New Take control of your patients’ ocular surface with Lacrifill®:
Ocular surface control starts with Lacrifill®
✔ Hyaluronic acid canalicular gel1
✔ Maintains natural lubricating tears on the ocular surface1
✔ Each administration provides dry eye relief for 6 months1
THIS ISSUE:
Celebrating Hospital Pharmacy Day Page 4 EDUCATION: Advancing Healthcare with New Programme Page 6 FEATURE: Designing Safer Pain Pathways Page 14 TRAINING: Training and Retaining the Future Medical Workforc Page 18 CPD: EGFR-mutated Non-Small Cell Lung Cancers Page 29 INTERVIEW: Surgical Innovation at Mater Hospital Page 38 AWARDS: Celebrating Hospital Pharmacy Page 51
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Contents Foreword
Future of Medical Logistics with Drone Delivery
P4
Turning Economic Strength into Patient Impact P7
We talk with Dr Tafadzwa “Dr Taffy” Mandiwanza P8
First Cohort of Advanced Specialist Pharmacists P12
Training and Retaining the Future Medical Workforce P18
World’s largest lung cancer clinical trial opens P20
Ophthalmology Advances Take Focus P24
How HIHI Supports Clinician-Led Product and Service Assessment Across Irish Hospitals P34
REGULARS
CPD: EGFR-Mutated NSCLC P29
Feature: Rapid Access, Triage and Risk-Stratification Models P36
Feature: CardiovascularInnovation in Action P42
Feature: Penicillin Allergy P46
Clinical R&D: P60
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only.
All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
This issue of Hospital Professional News comes at a time of significant progress and momentum within Irish hospital pharmacy, as the profession continues to evolve in response to increasing clinical demands, system pressures and opportunities for innovation.
A major milestone featured in this issue is the formal introduction of the Advanced Specialist Pharmacist (ASP) role—arguably the most significant reform of hospital pharmacy career structures in over four decades. Fourteen years on from the McLoughlin Report, this longawaited development marks a pivotal shift in recognising advanced clinical expertise within the profession. The appointment of the first cohort of ASPs signals not only progress in career progression, but also a strengthened capacity within hospital pharmacy to deliver high-quality, patient-centred and cost-effective care.
This advancement was further reflected at the recent HPAI Engagement Day for Managers of Advanced Specialist Pharmacists, which brought together leaders from across the country to focus on governance, leadership and service development. Importantly, the event acknowledged that supporting this new grade extends beyond heads of department, highlighting the need for a coordinated, system-wide approach to embedding advanced practice successfully within hospital pharmacy services.
Alongside developments within the profession itself, the broader pharmaceutical landscape continues to demonstrate its critical importance to Ireland’s economic and healthcare systems. As outlined in new analysis from the Irish Pharmaceutical Healthcare Association (IPHA), the sector has reached record levels across employment, output, exports and tax contribution. Against a backdrop of global uncertainty and ahead of Ireland’s Presidency of the Council of the EU, this reinforces the strategic role of the pharmaceutical industry in supporting national and European resilience.
Encouragingly, this economic strength is increasingly being aligned with improvements in patient access to innovative medicines, supported by the recently concluded IPHA Framework Agreement. For hospital pharmacists, this represents a meaningful opportunity to translate innovation into improved clinical outcomes, ensuring that patients benefit more quickly from advances in treatment.
Research and innovation also remain central to the advancement of patient care. This issue highlights the expansion of the TOURIST platform trial—one of the world’s largest clinical trials in metastatic lung cancer— which is now open to recruitment in Ireland. As the first international site outside the UK, this development underscores Ireland’s growing role in global clinical research and offers patients access to cutting-edge treatment pathways.
Finally, we are pleased to announce the launch of the Irish Pharmacy Awards 2026, now open for entries. Reflecting the continued evolution of the profession, this year sees the introduction of dedicated hospital pharmacy categories, recognising the vital contribution of hospital pharmacists, technicians and teams. This expansion ensures that excellence across all areas of pharmacy practice is acknowledged and celebrated at a national level.
Together, these developments reflect a profession that is advancing with purpose—strengthening its clinical impact, expanding its role within healthcare and continuing to deliver meaningful improvements in patient care. As always, we remain committed to bringing you the insights, developments and achievements that matter most to hospital pharmacy practice in Ireland.
Hospital Pharmacy Day
March 27th marked Hospital Pharmacy Day, a day created to highlight the importance and to celebrate the work done by hospital pharmacies. This day wants to celebrate all hospital pharmacy teams.
This year’s theme, 'All In for Our Patients', highlights the dedication of pharmacists, pharmaceutical technicians, administrative staff and portering teams who work together every day to support patient care.
Across Europe, hospitals mark the day by showcasing services, sharing achievements and engaging with colleagues.
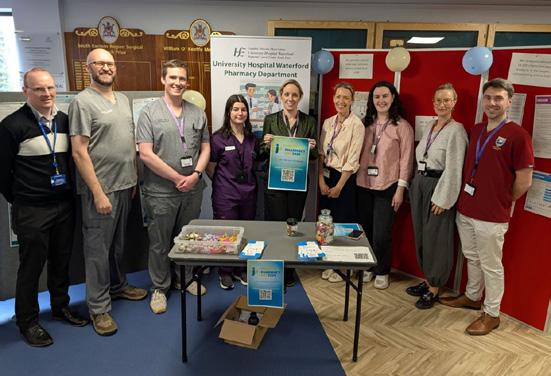
At University Hospital Waterford, pharmacy staff met with staff, patients and visitors to share insights into the essential work they do.
St Patrick’s University Hospital also marked the day. At St Patrick’s Mental Health Services, a pharmacist is part of every multidisciplinary team across both St Patrick’s University Hospital and St Patrick’s Hospital Lucan,
contributing to personalised care and treatment plans to help manage mental health symptoms and support recovery. Said a spokes person, “Thank you to our pharmacy team for your ongoing commitment, expertise, and care.”
Pictured are members of our pharmacy team;
Future of Medical Logistics with Drone Delivery
A flight simulation of medical drone delivery has taken place in Dublin, demonstrating the potential for rapid aerial transport of blood and other life-saving medical supplies between hospitals.
Led by the clinical expertise of Rotunda Hospital and enabled by Manna’s drone delivery platform - with software and drones built in Ireland - the demonstration simulated a delivery to Connolly
Hospital in Blanchardstown. The medical partners are driving the ambition to explore how drones can safely deliver between two hospital sites. This simulation is designed to show what is now technically possible and how it could support faster, cleaner and more connected healthcare in the near future.
On the simulation John O’ Loughlin, Laboratory Manager at
John O'Loughlin, laboratory manager at the Rotunda Hospital with a Manna drone.
Photograph: Lensmen
Rotunda Hospital said, “The ability to move blood, samples and other critical supplies between hospitals at speed could transform how we support emergency and planned care in Ireland. Today’s simulation is a glimpse of that future.”
The test reflects an ambition to upgrade how Irish hospitals operate as a system - moving vital supplies such as blood, pathology samples and emergency medicines in minutes, not hours. At a time when clinical pressure and population needs are growing.
Bobby Healy, Chief Executive Officer at Manna Air Delivery said, “We’ve proven this technology works at scale. What we’re showing now is how it can be applied in healthcare where minutes matter.
Ireland is well-placed to lead the way, and this simulation is about building trust and momentum toward full integration.”
In the UK, NHS trials have shown how drone technology can transform hospital logistics and clinical outcomes. In London, blood sample transport times between Guy’s Hospital and St Thomas’ Hospital were reduced from over 30 minutes by road to under 2 minutes by droneenabling faster diagnostics for high-risk surgical patients and accelerating decision-making at the point of care . In Dorset, a study found that drones serving 13 GP surgeries achieved an 83% reduction in average delivery time compared to traditional van routes. While live operations between hospitals are subject to regulatory approval, the underlying platform is already in use in Ireland. Manna has operated safely across suburban communities under IAA and European oversight delivering groceries, over the counter pharmacy items and other time-sensitive goods daily. Medical deliveries are the next evolution.
Members of the Hospital Pharmacy team at Waterford University Hospital
Valeria Sotgiu, Fionn Cullinane, Melissa Carthy, Lorraine McSweeney, Nuala Stenson, Ciara Ni Dhubhlaing, Áine Breen, Gary Brown, Orla Tyrrell, Helen Glassett
HPAI Engagement Day
On 5 February 2026, hospital pharmacy leaders from across the country gathered for the HPAI Engagement Day for Managers of Advanced Specialist Pharmacists, an event that signals the continued evolution of advanced practice within Irish hospital pharmacy.
Hosted by the Hospital Pharmacists Association of Ireland (HPAI), the engagement day brought together line managers overseeing Advanced Specialist Pharmacists (ASPs) for a focused discussion on leadership, governance and service development. Importantly, attendance extended beyond heads of department, recognising that responsibility for supporting this new grade sits across
multiple layers of hospital pharmacy management.
The introduction of the Advanced Specialist Pharmacist grade has been a significant structural development within Irish hospital services. Designed to reflect increasing clinical complexity and the expansion of pharmacistled care, the role acknowledges pharmacists practising at an expert level in areas such as oncology, antimicrobial stewardship, cardiology, critical care and other highacuity specialties. As services continue to evolve, so too does the need for clear management frameworks, defined scopes of practice and sustainable career pathways.
The engagement day provided a forum for managers to share early experiences of implementing the grade, explore practical challenges and consider how best to embed ASPs within multidisciplinary teams. Discussions reportedly centred on performance expectations, professional autonomy, service impact measurement and alignment with national workforce planning.
With hospital services operating under sustained pressure, advanced practice roles are increasingly viewed not simply as professional recognition but as strategic assets. ASPs are positioned to lead clinical initiatives, contribute to guideline development, support medicines
IHCA Publish Consultant Action Plan
A new clinician-led Action Plan for Health has been by the Irish Hospital Consultants Association (IHCA), focusing on improving access, safety and patient outcomes across the health service.
Unveiled at the IHCA FutureCare Conference in Dublin, the 10-point Action Plan is a clinician-led alternative to the almost decadeold, politician-driven Sláintecare policy, much of which has yet to be delivered. The IHCA says its plan provides a sustained, structured focus on real world policies that are shaped by those who see, first-hand, how system design affects patients on wards, in emergency departments and on waiting lists.
Taking place at the Dublin Royal Convention Centre, FutureCare 2026 heard from international speakers from the Mayo Clinic and the Cleveland Clinic in the US and from Germany on how leadership, governance, digital health and funding models can be aligned to improve patient outcomes and system performance.
The IHCA’s 10-point FutureCare Action Plan sets out a number of clear priorities including:
• The immediate and sustained expansion of hospital and critical care capacity, including the full delivery of all elective hospitals and surgical hubs
Professor Gabrielle Colleran, President, IHCA
• A doubling in the level of NTPF funding from ¤200m to ¤400m to provide timely care to an additional 143,000 patients
• Mandatory, internationally recognised accreditation and quality standards
• Clinician-led governance at hospital and system level
• Accelerated delivery of national Electronic Health Records
• Significant increases in consultant and other medical staff to delivery timely patient care.
Results from a new IHCA survey reveal that 86% of consultants are working longer than their contractual hours, with 40% working 45 hours or more per
optimisation and enhance patient safety in complex care settings.
The HPAI’s decision to convene managers at this stage reflects a recognition that the success of advanced practice depends not only on individual capability but on organisational support. As the ASP grade becomes more established, structured engagement of this nature will likely play a key role in shaping its long-term sustainability.
For hospital pharmacy in Ireland, the message from the day was clear: advanced practice is here, and thoughtful leadership will determine how effectively it delivers for patients and services alike.
Read more about this on page 12.
week. When asked to quantify the level of extra work or ‘discretionary effort’ they provide each week on a voluntary basis ‘above and beyond’ their contractual hours, 41% said they are working 7 hours or more extra per week, with a quarter (24%) providing 10 or more hours in ‘discretionary effort’ and 11% working an additional 13 hours or more.
The Association warns that continued reliance on such goodwill from consultants and crisis management from health officials is no longer tenable, and that failure to act now will carry
significant clinical, human and economic costs.
Professor Gabrielle Colleran, President of the Irish Hospital Consultants Association, said: “Ireland’s health service is operating at – and too often beyond – the limits of safe capacity. This is not a short-term pressure but a structural problem that requires structural solutions.
“FutureCare 2026 is about confronting that reality honestly and setting out a clinician-led roadmap for reform that focuses on capacity, governance and sustainable funding.”
Advancing Healthcare Education with New Pharmacy Programme and Medical School Investment
University of Galway is strengthening its position as a key provider of healthcare education with the launch of a new MPharm programme and significant Government investment in a new School of Medicine building. Dr Martina Ní Chúlain outlines how these developments will support workforce expansion, innovation, and future models of care.
University of Galway is set to play an increasingly important role in shaping the future of healthcare education in Ireland, following the recent announcement of Government funding under the Healthcare Education Activation Programme (HEAP). The investment, part of a ¤75 million capital programme under Project Ireland 2040, will support the development of a new School of Medicine building and the continued expansion of healthcare training across the University.
A key milestone in this expansion has already been achieved, with the launch of the University’s new Master of Pharmacy (MPharm) programme. The first intake of students commenced in September 2025, marking a significant step forward for both the University and the wider region.
According to Dr Martina Ní Chúlain, Director of Strategic Development and Process Improvement, the programme represents a major achievement, not least because it was the first pharmacy programme to be delivered through the Government’s Healthcare Activation Programme.
Addressing Workforce Needs Through Education
The introduction of the MPharm
Dr Martina Ní Chúlain, Director of Strategic Development and Process Improvement
ready to contribute to patientcentred care from the very beginning of their careers.”
Students will also benefit from Ireland’s established national placement system through the APPEL model. This interinstitutional framework provides structured, high-quality clinical placements across a range of settings, including community pharmacy, hospital practice, industry, and research.
to play a significant role in improving access to healthcare in underserved regions.
Drawing on international best practice, including models used in Scotland and other jurisdictions, the programme is designed to train doctors in rural settings with the aim of encouraging them to build long-term careers in those communities.
programme forms part of a broader strategic response to workforce shortages across healthcare professions.
Dr Ní Chúlain explains that the programme aligns closely with the University’s College FutureCare Strategy (2022–2025), which was reshaped in the aftermath of the Covid-19 pandemic to address growing workforce challenges.
“Our approach has been to expand capacity where we can and to develop new programmes where there is a clear regional need and strong alignment with our strengths,” she notes.
Pharmacy was identified as a natural fit within the University’s existing education and research portfolio. The programme has been developed in close collaboration with the regional health authority, with strong input from local pharmacy teams to ensure it reflects both current practice and future workforce requirements.
Preparing Practice-Ready Graduates
A defining feature of the new MPharm programme is its focus on producing graduates who are equipped for evolving clinical roles.
Dr Ní Chúlain highlights that prescribing competencies are embedded throughout the curriculum from the outset, reflecting the growing role of pharmacists as clinical practitioners within integrated healthcare systems.
“This investment reflects the increasing recognition of pharmacists as essential members of the healthcare team,” she says. “Our programme is designed to ensure graduates are
This exposure will support students in developing the practical skills and experience needed to pursue diverse and flexible career pathways within the profession.
Enhancing Learning Through Infrastructure
The development of a new School of Medicine building will further strengthen the University’s capacity to deliver high-quality healthcare education.
The facility will provide dedicated teaching spaces, including rooms designed specifically for small-group learning—an essential component of modern healthcare education. It will also enable greater opportunities for interdisciplinary and interprofessional training, reflecting the collaborative nature of realworld healthcare delivery.
“Students will be trained in ways that mirror how healthcare teams operate in practice,” Dr Ní Chúlain explains, highlighting the importance of preparing graduates for integrated care environments.
Beyond teaching, the new building will support the expansion of research and innovation activities. In particular, it will enhance the University’s capabilities in areas such as digital health and connected health—fields that are expected to play an increasingly important role in the future of healthcare.
Alongside the expansion of pharmacy education, the University is also progressing initiatives aimed at addressing broader workforce challenges, particularly in rural and remote areas.
The introduction of a Rural and Remote Graduate Entry Medicine Stream is expected
Dr Ní Chúlain notes that this approach has been shown to improve retention and support more sustainable workforce planning in rural healthcare systems.
Driving Innovation in Healthcare Education
The investment under HEAP is also enabling the University to accelerate innovation in how healthcare professionals are educated.
As healthcare continues to evolve, there is a growing need for graduates who are not only clinically competent, but also adaptable, digitally literate, and comfortable working within new models of care.
“This is an opportunity to develop graduates who are digitally ready and prepared for the future of healthcare,” Dr Ní Chúlain says. By integrating digital health, innovation, and interdisciplinary learning into its programmes, the University aims to ensure that graduates are equipped to meet the changing demands of healthcare delivery.
The combination of new programme development and infrastructure investment represents a significant step forward for University of Galway and for healthcare education in Ireland more broadly.
For pharmacy, in particular, the introduction of the MPharm programme signals a continued shift towards expanded clinical roles, greater integration within healthcare teams, and a stronger focus on patient-centred care.
As these developments take shape, they are expected to contribute not only to addressing workforce shortages, but also to enhancing the quality, accessibility, and sustainability of healthcare services across the country.
Turning Economic Strength into Patient Impact
The Irish Pharmaceutical Healthcare Association (IPHA) has published new analysis demonstrating the exceptional economic and strategic contribution of the pharmaceutical sector to Ireland, as industry leaders gathered for the IPHA Annual Conference 2026 –“Steering Through Disruption” at the Dublin Royal Convention Centre.
Against a backdrop of geopolitical uncertainty, shifting global trade dynamics and preparations for Ireland’s upcoming Presidency of the Council of the EU, the Goodbody Economic Report for IPHA shows that the pharmaceutical sector has reached record levels of employment, output, exports and tax contribution, underscoring its central role in Ireland’s and Europe’s economic resilience.
Crucially, the recent conference highlighted how this economic strength can now be matched by a system that delivers faster access to innovative medicines for Irish patients, supported by the newly concluded IPHA Framework Agreement.
The report confirms that the pharmaceutical industry is a cornerstone of Ireland’s economy, revealing that the sector continues to outperform all historic benchmarks:
• ¤139 billion in pharma exports in 2025, representing 53% of all goods exports – the highest on record.
• Pharma exports accounted for 41% of Ireland’s GNI* in 2025, with exports to the US alone representing 25% of GNI*.
• 75,000 workers are employed directly and indirectly in pharma and related activities, with sectoral employment growing three times faster than the wider labour market. *
• The industry paid an estimated ¤6 billion in total taxes in 2023, including an estimated 18% of all corporation tax receipts. ¤4.1bn in corporation tax was paid in 2024.
Ireland is now the EU’s second largest pharmaceutical exporter and hosts the highest number of FDA registered drug manufacturing sites per capita in Europe, reflecting its global leadership in high value biologics, advanced therapeutics and complex manufacturing.
As Europe seeks to compete globally in advanced therapies,
biologics and next generation medicines, the report shows that Ireland is one of the continent’s strongest and most competitive life sciences hubs, with deep expertise in high value biologics, sterile injectables and advanced therapeutics manufacturing.
A central theme of the conference was turning this economic strength into patient impact, faster, fairer, and more predictable access to innovative medicines.
The newly concluded IPHA Framework Agreement is designed to deliver precisely that:
• creating structural reforms in pricing and reimbursement so that Ireland complies with the 180 day timing for HSE decisions on reimbursement;
• enabling sustainable investment in innovation;
• supporting Ireland’s competitiveness as a location for manufacturing and R&D; and
• so that patients in Ireland can access the newest treatments at the same pace as other leading European countries.
The Agreement also aligns with Ireland’s priorities for its forthcoming EU Presidency, where regulatory efficiency, innovation pathways and Europe wide patient access will be central policy themes.
Industry leaders emphasise that the Agreement is a directional change — shifting Ireland toward a system that values innovation, supports long term investment, and strengthens Ireland’s role as a global manufacturing and R&D hub.
sector is one of the most competitive anywhere in the world – powered by exceptional talent, deep expertise and a strong track record of delivery. We are committed to improving the health and wellbeing of people across Ireland, while also making a major contribution to jobs, growth and the economy. Today’s Goodbody report shows just how important our sector has become, not just for Ireland, but for Europe, and for global healthcare.
“The challenge now is to ensure patients can access innovation as quickly as we deliver it. The new Framework Agreement is a critical step forward in supporting patients in Ireland gain faster access to innovative and life-changing medicines, whilst empowering clinicians to provide the best care available. The Agreement is the result of a shared ambition and significant collaboration between Government and our sector –creating the basis for a lasting
strategic partnership that backs innovation, strengthens supply chains, and, above all, improves outcomes for patients.”
IPHA Chief Executive Oliver O’Connor, added, “This report confirms that the pharmaceutical industry is one of Ireland’s greatest strategic strengths. It is an engine of stability and growth — delivering record exports, high value employment and major tax contributions — even as the global environment becomes more uncertain.
“This economic strength should clearly translate into patient benefit. The new IPHA Framework Agreement marks a decisive shift towards a system that values innovation and ensures patients in Ireland can access breakthrough medicines faster. With Ireland soon taking up the EU Presidency, we have a major opportunity to lead Europe toward a more competitive, innovation friendly, and patient focused future.”
IPHA President Shane Ryan
Six Hundred Children. Four Consultants. One National Service.
On any given week at Children’s Health Ireland at Temple Street, the work is exacting, highstakes and quietly relentless. Around 580 to 600 children pass through Ireland’s only paediatric neurosurgical service each year. Behind that number stands a team of four consultants, two of whom practise full-time paediatric neurosurgery. Dr Tafadzwa “Dr Taffy” Mandiwanza is one of them. Dr Mandiwanza recently made history when she was appointed as the first female pediatric neurosurgeon in Ireland. She works at Temple St Hospital, the only pediatric neurosurgery center in Ireland.
“It sounds like a lot when you say it out loud,” she says, reflecting on the figures. “Four consultants. Six hundred patients. Sometimes you’re one in three or one in four on call. That can be intense.”
And yet, the pressure is not quite what outsiders might expect. There is no spiralling waiting list. Theatre access is reliable. The average wait for surgery is around six weeks, shorter where clinical urgency demands. “If a child needs to be seen sooner, they are seen sooner,” she explains. “Space is made.”
The challenge is less about infrastructure and more about manpower. A national service concentrated in a small team inevitably creates intensity. Paediatric neurosurgery in Ireland is centralised, operating primarily from CHI at Temple Street, with collaboration across CHI at Crumlin. It is niche by design. There is no parallel
centre elsewhere in the country. Transfers from regional hospitals are routine, and while stabilisation at referring sites is strong, geography remains an operational reality. Getting a critically unwell child to Dublin in time will always require coordination.
What has changed in recent years is not the nature of pathology but the pace. “The type of work hasn’t fundamentally shifted,” Dr Mandiwanza says. “But we are busier.” Epilepsy surgery in particular has expanded, supported by increasingly sophisticated image-navigation systems and robotic-assisted approaches linked with specialist centres such as Beaumont Hospital. The field is evolving, and technology is moving fast.
If volume is rising, innovation is accelerating alongside it. Few developments illustrate this better than intraoperative MRI in paediatric neuro-oncology. “You think you’re done with the operation,” she explains, “and then you scan. If there’s residual tumour, you can go back immediately.” In children, where margins matter and long-term outcomes are shaped in millimetres, that capacity is transformative. It shifts the conversation from ‘good enough’ to ‘maximal safe resection’ in real time.
The forthcoming National Children’s Hospital will, in her view, amplify that capability. Complex children with long, multi-year clinical histories stand to benefit most from integrated infrastructure and high-spec radiology embedded within
surgical pathways. “It will be a game changer,” she says, without hyperbole.
Technology is also reshaping how surgeons communicate with families. Using advanced 3D modelling and virtual visualisation systems, tumours can be reconstructed digitally, allowing clinicians to walk parents through the exact anatomy and surgical approach. “We can show them precisely where the tumour is and how we plan to remove it,” she says. In a specialty where fear can overwhelm information, clarity matters.
Dr Mandiwanza brings an international perspective to this landscape. Originally from Zimbabwe, she trained in leading paediatric centres in London before establishing her consultant practice in Ireland. Some of the management paradigms she encountered abroad have translated seamlessly into Irish care. Others required adaptation. But she is clear on one point: clinically, Ireland stands strong.
“There’s a lot of negative talk about the health system,” she says. “But in paediatrics, clinically, we are on par.” Where she sees room for growth is in research output rather than bedside standards. The gap, she suggests, is academic rather than clinical.
Her appointment as Ireland’s first female paediatric neurosurgeon marked a milestone not because of symbolism alone, but because of what representation signals to a changing workforce. “When I was training, there weren’t many women or immigrants in surgical consultant roles,” she reflects. “The medical workforce now looks different. Leadership should reflect that.”
Diversity at consultant level is not about optics, she argues, but perspective. “I bring something different. I love my colleagues, but it’s important to have different viewpoints in leadership.”
For junior doctors navigating
competitive specialties, visible pathways matter. Seeing someone who has traversed similar terrain can recalibrate what feels possible.
If neurosurgery carries a reputation for ego, she challenges it gently. “There’s this idea that neurosurgeons are egotistical,” she says, smiling. “But we’re actually very approachable.”
In paediatrics, hierarchy gives way to collaboration quickly. “We are not the boss of the MDT.” Complex cases frequently require endocrinology, oncology, neuropsychology, intensive care and therapy input. Children can deteriorate rapidly. Decisions are rarely unilateral. “It would be a disaster without the team. We depend on each other.”
Despite the acuity, she describes the culture with surprising lightness. Four and a half years into her consultant role, she still finds it “fun to come to work”. It is not flippant. It is grounded in teamwork and purpose.
Her own career might easily have taken a different turn. At one stage, she considered returning to Zimbabwe. It was mentorship that shifted the trajectory. “When someone points you in the right direction, it’s gold,” she says. “It’s essential.”
She believes Ireland would benefit from more formalised mentorship structures within surgical training, while acknowledging that effective mentorship depends on genuine connection. “You have to gel. It’s a special relationship.” Her journey stands as an example of what that relationship can unlock.
For those contemplating neurosurgery, or any steep professional climb, her advice is unsentimental. “Life is too short to do something you’re not interested in or don’t enjoy.” The path will be demanding. “You will take some hits,” she says. “But staying resilient matters.”
Six hundred children. Four consultants. One national service. In a specialty defined by precision and pressure, Dr Tafadzwa Mandiwanza is clear-eyed about the realities. The workload is intense. The technology is advancing. The research base must grow. But clinically, she believes Ireland has reason to be proud. And for now, at least, the work still feels worth showing up for.
Dr Tafadzwa “Dr Taffy” Mandiwanza
For healthcare professionals in Ireland only. Abbreviated Prescribing Information can be found below.
Generic Product Launch
Nintedanib Teva
Soft Capsules
nintedanib
High Tech Prescription Medicine
Indications
Nintedanib Teva is indicated in adults for the treatment of idiopathic pulmonary fibrosis (IPF).
Nintedanib Teva is also indicated in adults for the treatment of other chronic fibrosing interstitial lung diseases (ILDs) with a progressive phenotype.
Nintedanib Teva is indicated in adults for the treatment of systemic sclerosis associated interstitial lung disease (SSc-ILD).
Nintedanib Teva Soft Capsules Abbreviated Prescribing Information. Presentation: Each soft capsule contains nintedanib esilate equivalent to 100 mg and 150 mg nintedanib. Indications: Nintedanib Teva is indicated in adults for the treatment of idiopathic pulmonary fibrosis (IPF); for the treatment of other chronic fibrosing interstitial lung diseases (ILDs) with a progressive phenotype; the treatment of systemic sclerosis associated interstitial lung disease (SSc-ILD). Dosage and administration: For oral use. Treatment should be initiated by physicians experienced in the management of diseases for which Nintedanib Teva is approved. Adults: The recommended dose is 150 mg nintedanib twice daily administered approximately 12 hours apart. The 100 mg twice daily dose is only recommended to be used in patients who do not tolerate the 150 mg twice daily dose. The recommended maximum daily dose of 300 mg should not be exceeded. Children: Nintedanib should not be used in children. Elderly: No overall differences in safety and efficacy were observed for elderly patients. No a-priori dose adjustment is required in elderly patients. Patients ≥75 years may be more likely to require dose reduction to manage adverse effects. Renal impairment: Adjustment of the starting dose in patients with mild to moderate renal impairment is not required. The safety, efficacy, and pharmacokinetics of nintedanib have not been studied in patients with severe renal impairment (<30 ml/min creatinine clearance). Hepatic impairment: In adult patients with mild hepatic impairment (Child Pugh A), the recommended dose of Nintedanib Teva is 100 mg twice daily approximately 12 hours apart. In patients with mild hepatic impairment (Child Pugh A), treatment interruption or discontinuation for management of adverse reactions should be considered. The safety and efficacy of nintedanib have not been investigated in patients with hepatic impairment classified as Child Pugh B and C. Treatment of patients with moderate (Child Pugh B) and severe (Child Pugh C) hepatic impairment with Nintedanib Teva is not recommended. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions and warnings: Serious cases of diarrhoea leading to dehydration and electrolyte disturbances have been reported in the post-marketing. Patients should be treated at first signs with adequate hydration and antidiarrhoeal medicinal products, e.g. loperamide, and may require dose reduction or treatment interruption. Nintedanib Teva treatment may be resumed at a reduced dose or at the full dose. In case of persisting severe diarrhoea despite symptomatic treatment, therapy with Nintedanib Teva should be discontinued. Nausea and vomiting are frequently reported gastrointestinal adverse reactions, with most patients experiencing mild to moderate intensity. If symptoms persist despite appropriate supportive care (including antiemetic therapy), dose reduction or treatment interruption may be required. The treatment may be resumed at a reduced dose or at the full. In case of persisting severe symptoms therapy with Nintedanib Teva should be discontinued. Cases of drug-induced liver injury have been observed with nintedanib treatment, including severe liver injury with fatal outcome. The majority of hepatic events occur within the first three months of treatment. Therefore, hepatic transaminase and bilirubin levels should be investigated before treatment initiation and during the first month of treatment with Nintedanib Teva. Patients should then be monitored at regular intervals during the subsequent two months of treatment and periodically thereafter, e.g. at each patient visit or as clinically indicated. Elevations of liver enzymes and bilirubin were reversible upon dose reduction or interruption in the majority of cases. If transaminase elevations > 3x ULN are measured, dose reduction or interruption of the therapy with Nintedanib Teva is recommended and the patient should be monitored closely. Once transaminases have returned to baseline values, treatment with Nintedanib Teva may be resumed at the full dose or reintroduced at a reduced dose which subsequently may be increased to the full dose. If any liver test elevations are associated with clinical signs or symptoms of liver injury, e.g. jaundice, treatment with Nintedanib Teva should be permanently discontinued. Alternative causes of the liver enzyme elevations should be investigated. Adult patients with low body weight (<65 kg), Asian and female patients have a higher risk of elevations of liver enzymes. Nintedanib exposure increased linearly with patient age, which may also result in a higher risk of developing liver enzyme elevations. Close monitoring is recommended in patients with these risk factors. Cases of renal impairment/failure, in some cases with fatal outcome, have been reported with nintedanib use. Patients should be monitored during nintedanib therapy, with particular attention to those patients exhibiting risk factors for renal impairment/failure. In case of renal impairment/failure, therapy adjustment should be considered. Vascular endothelial growth factor receptor (VEGFR) inhibition might be associated with an increased risk of bleeding. Patients at known risk for bleeding including patients with inherited predisposition to bleeding or patients receiving a full dose of anticoagulative treatment were not included in the clinical trials. Nonserious and serious bleeding events, some of which were fatal, have been reported in the postmarketing period (including patients with or without anticoagulant therapy or other medicinal products that could cause bleeding). Therefore, these patients should only be treated with Nintedanib Teva if the anticipated benefit outweighs the potential risk. Patients with a recent history of myocardial infarction or stroke were excluded from the clinical trials. Caution should be used when treating patients at higher cardiovascular risk including known coronary artery disease. Treatment interruption should be considered in patients who develop signs or symptoms of acute myocardial ischemia. The use of VEGF pathway inhibitors in patients with or without hypertension may promote the formation of aneurysms and/or artery dissections. Before initiating Nintedanib Teva, this risk should be carefully considered in patients with risk factors such as hypertension or history of aneurysm. Due to the mechanism of action of nintedanib patients might have an increased risk of thromboembolic events. Due to the
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Freephone: 1800 - 201 700 | Email: info@teva.ie
mechanism of action of nintedanib, patients might have an increased risk of gastrointestinal perforations. Cases of gastrointestinal perforations and cases of ischaemic colitis, some of which were fatal, have been reported in the postmarketing period. Particular caution should be exercised when treating patients with previous abdominal surgery, previous history of peptic ulceration, diverticular disease or receiving concomitant corticosteroids or NSAIDs. Nintedanib Teva should only be initiated at least 4 weeks after abdominal surgery. Therapy with Nintedanib Teva should be permanently discontinued in patients who develop gastrointestinal perforation or ischaemic colitis. Very few cases of nephrotic range proteinuria with or without renal function impairment have been reported postmarketing. Histological findings in individual cases were consistent with glomerular microangiopathy with or without renal thrombi. Reversal of the symptoms has been observed after nintedanib was discontinued, with residual proteinuria in some cases. Treatment interruption should be considered in patients who develop signs or symptoms of nephrotic syndrome. Some cases of posterior reversible encephalopathy syndrome (PRES) have been reported postmarketing. PRES is a neurological disorder (confirmed with magnetic resonance imaging) which can present with headache, hypertension, visual disturbances, seizure, lethargy, confusion and other visual and neurologic disturbances, and can be fatal. PRES has been reported with other VEGF inhibitors. If PRES is suspected, nintedanib treatment must be discontinued. Administration of Nintedanib Teva may increase blood pressure. Systemic blood pressure should be measured periodically and as clinically indicated. Nintedanib Teva should not be used in patients with severe pulmonary hypertension. Close monitoring is recommended in patients with mild to moderate pulmonary hypertension. No increased frequency of impaired wound healing was observed in the clinical trials. Based on the mechanism of action nintedanib may impair wound healing. No evidence of QT prolongation was observed for nintedanib in the clinical trial programme. As some other tyrosine kinase inhibitors are known to exert an effect on QT, caution should be exercised when nintedanib is administered in patients who may develop QTc prolongation. Interactions: Nintedanib is a substrate of P-gp. If coadministered with Nintedanib Teva, potent P-gp inhibitors (e.g. ketoconazole, erythromycin or cyclosporine) may increase exposure to nintedanib. In such cases, patients should be monitored closely for tolerability of nintedanib. Management of adverse reactions may require interruption, dose reduction, or discontinuation of therapy with nintedanib. Potent P-gp inducers (e.g. rifampicin, carbamazepine, phenytoin, and St. John’s Wort) may decrease exposure to nintedanib. Selection of an alternate concomitant medicinal product with no or minimal P-gp induction potential should be considered. Only a minor extent of the biotransformation of nintedanib consists of CYP pathways, therefore, the likelihood of drug-drug interactions with nintedanib based on CYP metabolism is considered to be low. Co-administration of nintedanib with oral hormonal contraceptives did not alter the pharmacokinetics of oral hormonal contraceptives to a relevant extent. Co-administration of nintedanib with bosentan did not alter the pharmacokinetics of nintedanib. Pregnancy and lactation: Nintedanib may cause foetal harm in humans. Women of childbearing potential should be advised to avoid becoming pregnant while receiving treatment with Nintedanib Teva and to use highly effective contraceptive methods at initiation of, during and at least 3 months after the last dose of Nintedanib Teva. The efficacy of oral hormonal contraceptives may be compromised by vomiting and/or diarrhoea or other conditions where the absorption may be affected. Women taking oral hormonal contraceptives experiencing these conditions should be advised to use an alternative highly effective contraceptive measure. As nintedanib may cause foetal harm also in humans, it must not be used during pregnancy and pregnancy testing must be conducted prior to treatment with Nintedanib Teva and during treatment as appropriate. Female patients should be advised to notify their doctor or pharmacist if they become pregnant during therapy with Nintedanib Teva. If the patient becomes pregnant while receiving Nintedanib Teva, treatment must be discontinued and she should be apprised of the potential hazard to the foetus. Breast-feeding should be discontinued during treatment with this medicinal product. Effects on ability to drive and use machines: Nintedanib Teva has minor influence on the ability to drive and use machines. Patients should be advised to be cautious when driving or using machines during treatment with nintedanib. Adverse reactions: Thrombocytopenia, myocardial infarction, bleeding, pancreatitis, colitis, hyperbilirubinaemia, renal failure, PRES. Very Common: Diarrhoea, nausea, abdominal pain, vomiting, hepatic enzyme increased. Common: Weight decreased, decreased appetite, hypertension, alanine aminotransferase (ALT) increased, aspartate aminotransferase (AST) increased, gamma glutamyl transferase (GGT) increased, blood alkaline phosphatase (ALKP) increased, rash, headache. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: There is no specific antidote or treatment for nintedanib overdose. Two patients in the oncology programme had an overdose of maximum 600 mg twice daily up to eight days. Observed adverse reactions were consistent with the known safety profile of nintedanib, i.e. increased liver enzymes and gastrointestinal symptoms. Both patients recovered from these adverse reactions. In the INPULSIS trials, one patient was inadvertently exposed to a dose of 600 mg daily for a total of 21 days. A non-serious adverse event (nasopharyngitis) occurred and resolved during the period of incorrect dosing, with no onset of other reported events. In case of overdose, treatment should be interrupted and general supportive measures initiated as appropriate. Legal category: POM. Marketing Authorisation
Job Code: MED-IE-00106. Date of Preparation: February 2026.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie.
Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Product subject to prescription which may not be renewed (A) Further information is available on request or in the SmPC. Product Information also available on the HPRA website.
Date of Preparation: March 2026 | Job Code: GEN-IE-00179
Ireland can ‘Lead the Way’
Ireland has an opportunity to lead the way in tackling sepsis, rather than continuing to react to its devastating impact, RCSI’s Professor Steven Kerrigan told the Joint Oireachtas Committee on Public Petitions and the Ombudsmen.
Addressing the Committee on the growing threat posed by the condition, Professor Kerrigan, Professor at the School of Pharmacy and Biomolecular Sciences at RCSI University of Medicine and Health Sciences, warned: “Sepsis does not wait for reform cycles. It does not wait for capacity reviews. And it does
Professor Kerrigan, Professor at the School of Pharmacy and Biomolecular Sciences at RCSI
not wait for the ‘right time’. Every delay costs lives, quietly, and often invisibly. Ireland has an opportunity not just to respond, but to lead.”
Professor Kerrigan noted that Ireland’s forthcoming Presidency of the Council of the European Union in July 2026 presents a unique opportunity to elevate sepsis on the European health agenda. He suggested that Ireland could use its Presidency to convene a European discussion on sepsis prevention, early recognition and antimicrobial resistance, positioning the country as a leader in patient safety and public health.
Sinead O’Reilly, who addressed the Committee alongside Professor Kerrigan, shared her family’s experience of losing her sister-in-law Sarah to sepsis in 2022 following failures in recognition and escalation of care. She called for national improvements in early detection, education and accountability to prevent similar tragedies.
Sepsis is a life-threatening condition in which the body’s response to an infection damages its own tissues and organs. Triggered most often by bacterial or viral infections, it occurs when pathogens enter the bloodstream and spread throughout the body, provoking an extreme immune reaction that can lead to organ failure and death without prompt treatment.
With nearly 50 million cases and 11 million deaths globally each year, sepsis represents a significant health crisis in Ireland and around the world. Despite its prevalence and severity, the condition remains difficult to diagnose due to a lack of a definitive biomarker that can reliably confirm a diagnosis in its early stages. Clinicians must rely on other signs and symptoms, along with the laboratory tests, to diagnose sepsis.
EMA Greenlights Higher-Dose Wegovy®
The European Medicines Agency (EMA) has approved a new 7.2 mg once-weekly dose of Wegovy® (semaglutide) for weight management in adults living with obesity, marking a further development in the pharmacological management of obesity as a chronic condition.
The higher-dose formulation is indicated as an adjunct to a reduced-calorie diet and increased physical activity for weight management, including weight loss and maintenance, in adults with an initial body mass index (BMI) of ≥30 kg/m2 As with existing GLP-1 receptor agonist therapies, treatment must be initiated on prescription by a healthcare professional and dispensed through pharmacies.
The approval is supported by clinical evidence from the STEP UP trial programme conducted
by Novo Nordisk. In the study, participants treated with semaglutide 7.2 mg achieved a mean weight reduction of 20.7% from a baseline body weight of 113 kg over 72 weeks, compared with a 17.5% reduction in those receiving the currently available 2.4 mg dose and 2.4% with placebo, when adherence to treatment was maintained.
Further analysis within the trial demonstrated that approximately 84% of total weight loss was attributable to reductions in fat mass, with preservation of muscle function also observed. These findings may be of particular clinical relevance in long-term weight management, where maintenance of lean body mass is an important consideration.
As with other GLP-1 receptor agonists, gastrointestinal adverse
events were the most commonly reported side effects. These occurred in 70.8% of participants receiving semaglutide 7.2 mg, compared with 61.2% in the 2.4 mg group and 42.8% in the placebo arm. Dysaesthesia was also reported more frequently at the higher dose. Serious adverse events were recorded in 6.8% of those receiving semaglutide 7.2 mg, compared with 10.9% for the 2.4 mg dose and 5.5% with placebo.
At present, the 7.2 mg dose is delivered as three separate 2.4 mg injections. Novo Nordisk has submitted an application to the EMA for a single-dose device designed to administer the full 7.2 mg in one injection, which may have implications for adherence and patient convenience if approved.
When a patient has sepsis, early diagnosis is key for survival. Cases in Ireland, across Europe and globally are rising, and the ability to treat infection is being hampered by antibiotic resistance.
In his presentation to the Committee, Professor Kerrigan noted that the healthcare system is not currently structured to detect sepsis early, deliver a consistent response, or provide adequate support for patients and families in the aftermath. He also highlighted that clinicians are increasingly encountering sepsis in older, sicker patients, often linked to infections that are less responsive to first-line treatments. This is contributing to longer hospital stays, higher costs, greater complications and higher numbers of deaths.
“Sepsis is not just an acute medical emergency; it is a lifealtering event.”, Professor Kerrigan stated. “Survivors often live with cognitive impairment, physical disability, PTSD, anxiety and depression. Families are changed forever. Careers end. Lives shrink.” Professor Kerrigan said that Ireland has the opportunity to lead by delivering a fully resourced national sepsis strategy focused on prevention, early detection, public awareness, professional training and post-sepsis care.
Commenting on the approval, Dilek Dogan Gurluk, General Manager of Novo Nordisk Ireland, described obesity as a complex medical condition requiring evidence-based, long-term management and noted that the availability of a higher semaglutide dose represents an important clinical development in the treatment landscape.
The approval comes amid rising obesity prevalence across Ireland, with increasing recognition of obesity as a chronic disease requiring multidisciplinary management. For community pharmacists, the introduction of a higher-dose semaglutide option is likely to further expand their role in supporting patients with weight management, including counselling on adherence, adverse effect management, and the importance of concurrent lifestyle interventions.
Wegovy® delivers quality weight loss1,2,5 and provides cardiovascular risk reduction1,3ɬ
Safety and tolerability profile comparable to the GLP-1 RA class in general1
Wegovy® is recommended in the ESC CCS guidelines for cardiovascular risk reduction4
tThis product is subject to additional monitoring. ESC = European Society of Cardiology. CCS = Chronic Coronary Syndrome. GLP-1 RA = Glucagon Like Peptide 1 Receptor Agonist.
Wegovy®t(semaglutide) Please refer to the full Summary of Product Characteristics (SmPC) before prescribing. Wegovy® 0.25 mg FlexTouch® solution for injection in pre-filled pen. Wegovy® 0.5 mg FlexTouch® solution for injection in pre-filled pen. Wegovy® 1 mg FlexTouch® solution for injection in pre-filled pen. Wegovy® 1.7 mg FlexTouch® solution for injection in pre-filled pen. Wegovy® 2.4 mg FlexTouch® solution for injection in pre-filled pen. Indication(s): Adults: Wegovy® is indicated as an adjunct to a reduced-calorie diet and increased physical activity for weight management, including weight loss and weight maintenance, in adults with an initial Body Mass Index (BMI) of ≥30 kg/m2 (Obesity) or ≥27 kg/m2 to <30 kg/m2 (overweight) in the presence of at least one weight-related comorbidity e.g. dysglycaemia (prediabetes or type 2 diabetes mellitus), hypertension, dyslipidaemia, obstructive sleep apnoea or cardiovascular disease. For trial results with respect to cardiovascular risk reduction, obesity-related heart failure, and populations studied, see section 5.1. of the Wegovy® SmPC. Adolescents: Wegovy® is indicated as an adjunct to a reduced-calorie diet and increased physical activity for weight management in adolescents ages 12 years and above with obesity* and body weight above 60 kg. Treatment with Wegovy® should be discontinued and re-evaluated if adolescent patients have not reduced their BMI by at least 5% after 12 weeks on the 2.4 mg or maximum tolerated dose. *See table 1 in the Wegovy® SmPC for BMI cut-off points for obesity by sex and age. Posology and administration: Administered once weekly at any time of the day, with or without meals. Injected subcutaneously in the abdomen, in the thigh or in the upper arm. The injection site can be changed. It should not be administered intravenously or intramuscularly. For the 7.2 mg dose, inject three doses of 2.4 mg one after each other. The injections can be administered in the same body area but should be at least 5 cm apart. Injection sites should always be rotated to reduce the risk of injection site amyloid deposits. The day of weekly administration can be changed if necessary, as long as the time between doses is at least 3 days (>72 hours). After selecting a new dosing day, once-weekly dosing should be continued. Adults: The maintenance dose of semaglutide 2.4 mg once-weekly is reached by starting with a dose of 0.25 mg. To reduce the likelihood of gastrointestinal symptoms, the dose should be escalated over a 16-week period to the maintenance dose. If needed, the dose can be increased to 7.2 mg once weekly after a minimum of 4 weeks on the 2.4 mg dose in adults with BMI ≥ 30 kg/m2 at treatment initiation. If no additional clinical improvement in body weight is observed with 7.2 mg, lower the dose to 2.4 mg once weekly. In case of significant gastrointestinal symptoms, consider delaying dose escalation or lowering to the previous dose until symptoms have improved. Adolescents: For adolescents ages 12 years and above, the same dose escalation schedule as for adults should be applied. The dose should be increased until 2.4 mg (maintenance dose) or maximum tolerated dose has been reached. Weekly doses higher than 2.4 mg are not recommended in the adolescent population. Patients with type 2 diabetes: When initiating Wegovy®, consider reducing the dose of concomitantly administered insulin or insulin secretagogues (such as sulfonylureas) to reduce the risk of hypoglycaemia. Missed dose: If a dose is missed, it should be administered as soon as possible and within 5 days after the missed dose. If more than 5 days have passed, the missed dose should be skipped, and the next dose should be administered on the regularly scheduled day. If more doses are missed, reducing the starting dose for re-initiation should be considered. Elderly: No dose adjustment is required based on age. Renal impairment: No dose adjustment is required for patients with mild or moderate renal impairment. Experience in patients with severe renal impairment is limited. Semaglutide is not recommended for use in patients with severe renal impairment (eGFR <30 mL/min/1.73m2) including patients with end-stage renal disease. Hepatic impairment: No dose adjustment is required for patients with mild or moderate hepatic impairment. Experience in patients with severe hepatic impairment is limited. Semaglutide is not recommended for use in patients with severe hepatic impairment and should be used cautiously in patients with mild or moderate hepatic impairment. Paediatrics: The safety and efficacy of semaglutide in children below 12 years of age have not been established. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Special warnings and precautions for use: Cases of pulmonary aspiration have been reported in patients receiving GLP-1 receptor agonists undergoing general anaesthesia or deep sedation. Therefore, the increased risk of residual gastric content due to delayed gastric emptying should be considered prior to performing procedures with general anaesthesia or deep sedation. Use of GLP-1 receptor agonists may be associated with gastrointestinal adverse reactions. This should be considered when treating patients with impaired renal function, as nausea, vomiting, and diarrhoea may cause dehydration, which in rare cases can lead to a deterioration of renal function. Patients treated with semaglutide should be advised of the potential risk of dehydration in relation to gastrointestinal side effects and take precautions to avoid fluid depletion. Acute pancreatitis has been observed with the use
of GLP-1 receptor agonists. Patients should be informed of the characteristic symptoms of acute pancreatitis. If pancreatitis is suspected, Wegovy® should be discontinued; if confirmed, Wegovy® should not be restarted. Caution should be exercised in patients with a history of pancreatitis. In the absence of other signs and symptoms of acute pancreatitis, elevations in pancreatic enzymes alone are not predictive of acute pancreatitis. Data from epidemiological studies indicates an increased risk for nonarteritic anterior ischaemic optic neuropathy (NAION) during treatment with semaglutide. There is no identified time interval for when NAION may develop following treatment start. A sudden loss of vision should lead to ophthalmological examination and treatment with semaglutide should be discontinued if NAION is confirmed. Wegovy® should not be used as a substitute for insulin in patients with type 2 diabetes. Wegovy® should not be used in combination with other GLP-1 receptor agonist products. Patients treated with Wegovy® in combination with a sulfonylurea or insulin may have an increased risk of hypoglycaemia. The risk of hypoglycaemia can be lowered by reducing the dose of sulfonylurea or insulin when initiating treatment with a GLP-1 receptor agonist. In patients with diabetic retinopathy treated with semaglutide, an increased risk of developing diabetic retinopathy complications has been observed. Patients with diabetic retinopathy using semaglutide should be monitored closely and treated according to clinical guidelines. There is no experience with Wegovy® in patients with type 2 diabetes with uncontrolled or potentially unstable diabetic retinopathy. In these patients, treatment with Wegovy® is not recommended. Semaglutide treated patients with gastroparesis may experience more serious or severe gastrointestinal adverse events. Semaglutide should be used with caution in these patients, and semaglutide is not recommended if gastroparesis is severe. The safety and efficacy of Wegovy® has not been investigated in patients treated with other products for weight management, with type 1 diabetes, with severe renal or hepatic impairment or with congestive heart failure New York Heart Association (NYHA) class IV. Use in these patients is not recommended. There is limited experience with Wegovy® in patients aged 85 years or more, with mild or moderate hepatic impairment, with inflammatory bowel disease. Use with caution in these patients. If semaglutide is used in combination with a sulfonylurea or insulin, patients should be advised to take precautions to avoid hypoglycaemia while driving and using machines. Fertility, pregnancy and lactation: Women of childbearing potential are recommended to use contraception when treated with semaglutide. There are limited data from the use of semaglutide in pregnant women. Therefore, semaglutide should not be used during pregnancy. If a patient wishes to become pregnant, or pregnancy occurs, semaglutide should be discontinued. Semaglutide should be discontinued at least 2 months before a planned pregnancy due to the long half-life. In lactating rats, semaglutide was excreted in milk. A risk to a breast-fed child cannot be excluded. Semaglutide should not be used during breast-feeding. Effect on fertility unknown. Undesirable effects: Very common (≥1/10): Headache, vomiting, diarrhoea, constipation, nausea, abdominal pain, fatigue. Common (≥1/100 to <1/10): Hypoglycaemia in patients with type 2 diabetes, dizziness, dysgeusia, dysaesthesia, diabetic retinopathy in patients with type 2 diabetes, gastritis, gastrooesophageal reflux disease, dyspepsia, eructation, flatulence, abdominal distension, cholelithiasis, hair loss, injection site reactions. Uncommon (≥1/1,000 to <1/100): Hypotension, orthostatic hypotension, increased heart rate, acute pancreatitis, delayed gastric emptying, increased amylase, increased lipase. Rare (≥1/10,000 to <1/1,000): Anaphylactic reaction, angioedema. Very rare (<1/10 000): Non-arteritic anterior ischaemic optic neuropathy (NAION). Not known (cannot be estimated from the available data): Intestinal obstruction. The SmPC should be consulted for a full list of side effects. MA number(s): Wegovy® 0.25 mg FlexTouch® EU/1/21/1608/006. Wegovy® 0.5 mg FlexTouch® (1.5 ml cartridge) EU/1/21/1608/007. Wegovy® 0.5 mg FlexTouch® (3 ml cartridge) EU/1/21/1608/012. Wegovy® 1 mg FlexTouch® EU/1/21/1608/008. Wegovy® 1.7 mg FlexTouch® EU/1/21/1608/009. Wegovy® 2.4 mg FlexTouch® EU/1/21/1608/010. Legal category: Product subject to prescription which may not be renewed. For complete prescribing information please refer to the SmPC which is available on www.medicines.ie or by email from infoireland@novonordisk.com or from the Clinical, Medical and Regulatory Department, Novo Nordisk Limited, 1st Floor, Block A, The Crescent Building, Northwood Business Park, Santry, Dublin 9, Ireland. Date last revised: February 2026. IE26SEMO00055.
tThis medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Adverse events should be reported to the Health Products Regulatory Authority. Information about adverse event reporting is available at www.hpra.ie. Adverse events should also be reported to Novo Nordisk on Tel: 01 8629700 or complaintireland@novonordisk.com.
*From baseline to week 72. Data presented here from the STEP UP trial are based on the trial product estimand, which describes the treatment effect if all people adhered to treatment, whereas the primary treatment policy estimand describes the treatment effect regardless of treatment adherence. When applying the treatment policy estimand, people treated with Wegovy® 7.2 mg achieved a superior weight loss of 18.7% vs placebo of 3.9%. The proportion of patients with a body weight reduction of ≥25% was greater with Wegovy® 7.2 mg (31.2%), vs placebo (0%).1
ɬ People living with overweight or obesity and established cardiovascular disease without diabetes.
Ŧ The co-primary endpoints were percentage change in body weight and the proportion of patients with a body weight reduction of 5% or greater for Wegovy® 7.2 mg vs placebo.1
Applying the trial product estimand, the proportion of patients with a body weight reduction of ≥5% was greater with Wegovy® 7.2 mg (93.2%), vs placebo (35.7%).1
¥Confirmatory secondary endpoint.
References: 1. Wegovy® Summary of Product Characteristics www.medicines.ie 2. Wharton S, Freitas P, Hjelmesæth J, et al. Once-weekly semaglutide 7.2 mg in adults with obesity (STEP UP): a randomised, controlled, phase 3b trial. Lancet Diabetes Endocrinol. 2025; S2213-8587(25)00226-8. 3. Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232 4. Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45(36):3415-3537. 5. Hjelmesæth J, Bhat S, Garvey WT, et al. Effect of semaglutide on body composition and proximal muscle strength: the STEP UP trial. Presented at: The 61st European Association for the Study of Diabetes (EASD) Annual Meeting; September 15-19, 2025; Vienna, Austria.
First Cohort of Advanced Specialist Pharmacists Appointed Across HSE Hospitals
A milestone in Irish hospital pharmacy has been reached with the appointment of the first cohort of Advanced Specialist Pharmacists, marking the most significant reform of the profession’s career structure in over four decades.
A Long-Awaited Development
Fourteen years after the landmark McLoughlin Report (2011) called for a new grade of pharmacist above senior level, the Health Service Executive (HSE) has formally introduced the Advanced Specialist Pharmacist role. The report highlighted the importance of this grade in delivering highquality, cost-effective care and in retaining experienced pharmacists in frontline positions.
This development is part of a broader overhaul of the pharmacy career framework, last updated in 1978. Following the initial recommendations, further work in 2017–2018 defined role descriptions, while an industrial relations process culminated in agreement under the Public Service Agreement: Building Momentum (2021–2022). The revised structure aims to strengthen governance, enhance medication management, and improve healthcare utilisation costs, ultimately delivering better patient outcomes.
Advanced Practice in Pharmacy
Advanced practice has become a cornerstone of healthcare professions worldwide, and pharmacy is no exception. The International Pharmaceutical Federation (FIP) has issued guidance, competencies, and a toolkit that helped to inform Ireland’s approach. A working group comprising representatives from the HSE, academia, and the Hospital Pharmacists Association of Ireland (through Forsa) developed competency-based criteria tailored to the Irish health system. The Department of Health approved the resulting framework for implementation in November 2023.
The six pillars of performance for Advanced Specialist Pharmacist Practice, aligned with FIP
Advanced Level II:
1. Expert Professional Practice
2. Working with Others
3. Leadership
4. Management
5. Education and Training
6. Research and Evaluation
Implementation and Validation
Unlike regulatory processes overseen by the Pharmaceutical Society of Ireland (PSI), this initiative is workplace-based and linked to the pharmacist’s role. Many experienced pharmacists were already working at advanced levels without formal recognition, and the new grade provides a structured pathway to acknowledge their expertise.
Implementation is being rolled out in two phases:
• Phase 1: Validation of current post-holders already working at advanced practice level.
• Phase 2: Future appointments aligned with Pay and Number policy or Department of Healthapproved service developments.
During Phase 1, eligible pharmacists submitted evidence of their work across the six competency areas, verified by their Pharmacist Executive Manager. The process was supported by the National Recruitment Service,
with applications anonymised and assessed by an expert panel using a structured scoring system.
Of those who applied, 235 pharmacists nationwide were successful, representing 70% of candidates who passed the eligibility stage. The strong success rate reflects both the depth of postgraduate education within the profession and the high level of expertise built up through years of specialised practice.
Not all applicants met the required standard at this time, a result anticipated given the short leadin period and varying stages of professional development.
Looking Ahead
The introduction of the Advanced Specialist Pharmacist grade marks a pivotal step in strengthening the HSE’s pharmacy workforce at a time of increasing complexity in medication use. The revised career structure offers a sustainable pathway for workforce development, encouraging deeper collaboration between pharmacists, multidisciplinary colleagues, and patients.
As implementation progresses, the impact of these changes promises to enhance clinical care, optimise healthcare resources, and support safer, more effective medication use for patients across the Irish healthcare system.
Consultant Executive Leadership Programme (CELP) –Applications Now Open
The Irish Hospital Consultants Association, in partnership with Trinity Executive Education, is pleased to announce that applications are now open for the inaugural cohort of the Consultant Executive Leadership Programme (CELP).
CELP is a consultant-led leadership programme designed to support hospital consultants in navigating the increasing complexity of modern healthcare systems. As clinical leadership becomes central to system performance, the programme provides a structured opportunity to develop the skills required to influence decision-making, lead multidisciplinary teams, and contribute to system-level reform.
Consultants operate at the intersection of clinical care, governance, and system design. However, formal training in leadership, strategy, and organisational influence is often limited.
CELP has been developed to address this gap, with a focus on:
Leading effectively within complex healthcare systems
Influencing policy, governance, and organisational direction
Building and managing highperforming teams
Developing strategic thinking and decision-making capability
Strengthening communication and executive presence
The programme is grounded in real-world healthcare challenges and delivered in a format that enables meaningful peer discussion across specialities.
Programme Structure
The inaugural programme will run across three in-person modules:
22–24 June 2026 – Trinity Executive Education, Dublin
27–29 September 2026 –Farnham Estate, Cavan
30 November – 2 December 2026 – Final module
Each module combines expert-led sessions, case-based discussion,
and peer learning, with a strong emphasis on practical application.
CELP is designed for:
Hospital consultants across all specialties
Clinical leaders seeking to expand their influence within their organisation
Consultants interested in contributing to system-level change
Those preparing for formal or informal leadership roles
Applications - Places are limited, and demand is expected to exceed capacity.
Early application is strongly encouraged. Visit www.ihca.ie to apply.
Muriel Pate
For healthcare professionals in Ireland only. Abbreviated Prescribing Information can be found below.
Generic Product Launch
Eltrombopag Teva
Film-coated tablets eltrombopag
High Tech Prescription Medicine
Indications
The treatment of adult patients with primary immune thrombocytopenia (ITP) who are refractory to other treatments (e.g., corticosteroids, immunoglobulins).
The treatment of paediatric patients aged 1 year and above with primary immune thrombocytopenia (ITP) lasting 6 months or longer from diagnosis and who are refractory to other treatments (e.g., corticosteroids, immunoglobulins).
In adult patients with chronic hepatitis C virus (HCV) infection for the treatment of thrombocytopenia, where the degree of thrombocytopenia is the main factor preventing the initiation or limiting the ability to maintain optimal interferon-based therapy.
Eltrombopag Teva Film-coated Tablets Abbreviated Prescribing Information. Presentation: Each film-coated tablet contains eltrombopag olamine equivalent to 25mg and 50mg eltrombopag respectively. Indications: Indicated for the treatment of adult patients with primary immune thrombocytopenia (ITP) who are refractory to other treatments (e.g. corticosteroids, immunoglobulins). Indicated for the treatment of paediatric patients aged 1 year and above with primary immune thrombocytopenia (ITP) lasting 6 months or longer from diagnosis and who are refractory to other treatments (e.g. corticosteroids, immunoglobulins). Indicated in adult patients with chronic hepatitis C virus (HCV) infection for the treatment of thrombocytopenia, where the degree of thrombocytopenia is the main factor preventing the initiation or limiting the ability to maintain optimal interferon-based therapy. Dosage and administration: Oral use. Should be initiated by and remain under the supervision of a physician who is experienced in the treatment of haematological diseases or the management of chronic hepatitis C and its complications. Immune (primary) thrombocytopenia: The lowest dose of eltrombopag to achieve and maintain a platelet count ≥50 000/μl should be used. Dose adjustments are based upon the platelet count response. Eltrombopag must not be used to normalise platelet counts. Adults and Children (aged 6 years and above): 50mg once daily. For patients of East-/Southeast-Asian ancestry, eltrombopag should be initiated at a reduced dose of 25mg once daily. Children (aged 1 to 5 years): 25mg once daily. After initiating eltrombopag, the dose must be adjusted to achieve and maintain a platelet count ≥50 000/ μl as necessary to reduce the risk for bleeding. A daily dose of 75mg must not be exceeded. Discontinuation: Treatment with eltrombopag should be discontinued if the platelet count does not increase to a level sufficient to avoid clinically important bleeding after 4 weeks of eltrombopag therapy at 75mg once daily. Chronic hepatitis C (HCV) associated thrombocytopenia: Eltrombopag should be initiated at a dose of 25mg once daily. No dosage adjustment is necessary for HCV patients of East-/Southeast-Asian ancestry or patients with mild hepatic impairment. If after 2 weeks of eltrombopag therapy at 100mg the required platelet level to initiate antiviral therapy is not achieved, eltrombopag should be discontinued. Children and Adolescents: Eltrombopag is not recommended for use in children under the age of one year with ITP due to insufficient data on safety and efficacy. The safety and efficacy of eltrombopag has not been established in children and adolescents (<18 years) with chronic HCV related thrombocytopenia. Elderly: There are limited data on the use of eltrombopag in ITP patients aged 65 years and older and no clinical experience in ITP patients aged over 85 years. There are limited data on the use of eltrombopag in HCV patients aged over 75 years. Caution should be exercised in these patients. Renal impairment: No dose adjustment is necessary in patients with renal impairment. Patients with impaired renal function should use eltrombopag with caution and close monitoring. Hepatic impairment: Eltrombopag should not be used in ITP patients with hepatic impairment (Child-Pugh score ≥5) unless the expected benefit outweighs the identified risk of portal venous thrombosis. If the use of eltrombopag is deemed necessary for ITP patients with hepatic impairment the starting dose must be 25mg once daily. After initiating the dose of eltrombopag in patients with hepatic impairment an interval of 3 weeks should be observed before increasing the dose. East-/Southeast-Asian patients: For adult and paediatric patients of East-/Southeast-Asian ancestry, including those with hepatic impairment, eltrombopag should be initiated at a dose of 25mg once daily. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions and warnings: Safety and efficacy have not been established in combination with direct-acting antiviral agents approved for treatment of chronic hepatitis C infection. Eltrombopag administration can cause abnormal liver function and severe hepatotoxicity, which might be life-threatening. Serum alanine aminotransferase (ALT), aspartate aminotransferase (AST) and bilirubin should be measured prior to initiation of eltrombopag, every 2 weeks during the dose adjustment phase and monthly following establishment of a stable dose. Caution is required when administering eltrombopag to patients with hepatic disease. In ITP and SAA patients a lower starting dose of eltrombopag should be used. Close monitoring is required when administering to patients with hepatic impairment. Chronic HCV patients with liver cirrhosis may be at risk of hepatic decompensation when receiving alfa interferon therapy. In patients with low albumin levels (≤ 35g/l) or with a MELD score ≥10 at baseline, there was a 3-fold greater risk of hepatic decompensation and an increase in the risk of a fatal adverse event compared to those with less advanced liver disease. In addition, the benefits of treatment in terms of the proportion achieving SVR compared with placebo were modest in these patients (especially for those with baseline albumin ≤35g/l) compared with the group overall. Eltrombopag should only be administered to such patients after careful consideration of the expected benefits in comparison with the risks. Patients with these characteristics should be closely monitored for signs and symptoms of hepatic decompensation. In controlled studies in thrombocytopenic patients with HCV receiving interferon-based therapy (n=1 439), 38 out of 955 patients (4%) treated with eltrombopag and 6 out of 484 patients (1%) in the placebo group experienced thrombotic/thromboembolic events (TEEs). Reported thrombotic/thromboembolic complications included both venous and arterial events. The majority of TEEs were non-serious and resolved by the end of the study. The risk of TEEs has been found to be increased in patients with chronic liver disease (CLD) treated with 75mg eltrombopag once daily for 2 weeks in preparation for invasive procedures. Eltrombopag should not be used in ITP patients with hepatic impairment (Child-Pugh score ≥5) unless the expected benefit outweighs the identified risk of portal venous thrombosis. When treatment is considered appropriate, caution is required when administering eltrombopag to patients with hepatic impairment. Thrombocytopenia is likely to reoccur in ITP patients upon discontinuation of treatment with eltrombopag. Following discontinuation of eltrombopag, platelet counts return to baseline levels within 2 weeks in the majority of patients, which increases the bleeding risk and, in some cases, may lead to bleeding. This risk is increased if eltrombopag treatment is discontinued in the presence of anticoagulants or anti-platelet agents. Platelet counts must be monitored weekly for 4 weeks following discontinuation of eltrombopag. Eltrombopag may increase the risk for development or progression of reticulin fibres within the bone marrow. Prior to initiation of eltrombopag, the peripheral blood smear should be examined closely to establish a baseline level of cellular morphologic abnormalities. If the patient develops new or worsening morphological abnormalities or cytopenia(s), treatment with eltrombopag should be discontinued and a bone marrow biopsy considered, including staining for fibrosis. The effectiveness and safety of eltrombopag have not been established for the treatment of
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Freephone: 1800 - 201 700 | Email: info@teva.ie
Product subject to prescription which may not be renewed (A)
thrombocytopenia due to myelodysplastic syndrome (MDS). Cytogenetic abnormalities are known to occur in SAA patients. It is not known whether eltrombopag increases the risk of cytogenetic abnormalities in patients with SAA. Bone marrow examination with aspirations for cytogenetics is recommended prior to initiation of eltrombopag, at 3 months of treatment and 6 months thereafter. If new cytogenetic abnormalities are detected, it must be evaluated whether continuation of eltrombopag is appropriate. Routine ophthalmologic monitoring of patients is recommended. In controlled studies in thrombocytopenic patients with HCV receiving interferon therapy (n=1 439), progression of pre-existing baseline cataract(s) or incident cataracts was reported in 8% of the eltrombopag group and 5% of the placebo group. Retinal haemorrhages, mostly Grade 1 or 2, have been reported in HCV patients receiving interferon, ribavirin and eltrombopag (2% of the eltrombopag group and 2% of the placebo group. Haemorrhages occurred on the surface of the retina (preretinal), under the retina (subretinal), or within the retinal tissue. QTc interval prolongation has been reported in clinical studies of patients with ITP and thrombocytopenic patients with HCV. A loss of response or failure to maintain a platelet response with eltrombopag treatment within the recommended dosing range should prompt a search for causative factors, including an increased bone marrow reticulin. Eltrombopag is highly coloured and so has the potential to interfere with some laboratory tests. Serum discolouration and interference with total bilirubin and creatinine testing have been reported in patients taking eltrombopag. Interactions: Administration of eltrombopag 75mg once daily for 5 days with a single 10mg dose of the OATP1B1 and BCRP substrate rosuvastatin to 39 healthy adult subjects increased plasma rosuvastatin Cmax 103%. Interactions are also expected with other HMG-CoA reductase inhibitors, including atorvastatin, fluvastatin, lovastatin, pravastatin and simvastatin. When co-administered with eltrombopag, a reduced dose of statins should be considered and careful monitoring for statin adverse reactions should be undertaken. Concomitant administration of eltrombopag and OATP1B1 (e.g. methotrexate) and BCRP (e.g. topotecan and methotrexate) substrates should be undertaken with caution. eltrombopag (up to 100mM) showed no in vitro inhibition of the CYP450 enzymes 1A2, 2A6, 2C19, 2D6, 2E1, 3A4/5, and 4A9/11 and was an inhibitor of CYP2C8 and CYP2C9. No clinically significant interactions are expected when eltrombopag and CYP450 substrates are co-administered. Dose adjustment is not required when eltrombopag is co-administered with either telaprevir or boceprevir. A decrease in eltrombopag exposure was observed with co-administration of 200mg and 600mg ciclosporin (a BCRP inhibitor). Eltrombopag chelates with polyvalent cations such as iron, calcium, magnesium, aluminium, selenium and zinc. Eltrombopag should be taken at least two hours before or four hours after any products such as antacids, dairy products or mineral supplements containing polyvalent cations to avoid significant reduction in eltrombopag absorption. Co-administration of eltrombopag with lopinavir/ritonavir may cause a decrease in the concentration of eltrombopag. Platelet count should be closely monitored to ensure appropriate medical management of the dose of eltrombopag when lopinavir/ritonavir therapy is initiated or discontinued. Eltrombopag is metabolised through multiple pathways including CYP1A2, CYP2C8, UGT1A1, and UGT1A3. Medicinal products that inhibit or induce a single enzyme are unlikely to significantly affect plasma eltrombopag concentrations, whereas medicinal products that inhibit or induce multiple enzymes have the potential to increase (e.g. fluvoxamine) or decrease (e.g. rifampicin) eltrombopag concentrations. Co-administration of repeat doses of boceprevir 800mg every 8 hours or telaprevir 750mg every 8 hours with a single dose of eltrombopag 200mg did not alter plasma eltrombopag exposure to a clinically significant extent. Platelet counts should be monitored when combining eltrombopag with other medicinal products for the treatment of ITP in order to avoid platelet counts outside of the recommended range. Pregnancy and lactation: Eltrombopag Teva is not recommended during pregnancy and is not recommended in women of childbearing potential not using contraception. A decision must be made whether to discontinue breastfeeding or to continue/abstain from eltrombopag therapy, considering the benefit of breast-feeding for the child and the benefit of therapy for the woman. Effects on ability to drive and use machines: negligible influence on the ability to drive and use machines. The clinical status of the patient and the adverse reaction profile of eltrombopag, including dizziness and lack of alertness, should be borne in mind when considering the patient’s ability to perform tasks that require judgement, motor and cognitive skills. Adverse reactions: Pneumonia, rectosigmoid cancer, leukocytosis, thrombocytopenia, haemolytic anaemia, hypersensitivity, toxic neuropathy, retinal haemorrhage, acute myocardial infarction, electrocardiogram QT prolonged, deep vein thrombosis, haematoma, embolism, pulmonary embolism, pulmonary infarction, hyperbilirubinaemia, hepatic function abnormal, cholestasis, hepatic lesion, hepatitis, drug-induced liver injury, thrombotic microangiopathy with renal failure, renal failure, leukocyturia, lupus nephritis, hepatic neoplasm (malignant), hepatic encephalopathy, neutropenia, splenic infarction, syncope. Very Common: Nasopharyngitis, upper respiratory tract infection, cough, nausea, diarrhoea, back pain, headache, dizziness, anaemia, decreased appetite, pruritus, myalgia, pyrexia, fatigue, influenzalike illness, asthenia, chills, oropharyngeal pain, rhinorrhoea. Common: Pharyngitis, influenza, oral herpes, sinusitis, tonsillitis, respiratory tract infection, gingivitis, Anaemia, eosinophilia, haemoglobin decreased, white blood cell count decreased, hypokalaemia, decreased appetite, blood uric acid increased, sleep disorder, depression, paraesthesia, hypoaesthesia, somnolence, migraine, dry eye, vision blurred, eye pain, visual acuity reduced, ear pain, vertigo, hot flush, oropharyngeal pain, rhinorrhoea, mouth ulceration, toothache, vomiting, abdominal pain, mouth haemorrhage, flatulence, rash, alopecia, hyperhidrosis, pruritus generalised, petechiae, myalgia, muscle spasm, musculoskeletal pain, bone pain, menorrhagia, pyrexia, chest pain, asthenia, hypoglycaemia, anxiety, epistaxis. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: In the event of overdose, platelet counts may increase excessively and result in thrombotic/thromboembolic complications. In case of an overdose, consideration should be given to oral administration of a metal cation-containing preparation, such as calcium, aluminium, or magnesium preparations to chelate eltrombopag and thus limit absorption. Platelet counts should be closely monitored. Because eltrombopag is not significantly renally excreted and is highly bound to plasma proteins, haemodialysis would not be expected to be an effective method to enhance the elimination of eltrombopag. Legal category: POM. Marketing Authorisation Number: PA22579/003/001-002. Marketing Authorisation Holder: TEVA GmbH, Graf-Arco-Str. 3, 89079 Ulm, Germany. Job Code: MED-IE-00103. Date of Preparation: November 2025
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie.
Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Date of Preparation: December 2025 | Job Code: GEN-IE-00167
Further information is available on request or in the SmPC. Product Information also available on the HPRA website.
Designing Safer, Kinder Pain Pathways in 2026
The human moment at the centre of a pathway
Pain changes how a person can see the world. What was once filled with opportunities now becomes restricted, limited by the prison of a symptom that defines how life can be lived. Pain should never be simplified to a score out of ten or an analgesic dose. We see its impact in so many immeasurable ways. It is the pause of apprehension before standing, the protective hand hovering over a wound in trepidation when needing to cough and the look of cautious hope in the eyes of families searching for reassurance that today will be a better day. As clinicians in Pain Medicine, we sit at the point where policy meets lived experience. Therefore, the conversation about pain pathways in Ireland is a conversation about how we can protect dignity, restore function and make recovery feel possible.
Chronic pain affects roughly 13–36% of the Irish population. The consequences are evident in hospitals daily with patients experiencing deconditioning, delayed discharge, polypharmacy and anxiety that persists long after injuries have healed. In 2021, a national survey of Irelands publicly funded pain services painted quite a stark picture of long waiting lists, staffing gaps and disparities in access to specialist multidisciplinary care. Shortages in nursing, physiotherapy and psychology were especially concerning with a quarter of outpatients waiting over 18 months at that time. Pain also features much earlier in the patient journey with the National Ambulance Service having now made pain one of its clinical KPIs and emphasises how basic
Written by Anna Marie Kiernan, RANP
in Pain Medicine and a National Nursing & Midwifery Innovation Fellow with the HSE Spark Innovation Programme. Based at Croom Orthopaedic Hospital Limerick
assessment, documentation and access to appropriate analgesia contributes to better care.
Sláintecare aims to make sure people get the right care, in the right place, when they need it and pain care now sits squarely inside that promise. The national Model of Care for Acute and Chronic Pain is currently being drafted with the aim of setting out clear integrated, multidisciplinary pathways across hospital and community. However, in the interim, we already have strong, actionable guidance to base care upon. The National Clinical Programme for Anaesthesia (NCPA) advises on the safe prescribing of opioid therapy in the acute and post operative settings. Also, the HSE Medicines Management Programme (MMP) explains how medicines should be managed safely for people living with long term, non cancer pain. In combination, they make quite clear that multimodal analgesic treatment should only be part of the foundation and that opioids must be used with caution in the short term with clear stop dates. Why pathways matter and how we feel it when they fail
Identifying how robust a pain pathway is becomes evident in quicker recovery times, better levels of mobility on the ward and clear instructions at discharge. This becomes particularly visible during inpatient episodes where variations in analgesic assessment or delayed escalation can significantly alter recovery trajectories. Where pathways are fragmented, individualised pain care plans becomes inconsistent which makes managing a complex symptom more complicated. With assessment style varying by person measuring and prescribing decisions at times ad hoc, GPs receive discharge letters that can raise more questions than they answer. Irish audits and quality improvement projects have repeatedly highlighted this concern. A one day point prevalence survey in a tertiary hospital found that 27% of surgical opioid prescriptions were in the slow release form
and 30% of prescriptions continued for more than a week. Both findings misaligned with national guidance. In contrast, implementation work in Tallaght University Hospital demonstrated through a service based QI project how implementation of a set of brief postoperative guidelines could improve standards of pain management. The suggested prioritising of immediate release opioids for short durations, mandatory stop dates and supportive patient education changed practice quickly across surgical wards. This demonstrated that good pathways do not demand perfection but they do need a human centred design focus. This ensures that services are designed with safety integral in routine care and makes the safest analgesia choice the easiest one. From policy to practice: what actually makes pathways work Effective pain pathways start with people. Those who implement it and also those impacted by it. However, pathways will live or die
based on communication. Lack of engagement with key stakeholders within the process impacts on the delivery of best care. Failure of pathways are often as a result of lack of engagement, lack of education and unaddressed lack of confidence. The development of relevant ward friendly algorithms, clear patient leaflets and prompts at the point of prescribing do more to change practice than lengthy policies. Embedding these tools directly into hospital prescribing workflows, such as during consultant rounds or pharmacist led medication reviews, helps ensure consistent escalation or deprescribing across multidisciplinary teams. For hospitals looking to strengthen pain pathways now, the core components are well established: (See table 1)
This list looks deceptively simple but that is the intention. Introducing complexity into the
Table 1
care pathway will overwhelm both service provider and user when under pressure so maintaining clarity on the proposed plan ensures safest care.
Perioperative planning: small decisions, large effects
Pre assessment care plans offer an impactful opportunity to set clear and attainable expectations. Within peri operative surgical pathways, these plans allow anaesthesiology and surgical teams to clearly communicate expected analgesic strategies and postoperative functional goals to inpatient ward staff. Identifying that pain postoperatively is normal but how individualised analgesic plans will be implemented to best manage the symptom. Clarifying the collaborative role of the patient and how opioids may be used and stopped. This supports the development of trust as patients’ value honesty over reassurance. Feeling prepared reduces anxiety and improves engagement with clinicians.
Maintaining consistency in the approach to care matters more than novelty of treatments available. There are procedure specific multimodal plans which can be reliable in treatment and are strongly associated with early mobilisation and lower opioid use when implemented appropriately. However, flexibility to pivot is essential, especially with vulnerable cohorts such as the elderly. Frailty, impaired renal function and delirium risk complicating prescribing at both ends of the spectrum.
Under treatment of pain will impair recovery while sedating analgesic regimes can increase the rate of falls and incidence of confusion. Careful and monitored dosing allows for early escalation rather than adjustments being made at the point of negative impact. Utilising multimodal algorithms such as the WHO analgesic ladder outperform procedure specific
Opioid stewardship means:
• No slow release opioids for acute or postoperative pain
• No “just in case” discharge prescriptions
• Explicit stop dates and tapering plans when integrated into care plans
• Patient education that respects autonomy and understanding of treatments
protocols as they respond to the individual patients need rather than the planned procedure.
Chronic pain: committing fully to a biopsychosocial model
Chronic pain never fits neatly into a diagnostic or treatment plan. Despite similar diagnosis and imaging, patients can have profoundly different experiences and outcomes. This variability as a result of personal circumstances is precisely why the biopsychosocial model of care must always be implemented. Holistic assessment should habitually consider neuropathic pain features, fear avoidance, mood disturbance, sleep dysfunction and current social context. For patients repeatedly admitted with pain crises, applying this biopsychosocial lens within the acute hospital setting helps reduce unnecessary investigations, refine prescribing decisions, and support safer discharge planning. EFIC’s recent definition of multimodal pain care reinforced the ideal that appropriate and effective treatment must integrate physical, psychological and social interventions and supports in addition to pharmacological management. Non pharmacological strategies are as impactful as pharmacological treatment and should be foundational in care. Incorporating specialist physiotherapy, pacing, psychologically informed supports and an expanding range of digital and immersive tools which support relaxation and self-management. Pharmacology should only have a supporting role in a complex plan which works symbiotically to increase independence and coping skills. Simple analgesics may be appropriate when clearly indicated yet opioids should only be considered in exceptional circumstances.
The HSE Medication Management
Policy guidance on chronic non cancer pain clearly outlines the risks of long term opioid therapy and clarifies the importance of deprescribing when benefits do not outweigh harms. The inclusion of Interventional procedures does hold benefit but only when used in conjunction with a comprehensive multidisciplinary team plan. Without this contextual based approach, the benefit is often temporary.
Opioid stewardship: kindness through design
Opioid stewardship is sometimes presented as restrictive but in truth it is a gentler, more compassionate approach to better care. It asks us to start with multimodal strategies
and to weigh the benefits of use against the true risks. The use of opioids should be done transparently, briefly and safely. Clear escalation and deprescribing thresholds which are visible within ward based drug charts or electronic prescribing systems, support safer, real time decision making for rotating clinical teams. System design matters. Setting organisational standards supports changes in clinician prescribing behaviour. This is particularly relevant in acute hospital workflows where clear escalation or deprescribing instructions must be available to ward teams during inpatient episodes. E discharge templates which require opioid duration to be documented and patient leaflets written in conversational language help to passively reshape and ground best behaviour for best outcome even on the busiest days.
The value and importance of opioid stewardship is further reinforced by regulatory partners. Health Products Regulatory Authority reporting supports vigilance with pharmacological prescribing. The Pharmaceutical Society of Ireland provides guidance which informs the safe supply of methadone and buprenorphine nationally. For patients on opioid substitution treatment, perioperative planning is integral to protecting patients from destabilisation while maintaining compassionate holistic care.
Communication: the quiet infrastructure of safety
Robust pain pathways are built on communication. The ideal Hospital pathway supports multidisciplinary alignment preoperatively to develop cohesive analgesic plans with ward based teams reviewing pain control daily to support escalation or deprescribing when clinically indicated and strong discharge communication which holds function as a potential future manual of care rather than a record of events. This is especially critical when transitioning patients from inpatient care to community based follow up, ensuring GPs receive guidance on analgesic duration, tapering steps, and red flags for re escalation.
Patient communication is equally as important. Clearly written informative leaflets explain not only side effects but explain why opioids must be limited. They outline how multimodal approaches to care works and what patients can do to support their recovery. Many clinicians recognise the quiet success of a patient acknowledging and understanding their proposed treatments as the instructions are clear and explanatory. That
reassurance is not coincidental but it is designed to support compliance with best care.
Looking ahead as the Model of Care takes shape
The emerging Model of Care for Acute and Chronic Pain represents a critical opportunity to reduce variation in approaches to impactful care while supporting local innovation. Key priorities may include:
• MDT led pathways spanning hospital and community with workforce planning that addresses clear gaps to multidisciplinary and multidimensional care.
• Embedding the principles of the Health Products Regulatory Authority and the Pharmaceutical Society of Ireland to support best pharmacological management
• Additional supports in the form of transitional pain services for high risk cohorts to prevent persistent postsurgical pain and analgesic dependency
• Strengthened and streamlined access to specialist pain psychology and physiotherapy services to support a true biopsychosocial approach to care
• Scaling non pharmacological and digital tools alongside traditional services to incorporate supportive selfmanagement by patients
• Routine opioid stewardship audit within acute care with visible feedback and co leadership by pharmacy and clinicians to reduce unnecessary risk to vulnerable patients
For organisations starting this journey, a pragmatic approach is crucial for consistency. A multidisciplinary approach remains the strongest foundation for high-quality multidimensional pain care. It is the bringing together of the expertise of medical, nursing, psychological, and rehabilitative teams to deliver truly integrated treatment. Prioritisation of the needs of vulnerable cohorts ensures that pain management is both safe and inclusive. Embedding opioid stewardship practices further strengthens clinical practice and balances effective analgesia with responsible prescribing techniques. Together, these principles create a resilient framework which supports consistent, compassionate, and evidence-based pain management across acute hospital settings, including peri operative care, inpatient pain management, and safe communication of analgesic plans at discharge while maintain the patient at the heart of approach.
Medicines for Ireland new Leadership Team
Medicines for Ireland (MFI), the representative body for the suppliers of the majority of medicines in Ireland, has announced its new senior leadership team, with Mr Donagh O’Leary appointed as Chairperson and Mr Joe Keane as Vice-Chairperson.
Joe Keane, Vice-Chaiperson, MFI
Since its foundation in 2016, Medicines for Ireland has been promoting the benefits of the increased use of generic, biosimilar, and value-added medicines in Ireland. The organisation’s core objective is to improve the way Ireland procures and supplies medicines, in order to expand patient access to affordable treatment.
As Managing Director of Clonmel Healthcare Ltd, Mr Donagh O’Leary has been elected Chairperson of the trade association, having previously served in the role of ViceChairperson. He brings over 25 years of experience in the pharmaceutical sector across Ireland and the UK. During his tenure at Clonmel Healthcare Ltd, Mr O’Leary has expanded the business to become Ireland’s largest supplier of consumer healthcare products and generic medicines.
New Pharmacy Toolkit
Mr O’Leary and Mr Keane’s appointments follow the conclusion of the new Framework Agreement on the Pricing and Supply of Medicines, a landmark agreement that marks a significant step forward in strengthening Ireland’s pharmaceutical sector. Developed in partnership with the Department of Health, the Department of Public Expenditure and the HSE, the Agreement sets out a comprehensive package of measures to improve security of supply, enhance affordability, and support a more predictable and competitive market environment through to 31 December 2029.
Taken together, the measures have the potential to generate up to ¤1.4 billion in value, which can be reinvested to support innovation and frontline patient services.
Mr O’Leary comments, “With the new framework agreement now in place, we are entering a fresh phase of growth that will strengthen our impact and sharpen our strategic direction.
I look forward to harnessing this opportunity to build momentum, deepen collaboration across the sector, and deliver meaningful progress for our members.”
Joe Keane, who has been elected Vice-Chairperson, is Head of Ireland Operations at Sandoz, trading as Rowex in Ireland.
Mr Keane has led the Bantry operation for almost two decades and brings extensive experience in the pharmaceutical industry.
Also speaking at the recent MFI EGM, Mr Keane expressed his gratitude to members for their support, adding that he “looked forward to working closely with members to address both the opportunities and challenges facing the sector.” He highlighted the importance of tackling emerging issues, including the EU’s Urban Wastewater Treatment Directive, noting that a proportionate transposition is imperative to protecting the sustainability of medicine supply in Ireland.
Vaccination remains one of the most effective public health interventions for preventing infectious diseases and reducing morbidity and mortality. Yet vaccination coverage, particularly among adults, remains below recommended targets in many countries.
Existing literature shows that recommendations from healthcare providers are one of the strongest drivers of vaccine acceptance and uptake. To support pharmacists in this role, FIP has launched a new toolkit and accompanying infographic on vaccination communication today. The toolkit focuses on three key areas of communication: pharmacist–patient, pharmacist–public, and pharmacists–other healthcare professionals communication.
“Pharmacists are among the most accessible healthcare professionals and are one of the first points of contact for people seeking advice about vaccines,” said Ms Nisa Masyitah, FIP Data and Intelligence Manager. “Effective communication skills are therefore essential for improving vaccine uptake, and this toolkit provides practical guidance to support pharmacists in having those conversations with confidence.”
Effective communication is therefore central to pharmacists’ capacity to support vaccination uptake. Conversations about vaccines may involve addressing concerns, correcting misinformation, providing clear and evidence-based recommendations, and collaborating with other healthcare professionals.
This toolkit has been developed to support pharmacists in their communication role within vaccination programmes. Building on evidence that healthcare provider recommendation is a key driver of vaccination uptake, it focuses on strengthening pharmacists’ capacity to communicate effectively about vaccines with different audiences, including patients, the public, and other healthcare professionals with whom they collaborate.
The toolkit also aligns with FIP Development Goal 16 on Communicable Diseases, which emphasises expanding the role of the pharmacy workforce in the prevention, surveillance, and management of communicable diseases.
Medical Affairs Masterclass
The Pharmaceutical Managers’ Institute is holding a Medical Affairs Masterclass April 29th, 2026 from 9.30-4.30pm at the Irish Management Institute, Sandyford Dublin.
Key topics will include Metrics and data management in Medical Affairs; Balancing field and office responsibilities; Medical Affairs & Market Access partnerships; Career progression in Medical Affairs and, Making an impact as an affiliate.
While this masterclass is open to all PMI members, it will be particularly relevant for Medical Science Liaisons, Medical Advisers and Medical Managers. Visit www.thepmi.com for further information.
Paul Reid Appointed Independent Chair of IMVO Board
The Irish Medicines Verification Organisation (IMVO) has announced the appointment of Paul Reid as Independent Chair of its Board.
Paul brings extensive leadership experience across the public, private and not-for-profit sectors. Paul previously served as CEO of the Health Service Executive (HSE) from May 2019 to December 2022, where he led Ireland’s health service through the Covid-19 global pandemic and a significant criminal
Paul Reid
cyber-attack, while acting as a key advisor to Government and a key communicator to the public.
With deep expertise as a board chairperson, non-executive director and CEO, he is currently Chair of An Coimisiún Pleanála, Ireland’s national and independent planning authority, and Chair of Ashdale Care, a sector leader in the provision of specialist residential care services for children and young people.
Commenting on his appointment, Paul Reid said: "I'm delighted to be joining the board of IMVO as Chair. The organisation plays a key role in protecting the public and patients, which is something that I'm highly committed to".
Leonie Clarke, Chief Executive of IMVO, welcomed the appointment saying: "We are
delighted to welcome Paul as Independent Chair of IMVO. His depth of experience, knowledge of healthcare in Ireland and unwavering commitment to public service will be invaluable as we work towards our vision of a secure and sustainable medicines supply chain where patients are confident about the authenticity of prescription medicines they receive in the Irish healthcare system.”
IMVO was established in 2017 to manage the Irish Medicines Verification System (IMVS) and works to ensure a secure and effective medicines verification system that protects patients from falsified medicines entering the legitimate supply chain in Ireland.
Paul succeeds Professor Pat O’Mahony, who served as Independent Chair from June 2017 until his unexpected passing in August 2025.
New Medical Council Training Survey now open
The Medical Council is inviting interns and trainees to complete the Medical Council Training Survey, which officially opened this month.
The survey is open to all interns and Non-Consultant Hospital Doctors (NCHDs) on a formal, Medical Council approved training scheme – that is, doctors who are on the internship and trainee specialist divisions of the register.
The survey covers key aspects of intern and postgraduate medical education, including how clinical
training sites support education and training, professional development, and wellbeing. The initiative is led by members of the Medical Council’s Education & Training team and supported by colleagues across Council, who have been redeveloping the survey over the past couple of years. It will be open for a period of four weeks, until Wednesday 6 May.
All responses are anonymous. No personal data is requested and reports produced by the Medical Council will present findings
Rare Disease Day
at group level only and will not identify individual respondents.
Dr Maria O’Kane, CEO, Medical Council addressed interns and trainees, “The survey tagline is ‘Your Training, Your Voice’ because we want to hear directly from interns and trainees about their experiences on the ground.
“This survey is your opportunity to shape how clinical training in Ireland develops, and strong participation makes that possible. I’d strongly encourage you all to complete it. In doing so, you will
be contributing directly to future improvements in safer clinical environments for yourselves and for patients.
“Hearing from interns and trainees will also help the Medical Council to highlight areas of good practice in medical education and training; and share learnings among key stakeholders such as sites, intern training networks and postgraduate training bodies”, Dr O’Kane concluded.
The survey can be accessed at: www.medicalcouncil.qualtrics.com
The Minister for Health Jennifer Carroll MacNeill TD has highlighted the areas of progress made since the publication of the National Rare Disease Strategy 2025-2030 and re-affirmed her commitment to improving services for the estimated 300,000 people in Ireland living with a rare disease.
Minister Carroll MacNeill said, “I have met with and listened to many people across Ireland living with rare disease s and their families. I am very aware of the challenges they face in accessing quality treatment and care as has been highlighted in Rare Disease Ireland’s recent survey.
“We have a long way to go to turn the vision of our strategy into reality. Rare disease services must be embedded into our healthcare service right across a patient’s life, starting with newborn bloodspot screening. The earlier we can detect, diagnose and treat rare diseases, the better the outcomes for patients. That is why I am pleased that the expansion of screening for both Severe Combined Immunodeficiency (SCID) and Spinal Muscular Atrophy (SMA) is expected to commence in April this year. But we must do more.
“As well as increasing education among our healthcare professionals and investing in research, we are also collaborating with international partners to enable patients in Ireland to benefit from clinical trials, and the development of innovative treatments.
“I want to assure the one in 17 people in Ireland living with a rare disease that progression of this work is a priority for me, not just today on Rare Disease Day, but every day.”
The Department of Health building in Dublin is lit up in blue today as part of the “Light Up for Rare” campaign, acknowledging the estimated 300 million people globally living with a rare disease.
Chief Medical Officer Professor Mary Horgan said, “Building greater awareness and knowledge across the public and healthcare professionals will be a core component of the implementation of the National Rare Disease Strategy.”
Training and Retaining our Future Medical Workforce
The key issue in Healthcare is access to skilled clinicians working in a well-equipped and supported health service. It is recognised that healthcare demands continue to exceed supply globally. In Ireland, there is a significant reliance on non-permanent internationalgraduate clinical staff to deliver healthcare, and there are major infrastructural deficits in many areas. A key element of health policy is that more care should be delivered outside of acute settings.
National Doctors Training and Planning (NDTP), a unit of the HSE, is tasked with considering future medical workforce demand, and supporting the training pipeline of doctors equipped with the skills and abilities to meeting this demand. Key elements of the NDTP strategic plan 2022-27 include: collecting high quality data on the medical workforce, supporting training, and planning for the future medical workforce.
Healthcare requires long-term planning; buildings take a long time to develop and doctors take a long time to train. The average age of new permanent consultants in Ireland is 39. Projecting and planning for the future medical workforce is a core function of NDTP. NDTP have collaborated with the Clinical Programmes for each of the 50 specialties to produce a set of workforce plans that outline the projected demand for consultants over the next 15 years. These projections examine the drivers of demand for consultants for each specialty, some are generic to all specialties, and some a specific to each specialty. Population growth, demographic aging, epidemiology
and configuration of the health service are key underlying drivers of increasing workload. The expansion of the public consultant workforce over the last 5 years, increasing from 71 to 90 per 100,000, has closed the gap between consultant staffing levels in Ireland and international peers. However, significant gaps remain in many specialties and demand continues to grow.
There is a strong rationale for seeking to train this future consultant workforce in Ireland. The medical training system in Ireland produces high quality doctors that are highly regarded internationally. Given the global shortages of doctors, Ireland cannot rely on attracting doctors from abroad into the future. For many specialties there is clearly a limited supply of consultants both Irish trained and from abroad. This forms the basis of linking supply with demand, and as such aligning training with workforce projections. As doctor training takes between 10 and 15 years, the NDTP workforce projections discussed previously are vital to guide trainee intake into training programme today to build a sufficient appropriately skilled workforce into the training programmes today. While training is critical, retention of the trained workforce is equally essential. This requires systems to monitor retention rates, and an understanding of key determinants of retention. NDTP maintains the Doctors Integrated Management E-System (DIME) database of consultants and Non-Consultant Hospital Doctors (NCHDs) working in the publicly funded health services. This longitudinal
Written by Professor Anthony O’Regan, Medical Director, National Doctors Training and Planning. HSE Consultant General and Respiratory Physician, University Hospital Galway
Professor of Postgraduate Clinical Education, WNW Health Region & University of Galway.
both on training and not on training schemes, indicates that over 90% wish to remains working as a doctor in Ireland long-term.
database allows for individual doctors to be followed over time to quantify the flows of doctors out of, and back into the Irish health system. This data is now reported annually in The Medical Recruitment & Retention report.
The report shows, for example, that while 60% of doctors leave the country after internship, 80% subsequently return for further training in Ireland. There is a substantial difference between the retention rates of Irish and both UK/EU and Non-EU interns; the retention rate of Irish nationality interns is over 20% higher than the other groups.
After completion of specialist training (CSCST) most doctors leave the country; 58% of doctors who received CSCST in 2024 were not in a public post in 2025. However, over three quarters return to take up a consultant post in subsequent years.
NCHDs who are not enrolled on a training programme comprise a major component of Ireland’s medical workforce. Over the last 25 years various reports have recommended reducing or phasing out non-training scheme posts. Since 2011, the number of doctors on a training scheme has increased by 70% percent from 3,412 to 5,791. Despite this the number of doctors not on a training scheme increased by 180% percent from 1,524 to 4,018 over the same period. This diverse cohort can be categorised as two distinct groups. The first group are NCHDs between training programmes e.g. Basic Specialist Training and Higher Specialist Training. The second group typically come to Ireland from abroad, stay for a short period and then leave the country. However, after 5 years 25% of this second group remain working in the public health system. A survey of NCHDs,
With a view to developing a better understanding of the determinants of recruitment and retention, NDTP have recently carried out a qualitative study of doctors who trained in Ireland. The study highlighted the importance of personal factors, such as proximity to family in migration decisions. However, the study also showed that there is a limited time window in which doctors are likely to return to Ireland; once they get settled abroad it becomes increasingly difficult to attract them back. This underlines the importance of clarity on the delivery of consultant posts that is aligned to the training pipeline. The study also highlighted the need to make posts in Model 3 hospitals more attractive to Irish trained doctors.
Having accurate data is also vital to supporting informed decision making. The medical workforce report, published by NDTP annually, provides a national, regional and site level overview of the current medical workforce. This report demonstrates the size and growth in the consultant and NCHD workforce in recent years. Currently there are almost 5,000 consultants and almost 10,000 NCHDs employed in the publicly funded health services. Over the past 5 years the number of consultants and NCHDs have expanded at an average rate of 9 and 6% per year respectively. Within the NCHD category, this report also documents the expansion of NCHDs on a postgraduate training scheme and those not on a training scheme.
NDTP commissioned a large-scale survey of NCHDs in 2024. This survey explored, career intentions, supports for doctors not on a training programme, training and teaching, and site conditions. The Taskforce on NCHD workforce provided funding to address many of the issues highlighted in the survey, for example in sites where access to food, water, rest, showering, and changing facilities were inadequate. This survey will be carried out again in 2026.
NDTP does not have a role in consultant post creation but recognises the need by trainees for clarity on future consultant workforce plans. It is expected that the new health service regional structures will play a large role
in new consultant post creation. NDTP aims to support the regions in developing workforce planning functions. The development of regional workforce plans will inform national training plans. The linking of the training pipeline with future consultant post
creation plans is key to retaining our trainees; in the short term we need to ensure that regional workforce plans when aggregated are consistent with the number of recently qualified specialist trainees (CSCST); in the longer term we need to train enough
doctors within each specialty to meet future service needs.
From national policy to regions and sites, the health service needs reliable data to make good decisions. We also need to recognise that the problems in
NEWS - Monthly Waiting list Figures
the health service cannot be fixed quickly. A long-term strategic approach focused on the future medical workforce, its composition and distribution across regions is essential and NDTP seeks to support stakeholders across the health system in these aims.
The latest hospital waiting list figures for February 2026 were published recently by the National Treatment Purchase Fund (NTPF).
The multi-annual Action Plan approach initiated in September 2021 is focussed on improving waiting times for patients, and the Waiting Time Action Plan (WTAP) 2026, published by Minister Carroll MacNeill on 30 January 2026 embodies the Government’s commitment to reducing waiting times for patients, thereby improving access to hospital care.
The 2026 Plan acts as a key enabler for each of the Health Service Executive (HSE) Regions to improve planned care delivery.
Under the reformed health service structures, HSE Regional Executive Officers have a key leadership role to drive and oversee the necessary productivity and performance improvements across each Region, including through increasing efficiencies and reducing regional variation (e.g. via shared learning) and ultimately increasing access to scheduled care across the health service.
The health service has seen significant progress in reducing the length of time patients are waiting under the multi-annual Action Plan approach, including a reduction of circa 55% or circa155,000 less patients waiting over 12 months since September 2021. In the same period there was an improvement of circa 43% or 5.3 months in the Weighted Average Wait Time (WAWT) that patients across lists have been waiting.
Notwithstanding these longer-term improvements, waiting lists more recently have been impacted by the ongoing trend of higher demand and increased referrals, which has offset the significantly increased levels of activity that are being delivered in acute hospitals.
Signs of progress in waiting list performance seen towards the end of last year, have not continued into 2026, having been impacted by the anticipated multi-annual trend arising from the winter surge in demand for unscheduled and emergency care.
The Department will continue to work to improve waiting list performance through ongoing engagement with the HSE and the NTPF. This will include engagement through the Waiting List Task Force, which is responsible for the governance and implementation of WTAP 2026.
World’s largest lung cancer clinical trial opens in the Republic of Ireland
A major research study using radiotherapy in the treatment of metastatic lung cancer is being offered to patients outside of the UK for the first time.
The TOURIST platform trial is the world’s largest lung cancer clinical trial, funded by a £3.4m grant from the National Institute for Health and Care Research (NIHR), and is now open to recruitment in the Republic of Ireland, the first international location, meaning more people with the disease will have the chance to take part in this world-leading research.
The trial, which is sponsored by The Christie NHS Foundation Trust in Manchester and managed by Southampton Clinical Trials Unit, is looking at whether modern radiotherapy treatments can improve outcomes for patients with advanced disease, who often have a poor prognosis and typically have about a year to live.
The TOURIST platform has recently opened to recruitment at the St Luke’s Radiation Oncology Network (SLRON) in Dublin, where it is being led by Principal Investigator Gerry Hanna, Consultant in Radiation Oncology at SLRON, Marie Curie Professor of Clinical Oncology at Trinity College Dublin, and Vice-Clinical Lead of Cancer Trials Ireland.
“Thanks to the Irish Research Radiation Oncology Group
(IRROG), we are really excited to be opening the TOURIST study at St. Luke’s Radiation Oncology Network, in collaboration with Cancer Trials Ireland and the Southampton Clinical Trials Unit,” says Professor Hanna.
“TOURIST is an important study evaluating the role of modern lung radiotherapy for people with advanced non-small cell lung cancer. We hope by using modern radiotherapy routinely we can improve outcomes and quality of life for such patients and we are delighted to be able to offer this opportunity to patients in Ireland.”
Lung cancer is the 4th most common cancer in Ireland with around 2,600 people diagnosed each year*. However, it is the leading cause of cancer deaths in the country in both men and women**.
Between 85 and 90 per cent of lung cancer cases diagnosed are non-small cell lung cancer (NSCLC) and nearly half of these cancers are diagnosed at a late stage when the disease has spread and is incurable, meaning treatment focuses on controlling symptoms and extending life, rather than curing patients.
Prof. Gerry Hanna, Principal Investigator and Consultant in Radiation Oncology at St Luke’s Radiation Oncology Network, Marie Curie Professor of Clinical Oncology at Trinity College Dublin, and ViceClinical Lead of Cancer Trials Ireland
TOURIST is the first trial in 20 years to look at how radiotherapy could benefit late-stage metastatic lung cancer patients.
It uses a technique called ‘VMAT’ (volumetric modulated arc therapy) which is a form of radiotherapy that uses multiple beams of varying strengths to treat cancer. A device called a linear accelerator (LINAC) delivers high-energy beams while rotating around the patient to treat the tumours.
Professor Sinead Brennan, Clinical Lead for the Irish Research Radiation Oncology Group (IRROG) and Director of Research at SLRON, commented, “IRROG is delighted to announce the opening
Professor Sinead Brennan, Clinical Lead for the Irish Research Radiation Oncology Group and Director of Research at St Luke’s Radiation Oncology Network
of the TOURIST study at St. Luke’s Radiation Oncology Network and looks forward to its activation at University Hospital Galway. Expanding this important trial to the West of Ireland is a major step towards ensuring equitable access to clinical research for patients with advanced lung cancer. By supporting the national rollout of TOURIST, IRROG is helping patients access innovative radiotherapy closer to home, reducing travel while maintaining the highest standards of researchled care.”
Angela Clayton-Lea, CEO at Cancer Trials Ireland, said:
“Cancer Trials Ireland is proud to act as the local Sponsor for the TOURIST study and delighted to open this important international trial across our national network. As sponsor in Ireland, we led contract and budget negotiations and completed the regulatory submissions required to enable site activation. We look forward to providing ongoing national governance and coordination for TOURIST, working closely with IRROG to ensure patients in Ireland can access innovative radiotherapy treatment.”
The TOURIST platform*** has been set up to see if radiotherapy, alongside other treatments, improves outcomes and quality of life for lung cancer patients. It currently has two trials recruiting patients through the platform: PRINCE and QUARTZ LUNG.
Angela Clayton-Lea, CEO, Cancer Trials Ireland
Eating Disorders
Compassion, Consistency and Collaboration: The Role of Bodywhys in Partnership with the HSE National Clinical Programme for Eating Disorders
Harriet Parsons – Chief Executive Officer at Bodywhys – Harriet is an accredited psychotherapist and CEO of Bodywhys. She joined the organisation in 2005 and has been with the organisation ever since, accumulating over 21 years of service. Previously, she served as Training and Development Manager, where her responsibilities included providing the support component for the HSE National Clinical Programme. As CEO, Harriet remains dedicated to the organisation’s support services and continues to deliver professional training for clinicians across various roles within the healthcare sector.
Ellen Jennings – Communications, Research and Policy Manager at Bodywhys - Ellen joined the organisation in 2020, initially volunteering with the email support service. In 2021, she was appointed Communications Officer and has since progressed to a managerial role overseeing communications, research and policy. Ellen holds an MSc in Human Nutrition and a BSc in Health Science, alongside a professional background in communications. She supports the development and dissemination of evidence-based communications and policy engagement, integrating research evidence and lived experience perspectives to strengthen awareness and understanding of eating disorders and inform public and policy discourse.
This established a national strategy for the provision of treatment for people with an eating disorder in Ireland. The programme aims to ensure timely access to highquality, evidence-based treatment services nationally, across all stages of illness, delivered through a four-tier stepped-care model.
A defining feature of the model is its formal partnership with Bodywhys – The Eating Disorders Association of Ireland, the national voluntary organisation supporting individuals affected by eating disorders and their families. Founded in 1995, Bodywhys has long advocated for the rights and healthcare needs of people affected by eating disorders. Today, its collaboration with the HSE NCP-ED embeds lived experience and community support directly into the clinical pathway.
