






HOLLY PAYNE
On a day of health announcements, Health
Minister Mark Butler allocated over $500 million for cancer care in a bid to “reduce the burden of lung cancer in Australia and drive equitable cancer outcomes for Aboriginal and Torres Strait Islander people”.
Mr Butler announced $263.8 million for a national lung cancer screening program, the first new national cancer screening program
in nearly 20 years.
Starting by July 2025, the program will target high-risk individuals “to detect lung cancer in its early stages to increase the likelihood of successful treatment and improve lung cancer outcomes”.
“Lung cancer is Australia’s biggest cancer killer, and we know that early detection is key to improving survival rates,” said Professor Dorothy Keefe, CEO of Cancer Australia in response to the announcement.
“Australia’s new National Lung Cancer Screening Program is the among the first in the world, representing a significant step forward in the global effort to tackle lung cancer and positioning Australia as a world leader in this area.”
In Australia, the average five-year survival rate after lung cancer is
20%, according to figures from the Australian Institute of Health and Welfare.
Research has shown that patients diagnosed early had a 20-year survival rate of 80%. A report published by Cancer Australia in 2020 showed that targeting highrisk people was the most clinically effective and cost-effective way to roll out the program.
More than 8600 Australians died from lung cancer in 2022, and the burden is even greater for First Nations people, who are twice as likely to be diagnosed than nonIndigenous Australians, and twice as likely to die from it.
The new screening program has been co-designed with First Nations people.
In addition, Mr Butler announced nearly $238.5 million to support achieving equity in overall







than 60 minutes, a longsought acknowledgment of the complexity of some GP appointments.
Medicare items will also receive a boost in July and in November, amounting to a 4% increase. But where the budget giveth, the budget also taketh away.
The government estimates that it will save $301.9m over three years by “streamlining and modernising” chronic disease management items. This may be tied to the long-anticipated voluntary patient enrolment system to be called MyMedicare, which will use a blended funding model to encourage “wraparound primary care” for people who frequently end up in hospital.
A sum of $99m over four years to “connect frequent hospital users to a general practice to receive comprehensive, multidisciplinary care in the community which will reduce the likelihood of hospital readmission” appears to be the seed funding for the scheme.
The implementation of MyMedicare has been allotted $19.7m over four years and $3.2m a year ongoing.
Primary Health Networks will receive $79.4m over four years, which will be used to improve access to multidisciplinary care teams for patients with chronic conditions.
Despite a passionate last-minute campaign from the Pharmacy Guild of Australia, 60-day dispensing for 320 PBS-listed medicines was included in the federal budget.
The change will allow patients
to access double the amount of medicines per script, saving an estimated $1.2bn in dispensing fees over five years.
Mr Butler pledged that any savings from the measure would be reinvested into community pharmacy, and the budget papers uphold that promise.
Pharmacists can also expect $377.3m in funding over the next four years to help run the PBSfunded opioid treatment program and can now deliver National Immunisation Program vaccines at $19 a pop.
Following the report by Dr Pradeep Philip into Medicare compliance sparked by media reports last year, a new taskforce will be established in the Department of Health “to identify and disrupt instances of fraud and serious non-compliance before they occur”.
This taskforce will, according to the budget papers: - limit the duration of backdated patient-billed claims through practices, to prevent fraudulent claims being submitted through practices;
- permit appropriate data sharing with Services Australia to allow entit ies and bank accounts associated with known fraud to be blocked from receiving claims payments; and
- enable the Department of Health and Aged Care to audit providers by removing the requirement for external consultation with peak bodies to occur before issuing a notice to produce.
Already announced was continued funding for Heart Health Check, $19m for HIV testing, treatment and information, and $350m for community pharmacist outreach into residential aged care.
The big news for cancer was announced before budget night – $263m for a lung cancer screening program and $238m to address inequity in cancer outcomes for First Nations people.
There’s a big focus on smoking and vaping: $737m for control measures, including $141m to extend the Tackling Indigenous Smoking program, $29m on quit programs, $68m on a public health campaign, and taxing all tobacco products at the same increased rate.
Other announcements from the budget worth noting include:
- $118.2m over five years for clinical services including genomic testing for recurrent breast cancer risk and subsidies for egg, sperm and embryo storage for cancer patients of reproductive age - $40m over four years for the National Clinical Quality Registry Program
- Gardasil will be available to eligible patients up to the age of 25. The recommended dose schedule for some patients will reduce from two to one.
- New/amended medicines listed on the PBS include: Nivolumab (Opdivo) for the adjuvant treatment of
Primary Health Networks will receive $79.4m over four years, which will be used to improve access to multidisciplinary care teams for patients with chronic conditions.
patients with oesophageal cancer or gastroesophageal junction cancer, Asciminib (Scemblix) for chronic myeloid leukaemia, nivolumab + ipilimumab for Stage III or IV malignant melanoma, and Apalutamide (Erlyand) for metastatic hormone sensitive prostate cancer.
- $31m over two years to trial enhanced training arrangements to support international medical students working in rural and remote locations
- $18.5m for testing genetic variants in patients suspected of having either a myeloid or lymphoid haematological malignancy and $16.8m for a new MBS item for an EndoPredict gene expression profiling test to determine risk of recurrent breast cancer
- $59.5 million over 5 years to fund ICT infrastructure for a national worker screening and registration scheme from 1 July 2024
- $429m over two years to modernise My Health Record (MHR), including a new National Repository platform for better data sharing across healthcare settings, investment to improve the sharing of pathology and diagnostic imaging information and increasing allied health professionals’ connection to MHR
- $325.7m over four years in continued funding for the Australian Digital Health Agency
HOLLY PAYNE
Health Minister Mark Butler has pledged to put an end to pink unicorns, highlighters and bubble gum, at least as far as nicotine vapes go.
As part of the process, GPs will end up with more power to prescribe the devices for smoking cessation.
In a rousing address to the National Press Club, Mr Butler outlined a new plan to quash the sale of illegal vapes at corner stores and newsagencies, putting the current regulations on blast.
“It’s a so-called prescription model with next to no prescriptions, a ban with no real enforcement and an addictive product with no support to quit,” Mr Butler said.
Former Health Minister Greg Hunt attempted to crack down on illegal vapes, eventually passing a ban on the importation of nicotine vaping liquids without a doctor’s prescription.
Plans to block the importation of some vaping devices in the same fell swoop were reportedly abandoned under pressure from other members of the Coalition.
The budget includes $30 million for smoking cessation support programs and a further $63 million for an education campaign aimed at warning young people about the dangers of nicotine addiction and smoking.
Stopping imports at the border will be a priority for Mr Butler, who proposes new regulations that would require importers to prove that the vapes they are selling are bound for a pharmacy and meet TGA-certified plain packaging and flavour standards.
“These are supposed to be pharmaceutical products so they will have to present that way – no more bubble gum flavours, pink unicorns or vapes disguised as highlighter

pens for kids to hide in their pencil cases,” he said.
“Instead, we will have [pharmaceutical style] packaging with plain flavours.”
Another legacy of the previous government is a requirement for doctors who do wish to prescribe nicotine vapes for the purpose of smoking cessation to take part in an authorised prescriber scheme.
Mr Butler has pledged to do away with this measure as well.
“A script is hard to come by,” he said. “Only one in 20 doctors are authorised by the TGA to prescribe vapes to those who need it.”
To solve that problem, the Department of
➥ $500M boost for lung cancer– from Page 1
cancer outcomes for First Nations people.
“This investment will build the capacity and capability of the Aboriginal CommunityControlled Health Services (ACCHS) sector to support cancer care needs on the ground, tailored to local need and priorities; and ensure mainstream cancer care services are culturally safe and accessible to Aboriginal and Torres Strait Islander people,” said the DoHAC press release.
“We know that different communities have different needs and perspectives when it comes to cancer prevention and treatment,” said Professor Keefe.
“By working together with Aboriginal and

Torres Strait Islander people, we can ensure that health services are tailored to the needs of different communities and achieve equity in cancer outcomes.”
“We have been duped.” ,
Minister Mark Butler
A spokesperson from the Department of Health and Aged Care has confirmed that high risk individuals will be identified by a GP or Aboriginal health practitioner or worker. High risk individuals eligible for screening are those:
• aged 50 to 70 years; and
• asymptomatic (no signs or symptoms of lung cancer); and
• have a history of cigarette smoking of at least 30 pack-years; and
• if a former smoker, have quit within the past 10 years.
GPs will be able to refer qualifying patients to
Health will be removing the restrictions so that “all doctors can write a script for those who really need it”.
Pharmacies will also be investigated as a potential pathway to obtaining a vaping script.
“We have been duped,” Mr Butler said.
“The difference between vaping and cigarettes is that cigarettes have been with us longer.
“If we knew [the dangers] back then, when cigarettes were being introduced, I would hope that governments would have snuffed it out immediately, which is what I want to do to vapes.”
a radiology provider for screening and a new MBS item number for low-dose computed tomography for lung cancer screening will be created.
“The implementation of the program will also explore the ability for Aboriginal Health Practitioners or Workers to refer for screening,” the spokesperson said.
The department said a program of education resources will be developed to support the health workforce in learning about the screening program and eligibility.
In addition, there will also be new nationally endorsed clinical guidelines for detection and treatment of lung cancer.
*5-YEAR POST-HOC ANALYSIS (34.2 months median follow-up): of patients progression-free with IMFINZI (vs 19% placebo, HR 0.55 95% CI 0.45-0.68); P=not reported 1 33% of patients alive with IMFINZI (vs 33% placebo, HR 0.72 95% CI 0.59-0.89); P=not reported 1 43%


PBS Information: Authority required (STREAMLINED) for NSCLC. Refer to PBS Schedule for full authority information. BEFORE PRESCRIBING, PLEASE REVIEW FULL PRODUCT INFORMATION AVAILABLE ON REQUEST FROM ASTRAZENECA ON 1800 805 342 OR www.astrazeneca.com.au/PI
This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse events at www.tga.gov.au/reporting-problems.

IMFINZI® (durvalumab) Minimum Product Information. 120mg/2.4mL or 500mg/10mL, Concentrated Solution for Infusion in a Single-Dose Vial. INDICATION: For the treatment of patients with locally advanced, unresectable non-small cell lung cancer (NSCLC) whose disease has not progressed following platinum-based chemoradiation therapy. DOSAGE AND ADMINISTRATION: 10 mg/kg every 2 weeks or 1500mg every 4 weeks administered as an IV infusion over 60 minutes, for one year or until disease progression or unacceptable toxicity Patients with a body weight of 30kg or less must receive weight-based dosing, equivalent to IMFINZI 10 mg/kg every 2 weeks as monotherapy until weight increases to greater than 30kg. Administer IMFINZI prior to chemotherapy when given on the same day. IMFINZI should be diluted prior to infusion, see full PI for compatible diluents. No dose reduction or escalation for IMFINZI is recommended. In general, withhold IMFINZI for severe (Grade 3) immune-mediated adverse reactions. Permanently discontinue IMFINZI for life-threatening (Grade 4) immune-mediated adverse reactions, recurrent severe (Grade 3) immune-mediated reactions that require systemic immunosuppressive treatment, or an inability to reduce corticosteroid dose to 10 mg or less of prednisone or equivalent per day within 12 weeks of initiating corticosteroids. See full PI for recommended treatment modifications and specific management for immune-mediated adverse reactions. IMFINZI has not been studied in patients with severe renal impairment. CONTRAINDICATIONS: Hypersensitivity to the active substance or to any of the excipients. SPECIAL WARNINGS AND PRECAUTIONS FOR USE: Immune-mediated adverse reactions (imARs): Immune checkpoint inhibitors, including durvalumab, can cause severe and fatal imARs, which may involve any organ system. Patients should be monitored for signs and symptoms associated with imARs including: immune-mediated pneumonitis/interstitial lung disease, *radiation pneumonitis, hepatitis, colitis, immune-mediated endocrinopathies including hypothyroidism/hyperthyroidism/thyroiditis adrenal insufficiency, type 1 diabetes mellitus, hypophysitis/hypopituitarism, nephritis, dermatological adverse reactions, and other immune-mediated adverse reactions *(including pancreatitis, encephalitis). See full PI for further information on monitoring and management recommendations for imARs. Infusion-related reactions: Monitor patients for signs and symptoms, severe reactions have been reported. Efficacy in patients with PD-L1 expression <1%: efficacy may be different, see full PI. Paediatric use: safety and efficacy not established in patients less than 18 years. Use in pregnancy: Category D. Durvalumab has the potential to impact maintenance of pregnancy and may cause foetal harm. Not recommended during pregnancy; women of childbearing potential should use effective contraception during treatment and for at least 3 months after the last dose. Use in lactation: lactating women should be advised not to breastfeed during treatment and for at least 3 months after the last dose. ADVERSE REACTIONS: IMFINZI monotherapy pooled data: Very common (≥10%, any grade): cough/productive cough, diarrhoea, rash, pyrexia, upper respiratory tract infections, abdominal pain, pruritus, hypothyroidism. Common (≥1% and <10%, any grade): Pneumonia, oral candidiasis, dental and oral soft tissue infections, influenza, hyperthyroidism, pneumonitis, dysphonia, aspartate aminotransferase or alanine aminotransferase increased, night sweats, myalgia, blood creatinine increased, dysuria, peripheral oedema, infusion related reaction. See full PI for other listed adverse reactions including immune-mediated adverse reactions. Date of first approval: 2 October 2018. *Note changes in Product Information.
CI: confidence interval; CRT: chemoradiation therapy; HR: hazard ratio; NSCLC: non-small cell lung cancer; Q2W: every 2 weeks; Q4W: every 4 weeks. References: 1. Spigel DR, et al. J Clin Oncol 2022;40:1301-1311. 2. Antonia SJ, et al. N Engl J Med 2018;379:2342-2350. 3. Antonia SJ, et al. N Engl J Med 2017;377:1919-1929. 4. IMFINZI Approved Product Information. IMFINZI ® is a registered trademark of the AstraZeneca group of companies. Registered user AstraZeneca Pty. Ltd. ABN 54 009 682 311. 66 Talavera Road, Macquarie Park, NSW 2113. www.astrazeneca.com.au. For Medical Information enquiries or to report an adverse event or product quality complaint: Telephone 1800 805 342 or via https://contactazmedical.astrazeneca.com or email Medical Information enquiries to medinfo.australia@astrazeneca.com. AU-16254. ASTR0892/EMBC Date of preparation: April 2023
One of
CATE SWANNELL
Our inability to tolerate even a single instance of failure by doctors is an important cultural driver in the continuing overdiagnosis of melanoma in situ in Australia, according to a leading epidemiologist.
Professor David Whiteman, senior scientist and cancer control group leader at QIMR Berghofer in Brisbane, told OR that overdiagnosis of melanoma in situ was “a fact of life”.
“Overdiagnosis is like gravity – it’s no good if you’re falling out a window, but it’s good for a lot of other reasons,” he said.
“It just exists and is a feature of any program of systematic screening or surveillance.
“In epidemiological terms, in the case of melanoma, overdiagnosis is the detection of a lesion that meets all the criteria – it looks like and feels like melanoma, but doesn’t display the biological behaviour of progressing to the point where it can cause death.”
Speaking at the Australasian Melanoma Conference in Brisbane last month, Professor Whiteman and other presenters referred to a graph published by Welch et al. in the New England Journal of Medicine in 2021, showing the incidence of melanoma in situ increasing over time while the mortality rate remained steady.
“You can interpret that graph two ways,” Professor Whiteman told OR
“If we had not diagnosed those cases then the mortality rate would have gone up. That’s the optimistic view – that we have prevented many deaths.
“The other view is that finding all those cases has not decreased the mortality rate, so perhaps we could have done nothing to those lesions.

