Human Motion & Essential Co-factors for Performance Optimisation


leaders and innovators in motion science, performance & injury solutions
The Science & Art of Human Motion
This narrative hopes to provide basic insight into the world of sports performance and rehabilitation to all those who may be interested in this subject either as: students, sports science, therapist, sports enthusiasts, institutions, or as consumers of health and sports performance services.
This narrative is delivered with the purpose of stimulating thought, interest and collaborative effort into the Science and Art of Human Movement, and hopes to expand the realm of Kinaesthetic Intelligence, Performance, & Recovery Management. This narrative is by no means definitive or complete, and does not constitute as being medical advice in any
(Excerpts of Corporate Creed) Kompass Health Associates© 2002
manner or form.
“The sharing and impartation of discoveries and ideas with others is possibly the most profound and rewarding aspect of science and life. By the sharing of discoveries and ideas, knowledge is strengthened and empowered to grow. The very growth and expansion of our knowledge may be the essence that brings about the wisdom of appropriate intervention, for the wellbeing of our society”.
- Kenneth Craig
Throw a stone into the sports and rehabilitation arena today an you will most like likely hit someone who is conducting a biomechanics assessment or motion analysis on either an injured party hoping to recover, or an athlete wanting answers to performance issues.
So then; What is Biomechanics and what role does it play in sports performance and rehabilitation?
Some consider biomechanics in a mechanical manner, where the body is a machine influenced by internal and external forces, acting on it to produce a given motion and pattern. However this is only partially true, as a machine regardless of its complexities and efficiency is most certainly NOT alive. Therefore, human Bio-Mechanics which is indeed highly complex, must consider the bio-neurological, bio-chemical, bio-physical, and psycho-social aspect of each individual as illustrated in the diagram below.

Biomechanics assessments may be carried out either qualitatively or quantitatively. Bartlett (2007), commented that most graduates from various rehabilitative and sports disciplines would in the majority be conducting qualitative assessments rather than quantitative ones. This in my view is inadequate, and may be the choice or trend where there is little or no need for precision. However if precision is required, then quantification and verification becomes necessary, and this can only be accomplished utilising sound cutting edge techniques and technology.
As emphasised earlier human movement is a highly complex function, right from the default movement pattern of everyday gait (walking), to pole-vaulting as an example.
This narrative focuses specifically on The Laws of Motion and the essential co-factors that produce the efficiency of motion and performance. It does not address the co-essential factor of nutrition, environment & equipment.

©Kompass Health Associates 2013
Motion in its very nature be it in sports or activities of daily living, requires constant change in bodily positions, balance, speed, velocity etc.

When measuring motion several components are required:
Distance in either liner or curved motion
Balance & Displacement
Speed
Velocity
Acceleration
Momentum
This already highlights the insufficiencies of a purely qualitative assessment. (Note: video analysis alone does NOT constitute a quantitative analysis)
©Kompass Health Associates 2013
Basic Axis of Movement
‘X’ axis (coronal axis) describes pitch rotation and lateral motion.

‘Y’ axis (sagittal axis) describes roll rotation and anterior & posterior motion.
‘Z’ axis (vertical axis) describes upward and downward motion
In any given movement (eg walking), the body is moving through each axis in varying proportions simultaneously.
Note:
Therefore a lower limb ‘biomechanics’ assessment without taking into account whole body movement is a ridiculous concept and completely unreliable. It is not a biomechanics assessment at all, but merely some form of professional guess work at best.
©Kompass Health Associates 2013
Laws of Motion
Inertia the resistance of the body to change its state of motion. This becomes important when examining the forces to change the state of motion (eg. tackled by an opponent & wind direction). The weights held by the lifter in the diagram below is in a state of inertia, until force due to muscle contraction results in a push upward changing its state of motion.
Acceleration is comprised of the relationships of: force, mass and acceleration, which in-turn is linked to momentum.

Action & Reaction the factor of force working in pairs. The term every action, has an equal and opposite reaction is not exactly true. Eg. When you land from a jump, you exert a force onto the ground on which you land...BUT the force returning up your body is not equal but greater, because the earth beneath you is far larger and heavier. Therefore, optimizing the appropriate resistive muscle groups, and utility of correct techniques and equipment become pertinent points for consideration. Inertia

©Kompass Health Associates 2013
Acceleration, Action / Reaction, & Momentum
The essential co-factors – for efficient motion & performance
Balance & Stability

Translation of gravity
Mass
Energetics (force production and translation)
“Biomechanics is a component of bio-kinesiology where each component of the living human organism must act in concert to produce the various efficient symphonies of motion”.
©Kompass Health Associates 2013
Kenneth Craig, 2013
Balance & Stability
This has a direct effect on each individual's motion pattern and ability to perform. Balance and stability is an essential asset for high-performance athletes across every sporting discipline. It is pertinent for control, where the loss of control can affect factors such as force production, endurance and accuracy.

