Foundations for Direct Support Master Trainer Manual 2025
Dear participants,
Welcome to Foundations of Direct Support: A National Training for Direct Support Practitioners, Training of Master Trainers.
On behalf of Keystone Institute India, we would like to thank you for setting aside significant time and commitment to become master trainers of this rich and new development course to promote the competence of direct support practitioners across India. We realize that time away from typical responsibilities is a major investment of your time and energy, and we are glad that both you and your organization have committed to learning about and teaching Foundations of Direct Support for a new and respected profession within India, all working towards rich, full lives for people with intellectual and developmental disabilities.
In keeping with our commitment to providing high-quality, value based training, Keystone Institute India brings to you a comprehensive training program that will create the third cadre of Master Trainers – YOU are one of them – and who will go on to develop highly competent and sensitive Direct Support Practitioners who can support and empower people with disabilities to lead rich, valued, and meaningful lives.
We are fortunate to have excellent faculty who bring with them decades of experience both on the ground and in training for this course. Many of our faculty are content experts and leaders in this space and are passionate about implementing and training in best practices.
We are also happy and honored that you have taken the time to invest in this rigorous and demanding training course, and we hope that you will leave this event with a passion and commitment to teach others and learn more. We are excited to partner with you and support your endeavours in enhancing the lives of the people you serve.
Elizabeth Neuville and Chitra Paul
eneuville@khs.org
Keystone Institute India cpaul@khs.org
M-14 A, Second Floor, South Extension Part-2
New Delhi-110049
Tel: 011 45649719/45644368
acKnowledgements
This course curriculum and content is a labour of love and intensive research. It brings together the ideas and voices of leading experts across the world including India. We are deeply appreciative to Leela Raj, during her tenure as Project Leader at KII, for her work as the developer of this curriculum and the primary designer and editor of these materials. Our heartfelt gratitude to content experts Aparna Das, Shampa Sengupta, Parul Kumtha, Nirupa Bhangar, and Milton Tyree and Darcy Elks in the USA. This crucial training would not have been possible without the critical insights and expert reviews from Betsy Neuville, Executive Director, Keystone Institute, Poonam Natarajan, Merry Barua, Dr Nidhi Singhal, Dr Neelam Sodhi, Geeta Mondol, and Joy Hopkins in Georgia, USA and to them we offer our heartfelt appreciation. Our sincere thanks to Nidhi Anand who made the materials come alive with powerful, visually appealing PowerPoint slide decks. And last but not the least, we offer our gratitude to all the individuals and organizations who willingly contributed their time and feedback in our pilot series the results of which are evident in this training. Finally, gratitude to the Rural India Supporting Trust, our partners in creating change across India in the lives of people with disability and their families. Please respect the work and do not copy or disseminate further. All materials herein are taught with permission from the developers.
2. Module 1a: A Deeper Look at Disability: Disability is Natural
3. Module 1b: A Deeper Look at Disability: Myths and Facts about Disability
4. Module 1c: A Deeper Look at Disability: Models of Disability
5. Module 1d: A Deeper Look at Disability: An Overview of Developmental Disabilities
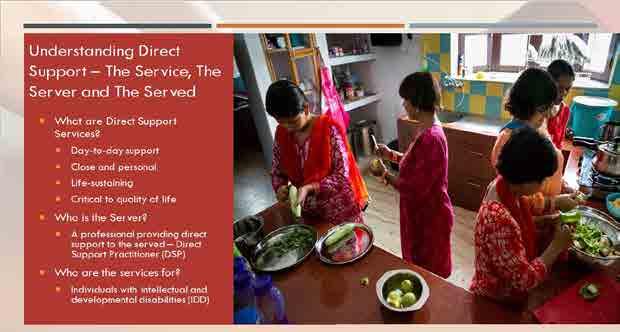
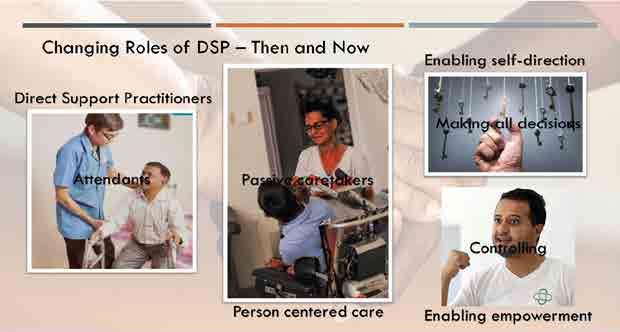
6. Module 2: Understanding Direct Support Services
7. Module 3: Code of Ethics
8. Module 4: Person-Centred Thinking
9. Module 5: The Basics of Social Role Valorization
https://www.youtube.com/ watch?v=Cq8rkqKZiyI
https://youtu.be/sZWV6_ C5MY0
...People learn very quickly when they have a need for the skills and information. If it will change their lives, if it will help them accomplish what is important to them, everyone can become a good learner. We learn complex competencies and knowledge in a matter of weeks, not months or years. And people learn best in community, when they are engaged with one another, when everyone is both student and teacher, expert and apprentice, in a rich exchange of experiences and learnings.
- Margaret Wheatley
course overview
Purpose of Course
The Foundations of Direct Support: A National Training Program for Direct Support Practitioners is a Training Course for Master Trainers. This course seeks to create a powerful cadre of Master Trainers who will contribute to realizing our shared vision of developing a highly competent professional workforce of Direct Support Practitioners (DSP).
The overarching goal of this course is to create a respected and valued profession of direct support service in India. Grounded on principles of person-centred approaches and Social Role Valorization, this comprehensive training program seeks to develop a professional community of Direct Support Practitioners that is not just sensitive and caring but is also competent and ethical – a trained workforce of professionals who work alongside people with intellectual and developmental disabilities to support and empower them to live rich, full, and meaningful lives.
