You can rely on Avant’s medico-legal expertise, support and resources.
•Access medico-legal experts, 24/7 in emergencies
• Leading defence, with local support from Avant Law’s 80+ medico-legal solicitors nationwide
•Medical advisors for peer support in a claim
•Personalised advice to reduce your claims risk
By your side, with support to protect your career.
Dr Matt Doane Avant member
We need to fix the system
Australia may not be facing the avalanche of patient demand the NHS is, but we also cannot wait for it to get that bad.
Complete the self-reflection and claim your CPD time, please scan here
A few editions ago we reported on the true cost of doctor burnout – the impact it has on doctors and the knock-on effects for the health system.
Recently I was in London and caught up with a friend who works in the NHS. He mentioned something that caught my attention – the NHS Trust where he works is seeing many UK doctors returning from Australia because they are too burnt out by our health system here.
There were two reasons I found this interesting. One, the NHS is notorious for burnout among all staff, largely due to the huge strain on the system.
Two, Australia has long been seen as an oasis for healthcare staff in the UK, with many choosing to relocate. I wrote about that more times than I can count in my years reporting on the NHS.
Australia may not be facing the avalanche of patient demand the NHS is, but we also cannot wait for it to get that bad.
In WA we have a record number of GPs practising in rural areas, however, we know GP deserts are still causing major problems for both practitioners and patients in metro and rural areas.
Some local governments are currently calling for reforms to better financially support primary healthcare services in rural areas.
Additionally, recent reports show wait times for specialist care and urgent care are becoming too long.
It’s a vicious cycle of patient demand and doctor shortages. If we cannot keep our overseas trained doctors, we risk the situation becoming worse.
What is the solution? I’m keen to know your thoughts on this, or if you’re someone who is considering leaving WA. Email editor@mforum.com.au
SYNDICATION AND REPRODUCTION Contributors should be aware the publisher asserts the right to syndicate material appearing in Medical Forum on the mforum.com.au website. Contributors who wish to reproduce any material as it appears in Medical Forum must contact the publisher for copyright permission.
DISCLAIMER Medical Forum is published by Medforum Pty Ltd (Publisher) as an independent publication for health professionals in Western Australia. Neither the Publisher nor its personnel are medical practitioners, and do not give medical advice, treatment, cures or diagnoses. Nothing in Medical Forum is intended to be medical advice or a substitute for consulting a medical practitioner. You should seek immediate medical attention if you believe you may be suffering from a medical condition. The support of all advertisers, sponsors and contributors is welcome. To the maximum extent permitted by law, neither the Publisher nor any of its personnel will have any liability for the information or advice contained in Medical Forum. The statements or opinions expressed in the magazine reflect the views of the authors and do not represent the opinions, views or policies of Medical Forum or the Publisher. Readers should independently verify information or advice. Publication of an advertisement or clinical column does not imply endorsement by the Publisher or its contributors for the promoted product, service or treatment.
Advertisers are responsible for ensuring that advertisements comply with Commonwealth, State and Territory laws. It is the responsibility of the advertiser to ensure that advertisements comply with the Competition and Consumer Act 2010 (Cth) as amended. All advertisements are accepted for publication on the condition that the advertiser indemnifies the Publisher and its personnel against all actions, suits, claims, loss or damages resulting from anything published on behalf of the advertiser.
EDITORIAL POLICY This publication protects and maintains its editorial independence from all sponsors or advertisers. Medical Forum has no professional involvement with advertisers other than as publisher of promotional material. Medical Forum cannot and does not endorse any products.
this issue
THE NEWS
Keeping abreast of cancer care
Preparing for the
20 Close up: Medical student Navya Nukamreddy
Call for distinct bereavement services
52 Margaret River Open Studios 54 Scientist hums through the years
Wine review: Mr Barvel – Dr Craig Drummond MW
WINNERS ARE GRINNERS
This month we have a great Doctors Dozen prize to win, with a selection of fine wine from Mr Barval. Read the review by Dr Craig Drummond on page 55.
Five lucky readers are taking a friend to the Hurtigruten Scandinavian Film Festival this month. Keep an eye out next month for our next foreign film competition.
To enter our Doctors Dozen competition, scan the QR code or go to www.mforum.com.au and hit the competitions tab.
PUBLISHERS
Alice Miles – Director Fonda Grapsas – Director Tony Jones – Director tonyj@mforum.com.au
EDITORIAL TEAM
Managing Editor
Andrea Downey 0437 909 904 andrea@mforum.com.au
Clinical Editor
Dr Joe Kosterich 0417 998 697 joe@mforum.com.au
Graphic Design
Ryan Minchin ryan@mforum.com.au
ADVERTISING
Advertising Manager
Bryan Pettit 0439 866 336 bryan@mforum.com.au
Advertising Account Manager
Rita Murphy 08 9203 5222 rita@mforum.com.au
Clinical Services Directory
Alice Miles 08 9203 5222 alice@mforum.com.au
CONTACT MEDICAL FORUM
Suite 3/8 Howlett Street, North Perth WA 6006
Phone: 08 9203 5222 Fax: 08 6154 6488
Email: info@mforum.com.au www.mforum.com.au
Guest Columns
Hepatocellular Carcinoma and Chronic Hepatitis B: The GP’s Role.
By Adam Gregson Hepatology Nurse Practitioner, Royal Perth Hospital
Chronic hepatitis B (CHB) causes hepatocellular carcinoma (HCC)
CHB is the most common cause of HCC worldwide. For those living with CHB, the risk of developing HCC is up to 100 times higher than those who don’t. Liver cancer is the fastest growing cause of cancer death in Australia.
Between 20-25% of people with CHB die from complications of the disease, specifically cirrhosis and HCC. Globally that is one death every 44 seconds or about the time it takes to read this paragraph. With optimal monitoring and treatment, these deaths are largely preventable, and HCC can be detected early.
Overseas migrants and Aboriginal people are at highest risk of CHB and HCC
An estimated 220,000 Australians are living with CHB, with 10% in WA. Overseas migrants (61%) and Aboriginal and Torres Strait Islander people (11%) are the populations most affected, and also have the highest rates of HCC.
Antiviral medication is the best way to prevent HCC in CHB. When treatment is commenced at the right time, the risk of HCC is reduced by 30% in patients with cirrhosis and 80% in patients without.
Commencing eligible patients on treatment is only one part of the solution. Over 30% of people
with CHB remain undiagnosed, and fewer than 25% are engaged in regular monitoring. This is concerning for those marginalised yet overrepresented patient groups who already face a range of health inequities and worse outcomes. We are far from achieving the targets in the 4th National Hepatitis B Strategy, including 22% of patients with CHB to be receiving treatment (by 2025, and 27% by 2030).
Estimates from the Doherty Institute show WA only reaching 8.4%, possibly due to low GP confidence in interpreting CHB blood results, as well as a difficulty in maintaining competency when numbers of CHB patients at practices may be low.
GPs play a vital role in screening and diagnosis, and providing optimal lifelong monitoring of CHB, as well as timely antiviral therapy and HCC surveillance. Royal Perth Hospital has established an innovative statewide project to support GPs to manage CHB in their practices, providing training to build confidence and competence.
The role of GPs and primary health care
As a chronic disease, primary care is the ideal setting for CHB management. GPs are best placed to provide quality holistic chronic disease oversight acknowledging that involvement of s100 prescribers or specialists may be required along the way. Support is available to help guide your management:
HBsAg positive?
There is active infection – contact the Hep B Hub WA for advice
HBsAg negative?
Check immune status and vaccinate/boost if needed
• the ASHM Hepatitis B Decision Making Tool: www.ashm.org.au/ resources/decision-making-inhepatitis-b/
• Hep B Hub WA: a statewide clinical advice service that provides GPs with online and in-person support, education, and advice to manage CHB with responses within two business days. Hepatitis B medication prescribing can also be requested if you are not an s100 prescriber yourself. You can email HepBHubWA@health.wa.gov.au
• Hepatitis B Outreach clinics: currently available to metropolitan general practices and primary care health services, providing onsite support to manage and treat your CHB patients, including providing access to a Fibroscan® in your practice to guide care planning. Contact the Hep B Hub WA for more information.
• The following link will take you to an array of patient CHB resources that are invaluable in the provision of care and education to your patients: www.hepatitisb.org.au/ patient-resources/
The following patients with chronic hepatitis B are a high risk of HCC and need 6-monthly HCC surveillance comprising of an abdominal ultrasound and serum AFP:
People with cirrhosis
People 40+ years with a family history of HCC in a first degree relative
People from sub-Saharan African aged 20+ years
Aboriginal and Torres Strait Islander people aged 50+ years
Asian-Pacific males aged 40+ years and females aged 50+ years.
The important role of GPs in managing CHB can be broken down into three key areas:
1. Timely testing and diagnosis (or vaccination)
The biggest pitfall when testing a patient for CHB is insufficient ordering on pathology requests, and not acting on the results. It is not enough to write “Hep B serology”, as different labs will test different things.
To get the most out of your opportunity to test, request the following three items with “? chronic hepatitis B” or similar stated in the clinical details:
• Hepatitis B surface antigen (HBsAg)
• Hepatitis B surface antibody (HBsAb)
• Hepatitis B core antibody (HBcAb).
These three tests provide you with enough information to confirm active/previous disease and immunity. Following up with non-
immunity is important, and if there was a reason to test for CHB, there is often a reason to vaccinate if indicated.
It is essential that you offer testing to everyone who is susceptible. An accurate list of those groups, along with a guide to interpreting blood test results can be found on the ASHM Hepatitis B Decision Making Tool or by emailing the Hep B Hub WA.
2. Regular monitoring of CHB and treating when required There is no such thing as a “healthy carrier” for hepatitis B, but the myth persists. Anyone with a positive hepatitis B surface antigen (HBsAg) has active infection and requires sixmonthly monitoring.
CHB can seem complicated and overwhelming to clinicians who see it infrequently. Support is available using the ASHM Hepatitis B Decision Making Tool and resources from Hepatitis Australia.
HCC and Hepatitis B: Key Learnings
Hep B Hub WA can also be contacted to provide clinical advice and support with the aim of keeping CHB management within primary care. Treating at the correct time significantly reduces HCC risk and Hep B Hub WA will guide you through the process and can provide prescriptions if required. Training to become an s100 prescriber for CHB treatment can be accessed via ASHM: www.ashm.org.au/ prescriber-programs/hepatitis-b/
There are opportunities for patientfinding within your practice to help identify and re-engage patients with CHB who need linking back into care, and this process can form part of your CPD hours (in particular Measuring Outcomes (MO) and Reviewing Performance (RP)) required as part of your role. Contact the Hep B Hub WA for more details.
3. Six-monthly HCC surveillance
All patients with CHB should have an abdominal ultrasound as a baseline, and certain high-risk groups need six-monthly surveillance (as outlined in the grey box) consisting of abdominal ultrasound and serum AFP.
The use of AFP in HCC surveillance along with ultrasound has been disputed. But AFP is useful for early detection, to validate concerning ultrasound findings as well as highlighting potential HCC where there is no sonographic evidence.
1. CHB is a chronic disease and primary care is the ideal setting for its management.
2. Timely testing and diagnosis of CHB is vital and can be done by requesting the three main tests - HBsAg, HBsAb, HBcAb. Remember to check immunity and vaccinate if required, if HBsAg is negative.
3. There is no such thing as a "healthy carrier" for CHB. Everyone who is HBAg positive requires 6-monthly monitoring with antiviral treatment at the correct time.
4. Explain to your patients with CHB that they are at-risk from HCC. Those with cirrhosis and those with CHB at high-risk should have an abdominal ultrasound and serum AFP 6-monthly. Remember to do a baseline ultrasound on all patients with CHB whether on surveillance or not.
Need help?
Refer to the ASHM Hepatitis B Decision Making Tool: www.ashm.org.au/resources/decision-making-in-hepatitis-b/
Contact the Hep B Hub WA: a state-wide clinical advice service providing GPs with online and in-person support, education, and advice to manage and treat CHB with responses within 2 business days.
You can email: HepBHubWA@health.wa.gov.au
Rural councils footing bill
A group of six local governments from rural Western Australia are hoping to start a conversation around the issue of funding support for primary healthcare services in rural areas.
This action was prompted by the long-standing and growing issue being raised at this year’s National General Assembly of Local Government.
The Shire of Lake Grace, on behalf of six local governments in rural WA, called for reform to the distribution of Financial Assistance Grants to rural local governments supporting primary healthcare services.
Rural Health West said local governments were increasingly funding general practice and primary care to ensure access in rural communities.
In 2023, Rural Health West partnered with the Western Australian Local Government Association (WALGA) to survey the extent of this support across WA. It was found that 69 local governments were contributing $6.8 million (net) annually through financial and in-kind assistance to sustain local primary healthcare services.
More than three-quarters of this funding supported general practice of which 92% came from communities with fewer than 5000 residents.
Rural Health West chief executive Professor Catherine Elliott said the motion’s passing placed national focus on the pressing issue that affects communities across Australia.
She said while local governments were well-placed to welcome and support health professionals, facilitate integration into communities, and foster the liveability
Fewer jabs, more flu
WA’s flu vax hesitancy is starting to bite at the sharp end of our health system, but all eyes are nervously on Queensland, which has delayed elective surgery because of the number of hospitalised flu and RSV cases overwhelming its resources. Could the same thing happen here?
New AMA (WA)
president, Dr Kyle Hoath said the WA health system was already "bursting at the seams" and a record flu season, which early figures seem to indicate it could well be, would be "a disaster waiting to happen."
that attracts and retains workforce, “they should not need to directly fund primary healthcare services”.
“Such arrangements are often the result of market failure – local governments step in not because it is their responsibility, but because they know these services are vital to the wellbeing, sustainability and vitality of their towns.”
Professor Elliott said the data gathered with WALGA made clear what many in rural Australia already know – “local governments are propping up essential health services to meet their communities’ needs.”
RSV and COVID," he said. "With what's happening in Queensland we are trying to keep our finger on the pulse over here and keep an eye on what's happening in our backyard and try to stay a step ahead."
The WA Health Department has recorded more than 13,000 flu cases in July and the AMA (WA) says it anticipated cases to continue surging into August.
"We don't really have the capacity to deal with these increased incidents of things like influenza,
The previous peak in the past five years for flu cases in July was 15,796 in 2023.
"You've heard of the horror flu season thrown around and it really is what we are seeing, worse than it has been in a long time," Dr Hoath said. "I would expect these numbers to increase over the next
couple of weeks at least into the next month before we see any kind of relief from natural attrition.
"Flu vaccination rates are down this year, currently sitting at 25% when we could expect above 30% and this drop has been attributed to the high influenza numbers."
More delays for ADHD drug
Ongoing ADHD medication shortages come as several states, including WA, make moves to allow GPs to play a greater role in diagnosing and treating ADHD.
The TGA has told GPs that the current shortage of Concerta modified-release tablets to ADHD will extend until the end of 2026.
Passionate about prostates
An advocate for men’s health, Dr Tom Shannon likes to set a good example for his patients and encourage self-care for the prevention of illness.
Urologist and prostate cancer surgeon Dr Tom Shannon aims to be in his patient’s lives for the shortest time possible.
“I love the fact that I can be important to a patient for a very short period of time. The goal is not to need me and to get on with their lives, free of cancer, which is such a privilege to be part of. Our team makes a difference,” he says.
Tom has been a urologist for more than 25 years, specialising in prostate cancer diagnosis and treatment. He still loves his profession as much today, if not more than when he started.
From a young age Tom knew he wanted to be a doctor, even though it wasn’t something that was in his family. Fascinated with the human body, he was drawn to books about how the body worked.
Tom was also very clear he was going to be a physician during medical school, but exposure to some great surgical bosses in early years changed his view. As a young intern at Hollywood Hospital he had his own theatre list, developing a love for surgery.
“Hollywood was a great place to be a junior doctor. I had a great boss who gave true one-on-one mentoring. I learnt so much. When I finished my internship, I just started studying for surgery. I was really interested in cardiothoracics but after a year realised it wasn’t for
Associate Professor Tom Shannon Consultant Urologist
A/Prof Shannon is a graduate of the University of WA. He completed his Fellowship in Urology in 1999 and completed post-fellowship training in the UK and the US focusing on minimally invasive surgery and prostate brachytherapy. He was a pioneer of minimally invasive urological surgery in WA and is a leader in the development of prostate MRI. He is a strong advocate for men’s health and has been a board member of the Prostate Cancer Foundation of Australia (WA) for over 10 years.
me. I was sent to do urology for a rotation and remember complaining loudly. I was given great advice –the only way to know if I liked it was to approach it like I would be doing that job every day for the rest of my career.
Among other accomplishments, in 2004 Tom operated in WA with the pioneering French surgeon Professor Claude Abbou for the first demonstration of a laparoscopic radical prostatectomy. To date, the urologist has cared for more than 10,000 men and performed more than 3,000 open, laparoscopic and robotic surgeries.
A big advocate of self-care and the prevention of illness, Tom actively advocates for men’s health and prostate cancer. He has been involved with the Prostate Cancer Foundation of Australia since inception and holds an adjunct associate professor role with Edith Cowan University in exercise medicine.
