HEALTH: Testicular Disease Page 43 HONOURS: Red Carpet at the Hospital Professional Honours Page 56
BLUEFISH PHARMACEUTICALS LAUNCHES
Product Information: Meladura 2mg prolonged-release tablets (melatonin) |Marketing Authorisation Holder (MAH): Bluefish Pharmaceuticals AB, P O Box 49013 100 28 Stockholm, Sweden | Marketing Authorisation Number(s): PA1436/047/001 | Legal Category: Medicinal product subject to medical prescription | Date of Last Review of API : 25/06/2024 | Further information including the SPC is available on request from Bluefish Pharmaceuticals AB Adverse event details should be reported to: HPRA Pharmacovigilance, Website: www hpra ie
Contents Foreword
New Survey from Irish Hospital Consultants Association P5
Significant investment in new medicines P6
Almost 700 new White Coats P9
Priorities outlines for adults with Type I Diabetes P12
Eye Care in Focus at the ICO 2024 Conference P14
Royal College of Physicians Ireland Annual Conference P24
Environmental Health in Ireland P46
REGULARS
CPD: Venous Thromboembolism P29
Men’s Health: Cardiovascular Disease P33
Men’s Health: Understanding UTI’s P34
Editor
A new survey commissioned by the Irish Hospital Consultants Association (IHCA) has found that 56% of consultants believe their working environment rarely or never reflects a culture of mutual support, cohesion, or trust, with 76% saying that they are very often or always in ‘firefighting mode’.
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only. All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
The Association published the results in advance of its Annual Conference. When exploring the theme of compassionate leadership, 56% say that their workplace rarely or never reflects a culture of mutual support, cohesion and trust. This is despite 72% of consultants believing in collaborative leadership, yet only 16% feel that management seeks their input in decision-making.
Turn to page 5 to read the full story.
In other news on page 6, the Irish Pharmaceutical Healthcare Association (IPHA), the representative body for the researchbased biopharmaceutical industry in Ireland, welcomes the allocation of ¤30 million for new medicines in Budget 2025.
IPHA also welcomes in Budget 2025 the introduction of a Chicken Pox vaccination programme. Vaccination and immunisation programmes play a vital role in protecting people’s health and, as vaccines are the most effective preventative measure against infectious diseases, they have a positive impact on the wider healthcare system.
On page 24 we cover the recent Royal College of Physicians of Ireland Annual Conference. One of the keynote speakers, Professor Michaela Higgins, Consultant Medical Oncologist at St Vincents Hospital, provided stark evidence of the growing challenges in targeted cancer care.
“I know what treatment would be best for a patient but increasingly, I cannot prescribe it,” Professor Higgins said. As the prevalence of cancer increases, the drugs to treat it become more expensive, explained Prof Higgins, comparing cancer treatment to exorbitantly priced wedding shoes. “Just like weddings, there is a cancer premium,” she said.
Despite the challenges, Professor Higgins says it is not all bleak and there is something we can do. “Cancer, for the most part, if caught early, is curable,” she said.
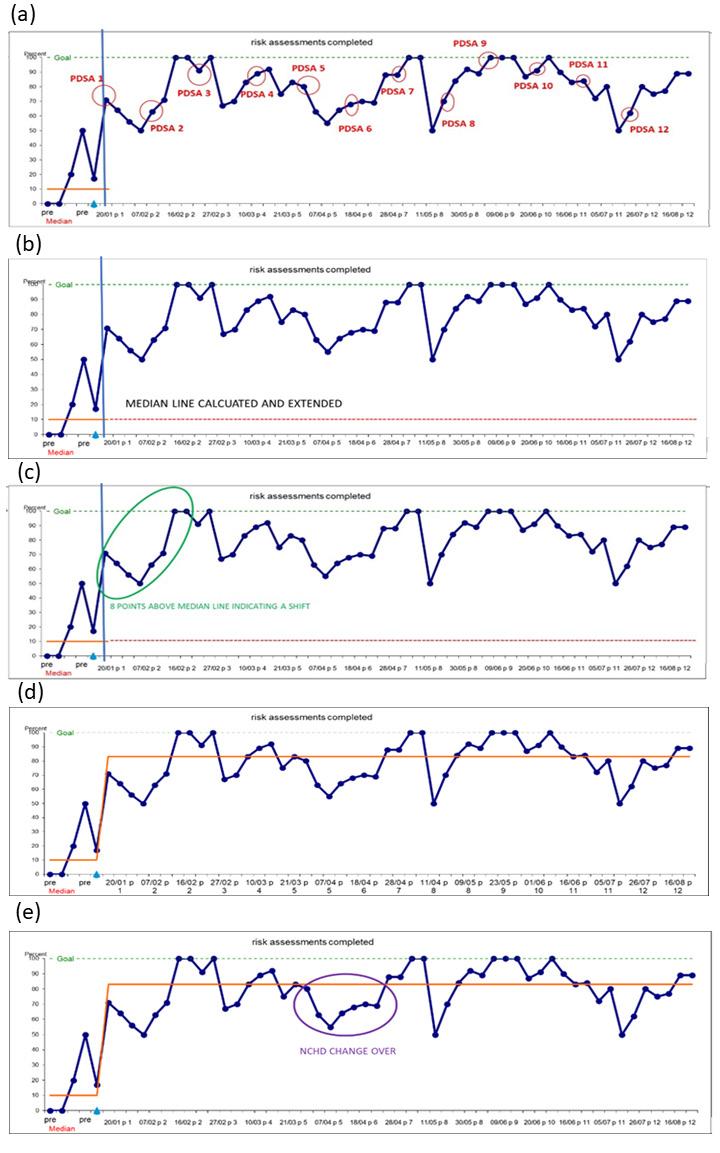
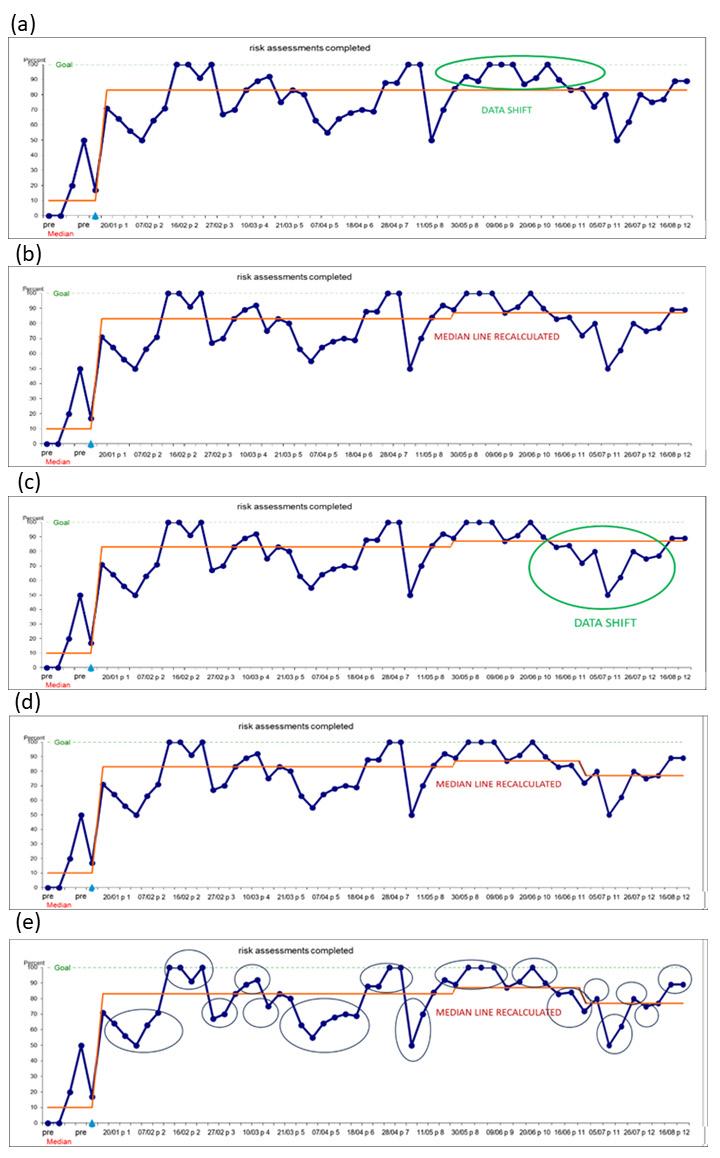
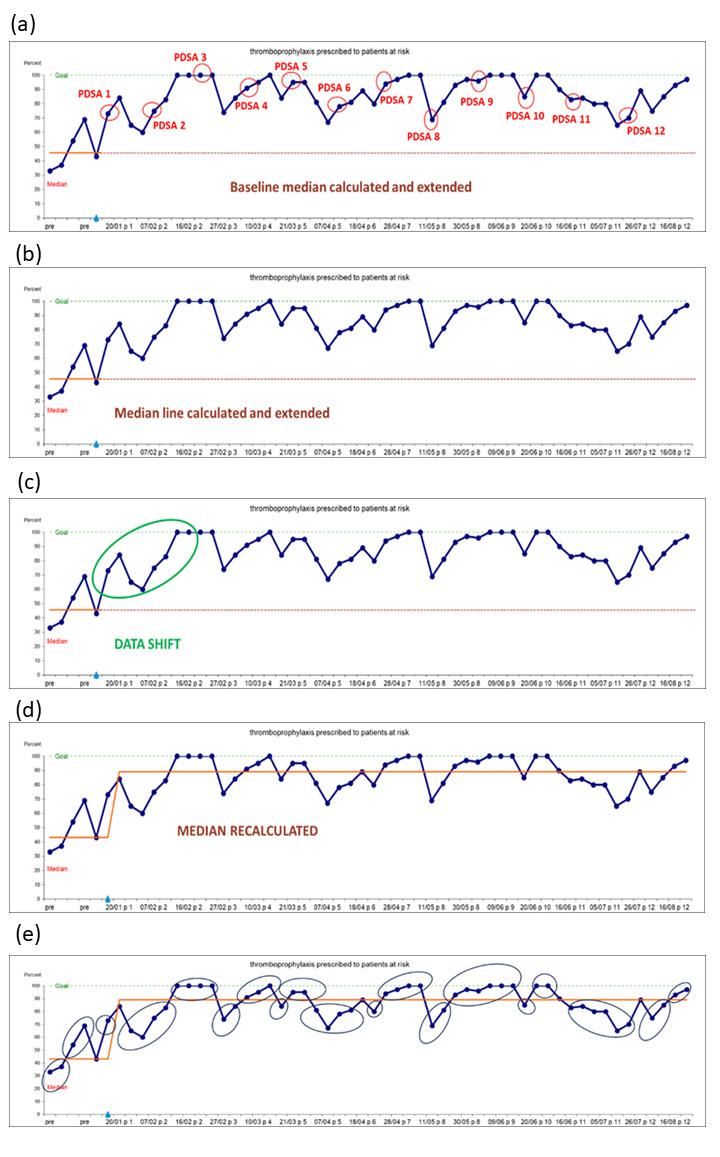
This issue also carries an excellent CPD authored by Carol Walsh, Advanced Nurse Practitioner and Emer O’Sullivan, Quality Risk & Patient Safety Officer, Bantry General Hospital which examines reducing hospital-associated venous thromboembolism. VTE is a significant cause of hospital-related death worldwide. It is estimated globally that there are 5 to 6 million HA-VTE annually and up to 70% of these could be prevented with appropriate thromboprophylaxis.
Turn to page 29 to read more.
I hope you enjoy the issue.
HPRA Launch Annual Report
The Health Products Regulatory Authority (HPRA) has published its 2023 annual report which details its activities across an extensive range of work programmes to regulate medicines, medical devices and other health products for the benefit of people and animals. The report outlines the HPRA’s core focus and achievements in each of the health product areas it regulates. It also details the organisation’s tailored and effective response to external developments that impacted on the wider health sector.
During 2023, the key activities undertaken by the HPRA included:
• The authorisation of 384 new human medicines following an assessment of their safety, quality and effectiveness.
• 19 new clinical trial authorisations under the EU Clinical Trials Directive (CTD) and 36 authorisations under the new EU Clinical Trials Regulation (CTR).
• Receipt of 7,793 suspected adverse reaction reports for human medicines.
• Assessment of 3,065 medical device vigilance reports.
• Recall of 65 medicines consisting of 59 human medicines and six veterinary medicines.
The HPRA’s active contribution at an EU and international level during 2023 included:
• Serving as one of the top 10 national contributors via the
Dr Lorraine Nolan, Chief Executive of the HPRA
European Medicines Agency (EMA) for lead assessment of centrally authorised human medicines and scientific advice, as was also the case last year. This included the assessment of 12 new human medicines applications – eight as rapporteur and four as co-rapporteur – and the co-ordination of 93 scientific advice procedures.
• Contributed to the effective application of the EU Medical Device Regulation and In Vitro Device Regulation at EU and national levels, gathering data on the challenges with implementation while working to ensure continued supply of essential devices.
Dr Lorraine Nolan, Chief Executive of the HPRA, said 2023 brought many opportunities, milestones and challenges for the organisation which at all times, and across all its operations and decisionmaking, maintained a clear, central focus on seeking to protect consumer and animal health.
“Medicine availability continues to be a top priority for the HPRA and our partners across the Irish health system. Over the course of 2023, all EU member states, and many countries globally reported an increased prevalence of medicines shortages, indicating this is by no means an issue that is unique to Ireland. We recognise and appreciate the issues that medicines shortages pose for patients and healthcare professionals, and this is central to our efforts to prevent and mitigate against shortages. As coordinator of the national Medicines Shortages Framework, the HPRA continues to collaborate with all stakeholders who have a part to play in reducing the impact of medicines shortages for Irish patients, including ensuring access to suitable alternative treatments, where possible. At EU level, the HPRA also actively contributes to numerous initiatives to address shortages and will continue to work towards our shared goal of strengthened medicines supply within Europe.”
Calls for Infrastructure Investment in Health
The Irish Medical Organisation (IMO) has called on the Government to use some of the proceeds from the Apple Tax windfall to address major infrastructural issues in the Irish health services.
Just last month, the Court of Justice of the European Union ruled that Apple must pay the Irish Exchequer ¤13 billion in backdated taxes.
Dr Denis McCauley, President of the IMO, said, “For over a decade the IMO has called for significant investment in our health infrastructure which has been a consequence of poor capacity and workforce planning and years of
austerity and under investment. With the significant growth in population over recent years and in particular the increase in the health needs of our older population we must use this opportunity to address the year round crisis in our health services.”
Dr McCauley continued, “This windfall tax provides a oncein-a-generation opportunity to undertake an aggressive investment programme that could finally deliver on increased bed capacity in our acute and rehabilitation services and upgrading current infrastructure to ensure it meets modern standards for the delivery of healthcare.”
Dr McCauley warned that as the Irish population increases and ages, pressure will increase significantly to provide beds and hospitals for those needing care.
In the last decade the population has grown by over 14% to 5.3 million in 2023, with over 15% of the population now aged 65 or over. There has been little or no increase in in-patient beds in the last 20 years and hospital waiting lists have almost tripled to over 896,000 in the decade between 2013 and 2023.
The recent pre-budget submission of the IMO called for action on a number of fronts and made the following calls in respect of infrastructure:
• Increase the number of new inpatient beds from 3,438 to 5,000 under the Acute Hospital Bed Capacity Expansion Plan to meet the needs of our growing and ageing population.
• Provide sufficient capital funding and planning to support the expansion of acute inpatient beds in full and on time.
• Develop and implement an adjacent plan to increase psychiatric inpatient beds to meet population needs.
• Increase the number of rehabilitative care beds, long-term nursing home beds and the financing of home care packages.
Majority of Consultants in ‘Firefighting Mode’
A new survey commissioned by the Irish Hospital Consultants Association (IHCA) has found that 56% of consultants believe their working environment rarely or never reflects a culture of mutual support, cohesion, or trust, with 76% saying that they are very often or always in ‘firefighting mode’.
The Association published the results in advance of its Annual Conference held recently in Kilkenny, which focused on the theme of compassionate leadership. Among the speakers attending the conference was the Minister for Health and international healthcare leadership experts, Professor Michael West and Professor Helen Thomas.
When exploring the theme of compassionate leadership, 56% say that their workplace rarely or never reflects a culture of mutual support, cohesion and trust. This is despite 72% of consultants believing in collaborative leadership, yet only 16% feel that management seeks their input in decision-making.
More than six in 10 (63%) consultants report a lack of access to necessary capacity and resources. Just 9% of the over 650 consultants who responded to the survey believe they have adequate time to forward plan in their roles.
Despite these challenges consistently being faced by consultants operating in difficult circumstances, almost threequarters (72%) state they feel they are making a valuable contribution to patient care, research and teaching.
Close to two-thirds (63%) of consultants feel a sense of worth
HCA President, Professor Gabrielle Colleran
in their work, while almost 70% say their work is very or completely meaningful to them. Overall, 70% stated that they find satisfaction in their roles, day to day.
Commenting, IHCA President, Professor Gabrielle Colleran said: “Healthcare can often feel consumed by contention and confrontation. Healthy debate has its place, but it should not define us.
“The path forward requires a new mindset—a shift towards collaborative and compassionate leadership. We all must play our part. We must foster a culture of connection, trust, and respect, because only through collective effort can we overcome the challenges ahead.”
The IHCA Annual Conference took place on Saturday, 12 October in Kilkenny. Guest speakers included Professor Michael West, who spoke on the core conference theme of ‘Leadership: a reset for Irish healthcare’ alongside Professor Helen Thomas, who focussed on Shaping Leadership and Culture Across NHS Wales.
Furthermore, Medical Council President Dr Suzanne Crowe and Consultant Dermatologist and former IHCA President Professor Alan Irvine will take part in a panel discussion titled ‘Leadership in Medicine – the lived experience’,
which was moderated by former RTÉ broadcaster Bryan Dobson. Minister for Health Stephen Donnelly also addressed the conference and partake in a panel discussion with IHCA President,
Calls for Reform of Medical Negligence
The President of the Irish Medical Organisation (IMO) has called for reform of the medical negligence system in Ireland, saying that the current system was leading to unnecessary trauma for patients in a highly legalised and adversarial system and a culture of over-referrals which was putting pressure on an already overburdened health system.
Dr Denis McCauley, a GP and Donegal Coroner, will chair an IMO
seminar in Dublin this evening (Thursday) to discuss the medicolegal environment in Ireland.
Dr McCauley said that the current system for medical negligence cases in Ireland, even taking into account recent legislative changes, is not in the best interests of patients or doctors with lengthy delays and costs leading to a change in how doctors will practice medicine. This is not
always in the best interests of the patient and the dangers of overreferral and a culture of “defensive medicine” are bad for doctors, patients and the health system as a whole.
To counteract these unsatisfactory measures, Dr McCauley recommended that a system of nofault compensation be introduced in Ireland, whereby the facts can be established and the patient
Professor Gabrielle Colleran, former Holles Street Master Dr Rhona O’Mahony, and HSE Chief Clinical Officer Dr Colm Henry on the future of care in Ireland, also moderated by Bryan Dobson.
can be compensated without the need to enter into lengthy costs legal battles which can compound the trauma for many years. “Such a system would be far more transparent, would enable the patient to have their issues addressed in a timely manner and would enable the doctor to concentrate on treatment and diagnoses without the overt threat of litigation.”
Budget 2025: ¤30m for new medicines is significant for patients as it will allow for the continuous flow of new life-enhancing treatments
The Irish Pharmaceutical Healthcare Association (IPHA), the representative body for the research-based biopharmaceutical industry in Ireland, welcomes the allocation of ¤30 million for new medicines in Budget 2025.