Components of balance & stability are:
posture
base of support
static balance
dynamic balance
In my opinion balance and stability conditioning must come before strengthening.
Consider this: from greatest buildings, ships, supercars, airplanes and rockets, the lack of stability will be disastrous regardless of their magnitude and power. Effective human motion is no different at all levels of moment, where greater need for balance is required at high-performance levels.
©Kompass Health Associates 2013
Translation of Gravity
Much has been focused on the centre of gravity, and rightfully so. However this is meaningless if this centre is ineffectively transferred or translated. The centre of gravity shifts with movement and can be inside or outside of the body depending on the movement pattern. In some sports, the centre of gravity shifts very rapidly. Wherever the given centre of gravity may be, drawing an imaginary line from that point straight down to ground level is considered as being the ‘line of gravity’. In order to effectively adapt to these gravitational translations, balance becomes the key as emphasised previously.
Point to consider: Besides the ‘central’ centre of gravity within the human body, individual body parts, such as limbs, also have their own centres of gravity.

 Centre of Gravity
Centre of Gravity
of Gravity ©Kompass Health Associates 2013
Line
Energetics & Force Translations
Simply put, in order for motion to exist it requires energy. This energy is produced mainly by the skeletal muscles in the body, transferred via the tendons to the skeleton to produce the desired movement. However there are other forces acting from within and outside the body, having an overall effect on the movement.



The four common properties of force are: line of action point of application

° Line of Action (action of force) Point of Application (point of force applied) Direction (angle of force) ©Kompass Health Associates 2013
direction
magnitude
Contact Forces
These are reaction forces involving contact and are divided into:
Contact forces
Non-contact forces (ie gravity and weight)
Before we proceed we need to clarify that weight and mass is not the same entity. Weight is dependant on the amount of gravity acting on and object or body. Mass is the constituent matter in an object or body. Therefore if you went into a vacuum negative gravity chamber, your body mass remains constant, while your body weight decreases due to lower gravity acting on it. We transfer forces in everyday life and in sports. The simplest actions such as turning around a street corner when walking, will require you to step a little harder to ensure sufficient pivot to change from a liner motion line (straight line), to a curved motion line (displacement: taking the turn). In sport, a rugby or tennis player will have to exert similar motion patterns with greater exertion of force in order to turn around or side-step.
Point to consider for therapists & coaches: If you cannot appreciate motion mechanics of daily living such as walking, a housewife in the kitchen, or an infant learning how to move, it will be of greater difficulty to understand motion in sports, as most movement patterns have great similarities, with the only variable being: acceleration and force.

©Kompass Health Associates 2013
Contact Forces
The majority of contact forces result from contact between objects and body mass, and may manifest as any one of the following types:
Ground reaction forces
Joint reaction forces
Friction forces
Fluid resistance forces
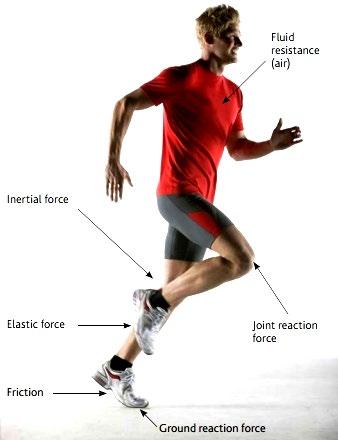
Inertial forces
Elastic forces
©Kompass Health Associates 2013
Friction force
Force Production & Summation

Most sports require an athlete to be able to generate and control forces. For sports where success is determined by achieving a maximum distance, it is necessary for athletes to produce as much force as possible, such as in a baseball pitch. While it is not always necessary for the force produced to be the maximum possible, certain principles may be used to produce the appropriate amount of force for the skill being performed.
To obtain maximum force it is essential to recruit force generated by as many body parts as possible, this is known as Force Summation.
Force summation is influenced by :
number of body parts involved.
timing and order of the involvement.
the force and velocity generated.
body balance and stability.
©Kompass Health Associates 2013
Assessment of Movement
Precision human motion assessment requires appropriate training, experience, and quantitative equipment to: assess, quantify and verify movement parameters. This strategic data helps provide optimal solution to complete the complex puzzle of movement, performance optimisation, recovery & rehabilitation.

