Contributors
Dina Al-Zubeidi, MD
Clinical Assistant Professor ofPediatrics Division of Gastroenterology
Stead Family Department ofPediatrics, Carver College ofMedicine University oflowa Iowa City, Iowa [16]
William Aughenbaugh, MD
Associate Professor and Program Director Department ofDermatology
Vice Chair ofEducation in the Department ofDermatology and Director ofSpecialty Clinical Medical Education and Residency Preparation
University ofWisconsin Madison, Wisconsin [33]
LaTisha L. Bader, PhD, LP, LAC,CC-AASP Center for Dependence, Addiction and Rehabilitation (CeDAR)
University ofColorado Hospital Aurora, Colorado [35]
Rebecca Benson, MD, PhD
Medical Director, Pediatric Pain and Palliative Care Program
Medical Director for Clinical Ethics and Director, Ethics Consult Service
Stead Family Department ofPediatrics University oflowa Children's Hospital, University oflowa Hospitals and Clinics Iowa City, Iowa [12]
James D. Burkhalter, LISW Director ofDBT Programming Social Work Specialist, Department ofPsychiatry Universityoflowa Hospitals and Clinics Iowa City, Iowa [29]
Gayathri Chelvakumar, MD, MPH
Nationwide Children's Hospital Section ofAdolescent Medicine Columbus, Ohio [1]
Paula Cody, MD, MPH
Assistant Professor Department ofPediatrics University ofWisconsin School ofMedicine and Public Health Madison, Wisconsin [1]
Cassandra J. Collins, BSW, LISW
Clinical Social Worker Department ofSocial Service
University oflowa Hospitals & Clinics Iowa City, Iowa [29]
Amy L. Conrad, PhD
Assistant Professor
The Stead Family Department ofPediatrics University oflowa Children's Hospital Iowa City, Iowa [6]
Linda J. Cooper-Brown, PhD
Clinical Associate Professor
Stead Family Department ofPediatrics, Division ofPediatric Psychology The University ofIowa Iowa City, Iowa [3]
Vanessa A. Curtis, MD
Clinical Assistant Professor Department ofPediatrics Division ofEndocrinology and Diabetes University ofIowa Carver College ofMedicine Iowa City, Iowa [11]
Anthony J. Fischer, MD, PhD
Assistant Professor
Department ofPediatrics Division ofAllergy, Pulmonology, and Immunology University oflowa Children's Hospital Iowa City, Iowa [32]
IX

Chris Hogrefe, MD, FACEP
Assistant Professor
Department ofMedicine-Sports Medicine
Department ofEmergency Medicine
Department ofOrthopaedic Surgery-Sports Medicine
Northwestern Medicine Northwestern University Feinberg School ofMedicine Chicago, Illinois [27]
Sandy D. Hong, MS, MD
Assistant Clinical Professor Division ofRheumatology Department ofPediatrics University oflowa Children's Hospital Iowa City, Iowa [7]
Erin Howe, MD
University oflowa Stead Family Department ofPediatrics Iowa City, Iowa [19]
Jennifer G. Jetton, MD
Clinical Assistant Professor
Division ofPediatric Nephrology, Dialysis and Transplantation
Stead Family Department ofPediatrics University oflowa Children's Hospital Iowa City, Iowa [31]
Kathleen Kieran, MD, MS
Associate Professor ofUrology Department ofUrology University ofWashington/Seattle Children's Hospital Seattle, Washington [18]
Todd Kopelman, PhD, BCBA
Clinical Assistant Professor Department ofPsychiatry University oflowa Hospitals and Clinics Iowa City, Iowa [6]
Kathy Lee-Son, MD, MHSc
Clinical Assistant Professor Pediatric Nephrology Department Stead FamilyUniversity oflowa Children's Hospital Iowa City, Iowa [31]
Ashley Loomis, MD
Assistant Professor, Pediatric Critical Care University ofMinnesota Minneapolis, Minnesota [8]
Rebecca L. Lozman-Oxman, DNP, APRN, MSN, BSN, MPH
Pediatric Nurse Practitioner Pediatrics, New London Hospital/Newport Health Center New London, New Hampshire [28]
Elizabeth H. Mack, MD, MS
Associate Professor ofPediatrics Division ofPediatric Critical Care Medical University ofSouth Carolina Charleston, South Carolina [25]
Jessie Marks, MD, FAAP
Clinical Assistant Professor University ofIowa Carver College ofMedicine Stead Family Department ofPediatrics, University oflowa Children's Hospital Iowa City, Iowa [14]
Ross Mathiasen, MD Department ofEmergency Medicine Department ofFamilyMedicine Institute for Orthopaedics, Sports Medicine, and Rehabilitation
The University ofIowa Carver College ofMedicine Iowa City, Iowa [35]
Satsuki Matsumoto, MD
Associate ofPediatrics Department ofPediatrics, Division ofNeurology and Developmental and Behavioral Pediatrics
Roy J. and Lucille A. Carver College ofMedicine University oflowa Iowa City, Iowa [23]
Jennifer McWilliams, MD
Child and Adolescent Psychiatrist Department ofBehavioral Health Children's Hospital and Medical Center Omaha, Nebraska [3]
Gary Milavetz, Pharm D, FCCP, FAPhA Associate Professor and Division Head The University ofIowa College ofPharmacy Department ofPharmacy Practice and Science Division ofApplied Clinical Sciences Iowa City, Iowa [26]
Sarah L. Miller, MD
Clinical Assistant Professor Department ofEmergency Medicine University oflowa Hospitals and Clinics Iowa City, Iowa [10]
Ashley A. Miller, MD, FAAP Pediatrician Pediatrics
Geisel School ofMedicine at Dartmouth Hanover, New Hampshire [28]
Lisa K. Muchard, MD
Assistant Clinical Professor Department ofDermatology University ofWisconsin Madison, Wisconsin [33]
X Contributors

Blaise Nemeth, MD, MS
Associate Professor (CHS)
Pediatric Orthopedics, American Family Children's Hospital
Department ofOrthopedics and Rehabilitation University ofWisconsin School of Medicine and Public Health Madison, Wisconsin [22]
Benton Ng, MD
Pediatric Cardiologist Pediatrics, All Children's Hospital St. Petersburg, Florida [5]
Erin A. Osterholm, MD
Assistant Professor ofPediatrics Department ofPediatrics, Division ofNeonatology University ofMinnesota Minneapolis, Minnesota [14]
Niyati Patel, MD
Assistant Professor, Pediatric Critical Care University ofMinnesota Minneapolis, Minnesota [8]
Andrew R. Peterson, MD, MSPH
Clinical Associate Professor
Stead Family Department ofPediatrics, Carver College ofMedicine University oflowa Iowa City, Iowa [30, 34]
Catherina Pinnaro, MD
Pediatrics Resident, Department ofPediatrics University oflowa Iowa City, Iowa [12]
Nathan Price, MD
Clinical Assistant Professor Pediatric Infectious Diseases
Stead Family Department ofPediatrics Iowa City, Iowa [20]
Gregory M. Rice, MD
Associate Professor ofPediatrics, Division ofGenetics and Metabolism
Co-Director, WSLH Biochemical Genetics Laboratory; Director, Medical Genetics Residency Program University ofWisconsin School ofMedicine and Public Health Madison, Wisconsin [17]
Eric T. Rush, MD, FAAP, FACMG
Departments ofPediatrics and Internal Medicine University ofNebraska Medical Center and Children's Hospital and Medical Center Omaha, Nebraska [21]
Judith Regine Sabah, MD, PhD, MBA Ophthalmologist-Comprehensive and Pediatric/Adult Strabismus
Operative Care, Eugene VA Healthcare System Eugene, Oregon [13]
Melanie A. Schmitt, MD
Assistant Professor ofPediatric Ophthalmology and Director ofOphthalmic Genetics Department ofOphthalmology and Visual Sciences University ofWisconsin-Madison Madison, Wisconsin [13]
Laura Steinauer, Pharm D Candidate Student Pharmacist The University ofIowa College ofPharmacy Iowa City, Iowa [26]
Natalie Stork, MD Assistant Professor University ofMissouri-Kansas City School ofMedicine Department ofOrthopedic Surgery and Department ofPediatrics
The Children's Mercy Hospital, Division ofOrthopedics Section ofSports Medicine Kansas City, Missouri [22]
Alex Thomas, MD Allergist/Immunologist Internal Medicine/Pediatrics Presence Sts. Mary and Elizabeth Medical Center, Advocate Children's Hospital Chicago, Illinois [2]
Amy 0. Thomas, MD Allergist/Immunologist Allergy and Immunology Department Dreyer Medical Clinic- Advocate Hospital System Aurora, Illinois [2]
Elizabeth C. Utterson, MD Assistant Professor ofPediatrics Division ofPediatric Gastroenterology, Hepatology and Nutrition Washington University St. Louis, Missouri [16]
Jeffrey Robert Van Blarcom, MD Assistant Professor Department ofPediatrics, Division ofInpatient Medicine University ofUtah Salt Lake City, Utah [15, 26]
Susan S. Vos, PharmD, BCPS, FAPhA Clinical Associate Professor The University oflowa College ofPharmacy Department ofPharmacy Practice and Science Division ofApplied Clinical Sciences Iowa City, Iowa [26]
Contributors XI
Tammy L. Wilgenbusch, PhD
Clinical Assistant Professor
Stead Family Department ofPediatrics, Division ofPsychology
University oflowa Children's Hospital Iowa City, Iowa [6]
Adam D. Wolfe, MD, PhD
Assistant Professor ofPediatric Hematology-Oncology
Baylor College ofMedicine
Children's Hospital ofSan Antonio San Antonio, Texas [4]
Kelly E. Wood, MD
Clinical Assistant Professor
Stead Family Department ofPediatrics Carver College ofMedicine
University oflowa Iowa City, Iowa [24, 29]
Leah Zhorne, MD
Clinical Assistant Professor Department ofPediatrics, Division ofNeurology and Developmental and Behavioral Pediatrics
Roy J. and Lucille A. Carver College ofMedicine University oflowa Iowa City, Iowa [23]
Derek Zhorne, MD
Clinical Assistant Professor ofPediatrics Division ofGeneral Pediatrics and Adolescent Medicine
Stead Family Department ofPediatrics Iowa City, Iowa [9]
XII Contributors
lh\1
llf\�IY\�Ii\�

TestesincreaseinsizePenisgrowsin Penisgrowsin width. Development iscomplete. AGERANGE 14.5-18y andskinofscrotum length. reddens
AGERANGE 10-13.5y
SEXUALMATURITY.........,,----.;;.2-,-..., 3 RATING
PUBICHAIR 4 5

Straighthair appearsat penisbase. AGERANGE 10-15y Hairbecomes Hairisfull, Fulldevelopment. curly,coarse, limitedinarea. anddark.
AGE11y 12y 13y 14y 15y AGERANGE 14.5-18y 16y 17y
FIGURE1-3. Adolescentmalesexualmaturationandgrowth.(ReproducedwithpermissionfromHayWW,LevinMJ,DeterdingRR,AbzugMJ,eds. Current Diagnosis and Treatment Pediatrics. 22nded.NewYork,NY:McGraw-HillEducation,Inc.,2014;Fig.4-3.)
Question 2-1
The most likely diagnosis for this patient is:
A) Pseudogynecomastia.
B) Testicular tumor.
C) Gynecomastia.
D) Normal puberty.
E) Phytoestrogen consumption.
Discussion 2-1
The correct answer is "C:' Gynecomastia is a common condition in adolescent males with a prevalence of 19.6% in 10.5-year-old males, increasing to 64.6% by age 14 years It is caused by an imbalance ofestrogen to testosterone in pubertal males. The relative increased estrogen leads to proliferation of glandular breast tissue. It is important to differentiate gynecomastia from pseudogynecomastia, which results from excess fat deposition as opposed to glandular tissue. In pseudogynecomastia, tissue tends to be more widely distributed and not localized to the nipple areolar complex. This patient has a normal testicular exam, making a testicular cancer unlikely. But take the opportunity to remind him to perform monthly selfexams as testicular cancer usually presents as a painless mass. Soyproducts contain phytoestrogen, but eating tofu won't give you breasts. Have you ever seen an orchidometer? To avoid confusion, be sure to explain that it is standard practice to compare the patient's testicles to wooden beads on a string to determine the testicular volume.
Question 2-2
Management for this patient would include:
A) Testicular ultrasound.
B) Reassurance and follow-up exam in 6 months.
C) Measurement ofgonadotropins.
D) Measurement ofprolactin.
E) Testosterone injections.
Discussion 2-2
The correct answer is "B:' Given that this patient has a normal testicular exam and no signs of exogenous estrogen exposure or underlying disease, reassurance and follow up is appropriate.
� QUICKQUIZ
You are seeing a 13-year-old boy who has testicular volume of 6 mL and light downy pubic hair. What is his SMR staging?
A) Testicular volume SMR 2; pubic hair SMR 2.
B) Testicular volume SMR 1; pubic hair SMR 2.
C) Testicular volume SMR 2; pubic hair SMR 3.
D) Testicular volume SMR 3; pubic hair SMR 3.
E) Testicular volume SMR 2; pubic hair SMR 1.
4 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS
AGE
Discussion
The correct answer is ''A:'
• HelpfulTip


The average age of menarche in the United States is 12.6 years, with rangeof 11.0to 14.1. Menarche occurs earlier in African American and Mexican American girls.
� QUICKQUIZ
What is the most common breast mass in adolescent females?
A) Fibroadenoma.
B) Fibrocystic changes.
C) Rhabdomyosarcoma.
D) Hemangioma.
E) Galactocele.
Discussion
The correct answer is "/\'. Most breast masses in adolescent girls are benign. A fibroadenoma feels like a rubbery, smooth, mobile, round mass. It is nontender and usually located in the upper outer quadrant of the breast. Other common benign masses include fibrocystic changes, cysts, abscesses, and fat necrosis from trauma. Options "D" and "E" are less common benign causes. Malignancy such as option "C" is a rare cause. Before a nipple is pierced or a hair is plucked, remember to counsel that both can cause an abscess.
TABLE1-2
SEXUAL MATU RITY RATING (SMR) IN FEMALES
SMRin PubicHair Breast
Females Development Development
No pubic hair Prepubertal breasts

You are seeing a 14-year-old girl in your office for her annual exam. When speaking with you confidentially, she mentions that she is concerned that she has not yet started her period like all of her friends. She reports breast development starting approximately 1 year ago. On exam she has palpable breast tissue extending just beyond her areola and pubic hair that is thick and curly and primarily midline in distribution.
Question 3-1
Which of the following most accurately describes her SMR staging?
A) Breast SMR 1; pubic hair SMR 2.
B) Breast SMR 3; pubic hair SMR 2.
C) Breast SMR 1; pubic hair SMR 4.
D) Breast SMR 3; pubic hair SMR 3.
E) Breast SMR 5; pubic hair SMR 5.
Discussion 3-1
The correct answer is "D:' The patient described in the vignette has breast and pubic hair development consistent with SMR 3.
(See Table 1-2 for details.)
2
Sparse, downy Formation of breast hair bud, glandular tissue palpable under areola; areola is slightly widened and projects as a small mound
3 Hair becomes Enlargement of breast thicker, longer, with elevation of and curlier, still breast contour and in limited mid- enlargement of areola line distribution
4 Adult type Areola forms a sechair in qual- ondary mound over ity but limited contour of breast distribution
5
Adult quality Fully mature breast hair with spread with continuous conto medial thighs tour between areola and breast
Data from Bordini B, Rosenfield R. Normal puberta development part II: Clinical aspects ofpuberty. Pediatr Rev. 201 1;32(7):281-292; and Neinstein LS,ed. Handbook ofAdolescent Hea/thcare. Philadelphia, PA: LippincottWilliams & Wilkins; 2009.
Question 3-2
The first sign ofpuberty in females is typically:
A) Breast development.
B) Development ofpubic hair.
C) Menses.
D) Body odor.
E) Acne.
Discussion 3-2
The correct answer is ''A:' Breast development (thelarche) is typically the first sign of puberty in girls and typically occurs between age 8 and 13 years (see Figure 1-2). Breast development typically precedes pubarche (pubic hair development) though in some girls pubarche may occur first or simultaneously. Pubarche typically occurs 1 to 1.5 years after breast development. Menarche occurs approximately 2.5 years after thelarche at an average age of 12.6 years in Caucasians and earlier in African Americans and Mexican Americans. Girls reach their peak height velocity of8.25 cm/y earlier than boys at approximately SMR 3. Peak height velocity in girls always precedes menarche. Peak height velocity occurs at approximately SMR 4 to 5 in boys.
CHAPTER1 • ADOLESCENTMEDICINE AND GYNECOLOGY 5
• HelpfulTip


The first stage of puberty for males is testicular 11 enlargement, defined as a testis volume of 4 mL or greater, or 2.5 em in diameter. For girls, it is the appearance ofbreast buds.
�QUICKQUIZ
Which ofthe following is correct?
A) Adrenarche results from testosterone secretion by the gonads.
B) Activation of the hypothalamic-pituitary-gonadal axis (HPA) causes gonadarche and adrenarche.
C) Estrogen secretion causes armpit hair development.
D) All ofthe above.
E) None ofthe above.
Discussion
The correct answer is "E:' Puberty encompasses gonadarche and adrenarche. Both are separate events, but the timing typically overlaps. Gonadarche, growth and maturation of the gonads (testes, ovaries), is under the control of the HPA secretion of gonadotropin-releasing hormone (GnRH). Before puberty, release of GnRH from the hypothalamus is inhibited. Adrenal androgen secretion (dehydroepiandrosterone [DHEA] and androstenedione) causes pubic and axillary hair development, acne, and body odor (adrenarche)
• HelpfulTip


