Usual daily dose: 24 mg to 48 mg in divided doses.2 REVIHIST 24 mg is indicated for the symptomatic treatment of vertigo associated with Meniere’s Syndrome.2 aural fullness in the affected ear 1
Second victim syndrome: bridging compassion and healing in healthcare
Impact of early vs. delayed initiation of dutasteride/tamsulosin combination therapy on the risk of acute urinary retention or BPH‑related surgery in LUTS/ BPH patients with moderate‑to‑severe symptoms at risk of disease progression
S D’Agate, C Chavan, M Manyak, JM Palacios‑Moreno, M Oelke, MC Michel, CG Roehrborn, OD Pasqua
Prostate safety events during testosterone replacement therapy in men with hypogonadism a randomized clinical trial
S Bhasin, TG Travison, KM Pencina, M O’Leary, GR Cunningham, AM Lincoff, SE Nissen, MS Lucia, MA Preston, M Khera, N Khan, MC Snabes, X Li, CM Tangen, KA Buhr, IM Thompson Jr
Direct
B
S
JJ Makhubele, JM Mokheseng, MC Kgokolo
S Afr Gen Pract
The South African General Practitioner (SAGP) circulates to general practitioners and family physicians in South Africa via Medicross and Intercare. This new title is a peer reviewed journal that publishes the contributions of local key opinion leaders and researchers. CPD articles, evidence based review articles, pharmaceutical product updates and original research address the information needs of the target audience. Sections include therapy in practice, focus on the young patient, practice management, home health care, chronic disease management, geriatric care and medical malpractice. Sure to become a valuable and widely-read resource, SAGP will provide your advertisement, insert or advertorial with the exposure and impact that you need to influence these very important therapeutic decision makers.
Manuscript submission office: www.medpharm.co.za
Published four times per annum and distributed to General Practitioners which includes Intercare and Medicross doctors
Medical and Pharmaceutical Publications (Pty) Ltd, trading as : Medpharm Publications, Ground Floor, Centurion Wine & Art Centre, 123 Amkor Road, Lyttelton Manor PO Box 14804, Lyttelton, 0157
S Afr Gen Pract 2024;5(2):55-57 https://doi.org/10.36303/SAGP.0510
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Second victim syndrome: bridging compassion and healing in healthcare
K Outhoff
Associate Professor, Department of Pharmacology, Faculty of Health Sciences, University of Pretoria, South Africa
Corresponding author, email: kim.outhoff@up.ac.za
In the intricate healthcare landscape, where compassion merges with complex medical decisions and procedures, second victim syndrome may lurk unnoticed and unaddressed.1 The psychological distress and emotional turmoil experienced by healthcare professionals after being involved in adverse patient events and near-misses remain largely silent, haunting healthcare professionals and leaving them vulnerable to subsequent health issues.2 This editorial delves into this second victim syndrome, shedding light on its profound impact, particularly in the context of medical malpractice and litigation, and exploring the potential of mindfulness in nurturing healing and resilience.
Adverse patient events, being iatrogenic in nature, result from medical care rather than an underlying disease.3 Consequently, they demand unforeseen patient monitoring, treatment, or hospitalisation.4 They may also result in patient death. These events, which include diagnostic errors, surgical complications, falls, healthcare-associated infections, pressure ulcers, or medication errors leading to adverse drug reactions, toxicity or treatment failure, can occur at any juncture of healthcare provision, spanning hospitals, clinics, nursing homes, outpatient facilities, and general practice.5 They may arise from communication errors, misdiagnoses, equipment failure, or systemic deficiencies within the healthcare delivery system.6
The fundamental priority of medicine lies in ensuring our patients’ rights to receive safe, dependable, and patientcentred care. Unforeseen complications and inadvertent errors are inherent to the medical system, however, stemming from the universal reality of human fallibility and technological limitations. While not all errors pose life-threatening risks, they have the potential to significantly undermine a patient’s quality of life.7 Adverse patient events are profound tragedies of healthcare delivery, often occurring despite adherence to best practices.8 Unfortunately, they are not uncommon; approximately a tenth of patients experience harm in hospitals, with half of these deemed preventable.9 These statistics offer little solace to healthcare professionals embarking on tortuous journeys of self-recrimination for their failings. The culture of perfectionism within healthcare further exacerbates the risk of second victim syndrome. Doctors often strive for perfection, driven by the desire to provide the best possible care for their patients. However, this relentless pursuit of perfection can lead to unrealistic expectations and a reluctance to acknowledge
mistakes. Patients and the public, who understandably expect their doctors to be infallible, may inadvertently reinforce this notion, denying the potential or existence of human error.1
In the aftermath of a medical error or adverse event, attention, support and condolences reasonably gravitate toward the patient (the first victim) and their loved ones. Yet, the ripple effects extend beyond the patient and their family, deeply impacting healthcare practitioners (the second victims).7 Up to 50% of doctors are affected by an adverse patient event in their career.10 Following such incidents, doctors often find themselves in a maelstrom of shock, grief, guilt, shame, self-doubt, remorse and fear.1 These emotional responses can significantly affect their well-being, job satisfaction, and ability to provide quality care to future patients.7,11,12, For many, witnessing harm to a patient shatters their sense of professional identity, prompting doubts about their competence and worthiness as caregivers. In the wake of such events, the psychological toll on doctors and other healthcare providers can be profound, leading to burnout, anxiety, depression, insomnia, post-traumatic stress disorder and thoughts or acts of suicide.1,12-15 The culture of silence and stigma surrounding medical errors exacerbates the isolation experienced by second victims, inhibiting their ability to seek support and cope with their trauma.1 Fearful of judgment and reprisal, healthcare practitioners may internalise their emotions, suffering in silence as they struggle to come to terms with their role in the adverse event. Left unchecked, this emotional burden can have serious consequences, not only for the well-being of individual healthcare workers but also for the broader healthcare system.
Fear of litigation adds another layer of stress to those already grappling with the emotional fallout of medical errors.10 The pending threat of legal action can exacerbate feelings of guilt and self-doubt, further contributing to the development of second victim syndrome. The legal process, while essential for accountability and justice, becomes a relentless source of stress for healthcare professionals, compounding their trauma and inhibiting their ability to heal. The adversarial nature of litigation pits healthcare providers against patients and plaintiffs, fostering an atmosphere of blame and distrust. In this hostile environment, the human element may be overlooked, as the focus shifts from understanding the complexities of medical practice to assigning culpability. The fear of professional repercussions
looms large, further exacerbating the anguish experienced by second victims. Despite their best intentions and dedication to patient care, healthcare providers find themselves thrust into a legal quagmire, grappling with the profound ramifications of a tragic event. This adversarial process not only adds to the stress and anxiety experienced by healthcare professionals but also challenges their professional integrity and credibility.16
While accountability is paramount in cases of medical negligence, it is imperative to recognise that not all adverse events are the result of substandard care. Medical practice is inherently complex, fraught with uncertainties and variables, often beyond the control of even the most skilled practitioners. As such, attributing blame solely to individuals may fail to acknowledge the systemic factors that contribute to adverse outcomes. Rather than fostering a culture of learning and improvement, the focus on assigning fault stymies efforts to address the root causes of medical errors and prevent future occurrences. To break free from this cycle, it is imperative to adopt a more compassionate and collaborative approach to addressing adverse patient events, one that prioritises the well-being of both patients and providers.
Six stages of recovery from an adverse patient event have been identified in healthcare practitioners.12 These are chaos and accident response, intrusive reflections, restoring personal integrity, enduring the inquisition, obtaining emotional first aid and moving on. In addressing the needs of healthcare practitioners affected by medical errors, interventions focused on psychological support and coping strategies are crucial. Healing involves a multifaceted approach that addresses the emotional, psychological, and professional needs of healthcare practitioners affected by adverse patient events. Several strategies have been proposed including peer support programmes, counselling and mental health services, educational interventions, organisational support, legal and professional support, and mindfulness-based interventions.10,12,17-19 Mindfulness practices have been shown to reduce stress and burnout, enhance emotional resilience and selfcompassion, and improve overall well-being among healthcare professionals.20,21 With its emphasis on present-moment awareness and non-judgmental acceptance, mindfulness may offer a promising avenue for fostering resilience among second victims. By incorporating mindfulness-based interventions into support programmes for second victims, healthcare organisations may help mitigate the psychological impact of medical errors and promote healing among their healthcare practitioners.
In addition to mindfulness-based interventions, addressing the systemic factors contributing to second victim syndrome is crucial. Healthcare organisations must strive to create environments that prioritise patient safety, learning, and improvement over blame and punishment. This includes implementing robust systems for reporting and analysing medical errors, as well as providing comprehensive support services for healthcare practitioners affected by adverse events. By shifting the focus from individual blame to system-level improvement, healthcare organisations
can create a more supportive culture for the well-being of both patients and providers.22
Furthermore, legal reforms may mitigate the fear of litigation that contributes to second victim syndrome. Alternative dispute resolution mechanisms, such as mediation and apology programmes, can offer a more compassionate and efficient approach to resolving medical malpractice disputes. By providing opportunities for open dialogue, reconciliation, and healing, these approaches can help reduce the adversarial nature of medical litigation and promote a culture of transparency and accountability.23,24
Second victim syndrome represents a significant yet often overlooked challenge within the healthcare system. By acknowledging the emotional toll of adverse medical events on healthcare providers and implementing mindful solutions, we can create a more supportive and robust environment for both patients and providers. Working together to foster a culture of compassion, learning, and improvement may create a healthcare system that prioritises the well-being of all.
ORCID
K Outhoff https://orcid.org/0000-0002-0851-4802
References
1. Wu A. Medical error: The second victim. Western Journal of Medicine. 2000;172:358-9. https://doi.org/10.1136/ewjm.172.6.358
2. Marchant-Short S. Adverse events in health care: examining the second victim experience: Memorial University of Newfoundland; 2017.
3. Enahoro QE. Empowering second victims: supporting healthcare professionals after adverse health events. International Journal of Health, Medicine and Nursing Practice. 2024;6(2):52-8. https://doi.org/10.47941/ijhmnp.1718.
4. Bates DW, Levine DM, Salmasian H, et al. The safety of inpatient health care. New England Journal of Medicine. 2023;388(2):142-53. https://doi.org/10.1056/ NEJMsa2206117
5. Insani WN, Whittlesea C, Alwafi H, et al. Prevalence of adverse drug reactions in the primary care setting: A systematic review and meta-analysis. PLoS One. 2021;16(5):e0252161. https://doi.org/10.1371/journal.pone.0252161
6. Soori H. Errors in medical procedures. Errors in Medical Science Investigations: Springer; 2024. p. 205-24. https://doi.org/10.1007/978-981-99-8521-0_11
7. Ozeke O, Ozeke V, Coskun O, Budakoglu II. Second victims in health care: current perspectives. Advances in Medical Education and Practice. 2019;10(null):593603. https://doi.org/10.2147/AMEP.S185912
8. Wu AW, Shapiro J, Harrison R, et al. The impact of adverse events on clinicians: what’s in a name? Journal of Patient Safety. 2020;16(1):65-72. https://doi. org/10.1097/PTS.0000000000000256.
9. Grimm CA. Adverse events in hospitals: A quarter of medicare patients experienced harm in October 2018. Office of Inspector General, I General. 2022;117.
10. Waterman AD, Garbutt J, Hazel E, et al. The emotional impact of medical errors on practicing physicians in the United States and Canada. The Joint Commission Journal on Quality and Patient Safety. 2007;33(8):467-76. https:// doi.org/10.1016/S1553-7250(07)33050-X
11. Busch IM, Moretti F, Campagna I, et al. Promoting the psychological well-being of healthcare providers facing the burden of adverse events: a systematic review of second victim support resources. Int J Environ Res Public Health. 2021;18(10):5080. https://doi.org/10.3390/ijerph18105080
12. Scott SD, Hirschinger LE, Cox KR, et al. The natural history of recovery for the healthcare provider “second victim” after adverse patient events. BMJ Quality & Safety. 2009;18(5):325-30. https://doi.org/10.1136/qshc.2009.032870
13. Whalen A, Collins C. Unmasking the silent struggle: Second Victim Syndrome among surgeons. American Journal of Surgery. 2024. https://doi.org/10.1016/j. amjsurg.2023.11.018
14. Stehman CR, Testo Z, Gershaw RS, Kellogg AR. Burnout, drop out, suicide: physician loss in emergency medicine, part I. West J Emerg Med. 2019;20(3):485. https://doi.org/10.5811/westjem.2019.4.40970
15. Li CJ, Shah YB, Harness ED, Goldberg ZN, Nash DB. Physician burnout and medical errors: exploring the relationship, cost, and solutions. Am J Med Qual. 2023;38(4):196-202. https://doi.org/10.1097/JMQ.0000000000000131
16. Vincent C, Young M, Phillips A. Why do people sue doctors? A study of patients and relatives taking legal action. Obstet Gynecol Surv. 1995;50(2):103-5. https:// doi.org/10.1097/00006254-199502000-00012.
17. Seys D, Wu AW, Gerven EV, et al. Health care professionals as second victims after adverse events: a systematic review. Eval Health Prof. 2013;36(2):135-62. https://doi.org/10.1177/0163278712458918
18. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516-29. https://doi. org/10.1111/joim.12752
19. Edrees HH, Paine LA, Feroli ER, Wu AW. Health care workers as second victims of medical errors. Pol Arch Med Wewn. 2011;121(4):101-8. https://doi.org/10.20452/ pamw.1033
20. Irving JA, Dobkin PL, Park J. Cultivating mindfulness in health care professionals: A review of empirical studies of mindfulness-based stress reduction (MBSR). Complement Ther Clin Pract. 2009;15(2):61-6. https://doi.org/10.1016/j. ctcp.2009.01.002
21. S Miller C, Scott SD, Beck M. Second victims and mindfulness: A systematic review. Journal of Patient Safety and Risk Management. 2019;24(3):108-17. https://doi.org/10.1177/2516043519838176
22. Chong RIH, Yaow CYL, Chong NZ, et al. Scoping review of the second victim syndrome among surgeons: Understanding the impact, responses, and support systems. Am J Surg. 2024;229:5-14. https://doi.org/10.1016/j. amjsurg.2023.09.045
23. Nwedamutsu T. Alternative dispute resolution in medical malpractice in South Africa. University of the Western Cape Library Services. 2020.
24. Yeh PH, Shen RN, Huang YY, Chen WW. A study on alternative medical malpractice dispute resolution in Japan-Focusing on non-governmental organization ADR. Angle Health Law Review. 2020;50:143-62.
S Afr Gen Pract 2024;5(2):58-62
https://doi.org/10.36303/SAGP.0597
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0]
http://creativecommons.org/licenses/by-nc-nd/4.0
Direct oral anticoagulants: the available agents and practical considerations
B Jordaan,1 S Louw2
1 Department of Pharmacology, University of Pretoria, South Africa
2 Department of Molecular Medicine and Haematology, University of the Witwatersrand and the National Health Laboratory Service, South Africa
Thrombosis remains one of the leading causes of death in the world, and South Africa is no exception. In addition, as the population across the globe is ageing, the burden of stroke due to cardiovascular disease and atrial fibrillation (AF) is proliferating exponentially. Infection with HIV, which is prevalent in Africa, contributes significantly to the risk of both venous and arterial thrombosis. Anticoagulation can prevent thrombotic events but careful consideration of the choice of drug is needed to ensure efficacy and safety in the multifaceted anticoagulation drug arena. Although warfarin is still widely used, the direct oral anticoagulants (DOACs) are becoming the agents of choice for acute and chronic anticoagulation. The DOACs are a group of individual drugs, and choice of agent, and even dose, will depend on therapeutic indication, renal and liver function, age, body weight, comorbidities, previous medical history and concomitant medication. In this article the key pharmacological characteristics, indications and contraindications of the available DOACs in South Africa are summarised with the aim to assist with choosing the right anticoagulant, for the right patient, at the right dose, for the right duration.
Keywords: direct oral anticoagulants (DOACs), warfarin, apixaban, dabigatran, rivaroxaban, dosage, body mass index, missed dose, renal function, hepatic function, bleeding, drug reversal
Globally, as well as in South Africa, one of the major cardiovascular diseases is venous thromboembolic disease (VTED) but despite the high burden of VTED, approximately a quarter of at-risk patients remain without prophylaxis.¹ The World Health Organization (WHO) further estimates that, in approximately six years, one in six people in both developing and developed countries will be over the age of 60 years with increased cardiovascular disease (CVD) risks.² Furthermore, stroke incidence has more than doubled in low- to middleincome countries in the last four decades, due to aggregating risk factors, including hypertension and AF, both of which are especially prevalent in Africa.³,⁴
For many patients with VTED events and AF, warfarin remains the anticoagulant of choice and healthcare professionals are well versed with the international normalised ratio (INR) for anticoagulation monitoring. Warfarin, however, has numerous drug and food interactions with slow on- and off-set of action and unpredictability of activity.⁵-⁸ These shortcomings in part motivated the development of the direct oral anticoagulants (DOACs). The currently available DOACs in South Africa are apixaban and rivaroxaban (direct factor-Xa inhibitors) and dabigatran (direct factor-IIa [thrombin] inhibitor).² The DOACs have more predictable pharmacological properties versus warfarin⁵-⁸ and routine anticoagulation activity monitoring is currently not advocated, although the results of ongoing research are awaited.⁹ The quick on- and off-set of actions of the DOACs are further advantages.⁵-⁸
DOACs mode of action
Apixaban and rivaroxaban prevent thrombin generation and thrombus development by directly inhibiting coagulation factor Xa (FXa). Activation of FX to FXa is pivotal in thrombus formation as FXa, together with factor Va (FVa), converts prothrombin to thrombin. This reaction leads to fibrin clot formation and activation of platelets. One molecule of FXa is able to generate more than 1 000 molecules of thrombin due to amplification in the coagulation cascade. In addition, the FXa activity is increased 300 000-fold when it binds to FVa resulting in an explosive burst of thrombin. Selective inhibitors of FXa, such as apixaban and rivaroxaban, terminate this augmented thrombin burst.10,11
Dabigatran is a direct thrombin inhibitor. Thrombin converts fibrinogen to fibrin, which is blood clot. The inhibition of thrombin therefore prevents the development of thrombus. Dabigatran inhibits free thrombin, fibrin-bound thrombin and also inhibits thrombin-induced platelet activation and aggregation.¹²
The indications, dosages and prescription considerations of the DOACs registered in South Africa are provided in Table I.¹⁰-¹²
The use of DOACs in elderly patients
The major concerns with DOAC use in elderly patients is renal dysfunction, which necessitates DOAC dose adjustments (Table II), as well as concomitant medications.
Apixaban
No routine dosage adjustment is required in elderly patients on apixaban therapy but in patients with at least two of the following characteristics, the dose should be decreased to
Table I: Indications, dosage and prescription considerations of the direct oral anticoagulants (DOACs) registered in South Africa¹⁰¯¹²
Treatment of DVT and PE and prevention of recurrent DVT and PE
Prevention of SPAF
Prevention of VTED after elective hip or knee replacement surgery
Treatment of DVT and PE and prevention of recurrent DVT and PE
Prevention of SPAF
Prevention of VTED after elective hip or knee replacement surgery
Treatment of DVT and PE and prevention of recurrent DVT and PE
Prevention of SPAF
Prevention of VTED after elective hip or knee replacement surgery
Registered indications
• 15 mg twice dly for 3 weeks after the acute event, then 20 mg dly
• 20 mg dly
• 10 mg dly starting 6–10 hrs after surgery
• In actively bleeding patient: delay therapy
• 150 mg twice dly after a parenteral anti-coagulant for at least 5 days after the acute event
• 150 mg dly
• 110 mg 1–4 hrs after surgery then 220 mg dly
• In actively bleeding patient: delay therapy
• 10 mg twice dly for 7 days after the acute event, then 5 mg twice dly
• 5 mg twice dly
• 2,5 mg twice dly starting 12–24 hrs after surgery
Dosage
• 36 months
* >6 months for patients with ongoing VTED risk
• Continue as long as risk for SPAF persists
• Hip surgery: 5 weeks
• Knee surgery: 2 weeks
• 3–6 months
• *>6 months for patients with ongoing VTED risk
• Continue as long as risk for SPAF persists
• If treatment not started on day of surgery: initiate with 220 mg daily
• 2.5 mg twice dly after at least 6 months of treatment for DVT or PE for prevention in patients with ongoing VTED risk
• In actively bleeding patient: delay therapy
• Hip surgery: 28 days
• Knee surgery: 10 days
• 10 mg: taken with or without food
• 15 and 20 mg: taken with food
• 2–4 hrs
• 9–13 hrs
• Taken with or without food with a full glass of water
• Do not open the capsule
• Taken with a meal and/or proton pump inhibitor if gastrointestinal symptoms develop
• 2–3 hrs
• 12–13 hrs
• 3-6 months
• *>6 months for patients with ongoing VTED risk
• Continue as long as risk for SPAF persists
• Hip surgery: 32–38 days
Treatment duration
• Knee surgery: 10–14 days
2,5 mg twice daily as opposed to 5 mg twice daily:¹⁰
• age ≥ 80 years
• body weight ≤ 60 kg
• serum creatinine ≥ 1,5 mg/dL (133 µmol/L)
Dabigatran
• Taken with or without food
Administration
• 1 hr
Peak effect
• 10–14 hrs
Effective half-life
VTED, venous thromboembolic disease; SPAF, stroke and systemic embolism prevention in non-valvular atrial fibrillation; DVT; deep vein thrombosis; dly, daily; hrs, hours; *ongoing treatment duration must be individualised.
Dabigatran is 80% renally excreted, and renal impairment is common in the elderly (i.e. > 75 years of age) and therefore kidney function should be assessed prior to therapy initiation and annually thereafter, in this group of patients.¹²
Rivaroxaban
Decreased renal function can result in rivaroxaban accumulation and bleeding and should therefore, be used with caution in patients with renal impairment (CrCl < 50 ml/min).¹¹
The use of DOACs at extremes of body mass index (BMI)
According to the registered package inserts of the DOACs, no routine dose adjustment is required based on body weight.¹⁰-¹²
According to Stats SA, in 2016 more than 30% of men and more than 60% of women were overweight or obese in South Africa.¹³ Obesity is a risk factor for arterial and venous thromboses. Previously, there were concerns regarding sub-therapeutic DOAC levels in patients weighing over 120 kg.¹⁴ New data on DOAC activity in overweight or obese patients published as a meta-analysis of 89 494 patients (45 427 on DOAC and 44 067 on warfarin therapy) indicates that DOACs at standard doses are effective and safe when compared with warfarin in morbidly obese patients.¹⁵ The International Society on Thrombosis and Haemostasis (ISTH) also published recommendations supporting the use of standard dose apixaban and rivaroxaban in patients weighing more than 120 kg.¹⁶ For patients between 120–150 kg, for SPAF or treatment of VTE, the National Health Scotland: Greater Glasgow and Clyde (NHSGGC) Drug and Therapeutics Committee consensus also supports standard dose apixaban. This recommendation is based on phase 4 post-marketing experience, but the
Dabigatran
Rivaroxaban
guidance does recommend for individualisation in patients >150 kg.¹⁷
The use of DOACs in patients with renal impairment
The percentage renal excretion of the DOACs is provided below:¹⁰-¹²
• Apixaban: 25%
• Dabigatran: 80%
• Rivaroxaban: 66%
According to the South African medicine, registration the use of dabigatran in patients with severe renal impairment (creatinine clearance [CrCl] < 30 mL/min) is contraindicated.¹² Rivaroxaban should be used with caution in patients with severe renal impairment (CrCl 15–30 mL/min).¹¹
However, various guidelines and reviews have recently been published with regards to DOAC dose adjustment in patients with renal dysfunction.¹⁸-²³ The recent guidelines from the American Heart Association (AHA) regarding DOAC dosing according to renal function is detailed in Table II.²⁴
The use of DOACs in patients with hepatic impairment
Since hepatic breakdown of drugs has an effect on the duration of drug activity, hepatic function is of importance especially in the prescription of anticoagulant drugs such as DOACs (Table III).