©Kompass Health Associates 2013
Synergistic Holistic Integrated Protocol (SHIP)™
We developed the SHIP™ formula which incorporates the combination of sound technique, innovative technology and philosophy, SHIP™ provides the basis to activate a myriad of healing and recovery processes simultaneously, improving performance and treatment outcomes within shorter timeframes with lasting outcomes survival. Helping you heal, recover and perform at optimal levels in a safe and sustained manner.

©Kompass Health Associates 2013
Kompass MotionLab 360°
In the past sports analytics and performance metrics technology was exclusive to multimillion dollar clubs and Ivy League institutions, having sophisticated measurement equipment that help athletes shave off seconds, increase endurance and power to optimise performance. Kompass Health Associates now make this technology available at your very door step.
The Delsys Trigno sensors are light-weight completely wireless digital sensors that are placed on various muscles to detect their activity, capacity and fatigue levels. Up to 8 different muscles may be tested in real-time tasks, both indoors and outdoors.

These sensors simultaneously detect accelerations in all three axes allowing for a more accurate assessment of the three pillars of motion. The data is then processed by the EMGWORKS software and can be used to develop and monitor rehabilitation and performance programmes.


Data can be acquired in actual ‘dry’ playing conditions and can be shared in real-time and may be simplified to be easily interpreted and communicated.

©Kompass
2013
Health Associates
Making sports news at the 2014 Soccer World Cup the dorsa Vi-Move system is used by most of the world’s leading youth and sports academies such as Manchester United, Real Madrid, Cricket Australia, The AFL and NFL among many others.
The dorsa Vi-Move assesses low back, knee and hamstring function, along with core stability and ground-reaction force assessments.


Detailed reports that are easily interpreted are generated to further monitor athletic and rehabilitation programmes and outcomes.

©Kompass Health Associates 2013
Our matrix module allows us to analyse biomechanics of running and gait both indoors and outdoors, and over short & sustained durations. It allows us to measure:


Ground Reaction Force (GRF)
Absolute Symmetry Index (ASI)
Load Over Time (LOT)
Initial Peak Acceleration (IPA)
Ground Contact Time (GCT)
Cadence
Speed Over Distance (SOD)
©Kompass Health Associates 2013
Extracorporeal Shockwave Therapy

Utilises specialised medical soundwaves that help the body recover, heal and perform better. It is a medical technology first utilised to break kidney stones, but has been adapted into many medical disciplines such as: orthopaedics, sports medicine, cardiology, complex wounds management, and pain among others. It is a safe drug-free treatment and rehabilitation option. We are the pioneers of ESWT in New Zealand and the Austral / Asian region with over 16 years of experience. We collaborate with many researchers and institutions locally and internationally in areas of: sports science and performance, musculoskeletal aging research, low back syndromes, neuropathy, complex pain syndromes, and diabetes. Focused electrohydraulic devices are the gold standard of treatment and we have the full range of devices.
 Treatment using ESWT
Treatment using ESWT
©Kompass Health Associates 2013
Electrohydraulic & Radial ESWT devices
Thermodynamic therapy utilises low and medium radio frequency signals that enhanced microcirculation and muscular action potential, and may be used on its own, or in combination with ESWT, movement therapy, training and nutrition programmes. It provides an effective performance, recovery, and pain management modality. Thermodynamic therapy is used by some of the world’s leading sporting institutions (ie. FC Barcelona; Juventus FC; Chelsea FC; Manchester City), and universities (ie. Milan; Lugano Switzerland; Kansas State) for sports performance, recuperation, as well as acute and chronic injuries.



©Kompass Health Associates 2013
The work we conduct in high-performance sports attracts both domestic and international attention.
The 2014 touring English rugby team’s high-performance coaches visited our clinic to understand more about our methods and protocols to help them prepare for the next Rugby World Cup. Sports researchers in Europe, The Untied States, and South America are some of the other sports science and performance networks with whom we are actively involved with many sports research projects.


©Kompass Health Associates 2013
Associates & Research Collaboration
We conduct research in several areas such as: sports injuries, sports performance optimisation, complex pain syndromes, diabetes, skeletal muscles in aging etc. We presently collaborate with:
Cristina d’Agostino
Orthopaedic Research Centre
International Medical University Milan, Italy
Robert SGM Perez
Head of Anaesthesiology



VU University Amsterdam, Holland
Daniel Poratt
Senior Lecturer, Podiatric Dept.

