Twins separated at last

Issue 2 10/2/2023Newsline More than just health

Editor’s note p.2
Twins separated at last p.3 - 4
Meet the Pediatric Intensivist and Emergency specialist at KNH p. 5 - 6
The ‘broken’ heart syndrome p.7 - 8
Against all odds: Meet Eunice Achieng
Owino, The Sickle Cell Champion p.9 - 10
Intern’s Experience p 10
Prime with Love: Through the eyes of a KPCC New Born Unit (NBU) nurse p.11
Pension in KNH p.12 - 13
KNH’s latest, fully-automated blood bank instrument (Immucor Neo Iris) p.14
The success story of the KNH
Comprehensive Care Centrep.15 -16
Our story in Pictures p.17
International day for zero tolerance of Female Genital Mutilation (FGM) p. 18 - 19
Kenyatta National Hospital spearheading specialized treatment and stigma reduction for patients with STIs p. 20 - 21
Positive mentions from KNH socials p. 22

KPCC PHARMACY open daily, 24 hours p. 23
Birthday Wishes p. 24 - 25
Comic zone p. 26
Design Concept Team:
Dave Opiyo, Edel Q. Mwende, Yvonne Gichuru & Collins Cheruiyot
Editorial Team:
Dave Opiyo , Edel Q. Mwende, Yvonne Gichuru, Luke Kung’u, Winfred Gumbo, Verah Mugambi, Shiphrah Njeri, Philip Etyang & Priscah Angwenyi
Stories:
Dave Opiyo, Verah Mugambi, Melody Ajiambo, Petterson Njogu, Yvonne Gichuru, Chebet Kwemoi, Joel Mokaya, Steve Arwa, Elizabeth Wambui, Bernice Njeri & Samira Yusuf
Design By: Collins Cheruiyot
Photos:
Nicholas Wamalwa, Steve Arwa, & Luke Kung’u
Tel: +254 20 2726300-9
Ext. 43121 or 43969
Fax: +254 20 272572
Email: caffairs@knh.or.ke knh.caffairs@gmail.com
The 14th of February will mark Valentines; a day of romance and love! Though love doesn’t need a single day to be ‘celebrated’, most people around the world acknowledge this special day by exchanging tokens of affection including chocolates, flowers, and gifts among loved ones, all in the name of St. Valentine. Whether you celebrate with friends, family, or a romantic partner, the day is a special one to express your affection for another person. Share this day with others by making them feel loved and appreciated. Treat yourself to things that make you feel good too. You define what each day means to you.

All the Newslines and Newsletters can be accessed online at: https://bit.ly/3uQGCcI

Ms. Yvonne N. Gichuru
Marketing & Communication Officer
Kenyatta National Hospital
Nairobi, February 2, 2023:
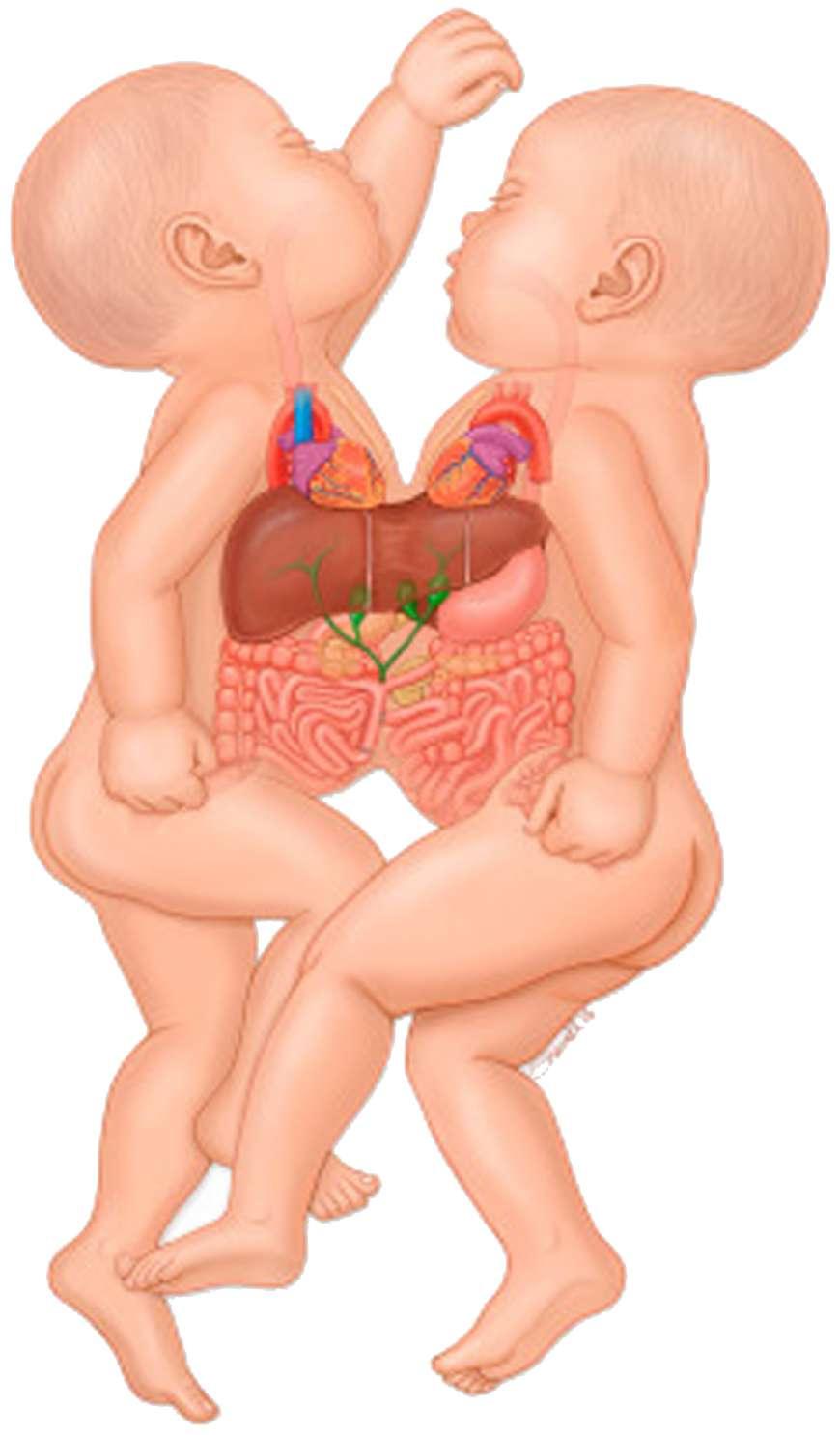
A pair of conjoined twins were successfully separated during a 15-hour complex surgery by a team of multidisciplinary medical experts at Kenya’s premier referral hospital.
The male infants, born four months ago in Bungoma County and who were joined at the chest and abdomen at birth, began a new life apart on Sunday after the delicate surgery at Kenyatta National Hospital (KNH).
The operation which began on Saturday night at a10pm ended on Sunday at midday.
It was conducted by a dedicated team of at least 38 medical experts from KNH and the University of Nairobi (UoN) led by peadiatric surgeon Dr. Joel Lessan. The team had 24 surgeons; Plastic and Reconstructive (5), Peadiatric Surgeons (14), Anaesthetists, and Cardiothoracic (1) as well as six nursing officers.

The twins have been under observation since September last year. Doctors described their condition as ‘Thoracoabdominocophagus’, a situation where twins are joined
face to face at the chest and abdomen.
Conjoined twins are the result of embryo cells that have not completely separated. Embryo cells develop when the egg (ovum) is fertilized by sperm. They multiply and differentiate to form different body organs and tissues. An alternative theory is that two separate embryos fuse in the early development of twins.
The exact cause of conjoined twins is unknown but it’s thought that genetic factors interacting with environmental ones may contribute. Another possibility is the medicines taken by the mother during pregnancy.
This type of conjoined twins often share a heart and may also share one liver and the upper intestine. This is one of the most common sites of conjoined twins globally.
In this case, however, the twins shared a liver and had two hearts in one cavity. Both hearts were abnormal. They similarly shared chest bones and muscles. In such cases, patients require close monitoring and treatment before a decision of their separation is duly agreed upon.
According to Dr. Lessan, the decision to operate on them came
on Saturday night as an emergency after one of them suffered cardiac arrest calling for a swift yet calculated move on how to save their lives.
He said both children had multiple holes in their hearts, with one of them having an abnormal blood vessel originating from the heart.
This, he said, was compounded by a life-threatening infection at two months that was diagnosed and treated early enough.
Even though the target time for safe separation was to be at six months, one of the twins, he said, developed high pressure in the lungs, exposing them to even greater danger including imminent heart failure.
“This informed our team, even at four months, to start plans for separation. The challenge at this level was how to cover the defects left behind on their line of separation,” he said.
“However, last week on Thursday, we successfully developed flaps to cover the separation lines. We were to wait for another eight weeks before attempting complete separation. Unfortunately, two days after raising the flaps, one of the twins suffered a heart attack.
We made an emergency decision to separate the twins because subsequent cardiac arrest would put the lives of the other twin in danger, hence. We mobilized the team, equipment, and medication culminating in the successful surgery on Sunday,”PHOTO | STEVE ARWA KNH Management being joined by the multi-discplinary team that performed the succesful twin seperation surgery
He was, however, successfully resuscitated.”
‘We made an emergency decision to separate the twins because subsequent cardiac arrest would put the lives of the other twin in danger, hence. We mobilized the team, equipment, and medication culminating in the successful surgery on Sunday,” he said.
Both infants are now under close monitoring and treatment at KNH’s ICU and are progressing well.
KNH’s Director of Surgical Service Dr. Kennedy Ondede attributed the success of the operation to surgical dexterity, teamwork, and dedication by the multi-disciplinary team.