Advances in medicines development are steadily growing and IPHA members expect to make applications for reimbursement for 36 medicines in 2025. Arising from this budget allocation, as many as 3,700 patients, along with their families and carers, could now benefit from access to therapeutic advances. These medicines would improve the standard of care for patients suffering from a number of diseases such as cancer –breast cancer, leukaemia, prostate cancer, multiple myeloma and others – Alzheimer’s, stroke, women’s health conditions, migraine, dermatitis, asthma, ulcerative colitis, type 2 diabetes and liver disease.
IPHA also welcomes in Budget 2025 the introduction of a Chicken Pox vaccination programme. Vaccination and immunisation programmes play a vital role in protecting people’s health and, as vaccines are the most effective preventative measure against infectious diseases, they have a positive impact on the wider
healthcare system.
As an industry we have been calling for greater transparency in the reimbursement system for quite some time. Therefore, we also welcome reports that an online medicines’ application tracker will be launched on the HSE website shortly. The purpose of this tracker will be to detail when a pricing application is received by the HSE and whether the application is progressing through the process. This level of transparency in the reimbursement process is vital for patients, clinicians and industry who will now be able to track a medicine as it progresses through each stage of the process.
While welcoming reported progress on the tracker, it is important that further steps are made to implement ‘indicative timelines’ for the completion of each stage of the reimbursement process. With this further initiative it should be possible for the all to see the HSE reaching a decision on the reimbursement of a lifeenhancing medicine within the legal requirement of 180 days, as set out in the Health Act 2013.
Commenting on Budget 2025 allocation for new medicines, Oliver O’Connor, Chief Executive of IPHA said, “We welcome the funding of ¤30 million for new
medicines which will greatly improve patient standards of care by ensuring they can avail of the latest innovative medicines available. We also welcome reported progress on the online medicines’ application tracker which will give everyone concerned greater visibility and transparency.
“IPHA members are very conscious of their responsibilities in ensuring a faster and continuous flow of life-enhancing new medicines for patients in Ireland. We believe that doctors should
Improving Access to Biologic Drugs
have the right medicine available for prescription for their patients at the right time. We are calling for parties in their General Election Manifestos to give a new voice for doctors in prioritising new medicines for patients. We believe that Involving clinicians from the outset of the process will allow medicines to be available for patients faster.
“We will continue to work with all stakeholders to improve the process and enhance healthcare outcomes for patients in Ireland.”
Minister for Health Stephen Donnelly met with Peter Goldschmidt, CEO of European medicines manufacturer STADA, to discuss how competition can improve patient access to cutting-edge biologic drugs, as well as STADA’s investments in Ireland through its Clonmel Healthcare affiliate.
Along with the head of STADA’s Irish subsidiary, Clonmel Healthcare, Donagh O’Leary, the Minister and Goldschmidt explored how biosimilar alternatives enable the health system to treat considerably more patients at the same or lower costs. The conversation also included investment opportunities in Ireland, following Clonmel’s recent opening of a ¤3 million warehouse in its home town.
Minister for Health Stephen Donnelly met with Peter Goldschmidt, CEO of European medicines manufacturer STADA, to discuss how competition can improve patient access to cutting-edge biologic drugs
IPHA Launches ‘Innovate for Life’
The Irish Pharmaceutical Healthcare Association (IPHA), which represents the international research-based biopharmaceutical industry, has launched a new campaign consisting of films and podcasts documenting the personal stories from patients who, because of new medicines, were able to experience moments in their lives which otherwise wouldn’t have been possible. Innovate For Life, which is in its sixth cycle, is the industry’s digital campaign demonstrating the impact of medicines innovation.
This year the campaign consists of photo montages of moments – both mundane and special – from the lives of patients which were possible because of new medicines. These are accompanied by podcasts from these same patients telling their personal stories.
The campaign, featuring four international biopharmaceutical companies with a presence in Ireland, centres around:
1. Pfizer’s work towards the cancer moonshot goal and how clinical trials can accelerate these breakthroughs. Featured is Patrick who, because of a successful cancer clinical trial, won’t miss a single precious family moment. During the podcast we hear Patrick tell his story to Pfizer Country Medical Director Orlaith Gavan, who also explains Pfizer’s cancer moonshot goal and the importance of clinical trials.
2. Novo Nordisk has a long history in the development of medicines to treat chronic disease. Featured is Carmel who, since 1997 when she was first diagnosed, has experienced
firsthand how new treatments have significantly improved her management of type 1 diabetes. She speaks to Professor Fidelma Dunne in the podcast on how new treatments have given her a sense of freedom and improved her quality of life.
3. Roche’s scientists are committed to finding new treatments that reduce the burden on patients with retinal diseases, which are a leading cause of sight loss. In these films Mary tells her story of how, because of access to new medicines, she can continue to be independent and enjoy doing what she loves most. During the podcast she discusses with Neil Ward, Fighting Blindness’ Head of Advocacy and Communications, how new medicines in ophthalmology can mean the difference between people losing and keeping their sight.
4. AbbVie’s researchers are driven to ensure that migraine sufferers have the option of new treatments that can help them live full lives. Featured in this campaign are Jen and Leona who, because of advanced migraine medicines, have both been able to experience more of life’s important little moments. In the podcast, they openly share their experiences of how migraine once impacted their lives – on being a mother, on their careers, on their relationships – and how transformational their treatment has been.
Eimear O’Leary, IPHA’s Director of Communications and Advocacy, said, “This Innovate For Life campaign is aimed at telling the personal stories of innovation and how new medicines can literally change the trajectory of someone’s lives. Unfortunately,
Digital Transformation in Hospital Pharmacy
Are you ready to Drive Digital Transformation in Hospital Pharmacy?
patient care in Ireland is not as good as it could be. IPHA believes that every patient in Ireland should have fast and fair access to the latest treatments available. To give them a chance at creating new memories, like the people featuring in these films.
“This campaign illustrates why IPHA are calling for a New Medicines Pledge to be adopted by the next Government– where doctors can have the right medicine available for prescription for their patients at the right time; where the number of clinical trials in Ireland are doubled; and where there is a levelling-up of care for patients with rare diseases.
“We are very grateful to the film’s eight-member cast who shared their personal stories and brought to life the impact of new medicines.”
The European Association of Hospital Pharmacy (EAHP) Synergy Masterclass, takes place on 29-30 November 2024 at the Sheraton Brussels Airport. This premier event is designed to empower hospital pharmacists and healthcare professionals with the knowledge and tools to revolutionize healthcare delivery.
What You’ll Gain:
Cutting-edge strategies for adopting advanced technologies in healthcare
Expert advice on hospital management, automation, and procurement
Hands-on workshops to build actionable business plans
As EAHP President Nenad Miljković emphasises, “Lead the digital transformation in your hospital and create lasting improvements in patient care.” Don’t miss your chance! Register now and take the next step in shaping the future of healthcare.
New research has revealed the firstever national data on the incidence of Sudden Unexpected Death in Epilepsy (SUDEP) in Ireland.
SUDEP is the sudden, unexpected death of someone with epilepsy, where no other cause of death can be found.
The study, led by Dr. Yvonne Langan of St. James’s Hospital Dublin & Trinity College Dublin, together with the HRB, examined data from all deaths referred to coroners in 2019, identifying those with a history of epilepsy. The research identified 33 cases of definite SUDEP in 2019, representing an incidence rate of
Peter Murphy, CEO of Epilepsy Ireland
1:1400 per annum among people living with epilepsy. Of the 33 cases, 21 were men and 12 were women, with ages ranging from 9 to 81.
Speaking on the importance of identifying Irish specific data, lead investigator Dr. Yvonne Langan said the study will shape the treatment of epilepsy patients in future.
She said: “Ireland-specific data is vital in shaping effective healthcare policies. The findings will help raise awareness of SUDEP within both the patient and medical community and I hope will support tailored interventions to reduce risk for patients in the future.”
New Appointment at SVHG
While the exact reasons for SUDEP occurring in some people with epilepsy is unknown, previous research has shown that having uncontrolled or untreated tonic-clonic seizures is the biggest risk factor. Epilepsy Ireland believes that with targeted action to improve access to specialist care, the incidence of SUDEP can be decreased.
Peter Murphy, CEO of Epilepsy Ireland, said not enough is known about SUDEP, even within the Irish epilepsy community.
He said, "This study is a significant step forward in our understanding of the extent of SUDEP in Ireland. SUDEP is the most devastating consequence of epilepsy and over the years, we have met with far too many bereaved families who were not aware of SUDEP until their loved one passed away.
“We know that at least some of these deaths can be prevented by ensuring that more people with epilepsy become seizure-free and remain that way. This can be achieved through faster access to diagnosis and treatment, improved dialogue between healthcare professionals and patients, and through enhanced efforts to improve education and selfmanagement about known SUDEP risk factors which are modifiable.
“To date, much of the action around SUDEP in Ireland has come from Epilepsy Ireland, supported by the fundraising efforts of bereaved families.
“The epilepsy community should not have to depend on the fundraising efforts of bereaved families to target this serious issue. This study tells us that a national, government-led strategy with input from clinicians and patients is urgently required and it is vital that these calls will be taken seriously by Government, the HSE and Department of Health.”
While this study has established the incidence SUDEP in Ireland for the first time, ongoing research will focus on identifying the total number of epilepsy-related deaths, including causes such as status epilepticus (prolonged seizures) and seizure-related injuries. It is currently estimated that over 130 epilepsy-related deaths occur annually in Ireland (including those from SUDEP). This data is expected to be published in the coming months and according to Epilepsy Ireland, will further highlight the urgent need to develop a new strategy to reduce SUDEP and epilepsyrelated deaths.
Breslin, Director, St Vincent's Healthcare Group
St Vincent’s Healthcare Group (SVHG) has announced the appointment of Mr Jim Breslin to the Board of the Group.
SVHG, is one of Ireland’s larger hospital Groups incorporating St Vincent’s University Hospital (SVUH), St Michael’s Hospital, (SMH), and St Vincent’s Private Hospital (SVPH). The Group offers a unique multi-disciplinary approach to patient care in the country’s only multi-hospital campus. In 2023 the Group provided care to over 500,000 people.
Mr Breslin who enjoyed a 30-year career in the Irish senior public service spent much of his career in the Irish health service including as National Director of the HSE and
six years as Secretary General of the Department of Health. He also served as Secretary General in the Department of Children and Youth Affairs and in the Department of Further and Higher Education, Research, Innovation and Science.
Jim Breslin said, “SVHG is one of the country’s leading teaching hospitals. It has a hugely important role to play within our health services in leading healthcare innovation and partnering with others to introduce new care models that are more accessible and patient focused. Volunteering alongside my fellow board members, I look forward to supporting the hospital’s leadership and staff in addressing national, regional and local health priorities. ”
The SVHG Board is: Conall O’Halloran (Chair), Orlaith Blaney, Jim Breslin, Ann Hargaden, Dr John Holian, Paul Lynch, Dr Rhona Mahony, Nicola McCracken, Imelda Reynolds and Mark Ryan.
Jim
Research Grant for Cystic Fibrosis
A project from RCSI University of Medicine and Health Sciences to investigate a new approach for the monitoring and treatment of early Cystic Fibrosis has been awarded ¤676,866 in funding under the Taighde Éireann –Research Ireland Frontiers for the Future Programme. The funding has been provided by Children’s Health Ireland as a Frontiers for the Future partner.
The funding was announced by Minister for Further and Higher Education, Research, Innovation and Science, Patrick O’Donovan TD, as part of a package of ¤26 million funding for 40 research projects.
The RCSI research team is led by Dr Judith Coppinger, Senior Lecturer at the School of Pharmacy and Biomolecular Sciences, RCSI and principal investigator at National Children’s Research Centre, Children's Health Ireland. The team will investigate the potential of small particles which are important in regulating
inflammation, to monitor and treat cystic fibrosis in its earliest stages. Inflammation occurs early in the lungs of children with cystic fibrosis, often before symptoms are present. This inflammation can cause significant damage if it is not detected and treated.
The project will look at the role of small particles called extracellular vesicles in causing this early inflammation and how we might unlock new treatments by learning how they do so.
Diverse research
Welcoming the announcement, Minister O’Donovan said: “I am pleased to announce the Research Ireland Frontiers for the Future projects, which support high-risk, high-reward research endeavours. The selected projects, spanning 12 research institutions, bring fresh and innovative ideas that will help boost business and benefit society.
“I would also like to commend Research Ireland and the Children’s
Health Foundation for their great partnership and their focus on advancing children’s health through this funding programme. I encourage others to create similar partnerships and collaborations.”
Celine Fitzgerald, Interim Chief Executive Officer, Research Ireland, commented: “The Research Ireland Frontiers for the Future programme helps to build research capacity, expertise and reputation. This latest round of grants will support a diverse range of research positions and represents a strong commitment to developing future talent in key areas. It has been a pleasure having Children’s Health Foundation as a funding partner in that drive to strengthen Ireland’s research pipeline.”
Future impact
Fionnuala O’Leary, Chief Executive Officer, Children’s Health Foundation, commented: “Children’s Health Foundation is a proud partner of Frontiers for the Future programme, and we are
delighted to co-fund paediatric research projects that will benefit sick children throughout Ireland. Working with Research Ireland, we are able to leverage the funds our incredible supporters raise, to deliver larger grants for research into childhood diseases.
“This ensures the tireless efforts of our fundraisers can result in kinder and more gentler treatments for sick children. Frontiers for the Future programme plays a key role in enabling us to fund paediatric research with the potential to deliver impact for sick children now and into the future.”
Professor Fergal O’Brien, DeputyVice Chancellor for Research and Innovation, RCSI, said: “RCSI is committed to driving translational research which has a real impact on patients, their outcomes and their quality of life. I extend my sincere congratulations to Dr Coppinger and her team. This research has the potential to make a real difference for children living with early cystic fibrosis and I wish the team every success.”
Almost 700 Take Part in White Coat Ceremony
Just under 700 students took part in traditional White Coat Ceremonies at RCSI University of Medicine and Health Sciences recently.
The White Coat Ceremony has featured at the start of the academic year at RCSI since the 1990s when the Students’ Union requested an event to formally acknowledge the introduction of students into the Anatomy Room. The ceremony has since developed into an inter-professional event to recognise professionalism for RCSI’s new students of medicine, physiotherapy, pharmacy, physician associates studies and advanced therapeutic technologies.
Professor Tracy Robson, Deputy Vice Chancellor for Academic Affairs, said: "I am proud to welcome our new students as they mark the beginning of their academic journey at RCSI. From their first day, our students begin to form the values, behaviours and attitudes that will underpin their future practice and enable them to have professional relationships with colleagues, promote public trust and enhance patient safety.
traditional
The White Coat Ceremony is a special milestone for our students, and I hope they remember this day throughout their time at RCSI and in their future careers."
The students were also addressed by Professor Denis Harkin, Head of the Centre for Professionalism in Medicine and Health Sciences; Professor Clive Lee, Professor of Anatomy; and Professor Celine Marmion, Deputy Dean for Student Engagement, all of whom offered their best wishes and advice to the students as they embark on their health sciences studies.
Professor Harkin told the students, "These white coats are symbolic of the trust that is placed in us by our patients and members of the public. This is a trust we must
work to maintain. Remember this each time you wear the coat while training in anatomy, working in the laboratory, when carrying out experiments and research, and in all areas of your clinical training."
During the ceremony, Avinash Nazareth, President of the RCSI Students' Union, and Rebecca Grealy, Events Officer, along with other student representatives, reflected on their experiences since their own White Coat
Ceremonies and shared stories and advice with the group.
Professor Deborah McNamara, RCSI President, then led the students in declaring their commitment to professionalism, mirroring the declaration they will recite on their conferring day. The declaration signals the responsibilities they must begin to undertake as future healthcare professionals and scientists from the start of their academic training.
The
White Coat ceremony took place at RCSI last month
Accelerating Medicine Delivery
University College Cork (UCC) research has received a grant to use modern computational methods to develop critical medicines for improving global health and equality.
A team of researchers at UCC has received ¤950,000 in funding from the Bill & Melinda Gates Foundation to use artificial intelligence (AI) and machine learning (ML) to accelerate the development of medicines for conditions that impact those in developing countries.
Access to life-saving medicines in developing countries is often fraught with obstacles. For major pharmaceutical companies, the financial incentive to develop treatments for smaller, underserved populations simply isn’t there. Local manufacturers, meanwhile, often grapple with a
Walsh Celebrates 40 Years of PR News
Walsh:PR, one of Ireland’s most trusted and established PR agencies, marked forty years in business with their clients at an intimate event in the Merrion Dublin last month. The event, MC’d by broadcast journalist Sarah McInerney, celebrated the agency’s significant milestone and offered clients across the food, health, sustainability and NGO sectors the opportunity to hear from a leading expert in behavioural change marketing, Peter Mitchell of Marketing for Change. Pictured at the event were Caroline Heywood of Walsh (centre) with Fiona Clancy and Niall Faul of Perrigo.
lack of technical expertise and resources needed to navigate the rigorous process of bringing a drug to market. The challenges are compounded by inadequate infrastructure and harsh climatic conditions, making the path to accessible medicines even steeper. Addressing this issue, a team from University College Cork’s School of Pharmacy - led by Professor Brendan Griffin, Dr Patrick O’Dwyer, and Dr Harriet BennettLenane - is driving forward the "Advancing Global Health Drug Formulation Development Using ML and AI" project. Their mission is to develop Artificial Intelligence (AI) and machine learning tools that can accelerate the creation of medicines for conditions that disproportionately affect those in developing countries, such as malaria and other tropical diseases.
Professor Brendan Griffin, Dr Patrick O’Dwyer and Dr Harriet Bennett-Lenane. Photos by Ruben Martinez (UCCTV)
The tools they are building will be made freely accessible via an open-source, web-based platform, ensuring that this technology can be leveraged worldwide. This ambitious project aligns to the UCC Futures thematic areas of Future Medicines and AI & Data Analytics.
Professor Brendan Griffin said, "We're building on the School of Pharmacy's strong foundation in AI and machine learning with this exciting project, which has the potential to reshape how medicines are developed for patients in developing countries. It ties in with our goal of using pharmaceutical innovation to create a more sustainable and accessible medicine supply for everyone."
A recent study by the UCC team has already demonstrated machine learning’s potential to predict the impact of taking medicine with food - an insight that will now be expanded upon to guide the development of optimal drug formulations tailored to the needs of patients in low-income regions. For the first time, these communities will benefit from AI-driven, predictive medicine
development, offering hope in the quest for global health equity.
Professor Helen Whelton, Head of the College of Medicine and Health at UCC congratulated the researchers on securing this funding support from the Gates Foundation.
"We are extremely proud of our exceptional researchers using AI and machine learning to develop critical medicines which will enhance the li ves of so many patients around the world. Their work reflects the vision of our UCC Futures framework to inspire, engage and enable our researchers to create future Medicines. This project shows how our research is impacting and transforming our approach to real-world health and social care. Their pioneering work will help transform human lives, advance economic development while addressing global grand challenges in health and disease, securing a better future for all."
Professor John Cryan, VicePresident for Research and Innovation at UCC, said: "Congratulations to the researchers from UCC’s School of Pharmacy on receiving this award from the Bill & Melinda Gates Foundation. This innovative research in the UCC Futures thematic areas of Future Medicines and AI & Data Analytics, will deliver future medicines to low-income countries. Through the open access nature of the work, this award will address key societal and economical challenges in the pharmaceutical sector."