Trainer Qualifications
Education/Work:
A bachelor’s degree in special education/psychology/occupational therapy/speech and language pathology/social work/physiotherapy, or social sciences like disability studies.
A professional with experience of working with people with intellectual & developmental disabilities for 3-5 years.
A caregiver with a bachelor’s or master’s degree in any subject with relevant professional work experience of 5 years minimum.
Additional Requirements:
Commitment to inclusive practices
Excellent proficiency in English (both speaking and writing skills are important)
Proficiency in any Indian language would be an added benefit.
The person should have prior experience of conducting trainings/workshops in the last 3 years.
Use of the Course Materials
These course materials may be used by persons approved by Keystone Institute India (KII) who have been duly trained.
Brief Course Reports will be submitted by trainers after any modules are taught so their use can be tracked.
Periodic revisions to the course materials will be made by KII and circulated to approved trainers.
The course is recommended to be taught with the modules in sequence.
Part 1 (Modules 1-5) should be taught in its entirety and in sequence. Part 2 (Module 6-14) may be taught in sections and in a flexible sequence, although Trainers are encouraged to use the recommended sequence.
Trainers may personalize the materials in minor ways such as adding trainer photographs, etc., especially in the opening and closing slide sets.
All materials must remain with the KII and RIST logos and with full credit for development in the materials and in the participants manuals.
Trainer materials and speaker notes must be protected and safeguarded – they may not be shared with others.
KII will provide each trainer with participants manual samples in English.
Powerpoint presentations will be available in Hindi (Phase 1 & 2), Tamil (Phase 1 & 2) and Bengali (Phase 1) in addition to English (Phase 1 & 2) for access on the FDS website for all credentialed Master Trainers.
Speaker notes are given as guidelines - trainers may adapt them to suit their own style.
Modules, Sections and Approximate Duration
Community is much more than belonging to something; it’s about doing something together that makes belonging matter.
- Brian Solis
Kii mentorship
kII Support for Trainers
As with all our trainings, KII will provide ongoing support and guidance as you move ahead teaching and training promising and aspiring Direct Support Practitioners:
Keystone Institute India will provide all materials, PowerPoints, speakers notes and trainer training for each module, downloadable and in print if needed.
Keystone Institute India will host an Online FDS Trainer’s Forum for the use of trainer communication, assistance, and networking.
KII is available to support individual trainers with planning and problem solving as needed via a helpline for FDS Trainers.
KII will periodically update and improve the materials based on Trainer experiences.
A helpline for trainer support will be provided.
To discover a new way of coming to know their clients as people, the participating staff must be introduced to a tool that is grounded in the values, beliefs and assumptions of typical citizenship and community.
- Jerry Kiracofe
welcoming & opening
Foundations of Direct Support
A National Professional Training Program for those working dire ctly with people with intellectual and developmental disabilities
About the Trainers
Pathway to Effective Direct Support Practice
Knowledge & Skill Development
Promoting Health & Wellbeing
Positive Approaches to Challenging Behaviour
Community Membership
Family Collaborations and Individual Voices
Laying the Foundation
A Deeper Look at Disability
Understanding Direct Support Services
Code of Values & Ethics
Person-CenteredThinking
An Orientation to Social Role Valorization
Promoting Competence
Sexual Wellbeing
Legal Framework
Advocacy and Activism
Taking Leadership
Wrap Up & Certification
Disability is a matter of perception. If you can do just one thing well, you’re needed by someone.
- Martina Navratilova module 1: a deeper look at disability
A Simple Fact
People to walk beside you…
• To care about your future
• To open some doors
• To appreciate your gifts
Your Task
Your group leader allows you a few minutes to reflect on the question, and each group members shares their thoughts.
The group then discusses and decides on ONE INSIGHT they have gained from their conversation.
Using wall, please write (or draw!) your group insight
Track time
The Role of Group Leader
All
Voices are Heard
Organize the Group to Complete the Task
Section 2: Myths and Facts
Myth or Fact?
Disability does not define the identity of the person.
Fact
Disability does not define the identity of the person. Disability is just one aspect of the person.
Myth or Fact?
Non-disabled people are obligated to “take care of” people with disabilities.
Myth
People may offer assistance to whomever they choose, but most people with disabilities prefer to be responsible for themselves.
Myth or Fact?
Wheelchair use is confining; people who use wheelchairs are “wheelchair-bound.”
Myth
A wheelchair, like a bicycle or an automobile, is a personal assistive device that enables someone to get around.
Myth or Fact?
People with disabilities are more comfortable with “their own kind.”
Myth
People with disabilities like anyone else are most comfortable with people they like and enjoy spending time with.
Myth or Fact?
People with disabilities are less likely to have accidents than other employees
Fact
Studies find that workers with disabilities perform significantly higher than their counterparts without disabilities in the area of safety.
Myth or Fact?
Curious children should never stare at or ask people about their disabilities.
Myth
Many children have a natural, uninhibited curiosity and may stare or ask questions that some adults consider embarrassing. But scolding curious children may make them think having a disability is “wrong” or “bad”.
Myth or Fact?
People with disabilities live totally different lives from people without disabilities.
Myth
People with disabilities are people first –they have the same needs, dreams, hopes, and desires like everyone else.
Myth or Fact?
Most people with disabilities cannot have sexual relationships.
Myth
People with disabilities, like other people, are sexual beings.
Myth or Fact?
People with disabilities deserve pity.
Myth!
People with disability do not suffer because of their disability. Having a disability does not automatically mean a poor quality of life.
Myth or Fact?
People with disabilities can lead a productive and a fulfilling life.
Fact!
People with disabilities are capable of participating fully in community life just like their peers without disabilities. The challenge is to focus on their abilities not on their limitations.
