2 Introducing the Bud and Sue Selig Hub for Surgical Data Science
4 Training for the Fight: Army Military-Civilian Trauma Team Training (AMCT3) and the Realities of Large Scale Combat Operations
6 Improvement in diastolic dysfunction after bariatric and metabolic surgery is associated with enhanced nitric oxide activity
9 A Collaborative Approach to Building a Pediatric Robotic Thoracic Surgery Program at Children’s
11 Integrating Mental Health in a Comprehensive Care Model for firearm Injury Patients
13 Utilizing Large Language Models for Surgical Case Length Prediction
15 Thoughts at the Scrub Sink: The More Things Change, the More They Stay the Same
16 Thoughts at the Scrub Sink: Treating the Human Spirit
17 New Faculty: Leading The Way
18 Remembering Robb Edwards
Faculty Listing
From Tim Ridolfi, MD, MS
A
Milestone Gathering: The Inaugural Meeting of the Edwin Ellison Surgical Society
On October 3, 2025, the Department of Surgery proudly hosted the inaugural meeting of the Edwin Ellison Surgical Society (EESS) at the Medical College of Wisconsin, marking the beginning of a new tradition connecting alumni, faculty, and trainees. Held just before the ACS Clinical Congress in Chicago, the event brought together more than 50 attendees from across the country to celebrate the legacy of MCW’s surgical training program.
Established in honor of Dr. Edwin H. Ellison, the first full-time Chair of Surgery at MCW, the society was created to foster mentorship, scholarship, and collaboration among generations of surgeons trained at the institution. The meeting reflected that mission through engaging presentations, meaningful discussion, and shared pride in the department’s history.
Dr. Steve Kappes (’82) opened the program with a historical perspective on the evolution of surgical training at MCW. He was followed by an outstanding group of alumni speakers, including Dr. Anahita Dua (’17), vascular surgeon and Associate Professor at Harvard Medical School; Dr. Kelly Collins (’13), transplant surgeon and Associate Professor at the University of Wisconsin–Madison; Dr. Rachel Greenup (’11), Chief of Breast Surgical Oncology at Yale’s Smilow Cancer Hospital; and Dr. Larry Bucshon (’93), cardiothoracic surgeon and former U.S. Congressman. Each shared insights from their careers and reflected on how their MCW training shaped their professional journeys.
The program concluded with the presentation of honorary memberships to Dr. Chris Ellison and Dr. Jon Ellison, the son and grandson of Dr. Edwin Ellison, recognizing their family’s enduring contributions to surgical education and leadership. The day ended with a reception at the Kimpton Journeyman Hotel in Milwaukee’s Historic Third Ward, where alumni, faculty, and residents reconnected and celebrated the shared heritage of the MCW Department of Surgery.
The inaugural meeting was a resounding success—honoring the department’s history while charting a vibrant course for future of the EESS. With strong enthusiasm and broad participation, the Edwin Ellison Surgical Society is poised to become a lasting forum for connection, mentorship, and collaboration.
Introducing the Bud and Sue Selig Hub for Surgical Data Science
Anai Kothari, MD, MS
Assistant Professor of Surgery, Division of Surgical Oncology
The intersection of data science, artificial intelligence, and surgical care represents one of the most promising frontiers in modern healthcare. Recognizing this potential, the Department of Surgery established the Bud and Sue Selig Hub for Surgical Data Science with a clear vision: to harness advanced analytics and AI to enhance surgical care delivery throughout Wisconsin and beyond. Officially launched in July 2024, the Selig Hub was founded on four core missions: fostering collaborative research across disciplines, solving time-sensitive data challenges, sharing knowledge to enhance data and AI literacy, and providing centralized data science support for surgical investigators.
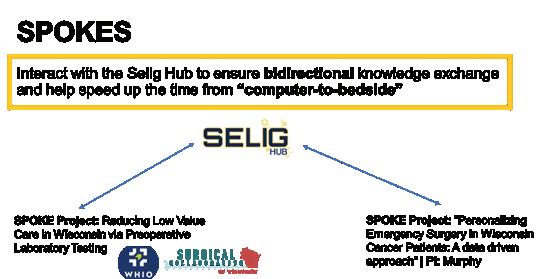
The Selig Hub has been designed to address real-world problems through practical applications of data science. This approach was based on how other successful technology implementations in healthcare and other industries have bridged the gap between innovation and practical utility. By focusing on actionable insights and user-centered solutions, the Selig Hub aims to ensure that discoveries directly impact patient outcomes, operational efficiency, and the overall quality of surgical care through a Hub and Spoke model. In this model, the Hub serves as a centralized resource that includes tools and expertise (“Co-Laboratories”) that can support Spoke Projects (Figure 1). Most importantly, however, is how to take all these buzzwords and operationalize them into a program that can realize this vision.
Figure 1. A schematic overview the “Hub and Spoke” design of the Selig Hub for Surgical Data Science.
Hub Infrastructure and Service Development
In its inaugural year, the Selig Hub has evolved from concept to functional entity, establishing several core “Hub” services that can support research and quality improvement initiatives Depart-
ment-wide.
Emma Staszkiewicz
Senior Administrative Assistant, Division of Surgical
Oncology
REDCap and Database Support Services: Data collection remains a fundamental challenge in surgical research. Through strategic collaboration with the Clinical & Translational Science Institute (CTSI), the Selig Hub can facilitate REDCap support for investigators. This includes establishing new REDCap projects, consultation on database design, implementation assistance, and training for research teams. Over time, this will evolve to streamline the database development process through standardizing data definitions and creating templated database builds.
Access to Large-Scale Surgical Datasets: Dr. Patrick Murphy created the first Selig Co-Laboratory to improve access to curated, surgically relevant datasets at scale that can be accessed using a virtual computing environment. These resources enable investigations that would be impossible within the constraints of single-institution data and reduces redundancy when using these datasets.
HIPAA-Compliant AI Access: Another service developed this year has been our partnership with MCW Information Technology and the AN.AI Lab to provide HIPAA-compliant access to generative AI models, including OpenAI's advanced language models. This infrastructure addresses a critical gap in the research ecosystem, where commercial AI tools offer tremendous potential but lack the security safeguards necessary for healthcare applications. By providing this access and a testing environment for using state-of-theart generative AI models almost immediately after their release in a secure and compliant environment.
"Surgiclinomics" EHR Data Access: Accessing and analyzing electronic health record (EHR) data can be a bottleneck for outcomes research and quality improvement initiatives. The Selig Hub has developed "Surgiclinomics," a streamlined process for accessing and analyzing clinical data to help move from question to insight. This includes standardizing regulatory approvals, data extraction queries, data pre-processing pipelines, and analytical templates. Through collaborations with both the CTSI and the Data Science Institute (Biostatistics), the Hub has created a more efficient pathway for investigators to use existing clinical data and reduce manual abstraction.
Spoke Projects will be able to use these support services and tools to complete projects that align with the goals of the Selig Hub, even
when project teams may not have the expertise immediately available to use data science and AI techniques.
Beyond F&MCW: External Collaboration Development
Recognizing that the most impactful innovations often emerge at the boundaries between disciplines and institutions, the Selig Hub is actively developing external collaborations to extend our capabilities and reach.
Academic Collaborations
The Selig Hub has initiated promising collaborations with UW-Milwaukee, Marquette University, and MSOE, each bringing unique strengths to our shared mission. These partnerships allow matching domain experts with specific challenges, creating multidisciplinary teams that can move quickly from concept to implementation. For example, a surgical workflow optimization project might combine MSOE's expertise in process engineering with MCW’s clinical knowledge and data infrastructure.
Inaugural Selig Symposium for Surgical Data Science
A key part of the hub is knowledge sharing and dissemination. The Selig Hub for Surgical Data hosted the inaugural symposium on September 28th, 2024. This 2-day event included a pre-conference social event at American Family Field and the main conference was held at the MCW Alumni Center. A total of 74 registrants from 19 regional and national institutions participated (Figure 2). Participants reviewed the fundamental mechanisms and capabilities of recent advances in artificial intelligence, specifically generative-type models, and how they could be integrated into surgical practice.
relationship between Surgeons in AI and entrepreneurship with a talk titled “From Scalpel to Silicon: Empowering Surgeons in AI and Entrepreneurship.” Finally, Dr. Tignanelli presented “A Comprehensive Journey Through the AI Lifecycle with Sepsis and Rib Fractures as Case Studies,” providing a deep dive into AI’s practical applications in clinical care. Together, these talks showcased the diverse ways AI is shaping the field of surgery.
Other national panelists included Dr. Tyler Loftus from the University of Florida and Dr. Majid Afshar from the University of Wisconsin-Madison. In addition to national thought leaders in AI and data science, several experts from Froedtert and the Medical College of Wisconsin participated in panels including Dr. Bill Hogan, Brad Taylor, Dr. Sam Thalji, Kevin Boggs, Dr. Rachel Morris, Debbie Cray, and Dr. Melek Somai.
Conclusion
In the first year, the Bud and Sue Selig Hub for Surgical Data Science has established itself as a valuable resource for the Department of Surgery, creating infrastructure and services that enhance our research capabilities and support our clinical mission. By bringing together expertise in data science, AI, and surgical care, the Selig Hub will continue to build capacity to address complex challenges and improve outcomes for surgical patients.
References for Utilizing Large Language Models for Surgical Case Length Prediction, Page 13
1. Childers CP, Maggard-Gibbons M. Understanding Costs of Care in the Operating Room. JAMA Surg. 2018;153(4):e176233-e176233. doi:10.1001/jamasurg.2017.6233
2. Macario A. What does one minute of operating room time cost? J Clin Anesthesia. 2010;22(4):233-236. doi:10.1016/j. jclinane.2010.02.003
3. Eijkemans MJC, Houdenhoven M van, Nguyen T, Boersma E, Steyerberg EW, Kazemier G. Predicting the Unpredictable. Anesthesiology. 2010;112(1):41-49. doi:10.1097/aln. 0b013e3181c294c2
4. Chung P, Fong CT, Walters AM, Aghaeepour N, Yetisgen M, O’Reilly-Shah VN. Large Language Model Capabilities in Perioperative Risk Prediction and Prognostication. JAMA Surg. Published online 2024. doi:10.1001/jamasurg.2024.1621
Dr. Heather Lyu from MD Anderson, Dr. Kevin Sexton from Vanderbilt University, and Dr. Chris Tignanelli from the University of Minnesota delivered three keynote presentations, each offering a unique perspective on the intersection of AI and surgery. Dr. Lyu, MD, MBI, presented “Automating Real-World Data Collection: Innovations and Transformations in Clinical Research,” and Dr. Sexton explored the
5. Shoham OB, Rappoport N. CPLLM: Clinical prediction with large language models. PLOS Digit Heal. 2024;3(12):e0000680. doi:10.1371/journal.pdig.0000680
Figure 2. Photos from the Inaugural Selig Symposium for Surgical Data Science.
Training for the Fight: Army Military-Civilian Trauma Team Training (AMCT3) and the Realities of Large Scale Combat Operations
Nathan Carlson, MD
Adjunct Assistant Professor of Surgery, Division of Trauma and Acute Care Surgery
As I prepare for my 6th Combat Deployment this coming fall, I look back at my time here at the Medical College of Wisconsin. As an Active-Duty Army General Surgeon, I was selected in 2019 to be part of an experiment by the Office of the Surgeon General. The Army Military-Civilian Trauma Team Training (AMCT3) at the Medical College of Wisconsin was a part of a rapidly expanding initiative throughout the military to partner with high-volume Level 1 trauma centers with the intention of sharpening the skills of military surgeons in anticipation of future conflict. With my prior assignment having been at a sleepy Army Community Hospital, the transition into a high-volume Level I trauma center marked a dramatic shift in clinical intensity, and it set the foundation for the next phase of my career. Now, five years later, I’ve completed a Trauma/Acute Care Surgery fellowship and am far more prepared for my military mission than ever.