Generic Product Launch
Ferric Carboxymaltose Teva
50 mg iron/mL
Dispersion for Injection/Infusion iron as ferric carboxymaltose
Indications
Ferric Carboxymaltose Teva is indicated for the treatment of iron deficiency when: oral iron preparations are ineffective. oral iron preparations cannot be used. there is a clinical need to deliver iron rapidly.
The diagnosis of iron deficiency must be based on laboratory tests.
Presentation: One ml of dispersion contains 50mg of iron (as ferric carboxymaltose). Indications: Ferric Carboxymaltose Teva is indicated for the treatment of iron deficiency when: oral iron preparations are ineffective; oral iron preparations cannot be used; there is a clinical need to deliver iron rapidly. The diagnosis of iron deficiency must be based on laboratory tests. Dosage and administration: For intravenous administration only by injection, infusion or during a haemodialysis session. Ferric Carboxymaltose Teva should only be administered when staff trained to evaluate and manage anaphylactic reactions is immediately available, in an environment where full resuscitation facilities can be assured. The patient should be observed for adverse effects for at least 30 minutes following each Ferric Carboxymaltose Teva administration. Adults and Adolescents (aged 14 years and older): A single Ferric Carboxymaltose Teva administration should not exceed: 15mg iron/kg body weight (for administration by intravenous injection) or 20mg iron/kg body weight (for administration by intravenous infusion); 1000mg of iron (20ml Ferric Carboxymaltose Teva). Children and Adolescents (aged 1 to 13 years): A single Ferric Carboxymaltose Teva administration should not exceed: 15mg iron/kg body weight; 750mg of iron (15 mL Ferric Carboxymaltose Teva). Children below 1 year of age: Not recommended for use. Hepatic and Renal impairment: In patients with liver dysfunction, parenteral iron should only be administered after careful benefit/risk assessment. Parenteral iron administration should be avoided in patients with hepatic dysfunction where iron overload is a precipitating factor, in particular Porphyria Cutanea Tarda (PCT). Careful monitoring of iron status is recommended to avoid iron overload. No safety data on haemodialysis-dependent chronic kidney disease patients receiving single doses of more than 200mg iron are available. Contraindications: Hypersensitivity to the active substance, to Ferric Carboxymaltose Teva or to any of the excipients. Known serious hypersensitivity to other parenteral iron products. Anaemia not attributed to iron deficiency, e.g. other microcytic anaemia. Evidence of iron overload or disturbances in the utilisation of iron. Precautions and warnings: Parenterally administered iron preparations can cause hypersensitivity reactions including serious and potentially fatal anaphylactic reactions. Hypersensitivity reactions have also been reported after previously uneventful doses of parenteral iron complexes. There have been reports of hypersensitivity reactions which progressed to Kounis syndrome (acute allergic coronary arteriospasm that can result in myocardial infarction). The risk is enhanced for patients with known allergies including drug allergies, including patients with a history of severe asthma, eczema or other atopic allergy. There is also an increased risk of hypersensitivity reactions to parenteral iron complexes in patients with immune or inflammatory conditions (e.g. systemic lupus erythematosus, rheumatoid arthritis). If hypersensitivity reactions or signs of intolerance occur during
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Freephone: 1800 - 201 700 | Email: info@teva.ie
Prescription Only Medicine.
administration, the treatment must be stopped immediately. Facilities for cardiorespiratory resuscitation and equipment for handling acute anaphylactic reactions should be available, including an injectable 1:1000 adrenaline solution. Additional treatment with antihistamines and/or corticosteroids should be given as appropriate. Symptomatic hypophosphataemia leading to osteomalacia and fractures requiring clinical intervention including surgery has been reported in the post marketing setting. Patients should be asked to seek medical advice if they experience worsening fatigue with myalgias or bone pain. Serum phosphate should be monitored in patients who receive multiple administrations at higher doses or long-term treatment, and those with existing risk factors for hypophosphataemia. In case of persisting hypophosphataemia, treatment with ferric carboxymaltose should be re-evaluated. Parenteral iron must be used with caution in case of acute or chronic infection, asthma, eczema or atopic allergies. It is recommended that the treatment with Ferric Carboxymaltose Teva is stopped in patients with ongoing bacteraemia. Therefore, in patients with chronic infection a benefit/risk evaluation has to be performed, taking into account the suppression of erythropoiesis. Caution should be exercised to avoid paravenous leakage when administering Ferric Carboxymaltose Teva Paravenous leakage of Ferric Carboxymaltose Teva at the administration site may lead to irritation of the skin and potentially long lasting brown discolouration at the site of administration. In case of paravenous leakage, the administration of Ferric Carboxymaltose Teva must be stopped immediately. Interactions: The absorption of oral iron is reduced when administered concomitantly with parenteral iron preparations. Therefore, if required, oral iron therapy should not be started for at least 5 days after the last administration of Ferric Carboxymaltose Teva. Pregnancy and lactation: A careful benefit/risk evaluation is required before use during pregnancy and Ferric Carboxymaltose Teva should not be used during pregnancy unless clearly necessary. Based on limited data on breast-feeding patients it is unlikely that ferric carboxymaltose represents a risk to the breast-fed child. Effects on ability to drive and use machines: Ferric Carboxymaltose Teva is unlikely to impair the ability to drive and use machines. Adverse reactions: Hypersensitivity, anaphylactic reactions, loss of consciousness, phlebitis, syncope, angioedema, hypophosphataemic osteomalacia. Common: Hypophosphataemia, headache, dizziness, flushing, hypertensions, nausea, injection/infusion site reactions. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: Administration of in quantities exceeding the amount needed to correct iron deficit at the time of administration may lead to accumulation of iron in storage sites eventually leading to haemosiderosis. Monitoring of iron parameters such as serum ferritin and transferrin saturation (TSAT) may assist in recognising iron accumulation. If iron accumulation has occurred, treat according to standard medical practice, e.g. consider the use of an iron chelator. Legal category: POM. Marketing Authorisation Number: PA1986/124/001. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00082. Date of Preparation: July 2024
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie.
Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Date of Preparation: July 2024 | Job Code: GEN-IE-00092
Further information is available on request or in the SmPC. Product Information also available on the HPRA website.
Diabetes
Priorities for Adults with Type I Diabetes
A new research paper titled “The Top Ten Priorities in Adults Living with Type 1 Diabetes in Ireland and the United Kingdom – A James Lind Alliance Priority Setting Partnership” has been published, shedding light on the most pressing concerns and priorities of adults living with Type 1 diabetes. This study builds on the work done by the James Lind Alliance and partners in 2011 and the ongoing efforts of Diabetes Ireland, Diabetes UK and Breakthrough T1D to bring person-centred care to the heart of diabetes research and ensure that the voices of those living with type 1 diabetes are heard and acted upon.
The paper comes as we approach World Diabetes Day, held on November 14th each year. This date marks the birthday of Sir Frederick Banting – one of the founding fathers of insulin. Insulin is a treatment that has saved millions of lives around the world. On this day over 100 years ago Frederick Banting and John Mcleod also won a Nobel Peace Prize for their discovery.
This year the theme for World Diabetes Day is ‘Empowering Global Health’. This theme not only centres on individual health but also stresses the importance of communities working together to combat this global issue.
The study, conducted through a collaborative effort by people living with diabetes, their families, diabetes charities and clinical professionals across Ireland and the United Kingdom, utilized the James Lind Alliance (JLA) Priority Setting Partnership (PSP) approach. This method brings together patients, caregivers, and clinicians to identify and prioritize the most critical uncertainties in healthcare that
require research attention, the JLA PSP approach ensured that the voices and experiences of those living with Type 1 diabetes were central to determining the most pressing research questions and care priorities.
Key Findings
The study revealed the top ten priorities for adults living with Type 1 diabetes, reflecting a range of concerns from daily management to long-term outcomes. These priorities are expected to shape the future of diabetes research and healthcare policy in the region.
Dr Newman the lead author of the study, emphasized the importance of these findings: “This study is a powerful example of how Public and Patient Involvement can shape the future of healthcare. This work highlights the real-world challenges and unmet needs of adults living with Type 1 diabetes. By focusing on these top ten priorities, we can ensure that future research and healthcare services are aligned with what truly matters to those affected by the condition.”
Top Ten Priorities
1. Can the use of artificial intelligence or fasting acting insulins help achieve fully closed loop insulin delivery?
2. Is time in range a better predictor of diabetes management and complications compared to HbA1c (an average reading of blood sugar over a 3-month period)?
3. What impact do hormonal phases such as the perimenstrual period and menopause play in glycaemic
management and what treatments are most effective for managing glucose levels around these times?
4. What interventions are the most effective for reducing diabetes related distress and burnout?
5. What are the long-term implications of frequent hypoglycaemia on physical and mental health?
6. What impact does type 1 diabetes (including frequent low blood sugar) have on memory and cognition in older adults?
7. How can health care professionals better take into account the physical, psychological and social aspects of type 1 diabetes in clinics?
8. How can access to potential therapies like stem cell therapy, transplants and medications that modify the immune systems be improved so that everyone with type 1 diabetes can be guaranteed access?
9. Why do some people with type 1 diabetes become insulin resistant and does resistance increase with the number of years a person has diabetes and if so, why?
10. Can technology assist to accurately count carbohydrates without having to weigh or measure all foods and drink?
Implications for Future Research and Policy
The identified priorities will serve as a roadmap for researchers,
funders, and policymakers, guiding future studies and interventions aimed at improving the lives of those living with Type 1 diabetes. This work underscores the critical need for patient involvement in research and highlights the value of the JLA PSP process in addressing complex healthcare challenges.
Significance for Research and Policy
The study’s PPI-driven approach ensures that the identified priorities are not only reflective of the community’s needs but are also poised to inform and direct future research, funding, and healthcare policy. This collaboration highlights the importance of engaging patients and the public in the research process, ensuring that outcomes are meaningful and relevant.
Public and Patient Involvement (PPI) is an approach that places patients and the public at the heart of research and healthcare planning. PPI is research done with or by the public rather than to/for/about them. By placing people with lived experience front and centre, PPI centred research ensures that research priorities and healthcare strategies are aligned with the real needs and concerns of those affected by specific conditions.
The James Lind Alliance is a nonprofit initiative that aims to bring patients, caregivers, and clinicians together to identify and prioritize the most important research questions affecting their health. By focusing on patient-centered outcomes, the JLA PSP approach ensures that research efforts are directed toward areas that will have the greatest impact on those living with the condition.
Record ¤25.8bn Budget for Health
The Minister for Health Stephen Donnelly, Minister for Mental Health and Older People, Mary Butler and Minister for Public Health, Wellbeing and the National Drug Strategy, Colm Burke have announced a record ¤25.8 billion health budget to support the continued delivery and expansion of quality, affordable healthcare services in 2025.
The funding represents an overall increase of ¤2.94 billion on the January 2024 allocation, recognising the challenges of inflation and the increased demand on services due to a growing and ageing population.
It will provide for more than 3,300 additional staff in our health and social care services, deliver 335 additional hospital beds, expand services, deliver increased productivity and continue the reductions in waiting lists and trolley numbers.
Budget 2025 includes significant increases on 2024 in areas such as:
• Acute Hospitals (up 22% to ¤9.9 billion)
• Mental Health (up 10% to a record ¤1.48 billion)
• Older Persons Services (up ¤349 million to ¤3 billion)
• Palliative Care (up 13% to ¤179 million)
• National Ambulance Service (up 13% to ¤280 million)
The 2025 health Budget includes ¤1.2 billion allocated for existing level of service, ¤1.5 billion additional funding for 2024 pressures and ¤335 million in additional new measures.
Highlights include:
• ¤49.5 million to provide 335 more hospital beds
• ¤33 million to develop cancer services including full funding for the National Cancer Strategy
• ¤21.5 million additional funding to increase Home Support hours to 24 million in 2025
• investment of ¤30 million in new medicines through increased savings in the medicines budget
• ¤35 million women’s health
‘Two for the Price of One’
package including provision of free Hormone Replacement Therapy (HRT) and expanded access to Assisted Human Reproduction (AHR) services
• ¤6 million to expand Injury Units
Budget 2025 also includes ¤0.9 billion of funding, initially introduced for one-off measures during the COVID-19 pandemic, that has now been made permanent. This will allow permanent funding to continue to reduce waiting lists. ¤420 million be allocated to the HSE and NTPF in 2025 for waiting list initiatives, a ¤60 million increase on 2024 funding.
Minister Donnelly said, "Investment in our health service is now at its highest level in the history of the State. Budget 2025 sees an increase of almost ¤3 billion on 2024, supporting the continued expansion and delivery of quality services as we continue to ensure everyone is able to get the health care they need, when they need it.
“Whether it’s an appointment with a GP, a home care package for a loved one, an X-ray or MRI, quick
Published recently in the leading journal Nature Metabolism, Professor Luke O’Neill and his team have found that a natural metabolite called Itaconate can stimulate immune cells to make interferons by blocking an enzyme called SDH.
Co-lead author, Shane O’Carroll, from Trinity’s School of Biochemistry and Immunology, based in the Trinity Biomedical Sciences Institute (TBSI), said: “We have linked the enzyme SDH to the production of interferons in an immune cell type called the macrophage. We hope our work will help the effort to develop better strategies to fight viruses because interferons are major players in how our innate immune system eliminates viruses – including COVID-19.”
Co-lead author, Christian Peace, from Trinity’s School of Biochemistry and Immunology, based in TBSI, added: “Itaconate is a fascinating molecule made by macrophages during infections. It’s already known to suppress damaging inflammation but now we have found how it promotes anti-viral interferons.”
Working with drug companies Eli Lilly and Sitryx Ltd, the next step is to test new therapies based on Itaconate in various diseases, with some autoimmune diseases and some infectious diseases on the likely list. And the work potentially extends to other disease contexts in which SDH is inhibited, such as cancer, and could reveal a new therapeutic target for SDH-deficient tumours.
Professor O’Neill, Professor of Biochemistry in the School of Biochemistry and Immunology, based in TBSI, said, “With Itaconate you get two for the price of one – not only can it block harmful inflammation, but it can also help fight infections. We have discovered important mechanisms for both and the hope now is that patients will benefit from new therapies that exploit Itaconate and its impacts.”
Clinical trials in patients are set to start next year.
The work is a collaboration led by Trinity, which also includes researchers from Children's Health Ireland at Crumlin; University of Valladolid, Spain; and Stanford School of Medicine, California, USA. It was funded by the European Research Council and Taighde Éireann – Research Ireland, formerly Science Foundation Ireland.
access to emergency care or a minor injury unit, an appointment with a hospital consultant or surgery, Budget 2025 is all about making this a reality for more and more patients and families. We are living longer and living better, but our growing and ageing population place additional demands on our services. We continue to respond to these challenges, and we are placing a strong focus on more productivity alongside investment in increased capacity and in workforce planning to ensure we can meet the needs of our healthcare service into the future."
The 2025 Health Budget will see spending on Mental Health rise to almost ¤1.5 billion. This marks the fifth consecutive year that an increase in funding has been provided to develop and support mental health services - an increase of 43.7% over the lifetime of this government. This clearly underscores the focus this government has placed on ensuring that our mental health services are safe, accessible, modern, and person-centered.
ICO Eye Care in Focus Conference 2024
The annual Eye Care in Focus Conference, hosted by the Irish College of Ophthalmologists, took place on Tuesday, 1st October at The Gibson Hotel, Dublin.
The 1-day clinical education meeting is designed for the multidisciplinary eyecare team working across community and hospital care in Ireland. It provides a unique opportunity for ophthalmologists, optometrists, orthoptists, ophthalmic nurses and technicians to come together to discuss current eye care pathways and developments, and facilitate a forum for shared learning across the disciplines..
Cataract Clinical Session
Talks at the cataract session outlined efficiencies and improvements to patient waiting times and care as a result of new cataract pathways in operation in Dublin North East (CHO9) and in Dublin South, Kildare and Wicklow (CHO7) regions. The pathway was reviewed under five areas to highlight how the process improvements were made in terms of referrals, referral management, pre-op assessment, day of surgery and post-op clinic.
Optometry Ireland President, Tania Constable gave key advice on how optometrists can improve
their referrals to ensure the right patients are seen in the cataract clinics and that they are prioritised according to their visual needs.
Paediatric Ophthalmology Clinical Session
At the paediatric session
Dr Geraldine Comer discussed the policies and procedures developed in the HSE CHOWest/ Galway region to facilitate the development of a modernised integrated paediatric eye care pathway. The pathway has ensured children in the west are seen in a timely manner in the most appropriate setting.
Dr Christine Bourke outlined the new pathways and services developed at CHI for children with Retinopathy of Prematurity, including links between tertiary and primary care. She
Ms Tania Constable, Clinical Optometrist, CHO7 and President, Optometry Ireland, Dr Geraldine Comer, Consultant Ophthalmologist, University Hospital Galway CHO2 West and Dr Christine Bourke, Paediatric Ophthalmology Clinical Fellow, Children's Health Ireland at Temple Street and Crumlin Hospitals, Dublin
highlighted the pathology of other eye conditions affecting premature children in the long term, namely cortical visual impairment (CVI) which is a commonly encountered condition.
Ms Tania Constable, Clinical Optometrist, CHO7 spoke to delegates about the
Keynote speakers at the Cataract Clinical Session, Dr Margaret Morgan, Dr Margaret Morgan, Consultant Ophthalmologist, CHO7 and Royal Victoria Eye and Ear Hospital, Dublin, Ms Lisa McAnena and Mr Tim Fulcher, Consultant Ophthalmologists, Mater Hospital and Beaumont Hospital, Mr John Doris (chair) President of the ICO, Ms Chriosa O'Connor, Clinical Optometrist, and Ms Tania Constable, Clinical Optometrist
considerations for adults with intellectual disabilities, who may have less contact with preventative services than the general population. Her presentation provided guidance on how to assess and manage adults with additional needs in the community with the aim of improving access to eye care, also discussing alternative clinical testing, different communication approaches, and management strategies.
Clinical Programme in Ophthalmology
The presentations provided a progress update on the strategy for eye care and developments following the implementation of new integrated care pathways that have significantly reduced patient waiting times in cataract and paediatric ophthalmology.
Pictured at the Irish College of Ophthalmologists ‘Eye Care in Focus’ Conference, The Gibson Hotel, Tuesday 1 October, Ms Aoife Doyle, HSE National Clinical Lead for Ophthalmology and Consultant Ophthalmic Surgeon, Royal Victoria Eye and Ear Hospital and St James's Hospital, Dublin, Ms Cathríona Ennis, Director of Nursing, Royal Victoria Eye and Ear Hospital, Dublin and Ms Sarah Spain, Senior Orthoptist, Health & Social Care Professions Lead for the National Clinical Programme in Ophthalmology
The development and support of the role of orthoptics, specialist and advanced nursing and a new ophthalmic technician grade as integral to the integrated eye care team were also discussed at the clinical programme update session.
Making your Practice more Sustainable
The ophthalmic field, like many others in healthcare, has a significant environmental footprint. Cataract surgery is the highest volume surgery performed in Ireland. From the disposal of single-use instruments to the energy consumption of diagnostic equipment, the impact is considerable. This session aimed to highlight the simple and practical steps eye care professionals can take in their clinics to help reduce their carbon footprint.
It follows the focus on sustainability at the ICO’s Annual Conference in May this year, and demonstrates the College’s commitment to placing a spotlight and ‘call to action’ on the impact of the specialty's carbon footprint to the full eye care team. The ICO has developed a new sustainability education resource on its members portal, aimed at
sign posting educational resources and providing helpful advice and practical tips on ways to reduce the carbon footprint in ophthalmology
Guest speaker Professor John Nolan, Director of the Nutrition Research Centre Ireland (NRCI)
Professor John Nolan, Director of the Nutrition Research Centre Ireland (NRCI) South East Technological University, with meeting chair Mr John Doris, President, ICO and Consultant Ophthalmic Surgeon, University Hospital Waterford
at the South East Technological University, discussed the role and evidence for targeted nutrition to improve visual function and also outlined plans for a New School of Optometry at South East Technological University in Waterford.
