy also saw it as a suitable, youthfriendly way to manage symptoms of mental ill-health. This was further supported by the high completion rates (87%), particularly when compared with other methods of mental health treatment. For instance, psychotherapy (talk therapy) has been reported to have a 28–75% drop-out rate for children and adolescents.
It’s early days
These early findings are promising. But given this was a pilot study, more research is needed with larger numbers of participants to confirm these outcomes and see if they generalise to broader populations.
We’d like to identify the best dose of surf therapy in terms of session frequency, duration, and program length.
We also need to understand the factors that maintain these initial positive changes in mental health, so any benefits can be sustained after the program finishes.
The recognition of surfing as a potentially effective and
acceptable mental health treatment among young people is also promising. But this finding does not preclude the more conventional clinical treatments, such as talk therapy and medication, which may work better for certain people.
Rather, surf therapy may be seen as an additional form of support alongside these approaches or an alternative for those who do not benefit from more traditional methods.
Tempted to try surfing?
If you think surfing might be for you, remember:
- surfing requires complete focus due to the ever-changing conditions of the ocean, making it a great way to step away from dayto-day life and wipe out the effects of stress
- for some people, surfing may reduce barriers to seeking mental health care
- surfing may not be for everyone, nor can it guarantee to reduce your symptoms. Even the best surfers can suffer from depression and may require external support
- don’t worry if you cannot access the ocean or a surfboard. Other nature-based activities, such as hiking and gardening, can also benefit your mental health.
It
’
s
almost like a second home :
why students want schools to do more about mental health
Authors Christine Grové Fulbright Scholar and Adjunct Senior Lecturer, School of Educational Psychology & Counselling, Monash University
Alexandra Marinucci
PhD Candidate, School of Educational Psychology and Counselling, Monash University
Psychological distress is on the rise among young people in Australia. The implications of COVID-19 and the strain on the training and availability of psychologists are likely to add to the mental health challenges and hinder young people’s ability to get help.
Social isolation, loneliness and uncertainty due to COVID-19 have contributed to a decline in the mental health of Australian youth. Young people in our research and other studies do not feel well equipped to manage their mental health. This is concerning as the onset of mental illness peaks at
Originally published on .
14.5 years of age, and about one in seven Australian youth experience mental illness.
Currently, schools address mental health and well-being through a social and emotional learning curriculum. Some have school counsellors or psychologists to offer students individual or group support.
However, research shows more than a third of young people with mental health problems do not seek professional help. This is due to limited mental health knowledge and awareness of how to seek help, and negative attitudes towards mental illness.
There is a need to address youth mental health through preventive approaches such as mental health literacy programs. Mental health literacy is the knowledge and awareness of mental health, help-seeking options and positive mental health behaviours. Mental health literacy programs aim to increase skills to achieve and maintain good mental health.
Schools are one setting to base such programs. Young people spend much of their childhood and adolescence in school where the environment is already geared towards supporting learning and development.
Young people need to be included in the development of these programs. Neglecting their voice in research leads to a risk of misinterpreting their needs and misguided approaches.
We used online group discussions as a forum for young people to give their perspective on current mental health education in the curriculum and whether
be experiencing mental health challenges for fear of crossing a boundary or saying the wrong thing.
Stigma is still a big problem
Stigma and negative attitudes towards mental illness exist despite many mental health initiatives and campaigns to normalise mental health challenges.
Young people described mental
it’s meeting their mental health literacy needs. Thirteen young Australians took part in these discussions in 2021.
What did the students tell us?
Our study participants expressed concern that they do not receive enough information about mental health in school. They also find it difficult to identify appropriate help sources. They told us:
“I haven’t been happy with […] how little they talk about mental health.”
“They don’t really talk about how you can help other people deal with it [mental health], so, like, then it […] is harder to help your friends.”
Informal sources of help such as family, friends and the internet were the most common avenues for seeking help. Young people were less likely to go to formal sources such as a mental health professional or general practitioner.
Young people are not confident about supporting a friend who may
health as a “hush-hush topic”, with language relating to the issue often framed negatively. A lack of mental health knowledge was seen as contributing to stigma. As one young person said:
“When people don’t understand something […] they become afraid of it.”
The youth in our study suggested discussing mental health in schools and normalising mental health difficulties can
reduce this stigma.
Though mental health can be a sensitive topic, young people believe it is important to understand and learn about it at school with others that are experts on mental health.