DOACs drug-drug interactions24
Care should be taken if patients on DOAC treatment are treated concomitantly with drugs such as antiplatelet agents (e.g. Aspirin) and nonsteroidal anti-inflammatories (NSAIDs).
In addition, apixaban and rivaroxaban should be administered with caution in patients receiving concomitant strong inhibitors of both Cytochrome 3A4 and P-glycoprotein, such as azole antifungals (e.g. ketoconazole, itraconazole, voriconazole and posaconazole), antiretrovirals (ARVs) for infection with human immunodeficiency virus (HIV) such as protease inhibitors (e.g. ritonavir), and additional drugs, including rifampicin, phenytoin, carbamazepine, phenobarbitone and St. John’s Wort
(Hypericumperforatum) as the anticoagulant action of these DOACs can be increased with these concomitant drugs.¹⁰
Dabigatran is not metabolised by the cytochrome P450 system, therefore, related interactions with, e.g. atorvastatin, diclofenac, rifampicin, carbamazepine or St. John’s Wort are not expected with dabigatran.¹²
DOACs missed dose¹⁰-¹²
If a dose is missed, the prescribed DOAC should be taken when patient remembers the omission and continue with the once or twice daily intake the next day. The dose should, however, not be doubled within the same day (24 hours) to make up for a missed dose.
For dabigatran, a missed dose may still be taken up to six hours prior to the next scheduled dose. From six hours onward prior to the next scheduled dose, the missed dose should be omitted. Patients should not take a double dose to make up for missed individual doses.¹²
DOACs
bleeding and reversal agents¹⁰-¹²
Idarucizumab, a specific reversal for dabigatran, is available in South Africa.¹² No specific reversal agents for apixaban and rivaroxaban is currently available in South Africa.¹⁰-¹² Should active haemorrhage occur, for instance during elective surgery, or invasive procedures that place patients at an increased risk of bleeding, apixaban or rivaroxaban should be delayed or discontinued as appropriate. The following supportive treatments are suggested: local compression (where possible), surgical intervention, fluid replacement and haemodynamic support (blood product or component transfusion). For lifethreatening bleeding that cannot be controlled with these measures, administration of a specific procoagulant reversal agent should be considered, such as prothrombin complex concentrate (PCC), activated prothrombin complex concentrate (APCC) or recombinant factor VIIa (r-FVIIa). However, there is currently very limited clinical experience with the use of these products in individuals receiving apixaban and rivaroxaban.¹⁰-¹² Administering activated charcoal can be considered.⁷ Dabigatran is dialysable because of its low plasma protein binding.¹²
Table III: DOAC therapy in patients with hepatic impairment²⁴
(Child Pugh Score)
Table II: American Heart Association (AHA) guidelines on DOAC dosing according to renal function²⁴
Conclusion
Thrombosis, including VTED and stroke, remains a leading cause of death in South Africa. DOACs as a therapeutic class of anticoagulants has become indispensable as substitute for warfarin for both prophylaxis and treatment. Additional trials and real-life post-marketing data will be included in DOAC treatment guidelines to improve patient outcomes.
ORCID
12. Pradaxa registered package insert, South Africa. Available from: https://pi-pilrepository.sahpra.org.za/wp-content/uploads/2022/08/pi-pradaxa-17aug2022. pdf.
13. National Department of Health, Statistics South Africa, South African Medical Research Council, and ICF. South Africa Demographic and Health Survey 2016: Key findings. Pretoria, South Africa, and Rockville, Md, USA: NDoH, Stats SA, SAMRC, and ICF, 2018. https://www.dhsprogram.com/pubs/pdf/SR248/SR248. pdf. Accessed 6 May 2024.
14. Martin K, Beyer-Westendorf MK, Davidson J, et al. Use of the direct oral anticoagulants in obese patients: guidance from the SCC of the ISTH. J Thromb Haemost. 2016.14(6):1308-1313. https://doi.org/10.1111/jth.13323
B Jordaan https://orcid.org/0009-0007-4921-4519
S Louw https://orcid.org.0000-0002-4315-1496
References
1. Danwang C, Temgoua MN, Agbor VN, Tankeu AE, Noubiap JJ. Epidemiology of venous thromboembolism in Africa: a systematic review. J Thromb Haemost. 2017;15:1770-81. https://doi.org/10.1111/jth.13769
2. World Health Organization. Fact Sheet - Ageing and health: World Health Organization, 2022. Available from: https://www.who.int/news-room/ fact-sheets/detail/ageing-and-health. Accessed 30 April 2024.
3. Pillay SC, Redant R, Umuneza N, et al. Factors affecting length of hospital stay in stroke survivors in South Africa: A call for a stroke unit. African Journal of Disability. 2022:11(0),a1065. https://doi.org/10.4102/ajod.v11i0.1065.
4. Smythe T, Inglis-Jassiem, G, Conradie T, et al. Access to health care for people with stroke in South Africa: a qualitative study of community perspectives. BMC Health Services Research. 2022;22:464. https://doi.org/10.1186/ s12913-022-07903-9
5. Semakula JR, Kisa G, Mouton JP, et al. Anticoagulation in sub-Saharan Africa: Are direct oral anticoagulants the answer? A review of lessons learnt from warfarin. Brit Jnl Clinical Pharma.2021;87:3699-3705. https://doi.org/10.1111/bcp.14796
6. Konstantinos NA, Hylek EM. Evidence gaps in the era of non-vitamin k oral anticoagulants. Journal of the American Heart Association. 2018;7(3):e007338. https://doi.org/10.1161/JAHA.117.007338.
7. Brouwer N, Mannaru K, Louw S. Monitoring, problems and pitfalls. Laboratory Medicine - Anticoagulation. The Specialist Forum. 2015;15(3):18,20.
8. Chen A, Stecker E, Warden BA. Direct oral anticoagulant use: a practical guide to common clinical challenges. J Am Heart Assoc. 2020;9(13):e017559. https://doi. org/10.1161/JAHA.120.017559
9. Beyer-Westendorf J, Köhler C. Direct oral anticoagulants: laboratory challenges and antidotes. Hamostaseologie. 2023;43:37-43. https://doi. org/10.1055/a-1987-3559
10. Eliquis registered package insert, South Africa. Available from: https://labeling. pfizer.com/ShowLabeling.aspx?id=10756.
11. Xarelto registered package insert, South Africa. Available from: https:// health4all.bayer.co.za/sites/g/files/vrxlpx21741/files/2021-06/16904%20XRL%20 PRESCRIBER_GUIDE_A5%20v4%20HR.pdf.
15. Mohammed M, Azizullah B, Ahmad AA, et al. Direct oral anticoagulants versus warfarin in morbidly obese patients with nonvalvular atrial fibrillation: a systematic review and meta-analysis. American Journal of Therapeutics. 2021;28(5):e531-e539. https://doi.org/10.1097/MJT.0000000000001403
16. Martin KA. Recommendations and guidelines. Use of direct oral anticoagulants in patients with obesity for treatment and prevention of venous thromboembolism: Updated communication from the ISTH SSC Subcommittee on Control of Anticoagulation. J Thromb Haemost. 2021;19:1874-1882. https:// doi.org/10.1111/jth.15358
17. NHS Greater Glasgow and Clyde Drug and Therapeutics Committee. Scotland, UK. DOAC prescribing and body weight. Published 1/5/2024. https:// ggcmedicines.org.uk/blog/medicines-update/doac-prescribing-and-bodyweight/. Accessed 6th May 2024.
18. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603. https://doi.org/10.1183/13993003.01647-2019.
19. Ortel TL, Neumann I, Ageno W, et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020;4(19):4693-738. https://doi.org/10.1182/bloodadvances.2020001830.
20. Weitz JI, Raskob GE, Spyropoulos AC, et al. Thromboprophylaxis with rivaroxaban in acutely ill medical patients with renal impairment: insights from the MAGELLAN and MARINER trials. Thromb Haemost. 2020;120(3):515-24. https:// doi.org/10.1055/s-0039-1701009
21. Yamashita Y, Morimoto T, Kimura T. Venous thromboembolism: Recent advancement and future perspective. J Cardiol. 2022;79(1):79-89. https://doi. org/10.1016/j.jjcc.2021.08.026
22. MacDougall K, Spyropoulos AC. Prevention of venous thromboembolism in acutely ill medical patients: a new era. Semin Respir Crit Care Med. 2021;42(2):308-15. https://doi.org/10.1055/s-0041-1723018
23. Martin KA, Beyer-Westendorf J, Davidson BL, et al. Use of direct oral anticoagulants in patients with obesity for treatment and prevention of venous thromboembolism: Updated communication from the ISTH SSC Subcommittee on Control of Anticoagulation. J Thromb Haemost. 2021;19(8):1874-82. https:// doi.org/10.1111/jth.15358
24. Joglar JA, Chungh MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS Guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2023;149(1).
S Afr Gen Pract 2024;5(2):63-71
https://doi.org/10.1007/s0034 5-020-03517-0
Open Access article distributed under the terms of the
Creative Commons License [CC BY-NC-ND 4.0]
http://creativecommons.org/licenses/by-nc-nd/4.0
Impact of early vs. delayed initiation of dutasteride/tamsulosin combination therapy on the risk of acute urinary retention or BPH‑related surgery in LUTS/ BPH patients with moderate‑to‑severe symptoms at risk of disease progression
S
D’Agate,1 C Chavan,2 M Manyak,3 JM Palacios‑Moreno,⁴ M
Oelke,⁵
MC Michel,⁶ CG Roehrborn,⁷ OD Pasqua1,8
1 Clinical Pharmacology and Therapeutics Group, University College London, BMA House, Tavistock Square, London WC1H 9JP, UK
2 Global Medical Urology, GlaxoSmithKline, Mumbai, India
3 Global Medical Urology, GlaxoSmithKline, Philadelphia, USA
⁴ Global Medical Urology, GlaxoSmithKline, Tres Cantos, Spain
⁵ Department of Urology, St. Antonius Hospital, Gronau, Germany
⁶ Department of Pharmacology, Johannes Gutenberg University, Mainz, Germany
⁷ Department of Urology, Texas Southwestern Medical Center, Dallas, TX, USA
⁸ Clinical Pharmacology Modelling and Simulation, GlaxoSmithKline, 980 Great West Rd, London TW8 9GS, UK
Corresponding author, email: odp72514@gsk.com
Purpose: To evaluate the effect of delayed start of combination therapy (CT) with dutasteride 0.5 mg and tamsulosin 0.4 mg on the risk of acute urinary retention or benign prostatic hyperplasia (BPH)-related surgery (AUR/S) in patients with moderate-to-severe lower urinary tract symptoms (LUTS) at risk of disease progression.
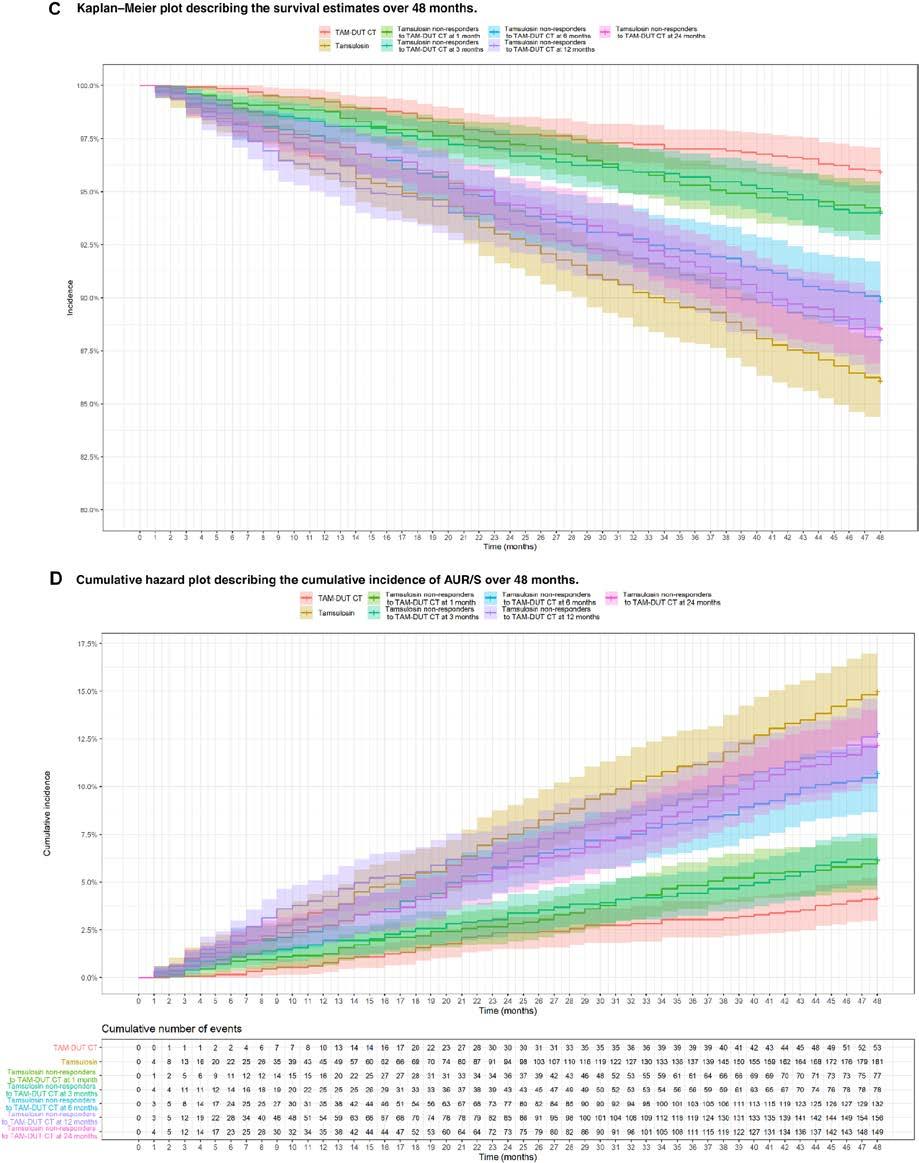
Methods: Using a time-to-event model based on pooled data from 10,238 patients from Phase III/IV dutasteride trials, clinical trial simulations (CTS) were performed to assess the risk of AUR/S up to 48 months in moderate-to-severe LUTS/ BPH patients following immediate and delayed start of CT for those not responding to tamsulosin monotherapy. Simulation scenarios (1 300 subjects/arm) were investigated, including immediate start (reference) and alternative delayed start (six scenarios 1–24 months). AUR/S incidence was described by Kaplan–Meier survival curves and analysed using log-rank test. The cumulative incidence of events as well as the relative and attributable risks were summarised stratified by treatment.
Results: Survival curves for patients starting CT at month 1 and 3 did not differ from those who initiated CT immediately. By contrast, significant differences (p < 0.001) were observed when switch to CT occurs ≥ 6 months from the initial treatment. At month 48, AUR/S incidence was 4.6% vs 9.5%, 11.0% and 11.3% in patients receiving immediate CT vs. switchers after 6, 12 and 24 months, respectively.
Conclusions: Start of CT before month 6 appears to significantly reduce the risk of AUR/S compared with delayed start by ≥ 6 months. This has implications for the treatment algorithm for men with LUTS/BPH at risk of disease progression.
Republished with permission: World Journal of Urology (2021) 39:2635–2643. https://doi.org/10.1007/s00345-020-03517-0
Introduction
Management of bothersome lower urinary tract symptoms (LUTS) constitutes the main focus of therapeutic interventions, including those patients who have confirmed diagnosis of benign prostatic hyperplasia (BPH).1 However, in patients at risk of disease progression, clinical deterioration is observed over time, with increasing LUTS severity (IPSS), reduction in maximum urine flow rate (Qmax), episodes of acute urinary retention (AUR), or the need for BPH‐related surgery.2,3 Currently, LUTS/ BPH management considers conservative, pharmacological and surgical treatments.1 Specifically, on pharmacological treatment for men with moderate or severe LUTS at increased risk of disease progression, i.e. higher prostate volume, higher PSA concentration, advanced age, higher PVR, lower Qmax, etc., the initial treatment of choice is a 5α-reductase inhibitor (5ARI) with or without an α-adrenoreceptor antagonist (α-blocker) or a
phosphodiesterase 5 inhibitor (PDE5I).1,4 In some cases, patients experiencing failure of pharmacological treatment or symptom deterioration may require minimally invasive or surgical procedures.5,6
While epidemiological data show that LUTS/BPH patients at risk of disease progression represent a significant proportion of the overall patient population,7 clinicians continue to use α-blocker monotherapy as a first-line treatment option to primarily manage LUTS/BPH symptoms, irrespective of the underlying rate of disease progression. Such a practice appears to contrast with robust evidence and current guidelines that support the use of combination therapy (CT) of α-blocker and 5ARI for LUTS/BPH patients with moderate or severe symptoms at risk of disease progression.1 The pharmacological basis for the use of CT relies on the fact that in addition to the effects of α-blockers on contractile properties of prostate smooth muscle, 5ARI
Impact
effectively reduces the serum and intraprostatic concentration of dihydrotestosterone, causing an involution of prostate tissue. These changes ultimately lead to a reduction in the long-term risk of AUR or BPH-related surgery (AUR/S) in patients at risk of disease progression.8
Different arguments have been identified for the underuse of CT of α-blocker and 5ARI at the time of diagnosis, in particular the effects of 5ARIs on sexual9,10 and mental function.11 Yet, there is limited awareness of the fact that the impact of CT of α-blocker and 5ARI on sexual function is primarily driven by changes in the ejaculation domain and modest impairment in the satisfaction, sexual activity and sexual desire domains, which are unlikely to be of clinical relevance.12,13 In addition, the use of α-blocker monotherapy as a first-line treatment underestimates long-term adverse outcomes, including higher incidence of AUR and prostate-related surgery, abnormal ejaculation and intraoperative floppy iris syndrome.14,15
Clinical evidence suggests that the delay in initiating a 5ARI may be associated with an increased likelihood of AUR and surgery.16–18 However, there are no accurate estimates of the effect of such a delay due to confounding factors and differences in medical practice.19,20 Recently, D’Agate and colleagues have shown the long-term effects of delayed onset of dutasteride and tamsulosin CT using clinical trial simulations (CTS).21 Their work reveals statistically significant differences in the proportion of patients who achieved clinical response (≥ 25% IPSS reduction relative to baseline) when switching from tamsulosin monotherapy at 6 months or later (79.7% vs. 74.1%, p < 0.001). Overall, these results support current guidelines recommendations to start CT of α-blocker and 5ARI in men who have moderate- to-severe LUTS and are at risk of disease progression. They also reflect the disease-modifying properties of 5ARIs and reinforce the importance of slowing down or even reverse disease progression.22,23
Here, we apply CTS to evaluate the effect of delaying the start of treatment with dutasteride and tamsulosin CT in patients with moderate or severe LUTS/BPH at risk of disease progression. Using a cohort of patients with baseline characteristics comparable to those enrolled in previous clinical trials, the incidence and time to first episode of acute urinary retention or BPH-related surgery (AUR/S) was assessed for a range of scenarios, including immediate and delayed initiation of treatment with CT. The analysis is based on a time-to-event (TTE) model that describes the time to first AUR/S, taking into account the potential effect of baseline covariate factors.24
Patients and methods
Data source
The baseline clinical and demographic data used in the CTS were obtained from six clinical trials (ARIA3001, ARIA3002, ARI40002, CombAT, CONDUCT and ARIB3003). The selection of these studies was based on the fact that protocols shared similar definitions of clinical events (i.e. AUR/S), patients had comparable medical history and study data included individual level information for
LUTS/BPH patients with moderate or severe LUTS (see Tables S1, S2 and S3 for details). In addition, CombAT and CONDUCT reflect current clinical guidelines1 for the treatment of LUTS/BPH patients.
Clinical trial simulations
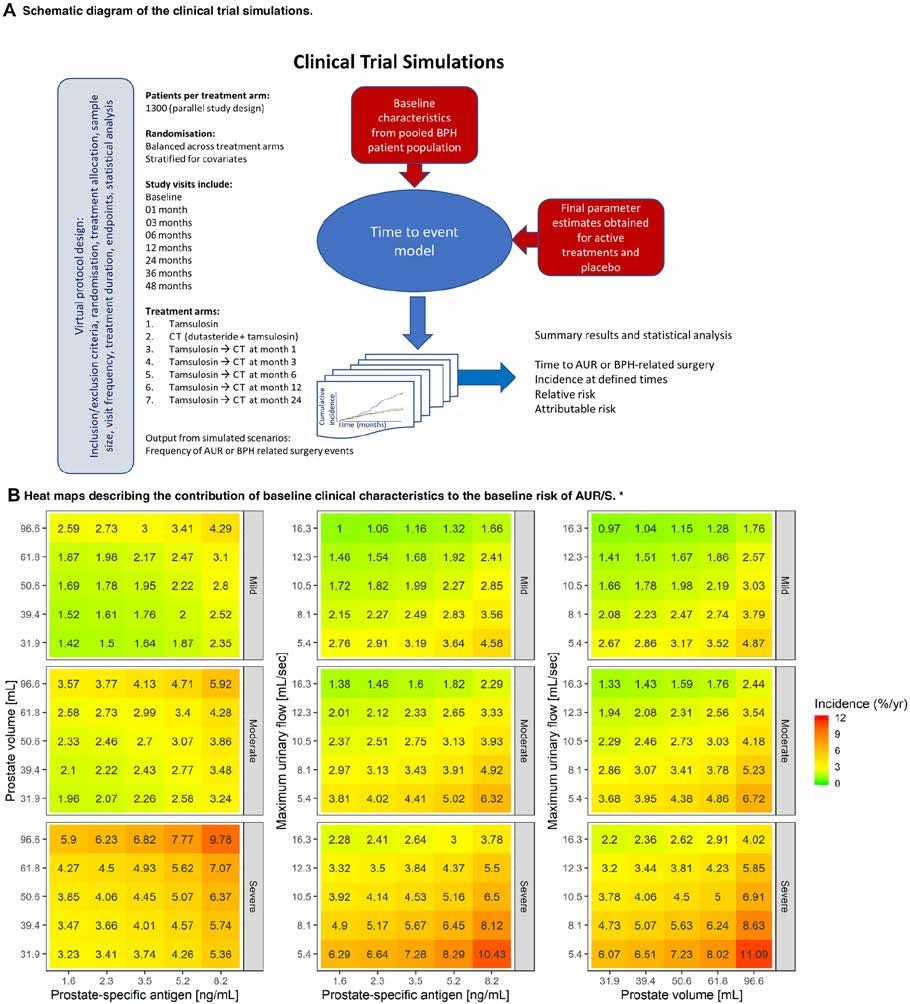
Final parameters of the TTE model previously developed by D’Agate et al.24 (Table S4) were used for the implementation of the simulation scenarios, which assess the potential implications of the delayed start of treatment with dutasteride and tamsulosin CT. Transition to CT was based on symptom improvement less than 25% or deterioration, as assessed by changes in IPSS relative to baseline.21 Only non-responders to tamsulosin, i.e. patients who showed a change in IPSS < 25% from baseline after the initial treatment, were assigned to CT. From a pharmacological perspective, these scenarios represent the effect of a drug with symptomatic properties (i.e. tamsulosin) prior to the addition of a drug with disease-modifying properties (i.e. dutasteride). The CTS results were subsequently analysed using Kaplan–Meier survival curves and log-rank test. An outline of the clinical trial simulation workflow is shown in Figure 1a. Additional details of each simulation scenario and protocol design characteristics are summarised in Table S5.
Results
Figure 1b shows the contribution of demographic and clinical baseline characteristics to the risk of AUR/BPH-related surgery at onset of treatment. An overview of the baseline characteristics of patients included in each treatment arm is presented in Table S6.
