This publication is available digitally at https://isass.org/category/news/ vertebral-columns/
From the Department of Orthopaedic Surgery at Rush University Medical Center in Chicago, Illinois.
Using Endoscopic Surgery For Thoracic Pathology:
Learning from Cervical and Lumbar Techniques
Unlike in the cervical and lumbar spine, pathology in the thoracic spine requiring surgery is not seen very often. Thoracic disc herniation (Figure 1) and stenosis are fairly uncommon with an estimated incidence of 1 case per 1,000,000 people.1 Patients may present with a variety of symptoms, such as back pain, radiculopathy, lower extremity weakness, urinary or bowel incontinence, and difficulty walking, which can make a correct diagnosis difficult.1–4 People with progressive myelopathic symptoms due to acute thoracic disc herniation or those with giant, heavily calcified herniations are often strongly recommended for surgery.1,2,5 Traditional surgical techniques, such as posterior decompression with instrumented fusion, anterior transthoracic approaches, or thoracoscopy are successful but carry with them significant rates of complications.1,6–8 In a systematic review, Court et al 1 found a significant rate of complications across several surgery techniques, including dural breach, worsening neurologic symptoms, intercostal neuralgia, and lung-related complications. A meta-analysis of 545 patients who underwent thoracoscopy for discectomy for thoracic herniation found that 24% experienced complications. This included pleural complications in 6% of cases and intercostal neuralgia in another 6% of cas -
Sagittal MRI of the thoracic spine showing disc herniation (arrow).
Source: Adapted from Corenman D. Herniated disc thoracic spine. NeckandBack.com. https://neckandback.com/conditions/herniated-disc-thoracic-spine/ es. 9 In a review of 17 patients undergoing mini-thoracotomy for thoracic disc herniation, Roelz et al found that 23% of patients experienced neurological deterioration in the postoperative period.10 In many places, the aforementioned approaches are still used to
Gregory Snigur, MS
John Sencaj, MD
Shriya Patel, BS
Sloane Ward, BS
Kern Singh, MD
Figure 1
address thoracic disc pathology. However, recent advancements in endoscopic spine surgery have offered a novel technique.
With a common patient preference for minimal invasiveness and modern improvements in technology, endoscopy has become increasingly pursued in spine surgery. Endoscopic techniques, such as unilateral biportal endoscopy or full endoscopy, have become popular among many spine surgeons performing decompressions in the cervical and lumbar spine.11–13 Early studies have demonstrated several potential benefits when compared to other minimally invasive surgery (MIS) techniques, including less tissue disruption, reduced blood loss, shorter postoperative length of stay, less postoperative pain, ambulatory capacity, enhanced visualization, and similar longterm patient-reported outcome measures.14–17
Regarding cervical spine studies, a meta-analysis of percutaneous endoscopic cervical discectomy (PECD) for cervical disc herniation performed by Zhang et al16 showed a high rate of successful treatment with a low incidence of adverse events or recurrence. Additionally, when compared to anterior cervical discectomy and fusion (ACDF), PECD demonstrated a higher rate of excellent outcomes (47% for PECD versus 39% for ACDF) and a lower average operative time and postoperative length of stay. In a retrospective review of 114 patients who underwent full endoscopic cervical spine procedures, Shen et al 15 reported similar improvements in NDI and VAS scores when compared to ACDF with no report of major complications. While the adoption of endo -
scopic techniques in cervical pathology is relatively new, the data suggest that outcomes are no worse if not better than outcomes with more established, traditional techniques. Recent data surrounding the implementation of endoscopic techniques in lumbar spine pathology is also marked by improved clinical outcomes, namely reduced recovery times, less postoperative pain, and lower risk of infection. In a meta-analysis comparing outcomes between endoscopic and MIS techniques in the treatment of lumbar stenosis, Perez-Roman et al found that patients who underwent endoscopic intervention appeared to report significantly less postoperative lower back pain and had a significantly reduced length of hospital stay after surgery.18 Additionally, they found no significant differences in visual analog scale (VAS) scores, Oswestry Disability Index (ODI) scores, or complication rates between groups, suggesting that longer term surgical outcomes are similar. Another systematic review found that outcomes following unilateral biportal endoscopic discectomy were comparable to lumbar microdiscectomy.19 Additionally, a retrospective cohort study comprising 99 patients treated with MIS-TLIF or Endo-LIF, showed no significant differences in VAS, ODI, and MacNab criteria at preoperative and at 1-month, 3-month, and 1-year postoperative intervals. 20 These findings suggest that outcomes with endoscopic interventions are similar, if not better, when considering that there is less incurred damage to surrounding tissues and quicker immediate postoperative recovery.
Although seen with a much less frequency, it is likely that these results have in part inspired the implementation of endoscopic techniques in thoracic pathology. There are several factors that make this transition challenging and deserving of careful examination. Surgeons widely recognize that interventional procedures at the thoracic level are inherently complex and technically demanding. Decompression surgeries in the thoracic spine pose greater challenges than those in the lumbar spine due to the anatomical complexity and proximity to vital structures, such as the Adamkiewicz artery. 5,21 The attachment of the rib cage, narrower spinal canal, and higher density of critical neural and vascular structures heightens the risk of complications. Moreover, thoracic vertebrae have denser cortical bone and unique morphology, necessitating specialized approaches.1,2,5 These factors collectively require meticulous planning and advanced surgical expertise for successful outcomes.
Several studies have demonstrated successful introduction of endoscopic techniques for thoracic pathology. 4,5,21,22 A retrospective case review of 8 patients who underwent fully endoscopic transforaminal and posterior approaches for severe stenosis of thoracic spinal canal showed great results. By combining both techniques, surgeons were able to achieve 360° decompression as an outpatient procedure under local anesthesia with intravenous sedation. 4 At final follow-up, all patients reported significant improvement in symptoms with an average VAS score of 2.7, an improvement from an average preoperative VAS score of 8.1.
There were also no reports of neurological deterioration. Despite successful decompression through both windows, the authors reported relatively longer operating times given limitations of instrumentation per endoscope channel. A retrospective cohort of 55 patients with thoracic disc herniation undergoing full endoscopic decompression showed similar symptom improvement in all patients. 23 Additionally, no serious complications were observed. The results of endoscopic surgery to address thoracic pathology have been promising. It is true that steep learning curves have been associated with adoption of endoscopic techniques, which may partly explain the slower adoption for this technique in thoracic pathologies, given the rarity of their presentation. Studies have shown that spine surgeons require 20 to 24 cases before becoming greater than 90% proficient in a given endoscopic technique.24,25 Some studies have also suggested that endoscopic spine surgery increases operative time and costs. 26 Given the challenge of acquiring enough cases to reach proficiency, the more extensive surgical planning required for thoracic pathologies, and initially greater surgical times associated with endoscopic techniques, consideration into the compounding prolongation of operative times should be undertaken. In summary, the use of endoscopic surgery techniques for thoracic spine pathologies, while complex and technically demanding, has shown promising results. The transition from traditional surgical approaches to endoscopic methods is driven by the benefits observed in cervical and lumbar spine sur-
geries, including reduced tissue disruption, less postoperative pain, and shorter recovery times. Early studies indicate that endoscopic techniques for thoracic pathologies can achieve significant symptom improvement with minimal complications. However, the
References
1. Court C, Mansour E, Bouthors C. Thoracic disc herniation: surgical treatment. Orthop Traumatol Surg Res . 2018;104:S31–S40.
2. Vanichkachorn JS, Vaccaro AR. Thoracic disk disease: diagnosis and treatment. J Am Acad Orthop Surg. 2000;8:159–169.
3. Linscott MS, Heyborne, R. Thoracic intervertebral disk herniation: a commonly missed diagnosis. J Emerg Med. 2007;32:235–238.
4. Shen J, Telfeian AE. Fully endoscopic 360° decompression surgery for thoracic spinal stenosis: technical note and report of 8 cases. Pain Physician. 2020;23:E659–E663.
5. Bae J, Lee SH, Wagner R, Shen J, Telfeian AE. Full endoscopic surgery for thoracic pathology: next step after Mastering lumbar and cervical endoscopic spine surgery? Biomed Res Int . 2022;2022, 8345736.
6. Dimar JR 2nd, Bratcher KR, Glassman SD, Howard,JM, Carreon LY. Identification and surgical treatment of primary thoracic spinal stenosis. Am J Orthop. 2008;37:564–568.
7. Oppenlander ME, Clark JC, Kalyvas J, Dickman CA. Surgical management and clinical outcomes of multiple-level symptomatic herniated thoracic discs. J Neurosurg Spine. 2013;19:774–783.
8. Machino M, Yukawa Y, Ito K, Nakashima H, Kato F. A new thoracic reconstruction technique ‘transforaminal thoracic interbody fusion’: a preliminary report of clinical outcomes. Spine 2010; 35;E1000–5.
9. Elhadi AM, Zehri AH, Zaidi HA, et al. Surgical efficacy of minimally invasive thoracic discectomy. J Clin Neurosci. 2015;22:1708–1713.
steep learning curve and the anatomical challenges of the thoracic spine necessitate meticulous planning and advanced surgical expertise. Continued research and refinement of these techniques will be essential to fully establish their efficacy and safety. l
10. Roelz R, Scholz C, Klingler JH, Scheiwe C, Sircar R, Hubbe U. Giant central thoracic disc herniations: surgical outcome in 17 consecutive patients treated by mini-thoracotomy. Eur Spine J. 2016;25:443–1451.
11. Kwon O, Yoo SJ, Park JY. Comparison of unilateral biportal endoscopic discectomy with other surgical technics: a systemic review of indications and outcomes of unilateral biportal endoscopic discectomy from the current literature. World Neurosurg. 2022;168:349–358.
12. Chang CJ, Liu YF, Hsiao YM, et al. Full endoscopic spine surgery for cervical spondylotic myelopathy: a systematic review. World Neurosurg. 2023;175:142–150.
13. Shepard NA, Protopsaltis T, Kim Y. Lumbar endoscopic spine surgery: a comprehensive review. Bull Hosp Jt Dis . 2021;79:35–42.
14. Gadjradj PS, Harhangi BS, Amelink J, et al. Percutaneous transforaminal endoscopic discectomy versus open microdiscectomy for lumbar disc herniation: a systematic review and meta-analysis. Spine. 2021;46:538–549.
15. Shen J, Telfeian AE, Shaaya E, et al. Full endoscopic cervical spine surgery. J Spine Surg. 2020;6:383–390.
16. Zhang J, Zhou Q, Yan Y, et al. Efficacy and safety of percutaneous endoscopic cervical discectomy for cervical disc herniation: a systematic review and meta-analysis. J Orthop Surg Res . 2022;17:519.
17. Compagnone D, Mandelli F, Ponzo M, et al. Complications in endoscopic spine surgery: a systematic review. Eur Spine J. 2024;33:401–408.
18. Perez-Roman RJ, Gaztanaga W, Lu VM, Wang MY. Endoscopic decompression for the treatment of lumbar spinal stenosis: an updated systematic review and meta-analysis. J Neurosurg Spine. 2022;36:549–557.
19. Özer Mİ, Demirtaş OK. Comparison of lumbar microdiscectomy and unilateral biportal endoscopic discectomy outcomes: a single-center experience. J Neurosurg Spine . 2024;40:351–358.
20. Silva JDS, Carelli LE, de Oliveira JAA, de Araújo RML. Full-endoscopic discectomy for thoracic disc herniations: a single-arm meta-analysis of safety and efficacy outcomes. Eur Spine J. 2023;32:1254–1264.
21. Gibson RDS, Wagner R, Gibson JNA. Full endoscopic surgery for thoracic pathology: an assessment of supportive evidence. EFORT Open Rev. 2021;6:50–60.
22. Silva JDS, Carelli LE, de Oliveira JAA, de Araújo RML. Full-endoscopic discectomy for thoracic disc herniations: a single-arm meta-analysis of safety and efficacy outcomes. Eur Spine J. 2023;32:1254–1264.
23. Ruetten S, Hahn P, Oezdemir S, et al. Full-endoscopic uniportal decompression in disc herniations and stenosis of the thoracic spine using the interlaminar, extraforaminal, or transthoracic retropleural approach. J Neurosurg Spine. 2018;29:157–168.
24. Chen L, Zhu B, Zhong HZ, et al. The learning curve of unilateral biportal endoscopic (UBE) spinal surgery by CUSUM analysis. Front Surg. 2022;9:873691.
25. Kang MS, Park HJ, Park SM, You KH, Ju WJ. Learning curve for biportal endoscopic posterior cervical foraminotomy determined using the cumulative summation test. J Orthop Surg Res . 2023;18:146.
26. Findlay MC, Hamrick FA, Kim RB, Twitchell S, Mahan MA. Hospital cost differences between open and endoscopic lumbar spine decompression surgery. J Neurosurg Spine . 2024;40:77–83.
From Somers Orthopaedic Surgery & Sports Medicine Group in Mt. Kisco, New York (Dr Perfetti), and the Texas Back Institute in Plano, Texas (Drs Satin and Derman).
Anterior cervical discectomy and fusion (ACDF) utilizing a cage and plate construct (CPC) is the established gold standard treatment for cervical degenerative disease. Ventral cervical plating enhances segmental stability, reducing the risk of collapse and kyphosis.1 However, plate placement extends surgical times and may require wider surgical exposure, increasing the risk of soft tissue swelling, esophageal injury, dysphagia, hematoma and adjacent segment disease.2
Zero-profile integrated ACDF devices (Figure) allow for decreased soft tissue dissection and retraction, decreased mass effect on retropharyngeal structures, and decreased adjacent segment degeneration.2 However, zero-profile cages may be more susceptible to cage subsidence, graft collapse, and cervical kyphosis. 3
Zero-profile stand-alone (SA) cages approach the biomechanical profiles of traditional CPCs for single-level disease. In the setting of multi-level constructs, CPCs are biomechanically stiffer with a significantly lower range of motion in flexion and extension compared to multi-level
anchored devices without plating.4 The primary objective of this review is to compare the clinical and radiographic outcomes of ACDF using SA cages versus conventional CPCs in single and multi-level constructs.