Schools are the right place to learn about mental health
Young people want schools to teach them how to recognise mental health challenges and practical coping strategies. They observed that discussions of mental health in school are often in response to crises or a stressful time such as exams. These discussions are usually rushed and not comprehensive.
There is a need to proactively talk about mental health with students throughout their schooling. This will build their mental health literacy, as one young person told us:
“If you’re equipped with everything you need to know prior to that experience [mental health issues] you could better tackle that and you could better bounce back from that difficult time in the future if you’re equipped with the knowledge of how to overcome that issue.”
Youth want to learn about mental health at all year levels. Some felt frustrated that they didn’t learnt appropriate coping skills before entering secondary school.
Students see schools as a safe place for supporting their mental health, suggesting schools have an obligation to provide a holistic education that includes mental health.
“It’s [school] almost like a second home, and within that second home mental health needs
to be the safe discussion topic.”
Good education includes mental health literacy
From the perspectives of the young people in our study, more needs to be done in schools to improve mental health literacy.
There is evidence that preventive mental health approaches are effective. School-based mental health literacy programs are one way to overcome the lack of mental health education in Australia.
Schools exist to support the learning and development of young people, which should include fostering good mental health and increasing mental health literacy.
Erling Haaland or Harry Kane?
Mo Salah or Marcus Rashford? Use the “triple captain” chip or save it?
This weekend (and pretty much every weekend until the end of May), millions of people around the world will be making these sorts of decisions, hoping the right call will take them a step closer to fantasy football glory.
Glory or not, fantasy football should be a fun, enjoyable hobby… right? Recent research –including a newly published study – sheds light on whether that really is the case.
A real-world virtual team
For the uninitiated, fantasy football (“soccer” in some parts of the English-speaking world) is a game in which you select real-world players for your virtual team, with their subsequent real-
Fantasy football can negatively affect your wellbeing, but research shows it doesn’t have to
world performance dictating your team’s score.
Many versions exist, but the basic premise is that points are awarded for doing good things (like scoring a goal) and deducted for doing bad things (like getting a red card). The virtual team with the most points by the end of the season, wins.
Fuelled by advances in smartphone technology and social media, fantasy football has rapidly grown to become a key meal in a fan’s football consumption.
You would think this would be a good thing, but take a quick scroll through the fantasy football “Twitter-verse” and you will soon find not everyone seems to be enjoying it for what it’s meant to be – a game.
This Twitter toxicity is what led colleagues and I to publish the
first scientific paper exploring the impact of fantasy football on mental health in October 2021.
Not all fun and games
In our study, 1,995 fantasy football players (representing 96 different nationalities) completed a questionnaire on their anxiety, low mood, daily functioning, and problematic behaviour in relation to the game. Importantly, players also told us about their engagement (primarily the time spent playing the game) and experience (the number of years playing the game).
The good news was that for most respondents, fantasy football did not seem to have a negative impact on mental health. However, given the popularity of the game, it is notable that 3.4% and 5.1% of the respondents reported having
Author: Luke Wilkins Lecturer in Sport and Exercise Science, La Trobe University Originally published on .
moderate to severe anxiety and low mood in relation to the game, respectively.
In a game played by over 10 million people, that could be hundreds of thousands of people negatively affected by what is meant to be a fun and enjoyable hobby.
Interestingly, while engagement and mental health concerns were positively correlated, experience and mental health concerns showed the opposite relationship. That is, the more time a player invested in the game, the greater the negative mental health concerns they reported; but the more years’ experience they had playing the game, the fewer negative mental health concerns they reported.
It’s unclear why this is, but we think it’s possible that over time, players develop coping mechanisms or even an emotional “numbness” towards the game.
Looking for positives
Our first study provided insights into fantasy football’s potential harmful effects on wellbeing, but failed to investigate the numerous positives that inevitably must exist (why else would it have become a global phenomenon?).
We decided to address this by carrying out a follow-up study.
This time, we took a qualitative, interview-based approach to paint a more holistic and detailed picture of what goes on when people take part in fantasy football. This paper has just
been published in the journal Entertainment Computing.