“Proper planning, expertise, and careful preparation of the various sub-specialties is a critical part of this kind of surgery,” said Dr. Ondede.
KNH Chief Executive Officer Dr. Evanson Kamuri hailed the KNH team for yet another milestone. “This is a landmark. On this historic day, we have achieved yet another achievement in fulfilling our mandate as a top premier referral


hospital,” he said.
“It was just amazing to see one set of conjoined twins turn into two separate children. We are dedicated to ensuring that their follow-up care nurtures them into happy and healthy children.
The KNH team seized the moment against all odds. We
“It was just amazing to see one set of conjoined twins turn into two separate children. We are dedicated to ensuring that their follow-up care nurtures them into happy and healthy children.PHOTO | STEVE ARWA Lead Paediatric Surgeon Dr. Joel Lessan addressing the Media after the succesful surgery
As the largest referral hospital in the country, we pride ourselves as a world-class patient-centered specialized care hospital. True to it, we have specialized doctors and nurses who are always committed to their duties.
It can be tense when kids are in the hospital and even more so in the Pediatric Intensive Care Unit (PICU). However, understanding the people and equipment in the PICU can help you feel better prepared to help your child.
In Kenya, we have only two pediatric intensivists & emergency specialists, and one works here at Kenyatta National Hospital. Meet Dr. Mukokinya Kailemia, a Pediatric Intensivist and an emergency specialist at KNH Pediatric Intensive Care Unit (PICU). She joined KNH three years ago as a Pediatrician before specializing in Pediatric Intensivist and Emergency.
According to Kenya Paediatric Association (KPA), a Pediatric Intensivist is a doctor with special training in diagnosing and treating children who are seriously ill or injured children. Pediatric intensivists use special procedures, treatments, and medicines to care for children in a pediatric intensive care unit of a hospital.
“Paediatric Intensive Care Unit (PICU) is an area in the hospital where very sick kids aged between two months to 13 years require intensive care or the highest level of medical care,” Dr. Kailemia stated in the interview with the Newsline team.
It differs from other parts of the hospital, like the general medical floors. In the PICU,
kids get intensive nursing care and close monitoring of heart rate, breathing, and blood pressure. These can include ventilators (breathing machines) and medicines used only under close medical supervision.
What types of patients are in PICU?
Diagnosis of patients admitted to the PICU includes trauma, sepsis, pneumonia, solid organ/ bone marrow transplants, post-neurosurgery, post-airway
Pediatricians) and PICU fellows (pediatricians training to be attending intensivists),” Dr. Kailemia explained.
Why pediatric Intensive & emergency specialists?
Dr. Kailemia: From med school, I felt pediatrics was one of the neglected areas. Most of the efforts are put toward adult medicine rather than pediatrics. Children are tomorrow’s future; remember, some are too young to speak for themselves,

think through what the patient is feeling… for me, that’s interesting.
Also, there is a need for an intensivist & emergency specialist combined in our hospital and the country. Another colleague and I were the first group in the country to do it blend; that pediatric intensivist & emergency medicine. Most people do it as separate courses.
Dr. Kailemia: First, we see very sick patients, and outcomes vary. Some go home, others are left with severe neuro issues, and unfortunately, others don’t make it. It takes a toll on you because the aim is to save all patients, but losing them is painful. Being unable to keep them all is the worst part of the day.
The worst part is that most of the conditions we deal with are not congenital… it
is not something someone is born with. Some of these diseases are preventable and also manageable. This is a bit discouraging because sometimes you feel that you could have saved the patient if you had gotten the patient earlier.
“Of late, we have been getting several positive outcomes, from the year 2022, we have had a reduction in our mortality, and that’s a big thing, especially for a public pediatric ICU. It’s a result of teamwork. We have an excellent team of nurses, consultants, and registrar all have been helpful,” she said with a smile.
What does it take to be a Paediatric intensivist and emergency specialist?
Pediatric intensivists have specialized training. After completing medical school as a pediatrician, one must

complete a three-year pediatric residency and then a three-year fellowship in pediatric critical care; you can do it separately or combined; pediatric urgent care or (&) emergency specialist. After that you work for one year then you get your recognition. Board certification examinations in pediatric critical care are offered every other year, and one must also maintain board certification in general pediatrics.

How do you deal with overwhelm?
As a team, we debrief each other or talk to colleagues outside the hospital because sometimes, if things go south, you wonder what did I miss? Where did I go wrong? I normalize spending time with family and friends, listening to music, exercising, etc.
According to Dr. Kailemia, there’s a need for more human resources among pediatric intensivists & emergency specialists. “These children are the future so I hope more doctors in medical schools focus on PICU,” she concluded.
Many of us can probably relate to someone that just got blindsided and broken up with the person they thought was ‘the one’.
They often get into some form of emotional shock or life crisis; barely getting out of bed, feeling and often looking miserable, spending hours of their day crying and moping around, and most likely, their work and social life begin to slip. It’s almost like they are going to die from a “broken heart”.
There are also scenarios where longtime married couples that have been together for decades, die within just a few days of each other. A tragedy or a love story?
Losing a loved one can be emotionally devastating. But, the most important question is how this emotional despair affects our health and our heart.
As extreme as it sounds, feeling broken hearted sucks. But are you being overly melodramatic when equating the connection of deep emotional pain with real physical pain or is there some truth to it?
Well, it’s possible to suffer from a real broken heart. Unfortunately, in some cases, a bad breakup or losing
someone very close to your heart can cause enough emotional trauma and stress that it will cause real physical damage to one’s actual heart. This is recognized in the medical field as a real phenomenon known as “broken heart syndrome”.
According to Dr. Martin MurageHead of the Cardiology Department at Kenyatta National Hospital, Broken heart syndrome, though rare is a temporary heart condition that’s often brought on by an automatic stressful emotional experience such as grief in most cases.
“People who are experiencing broken heart syndrome describe sudden heart attack-like symptoms that include chest pain and difficulty breathing. In some cases, it can be misdiagnosed as a heart attack since test results will show changes in rhythm and rising troponin levels consistent with a heart attack. But, unlike a myocardial infarction, other tests will not show blocked arteries.
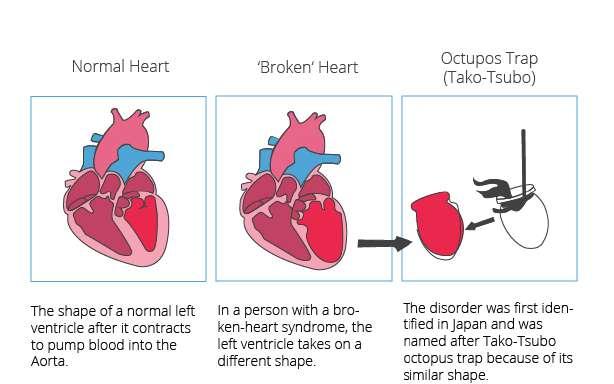
During Broken Heart Syndrome, the left ventricle will temporarily enlarge and does not pump enough blood. The remainder of the heart will function normally and may even contract more forcefully trying to make up for a poor function in the left ventricle.”
he added.
Events that have been known to trigger broken heart syndrome include car or other accident, Asthma attack, serious illness, surgery or medical procedure, death or serious illness or injury to a loved one, domestic violence, financial loss, intense fear, sudden surprise or even loss of a job.