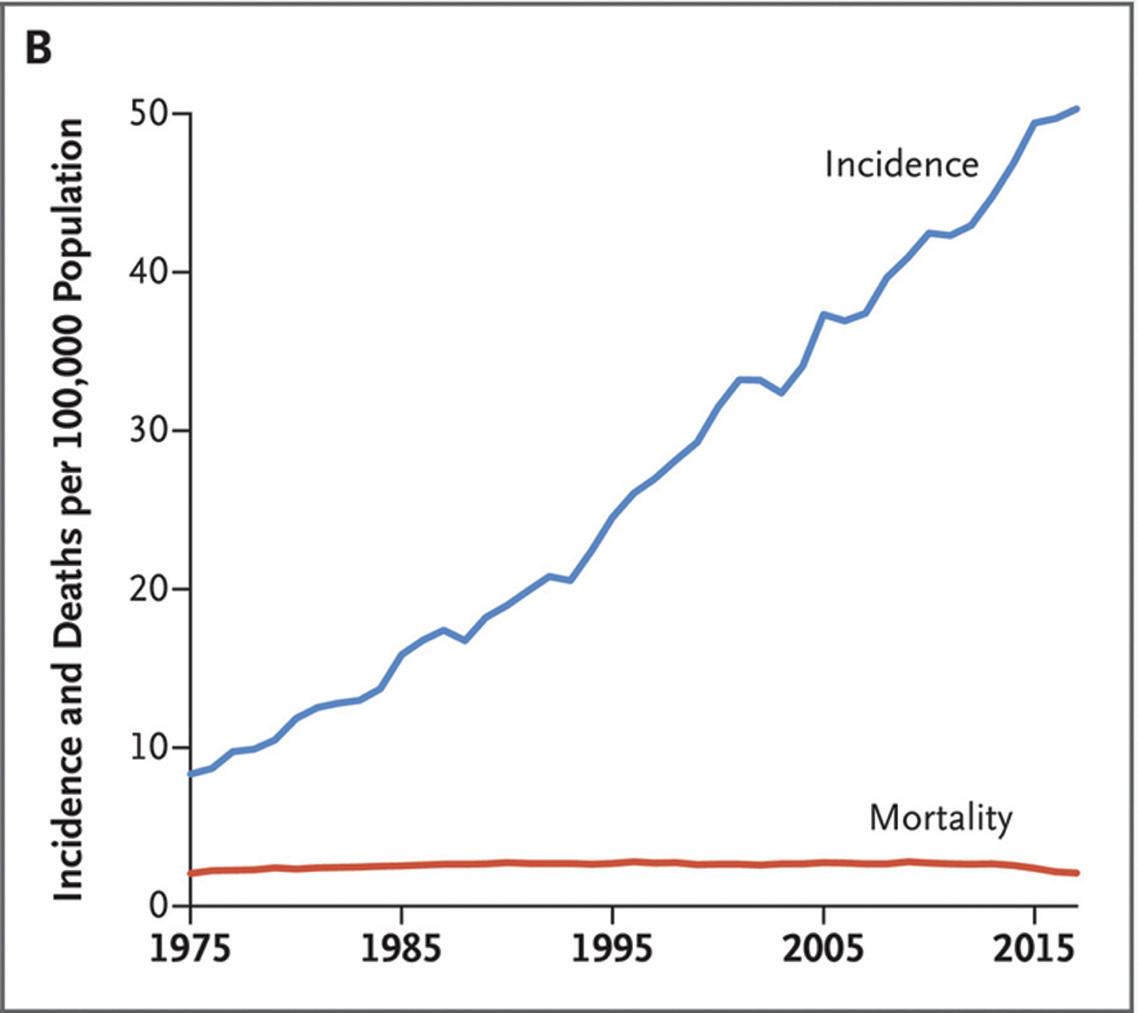
“Both of those things are going on, but we still see a rise in lethal melanomas [given the growth and ageing of the population].”
The clinical reality is that nobody wants to miss even one potentially lethal melanoma.
“We can’t change our advice because nobody has the acuity to predict the future biological behaviour of a lesion on the skin,” said Professor Whiteman.
“At least we can’t do it to the level that would offset the threat of a lawsuit if we get
it wrong. “If we had a more tolerant system, we would watch and wait more often, particularly in elderly patients, for example.
“But the reality is the system does not tolerate a single instance of failure, and that is an important cultural driver of overdiagnosis – apart from the fact that nobody wants our patients to suffer.”
A prominent practising GP told our sister publication, The Medical Republic , that missing a melanoma was “one of the top
three things that keep me awake at night”, suggesting that clinicians will continue to err on the side of caution when it comes to treating melanoma in situ aggressively.
One of the downsides of overdiagnosis is the financial strain on the Australian healthcare system.
Associate Professor Louisa Gordon, a health economist from QIMR Berghofer, told conference delegates that skin cancer was the most expensive cancer in terms of financial burden on the Australian health care system, costing approximately $1.8 billion per year.
Melanomas contribute about $259 million per annum to that cost.
“These costs are increasing,” she said. “We’ve got this ageing population. Baby boomers are now elderly and coming into the healthcare system in big numbers – they are the most common age group for treating skin cancers.
“But we’ve also got Gen X coming through. These are people born in the [1960s and 70s] who are now in their 50s and 60s. There are eight million Australians in that generation who are about to come on to the healthcare system with skin cancers.
“We’ve got this greater awareness of the need for skin checks and we’ve also got a lot of new technologies on the horizon. All of these things are going to contribute to higher costs for skin cancer in Australia.”
But the financial burden is not the only consequence of overdiagnosis, according to Professor Whiteman.
“Patients diagnosed with early melanomas can experience psychological harms,” he told OR
“They can become anxious, they may avoid going outside, perhaps they may withdraw from friends, family and social situations as a result. In some cases they may struggle to get insurance, or they may need to change jobs.
“Diagnosis is not without consequences, and right now we don’t have a good handle on the relative burdens of those consequences.
“We need to learn more about the biology of these lesions. We need to better harness the new technologies and the new pathology techniques to help us diagnose these lesions more accurately. It’s over to the research now.”
KARINA BRAY
PBAC has recommended the government subsidise Shingrix (GSK) on the PBS for immunocompromised patients aged 18 and over.
If the recommendation is approved by the health minister, which PBAC recommendations
almost always are, it would sharply increase access to the varicella zoster vaccine.
It would see the recombinant vaccine included on the National Immunisation Program for nonIndigenous people aged 70, Aboriginal and Torres Strait Islander peoples aged 50 or older and immunocompromised people aged 18 and older with conditions at high risk of herpes zoster infection.
Currently, the PBS covers Zostavax, but does not cover Shingrix at all.
Details about the eligible immunocompromised population are yet to be determined, and this will be finalised in consultation with ATAGI.
ATAGI has previously recommended Shingrix be given to immunocompromised people for whom the NIP-listed Zostavax live
vaccine is not suitable, although patients were liable for the costs.
This includes people currently taking mycophenolate, TNF inhibitors and other bDMARDS (such as anakinra, tocilizumab, abatacept and rituximab), and JAK inhibitors.
PBAC has deferred a decision to potentially include a broader population of immunocompromised people for whom the vaccine would
be cost effective, pending ATAGI advice. GSK’s request to include all (non-Indigenous) adults aged 65, with a catch-up program for adults over 65, was not recommended for those aged 65-69 and 71 or older.
PBAC considered they were a lower clinical priority and represented a large number of people, with consequent uncertainty about the cost-effectiveness of Shingrix in these populations being too high.
While Australian mortality rates have stayed steady for 30 years, more than double the rate of teens and young people are surviving
HELEN TOBLER
Deaths from cancer among adolescents and young adults have more than halved since the 1980s, but cancer remains the second biggest killer after injury, according to new Australian data.
The good news appears to be largely driven by better blood cancer survival, but is tempered by the ballooning rates of colorectal, thyroid and chronic myeloid cancer in this group.
Hodgkin lymphoma is now the most common cancer in people aged 15 to 24, making up 13% of all cancer cases, according to the Australian Institute of Health and Welfare’s Cancer in adolescents and young adults in Australia report. That’s followed by skin melanoma at 12%, testicular germ cell cancers (12%), thyroid cancer (11%) and colorectal cancer (10%).
Since the early 1980s, the mortality rate from all cancers has fallen from 62 deaths per one million down to 29 deaths per one million in the late 2010s. Mortality rates also increase with age.
“Mortality rates have been consistently higher for males than females, however the gap between the sexes has decreased over time,” the AIHW report said.
“While both sexes have experienced a decrease in mortality since 1981-1985, the decrease has been greater for males.”
The report said there was likely to be several reasons for the decrease in mortality, such as sun