Meeting chair Mr John Doris, President, Irish College of Ophthalmologists (2nd right) with keynote speakers at the Making your Practice more Sustainable session Ms Louise Doyle, Theatre Nurse, University Hospital Waterford, Dr Alison Greene, SpR Royal Victoria Eye and Ear Hospital, Dublin, and Ms Helen Curran, Head of Sustainability, Specsavers UK/IRE
Health & Safety
Supporting Frontline Workers: The Role of Safety Solutions in Modern Healthcare Facilities
The Irish healthcare system is at a critical juncture, with the Irish Nurses and Midwives Organisation (INMO) and other healthcare unions preparing to ballot members for industrial action. This development follows a month of ongoing protests and growing frustration among healthcare workers, largely over staffing shortages and deteriorating working conditions.
Here John McSwiggan, Sales Engineer for Pinpoint Ireland, explores the current challenges facing healthcare workers and examines how innovative safety solutions can improve staff morale and workplace safety.
Staffing Shortages and Deteriorating Conditions
At the core of the issue is a severe staffing shortage, exacerbated by recent Health Service Executive (HSE) policies. The INMO reports that crucial nursing positions in specialised areas such as cancer care, palliative care, paediatrics, and rehabilitation remain unfilled. This shortage is not a sudden occurrence but the result of years of underinvestment and insufficient workforce planning. The HSE's "Pay and Numbers Strategy" has drawn sharp criticism from unions, who view it as an all but confirmed freeze on recruitment. While the HSE asserts that staffing levels have increased, the experiences of frontline workers tell a different story.
Impact on Healthcare Workers
The impact of these staffing shortages is significant and farreaching. Nurses and midwives are frequently required to work on their days off and stay for extended unpaid periods after shifts. This unsustainable workload is contributing to burnout among healthcare professionals. The Practitioner Health Matters Programme (PHMP) revealed that 2023 saw a 48% increase in healthcare workers presenting to the service. According to the report, the most predominant concerns were anxiety, depression, and burnout. Research has shown that this can have severe consequences on patient safety with studies showing a significant association between burnout and patient safety [Hall LH, Johnson J, Watt I, Tsipa A, O’Connor DB (2016)].
Staff shortages not only directly impact patient care but also lead to longer wait times and reduced services.This often causes deep frustration for patients and their families, which can escalate into threats of violence and, in some cases, physical attacks on healthcare workers.
In response, the INMO and other unions have taken action. A series of lunchtime protests were staged nationwide to highlight the staffing crisis, and unions are now balloting their members for potential industrial action, emphasising the gravity of the situation.
Written by John McSwiggan, Pinpoint Ireland
Impact of Violence on Healthcare Staff
As Ireland's healthcare system faces these challenges, the INMO protests and potential industrial action serve as a critical wake-up call. In navigating this crisis, the HSE must recognise the importance of supporting current staff, especially during this apparent employment freeze. Implementing systems and processes to ensure that healthcare workers feel valued and supported is essential as demand for the healthcare system continues to grow.
A resulting rise in violence against healthcare workers
The rising tide of violence against healthcare workers has become an alarming concern, with significant implications for the HSE and the overall healthcare system. This troubling trend not only jeopardises the well-being of frontline workers but also strains an already burdened healthcare infrastructure.
Recent statistics paint a worrying picture of the situation. According to the INMO, over 4,000 nurses and midwives were assaulted in the workplace during a 13-month period from January 2023 to February 2024. These assaults ranged from verbal to physical and sexual in nature. Even more concerning is that many incidents likely go unreported.
The surge in violence against healthcare workers can be traced to several key factors, one of which is the fluctuation in staffing levels. This instability often leads to high-pressure situations, especially when healthcare staff are dealing with patients and families already under emotional strain. Prolonged wait times and delays in care further fuel frustration, which in many cases escalates into hostile behaviour directed at nursing staff.
The impact of this violence on healthcare workers is profound and multifaceted. Beyond the immediate physical harm, these incidents take a severe toll on mental health and overall well-being. The ripple effects of violence against healthcare workers extend far beyond individual incidents. It erodes workplace morale, increases stress-related sick leave, and ultimately contributes to staff turnover. Many nurses are now citing work-life balance as their primary reason for leaving the profession, rather than retirement – a significant shift from previous years.
In England alone, last year, the NHS witnessed a staggering 1.68 million sick days attributed to stress, with anxiety and depression emerging as the leading causes of illness among nurses. This burnout is further exacerbated by extended shift hours, chronic understaffing, and workplace abuse.
Protecting Healthcare Staff: Systems and Solutions
Healthcare institutions face a significant challenge in protecting their staff from violent attacks. As incidents of aggression toward healthcare workers continue to rise, it is imperative that these institutions implement comprehensive strategies to ensure the safety and well-being of their employees.
Security Presence and Technological Solutions
One of the most effective ways to improve security in healthcare settings is to ensure a strong and visible presence of trained security personnel. However, it is crucial that these security professionals receive specialised training in de-escalation techniques and crisis intervention specific to healthcare settings. In addition to human resources, technological solutions play a vital role in enhancing staff safety. Advanced closed-circuit television (CCTV) systems with live monitoring capabilities serve as both a deterrent and a means of rapid response to potential threats. Personal safety alarms for staff members, such as Pinpoint’s
Health & Safety
P2 System, allow employees to summon immediate assistance in the event of a threat or emergency.
Environmental Design and Policy Enforcement
Environmental design and clear policies also play crucial roles in staff protection. Healthcare institutions should implement strict access control measures, including ID badges, controlled entry points, and visitor management systems to limit unauthorised access. In addition, patient rooms and work areas should be designed with safety in mind, incorporating features like easily accessible panic buttons and escape routes.
Training and support for staff are equally important. Regular training on de-escalation techniques and recognising potential threats can empower employees to prevent incidents before they occur. Furthermore, implementing userfriendly incident reporting systems encourages staff to document threats and incidents, allowing for better risk assessment.
Pinpoint Staff Safety Systems: A Crucial Tool in Healthcare
Pinpoint staff safety alarms have become an essential tool in safeguarding healthcare workers from the rising incidents of violence in medical settings.
As aggression toward medical professionals escalates, these innovative systems offer a critical layer of security and peace of mind for those on the front lines of patient care. Pinpoint, a family-owned business with an Irish office in Blanchardstown, Dublin, has been at the forefront of addressing this issue for over 30 years. Their staff safety systems are now widely used across NHS healthcare trusts in the UK, as well as in healthcare facilities in Ireland and the US. The company's latest solution, the P2 System, marks a significant advancement in staff protection technology.
At the heart of Pinpoint's system is a wearable panic alarm. This device features two programmable buttons: a smaller one typically used to request assistance and a
larger one for emergencies. The alarms use infrared technology, ensuring reliable and accurate communication in healthcare environments. When activated, the system sends alerts to nearby colleagues, enabling a rapid response and intervention. This quick reaction time is crucial, as the Pinpoint system can call for security and support in less than 85 milliseconds. The proactive nature of this system allows staff to address potential conflicts early, significantly reducing the chances of an incident escalating.
Pinpoint's staff safety alarms are designed to be versatile and effective in various healthcare environments:
• Hospitals: The system equips nurses and hospital staff with a reliable device to prevent workplace violence initiated by patients.
• Mental health facilities: It fosters a safe and trusting environment during treatment sessions and daily interactions with clients.
• Residential rehabilitation centres: The alarms prioritise staff safety during therapeutic engagements with residents in rehabilitation programs
Pinpoint's staff safety systems are now a key feature in many healthcare facilities. Although they don’t solve broader healthcare challenges, they provide peace of mind, enabling staff to focus on patient care without worrying about their safety. By showing that employee well-being matters, these systems help create a more positive work environment, lower stress levels, and boost job satisfaction, leading to a more motivated and engaged workforce.
Case Studies: Pinpoint in Action
The following case studies showcase the real-world impact of Pinpoint staff safety alarms in different healthcare settings. These examples highlight how the systems have enhanced both staff safety and overall wellbeing, creating a more supportive environment for patient care. By looking at these cases, we can
better understand how effective staff safety systems can be in reducing risks and fostering a culture of safety within healthcare facilities.
St. Brigid’s Hospital, Ballinasloe, Galway
Located in Ballinasloe, Galway, The Creagh Suite in St. Brigid’s Hospital offers long-stay, continuing care for residents living with dementia and experiencing the psychological and behavioural symptoms of this illness.
The facility holds 14 beds for individuals who require ongoing care for severe mental health conditions and dementia. Staff at the hospital provide therapeutic activities, physical health monitoring and continuous support to allow residents to carry out their daily lives.
The Challenge
St. Brigid’s Hospital required a reliable, effective staff safety system to comply with Ireland’s health and safety legislation and protect the nursing staff on site. Pinpoint’s easy-to-use programme was chosen to meet the complex safety needs of the residents in Creagh Suite.
Aggressive behaviour can occur in people experiencing the behavioural and psychological symptoms of dementia. The confusion, hallucinations, memory loss and physical pain associated with the illness can cause a person to behave violently, often unintentionally.
To protect against this, Pinpoint’s staff safety systems were installed before the residents moved into the Creagh Suite.
The Solution
Meeting the high standards set by Ireland’s health and safety legislation, Pinpoint’s security systems were installed in St. Brigid’s Hospital to protect healthcare staff at risk of violence on the ward.
To minimise any interruptions to the daily running of the facility, the installation was carried out ahead of the residents moving into the building.
Twin Code Perpetual PITs were given to all staff members. Powered by a specialist energiser, these personal alarms could be used and recharged between shifts. The Perpetual PITs have two call levels, Assistance and Emergency, which correlate to the severity of the incident in question.
By activating the alarm, infrared signals are transmitted to receiver units found within the hospital, activating the system and alerting a response team to the exact location and type of call. Doing so reduces the risk of an incident escalating and limits harm to the staff member.
Every member of the team was then given comprehensive training on how to use the system and the protocol in place for responding to incidents. This was all carried out before the hospital opened to ensure staff were confident and competent in using the systems in case of an incident.
The Result
Installing Pinpoint’s staff safety system gave staff confidence in their safety on the ward. With the approval of the HSE, the advanced security system superseded the legal safety requirements for St. Brigid’s Hospital, providing reliable, full-proof coverage of the Creagh Suite and garden area.
Maria Donnellan, Clinical Nurse Manager 3 at St. Brigid’s Hospital, said
“With Pinpoint’s staff safety systems installed, staff are reassured of their safety at work and know they can call for help in the event of any emergency. If a resident becomes abusive toward a member of the team, or if a patient is choking, staff can quickly call for support and know it will soon be on its way”
“The systems help us all stay safe, and crucially, meet the high requirements of health and safety legislation in Ireland. The Health and Safety Authority was impressed during a recent visit to the facility”
To find out more about staff security systems used in hospitals across Ireland, please contact us at https://www.pinpoint.ltd.uk/ contact-us.
Smallwood Manor, North Staffordshire, England
Smallwood Manor is an independent tier 4 hospital in North Staffordshire. The country estate serves as a therapeutic environment for young people and their families to receive care and treatment.
Part of Cove Healthcare, the facility offers specialist inpatient support to young people experiencing mental health disorders, with a focus on general adolescent, high dependency and eating disorder services.
The Challenge
Smallwood Manor required highperformance safety systems to protect both healthcare staff and residents on site.
Levels of violence against staff in mental health trusts are continually higher than in any other type of NHS trust (Royal College of Nursing). This is partially due to the complex nature of mental health illnesses, which can result in patients becoming distressed and behaving aggressively toward staff. In these cases, healthcare workers need to be able to call for assistance rapidly to swiftly deescalate the situation and provide the necessary support.
Equally, residents required accessible, easy-to-use systems that would allow them to call for support in case of a medical or mental health crisis. Should a patient become distressed, it’s crucial they – or another resident –could summon assistance from a professional within an instant.
Due to the challenging nature of the environment, Cove Healthcare needed the highest quality security systems that would alert staff to potential issues on the ward without undue noise and disruption.
The Solution
Cove Healthcare identified the Pinpoint System as meeting the highest level of specification.
Personal Infrared Transmitters (PITs), which act as personal safety alarms, were given to all staff members to sound in case of an incident. Pinpoint’s PITs have two call levels, Assistance and Emergency, which correlate to the severity of the situation in question. By activating the alarm, infrared signals are transmitted to the Advanced Receiver Units installed within the hospital, triggering the system and alerting a response team to the exact location and type of the call. Doing so allows staff to intervene and de-escalate potentially dangerous situations, thereby reducing the risk of harm to workers and other residents.
Every member of the team was given comprehensive training on how to use the system and the protocol in place for responding to incidents. This was all carried out before the hospital opened to ensure staff were confident and competent in using the systems in case an incident were to occur.
Pinpoint’s Nurse Call Buttons were also built into the walls throughout the building for patients to use should they need
assistance. Placing these at regular, accessible intervals in Smallwood Manor meant that residents could easily call for help in any situation or emergency.
The Results
Installing Pinpoint’s staff safety systems throughout Smallwood Manor maximised staff and patient safety, and significantly reduced the risk of harm. As a result, staff could focus on delivering the highest quality of care, and thereby improve patient treatment outcomes.
By offering thorough training ahead of the hospital opening employees felt reassured in how to use the systems effectively and could teach other bank staff how to do the same.
Lee Smith, head of Cove Health and Smallwood Manor said of the system “I’ve worked with all manner of safety systems, but none of them come anywhere near Pinpoint. It gives staff confidence. These types of environments can be quite stressful, and people need the confidence that they are safe at work in order to do the best job.”
Conclusion: A Time for Change
The current crisis in Irish nursing is not just a problem for nurses; it's a critical issue that affects the entire healthcare system and, by extension, every citizen of Ireland. The HSE has a responsibility to its staff and the public, to take decisive action.
By implementing the practical measures outlined above, investing in staff safety and well-being, and learning from successful models elsewhere, the HSE can turn this crisis into an opportunity for positive change. The time for halfmeasures and stopgap solutions has passed. What is needed now is a comprehensive, systemic approach to valuing and protecting the nursing workforce.
As we move forward, it is crucial to remember that nurses are not just employees; they are the backbone of our healthcare system. Their well-being is intrinsically linked to the quality of care that patients receive. By investing in nurses, we invest in the health of the nation.
The protests we see today are a call to action. It is now up to the HSE and policymakers to answer that call with meaningful, lasting change. The future of Irish healthcare depends on it.
Management of Anaemia in Chronic Kidney Disease Anaemia
Dr Niamh Corcoran1 Specialist Registrar in Nephrology
Professor Austin Stack1,2 Professor of Medicine, Consultant Nephrologist
1Department of Nephrology, University Hospital Limerick, 2School of Medicine, University of Limerick
Introduction
The development and progression of anaemia is an almost universal consequence of chronic kidney disease (CKD) and worsens with progressive loss of kidney function. Anaemia is considered both a risk marker and a risk amplifier in that it accelerates the risk of major events such as hospitalisations, stroke, myocardial infarction, and death in patients who have anaemia compared to those who do not. The mechanisms through which anaemia develops in CKD are diverse and complex. Studies over the past 20 years have elucidated mechanistic pathways and generated novel therapeutic interventions. Defective erythropoiesis, iron deficiency, and abnormal iron regulation coupled with a heightened inflammatory system have all conspired to drive the development of anaemia in CKD. The management of anaemia has been revolutionised with the wide availability of recombinant erythropoietin and increased utilisation of intravenous iron. More recently the discovery of a novel set of drugs, the hypoxia-inducible factor prolyl hydroxylase inhibitors (HIF-PHIs), has added to these treatment strategies. Optimisation of anaemia management is associated with improved quality of life, exercise tolerance, and lower risks of adverse clinical outcomes.
Evaluation of Anaemia in CKD
Anaemia is defined as a haemoglobin of <13g/dL in men and <12g/dL in non-pregnant women.1 The prevalence of anaemia increases with advancing
age and with worsening kidney function.2 A recent study by Clancy et al found that the prevalence of anaemia among patients in the Irish health system increased from 8.2% in individuals with GFR > 90 ml/min/1.73m2 to 64% for those with advanced kidney disease eGFR < 30 ml/ min/1.73m2, compared with an overall prevalence of 12% in the general population.3 Once anaemia is diagnosed, a detailed evaluation should seek to identify underlying causes.
The majority of patients with CKD will have a multifactorial anaemia with contributions from iron deficiency and anaemia of chronic disease.4 A focused clinical evaluation should evaluate for blood loss, the presence of comorbidity, and prescribed medications especially the use of antiplatelet agents and anticoagulants. With more advanced CKD, erythropoietin deficiency becomes a more significant contributory factor. The routine full blood count may reveal a microcytic (MCV <80 fL) picture if iron deficiency is a predominant contributor. First-line investigations should include a full blood count (including white cell differential, platelets), absolute reticulocyte count, transferrin saturation (TSAT), ferritin, B12 and folate concentrations, as well as a faecal occult blood test.5
Importance of Iron Deficiency in CKD
Iron deficiency is common contributor to the anaemia of CKD with approximately 60%
of patients affected at the start of dialysis. It can present either as functional iron deficiency –inadequate iron supply to meet demand despite normal iron stores – or absolute iron deficiency – a reduction in stored iron. In general, the detection of iron deficiency requires measurement of transferrin saturation ratio (TSAT), which is a measure of functional iron deficiency, and the plasma ferritin which measures iron storage. Absolute iron deficiency in CKD is generally defined as a TSAT <20% and serum ferritin <100ng/ mL (or <200ng/mL in patients on haemodialysis). This cut off is higher in CKD compared with the general population because plasma ferritin levels increase in states of inflammatory stress such as chronic kidney disease.6 In functional iron deficiency, the TSAT is generally <20% and plasma ferritin levels are elevated.
Management of Anaemia in CKD
The management of anaemia of CKD depends on many factors and requires a balanced approach to treatment. The approach will vary according to stage of CKD, the severity of anaemia, the copresence of iron deficiency, and may differ according to practice patterns within countries. In general, guidelines recommend correction of iron deficiency in the first instance. Treatment with erythropoietin may be indicated where there is persistent anaemia in the setting of advanced CKD and a rise in haemoglobin level is desired. Oral iron supplementation should be considered in the initial treatment of absolute iron deficiency. Oral iron is cheap and easy to administer, but is associated with gastrointestinal upset, non-adherence, and poor absorption. Intravenous iron may be the preferred option in symptomatic or severe iron deficiency (TSAT <12%), and for those who do not tolerate or fail to respond to oral iron. Intravenous iron fully corrects iron deficiency, bypasses need for GI absorption and is incorporated more rapidly into RBCs than oral iron, and delays or avoids the need for erythropoietin therapy.6
The goal of treatment is to correct iron deficiency and increase the haemoglobin concentration. For
patients who are receiving dialysis, the target haemoglobin levels are generally between 10-12 g/ dl. There are no evidence-based target haemoglobin concentrations for patients with CKD and not requiring dialysis, but in general levels should not exceed 13 g/ dl, due to an association between higher haemoglobin levels and adverse clinical outcomes.7
Erythropoietin stimulating agents (ESAs) are generally indicated for the correction of anaemia where patients have persistent anaemia, (Hb <10g/dl) despite adequate iron stores. These agents are administered subcutaneously for patients with non-dialysis dependent CKD or intravenously for those on dialysis. ESA are contraindicated in patients with active malignancy or prior stroke, where the risks may outweigh the benefits.8
A new class of agent, the hypoxia-inducible factor prolyl hydroxylase inhibitors (HIF PHIs) has emerged for the treatment of CKD-associated anaemia. Their novel mechanism of action mimics the natural response of the body to hypoxia and stimulates the transcription of the endogenous erythropoietin gene. Evidence from randomised clinical trials have shown them to increase haemoglobin levels, reduce blood transfusions, and improve iron homeostasis, though there are some concerns regarding the higher risk of thromboembolic events.9, 10
Conclusion
Anaemia in CKD is highly prevalent and confers substantial burden on both patients and the healthcare system. The aetiology is multifactorial, and thus therapeutic strategies must be individualised. Targeted screening of high-risk groups should be performed on a routine basis. Simple measures should be implemented to correct deficiencies wherever possible. Novel therapies such as ESAs and HIF PHIs are emerging as treatments where first line measures are insufficient. Clinicians must remain vigilant and endeavour to continuously improve the identification and treatment of patients with anaemia and CKD. References available on request
Dr Niamh Corcoran
Professor Austin Stack
Patient Safety Network Launched
A new national patient safety research network, led by the School of Psychology at Trinity College Dublin, welcomed 100 patient partners, academics and healthcare professionals to Trinity for the EQUIPS network's first inperson event.