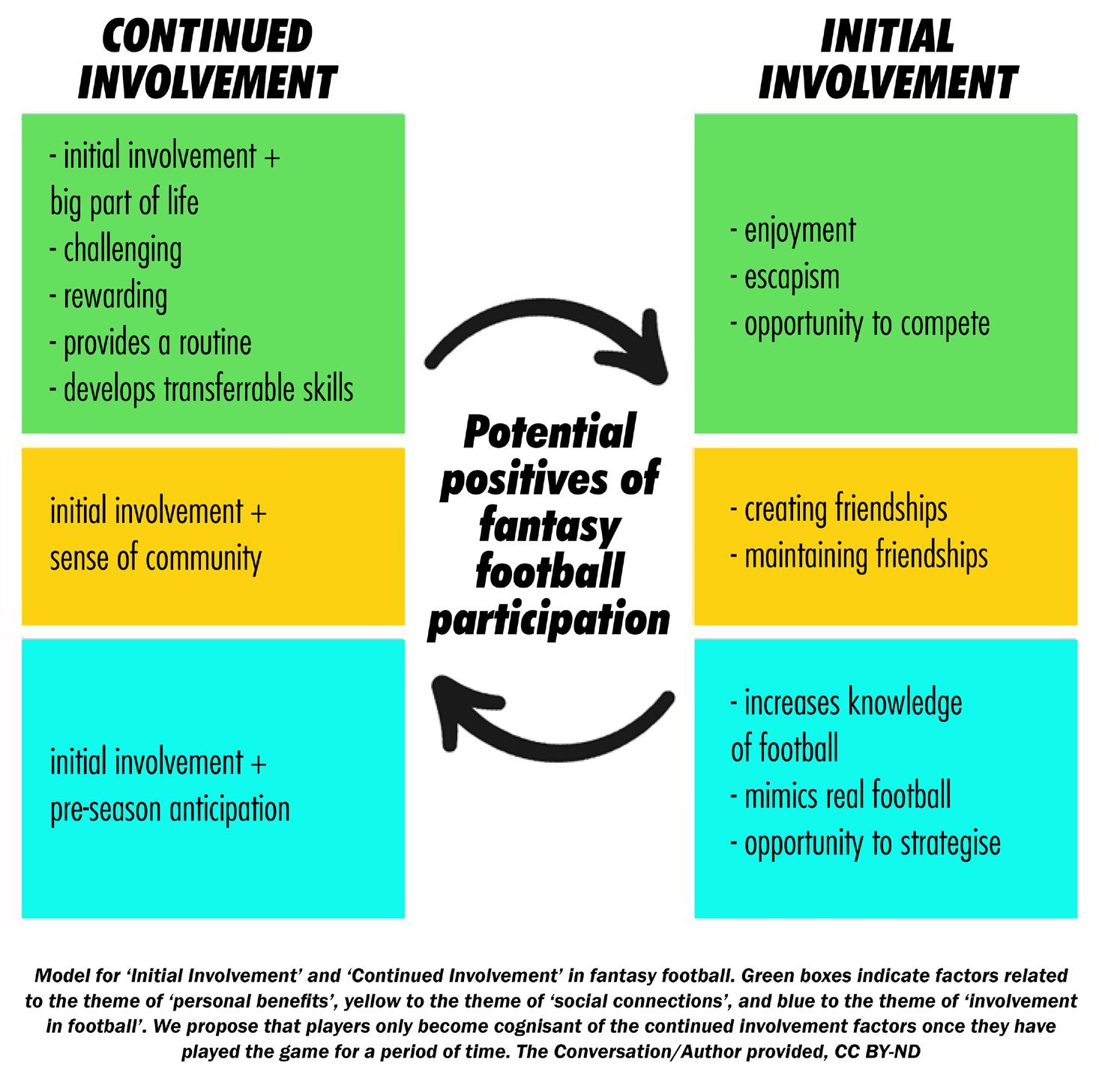
We interviewed 15 experienced male fantasy football players, and thematically analysed the resulting data. Overall, it was found the
game appears to have a much more positive than negative impact. Aside from the obvious enjoyment factor, benefits included the creation and maintaining of friendships; an increased knowledge of football; the opportunity to strategise, compete, and develop transferable skills (such as an understanding of maths and statistics); escapism; and the provision of structure and routine to one’s week.
Mitigating the negatives
We also teased out some negatives. Responses from all participants lent support to our original study which highlighted fantasy football’s potential harm to wellbeing. “Anxiety-provoking”, “frustrating”, “addictive”, “affects self-confidence” and “disappointment and regret” were prevalent enough to warrant sub-themes of their own within the analysis.