Myth or Fact?
People with disability are sick and in constant pain.
Myth!
People with disabilities are like people without disabilities –they get sick on occasion or sometimes may be in pain.
Myth or Fact?
Some disabilities may not be visible.
Fact
Not every disability is physical or can be easily seen.
The Moral/Religious Model
Act of God
Consequence of acts
Test of faith
Redemption
" some disabilities are the result of lack of adherence to social morality and religious proclamations that warn against engaging in certain behaviour some disabilities are the result of punishment from an allpowerful entity " - Henderson & Bryan, 2011
“Individuals and families are specially selected by God to receive a disability and are given the opportunity to redeem themselves through their endurance, resilience, andpiety "
-Niemann, 2005
The Medical Model
• Medical problem/diagnosis
• Abnormal/pathological
• Goal to cure
• Role of patient/client
"The medical model of interpretation of disability projects a dualism which tends to categorise the able-bodied as somehow 'better' or superior to people with disabilities "
-Johnstone, 2012
“Apersonal tragedy for both the individual and her family, something to be prevented and, if possible, cured. "
-Carlson, 2010
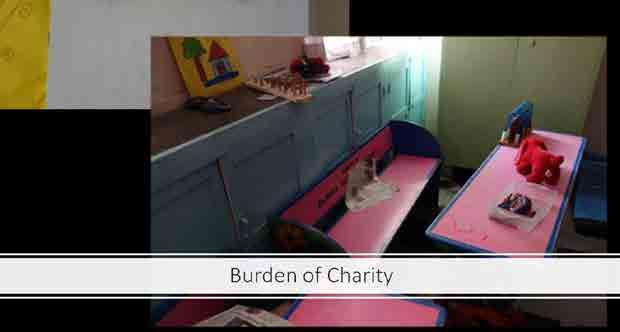
• Special services The Charity Model
• Victims of circumstances
• Objects of pity
• Assistance from able-bodied
"The Charity Model sees people with disabilities as victims of their impairment. Their situation is tragic, and they are suffering. "
-Duyan, 2007
The Social Model
• Social construct
• Social aspects of disability
• Impairment vs disability
• Strong influence on current social policies
“[D]isability is a situation, caused by social conditions, which requires for its elimination, (a) that no one aspect such as incomes, mobility or institutions is treated in isolation, (b) that disabledpeople should, with the advice and help of others, assume control over their own lives, and (c) that professionals, experts and others who seek to help must be committed to promoting such control by disabledpeople. ”
-Fundamental Principles of Disability, UPIAS, 1976
“[D]isabledpeople are people who are “disabled” by the society they live in and by the impact of society’s structures and attitudes ”
-Purtell, 2013
The Human Rights Model
"The human rights model focuses on the inherent dignity of the human being and subsequently, but only if necessary, on the person ’ s medical characteristics. It places the individual centre stage in all decisions affecting him/her and, most importantly, locates the main ‘problem’ outside the person and in society. "
-Quinn & Degener, 2002
the power oF words & respectFul language (handout)
PoSITIVE worDS
Winner Love Pride Fair Strength Enable Allow Able Unique Choice Possible Include Capable Potential Support Talent Assist Determined Empower Enduring Engage Accept Befriend Embrace Care Help
Words can make you feel a certain way. The words you use can affect how other people feel and how you act towards them. The positive words on this Worksheet can help you treat others in a more respectful way. YOU HAVE THE POWER TO CHOOSE HOW YOU USE WORDS.
The words we use when talking to or describing others can be very powerful. Sometimes the negative words we use about disability causes us to see what the person cannot do before we see their abilities. For example, when you say handicapped, you automatically look at that individual’s challenges. Instead, say someone with a disability… See the PERSON before the disability. People with disabilities are people like everyone else.
Disability is natural; it does not make a person less valuable to society. When we interact with people with disabilities we should focus on their unique personal characteristics instead of defining who they are based on their disability. Having a disability is not a “problem”, it is a natural part of life. The words we use have the power to build positive images about disability.
Respectful language is important to everyone and especially so for people with disabilities as it conveys respect and acknowledgement that they are viewed as a person with his or her unique identity and an identity beyond the disability. The words we use to describe one another can have an enormous impact on the perceptions we and others have, how we treat one another, mutual expectations, and how welcome we make people feel.
Here are a few guidelines that explain preferred terminology and offer suggestions for appropriate ways to describe people with disabilities.
1. Do not focus on a disability unless it is crucial to a situation. Avoid tear-jerking human interest stories about incurable diseases, congenital impairments, or severe injury. Focus instead on issues that affect the quality of life for those same persons, such as accessible transportation, housing, affordable health care, employment opportunities, and discrimination.
2. Do not portray successful people with disabilities as superhuman. Even though the public may admire super-achievers, portraying people with disabilities as superstars raises false expectations that all people with disabilities should achieve at this level.
3. Do not sensationalize a disability by saying afflicted with, crippled with, suffers from, victim of, and so on. Instead say person who has multiple sclerosis or man who had polio.
4. Do not use generic labels for disability groups, such as “the retarded,” “the deaf.” Emphasize people, not labels. Say “people with intellectual disabilities” or “people who are deaf”.
5. Put people first, not their disability. Say “woman with arthritis,” “children who are deaf,” “people with disabilities.” This puts the focus on the persons, not the particular functional limitation. Crippled, deformed, suffers from, victim of, the retarded, infirm, etc. are never acceptable under any circumstances.
6. Emphasize abilities, not limitations. For example, say: “uses a wheelchair/braces,” “walks with crutches,” rather than “confined to a wheelchair,” “wheelchair-bound” or “is crippled.” Similarly, do not use emotional descriptors such as “unfortunate,” “pitiful,” and so forth.