Embedding Lived Experience in Service Development
Christopher Cash – Training and Development ConsultantChristopher is a PhD candidate in Clinical Psychology at the Université Libre de Bruxelles, under the supervision of Professor Alan Carr (University College Dublin) & Prof. Salvatore D’Amore (Université Libre de Bruxelles), and a graduate member of the Psychological Society of Ireland (PSI). Christopher has been working with Bodywhys since 2021 and currently supports the provision of the Family Support Package.
Eating disorders are serious and complex mental illnesses that carry significant risks to a person’s physical, psychological and emotional health. They are associated with increased risk of suicide and mortality (Academy for Eating Disorders, 2021). Early assessment, timely access to evidence-based treatment and support significantly improve recovery outcomes. Specialist outpatient treatment is recognised as the most effective and efficient pathway to recovery for the
majority of individuals (National Institute for Health and Care Excellence (NICE), 2017). Within this context, integrated, specialist and person-centred care and support is essential.
The HSE National Clinical Programme for Eating Disorders
In 2016 the Health Service Executive (HSE) launched a National Clinical Programme for Eating Disorders (NCP-ED), and in January 2018, the Model of Care for the programme was published.
Bodywhys contributes to the NCP-ED at both strategic and operational levels. The organisation contributed a chapter on ‘The Patient Journey’ in the Model of Care, and staff members participate in the National Oversight and Implementation Group, supporting national service development, evaluation and quality improvement. The organisation also facilitates an “expert by experience” (eBe) group, ensuring that patient and carer perspectives inform policy, service design and implementation.
In addition, Bodywhys provides real-time service user feedback to the HSE NCP-ED, highlighting service gaps and emerging concerns. This feedback loop supports continuous quality enhancement and strengthens accountability within the system. Supporting Clinical Services Through Education and Support Partnership
Bodywhys serves as a national support partner to the NCP-ED, offering free therapeutic support, psychoeducation programmes, and caring skills training. Through non-judgemental listening and information services, it supports individuals and their families from pre-diagnosis through to recovery and beyond. This ongoing presence ensures that support is tailored to where individuals are on their journey, complementing clinical care through consistent engagement, communication, and support.
Bodywhys also serves as an educational liaison to healthcare professionals, providing training, webinars, literature, and podcasts to clinicians and allied health professionals. These activities support multidisciplinary teams operating within the NCP-ED programme as well as across the wider public health system nationwide. By providing consistent, evidence-informed resources, and building upon the working relationship with the NCPAUTHORS
ED, Bodywhys support services align with treatment approaches and help reduce variability in care delivery — an issue frequently identified by service users as a barrier to recovery. In short, this working partnership ensures that Bodywhys services support the work of the NCP-ED. Ultimately benefitting those using the services.
Listening to people with lived experience, Bodywhys promotes three essential components necessary for a successful national treatment programme for eating disorders:
• Clinical expertise and consistency
• Individualised and appropriate treatment
• Sufficient time to recover
Inconsistency in therapeutic approaches can disrupt recovery momentum. By promoting shared principles and continuity across settings, Bodywhys helps reinforce a unified, recoveryoriented approach.
Carer Testimonial: ‘CAMHS told us what to do and Bodywhys showed us how to do it.’
Bodywhys Family Support Package
Individuals supporting someone with an eating disorder play a vital role in the recovery process. It is equally important that they receive appropriate support to enable them to care effectively for the individual as well as to maintain their own well-being. Those caring for a person with an eating disorder have a very high ‘Burden of Care’, meaning they experience high levels of anxiety, and depression and can become isolated. Connecting with others experiencing similar situations can be beneficial for carers, helping them to feel less isolated and more supported in their role. With this in mind, Bodywhys developed a comprehensive Family Support Package (FSP), which provides psychoeducation, therapeutic support and skills-based training for parents, family members and
friends. The Bodywhys FSP is not only a vital service for carers, it also fills potential support gaps within treatment provision by NCPED and general C/AMHS teams.
The FSP comprises five integrated elements:
1. The PiLaR Programme – A structured four-week psychoeducational programme delivered over four evenings. It provides practical guidance and emotional support to carers navigating the challenges of supporting a loved one with an eating disorder. The programme was evaluated by the HSE National Clinical Programme for Eating Disorders in collaboration with University College Dublin in 2019 and was found to improve carers confidence, understanding and ability to cope.
2. Post-PiLaR Support Group – A weekly support space for carers who have completed the PiLaR programme, facilitating mutual learning, shared problem-solving, getting and giving support to one another, facilitated by Bodywhys staff.
3. New Maudsley Carer Skills Workshop Series – An eightworkshop series delivered over four months, based on skills originally developed at the Maudsley Hospital in London. The programme focuses on collaborative, skills-based approaches to supporting recovery. Delivery is supported by a dedicated workbook developed by Bodywhys to enhance engagement and practical application.
4. Regular New Maudsley Support Group – A monthly group for carers who have completed the workshop series, providing continued practice and consolidation of skills.
5. Conversations with Carers – A monthly themed group enabling carers to reflect on common challenges and share learning.
In 2026, Bodywhys will undertake a mixed-methods research evaluation
of the PiLaR Family Support Programme and New Maudsley Skills-Based Caring Workshop Series in collaboration with Professor Alan Carr at University College Dublin. This evaluation aims to ensure that programmes remain evidence-based, inclusive of diverse service users, and responsive to evolving need. In response to growing demand, Bodywhys is expanding FSP provision through additional monthly sessions and developing new services, including individualised carer support. These initiatives aim to strengthen early intervention, support individuals during active waiting periods, and reduce deterioration while awaiting specialist treatment.
Continuity Across the Four-Tier Model
A core strength of the partnership between Bodywhys and the NCP-ED lies in continuity of care. Bodywhys services both for carers and for people with an eating disorder, complement each tier of the HSE stepped-care model:
Transition into services: Confidential listening and information support individuals in taking initial steps toward professional help.
Between appointments (outpatient/inpatient): Ongoing support maintains engagement and mitigates risk of disengagement, particularly in early treatment phases.
Step-down and transitions: Regular support during movement between service intensities helps sustain recovery momentum.
Crisis support: Assistance is available to individuals and families during periods of acute distress.
This shared responsibility between statutory and community services reflects the understanding that no single service can meet the complex psychological and medical needs associated with eating disorders. Effective treatment and support require coordinated, multidisciplinary and community-linked responses.
Stakeholder Briefing – Common Conditions Services
A Collaborative Model for Complex Illness
Collaboration between statutory services and the voluntary sector can enhance clinical pathways. By integrating lived experience, providing carer training, strengthening continuity and supporting professional development, Bodywhys plays a pivotal role in the journey towards recovery.
For health professionals, this partnership offers a reminder that recovery from an eating disorder rarely occurs in isolation. It depends not only on specialist clinical expertise but also on informed carers, consistent messaging, accessible support and a system designed to protect individuals during vulnerable transitions.
As eating disorder services continue to evolve nationally, sustained collaboration between the HSE and Bodywhys will remain central to ensuring that individuals and families receive timely, evidence-based and compassionate care — and the best possible opportunity to move towards recovery.
So far, the feedback is positive. In 2024, Bodywhys surveyed the NCP-ED clinical teams to gather feedback on the working partnership. Feedback highlighted that when families access Bodywhys support services it improves understanding of the illness, treatment duration, ‘buy in’ or readiness to engage in treatment, understanding of treatment goals and importantly confidence in C/AMHS.
This positive feedback underscores the significant impact of integrated family support and emphasises the importance of this partnership as a key component of Ireland’s evolving eating disorder care pathway.
Bodywhys free, confidential support services are available to all, no diagnosis neccessary.
The Pharmaceutical Managers’ Institute is hosting a Stakeholder Briefing on April 23rd, 2026 at The Address Citywest in Dublin.
Community pharmacy is undergoing significant transformation, with the pharmacist’s role expanding across several key areas. The recently launched Common Conditions Service marks a policy shift towards an enhanced role for community pharmacy in supporting improved access to care.
This Stakeholder Briefing will explore developments across community pharmacy including: Vaccination rollout in pharmacy Shared care records ePrescriptions CPA 25 developments Introduction of Common Conditions services
There will also be an opportunity for questions from the floor. Speaking at the event will be Susan O’Dwyer, Head of Professional Services – Irish Pharmacy Union. Visit www.thepmi.com for further information.
Ophthalmology Advances Take Focus at RCSI Charter Meeting 2026
The RCSI Charter Meeting 2026 brought together Fellows, Members, trainees and healthcare professionals from across Ireland and internationally for a week of learning, collaboration and forward-thinking discussion. Held from 10–14 February at the Royal College of Surgeons in Ireland, this year’s meeting centred on the theme ‘Progress and Precision’, reflecting a strong focus on innovation, data-driven care and the evolving role of technology in modern surgical practice.
While the programme spanned a broad range of specialties and disciplines, ophthalmology featured as a key area of clinical advancement, with a dedicated session highlighting both the complexity and rapid progression of care within this field.
The ophthalmology session, chaired by Ms Christine Goodchild, Consultant Ophthalmic Surgeon at St Vincent’s University Hospital and Co-Programme Director for Ophthalmic Surgery, brought together leading clinicians to explore current challenges and emerging approaches across ophthalmic practice.
Opening the session, Ms Clare McCloskey, Consultant Ophthalmic Surgeon at Sligo University Hospital, presented on paediatric orbital lesions—an area requiring particular clinical
precision and multidisciplinary coordination. Her presentation underscored the importance of early diagnosis and tailored surgical intervention in paediatric populations, where both anatomical complexity and longterm outcomes must be carefully balanced. Advances in imaging and surgical planning were highlighted as critical tools in improving outcomes for these patients.
A strong emphasis on digital innovation followed, with Dr Bobby Tang, Consultant Ophthalmologist at Our Lady of Lourdes Hospital, Drogheda, and the Mater Hospital, Dublin, presenting on the development of a digital pathway for retinopathy of prematurity (ROP) in Ireland. This work represents a significant step forward in improving access to specialist care for vulnerable neonatal patients. By leveraging digital systems and structured pathways, the model aims to enhance early detection, streamline referrals and ensure timely intervention—key factors in preventing avoidable vision loss. The presentation reflected a broader trend across healthcare towards integrating digital solutions into clinical workflows to support both efficiency and patient safety.
The session concluded with a presentation from Ms Clare
Quigley, Consultant Ophthalmic Surgeon at the Royal Victoria Eye and Ear Hospital, Dublin, who addressed the investigation and management of orbital inflammation. Highlighting the diagnostic challenges associated with this condition, Ms Quigley outlined the importance of a systematic approach to investigation, incorporating imaging, laboratory testing and clinical assessment. Her discussion reinforced the need for clinical vigilance and multidisciplinary collaboration in managing complex inflammatory conditions that can have significant implications for patient outcomes.
Collectively, the ophthalmology session demonstrated the breadth of innovation currently shaping the specialty—from advances in paediatric care and complex diagnostics to the integration of digital pathways that are transforming how care is delivered. It also reflected the wider theme of precision medicine, with each presentation emphasising the importance of tailored, evidence-based approaches to patient management.
Beyond ophthalmology, Charter Meeting 2026 offered a comprehensive programme addressing key developments across surgical practice. The meeting opened with the National Office of Clinical Audit (NOCA) Annual Conference, focusing on how data and audit can drive measurable improvements in patient care. This was followed by the Health Service Quality
Improvement and Innovations Conference, which explored service redesign, digital enablement and system-wide transformation.
Innovation and technology were central themes throughout the week, particularly with the return of the Robotic and Technology Learning Village, where delegates had the opportunity to engage with next-generation surgical platforms. The launch of the RCSI Robotic Surgery Curriculum further highlighted the College’s commitment to preparing surgeons for an increasingly technologydriven future.
Speaking at the meeting, Professor Deborah McNamara, President of RCSI, emphasised the importance of equipping surgeons with the skills and knowledge required to navigate a rapidly evolving healthcare landscape. She noted that while innovation continues to accelerate, the core principles of quality, governance and patient safety remain fundamental to surgical practice.
The final days of the meeting focused on leadership, governance and clinical excellence, with keynote lectures addressing best practice in quality and safety. The Charter Meeting concluded with the Irish Surgical Training Group Meeting, which examined the full lifecycle of a surgical career, from training and development to leadership and wellbeing.
However, it was clear that ophthalmology remains a specialty at the forefront of many of these broader developments. The integration of digital care pathways, advances in diagnostic precision and continued innovation in surgical techniques all point towards a future where patient outcomes can be further improved through both technology and clinical expertise.
As Charter Meeting 2026 demonstrated, progress in ophthalmology is not occurring in isolation but as part of a wider shift across healthcare towards more precise, data-driven and patient-centred care. For clinicians working in this field, the insights shared during the meeting provide a valuable snapshot of where the specialty is heading—and the opportunities that lie ahead.
Professor Deborah McNamara
New
Ocular surface control starts with Lacrifill®
Take control of your patients’ ocular surface with Lacrifill®:
✔ Hyaluronic acid canalicular gel1
✔ Maintains natural lubricating tears on the ocular surface1
✔ Each administration provides dry eye relief for 6 months1 Safety issues should be reported to Nordic Pharma by email at lacrifill-vigilance@nordicpharma.com
For more information about Lacrifill® and the Instructions for Use, visit www.lacrifill.ie
http://www.hpra.ie
Modelling the impact of changes to prescription medicine cost-sharing schemes among middle aged and older adults
James Larkina b, Ciaran Prendergasta, Logan T. Murrya, Michelle Flooda, Barbara Clynec, Sara Burked, Conor Keegane, Fiona Bolandf, Tom Faheyb, Nav Persaudg h, Rose Anne Kennyi, Frank Moriartya i
aSchool of Pharmacy and Biomolecular Sciences, RCSI University of Medicine and Health Sciences, Dublin, Ireland
bDepartment of General Practice, RCSI University of Medicine and Health Sciences, Dublin, Ireland
cDepartment of Epidemiology and Public Health, School of Population Health, RCSI University of Medicine and Health Sciences, Dublin, Ireland
dCentre for Health Policy and Management, School of Medicine, Trinity College Dublin, Dublin, Ireland
eEconomic and Social Research Institute, Dublin, Ireland
fData Science Centre, School of Population Health, RCSI University of Medicine and Health Sciences, Dublin, Ireland
gDepartment of Family and Community Medicine, University of Toronto, Toronto, Ontario, Canada
hMAP Centre for Urban Health Solutions, St Michael's Hospital, Toronto, Ontario, Canada
iThe Irish Longitudinal Study on Ageing, Trinity College Dublin, Dublin, Ireland
Prescription medicine use has increased across countries1, 2, 3, 4, 5, 6 and concurrently, there has been increased development of expensive medicines,7 leading to increased medicine expenditure for countries and individuals. Medicines represent a significant proportion of out-of-pocket healthcare costs in Ireland and other countries,8, 9, 10 particularly for low-income groups.11 National prescription cost-sharing policies vary, reflecting differences in public financing and health insurance policies. Prescription medicines co-payment levels increased between 2009 and 2016 in Ireland following the financial crisis, due to changes to stateprovided schemes.12 Since 2016, however, co-payment levels were reduced due to further schemes changes,13,14 with more changes under consideration.15, 16, 17, 18
Increased out-of-pocket prescription medicine expenditure, linked to increased co-payment charges (even small increases), can lead to cost-related nonadherence,19 with negative impacts on health.20 Greater out-of-pocket healthcare expenditure can also force people to cut spending on essentials like food,21 further affecting wellbeing.21
Prescription cost-sharing and reform in Ireland
In Ireland, low-income individuals are eligible for the General Medical Services (GMS) scheme, which includes a reduced co-payment: ¤2.50 per prescription item in 2016, capped at ¤25 monthly per household. Income eligibility for this scheme depends on age
and household size, with higher thresholds for older adults.22 Those without GMS-scheme eligibility are eligible for the Drugs Payment Scheme (DPS), where they pay full price for medicines up to a monthly household cap (which peaked at ¤144 in 2016) with remaining costs covered by the state.23 In 2016, 36 % of the population were GMS-eligible and others were DPS-eligible.24 Additionally, those with 16 specific conditions (e.g. diabetes, Parkinson's) are eligible for the Long-Term Illness (LTI) scheme which provides for prescription medicines prescribed for that condition at no charge.25
In 2017, the Sláintecare Report from an all-parliamentary committee on Irish healthcare reform recommended large increases in public healthcare funding.18 One of its goals was to reduce outof-pocket prescription medicine costs.18 Following this report, prescription co-payment charges and monthly payment caps have been significantly reduced, but there has been limited assessment of the financial impact of these changes on individuals. Whilst Ireland's healthcare coverage system is relatively unique, this study is relevant for other countries facing challenges in providing affordable healthcare.26,27
Methods
This is a modelling study using Wave 4 data from The Irish Longitudinal Study on Ageing (TILDA), collected in 2016.28 TILDA is a nationally representative prospective cohort study charting the health, economic, and social circumstances of adults
in Ireland most of whom were aged ≥50 years when initially sampled between 2009-2011.29 A small number of participants aged <50 years were included, as the inclusion criteria were community-dwelling adults aged ≥50 years and their spouses (of any age). By wave 4 (2016), most participants were aged ≥56 years (<5 % of participants were aged <56 years). We chose TILDA data because older adults, on average, are prescribed more medicines,30 and to the authors’ knowledge, this dataset has the most comprehensive data on Irish outof-pocket prescription medicine expenditure. Wave 4 was the most recent data available where prescription medicine co-payment charges and caps were at their highest level since 2004.31 Between 2016 and 2022, changes to these charges and payment caps were implemented. Wave 4 data (2016) was used to model the financial impacts (i.e. savings) of these policy changes, by applying the post-2016 reforms to the pre-reform expenditure data.
Participants
Participants were initially recruited between October 2009–February 2011. Households were randomly selected using a national geodirectory. For this analysis, participants were those at Wave 4 free from significant cognitive impairment. Cognitive impairment was screened by trained interviewers using the Abbreviated Mental Test Score (score <7). We excluded a) those in residential care settings because their healthcare utilisation patterns likely differ from community-
dwelling adults, and b) participants who had not answered the outof-pocket prescription medicine expenditure question.
Results
There were 5,856 participants. After excluding those in residential care, and those with missing/ implausible out-of-pocket healthcare expenditure data, there were 5,668 eligible participants. Of the 5,668, 73.3% (n = 4,155) had out-of-pocket prescription medicine expenditure.
Mean annual out-of-pocket prescription medicine expenditure for those with DPS-cover, was ¤719 (SD = ¤571) when the ¤144 monthly cap was in place, which then decreased to ¤555 (SD = ¤325) when modelling the ¤80 monthly cap, i.e. mean annual savings of ¤164 (SD = ¤296).
Mean savings associated with each DPS change are in Fig. 1. The largest mean savings occur for those on ≥6 regular medicines (¤490, SD = ¤331), with 36.5% (mean = ¤179, SD = ¤102) of savings resulting from the ¤100 to ¤80 change in cap. For those aged ≥80 years, mean savings were ¤292 (SD = ¤340) with 39.9% (mean = ¤117, SD = ¤118) of savings resulting from the ¤100 to ¤80 change in cap. Details of percentage savings are in eFigure 1.
Mean savings associated with each GMS-scheme change are in Fig. 2. Mean expenditure for those with GMS-scheme cover was ¤117 (SD = ¤76) at baseline, which decreased to ¤55 (SD = ¤36) under change 3, i.e. a mean annual savings of ¤62 (SD = ¤44). The largest savings occur for those
Fig. 1. Mean savings associated with each change to Drugs Payment Scheme monthly caps
Note: Equiv. HH Inc. Quint = Equivalised Household Income Quintile. DVC=General Practitioner Visit Card. LTI = Long Term Illness. PHI=Private Health insurance.
on ≥6 regular medicines (mean = ¤122, SD = ¤32), with 36.6% (mean = ¤45, SD = ¤9) of these savings occurring due to change 3. For those aged ≥80 years, their mean savings were ¤81 (SD = ¤47) with 33.3% (mean = ¤37, SD = ¤16) of savings resulting from change 3. eFig. 2 provides further details of percentage savings.
Summary
The changes to co-payment charges and caps for prescription medicines in Ireland since 2016 likely led to large reductions in out-of-pocket prescription medicine expenditure. The effect is strong for those with DPS-cover: reducing the monthly payment cap
from ¤144 to ¤80 is estimated to have reduced average expenditure from ¤719 to ¤555, translating to mean annual savings of ¤164. Mean reductions ranged from ¤50 to ¤490 across demographic groups, with reductions necessarily concentrated amongst higher spenders.
For GMS-cover, estimated reductions were smaller in absolute terms, with mean expenditure reducing from ¤117 to ¤55, and estimated mean annual savings of ¤62. However, as this group has lower incomes, these savings may be more impactful. Estimated mean reductions
Note: GMS=General Medical Services. Equiv. HH Inc. Quint = Equivalised Household Income Quintile. DVC=General Practitioner Visit Card. LTI = Long Term Illness. PHI=Private Health insurance.
The GLM, adjusting for participant characteristics, showed that DPS-scheme eligibility was associated with 280% (exp(1.335)) higher savings when compared to GMS-eligible participants. In absolute terms, this is ¤108 more savings for DPS-eligible participants. In the sensitivity analysis the coefficients were similar to those in the primary analysis.
ranged from ¤10 to ¤123 across demographic groups. This difference persisted with ¤108 more savings for DPS-eligible participants versus GMS-eligible, after controlling for other factors.
Estimated savings across income quintiles were similar in both schemes, despite potentially greater need for reductions among lower income groups, especially those in the GMSscheme, where small co-payment changes affect cost-related non-adherence.46 It is important to note that the two approaches to co-payment reductions differ: for the GMS-scheme both the monthly payment cap and co-payment charges were reduced, while for the DPS, only
the monthly payment cap was lowered, individual co-payment charges are not capped. In both groups the estimated savings were highest among those on ≥6 regular medicines.
Implications
There is still significant potential to reduce prescription co-payments. For example, Northern Ireland, has no prescription medicine co-payments.47 Further reductions should prioritise expanding GMS eligibility by raising the income threshold for eligibility to include those DPS-eligible individuals with low incomes. Though this may lead to significantly increased healthcare utilisation.48 Reductions should also prioritise those with GMS eligibility as they have lower
capacity to pay, even for small co-payment charges.12 Additional strategies, such as deprescribing interventions to reduce the number of regular medicines safely,49 could further alleviate prescription cost burdens. Future research could model possible changes to prescription cost-sharing schemes including those proposed by political parties15, 16, 17, 18 or policies in other countries. This could also involve modelling the potential administrative savings associated with simplified universal entitlements.50 Future research could model expenditure for younger adults, who have different patterns of entitlements24 and prescription medicine use.30
Conclusion
Changes to prescription medicine co-payments and caps under various government schemes in Ireland have likely led to large savings on out-of-pocket prescription medicine expenditure. These savings were estimated to be higher in absolute terms for those with DPS-cover but were perhaps more impactful for those with GMS-scheme cover given their lower incomes. There is still a high prescription medicine cost burden for individuals in Ireland, compared to other European countries, and consideration could be given to further reductions in monthly payment caps and copayment charges, particularly for those with low incomes.
References available on request
Fig. 2. Mean savings associated with each GMS change
CPD
CPD
60 Second Summary
Lung cancer was the leading cause of cancer death in Ireland between 2020 and 2022, accounting for approximately 20% of cancer deaths.
Epidermal growth factor receptor (EGFR) mutations have been identified as a key driver oncogene in non small cell lung cancer (NSCLC). EGFR was first cloned in 1984; however, activating mutations targetable by modern cancer therapeutics were not discovered until 2004. The identification of EGFR mutations predicts biomarker guided response to EGFR targeted drugs and has transformed EGFR mutated NSCLC into a targetable disease.
In many cancers, EGFR signalling becomes constitutively activated through receptor overexpression, gene amplification or activating mutations, driving uncontrolled cell growth.
Concurrent genomic alterations within EGFR mutant lung cancers can influence mechanisms of resistance and overall outcomes. Studies have shown that EGFR mutant tumours with TP53 mutations are associated with lower response rates and shorter overall survival (OS).
As treatment options for EGFR mutant NSCLC expand across disease stages, well designed care pathways are essential to ensure timely diagnosis, appropriate treatment selection and safe delivery of therapy.
Reflex molecular testing using NGS at diagnosis is now a core component of modern lung cancer management and should be performed in all patients with non squamous NSCLC and in selected patients with squamous histology.
Authors: Dr Kate Coakley, Dr Rionagh Lynch, Oncology Registrars, Mater Misericordiae University Hospital, Dublin and Dr Jane Sui, Consultant Medical Oncologist, Mater Private Network Dublin
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may
EGFR-mutated
non-small cell lung cancers: From Molecular Testing to Optimised Targeted Therapy
Introduction and epidemiology
Lung cancer was the leading cause of cancer death in Ireland between 2020 and 2022, accounting for approximately 20% of cancer deaths. Epidermal growth factor receptor (EGFR) mutations have been identified as a key driver oncogene in non small cell lung cancer (NSCLC). EGFR was first cloned in 1984; however, activating mutations targetable by modern cancer therapeutics were not discovered until 2004. The identification of EGFR mutations predicts biomarker guided response to EGFR targeted drugs and has transformed EGFR mutated NSCLC into a targetable disease.
EGFR mutations are more commonly found in non smokers and occur more frequently in younger patients and women. Overall, these mutations are present in 10–15% of non squamous NSCLC in Caucasian populations and in up to 50% in Asian populations. In Ireland, approximately 53% of patients with advanced NSCLC have an actionable genomic alteration identified, with EGFR mutations detected in 8.8% of cases.
EGFR as an oncogenic driver in NSCLC
EGFR is a single pass transmembrane glycoprotein comprising an extracellular ligand binding domain, a transmembrane helix, an intracellular tyrosine kinase domain and a C terminal regulatory tail. In the absence of ligand, EGFR is predominantly in a basal, inactive conformation with low kinase activity. Ligand binding induces a conformational change that promotes receptor dimerisation and asymmetric activation of the intracellular kinase domains, leading to autophosphorylation of multiple
tyrosine residues in the C terminal tail and initiation of downstream signalling pathways that regulate proliferation and survival.
In many cancers, EGFR signalling becomes constitutively activated through receptor overexpression, gene amplification or activating mutations, driving uncontrolled cell growth. Small molecule EGFR tyrosine kinase inhibitors (TKIs) bind competitively within the ATP binding pocket of the kinase domain, thereby preventing receptor autophosphorylation and attenuating downstream signalling.
Oncogenic driver mutations in EGFR typically occur in exons
Dr Jane Sui
Dr Rionagh Lynch
Dr Kate Coakle
30 CPD 123: LUNG THERAPY
18–21. Mutations involving L858R or exon 19 deletions are termed “classical” or sensitising mutations. Patients with uncommon EGFR mutations such as S768I, L861Q, G719X or exon 20 insertions tend to show reduced response to EGFR TKIs compared with those harbouring classical mutations. Recent study suggests that a structure–function based classification better predicts sensitivity to targeted treatment than simple exon based categorisation. Four molecular subgroups have been proposed: classical like, T790M like, exon 20 loop insertion (near and far loop), and P loop αC helix compressing.
Concurrent genomic alterations within EGFR mutant lung cancers can influence mechanisms of resistance and overall outcomes. Studies have shown that EGFR mutant tumours with TP53 mutations are associated with lower response rates and shorter overall survival (OS). RB1 alterations in EGFR mutant lung cancers almost always occur in combination with TP53. When EGFR, TP53 and RB1 alterations co exist, the risk of small cell
transformation during the disease course is increased, occurring in approximately 5% of cases.
Importance of molecular testing
According to the 2025 ESMO guidelines, EGFR mutation testing is recommended for patients with stage IB–IV NSCLC. EGFR testing is also advised for patients being considered for neoadjuvant chemo immunotherapy, since patients with classical EGFR mutations were excluded from key trials evaluating this approach. Biomarker testing should be carried out promptly as part of the pre operative evaluation, with broad next generation sequencing (NGS) recommended where feasible. At present, circulating tumour DNA (ctDNA) detection or clearance after curative intent treatment is not advised to guide treatment decisions outside clinical trials.
In metastatic NSCLC, both tissue and liquid biopsy are used to identify actionable alterations such as EGFR mutations. Liquid biopsy has not yet been validated for early stage disease. The difference in turnaround time between the two methods is striking: liquid biopsy
typically yields results in about 8 days, versus around 32 days for tissue biopsy. A 2026 study of 425 patients reported sensitivity and specificity of 98% and 45% for liquid biopsy, compared with 99% and 53% for tissue biopsy.
Tissue biopsy offers the advantage of assessing tumour cellularity and histology but may be limited by necrosis and insufficient sampling. Extensive immunohistochemistry panels can sometimes deplete tissue such that insufficient material remains for NGS. Liquid biopsy, while less invasive and faster, carries risks of false negatives due to low DNA shedding and may require tissue confirmation in cases of negative results, which can prolong the time to definitive diagnosis.
Treatment landscape of EGFR mutant lung cancers
Classical or sensitising EGFR mutations
EGFR TKIs are a cornerstone of therapy across stages of EGFR mutant lung cancer, from early operable disease to advanced or metastatic settings
Early stage disease (neoadjuvant and adjuvant)
NeoADAURA is a phase III study, randomised patients with resectable non squamous stage II–IIIB (N2) EGFR mutant NSCLC to neoadjuvant osimertinib plus chemotherapy (pemetrexed with cisplatin or carboplatin), osimertinib alone, or chemotherapy alone. Major pathological response rates were 26% with osimertinib plus chemotherapy, 25% with osimertinib alone and 2% with chemotherapy alone, with event free survival (EFS) favouring the osimertinib containing arms, although EFS data are not yet mature.
In the adjuvant setting, the ADAURA trial randomised patients with resected stage IB–IIIA EGFR mutated NSCLC to 3 years of osimertinib or placebo. At 4 years, disease free survival was 70% with osimertinib versus 29% with placebo, and 5 year OS was 88% versus 78% (HR 0.49, p<0.001), establishing adjuvant osimertinib as the standard of care.
Locally advanced disease after chemoradiation
Durvalumab, an anti PD L1 antibody, became standard consolidative therapy after chemoradiation based on the PACIFIC trial. However, post hoc analyses in EGFR mutant subgroups showed no clear benefit in progression free survival (PFS) or OS for durvalumab over placebo. Retrospective data further suggest limited PFS benefit and relatively high rates of immune related adverse events, including pneumonitis, particularly when patients are subsequently exposed to EGFR TKIs such as osimertinib. Given this lack of proven efficacy and the toxicity profile, many clinicians avoid durvalumab consolidation in EGFR mutant disease.
Phase III LAURA trial evaluated osimertinib versus placebo in EGFR mutant patients with unresectable stage III NSCLC who had completed concurrent chemoradiation. Osimertinib significantly improved median PFS (39.1 vs 5.6 months), representing a major advance in this setting.
Advanced and metastatic disease
Immunotherapy has limited efficacy in metastatic EGFR mutant NSCLC. Treatment has therefore evolved from first generation TKIs to newer third generation agents and combination strategies, with ongoing efforts to overcome resistance.
First and second generation EGFR TKIs
First generation reversible EGFR TKIs such as gefitinib and erlotinib were the standard first line therapy for metastatic EGFR mutated NSCLC before osimertinib. They demonstrated clear advantages over platinum based chemotherapy, with higher response rates and longer PFS in patients with classical sensitising mutations. EGFR TKIs generally have a more favourable toxicity profile than chemotherapy, with less myelosuppression but more dermatological and gastrointestinal toxicity.
Second generation TKIs (afatinib, dacomitinib) are irreversible pan ErbB inhibitors and show longer PFS than first generation agents. However, broader kinase inhibition is associated with more pronounced toxicities, especially diarrhoea, mucositis and skin rash, limiting routine use. These limitations and the emergence of resistance—particularly the T790M mutation—paved the way for third generation TKIs such as osimertinib to move into the frontline setting.
Osimertinib and combination strategies in the frontline Osimertinib, a third generation EGFR TKI, targets both sensitising EGFR mutations and de novo or acquired T790M. In the phase III FLAURA trial, osimertinib significantly prolonged median PFS (18.9 vs 10.2 months) and median OS (38.6 vs 31.8 months; HR 0.80, p=0.046) with a similar or better tolerability profile than first generation TKIs. Phase III FLAURA2 trial compared osimertinib monotherapy with osimertinib plus platinum–pemetrexed chemotherapy. The combination yielded longer median PFS (24.0 vs 15.3 months) and median OS (47.5 vs 37.6 months),
suggesting a survival benefit in selected patients, for example those with high tumour burden or brain metastases. However, more adverse events led to higher rates of dose reductions and treatment discontinuations, so this regimen should be reserved for carefully selected individuals.
In the phase III MARIPOSA trial randomised treatment naïve patients to amivantamab plus lazertinib, osimertinib monotherapy, or lazertinib alone. Amivantamab–lazertinib significantly improved median PFS versus osimertinib (23.7 vs 16.6 months; HR 0.70) and produced an absolute 3 year OS gain of about 9%, establishing this EGFR–MET bispecific antibody plus third generation TKI as a compelling first line option with strong CNS activity, though with higher rates of infusion reactions, rash, paronychia and venous thromboembolism.
Alternative third generation EGFR TKIs
Beyond osimertinib, newer third generation EGFR TKIs such as furmonertinib and aumolertinib have entered clinical practice, particularly in Asia. These agents are irreversible inhibitors with strong CNS penetration and activity against common sensitising mutations and T790M and contribute to an increasingly diverse treatment landscape.
Post osimertinib progression
Despite advances with third generation TKIs, acquired resistance develops in almost all patients. For those progressing on first line osimertinib monotherapy, platinum–pemetrexed chemotherapy has historically offered limited benefit. The COMPEL trial evaluated continuation of osimertinib with chemotherapy versus chemotherapy alone after progression on first line osimertinib. The osimertinib containing regimen improved median PFS (8.4 vs 4.4 months; HR 0.43), supporting continuation of osimertinib beyond progression in selected patients.
The MARIPOSA2 trial assessed patients with metastatic EGFR mutant NSCLC after osimertinib, comparing chemotherapy alone
with amivantamab–chemotherapy or amivantamab–lazertinib–chemotherapy. Amivantamab–chemotherapy significantly improved OS (17.7 vs 15.3 months; HR 0.73, p=0.039), median time to treatment discontinuation (10.4 vs 4.5 months; HR 0.42, p<0.0001) and median time to subsequent therapy (12.2 vs 6.6 months; HR 0.51, p<0.0001).
In selected patients with limited sites of progression, local ablative therapy may allow continuation of osimertinib beyond progression. Radiotherapy or surgery for oligoprogressive disease can delay the need to switch systemic therapy and preserve the benefit of a well tolerated targeted agent.
Uncommon EGFR mutations
Approximately 14% of EGFR mutant NSCLC cases harbour uncommon EGFR mutations. The LUX Lung trials evaluated afatinib in treatment naïve patients with uncommon mutations, including point mutations and duplications in exons 18–21, de novo T790M, or exon 20 insertions. Afatinib showed clinically meaningful activity for G719X, L861Q and S768I, with a median PFS of 10.7 months and median OS of 19.4 months, but limited benefit in de novo T790M or exon 20 insertions.
Phase II, non randomised UNICORN trial demonstrated that osimertinib achieved an objective response rate (ORR) of 50% and median PFS of 9.4 months in uncommon EGFR mutant NSCLC (excluding exon 20 insertions), providing an additional option for this subgroup.