safety campaigns and improvements in cancer detection, treatments and prevention.
But while mortality rates have fallen, the rates of all cancers in young people aged 15 to 24 have remained steady over the last 30 years, at around 315 to 335 cases per one million.
Between 1984 and 2013, melanoma was the most common cancer in young people, but it’s now the second most common after Hodgkin lymphoma.
During the 30 years up to 2018, the rates of colon and rectum cancer quadrupled in young people, from nine to 33 cases per one million. Rates almost tripled for thyroid cancer and chronic myeloid cancer and doubled for mature non-Hodgkin lymphoma.
But for cervical cancer, cancer of the head and neck and melanoma of the skin, the incidence more than halved during that period.
For people aged 15 to 24, five-year survival for
all cancers rose from 79% to 90% in the 20 years to 2018.
“The increase in survival for all cancers combined has been largely driven by improved relative survival for blood cancers,” the report said.
“Bone cancer and central nervous system cancer were the leading causes of cancer death among people aged 15–24, followed by soft tissue sarcoma, acute lymphoblastic leukaemia/ lymphoma, and acute myeloid leukaemia,” the report said.
“Mortality tended to increase with age, however, people aged 15–24 had higher mortality rates than people aged 25–39 for acute lymphoblastic leukaemia and bone cancer.”
Bone cancers and central nervous system cancers were the largest causes for cancer death in 2013-2017, causing 17% of deaths each, while sarcomas caused 15% of deaths.
“For people aged 15 to 24, five-year survival for all cancers rose from 79% to 90% in the 20 years to 2018.”
In 2020–21, there were 11,300 hospitalisations of young people for cancer treatment, and 70% of those were same-day admissions. There were also 37,000 services at hospital outpatient clinics during that period.
According to the report, the cancers most commonly associated with hospital admission were acute lymphoblastic leukaemia (16%), Hodgkin lymphoma (14%) and bone cancer (11%), followed by testicular cancer for males and acute myeloid leukaemia for females.
Young people who have had cancer also have a higher risk of developing a second primary cancer, at a rate 1.9 times higher than the general population.
Among people who went on to develop a subsequent cancer, about 20% had previously had Hodgkin lymphoma, followed by melanoma (19%), testicular germ cell cancer 8% and thyroid cancer (6%).
CATE SWANNELL
The numbers are clear – melanoma is the third most commonly diagnosed cancer in Australia; it kills about 1400 of us every year; and we have the highest incidence in the world, with a rate approximately 8.7 times the global average.
Why then do we not have a national screening program, as we do for bowel cancer, breast cancer and cervical cancer?
“In Australia, there are already a lot of people getting skin checks,” said Professor Anne Cust during her recent presentation to the Australian Melanoma Conference in Brisbane.
“From 2006 to 2016, the proportion of people aged 45 to 69 who had a skin check in the past 12 months increased from 29% to 37%.
“Perhaps we’re doing well enough without an organised, targeted screening program? Maybe we just need to encourage the right people to get a skin check.”
The problem with that if-it-ain’t-brokedon’t-fix-it model is that on closer inspection there are some quite important broken bits.
“What we have is an opportunistic screening scenario in which it might be the doctor or the patient who initiates a skin check,” said Professor Cust, a cancer epidemiologist and deputy director of the Daffodil Centre, a joint venture between Cancer Council NSW and the University of Sydney.
“There are several problems with that opportunistic system. It’s very costly –almost $2 billion a year is now spent on skin cancer.
“We know that there is inequity in who accesses skin checks, who’s got access to a specialist, who has access to new
technologies, and that results in overscreening of some population sub-groups and under-screening in others.
“There are also lost opportunities to embed primary prevention alongside early detection.”
An organised screening program solves many of those knotty issues.
“Everyone who is eligible can access that regardless of how much money they have,” Professor Cust told Oncology Republic
“[You also get] an assessment of the quality of the skin check that people are getting … reminder systems, call-backs, and data collection. And there is a very clear pathway for what happens after diagnosis,” she said.
“You can’t avoid overdiagnosis in a screening program. But you’re also preventing people dying from cancer.”
The key, perhaps, is a risk-stratified, targeted screening program rather than implementing population-wide program
similar to breast, colon and cervical cancer.
“A targeted program would be focused on people at higher risk of skin cancer in whom we think the benefits of having a regular skin check would outweigh the potential negatives or harms of having a skin check,” she said.
Identifying high-risk groups, what risk factors are most predictive of benefit, and how the program would be managed are just some of the questions for research projects around the country.
Professor Cust said it was “relatively easy” to assess melanoma risk with online tools such as that on the Melanoma Institute Australia website and at QSkin.
“We’re doing some modelling at the Daffodil Centre, trying to work out whether [a targeted screening program] would be cost effective,” she said.
“We’re hoping to have some preliminary findings on the risk-stratified screening program by the end of the year.”
KARINA BRAY
Immune checkpoint inhibitors (ICI) can cause immune-related adverse events, and patients with pre-existing autoimmune disease may be at increased risk.
However, a retrospective cohort study of patients with pre-existing rheumatoid arthritis (RA) undertaking ICI therapy for cancer has suggested they are not at increased risk of immunerelated adverse events (AEs) compared to similar cancer patients without RA.
“Our results suggest that pre-existing rheumatoid arthritis should not be considered a contraindication for receiving immune checkpoint inhibitors for cancer treatment,” wrote the authors, led by Dr Kaitlin McCarter of Brigham and Women’s Hospital in Boston.
The researchers included 87 RA patients from among almost 12,000 patients in data repositories who’d initiated ICI for cancer. Each RA patient was matched with up to three patients without RA based on sex, calendar year, ICI target, and cancer type and stage.
“To our knowledge, this study is the largest to date to focus on patients with a single pre-existing autoimmune condition who initiated immune checkpoint inhibitors for cancer that also includes a comparator group matched by age, sex, year, target of immune checkpoint inhibitor, and cancer type and stage,” wrote the authors in The Lancet Rheumatology
The median age was around 71 years, 61% of participants were female and around 92% were white. The most common ICI target was PD-1 and the most common cancers were lung cancer (about half of patients) and melanoma (about one quarter). The median duration of RA was around nine years, and most patients were in remission or low disease activity upon ICI initiation.
Primary outcomes were time to mortality and time to first immune-related adverse event, and secondary outcomes were number, severity and specific types of immune-related adverse events.
Researchers found there was no difference in mortality between the two
groups: among patients with RA, 69% died, compared to 63% in the comparator group. Median survival time was 13.5 months for the RA group and 17.2 months for the comparator group (a non-significant difference).
There was also no difference between the groups for more serious (grade 3 or above) immunerelated adverse events (14%
in the RA group vs 15% in the comparator group).
Those in the RA group were more likely to experience any-grade immune-related adverse events (61% of the RA group vs 49% of the comparator group; adjusted HR=1.72, 95%CI 1.20-2.47). However, the difference was mainly down to RA flares: 48% of RA patients experienced flares, which
were mostly mild, while 7% of the comparator group experienced inflammatory arthritis. After excluding flares and inflammatory arthritis, the RA group was significantly less likely to experience any-grade immune-related adverse events. RA patients were at lower risk of some types of immune-related adverse events: they were
significantly less likely than the comparator group to experience rash or dermatitis, endocrinopathy and hepatitis, and numerically less likely to have colitis or enteritis.
Dr David Liew, deputy chair of the international Rheumatic Immune-related Adverse Event Classification Criteria Initiative, said, rheumatoid arthritis patients
should have access to the best systemic therapy for their cancer.
“It does behove us as rheumatologists, however, to support our patients during that inherently stressful time, to make sure we are ready to manage their RA flares if they do come up,” added Dr Liew, who is also deputy editor of Rheumatology Republic.

*Optimal dosing of Creon® can lead to an improved quality of life.1–5 Creon® can optimise nutritional status and normalise digestion, pain, and bowel movements, which may improve QoL in patients with PEI.5,6
Suggested adult maintenance dosing: 1,5
PEI, pancreatic exocrine insufficiency; QoL, quality of life.
Meals 2 x Creon® 35000
Snacks 1 x Creon® 35000
PBS Information: Creon is listed on the PBS as a digestive enzyme preparation (10 repeats).
Restricted benefit: for cystic fibrosis patients under a GP Management Plan or Team Care Arrangement (21 repeats).
Before prescribing please review the full product information available on request from Viatris or telephone 1800 314 527
MINIMUM PRODUCT INFORMATION: CREON® CAPSULES (pancreatic extract 10,000, 20,000* 25,000, 35,000, 40,000* BP) CREON® MICRO enteric coated granules (Pancreatic Extract)
INDICATIONS: Pancreatic enzyme replacement in paediatric and adult patients with pancreatic exocrine insufficiency (PEI). PEI is often associated with, but not limited to cystic fibrosis, chronic pancreatitis, pancreatic surgery, gastrointestinal bypass surgery (eg. Bilroth II gastroenterostomy), ductal obstruction of the pancreas or common bile duct (e.g. from neoplasm). CONTRAINDICATIONS: Hypersensitivity to porcine protein or any of the ingredients. PRECAUTIONS: Fibrosing Colonopathy, Pregnancy, Lactation. INTERACTIONS WITH OTHER MEDICINES: Antacids: Antacids should not be taken at the same as time as with Creon. If necessary, it is recommended that at least one hour should elapse between use. ADVERSE EFFECTS: The most commonly reported adverse reactions were gastrointestinal disorders and were primarily mild or moderate in severity. Common adverse reactions included, nausea, vomiting, constipation, diarrhoea, abdominal distention, rash, pruritus, urticaria, abdominal pain. Some of these adverse events are similar to the symptoms associated with PEI and underlying conditions. DOSAGE AND ADMINISTRATION: The capsules: Capsules should be swallowed without crushing or chewing, with enough fluid during meals. If unable to swallow capsules, open and add minimicrospheres to acidic soft foods and consume immediately. Do not chew or crush minimicrospheres. Ensure that none is retained in mouth. The dosage should be individually titrated and depends on the severity of the disease and the composition of food. Cystic fibrosis: 1,000 lipase units/kg/meal for children less than four years old; 500 lipase units/kg/meal for those over age four. For adult patients with PEI associated with other conditions, initiate at 25,000 to 40,000 BP units of lipase per meal and half of that dose for snacks. If required, 80,000 BP units of lipase per meal and half of that dose for snacks. Max dose 10,000 units lipase/kg body weight. The granules: Can be added to acidic soft food. The scoop provides 100 mg or 5,000 units of lipase. Any mixture of the granules with food or liquids should be used immediately. The dose is adjusted to the fat content of the meal and the severity of the disease. Cystic fibrosis: 1,000 lipase units/kg/meal for children less than four years old; 500 lipase units/kg/meal for those over age four. Most patients should remain below 10,000 lipase units/kg body weight per day or 4,000 lipase units/gram fat intake. *Not currently marketed in Australia. Minimum PI updated: 21 April 2021.
References: 1. Smith RC, et al. Australasian guidelines for the management of pancreatic exocrine insufficiency. Australasian Pancreatic Club, October 2015. Available at: https://www.pancreas.org.au/resources [Accessed January 2023]. 2. Sikkens EC et al J Gastrointest Surg 2012; 16:1487-92. 3. Kuhlmann L et al. JOP J Pancreas (Online) 2018; 19(4):183-89. 4. Keller J et al. Gut 2005; 54(Suppl VI):vi1-vi28 5. Creon® Product Information. 24 January 2022. 6. Ramesh H et al. Pancreatology 2013; 13(2):133-39.
Creon® is a Viatris company trademark. Copyright © 2023 Viatris Inc. All rights reserved. Viatris Pty Ltd. Level 1, 30-34 Hickson Rd Millers Point, NSW 2000, Australia. ABN: 29 601 608 771. Call: 1800 314 527. Date of preparation: January 2023. CRE-2022-1127. MYL0718.
Two years down the track, sonographers are ready to try again, with a revamped submission seeking a sponsor
CATE SWANNELL
Two years after their last attempt, sonographers are trying once more to be added to the list of imaging professions regulated by AHPRA, with a recent survey showing public trust plummets when patients learn the person wielding the transvaginal wand may be completely unregulated.
While a quarter of sonographers are also radiographers and therefore regulated by the Medical Radiation Practice Board of Australia under the AHPRA umbrella, the rest are guided by a national code of conduct for unregulated health professions, in some states and territories.

learning sonographers were unregulated.
The Australasian Sonographers Association (ASA) recently commissioned a nationally representative online survey to understand the impact of the profession’s lack of regulation on public trust and confidence.
Those surveyed almost universally (97%) believed ultrasounds were an important diagnostic tool, with 71% believing the skills and experience of the sonographer were important to the outcome of the ultrasound. However, 70% believed sonographers were regulated before taking the survey. Ninety-six percent believed they should be regulated (up 8% since 2019) and 76% were concerned that they are not.
Before respondents knew sonographers were unregulated, 50% reported very high trust in the profession. Once they were informed about the lack of regulation, however, that dropped to just 23%, with 44% saying their trust in the health system as a whole dropped after
The big hurdle for the profession in gaining entry into the AHPRA stable remains catching the attention of the nation’s health ministers, who must agree the profession needs regulating before a regulatory impact assessment can be carried out.
Persuading all nine ministers to agree means getting the issue on to the agenda of the next Health Ministers’ Meeting, and that requires a minister or chief health executive to sponsor the sonographers’ submission.
In 2021, after negotiating with then health minister Greg Hunt, the group’s submission failed to find a sponsor and was rejected by the federal Department of Health, who requested it be made “more robust”.
Two years down the track, sonographers are ready to try again, with a revamped submission seeking a sponsor.
“Ultrasound is operator-dependent,” said Jodie Long, CEO of the ASA. “The sonographer is scanning in real time trying to determine what is normal and what is abnormal. The responsibility is on the sonographer to pick
up something is abnormal, and then take representative pictures of it.
“There is quite a substantial amount of trust between the reporting doctor and the sonographer, which is why we have the backing of the AMA, RANZCOG and RANZCR,”
Ms Long told Oncology Republic “They are so reliant on the sonographer being held to a higher account.”
The new submission has been prepared by a working group consisting of the ASA, the Australasian Society for Ultrasound in Medicine, the Australian Sonographer Accreditation Registry (ASAR) and Jenny Parkes, the senior sonographer representative.
The submission lists the “risks of harm to the public health and safety” of being unregulated as: delayed treatment, more advanced and complex medical conditions, additional costs, unnecessary surgery or treatment, reduced quality of life, significant physical and emotional harm, and ultimately death due to missed or misdiagnosis; personal injury, harm or patient distress from misuse of the transducer (or probe) and other failures
in professional practice; physical harm and immediate and ongoing emotional harm due to unprofessional behaviour, including inappropriate, unethical or illegal conduct; the risk of death or significant physical and emotional harm from a failure to act appropriately, such as providing timely and appropriate communication of urgent or unexpected findings; avoidable infection of individuals and between patients and the public from a failure to follow infection control standards and procedures; and immediate and lifelong injury and disability caused by biological effects due to misuse of the technology.
“Currently there are no nationally enforceable standards of practice that set the minimum expectations of ultrasound examinations performed by Australian sonographers, putting the public’s health and safety at risk,” says the submission.
“The only existing system that comes close to providing an effective system of public protection is the regulation system and the processes administered by the National Registration and Accreditation Scheme Medical Radiation Practice Board of Australia – however, this only applies to the 24.5% of sonographers who are also registered medical radiation practitioners.”
The National Code of Conduct for Health Care Workers does not cover the activities of sonographers, self-regulation is a non-starter, and credentialling organisations such as the ASAR and the Australian Society of Medical Imaging and Radiation Therapy do not have regulatory functions, nor do they take complaints.
“We’ve spoken to every jurisdiction,” Ms Long told OR . “We’ve spoken to health ministers and to chief health executives. They are all sympathetic to our need.
“The issue now is making it a priority for them. That’s where we’re at – this needs to be made a priority, by putting it on to the Health Ministers’ Meeting agenda, because there are over 11 million ultrasounds performed by sonographers in Australia every year.”
LAURA WOODROW
An ultrasound device implanted in the skull and intravenous microbubbles enable researchers to open the blood-brain barrier and target glioblastoma with chemotherapy for the first time.
Treatment of aggressive malignant gliomas has long been hindered by the inability of most strong chemotherapy drugs to cross the blood-brain barrier. Now researchers have been able to use low-intensity pulsations of ultrasound to open the blood-brain barrier and deliver albumin-bound paclitaxel into the brains of patients with recurrent glioblastoma.
“Large size drugs that previously were not used for gliomas could now be considered
for the treatment of diseases in the brain, including glioblastoma,” the researchers wrote in The Lancet Oncology this month.
The researchers said they demonstrated drug penetration to a brain area nine times larger than in previous studies, which is more closely reflective of the treatment area for post-surgical chemotherapy. The chemotherapy was able to reach deep, critical brain areas including the thalamus and basal ganglia.
In the dose-escalation phase I clinical trial, 17 adults with recurrent glioblastoma with a diameter of 70mm or smaller were implanted with ultrasound devices in their skulls after tumour resection.
The researchers monitored blood-brain barrier opening, safety and pharmacokinetics during the sonication-coupled chemotherapy
with either albumin-bound paclitaxel or carboplatin. These cytotoxic agents have previously been associated with neurotoxicity when administered to the brain via injection.
Participants had an average of three treatment cycles.
Brain concentrations of the drugs increased between three and six times when administered with sonication, depending on the molecular weight of the drug, they said.
“We report that large-volume blood–brain barrier opening is safe, reproducible, and can be repeated over multiple cycles of chemotherapy,” the researchers said.
The most common side-effect was transient headache, which 71% of patients experienced, and the most common adverse events were neutropenia (47% of patients), leukopenia (29%) and hypertension (29%).
There were no treatment-related deaths during the 12-month follow-up period and no progressive neurological deficits associated with the technique, the authors said.
The researchers said the blood-brain barrier was restored within 30 to 60 minutes after they stopped sonication, which showed there was a critical time window in which to administer drugs.
They also noted that the method may fall short in the case of larger tumours due to the limited scale for the device, despite being larger than previous devices, and the dynamics of the drugs following lowintensity pulsed ultrasound remain poorly characterised, they said.
A follow-up phase 2 study investigating treatment with a combination of paclitaxel and carboplatin is currently underway.

