Page
Page


Page
Page
Page
The SMART AMI app has been used by Hamilton General Hospital and the region’s emergency departments since 2020 as part of two pilot projects led by Dr. Hassan Mir and Dr. Madhu Natarajan (pictured), an interventional cardiologist at HGH. Created by cardiologists, the secure communications system is now being deployed in the Ottawa region, and could also be adopted internationally. SEE STORY ON PAGE 5.
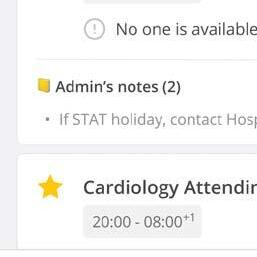
linical staff at Health Sciences North (HSN) in Sudbury, Ontario, surrendered their pagers on November 1 when the hospital went live with Hypercare’s cell phone and web-based communication software.
“HSN had a burning need to replace physician pagers and improve page request turnaround times, which were not up to par with the needs of our clinical care teams,” said Lindsay Cooper, the HSN project manager who supported the implementation.
Using pagers, clinical teams wouldn’t know if their page requests were read or even received. Nor could they communicate the urgency of a call. Now, they can see a clear indicator in the app confirming a mes-
sage has been sent, delivered or read and they can see whether the message priority was normal, urgent or stat.
“When clinicians see a read receipt on their message, that’s live feedback they weren’t getting before,” said Cooper.
The Hypercare solution also improves staff scheduling, and shows changes in real-time.
The hospital-wide deployment has physicians using their own cellphones and nurses using Hypercare primarily on nursing station computers.
The HIPAA and PHIPA-compliant Hypercare solution also frees HSN staff from using Excel spreadsheets for on-call
schedules that were only accessible on the hospital’s intranet or printed and posted on bulletin boards. Using Hypercare, the on-call schedule is on the app and is updated in real-time when a physician changes their shift. This ensures clinicians are referring to the most up-to-date oncall schedule.
“Our project team began researching possible solutions through the winter/spring of 2023 to see what options were out there,” said Cooper. “Hypercare popped up as part of that research and a decision to go with them was made in August.”
Toronto-based Hypercare’s CEO, Albert Tai, was effusive in his praise for HSN and its project team for the rapid deployment. “HSN did a fantastic job making decisions
CONTINUED ON PAGE 2
and moving the process forward,” said Tai. “If all healthcare organizations moved that fast, healthcare wouldn’t be this broken. HSN was very clear about what needed to be deployed right away and didn’t try to boil the ocean, so that helped us deploy the solution very quickly to solve their immediate pain points.”
Cooper is equally complimentary about how the two teams worked together to deploy the application in record time.
“We quickly built a strong team dynamic between our HSN project team and the Hypercare team which allowed us to work quickly and effectively together,” said Cooper. “The Hypercare team was flexible in adapting to our project needs and provided hands on support directly with our clinicians.”
The HSN project team consulted widely on the policies and procedures for using the application, inviting input from clinicians and Hypercare staff.
Policies included expected response times for normal, urgent and stat messages, how changes to on-call schedules

would be made after hours and whether physician orders could be processed through Hypercare messaging.
“Our project team was instrumental to HSN’s deployment and consisted of members across Information Technology,
Issue DateFeature ReportFocus Report
April Mobile SolutionsArtificial Intelligence
May EHR / EMR TrendsPrecision Medicine
June/July IT Resource GuidePoint-of-Care Systems
September Community CareStart-ups
October Virtual CarePhysician IT
Nov/Dec AI / AnalyticsCardiology
Zeidenberg, Publisher, jerryz@canhealth.com
www.canhealth.com
Telecommunications, Switchboard, Medical and Academic Affairs, Quality and Patient Safety, Medical Staff and Nursing,” said Cooper.
“HSN’s policies and procedures are the most sophisticated and comprehensive

Address all correspondence to Canadian Healthcare Technology, 1118 Centre Street, Suite 204, Thornhill ON L4J 7R9 Canada. Telephone: (905) 709-2330. Fax: (905) 709-2258. Internet: www.canhealth.com. E-mail: info2@canhealth.com. Canadian Healthcare Technology will publish eight issues in 2024. Feature schedule and advertising kits available upon request. Canadian Healthcare Technology is sent free of charge to physicians and managers in hospitals, clinics and nursing homes. All others: $67.80 per year ($60 + $7.80 HST). Registration number 899059430 RT. ©2024 by Canadian Healthcare Technology. The content of Canadian Healthcare Technology is subject to copyright. Reproduction in whole or in part without prior written permission is strictly prohibited. Send all requests for permission to Jerry Zeidenberg, Publisher. Publications Mail Agreement No. 40018238. Return undeliverable Canadian addresses to Canadian Healthcare Technology, 1118 Centre Street, Suite 204,
Publisher & Editor Jerry Zeidenberg jerryz@canhealth.com
Office Manager Neil Zeidenberg neilz@canhealth.com
that I have seen, and a lot of other hospitals are now building their policies based on HSN’s. It’s amazing for them to share their knowledge,” said Tai.
Clinicians can also include photos, videos, diagnostic images and documents with their Hypercare messages. It could be a photo of a wound that’s sent to a dermatologist, for example, or an emergency doc sending a photograph of a patient’s burn to a plastic surgeon.
To ensure privacy, users click on a camera icon within the Hypercare app, so the photo is saved in Hypercare – not stored on the cell phone’s photo reel.
Ontario Health Teams may be eligible for funding from the province to cover the cost of a Hypercare deployment as the application has been identified by the Ontario Centre of Innovation as a solution capable of improving their operations.
To date, Hypercare has been deployed by 30 hospital systems in Ontario representing 20 percent of hospitals in Ontario, including Michael Garron Hospital in Toronto, Royal Victoria Regional in Barrie, Southlake in Newmarket, Joseph Brant Hospital in Burlington, and the Huron Perth Healthcare Alliance in southwestern Ontario. Other deployments are in the works across Canada and the U.S.
Feedback from HSN staff has been extremely positive, said Cooper. “It was exciting to see clinical team members’ eyes light up when they started playing with the app. I can remember onboarding a nurse and watching her message a physician she was working with. Within seconds she received a response and looked at me in disbelief. Real-time communication and collaboration was something they never had before when using pagers.”
Contributing Editors
Dianne Craig dcraigcreative@yahoo.ca
Dianne Daniel dianne.l.daniel@gmail.com
Dr. Sunny Malhotra Twitter: @drsunnymalhotra
Norm Tollinsky tollinskyn@gmail.com
Art Director Walter Caniparoli art@canhealth.com
Art Assistant Joanne Jubas joanne@canhealth.com

Our care enables us to provide attention where it’s needed. We believe in innovation that continues to build a world where healthcare has no limits.
ARRIE,
ONT.– When a patient –often elderly – no longer requires acute care services in hospital, they can remain in bed for months as staff search for a place in a community or long-term care facility. Unfortunately, when these ALC (Alternate Level of Care) patients have prolonged hospitalization, they prevent others from getting a hospital bed, leading to delays and logjams in the healthcare system.
An innovative program at the Royal Victoria Regional Health Centre (RVH), in Barrie, is using technology to move these patients into their own homes and to monitor them remotely as they rehab safely and more comfortably.
“RVH@Home is a 16-week restorative program that creates a seamless transition of quality care from hospital to home,” said Dana Naylor, vice president, clinical. “It promotes patient independence after 16 weeks of rehabilitative care, in the familiarity of a patient’s home. They eat their own food, sleep in their own bed, all while being surrounded by family and pets.”
The program was established in November 2022 and to date has enrolled 350 patients. “Given the rate of referrals, we expect to enroll over 400 patients before our fiscal year end, March 31, 2024,” Naylor added.
Monitoring of patients in their homes is managed by Toronto Grace Health Centre’s Remote Care Monitoring (RCM) program – which launched in 2020 and has over 10,000 active clients in all five regions of Ontario. The main goal of the program is to help older adults stuck in hospital get back home living safely and independently.
“It’s about improving flow,” said Jake Tran, president & CEO, Toronto Grace Health Centre. “When patients can transition quickly to more appropriate care settings, they experience better health outcomes.
“And by providing patients with a combi-

nation of in-person and virtual care, coupled with 24/7 medical and non-medical monitoring, we’re helping them to avoid returning to an acute care facility,” Tran added.
The technology includes an SOS/falls pendant, worn around a client’s neck or wrist to detect falls, an emergency or patient wandering, and an automated medication dispensing device to help clients stay on track with their meds.
The pendants use GPS to create a virtual perimeter, safely tracking the movements of an individual at home.
“The pendants work on cellular twoway communication technology, and no cameras are used so patients maintain their privacy,” said Danielle Kilby-Lechman, manager, Remote Care Monitoring, Toronto Grace Health Centre. “If a patient falls or no movement is detected, or if a patient moves beyond a virtual barrier, an alert by text message is sent automatically to our 24-hour call Centre.”
At that point it will be determined if there is an emergency, or a false alarm, and staff can respond accordingly. In many