EGFR exon 20 insertions
Exon 20 insertions account for up to 12% of EGFR mutant NSCLC. These mutations cause conformational changes in the kinase active site that restrict binding of conventional EGFR TKIs, rendering them largely insensitive to agents approved for classical EGFR mutations. Until recently, first line therapy for these patients remained platinum based chemotherapy, with limited benefit from immunotherapies.
Amivantamab was approved for EGFR exon 20 insertions based on the phase I CHRYSALIS trial, which reported an ORR
of 40%, median PFS of 8.3 months and median OS of 22.8 months. The phase III PAPILLON trial showed that adding amivantamab to chemotherapy significantly improved PFS versus chemotherapy alone (median 11.4 vs 6.7 months; HR 0.40, p<0.001), establishing this as a new first line standard.
Sunvozertinib, an oral third generation EGFR TKI, received FDA accelerated approval based on the WU KONG 1B trial, which reported an ORR of 46% and duration of response (DOR) of 11.1 months in chemotherapy pretreated patients. The ongoing phase III WU KONG 28 trial is comparing sunvozertinib with chemotherapy in treatment naïve patients. Other phase III trials under investigation include REZILIENT 1 (zipalertinib plus platinum–pemetrexed chemotherapy) and FURVENT (furmonertinib versus platinum based chemotherapy) in previously untreated patients.
Mechanisms of osimertinib resistance
In Ireland, first line osimertinib monotherapy remains the standard approach for advanced EGFR mutant NSCLC. However, acquired resistance is almost inevitable. Resistance mechanisms are heterogeneous and can be broadly classified as on target, off target or histological transformation. Analyses of tumours progressing on osimertinib show no single predominant mechanism, underscoring the biological complexity of the disease.
On target resistance most commonly involves tertiary EGFR mutations that impair drug binding, with C797S the best characterised alteration following osimertinib exposure. Other changes include EGFR amplification and G724S. Off target resistance arises through activation of alternative signalling pathways, such as MET amplification, which restores downstream proliferation despite EGFR inhibition. Additional mechanisms include HER2 amplification, KRAS or PIK3CA mutations, BRAF alterations and acquired gene fusions.
Histological transformation, most commonly to small cell lung cancer, is another recognised
32 CPD 123: LUNG THERAPY
mechanism and is often associated with co alterations in TP53 and RB1, which may signal a more aggressive clinical course. Transformations to squamous cell carcinoma or large cell neuroendocrine carcinoma also occur, reinforcing the importance of repeat tissue biopsy at the time of progression on osimertinib when feasible.
Optimising care pathways
As treatment options for EGFR mutant NSCLC expand across disease stages, well designed care pathways are essential to ensure timely diagnosis, appropriate treatment selection and safe delivery of therapy. Reflex molecular testing using NGS at diagnosis is now a core component of modern lung cancer management and should be performed in all patients with non squamous NSCLC and in selected patients with squamous histology. Early identification
of actionable mutations allows prompt initiation of targeted therapy and reduces the risk of inappropriate empiric treatment.
An integrated approach combining tissue and liquid biopsy can improve mutation detection and reduce delays in treatment initiation and at progression. Tissue biopsy remains important for histological diagnosis and comprehensive genomic profiling, but may be limited by tumour cellularity, necrosis or insufficient material. Liquid biopsy offers a rapid, minimally invasive alternative, particularly at progression, although negative plasma results should be interpreted cautiously and tissue confirmation pursued whenever possible. Given the diversity of resistance mechanisms, repeat biopsy and molecular testing at progression are recommended where feasible to guide switching TKIs, adding targeted agents or enrolling patients in clinical trials.
Multidisciplinary input is increasingly important. Regular multidisciplinary team discussion supports accurate interpretation of molecular results, consideration of re biopsy, evaluation of oligoprogression for local therapy and identification of suitable clinical trials. Close collaboration between respiratory medicine, pathology, radiology, thoracic surgery, radiation oncology and medical oncology is essential to optimise care, particularly now that targeted therapy is being incorporated into earlier stage disease.
Patient education and adherence support are also critical, as EGFR TKIs are administered orally over prolonged periods, often in the outpatient setting. Patients should receive clear counselling on dosing schedules, potential drug interactions and expected toxicities, and be encouraged to report adverse effects early. Although generally well tolerated, EGFR inhibitors may cause
rash, diarrhoea, nail toxicity and fatigue, while less common but clinically significant toxicities such as interstitial lung disease, QTc prolongation or cardiotoxicity require prompt recognition. Structured follow up and clear toxicity management pathways help maintain treatment intensity while preserving quality of life.
Conclusion
The management of EGFR mutated NSCLC has evolved substantially over the past two decades, driven by advances in molecular characterisation, improved diagnostic techniques and the development of highly effective targeted therapies. A detailed understanding of EGFR biology, together with accurate and timely molecular testing, is now central to treatment selection across all stages of disease, including neoadjuvant, adjuvant, locally advanced and metastatic settings. The introduction of osimertinib has significantly improved outcomes, with meaningful gains in survival and central nervous system control compared with earlier therapies. Despite these advances, acquired resistance remains a major challenge, and the mechanisms underlying resistance are increasingly recognised as biologically complex and heterogeneous. As newer agents and novel combinations continue to emerge, the ability to individualise therapy based on tumour biology will remain a key principle of care.
Optimising outcomes for patients with EGFR mutated lung cancer depends not only on access to effective drugs, but also on the strength of the surrounding care pathway. Reflex molecular testing, multidisciplinary review, appropriate use of tissue and liquid biopsy, patient education, and proactive toxicity management are all essential components of modern practice. As the field continues to develop, integrating advances in molecular science with efficient clinical pathways will be fundamental to delivering high quality, personalised care for patients with EGFR mutated NSCLC.
More than a Headache Migraine Moves Up the European Health Agenda: Continued Advocacy from EMHA in 2026
Migraine and headache disorders are increasingly being recognised as a major public health issue across Europe, with ongoing advocacy efforts helping to reshape how these conditions are understood, prioritised and managed within healthcare systems. While 2026 has not yet produced a single defining headline moment, activity across the sector—particularly from the European Migraine and Headache Alliance (EMHA) under the leadership of its President, Patrick Little—continues to build momentum around awareness, policy engagement and patientcentred care.
Migraine is now widely acknowledged as one of the most prevalent neurological conditions globally, affecting an estimated one in seven people across Europe. Despite this, it remains historically underdiagnosed, undertreated and often misunderstood, both within healthcare systems and society more broadly. In recent years, EMHA has played a central role in challenging this perception, advocating for migraine to be recognised not as a minor or episodic complaint, but as a serious and often debilitating neurological disease with significant personal, social and economic consequences.
Under Patrick Little’s presidency, EMHA has continued to position migraine firmly within the broader European brain health agenda. This includes participation in key neurological and policy discussions, where migraine is increasingly being considered alongside other chronic neurological conditions in terms of its burden and impact. The reframing of migraine as a chronic neurological disease marks an important shift, with implications for how it is prioritised in health policy, funding decisions and service design.
A key focus of ongoing advocacy has been engagement at European Union level, where EMHA continues to work with policymakers, clinicians and stakeholders to improve recognition and access to care. This includes calls for earlier diagnosis, better treatment pathways and more equitable
access to innovative therapies across member states. Variability in access remains a significant challenge, with patients in different regions experiencing markedly different levels of support and treatment availability.
In parallel, there has been a growing emphasis on the role of migraine in workforce health and productivity. Migraine is one of the leading causes of disability worldwide, particularly among working-age populations. The condition can have a profound impact on an individual’s ability to work, contributing to absenteeism, reduced productivity and, in some cases, long-term withdrawal from the workforce. As a result, migraine is increasingly being recognised not only as a healthcare issue, but also as an economic one—an area that EMHA continues to highlight in its policy engagement.
Patrick Little has also highlighted the need for greater awareness among healthcare professionals of the significant impact migraine and headache disorders have on patients’ daily lives.
Another important theme emerging in 2026 is the role of digital health and innovation in improving migraine care. There is increasing interest in the development of digital tools and structured care pathways that support earlier identification, ongoing monitoring and more personalised management of migraine. Patrick Little has previously emphasised the importance of ensuring that patients are actively involved in the design and development of these solutions, highlighting the value of lived experience in shaping effective and accessible care models.
This focus on patient-centred care reflects a broader shift within healthcare systems towards more inclusive and collaborative approaches. For migraine in particular, where symptoms can vary significantly between individuals, personalised care is essential. The integration of digital solutions—such as symptom tracking, telemedicine consultations and remote monitoring—offers opportunities to improve both clinical outcomes
“Patrick Little has also highlighted the need for greater awareness among healthcare professionals of the significant impact migraine and headache disorders have on patients’ daily lives”
require continued collaboration between policymakers, clinicians, patient organisations and industry stakeholders. EMHA’s ongoing work in this space, supported by leadership at both national and European levels, will be critical in sustaining momentum and driving meaningful change.
and patient engagement, particularly for those who may face barriers to accessing traditional in-person services.
Awareness campaigns also continue to play a critical role in maintaining visibility for migraine and headache disorders. Initiatives such as European Migraine Day of Action and International Headache Awareness Week provide important platforms to engage policymakers, healthcare professionals and the public. These campaigns aim not only to raise awareness, but also to challenge persistent stigma and misconceptions that can prevent individuals from seeking appropriate care.
Despite this progress, significant challenges remain. Many patients still experience delays in diagnosis, limited access to specialist services and inconsistent treatment pathways. Addressing these issues will
Looking ahead, the trajectory for migraine care in Europe appears to be one of gradual but meaningful advancement. The increasing recognition of migraine as a serious neurological condition, combined with growing investment in innovation and a stronger emphasis on patient involvement, suggests that the landscape is evolving in a positive direction. However, translating this progress into tangible improvements in patient outcomes will depend on continued advocacy, policy action and system-level change.
In this context, the work of organisations such as EMHA— and the leadership provided by figures like Patrick Little— remains central. While 2026 may not yet have delivered a single defining milestone, it is clear that the foundations for longterm progress are continuing to be built, with migraine firmly established as a priority within the European health agenda.
Make sure to catch the May issue of Hospital Professional News featuring an authored article by Patrick Little on “Early Identification and Intervention in Migraine.”
Patrick Little, President, EMHA
Evaluating Innovation in Practice: How HIHI Supports Clinician-Led Product and Service Assessment Across Irish Hospitals
Health Innovation Hub Ireland (HIHI) operates at the intersection of clinical need and commercial innovation. Its evaluation framework goes beyond traditional product validation, it rigorously assesses how innovations perform within real healthcare workflows, what they deliver to patients and staff and what the barriers and opportunities are to scale across a small but complex health system. For clinicians, hospital managers and multidisciplinary teams (MDTs), understanding HIHI's approach offers valuable insights into how healthcare innovations are vetted, what evidence they generate and how lessons learned in one site can inform scaling and adoption elsewhere. For clinical experts and decision makers assessing whether a new product is safe, usable and worth adopting, this real world evidence is critical. Since 2016, HIHI has logged 2,181 engagements with health innovation developers, supported 1,284 new innovations and worked with 745 companies - generating 9,205 jobs supported and helping HIHI engaged SMEs, startups and researchers raise a combined ¤234 million in funding.
HIHI's evaluation model is fundamentally clinician led, embedding innovations directly with clinical teams in sites to assess real world performance. Rather than relying solely on manufacturer claims or controlled test conditions, HIHI facilitates pilots and clinical evaluations that engage frontline healthcare professionals, consultants, clinical
Written by Eimear Galvin, HIHI Regional Manager (Dublin)
nurse specialists, biomedical engineers, pharmacists and allied health staff as active evaluators. The model operates across three support tiers. Early stage concept assessment helps refine nascent ideas and whether they address genuine healthcare needs. Clinical and end user evaluations brings together experts to provide structured feedback on developing solutions, examining usability, clinical efficacy and workflow integration. Full pilots test market ready products in real healthcare environments, measuring tangible outcomes across clinical, operational, financial, interoperability and sustainability. To date, this tiered model has produced 369 formal projects: 183 idea assessments, 110 clinical evaluations and 76 product pilots, supported by more than 2,000 clinical staff across 208 healthcare sites nationwide. This approach ensures that innovations are not assessed in isolation but within the often messy reality of healthcare delivery. Over a decade of operations, across four hubs, HIHI has evaluated solutions ranging from sustainable surgical equipment and AI-driven chemotherapy toxicity screening to anaesthetic gas capture systems and reusable medical devices. Each evaluation generates evidence that companies can use for regulatory submissions, procurement discussions and investor presentations, simultaneously exposing Irish healthcare teams to the latest innovations and generating data that can inform adoption feasibility.
Central to HIHI's evaluation process is a structured risk/ benefit assessment that considers multiple dimensions of impact. This is not limited to clinical safety, although patient safety remains paramount, but extends to operational, financial, and system level considerations. HIHI assesses innovations across five core domains:
Clinical pathway value: Does the innovation improve patient access, outcomes, or experience? For instance, the eAltra AI chatbot for pre-chemotherapy assessments eliminated unnecessary patient
journeys by identifying unsuitable candidates 24 hours before scheduled appointments, sparing vulnerable patients travel costs and reducing wait times by up to two hours through timed chemotherapy production.
Workflow efficiency: Does it save time or reduce administrative burden for healthcare teams? The eAltra system achieved 98% concordance with gold-standard nurse-led assessments while saving a minimum of 3.5 hours per treatment day. The Safe Clean Box pre-cleaning system reduced cleaning time by 40 minutes daily and halved non-conformances in sterilised instruments.
Financial impact: What are the cost implications? HIHI pilots can quantify savings with precision. Safe Clean Box generated ¤32,000 in annual savings through reduced PPE usage (¤20,000), eliminated wire brushes (¤8,661), labour efficiency (¤3,211 - ¤3,754), and lower incineration costs (¤158), offsetting its ¤60,000 purchase price in two years. Meanwhile, Ecco Spray's sustainable ultrasound gel replacement saved ¤0.24 per scan - scaling to ¤461 annually in one urology department and potentially thousands of euro hospital wide for point of care ultra sounds.
Interoperability: How does the solution integrate with existing IT systems, equipment, and workflows? eAltra's HL7-compliant web application integrates seamlessly with CERNER/ORACLE HEALTH and EPIC electronic patient record systems.
Sustainability: What is the environmental footprint? Safe Clean Box achieved an 82% reduction in energy consumption versus ultrasonic cleaners and saved 1,200 litres of water daily. Ecco Spray eliminated singl -use gel sachets entirely, delivering a 95% reduction in gel volume and removing all associated paper towel waste. EnviroMedical's anaesthetic gas capture systems target F-gases with up to 99.9% capture efficiency and nitrous oxide with >99% destruction rates.
Risk assessment is equally granular. HIHI evaluations consider patient safety implications - does the innovation introduce new clinical risks? Regulatory compliance pre pilot is
non-negotiable: is it CE marked, MDR compliant, GDPR adherent? Operational disruption - will it require staff retraining or workflow redesign. Implementation complexity - who manages maintenance, consumables, technical support? HIHI's evaluation framework produces evidence that is immediately actionable for clinical MDTs, procurement teams and health system planners. Each pilot generates:
• Quantified clinical outcomes: Agreement rates with gold standards, patient satisfaction scores, safety metrics, and impact on care quality.
• Operational metrics: Time savings per procedure, reduction in non-conformances, workflow disruption assessments, and staff usability feedback.
• Environmental impact data: Energy consumption, water usage, waste generation, CO2 emission reductions, and alignment with HSE sustainability mandates.
• Implementation guidance: Installation requirements, training needs, technical support considerations, and maintenance protocols.
For MDTs, this translates into confident, evidence based adoption decisions, proactive identification of workflow risks, robust procurement justification, and the benefit of shared national learning.
One of HIHI’s most significant lessons is the variability in governance thresholds across Irish healthcare sites. While Ireland operates a small health system by international standards, governance requirements for innovation adoption are not uniform. For innovators, this variability creates friction. A solution that secures rapid ethical approval at one university hospital may face months of additional review at another. Procurement processes differ in
requirements for clinical evidence, health technology assessments and budgetary sign off. Legacy systems make interoperability a major challenge – often requiring bespoke configurations per hospital site. HIHI's role as a national intermediary mitigates some of this complexity. By standardising evaluation protocols, providing project management expertise and leveraging relationships across the HSE's acute, primary and community sites, HIHI helps companies navigate inconsistencies. HIHI's project agreement documents specify evaluation scope, data collection methods and deliverables upfront, reducing ambiguity. However, the underlying governance heterogeneity persists, and HIHI's evidence base documents these barriers as clearly as it documents clinical outcomes.
For healthcare systems, this variability highlights an opportunity. Sites with streamlined governance can pilot innovations faster, generating evidence that other sites can leverage. Conversely, overly rigid processes risk delaying adoption of beneficial technologies. Ireland's small health system size creates both advantages and challenges. In theory, innovations proven in one site should scale rapidly up through an innovation pathway for multiple site use. In reality,
there is persistent duplication of effort and missed opportunities for knowledge transfer. Multiple sites may independently evaluate similar technologies, repeating pilots unnecessarily rather than sharing learnings. Procurement teams at different hospitals negotiate separately with the same vendors, missing opportunities for collective bargaining or shared service contracts. Clinical engineering departments assess identical equipment compatibility issues without coordinating findings. Even sustainability initiativeswaste management systems, reusable device protocols, green anaesthesia programmes are developed in silos despite addressing identical challenges.
HIHI's cross-site network begins to address this. By publishing case studies, project reports and pilot findings, HIHI creates a repository of validated evidence that other sites can reference. Clinicians contemplating Safe Clean Box adoption can review the Mater Hospital's quantified savings. Teams interested in AI chatbots can examine Tallaght Hospital’s eAltra data on concordance rates and usability feedback. Anaesthetists considering gas capture systems can draw on the clinical evaluation findings from clinical experts in Cork and Galway regarding compatibility, workflow integration and regulatory
compliance. Despite this, crosssite adoption remains sluggish. HIHI's role increasingly involves not just evaluation but active dissemination, presenting findings at national forums, connecting early adopters with later stage sites and demonstrating returnon-investment calculations that finance teams require.
Ireland’s six Regional Health Authorities (RHAs) offer a structural opportunity to redesign how healthcare innovation is evaluated and scaled. For MDTs and clinicians, this shift offers practical advantages. RHAs function as natural scaling platforms, combining defined populations, consolidated budgets and independent procurement authority. This enables innovations to be evaluated once at regional level, using robust, clinicianled HIHI methodologies and where successful, implemented consistently across multiple sites rather than through fragmented single hospital pilots. HIHI is uniquely positioned to support this regional approach. Its established evaluation and testing framework, which generates evidence across clinical, operational, financial, and sustainability domains, can be deployed at RHA scale without the need for each region to build separate assessment infrastructure. For clinicians, this reduces duplication of local
evaluation effort, accelerates access to proven technologies and provides clearer evidence to support safe adoption in practice. For MDTs, it strengthens procurement decisions through shared regional data, distributes implementation risk across organisations and shortens the pathway from pilot to routine care. The economic case for scaling is clear: HIHI-supported companies have raised ¤160 million in funds since engaging with HIHI and created 578 new jobs — outcomes that can be accelerated by regional level adoption infrastructure.
HIHI's evaluation and reports can support answers to the critical question: "Should we adopt this?" They provide evidence that survives scrutiny from clinical governance committees, finance teams, procurement boards and investors. For healthcare professionals, HIHI offers validated insights into what works, what costs, what saves and what scales. For the health system, it provides a mechanism to accelerate cross-site learning and reduce inefficiencies. Irish healthcare innovation need not be a leap of faith. Though HIHI’s structured evaluation, transparent risk/benefit assessment and cross site knowledge sharing, Irish healthcare can adopt solutions that genuinely improve outcomes while delivering financial and environmental sustainability.
Rapid Access, Triage and Risk-Stratification Models: The Role of Rapid Cardiac Care in Contemporary Chest Pain Pathways
Written by Marina Gomes, Candidate ANP in Cardiology, Hermitage Clinic
Marwa
Al Habsi, Cardiac Imaging/RCPI Fellow, Hermitage Clinic
Tora Leong,
Consultant
Marina Gomes, Candidate ANP in Cardiology, Hermitage Clinic
Introduction
Healthcare systems in high-income countries continue to experience sustained increases in demand, driven by population ageing, rising multi-morbidity, and advances in diagnostic and therapeutic interventions (OECD, 2023). These pressures are particularly evident in Emergency Departments (EDs), where attendance rates have risen steadily over the past two decades and case complexity continues to grow, particularly among older adults and people with multimorbidity (Stewart, 2025; PubMed, 2024). ED overcrowding is now recognised as a global systemslevel challenge, associated with prolonged waiting times, delayed diagnosis, increased risk of adverse events, staff burnout, and reduced patient satisfaction (Darraj et al., 2023; Pearce et al., 2024). In parallel, modern patients increasingly expect timely access to specialist care, efficient service delivery, and flexibility in how and where care is provided. Together, these factors necessitate the development of innovative models of care that improve patient flow while maintaining safety, quality, and appropriate resource utilisation. Rapid access, triage, and risk-stratification models have emerged as key strategies for addressing these challenges. By facilitating early assessment,
identifying patients at greatest risk, and directing care to the most appropriate setting, these models aim to reduce avoidable hospitalisation, optimise use of specialist resources, and improve patient outcomes (BMC Emergency Medicine, 2024).
Chest Pain Presentations and the Limitations of Traditional Pathways
Chest pain remains one of the most common reasons for ED presentations worldwide and represents a substantial proportion of acute medical admissions (Stepinska et al., 2020; OECD, 2023). While the incidence of acute coronary syndrome (ACS) is projected to decline in high-income countries due to improvements in primary prevention and secondary risk reduction, the absolute number of hospital presentations for chest pain has increased, alongside a rising mean age of patients (OECD, 2023; Roth et al., 2020). This reflects the growing prevalence of chronic cardiovascular disease, multi-morbidity, and non-cardiac causes of chest pain in ageing populations (Roth et al., 2020).
Despite this epidemiological shift, management pathways for chest pain in many settings remain conservative and admissionfocused. Observational studies consistently demonstrate high
admission rates with relatively low diagnostic yield for ACS (Goodacre et al., 2005; Rui et al., 2023). In one large study, 96% of patients presenting with chest pain were admitted to hospital, yet only 11% were ultimately diagnosed with ACS (Goodacre et al., 2005). Importantly, 30-day adverse event rates were 0% among low-risk patients and 2% among intermediate-risk patients, compared with 20% among high-risk patients. These findings highlight the potential for more selective admission strategies based on robust risk stratification (Poldervaart et al., 2017; Mahler et al., 2018).
Hospitalisation is associated with significant direct and indirect costs, including bed occupancy, investigations, and staffing demands, as well as patient-level harms such as hospital-acquired infection, functional decline, anxiety, and disruption to social and occupational roles (OECD, 2023; Krumholz, 2013). These risks have driven interest in alternative models of care that enable safe early discharge or outpatient management for appropriately selected patients (Mahler et al., 2018; Stepinska et al., 2020).
In the public sector in Ireland, waiting times to see a specialised cardiology consultant are typically several months, with national data showing many patients
waiting beyond six months for an outpatient appointment — and in some localities over a year — reflecting ongoing pressures on cardiology services (HSE.ie, 2026)
Triage Systems: Strengths and Persistent Limitations
Triage systems are fundamental to ED operations and serve as the primary point of clinical prioritisation for patients presenting for unscheduled care. Most contemporary EDs employ five-level triage systems, including the Australasian Triage Scale, Manchester Triage System, Emergency Severity Index, and Canadian Triage and Acuity Scale. These systems have demonstrated acceptable reliability and validity in identifying high-acuity patients requiring immediate intervention (Christ et al., 2010; Mirhaghi et al., 2015).
However, a key criticism is their limited discriminatory capacity within mid-acuity categories, where heterogeneous groups of patients with differing risk profiles may be clustered together. This limitation reduces precision in predicting adverse outcomes and may delay assessment for patients with time-sensitive but initially subtle pathology (Dugas et al., 2016). Such challenges undermine the core objective of triage—to meaningfully differentiate urgency beyond broad categorisation.
Triage decisions are also influenced by clinician experience, cognitive bias, workload, and environmental pressures. ED crowding, time constraints, and competing clinical demands have been shown to negatively affect triage accuracy and increase the risk of under-triage (Sun et al., 2013; Morley et al., 2018). Evidence further suggests that clinical deterioration during ED waiting periods is not uncommon, particularly among patients initially classified as intermediate acuity (Considine et al., 2017).
These limitations have prompted calls for more dynamic triage approaches that incorporate structured reassessment, physiological early warning
Marwa Al Habsi, Cardiac Imaging/ RCPI Fellow, Hermitage Clinic
systems, and objective riskprediction tools rather than relying solely on initial acuity categorisation (Islam et al., 2022). Integrating serial assessment and data-driven risk stratification may enhance sensitivity for early deterioration while preserving operational efficiency.
Risk Stratification in Cardiovascular Care
Risk stratification provides a structured approach to addressing the shortcomings of traditional triage by estimating an individual patient’s likelihood of adverse outcomes and aligning care accordingly. In cardiology, risk stratification is central to clinical decision-making across the spectrum of disease, from primary prevention to acute coronary syndromes and chronic heart failure.
Effective risk stratification enables clinicians to:
identify patients at high risk of adverse cardiovascular events,
tailor diagnostic and therapeutic interventions,
allocate specialist resources more efficiently,
reduce unnecessary investigations and admissions in low-risk patients,
and improve patient outcomes and quality of life.
In the context of chest pain assessment, validated risk scores, biomarkers, and physiological parameters can be combined to improve prognostic accuracy. Integration of objective data such as serial electrocardiography, cardiac biomarkers, vital sign trends, and clinical risk scores has been shown to outperform clinician judgement alone. Importantly, risk stratification supports a shift from purely acuity-based decisionmaking toward needs-based and outcome-focused care pathways.
Rapid Access Models and the Emergence of RAC Services
Rapid Access Cardiology (RAC) services have emerged as a practical application of riskstratified care. These services provide timely specialist assessment and investigation for patients with suspected cardiac pathology who do not require immediate hospital admission. In the United Kingdom, RAC clinics are embedded within national guidance from the National Institute for Health and Care Excellence and are the standard outpatient model for the assessment of suspected stable angina following updated chest pain pathways (NICE, 2016; updated 2019).
A review of 21 studies evaluating RAC services demonstrated that early specialist assessment of low-to-intermediate risk chest pain is safe, reduces hospitalisation rates, and is cost-effective (Goodacre et al., 2004; Lau et al., 2010). Patients managed through RAC pathways experience shorter time to diagnosis, high satisfaction rates, and no increase in short-term adverse cardiac events compared with traditional inpatient strategies (Sekhri et al., 2007; Goodacre et al., 2004). These findings align with broader European recommendations from the European Society of Cardiology, which support structured outpatient investigation for appropriately selected patients with suspected chronic coronary syndromes (ESC, 2019; ESC, 2020).
Collectively, the evidence supports the wider adoption of rapid access, risk-stratified models of care that reduce unnecessary admission while maintaining clinical safety.
Rapid Cardiac Care at the Hermitage Clinic
The Rapid Cardiac Care (RCC) Clinic at the Blackrock Health Hermitage Clinic (BHHC) represents an integrated application of rapid access and risk-stratification principles outlined above within a local healthcare setting. The clinic was developed in response to increasing ED attendances for cardiac symptoms, prolonged waiting times for outpatient cardiology review largely increased demand for cardiological assessment, and a recognised need to streamline cardiological investigations and in many cases, may lead to reduction in hospital admissions while maintaining patient safety, and of course, higher levels of patient satisfaction in expedited cardiac investigations and treatment.
Rapid Cardiac Care (RCC): Design and Access Pathways
The RCC operates as a flexible, open-access service which accepts both referrals from general practitioners and the ED after initial triage, and also self-referred patient walk-in attendance. This model allows patients with cardiac symptoms to access specialist assessment without the delays associated with traditional referral pathways. Following referral or presentation, all patients undergo an initial structured screening process designed to support early cardiovascular risk stratification. This may even be over the phone on initial patient or GP phone contact. Screening/ triaging incorporates referral
information, presenting symptoms, cardiovascular risk factors, past medical history, and very importantly, electrocardiography (ECG) on arrival, and later, relevant laboratory findings. This information is used to risk stratify more urgent assessment pathways for acute coronary syndrome and malignant arrhythmias and to identify features suggestive of clinical instability.
After initial triage/risk assessment, full clinical initial assessment is made by clinical nurse specialists or advanced nurse practitioners and appropriate investigations organised after clinical history and examination.
Patients identified as having higher-risk or concerning features such as ongoing or recurrent chest pain, dynamic electrocardiographic changes, abnormal biomarkers, haemodynamic instability, or significant comorbidity, are prioritised for early/immediate discussion with a cardiologist immediately after initial triage/risk assessment.
Patients triaged as lower risk with stable symptoms are assessed and offered appropriate general cardiac investigations. A defining feature of the service is the capacity to provide same-day or next-day appointments without reliance on conventional outpatient waiting lists. This immediate access model enables dynamic risk stratification, allowing clinical decisions to be refined rapidly as new information becomes available. Review by a cardiologist usually happens after assessment.
By combining structured risk assessment with rapid access to specialist review and diagnostics, the clinic can quickly come to a diagnosis, a ‘rule-out’ and also, safely divert appropriate patients from inpatient admission, of particular relevance to chest pain and heart failure attendances, and maintain a high standard of patient-centred cardiovascular care. Some chronic conditions may need longer term follow-up in which case the patients are seen in cardiologist clinics after.
Rapid Access Diagnostics
A defining feature of the RCC at the Hermitage clinic is the availability of same-day or next day rapid-access diagnostic testing. Based on their clinical indication after assessment, patients may undergo a number of non-invasive cardiac investigations including:
Transthoracic echocardiography
Treadmill Exercise stress testing
24- or 48-hour Holter monitoring
24-hour ambulatory blood pressure monitoring
These investigations facilitate early identification of structural heart disease, arrhythmias, and inducible ischaemia, allowing prompt reassurance or escalation of care. Rapid access to diagnostics reduces uncertainty, a key driver of hospital admission in chest pain presentations.
For patients identified as needing more advanced cardiac investigations, the RCC Clinic facilitates expedited access to advanced cardiac imaging such as:
CT Coronary Angiogram (CTCA)
Cardiac MRI (CMR) both stress perfusion and structural
This is where the Hermitage Clinic can make a difference by offering fast, clinically-driven advanced cardiac imaging tests such as CTCA and CMR in a matter of days or a couple of weeks, and sometimes even same-day CTCA/ CMR specially for RCC patients.
Of course, timely access to invasive coronary angiography is also available same day if needed, or within a few days, and it is this expedited access of a armamentarium of tests along with senior clinical decision making that can quickly arrive at a diagnosis and in some cases, avoid hospital admission even for unstable angina.
CONCLUSIONS
Through structured risk stratification and rapid access to specialist assessment and diagnostics, a model such as our RCC Clinic can contribute to improved patient flow and reduce pressure on acute services. Patients who can be safely managed outside the inpatient setting are identified early, reducing ED attendances, length of stay and avoiding hospital admissions. From a system perspective, the RCC Clinic supports more efficient utilisation of cardiology and diagnostic resources by aligning intensity of investigation with clinical risk. For patients, the model offers timely reassurance, early diagnosis, and clear management plans, reducing anxiety and improving the overall patient care and experience.
This model reflects a broader shift in acute care toward dynamic, outcome-focused pathways that extend beyond the ED. As healthcare demand continues to rise, such approaches are likely to become increasingly important in balancing safety, efficiency, and patient-centred care.
“From Dependence to Independence”: How Surgical Innovation at the Mater Hospital is Redefining Possibility in Spinal Cord Injury Care
An interview with Dr Gráinne Colgan, Consultant in Plastic and Reconstructive Surgery, and Dr Emer Smith, Consultant in Rehabilitation Medicine
Dr Gráinne Colgan
For patients living with spinal cord injury, the loss of hand and arm function is often one of the most devastating consequences of their condition. It is not simply a clinical deficit, but a profound shift in autonomy, identity, and daily life. The ability to feed oneself, to use a phone, to perform even the smallest personal tasks, can disappear in an instant, replaced by a long and often uncertain path of adjustment.
Against this backdrop, a specialised programme at the Mater Hospital is quietly changing what recovery can look like. Through a combination of nerve and tendon transfer surgery, delivered within an integrated hospital pathway, clinicians are restoring meaningful function in patients who would otherwise have limited options.
What makes this work particularly striking is not just the surgical innovation, but the context in which it exists. In spinal cord
Dr Emer Smith
injury care, there are currently no interventions globally that can reliably restore neurological or functional recovery once injury has occurred. Treatment pathways focus on stabilisation, prevention of complications, and rehabilitation, but not reversal.
“There is nothing that we can give patients with a spinal cord injury that will improve their neurological or functional recovery,” explains Dr Emer Smith, Consultant in Rehabilitation Medicine. “That’s why something like this is so important. It’s not an intervention on the spinal cord itself, but it’s a way of working around it to restore function.”
It is a statement that frames the significance of the programme. In a field defined by limitation, even partial restoration becomes transformative.
Access to such reconstructive approaches, however, remains limited worldwide. It is estimated that only a small proportion of
“There is nothing we can give patients with a spinal cord injury that restores function. That’s why this work matters.”
“Only about 10% of patients who could benefit from reconstructive surgery ever reach it.”
eligible patients ever reach surgery, not due to lack of need, but because of systemic barriers.
“Only about 10% of patients who could benefit from reconstructive surgery actually get to surgery,” says Dr Gráinne Colgan, Consultant in Plastic and Reconstructive Surgery. “There are many reasons for that, including lack of awareness, lack of referral, and lack of expertise.”
What has been developed at the Mater Hospital is an attempt to address those barriers directly. Rather than positioning surgery as a standalone intervention, the programme is built as part of a continuous pathway, linking acute care, surgical decision-making, and long-term rehabilitation.
Because the surgical and rehabilitation teams are embedded within the National Spinal Cord Injury Unit and closely connected to the National Rehabilitation Hospital, patients can be identified early and followed throughout their journey. This removes one of the most significant obstacles seen in other systems, where patients are often never referred or considered for reconstructive options.
“We are able to link with patients from the very beginning,” Dr Colgan explains. “That doesn’t mean they will necessarily go on to have surgery, but it means they are
aware of the option. Our aim is to make sure that opportunity exists.”
Timing is critical in this context. Surgery is not typically performed immediately after injury, but rather considered at least a year later, once neurological recovery has stabilised and patients have adapted to the initial impact of their condition. This allows clinicians to better understand each patient’s baseline function and recovery trajectory, which in turn informs surgical planning.
Advances in data have strengthened this process.
Longitudinal studies now allow clinicians to predict, with reasonable accuracy, the likely course of recovery in the absence of intervention. This predictive capability supports more informed conversations with patients and more precise identification of those who may benefit from surgery.
“We can now say with some certainty what recovery is likely to look like within the first year,” Dr Smith notes. “That gives us a clearer picture of where surgery might add value.”
At the centre of the programme is a nuanced approach to surgical reconstruction, one that moves beyond simple technique selection and instead focuses on functional outcomes. The use of tendon and nerve transfer surgery is not framed as a binary choice, but as a complementary strategy tailored to the individual.
“We are not deciding between procedures. We are building a strategy around the patient.”
“If we can restore pinch, patients can perform up to 90% of daily tasks independently.”
“The emphasis is always on patient-centred goals,” says Dr Colgan. “We are not deciding between procedures in isolation. We are building a strategy based on what the patient has available and what they want to achieve.”
Tendon transfer surgery offers the advantage of immediacy. By redirecting a functioning muscle to replace the role of a paralysed one, it can deliver relatively rapid functional gains. However, this comes with the need for early and intensive rehabilitation, as patients must learn to use the transferred muscle in a new way.