Clinical Outcomes
Stand-alone cages have exhibited statistically significant advantages over CPCs in several perioperative outcomes. A recent meta-analysis comparing SA to CPC cohorts found significant differences regarding operative time, intraoperative blood loss, and length of stay in favor of the SA cohort.5 The clinical difference in minutes or millimeters was not further characterized. Presumably, as the number of levels increases, so too would the differences in surgical duration, intraoperative bleeding, and length of stay. When comparing SA devices versus CPCs for 3-level constructs, Zhu et al found the SA self-locking cohort had shorter operative times (100.8 ± 24 min) compared with the CPC fixation group (130 ± 18) ( p < 0.05).6 Interestingly, there were no differences between the 2 groups in blood loss, postoperative drainage, or hospital stay (p > 0.05).6 Moreover, no statistically significant differences in neck pain visual analog scale (VAS) scores, Japanese Orthopaedic Association (JOA) scores, or Neck
Figure. Example of a zero-profile anterior cervical discectomy and fusion device. Image courtesy of DeGen Medical, Charleston, SC.
Dean C. Perfetti, MD, MPH
Alexander M. Satin, MD
Peter B. Derman, MD, MBA
CERVICAL SPINE
Disability Index (NDI) scores were observed at 3-month follow-up.6 A large meta-analysis also found no statistical difference between SA and CPC in terms of operative time, length of stay, and patient-reported clinical outcomes including VAS neck score, VAS arm score, JOA score, and NDI score.7 Both techniques effectively decompress the cervical spine and promote neurologic recovery as exhibited by comparable JOA, NDI, and VAS scores at 6-month follow up.5
Dysphagia and dysphonia are known complications after an anterior-based approach, with an incidence as high as 50%.8 The most prevalent clinical difference in the aforementioned studies comparing SA and CPCs is the increased incidence of postoperative dysphagia in CPCs. 5,7 Zavras et al found that their CPC cohort patients reported worse swallowing at 6 weeks in both 1-level ACDF ( p = 0.05) and 2-level ACDF ( p = 0.038) compared to the SA cohort. 9 While Mean Voice Handicap Index and Eating Assessment Tool scores improved significantly from discharge to last follow-up in both single-level groups (p < 0.05), at 6-month follow up, SA patients demonstrated greater improvements in their Voice Handicap Index.10
Hofstetter et al utilized prevertebral space swelling on postoperative radiographs as a proxy for dysphagia and found significantly more swelling in the prevertebral space (20.4 ± 0.9 mm) after implantation of an anterior locking plate compared to the zero-profile device (15.6 ± 0.7 mm, p < 0.001).11 This difference remained significant at 6-month follow-up (p = 0.035).11 Cheung et al found in their meta-analysis that dysphagia within 3 months of surgery was significantly less common in the SA group compared to the CPC group (OR 0.32; p < 0.01).7
Radiographic Outcomes
Radiographic parameters to consider when comparing the two techniques are subsidence, fusion, sagittal alignment, and adjacent segment disease. CPC require more extensive exposure to accommodate the plate, which may encroach on adjacent disc levels. However, CPCs have also been shown to better preserve sagittal Cobb angles, the loss of which has been linked to postoperative functional disability.3 A meta-analysis comparing postoperative C2-C7 Cobb angles found a significantly lower Cobb angle in the SA group compared to the CPC group (difference of 1.4°, p = 0.04).7 Parameters for subsidence differ across studies but are generally defined as a >3 mm reduction in intervertebral body height or >3 mm reduction between the midpoint of the upper margin of the upper vertebral body and lower margin of the lower vertebral body.7 A meta-analysis including single- and multi-level fusions determined that CPCs had significantly higher vertebral fusion rates (OR 1.98, 95% CI 1.16-3.37) with lower subsidence rates (OR 0.31, 95% CI 0.18-0.52) compared to SA patient cohorts.12 However, the literature remains divided when performing sub-analyses on these patient cohorts. A recent study showed no difference in radiographic parameters for both 1- and 2-level ACDF SA and CPC constructs, specifically for fusion rates, subsidence rates, disc height correction, and sagittal parameters.9 However, this study was underpowered with fewer than 12 patients in each of the 4 arms.9 Mari et al showed that single-level SA cages do not statistically differ in the rate of subsidence (50% SA, 33.3% CPC, p = 0.32), although 2-level SA fusions exhibited an increased subsidence risk at 12 months (75%
vs 28.5%, p = 0.046).13 An early study comparing 2-level ACDF in 54 patients (28 SA to 26 CPC) found no significant differences in fusion rates (96% for both, p > 0.05) or segmental kyphosis of greater than 5° (14.3% SA vs 7.7% CPC, p > 0.05).14 However, subsidence was significantly increased in the SA group (35.7% vs 11.5%, p < 0.05).14 Ji et al performed a 2-year follow-up study on 2-level constructs and found that, while the SA patient cohort had a similar fusion rate compared to the CPC cohort (95% vs 100%, p = 0.335), there was an increased rate of ASD in the CPC group.15 Additionally, a recent meta-analysis comparing SA to CPC cohorts in single- and multi-level fusions found a lower
References
1. Ugokwe K. Anterior subaxial cervical fixation techniques. In: Benzel E, ed. Benzel’s Spine Surgery: Techniques, Complication Avoidance and Management. 4th ed. Elsevier; 2016.
2. Sang-Soak Ahn, Ho-Kyu Paik, et al. The fate of adjacent segments after anterior cervical discectomy and fusion: the influence of an anterior plate system. World Neurosurg. 2016;89:42-50.
3. Kwon WK, Kim PS, Ahn SY, et al. Analysis of associating factors with C2-7 sagittal vertical axis after two-level anterior cervical fusion: comparison between plate augmentation and stand-alone cages. Spine (Phila Pa 1976). 2017;42:318-325.
4. Scholz M, Schleicher P, Pabst S, Kandziora F. A zero-profile anchored spacer in multilevel cervical anterior interbody fusion: biomechanical comparison to established fixation techniques. Spine (Phila Pa 1976). 2015;40(7):E375-E380.
5. Elias E, Daoud A, Smith J, Elias C, Nasser Z. Assessing surgical outcomes for cage plate system versus stand-alone cage in anterior cervical discectomy and fusion: a systematic review and meta-analysis. World Neurosurg. 2024;185:150-164.
CERVICAL SPINE
rate of ASD in the SA group (OR 0.33, 95% CI 0.18-0.58, p = 0.0001).5
Conclusion
Both SA and CPC techniques exhibit comparable effectiveness in a majority of short-term perioperative clinical and radiographic outcomes. However, SA techniques significantly reduce the incidence of postoperative dysphagia and adjacent segment disease. This may come at the expense of cage subsidence and decreased ability to preserve cervical lordosis, especially in multi-level cases. Studies with higher levels of evidence and long-term follow-up are needed to better characterize these differences. l
6. Zhu D, Zhang D, Liu B, Li C, Zhu J. Can self-locking cages offer the same clinical outcomes as anterior cage-with-plate fixation for 3-level anterior cervical discectomy and fusion (ACDF) in mid-term follow-up? Med Sci Monit. 2019;25:547-557.
7. Cheung ZB, Gidumal S, White S, et al. Comparison of anterior cervical discectomy and fusion with a stand-alone interbody cage versus a conventional cage-plate technique: a systematic review and meta-analysis. Global Spine J. 2019;9(4):446-455.
8. Bazaz R, Lee MJ, Yoo JU. Incidence of dysphagia after anterior cervical spine surgery: a prospective study. Spine (Phila Pa 1976). 2002;27(22):2453-2458.
9. Zavras AG, Nolte MT, Sayari AJ, Singh K, Colman MW. Stand-alone cage versus anterior plating for 1-level and 2-level anterior cervical discectomy and fusion: a randomized controlled trial. Clin Spine Surg. 2022; 35(4):155-165.
10. Panchal RR, Kim KD, Eastlack R, et al. A clinical comparison of anterior cervical plates versus stand-alone intervertebral fusion devices for single-level anterior cervical discectomy and fusion procedures. World Neurosurg. 2017;99:630-637.
11. Hofstetter CP, Kesavabhotla K, Boockvar JA. Zero-profile anchored spacer reduces rate of dysphagia compared with ACDF with anterior plating. J Spinal Disord Tech. 2015;28(5):E284-E290.
12. Oliver JD, Goncalves S, Kerezoudis P, et al. Comparison of outcomes for anterior cervical discectomy and fusion with and without anterior plate fixation: a systematic review and meta-analysis. Spine (Phila Pa 1976). 2018;43(7):E413-E422.
13. Mari AR, Zeeshan QM, Uddin MM, Zulfiqar F, Kumar R, Ali MM. Comparison of radiological outcome in anterior cervical discectomy and fusion: cage-only v/s cage and plate fixation. Pakistan J Med Health Sci. 2022;16(5):1033-1035.
14. Oh JK, Kim TY, Lee HS, et al. Standalone cervical cages versus anterior cervical plate in 2-level cervical anterior interbody fusion patients: clinical outcomes and radiologic changes. J Spinal Disord Tech. 2013;26(8):415-20.
15. Ji GY, Oh CH, Shin DA, Ha Y, Kim KN, Yoon DH, Yudoyono F. Stand-alone cervical cages versus anterior cervical plates in 2-level cervical anterior interbody fusion patients: analysis of adjacent segment degeneration. J Spinal Disord Tech. 2015;28(7):E433-E438.
From the Department of Orthopaedics Spine at UC Davis Health in Sacramento, California.
Iliac Crest Autograft
No
Longer the Gold Standard—How to Evaluate Osteobiologics in 2024
For decades, the iliac crest autograft has been considered the gold standard in bone grafting due to its osteogenic potential and clinical reliability. However, with advancements in osteobiologic materials and techniques, the landscape of osteobiologics is rapidly evolving. In 2024, evaluating bone graft options requires a multifaceted approach that goes beyond traditional methods. Surgeons must consider regulatory pathways, levels of evidence, product variability, safety concerns, and cost to make informed decisions. The present article serves as a quick overview of the mechanisms and regulatory pathways, based on available evidence, guiding surgeons in selecting the most effective graft materials for their patients.
Key Factors in Evaluating
Osteobiologics: Regulatory Pathways, Evidence, and Costs1–5
Regulatory Pathways
Each osteobiologic category comes with distinct mechanisms and regulatory requirements. Nonstructural allografts and cellular-based allografts, regulated under Human Cells, Tissues, and Cellular and Tissue-Based Products, require no premarket Food and Drug Administration (FDA)
review but rely on long-standing clinical experience. Demineralized bone matrices (DBMs) and synthetic bone grafts follow the 510(k) pathway as autograft extenders in posterior lumbar fusion (PLF), supported by animal studies and limited clinical data. Autologous cellular grafts, approved via 510(k) for concentration devices, and Class III drug-device combination products like bone morphogenetic protein 2 (BMP-2) and P-15 peptides, necessitate robust human clinical studies, such as investigational device exemption and premarket approval, to ensure high safety and efficacy.
Levels of Evidence
Evaluating the evidence is crucial in determining the effectiveness of osteobiologics. The hierarchy of evidence ranges from Level 1, characterized by high-quality randomized controlled trials (RCTs), to Level 5, which includes expert opinions and consensus. Level 1 evidence is marked by sufficient sample sizes to reduce bias, blinded study designs to eliminate evaluator bias, comprehensive follow-up periods beyond 1 year, CT scans as the gold standard for imaging, and representative population inclusion with subgroup analyses of high-risk patients. These characteristics are essential to ensure the reliability and validity of the study outcomes.
Safdar N. Khan, MD
Hania Shahzad, MD
Costs
Cost is another significant factor in the evaluation process, with prices varying widely across different osteobiologics. BMP, platelet-derived growth factor (PDGF), and P-15 peptide products are the most expensive, ranging from $3,500 to $4,000, followed by cellular-based allografts at approximately $2,000. Second-generation synthetic grafts average around $1,500, while first-generation synthetics range from $1,000 to $1,200. DBMs are priced slightly higher than first-generation synthetics, around $1,200 to $1,300, and allografts are the most cost-effective at approximately $200. The high cost of advanced products like BMP-2 and P-15 peptides must be weighed against their substantial evidence base and clinical benefits.
Comparative Evaluation of Osteobiologics: Efficacy, Safety, and Level of Evidence
DBM
DBM is an allograft bone devoid of its mineral phase, consisting of collagen and non-collagenous proteins, available in formats such as putty, gel, and flexible sheets. Its osteoinductive potential relies on proteins such as BMP-2 and BMP-7, which vary significantly among donors and manufacturers. This variability, up to 4-fold in BMP-2 content, along with processing and sterilization, can greatly decrease osteoinductivity. DBMs must be tracked as donor-derived products. 2,6–8 Clinical evidence for DBM efficacy is limited with few Level 1 studies available. 9 Grafton
DBM, mixed with allograft/local autograft, has been examined in 3 randomized controlled trials (RCTs).10–12 The most recent Level 1 study compared Grafton DBM with local autograft to iliac crest bone graft in single-level PLF procedures and found no statistically significant difference between groups at the final 2-year analysis.10 However, this study excluded smokers and included few diabetic patients, with no power calculation reported, limiting its reliability and generalizability. No Level 1 studies have evaluated Grafton as a standalone bone graft, raising questions about the direct contribution to fusion outcomes. While DBM is a cost-effective and safe osteobiologic, its limited evidence and product variability necessitates cautious interpretation of its clinical efficacy. More comprehensive, high-quality studies are needed to fully establish their role in bone grafting procedures.
Synthetic Bone Grafts
Synthetic bone graft materials, particularly early-generation calcium phosphate–based ceramics, have a composition similar to the inorganic component of bone, making them osteoconductive and supportive of bone growth on their surface. These materials elicit minimal immunologic reactions, exhibit negligible systemic toxicity, are easy to sterilize, and come in various sizes and shapes. 2,6,13 Early synthetic ceramics were also relatively inexpensive. Later-generation synthetics have demonstrated osteoinductive capacity in animal models, indicating their ability to induce
The iliac crest autograft is no longer the exclusive gold standard in bone grafting.