cases, call Centre staff can assist clients without involving EMS. All alerts are documented and added to a client’s record.
A medication dispensing device works by dispensing multi-pouch medication strips pre-loaded into a dispenser cartridge. It ensures clients get the right medication dispensed at the right time. A musical alert tells clients when it’s time to take their meds, and if a dose is missed, an alert is automatically sent to Toronto Grace RCM 24/7 call Centre.
Care providers assisting patients in their home include:
•Registered Nurses (RN)
•Registered Practical Nurses (RPN)
•Personal Support Workers (PSWs); and
•Occupational therapists who help to execute a rehabilitation plan.
The nursing team is not from the hospital, but rather from leading home care agencies.
Patients receive a care plan upon discharge from hospital, so they know exactly which services they’ll receive for the first two weeks. During that time, patients re-
ceive visits from nurses or PSWs about two to three times per day. After this period, as patients improve, they may only require visits once or twice per week.
Being able to recover at home has many benefits. It provides patients with comfort and familiarity in their own surroundings; promotes a positive mindset, independence and improved overall quality of life.
Moreover, home care rehab programs cater to the individual needs of patients. “Therapists assess the home environment and tailor rehabilitation plans accordingly, ensuring that each patient receives personalized and targeted care,” said Naylor. “This unique approach enhances the effectiveness of rehabilitation, leading to faster and more sustainable recovery.”
Naylor added the program is progressing and evolving. Pendants are now provided to every patient, and remote care management is tailored to every patient’s needs. “RVH@Home forces us to think about patient care in a different way,” said Naylor. “It’s time to expand the ways in which patients receive care.”
THUNDER BAY, ONT. – As the largest and least populated region of the province, Northwestern Ontario has a unique set of challenges in meeting the needs of its diverse and geographically dispersed patient population. While most of the area’s 238,000 residents will visit Thunder Bay Regional Health Sciences Centre (TBRHSC) at some point in their lifetime, the vast majority will also seek healthcare elsewhere with PCPs, specialists, or referral organizations.
TBRHSC understands the importance for health data, especially medication history, to follow patients between all venues of care, so they developed a Digital Health Strategic Roadmap.
After meeting with groups of patients and providers, TBRHSC recognized that a new EHR platform, data more accessible for decision making, and transitions
between facilities smoother.
The health system recently began implementing the first phase of their roadmap, which will establish a single, person-centered digital record with a new electronic health record – for seamlessly exchanging health information between providers.
The EHR will also serve as the foundation for advanced analytics and research to improve outcomes and health equity.
“Providers should be able to access timely clinical information from a variety of sources, through a single, more meaningful view,” said Thunder Bay Regional Health Sciences Centre’s Regional chief information officer Cindy Fedell. “This comprehensive patient record will provide a more complete picture of our patients at the point of care and enable more shared care planning.”
TBRHSC selected MEDITECH Ex-
panse to establish an integrated EHR across its hospital, ambulatory, and primary care providers. In addition to providing more connected care and new digital tools, the EHR will bridge the workflow between provincial and federally orga-
TBRHSC and dozens of other healthcare providers are planning to join ONE Healthcare Technology Services.
nized care. It will also enable TBRHSC to connect to the Provincial Health Record.
As part of its digital transformation, the North West – comprised of TBRHSC and dozens of other healthcare providers across the region – is planning to join ONE Healthcare Information Technology Services (ONE HITS), which oper-
ates one of MEDITECH’s largest Expanse instances. ONE HITS has already brought more than 20 hospitals together to share resources and develop standard order sets, documentation templates, and dictionaries.
“We would all like to reduce the amount of time doctors and nurses spend administrating or navigating disparate systems,” said ONE Healthcare Information Technology Services CEO Brenda Muto.
“The goal has always been to improve the experience for clinicians and give them back more time on direct patient care. We are partnering with TBRHSC to achieve this goal by providing a comprehensive view of the patient record, enabling clinicians to make more informed decisions while also increasing their efficiency. They shouldn’t have to jump through hoops to
The Ontario Centre of Innovation recently announced $500,000 in provincial funding to expand a made-in-Hamilton smartphone application into the Ottawa region. Funding is aimed at fast-tracking digital health innovations in Ontario.
The Hamilton-born SMART AMI app by Sayhut Inc. streamlines how hospital emergency department doctors share electrocardiogram (ECG) images with on-call interventional cardiologists at regional cardiac centres for real-time review and decision making.
The app has the potential to expand to hospital systems provincially, nationally and internationally. This funding is part of an $8.2 million investment of 13 approved projects designed to revolutionize healthcare delivery across the province.
APP-reciation for innovation: It was mid-October when Burlington resident Paul Cropper awoke in the middle of the night with abdominal pain, and then noticed other alarming symptoms. “I was sweating. I felt nauseated and my chest was feeling tight,” recalls the 81-year-old man.
Based on Cropper’s ECG images, the emergency department doctor at Burlington’s Joseph Brant Hospital suspected he was experiencing a potentially deadly type of heart attack called a STEMI (ST-Elevation Myocardial Infarction), where the coronary artery is completely blocked.
In order to confirm the diagnosis, and plan next steps, the emergency department doctor used an innovative new made-inHamilton smartphone app to instantly and securely share Cropper’s ECG images with the on-call interventional cardiologist at Hamilton Health Sciences (HHS), Hamilton General Hospital (HGH), the regional cardiac centre for south-central Ontario.
The cardiologist was able to quickly confirm a STEMI, and Cropper was rushed by ambulance to HGH where the region’s cardiac catheterization lab is located, for emergency angioplasty to open the blocked artery.
“Everything happened really smoothly and efficiently,” says Cropper, who has since recovered and is back home. “The paramedics were very thorough and caring, and the catheterization lab team at Hamilton General Hospital was ready for me as soon as I arrived.”
SMART AMI app by Sayhut Inc.: The SMART AMI app has been used in two Hamilton-based trials over the past four years. This fast, secure, easy-to-use and privacy-compliant smartphone app allows for real-time ECG review and decision making for STEMI patients. The app also helps improve hospital efficiency by ensuring that only those patients needing emergency angioplasty treatment are brought to the catheterization lab.
“The success of the SMART AMI app underscores the vital role clinicians play in turning ideas to innovation driving better health outcomes in our community and beyond,” says Dr. Ted Scott, vice president of innovation and partnerships for HHS.
Innovative thinking: The app is the brainchild of Dr. Hassan Mir and Dr. Talha Syed, who came up with the idea when
they were resident doctors at McMaster University from 2015 to 2018, with placements at HGH’s cardiology department.
Mir is now an academic cardiologist, clinician investigator, and assistant professor at the University of Ottawa Heart Institute. He is also co-founder of Sayhut Inc.,

the mobile health start-up company he established to develop the SMART AMI app. The company has since branched out to develop other smartphone healthcare apps aimed at improving access, efficiency, and patient outcomes.
Syed leads a large and diverse cardiol-




ogy practice at Oakville Trafalgar Memorial Hospital and remains involved with the app project through ongoing consulting.
Recognizing potential for improvements: Across Ontario and Canada, fax machines or hospital-based e-mail are still con-


March is Fraud Prevention Month.
Rosemary Rofail, a pharmacist in the Greater Toronto Area, discusses the challenges pharmacists face in curtailing prescription fraud and how implementing PrescribeIT® can help.
How does prescription fraud affect our healthcare system?
Every year in Canada, over 250 million new and renewed prescriptions are issued by prescribers to patients and at the core, the role of the pharmacy is to ensure those medications are dispensed safely and accurately to the right patient. Any controlled substance can be a target for prescription fraud but opioids are by far the biggest target.
Pharmacies are one of the primary gateways to ensuring that drugs are being dispensed to the right people and not being diverted elsewhere. As we see the opioid epidemic continue to worsen, it puts extra strain on pharmacists to ensure we are confident in the provenance of the prescriptions we’re filling.
What are some of the biggest challenges to curbing prescription fraud?
Time is a big limiting factor. For pharmacists like myself in Ontario and in other provinces like B.C., we now have an expanded scope of practice. It becomes difficult to navigate your time between treating minor ailments, administering vaccines, dispensing and then doing detective work to verify the legitimacy of a prescription.
Many people engaging in prescription fraud have become very sophisticated at mimic-
king a prescription faxed by a doctor – how the headings look, what information is required on a prescription – causing fraudulent scripts to be increasingly challenging to identify. You can easily spend 15-20 minutes trying to determine whether a prescription is valid, researching the clinic and trying to track down the prescriber.
Why is technology like PrescribeIT valuable in combating prescription fraud?
It’s very difficult to verify that a fax is coming from the right person and even more so since the pandemic, when it became more common for physicians to work from home – so faxes are not necessarily coming from their office number.
PrescribeIT, a national e-prescribing service, connects community-based prescribers to retail pharmacies, enabling the secure, digital transmission of prescriptions, so we can see exactly where it originated from and I am guaranteed that it came from a legitimate prescriber.
PrescribeIT also has an integrated, secure messaging feature that allows us to communicate directly with the prescriber if any questions arise. I find prescribers are much more responsive on PrescribeIT than they are through fax so I’m not spending a chunk of time trying to track a prescriber down when I need to verify something – especially helpful now that we’re seeing more ehealth services with physicians working out of multiple clinics.