Not a real patient, for illustrative purposes only. Not representative of every patient’s experience. PHN=post-herpetic neuralgia.
Indication1 : SHINGRIX is indicated for the prevention of herpes zoster (HZ) and post-herpetic neuralgia in:
- adults 50 years of age or older;
- adults 18 years of age or older at increased risk of HZ.
Dosing1 : The primary vaccination schedule consists of two doses; an initial dose, followed by a second dose 2 to 6 months later. For subjects who are immunodeficient, immunosuppressed or likely to become immunosuppressed due to known disease or therapy, and who would benefit from a shorter vaccination schedule, the second dose can be given 1-2 months after the initial dose.
Safety1 : Very common (≥10%) solicited local adverse reactions and solicited general adverse events were pain, redness, and swelling at the injection site; and myalgia, fatigue, headache, shivering, fever, and gastrointestinal symptoms, respectively.
Please review full Product Information before prescribing. Product Information can be accessed at www.gsk.com.au/shingrix or by scanning the QR code.

This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse events at www.tga.gov.au/reporting-problems. PBS Information: This product is not listed on the PBS or the National Immunisation Program (NIP).
HZ=herpes zoster
Reference: 1. SHINGRIX Approved Product Information.
For information on GSK products or to report an adverse event involving a GSK product, please contact GSK Medical Information on 1800 033 109. Trade marks are owned by or licensed to the GSK group of companies. © 2023 GSK group of companies or its licensors. GlaxoSmithKline Australia Pty Ltd, Melbourne, VIC. ABN 47 100 162 481. PM-AU-SGX-ADVT-230003. Date of approval: February 2023.
Delays in referral and diagnosis and a lack of continuity of care cause anxiety and a waste of money and time
Poor communication, long wait times and conflicting medical advice cause unnecessary anxiety for lung cancer patients and their carers, research shows.
An analysis of patient experience, published in Internal Medicine, found that patients may have multiple medical appointments which could lead to delays in diagnosis and treatment, and those challenges were magnified in rural, remote and regional areas.
The Townsville researchers also found that lung cancer patients may be sent to oncology appointments before having the appropriate tests.
The researchers interviewed newly diagnosed patients and their carers about their experiences as part of an analysis of a lung cancer referral pathway implemented by Townsville Hospital that enables GPs to refer cancer patients. They found that patients were unhappy with poor communication from GPs and specialists and with delays in being told about test results. Patient experiences would be improved by addressing barriers including perceived delays in diagnosis and specialist appointments, frequent turnover and lack of clinician time, improper communication and use of telephone consultations and lack of adequate psychosocial support, they said.
“Patients and their carers in this study indicated high satisfaction with care if they had every step of the lung cancer referral pathway clearly explained to them,” they wrote in the

Internal Medicine Journal. “Our study also suggests that avoiding delays in investigations and informing them about test results as soon as available can reduce patient anxiety and distress.”
They said these delays caused significant anxiety and distress to some patients and carers.
“Many patients felt that since their GPs did not take their symptoms seriously during initial consultations, their diagnosis and treatment were delayed,” the researchers said.
Some patients said that frequent turnover of GPs in their rural area resulted in delayed diagnosis. “Another concern voiced by some patients was that the delays may have caused their tumours to grow while they were waiting, which led to worse outcomes.”
Lead author and medical oncologist Dr Zulfiquer Otty said a cancer referral pathway enabled GPs to refer patients and help avoid
unnecessary tests, travel and inappropriate referrals to specialists, such as referring patients to oncologists without doing an X-ray or CT scan.
“Sometimes patients come directly to the oncology clinic, which is actually not appropriate, and we see benign cases that fill up our clinics with non-cancer cases, when this person needs to be ideally seen by a respiratory specialist first and investigated and diagnosed before they are sent to an oncologist or surgeon.”
Dr Otty told OR that even after patients were referred to a specialist clinic there could be delays, especially in rural and regional areas.
“Delaying diagnosis is shown to reduce survival. If patients are diagnosed early, they can be cured. If there is a delay even by a few months, it can become incurable,” he said.
“The lung cancer pathway, which is available online for all GPs to refer the patient to appropriate specialists, could reduce delays in
care and improve the satisfaction of patients,” said Dr Otty, staff specialist in medical oncology at Townsville Cancer Centre and senior lecturer and PhD candidate at James Cook University.
Dr Otty said it was important for doctors to understand the individual needs of patients regarding information and levels of detail, and concerns they may have other than the diagnosis and treatment.
“Some patients are not very concerned about the details, and they just want the diagnosis and treatment as soon as possible, while other patients or their carers would like to have more involvement in the decision-making and need more information.”
Some patients reported that the information they received was too technical, he said.
“Many of the specialists or even the GPs don’t have much time to spend with patients so sometimes they are abrupt and don’t take into account what the concerns of the patients are.”
If patients saw different GPs due to a high turnover of GPs and specialists in rural and regional areas, that could lead to poor continuity of care and delays in diagnosis.
For example, Dr Otty said a patient may be diagnosed with a lung infection and be prescribed antibiotics, then later return and see a different GP who also treated it as a chest infection, delaying a cancer diagnosis.
“Long-term GPs who know the patients well will be supportive of the patients and will try to get specialist appointment as soon as possible,” he said.
Dr Otty said the period of waiting for a diagnosis caused the most distress for patients and families.
“Most of our patients told us that during delays they feel that the cancer is growing and might be spreading to other places,” he said.
“Once they have a diagnosis and plan of treatment, they’re a bit more certain of what is going to happen.”
Better coordination between hospitals would also improve patient experiences, he said.
LINCOLN TRACY
Haematology patients can mount strong cellular immune responses against covid after being vaccinated, despite their immunocompromised status.
A paper published in Cell Reports Medicine shows that the immune response, driven by T cells, is equal to that of healthy controls, and provides important insight into future immunisation strategies which typically activate B cell immune responses.
Dr Oanh Nguyen, senior research fellow at The Doherty Institute and co-lead author on the study, said the findings were “really important and super exciting for cancer patients.”
As part of the study, researchers compared immune responses in 153 initially covid-free people prior to and after they received their first, second, and third covid vaccines.
Blood cancer patients, particularly those who are immunocompromised, have an increased risk of developing viral respiratory tract infections, including covid. Certain therapies, such as chimeric antigen receptor therapy, can further enhance this risk by impacting protective responses obtained through vaccination.
The 95 haematology patients displayed reduced antibody and B cell responses following covid vaccination compared to the 58 healthy controls, although this was somewhat expected due to their disease state and potentially immunocompromising treatments.
Haematology patients displayed high levels
of antibody-secreting and T-follicular helper cells after their second vaccine does, as well as high levels of CD4+ and CD8+ T cell responses after their third vaccine dose. The T cell increase was a similar size to that seen in healthy controls.
Twelve of the 95 haematology patients developed covid during the course of the study and generated higher antibody responses than their uninfected counterparts.
Associate Professor Benjamin Teh, infectious disease physician at the Peter MacCallum Cancer Centre and co-senior author on the current study, said the findings should give clinicians confidence that covid vaccination is safe and beneficial in this patient population.
“Regardless of their diseases and treatments, COVID-19 vaccination generates strong T cell immunity in this group,” he said in a statement.
KEYTRUDA , in combination with LENVIMA , for the first-line treatment of adult patients with advanced renal cell carcinoma (RCC) 1
*In the KEYNOTE-581/CLEAR trial, KEYTRUDA + LENVIMA demonstrated superior PFS vs sunitinib:
• HR 0.39 (95% CI: 0.32–0.49), p<0.00011
• Median PFS: 23.9 months (95% CI: 20.8–27.7) vs 9.2 months (95% CI: 6.0–11.0)1
• Events observed: 45% (160/355) vs 57% (205/357)1
ORR (secondary endpoint):
• 71% (95% CI: 66–76) with KEYTRUDA + LENVIMA vs 36% (95% CI: 31–41) with sunitinib; nominal p<0.00011
SCAN QR CODE to view the KEYNOTE-581/CLEAR Study Design



KEYNOTE-581/CLEAR trial adverse events: AEs of any cause that emerged or worsened during treatment in at least 25% of patients in the KEYTRUDA + LENVIMA group were: diarrhoea, hypertension, hypothyroidism, decreased appetite, dysphonia, stomatitis, nausea, fatigue, decreased weight, proteinuria, palmar-plantar erythrodysesthesia syndrome, arthralgia, rash, vomiting, and constipation.1
Grade 3 or higher AEs occurring in 10% or more of patients in any treatment group included diarrhoea, hypertension, elevated lipase levels, and hypertriglyceridaemia.1
KEYTRUDA Selected safety information
Precautions: Immune-mediated adverse reactions (ImARs), incl. severe and fatal cases, have occurred in patients receiving KEYTRUDA. These have included, but not limited to: pneumonitis, colitis, hepatitis, nephritis, endocrinopathies, severe skin reactions (Stevens-Johnson syndrome, toxic epidermal necrolysis and bullous pemphigoid), uveitis, myositis, GuillainBarre syndrome, pancreatitis, encephalitis, sarcoidosis, myasthenic syndrome/myasthenia gravis (incl. exacerbation), myelitis, vasculitis, hypoparathyroidism, myocarditis, pericarditis and pericardial effusion, peripheral neuropathy, sclerosing cholangitis, solid organ transplant rejection, severe infusion reactions (hypersensitivity, anaphylaxis) and complications of allogeneic HSCT.1
ImARs have occurred after discontinuation of treatment with KEYTRUDA.1 ImARs can affect more than one body system simultaneously.1
Contraindications: None.1
Please review the Product Information before prescribing, available at www.msdinfo.com.au/keytrudapi or by scanning the QR code
This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse events at www.tga.gov.au/reporting-problems.
Warnings and precautions: Gastrointestinal toxicity: diarrhoea and dehydration; hypertension; proteinuria; renal failure and impairment; aneurysms and artery dissections; cardiac dysfunction; posterior reversible encephalopathy syndrome/Reversible Posterior Leucoencephalopathy Syndrome; hepatotoxicity; haemorrhagic events and thrombocytopenia; arterial thromboembolic events; wound healing complications; gastrointestinal perforation and fistula formation; non-gastrointestinal fistula; QT interval prolongation; impairment of TSH suppression/Thyroid dysfunction; osteonecrosis of the jaw.4
Contraindications: Hypersensitivity to the active substance or any of the excipients.4
Please review the Product Information before prescribing, available at www.eisai.com.au/PI or by scanning the QR code
KEYTRUDA in combination with LENVIMA is PBS listed for certain patients with renal cell carcinoma. Criteria apply, see www.pbs.gov.au
AE: adverse event. HSCT: haematopoietic stem-cell transplantation. IO: immuno-oncology. ORR: objective response rate. PFS: progression-free survival. TKI: tyrosine kinase inhibitor. TSH: thyroid-stimulating hormone.
References: 1. KEYTRUDA Product Information, www.msdinfo.com.au/keytrudapi. 2. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Available at www.pbs.gov.au. 3. Data on File (PBS) (REF-194017), MSD. 4. LENVIMA Product Information, www.eisai.com.au/PI.
Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved. Merck Sharp & Dohme (Australia) Pty Limited. Level 1 – Building A, 26 Talavera Road, Macquarie Park NSW 2113.
Lenvima® is a registered trademark of the Eisai Group, whose affiliate company in Australia is Eisai Australia Pty Ltd, Level 2, 437 St Kilda Road, Melbourne VIC 3004. ABN 73 117 970 993. Eisai Australia Medical Information: 03 9832 9100 or medinfo_australia@eisai.net. Adverse Events can also be reported to safety_australia@eisai.net. AU-RCC-00092. Issued May 2023. 2003469.
Clinical outcomes for low-risk disease are the same for surgical, radiation and surveillance options, but very different for quality of life
MARIELLA ATTARD
Active surveillance is the best option for many men with low-risk prostate cancer, according to a long-running UK study.
The findings support the approach given to around 80% of Australian men who fall into this category, said Professor Jeff Dunn AO, from the Prostate Cancer Foundation of Australia.
“This trend largely reflects recent advances in diagnostic approaches which have strengthened our ability to determine the aggression of different prostate cancers and weigh this against the likelihood they will cause harm in the short and long term,” said the Foundation’s chief of mission and head of research.
The study of 80,000 middle-aged UK men who took a PSA test found that those undergoing active surveillance had the same rates of death from prostate cancer as those who underwent prostatectomy or radiology treatment.
Around 3% of the study participants were diagnosed with localised prostate cancer with a life expectancy of at least 10 years, with a median PSA level of 4.6ng per millilitre (range, 3.0 to 18.9).
The men deemed to be at low-risk were randomly assigned to receive either active monitoring, prostatectomy radiotherapy, in addition to three to six months of androgendeprivation therapy. Researchers found that the incidence of death was low over the 15-year follow up, at 3.1% in the active monitoring group, 2.2% in the prostatectomy group and 2.9% in the radiotherapy group.
One surprising finding was that while 9.4% of the active monitoring group eventually metastasised, which was almost double the other groups, this had little effect on mortality.
“The higher incidence of metastatic disease in the active-monitoring group at 10 years was anticipated to have an effect on prostate cancer-specific mortality at 15 years, but this was not the case,” the authors wrote.
“Among the 40 men in whom metastatic disease had been diagnosed at 10 years, the risk of death from prostate cancer was lower among those in the active monitoring group (3 of 22 [13.6%]) than in either the prostatectomy group (2 of 8 [25.0%]) or the radiotherapy group (7 of 10 [70.0%]).
“Our findings indicate that depending on the extent of side effects associated with early radical treatments, more aggressive therapy can result in more harm than good. Clinicians may avoid overtreatment by ensuring that men with newly diagnosed, localized prostate cancer consider critical trade-offs between short-term and long-term effects of treatments on urinary, bowel, and sexual function, as well as the risks of progression.”

