We can help you reach San Diego’s physicians and medical leadership through our comprehensive print and digital channels. Our print channels are great for brand awareness and explaining your message, while digital gives you the option to drive website traffic. An advertising package with the San Diego County Medical Society is your best bet to influence the purchasing decisions — both professional and personal — of this influential audience. Learn more. Contact Jennifer Rohr today: (858) 437-3476 or Jennifer.Rohr@SDCMS.org
Editor: William T–C Tseng, MD, MPH
Editorial Board: James Santiago Grisolia, MD; David E.J. Bazzo, MD; William T-C Tseng, MD; Holly B. Yang, MD, MSHPEd, HMDC, FACP, FAAHPM
Marketing & Production Manager: Jennifer Rohr
Art Director: Lisa Williams
Copy Editor: Adam Elder
OFFICERS
President: Preeti S. Mehta, MD
President–Elect: Maria T. Carriedo-Ceniceros, MD
Immediate Past President: Steve H. Koh, MD
Secretary: Karrar H. Ali, DO, MPH
Treasurer: Rakesh R. Patel, MD, FAAFP, MBA
GEOGRAPHIC DIRECTORS
East County #2: Rachel B. Van Hollebeke, MD
Hillcrest #1: Vikant Gulati, MD
Hillcrest #2: Stephen R. Hayden, MD (Delegation Chair)
Kearny Mesa #1: Anthony E. Magit, MD, MPH
Kearny Mesa #2: Dustin H. Wailes, MD
La Jolla #1: Toluwalase (Lase) A. Ajayi, MD
La Jolla #2: Audra R. Meadows, MD
La Jolla #3: Emily A. Nagler, MD
North County #1: Arlene J. Morales, MD (Board Representative to the Executive Committee)
North County #2: Phil E. Yphantides, MD
North County #3: Nina Chaya, MD
South Bay #1: Paul J. Manos, DO
South Bay #2: Latisa S. Carson, MD
AT–LARGE DIRECTORS
#1: Steven L.W. Chen, MD, FACS, MBA (Board Representative to the Executive Committee)
#2: Kelly C. Motadel, MD, MPH #3: Kyle P. Edmonds, MD #5: Daniel D. Klaristenfeld, MD #6: Alexander K. Quick, MD
#7: Karl E. Steinberg, MD, FAAFP #8: Alejandra Postlethwaite, MD
ADDITIONAL VOTING DIRECTORS
Young Physician: Quinne C. Sember, MD
Retired Physician: Mitsuo Tomita, MD
Medical Student: Christina Noravian
CMA OFFICERS AND TRUSTEES
Trustee: Sergio R. Flores, MD
Trustee: Timothy A. Murphy, MD
Trustee: Holly B. Yang, MD, MSHPEd, HMDC, FACP, FAAHPM
AMA DELEGATES AND ALTERNATE DELEGATES
District I: Mihir Y. Parikh, MD
District I Alternate: William T–C Tseng, MD, MPH
At–Large: Kyle P. Edmonds, MD
At–Large: Sergio R. Flores, MD
At–Large: Robert E. Hertzka, MD
At–Large: Theodore M. Mazer, MD
At–Large: Albert Ray, MD
At–Large: Holly B. Yang, MD, MSHPEd, HMDC, FACP, FAAHPM
CMA DELEGATES
District I: Christopher M. Bergeron, MD, FACS
District I: Corrie D. Broudy, MD
District I: Mojgan Hosseini, MD
District I: Quinn K. Lippmann, MD
District I: Yolanda Marzan, MD
District I: Bijal V. Patel, MD
District I: Eric L. Rafla-Yuan, MD
District I: Ran Regev, MD
District I: Kristen N. Rice, MD
District I: Kosala Samarasinghe, MD
District I: Mark W. Sornson, MD
District I: Wynnshang (Wayne) C. Sun, MD
District I: Patrick A. Tellez, MD, MHSA, MPH
District I: Randy J. Young, MD
District I: Nicholas (dr. Nick) J. Yphantides, MD, MPH
RFS Delegate: Shawn A. Ali, MD
Opinions expressed by authors are their own and not necessarily those of SanDiegoPhysician or SDCMS. SanDiegoPhysicianreserves the right to edit all contributions for clarity and length as well as to reject any material submitted. Not responsible for unsolicited manuscripts. Advertising rates and information sent upon request. Acceptance of advertising in SanDiegoPhysicianin no way constitutes approval or endorsement by SDCMS of products or services advertised. SanDiegoPhysicianand SDCMS reserve the right to reject any advertising. Address all editorial communications to Editor@SDCMS.org. All advertising inquiries can be sent to DPebdani@SDCMS.org. SanDiegoPhysicianis published monthly on the first of the month. Subscription rates are $35.00 per year. For subscriptions, email Editor@SDCMS.org. [San Diego County Medical Society (SDCMS) Printed in the U.S.A.]
FEATURES
4
Tackling the Ongoing Challenges of Clostridioides difficile
By Behnam Moein Jahromi, MD, FACP, Elizabeth Anne Jefferson, BS, PhD, CIC, Mariah Maier, BSN, RN, and Mike Preziosi, MD
8
Efficacy of Daily CHG Bathing in Place of Isolation in Prevention of MDRO Transmission in Acute-Care Settings
By Lisa Kilgore, MBA-HCM, CIC, Ashley Homesley, BSN, RN, PHN, CIC, and Brianna Scott, DrPH, MPH
12
Drug-Resistant Yeast Along for the Ride: Patient Care Implications of Candida auris Colonization and Infection
By Ahnika Kline, MD, PhD, D(ABMM) and Sinem Beyhan, PhD
17
‘It’s Ok to Have a Dirty Urine’ (aka Asymptomatic Bacteriuria)
By Jessica Merchant, DNP, AGPCNP-BC, Bridget Olson, ID/ASP pharmacist consultant, CDPH, and Raymond Chinn, MD, FIDSA, FSHEA
DEPARTMENTS
2
Briefly Noted: Public Health • Federal Issues
20 Classifieds
West Coast States Launch New Alliance to Uphold Science in Public Health
CALIFORNIA, OREGON, AND WASHINGTON announced the launch of a new West Coast Health Alliance to ensure public health decisions remain grounded in science. The move follows the Trump Administration’s removal of the Centers for Disease Control and Prevention (CDC) director and shakeup of the Advisory Committee on Immunization Practices (ACIP), which state leaders warn threatens the health and safety of communities across the country.
“President Trump’s mass firing of CDC doctors and scientists — and his blatant politicization of the agency — is a direct assault on the health and safety of the American people,” Governors Gavin Newsom, Tina Kotek and Bob Ferguson said in a joint statement. “California, Oregon, and Washington will not allow the people of our states to be put at risk.”
The day after the Alliance was announced, Hawaii joined as the fourth member state. “By joining the West Coast Health Alliance, we’re giving Hawaii’s people the same consistent, evidence-based guidance they can trust to keep their families and neighbors safe,” said Hawaii Governor Josh Green, MD.
State public health leaders emphasized that the Alliance is intended to restore trust and provide residents with clear, consistent vaccine recommendations rooted in evidence. “The dismantling of public health and dismissal of experienced and respected health leaders and advisers, along with the lack of using science, data, and evidence to improve our nation’s health, are placing lives at risk,” said California State Public Health Officer Erica Pan, MD.
The four Alliance states will coordinate health guidelines and align immunization recommendations informed by respected national medical organizations, while respecting tribal sovereignty over vaccine services. In the coming weeks, they will finalize shared principles to strengthen public confidence in vaccines and public health.
The California Medical Association (CMA), which has long supported public health policies guided by scientific evidence, welcomes the formation of the Alliance.
“Public health only works when it is rooted in science, transparency, and trust. The erosion of the CDC’s credibility puts patients and communities at risk, but California and our West Coast partners are stepping up to ensure that health policy is guided by evidence, not ideology,” says CMA President Shannon Udovic-Constant, MD. “CMA will continue advocating for sciencebased decisions that safeguard our patients and communities and restore confidence in our public health system.”
FEDERAL ISSUES
New HHS Rule Promises to Enhance Drug Price Transparency and Electronic Prior Authorization
THE U.S. DEPARTMENT OF Health and Human Services (HHS) has finalized the Health Data, Technology, and Interoperability rule, which will require certified electronic health records (EHR) systems to offer real-time drug cost information and support electronic prior authorization — streamlining clinician workflows, reducing patient surprises and advancing administrative efficiency.
This rule will require certified EHR vendors to embed prior authorization, benefit verification, and e prescribing within their EHRs — enabling smoother workflows and eliminating burdensome manual steps like faxing and portal hopping. The updated e-prescribing standards are also intended to improve patient safety by reducing medication errors, providing clearer prescribing directions, and ensuring more accurate dispensing across pharmacies. By integrating prior authorization directly into the prescribing process, physicians will spend less time navigating outdated systems and more time focused on patient care.
Key provisions of the rule include:
• Real-time cost visibility: Physicians and patients will be able to view patient-specific drug pricing and compare alternatives across pharmacies at the point of prescribing.
• Prior authorization: Certified EHR systems must enable physicians to check coverage requirements, compile documentation, and submit and track requests
electronically within their existing workflows.
• Interoperability: The rule establishes standardized data flows among EHRs, payers, and pharmacies, replacing inefficient legacy processes.
• Modernized e-prescribing: New prescribing tools will help reduce errors, streamline medication management, and improve coordination between prescribers and pharmacies.
The new rule builds on the 2024 Interoperability and Prior Authorization Final Rule and reflects months of engagement between HHS, CMS, and major health insurers.
The California Medical Association (CMA), American Medical Association and others in organized medicine have made widespread calls over the past decade for meaningful prior authorization reform. AMA has called this final rule a major win for physician practices. “Not to overstate it, but this new policy could contribute to the demise of the fax era in medicine,” said AMA President Bobby Mukkamala, MD. “By replacing phones, faxes, and portal-hopping with standardized, interoperable EHR connection points, HHS’ new policy turns AMA advocacy into measurable workflow relief and faster decisions.”
CMA will monitor implementation of this new rule and will continue to advocate for policies that reduce administrative burdens, protect physician autonomy, and improve patient access to care.