With around 26,400 cases diagnosed in 2024, prostate cancer is estimated to account for 28% of the cancers to be diagnosed in
males for the year. Because prostate cancer survival rates are high, Tom says it’s a rewarding field to be working in.
He says there’s still work to do to bring equality to early detection. There’s excellent data showing the benefits of Prostate-Specific Antigen (PSA) testing and new Australian guidelines advocate men start testing at 40 and at regular intervals after, depending on personal risk. Tom argues that we could achieve significant gains with simple, but uniform changes.
“The goal is to find significant cancers early and cure them. Cures are achieved by complete surgical resection, which is a challenge, because you get one chance to do it really well. There are minimal margins for the cancer. To cure and retain continence and sexual function, you must be precise. The trifecta is the goal. Cure avoids needing testosterone suppression, which can be devastating.”
"Methylphenidate products will continue to be available during the shortage but there will be periods when the supply is limited and some products are unavailable," the TGA advised.
The TGA is aiming to reduce the impact on patients by working with wholesalers to ensure fair distribution of existing stock and pharmaceutical companies. It is also developing clinical management advice about alternatives during the shortage.
Prescribers can be kept informed with the latest information on the Federal Government’s website as well as the Medicine Shortage Reports Database, where 368 medicines are currently in shortage.
DIAmONDs for WA
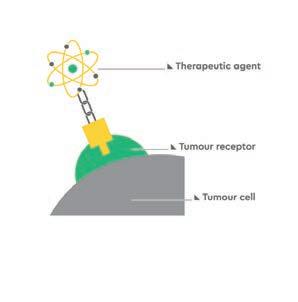
Several WA patients have taken part in an immunotherapy drug trial which has shown promising results in the treatment of HER2 positive metastatic breast cancer.
Results from the DIAmOND clinical trial have shown that adding dual immunotherapy to existing treatments could be promising for selected women and men with advanced HER2-positive breast cancer.
The trial was conducted by Breast Cancer Trials, Australia’s largest independent oncology clinical trials research group.
The study was developed by Australian researchers as a worldfirst clinical investigation into whether giving patients dual immunotherapy, in combination with drug trastuzumab (commonly known as Herceptin), can prolong cancer control in patients with advanced HER2-positive breast cancer that has become resistant to trastuzumab.
Various regimens of tremelimumab followed by durvalumab were administered in addition to trastuzumab.
The combination of the two drugs has been given previously to people with lung cancer, but this is the first clinical trial that has tested the combination of these two drugs in people with breast cancer.
Researchers have found that
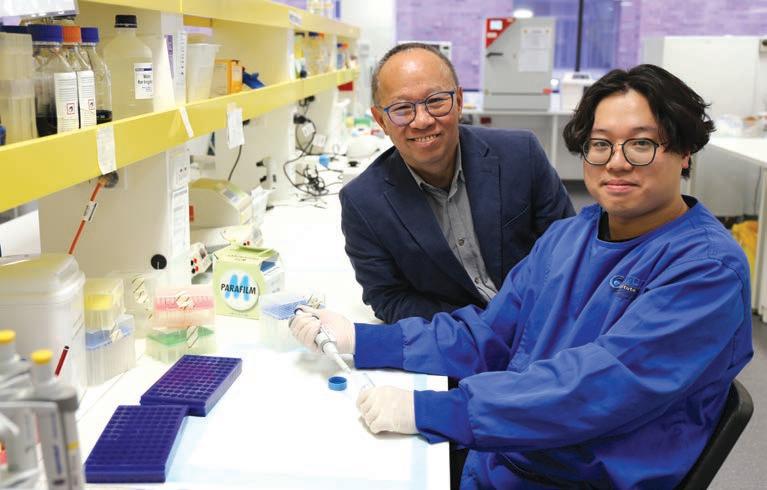
Exercise clues to health
Scientists at UWA and the Perron Institute have made a breakthrough in understanding how cells in the body respond to physical activity and exercise.
They have discovered a direct mechanical signal that travels from outside the cell into the energy-producing parts of the cell, which could change the way we think about exercise and its benefits.
The international study, led by Dr Ziming Chen and Professor Minghao Zheng, found that a protein production factory in the cell, called the endoplasmic reticulum (ER), can sense external mechanical forces, such as stretching or strain, and transmit them deep into the cell. This process helps regulate energy production in the cell and maintains tissue health.
“Cells constantly experience physical forces, especially in load-bearing tissues such as tendon, muscle, and lung,” said Dr Chen. “We found that the ER plays a central role in converting these mechanical cues into metabolic responses, controlling how cells produce energy and prevent tissue damage.”
The team discovered that while moderate physical activity and exercise can enhance energy production in cells, excessive strain or injury can disrupt this process, leading to cellular damage. They identified a "sweet spot" of mechanical loading that can boost energy production and promote cellular health.
Professor Zheng said the research had significant implications for understanding how tendons and ligaments responded to exercise and physical activity.
among the 68 trial participants – seven of them treated at Fiona Stanley Hospital – the new treatment combination showed an overall response rate of 27% in those with oestrogen receptor positive cancer.
Patients whose cancer was estrogen receptor (ER)-positive and had high levels of tumour infiltrating lymphocytes (TILs) showed significantly better outcomes, with an overall response rate of 63%.
Some patients had their cancer controlled for up to 30 months, indicating the potential longterm benefits of this treatment combination.
Headache help
The Neurological Council of WA has launched a nurse practitioner-led headache and migraine clinic.
Headache disorders, including migraines, are among the
Professor Zheng and Dr Chen in the Perron Institute lab
most prevalent and disabling neurological conditions globally, with significant impacts on daily functioning, relationships, productivity and quality of life.
The clinic aims to complement primary and tertiary care headache and migraine management, to reduce wait times for patients and provide interventions and care for managing acute migraine attacks and preventing chronic headache disorders.
It is led by nurse practitioner Adrienna Elliot and the team will work in collaboration with GPs, neurologists, paediatricians and other treating professionals.
Part of their role will be to evaluate new patients by documenting symptoms, functional impairment and medical history, undertake neuro-nursing assessments, order tests and diagnostic imaging, and determine the type of headache or migraine and any underlying conditions.
They will consult and refer patients to other specialists, such as neurologists, for more complex cases, secondary neurological issues or for specialised treatments.
Patients can self-refer or be referred by their healthcare practitioner. Services are bulk billed through Medicare without any outof-pocket costs.
Appointments can be made by calling the Neurological Council of WA NeuroCare TeleNurses on 1800 645 771 or completing an online referral form.
From the UK to the Pilbara
The first of 10 doctors expected to take up roles in rural WA as part the Expedited Specialist Pathway (ESP) is settling into a role in Pilbara.
Dr Marcus Stevens, who is from the UK, arrived in Newman in June to take up a role as GP at Puntukurnu Aboriginal Medical Service (PAMS).
In his role Dr Stevens is providing services to a population that is 98% Indigenous across Newman and surrounding communities.
“It’s an amazing part of the world with a fascinating history and culture to work within. Medically, there is a lot to learn. In the UK we don’t see rheumatic heart disease, which is a big part of the work here, and while in most parts of the world trachoma has been eradicated, we deal with that a lot that up here too.”
The expedited pathway allows doctors from approved countries to apply for registration with the regulator without first being assessed by the RACGP.
Figures from the Medical Board show a total of 150 specialists have been granted registration, with 17 having WA listed as their principal place of practice.
NEW ROLES IN WA
Infertility and IVF specialist Dr Sebastian Leathersich is new medical director at Concept Fertility. His most recent role was at the world-renowned Dexeus Fertility Institute in Barcelona.
The AMA (WA) has a new president, with psychiatrist Dr Kyle Hoath taking over from Dr Michael Page for a two-year term.
WA’s Perron Institute has a new medical director, neurologist Professor Merrilee Needham, who takes over from Clinical Professor David Blacker
Dr Sebastian Leathersich
Professor Merrilee Needham and Professor David Blacker
Rural Health West chief executive Catherine Elliot with Dr Marcus Stevens
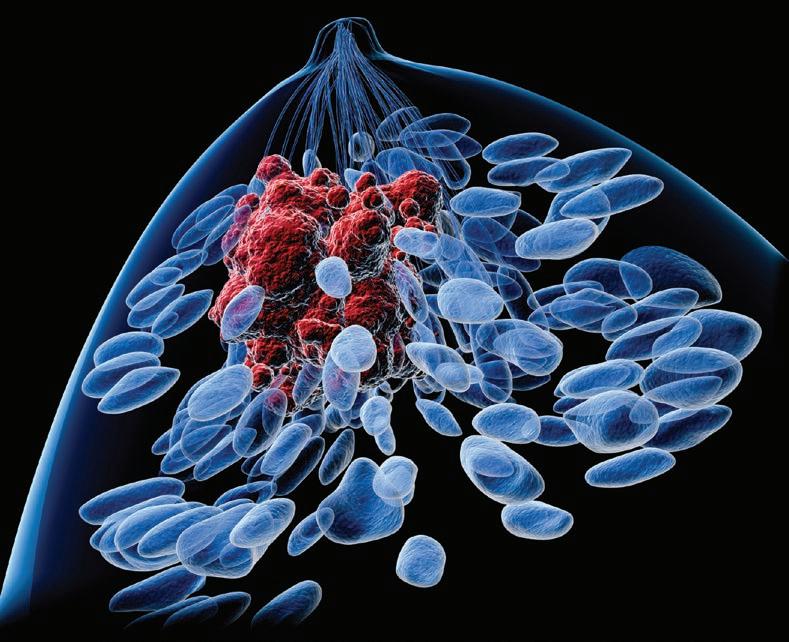
Keeping abreast of cancer care
With GPs recently updated on the prevention and early detection of breast cancer, debate about how to manage breast density has come under the spotlight once again.
By Cathy O’Leary
The statistics for breast cancer in Australia are sobering. Not only is it the most common cancer in women – responsible for more than 21,000 new cases a year – it is also the second leading cause of death.
The lifetime risk of the disease is now nudging one in seven for women by the age of 85 – compared to about one in 12 in the 1990s – and there has been an increase in cases in younger women.
While treatments for breast cancer have gone ahead in leaps and bounds, the stark rates of the disease highlight the urgent need for better prevention, and educator Dr Sandy Minck is part of the push to bring GPs up to speed.
The Brisbane-based doctor contributed to new breast cancer guidelines recently published by the Royal Australian College of GPs in its Australian Journal of General Practice
An article by Dr Minck, who is a member of BreastScreen Queensland’s Clinical Standards and Excellence Committee, guides GPs on evidence-based strategies for breast cancer prevention.
“More than 75% of cases occur in patients over 50, but there has been a 10% increase among patients under 50 in the past 20 years, so breast cancer will be a concern for younger patients too,” she said.
Dr Minck is a strong advocate of personalised risk assessment and promotes advice about modifying the impact of lifestyle factors such as alcohol, obesity and physical inactivity.
She said that in higher risk women, two main categories of medication – selective oestrogen receptor modulators and aromatase inhibitors – could decrease breast cancer risk by 30-60%.
“These are an effective risk-reducing strategy for patients who do not want to undergo, or want to postpone, mastectomy,” she said.
“Risk-reducing surgery is an option for those at very high risk of developing breast cancer. This can be overwhelming, and GPs can support women to make their own informed decision based on their individual risk, values, circumstances and the potential benefits and risks of surgery.”
Breast density role
The latest RACGP breast cancer advice weighs into the ongoing debate about managing breast density – the proportion of fibroglandular tissue measured on a mammogram.
Dense breast tissue, like cancer, appears as white on a mammogram, making it hard to pick up cancer and potentially delaying diagnosis and resulting in more advanced cancers. It is also itself an independent risk factor for developing the disease.
Breast density is not related to breast size or the ‘breast aware’ message promoted to women because it cannot be determined by feel or touch.
About 10% of Australian women have extremely dense breasts and they are four to six times more likely to get breast cancer than those with fatty breasts.
The RACGP guidance concludes that while women with dense breasts are more likely to benefit from supplemental screening, there
is not enough evidence to routinely recommend this.
But the issue of whether women who are found to have dense breasts during their mammograms should at least be notified of this information has recently gained more clarity.
In what many doctors regard as a significant shift in position, Australia’s government-funded BreastScreen service now recommends that women with dense breasts be advised in writing and encouraged to talk to their doctor.
Western Australia has long been acknowledged as a trailblazer in this area – having quietly introduced a similar policy more than 15 years ago.
Poorly understood
According to Australian research, most GPs know little about breast density.
A BMJ Open study looked at GPs’ understanding of breast density and the value of discussing it with their patients – and found poor knowledge overall.
There were also mixed views about the benefit of notifying patients of their breast density, with some GPs believing it would create unnecessary anxiety.
Dr Minck has her own back story, having undergone a risk-reducing mastectomy in 2023. At the time of
her treatment, she spoke out publicly about the lack of information given to women about the significance of breast density.
She believes she survived because she sought out private breast imaging, later self-funding an MRI and a clinical genetic consultation which found a mutation.
Dr Minck argues that while mammograms do not prevent cancer, they are a vital tool in early detection which can alter the outcomes for patients.
She told Medical Forum she welcomed the recent position announcement by BreastScreen Australia, acknowledging WA was the first State to notify women found to have dense breasts, with South Australia, Victoria and New South Wales since adopting the policy.
“BreastScreen Australia currently has a policy and funding review, and we’re anxiously awaiting the report, but while previously it was really about your sex and your age, which are the two biggest risk factors for breast cancer, there’s been a huge amount of work going into risk stratification screening,” she said.
Personalised risk
“What I’m advocating for is increased awareness and education so that women understand the breast cancer risk factors,
Keeping abreast of cancer care
continued from Page 13
particularly the ones they can do something about like alcohol, which sadly is a significant one, yet many women are completely unaware of this.
“There are multiple risk factors, and the more women have that information and knowledge, the more they can work out with their health care professional what screening strategy is best for them.
“The current one-size-fits-all approach for breast screening fits no one.” Dr Minck said that while there was evidence that other screening technologies improved mortality, very long-term data was needed to prove this.
“But with all the women I speak to, it’s about more than death, there’s quality of life, and we all know that the earlier you pick up cancer the less aggressive options you need to treat it, and we are very successful at treating breast cancer.
“There are lot of trials overseas that show that MRI and contrastenhanced mammography pick up many more cancers than mammography and even ultrasound.
“So, my argument would be not just taking breast density in isolation but doing a risk assessment and if someone is in the high-risk category and under the age of 60, they will meet the Medicare criteria for an MRI rebate.”
Dr Minck said she went to many GP education events and every breast surgeon or a radiologist at them talked about breast density. It was something doctors had known about for 50 years, but some were more informed than others.
“That’s why I’ve been raising awareness and informing GPs and also educating women so they can talk to their GP, but it is hard to talk about all the risk factors in a 10-minute consultation.
“It’s not just about GPs saying to women you should drink less, it’s about making women more aware of the risks and promoting healthy lifestyle choices so that women are living their best life.”
Dr Minck said women should be encouraged to be ‘breast aware’ and know what their breasts usually
look like and feel like so if they see a change they can get it looked at quickly.
“I’ve been critical of BreastScreen in the past for not reporting breast density, but we are fortunate to have that service, and if it takes on that role in education and health promotion there will be more trust and participation rates will increase," she said.
“GPs are the part of the healthcare system that are most able to look at preventive interventions, because once you’re in the hospital system you’re sick, you’ve missed the boat.
“But I recognise it’s very challenging for GPs to manage everything, and for patients the out-of-pocket costs have gone up significantly and it’s harder to get in and see your GP so that means it’s becoming harder to access GPs and get this advice.”
She said that in the public system, BreastScreen WA had been the only one initially reporting breast density back to women, and then South Australia came on board in 2023 and NSW and Victoria had followed suit.
to me a harm is something really serious.
“And while having biopsies can be inconvenient, uncomfortable and expensive, if this is a person making an informed decision on what is best for them and how they want to proceed, it takes away from that whole view of ‘well if we can’t do it for everyone, then we can’t do it’.
“I think most women would prefer to be overdiagnosed than underdiagnosed.”
Calls for uniformity
Breast Cancer Network Australia also welcomed BreastScreen Australia’s new position on breast density, describing it as a significant step forward for transparency.
Director of policy, advocacy and support services Vicki Durston commended WA, South Australia, Victoria and New South Wales for leading the way, but called on Queensland, Tasmania, Northern Territory and the ACT to report breast density without delay.
“But having BreastScreen Australia recommend it from a national perspective is important,” she said.
“We’re on the right track and things are improving, but the more we talk about it the more GPs will become aware and then women will become aware, so we’re on this pathway to hopefully having more personalised risk assessment and screening.
“Every woman has the right to know her breast density and understand her breast cancer risk, and we need every state and territory to act now to provide this information, along with clear pathways for supporting women at higher risk,” Ms Durston said.
Dr Emmeline Lee, director of BreastScreen WA, said that in 2008 the WA service became the first breast cancer screening program in Australia to provide information on mammographic breast density to women screened, and notify those found to have dense breasts.
“And that may lead to more people being able to take advantage of riskreducing medication or surgery if that’s what they want, but also early intervention.