In the evolving landscape of global conflicts, the U.S. Army has recognized the imperative to prepare its medical personnel for the complexities of large-scale combat operations (LSCO). LSCO is conflict with a near-peer military force, characterized by limited freedom of mobility secondary to the threat environment, uncertain air superiority, and high volumes of casualties. This is in distinct contrast to the last 20 years of counterinsurgency (COIN) combat operations which saw patient movement from the point of injury to the continental USA in as few as 3 days. Central to this preparation is the Army Military-Civilian Trauma Team Training (AMCT3) program, designed to embed military medical professionals within high-volume civilian trauma centers. This initiative not only enhances the clinical skills of Army trauma surgeons but also addresses the challenges highlighted in recent analyses of battlefield medical care timelines.
The AMCT3 Program: Bridging Military and Civilian Expertise
Joshua Dilday, DO
Adjunct Assistant Professor of Surgery, Division of Trauma and Acute Care Surgery
Initiated in response to directives from the 2017 National Defense Authorization Act, the AMCT3 program aims to sustain and advance the trauma care competencies of Army medical personnel. By partnering with leading civilian trauma centers, the program offers Army surgeons, nurses, and medics exposure to a diverse array of traumatic injuries, many of which mirror the complexities encountered in combat scenarios.
A program similar to MCW, at Vanderbilt University Medical Center (VUMC), Army physicians, certified registered nurse anesthetists (CRNAs), and registered nurses are embedded for approximately three years. During this tenure, they function as full-time staff, gaining invaluable experience in a high-acuity Level I trauma center. This collaboration ensures that military medical professionals maintain readiness for deployment, equipped with the skills honed in a demanding civilian environment. This partnership not only benefits the military personnel by providing hands-on experience with severe trauma cases but also enriches the civilian institutions through the infusion of military medical expertise.
Challenging the "Golden Hour to Golden Day" Paradigm
Recent discourse in military medical circles has scrutinized the applicability of the "golden hour" concept to LSCO scenarios. In their article, "'Golden day' is a myth: rethinking medical timelines and risk in large scale combat operations," Joshua Dilday and colleagues argue that extending the "golden hour" to a "golden day" misrepresents the physiological realities of trauma care. They emphasize that delays in evacuation and treatment inherent in LSCO can significantly increase mortality rates, underscoring the need for timely medical interventions.
This analysis reinforces the importance of programs like AMCT3, which prepare military medical personnel to operate effectively even when traditional evacuation timelines are compromised. By training in civilian trauma centers where they encounter a broad spectrum of injuries and treatment scenarios, Army medical teams develop the adaptability and proficiency required to manage casualties in prolonged field care situations.1
Measurable Outcomes and Future Directions
The efficacy of the AMCT3 program is evident in the clinical activity of its participants. A study conducted at the University of Chicago reported that embedded Army trauma surgeons engaged in over 400 trauma evaluations and approximately 190 operative cases annually. These cases included a significant number of laparotomies, thoracotomies, and vascular procedures—critical skills for battlefield surgery. Such exposure ensures that military surgeons not only meet but exceed the readiness metrics established for deployment.2
Looking ahead, the Army aims to expand the AMCT3 program, establishing additional partnerships with civilian trauma centers nationwide. This strategic initiative seeks to create a robust network of training sites, ensuring that Army medical personnel across various specialties have access to the clinical experiences necessary for combat readiness.
Conclusion
As the nature of warfare evolves, so too must the preparation of military medical personnel. The AMCT3 program exemplifies a forward-thinking approach, leveraging civilian partnerships to enhance the trauma care capabilities of Army medical teams. By embedding within high-volume trauma centers, these professionals gain the critical experience needed to save lives on the battlefield, even in the challenging contexts of large-scale combat operations. Such collaborations not only bolster military medical readiness but also foster a mutual exchange of knowledge that benefits both military and civilian healthcare systems.
See page 12 for references.
@MCWSurgery
@MCWSurgOnc
@MCWMIGS
@MCWTraumaACS
@MCWPancreasProgram
Referemces for Integrating Mental Health in a Comprehensive Care Model for firearm Injury Patients, Page 11
1. Wintemute, GJ. (2015) The epidemiology of firearm violence in the twenty-first century United States. Annual Review of Public Health, 36, 5-19.
2. Semenza, D. C., Stansfield, R., Silver, I. A., & Savage, B. (2023). Reciprocal neighborhood dynamics in gun violence exposure, community health, and concentrated disadvantage in one hundred US cities. Journal of urban health, 100(6), 11281139.
3. deRoon-Cassini, T. A., Mancini, A. D., Bonanno, G. A. & Rusch, M. D. Psychopathology and resilience following traumatic injury: a latent growth mixture model analysis. Rehabil. Psychol. 55, 1–11 (2010).
4. Timmer-Murillo, S. C., Melin, S. J., Tomas, C. W., Geier, T. J., Brandolino, A., Schramm, A. T., ... & deRoon-Cassini, T. A. (2023). Mental health and health-related quality of life after firearm injury: a preliminary descriptive study. Annals of internal medicine, 176, 1010-1012.
5. Timmer-Murillo, S. C., Schroeder, M. E., Trevino, C., Geier, T. J., Schramm, A. T., Brandolino, A. M., ... & deRoon-Cassini, T. A. (2023). Comprehensive framework of firearm violence survivor care: a review. JAMA surgery.
6. Brandolino, A., deRoon-Cassini, T. A., Biesboer, E. A., Tomas, C. W., Woolfolk, M., Wakinekona, N. A., ... & Trevino, C. M. (2024). Improved follow-up care for gun violence survivors in the Trauma Quality of Life Clinic. Trauma Surgery & Acute Care Open, 9(1), e001199.
7. Williams, J. L., Hambrick, E. P., Gleason, V. L., Hardt, M. M., Henschel, A. V., Wilfred, S. A., ... & Moncure, M. (2024). Evaluating skills for psychological recovery with gunshot injury survivors in a hospital-based early intervention program. American journal of orthopsychiatry, 94(2), 159.
8. Williams, J. L., Gleason, V. L., Wilfred, S. A., Friend, R., Howard, J., Freese, S. A., ... & Peters Baker, J. (2024). Development and Overview of a Hospital-Based PTSD Screening and Early Intervention Program for Gunshot Injury Survivors: The RISE Program. Illness, Crisis & Loss, 10541373241269029.
CONNECT WITH MCW SURGERY
@MCWSurgery
@MCWEndoSurg
@MCWMIGS
@MCWPancProgram
@MCWPedSurg
@MCWTraumaACS
@MCWSurgResearch
@MCWSurgOnc
@MCWVascSurg
@MCWSurgery
@MCWGenSurg_Residents
Improvement in diastolic dysfunction after bariatric and metabolic surgery is associated with enhanced nitric oxide activity
Sarah Suh, MD
General Surgery Resident
Heart failure with preserved ejection fraction (HFpEF) affects greater than 50% of people with heart failure, and its prevalence has been increasing over time1. HFpEF is characterized by diastolic dysfunction and impaired ventricular relaxation2. There are a variety of risk factors that contribute to HFpEF, with obesity-associated heart failure representing more than 70% of HFpEF patients1. A key mechanism underlying obesity-associated HFpEF is the accumulation of excess visceral fat, which triggers inflammatory pathways, such as interleukin-6 (IL-6) that elevates reactive oxygen species (ROS) production. This leads to endothelial-cardiomyocyte dysfunction by reducing nitric oxide (NO) bioavailability, which reduces NO-dependent cyclic guanosine monophosphate (cGMP)-protein kinase G (PKG) signaling between endothelial cells and cardiomyocytes, ultimately leading to cardiac hypertrophy, stiffness, and HFpEF2.
Metabolic and bariatric surgery (MBS) significantly improves diastolic dysfunction associated with HFpEF, but the mechanism of improvement remains unknown3. Studies have demonstrated that while weight loss through caloric restriction may alleviate symptoms in HF patients, it often fails to produce significant changes in cardiac structure or function4. In the STEP-HFpEF trial, semaglutide alleviated symptoms, reduced physical limitations, enhanced exercise capacity, and promoted weight loss in patients with obesity and HFpEF, with the extent of benefits correlating to the degree of weight reduction5. Although weight loss is beneficial, we have previously published in a rodent model of sleeve gastrectomy, obesity, and cardiac dysfunction, that diastolic dysfunction in rats improves independent of weight loss or calorie restriction3. While studies have found a positive effect of sleeve gastrectomy on IL-6 and TNF-α, the weight-loss independent impact of sleeve gastrectomy on endothelial function and ROS have not been examined in a model of diastolic dysfunction6. The purpose of this study was to test the hypothesis that sleeve gastrectomy in rodents improves diastolic dysfunction by enhancing NO signaling in a weight-loss independent manner.
We obtained five-week-old, male C57BL/6J mice, and they were fed either a high-fat diet (n=36) or a low-fat diet (n=12) for ten weeks prior to sleeve gastrectomy or sham surgery. Four experimental groups were created: (1) high-fat diet ad-libitum sleeve gastrectomy (SG) (n=12), (2) high-fat diet pair-fed sham surgery (SHPF)
Tammy Kindel, MD, PhD
Vice Chief, Division of Research, Associate Professor of Surgery, Division of Minimally Invasive and Gastrointestinal Surgery
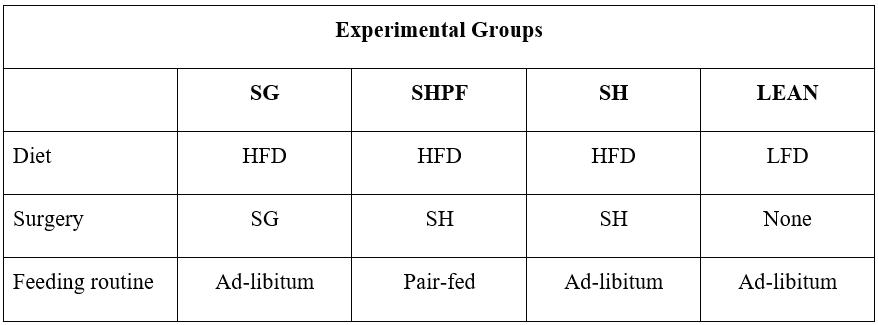
(n=12), (3) high-fat diet ad-libitum sham surgery (SH) (n=12), and (4) low-fat diet mice who did not undergo an operative intervention (LEAN) (Table 1). To control for the effect of weight loss and calorie restriction on surgical outcomes, the SHPF group was fed the average daily food intake of the SG mice on the same corresponding post-operative day to induce a similar weight loss and body weight as SG by forced calorie restriction instead of gastrectomy. At twelve weeks post-surgery, mice were euthanized, and blood and tissue samples (left ventricle, aorta, liver, urine, mesenteric resistance arteries) were collected for molecular analysis.