Associate Professor Weranja Ranasinghe, spokesperson for the Urological Society of Australia and New Zealand, said that doctors were now better able to identify the patient’s risk profile accurately, thanks to both technology such as MRI and PSMA scans, as well as many risk stratification tools that take into account factors like age, family history, biopsy results, digital rectal examination and PSA density.
“The key message now is to identify prostate cancer early in order to utilise these new tools and help patients make the right decisions about whether to undergo active surveillance or pursue active treatment,” said Professor Ranasinghe.
It also helped to remind patients that active surveillance was not a hands-off approach.
“The fact that you’re regularly monitoring them with PSA tests, clinical examinations, MRI, and plus or minus biopsies is quite reassuring to a lot of patients,” he said.
Some patients who needed treatment were very focussed on the surgical option, and could be resistant to considering other options, Professor Ranasinghe said. Urologists discuss all options with their patients and most of them would be offered a radiation oncology appointment, he said, though some refused.
“Surgery and radiation have similar cancer outcomes, so treatment depends on what’s important to the patient. The side effect profile of the treatment plays a huge role in determining which treatment you choose, and in appropriate patients, surveillance offers a great option to reduce or avoid the side effects associated with treatment,” said Professor Ranasinghe.
Radiation oncologist Professor Jeremy Millar, clinical lead at the Prostate Cancer Outcomes Registry Australia and New Zealand, said that evidence on side-effects and outcomes, and patient anxiety weren’t the only things driving patient choices.
“Even important high-quality long-term work like this does not change practice quickly — patterns of practice have a momentum of their own, determined by fashion, tradition, surgical or radiation dogma and conservatism,
,Professor Jeremy Millar “Even important high-quality long-term work like this does not change practice quickly -patterns of practice have a momentum of their own.”
training and availability, public perceptions and marketing, policy and financial frameworks, constraints and incentives, and availability of treatments and expertise,” he told OR
“In practically any dimension of adverse outcome in which there is a discernible gap between RT [radiotherapy] and RP [radical prostatectomy], RP is worse at practically every time point than radiation.
“This is particularly true in the dimensions where there are larger problems (GU and sexual) and [side effects] men really care about: sexual function and incontinence.
“If you have your prostate removed then this does marginally improve the amount of nocturia and the frequency compared with no treatment or RT. In bowel function, the scores are reasonably good for all treatments (including observation) apart from an increasing bowel leakage. Here, about 12% reported once or more a week, compared with 6% with RP.”
Research published last year from the same trial suggested seed brachytherapy has a more favourable side-effect profile than radiation therapy — fewer sexual side-effects, less faecal incontinence, fewer loose stools and fewer bloody stools. But its use had declined by about two-thirds in the last decade, despite increasing prostate cancer cases, “almost entirely for the other factors I mentioned above”, Professor Millar said.
“This sort of work might be a stimulus to turn this around, but the decline has a momentum that won’t change too quickly,” he said.
According to the PCFA, newly diagnosed Australian men don’t tend to be aware of their treatment options. The organisation provides specialised support through prostate cancer specialist nurses.
“[Their role] is to help raise understanding and inform treatment decisions, minimising all risks of harm and ensuring that the man’s clinical and psychological needs are immediately addressed and supported over the long-term,” Professor Dunn said.
“Health professionals and researchers who have questions about the treatment of prostate cancer are welcome to contact PCFA via 1800 22 00 99 or email Telenurse@pcfa.org.au.”


tipped to make a “significant difference”
HELEN TOBLER
Adrug that doubles the time before relapse for people with gastrooesophageal cancer has been listed on the PBS, making it accessible to patients who could not afford the $120,000 annual cost.
From 1 April, nivolumab (Opdivo, BristolMyers Squibb) was listed on the PBS for people with resected oesophageal cancer or gastrooesophageal junction cancer who have had neoadjuvant chemoradiotherapy.
The adjunct immunotherapy turns the immune system back on, enabling it to recognise the cancer as foreign.
Medical oncologist, pharmacologist and translational researcher Professor
Stephen Clarke said prior to the PBS listing of nivolumab, the standard treatment for operable oesophageal cancer was chemotherapy and radiation therapy followed by surgery.
“Then we weren’t doing any additional treatment postoperatively, and in spite of pretty good surgical results, patients were still relapsing subsequently. And if that occurs, they’re no longer curable by standard treatments,” said Professor Clarke from GenesisCare in Sydney.
“So we needed some way to try and enhance the effectiveness of the local treatments and stop metastatic cancer from occurring and make patients live longer.”
Professor Clarke said for the almost 75% of patients whose tumours did not show a complete therapeutic response, the risk of recurrence was high, which is why the reimbursement of nivolumab was a significant milestone in addressing this high clinical unmet need.
Immunotherapy has been used to treat cancers such as melanoma for around 10 to 15 years and was being expanded to include

other cancer types such as head and neck cancer, kidney cancer and now oesophageal and gastric cancer, he said.
“This has been the single most significant development during my working lifetime. This has been very exciting.”
Professor Clarke said a study in the NEJM found that after one year, the median diseasefree interval of patients taking nivolumab was 22 months compared to 11 months for patients in the placebo group.
The randomised, double-blind, interventional trial compared adjuvant nivolumab after neoadjuvant chemoradiotherapy and surgery with matching placebo.
Patients included in the CheckMate-577 study had resected stage II or III oesophageal or gastro-oesophageal junction cancer.
The study also showed that nivolumab had an acceptable toxicity profile, and the occurrence rate of grade 3 or 4 adverse events was 13% in the nivolumab group compared to 6% in the placebo group.
Professor Clarke said other research has shown that metastasis-free survival and
recurrence-free survival were more than 60 months for the nivolumab group compared to “tens of months” for the placebo group.
“It looks like it’s going to make a significant difference to this patient population and mean survival is going to be better for those receiving this treatment. It’s only 12 months of treatment and it’s pretty well tolerated.”
Professor Clarke said there are 1700 new patients with oesophageal cancer each year in Australia.
Oesophageal adenocarcinoma has an overall five-year survival of 23% in Australia and is the seventh most common cancer globally.
Professor Clarke said rates of squamous cell cancers of the oesophagus which are related to smoking and drinking alcohol were falling in Australia, thanks to declining smoking rates.
“Oesophago-gastric cancer is one cancer that’s increasing in incidence in Australia because of obesity leading to increased reflux and the acid coming into the stomach is leading to the development of these malignancies,” he added.



Diabetes patients taking the common medication had better non-small cell lung cancer survival, early research has found HELEN TOBLER
Taking sodium-glucose cotransporter 2 inhibiters has been linked to better survival rates in people with nonsmall cell lung cancer, research suggests.
The US study of 2400 patients (aged over 65) with both lung cancer and pre-existing diabetes also found a dose-response relationship, with survival better among those who took SGLT2 inhibitors for a longer duration.
Over an average follow-up of 21 months, those who were taking SGLT2 inhibitors had a 32% lower risk of dying compared to those who were not taking the medication.
The benefits remained regardless of demographics, tumour characteristics and type of cancer treatment.
“This study is among the first epidemiological evaluation of the association between SGLT2 inhibitors and cancer survival using large nationally representative datasets,” the researchers wrote in the British Journal of Cancer
The study findings support previous research that has suggested this class of

drugs may be of benefit in a broad range of cancers.
“Early clinical evidence indicates SGLT2 inhibitors may have anti-cancer benefits for gastrointestinal, lung, pancreas, prostate and liver cancers,” the study authors said.
The researchers said further studies were needed to determine the mechanisms, but they could include glycaemic-dependent pathways.
“Glucose is required for cancer cell
survival and growth,” they said. “Lung cancer cells show increased glucose uptake and utilisation compared to normal lung cells.”
Previous research has shown that the inhibition of glucose uptake and glucose deprivation have induced apoptosis, they said.
“It may be possible to induce apoptosis of tumour cells by inhibiting glucose uptake,” they wrote.
Commenting on the study, respiratory researcher Professor Brian Oliver told Oncology Republic more research was needed to determine which cancer patients would benefit.
“I would be amazed if this becomes a frontline treatment for lung cancer,” said Professor Oliver, head of the respiratory cellular and molecular biology group at the Woolcock Institute of Medical Research.
“But maybe, with future research and more careful investigation as to who’s going to benefit the most, maybe it would become a therapeutic option for the treatment of lung cancer.”
Professor Oliver said previous research had shown a benefit of SGLT2 inhibitors in other cancers, but this was the first in lung cancer.
“There’s a lot of evidence in animal models. It’s the first time it’s been shown in lung cancer, which is, from a lung cancer perspective, very interesting.
“This is very exciting, but it’s early-stage research.”
Professor Oliver said the mechanism was unknown, but agreed that the SGLT2 inhibitors could quell cancer growth by controlling blood glucose levels.
“Because cancer cells are so metabolically active, if you reduce blood glucose, the theory is that that would inhibit cancer cell proliferation,” he said.
“The other possibility is that those drugs are acting directly on the tumour cells and causing an anti-tumour effect. And in invitro studies, there is evidence of that with various tumours.”
The combined oral contraceptive pill and the progesterone-only pill both increase the risk of breast cancer, but only marginally, new research suggests.
An analysis involving almost 30,000 women found that among those who used hormonal contraceptives for 15 years, an additional eight to 265 per 100,000 women developed breast cancer compared to those who did not use hormonal contraceptives.
The UK-based nested casecontrol study found an increase in the 15-year absolute excess incidence of breast cancer associated with five years of hormonal contraceptive use.
Researchers reported in PLOS Medicine that the incidence increased from 0.08% to

Oral contraceptives have been linked to breast cancer risk
0.09% in women aged 16 to 20, corresponding to approximately eight additional breast cancer cases per 100,000 hormonal contraception users over that period.
A larger increase was observed in women aged 35 to 39, where the incidence increased from 2.0% to 2.2%, meaning 265 additional women in every 100,000 would receive a diagnosis.
“Similar levels of risk have been found with being overweight or drinking more than one standard drink of alcohol per day,” said
Professor John Boyages, a radiation oncologist based at the Icon Cancer Centre in Sydney.
“The main finding in this study is that the risk was similar irrespective of contraceptive type and not to say that the pill was a major risk factor for breast cancer,” Professor Boyages told Oncology Republic
Combined oral contraceptives have previously been linked to increases in breast cancer risk, but less is known about the effect of progestogen-only contraceptive approaches on breast cancer risk,
despite their substantial increase in usage over the last decade.
Almost half of breast cancer patients and 39% of cancer-free women received one or more prescriptions for a hormonal contraceptive prior to receiving their diagnosis. About half of the prescriptions were for progestogen-only contraceptives.
Women with at least one prescription for hormonal contraceptives had a 25% increase in the relative odds of developing breast cancer compared to women who did not use hormonal contraceptives.
Similar increases in the odds of developing breast cancer were reported when the type of hormonal contraceptive was considered: combined oral preparations by 23%, progestogenonly oral preparations by 26%, injectable progestogen by 25% and progestogen IUDs by 32%.
The meta-analysis of 12 studies from high-income countries
explored the association between progestogen-only contraceptive use and breast cancer, and found an increase in similar magnitude with respect to relative breast cancer risk.
The inclusion of other highincome countries in the metaanalysis meant it was “reasonable” to say the findings were transferrable to an Australian population, said Professor Deborah Bateson, a clinical researcher from the University of Sydney.
Professor Bateson said the findings should not be a cause for concern and that the slight increase in breast cancer risk should be communicated to patients in an appropriate way.
“This is an important study, but there is no cause for alarm and no reason for people to stop using their preferred method of contraception – or for GPs to change their prescribing practices,” she said.