“We do hear about overdiagnosis and overtreatment, and critics of mammography often bring up the so called ‘harms’ and I get quite upset when I hear that term because
“While reporting breast density can enhance awareness and potentially lead to earlier detection through additional screening, the direct impact on saving lives is still a subject of ongoing research,” Dr Lee told Medical Forum
“But having said that, I know of specific cases where informing a woman that she had dense breasts has led to her being seen by her GP for a consultation and clinical breast examination which found a lump that turned out to be a breast
cancer that was hidden by the breast density on the mammogram.”
She said it was important for women to have information because mammographic breast density could make it harder to detect abnormalities on screening mammograms, potentially leading to delayed diagnoses.
Women with dense breasts also have a higher risk of developing breast cancer compared to those with less dense breasts, however, this did not necessarily translate to a higher risk of death from breast cancer.
Informing women about their breast density could lead to more personalised screening strategies for some women and awareness of risk factors for breast cancer.
Next steps
Dr Lee said that if women have dense breasts, BreastScreen WA recommends they see their GP for a consultation and clinical breast examination.
A recent study published in The Lancet found that offering additional scans to women with very dense breasts – contrast enhanced mammography (CEM), abbreviated magnetic resonance imaging (ABMRI) and automated whole breast ultrasound (ABUS) could detect 3500 extra breast cancers a year in the UK.
The trial showed that CEM and AB-MRI were particularly effective, detecting 17-19 cancers per 1000 women that were not seen in mammograms.
But Dr Lee said there were a few points of concern, including the logistical challenges of implementing additional scans like AB-MRI and CEM into routine practice because of limited availability of MRI scanners and the need for contrast agents, particularly in big jurisdictions like WA where more than “10 UKs could fit into our State”.
Other issues were cost and accessibility, false positives and overdiagnosis, and rare adverse reactions to the contrast agents in CEM.
Dr Lee said more research was needed to confirm whether additional scans would reduce the number of deaths, as cancers detected through screening were not always life-threatening.
“GPs have a crucial role in breast cancer detection, from ensuring eligible patients have their regular screening mammograms with BSWA to following an appropriate assessment strategy such as the Triple Test to investigate a new breast symptom,” she said.
“Women and their GPs might benefit in considering using iPrevent and CanRisk – online tools that enable the calculation of an individual's future risks of developing breast cancer using cancer family history, genetic and other risk factors.
“By combining regular mammograms with these additional strategies and the support of their GPs, women can significantly enhance their chances of early cancer detection.”
Dr Lee said WA had a wellestablished multidisciplinary group of breast specialists to support GPs looking after their patients with breast issues.
No ‘best’ approach
Dr Minck said that when it came to supplementary screening such as MRI or contrast-enhancing mammography, her view was that there was no ‘best’.
“It’s about what is going to work depending on your circumstance, and MRI is not going to work if you’re in a remote area and you have to travel thousands of kilometres,” she said.
“It’s about saying here are the options and the advantages and disadvantages and letting women and their GPs make that choice.
“We’re moving in the right direction, and it’s a big move by BreastScreen Australia, which has listened to patient advocates and consumers, and that is fabulous.
“Ultimately awareness is the first step, so women should be encouraged to discuss any family history of breast cancer with their GP, become familiar with the normal look and feel of their breasts, and promptly speak to their GP about any new or unusual changes.”
Resources:
The first step in personalised breast cancer prevention is risk assessment. iPrevent, developed in Australia, is recommended by Cancer Australia and is a clinical resource accepted by the RACGP. It can be completed online by women and/or their GPs. www.petermac.org/patients-and-carers/health-services-forcancer-patients/cancer-prevention/iprevent
A separate article in the RACGP breast cancer guidance updates GPs on the early detection of breast cancer, informed by the 10th edition of the RACGP’s Red Book preventive health guidelines for breast cancer.
Cancer care –are we prepared?
Is WA ready for the projected surge in cancer cases? With the new bowel and lung cancer screening programs up and running, what is being done well, and what can be improved?
By Suzanne Harrison
It wasn’t until she had severe stomach pain that Cherie Salter presented to emergency in 2022. The now 55-year-old cannot believe she waited so long to get the right medical help for what was eventually diagnosed as stage 4 bowel cancer.
Cherie, a Badimia Yamatji Wadjak Ballardong Nyoongah woman who works for the Smith Family, started experiencing symptoms in her 40s, ignoring them for two to three years and putting it down to irritable bowel syndrome.
After the pain became unbearable, it was found the cancer had spread to other parts of her body. She has since undergone chemotherapy, surgery and radiotherapy.
Luckily, Cherie no longer has bowel cancer symptoms, is receiving the regular care she needs and has returned to work.
“There has been a lot of campaigning to get us tested with pap smears and mammograms, but we haven’t got to that stage with bowel cancer,” said Cherie, adding there is still a stigma attached to bowel-related testing.
“I was doing the pap smears and breast checks, but I didn’t have what I thought was typical bowel cancer symptoms. We’ve all heard the stories of prepping for a colonoscopy, and that can be embarrassing.”
Now, Cherie’s message is simple: do not ignore anything unusual when it comes to your bowel.
Surge in cases
Cherie’s message couldn’t come at a better time. Earlier this year, Cancer Council research in Australia showed more than 4.5 million new cancer cases are projected to be diagnosed between 2020 and 2044, putting a significant burden on the healthcare system.
The same research found nearly one in two (45%) Australians believe the country’s health system is unprepared for what will be a significant rise in cancer cases over the coming years.
Data showed that Australians were significantly concerned about their cancer risk, with seven in 10 surveyed saying they were worried about developing cancer in their lifetime.
While cancer risk increases with age, eight in 10 Australians aged 25-34 and more than seven in 10 Australians aged 35-49 are concerned about developing cancer in their future.
Cancer Council is calling on the Federal Government to commit to four key priorities to reduce the impact of cancer for all Australians. These include tackling the rise of obesity to reduce the incidence of 13 types of cancer, investing in skin cancer prevention campaigns towards a future free from skin cancer, increasing participation in the National Bowel Screening Program, and providing equitable access to cancer care by reducing the financial burden through improved services and support.
More screen time
This data comes hot on the heels of the new National Lung Cancer Screening Program, introduced on July 1, targeting people considered to be at high risk in the hope of detecting cases early, before they become incurable.
Lung cancer is the fifth most commonly diagnosed cancer in Australia, with about 15,100 cases diagnosed in 2024, according to the Australian Institute of Health
and Welfare (AIHW). It is still the deadliest cancer of those most commonly diagnosed – just 26% of people survive past five years.
In WA, latest data suggests more than 1000 cases of lung cancer are diagnosed in the State every year, but many more cases could be going undiagnosed. It is expected that with the new screening program, more will be diagnosed at an earlier stage.
Yet Prof Fraser Brims, Consultant Respiratory Physician at Sir Charles Gairdner Hospital, said WA was well prepared to implement the program and deal with an increase in diagnoses.
One of the aims of the program, he says, is to target the hard-to-reach populations.
“Lung cancer is a disease of inequity and we know that rural and remote areas and Indigenous populations have higher rates,” he said.
As a result, WA will have its first national mobile low-dose CT scanner truck – commissioned through Heart of Australia – as of November. It will be on the road in predominantly northern WA.
In terms of what can be done better, Professor Brims notes the introduction of LUCAP, a patientfocused research group developing a national clinical-quality data platform for lung cancer that collects, analyses and reports on information.
This includes such things as the pace of screening, the type of tests done and how quickly people are treated.
“LUCAP maps our care pathways, collects data across different centres and compares it,” Prof Brims said. “It enables physicians to monitor the impact of lung cancer screening, offering a real-time process across public hospitals, looking at numbers coming through, wait times for surgery and demand for CT scans.”
For example, lung cancer –or potential lung cancer – can be identified early, but if the system can’t process people in a timely enough manner to avoid it going beyond early stage by the time they go for treatment, it misses the point of screening, he said.
awareness front gradually, and that every healthcare provider has a role in ensuring the message to prevent –especially around smoking cessation – is powerful.
“Everyone – not just GPs, even the receptionist – has a role to play in talking about smoking cessation. The more patients who hear that message, the better.”
Bowel screening updates
Meanwhile, Bowel Cancer Australia data shows 1716 Australians are diagnosed with the disease under age 50 each year. In response, the National Bowel Cancer Screening Program (NBCSP) recently lowered its screening age to adults aged 45 to 74, from 50 to 74.
Early statistics show that while there is still a way to go in participation, there has been some impact.
In June, AIHW reported that initial data showed 77,551 home kits were requested between July and December 2024 for eligible people aged 45–49.
Of the 6.3 million people invited to take part in screening between January 2022 and December 2023, there was a marginal increase in participation to 41.7% – up from 40% in 2022.
In November 2024, the Department of Health, Disability and Ageing said many healthcare providers were already issuing program kits directly to patients but encouraged more practices to bulk order test kits and speak to eligible patients about screening.
“To put into context how impactful talking about bowel screening with patients can be: if we can increase participation to 60%, over 84,000 lives could be saved by 2040,” the department said in a statement.
An allied approach
While the increases in cancer cases are cause for alarm, experts suggest the health system is in a good position to support these patients.
The roll-out of the screening program will pick up the pace on the
Associate Professor Kynan Feeney, Head of Department Oncology, Haematology and Palliative Care at St John of God Hospital Murdoch, is hopeful for the future, saying a
Cancer care – are we prepared?
continued from Page 17
multi-disciplinary approach to the projected surge in cancer cases is a way forward.
“As we’ve improved our treatments and patients survive for longer, we’ve become busier,” A/Prof Feeney said.
“We do have the foundations to support that busyness and increase in care, not just necessarily keeping people from death, but keeping them alive and well when they do survive.
“More and more we are saying that we can make a big difference, not only in quality of life but also their survival by non-medically directed therapies, such as improving diet, exercise, reducing alcohol consumption, no smoking.”
Utilising a multidisciplinary team can also help take the load off other physicians.
“For example, medical oncologists are not very well trained in dealing with some of the mental health issues when it comes to cancer patients. For some people, cancer can bring up other past traumas, which is why we have a clinical psychologist in our practice.”
When it comes to GPs, Melissa Ledger, Cancer Council WA Cancer Prevention and Research Director, told Medical Forum that with shared risk factors for several chronic conditions and myriad of other acute and chronic health issues, “discussing risk factors for cancer is an important part of a GP’s role”.
the last 20 years, funded by Cancer Network WA.
Breast cancer funding
Amid the projected surge in cases and patients living better for longer, Breast Cancer Care WA (BCCWA) said it is vital patients and their families or carers are advised on how to move forward with a healthier lifestyle after a diagnosis.
However, it faces a new challenge amid a rise in breast cancer cases –it is facing a funding challenge for the first time.
It’s estimated that about one third of cancers can be prevented, and risk can be modified, she said.
“Behavioural risk factors and all risk factors could form part of GP ‘preventive health’ consultations and patient advice.”
She adds that there are numerous opportunities for GPs and primary care professionals to upskill, from prevention to supportive and palliative care.
Cancer Council WA has delivered a primary care education project for
For 25 years BCCWA has provided specialist support across WA. In 2024, more than 1900 people and their families approached BCCWA, all provided free of charge.
Sally Dare from BCCWA said: “The incidence of breast cancer diagnoses among Australians is on the rise and the survival rate has increased to 92% for the 2016-2020 period,” said Ms Dare.
“BCCWA helps ease pressure on time-constrained WA health services by offering ongoing, person-centred support and vital information to WA people navigating breast cancer.”
BCCWA spokesperson Jess Hicks told Medical Forum the charity was hopeful that State government funding would come their way.
“For that whole 25 years, we’ve been able to fundraise ourselves,
but now with the increasing numbers of cancer patients we’re seeking that extra support.”
“We receive 70% of our referrals from public and private hospitals. That demonstrates the critical gap we are filling.”
Talk about it
As for Cherie, she can’t speak highly enough about the care she has received, and continues to benefit from, at Joondalup Hospital.
“I no longer have shortness of breath, I have an amazing sense of relief that I can work in a job I love, be in the community and no one would know.
“That’s really helped me accept what is in my body and deal with my physical and mental health.”
Cherie discusses her experience publicly in a bid to help others who may feel too ashamed to admit they are worried.
“It’s better to be overly zealous than ignore things,” she said.
“Inform yourself about what the real symptoms are. Speak to your doctor, don’t just Google search. Be frank and honest with your GP. Insist on an investigation.”
As Cherie rightly concludes: “Let’s talk crap!”
Bowel cancer surviver Cherie Salter urges people to check-in with their GP
A driving desire to help
Third-year medical student Navya Nukamreddy has a big heart and is passionate about hearing from and caring for her future patients.
By Ara Jansen
As a young girl Navya Nukamreddy was inspired by the idea of helping and comforting others, ideas she correlated to the role of a doctor and they have been her drivers to become one.
When she was 12, a chin injury sent Navya to the ER. There was plenty of blood but what she remembers clearly was the kindness and empathy of the doctors who treated her.
A subsequent visit to an orphanage in India gave her firsthand insights into healthcare inequalities. The lack of basic necessities such as sanitary pads forced women to create unhygienic period underwear, something that could increase the risk of infection. This sparked her interest in one day contributing to global health.
Almost two decades later Navya is making her contribution. She’s driven by a desire to help people feel better and is currently a thirdyear medical student at Curtin University.
“I realised I wanted to make other people feel the way those doctors had made me feel,” says Navya, who is the first person in her extended family to pursue medicine.
Born in India, Navya and her family moved to Perth for her first nine years. The Nukamreddys then moved to Dubai and returned to Perth in 2020 for Navya to finish school and start her medical studies.
On Navya’s list for her future career are obstetrics and gynaecology, being a GP, or focusing on children’s health. Her experience in the former has re-enforced her
“I realised I wanted to make other people feel the way those doctors had made me feel.”
interest in women’s health, while the idea of being the first port of call as a GP, never knowing what you might have to treat and getting to know patients over many years, is highly attractive.
Her parents’ generosity, especially when it comes to helping others – such as in orphanages and asylums – has deeply influenced Navya and her desire to make a meaningful impact. That includes
being active in the advocacy space and with her extracurricular activities such as being secretary for the Pre-Vocational Obstetrics & Gynaecology Society WA and the National Coordination WA representative for AMSA Global Health.
Her past work and contributions include being a UCAT tutor (University Clinical Aptitude Test) for Year 11 and 12 students, the 2024 Curtin University junior representative and Vampire Cup representative for the Australian Medical Students Association and the past President of the General Practice Students Network (GPSN) at Curtin.
Earlier this year, she visited the Indian Institute of Mother and Child (IIMC) in Kolkata and says the visit taught her a lot and reaffirmed medicine and caring for people are her passion and that she wants to maintain this type of connection. Navya believes in holistic medicine and listening to patients rather continued on Page 23
Dr Shane La Bianca
Dr Andrew Tan
Dr Jeff Thavaseelan
Dr Trent Barrett
Dr Matt Brown
Dr Manmeet Saluja
Dr Alarick Picardo
Dr Steve McCombie
Dr Sarah O’Neill
A driving desire to help
continued from Page 21
than being hellbent on a diagnosis without hearing what’s actually being said.
“In the future I very much want to be involved in research, in particular around women’s health, and I’d like to be able to bring that new knowledge and awareness to wider populations. I’d like more women to feel heard.”
Juggling her studies, extracurricular activities and just life in general has forced the medical student to become highly organised. Navya likes to sit down every week and make up a plan and a schedule –ensuring nothing is forgotten or accidentally ignored.
“I write down everything I need to do, and I allocate time for it. I map it out, allocate colours to activities. Plus, I have to make sure I allocate free time as well. I didn’t always do that in high school and I think it took a toll on me. I do give myself some leniency, but I definitely like to have structure and acknowledge when I need a rest.
“I get support from my friends and family. They know when I’m in study mode and when I won’t reply for a while. With my friends from Dubai, they tell me when they are going to call, so we plan ahead.”
This year Navya has done her GP placement. She enjoyed learning how a GP and a practice work.
“The doctor has a lot of knowledge and was very adept at sharing it with patients. He helped the patients feel good about their health, so I learnt a lot of things that can help me help patients feel better.
“I always think ‘today I’m going to learn something that might possibly help someone in the future’. That’s what stuck with me. It’s a learning process and it’s about getting to know people.
“It’s the same environment that Curtin provides. It’s not just about seminars and interactive sessions that help you learn, it’s engaging with all the people you come across.”
The chef of the house, Nayva lives with her parents and
younger brother. She’ll put on her headphones and create a three-course dinner as a way to relax. Apparently, her Pad Thai is excellent.
“When I’m cooking, my family are happy because they know they are going to get a good meal. I love making pasta – it always feels warm and healing – and chicken stir fry.”
Things don’t always go to plan in the kitchen though, a recent experiment to make a peach
cobbler turned out more salty than sweet because Navya had her mind on her studies.
To relax and keep fit, Navya plays badminton, enjoys walking around her neighbourhood and loves to talk.
“I talk a lot. My friends know that. I love a good debrief and I’m there for my friends as well, even if I’m in the middle of studying about the radial nerve.”
You speak, we’re listening
A big thanks to everyone who took part in our readership survey*. We value the feedback and suggestions in the hundreds of responses we received.