7. Do not imply disease when discussing disabilities that result from a prior disease episode. People who had polio and experience its aftereffects years later have a post polio disability. They are not
currently experiencing the disease. Do not imply disease with people whose disability has resulted from anatomical or physiological damage (e.g., person with spina bifida or cerebral palsy). Reference to a disease associated with a disability is acceptable only with chronic diseases, such as arthritis, Parkinson’s disease, or multiple sclerosis. People with disabilities should never be referred to as “patients” or “cases” unless their relationship with their doctor is under discussion.
8. Promote that people with disabilities are active participants of society. We know that persons with disabilities interacting with non-disabled people in social and work environments help break down barriers and open lines of communications.
9. And last, but most importantly, respect the person’s preference in the way they are referred to or described.
Examples of respectful Language (by kathie Snow)
SAY INSTEAD of
People with disabilities
He has a cognitive disability/intellectual disability
She has autism
He has Down syndrome
She has a learning disability
He has a physical disability
She’s of short stature/she’s a little person
He has a mental health condition
She uses a wheelchair
He receives special ed services
She has a developmental delay
Children without disabilities
Communicates with her eyes/devices/etc.
Congenital disability
Brain injury
Accessible parking, hotel room, etc.
She needs…. or she uses…..
The handicapped or disabled
He’s mentally retarded
She’s autistic
He’s Down’s; a mongoloid
She’s learning disabled
He’s a quadriplegic/is crippled
She’s a dwarf/midget
He’s emotionally disturbed/mentally ill
She’s confined to/is wheelchair bound
He’s in special ed
She’s developmentally delayed
Normal or healthy kids
Is non-verbal
Birth defect
Brain damaged
Handicapped parking, hotel room, etc.
She has a problem with….
She has special needs
respectFul language exercise
Handout to be given to participants prior to this exercise.
HANDoUT (Power of words and respectful language)
Respectful Language Exercise
Cut out the word pieces for each group:
y Group 1: Jaspreet is a talented student who uses a wheelchair because she has paraplegia.
y Group 2: Kishore has a learning disability which makes reading a challenge for him.
y Group 3: Chandni assists her friend who has a visual impairment through the dark passage.
y Group 4: Sarita has cerebral palsy and uses an electronic device to communicate.
y Group 5: Harpreet has intellectual disability and needs help with daily living skills.
y Group 6: Yami has ADHD which makes it difficult for her to concentrate in class.
Put the word pieces for each group into separate bags (e.g. Ziploc) and label the bags with group numbers.
Divide the participants into groups.
Instructions for students:
y Create sentences from the word pieces in the bag assigned to you.
y There are no punctuation marks so it is your responsibility to put them in where required.
y The sentences you create should NOT use negative words.
y You may refer to the “Power of Words” handout you have received for help.
group 1
Best possible sentence: Jaspreet is a talented student who uses a wheelchair because she has paraplegia
Jackie is a talented student who uses a wheelchair because she has paraplegia handicapped confined is crippled restricted lazy loser
group 2
Best possible sentence: Kishore has a learning disability which makes reading a challenge
Kiran has a learning disability which makes reading a challenge for him is disabled weakness impossible students ignore him reject learning group 3
Best possible sentence: Chandni assists her friend who has a visual impairment through the dark passage
Cathy assists Her friend who has a visual impairment through the dark passage suffers from avoids in is unable to help group 4
Best possible sentence: Sarita has cerebral palsy and uses an electronic device to communicate
Savita has cerebral palsy and uses an electronic device to communicate is crippled relies on is restricted using is a loser
group 5
Best possible sentence: Harpreet has intellectual disability and needs help with daily living skills
Harpreet has intellectual disability and needs help with daily living skills is mentally retarded disabled is stupid she has no friends
group 6
Best possible sentence: Yami has ADHD which makes it difficult for her to concentrate in class
Yami has ADHD which makes it difficult for her to concentrate in class impossible restricts learning is a weakness handicap
Activity (10 minutes)
Break up the participant group into smaller groups of 4 each.
Give each group a Respectful Sentence Activity word bag.
Explain the activity to the participants.
Give participants 5 minutes to create their “Respectful” sentence.
After each group has created their sentence, have a member from each group write their sentence on the board.
As a group, go over each sentence making corrections and revisions as necessary.
reflection (5 minutes)
Have participants engage in discussion about the activity. Sample questions to ask:
What was the experience like to create the sentence?
Was it easy to separate the words that brought up positive images from the negative ones?
Do you think you can practice Respectful Language when communicating with others?
disability awareness & sensitization activities
Autism & Attention Deficit/Hyperactivity Disorder
This activity is designed to show how people with autism and/or ADHD are bothered by things most people don’t notice and in people with the latter affect their ability to concentrate. People with autism are often extra sensitive to noise, movement and even things like background noises most of us don’t notice. Remember, not everyone with autism or ADHD has these problems.
Divide the class into groups of 5. Explain that they will each have a job to do. Go over their jobs and tell them they will start when you give the signal.
One participant in each group will play the part of someone with autism. The other 4 people each have different jobs:
Person #1 - You will play the part of a person with autism. Your job is to try and listen to what Person #5 is reading to you so you can take a test on the material. Try to ignore everyone else.
Person #2 - Stand behind the participant playing the part of someone with autism. Rub the edge of an index card (or piece of cardboard) against the back of their neck. You do not need to rub hard, but keep doing it over and over.
Person #3 - Grab a book (any book will do), lean close to Person #1 and read in a loud voice the entire time.
Person #4 - Pat Person #1 on the head and shoulder the entire time.
Person #5 - Using a normal voice, read a paragraph to Person #1 then ask them questions about what you read. Do NOT try to drown out the other noises.