How one doctor’s experience with racism inspired a new clinic
Istill remember the first day I met a First Nations doctor. It was a profound moment that led to my decision to study medicine – a career I had always wanted but which never truly felt achievable up until that moment.
I cannot do justice to the protective benefit that having First Nations people in medicine, particularly at senior levels, has had upon me. It was First Nations doctors who stood beside me when I had to reconcile myself with the deeply distressing impact of racism from my medical peers.
For a long time, I felt that racism in medicine was a dirty little secret; something spoken about in short snippets as hurried conversations in corridors that usually went nowhere other than the sad glance of a sympathetic colleague, clearly distressed by the account of racism but unsure how to advocate for change.
If you ask First Nations people about their experiences of our hospitals, their accounts are damning. There is no question that racism impacts the care people receive in our hospitals. This racism costs lives, such as that of Wiradjuri woman, Naomi Williams, and her unborn baby. 1 For myself, comments on my appearance as an Aboriginal doctor have always been hurtful and undermined my safety and confidence while training.
My most defining experience of racism, however, occurred after I made a genuine disclosure of life-threatening family violence and sought support from my senior colleagues during this time. I received not so much as a text message, a phone call or even a cup of coffee from my training supervisor, and limited on-call cover and bullying from another who, even in the face of serious and life-threatening family violence, felt that my priority should be listing off differential diagnoses and mnemonics for my exam.
The fact that doctors manage disclosures of family violence poorly should not be a surprise to anyone who works in medicine. What training have we had? For most of us, very little. Family violence training was never part of my medical school or specialist training.
None of my clinical supervisors prior to my disclosure had family violence training and were, I assert, predictably inadequate in their responses.
First Nations women and children do experience higher rates of family violence but are not the only group affected – many people of different backgrounds and statuses suffer from it, mostly woman and their children.2, 3 At what point does our reluctance to adequately train doctors who have the expertise to manage

disclosures of family violence continue to perpetuate this gender and health inequity?
All in all, my experience of racism left me wondering whether, if I had been a doctor of any racial background other than Aboriginal, would the lives of my family members have been valued more?
Would I have received more support? Would my colleagues have been more willing to cover my on-call?
The answers to these questions may be academic to others but are deeply personal to me. This is the sometimes-non-quantifiable racism experienced every day by First Nations people who interact with the hospital system, clinical supervisors and training providers.
For me, it informed my decision to establish a clinic dedicated to First Nations people within the Royal Melbourne Hospital, where First Nations people are seen by a First Nations doctor in a space where the care and dignity of the individual are prioritised above racism and bias. I am pleased to announce that the clinic has an ongoing community partnership with Victorian Aboriginal Community Controlled Health Organisation (VACCHO) following their generous support and has secured five years of funding to allow it to become a more permanent place within the hospital.
There is a dedicated space where First Nations people are welcome, and I am allowed to speak about the impact of racism with my colleagues and the generations of new doctors coming through.
Overwhelming, my hope for the future is that hospitals, medical schools and specialist training providers recognise that family violence is an important health issue and embrace our role as medical professionals in supporting and advocating for victims
The fact that doctors manage disclosures of family violence poorly should not be a surprise to anyone who works in medicine.
and survivors of family violence. Let’s pledge a commitment to train doctors and clinical supervisors capable of managing family violence disclosures as part of our commitment to the safety of women, children and priority community groups.
Lastly, I hope that no other trainee is ever treated in the inexcusable way I was treated by my hospital colleagues in response to a family violence disclosure.
By talking about these things openly, I hope we demand a higher standard of ourselves as doctors and petition our training providers to produce graduates and clinical supervisors up to this critical task.
Dr Williams is a Wiradjuri woman, consultant dermatologist and clinical lead of the First Nations Teledermatology Clinic at the Royal Melbourne Hospital located on the lands of the Wurundjeri people of the Kulin Nations. She also provides a visiting specialist service to the Northern Territory and sits on the Board of Directors of the Australian Indigenous Doctors’ Association.
This article first appeared in the Australian Healthcare and Hospitals Association (AHHA) magazine The Health Advocate and is reproduced with permission.
References:
1. Inquest into the death Naomi Williams: https:// coroners.nsw.gov.au/coroners-court/download. html/documents/findings/2019/Naomi%20 Williams%20findings.pdf
2. Victorian Royal Commission on Family Violence Report: https://www.vic.gov.au/about-royal-commission-family-violence
3. Link to AIHW Report on Family, domestic and sexual violence in Australia: continuing the national story 2019: https://www.aihw.gov.au/ reports/dome
Cate Swannell

Reform inertia in Australian healthcare system over the past 20 years has been maintained by a fear of someone “losing”, says one of the country’s leading health economists.
Professor Martin Hensher, the Henry Baldwin professorial research fellow in health system sustainability at the Murdoch Institute for Medical Research, told our sister publication, The Medical Republic, that politicians, health reformers and policy makers have “failed for a generation”.
“The expectation has been that major reform cannot be done if anybody loses,” Professor Hensher said.
“The truth is, it’s been a very abnormal period in history when you could do reform and everybody wins. Somebody’s going to lose something. You have to have sensible conversations.”
Professor Hensher was responding to an article by Associate Professor Emily Callander, published in the Medical Journal of Australia
“In Australia, out-of-pocket fees make up a larger proportion of overall health expenditure than in these other countries [with similar systems, such as New Zealand, France, Ireland, Germany, the Netherlands and the UK],” wrote Professor Callander.
“The increasing out-of-pocket expenditure by patients is concerning in light of international experience in the United States, where there is a reliance on private or market-based health care, and health care costs are the leading cause of bankruptcy.
“Varied viewpoints range from the impact of high fees on a patient’s ability to access care and the equity implications of high fees, to the right of private providers to set their own fees in an open market and to recover costs of providing care.”
Professor Hensher said Australia’s reliance on out-of-pocket costs is anomalous — given that we are one of the richest countries in the world.
“When you look globally at different countries, from low-income through middle-income up to high-income, one of the distinguishing features is that in the poorest countries, healthcare is funded overwhelmingly by out-of-pocket payments,” he said.
“As countries begin to escape poverty and move into middle income, they very quickly move away from out-of-pocket costs and into government-

funded healthcare and social insurance.
“Our out-of-pocket costs are beginning to be anomalous – they’re beginning to not be consistent with having a high income, and it’s actually the out-of-pocket payments that have to go.
“If some of the infrastructure has to be pulled down to make that happen, so be it.
“Because if we stay tracking this way, we do go towards the US system, not just in the usual way that we talk about the US, but the way the US actually is, which is that many of its people effectively live in a lower-middle-income country which also happens to have the richest people in the world in it.
“And we don’t we don’t want to go that way.”
Professor Hensher acknowledged that there were “terrible problems” in general practice, but suggested that out-of-pocket costs were even more of a problem for specialists, citing his recent narrative review, published in the MJA
“The major causes of out-of-pocket costs were non-PBS pharmaceuticals, and dental and medical services; in the non-hospital Medicare category, the major contributors were specialists’ services (33.7%), GP services (24.6%), and diagnostic services (12.3%),” Hensher et al. wrote.
“Some specialists charge patients more than twice the relevant MBS fees, and some surgeons more than three times the MBS rate for common procedures. Specialists often do not discuss outof-pocket costs with patients in advance, which can result in unexpectedly large costs for the patient.
“The Australian Bureau of Statistics 2016–17 Patient Experiences Survey found that 7.6% of people aged 15 years or more (1.3 million people) deferred or did not use specialist, general practice, imaging, or pathology services because of the cost involved.
“People with chronic conditions were more likely to forgo health care because of cost than people in other high-income … countries. Some people skipped appointments or did not use prescribed medication because of cost, reported they could not pay for other living expenses, or drew on their savings or superannuation or sold assets to pay for health care.”
Speaking with TMR , Professor Hensher said it was time for some courage and action from those at the top levels of Medicare and health system reform.
“There is no alternative, but quite deep structural solutions,” he said.
“The Callander paper draws all the right conclusions – without being alarmist, [out-ofpocket costs are] the thing that will take us into US-style territory, combined with corporates and private equity ownership of practices, which we already know is accelerating.
“There’s a worst-case scenario, which a lot of doctors are falling into because of the pressures that they face – they’re selling up to big chains, many of whom increasingly are private equityowned. Their only interest is extracting profit and they will do that any way they can include including by maximising out-of-pocket fees.
“Lots of people may soon start falling out of the healthcare system, because the safety net programs are targeted at very poor people. But people who are not very poor, yet can no longer afford their care, will find that they are not helped by those programs. That [scenario] will be coming quite soon.”
“The things they’re talking about in the Strengthening Medicare Taskforce report, they’re very nice,” said Professor Hensher.
“But they’re no way big enough to meet the scale of the problem. And they’re only talking about general practice. The rest is not even being
Professor Martin Hensher
“It’s been a very abnormal period in history when you could do reform and everybody wins. Somebody’s going to lose something.”
addressed. Out-of-pocket costs are only one problem, but it’s a problem that’s just going to get worse and worse over years to come unless we intercept it.”
So, what are the solutions?
“The problem is political will, and this misplaced fear that if you get it wrong, there’ll be this enormous flood of people into the public sector that we won’t be able to deal with,” said Professor Hensher.
“I would put the argument the other way: we’re handing over enormous amounts of public subsidy to the private sector, private health insurance and private doctors, with no real visible benefit.
“If you took that money and put it into public provision systems, you might actually get a better outcome and a more efficient solution.
“To be blunt, we’ve got extremely rich stakeholders who benefit from the status quo. It’s not a coincidence surgeons are always the highest-paid income group.
“Yes, doctors need to be well paid. Do they need to be that well paid? Probably not.”
Which brings the debate back to who loses if major reform is undertaken?
“In the long sweep of history, the medical profession is never really going to lose out,” said Professor Hensher.
“Maybe you need to take a little bit less. All roads lead back to having everything on the table. Cost caps, or even bans on out-of-pocket costs, capitation models, all of it.
“Over the next two or three years, there’s got to be a real and different discussion about do we want universal health care in this country? And if we do, what is it?
“We can’t carry on pretending – whichever way we jump, there will be losers. And that’s the conversation we need to start having.”
Danger lies in AI’s inability to comprehend the material it analyses
FRANCIS WILKINS
Alandmark study published in the UK this week has proposed a comprehensive set of practices and principles designed to ensure artificial intelligence (AI) is used ethically in healthcare and medicine.
The study calls for AI-generated content to be clearly labelled as such; for copyright, liability and accountability frameworks to be established where appropriate; and for AI to always be considered as a tool to assist human decision makers, not replace them.
Published in The Lancet’s eBioMedicine journal, it details how large language models (LLMs) could potentially transform information management, education and communication workflows in healthcare and medicine. LLMs are a key component of generative AI applications that create new
content, including text, imagery, audio, code and videos, in response to text or voice prompts, such as ChatGPT.
But according to the paper’s author, Australian AI ethicist Dr Stefan Harrer, LLMs also remain one of the most dangerous and misunderstood types of AI.
The study, he says, is “a plea for regulation of generative AI technology in healthcare and medicine and provides technical and governance guidance to all stakeholders of the digital health ecosystem: developers, users, and regulators – because generative AI should be both exciting and safe”.
According to Dr Harrer, there is an inherent danger in LLM-driven generative AI, since it can authoritatively and convincingly generate and distribute false, inappropriate and dangerous content on an unprecedented scale.
But that point is getting lost in the noise surrounding the newest generation of powerful chatbots, such as ChatGPT, he says.
Dr Harrer emphasises this danger lies in AI’s inability to comprehend the material it analyses.
“In the generation of medical reports, what is currently a manual process –
ploughing through records from various sources in various forms – can with this technology, theoretically, become an instruction to the AI to potentially read all those documents and then produce a summary or a diagnostic and medical report,” he said.
“There are two steps: the clinician giving the prompt, and the AI responding to it.
“That’s very, very tempting, but the thing is the generative AI does not understand the content, the language is not comprehended by the AI. It has no way to assess whether any of the content it created is correct, whether it omitted something, or whether it created an incorrect statement in its output.
“This means that every output created by generative AI needs to be closely vetted by human subject matter experts to make sure there’s no misinformation or wrong information in there.”
Dr Harrer – who is chief innovation officer of the Digital Health Cooperative Research Centre, a major Australian funder of digital health research – proposes a regulatory framework with 10 principles to mitigate the risks:
• Design AI as an assistive tool for
augmenting the capabilities of human decision makers, not for replacing them.
• Design AI to produce performance, usage and impact metrics explaining when and how AI is used to assist decision making and scan for potential bias.
• Study the value systems of target user groups and design AI to adhere to them.
• Declare the purpose of designing and using AI at the outset of any conceptual or development work.
• Disclose all training data sources and data features.
• Design AI systems to clearly and transparently label any AI-generated content as such.
• Audit AI on an ongoing basis against data privacy, safety, and performance standards.
• Maintain databases for documenting and sharing the results of AI audits, educate users about model capabilities, limitations and risks, and improve performance and trustworthiness of AI systems by retraining and redeploying updated algorithms.
• Apply fair-work and safe-work standards when employing human developers.
• Establish legal precedence to define under which circumstances data may be used for training AI, and establish copyright, liability and accountability frameworks for governing the legal dependencies of training.
The study scrutinised several AI tools for ethical design, release and use principles, and performance, including OpenAI’s chatbot ChatGPT, Google’s chatbot MedPALM, Stability AI’s imagery generator Stable Diffusion, and Microsoft’s BioGPT bot.
“As impressive as their performance is in many ways, you cannot use them in an evidence-based sector, such as healthcare and medicine, without a mechanism in place – a human in the loop – to check the outputs before you act on them,” Dr Harrer says.
“The problem we see right now is that the latest generation of generative AI has essentially been unleashed onto the public but, generally, with very insufficient guardrails, often with insufficient education of users as to how they work, what they are and what they are not. People have essentially been invited to experiment with these tools widely.”
Distributing incorrect data can have a further, compounding effect, he says.
“If you ingest, re-ingest or amplify incorrect content created by generative AI and then return it to contaminate the public knowledge database, then use it as you go forward to train generative AI or to feed into other AI, you amplify the falsification in the source data – and that’s worrying as it is.
“But if you think about the scale at which
this can happen with the generative AI tools that we have now, then it’s truly worrisome.”
The study highlights and explains many key applications within healthcare and medicine, including:
• assisting clinicians with the generation of medical reports or pre-authorisation letters;
• helping medical students to study more efficiently;
• simplifying medical jargon in clinicianpatient communication;
• increasing the efficiency of clinical trial design;
• helping to overcome interoperability and standardisation hurdles; and
• making drug discovery and design processes more efficient.
Dr Harrer isn’t pessimistic about the development of ethical AI models in healthcare and medicine. He predicts the field will move from the current “arms race” to a phase of more nuanced, risk-conscious experimentation with research-grade generative AI applications.
However, a paper published by Monash University in the Journal of Applied Gerontology last month has found that introducing AI into aged care homes can exacerbate ageism and social inequality. The technology has been used in areas ranging from addressing the loneliness of residents through chat, video and image sharing, through to medical diagnosis and assessments tools. But its value can be compromised by the choices of carers on
,Dr Stefan Harrer
“Everyone needs to take a step back, take a deep breath and think about how to develop this from here on in a responsible, ethical way.”
how best to use technology for older people in these settings.
“AI can perpetuate ageism and exacerbate existing social inequalities,” says lead author Dr Barbara Barbosa Neves, senior lecturer in sociology and anthropology at Monash.
“When implementing AI technologies in aged care, we must consider them as part of a suite of care services and not as isolated solutions.”
More work is needed to better incorporate how older people are viewed in the design and implementation of AI technologies. The findings show ageism can be generated by design that includes views of older people as dependent, incompetent, and disinterested in technology.
“The use of AI in aged care must be done with consideration of the potential impact of these technologies on wellbeing, autonomy, and dignity of older residents,” Dr Neves says.
According to Dr Harrer, the enthusiasm with which some AI applications have been received has meant the area is “extremely supercharged right now”.
“But what that means is everyone needs to take a step back, take a deep breath and think about how to develop this from here on in a responsible, ethical way,” he says.
“If we don’t, I believe it would be one of the greatest missed opportunities in the field of science – churning out ever-more complex models trained on ever-more data but forgetting ethical and responsible design, deployment and use frameworks.”