The big takeaway for us is how much you value the magazine for its up-todate news and clinical content, particularly from its unique local perspective as WA’s only medical publishing house, with 94% of the respondents saying Medical Forum is their go to for local medical news.
It’s also exciting to see that 70% of those surveyed look to our weekly digital newsletter and our website, as well as our podcasts and social media, to keep themselves fully informed on the news that affects their professional lives.
The consistent response about the value of our clinical articles, many written by specialist colleagues in their fields, has resulted in our seeking and being approved to offer CPD points for clinical content in the magazine, our digital channels and podcasts.
This thirst for continuing clinical education will see Medical Forum offerings expand next year to in-person events with local specialists and on-demand online modules with hours for MO and RP.
At Medical Forum, we will always strive to focus on WA and the incredible group of doctors and allied support teams who provide world class care in our State, by both informing and entertaining our readers.
*n = 241 respondents unaudited
84% of respondents say they read every or most issues of Medical Forum magazine
How often do you read Medical Forum magazine?
Over 84% find Medical Forum clinical updates keep them abreast of changes to clinical practice
I find the clinical updates useful to stay abreast of changes to clinical practice
94% of respondents say they read Medical Forum to keep up-to-date with WA health news
We asked our readers what publications they read to keep across Western Australian medical news. They said:
We asked our readers how they like to access Medical Forum content:
CONGRATULATIONS DR MOJDEH BASSIRI – THE LUCKY PRIZE WINNER OF A $1000 LUXURY ESCAPES VOUCHER!
70% of respondents say they read the weekly digital e-newsletter
Call for distinct bereavement services
People with insight into the complexities of bereavement are questioning whether greater consideration is needed around how care is delivered, including the role of GPs.
By Aleisha Orr
The release of a WA Government document earlier this year canvassing bereavement support after an expected death has been welcomed by many, it has also prompted wider discussion.
The framework was designed to provide a strategic guide for services providing end-of-life and palliative care in supporting bereaved families and carers in such situations.
Dr Margaret Sealey, a thanatologist and a member of Palliative Care WA spoke to Medical Forum about how her work led her to form the view that bereavement care would benefit from being separate to palliative care, while the RACGP’s Dr Joel Rhee spoke about challenges GPs face in providing such care.
Dr Sealey studied psychology and says she was driven to carry out her PhD in the area of palliative care out of frustration with how bereavement was dealt with.
She spent decades working in palliative care and recalled weekly meetings.
“They’d say, ‘right Mr Smith, he died, he was in bed two, right... Mrs Smith, oh, yes, I remember Mrs Smith, yes, she was crying appropriately so we don't need to follow her up’,” she said.
"The psychologist part of me thought I'd no sooner look at somebody and assume to know what was going on in their head and their heart than I would fly to the moon.”
The framework
Bereavement support was recognised as an essential component of end-of-life and palliative care services in the State’s current end of life and palliative care strategy released in 2018 and this is what prompted the new framework.
It also follows the 2021 introduction of the legal voluntary assisted dying process in the State.
The document is not designed to be a clinical guideline, instead it aims to increase awareness and understanding of the service considerations associated with the provision of bereavement support after an expected death.
Considerations touch on personcentred and equitable bereavement support for the family and carers of those who die from an expected death across diagnoses, cultural backgrounds, and locations within the State.
They highlight that such support should be delivered in a coordinated manner, that all staff dealing with family members should have an understanding of bereavement, and that communities should also be supported and empowered to be part of griefrelated support.
However, the framework itself notes “Bereavement services are seldom recognised as part of the clinical workload because the recipient is not an admitted patient of the palliative care services.”
Dr Sealey says bereavement care has always been seen as part of palliative care.
“It's in the World Health Organization definition, in the national palliative care standards, it's in all of these policies, yet it's
Bereavement support was recognised as an essential component of end-of-life and palliative care services in the State’s current end of life and palliative care strategy released in 2018 and this is what prompted the new framework.
totally unrealistic because services need to stick to doing what they do best, which is palliative care and end-of-life care.
“Yes, the families and loved ones should also be a part of that care, but palliative care services don't have the expertise to do that, they don't have the funding to do that.”
“The problem is we don't have a service pathway here, it's up to each individual professional to decide where to send people.”
She said that while palliative care and bereavement support were related, they were not the same, and there needed to be a whole infrastructure around bereavement care. Extensive research on who needed bereavement care and what supports were necessary, had also been done in recent years, so the evidence already existed.
GPs part to play
The framework notes primary care should be recognised as best placed to provide access to specialist therapeutic support.
Dr Sealey says GPs are the frontline of healthcare and the “prime” people to track and assist bereaved people in how they work through their grief, given they are already likely to be seeing them for other health matters.
While the framework suggests assessment and pre-screening around bereavement start at first contact with palliative care, Dr Sealey suggests GPs were better placed to do the pre-screening and follow up.
Dr Sealey says she does not think the framework goes far enough by simply listing service considerations against the end of life and palliative care strategy priorities.
Dr Joel Rhee, chair of the RACGP Cancer and Palliative Care network, says implementing practical models on the ground would be the obvious next step beyond the framework.
He says while the document is a good start there is room for improvement, much of it around principles and priorities, but the other issue is actually implementing practical models.
Connecting the pre-screening of family and loved ones done within palliative care settings to GPs and services was “tricky”, he said.
“Who do they pass the information to? Because the person who may require further support later with bereavement issues are going to have their own GP, who is probably different to the patient's GP.
“The palliative care service will need to have a consent process so information can be passed on to the patient's GP and sometimes that can be challenging. It's something that needs careful consideration and forward planning.”
He wants to see a secure national messaging system created where public health and palliative care services can be linked.
When contacted about referral pathways, the Australian Government Digital Health Agency referred Medical Forum to the WA Health Department.
World-class comprehensive cancer care in Western Australia
Radiation Oncology | Medical Oncology | Haematology
Led by a collegial network of experienced specialists, our state-of-the-art centres deliver seamless, multidisciplinary cancer care - all under one roof. With no wait list for consultation or treatment, your patients receive timely, world-class care closer to home.
Our leading technology and treatments
• Stereotactic radiation therapy, including HyperArc® for brain metastases
• RapidArc Dynamic – faster, highly targeted technique that minimises impact on healthy tissue
• Deep Inspiration Breath Hold (DIBH) for leftsided breast cancer
• Brachytherapy for prostate cancer
• Integrated day oncology and haematology
• Access to pharmaceutical-sponsored clinical trials and research
Icon Cancer Centre Midland
6 Centennial Place
Midland WA 6056
P 08 6317 3400
F 08 9250 3287
E admin.midland@icon.team
HealthLinkID: iconmidl
Your patients benefit from
• No wait list for consultation or treatment
• Bowel, breast and prostate care nurses
• Palliative care nurse practitioner
• Access to allied health services: exercise physiology, dietetics, psychology
How to refer
Specialist and GP referrals are accepted for all cancer types. Referrals can be made via IconDoctorApp.com or HealthLink
Icon Cancer Centre Rockingham
2 Civic Boulevard
Rockingham WA 6168
P 08 9500 7800
F 08 8490 2305
E admin.rockingham@icon.team
HealthLink ID: iconrock
Icon Cancer Centre Subiaco St John of God Subiaco Hospital Coming soon
Icon Cancer Centre Hollywood WA’s first private theranostics & molecular imaging centre
Coming soon
Call for distinct bereavement services
continued from Page 27
Prolonged grief
The framework states that there is an ongoing need throughout to identify family and carers who are at risk of severe or prolonged grief and need professional treatment and support.
Dr Sealey says if family or friends were after more than a year after their loss “still disabled by their grief to the point that they can't go back to work, they can't earn a living, they can't get out of bed, they can't socialise with other people, then they need proper assessment and treatment by a psychologist or a psychiatrist.”
However, in Dr Sealey’s research she found that even the service that recorded the longest contact with family of those who had died kept in touch for five months at the most.
“If, six months after a death, you're running an inventory to check if somebody's got prolonged grief or some sort of problem, you don't have a file to put that into.”
At the same time, she says, many family members do not want to be contacted by the service that they associate with the end of their loved one’s life and for those reasons she did not think palliative care services should “be going anywhere near prolonged grief”.
Understanding grief
Dr Sealey says a better general understanding about grief was needed in the community in order for more meaningful communitybased support, including support groups and grief cafes.
Dr Sealey says many people, even within the health system still “bought into the five stages of grief as a model for bereavement care”, which research has found to be scientifically inaccurate.
“That can keep them stuck in their grief, because everybody's saying, you should get to acceptance at some point. They might acknowledge a new reality but to accept, that’s quite a big ask,” she says.
Shes adds that better understanding that different people experienced different types of grief in different situations is also required.
Challenges as a GP
Dr Rhee acknowledges the importance of the GP in bereavement support while noting the challenges experienced.
Sometimes the GP may not even be aware of a bereavement issue, because the chances that they were also the deceased person’s GP are not high, he explained.
“They wouldn't know unless their patient tells them, so there can be challenges, but asking questions, taking time to just ask how the patient's going, how are they coping? Those common-sense questions would be useful for GPs to do,” he says.
“People may not be aware that what they're experiencing right now may not be quite normal, or what may be expected for a person who's experiencing grief.”
Dr Rhee says that while a GP having good links with local mental health services can be of assistance, issues associated with accessing such services play a role in getting support in situations of prolonged grief.
“When you look at the framework, priority three is about having referral pathways, and it talks about primary care providing access to mental health providers, but sometimes that's easier said than done.”
Prolonged waiting lists for psychologists and counsellors as
“Having an understanding of the client’s journey can make a significant difference during the early stages of grief.”
well as associated costs, including gap fees, can delay or prohibit the delivery of those services.
“GPs or nurses within clinics are often providing that sort of counselling and support, basically holding the patient or holding the person and making sure that they're socially and otherwise supported while waiting for those mental health services to kick in,” he says.
Service delivery
Silverchain has operated palliative care services in WA for more than 40 years and has a partnership with the WA Government to provide them.
While the organisation did not say whether it would support a separate infrastructure around bereavement support outside of palliative care services, its WA executive director Renae Lavell told Medical Forum that “bereavement support is an essential component of providing comprehensive and compassionate palliative care”.
“To ensure continuity of care, bereavement services are initiated by the specialist palliative care provider. Having an understanding of the client’s journey – and an existing relationship with the family – can make a significant difference during the early stages of grief.”
While she acknowledges a holistic and coordinated approach is required, especially because the onset of grief may not fully surface until after their loved one has passed and their contact with the palliative care provider has ended, she did not specify what communication or referral pathways were currently in place to ensure this is facilitated.
“Together with their specialist palliative care team and their GP, we can help facilitate additional support and referrals to psychiatrists, counsellors and psychologists as needed,” she says.
WA’s Department of Health was contacted for comment and has yet provided a response.
Patients given wrong jabs in RSV error
Health practitioners are urged to ensure they understand the different types of respiratory syncytial virus (RSV) vaccines and who they can be administered to after some patients in Western Australia received the wrong jabs.
While the WA Department of Health did not provide exact numbers on how many patients had been given the incorrect vaccines, it confirmed that 0.07% of the RSV immunisations provided in the State throughout a four-month period this year were delivered incorrectly.
The different RSV vaccines available in Australia are approved for use in certain patient groups, including babies.
The department did not say whether those who received incorrect vaccines in WA were babies or adults.
The Therapeutic Goods Administration (TGA) issued advice on June 23 that it had received reports about administration errors related to RSV prevention products.
Nationally ss of June 13 there had been 90 reports of administration errors related to the three relatively new RSV prevention products.
The TGA reminded prescribers and vaccination providers that each of these were “specifically indicated for different patient groups”.
It advised that Arexvy is to be used to prevent lower respiratory tract disease in individuals aged 60 years and older, or those aged 50–59 years who are at increased risk of RSV disease.
Abrysvo, which this year was added to the National Immunisation Program, is given to pregnant women to prevent lower respiratory tract disease caused by RSV in infants from birth through to 6 months of age.
The TGA’s advice said Abrysvo was
also approved for use in individuals aged 60 years and older.
It outlined that Beyfortus (nirsevimab) is given to infants and children to prevent RSV lower respiratory tract disease.
The TGA confirmed the incorrect vaccinations were thought to have occurred due to administration errors.
"An administration error generally occurs when one of these products is given outside the indications approved by the TGA,” it said in a statement.
The errors included 24 reports of Arexvy being given in pregnancy, 24 reports of Abrysvo being administered to children less than 12 months old, and 36 reports of Beyfortus being administered to females aged 15–54 years.
While WA Health was not aware of any “adverse events” from local cases where administration errors occurred, the TGA noted some adverse reactions were reported in some of the patients that received incorrect vaccines nationally.
For the reports of Arexvy being given during pregnancy, the TGA received five reports where an adverse event was also reported following vaccination.
Fatigue, lethargy, pain at the vaccination site, shortness of breath and a single report of chest pain were among the adverse effects experienced following the vaccination.
For Abrysvo being given to newborns and infants, there were four reports of adverse events that included irritability, sleepiness, fever, and rash; a single report of vomiting; and a single report where the baby had an increased heart rate and increased breathing rate.
The TGA also noted the errors “may lead to various problems, including unknown levels of protection for vaccine recipients”.
Immunisation Foundation of
Australia Director Catherine Hughes said the errors were concerning.
"We urge the Department of Health and vaccine manufacturers to collaborate on clearer, more consistent information and training for all immunisation providers,” she said.
“Ensuring the right vaccine is given to the right patient is paramount for public safety and maintaining confidence in immunisation programs.”
WA Health Chief Health Officer Andrew Robertson said the WA community could be confident that the maternal and infant RSV immunisation programs were “safe and effective – and the best way to prevent babies from ending up in hospital very sick with RSV”.
Dr Robertson said WA Health remained committed to the safe and effective delivery of vaccines and continued to work with immunisation providers to support best practice and safeguard public health.
WA became the first State in the country to provide free RSV immunisation to infants in 2024
when it rolled out its vaccination program to administer Beyfortus.
The immunisation program was made free for another year this year. State Government figures show 22,000 babies were protected during the 2024 RSV season.
A $7.6 million investment as part of the 2025-2026 State budget will fund the program.
The continuation of the program will be boosted by the Commonwealth’s newly funded maternal RSV vaccine for pregnant women, delivering additional protection.
The Australian Immunisation Handbook recommends RSV vaccination for pregnant women, all people over 75 years of age, and anyone over 60 who is Aboriginal or Torres Strait Islander or who has medical risk factors for severe RSV disease.
Australia has recorded more than 63,000 cases of RSV so far this year.
oncology team are involved in private and public multidisciplinary meetings across all facets of oncology
Addressing healthcare gaps for tic disorders
People living tic dissorders are waiting too long for diagnosis, treatment and understanding says Dr Melissa
Licari
.
A young patient presents to their GP, accompanied by a concerned parent. The child has been experiencing sudden, involuntary movements and sounds – facial grimacing, head jerking and throat clearing – that are becoming increasingly noticeable. The parent is anxious, unsure whether these behaviours are a sign of something serious. The GP attributes them to anxiety, recommending a watchand-wait approach and advising stress reduction, but offers no further investigation or referral.
It's an all-too-common scenario for children with tic disorders. While for some, tics resolve quickly, for others they persist or worsen. In Australia, about one in 100 children will experience persistent tics.
Of these, 75% will see symptoms peak between ages 10–12, after which their tics often gradually reduce. However, the remaining 25% will continue to experience tics for life. Currently, about 50,000 Australians live with a lifelong tic disorder.
Australia’s first national survey evaluating the unmet needs of people with tic disorders – Impact for Tourette’s, led by The Kids Research Institute Australia and UNSW Sydney – has revealed worrying gaps in the healthcare system. Delays in diagnosis, inconsistent access to care, a lack of knowledge among medical professionals, and limited availability of evidence-based interventions are having a profound impact on the lives of people with tic disorders.
Dealing with delays
Many individuals with tic disorders experience significant delays in diagnosis. Our survey found one in four individuals waited more than two years for a diagnosis, with some waiting up to four years.
Poor understanding of tic disorders within the healthcare system
While there is no cure, tic disorders can be effectively managed and sometimes even significantly reduced through evidence-based treatments and therapies.
exacerbates the issue. When patients with severe tics or tic attacks present to emergency departments, they are often misidentified as intoxicated or experiencing a mental health crisis, leading to unnecessary treatments or dismissal. Similarly, when patients see specialists, they often leave with a prescription for medication but no guidance on managing their condition.
Although tic disorders like Tourette syndrome are lifelong for many, early intervention can make all the difference – improving understanding, reducing tic severity, and boosting quality of life. Instead, many patients report being dismissed or not believed, with symptoms often attributed to
anxiety or stress – delaying proper care and prolonging unnecessary suffering.
The GPs’ role
As the frequent first point of contact, GPs play a critical role in early diagnosis, support and referral.
Lack of knowledge can result in missed opportunities for timely intervention. Considering tic disorders as a possible diagnosis rather than attributing symptoms to anxiety, GPs can refer patients to paediatricians, neurologists, or psychiatrists who specialise in tic disorders for further evaluation. While there is no cure, tic disorders can be effectively managed and
Dr Melissa Licari with Vicky and Max Radcliffe, who has Tourette syndrome
sometimes even significantly reduced through evidence-based treatments and therapies. While medication can be effective for some individuals, first-line interventions such as Comprehensive Behavioural Intervention for Tics (CBIT) and Exposure and Response Prevention (ERP) can reduce symptoms and improve quality of life.