Evaluating modern osteobiologics, including DBM, synthetic bone grafts, CBAs, BMPs, and P-15 peptides, requires a thorough consideration of regulatory pathways, evidence levels, product variability, safety, and cost.
new bone formation.13 However, most lack published Level 1 evidence, with Vitoss and AttraX Putty being notable exceptions. An RCT evaluated AttraX Putty in PLF, comparing it to iliac crest/local autograft in 87 patients.13 The trial showed a 1-year fusion rate of 55% for AttraX and 52% for autograft, with an overall rate of 72% ( p = 0.617). Despite being a Level 1 study, it had several limitations: a short follow-up period of 1 year, no subgroup analysis of high-risk patients, and inconsistent unilateral fusion rates. The intra-patient study design also meant clinical outcomes and adverse events could not be separately attributed to the treatment conditions. Synthetic bone grafts benefit from reduced product variability due to standardized manufacturing processes and have minimal safety concerns compared to control groups. While it is more costly than DBMs, synthetics offer a reliable and uniform option. However, the lack of comprehensive, long-term studies and subgroup analyses of high-risk patients highlights the need for
further research to confirm their long-term efficacy and clinical outcomes in diverse patient populations.
Cellular-Based Allografts (CBAs)
CBAs combine osteoconductive carriers with cryopreserved allogeneic stem cells. 2 However, their effectiveness in promoting bone fusion has been questioned due to significant variability in clinical outcomes and potential safety concerns related to pathogen transmission.14 Animal studies have raised doubts about the cellular component’s role in successful fusion, with research indicating that DBM is the primary contributor to fusion, regardless of whether live or dead cells are used. 15 Currently, no Level 1 studies exist for CBA stem cell products. 2 Nonetheless, representative studies provide some insight into their clinical efficacy. For instance, a study on OsteoCel reported a 90.5% fusion rate at 1 year using the Trinity Elite matrix in an uncontrolled, prospective, multicenter, open-label trial.16 Despite the high fusion rate, the study was not randomized or controlled and included 274 patients, of whom only 62% underwent a single-level procedure. In the patient cohort, 15% were smokers and 20% had diabetes, which can significantly impact fusion outcomes. Moreover, no power calculation was reported, further limiting the study’s reliability. Although current procedures aim to limit the spread of known pathogens,14 in 2021, a multistate outbreak of tuberculosis was linked to a single lot of the CBA product FiberCel by Aziyo Biologics, resulting in
infections in at least 19 patients and more than 100 healthcare workers, leading to a product recall.17–19
Studies on CBAs, including those on products such as the Trinity Elite matrix, lack rigorous design elements such as randomization and control groups, making it difficult to draw definitive conclusions about their efficacy and safety. The high cost of CBAs poses a barrier to their widespread adoption. The economic burden associated with these products needs careful consideration, especially given the limited evidence supporting their use. More comprehensive, high-quality studies are necessary to fully establish the role of CBAs in bone grafting procedures.
BMPs
Recombinant BMPs are potent bone-forming agents that drive mesenchymal stem cells into the osteoblastic lineage, crucial for bone formation and healing. They can be integrated into carrier matrices to enhance their effectiveness. 2,6 Recombinant BMP-2 (rhBMP-2) has been extensively studied for its efficacy in promoting spinal fusion. Since the first RCT by Boden et al in 2000, more than 20 RCTs have compared rhBMP-2 with iliac crest bone graft. 6,20 These studies collectively support rhBMP-2’s efficacy in enhancing fusion rates, despite some limitations such as inconsistent reporting of randomization and allocation methods and a lack of independent blinding in most trials. A representative multicenter, prospective, randomized trial involving 279 patients undergoing single-level anterior
lumbar interbody fusion compared the use of INFUSE (rhBMP-2) with iliac crest autograft. 21 Patients and surgeons were unblinded, but radiographic assessments were blinded. The trial showed a fusion rate of 94.5% for INFUSE at 2 years compared to 88.7% for iliac crest autograft. Overall success at 2 years was 57.1% for INFUSE and 56.7% for iliac crest autograft. 22 Despite the robust sample size and blinded radiographic assessments, the study’s lack of blinding for patients and surgeons was a limitation. It was also among the first to use thin-cut CT for more precise fusion assessment. The high fusion rates observed with INFUSE underscore its efficacy, though the marginal difference in overall success rates compared to iliac crest autograft suggests a need for further investigation into other contributing factors. Furthermore, notable safety concerns, including heterotopic bone formation, radiculitis, and dysphagia, have emerged. 23 Additionally, there is an ongoing debate about the potential increased risk of cancer, necessitating further investigation. The high cost of BMPs is another significant consideration for healthcare providers and patients when evaluating their overall value and feasibility in clinical practice.
P-15 peptide
P-15 peptide, a 15-amino acid sequence found in human type I collagen, facilitates the attachment and activation of osteogenic cells, accelerating bone regeneration. 24–26 The evidence supporting P-15 is robust, derived from Level 1 investigational drug
exemption studies, including an RCT for P-15/ABM in ACDF. 26 This trial demonstrated superior overall success compared to local autograft, with consistent efficacy and safety observed over a 6-year follow-up period. 27-29 Safety assessments have shown no significant concerns compared to the control group, reinforcing its reliability for clinical use. Despite its high cost, P-15 peptide offers a valuable option in spinal fusion surgeries, with substantial evidence backing its effectiveness and safety.
Conclusion
The iliac crest autograft is no longer the exclusive gold standard in bone grafting.
Evaluating modern osteobiologics, including DBM, synthetic bone grafts, CBAs, BMPs, and P-15 peptides, requires a thorough consideration of regulatory pathways, evidence levels, product variability, safety, and cost (Table). DBM and synthetics are cost-effective but have variable efficacy and limited evidence. CBAs offer potential but are challenged by variability and safety concerns. BMPs demonstrate strong efficacy but are associated with high costs and safety issues. P-15 peptides are effective and safe but also expensive. Comprehensive, high-quality studies are essential to confirm the long-term outcomes and clinical utility of these alternatives. l
HCT/P
Safety concerns None vs Control
None vs Control Pathogen transmission Heterotopic bone formation, radiculitis, dysphagia, potential for increased cancer risk vs control None vs Control
Abbreviations: BMP, bone morphogenic protein; CBA, cellular-based allograft; DBM, demineralized bone matrix; HCT/P, human cells, tissues, and cellular and tissue-based products; IDE, investigational drug exemption; PMA, premarket approval.
Table. Comparative Analysis of Osteobiologics: Regulatory Pathways, Evidence, and Considerations
References
1. Basic principles of bone grafts and bone substitutes. Accessed June 4, 2024. https://medilib.ir/uptodate/show/134456
2. Abjornson C, Brecevich A, Callanan T, Dowe C, Cammisa FP, Lorio MP. ISASS recommendations and coverage criteria for bone graft substitutes used in spinal surgery. Int J Spine Surg. 2018;12(6):757-771.
3. Levels of evidence for primary research question. North American Spine Society. https://www.spine.org/documents/researchclinicalcare/levelsofevidence.pdf
4. Kitchen D, Rao PJ, Zotti M, et al. Fusion assessment by MRI in comparison with CT in anterior lumbar interbody fusion: a prospective study. Glob Spine J. 2018;8(6):586-592.
5. Khan SN, Shahzad H. Osteobiologics and value-based care: challenges and opportunities. Int J Spine Surg. 2023;17(S3):S44-S52.
6. Gupta A, Kukkar N, Sharif K, Main BJ, Albers CE, El-Amin III SF. Bone graft substitutes for spine fusion: A brief review. World J Orthop. 2015;6(6):449-456.
7. Bae H, Zhao L, Zhu D, Kanim LE, Wang JC, Delamarter RB. Variability across ten production lots of a single demineralized bone matrix product. JBJS . 2010;92(2):427.
8. Bae HW, Zhao L, Kanim LEA, Wong P, Delamarter RB, Dawson EG. Intervariability and intravariability of bone morphogenetic proteins in commercially available demineralized bone matrix products. Spine . 2006;31(12):1299.
9. Shepard NA, Rush AJ, Scarborough NL, Carter AJ, Phillips FM. Demineralized bone matrix in spine Surgery: a review of current applications and future trends. Int J Spine Surg. 2021;15(s1):113-119.
10. Kang J, An H, Hilibrand A, Yoon ST, Kavanagh E, Boden S. Grafton and local bone have comparable outcomes to iliac crest bone in instrumented single-level lumbar fusions. Spine . 2012;37(12):1083.
11. An HS, Simpson JM, Glover JM, Stephany J. Comparison between allograft plus demineralized bone matrix versus autograft in anterior cervical fusion: a prospective multicenter study. Spine . 1995;20(20):2211.
12. Cammisa FPJ, Lowery G, Garfin SR, et al. Two-year fusion rate equivalency between Grafton® DBM gel and autograft in posterolateral spine fusion: a prospective controlled trial employing a side-by-side comparison in the same patient. Spine . 2004;29(6):660.
13. Lehr AM, Oner FC, Delawi D, et al. Efficacy of a standalone microporous ceramic versus autograft in instrumented posterolateral spinal fusion: a multicenter, randomized, intrapatient controlled, noninferiority trial. Spine . 2020;45(14):944.
14. Campana V, Milano G, Pagano E, et al. Bone substitutes in orthopaedic surgery: from basic science to clinical practice. J Mater Sci Mater Med. 2014;25(10):2445-2461.
15. Abedi A, Formanek B, Russell N, et al. Examination of the role of cells in commercially available cellular allografts in spine fusion: an in vivo animal study. JBJS . 2020;102(24):e135.
16. Wind J, Park D, Lansford T, et al. Twelvemonth results from a prospective clinical study evaluating the efficacy and safety of cellular bone allograft in subjects undergoing lumbar spinal fusion. Neurol Int . 2022;14(4):875-883.
17. Urgent Voluntary Notification: FiberCel Fiber Viable Bone Matrix (“FiberCel”) - Lot Number: NMDS210011. Food & Drug Administration. Published June 8, 2021. Accessed June 4, 2024. https:// www.fda.gov/vaccines-blood-biologics/ recalls-biologics/urgent-voluntary-notification-fibercel-fiber-viable-bone-matrix-fibercel-lot-number-nmds210011
18. Li R. Notes from the field: tuberculosis outbreak linked to a contaminated bone graft product used in spinal surgery — Delaware, March–June 2021. MMWR Morb Mortal Wkly Rep. 2021;70.
19. Wortham JM. Second nationwide tuberculosis outbreak caused by bone allografts containing live cells — United States, 2023. MMWR Morb Mortal Wkly Rep. 2024;72.
20. Liu S, Wang Y, Liang Z, Zhou M, Chen C. Comparative clinical effectiveness and safety of bone morphogenetic protein versus autologous iliac crest bone graft in lumbar fusion: a meta-analysis and systematic review. Spine . 2020;45(12):E729.
21. Burkus JK, Gornet MF, Dickman CA, Zdeblick TA. Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. Clin Spine Surg. 2002;15(5):337.
22. Summary of Safety and Effectiveness Data [InFUSE Bone Graft/LT-CAGE Lumbar Tapered Fusion Device]. Food and Drug Administration. https://www.accessdata. fda.gov/cdrh_docs/pdf/p000058b.pdf.
23. Simmonds MC, Brown JVE, Heirs MK, et al. Safety and effectiveness of recombinant human bone morphogenetic protein-2 for spinal fusion. Ann Intern Med. 2013;158(12):877-889.
24. Hennessy KM, Pollot BE, Clem WC, et al. The effect of collagen I mimetic peptides on mesenchymal stem cell adhesion and differentiation, and on bone formation at hydroxyapatite surfaces. Biomaterials . 2009;30(10):1898-1909.
25. Nguyen H, Qian JJ, Bhatnagar RS, Li S. Enhanced cell attachment and osteoblastic activity by P-15 peptide-coated matrix in hydrogels. Biochem Biophys Res Commun. 2003;311(1):179-186.
26. Qian JJ, Bhatnagar RS. Enhanced cell attachment to anorganic bone mineral in the presence of a synthetic peptide related to collagen. J Biomed Mater Res. 1996;31(4):545-554.
27. Arnold PM, Sasso RC, Janssen ME, et al. Efficacy of i-Factor bone graft versus autograft in anterior cervical discectomy and fusion: results of the prospective, randomized, single-blinded Food and Drug Administration investigational device exemption study. Spine . 2016;41(13):1075.
28. Arnold PM, Sasso RC, Janssen ME, et al. i-Factor bone graft vs autograft in anterior cervical discectomy and fusion: 2-year follow-up of the randomized single-blinded Food and Drug Administration investigational device exemption study. Neurosurgery. 2018;83(3):377.
29. Instructions for use [i-Factor]. Cerapedics. https://www.cerapedics. com/sites/default/files/documents/40002-07-2%20Putty%20IFU%20 USA%20-%202019%20version.pdf
From the Department of Orthopaedic Surgery at Rush University Medical Center in Chicago, Illinois.
Acute Spinal Cord Injury Treatment
Acute spinal cord injury (ASCI) is a relatively rare event that remains a significant cause of disability and healthcare expenditures worldwide. In the United States, approximately 54 out of every 1 million people suffer from ASCI, and the estimated lifetime cost ranges from $1.4 million to $6 million.1 The majority of ASCIs are sustained by men aged in their 40s due to falls or motor vehicle accidents, and only 18% of these patiets are employed 1 year after their injury.1 As the burden of spinal cord injury (SCI) remains high, optimizing patient outcomes is crucial and requires a multidisciplinary approach. Patients with ASCI undergo several phases of care depending on the amount of elapsed time since the injury and the degree of neurologic impairment, including initial trauma management, surgical intervention, and perioperative medical management.
Pathophysiology
There are 2 distinct phases in SCI: direct mechanical injury and acute inflammatory response. Mechanical injury to the spinal cord may be due to laceration, distraction, shearing, and, most commonly, compression from discoligamentous structures or bone. 2 The initial neurological injury results in the destruction of spinal cord microvasculature, leading to delayed and progressive tissue
damage, which characterizes the second phase of SCI. This secondary inflammatory response and propagation of neurologic dysfunction can last from minutes after the injury to several days or months. Within minutes, there is ischemia, hemorrhage, and local acidosis. Proapoptotic factors are released and disruption of the blood–spinal cord barrier leads to the influx of inflammatory cells and cytokines, including tumor necrosis factor- α (TNF- α), interleukin-1α (ILα), interleukin-1β (IL-1β), and interleukin-6 (IL6). 2 As cellular necrosis ensues, adenosine triphosphate, free DNA, and potassium infiltrate the zone of injury, further leading to a cytotoxic environment. This activates microglia to summon phagocytes, resulting in the production of free radicals and the release of excess glutamate as macrophages and polymorphonuclear leukocytes phagocytose injured cells. 3 Subsequently, excessive glutamate release and impaired reuptake by astrocytes lead to excitotoxicity in neighboring neurons. 4,5 Following the acute inflammatory response, the spinal cord injury progresses to intermediate and chronic phases. As parenchymal volume is lost, cystic cavities coalesce and glial scar tissue extends, creating a physical barrier to cell migration for regenerative factors. 6,7 The lack of a structural framework for remyelination and axonal regeneration may result in long-term Wallerian degeneration.
