DSP Phase 2 Key Stone Training Manual_Volume 3_Final
Welcome to Phase 2 of the Foundations of Direct Support: A National Training for Direct Support Practitioners, Training of Trainers.
On behalf of Keystone Institute India, we would like to thank you for setting aside significant time and commitment to become master trainers of this rich and new development course to promote the competence of direct support practitioners across India. We realize that time away from typical responsibilities is a major investment of your time and energy, and we are glad that both you and your organization have committed to learning about and teaching Foundations of Direct Support for a new and respected profession within India, all working towards rich, full lives for people with intellectual and developmental disabilities.
This second phase of the Training for Trainers of the National Training for Direct Support Practitioners is a deep dive into critical subject areas that are key to person-centered support and empowerment of people with disabilities.
YOU belong to the third cadre of Master Trainers taking this high-quality, value based training to develop highly competent and sensitive Direct Support Practitioners who can support and empower people with disabilities to lead rich, valued, and meaningful lives.
We are privileged to have excellent faculty who bring with them decades of experience both on the ground and in training for this course. Many of our faculty are content experts and leaders in this space and are passionate about implementing and training in best practices.
We are also happy and honored that you have taken the time to invest in this rigorous and demanding training course, and we hope that you will leave this event with a passion and commitment to teach others and learn more. We are excited to partner with you and support your endeavours in enhancing the lives of the people you serve.
Elizabeth Neuville and Chitra Paul
eneuville@khs.org
Keystone Institute India cpaul@khs.org
M-14 A, Second Floor, South Extension Part-2
New Delhi-110049
Tel: 011 45649719/45644368
SCHEDULE
PHASE 2 Trainer Preparation
WEEk 1: SEPTEmbEr 8–12, 2025 Day Time Activity
Day 1: 8 September 2025 05.00 PM – 06.00 PM Welcome & Opening of Phase 2
Day 2: 11 September 2025 03.00 PM – 05.00 PM • Open House
• Live online presentation of Module 6 - Promoting Health and Wellbeing Section 1:
– Assessing Healthcare Needs
Until next meeting
• Participants to review Module 6Promoting Health and Wellbeing Section 2:
– Assisting with Activities of Daily Living
Day 3: 12 September 2025 03.00 PM – 05.30 PM • Open House
• Live online presentation of Module 6 - Promoting Health and Wellbeing Section 3:
– Common Health Problems & Interventions
Until next meeting
WEEk 2: SEPTEmbEr 15–19, 2025
• Participants to review Module 6 - Promoting Health and Wellbeing
– Health & Safety
– Health & Wellness
– Mental Health Wellness
Day 1: 15 September 2025 03.00 PM – 5.30 PM • Open House
• Live online presentation of Module 7 - Positive Approaches to Challenging Behaviour
Day 2: 16 September 2025 03.00 PM – 6.00 PM
Day 3: 17 September 2025 03.00 PM – 06.00 PM
• Open House
• Live online presentation of Module 9 - Family Collaboration
• Module 9 - Family Collaboration
Day 4: 18 September 2025 02.00 PM – 06.00 PM • Open House
• Live online presentation of Module 12 - Sexual Wellbeing
Day 5: 19 September 2025 03.00 PM – 05.30 PM • Open House
• Live online presentation of Module 8 - Community Membership
Until next meeting
WEEk 3: SEPTEmbEr 22–25, 2025
Day 1: 22 September 2025 03.00 PM – 5.00 PM
• Participants to review Module 10 - Legal Framework
• Open House
• Live online presentation of Module 11 - Advocacy & Activism
Day 2: 23 September 2025 03.00 PM – 6.00 PM • Open House
• Live online presentation of Module 13 - Promoting Competency Day 3: 24 September 2025
Day 4: 25 September 2025 03.00 PM – 6.00 PM • Open House
• Live online presentation of Module 14 – Taking Leadership
• Phase 2 Wrap Up
Phase 2: PrACTiCUm (in-Person New Delhi)
18–19 November 2025
• Welcome
• Pre-assigned Team Presentations
• Grand Finale
1. Module 6: Section 1Assessing Healthcare Needs
2. Module 6: Section 2Assisting with Activities of Daily Living
3. Module 6: Section 3Common Health Problems & Interventions
...People learn very quickly when they have a need for the skills and information. If it will change their lives, if it will help them accomplish what is important to them, everyone can become a good learner. We learn complex competencies and knowledge in a matter of weeks, not months or years. And people learn best in community, when they are engaged with one another, when everyone is both student and teacher, expert and apprentice, in a rich exchange of experiences and learnings.
- Margaret Wheatley
phase 2: module structure
Take care of yourself, be healthy, and always believe you can be successful in anything you truly want.
- Alessandra Amrosio
module 6: promoting health & Wellbeing
Health and Wellbeing
SECTION 1: Assessing Health Care Needs of People with Intellectual & Developmental Disabilities
Agenda
• Health Outcomes for People with Disabilities
• Assessing Health Needs
• Behavior as an Indicator of Illness
• Vital Signs
• Accuracy in Assessing Vital Signs
• Special Considerations for People with Disabilities
Health Outcomes for People with Disabilities
A young woman with a mild level of intellectual disability developed an earache. Her mum took her to a general physician who prescribed antibiotics for her. However, the pain continued and got worse.
Her mum then took her to the emergency department. They had to wait over five hours to be seen, and as time progressed, the pain worsened. The young woman found it difficult to cope with her pain and expressed this by sitting on the floor, rocking, making sounds, and holding her head. When the doctor came the mum tried to explain, but she was dismissed. And the doctor wrote in her chart that the woman was having a temper tantrum.
The young woman and her mum were asked to leave and return after she ‘settled down’. She died six hours later in her mum’s arms. An investigation into the cause of death identified that she had died as a result of undiagnosed meningitis.
Assessing Health Needs
Something isn’t right…
SIGNS
SYMPTOMS
Signs on eyes/ears/nose
Changes in eating habits
Urinary changes
Signs specific to men
Signs on skin
Signs in breathing/respiration
Change in bowel habits
Signs specific to women
Behavior as an Indicator of Illness
General
Aggression or any self-injurious behaviour
Specific Behaviour
Refusing
Holding
Rubbing
Jerky
Limping
Hitting
Body Positioning
Outstretched Twisted Bent
Foetal
Changes in energy levels or losing interest in activities
Changes in sleep habits, moods or appetite
Behaviour changes and trigger points for same
What should you do now?
What should you do first?
What should you say to John and the doctor?
∙ Tell John not to talk
∙ Talk to John about going for a blood test
• Take John immediately to the hospital
• Talk to John’s family
∙ Call John’s doctor immediately and schedule a test
• Review John’s medical history
∙ Make sure he understands what the doctor is saying, and let the doctor know he is confused by this
∙ Don’t say anything
∙ Don’t do anything, it’s John’s choice if he wants to take the test
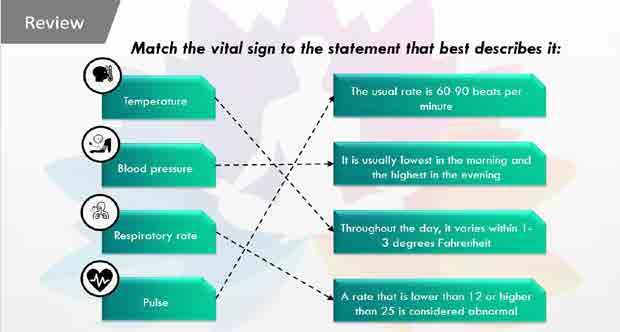
Vital Signs
Factors Affecting
Ways to Assess
Ways to Measure Pulse
Radial
Brachial
Factors Affecting BP
Age & Gender
Weight
Emotions
Heredity
Medications
Disease
conditions
Viscosity of Blood
Conditions of Blood Vessels
Blood Pressure
Accuracy in Assessing Vital Signs
Gayatri has autism. During a routine check-up, the nurse briskly walked into the room and immediately placed the blood pressure cuff onto Gayatri’s arm.
This frightened her (who did not understand what the doctor was doing), which elevated her BP during the assessment. In turn, the doctor incorrectly diagnosed Gayatri with hypertension.