GPs can also provide families with educational resources and offer guidance on managing the condition more effectively.
The emotional toll
Having a tic disorder takes away control of your body. It can cause pain and injury and affect your ability to concentrate, perform simple daily tasks, relax or even sleep. Compounding this, limited access to treatment and support, being turned away by the NDIS, bullied at school, unable to work, and constantly stared at by a society that does not understand, and you begin to grasp just some of the burden being carried by individuals living with tic disorders, and their caregivers.
Unsurprisingly, these challenges in turn impact mental health. Our national survey revealed 70% of people with tic disorders have an anxiety disorder, one in three experience depression, more than half have thought about ending their life, and one in four adults and one in 10 children have attempted suicide. Access to psychologists specialising in tic disorders is critical.
The survey also revealed almost 80% of caregivers face mental health issues, often due to the significant care burden. Caregivers also need support.
Immediate action is needed to address health system gaps. By proactively considering tic disorders as a potential diagnosis, GPs can ensure timely referrals to specialists and early intervention.
Medical professionals, including tic specialists, should also provide individuals and families with educational resources – readily available from the Tourette Syndrome Association of Australia (TSAA) – and offer guidance on managing the condition effectively.
Given the common co-occurrence of mental health issues such as anxiety and depression, healthcare professionals should screen for these conditions and refer patients to appropriate mental health support when needed. Additionally, when patients present at EDs or seek specialist care, it is vital that all healthcare professionals recognise tic disorders – avoiding misdiagnosis and ensuring appropriate treatment and support.
While broader systemic changes, such as the development of a National Clinical Guideline, are needed for long-term improvements, healthcare professionals can make a significant difference today. By improving early recognition, offering timely referrals, and providing holistic care, they can reduce delays, improve treatment, and ensure patients with tic disorders receive the care they need.
ED: Dr Licari is a senior research fellow at the Kids Research Institute Australia
Supporting cancer patients beyond diagnosis
It takes a village to support a cancer patient through the journey, and Cancer Council WA’s Melanie Marsh urges doctors to share the load through its support line.
When a patient hears the words, “you have cancer,” it changes everything. For many, the days and weeks that follow are filled with fear, confusion and unanswered questions. As a GP or specialist, you may be one of the first trusted voices they hear — a steady presence during a deeply uncertain time. But you don’t have to support them alone.
One of the most powerful — and often underutilised — services available to WA health professionals is our Cancer Council WA 13 11 20 Information and Support Line.
This free, confidential service exists to support not only people with cancer, but also their carers, families and their healthcare providers.
Our services can assist with the physical, emotional and practical impact a cancer diagnosis can bring. We provide tailored information relevant to each patient’s needs, including referrals to local programs and support options.
More than a helpline
For GPs and specialists, the helpline can act as an extension of care — a bridge between the clinical setting and the supportive care services patients often desperately need. Health professionals can access the service by phone, email, or by completing a health professional referral form on the Cancer Council WA website.
The service is particularly useful for time-poor clinicians, or in cases where a patient needs support and information beyond what’s possible in a standard appointment.
We’ve had GPs contact us directly to request information about Cancer Council WA’s support services. We’ve also had GPs encourage their patients to call for emotional support or practical
guidance — and the impact of those referrals can be life-changing.
Whether it’s connecting someone with a counsellor, assisting with transport to treatment, or simply providing information, we ensure no person needs to navigate cancer alone.
A life-changing call
Each call is unique because every cancer experience is different. Some people are seeking practical help, such as financial advice or accommodation near a treatment centre. Others just need someone to talk to who understands.
One such caller was Nan Samy, who was diagnosed with ovarian cancer during a routine check-up. Nan accessed Cancer Council WA’s counselling services and described the experience as transformative.
“The session helped me reflect on myself. The questions the counsellor asked made me think, and that gave me more clarity,” Nan said.
“I feel some people being diagnosed with cancer will find it useful because they can have someone to speak to not only to share their grief but also to get them thinking about what is next
Nan Sammy accessed counselling service through Cancer Council WA's helpline
“The session helped me reflect on myself. The questions the counsellor asked made me think, and that gave me more clarity.”
and how to accept the situation through self-reflection.”
Inspired by the support she received, Nan went on to complete a Graduate Certificate in Counselling at ECU and now helps others through life coaching and mindfulness.
Stories like Nan’s highlight how a single phone call — often made at one of the most vulnerable moments in a person’s life — can set someone on a path toward empowerment and healing.
Helping patients ask the right questions
In addition to the helpline, Cancer Council WA has developed practical tools to help people navigate their cancer journey from the very beginning. One such resource is our Questions to Ask Your Doctor
After a Cancer Diagnosis guide — a straightforward, downloadable list designed to support patients during those crucial first conversations.
It includes questions such as:
• What type of cancer do I have?
• What are the treatment options, and what do you recommend?
• What are the side effects?
• What support services are available?
GPs and specialists are encouraged to print or email the guide to newly diagnosed patients. Resources like this empower people to participate in their care with more confidence.
Patients often leave appointments with a head full of information but very little clarity, however this guide helps them feel more in control, more informed, and less overwhelmed.
For any GP or specialist who hasn’t yet referred a patient, our message is clear: refer. It’s one of the easiest and most impactful things you can do to support your patients.
With cancer affecting one in two Australians during their lifetime, the demand for emotional, practical and psychosocial support is growing. Referring patients ensures they are connected with a team of cancer nurses, counsellors, and support staff who can walk beside them — from diagnosis through treatment and beyond.
Importantly, it also takes pressure off clinicians by giving patients another trusted place to turn for guidance, reassurance and connection.
To find out more or refer a patient, visit www.cancerwa.asn.au or call 13 11 20
ED: Melanie Marsh is the Cancer Council WA’s Supportive Care Director
UNDER CONSTRUCTION | COMPLETION Q4 2027
SECURE YOUR HOME WITH ONLY A 10% DEPOSIT
Experience the height of luxury living.
Discover Somerset at Burswood Point - luxurious riverfront living just 3.5km from Perth CBD. These stunning residences offer sweeping views, premium finishes and access to resort-style amenities including a 20m infinity pool and spa, gymnasium, yoga studio and private lounges. Live a lifestyle like no other.
As a thank you for the care you provide WE’RE PLEASED TO OFFER MEDICAL FORUM SUBSCRIBERS EXCLUSIVE PRICING. ENQUIRE TODAY TO FIND OUT MORE
WED: 10AM - 2PM & 4PM - 6:30PM | THUR TO SUN: 10AM - 2PM OR BY PRIVATE APPOINTMENT Lillian Babich 0402 708 003 | Zoey Lim 0420 870 087
Delivering health equity for rural WA must be more than a slogan, writes Professor Catherine Elliott, newly appointed chief executive at Rural Health West.
Across rural and remote Western Australia, access to healthcare is still too often determined by postcode.
Life expectancy drops by up to five years the further you live from a metropolitan centre. Rates of preventable hospitalisation, chronic disease, and early death remain unacceptably high. In some communities, there is no local access to GPs, mental health support or culturally safe care – with more than 10,000 West Australians living over an hour from the nearest GP.
This is not a new problem, but it is one we have failed to meaningfully shift. If we are serious about equity, we must plan, prioritise, fund, and work together to deliver it.
Growing up in remote areas, I saw the impact of families doing their best without access to care. Those experiences shaped my career – first as a clinician, then as a researcher focused on early intervention for children with developmental needs.
Now at Rural Health West, I’m focused on the fundamental question: how can we ensure everyone, no matter where they live, has access to quality care based on the best evidence?
Strong primary care pays off
This is the promise of a strong primary care sector. A wellsupported, well-connected rural primary care system doesn’t just deliver better local care – it reduces the burden on our overstretched tertiary hospitals, delivers care earlier, and prevents small problems becoming major health crises.
We need to provide opportunities for primary care providers and communities to design and implement research and clinical services relevant to local needs.
We also need dedicated and funded
clinical networks, communities of practice, and knowledge translation to turn evidence, research and lived experience feedback into action in the places it’s needed most.
Our Health Professionals Networks (HPNs) help bridge that gap. These grassroots networks bring together GPs, nurses, allied health professionals and hospital staff across WA to connect with one another, access expert knowledge, and support each other through some of the toughest challenges in rural care.
The HPNs are communities of practice in action. They help rural clinicians stay up to date, connected to experts in specific fields, and better equipped to meet the changing needs of their communities. This is about equitable access to knowledge and, in turn, more equitable care.
Value of support
Clinicians who feel supported, connected and professionally nourished stay longer. Services become more stable, care more coordinated, and patient outcomes improve.
This isn’t theory – it’s happening, and it’s affordable. With under $600,000 annually, HPNs support over 4500 rural health professionals.
At last year’s WA Rural GP Summit, Rural Health West convened clinicians, health leaders and stakeholders to identify actions to strengthen rural general practice. The message was clear: the pressure on rural general practice is real, but so are the solutions.
One key priority was better support for international medical graduates (IMGs), who make up 52% of WA’s rural GP workforce. These doctors face steep challenges like navigating red tape, building trust in new communities and supporting their
families. Without tailored support, many leave, especially as DPA changes make metro practice more accessible.
Speaking at the Summit, Nepaleseborn Dr Ajit Chaurasia said: “It can be difficult for the spouse and children to build meaningful connections and there is not always clear support for them.”
The recent Kruk review creates an opportunity to make Australia more competitive globally for healthcare talent, but without funding and local support we risk repeating the pattern of rural WA being left behind while new doctors – whether they be IMGs or our locally-grown trainees –move to cities.
We’ve called on the WA Government to invest in scaling HPNs and properly resourcing the integration of new rural arrivals. These are essential. Modest investment now could deliver lasting returns in workforce stability, patient care and system resilience.
We’re ready to work with government, clinicians and communities to make this happen. But we need a coordinated approach, one that recognises rural health as a shared responsibility.
Rural funding too often falls between State and Federal cracks, but in country communities those boundaries blur. We can’t let this grey zone continue to excuse underinvestment in rural WA.
Health equity in WA shouldn’t depend on where you live. Let’s stop talking around it and start delivering it.
Advert removed in compliance with Medicines Australia's Code of Conduct and the Therapeutic Goods Administration's Therapeutic Goods Act.
What gets lip service is that around 90% of cancers have an underlying lifestyle cause.
Numbers tell a story
In 1971, then President Nixon declared a war on cancer with the aim of eliminating it by 1976. How are we doing?
According to the Cancer Council, in 2024 there were around 169,500 new cancer diagnoses and 52,700 cancer deaths. State figures are hard to come by, but WA likely accounts for roughly 10% of these.
More disappointingly, according to AIHW data, the number of cancer diagnoses has increased each year since 2000, with the average being an additional 3200 each year.
The number of new cases in 2024 was double that of 2000. In fairness, some of this could be attributed to a growing and ageing population and better detection.
It’s not all bad news though. Total five-year survival is now 71%. This overall figure does hide the fact that some cancers, like breast, now have very high survival rates whilst others, like lung and pancreas, remain low.
The national lung cancer screening program kicked off on July 1 and hopefully this will lead to improvements in lung cancer detection and, in turn, survival.
Treatments have improved in lung cancer as I discussed with Dr Tim Clay on a recent Medical Forum podcast. However, rate of lung cancer in never smokers has been increasing and this group sits outside the screening program.
What gets lip service is that around 90% of cancers have an underlying lifestyle cause. Not smoking, not drinking alcohol excessively, eating sensibly, not carrying too much excess weight, doing regular exercise and not getting sunburned are all ways to reduce cancer risk. Yet the numbers suggest that collectively we are not succeeding with these.
It’s a cliché but an ounce of prevention goes a long way. Perhaps never further than with reversing the trends in cancer diagnosis.
Want to stay up to date on clinical news?
Sign up to our Wednesday clinical newsletter to get the latest updates from your local specialists.
Head to our website and click the subscribe button or scan the QR code
Personalising liver cancer care: a WA-led collaborative effort
By Prof Nina Tirnitz-Parker AM and Prof Peter Leedman AO Co-Directors, Liver Cancer Collaborative
Liver cancer, of which the majority of cases are hepatocellular, is one of the fastest-growing causes of cancer-related death in Australia. Despite intensive research worldwide, progress has lagged behind that in many other cancers. This reflects the unique challenges of liver cancer.
It is highly heterogeneous, and the liver’s ability to compensate for damage often masks symptoms until the disease is advanced. For many patients with late-stage disease treatment options are limited and often non-curative.
Survival rates remain poor, and there are still no established tools to reliably predict individual risk or determine which treatments are most likely to be effective. A key reason is that the molecular basis of liver cancer is still not fully understood, as, in contrast to almost all other tumours, biopsy has not been routine to establish the diagnosis. That gap is now being addressed through collaborative research efforts that bring clinicians, researchers, and data scientists together.
The Liver Cancer Collaborative (LCC) was established in 2020 to drive an integrated, multidisciplinary approach in WA. Funded by several organisations, primarily the local Cancer Research Trust (CRT), the LCC links major hospitals, universities, and research institutes across the state to improve outcomes for people at risk of, or living with, liver cancer.
By embedding research into clinical practice and working across disciplines, the LCC focuses on understanding how liver cancer develops, progresses in real time, and on discovering new therapeutics.
A key LCC strength is its longitudinal infrastructure, including an ethically governed clinical database and biobank. These platforms support
clinical information collections and matched biological samples from individuals with liver disease or liver cancer over time. Laboratory analyses are linked with clinical, pathology, and imaging data, together with advanced molecular genomic profiling, and are closely integrated with WA’s public health system and the clinicians providing care.
The LCC is exploring why some tumours respond to certain therapies while others do not, the reasons some patients develop resistance, and markers that could help detect cancer earlier.
Laboratory models using patient tumour samples and patient-derived organoids have been developed to rapidly assess how individual cancers respond to treatments, aiming to support personalised decision-making in the future. Parallel, efforts are underway to develop a blood-based test for earlier detection, particularly in highrisk groups.
Alongside biological research, new digital and imaging tools are being explored. A mobile app is in development to help people with chronic liver disease track symptoms and prompt timely clinical review. It also includes developing a tool to integrate all of the above data to assist clinicians with treatment selection.
Advanced imaging techniques are also being explored, including radiomics and artificial intelligence, which may enable earlier detection of disease-related changes not visible with standard methods.
The LCC’s growing database links clinical, molecular, and imaging data to support the discovery of clinically relevant patterns. The collaborative works closely with national and international experts who ensure that the new tools developed in WA can be applied in a broader clinical context. The database is emerging as one of the most comprehensive of its kind.
Ultimately, the goal is to shift the trajectory of liver cancer care through data-driven, patient-specific treatment. By linking clinical insight with molecular and imaging-based understanding, and by capturing changes over time within individual patients, the LCC is helping to move the field towards more precise and timely interventions.
Although many challenges remain, the collaborate provides the basis for improving surveillance in high-risk populations, supporting earlier and potentially curative interventions, and enabling better matching of therapies to the biology of each patient’s disease.
The future of liver cancer care will depend on our ability to interpret complexity rather than simplify it. Progress will come from working together across traditional boundaries and building systems that are both scientifically rigorous and clinically informative.
More information, enquiries, and a list of funders and supporters, available at www.livercancercollaborative.au
Author competing interests – nil
Human liver cancer organoid used for drug screening. Picture: Dr Nathan Main & Dr Ben Dwyer
Exercise in cancer care: It is time to deliver
By Mary Kennedy, PhD Exercise Physiologist
The days when rest was considered the best option for people with cancer are long past. Decades of research demonstrates clear benefits of exercise to improve health outcomes before, during, and after cancer treatment.
A 2019 review showed exercise has a role in positively impacting eight common side effects of cancer treatment, including improved health-related quality of life and physical function, bone health, and sleep, and decreased cancer related fatigue, anxiety and depression. Further research supports the role of exercise in the improved survival rates of breast, colon, and prostate cancer.
Yet some clinicians still question the true impact of exercise due to the observational nature of most exercise oncology studies. A recent randomised controlled trial (889 people, 55 centres primarily in Canada and Australia) investigated if structured exercise could improve survival outcomes for people with stage III or high-risk stage II colon cancer after the completion of surgery and chemotherapy.
Participants were randomly assigned to either a three-year supervised exercise program (intervention group) or received health education materials only (control group). The results demonstrated significantly longer disease-free survival for people in the exercise group and were consistent with longer overall survival for exercisers too.
This is the first randomised trial showing that exercise can directly improve survival in people with colon cancer – reinforcing the importance of providing exercise as part of cancer care.
The Clinical Oncology Society of Australia (COSA) calls for exercise to be embedded as a standard part of cancer care. COSA encourages all healthcare professional to talk about exercise, recommend it, and
Key messages
Exercise is medicine for people with cancer
A substantial body of evidence supports integrating exercise into clinical care
Start the conversation about exercise with your patients today.
refer patients to accredited exercise physiologists or physiotherapists.