Earlier this year, Trinity was successful in securing funding from the Health Research Board (HRB) and Health Services Executive (HSE) National Quality and Patient Safety Directorate (NQPSD) to facilitate a new Evidence-Based Quality Improvement and Patient Safety (EQUIPS) Research Network.
EQUIPS aims to bring together academics, healthcare staff, and patient partners to coordinate and accelerate healthcare quality and patient safety research in Ireland.
The EQUIPS Research Network has grown steadily and this month the network welcomed one hundred delegates to the Dargan Theatre in Trinity Business School for their inaugural in-person event.
The audience consisted of knowledge users, patient partners, and academics from institutions and healthcare organisations around Ireland. The aim of this event was to provide a unique opportunity for EQUIPS’ three stakeholder groups to connect with one another and discuss quality and patient safety research in Ireland.
EQUIPS team from the Centre for Innovative Human Systems.
L-R Prof. Sam Cromie, Dr Jill Poots, Prof. Siobhan Corrigan, Rory Carrick and Paula Hicks
The event opened with talks from representatives of each of the network’s stakeholder groups. Professor Sam Cromie (Principal Investigator, Centre for Innovative Human Systems, Trinity College Dublin) provided an overview of the scope of EQUIPS Research Network and emphasised bringing together patients, academics, and knowledge users as key to EQUIPS’ success.
Lead Knowledge User Dr Orla Healy, National Clinical Director for Quality and Patient Safety in the HSE, outlined HSE's patient safety strategy, commitments, and priorities, which are reflected in the work of EQUIPS. EQUIPS
Patient Partner, Anne Lawlor, Chairperson for 22q11 Ireland and Co-chair HSE Patient Forum shared her own personal journey, the role that research has played, and her vision for EQUIPS, encouraging researchers to think of ‘what matters’ to patients when conducting QPS research.
A priority area for EQUIPS is Sociotechnical Systems Design. To introduce this concept Professor Paul Bowie, from the University of Staffordshire and NHS Education for Scotland, gave the inaugural keynote speech to the EQUIPS Research Network. This talk provided an introduction to the use of Human Factors (‘systems thinking’) in quality improvement and patient safety research.
The event was carefully curated to emphasise networking between attendees, from registration to close. Attendees had the opportunity to draft a vision for EQUIPS and discussed research conducted by EQUIPS member Professor Paul O'Connor (University of Galway), which describes barriers and facilitators to quality and patient safety research.
Finally, with the aim of addressing some of the proposed barriers to research, the event closed with a panel on ‘The Practicalities of Quality and Patient Safety Research. The panellists were: Prof Sam Cromie (PI, TCD), Dr Orla Healy (Lead Knowledge User, HSE NQPSD), Prof Paul Bowie (University of Staffordshire), Dr Padraig Carroll (PPI Ignite, TCD), Dr Olga Cleary (HSE Research and Development), Anne Lawlor (Patient
Partner, 22q11) & Dr Teresa Maguire (Health Research Board).
Network Manager Dr Jill Poots (Centre for Innovative Human Systems, TCD) described the day as a success stating:
“The EQUIPS operations team is delighted with the success of our inaugural in-person event. It was great to see new connections being made, and feedback from attendees has been positive. I look forward to seeing the network continue to grow.”
EQUIPS Lead Knowledge User, Dr Orla Healy, National Clinical Director for Quality and Patient Safety said:
“I was delighted to speak at the inaugural in-person EQUIPS event and see staff from across the health regions attending and engaging with researchers and patient partners. EQUIPS is cofunded by the National Quality and Patient Safety Directorate to bring these groups together so that we can better align QPS research with the needs and priorities of our health services and so that high quality research is translated into service improvements for patient safety . EQUIPS will also provide new opportunities for healthcare staff to participate and build their own QPS research skills.”
The EQUIPS Research Network is open to anyone interested in Quality and Patient Safety Research, including Trinity staff, students, and members of the public. To register your interest, see www.tcd.ie/cihs/equips.
Infectious Diseases
Reducing Infectious-Disease Stigma
Written by Dr Pádraig Morrissey,
Consultant
in Infectious Diseases
Senior House Officer in Infectious Diseases, and Dr Eoghan de Barra,
At the onset of a worldwide public health crisis in the late 80s, a series of adverts were designed to raise awareness of the AIDS epidemic in the United Kingdom. The UK government’s Don’t Die of Ignorance campaign is etched in the memories of many. Opening with the eruption of a volcano and dark ominous music accompanied by a voiceover from John Hurt, it described a deadly disease which could be spread from an “infected person” and how “anyone can get it”. It warned the British public to protect themselves and not to die of ignorance, as a bouquet falls on a tombstone with “AIDS” etched across it. Although the advertisement saved lives, it likely contributed to the stigma that still surrounds HIV more than thirty years later.
The advances in HIV care with antiretroviral therapy have dramatically improved the lives of people living with HIV. Early diagnosis and treatment have led to people living with HIV having the same health and life expectancy as the general population. In addition, successful treatment can prevent onwards transmission of HIV, known as U=U (Undetectable equals Untransmittable). This public health message has the power to help tackle some of the antiquated stigma faced by persons living with HIV. Living with HIV is not a barrier to any form of employment and is not a barrier to having children, as effective therapy means babies born to
mothers living with HIV do not have the infection.
The Health Protection Surveillance Centres (HSPC) most recent annual data for 2022 showed a large increase (68%) in the overall number of diagnoses of HIV in Ireland, compared to pre-pandemic year 2019. This is largely attributable to an increase in diagnoses amongst people with a previous diagnosis outside of Ireland. Amongst new diagnoses, 84% reported their region of birth to be – Latin America or Caribbean (32%), sub-Saharan Africa (27%) or Eastern Europe (25%). While this group are unlikely to have benefitted from HIV prevention strategies in Ireland, it is imperative that they are promptly linked with HIV care to on arrival in Ireland for their own benefit and to prevent onward transmission.
The rate of first-time HIV diagnoses (3.4 per 100,000 population) decreased by 16% in 2022 compared to pre-pandemic year 2019 and is lower than the rates between 2012 and 2018. The key population group affected by HIV in Ireland remain gay, bisexual and other men who have sex with men (gbMSM), accounting for 58% of first-time diagnoses in 2022. Eighty percent of first-time diagnoses in gbMSM in 2022 occurred in those born in either Ireland (41%) or Latin America and Caribbean (39%).
Heterosexuals accounted for 34% of first-time diagnoses in 2022 and
the number of first-time diagnoses among heterosexuals is 33% lower than the peak in 2018. Over two thirds of diagnoses among heterosexual females (69%) are in those born in sub-Saharan Africa while the largest proportion of diagnoses among heterosexual males were born in Ireland (50%).
The number of first-time diagnoses among people who inject drugs (PWID) remains low and accounts for <5% of new diagnoses.
Among people with a first-time HIV diagnosis, 45% were diagnosed late (CD4 count <350 cells/µl) which is similar to the proportion diagnosed late in recent years. This is of concern as it has been shown that late HIV diagnosis is associated with poorer outcomes and an increased likelihood of ongoing HIV transmission. Groups with a higher proportion presenting late in 2022 were: females; those aged 50+years; those born in sub-Saharan Africa; living outside HSE East; PWID; and heterosexual males.
In 2019, the four cities Dublin, Cork, Galway and Limerick, signed up to the HIV Fast-Track Cities (FTC) Initiative, committing to scale up local HIV responses to help end the HIV epidemic by 2030. As people living with HIV are living longer, the total number of people living with HIV in Ireland, who require HIV care and support services, continues to increase.
In 2022, the HSE Sexual Health and Crisis Pregnancy Programme (SHCPP) conducted a scoping study of available HIV data, services and support in the four Fast-Track Cities, to provide a baseline description of existing HIV prevention and support services, to document the current challenges and gaps, and make recommendations to inform the development of Fast-Track City implementation plans.
The report published in August 2024 brings together findings from 193 participants across public health, adult public HIV clinical services, NGOs and community organisations, people living with HIV, HIV networks/member organisations, and city-level public structures. The report identifies a range of challenges and gaps
across all stakeholder groups. One key recommendation from the report outlined the need to address HIV related stigma to improve access to HIV prevention, care and community support services.
A recent survey conducted by RCSI identified a significant lack of knowledge amongst healthcare workers regarding HIV and found that 75% of those surveyed had witnessed stigma from colleagues in relation to those living with an infectious disease.
The survey was conducted in the development of a new module for healthcare workers and students on HIV stigma by the RISE project, via the Department of International Health and Tropical Medicine. Carried out between June and November 2023, the study was aimed at both healthcare workers and healthcare students in Ireland. It had 117 responses – 67 healthcare workers, 20 students and 20 ‘other’.
Responses in the survey included examples of stigma witnessed, which included overuse or unnecessary use of personal protective equipment and double gloving for persons living with HIV. Other anecdotes included reluctance regarding carrying out surgical procedures or phlebotomy on persons living with HIV or placing those patients last on procedure lists. Other worrying examples from a nurse in the survey outlined witnessed stigma of “nursing staff wearing gloves when touching patients, contact precaution signs on room doors of persons living with HIV and being quick to change resuscitation statuses on younger patients on which they normally wouldn’t”.
Participants in the survey also outlined that there was an assumption of an association with “risky behaviours, such as intravenous drug use or sexual promiscuity and persons living with HIV”. 85% of participants ranked HIV as either the first or second most stigmatised against disease and also indicated that patients can feel unsure of disclosing their HIV status due to a negative reaction and also worry that their disclosure will not be treated confidentially.
Dr Pádraig Morrissey
Dr Eoghan de Barra
Overall, a lack of knowledge was identified amongst healthcare workers about HIV transmission and risk factors, with only 42% of healthcare workers and 27% of healthcare students receiving education on HIV stigma and discrimination. Only 45% of healthcare workers reported completing further training or CPD related to HIV since qualifying, however of those who have not engaged with CPD on HIV, 68% said they would if available. It is vital that there is a continued focus on HIV prevention to meet UNAIDS targets for zero new infections by 2030. Ireland has free HIV treatment available to all persons living with HIV and a national PrEP (pre-exposure prophylaxis) programme since 2019. Free HIV testing is available through a number of services in Ireland, including both healthcare and community based settings. The National HSE home STI testing provides home testing and the MPOWER programme within HIV Ireland has a HIV self-testing programme for gbMSM.
The future of HIV medicine continues to ever expand with ongoing research and breakthroughs in treatment. Research presented at the Conference on Retroviruses and Opportunistic Infections (CROI) highlighted advances in longacting oral HIV treatments and injectables. In a large clinical trial in Africa (CARES study), injectable HIV treatment proved as effective in maintaining viral suppression as standard oral antiretroviral treatment. The first injectable regimen, consisting of an integrase inhibitor cabotegravir and a NNRTI rilpivirine, is already approved in Europe and North America and consists of intramuscular injection every two months. Another study also showed that a once-weekly oral regimen of lenacapavir and islatravir can keep HIV suppressed as effectively as daily pills.
A new case of long HIV remission was reported at the 25th International AIDS Conference (AIDS 2024), fuelling optimism for an eventual cure. In 2007, the first Berlin patient was the first person
considered to be cured of HIV. He underwent a stem-cell transplant to treat leukaemia from a donor with the rare genetic mutation CCR5-delta 32, which is known to provide genetic resistance to HIV. The success of this treatment was followed by four similar treatments resulting in sustained remission. A fifth case was reported in 2023 with prolonged HIV remission from a donor with the genetic mutation. The most recent case presented was in a 60-year old German man with acute myeloid leukaemia who underwent a blood stem cell transfer from a donor with a single CCR5-delta 32 mutation, meaning not all cells were fully immune to HIV. He discontinued his antiretrovirals in 2018 and HIV has not been found in multiple tissue samples since. Although this does not have direct clinical implications as stem cell transplants are reserved only for patients requiring same for malignancy, it does pose questions regarding ongoing research in gene-editing techniques to stimulate these resistant cells to eventually develop a cure for HIV.
#MetastaticMatters campaign
A new ¤5 million research programme focused on advanced breast cancer has been announced, aiming to improve survival rates and quality of life for patients with this challenging form of breast cancer. The PRISM (Precision Oncology Research Initiative for Metastatic Breast Cancer) programme, which brings together research scientists from collaborating universities, a pharmaceutical company and Breast Cancer Ireland, will be led by Professor Leonie Young, as Director and Dr Damir Vareslija as Co-Director of the Beaumont RCSI Cancer Centre.
Breast Cancer Ireland, which is Ireland’s leading breast cancer charity, is one of the lead partners of this pioneering four year-long research project into metastatic disease (alongside Research Ireland Strategic Partnership Programme and Carrick Therapeutics) with the charity itself having invested ¤1.8m of funding into the programme as part of their ongoing #MetastaticMatters campaign.
In Ireland, more than 3,700 new cases of breast cancer are diagnosed each year, with 1 in 7 women and 1 in 720 men developing the disease in their lifetime, a portion of which
Pictured at the announcement were (left-right): Aisling Hurley, CEO Breast Cancer Ireland; Dr Damir Vareslija, PRISM Co-Director; Prof. Leonie Young, Scientific Director of the Beaumont RCSI Cancer Centre and PRISM Director, Minister Patrick O’Donovan TD; Dr Aisling McEvoy, Head of Enterprise Partnerships at Research Ireland; Claire Noonan, COO Beaumont RCSI Cancer Centre; and Seamus Browne, Head of Industry Partnerships at RCSI.
Picture: Jason Clarke Photography
progress to metastatic disease –where the tumour evades initial treatment and reappears in major organs of the body.
Aisling Hurley, CEO of Breast Cancer Ireland, commented “Breast Cancer Ireland is proud to co-fund the PRISM Programme, which brings together a highly qualified team of scientists and research experts working on the first national longitudinal study for advanced breast cancer patients, to better understand and target the mechanisms of breast cancer spread (metastasis) and consequently develop new, more effective treatments - ultimately changing outcomes for patients with metastatic breast cancer into the future. In this way, we
All healthcare workers should continue to be educated and updated regarding HIV and the ongoing initiatives to reduce new infections, onwards transmission and HIV-related stigma. With the upcoming World AIDS Day on December 1st, it should prompt all healthcare workers to initiate conversations regarding HIV, the significant work currently underway both in Ireland and globally and how best we can advocate for and improve the lives of persons living with HIV. It should lead to expanded testing to ensure people get diagnosed early, get care needed and to prevent onward transmission.
aim to bring much needed hope to metastatic patients and their families, which aligns with our overall aim of ensuring that breast cancer becomes a treatable illness for ALL of those impacted by this dreadful disease.”
Professor Fergal O’Brien, Vice Chancellor of Research and Innovation at Beaumont RCSI Cancer Centre said “Through this strategic partnership, our researchers are embarking on a journey that aligns with RCSI’s aim to find innovative solutions that translate into new technologies for the benefit of patient health."
“Partnership is so often a critical factor in determining the success of research endeavours. I am confident that this breast cancer research collaboration will enhance understanding and treatment of this disease” added Minister for Further and Higher Education, Research Innovation and Science, Patrick O’Donovan, TD speaking at the announcement of the funding today.
Other key collaborators include University College Dublin, University College Cork, the University of Galway and Cancer Trials Ireland.
New Frontiers in Medicine - RCPI Conference
Five innovators in medical practice and education spoke at the St Luke’s Symposium recently, as part of the Royal College of Physicians of Ireland’s Conference.
The session titled “New Frontiers in Medical Practice and Education” gathered professionals working across different domains of medicine.
Professor Diarmuid O’Donovan (director of National Health Improvement, HSE Public Health) gave an update on the rollout of a new global health curriculum. Global health is the area of study, research, and practice that prioritises health equity for all people worldwide.
The curriculum is currently being integrated with specialty training programmes offered by the postgraduate medical training bodies. According to Prof O’Donovan, a new global health e-module has been designed and will soon be launched.
Ms Isabel Simpson, executive director of Médecins Sans Frontières/ Doctors Without Borders Ireland, presented on that organisation’s responses to conflict in Sudan and Palestine.
“Women and children are bearing the brunt of the full-blown war on people raging across Sudan, and particularly throughout Darfur,” said Ms Simpson.
Her presentation showed maternal and neonatal mortality on the rise, with maternal deaths increased more than 50% across two Médecins Sans Frontièressupported maternity services. Parties in the war are blocking or restricting access to lifesaving aid.
In Palestine, Ms Simpson said, it took more than six months to get permission to establish a second Médecins Sans Frontières field hospital in the Gaza Strip.
“Up to 18 September 2024, 504 attacks were recorded on healthcare sites, and nearly 1100 health workers killed,” she said. “In Gaza, the dismantling of the health system by Israeli forces is leaving people without healthcare access. Our work is often unable to meet the needs of what we’re confronted. This is healthcare in paralysis.”
In her presentation, Dr Emily Buckley, a RCPI Trainee on the Higher Specialist Training in Geriatric Medicine programme,
discussed the benefits of simulation-based training.
“Simulation has been suggested by studies to train doctors in technical and non-technical skills – from non-technical skills such as communication skills, to technical skills such as how to manage an acute stroke,” she said.
Dr Buckley shared findings from a pilot study she created, asking hospital doctors about the potential of simulation-based training.
As a next step for the study, she is identifying gerontological competencies to prioritise.
Dr Blánaid Hayes, a retired consultant occupational physician, delivered a presentation on workplace wellbeing. “It’s only in the last decade we’ve become aware of its importance to physicians,” she said.
In her presentation, Dr Hayes referenced recent research papers measuring doctors’ wellbeing. 21% of respondents to a survey admitted to experiencing burnout. Another paper examined ‘coping’ amongst doctors as a set of cognitive and behavioural strategies dealing with challenges in life and in work.
Professor Diarmuid O’Donovan, Ms Isabel Simpson, Dr Emily Buckley, Dr Blánaid Hayes, Associate Professor Catherine Quinlan and speakers/organisers from the RCPI Annual Conference 2024
“It’s the organisational interventions that have the most impact,” said Dr Hayes. “When an organisation actively promotes wellbeing.”
Finally, a presentation by Associate Professor Catherine Quinlan, a paediatric nephrologist at the Royal Children’s Hospital Australia, encouraged embracing genetics in patient care. She spent the last 10 years building an evidence base for utilising geonomics in nephrology.