Points to Note
1 2 3 4
Person’s appearance and behavior
Skin appearance and temperature
Timing of medication just before assessment What’s “Normal” for the person
Factors Affecting Accuracy of Vital Signs
Special Considerations for People with Disabilities
Health and Wellbeing
SECTION 2: Assisting with Activities of Daily Living
AGENDA
▪ What are Activities of Daily Living
▪ Assisting with Eating
▪ Assisting with Personal Care
▪ Bathing
▪ Dental Care
▪ Hair Care
▪ Toileting
▪ Nail Care
▪ Menstrual Care
▪ Clothing
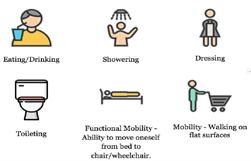
ACTIVITIES OF DAILY LIVING
▪ What are activities of daily living (ADL)?
▪ Eating
▪ Dressing
▪ Hygiene
▪ Mobility
▪ What are instrumental activities of daily living (IADL) ?
ADL and Support
Potential Needs of People with IDD
Need for consistency
Reminders to perform personal care tasks
Assistance in making changes
Encouragement or acceptance
Reminders of how to perform tasks
Assisting with Eating
Positioning
1 Maintain good body alignment
2 Provide comfort
3 Inhibit unhelpful reflex patterns
4 Decrease respiratory problems
Positioning Essentials
Ensure body as upright as possible
Ensure chair fits the individual
Prevent head from tipping back
Ensure feet are supported
Ensure individual is relaxed
Alert individuals before positioning
Reposition if required
Ensure upright position post eating
Personal Care
Important Considerations
Review
Precautions
✔ Allow as much independence as possible
✔ Familiarise yourself with person-centred plan
✔ Consider use of special equipment
✔ Check water temperature
✔ Poor bathing habits increase chances of bed sores/infections
✔ Examine skin for injuries/indications
✔ Honour personal choice
✔ Wash your own hands
✔ Inadequate drying after the bath can cause fungal infections
You are helping Kantha get ready for her evening bathing routine. She requires assistance transferring from her walker to the shower chair, but otherwise performs all her own bathing activities. In the past, Kantha had slipped on the bathroom floor because the floor was wet. What should you do before assisting Kantha to the shower chair to ensure she does not slip this time?
✔ Demonstrate correct bathing procedure
A. Remove the shower curtain
✔ Close windows to prevent drafts
✔ Be wary of scrubbing the body too hard or using products that may irritate the skin
B. Spread a small towel across the floor
✔ Ensure privacy - draw curtains, close doors
C. Place the bathmat on the shower floor
✔ Gather all supplies beforehand
✔ Encourage use of toilet before bathing
✔ Guard against spreading bacterial infection from one body part to another
✔ Place a mat/towel on bathroom floor
✔ Follow top-to-bottom approach
✔ Ensure use of after-bath products to keep skin healthy
✔ Watch out for any skin irritations; report if any
✔ When finished, wash hands and straighten bath area
Guidelines
✔ Wash your hands before and after physically assisting the individual
✔ Place the head of the toothbrush alongside the teeth with the bristles at 45º angle
✔ Use a back and forth ‘vibrating’ / up and down / circular motion
✔ Brush the outer side of each tooth with this technique
✔ Repeat this technique on the inside surfaces
✔ For the inside surfaces of the front teeth, tilt the brush vertically and brush up and down using the front part of the brush head
✔ Brush the tops of the teeth using a back and forth motion
✔ Brush the tongue
Even individuals who do not have any teeth or dentures need mouth care. This would include at least a daily, gentle brushing and rinsing of the gums, tongue and roof of the mouth.
✔ Don’t brush too hard
✔ Best remedy for bleeding gums is to keep brushing gently
MENSTRUAL CARE
NAIL CARE
TOILETING
Guidelines
✔ Teach and assist with drying hair and applying hair products
✔ Section long hair to avoid pulling and tugging
✔ Teach and assist the individual to comb or brush hair from scalp to ends
✔ Special care while handling curly hair
✔ Gentle touch
✔ Ensure cleanliness of comb/hair brush
ORAL CARE HAIR CARE
BATHING
MENSTRUAL CARE
NAIL CARE
✔ Ensure safety and dignity always
✔ Promote independence
✔ Never leave the person served out of hearing range
✔ Familiarise yourself with adaptive equipment used
✔ Follow hygiene practices
TOILETING
ORAL CARE HAIR CARE
BATHING
Keep in mind Guidelines
✔ Female staff only
✔ Ensure use of product as per directions on packing
✔ Nail care important for overall health
✔ Medications
✔ People with diabetes may require help of health professional
✔ Consent and clear communication
✔ Period flow
✔ Pads – Used externally; many varieties and brands available; depends upon specific features – high absorbency, with wings, thin, etc
✔ Advisable to trim nails every fortnight
✔ Mark the date
✔ Skipped cycles
✔ Pre-menstrual symptoms
✔ Not changing products timely can cause deadly infections
✔ Report unusual conditions
CLOTHING
Health and Wellbeing
SECTION 3: Common Health Problems and Interven�ons
Agenda
• The Crucial Four
• Aspiration
• Dehydration
• Seizures
• Constipation
• Other Common Health Issues
• Incontinence and UTI
• Pressure Injuries
• Allergies and Asthma
• Diabetes
The Crucial Four
Aspiration
Choking
Dysphagia
Dehydration
Aspiration Signs
Constipation Seizures
Aspiration
Choking
Dysphagia
Aspiration
Dehydration
Indications
Constipation Seizures
Dysphagia Aspiration
Aspiration
Dehydration
Constipation
Example
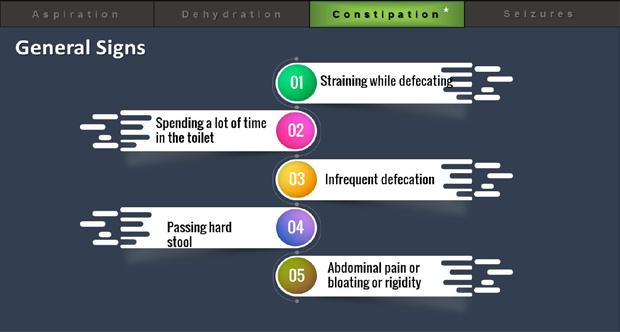
General Signs
Specific Signs
Risk Factors
Alerts
Influencing Factors
Prevention
Treatment
Review
Example Risks Dehydration
Constipation
Seizures
Causes Triggers Signs
Treatment Response
Seeking Medical Help Helping Manage Reporting and Documenting
Choking - Signs
Dysphagia
Indications of Dysphagia
Sarla has cerebral palsy
Sarla loves cup cakes
She has trouble swallowing and her food is pureed
She longs for ‘real’ food and has a history of grabbing food
Neighbour brings cupcakes for a birthday party
Sarla grabs one when you are not looking
Sarla looks agitated and soon becomes unconscious.
You give CPR and call for help, but .it’s too late!
Behavioural Indications
Risk Factor - Foods
Review
Based on your knowledge of swallowing problems, what could have gone wrong?
- Dhoni should have been hospitalized when he got a chest cold
- The thickened orange juice Dhoni drank did not allow him to swallow pills effectively
- Dhoni should not have had his medication in a tablet form
- Dhoni should have had medications before his breakfast
Aspiration
Prevention
Regularly offer water throughout the day
Understand the person’s communication style
Be aware of other medical conditions
Interventions
Pay attention to any weather changes
Urine or stool pattern changes
Medications
Offer fluids if the person is alert and can drink safely Else contact healthcare professional for intravenous fluids
Example
Wilson – 24 year old with moderate intellectual disability
Lives with 4 roommates; attends a day program
Works with Mukesh – a DSP at the day program
Mukesh notices Wilson spending a long time in bathroom
Wilson’s behavioural outbursts
Mukesh’s concern
Review
At the suggestion of Wilson’s physician, Mukesh helps him track his food and fluids for two weeks. Mukesh shows Wilson that he is eating balanced meals but is not drinking enough fluids. Mukesh encourages Wilson to drink more water throughout the day. Wilson’s physician also prescribed him a laxative that he could take as needed. Because of Wilson’s depression, he was not getting as much physical activity as he needs. Mukesh helped Wilson choose activities that he enjoyed and could practice every day, including taking walks around his neighborhood.
Meet Meena and Richard
Richard - a 35-year old man with a mild intellectual disability who lives in the community.