Yet, a recent study found that while 94% of healthcare professionals agree exercise is beneficial, only 35% routinely apply COSA’s recommendations in practice. The reason for the low participation rate? Many feel it is not their role, or they lack the time, training, or resources.
But patients report they trust their care team, so even a brief conversation or referral can make a difference.
Exercise isn’t just a “nice to have” –it’s evidence-based care, and health professionals need to promote that message.
Helpful resources
Whilst not necessary to upskill as an exercise professional to promote exercise to patients, it is important to start the conversation reinforcing that exercise is an important part of care, not an optional extra.
Exercise is Medicine Australia offers a variety of resources to guide healthcare professionals to incorporate exercise screening, assessments, discussions, and referrals into their practice. The practical tools are free and are designed to be integrated into clinical care.1
The Exercise and Sports Science Australia (ESSA) Professional Directory is a practical tool helping locate qualified providers, making referrals easier and more accessible. The tool allows for screening by location and
specialty area (e.g. cancer) of the professional. 2
Cancer Council WA offers the Life Now Exercise program—a free 12week supervised group program for people diagnosed with cancer and their primary carers. 3
General practitioners have a particularly important role in providing exercise for people living with and beyond cancer. A Chronic Disease Management Plan (CDMP), allows eligible patients, including anyone with a cancer diagnosis, to access Medicare-funded exercise sessions.
People are eager to receive exercise guidance. A recent focus group in Western Australia explored the experience and desires of breast and prostate cancer survivors for receiving exercise information from their health care providers. A key finding from the study: people wanted more. One breast cancer survivor noted: "I would like to be referred to someone… to help me with everything, like, how to exercise, what kind of exercises."
Author competing interests – the author is supported by a Cancer Council of Western Australia Postdoctoral Fellowship and serves on the ACSM Exercise is Medicine® Moving Through Cancer Task Force.
Focal therapy for prostate cancer: Precision with fewer side effects
By Dr Andrew Tan , Urologist, Prostate & Kidney Surgeon, Nedlands
Over the past decade, the management of clinically significant, localised prostate cancer has undergone a significant evolution.
While radical prostatectomy and external beam radiotherapy remain the gold standards for many patients, the associated morbidity – particularly impacting sexual function and urinary continence – has prompted interest in less invasive strategies.
Focal therapy has emerged as a promising middle ground, offering the potential for effective cancer control with minimal impact on quality of life.
Focal therapy is a precise, imageguided treatment that targets the dominant prostate cancer lesion, aiming to ablate the tumour while preserving surrounding healthy tissue.
The goal is to maintain erectile and urinary function by avoiding wholegland treatment. This targeted approach is supported by improved imaging and biopsy techniques allowing better identification and characterisation of clinically significant lesions.
Despite technical advances in surgery and radiotherapy, functional side effects remain common. The Prostate Cancer Outcomes Registry (2023) provides sobering data:
• One year after radical prostatectomy, 45% of men reported sexual function as a problem; only 22% achieved a fair to very good erection. 20% experienced more than one urinary leak per day, and 31% needed more than one pad daily.
• After radiotherapy, 34% of patients still had sexual function issues, with only 24% reporting erections adequate for intercourse. 10% experienced significant urinary leakage.
Treatment approaches that better preserve quality of life, especially in men with intermediate-risk, organconfined disease are needed.
The focal therapy opportunity
Focal therapy can treat prostate cancer while minimising side effects, preserving future treatment options if necessary. While most prostate cancers are multifocal, about 20–25% of cases are unifocal. However, the concept of the index lesion – the dominant tumour driving disease progression – has expanded the potential use of focal therapy beyond unifocal cases. Treating this main lesion may significantly alter disease trajectory, even if smaller secondary foci remain.
Ideal candidates for focal therapy are carefully selected and wellcounselled. Criteria include ISUP Grade Group 2 (Gleason 3+4=7), PSA <15 ng/mL, organ-confined (T2) disease, life expectancy ≥10 years, ability to comply with rigorous follow-up protocols and
enrolment in a data registry and understanding of the lack of longterm outcome data.
Patients with low-risk disease, for exampe low-volume Gleason 6, are better managed with active surveillance. Those with high-risk or locally advanced cancers typically require whole-gland treatment.
The feasibility of focal therapy has been significantly improved by technological advancements, allowing more accurate detection, localisation, and staging of disease. These include multi-parametric MRI (mpMRI) for lesion detection and staging, PSMA PET/CT for detecting disease outside the prostate and ensuring concordance with MRI, MRI-ultrasound fusionguided biopsies for targeted sampling and transperineal roboticassisted biopsy platforms currently emerging.
Key messages
Focal therapy can offer curative intent in a minimally invasive, function-preserving format, suited to selected patients with intermediate-risk disease
Whilst long-term data is evolving, focal therapy is increasingly supported by modern imaging, precision biopsy, and growing clinical experience
For the right patient, this approach can mean avoiding the morbidity of whole-gland treatment without compromising on cancer control.
Together, these tools reduce the risk of under-staging and increase confidence in patient selection.
Focal therapy modalities
A range of focal therapy techniques are available; all typically performed as day-case procedures with minimal downtime and side effects. These include:
• Cryotherapy: Employs rapid freezing to destroy cancer cells.
• Irreversible Electroporation (Nanoknife): Uses electrical pulses to disrupt cancer cell membranes without heat.
• Focal Laser Ablation: Applies laser energy to precisely ablate the lesion under image guidance.
• Focal Brachytherapy: Involves placing radioactive seeds into the tumour zone for localised radiation delivery.
Currently, only focal brachytherapy is fully reimbursed by private health insurers in Australia. There is no high-level evidence yet to suggest one modality is superior; choice often depends on surgeon experience, tumour location and technological availability, for example HIFU is ideal for posterior lesions.
Post-treatment surveillance and outcomes
Patients require ongoing monitoring with regular PSA testing, post-treatment mpMRI and repeat biopsies to assess both in-
field and out-of-field recurrence. Recurrence can be managed with repeat focal ablation or salvage whole-gland therapy (radical prostatectomy or radiotherapy). Importantly, salvage treatments remain feasible and reasonably safe, although functional outcomes are understandably reduced, as with upfront whole-gland treatment.
Most published data are from prospective studies with short- to medium-term follow-up. The results are encouraging, with continence preserved in over 90% of cases, erectile function preserved in up to 100% in some series, five-year failure-free survival ~83% and treated zone control 85–90%, with most recurrences occurring outside the treated area
These outcomes suggest that focal therapy offers excellent functional preservation with reasonable oncologic control in the short term. As imaging and biopsy techniques continue to evolve, we may reduce out-of-field failures due to undersampling or staging errors.
Author competing interests – nil
What is Theranostics?
Theranostics refers to the combination of two words, therapy and diagnostics.
In broader terms, usually PET-based targeted molecular imaging is applied to localise the tumour followed by targeted radionuclide therapy to the identified tumour cells. The therapeutic radiopharmaceutical is generally administered intravenously but other routes are also applicable. The treatment is often provided in courses of multiple cycles with a few weeks apart.
Treatment effect can be monitored using respective tumour markers and restaging with the same nuclear imaging agent (PET or non-PET) used for staging and patient selection for therapy. Recently, 177Lutetium Prostate Specific Membrane Antigen (177Lu PSMA) has been added to the Medicare Benefit Scheme. Other treatment options are still fully self-funded through the Special Access Scheme (SAS) or through clinical trials.
Current Theranostics program at GenesisCare, Murdoch, WA
GenesisCare are currently offering 177Lutetium- PSMA (Pluvicto)® for Metastatic Castrate Resistant Prostate Cancer and 177Lutetium-DOTA- somatostatin receptor agonist treatment for neuroendocrine neoplasm (NENs) patients. Additionally, for various other types of advanced progressive tumours, theranostics may be suitable for those patients who have not responded to conventional treatments as standard of care. Current real-world studies and clinical trials data suggest that targeted radionuclide therapies can increase overall survival, progression-free survival, and disease control rates, even in late-stage disease along with improvement in quality-of-life and symptom alleviation. Currently available literature suggests targeted radionuclide therapies for patients with metastatic prostate cancer and neuroendocrine tumours.1-4 Patients with other tumour and malignancies may be suitable for inclusion into Theranostics related clinical trials.
Your GenesisCare, Murdoch Nuclear Medicine Physician will determine if Theranostics may be suitable for your patients.
GenesisCare has several Theranostics facilities in Australia including a facility at Murdoch in Perth with PET and SPECT imaging provided by SKG at the one location for ease of access to patients.
Where to find us
GenesisCare
St John of God Murdoch Hospital 100 Murdoch Dr, Murdoch, WA, 6150 Australia
GenesisCare is involved in several Theranostics Clinical Trials. To learn more, click here.
Introducing our Clinical Director of GenesisCare Theranostics and Clinical Head of Theranostics and Nuclear Medicine
Prof Joe Cardaci
Clinical Director of Theranostics, GenesisCare MBBS, FRACP, AANNMS
Prof Joe Cardaci is a Nuclear Medicine Physician with a long-standing interest in Theranostics. Prof Cardaci was involved in the early development of SIRT therapy for liver cancer and continues to offer a clinical service for complex liver tumours. He has been involved in multiple international research trials advancing the field of radionuclide therapy in advanced malignancies. Prof Cardaci’s clinical interests include advanced prostate cancer, neuroendocrine tumours (NETs), liver cancer, and non-melanoma skin cancer.
Dr Aviral Singh
Clinical Head of Theranostics and Nuclear Medicine, GenesisCare MD PGDipCard, MSc, FAfNM, FRACP
Dr Aviral Singh is based in Murdoch, WA as our Clinical Head of Theranostics and Nuclear Medicine. He has extensive experience in the field of Theranostics, both as a clinician and researcher, with more than 45 peer reviewed scientific papers and over 100 scientific abstracts presented at various international medical societies. Dr Singh has taken part in several first-in-human clinical studies, some of which have translated to real-world clinical application. His clinical interests include targeted radionuclide imaging and therapy of neuroendocrine neoplasms, prostate cancer, and other difficult to treat advanced progressive oncological entities.
References: 1. Strosberg J., et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N Engl J Med 2017;376:125-135. (NETTER-1 Trial) 2. Singh S., et al. [177Lu]Lu-DOTA-TATE plus long-acting octreotide versus highdose long-acting octreotide for the treatment of newly diagnosed, advanced grade 2-3, well-differentiated, gastroenteropancreatic neuroendocrine tumours (NETTER-2): an open-label, randomised, phase 3 study. Lancet 2024;403(10446):2807-2817. 3. Sartor O., et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2021;385:1091-1103. (VISION Trial) 4. Sathekge MM., et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): a multicentre, retrospective study. Lancet Oncol 2024;25(2):175-183.
Disclaimer: Some radiopharmaceuticals used for Theranostics are not currently included in the Australian Register of Therapeutic Goods.
Scan the QR code for more information
Ten-minute consult – iron deficiency in children
By Dr Amit Saha , Paediatric Gastroenterologist, Hollywood
A recent study conducted with children in Western Australia revealed that one third of oneyear-olds and nearly two thirds of three-year-olds had iron deficiency, presumed to be predominantly nutritional.
The subtle but serious implications of iron deficiency include potential harm to neurodevelopment, a weakened immune system and impaired overall health. Early detection and correction is vital.
The causes of iron deficiency in children generally fall into five main categories: insufficient dietary intake, chronic blood loss, rapid growth spurts, malabsorption, and genetic factors like TMPRSS6 gene mutation.
Infants, toddlers, and adolescent girls face increased risks of iron deficiency due to heightened iron needs during times of rapid growth or menstruation.
Prevalence is also influenced by factors such as age, socioeconomic background, and ethnicity.
Indigenous Australian children and those from low-income families are disproportionately affected by iron deficiency.
Left untreated, iron deficiency can progress to iron deficiency anaemia (IDA) with notable implications on growth; cognitive, psychomotor, and neurodevelopmental outcomes; mortality, and overall quality of life.
Refractory iron deficiency arises from mutations within the TMPRSS6 gene, which causes elevated hepcidin levels impeding iron absorption and storage. This culminates in ironrefractory iron deficiency anaemia (IRIDA), a subgroup characterised by persistent, lifelong iron deficiency anaemia despite adequate supplementation.
Diagnosis
Diagnosing iron deficiency anaemia in children requires a comprehensive approach that combines clinical evaluation, laboratory testing, and exploration of possible underlying factors.
A detailed medical history should include dietary patterns, growth trends, history of bleeding or chronic health issues. A physical examination might uncover signs such as pallor, fatigue, irritability, and delayed developmental milestones.
Although these indicators are not exclusively tied to iron deficiency, neither their absence eliminates the possibility.
Laboratory analysis is crucial for confirming the diagnosis and determining the severity of anaemia. A complete blood count shows decreased haemoglobin levels, a lower red blood cell count, and altered red blood cell indices (MCV and MCH).
Serum iron measures the amount of iron circulating in the blood, bound to transferrin. However, it fluctuates diurnally and is affected by recent iron intake, making it a less reliable indicator of overall iron status.
Ferritin, an intracellular protein that stores iron, reflects the body's iron reserve.
A low ferritin level is generally considered the most specific indicator of depleted iron stores. However, ferritin is also an acutephase reactant, meaning that its levels can be elevated in the presence of inflammation, infection, liver disease or malignancy, masking underlying iron deficiency.
In these situations, additional parameters can yield vital information. In iron deficiency, the total iron-binding capacity (TIBC) and transferrin levels are often elevated – the body increases transferrin production to compensate for lack of iron –while transferrin saturation – the percentage of transferrin carrying iron – is typically reduced.
Management
The cornerstone is identifying the root cause and replenishing iron stores through dietary modifications, iron supplementation, or, in severe cases, intravenous iron infusions. Dietary approaches focus on increasing the intake of iron-rich
foods like lean meats, poultry, fish, beans, and fortified cereals. Increasing intake of foods high in vitamin C can enhance iron absorption improving overall iron status.
Oral iron supplementation is typically prescribed to correct iron deficiency either prophylactically at a dose of 1-2mg/Kg/day, or to treat IDA at 3-6mg/Kg/day.
Higher oral doses of up to 10mg/ Kg/day or iron infusions can be used for severe anaemia or IRIDA. Supplementation should continue at least three months after anaemia has been corrected, to replenish stores. Poor compliance is the leading cause of treatment failure – be mindful of this.
It is crucial to inform parents about possible side effects, including gastrointestinal discomfort, blackish discoloration of stool, staining of teeth and constipation.
Additionally, addressing underlying medical conditions that may contribute to iron deficiency, such as coeliac disease or inflammatory bowel disease, is essential for longterm management. Refer for further specialist workup if suspected.
Prognosis in children is generally favourable with timely diagnosis and appropriate management. Early intervention can prevent or reverse many of the adverse effects associated with iron deficiency, including cognitive impairment and developmental delays.
Emerging therapies targeting hepcidin pathways offer hope for personalised management in IRIDA in the near future.
Preventing iron deficiency through public health initiatives, for example food fortification and iron supplementation programs along with vitamin C, is important.
Community based education, screening and early intervention is crucial for reducing the burden of iron deficiency in toddlers and children, with specialist input in refractory cases as needed.
Author competing interests – nil
Helping to expand the acute stroke treatment window
By Dr Liz Dallimore, Neuroscientist, Nedlands
Acute stroke remains a leading cause of death and disability worldwide, where rapid intervention can mean the difference between recovery and permanent brain damage.
While thrombolysis and thrombectomy remain the foundation of ischaemic stroke treatment, a West Australiandeveloped neuroprotective drug may soon offer clinicians a new tool to preserve brain tissue in the crucial early hours as well as after treatment.
The current acute stroke workflow in emergency departments prioritises rapid recognition and imaging, with non-contrast CT and CT angiography used to assess eligibility for reperfusion therapies.
Patients with a confirmed large vessel occlusion (LVO) may receive intravenous thrombolysis within 4.5 hours of onset, and/or endovascular thrombectomy up to 24 hours of onset, per imaging criteria.
These treatments are highly timesensitive and often inaccessible to patients in regional or remote areas, where delays in transfer may result in missed intervention windows. Even when performed promptly, reperfusion injury can contribute to ongoing neurological damage.
A new agent
A new neuroprotective peptide drug is currently being developed by a Perth biotechnology company, based on a decade of research from the Perron Institute and UWA.
Unlike existing therapies that target clot removal, this new drug is designed to protect brain cells from damage during and after ischaemia, offering a novel approach to stroke care.
Administered via intravenous infusion, the drug can be given prior to reperfusion therapy, potentially in emergency departments or even pre-hospital settings.
Its aim is two-fold:
• Preserve the ischaemic penumbra while awaiting reperfusion, potentially extending
the time-window for current treatments
• Mitigate damage from posttreatment oxidative stress and inflammation.
This mechanism makes it complementary – not competitive – with existing standards of care, fitting ideally into current stroke treatment workflows.
Current and planned research
In April 2025 patient dosing in a Phase Two clinical trial of the peptide drug in acute ischaemic stroke patients was completed across multiple Australian stroke centres, including Sir Charles Gairdner Hospital and Fiona Stanley Hospital in WA.