Auckland, New Zealand
Wayne Hing
Programme Leader
Faculty of Health Science & Medicine
Sydney, Australia
Bruce Twaddle
Professor In Chief, Sports Medicine Department

Washington State University, USA
(Past) Head of Orthopaedics, Auckland Hospital.
Dominic Sainsbury
Education Director
Auckland, New Zealand
Jo Vogl
Lecturer, Sports Department
German Sports Institute

Koln, Germany
Noel Manning
Director, Technical Adviser

New Zealand

Austrian Workman’s Compensation Insurance: collaborative research project on spinal cord injury rehabilitation utilizing ESWT

Woflgang Schaden Sr. Surgeon & adj. Prof.
Ludwig Boltzmann Institute for Experimental and Clinical Traumatology.
David Hercher PhD. Researcher Ludwig
Boltzmann Institute for Experimental and Clinical Traumatology.

Stephen Buckley High Performance NZ Coach and performance coach to Breakers
Basketball Academy, Auckland, New Zealand
Richard Patterson Director Functional Strength (Olympic Weightlifter & 2014

Commonwealth Games Gold Medallist)

Research projects 2015 / 2016:
Golf swing optimisation among professional golfers.
Craig K (Kompass Health Associates)
Manning N (Golf Technologies, New Zealand / Australia)
Sainsbury D (New Zealand PGA)
The potential to reverse age related skeletal muscle atrophy and sarcopenia improving quality of life utilising medical shockwaves.
K Craig, Huges J, Takai B, Wong R. (Kompass Health Associates)
d’Agostino CM (Institutico Clinico Humanitas, International Medical University Milan, Italy)
Treatment of thoracic level spinal cord injury utilising extracorporeal shockwave therapy: a multi-centre trial.
Schaden W, Mittermyer R, Ponochey-Selger E. Hufgard J. Grazer A (Ludwig Boltzmann Institute, Austria)
Craig K, Takai B, Sajjakovich S, (Kompass Health Associates, New Zealand)
Furia J, Weaver H (Atlanta Spinal and Orthopaedics, USA)
The homeostatic return of pancreatic insulin excretion in Type-1 diabetes mellitus utilising three different therapeutic approaches: an original exploratory case series in a Middle Eastern population.
Belal K (Prof. Medical University of Kuwait) & Craig K (Kompass Health Associates)
Invitation of Wisdom:
“Call to Me, and I will answer you. I will show you great and unsearchable things that you do not yet know”
Publication and conference presentation:
Craig K. Biopsychosocial Approach in Pain Management (2010) New Zealand Pain Society Publication Summer Edition.
Craig K & Miller A. Extracorporeal shockwave therapy (ESWT) an option for chronic tendinopathy management: a clinical perspective (2011). New Zealand Pain Society Publication Winter Edition.
Craig K & Walker M. Medical Shockwaves for the treatment of peripheral neuropathic pain in a Type II diabetic: a case report (2012). New Zealand Pain Society Publication Winter Edition.
Craig K, d’Agostino CM, Poratt D & Walke M. Original hypothesis: Extracorporeal shockwaves as a homeostatic autoimmune restorative treatment (HART) for Type 1 diabetes mellitus (2014). Medical Hypotheses
Craig K, d’Agostino CM & Schaden W. Extracorporeal shockwave therapy a potential treatment option for complex pain syndromes (2015). Medical Hypotheses. (In-press)
Craig K, d’Agostino CM & Takai B. Induction of endogenous progenitor cells via acoustic soundwave mechanotransduction (2015). Journal of Stem Cell Research and Therapy (Open Access) (In-press)
D’Agoistinio CM, Craig K, Tibalt E & Respizi S. Shockwave as a Biological Therapeutic Tool: from Mechanical Stimulation to Recovery and Healing, through Mechanotransduction (2015). International Journal of Surgery (In Press).
Craig K. Mini Review: Obesity & Diabetes – Internal Medicine: Open Assess (Special Issue: Obesity & Diabetes). (In-press)
Craig K, Takai B, MacDonald D, Craig J & Pelham S. Medical shockwaves for chronic low back pain: a case series. Presented at the International Society of Medical Shockwave Treatment Conference, Argentina 2015
Craig K, Takai B, Sainsbury D, Patterson R, Craig J, MacDonald D, Buckley S & Wong R. The influence of medical shockwaves on muscle activation patterns and performance in healthy athletes: a preliminary report. Presented at the International Society of Medical Shockwave Treatment Conference, Argentina 2015
Craig K, Poratt D & Takai B. ESWT for the treatment of Complex and Neuropathic Pain Conditions? Presented at the International Society of Medical Shockwave Treatment Conference, Italy 2014
Craig K. Extracorporeal shockwave therapy for the treatment of chronic diabetic ulcers: a clinical perspective. Presented at the New Zealand Society for Study of Diabetes Conference 2012.
Craig K. Extracorporeal shockwave therapy for the treatment of complex regional pain syndrome I. Presented at the New Zealand Pain Conference 2012.
Craig K, Poratt D, Lewis G, Hing W & Walker M. Original Research: An attempt to restore peripheral sensitivity in a type I diabetic foot: a case study. Presented at the International Society of Medical Shockwave Treatment Conference, Columbia 2010.
Journal author and reviewer:
International Journal of Diabetes & Clinical Research
Editorial Board Member & Reviewer
International Journal of Autoimmune Disorders & Therapy
Editorial Board Member & Reviewer
Autoimmune Diseases & Therapeutic Approaches
Editorial Board Member & Reviewer
Medical Hypotheses
Author / Reviewer
OMICS Publishing Group - Medical Sciences