A leading researcher for the Kidney Flagship, an initiative committed to end kidney failure in childhood, Associate Professor Quinlan secured federal funding for genomic sequencing for adults and children across Australia.
She and her colleagues designed a series of explainers to assist nephrologists in reading genomic reports, and identifying patients who would benefit from geonomics.
In her presentation, she shared some of those new resources they have developed, including an interactive learning platform, and a new ‘classification’ tool for nephrologists to identify patients as requiring a genetics test.
“My mantra is: it needs to be as easy to order a genetics test as it is to order an MRI,” she said.
Not all Cancer Patients are Equal Access to gold standard oncology treatments is inequitable in Ireland
Speaking at the Royal College of Physicians Ireland (RCPI) Annual Conference, Professor Michaela Higgins, Consultant Medical Oncologist at St Vincents Hospital, provided stark evidence of the growing challenges in targeted cancer care.
“I know what treatment would be best for a patient but increasingly, I cannot prescribe it,” Professor Higgins said.
As the prevalence of cancer increases, the drugs to treat it become more expensive, explained Prof Higgins, comparing cancer treatment to exorbitantly priced wedding shoes.
“Just like weddings, there is a cancer premium,” she said.
“We have seen a sharp increase in oncology drug prices. Yes, a lot goes into the research to develop the drugs but the price of a drug to treat cancer will be higher than the price of drugs to treat other diseases.”
Growing Divide
Once a drug is approved by the European Medicines Agency (EMA), the licence-holder must apply for approval for it to be reimbursed for public patients in Ireland, a process which is currently taking 22 months or longer for oncology medicines.
Since June 2023, three of Ireland’s leading private insurance providers have made EMA-approved cancer drugs immediately available to those with private coverage, while public patients could have to wait up to two years for access to the same drug treatment.
Doctors are in an untenable position – prescribe a less effective treatment protocol, knowing the patient has a higher chance of losing their battle with cancer. Without health insurance to cover the cost of the drugs, patients have no other choice.
The gap widens when you compare Ireland to other countries.
“In the majority of other European countries, the wait time is considerably lower. Germany, for example, is approving the drugs within about 4 months.”
“So, the public vs private access to care issue is exacerbated by the speed at which approval is happening in Ireland compared to the rest of the world.”
A Call to Action
Despite the challenges, Professor Higgins says it is not all bleak and there is something we can do.
“Cancer, for the most part, if caught early, is curable,” she said.
Cancer screening programmes are hugely successful in early identification and the HPV vaccine is highly effective in protecting against cervical cancer. More resources are needed to provide screening for lung cancer.
Budget 2025 offered renewed commitment for the National Cancer Strategy, including ¤10 million for new cancer drugs. There will also be a shared EU technology assessment process for new drugs beginning in January 2025.
“I am very grateful and welcome the cancer strategy funding in Budget 2025, but we need to see ring fenced funding year on year,” Prof Higgins said.
She also argued for the need to optimise oncology drug expenditure.
“We need to practice evidencebased medicine,” she said.
This includes clinical trials and expanded access programmes, vial-sharing, and weight-based
Professor Michaela Higgins, Consultant Medical Oncologist at St Vincents Hospital
“In the majority of other European countries, the wait time is considerably lower. Germany, for example, is approving the drugs within about 4 months.” “So, the public vs private access to care issue is exacerbated by the speed at which approval is happening in Ireland compared to the rest of the world”
vs fixed-dose immunotherapy dosing, which would result in significantly less wastage – a common problem currently.
Finally, she issued a call to action to the doctors in the room.
“Use your voice,” she said.
“Advocate for patients, lobby our leaders for overhaul of the drug reimbursement process, and insist on reasonable pricing of cancer drugs.”
One in two people have a chance of developing cancer at some point in their lives.
Cancer effects everyone equally but only the fortunate can access the best targeted care for them.
Leadership Can be Taught Cathleen Biga told the RCPI Conference that leadership can be taught
“I have been nearly around the globe completely now, and I haven’t found a healthcare system that works,” said Cathleen Biga, during a presentation at the Royal College of Physicians of Ireland’s Conference.
As part of the St Luke’s Symposium at the conference, Ms Biga was delivering a presentation titled: “Leading Teams to Improve Patient Outcomes.”
Originally working as a critical care nurse, Ms Biga is the first non-physician president of the American College of Cardiology and is President and Chief Executive Officer of Cardiovascular Management of Illinois – a cardiology physician practice management company.
At a time when populations are ageing, Ms Biga is focused on the subject of leadership, and how that can best transform access to care. In her presentation, she made a distinction between management and leadership: “I can teach you to manage a budget but leadership is different: it’s not telling people what to do; it’s convincing them it’s what they want to do.”
She encouraged the symposium audience to consider non-clinical competencies that lead to good leadership, such as emotional intelligence. (“It is the key to leadership. Whether in the clinic or at home, understanding who you are is really important”). Using
‘mirror theory’ – depending on personal reactions to others as a reflection – is a way to heighten self-awareness. “You can ask someone: how am I really, when in the thick of things? When things are spinning out of control, how well do I manage my team?” she said.
Can leadership be taught? “I really do believe it can,” she said. She believes around 70% of the education is done during events that happen day-to-day, and securing opportunities for team members to make presentations and contribute. “Not only should we be mentoring our young people; we should be sponsoring them,” she said.
Ms Biga’s presentation was one of several as part of a panel titled “Pathways, Progress in Medicine and Leadership Insights.” Other medical professionals’ journeys were highlighted. RCPI Keeper of Collections Harriet Wheelock presented on the medical career of college founder John Stearne. Dr Karen Dennehy, a Trainee on the Higher Specialist Training (HST) in Geriatric Medicine programme, shared her experiences travelling as a doctor, from treating patients in the Peruvian Andes to assisting South Pole-evacuees in a New Zealand Hospital.
Dr Nataliya Kononenko, an occupational health physician at the HSE’s Workplace Health
Cathleen Biga, the first nonphysician president of the American College of Cardiology and is President and Chief Executive Officer of Cardiovascular Management of Illinois
and Wellbeing Unit, presented on the damage done to the hospital infrastructure in her home country Ukraine during the war. Dr Sarah Kyne spoke of her experience on a RCPI Management Fellowship, and Dr Ali Almajrafi spoke of his experience on the International Clinical Fellowship Programme in Infectious Diseases.
Ms Biga, at the end of her presentation, shared a snapshot of the team-based care model she implemented in Illinois. She showed the structure for an APP-Led Heart Function Clinic, integrating cardiologists with other professionals as needed: an endocrinologist, an obstetrician, nurse staff, a pharmacist and nutritionist. “A patient can come to one place where they receive all the interprofessional help they need,” she said.
Looking Back to 17th Century
During a session at the Royal College of Physicians of Ireland’s Conference, a physician from the early-17th century was quoted as saying: “There are certainly more persons in Dublin at the present day practising the Art of Medicine than any other art, yet there are very few of them with the qualifications which Hippocrates requires in a Medical Doctor.”
That observation was made in the years before physician John Stearne founded RCPI – then the Fraternity of Physicians of
Trinity Hall – in 1654. In a session marking the 400th anniversary of Stearne’s birth year, the college was shown as emerging from a period of immense political turmoil. In a presentation titled “Ireland in the Age of John Stearne (162469),” Prof Robert Armstrong (Associate Professor in History, Trinity College Dublin) outlined how Irish society was changing at the time. Stearne’s mother was “Old English,” her family embedded in Ireland for generations, while his father was “New English,” recently arrived to the country to take-up a position as official of Church of Ireland.
Since the surrender of Hugh O’Neill ended the Nine Years’ War, a collapsed Lordship system saw new generations become professionals, benefitting from being able to pay rent as “freeholders” and live in a country with a more commercial trade system. According to Prof Armstrong, Stearne came to embody this more fluid society.
Shortly after the onset of the Irish Confederate Wars in 1641, in opposition against Charles I’s attempts to impose religious policies across the kingdom, Stearne left Ireland. A presentation by Prof Joe Harbison (Associate Professor, Medical Gerontology, Trinity College Dublin) showed the young physician being enrolled at Cambridge during the conflict.
GO BEYOND LOWERING LDL-C
ADD ON TO REDUCE CV RISK
When statins* and ezetimibe are not enough, add on once daily oral Bempedoic Acid earlier, to help your patients go even further.1,2Δ
* Concomitant use with simvastatin >40 mg daily is contraindicated; please refer to the relevant SmPC for more information.1,2
Δ NILEMDO® and NUSTENDI® are indicated in adults with established, or at high risk for, ASCVD to reduce CV risk by lowering LDL-C levels, as an adjunct to correction of other risk factors, who are on maximally-tolerated statins, or statin-intolerant, or statin-contraindicated with or without ezetimibe or not adequately controlled with ezetimibe treatment.1,2
▼These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information. Refer to Summary of Product Characteristics (SmPC) prior to prescribing.
Presentation: Each Nilemdo film-coated tablet contains 180 mg bempedoic acid. Each Nustendi filmcoated tablet contains 180 mg of bempedoic acid and 10 mg of ezetimibe. Indications: Hypercholesterolaemia and mixed dyslipidaemia: Nilemdo/Nustendi are indicated in adults with primary hypercholesterolaemia (heterozygous familial and non-familial) or mixed dyslipidaemia as an adjunct to diet: In combination with a statin (Nilemdo: or statin with other lipid-lowering therapies) in patients unable to reach LDL-C goals with the maximum tolerated dose of a statin; alone or in combination with other lipid-lowering therapies in patients who are statin-intolerant, or for whom a statin is contraindicated (Nustendi: and are unable to reach LDL-C goals with ezetimibe alone). Cardiovascular disease: In adults with established or at high risk for atherosclerotic cardiovascular disease to reduce cardiovascular risk by lowering LDL-C levels, as an adjunct to correction of other risk factors: in patients on a maximum tolerated dose of a statin and not adequately controlled with additional ezetimibe or, in patients who are either statin-intolerant, or for whom a statin is contraindicated (Nustendi in patients already being treated with the combination of bempedoic acid and ezetimibe as separate tablets with or without statin.) Posology and method of administration: The recommended dose is one tablet of 180 mg Nilemdo or 180 mg/10 mg Nustendi taken once daily, with or without food. Tablet should be swallowed whole. Concomitant simvastatin therapy: When Nilemdo/Nustendi are co-administered with simvastatin, simvastatin dose should be limited to 20 mg daily (or 40 mg daily for patients with severe hypercholesterolaemia and high risk for cardiovascular complications, who have not achieved their treatment goals on lower doses and when the benefits are expected to outweigh the potential risks). Coadministration with bile acid sequestrants: Dosing of Nustendi should occur either at least 2 hours before or at least 4 hours after administration of a bile acid sequestrant. Patients with renal impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild or moderate renal impairment. Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment and patients with end-stage renal disease (ESRD) on dialysis when Nustendi is administered. Patients with hepatic impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild hepatic impairment (Child-Pugh A). Treatment with Nustendi is not recommended in patients with moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment due to the unknown effects of the increased exposure to ezetimibe. Contraindications: Hypersensitivity to the active substance or any of the excipients (see SmPC); pregnancy; breast-feeding; concomitant use with simvastatin > 40 mg daily. When Nustendi is co-administered with statin in patients with active liver disease or unexplained persistent elevations in serum transaminases; when Nustendi is co-administered with a statin, consult the SmPC for that particular statin therapy. Warnings and precautions: Potential risk of myopathy with concomitant statins: Bempedoic acid increases plasma concentrations of statins. Patients receiving Nilemdo and a statin should be monitored for adverse reactions that are associated with high doses of statins. Statins occasionally cause myopathy. In rare cases, myopathy may take the form of rhabdomyolysis with or without acute renal failure secondary to myoglobinuria and can lead to fatality. In post marketing experience with ezetimibe, very rare cases of myopathy and rhabdomyolysis were reported. Most patients who developed rhabdomyolysis were taking a statin with ezetimibe. Patients receiving Nilemdo/Nustendi and a statin should be advised of the potential increased risk of myopathy and told to report promptly any unexplained muscle pain, tenderness, or weakness. If such symptoms occur, a lower maximum dose of the same statin or an alternative statin, or discontinuation of Nilemdo/Nustendi and initiation of an alternative lipid-lowering therapy should be considered under close monitoring of lipid levels and adverse reactions. If myopathy is confirmed by creatine phosphokinase (CPK) > 10× upper limit of normal (ULN), immediately discontinue Nilemdo/ Nustendi and any statin. Doses of simvastatin > 40 mg should not be used with Nilemdo/Nustendi. Increased serum uric acid: Bempedoic acid may raise serum uric acid due to inhibition of renal tubular OAT2 and may cause or exacerbate hyperuricaemia and precipitate gout in
patients with history of gout or predisposed to gout. Discontinue Nilemdo/Nustendi if hyperuricaemia accompanied with symptoms of gout appear. Elevated liver enzymes: Liver function tests should be performed at initiation of therapy. Discontinue Nilemdo/Nustendi if increase in transaminases > 3× ULN persists. Renal impairment: Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment (eGFR < 30 mL/min/1.73 m2) or patients with ESRD on dialysis. Hepatic impairment: Periodic liver function tests should be considered for patients with severe hepatic impairment (Child-Pugh C) taking Nilemdo. Nustendi is not recommended in moderate to severe hepatic impairment (Child-Pugh B and C) due to unknown effects of increased exposure to ezetimibe. Fibrates: If cholelithiasis is suspected in a patient receiving Nustendi and fenofibrate, gallbladder investigations are indicated, and therapy should be discontinued. Ciclosporin: Caution when initiating Nustendi in the setting of ciclosporin. Ciclosporin concentrations should be monitored. Anticoagulants: Appropriately monitor INR if Nustendi is added to warfarin, other coumarin anticoagulants, or fluindione. Contraception: Women of childbearing potential must use effective contraception during treatment. Patients should be advised to stop Nilemdo/ Nustendi before stopping contraceptive measures if planning to become pregnant. Excipients: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take Nilemdo/Nustendi as it contains lactose. Patients at high risk of cardiovascular disease: Evidence for the use of the fixed combination medicinal product of bempedoic acid with ezetimibe in patients at high risk of cardiovascular disease is only available for the lipid-lowering effect in absence of any cardiovascular risk reduction estimation for ezetimibe in primary prevention patients. Driving and use of machines: Nustendi has minor influence on ability to drive and use machines. Dizziness has been reported. Interaction with other medicinal products: Refer to SmPC for full information on interactions. Adverse reactions: Nilemdo: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, gout, hyperuricaemia (includes blood uric acid increased), AST increased, pain in extremity. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, haemoglobin decreased, ALT increased, liver function test increased, blood creatinine increased, blood urea increased, Consult Nilemdo SmPC in relation to other adverse reactions. Nustendi: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, decreased haemoglobin, hyperuricaemia (includes uric acid increased), decreased appetite, dizziness, headache, hypertension, cough, constipation diarrhoea, abdominal pain, nausea, dry mouth, flatulence, gastritis, liver function test increased (includes liver function test abnormal), back pain, muscle spasms, myalgia, pain in extremity, arthralgia, blood creatinine increased, fatigue, asthenia, gout, AST increased (for bempedoic acid), blood CPK increased. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, ALT increased, blood urea increased, hot flush, dyspepsia, gastrooesophageal reflux disease, AST increased (for ezetimibe), GGT increased, pruritus (with statin), neck pain, muscular weakness (with statin), chest pain, pain, oedema peripheral (with statin). Frequency not known: Thrombocytopaenia, hypersensitivity (including rash, urticaria, anaphylaxis, angio-oedema), depression, paraesthesia (with statin), dyspnoea, pancreatitis, hepatitis, cholelithiasis, cholecystitis, erythema multiform, myopathy / rhabdomyolysis. Consult Nustendi SmPC in relation to other adverse reactions. Legal Classification: POM. Package quantity, marketing authorisation (MA) number: Nilemdo 28 tablets: EU/1/20/1425/002. Nustendi 28 tablets: EU/1/20/1424/002. MA Holder: Daiichi Sankyo Europe GmbH, Zielstattstrasse 48, 81379 Munich, Germany. Further information available on request from Daiichi Sankyo Ireland Ltd. D09 YF97. Telephone: (01) 489 3000. Fax: (01) 489 3033. Email: medinfo@daiichi-sankyo.ie Date of Preparation: May 2024 JOB ID: IE/BIL/05/24/0004
▼ These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information. Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events or a product complaint about a Daiichi Sankyo medicine can also be directly reported to Daiichi Sankyo Ireland Ltd. D09 YF97 by telephone: +353 (1) 4893000
In his presentation titled “The Life and Legacy of John Stearne: ‘Philosopher, Physician, and consummate Theologian,” Prof Harbison explained that during the wars, Stearne spent several years being active in Cambridge, Oxford and Bedford
The Battle of Rathmines in 1649 saw the beginning of the Cromwellian invasion, whose forces brought the Bubonic Plague with them to Dublin, leading to a public health crisis.
In the early 1650s, Stearne returned, as registrar of Trinity College Dublin. The college was planning to sell one of its buildings – an empty hall – but the physician suggested an alternative: to restore the building into a centre to teach medicine. The Fraternity of Physicians of Trinity Hall was founded in 1654, with Stearne as its first president.
The Fraternity of Physicians of Trinity Hall was a major part of Stearne’s final years – he died in 1669, aged 45.
According to Prof Harbison, Stearne wrote many books in that period, most of which concerned philosophy.
In Aphorismi de Felicitate (Aphorisms on Happiness), published in 1664, Stearne compiled an extensive list of pithy statements. One aphorism seems to summarise an entire philosophy on how to live a happy life: “Health, bodily pleasure, clothing, and home are to be considered.”
33 Fellows Welcomed
The Royal College of Physicians of Ireland (RCPI) celebrated the conferring of 33 new Fellows from Pakistan, India, Malaysia, the United Kingdom, and Ireland at a special admission ceremony during the Annual Conference on Wednesday, 16 October 2024.
Dr Diarmuid O’Shea, President of the Royal College of Physicians of Ireland, acknowledged the significant contribution of the doctors in the room who have worked in earnest to earn the postnominal FRCPI.
“Your career in medicine is one that requires continual growth, reflection and a deep commitment to your patients and the field of medicine. Stay positive for yourself, curious about health and healthcare delivery and focused on your patients. Work collaboratively and collegially. Be open to change and inspire others. Imagine aspects of healthcare training and health care delivery you want to improve, reform or simply do better, and help us lead the changes required.”
The college also welcomed two esteemed Honorary Fellows, Cathleen Dalton Biga, President of the American College of Cardiology, and Professor David Burn, Pro-Vice Chancellor, Faculty of Medical Science at Newcastle University.
Ms Cathleen Biga is a proud member of the Irish American diaspora. She spent 15 years in a critical care unit as a nurse and she is also a former cardiovascular service line leader, hospital president, and Chief Executive Officer. She has focused on uniting all constituencies of the healthcare enterprise in promoting patient access, optimizing outcomes and experience, maximizing the value of team-based care, and ensuring the professionalism and well-being of the entire medical team.
Her 41-year experience in health care delivery, innovation, quality, and economic sustainability brings fresh perspectives in her current role as President of the 56,000 member American College of Cardiology.
Ms Biga is a leader who exemplifies the critical and expanding role of team-based care and who has already received global recognition for her leadership and how working together we can transform cardiovascular care and improve heart health for all.