The double-blind trial involved 92 AIS patients with LVO, each receiving the drug or placebo prior to undergoing thrombectomy. The key endpoints included:
• Infarct volume reduction, assessed on imaging at 48 hours
• Functional outcomes, measured at 90-day follow-up.
Trial data is currently blinded, however, all results are expected in September this year.
Following successful results from the Phase Two trial, the drug trials will progress to a Phase 2b/3 clinical trial. Preparation is underway for this trial, which is expected to recruit around 1000 patients across Australia, the US, Europe, Canada, and China, commencing in mid to late 2026.
It will evaluate efficacy across a broader population and refine patient selection criteria. If proven successful, it could mark the world’s first clinically approved neuroprotective drug for acute stroke.
The development of this novel drug underscores WA’s leadership in translational neuroscience. The drug has already shown up to 70% reduction in brain cell death in preclinical studies.
The potential applications may extend beyond stroke, with ongoing preclinical research into traumatic brain injury (TBI), hypoxic ischaemic encephalopathy (HIE), and neurodegenerative conditions.
Author competing interests- the author is the Managing Director of Argenica Therapeutics and is actively involved in the drug development and clinical research.
Can aspirin prevent hepatocellular carcinoma in people with cirrhosis?
By Prof John Olynyk , Curtin University
Hepatic cirrhosis and hepatocellular carcinoma (HCC) are rapidly increasing causes of premature morbidity and death globally. In 2021, Deloitte Access Economics reported costs of HCC to the health system, productivity and loss of wellbeing in Australia were $140m, $382m and $4.3b a year, respectively. HCC is the second most common global cause of years-of-life-lost due to malignancy, and the commonest cause of death in cirrhosis.
Globally, the incidence of HCC is increasing at a far greater rate than all other malignancies. Between 2000 and 2015 the liver cancer death rate increased by 50% in men and women, especially in those of lower socioeconomic groups.
In Australia, HCC is now the second leading cause of cancerrelated death in men, and of higher incidence in Aboriginal, regional and culturally and linguistically diverse communities. The peak age of incidence is 70 years.
Over 90% of cases of HCC occur in the setting of established cirrhosis. Chronic viral hepatitis B or C, and the chronic steatotic liver diseases (SLDs), which encompass the spectrum of metabolic-associated (MASLD, previously known as nonalcoholic fatty liver disease) through to alcohol-related liver disease, are the commonest aetiologies leading to the development of cirrhosis and HCC.
The clinical impact of HCC is devastating – 90% of all individuals who develop HCC die of the disease – the highest mortality rate of all cancers. Even with the development of cancer surveillance and new treatments, the World Health Organization predicts that the incidence of HCC will increase by 60% over the next 30 years and the mortality will remain approximately 90%.
Clearly, there is a significant gap in the provision of current care, with the only effective way to reduce the future burden of disease being through prevention of HCC in people with cirrhosis.
Key messages
Hepatocellular carcinoma is the commonest cause of mortality in people with cirrhosis and the second most common cause of years-of-life-lost due to malignancy after lung cancer world-wide
Most cases of hepatocellular carcinoma occur in the setting of cirrhosis and are diagnosed at an incurable stage with mortality approximating 90%
Potential prevention of hepatocellular carcinoma in people who have cirrhosis could reduce the incidence by up to 50%. We will conduct a prospective, placebo-controlled trial of aspirin to determine if this is possible.
Based on compelling epidemiological data there is a strong rationale for a randomised clinical trial to test the benefits of aspirin for prevention of HCC. Low dose aspirin consumption (100mg daily) has been associated with a 50-70% reduction in the incidence of HCC.
The longer the duration of treatment, the greater the reduction in incidence. Similar benefits were observed in men and women. Cessation of aspirin therapy was associated with a reversion back to the general population risk of HCC, suggesting that aspirin was inducing the protective effect.
The 10-year liver-related mortality was also reduced by 30%. The magnitude of benefit associated with aspirin was significantly stronger in subjects with cirrhosis. Thus, aspirin represents an ideal low-risk agent to systematically evaluate in the prevention of HCC in cirrhotic subjects.
Whilst aspirin was safe, with no increased risk of gastrointestinal bleeding in aspirin-users compared with non-users, concerns remain regarding its safety in routine clinical care.
We will conduct a prospective, randomised clinical trial over four years to evaluate the effects of daily aspirin compared with placebo therapy on the incidence of HCC in 890 stable, well-compensated cirrhotic subjects attending hospital outpatient clinics and otherwise receiving standard of care treatment. Five large Australian hospitals and two UK sites will participate in the research program.
If successful, our trial will deliver significant health impact through change in practice, providing a clinical indication for aspirin prophylaxis to become standardof-care for the prevention of HCC in people with cirrhosis, and reduce the incidence and mortality of HCC by at least 50%. These important outcomes will deliver significant economic impact, saving the Australian economy at least $70m a year in direct health care costs.
Author competing interests – the author is involved in the research described
Immunotherapy related cutaneous toxicity
By A/Prof Tony Caccetta & Dr Helena Collgros, Dermatologists
Immunotherapy has transformed cancer treatment by shifting the focus from directly killing cancer cells to activating the immune system to fight cancer – improving survival in many advanced cancers without chemotherapy related side effects. However, immunotherapy related adverse events (irAEs) are common and may be serious or lifethreatening.
Immune checkpoint inhibitors (ICIs) (e.g. ipilimumab, nivolumab, pembrolizumab, atezolizumab) may cause cutaneous toxicity in 3050% of patients. Often occurring in the first few weeks or months of treatment, the onset can be unpredictable occurring at any time.
Most cases are mild and manageable, not requiring systemic corticosteroids or immunotherapy interruption/ cessation (interventions which may shift the tipping point for durable cancer response). We present some of the more common and serious presentations of ICI-related cutaneous toxicity below.
Psoriasis
Immunotherapy has the potential to trigger or exacerbate existing psoriasis. It is essential to ask about a personal or family history of psoriasis before commencing immunotherapy.
Immunotherapy related psoriasis may be widespread, however can often be managed effectively with skin directed treatments such as topical steroids, phototherapy and/ or oral acitretin (retinoid).
A lack of response or the development of arthritis may require treatment escalation with immunosuppressive agents such as methotrexate or biologic therapy. Oral prednisolone or intravenous methylprednisolone can potentially destabilise psoriasis upon withdrawal, with rebound/unstable flares, which may be sometimes pustular or erythrodermic.
1: A patient with a personal and family history of psoriasis, late onset Grade 2 psoriasis flare with pembrolizumab. Pembrolizumab dose held, and high dose oral prednisolone given. Unstable psoriasis upon taper of prednisolone. Psoriasis did not improve with topical steroids initially, however cleared following 8 weeks phototherapy and acitretin.
Vitiligo
Vitiligo (an autoimmune disease) can be triggered or exacerbated by immunotherapy treatment targeting melanocytes. It may be a good prognostic sign and marker of treatment response in melanoma patients. Treating vitiligo can be challenging and the response unpredictable. However, topical steroids, topical calcineurin inhibitors and phototherapy may trigger repigmentation in these patients.
Spontaneous re-pigmentation can also occur without specific treatment. While vitiligo can be a very significant adverse event for patients, immunosuppressive treatments (e.g. emerging oral JAK inhibitors) should currently be avoided in this setting.
Lichenoid eruption
Lichenoid immunotherapy eruptions often present as violaceous flat-topped papules or plaques which may coalesce, often affecting the limbs and trunk. They often occur 6-12 weeks after
ICI commencement. Skin biopsy and lupus serology can be helpful to distinguish a lichenoid reaction from immunotherapy induced subacute cutaneous lupus (SCLE). Skin directed treatment includes topical steroids, phototherapy and acitretin.
Lichenoid eruptions can often be managed without systemic corticosteroids or immunotherapy interruption/cessation. Phototherapy should be avoided in SCLE and topical steroids +/oral hydroxychloroquine are often considered. SCLE management would be escalated if associated with systemic lupus erythematosus.
Pruritus
Pruritus in this setting is often multifactorial. It can be related to immunotherapy, but often there is an underlying contributing factor, commonly dry skin. Not all skin related presentations are due to immunotherapy side effects. A co-existing morbilliform or other rash, related or unrelated to immunotherapy, may also contribute to pruritus. General skin care measures (e.g. soap-free wash and moisturising immediately following showering) are simple and often helpful.
Anti-pruritic creams containing menthol can be very soothing and used regularly. If there is an underlying dermatosis, specific treatment will improve pruritus. Pruritus and morbilliform rash can often be managed without systemic corticosteroids or immunotherapy interruption/cessation.
Bullous pemphigoid
Bullous pemphigoid is an immunobullous disorder that commonly affects older people and presents with a prodromal urticarial eruption (pre-bullous pemphigoid) before evolving into tense blisters on an erythematous base. Immunotherapy may trigger bullous pemphigoid at any time during treatment. However, delayed presentations are common.
Figure
Key messages
Rapid access pathways to dermatologist care can improve QOL for cancer patients
Skin directed treatments are often safe and effective and may provide options prior to considering systemic corticosteroids and immunotherapy interruption/ cessation
Not all cutaneous eruptions are related to immunotherapy.
It requires a diagnostic biopsy sent for histopathology and direct immunofluorescence. Treatments include topical steroids, doxycycline + nicotinamide or off-label dupilumab (IL-4 and IL-13 inhibitor). If not controlled by the above, oral prednisolone, methotrexate, IVIG and rituximab may be considered. Immunotherapy interruption/ cessation may be required.
threatening adverse reaction to immunotherapy. Immediate cessation of immunotherapy is required upon suspicion of SJS/ TEN. All medications require review as potential culprits. Skin pain, flaccid blistering with a positive Nikolsky’s sign and mucosal involvement are important diagnostic features. A skin biopsy can be useful. Admission to a tertiary hospital with experience in supportive care and SJS/TEN management is required.
When managing ICI related cutaneous toxicity, the risks of continuing or resuming immunotherapy treatment are carefully considered and may include:
1) Worsening of cutaneous toxicity, which may potentially become treatment refractory and permanent.
2) The development of other systemic toxicities (e.g. colitis, hepatitis, pneumonitis, endocrinopathies), which may also potentially become treatment refractory and permanent.
Most cancer patients developing
PERTH OROFACIAL PAIN & TMJ CLINIC
welcomes Dr Guru O to
our
practice at St John of God Hospital, Subiaco
dermatological issues are not referred to a dermatologist. Improving timely access to dermatology services for oncology patients with cutaneous toxicity is required.
The interval between immunotherapy doses, often 2-4 weeks, is when skin directed therapies may be trialled, with close dermatology monitoring for skin progression and oncology monitoring for other systemic toxicities. Even if a grade 2/3 cutaneous toxicity improves significantly with skin directed treatments, continuing or resuming immunotherapy comes with careful consideration and caution.
Rapid access dermatology services for assessment of ICI cutaneous toxicity, allows for timely and accurate diagnosis and offers oncology patients effective skin directed treatment options. This can improve quality of life (QOL) and potentially avoid systemic corticosteroids and immunotherapy interruptions/cessation for advanced cancer patients.
Author competing interests – nil
Dr Guru O is a highly trained Oral Medicine Specialist bringing a wealth of experience from both Australia and overseas. With a career built on compassion, precision, and academic excellence, Dr Guru specialises in: Orofacial Pain Temporo-mandibular Disorders (TMD) Dental management of obstructive sleep apnoea Oral mucosal diseases
Perth Orofacial Pain and TMJ Clinic is a well-known specialist practice focusing on the diagnosis and management of complex oral and facial pain conditions. We work collaboratively with medical, dental and other health care professionals across disciplines to deliver integrated care for patients with persistent pain and jaw dysfunction.
Dr Guru O graduated from the University of Adelaide with a Bachelor of Dental Surgery in 2012. He gained valuable experience in Singapore before completing a Masters in Orofacial Pain at the University of Sydney and his Doctor of
Clinical Dentistry in Oral Medicine at the University of Western Australia. He has gained experience in multiple hospital departments including pain medicine, immunology, dermatology, rheumatology, and sleep medicine, and continues to publish in peer-reviewed journals and book chapters.
We are delighted to welcome Dr Guru to our clinic at St John of God Hospital, Subiaco. His commitment to education and excellence in delivering evidence-based, patient-centred care makes him a valued member of our team.
St John of God Hospital – Subiaco Clinic Suite 319, 25 McCourt Street Subiaco, WA 6008
By A/Professor Rob Paul, Ophthalmologist, Melville & Nedlands
It’s hard to believe the first laser eye surgery keratorefractive procedure on humans was performed 40 years ago. It was called PRK (photorefractive keratectomy) and involved manual removal of the corneal epithelium then reshaping of the corneal stroma with an excimer laser.
The procedure was exceptionally painful and had a prolonged recovery. This was superseded by LASIK (laser assisted in-situ keratomileusis) which involved cutting a corneal flap with a mechanical blade and then applying the excimer laser to the underlying cornea. This procedure carried a higher complication rate.
The introduction of the femtosecond laser to perform laser refractive surgery has been one of the greatest modern advances in ophthalmology and its multiple uses extends to cataract surgery and the correction of reading problems.
LASIK and SMILE
LASIK is still a premium treatment for most types of vision errors. Short-sightedness (myopia), astigmatism, long-sightedness (hyperopia) and reading problems (presbyopia) can successfully be treated. A femtosecond laser creates a flap on the cornea. This flap is then lifted and an excimer laser reshapes the corneal bed. The femtosecond laser creates the flap in eight seconds and is painless.
Over 40 million people have benefited from this surgery, including Tiger Woods, Usher, Taylor Swift, Brad Pitt and numerous sportspeople.
Myopia up to 12 points, hyperopia up to six points and astigmatism up to six points can be treated, with 20/20 vision rates between 95-98% the day after surgery.
Small incision lenticule extraction (SMILE) is the next generation in laser eye surgery procedures. It is essentially keyhole laser eye surgery and involves a femtosecond
laser creating a lenticule of tissue under the corneal surface and then removal of the tissue through a 3mm incision.
There is no LASIK-like flap or painful scraping of the surface such as in photorefractive keratectomy surgery (PRK).
One of the benefits of this surgery is that it is essentially pain free and takes 10 seconds. Patients
experience minimal to no dry eye. Contact sports pose no risk of flap dislodgement unlike LASIK.
There is less biomechanical weakening of the cornea with SMILE as opposed to LASIK. The latter is important as in some patients, laser can lead to an ectasia/keratoconus syndrome which adversely impacts on vision. Clinical studies suggest results of SMILE are better than LASIK for higher levels of myopia. SMILE can now treat hyperopia.
More than 10 million SMILE procedures have been performed worldwide, and it is the gold standard for this keyhole laser surgery.
Lens pulses creating cleavage plane
Image-guided capsulotomy, incisions, and lens division
Key messages
Femtosecond lasers are the standard of care in Lasik surgery and have allowed the evolution of SMILE keyhole laser surgery
Cataract surgery is made easier and potentially safer in some cases with FLACS
health funds do not cover the cost of $1000 per eye. It can be combined with multi-focal implants to maximise near/distance vision. It is useful in very dense cataracts or complicated eyes such as those with corneal endothelial dysfunction (Fuchs Dystrophy) or very shallow anterior chambers.
Presbyopic Lasik Correction
Presbyopia and the requirement for reading glasses/correction will affect all of us to some degree after the age of 40. It is 100% guaranteed, just like death and taxes.
problems. It uses a sophisticated excimer laser algorithm that controls the spherical aberration of the eye. It increases depth of focus by creating distance and computer vision in the dominant eye and reading and computer vision in the non-dominant eye. This increases depth perception and minimises distance blur compared to Lasik monovision.
Femtosecond laser assisted cataract surgery (FLACS)
Bladeless laser femtosecond treatment for cataract and lens replacement surgery is extremely useful. The laser surgery takes 30 seconds to complete and the subsequent cataract surgery under seven minutes. The laser creates computer-generated incisions, as well as breaking up the cataract,
Lasik has been used to treat reading problems in the past. Traditionally this involves setting one eye for near and one for distance. Whilst this is effective in some it can reduce depth perception and cause an imbalance. More importantly patients may complain of reduced distance vision or a monocular blur and may not adapt. Studies show that only 70% of patients are satisfied with Lasik monovision.
Presbyond Laser Blended vision is the fastest growing laser procedure worldwide to correct reading
Hepatocellular carcinoma and chronic Hepatitis B
Iron deficiency in children
Advances in laser surgery
Immunotherapy related cutaneous toxicity
Focal therapy for prostate cancer
Cancer care and exercise
Presbyopic laser treatments are a huge advance in laser correction of reading problems. Complete the self-reflection and claim your CPD time, please scan here
Presbymax is another procedure where one or both eyes can have a multifocal-type laser treatment so that depth perception and distance is not compromised significantly. It can also be reversed if patients are not fully satisfied.
It’s no surprise the inventors of femtosecond technology are Nobel laureates.
Author competing interests – nil
Aspirin and hepatocellular carcinoma
RACGP advice on breast cancer
Supporting patients after a cancer diagnosis
Tic disorders
Aortic stenosis
Radiation oncology
Meet the artist in their studio
Natalie Briney is one of more than 150 artists you can meet and buy work from at this year’s Margaret River Region Open Studios.