Luis M. Salazar, MD
Gregory Lopez, MD
Initial Management
The initial evaluation of patients with SCI begins with securing the airway and thus ensuring breathing and circulation, followed by adequate cervical spinal immobilization. Early radiographic evaluation in the form of 3-view cervical spine x-ray images and a computed tomography image of the cervical, thoracic, and lumbar spine is recommended to ensure the detection of any noncontiguous injuries. Although the role of magnetic resonance imaging in the initial workup of patients with SCI remains an area of ongoing investigation, magnetic resonance imaging is recommended before surgery, particularly in the setting of unexplained neurologic deficits, to ensure that ongoing cord compression or ligamentous injuries are not missed. 8 The patient should be transferred promptly to an intensive care unit for adequate resuscitation and maintenance of a targeted mean arterial pressure (MAP) of 85 to 90 mm Hg. Although most of the benefits attributed to maintaining this target MAP are seen within the first 3 days, the current American Academy of Neurologic Surgeons (AANS) guidelines recommend maintaining a target MAP for 7 days.9,10 Furthermore, if possible, commencing anticoagulant thromboprophylaxis with low molecular weight heparin is also recommended within the first 72 hours after injury.11 The foundation of ASCI management is early surgical decompression and stabilization. Notably, in an alert and oriented patient with neurologic deficits and compression due to a fracture/dislocation, acute closed reduction with axial traction should be considered prior to surgery. The 2013 AANS guidelines
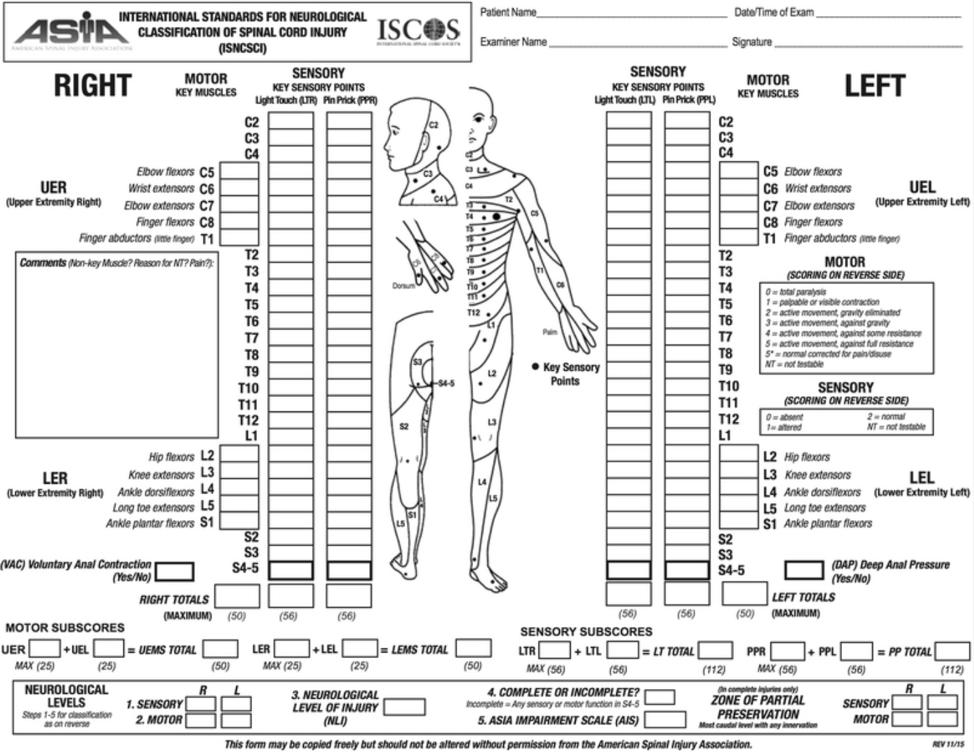
recommend transferring patients with ASCI to medical facilities capable of providing definitive surgery and postsurgical care as early as possible.12 The primary aim of early surgical decompression is to alleviate mechanical compression of the spinal cord that leads to local ischemia, restoring perfusion and reducing the zone of secondary injury expansion. The Surgical Timing in Acute Spinal Cord Injury Study was a landmark multicenter trial demonstrating the important role of early decompression after ASCI.13 The trial prospectively evaluated the outcomes of 313 patients with a cervical SCI who underwent early (<24 hours) versus late intervention. At 6 months, those who underwent early decompression had a 2.8 times higher chance of experiencing a two-grade improvement in the American Spinal Injury Association (ASIA) Impairment Scale (AIS; Figure). Furthermore, a recent meta-analysis
Figure. The American Spinal Injury Association Impairment Scale provides a standardized way to classify the severity of a spinal cord injury and helps healthcare providers develop a treatment plan and predict the patient’s outcome.
from 4 independent, prospective, multicenter data sources from 1991-2017 evaluated 1,548 patients with acute cervical SCI undergoing early versus late surgical decompression.14 Their study demonstrated that patients who underwent early surgery had better recovery and AIS scores 1 year after spinal injury. Patients with delays in surgical intervention in the first 24-36 hours after injury experienced a steep decline in motor recovery, with a plateau in motor recovery after 36 hours.
Neuroprotective Medical Therapy
Methylprednisolone
The goal of methylprednisolone (MP) therapy in the early management of ASCI is intended to mitigate the secondary inflammatory response in the zone of injury and decrease damage to the spinal cord. The National Acute Spinal Cord Injury Study (NASCIS) consisted of three multicenter, double-blinded randomized trials that have served as the primary foundation supporting the administration of MP.15–17 The first NASCIS, published in 1984, compared high-dose MP to low-dose MP and found no difference in patient outcomes, but the high-dose MP cohort was more likely to experience wound infections, pulmonary embolism, sepsis, or death.15 In 1990, the second NASCIS randomized patients to receive steroids, naloxone, or placebo and found significant improvement in motor function, pinprick, and touch compared with placebo if treatment was started within 8 hours of the injury.16 However, patients receiving steroids were more likely to develop wound infections and gastrointestinal bleeding.
The most recent NASCIS, published in 1997, compared patients within 8 hours of injury receiving steroids for either 24 or 48 hours and found greater recovery in motor function in the 48-hour regimen group.17 Yet, there was also a higher likelihood of developing severe sepsis and/or severe pneumonia in this cohort. In that light, the 2013 AANS guidelines recommend against routine MP administration for ASCI due to the lack of substantial evidence supporting the benefits of MP.18 The most recent clinical practice guidelines supported by AANS and AO Spine suggest that the NASCIS II protocol confers no benefit in neurologic recovery, but the guidelines offered a weak recommendation for the 24-hour infusion of MP in patients presenting within 8 hours of injury.19
Riluzole
Riluzole is a medication primarily used to treat amyotrophic lateral sclerosis and is currently under investigation for the treatment of ASCI. Riluzole is a sodium channel blocker that reduces intracellular calcium influx after axonal injury, thereby reducing neuronal apoptosis as it mitigates glutamate release. 20 Grossman et al undertook a phase I/IIa clinical trial demonstrating that 50 mg riluzole twice daily for 2 weeks was safe. 21 In 2014, a phase III trial was initiated to test the efficacy of Riluzole in patients with AIS A-C and a cervical SCI within 12 hours from injury. 22 The study was originally designed to enroll 351 patients, but due to the COVID-19 pandemic, it was terminated in 2021. Therefore, although the study did not reach its primary efficacy endpoint of a
change in upper extremity scores at 6 months, the authors owed this to an underpowered study as only 193 patients were randomized. However, secondary analysis of subgroups revealed that all cervical SCI subgroups (AIS grades A, B, and C) showed significant improvement in functional recovery.
Minocycline
Minocycline is a tetracycline antibiotic with anti-inflammatory properties that has demonstrated neuroprotective properties in preclinical studies for patients with Huntington’s disease and multiple sclerosis. 23 The neuroprotective effects of minocycline are due to its ability to inhibit tumor necrosis factor- α , IL-1b, cyclooxygenase-2, nitric oxide synthase, and microglia. 23 Recently, a phase II trial that randomized 52 patients with cervical ASCI revealed greater motor recovery in patients who received intravenous minocycline compared with placebo. 24 Furthermore, the investigators discovered that the use of minocycline led to better functional outcomes, but the results were not statistically significant. A phase III clinical trial is currently underway.
Neuroregenerative Medical Therapy
Several current investigations explore medications that promote neuronal proliferation by targeting the inhibition of the Rho-ROCK pathway. The blockade of the Rho-ROCK pathway inhibits myelin-associated axon growth inhibitors, thereby promoting regeneration. 25 Early evidence suggests that nonsteroidal anti-inflammatory drugs (NSAIDs) and BA-210 (Cethrin) may have a
neuroregenerative role through inhibition of the Rho-ROCK pathway. A systematic review of animal models indicates that NSAIDs improve neurologic function recovery in 70% of studies compared to control groups. 26 Additionally, phase I and phase II trials evaluating Cethrin as a direct Rho inhibitor revealed increases in ASIA motor scores in cervical SCI patients at 12 months. 27
In addition to therapies targeting the Rho-ROCK pathway, stem cell therapy is currently being investigated for treating ASCI. Such investigations include the use of bone marrow mesenchymal stem cells (MSCs), which comprise more than 60% of currently registered trials investigating MSCs in SCI. MSCs are multipotent cells that can differentiate into various cell types, such as myocytes, osteoblasts, chondrocytes, and adipocytes. They have been studied extensively for their potential to treat ASCI both as a neuroprotective and as a regenerative agent. However, despite the significant heterogeneity observed in clinical trials of MSCs, there has been no clear benefit in their ability to treat SCI. 28,29
Summary
ASCI is a life-altering event leading to significant functional limitations and healthcare expenditures. The foundation of ASCI treatment is early decompressive surgery. The medical and pharmacologic management of ASCI remains controversial. Ongoing clinical trials and translational studies exploring neuroprotective and neuroregenerative agents offer hope for improving the care of individuals with ASCI in the future. l
TRAUMA
References
1. National Spine Cord Injury Statistical Center. Traumatic spinal cord injury facts and figures at a glance. Accessed May 7, 2024. https://www.nscisc.uab.edu/
2. Ahuja CS, Nori S, Tetreault L, et al. Traumatic spinal cord injury-repair and regeneration. Neurosurgery. 2017;80(3S):S9-S22.
3. Ahuja CS, Martin AR, Fehlings M. Recent advances in managing a spinal cord injury secondary to trauma. F1000Research. 2016;5(F1000 Faculty Rev):1017.
4. Li S, Stys PK. Mechanisms of ionotropic glutamate receptor-mediated excitotoxicity in isolated spinal cord white matter. J Neurosci. 2000;20(3):1190-1198.
5. Li S, Mealing GA, Morley P, Stys PK. Novel injury mechanism in anoxia and trauma of spinal cord white matter: glutamate release via reverse Na+-dependent glutamate transport. J Neurosci. 1999;19(14):RC16.
6. Milhorat TH, Capocelli AL, Anzil AP, Kotzen RM, Milhorat RH. Pathological basis of spinal cord cavitation in syringomyelia: analysis of 105 autopsy cases. J Neurosurg. 1995;82(5):802-812.
7. Yuan YM, He C. The glial scar in spinal cord injury and repair. Neurosci Bull. 2013;29(4):421-435.
8. Lambrechts MJ, Issa TZ, Hilibrand AS. Updates in the early management of acute spinal cord injury. J Am Acad Orthop Surg. 2023;31(17):e619-e632.
9. Walters BC, Hadley MN, Hurlbert RJ, et al. Guidelines for the management of acute cervical spine and spinal cord injuries: 2013 update. Neurosurgery. 2013;60(CN_suppl_1):82-91.
10. Weinberg JA, Farber SH, Kalamchi LD, et al. Mean arterial pressure maintenance following spinal cord injury: Does meeting the target matter? J Trauma Acute Care Surg. 2021;90(1):97-106.
11. Fehlings MG, Tetreault LA, Aarabi B, et al. A clinical practice guideline for the management of patients with acute spinal cord injury: recommendations on the type and timing of anticoagulant thromboprophylaxis. Global Spine J. 2017;7(3 Suppl):212S-220S.
12. Middleton PM, Davies SR, Anand S, Reinten-Reynolds T, Marial O, Middleton JW. The pre-hospital epidemiology and management of spinal cord injuries in New South Wales: 20042008. Injury. 2012;43(4):480-485.
13. Fehlings MG, Vaccaro A, Wilson JR, et al. Early versus delayed decompression for traumatic cervical spinal cord injury: results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PLoS ONE . 2012;7(2):e32037.
14. Badhiwala JH, Wilson JR, Witiw CD, et al. The influence of timing of surgical decompression for acute spinal cord injury: a pooled analysis of individual patient data. Lancet Neurol. 2021;20(2):117-126.
15. Bracken MB, Collins WF, Freeman DF, et al. Efficacy of methylprednisolone in acute spinal cord injury. JAMA. 1984;251(1):45-52.
16. Bracken MB, Shepard MJ, Collins WF, et al. A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. Results of the Second National Acute Spinal Cord Injury Study. N Engl J Med. 1990;322(20):1405-1411.
17. Bracken MB, Shepard MJ, Holford TR, et al. Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the third National Acute Spinal Cord Injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA . 1997;277(20):1597-1604.
18. Hurlbert RJ, Hadley MN, Walters BC, et al. Pharmacological therapy for acute spinal cord injury. Neurosurgery. 2013;72(Suppl 2):93-105.
19. Fehlings MG, Wilson JR, Tetreault LA, et al. A clinical practice guideline for the management of patients with acute spinal cord injury: recommendations on the use of methylprednisolone sodium succinate. Global Spine J. 2017;7(3 Suppl):203S-211S.