Tackling the Ongoing Challenges of Clostridioides difficile
What Experts Are Saying
By Behnam Moein Jahromi, MD, FACP, Elizabeth Anne Jefferson, BS, PhD, CIC, Mariah Maier, BSN, RN, and Mike Preziosi, MD
CLOSTRIDIOIDES DIFFICILE (C. DIFF.) IS A GRAMpositive, spore-forming, anaerobic, toxin-producing bacterium found in the environment and in the gastrointestinal tracts of both humans and animals. Although first recognized as a cause of human disease in 1978, C. diff. remains one of the most prevalent healthcare-associated infections (HAIs) today.1,2
A hospital-onset (HO) C. diff. case is defined as a positive laboratory result occurring four or more days after admission to a healthcare facility. In contrast, a community-onset (CO) case is identified when a positive result occurs within the first three days of admission. The financial burden of a single HO onset C. diff. case is significant, costing the U.S. healthcare system an estimated $9,341 to $25,180 per case, and has implications for hospitals participating in the Centers for Medicare and Medicaid Services (CMS) Hospital-Acquired Condition Reduction Program and the Hospital Value-Based Purchasing Program.3
Our hospital has excellent nurse-led protocols in place to ensure timely identification of CO C. diff. cases. Hospitalonset C. diff. cases are now rare. When they do occur, they trigger a multidisciplinary review in which opportunities for improvement are identified and shared—from frontline staff to senior hospital leadership. Patients with a C. diff. infection are immediately placed on transmission-based precautions, which include the use of gowns and gloves, as well as hand hygiene with soap and water since alcohol-based hand sanitizers are ineffective against C. diff. spores. Upon discharge, the patient’s room undergoes terminal cleaning, including bleach disinfection of all surfaces and ultraviolet (UV) light decontamination. Educational materials and instructions are given to patients to support safe practices and reduce the risk of C. diff. transmission after discharge. While hospital-acquired C. diff. infections have declined
As a gastroenterologist, I often get involved when a patient doesn’t respond to initial treatment or begins INFECTIOUS DISEASES
Interview with Behnam Moein Jahromi, MD, FACP, Division of Gastroenterology and Hepatology, Scripps Clinic, La Jolla
due to our rapid improvement approaches4, the continued burden of C. diff. in the community remains concerning. Many patients are now admitted with infections that began outside the hospital. In outpatient settings, providers can encounter C. diff. in patients who have recently received antibiotics or who develop diarrhea following a surgical procedure or hospitalization. A recent publication also identified a wide range of sources for community-onset (CO) C. diff., including zoonotic reservoirs (such as companion animals and livestock), contaminated food, and environmental sources like soil, water, wastewater, and public areas.⁵
To better understand why C. diff. remains so difficult, we spoke with a gastroenterologist and an infectious disease specialist to gain their insight into the clinical and systemic challenges that surround this complex infection.
What is your biggest concern with C. diff.?
The biggest concern is the growing prevalence of C. diff. and the rise in recurrent infections, which are partly driven by widespread antibiotic use disrupting the gut microbiome. Recurrence occurs in up to 30% of cases after initial treatment, with risk increasing after each episode, and is associated with higher complication rates, healthcare costs, and treatment difficulty. Keeping C. diff. in mind when prescribing antibiotics and focusing on prevention through antibiotic stewardship and targeted strategies is essential.
At what point do you become involved in the management of C. diff.? There’s definitely overlap between gastroenterology and infectious disease when it comes to C. diff. infection.
to experience recurrent infections. However, in more severe cases, especially when there’s concern for complications, we’re involved from the very beginning.
Are there any therapies in gastroenterology that hold promise for C. diff. treatment?
Antibiotics remain the mainstay of treatment for C. diff. colitis, but there is growing interest in microbiome-based therapies like fecal microbiota transplantation (FMT). While no FMT product is FDA-approved specifically for treatment, two live biotherapeutic products have been approved for the prevention of recurrent C. diff. infection in select patient populations. These therapies represent a promising shift toward restoring a healthy gut microbiome to prevent relapse.
What is your biggest challenge when treating a patient for C. diff.?
The biggest challenge is managing the risk of recurrent infection, which has become increasingly common over the past several years. Even after successful initial treatment, many patients go on to have relapses, which are often harder to treat and can significantly impact their quality of life.
What are your criteria for recommending FMT?
Currently, fecal microbiota transplantation (FMT) is FDA-approved only for the prevention of recurrent C. diff. infection, not for initial treatment. At this time, treatment of C. diff. with FMT should be performed solely within the context of a clinical trial. However, offlabel use of FDA-approved FMT products for treating severe or recurrent C. diff. may be available at select institutions.
What are the benefits of FMT?
The benefits of FMT are still being actively studied. The concept is that by transplanting healthy gut flora from one person to another, we can help restore microbiome balance and potentially treat certain conditions. While there’s growing interest in its use for various diseases, the only current FDAapproved use of FMT-based products is for preventing recurrent C. diff. infection.
Does FMT have any risks?
Yes, FMT does carry risks. We are essentially transplanting one person’s microbiome into another, and despite rigorous donor screening, there’s still a potential risk of transferring unknown or emerging pathogens. Allergic reactions, as well as immediate
and long-term side effects, are also possible. For these reasons, FMT should currently be limited to specific, approved indications and performed in controlled clinical settings.
What are your thoughts on the use of probiotics to prevent C. diff.?
I believe the future of microbiome-based therapies, including probiotics and prebiotics, is promising, and ongoing research continues to explore their potential. While the idea of using probiotics to prevent C. diff. is appealing, we still lack large, high-quality randomized controlled trials to clearly support their effectiveness. For now, their use remains largely theoretical or based on small studies. That said, probiotics are generally considered safe, which is why they continue to be explored as a preventive option.
If you don’t routinely recommend probiotics for your C. diff. patients, are there any alternatives you suggest?
I’m a big fan of food-based probiotics. These are natural, fermented foods that serve as a great source of beneficial bacteria. Examples include kimchi, sauerkraut, pickles, kombucha, and kefir. They’re often inexpensive, have fewer additives than supplements, and can be a delicious way to support gut health. While the evidence is still evolving, incorporating these foods into the diet is a simple, low-risk measure I often encourage.
Are there any GI disorders that increase your chances of C. diff.?
Yes. One of the most notable examples is inflammatory bowel disease (IBD), which includes ulcerative colitis and Crohn’s disease. Patients with IBD are at higher risk for C. difficile infection due to several factors, including chronic inflammation of the gut, frequent use of immunosuppressive medications, and a disrupted gut microbiome.
What makes this especially important is that C. diff. can both mimic and trigger an IBD flare, making it difficult to distinguish between the two. Because of this, clinicians should have a lower threshold to test for C. diff. in IBD patients who present with worsening diarrhea, abdominal pain, or systemic symptoms like fever, even if they haven’t had recent antibiotic exposure or hospitalization. It’s a tricky overlap, but recognizing it early is key. C. diff. tends to be more severe in patients with IBD, and delays in diagnosis can lead to serious complications.
In one sentence, how can we prevent C. diff. infection?
Avoid unnecessary antibiotics and let your good bacteria keep the peace. Trust your gut’s bouncers; don’t kick them out by unnecessary antibiotics!
Interview with Michael Preziosi, MD, DIO of graduate medical education, Scripps Clinic/Scripps Green Hospital, and associate clinical professor of medicine, Scripps Clinic Medical Group, La Jolla
What is your biggest challenge when treating a patient for C. diff.?
The recurrence rate is the biggest challenge. As Dr. Moein mentioned, the recurrence rate can be up to 30 percent after an initial episode, but actually goes up after a first recurrence. An antibiotic called fidaxomicin is associated with fewer recurrences if used as initial treatment but is prohibitively expensive for many patients. Fecal microbiota transplantation has been shown to be very effective for treating and preventing recurrent C. diff. This has become increasingly available in the last decade but has historically been administered through colonoscopy by GI doctors. Since I don’t do colonoscopies, I need to coordinate care with GI doctors. There are newer FDA approved products that have been approved for C. diff. prevention that do not require an invasive procedure and will become cheaper and more widely available in coming years.
What can PCPs do to prevent C. diff. in their patients?
The number one risk factor for C. diff. is antibiotic use. The risk goes up with each day of antibiotics. PCPs can help prevent C. diff. by being judicious with antibiotics — not prescribing antibiotics for URIs or sinusitis in which the pathogen is clearly viral, avoiding antibiotics for asymptomatic bacteriuria, and when antibiotics are necessary, using the shortest course of the most narrow-spectrum antibiotic possible. Most bacterial infections encountered in primary care can be treated with a five-day course of antibiotics.
What do you wish PCPs knew about C. diff.?
In patients who have a history of C. diff. and are at risk for recurrence but have a clear need to be treated with antibiotics, simultaneously giving oral vancomycin 125mg daily has been shown to decrease the risk of recurrence.
What makes the difference whether you prescribe fidaxomicin or vancomycin for C. diff.?
Both antibiotics seem to work just as well to treat the initial episode, but it seems that fidaxomicin is associated with fewer recurrences. However, a 10-day course of fidaxomicin can be very expensive: up to $5,000 if paid out-of-pocket. As such, I tend to only use it in an initial episode in a patient that is very high risk for recurrence. The three primary risk factors are advanced age, immunocompromise, and severity of disease. So I might use it first-line in an elderly immunocompromised patient with a severe episode, or perhaps in someone with fewer risk factors but who nonetheless has had a recurrence. Still, I’m usually checking to see if insurance will cover it first.
Are there questions you recommend we ask you? What are they and how would you answer them?
I get asked about probiotics a lot and if they are effective to prevent C. diff. The answer is no. No studies of probiotics have been shown to decrease the incidence of C. diff. in patients who are prescribed antibiotics. While many commercial formulations of probiotics state that they contain, for example, “billions of colony-forming units of lactobacillus,” your gut microbiome has trillions of colony-forming units of a huge variety of species of bacteria. Nobody has shown that lactobacillus or saccharomyces somehow unlock the diversity of your gut ecosystem. In fact, your gut ecosystem is very resistant to change, and most probiotics come out in the stool unchanged. I’m often heard saying “people who take probiotics have very expensive poop.” Of note, when we do an FMT, we transplant an entire stool ecosystem, not just one species. I am not opposed to patients taking probiotics as they are
essentially harmless, but we have not yet “cracked the code” when it comes to probiotics preventing C. diff. The very effective fecal microbiota transplant involves an entire bacterial ecosystem — not just one species.
References:
1. “CDC C. diff. (Clostridioides difficile)”, accessed June 18, 2025, https://www.cdc.gov/c-diff/index.html
3. Agency for Healthcare Research and Quality (AHRQ), accessed June 26, 2025, Results | Agency for Healthcare Research and Quality
4. Sharieff GQ, Uejo C. Sprint Team Approach Yields Rapid Improvement in Leapfrog Quality Indicators. J Healthc Manag. 2024 Mar-Apr 01;69(2):156-163. doi: 10.1097/JHMD-22-00223. PMID: 38467028.
5. Alshannaq AF, Kates AE, Keating JA, Mckinley LL, Dixon JW, Safdar N. Diverse Sources and Latent Reservoirs of Community-Associated Clostridioides difficile Infection. Clin Infect Dis. 2025 Feb 5;80(1):37-42. doi: 10.1093/cid/ciae429.
Dr. Jahromi is a dual board-certified physician in internal medicine and gastroenterology at Scripps Clinic in La Jolla, where he is recognized for his compassionate patient care. His academic contributions include several peerreviewed publications and presentations at national and international conferences. He is actively involved in clinical research and quality improvement initiatives, and serves as a passionate educator to residents and fellows. Elizabeth A. Jefferson is the manager of epidemiology at Scripps Green Hospital. She joined Scripps in 2018, bringing 17 years of experience as a medicinal chemist in the biotechnology industry, where she authored more than 40 peer-reviewed publications. Her unique background blends deep scientific expertise with evidence-based infection prevention strategies, advancing patient safety and improving quality of care. Mariah Maier is an infection preventionist at Scripps Green Hospital with two years of experience in healthcare-associated infection prevention, safeguarding immunocompromised patients, and promoting employee health and safety. She brings a strong clinical background in critical care nursing and solid organ transplant coordination to infection prevention. Dr. Preziosi is a clinical associate professor of medicine in the division of infectious diseases in the Scripps Clinic Medical Group. His expertise is in the diagnosis and management of infectious diseases. He is also the director of graduate medical education at Scripps Clinic Medical Group.