PrescribeIT’s own data from the recent user survey shows that 83 percent of pharmacists and 65 percent of prescribers believe that Pre-
Rosemary Rofail
scribeIT reduces the number of stolen and fraudulent prescriptions.
Does technology like PrescribeIT have a role to play in fighting the opioid epidemic?
Absolutely. Implementing systems like PrescribeIT is the logical next step towards eliminating the risk of prescriptions getting into the hands of people where the need is not warranted. In many states in the U.S., they are not even allowed to fill prescriptions for controlled substances without it being an e-prescription and I believe that we should be following suit and requiring every prescription for any controlled substance be issued through eprescribing.
This sentiment is also echoed among my colleagues – 87 percent of pharmacists and 78 percent of prescribers recently surveyed by Canada Health Infoway expressed
enhanced confidence in transmitting and receiving prescriptions for opioids and controlled substances via PrescribeIT.
What are the risks of continuing to rely on analog methods to prevent prescription fraud?
If we continue to rely on analog methods, the status quo will continue and we are at risk of the problem getting out of control, as we’re already seeing in Vancouver. During the pandemic when the rules were changed to allow prescriptions for certain medications to be called in, it was shocking how many we’d receive that were clearly fraudulent.
We need to be more stringent and take the steps necessary to close the loopholes. Tools like PrescribeIT that can reduce that time burden and ensure accuracy make life immensely easier and safer for everybody.
Toronto-based start-up KeyOps has created an online platform that enables pharma companies to interact with physicians online, instead of the old-fashioned method of timeconsuming lunches, dinners and off-site presentations and Q&A sessions. By alerting physicians to online surveys, which they can complete in a matter of minutes, doctors gain extra dollars in compensation and the pharmaceutical companies obtain valuable insights from key influencers.
Company CEO Peter Doulas noted that it’s important for the pharmaceutical companies to gain feedback from doctors about how their therapies are being used and how they might further support clinicians and patients. Communicating with physicians also helps them learn
about the competition and how they might improve their own performance.
“After a drug is released, for example, pharma companies want physician insights,” said Doulas. “It’s important to continuously monitor the therapeutic landscape and physicians are in the best position to offer pharmaceutical companies on how to improve.”
However, in recent years, doctors have been overwhelmed by their patient workloads, paperwork and the problem of balancing their personal lives with their professional careers. They just don’t have time for meetings with companies – even using Zoom or Teams – that take hours away from their schedules.
“With KeyOps, we created a solution that’s empathetic to this problem and hassle free,” said Doulas.
Indeed, KeyOps was the brainchild of two Toronto-based physicians – Dr. Sam
Doctors can complete pharma related surveys online in a matter of minutes, for which they are quickly compensated.
Elfassy (a gastroenterologist) and Dr. Saeed Darvish-Kazem (a cardiologist) –who realized a better solution was needed. They teamed up with Doulas, a long-time Microsoft executive with experience in launching and growing startups, and Darren Anderson, who brought over 25 years of pharmaceutical expertise to the founding team.
Since 2020, the company has grown to 22 employees and recently raised $4 million in seed capital. The company works with numerous pharma and medical device companies, including Biosyent,
GlaxoSmithKline, Sanofi Canada, and Becton Dickinson and Company (BD).
They’re reaching physicians across Canada, and they’ve begun marketing the system to doctors in the United States, along with additional pharma and medical device companies. “We’re working in about a dozen different therapeutic areas across Canada, and we’re expanding into the United States,” said Doulas.
The system provides substantial benefits for physicians and companies.
“The physician logs into the dashboard, and sees which opportunities are available, along with the honorarium that goes with it – usually $100 to $200,” said Doulas. They can complete the survey in about 10 minutes at their desktop or even on the go using their mobile device.”
The surveys are targeted at various kinds of clinicians, such as GPs, oncolo-









CHICAGO – One of the most instructive sessions at the annual RSNA conference is the Fast Five event. In it, five diagnostic imaging professionals are each given five minutes to make their case on a non-clinical topic of interest – such as a social or technological development that’s having an impact on radiology.
For example, at the most recent RSNA, Dr. Anne Williams Darrow spoke about the importance of keeping up with LGBT issues in a time of growing importance of sexual and identity awareness and politics. Dr. Darrow is a radiology resident at the University of Chicago and has helped build an Illinois-based organization called MORE, short for Mentoring, Outreach & Resources for Equity.
In particular, the group is seeking to help radiologists become more aware of LGBT medical issues in their practices.
Dr. Darrow is married to a trans-male and both became pregnant at the same time, just before she entered medical school. “I am cis-feminine, and my spouse is trans-masculine. We were so lucky to have conceived at the same time,” she said.
However, during their pregnancies and after delivering, the women discovered that medical professionals were often confused about how to treat them and even how to address them. “Even the most wellintentioned doctors, nurses and other professionals we interacted with sometimes stumbled through their interactions with us.”
After getting into medical school, Dr. Darrow noticed there wasn’t much education about LGBT issues and concerns. It was then she decided to try to make changes in the system.
“We can create a more inclusive environment in our radiology departments, and we can use correct pronouns in our imaging reports,” she said. “It really makes a difference to patients.”
Trans-feminine and trans-masculine individuals may pursue therapies that include hormones, breast augmentation or reduction, facial and body modification, and vaginoplasty or phalloplasty.
A radiologist, for example, may receive a call from a primary care provider asking for a recommendation for breast cancer screening for a male who has transitioned to a woman – a trans-feminine patient.
She noted that the American College of Radiology has now released “appropriateness criteria” for transgender breast cancer screening.
“So, if a trans woman has been on hormonal therapy for at least five years, for example, and has average risk, we may recommend similar screening as for a cis female patient,” she said.
She mentioned that it is extremely useful to be aware of surgical procedures used in gender transitioning, as well.
“Similarly, we may want to do an ultrasound if we’re doing a paracentesis on a patient to look for the inferior epigastric artery, to make sure we’re not causing harm.”
She added, “That same vessel may be the arterial supply for a trans-masculine patient, if they’ve had a surgical neophallus created from an anterior abdominal flap.”
Dr. Darrow noted there are three main procedures that surgeons use to create a neophallus – the anterior abdominal flop, the anterior thigh and radial flap.
“As radiologists, it’s important for us to know what the donor site may be, as well as the surgical and hormonal history of the patient,” she asserted. Overall, it results in better medical care when radiologists are up to date on LGBT medical treatments. It also makes patients feel better to be addressed in the right way and “it gives them more confidence in their care,” said Dr. Darrow.
ANOTHER SPEAKER asked if more working radiologists should be spending time educating residents and fellows. With growing patient lists and increasing burnout, fewer radiologists may be taking time for teaching.
Dr. Kara Gaelke-Udager, an associate professor of musculoskeletal radiology at the University of Michigan and program director of the MSK division,
having a trainee ask you a question at the workstation that you should have had the answer to. We all get better in this way.”
As a result, she said, when you are teaching, you are not just giving. You are building on what you know and learning new things. “You can’t become stagnant because you have bright trainees keeping you on your toes,” she said.
Teaching up-and-coming radiologists also helps reduce the transactional feeling that can surround radiology today. By teaching, there’s constant human interaction, said Dr. Gaelke-Udage.
Instead of losing time and money through teaching, experienced radiologists are gaining, she concluded. “You are gaining outstanding future colleagues while building an incredible culture at work. You’re gaining clinical expertise, constant inspiration