Table 1. Diet, post-operative feeding routine and surgical intervention for experimental groups
SG: high-fat diet ad-libitum sleeve gastrectomy, SHPF: high-fat diet pairfed sham surgery, SH: high-fat diet ad-libitum sham surgery, LEAN: lowfat diet mice who did not undergo an operative intervention
For SG animals, a midline laparotomy was created, and the fibro-fatty tissue of the greater curvature was taken up to the gastroesophageal junction with scissors. A large vascular orange hemoclip was used to remove the lateral stomach tissue including the greater curvature of the lateral stomach. The abdomen was closed with suture. For sham animals, the same procedure was performed except the stomach was not divided. Rodent TTE was performed in anesthetized mice at 11 weeks of age (1 week pre-operatively) and at 11 weeks post-operatively. Molecular analysis was performed on preserved tissue from the thoracic aorta, left ventricle, urine and mesenteric resistance arteries to assess protein expression and activity via histology, enzyme-linked immunosorbent assay, and western blot.
SG (66%), 9 SHPF (75%), 10 SH (83%), and all 12 LEAN mice survived surgery. Prior to surgery, there were no significant differences
in body weight for all three mouse groups fed a high-fat diet: SG 32.8 ± 3.1 g, SHPF 30.9 ± 2.6 g, SH 32.8 ± 3.4 g, p = 0.32. All highfat diet groups weighed significantly more than those fed a low-fat diet prior to surgery (28.1 ± 2.0, p = 0.004). Postoperatively, SG and SHPF groups did not differ in body weight after two weeks. At the study end, the SH group weighed significantly more than the other surgical groups (Figure 1).
Figure 1. Percentage total body weight change from post op day 0 for experimental groups
SG: high-fat diet ad-libitum sleeve gastrectomy, SHPF: high-fat diet pairfed sham surgery, SH: high-fat diet ad-libitum sham surgery, LEAN: lowfat diet mice who did not undergo an operative intervention
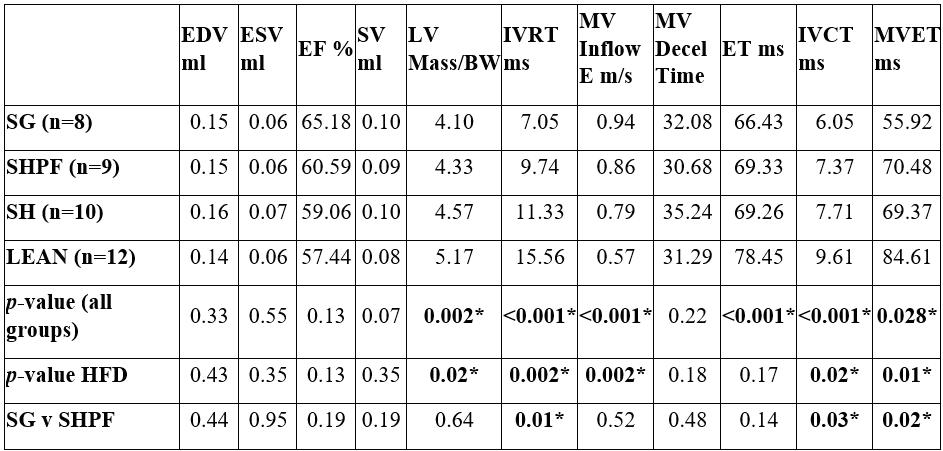
As seen in Table 2, post-operatively, there was significance among high-fat diet surgical groups for isovolumetric relaxation time (IVRT) (p < 0.001) and this difference remained significant on post-hoc analysis specifically comparing SG to the SHPF mice (p = 0.01, p = 0.03, and p = 0.02 respectively).
Table 2. A comparison of post-op cardiac structure and function between experimental groups
SG = sleeve gastrectomy, SHPF = sham pair fed, SH = sham, EDV = end diastolic volume, ESV = end systolic volume, EF = ejection fraction, SV = stroke volume, LV Mass/BW = left ventricular mass divided by body weight, IVRT = isovolumetric relaxation time, MV inflow velocity, MV decel time = MV deceleration time, ET = ejection time, IVCT = isovolumetric contraction time, MVET = mitral valve ejection time
As the observed improvements in diastolic function appeared to occur independent of weight loss and calorie restriction, our molecular analysis focused on comparing the SG and SHPF groups (Table 3). There was no statistically significant difference noted in ROS fluorescence in the thoracic aorta between SG and SHPF groups. NO expression in the mesenteric resistance artery was also similar between groups. Total urine nitrates/nitrites were significantly high-
er among the SG mice compared to SHPF (p = 0.03), and cardiac cGMP expression was greater among the SG mice (p = 0.02).
Table 3. Outcomes of molecular assays between SG and SHPF groups
This study demonstrates that SG significantly improves diastolic function in mice with diet induced obesity and metabolic syndrome, confirming our prior studies in rats and existing clinical observations of the beneficial impact of MBS on HFpEF3. Our findings reveal that this improvement in diastolic function, as evidenced by IVRT on echocardiogram, is achieved independent of weight loss, as the SG group exhibited statistically significant improvements in diastolic parameters compared to the SHPF group despite similar post-operative weight trajectories. This weight-loss independence suggests that mechanisms beyond simple caloric restriction contribute to the cardiac benefits of SG.
While our initial hypothesis posited that enhanced arterial NO bioavailability would mediate improved endothelial-cardiomyocyte crosstalk and subsequent diastolic function recovery, our results present a more nuanced picture. We did not observe a significant increase in NO expression in the mesenteric resistance artery in the SG group compared to the SHPF group, nor did we detect differences in ROS within the thoracic aorta. This suggests that the anticipated reduction in oxidative stress and enhancement of arterial NO in this specific vascular bed may not be the primary driver of the observed diastolic improvements in this model within the study timeframe.
Despite the lack of significant change in mesenteric resistance arterial NO, we found that the SG group exhibited significantly elevated urine nitrate/nitrite levels and increased cardiac cGMP expression compared to the SHPF group. Urine nitrate/nitrite levels are often used as a proxy measure for systemic NO production7. cGMP is a key downstream second messenger molecule of NO in cardiomyocytes, primarily regulating cardiac contractility and preventing hypertrophy8. The concurrent elevation of these markers in the SG group raises the possibility that SG may enhance NO signaling through pathways that are not primarily localized to the endothelium as we found no difference in NO or ROS in two vascular structures, mesenteric resistance artery and thoracic aorta. This could involve increased NO production from other sources such as parenchymal
hepatocytes, kidney or the intestine itself9. Several emerging therapeutic strategies aim to modulate NO/cGMP signaling to counteract the pathways driving cardiovascular disease development. These include folate supplementation to restore and enhance NO synthase activity, as well as soluble guanylyl cyclase stimulators to boost cGMP production10. The potential of SG to simultaneously influence both aspects of this pathway presents a promising therapeutic approach for heart failure in the future.
The findings in our study demonstrated that SG improves diastolic dysfunction independent of weight loss by enhancing systemic NO and cGMP mediated signaling in cardiac tissue. SG represents a promising intervention for obesity related HFpEF, offering unique metabolic and cardiovascular benefits beyond weight reduction in comparison to glucagon-like peptide-1 receptor agonists, which are largely weight dependent11. As these findings are novel and unexplored in existing literature, future research is necessary to identify additional molecular pathways contributing to these cardioprotective effects and to explore their clinical relevance in patients with HFpEF.
Note: Significant portions of this text have been submitted to Surgical Endoscopy for publication and are currently under review.
References
1. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM (2006) Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 355:251-259.
2. Zile MR, Baicu CF, Ikonomidis JS, Stroud RE, Nietert PJ, Bradshaw AD, Slater R, Palmer BM, van Buren P, Meyer M, Redfield MM, Bull DA, Granzier HL, LeWinter MM (2015) Myocardial stiffness in patients with heart failure and a preserved ejection fraction. Circulation. 131:1247-1259.
3. Kindel TL et al. (2019) Sleeve gastrectomy in obese Zucker rats restores cardiac function and geometry toward a lean phenotype independent of weight loss. J Card Fail. 25(5):372-379.
4. de las Fuentes L, Waggoner AD, Mohammed BS, et al. (2009) Effect of Moderate Diet-Induced Weight Loss and Weight Regain on Cardiovascular Structure and Function. J Am Coll Cardiol. 54(25):2376–2381.
5. Borlaug BA, Kitzman DW, Davis MJ, Rasmussen S, Barros E, Butler J, Einfeldt MN, Hovingh GK, Moller DV, Petrie MC, et al. (2023) Semaglutide in HFpEF across obesity class and by body weight reduction: a prespecified analysis of the STEP-HFpEF trial. Nat Med. 29(9):2358-2365.
6. Viana EC et al. (2013) Gastric bypass and sleeve gastrectomy: the same impact on IL-6 and TNF-α. Prospective clinical trial. Obes Surg. 23(8):1252-61.
7. Tsikas D (2007) Analysis of nitrite and nitrate in biological fluids by assays based on the Griess reation: appraisal of the Griess reaction in the L-arginine/nitric oxide area of research. J Chromatogr B analyt Technol Biomed Life Sci. 851(1-2):5170.
8. Francis SH (2011) The role of cGMP-dependent protein kinase in controlling cardiomyocyte cGMP. Circ Res. 107(10)11641166.
9. Bultinck J, Sips P, Vakaet L, Brouckaert P, Cauwels A (2006) Systemic No production during (septic) shock depends on parenchymal and not on hematopoietic cells: in vivo iNOS expression pattern in (septic) shock. FASEB J. 20(13):23632365.
Scan to learn more about “The Word on Medicine”, a weekly radio show hosted by Drs. Douglas Evans and Rana Higgins, highlighting innovation and discovery across MCW! Past episodes are available in podcast format on iHeartRadio.
10. Blanton R (2020) cGMP signaling and modulation in heart failure. Journal of Cardiovascular Pharmacology. 75(5):385-398.
A Collaborative Approach to Building a Pediatric Robotic Thoracic Surgery Program at Children’s
Caroline Maloney, MD, PhD
Assistant Professor of Surgery, Division of Pediatric Surgery
Robotics has transformed the field of adult thoracic surgery, and its utilization has only accelerated over the last two decades. The translation of robotic thoracic surgery to the pediatric population presents unique challenges due to differences in patient size, available robotic instrumentation, and case volume. At Children’s Hospital of Wisconsin in collaboration with Froedtert Medical Center, we are pioneering a dedicated pediatric robotic thoracic surgery program, integrating advanced robotic technology to meet the unique needs of our young patients. Through collaboration, innovation, and thoughtful adaptation of robotic techniques, we aim to expand minimally invasive options for children requiring complex thoracic procedures, improving outcomes by reducing pain and recovery time. This article highlights our experience, early successes, and the future of robotic thoracic surgery in pediatric care.