Author / Reviewer
Journal of Stem Cell Research & Therapy
Author / Reviewer
International Journal of Surgery
Author
New Zealand Pain Society Publication
Author
International Journal of Neurorehabilitation
Reviewer
Biology and Medicine
Reviewer
Journal of Trauma and Treatment
Reviewer
International Journal of Physical Medicine and Rehabilitation
Reviewer
International Journal of Sports Science
Reviewer
Occupational Medicine Health Affairs
Reviewer
International Journal of Physical Medicine & Rehabilitation
Reviewer
Memberships & Affiliations:
International Society for Medical Shockwave Treatment




European College of Sports Science

Fascia Research Society


International Diabetes Federation

Stem Cell Research Collaboration

Community Focus
We recognise that there are some in society who may not have equal access to health and the privilege of modern technology.

This is why Kompass Health, our associates and partners as responsible corporate members of society play an active role among the youth of our community.
Our Youth Health & Sports Programme help Kiwi’s in lower decile schools gain access to sporting equipment, training and nutrition. Our programmes are conducted alongside local charities and the Ministry of Social Development, to help ensure that talent in these schools are not lost, but offered the opportunity to gain exposure, information and guidance, to focus and achieve both sporting and academic excellence.
Youth and selected teams are provided with appropriate sporting equipment, motivational talks, and access to high-performance training and technology, to hopefully ignite a positive self image, vision, and ambition.
We hope to expand this programme beyond Auckland to help the youth of New Zealand become high achievers both domestically and internationally, who would then in turn contribute back to society in their own individual fashion.
Contact Us
T. 64 9 6240281 / 9 3203846
F. 64 9 6241082
E. nopain@xtra.co.nz
Clinic Locations:
Auckland City & North Shore, New Zealand
“Knowledge defines our possibilities, Philosophy defines our goals. Together they provide a basis for sound healthcare techniques and appropriate intervention”
David Manning & Kenneth Craig, 2012
The Information in this Document in Its Entirety Does Not Constitute Medical Advice
Reference
Learch C. & Matthie F. (2013). The Potential of Biomechanical Movement Analyses in Therapy Process. Journal for Unified Manual Healthcare, 1(1), 36 – 37.
Kenji Doma , Glen B. Deakin & Kevin F. Ness (2013): Kinematic and electromyographic comparisons between chin-ups and lat-pull down exercises. Sports Biomechanics, DOI:10.1080/14763141.2012.760204
Liang- Ching Tsai & Christopher M. Powers (2013). Increased Hip and Knee Flexion During Landing Decreases Tibiofemoral Compressive Forces in Women Who Have Undergone Anterior Cruciate Ligament Reconstruction. The American Journal of Sports Medicine 41(2), 423 - 429.
Wyndowa, S.M. Cowan, T.V. Wrigley & K.M. Crossley (2013). Triceps surae activation is altered in male runners with Achilles tendinopathy. Journal of Electromyography and Kinesiology 23 (2013) 166–172.
S.A. Jobson, J. Hopker, M. Arkesteijn & L. Passfield (2013). Inter- and intra-session reliability of muscle activity patterns during cycling. Journal of Electromyography and Kinesiology 23 (2013) 230–237.
Theodoros Ntousis, Dimitris Mandalidis, Efstathios Chronopoulos & Spyros Athanasopoulos (2013). EMG activation of trunk and upper limb muscles following experimentally-induced overpronation and oversupination of the feet in quiet standing. Gait & Posture 37, 190 - 194.