20. Fehlings MG, Nakashima H, Nagoshi N, Chow DSL, Grossman RG, Kopjar B. Rationale, design and critical end points for the Riluzole in Acute Spinal Cord Injury Study (RISCIS): a randomized, double-blinded, placebo-controlled parallel multi-center trial. Spinal Cord. 2016;54(1):8-15.
21. Grossman RG, Fehlings MG, Frankowski RF, et al. A prospective, multicenter, phase I matched-comparison group trial of safety, pharmacokinetics, and preliminary efficacy of riluzole in patients with traumatic spinal cord injury. J Neurotrauma. 2014;31(3):239-255.
22. Fehlings MG, Moghaddamjou A, Harrop JS, et al. Safety and efficacy of Riluzole in Acute Spinal Cord Injury Study (RISCIS): a multi-center, randomized, placebo-controlled, double-blinded trial. J Neurotrauma. 2023;40(17-18):1878-1888.
23. Festoff BW, Ameenuddin S, Arnold PM, Wong A, Santacruz KS, Citron BA. Minocycline neuroprotects, reduces microgliosis, and inhibits caspase protease expression early after spinal cord injury. J Neurochem. 2006;97(5):1314-1326.
24. Casha S, Zygun D, McGowan MD, Bains I, Yong VW, Hurlbert RJ. Results of a phase II placebo-controlled randomized trial of minocycline in acute spinal cord injury. Brain. 2012;135(Pt 4):1224-1236.
25. Tan HB, Zhong YS, Cheng Y, Shen X. Rho/ ROCK pathway and neural regeneration: a potential therapeutic target for central nervous system and optic nerve damage. Int J Ophthalmol. 2011;4(6):652-657.
26. Lambrechts MJ, Cook JL. Nonsteroidal anti-inflammatory drugs and their neuroprotective role after an acute spinal cord injury: a systematic review of animal models. Global Spine J. 2021;11(3):365-377.
27. Fehlings MG, Theodore N, Harrop J, et al. A phase I/IIa clinical trial of a recombinant Rho protein antagonist in acute spinal cord injury. J Neurotrauma. 2011;28(5):787-796.
28. El-Kheir WA, Gabr H, Awad MR, et al. Autologous bone marrow-derived cell therapy combined with physical therapy induces functional improvement in chronic spinal cord injury patients. Cell Transplant . 2014;23(6):729-745.
29. Oh SK, Choi KH, Yoo JY, Kim DY, Kim SJ, Jeon SR. A phase III clinical trial showing limited efficacy of autologous mesenchymal stem cell therapy for spinal cord injury. Neurosurgery 2016;78(3):436-447; discussion 447.
Tarlov Cysts
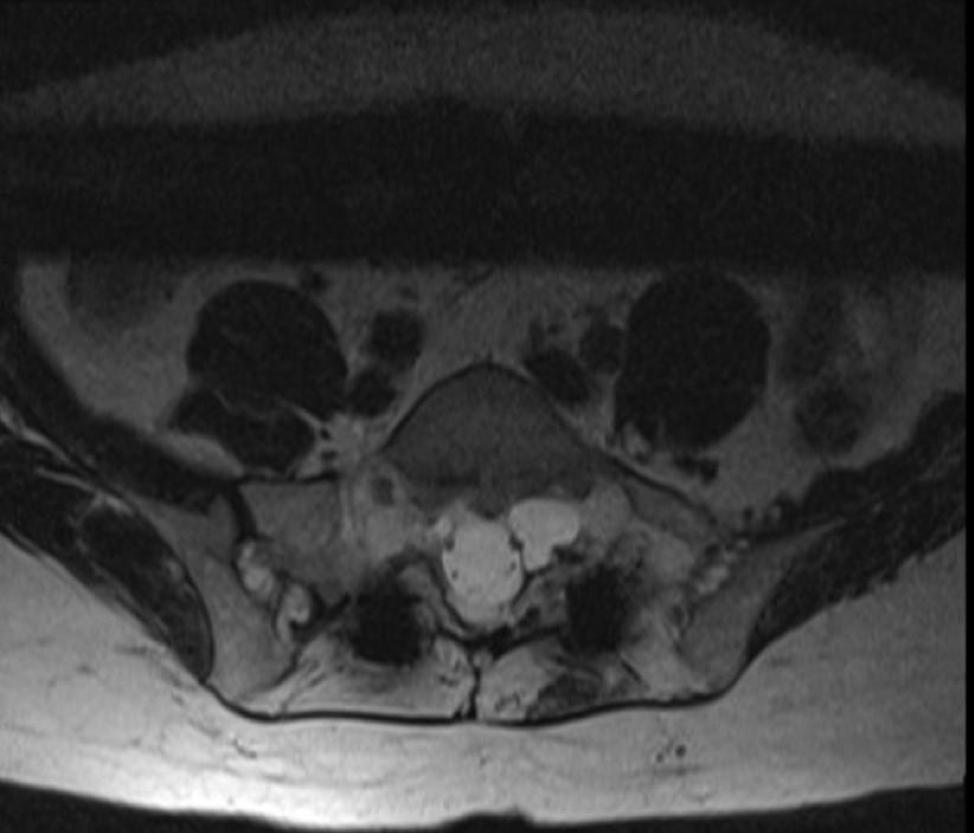
Tarlov cysts were first described by Isadore Max Tarlov in 1938. Tarlov was a neurosurgeon who worked at McGill University and discovered these perineural cysts while dissecting cadavers. He initially described these lesions as anatomic variants with unclear clinical significance. These cysts are filled with cerebrospinal fluid (CSF) and pouch out from the nerve roots. The cysts form in the layers between the perineurium and the endoneurium. They most commonly occur at the sacral level but can also occur in the lumbar and cervical spine (Figure).
The etiology of Tarlov cysts remains unclear. Many theories exist regarding their formation, including inflammation, trauma, congenital, and degenerative processes as possible origins. But how they form still remains a mystery. Their prevalence is also a mystery because they are often asymptomatic and are typically picked up as incidental findings on magnetic resonance images. Prevalence estimates range from 1.5%-13.2%.1
Traditionally, Tarlov cysts were thought to be asymptomatic because they were frequently identified incidentally. However, there is growing evidence that Tarlov cysts can be a source of pain and dysfunction. It is believed that Tarlov cysts can become symptomatic as they increase
in size. As Tarlov cysts grow, they may press on adjacent nerves and cause pain and dysfunction. Tarlov cysts may also become large enough to erode surrounding bone, leading to pain and even sacral insufficiency fractures.
Treatment options for symptomatic Tarlov cysts include nonsteroidal anti-inflammatory drugs and neuropathic medications (gabapentin or pregabalin), acupuncture, and surgery. In patients who have failed standard oral medication and physical therapy, epidural steroid injections may be an option.
From UCI Health in Orange County, California.
Figure. Axial magnetic resonance image of left S1 nerve Tarlov cyst.
Yu-Po Lee, MD
References
SPINAL GROWTHS
Studies have reported positive results with this treatment. In a case series by Mitra et al, the authors reported positive results with oral steroids and epidural steroid injections.1 In some cases, a series of injections may be necessary before patients experience relief. One benefit of epidural steroid injections is that the injections can act as a confirmatory test and indicate whether the Tarlov cysts are a likely source of the patient’s pain.
In patients who report intractable pain despite physical therapy and epidural steroid injections, percutaneous aspiration and injection of fibrin sealant has been reported as an option with positive results. In a retrospective study by Jiang et al, the authors reviewed the outcomes for 82 patients who were treated with aspiration of Tarlov cysts. 2
In a subset of these patients who received percutaneous fibrin gel injection, 34 patients (61%) had complete resolution and 22 patients (39%) had substantial resolution. No CSF leakage or recurrence occurred.
Surgical treatment has also been described for Tarlov cysts. However, there is no consensus on the optimal surgical strategy. Laminectomy followed by varying techniques to decrease the cyst size have been reported. In a study by Xu et al, the authors performed at
1. Mitra R, Kirpalani D, Wedemeyer M. Conservative management of perineural cysts. Spine (Phila Pa 1976). 2008;33(16):E565-E568.
retrospective review on 15 patients who were treated for Tarlov cysts.4 Six patients were treated with microsurgical cyst fenestration and cyst wall imbrication. These patients reported good results. However, 1 patient’s symptoms reappeared 8 months after the operation. Another patient experienced a postoperative cerebrospinal fluid leak. Therefore, surgery can be a consideration for patients with Tarlov cysts, but the risk of complications can be relatively high. In a study by Kameda-Smith et al, the authors performed a meta-analysis on patients treated surgically for symptomatic Tarlov cysts. The authors found a complication rate of 16.9% and cyst recurrence rate of 8.5%. The most frequent complication was the development of a surgical site infection and/or CSF leak.
The treatment of Tarlov cysts is an evolving area of study in spine surgery. There is the growing belief that Tarlov cysts can be symptomatic and therefore a source of pain. Treatment typically involves oral medications, physical therapy, and epidural steroid injections. In refractory cases, percutaneous aspiration and injection of fibrin glue has been reported with good results. Surgery is also an option, but complication and recurrence rates are relatively high. l
2. Jiang W, Hu Z, Hao J. Management of symptomatic Tarlov cysts: a retrospective observational study. Pain Physician. 2017;20(5):E653–E660.
3. Xu J, Sun Y, Huang X, Luan W. Management of symptomatic sacral perineural cysts. PLoS One . 2012;7(6):e39958.
4. Kameda-Smith MM, Fathalla Z, Ibrahim N, Astaneh B, Farrokhyar F. A systematic review of the efficacy of surgical intervention in the management of symptomatic Tarlov cysts: a meta-analysis. Br J Neurosurg. 2024;38(1):49-60.
From the Hospital for Special Surgery and Weill Cornell Medicine in New York, New York.
DEGENERATIVE DISEASE
Global Alignment in Isolated Decompression
Does It Matter?
Degenerative changes of the spine include a diagnostic classification with diverse clinical and radiographic presentations. Over the past few decades, scoring methods and classification guidelines have been established to describe these degenerative changes and compare treatment outcomes.1–3 Recent literature has also demonstrated that global spinal alignment parameters and clinical symptoms are inextricably linked. 2,4 Global alignment involves a complex interplay between spinal and pelvic parameters, which are critical in maintaining a balanced upright posture and minimizing compensatory mechanisms that can lead to pain and disability. 5
The importance of these parameters has been underscored in contemporary clinical practice, where a thorough understanding of global spinal alignment is fundamental to optimizing treatment outcomes after spine surgery. Within the deformity literature, various robust frameworks exist for classifying spinal deformities. These classifications incorporate sagittal modifiers and are designed to closely correlate specific spinal
alignment types with clinical and surgical outcomes. While this area of research is ever-evolving, improved classifiers provide a predictive framework that may assist surgeons in planning interventions tailored for individual patients. 6
In recent years, the scope of global spinal alignment considerations has expanded to include minimally invasive surgery (MIS) techniques, especially in the treatment of degenerative spinal conditions. 3,7–9 MIS approaches offer the potential to correct spinal alignment with minimal disruption to patient anatomy, which is particularly crucial in managing degenerative changes without extensive surgical interventions. Emerging evidence suggests that even with the conservative scope of MIS, significant improvements in global and sagittal alignment can be observed, which may halt the progression of spinal disability and enhance patient recovery and function. Despite the evolving landscape of spine surgery, this shift toward less invasive techniques continues to support the principles of optimal spinal alignment. In this review, we examine the role of global
Tejas Subramanian, BE
John Lama, BS
Robert A. Cecere, BS
Robert N. Uzzo, MBA
Tomoyuki Asada, MD, PhD
Sheeraz A. Qureshi, MD, MBA
DEGENERATIVE DISEASE
alignment parameters on outcomes following isolated MIS decompression.
Does preoperative alignment impact MIS decompression outcomes?
With the growing interest in the importance of global spinal alignment in MIS, recent studies have analyzed the relationship between preoperative alignment and postoperative outcomes in patients undergoing minimally invasive decompression procedures. It is generally thought that optimal restoration of sagittal balance is associated with improved outcomes, yet in isolated decompression, when the goal of surgery is to target a specific pain generator unrelated to the patient’s deformity, the importance is less clear.
Various studies have focused on the impact of sagittal alignment on postoperative outcomes following isolated decompression. Song et al published a cohort of 52 patients analyzing sagittal imbalance as defined by the age-adjusted alignment goals for pelvic incidence-lumbar lordosis (PI-LL).10 In their analysis, no differences in long-term outcomes were observed between preoperative balanced and imbalanced patients. Divi et al studied a similar question, similarly finding pelvic incidence (PI) greater than 10° degrees and pelvic tilt (PT) greater than or equal to 20° were not predictive of worse postoperative outcomes at 1 year.11 Hikata et al and Ogura et al both categorized patients as malaligned by preoperative sagittal vertical axis (SVA) greater than 50 mm.12,13 Interestingly, the 2 analyses found differing outcomes. Hikata et al demonstrated no difference in postoperative pain scores and physical function while Ogura showed that these malaligned patients demon-
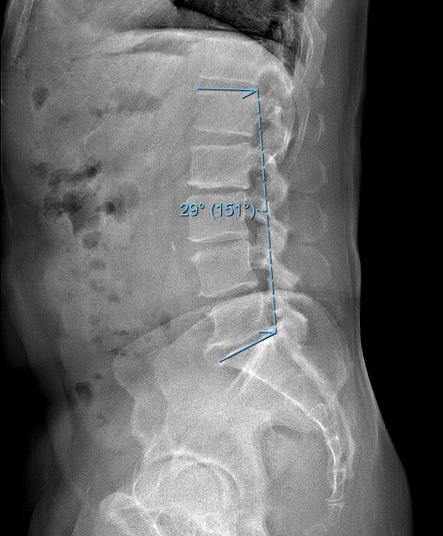
Figure. (A) Preoperative and (B) 6-month postoperative lateral radiographs demonstrating change in lumbar lordosis after isolated decompression.
DEGENERATIVE DISEASE
strated significantly worse postoperative Japanese Orthopedic Association recovery rate, physical function, and back pain. Kawai et al utilized a sagittal age-adjusted score (SAAS) less than or equal to -2 to define preoperative malalignment.14 This analysis found that malaligned patients significantly improved postoperatively. However, they also experienced lesser rates of minimal clinically important difference (MCID) improvement for the lumbar function subdomain of the Japanese Orthopedic Association Back Pain Evaluation Questionnaire. Despite the growing literature, the impact of preoperative sagittal imbalance on outcomes following isolated decompression remains unclear.