Robotics has pushed the limits of minimally invasive surgery (MIS) through enhanced visualization, improved precision and dexterity, enabling surgeons to perform increasingly complex operations through smaller incisions. Over the last two decades the utilization of robotics in thoracic surgery has grown exponentially. A recent report from the Society of Thoracic Surgery General Thoracic Surgery Database (GTSD) reports a yearly increase in utilization of 15-34% since 2019 across all thoracic procedures in North America.1 Although data shows it is at least equivalent to video assisted thoracoscopic surgery (VATS) when it comes to oncologic outcomes, robotic approaches have a lower likelihood of converting to an open procedure and may facilitate an MIS approach for complex operations such as sublobar resections or sleeve lobectomy.2 As a result, robotic-assisted surgery is quickly becoming the standard of care for lung cancer operations and has been applied to nearly all procedures in the chest, including surgery of the esophagus and mediastinum with outstanding short-term results published by high-volume robotic surgeons.3
Pediatric surgery is often considered the last bastion of general surgery as it encompasses a wide array of congenital, infectious, malignant, and acquired conditions in the abdomen and chest of children- from neonates to young adults. With its numerous advantages over traditional straight stick endosurgery – including 3D visualization, 10-15X magnification, tremor filtration, and dexterity in even the smallest of spaces— robotic-assisted surgery, in theory, should be ideal for managing the diverse procedures that encompass a pediatric surgical practice. However, its widespread adoption within pediatric surgery has been slow.4 The biggest limitation in the application of robotic technology relates to the inappropriate size of the instruments for small children and infants (smallest
Paul Linsky MD
Associate Professor of Surgery, Division of Cardiothoracic
Surgery
Program Director, Cardiothoracic Surgery Fellowship
available instruments are 8mm). As a result, pediatric surgeons typically turn to laparoscopy or VATS using 3 or 5mm instruments.4 Despite these challenges, robotic utilization in pediatric abdominal surgery and urology is steadily rising. A review of the Pediatric Health Information System (PHIS) database from 2010-2019 revealed a 7.5% growth in the number of pediatric surgeons operating robotically with foregut, colon and biliary representing the most common procedures.5 However, pediatric robotic thoracic surgery is much less common and literature on the topic is scare.6 While VATS is commonly used for congenital lung lesions, esophageal anomalies and spontaneous pneumothorax in adolescents, more complex thoracic procedures in older children are often referred to adult thoracic surgery centers for robotic expertise or performed open.
In 2023 Children’s Wisconsin began developing one of the first dedicated pediatric robotic thoracic programs in the nation. To accomplish this, we have established a novel model of close collaboration and mentorship between a pediatric surgeon (Dr. Caroline Maloney) and a thoracic surgeon with significant robotic experience (Dr. Paul Linsky). Although pediatric surgical training includes MIS and open thoracic surgery, adult thoracic surgery has evolved into a distinct subspecialty with a dedicated two-year fellowship and an increasing emphasis on robotics. During this specialized training a thoracic surgeon gains experience not only with the complexity and variations of lung and mediastinal anatomy, but also navigating the robotic arms, depth perception through a 3D console, and the lack of direct tactile feedback within the narrow confines of the chest where inadvertent injury to the airways or blood vessels can be catastrophic. In pediatric cases, these challenges are further compounded by the smaller size of the thorax. Our goal is to forge a long-term collaboration that aims to safely expand the MIS options offered at Children’s Wisconsin, enhancing the surgical care for complex thoracic disease in children and adolescents. With the help of our Robotic Surgery Working Group at Children’s lead by Dr. John Densmore, we have taken a measured and stepwise approach to the translation of robotic thoracic surgery to the pediatric arena.
The first step we took was to establish a working relationship with our adult robotic thoracic surgery colleagues. The involvement of local robotic experts in the planning phase of programmatic development has been invaluable not only for the implementation of new technology, but also for preoperative planning to help to avoid inefficiencies that can prolong operative and turnover time.
They recommended creation of a consistent robotic team as well as standardized protocols of bed and patient positioning, anesthesia care, monitoring, port placement, and instrument choice—all independent factors involved in streamlining the process. Observational training at Froedtert, not only for the pediatric surgeon but the entire robotic team, was performed early and often. A dedicated bedside assistant at Children’s, Ruth Povlich PA-C, was identified and got direct training from experienced thoracic surgery PAs. The importance of the robotic team cannot be overstated, and their active participation in programmatic development is crucial to good outcomes, shorter operative times, and the ultimate success of robotic thoracic surgery at Children’s.
Aside from the prerequisite simulation required for credentialing, we found that frequent practice on the Da Vinci simulator, particularly learning to maneuver within the confines of the thorax and perform various lung exposures, was helpful in establishing surgeon comfort. Credentialing for the surgeons at each other’s institutions facilitated early proctored cases as well as pediatric surgeon participation in more complex adult cases prior to their adaptation of these procedures in children. The dual console of the Da Vinci platform allows the experienced proctor and learner to have not only the same view but essentially has the same hands. The learner can observe and participate in the operation with graduated autonomy, yet it allows for the proctor to assume control of the robotic arms in an instant, ultimately providing an extra level of safety to the patient. This allowed the pediatric surgeon to develop confidence and robotic surgical proficiency under the guidance of experienced adult robotic surgeons and robotic manufacturer representatives simultaneously.
Prior to the performance of any robotic thoracic cases at Children’s, the parameters for appropriate patient and case selection were established. It can be useful to classify thoracic operations by level of difficulty as reported by Geraci et al.8,7 For our first cases at Children’s, we chose “beginner” level operations in adolescents, which we are accustomed to performing using a VATs approach as pediatric surgeons. These included peripheral lung wedge resections for spontaneous pneumothorax and metastatic nodules as well as an apical chest wall tumor. When performing more intermediate to advanced procedures such a lobectomy or the repair of a recurrent traumatic diaphragmatic hernia, we focused on completing the procedure in a step-wise fashion— the pediatric surgeon learner performing the more basic parts of the operation and our thoracic
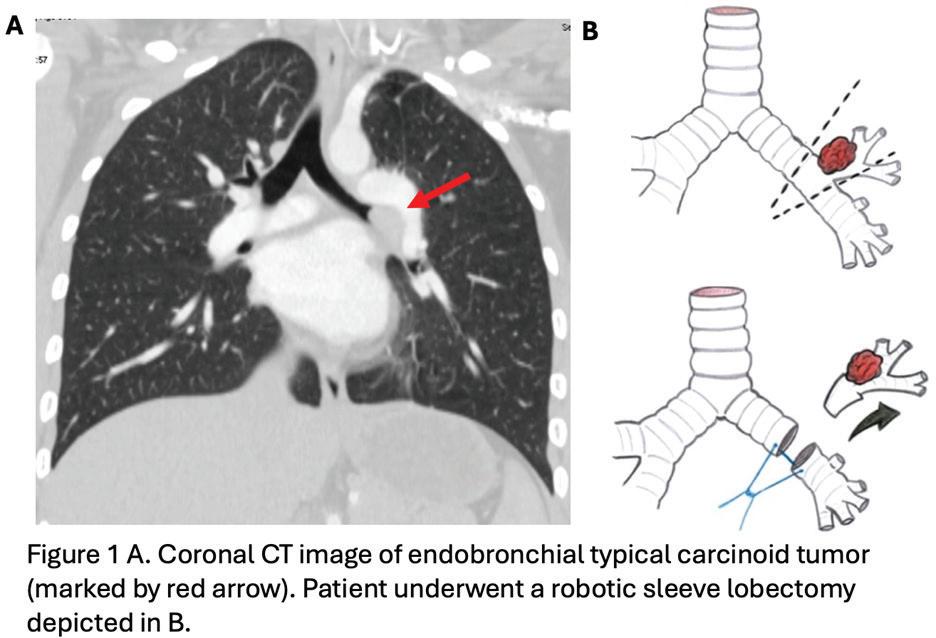
surgeon taking over to demonstrate the more difficult aspects of the case.7 Our hope is that with time and experience the pediatric surgeon will slowly develop these skills under the mentorship of the adult thoracic team. In the nascency of our program, we were referred a
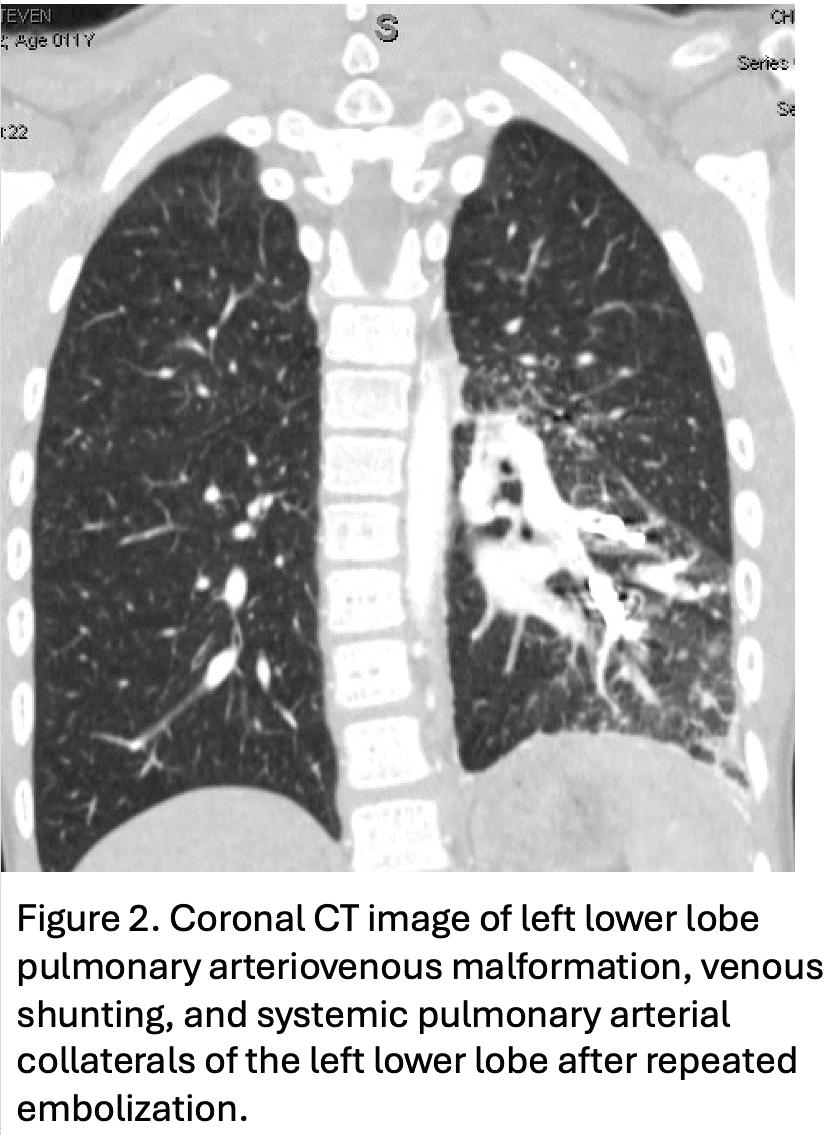
few complex procedures including an endobronchial carcinoid tumor requiring a sleeve lobectomy (Fig 1) and a pulmonary arteriovenous malformation with extensive large collaterals that had failed multiple embolization attempts and required left lower lobectomy (Fig 2). Rather than perform these extremely complex and high-risk procedures with a relatively new team at Children’s, we elected to perform these cases at the adult hospital. We believed this approach accomplished our goal of expanding the MIS options available to these children while simultaneously adding to the experience for the pediatric surgeon who was still able to participate in the operation at Froedtert.