Athanasios Katis, Emmanouil Giannadakis, Theodoros Kannas, Ioannis Amiridis, Eleftherios Kellis & Adrian Lees (2013). Mechanisms that influence accuracy of the soccer kick. Journal of Electromyography and Kinesiology 23 125–131.
Derek J. Rutherford, Cheryl L. Hubley-Kozey & William D. Stanish (2013). Changes in knee joint muscle activation patterns during walking associated with increased structural severity in knee osteoarthritis. Journal of Electromyography and Kinesiology.
Han-Yi Huang, Jiu-Jenq Lin, Yueliang Leon Guo, Wendy Tzyy-Jiuan Wang & Yu-Jen Chen (2013). EMG biofeedback effectiveness to alter muscle activity pattern and scapular kinematics in subjects with and without shoulder impingement. Journal of Electromyography and Kinesiology 23 (2013) 267–274
Fernando Diefenthaeler , Edward F. Coyle , Rodrigo Rico Bini , Felipe Pivetta, Carpes & Marco Aurélio Vaz (2012): Muscle activity and pedal force profile of triathletes during cycling to exhaustion, Sports Biomechanics, 11:1, 10-19.
Erik Giphart, Justin D. Stull, Robert F. LaPrade, Michael S. Wahoff & Marc J. Philippon (2012). Recruitment and Activity of the Pectineus and Piriformis Muscles During Hip Rehabilitation Exercises: An Electromyography Study. The American Journal of Sports Medicine 40(7), 1654 - 1663.
Ruth Barn, Daniel Rafferty, Deborah E. Turner & James Woodburn (2012). Reliability study of tibialis posterior and selected leg muscle EMG and multi-segment foot kinematics in rheumatoid arthritis associated pes planovalgus. Gait & Posture 36, 576 - 571.
32
Young-Tae Lim , John W. Chow & Woen-Sik Chae (2012): Lumbar spinal loads and muscle activity during a golf swing, Sports Biomechanics, 11:2, 197-211
Jay Dicharry (2010). Kinematics and Kinetics of Gait: From: Lab to Clinic. Clinics in Sports Medicine 29, 347 - 364.doi:10.1016/j.csm.2010.03.013J.
Erik Giphart, Justin D. Stull, Robert F. LaPrade, Michael S. Wahoff & Marc J. Philippon (2012). Recruitment and Activity of the Pectineus and Piriformis Muscles During Hip Rehabilitation Exercises: An Electromyography Study. The American Journal of Sports Medicine 40(7), 1654 - 1663.
Knudson D. (2007). Fundamentals of Biomechanics, (2 Ed.), Springer, USA.
Herr, H. W. (2008). ‘Crushing the stone’: a brief history of lithotripsy, the first minimally invasive surgery. British Journal of Urology International 102(4) 432 – 435.
Amelio, E. & Manganotti, P. (2010). EFFECT OF SHOCK WAVE STIMULATION ON HYPERTONIC PLANTAR FLEXOR MUSCLE IN PATIENTS WITH CEREBRAL PALSY: A PLACEBO-CONTROLLED STUDY. Journal of Rehabilitative Medicine 42 (4) 339 -343.
Angehrn, F., Kuhn, C., Sonnabend, O. & Voss, A. (2008). Impact of extracorporeal shockwaves on the human skin with cellulite: A case study of an unique instance. Clinical Interventions in Ageing, 3 (1) 175 – 182.
Chen, Y. J., Wang, C. J., Yang, K. D., Kuo, Y. R., Huang, H. C., Huang, Y. T., Sun, Y. C. & Wang, F. S.(2004). Extracorporeal shock waves promote healing of collagenase-induced Achilles tendinitis and increase TGF-b1 and IGF-I expression. Journal of Orthopaedic Research, 22(4) 854 – 861.
Ronchi AJ, Lech M, Taylor NF & Cosic I. A Reliability Study of the Back Strain Monitor Based on Clinical Trials. 2008. 30 th Annual International IEEE EMBS Conference. August 20 – 24, Vancouver, Canada.
Furia, J. P. (2006). High-Energy Extracorporeal Shock Wave Therapy as a Treatment for Insertional Achilles tendinopathy. The American Journal of Sports Medicine 34(5) 733 – 740.
Furia, J. P. (2008). High Energy Extracorporeal Shock Wave Therapy as a Treatment for Chronic Non- nsertional Achilles Tendinopathy. The American Journal of Sports Medicine 36(3) 502 – 508.