Detection ofnocturnal luteinizing hormone (LH) pulses is the first hormonal sign that puberty has started. At puberty, the hypothalamus is no longer inhibited and releases GnRH in a pulsatile fashion. GnRH stimulates the anterior pituitary to secrete gonadotropins-LH first, then follicle-stimulating hormone (FSH). FSH and LH stimulate the gonads to produce gametes (eggs or sperm) and sex hormones (estradiol ortestosterone).
Question 3-3
What is the next step in management ofthis patient?
A) Bone age.
B) Measurement ofgonadotropins.
C) Reassurance and followup in 6monthsto ayearifno menses.
D) Thyroid studies.
E) CBC.
Discussion 3-3
The correct answer is "C:' This patient is progressing through the stages ofpuberty and willlikelyattain menarche in the next 6 months to 1 year. Ifno menses occur by age 16 further workup would be warranted.
• HelpfulTip

Don't forget that isolated GnRH deficiency has been 11 associated with both Kallman syndrome and anosmia.
A mother brings her 17-year-old son for his annual health maintenance exam. When you ask if she has any concerns about him, she mentions that he sleeps all the time. She also states that he was always a happy child but recently has become more withdrawn and always seems tired. She reports that his grades have been declining, and he does not seem to enjoy activities he previously enjoyed, such as playing soccer and video games with friends.
Question 4-1
The next step in diagnosing this patient is:
A) Obtaining a CBC and iron studies.
B) Obtaininga complete psychosocialhistoryfrom the patient.
C) Thyroid testing.
D) Intelligence testing.
E) Completion ofVanderbilt forms by parents and teachers
Discussion 4-1
The correct answer is "B:' Adolescence is time of rapid growth and development. It can be a stressful time, manifesting as anxiety, withdrawal, aggression, somatic complaints, depression, or poor copingskillssuch as usingdrugs. The most common causes of morbidity and mortality in adolescence are related to the risk-taking behavior and experimentation that is a normal part ofadolescent development. Obtaining a thorough psychosocial history is important in screening forthese risk-taking behaviors and identifying protective factors The symptoms the mother has described raise concern about depression in this patient. A thorough psychosocial assessment using the HEADSSS screening tool with a follow-up depression screenwilllikely reveal the cause ofhis symptoms. How many knew that Vanderbilt scales assess for attention deficit hyperactivity disorder (ADHD)?
• HelpfulTip


HEADSSS was developed as a psychosocial screening 1 tooL
H- Home (Who lives with the teen? How does the teen get along with family?)
E - Education (Is the teen in school? How is he or she performing in school? School performance can be an important indication ofhowa teen is functioning.)
E- Eating (meal consistency; body image)
A- Activities
D- Drugs (alcohol,tobacco, marijuana, and other drug use, including prescription and over-the-counter)
6 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS

S - Sexua ity (Sexual attraction: Are you attracted to males, females, both, neither? Sexual behavior: Have you ever had sex, how many partners, history of sexually transmitted infection diagnosis and testing, condom use, contraceptive use, last sexual activity, history offorced sex?)
S- Suicide/Depression
S- Safety (Does the teen feel safe at home or school? What is his or her exposure to violence?)
Through the HEADDSS assessmentyoulearn that thepatient is attracted to males and recently entered a relationship with a boy at school. He wrote a letter to the boy which another student found and shared with the whole class. Since then the patient reports that he is teased by many ofhis classmates and has been skipping classes to avoid being teased. His depression screen is positive for sadness, anhedonia (no pleasure in activities), excessive sleeping, and feelings of guilt. He denies anythoughts of self-harm or suicidality.
Question 4-2
Adolescents who identify as lesbian, gay, or bisexual are at increased risk for which of the following?
A) Eating disorders.
B) Substance abuse.
C) Depression.
D) Bullying.
E) All ofthe above.
Discussion 4-2
The correct answer is "E:' Sexual development is one part ofadolescent development. During early adolescence pubertal developmentisjust beginning. Atthis stage ofdevelopment adolescents are very focused on changes occurring in their bodies and questioningwhethertheyare normal. Adolescents maybegin to experience sexual fantasies and experience sexual pleasure through masturbation. Sexual intercourse at this stage is uncommon, but may occur. Adolescents often experience crushes, which may be same sex or opposite sex. These patterns of attraction may or may not persist into future stages. In middle adolescence physical development is nearing completion; atthis stage adolescents are formingtheir sexual orientation and identity. Sexual experimentation is common at this stage and many adolescents mayhave intercourse for the first time. By late adolescence the goal is to become a sexually healthy adult with the ability to form long-lasting relationships. Sexual orientation refers to an individual's pattern of physical and emotionalattractions to others and involves complex components such as fantasies and feelings. Personal, family, cultural, developmental, and social factors can affect an individual's ability to identify, accept, and act on his or her attractions. Adolescents who identify as lesbian, gay, or bisexual are at an increased risk for a number of conditions, including eatingdisorders, substance abuse, and mentalhealthillnesses, particularly depression and anxiety. The patient has questions about how to stay safe when he does become sexually active with his partner.
Question 4-3
Which of the following is true about sexually transmitted infection (STI) transmission?
A) HIV transmission rates are low with receptive anal intercourse.
B) STis cannot be transmitted through oral sex.
C) Women who have sexwithwomen are at a low risk for STis. D) Condoms are effective at reducing STI transmission.
Discussion 4-3
The correct answer is "D:' HIV transmission rates are high with receptive anal intercourse due to microtrauma during intercourse. STis can be transmitted through oral sex, and it is important to educate patients to use condoms when havingoral sex to reduce the risk ofcontracting an STI. Studies have shown that women who have sex with women are at an increased risk of contracting human papillomavirus (HPV), trichomoniasis, and HIV Condoms are an effective method of STI prevention and when properly used have been shown to reduce rates of transmission of HIV, gonorrhea, chlamydia, trichomonas, and hepatitis B. They can also be effective at preventing STis transmitted by skin-to-skin or mucosal contact, such as herpes simplex virus (HSV), syphilis, and HPV, but onlyifthe affected area is covered by the condom. Equally important is making sure adolescents know how to put on a condom. Pregame practice is a good idea.
Question 4-4
You also counsel the patient that the most common cause of mortality in the adolescentpopulation is:
A) Cardiac disease.
B) Unintentional injuries
C) Suicide.
D) Homicide.
E) Cancer.
Discussion 4-4
The correct answer is "B:' The leading cause ofdeath in the adolescent population is unintentional injuries, with motor vehicle collisions being the most frequent cause of such injury in this population. (See Figure 1-4.) Homicide is the second leading cause of death, followed closely by suicide. Organic disease is a less frequent cause of mortality in this age group. Screening for risk factors such as substance use, mental illness, and exposure to violence is important in this population to address the leading causes of mortality. Good driving habits, including no texting while driving, should be discussed.
� QUICKQUIZ
Which ofthe following is a risk factor for suicide?
A) Bullying.
B) Witnessing violence.
C) Social isolation.
D) Mental illness.
E) All ofthe above.
CHAPTER1 • ADOLESCENT MEDICINE AND GYNECOLOGY 7
Unintentionalinjury