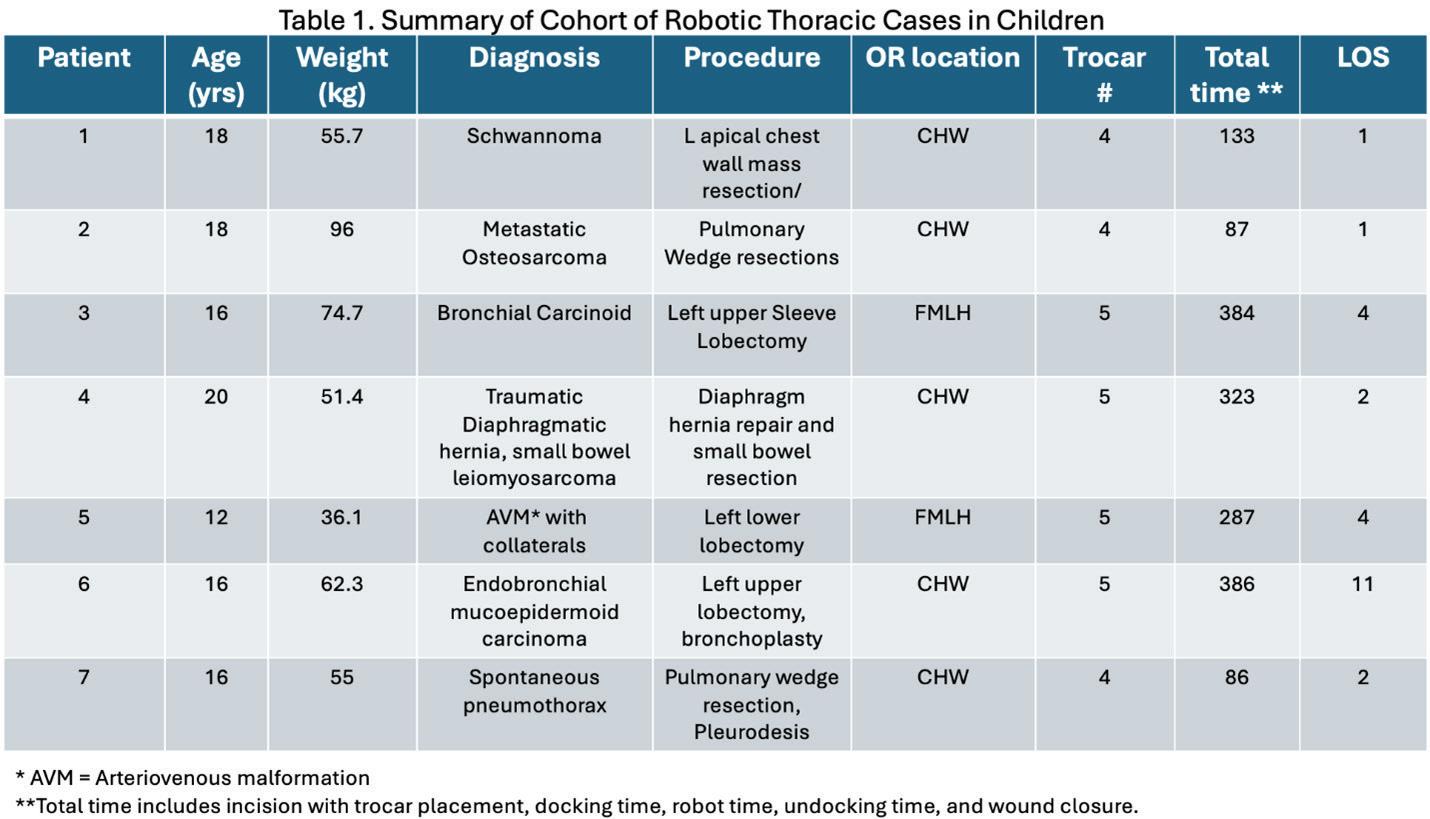
Utilizing this framework of collaboration and shared expertise has allowed for the successful development of a pediatric robotic surgery team over the course of the last year. Since April 2024 we have completed 7 collaborative robotic thoracic cases in our pediatric patients, with 5 of them occurring at Children’s Wisconsin (Table 1). Our approach, emphasizing safety and progressive skill expansion in the setting of institutional collaboration, has strengthened the robotic surgery teams across both medical centers. As technology advances (and downsizes) we can expect a broader application of these techniques, ultimately improving outcomes for our youngest patients and we are proud to be leading the way.
See page 14 for references.
Integrating Mental Health in a Comprehensive Care Model for firearm Injury Patients
Sydney Timmer-Murillo, PhD
Assistant Professor of Surgery, Division of Trauma and Acute
Care Surgery
Firearm violence is a public health crisis in the United States, deleteriously impacting our communities in a myriad of ways.1,2 A vital yet often unexamined aspect of firearm injury prevention is the tertiary prevention efforts aimed to limit the impact and spread of violence. Simply put, we know very little about the experiences of interpersonal firearm injury survivors and their post-injury needs. Constraints in funding have restricted knowledge on the aftermath of firearm injury, making the literature sparse regarding long-term effects of firearm injury, particularly as it relates to mental health outcomes.²
What we do know is firearm injury rates are disparate in our community, and furthermore, those who are shot are often plagued by socioenvironmental risk factors that adversely impact recovery and quality of life.² After any traumatic injury chronic non-remitting mental health concerns, including posttraumatic stress disorder (PTSD) and depression, occur in approximately 20% of patients.3 Given the initial evidence, in relatively recent years, firearm injury has been understood through a biopsychosocial disease model.1 This approach thus encourages the exploration of risk factors and socioenvironmental contexts that influence recovery and aims to mitigate the ripple effects of firearm injury, prevent both physical and psychological complications, and reduce the likelihood of recurrence. Whereas previous research tends to silo factors that relate to firearm injury, this neglects the meaningful intersections of recovery that may shape healthcare.
Mental Health Trajectories after Firearm Injury
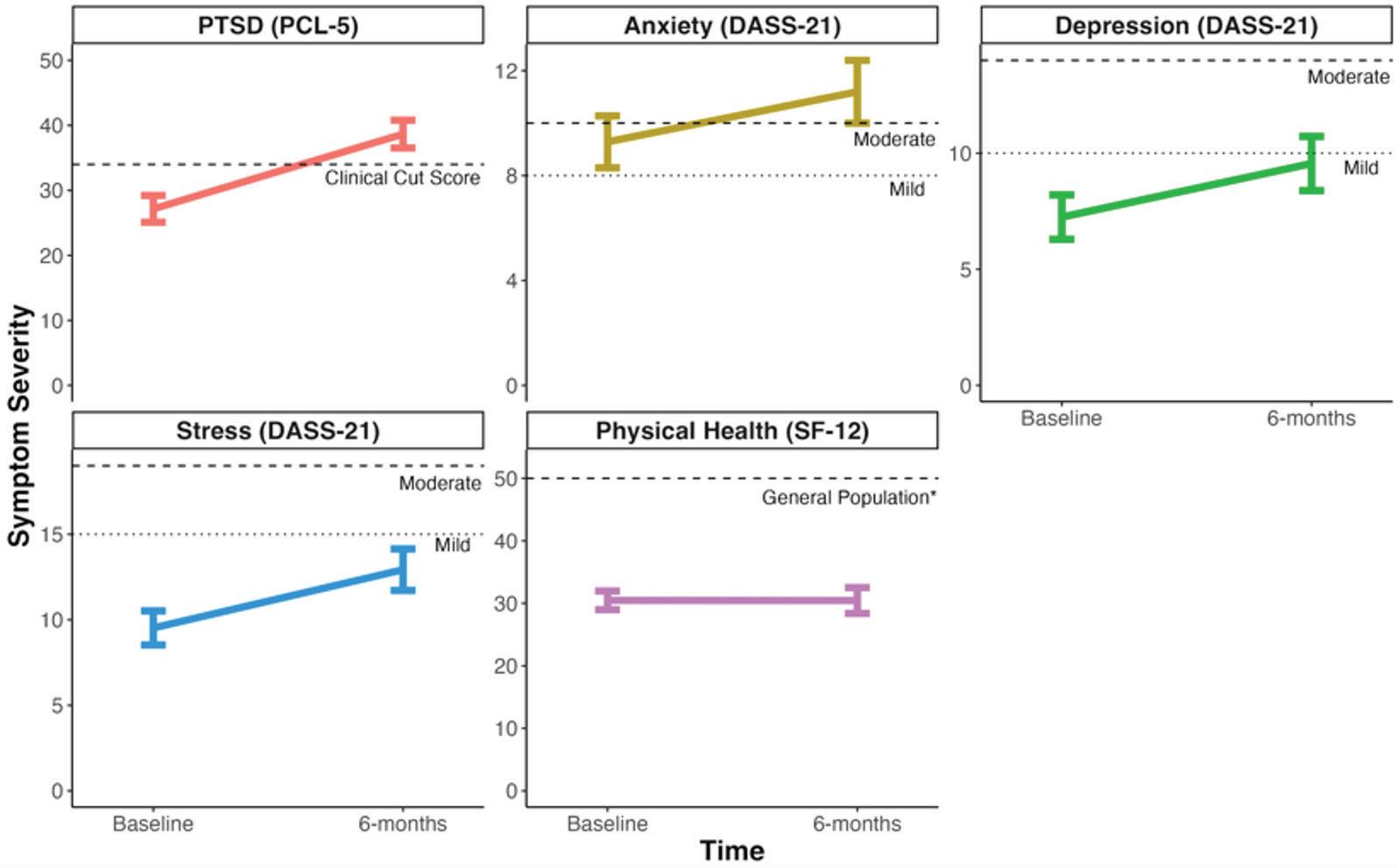
Our team has evaluated mental health and quality of life outcomes acutely after firearm injury and 6 months post-injury, comparing them with outcomes of patients injured in motor vehicle collisions (MVCs). Findings indicate that, contrary to general trauma literature, symptoms of anxiety, depression, and PTSD often persist or worsen among firearm injury survivors4 (see Figure 1), whereas MVC survivors typically show symptom decline over time. These findings align with research showing increased Medicaid claims for psychological diagnoses in the year following firearm injury.
This further aligns with the evidence highlighted in our JAMA Surgery publication5, which highlights that the psychological burden of firearm violence is significantly greater than that of nonviolent injuries, with survivors of assaultive injuries being twice as likely to experience long-term disability. Importantly, over half of these
Timothy Geier, PhD
Assistant Professor, Director, Outpatient Trauma and Acute Care Surgery Psychology Services; Director, Trauma and Health Psychology Rotation for Residency Program
survivors develop persistent PTSD and/or depression, underlining the urgent need for timely and accessible mental health care.