asserted that radiologists are now asking, “What’s in it for me?”
In her allotted five minutes, she argued that there’s a lot to be gained.
“I’m here to say that teaching can benefit you, the teacher. It’s not all altruism,” she said.
Train your residents well and they will take outstanding care of your shared patients while they’re in your program, Dr. Gaelke-Udager contended. Train them well, she added, because one day they’ll be your fellow or colleague. You could even benefit from their expertise if they’re taking care of one of your family members – or one day, caring for you!
On another note, teaching creates research questions and produces creative ideas. “Trainees have lots of questions,” she said. “They don’t accept our answers of, ‘because we’ve always done it that way’. They see the flaws in those arguments,” she averred.
Dr. Gaelke-Udage added that trainees know the problems with our systems and many times, they have the best solutions. “They show us the way forward.”
She said, “Teaching keeps you sharp and skilled. It makes you a better radiologist. There’s nothing like
and innovative thinking. You’re gaining a practice that everyone would love to be part of.”
COOPER GAMBLE, a first-year biophysics student at the University of Southern California is also working in the Mayo Clinic’s radiology informatics lab building Deep Learning tools. He addressed the limits of artificial intelligence in an address titled, ‘AI needs to know what it doesn’t know.’
Gamble gave an example of how an AI algorithm might bump up against the unknown and make a mistake.
A radiologist could be given a particularly difficult case – perhaps an ER patient who presented with a severe headache, vomiting and a loss of balance. “So, you know you’re looking for a haemorrhage, but you just can’t find it,” said Gamble.
He continued, “The first thing you notice are some small, high intensity regions around the midline, but you can’t say for sure whether it’s bleeding or calcification.”
As well, you notice that some of the skull seems to leak into the parenchyma, but you can’t definitively
conclude that it’s an epidural hematoma.
While you’re stuck, and uncertain about the answer, Gamble said this is a critical difference between humans and AI systems.
An AI algorithm will, instead, suggest a diagnosis. It will give its solution a measure of accuracy, say 99 percent.
“However, in a case as challenging as this one, it would probably be wrong,” said Gamble. “It’s in these 1 percent of cases where uncertainty becomes critically important.”
He said that AI must be made more trustworthy by using uncertainty quantification, also known as UQ.
“You could think of UQ as a lingua franca between humans and AI,” said Gamble. “It communicates the amount of unknown information about a given problem.”
It would have been better for the AI system to have told us it didn’t have enough information to make a definitive diagnosis and needed additional review from a human physician.
Gamble noted that in the past three years, only 3 percent of all AI-related articles in the esteemed Journal Nature have referenced UQ.
And only 8 percent of AI-related articles in Radiology have discussed UQ.
Gamble stated: “So you may ask, what can I as a physician whose closest contact with AI has been this Fast Five talk, do to shine light on the uncertainty quotient? It’s simple, talk about it.”
Actually, AI and its limitations have been avidly discussed by radiologists for the past five years. Nearly every hospital radiology department has test projects under way, and the RSNA conference itself has held dozens of educational sessions and workshops. Moreover, the keynote speaker at last year’s conference, Dr. Siddartha Mukherjee, addressed the issue of trustworthiness of AI systems in medicine.
Nevertheless, one must give Gamble credit for speaking at the Fast Five and for publicizing the idea of the uncertainty quotient (UC).
DR. SAURABH JHA, an associate professor of radiology at Penn Medicine, in Philadelphia, described Project Khumba, a 10-day trek in April 2022 to provide AI-powered X-ray services in the remote and underserved region surrounding Mount Everest.
Dr. Jha, along with colleagues from AIcompany Qure and portable X-ray developer MinXray, investigated the lack of medical care there and gave X-rays to patients in the region, including the Everest Base Camp. They believe it might be something for the Guiness Book of Records, with both X-rays and AI used at the highest altitude ever – nearly 18,000 feet.
“Along with our Sherpa partners, we did something very audacious,” said Dr. Jha. “We pushed the limits of imaging … in one of the most inhospitable terrains, where the practice of medicine is constrained by the environment.”
He noted that MinXray has been able to create a compact X-ray machine that can fit into a backpack. It’s wireless and is powered by a battery; it is also equipped with AI from Qure that’s able to help analyze X-rays.
The whole Khumba region surrounding Mount Everest has only three physicians, none of whom are radiologists. In future, technology of this kind could help them make accurate diagnoses.

Dr. Jha, a specialist in chest X-rays, described the importance of this. A Sherpa employed with fixing ropes for people climbing up the mountain – a very dangerous job – had a progressive cough “which he ignored until he could ignore it no more.”
The group X-rayed him at Base Camp and determined that it was HAPE – high altitude pulmonary edema, a potentially dangerous medical problem.
“It is a diagnosis that’s delayed in Sherpas because if one makes a false diagnosis of HAPE, the Sherpa loses his livelihood.”
Dr. Jha added, “So doctors are very reluctant to make this diagnosis until they’re sure. And often when they’re sure, it becomes quite life-threatening.”
By diagnosing the Sherpa’s problem, they may have saved his life.
Dr. Jha observed that the group X-rayed people along the way to the Base Station, stopping at several Sherpa settlements. At the main outpost, he quipped, there were more Irish pubs than doctors – a sign of the many tourists and mountaineers who clamber through each year.
“Our goal was to bring the X-ray to the people,” he said. “If we are to democratize imaging, we need to get to the patients when the patients cannot come to us.”
Even equipped with a backpack-sized X-ray machine, it’s still difficult to deliver
CONTINUED FROM PAGE 6
gists, dermatologists, gastroenterologists and other specialists, and offer questions germane to their areas of expertise.
For example, a dashboard for dermatologists – at the time this article was written – included questionnaires about atopic dermatitis and skin cancer.
After completion, the payment is processed within a few hours, while a face-to-face meeting would normally take weeks to process.
Meanwhile, the pharma and medical device companies that posted the surveys can see results in real-time, as the survey is picked up by clinicians, and they can analyze the data in many ways – comparing results by province or over time.
So, a company could run a similar
care. There are places with rocks, where doctors and staff need to jump from one to the other.
The group demonstrated how useful portable X-ray and AI could be in a remote territory. While Mount Everest is an extreme example, in terms of altitude, there are many more areas around the world that could benefit from the technology.
“Never before was I more proud of being a radiologist than when I was at 18,000 feet,” said Dr. Jha. “I realized that imaging is not an indulgence for the rich but a necessity for the poor.”
DR. JESSICA WEN, a radiology resident at Stanford University, aimed to convince her audience to report the ethnic and racial breakdown of their cohorts – the groups being studied – when they conduct research. Dr. Wen is also the creator of RISE, an initiative that’s striving for racial justice in medical research.
She stated that since the Second World War, medical researchers have chosen to be colourblind, thinking it would be helpful for racial minorities. However, Dr. Wen pointed out numerous areas where racial and ethnic minorities have different medical problems than Whites.
“During the COVID-19 pandemic, all populations of colour, including Black, His-
question in three different surveys, for example, and then compare the responses.
“That kind of analysis could normally take a research company months,” said Doulas. Using KeyOps, the answers are obtained in days or even minutes.
To do so, the system makes use of artificial intelligence, something that
Research that used to take months to roll out and compile can now be done in a matter of days.
Doulas says differentiates KeyOps from its competitors. “We’re the first in the market with this,” he said.
KeyOps also benefits from a strong management team. With two physicians on board, the company can quickly check on whether its surveys and out-
panic, and Asian Americans, experienced case fatality rates two to three times higher than non-Hispanic Whites,” she said.
She asserted that pulse oximeters, “a fundamental and pervasive healthcare device”, were built colourblind.
Because they weren’t as effective for non-White minorities, pulse oximeters resulted in a phenomenon called hidden hypoxemia. “And that resulted in clinically delayed care for all populations of colour, with the Black and brown populations suffering the worst disparities,” said Dr. Wen.
She noted that with the rise of artificial intelligence and genomics, we’ve discovered that the relationship between race, ancestry and healthcare is complex.
“Allow me to use my own population as an example,” said Dr. Wen. “Due to socioeconomic factors, one in 12 east and southeast Asian Americans are chronically infected with hepatitis B.”
That compares with just one in 1,000 non-Hispanic Whites. As well, due to genetic factors, Asian women have higher breast densities than non-Hispanic Whites. And women with high breast densities have up to a six-fold increased risk for breast cancer.
“Now, knowing this as a physician and a radiologist, I will be doing a disservice to my population – and all populations of colour – by failing to seek out and incorporate such disparities in disease screening and surveillance,” Dr. Wen said.
She noted that in 2022, the U.S. Federal Drug Agency mandated that all clinical trials report the ethnic and racial breakdown of their research cohort as part of their diversity action plans. She believes that radiologists should be doing this too, in their research studies.
In helping with population health and combatting social inequities, Dr. Wen said radiologists can make a significant difference.
“As radiologists we are the gatekeepers of disease screening, disease diagnosis, and treatment response,” she said. “We are also leaders in AI-assisted healthcare and Big Data.”
She continued, “It is our duty to ensure that we are not overlooking the 40 percent and growing population [in America] that is a population of colour.”
reach methods will appeal to doctors.
“They’re able to tell us a lot about the software, whether it’s easy to use and how best to engage the physician community,” said Doulas. “They also provide us with their medical expertise.”
Doulas commented that the KeyOps solution is particularly useful for companies that want fast insights. In future, the company will expand its reach to physicians south of the border. As well, KeyOps is looking at solutions that connect drug companies with pharmacists.
“There have been a lot of regulatory changes in the pharmacy sector,” said Doulas. For example, many provinces are expanding the scope of practice for pharmacists, enabling them to diagnose patients and prescribe therapies as well as dispensing them. The KeyOps platform could provide drug companies with more information about how pharmacists plan to adapt to these changes.
ccording to Gartner, who publish the now well-recognized “hype cycle” of emerging technologies and their relative maturity and adoption, generative AI and AIaugmentation are approaching their peak in hype, which is unlikely to surprise anyone.
Generally speaking, the buzz is exceeding delivery of value from AI at the present moment, particularly when we talk about primary care.
With that said, let’s dive into talking about what I think lies ahead in the near future. Here are some of my thoughts for how AI will impact preventative and primary care in 2024, broken down by the perspective of different players in the care delivery system:
Clinics and administrative staff: LLM-based tools will begin to become the patient’s “front door” for tech-savvy care delivery organizations; the key value will be reduction of admin burden, which will translate to improved work experience for admin staff as well as cost savings for clinics (reduced staff).
Patients: People will slowly become more comfortable with LLMs as their first stop for general medical advice (compared to a Google search).
The availability of medical-specific LLMs will additionally mean more trust and credible options for the public to have their questions answered.
However, my guess is that by year end, Google search will still remain the primary resource for searching for medical information.
Bard (Google’s general purpose LLM), which is currently only available in the US, will eventually become more deeply integrated into Google, though my guess is Google will retain both classic search along with Bard results, given how deeply their legacy search in entrenched in their business model as well as with the general public.
Additionally, on average, use of an LLM for medical information will not tangibly make patients more “informed” than if they had used a Google search, and it will not appreciably decant patients away from basic primary and preventative care.
Clinicians: The dominant forms of LLM utilization by primary care clinicians will be ambient scribe
and general LLM use for medical reference purposes.
Penetration of ambient scribe usage in the market will increase over the year, though I think by year end that number is unlikely to be more than 20-30 percent in North America (certainly it won’t be the majority).
There will also be an increased utilization of stand-alone LLM usage for medical reference and clinical decision support, as the market gets flooded with “medically fine-tuned” GPTs on OpenAI’s store, and there is a proliferation of other LLMs that are either medical foundational models or fine-tuned for usage with medical knowledge. We will see trusted
Ambient scribe tools will soon show additional functionality, such as the ability to create automated post-visit letters, billing and coding.
brands bring their own models into the public market, and I anticipate Mayo Clinic and UpToDate to be amongst those throwing their hat in the mix.
Medical schools and academia: The pressure to incorporate and respond to the acceleration of AI into medical education will begin to rise dramatically in this year. Beyond isolated sessions,
I doubt significant real progress will be seen this year (nor will AI become a core competency for clinical trainees in 2024, as I advocated for here).
The exception to this will be newer programs/schools that may benefit from starting with a clean slate (examples being the Kaiser Permanente School of Medicine and the Toronto Metropolitan University School of
Dr. Puneet SethMedicine). We will continue to see a rise in continuing education programs and certificates in relation to AI in medicine come onto the market for healthcare providers already in practice that are looking for a primer.
Technology: If 2023 was defined as the year of LLM experimentation and ambient scribe’s entry to the market, 2024 will be the year of maturation and specialization.
Ambient scribe penetration in the market will increase (though a significant fraction of the market will be impervious to the change).
Ambient scribe tools that benefit from EMR integration will be able to demonstrate their value-add more clearly, with the release of functionality such as automated post-visit tasks (letter generation, billing, coding, etc.)
Ecosystem: Major corporate players (who have historically failed to make a meaningful entrance into primary care delivery) will be more likely to succeed in the present climate.
It will be interesting to follow of the progress of Walmart Health and Amazon Clinic in particular.
Bottomline, my prediction for 2024 is that while we will see an increased usage of AI tools in primary care this year, the gap between what AI can do and its real-world usage in clinics will only widen.