Have all the participants take a turn being Person #1 before you discuss it. How did it feel to have so much commotion going on? Did it make them want to scream or get away? Were they able to concentrate on the paragraph being read? What might have helped?
Autism is a developmental disability that usually appears during the first three years of life. The cause is unknown. It affects how a person’s brain works, but not all people with autism are affected the same way.
Intellectual Disability
Activity 1 – Difficulty understanding
Have 2 participants sit back to back. Give one participant a paper with an abstract shape on it (page 11 of Disability Awareness Packet). Without seeing each other, he/she must explain to the other participant how to draw the shape.
Give the second participant a pencil and piece of paper. He/she must draw the shape following the first participant’s directions.
What were the problems? What would have helped?
Activity 2 – How it feels
Make a paper copy for each participant of the “German Test” on page 12 and “Test your awareness” on page 13 of the Disability Awareness Packet.
Hand out the “German Test”. Tell them they have 5 minutes to read the paragraph and answer the questions. Tell them it is an easy test and all the answers are right there in the paragraph. When participants complain they can’t do it, tell them to “try harder”. As soon as the time is up, take up their papers.
Hand out “Test Your Awareness.” Tell participants to follow the directions on the page. Tell them this test should be very easy because it is in English.
When they are finished, have them raise their hands to show if they found 3 Fs. How many found 4 Fs? 5 Fs? Did anyone find more? The correct answer is 6. Most people miss the Fs in the word “OF”. This is because we pronounce this as “ov” so our brain skips right over this when we are looking for “f.”
Discuss how it felt to be given a German test and told to “try harder.” Did that help them do it? How many people stopped trying when they saw what the test was? How did it feel to realize they didn’t count all the Fs? How did it feel to have your brain “trick” you on this test? How would it feel if this happened to you all the time, every day?
When a person has an intellectual disability, it means that they learn slower. Because they learn more slowly, they don’t learn as much as other people might. There are over 200 known causes for intellectual disability. About one-third of the time, no one knows what caused it. Not everyone with an intellectual disability is alike. One person can have mild problems while another may have severe problems.
Cerebral Palsy/Physical Disabilities
Activity 1 – In a wheelchair
Borrow a wheelchair from a disability agency or a hospital nearby.
Have each participant take a turn sitting in the chair. Have them try different activities:
Going from one part of the building to another, pushing the wheelchair with their hands
Going through the lunch line
Getting a book off the top shelf in the library
Going to the bathroom
Going through an outside door
Being in a group where everyone else is standing up
Discuss how being in the wheelchair felt. What would have made things better?
Students in wheelchairs are often left out of games or PE or given the job of keeping score. Discuss how this would feel. What if you hate keeping score?
No one likes to be treated as if they are helpless. If you see someone in a wheelchair, don’t just do things for them. Ask if they want help first.
Activity 2 – Using one hand
Have participants try different activities using only one hand:
Eating lunch
Opening a jar that has a screw-on lid
Playing catch
Holding a stack of papers and handing out one at a time
Going to the bathroom
Discuss the problems the participants had. What if they couldn’t use either hand? What problems would there be if they were in a wheelchair AND couldn’t use their hands?
SECTION 4:
Intellectual and Developmental Disabilities: An Overview A DEEPER LOOK AT DISABILITY
Learning Objectives
At the end of this section, you should be able to:
• Define key terms
• Identify common causes of disability
• List key features and support needs of different disabilities
Some Questions to Think About…
“Can you imagine pain that comes from the stigma and the discrimination that you face everyday which disables you from even moving out from your bed in the morning?
Can you imagine yourself requiring assistance for even daily activities?
What is a Disability?
Defining Disability
• A condition that makes it harder to perform major life activities and interact with the world
• Difficulty with:
• Vision / Hearing / Communication
• Movement (muscle control)
• Social relationships
• Thinking / Learning / Remembering
• Mental health
Impact of Disability
Spectrum disorders
•Mild affect to severe affect
Important to know how a condition affects a person
Disabilities affect a person in two ways:
Physical abilities: Change the way a person’s body works.
Mental abilities: Change the way a person’s brain works.