Effect of early vs. delayed onset of treatment with dutasteride and tamsulosin CT
The simulated scenarios reveal the effect of delayed onset of treatment with CT on the risk of AUR/S. Having taken into account the contribution of baseline characteristics, no other factor than the delayed onset of treatment with CT was identified, which explains the increased risk in patients switching from tamsulosin after 6, 12, or 24 months. The number of subject switching to CT at the different visits is summarised in Table I, along with the number of events at the end of the study and 90% CIs from ten trial replicates. The relative and attributable risks are also shown for each treatment arm, with tamsulosin and dutasteride CT as reference arm. These results are complemented by estimates for a single trial replicate (Table S7).
Figure 1c shows the Kaplan–Meier survival curves in each treatment scenario. The different curves indicate that switching treatment from tamsulosin to CT at 6 months or later from the start of treatment has a significant effect on the proportion of events at completion of the study at month 48. As summarised in Figure 1d, the impact of the delayed onset of treatment with CT is also reflected in the cumulative hazard plot. Along with it, the figure shows the cumulative number of events for each treatment scenario.
CombAT INCONVENIENCE
INDICATED FOR THE TREATMENT OF MODERATE TO SEVERE SYMPTOMS OF BENIGN PROSTATIC HYPERPLASIA (BPH)
The 4-year CombAT study provides support for the long-term use of dutasteride and tamsulosin combination therapy in men with moderate to severe LUTS* due to BPH and prostatic enlargement1 *LUTS – Lower urinary tract symptoms
Fig. 1 Overview of the steps for the implementation of the clinical trial simulation scenarios, covariate factors affecting baseline risk of AUR/S and main findings. a Schematic diagram of the clinical trial simulations based on a hazard model describing the time to first AUR/S. b Heat maps illustrating the contribution of baseline clinical characteristics to the baseline risk of AUR/S. * Whilst heat maps allow visualisation of the effect of the interaction between some baseline characteristics, an assessment of the baseline risk of AUR/S for individual patients, which takes into account all these factors concurrently (i.e. IPSS, PSA, PV and Qmax) requires the use of the TTE model (Table S4). Even though each panel shows scales that include mild IPSS symptoms scores and normal ranges for the other baseline characteristics, defining a patient at risk of disease progression implies not only the resulting contribution of all these covariates, but also other factors than the risk of AUR/S. c Kaplan–Meier plot describing the survival estimates over 48 months stratified by treatment arm. Survival
(y-axis) indicates the proportion of patients who have not had an event; at time zero the survival is 100% (i.e. no patient has experienced an AUR/S). The solid lines describe the predicted median time to first AUR/S over the period of 48 months across the different treatment arms. Shaded areas show 95% confidence intervals. The number of patients in each cohort is summarised in Table S4. d Cumulative hazard plot describing the cumulative incidence of AUR/S over 48 months stratified by treatment arm. Cumulative incidence of AUR/S across different treatment arms. Lines represent the median cumulative incidence of AUR/S over time. Shaded areas show the 95% confidence intervals. The table below the panel shows the cumulative number of events over time. The number of patients in each cohort is summarised in Table S4. TAM-DUT CT: tamsulosin and dutasteride combination therapy
Figure 1: Overview of the steps for the implementation of the clinical trial simulation scenarios, covariate factors affecting baseline risk of AUR/S and main findings. a Schematic diagram of the clinical trial simulations based on a hazard model describing the time to first AUR/S. b Heat maps illustrating the contribution of baseline clinical characteristics to the base- line risk of AUR/S. * Whilst heat maps allow visualisation of the effect of the interaction between some baseline characteristics, an assessment of the baseline risk of AUR/S for individual patients, which takes into account all these factors concurrently (i.e. IPSS, PSA, PV and Qmax) requires the use of the TTE model (Table S4). Even though each panel shows scales that include mild IPSS symptoms scores and normal ranges for the other baseline characteristics, defining a patient at risk of disease progression implies not only the resulting contribution of all these covariates, but also other factors than the risk of AUR/S. c Kaplan–Meier plot describing the survival estimates over 48 months stratified by treatment arm. Survival (y-axis) indicates the proportion of patients who have not had an event; at time zero the survival is 100% (i.e. no patient has experienced an AUR/S). The solid lines describe the predicted median time to first AUR/S over the period of 48 months across the different treatment arms. Shaded areas show 95% confidence intervals. The number of patients in each cohort is summarised in Table S4. d Cumulative hazard plot describing the cumu- lative incidence of AUR/S over 48 months stratified by treatment arm. Cumulative incidence of AUR/S across different treatment arms. Lines represent the median cumulative incidence of AUR/S over time. Shaded areas show the 95% confidence intervals. The table below the panel shows the cumulative number of events over time. The number of patients in each cohort is summarised in Table S4. TAM-DUT CT: tamsulosin and dutasteride combination therapy
Impact of early vs. delayed initiation of dutasteride/tamsulosin combination therapy on the risk of acute urinary retention
Discussion
Currently, LUTS/BPH management considers conservative, pharmacological and surgical treatments. The strength of each recommendation is determined by the balance between desirable and undesirable consequences of alternative management strategies and the quality of the evidence. Whilst guidelines are available, the choice of treatment should be reached in a shared decision-making process between the physician and patient.1,25,26
Specifically, for men with moderate or severe LUTS at risk of disease progression, 5ARI with an α-blocker is an initial treatment of choice recommended by clinical guidelines.1 Nevertheless, in clinical practice patients with moderate or severe LUTS at risk of disease progression continue to be treated initially with only an α-blocker.27 Little attention has been given to the impact of variable disease progression rates on LUTS deterioration and subsequent implications for the risk of AUR/S following delayed initiation of 5ARIs.28,29
Fig. 1 (continued)
Figure 1 (continued)
Table I: Proportion of patients who switch to combination therapy and summary of the results from 10 clinical trial replicates for the different treatment arms
Treatment duration Transition to CT
Start of treatment 0
01 month
1272 (1269, 1280)
03 months 1111 (1102, 1139)
06 months 716 (700, 753)
12 months
24 months
(424, 472)
(395, 439)
36 months 0
48 months 0
Treatment arm
Upper panel: Overview of the patient population that switches to combination therapy (CT) due to non-response to tamsulosin monotherapy, as defined by a change in IPSS < 25% relative to baseline. Lower panel: number of events, incidence, relative risk, attributable risk and time to comparable progression for 10 trial replicates. Results are shown as medians (90%-confidence intervals)
*p < 0.001 log-rank test on survival curve; Bonferroni-corrected α = 0.0083
aTime at which the incidence of AUR/S is comparable to that observed at 48 months after immediate start of treatment with tamsulosin and dutasteride CT
Even though the risk and incidence of complications may vary due to the contribution of different risk factors, AUR, which often presents as an emergency, remains an important complication for patients at risk of disease progression with financial, emotional and health-related consequences.30,31 On the other hand, BPHrelated surgery is primarily a consequence of the perceived severity of the condition. In fact, irrespective of considerable variation between studies in the reported incidence of AUR in male patients, AUR results in prostatectomy in only 24–42% of men,28 while those who avoid surgery through a successful trial without catheter were found to be at high risk of requiring surgery within a year.29
The benefits of CT of α-blocker and 5ARI for this group of patients have been evaluated extensively in different investigations, which have also shown a statistically significant reduction in the incidence of AUR/S.32,33 These findings are further supported by a large retrospective study, which identified that patients who received dutasteride following a urologist referral had a lower risk of BPH-related prostate surgery than those treated with finasteride.30 In line with the aforementioned findings, the results from our simulations indicate that tamsulosin does not reduce the risk of AUR/S, and that delaying the start of treatment with CT by ≥ 6 months results in a statistically significant increase in the incidence of events.
Using scenarios which reflect a real clinical trial setting where patients are often randomized to different treatment arms, it was possible to demonstrate that drugs with disease modifying properties reduce the risk and incidence of AUR/S. Early onset of treatment with dutasteride and tamsulosin CT (i.e. < 6 months delay) leads to approximately three-fold decrease in relative risk compared to tamsulosin.22 This effect wanes progressively with delayed transition from tamsulosin to CT; the longer the delay, the higher the incidence of events. This benefit is complemented by the effect of dutasteride and tamsulosin CT on symptom deterioration as assessed by IPSS. Early onset of treatment with tamsulosin and dutasteride CT does not only result in a significantly higher responder rate relative to tamsulosin (p < 0.001); it also shows a larger proportion of patients with larger LUTS improvement (i.e. ≥ 50% change in IPSS relative to baseline) than when CT is delayed by ≥ 6–24 months (60.8% vs. 48.4–52.7%).21
Our analysis also shows that baseline characteristics affect baseline hazard rate and as such contribute to the instantaneous risk (Figure 1b), but are not predictive of the overall response to an intervention, which is determined by treatment type. In fact, baseline demographic and clinical characteristics in nonresponders to tamsulosin do not differ significantly from patients on CT. This implies that the risk of progression at the time of
diagnosis will be miscalculated if only baseline characteristics are used to predict treatment response.
From a methodological perspective, we acknowledge that to address the key research question from this investigation, it is essential to discriminate the contribution of multiple interacting factors to the instantaneous risk of AUR/S, including baseline covariates, trial design and treatment type. Whereas these factors may not be easily controlled in a prospective clinical trial, CTS do offer an opportunity to control and eventually assess the effect of confounding or uncontrolled factors.34 In this regard, it should be emphasised that it may not be possible to accurately assess the magnitude of the effect of delayed start of CT on the incidence of AUR/S based on a prospective or retrospective clinical trial. In addition to the large sample size and logistic challenges associated with patient monitoring and follow-up, prospective clinical studies may not be considered ethically acceptable, especially when guidelines recommend it for men who have moderate-to-severe LUTS and are at risk of disease progression (i.e. higher prostate volume, higher PSA concentration, advanced age, higher PVR, lower Qmax, etc.).1 Likewise, any attempt to use retrospective data from randomised controlled clinical trials or real-life clinical settings will be fraught with difficulties, as one needs to consider the effect of censoring and other deviations, which cannot be easily accounted for during data analysis. These limitations are illustrated by a recent investigation on the effects of early (≤ 6 months after starting any medical treatment for BPH [baseline]), intermediate (between > 6–24 months from baseline) and late (24 months after baseline) initiation of addon dutasteride therapy on the incidence of AUR/S in Japanese patients with moderate-to-severe BPH.18 The relatively small sample size and striking differences in the incidence of BPHrelated surgery across sites have resulted in confounding and consequently made it very difficult to disentangle the effect of varying medical practice from delayed start of CT on overall treatment outcome.
Hence, the differences observed across CTS scenarios may have further relevance in real life. Considering the chronic nature of the disease, on a longer time scale the effect of diseasemodifying properties of dutasteride cannot be compensated by symptomatic interventions. Patients who are eligible to initiate CT miss the benefit over long term, as shown by the difference in the cumulative incidence, relative and attributable risk in treatment arms with patients who switch from tamsulosin at ≥ 6 months.
Limitations
Undoubtedly, there are limitations in our work. Whereas the protocol conditions and criteria outlined for the evaluation of early and delayed onset of treatment with CT may not be easily implemented in real life due to ethical and practical challenges, assumptions had to be made regarding trial characteristics, model parameter precision, and generalisability of the findings from the different simulation scenarios. An overview of the main assumptions and limitations is summarised in Table S4. Moreover, it should be noted that prior to implementing the simulation
scenarios, an attempt was made to assess the predictive performance of the model by simulating the survival estimate over time for a subset of patients (n = 1405) who switched from placebo treatment (randomised phase) to dutasteride monotherapy (Fig. S1). These data were not used during model development. There were no other controlled studies in which patients on monotherapy were switched to CT.
From a statistical perspective, we have assumed no carry over effect for treatment with drugs showing symptomatic improvement only (i.e. tamsulosin). In addition, as transition from tamsulosin to CT was implemented by design, i.e. switching at pre-specified times for each treatment arm, no additional statistical methods were used for adjustment or correction of potential bias in estimates.35
Conclusions
The use of CTS enabled the evaluation of the implications of delayed start of CT with tamsulosin and dutasteride. Delaying the start of treatment with CT by ≥ 6 months significantly increases the risk of AUR/S relative to those who start immediately on CT. Together with previous findings from a longitudinal model describing individual IPSS trajectories, these results show that early start of CT does not only ensure higher response rate and overall symptoms improvement;36 it also slows down disease progression, reducing the risk of AUR/S. However, such benefits need to be weighed for individual patients taking into account the risk of progression and susceptibility to the adverse events of treatment as well as patient preferences.
Author contributions
SD contributed to project development, data analysis and manuscript writing and editing; CC contributed to interpretation of study results and critical revision of the manuscript; MM contributed to project development, interpretation of study results and critical revision of the manuscript; JMPM contributed to project development, interpretation of study results and critical revision of the manuscript; MO contributed to interpretation of study results and critical revision of the manuscript; MCM contributed to interpretation of study results and critical revision of the manuscript; CGR contributed to interpretation of study results and critical revision of the manuscript; ODP contributed to project development, interpretation of study data and manuscript writing and editing.
Compliance with ethical standards
Conflict of interest
S. D’Agate has none to declare; M. Oelke has been a speaker, consultant and/or trial investigator for Apogepha, Astellas, Ferring, GSK, Pierre Fabre and Pfizer and received research grants from Astellas and Pfizer; M.C. Michel has been a speaker and consultant for Apogepha, Astellas, Dr. Willmar Schwabe, Ferring, GSK, Recordati and Velicept; he is a past employee of Boehringer Ingelheim and a current shareholder of Velicept; C.G. Roehrborn was previously employed as a consultant for GSK; C. Chavan, M. Manyak, J.M. Palacios-Moreno and O. Della Pasqua are GSK employees and hold stocks/shares in GSK.
Impact of early vs. delayed initiation of dutasteride/tamsulosin combination therapy on the risk of acute urinary retention
Human and animal rights
The current investigation describes the results from computer simulations and as such does not involve human participants and/or animals. Patient baseline characteristics used as basis for resampling were obtained from the pooled population enrolled in the clinical trials listed in the supplementary materials, all of which have been performed according to relevant ethical and clinical guidelines.
Informed consent
All participants enrolled into the original clinical trials have given informed consent. The terms of consent include the scope of the research presented here.
Open Access
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/ by/4.0/.
References
1. Gravas S, Cornu J, Gacci M, Gratzke C, Herrmann T, Mamoulakis C, Rieken M, Speakman M, Tikkinen K (2020) EAU guidelines on the management of non-neurogenic male lower urinary tract symptoms (LUTS), incl. benign prostatic obstruction (BPO). https://uroweb.org/guideline/treatment-of-non-neurogenicmale-luts/. Accessed 14 Apr 2020
2. Fitzpatrick JM (2006) The natural history of benign prostatic hyperplasia. BJU Int 97(s2):3–6
3. Roehrborn CG (2008) BPH progression: concept and key learning from MTOPS, ALTESS, COMBAT, and ALF-ONE. BJU Int 101(s3):17–21
4. Oelke M, Martinelli E (2015) Medikamentöse Therapie des benignen Prostatasyndroms. Der Urol 55(1):81–96
6. Woodard TJ, Manigault KR, McBurrows NN, Wray TL, Woodard LM (2016) Management of benign prostatic hyperplasia in older adults. Consul Pharm 31(8):412–424
7. Presicce F, De Nunzio C, Tubaro A (2017) Can long-term LUTS/ BPH pharmacological treatment alter the outcomes of surgical intervention? Curr Urol Rep 18(9):72
8. Roehrborn CG, Siami P, Barkin J, Damião R, Major-Walker K, Nandy I, Morrill BB, Gagnier RP, Montorsi F (2010) The effects of combination therapy with dutasteride and tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4-year results from the Combat study. Eur Urol 57(1):123–131
9. Kruep EJ, Hogue SL, Eaddy MT, Chandra MD (2011) Clinical and economic impact of early versus delayed 5-alpha reductase inhibitor therapy in men taking alpha blockers for symptomatic benign prostatic hyperplasia. P T 36(8):493–507
10. Rosen RC, Wei JT, Althof SE, Seftel AD, Miner M, Perelman MA (2009) Association of sexual dysfunction with lower urinary tract symptoms of BPH and BPH medical therapies: results from the BPH registry. Urology 73(3):562–566
11. Muderrisoglu AE, Becher KF, Madersbacher S, Michel MC (2019) Cognitive and mood side effects of lower urinary tract medication. Expert Opin Drug Saf 18(10):915–923
12. Roehrborn CG, Manyak MJ, Palacios-Moreno JM, Wilson TH, Roos EP, Santos JC, Karanastasis D, Plastino J, Giuliano F, Rosen RC (2018) A prospective randomised placebo-controlled study of the impact of dutasteride/tamsulosin combination therapy on sexual function domains in sexually active men with lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH). BJU Int 121(4):647–658
13. Rosen RC, Roehrborn CG, Manyak MJ, Palacios-Moreno JM, Wilson TH, Lulic Z, Giuliano F (2018) Evaluation of the impact of dutasteride/tamsulosin combination therapy on libido in sexually active men with lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia ( BPH ): a post hoc analysis of a prospective randomised placebo-controlled study. Int J Clin Pract 73(9):1–9
14. Pinto F, Racioppi M, Sacco E, Totaro A, Brescia A, Volpe A, Gardi M, Bassi PF (2009) Progression, risk factors and subsequent medical management of symptomatic benign prostatic hyperplasia. Arch Ital Urol Androl 81(1):1–8
15. Sountoulides P, Gravas S (2015) The impact of combination therapy with α-blockers and 5ARIs on the progression of BPH. Curr Drug Targets 16(11):1172–1179
16. Morlock R, Goodwin B, Gomez Rey G, Eaddy M (2013) Clinical progression, acute urinary retention, prostate-related surgeries, and costs in patients with benign prostatic hyperplasia taking early versus delayed combination 5α-reductase inhibitor therapy and α-blocker therapy: a retrospective analysis. Clin Ther 35(5):624–633
17. Naslund M, Eaddy MT, Hogue SL, Kruep EJ, Shah MB (2009) Impact of delaying 5-alpha reductase inhibitor therapy in men on alpha-blocker therapy to treat BPH: assessment of acute urinary retention and prostate-related surgery. Curr Med Res Opin 25(11):2663–2669
18. Shima Y, Kawano Y, Kobayashi A, Yamanishi T, Takeda H, Palacios-Moreno JM, Yamada M, Masumori N, Fukuta F, Nanri M, Nishino Y, Sagiyama K, Tsujimoto Y, Arai Y, Ohoka H, Yamaguchi T, Nagao K, Noma Y, Suzuki K, Okamoto T, Enomoto Y, Sakuma T, Sakai I, Nagae H, Torii S, Hiura M, Matsushita M, Nozawa E, Kurokawa S, Mitsui Y, Miyakoda K, Kato S, Yoshikawa K, Kuwahara Y, Sakai H, Hagiwara N, Kasuya Y, Miyamae K (2019) Comparison of the clinical effect of dutasteride therapy for benign prostatic hyperplasia when initiated at different time points: a multicentre, observational, retrospective chart review study. Int J Clin Pract e13418
19. Colditz GA (2010) Overview of the epidemiology methods and applications: strengths and limitations of observational study designs. Crit Rev Food Sci Nutrit 50(sup1):10–12
20. Munnangi S, Boktor SW (2019) Epidemiology of study design. StatPearls. StatPearls Publishing, Treasure Island
21. D’Agate S, Wilson T, Adalig B, Manyak M, Palacios-Moreno JM, Chavan C, Oelke M, Roehrborn C, Della Pasqua O (2019) Impact of disease progression on individual IPSS trajectories and consequences of immediate versus delayed start of treatment in patients with moderate or severe LUTS associated with BPH. World J Urol 38(2):463–472
23. Ploeger BA, Holford NHG (2009) Washout and delayed start designs for identifying disease modifying effects in slowly progressive diseases using disease progression analysis. Pharm Stat 8(3):225–238
24. D’Agate S, Chavan C, Manyak M, Palacios-Moreno JM, Oelke M, Michel MC, Roehrborn CG, Della Pasqua O (2020) Model-based meta-analysis of the time to first acute urinary retention or BPHrelated surgery in patients with moderate or severe symptoms. Br J Clin Pharmacol. https://doi.org/10.1111/bcp.14682
25. Juliao AA, Plata M, Kazzazi A, Bostanci Y, Djavan B (2012) American Urological Association and European Association of Urology guidelines in the management of benign prostatic hypertrophy: revisited. Curr Opin Urol 22(1):34–39
26. Clinical guideline (2010) Lower urinary tract symptoms in men: management. https://www.nice.org.uk/guidance/cg97. Accessed 14 June 2020
27. Gacci M, Sebastianelli A, Spatafora P, Corona G, Serni S, De Ridder D, Gravas S, Abrams P (2017) Best practice in the management of storage symptoms in male lower urinary tract symptoms: a review of the evidence base. Ther Advan Urol 10(2):79–92
28. Fujimura T, Kume H, Nishimatsu H, Sugihara T, Nomiya A, Tsurumaki Y, Miyazaki H, Suzuki M, Fukuhara H, Enomoto Y, Homma Y (2011) Assessment of lower
Impact of early vs. delayed initiation of dutasteride/tamsulosin combination therapy on the risk of acute urinary retention
urinary tract symptoms in men by international prostate symptom score and core lower urinary tract symptom score. BJU Int 109(10):1512–1516
29. Glass AS, Hilton JF, Cowan JE, Washington SL, Carroll PR (2014) Serial prostate biopsy and risk of lower urinary tract symptoms: results from a large, singleinstitution active surveillance cohort. Urology 83(1):33–39
30. Kuiper JG, Bezemer ID, Driessen MT, Vasylyev A, Roehrborn CG, Penning-van Beest FJA, Herings RMC (2016) Rates of prostate surgery and acute urinary retention for benign prostatic hyperplasia in men treated with dutasteride or finasteride. BMC Urol. 16(1):53
31. van Exel NJA, Koopmanschap MA, McDonnell J, Chapple CR, Berges R, Rutten FFH (2006) Medical consumption and costs during a one-year follow-up of patients with LUTS suggestive of BPH in six European countries: report of the TRIUMPH study. Eur Urol 49(1):92–102
32. Roehrborn CG, Barkin J, Tubaro A, Emberton M, Wilson TH, Brotherton BJ, Castro R (2014) Influence of baseline variables on changes in International Prostate Symptom Score after combined therapy with dutasteride plus tamsulosin or either monotherapy in patients with benign prostatic hyperplasia and lower urinary tract symptoms: 4-year results. BJU Int 113(4):623–635
33. Roehrborn CG, Oyarzabal Perez I, Roos EPM, Calomfirescu N, Brotherton B, Wang F, Palacios JM, Vasylyev A, Manyak MJ (2015) Efficacy and safety of a fixed-dose combination of dutasteride and tamsulosin treatment (Duodart®) compared
with watchful waiting with initiation of tamsulosin therapy if symptoms do not improve, both provided with lifestyle advice, in the management of t. BJU Int 116(3):450–459
34. Della Pasqua OE (2010) PKPD and disease modeling: concepts and applications to oncology. In: Kimko H, Peck C (eds) Clinical trial simulations. AAPS Advances in the Pharmaceutical Sciences Series. Springer, New York, pp 281–306
35. Branson M, Whitehead J (2002) Estimating a treatment effect in survival studies in which patients switch treatment. Stat Med 21(17):2449–2463
36. D’Agate S, Wilson T, Adalig B, Manyak M, Palacios-Moreno JM, Chavan C, Oelke M, Roehrborn C, Della Pasqua O (2020) Model-based meta-analysis of individual international prostate symptom Score trajectories in patients with benign prostatic hyperplasia with moderate or severe symptoms. Br J Clin Pharmacol 86(8):1585–1599
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary files available online https://doi.org/10.1007/s0034 5-020-03517-0
S Afr Gen Pract 2024;5(2):72-82
10.1001/jamanetworkopen.2023.48692
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Prostate safety events during testosterone replacement therapy in men with hypogonadism - a randomized clinical trial
S Bhasin,1 TG Travison,2 KM Pencina,1 M O’Leary,1 GR Cunningham,3 AM Lincoff,⁴ SE Nissen,⁴ MS Lucia,⁵ MA Preston,⁶ M Khera,3 N Khan,⁷ MC Snabes,⁷ X Li,⁷ CM Tangen,⁸ KA Buhr,⁹ IM Thompson Jr10
1 Research Program in Men’s Health: Aging and Metabolism, Boston Claude D. Pepper Older Americans Independence Center, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts
2 Marcus Institute for Aging Research, Hebrew Senior Life, Division of Gerontology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts
3 Baylor College of Medicine, Houston, Texas
⁴ Cleveland Clinic Coordinating Center for Clinical Research (C5Research), Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, Ohio
⁵ Department of Pathology, University of Colorado, Aurora
⁶ Division of Urology, Brigham and Women’s Hospital, Boston, Massachusetts
⁷ AbbVie Inc, North Chicago, Illinois
⁸ Fred Hutchison Cancer Center, University of Washington, Seattle
⁹ Statistical Data Analysis Center, Department of Biostatistics and Medical Informatics, University of Wisconsin, Madison
10 CHRISTUS Santa Rosa Health System and The University of Texas Health Science Center, San Antonio Corresponding author, email: sbhasin@bwh.harvard.edu
Importance: The effect of testosterone replacement therapy (TRT) on the risk of prostate cancer and other adverse prostate events is unknown.