There are many reasons for this, for which the baseline inertia to change in healthcare being just one point. A more nuanced factor is that the pace of change with which AI-based technologies (LLMs in particular) are advancing is putting virtually every industry on edge.
Even though the state of primary care is dire in both the US and Canada, healthcare is simply not designed in current configuration to be able to handle such a velocity of change.
Remember that fax machines are still pervasive in healthcare, despite the fact that more compelling technology has been available for decades.
This article was excerpted from Dr. Puneet Seth’s original article on Substack.
https://puneetseth.substack.com/
The healthcare sector has always been at the forefront of technological advancement, from leveraging the first computers in clinical research to the development of robotic surgery. Medical professionals have a culture of innovation and adaptability when exploring the latest therapies and surgical devices.
Paradoxically, these same professionals often use outdated administrative systems and platforms.
Many medical practices continue
to use devices like fax machines to send important documents. Canadian doctors already spend 18.5 million hours per year on unnecessary administrative work, equal to more than 55 million patient visits. Referrals and forms are often completed manually or using outdated technology, further slowing the process.
Yet doctors are still reluctant to transition away from these older methods. Why are tech-friendly medical professionals so hesitant to update their administrative processes, and what techniques can healthcare providers use to over-
come any hurdles to implementing new technology?
The biggest barrier to digital transformation: For many healthcare professionals, avoiding administrative upgrades stems more from psychological resistance than practical considerations. Some worry that
Physicians worry that adopting new systems and leaving their faxes behind will disrupt workflow.
replacing outmoded systems could disrupt workflow, so they continue using legacy administrative procedures even when more efficient digital solutions are available. With this mindset, change only occurs when systems become irretrievably broken.
Just because a process is well-established does not mean it is efficient or secure. Doctors believe the integration of new technology will lead to confusion or errors, but legacy systems jeopardize patient data security.
For example, misdirected faxes are the leading cause of unauthorized
Imagine a city with mismatched pipes. The pipes from the lake don’t line up with the pipes at the water treatment plant. And the pipes from the water treatment plant, don’t line up with the pipes connected to your home. You can access water in your kitchen, but you can’t in your bathroom.
With such a misaligned and inaccessible system, you wouldn’t be able to drink a glass of water. A city couldn’t function like this, and neither can our healthcare system.
That’s where interoperability comes in. Interoperability enables information to flow seamlessly between care providers and solutions (a.k.a. have matching pipes and drinkable water).
And when different parts of the health system are interoperable with one another, health information can be exchanged seamlessly. This improves continuity of care, collaboration between health providers, and patient access to their health information.
By breaking down data silos, it also reduces inefficiencies within the health system.
To support this goal, Canada Health Infoway, in partnership with Health Canada and the provinces and territories, developed the Shared Pan-Canadian Interoperability Roadmap.
This Roadmap provides guidance to governments, health system managers and industry on common standards needed to support the secure transfer of health information from different systems and to patients themselves.
Once implemented, it will improve the quality and safety of patients’ care by standardizing health information so that it can be securely accessed wherever patients go for care. Using standards for health information will also help administrators, researchers and decision makers better understand and compare aggregated, de-personalized health data across Canada, providing valuable insights needed to improve the health system and inform public health responses.
The Roadmap identifies common priorities and programs that are essential to enhance the experience of clinicians and patients across the country. One example that highlights the potential of an interoperable system can be found with patient summaries.
Patient summaries are simple, yet quite impactful: they are a portion of an individual’s health record, comprised of the most important information a care team would need at the point of care, such as a patient’s medications, allergies, immunizations, and more.
Standardizing this important data is an effective and sustainable way to help data flow and improve the coordination of care, clinical workflow efficiencies, and better health outcomes. including patient safety. Without this standard, healthcare domains remain siloed and unable to easily communicate with each other.
When patient data is not available, clinicians must deploy various workarounds. Reconstructing patient histories for each encounter represents considerable time
and effort spent on the part of the clinician. In some cases, clinicians contact the patient’s last point of care to seek information directly.
Clinicians may also rely on the patients themselves to provide their history. Not only does such an approach risk important health information being omitted or misunderstood, but it can also undermine patient confidence in their care team.
To address this gap, Infoway led the development of the pan-Canadian Patient Summary Specification (PS-CA) based on the IHE International Patient Summary specification and the HL7 IPS Implementation Guide. Once implemented, Canada’s Patient Summary standards can expect to deliver:
•Enhanced communication between health providers: Bridged silos within the health system enable more effective coordination and transitions of care, in addition to improved support for clinical decision-making. The ability to communicate between different solutions, and/or different jurisdictions also facilitates cross-jurisdictional patient flows.
•Improved provider experience and increased satisfaction: More accessible and better-organized patient information leads
to significant time savings, freeing time to spend with patients. Reduced administrative burden, improved workflow efficiencies and more targeted, effective use of practice hours helps prevent clinician burnout and facilitate clinician work-life balance.