Malignantneoplasms
Heartdisease
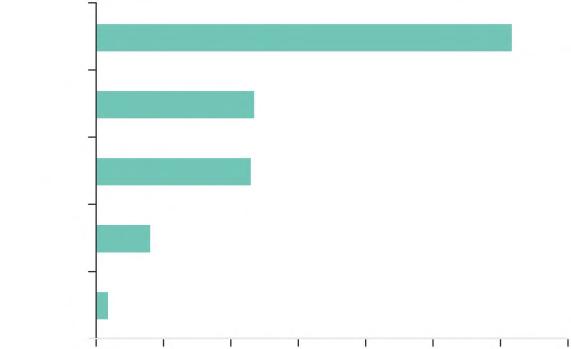
0 2000 4000 6000 8000 10000 12000 14000
FIGURE1-4. 2010Leadingcausesofdeathinyouthages15to24yearsof ageintheUnitedStates.(ReproducedwithpermissionfromtheCentersfor DiseaseControlandPrevention,NationalCenterforInjuryPreventionand Control,Web-basedInjuryStatisticsQueryandReportingSystem(WISQARS). AccessedJanuary28,2015fromhttp://www.cdc.gov/injury/wisqars/.)
Discussion
The correct answer is "E:' Additional risk factors include family history of suicide, history of abuse, previous attempt, access to means such as firearms, alcohol and drug use, stressful events, and sexual identification other than heterosexuality.
The patient's mother mentions that she recently caught him smoking pot in the garage with some friends. She is requesting that you drug test him without letting him know.
Question 4-5
Your next step is to:
A) Do as the mother requests.
B) Notify the patient and perform testing regardless of his wishes.
C) Notifythe patient and perform the testing ifhe agrees.
D) Refuse to perform drug testing.
E) Reassure the mother that catching him guarantees he will stop using.
Discussion 4-5
The correct answer is "C:' Recreational drug use is an underrecognized cause of morbidity and mortality in adolescents. Indications for drug testing in the acute care setting include acute presentation with altered mental status, suicide attempt, unexplained seizures, syncope, arrhythmias, or the presence of toxidromal signs. In the primary care setting voluntary drug testing can be helpful for assessment, therapy, and monitoring. The American Academy ofPediatrics (AAP) currently cautions against involuntary drug testing ofadolescents in nonemergent settings. Testing of competent adolescents without their knowledge is unethical and illegal, and without their consent is impractical. If a pediatrician suspects that a patient is abusing drugs and the patient refuses drug testing, documentation ofthe refusal and referral to a mental health or addiction specialist may be warranted. Given the limitations of currently available drug tests, a thorough substance abuse historyoften provides more useful information on drug abuse/ use than a drug test.
A 16-year-old girl and her mother present to your office with concerns about irregular periods. The patient had her first menses at 12 years of age and had regular monthly periods until 6 months ago when her periods stopped. She has had an accompanying 50-pound weight loss over the past 6 months. When asked further about the weight loss, she reports that she has been working on more healthful eating, has cut all desserts and junk foods out ofher diet, and eats a low-fat and low-carb diet. In addition she has started running 3 miles a day in order to "get healthy?' On physical exam her vital signs are temperature 36.4°C {97.5°F), heart rate 44 beats per minute, blood pressure 96/60 mm Hg, andrespirations 16 breaths per minute. She appears thin, with sallow-looking skin and dry hair. She is bradycardic on exam, with no murmurs and a regular rhythm. Her heart rate increases by 19 beats during positional changes from sitting to standing, with minimal change in her blood pressure. Her pulses are strong and symmetric while her fingers and toes are cool to touch.
Question 5-1
Which ofthe followingis the most likely causeofthis patient's symptoms?
A) Thyroid disease.
B) Anorexia nervosa.
C) Bulimia nervosa.
D) Diabetes mellitus.
E) Coarctation ofthe aorta.
Discussion 5-1
The correct answer is "B:' Eating disorders are a common but often underdiagnosed condition in the pediatric population. The 12-month prevalence ofanorexia nervosa among young females in approximately 0.4%, the prevalence of bulimia nervosa is approximately 1% to 1.5%. Anorexia nervosa has a mortalityrate of 5% to 6%, the highest ofanypsychiatric illness. Patients with anorexia nervosa generally present with rapid weight loss secondary to caloric restriction, which may present as elimination of "junk food" from the diet; avoidance of certain food groups, such as carbohydrates and fats; or changing to a restrictive vegan or vegetarian diet. Patients may also try and reduce weight by over-exercising or purging through self-induced vomiting or use of diuretics and laxatives. In contrast, patients with bulimia nervosatypicallypresentwith cycles ofbinging that trigger purging or inappropriate compensatory behaviors. Compensatory behaviors could include self-induced vomiting, use of diuretics, use oflaxatives, fasting, or over-exercising. Patientswith bulimia nervosa are typically of normal weight or overweight. Patients with anorexia nervosa often present with signs of malnutrition (eg, bradycardia); hair, skin, and nail changes, often manifesting as dryandbrittlehair,nails, and skin; menstrual irregularities (eg, amenorrhea and oligomenorrhea); orthostaticvital sign changes; cold intolerance; acrocyanosis; mood changes; and fatigue. The DSM is revised periodically and eating disorder diagnostic criteria often change. Due to copyright restrictions, we are unable to print the DSM-5 diagnostic criteria for anorexia and bulimia.
8 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS
1--------------
Homicide I Suicide I
TA
BLE1-3 COMMON FEATURES OF ANOREXIA NERVOSA
• Restricted eating
Low body weight for age and sex
• Fear of gaining weight or becoming fat
• Behaviors that interfere with gaining weight
• Disturbance of body image
• Excessive influence of body weight or shape on self-evaluation
• Lackof recognition ofthe seriousness oflow body weight
Summaries oftheir common features are included in Tables 1-3 and 1-4. But the reader should make themselves familiarwith the current DSM criteria forboth conditions.
Question 5-2
Which ofthe following would be a reason for inpatient hospitalization for this patient?
A) Hypertension.
B) Bradycardia.
C) Hypokalemia.
D) Rapid weight loss.
E) Amenorrhea.
Discussion 5-2
The correct answer is "B:' The AAP suggests that the following signs and symptoms warrant inpatient hospitalization: For anorexia nervosa:
• Bradycardia (<45 bpm daytime or <45 bpm nighttime)
• Hypotension (<90 mmHg systolic)
• Arrhythmia
• Hypothermia
• Weight <75% ideal body weight
• Body Fat < 10%
• Refusal to eat
• Failure ofoutpatient treatment
For bulimia nervosa:
• Syncope
• Hypokalemia
• Severe hypochloremia (<88 mmol!L)
• Esophageal tears
• Arrhythmia
• Hypothermia
• Suicidality
• Intractable vomiting
• Hematemesis
• Failure ofoutpatient treatment
This patient warrants inpatient treatment due to her bradycardia. Note that the AAP endorses electrolyte abnormalities as admission criteria for bulimia, but not anorexia. In reality, a patient with anorexia and severe electrolyte abnormalities would also likelybe admitted to the hospital. Also ofinterest is that hypothermia is defined for one but not both disorders The goal in hospital admission is medical stabilization, which is usually achieved through nutritional rehabilitation and correction of any underlying electrolyte abnormalities. Fluid and electrolyte shifts can occur with the reintroduction of nutrition in a patient who has been malnourished. This is called refeeding syndrome and most typically manifests as decrease in phosphate, magnesium, and potassium, as well as an increase in extracellular volume causing peripheral edema or congestive heart failure, or both. These fluid and electrolyte shifts can lead to cardiac arrhythmias; thus monitoring ofcardiac status, electrolytes, and fluid status is important in the inpatient setting.
Question 5-3
Which of the following will likely NOT be a part of this patient's treatment?
A) Nutritional rehabilitation.
B) Psychotherapy.
C) Medical monitoring for complications ofillness.
D) Use ofan appetite stimulant.
E) Family therapy.
Discussion 5-3

TABLE1-4 COMMON FEATURES OF BULIMIA NERVOSA (MUST BE PRESENT AT LEAST ONCE A WEEK FOR 3 MONTHS)
• Eating a large amount offood over a short amount of time
• Lackofcontrol during the episode-feels as though one cannot stop eating
• Behaviors to compensate for episodes of binge eating.
• Excessive influence of body weight or shape on self-evaluation
• Diagnosis is not better explained by a diagnosis of anorexia nervosa
The correct answer is "D:' Treatment ofeating disorders is multidisciplinary and includes medical monitoring for complications of the illness such as refeeding syndrome; psychotherapy to address eating disorder thoughts and body image concerns; and nutritional rehabilitation, which involves reintroducing meals and snacks in a stepwise fashion with a goal of restoring body weight. The use of appetite stimulants is not recommended as this does not address the disordered thoughts and behaviors that are a part ofthe eating disorder. Treatment goals include medical stabilization; nutritional rehabilitation as measured by restoration ofbody weight, usually at a rate of 0.25 to 1 kg per week in the outpatient setting; decrease in eating disorderthoughts and behaviors; and improvement in bodyimage. Healthy family involvement is always good.
CHAPTER1 • ADOLESCENT MEDICINE AND GYNECOLOGY 9
• HelpfulTip