Objective: To compare the effect of TRT vs placebo on the incidences of high-grade prostate cancers (Gleason score >4 + 3), any prostate cancer, acute urinary retention, invasive prostate procedures, and pharmacologic treatment for lower urinary tract symptoms in men with hypogonadism.
Design, setting, and participants: This placebo-controlled, double-blind randomized clinical trial enrolled 5246 men (aged 45-80 years) from 316 US trial sites who had 2 testosterone concentrations less than 300 ng/dL, hypogonadal symptoms, and cardiovascular disease (CVD) or increased CVD risk. Men with prostate-specific antigen (PSA) concentrations greater than 3.0 ng/mL and International Prostate Symptom Score (IPSS) greater than 19 were excluded. Enrollment took place between May 23, 2018, and February 1, 2022, and end-of-study visits were conducted between May 31, 2022, and January 19, 2023.
Intervention: Participants were randomized, with stratification for prior CVD, to topical 1.62% testosterone gel or placebo.
Main outcomes and measures: The primary prostate safety end point was the incidence of adjudicated high-grade prostate cancer. Secondary end points included incidence of any adjudicated prostate cancer, acute urinary retention, invasive prostate surgical procedure, prostate biopsy, and new pharmacologic treatment. Intervention effect was analyzed using a discrete-time proportional hazards model.
Results: A total of 5204 men (mean [SD] age, 63.3 [7.9] years) were analyzed. At baseline, the mean (SD) PSA concentration was 0.92 (0.67) ng/mL, and the mean (SD) IPSS was 7.1 (5.6). The mean (SD) treatment duration as 21.8 (14.2) months in the TRT group and 21.6 (14.0) months in the placebo group. During 14 304 person-years of follow-up, the incidence of high-grade prostate cancer (5 of 2 596 [0.19%] in the TRT group vs 3 of 2 602 [0.12%] in the placebo group; hazard ratio, 1.62; 95% CI, 0.39-6.77; p = .51) did not differ significantly between groups; the incidences of any prostate cancer, acute urinary retention, invasive surgical procedures, prostate biopsy, and new pharmacologic treatment also did not differ significantly. Change in IPSS did not differ between groups. The PSA concentrations increased more in testosterone-treated than placebo-treated men.
Conclusions and relevance: In a population of middle-aged and older men with hypogonadism, carefully evaluated to exclude those at high risk of prostate cancer, the incidences of high-grade or any prostate cancer and other prostate events were low and did not differ significantly between testosterone- and placebo-treated men. The study’s findings may facilitate a more informed appraisal of the potential risks of TRT.
Republished with permission: JAMA Network Open. 2023;6(12):e2348692. 10.1001/jamanetworkopen.2023.48692
Key Points
Question: Does testosterone replacement therapy in men with hypogonadism increase the risk of high- grade or any prostate cancer or other adverse prostate events?
Findings: During 14 304 person-years of follow-up of 5 204 men (aged 45–80 years) with hypogonadism in this randomized clinical trial, incidences of high-grade or any prostate cancer, acute urinary retention, invasive surgical procedures, and new pharmacologic treatment were low and did not differ significantly between groups.
Meaning: The study’s findings will facilitate a more informed appraisal of the potential prostate risks of testosterone replacement therapy.
Introduction
The relationship between testosterone replacement therapy (TRT) and the risk of prostate cancer remains incompletely studied.1-3 Epidemiologic studies have not found a consistent association between prostate cancer risk and testosterone levels or polymorphisms in genes involved in androgen action.4-13
Prostate events were not adjudicated in any testosterone trial, and none have reported the incidence of high-grade prostate cancer or other prostate events, such as acute urinary retention, invasive prostate procedures, or initiation of new pharmacologic therapy for benign prostatic hyperplasia (BPH).1,14 Because of uncertainty about the risk of prostate events during TRT, most professional society guidelines recommend against TRT in men with a history or increased risk of prostate cancer.1,2,15
In 2015, the US Food and Drug Administration required testosterone manufacturers to conduct a randomized clinical trial to determine the effect of TRT on major adverse cardiovascular events (MACEs).16 The Testosterone Replacement Therapy for Assessment of Long-Term Vascular Events and Efficacy Response in Hypogonadal Men (TRAVERSE) study was designed to meet this regulatory requirement.17 Because of its large size and longer duration, the TRAVERSE study offered a unique opportunity to evaluate the effects of TRT on prostate safety events.17 The study compared the effects of TRT and placebo on the incidences of high-grade prostate cancer, any prostate cancer, acute urinary retention, invasive prostate surgical procedures for BPH, and initiation of pharmacologic therapy for BPH. Prostate events were recorded using a structured protocol and adjudicated. To minimize ascertainment bias due to greater likelihood of urologic referral for prostate biopsy because of testosterone-induced elevation in prostate-specific antigen (PSA) concentrations, the TRAVERSE study protocol prespecified procedures for managing PSA elevations and urologic referrals.
Methods
This randomized clinical trial’s design, as well as the MACEs and overall safety results, have been previously published.17,18 Briefly, this placebo-controlled, double-blind, parallel-group randomized clinical trial enrolled men, aged 45–80 years, with 2 fasting, morning testosterone concentrations, measured using liquid chromatography–tandem mass spectrometry, less than 300 ng/dL (to convert to nanomoles per liter, multiply by 0.0347) in a central laboratory certified by the Hormone Standardization Program for Testosterone, 1 or more symptoms
of hypogonadism, and prior cardiovascular disease (CVD) or increased risk of CVD.17 Men with history of prostate cancer, PSA concentrations greater than 3.0 ng/mL (or >1.5 ng/mL if receiving a steroid 5α-reductase inhibitor [5ARI] [to convert to micrograms per liter, multiply by 1]), severe lower urinary tract symptoms (LUTSs) (International Prostate Symptom Score [IPSS] >19), or a prostate nodule or induration were excluded. A PSA cutoff of 3 ng/mL was established to exclude men at increased prostate cancer risk.19 Participants were randomized in a 1:1 ratio with stratification for preexisting CVD to receive 1.62% transdermal testosterone gel or matching placebo gel for the duration of the study. Testosterone dose was adjusted, while maintaining blinding, based on on-treatment testosterone and hematocrit levels to maintain testosterone concentrations between 350 and 750 ng/dL and hematocrit levels less than 54% (to convert to a proportion of 1.0, multiply by 0.01).17,18 Participants’ self-reported race and ethnicity were collected because racial differences in the incidence of clinical prostate cancers are well recognized. The trial was conducted at 316 US sites. Enrollment took place between May 23, 2018, and February 1, 2022, and end-of-study visits were conducted between May 31, 2022, and January 19, 2023. The study protocol was approved by the national and local institutional review boards for human subjects research. All participants provided written informed consent. An independent data and safety monitoring board reviewed safety data every 6 months.
Prostate safety monitoring plan
The prespecified prostate safety monitoring plan is provided in Supplement 1. The PSA levels were measured at baseline, 3 months, 12 months, and annually thereafter, and IPSS was assessed at baseline, 3 months, 12 months, 36 months, and the end of the study. Digital prostate examinations were performed at baseline, 12 months, 36 months, and end of study. At each visit, participants were asked structured questions about LUTS and prostate procedures. If a prostate procedure was reported, an attempt was made to obtain pathology reports and tissue.
To minimize the ascertainment bias attributable to the increased risk of being referred for a prostate biopsy because of testosterone-induced increase in PSA levels, the criteria for urologic referral were prespecified. The participants were referred for urologic evaluation and possible biopsy if they had any of the following: (1) confirmed PSA increase more than 1.4 ng/mL above baseline in the first year of treatment (or >0.7 ng/mL in 5ARI-treated men); (2) confirmed PSA concentration greater than 4.0 ng/mL at any time (>2.0 ng/mL in 5ARI-treated men); (3) for men aged 45 to 54 years with a baseline PSA concentration less than 1.5 ng/mL, a PSA level increasing to 3.0 ng/mL at any time (<0.75 ng/mL increasing to 1.5 ng/mL for 5ARI-treated men); or (4) prostate nodule or induration at any time. For criteria 1, 2, and 3, elevations in PSA concentrations were confirmed by repeating the test.20,21 For the men who met these criteria, prostate cancer risk was estimated using the Prostate Cancer Prevention Trial Risk Calculator, version 2.0 (UT Health San Antonio), and participants were provided an institutional review board–approved video that
Prostate safety events during testosterone replacement therapy in men with hypogonadism - a randomized clinical trial
described the potential benefits and risks of prostate biopsy22 to facilitate informed decision-making regarding prostate biopsy.
Prostate safety end points
The primary prostate safety end point was the incidence of highgrade prostate cancer (Gleason score 4 + 3 or higher). Secondary end points included the incidence of any prostate cancer, acute urinary retention, invasive prostate surgical procedure for BPH, prostate biopsy, and new pharmacologic treatment for LUTSs. The LUTSs were evaluated using the IPSS. Changes in PSA concentrations from baseline and from month 12 were determined.
Adjudication of prostate safety end points
A blinded Prostate Adjudication Committee adjudicated prostate cancer diagnosis and Gleason score, acute urinary retention, and invasive prostate surgical procedure for BPH. The diagnosis of prostate cancer was based on evaluation of tissue from prostate biopsy specimens and surgical procedures by the Prostate Adjudication Center at the University of Colorado. If tissue or slides were not available, the Prostate Adjudication Committee reviewed site pathology reports. High-grade prostate cancer was defined as a Gleason score of 4 + 3 or higher.23 Acute urinary retention was defined as inability to voluntarily pass urine, requiring a visit to the emergency department, and/or placement of a catheter, ascertained by participant self-report and verified by medical record. An invasive prostate procedure was defined as any surgical procedure for BPH other than a prostate biopsy, verified by medical record.
Statistical analysis
The trial’s statistical analysis plan is available in Supplement 2. Analyses used SAS software, version 9.4 (SAS Institute Inc) and R, version 4.2.1 (R Foundation for Statistical Computing).24 Descriptive analyses of baseline characteristics were conducted in the full analysis set, which included all randomized participants. Prostate safety analyses were conducted in the safety set, which included all randomized participants who received at least 1 dose of the study drug. The data analysis and interpretation of the data were performed by the statisticians associated with the Prostate Substudy Committee (K.B., K.M.P., and T.G.T.).
Analysis of the primary safety end point and event-based secondary end points used a discrete- time proportional hazards model25 with event intervals based on scheduled visits. All postrandomization events were included. Hazard ratios (HRs) for treatment effect and associated 95% CIs and Wald P-values were calculated, adjusting for prior CVD. The discrete-time model was prespecified under the assumption that exact event times might not be consistently available for analysis during the COVID-19 pandemic, a concern that proved unfounded, so an additional post hoc Cox proportional hazards analysis using actual time of events was conducted. Aalen-Johansen estimates of cumulative incidence of prostate events with death as a competing risk were calculated. Post hoc sensitivity analyses of events occurring within 1 year and within 30 days of the last dose of the study drug were also conducted.
Changes over time in IPSSs, PSA levels, and hormone levels were analyzed using linear mixed- effects models with fixed effects for treatment, visit, treatment × visit interaction, baseline value, CVD status, and a random-subject effect using an unstructured covariance. Least-squares means estimates, 95% CIs, and P-values for treatment effect were computed using an F test. For PSA, a mixed model was used to test whether treatment difference continued to increase after month 12 by comparing month 12 with the mean of later visits. All hypothesis tests used a 2-sided significance level of p < .05.
The study was powered to establish noninferiority for the MACE end point within a noninferiority margin of an upper confidence limit of the HR less than 1.5. Approximately 6 000 individuals were to be recruited to accrue 256 MACEs (90% power) under the initial assumptions of annual event rate, accrual rate, and discontinuation rate.17
Results
Among 32 152 screened men, 50 (0.16%) were excluded because of a history of prostate or breast cancer, 1201 (3.74%) for PSA concentrations greater than 3.0 ng/mL (or >1.5 ng/mL if receiving 5ARIs), 549 (1.71%) for IPSSs greater than 19, and 57 (0.18%) for prostate nodule or induration; these percentages should be interpreted with caution because men who failed screening at earlier screening visits did not complete subsequent screening assessments. Among 5 246 identification numbers of randomized men, 42 were attributed to 20 participants with duplicate enrollment. After excluding these duplicates, the full analysis set included 5204 participants (mean [SD] age, 63.3 [7.9] years; self-reported race: 877 [16.9%] Black, 4 154 [79.8%] White, and 173 [3.3%] other; self- reported Hispanic or Latinx ethnicity, 848 [16.3%]), with 2 601 in the TRT group and 2 603 in the placebo group. The safety set included 5198 participants (2 596 in the TRT group and 2602 in the placebo group) who received at least 1 dose of study medication (Figure 1).
As reported earlier,18 the mean (SD) follow-up duration was 33.0 (12.1) months. Of 5 204 participants in the full analysis set, 4 804 (92.3%) were followed up for at least 1 one year, 3 842 (73.9%) for 2 years, 2974 (57.2%) for 3 years, and 85 (1.6%) for 4 years, yielding 14 304 person-years of follow-up. The mean (SD) treatment duration was 21.8 (14.2) months in the TRT group and 21.6 (14.0) months in the placebo group, and treatment discontinuation rates were similar between the 2 arms.
Baseline characteristics of the participants have been previously published.18 The mean (SD) PSA concentration was 0.92 (0.67) ng/mL. Of 5 182 men with nonmissing baseline PSA values, 3 347 (64.6%) had PSA concentrations less than 1 ng/mL, 1 355 (26.1%) had PSA concentrations between 1.00 and 1.99 ng/mL, and 480 (9.3%) had PSA concentrations between 2 and 3 ng/mL. The mean (SD) baseline IPSS was 7.1 (5.6).
High-grade and all prostate cancers
As reported previously in the trial’s overall safety events,18 during 14 304 person-years of follow-up, there were 5 participants with high-grade prostate cancer in the TRT group and 3 in the
Prostate safety events during testosterone replacement therapy in men with hypogonadism - a randomized clinical trial
placebo group. The incidence of high-grade prostate cancer did not differ significantly between groups (5 of 2 596 [0.19%] in the TRT group vs 3 of 2 602 [0.12%] in the placebo group; hazard ratio, 1.62; 95% CI, 0.39-6.77; p = .51) (Figure 2 and Figure 3). Among the 8 participants with high-grade cancer, 3 had baseline PSA concentrations between 1 and 1.99 ng/mL and 5 between 2 and 3 ng/mL.
The number of participants with any prostate cancer did not differ between the TRT (12 [0.46%]) and placebo (11 [0.42%]) groups (HR, 1.07; 95% CI, 0.47-2.42; p = .87). Among 23 men with prostate cancer, 1 had a baseline PSA concentration less than 1 ng/mL, 8 between 1 and 1.99 ng/mL, and 14 between 2 and 3 ng/mL. The highest postbaseline PSA concentration before biopsy in these 23 men is shown in eTable 1 in Supplement 3
Other secondary prostate safety end points
Twenty testosterone-treated men (0.77%) and 16 placebotreated men (0.61%) developed acute urinary retention, with no significant difference between groups (HR, 1.25; 95% CI, 0.65-2.41; p = .50). Twenty-three men (0.89%) in the TRT group underwent an invasive surgical prostate procedure compared
with 12 (0.46%) in the placebo group (HR, 1.91; 95% CI, 0.95-3.84; p = .07). Rates of new pharmacologic therapy for LUTSs did not differ significantly between the TRT and placebo groups (101 [3.89%] vs 87 [3.34%]; HR, 1.16; 95% CI, 0.87-1.54; p = .32) (Figure 2 and Figure 3).
Eighty-five men (1.6%) met the criteria for referral for urologic evaluation, 57 (2.2%) in the TRT group vs 28 (1.1%) in the placebo group. Sixty men (39 in the TRT group and 21 in the placebo group) had confirmed PSA concentrations greater than 4.0 ng/ mL, 37 men (25 in the TRT group and 12 in the placebo group) had confirmed increases in PSA concentrations greater than 1.4 ng/mL above baseline during the first year (or >0.7 ng/mL for those taking 5ARIs), 5 men (4 in the TRT group and 1 in the placebo group) had a new prostate nodule or induration, and 1 man (in the TRT group) had a PSA concentration that increased from less than 1.5 ng/mL at baseline to greater than 3.0 ng/mL.
Of the 85 men who met the criteria for urologic referral, 16 (18.8%) elected to undergo prostate biopsy; an additional 14 men who did not meet these criteria also underwent biopsy. The numbers of prostate biopsies (16 in the TRT group vs 14 in the placebo
5 246 Patients assessed for eligibility
42 Excluded with duplicate enrolment
5 204 Randomised
2 601 Randomised to testosterone
2 596 Received testosterone (99.8%)
5 Did not receive testosterone (0.2%)
1 003 Completed study drug
1 593 Discontinued study drug
650 Withdrawal by subject 332 Lost to follow-up
238 Adverse event
65 Lack of efficacy
1 594 Completed study 1 Died
95 Met protocol criteria 213 Other 1 007 Discontinued study drug
143 Died
308 Withdrawal by subject 439 Lost to follow-up
16 Adverse event
65 Lack of efficacy
89 Other
2 Missing reason
Included in analysis
2 601 Full analysis set (100%)
2 596 Safety set (99.8%)
2 601 Randomised to testosterone
2 596 Received testosterone (99.8%)
5 Did not receive testosterone (0.2%)
997 Completed study drug
1605 Discontinued study drug 764
Withdrawal by subject 364 Lost to follow-up
209 Adverse event 87 Lack of efficacy 12 Met protocol criteria
169 Other
1 508 Completed study 1 Died
1 023 Discontinued study drug
147 Died
343 Withdrawal by subject 445 Lost to follow-up
15 Adverse event
21 Lack of efficacy
49 Other
3 Missing reason
Included in analysis
2 603 Full analysis set (100%) 2 602 Safety set (99.8%)
Prostate safety events during testosterone replacement therapy in men with hypogonadism - a randomized clinical trial
Discrete-time proportional hazards model estimates of hazard ratios (95% CIs) quantifying differential risk in testosterone replacement therapy (TRT) relative to placebo are shown in the forest plot. The hazard ratios are the hazard in the TRT group over the hazard in the placebo group, so a value greater than 1 indicates an excess of prostate events in the TRT group. BPH indicates benign hyperplasia.
Aalen-Johansenestimatesofcumulativeincidencewithdeathasacompetingrisk, togetherwithpointwise95%CIs,areshown.Hazardratios(HRs)andassociated95%CIs and P valuesbasedonthediscreteproportionalhazardsmodelarealsoshown.
Aalen-Johansen estimates of cumulative incidence with death as a competing risk, together with pointwise 95% CIs, are shown. Hazard ratios (HRs) and associated 95% CIs and P values based on the discrete proportional hazards model are also shown.
Aalen-Johansenestimatesofcumulativeincidencewithdeathasacompetingrisk, togetherwithpointwise95%CIs,areshown.Hazardratios(HRs)andassociated95%CIs and P valuesbasedonthediscreteproportionalhazardsmodelarealsoshown.
o ownnloaded from jamanetwork com by guest on 01/02/2024
Doownnloaded from jamanetwork com by guest on 01/02/2024
group) did not differ between groups (0.62% vs 0.54%; HR, 1.13; 95% CI, 0.55-2.31; p = .74). Eighteen men who underwent biopsy had baseline PSA concentrations between 2 and 3 ng/mL.
Post Hoc Sensitivity Analyses
December27,20236/14
Lower Urinary Tract Symptoms
The IPSS increased over time in both groups (Figure 4); change from baseline in IPSS did not differ significantly between groups. Of 4809 men with any postbaseline IPSS, 378 (7.9%) had a score greater than 19 (180 [7.5%] in the TRT group and 198 [8.2%] in the placebo group).
Post hoc analysis for primary and secondary event end points using a Cox proportional hazards regression model (eFigure 1 in Supplement 3) yielded results similar to those of prespecified analyses. Similarly, the results of the sensitivity analyses in which events 1 year and 30 days after the end of treatment were censored (eFigures 2 and 3 in Supplement 3) were similar to those of prespecified analyses.
Figure 4: Changes in lower urinary tract symptoms over time
Table: Change from baseline in serum PSA levels in study participants categorized by baseline PSA levels
wnnloaded from jamanetwork com by guest on 01/02/2024
Treatment No. PSA level, mean (SD)
Baseline PSA <1 ng/mL
Month 0
3
Month 12
Change from baseline, least-squares mean (95% CI)
December27,20237/14
Treatment difference, least-squares mean (95% CI)
Month 12
Month 24
Table: Change from baseline in serum PSA levels in study participants categorized by baseline PSA levels (continued)
Treatment
Month 36
Month 48
Baseline PSA 2-3 ng/mL Month 0
PSA levels
Testosterone treatment was associated with a greater increase in PSA levels than placebo (estimated between-group difference, 0.11 [ 95% CI, 0.07-0.15] ng/mL at 3 months; 0.15 [95% CI, 0.080.21] ng/mL at 12 months; 0.11 [95% CI, −0.01 to 0.21] ng/mL at 24 months; 0.01 [95% CI, −0.09 to 0.10] ng/mL at 36 months; and 0.09 [95% CI, −0.04 to 0.22] ng/mL at 48 months; omnibus test p < .001) (eFigure 4 in Supplement 3) regardless of baseline PSA concentration (Table). There was no significant between-group difference in PSA levels after month 12; the difference at time points after month 12 was significantly smaller than difference at month 12.
Hormone levels
Mean (SD) total testosterone was 220 (48) ng/dL at baseline.18 As reported, testosterone and estradiol levels,18 as well as dihydrotestosterone levels (eTable 2 in Supplement 3), increased significantly in testosterone-treated men but did not change in placebo-treated men.
Discussion
The TRAVERSE study is, to our knowledge, the largest randomized trial of TRT conducted to date, with prospectively recorded and adjudicated prostate safety outcomes. Among middle-aged and older men with hypogonadism who had or were at increased risk
Change from baseline, least-squares mean (95% CI)
Treatment difference, least-squares mean (95% CI)
of CVD, the incidence of high-grade or any prostate cancer in TRTtreated men with a baseline PSA concentration less than 3.0 ng/ mL was low and not significantly different from that in placebotreated men. This group of men whose PSA concentration is less than 3.0 ng/mL represents most of the aging US population.26 Similarly, incidences of acute urinary retention, invasive surgical procedure for BPH, or new pharmacologic treatment for LUTSs did not differ between the treatment groups. The invasive prostate surgical procedures were more common in the TRT group compared with the placebo group, although the difference was not significant. Consistent with meta-analyses of smaller testosterone trials, TRT did not increase IPSSs.14,27 Although PSA concentrations increased more among the TRT group than the placebo group, the mean increase was small and between-group difference did not widen after 12 months. Thus, in a population men with hypogonadism and PSA concentrations less than 3 ng/ mL who were evaluated carefully to exclude those at increased prostate cancer risk, TRT was associated with low risk of adverse prostate events, including cancer.