Figure 1. Mental Health Outcomes across Time for Firearm Injury
Patients
A Framework for Comprehensive Care
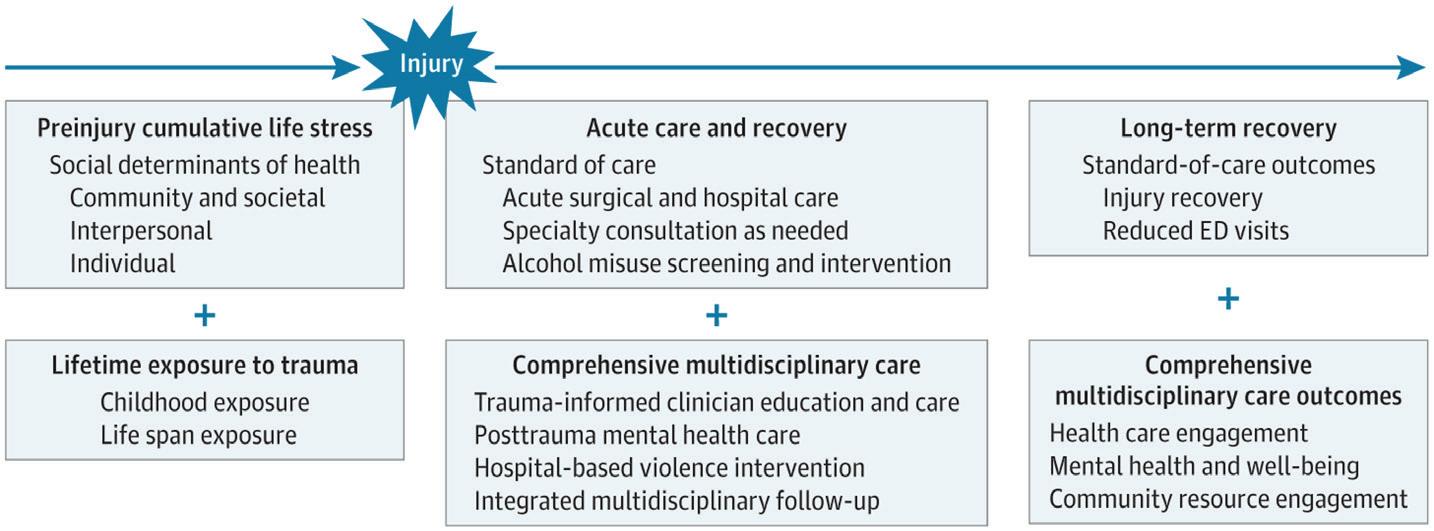
In response to the evidence of need, a collaborative team from the Divisions of Trauma and Acute Care Surgery and the Emergency Medicine developed and published a model in JAMA Surgery, outlining how trauma centers can deliver comprehensive care to survivors of firearm injury5. This model includes a thorough review of the latest literature, highlighting key clinical considerations for trauma centers (Figure 2). The review emphasizes the importance of understanding the patient’s history of pre-injury stress and trauma, implementing holistic, trauma-informed care, and integrating psychological services and violence-prevention programs. These elements aim to address the biopsychosocial nature of firearm injury and demonstrate how tailored patient care can enhance outcomes for survivors. The proposed model is structured into three pillars:
• Pillar A) acknowledging pre-injury trauma history;
• Pillar B) providing comprehensive acute care
• Pillar C) offering comprehensive long-term care.
This three-pillar model accounts for the socioecological context
of firearm violence, acknowledging that its impact is not evenly distributed across populations. As documented in our JAMA Surgery review, Black or African American individuals are more likely to experience nonfatal firearm injury than any other racial or ethnic group, and survivors of firearm violence remain at heightened risk of being shot again.
efficacy and outcomes of the model is critical for promoting and refining best practice guidelines and informing national implementation.
Looking Forward
Moving forward through a Comprehensive Injury Center pilot award, we will be able to test this model using data collected in the past two years. The data collected through this pilot study will be particularly valuable given the 2022 guidelines from the American College of Surgeons Committee on Trauma, which now require all trauma centers to screen for risk of psychopathology and provide referral to intervention.
Figure 2: Model for Comprehensive Care to Patients of Firearm Injury
From: Comprehensive Framework of Firearm Violence Survivor Care: A Review. JAMA Surg. 2023;158(5):541-547. doi:10.1001/jamasurg.2022.8149
Implementation at Froedtert & MCW
At Froedtert & MCW, we operationalize this in several ways. First, our Trauma Psychology services provide both inpatient and outpatient treatment for firearm injury survivors. The Trauma Quality of Life (TQOL) clinic, led by Dr. Colleen Trevino, also addresses patients’ comprehensive needs through appointments 7-10 days post-discharge with a multidisciplinary team.6 The clinic’s team — including a trauma nurse practitioner, psychologist, physical therapist, social worker, and hospital-based violence interrupter — ensures a patient-centered, trauma-informed approach. This approach allows subsequent follow-up visits to be tailored to patients' individual needs, addressing both the physical and psychological aspects of recovery.
Beyond direct patient care, implementing this model has significant implications for how we train future trauma care providers. At Froedtert & MCW, we have developed interdisciplinary educational modules that teach trauma-informed care principles across specialties. Surgeons, nurses, psychologists, residents and social workers participate in shared learning experiences that break down traditional silos and foster collaborative, holistic approaches to complex cases.
This framework has begun to be implemented nationally, yet there is still limited research evaluating data across the three pillars.7,8 Although Froedtert & MCW’s pioneering comprehensive trauma program — including Trauma Psychology and the TQOL clinic — has been in effect for several years, we have yet to evaluate the whole of our programming based on this model. Assessing the
Our comprehensive care model not only meets these requirements but exceeds them by addressing the unique needs of firearm injury survivors. By systematically and rigorously evaluating our approach across all three pillars of the model, we aim to develop evidence-based recommendations for trauma centers nationwide. This work has the potential to transform how we conceptualize and foster recovery from firearm injury, moving beyond a focus solely on physical healing to a truly biopsychosocial approach that acknowledges the complex interplay between trauma history, acute care experience, and long-term outcomes.
As we continue to refine and expand our implementation of this comprehensive care model, the lessons learned from our division’s programming will inform not only our upcoming Comprehensive Injury Center pilot study but also the broader national conversation about best practices in trauma care for this vulnerable population. By bridging research and practice, we can continue advancing a care model that prioritizes holistic recovery and long-term well-being.
References for Training for the Fight: Army Military-Civilian Trauma Team Training (AMCT3) and the Realities of Large Scale Combat Operations, Page 4
1. Dilday J, Webster S, Holcomb J, Barnard E, Hodgetts T. 'Golden day' is a myth: rethinking medical timelines and risk in large scale combat operations. BMJ Mil Health. 2024 Nov 21:e002835. doi: 10.1136/military-2024-002835. Epub ahead of print. PMID: 39578018
2. Plackett TP, Jaszczak N, Hampton DA, Prakash P, Cone J, Benjamin A, Rogers SO, Wilson K. Trauma surgical skill sustainment at the University of Chicago AMEDD Military-Civilian Trauma Team Training Site: an observation report. Trauma Surg Acute Care Open. 2024 Jan 24;9(1):e001177. doi: 10.1136/tsaco-2023-001177. PMID: 38287924; PMCID: PMC10824070.
Utilizing Large Language Models for Surgical Case Length Prediction
Introduction
Adhitya Ramamurthi, MD, MS
General Surgery Resident
Operating room (OR) scheduling is a complex and nuanced endeavor. Even small errors in predicting surgical case lengths can cause patient delays, overtime for staff, postponed procedures, and substantial financial costs.1 It is estimated that each minute of idle or underutilized OR time costs between $15–$20.2 Historically, hospitals have relied on surgeon estimates and institution-specific electronic health record (EHR) algorithms to determine case length. Yet these methods often leave room for improvement, leading to wasted resources and suboptimal OR efficiency.3
Recent advances in artificial intelligence (AI), especially in large language models (LLMs), offer new possibilities. While traditional machine learning (ML) models focus on structured inputs (e.g., data found in a tabular format), LLMs have the ability to process and understand unstructured data (e.g. clinical notes). LLMs are what tools like OpenAI’s ChatGPT, Google’s Gemini, and Anthropic’s Claude use to enable natural language understanding to complete tasks like answering questions, generating new content, and engaging in conversational interactions. An emerging capability is for LLMs to make direct predictions on input data, which may provide a novel approach for surgical case length prediction.4-5 The hypothesis is that unstructured data contain information relevant to surgical case length such as comorbidities, surgical risk factors, imaging findings, or even subtle contextual clues often lost in discrete data fields. By using an LLM to process this unstructured clinical data, we may have the ability to improve the accuracy of surgical case length prediction.
In our recent retrospective study using data from Froedtert&MCW, we explored how both base and custom fine-tuned LLMs compared to our current scheduling methods. We analyzed 2,500 elective surgical cases from 2017 to 2023. Each case included at least one year of clinical notes, such as history and physicals, consult reports, operative note, and discharge summaries. Because the sheer volume of text often exceeded LLM context-window limits (e.g. the maximum amount of information an LLM can parse at once), a summarization pipeline was developed. We used a general-purpose LLM to condense the patient’s clinical history, ensuring the model retained relevant data while discarding redundancy.
Eleven different LLMs were assessed, including several “base” (not
Anai Kothari, MD, MS
Assistant Professor of Surgery, Division of Surgical Oncology
domain-adapted) versions (GPT-4o, GPT-4, GPT-3.5, Claude 3.7, Mistral, Llama-3, Phi-3) and two “fine-tuned” LLMs (GPT-4-FineTune and GPT-3.5-Fine-Tune). We then compared each model’s predictions to two real-world baselines: (1) “EHR-Estimated”, automatically generated case length prediction by our institution’s electronic health record (Epic), and (2) “OR-Scheduled”, the final case length estimate used by our OR scheduling staff (based on EHR data, surgeon input, and scheduler expertise).
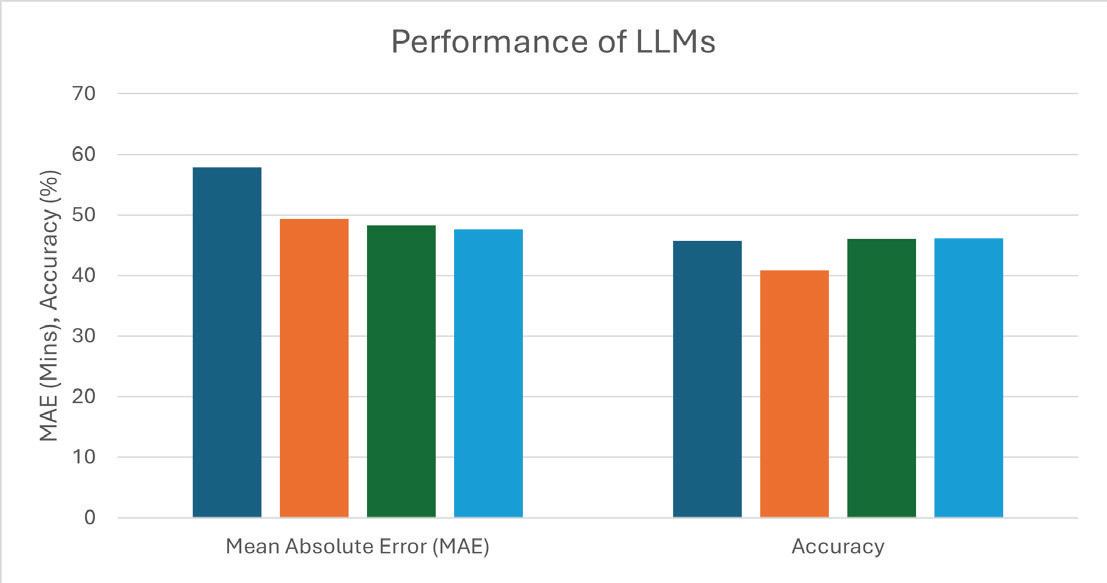
Key Findings
1. Fine-Tuned LLMs Outperform Standard Methods: GPT-4Fine-Tune and GPT-3.5-Fine-Tune achieved predictive accuracy (i.e., predicted length within 20% of the actual) of approximately 46%. This surpassed our OR-Scheduled estimate (~41% accuracy) and on par with the EHR-Estimated approach (~46% accuracy). While the fine-tuned models had only a slight edge in average error compared to OR-Scheduled times (~48 minutes), their higher accuracy rate across various case types was statistically significant. (Figure 1)
2. Base Models Lagged Behind: Non-fine-tuned GPT-4 and Claude 3.7 performed comparably or slightly better than the EHR’s baseline estimates, but none of the other base models matched the performance of the fine-tuned LLMs. Smaller and older models performed significantly worse than the newer, larger, reasoning LLMs.
3. LLM Performance Varies by Surgical Specialty: Our fine-tuned models noticeably improved performance in average error and accuracy with vascular surgery (-8.57 min average error, +14.29% accuracy) and general surgery (-5.01 min average
error, +10.67% accuracy) when compared to OR-Scheduled. All models (including fine-tuned ones) were less accurate in predicting case lengths for highly complex procedures such as transplant and cardiac surgery. This suggests that further domain-specific training or specialized data engineering might be needed for certain surgical subfields.