Meena - a new DSP working with him
Meena’s been told Richard has seizure disorder; limited details given by her supervisor
Richard’s seizure during grocery shopping
Dazed look
Lip smacking
Loss of bladder control
Meena is clueless and helpless
Meena realizes there’s a lot she needs to learn
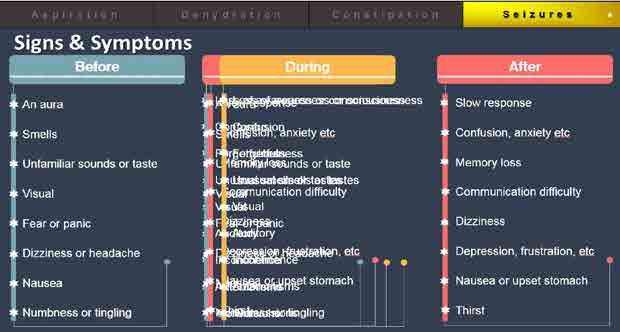
Seizures
• Epilepsy is another name for seizure disorder
• More prevalent for people with developmental disability
• May impact daily living skills
• Is a spectrum condition
• Seizures vs Convulsions
Response to seizure
Stay with the individual until the seizure is over
Call for medical help if seizure lasts for more than 5 minutes
Keep the individual comfortable and safe from injury
If in public, keep onlookers away
Don’t hold the person down or put anything in their mouth
Don’t give any pills/water/food until the individual is fully alert
Stay
When to call for medical help
Multiple seizures happen one after the other without the person regaining consciousness between seizure episodes
Seizures happen closer together than usual for that person
If the individual appears to be choking or having trouble breathing
The seizure happens in a body of water, such as a pool or bathtub
The person injures themselves during a seizure
This is the first seizure the person has ever experienced
Seizures that last for five minutes or longer
Helping to Manage
Community
Empowerment
Constipation Seizures
Reporting and Documenting
Be aware of likely triggers
Provide appropriate assistance
Record conditions and description
Constipation
What to document
Time of the seizure
Any drug or alcohol use
Parts of the body affected
Types of movement
Antecedent conditions
Impairment in consciousness
Changes in skin colour
Any resulting injuries
Condition after the seizure
Any difficulty with recall
Who the seizure was reported to
Other Common Health Issues
Urinary / Faecal Incontinence
Urinary Tract Infection (UTI)
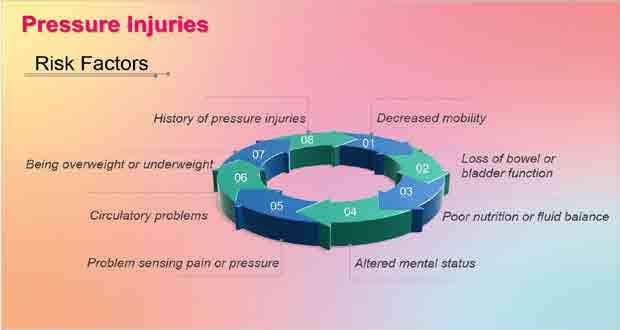
Pressure Injuries
Breakage in area of skin
Sore or intact skin Common areas
Asthma
Cause
Symptoms
Prevention
and Treatment
Health and Wellbeing
Agenda
• Safety
• Privacy
• Dignity
• Communication
• Independence
• Infection Control
• Fire safety
• First Aid
Safety
- Preventing Falls
- Preventing Shocks and Electrocution
- Preventing Burns and Scalds
- Preventing Poisoning or Chemical Accidents
- Preventing other Household Injuries
Assist people who might fall
Preventing Falls
Pick up things dropped on floor
Clean up floor spills
Remove potential tripping hazards
electricals when not in use
Unplug
Place rubber mats in bathrooms
Limit use of extension chords
Straighten carpets/rugs/throws
Install grab rails
Ensure good lighting
Clear entrances and passages
Exercise/physiotherapy can help
Use walkers/canes for support
Use special equipment for emergency alert
Preventing Shocks and Electrocution
Preventing Burns and Scalds
Preventing other Household Injuries
Teach Safety
- Modelling
- Using every teachable opportunity
- Providing positive reinforcement
Do not discuss personal issues
Respect confidentiality
Respect personal space and belongings Knock and wait
Close door before assisting
Dignity
Communicatio n
Independence
Infection Control
Controlling spread of germs
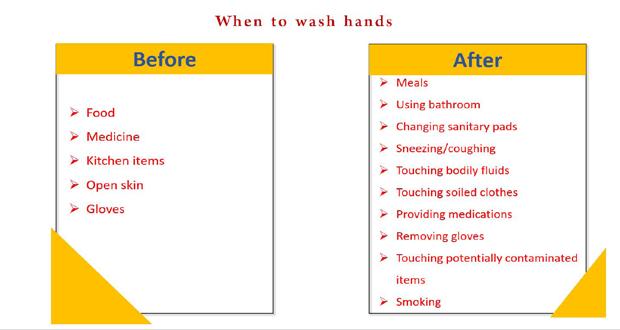
• Hand washing
• Choice of soap
•Remove any protective equipment
•Moisturizing
Fire Safety
Response to Fire
Remember to RACEE
If you smell smoke or discover a fire at your site, you must do the following in the order outlined:
• Remove/Rescue
• Alert (contact)
• Contain (control)
• Extinguish (put out)
• Evacuate (leave)
In the Event of a Fire
www.youtube.com/c/powerupwithpowerpoint
Health and Wellbeing
Health and Wellness
Wellness and Healthy Lifestyle
A healthy lifestyle
In your opinion, are Shashi’s decisions helpful or not?
▪ Shashi baked a cake to celebrate Devi’s first night at the home.
▪ Shashi told Devi that “lights out” was at 10.00 and he must comply.
▪ Shashi told Devi he could not watch television in his bedroom.
▪ Shashi decided that she should get Devi’s bath ready for her.
Dis(ability)
Good Nutrition
Preparation Method
Smaller plates
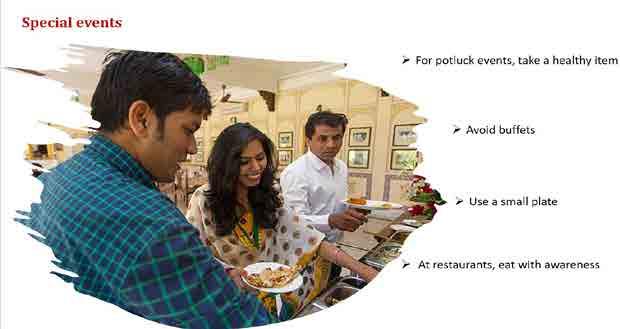
Smaller serving utensils
Condiments from bowls
Portion large items
Extra food out of sight
For a healthy body & mind
Aerobic activity
Muscle strengthening activity
Balance and Flexibility
Other Strategies
Think of one person you support who would benefit from increased exercise – Come up with one exercise idea to try with that person that is new to them.
Supporting healthy lifestyles
Model Healthy Choices Support Choices
Health and Wellbeing
Mental Health
Wellness
What are mental health conditions?
Can take many forms
Conditions that impact a person’s thinking, feeling or mood
Diagnosis requires clinical judgement
When a person has both a developmental disability and a mental health condition, the person is said to have a “co-occurring diagnosis of a mental health condition”.
aspects
Biopsychosocial Approach
Biological Aspects
Genetic, biological component
Family history
Psychological Aspects Social Aspects
Psychological challenges
Social connections
Physical illness
Verbal communication
challenges
Opportunity to contribute
Recreation
Communication
Functional challenges
Role of DSP
Stressful life events
Challenges with control and regulation
Behaviour
Healthy habits
A 35 year old woman, Lakshmi, has moved into an apartment in the community, sharing the apartment with two other women in their 30s. It’s been a couple of months since Lakshmi moved here from an institution where she lived since she was 10. The women are supported by direct support staff. Lakshmi is mostly withdrawn, aloof, and cries frequently. One day she screams at her roommate and throws things around the room for no apparent reason. Another day she seemed disoriented when they were getting down to having lunch around 2 pm.
Lakshmi has intellectual disability. She has diabetes for which she takes medication. At the institution, she was used to having lunch at 12 and followed a strict routine around food. She had a couple of good friends at the institution.
Please share your thoughts using the biopsychosocial approach.