Efficacy of Daily CHG Bathing in Place of Isolation in Prevention of MDRO Transmission in Acute-Care Settings
By Lisa Kilgore, MBA-HCM, CIC, Ashley Homesley, BSN, RN, PHN, CIC, and Brianna Scott, DrPH, MPH
WHAT IS CHLORHEXIDINE GLUCONATE, ALSO known as CHG? CHG is a broad-spectrum antiseptic that is Food and Drug Administration (FDA) cleared for use in various medical and healthcare applications to reduce microbial load on the skin, mucous membranes, and certain devices. CHG works by disrupting microbial cell membranes (at low concentrations) and irreversible aggregation of intracellular contents (at high concentrations), leading to cell death, particularly of vegetative bacteria, fungi, and some viruses. Though CHG is commonly used in the inpatient/clinical settings, outpatient physician offices also prescribe over-thecounter (OTC) CHG for patients to use the night before and the morning of a procedure. Due to the increased usage of OTC CHG, the FDA issued a warning that rare but serious allergic reactions have been reported with commonly used skin antiseptic products containing chlorhexidine gluconate1. According to Medscape, CHG comes in multiple forms and concentrations and has been used in healthcare settings for more than 60 years as a versatile tool in infection prevention and control2. CHG is often used as:
• Skin antiseptic solutions (e.g., 2% or 4% CHG)3
• Surgical scrubs and pre-op skin preps
• Bathing cloths/wipes (commonly used for ICU)
• Oral rinses (e.g., for prevention of ventilator-associated pneumonia)
• CHG-impregnated products:
o Catheter dressings
o IV catheters
o Surgical meshes and sponges
It is important to note that CHG is not sporicidal, and does not kill pathogens like Clostridioides difficile (C. diff) or mycobacteria (e.g., M. tuberculosis). CHG was introduced as a key preventative against specific organisms and for certain procedures such as:
Daily CHG bathing is used as a universal decolonization (nose to toes) strategy, especially in ICUs, due to its broadspectrum coverage, and its efficacy in preventing the transmission of organisms. According to the American Association of Critical-Care Nurses consistent daily use of 4% CHG in ICU settings was associated with a 52% reduction in HAIs and a 32% reduction in CLABSIs and other bloodstream infections (BSIs) 4
The CHG body map (Figure 1.) provides step by step instructions for the
proper application of CHG. As with any medical treatment, the use of CHG comes with risks and benefits which should be evaluated carefully for each patient and clinical scenario. Benefits of CHG bathing include reduced infection risk, preventing specific types of infections in high-risk populations, effectiveness against resistant bacteria, improved patient outcomes, low cost, and persistence of action at the application site. CHG bathing significantly reduces the spread of infections in hospitals, including those on the forefront like methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococcus (VRE), by killing germs on the skin. CHG continues to kill bacteria for up to 24 hours after the treatment, due to the binding of the CHG cationic molecules to the negatively charged components of the bacterial cell wall5. It also helps prevent infections related to central venous catheters (CVC), surgical sites (SSI), and ventilators. In one research study, CLABSI cases which utilized CHG baths were reduced by 48% as compared with those which utilized conventional bed-bathing6. By preventing infections, CHG bathing may shorten hospital stays and improve patient outcomes. These reductions translate into significant cost savings, as HAIs are among the most expensive complications in
Figure 1.
CHG bathing: Top highlighted points
• Work from clean to dirty in each 6 areas
• Color coding sections with correct order of operations.
• Wipe #2 for BOTH arms, use one side per arm.
• Clean closest 6” of lines (central line, foley, etc.) nearest to the patient with the same wipe as the level you are cleaning.
• You may require more than 6 wipes based on the patient size, condition, etc.
healthcare, with an average annual cost per HAI ranging from $28.4 to $45 billion in the US and $20,000 to over $45,000 per case, depending on the infection type7. By reducing infections, CHG use can help to:
• Lower ICU length of stay
• Reduce antibiotic usage
• Prevent costly complications and readmissions
• Improve patient outcomes and hospital safety scores
Risks associated with CHG bathing include skin irritation/ dryness, potential for treatment resistance, age and skin related contraindications, and allergic reactions (rare). While not a risk, patient preference for soap and water may also play a role in treatment compliance and requires education from clinicians on the preference for CHG in the hospital setting. Education and assistance by healthcare workers have been proven to improve CHG bathing compliance8. CHG should be kept out of the eyes and ears, and can cause permanent injury if it comes in prolonged direct contact with nerves9. The most common side effect is skin dryness with prolonged use. Mild skin rashes and irritation can also occur. Heavy and widespread use of CHG may, over time, lead to the development of bacteria that are resistant to the treatment. It is generally not used in babies younger than 2 months old and CHG baths may not be suitable for individuals with serious skin problems, irritation, or burns. The ‘sticky feeling’ reported is temporary and is due to lotion or aloe vera in the cloths, which moisturizes your skin while it cleans10. This discomfort typically goes away completely when dry. CHG bathing is not a complete replace-
ment for other critical infection control practices like hand hygiene. Also noted by the ARHQ Task Force for Combating AntibioticResistant Bacteria (CARB): “Every infection prevented is one less instance of antibiotic use, and using fewer antibiotics significantly reduces the risk for resistant infections,” which has been a national goal for a decade11 Multi-drug-resistant organisms (MDROs) resistant to last-resort antibiotics continue to rise in healthcare settings and pose a significant risk. According to the Centers for Disease Control and Prevention (CDC), MDROs infect an estimated 2.8 million individuals annually in the U.S. and cause 35,000 deaths each year12. In addition to increased prevalence and preventable deaths, MDROs
cause incremental costs for Acute Care Hospitals. CDC estimates the national cost of treating infections associated with MDROs in the hospital setting to be $2.4–3.4 billion annually13 To decrease the transmission of MDROs, the CDC has developed horizontal infection control strategies to limit the transmission and prevalence of MDROs, including hand hygiene, environmental cleaning, isolation, and chlorhexidine bathing14. According to a recent study, the use of hand hygiene, environmental cleaning, and patient isolation yielded little impact on the prevalence of MDROs. However, such strategies contributed to a decrease in trends when used together14 Notably, CHG bathing has shown considerable efficacy in reducing MRSA clinical
Men > Groin > Perenium One wipe for right front/back: Thigh > Knee > Foot
INFECTIOUS DISEASES
cultures compared to MRSA screening and the use of Contact Precautions (CP)15. Research shows that CHG bathing has emerged as a less disruptive strategy for reducing transmission and its potential as a substitute for isolation in the prevention of MDRO transmission.
Isolation precautions have evolved into an effective practice for reducing the transmission of MDROs. Specifically, CP, which include the use of gloves and gowns, prevent the spread of pathogens16. Nevertheless, research has found a lack of rigorous data to support a relationship between the use of CP and the prevention of MDROs, such as MRSA or VRE; instead, it raises concerns. Through a systematic review of the effectiveness of CP, a research study found that the use of CP included “decreased time spent with patients, delay in patient transfer, excess length of stay, increased re-admission stays, and patients’ perception of poor-quality care15.” Furthermore, researchers argued that facilities with strong horizontal infection prevention strategies can safely discontinue CPS for MDROs such as MRSA and VRE.
To support this shift in prevention strategies, the implementation of daily CHG bathing has proven effective in lowering costs and reducing the acquisition of MDROs. According to a research study published in the Journal of Patient Safety, daily CHG bathing significantly reduced CRE colonization in a hospital setting, from 26.8% to 9.3%17. Not only does CHG bathing reduce MDRO prevalence immediately, but it is also a low-cost implementation and has rare adverse events. Lastly, daily CHG bathing has proven to be not only more effective in decreasing the prevalence of MDROs but also offers an immediate reduction in MDRO prevalence than isolation. A research study published in the American Journal of Infection Control found that after implementing daily CHG bathing during a two-month period. VRE incidence decreased from 15.8% to 9.6%, and fluoroquinolone-resistant gram-negative bacilli (FQRGNB) incidence decreased from 10.1% to 5.5%18. This study also supports the implementation of daily CHG bathing as an effective measure against both Gram-positive and Gram-negative bacteria, making it effective for the majority of MDROs18.
Daily CHG bathing has proven effective in reducing the transmission of MDROs. It can serve as an alternative to isolation, particularly in healthcare settings with robust horizontal infection prevention strategies. However, many limitations exist for the direct study of solely using CHG bathing as a replacement for isolation, and future studies should examine this through CHG bathing-only protocols as a replacement for isolation practices. Nevertheless, CHG bathing offers a promising evidence-based strategy for preventing MDROs in acute care settings.
References
1. U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA warns about rare but serious allergic reactions with the skin antiseptic chlorhexidine gluconate. Published February 2, 2017. Accessed July 16, 2025. https://www.fda.gov/drugs/drug-safetyand-availability/fda-drug-safety-communication-fdawarns-about-rare-serious-allergic-reactions-skinantiseptic
2. Stokowski LA. Chlorhexidine in Healthcare: Your Questions Answered. Medscape. Published August 4, 2010. Accessed July 16, 2025. https://www.medscape. com/viewarticle/726075
3. Stryker. Sage 2% Chlorhexidine Gluconate (CHG) Cloths. Published [year not specified]. Accessed July 16, 2025. https://www.stryker.com/us/en/sage/products/ sage-chg-cloths.html
4. Chapman L, Hargett L, Anderson T, Galluzzo J, Zimand P. Chlorhexidine gluconate bathing program to reduce health care–associated infections in both critically ill and noncritically ill patients. Crit Care Nurse. 2021;41(5):e1–e8. doi:10.4037/ccn2021340. Accessed July 16, 2025
5. Edmiston CE Jr, Bruden B, Rucinski MC, Henen C, Graham MB, Lewis BL. Reducing the risk of surgical site infections: does chlorhexidine gluconate provide a risk reduction benefit? Am J Infect Control. 2013 May;41(5 Suppl):S49–S55. doi:10.1016/j.ajic.2012.10.030. PMID: 23622749. Accessed July 16, 2025.
6. Peixoto EAC, Poveda VB, Gnatta JR, Oliveira RA. Bathing with wipes impregnated with chlorhexidine gluconate to prevent central line–associated bloodstream infection in critically ill patients: a systematic review with metaanalysis. Am J Infect Control. 2024 Jun;52(6):731–738. doi:10.1016/j.ajic.2024.01.019 E pub 2024 Feb 10. PMID: 38342345
7. Nevoa Inc. How Much Are HAIs Really Costing Your Healthcare Facility? Published June 17, 2024. Accessed July 16, 2025. https://nevoainc.com/hai-costing-healthcare-facility/
8. Vanhoozer G, Lovern I, Masroor N, et al. Chlorhexidine gluconate bathing: Patient perceptions, practices, and barriers at a tertiary care center. Am J Infect Control. 2019;47(3):349–350. doi:10.1016/j.ajic.2018.08.002. PMID: 30322813. Accessed July 16, 2025.