Professor David Burn is Pro-Vice Chancellor of the Faculty of Medical Sciences in Newcastle University and Professor of Movement Disorders Neurology and Honorary Consultant Neurologist for Newcastle upon Tyne Hospitals NHS; He is also Director Of Newcastle Health Innovation partners, the Academic Health Sciences Centre for Northeast of England & North Cumbria; Chair, Board of Northern Health Sciences Alliance; Director of Newcastle Health Innovation Partners NIHR/NHS-E Academic Health Science Centre and Emeritus NIHR Senior Investigator. He is a past President of the Association of British Neurologists 2019-2021 and Fellow of the Academy of Medical Sciences.
He is a careful, thoughtful and outstanding clinician. He is a brilliant clinical scientist and innovator with a deserved national and international reputation in Movement Disorders, and neurodegenerative disease including Parkinson’s disease, and Lewy body dementia. He has published over three hundred peerreviewed papers, thirty chapters/books in Neurology.
In recognition of his global standing, he is the incoming President of the MDS, the largest movement disorder organization globally in education, training, and research.
Pictured are the 33 new Fellows from Pakistan, India, Malaysia, the United Kingdom, and Ireland
60 Second Summary
AUTHORS: Carol Walsh, Advanced Nurse Practitioner and Emer O’Sullivan, Quality Risk & Patient Safety Officer, Bantry General Hospital
Hospital-associated venous thromboembolism (HA-VTE) is a preventable yet potentially life-threatening complication. A quality improvement (QI) initiative was launched in 2023 at Bantry General Hospital to reduce HA-VTE rates. Using the Model for Improvement and Plan-Do-Study-Act (PDSA) cycles, the project focused on improving VTE risk assessments and thromboprophylaxis prescriptions. Initial audits revealed low rates of VTE risk assessment (17%) and thromboprophylaxis prescribing (43%) on admission. Through 12 PDSA cycles, the hospital improved these rates, with median risk assessment completion reaching 85%, and thromboprophylaxis prescribing rising to 89%.
Challenges included staff resistance, lack of education on VTE risk, and inconsistent national data collection. Education sessions were implemented, and HA-VTE prevention was integrated into daily hospital practices.
Although the target of zero HA-VTE within six months was not achieved, HA-VTE rates improved substantially, dropping from 32.53 per 1000 discharges in Q1 2022 to 20.8 in Q1 2023. The initiative demonstrated the importance of sustained education and auditing to prevent HA-VTE and improve patient safety and outcomes.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
Venous thromboembolism (VTE) is an umbrella term for blood clots that form within a vein. These blood clots normally form in a deep vein in one of the lower limbs, called deep vein thrombosis (DVT), but may also form in the upper limbs. Part of a DVT can break off and travel to another part of the body, usually to the lungs. These are called pulmonary embolisms (PE). It is estimated that there are 10 million cases of VTE worldwide annually.1, 2 In the US, deaths related to VTE amount to approximately 100,000.3 While Europeans experience nearly half a million deaths a year due to VTE.4
About 4,000 of these VTE-related deaths occur annually here in Ireland.5 Numerous risk factors increase a person’s chance of developing VTE, one of which is a hospital stay. It can occur during hospital admission or in the 90 days after hospitalisation. It is estimated that between 50 and 60% of all VTE cases are hospitalassociated and that 70% of these are avoidable with appropriate preventive measures.6
VTE is a significant cause of hospital-related death worldwide. It is estimated globally that there are 5 to 6 million HA-VTE annually and up to 70% of these could be prevented with appropriate
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings. Published by HPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
thromboprophylaxis.6, 1 This equates to 4 million people who could have avoided a HA-VTE. NICE guidelines require that all patients be assessed for their risk of HA-VTE while in hospital.7 It is recommended that a validated risk assessment tool be used on admission to the hospital. If the patient is deemed at risk for HA-VTE and has no contraindications, then they should receive thromboprophylaxis within 14 hours of admission. Despite these guidelines, HA-VTE rates continue to be high. This is likely due to patients not being riskassessed or thromboprophylaxis not being used.1
In Ireland, HA-VTE rates are monitored through an HSE data management system called HIPE, this data is captured on-site from patients’ medical notes and discharge documentation, and it is published monthly as part of the Hospital Patient Safety Indicator Report (HPSIR). However, data collection in Ireland for HA-VTE is limited due to the inability of HIPE data to capture HA-VTE cases that occur in the 90 days post-discharge unless it is documented as a HA-VTE in the medical notes. Given this, it is probable that the actual rates are higher than currently
indicated. With the available data, it is proposed that there are approximately 11,000 VTE a year and 63% of that is HA-VTE.6 This equates to approximately 6,930 cases of HA-VTE. This means that potentially 5000 cases of HA-VTE are preventable. The national average rate of HA-VTE in Ireland is 8 cases per 1000 hospital discharges.6 To date, there are no known reports on the economic impact of HA-VTE in Ireland. However, it must be presumed that there is a significant financial burden to both the patient and the Health Service. HA-VTE increases patient lengths of stay, requires patients to have further imaging and treatment, requires increased outpatient follow-up, and limits patients’ activities, lifestyle, and possibly their livelihood while on anticoagulation due to potential bleeding risks. European reports8 on HA-VTE state that at least 400,000 people could potentially suffer long-term complications because of VTE, such as pulmonary hypertension, or postthrombotic syndrome. In the US, the Agency for Research and Quality9 reported that up to 30% of patients will have a recurrence of VTE. Up to 50% of patients will go on to develop post-thrombotic syndrome10 and approximately 4%
30 CPD 113: VTE
Figure 1. (a.) Run chart for % of risk assessments completed, annotated with each PDSA cycle (b.) The median line was calculated to 10%. (c.) A shift in the data after PDSA 1. (d.) The median line was recalculated to 83%. (e.) 7 points are seen below the median line during PDSA 5 and 6
of patients with VTE will eventually be diagnosed with post-thrombotic pulmonary hypertension.11
At Bantry General Hospital, the rate is much higher than the national average with local rates ranging from between 7.5 to 34.9 per 1000 discharges and an approximate average per quarter of 24 per 1000 discharges. As a measure to reduce the incident of HA-VTE, a new medication chart was developed to be used in all hospital sites within the group in 2020. This medication chart included a VTE risk assessment and a preprinted thromboprophylaxis prescription to prompt prescribers. Unfortunately, this failed to improve the rates of HA-VTE. When it was initially rolled out, no education was provided in the hospital on HA-VTE or how to complete the risk assessment. However, it is unclear if this was provided for rotating NCHDs at other sites within the hospital group. Locally, an audit was performed, which looked at VTE risk assessment of new admissions to the hospital (inpatients >14 hours). It showed that 85.7 % of patients did not have a VTE risk assessment performed on admission and 69.2% of the patients, who were at risk of HA-VTE and suitable for thromboprophylaxis, had none prescribed. Of the 30.8 % that had been prescribed thromboprophylaxis, two patients had been prescribed an incorrect dose. The patients with the risk assessment performed were appropriately prescribed anticoagulation at the correct dose.
Aim
Given the persistently high rates of HA-VTE locally, a quality improvement initiative was launched in 2023 to reduce hospital-associated venous thromboembolism to zero within 6 months of starting the project.
Methodology
Using the Model for Improvement, the project applied a structured approach to evaluate and enhance thromboprophylaxis prescription practices. This methodology is widely recognised in healthcare
settings for its focus on continuous learning and iterative testing of change ideas.
Step 1: Define the Problem – "What are we trying to accomplish?"
The first step of the model focuses on understanding the problem at hand, which was rising HA-VTE rates. To address this, several assessment tools were used to identify the barriers to optimal thromboprophylaxis prescription and risk assessments.
Baseline Audits were conducted to quantify the problem. Five audits were performed, each focusing on patients admitted within the previous 24 hours. These revealed that a median of 17% of patients had a VTE risk assessment completed, and 43% of at-risk patients received thromboprophylaxis within 14 hours of admission. HA-VTE rates from 2021 to 2022 showed variability. In quarter one, HA-
A process map was then developed to visualise the steps involved in patient admission and risk assessment during the first 24 hours. This exercise highlighted inconsistencies in thromboprophylaxis prescription practices, with some patients receiving prophylaxis upon admission, others only after an NCHD review or consultant rounds, and some receiving no prophylaxis at all due to incomplete risk assessments.
Fishbone diagrams were mapped out to systematically explore the causes behind the high HA-VTE rates. This brainstorming session identified key contributors such as staff knowledge gaps, inconsistent practices, workload pressures, and a lack of clear local guidance.
A survey was distributed among hospital staff through WhatsApp and email, yielding a 40% response rate. Findings indicated that 80% of respondents cited workload as a barrier to completing VTE risk assessments, and 34% reported anxiety surrounding anticoagulation prescriptions.
Step 2: Measuring Improvement – "How do we know that a change is an improvement?"
This step focused on identifying key metrics to track progress. The outcome measure was the overall HA-VTE rates, but since national data is released quarterly, alternative process measures were determined to assess more immediate progress. These included:
VTE rates dropped slightly from 34 per 1,000 discharges in 2021 to 32.53 per 1,000 discharges in 2022. However, quarter two rates increased from 14.6 per 1,000 in 2021 to 26.3 per 1,000 discharges in 2022.
These results were then analysed using a Pareto chart, which helped to prioritise areas of improvement. The two biggest opportunities identified were increasing the completion rates of risk assessments and ensuring correct prophylaxis prescriptions.
A stakeholder map and communication plan were created to identify all key stakeholders, including healthcare professionals and hospital administrators, and project champions were recruited from the Medical Assessment Unit. These early adopters played a key role in driving the initiative by leading by example and promoting the importance of HAVTE prevention.
• VTE Risk Assessments: The percentage of VTE risk assessments completed within 14 hours of patient admission was selected as an immediate indicator of improvement.
• Thromboprophylaxis
Prescription Rates: The percentage of at-risk patients receiving thromboprophylaxis was also tracked regularly.
• To monitor potential side effects of increased anticoagulation prescriptions, incident reports of major bleeding events were reviewed monthly. Ensuring patient safety while increasing prophylaxis prescribing was a core focus of the QI project.
Data collection involved twiceweekly audits of medication charts for all patients admitted within the previous 24 hours. This information was then visualised using run charts to track trends and nonrandom variations, such as shifts or trends, which would signal successful interventions.
Figure 2. (a.) A shift in the data during PDSA 8,9, and 10. (b.) The median line was recalculated to 85.5%. (c.) A shift in the data during PDSA 11. (d.) The median line was recalculated to 78.5%. (e.) 16 runs were noted on the run chart, indicating non-random variation
Step 3: Identifying and Testing Change Ideas – "What changes can we make that will result in an improvement?"
This step required the development of change ideas, for this, we used driver diagrams. Which were used to examine the cause and effect of various interventions on the desired outcome and develop theories of change. In total three driver diagrams were developed. The first focused on change ideas to improve the identification of patients at risk for HA-VTE. The second focused on change ideas to improve the mitigation of the risk from HA-VTE. The last driver diagram developed change ideas to ensure appropriate escalation of patient care when deemed to be at risk for HA-VTE. The second part of the model for improvement then focuses on testing those change theories. These tests of change were structured by Plan, Do, Study, Act cycles (PDSA). The PDSA cycles were planned before starting the QI project. The “DO” stage required the implementation of interventions or strategies that were developed and agreed upon during the group sessions while developing the driver diagrams. A total of ten PDSA cycles were designed. However, at times PDSA cycles were redesigned or new PDSA cycles were developed from the learning gained during the “STUDY” phase of the previous cycle.
Part of the project involved providing educational material for patients attending the hospital on the risks of, and the signs and symptoms of HA-VTE, it was imperative that patients’ opinions were sought as to what methods of education would be the most beneficial. A patient survey was distributed to all patients within the hospital. This was done over one day. All inpatients and patients attending outpatients’ services.
Results
HA-VTE rates.
HA-VTE rates for the hospital were compared with quarterly data for the same quarter in previous years. HA-VTE rates for quarter
one of 2023 have reduced to 20.8 per 1000 discharges from 32.53 in 2022 and 34 in 2021. While quarter two of 2023 rates for HA-VTE reduced to 15.46 per 1000 discharges from 26.3 in 2022. However, they are slightly increased from 2021 rates of 14.6 per 1000 discharges.
Percentage of risk assessments completed for patients.
A run chart (fig.1) was plotted with the percentages of risk assessments completed at each audit and annotated for each PDSA cycle (fig.1). A median line from the baseline results was calculated and extended along the chart. The median of the baseline data was 10%. A shift in data was seen following PDSA 1 and at the beginning of PDSA 2 with more than 8 data points above the median line (fig.1). This also indicates that the median line should be recalculated. The recalculated median line is increased to 83% (fig.1). During
line. There are 16 runs seen on the chart (fig.2). Which is too few runs and is a statistical signal of non-random variation [15]. This indicates that a shift in the process has happened.
Percentage of patients prescribed thromboprophylaxis.
A run chart (fig.3) was plotted with the percentages of thromboprophylaxis prescribed for patients deemed to be at risk from HA-VTE at each audit and annotated for each PDSA cycle. A median line from the baseline results was calculated and extended along the chart. The median of the baseline data was 43% (fig.3). Data collected from PDSA 1 and 2 revealed a data trend suggesting that the median line should be recalculated (fig.3). The median line was recalculated to 89%. On reviewing the data, it was noted that on 12 occasions audits revealed that compliance with prescribing of thromboprophylaxis reached 100%. To date, no further data shifts have been observed. In total, the run chart had 56 data points, with 5 of these data points on the median line (fig.3). The run chart had 19 data runs, which statistically signals that nonrandom variation has occurred (fig.3). No downward or upward data trends have been noted during the QI project to date. No upward or downward astronomical points were seen either.
Percentages of VTE risk assessment completed correctly.
All VTE risk assessments audited were completed correctly.
PDSA 5 and PDSA 6, it was noted that there were 7 data points below the median (fig.1). There were not enough data points to recalculate the median. A second data shift occurred during PDSA 8, 9, and 10 (fig.2). The percentage of risk assessments completed regularly reached 100%. The median line was recalculated and increased to 85.5% (fig.2). Another data shift was seen during PDSA 11. This data shift, however, was below the median line (fig.2). The median line was recalculated and was reduced to 78.5% (fig.2). No downward or upward trends have been seen during the QI project to date.
There were two astronomical points. One upgoing astronomical point was seen during the baseline data, and one downward astronomical point was seen at the beginning of PDSA 8. The previous data point was 100%.
The run chart has 56 data points 50 of which are not on the median
The number of major bleeding events reported.
There was no major bleeding events reported.
Discussion
To date the overall aim of the project, to reduce HA-VTE to zero within 6 months (June 2023), has not been reached. However, HA-VTE rates have improved substantially. As new practices become embedded and there is a new increased awareness of the rates and risk of HA-VTE, it is expected that rates should continue to fall. However, given that evidence suggests [6] that at least 30% of HA-VTE is not preventable it is unlikely that rates will ever be reduced to zero. The specific objectives, 100% of patients will have risk assessments and thromboprophylaxis prescribed, reached the projected aim of 100% on several occasions. However, the median was below
Figure 1. (a.) Run chart for % of risk assessments completed, annotated with each PDSA cycle (b.) The median line was calculated to 10%. (c.) A shift in the data after PDSA 1. (d.) The median line was recalculated to 83%. (e.) 7 points are seen below the median line during PDSA 5 and 6
the target in both objectives. The rates of VTE risk assessments completed on admission had a median of 85% at the highest and 78.5% at the lowest. While the rates of thromboprophylaxis prescribed for patients at risk for VTE had a steady median of 89%. This could be in part due to more senior NCHDs prescribing thromboprophylaxis without the need to complete the VTE risk assessments. However, this was not examined as part of the QI project. The steady median shows that improvement occurred and was sustained during the QI project. Both run charts showed too few runs, which is a statistical signal of non-random variation and means that something has affected the process. Also, both run charts show shifts in the data. A shift in data points is equal to a p-value of 0.05, which indicates that the shift is statistically unlikely to occur by chance. Given this, changes in data must be due to changes made by the QI project There were two downward runs observed in both run charts. These coincided with the NCHD changeover. Rates then improve quickly following brief education sessions. This suggests that the NCHDs have a poor awareness of the risks and incidence of HAVTE. This shows the benefit of developing mandatory education on HA-VTE for NCHDs, and potentially the wider MDT. Rates of VTE risk assessment data showed a downward astronomical point in PDSA 8. When examined it became apparent that one NCHD, while rostered to the MAU, had failed to do any risk assessments, and did not correctly identify patients who required thromboprophylaxis. Numerous
focused education sessions failed to improve resistance to change with this individual. This astronomical point did not impact the overall rate of thromboprophylaxis prescribing.
A cost comparison between treating and preventing HA-VTE was conducted for a typical patient admitted with pneumonia. Treating a major PE costs approximately ¤6,818.40, including follow-up care, while preventing HA-VTE with prophylactic anticoagulation, IPC devices, and in-house educational materials costs ¤45.62 per patient. This demonstrates a potential saving of ¤6,772.78 per patient by preventing HA-VTE.
The project team prioritised equity throughout all stages by examining VTE prevention and management data across various demographic groups, including race, gender, ethnicity, age, and socioeconomic status. To address health literacy, patient preferences for educational
Conclusion
HA-VTE is a potentially lifethreatening complication that can be prevented through VTE risk assessment and appropriate thromboprophylaxis, reducing HA-VTE incidence by up to 70%. This quality improvement project used PDSA cycles to enhance VTE risk assessment and thromboprophylaxis prescribing, resulting in fewer HA-VTE cases. Cost-neutral interventions were introduced to improve patient outcomes, prevent complications, and standardise care. Challenges included resistance to change, difficulty accessing national data, and maintaining the improvements.
To sustain the changes, HA-VTE prevention is being integrated into routine care, with quarterly audits and monitoring through the hospital's VTE committee. Mandatory education on HAVTE has been implemented, starting with NCHDs. All HAVTE cases are reviewed for learning opportunities, and new nursing care plans have been developed. Local data analysis revealed some HA-VTE cases were due to incorrect discharge documentation, prompting efforts to address this issue.
Questions
What is HA-VTE, and why is it important to prevent it?
materials and methods were assessed, and resources were provided in multiple languages to overcome language barriers. Data analysis revealed no disparities in VTE outcomes among different demographic groups.
The environmental impact of the project was taken into consideration, with ongoing monitoring of waste generation. At this stage, the estimated impact is low. Prevention treatments for VTE, such as single-use syringe cases and IPC sleeves, produce recyclable or biodegradable waste. In contrast, treatment involves prolonged medication use in non-recyclable blister packs and frequent follow-up appointments, contributing to a higher environmental cost. Due to limited public transport in rural West Cork, single-car journeys are common for hospital and pharmacy visits, further adding to the carbon footprint.
How effective is appropriate thromboprophylaxis in preventing HA-VTE?
What was the main aim of the quality improvement (QI) project initiated at Bantry General Hospital?
What methodologies were used in the project to achieve its goals?
What were the key outcomes of the QI project, and did it achieve its goal of reducing HA-VTE?
Cardiovascular Disease on Men’s Health
The impact of cardiovascular disease on men’s health is staggering. According to the findings from the Central Statistics Office (CSO) in 2023 over 5,000 men died from cardiovascular disease.
One in three men lose their lives to heart disease or stroke. It is widely recognised that men are often less likely to engage with heart health supports, and historically have not prioritised their cardiovascular well-being, this narrative does not need to persist. Shifting the focus to prevention, education, and awareness can help men take greater ownership of their heart health.
The good news is that 80% of premature deaths from cardiovascular disease is preventable through embracing healthier lifestyles.
Making minor changes now can lead to a long-term healthier lifestyle. Start by being more physically active, focusing on a nutritious diet, and getting regular health checks for blood pressure and cholesterol. Additionally, follow health guidelines on alcohol consumption and avoid smoking. These steps will set the foundation for better heart health and overall well-being. Your future self will thank you for it.