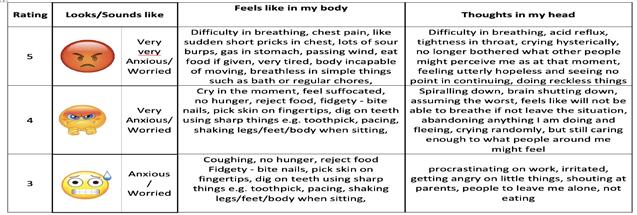
Specific Mental Health Conditions
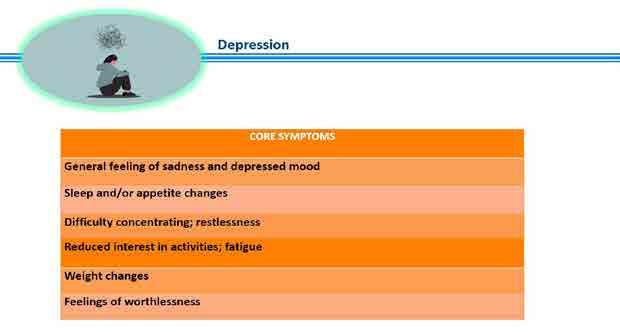
Depression
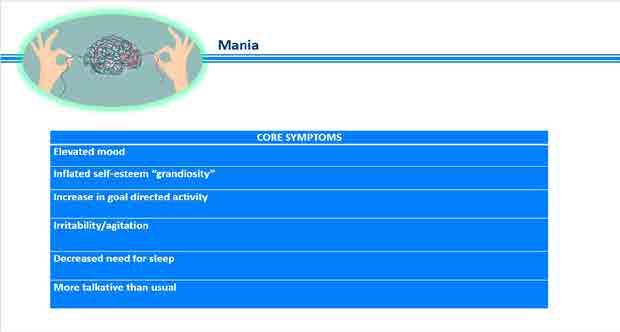
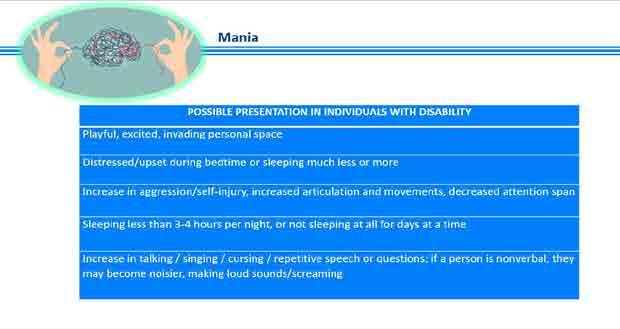
Mania Anxiety Disorder s
Jamal has recently been giggling a lot, talking non-stop and pacing; he also made several remarks toward female DSPs, which is not usual for him. He offered to take Anita, his DSP, to Mauritius on his jet. As his DSP, and from you just learned what would be best to do?
Concerned
Worried
Apprehensive
Afraid
Scared
Restless
Stressed
Panicked
Nervous
• Which of the following are common mental health conditions among people with IDD?
o Depression
o Anxiety
o Bipolar disorder
o All of the above
• Shanti gets easily stressed and hits others when she is asked to do household chores. Shanti has many interests and strengths, one of which is drawing. How might you best support Shanti if she shows signs of becoming agitated?
o Offer Shanti opportunities to draw, but when she shows signs that she is becoming stressed, take the drawing materials away
o Let Shanti know that if she does not hit others, she can have the drawing materials after she does her chores
o Allow Shanti the opportunity to draw when she starts to become stressed and at other times during the day when she isn’t doing chores
o Don’t let Shanti have drawing materials until she shows that she will not hit others for one week
• True or False: Intellectual disabilities are typically present at birth or appear during the developmental period.
• When someone has both an IDD and a mental health condition, this is commonly referred to as
o Double diagnosis
o Multiple medical challenges
o Simultaneous conditions
o Co-occurring conditions
There is no greater disability in society than the inability to see a person as more.
- Robert M. Hensel
module 7: positive approaches to challenging Behaviour
POSITIVE APPROACHES TO CHALLENGING BEHAVIOUR
POSITIVE APPROACHES TO BEHAVIOURS THAT SEEM CHALLENGING
Not just semantics…
Defining Behaviour
Lets’s Identify Behaviours
Pritam coloured in his picture book with crayons.
Observable:
•What do you see or hear?
•Physical movements
•Action verb
Measurable:
•Frequency
•Duration
•Intensity
Mamta behaves very well in the history class. When the teacher asks a question, Mamta raises her hand to answer.
Vineeta is often aggressive in the park
When children pull Vineeta to come play with them, Vineeta pushes them hard.
Whenever, Sachin hears the siren, he closes his ears and starts shouting loudly.
In people with disability…
Tendency to see ALL behaviours as challenging
• “In the absence of language use of the word behaviours has become associated primarily with meltdowns, self-injurious stimming, and other obvious signs of distress.”
Socially isolates –Interferes with participation in the community
• Interferes with learning
• Compromises safety of self or others
• Decreases independence
• Socially isolates
Which behaviours might need changing?
Anita rocks while doing her worksheet
Bunty spits on his classmates during math class.
At the gym, Abdul wears his gym-shirt inside out.
Tanisha first eats up all her vegetables and then eats her roti.
Bharat likes to stand in one spot in the family room.
Twenty-year-old Vanita likes to stroke her cheek with a round pebble at bedtime.
Abby cries and shouts when she does not get to go out with her friends.
WHY before WHAT and HOW
Understand the “Why?”; there must be a reason
Behaviour = Communication?!
GET Something | AVOID Something
Attention: Adult / Peer
Object, activity, setting, event
Sensory Stimulation: Seek what is needed or avoid painful or uncomfortable experiences - Crying in an OT room?
All Behaviour ≠ Communication
Self Regulation
Emotional Regulation
Sensory Regulation
Leisure
Stimming: is usually not about communication, but typically about self-regulation, sensory seeking, or self-expression
Meltdowns or shutdowns: overwhelmed to the point of dysregulation, and very much needs NOT to communicate or interact
All Behaviour ≠ Communication
Obsessive compulsive need
Impulsivity or motor control
Body control ‘I know you want me to go over there, and I’m trying to go over there, but I can’t get my body to initiate the movement - I’m not being defiant.’”
“My understanding is not based on neurotypical experience, reasoning and cultural norms”
• Are you rewarding a behaviour without meaning to?
(Giving something to make her quiet and easier)
Antecedent
• What happened before
So think about this….
WHY WHAT HOW
The ABC Format
Behavior
• What happened C Consequence
• What happened after
Wrong Patterns
Difficult behaviors get faster results
So
Difficult behaviours occur again and again
Theory of Reinforcement
Reinforcer
Not just a reward
Not only about whether a consequence is pleasurable
Always defined by the effect the consequence has on future responses.
(Are the responses being ‘strengthened’, gone up?)
Strategies to Provide Positive Behaviour Support
NOT situation specific, ACROSS THE BOARD
• Enjoy the person
• Mind the language
• Enhance motivation
• Up skill
• Prepare for changes
1. Enjoy the Person
Manage your expectations
• Too many demands on the individual?
• Demands being placed reflect lower expectations?
• Demands being placed exceed the skills?
2. Mind the Language
Park
Rally
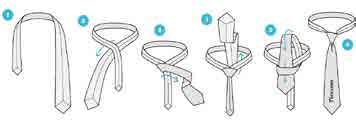
Drape both ends over your neck ensuring the wider end is towards the right Now, cross the right end (the wide one) over the narrow end. In one swift motion, bring the wide end inward, and take it up, further passing it through the intersection/hole formed at the centre due to the previous crossingover step
Step 1: Drape both ends over your neck ensuring the wider end is towards the right.
Step 2: Now, cross the right end (the wide one) over the narrow end.
Step 3: In one swift motion, bring the wide end inward, and take it up.
Step 4: Further pass it through the intersection/hole formed at the due to the previous crossing-over step.
Sona
PHYSICAL ENVIRONMENT
Make it Visual
COMMUNICATE NEEDS, THOUGHTS, DESIRES, FEELINGS GENERATE PREDICTABILITY FUNCTION INDEPENDENTLY SELF-REGULATE
Schedule / Time Table / Things -to-do
Self - Care
Teaching Rules
Class Rules
1. When the Teacher is in class everyone sits
2. When the Teacher is talking no one talks
3. If I need to go to the Toilet or drink water I put up my hand and ask permission
4. If I want to say anything about any one in the class I put up my hand and ask permission
Class Rule for Rahul: I can raise my hand to -
1. Answer question
2. Ask question
3. To go to the toilet or get a drink of water
3. Enhance Motivation
Motivation
• May not be ‘as’ socially motivated
• Intrinsic motivation: interest-based
• May be short-circuited due to confusion, stress, anxiety
Provide with external tangible and intangible motivators / reinforcers
Have fun
Embed interests in activities
Provide clarity, predictability through visualization of expectations and information
Intersperse difficult non-motivating with easy motivating activities
Structure for success
4. Up Skill
Provide Agency and Control
4. Up Skill
Teach appropriate ways to Communicate for attention/ comfort/ help /object / activity
Prepare for exposure to difficult activities /events. Respect and minimize exposure.