It can also be triggered by a difficult breakup, a long physical separation from a loved one, an act of strong betrayal, or a romantic rejection. All of these examples have some sort of negative emotional or physical connotation to them.
“The syndrome can lead to severe, short-term heart failure. Most will make a full recovery within several weeks. However, there is no standard treatment. Instead, clinicians depend on other symptoms, such as arrhythmia (a condition characterized by abnormal heart rhythm) to determine treatment options.” said Dr. Murage.
Another name for broken heart syndrome is ‘Takotsubo cardiomyopathy’. The word ‘takotsubo’ was derived from the name for a pot used by Japanese fishermen to trap octopuses. When the left ventricle of
The human heart is considered the center of all of our emotions and is associated the most with love. What is the connection between the human heart and love? Can you die from a ‘broken’ heart?
the heart changes shape, it develops a narrow neck and a round bottom making it looks similar to the octopus trap just like the pot-like shape of the stunned heart in broken heart syndrome as depicted below:
that will eventually lead to cardiogenic shock - when the heart is suddenly dramatically weakened and is unable to pump enough blood throughout the body to meet its needs to function normally. This
“People who are experiencing broken heart syndrome describe sudden heart attack-like symptoms that include chest pain and difficulty breathing. In some cases, it can be misdiagnosed as a heart attack since test results will show changes in rhythm and rising troponin levels consistent with a heart attack. But, unlike a myocardial infarction, other tests will not show blocked arteries.
again.” he concluded.
In conclusion, Is it true that you can have a heart attack or stroke from a broken heart?
This drew the attention of scientists in the West who later named the condition broken heart syndrome in reference to those who experience the condition after the death of a loved one. It is key to note after the spread of COVID-19, the prevalence of depression, anxiety, and stress and the general population rose significantly.
Surprisingly, this syndrome can even happen in people who are considered very healthy and have no previous history of any cardiovascular or heart disease as this is the case for the majority of people suffering from broken heart syndrome; Individuals that go the majority of their life with a perfectly healthy heart, but then after experiencing a very specific stressful event they all of a sudden suffer from symptoms of massive heart attack or even go into complete heart failure.
“In general, menopausal women are much more likely to suffer from broken heart syndrome. More than 90 percent of the reported cases occur in women ages 58 to 75 as they are more susceptible to this condition due to reduced levels of estrogen after menopause” Dr. Murage stated.
Fortunately, for the majority of cases, broken heart syndrome is usually only temporary and most people can fully recover within just weeks. And although death from a “broken heart” is extremely rare, it’s still possible in some cases.
“It can cause irregular heartbeats
shock to the body is dangerous and without immediate treatment, it can be fatal. It’s also the most common cause of death when one dies from a heart attack. But the good news is, unlike a person experiencing a heart attack, once a person recovers from their “broken heart”, they are at very low risk of forever experiencing it
Although rare, it can happen. The reality of a real broken heart is to show you just how big of a role stress, emotional or physical, can play in affecting your heart health, as well as your mental health and social support. The condition is temporary and most people recover within two months.
 By Melody Ajiambo
By Melody Ajiambo
Eunice Achieng Owino is one bubbly soul. When you see her smile as she expresses herself, it is hard to imagine that she is living with Sickle Cell Disease (SCD).
SCD is an inherited red blood cell disorder. With SCD, the hemoglobin (a protein that carries oxygen in the red blood cell) is abnormal, which causes the red blood cells to become hard, and sticky and look like a C-shaped farm tool called a sickle.
These sickle cells, unlike the round healthy red blood cells, can cause serious health complications; when they travel through small blood vessels, their shape causes them to get stuck and clog the blood flow. Moreover, sickle cells die early, which causes a constant shortage of red blood cells. The result is anemia and immense pain.
For Ms. Eunice, the journey has not been easy. In October 1981, at the tender age of eight months, she was diagnosed with SCD type “SS” at Kenyatta National Hospital (KNH). Eunice took time to talk to Newsline about her experience living with the disease.
While recounting her story, Eunice expressed how grateful she was that her family had been very supportive. Being the fourth born in a family of five children, she had seen her loving and caring family stand by her side unwaveringly. With teary eyes, she recounted how her mother would travel long distances just to get her to the Hospital for her clinic appointments.
When she turned 13 years, Eunice began to understand her condition. She also began to take care of herself better, and manage the disease by keeping warm during cold seasons, drinking enough water, eating vegetables, and fruits, taking medication at the right time and going for her regular checkups after every three months. She tells us that this is how she has managed to live with the disease
to date.
According to Dr. Kibet Shikuku, a lecturer at the University of Nairobi’s Human Pathology, Hematology, and Blood Transfusion Unit, a fetus can be diagnosed with sickle cell disease under the right circumstances. Dr. Kibet currently works with the Paediatric Unit at KNH, treating children with hematological disorders, including SCD.
Expounding on the subject, Dr. Kibet explained that Sickle Cell Disease is a genetic condition caused by a mutation in
hemoglobin. While it is prevalent in some parts of the country, like the Western and Nyanza regions, SCD can affect anyone who inherits the hemoglobin ‘S’ from one parent and another gene that codes for another abnormal type of hemoglobin from the other parent.
The most common and often severe type of the disease is the ‘hbSS’ (the one Eunice has) and is inherited if both parents have hemoglobin ‘S’. Dr. Kibet says that the only way to prevent the disease is to get tested early to determine if both parties have the dormant genetic condition, and avoid
conceiving children together. There is a lot of stigma surrounding Sickle Cell Disease, but Eunice has found a way to weather the storm. “I live my life as normal as any other person. I lost my father when I was 19 years old and most people thought I would get very sick, but I thank God I never had any crisis at that time,” she said.
Unfortunately, in 2003, Eunice began feeling pain in the hip. Upon check-up, a crack was discovered on her hip joint. To reduce or stop the pain and maintain joint mobility, she would; elevate and rest the joint, go for physical therapy, and take pain relief medicine. In 2014, however, she underwent total hip replacement surgery. This was necessitated by Avascular Necrosis (AVN), commonly known as aseptic bone necrosis- the death of the bone tissue due to lack of enough blood and oxygen supply. The surgery left her with some scars; now she walks with a slight limp.
Eunice recounted how she has experienced other challenges, like discrimination at the workplace, school, among friends, and
from some relatives who don’t understand her situation. Also, not being able to have a romantic relationship because of this lifelong condition.
“My experience as a person living with SCD led me to become a Sickle Cell Warrior and a voice for the Sickle Cell Community. Together with other patients, we have formed the Sickle Cell Warriors Association which seeks to advocate and raise awareness of the disease in Kenya by educating the public on the disease. We also share information on how patients can find sustainable medical care and how to care for people living with sickle cell disease. So far, we have done sensitization in a few counties and we hope to reach the entire country,” she tells us.
Eunice is now a sickle cell advocate. She is the Executive Director / Founder of the Sickle Cell Uhuru Trust (SCUT) and SCUT Company which have been in existence for more than 5 years. Both have been registered in Kenya and are working to create awareness of SCD. She is also on the Board of Directors at The Sickle
She explains that SCUT has several activities which include;
• Monthly support group meetings
• Home and hospital visits to patients
• Fun days where the ‘warriors’ meet, greet and have fun, both in Nairobi and other counties
• Training and empowering warriors through a partnership with Google to train adult sickle cell patients on how to generate income through Google
• Collaborating with other sickle cell organizations aimed at creating awareness of sickle cell disease. SCUT also played a role in the establishment of the Sickle Cell Federation of Kenya, which is the umbrella body of sickle cell organizations in Kenya
Eunice laughs as she shares her daily motto with us, “’ Live a day at a time.’ Sickle Cell is not a death sentence, enjoy your life and find what makes you happy,” She concluded.
Department: Marketing & Communication (This is the face of the hospital that coordinates, creates, and disseminates all materials representing the Hospital).
Tasks
Managing customer serving desks, assisting and directing visitors and patients accordingly, managing patient visitations in accordance with hospital guidelines, photography, and videography.
The learning experience at KNH
What I love about KNH
It is an encouraging environment to work in, and the doctors are neat and excellent. Also helpful supervisors (a nod to my supervisor, Mr. Ruto). Welcoming colleagues and an amazing work environment.
Plans?
I want to start a podcast after campus. I’m also planning to be self-employed rather than diving into employment in media and communications.
By Elizabeth Wambui & Bernice NjeriName: Alfonse Odhiambo

Education: Journalism & Media Studies
The learning experience has been amazing so far. I have improved my communication skills. The clients here are mostly anxious, so one needs to develop more empathetic communication skills to serve patients and relatives well. It has been an interesting journey.
Parting shot?
I will urge my fellow interns to perform their duties well to build experience and connections. Follow the rules and be as present as possible. Follow your dreams.
 By Petterson Njogu
By Petterson Njogu
Meet Eddah Wambui, a dedicated neonatal nurse who works in the New Born Unit at KNH Prime Care Center (KPCC). She has been working in the unit for over four years.
After normal pleasantries, we dove into understanding who a neonatal nurse is, and their role in the care process of a newborn:

A neonatal nurse is specialized in neonatal care (newborn babies who are born prematurely); those that are between the ages of 0-28 days old.
Various types of nurses work very closely with doctors to ensure that babies recover fast. They include; neonatal nurses, Intensive Care Unit (ICU) nurses, and general nurses.
“Neonatal nurses in particular handle different kinds of cases such as preterm neonates- these are babies who are born before 37 complete gestation weeks. We also have neonates with congenital anomalies- birth defects or disorders that may develop after birth. For instance, babies born with cleft lip and palate, club foot, and limb deficiencies just to highlight a few,” she explained.
Additionally, all sick babies between the ages of 0-28 days who have not gone home may find their way to our NBU. The reason behind this is to strictly mitigate risks that may be brought about by unknown infections. Infection Prevention Control measures oftentimes take precedence in such situations.
These unwell babies mostly suffer from a condition called neonatal sepsis (blood infection amongst infants) and jaundice. Infant jaundice occurs when the baby’s blood contains excess bilirubin – a yellowish pigment of red blood cells. Another common condition in babies who develop Hypoxic-Ischemic Encephalopathy (HIE) is when a baby does not cry after birth; this may be a sign of brain damage. Also, the newborn may contract respiratory distress
that is caused by a low supply of oxygen.
For all the aforementioned medical conditions that the babies may face, KPCC NBU is wellequipped to handle such cases with the help of highly experienced and dedicated professionals, added Eddah.
Despite Eddah’s warm and upbeat demeanor, her job involves long hours, stressful situations, and most importantly emotional toll that comes with her line of work.
She vividly recalls baby Rachel who was born weighing 600g sometime back at KPCC. The baby was emaciated, dehydrated, and had a skin infection and breathing complications. Baby Rachel’s survival chances were slim but Eddah took her under her wing. She would spend every moment she could spare with her, holding her, and talking or singing to her.
Days turned into weeks, and baby Rachel started gaining weight and strength. Her parents were also delighted to see the difference in their baby’s health. After two months of thorough nursing care provided by Eddah and her team, the baby was eventually strong enough to go home weighing two (2) kilograms.
Watching Baby Rachel get discharged to go home with her parents made Eddah realize that she and her team may not have all the answers but one thing remains for sure- every baby that comes to her is a miracle, and she’s honored to be part of their journey to good health.
Eddah is still in touch with Baby Rachel and her parents. She constantly receives major milestones in Rachel’s life; videos of her when she started weaning and taking her first steps, the latest being her second birthday celebration photos.
On the downward also, the job comes with its share of emotional demands. She mentioned the
heartbreak she experiences when a baby doesn’t make it out of the NBU and seeing couples devastated after hearing the devastating news.
At that moment it dawns on her that hers is more than a job, she also provides love and comfort to families going through difficult moments.
“Do not save what is left after spending, but spend what is left after saving”. This is a famous quote by Warren Buffett. In this regard, we need to know how to save for our future.
Newsline got the opportunity to interview Ms. Lilian Gitau, KNH’s Pensions Manager, who gave us great insights on the subject.
What is a Pension?
This is a question that lingers in people’s minds, especially in the corporate world. Pension is defined as a fund into which a sum of money is added during an employee’s employment years and from which payments are drawn to support the person’s retirement from work in the form of periodic payments. This should not be confused with a Retirement Plan.
A retirement plan is an arrangement to provide individuals with an income during retirement when they are no longer earning a steady income from employment.
There are two main types of retirement plans:
1. Employer-Sponsored plans are formed by employers for the benefit of their employees to provide income at the point of retirement and benefits to dependents in the unfortunate event of the death of an employee.
2. Individual Pension Plans for employed individuals who are not in an employer-sponsored scheme, as well as self-employed individuals.
“It is key to note that it is not compulsory for employers to form pension schemes and most employers in Kenya have not set up retirement schemes meaning that their employees have to plan for their retirement savings,” said Ms. Gitau.
Kenyatta National Hospital operates two pensions scheme under Irrevocable Trusts for its employees namely the Kenyatta National Hospital Staff Superannuation Scheme (Defined Benefit (DB) Scheme) and the Kenyatta National Hospital Staff Retirement Benefits
Scheme (Defined Contribution (DC) Scheme).
“The KNH Staff Superannuation Scheme was established on 1st January 1991 and was closed to new entrants on 30th June 2011 following a government directive that all DB schemes be converted and be operated as DC schemes. Therefore, the Kenyatta National Hospital Staff Retirement Benefits Scheme was set up for employees 45 years and below and those employed after 1st July 2011,” continued Ms. Gitau.
Benefits of pension;
i. Provision of income at retirement
When employees retire, they experience a reduction in income and pension makes up for part of this loss of income.
ii. Safeguarding the interests of beneficiaries
In the unfortunate event of your death, a pension protects dependents in the form of lump sums or monthly pensions.
iii. Disciplined Savings
Savings put away in a pension scheme are not readily available
for withdrawal, unlike money in a bank account.
iv. Enjoy Taxation Benefit
Employees enjoy tax relief on pension contributions of up to Kshs. 20,000 per month. For instance, an individual earning Kshs. 30,000 making a monthly contribution of Ksh. 2,250 will be taxed on Kshs. 27,750. The return earned on the investment of these contributions is also tax-exempt.
v. Compound Interest
Pension benefits are only accessible when one exits employment by way of resignation, dismissal, retrenchment, retirement, ill-health retirement, migration, or upon death. Hence, it means benefits earn compounded income year-on-year as no benefits are withdrawn during an employee’s working life.
When should one start saving?

“The best time to plant a tree was 20 years ago. The second-best time is today.” Chinese Proverb
An individual should start saving
early in their career, if possible, from the first day of employment.
One of the main advantages of starting to save early is the power of one percent stemming from the ‘magic’ of compound interest. Compound interest, in simple terms, is where your interest earns interest. In other words, after the first year, your savings will have grown with interest. In the second year, the first year’s interest is part of your savings, and hence will also earn interest in the second year – hey Presto! Compound interest.
To show you the impact of compound interest, let’s use a simple numerical example. Let’s assume at age 30 you start saving a fixed amount of KShs. 2,000 every month for 30 years, the table below shows your savings balances after 30 years of applying different net investment returns:
On a different angle, if you start saving at the age of 40 the same fixed amount of KShs. 2,000 every month for the next 20 years, the below table shows your savings balance after 20 years of applying different net investment returns:
greatly impacts the replacement ratio.
Gross Replacement Ratio (GRR) measures the adequacy of a retirement benefits arrangement. It is the gross income after retirement divided by the gross income just
It is key to note from the table above just how much of your balance is made up of interest. Remember, in all three examples above, your capital is only KShs. 720,000.
This shows that when you delay your savings plan you will not be able to save as much, and you will need to increase your monthly savings amount to attain the same target. When you start saving early, a little can go a long way to retire comfortably at the age of 60. The power of compounding, the amount of savings, and a long investment
before retirement and experts recommend a GRR of 60% - 70%. For instance, say your last salary at the date of retirement is KShs. 100,000.00 your ideal GRR would be an amount between KShs. 60,000.00 and KShs. 70,000.00. This will ensure one can maintain their pre-retirement lifestyle.


>>> Part two continues in edition 3

Kenyatta National Hospital, being one of the largest referral health facilities in the region and especially with the high number of its specialty clinics, blood transfusion is a common and key procedure in treatment and medical interventions.
In December 2022, the hospital acquired an advanced version of the NEO Galileo machine which is already in operation.
An analysis in 2020 found that about 40 percent of hospital admissions were based on maternity, oncology, and other disorders. This excludes the admissions or patients due to other reasons of accident emergencies. In addition, the report showed that 100 percent of new admissions get a blood typing to determine the blood group and a blood antibody screening.
The sensitivity of blood transfusion and the risks to be eliminated and checked and the workload of the facility could only be handled by blood bank automation.
Apart from testing of infectious diseases on donated blood for transfusions like Hepatitis B, C, E, syphilis, and HIV/AIDS, the blood sample undergoes some other comprehensive and sensitivity confirmation before the final transfusion to a recipient (patient).
Depending on the case of transfusion, at least six other tests are done on the donated blood sample to determine the safety of the blood to the recipients. These include blood group testing, Rhesus testing, antibody screening, weak D testing (on RH-VE blood), IgG DAT, and crossmatch or compatibility testing.
The complexity and sensitivity of a transfusion procedure allow no room for error or even delay from the blood donation room to the lab testing and the final transfusion procedure.
Neo iris is a fully automated blood bank equipment that can do all the pre-transfusion tests in a blood bank testing laboratory. Just like Immucor ® is the leading manufacturer globally in both transfusion and organ transplant medicine, Neo Iris is the
most productive, fully-automated blood bank instrument with the highest type and screen throughput in the market.
The equipment uses CAPTURE ®, a patented technology to its manufacturer IMMUCOR® which is ranked as the most sensitive and highly accurate principle in the market to detect the most clinically significant antibodies in the blood.
Neo Iris is a ‘Next Generation of equipment with high productivity and throughput allowing a dynamic workflow and resource handling, improved flexibility for emergency testing, continuous loading of
“ Neo iris is a fully automated blood bank equipment that can do all the pre-transfusion tests in a blood bank testing laboratory. Just like Immucor ® is the leading manufacturer globally in both transfusion and organ transplant medicine, Neo Iris is the most productive, fully-automated blood bank instrument with the highest type and screen throughput in the market.”
additional samples as others proceed with testing as well as more customized profiles.
The principle and technology of the equipment allow the use of fewer resources and consumables per test, hence cutting down on the cost of reagents and in turn enhancing costeffectiveness.
At a go, the equipment can support at least 165 blood samples in the improved sample rack loading bays.
The flexibility of the machine allows the running of the aforementioned tests as single tests or a combined series of tests per sample, allowing all the tests to be done on all the samples at a go. This increases the throughput as well as reduces the Turn Around Time on both the routine and emergency samples.