4. External Validation Appears Promising: We replicated our methods at an affiliated community hospital, finding consistent benefits of fine-tuned LLMs across a smaller cohort of 500 cases. This supports that our model can generalize to different practice settings if institutional data is readily available.
Practical Implications & Next Steps
From an operations perspective, more accurate estimates of case length can lead to reduced overtime, fewer scheduling issues, and a less stressful work environment for clinical teams. Patients also benefit from shorter waiting times and fewer last-minute rescheduling. By focusing on free-text clinical documentation that is already part of standard practice, the pipeline can integrate seamlessly without needing extensive new data entry. Additionally, this approach has the potential to improve even further with improvements and evolution in LLMs (which still are a relatively new model type).
Despite promising results, some areas would benefit from deeper investigation. For instance, interpretability remains a concern. Many clinical and administrative leaders want explanations beyond a numeric estimate that justify the predictions. Researchers could develop user-friendly interfaces or dashboards offering supporting “rationales” derived from the model’s reasoning. Additionally, specialty areas like liver and kidney transplant or highly complex cardiovascular surgery had less reliable performance. Further fine-tuning on subspecialty cases, or a more targeted approach that harnesses domain-specific data, may bolster accuracy for these difficult to predict procedures. Finally, confidentiality and security remain essential as the pipeline inevitably involves sensitive patient information.
Our study illustrates that LLMs, when domain-adapted, can strengthen surgical case length prediction. Many challenges still persist including improving accuracy of predictions and interpretability, however these tools still show remarkable potential. Over time, they may help reduce unnecessary expenditure, streamline operations, and improve patient care.
See page 3 for references.
References for A Collaborative Approach to Building a Pediatric Robotic Thoracic Surgery Program at Children’s, page 9
1. Towe, Christopher W et al. “The Society of Thoracic Surgeons General Thoracic Surgery Database: 2024 Update on Outcomes and Research.” The Annals of thoracic surgery vol. 119,4 (2025): 733-743.
2. Servais, Elliot L et al. “Conversion to Thoracotomy During Thoracoscopic vs Robotic Lobectomy: Predictors and Outcomes.” The Annals of thoracic surgery vol. 114,2 (2022): 409-417.
3. Oh, Daniel S et al. “Robotic-Assisted, Video-Assisted Thoracoscopic and Open Lobectomy: Propensity-Matched Analysis of Recent Premier Data.” The Annals of thoracic surgery vol. 104,5 (2017)
4. Jacobson, Jillian C, and Samir R Pandya. “Pediatric robotic surgery: An overview.” Seminars in pediatric surgery vol. 32,1 (2023
5. Richards, Holden W et al. “Trends in robotic surgery utilization across tertiary children's hospitals in the United States.” Surgical endoscopy vol. 35,11 (2021): 6066-6072
6. Svetanoff, Wendy Jo et al. “Robotic-assisted resection of mediastinal tumors in pediatric patients.” Seminars in pediatric surgery vol. 32,1 (2023)
7. Linsky, Paul L, and Benjamin Wei. “Training in robotic thoracic surgery.” Journal of visualized surgery vol. 4 1. 4 Jan. 2018
8. Geraci, Travis C et al. “Beyond the learning curve: a review of complex cases in robotic thoracic surgery.” Journal of thoracic disease vol. 13,10 (2021)
Referrals, Transfers, and Consultations
ADULT PATIENTS
All Non-cancer Requests Referrals: 800-272-3666
Transfers/Consultations: 877-804-4700
Clinical Cancer Center Referrals: 866-680-0505
Transfers/Consultations: 877-804-4700
PEDIATRIC PATIENTS
Referrals/Transfers/Consultations: 800-266-0366
Acute Care Surgery: 414-266-7858
For more information, please visit mcw.edu/surgery.
Thoughts at the Scrub Sink: The More Things Change, the More They Stay the Same
Mallory Hunt, MD, MSTR
Assistant Professor of Surgery, Division of Cardiothoracic Surgery
Last week I found myself sitting in the operating room early on a Thursday morning, reviewing my patient’s imaging while she was wheeled into the room and moved to the OR table. As I scrolled through her CT, half of my brain created a mental roadmap for the procedure and the other half was listening to the usual sequence play out around me: the nurses introducing themselves and asking if she would like some warm blankets; the anesthesia team pre-oxygenating the patient; the clinking of instruments being removed from sterile trays and aligned on the table; the moment of silence following “Ma’am, can you hear me?” followed by intubation. Time to stand up, I thought to myself. Like clockwork I walked over to the bedside. Bronchoscopy to confirm the double lumen tube. Lines in order? Excellent. Time to rock and roll.
It's been a little over six months since I joined the team here at Froedtert and began my career as a junior thoracic surgery attending. I remember finishing up my fellowship in Philadelphia and thinking to myself – how is this ever going to work? I had been at the same institution for 12 years. It was where I opened my first medical textbook, where I completed all of my clerkship rotations, where I graduated medical school and started residency. It was where I spent years walking in the same hallways day in and day out, operating with the same faces, looking out the same windows, staring at the same clocks late into the nighttime hours. Where I met my husband and grew our family. I knew nothing of what it would be like anywhere else, or how I would transition to someplace new. On the eve of my first day as an attending I asked my closest mentor for advice. He said to me: “be yourself. And remember, the more things change, the more they stay the same.”
I’ve thought a lot about his words over the last six months, and I think I am starting to finally realize what he meant. While the physical structure and the faces may be different, there is an oddly comforting consistency to the operating room that I suspect is one of the reasons I fell in love with surgery in the first place. It doesn’t matter where you are or what team you are on: in the operating room, there is an unspoken “code,” a set of rules and a sequence of events that never changes and provides familiarity and routine. It is not surprising to me that many surgeons are former or current athletes. We are people who thrive in the environment of a team, taking turns leading and following, our “pre-game” routines playing out in almost ritualistic fashion. We scrub with purpose, put our gloves on the same way every single time, fix the OR lights just so, arrange our instruments in a line. We “do it the same way every time,” in concert and, most importantly, never alone.
And so now, six months in, I find myself not only appreciative of this consistency but also grateful for the opportunity to land somewhere new. Building upon the familiar customs and integrating new techniques or approaches, all the while supported by a fantastic team, has been so rewarding for me. I am so appreciative of the opportunities that you all have given me to grow, and look forward to everything that is to come.
References for Thoughts at the Sink: Treating the Human Spirit, page 16
1. Halaszynski TM, Juda R, Silverman DG. Optimizing postoperative outcomes with efficient preoperative assessment and management. Critical care medicine. 2004 Apr 1;32(4):S7686.
2. Kamarajah SK, Bundred J, Weblin J, Tan BH. Critical appraisal on the impact of preoperative rehabilitation and outcomes after major abdominal and cardiothoracic surgery: a systematic review and meta-analysis. Surgery. 2020 Mar 1;167(3):5409.
3. Poldermans D, Hoeks SE, Feringa HH. Pre-operative risk assessment and risk reduction before surgery. Journal of the American College of Cardiology. 2008 May 20;51(20):191324.
4. DiMatteo MR. Social support and patient adherence to medical treatment: a meta-analysis. Health psychology. 2004 Mar;23(2):207.
5. Brown-Johnson C, Cox J, Shankar M, Baratta J, De Leon G, Garcia R, Hollis T, Verano M, Henderson K, Upchurch M, Safaeinili N. The Presence 5 for Racial Justice Framework for anti-racist communication with Black patients. Health Services Research. 2022 Dec; 57:263-78.
Thoughts at the Scrub Sink: Treating the Human Spirit
Adrienne Cobb, MD, MS
Assistant Professor of Surgery, Division of Surgical Oncology
There are many milestones and competencies to be met during medical training. In medical school, your grades, test scores and rotation evaluations are the priority. Once you have decided on a specialty, survived match day, and entered your field of choice, your focus shifts to being the best at that specialty. I think this is particularly true of surgical specialties. Not only do you have to be able to care for patients on the floor, in the ICU, and in the clinic, but you must learn, and at least partially master, a myriad of procedures to be considered a safe and competent surgeon. It is a daunting task that we have all completed to take care of patients. With the advent of Entrustable Professional Activities (EPAs) by the American Board of Surgery, even more emphasis will be placed on trainees’ ability to complete the technical/clinical aspects of surgery. While I think technical proficiency is paramount to a career in surgery, I would assert that there is another curriculum that remains neglected.
I completed my General Surgery residency at Loyola University Medical Center in Maywood, IL. One of the primary mantras for the hospital was “Treat the human spirit”. Admittedly, my coresidents and I would mildly scoff at the notion of treating the human spirit in hour 28 of a brutal trauma call, but as I have gained more perspective in treating patients that motto rings true. After many years of stressing about learning the steps of a Whipple, I now know that surgery is often the most straightforward portion of the patient’s care. It is not enough to be able to successfully perform a life-changing surgery if you cannot get the patient to the operating room. We know that preoperative risk assessment, prehabilitation and ensuring appropriate postoperative care are integral to the patient’s long-term outcomes.1-3
What do we do with the patient who does not seem to want to help themselves? We have made the referrals, explained the plan, given time for questions, involved our social work and case management colleagues to help facilitate transportation or address financial concerns, and still can’t seem to make progress toward surgery. I believe the innate response in these cases is that the patient is not invested in their care, doesn’t want to be well, and perhaps is not worth the resources being used to help them through this process. Patients get lost to follow up, and in the case of cancer care, often meet an unnecessary demise because we do not go looking for them or miss an opportunity early on to intervene. Often, the patients most impacted are those that present with significant social challenges.
Dr. Robin DiMatteo defines patient compliance or adherence as patient acceptance and follow-through with treatment recommendations.4 The canon of Psychology literature regarding the science of patient adherence is vast. In a review of the literature from 1948 to 2001, Dr. DiMatteo found that patient adherence to medical recommendations was correlated with structural (ex. marital status, living arrangement) and functional (emotional, family cohesion) social support. The odds of adherence are 3.6 times higher in patients with practical support. Additionally, poor social support, family cohesion and a high level of familial conflict all increased the patient’s odds of noncompliance.
I am not naïve enough to believe that we can save every patient. However, I am hopeful that we can do more to meet patients where they are. A group at Stanford developed The Presence 5 for Racial Justice Framework designed to promote anti-racist communication with Black patients but can be applied broadly as well5. The five practices include:
1. Prepare with intention by reflecting on identity, bias, and power dynamics; and creating structures to address bias and structural determinants of health
2. Listen intently and completely without interruption and listen deeply for the potential impact of anti-Black racism on patient health and interactions with health care
3. Agree on what matters most by having explicit conversations about patient goals, treatment comfort and consent, and referral planning
4. Connect with the patient's story, acknowledging socioeconomic factors influencing patient health and focusing on positive efforts
5. Explore emotional cues by noticing and naming patient emotions, and considering how experiences might influence emotions.
There are adjustments to be made at every level: system, hospital, provider, and patient. As surgeons, we can lead the way by treating the human spirit.
See page 15 for references.