Anorexic patients are at risk for refeeding syndrome. Hypophosphatemia is the hallmark and the primary culprit ofrefeeding syndrome.
Question 5-4
Which of the following laboratory findings would NOT be expected in a patient with anorexia nervosa?
A) Hyperkalemia.
B) Leukopenia.
C) Normal laboratory results.
D) Hypoglycemia.
E) Elevated liver enzymes.
Discussion 5-4
The correct answer is "A:' Most patients with eating disorders have normal laboratory findings. General laboratory workup includes a CBC with white blood cell count differential; full chemistry panel, including liver and renal studies; thyroid studies; nutritionalmarkers, such asvitamin D and prealbumin; and coagulation studies. Don't forget an ECG. Technically it isn't a lab test but we needed to include it somewhere! Additional testing maybe indicated to excludealternative diagnoses. Common laboratory abnormalities thatmaybe seen in patients with anorexia include hypokalemia (not hyperkalemia) and hypochloremic metabolic alkalosis secondary to purging. Hypoglycemia can be seen secondary to malnutrition. Hyponatremia maybe seen as a sign ofwater-loading or excessive water intake. Leukopenia can be seen, and in severe cases pancytopenia. Mild elevation of liver enzymes can also be seen secondary to malnutrition.
�QUICKQUIZ
What is NOT a complication of anorexia nervosa?
A) Diarrhea.
B) Gastroparesis.
C) Osteopenia.
D) Brain atrophy.
E) Pericardia! effusion.
Discussion
The correct answer is "A:' Anorexia causes constipation, not diarrhea (unless the patient is taking laxatives).
sit out practice and competitions for the past few weeks, she has kept active by riding a stationary bike and swimming. She isotherwisehealthyandtakes no medication. The patient's breast development began at about 12 years of age and pubic hair 2 years ago. Her brother has insulin-dependent diabetes mellitus and her mother has hypertension. The mother states that her own menses started at 14 years of age. The patient is a sophomore in high school and is getting straight Xs. She has a boyfriend but denies sexual activity. She denies all substance use. Review ofsystems is negativeforheadaches, nausea, vomiting, abdominal pain, constipation, diarrhea, or vaginal discharge. On physicalexam she is 5 feet, 6 inches tall and weighs 110 pounds, with a heart rate of 56 bpm and a blood pressure of 110/70 mm Hg. She is SMR 3 for breasts and pubichair. The rest ofher exam is normal.
Question 6-1
The definition of primary amenorrhea includes absence of menses by what age, assuming normal secondary sexual development?
A) 12 years.
B) 14 years.
C) 16 years.
D) 18 years.
Discussion 6-1
The correct answer is "C." Primary amenorrhea refers to the absence of menses (1) by age 16 years with normal secondary sexual development; (2) by age 14 years in the absence of any breast maturation; or (3) despite having attained SMR 5 for 1 year or more, or despite the onset of thelarche 4 years previously. Focus on remembering the first and second criteria.
Question 6-2
The most likely cause ofprimary amenorrhea in this patient is:
A) Hypothalamic amenorrhea.
B) Hypothyroidism.
C) Hyperprolactinemia.
D) Hypopituitarism.
E) Imperforate hymen.
Discussion 6-2
A 16-year-old Caucasian girl comes to the adolescent clinic for the first time because she has never had a menstrual period. She is a runneron her school's cross-countryteam and recently was diagnosed with a stress fracture. Although she has had to
The correct answer is "A." Causes of primary amenorrhea include conditions resulting from central dysfunction (hypothalamic or pituitary), ovarian dysfunction, or anatomic abnormalities ofthe genital tract. Given this patient's clinical presentation, the most likely diagnosis would be functional hypothalamic amenorrhea, due to partial or complete inhibition of GnRH release. This inhibition can be due to nutritional deficiencies, cystic fibrosis, eating disorders, excessive exercise, stress, or severe or prolonged illness. Excessive exercise is to blame in this teenage girl. She has developed a stress fracture from excessive running. Signs and symptoms of hypothyroidism include constipation, dry skin, weight
10 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS

gain, and increased sensitivity to cold. When hypothyroidism is present in children and teens, one may also see delayed puberty and poor growth, resulting in short stature. Hyperprolactinemia is usually due to a prolactin-secreting adenoma that also may cause headaches, visual changes (bitemporal hemianopsia), and galactorrhea. Hyperprolactinemia can also be caused by physiologic hypersecretion of prolactin (pregnancy), hypothalamic-pituitary stalk damage, certain systemic disorders, or drug-induced hypersecretion (eg, risperidone). With hypopituitarism, the pituitary gland fails to produce or does not produce enough of one or more of its hormones, and multiple body functions can be affected. If the complaint relates to menstruation, always make sure everything is anatomically correct. Young women need "girl parts" to have periods and an open outflow path (eg, no imperforate hymen).
Question 6-3
If this patient lacked breast development, which of the following would be included in the diagnosis?
A) Agenesis ofmiillerian structures.
B) Complete androgen insensitivity syndrome.
C) Asherman syndrome.
D) Pure gonadal dysgenesis (46,XXwith streak gonads).
Discussion 6-3
The correct answer is "D:' With pure gonadal dysgenesis, the streak gonads are unable to produce sex hormones. In a female with pure gonadal dysgenesis, the ovaries do not produce estrogen, resulting in absence of breast development. Agenesis of miillerian structures impacts the formation of the internal reproductive tract (uterus, fallopian tubes, and upper third of the vagina), not the ovaries, and has no effect on breast development. Individuals with complete androgen insensitivity syndrome are resistant to testosterone due to defective androgen receptors. They do not develop testosterone-dependent male sexual characteristics, and the testosterone produced by the testes is aromatizedinto estrogen, leading to phenotypicallyfemale appearance with normal breast development. Their genotype is male (46,XY) but their external genitalia look female. Internal female structures such as a uterus are not present as the testes make miillerian-inhibiting substance. Asherman syndrome occurs when uterine synechiae or adhesions obstruct or obliterate the uterine cavity, leading to amenorrhea. Adhesions may develop after uterine infection or other disruption. Breast development is not affected.
� QUICKQUIZ
Which of the following clinical characteristics would NOT be seen in a patient with complete androgen insensitivity syndrome?
A) Absent menses.
B) Normal breast development.
C) Tanner 3 pubic hair.
D) Normal linear growth.
Discussion
The correct answer is "C' Patients with complete androgen insensitivity syndrome are (46,XY) and have a defect in androgen receptors. Thus theydo not develop testosterone-dependent male sexual characteristics, such as pubic and axillary hair.
Question 6-4
What tests should you order to assess primary amenorrhea in this patient in order to confirm your diagnosis?
A) Pregnancy test.
B) Follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
C) Prolactin.
D) Thyroid-stimulating hormone (TSH).
E) All ofthe above.
Discussion 6-4
The correct answer is "E:' Pregnancy should always be excluded, even in patients who deny sexual activity. It is useful to obtain FSH and LH levels to differentiate between hypothalamic (low or normal LH and FSH) and ovarian insufficiency (elevated LH and FSH). A prolactin level would confirm the presence of a pituitary microadenoma, which might (or might not) also cause headache, galactorrhea, and bitemporal hemianopsia (decreased vision in the outer half) TSH level is used to diagnose thyroid abnormalities, which may impact menses. Even though you suspect hypothalamic amenorrhea (suppression from excessive exercise), you should rule out both hyperprolactinemia and thyroid abnormalities.
Question 6-5
Which of the following would make Turner syndrome an unlikely diagnosis in a patient with amenorrhea?
A) Short stature.
B) Hypogonadotropic hypogonadism.
C) Hypergonadotropic hypogonadism.
D) Webbed neck.
E) Widely spaced nipples.
Discussion 6-5
The correct answer is "B:' Tuner syndrome (45,XO) is the most common cause of primary gonadal failure (primary hypogonadism) in adolescent girls and is characterized by ovarian dysgenesis (accelerated stromal fibrosis and decreased or absent oocyte production), short stature, and a wide variety ofphenotypical abnormalities (widely spaced nipples, webbed neck, coarctation of the aorta, lymphedema), and elevated gonadotropins The hypothalamus and pituitary function normally but the ovary does not, so FSH and LH are elevated. Most women with Turner syndrome do not develop breasts or have periods (primary amenorrhea) but some develop normally with secondary amenorrhea as their presenting symptom. Short stature is a big clue.
CHAPTER 1 • ADOLESCENT MEDICINE AND GYNECOLOGY 11
• HelpfulTip