www.oncologyrepublic.com.au /newsletter-sign-up/

up here for Oncology Republic’s award-winning journalism, expert opinions, in-depth analysis and more.
It’s our health system, not the science, that’s preventing equity of access to personalised cancer treatment
MARIELLA ATTARD
Precision medicine is within the reach of Australian cancer patients. The system just needs a push in the right direction, according to experts gathered at the inaugural Victorian Precision Oncology Summit held in Melbourne last month.
Personalised molecular testing allows people with cancer to be matched to treatment that targets their specific tumour according to its genomic profile. Not only are survival rates improved, but patients are saved exposure to toxicities and wasted time on treatments that are not likely to work for them.
But in Australia, testing and treatment outside the standard of care are not covered by the PBS, leaving patients and oncologists to work out access as best as they can. Hardly a recipe for equity.
“The problem is not the targets. It’s not the state of science,” Professor David Thomas, the recently appointed Director of the Centre of Molecular Oncology at the University of NSW, told delegates.
“It’s about getting access to the drugs for these patients who would benefit from it, which means more trials because we don’t have an article 71.”
Article 71 is the part of Swiss law (Ordinance of 27 June 1995 on Health Insurance) which requires insurance companies and drug providers to negotiate to cover non-standard treatment where needed.
“In terms of accessing a treatment based on the molecular profile and data analytics, I think we are very lucky in Switzerland to have this article. That helps us a lot,” said keynote speaker Professor Olivier Michielin, who heads the Centre for Precision Oncology at Lausanne University Hospital in Switzerland.
Professor Michielin described Australia as a “jewel of translational research and patient care”. But in reality, Switzerland is streets ahead in providing equitable access to personalised cancer treatment to its citizens, due to its legal, health and data systems.
In Professor Michielin’s home country, insurance covers both standard of care and off-label therapies in precision oncology. This includes the standard 52 gene hotspot

molecular testing panel, as determined by an organ specific tumour board – a process which is also covered by insurance – and a 400 full length gene panel used by the molecular tumour board to recommend individual treatments.
“I think this creates an interesting scenario, because, of course, it’s advantageous for those companies to invest in the analytics if that analytics allows you to have a more rational use of the drugs at the end,” Professor Michielin pointed out.
Patient care is the priority, but precision oncology makes financial sense too, Professor Michielin reminded delegates.
“Sometimes those [predictive] biomarkers will allow you to pinpoint the patient who will not benefit from your therapy. And as the therapies are extremely expensive, the
amount you invest in the analytics might be actually well invested, because you’re going to spare treatment costs for many patients as well,” he said.
‘WE
Professor David Thomas, who followed the Swiss professor on the stage, admitted he was “green with envy”. And he wasn’t the only one who found the comparison between systems hard to bear.
“It’s always difficult to hear,” Dr Kortnye Smith, a medical oncologist at Peter MacCallum Cancer Centre, told Oncology Republic
Dr Smith, who gave delegates a picture of what it’s like for clinicians to try and access molecular testing in Victoria, has researched ways to integrate complex
genomic sequencing into cancer therapy and facilitate access to genomics.
“From my point of view, it seems like it would be a reasonably straightforward test to deliver to patients to give improved outcomes. And we’re a long way from being able to deliver that in a way that is equitable for everybody and not determined by which hospital they happen to have their care directed through.”
Lack of public funding for non-standard testing and therapy can put oncologists in a difficult position when their patient is not financially well off, but “all the data certainly tells us that patients would prefer to be told if there are things that are available for them, even if that is at a cost,”
Dr Smith told OR
The price tag on molecular tests is not
much higher than for a PET scan, which is covered on the PBS, Dr Smith pointed out.
“When cancer drugs can cost $8000 to $16,000 a month, $3000 to $5000 to make sure that we get patients on the right drug does seem like a valuable investment,” she said
The way Australian advisory bodies evaluate new tests or therapies and make recommendations about funding is part of the problem, she suggested.
“Genomics really hasn’t been able to fit into the way that the boards evaluate what efficacy is,” she said.
“While we can show that patients are living longer after having these tests, it’s [about]

the comparator. And it’s hard to provide them with the kind of data that’s required for that.”
The Australian government is currently undertaking a Health Technology Assessment Policy and Methods review, described as “an important opportunity to develop specific reforms to how health technologies are assessed and funded to help ensure that Australia’s subsidy schemes and funding programs continue to meet the needs of Australians into the future.”
Professor John Zalcberg, chair of the Australian Clinical Trials Alliance and editor of this publication, has exhorted clinicians and, more importantly, consumers to get onto the website and make submissions before the end of the first consultation round on 6 June 2023.
“Article 71 is in our grasp,” Professor Zalcberg said. “But there needs to be a groundswell of support from the community to say that what we have currently doesn’t provide for the future of medicine and the future of oncology.
“This is a once in a lifetime opportunity for the community to say that what we have is not good enough. We’ve got to do better and we can do better. Lots of countries do better.
“But we’ve got to convince the people doing this review that the support is there.”
As the CEO of the Australian Genomic Cancer Medicine Centre and of Omico, a not-for-profit set up to match patients with trials, Professor Thomas has been working
,Professor David Thomas
“We should use the same ferocity of focus on the system as we do on research.”
But while almost 40% of the Omico cohort had biomarkers that would be expected to see those high survival rates, under 6% were getting access to treatment.
“That for me is still an unresolved problem – equity of access; not to the genomics, but to the treatments upon which genomics are predicated,” he told those gathered.
Dr Smith said the program was a very good option for patients, but not all oncologists felt confident about what to do with the test results and the recommendations made by the molecular board, let alone explaining them to patients.
Currently, there isn’t even an MBS item number for discussing those results with patients.
“Managing the information and giving the best advice to a patient to make a decision can be really tricky,” she told OR . “And accessing the drug is really challenging. It’s still your job to find access to programs or try and get the patient on a clinical trial, to make the right decision in terms of whether they’d be better off on chemo. So there’s still lots of bits and pieces in terms of what is appropriate.”
Dr Smith said education about how genomic testing works would go some way to help.
“There are some types of cancers where it is much more likely that you’re going to find a molecular variant,” she said.
“So when you do get a patient that has, for example, a thyroid cancer, where we know that the rates of mutations are high, you could say this is a patient I’m going to chase down a clinical trial for, or commercial testing, and talk to the patient about the value of it.
“You’ll know when it’s worthwhile asking for that extra effort to get people where we want them to be.”
Education was unanimously recommended by forum participants as a way to improve equity of access, for and by clinicians and consumers alike, along with standardisation and centralisation.
Dr Smith told delegates that even standard of care tests are handled and reported differently across laboratories and hospitals.
Of course, data standardisation is complicated, even the Swiss would agree.
“The solution we found was to actually project the data from each hospital into a common vocabulary and that common vocabulary has been determined among us. It took us three years to agree on everything but now we have this common data set that we use,” Professor Michielin told the gathered experts.
gathered from both standard and nonstandard panel tests, including raw patient data.
And its data sharing infrastructure allows clinicians to squeeze as much as they can from it, with analysis done by both the pathology department at the university hospitals and bulk RNA sequencing by the Genomic Centre in Geneva.
It also makes it possible to quickly integrate new innovations such as the rapidly evolving field of spatial transcriptomics, which adds spatial information to RNA sequencing.
All of this data is integrated as a reference data set for use by molecular oncology tumour boards, which include bioinformaticians, geneticists, pathologists, and medical oncologists.
They consider panel next generation sequencing and use technologies such as data science to make educated decisions about treatment for individual patients, which is then fed back to the referring oncologist and the patient to decide next steps. The loop is closed by collecting and reporting data from patient treatment and experience.
Thanks to the development of the Swiss Personalised Health Network initiative, the data set is being expanded to include data from non-university public hospitals and private hospitals around the country.
The goal is interoperability – the capacity to compare clinical and genomic data for any patient, being treated anywhere, with the data set.
“We have created a system by which we can gather the material and also at the same time, through flying data managers in a different system, to collect the relevant clinical information, to get what is needed to make the decision through data mining”, Professor Michielin explained.
Over the last seven years, 46% of patients have had off-label treatment administered at their usual location, without needing to travel, and 45% enrolled in a clinical trial.
“So I think we are now pretty happy because we have secured access to every patient to this large data set, and there is absolutely no cost [to the patient],” Professor Michielin said.
“All of these cases are discussed at a joint tumour board, either at the national or regional level. And thanks to specific articles, like the article 71, we now have the possibility to treat, I think, probably every patient with an off-label drug or a clinical trial.”
Back in Australia, access to standard of care molecular testing varies, let alone nonstandard of care.
to connect as many people as possible with treatment within the system we have.
The government-backed program started in Victoria and went national in 2019.
It now involves 23 cancer centres across the country and patients can be referred from anywhere in Australia.
The program is expected to reach 3000 people by the end of this year and has already had 7300 referrals.
“Trial matching works,” Professor Thomas said, pointing to slides showing impressive survival data, in some cases doubling.
“Imagine if [these results were not for] a model of care, but rather a drug. This magnitude of effect in a terminal population who had exhausted treatment options would get that drug approved in every jurisdiction around the world.”
Health data is well organised in Switzerland. For starters, electronic health records work. “There is really an opportunity to directly question the general population through electronic patient records, and to be able to complement some of the molecular testing,” said Professor Michielin.
Information collected includes clinical data on efficacy, patient reported outcomes and, importantly, digital pathology images and radiomics.
“Images are really standard. All patients have these images,” he said.
“And if we can base biomarkers on images, in addition to genomic testing, this is, of course, a great opportunity to create a system that will have equity at its roots.”
The country is building an accessible, extremely valuable data system around the analytics from genomics information
We are still seeing pronounced disparities in access to precision medicine, depending on factors including postcode, financial means, whether patients are getting care through the public or private system, the language they speak, the particulars of their tumour, their oncologist, and timing.
“We should use the same ferocity of focus on the system as we do on research,” Professor Thomas told the assembled oncology community.
“We can work with policymakers, government leaders and community leaders to come up with a viable, fundable solution that will solve not just the survival challenges, but those sustainability challenges.
“It shouldn’t be beyond us. If we can actually find a solution to cancer by developing a treatment, surely we can solve the social problems that might stop us from applying it.”
The idea for a radical type of organ transplantation was born in Australia
HELEN TOBLER
Three decades ago, a young Swedish doctor training in gynaecological cancer surgery at Royal Adelaide Hospital had to break the news to a 25-yearold cervical cancer patient that she needed a radical hysterectomy to save her life.
Professor Mats Brännström explained to her that surgeons could preserve her ovaries but that she could never carry her own pregnancy.
“And then she actually suggested to me, ‘can’t you do a uterus transplantation?’ And I was astonished because I had never thought about the concept of uterus transplantation,” he remembers.
That conversation changed the course of Professor Brännström’s career, and like so many simple but wonderfully complex ideas, like spray-on skin and cochlear implants, uterus transplantation has its roots firmly in Australian soil.
Professor Brännström made that idea his life’s work, returning to Sweden and spending almost 20 years researching and trialling uterus transplants in animals. In 2014, he performed the first human uterus transplant that resulted in a live birth.
And on 10 January this year, his vision came full circle, when Coffs Harbour woman Kirsty Bryant, 30, received the uterus of her mother Michelle Hayton, 54, in a 16-hour dual surgery at the Royal Women’s Hospital in Sydney.
Lead surgeon, Sydney paediatric and adolescent gynaecologist Dr Rebecca Deans has been working with Dr Brännström for more than 10 years and he and his team were there to oversee the marathon surgery.
The hospital is home to one of two teams in Australia that have secured $1 million in research project funding to perform six uterus transplants this year. They have approval for another six, which will be dependent on more funding.
Uterine transplantation offers the chance of conception for women for whom conception and pregnancy are impossible. That includes women who have had a hysterectomy due to gynaecological cancer, postpartum bleeding or severe endometriosis, for example, or the one in 500 women with absolute uterine factor infertility (AUFI) in which there is either no uterus or the organ isn’t functioning.
Dr Deans has seen women with congenital absence of the vagina or uterus, known as Mayer-Rokitansky-Küster-Hauser (MRKH) Syndrome, at the Royal Hospital for Women
for nearly 20 years. Dr Deans and her team perform vaginal dilation and surgical procedures to create a vagina for women who are born without one at Australia’s only inpatient vaginal dilation service.
Participants in the uterus transplant trial have come from the MRKH clinic and through the Uterus Tx Australia and Royal Hospital for Women Foundation websites.
“The patients really drive this,” Dr Deans tells Oncology Republic . “The patients really do want it.
“It’s really about that improvement of quality of life. And I think that in Australia where surrogacy is pretty hard to achieve, it gives another option for women.”
The projects at the Royal Women’s and at Sydney’s Royal Prince Alfred Hospital are operating under research funding, and there are no plans for uterus transplants to become widely available or publicly funded. But even for those people who hope to take part, many of them don’t fit the criteria, Dr Deans says.
“They’re either too old for inclusion or they don’t have a donor,” she says.
,Dr Rebecca Deans
“In Australia, where surrogacy is pretty hard to achieve, it gives another option for women.”
Professor Brännström’s commitment to his patients is clear. As he tells OR, he receives Christmas cards in the mail each year from the families of babies who wouldn’t exist without a donated uterus. The baby born from his first successful uterus transplant bears his name.
He says that from the very first conversation he had with his young Australian cancer patient he felt confident it was possible to master the technique.
After returning to Sweden, he worked on developing the technique in animals in 1989, first in mice, then bats, pigs, sheep and baboons for a non-human primate model.
“In my project, the donors can be either deceased or living and a lot more people want a deceased donor because they don’t have an eligible living donor – like most transplants. Some are lucky enough to have one.”
It was slow and painstaking research that took decades. Dr Deans first heard about Dr Brännström’s research in 2009 was inspired to go to Sweden to train with him in the animal trials. A few years later she assisted with human transplants.
“It was a great experience training in the sheep model and then scrubbing in to do the human transplant surgeries in Sweden,” she says.
Professor Brännström recalls the first hysterectomy in a woman took longer than the team expected.
“We thought it could take four to six hours,” says the professor and chairman in the department of obstetrics and gynaecology at Sahlgrenska Academy, University of Gothenburg.
“It actually took 11 hours, so it was a lot more difficult than we thought.”
That transplant was a success and resulted in two pregnancies and healthy babies. Since then, 12 babies have been born in Sweden thanks to uteruses donated by mothers, sisters, aunts, cousins and good friends of the recipients.
“Even kidney transplants in a sense are about quality of life because it’s about getting people off dialysis rather than necessarily saving lives,” Dr Lotz, who gave ethical advice to the uterus transplant team and the patient safety and data monitoring board, says.
Dr Lotz was reticent about the idea of uterus transplantation at first.
“I felt that it was best to be involved rather than to be standing on the sidelines,” she says.
“I felt like if it is going to happen, then it needs to be as ethical as possible, and we need to make sure that there are no unscrupulous providers here. We need to make sure that proper processes are in place to ensure that the women who are undertaking the procedure