Prostate cancer is highly prevalent among older men, but only a small fraction have high-grade tumors.19 Androgen receptor signaling plays a central role in prostate cancer biology, and testosterone treatment promotes the growth of metastatic prostate cancer.28 A mendelian randomization analysis found an increased incidence of prostate cancer in men with higher
genetically determined testosterone level29; conversely, men with Klinefelter syndrome have lower risk of prostate cancer.30 These data have led to concerns that TRT could promote progression of subclinical low-grade prostate cancer.1 Because TRT increases PSA in men with hypogonadism, PSA elevations in older men receiving TRT could lead to prostate biopsy and detection of a subclinical low-grade prostate cancer.1 To minimize the risk of unnecessary prostate biopsies and mitigate ascertainment bias, while enabling detection of prostate cancers for which clinical management may reduce long-term diseaserelated morbidity and mortality, the study protocol specified PSA elevation thresholds for referral to a urologist.21,31 Elevations in PSA concentrations above these thresholds were verified, and participants with confirmed PSA elevation were asked to watch a video on the significance of PSA elevation and the benefits and risks of prostate biopsy to facilitate a shared decision on prostate biopsy. This approach was effective in reducing the number of prostate biopsies in both treatment groups; the small number of biopsies and high percentage of positive biopsy results in the trial support its usefulness in facilitating shared decision-making before prostate biopsy in men receiving TRT.
Limitations
The trial has some limitations. These findings should not be applied to patients with known prostate cancer, those with higher PSA values, or men who do not have confirmed hypogonadism. Although the TRAVERSE study was longer than most other randomized clinical trials of TRT, carcinogens may require many years to induce malignant neoplasms. The trial’s structured evaluation of men after PSA testing did not include prostate imaging or other biomarker tests that may influence the decision to perform a biopsy. It is possible that shared decision-making played a role in lower rates of prostate biopsy; results could be different in a setting in which shared decisionmaking is not made available. Although the trial’s sample size is the largest of any randomized testosterone trials to date, the numbers and incidences of any prostate cancer and highgrade prostate cancer were low. Because of the small number of prostate cancer events, these findings should not be interpreted to imply that the risk of prostate cancer in the testosterone and placebo groups was similar. The trial’s findings indicate that in men with hypogonadism who were screened and monitored carefully using a structured protocol, the risk of high-grade or any prostate cancer and other prostate events is low. The trial’s findings do not apply to men at high risk of prostate cancer, who were excluded. Rates of study medication discontinuation and loss to follow-up were high, although not dissimilar from those in randomized trials in other symptomatic conditions32,33 or in hypogonadal men prescribed TRT.34 The trial was conducted during the COVID-19 pandemic, which affected retention. However, nonretention rates were similar in the 2 groups. Among participants who discontinued trial participation, nearly half did so after end-of-study visits had started, and findings were similar in sensitivity analyses limited to follow-up durations of 1 month or 1 year after the last administered dose. The study population met the Endocrine Society’s criteria for hypogonadism1 but had high rates of diabetes, obesity, and other comorbid conditions,
not dissimilar from men with hypogonadism35 receiving TRT in the US.36
Conclusions
In this randomized clinical trial of men with hypogonadism who were carefully evaluated to exclude those at high risk for prostate cancer and followed using a standardized monitoring plan, TRT was associated with low and similar incidences of high grade or any prostate cancer, acute urinary retention, and invasive surgical procedures for BPH compared with a placebo. Testosterone replacement therapy did not worsen LUTSs. The concern about prostate risk heavily influences decision-making by clinicians and patients who are considering TRT for hypogonadism. The study’s findings will facilitate a more informed appraisal of the potential risks of TRT.
Drs Bhasin and Buhr had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Drs Travison and Pencina contributed equally to this work.
Wrote protocol drafts for original protocol Snabes.
Conflict of interest disclosures
Dr Bhasin reported receiving grants from Metri International Biotech and Function Promoting Therapies and consulting fees from OPKO and Versanis outside the submitted work; in addition, Dr Bhasin holds a patent as a co-inventor of a method for free testosterone measurement. Dr Lincoff reported receiving grants from Esperion, Commonwealth Serum Laboratories, Ltd., Novartis, and AstraZeneca; personal fees from Eli Lilly as a trial steering committee member; personal fees from Novo Nordisk as a trial steering committee member and consultant; consulting fees from Recor, Ardelyz, GlaxoSmithKline, Akebia, Endologix, Fibrogen, Provention, Becton Dickson, and Medtronic outside the submitted work. Dr Khera reported receiving personal fees from Tolmar, AbbVie Inc, Halozyme, Marius, and Endo Pharmaceuticals outside the submitted work. No other disclosures were reported.
Funding/support
The trial was funded by a consortium of testosterone manufacturers led by AbbVie Inc with additional financial support provided by Endo Pharmaceuticals, Acerus Pharmaceuticals Corp, and Upsher-Smith Laboratories. Dr Bhasin was supported in part by grant 3P30AG031679 from the Boston Claude D. Pepper Older Americans Independence Center.
Role of the funder/sponsor
The prostate substudy design and analysis plan were crafted by the TRAVERSE Prostate Substudy Committee led by the Research Program in Men’s Health at the Brigham and Women’s Hospital, Boston, Massachusetts (eAppendixes 1 and 2 in Supplement 3). The funder reviewed and made suggestions to the prostate substudy design and statistical analysis plan and oversaw the conduct, data collection, and management of the trial. The data analysis and interpretation of the data were performed by the statisticians associated with the Prostate Substudy Committee (K.B., K.M.P., T.G.T.). The first author (S.B.) wrote the first manuscript draft and all co-authors reviewed and approved the manuscript. The decision to submit the manuscript for publication was made by the academic leadership of the TRAVERSE Prostate Substudy Committee. The funder reviewed the manuscript, made suggestions on the content, and approved the final version of the manuscript.
Additional contributions
The members of the Prostate Adjudication Committee are as follows: Michael O’Leary, MD (chair), Scott Lucia, MD, Mark A. Preston, MD; A. John Kellog Parsons, MD, MHS. The members of the Data Monitoring Committee are as follows: John H. Alexander, MD, MHSc (chair), Duke Clinical Research Institute, Duke University, Durham, North Carolina; William Bremner, MD, PhD, University of Washington, Seattle; Eric Klein, MD, Cleveland Clinic, Cleveland, Ohio; Darren K. McGuire, MD, MHSc, University of Texas Southwestern Medical Center, Dallas; Janet Wittes, PhD, Wittes LLC, Washington, DC; Renato D. Lopes, MD, PhD (observer, nonvoting), Duke Clinical Research Institute, Durham, North Carolina; Andrew Armstrong, MD, ScM (ad hoc consult), Duke University Medical Center, Duke Cancer Institute Center for Prostate and Urologic Cancers, Durham, North Carolina.
References
1. Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744. doi:10.1210/jc.2018-00229
2. Wang C, Nieschlag E, Swerdloff R, et al; International Society of Andrology (ISA); International Society for the Study of Aging Male (ISSAM); European Association of Urology (EAU); European Academy of Andrology (EAA); American Society of Andrology (ASA). Investigation, treatment, and monitoring of late-onset hypogonadism in males: ISA, ISSAM, EAU, EAA, and ASA recommendations. J Androl. 2009;30(1):1-9. doi:10.2164/jandrol.108. 006486
3. Liverman C, Blazer DG, eds. Testosterone and Aging: Clinical Research Directions National Academies Press; 2004.
4. Roddam AW, Allen NE, Appleby P, Key TJ; Endogenous Hormones and Prostate Cancer Collaborative Group. Endogenous sex hormones and prostate cancer: a collaborative analysis of 18 prospective studies. J Natl Cancer Inst 2008;100(3):170-183. doi:10.1093/jnci/djm323
5. Lenfant L, Leon P, Cancel-Tassin G, et al. Testosterone replacement therapy (TRT) and prostate cancer: an updated systematic review with a focus on previous or active localized prostate cancer. Urol Oncol. 2020;38(8): 661-670. doi:10.1016/j. urolonc.2020.04.008
6. Elliott J, Kelly SE, Millar AC, et al. Testosterone therapy in hypogonadal men: a systematic review and network meta-analysis. BMJ Open. 2017;7(11):e015284. doi:10.1136/bmjopen-2016-015284
7. Gann PH, Hennekens CH, Ma J, Longcope C, Stampfer MJ. Prospective study of sex hormone levels and risk of prostate cancer. J Natl Cancer Inst 1996;88(16):1118-1126. doi:10.1093/jnci/88.16.1118
8. Nomura AM, Stemmermann GN, Chyou PH, Henderson BE, Stanczyk FZ. Serum androgens and prostate cancer.
9. Cancer Epidemiol Biomarkers Prev. 1996;5(8):621-625.
10. Vatten LJ, Ursin G, Ross RK, et al. Androgens in serum and the risk of prostate cancer: a nested case-control study from the Janus serum bank in Norway. Cancer Epidemiol Biomarkers Prev. 1997;6(11):967-969.
11. Dorgan JF, Albanes D, Virtamo J, et al. Relationships of serum androgens and estrogens to prostate cancer risk: results from a prospective study in Finland. Cancer Epidemiol Biomarkers Prev. 1998;7(12):1069-1074.
12. Mohr BA, Feldman HA, Kalish LA, Longcope C, McKinlay JB. Are serum hormones associated with the risk of prostate cancer? prospective results from the Massachusetts Male Aging Study. Urology. 2001;57(5):930-935. doi:10.1016/ S0090-4295(00)01116-X
13. Platz EA, Leitzmann MF, Rifai N, et al. Sex steroid hormones and the androgen receptor gene CAG repeat and subsequent risk of prostate cancer in the prostate-specific antigen era. Cancer Epidemiol Biomarkers Prev. 2005;14(5):12621269. doi:10.1158/1055-9965.EPI-04-0371
15. Ponce OJ, Spencer-Bonilla G, Alvarez-Villalobos N, et al. The efficacy and adverse events of testosterone replacement therapy in hypogonadal men: a systematic review and meta-analysis of randomized, placebo- controlled trials. J Clin Endocrinol Metab. Published online March 17, 2018. doi:10.1210/jc.2018-00404
16. Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol . 2018;200(2):423-432. doi:10.1016/j.juro.2018.03.115
17. US Food and Drug Administration. FDA Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use. Accessed November 17, 2023. https://www.fda.gov/drugs/ drug-safety-and-availability/ fda-drug-safety-communication-fda-cautionsabout-using-testosterone-products-low-testosterone-due
18. Bhasin S, Lincoff AM, Basaria S, et al; TRAVERSE Study Investigators. Effects of long-term testosterone treatment on cardiovascular outcomes in men with hypogonadism: Rationale and design of the TRAVERSE study. Am Heart J 2022;245:41-50. doi:10.1016/j.ahj.2021.11.016
19. Lincoff AM, Bhasin S, Flevaris P, et al; TRAVERSE Study Investigators. Cardiovascular safety of testosterone- replacement therapy. N Engl J Med 2023;389(2):107-117. doi:10.1056/NEJMoa2215025
20. Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of prostate cancer among men with a prostate- specific antigen level <4.0 ng per milliliter. N Engl J Med. 2004;350(22):2239-2246. doi:10.1056/NEJMoa031918
21. Riehmann M, Rhodes PR, Cook TD, Grose GS, Bruskewitz RC. Analysis of variation in prostate-specific antigen values. Urology . 1993;42(4):390-397. doi:10.1016/0090-4295(93)90364-G
22. Cunningham GR, Ellenberg SS, Bhasin S, et al. Prostate-specific antigen levels during testosterone treatment of hypogonadal older men: data from a controlled trial. J Clin Endocrinol Metab. 2019;104(12):6238-6246. doi:10. 1210/ jc.2019-00806
23. Ankerst DP, Hoefler J, Bock S, et al. Prostate Cancer Prevention Trial risk calculator 2.0 for the prediction of low- vs high-grade prostate cancer. Urology 2014;83(6):1362-1367. doi:10.1016/j.urology.2014.02.035
24. Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA; Grading Committee. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol 2016;40(2): 244-252. doi:10.1097/PAS.0000000000000530
25. R Core Team. A Language and Environment for Statistical Computing . R Foundation for Statistical Computing; 2021.
26. Prentice RL, Gloeckler LA. Regression analysis of grouped survival data with application to breast cancer data.
28. Espaldon R, Kirby KA, Fung KZ, et al. Probability of an abnormal screening prostate-specific antigen result based on age, race, and prostate-specific antigen threshold. Urology. 2014;83(3):599-605. doi:10.1016/j.urology. 2013.10.051
29. Kathrins M, Doersch K, Nimeh T, Canto A, Niederberger C, Seftel A. The relationship between testosterone- replacement therapy and lower urinary tract symptoms: a systematic review. Urology. 2016;88:22-32. doi:10. 1016/j. urology.2015.11.006
30. Fowler JE Jr, Whitmore WF Jr. The response of metastatic adenocarcinoma of the prostate to exogenous testosterone. J Urol. 1981;126(3):372-375. doi:10.1016/ S0022-5347(17)54531-0
Prostate safety events during testosterone replacement therapy in men with hypogonadism - a randomized clinical trial
31. Ruth KS, Day FR, Tyrrell J, et al; Endometrial Cancer Association Consortium. Using human genetics to understand the disease impacts of testosterone in men and women. Nat Med. 2020;26(2):252-258. doi:10.1038/ s41591-020-0751-5
32. Swerdlow AJ, Schoemaker MJ, Higgins CD, Wright AF, Jacobs PA; UK Clinical Cytogenetics Group. Cancer incidence and mortality in men with Klinefelter syndrome: a cohort study. J Natl Cancer Inst . 2005;97(16): 1204-1210. doi:10.1093/jnci/dji240
33. Snyder PJ, Bhasin S, Cunningham GR, et al; Testosterone Trials Investigators. Effects of testosterone treatment in older men. N Engl J Med. 2016;374(7):611624. doi:10.1056/NEJMoa1506119
34. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288(3):321-333. doi:10.1001/ jama.288.3.321
35. Nissen SE, Wolski KE, Prcela L, et al. Effect of naltrexone-bupropion on major adverse cardiovascular events in overweight and obese patients with cardiovascular risk factors: a randomized clinical trial. JAMA. 2016;315(10): 990-1004. doi:10.1001/jama.2016.1558
36. Schoenfeld MJ, Shortridge E, Cui Z, Muram D. Medication adherence and treatment patterns for hypogonadal patients treated with topical testosterone therapy: a retrospective medical claims analysis. J Sex Med . 2013;10(5): 1401-1409. doi:10.1111/jsm.12114
37. Mulligan T, Frick MF, Zuraw QC, Stemhagen A, McWhirter C. Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract 2006;60(7):762-769. doi:10.1111/j.1742-1241.2006.00992.x
38. Jasuja GK, Bhasin S, Reisman JI, et al. Who gets testosterone? patient characteristics associated with testosterone prescribing in the Veteran Affairs system: a cross-sectional study. J Gen Intern Med. 2017;32(3): 304-311. doi:10.1007/s11606-016-3940-7
Supplementary files available here.
Please note: Only Testosterone 1% gel (ANDROGEL®) is currently registered by SAHPRA.
Register for free to access all resources
S Afr Gen Pract 2024;5(2):83-85
https://doi.org/10.36303/SAGP.0511
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Assessing the clinical impact of sodium-glucose cotransporter type 2 (SGLT2)inhibitors in treating heart failure with reduced ejection fraction
JA Ker,¹ K Outhoff²
¹ Emeritus Professor of Internal Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
² Associate Professor, Department of Pharmacology, Faculty of Health Sciences, University of Pretoria, South Africa
Corresponding author, email: jaker@lantic.net
Heart failure with reduced ejection fraction (HFrEF), often considered life-threatening, presents a significant risk to patient health. Guideline-directed medical therapy (GDMT), comprising a four-drug regimen, is currently widely recommended to optimise patient outcomes. This article seeks to elucidate the absolute benefits of SGLT2-inhibitors in the management of HFrEF and their integration into GDMT protocols.
Keywords: heart failure with reduced ejection fraction (HFrEF), SGLT2-inhibitors, guideline-directed medical therapy (GDMT)
Heart failure
Heart failure manifests through a spectrum of symptoms reflecting its complex pathophysiology. Classification of heart failure is primarily based on ejection fraction (EF), though, dividing it into two main categories: heart failure with reduced ejection fraction (HFrEF), characterised by EF ≤ 40%, and heart failure with preserved ejection fraction (HFpEF), where EF is ≥ 50%. An intermediate category, heart failure with mid-range ejection fraction (HFmrEF), falls between these two extremes with EF ranging from 41%–49%. This classification guides treatment decisions and helps tailor management strategies to address the underlying mechanisms and severity.
Heart failure is a serious syndrome associated with significant mortality and morbidity, diminished quality of life, compromised functional capacity, and considerable financial burden. The Global Burden of Disease study has revealed a heart failure prevalence of 1–3% within the general population, a figure that escalates notably with advancing age, affecting at least one in 10 individuals aged over 70 years.1 Moreover, the global prevalence of heart failure is on the rise. The incidence is 1–20 cases per 1 000 person-years or per 1 000 of the population. Regrettably, there is a notable scarcity of data concerning heart failure in developing nations.
Mortality rates linked to heart failure are concerning, with a 30-day mortality ranging from 2–3%, a one-year mortality of 15–30%, and a five-year mortality reaching 50–75%.1 Undoubtedly, heart failure poses a significant threat to life.
Heart failure in Type-2 diabetes mellitus
Type-2 diabetes mellitus (T2D) presents a considerable symptom burden and elevates the risk of cardiovascular and renal complications, as well as mortality. A multinational cohort study of patients from Norway, Sweden, Germany, the Netherlands, the United Kingdom, and Japan, evaluated a total of 1 177 896 individuals with T2D.2 Among them, 772 336 (66%) were initially
free of cardiovascular-renal disease (CVRD) at the study’s onset. Over a mean follow-up period of 4.5 years, the incidence of a first chronic kidney disease event was 36%, while that of heart failure was 24%. Incidences of stroke (16%), myocardial infarction (14%), and peripheral arterial disease (10%) were comparatively lower. The study’s conclusion stresses that heart failure and chronic kidney disease were consistently the most prevalent initial cardiovascular disease manifestations in patients with T2D.
Guideline-directed medical therapy
Guideline-directed medical therapy (GDMT) for HFrEF, defined by an EF ≤ 40%, advises the utilisation of four specific medication classes to achieve optimal treatment outcomes.3 These encompass the following:
1. Renin-Angiotensin-Aldosterone-System inhibitors such as ACE-inhibitors, ARB’s, ARNI (ARB plus Neprilysin inhibitor)
In a landmark study assessing the lifetime benefits of this GDMT approach, researchers conducted a cross-trial analysis using published randomised trials in a collaboration between the United Kingdom, United States of America, Portugal, and France.4 This study compared the GDMT method with conventional therapy and found that GDMT was associated with a favourable hazard ratio (HR) of 0.38 (95% CI: 0.30–0.47) for cardiovascular death and first hospitalisation for worsening heart failure. The study estimated that GDMT provided an additional 2.7 years free from cardiovascular death or first hospitalisation due to heart failure for an 80-year-old patient, and 8.3 additional years for a 55-year-old.
In this enhanced management strategy for HFrEF, the role of SGLT2-inhibitors becomes a pivotal aspect to explore. Two randomised controlled trials involving SGLT2-inhibitors for HFrEF aimed to address this and other relevant research inquiries.
Assessing the clinical impact of sodium-glucose cotransporter type 2 (SGLT2)-inhibitors in treating heart failure with reduced ejection fraction
The primary endpoint for both trials was the combination of cardiovascular death or hospitalisation for worsening heart failure. Both trials yielded statistically significant results: Dapagliflozin in HFrEF (DAPA-HF)5
A total of 4 744 patients diagnosed with HFrEF were enrolled in a study comparing the effects of dapagliflozin 10 mg daily versus placebo over a duration of 18.2 months.
Empagliflozin in HFrEF (EMPEROR-REDUCED)6
There were 3 730 patients with HFrEF who participated in this trial comparing empagliflozin 10 mg daily to placebo over a period of 16 months.
Number Needed to Treat (NNT) for dapagliflozin was 21 over 18.2 months; and for empagliflozin, the NNT was 19 over 16 months (See Box 1).
Event rate per 1 000 patient-years: dapagliflozin prevented four patients from experiencing the primary endpoint per 1 000 patients treated for one year; and empagliflozin prevented five patients from experiencing the primary endpoint per 1 000 patients treated for one year.
The differences between the two, while not statistically significant, could be attributed to the fact that enrolled patients receiving empagliflozin presented with more severe heart failure, as evidenced by their lower EFs.
Box 1: Number Needed to Treat (NNT)
The NNT assesses the effectiveness of a treatment. It represents the number of patients who need to be treated –in this case with an SGLT2-inhibitor – over a specific period to prevent one additional adverse cardiovascular outcome or to achieve one additional beneficial outcome compared to those not receiving the treatment. The NNT provides valuable information about the magnitude of the treatment effect and helps to evaluate the clinical significance of interventions. Lower NNT values indicate that a treatment is more effective, while higher NNT values suggest that more patients need to be treated to achieve the desired outcome.
Meta-analysis of these two trials7
A meta-analysis of these two trials involving a combined total of 8 474 patients with HFrEF yielded the following HRs (Box 2):
• Primary endpoint of cardiovascular death or hospitalisations for heart failure: HR 0.74 (95% CI: 0.68–0.82).
These findings suggest that SGLT2-inhibitors may effectively reduce cardiovascular events in patients with HFrEF, providing reassurance regarding their therapeutic benefit.
Box 2: Hazard ratio (HR)
HRs are commonly used in survival analyses and clinical trials to compare the timing of events between two groups. HRs are often used to assess the relative risk of an event (such as death, disease progression, or treatment failure) occurring in one group compared to another.
The HR represents the ratio of the hazard rates (or risks) of the event between two groups. A HR greater than 1 indicates a higher risk or hazard of the event in the first group compared to the second group, while a HR less than 1 indicates a lower risk or hazard in the first group compared to the second group.
HRs are often accompanied by confidence intervals (CI), which provide a range of values within which the true HR is likely to lie. A HR with a CI entirely above or below 1 is typically considered statistically significant.
Example:
A clinical trial comparing two treatments for heart failure finds a HR of 0.80 for cardiovascular mortality, with a 95% CI of 0.70 to 0.90.
In this example:
The HR of 0.80 suggests that patients receiving Treatment A have a 20% lower risk of cardiovascular mortality compared to those receiving Treatment B.
The 95% CI of 0.70 to 0.90 indicates that we can be 95% confident that the true HR lies somewhere between 0.70 and 0.90.
Since the CI does not include 1 (which represents no difference between the two groups), the HR of 0.80 is statistically significant, suggesting a meaningful difference between the treatments in terms of reducing cardiovascular mortality.
The absolute benefit of SGLT2-inhibitors in HFrEF
Drawing from a comprehensive study analysing data from 71 545 patients across 10 randomised controlled trials of SGLT2inhibitors,8 the following outcomes were observed when treating 1 000 patients with HFrEF for one year: 56 fewer heart failure hospitalisations, 11 fewer cardiovascular deaths, 13 fewer total deaths, and seven fewer instances of renal deterioration. These benefits should be weighed against the potential costs, which included two urinary tract infections, three mycotic genital infections, eight episodes of volume depletion, two major hypoglycaemic events, one amputation, and one fracture.