Moretti, B., Notarnicola, A., Maggio, G., Moretti, L., Pascone, M., Tafuri, S & Patella, V. (2009). The management of neuropathic ulcers of the foot in diabetes by shock wave therapy. BMC Musculoskeletal Disorders 10 (54).
Moretti, B., Notarnicola, A., Maggio, G., Moretti, L., Pascone, M., Tafuri, S & Patella, V. (2009). A volleyball player with bilateral knee osteochondritis dissecans treated with extracorporeal shock wave therapy. Musculoskeletal Surgery 93(1) 37 – 41.
Moretti, B. (2010). Shockwave therapy in the management of complex regional pain syndrome in medial femoral condyle of the knee. Ultrasound in Medicine & Biology, 36 (6) 874 – 879.
Ogden, J. A., Alvarez, R. G., Levitt, R. L ., Johnson, J. E. & Marlow, M. E. (2004). Electrohydraulic High-Energy Shock-Wave Treatment for Chronic Plantar Fasciitis. Journal of Bone and Joint Surgery 86-A (10) 2216 – 2228.
33
Sagginni, R., Figus, A., Troccola, A., Cocco, V., Sagginni, A. & Scuderi, N. (2008). EXTRACORPOREAL SHOCK WAVE THERAPY FOR MANAGEMENT OF CHRONIC ULCERS IN THE LOWER EXTREMITIES. Ultrasound in Medicine and Biology, 34(8) 1261 – 1271.
Schaden, W., Fisher, A. & Sailler, A. (2001). Extracorporeal Shockwave Therapy of Nonunion or Delayed Osseous Union. Clinical Orthopaedics and Related Research, 387; 90 – 94.
Schaden, W., Thiele, R., Kölpl, C., Pusch, M., Nissan, A., Attinger, C. E., Maniscalo-Theberge, M.E., Peoples, G. E., Elster, E. A. & Stojadinovic , A. (2007). Shock Wave Therapy for Acute and Chronic Soft Tissue Wounds: A Feasibility Study, 143 (1) 1 – 12.
Skaler, T. (2008). EXTRA-CORPOREAL SHOCKWAVE THERAPY (ESWT) IN TREATMENT OF SELECTED MUSCULOSKELETAL CONDITIONS. Evidence Based Review, ACC.
Taki, M., Iwata, O., Shiono, M., Kimura, M. & Takagishi, K. (2007). Extracorporeal Shock Wave Therapy for Resistant Stress Fracture in Athletes. The American Journal of Sports Medicine, 35 (7) 1188 – 1192.
Tizanni, E., Amelio, E., Marangoni, E., Guerra, C., Puccetti, A., Codella, O. M., Simeoni, S., Cavalieri, E., Montagnana, M., Adani, R., Corrocher, R. & Lunardi, C. (2010). Effects of shock wave therapy in the skin of patients with progressive systemic sclerosis: a pilot study. Rheumatology International, 12.
Trompetto, C., Avanzino, L., Bove, M., Marinelli, L., Molfetta, L., Trentini, R. & Abbruzzese, G. (2009). External shock waves therapy in dystonia: preliminary results. European Journal of Neurology, 16 (4) 517 – 521.
Vasyuk, Y. A., Hadzegova, A. B., Shkolnik, E. L., Kopeleva, M. V., Krikunova, O. V., Iouchtchouk, E.N., Aronova, E. M. & Ivanova, S. V. (2010). Initial Clinical Experience With Extracorporeal Shock Wave Therapy in Treatment of Ischemic Heart Failure. Original Research.
Wang, F. S., Yang, K. D. & Chen, R. F. (2002). Extracorporeal shock wave promotes growth and differentiation of bone-marrow stromal cells towards osteo-progenitors associated with induction of TGF-β1. Journal of Bone and Joint Surgery British Volume, 84(3) 457 – 461.
Wang, C. J ., Liu, H. C. & Fu, T. H. (2007). The effects of extracorporeal shockwave on acute high-energy long bone fractures of the lower extremity. Archives of Orthopaedic Trauma and Surgery, 127 (2) 137 – 142.
Weil, L. S. Jr., Roukis, T. S., Weil, L. S. Sr., & Borelli A. H. (2002). Extracorporeal Shock Wave Therapy for the Treatment of Chronic Plantar Fasciitis: Indications, Protocol, Intermediate Results, and a Comparison of Results to Fasciotomy. Journal of Foot and Ankle Surgery 41(3) 166 –172.