Intellectual and Developmental Disabilities
Group
• Person may require services and/or support -lifelong or for extended period
• Lasts throughout lifetime; cannot be “cured”
Causes and Risk Factors
7654321
Genetics and Syndromes
Parental Health
Parental Behavior
Birth Complications
Infections in mother
Early infections in child
Environmental Causes
Intellectual Disability
Attention Deficit/Hyperactivity Disorder
Autism Spectrum Disorder
Cerebral Palsy
Multiple Disabilities
Intellectual Disability
Manifests during developmental period
Below average intellectual functioning
`
Impairment in adaptive functioning
Classification of severity
Can be caused by injury, disease or other conditions in the brain
REMEMBER: Regardless of a person’s IQ, new skills can be learned
Intellectual Functioning
A person’s ability to learn, reason, plan, solve problems Affects experiential learning Affects social learning Affects academic learning Affects social and emotional functioning
Conceptual skills –
• Language & literacy
• Money, time, numbers
• Self-direction
Social skills –
• Interpersonal skills
• Social responsibility
• Problem solving
Practical skills –
• Daily living activities
• Occupational skills
• Healthcare
• Independent living skills
Adaptive Functioning
Severity of Intellectual Disability
Mild
Moderate
Severe Profound
Intellectual disability versus Learning disability
Attention-Deficit / Hyperactivity Disorder
• One of the most common development disorders of childhood
• Persistent pattern of inattention and/or hyperactivity-impulsivity
• Three types of ADHD
Poor inter-personal skills
Impatience
Gullible to temptation
Common Behavioural Traits
Day dreaming / Forgetfulness
Fidgety
Excessive talking
Carelessness/Risk taking
Poor executive functions
Types of ADHD
Predominantly Inattentive Presentation
Predominantly HyperactiveImpulsive Presentation
Combined Presentation
Basic Supports
• Individualized supports
• Attention strategies
• Organization and time management aids or tools
Autism Spectrum Disorder
⮚ An invisible disability
⮚ A spectrum disorder
⮚ Affects person’s interaction with environment and people
⮚ Abilities can range from highly gifted to severely challenged
⮚ Common characteristics:
⮚ Difficulty in social communication & interaction
⮚ Restricted repetitive behaviours and interests
⮚ Different ways of learning and reacting
Some common features
Social-emotional reciprocity
Non-verbal communication
Relationships
Repetitive behaviours
Routines
Interests
Sensory processing
Positive Behaviour Support
• Behavioral challenges
• Understand underlying cause
• Appropriate support
My name is Danny and I have autism…
• Routines
• Communication
• Social
Basic Supports
• Sensory
Cerebral Palsy
• Neurological disorder due to brain damage
• Mostly affects motor function
• Causes physical impairment
• Permanent but not progressive
• With or without cognitive impairment
Classification: type of movement disorder
• Spastic cerebral palsy
• Dyskinetic cerebral palsy
• Ataxic cerebral palsy
• Mixed
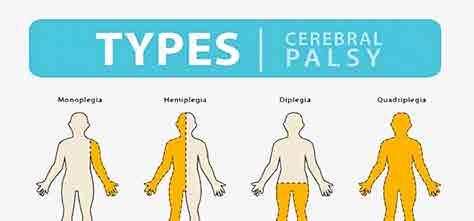
Classification: body part(s) affected
• Hemiplegia
• Diplegia
• Quadriplegia
Affects one limb, usually an arm
Affects one side of the body, including one arm, leg and trunk
Affects symmetrical part of the body (legs or arms)
(ref: relias-An overview of Different Types of Disabilities)
Intellectual Disability has four levels of severity:
These categories used to be based on a person’s IQ score. However, the modern approach bases severity on a person’s adaptive skills. A person with a mild intellectual disability will have more skills and need less support than a person with profound intellectual disability.
The level of intellectual disability a person has will give you an idea about what support they might need. However, it’s important to remember that all people are different and one must learn about their individual needs.
Level
Mild
Skills
Can complete basic hygiene & household tasks on their own.
Can hold jobs and live quite independently within familiar routines, people, locations.
May have difficulty regulating or controlling their emotions or behavior.
Can develop friendships and romantic relationships.
Support needs
To complete complex tasks such as managing finances, planning and preparing meals, coordinating transportation.
To handle unfamiliar situations, set priorities, solve problems. Moderate
Need extensive teaching to gain basic skills.
May have simple reading or math skills but may need help to apply them in daily life.
May use language more simply than their peers and will often misunderstand social cues.
Friendships and romantic relationships are often with others who have ID.
Often need ongoing support to complete daily tasks or hold a job.
Complex tasks, problem solving, or using judgment may be difficult even with support.
May rely on others to make major life decisions.
Mild Moderate Severe
Profound
Level Skills
Severe Limited movement or speech.
Communication in single words or phrases.
Focus is on concrete, not abstract concepts.
Understanding of time, money, or written words is very simple.
Profound Significant needs in all areas of life.
Many have complex medical conditions that may limit their movement and activity.
May participate in tasks and activities but usually cannot complete them on their own.
May understand simple speech but generally do not speak. Some may communicate with gestures.
Do not understand abstract concepts like time, money, and writing.
Support needs
Can learn simple skills but will need support to complete most tasks.
Most will need constant supervision to keep them safe.
Depend on constant supervision and support from others.
By empowerment I mean connecting with a community of peers and caregivers on a mutually respectful level, and fully participating in the decisions affecting one’s life.
- David Fisher
module 2: understanding direct support services
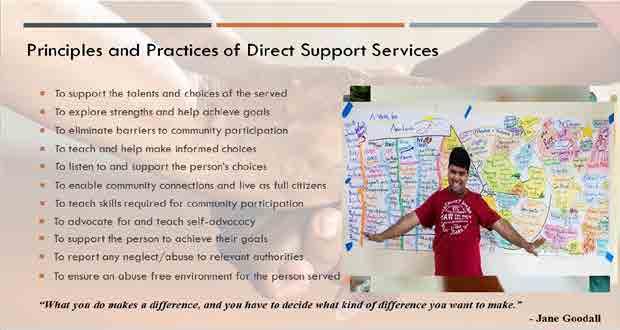
What you do makes a difference, and you have to decide what kind of difference you want to make.
- Jane Goodall
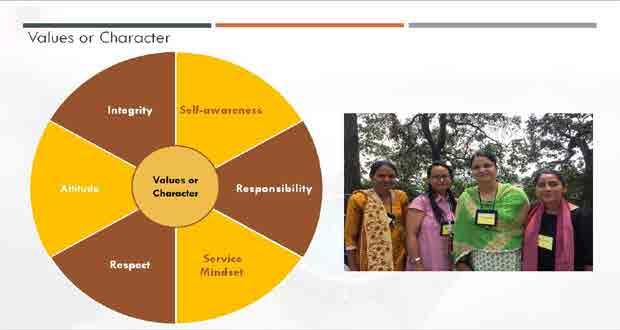
module 3: code of values & ethics
CODE OF ETHICS
A person unaccustomed to sharing a dream needs a careful listener. A person whose dream calls for a change in his relationship with an important helper, needs respectful validation and the listener’s willingness to figure out a changing relationship.