In their guideline on heart failure treatment, the Heart Failure Society of America calculated the NNT over 36 months for the four classes of drugs used in GDMT as follows:9 ARNI (ARB plus neprilysin inhibitor): 27; ACE-inhibitor or ARB: 26; SGLT2inhibitor: 22; Beta-blocker: 9; and Mineralocorticoid receptor antagonist (MRA): 6.
One expert noted that the two heart failure trials involving SGLT2-inhibitors (DAPA-HF and EMPEROR-REDUCED) prevented five to eight hospitalisations per 100 patients treated for one year.10 Referring to the publication from the Heart Failure Society
Assessing the clinical impact of sodium-glucose cotransporter type 2 (SGLT2)-inhibitors in treating heart failure with reduced ejection fraction
of America,9 this article further indicated that SGLT2-inhibitors, when used in 100 patients for three years, would prevent four to five deaths, while MRAs would prevent 17 deaths, and beta blockers would prevent 11. The author concluded by stating that while SGLT2-inhibitors are a valuable addition to other treatments for HFrEF, they are not superior to many others. These data highlight the maximal benefit achievable through GDMT, consisting of four drugs, for HFrEF.
Summary points
1. HFrEF is a life-threatening condition.
2. GDMT comprises four drug classes: RAAS-inhibitor (ARNI or ACE-Inhibitor or ARB), Beta-blocker, MRA, and SGLT2-inhibitor. Evidence supports the superiority of GDMT over conventional therapy in reducing clinical events and extending lifespan. Efforts should be directed toward promoting wider adoption of GDMT.
3. When considering SGLT2-inhibitors, their calculated absolute benefits are weighed against potential harms. While SGLT2 inhibitors provide benefits that may be less pronounced than those offered by the other three components of GDMT, they are still regarded as valuable additions to complete the fourdrug therapy regimen for HFrEF.
ORCID
References
1. Savarese G, Becher PM, Lund LH, et al. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Research. 2022;118:3272-3287. https://doi.org/10.1093/cvr/cvac013
2. Birkeland KI, Bodegard J, Ericsson JW, et al., Heart failure and chronic kidney disease manifestation and mortality risk associated in type 2 diabetes: a large multinational cohort study. Diabetes Obes Metab. 2020;1607-1618. https://doi. org/10.1111/dom.14074.
3. 2022 AHA/ACC/HFSA Guideline for the management of heart failure: Executive summary. Journal of American Coll Cardiol. 2022;79:1757-1780. https://doi.org/10.1016/j.jacc.2021.12.011
4. Vaduganathan M, Claggett BL, Jhund PS, et al. Estimating life-time benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure and reduced ejection fraction: a comparative analysis of three randomised controlled trials. Lancet. 2020;396:121-128. https://doi.org/10.1016/ S0140-6736(20)30748-0
5. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. (DAPA-HF) New Engl J Med. 2019;381: 1995-2008. https://doi.org/10.1056/NEJMoa1911303
6. Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with Empagliflozin in heart failure (EMPEROR-REDUCED). New Engl J Med. 2020;383: 1413-1427. https://doi.org/10.1056/NEJMoa2022190
7. Zannad F, Ferreira JP, Pocock SJ, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: a meta-analysis of the EMPERORREDUCED and DAPA-HF trials. Lancet. 2020;396:819-829. https://doi. org/10.1016/S0140-6736(20)31824-9
8. Chiang B, Chew DP, De Pasquale CG. Outcome trial data on sodium glucose cotransporter-2 inhibitors: Putting clinical benefits and risks in perspective. International J Cardiol. 2022;349:96-98. https://doi.org/10.1016/j. ijcard.2021.12.015
9. Bozkurt B, Ahmad T, Alexander KM, et al. Heart failure epidemiology and outcomes statistics: A report of the Heart Failure Society of America. J Cardiac Fail. 2023;29:1413-1451. https://doi.org/10.1016/j.cardfail.2023.07.006.
JA Ker https://orcid.org/0000-0002-6303-9848
K Outhoff https://orcid.org/0000-0002-0851-4802
10. Cleland JGF. Editorial: Nature and magnitude of the benefits of Dapagliflozin and Empagliflozin for heart failure. Circulation. 2024;149:839-842. https://doi. org/10.1161/CIRCULATIONAHA.123.068089
S Afr Gen Pract 2024;5(2):86-91
https://doi.org/10.36303/SAGP.0432
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Self-reported practices and learning needs of private general practitioners during the pandemic in South Africa
JM Musonda,1 JS Musonda2
1 Department of Family Medicine and Primary Care, University of the Witwatersrand, South Africa
2 Department of Family Medicine and Primary Care, University of Pretoria, South Africa
Background: General practitioners (GPs) are the first contact when seeking medical treatment for any symptom. However, their clinical practices and learning needs in the pandemic remain unknown in South Africa. We aimed to evaluate private GP practices and learning needs during the pandemic in South Africa. The objectives described and determined participant characteristics, skills, and roles and identified gaps.
Methods: The online survey conducted a cross-sectional descriptive study of private general GPs in South Africa between 30 June and 30 July 2021. Overall, 7 782 subscribed to the e-mail marketing network, which conducted a single-stage cluster sampling. A validated data collection tool and COVID-19 scorecard on the Likert scale were utilised. Data analyses used R and R Studio (v 2021.09.0+351) (R Core Team, 2019) and Microsoft Excel (v 2019).
Results: Respondents completed 88 questionnaires (40 males, 48 females, median age 47 years). The median clinical practice was 60%. The best-performing domain was medical products and technologies, at 69% (n = 61). The lowest was service delivery, at 47% (n = 41). Most reported training and practice in administration, communication, consultation, women’s health, and emergencies. Most did not practice obstetrics and paediatrics and lacked forensic medicine training and skills. Significant GP roles were competent clinician, capacity builder, and critical thinker. The minors were collaborators, community advocates, and the slightest change agents.
Conclusion: Most private GPs are trained in most disciplines with limited exposure to forensic medicine. Similarly, most competencies are performed except as change agents. However, gaps exist in obstetrics, paediatrics, and forensic medicine skills. Further research is recommended.
Keywords: private, general practitioners, skills, roles, competencies, learning needs, COVID-19 pandemic, South Africa
Introduction
The COVID-19 pandemic emphasised the need for a coordinated national response that harnesses the resources of the current two-tier health system in South Africa.1 Success in managing the spread of the coronavirus was achieved with a coordinated and integrated health systems approach involving private general practitioners (GPs). A coordinated national response may have provided a framework for future public health emergencies.2 Improving the efficiency and effectiveness of the healthcare system by allocating adequate resources, particularly during a pandemic, promotes a better quality of service for everyone in South Africa.3,4
Universal health coverage (UHC) is one of the health targets of the Sustainable Development Goals set by the United Nations. It is core to achieving improved quality and distribution of healthcare by GPs and others.5,6,7 National Health Insurance (NHI) is a funding designed to guarantee access to quality health services for everyone in South Africa, irrespective of socioeconomic status, and based on individual healthcare needs.8,9 The World Health Organization (WHO) member states commit to realising universal health coverage.10 Hence, the priority in South Africa is to re-engineer the primary healthcare system to address the burden of diseases and prepare for future pandemics. The private
GPs are vital to those aspirations.3,4 The skills and learning needs of private GPs in the pandemic remain unknown. Understanding that may prepare the healthcare system better for the future.
The study aimed to evaluate private GP practices and learning needs during the COVID-19 pandemic in South Africa. The objectives described and determined participant characteristics, clinical skills, and roles and identified gaps considering the pandemic.
Materials and methods
Research design
This was a cross-sectional descriptive study of primary care doctors, specifically private GPs in South Africa.
Study site
We recruited private GPs in South Africa from the Medpages healthcare database. It actively managed 509 258 healthcare provider records (public and private sector) across Africa. There were 14 456 registered private GPs in the South Africa Medpages database.11
Study population
Private GPs registered on the Medpages database across all provinces in South Africa were surveyed.
Sampling strategy
Overall, 7 782 private GPs were subscribed to the e-mail marketing network on the Medpages database, which provided a once-off opportunity to survey 7 782 GPs using a single-stage cluster sampling.11
Data collection tool/instrument
The survey tool addressed the study objectives and adapted relevant publications. The GPs’ practice changes during the pandemic were described by adopting a COVID-19 - Score designed to gauge the healthcare system’s response during the pandemic.2 For each statement on the scorecard, respondents were asked to select one response on a Likert scale: 1 – I strongly disagree with this statement; 2 – I disagree with this statement; 3 – I feel neutral towards this statement; 4 – I agree with this statement; 5 – I strongly agree with this statement. The statements were scored in six domains: leadership and governance, health workforce, health information systems, medical products and technologies, financing, and service delivery.12,13,14.
Relevant skills were extracted from the national list related to training family physicians in South Africa to describe skills needed during the pandemic.10 The skills focused on emergency care, communication and consultation, administrative, forensic, maternal health, and paediatric care. We asked GPs to assess their ability to perform the skills by selecting each skill category from a Likert scale: 1 – I have not had training in the skill; 2 – I have received training but have not performed the skill in the last year; 3 – I have performed the skill in the previous year; 4 – I have taught the skill to others in the past year.
The competencies were described by adapting the blueprint for the National Diploma in Family Medicine.13,15,16 We asked GPs to rate their confidence in performing competencies related to the six roles for each role from a Likert scale: 1 – Not confident (I have never taken on this role); 2 – Some confidence (I have taken on this role in the past, but not in the previous year); 3 – Confident (I have taken on this role in the last year); 4 – Very confident (I could be a role model to others).
Data collection process
We contacted GPs through the healthcare provider contact information supplied by the Medpages database and invited the 7 782 private GPs to participate in the survey. We requested that they complete the survey electronically on a secure online platform using Google Forms. The survey questionnaire was distributed once to each GP, and access to the survey link was open between 30 June 2021 and 30 July 2021 (Figure 1).
Pilot study for testing the measurement tool.
We tested the feasibility of the survey with members of the research team and a biostatistician at the Faculty of Health Sciences, University of the Witwatersrand. The pilot study was
Private GPs on SA Medpages = 14 465. Single-stage cluster e-mail marketing 7 782 (54%)
Total e-mails sent on 30 June 2021 = 7 651 (98%)
Total click-through = 2 063 (27%)
Total respondents who completed the questionnaire on 30 July 2021 during the pandemic = 88 (1%)
Total undelivered = 131 (2%)
Total unsubscribes = 15 (2%)
conducted between January and February 2021, validated the survey’s content and construct, identified unanticipated problems, and thoroughly checked the planned analytical and statistical procedures.
Statistical methods
The sociodemographic details of the participating GPs and data on an ordinal Likert scale, were scored from 1 to 5 and 1 to 4 for each entry. We included six sociodemographic variables: age (years); gender (female, male, non-binary); population group (Black African, Coloured, White, Indian/Asian); practice type (solo, group, independent practitioner association or IPA); community served (lower income; lower-middle income; middle-upper income; and not applicable); and the year of graduation.
The population groups were assigned based on self-identified ancestry, such as Black African (African ancestry), White (European ancestry), Coloured (mixed ancestry, this is a uniquely South African classification), and Indian/Asian (East Asian ancestry, predominantly the Indian subcontinent). Those who did not fall into the above were designated “other”. Categorical data was reported as frequencies and numbers. Data was analysed using descriptive statistics with the help of a biostatistician at the Faculty of Health Sciences, University of the Witwatersrand. The ordinal data was reported as frequencies. All statistical analyses were computed using R and R Studio (v 2021.09.0+351) and plotted in Microsoft Excel.17
Results
Sociodemographics
The respondents who completed the online survey questionnaire were 88 (males 40, females 48, median age 47 years), with 440 potential responses. The majority were White (72%, n = 63), followed by Black Africans (18%, n = 16), and Indians/Asians (10%, n = 9). The most frequent age group of respondents was between 37 and 57, with a median age of 47 years, and most having graduated between 1986 and 2005. Nearly 40% (n = 35) of respondents were based in Gauteng Province, followed by the Western Cape 26% (n = 23), KwaZulu-Natal 10% (n = 9),
Figure 1: A flow diagram depicting the data collection process.
Mpumalanga 7% (n = 6), Eastern Cape 6% (n = 5), Free State 6% (n = 5), Limpopo 3% (n = 3), and North west 2% (n = 2).
For the practice type, 55% (n = 48) of respondents worked in solo practices, 10% (n = 9) in independent practitioner associations, and 35% (n = 31) in group practices. Regarding the type of community served, 11% (n = 10) of respondents reported the lower income community, 41% (n = 36) the lower-middle income community, and 41% (n = 36) the middle-upper income group (Figure 2).
Clinical practice and the pandemic
The overall median score for the clinical practice response was 60%, with most scores falling between 50% and 70%. However, some scores were as low as 36% and as high as 94%.
The domains derived from the Likert scorecard showed medical products and technologies had a median score of 69% (the highest) with an upper quartile of 80% and a lower quartile of 60%. In contrast, service delivery had a median of 47% (the lowest), with an upper quartile of 58% and a lower quartile of 38% (Table I).
Figure 2: Distribution of private general practitioners by the community they served.
Table I: The pandemic health systems domain scores by private general practitioners
Figure 3: A cluster bar chart depicting each competency category’s frequency of Likert options.
1
2
3
4 - Trained (taught others)
Roles and competencies of general practitioners
For the overall rating of performing the roles collectively, the median score was 75%, with most falling between 54% and 91%. However, some scores were as low as 25% and others as high as 100%. Most GP role scores were relatively high, with a broader variability than the clinical skills categories.
Similarly, the Likert options of the GP roles showed the most confidence in performing them as competent clinicians, followed by capability builders, critical thinkers, community advocates, and collaborators. The least confidence in GP roles was as a change agent (Figure III).
Learning needs of general practitioners
For the overall ability to perform clinical skills collectively, the median score was 65%, with most falling between 54% and 75%. However, some scores were as low as 33% and as high as 100%.
The frequency of the Likert options in each clinical skills category showed that the taught skill category was administration, followed by communication and consultation, feminine or women’s health, and emergency. Similarly, private GPs had the most training and clinical performance in those skills. In the obstetrics and paediatrics skills category, most respondents indicated that they had been trained but had not performed the skill the previous year. Significantly, most respondents indicated lacking training in the forensic skill category (Figure 4).
Discussion
Main study findings
Overall, 7 782 private GPs were requested to complete the survey, and 88 completed the questionnaire. The best-performing domain was medical products and technologies, at 69% (n = 61), and the lowest was service delivery, at 47% (n = 41). Most
reported training and performance or practice in administration, communication, consultation, women’s health, and emergency care. Despite training, the majority did not practice obstetrics and paediatrics. However, most reported lack of training postgraduation from medical school. Significant GP roles included competent clinician, capacity builder, and critical thinker. The minor roles were a collaborator and community advocate; the least was a change agent, in that order.
Interpretation of findings
Sociodemographics
According to one study, 59.4% of medical doctors in South Africa were male, and 40.6% were female.17 The converse is true of the present survey responses, where the majority are female. As of 2019, the doctor population in South Africa was 44.8% white, 28.7% black, and 15.4% Indian/Asian.15 It follows that respondents in the current study were not aligned with the reported distribution of doctors by race in South Africa because nearly three-quarters of respondents were white, meaning black African and Indian/Asian doctors were under-represented for different reasons, which may range from lack of interest in the topic, time constraints, connectivity challenges or lack of equipment and so forth.
The lack of data hardly describes the distribution of private GPs by type of practice and population group served in South Africa. The current study adds value to that understanding. The finding that most private GPs work in solo practice and serve middleincome groups is not surprising but may provide some insight into private GP distribution because a significant number of GP practices are found in urban areas of South Africa. Furthermore, the distribution of respondents by SA provinces in the current study showed the majority practised in Gauteng and the Western Cape, as reported previously.18
Figure 4: A clustered bar chart depicting the frequency of Likert options of the clinical skills category and learning needs.
Less than two-thirds of respondents reported readiness in different aspects of healthcare provision in a pandemic, with five out of the six category medians above 60%. The finding may suggest most GPs consider themselves capable of performing duties during a pandemic because there is sufficient access to services and the use of the necessary medical supplies and equipment. On the contrary, most GPs perceive that service delivery may be compromised during the pandemic because the doctor-to-patient ratio and quality of care may decrease. Ideally, comparison to health systems from other countries may give us insight into the level of preparedness of South African doctors, evaluating health issues and the need for changes to the national healthcare framework. While the overall median shows a relatively low level of preparation and readiness for the pandemic, it remains unclear what specific improvements need to be made in the relevant areas of the pandemic.20, 21.
Clinical
skills and the pandemic
The finding that most respondents reported having trained and practised in four of the six clinical skills surveyed is interesting. However, only 17% of respondents reported that all six skills were learned and practised, and GPs could confidently teach the skills to others. That observation suggests most GPs in the current study are competent in the necessary and relevant clinical skills but may not teach the same. Lack of knowledge in those fields, thus preventing teaching or the workload pressure during the pandemic, may be the reason. The above may also provide some insight into the learning needs of GPs during a pandemic. Furthermore, confidence in teaching, availability of time to teach, and accessibility of trainees may have contributed to the weak findings.
Although most private GPs are trained in obstetrics and paediatrics, they do not practise those clinical skills. It is unclear whether that is due to insufficient training, clinical exposure, lack of opportunity, or necessity to perform them. However, the finding suggests that a curriculum change focusing on obstetric and paediatric clinical skills may be beneficial. Most GPs ultimately had no training in forensic medicine skills. While more significant and inclusive studies must be conducted to confirm this finding, it preliminarily suggests a clear need in the education system to include more comprehensive forensic medicine training to ensure more competent healthcare providers.
General practitioners’ roles or competencies
Family physicians are required to master several clinical roles or competencies to become competent healthcare providers.12,13,14 While the study specifically focused on postgraduate training, the roles apply to all primary care doctors, including GPs, in assessing their competencies as clinicians in a primary care setting. Private GPs were, at minimum, competent in five out of the six roles, as highlighted in Figure 3. The observation correlates well with previous reports and implies that the majority of private GPs in South Africa can provide quality healthcare that is holistic and collaborative when they are trained on a variety of skills and competencies.12,13,14 However, in the role of “change agent,” most respondents indicated they had “some confidence” in
performing a given skill. The finding suggests that most doctors surveyed may have had some confidence in the change process, both on practical and administrative levels.
Learning needs of general practitioners
Generally, medical doctors in South Africa contribute to and are champions of improved healthcare for better healthcare. Most respondents reported that they practised the role of “collaborator” very confidently. That may imply that private GPs “champion collaborative practice and change”, essential to successful healthcare reforms. Besides, the finding supports a study that reported that the medical school curriculum in South Africa provided adequate training. Other studies that focused on the learning needs of family physicians in South Africa confirmed that medical education in South Africa was sufficient regarding clinical roles.12,13,14.
Moreover, private GPs show competencies in most clinical roles, except for the lack of practise in obstetrics and paediatrics, despite having participated in theoretical training. Additionally, there is a lack of training in and practise in clinical forensic medicine. There are several reasons for the findings. However, the standard features across obstetrics, paediatrics, and clinical forensic medicine are that they are all highly specialised and prone to medicolegal risk, and less attractive GPs. Reasonable exposure and targeted training at both undergraduate and postgraduate levels may help to mitigate the apparent gap in the private GP practice and roles.14,15,16
Potential strengths and limitations
The study did have some strengths. Perspectives from GPs may provide insights into parts of a health system framework, such as service delivery, financing, leadership and governance, health information systems, and medical products and technologies. The views may have highlighted critical inadequacies in the health system resilience and pandemic preparedness.2, 20,21 Therefore, addressing the shortcomings may improve the healthcare system’s response to future pandemics and strengthen it to implement the NHI.9,10,19
The study did have some limitations. The low response rate may be attributed to the peak of the COVID-19 pandemic. The small sample size affected the power of the study and did not represent all private GPs. Hence, our study findings are not generalisable to all private GPs. Moreover, the single-stage cluster sampling may have affected our chances of reaching more private GPs because we were limited to one mode of communication. Furthermore, our limited period for data collection and lack of reminders may have reduced our chances of reaching a high response rate.
Performing a clinical skill recently does not imply the performance is at a level of competence. Direct observation may be the only acceptable assessment technique. It is plausible that GPs may have overestimated their competencies, particularly the scope of practice and clinical skills, in a self-reported scoring system. Although we aimed to select a diversity of GPs, we may
have missed GPs who could have contributed more viewpoints to our findings.
Conclusion
The study shows that most private GPs adequately practise most clinical disciplines besides obstetrics, paediatrics, and forensic medicine. Similarly, most roles or competencies are performed except as change agents. The identified gaps suggest learning needs, which may be addressed through continuous professional development. Further research to understand specific experiences by private general practitioners is recommended.
Acknowledgements
The study emanated from a research project. The authors thank the participants, Medpages, and the University of the Witwatersrand, Department of Family Medicine, and Primary Care. Special thanks to Prince Chikezie, Meghan Britz, Gabriel Desjardins, Muhammad Essack, Mpumelelo Ngele, and Lesego Phiri, who participated in the data collection and report compilation.
Conflict of interest
No conflict of interest is to be declared.
Funding source
No funding source is to be declared.
Ethical approval
The ethical approval for the study protocol was obtained from the Human Research Ethics Committee of the University of the Witwatersrand certificate no. M200817. Each respondent was availed of participant information and an option to consent and opt out at any stage of the study. Information collected was anonymous, confidential, and secured by the researchers, who acknowledged that respondents may have experienced discomfort and lost time when completing the questionnaires.
ORCID
5. Smith A, Ranchod S, Strugnell D, Wishnia J. Human resources for health planning and National Health Insurance: the urgency and the opportunity. South African Health Review. 2018;23-31.
6. Kavanagh MM, Erondu NA, Tomori O, et al. Access to lifesaving medical resources for African countries: COVID-19 testing and response, ethics, and politics. Lancet. 2020;395(10238):1735-1738. https://doi.org/10.1016/S0140-6736(20)31093-X.
7. Tangcharoensathien V, Mills A, Palu T. Accelerating health equity: the key role of universal health coverage in the Sustainable Development Goals. BMC Medicine. 2015;13(1):101. https://doi.org/10.1186/s12916-015-0342-3.
8. South African Government. National Health Insurance - NHI. Pretoria; South Africa. 2015. Available at: http://www.health.gov.za/index.php/nhi. Accessed 5 July 2020.
9. Department of Health. White paper: National Health Insurance for South Africa: Towards universal health coverage. Government Gazette. Version 40. Friday, 11 December 2015. http://www.gpwonline.co.za. Accessed 5 July 2015.
10. Mathew S, Mash R. Exploring the beliefs and attitudes of private general practitioners towards national health insurance in Cape Town, South Africa. Afr J Prim Health Care Fam Med. 2019;11(1):e1-e10. https://doi.org/10.4102/phcfm. v11i1.2189.
11. Medpages. Statistics - medical professionals in South Africa. 2020. Available from: http://www.medpages.info/sf/index.php? page = category stats & country id = 1&categoryid = 1. Accessed 20 July 2020.
12. Malan Z, Cooke R, Mash R. The self-reported learning needs of primary care doctors in South Africa: A descriptive survey. S Afr Fam Pract. 2015;57(1):35-43. https://doi.org/10.1080/20786190.2014.1002677.
13. Mash R, Malan Z, von Pressentin K, Blitz J. Strengthening primary health care through primary care doctors: designing a national postgraduate diploma in family medicine. S Afr Fam Pract. 2016;58(1):32-36. https://doi.org/10.1080/207 86190.2015.1083719.
14. Akoojee Y, Mash R. Reaching national consensus on the core clinical skill outcomes for family medicine postgraduate training programs in South Africa. Afr J Prim Health Care Fam Med. 2017;9(1):a1353. https://doi.org/10.4102/phcfm. v9i1.1353.
15. Couper I, Mash R. Obtaining consensus on core clinical skills for training in family medicine. S Afr Fam Pract. 2008;50(6):69-73. https://doi.org/10.1080/20786204.2 008.10873796.