The identification of samples by unique barcodes by the equipment reduces significantly the mix-up of results and samples as a human error, which in turn could lead to fatal results due to erroneous transfusions.
Blood bank automation has, according to global statistics, reduced HTRs due to wrong or inaccurate transfusions by more than 80 percent.
Neo Iris provides more testing panels that will be of great significance as more procedures develop at KNH, such as more organ transplants.
It is 05:30 am and already a few people are seen arriving at Kenyatta National Hospital (KNH) Comprehensive Care Centre (CCC). The Centre, which is dedicated to the care and management of HIV/AIDS patients, has been in operation for the last 21 years since its inception in 2002.
The Centre currently serves over 10,000 clients, which constitutes the bulk of those seen in Nairobi. In the early 1990s, KNH was already caring for the largest pool of HIV/AIDS Patients in the country.

Dr. Dorothy Aywak, the Acting Head of the Unit at the CCC, said the facility’s mandate is to provide comprehensive HIV care and treatment services, facilitate HIV/AIDS training and research, and participate in national health planning and policy.
“Implementing a family-centered HIV/AIDS care model- besides linking children and caregivers to relevant services. We host Family Open day that allows us to interact with the clients in a more relaxed setting which enables the provision of psychosocial support,” she said.
As part of the comprehensive services offered at the CCC, they also provide:
• COVID -19and Human Papillomavirus vaccines
• Conduct Non-Communicable Disease screening
• Cervical cancer screening
In the late 1990s, the KNH management started an initiative dubbed “KNH AIDS initiative 2000 and beyond,” a program that helped in the management of the HIV/AIDS pandemic. However, the Hospital management, through the CCC has since then adopted many other strategies to help reduce and control the spread of the virus.
“KNH is leading in the fight against HIV/AIDS through identification
of people living with HIV through voluntary testing in the VCT, through provider-initiated testing in the in-patient wards where patients admitted in the wards are tested and through the provision of selftest HIV kits where people can test themselves at home and encouraged to repeat the test in a health facility should they turn positive,” Dr. Aywak maintained, adding; “Through these initiatives, KNH is now rated top among health facilities that diagnose the most people living with HIV. We not only test but also link those who test positive to treatment in our CCC.”
Mr. Isaac Makumi, the Human Resource Administrator at CCC linked the success of the Hospital management’s strategies to reduce the virus through the deployment of CCC staff all around the Hospital.
“Our staff are distributed across the hospital. Because we have the mandate of running the HIV service in this hospital. We have staff at the wards, Casualty, levels 2,4,5,6, and even a sister unit; the HIV Prevention Unit. We have staff at the Youth Centre, Reproductive Clinic, Clinic 66,
GFD, Blood Transmission Unit, and many more other points within the hospital,” he said.
On her part, Dr. Anne Mungai, a pediatrician attached to the CCC and who has seen the Centre grow from inception, said that she is encouraged because the facility has been able to prevent at least 95 percent of patient suppression.
“I have been working here since 2002. The CCC started in the old hospital where the Patient Support Centre is located. The VCT had already been established and of course, there was a gap in care for those who tested positive, especially among our KNH staff. When that clinic was established primarily it was a KNH clinic for their staff,” Dr. Mungai said.
She revealed that initially, CCC used to source drugs for staff members only, but then later they opened up to the rest of the public.
“In 2003, a government-sponsored program came into place and we started getting a lot of training which formed our basis for starting other CCCs in other counties. With the
support of the National AIDS/STD Control Program, we train very many people even within the Hospital and outside,” Dr. Mungai revealed.

The CCC at KNH has also proven beyond doubt that they are a first among many. The Centre was an early adopter of the Electronic Medical Records (EMR) system.

“Early adopters of the EMR system. The clinic initially moved to electronic records with the rest of the Hospital just recently began the journey of moving to electronic medical records and we look forward to the integration of the same and enhanced patient management,” Dr. Aywak said.
The CCC also was the first to pilot the Queue Management System, before the rest of the hospital adopted it. The system is patientcentered where patients pick a number to be called out before being seen.
“We are first in many things at the Hospital. For example, the Queue Management System started here. It was benchmarked here, even the Electronic Medical Records (EMR). We started in 2004 and are purely paperless within the clinic. We have
eliminated paper within our sites. Our staff carry tablets which they can access the EMR,” Mr. Makumi added.
The CCC is also host to the Nairobi County HIV Technical Working group, a group of specialists drawn from Nairobi County. The vibrant multi-disciplinary team meets every Monday to discuss complex HIV/AIDS
cases in the clinic and from Nairobi County.
“In light of this, the success of CCC is attributed to the team of committed staff deployed at the unit. Isaac Makumi our Human Resource Administrator is the metaphorical linchpin as he keeps all our gears turning, he has been working at the unit since 2010,” Dr. Aywak said.
Dr. Ann Mungai deserves special mention, Dr. Aywak said because of her longstanding commitment to the Centre since its establishment back in 2002. Dr. Wangui Kamau from Pediatrics and the CCC lead on Care and Treatment as well as the Continuous Quality Improvement CQI initiatives as being one of the pillars for their success.
“Other staff members that have shown great commitment to their work at the CCC are Mr. John M and Ms. Brenda; who have been complimented several times by clients. Without the diligence and commitment demonstrated by all the staff here, there would be no success to speak of. No one can whistle a symphony. It takes a whole orchestra to play it,” she concluded.







Female Genital Mutilation (FGM) comprises all procedures that involve altering or injuring the female genitalia for non-medical reasons and is recognized internationally as a violation of the human rights of girls and women.


The International Day of Zero Tolerance to Female Genital Mutilation is an awareness day marked annually every 6th of February to educate the public on issues of FGM and mobilize political will and resources to eradicate it.
This year’s theme is; “Partnership with Men and Boys to transform Social and gender Norms to End FGM.” The theme is a call to mobilize and involve everyone in eradicating FGM and promoting positive gender
(KDHS), 2022, the prevalence among women aged 15-49 fell from 38 percent in 1998, 32% in 2003, 21% in 2014, and further down to 15 percent in 2022. The declining trend results from massive investment in programmatic, policy, and legal measures toward eliminating this practice.
Newsline had a one-on-one with Dr. Stephen Mutiso, KNH’s obstetrician-gynecologist, for ten years and expounded on FGM.
What is the history of FGM, and why was it performed?
FGM is an outdated cultural practice that has been there in most of our communities. It was and is being practiced as a rite of passage to signify a woman maturing from childhood. In some communities, this practice aims to ‘tame’ women sexually.
How do you treat patients who have undergone FGM?
Girls who undergo female genital mutilation face short-term complications such as severe pain, shock, excessive bleeding, infections, and difficulty in passing urine, as well as long-term consequences for their sexual and reproductive health and mental health, i.e., most complain of experiencing much pain during sex due to the narrowing of the genitalia. In such cases, reconstructive surgery can be done to remove the scar tissue and enlarges the genitalia for better sexual function.
Also, for women in labor, scarring poses difficulties in delivery as the passage loses elasticity. In such cases, episiotomy is done to widen the birth canal; this procedure can sometimes be performed in subsequent births.
We have had cases of some women come later in life who want their sexual function to be restored. In most cases, the clitoris is severely trimmed or removed. A restorative procedure called clitoroplasty can be done to reconstruct the clitoris. This procedure generally has good results, with most patients reporting improved sexual function.
How do you help FGM victims deal with psychological trauma?
For most girls and women, FGM
happens without consent; hence, much psychological trauma is attached. Also, in most cases, anesthesia is not used; therefore, there is intense and severe pain experienced by the girl in the event of FGM, which can cause severe mental trauma.
While treating FGM complications, we involve mental health specialists for counseling and psychological therapy of the patient.
Are there different forms of FGM?
The procedure of FGM varies from community to community. Remember, FGM is any alteration of the female genitalia for non-medical purposes. This may involve removing part of the clitoris (clitoridectomy) and the labia minora and labia mijora. Stretching of parts of the female genitalia is also considered FGM.
Is there any connection between FGM and the risk of getting HIV/ AIDS?
Yes, a high risk. Since FGM practices occur at the community level, the blades and other tools are not sterilized and can pass infections. There is also the aspect of sharing instruments between the different girls during the procedures.
Does FGM affect the flora
of the female genitalia?
FGM may not necessarily affect the vaginal flora. However, FGM practices encourage other cultural forms of treatment which may affect vagina flora. For example, when a girl has an excessive discharge, they are advised to introduce foreign objects to their genitalia, yogurt, among others. FGM scarring can also create a covering on the urethra that prevents the free flow of urine, which leads to urinary tract infections.
In your opinion, what’s the best way to eradicate FGM?
FGM is a deeply rooted cultural practice; hence, I believe the best way to eradicate it is by creating awareness on the grass root. Sensitization and frequent education on FGM’s short-term and longterm effects can go a long way to eliminating it. It is a harmful practice that should stop. It has no benefit whatsoever.