Does MIS decompression impact postoperative global alignment? How does postoperative alignment impact outcomes?
Evolving literature supports changes in global alignment postoperatively following MIS decompression. Due to the propensity of patients with lumbar spinal stenosis to lean forward and expand the spinal canal for pain relief, the compensatory reduction in lumbar lordosis (LL) has been thought to induce global malalignment. In a retrospective study of 88 patients who underwent lumbar decompression without fusion, Fujii et al reported significantly increased LL and thoracic kyphosis with postoperative decreases in SVA, PI-LL, and PT at 1 year. 8 The 1 cervical parameter measured, occipital 7th cervical angle (OC7A), did not change at the postoperative time point. In this cohort, 65 patients were defined with preoperative malalignment in accordance with the Scoliosis Research Society-Schwab (SRS-Schwab) classification. Of the 65
In patients with coronal deformities, the resulting instability of the spine may impact the utility and long-term outcomes following isolated decompression. Asada et al evaluated a cohort of 253 degenerative scoliosis patients with a Cobb angle greater than 20° who underwent MIS decompression, and they found that degenerative scoliosis patients exhibited a lower rate of Oswestry Disability Index (ODI) MCID achievement with decompression within the Cobb angle being an independent predictor of MCID non-achievement. Other studies also investigating degenerative scoliosis have found varying levels of success for isolated decompression. Transfeldt et al showed that patients with isolated decompression experienced improvement in postoperative clinical outcomes with low revision rates.15 However, these patients did experience the lowest satisfaction when compared to short and longer segment fusions.15 Liu et al similarly compared decompression alone to short and long fusions in patients with degenerative scoliosis.16 In their cohort of 85 patients, those who underwent decompression alone experienced lower ODI improvements. Taken together, in patients with significant coronal deformities resulting from degenerative processes, decompression alone may be less successful and thus should be taken into account with the rest of the clinical context when making surgical decisions.
patients, 43% improved to normal global alignment postoperatively. Preoperative PI-LL greater than 21.5° and preoperative SVA greater than 69 mm were predictors of postoperative malalignment in patients undergoing isolated decompression. Notably, of the patients who were malaligned postoperatively, 54% reported good pain score outcomes.
Madkouri et al also showed severe preoperative imbalance, SVA greater than 100 mm, was predictive of persistent imbalance after surgery.17 Salimi et al similarly reported longer term alignment outcomes after isolated decompression, also finding that LL significantly increased while SVA decreased at 2 and 5 years postoperatively. 9 Overall, 42.6% of patients with preoperative malalignment developed normal alignment postoperatively, maintaining proper alignment up to the 5-year follow-up. In this cohort, postoperative malalignment was associated with significantly worse VAS back pain scores at long-term follow-up. These findings are consistent with those of Hikata et al and Ogura et al, who reported similarly sustained transitions to improved sagittal alignment following isolated decompression of 52.3% and 44.8%, respectively, at 2-year follow-up. 12,13 Ogura et al further reported that continued positive postoperative SVA had negative implications on clinical outcomes and patient-reported quality of life. Along with improvements in sagittal alignment, Bouknaitir et al found significant concomitant reductions in PI-LL at 6-month follow-up, which
was further studied by Minamide et al and Chang’s report of LSS patients being more likely to have satisfactory clinical outcomes with decompression alone if the PI-LL mismatch is minimized. 18–20 A separate analysis by Chang demonstrated a correlation of 10° increase in lumbar lordosis after decompression surgery was associated with a 5-point improvement in physical function scores. 21
Some of the sagittal malalignment in patients with lumbar spinal stenosis is irreversible, with older age, higher decompression levels, pelvic retroversion, and higher PI-LL mismatch increasing the risk for postoperative SVA exacerbation.13 So, while isolated decompression can improve postoperative global alignment, the severity of preoperative malalignment limits its corrective potential.
Does global alignment matter in isolated decompression?
The literature regarding global alignment supports the significant role that decompression can play in restoring malalignment. Patients over time learn to compensate for degenerative processes in an attempt to alleviate pain. Successful decompression surgery allows some subset of patients to regain their optimal alignment. Generally, therefore, it seems as though those with minimal imbalance do not experience worse postoperative outcomes. In these patients, “smaller” isolated decompression surgery rather than more invasive options to address specific pain symptoms is appropriate. Most of these patients likely correct to a
more optimal alignment postoperatively. Contrastingly, patients with significant preoperative deformities likely fall into a different group of patients that cannot fully correct after an isolated decompression. These patients who maintain a poor
References
1. Cho Y, Jo DJ, Hyun SJ, Park JH, Yang NR. From the spinopelvic parameters to global alignment and proportion scores in adult spinal deformity. Neurospine . 2023;20(2):467-477.
2. Iyer S, Sheha E, Fu MC, et al. Sagittal spinal alignment in adult spinal deformity: an overview of current concepts and a critical analysis review. JBJS Rev. 2018;6(5):e2.
3. Diebo BG, Balmaceno-Criss M, Lafage R, et al. Sagittal alignment in the degenerative lumbar spine: surgical planning. J Bone Joint Surg Am. 2024;106(5):445-457.
4. Diebo BG, Oren JH, Challier V, et al. Global sagittal axis: a step toward full-body assessment of sagittal plane deformity in the human body. J Neurosurg Spine . 2016;25(4):494-499.
5. Hasegawa K, Dubousset JF. Cone of economy with the chain of balance-historical perspective and proof of concept. Spine Surg Relat Res . 2022;6(4):337-349.
6. Jacobs E, van Royen BJ, van Kuijk SMJ, et al. Prediction of mechanical complications in adult spinal deformity surgery-the GAP score versus the Schwab classification. Spine J. 2019;19(5):781-788.
7. Trenchfield D, Lee Y, Lambrechts M, et al. Correction of spinal sagittal alignment after posterior lumbar decompression: does severity of central canal stenosis matter? Asian Spine J. 2023;17(6):1089-1097.
8. Fujii K, Kawamura N, Ikegami M, Niitsuma G, Kunogi J. Radiological improvements in global sagittal alignment after lumbar decompression without fusion. Spine (Phila Pa 1976). 2015;40(10):703-709.
DEGENERATIVE DISEASE
alignment after surgery may be at greater risk for poorer outcomes. Surgeons should therefore consider a patient’s global alignment for surgical decision-making, adequate preoperative counseling, and expectation management. l
9. Salimi H, Toyoda H, Yamada K, et al. The effect of minimally invasive lumbar decompression surgery on sagittal spinopelvic alignment in patients with lumbar spinal stenosis: a 5-year follow-up study. J Neurosurg Spine . 2021;35(2):177-184.
10. Song J, Samuel A, Shahi P, et al. The impact of preoperative sagittal imbalance on long-term postoperative outcomes following minimally invasive laminectomy. HSS J. 2024;20(2):222-229.
11. Divi SN, Goyal DKC, Bowles DR, et al. How do spinopelvic parameters influence patient-reported outcome measurements after lumbar decompression? Spine J. 2020;20(10):1610-1617.
12. Hikata T, Watanabe K, Fujita N, et al. Impact of sagittal spinopelvic alignment on clinical outcomes after decompression surgery for lumbar spinal canal stenosis without coronal imbalance. J Neurosurg Spine . 2015;23(4):451-458.
13. Ogura Y, Shinozaki Y, Kobayashi Y, et al. Impact of sagittal spinopelvic alignment on clinical outcomes and health-related quality of life after decompression surgery without fusion for lumbar spinal stenosis. J Neurosurg Spine . 2019;30(4):470-475.
14. Kawai M, Yagi M, Okubo T, et al. The effect of age-adjusted sagittal alignment on the result of posterior decompression surgery for lumbar spinal canal stenosis. Spine (Phila Pa 1976). Published online September 27, 2023. doi:10.1097/BRS.0000000000004836
15. Transfeldt EE, Topp R, Mehbod AA, Winter RB. Surgical outcomes of decompression, decompression with limited fusion, and decompression with full curve fusion for degenerative scoliosis with radiculopathy. Spine (Phila Pa 1976). 2010;35(20):1872-1875.
16. Liu W, Chen X sheng, Jia L shun, Song D wen. The clinical features and surgical treatment of degenerative lumbar scoliosis: a review of 112 patients. Orthop Surg. 2009;1(3):176-183.
17. Madkouri R, Brauge D, Vidon-Buthion A, et al. Improvement in sagittal balance after decompression surgery without fusion in patients with degenerative lumbar stenosis: clinical and radiographic results at 1 year. World Neurosurg. 2018;114:e417-e424.
18. Bouknaitir JB, Carreon LY, Brorson S, Andersen MØ. Change in sagittal alignment after decompression alone in patients with lumbar spinal stenosis without significant deformity: a prospective cohort study. J Neurosurg Spine . 2022;37(1):57-63.
19. Minamide A, Yoshida M, Iwahashi H, et al. Minimally invasive decompression surgery for lumbar spinal stenosis with degenerative scoliosis: predictive factors of radiographic and clinical outcomes. J Orthop Sci. 2017;22(3):377-383
20. Chang HS. Effect of sagittal spinal balance on the outcome of decompression surgery for lumbar canal stenosis. World Neurosurg. 2018;119:e200-e208.
21. Chang HS. Influence of lumbar lordosis on the outcome of decompression surgery for lumbar canal stenosis. World Neurosurg. 2018;109:e684-e690.
From The CORE Institute in Phoenix, Arizona.
Return to Golf After Lumbar Surgery
In April 2019, Tiger Woods shot a 70 in the final round of the Masters Tournament to claim his 15th major Professional Golf Association (PGA) Tour win. This victory stands among the greatest comeback stories in golf history, as Woods was only 24 months removed from his fourth lumbar surgery, an L5-S1 anterior lumbar interbody fusion (ALIF), and had not had a major PGA Tour win since 2008. Although the 5-time Masters champion dealt with a variety of ailments during his career, none were as disruptive to his play as his lumbar spine injuries.
Although some may view golf as a leisurely, low impact sport, the modern golf swing places tremendous force across the lumbar spine and its supporting structures. A widely quoted study of swing biomechanics found that high-level golfers create compression loads across the lumbar segments of up to 8 times their body weight, approaching that seen in football linemen during blocking drills.1 Commonly taught swing mechanics involve maintaining the hips and lower extremities fixed while emphasizing shoulder turn in the backswing, creating a coiling effect meant to drive club speed and power in the downswing. This increasingly popular technique loads the lumbar spine, subjecting it to significant torsional and shear forces. 2,3
The global population seeking spine care continues to age and expects to remain more active later in life compared with past older populations. 4 As a result, spine surgeons increasingly field questions from patients regarding their return to golf and other sporting activities. For surgeons practicing in communities with a high proportion of retirees, the timing and likelihood of return to golf often becomes a critical factor in patients’ decision to proceed with surgical treatment. 5,6 Despite the popularity of golf within the spine surgery patient population, few objective data exist to guide return to play after lumbar surgery.
While many articles address return to sport after lumbar surgery,7–11 few studies have specifically analyzed return to golf. A 2011 study surveyed members of the North American Spine Society (NASS) regarding recommendations on returning to golf in four different hypothetical patient scenarios.12 Multiple-choice questions were posed regarding the time point at which they would expect patients to return after lumbar laminectomy, lumbar microdiscectomy, and L4-5 laminectomy and instrumented posterolateral fusion. A variety of hypothetical patient types were presented in association with each procedure. These patients ranged from young professional or collegiate golfers to retirement age recreational golfers. All
Brandon Hirsch, MD
hypothetical patients were asymptomatic other than typical incisional pain. The authors received responses from 523 surgeons (52% response rate). After microdiscectomy, the most common time point recommended for return to golf was 4-8 weeks, regardless of the patient’s athletic performance level. In subanalysis a higher proportion of respondents (21%) recommended return in 2-4 weeks for the high-level athlete scenarios when compared with the recreational patient scenarios (13%). In the scenarios involving laminectomy surgery, the most common recommendation was also to return at 4-8 weeks, regardless of patient type. The most popular response for return time frame after L4-5 laminectomy and fusion was also similar across patient types, with 6 months being the most common recommendation. A larger proportion of respondents (38%) felt high-level athletes could return to golf at 2-3 months when compared with recreational athletes (33%). In the open-ended portion of the survey, respondents indicated that evidence of bony union on imaging would be an essential requirement for return to play after fusion.
Patients’ real-world experiences with return to golf after lumbar surgery have also been studied in several case series. In the first and largest study of its kind, Shifflett et al surveyed 34 golfers following 1- or 2-level lumbar fusion surgery. 5 Among these patients, 79% stated that their preoperative symptoms affected their golf play and 47% stated that golf played a role in deciding whether to undergo surgery. More than half of patients reported returning to course play within 12 months of surgery. Only 24% of
patients reported playing golf less frequently following lumbar fusion.
A 2020 study analyzed return to several common sports following lumbar fusion and included a cohort of 13 golfers.13 In this cohort, all patients were able to return to play within 9 months of surgery. These patients reported a reduction in driving distance of 10 yards as well as an increase in handicap following surgery. Another case series by Zuckerman et al reported on 5 patients’ experiences returning to golf after either thoracolumbar fusion or single level fusion at L4-5.14 All patients returned to golfing within 15 months of surgery, and all patients were able to return to the same or greater frequency of play. Only one patient in this series reported worsening of their handicap following surgery.
Figure. The modern golf swing maximizes shoulder turn while keeping the pelvis and lower extremities mostly stationary. This “coiling effect” generates club head speed during the downswing but applies significant torsional force across the lumbar spine.
References
Data gathered from surveys of both patients and surgeons indicated that the majority of patients undergoing lumbar surgery can expect to return to golfing within 12 months of their operation. While no reports exist on patients’ experiences after nonfusion lumbar surgery, most surgeons recommend a return to golf during the second postoperative month. Patients’ experiences with returning to golf in the 6-12 months following lumbar fusion are consistent with the 2011 survey12 of surgeons’ recommendations. The available data suggest that most patients are able to play as much or more than they did prior to lumbar fusion.