Nerve transfer surgery, by contrast, is a slower process. It involves rerouting functioning nerves to reanimate paralysed muscles, with recovery typically emerging over 12 to 18 months as the nerve regenerates and patients relearn movement patterns.
Each approach has its advantages and limitations. Tendon transfer can deliver quicker results but may involve trade-offs in muscle function. Nerve transfer preserves muscle function and can offer more natural movement, but requires patience and carries a longer timeline.
“The international consensus is moving towards combining both,” Dr Colgan explains. “It’s not usually a case of one or the other. It’s about using both in a way that best serves the patient.”
Patient selection remains a critical component of the process. Not every individual with spinal cord injury is a suitable candidate, and decisions must take into account not only the level and severity of injury, but also the patient’s capacity to engage with rehabilitation.
“This is not for everybody,” Dr Smith says. “It depends on the injury, but also on the person. They need to be able to participate in the rehabilitation process, because that is essential to achieving a good outcome.”
Functional baseline also plays a role. Patients who retain some degree of movement early on are more likely to benefit from
reconstructive approaches, as there is more existing function to build upon.
The outcomes themselves are best understood not in abstract clinical terms, but through the restoration of everyday actions. One of the most significant goals is the return of pinch function between the thumb and index finger.
“If we can restore pinch, patients can perform up to 90% of daily tasks independently,” Dr Colgan explains.
This includes activities that are often taken for granted, such as holding utensils, using a mobile phone, or controlling a wheelchair. For patients, these changes represent far more than functional improvements; they represent a return of autonomy.
Patients often define their goals in deeply personal terms.
“They will say, ‘I want to be able to cut my food,’ or ‘I want to be able to blow-dry my hair,’” she says. “From that, we work backwards to understand what needs to be restored.”
Even modest gains can have a profound impact.
“Moving from complete dependence to even a small level of independence makes a huge difference. It’s very difficult to quantify, but the impact is enormous.”
What becomes clear through these conversations is that success is not measured by full restoration, but by meaningful change. The ability to perform even one task independently can shift the experience of daily life.
While surgical innovation sits at the centre of the programme, both clinicians are quick to emphasise that outcomes are inseparable from the work of the wider multidisciplinary team. Physiotherapists and occupational therapists play a central role, particularly in the post-operative phase, where patients must learn to use transferred muscles effectively.
“They are the ones who do the hard work,” Dr Smith says. “They spend the time with patients, helping them relearn movement and maximise the benefit of surgery.”
This rehabilitation is not generic. It requires specific expertise and familiarity with the surgical techniques involved. The relationship between surgical and rehabilitation teams is continuous and collaborative, rather than sequential.
“This is not surgery followed by rehab,” she adds. “It is a coordinated process throughout.”
The Mater Hospital’s ability to deliver this level of care is rooted in a convergence of factors. As the National Spinal Cord Injury Unit, it brings together specialised surgical expertise, experienced nursing teams, anaesthetic support, and direct links with rehabilitation services.
“It’s really a combination of everything,” Dr Colgan explains. “We have the expertise, the infrastructure, and the institutional support to deliver this type of care.”
High-quality baseline care also contributes to outcomes. Patients treated within the unit are less likely to develop secondary complications, such as infections or pressure injuries, which can compromise recovery and limit eligibility for surgery.
“That level of care sets patients up better for any intervention,” Dr Smith notes. “It means they are in a stronger position to recover.”
In Ireland, the number of patients sustaining cervical spinal cord injuries each year is relatively small, estimated at around 20 to 25 individuals. However, the ambition of the programme is not defined by volume, but by access.
“Moving from complete dependence to even a small level of independence makes a huge difference.”
“Not every patient will have surgery, but every patient should have the opportunity.”
“We would like every patient to at least have the opportunity to explore their options,” Dr Colgan says.
This reflects a broader shift in thinking. Rather than reserving reconstructive surgery for a select few, the aim is to embed it within standard care pathways, ensuring that no patient is excluded simply due to lack of awareness or referral.
At present, much of the work required to sustain the service happens behind the scenes, through coordination, collaboration, and ongoing development of pathways. The next phase will involve formalising these processes, making them more visible and accessible within the wider healthcare system.
“We are moving towards a more structured model,” Dr Colgan explains. “We want this to become seamless.”
Looking ahead, both clinicians see significant potential for growth.
“We want to go from strength to strength,” Dr Smith says. “The goal is to ensure that every patient who could benefit has the opportunity to do so.”
In a field where therapeutic options remain limited, the significance of this work lies not in dramatic breakthroughs, but in incremental, meaningful change. It challenges longstanding assumptions about what is possible after spinal cord injury, offering a pathway that moves beyond adaptation towards restoration.
For patients, that shift can redefine daily life.
For clinicians, it represents a reminder that even within the constraints of complex conditions, there is still space for innovation, collaboration, and progress.
Nutrition and Parenteral Support in Complex Patients
Malnutrition remains a significant yet often under-recognised challenge within hospital settings, particularly among patients with complex medical conditions. Across Europe, disease-related malnutrition is estimated to affect up to 30–50% of hospitalised patients, and Irish data suggests a comparable burden, particularly among older adults and those with chronic illness. Despite advances in medical care, the identification and management of nutritional risk is frequently inconsistent, leading to poorer clinical outcomes, prolonged hospital stays and increased healthcare costs.
In Ireland, malnutrition is estimated to cost the healthcare system in excess of ¤1.4 billion annually, largely driven by increased length of stay, higher complication rates and readmissions. The consequences are far-reaching, impacting immune function, wound healing, muscle strength and overall recovery. Within this context, early nutritional assessment and appropriate intervention are essential components of highquality patient care.
Nutrition is not merely supportive care; it is a fundamental aspect of treatment. For patients with complex needs, including those with gastrointestinal disorders, malignancy, critical illness or postsurgical complications, nutritional support plays a pivotal role in improving outcomes. However, despite its importance, nutrition is often underprioritised within clinical workflows.
Early identification of malnutrition risk is the first step in effective management. Screening tools such as the Malnutrition Universal Screening Tool (MUST) are widely recommended and endorsed within Irish clinical guidance.
Written by Professor Kieran O’Connor, Clinical Nutrition/ Consultant Gastroenterologist
However, audits across acute hospital settings have shown that routine nutritional screening is not consistently implemented, with missed opportunities for early intervention particularly evident in high-turnover admission settings.
A key challenge lies in recognising that malnutrition does not always present in obvious ways. Patients may have a normal or elevated body mass index yet still be nutritionally compromised. This is particularly relevant in patients with chronic disease, where inflammation and metabolic changes can lead to significant nutritional deficits despite preserved body weight. In older Irish populations, sarcopenia and frailty further complicate assessment, requiring a more nuanced clinical approach.
Once identified, nutritional support should be initiated promptly. Oral nutritional support, including dietary modification and supplementation, is typically the first-line approach. However, for many complex patients, oral intake alone is insufficient to meet nutritional requirements.
Enteral nutrition, delivered via feeding tubes, is generally preferred where the gastrointestinal tract is functional. It supports gut integrity, reduces the risk of infection and is associated with improved clinical outcomes compared to parenteral nutrition. Within Irish hospitals, enteral feeding is widely used, particularly in patients with neurological conditions, strokerelated dysphagia and critical illness.
However, there are circumstances where enteral nutrition is not feasible or adequate. In such cases, parenteral nutrition becomes a critical intervention.
Parenteral nutrition involves the intravenous delivery of nutrients, bypassing the gastrointestinal tract entirely, and is indicated in patients with non-functioning or inaccessible gastrointestinal systems, including those with bowel obstruction, severe malabsorption or complex surgical complications.
The decision to initiate parenteral nutrition requires careful clinical judgement. Evidence suggests that delayed initiation in highrisk patients is associated with increased complications and poorer outcomes. Conversely, inappropriate use exposes patients to unnecessary risks and resource utilisation. Clear clinical pathways and early specialist input are therefore essential.
Parenteral nutrition is a complex intervention that requires meticulous management. It is associated with risks, including catheter-related bloodstream infections, metabolic disturbances and hepatobiliary complications. In Ireland, infection prevention remains a key priority within acute services, and strict adherence to central line protocols is essential in mitigating these risks.
Central venous access is typically required for parenteral nutrition, and careful line management is critical. Regular biochemical monitoring is also required to prevent complications such as refeeding syndrome, electrolyte imbalance and hyperglycaemia, all of which can significantly impact patient outcomes if not identified early.
The role of the multidisciplinary team is central to the success of nutritional support strategies. Dietitians are essential in assessing nutritional requirements and tailoring interventions, while pharmacists contribute expertise in compounding and monitoring parenteral formulations. Nursing staff play a critical role in administration, monitoring and patient education.
In Ireland, multidisciplinary nutrition support teams have been associated with improved outcomes, including reduced complication rates and more appropriate use of parenteral nutrition. However, access to such teams is not uniform across all hospitals, and service variability remains a challenge.
Another important consideration is the transition of care. Patients
receiving nutritional support in hospital often require ongoing management following discharge. In Ireland, this may involve coordination with community dietetic services, general practice and, in some cases, home parenteral nutrition programmes. Effective communication at discharge is therefore essential to ensure continuity of care.
The integration of nutritional care into broader clinical pathways is also critical. In surgical patients, preoperative nutritional optimisation has been shown to reduce postoperative complications and length of stay. Similarly, in oncology, early nutritional intervention is associated with improved tolerance to treatment and better overall outcomes.
Despite clear evidence supporting nutritional intervention, barriers to implementation persist. These include time constraints, limited staffing, competing clinical priorities and variable awareness among healthcare professionals. Addressing these challenges requires both organisational support and cultural change within hospital settings.
Education and training are essential in supporting this shift. Clinicians must be equipped with the skills to recognise malnutrition, initiate appropriate interventions and understand when to escalate care. In Ireland, increasing emphasis is being placed on nutrition as a core component of clinical care, but further integration into routine practice is required.
From a health system perspective, improving nutritional care represents a significant opportunity to enhance efficiency. Studies have shown that appropriate nutritional intervention can reduce hospital length of stay by several days and decrease complication rates, translating into meaningful cost savings for healthcare systems.
Optimising nutritional care in complex patients requires a structured and proactive approach. Routine screening, early intervention, multidisciplinary collaboration and clear escalation pathways are all essential components. By embedding these principles into clinical practice, hospitals can improve outcomes for some of their most vulnerable patients.
References available on request
When the Wards Grow Quieter: How CFTR Therapy Is Changing Cystic Fibrosis News
Cystic fibrosis has long occupied a distinct and often emotional space within hospital medicine. For decades, respiratory wards were shaped by repeated admissions, intravenous antibiotics and the steady progression of lung disease in young patients.
Today, that rhythm is changing.
A recent scientific media briefing led by Fredrick Van Goor, Ph.D., Vice President and Head of Cystic Fibrosis Research at Vertex Pharmaceuticals, focused not on a single therapy, but on a broader question: how far has cystic fibrosis research truly come, and what remains unresolved?
For Irish hospital professionals, the impact is no longer theoretical. It is visible in reduced admissions, altered care pathways and changing patient trajectories.
Understanding cystic fibrosis
Cystic fibrosis (CF) is a rare autosomal recessive genetic condition caused by mutations in the CFTR gene. The CFTR protein functions as a chloride channel across multiple organ systems, including the lungs, pancreas and gastrointestinal tract.
When CFTR function is impaired, thick, dehydrated mucus accumulates, leading to chronic lung disease, recurrent infections, pancreatic insufficiency and systemic complications.
Historically, CF was considered a fatal childhood condition. Advances in multidisciplinary care gradually improved survival, but the introduction of CFTR modulators has accelerated this shift. Increasingly, CF is now managed as a chronic adult condition.
From symptom control to molecular correction
The discovery of the CFTR gene in 1989 transformed understanding of the disease, but treatment
remained focused on managing symptoms for many years.
A critical breakthrough came with the realisation that even partial restoration of CFTR function could significantly alter disease progression.
More than 2,000 CFTR variants exist, with over 700 diseasecausing. The most common mutation in Ireland, F508del, results in misfolding of the CFTR protein, preventing it from reaching the cell surface.
Modern therapies target these defects directly. CFTR modulators work by improving protein folding, enhancing trafficking or increasing channel activity, shifting treatment from symptom management to addressing the root cause.
Measuring impact: biomarkers and biology
Sweat chloride testing remains a diagnostic cornerstone and now serves as a key pharmacodynamic marker.
In CF, defective CFTR leads to elevated sweat chloride levels. When modulators restore function, these levels decrease, providing measurable biological evidence of treatment effect.
As patients begin therapy earlier and remain stable longer, researchers are now exploring additional endpoints, including long-term organ preservation and quality-of-life outcomes.
Triple therapy and earlier intervention
Triple combination CFTR modulators represent a major milestone, particularly for patients with at least one F508del mutation.
Clinical development has progressed from adults to paediatric populations, with increasing focus on initiating treatment earlier in life. The rationale is clear: correcting CFTR
dysfunction before irreversible damage occurs may fundamentally change lifetime outcomes.
Changing hospital realities
One of the most tangible shifts for hospital teams has been the reduction in inpatient burden.
Historically, CF care involved frequent hospitalisations for pulmonary exacerbations. With improved baseline lung function and fewer exacerbations in patients receiving modulators, many centres now report fewer admissions and longer intervals between reviews.
For Irish respiratory services under ongoing capacity pressure, even incremental reductions represent a meaningful operational shift.
Ageing with cystic fibrosis
Longer survival brings new challenges.
Adult CF populations are growing, and hospital teams are increasingly managing CF-related diabetes, bone disease, liver complications and reproductive health considerations.
The transition from paediatric to adult care has become a critical point in the patient journey, requiring more structured long-term planning and multidisciplinary coordination.
The human dimension
While clinical outcomes have improved, the psychosocial landscape is also evolving.
As CF shifts from a terminal to a chronic condition, patients face new realities around identity, future planning and long-term expectations. This transformation mirrors broader patterns seen in chronic disease management.
Cystic fibrosis is no longer defined solely by lung function curves, but by education, employment, family life and ageing.
The remaining gap
Despite significant progress, approximately 5% of individuals with CF do not currently benefit from available modulators.
For this group, research is focused on genetic and mRNAbased therapies aimed at restoring CFTR function where protein production is minimal or absent. Challenges remain around
delivery, durability and safety, particularly within lung tissue.
The ambition remains comprehensive: effective treatment across all genotypes.
Infection and stewardship
Chronic infection remains a defining feature of CF.
While modulators reduce exacerbation frequency, issues such as persistent bacterial colonisation, non-tuberculous mycobacterial infections and antimicrobial resistance continue to require careful management.
Antibiotic stewardship remains central to hospital-based CF care, even as treatment paradigms evolve.
Looking ahead
Since the identification of the CFTR gene in 1989, cystic fibrosis research has progressed from gene discovery to targeted molecular therapies, with genetic approaches now on the horizon.
For Irish hospital professionals, the transformation is already visible: fewer admissions, ageing patient populations and evolving service demands.
The landscape has shifted. The story, however, is still being written. CF in Ireland: a shifting profile
Data from the Cystic Fibrosis Registry of Ireland reflects this transformation. More than half of people living with CF in Ireland are now adults, supported by newborn screening, specialist centres and access to CFTR modulators.
This demographic shift places increasing demand on adult respiratory services and highlights the need for long-term, multidisciplinary care models.
Understanding F508del
F508del remains the most common CF-causing mutation in Ireland. It results in misfolding of the CFTR protein, preventing it from reaching the cell surface.
Corrector therapies improve protein folding and trafficking, while potentiators enhance channel function. Given its prevalence, therapies targeting F508del have had significant impact at a population level, particularly in reducing hospital admissions and disease burden.
Cardiovascular
Innovation in Action: Powering Advanced Nursing and Midwifery Introduction
Innovation is not a concept that has evolved with modern technology. From hygiene reform, to clinical academia development to evolution into scientific advancements, Innovation has progressively become woven into the fabric of current healthcare. It is no longer a side project or a luxury for those with resources. Innovation has become essential to ensuring the delivery of safe and effective care in hospitals across the country. As clinicians, with an ever-aging population we feel the increasing demand on already stretched services. Escalating multimorbidity, limited bed availability and increasing waiting lists are creating a critical need for innovative strategies to strengthen patient care.
Yet, the progression of nursing and midwifery through innovation is what is truly reshaping the landscape of acute hospital care in Ireland. The emergence and strengthening of advanced specialist roles in Nursing and Midwifery is not only directly enhancing patient outcomes but is creating a blueprint for others to follow. Over the past decade, Ireland has made it a national priority in implementing Advanced Nurse/Midwife Practitioner (ANMP) roles, transitioning from less than 0.2% of the workforce practising at an advanced level to becoming recognised as a global leader in advanced practice development. This shift has been fuelled by targeted government investment,
Written
by
Anna
Marie Kiernan, RANP in Pain Medicine and a National Nursing & Midwifery Innovation Fellow with the HSE Spark Innovation Programme. Based at Croom Orthopaedic Hospital Limerick.
Anna Marie Kiernan is an RANP in Pain Medicine and a National Nursing & Midwifery Innovation Fellow with the HSE Spark Innovation Programme. Based at Croom Orthopaedic Hospital Limerick, she has led service redesign initiatives that significantly reduced patient wait times. With postgraduate qualifications in Pain Management, Healthcare Innovation, and Service Design, she focuses on sustainable, human-centred care. She has codeveloped extended reality tools for chronic pain self-management in the areas of procedural pain and incidental pain management support. As a national fellow, Anna Marie is focused on developing innovation literacy and skills in healthcare and supporting frontline staff-led innovation.
national reform programmes and policy frameworks, which have streamlined and strengthened the pathway towards advanced practice roles
From caring to creating change
Empowering nurses and midwives to recognise service barriers and develop solutions rooted in day-to-day clinical experience is becoming an essential driver of improvement across the health system. Initiatives such as the HSE Spark Innovation Programme gives frontline workers the confidence, support and the space to question safely and refine ideas that respond directly to the challenges they encounter in acute healthcare. By enabling clinicians to lead in transformative change, the programme helps build a stronger sense of ownership and encourages creative problem-solving to accelerate practical improvements, which benefit both the patient and the organisation.
The growth of advanced practice roles in nursing and midwifery across Ireland reflects a significant shift in how care is delivered. Over two decades ago, nursing was still widely seen as a supportive and largely subordinate profession where nurses and midwives were perceived as assisting doctors rather than autonomous practitioners. The reform of healthcare education had a profound and often underestimated influence on the evolution of nursing and midwifery. Reflecting on this progression, it becomes clear that the shift from apprenticeship-based training to university based and research informed programmes shaped the
progression from roles previously identified as vocational to true professionals. It modernised and reshaped the professional identity and perceived value of the disciplines. It legitimised nursing and midwifery as knowledge-generating disciplines and positioned them as integral leaders in health-system improvement. As postgraduate pathways have expanded, advanced practice roles emerged. Professions supported by robust theoretical foundations and clinical competence frameworks. These roles demonstrate the professions’ capacity for complex decision-making, prescribing, diagnostics and leadership across multidisciplinary teams. With education as the catalyst, nursing and midwifery moved from reactive disciplines to proactive drivers of innovation, patient safety, and service redesign. The use of critical enquiry and evidence-based practice has enabled practitioners to interpret clinical presentations through analytical reasoning rather than anecdotal habit and enabled the thoughtful contribution to diagnostic and therapeutic discussions.
Innovation is not a decoration around advanced practice, it is its backbone. It is the foundation on which the role was developed. Advanced roles require autonomy, streamlined systems and reconfigured pathways that leverage their full scope. Without innovation, advanced practice becomes constrained by legacy systems.
Innovation as the backbone of advanced practice
Across Ireland, the growth of advanced nursing and midwifery
practice has been extraordinary. What was once a small, niche cohort has expanded into a diverse workforce of ANPs across emergency care, rheumatology, respiratory, oncology, cardiology, fracture liaison services and chronic disease management to name but a few. The specialities are endless. This evolution did not happen by chance. It emerged from national policies, structured frameworks and local teams willing to trial new models of care.
The expansion of advanced practice roles represents a transformative innovation within Irish healthcare. Based on the Department of Health’s Final Evaluation Report there has been substantial impact. It has been shown that ANPs reduce specialist waiting lists by 3.9 patients per week, prevent approximately 4.3 hospital admissions weekly and also shorten the emergency care patient experience time by up to 2 hours and 43 minutes. Ninety-five percent of patients reported positive experiences with ANP-led care. The expansion of ANMP roles also facilitates access to diagnostics, prescribing and independent decision-making, which as a result enhances the efficiency in acute hospital pathways.
From a personal reflective standpoint, the integration of advanced practice has demonstrated how innovation is not solely technological but can be based in process, profession and structure. It has reconfigured traditional clinical hierarchies and amplified the leadership capacity of nurses and midwives, which has embedded specialist expertise directly at the point of care. This aligns with international guidance and Ireland’s broader strategic
priorities for integrated and person-centred care.
As Ireland continues to invest in specialist nursing and midwifery roles, sustaining innovation ecosystems that empower frontline professionals remains vital. By harnessing the insight of those who experience service barriers first-hand, the health system ensures that innovation is meaningful, grounded, and impactful which ultimately strengthens0 acute hospital care and advancing the future of the profession.
Innovation creates space for progressive clinical autonomy
When systems continually improve, advanced practice clinician roles evolve and progressively thrive. Within the authors outpatient chronic pain management service, a redesigned triage process and the integration of structured digital assessment has enabled ANP-led review of neuropathic pain presentations. This has supported a continuously improving service model, resulting in shorter waiting times to effective treatment and earlier clinical intervention for patients. Nationally the same pattern is evident:
• Emergency departments have redesigned triage and patient flow models to support Advanced Nurse Practitioners (ANPs) in independently managing minor injury presentations. This approach has contributed to reduced patient length of stay and helped relieve pressure on overcrowded clinical areas, supporting safer and more efficient care delivery.
• Rheumatology and respiratory services have implemented nurse-led biologics review clinics and structured chronic disease management pathways, enabling more efficient use of specialist nursing expertise and releasing consultant capacity to focus on patients with complex care needs.
• Oncology services have implemented Advanced Nurse Practitioner led toxicity management pathways, supporting early identification and intervention for treatment-related side effects and contributing to a reduction in unplanned hospital admissions.
• Late-effects and survivorship clinics led by advanced practitioners provide structured, proactive follow-up for patients living beyond breast cancer,
haematological malignancies and prostate cancer. These clinics support ongoing symptom management, surveillance and timely escalation where needed. It also streamlines long-term follow-up and frees specialist teams to focus on complex care.
Across these examples, innovation has enabled the role rather than other way around. Advanced practice has emerged as a means of bringing structure and safety to previously fragmented or high pressure care environments. The roles often serve as the connective tissue within redesigned pathways. However, the Covid 19 pandemic disrupted and challenged long-established as well as evolving ways of working to expose the limits of traditional, face-to-face models of care. As a response, we saw services rapidly adopt digital and emerging innovative technologies to sustain essential services. Since then, these technologies have evolved beyond being reactive solutions to now becoming strategically embedded to sharpen service delivery.
Research and innovation hubs With the need to translate sitespecific transformative innovation into practice, a new ecosystem of identifying innovation quality through supported design and implementation began to emerge. In response, research and innovation hubs began develop to provide structured environments where clinical challenges could be addressed through collaboration, testing, and evaluation. Partnerships developed between hospitals and universities, such as Trinity’s innovation centre, the Mater Pillar Centre and hospital innovation offices to support the design and pilot of frontline projects.
Research and innovation hubs provide practical spaces where frontline staff can work together with designers to develop and test new ideas grounded in everyday service needs. Through this collaborative approach, digital tools such as oncology toxicity decision-support systems and remote monitoring platforms have been introduced and refined. Other developments include digital pain diaries used ahead of consultation and support on redeveloping human centred design based pathways to care. Collectively, these innovations improve safety and support an individualised approach to care while giving the opportunity for advanced
practitioners to practice at the top of their scope.
Virtual reality innovation extending pain management beyond the acute setting
In several Irish hospitals, virtual reality is being used to support patient care. In the Pain Excellence Centre, Limerick, Virtually Pain Free is an ANP led virtual reality initiative delivering measurable improvements in pain outcomes across acute and community pathways. The ShineVR platform is accessed with phones used via a mobile phone mountable headset, creating the affordable and accessible 360 virtual reality based platform which provided distraction techniques and psychoeducation for pain conditions such as chemotherapy induced peripheral neuropathy. Evaluation of data to date shows that 76% of users experience an improvement across all outcome measures, with average reduction in pain intensity of 19% and pain interference scores of 33%. Success in the field has resulted in diffusion to other areas to reduce anxiety secondary to the environment and from procedures. Innovative digital monitoring supporting earlier intervention in heart failure care
Fluid Heart Tracker, a CE approved app developed by Norma Caples, Registered Advanced Nurse Practitioner in Heart Failure at University Hospital Waterford, is supporting earlier intervention across Irish acute heart failure services. The app automatically identifies clinically significant weight gain (≥2 kg over seven days), a recognised trigger for acute decompensation, addressing a key gap in paper based monitoring where up to 66% of patients have cognitive or numeracy difficulties. Multicentre Irish evaluation across 12 acute hospital sites (n=179) demonstrated improved daily monitoring engagement and earlier help seeking compared with traditional logbooks, a recognised factor in reducing avoidable admissions. The app is now referenced within Ireland’s National Model of Care for Heart Failure, highlighting the impact of ANP led digital innovation on acute service demand.
Strengthening cancer surveillance pathways in acute services through human centred redesign
At the South Infirmary Victoria University Hospital (SIVUH) in Cork, an Advanced Nurse
Practitioner led Head and Neck Oncology service have redesigned cancer surveillance within the acute setting. The ANP independently delivers outpatient surveillance clinics, manages new referrals and assesses patients presenting to ENT casualty with suspected recurrence or treatment-related complications. Service evaluation demonstrated that almost 2,000 patients were managed through ANP-led clinics over a two-year period with high patient satisfaction and timely identification of recurrence and second primary tumours. By shifting routine surveillance and urgent assessment to advanced nursing practice, the service has reduced pressure on consultant-led clinics, improved patient flow and enhanced continuity of care within acute oncology pathways.
Advanced practice emerges from recognising the unmet needs of specific patient cohorts and addressing this through the delivery of responsive services designed to support them. Moving beyond meeting these deficits, advanced practitioners bring an ability to subtly, yet progressively improve care delivered beyond initial design by addressing the needs of service users while being informed by daily clinical realities. When this practitioner insight is combined with empathy and an understanding of the wider system, innovation emerges that balances patient experience, workforce sustainability and organisational needs. In this way, advanced practice enables models of care, which are not only clinically effective but also aligned with the needs of all stakeholders across the health service.
Building Innovation That Lasts: Supporting sustainability
Irish hospitals do not need to start from scratch to support the delivery of meaningful innovation into advanced practice. Well-established national frameworks already provide a strong foundation to the professions that can be adapted locally. Governing bodies such as the Nursing & Midwifery Board of Ireland (NMBI) and the Office of Nursing & Midwifery Services Director (ONMSD) offer guidance and policy, which offers clear pathways for role development, accountability and integration. Sláintecare principles and National Clinical Programme models of care provide a practical blueprint for implementing innovation. This is by setting out clear priorities for integrated, patient-centred
Cardiovascular
and care-closer-to-home service delivery. When used as guidance, these documents help align new initiatives with national policy which ensures innovations are clinically grounded, scalable and embedded within established pathways rather than developed in isolation.
Equally important is the recognition that innovation thrives more through support and engagement than through oversight and governance. While governance does provide safety and structure, progress in innovation is accelerated when staff are enabled and actively involved in shaping
solutions and trusted to implement them. Hospitals that foster interdisciplinary collaboration and clinical champions consistently report stronger momentum and uptake. A supported workforce is an engaged workforce. Engagement drives ownership, creativity and sustainability. By prioritising empowerment alongside governance, organisations can create an environment where advanced practice innovation becomes an integrated part of everyday service improvement rather than an exceptional activity.
From the Frontline to the Future
Innovation in advanced nursing and midwifery practice is no longer emerging in silos within healthcare. It is shaping how care is delivered and progressed. Anything is possible when clinical insight, advanced education and supportive structures align. Advanced practitioners are uniquely positioned to see service gaps early. There is the experience to respond with empathy and design solutions which improve outcomes for patients while strengthening the
wider health service. When these efforts are nurtured through trust and clear national direction then innovation becomes sustainable rather than occasional. As Irish healthcare continues to navigate rising demand and complexity, empowering advanced practice is not simply an investment in roles. It is a means of supporting safer pathways, better experiences and a more adaptable system. The future of healthcare will be built by those closest to care who will be supported to lead meaningful change.
Innovative National Osteoarthritis Pathway
Results from a review of a new osteoarthritis pathway for hip and knee patients shows faster access to care, improved patient outcomes and major cost savings across two pilot sites, transforming how osteoarthritis is treated in Ireland.
The National Osteoarthritis Hip and Knee Pathway was developed by the RCSI HSE National Clinical Programme for Trauma and Orthopaedic Surgery in collaboration with the HSE Modernised Care Pathway Programme.
Between April 2023 and May 2025, more than 2,000 patients were managed through the pathway. 1,059 (51%) were direct
GP referrals, from 67 GP practices participating across the two pilot sites.
58 (5.5%) patients required a specialist outpatient appointment with an orthopaedic surgeon. Each of these appointments were scheduled within 10 weeks of referral in line with Sláintecare targets. Only 25 (2.36%) patients proceeded to a surgical intervention.
1,197 (58%) patients participated in group-based interventions which were facilitated by either a physiotherapist/dietitian or both within 10 weeks of referral. More than 130 group sessions and education classes were delivered in seven community-
based locations across the pilot sites during the project period. Group capacity varied from 10–20 participants depending on available facilities and staffing resources. 23% of patients engaged with the dietitian for advice and support. Over 85% reported a high level of satisfaction with the group interventions. Prior to the introduction of this model, the average time patients were waiting for a first orthopaedic appointment was 16 months at University Hospital Waterford and 27 months at Our Lady’s Hospital, Navan.
Throughout the project, Patient Reported Outcomes Measures were collected and aligned with data collected by the Irish National Orthopaedic Register. Current available data from the two sites demonstrates that when the Oxford hip score/ knee score was used, more than 72% of patients reported positive changes in terms of pain reduction and improved function.
Efficient, patient-centred care
The pathway has also delivered significant financial efficiencies, generating estimated cost savings of ¤220,220 through the avoidance of 1,001 outpatient appointments. The reduction in repeat GP attendances, more efficient use of consultant time, and the ability for physiotherapists and dietitians to work to the top of their scope, further contributed to the project’s success.
Funded through the Department of Health’s Sláintecare Integration Innovation Fund, the pathway was tested between January 2023 and June 2025 at Our Lady’s Hospital, Navan, University Hospital Waterford and within the Community Healthcare Network regions of Carlow, Kilkenny and Meath.
In line with Sláintecare principles, the integrated care pathway focuses on providing the right care in the right place at the right time by the right team. This improves timely access for patients to the most appropriate non-surgical interventions such as physiotherapy and dietetics in a community-based setting. Patients were referred directly from their GP into the pathway as an appropriate alternative to joining an outpatient waiting list. This is the first Irish project that has a dedicated dietitian working with patients with musculoskeletal conditions.
Mr Alan Walsh, Consultant Orthopaedic Surgeon Our Lady’s Hospital, Navan and clinical advisor for the National Clinical Programme for Trauma and Orthopaedic Surgery, added: “The Sláintecare funding has been critical in making this progress possible. It gave us the resources and flexibility to trial a new way of delivering care, one that puts patients at the centre, reduces pressure on hospitals, and makes better use of the wider healthcare team.”
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Allergies
Label, Question, Remove: The International Push to Rethink Penicillin Allergy
Introduction
Approximately 10% of inpatients are labelled as penicillin allergic; however, the vast majority have not experienced a true allergic reaction, but rather another type of adverse drug event. Carrying an inaccurate penicillin allergy label often results in the use of sub optimal alternative antibiotics, which may lead to poorer outcomes for both patients and healthcare systems—for example, increased morbidity, higher healthcare costs, antimicrobial resistant infections, prolonged hospital stays, higher readmission rates, and more frequent critical care admissions. These consequences are largely attributed to the use of broader spectrum non penicillin antibiotics. It is therefore essential to assess whether patients have experienced a true allergic reaction and to remove the penicillin allergy label when appropriate.1
Penicillin allergy de labelling (PADL) is a well established process, widely reported in peer reviewed literature and supported by national and international allergy organisations.1-2 For patients with a history of low risk allergy, supervised direct oral challenge (DOC) allows safe de labelling, and this can be carried out by non allergy specialists. Two studies published in the Journal of Antimicrobial Chemotherapy in 2019 demonstrated that a pharmacist led PADL service in the hospital setting offers a safe and effective method to promote antimicrobial stewardship, ensure appropriate allergy labelling, and reduce the use of broad spectrum antimicrobials.3-4 One study found that 98% of patients who were de labelled experienced no adverse events on subsequent
Biography
Maura Hegarty is an Advanced Specialist Pharmacist in Antimicrobials at Cavan and Monaghan Hospital. She has a strong foundation in clinical pharmacy and works as part of the multidisciplinary antimicrobial stewardship team, providing evidence based guidance on targeted antimicrobial therapy to reduce antimicrobial resistance and support optimal patient care. She also leads key antimicrobial stewardship initiatives within the hospital.
One of the team’s primary areas of focus is penicillin allergy de labelling, an important intervention that promotes safe, accurate allergy documentation and improves antibiotic prescribing practices. Maura serves as the principal investigator for her site in the International Network of Antibiotic Allergy Nations (iNAAN) study—an international clinical research initiative centred on penicillin allergy evaluation and de labelling. This work aims to safely identify individuals who are not truly allergic to penicillin and to remove incorrect allergy labels from their medical records, enabling access to first line beta lactam therapies and supporting global antimicrobial stewardship efforts.
penicillin administration.3 PADL is now recommended as a key antimicrobial stewardship intervention by several international organisations, with multiple guidelines available to support safe implementation.5-9
In Ireland, where access to immunology services is limited, pharmacist led PADL pathways have been established in many sites across the acute sector. The HSE Antimicrobial Resistance and Infection Control (AMRIC) team has further supported primary care by endorsing the internationally validated PEN FAST tool and providing educational materials via www.antibioticprescribing.ie.10
Methods
In 2022, antimicrobial pharmacists introduced a penicillin allergy de labelling service for adults in Cavan and Monaghan Hospital (CMH). This initiative was supported by the antimicrobial stewardship and pharmacy teams, alongside clinicians, nursing staff, and hospital management. Clinical immunology guidance was provided by Dr Niall Conlon, Consultant Clinical Immunologist at St James’s Hospital. The HSE AMRIC team awarded grant funding to support the project.
The Scottish Antimicrobial Prescribing Group (SAPG) penicillin allergy toolkit was adapted to meet local governance requirements.2 Designed for use by non allergy specialists, the toolkit supports identification and removal of penicillin allergy labels in patients without histories suggestive of Type I or Type IV hypersensitivity. Patients with low risk allergy histories were de labelled either through:
• Direct Oral Challenge (DOC): A supervised oral dose of a penicillin (usually amoxicillin), suitable for patients with non severe skin reactions occurring more than 10 years previously
or historical reactions with no severe features such as hospitalisation, adrenaline use, blistering, or desquamation.
• Direct De label (DDL): Used for intolerance symptoms (e.g., nausea, vomiting), as well as cases where patients had subsequently tolerated penicillin, provided their history met low risk criteria.