9. Agency for Healthcare Research and Quality. Universal ICU Decolonization: An Enhanced Protocol. Content last reviewed September 2013. Accessed July 16, 2025. https://www.ahrq.gov/hai/universal-icu-decolonization/index.html
10. Agency for Healthcare Research and Quality. Toolkit for Decolonization of NonICU Patients With Devices. Content last reviewed March 2022; originally created February 2022. Accessed July 16, 2025. https://www. ahrq.gov/hai/tools/abate/index.html
11. Agency for Healthcare Research and Quality. Combating AntibioticResistant Bacteria. Content last reviewed May 2022; originally created September 2020. Accessed July 16, 2025. https://www.ahrq.gov/hai/carb/ index.html
12. Centers for Disease Control and Prevention. Preventing Multidrug-Resistant Organisms (MDROs) in Healthcare Settings. Updated December 11, 2024. Accessed July 16, 2025. https://www.cdc.gov/healthcare-associated-infections/php/preventing-mdros/index.html
13. Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2019. Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2019. Accessed July 16, 2025. https://www.cdc. gov/antimicrobial-resistance/media/pdfs/2019-arthreats-report-508.pdf
14. Huang W, Qiao F, Cai L, Zong Z, Zhang W. Effect of daily chlorhexidine bathing on reducing infections caused by multidrugresistant organisms in intensive care unit patients: A semiexperimental study with parallel controls. J Evid Based Med. 2023 Mar;16(1):32–38. doi:10.1111/ jebm.12515. PMID: 36779575. Accessed July 16, 2025.
15. Marra AR, Edmond MB, Schweizer ML, Ryan GW, Diekema DJ. Discontinuing contact precautions for multidrug-resistant organisms: a systematic literature review and meta-analysis. Am J Infect Control. 2018 Mar;46(3):333–340. doi:10.1016/j.ajic.2017.08.031. PMID: 29031432. Accessed July 16, 2025.
16. Centers for Disease Control and Prevention. Transmission-Based Precautions. Updated April 8, 2025. Accessed July 16, 2025. https://www.cdc.gov/infection-control/hcp/ basics/transmission-based-precautions.html
17. Gall E, Long A, Hall KK. Chlorhexidine Bathing Strategies for MultidrugResistant Organisms: A Summary of Recent Evidence. J Patient Saf. 2020 Sep;16(3S Suppl 1):S16–S22. doi:10.1097/PTS.0000000000000743. PMID: 32809997. Accessed July 16, 2025.
18. Musuuza JS, Sethi AK, Roberts TJ, Safdar N. Implementation of daily chlorhexidine bathing to reduce colonization by multidrugresistant organisms in a critical care unit. Am J Infect Control. 2017;45(9):1014–1017. doi:10.1016/j.ajic.2017.02.038
Lisa Kilgore has 25 years of experience marked by a deep commitment to healthcare quality, infection prevention and control, emergency preparedness, and addressing healthcare disparities — demonstrated through her leadership roles and specialized expertise. Ashley Homesley has 22 years of clinical experience in varied ambulatory and inpatient settings as a perioperative nurse and infection preventionist. Most of her patient care experience was focused on delivering total nursing care to the perioperative patient in varied specialties with a strong focus in orthopedics, spine, pain management and general surgery. Her role for the last decade has been as an infection control coordinator on a corporate surveillance team for a five-hospital health system in San Diego. Ashley is a licensed registered nurse and public health nurse, holds a bachelor of science in nursing, and is board-certified in infection control and epidemiology. Brianna Scott has several years of experience in the public health sector, specializing in infectious disease prevention, outbreak response, and humanitarian epidemiology. She is currently a manager of epidemiology for a health system in San Diego and previously served as an epidemiologist in the government health sector, leading infection prevention and outbreak response efforts. Brianna holds a bachelor of science in public health, a master of public health, and a doctor of public health (DrPH).
Drug-Resistant Yeast Along for the Ride
Patient Care Implications of Candida auris Colonization and Infection
By Ahnika Kline, MD, PhD, D(ABMM) and Sinem Beyhan, PhD
FUNGAL INFECTIONS POSE A SIGNIFICANT HEALTH threat globally, as they present challenges in treatment due to the limited number of antifungals available in the clinical setting. Fungal infections are also frequently recurrent, which leads to repeated exposure to antifungals and increases the acquisition of antifungal resistance by pathogens.
Candida auris: An Emerging Fungal Pathogen
The yeast pathogen Candida auris is a rapidly emerging human pathogen. It has been classified within the critical pathogen group — the highest risk group — according to the World Health Organization’s first fungal pathogens list1. More recently, C. auris has been assigned to a newly created genus Candidozyma and has been renamed as Candidozyma auris2
Since its first characterization in 2009 from an external ear canal of a patient in Japan3, C. auris has been isolated from patients worldwide, including five continents (Asia, Africa, Europe, South America, and North America)4. In the U.S., it was first described in 20135. However, retrospective studies suggest that C. auris was present among patients much earlier than it was originally thought, dating back to 1996 in a blood culture sample from a patient in South Korea6. Unfortunately, the diagnostic methods used by clinical microbiology laboratories at that time were not sensitive enough to classify C. auris as a new species. Thus, it is possible that C. auris emerged much earlier than 1996, but was not recognized until 2009.
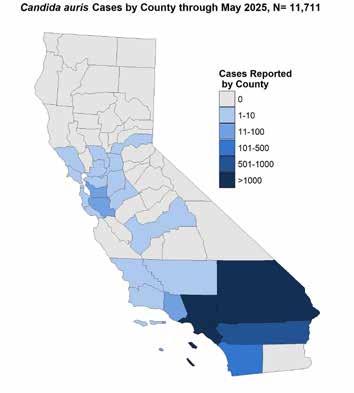
In the U.S., the initial C. auris cases were reported from the states of New York, Illinois, Maryland, and New Jersey5. The Centers for Disease Control (CDC) has been actively tracking cases nationwide since 2016. In California, C. auris detection is notifiable to both the CDC and the California Department of Public Health (CDPH). As of 2023, there were 10,788 clinical cases nationwide and an additional 22,931 identified by screening patients7. In California, from January 2017 through May 2025, there have been 11,711 patients with C. auris, with 413 cases reported in San Diego County (Figure 1)8.
C. auris Is an AzoleResistant Yeast C. auris infections are notoriously difficult to treat due to the pathogen’s high rates of resistance to the antifungal drugs used in clinical practice. It is estimated that 90% of C. auris clinical isolates in the U.S. are resistant to fluconazole9 Both culture-based and molecular methods can be used to detect C. auris from clinical samples10. Clinical diagnostic laboratories may elect to perform susceptibility testing in which C. auris is incubated with increasing concentrations of antifungal drugs to determine a minimal inhibitory drug concentration (MIC); however, there are no FDA-approved breakpoints for C. auris to interpret the MIC values and classify the isolates as susceptible or resistant to a given antifungal11. Clinicians looking to interpret MIC results for C. auris may find some utility from the CDC, which has published guidance for interpretation9. Notably, fluconazole testing is recommended as a
Figure 1. C. auris cases by county through May 2025, N=11,711 (source: CDPH)
surrogate for susceptibility to all other azoles; however, some in vitro data suggest that voriconazole and micafungin can act synergistically even against resistant isolates 12. Given the high rates of fluconazole resistance, echinocandins represent the mainstay of treatment, and fortunately, less than 2% of the clinical isolates in the U.S. are echinocandin resistant9. Unfortunately, 30% of isolates also exhibit reduced susceptibility to amphotericin B9 C. auris resistant to all three classes of antifungals was described in New York in 201913. Among the recently developed antifungals, ibrexafungerp, which
Figure 1. C. auris cases by ounty through May 2025, N=11,711 (source: CDPH)
has been recently approved by the FDA for the treatment of vaginal candidiasis, and fosmanogepix, which is not yet approved by the FDA, may offer promise as alternative treatments for these infections14.
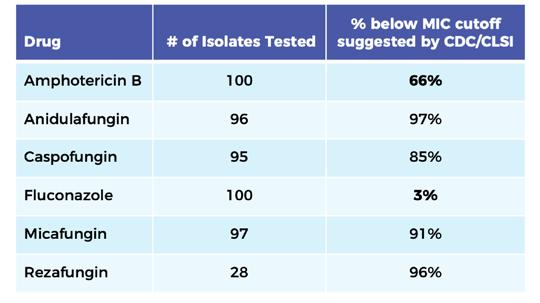
The antifungal susceptibility testing results performed in UC San Diego Center for Advanced Laboratory Medicine (CALM) from initiating testing in 2022 through August 2025, suggest that 97% of clinical isolates from UC San Diego hospitals are fluconazole resistant and micafungin resistance is observed only in 9% of clinical isolates (Table 1). Based on the antifungal susceptibility profiles of the current clinical isolates in UC San Diego hospitals, echinocandins remain the drug of choice for the treatment of C. auris infections.
C. auris Colonization and Its Impact on Patient Care
Like most pathogenic yeasts, C. auris has the ability to colonize humans. However, in contrast to Candida albicans, which is also in the WHO critical priority pathogens group, C. auris does not make hyphae, the filamentous fungal form that is used by C. albicans to invade host tissues3,15,16. C. auris exhibits a competitive advantage in colonization compared to C. albicans, potentially due to its ability to make aggregates and biofilms17,18 Colonization
precedes opportunistic infection, often in patients with compromised immune systems or those who have central lines placed. C. auris biofilms pose an additional challenge for patients with central lines. Additionally, the reduced penetration of echinocandins, the firstline therapy for C. auris, in urine, cerebral spinal fluid, and pleural fluid creates a barrier to treating C. auris in these locations, even if the isolates are deemed echinocandin-susceptible based on in vitro testing19.
Many healthcare systems have opted to isolate and screen patients for C. auris colonization to try to prevent transmission, since initial colonization of the patients poses the highest risk for C. auris infections. The CDC and CDPH recommend empiric contact or
enhanced barrier precautions for select patients in many healthcare facilities, including long-term acute care hospitals (LTACHs), ventilator-equipped skilled nursing facilities (vSNFs), and acute care hospitals (ACHs) until the diagnostic test results for C. auris are obtained for these patients20. At UC San Diego, patients are isolated and screened if they have stayed overnight in a healthcare facility outside of the U.S. in the past year, a U.S. hospital or SNF in the past six months, or were transferred from an LTACH.
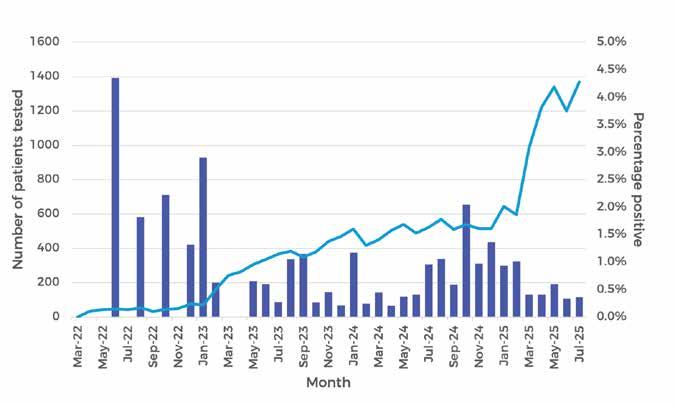
At many hospitals, diagnostic testing for screening purposes involves swabbing both axilla and inguinal creases. In the clinical laboratory, multiple methodologies may be used to identify C. auris, including culture-based methods and molecular techniques such as PCR. PCR can be advantageous with faster turnaround times and significantly increased sensitivity for the detection of C. auris21. However, if antifungal susceptibility testing is required, culturing the isolates on chromogenic Candida growth medium may be preferred either as a primary screening method or as reflex testing on specimens positive by PCR. On these indicator plates, C. auris is quickly differentiated from other pathogenic Candida species22. At UC San Diego Health, we currently process the screening samples by PCR and subculture PCR-positive specimens on selective media to be able to perform susceptibility testing and inform clinicians regarding the potential resistance to antifungals. Within the last three years, we have screened over 17,000 patients and are currently testing over 1,000 patients a month. Of particular importance, less than
Table 1. C. auris antifungal susceptibility test results at UC San Diego
0.5% of patients tested positive for C. auris colonization within the last six months (Figure 2).