Given the popularity of golf in the aging population and the unique stresses the
1. Hosea TM, Gatt CJ. Back pain in golf. Clin Sports Med. 1996;15:37–53.
2. Gluck GS, Bendo JA, Spivak JM. The lumbar spine and low back pain in golf: a literature review of swing biomechanics and injury prevention. Spine J. 2008;8:778-788.
3. Walker CT, Uribe JS, Porter RW. Golf: a contact sport. Repetitive traumatic discopathy may be the driver of early lumbar degeneration in modern-era golfers. J Neurosurg Spine . 2019;31:914–917.
4. Fehlings MG, Tetreault L, Nater A, et al. The aging of the global population: the changing epidemiology of disease and spinal disorders. Neurosurgery. 2015;77:S1–S5.
5. Shifflett GD, Hellman MD, Louie PK, et al. Return to golf after lumbar fusion. Sports Health. 2017;9:280–284.
sport places on the lumbar spine, more granular data are needed to guide patients who are interested in early return to golf after lumbar surgery. Unanswered questions remain as to whether surgical techniques (i.e., minimally invasive fusion, endoscopy) influence the timeline of a patient’s return to the course. Further prospective analyses of patient factors affecting their ability to resume golfing would also be of help when counseling patients preoperatively. Given that patients’ expectations regarding return to golf often influence their decision-making with respect to surgery, surgeons may wish to consider incorporating the topic into their preoperative discussion with golfers prior to lumbar surgery. l
6. Haddas R, Pipkin W, Hellman D, et al. Is golf a contact sport? Protection of the spine and return to play after lumbar surgery. Global Spine J. 2022;12:298–307.
7. Siepe CJ, Wiechert K, Khattab MF, et al. Total lumbar disc replacement in athletes: clinical results, return to sport and athletic performance. Eur Spine J. 2007;16:1001–1013.
8. Watkins RG, Williams LA, Watkins RG. Microscopic lumbar discectomy results for 60 cases in professional and Olympic athletes. Spine J. 2003;3:100–105.
9. Anakwenze OA, Namdari S, Auerbach JD, et al. Athletic performance outcomes following lumbar discectomy in professional basketball players. Spine (Phila Pa 1976). 2010;35:825–828.
10. Matsunaga S, Sakou T, Taketomi E, et al. Comparison of operative results of lumbar disc herniation in manual laborers and athletes. Spine (Phila Pa 1976). 1993;18:2222–2226.
11. Iwamoto J, Sato Y, Takeda T, et al. The return to sports activity after conservative or surgical treatment in athletes with lumbar disc herniation. Am J Phys Med Rehabil. 2010;89:1030–1035.
12. Abla AA, Maroon JC, Lochhead R, et al. Return to golf after spine surgery: clinical article. J Neurosurg Spine . 2011;14:23–30.
13. Jain NS, Lin CC, Halim A, et al. Return to recreational sport following lumbar fusion. Clin Spine Surg. 2020;33:E174–E177.
14. Zuckerman SL, Gillespie A, Kerolus MG, et al. Return to golf after adult degenerative and deformity spine surgery: a preliminary case series of how surgery impacts golf play and performance. J Spine Surg. 2021;7:289–299.
From the Weill Cornell Medical College and the Hospital for Special Surgery in New York, New York.
Advancements in Spine Surgery Navigation Systems
Since the 1990s, computer-assisted navigation (CAN) has become a routine tool in spine surgery. Initially, CAN systems were used to improve accuracy of implant placement during knee and hip arthroplasties1; later, they were used for pedicle screw placement in spine surgery. 2,3 Recently, advancements in imaging and software have pushed CAN to the forefront of medical innovation. Modern CAN systems are now able to construct intraoperative models with granular details of patient anatomy, providing surgeons with real-time, 3-dimensional (3D) guidance during complex procedures. The use of CAN has also allowed for a wider adaptation of minimally invasive surgery (MIS) for the spine, which allows surgeons to navigate patients’ anatomies without conventional open visualization requiring large soft tissue dissection.4
Fundamental Principles of CAN
While various models of CAN currently exist, they often operate based on similar fundamental principles, including image acquisition, registration, and device calibration. In many CAN systems, a procedure-specific digital map is created via pre- or intraoperative imaging by C-arms or O-arms, which are able
to construct intraoperative 3D images. In registration, the constructed map is matched precisely to the patient’s anatomy with tracking markers, also known as a reference array. These markers are affixed to the patient’s skin or via a surgically implanted pin in a spinous process or the iliac crest; subsequently, they are recognized by the CAN system’s stereotactic camera or other type of sensor, facilitating the imposition of the constructed digital map onto the patient’s anatomy in real-time. On this map, surgical instruments equipped with their own tracking markers are also calibrated and tracked with accuracy (often on a millimeter scale) by the CAN sensor and/or camera. A pointing device may also be used to identify predetermined landmarks to further ensure an accurate correlation of the patient’s anatomy with the digital map.5 Combined, these factors allow CAN to augment surgeons’ accuracy and consistency, especially during procedures that require a high degree of precision, making them a mainstay of spine surgery.
Clinical Applications
The ability to visualize patient anatomy in real-time through CAN has led to extensive expansion of MIS techniques
Eric Zhao, BS
Eric Mai, BS
Arsen Omurzakov, BA
Tim Xu, BS
Tomoyuki Asada, MD
Sravisht Iyer, MD
in spine surgery. CAN assists surgeons during MIS procedures that require great accuracy, such as placing spinal instrumentation for fusion and localizing and assessing adequacy of decompression.4,6 In a study comparing open versus CAN screw placement, Lee et al found that CAN via fluoroscopy or CT was more accurate than the traditional “open” technique.7 Additionally, percutaneous endoscopic approaches to laminotomy and decompression have begun incorporating CAN technology with promising results.8 Navigation has also been applied in the setting of spinal tumor resection with several studies supporting its safety, accuracy, and efficacy. 9,10 A prospec-
tive study reporting on primary spine tumor resection using navigation demonstrated no intraoperative complications, screw misplacements, or mechanical implant failure, as well as no local recurrence.11 Additionally, Smitherman et al described a safe method for 4-level sagittal vertebral osteotomy for en bloc resection of large tumors involving the thoracic spine with clear margins using navigation.12
CAN vs Traditional Fluoroscopy
One of the most well-documented advantages of CAN is improved accuracy of pedicle screw placement compared to non-navigated techniques.13-17 In a meta-analysis including more than 7,500 pedicle screws, Tian et al reported 90.8% and 85.5% screw placement accuracy for navigation and fluoroscopic groups, respectively.18 Shin et al studied more than 8,500 screws in another meta-analysis and also reported advantages of CAN, demonstrating a significant difference (6% versus 15%) in screw perforation rates for navigation and traditional techniques, respectively, though no difference in neurologic complications was found.19 Meta-analyses by Verma et al of more than 5,900 screws also found no significant differences in neurological complications between navigated and nonnavigated screw placement. 20 Overall, the available literature suggests improved screw placement accuracy with lower rates of breaches using navigation. However, the clinical significance with respect to neurologic or vascular complications, fusion rates, and functional outcomes remains unclear and requires further investigation.14,21 CAN may be superior to traditional fluoroscopic approaches in other regards, such as
Figure. Example of navigation-assisted spine surgery. Intraoperative sagittal screw projections are demonstrated on the screen (red circle). The reference array is also shown (red arrow). Surgical instruments may also be equipped with their own tracking markers (not shown).
operative time and surgical blood loss. In both cervical and lumbar cases, previous studies have demonstrated shorter operative times using navigation versus fluoroscopy.22,23 One retrospective review by Vaishnav et al reported significantly shorter operative times (92 versus 108 minutes) and less blood loss (25 versus 50 mL) during minimally invasive transforaminal lumbar interbody fusions (MIS-TLIF) for the navigation group compared to the fluoroscopy group.24 Less operative blood loss has also been observed in navigation-guided thoracic pedicle screw placement.25
The available literature is inconclusive regarding radiation exposure. Kim et al demonstrated reduced fluoroscopy time by 90 seconds per MIS-TLIF with CAN, though procedures were performed on cadaveric samples, not patients. 26 In a study of 38 patients, Gebhard et al demonstrated decreased patient radiation exposure when various modalities (eg, CT-based, C-arm-based) of CAN were compared to traditional fluoroscopy. 27 In this study, however, study cohorts were not uniform in terms of surgical region (cervical, thoracic, and lumbar), making the results more difficult to interpret. In contrast, in a randomized controlled trial of 41 patients undergoing MIS-TLIF, Klingler et al found that surgeons experienced a nonsignificant reduction in radiation while patients’ radiation actually increased.28 Radiation usage and exposure is also multifactorial, dependent on surgeon skill and detection methods (eg, placement and type of sensor), among other factors. Further subgroup analysis is needed to elucidate the impact of CAN on radiation exposure for both the patient and operating
room personnel during different types of spine surgery.
Limitations of CAN
Although CAN has existed for more than 30 years, the adoption of CAN worldwide has been inconsistent. 29 In a global survey conducted over 5 major geographical regions (Asia Pacific, Europe, Latin America, Middle East, North America), Härtl et al reported high costs as a major reason why spine surgeons have not implemented CAN in their operating rooms. Interestingly, a study by Watkins et al of the first 100 patients to undergo navigation-guided thoracolumbar pedicle screw instrumentation at their institution showed that navigation reduced costs, rates of revision surgery, and time for pedicle screw placement. 30 Another limitation to CAN implementation is the initial disruption of surgical workflow. In the same global study, the authors cited disruption of workflow as a major contributor to frustration when using CAN, especially when surgeons first become accustomed to CAN. Indeed, Bai et al showed that although perforation rates and operative times decreased over time with CAN compared to traditional fluoroscopy, the learning curve to show substantial benefits required 6-12 months of use. 31 Of note, both Watkins and Härtl emphasized the idea that high-volume practices tend to be better suited for adopting CAN. Perhaps in order for CAN to be worthwhile both financially and outcomes-wise, surgeons must be able to efficiently adapt and overcome this learning curve and perform enough surgeries annually to offset the additional costs of implementing CAN, which may be substantial. Finally,
References
one may also imagine that certain operating rooms are simply not large enough to fit the additional equipment necessary for CAN without potentially obstructing the line of sight of the detection camera or disturbing the reference array. As CAN technology continues to develop, these limitations may have less of an impact on CAN implementation.
Recent Developments and Future Directions
The most recent models of CAN may only consist of a small portable computer workstation, a mobile arm, and surgical light source
1. Deep K, Shankar S, Mahendra A. Computer assisted navigation in total knee and hip arthroplasty. SICOT J. 2017;3:50.
2. Nolte LP, Visarius H, Arm E, Langlotz F, Schwarzenbach O, Zamorano L. Computer-aided fixation of spinal implants. J Image Guid Surg. 1995;1(2):88–93.
3. Lavallée S, Sautot P, Troccaz J, Cinquin P, Merloz P. Computer-assisted spine surgery: a technique for accurate transpedicular screw fixation using CT data and a 3-D optical localizer. J Image Guid Surg. 1995;1(1):65–73.
4. Virk S, Qureshi S. Navigation in minimally invasive spine surgery. J Spine Surg. 2019;5(Suppl 1):S25–S30.
5. Gebhard F, Weidner A, Liener UC, Stöckle U, Arand M. Navigation at the spine. Injury. 2004;35(Suppl 1):S-A35-45.
6. Rawicki N, Dowdell JE, Sandhu HS. Current state of navigation in spine surgery. Ann Transl Med. 2021;9(1):85.
7. Lee GYF, Massicotte EM, Rampersaud YR. Clinical accuracy of cervicothoracic pedicle screw placement: a comparison of the “open” lamino-foraminotomy and computer-assisted techniques. J Spinal Disord Tech. 2007;20(1):25–32.
with built-in stereoscopic cameras.32 Not only are these machines more efficient regarding space occupation, but they also increase surgical efficiency by having simple and quick registration processes in case the reference array is purposefully or accidently moved. 33 While these developments are impressive, Dr Iain Kalfas, a neurosurgeon at the Cleveland Clinic, believes that in the future, CAN may be able to help in detecting erroneous-level spine surgeries and providing real-time feedback on coronal and sagittal alignment to aid in deformity surgery.32 Recent developments also include robot-assisted navigation, in which
8. TY Ho, Lin CW, Chang CC, et al. Percutaneous endoscopic unilateral laminotomy and bilateral decompression under 3D real-time image-guided navigation for spinal stenosis in degenerative lumbar kyphoscoliosis patients: an innovative preliminary study. BMC Musculoskelet Disord. 2020;21(1):734.
9. Arand M, Hartwig E, Kinzl L, Gebhard F. Spinal navigation in tumor surgery of the thoracic spine: first clinical results. Clin Orthop Relat Res . 2002; 399:211–218.
10. Van Royen BJ, Baayen JC, Pijpers R, Noske DP, Schakenraad D, Wuisman PIJM. Osteoid osteoma of the spine: a novel technique using combined computer-assisted and gamma probe-guided high-speed intralesional drill excision. Spine . 2005;30(3):369–373.
11. Ando K, Kobayashi K, Machino M, et al. Computed tomography-based navigation system-assisted surgery for primary spine tumor. J Clin Neurosc i. 2019;63:22–26.
12. Smitherman SM, Tatsui CE, Rao G, Walsh G, Rhines LD. Image-guided multilevel vertebral osteotomies for en bloc resection of giant cell tumor of the thoracic spine: case report and description of operative technique. Eur Spine J. 2010;19(6):1021–1028.
13. Costa F, Cardia A, Ortolina A, Fabio G, Zerbi A, Fornari M. Spinal navigation: stan -
dard preoperative versus intraoperative computed tomography data set acquisition for computer-guidance system: radiological and clinical study in 100 consecutive patients. Spine . 2011;36(24):2094–2098.
14. Amiot LP, Lang K, Putzier M, Zippel H, Labelle H. Comparative results between conventional and computer-assisted pedicle screw installation in the thoracic, lumbar, and sacral spine. Spine 2000;25(5):606–614. https://doi. org/10.1097/00007632-200003010-00012.
15. Overley SC, Cho SK, Mehta AI, Arnold PM. Navigation and robotics in spinal surgery: where are we now? Neurosurgery. 2017;80(3S):S86–S99.