To differentiate between primary and secondary hypogonadism, use FSH and LH to guide your thinking. In hypogonadotropic hypogonadism, the problem is central (hypothalamusorpituitary,orboth)and FSH and LH levels will be low or normal. In hypergonadotropic hypogonadism, the problem is the gonads (testes or ovaries) and FSH and LH will be elevated.
You decide to proceedwith a progesterone challenge in your patient, which does NOT result in a withdrawal bleed.
Question 6-6
Which of the following are possible causes for failure of a progesterone challenge?
A) Elevated estrogen level.
B) Ovarian cyst.
C) Transverse vaginal septum.
D) Septate hymen.
E) Bicornate uterus.
Discussion 6-6
The correct answer is "C:' A progesterone challenge helps determines thelevel ofendogenous estrogen and confirm the patencyof the outflow tract. Ifno bleeding occurs after a progesterone challenge, either the anatomyis disrupted (imperforate hymen, vaginal atresia, vaginal septum, miillerian agenesis, absent uterus) or there is not enough circulating estrogen. Estrogen stimulates buildup of the uterine lining, which is shed in the progesterone challenge. A transverse vaginal septum is a thin horizontal membrane in the vagina that may cause obstruction. A septate hymen has an extra band oftissue in the middle that causes two vaginal openings but not obstruction. A bicornate uterus is just shaped funny.
A 17-year-old girl presents to the adolescent clinic complaining ofirregular periods for the past 6 months. Menarchewas at 11 years ofage. Menseshavebeen regular, comingeverymonth and lasting 5 days for the past 4 years until 6 months ago. In the past 6 months, she has had only 2 periods, the last one was 2weeksago and lasted 10 days. Shehas gained 25 pounds in the pastyear (current BMI is 33 kg/m2). She has noticed increasing acne and dark, velvety skin in her neck and axilla. She is sexually active with boyfriend of 1 year and uses condoms consistently. The last sexual activity was about 3 weeks ago.
Question7-1
Which of the following qualifies as dysfunctional uterine bleeding?
A) Menstrual cycles occurring 19 days apart.
B) Menstrual cycles occurring 35 days apart.
C) Menstrual cycles lasting 7 days.
D) Menstrual cycles resulting in blood loss of60 mL.
Discussion 7-1
The correct answer is ''A:' Dysfunctional uterine bleeding (DUB), also known as anovulatory abnormal uterine bleeding, is defined as menstrual cycles occurring less than 20 days or more than 45 days apart, and lasting longer than 8 days, or menstrual cycles resulting in blood loss ofgreater than 80 mL. DUB is characterized as (1) oligomenorrhea-too few periods (> 45 days apart), (2) polymenorrhea-too many periods (< 20 days apart), (3) metrorrhagia-too-frequent bleeding irregularly or between periods, (4) menorrhagia-too-heavy blood loss (> 80 mL or lasting > 7 days), and (5) menometrorrhagia-too-frequent and heavyblood loss. Anovulationis a common cause ofDUB in adolescents. Without ovulation, progesterone secretion is disrupted, resulting in estrogen-induced overgrowth ofthe endometrial lining. The thickened lining outgrows it blood supply and then is shed irregularly.
• HelpfulTip


Anovulatory cycles are common in early menstrual cycles and are characterized by large variations in estrogen levels and lack of progesterone. During the first 2 years following menarche, anovulation is associated with 50% to 80%of bleeding episodes.Two to4yearsaftermenarche,anovulation is associatedwith 30% to 55% of bleeding episodes. Four to 5 years after menarche, 20% ofbleeding episodes are anovu atory.
• HelpfulTip


The female athlete triad includes osteoporosis, amenorrhea, and disorders of nutritional intake.
A urine pregnancy test was negative. Based on the clinical picture, you suspect polycystic ovary syndrome (PCOS).
Question 7-2
What test shouldyou order to help confirm the diagnosis?
A) CBC.
B) Estradiol level.
C) Total and free testosterone.
D) FSH level.
E) Ovarian ultrasound.
Discussion 7-2
The correct answer is "C:' Obesity, acanthosis nigricans (see Figure 1-5), andmenstrualirregularitiessuggestPCOS. There are several diagnostic criteria for PCOS. Essentially, there needs to be evidence ofovulatory dysfunction and clinical or biochemical
12 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS

FIGURE1-5. Acanthosisnigricansonthebackoftheneck.(Reproduced withpermissionfromHoffmanBL,SchorgeJO,SchafferJl,HalvorsonLM, BradshawKD,CunninghamFG,CalverLE,eds. William's Gynecology. 2nded. NewYork,NY:McGraw-HillEducation,Inc.,2012;Fig.17-6.)
signs ofandrogen excess. Ultrasound evidence ofpolycystic ovaries is suggestive but not required for the diagnosis. Women with PCOS often have an increased level ofboth total testosterone and free testosterone. FSH level will not be helpful on its own; however, in combination with LH level it may be helpful as half of patients with PCOS have an LH:FSH ratio of2.5:1. Most women with PCOS have normal estradiol levels.
Question 7-3
Additional laboratory studies that should be ordered in patients with PCOS include:
A) Glucose.
B) Lipid panel.
C) Insulin.
D) Glucose tolerance test.
E) All ofthe above.
Discussion7-3
The correct answer is "D:' PCOS patients are at higher risk for impaired glucose tolerance and insulin resistance, as well as metabolic syndrome, which is a group of cardiovascular risk factors that include dyslipidemia, type 2 diabetes mellitus, hypertension, and obesity.
Question 7-4
The type of cancer that people with PCOS are at risk for includes:
A) Endometrial cancer.
B) Ovarian cancer.
C) Breast cancer.
D) Cervical cancer.
E) None ofthe above.
Discussion 7-4
The correct answer is "A:' Womenwith PCOS have an increased risk of developing endometrial cancer. A major factor for this
increased malignancy risk is the prolonged exposure of the endometrium to unopposed estrogen that results from anovulation. Women with PCOS are not at increased risk of ovarian, breast, or cervical cancer.
Question 7-5
Other conditions that may show evidence of excess androgen include:
A) Adrenal tumor.
B) Late-onset congenital adrenal hyperplasia.
C) Anabolic steroid use.
D) All ofthe above.
Discussion7-5
The correct answer is "D:' Adrenal tumors can manifest as virilization and can be diagnosed by means of an elevated dehydroepiandrosterone sulfate (DHEA-S) level. Late-onset congenital adrenal hyperplasia may become apparent during mid-childhood and can lead to early pubic hair, accelerated bone age, hirsutism, and possible mild clitoral enlargement. This can be diagnosed based on elevated serum 17-hydroxyprogesterone. Anabolic steroids have effects similar to testosterone in the body.
� QUICKQUIZ
Which is a clinical feature of PCOS?
A) Acanthosis nigricans.
B) Hirsutism.
C) Acne.
D) Obesity.
E) All ofthe above.
Discussion
The correct answer is "E:' Obesity, menstrual irregularities, and infertility are common. Hirsutism, male pattern alopecia, and acne result from androgen excess. Acanthosis nigricans, as seen in the patient inthis case, is a manifestation ofinsulin resistance.

The mother of a 14-year-old girl calls the clinic stating that her daughter's first period began 2 weeks ago and she continues to bleed heavily. Her daughter is complaining of feeling increasingly tired. Review of the girl's chart shows that the 14-year-old was previously healthy. She has never had any surgical procedures. The family history indicates that both the mother and maternal grandmother had hysterectomies in their 30s due to heavy menstrual bleeding. You tell the mother to bring her daughter to the clinic. At arrival, the girl's vital signs are heart rate of 120 bpm and blood pressure of 100/70 mm Hg. On exam, her skin is pale andvaginal exam shows active bleeding from the cervix.
CHAPTER 1 • ADOLESCENT MEDICINE AND GYNECOLOGY 13
Question 8-1
Which ofthe following conditions would be an unlikely cause ofabnormalvaginal bleeding in this patient?
A) Endometrial cancer.
B) Pregnancy-related condition.
C) Sexuallytransmitted infections.
D) Anovulatory cycle.
E) Bleeding disorder.
Discussion 8-1
The correct answer is "A:' Most cases of abnormal vaginal bleeding in adolescence are secondary to dysfunctional uterine bleeding from anovulatory cycles. Genital cancers are very rare in young adolescents. The differential diagnosis includes:
• Pregnancy-related conditions (intrauterine or ectopic pregnancy, spontaneous abortion, and molar-trophoblastic disease)
• Infections (vaginitis, cervicitis, endometritis, salpingitis, and pelvic inflammatory disease)
• Other gynecologic conditions (ovarian cyst, genital cancers, breakthrough bleeding associated with contraceptive use, ovulation bleeding, polyps, endometriosis)
• Systemic disease (renal and liver failure)
• Bleeding disorders
• Direct trauma and foreign body
• Medications (anticoagulants and platelet inhibitors)
Question 8-2
The following tests should be included in the workup of this patient:
A) Pregnancy test.
B) Hemoglobin/hematocrit.
C) Coagulation studies.
D) Nucleic acid amplification testing (NAAT) for gonorrhea and chlamydia.
E) All ofthe above.
Discussion 8-2
The correct answer is "E:' A pregnancytest is essential to exclude complications of pregnancy. Hemoglobin and hematocrit values will help determine the magnitude ofbleeding. Coagulation studies may reveal coagulopathies or blood dyscrasias, particularly in this case of heavy bleeding since onset of menarche and a family history of abnormal vaginal bleeding. STis such as gonorrhea and chlamydia are common causes of prolonged or irregular vaginal bleeding. Other causes to consider include endocrine abnormalities such as hypothyroidism.
The pregnancy testwas negative. Her hemoglobin is 8.5 g/dL.
Question 8-3
What is the next appropriate step?
A) Reassurance.
B) Start a multivitamin with iron.
C) Start a combined oral contraceptive pill daily.
D) Admit to hospital for higher doses ofestrogen and possible blood transfusion.
E) Uterine dilational and curettage.
Discussion 8-3
The correct answer is "D." Treatment of abnormal uterine bleeding depends on the severity of the bleeding, hemoglobin level, and degree of associated hemodynamic changes. Mild cases associated with a hemoglobin level of 12g/dL or higher require only reassurance, a multivitamin with iron, and close follow up. Individuals with a hemoglobin level of 10 to 12 g/dL should take a combined oral contraceptive pill (OCP) every 6 to 12 hours for 24 to 48 hours until the bleeding stops, taper to one pill per day, and then continue daily OCPs for 3 to 6 months. Patients with a hemoglobin level of less than 10 g/dL may require hospitalization and initial treatment of higher doses of estrogen if hemodynamically unstable. This patient has anemia and is subsequently tachycardic. She needs aggressive management.
Question 8-4
The most common inherited bleeding disorder, which often presents as menorrhagia in adolescent females is:
A) Factor VIII deficiency.
B) Factor IX deficiency.
C) von Willebrand disease.
D) Protein C deficiency.
E) Antiphospholipid syndrome.
Discussion 8-4
The correct answer is "C:' The most common inherited bleeding disorder in the United States population is von Willebrand disease, with an estimated prevalence of 1% to 2%. The prevalence ofvon Willebrand disease rises in studiesinvolvingwomen with menorrhagia, with estimates ranging as high as 10% to 20% in Caucasian women, and 1% to 2% among African American women. VonWillebrand factor helps with formation ofthe initial blood clot (binds platelets and factor VIII). Other bleeding disorders seen in adolescents with menorrhagia are disorders of inherited platelet dysfunction, clotting factor deficiencies, thrombocytopenia, and disorders of the fibrinolytic pathway. People with antiphospholipid syndrome and protein C and S deficiencies are at increased risk for thromboembolism, not menorrhagia.