While diagnostic testing for screening purposes is helpful in preventing the spread of C. auris colonization, the turnaround times for screening tests critically affect patient flow rates, as patients may require an individual room where contact precautions can be achieved until the results are negative. In order to allow for faster and more frequent testing, the UC San Diego CALM laboratory has recently adapted a smaller per-run assay (Simplexa® C. auris Direct, Diasorin), instead of large, batched testing, which would be done less frequently. Patient rooms, where a patient with a positive test for C. auris was admitted, require a terminal clean with an agent that has activity against C. auris, such as hydrogen peroxide or sodium hypochlorite23
The Future of C. auris Infection Prevention
Despite all efforts on active surveillance, patient isolation, and room cleaning, it is likely that C. auris will continue to spread in hospitals. Biofilm-forming capacity of C. auris makes it a very successful colonizer of abiotic surfaces in addition to human skin (reviewed in24). C. auris biofilms are also thought to contribute to rapid re-colonization of patients despite the chlorhexidine baths given to patients to eliminate C. auris25 .
Due to the difficulties in patient decolonization, a potential transmission event within a hospital setting remains a potential concern for healthcare providers. However, even if a transmission event is suspected, it is difficult to determine the relatedness of any given C. auris isolates. Determining that two isolates are clonal requires genomic sequencing and comparison, which is significantly more laborious in eukaryotic pathogens like C. auris, compared to bacteria. Due to the differences in DNA repair mechanisms between fungi and bacteria, fungi are more prone to chromosomal rearrangements and mutations as they propagate. Thus, even clonal isolates may have few mutations as they grow independently. While there are published studies trying to identify the threshold for the number of mutations to determine clonality, it is difficult to shed light on transmission patterns due to the lack of sequencing and culturing standards.
Lastly, C. auris likely has environmental reservoirs outside of the patient facilities, as it has been recovered from marine environments26 and detected in community wastewater27. Phylogenetic analyses suggested potential relatedness between the clinical and wastewater isolates27. However, future studies will determine whether the marine and clinical isolates have any genomic relatedness and whether environmental reservoirs of C. auris pose a risk for human health.
Figure 2. C. auris nucleic acid tests performed at UC San Diego
Funding
Dr. Beyhan is funded by the CDC Prevention Epicenters Program (1U54CK000603-01).
References
1. WHO fungal priority pathogens list to guide research, development and public health action. World Health Organization; 25 Oct 2022 [cited 24 Aug 2025]. Available: https://www.who.int/publications/i/item/9789240060241
2. Liu F, Hu Z-D, Zhao X-M, Zhao W-N, Feng Z-X, Yurkov A, et al. Phylogenomic analysis of the Candida auris-Candida haemuli clade and related taxa in the Metschnikowiaceae, and proposal of thirteen new genera, fifty-five new combinations and nine new species. Persoonia. 2024;52: 22–43. doi:10.3767/persoonia.2024.52.02
3. Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009;53: 41–44. doi:10.1111/j.1348-0421.2008.00083.x
4. Jeffery-Smith A, Taori SK, Schelenz S, Jeffery K, Johnson EM, Borman A, et al. Candida auris: A review of the literature. Clin Microbiol Rev. 2018;31. doi:10.1128/CMR.00029-17
5. Vallabhaneni S, Kallen A, Tsay S, Chow N, Welsh R, Kerins J, et al. Investigation of the first seven reported cases of Candida auris, a globally emerging invasive, multidrugresistant fungus-United States, May 2013-August 2016. Am J Transplant. 2017;17: 296–299. doi:10.1111/ajt.14121
6. Lee WG, Shin JH, Uh Y, Kang MG, Kim SH, Park KH, et al. First three reported cases of nosocomial fungemia caused by Candida auris. J Clin Microbiol. 2011;49: 3139–3142. doi:10.1128/JCM.00319-11
7. CDC. Tracking C. auris. In: Candida auris (C. auris) [Internet]. 8 Aug 2025 [cited 24 Aug 2025]. Available: https:// www.cdc.gov/candida-auris/tracking-c-auris/index.html
8. Department of Public Health. California Department of Public Health. [cited 24 Aug 2025]. Available: https://www. cdph.ca.gov/Programs/CHCQ/HAI
9. CDC. Antifungal Susceptibility Testing for C. auris. In: Candida auris (C. auris) [Internet]. 30 Apr 2024 [cited 24 Aug 2025]. Available: https://www.cdc.gov/candida-auris/ hcp/laboratories/antifungal-susceptibility-testing.html
10. Hsu C, Yassin M. Diagnostic approaches for Candida auris: A comprehensive review of screening, identification, and susceptibility testing. Microorganisms. 2025;13. doi:10.3390/microorganisms13071461
11. Center for Drug Evaluation, Research. Antifungal Susceptibility Test Interpretive Criteria. In: U.S. Food and Drug Administration [Internet]. FDA; 19 Aug 2025 [cited 24 Aug 2025]. Available: https://www.fda.gov/drugs/developmentresources/antifungal-susceptibility-test-interpretive-criteria
12. Fakhim H, Chowdhary A, Prakash A, Vaezi A, Dannaoui E, Meis JF, et al. In vitro interactions of echinocandins with triazoles against multidrug-resistant Candida auris Antimicrob Agents Chemother. 2017;61. doi:10.1128/AAC.01056-17
13. Ostrowsky B, Greenko J, Adams E, Quinn M, O’Brien B, Chaturvedi V, et al. Candida auris isolates resistant to three classes of antifungal medications - New York, 2019. MMWR Morb Mortal Wkly Rep. 2020;69: 6–9. doi:10.15585/ mmwr.mm6901a2
14. Hoenigl M, Sprute R, Egger M, Arastehfar A, Cornely OA, Krause R, et al. The antifungal pipeline: Fosmanogepix, ibrexafungerp, olorofim, opelconazole, and rezafungin. Drugs. 2021;81: 1703–1729. doi:10.1007/s40265-021-01611-0
15. Borman AM, Szekely A, Johnson EM. Comparative pathogenicity of United Kingdom isolates of the emerging pathogen Candida auris and other key pathogenic Candida species. mSphere. 2016;1. doi:10.1128/mSphere.00189-16
16. Chowdhary A, Sharma C, Duggal S, Agarwal K, Prakash A, Singh PK, et al. New clonal strain of Candida auris, Delhi, India. Emerg Infect Dis. 2013;19: 1670–1673. Available: http:// wwwnc.cdc.gov/eid/article/19/10/13-0393_article.htm
17. Bing J, Guan Z, Zheng T, Ennis CL, Nobile CJ, Chen C, et al. Rapid evolution of an adaptive multicellular morphology of Candida auris during systemic infection. Nat Commun 2024;15: 2381. doi:10.1038/s41467-024-46786-8
18. Horton MV, Johnson CJ, Kernien JF, Patel TD, Lam BC, Cheong JZA, et al. Candida auris forms high-burden biofilms in skin niche conditions and on porcine skin. mSphere. 2020;5: 134–138. Available: https://msphere.asm. org/lookup/doi/10.1128/mSphere.00910-19
19. Echinocandins. Meyler’s Side Effects of Drugs. Elsevier; 2016. pp. 6–14. doi:10.1016/b978-0-444-53717-1.00672-7
20. CDC. Implementation of Personal Protective Equipment (PPE) Use in Nursing Homes to Prevent Spread of Multidrug-resistant Organisms (MDROs). In: Long-term Care Facilities (LTCFs) [Internet]. 18 Mar 2025 [cited 25 Aug 2025]. Available: https://www.cdc.gov/long-term-carefacilities/hcp/prevent-mdro/PPE.html
21. Komorowski AS, Aftanas P, Porter V, Katz K, Kozak RA, Li XX. Verification, analytical sensitivity, cost-effectiveness, and comparison of 4 Candida auris screening methods. Open
Forum Infect Dis. 2024;11: ofae017. doi:10.1093/ofid/ofae017
22. CHROMagarTM Candida Plus. In: Chromagar [Internet]. 9 Nov 2021 [cited 25 Aug 2025]. Available: https://www. chromagar.com/en/product/chromagar-candida-plus/
23. Us Epa O. EPA’s Registered Antimicrobial Products Effective Against Candida auris [List P]. In: US EPA [Internet]. 28 Oct 2020 [cited 25 Aug 2025]. Available: https://www. epa.gov/pesticide-registration/epas-registered-antimicrobial-products-effective-against-candida-auris-list
25. Schelenz S, Hagen F, Rhodes JL, Abdolrasouli A, Chowdhary A, Hall A, et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob Resist Infect Control. 2016;5: 1–7. doi:10.1186/s13756-016-0132-5
26. Arora P, Singh P, Wang Y, Yadav A, Pawar K, Singh A, et al. Environmental isolation of Candida auris from the coastal wetlands of Andaman Islands, India. MBio. 2021;12.
doi:10.1128/mBio.03181-20
27. Rossi A, Chavez J, Iverson T, Hergert J, Oakeson K, LaCross N, et al. Candida auris discovery through community wastewater surveillance during healthcare outbreak, Nevada, USA, 2022. Emerg Infect Dis. 2023;29: 422–425.
doi:10.3201/eid2902.221523
Dr. Kline is an assistant professor at UC San Diego. She is the associate director of the Clinical Microbiology Laboratory for UC San Diego Health and also a practicing infectious disease physician. Dr. Beyhan is an associate professor in the department of infectious diseases at the J. Craig Venter Institute, where she serves as a principal investigator in the JCVI Prevention Epicenter funded by the CDC. She is also an assistant adjunct professor in the department of medicine at UC San Diego and a research biologist at the Veterans Affairs San Diego Healthcare System.
‘It’s Ok to Have a Dirty Urine’ (aka Asymptomatic Bacteriuria)
By Jessica Merchant, DNP, AGPCNP-BC, Bridget Olson, ID/ASP pharmacist consultant, CDPH, and Raymond Chinn, MD, FIDSA, FSHEA
DESPITE AGGRESSIVE CAMPAIGNS NOT TO TREAT asymptomatic bacteriuria (ASB), many clinicians continue to do so. ASB is defined as the presence of bacteria in the urine, in the absence of any signs or symptoms of infection. Treatment of ASB is recognized as one of the most important contributors to antibiotic overuse, and consequently, promotes the emergence of multidrug-resistant organisms (MDROs).
We would like to discuss ASB from three perspectives: (1) treatment of ASB in the emergency department (ED); (2) the myths associated with the diagnosis of UTI; and (3) the emergence of resistance resulting from treatment.
Childers and colleagues conducted an observational study reviewing patients at risk of UTI misdiagnosis in the ED.1 In this cohort, only 15% of patients who were treated for UTI actually had UTIs based on the presence of UTI symptoms and positive urine cultures, suggesting that 85% of patients did not have a UTI.