- John & Connie Lyle O’Brien
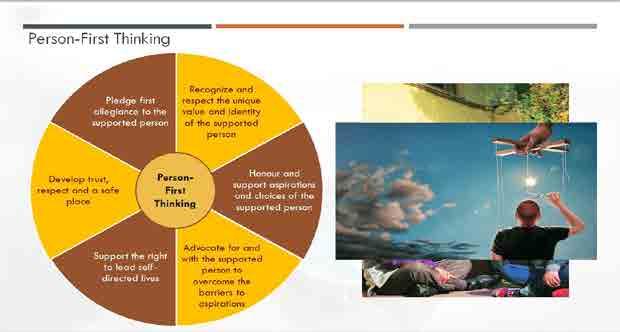
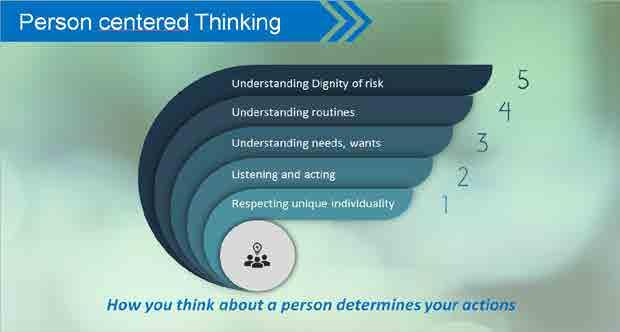
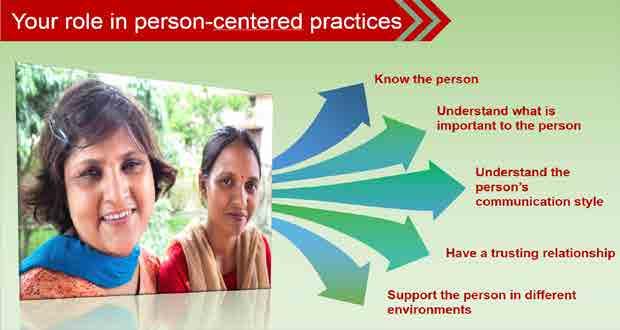
module 4: person-centred thinking
Person Centered Thinking & Planning
Person‐CenteredThinking can Guide Us…
Towards a vision of a full life
Towards a community of support to walk alongside people
Towards a society where everyone’s gifts are welcomed and offered
Towards the steps needed to help a person move into the life they desire
Towards a positive and possible future for someone we care about
What is Typical?
Programs and services for people with disabilities tend to be focused on their system….
System‐Centered….. Tries to fit people into programs….
Programs often want to “service people”
And the program sets about trying to fix the person….
Then and only then….
Can the person join regular community life…..
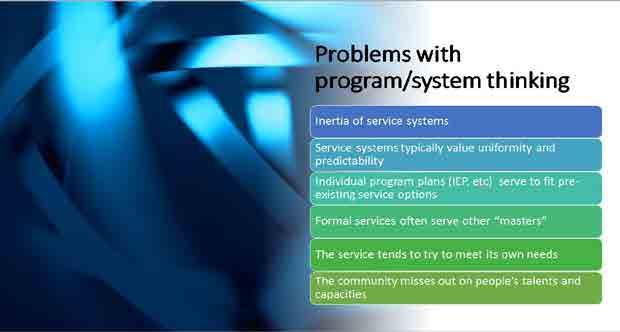
Problems with program/system thinking
• Many people get stuckforever in segregated settings
• People miss out on life todayand tomorrow
• The service tends to try to meet its ownneeds
• People get seen as all the same
• People who don’t get “fixed” frustratepeople
• The community misses out on people’s talents and capacities
Person Centred Thinking takes a VERY DIFFERENT perspective…
People Belong to Themselves….
Their Families
and their Communities….
Beth Mount, 2019
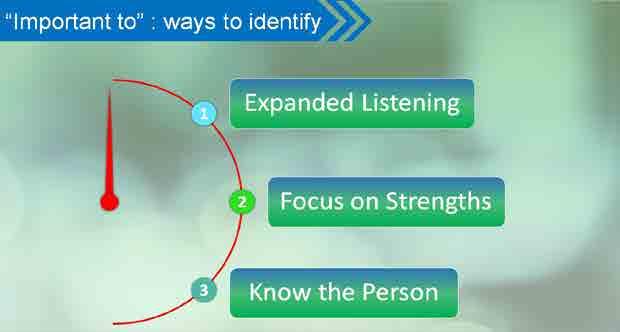
“Important To” and “Important For” BETSY
Important to Me?
1. Living in the countryside
2. Having pet animals (dog cat, etc)
3. Taking one family trip every year
4. Morning routine
Important for Me?
1. Resist impulsive ideas
2. Save money
3. Exercise 5 times weekly
4. Keep in touch with extended family
“Important To” and “Important For”
to Me?
for Me?
How about one person with a disability you work with?
Important to:
Important for:
Ajit’s Strengths….
How well do you know the person you support?
• The person’s “story” and life experiences
• Capacities and Gifts
• “What Works” and “What Doesn’t Work” in the person’s life
• What the person needs to be safe and healthy –at her best
• Interests and passions
• Important life moments
• Dreams and Desires
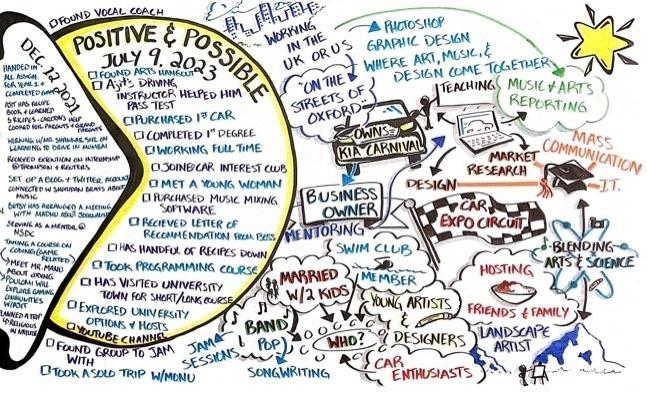
“A person‐centered plan can help those involved with the focus person
see the total person, recognize his or her desires and interests, and discover completely new ways of thinking about the future of the person.”