A 16-year-old girl comes to your clinic requesting birth control. She just started having sexual intercourse with her boyfriend of 1 year. They have used condoms with each episode ofvaginal intercourse. Menarche was at 12 years of age. Menses occurs every month, lasts for 5 days, and is associated with mild cramps. Her past medical history consists of
14 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS
well-controlled absence seizures diagnosed at 16 years of age for which she takes a medication. She had an appendectomy in the past year; imaging during the diagnostic evaluation showed a left ovarian cyst measuring 1.6 x 2 x 1.8 em. Her mother takes medication for high blood pressure and her father has high cholesterol.
Question 9-1
Which of the following contraceptive options has the lowest failure rate during typical use in adolescence?
A) Male condom.
B) Combined OCPs.
C) Implantable etonogestrel rod.
D) Injectable depo-medroxyprogesterone.
E) Progestin-only pills.
Discussion 9-1
The correct answer is "C' See Table 1-5 for failure rates ofdifferent methods of contraception. With so many choices, why aren't all sexually active adolescents using contraception and STI protection? Perhaps the adolescent has difficultly planning ahead, fails to recognize potential consequences, lives in the moment, fears a pelvic exam or side effects, or has concerns over confidentiality.
Question 9-2
Combined OCPs can safely be used byan adolescent with any of the following conditions EXCEPT:
A) Migraine with aura.
B) Blood pressure of 135/80 mm Hg.
C) Hypothyroidism.
D) History ofovarian torsion.
E) Asthma.
Discussion 8-2
The correct answer is "A:' According to the Centers for Disease Control and Prevention's (CDC) US Medical Eligibility Criteria for Contraceptive Use, absolute (level 4) contraindications to combined OCP use include current breast cancer or estrogendependent tumor, thromboembolic disease or high risk for thromboembolism (thrombogenic mutation, antiphospholipid antibody), migraine with aura, blood pressure of 160/100 mm Hg or higher, cardiovascular disease, liver disease, and cerebrovascular events.
�
QUICKQUIZ
Which is a noncontraceptive benefit of estrogen-progestincontaining birth control?

TABLE1-5 FAILURE RATES WITH PERF ECT USE AND TYP ICAL USE OF DIFF ERENT CO NTRACEPTIVE METHODS
A) Increased risk ofovarian cancer.
B) Increased acne.
C) Worsening menstrual cramps.
D) Decreased bone density.
E) Prevents menstrual migraines without aura.
Discussion
The correct answer is "E" Combined hormone-containing pills, patch, and vaginal ring improve bone density and decrease (1) risk of ovarian and endometrial cancer; (2) menstrual cycle disorders, including menorrhagia and dysmenorrhea; (3) acne; and (4) pelvic pain from endometriosis.
Question 9-3
Which ofthe following antibiotics interferes with the contraceptive effectiveness of the OCP?
A) Amoxicillin.
B) Rifampin
C) Cephalosporin.
D) Sulfonamides.
Discussion 9-3
DMPA, depot medroxyprogesterone acetate; IUD, intrauterine device; OCP, oral contraceptive pill.
Data from Hatcher RA,Trussell J, Nelson AL, etal. Contraceptive Technology. 20th rev ed. New York, NY: Ardent Media; 201 1.
The correct answer is "B:' Rifampin is the onlyantibiotic proven to decrease the contraceptive effectiveness ofthe pill. Amoxicillin, cephalosporins, and sulfonamides do not affect birth control effectiveness. Griseofulvin, an antifungal medication used to treat tinea infections, also speeds up metabolism of OCPs, decreasingtheir effectiveness.
FailureRate WithPerfect WithTypical Contraceptive Use(%) Use(%) Withdrawal method 4 22 Rhythm method/ 5 24 periodic abstinence Male condom 2 18 Female condom 5 21 Combined OCPs 0.3 9 Combined transder- 0.3 8 mal patch Combined vaginal 0.3 8 ring Progestin-only pill 0.3 9 Injectable DMPA 0.2 6 Implantable 0.05 0.05 etonogestrel rod Levonorgestrei iUD 0.2 0.2 Copper IUD 0.6 0.8
CHAPTER 1 • ADOLESCENT MEDICINE AND GYNECOLOGY 15
Question 9-4
Which ofthe following antiseizure medications decreasesthe contraceptive effectiveness ofthe OCP?
A) Gabapentin.
B) Phenobarbital.
C) Valproate.
D) Levetiracetam.
E) All ofthe above.
Discussion 9-4
The correct answer is "B:' Antiepileptics that induce the cytochrome P450 system (increasing metabolism), and therefore make the birth control pill less effective, include carbamazepine, felbamate, phenobarbital, phenytoin, primidone, and topiramate. Lamotrigine clearance is increased in presence of estrogen-containing birth control options, meaning the effectiveness ofthe seizuremedication is decreased.
Your patient does not think she would remember to take a birth control pill every day and would like to hear about the other options.
Question 9-5
Which of the following correctly matches the contraceptive with its duration of action?
A) Transdermal patch; 3 weeks.
B) Vaginal ring; 3 months.
C) Levonorgestrel intrauterine device (IUD); 10 years.
D) Copper IUD; 10 years.
E) None ofthe above.
Discussion 8-5
The correct answer is "D:' The birth control patch needs to be changed weekly. The birth control ring is typically replaced after 3 weeks. There are two different levonorgestrel IUDs; one lasts for 3 years and the other for 5 years. The copper IUD is replaced every 10 years.
She returns 6 months later and tells you that she is pregnant.
Question 9-6
Which of the following would put her at higher risk for an ectopic pregnancy?
A) Prior episode ofpelvic inflammatory disease.
B) History ofOCP use.
C) History oflabial adhesions requiring estrogen cream.
D) Frequent yeast infections.
E) All ofthe above.
Discussion 9-6
The correct answer is ''A:' Risk factors for ectopic pregnancies include previous ectopic pregnancy; infection of the uterus, fallopian tubes, or ovaries (pelvic inflammatory disease); pregnancywhen an IUD is in place; or pregnancyafter tuballigation.
She hasn't told anyone about her pregnancy. Upon further questioning, she discloses that she was sexuallyassaulted by a
classmate while at a party 3 months ago. She has not told anyone about the assault and still sees the person who assaulted her at school. She does not want to report the incidence because she doesn't want her boyfriend to know that he may not be the father ofher child.
Question 9-7
Legally, you:
A) Agree to her wishes to not disclose the assault.
B) Arrange for her boyfriend to undergo paternity testing.
C) Inform her that it is your legal obligation to report the assault to the authorities because she is a minor.
D) Inform her that you are going to tell her parents.
Discussion 9-7
The correct answer is "C:' All sexual assaults involving a minor must be reported to authorities, even ifthe minor does not want the assault disclosed.
� QUICKQUlZ
True or false: Pregnancy related risks in adolescents are age dependent.
A) True.
B) False.
Discussion
The correct answer is ''A:' Younger adolescents are at increased risk for pregnancy complications, including poor weight gain, anemia, pregnancy-induced hypertension, and poor prenatal care; are less likely to finish high school; and are more likely to be single parents. They may lack the maturity to care for an infant. Infants of adolescent mothers are at increased risk for prematurity and low birth weight. Pregnant adolescents are more likely to live in poverty, not finish high school and require governmental assistance. Care should be multidisciplinary, involve community resources, stress the importance of school, and provide positive reinforcement for successes.