Participants were also keen to mention the negative online impact – particularly through social media
– that accompanies the game, as well as the intensity of involvement the game was perceived to require.
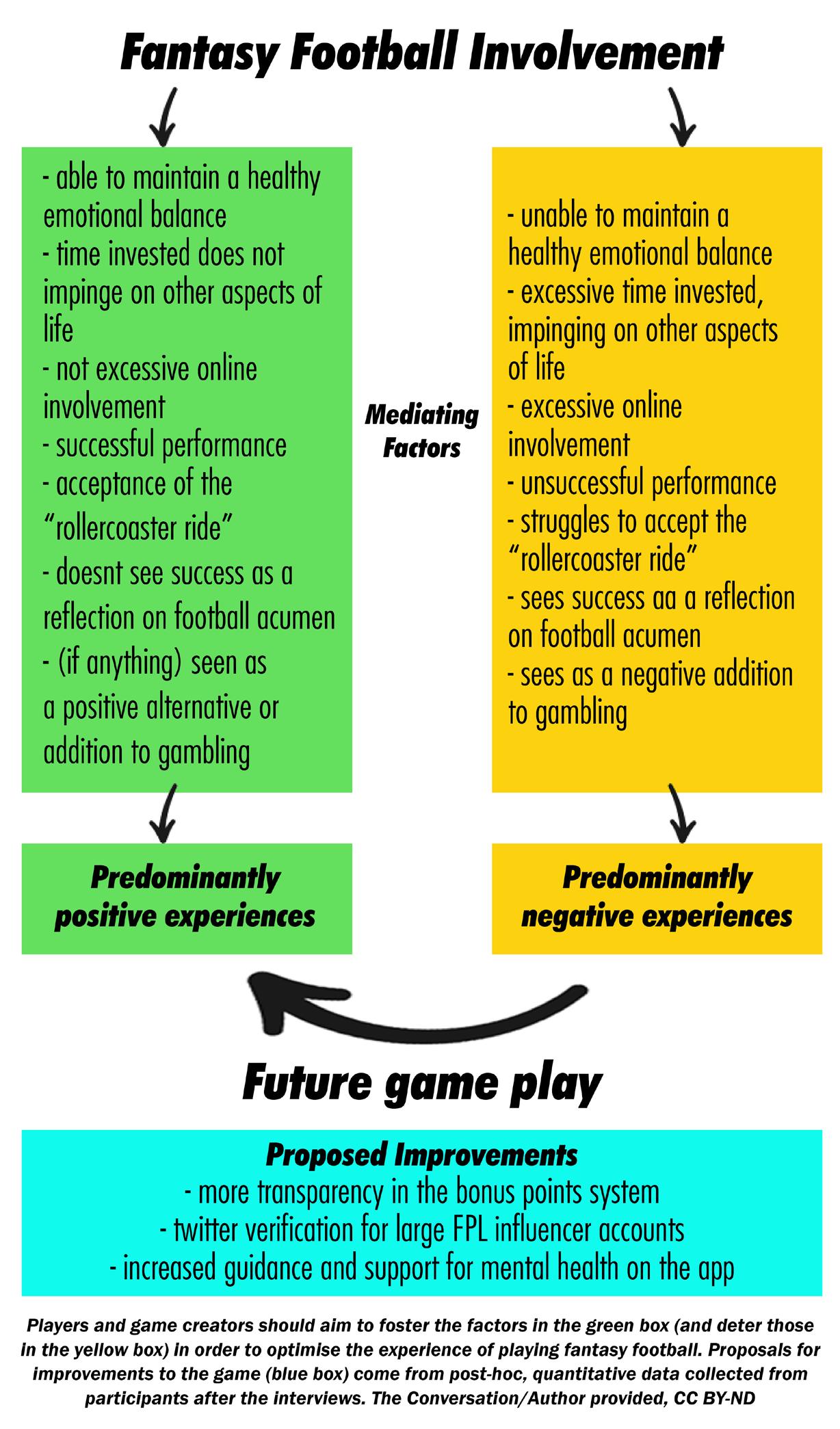
Perhaps of most importance was the identification of seven factors which we believe can be used by game creators and game players alike to help optimise participation in fantasy football.
For instance, we propose that if you think success in the game reflects your knowledge of football in the real world, it will lead to predominantly negative
experiences. Likewise, it’s not wise to invest excessive time at the expense of other areas of life.