16. Ishikawa Y, Kanemura T, Yoshida G, Ito Z, Muramoto A, Ohno S. Clinical accuracy of three-dimensional fluoroscopy-based computer-assisted cervical pedicle screw placement: a retrospective comparative study of conventional versus computer-assisted cervical pedicle screw placement. J Neurosurg Spine . 2010;13(5):606–11.
17. Rajasekaran S, Vidyadhara S, Ramesh P, Shetty AP. Randomized clinical study to compare the accuracy of navigated and non-navigated thoracic pedicle screws in deformity correction surgeries. Spine. 2007;32(2):E56-E64.
robotic arms are integrated with the navigation system, allowing for greater fine-tuned control of instrument positioning.34 Furthermore, the combination of augmented reality with CAN has opened new possibilities for surgeons, as augmented reality–assisted CAN allows surgeons to visualize 3D anatomical structures in real-time overlaid upon the surgical field. This may further help with pedicle screw placement, especially in novice surgeons. 35
Conclusion
CAN has revolutionized the world of spine surgery. Advantages of CAN include improved
screw placement accuracy, decreased blood loss, and shorter operative times, among others. However, these factors may depend on a surgeon’s ability to overcome the initial learning curve. Further investigations are needed to elucidate the impact of CAN on factors such as radiation exposure. As CAN continues to evolve, we anticipate that the advancements in CAN technology will continue to translate into better outcomes for our patients. Furthermore, with progress in CAN technology, we hope to see a decreased barrier to implementing CAN in operating rooms around the world. l
18. Tian NF, Xu HZ. Image-guided pedicle screw insertion accuracy: a meta-analysis. Int Orthop. 2009;33(4):895–903.
19. Shin BJ, James AR, Njoku IU, Härtl R. Pedicle screw navigation: a systematic review and meta-analysis of perforation risk for computer-navigated versus freehand insertion. J Neurosurg Spine. 2012;17(2):113–122.
20. Rajeev V, Krishan S, Haendlmayer K, Mohsen A. Functional outcome of computer-assisted spinal pedicle screw placement: a systematic review and meta-analysis of 23 studies including 5,992 pedicle screws. Eur Spine J. 2010;19(3):370–375.
21. Gelalis ID, Paschos NK, Pakos EE, et al. Accuracy of pedicle screw placement: a systematic review of prospective in vivo studies comparing free hand, fluoroscopy guidance and navigation techniques. Eur Spine J. 2012;21(2):247–255.
22. Richter M, Cakir B, Schmidt R. Cervical pedicle screws: conventional versus computer-assisted placement of cannulated screws. Spine 2005;30(20):2280–2287.
23. Lutfi AK, Shweikeh F, Pashman R, Johnson JP, Kim TT, Drazin D. Economics of image guidance and navigation in spine surgery. Surg Neurol Int . 2015;6(Suppl 10):S323-S326.
24. Vaishnav AA, Merrill RK, Sandhu H, et al. A review of techniques, time demand, radiation exposure, and outcomes of skin-anchored intraoperative 3D navigation in minimally invasive lumbar spinal surgery. Spine. 2020;45(8):E465–E476.
25. Meng XT, Guan XF, Zhang HL, He SS. Computer navigation versus fluoroscopy-guided navigation for thoracic pedicle screw placement: a meta-analysis. Neurosurg Rev. 2016;39(3):385–391.
26. Kim CW, Lee YP, Taylor W, Oygar A, Kim WK. Use of navigation-assisted fluoroscopy to decrease radiation exposure during minimally invasive spine surgery. Spine J. 2008;8(4):584–590.
27. Gebhard FT, Kraus MD, Schneider E, Liener UC, Kinzl L, Arand M. Does computer-assisted spine surgery reduce intraoperative radiation doses? Spine 2006;31(17):2024–2027; discussion 2028.
28. Klingler JH, Scholz C, Krüger MT, et al. Radiation exposure in minimally invasive lumbar fusion surgery: a randomized controlled trial comparing conventional fluoroscopy and 3D fluoroscopy-based navigation. Spine. 2021;46(1):1–8.
29. Härtl R, Lam KS, Wang J, Korge A, Kandziora F, Audigé L. Worldwide survey on the use of navigation in spine surgery. World Neurosurg. 2013;79(1):162–172.
30. Watkins RG, Gupta A, Watkins RG. Cost-effectiveness of image-guided spine surgery. Open Orthop J. 2010;4:228–233.
31. Bai YS, Zhang Y, Chen ZQ, et al. Learning curve of computer-assisted navigation system in spine surgery. Chinese Med J. 2010;123(21):2989–2994.
32. Kalfas IH. Machine vision navigation in spine surgery. Front Surg. 2021;8:640554.
33. Faraji-Dana Z, Mariampillai ALD, Standish BA, Yang VXD, Leung MKK. Machine-vision image-guided surgery for spinal and cranial procedures. In: Handbook of Robotic and Image-Guided Surgery. Elsevier; 2020:551–574.
34. Huang M, Tetreault TA, Vaishnav A, York PJ, Staub BN. The current state of navigation in robotic spine surgery. Ann Transl Med. 2021;9(1):86.
35. Cyrill D, Jaberg L, Spirig J, et al. Augmented reality-based navigation increases precision of pedicle screw insertion. J Orthop Surg Res . 2020;15(1):174.
From the Department of Orthopaedic Surgery at Rush University Medical Center in Chicago, Illinois.
Artificial Intelligence in Spine Surgery
Over the past decade, artificial intelligence (AI) and machine learning (ML) have become increasingly prominent in the scientific community, including spine surgery. AI involves replicating human intelligence through specialized programs and computers that mimic cognitive functions. ML, a subset of AI, involves algorithms that learn from data, improving performance over time. The rapid increase in both the collection and availability of patient data presents a challenge for efficiently processing and analyzing information to determine the best therapeutic approaches for spine-related issues. Areas of interest have included spine deformity classification, 1,2 intraoperative modeling for pedicle screw placement, 3,4 and predictive algorithms for treatment outcomes, 5,6 to name a few. Ultimately, the goal is to significantly improve spine surgery outcomes, lower costs for hospitals and patients, and reduce potential risks. This brief review explores the current utilization of AI in spine imaging, ethical considerations, and clinic-based applications.
Utilization in Spine Imaging
From identifying, classifying, and differentiating between spinal pathologies to predicting clinical outcomes, the role of AI in spine imaging is multifaceted and applicable to a variety of clinical scenarios. Forsberg et al sought to detect and label vertebrae in MR images using a single institution training set of 475 lumbar and 245 cervical cases.7 They demonstrated high labeling accuracy (96%-97%), which was on par, if not better, than previously reported AI models. 8,9 Roth et al used a dataset of 55 displaced posterior-element fractures in 18 trauma patients to train a deep convoluted neural network to detect posterior-element spine fractures from CT images. 10 The authors achieved an area under the curve of 0.857, which corresponds to a sensitivity of 71% or 81% at 5 or 10 false-positives per patient, respectively.
AI tools have extended to include analysis of spinal tumors and infection as well. Chmelik et al trained a deep-learning model using 2125 CT images of 79 patients to classify different osteolytic and osteogenic metastatic spinal tumors and reported an accuracy of 87.2% and a precision of 94.8%. 11 Kim et al trained a deep neural network using 161 spine MR images to differentiate tuberculous and
Daniel Shinn, MD
Vincent P. Federico, MD
Arash Sayari, MD
pyogenic spondylitis. 12 The performance of their AI model was comparable to that of 3 skilled radiologists. To improve the classification in adolescent idiopathic scoliosis (AIS), Shen et al used a clustering algorithm to identify subgroups based on 10 parameters measured on 3-dimensional reconstructions of the spine. This AI model resulted in 11 sub-groups with a population size for each cluster that varied from 11 to 290.13 Although this implementation of AI is a step up from binary detection, there is still a need for clinical validation to determine its usefulness.
Ethical Considerations
The development of AI tools raises ethical concerns about its side effects on clinicians, patients, and regulatory/governing parties. As with any clinical decision-making tool, the principles of autonomy, nonmaleficence, beneficence, and justice should be upheld. First, AI models generally rely on large datasets to create accurate and generalizable conclusions. It is the responsibility of all parties, including clinicians, statisticians, and corporations, to ensure patient-protected health information (PHI) is collected with consent and maintained
From identifying, classifying, and differentiating between spinal pathologies to predicting clinical outcomes, the role of AI in spine imaging is multifaceted and applicable to a variety of clinical scenarios.
securely. This is especially important for multi-institutional studies where PHI may be transferred to a third party. Second, these large datasets have significant inherent biases, typically because it’s unclear whether the data reflects the entire population or just a specific subset. If minority groups are under- or misrepresented, the training data becomes flawed, ultimately leading to inaccurate algorithms. To promote health equity, researchers should, at the minimum, acknowledge such structural inequalities. In the same vein, clinicians must understand the scope of any AI tool in their arsenal. Another important ethical consideration arises when AI contradicts conventional indications, diagnoses, or treatments. Physicians must critically evaluate these cases to avoid causing harm to the patient. For instance, if an AI model suggests decompression alone to treat a patient with degenerative lumbar spondylolisthesis, but standard of care calls for a single-level fusion, the surgeon should carefully consider possible reasons
for the discrepancy and not immediately dismiss either option. Last, government and administrative bodies can foster a trust in AI tools by defining legal responsibilities, promoting transparency, and providing constructive infrastructure.
Clinic-Based Applications
The application of AI is not limited to purely academic discussions and imaging analysis. AI can play a role in patient selection for various spinal procedures. With patient data becoming more available, clinical decision-making has become increasingly multifactorial. In the clinic, AI tools can be deployed to efficiently weigh preoperative patient factors to offer the best treatment and optimize patient outcomes. AI can also be used when discussing periand postoperative risks with patients. Karhade et al developed ML algorithms for prediction of in-hospital and 90-day postdischarge mortality in patients with spinal epidural abscess, reporting a c-statistic of 0.89 (ranges from 0 to 1; greater than 0.8 represents good performance).14 The variables used for prediction of 90-day mortality, ranked by importance, were age, albumin, platelet count, neutrophil to lymphocyte ratio, hemodialysis, active malignancy, and diabetes. Additional studies are needed to validate the clinical utility of this model. However, it demonstrates the integration of variables that may not have been considered when discussing postoperative complications. Khan et al used ML to predict which patients with mild myelopathy would benefit most from
surgery, using minimal clinically important differences of Short Form-36 mental component summary (MCS) and physical component summary (PCS) at 1-year after surgery as the primary outcome. The ML model had moderate performance and found that female patients with a low initial MCS were less likely to experience significant improvement in MCS compared with male patients.15
Conclusion
AI and ML have made remarkable strides in spine surgery, enhancing diagnostic
References
1. Jamaludin A, Fairbank J, Harding I, et al. Identifying scoliosis in population-based cohorts: automation of a validated method based on total body dual energy X-ray absorptiometry scans. Calcif Tissue Int. 2020;106:378–385.
2. García-Cano E, Arámbula Cosío F, Duong L, et al. Prediction of spinal curve progression in adolescent idiopathic scoliosis using random forest regression. Comput Biol Med. 2018;103:34–43.
3. Esfandiari,H, Newell R, Anglin C, Street J, Hodgson AJ. A deep learning framework for segmentation and pose estimation of pedicle screw implants based on C-arm fluoroscopy. Int J Comput Assist Radiol Surg. 2018;13(8):1269–1282.
4. Burström G, Buerger C, Hoppenbrouwers J, et al. Machine learning for automated 3-dimensional segmentation of the spine and suggested placement of pedicle screws based on intraoperative cone-beam computer tomography. J Neurosurg Spine. 2019;31(1):147–154.
5. Arvind V, Kim JS, Oermann EK, Kaji D, Cho SK. Predicting surgical complications in adult patients undergoing anterior cervical discectomy and fusion using machine learning. Neurospine. 2018;15(4):329–337.
accuracy, predicting clinical outcomes, and optimizing treatment plans. These technologies promise significant improvements in patient outcomes, cost reduction, and risk minimization. Importantly, the ethical implications, including data biases and patient privacy, should be continuously considered to ensure responsible implementation. Additionally, clinicians need to understand AI’s limitations and validate its clinical utility. With ongoing research, AI can be effectively integrated into clinical practice, revolutionizing spine surgery and advancing patient care. l
6. Kim JS, Merrill RK, Arvind V, et al. Examining the ability of artificial neural networks machine learning models to accurately predict complications following posterior lumbar spine fusion. Spine. 2018;43(12):853–860.
7. Forsberg D, Sjöblom E, Sunshine JL. Detection and labeling of vertebrae in MR images using deep learning with clinical annotations as training data. J Digit Imaging. 2017;30(4):406–412.
8. Cai Y, Osman S, Sharma M, Landis M, Li S. Multi-modality vertebra recognition in arbitrary views using 3D deformable hierarchical model. IEEE Trans Med Imaging. 2015;34(8):1676–1693.
9. Cai Y, Landis M, Laidley DT, Kornecki A, Lum A, Li S. Multi-modal vertebrae recognition using Transformed Deep Convolution Network. Comput Med Imaging Graph. 2016;51:11–19.
10. Roth HR, Wang Y, Yao J, Lu L, Burns JE, Summers RM. Deep convolutional networks for automated detection of posterior-element fractures on spine CT. SPIE Med Imag. 2016:9785:165-171.
11. Chmelik J, Jakubicek R, Walek P, et al. Deep convolutional neural network-based segmentation and classification of difficult to define metastatic spinal lesions in 3D CT data. Med Image Anal. 2018;49:76–88.
12. Kim K, Kim S, Lee YH, Lee SH, Lee HS, Kim S. Performance of the deep convolutional neural network based magnetic resonance image scoring algorithm for differentiating between tuberculous and pyogenic spondylitis. Sci Rep. 2018;8(1):13124.
13. Shen J, Parent S, Wu J, et al. Towards a new 3D classification for adolescent idiopathic scoliosis. Spine Deform. 2020;8(3):387–396.
14. Karhade AV, Shah AA, Bono CM, et al. Development of machine learning algorithms for prediction of mortality in spinal epidural abscess. Spine J. 2019;19(12):1950–1959.
15. Khan O, Badhiwala JH, Witiw CD, Wilson JR, Fehlings MG. Machine learning algorithms for prediction of health-related quality-of-life after surgery for mild degenerative cervical myelopathy. Spine J. 2021;21(10):1659–1669.