There are two scenarios that compel clinicians to treat ASB in the ED: pyuria and delirium. Bixby and colleagues observed that a significant number of ED visits led to the treatment of ASB, with pyuria being the only independent risk factor linked
to this treatment. Among the 254 ED patients with positive urine cultures who met the criteria for ASB, 80.7% were empirically treated for presumed UTI.2
A study done in the Netherlands examined the reasons behind the frequency of urine testing in the ED. It found that the urinalysis (UA) is often viewed as a rapid, non-invasive diagnostic tool and is commonly performed in EDs to promote a fast work process, even before a clinician’s examination.3 Frequently, an abnormal UA reflexes to a urine culture, which can often reflect colonization or contamination. Therefore, diagnostic stewardship, or “the culture of not culturing,” is an effective strategy to reduce the treatment of ASB.4
A “new onset” of delirium in an elderly person or a nonverbal resident from a skilled nursing facility (SNF) with an indwelling urinary catheter, even in the absence of UTI symptoms, often leads to a presumptive diagnosis of UTI in the ED. Such presentations may fulfil the Loeb criteria for initiation of antibiotic therapy, and they are most likely accompanied by pyuria.5
However, some facilities have successfully implemented a “watchful waiting” program, where UTI treatment is deferred
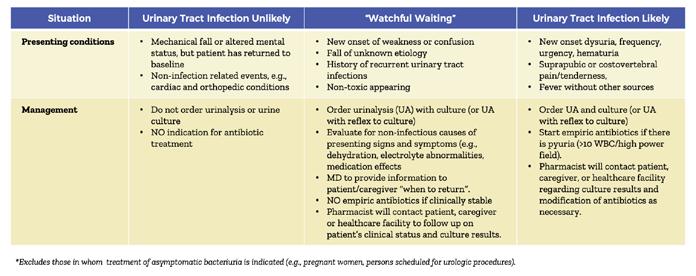
Figure 1. ‘Watchful waiting’ algorithm for ED evaluation of patients suspected of UTI, adapted from Scripps Healthcare ASP Guidelines*
INFECTIOUS DISEASES
for nontoxic patients. This approach includes a “safety net” of follow-up by a pharmacist, once urine culture results are available. Over the course of one year at one facility, out of 87 ED patients assigned to “watchful waiting,” only 15 (17%), were subsequently started on antibiotics after the pharmacist contacted the patient or facility, once the culture results were available. This approach necessitates considerable trust and collaboration among ED staff, the pharmacists, and the patients or outside facilities, (Fig 1).6
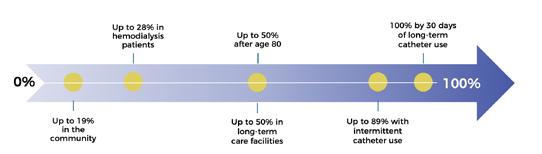
The chance of a positive urine culture (or an abnormal UA in the ED) is high, notably in the elderly or those transferring from SNFs, (Fig 2)7. A positive urine culture is often interpreted as a true UTI, despite the absence of localizing urinary symptoms, such as suprapubic or flank pain, new or worsening urgency or frequency, dysuria or hematuria. It is challenging for a provider to determine whether an older
patient and/or one with cognitive impairment may be symptomatic if he or she is unable to report localizing symptoms. Misdiagnosis can trigger inappropriate antibiotic prescribing. This can result in antimicrobial resistance, exposing patients to harmful side effects, escalating costs, and most importantly, delaying the correct diagnosis and effective therapy. Additionally, Childers found that urine testing was associated with
an increased length of stay in the ED.1
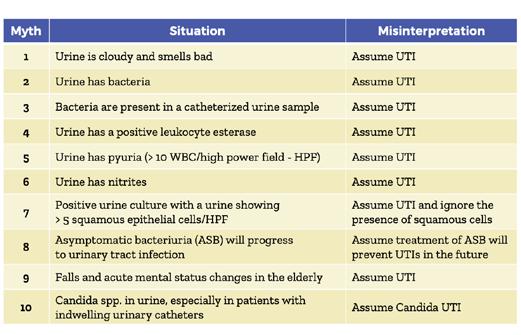
Myths surrounding the diagnosis of UTI in asymptomatic patients are common in clinical practice. (Fig 3).8 Possibly the most common is that cloudy and/ or malodorous urine (Myth 1) are indicative of a UTI; this has resulted in many calls from the nursing staff and family members to practitioners requesting urine testing. Although purulent urine may be cloudy and malodorous, these characteristics are more commonly reflective of diet and medications or hydration status. UAs associated with abnormal infection markers (Myths 2-6) may all be positive in the presence of a bacterial colonization of the urine. The presence of pyuria (UA WBC > 10) is the driver of most antibiotic initiations (Myth 5). Although pyuria has a strong negative predictive value for excluding urinary tract infection, its presence may reflect a range of non-infectious conditions — including biofilm formation in indwelling catheters, interstitial cystitis, pneumonia, nephrolithiasis, chronic inflammatory disorders — and may also be drug-induced by medications such as non-steroidal anti-inflammatory drugs, proton pump inhibitors, diuretics, and certain antibiotics.9 The detection of more than five squamous epithelial cells per high-power field suggests specimen contamination, with any resulting positive urine culture
Figure 3. Ten Common Myths Associated with the Diagnosis of Urinary Tract Infection (UTI) in the Asymptomatic Patient
Figure 2. The prevalence of asymptomatic bacteriuria (ASB) in select populations7 Adapted from Palomar Healthcare Antimicrobial Stewardship Program with permission.
potentially reflecting perineal or vaginal flora, rather than true urinary pathogens (Myth 7). Evidence does not support the assumption that asymptomatic bacteriuria can progress to a UTI if untreated (Myth 8). Falls and acute altered mental status changes (Myth 9) should not be attributed to infection (UTI) without investigating the many possible causes other than infection. And lastly, Candida spp. is especially common in patients with indwelling urinary catheters, often representing colonization. Patients with Candida upper tract infection or systemic infection associated with a UTI are almost always symptomatic (Myth 10).
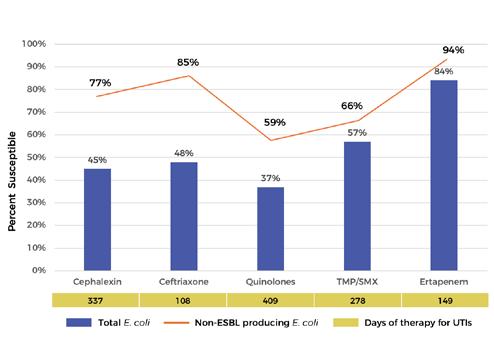
A composite of Escherichia coli susceptibilities from 3 ventilator-equipped skilled nursing facilities in 2002 reveals an alarming trend showing overall low antibiotic susceptibilities, including resistance to the quinolones of 37% and the carbapenems like ertapenem with 84% susceptibility. The carbapenems are the last line of therapy for many MDROs. (Figure 4). E. coli, representing 30% of the total isolates (237), is the most common organism isolated from urine. These isolates include 43% that were extended-spectrum beta-lactamase (ESBL) producing or carbapenem resistant, accounting for the low overall beta-lactam susceptibility. The susceptibilities are similar or lower for Proteus mirabilis, the second most common (28%) urinary isolate. For non-ESBL producing E. coli, the susceptibility pattern is such that the cephalosporins may be reasonable treatment options in these patients.
The upward trajectory of MDROs likely results from the overuse of antibiotics during the COVID-19 pandemic. As clini-
cians, it is important to obtain urine studies only in symptomatic individuals, except in the population where treatment of ASB is recommended. In addition to facilitating the emergence of MDROs, treatment of ASB is associated with the unintended consequences of patient harm from adverse reactions to antibiotics, increased costs, increased length of stay in the ED and missing the actual diagnosis. For nontoxic and nonverbal patients who present to the ED with nonspecific symptoms, “watchful waiting” is a strategy that, if successfully implemented, will have an impact on the treatment of ASB. Dispelling the myths associated with the diagnosis of UTI that leads to treatment of ASB requires ongoing educational efforts.
References:
1. Childers R, Liotta B, Brennan J, et.al. Urine testing is associated with inappropriate antibiotic use and increased length of stay in emergency department patients. Heliyon 2022;8(10):e11049. doi: 10.1016/j.heliyon.2022.e11049. PMID: 36281377; PMCID: PMC9587269.
2. Bixby M, Raux B, Bhalla A. Opportunities for antibiotic stewardship in emergency department or hospitalized patients with asymptomatic bacteriuria: identifying risk factors for antibiotic treatment. Antimicrob Steward Healthc Epidemiol 2022;31:1-4
3. Van Horik T, Laan B, Huizinga A, et al. Why are we frequently ordering urinalysis in patients without symptoms of UTI in the emergency department? Int J Environ Res Public Health 2022;19:10757.
Quinolones: ciprofloxacin and levofloxacin
TMP/SMX: trimethroprim/sulfamethoxazole
Comments:
• E.coli represented 30% of all isolates (N-237) in 2023; of these 43% were carbapenemresistant or extended-spectrum betalactamase producers.
• Quinolones are the most frequently prescribed antibiotic for UTI (DOT = 409) and associated with the lowest susceptibility profile (37%).
• The linear line depicts the antibiotic susceptibilities of non-ESBL producing E. coli.
Figure 4. A composite of Escherichia coli susceptibilities from 3 ventilator-equipped skilled nursing facilities in San Diego County
INFECTIOUS DISEASES
4. Vaughn V, Gupta A, Petty L, et. al. A statewide quality initiative to reduce unnecessary antibiotic treatment of asymptomatic bacteriuria. JAMA Intern Med.2023;183(9):933-941.
5. Loeb M, Bentley DW, Bradley S, et al. Development of minimum criteria for the initiation of antibiotics in residents of long-term-care facilities: results of a consensus conference. Infect Control Hosp Epidemiol 2001;22:120–124.
6. Personal Communication with Justin Lin, PharmD, Scripps Mercy Medical Center, San Diego, CA
7. Clinical Practice Guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Disease Society of America. Clin Infect Dis 2019;68:e83-e110.
8. Schulz L. Top ten myths regarding the diagnosis and treatment of urinary tract infections. J Emerg Med 2016;51:25-30
9. Wallace D, Hudson B, Delaney M. Urinalysis: A Simple Test with Complicated Interpretation. J Urgent Care Med July 1, 2020.
10. Facility-specific 2022 Antibiogram data from 3 ventilatorequipped skilled nursing facilities in San Diego County.
Jessica Merchant earned her doctorate of nursing practice at ECU and is currently working as a nurse practitioner at a very busy infectious disease practice, covering both inpatient and outpatient consultative services. Bridget Olson worked at Sharp Healthcare as an infectious disease pharmacist before joining the California Department of Public Health (CDPH) in 2022 for an ASP initiative aimed at improving antimicrobial stewardship in six ventilatorequipped skilled nursing facilities (vSNFs). This effort led to a collaboration between vSNFs, acute care emergency departments, and ASP teams across San Diego County to reduce the unnecessary treatment of asymptomatic bacteriuria. Dr. Chinn, a fellow of the Infectious Disease Society of America and the Society of Healthcare Epidemiology of America, was the medical director of infection prevention and clinical epidemiology for the Sharp Metropolitan Medical Campus, where he started the Antimicrobial Stewardship Program. His clinical interests include prevention of healthcare-associated infections, management of HIV infection, infections in transplant recipients, and infections involving vascular devices. Dr. Chinn joined the HealthcareAssociated Infections Program in the epidemiology and immunization services branch with the San Diego County Health and Human Services Agency as a medical consultant in 2019. He has assisted in COVID-19 mitigation efforts for long-term care facilities and has participated in outbreak investigations of healthcare-associated infections.