4. Up Skill
Provide Agency and Control
Teach Making Choices & Respect those choices
- Yes / No
- Daily activities (what to wear, what to eat, decorating my room)
- Activities (Work, leisure)
- Places (which restaurant to go to)
- People
Express Choices
4. Up Skill
Provide Agency and Control
Teach Strategies for selfregulation (sensory & emotional)
- How can I express my distress?
- What helps me calm down?
5. Prepare in Advance
• Sudden unplanned activities and changes can cause immense anxiety
• Especially when the person may not have the ability to ask requisite questions
• Provide information ahead of time
• Give predictability and clarity with regard to expectations (what to do, how to do it, how long, what next)
• Teach about alternatives
Busy Brain
Visualise Changes
Play Time
Work Time
Snack Time X
Computer Time
Avik works at a Bakery
Avik gives his exams
Avik does not clear his exams
AVIK is in a NO-LOSS WIN-WIN SITUATION
Avik clears exams
Avik gets a promotion
Using Punishment
Punishment doesn’t result in learning. It only temporarily suppresses behaviour.
It isn’t fair to punish for a behaviour, because the behaviour is there for a reason. If you deal with the reason, then the behaviour will change anyway.
Using Punishment
Short-lived not eliminated, just suppressed in the presence of the punisher
It does not teach them WHAT TO DO!
Focus is to escape / avoid / fear the punisher - not a conducive learning environment
Punishment and Modeling - venting frustration is a solution to problems
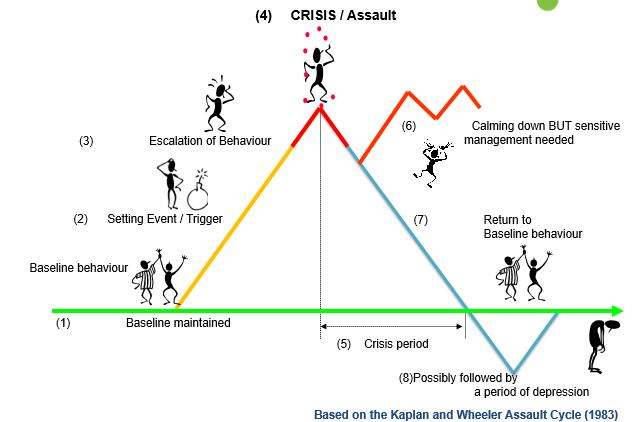
• Can you think of what behaviours you might see at each stage?
Our Role
Surface Management…..In The ‘Rumbling’ Stage
• Remain calm
• Take deep breaths
• Acknowledge
• Use a quiet voice
• Minimal words
• Be conscious of your nonverbal cues
• Be Flexible, meet halfway - Stop from Escalation
• Support from visuals / learnt routines e.g. social story
• DO NOT berate the person
• DO NOT ask questions repeatedly (“What happened?”, “Why are you getting angry?
Our Role
Surface Management….. In The ‘Rage’ Stage
• Remain calm
• Take deep breaths
• Be conscious of your nonverbal cues
• Protect person and others
• Remove audience
• Follow a Plan
• Support from visuals/ learnt routines e.g. social story
• Give the person time/ space to recover
• Give yourself time/ space to recover
• DO NOT berate the person
• DO NOT ask questions (“Are you ok?”, “What happened?”, “Why are you getting angry?” over and over again)
• Try not to talk to the person (in that minute)
• Acknowledge, talk about it later
Our Role
Return to ‘baseline’ stage
• Go back to the drawing board
• Reflect and Analyse What happened What did I do/ say? What could I have done / said differently What can I do the next time
• Put positive behaviour supports in place
To Summarize
There are no recipes for modifying or changing behaviours
It cannot be based on a mechanical use of any prescribed ‘strategy’ or ‘intervention’.
Provide Positive Behaviour Support
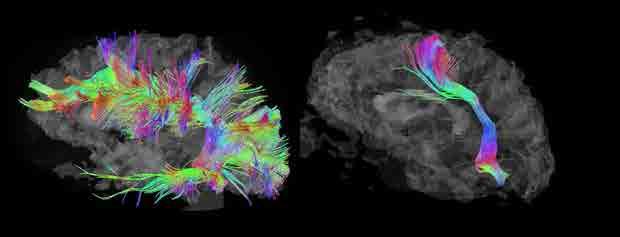
Understand the learning style
A different neurobiology
Perceive, understand and react to the world in a different manner
Learn differently
Understand the individual
Strengths, needs, learning style
Ascertain Communicative Function for specific behaviours/situations
To provide precise supports for those specific situations
Provide support to minimize difficulties/ challenges faced
Minimise triggers
Teach skills
Thereby reduce the need to communicate through ‘challenging behaviours’!
Some people think they are in community, but they are only in proximity. True community requires commitment and openness. It is a willingness to extend yourself to encounter and know the other.
- David Spangler
module 8: community membership
Community is a group of people who come together for a common reason.
Everyone needs Community. Community needs everyone.
A community that excludes even one of its members is no community at all – Dan Wilkins
Community involvement
Role of Human Service Client History
Services
Especially important to people with disabilities
In (but not of) the
Community -
• Aditya lives in a group home with nine other adults who have disabilities. On some days he attends a day centrewith 20 other people also with disabilities. His support worker is encouraging him to research training programs that could eventually lead to employment. The program provides computers where he can conduct his research. On weekends, his family sometimes picks him up to spend time at their house.
Physical integration does not necessarily lead to social integration
–Lemay, 2006
• Prabha lives in an apartment with a roommate in a program that provides support services. She is currently unemployed and is looking for either a part time job or an interesting volunteer opportunity. Because she doesn’t have a computer, she goes to the cyber café a few days a weekto search for jobs and work on her resume and surf the internet for areas that interest her. She has gotten to know one of the staff there and they often take a break together for coffee or just a walk. On weekends, Prabha and her roommate often host potluck dinners for friends and/or family.
Being part of a Community
What Does Community Inclusion Encompass?
Education
Family Roles
Friendships
Leisure & Recreation
Spirituality
Civic Life
Work & Career
Elements of Community Inclusion
Barriers to Community Engagement
People with disabilities segregated, congregated, distanced
Mindsets, attitudes, stigmatization and discrimination
Autonomy, self-determination and expectations
Accessibility and other barriers Other
-(Hastabackaet al., 2016)
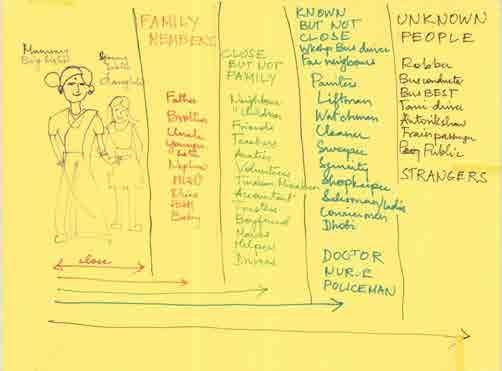
Connections with Community
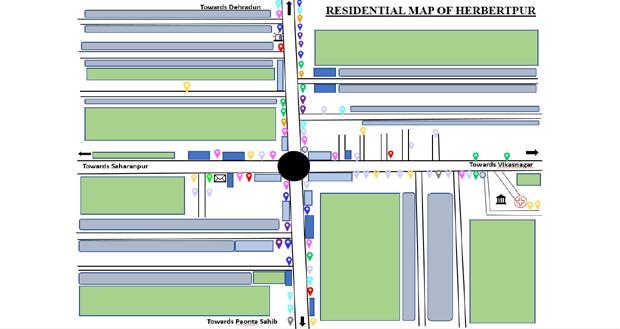
Community Mapping helps figure out what talents, gifts, skills, and capacities lie within a community, and find ways that the community can strengthen itself by “bringing” out those gifts and using the capacities that already exist.
Town of Herbertpur
Located on the bank of river Asan.
As of 2011India Census, Herbertpur had a population of 9,782.
Languages spokenHindi, Punjabi,English,Garhwali and Tibetan.
Self sufficient town
Here you find diversity in religious beliefs
Celebrations happen here !!
Community Gathering
Café | Restaurants
Bakery
What do people do for a living ?
Major Local Businesses
Domestic Connectivity
Passing time ??
Where do people study ?
Healthcare Services
Digital Seva Kendra & Postal Services
Standard of Living
Educational Institutions
Farm Area/ unoccupied Space
Residential Area
Religious places
Medical Stores/Clinics/Individual practitioners
Banks and ATMs
Departmental Stores
Eateries, bakeries and confectionary stores
Selfcare and Beauty Services
Celebration Hall
Other Small Business Shops (Electrical, furniture &Plywood, marble work, iron work, etc.)