16. Mash B, Couper I, Hugo J. Building consensus on clinical procedural skills for South Africa family medicine training using Delphi technique. S Afr Fam Pract. 2006;48(10):14a-e. https://doi.org/10.1080/20786204.2006.10873475.
17. R Core Team. A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing. 2019. Available from: https:// www.r-project.org/ Accessed 18 July 2020.
JM Musonda https://orcid.org/0000-0003-2942-1039
JS Musonda https://orcid.org/0000-0002-8125-6723
References
1. Rispel LC, Shisana O, Dhai A, et al. Achieving high-quality and accountable universal health coverage in South Africa: a synopsis of the Lancet National Commission Report. South African Health Review. 2019;69-80.
2. Lazarus JV, Binagwaho A, El-Mohandes AE, et al. Keeping governments accountable: the COVID-19 Assessment Scorecard (COVID-SCORE). Nature Medicine. 2020;1-4. https://doi.org/10.1038/s41591-020-0950-0.
3. Mayosi BM, Lawn JE, van Niekerk A, et al. Health in South Africa: changes and challenges since 2009. Lancet. 2012;380(9858):2029-2043. https://doi. org/10.1016/S0140-6736(12)61814-5
4. Van Rensburg HCJ. South Africa’s protracted struggle for equal distribution and equitable access - still not there, Human Resources for Health, BioMed Central. 2014;12(1),26. https://doi.org/10.1186/1478-4491-12-26
18. Tiwari R, Wildschut-February A, Nkonki L, et al. Reflecting on the current scenario and forecasting the future demand for medical doctors in South Africa up to 2030: towards equal representation of women, Human Resources for Health. 2021;19(1):27. https://doi.org/10.1186/s12960-021-00567-2.
19. Mofolo N, Heunis C, Kigozi GN. Towards national health insurance: Alignment of strategic human resources in South Africa. Afr J Prim Health Care Fam Med. 2019;11(1):7. https://doi.org/10.4102/phcfm.v11i1.1928.
20. Corlette S, Wengle E, Houston M, Thomas TW. The impact of the COVID-19 pandemic and recent federal policies on small business health insurance. 2021. Available from: https://www.urban.org/research/publication/impact-covid19-pandemic-and-recent-federal-policies-small-business-health-insurance. Accessed 2 October 2021.
21. Verhoeven V, Tsakitzidis G, Philips H, van Royen P. Impact of the COVID-19 pandemic on the core functions of primary care: Will the cure be worse than the disease? A qualitative interview study in Flemish GPs, BMJ Open. 2020;10(6):e039674. https://doi.org/10.1136/bmjopen-2020-039674.
S Afr Gen Pract 2024;5(2):92-95 https://doi.org/10.36303/SAGP.0565
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Acne vulgaris and variants
JJ
Makhubele, JM Mokheseng, MC Kgokolo
Department of Dermatology, Faculty of Health Sciences, Steve Biko Academic Hospital, University of Pretoria, South Africa
Corresponding author, email: jmakhubele@gmail.com
Acne vulgaris is a multifactorial, inflammatory disease of the pilosebaceous unit (comprising the hair follicle and sebaceous gland), primarily involving the face, chest, and back. It is a chronic disease with a potentially severe impact on the quality of life and self-image of all age groups affected. It has been associated with increased rates of anxiety, depression, and suicidal ideation. Therefore, clinicians must be well informed on the pathogenesis, clinical diagnosis, grading of severity, treatment algorithm, and pharmacology of the medications used for acne.
Keywords: acne vulgaris, common skin condition
Introduction
Acne vulgaris is a common skin condition that affects all skin types and ethnic groups. Although perceived to be a teenage disease, acne often persists into adulthood and can result in significant scarring.1 The condition typically begins at puberty when sex hormones begin to be produced, with the prevalence of acne in boys increasing from 40% at age 12 years to 95% at age 16 years, and the prevalence increases similarly from 61% to 83% in girls.2
The presence of acne has an important impact on emotional functioning, social functioning, relationships, leisure activities, daily activities, sleep, school, and work, particularly in adolescents. Suicidal ideation has been documented in ~7.1% of affected individuals.3,4 The negative impact on the quality of life further illustrates the importance of early and aggressive treatment.1 The risk factors for acne include genetics, hyperandrogenism, polycystic ovarian syndrome, medications such as antiepileptics, lithium, progesterone-only contraception, isoniazid, oral and topical corticosteroids, vitamin B12, the application of oily products and a high glycaemic-index diet.5,6
Variants of acne vulgaris include acne fulminans, acne conglobata, acne excoriée, drug-induced acne, acne mechanica, pomade acne, occupational acne, chloracne, neonatal and infantile acne.1
Pathogenesis
The pathophysiology of acne is multifactorial and is still not well understood. It is a chronic inflammatory condition that usually occurs at the onset of puberty due to increased production of androgens by the adrenals and gonads and/or increased sensitivity of androgen receptors.
The main pathogenetic factors important for acne include:7,8
• Androgen stimulation of sebaceous glands
• Hypersecretion of sebum
• Hyperkeratosis and occlusion of the duct that drains sebum into the hair follicle
• The formation of the invisible microcomedo
• Inflammatory mediators (Interleukin 1, etc) released after stimulation of toll-like receptor 2 by Cutibacterium acnes (formerly Propionibacterium acnes)
• Neutrophilic response to rupture of comedones and inflammation induced by free fatty acids in sebum
• Proliferation of Cutibacterium acnes
• Inflammatory tissue damage by matrix metalloproteinases
Clinical presentation
Acne vulgaris affects areas with a high density of sebaceous glands, i.e. the face, chest, and back, and the skin lesions can be inflammatory or non-inflammatory. It is a clinical diagnosis. Noninflammatory acne is characterised by both open (blackheads) and closed (whiteheads) comedone formation.5 Melanin deposition and lipid oxidation within the debris is responsible for the black discolouration.
The inflammatory lesions of acne originate with comedo formation but then expand to form papules, pustules, nodules, and cysts of varying severity. As the severity of lesions progresses, nodules form and become markedly inflamed, indurated, and tender. The acne cysts are deeper and filled with a combination of pus and serosanguineous fluid. In patients with severe nodulocystic acne, these lesions may form massively inflamed complex plaques and sinus tracts.7
Acne can be clinically graded and classified to assess overall disease severity, help facilitate therapeutic decision-making, and assess and evaluate treatment response.6
Scars are visible and persistent reminders of acne. This dreaded outcome can occur in all grades of acne. Early and appropriate treatment is best to minimise the potential for acne scarring. Scars form at the site of tissue injury and may be hypertrophic or atrophic. Atrophic scars are divided into three types: ice-pick, rolling, and boxcar.1
The scar: scar characteristics usually determine the treatment approach and may involve resurfacing, surgical revision, and dermal fillers. In many cases, topical retinoids are a useful adjunct to procedures in managing scarring.1,2 Pigmentary complications are also of important cosmetic concern for all patients regardless
Dermatology 2nd edition; Bolognia
Picture 1: Closed comedone (black arrow) and open comedone (blue arrow)
Courtesy of Dr AV Chateau
Picture 2: Papule
Picture 3: Pustule (black arrow) and nodule (blue arrow)
of skin colour, and inflammation is an important factor in postacne hyperpigmentation.9
Management
There is currently vast literature and several guidelines for management of acne vulgaris (Table I).
Table I: Pathogenic factors in acne and relevant treatment
Pathogenic factor
Androgen stimulation of sebaceous glands
Hypersecretion of sebum
Hyperkeratosis and occlusion of the duct that drains sebum into the hair follicle
Formation of the invisible microcomedo
Inflammatory mediators released
Neutrophilic response to rupture of comedones and inflammation
Proliferation of P. acnes (Cutibacterium)
Inflammatory tissue damage by metalloproteinases
S Afr Fam Pract 2017;59(1):24–29
Medication
Cyproterone acetate
Oral isotretinoin
Topical retinoids
Topical retinoids
Topical retinoids; oral isotretinoin
Oral cyclines; oral and topical dapsone; oral macrolides
• Tetracyclines – contraindicated below 9 years of age
J Am Acad Dermatol Volume 90, Number 5 2024
Laboratory monitoring during isotretinoin treatment
Includes – liver function test, fasting lipid profile and pregnancy test (if applicable).
Side effects of isotretinoin
• Teratogenicity (pregnancy test before initiation and effective contraception)
• Mucocutaneous side effect
• Photosensitivity
Picture 4: Types of acne scarring: Ice pick scarring (white arrow); boxcar (blue arrow); rolling (black arrow)
• Ocular complications
• Deranged liver enzymes and dyslipidaemia
• Raised intracranial pressure when combined with tetracyclines
• Myalgia and arthralgia
• Gastrointestinal side effects
• Mood disturbances
Maintenance treatment
Maintenance therapy is necessary post successful treatment of acne. A cure rate of 38% is seen in patients treated with oral isotretinoin. Maintenance should continue until a patient no longer develops new lesions. Topical retinoids are ideal for maintenance and are the only registered products for this indication as they eradicate inflammatory and non-inflammatory microcomedones. Topical retinoids can be combined with topical benzoyl peroxide (combination therapy) or as a single product (BPO in the morning and retinoids at night). Benzyl peroxide should not be used as monotherapy as it does not target the microcomedones and does not have non-inflammatory effects like retinoids. Azelaic acid can also be used if topical retinoids cannot be tolerated.1,10
Take home message
Acne vulgaris is not a self-limiting condition. Early and effective treatment can improve the patient’s well-being and may prevent permanent scars or pigment changes.1
JM Mokheseng https://orcid.org/0009-0001-9104-8303
MC Kgokolo https://orcid.org/0000-0003-0362-1497
References
1. Thiboutot D, Gollnick H, Bettoli V, et al. New insights into the management of acne: An update from the Global Alliance to Improve Outcomes in Acne Group. J Am Acad Dermatol. 2009;60(5):S1-S50. https://doi.org/10.1016/j. jaad.2009.01.019
2. Eichenfield DZ, Sprague J, Eichenfield LF. Management of acne vulgaris. A review. JAMA. 2021;326(20):2055-2067. https://doi.org/10.1001/ jama.2021.17633
3. Archana NH. The psychosocial impact of acne vulgaris. Indian J Dermatol. 2016;61(5):515-520. https://doi.org/10.4103/0019-5154.190102.
4. Zulu TP, Mosam A, Balakrishna Y, Dlova NC. Acne in South African black adults: A retrospective study in the private sector. S Afr Med J. 2017;107(12):1106-1109. https://doi.org/10.7196/SAMJ.2017.v107i12.12419
5. Santer M, Ravenscroft J. Managing acne vulgaris: an update. Drug and Therapeutics Bulletin, January. 2024;62:1. https://doi.org/10.1136/ dtb.2023.000051
6. Sinclair W. Guidelines for the management of acne vulgaris. South African Family Practice. 2017;59(1):24-29. https://doi.org/10.4102/safp.v59i1.4629
7. Bolognia JL, Rapini RP. Dermatology. Second edition ed: British Library Cataloguing in Publication Data; 2008.
8. Beylot C, Poli F, Claudel J-P, et al. Propionibacterium acnes: an update on its role in the pathogenesis of acne. JEADV. 2014;28:271-278. https://doi.org/10.1111/ jdv.12224
9. Al-Qarqaz F, Badoor K, Baba A, et al. Post-acne hyperpigmentation: Evaluation of risk factors and the use of artificial neural network as a predictive classifier. Dermatology Reports. 2021;13:8223. https://doi.org/10.4081/dr.2021.8223
10. Reynolds RV, Yeung H, Cheng CE. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):P1006.E1. https://doi.org/10.1016/j. jaad.2023.12.017.
S Afr Gen Pract 2024;5(2):96-97 https://doi.org/10.36303/SAGP.0605
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
The link between thyroid hormones and cutaneous squamous cell carcinoma
S Khan,1 H Parkar2
1 Bophelong Clinic, Tshwane District Offices, South Africa
2 Department of Pharmacology, Faculty of Health Sciences, University of Pretoria, South Africa
This case study aims to improve clinical practice by highlighting hypothyroidism as a possible risk factor for the development of squamous cell carcinoma (SCC), particularly in people of colour. A 65-year-old Black female presented with generalised weakness and confusion. Examination revealed a left-sided oculomotor nerve palsy. Laboratory tests indicated central hypothyroidism with a CT brain scan showing a cystic lesion in the suprasellar region. Patient history revealed that a malignant growth had been excised from her left leg eight months earlier and biopsy results revealed SCC. This case study underlines the connection between hypothyroidism and SCC, emphasising the complex role of thyroid hormones in cancer development.
A 65-year-old Black female was brought to the emergency centre with a history (~1 year) of generalised body weakness and occasional confusion. The family described that the patient was previously independent and capable of performing all the activities of daily living but had steadily declined in her ability to do so. They confirmed that she had deviated from her cognitive baseline and reported a history of lethargy and occasional confusion. The patient’s family had assumed that the initial symptoms observed were attributed to age but expressed concern due to the significant worsening of her symptoms in the last six weeks. A general examination revealed an area of mild hypopigmentation on the left leg with no other skin lesions noted. The thyroid examination was within normal limits and no stigma of immunecompromised state or chronic disease was observed. A focused neurological examination revealed an isolated left-sided oculomotor nerve palsy. The rest of the physical examination was unremarkable. Noteworthy patient history included a skin lesion on the left lower leg eight months prior. The histological biopsy revealed a malignant neoplasm characterised by malignant cells growing in large nests and surrounded by fibrosis, the borders of which had infiltrated 14 mm into the reticular dermis. The entire tumour, measuring 130 ×15 ×25 mm was completely excised with good margins and had healed well.
The patient was admitted, and special investigations included a delirium workup. Included in this were thyroid function tests for thyroid stimulating hormone (TSH) and thyroxine (T4), vitamin B12, urea and electrolytes and a septic screen. Laboratory results revealed a TSH level of < 0.01 mIU/L and T4 level of 10.0 pmol/L indicative of central hypothyroidism. The rest of the biochemistry was within a normal range, with a negative septic workup. Imaging was requested, and an uncontrasted CT brain scan revealed a poorly defined cystic lesion in the suprasellar region of the brain, suggestive of central hypothyroidism. Results from a lumbar puncture were unremarkable, aside from raised protein
levels of 2.89 g/L. Unfortunately, the patient demised prior to an MRI scan being performed.
The question was then posed whether thyroid dysfunction is an identifiable risk factor for the development of cutaneous squamous cell carcinoma (SCC). The following discussion aims to explore this.
Discussion
There are multiple risk factors strongly associated with the development of SCC. The most well-known are the phenotypic characteristics: red hair, fair skin (with long exposure to UV radiation), suntanning, HIV, as well as other genetic or immune and environmental risk factors.1,2 In the African population, high levels of melanin serve as a protective factor against UV rays.3 However, SCC is still a frequently diagnosed dermatological malignancy, developing in sun-protected areas of the body such as the lower leg, particularly in sites of chronic ulceration and previous burns that are not related to sunburns.2,4 The development of SCC occurs by malignant transformation of epidermal skin cells. UV rays damage DNA in cells, leading to genetic defects with ongoing replication.5
Primary hyperthyroidism is defined as low levels of TSH and elevated levels of 3, 5, 3’-triiodo-L-thyronine (T3) and T4, while hypothyroidism is diagnosed when the TSH is elevated and the T4 is low.6 Central hypothyroidism is characterised by low levels of both TSH and T4.7 Clinical manifestations on the target organ in both hyper- and hypothyroidism are as a result of T4 levels. The cutaneous manifestations of hypo- and hyperthyroidism are mainly attributed to the dysregulation of epidermal homeostasis resulting in either dry and course skin with myxoedema or smooth skin with thyroid acropachy, respectively.8
Thyroid dysregulation has long been implicated in the pathogenesis of cancer. The link between thyroid dysregulation and cancer involves complex interactions that influence both cancer risk and progression. There is more evidence supporting
Table I: Effect of thyroid enzymes on T4 and their link to squamous cell carcinoma17
Thyroid enzyme Effect on T4 Effect on SCC
Increased expression of D2 Activates conversion of T4 to T3
Increased expression of D3 Inactivates T4 or T3
the role of hyperthyroidism in the pathogenesis of cancers, with hypothyroidism having an inhibitory effect in some cancers.9 This case report postulates that hypothyroidism is implicated in the development of SCC.
A study conducted by Ahadiat et al., 2018 highlighted a prominent link between hypothyroidism and the development of cutaneous SCC as seen in this case report. The retrospective review showed that 31% of patients with SCC were previously diagnosed with hypothyroidism.10 It was concluded that individuals with SCC are more likely to have a history of hypothyroidism compared to the general population.
Lobl et al., 2022 conducted a multi-institutional, case-controlled study of 65 cutaneous SCCs with known lymph node metastasis matched with 195 cutaneous SCCs without lymph node metastasis. Hypothyroidism was identified as a key risk factor for SCC in lymph node metastasis (OR 2.7 CI 95% 1.04–7. 0).11
Hypothyroidism has been associated with several types of cancer, including thyroid cancer, colon cancer, breast cancer, and hepatocellular carcinoma. Studies have indicated connections between hypothyroidism and these cancers, though the precise nature of these relationships is still being explored.9,10,12-16 Currently, there is limited evidence linking hypothyroidism to any type of skin cancer, specifically SCC.
Despite extensive research on hypothyroidism, there is a need for larger studies to establish a conclusive connection between hypothyroidism and any type of skin cancer, including SCC. However, given the significant impact hypothyroidism has on the skin, exploring a potential link between hypothyroidism and skin cancer is a logical area for further investigation.10
Possible mechanisms to explain the pathogenesis of hypothyroidism-induced cancers involve the expression levels of the thyroid enzymes. Thyroid enzymes iodothyronine deiodinases type 1 and 2 (D1 and D2) have a role in activating thyroid hormone T4 to its more active form, T3, and deiodinsases D3 and D4 are responsible for inactivating it, thus maintaining homeostasis.17
A study conducted by Miro et al., 2019 showed the correlation of D2 and D3 to tumour behaviour by introducing SCC into mouse subjects. Tumour behaviour was then monitored by depleting the mice of the respective enzymes. The main findings of the study are summarised in Table I which highlight the link between thyroid enzymes, T4 and their effects on SCC.17
This supports the hypothesis that thyroid hormone (activated by D2 – cited as a “metastasis promoter”) appears to be central in the progression of tumours to the metastatic stage. Based on this research, the previously accepted linear model of tumour
Tumour growth and increase in size (tumour size)
Correlates with tumour grade and increased rate of post-surgical relapse
Tumour initiation (number of tumours)
progression is challenged, particularly regarding SCC. Thyroid hormone plays a crucial role in promoting cell migration and accelerating metastasis. This conclusion is further supported by observations that reducing thyroid hormone accelerates tumour formation but decreases invasiveness.17
The aforementioned examples explore the way in which thyroid hormone levels affect tumour behaviour. Another earlier publication by Ellerhorst et al., 2006 explored the role of TSH in melanoma. Findings showed that TSH receptors (TSH-R) on melanoma cells are functional and hypothesised that TSH could be a growth factor for melanoma cells. It is postulated that in SCC, hypothyroidism may act in a similar manner due to the patients having a certain degree of immune dysfunction.
While pathogeneses are well described in other cancers, the exact mechanisms in skin cancer, specifically SCC, are not well understood.9 There is a lack of sufficient case studies and population studies to indicate the link between SCC and hypothyroidism and, therefore, the statistical power is not strong enough to conclusively establish causality. Therefore, more studies are required to strengthen the body of evidence linking hypothyroidism to SCC.
Conclusion
This case study has highlighted the link between hypothyroidism and SCC and emphasises the multifaceted role of thyroid hormones in cancer development. This report underscores the value of thyroid function testing in patients with newly discovered malignant tumours, specifically SCC, with special consideration in people of colour, where SCC is not often expected. Current evidence in literature is not sufficient to prove causality and requires further investigation, particularly in people of colour. The mechanisms discussed are part of ongoing research and continue to contribute to the understanding of cancer pathogenesis.
Conflict of interest
Authors have no conflict of interest to declare.
Funding source
None to declare.
ORCID
S Khan https://orcid.org/0009-0007-8440-2216
H Parkar https://orcid.org/0000-0003-3732-1409
References
1. Leiter U, Garbe C. Epidemiology of melanoma and nonmelanoma skin cancerthe role of sunlight. Sunlight, vitamin D and skin cancer. 2008:89-103. https://doi. org/10.1007/978-0-387-77574-6_8
Full list of references available on request
S Afr Gen Pract 2024;5(2):98-100
https://doi.org/10.36303/SAGP.0470
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Unveiling the grip of opioid addiction in South Africa: a call for community-centred interventions
T Khumalo
Discipline of Psychology, University of KwaZulu-Natal, South Africa
Corresponding author, email: khumalor@ukzn.ac.za
In anticipation of the forthcoming rollout of opioid substitution therapy (OST), this paper discusses the nature of heroin, which is commonly referred to as whoonga or nyaope in South Africa, examining its addictive properties as a foundation for community interventions, including harm reduction. Analysing its chemical composition enables the classification of the main substance as an opioid. Identifying common cheaper adulterants added to produce or sell more product, to make it less potent or to mimic its effects and potentially increasing its desirability to consumers, helps to dispel misconceptions such as the inclusion of rat poison or antiretroviral agents, and aids in relevant treatment approaches and strategies. This paper further seeks to initiate crucial conversations to raise awareness of the drug and its effects. The emphasis is on psychoeducation as a foundational step in enabling communities to comprehend the complexities of opioid addiction, its pervasive grip on individuals, and the formidable obstacles to cessation. Such understanding fosters empathy and lays the groundwork for comprehensive and supportive care for individuals struggling with opioid addiction. Drawing from successful models in other countries, the paper supports proposals of expanding OST to the community and primary healthcare settings, involving primary healthcare nurses, clinical associates, and mental health professionals not only to increase access to treatment but also to enhance support for those affected by opioid addiction.
Opioid addiction has emerged as a formidable challenge within the fabric of South African society, particularly ensnaring the vulnerable and communities. As the nation is due for the imminent rollout of opioid substitution therapy (OST), notably in the form of replacement agonists such as methadone, it prompts a critical reflection on combating the pervasive grip of opioid addiction among South Africa’s youth. Amidst this backdrop, there arises a compelling need for a coherent understanding and clear delineation of the complex nature of a potent opioid known as whoonga or nyaope. This introductory discourse aims to provide a guiding framework amidst the ambiguity surrounding the “white powder,” whose elusive contents have baffled many, even as its consistent and debilitating effects unmistakably categorise it as a hard drug. The urgent call for clarity extends beyond mere identification to untangling the web of adulterants with which it has become intertwined, ranging from antiretroviral (ARV) medication to rat poison. Establishing a definitive understanding of the addictive nature of opioids is not only a strategic imperative for psychoeducation but also a cornerstone in the comprehensive rollout of intervention strategies. By unravelling the mechanisms and intricacies underlying opioid addiction, this paper seeks to shed light not only on the substance itself but also on the formidable challenges it presents in cessation efforts and, crucially, how individuals ensnared by its grip can be effectively supported.
OST in communities
The suggestion to make OST available to communities in various ways often arises from resource limitations that may not adequately accommodate the number of people addicted to drugs.1 As a result, community interventions following a primary healthcare model have been proposed. Such models often involve the provision of health services through mobile clinics, but also mental health centres where such mobile clinics are resourced.2 To further enhance access in contexts facing similar challenges, some regions have implemented waivers allowing intermediary professionals to prescribe OST.3 This approach not only facilitates the treatment of concurrent conditions that addiction may entail but also ensures comprehensive care for individuals struggling with drug addiction, incorporating intervention within existing infrastructure.