Some of these are clearly easier said than done, and others may actually be incompatible with one another.
Nevertheless, we believe through identifying these factors, we can help players become more mindful of their fantasy football involvement, and the impact it may have on their mental health.
Like with most things in life,
balance is key for fantasy football. The growth of the game shows no sign of slowing down, so it’s important for players and game creators alike to act now to improve the playing experience.
If we don’t, making that call on Haaland or Kane will continue to have a greater consequence than it ought to.
Back-to-school blues
are normal, so how can you tell if it’s something more serious?
Author: Vanessa Cobham Professor of Clinical Psychology, The University of Queensland
Originally published on
Many children come down with a case of the back-to-school blues as summer slips away. Having spent the holidays staying up late and having fun with friends and family, it can be a struggle to get back into a routine.
For some children, going back to school can also be daunting if they are worried about keeping up with schoolwork, friendship problems or how they might go with a new teacher and class. Nerves about returning to school can manifest in a number of ways, from irritability to tears at the school gates.
How can you cope with this routine challenge? And how do you tell if is it something more serious?
How to tackle black-to-school blues
There are a few ways you can support your child and the family as you all head back the daily routine of school.
Plan ahead together
There are lots of ways you can gently work in a new routine – from encouraging kids to pack their bag the night before, to thinking of lunchbox ideas together.
Giving your child choices and the chance to be part of the decisionmaking process around routines will give them a sense of ownership and independence. For example, you could negotiate bedtime for the school term.
There are other fun, simple ways you can support them through this
kids will find it easier to remain calm and positive, too.
When is it more than the blues?
Nervousness about returning to school is normal. But some children will experience a level of anxiety about going to school that causes them significant problems. Because everybody feels worried or anxious from time to time, it can be really tough to know how to distinguish between “normal” nervousness and problematic (or clinically
time. For example, you could could create a music playlist for the school run, set aside a regular time after school to do something you both enjoy (like a play at the park, seeing friends or buying an icecream) or set up a reward system for getting homework done on time.
Chat about school
Check in regularly with your child about how they are feeling, particularly in the early weeks. Try to do this in a way that shows that you’re interested rather than concerned. For example, keep the questions open-ended: “what happened in your day?”. And keep a positive focus: “what was the best bit of your day?”
Look after yourself
With a hundred different things to think about, many parents and carers often forget about their own needs. But it is crucial to give yourself time to recharge, and reach out for support from friends, family or a health professional if needed. If you are calm and positive, your
significant) anxiety.
There are two key ideas to keep in mind: are the feelings causing high and persistent levels of distress? Are they stopping your child from doing what they want or should be able to do?
What should I look for?
When it comes to school-related anxiety, here are some specific signs to look for:
- frequently feeling physically sick (such as a tummy or headache) and unable to go to school. Anxiety causes real physical changes in our bodies, so when kids say they’re feeling sick, they’re telling the truth. It’s just they might be describing “worry sick” as opposed to “doctor sick”
- becoming teary, angry or aggressive when thinking or talking about school
- being uncharacteristically slow to get moving on school mornings
- avoiding activities that relate to school, such as joining a sporting team, putting on their uniform or going on a play date.
Is this school refusal?
School refusal or avoidance (when a child regularly fails to attend class for some or all of the day) has anecdotally been on the increase since COVID. The Senate is currently conducting an inquiry into the issue, with a report due in March.
If you’re starting to think your child’s anxiety may be falling into the problematic zone, you are not the only one. Anxiety is the second most common mental health problem experienced by all children in Australia (among girls, it takes first place).
Without treatment, children with clinically significant anxiety don’t tend to “just grow out of it”. Anxiety (often together with ADHD), tends to be the cause of school reluctance or refusal.
Next steps
If you notice your child is struggling to get to school, it’s important to act quickly. The more time kids miss in school, the harder it becomes for them to return.
The first thing to do is work with school staff. Your child’s classroom teacher will be able to tell you if they or someone else in the school is the best person to be talking to. If necessary, seek further support from a health professional. You can start with your GP, who may suggest a referral to a psychologist. There are also free, evidence-based programs been developed by clinical psychologists for parents of children who are experiencing anxiety.
Although it can be daunting, it is important to know you are not alone and there are interventions that can help.
If this article has raised issues for you or someone you know, you can call Lifeline on 13 11 14 or Kids Helpline on 1800 55 1800.