• Improved patient experience: Patients will not need to repeat/explain their clinical histories at each new clinical encounter; a greater proportion of the visit can be devoted to strengthening the patient-provider relationship and to the health issue at hand. Patients who are travelling or otherwise outside of their home jurisdiction will find it easier to seek care, as extra-jurisdictional clinicians will have better access to their pertinent health information.
•Improved data quality and patient safety: Clear, consistent records of past tests and results enable more focused investigations and testing, with reduced redundant/duplicative tests. Patient safety is improved through the availability of more
timely, accurate information about the patient’s medical history, potentially preventing harm, delayed care or inappropriate treatments.
•Supports the provision of virtual care: Providers delivering care through different modalities/solutions can access the same health information about a patient.
Consistent access to information and better communication also facilitates encounters with unfamiliar providers at the point of care (i.e., a provider delivering care on a telehealth platform to a patient without a regular primary care provider).
•Better health outcomes: Consistent access to health information aids decisionmaking for clinicians and patients and supports proactive health management. Better coordination and transitions of care help to increase patient safety by improving timeliness of care, reducing duplicative testing and preventing instances of contraindicated medications and/or treatments.
More effective care is received quickly, across healthcare settings.
Abhi Kalra is Executive Vice-President of Digital Health Interoperability at Canada Health Infoway.
Asurgical team at St. Joseph’s Health Care London, led by Dr. George Athwal, has advanced the use of mixed reality in the operating room using VR headsets and hologramlike images to dramatically improve the accuracy of shoulder implants.
Using cameras, a computerized headset and tracking technologies, Dr. Athwal is able to “project” the patient’s pre-surgical plan – using CT images – onto his or her anatomy during the operation.
While simultaneously watching the projection and conducting the surgery, the orthopedic surgeon can improve the accuracy of the procedure by a quantum leap – especially in more difficult cases.
“Even in normal surgeries, humans can be off by as much as 10 to 15 degrees [in placing the implant] or as much as 5 millimetres,” said Dr. Athwal. “Sometimes it’s as much as a centimetre. But using this mixed reality solution, we’re getting as close as 1.5 millimetres to where we want to be.”
Dr. Athwal said orthopedic surgeons are quite good at what they do but asserted that this technology can “make us even better surgeons.”
For several years, Dr. Athwal has been helping global medical technology giant Stryker to develop the mixed reality orthopedic surgery system, called the Stryker Blueprint MR Guidance solution. He and another orthopedic surgeon at the Mayo Clinic in the U.S., Dr. Joaquin Sanchez-Sotelo, were the first worldwide to deploy the latest system.
Three years ago, Dr. Athwal was the first in Canada to use the previous ver-
sion of the solution, in which the presurgical CT images could be viewed as a reference for the surgeon.
In the latest iteration, the 3D computed tomography scans appear as an overlay on the patient and show the surgeon the underlying anatomy. They also guide the surgeon, showing him when he is off the mark and enabling him to get back on track.
“The operations are normally done through a small incision, and we can’t see

all of the bones and underlying structures,” said Dr. Athwal. “Now we can see all of the bones. I can see when I’m off, and I can correct my positioning.”
Dr. Athwal, a surgeon with St. Joseph’s renowned Roth McFarlane Hand and Upper Limb Centre, said he has a passion for developing new solutions that apply mixed reality to surgery. He is also a professor at Western University’s School of
Medicine, where he supervises engineering students working on novel biomedical technologies, along with medical students.
He said the Stryker solution, which he helped devise, could be adapted to other orthopedic surgeries, such as knee, hip and spine.
While it’s a new method of conducting surgeries, and one that has a futuristic appearance with surgeons wearing headsets as they work, Dr. Athwal said it’s likely to become “the standard of care in five to ten years.”
That’s because the improvements in accuracy that it enables are so profound.
Dr. Athwal was part of a team that worked with Stryker, a manufacturer of shoulder implants, and Microsoft Corporation, manufacturer of the HoloLens 2 – a holographic headset – to develop the mixed reality shoulder replacement technique.
He has since performed numerous surgeries using the initial version of the technology and is in demand to provide demonstrations worldwide.
Involved in the development of this software and technology for the past 10 years, the London surgeon says, “it feels like you’ve been watching your child grow and become increasingly successful at every stage.” He envisions this next generation of the system being particularly instrumental for more complex shoulder replacement patients – those with the greatest amount of bone deformity and disease.
“For the most challenging cases, where implant positioning is critical to successful patient outcome, this technology is a game changer.”
Researchers are also creating facilities to test hospital-at-home technologies before they’re implemented.
BY DIANNE DANIELIt’s been more than two years since Montreal’s Jewish General Hospital launched its innovative hospital-at-home program (Hospital@Home) to help patients recover at home while being remotely monitored using digital technology.
What started as an effort to free up bed capacity and keep people safe during the pandemic is now a burgeoning multidisciplinary program, treating 800 patients from January 2022 to January 2024 with a 93 percent patient satisfaction score. Unanimous feedback is that virtual care is preferred over a hospital stay.
“We’re really aligning with the vision we have in our organization, which is to provide care everywhere,” said Erin Cook, director of Quality, Transformation, Evaluation, Value, Ethics and Virtual Care for CIUSSS Ouest-de-l’Île-de-Montréal, the regional integrated university health and social services centre to which Jewish General belongs.
There’s no magic recipe to follow, she added, but there are ingredients she believes are contributing to and supporting the successful rollout of hospital-at-home services at the hospital.
For one, the hospital has adopted a strong culture of innovation that encourages engagement and transformation. The organization is also certified in lean six sigma principles, and staff are trained in both value-based care and the Agile methodology for project management.
Transformation goals are supported from the top down, fostering strong collaboration between all professional teams. Home care nursing staff as well as medical partners from surgery, family medicine, emergency medicine, palliative care and cardiology are all playing an instrumental role in advancing Hospital@Home, said Cook.
Patient participation in the program remains voluntary. People are screened for admissibility based on their acuity and medical condition, and on the exclusion criteria set by each of practice area. To date, the hospital has 30 different trajectories of care that allow for safe transition of patient care from hospital to home, using the in-house command centre to help identify potential candidates and facilitate admission.
quire a digital thermometer, weight scale or equipment to deliver IV therapies.
New in the past year is the introduction of pointof-care home testing for influenza, RSV and COVID-19 for vulnerable elderly, with the ability to onboard seniors directly to the Hospital@Home program if they test positive for illness and require medical attention.
The rapid evolution of virtual care within the healthcare organization has prompted the creation of other innovative services. For example, a tele-rehabilitation program enables people with chronic pulmonary disease to receive care from the comfort of home, and an innovative pilot program at a Quebec long-term care facility is using virtual reality goggles to help remote physicians administer care to 78 elderly residents.
“Whether they are needing regular checkups or something more serious, we don’t have to transfer them to hospital,” explained Cook, adding that the
the value we were creating, the ministry in turn funded our project,” she said.
Cook emphasizes that one remaining challenge is the lengthy regulatory approval process facing healthtech companies who are looking to advance their remote monitoring devices and are seeking approval from Health Canada to grow their services here. “It’s not the same business model as the U.S.,” she said. “There’s a shift happening, but it’s taking time for this technology to be adopted across the country.”
As part of its effort to free up hospital beds and improve the quality of healthcare in Quebec, the provincial government announced plans to roll out hospital-at-home services to eight health networks in the greater Montreal and Quebec City areas in May. An estimated $100 million is to be invested in the project over the next three years, demonstrating the value of the pioneering work accomplished by Jewish General Hospital.
To help alleviate emergency overcrowding, for example, Jewish General has created a direct admission from triage to Hospital@Home. Patients arriving in the ER who require short-term observation are able to return home under the remote care of an emergency physician, supported by whatever technology is required, including an iPhone or iPad that connects them to their virtual care team.
Hospital@Home is also helping to provide around-the-clock monitoring of palliative care patients, making it easier to keep people at home with their loved ones as they near end of life. “It’s a nice, patient-centred initiative,” said Erin. “It’s nice for families and it provides them with reassurance.”
Digital devices required to support people at home are prescribed by admitting physicians within each care discipline. Some patients may be issued automated blood pressure cuffs, finger probes for oxygen monitoring, and the BioBeat chest patch for continuous vital sign monitoring, while others may re-
long-term care staff learned how to use the Microsoft HoloLens technology within hours.
“For the physician, it’s as if they are looking through the eyes of the staff member and they can go into Microsoft Teams and have an accurate visualization of everything in the room,” she added. The system also enables wound care specialists to remotely guide staff through procedures they don’t often encounter.
As an early adopter of Hospital@Home, Jewish General faced several administrative challenges but has since worked through many of them. Cook credits strong support from the provincial ministry of health as a key contributor to their success, by allowing for physicians to use the same billing code for patients receiving virtual care that they do for hospitalized patients, for example.
Comparing a 20-bed hospital unit to a 20-bed virtual unit, Cook did the math to show annual operating savings of roughly $1.5 million and a staff reduction of 46 percent. Length of hospital stay has also decreased. “As we showed results and demonstrated
Manitoba is another Canadian province looking to expand virtual care. Last November, the University of Manitoba and the Health Sciences Centre (HSC) Foundation announced the creation of a new research hub dedicated to studying how technology can support patients in recovery, people with disabilities and older adults who want to live independently at home.
Jacquie Ripat, professor of occupational therapy at the College of Rehabilitation Science and vicedean, academic affairs, of the Rady Faculty of Health Sciences, was appointed endowed chair of the new technology for assisted living (TAL) program.
Over the next five years, researchers will be exploring how existing and emerging technologies can be used to make living spaces more accessible for people with different needs.
The interdisciplinary projects include national and international collaborations primarily aimed at helping seniors and patients with chronic illnesses, rehabilitation or disability needs, as well as their families.
What’s exciting, said Ripat, is the creation of a smart living lab environment at the faculty of Health Sciences’ College of Rehabilitation Sciences. The virtual suite replicates everyday living quarters, including a kitchen, living room and two bathrooms, and is outfitted with lift systems, remote controls to operate lights, TVs and window coverings, smart floor mats and motion sensors to detect time, location and frequency of movement.
Whereas smart home technologies are sometimes viewed as a modern-day convenience, for those facing health challenges they can be life changing.
It might be as simple as using automated solutions to provide reminders to take medications, alert if a stove is left on, or enable someone to see who’s at their door before using a remote locking mechanism to allow entry, but the over-arching goal is to pro-
mote autonomy, participation and inclusion for people in need, she said.
The smart suite is both a place where researchers can test solutions and where patients can practice them. A future goal is to use the room as a temporary discharge suite, so that patients who are being discharged from the HSC rehabilitation hospital can trial equipment to see what solutions work best for them.
“There is an individual perspective that needs to be taken in all of this,” said Ripat. “It’s not just, go out to Best Buy, purchase a whole bunch of stuff and put it in place. It’s about knowing your physical, cognitive and healthcare needs – it’s a very complex picture.”
One project is exploring how smart home technologies can support people with brain or spinal cord injuries. Another study looked at kitchen designs to support aging in place by incorporating seated workstations, easy-access storage solutions and accommodation for mobility devices. Researchers are also considering how telepresence robots can be used to remotely support people living with dementia.
“If you had a robot in your older relative’s home … you would have the app on your phone and you could drive it to follow mom or dad, or to go look for something,” explained Ripat, noting that most robots are equipped with a computer tablet as a ‘face,’ so a loved one can see their caregiver’s face as they operate it.
“I think there are a lot of possibilities,” she added. “We’ll have to see where things go with price and availability. Acceptance will be a big one too.”
Research is also being conducted in a unique outdoor testing area where researchers can observe people using mobility devices as they navigate an obstacle course under different weather conditions. “There are labs that simulate winter, but this is ‘au natural,’” said Ripat. “It allows us to trial technology in authentic conditions, but in a safe place.”
As university researchers work to better understand how technology can serve as an interface between patients and the health system, the HSC Foundation intends to leverage their findings to support a broader rollout of virtual care services that were introduced during the pandemic.
The Virtual COVID-19 Outpatient Program (VCOP) launched in December 2020 with the foundation providing funding for the tablets, oximeters and thermometers to make it possible in the initial phase, enabling COVID patients to safely recover at home. Patients reported being “happy at home, in a comfortable, quiet place” while also feeling that they were “getting optimal medication attention.”
The TAL program builds on that success, said HSC Foundation CEO Jonathon Lyon. “It’s a matter of taking the program we have for assisted living and expanding it to a broader realm of virtual care. That’s really the next frontier,” said Lyon. “There’s no question that we know virtual care is a necessary component for healthcare going forward because we have these enormous demands.”
Lyon sees virtual care as one way to address hospital bed capacity challenges, as long as people continue to receive quality care. Moving forward, the foundation will
continue to work closely with hospital leadership to identify future opportunities for virtual care, including studying ways to make some healthcare procedures more accessible to people living in rural communities or on remote First Nations.
“Whether you live five minutes from a care facility or five hours away, home is always a better option,” said Lyon. “The pandemic blew virtual care wide open and
made it not something we were kind of interested in, but something we need to take the lead on.”
Ripat will also be focusing some of the research effort on training future health providers to start including home-based technology as part of their practice and thinking about it as a good option for their patients.
“It’s fine to have all of these technolo-