CLASSIFIEDS
PRACTICE ANNOUNCEMENTS
CRANIO/MAXILLOFACIAL AND HEAD & NECK SURGERY: Accepting new adolescent and adult patients seeking evaluation and management of head and neck masses, multidisciplinary assessment of oral/facial cancers and reconstruction, nasal airway assessment and functional rhinoplasty, corrective jaw surgery including jaw advancement for obstructive sleep apnea, cleft and craniofacial reconstruction, maxillofacial fracture management and secondary facial and jaw reconstruction. We work with Medicare, Tricare, most PPO insurance plans, and some HMO plans. Referrals may be called in to (619) 452-7332, or emailed to jaw@ scrippshealth.org. [2887-0808]
VIRTUAL SPEECH THERAPY AVAILABLE: Accepting new pediatrics and adult patients. We accept FSA/HSA, Private pay, Medicare, Medi-Cal, and several commercial insurance plans pending credentialing. Visit virtualspeechtherapyllc.org or call (888) 855-1309.
PSYCHIATRIST AVAILABLE: Accepting new patients for medication management, crisis visits, ADHD, cognitive testing, and psychotherapy. Out of network physician servicing La Jolla & San Diego. Visit hylermed.com or call (619) 707-1554.
PHYSICIAN OPPORTUNITIES
UCSD DEPARTMENT OF FAMILY MEDICINE | FACULTY POSITIONS AVAILABLE: UCSD Department of Family Medicine seeks motivated faculty to join our team in clinical, teaching, and scholarly roles. Faculty participate in comprehensive patient care, resident and fellow education, and research or quality improvement initiatives. We welcome candidates with diverse experiences and a passion for family medicine, community engagement, and academic medicine. Opportunities are available at various academic ranks, with salary commensurate with experience, rank, and step. Join a collaborative, supportive environment committed to excellence in primary care and education. Apply here: https://apol-recruit.ucsd.edu/JPF04341. [2889-0822]
OB/GYN PHYSICIAN | PHMG ESCONDIDO: Palomar Health Medical Group is seeking a full–time, board–certified/eligible Obstetrics and Gynecology Physician to deliver comprehensive reproductive care, including labor and delivery management, gynecologic surgeries, and OB call rotations. The ideal candidate will possess strong surgical skills, California licensure, and a commitment to maternal health. We offer competitive compensation, performance–based incentives, and a collaborative team environment. Please email CV to clayton.trosclair@ palomarhealth.org or phil.yphantides@phmg.org. [2882-0626]
FAMILY MEDICINE/INTERNAL MEDICINE PHYSICIAN | PHMG RANCHO PENASQUITOS: Palomar Health Medical Group is seeking a Family Medicine or Internal Medicine Physician (MD/DO) to join our multi–specialty practice at our Rancho Penasquitos clinic location. Experienced physicians and new graduates are encouraged to apply. Clinic schedule is Mon — Fri, outpatient only, no weekends or holidays. We offer competitive salary of $300k/ year or more depending on experience. In addition, we offer productivity and other bonuses, PTO, CME reimbursement, health, dental, vision insurance, participation in 401K with partial employer match, short and long–term disability, and life insurance. Student loan repayment assistance is also available. Join Palomar Health Medical Group, where we’re reimagining healthcare with compassion, excellence, and integrity. Please email CV to clayton.trosclair@ palomarhealth.org or phil.yphantides@phmg.org. [2881-0626]
FAMILY PRACTICE | INTERNAL MEDICINE PHYSICIAN: La Jolla Village Family Medical Group is seeking a PT/FT primary care physician to join our well–established private practice. We’ve been caring for our La Jolla/UTC area neighbors for 35+ years providing comprehensive, longitudinal care to patients of all ages. Call responsibilities are minor; hours consistent with a healthy work/life balance. Our office is new, clean, modern, and well-appointed. Our clinical team is collegial, passionate, and close-knit, with a supportive, cohesive support staff. A true private practice where physicians practice artfully and build enduring relationships with patients and colleagues. Seeking a Board-certified, California-licensed MD/DO physician, passionate about medicine and looking to establish roots in a practice dedicated to the art of good medicine. Competitive salary and excellent benefits including medical, dental, vision, and retirement. Send a cover letter and CV to jcataluna@lajollafamilymedical.com. [2880-0520]
CLINICAL DIRECTOR | BEHAVIORAL HEALTH SCIENCES | COUNTY OF SAN DIEGO: The County of San Diego is seeking a dynamic physician with a passion for building healthy communities. This is an exceptional opportunity for a California licensed, board-certified Physician to help transform the local behavioral health continuum of care and lead important work within the Health and Human Services Agency’s Behavioral Health Services department. Visit our website to view a detailed brochure outlining the duties and responsibilities of the position. Anticipated Hiring Range: $310,000 to $320,000 annually. In addition to the base salary, the incumbent may receive a 10 % premium for Board Certification or a 15 % premium for Board Certification and Sub–specialty. [2877-0225]
VENOUS DISEASE SPECIALIST | NORTH COUNTY: La Jolla Vein & Vascular, the premier vein care provider in San Diego, is seeking a highly skilled and experienced Venous Disease Specialist to join our team at our newest location in Vista, CA, nestled in the stunning coastal region of North County San Diego. This full-time position offers competitive salary and benefits, including profit-sharing and a 401(k). Our state-of-the-art facility operates Monday through Friday, with no weekend or night shifts, promoting an excellent work-life balance. Ideal candidates may also consider a locum or locum-to-hire arrangement. Join us in making a difference in our patients’ lives while enjoying your dream location! Email cv to jobs@ljvascular.com. [2875-1030]
PART–TIME PRIMARY CARE PHYSICIAN: Primary Care Clinic in San Diego searching for part-time physician for 1 to 2 days a week, no afterhours calls. Please send CV to medclinic1@ yahoo.com. [2872-0909]
OB/GYN POSITION AVAILABE | EL CENTRO: A successful Private OBGYN practice in El Centro, CA seeking a board eligible/ certified OB/GYN. Competitive salary and benefits package is available with a tract of partnership. J-1 Visa applicants are welcome. Send CV to feminacareo@gmail.com or call Katia M. at (760) 352-4103 for more information. [2865-0809]
COUNTY OF SAN DIEGO PROBATION DEPT. MEDICAL DIRECTOR: The County of San Diego is seeking dynamic physician leaders with a passion for building healthy communities. This is an exceptional opportunity for a California licensed, Board-certified, physician to help transform our continuum of care and lead essential medical initiatives within the County’s Probation Department. Anticipated Hiring Range: Depends on Qualifications Full Salary Range: $181,417.60 - $297,960.00 annually. As part of the Probation Administrative team, the Medical Director is responsible for the clinical oversight and leadership of daily operations amongst Probation facilities’ correctional healthcare programs and services. As the Medical
Director, you will have significant responsibilities for formulating and implementing medical policies, protocols, and procedures for the Probation Department.
PART–TIME CARDIOLOGIST POSITION AVAILABLE: Cardiology office in San Marcos seeking part–time cardiologist. Please send resume to Dr. Keith Brady at uabresearchdoc@yahoo.com. [2873-0713]
INTERNAL MEDICINE PHYSICIAN: Federally Qualified Health Center located in San Diego County has an opening for an Internal Medicine Physician. This position reports to the chief medical officer and provides the full scope of primary care services, including diagnosis, treatment, and coordination of care to its patients. The candidate should be board eligible and working toward certification in Internal Medicine. Competitive base salary, CME education, four weeks paid vacation, year one, 401K plan, No evenings and weekends, Monday through Friday 8:00am to 5:00pm. For more information or to apply, please contact Dr. Keith Brady at: uabresearchdoc@yahoo.com. [2874-0713]
FAMILY MEDICINE/INTERNAL MEDICINE PHYSICIAN: San Diego Family Care is seeking a Family Medicine/Internal Medicine Physician (MD/DO) at its Linda Vista location to provide outpatient care for acute and chronic conditions to a diverse adult population. San Diego Family Care is a federally qualified, culturally competent and affordable health center in San Diego, CA. Job duties include providing complete, high quality primary care and participating in supporting quality assurance programs. Benefits include flexible schedules, no call requirements, a robust benefits package, and competitive salary. If interested, please email CV to sdfcinfo@sdfamilycare.org or call us at (858) 810-8700.
PHYSICIAN POSITIONS WANTED
HOSPITAL BASED GROUP SEEKING A BOARD ELIGIBLE/ BOARD CERTIFIED PSYCHIATRIST IN SAN DIEGO. Competitive base salary with performance based bonus. Comprehensive benefits package is available. Send CV to sdpcc@yahoo.com
PART–TIME CARDIOLOGIST AVAILABLE: Dr. Durgadas Narla, MD, FACC is a noninvasive cardiologist looking to work 1-2 days/ week or cover an office during vacation coverage in the metro San Diego area. He retired from private practice in Michigan in 2016 and has worked in a San Marcos cardiologist office for the last 5 years, through March 2023. Board certified in cardiology and internal medicine. Active CA license with DEA, ACLS, and BCLS certification. If interested, please call (586) 206-0988 or email dasnarla@gmail.com.