Small Shops
Police Station
Post office
Hospital, Local Court
Bus Stand
Final Thoughts
Authentic inclusion is not likely to happen when people with disability “visit community” in large groups.
It IS likely to happen if people with disability are introduced to people, places, and activities which are a good fit for them…individually, one person at a time. Just because this is a challenge does not mean it is not true.
So…get out there, see what’s around, see who’s around and your life will get richer and more included as well!
Before you start to judge me, step into my shoes, walk the life I’m living and if you get as far as I am, just maybe you will see how strong I really am.
- Anonymous
module 9: Family collaboration
INTRODUCTION
Family Collaboration
Purpose
Goal
Structure
Developed by Darcy Elks For Keystone Institute India
What You Will Learn:
► The importance of collaborative relationships with families
► The importance of understanding the kinds of hurtful experiences families may have had
► What families want from direct support staff
► Some possible challenges you may encounter when collaborating with families
► Some guidelines to foster collaboration between staff and families
Part 1: Creating the Context
Focus on Family: a Mindset
► The importance/value of family relationships for all people, especially vulnerable people
► Vision for collaborative staff family relationships
► Understanding Family Experiences
► Reflecting on our role and responsibility in the life of the person with a disability
Part 2: Fostering Collaborative Relationships
► Brief review of key ideas in part 1
► Some possible challenges that could impact staff/family relationships
► General guidelines to help develop collaborative relationships
► Family and staff presentations of positive examples
► Working through some situations
► Conclusion
Part 1: Creating the Context
Focus on Family: a Mindset
► The importance/value of family relationships for all people, especially vulnerable people
Reflection Questions:
1. Think about the importance of family in your own life.
2. What would your life be without your family?
Write down your thoughts and we will have a brief sharing afterwards.
A Family Is……
❖ A Changing Life Mobile
❖ A Balanced Environment
❖ A Birthplace of Creativity
❖ A Formation Center of Human Relationships
❖ A Shelter in the Time of Storm
❖ An Education Center
❖ A Museum of Memories
❖ A Mutual Admiration Society
From Edith Schaffer
VISION FOR COLLABORATIVE FAMILY/STAFF RELATIONSHIPS: PARTNERSHIP
Partner = someone associated with another in a common undertaking, partnership implies relationship
Being in partnership means:
► Working together for good of person with disability
Working Together
► Being open, willing to listen to each other
► Having a shared vision
► Having a sense of one another’s vulnerabilities, pressures, etc.
► Willingness to accept challenges from one another
► Willingness to try to understand one another ’s point of view
► Others you can think of:
IT IS IMPORTANT TO REMEMBER THAT:
While some families may contribute to hurtful life experiences of a person with a disability, for example:
• Rejection
• Participating in segregation
• Denial of autonomy
• Contributing to life-wasting
• Conveying to person that he/she stresses the family A family also has tremendous potential to:
• Protect from some wounding
• Share the suffering which comes from wounding life experiences
• Offset some of the negative effects of wounding
SOME TYPICAL DIFFICULT EXPERIENCES OF FAMILIES WHO HAVE A MEMBER WITH A DISABILITY
Dealing with the “differentness” of your family member
Experiencing negative attitudes towards your family member from others
Experiencing value crisis and disagreements
Needs of family member may be hard to meet at times
Getting a reputation as “difficult”
Living with the impact on the whole family that even a small negative experience can generate
Having to ask for help
SOME TYPICAL DIFFICULT EXPERIENCES OF FAMILIES WHO HAVE A MEMBER WITH A DISABILITY (cont. ’d)
Having to see your family member be wounded
Having your vision for your family member dampened or even scoffed at
Being let down by the very services that say they are there to help
Being humiliated by service professionals
Having to endure the self righteousness of others (e.g., professionals, other family members, friends)
SOME TYPICAL DIFFICULT EXPERIENCES OF FAMILIES WHO HAVE A MEMBER WITH A DISABILITY (cont. ’d)
Experiencing some of the same wounds your family members with a disability experience (e.g., rejection, cast into negative roles, etc.)
Feeling guilt/inadequate
Coping with the vulnerability of your family member with a disability
Being judged by others
Being fearful of
•The future
The effects of advocacy
•Placing the life of your family member in someone else’s hands
WHAT FAMILIES WANT FROM STAFF
An honest interest in getting to know their family members
Genuine concern that their family member be loved and have a full, meaningful life
Openness and willingness to learn from the family
Honesty – even if painful
Expertise Patience
Humility
SOME POSSIBLE CHALLENGES THAT COULD IMPACT STAFF/FAMILY RELATIONSHIPS
Role Confusion (role of staff/family) e.g., staff as cleaner
Supporting the person with a disability when there is a difference of opinion between the person and family
When there is a difference of opinion between what you think is best and what the family thinks is best
Honoring a family’s traditions and spirituality if they are different (maybe in conflict) with yours
There is poor communication between you and the family
Some Possible Challenges That Could Impact Staff/Family Relationships
The person you work with shares a confidence with you and you think that the family should have the information, but the person does not want you to share it.
The family is committed to traditional ways of doing things and is not willing to let their family member try to do things differently
You do not know much about the past experiences of the person you are supporting
Sharing of Two Stories About Collaboration Between Staff and Family
Staff/family share story #1
What did I learn from this story?
Staff/Family share story #2
What did I learn from this story?
Some Ideas To Help Develop Collaborative Staff Family Relationships
► Really listen to what family members (e.g., parents, siblings, grandparents) are saying
► Try to put yourself in the shoes of family member(s) and the person you are supporting
► Be respectful and patient
► Remember the importance of your role in the life of the person with a disability
► Don’t jump to conclusions
Some Ideas To Help Develop Collaborative Staff Family Relationships
► Be open to suggestions of family members
► Let the past be the past
► Be interested in learning from the family
► Encourage family members
► Be positive
► How are family members responding to the situation?
► Why might the family be responding in this way?
► How can you respond in a way that is respectful of the family and the family member with a disability?
► Is there a way that you can respond which will build trust with the family?
► Is there a way that you can respond which will affirm and strengthen your relationship with the family and the person with a disability?
► Is the person with a disability and a vision of a full meaningful life at the heart of the conversation?
► What can staff and family do on a regular basis to nurture and build a collaborative relationship?
Questions To Guide Our Actions When Thinking About A Specific Challenging Situation
Concluding Thought
Alone we can do so little. Together we can do so much.
…Hellen Keller
THANK YOU!
The marvelous richness of human experience would lose something of rewarding joy if there were no limitations to overcome. The hilltop hour would not be half so wonderful if there were no dark valleys to traverse.
- Helen Keller
module 10: legal Framework
Legal Provisions Rights of Persons with Disabilities Act
Historical Background
No Specific Law till 1995
Ratification of UNCRPD by India
In 2010, Government agrees to bring new Disability Law
Rights of Persons with Disabilities Act passed in 2016
Salient features
Definition of disability changed from medical model of disability to rights based model
Focus on barriers
21 categories of disabilities named
Clauses on Rehabilitation, Health, Education
Separate Clauses on Women/Children
Punishment Clause
RPD mentions :
• Equality and non-discrimination
• Protection from cruelty and inhuman treatment
• Accessibility in voting
• Time-limit for compliance with some of its substantive provisions
Education
Free Education for children with Disabilities aged 6-18
Choice to select Special Education or Inclusive Education
5% reservations in Higher Education
Employment
4% reservation in employment
Reservation category includes autism, intellectual disabilities
What steps can be taken so that Kavita can cast her vote?
So many of our dreams at first seem impossible, then they seem improbable, and then, when we summon the will, they soon become inevitable.
- Christopher Reeve
module 11: advocacy & activism
All persons with intellectual disabilities can be selfadvocates.
I've got a voice and even without a voice I can communicate in other ways.
Persons with intellectual disabilities can work and earn money. Obviously they will take decisions of their lives in such a scenario.
DevanshiJoshi, a young woman with Downs Syndrome, said in a video interview that she thinks earning money is an important part of her life.
We are seeing groups of self-advocates with different developmental disabilities in India these days.
I can take a risk, have a relationship
People must listen to me.
I can go to the shop with support and if required, can take help from others.
I can think for myself
I am not incapable and take decisions of my own
As care-givers, we sometimes think we need to take decisions on behalf of persons with intellectual disabilities.
Sometimes, we treat them as “children” even when they are adults.