Zelle, B. A., Gollwitzer, H., Zlowodski, M. & Buhren, V. (2010). Extracorporeal Shock Wave. Therapy: Current Evidence. Journal o f Orthopaedic Trauma 24(3)S 66 – 70.
Andrzejewski, Marcin, et al. Analysis of sprinting activities of professional soccer players. The Journal of Strength and Conditioning Research. 2013; 27(8); 2134 – 2140.
34
Sagginni, R., Figus, A., Troccola, A., Cocco, V., Sagginni, A. & Scuderi, N. (2008). EXTRACORPOREAL SHOCK WAVE THERAPY FOR MANAGEMENT OF CHRONIC ULCERS IN THE LOWER EXTREMITIES. Ultrasound in Medicine and Biology, 34(8) 1261 – 1271.
Notarnicola, A., Moretti, L., Tafuri, S., Panella, A., Filipponi, M., Casalino, A., Panella, M. & Moretti, B. (2010). Shockwave therapy in the management of complex regional pain syndrome in medial femoral condoyle of the knee. Ultrasound in Medicine & Biology, 36 (6) 874 – 879.
Yardi, Y., Appel, B., Jacob, G., Massarwi, O. & Gruenwald, I. (2010). Can low-intensity Extracorporeal Shockwave Therapy Improve Erectile Function? A 6-Month Follow-up Pilot Study in Patients with Organic Erectile Dysfunction. European Urology, 58: 243 –248.
D’Agostino, C. Romeo, P., Amelio, E. & Sansone, V. (2011). Effectiveness Of ESWT In The Treatment Of Kienbock’s Disease. Ultrasound in Medicine and Biology, 37(9), 1452 – 1456.
Craig, K., D’Agostino, C., Poratt, D., Lewis, G. & Hing, W. (2012). Original Exploratory Case Study: Utilization of ESWT to Restore Peripheral Vibrosensory Perception in a non-Sensitive Type I Diabetic Foot. Paper Presented at the 15th International Society for Medical Shockwave Treatment Congress, Cartagena, Columbia.
Mittermayr R, Hartinger J, Antonic V, Meinl A, Pfeifer S, Stojadinovic A, Schaden W & Redl H. Extracorporeal Shock Wave Therapy (ESWT) Minimises Ischemic Tissue Necrosis Irrespective of Application Time and Promotes Tissue Revascularisation by Stimulating Angiogenesis. Annals of Surgery. 2011; 253(5): 1024 – 1032.
Mariotto, S., Cavaleri, E., Amelio, E., Ciampa, A. R., de Pratti, A. C., Marlinghaus, E., Russo, S. & Suzuki, H. (2005). Extraco rporeal shock waves: From lithotripsy to anti-inflammatory action by NO production. Nitric Oxide 12(2) 89 – 96.
Moretti, B., Iannone, F., Notarnicola, A., Lapadula, G., Moretti, L., Patella, V. & Garofalo, R. (2008). Extracorporeal shock waves down-regulate the expression of interleukin-10 and tumor necrosis factor-alpha in osteoarthritic chondrocytes. BMC Musculoskeletal Disorders 9:16.
Notarnicola A & Moretti B. The biological effects of extracorporeal shock wave therapy (eswt) on tendon tissue. Muscles, Ligaments, and Tendons Journal. 2012; 2(1): 33 – 37.
Berta FR. Biological Effects of Extracorporeal Shock Waves on Fibroblast: A Review. Muscles, Ligaments and Tendons Journal. 2011; 1(4): 137 –146.
Berta L, Fazzari A, Ficco AM, et al. Effect of extracorporeal shock wave enhance normal fibroblast proliferation in-vitro and activate mRNA expression for TGF-B1 and collegen types I and III. Acta Orthpaedica. 2009; 80(5): 612 – 617.
Race O, Shell K, Goessi A, et al. Effect of extracorporeal shock wave on proliferation and differentiation of equine adipose tissue-derived mesenchymal stem cell in vitro. American Journal of Stem Cells. 2013; 8;2(1): 62 – 73.
Zadpoor, Abbas A & Nikooyan AA. Modeling muscle activity to study the effects of footwear on the impact forces and vibrations of the human body during running. Journal of Biomechanics 2010; 43(2): 186 – 193.
Logan et al. Ground reaction force difference between running shoes, racing flats, and distance spikes in runners. Journal of Sports Science and Medicine. 2010; 9(1): 147
35


Motionlab360° Kompass OrthoShock