A 16-year-old girl presents to clinic with dysuria and vaginal discharge. She has had four sexual partners in her lifetime: three male and one female. She started having sex at 12 years of age. The pH of the vaginal discharge obtained during saline mount (wet prep) collection is 7.
Question 1 0-1
Which of the following is an unlikely cause of the vaginal discharge?
A) Bacterial vaginosis.
B) Trichomoniasis.
16 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS
C) Vaginal candidiasis.
D) Gardnerella vaginalis.
E) None ofthe above.
Discussion 1 0-1
The correct answer is "C:' The pH for yeast infection is less than 4.5 (acidic), and budding yeast or pseudohyphae can be seen on KOH prep. The pH for bacterial vaginosis (caused by Gardnerella vagina/is) and trichomoniasis is greater than 4.5.
On speculum exam, you see a red and friable cervix and white, frothy discharge in the cul-de-sac.
Question 1 0-2
On thewet mount,you are likely to find:
A) Trichomonads.
B) Buddingyeast.
C) Pseudohyphae.
D) Clue cells.
E) No-clue cells.
Discussion 1 0-2
The correct answer is "A:' The clinical appearance of the discharge provides important clues to the diagnosis. Gray, frothy discharge is consistent with trichomoniasis (along with the appearance of the red, friable cervix, or "strawberry cervix"). The discharge associated with yeast infections is usually described as thick and curdlike, and adheres to vaginal walls. The discharge associated with BV is usually described as thin, grayish, and foul smelling. With BV, clue cells are present on wet prep and the whifftest is positive. No one likes a fishy odor. Ifyou chose option "E;' it suggests that you were clueless about this question.
Question 1 0-3
What additional diagnostic tests should you order?
A) Urine pregnancy test.
B) NAAT for gonorrhea.
C) NAAT for chlamydia.
D) HIV.
E) All ofthe above.
Discussion 1 0-3
The correct answer is "E:' The patient admits to having unprotected sex and already has been diagnosed with one STI (trichomonas). She is at risk for other infections as well as pregnancy. The CDC's STI screening guidelines for sexually active adolescents include (1) annual Chlamydia trachomatis screening for all females younger than 25 years old, (2) C. trachomatis screening ofmales in certain settings, and (3) annual Neisseria gonorrhoeae screening in all at-risk females. HIV screening should be discussed and encouraged for sexually active adolescents and those who use injection drugs. Screening for certain STis in asymptomatic adolescents (eg, syphilis, trichomoniasis, hepatitis B) is not recommended.
� QUICKQUlZ
Which is NOT an indication for a pelvic exam?
A) Amenorrhea.
B) Pregnancy.
C) Yearly checkup.
D) Persistent vaginal discharge.
E) Dysuria in a sexuallyactive female.
Discussion
The correct answer is "C". The guidelines for Papanicolaou (Pap) testing have changed and noninvasive STI testing is available, so fewer adolescents need pelvic exams. (See Table 1-6.)
A Pap smear and pelvic exam are no longer required at the onset of sexual activity or before prescribing birth control. Current guidelines recommend performing the first Pap test at age 21 years, with these exceptions: (1) immunocompromised (includes HIV) adolescents need annual tests once sexually active, and (2) adolescents who have alreadybeen found to have cervical intraepithelial neoplasia (CIN) 2 or 3 or carcinoma need periodic screening and, in the case ofCIN 3, treatment.
• HelpfulTip


Consider acute retroviral syndrome in any sexually active adolescent with nonspecific viral symptoms, including fever, malaise, lymphadenopathy, and skin rash. The syndrome occurs in the first few weeks of infection, before antibody testing is confirmed as positive.The testto orderforacute retroviral syndrome is an HIV PCR-DNA or HIV plasma RNA. Acutely infected patients are highly contagious during this stage.
The patient does not want her parents to know that she is being tested for STis.
TABLE1-6 IND ICATIONS FOR PELVIC
EXAMI NATION
Persistent vaginal discharge

Dysmenorrhea not helped by NSAIDs
Abnormal vaginal bleeding
IUD or diaphragm contraceptive counseling
Suspected or reported /rape or sexual abuse
Sexually active with dysuria or urinary tract symptoms
Amenorrhea
Lower abdominal pain
Perform Pap test
Pregnancy
IUD, intrauterine device; NSAID, nonsteroidal anti-inflammatory drug.
CHAPTER 1 • ADOLESCENT MEDICINE AND GYNECOLOGY 17

Question 1 0-4
You tell her:
A) Minors can consent to STI testing without parental notification.
B) Minors require parent or guardian consent for STI testing.
C) Minors can consent to STI testing but parents must be notified.
D) None ofthe above.
Discussion 1 0-4
The correct answer is ''A:' All 50 states and the District of Columbia allow minors to consent to STI services without parental notification. Eighteen states allow, but do not require, a physician to inform a minor's parents that he or she is seeking or receiving STI services when the physician deems it in the minor's best interests. A key consideration is that you can't control what is on the insurance claims.
The patient wants to knowwhat type ofcomplications could occur if she was exposed to gonorrhea.
Question 1 0-5
You explain that gonorrhea can cause all of the following EXCEPT:
A) Rash.
B) Arthritis.
C) Pelvic inflammatory disease.
D) Painless ulcer.
E) Perihepatitis.
Discussion 1 0-5
The correct answer is "D:' Gonorrhea infection can cause mucopurulent cervicitis, intermenstrual bleeding, and pelvic inflammatory disease. Disseminated gonococcal infection occurs in 1% to 3% ofindividuals with gonorrhea. It can present as petechial or pustular skin lesion, tenosynovitis, septic arthritis, and perihepatitis (Fitz-Hugh-Curtis syndrome). A painless ulcer is indicative of primary syphilis (chancre), granuloma inguinale, or lymphogranuloma venereum.
The patient's boyfriend has a history ofchlamydia, whichwas picked up on routine screening.
Question 1 0-6
What is the treatment of chlamydial infections in men?
A) Azithromycin.
B) Ceftriaxone.
C) Penicillin.
D) Metronidazole.
E) Fluconazole.
Discussion 1 0-6
The correct answer is ''A:' The preferred treatment ofchlamydia consists of a single 1 g oral dose of azithromycin or a 1-week course of doxycycline (100 mg twice daily). Those who test positive for chlamydia or gonorrhea should have a test of cure
3 months after treatment. Reinfection rates are high, especially ifpartners are not treated.
• HelpfulTip


Empiric antibiotic prophylaxis after possible STI exposure includes ceftriaxone (250 mg intramuscular injection) for gonorrhea, azithromycin (1 g orally) or doxycycline(100mgtwicedailyfor7days)forchlamydia, and metronidazole (2 g orally)fortrichomoniasis.
The patient is seen in the emergency department 2 months later with a 3-day history offever and abdominal pain, but no dysuria, vomiting, or diarrhea. She states that a new vaginal discharge developed 1 week ago. She continues to be sexually activewith sporadic use ofcondoms andhas had onenewmale sexualpartner. Herlastepisode ofunprotected sexwas 2weeks ago. On exam, she is febrile to 38.5°C (101.3°F) and has pain and rebound tenderness in the left lower quadrant. On pelvic exam, her SMR is 5 with normal external genitalia. On speculum exam, there is discharge coming from the cervical os. On bimanual exam, cervical motion tenderness and fullness of the left adnexa are present.
Question 10-7
Which is NOT a diagnostic criterion for her acute condition?
A) Uterine tenderness.
B) Adnexal tenderness.
C) Lower abdominal pain.
D) History ofsexual activity.
E) Positive result for Neisseria gonorrhoeae.
Discussion 1 0-7
The correct answer is "E:' Pelvic inflammatory disease (PID) is an infection of the upper reproductive tract, including endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis Adolescent girls are disproportionately affected. Infection occurs when lower genital tract (vagina, cervix) bacteria move into the upper genital organs. Symptoms range from mild to severe. The CDC recommends treatmentfor presumed PID in a sexually active woman at risk for STis presenting with the minimum clinical criteria of (1) lowerabdominal or pelvic pain and (2) uterine, adnexal, or cervical motion tenderness. Supportive criteria include fever (> 38.3°C [100.9°F]), mucopurulent discharge (vaginal, cervix), white blood cells on saline microscopy, elevated inflammatory markers, and known positivity for N. gonorrhoeae or C. trachomatis. Don't forget you have to rule out alternative causes first. (See Table 1-7.)
Question 1 0-8
Which is a bacterial cause of PID?
A) Neisseria gonorrhea.
B) Chlamydia trachomatis.
C) Ureaplasma urealyticum.
D) Haemophilus influenzae.
E) All ofthese bacteria can cause PID.
18 MCGRAW-HILL EDUCATION SPECIALTY BOARD REVIEW: PEDIATRICS