We need to change our mindset and understand everyone has equal legal capacity i.e. right to be an adult individual with personal choices and thoughts.
According to our law, a person with any kind of disability can take action if his/her rights are violated.
Care-givers can also lodge similar complaint if they see any violation.
This can be done after discussing the same with the person violated.
Care-givers can support the person with intellectual disabilities to become a self-advocate in such cases.
Case Study I
A popular TV serial shows a character with intellectual disabilities as a very incompetent/childish person. Everyone talks to her in the serial as if she is a baby although she is an adult. The other characters use the term “mentally retarded” when they talk about her.
What activities can self-advocates do after watching this serial?
Case Study II
Private buses do not stop at a particular bus-stop even though many passengers wait there. The conductor of the bus says that since this is the time when a special school nearby closes, most of the passengers at the bus-stop are disabled. Disabled students have bus-passes and do not need to buy tickets. So, if many of them take the private bus, they will run at a loss.
How can one find a solution to this problem?
Case Study III
The corporation office of a metro city decides to make a list of vulnerable people so that they can be given preference at the time of a medical emergency like Covid-19. They have enlisted the elderly and transgenders but left out those with disabilities. They are starting the survey in seven days time.
How can self-advocates act as change agents in this kind of scenario?
Our lives begin to end the day we become silent about things that matter.
- Martin Luther King, Jr.
module 12: sexual Wellbeing
Sexual Wellbeing
Let’s get to know each other
Stand by your opinion
People with developmental disabilities do not feel the desire to have sex.
People with developmental and physical disabilities are asexual, childlike, sexually innocent.
People with developmental disabilities are sexually impulsive, aggressive men & women promiscuous.
People with developmental disabilities will not marry or have children so they have no need to learn about sexuality.
It is not really necessary to broach the subject of intercourse since people with developmental disabilities are simply not capable of a close relationship, let alone a sexual encounter.
Stand by your opinion
They will be accompanied all their life by a support worker, so there is practically no chance that they will have sex.
People with developmental disabilities who are intellectually much behind their age or are very young, do not need to know about sex or sexuality. This type of information can be given to them much later - five years or even later.
Persons with disabilities should not be allowed to masturbate because it can become a habit.
It is not natural for women to be sexually attracted to women or men to be sexually attracted to men.
Self awareness and introspection Self awareness and Introspection related to sexuality and sharing
Let
What do they feel about themselves?
Self image
Gender identification
Sharing with others
Possibility of physical relationships
How is their body experience?
Openness towards self-pleasure/ sexual relationship
Opportunities for physical contact
- Understanding puberty - In relation with people with disabilities
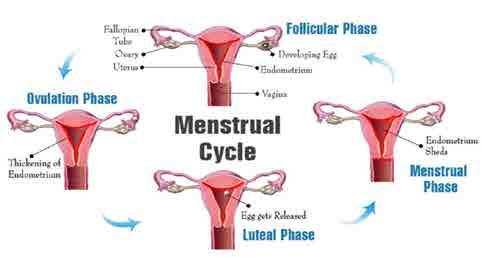
What is Puberty?
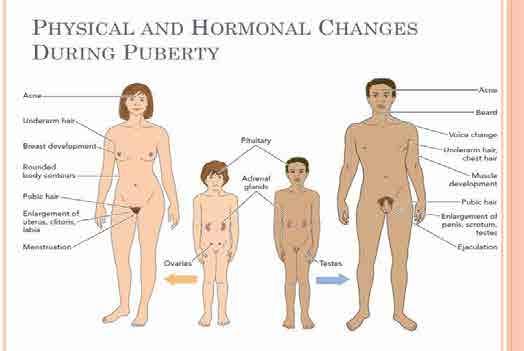
Puberty is the time in life when a young person starts to become sexually mature.
- Final stages of development - Menstrual cycle and ovulation have begun
- Pubic hair growth
- Breast growth continues - Vagina enlarging - Produces discharge
- Breast growth - Height & weight gain
Usually begins
Nearing adult appearance
Development continues
-Penis begins to grow in length -Changes in hair, height and voice
Testicles and scrotum begin enlarging
Usually begins
Menstrual Cycle
Masturbation
A perfectly normal stage of a child’s development.
Self-pleasure
•Masturbation should only be considered a problem if it is:
•Done in public places
•Excessive (causing pain, interfering with other daily activities such as school, therapy, training and work )
•Causing other behavioral issues
•Upsetting for the child.
Wet Dreams/Nocturnal Emissions
A wet dream is also known as a nocturnal emission. Nocturnal means “at night” and emission means “discharge.”
Puberty: social and emotional development
Changes in social interactions during adolescence
Every child’s social and emotional development differs
Unique combination of genes, brain development, environment, social experiences, community and culture
Puberty issues
• Have difficulties monitoring and expressing emotions
• Difficulties balancing emotions and behavior
• Moodiness, has more arguments with you
• Sees things differently from you
• Difficulties with peer and social relationships
• Might have difficulties making and keeping friends
• Antisocial behavior and risk-taking behavior
• Wants to spend less time with family
Biological
Emotional & Social Cognitive
Adolescent development
Without disabilities
-Puberty development the same
-Mood swings -Social-sexual changes
- A variety of ways to express feelings - May understand more complex language
With disabilities
-Puberty development the same
-Mood swings
-Social-sexual changes
- More challenging to express feelings -Need more concrete language
Snippets 2
Impulsive
Poor self-esteem
Depression
Part 2
Harmful effects of repressing of sexual expression
Emotional instability
Anger
Child Abuse
Aggression
Criminal behaviour
Isolation
Inferiority complex
Related physical problems
Frustration, confusion
Misconduct
At-risk behaviour
Poor decision making
Loneliness
Anxiety
Physical discomfort
Mental health issues
Scenarios
Ajay is a young man who is exploring his sexuality. This leads to frequent self pleasuring, which is often done in socially inappropriate situations e.g., in the garden when taking a walk.
An attempt was made to stop his behavior by calling in a policeman who threatened Ajay with prison and beatings if he was found doing this again. Ajay is now terrified of being caught.
Bhagyashree is a young lady who has been constantly stopped and scolded for self pleasuring at home.
As a result, she had taken to pleasuring herself in the shower cubicle of the swimming pool she visited, with a hanger.
At an overnight picnic from a school, Chanda, a very sociable and talkative person was caught fondling with her room mate by mutual consent, at night after lights out. The room mate was also a young lady. Her parents were called and she was shamed in front of the whole class and parents. She carried the humiliation for years.
Dheeraj and Ekam are very fond of each other and are colleagues. They only meet at work. On one occasion, when the sheltered workshop had gone on a picnic, the two were seen being cozy with each other. Dheeraj was sitting on a garden bench and Ekam was lying down with his head in her lap. The staff immediately broke them up and scolded them for their behavior. They experienced guilt and became very secretive.
Firuza used a wheelchair. She had a crush on a boy at her college and wanted to look special for him on a particular day. She needed help bathing so that day, she asked her mother to shampoo her hair. Her mother, who needed to drive Firuza to college before reporting to her work, scolded Firuza for asking for a shampoo on Wednesday when she knew that Sunday was shampoo day. Firuza felt dejected and angry at her mother.
Gurpreet, a middle aged woman was very terrified of any workers in her home. She would become very agitated and it was very difficult for her family to get any repair or renovation work done. This was directly the result of a childhood experience when her building was being renovated and a worker had climbed into her room from the scaffolding and molested her.
Need for social-sexual education
A
Decreases the Likelihood of Abuse
Need for social-sexual education
Combats myths and misinformation
Need for social-sexual education
Promotes personhood, pleasure, etc. C
Need for social-sexual education
Reduces fear, anxiety, worry, etc.