How many cases of FGM do you get?
Kenyatta being a referral hospital, we get the most complicated cases of FGM who come in as referrals. The patients are first attended at the
 By Steven Arwa
By Steven Arwa
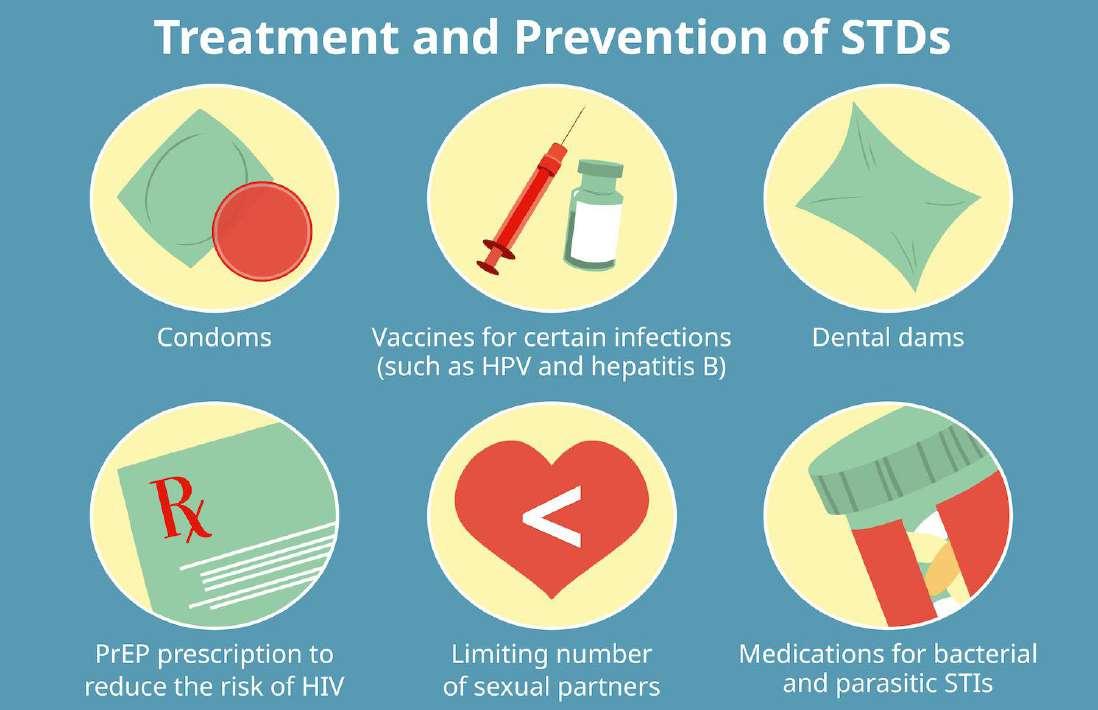
When one hears about Sexually Transmitted Infections the first thing that comes to mind is HIV/AIDS and Immunodeficiency Syndrome, but the world today has greatly evolved and HIV/AIDS is not the only disease that can be transmitted sexually. There are other numerous sexually transmitted infections.
Our focus will be on other sexually transmitted bacterial infections and in this case Gonorrhea. In December 2022, super gonorrhea trended on different social media platforms invoking intriguing conversations among the public, most very debatable but also raising questions concerning how people perceive the whole concept of Gonorrhea and super Gonorrhea.
Newsline got an opportunity to have a sit down with Dr. Phoebe Juma, Head of the Infectious Disease Unit at Kenyatta National Hospital (KNH). (Live video feed on Facebook can be accessed at: https://www. facebook.com/KenyattaNationalHospital/videos/5289544171148771/?flite=scwspnss ) where she got to expound more in detail on the
trending super gonorrhea bacterial infection, how it comes about, how it spreads, is prevented, and is treated once a person tests positive.
While this was well covered by Dr. Juma another question arose from the interview concerning whenever a person wants to come for testing or when they are aware of their predicament and want to come for treatment at KNH, where do they start? Newsline felt that this subject needed more clarification and
therefore went out in search of more information.
To any person visiting the Hospital for the first time, being able to locate where they can get the right services in terms of testing and treatment. Stationed at the clinics section Ms. Joan Macharia, a Marketing and Communication officer at the Hospital who has vast experience through her interactions with clients over the years, said part of her duties involve working with clients to try to help
them reach their areas of destination.
“But it becomes a huge challenge when they are not truthful or forthcoming in terms of providing genuine information therefore in some instances leading to cases of misdirection. If such visitors do not seek other relevant help from our various customer care points, they normally spend a lot of time going round and round the Hospital eventually giving up, all this mostly due to fear of being stigmatized,” said Ms. Macharia.
According to medical experts like Dr. Dorothy Aywak Acting Head of Unit KNH Comprehensive Care Centre (CCC) and Mr. M. Gikonyo, Senior Nursing Officer at Clinic 18, whenever one comes to KNH for the first time, for the case of adults they undergo comprehensive testing at our Accident and Emergency Department which is open 24 hours a day where they will get appropriate medical assistance from a Clinical Officer deployed by the CCC Unit.
If found positive they are immediately put under the right medication. When it comes to the youth, KNH has designated an appropriate and adolescent-friendly center (KNH Youth Centre) located on the ground floor of the tower block and is open every day from 8:00 am to 4:30 pm. At the unit,
youth are provided with free testing services, and if found positive, are referred to the Accident and Emergencies (A&E) for treatment. This is done free of charge to reduce instances where youth might shy away from treatment due to fear of not being able to afford the payment.
It is also vital to understand that whenever a person reports to the A&E and tests positive for other medical complications brought about by Gonorrhea such as infertility, necessary laid-down procedures will be followed. First, they will be directed to the appropriate specialized medical clinic such as the Medical Outpatient Clinics or General Outpatient Clinics where they can receive the much-needed critical specialized treatment.
Therefore, KNH through its Clinics like CCC has continued to expand its services, making them easily available as much as possible to patients and this has seen successful disbursement of medical personnel to all critical units like Clinics 18, 66, A&E, Wards, and the Blood Transfusion Unit. This has greatly helped in early identification processes hence allowing medical personnel the capacity to provide the right treatment to patients.
According to Mr. Isaac M. Njubi Human Resource Administrator at CCC clinic, over the years advancement in technology and adoption of new ways of operations being used are providing cutting-edge approaches to tackling emerging challenges and allowing advancement in ways of handling patients that take into account their mental health.
Issues concerning fear of stigmatization can be tackled by taking into account the patient’s state of mental health. As Ms. Macharia had stated and also Dr. Phoebe Juma in her Facebook video interview, one of the many reasons why the issue of stigmatization is at the forefront of matters concerning STIs, is fear, fear of being judged and discriminated against.
But one thing stands out, one cannot get the much-needed medical assistance if they are not ready or willing to ask the right questions therefore, KNH through its units like the Youth Centre and Comprehensive Care Center is working hard to create an environment where patients and visitors can feel not judged but rather well received hence going a long way in reducing fear and stigmatization among clients visiting the hospital in search of medical services.