By Ara Jansen
She’s not really sure why, but the women featured in Natalie Briney’s paintings usually have white hair. They are not old though and the Margaret River artist prefers to think of them as soft but fierce.
“I just find I’m drawn to women with white hair,” says Natalie. “Maybe it’s a purity thing or maybe it just gives them this sense of peace.”
Natalie works with mixed media and texture and often uses sheet music or other old, printed pages like hymn books as the undercoat or primer for her work, covering it and revealing it as the piece demands.
“I fell in love with hand-written musical notes, which are like veins under the skin. I kept playing with that. The music also covers the canvas as I don’t like the texture of it. Then I build up from there and draw on the girls.”
Natalie is one of 151 artists who are opening their studios and their practices to the public as part of the award-winning annual Margaret River Region Open Studios event. Taking place from September 13 to 28, visitors will be able to visit studios from Busselton to Yallingup
and Dunsborough through to Cowaramup, Magaret River and Augusta.
Almost 30 artists are taking part for the first time alongside veterans like Rebecca Cool, Christian Fletcher, Leon Pericles, Fi Wilkie and Lesley Meaney. The artists opening their spaces are ceramicists, illustrators, furniture makers, glassmakers, installation artists, jewellers, metalwork, milliners, mixed media artists, mosaicists, painters, photographers, potters, printmakers, sculptors, textile
creators, upcyclers and timber craftspeople.
All visits are free in Australia’s largest open studios event and organisers expect more than 12,000 people will hit the art trail, clocking up more than 110,000 studio visits.
Natalie says she has felt hugely encouraged by the local arts community since she settled back in Margaret River after living in the North-West for eight years. This is her fourth open studios event.
Giving up finance and administration, Natalie became a full-time artist after watching the 2014 Lindt Café siege in Sydney. It caused her to seriously reevaluate and consider what she would regret not doing with her life.
Last year, inspired by Sadako Sasaki and the Japanese story of the 1000 paper cranes, Natalie started her Geisha Collection. The pieces feature heads of geishas with white hair and those printed sheets still live underneath the work.
With a wish for peace in her heart, a paper crane has become a new and recurring theme in Natalie’s work. She’s also inspired by Gustav Klimt and Frida Kahlo and is a long time Ken Done fan.
“Over the Christmas and New Year period of 2023/24, I was really struggling. I needed something positive, and I remembered that story. While she did it for different reasons, I realised I could put all my feelings of angst and what I was feeling into the work. So, I kept working out my feelings through painting.
“As artists we are pretty internal and do a lot of stuff in our heads. Painting has become my way of working through hard times. I like to think of my ladies as having a quiet strength and a sense of beauty as well. I think there’s a positive strength to the work. Sometimes I think I’m painting myself – all these different versions of myself in different forms.”
Plan your Margeret River Region Open Studios visits and find out about the artists at www.mrropenstudios.com.au or pick up a copy at Jacksons Drawing Supplies stores around WA. They will also be available in regional visitor centres closer to the event.
Humming through the years
Shey Marque releases her third poetry collection – and it has an unexpected scientific link.
By Ara Jansen
As a child, Shey Marque didn’t voluntarily write poetry. Even as an adult it wasn’t really her cup of tea. That was until a fellow writing student suggested she try reading some contemporary works.
When she discovered Dorothy Parker’s verse novel, The Monkey’s Mask, everything changed. Halfway between a novel and a book of poetry, a whole new world opened up. Shey was no longer going to be a novelist but would be a poet.
The Hum Hearers, recently released and shortlisted for the 2023 Dorothy Hewett Award for unpublished manuscripts, is her third collection. The collection evolved from her final Masters university work, a chapbook of all the stories she had collected about her family dating back to Victorian England.
The award-winning poet is a former clinical haematology and medical research scientist. While one might think that never the twain shall meet, The Hum Hearers, explores the writer’s interest in epigenetics and cellular memory.
The collection explores her family tree and imagines the women before her, creating poetic narratives around their lives and troubles, moving through time to poems about the 2022 death of Shey’s mother from a brain tumour.
Shey writes in the introduction to her book that “our DNA carries a vibrational energy (I’m calling it
the hum)” and through her poems suggest that this hum can move through bloodlines and generations. She set about to trace family memory by following the women in her mother’s line back to Victorian London. That history began in a Covent Garden music hall owned by a maternal forefather John (Paddy) Green from 1842.
Cholera and tuberculosis, bankruptcy, abandonment, migration, war and domestic violence were some of the traumatic events peppering the family history. Shey’s mother’s passing meant the end of any of her stories which might have furthered the family narrative.
“As I wrote these poems over six years, I started to form a personal connection between myself and these women from a couple of centuries ago,” says Shey. “Are the things which happened to these women a coincidence or is it an epigenetic carry-over? What has happened since then is quite significant so I decided that would inform the collection as well, all that imprinting. What carries on to future generations, even if they haven’t been exposed to the same thing.
“My three times great grandmother spoke French and played the violin while her father ran the music hall in Covent Garden. I’ve lived in France, speak French, chose to pick up the violin as an adult and even married a man who creates music hall-style
productions. These are essential things to my life, and I made these choices before I knew anything about these family stories.”
While Shey admits that you never know how accurate the old family stories are, equally she would have never found out anything about her family if she hadn’t embarked on researching them.
“With poetry you are able to transcend the usual limitations of language and explore all these different hypotheses on paper. You can suggest whatever you want and don’t have to wait for proof of anything. The non-linear storytelling aspect of prose poetry means it’s suited to going back and forth in time, entangling past and present and benefits from speculative notions.
“DNA is not silent. You can record it, and it vibrates – it’s a living thing. I most likely have a piece of DNA from these ancestors, even if it’s small.
“You also don’t know how much of it is passed along. There’s some thought that even though these traits are carried through generations, sometimes they can be reversible. I’ll be very interested to continue reading about future scientific advancements on this subject.”
The Hum Hearers (RRP $24.99) is published by UWA Publishing.
Mr Barval – an evolving Margaret River gem
Mr Barval Fine Wines is an exciting newish producer located off Caves Road in the Witchcliffe subregion, right in the heart of the Margaret River wine region. In 2022, Robert Gherardi and family purchased the property from Mr Barval. Rob comes with considerable experience in viticulture and oenology, gained both in the Margaret River region and also a number of vintages in the Piedmonte region of Italy.
At Mr Barval, Rob has reinvigorated one hectare each of Sauvignon Blanc and Shiraz. In 2023 a further 2.5ha of plantings were undertaken, which include Chardonnay, Nebbiolo, Marsanne and Roussanne. However, most of the fruit is purchased from growers in the subregions Wilyabrup, Wallcliffe and Karridale. All winemaking is onsite.
The reviewed wines are all interesting and of very good quality. I love the European influences in his wines. Winemaking is traditional, with minimal intervention. Ferments are with wild yeasts, varieties are often blended, with the introduction of some lesser-known European varieties. Ferments are often initiated with a petit cuvee a week prior to harvest. Oaking is predominantly in seasoned oak.
Mr Barval 2024 Rose Margaret River (RRP $33)
Made from Shiraz grown on the home estate. The style of this wine takes me back to Tavel in Southern France. Shows attractive salmon skin colour. Aromas are restrained, savoury and complex. Palate displays fresh, crisp acidity and minerality. Underlying secondary red berry flavours come through. A really good drink-now Rose style.
Mr Barval 2023 Vino Rosso Margaret River (RRP $33)
Blend of Petit Verdot 57%, Malbec 24%, Merlot 19%.
The aim of this wine is early drinkability, but with some ageing potential, using Bordeaux varieties but excluding Cabernet Sauvignon. I think this has been achieved. Displays a deep beetroot purple colour. Aromatics are savoury, bucolic, brambly, with a touch of soy. Palate shows vibrant fruit – black cherry, satsuma plum. Gamey. Supple and soft. Harmony of all elements.
Mr Barval 2022 Cabernet Malbec Margaret River (RRP $40)
My favourite wine of this tasting. A real Bordeaux blend of Cabernet Sauvignon 70%, Malbec 20%, Merlot 5% and Petit Verdot 5%. The nose is ‘elevated’. Spice, blackcurrant. Cedar from oak. Fruit flavours of blueberry, mulberry, and a touch of allspice. The tannins are fine grained and ‘dusty’. Oak is integral. Firm acid brings everything together. This wine is balanced, integrated and very harmonious. Has the structure to drink well for another 10 years . A very good wine.
Mr Barval 2024 Mistral Margaret River (RRP $40)
A blend of Viognier 73% and Marsanne 27%. Perfumed floral aromas, apricot, peach and coriander stalk. Palate is textural and mineral. Dried apricot and marzipan. A clean acid finish. This is a fascinating wine. Often these Rhone varieties are overtly unctuous. Good viticulture and winemaking have contained that. When the home estate Roussanne is ready (the third Rhone white variety) it will add another dimension to this blend.
Mr Barval 2024 Chardonnay Margaret River (RRP $55)
Fruit for this wine came from Wilyabrup and Karridale, which is the most southerly and coolest subregion giving grapes of high acidity. On the nose the cool climate fruit characters – Nashi pear , nectarine – abound. Palate shows nice weight. Granny Smith apple, rockmelon. A touch of oatmeal from lees contact. Creamy texture from malolactic ferment and battonage. Has had 10 months in French oak, but only 14% was new oak, so oak characters are not overt, but add to the nice balance in this wine.
Mr Barval 2024 Prima Alba Margaret River (RRP $33)
Made from the first Sauvignon Blanc off the estate vineyard. The nose instantly says this is something different for a Margaret River Sauvignon Blanc. Piercing intensity, yet with complexity. Citrus lemon and grapefruit abound. Matured in seasoned oak, and three months on lees have created this style. Palate is pristine and pure. Charming to drink now, with the structure to go 3-4 years. Review by Dr Craig Drummond Master
Medical Forum Podcast
Our podcasts bring you the latest updates and key insights into new treatment options available.
Join our clinical editor Dr Joe Kosterich in conversation with WA specialists to learn more about developments to improve patient outcomes. Our podcasts are now CPD verified. Look for the CPD logo to complete your self-reflection and claim your time.
Topics covered in this series:
Difficult-to-treat depression with Dr Kyle Hoath
Advances in lung cancer management with A/Prof Tim Clay
Holistic management of osteoarthritis with Dr Arash Taheri
Improving outcomes of Aortic Stenosis with Dr Kevin Chung
Managing acute and chronic knee pain with Dr Jean Louis Papineau
Listen on your favourite podcast platform – scan the QR code to follow us!
WINTHROP
CONTACT
Sharon: P: 08 9310 4400
Full-Time General Practitioner
To replace departed Male GP and long-established GP also reducing hours.
• Private Billing Practice
• Well established small but busy General Practice
• Individual large room available in comfortable and relaxed setting
• Fully Accredited
E: admin@hatherleymedical.com.au
Scan QR code for more details
COMO
CONTACT
Practice Manager:
P: 08 6165 2444
E: reception@comogp.com.au
Scan QR code for to email
Opening for VR GP - F/time or P/time Full Private List Available
Unique opportunity to join our family orientated practice in one of Perth’s fastest-growing suburbs.
• FRACGP essential
• Up to 70% private billings
• Enjoy working for a doctorowned, non-corporate, well support, and accredited practice.
Key Features:
• Pathology onsite
• Excellent nursing and administrative support
• Wide variety of patients and strong demand
• Family-friendly, flexible working hours
• Practice is happy to support special interests
• Team-building activities and supportive culture
• Opportunity for your own consulting room if full-time.
General Practitioner (Full-time or Part-time)
Immediate start, $200/hour minimum guarantee (first 3 months), then 68% of billings.
We are a busy, GP-owned, noncorporate practice seeking a motivated and caring GP to join our friendly and supportive team. Whether you’re looking for full-time or part-time work, we offer flexibility, excellent earning potential, and a positive team environment. You’ll be stepping into a practice with full books, and we’ll open to new patients once you start.
About You:
Vocationally Registered (FRACGP or equivalent), AHPRA registration, Strong communication skills and a collaborative mindset.
General Practitioner
Convenient location with adjacent pharmacy and allied health services.
• $200–$300 per hour with 6–7 sessions available
• Modern, well-equipped working environment with excellent facilities
• Skilled nursing staff and onsite non-dispensing pharmacist.
CONTACT
Practice Manager Rachael Hadlow: E: rhadlow@3rdave.com.au www.thirdavenuesurgery.com.au
Scan QR code for more details
PERTH METRO
CONTACT
Sue Stark: P: 08 9346 9325
Western Cardiology is looking for a GP to supervise Exercise ECG and Stress echos on Monday pm and Wednesday am, training provided and access to cardiologists.
E: sues@westerncardiology.com.au
Scan QR code for more details
CONTACT
Please email your CV to Debi: P: 08 6478 3955
E: practicemanager@balcattafamilypractice.com.au
Scan QR code for more details
SCARBOROUGH
What We Off er:
• Supportive work environment with a focus on work-life balance
• Nursing support
• No weekends or afterhours work
• Modern facilities and equipment
• Best Practice software
• Mentorship and training opportunities should you wish to develop skin cancer management skills.
Doctor Opportunity at The Woods Medical Centre
We are looking for an enthusiastic and experienced GP to join our growing team.
The Ideal Candidate:
Strong General Practice Skills:
• Proven experience in providing high-quality patient care
• Excellent clinical skills and a commitment to preventative healthcare
• Experience in managing chronic diseases effectively
• A keen interest in skin cancer management preferred but not essential.
Team Player and Communicator:
• Ability to collaborate effectively
• Excellent interpersonal and communication skills to build rapport with patients.
Essential Requirements:
• FRACGP qualification
• Vocational Registered
• AHPRA registration.
CONTACT
Practice Manager: P: 0478 021 910
E: practicemanager@thewoodsmedical.com.au
Scan QR code for more details
MOUNT LAWLEY
BALCATTA
SWAN VIEW
What We Off er:
• Current AHPRA registration and right to work in Australia
• FRACGP (or equivalent), VR General Practitioner. Non-VR on pathway to achieving VR registration are welcome to apply
• Current medical indemnity insurance.
Eastern Perth Metro GP Practice looking for FT or PT GPs
We are looking for an enthusiastic and experienced GP to join our growing team.
What we can off er You:
• DPA location – suitable for doctors under the 10-year moratorium
• Experienced and well-trained staff
• VERY Competitive service fee rates
• Agreed Guarantee period. 70% Tops of Mixed Billing
• Supportive GPs
• Family friendly culture, with great community links
• Reliable clinical software
• Potential Pathway to equity options.
CONTACT
Forward CVs to Practice Manager: E: practice.manager@swanviewfp.com.au
Scan QR code for more details
MEDIICAL C CE ENTRRE FOR R LEASE - MAANDUURAH
Positioned in the heart of Mandurah, this purpose-built 505sqm Medical Center offers an exceptional opportunity for healthcare providers seeking a prime location.
With its spacious layout, modern amenities, and patient-friendly design, this facility is ideal for a range of medical, allied health, or specialist services.
Building
Current
2
Reverse
$220,000.00
Outgoings: $50,000.00
Available:
Development Approved for Medical Centre
Estimated completion August 2026
Excellent street frontage exposure
27 Parking Bays
We are seeking Expressions of Interest from experienced medical operators for: Medical Centre 495m2
Pharmacy 200m2
This exciting site offers plenty of traffic exposure and convenience making it a key location at the northern entry to the growing communities of Anketell, South Wandi and surrounding areas.
Contact exclusive Leasing Agent Kong Wai Wong on 0421 883 338 to secure
Onsite parking
GP, Physio and Psychology in same building
Includes use of waiting area, kitchen
$200 half day; $300 full day
Admin
advantage
character of the
–
since
Building, built 1898 & just a short distance from the Murray St Mall. With plenty of pharmacies, medical centres, dentists, physios, and allied health services, this office would suit a medical business well, bringing you into the heart of the City* (subject to council approval).
Set up now to take advantage of the City Centre University campuses & Student Accommodation soon to open (estimated 1st Semester 2026). 180sqm (approx), set over 2 floors with large open display room, service area & 2 separate appointment rooms downstairs. 1st floor has an office and open plan area with male & female toilets. Designated parking for 1 car off private, gated laneway adjacent to the building.
Plenty of foot traffic passing by, client parking available in nearby Wilson & CPP Parking.
East End revival is happening! Make this space your own (STCA if required).
Rent from $300psqm + GST = $54,000p.a + GST
Budget Outgoings = $26,000p.a + GST
Parking $300 per bay/pcm + GST
* Subject to council change of use approval
HERE FOR GOOD
Partner with Australia’s largest independent practitioner network and experience freedom over your billings, appointment types, and clinic care.
Explore our WA GP vacancies
WHAT DOES YOUR FOREVER HOME LOOK LIKE?
At Humphrey Homes, every home we design and build starts with listening. We take the time to understand your vision, your lifestyle and your budget - then translate that insight into thoughtful spaces that are beautifully crafted. By integrating architecture, interior design and construction under one roof, we make the journey to your forever home harmonious, effortless and deeply personal
To experience our creativity and craftsmanship firsthand, don’t miss our upcoming Open House Event on 16/17 and 23/24 August. Register your interest at humphreyhomes.com.au