“They are all healthy and normal weight,” Professor Brännström tells OR by phone as he catches public transport to work in Gothenburg.
“The oldest is now eight years old and we haven’t seen any differences and he seems to be healthy. And we follow the donors for five years afterwards and they’re fine both physically and mentally.
“I can see that I actually helped to create a family which they thought was impossible. I’m happy that I can help patients who were not able to have that before.”
The concept of uterus transplants is certainly not short of ethical questions, and one of the most common is around the issue of whether a uterus transplant is medically necessary.
While uterus transplantation is the only reproductive transplant available, it’s certainly not the only non-life-saving transplant – face, hand and even penis transplants are now possible, Dr Mianna Lotz, associate professor of philosophy at Macquarie University, says.
less likely to psychologically reject it,” she says.
“To the best of my knowledge, we’ve got no cases of psychological rejection in recipients in the case of uterus transplants. This is partly because it is transient and temporary, and partly because it’s not visible.”
As with any organ transplant, recipients need to take immunosuppression therapy, but for women with transplanted uteruses that immunosuppression is kept at levels that are safe for the baby.
“With a uterus transplant the recipient only keeps the transplanted organ in to have a baby, or at most two,” Dr Lotz says.
“So you don’t have the extended exposure to immunosuppression and you also don’t need as high a dose of immunosuppression as compared to permanent transplants and face or hand transplants,” Dr Lotz says.
She says that if conception is successful, immunosuppression is carefully monitored.
“That has to be monitored extremely closely to ensure that the recipient is not getting infections through loss of immune response, but the level of immunosuppression can be reduced to a level that’s deemed compatible with the wellbeing of the fetus developing in utero,” she says.
And it’s only temporary. Once the recipient has a baby (or two), the uterus is removed, and that temporary nature of the transplant brings the advantage of limiting the need for immunosuppression to five years, at the most.
For the recipient, there’s a long road to recovery and then once menstruation has started they will try to conceive via IVF and embryo transfer.
As for the organ itself, that’s the end of its service, but Dr Deans says research is being planned by other teams to see whether uteruses can be donated to a second person.
Internationally, around 75% of all transplants have been from living donors, and the Royal Hospital for Women project has approval to use both living and deceased donors, Dr Deans says.
Dr Lotz says there are pros and cons for both.
“I regard it to still be a genuine matter of research equipoise and for that reason, we should be going ahead with developing the research for both the deceased donor and the living donor model,” she says.
For instance, using living donors has the advantage of enabling the surgical team to be well rested and reducing the ischemic time, thus improving the success rate of the transplant.
Dr Brännström says data shows that if the transplant and embryo transfers are successful, the take-home baby rate is about 85%.
“That’s a very high success rate for fertility treatment,” he says.
A review of the first five years of uterus transplants in the US found there was no donor or recipient mortality, and one-year graft survival was 74%. Among the 33 recipients, 19 delivered 21 live-born children.
“Uterus transplant is safe for mother and child; success is reproducible and not limited to single centres; success is achieved with both DDs and LDs; and success rate is comparable with the most effective infertility treatments,” the JAMA Surgery review concluded.
Whether uterus transplants will one day be publicly funded raises the broader ethical concern that relates to all fertility services: that it’s more accessible to wealthier people, Dr Lotz says.
“There’s the concern that if we don’t make it publicly funded, then that means that only those who can privately afford it get access to it,” she says.
“And if we do, we may be signalling something that is perhaps concerning around making a priority of something that has the risk profile that it does, that isn’t life-saving and uses the resources that it does.
“At this point, my view on it is that at the research level, it’s appropriate to apply for National Health and Medical Research Council funding and government funding through that. But I’m remaining on the fence about whether it should be Medicare funded in the future. And I think opinion definitely diverges on that question.”
When it comes to deceased donation, there’s also the question of whether the uterus could one day be included in the organ donor list.
That’s still some way down the track, and it will depend on the results of the trials in Australia which are still in the research phase, according to a spokesperson for the Organ and Tissue Authority.
“Once the results of these trials are finalised our medical experts can begin the process of reviewing the findings and determine the next steps,” the spokesperson says.
Dr Lotz says that while the uterus would be part of multi-organ retrieval, it would be retrieved only after the life-supporting organs had been removed.
are fully informed, not coerced, not feeling compelled or pressured.”
It’s a major procedure for both the recipient and the living donor, for whom the procedure is a much bigger deal than a standard hysterectomy, Dr Deans says.
“It’s long surgery of eight to 12 hours,” she explains.
“There’s a higher risk of vessel and ureteric injury as well as shortening of the vagina as the upper cuff is removed also, so there are possible sexual function impacts.”
There are also potential psychological impacts for the donor if the uterus doesn’t function well or fails after transplant and there’s the potential psychological rejection of the organ, which has been known to occur with a hand transplant.
But worldwide, no women who have had the procedure have psychologically rejected the uterus, Dr Lotz says.
“It’s not visible to the patient so that they are
On the other hand, using living donors involves major surgery for someone who doesn’t medically need any intervention, exposing them to potential harms and risks. There are also the potential psychological and emotional impacts on the donor if something goes wrong or if there are poor outcomes for the recipient, pregnancy or baby.
Using organs from deceased donors allow surgeons to remove longer lengths of vasculature, a process which carries a risk of injury when carried out in a living donor.
“For the living donor there is a concern that we’re putting a perfectly healthy person through a significant and lengthy surgery. Whether a donor is known to the recipient or not, it’s a lot to go through,” Dr Lotz says.
“We’re only taking peri-menopausal women as living donors, to ensure they have finished with their own reproductive plans. But still, it’s a big surgery and it’s one that they are not medically indicated for.”
As uterus transplants are done in more and more countries and the data accumulates, evidence grows to support its efficacy.
“Uterus removal for transplantation would never jeopardise the ability for life-saving organs to be taken and utilised first, and that’s pretty standard for quality-of-life transplants,” she says.
For now, all eyes are on Ms Bryant, who Dr Deans says has a good chance of conceiving by the end of the year.
While there were no major complications during the two surgeries, Ms Bryant had significant blood loss 24 hours after the surgery and needed blood transfusions, while her mother had a serious infection and lack of sensation in her bladder.
Ms Bryant told media that she started menstruating 32 days after the transplant in January. All going well, about three to six months after the transplant she will try to conceive through IVF using embryos frozen before the transplant.
“There is a good number of women coming forward saying, ‘I really would love to do this. I don’t have other options. We desperately want to have another child and we’d really love to be considered’,” Dr Deans told media.
“I’d love to be able to offer this to women in Australia.”

Australian healthcare is stretched to breaking point, with patients having to wait for weeks to see their GP, sitting for hours in crowded emergency rooms and waiting months or years for elective surgery.
“Providing cutting-edge health care is both technologically and economically expensive,” medical historian Professor Candid told us, “but the federal government is constantly on the lookout for sources of cheap labour and today they’ve announced that they’ll be reinstating barber surgeons.
“Barbers cut hair and occasionally trim eyebrows,” Professor Candid continued, “but it hasn’t always been this way. Two hundred and fifty years ago barbers were in the same guild as surgeons. They were highly skilled professionals who could treat buboes, lance boils, pull teeth, insert enemas, set fractures and apply leeches.
“It’s hoped that by reclaiming their barber surgeon status the high-street hairdresser will once again be able to ease the pressure on GPs and even shorten surgical waiting lists.”
We spoke with Colin, one of the first patients to visit Sweeney Todd’s, a newly opened barber surgeon in a trial of the scheme in northern Queensland.
“When I arrived everything seemed pretty normal,” Colin said. “There were piles of hair on the floor and faded pictures of Cher on the wall – but then I heard a blood-curdling scream coming from the back of the shop.”
Before he knew it the barber surgeon had strapped Colin into a chair.
“He shaved off all my hair and then tried to saw off the top of my head with a piece of cheese wire,” Colin recalled.
“I must have passed out because when I woke up I had a neat scar on my scalp and I couldn’t remember my name … What is my name by the way? And where have all my teeth gone?”
“We’re entering a new age in healthcare,” explained Professor Candid. “A cheaper, less qualified age, where the government is all too willing to replace your experienced but expensive doctor with a bulk-billing barber-surgeon.”
- Dr Kevin Hinkley

As is the disposition of tech enthusiasts the world over, news from earlier in the year that detailed how AI chatbot ChatGPT had passed the US medical licensing exam sparked a flurry of commentary portending the imminent demise of actual physicians. Folks with skin in the game, such as OpenAI head honcho Sam Altman, the outfit that developed ChatGPT, suggested the digital dynamo could one day serve as “medical adviser” for those unfortunate enough to live in the US and not be able to afford proper healthcare. As harebrained as this sounds, people were taking it seriously enough to prompt boffins at the US’s Stanford University to test how well this souped-up Dr Google could perform in real-life medical scenarios. The short answer? Really, really badly. They found nearly 60% of ChatGPT’s answers to actual medical situations either disagreed with a human expert’s opinion or weren’t relevant enough to be helpful. Call us a Luddite, but we reckon the chances of ChatGPT becoming ChatGP anytime soon seems low.

Are country-raised kids healthier than city-bred children? If your gut instinct says “yes”, then chances are your perceptions have been swayed by romanticised portrayals of rural idylls and dark and demonic depictions of urban slum life. The reality, however, is that historically children and teenagers across the globe have tended to have better growth and physical development if they lived in cities than if they lived in rural areas. Boring health statistics show that the life of a peasant child overall could often be even more crappy than that of a city-based Dickensian urchin. Which is why a recent study by Australian and international authors suggesting the balance may now be tipping the other way is quite interesting. Using height and weight as a general indicator of development across more than 70m young folk from around 200 nations, the boffins found that while urban children were taller than their rural counterparts in almost all countries in 1990, this advantage had subsequently decreased in most countries, and even reversed in places such as the UK and US by 2020. So could it be time to dust off the old Escape to the Country fantasies again?