The toolkit includes a protocol, a risk assessment algorithm, standard procedures for DOC, patient information leaflets, consent forms, post test advice sheets (for positive or negative outcomes), guidance on managing allergic responses, clinician FAQs, and template letters for communication with general practitioners and community pharmacists.2
Findings
Antimicrobial pharmacists maintained a password protected database of patients reviewed between 18 October 2022 and 6 March 2026.
• 131 patients were screened.
• 83 were eligible for de labelling.
• 77 were successfully de labelled.
• 27 underwent DOC, with no adverse drug events observed.
• 50 were de labelled via DDL, as their histories suggested no greater likelihood of penicillin allergy than the general population.
iNAAN Study
Beaumont Hospital; Cavan and Monaghan Hospital; Connolly Hospital; and Our Lady of Lourdes Hospital in the Dublin North East Hospital Group are now building on this work by participating in the International Network of Antibiotic Allergy Nations (iNAAN) study. This major international research initiative, embedded within Australia’s National Antibiotic Allergy Network (NAAN), focuses on penicillin allergy evaluation and de labelling.11 Dr Fionnuala Cox, Consultant Immunologist at Beaumont Hospital, serves as Chief Investigator for the Irish sites.
iNAAN study aims
• To assess the safety and effectiveness of direct oral penicillin challenge in labelled patients.
• To evaluate implementation and sustainability of multidisciplinary PADL programmes.
• To generate evidence to inform antimicrobial stewardship policy and improve antibiotic prescribing globally.
This is a type 2 hybrid effectiveness implementation multicentre study, examining both the clinical performance of DOC and its real world implementation using a digital penicillin allergy assessment toolkit within a smartphone application.
Participating health systems include Australia, the UK, South Africa, Malaysia, Hong Kong, Canada, the USA, and New Zealand. The aforementioned Irish hospitals will be the first national participants.
Preliminary results from 9 November 2022 to 7 June 2024 demonstrate:
• 97% negative DOCs (successful de labelling).
• No serious adverse events
• 1,603 assessments and 545 DOCs across 29 Australian and 3 international health services.
• Extensive multidisciplinary involvement from physicians, pharmacists, and nurses. 11
Alignment with National and International Goals
PADL programmes delivered through the iNAAN network align with Ireland’s third One Health National Action Plan on Antimicrobial Resistance 2026–2030 (iNAP3) by:
1. Enhancing appropriate antibiotic use through correction of inaccurate allergy labels and increased use of first line penicillin’s.
2. Advancing research and innovation via multicentre
evaluation of PADL implementation.
3. Promoting awareness and behaviour change among clinicians and patients.12
These initiatives also support the WHO AWaRe antimicrobial stewardship framework, reaffirmed during the 2024 UN General Assembly High Level Meeting on AMR.13 Removing inaccurate penicillin allergy labels reduces inappropriate use of Watch and Reserve antibiotics and supports increased use of Access antibiotics.
Conclusion
The pharmacist led penicillin allergy de labelling service at our hospital demonstrates that structured allergy assessment can be safely integrated into routine antimicrobial stewardship practice. Our findings indicate that
New Health Equity Research Alliance
A new Health Equity Research Alliance (HERA) has been launched by RCSI, uniting researchers, international experts and people with lived experiences in advancing equity-informed and inclusive health research.
The launch, which took place on 26 February, marks a significant step in strengthening collaboration to tackle the structural barriers to equitable health research and, in turn, reduce unfair health inequalities. Health equity is becoming a defining priority for the future of health research, driving efforts to confront historical exclusion and create more inclusive and representative evidence. According to HERA member Dr Olga Cleary, Cameron Lecturer at RCSI: “We know that health outcomes are not the same for everyone, and many population groups remain under-represented in research. When people are overlooked, the evidence we rely on can miss what matters most in their lives. The launch of HERA is about changing this – embedding inclusion into how research is designed and carried out so it better reflects people’s lived realities and helps improve health for all.”
Professor Edward Gregg, Head of RCSI’s School of Population Health, formally launched the Alliance and underscored its importance: “The launch of the Health Equity Alliance is an initiative I am proud to be a part of.
It showcases HERA’s commitment to creating health research that aims to uncover and understand the systemic inequalities in population health and prioritise the approaches to reduce them. I am excited about what this initiative can do over the coming months, enhancing not only RCSI’s research ethos but also health equity across Ireland.”
The launch event featured a masterclass opened with international health equity leader Mr Jordi Pardo Pardo, who spoke on practical approaches to operationalising equity in health research and the challenges of implementation. He was followed by Mr Omar Dewidar, GRADE-Equity Coordination Lead with the Campbell and Cochrane Equity Methods Group at the University of Ottawa, who discussed how STROBE-Equity strengthens the standardised reporting of observational studies in epidemiology. The masterclass concluded with a presentation from Ms Liz Hughes, Head of Equality, Diversity and Inclusion at RCSI.
Closing the day, a panel discussion examined what Ireland needs to prioritise to enable equitable health research. It was chaired by HERA member, Dr Eunice Phillip, Global Health Researcher in the RCSI School of Population Health, who is contributing to health equity in Ireland and internationally as an expert in participatory research approaches.
multidisciplinary PADL can reliably identify and remove inaccurate penicillin allergy labels, facilitating first line antibiotic use and improving prescribing practices. However, limited staffing resources and constraints in information technology infrastructure remain barriers to broader implementation. Addressing these challenges will be essential for sustainable integration of allergy assessment into routine care.
Participation in the international iNAAN collaboration offers an opportunity to contribute to a growing evidence base evaluating PADL safety, effectiveness, and implementation across diverse healthcare settings. Such programmes represent a pragmatic and impactful strategy to optimise antibiotic use and advance global antimicrobial stewardship priorities. References available on request
Professor Edward Gregg, Head of School of Population Health,
The panel of speakers included Christopher Carroll from the HSE, Greg Straton from the Department of Health and Siobhan Gaffney, a patient and public involvement (PPI) representative who is working with the Converge Research Centre at RCSI.
According to Siobhan Gaffney: “Patient and public involvement in research has come a long way, but to make sure research delivers real impact for everyone, we need to view research through an equity lens. So-called ‘hardto-reach’ groups are not hard to
Group, Toronto
find, too often our systems have not spoken to them in ways that resonate, or listened when they share their experiences.”
HERA’s launch marks a commitment to enhancing health equity, coinciding with other initiatives prioritising health equity at a national level to create a more inclusive knowledge base. HERA emphasises that this vision can only be achieved collectively to create the platform where our work, practice, and policies embed and address unfair health gaps.
Pictured at the launch of the Health Equity Research Alliance at RCSI (l-r):
RCSI; members of the HERA steering committee Dr Siobhán McCarthy, Dr Samira Jabakhanji, Dr Eunice Phillip, Dr Olga Cleary, and Dr Jennifer Pallin; together with Jordi Pardo Pardo, Senior Advisor, Cochrane Health Equity Thematic
Vaccination in Adults: Optimising Hospital Programmes
Vaccination is one of the most effective public health interventions, yet adult immunisation remains an underutilised strategy within hospital settings. While paediatric vaccination programmes are well established and widely implemented, adult vaccination pathways are often fragmented, opportunistic and inconsistently applied. This gap represents a missed opportunity to prevent serious illness, reduce hospital admissions and protect vulnerable patient populations.
In Ireland, the importance of vaccination has been underscored by recent public health challenges, including the COVID-19 pandemic and ongoing concerns around seasonal influenza and pneumococcal disease. Despite this, adult vaccination uptake remains suboptimal across several key groups, including older adults, individuals with chronic
conditions and those who are immunocompromised.
Hospitals play a critical role in addressing this gap. As points of contact for high-risk patients, they are uniquely positioned to identify individuals who would benefit from vaccination and to deliver immunisation in a timely and structured manner. Optimising hospital-based vaccination programmes is therefore a key component of improving population health outcomes.
Adult vaccination encompasses a broad range of vaccines, including influenza, pneumococcal, COVID-19, shingles (herpes zoster), pertussis and, in certain cases, hepatitis and HPV. The National Immunisation Advisory Committee (NIAC) provides guidance on vaccine recommendations in Ireland, identifying priority groups and outlining best practice
In collaboration with Professor Karina Butler, Chair of National Immunisation Advisory Committee (NIAC)
BIO: Prof Karina Butler is UCD Clinical Professor of Paediatrics, Consultant Paediatrician and Infectious Diseases Specialist at Our Lady's Children's Hospital Crumlin and Temple Street Children's University Hospital. She is a member of the national tuberculosis and scientific advisory committees of the Health Protection Surveillance Centre and a steering committee member of the Paediatric European Network for Treatment of AIDS and Infectious Diseases (PENTA-ID). Her clinical research has focussed on prevention and management of HIV infection in children and adolescents. As Chair of the National Immunisation Advisory Committee she is committed to the prevention of infectious diseases using safe and effective vaccines, thus protecting the health of our population.
part of patient evaluation, clinicians can identify gaps in immunisation and act accordingly.
Standing orders and protocoldriven approaches have been shown to significantly improve vaccination rates in hospital settings. These allow appropriately trained healthcare professionals, including nurses and pharmacists, to assess eligibility and administer vaccines without requiring individual physician orders for each patient. Such models not only streamline delivery but also reduce the burden on medical staff.
Multidisciplinary collaboration is central to the success of hospital vaccination programmes. Pharmacists, in particular, play an increasingly important role in medication management and patient education, and are well positioned to support vaccination efforts. Nursing staff are often the primary point of patient contact and can facilitate both assessment and administration. Engaging the entire healthcare team ensures that vaccination is seen as a shared responsibility rather than an isolated task.
for implementation. However, translating these recommendations into routine hospital practice remains a challenge.
One of the primary barriers to effective adult vaccination in hospitals is the lack of systematic processes. Vaccination status is not always routinely assessed on admission, and opportunities to vaccinate during inpatient stays are frequently missed. This is particularly relevant for patients admitted with conditions that increase their risk of vaccinepreventable disease, such as chronic respiratory illness, cardiovascular disease or diabetes. Integrating vaccination assessment into standard clinical workflows is a critical first step. This may involve incorporating vaccination status into admission documentation, electronic health records or nursing assessments. By making vaccination a routine
Patient education is another key component. Vaccine hesitancy remains a significant barrier, even within hospital settings. Patients may have concerns regarding safety, efficacy or side effects, often influenced by misinformation or previous experiences. Clear, evidencebased communication from trusted healthcare professionals is essential in addressing these concerns and supporting informed decision-making.
Hospitalisation represents a unique window of opportunity to engage patients in discussions about vaccination. During this time, patients may be more receptive to health interventions and more aware of their vulnerability to illness. Leveraging this moment can improve uptake and reinforce the importance of preventive care.
Targeting high-risk groups is particularly important in adult vaccination strategies. Older adults, especially those over 65, are at increased risk of complications from influenza and pneumococcal disease. Individuals with chronic conditions, including respiratory disease, cardiovascular disease and diabetes, also face higher
risks. Immunocompromised patients, whether due to underlying conditions or immunosuppressive therapies, require tailored vaccination approaches.
The introduction of newer vaccines, such as recombinant zoster vaccine for shingles prevention, has expanded the scope of adult immunisation. Ensuring that clinicians are aware of these developments and understand their role in prevention is essential. Ongoing education and access to updated guidelines support this process.
From a systems perspective, data collection and monitoring are essential for evaluating the effectiveness of vaccination programmes. Electronic health records can facilitate tracking of vaccination status, identification of eligible patients and measurement of uptake rates. In Ireland, improving data integration across primary and secondary care remains a priority, as fragmented systems can hinder continuity of care.
Discharge planning provides another opportunity to reinforce vaccination strategies. For patients who are not vaccinated
during their hospital stay, clear communication with primary care providers is essential. Including vaccination recommendations in discharge summaries ensures that follow-up can occur in the community setting.
The COVID-19 pandemic demonstrated the capacity of the Irish healthcare system to deliver large-scale vaccination programmes when required. Lessons learned from this experience, including the importance of coordination, communication and accessibility, can be applied to broader adult vaccination efforts within hospitals.
Healthcare worker vaccination is also a critical component of hospital-based programmes. Ensuring high uptake among staff not only protects healthcare workers but also reduces the risk of transmission to vulnerable patients. Hospitals must therefore prioritise staff education, accessibility of vaccines and supportive workplace policies.
Barriers to implementation must be acknowledged and addressed. These include resource constraints, competing clinical priorities and logistical challenges
related to vaccine storage and administration. However, the long-term benefits of improved vaccination uptake, including reduced hospital admissions and improved patient outcomes, justify investment in these programmes.
From a public health perspective, strengthening adult vaccination programmes aligns with broader goals of disease prevention and healthcare sustainability. By reducing the incidence of vaccinepreventable diseases, hospitals can alleviate pressure on acute services and contribute to more efficient use of resources.
Optimising hospital vaccination programmes requires a shift from opportunistic to systematic approaches. This involves embedding vaccination into routine care, leveraging multidisciplinary teams and utilising data to inform practice. It also requires a cultural shift, recognising vaccination as a fundamental component of adult healthcare rather than an optional add-on.
As Ireland continues to navigate evolving public health challenges, the importance of adult vaccination will only increase. Hospitals, as central pillars of the healthcare
system, have a critical role to play in this effort. By strengthening vaccination programmes within hospital settings, clinicians can protect vulnerable populations, improve patient outcomes and contribute to the overall resilience of the healthcare system.
References
1. National Immunisation Advisory Committee (NIAC), Ireland –Immunisation Guidelines.
2. Health Service Executive (HSE) National Immunisation Office.
3. World Health Organization. Vaccines and immunisation overview.
4. European Centre for Disease Prevention and Control (ECDC) –Adult Immunisation Strategies.
7. CDC Adult Immunization Schedule (for comparative best practice).
8. MacDougall DM et al. Hospitalbased vaccination programmes: impact and implementation.
Vaccines
Shingles Vaccination: A Missed Opportunity in Preventative Care?
Shingles is a viral infection caused by the reactivation of the varicella-zoster virus—the same virus responsible for the common childhood illness, chickenpox. Following initial infection, the virus does not leave the body but instead remains dormant in nerve cells, often for decades.
As individuals age or experience a weakening of the immune system, the virus can reactivate. When this occurs, it travels along nerve pathways to the skin, producing the characteristic blistering rash typically seen on one side of the body or face. This process is often accompanied by intense pain, which can persist even after the visible rash has resolved. In some cases, this leads to postherpetic neuralgia, a debilitating condition that can significantly impact quality of life. A vaccine for shingles has been available for approximately 20 years, with a newer, more effective version introduced in 2017. This updated vaccine offers around 90% protection against infection and represents a major advancement in the prevention of shingles and its complications. While the primary aim of vaccination is to prevent shingles itself, emerging research suggests that its benefits may extend beyond this. A recent large-scale study in Wales, which compared vaccinated and unvaccinated older adults, found that those who received the shingles
vaccine had a 20% lower risk of developing dementia. This may be linked to the role of the varicella-zoster virus in triggering chronic inflammation in the brain, which has been associated with neurodegenerative processes.
In addition, research from Korea has indicated a 26% reduction in cardiovascular events among individuals who had been vaccinated against shingles. This may be explained by the fact that shingles infection can contribute to blood vessel damage, inflammation, and clot formation— factors known to increase the risk of heart disease. By preventing infection, vaccination may therefore help reduce these downstream risks.
The Role of Pharmacy in Vaccine Delivery
Community pharmacy has played an increasingly important role in vaccine delivery in Ireland over the past decade. Pharmacists first became involved in national vaccination efforts in 2011 with the rollout of the influenza vaccine. Their role expanded significantly during the Covid-19 pandemic, when pharmacy teams were instrumental in delivering vaccines at scale across the country.
Pharmacies are deeply embedded within communities and have established, trusted relationships with patients—particularly older adults, who are most at risk from shingles. This accessibility and trust
Written by Professor Christine Loscher, Head of School and Full Professor of Immunology, School of Biotechnology, Dublin City University
The Case for Prevention
The growing body of evidence linking shingles vaccination to reduced risks of dementia and cardiovascular disease adds further weight to the case for wider access. These findings suggest that the benefits of vaccination extend beyond infection control and into broader areas of public health.
Preventative medicine offers significant long-term value, both in improving patient outcomes and reducing pressure on healthcare systems. However, it is not always prioritised in funding decisions.
are key reasons why pharmacyled vaccination programmes have proven so effective.
Given this track record, community pharmacy is well positioned to support the delivery of a national shingles vaccination programme, should one be introduced. Pharmacists have the clinical expertise, infrastructure, and patient engagement necessary to improve access and uptake.
Access and
Affordability:
A Key Barrier
Despite the availability of an effective vaccine, access remains a significant challenge in Ireland.
The National Immunisation Advisory Committee (NIAC) has approved the shingles vaccine for use in Ireland. However, it has not yet been prioritised for inclusion in a publicly funded national programme. As a result, the vaccine is currently only available on a private basis, at a cost of approximately ¤500 for the required two-dose course.
For many patients—particularly older adults—this cost represents a substantial barrier. The consequence is that a highly effective preventative intervention remains out of reach for a large proportion of the population.
This situation is in stark contrast to other countries. The shingles vaccine is available free of charge in several healthcare systems, including those in the UK, the United States, Canada, Australia, and a number of European countries. These programmes recognise not only the direct benefits of preventing shingles, but also the wider health and economic benefits associated with reducing complications and hospitalisations.
Ireland has a strong and successful childhood vaccination programme, but adult vaccination remains more limited. Vaccines such as influenza and shingles are often not publicly funded, leaving patients to bear the cost themselves. This has a direct impact on uptake, particularly among those who may benefit most.
Lower uptake not only increases the burden of disease but also contributes to seasonal pressures on healthcare services, as seen each winter with influenza.
Looking Ahead
The current situation presents a clear opportunity for policy reconsideration. The availability of an effective shingles vaccine, combined with emerging evidence of wider health benefits, strengthens the argument for its inclusion in a national vaccination programme.
Community pharmacy stands ready to support such an initiative. With its accessibility, trusted relationships, and proven track record in vaccine delivery, pharmacy could play a central role in improving uptake and ensuring equitable access.
Ultimately, the question is not whether the shingles vaccine works—it does—but whether it should be made more widely available to those who need it most.
As the focus of healthcare increasingly shifts towards prevention, ensuring access to effective vaccines such as this will be critical in improving long-term health outcomes for the population.
The Irish Pharmacy
Awards 2026
One Profession. One Celebration. The Irish Pharmacy Awards 2026
The Irish Pharmacy Awards 2026 – Now Open for Entries, with Dedicated Hospital Pharmacy Categories
As Ireland’s leading pharmacy publications, Irish Pharmacy News and Hospital Professional News are proud to officially launch the Irish Pharmacy Awards 2026 — the most prestigious and anticipated celebration of pharmacy excellence across the entire profession.
For the first time, the Awards will expand to fully reflect the evolving pharmacy landscape, with the introduction of dedicated hospital pharmacy categories recognising the vital contribution of hospital pharmacists, technicians and multidisciplinary teams. This marks an important step in ensuring that excellence across all areas of pharmacy practice is acknowledged and celebrated at a national level.
Each year, the Awards shine a spotlight on the individuals and teams who deliver exceptional care and drive continuous improvement within healthcare. Within hospital pharmacy, this excellence is seen through clinical leadership, medicines optimisation, patient safety initiatives, research, innovation and the critical role pharmacists and technicians play within multidisciplinary teams. In an increasingly complex healthcare environment, hospital pharmacy continues to demonstrate its value at every stage of the patient journey.
The Irish Pharmacy Awards are more than a ceremony — they are a national platform for recognition, collaboration and professional pride. They celebrate
those who are advancing clinical practice, improving patient outcomes and contributing to the delivery of safe, effective and innovative healthcare services across Ireland.
In 2026, the Awards will once again bring together over 650 pharmacy professionals from across community, hospital and industry settings for an evening of celebration, networking and industry recognition at the Clayton Hotel, Burlington Road, Dublin on Saturday 6th June 2026.
Entries are now officially open across all categories, including the newly introduced hospital pharmacy awards:
• Medisource Hospital Pharmacy Technician of the Year
• Hospital Pharmacist of the Year
• Hospital Pharmacy Team of the Year
Alongside a wide range of established categories recognising excellence across the wider pharmacy profession.
Whether you are recognising an outstanding colleague, celebrating the achievements of your department, or showcasing innovation within hospital pharmacy practice, the Irish Pharmacy Awards provide a unique opportunity to highlight excellence, share best practice and inspire the profession nationwide.
We look forward to receiving your entries and to celebrating with you in June 2026.
Medisource Hospital Pharmacy Technician of the Year 2026
Hospital Pharmacy Technicians are playing an increasingly vital role within modern healthcare. As pharmacists spend more time delivering direct patient care, leading clinical services and engaging with multidisciplinary teams, pharmacy technicians provide the operational, technical and professional backbone that ensures safe, efficient and high-quality medicines management within the hospital setting.
The evolving focus of hospital pharmacy — from traditional dispensing functions towards enhanced clinical service provision — has placed greater emphasis on teamwork, adaptability and innovation. Hospital Pharmacy Technicians exemplify this collaborative spirit in their daily practice, supporting patient safety, workflow optimisation and service delivery while contributing meaningfully to the wider objectives of the department.
This Award recognises the outstanding contribution of an individual Hospital Pharmacy Technician who has demonstrated leadership, professionalism and a commitment to advancing the technician role. The recipient will embody excellence in practice, promote the value of the technician profession within hospital pharmacy, and act as a role model for colleagues across the sector.
Judges will be seeking evidence of forward-thinking practice, innovation, and a clear commitment to raising standards within hospital pharmacy. The successful entrant’s achievements should inspire peers, support the development of innovative practice, and reflect the professionalism and dedication that define the hospital pharmacy technician profession.
How to Enter:
The judges will be looking for a Hospital Pharmacy Technician who can clearly demonstrate their impact on patient care, their contribution to service development, and their commitment to advancing the technician role within hospital pharmacy. Evidence of leadership, innovation and professionalism will be key, alongside examples of how the entrant has championed excellence and inspired colleagues through their work.
Judges will be looking for:
1. How their work has delivered measurable benefits to patients and/or colleagues, contributing to safer, more efficient or improved pharmacy services.
2. Evidence of promoting and advancing the role of the Hospital Pharmacy Technician within their organisation and the wider profession.
3. Examples of projects, initiatives or service developments that demonstrate excellence in quality, innovation, productivity or prevention.
4. A clear display of the values, teamwork and professional principles underpinning their success, including mentoring, training or supporting colleagues.
Applications Close - Friday, April 27th, 2026 Send your entries to - kelly-jo@ipn.ie Download application forms from: https://irishpharmacyawards.ie/
Pharmasource Hospital Pharmacist of the Year 2026
The Pharmasource Hospital Pharmacist of the Year Honour recognises a hospital pharmacist who demonstrates leadership and exemplifies the evolution of the pharmacy profession towards an expanded role in healthcare.
The winner will demonstrate significant contributions to the pharmacy industry overall resulting in meaningful improvements in the quality of patient care and improved delivery models as well as the role of pharmacy in the healthcare team.
Who Can Enter:
This category is open to all hospital pharmacists working within the hospital sector in Ireland. Applications can be through nominating an individual or yourself.
Each submission will be judged by an independent judging panel. There will be no personnel from any of the sponsoring companies or IPN Communications LTD on the judging panel. Short-listed finalists will be invited to the Irish Pharmacy Awards at the Clayton Hotel (Burlington) on Saturday, June 6th, 2026.
Entries can be submitted by post or email. All entries will be handled in the strictest confidence and will not be made available to any party not involved with judging the Awards. If your entry is shortlisted, the organisers may wish to reproduce a summary of your entry, photographs and any other supporting materials in the finalists’ booklet or within other materials they produce to promote the awards including all press materials.
Judges will be looking for:
1. Evidence of long-term, consistent dedication and outstanding achievements that have led to the advancement of the profession of pharmacy and public health.
2. Evidence of a large variety of skills, attributes and accomplishments.
3. Evidence of an individual strong in character, cumulative professional accomplishments and the ability to properly represent and model what pharmacy as a profession encompasses.
4. Evidence of an understanding of the goals of pharmacy and significantly contributing to how these goals may be achieved.
Hospital Pharmacy Team of the Year 2026
There are many key elements to building a productive team including communication and co-operation. Good communication means everyone is aware of their own responsibilities and what the team’s goals are whilst cooperation leads to increased productivity.
A team which excels is the one who work together to improve their efforts. They comprehend the importance of ongoing improvements and how this helps to support the overall objectives of the department.
This Award is open to any hospital pharmacy team with a minimum of three team members.
Who Can Enter:
This category is open to all pharmacy teams working within any hospital in Ireland. Applications can be through nominating an individual or yourself. Each submission will be judged by an independent judging panel. There will be no personnel from any of the sponsoring companies or IPN Communications LTD on the judging panel. Short-listed finalists will be invited to the Irish Pharmacy Awards at the Clayton Hotel (Burlington) Dublin on Saturday, June 6th, 2026.
Entries can be submitted by post or email. All entries will be handled in the strictest confidence and will not be made available to any party not involved with judging the Honours. If your entry is shortlisted, the organisers may wish to reproduce a summary of your entry, photographs and any other supporting materials in the finalists’ booklet or within other materials they produce to promote the awards including all press materials.
Judges will be looking for:
1. Effective communication skills with both staff and patients.
2. Demonstration of a commitment to mentoring or other leadership activities.
3. Operation within their own pharmacy liaising with key staff members and management and developing key communication skills.
4. A dedication and commitment to furthering the profession into the future.
Applications Close - Friday, April 27th, 2026 Send your entries to - kelly-jo@ipn.ie
Download application forms from: https://irishpharmacyawards.ie/
IPSON annual conference 19th & 20th March 2026
Written by Aoife Mc Namara, IPSON President
PsychoSocial cancer care is unique in that every professional working in cancer care provides psychosocial care to cancer patients in their daily practice. Every meaningful interaction with patients involves identifying or addressing one or some of their psychosocial needs. If you are a professional working with cancer patients, IPSON is for you.
given to Noreena Coyle from DCU on her poster titled ‘A systematic Review of Unmet Supportive Care Needs, Barriers, and Facilitators for People with Physical Disabilities and Cancer’. Laura Curran from Maynooth University was also commended for her poster titled ‘A Systematic Review of The Impact of Premature and Early Menopause Resulting from Cancer Treatment on Psychological Wellbeing’.
First prize was awarded to Dr Sonya Collier, SJUH/TCD for her poster titled ‘Emotional prehabilitation for patients and family members facing haematopoietic stem cell transplant – a feasibility and acceptability study’.
Congratulations to all the winners.
The 3rd annual IPSON conference was held in the National College of Ireland, Dublin 1 on Thursday 19th March and Friday 20th March 2026. The Irish PsychoSocial Oncology Network (IPSON) is an interdisciplinary organisation that represents professionals working in cancer care. This includes professionals working in clinical settings, community centres, academia, research, primary care, palliative care and public policy. Our mission is to promote and advocate for psychosocial excellence in cancer care in Ireland. We do this through supporting a thriving community of psychosocial oncology professionals who collaborate on clinical practice, education, policy, advocacy, and research. Our annual conference is an excellent opportunity to share knowledge and foster collaboration within the community.
A model of care for Psycho-Oncology, Ireland (2020) states that ‘Cancer and its treatment have the potential to significantly impact on mental health, physical health and socioeconomic status in multiple ways. Most people will use a variety of resources to cope including their own emotional resources, often accessing the advice of healthcare professionals and other support systems such as family, friends, and community cancer support centres’.
The theme of the conference was ‘Stories that shape us: bridging science and humanity in psychosocial oncology’ and included keynote talks, panel discussions, academic poster viewing sessions and networking. Keynote speakers included Dearbhaile O’Hare and Laura Foran. Dearbhaile is a breast cancer survivor and advocate. She delivered an incredibly engaging presentation on her diagnosis and experience of cancer treatment. Her poetry was interspersed throughout her story. Dearbhaile’s book ‘Things went t*ts up’ is available at www. thingswenttitsup.ie Laura Foran is a social worker and manager of the CALM (Cancer and Living Meaningfully) National Program in Ontario, Canada. Laura highlighted gaps in care in clinical settings where very little time and space are available to patients to process their feelings. The CALM program is designed to address this gap, focusing on four domains, symptom management and communication with healthcare professionals, self-concept, identity and relationships, spirituality and sense of meaning and thoughts, fears and hopes about mortality. In addition to an excellent conference presentation, Laura delivered a post-conference workshop on CALM on Friday 20th March where we had the opportunity to delve into the program design in detail.
The second workshop on Friday was from Anna Nissyraiou and Maria Vsilopoulou from the Centre for Research and Technology Hellas, Greece. This workshop explored the concept of post traumatic growth, examining how growth-related processes might emerge alongside distress, uncertainty and ongoing treat in psychotherapy and how this can be recognised and supported. The interactive element of the workshop sparked lots of thoughtful discussion. This is just a snapshot of our conference, the full agenda can be found on www.ipson.ie.
It is important to us in IPSON to recognise the calibre of our colleagues here in Ireland and our conference gives us an opportunity to do just that. Our poster competition was of a very high standard this year, showcasing research from around the country. Commendations were
Another popular feature of the IPSON conferences has been the awards. These awards are an important recognition of the work done by our colleagues in psychosocial care.
Congratulations to all the 2025 award winners:
Outstanding Clinical Care Award: Dr Chiara Besani
Outstanding Clinical Care Award: Dr Nicola Elmer
Outstanding Research Award –Student/Trainee: Ms Avril Deegan
Outstanding Service Award: Ms Tracy McDaid
Outstanding Service Award: Mr Martin Sweeney
IPSON cannot grow without the support of our members. To join and benefit from our upcoming webinars, newsletters and more, please register at: www.ipson.ie/membership
IPSON executive committee
HSE West and North West Conference
How healthcare can positively impact climate and sustainability
The impact of healthcare on our climate and how to make improvements formed the basis of the HSE West and North West climate and sustainability conference in Sligo recently.
Initiatives such as turning clinical waste into reusable needle bins, auditing inhaler use to reduce CO2 emissions and turning Emergency Departments Green were just some of the topics touched on by the speakers.
Tony Canavan, REO HSE West and North West said “Climate change is a health issue and it’s important that the HSE makes that connection. I’d like to thank the people who will pick up the baton and carry it and pass it on within our health services. I’m pleased that this region is showing leadership in relation to climate change and by showing leadership we are encouraging others to join us.”
John Fitzmaurice, HSE Integrated Healthcare Area Manager, Sligo. Leitrim, South Donegal, West Cavan said “We all need to ask ourselves the question, is there one thing I can do? Simple interventions can have big results. We are working on our Regional Green Plan which will outline a structured approach to reducing our Greenhouse Gas (GHG) emissions, along with our planned actions over the next three years (covering the 2026 to 2029 period). This three-year horizon is designed to strike a balance between delivering immediate reductions in some areas while building longterm capabilities in others.”
Public Health Specialist working with Trinity College Dublin and the HSE, Dr. Teresa O’Dowd,
discussed how reducing the carbon footprint of inhaler prescribing is an important step in tackling healthcare’s contribution to climate change. Educational interventions were used to switch patients from high carbon to low carbon inhalers resulting in estimated carbon saving of 21,448kg of CO2
Professor Francis Finnucane, Consultant Endocrinologist at Galway University Hospitals, discussed the obesity crises and environmental links. He said that the change in our food environment has changed eating patterns and the use of pesticides are damaging our environment. A solution to some of these issues, he recommended, is the adoption of a plant-based diet, the improvement public transport and the development of more greenways.
Programme Manager for the HSE Climate Action and Sustainability Programme, Roisin Breen, discussed the HSE’s Green Plan which aims to deliver measurable carbon reduction, improve resilience, and embed sustainability into regional healthcare while her colleague Niall Walsh, Project Manager with the HSE Climate and Sustainability Programme said the focus of 2026 was the establishment of national forums to keep the climate conversation going.
Dr Niall McCormick, Core Speciality Trainee in Emergency Medicine, spoke about ED’s at GUH and MUH receiving Bronze accreditation for Green ED’s from the Royal College of Emergency Medicine. Some of their changes mean they now use 100% recycled paper, climate health
communications provided to staff and patients, waste streams are reviewed and initiatives to improve segregation have started. He also discussed how on-site energy consumption has been reduced and they have eliminated unnecessary canulation.
Fiona Dowling, Commercial Director with Stericycle, described how they supply reusable sharps containers across 65 public and private hospitals in Ireland. These reusable containers, which themselves are made from recycled waste can be reused 600 times after washing and decontamination.
Ailbhe Healy, Water Stewardship Advisor discussed the Water Stewardship Programme which promotes the use of water as it is socially and culturally equitable, environmentally sustainable and economically beneficial. This she said is achieved through a stakeholder-inclusive process that includes both site and catchmentbased actions.
HSE West and North West Green Committee- Organisers of the Conference L-R- Kevin Fitzmaurice, Martin Casserly, John Nally, Tracy Shannon, Siobhan Patten, Paul McGinley, Dean Flynn, John Fitzmaurice, Nadine Dabbagh, Peter Keane, Pauline Conroy, Michael O’Brien, Catherine Flynn and Marion Gady
Declan McGoldrick, HSE Capital and Estates Energy Manager, outlined the HSE’s Deep Retrofit Programme to refurbish and upgrade HSE accommodation. Finally Dr Annmarie Crosse, Sláintecare Healthy Communities Coordinator, discussed placing communities at the centre of integrated climate and health action in Donegal. She outlined the importance of nature and health connections as ecological determinants within local healthy community plans.
Tony Canvan, REO HSE West and North West- Tony Canvan, REO HSE West and North West speaking at the HSE West and North West Climate and Sustainability Conference
affected by asthma in Ireland. Previous estimates grossly under-estimated the number of people with asthma in Ireland. The annual economic burden of asthma is a staggering €472million. 2017 saw 2.4 million GP and 625,000 practice nurse asthma consultations respectively, 421,000 specialist visits, 133,000 emergency department visits and 8,000 hospital admissions. There was one attendance at emergency departments every 4 minutes by a person with asthma.
Asthma Management in Adults and Young People
The exact cause of asthma remains unknown. However, risk factors such as smoking, obesity, family history and atopy all increase the risk of developing asthma (Shamanthi et al, 2025). There are numerous triggers which can cause symptoms and these differ from person to person (Figure 1).
Asthma is a heterogeneous disease, usually characterised by chronic airway inflammation defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation (GINA, 2025).
Wintertime can be particularly challenging for people with asthma due to cold air and common viruses being common triggers. As Spring emerges, this can also be a challenging time as various tree pollen levels start to increase. Some people with asthma may need to increase their controller medication over the winter months to help manage their symptoms.
Symptoms
The clinical features of asthma (wheeze, cough, shortness of breath and chest tightness) result from changes in the airways as a result of abnormal sensitivity called bronchial hyperreactivity. The muscle of the bronchial walls becomes hypertrophied causing occlusion of the airway resulting in contraction of the muscle causing bronchospasm. Secondly, in the mucosal, submucosa and smooth muscle layers of the bronchi and bronchioles inflammatory cells infiltrate. Eosinophils, neutrophils, macrophages, mast cells and plasma cells are found in varying numbers. All of these cells contain chemical mediators that produce the “asthmatic response”. With the increase in secretions, plugging of the smaller airways result. Asthma is a condition where not only bronchospasm occurs but muscle constriction, mucosal swelling and an increase in secretions in the lumen in the airways (Figure 2).