Available reports, including clinical trials, indicate that the country is ready for this rollout of agonists that ease dependence on heroin or other opioids. To assist recovery and to reduce harm, it must be argued that the drug in question is an opioid, or at the very least, an opioid-based entity. While presenting symptoms may vary between heroin-derived drugs mixed with other substances or base ingredients, or consumed by different methods, similarities can be drawn with drugs like krokodil (the semi-synthetic opioid, desomorphine) or oxycontin. Thus, it is important to note that despite these differences, they are all still opioids.4
Identifying the drug can be achieved by synthesising tests conducted so far.5,6 In this paper, we draw primarily from
Strauss,7 to provide insight into the signs and symptoms, while leveraging the works of Myers, Petersen8 and recommendations by Scheibe, Shelly9 to propose and assert how community and community health interventions would feature in the provision of a comprehensive plan.
That this drug is an opioid: the origins and composition of nyaope
The origin of the popular names of the drug sheds light on its journey to South Africa, originating in the Middle East before traversing through East Africa via the Eastern Coast trade route.10 This drug, often appearing as a whitish powder, garnered names such as nyaope and whoonga, derived from KiSwahili, reflecting both its colour and composition. As elucidated by Eligh,10 these names translate to “white” and “flour,” aligning perfectly with the drug’s appearance. Despite its predominantly white form, variations in colour are evident, with the brownish version typically associated with smokable heroin. Interestingly, coffee may play a role not only in bulking the drug but also in imparting this brownish hue, as its composition in nyaope is indicated by laboratory tests conducted on nyaope samples.5 However, regardless of colour, the presence of morphine and heroin remains consistent, reaffirming nyaope’s foundation as a heroin-based entity.11
The transition from smoking to injecting nyaope reflects global trends in heroin consumption and addiction progression, underscoring the potent and addictive nature of this substance.12 Despite its evolving forms, packaging and methods of consumption, nyaope remains unequivocally classified as an opioid, with morphine and heroin identified as its pervasive, primary and active ingredients.
Administration methods and effects
The initial and ongoing method of consuming the drug involves sprinkling it onto cannabis, reminiscent of the “white pipe” method used for Mandrax (Quaaludes). The prevalence of cannabis use prior to nyaope’s emergence may have facilitated its introduction and popularity, particularly among youth. “Chasing the dragon” involves inhaling the vapours which arise when heating the drug, usually on tin foil over a flame. Industrialised drug distribution is exemplified by the formulation of heroin in capsules, and more recently, specialised and reusable glass dispensers used for smoking the drug. Reports indicating intravenous use are consistent with the progression of opioid use around the world.12,13
Despite the initial pleasantness of the high experienced upon first encounter, addiction ensues as individuals find it increasingly difficult to achieve the same level of euphoria with subsequent doses. This tolerance reflects the nervous system’s adjustment to the drug, leading to escalating consumption and subsequent withdrawal symptoms when the drug is stopped. The effects of nyaope are often characterised as a “euphoric depressant”, inducing feelings of contentment and lethargy. Its allure is rooted in the intense euphoria produced by heroin, which drives individuals to desperate measures in pursuit of this fleeting high. However, this pursuit often leads to addiction, as diminishing
returns prompt individuals to increase their drug intake in a relentless quest for the same effects. This cycle of escalating consumption results in an inability to function without heroin.
Despite the negative consequences of nyaope addiction, individuals find themselves trapped in a cycle of dependence and withdrawal, unable to break free from its grip. Attempts to quit are thwarted by debilitating withdrawal symptoms, including stomach cramps, generalised pain, and diarrhoea,7 driving individuals back to the drug in a desperate attempt to alleviate their suffering. Tragically, deaths from drug overdose are all too common among people addicted to nyaope, an indication of the devastating toll of opioid addiction on individuals and communities alike.
The multifaceted impact of nyaope addiction
Addiction to nyaope manifests in a grim array of physical, psychological, and social symptoms. Nyaope is not associated with the lurid symptoms of krokodil (a “bathtub desomorphine chemistry” of codeine tablets, alkali solutions, organic solvent, acidified water, iodine and red phosphorus) that may cause thrombophlebitis, ulcerations, skin necrosis and gangrene. Rather, physical effects of nyaope are often related to withdrawal, which include stomach cramps as a key indicator. Gastrointestinal issues may further link to poor eating habits and malnutrition that are common among chronic users due to social and financial constraints. While users may initially experience euphoria and anxiety relief, this is overshadowed by slowed respiration and the risk of respiratory depression. Dry mouth, cognitive impairment and slurred speech are notable symptoms. Profuse sweating, itching, nausea, and vomiting may also occur.7 Social withdrawal is profound, leading to isolation and estrangement from loved ones. Financial struggles often drive users to desperate measures and side hustles. Ultimately, addiction may lead to homelessness and a decline in appearance and well-being.
Community-centred interventions
Community-centred interventions play a crucial role in addressing the chronic relapsing nature of nyaope addiction, emphasising the adoption of a disease model approach that extends beyond individual treatment to encompass the broader community. Understanding the drug and its effects promotes knowledge of what we are dealing with and does not only assist parents, caregivers and the community to identify symptoms, understand why it is difficult to quit the drug, but further enacts prevention as a necessary proactive measure.
Proposals to integrate treatment into primary healthcare systems aim to enhance accessibility and provide comprehensive care for people addicted to the drug. For Myers et al. (2012),8 integrating treatment services into existing primary healthcare structures would ensure a continuum of care catering to the diverse needs of individuals grappling with addiction. Legislative measures, including granting waivers to nursing practitioners and physician assistants and clinical associates in this country9 to prescribe opioid substitution medications like methadone and buprenorphine (a partial opioid agonist) have been implemented
Unveiling the grip of opioid addiction in South Africa: a call for community-centred interventions
to expand access to treatment.3 Moreover, leveraging community health centres and outreach programmes offers a promising avenue for reaching vulnerable populations and delivering essential services. By utilising existing pharmacological chains and involving clinical associates and primary healthcare nurses in dispensing and treating concomitant conditions, these interventions effectively bridge gaps in care and improve outcomes for individuals affected by nyaope addiction.
Conclusion
Nyaope presents a complex and potent opioid-based entity, with heroin and morphine, derived from the manufacturing process, serving as its primary active ingredients. By deepening our understanding of nyaope, this paper provided insights into its addictive nature. Addressing the complexities of opioid addiction demands a comprehensive and collaborative approach that encompasses psychoeducation, hence the need to understand the drug is important. Expanding access to treatment and engaging healthcare professionals within community health settings also tackles other health issues. As South Africa prepares for the rollout of OST, embracing a holistic approach to care and fostering empathy within communities, we can navigate the challenges posed by nyaope addiction and pave the way for healing and recovery for all affected individuals.
ORCID
2000: A Systematic Review. Social and Health Sciences. 2024:12481. https://doi. org/10.25159/2957-3645/12481
2. Khumalo T, Shumba K, Mkhize N. Ecological and recovery approaches to curbing whoonga addiction in South Africa: A critical hermeneutical review of literature. Journal of Addiction Research & Therapy. 2019;10(4:388).
3. Andrilla CHA, Jones KC, Patterson DG. Prescribing practices of nurse practitioners and physician assistants waivered to prescribe buprenorphine and the barriers they experience prescribing buprenorphine. J Rural Health. 2019. https://doi. org/10.1111/jrh.12404
4. Cole M. Monkey dust, krokodil, nyaope: why new drug concoctions keep appearing. The Coversations. 2014.
5. Mthembi PM. Chemical profiling of the street cocktail drug ‘nyaope’ in South Africa using gas chromatography-mass spectrometry (GC-MS): University of the Free State; 2020.
6. Khine AA, Mokwena KE, Huma M, Fernandes L. Identifying the composition of street drug Nyaope using two different mass spectrometer methods. African Journal of Drug and Alcohol Studies. 2015;14(1):49-56.
7. Strauss L. Nyaope and anaesthesia. South Afr J Anaesth. 2022;28(5):S150-S5.
8. Myers B, Petersen Z, Kader R, Parry CD. Moving beyond access: towards a qualityorientated substance abuse treatment system in South Africa. S Afr Med J. 2012;102(8):667-8. https://doi.org/10.7196/SAMJ.5990
9. Scheibe A, Shelly S, Hugo J, et al. Harm reduction in practice - The community oriented substance use programme in Tshwane. Afr J Prim Health Care Fam Med. 2020;12(1):e1-e6. https://doi.org/10.4102/phcfm.v12i1.2285
10. Eligh J. A shallow flood: The diffusion of heroin in eastern and southern Africa. Global Initiative against transnational organized crime; 2020.
11. Smillie S. Alarming rise in SA heroin abuse. Independent Newspapers SA. 2013 June 28.
T Khumalo https://orcid.org/0000-0002-7222-5300
References
1. Khumalo T, Mtambo T, Van Deventer M, Mdluli N, Makhathini N. Discourses on opioid addiction and its treatment and management in South Africa Since
12. Strang J, Griffiths P, Gossop M. Heroin smoking by ‘chasing the dragon’: origins and history. Addiction. 1997;92(6):673-83; Discussion 85-95. https://doi. org/10.1111/j.1360-0443.1997.tb02927.x
13. Meel R, Peters F, Essop MR. Tricuspid valve endocarditis associated with intravenous nyoape use: a report of 3 cases. S Afr Med J. 2014;104(12):853-5. https://doi.org/10.7196/SAMJ.8291.
S Afr Gen Pract 2024;5(2):101-102 https://doi.org/10.36303/SAGP.0596
Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
"It is fabled that we slowly lose the gift of speech with animals, that birds no longer visit our windowsills to converse. As our eyes grow accustomed to sight they armor themselves against wonder."
Leonard Cohen. The Favorite Game.
In the 1970s, I did a weekly rural clinic in the Injasuti Valley in the Drakensberg mountains. The clinic was near the river and outside were some tall gum trees that quietly sang when the warm summer winds came sweeping down the valleys. There were usually some cattle slowly cropping the grass near the clinic while unperturbed goats would tug at the lower branches of a thorn tree under which the patients sat, discussing the affairs of the day. They were what the prophet Zechariah called “the days of small things”.
The patients had either walked for miles or saved up to get a communal ride to see the doctor. Very few, especially the older patients, spoke or understood English.
My days were spent treating worn-out hands and backs, listening to the heartbeats of unborn babies, pulling teeth and examining children with wide innocent eyes as they looked into the faces of their African mothers.
One day, a traditional healer (sangoma) came in to see me as a patient. She requested that I give her some medicine to reduce the number of voices she was hearing.
I was not experienced enough at the time to ask her about the voices and what they said, but she was otherwise mentally normal. She had a large practice of her own and was accompanied by two young women who she was training as interns (ithwasa).
I had with me a Zulu interpreter/assistant, whose name was Joel Maphanga. He often helped me with interpreting the cultural aspects of the patient’s illnesses. Unfortunately, in these consultations, I never really got around to asking her whether she was hearing voices (izwi), or dreams (phupha) or was overthinking (cabanga kakhulu). I prescribed a phenothiazine (antipsychotic) and at subsequent visits she said that they helped her a lot.
I have since wondered about the line between rural indigenous people hearing voices and the auditory hallucinations of the
schizophrenic spectrum disorders. The boundaries are often blurred and difficult to separate.
On one end of the spectrum are the obvious schizophrenic hallucinations that are bizarre and out of context accompanied by other features of schizophrenia that make the diagnosis of schizophrenia more likely. I am reminded of a patient who heard voices coming out of her vagina and the voices sang songs to her. This is when the dark riders of true madness are chasing out the voices of reason and sanity.
On the other end of the spectrum are people in rural communities with often little or no education, whose culture accepts and allows them to hear the voices of deities, spirits and ancestors. Their cosmology and world views are connected more to the natural world around them as well as the supernatural world. If your ancestors or spirits are an integral part of your daily life then it stands to reason that one’s connectedness to the numinous and supernatural allows thoughts, voices and dreams to acquire a measure of formed reality. One of the problems in this area is when does a thought become a voice and how do you explain it to the external world.
Formal education in school may also suppress these indigenous thought processes and voices. In school we learn linear cause and effect reasoning and logical and rational thought processes. With education the pathways in our neurocircuitry become more focused and goal-directed along with the increased load of information that we now have to process.
In these rural communities voices from spirits and ancestors may help guide or warn them and may be accepted as normal. AxelIvar Berglund in his book Zulu Thought-Patterns and Symbolism describes the communion with clan ancestors (referred to as “shades”) by visions and dreams but does not specifically mention voices, although there is the culture-bound syndrome of ukuthwasa which is the “calling” of a person to become a traditional healer (sangoma).
One must also be careful to rule out medical diseases as a cause of hearing voices. Hearing voices can be caused by stress, sleep deprivation and medication side effects as well as specific medical and neurological conditions.
Chris Ellis
When I started practice, I occasionally saw patients with pellagra, which is due to the deficiency of niacin (vitamin B3). We were taught that the symptoms of pellagra were the 3 Ds of Dementia, Diarrhoea and Dermatitis. When I suspected that a patient had pellagra, I would ask them if they dreamed a lot (uyaphupha ebusuku?) which is the stage before the dementia. Those with pellagrinous predementia would enthusiastically reply in the affirmative.
My patients who I treated at the clinic in the 1970s, which is now 50 years ago, lived in a different world to that of today. There was no television and very little radio reception and no Ctrl-AltDelete-Enter. They lived a traditional rural life in the mountains that was relatively untouched by modern Western influences except for those younger ones who went to work in the cities or mines and came back to visit them.
I sensed that they also lived in a different dimension of time. The soft chattering of the patients waiting and sitting on the grass outside the clinic had an unhurried acceptance of just waiting. In the consultation when I asked when their symptoms started (kuqale nini?) they would sometimes refer to the season or the moon as their reference. I myself was living in a rushed ,measured tick-tock time and wanted exact answers framed in the precision of the Gregorian calendar.
Their time frame was different and their symptoms started at the time of the moon when the yellow-billed kites were nesting (inyanga uNhloyile) or at inKhwenkwezi, when the bright star of Canopus first appeared in the predawn sky, in the third week of May. They travelled lightly through the timeless African days and nights.
There was also this well documented connection that rural people have with the animals around them, especially cattle.
This extended to the surrounding environment and the trees as sentient beings breathing for our increasingly fragile planet. It is from these trees that the forked-tailed drongo still calls out the praise names of the cattle, as the sun sets slowly over the horizon.
There also appeared to be, in those days, a strong architecture of social relationships. The hierarchy and discipline of the traditional family was yet to be displaced by the modern stressed triad of grandmother, single mother and one child. They had not yet stepped through the looking glass into the new world.
In the past, philosophers such as Jean Jacques Rousseau, romanticised these rural lives into a sort of untroubled garden of Eden, but their lives were mostly hard and poverty-stricken. Even so their expectations of life appeared less than today. Their trust and beliefs were less questioned and unexamined compared to today’s almost ceaseless media dissection and analysis of life and its contingencies.
The world had not yet become the complicated surveillance state it is now, saturated by noise, contradictory opinions and fake news. Nowadays the outside world enters their lives shouting and asking questions, trampling on their thoughts and words. Sirens wail, phones ring, appliances bleep and gates are rattled while roadworks roar in the distance.
One can hear the voices better when there is less of this “noise” and “traffic” of modern life. Our thoughts and voices can then become clearer when there is silence in the magic gardens of our minds.
When I am back in the mountains, I have learned to listen to the wind sing again in the trees. Sometimes, in the quiet of a starry night, I sing along with it.
SAGP
6. The study population was all private general practitioners who were registered on the Medpages database across all provinces in South Africa at the time of the survey. Which province contributed the least respondents?
a KwaZulu-Natal
b Mpumalanga
c Northern Cape
d North West
e Western Cape
7. In assessing their competencies as clinicians in a primary care setting, private general practitioners were, at minimum, competent in five out of the six roles. Which competence scored the least?
a Capacity builder
b Change agent
c Collaborator
d Competent clinician
Assessing the clinical impact of sodium-glucose cotransporter type 2 (SGLT2)-inhibitors in treating heart failure with reduced ejection fraction
1. What is the current global prevalence of heart failure?
a 5–15%
b 1–3%
c 15–20%
d Less than 1%
2. Heart failure classification is currently based on the level of the ejection fraction. What is the ejection fraction of heart failure with reduced ejection fraction?
a Less than 60%
b Less than 55%
c Less than 40%
d Less than 80%
3. Guideline-directed medical therapy (GDMT) for heart failure is associated with a better outcome than conventional therapy. Which of the following drugs is not part of GDMT?
a Digoxin
b Renin-angiotensin-aldosterone system inhibitors
c Mineralocorticoid receptor antagonists
d Beta-blockers
4. The SGLT2-inhibitors, Empagliflozin and Dapagliflozin available in South Africa, have been tested in heart failure with reduced ejection fraction (HFrEF). What was the NNT (Numbers-needed-totreat) for the event reduction over 16–19 months of treatment?
a 50–70
b 50–100
c 19–21
d 5–10
Self-reported practices and learning needs of private general practitioners during the pandemic in South Africa
5. One of the health targets for the Sustainable Development Goals set by the United Nations is the realisation of universal health coverage (UHC). Which is the correct statement relating to South Africa?
a Access to quality health services for some poor South African citizens is guaranteed.
b Health National Insurance (NHI) is the funding which will pay for the services.
c Current skills and competencies of general practitioners prepare them for pandemics.
d The implementation of re-engineering of the primary healthcare services is to follow.
e Future pandemics may not occur when the UHC is fully implemented in the country.
e Critical thinker
8. The GP’s practice changes during the pandemic were described by adopting a COVID-19-Score designed to gauge the healthcare system's response during the pandemic. Which pandemic health systems’ domain has the second-lowest median score?
a Finance
b Health information systems
c Health workforce
d Leadership and governance
e Service delivery
Direct oral anticoagulants: the available agents and practical considerations
9. What percentage of renal excretion do the DOACs have?
a Apixaban: 66%, Dabigatran: 25%, Rivaroxaban: 80%
b Apixaban: 25%, Dabigatran: 80%, Rivaroxaban: 66%
c Apixaban: 66%, Dabigatran: 80%, Rivaroxaban: 25%
d Apixaban: 80%, Dabigatran: 25%, Rivaroxaban: 66%
10. Which DOAC is a direct thrombin inhibitor?
a Apixaban
b Dabigatran
c Rivaroxaban
d Warfarin
11. What should patients do if they miss a dose of the prescribed DOAC?
a Skip the missed dose and do not take the next dose until 24 to 48 hours later
b Double the missed dose within the same day (24 hours)
c Take the missed dose as soon as they remember, but do not double the dose within the same 24 hours
d Take the missed dose immediately and double the prescribed dose.
12. Which one of the following statements is false regarding drug-drug interactions with DOACs?
a Since dabigatran is not metabolised by the cytochrome P450 system, interactions with, for example, atorvastatin and carbamazepine are not expected with the use of dabigatran.
b Apixaban and rivaroxaban should be administered with caution in patients receiving concomitant strong inhibitors of both Cytochrome 3A4 and P-glycoprotein such as azole antifungals (e.g. ketoconazole) as well as anti-retrovirals such as ritonavir, since the anticoagulant action of these DOACs may be increased.
c The anticoagulant action of both apixaban and rivaroxaban may be increased when administered concomitantly with phenytoin or rifampicin.
d Dabigatran is metabolised by the cytochrome P450 system and therefore interactions with, for example, diclofenac and St. John’s Wort may occur.
Acne vulgaris and variants
13. Which of the following is correct concerning the correlation of pathogenic factor and relevant treatment in acne?
a Hypersecretion of sebum – oral cyclines
b Neutrophilic response to rupture of comedones and inflammation – cyproterone acetate
c Proliferation of Cutibacterium acnes – oral macrolides
d Androgen stimulation of sebaceous glands – topical retinoids
14. Indications to use oral isotretinoin include the following:
a Grade 2 acne vulgaris
b Lesser grade with significant scarring
c Lesser grading of acne that failed only topical treatment
d Microcomedomal acne vulgaris
15. The important laboratory monitoring tests for a patient on isotretinoin include:
a Full blood count
b Renal function test
c Fasting lipid profile
d Erythrocyte sedimentation rate
16. The following medication can exacerbate acne vulgaris except:
a Lithium
b Isoniazid
c Systemic steroids
d Minocycline
The link between thyroid hormones and cutaneous squamous cell carcinoma
17. In this case study, the patient presented with which of the following symptoms of hypothyroidism?
a Generalised body weakness and confusion
b Weight gain
c Constipation
d Hair loss and thickened skin
18. Laboratory findings were in keeping with:
a Primary hypothyroidism
b Central hypothyroidism
c Vitamin B12 deficiency
d Systemic infection
19. The aim of this article is to:
a Discuss UV radiation as a novel risk factor for cutaneous squamous cell carcinoma
b Explore hypothyroidism as a risk factor for cutaneous squamous cell carcinoma
c Discuss the general clinical cutaneous manifestations of hypothyroidism
d Explore burns as a risk factor for cutaneous squamous cell carcinoma
20. The clinical importance of this case report is :
a Thyroid testing in patients with newly diagnosed malignant tumours
b Do thyroid function tests in red-haired patients
c To expect a linear model of progression of squamous cell carcinoma in patients with thyroid dysfunction
d Do thyroid function testing in all HIV patients.
Prostate safety events during testosterone replacement therapy in men with hypogonadism – a randomized clinical trial
21. The TRAVERSE study evaluated the effects of testosterone replacement therapy (TRT) on prostate safety events. The study compared the effects of TRT and placebo on the incidences of which of the following?
a High-grade prostate cancer and any prostate cancer
b Acute urinary retention
c Invasive prostate surgical procedures for benign prostatic hyperplasia (BPH)
d Initiation of pharmacological therapy for BPH
e All of the above
22. The study design of the TRAVERSE study of TRT on major adverse prostatic events was which one of the following?
a Retrospective, case-controlled study
b Double-blind, randomised, placebo-controlled
c Prospective cross-over study
d Cross sectional survey
e All of the above
23. The following statement is/are true:
a Prostate cancer is highly prevalent among older men, but only a small fraction have high-grade tumours.
b Androgen receptor signalling plays a central role in prostate cancer biology, and testosterone treatment promotes the growth of metastatic prostate cancer.
c There were concerns that testosterone replacement therapy could promote progression of subclinical low-grade prostate cancer.
d Testosterone treatment was associated with a greater increase in PSA levels than placebo in the TRAVERSE study until month 12 of follow-up, when differences became non-significant.
e All of the above
24. The TRAVERSE study of men with hypogonadism who were carefully evaluated to exclude those at high risk for prostate cancer and followed using a standardised monitoring plan, concluded that:
a Compared with a placebo, testosterone replacement therapy was associated with low and similar incidences of high grade or any prostate cancer, acute urinary retention, and invasive surgical procedures for BPH.
b TRT did not worsen lower urinary tract symptoms (LUTS).
c The concern about prostate risk heavily influences decisionmaking by clinicians and patients who are considering TRT for hypogonadism.
d The study’s findings will facilitate a more informed appraisal of the potential risks of TRT.
e All of the above
To complete and submit this CPD activity go to www.mpconsulting.co.za
Note that from the 2nd of April 2024 MPC is now offering a comprehensive CPD compliance solution under their new brand as Vertice Software Solutions. This is an annual subscription offered to HCPs to:
• Gain access to all relevant CPD medical journals published on the Sabinet African Journals Platform with full functionality and seamless integration to support medical research.
• Complete CPD assessments for all accredited medical journals (excluding those associated with Association or Society Memberships) on the Vertice Software Solutions’ system.
• Receive CPD Compliance Support services to HCPs requiring assistance with their CPD compliance status at the Health Professions Council of South Africa (HPCSA), where HCPs complete CPD assessments for Medical Journals. This support service is provided by Vertice Software Solutions.
To subscribe to this service, or more information please contact the Vertice support team support@vertice.software
DID YOU KNOW?
All of our journals are available digitally and can be read online.
We have recently updated our journal viewer website to enhance your reading experience.
Please reregister on the link below to gain access to all of our journals.