Happy birthday to the 354+ February babies! From Marketing & Communication team

1. MRS. EMILY KAWIRA NGUGI
2. MR. DAVID MAURICE MBATHA
3. MR. SIMON MUTUKU MUTISO
4. MRS. LEAH WAMUYU WAWERU
5. MR. ERNEST ACHANDO MIRUYA
6. DR.(MISS) MARY MWANISA OMUTSANI
7. MR. PETER MOENGA NYAMASEGE
8. MISS. MARGARET NJOKI MBUGUA
9. MISS. PRISCILLA CHERONO
10. MR. PAUL KARUGA KAHARI
11. MR. GERALD MBURIA NJAGEH
12. DR. JOSEPH MAINA KIRAGU
13. MR. PRESTER CHARLES MAUGO
14. MR. JOHN FLANCO ARISA
15. MR. STEPHEN GUCHU MUIRURI
16. MISS. MARGARET AKINYI AYARA
17. MR. CHARLES GIKONYO MWANGI
18. MRS. JANE WANJIRU MUSYOKA
19. MISS. ADELAIDA MUNYIVA LEMBA
20. MRS. JOSEPHINE WAMBUI MBUGUA
21. MRS. IRENE WANGUI GITIBA
22. MISS. HELLEN GATUIRI GITONGA
23. MISS. ANICETA RUGURU BORONA
24. MISS. NAOMI WAIRIMU IRUNGU
25. MISS. ROSEMARY WANGUI WANJOHI
26. MR. JULIUS LABAN MURIITHI
27. MRS. HELLEN WAMBUI MUNA
28. MR. PHENEAS KARANI NYAGA
29. MISS. JENNIFER OGUTU
30. MR. ANTHONY MWAU FOLINGI
31. MR. DAVID BARASA BENGI
32. MISS. EMMA MUTHONI KARATAI
33. MISS. MARGARET LOICE MAYWAKA
34. MR. PHILEMON ODHIAMBO OMUNGU
35. MISS. MILDRED AMONDI AGOLA
36. MR. STANLEY NELSON NGANGA MUTHONI
37. MISS. PATRICIA KALEKYE MUTISO
38. DR. PRAXADES P. MANDU OKUTOYI
39. MRS. JANE WANJIKU NDIANGUI
40. MISS. ANGELYN NDUTI MUSEE
41. MR. PETER GAKERE KURIA
42. MR. VICTOR KITHOME NGIE
43. MRS. FAUSTINE AJIAMBO OJIAMBO
44. MR. PAUL MUIRURI KIARIE
45. MR. EUSTACE KIRIMI MUTEGI
46. MR. STEPHEN MUTUA MAINGI
47. MRS. JOSEPHINE VIKI NZOMO
48. DR. ROSE ACHIENG NYABANDA
49. MR. YUSSUF ODHIAMBO NGAU
50. MR. MATHEWS OMONDI OMITO
51. MISS. EVALYNE AUMA SUMBA
52. MR. KINYUA KAMURI
53. MR. JOEL KIPLAGAT
54. MR. SAMUEL NKULA ITUAMWARI
55. MRS. FAITH GATWIRI GICHURU
56. MRS. ROSEMARY WAMBUI CHEGE
57. MISS. NAOMI KARINTHONI M’IRINGO
58. MISS. MONICA NDUKU NDUVA
59. MR. ERIC OKELO WANGAJI
60. MISS. JANE NJERI NDUNGU
61. MISS. MILKA KERUBO ONTITA
62. MISS. FELISTUS NUSU MATINGI
63. MISS. RACHAEL SHISIA MUTIMBA
64. SR. THERESIA NDUNGE MUTUI
65. MR. GERALD MWITI M’RIRIA
66. MR. HERBERT KAMADI MWANJI
67. MISS. CHRISTINE ORANGI
68. MR. BENJAMIN ORENI KENYENGA
69. MISS. NANCY MURUGI KAHIRO
70. MR.PATRICK KWATEMBA OPISA
71. MISS. PRISCAH NDINDA MULILI
72. MR. ARTHUR NJOROGE KAMAU
73. MR. JAMES MUTHAMA KYENGO
74. MR. BERNARD MUNYUA WANGUI
75. MRS. ANNE NJIRU MAINA
76. MISS. FLORENCE AUMA OKECH
77. MR. PATRICK KILILE MUSYOKA
78. MISS. JANE NASIMIYU MUSUNGU
79. MISS. ANN JANET NYAWIRA KAMURI
80. MR. JOASH NYANYUKI OBAGA
81. MR. TELESPHORUS MATEKWA SHILEHWA
82. MISS. DORCAS ATIENO MIYOMBE
83. MISS. EMILLY ATIENO ONYURO
84. MISS. JOYCE MUTETE
117. MR. MICHAEL GITONGA KIRAITHE
118. MISS. ELIZABETH MUMBI MUTEMI
119. MISS. JUDY NABULU LENGETE NKURNE
120. DR. GIDEON JACOB NDERI
121. MISS. BISHARO HASSAN DUBA
122. MR. HILLARY KIPKOECH BETT
123. MR. PHINEAS KINOTI KIRIMI
124. MRS. MERCY KATHURE GICHURU
125. MISS. MARY NJERI WAWERU
126. MISS. ROSE GATWIRI MUTEA
127. MISS. LUCY NTHAMBI THOMAS
128. MISS. ESTHER WANJIRU KIMARU
129. MISS. MARTINA NGINA KIMEU
130. MR. MATHEW ANTHONY MWANGI MBURU
131. MISS. VIOLET ABISINA OKOVA
132. MISS. PHYLIS KAGWIRIA MARETE
133. MR. LENSON MACHARIA WAMBUI
134. MISS. JOYCE WANJIRU KARIUKI
135. DR. DAVID KABAA KIMANI
136. MR. DAVID KAZI JUMA
137. DR. PAUL ETAU EKWOM
138. MISS. MARY NYAGUTHII WACHIRA
139. MISS. EMMY TALAM
140. MISS. SERAH MUNYIVA KATANGA
141. MR. NICHOLAS KYALO KITHIKII
142. MISS. WINNIE CHEROTICH KOSKEI
143. MISS. SUSAN WAMBUI
144. MISS. MONICA JEPKONGA KOSGEI
145. MR. BENBELLA ONYINO AHURA
146. MISS. JULIET WAMBUI KIBUCHI
147. MR. DOMINIC OMONDI ACHUNGO
148. MR. JOHN MURIITHI NJIRU
149. MISS. JUDITH WAKESHO MWASHEGWA
150. MRS.ALICE MWIKALI MBEVI
151. DR. JANE WANGUI MACHIRA
152. MISS. JACINTA KIENDE MWARANIA
153. MR. ZABLON ONSEMBE GICHABA
154. MRS.CAROLYNE MMBOGA KIMIYA
155. MR. DENNIS ISABOKE ONG’ERA
156. MISS. JANE KOIMA JEPKOECH
157. MISS. JANE WANJIRU GITHINJI
158. DR.JECINTER ACHIENG MODI
159. MISS. LILIAN AUMA MBORI
160. MISS. ALICE MUTHONI WANJIKU
161. MR. JULIUS KANYI NDEGWA
162. MISS. CAROLINE JEPNGETICH LEL
163. MR. HAROLD NIXON ODHIAMBO
164. MR. STEPHEN NGUGI
165. DR. NICHOLAS OCHIENG OKUMU
166. MR. DALMUS OLOO
167. MR. IBRAHIM OMERIKIT PAPAI
168. MISS. FLORENCE NYATICHI NYAGETARI
169. MISS. JANET WANJA CHEGE
170. MR. FELIX KANGOGO CHEPKONGA
171. MR. KIMUTAI ROBERT TOO
172. MR. ALFRED AWINO OGAK
173. MR. CHARLES NYAGONA SINA
174. MISS. REGINA WANGUI NDUNGU
175. MRS. JOSEPHINE MWENDE NGILA
HAPPY BIRTHDAY FEBRUARY BABIES
176. DR. LEONIDA MUTINDA MBUVI
177. MISS. ALICE WAWIRA NJOMO
178. MR. AMOS BELIO SIMOTWO
179. MRS.ALICE ADHIAMBO OTIENO
180. MR. ROLLAND SHAMALLA SHIVACHI
181. MR. MARTIN MAINA KIBUI
182. MISS. GLORIA KALUMU MWANDIKWA
183. MRS.ELIZABETH WANGU NJORO
184. DR.TERESIAH WANJIRU NJOROGE
185. MISS.SHEILA WABOSHA MJOMBA
186. MISS. CATHERINE WANJA IRERI
187. MRS.CHRISTINE LILIAN MAINA
188. MR.VICTOR MUNYAO OMIDO
189. MISS. ANGELA NANEU KONE
190. MR. NATHAN MWENDA MUTABARI 191. MISS. WINNY CHEPKEMOI 192. MISS.ANN WANJA MURIITHI 193. MISS. ROSELYNE ASIKO AMUNGA
194. MISS. MERCY WOTHAYA WANGAI
195. MR. ALBANUS MUINDE MUTHIANI
196. DR.ESTHER WANJIKU NDUNGU
197. MR. IBRAHIM JUMA
198. MR. THEODORE COLLINS OWINO
199. MR. GEOFFREY KIOKO ZAKAYO
200. MR. ALFRED APIEMI APIEMI
201. MRS. ELIZABETH WANJIRU OUMA
202. MISS.NAUMI KALEKYE KILONZO
203. MR. PATRICK MUKHUYU MAKOVI
204. MISS. REGINA KAGWIRIA KAURA
205. MR. LEWIS KIRIMI GIITU
206. DR. MARK PATRICK KARANJA THARAO
207. MISS. MARY WANJIRU MARIGI
208. MISS. ESTHER ANYANGO OKUMU
209. MR. JAPHET NGIRI NTONG’ONDU
210. MRS. LYDIA MORAA ARIGA
211. MR. BENSON MWANZA MICHAEL
212. MISS. MERCYLINE BOSIBORI OMETE
213. MR. ALPHONCE KIOKO MWELELI
214. MRS.BERNADETTA WACEKENGUGI WANYOIKE
215. MISS. KEZIA SAYO KIPANDE
216. MRS.VERAH JOYCE OTIENO
217. MISS. SCHOLARSTICA AMUSUGUT ETYANG
218. MRS.JUDY EFFETA MREMA
219. DR.LUCIA APIYO AMOLO
220. MISS. ELNORAH IGHANA MWASHIGHADI
221. MISS. MARYGORRETY AWINO NYAWANDA
222. MR.LAWRENCE FELIX MUNENE KATHENYA
223. MRS.LYDIA AKINYI OGOWA
224. DR. JOSIAH OYIEKE ODUOR
225. MRS.ELIZABETH NYARINDA MATAGARO
226. MISS. DAMARIS WANJIRU KUNYIHA
227. MISS. TABITHA MWENDE MUSILA
228. MISS.LUCY WAHU WAIRIMU
229. MISS. LILIAN WAMBURA MUTHEE
230. MR. RICHARD MUTHUI THUITA
231. MR. SIMON KIPROP TOO
232. MR. VICTOR MAHASI SERENGE
233. MR. JAMLICK BURUGU GIKONYO
234. REV.KENNEDY OWINO OCHIENG
235. MISS. MARY EDNA RUNYENJE
236. MR. JOSEPH MULI MUTUKU
237. DR.DAISY ATIENO ODUNDO
238. MRS.HALIMA WATO DUBA
239. MRS.JUDY WANJIKU MUNYASYA
240. MISS.EDNA OMONDI
241. MISS. SARIAH CHESIRO CHEMONI KAPSAN
242. DR.GRACE NJERI MWANGI
243. MR. VICTOR ONYANGO MURONO
244. MRS.JANE WANGUI MUTUNGA
245. DR. DANIEL GAKUO NJENGA
246. MR. ANTONY LEMISO SERPEN
247. MISS. ESTHER NJERI KAROKI
248. MRS. CATHERINE WANGUGI
249. MISS. ELIZABETH WAMBUI NJAGI
250. DR. PAUL MBUVI MUTUA
251. MISS. MAUREEN CHEROTICH SONIT
252. DR.JOHN WAMUTITU MAINA
253. MISS. LILIAN ANYANGO ADALLA
254. MR. ALEX LETTING
255. MISS.BOLE MUSE ADO
256. MR.HARRISON MUTWIRI NTHIA
257. MR. PKENDEN MOTWOI OMEGA
258. MISS. JACKLINE WANINA NJOROGE
259. MRS.TERESA WANJIRU MUCHANGI
260. MISS. MARYANNE SYOKAU
261. MR. WALTER OTIENO ODIPO
262. MR. AUSTUS NJOROGE NGARUIYA
263. MR.ALEX MUTUNGA KATUMO
264. MRS.LUCY KARIRA KINYANJUI
265. MISS. SILVIA AWUOR KOLA
266. MR. MOSES MUCHIRI MUMBI
267. MR. JUSTIN NJENGA NGUGI
268. MRS. HANAN HUDOW HASSAN
269. MISS. DOROTHY MORAA MONGA’RE
DR.SIELE SHEILA
MISS. ANNE ANYANGO ACHIENG
MR. KELVIN MAINA MUMENYA
MR. VINCENT ONDERE CHAGARA
MR.KELVIN WAMAE MBUTHIA
KIBET RUTTO
MRS. RIGIRI FAITH KATHIARI
NJERI MBUGUA
NAMUKHOSI NABENDE
MUNALA
288. MRS.CAROLINE NJERI NJUE
289. MRS.WINNIE SAYO MUSERA
290. MRS.TERESIAH OSOFORI NYANJAMA
291. MR. CHARLES KIPRONO SANG
292. MR.DANIEL KATUA SAMSON
293. MISS.DAISY ATIENO ONGETE
294. DR. GEORGE TENDE ODUMA
295. MISS.CATHERINE NJOKI RUNYORA
296. DR. EBBY CHELANGAT MUTAI
297. MR. JOE MURITHI NDIRANGU
298. MRS.HANNAH WANGUI KIARIE
299. MRS.JACQUELINE KINA MBUGU
300. MISS.BALAFU GALMA GODANA
301. MR. JOHNHUSS VICTOR ANDONYI
302. MRS. PURITY WANJIRU NDUMIA
303. MISS.PATRICIA MUSENYA MBEVI
304. MR.DENIS GITONGA NJAGI
305. DR.PENINA NTHAMBI KATUNDA
306. DR. DAVID MBOTA SABAI
307. DR.STELLA JEPKORIR RONO
308. MR.DANIEL OGEMBO NYARIBARI
309. MR.CHARLES MWENDWA SEKENI
310. MRS. KETRY IHADO LUVAGA
311. MR.WILBERT BOTA GARI
312. MRS. ELIZABETH SIALO KURRARU
313. DR.WYCLIFF OYIEKO AUKA
314. MISS. MERCY CHEBET NGENY
315. MISS.JACKLINE NJERI NGANGA
316. MISS. DIANA BIBI MUTISO
317. MR. BRIAN MUCHAI MABONGA
318. MISS. KADIJA ABDIKARIM ISSA
319. MRS.DAMARION KERUBO NYAKUNDI
320. DR.KAREN WAITHERA WAINAINA
321. MISS.LUCY ONGACHI OSINDE
322. MR JOB ANYONA KANGWANA
323. MISS.NORAH KHALIFWA WASAKWA
324. MISS. EDITH JERUTO KORIR
325. MISS.LUCY WAMAITHA NJOROGE
326. MISS.BABRA MIGIDE ETENYI
327. MISS.PURITY MUTANU NZIOKA
328. MISS.MARIAN MORAA MECHEO
329. MISS. CAROLINE WAITHIRA KIMANI
330. MISS.BRENDAH ANYANGO MUKARA
331. MR. BENJAMIN KIPROTICH KOECH
332. MISS. GRACE WAITHIRA GATUMA
333. MR. LEE KIMAITA MUGAMBI
334. MISS. PHYLIS WANGARI NJOROGE
335. MR. WILSON MWANIKI KIMEMIA
336. MR. COLPHASE LINAGALA SHINAKA
337. MR.PAUL WILSON AMUHINDA
338. MISS.MOUREEN NAKUYA EMOOT
339. MR. NICHOLAS MAKIYO EGESA
340. MR. RICHARD CHOGO MWACHI
341. MISS. RISPER CHEPTALAH LUBANGA
342. MISS. MERCY MONGELI WANYONYI
343. MRS.MARY MWENDE MUTUA
344. MR. VICTOR KIAMA NDERITU
345. MISS. CAROLINE NJERI MWANIKI
346. MR. KEVIN WABILI SAMITA
347. MR. KEVIN WABILI SAMITA
348. MISS. TERESA LUSENO IYAYA
349. MR. AMOS MWIRIGI MUIYURO
350. MISS.BENEDINE JEPKEITICH YATOR
351. MISS. ESTHER WANJIRU MBURU
352. MR. DERRICK MWENDA KIMATHI
353. MR. BENEDICT NANDWA AKUNDA
354. MRS. MERCY CHEPKEMOI