Beth Mount & Kay Zwernik, 1988
If we have no peace, it is because we have forgotten that we belong to each other.
- Mother Teresa
module 5: orientation to social role valorization
Direct Support Professionals have a BIG impact
• You know the people you serve differently than anyone else
• You spend a great deal of time with people in everyday situations
• How you interact with people with disabilities teaches others
Agenda
Part 1 Our Goal: The Good Things of Life
Part 2: What Stands in the Way?
Part 3: How Can Direct Support Practitioners Help?
“What do you think are the “good things of life” that you think most people are hoping to gain?”
What Stands in the Way?
The problem is…..
These good things of life are often NOT easily available to people with disabilities in most societies.
Social Devaluation
Means that people with disability are judged as being of less value than other people…..
Usually on the basis of a characteristic (like a physical disability, an intellectual disability, autism, a mental illness, the color of their complexion, etc.)
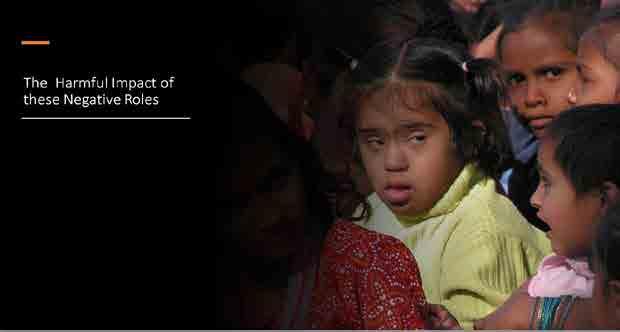
The
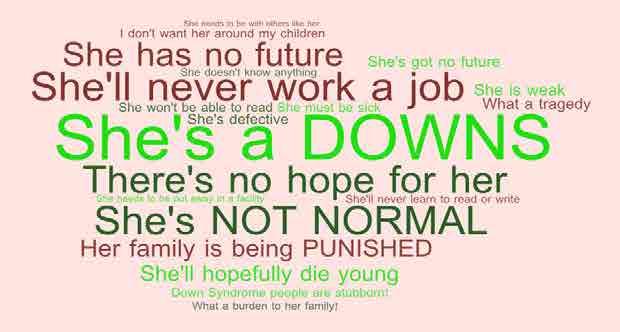
“Wounds” of Devaluation
1. People get defined by their disability
What are some of the negative stereotypes you are aware of?
Those people with disabilities are
The “Eternal Child”
Object of Pity
Object of Ridicule
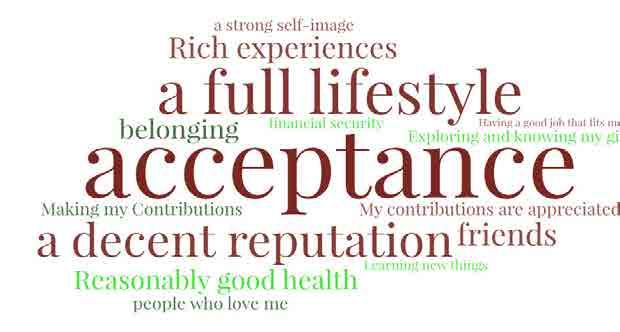
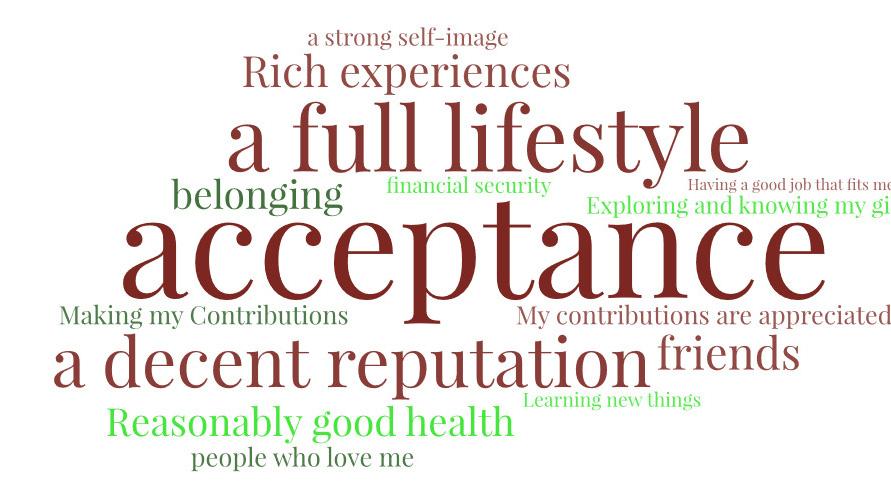
And What ARE the Good Things of Life?
“What are the qualities and characteristics of a good life?”
“What do you think are the “good things of life” that most peop le are hoping to gain?”
“What are the most important ‘good things’ of life that you che rish and hold dear?”
“At the end of your life, what do you think that you would like to say you have accomplished and experienced?”
“What do you love about your life?”
EMPLOYEE
EMPLOYEE
Money/Benefits
Opportunities
Friends and Colleagues
Reputation and SelfImage
Belonging
Personal Growth
Going Swimming
But being a SWIMMER is a Social Role
How Can Direct Support Practitioners Help?
Think Age‐Appropriate!
• Think of roles that enhance the person’s AGE
An Adult Artist
Small Groupings are generally better
Who Might Bhawna Become?
What roles might Bhawna try out and COULD be a good fit?