gies, but someone is going to have to provide that service, someone is going to have to make that match and help people figure out whether it’s the right technology, and how to use it and support it,” she said. “In a person’s life, interaction with the healthcare system is just a blip for the most part. Let’s reduce those blips and help them function in their lives the best they can.”



ORONTO – Patients and providers can all agree, many people prefer to receive care at home, instead of in hospital, when they can.
For its part, North York General’s (NYGH) transitional care and “at home” programs are putting digital technologies and other tools to work to enable more patients to heal and age at home. In the process, they are redefining the hospital’s role in community care.
“People who are seriously ill or need emergency care will always receive excellent and compassionate care at our hospital,” said Zahra Ismail, NYGH’s director for Transitional Care, Community Integration and Ambulatory Care.
“Our goal is to provide each person with the right care in the right place. So, when the patient no longer needs acute care, we help them to flourish at home or in a community environment.”
NYGH serves a population of 500,000, which includes Toronto’s highest concentration of seniors. Looking to the future, NYGH needs to meet the needs of a growing and increasingly diverse population that is living longer with multiple chronic diseases.
In addition to being a more comfortable and convenient option for patients and their caregivers, care at home has allowed NYGH to reduce the rate of patients waiting in a hospital bed for alternative care in the community.
This is freeing up nurses, physicians and other vital human resources, as well as hospital beds for other patients and has a positive impact on wait times.
NYGH has the lowest ambulance of-