OFFICE SPACE / REAL ESTATE AVAILABLE
AVAILABILITY OF UTC MEDICAL OFFICE: Office in UTC area. 2-3 exam rooms, ample waiting room, 2 private offices. Ground floor location. Just one block from 805 exit. Close to Genesee Ave, all major shopping and restaurants in UTC. Parking available. Ground floor office, handicapped accessible. Six month-one year lease available with possibility to renew. Call (619) 585-0476. Ask for Alisha. [2890-0825]
MEDICAL OFFICE FOR SALE OR LEASE: Up to $2,000 Cash Finder’s Fee for referring a colleague | Class A Nordahl Medical Center near Palomar Medical Center | First floor office with waiting room, private restroom and several office/exam rooms newly built out with high end finishes. Abundant 5/1000 parking and natural light with expansive window line in exams/offices and waiting room/reception area. Walking distance to retail centers, which is great for staff to take a walking lunch break and/or patients to visit before or after an appointment. Listing Agent for details: Joshua J Smith (619) 797-1322 | Joshua.Smith@SVN.com | DRE#01476024 [2884-0804]
GORGEOUS BOUTIQUE OFFICE SPACE IN PRIME LOCATION FOR PER DIEM RENTAL: A newly remodeled and meticulously decorated medical office in University Heights, close to UCSD and Scripps Mercy, available for share including one large furnished patient exam room plus ample shared space (front office, patient wait room, kitchen). Looking for specialty physician preferably and able to do per diem or monthly agreement. The office is shared with 1 other provider and is located on Park Blvd near Adams Ave. Available immediately and turnkey ready. Please contact info@prosperaima.com or (619) 206-4232 for more information. [2883-0804]
OFFICE SPACE FOR LEASE | AESTHETIC SETTING: Take your practice to the next level with this beautifully appointed office space available in a modern, fully equipped clinical environment. Whether you’re already in aesthetics or starting an aesthetic practice, we offer flexible, high-end rental options. Rentals include use of PicoSure Pro Laser and Potenza Microneedling with Radiofrequency, two private treatment rooms and staff breakroom in a professional, clean and serene setting. Available Mondays, Tuesdays, Thursdays & Fridays at $1,000/day between the hours of 8:30am–5:00pm. Ideal for dermatologists/plastic surgeons, cosmetic physicians, nurse injectors or other licensed professionals in the aesthetic field. Must see to appreciate the quality and atmosphere. Contact us today at Vivian@sandiegomobiledoctor.com to schedule an in-person tour of this great opportunity. [2886-0804]
OFFICE SPACE FOR LEASE | MEDICAL SETTING: Take your practice to the next level with this beautifully appointed office space available in a modern, fully equipped clinical environment. Whether you’re in primary care or specialty medicine, we offer flexible, high-end rental options. Rentals include use of two medical exam rooms and waiting (lobby) area in a clean, professional setting. Available Mondays, Tuesdays, Thursdays and Fridays at $350/half day or $600/day between the hours of 8:30am–5:00pm. Ideal for primary care physicians and specialists seeking flexible space. Must see to appreciate the quality and atmosphere. Contact us today at Vivian@sandiegomobiledoctor.com to schedule an in–person tour of this great opportunity. [2885-0804]
LA JOLLA/XIMED OFFICE TO SUBLEASE: Modern upscale office on the campus of Scripps Hospital — part or full time. Can accommodate any specialty. Multiple days per week and full use of the office is available. If interested please email kochariann@yahoo. com or call (818) 319-5139. [2866-0904]
SUBLEASE AVAILABLE: Sublease available in modern, upscale Medical Office Building equidistant from Scripps and Sharp CV. Ample free parking. Class A+ office space/medical use with highend updates. A unique opportunity for Specialist to expand reach into the South Bay area without breaking the bank. Specialists can be accommodated in this first floor high-end turnkey office consisting of 1670 sq ft. Located in South Bay near Interstate 805. Half day or full day/week available. South Bay is the fastest growing area of San Diego. Successful sublease candidates will qualify to participate in ongoing exclusive quarterly networking events in the area. Call Alicia, (619) 585-0476.
MEDICAL OFFICE FOR SALE OR SUBLEASE: A newly remodeled and fully built-out primary care clinic in a highly visible Medical Mall on Mira Mesa Blvd. at corner of Camino Ruiz. The office is approximately 1000 sq ft with 2 fully equipped exam rooms, 1 office, 1 nurse station, spacious and welcoming waiting room, spacious reception area, and ADA accessible restroom. All the furniture and equipment are new and modern design. Ample parking. Perfect for primary care or any specialty clinic. Please contact Nox at (619) 7765295 or noxwins@hotmail.com. Available immediately.
RENOVATED MEDICAL OFFICE AVAILABLE | EL CAJON:
Recently renovated, turn-key medical office in freestanding singlestory unit available in El Cajon. Seven exam rooms, spacious waiting area with floor-to-ceiling windows, staff break room, doctor’s private office, multiple admin areas, manager’s office all in lovely, droughtresistant garden setting. Ample free patient parking with close access to freeways and Sharp Grossmont and Alvarado Hospitals. Safe and secure with round-the-clock monitored property, patrol, and cameras. Available March 1st. Call 24/7 on-call property manager Michelle at the Avocado Professional Center (619) 916-8393 or email help@avocadoprofessionalcenter.com.
OPERATING ROOM FOR RENT: State of the Art AAAASF Certified Operating Rooms for Rent at Outpatient Surgery of Sorrento. 5445 Oberlin Drive, San Diego 92121. Ideally located and newly built 5 star facility located with easy freeway access in the heart of San Diego in Sorrento Mesa. Facility includes two operating rooms and two recovery bays, waiting area, State of the Art UPC02 Laser, Endoscopic Equipment with easy parking. Ideal for cosmetic surgery. Competitive Rates. Call Cyndy for more information (858) 658-0595 or email Cyndy@roydavidmd.com.
PRIME LOCATION | MEDICAL BUILDING LEASE OR OWN OPPORTUNITY IN LA MESA: Extraordinary opportunity to lease or lease-to-own a highly visible, freeway-oriented medical building in La Mesa, on Interstate 8 at the 70th Street on-ramp. Immaculate 2-story, 7.5k square foot property with elevator and ample free onsite parking (45 spaces). Already built out and equipped with MRI/ CAT machine. Easy access to both Alvarado and Sharp Grossmont Hospitals, SDSU, restaurants, and walking distance to 70th St Trolley Station. Perfect for owner-user or investor. Please contact Tracy Giordano [Coldwell Banker West, DRE# 02052571] for more information at (619) 987-5498.
KEARNY MESA OFFICE TO SUBLEASE/SHARE: 5643 Copley Dr., Suite 300, San Diego, CA 92111. Perfectly centrally situated within San Diego County. Equidistant to flagship hospitals of Sharp and Scripps healthcare systems. Ample free parking. Newly constructed Class A+ medical office space/medical use building. 12 exam rooms per half day available for use at fair market value rates. Basic communal medical supplies available for use (including splint/ cast materials). Injectable medications and durable medical equipment (DME) and all staff to be supplied by individual physicians’ practices. 1 large exam room doubles as a minor procedure room. Ample waiting room area. In office x-ray with additional waiting area outside of the x-ray room. Orthopedic surgery centric office space. Includes access to a kitchenette/indoor break room, exterior break room and private physician workspace. Open to other MSK physician specialties and subspecialties. Building occupancy includes specialty physicians, physical therapy/occupational therapy (2nd floor), urgent care, and 5 OR ambulatory surgery center (1st floor). For inquiries contact kdowning79@gmail.com and scurry@ortho1. com for more information. Available for immediate occupancy.
LA JOLLA/UTC OFFICE TO SUBLEASE OR SHARE: Modern upscale office near Scripps Memorial, UCSD hospital, and the UTC mall. One large exam/procedure room and one regular-sized exam room. Large physician office for consults as well. Ample waiting
room area. Can accommodate any specialty or Internal Medicine. Multiple days per week and full use of the office is available. If interested please email drphilipw@gmail.com.
ENCINITAS MEDICAL SPACE AVAILABLE: Newly updated office space located in a medical office building. Two large exam rooms are available M-F and suitable for all types of practice, including subspecialties needing equipment space. Building consists of primary and specialist physicians, great for networking and referrals. Includes access to the break room, bathroom and reception. Large parking lot with free parking for patients. Possibility to share receptionist or bring your own. Please contact coastdocgroup@ gmail.com for more information.
NORTH COUNTY MEDICAL SPACE AVAILABLE: 2023 W. Vista Way, Suite C, Vista CA 92082. Newly renovated, large office space located in an upscale medical office with ample free parking. Furnishings, decor, and atmosphere are upscale and inviting. It is a great place to build your practice, network and clientele. Just a few blocks from Tri-City Medical Center and across from the urgent care. Includes: multiple exam rooms, access to a kitchenette/break room, two bathrooms, and spacious reception area all located on the property. Wi-Fi is not included. For inquiries contact hosalkarofficeassist@gmail.com or call/text (858) 740-1928.
MEDICAL EQUIPMENT / FURNITURE FOR SALE
FRIDGE & FREEZER EQUIPMENT AVAILABLE | MINT CONDI-
TION: Pristine medical cold storage refrigeration equipment available for purchase by Champions for Health, SDCMS’ philanthropic 501(c)3. Used to store vaccines. Includes 2 (two) commercial-grade Accucold ARG49ML 49 cu ft upright pharmacy refrigerators each with two glass doors, automatic defrost, digital thermostat and stainless steel cabinets (83.75” H x 55.25” W x 31.0” D), plus 1 (one) pharmaceutical–grade TempArmour BFFV15 compact freezer built to ensure stable temperatures and virtually eliminate supply losses (26.5” H x 25.0” W x 31.0” D). All units were acquired new, in use between 2-4 years and in very gently used condition. Units meet all CDC guidelines for vaccine storage. Asking price for each fridge is $4,000 OBO and $2,500 OBO for the freezer. Purchase individually or as a set. Contact Adama at (858) 300–2780 or adama.dyoniziak@championsfh.org. [2879-0502]
NON–PHYSICIAN POSITIONS AVAILABLE
NURSE PRACTITIONER | PHYSICIAN ASSISTANT: Open position for Nurse Practitioner/Physician Assistant for an outpatient adult medicine clinic in Chula Vista. Low volume of patients. No call or weekends. Please send resumes to medclinic1@yahoo.com. [2876-1121]
POSTDOCTORAL SCHOLARS: The Office of Research Affairs, at the University of California, San Diego, in support of the campus, multidisciplinary Organized Research Units (ORUs) https:// research.ucsd.edu/ORU/index.html is conducting an open search for Postdoctoral Scholars in various academic disciplines. View this position online: https://apol-recruit.ucsd.edu/JPF03803. The postdoctoral experience emphasizes scholarship and continued research training. UC’s postdoctoral scholars bring expertise and creativity that enrich the research environment for all members of the UC community, including graduate and undergraduate students. Postdocs are often expected to complete research objectives, publishing results, and may support and/or contribute expertise to writing grant applications https://apol-recruit.ucsd. edu/JPF03803/apply. [2864-0808]
RESEARCH SCIENTISTS (NON–TENURED, ASSISTANT, ASSOCIATE OR FULL LEVEL): The University of California, San Diego campus multidisciplinary Organized Research Units (ORUs) https://research.ucsd.edu/ORU/index.html is conducting an open search for Research Scientists (non–tenured, assistant, associate or full level). Research Scientists are extramurally funded, academic researchers who develop and lead independent research and creative programs similar to Ladder Rank Professors. They are expected to serve as Principal Investigators on extramural grants, generate high caliber publications and research products, engage in university and public service, continuously demonstrate independent, high quality, significant research activity and scholarly reputation. Appointments and duration vary depending on the length of the research project and availability of funding. Apply now at https://apol-recruit.ucsd.edu/JPF04188/apply. [2867-0904]
PROJECT SCIENTISTS: Project Scientists (non-tenured, Assistant, Associate or Full level): The University of California, San Diego, Office of Research and Innovation https://research.ucsd.edu/, in support of the Campus multidisciplinary Organized Research Units (ORUs) https://research.ucsd.edu/ORU/index.html is conducting an open search. Project Scientists are academic researchers who are expected to make significant and creative contributions to a research team, are not required to carry out independent research but will publish and carry out research or creative programs with supervision. Appointments and duration vary depending on the length of the research project and availability of funding: https:// apol-recruit.ucsd.edu/JPF04189/apply. [2868-0904]
8690
Day at the Races
Del Mar Thoroughbred Club – Crosby Celebrity Suite Friday, November 21, 2025
Join us for Champions for Health’s Day at the Races at the Del Mar Thoroughbred Club. Enjoy an exclusive afternoon of exciting horse racing, delicious food, and refreshing drinks while supporting vital healthcare programs for San Diego’s underserved communities.
12:00 pm – 4:00 pm (1st race is at 12:30 pm)
Del Mar Fairgrounds 260 Jimmy Durante Blvd, Del Mar, CA 92014 For sponsorship information, please contact Gabriela Stichler at gabriela.stichler@championsfh.org or at 858-300-2789 • Race4Health.givesmart.com