Asthma affects over 450,000 people in Ireland. 7.1% of Irish adults have asthma with 890,000 likely to experience it sometime in their lifetime. In 2024, two people lost their lives from asthma in Ireland every week despite advances in the knowledge of the mechanisms of asthma and pharmacology. In 2019, the Asthma Society of Ireland published Easing the Economic Burden of Asthma –The Impact of a Universal Asthma Self-Management Programme. The report, for the first time,
published confirmation of the enormity of the burden of asthma and contains, up-to-date figures on the number of people affected by asthma in Ireland. Previous estimates grossly under-estimated the number of people with asthma in Ireland. The annual economic burden of asthma is a staggering ¤472million. 2017 saw 2.4 million GP and 625,000 practice nurse asthma consultations respectively, 421,000 specialist visits, 133,000 emergency department visits and 8,000 hospital admissions. There
was one attendance at emergency departments every 4 minutes by a person with asthma.
The exact cause of asthma remains unknown. However, risk factors such as smoking, obesity, family history and atopy all increase the risk of developing asthma (Shamanthi et al, 2025). There are numerous triggers which can cause symptoms and these differ from person to person (Figure 1).
Wintertime can be particularly challenging for people with asthma
Written by Ruth Morrow, Respiratory Nurse Specialist, Asthma Society of Ireland
due to cold air and common viruses being common triggers. As Spring emerges, this can also be a challenging time as various tree pollen levels start to increase. Some people with asthma may need to increase their controller medication over the winter months to help manage their symptoms.
Symptoms
The clinical features of asthma (wheeze, cough, shortness of breath and chest tightness) result from changes in the airways as a result of abnormal sensitivity called bronchial hyper-reactivity. The muscle of the bronchial walls becomes hypertrophied causing occlusion of the airway resulting in contraction of the muscle causing bronchospasm. Secondly, in the mucosal, submucosa and smooth muscle layers of the bronchi and bronchioles inflammatory cells infiltrate. Eosinophils, neutrophils, macrophages, mast cells and plasma cells are found in varying numbers. All of these cells contain chemical mediators that produce the “asthmatic response”. With the increase in secretions, plugging of the smaller airways result. Asthma is a condition where not only bronchospasm occurs but muscle constriction, mucosal swelling and an increase in secretions in the lumen in the airways (Figure 2). burden of asthma and contains, up-to-date figures on
Figure 1: Asthma triggers
Figure 1: Asthma triggers
Figure 2: Pathology of asthma
Figure 2: Pathology of asthma
Asthma
Management of stable asthma
The goals of asthma management are:
1. Symptom control: to achieve good control of symptoms and maintain normal activity levels
2. Risk reduction: to minimise future risk of exacerbations, fixed airflow limitation and medication side-effects (GINA 2025)
Assessment of asthma control involves assessing symptoms over the previous 4 weeks using the GINA Assessment of Asthma Control, the Asthma Control Test (ACT) and assessing risk factors for poor outcomes. Treatment issues should also be addressed at every visit and should include:
• Assessment of the patient’s symptoms, medication usage and impact of asthma on daily life
• Review of inhaler technique and adherence
• Asking about side-effects
• Reviewing and updating the patient’s written asthma action plan
• Exploring the patient’s attitudes and goals for their asthma
The treatment and management of asthma should incorporate the following elements:
• Education on the disease process
• Management of trigger factors
• Medication management – mode of action, inhaler technique, adverse events and adherence
• Asthma Action Plan
• Management of acute flare-ups of asthma
The goal of asthma management is for the patient to be optimally controlled on the minimum amount of medication. GINA (2025) provides health care professionals with a management approach based on control using a step wise approach. This assists health professionals with the titration of medications using a step down or step up approach in attempt to achieve this goal.
The cornerstone of asthma treatment is inhaled therapy as medications are directly targeted at the airways and therefore, are more effective. This also limits the amount of systemic absorption and reduces adverse events. Patients should be commenced on the appropriate step of the treatment guidelines which is dependent on the severity of their
symptoms (GINA, 2025). Based on the severity of their symptoms at presentation, the patient is assigned to one of five treatment steps. Patients may move up or down the steps depending on symptoms and the amount of reliever therapy being used. Inhaled glucocorticosteroids (ICS) are the cornerstone of asthma treatment and are the most effective controller medications available. However, there are additional oral medications such as leukotriene receptor antagonists which can be added on and are very useful in patients who have an allergic component to their asthma, experience cold air bronchoconstriction and have exercise induced symptoms. These medications are also licensed for use in allergic rhinitis, a condition which 85% of people with asthma also have. House dust mite sublingual immunotherapy is also now recommended at all steps of the guideline depending on the patient’s asthma phenotype. Anti-inflammatory (AIR) and Maintenance and Reliever Therapy (MART)
In their review of the literature, GINA found no evidence to support a Step 1 SABA-only approach. The lack of evidence for short acting beta-agonist only treatment (SABA) contrasted with the strong evidence for safety, efficacy and effectiveness of inhaled corticosteroid (ICS) and inhaled corticosteroid and longacting beta agonist ICS/LABA). For safety reasons, GINA no longer recommends SABA-only treatment for Step 1. It is now recommended that all adults and adolescents with asthma should receive symptomdriven or regular low dose combination LABA/ICS-containing controller treatment, to reduce the risk of serious exacerbations (GINA, 2025).
Patients who have symptoms more than twice a month should be prescribed ICS/LABA twice daily (Step 2-5) known as Maintenance and Reliever Therapy (MART therapy) and patients who have symptoms less than twice a month should use ICS/LABA on “an as-needed basis” (Step1) known as Anti-inflammatory Reliever Therapy (AIR therapy). For patients on AIR therapy who use their inhaler more than twice a week indicates uncontrolled asthma and should be titrated up to MART therapy. For patients on MART who are well controlled and have had no exacerbations in the previous 12 months, can be titrated down to AIR therapy. Level 1 scientific evidence of the greater efficacy and safety of ICS/formoterol versus SABA
reliever therapy across the range of asthma severity allows Grade A recommendations to be made for its use as the preferred reliever therapy in adults and adolescents (Beasley et al 2024)
The synergistic effect of ICS and LABA has been known for some time (Barnes, 2002). This effect allows for lower doses of ICS to be used with maximum benefit to the patient and reducing the risk of unwanted side effects. Higher doses of ICS/LABA do not improve asthma control and increases the risk of adverse events. Beasley et al (2024) acknowledged the available evidence suggests that medium dose ICS/formoterol MART has a superior efficacy/safety profile than high dose ICS/LABA plus SABA (Beasley et al 2024).
Further support comes from a meta-analysis by Sobieraj et al (2018) that included 22 524 patients aged 12 years or older and 341 children aged 4 to 11 years with persistent asthma. MART was associated with a significantly lower risk of asthma exacerbations compared with a higher dose of inhaled corticosteroids and LABA as controller therapy. Why this change?
Inhaled SABA (Salbutamol, Terbutaline) have been firstline treatment for asthma for 50 years. Traditionally asthma was thought to be a disease of bronchoconstriction with SABA being the drug of choice. Added to this, rapid relief of symptoms, reliance on, patient satisfaction and their low cost have meant that SABAs were widely used, overused and over-relied upon. The perception by patients that their reliever “gives me control over my asthma”, so much so that they often don’t see the need for other treatment. However, research over the past number of years has shown that regular and frequent use of SABAs decrease bronchoprotection, increase rebound hyperresponsiveness, and decrease bronchodilator response. Patients with apparent mild asthma are at risk of serious adverse events such as near fatal asthma, acute asthma and death from asthma. Patients who get 3 or more canisters of SABA per year (average 1.7 puffs/day) are associated with higher risk of attendance to the emergency department (Stanford, AAAI 2012) and patients who receive 12 or more canisters per year are associated with higher risk of death (Suissa, AJRCCM 1994). A meta-analysis by Crossingham et al (Cochrane 2021) of four RCTs involving 9,565 patients demonstrated the benefits of
LABA/ICS combination therapy showing a 55% reduction in severe exacerbations compared with SABA alone. ED visits or hospitalisations were 65% lower than with SABA alone and 37% lower than with daily ICS.
Non-pharmacological management
The non-pharmacological management of asthma include management of trigger factors, smoking cessation, management of obesity and gastroesophageal reflux disease. Influenza vaccination is recommended for those with more severe asthma. Gastroesophageal reflux can worsen asthma symptoms and treatment of reflux may improve asthma symptoms.
Adherence with medication regimes and inhaler technique
One of the biggest challenges in asthma management is adherence to medication as many patients may be asymptomatic and therefore “don’t feel the need to use their medication daily” Exploring the patient’s beliefs and attitudes can be useful in determining a rationale for non-adherence to medication regime. Saving medication until it is needed, fear of becoming addicted or the health professional didn’t listen are amongst reasons given by patients in the INCA study (Sulaiman et al, 2014). In the current climate, cost is a significant factor even for the person who has a medical card and should not be overlooked. Two proven ways to address non-adherence are shared decision-making between the health professional and the patient and motivation interviewing. Using motivational interviewing, the health professional can assess the individual’s likelihood to adhere to their medication or to nonpharmacological interventions.
Inhaler technique should be checked at every opportunity as errors frequently occur even in patients who are taking inhaled medication for years. Care and maintenance of devices should also be addressed. Inhaler technique videos are available on www.asthma.ie.
Risk factors for poor outcomes
Patients who experience uncontrolled asthma symptoms, had one or more exacerbations in the previous year, the start of the patient’s usual ‘flare-up’ season (especially if autumn), has major psychological or socio-economic problems, poor adherence with controller medication and/or incorrect inhaler technique are at risk of an exacerbation in the coming months.
Symptoms Mild Severe
Altered consciousness No
Oximetry on presentation (SaO2)
Speech Sentences
Pulse rate
Peak Flow Pulse rate
Agitated, confused or drowsy
Words
>50% predicted or best <50% of predicted or best
Central cyanosis Absent Likely to be present
Wheeze intensity Variable Chest may be quiet
Table 1: Assessment of acute exacerbation of asthma (GINA, 2025)
People who have questions about managing their asthma are encouraged to send a WhatsApp message to Asthma WhatsApp service on 086 059 0132 or freephone the Asthma Society’s HSE-funded Asthma Adviceline on 1800 44 54 64. Both services are free and allow users to communicate directly with an asthma nurse specialist (Figure 3).
Patients can self- refer to the Adviceline using the following link: https://www.asthma.ie/book-anurse-call/
Assessment and Management of Acute asthma
3. Persisting tachypnoea despite 3 administrations of inhaled SABA,
Table 1: Assessment of acute exacerbation of asthma (GINA, 2025)
Conclusion
Accurate and timely assessment of acute asthma exacerbations should be carried out to ensure a successful outcome. Table 1 differentiates between a mild and severe acute exacerbation.
The management of acute asthma includes:
4. Unable to be managed at home
Follow-up post exacerbation
1. Oxygen therapy - 24% delivered by face mask (usually 1L/min) to maintain oxygen saturation 93-95%
The management of acute asthma includes:
This article has addressed stable and acute asthma management. The rationale for the introduction of ICS/Formoterol combination therapy has been explored following the changes to the GINA guidelines in 2019.
Healthcare Professionals can refer patients to the Adviceline using the following link: https://www. asthma.ie/health-professionals/ patient-referral/
E-referrals can also be made by clicking the e-referral tab on www.asthma.ie
2. Inhaled short-acting bronchodilator – 4-10 puffs of Salbutamol by spacer, or 5mg by nebulizer, every 20 min for first hour, then reassess severity. If symptoms persist, deteriorate or recur, give an additional 10 puffs per hour and admit to hospital
3. Oral corticosteroids – max 50mgs of oral steroids and continue for 5 -7 days
1. Oxygen therapy - 24% delivered by face mask (usually 1L/min) to maintain oxygen saturation 93-95%
2. Inhaled short-acting bronchodilator – 4-10 puffs of Salbutamol by spacer, or 5mg by nebulizer, every 20 min for first hour, then reassess severity. If symptoms persist, deteriorate or recur, give an additional 10 puffs per hour and admit to hospital
References available on request
4. Additional treatments can include - For moderate/severe exacerbations, Ipratropium bromide 80mcg (or 250mcg by nebulizer) every 20 minutes
Criteria for immediate transfer to secondary care include:
1. Features of severe exacerbation at initial or subsequent assessment
Patient is unable to speak or drink
Cyanosis
All patients should be followed up regularly after an exacerbation, until symptoms and lung function return to normal. Patients are at increased risk during recovery from a further exacerbation. This provides an opportunity to review and update the patient’s asthma action plan, review inhaler technique and adherence and to ascertain if there was a cause for this flare-up eg new trigger factors, poor adherence, poor inhaler technique, medication cost. This might be helpful in preventing future flare-ups.
Subcostal retraction
At follow-up visit(s), the asthma review should include:
Oxygen saturation <92% when breathing room air
3. Oral corticosteroids – max 50mgs of oral steroids and continue for 5 -7 days
Silent chest on auscultation
• The patient’s understanding of the cause of the flare-up
2. Lack of response to initial bronchodilator treatment
3. Persisting tachypnoea despite 3 administrations of inhaled SABA,
4. Additional treatments can include - For moderate/severe exacerbations, Ipratropium bromide 80mcg (or 250mcg by nebulizer) every 20 minutes
4. Unable to be managed at home
Follow-up post exacerbation
Criteria for immediate transfer to secondary care include:
• Modifiable risk factors, e.g., smoking, weight loss if indicated, addressing new triggers
• Adherence with medications, and understanding of their purpose
All patients should be followed up regularly after an exacerbation, until symptoms and lung function return to normal. Patients are at increased risk during recovery from a further exacerbation. This provides an opportunity to review and update the patient’s asthma
1. Features of severe exacerbation at initial or subsequent assessment
• Patient is unable to speak or drink
• Cyanosis
• Subcostal retraction
• Oxygen saturation <92% when breathing room air
• Silent chest on auscultation
2. Lack of response to initial bronchodilator treatment
• Reliever should be being used as-needed rather than routinely
• If controller medication was increased, the increased dose should be maintained for 3 weeks and possibly longer particularly, if flare-up was during the winter or during pollen season
• Inhaler technique skills
• Written asthma action plan
Figure 3: Resources for people with asthma
Figure 3: Resources for people with asthma
Clinical R&D
BEONE’S TISLELIZUMAB NOW AVAILABLE IN IRELAND, OFFERING A NEW FIRST LINE IMMUNOTHERAPY OPTION FOR ADVANCED OESOPHAGEAL CANCER
BeOne Medicines (Nasdaq: ONC; HKEX: 06160; SSE: 688235), a global oncology company, revently announced that the Health Service Executive (HSE) in the Republic of Ireland has approved reimbursement of tislelizumab, in combination with platinumbased chemotherapy, for the first-line treatment of eligible adult patients with unresectable, locally advanced recurrent or metastatic oesophageal squamous cell carcinoma (OSCC) whose tumours express PD-L1.
From 10 March 2026, tislelizumab will be available to prescribe to eligible patients across Ireland through HSE-funded hospital oncology services, in line with reimbursement approval.
Oesophageal cancer has a relatively low five-year survival and, according to the National Cancer Registry Ireland, approximately 500 patients are diagnosed each year. OSCC is the most common subtype, accounting for nearly 90% of cases. Squamous cell carcinoma represents one of the primary histological subtypes of oesophageal cancer globally.
The HSE reimbursement decision is based on results from the Phase 3 RATIONALE-306 trial, a randomised, double-blind, placebo-controlled study evaluating tislelizumab in combination with chemotherapy as a first-line treatment in 649 patients with unresectable, locally advanced recurrent or metastatic oesophageal squamous cell carcinoma.
The study met its primary endpoint and demonstrated a statistically significant improvement in overall survival in the intention-to-treat population. Median overall survival was 17.2 months for patients receiving tislelizumab in combination with chemotherapy compared with 10.6 months for those receiving chemotherapy alone (hazard ratio 0.66; 95% CI 0.54–0.80). In patients with PD-L1 expression ≥5%, median overall survival was 19.1 months versus 10.0 months, respectively (HR 0.62; 95% CI 0.49–0.79).
The safety profile of tislelizumab in combination with chemotherapy was consistent with the known profile of the individual agents.
The most frequent serious adverse reactions (≥2%) were pneumonia, dysphagia, diarrhoea, fatigue and oesophageal stenosis. The most common adverse reactions were anaemia, fatigue, decreased appetite, nausea, constipation,
decreased weight, diarrhoea, peripheral sensory neuropathy, vomiting and stomatitis.
James Harris, Interim General Manager, BeOne Medicines UK & Ireland, said: “This approval marks our first launch in solid tumours in Ireland and reflects our commitment to supporting patients with advanced oesophageal squamous cell carcinoma. We are pleased that eligible patients will now have access to tislelizumab as a treatment option, and we remain focused on working with the oncology community to support patient care in Ireland.”
Tislelizumab first received approval by the European Commission on 15 September 2023 for the second-line treatment of OSCC. It is approved in multiple advanced cancer indications across Europe, including in gastric and gastro-oesophageal junction adenocarcinoma, non-small cell lung cancer (NSCLC), extensivestage small cell lung cancer (SCLC) and nasopharyngeal carcinoma.
PATIENTS WILL PAY THE PRICE FOR THE LACK OF URGENCY AROUND NATIONAL CANCER STRATEGY, WARNS IRISH CANCER SOCIETY
The Irish Cancer Society is calling on Government to provide clarity on its plans to develop a new and adequately funded National Cancer Strategy. The charity’s call comes ahead of a Dáil debate this evening following a Sinn Féin motion on Cancer Services.
The Society has consistently highlighted the lack of ringfenced funding for the current National Cancer Strategy, which has caused staffing shortages, outdated cancer care equipment and a lack of progress reporting on the Strategy's defined targets. The result is that patients continue to experience chronic delays for diagnostics, treatment and access to medicines.
Steve Dempsey, Director of Advocacy & Communications at the Irish Cancer Society, said:
“Previous national cancer strategies have worked. In the 90s just 44% of Irish people were alive five years after a cancer diagnosis. By 2018, after our first two National Cancer Strategies, this had increased to 65%. Planning and centralisation have worked. Patients have benefited from multidisciplinary services in one location, treating cancer in its complexity, including surgery, radiation therapy and medical oncology.
“With cancer effecting one in two of us, and incidences projected to rise in the coming years, it’s vital that the Government builds on the good work of the first two cancer strategies and doesn’t take progress for granted. This means vision, long-term planning and modelling the investment needed to minimise delays, improve outcomes, and save lives. On behalf of cancer patients and their families, we’re calling on Government to urgently provide clarity and timelines on how it will develop and resource a new National Cancer Strategy.”
EDUCATION SERVICES FOR CHILDREN AT THE NEW NATIONAL CHILDREN’S HOSPITAL IRELAND
Minister for Education and Youth Hildegarde Naughton and Minister for Health Jennifer Carroll MacNeill have announced details of education services for children and young people at the new National Children’s Hospital Ireland (NCHI).
The new hospital school being established at the NCHI will bring together and build on the strengths of the four existing hospital schools currently located at the Children’s Health Ireland hospitals at Temple Street, Crumlin, and Tallaght and at Beaumont Hospital. All paediatric services under CHI will transition from their current locations to the NCHI, bringing these services together under one state of the art facility.
The new hospital school will provide enhanced educational support for children and young people during their care. The school’s patron will be the City of Dublin Education and Training Board (City of Dublin ETB).
Minister for Education and Youth Hildegarde Naughton and Minister for Health Jennifer Carroll MacNeill
On a visit to NCHI, Minister Naughton said:
“I want to express my deep appreciation for the outstanding support, dedication and guidance shown across all of the hospital schools involved in this exciting development. I am acutely aware of the unique environment in which hospital schools operate and I greatly admire the vocation, compassion, and professionalism demonstrated by every member of staff. I would also like to sincerely thank each of the patrons and their representatives for their constructive and collaborative engagement throughout this process - engagement that has brought us to today’s important announcement.
“The National Children’s Hospital Ireland represents the most significant capital investment in our healthcare system in the history of the State. It will unite existing services within a modern, purpose built, digital hospital on the St. James’s campus, providing the very best care and treatment for Ireland’s sickest children and young people. Education will be at the heart of this new facility, and the new hospital school will play a vital role in supporting the holistic care of every child and young person who attends.
“I want to record my sincere gratitude to Archbishop Farrell and Archbishop Jackson for their invaluable stewardship as patrons of the Temple Street Children’s Hospital School and Tallaght University Hospital School, and indeed for their wider contributions as patrons of so many schools across the country. Their leadership has supported generations of children at the intersection of health and education.
“I also want to thank the City of Dublin ETB for its dedicated work as patron of the hospital schools at Beaumont and Crumlin, and I wish the City of Dublin ETB every success as it assumes patronage
of the new hospital school at the NCHI.
“My department will continue to fully support all patron bodies as they progress the patronage transfer and amalgamation processes. We will work closely together to ensure that all necessary arrangements are in place in the weeks ahead so that the new hospital school is ready to open in line with the opening of the NCHI.
“My department will also continue our strong partnership with the HSE, and I am grateful to Linn Dara School for extending its specialist provision into the NCHI.”
NEW NATIONAL FRAMEWORK TO STRENGTHEN EMERGENCY CARE FOR OLDER ADULTS
A new national quality improvement framework aimed at ensuring that every older person receives safe, timely and respectful emergency care, regardless of when or where they attend, has been published by the National Clinical Programme for Emergency Medicine in the Royal College of Surgeons of Ireland (RCSI). The framework was developed in response to the steady and sustained increase in Emergency Department and Injury Unit attendances by older adults. In 2025, more than 560 people aged 75 years and over present to EDs nationally each day, reflecting the evolving patterns of emergency care demand.
The framework is informed by national data and earlier work led by the National Clinical Programme for Emergency Medicine, which highlighted that many patients aged 75 and over are triaged to lower acuity categories despite complex clinical needs, often resulting in prolonged Emergency Department stays and delayed care.
The National Quality Improvement Framework (QIF) for the Care of Older Adults in Emergency Departments and Injury Units sets out a structured, evidenceinformed approach, translating national policy and international standards into practical actions that can be implemented at site level, even in the context of ongoing system pressures. By strengthening post-triage assessment and standardising age-attuned practices, the framework aims to improve patient experience and outcomes while supporting more effective use of existing resources.
Dr Rosa McNamara, Clinical Lead, National Clinical Programme for Emergency Medicine said that “providing emergency care to older adults is a core responsibility of
Emergency Departments and Injury Units. As we evolve to meet the changing needs of the populations we serve, this document offers clear guidance and direction on minimum standards, best practices, and aspirational care.”
Professor Deborah McNamara, President, RCSI, welcomed the publication of the framework: “Ireland’s ageing population is reshaping the demand for emergency care, and our health services must evolve accordingly. This Quality Improvement Framework provides practical, evidence-informed guidance to support Emergency Departments and Injury Units in delivering safe, timely and respectful care for older adults. RCSI is proud to support this important step towards more age-attuned emergency services nationwide.”
The framework builds on the Emergency Medicine Programme Model of Care (HSE, 2025) and aligns with Delivering an Age-Friendly Health System (Department of Health and HSE, 2025), as well as international best practice outlined by the International Federation for Emergency Medicine (IFEM). The framework focuses on three priority areas:
• Minimum Care Standards to ensure that all older adults have access to essentials such as hydration, appropriate seating, timely clinical assessment and clearly documented discharge and follow-up plans.
• Post-Triage Assessment and Bundles of Care, including frailty and delirium screening, to support early identification of risk, prompt intervention and avoidance of deterioration during Emergency Department stays.
• Education and Workforce Development, promoting Geriatric Emergency Medicinefocused training for all Emergency Department staff, supported by dedicated clinical leads and simulationbased learning.
The framework provides clarity on core requirements while allowing flexibility for local adaptation. Accompanying tools and implementation resources have been developed to support sites in embedding improvements in a sustainable way.
Examples of effective practice already operating within Irish Emergency Departments and Injury Units demonstrate that meaningful improvements are achievable, even within constrained environments. Some of these case studies are featured in the document.
Under the National Clinical Programme for Emergency Medicine in RCSI, this Quality Improvement Framework and accompanying resources have been developed by frontline staff in Emergency Departments and Injury Units and provide a clear, practical pathway to consistently highquality emergency care for older adults across Ireland, supporting frontline teams to meet changing patient needs while remaining mindful of the significant pressures faced by emergency services.
MATER PRIVATE NETWORK ANNOUNCES EXPANDED DIAGNOSTIC OFFERING AT CHERRYWOOD DAY HOSPITAL
Mater Private Network has unveiled the latest offering in its Cherrywood Day Hospital, a new, cutting-edge CT scanner which offers both general and cardiac CT imaging. The new scanner offers
quick turnaround and convenient access, improving the patient experience, while significantly enhancing diagnostic capabilities and patient experience.
Mater Private Network is continually investing in new services and technologies to improve patient experience and care. In addition to the standard CT offering, the new scanner offers enhanced cardiac diagnostic capabilities including highresolution images of the heart to identify calcium buildup, coronary artery disease, blockages, and structural issues.
With the hospital group’s longstanding reputation for diagnosing and treating Ireland’s most complex cardiovascular cases, this state-of-the-art CT scanner significantly expands cardiac diagnostic capacity in South County Dublin by initially offering 160 extra scans a month, and scaling up to 450 as required.
A new DEXA scanner in the Cherrywood Day Hospital also improves diagnostic access for patients with conditions such as osteoporosis, rheumatoid arthritis and fracture risk.
Commenting on the new offering, David Slevin, Deputy CEO of Mater Private Network said, “At Mater Private Network we are continually looking at how we can improve our patient services. This new CT scanner will offer enhanced diagnostic capabilities, with quick turnaround times to give our patients peace of mind. This marks the latest in a series of recent investments for Cherrywood – in the past year we have opened
David Slevin, Deputy CEO of Mater Private Network at the openin
Clinical R&D
new clinics in geriatric medicine, rheumatology, urogynaecology, neurology, pain medicine and an orthopaedic foot & ankle clinic. Work is also currently underway on a new oncology suite and endoscopy suite in our Northern Cross Day Hospital, due to come on stream from September 2026.
“Our day hospitals mean that patients can access specialised care from same day clinic appointments to diagnostics and treatment plans from leading experts, without lengthy waiting times. Patients also have the reassurance that as part of our wider care network, they will have access to our full suite of hospitals and specialist teams, should the need for more acute treatment arise.”
Additional radiology services available in Cherrywood include MRI, X-ray, Ultrasound and CT. Advanced cardiac testing is also available, including cardiac MRI and cardiac CT, as well as ECG, Echo and stress testing. Treatment options include ultrasound-guided and fluoroscopic-guided joint injections for orthopaedic, rheumatology and spine pain management, while a physiotherapy clinic offers full musculoskeletal (MSK) assessments and reviews.
In 2025, Cherrywood Day Hospital saw over 15,000 patients across clinic appointments, diagnostic scans, and treatment.
FIRST INTERNATIONAL GUIDELINE ON FIRST-LINE ANTIPSYCHOTIC TREATMENT FOR FEMALES
Researchers at St John of God University Hospital’s Research & Innovation Hub, UCD Centre for Psychosis Research and University Medical Centre Groningen in the Netherlands have developed the first international clinical practice guideline specifically focused on the choice of first antipsychotic medicine for females experiencing a first episode of psychosis. The recommendations were developed by an international multidisciplinary panel of clinicians, researchers and experts-by-experience from Europe, North America and Australia. These guidelines are developed as part of the PROGRESS research group that has been funded by the Health Research Board.
Published in this month’s Schizophrenia Bulletin, the guideline responds to longstanding gaps in prescribing guidance, where sex-specific risks and side-effect profiles have not been adequately reflected in clinical recommendations. The recommendations are designed to support clinicians and patients
to make safer, more personalised treatment choices at the earliest stage of care.
Psychosis most commonly begins in early adulthood, with the median age of onset around 20 years. Symptom onset is often later in females, with a second peak after age 50. Early intervention at first onset is considered the gold standard of care, with antipsychotic medicines forming a key component of treatment alongside psychological, social, occupational and educational supports.
Caroline Hynes-Ryan, lead author and pharmacist at St John of God University Hospital, said “Firstepisode prescribing is a crucial window to get treatment right. By prioritising outcomes that matter for females - particularly hormonal and cardiometabolic effects - this guideline helps clinicians choose options with a lower long-term burden and supports females to stay on treatment that is both effective and acceptable.”
Professor Brian O’Donoghue, Director of the UCD Centre of Psychosis Research at the School of Medicine in UCD and lead of the PROGRESS group, said “Response rates to antipsychotic medications are high and therefore the choice of first antipsychotic medication needs to be based on the expected side-effects and tolerability. There is a very real differences in side-effect vulnerability for females and therefore, these sex specific guidelines should result in females being prescribed lower risk medications from the outset and
will have longer term benefits for physical health. This guideline brings together international evidence and expert consensus to support safer first-choice antipsychotic medicine, better shared decision-making, and more equitable care from day one.”
Addressing sex-specific risk from the start
The guideline highlights that females can experience distinct vulnerabilities to certain antipsychotic side-effectsparticularly hormonal disruption (including prolactin elevation) and cardiometabolic risk - with potential long-term implications for bone health, fertility and overall physical health.
The guideline was developed using the GRADE-ADOLOPMENT methodology and AGREE II framework, involving an international multidisciplinary panel including clinicians, researchers and experts-by-experience.
The aim of the guideline is to improve treatment acceptability and adherence, support better long-term physical health outcomes, and advance equity in psychosis care.
This work is part of the Research & Innovation Hub’s mission to translate evidence into improved patient care across the mental health sector.
THE GLOBAL ONCOLOGY & HAEMATOLOGY CONGRESS
The Network for Collaborative Oncology Development & Advancement (NCODA) recently
brought together international leaders across oncology, haematology, pharmacy, diagnostics and healthcare innovation for day two of its inaugural Global Oncology & Haematology Congress, held at The Shelbourne Hotel, Dublin.
The two-day Congress convened a carefully curated group of experts from Europe, North America and beyond for high-level dialogue, collaboration and clinically relevant education focused on improving patient outcomes worldwide. Discussions explored key issues shaping the future of cancer care, including precision oncology, AI-driven healthcare, treatment sequencing, sustainable oncology and multidisciplinary, patientcentred care models.
The Global Oncology & Haematology Congress reflects NCODA’s ongoing commitment to advancing quality, safety and access in cancer care through collaboration, education and realworld innovation, strengthening partnerships across disciplines and geographies.
Pictured at the Congress are Michael Reff, RPh, MBA, Founder and Executive Director of NCODA, alongside Dave Shanahan, a member of the Global Steering Committee and CEO of Athena Pharmaceuticals, Orla Dolan, CEO of Breakthrough Cancer Research, and Amy Nolan, Director of Clinical Affairs at the Irish Cancer Society.
HSE ENCOURAGES SMOKERS IN THE WEST TO QUIT SMOKING
To mark National No Smoking Day on Wednesday, 18 February the HSE was reminding people in the West that HSE Stop Smoking Advisors are ready to help you start your QUIT plan and support you every step of the way.
The HSE Stop Smoking Services are free and available all year round. The HSE provide personalised, evidence-based stop smoking plans, tailored to people’s individual needs. When you engage with the HSE Stop Smoking service you can avail of:
• Free confidential one to one behavioural support with your own trained stop smoking advisor
• Free ongoing Carbon Monoxide Testing to show your improvement over time
• FREE stop-smoking Nicotine Replacement Therapy (NRT) medications to help deal with cravings
• Follow up appointments for one full year in-person, over the phone or online
• Motivational tips to keep you on track
Ann Marie McGarry, Smoking Cessation Advisor, Galway University Hospitals said: “Pauline’s achievement shows that with the right support and determination, quitting smoking is possible. Stopping smoking is one of the most important lifestyle changes smokers can take to improve their health. It reduces the risk of heart disease, stroke,
Marie McGarry, Smoking Cessation Advisor, Galway University Hospitals and Pauline Connor, Member of Staff at University Hospital Galway
cancer and respiratory illness, improves overall wellbeing and has immediate benefits such as better breathing and increased energy.
“Stop Smoking Advisors in Galway, Roscommon and Mayo are here to provide practical tools, NRT, guidance and encouragement to help people at every stage of their quit journey.”
RCSI LAUNCHES IRELAND’S FIRST NATIONAL ROBOTIC
SURGERY CURRICULUM
The Royal College of Surgeons in Ireland (RCSI) has today launched Ireland’s first national programme for robotic surgical training. The new National Robotic Surgery Curriculum marks a significant advance in robotic surgery education in Ireland, supporting consistent standards of practice nationwide by ensuring that trainees develop a shared foundation in robotic safety, technical competence and nontechnical skills.
Formally launched at the Robotic and Technology Learning Village, which is part of RCSI’s annual Charter Week meeting, the curriculum is supported by a ¤2.3m institutional investment from RCSI in robotic surgical education. This includes the purchase of three robotic platforms and the opening of a new robotic education space at the National Surgical and Clinical Skills Centre on RCSI’s St Stephen’s Green campus.
Deliberately vendor-agnostic, the curriculum focuses on transferable skills that allow surgeons to adapt as robotic technologies continue to evolve. This approach reflects the rapid growth of robotic surgery across multiple specialties and the increasing number of platforms entering clinical practice and ensures that trainees are prepared not only for current systems but for future innovations.
Delivered through a staged and progressive programme, trainees
are introduced to the principles of robotic surgery, including system setup, ergonomics, and safe workflow. They then develop core console skills such as camera control, instrument handling, dissection, and suturing through advanced simulation and modelbased training.
Equal emphasis is placed on the human factors that are critical in robotic operating theatres, including communication, teamwork, situational awareness, and emergency management. This recognises the unique challenges posed by the physical separation between the surgeon and the patient.
The curriculum, supported by RCSI’s investment in hands-on training, is a key enabler of the National Governance Framework for Robotic Surgery published by RCSI in 2025 to provide national standards for safety, oversight and quality in robotic surgical practice.
Professor Deborah McNamara, President of RCSI, said: “Robotic surgery is rapidly becoming a core component of modern surgical practice. With the launch of this national curriculum, RCSI is ensuring that innovation is supported by education, safety, and consistency. This programme reflects our commitment to preparing surgeons for the future of patient care and maintaining the highest standards of surgical training.”
Professor Barry McGuire, Professor of Postgraduate Surgical Education and Academic Development at RCSI, said: “This curriculum is about more than learning how to use a robot. It is about developing safe, adaptable surgeons who understand both the technical and human factors that define modern robotic surgery.
Looking ahead, RCSI aims to develop a nationally distributed learning model, with education
delivered centrally from RCSI and accessed remotely through consoles located across the country. This approach will allow trainees to learn, practise and be supervised without geographical barriers, supporting equitable access to high-quality training nationwide”, Professor McGuire added.
PORTIUNCULA UNIVERSITY HOSPITAL APPOINTS ADVANCED NURSE PRACTITIONER IN ONCOLOGY
Portiuncula University Hospital (PUH) welcomes the appointment of Sarah Ennis as Advanced Nurse Practitioner (ANP) in Oncology, further enhancing its nurse-led oncology services and improving access to specialist cancer care for patients across the region.
In her new role, Sarah is responsible for the assessment, diagnosis and management of patients receiving oral anti-cancer therapies. She provides care to patients with a wide range of cancers, including breast, ovarian, colorectal, prostate, lung, brain and neuroendocrine cancers, and works closely with two Consultant Medical Oncologists in dedicated Medical Oncology Clinics.
The Oncology Department at PUH operates as a fully nurse-led service and continues to expand its capacity to meet growing demand. As the department’s second Advanced Nurse Practitioner, Sarah practises independently as part of an experienced multidisciplinary nursing team, including a Clinical Nurse Manager, Clinical Nurse Specialists and Staff Nurses, supporting the delivery of timely, high-quality care closer to patients’ homes.
Ann
Sarah Ennis, Advanced Nurse Practitioner (ANP) in Oncology