Leading The Way
Division of Colorectal Surgery
Katherine Hu, MD, joined the Department of Surgery in October 2024 as an Assistant Professor of Surgery. Dr. Hu received her medical degree from the University of Iowa before completing her general surgery residency here at MCW. She then completed a fellowship in colon and rectal surgery at the Cleveland Clinic in Cleveland, Ohio, where she spent an additional year as a Clinical Associate staff to gain further experience in management of complex colorectal disease. Dr. Hu has a special interest in inflammatory bowel disease and is dedicated to multidisciplinary patient-centered care to optimize outcomes for patients with complex or recurrent disease. Dr. Hu is excited to return to Milwaukee. She provides care to patients at Froedtert Hospital main campus.
Division of Congenital Heart Surgery
RDB “Jake” Jaquiss, MD, joined the Department of Surgery faulty in March of 2025 as a Professor of Surgery. He serves as the Co-Director of the Herma Heart Institute at Children’s Wisconsin where he holds the AO Nicholas Chair in Congenital Cardiac Care. Prior to joining the Medical College of Wisconsin faculty, Jaquiss held similar positions at the University of Texas Southwestern, Duke University, and the University of Arkansas for Medical Sciences. For him the move to Milwaukee is actually a return, as Jaquiss was Assistant and then Associate Professor at the Medical College of Wisconsin from 2000 to 2005. Beyond his work in Milwaukee, Jaquiss currently serves as the President of the Congenital Heart Surgeons’ Society.
Division of Minimally Invasive and Gastrointestinal Surgery
Ezra Teitelbaum, MD, MEd, joined the Department of Surgery faculty in June 2025 as an Associate Professor of Surgery. Dr. Teitelbaum completed his medical degree at the Mount Sinai School of Medicine, followed by general surgery residency at Northwestern University and minimally invasive surgery fellowship at Providence Portland Medical Center. Prior to joining MCW, he was an Associate Professor of Surgery at Northwestern University. Dr. Teitelbaum's clinical practice focuses on minimally invasive foregut, bariatric, and endoscopic surgery.
Division of Surgical Oncoloy
Yongwoo (David) Seo, MD joined the Department of Surgery faculty in October 2024 as an Assistant Professor. He completed medical school at the University of Michigan in Ann Arbor, general surgery training at University of Washington in Seattle, and fellowship training in Complex General Surgical Oncology at MD Anderson Cancer Center in Houston. Dr. Seo's research interests are in the field of pancreatic cancer – specifically, trying to use novel translational methods to understand how to better select patients for therapy and surgery.
Jasmine Walker, MD, MPH, joined the Department of Surgery faculty in September 2024, following a breast surgical oncology fellowship at the University of Michigan. Dr. Walker received her medical degree from Columbia University Vagelos College of Physicians and Surgeons. Prior to attending medical school, she spent three years teaching high school in Indiana. After medical school, Dr Walker completed general surgery residency at Vanderbilt University Medical Center in Nashville, TN. While at Vanderbilt, she also completed a Master of Public Health. Dr. Walker joins an amazing group of breast surgical oncologists at MCW, poised to make great progress in breast cancer care.
Division of Trauma and Acute Care Surgery
Kelly Boyle, MD joined the Department of Surgery faculty in October 2024 as an Assistant Professor of Surgery. Dr. Boyle earned her medical degree from the University of Wisconsin School of Medicine and Public Health, then completed her general surgery residency at the Medical College of Wisconsin. She went on to complete a surgical critical care fellowship and an American Association for the Surgery of Trauma (AAST) acute care surgery fellowship at the University of Southern California and Los Angeles County Medical Center (LAC+USC). Dr. Boyle is excited to return to MCW and her home state of Wisconsin, where she is passionate about advancing trauma care and leadership.
Remembering Dr. Robb Edwards
Patrick Hettinger, MD
Associate Professor of Surgery, Department of Plastic Surgery
Dr. Robb Edwards Assistant Professor Division of Trauma and Critical Care
The Medical College of Wisconsin recently lost an outstanding surgeon, Dr. Robb Edwards. Robb tragically passed away on August 25, 2025 following a motor vehicle crash. Robb was an excellent surgeon and mentor, and someone I was lucky enough to call a close friend. Robb grew up outside of Portland, Oregon. He attended a technical high school where he excelled in academics and athletics. A star on the field, Robb went on to play division one football in college as a wide receiver and defensive back. He carried his athleticism with him throughout life, completing national and international marathons and also competing in numerous triathlons. Although he would often win in his age group, his modesty did not allow him to brag, but only offer information when prompted.
After college, Robb went on to work in industry, but his scientific curiosity brought him back to medical school at a later age. When not buried in his books, Robb was always up for a pickup game of any sport, as he would nonchalantly defeat his opponents making it look easy. Robb completed medical school and matched into General Surgery Residency at the Medical College of Wisconsin where he completed his five years of surgical training.
After residency, Robb was always up for an adventure and practiced general surgery throughout the US; however, his roots brough him back to Milwaukee where he practiced with the Medical College of Wisconsin and Froedtert. For the past 2 years, Robb led the acute care and general surgery team while also directing trauma surgery at Froedtert Menomonee Falls Hospital. Robb participated in medical missions, touching the lives of patients and caring for those less fortunate. He provided outstanding care for all of his patients and was never one to shy away from putting in long hours and hard work.
Outside of medicine, Robb was genuine and full of life. He loved to travel to far-off destinations and immerse himself in other cultures, often in the company of his closest friends. He loved music and was a voracious reader, always eager to learn. He lit up every room he was in and was always willing to help friends and family in challenging times. He had an excellent sense of humor and was quite the dancer, frequently winning impromptu dance-offs among friends.
My heart goes out to all of Robb’s family, friends, and patients for this tragic loss. Selfishly, I am heartbroken because Robb was my dear friend. Although Robb’s loss is difficult to accept, I am comforted by the memories and stories that we shared together.
The Medical College of Wisconsin Department of Surgery Faculty by Specialty
Bariatric & Minimally Invasive Gastrointestinal Surgery
Amir Ghaferi, MD, MSc, MBA
Matthew Goldblatt, MD
Jon Gould, MD, MBA
Rana Higgins, MD
Andrew Kastenmeier, MD
Tammy Kindel, MD, PhD
Kathleen Lak, MD
Philip Redlich, MD, PhD
Wen Hui Tan, MD
Ezra Teitelbaum, MD, MEd
Cardiac Surgery
Ahmed Ali, MD
G. Hossein Almassi, MD
Lucian Durham III, MD, PhD
Viktor Hraska, MD, PhD
Robert Jaquiss, MD
Takushi Kohmoto, MD, PhD, MBA
James Mace, Jr., MD
Jorge Mascaro Carvajal, MD
Michael Mitchell, MD*
Paul Pearson, MD, PhD
Stefano Schena, MD, PhD
H. Adam Ubert, MD
Colorectal Surgery
Jed Calata, MD
Katherine Hu, MD
Kirk Ludwig, MD
Carrie Peterson, MD, MS*
Timothy Ridolfi, MD, MS
Community Surgery
Marina Affi Koprowski, MD
Marc de Moya, MD
Kaizad Machhi, MD
Allegra Saving, MD
Eric Soneson, MD
Mark Timm, MD
Pediatric General & Thoracic Surgery
John Aiken, MD*
Christina Bence, MD
Casey Calkins, MD*
Brian Craig, MD
John Densmore, MD*
Katherine Flynn-O’Brien, MD, MPH
David Gourlay, MD*
Tammy Kindel, MD, PhD
Christopher Laird, MD
Dave Lal, MD, MPH*
Caroline Maloney, MD, PhD
Jose Salazar Osuna, MD, PhD*
Jack Schneider, MD*
Amy Wagner, MD*
Research Faculty
Mohammed Aldakkak, MD
John Baker, PhD
Young-In Chi, PhD
Christian Kastrup, PhD
Gwen Lomberk, PhD
Nikki Lytle, PhD
Angela Mathison, PhD
Aoy Tomita Mitchell, PhD
M. Muska Nataliansyah, MD, PhD, MPH
Kirkwood Pritchard, Jr., PhD
Raul Urrutia, MD
Surgical Oncology – Breast Surgery
Adrienne Cobb, MD, MS*
Chandler Cortina, MD, MS*
Amanda Kong, MD, MS*
Caitlin Patten, MD*
Jasmine Walker, MD, MPH
Tina Yen, MD, MS
Surgical Oncology – Endocrine Surgery
Douglas Evans, MD*
Catherine McManus, MD, MS
Tracy Wang, MD, MPH*
Tina Yen, MD, MS
Surgical Oncology – Hepatobiliary & Pancreas Surgery
Kathleen Christians, MD
Callisia Clarke, MD, MS
Douglas Evans, MD*
Karen Kersting, PhD, LCP
David Seo, MD
Surgical Oncology – Regional Therapies
Callisia Clarke, MD, MS
T. Clark Gamblin, MD, MS, MBA
Alexandra Istl, MD, MPH
Anai Kothari, MD, MS
Ugwuji Maduekwe, MD, MMSc, MPH
Thoracic Surgery
Mario Gasparri, MD
Mallory Hunt, MD, MBE, MSTR
Paul Linsky, MD
Transplant Surgery
Emre Arpali, MD, PhD
Matthew Cooper, MD
Ty Dunn, MD, MS
Joohyun Kim, MD, PhD
Kondragunta Rajendra Prasad, MD, MS
Jenessa Price, PhD
Stephanie Zanowski, PhD
Trauma/ACS
Jeffrey Anderson, MD
Marshall Beckman, MD, MA*
Jacqueline Blank, MD*
Kelly Boyle, MD
Nathan Carlson, MD
Thomas Carver, MD*
Joshua Dilday, DO*
Marc de Moya, MD*
Terri deRoon-Cassini, PhD, MS
Christopher Dodgion, MD, MSPH, MBA*
Anuoluwapo Elegbede, MD, MS*
Timothy Geier, PhD, LP
Daniel Holena, MD, MCSE*
Allyson Hynes, MD MSCE
Katie Iverson, MD, MPH*
Jeremy Levin, MD*
Christina Megal, DNP, APNP
David Milia, MD*
Rachel Morris, MD*
Patrick Murphy, MD, MSc, MPH*
Todd Neideen, MD*
Jacob Peschman, MD, MSPE*
Andrew Schramm, PhD
Libby Schroeder, MD, MS*
Lewis Somberg, MD, MSS*
Sydney Timmer-Murillo, PhD
Colleen Trevino, MSN, FNP, PhD
Riley Westein, MD
Vascular & Endovascular Surgery
Shahriar Alizadegan, MD*
Kellie Brown, MD*
Mitchell Dyer, MD, MSc
Joseph Hart, MD, MHL
Momodou Jammeh, MD
Christopher Johnson, MD
Dean Klinger, MD
Nathan Kugler, MD*
Brian Lewis, MD
Mona Li, MD*
Michael Malinowski, MD, MEHP*
Peter Rossi, MD*
Abby Rothstein, MD*
Affiliated Institution Program Directors
Gary Sweet, MD (Wausau)
Nicholas Meyer, MD (Columbia St. Marys)
Chief Advance Practice Providers
Courtney Johnson, PA-C, Ambulatory Chief APP
Maria Wellenstein, APNP, Inpatient Chief APP
Chief Surgical Residents (20252026)
Elise Biesboer, MD
Administrative Chief Resident
Melissa Drezdzon, MD
Administrative Chief Resident
Taylor Jaraczewski, MD, MS
Santiago Rolon, MD
Ben Seadler, MD
Monica Seadler, MD
Brexton Turner, MD
Amanda Witte, MD
*Participates in Community Surgery/Off-Campus Locations.
Learn more at mcw.edu/ surgery or follow us on social media. @MCWSurgery