fload wait times in Toronto and is a provincial leader in Emergency Department wait times.
Integrated and team-based models of care, coupled with technology, are also enabling traditional hospital services to be delivered where people are, whether that is at home, a local clinic, and even at work.
“Through NYGH’s Digital Strategy, we are harnessing innovations across our hospital and six community sites to deliver the best outcomes for each individual,” said Duska Kennedy, NYGH’s vice president Strategy, Digital and chief digital officer. “We want people to experience NYGH as a hospital without walls – a trusted place to receive care throughout all life stages that also brings care into their communities and homes.”
NYG@Home: NYGH, in partnership with SE Health and Bayshore HealthCare, provides NYG@Home for seniors transitioning from hospital to home. The 16-
week program provides intensive home and community support, including individualized discharge and care plans.
In addition to in-person care, patients are supported through remote patient monitoring (RPM), using the patients’ phone, tablet or computer to monitor vital signs, blood sugar, and weight and relaying the information to the NYG@Home team.
“Remote patient monitoring allows the patient and their family to be involved in their own care,” said Angel Javonillo, NYG’s Integrated and Transitional care coordinator. “If RPM detects low blood pressure, a nurse will follow up, check for other symptoms and take the appropriate action.”
NYG@Home also educates patients and caregivers on what to do about abnormal readings. “It gives patients greater control,” added Javonillo.
North York CARES: North York Community Access to Resources Enabling Support (North York CARES) provides high-
intensity home care to patients with complex needs who are waiting to move to long-term care or another setting.
A collaboration between NYGH, Home and Community Care Support Services, VHA Home HealthCare and Bayshore HealthCare, the program allows patients with complex needs to remain at home for up to three months after a hospital stay.
Each patient receives a customized and integrated bundle of services designed to restore their health and ability to manage everyday activities. Services can include home and community care resources, restorative care, dementia care and caregiver support. It is also the first program of its kind to use RPM.
“The goal is to give the patient and family a better experience,” said Steve Burden, NYGH’s interim clinical team manager for Integrated Transitions. “North York CARES also reduces ED visits and readmissions to hospital.” The program, which began in 2000, supported 67 patients in 2023-24.
NYCAST: In summer 2023, NYGH and the North York Toronto Health Partners (Ontario Health Team) launched the North York Congregate Access and Support Team (NYCAST) to improve health outcomes for people living in North York’s eight long-term care (LTC) homes.
Again, technology is key to delivering the program. NYCAST’s specialized Nurse Practitioner-Led Outreach Team provides virtual and on-site clinical support for residents and caregivers, including primary care, injury and illness prevention, and palliative care.
Janine Hopkins is Chief Communications Officer & Executive Lead (NYGH), North York Toronto Health Partners.
Recently, I chaired a panel consisting of a cross section of healthcare specialists, experts, and innovators who have been at the forefront of change. They shared their experiences in their organizations and from across the healthcare spectrum.
Dr. Gregg S. Meyer, president of Community Division and executive vice president of Value-Based Care at Mass General Brigham Healthcare at Home talked about the exciting role of technology in moving care back to the home and highlighted its benefits.
“When people are in their home, they move around more than they do when they’re sitting in a hospital bed. Mobility is really important to health. It improves outcomes,” he said.
He added that not only does care delivered at home come with a lower price tag but it also “brings back joy to caregivers.”
Most notably, he underscored that, “Our ability to complement inpatient care with care at home actually gets us out of the current capacity crisis that many of us
experience. This is a greenfield opportunity that we’re not going to have again.”
Dr. Lawrence Rosenberg, president and CEO, Integrated Health and Social Services University Network at WestCentral Montreal Health expanded on the benefit for providers. When you deliver care in the patient’s home, in contrast to seeing them as out-patients at the hospital, higher quality information can be gathered.
The care provider can see how the patient lives and make decisions accordingly. “You can actually see, not just what a patient tells you about their diet, but actually look in their refrigerator. That gives you a level of insight that you don’t get from anything else,” said Dr. Rosenberg.
When speaking about the benefits for patients he added that, “Families are telling us that they have more face time with the treating team in the virtual program than they had experienced when they were being treated in the hospital.”
Scott Dulchavsky, chief of Surgery and CEO of Henry Ford Health System Innovation Institute, drew from his extensive experience as a principal investigator for NASA and for the National
Space Biomedical Research Institute in Houston, Texas.
“In space, during long duration missions, there are about 600 conditions that keep me up at night, and strangely enough, they’re the same conditions that we see on the planet,” he said.
He further noted the similarities between healthcare delivered in space and on Earth, saying that, I’ll give you a
Families say they have more face time with the treatment team in the virtual program than in the hospital.
quick example. “In space, we worry about collapsed lungs when we are out doing spacewalks and we don’t have an X-ray. That seems to be a problem. But we have an ultrasound machine, which showed that cute little thing about the echo. So, we said could we use this? Nobody had done that before. We did use it and it worked, and now it’s a terrestrial standard.”
John Torous, MD MBI, director of the
Digital Psychiatry Division, Department of Psychiatry at Beth Israel Deaconess Medical Center, talked about the opportunity for behavioral health.
“People have phones and sensors. So, we can bring a wealth of new data into our clinical teams. We can understand our patients’ behaviors, their sleep, their step count, what influences them and use that data to personalize care and make health at home a better care.”
Liz Fowler, who leads the innovation center at CMS, the largest healthcare player in the United States, talked about, “Providing regulatory waivers and more incentives for care to be delivered at the point where you’re actually meeting patients’ needs. When you’re meeting with the patients and their caregivers, you can see the environment where they live. Do they have heat? Do they have enough food? Do they have other needs that obviously impact health? This helps keep people out of the hospital.”
Dr. Alan John Forster, is VP in Innovation, Transformation and Director of Clinical Performance at McGill University Health Centre.
sidered standard way for emergency department doctors and on-call interventional cardiologists to share ECG images because they’re secure and protect patient privacy.
Using faxes or e-mail to communicate is inefficient for rapid point-of-care decision-making when time is of the essence, yet they remain the norm at most Canadian hospitals, says Mir.
Canadian guidelines say that once a STEMI patient arrives at a hospital emergency department, they need to be diagnosed and receive treatment at a regional catheterization lab within two hours, where appropriate, for the best chance of survival and to avoid major adverse cardiac events.
“These patients needed to be diagnosed as fast as possible and transferred to a catheterization lab if needed, but this wasn’t happening as efficiently as it could because we were using outdated technology,” says Mir.
Time is of the essence: Mir and Syed felt that a secure, privacy-compliant, point-ofcare tool would be a game-changer for hospitals and STEMI patients, so over the subsequent years during their off-hours, they developed the SMART AMI app. “It was something we did on our own time, after work and on weekends,” says Mir. “It became a passion project.”
The SMART AMI app has been used by HGH and the region’s emergency departments since 2020 as part of two pilot projects led by Mir and Dr. Madhu Natarajan, an interventional cardiologist at HGH. It has shown to speed up communication and get STEMI patients to HGH’s catheterization lab faster.
The first trial, from 2020 to 2022, allowed Niagara area emergency department doctors to send ECG images to
HGH on-call interventional cardiologists using the app. Based on that trial’s success, a grant was secured from the Hamilton Academic Health Sciences Organization for a two-year trial launched in 2022 to implement the app at the 14 hospitals in the region that send their STEMI patients to HGH.
The HHS-based Centre for Evidence Based Implementation trained the region’s more than 350 emergency doctors to use the app and supported the app during the evaluation process.
When the trial ends in the spring of 2024, the smartphone app is expected to remain at HGH as a leading-edge communications tool. There is also hope that the program can be expanded to help with communication between paramedics and interventional cardiologists when a STEMI
patient is identified on an ECG done by the paramedics in the patient’s home. Currently, only verbal rather than visual communication is used.
“Every single emergency department doctor in our region that refers STEMI pa-
The app helps emergency department doctors reach interventional cardiologists more efficiently.
tients to HGH has access to this app,” says Natarajan, who considers it an excellent tool. Natarajan is also the provincial task group chair for STEMI at the Ontario Health cardiac services team.
“This has been about more than just
building the technology of the app. Quick recognition is key, so patients can receive the most appropriate care. We’ve been able to navigate the many challenges in implementing such a tool across a complex healthcare system to help with rapid communication between different healthcare providers in helping patient management.”
The app’s many supporters also include Dr. Alim Pardhan, site lead at HGH’s emergency department.
“It definitely helps emergency department doctors reach interventional cardiologists more efficiently,” he says. “That’s especially helpful for emergency department doctors working in regional hospitals. It totally speeds things up in terms of getting the patient to where they need to be, faster and more efficiently. It has certainly been a very helpful tool.”
CONTINUED FROM
get all the necessary information.” Implementing one digital patient record will save time between nurse shift handovers as well as transfers between TBRHSC and other facilities in the ONE network.
“Our member facilities cover a large geographic area, but all of the ONE HITS sites are working together to put the patient at the center of their experience and break down facility barriers,” Muto said. “Transfer volumes are quite high within our membership right now, so if we can save time and reduce errors, that’s incredible improvement.”
The North West anticipates establishing a single patient record will improve clinician experience and ease of use. In Northwestern Ontario, many doctors and nurses
hold positions at several facilities – one day working at a hospital and another in a local family practitioner office. By joining ONE HITS and gaining access to a single MEDITECH Expanse instance, clinicians
The Expanse EHR has already been vetted by 23 plus hospitals and is customized for their specific populations.
will benefit from easier transitions as they move between sites.
“The Expanse EHR has already been vetted by 23 plus hospitals and designed specifically around how we work in remote and rural communities,” Fedell said. “And as we take it one step further by joining
ONE HIS, we can provide more efficiencies than we ever could independently.”
As part of its digital transformation strategy, TBRHSC will leverage Expanse to address health equity. Residents of Northwestern Ontario have higher than average rates of several chronic health issues, including diabetes, COPD, and alcohol use disorder. Various tools embedded in Expanse will provide advanced clinical decision support, alerts for possible drug interactions, and prompts for potential complications like sepsis.
“Thunder Bay and ONE HITS have a forward-thinking approach to meeting the unique challenges of the region,” said MEDITECH director Nick Palmieri. “We are excited to partner with them and share the goal of transforming healthcare delivery throughout the North.”
disclosure of personal health information in Ontario, according to the province’s Information and Privacy Commissioner. Nearly 5,000 privacy breaches related to misdirected faxes were reported to the commissioner’s office in 2021.
Today’s administrative software platforms are designed to minimize risk. Encrypted cloud-based systems actually offer higher security against unwelcome access and tampering than traditional methods of information sharing between healthcare professionals.
New administrative technology also reduces operating costs through streamlined operations. Unlike fax machines or regular mail, digital platforms are designed to be intuitive for today’s techsavvy workforce. These systems simplify complex interactions, expedite repetitive tasks, and even automate correspondence with third parties.
How to overcome uncertainty and embrace new technology: Despite compelling arguments for adopting new administrative software, physicians’ resistance to change requires a solution that
takes their emotional barriers into account. By working as a team, providers at a healthcare practice can combat the reluctance to step out of their comfort zone, ultimately making their practices more efficient and reducing unnecessary administrative burdens.
Dispel worry through research: At the prospect of implementing new technology, providers can be quick to think of potential problems and worst-case scenarios. It can be helpful to look up the new software and see if other users encountered those concerns or if the tool actually improved workflow. In most cases, the evidence will indicate that new technological solutions are a net benefit for any medical practice.
Talk it out together: Before adopting a new software tool, give everyone an opportunity to air and address any concerns. The team can go through the proposed technological solution’s information, performance statistics, and case studies as a group to understand the potential benefits of an upgrade. Those most opposed to the upgrade can play the ambassador for the product. By teaching the rest of the team
why a new upgrade is a good idea, they’ll also be working through their own reluctance.
Prepare for the change: Being proactive when implementing new technology is the key to preventing workflow issues down the line. Host an onboarding session with the product’s sales or training team. Not only will this directly counter fears about the new software taking too long to
It can be helpful to see if other users have encountered the concerns of naysayers, or if the tools improved workflow.
learn, it will also empower providers to make the most of the new software and help with smooth integration.
Ultimately, the better medical practitioners understand how to use new technology, the more they will embrace that technology in every aspect of their practices. Not taking steps to confront psychological barriers will only make the reluctance to upgrade last longer.
Medical innovation means adminis-
trative innovation: The key to overcoming psychological barriers lies in acknowledging the inherent resistance to change and addressing it with a combination of research, teamwork, and preparation. By understanding the benefits of new technology, healthcare providers can begin to dispel the fears associated with change.
The healthcare industry needs to extend its spirit of technological innovation to administrative practices. Digital solutions for healthcare administration not only streamline operations but also enhance patient data security, ultimately benefiting both their practice and their patients. The shift from outdated methods to modern systems is not just a technical upgrade, it’s a step toward a more secure, efficient, and patient-focused healthcare environment.
Gabriel Tick is the founder and CEO of Opifiny Corp. and has been a business leader and entrepreneur for nearly 30 years. He is dedicated to creating ‘Great Places to Work,’ and to building dynamic technology businesses that improve patients’ lives.




































Princes’ Blvd, Exhibition Place, Toronto