Relax, Jim
Right before surgery, the surgeon says, “Relax, Jim. It’s just a small scalpel incision. No reason to panic.”
The patient replies, “But, Doctor, my name is not Jim.”
The surgeon responds, “I know. I’m Jim.”
Nearing the end, old Ed is surrounded by his loved ones.
As the final moment approaches, he gathers all his strength and whispers, “I must tell you my greatest secret.”
His family members are all ears, urging him to go on.
“When I was young, I had it all,” explains Ed. “Fast cars, cute girls, and plenty of money. But a good friend warned me, ‘Get married and start a family. Otherwise, no one will be there to give you a glass of water to drink when you’re on your deathbed.’
So I took his advice. I traded the girls for a wife and beer for baby food. I sold my Ferrari and invested in college funds. And now here we are. And you know what?”
“What?” whispered the fascinated members of his family.
“I’m not even thirsty!”
1. “One word frees us of all the weight and pain of life: That word is love.”-Sophocles
2. “Begin doing what you want to do now. We are not living in eternity. We have only this moment, sparkling like a star in our hand and melting like a snowflake.” -Marie Beyon Ray
3. “The mind, properly controlled, can do just about everything. You can think your way through adversity, you can think your way through problems. It is a super powerful instrument that so few use to the maximum. And if the mind thinks with a believing attitude, one can do amazing things.”
-Norman Vincent PealeOUR VISION

A world class patient-centered specialized care hospital
OUR MISSION

4. “I am still learning…how to take joy in all the people I am, how to use all my selves in the service of what I believe, how to accept when I fail and rejoice when I succeed.” Audre Lorde
5. “Don’t be intimidated by what you don’t know. That can be your greatest strength and ensure that you do things differently from everyone else.”-Sara
Blakely6. “Please think about your legacy, because you’re writing it every day.”-Gary Vaynerchuk
7. “There’s no shortage of remarkable ideas; what’s missing is the will to execute them.”-Seth Godin
8. “Everyone has inside them a piece of good news. The good news is you don’t know how great you can be! How much you can love? What you can accomplish! And what your potential is.”- Anne
FrankTo optimize patient experience through innovative healthcare; facilitate training and research; and participate in national health policy formulation
OUR MOTTO We Listen, We Care