Need for social-sexual education
Increase self-awareness, gender comfort E
Need for social-sexual education
Allows for mature and healthy relationships
Challenges
TEA BREAK
Part 3
Exploring the body and bodily needs
Exploring the body and bodily needs
What are the aspects to be aware of
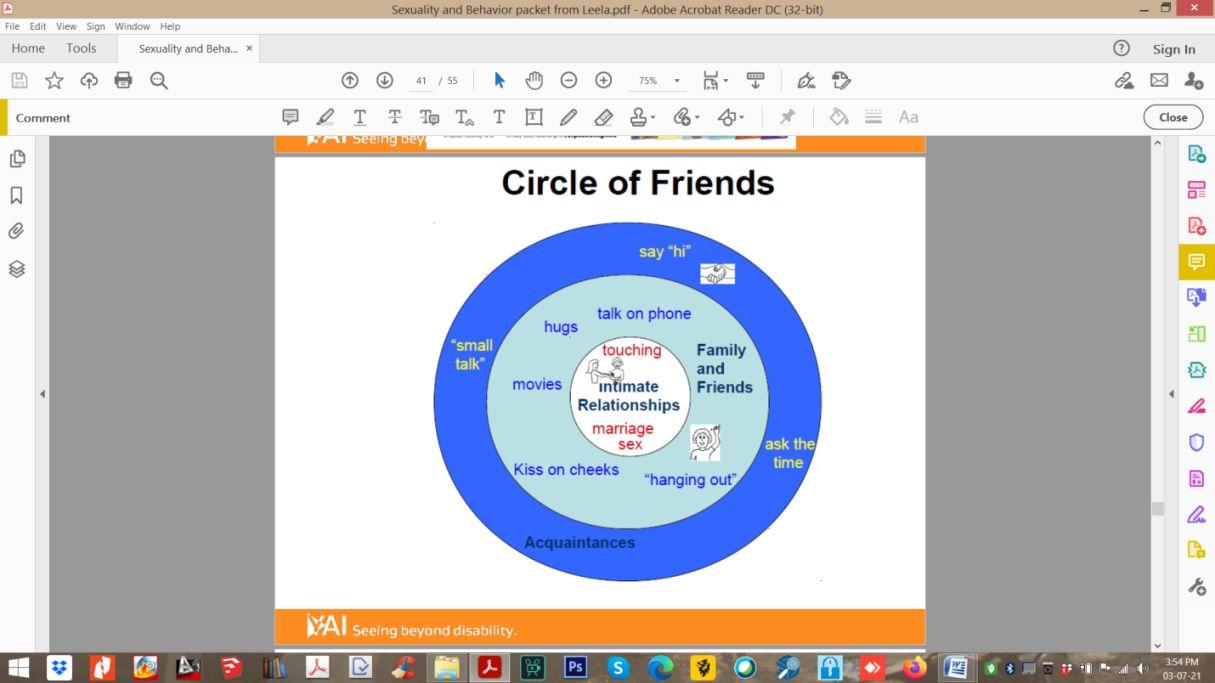
Body parts Self touch Private vs. Public Circle of trust Boundaries Good/bad touch Hidden social etiquette
Emotions as a tool for self awareness for the child/adult, explored as connected to sexuality
Significance of understanding complex emotions
Nidhi – make it
Empowerment
"I am the boss of my body"
angry when someone touches me like this
happy when someone touches me like this
scared when someone touches me like this
Where does the possibility of these arise?
Important points
Be proactive not reactive
• Normalize the discussion of sexuality!
• Use concrete language at their cognitive level & pictures
• Making it taboo encourages secrecy and increases vulnerability
• You may need to initiate the conversation
• Be honest and give correct information
• Respond to all sexual issues non-judgmentally
Addressing situations without creating guilt or shame
RESPONDING TO SITUATIONS
Gia, is a 35-year-old lady, who is in the practice of self pleasuring in the afternoons in her bedroom. She does not shut the bedroom door or draw the curtains.
On one such afternoon, you walk in on her.
Do you see an issue here? How would you address it?
Hiren, a young, adolescent lad has not been able to sleep well, and it has been disturbing his daily routine. You notice that he has been using up all his underwear, shorts, pajamas, pants through the night and putting them in the washer.
He has been saying “toilet” all day and going in, changing clothes and coming out without using the toilet.
He does not appear to have a stomach upset or a urinary tract infection.
Do you see an issue here? How would you address it?
Further examination tells you that he has been having nightfall and his sensory issues make it difficult for him to sleep with even slightly damp clothes.
What would you do? to explain what is happening and to restore his sleep needs
Yogesh, inappropriately puts his nose into the blouse fronts of women who might be using perfumes he likes.
This has led to him being called an “attacker” and women avoid him.
Do you see an issue here?
How would you address the situation?
Joginder, a 50-year-old man likes to surf YouTube videos on his cell phone and watch raunchy numbers.
His surfing often takes him to pornographic sites, which too he enjoys watching in the privacy of his room and by himself.
However, when he wants to maneuver his way back to where he started from, he finds that he cannot do it without assistance and lands up approaching his care giver for help.
Do you see an issue here? How would you address it?
Karthik, a middle aged man has been in a relationship with the liftman of their building. It has been going on for several years.
Recently, this young man decided to confide in you and tell you that the two of them meet often and that he likes this person’s company and the relationship.
Do you see an issue here? How would you address it?
One day, while going about your daily chores, you notice that Lalit, the person in your care is making physical and sexual advances towards you.
When you ask or observe closely, you are certain that you are not mistaken.
Do you see an issue here? How would you address it?
Mehtab, a man in your care, confides in you that he dearly loves a lady at his workplace and wants to marry her, hold her hand and kiss her.
But she is very firm that she only wants to be his friend. This is disturbing M a lot and he wants your help.
Do you see an issue here? How would you address it?
You come to know that Noel, a man in your care, follows a girl who travels on the same public bus with him and gets off at his stop, everyday, right up to her home.
This is unsettling to the girl, who has complained to you about Noel’s behavior.
Do you see an issue here? How would you address it?
A relook at our opinions
Stand by your opinion
People with developmental disabilities do not feel the desire to have sex.
People with developmental and physical disabilities are asexual, childlike, sexually innocent.
People with developmental disabilities are sexually impulsive, aggressive men & women promiscuous.
People with developmental disabilities will not marry or have children so they have no need to learn about sexuality.
It is not really necessary to broach the subject of intercourse since people with developmental disabilities are simply not capable of a close relationship, let alone a sexual encounter.
Stand by your opinion
They will be accompanied all their life by a support worker, so there is practically no chance that they will have sex.
People with developmental disabilities who are intellectually much behind their age or are very young, do not need to know about sex or sexuality. This type of information can be given to them much later - five years or even later.
Persons with disabilities should not be allowed to masturbate because it can become a habit.
It is not natural for women to be sexually attracted to women or men to be sexually attracted to men.
Closing Questions
Your present circumstances don’t determine where you can go; they merely determine where you start.
- Nido Qubein
module 13: promoting competency
If your actions inspire others to dream more, learn more, do more and become more, you are a leader.
- John Quincy Adams
module 14: taking leadership
SECTION 1: - Effective Leadership - Growing into Leadership
EXPLORING LEADERSHIP
THINK OF ONE WAY YOU HAVE INFLUENCED OTHERS IN YOUR CURRENT ROLE AS A DSP?
GROUP DISCUSSION
1. In each of the scenarios who do you think is a leader?
2. Why do you feel the person you chose is a leader?
3. Based on the understanding gained from the discussion around these scenarios, what do you think are the main differences between a manager and a leader?
GROUP DISCUSSION: CHARACTERISTICS OF GOOD LEADERS
EFFECTIVE LEADERSHIP
Share a vision
Create a collaborative environment
Engage with People you support, team members and allies
STRATEGIES TO LEAD WITH IMPACT
TAKE TIME TO BUILD CONNECTIONS
KEEP TRAINING AS A MAIN FOCUS
USE CLEAR AND RESPECTFUL COMMUNICATION
SUPPORT WELL - BEING
LINK THE WORK TO THE PURPOSE
Growing into
Leadership:
Personal Development for DSPs
“I am because we are.”
Why does Personal Development matter?
The Ripple Effect of Growth
Leadership is Collective
Leadership Strengths
Activity – Strengths Tree
Roots and Trunk – represent Core Values, Beliefs, and Motivations
Leaves – represent Strengths, Skills and Leadership qualities
Flowers – represent Achievements and Contributions
Fruits – represent Future growth aspirations and goals
From Strength to Stewardship: The Leadership Journey Ahead
Bridging lived experience with policy
Meet Asha, a seasoned DSP. Her strength lies in deep listening she notices the subtle shifts in mood, the unspoken needs, the quiet victories. Over time, her consistency builds trust not just with the person she supports, but with families, colleagues, and even the organisation’s leadership.
One day, a new initiative is proposed: changing the morning routine so that all personal care tasks must be completed by a fi xed early time, rather than allowing each person to choose when to start their day. While intended to improve scheduling, this shift could unintentionall y reduce autonomy for those she supports.
Asha speaks up not loudly, but clearly. She shares stories of how flexible mornings help people feel in control, data showing th e benefits of choice, and lived experiences from those directly affected. Her voice reshapes the conversation, leading to a plan that keeps efficie ncy without taking away personal choice.
Months later, she’s invited to co-design training modules. Her insights become part of the organizational DNA.