Let’s make the change and prioritise your heart health!
Move More – Every Move Counts
Physical activity is one of the most important things to help
reduce your risk of heart disease and stroke. Getting regular physical activity improves your cardiovascular fitness, reduces your blood pressure, and helps maintain a healthy weight. It is recommended that all adults should get 150 minutes a week of moderate intensity activity. That adds up at most 30 minutes per day for five days a week, which is less than three per cent of your day.
Healthy Diet = Healthy Heart
A healthy, balanced diet is essential for lowering the risk of heart disease and stroke. It is recommended to include plenty of fruits, vegetables, and whole grains in your meals. Minimise highly processed foods and limit consumption of foods and drinks high in sugar, fat and salt for better heart health.
Quit smoking and rethink your drinking
21% of men are more likely to smoke than their female counterparts according to Healthy Ireland, 2023. 1 in every 2 smokers will die of a tobacco related disease. The good news is that once you quit smoking you significantly reduce your risk of heart disease and stroke.
At least 1 in 3 adult men consume alcohol at least once a week. 37% of men binge drink according to statistics from Healthy Ireland, 2023. Alcohol is high in sugar and calories and consuming more than the recommended amounts can have a significant impact on
Written by Dáire Conway, Health Promotion Officer (Physical Activity) with the Irish Heart Foundation
your heart health. Be aware of the recommended low risk alcohol guidelines for men, consume less than 17 standard drinks across the week with at least two alcohol free days.
Check your blood pressure and cholesterol
High blood pressure (hypertension) is another major risk factor for heart disease and stroke. The normal level of blood pressure is about 120 over 80, with high blood pressure defined as 140 over 90 or higher. Known as the silent killer, 2 in 3 people over the age of 50 have undiagnosed high blood pressure, so it is important to get your blood pressure checked regularly by your GP or local pharmacy.
One of the best ways to prevent cardiovascular disease (such as stroke or heart attack) is to keep your cholesterol at a healthy level. Having high cholesterol affects people of all ages and it can be caused by many different things. Some things you can control like lifestyle habits, and others you
NEWS - Discussing UWWTD Impact on Pharma Sector
As a participating member of Medicines for Ireland (MFI), Donagh O’Leary, Managing Director at Clonmel Healthcare along with John Donnelly had the pleasure to meet with MEP Barry Andrews in conjunction with Paul Neill, Chairperson of MFI and Eimear O’Leary, Director of Communications and Advocacy at the Irish Pharmaceutical Healthcare Association (IPHA).
The meeting was held at the new European Parliament office in Dublin. Discussed at the meeting was the Urban Wastewater Treatment Directive (UWWTD), the impact on the pharmaceutical sector and what we believe to be the potential negative implications the Directive will have if introduced in Ireland for the industry.
Paul Neill (MFI), MEP Barry Andrews, Eimear O’Leary (IPHA), Donagh O’Leary, Clonmel Healthcare, John Donnelly, Clonmel Healthcare
can’t. Making small changes now can make a big difference to your life now and in the future, especially if you already have heart disease or a family history of it.
Irish Heart Foundation
The Irish Heart Foundation has a long-standing relationship of collaborating with men to meet their health needs and protect their heart health. Initiatives that support improved heart health for men have been designed and delivered in partnership with various stakeholders.
Our campaign “Reboot Your Life” encourages men to assess their lifestyle and make essential changes to improve their heart health. A booklet with heart healthy tips and information can be downloaded from irishheart.ie.
The Irish Heart Foundation offers a range of resources and support materials at irishheart.ie.
Understanding UTIs in men is crucial for effective diagnosis, treatment and prevention
Written by Helen Lake RN, UTI Information Nurse, The Urology Foundation
Email:
nurse@theurologyfoundation.org
Helpline: 0808 801 1108 (Tues and Thurs 10am-12noon)
Resources: nurse@theurologyfoundation.org
Urinary tract infections (UTIs) are one of the most common bacterial infections globally, affecting millions of people each year. It is estimated that UTIs account for over 150 million cases annually worldwide. UTIs are a frequent cause of GP consultations, particularly among women. Why specific strategies are needed for UTIs in men
Nearly 50% of women will have at least one UTI in their lifetime. While UTIs are more prevalent in women, they also represent a significant health concern for men, particularly as they age. The incidence of UTIs in men is lower than in women; however, when men do develop UTIs, these infections are often more severe and associated with underlying anatomical abnormalities, such as prostate enlargement, which can complicate treatment and increase the risk of recurrence.
The global and national burden of UTIs has been rising, partly due to the increasing prevalence of antibiotic-resistant pathogens,
which complicates treatment and leads to higher healthcare costs. The complexity of managing UTIs in men, coupled with the growing challenge of antibiotic resistance, underscores the need for ongoing research and tailored management strategies. Understanding UTIs in men is crucial for effective diagnosis, treatment and prevention. That’s why it is important for nurses to be given comprehensive information on the subject, to help improve patient care and encourage critical thinking about the unique challenges and considerations in managing UTIs in men.
Anatomy & Physiology
As a recap, the male urinary system includes the kidneys, ureters, bladder and urethra. Notably, the male urethra, which extends through the penis, is significantly longer than the female urethra. This anatomical difference provides a natural barrier to infection because the greater length of the male urethra makes it more difficult for bacteria to travel from the external environment to the bladder. However, the presence of the prostate gland introduces another layer of complexity in male urinary health. These anatomical features can create barriers to effective urine flow, contributing to a higher likelihood of complications such as prostatitis, urethral strictures and incomplete bladder emptying, all of which can increase the risk of recurrent infections.
Causes & Risk Factors
UTIs in men are commonly caused by bacterial infections, with E. coli being the most frequent pathogen. Other bacteria, such as Proteus,
Klebsiella and Enterococcus, can also cause UTIs. The category of adult male UTIs encompasses conditions including urethritis, prostatitis, orchitis, epididymitis, cystitis and infections related to urinary catheters.
Older men are more susceptible to UTIs due to several factors. Conditions such as neurological conditions, benign prostatic hyperplasia (BPH) and bladder neck muscular obstruction (BNO) can obstruct urine flow, leading to retained urine in the bladder and increasing the risk of infection. An incomplete bladder may lead to the formation of bladder stones, which can act as a reservoir for bacteria, increasing the risk of recurring UTIs and making it difficult to clear the infection. Kidney stones can also sometimes act as a reservoir for bacteria.
Men who use indwelling or selfcatheterisation need to ensure good standards of hygiene, a ‘no touch’ technique and regular reviews to monitor compliance to minimise UTI occurrence. There is evidence to suggest that men often struggle with compliance with intermittent selfcatheterisation (ISC), considering it a nuisance and time-consuming, and also struggle with toilet facilities when out and about. This is an important factor to consider when supporting male patients with ISC.
Additionally, a weakened immune system, often due to autoimmune conditions, or cancer, and health issues such as poorly controlled diabetes, can impair immune function and bladder emptying. It’s important to remember that several of these factors can coexist.
Dehydration is another significant risk, particularly in older patients. As we age, the sense of thirst can become blunted, partly due to changes in the regulation of antidiuretic hormone (ADH). This leads to a reduced ability to concentrate urine, which accelerates dehydration. Constipation is also a contributing factor as it can put pressure on the urinary tract, leading to incomplete bladder emptying. Both constipation and diarrhoea can cause bacterial contamination of the perineum increasing the risk of UTI.
Incidence of UTIs in Men
UTIs are a significant health issue, especially over the age of 50 with the incidence increasing with age. Older men experience higher rates of infection due to associated risk factors, such as an enlarged prostate and a weakened immune system. Recurrent UTIs in men are a concern, though specific recurrence rates are hard to capture and can vary based on individual health factors and underlying conditions.
Symptoms & Diagnosis
Men with UTIs may experience frequent urination, an urgent need to urinate and a pain or burning sensation during urination (dysuria). They may also experience lower abdominal, pelvic, and rectal pain, along with cloudy, foul-smelling, or bloody urine. If the infection reaches the upper urinary tract, symptoms may include fever and chills.
• Urinalysis – Limitations: While urinalysis can detect signs of infection, such as the presence of white blood cells (leukocytes) and nitrites, it does not directly detect bacteria. The reliability of urinalysis is increasingly coming under scrutiny due to its potential for false positives and negatives, which can lead to either unnecessary treatment or missed infections. False positives can occur due to contamination, while false negatives can occur if the bacteria are not present in sufficient concentrations in the sampled urine.
• Urine Culture and Diagnostic Challenges: Urine cultures,
which identify the specific pathogen and determine antibiotic sensitivity, remain the gold standard for diagnosis. However, it’s important to note that some culturing can be problematic if the laboratory’s parameters for bacterial count are set too high. For example, a common threshold for significant bacteriuria is 100,000 colony-forming units (CFU) per millilitre (10^5 CFU/mL). This threshold can sometimes miss infections in symptomatic patients who may have lower bacterial counts, such as 1,000 CFU/ mL (10^3 CFU/mL) or 10,000 CFU/mL (10^4 CFU/mL), which are still clinically significant. Laboratories can lower the threshold based on clinical context and patient symptoms to improve diagnostic accuracy.
• Emerging diagnostic methods: PCR (polymerase chain reaction) testing and advanced microbial analysis, are being explored for their potential to offer more accurate and rapid detection of urinary pathogens. Nurses should stay informed about these developments and their local availability to ensure the most effective diagnostic strategies are employed. Additionally, when interpreting culture results, it’s crucial to consider the patient’s symptoms and clinical history to make informed treatment decisions.
• Physical Examination: Physical examinations, including checking for prostate tenderness or enlargement, are crucial. If indicated, imaging
tests like ultrasound or CT scans help detect any obstructions or abnormalities in the urinary tract. Flexible cystoscopy is an essential diagnostic tool that should be routinely considered when evaluating men with suspected urinary tract obstructions or recurrent infections.
Treatment & Management
Treatment typically involves antibiotics such as trimethoprimsulfamethoxazole, ciprofloxacin, levofloxacin, or nitrofurantoin, tailored to the specific bacteria and resistance patterns. Unlike women, men generally require a longer antibiotic course, often 7-14 days, this is because good antibiotic penetration into the prostate tissue is a challenge, and the prostate is a likely reservoir for bacteria in the male urinary tract. A 3-day course of antibiotics in male patients should always be challenged. Pain relief with over-the-counter analgesics like ibuprofen can help alleviate discomfort during urination. Follow-up care ensures the infection is cleared, often through repeat urine tests. Completing the entire course of antibiotics, even if symptoms improve, is crucial so as to increase the likelihood of successful elimination of the UTI and reduce the risk of recurrence/ resurgence. Patients should be educated on maintaining proper hydration, especially older men who may have a blunted sense of thirst. Encouraging good hygiene and avoiding irritants like caffeine and alcohol are also important.
minimise the risk of bacterial contamination and infection. Urinating after intercourse can help flush out any bacteria that may have entered the urethra during sexual activity.
• Catheter Care: Men who use indwelling or self-catheterisation should practise good standards of hygiene, using a ‘no touch’ technique and not breaking the connections between drainage systems unnecessarily. It’s important to be aware of the signs of UTI and not necessarily go from the colour of the urine. Asymptomatic bacteriuria that is routinely picked up should not be treated with antibiotics.
Prevention Strategies
Preventing UTIs in men involves several strategies, some of which are similar to those recommended for women, but with additional considerations specific to men:
• Hydration and Diet: Staying well-hydrated helps flush bacteria from the urinary tract. Addressing constipation with diet and lifestyle changes is important to prevent additional pressure on the urinary tract. Instructing patients and their carers or family members on the importance of ensuring fluids are made available and encouraging regular intake.
• Hygiene: Good personal hygiene, particularly after bowel movements, is optimal. Uncircumcised men should be vigilant about gently pulling back the foreskin and washing the head of the penis with warm water daily. There is evidence that uncircumcised males have a greater lifetime risk of UTI than men who are circumcised as infants. While the use of non-perfumed soaps and products is often recommended for women to avoid irritation, similar precautions can be beneficial for men, particularly those with sensitive skin or recurring infections.
• Sex: Safe sexual practices are crucial. Couples who have anal sex should use condoms to reduce the risk of introducing bacteria into the urinary tract. Additionally, washing the genital and anal areas thoroughly before and after sex can help
• Flow Issues/Prostate Health: Men should be encouraged to check in with their GP if they experience urinary flow issues or discomfort, as these symptoms may indicate problems such as benign prostatic hyperplasia (BPH), prostatitis, or urethral stricture. Addressing these symptoms can help identify and manage conditions that contribute to incomplete bladder emptying and increase the risk of UTIs. Encouraging the use of the double void technique can be beneficial to men as well as women, to help with bladder emptying and thus helping to prevent UTIs.
• General Health: Managing underlying conditions such as diabetes and maintaining a healthy immune system and gut health, through a balanced diet and regular exercise, can help reduce the risk of UTIs.
Criteria for Complex UTIs in Men
Recurrent Infections: Frequent UTIs suggest underlying structural or functional abnormalities that require thorough investigation, including cystoscopy, imaging, flow studies and often long-term management strategies, which may include surgical intervention/correction.
Antibiotic-Resistant Pathogens: UTIs caused by multidrug-resistant organisms are more challenging to treat, necessitating alternative antibiotic regimens and sometimes longer durations of therapy.
Structural Abnormalities: The presence of anatomical issues such as strictures, stones or congenital abnormalities often requires surgical intervention or specialised treatments.
Immunocompromised Status: Conditions like diabetes, HIV the use of immunosuppressive medications for chronic conditions
such as rheumatoid arthritis or chemotherapy significantly increase the risk of complications and treatment failures.
Complicated Clinical Presentation: Symptoms extending beyond the lower urinary tract, such as fever, chills, flank pain and systemic symptoms, indicate a more severe infection that requires immediate and comprehensive treatment. Importantly, while women generally experience more cases of complicated and upper-tract UTIs (such as pyelonephritis), men can face a higher risk of mortality from these infections. Aside from men being less likely to seek medical intervention when ill, it is postulated that the increased risk may be influenced by sex hormones, with testosterone potentially dampening immune responses, while oestrogen in women may offer some protective effects. Additionally, millions of men suffer from acute and chronic bacterial prostatitis, further contributing to the overall burden of UTIs in male populations. Why UTIs in Men are Considered Complex
The complexity of UTIs in men stems from anatomical, physiological, and clinical factors. The longer urethra and the presence of the prostate gland, which can become inflamed or enlarged, often complicate infections. Conditions like BPH, prostatitis, urethral strictures, kidney stones and bladder stones obstruct urine flow and increase infection risk. Bladder dysfunction, including neurogenic bladder dysfunction, also contributes to incomplete emptying and bacterial growth. Diagnosing UTIs in men often requires differentiating them from sexually transmitted infections, which have different treatment protocols.
Clinical Presentation and Diagnostic Challenges in Men
Men treated for UTIs and recurrent UTIs in primary care settings may have underlying conditions such as bladder cancer that can be missed without prompt referral and investigation. While the greater risk appears to be older women in a missed diagnosis scenario, men are also at risk of delayed referral. These patients need to be referred more quickly for cystoscopy to ensure accurate diagnosis and appropriate management. Additionally, bladder pain in men can often overlap with symptoms of chronic prostatitis, making differential diagnosis challenging.
Infection may also be present in these cases, further complicating the clinical picture. Men often sit on symptoms for longer or may not be aware that their urinary symptoms are significant. This delay in seeking treatment can lead to complications.
Alternatives to Antibiotics for recurrent/chronic UTIs
Managing recurrent or chronic UTIs in men often requires exploring alternatives to traditional antibiotic therapies. Several nonantibiotic treatments and future prospects are being studied, although many have not been extensively researched in men:
Vitamin C: Vitamin C is believed to acidify the urine and create an inhospitable environment for bacteria. However, clinical evidence supporting its efficacy in preventing UTIs is limited, and again not specifically studied in men.
D-Mannose: D-mannose, a type of sugar, has been suggested to prevent bacteria from sticking to the walls of the urinary tract. Recent research indicates that D-mannose may not be effective in preventing recurrent UTIs in women in a primary care setting. The study findings cannot be applied to more complex cases highlighting the need for further investigation.
Methenamine Hippurate:
Methenamine acts as a urinary antiseptic by releasing formaldehyde in acidic urine. While it is used to prevent recurrent UTIs, its efficacy in men specifically has not been well-studied and requires further research.
Bladder Instillations: Intravesical treatments, where medications are directly instilled into the bladder, can include agents containing sodium hyaluronate and/or chondroitin sulphate. These treatments aim to reduce bacterial adherence and inflammation, although more research is needed to confirm their effectiveness. In complex cases intravesical administration of Gentamicin may also be used. Direct instillation into the bladder has the benefit of limited systemic absorption/side-effects and does not come with the additional concern of antibiotic resistance. Further studies are ongoing.
Uromune Vaccine: This vaccine is aimed at preventing recurrent UTIs by stimulating the immune system. It is composed of a combination of inactivated whole bacteria commonly associated with UTIs - Escherichia coli, Klebsiella pneumoniae, Enterococcus
faecalis and Proteus vulgaris. It is taken daily as a sublingual spray for 3 months. Currently, in the UK, it is only available via specialist NHS recurrent UTI clinics or on private prescription. More research is required to determine its longterm efficacy.
Phage Therapy: This treatment utilises bacteriophages, viruses that infect and kill bacteria, as a potential treatment for antibioticresistant infections. This innovative approach shows promise but needs extensive clinical trials.
Other Vaccines: Research into new vaccines targeting UTIcausing pathogens is ongoing, with the hope of providing longterm prevention.
Interdisciplinary Collaboration is Key
Managing UTIs in men often requires collaboration across various urological subspecialties and primary care. Nurses should get to know their fellow specialists and work closely with them to enhance patient outcomes. Collaboration with urologists, nephrologists, infectious disease specialists, endocrinologists, radiologists, microbiologists, community-based nurses and GPs is essential. Regular interdisciplinary meetings and open communication channels are ideal for successful management, along with improved collaboration with GPs and Primary Care.
Conclusions
Understanding UTIs in men is essential for providing effective nursing care, as these infections are often more complex and require a highly individualised approach. Nurses play a crucial role in educating patients, delivering targeted treatments and implementing both prevention strategies and prompt interventions tailored to each patient’s unique circumstances.
Continuous education and heightened awareness of the complexities associated with UTIs in men can significantly improve patient outcomes and reduce the incidence of these infections.
This includes how men engage with health services and their reluctance to seek help promptly. The complexities discussed in this article underscore the need for ongoing research and a more nuanced understanding of UTI manifestations in men.
It is hoped that this article has stimulated further thought and
discussion in this critical area of urology, encouraging nurses to consider the specific needs of male patients when addressing UTIs.
The Urology Foundation’s UTI Information Service is here to help
The Urology Foundation appreciates the challenges associated with UTIs and is dedicated to providing resources and guidance needed. That’s why we launched a dedicated nurseled UTI Information Service to support and guide both patients and healthcare professionals. It offers valuable resources for healthcare professionals seeking advice and information as well as a telephone helpline.
Do you have ideas for research on UTIs?
The Urology Foundation is committed to driving change in the field of UTIs and to improving the lives of and outlook for patients and their families. UTIs have been identified as one of the research priorities in our Research Strategy 2024 – 2028. Thanks to the generosity of a donor, The Urology Foundation has a fund of £250,000 to support research into UTIs. Expressions of interest are due on 15th November 2024 and we would be delighted to hear from those with ideas.
About The Urology Foundation
The Urology Foundation is the UK’s only charity representing all urological diseases including prostate, bladder, kidney and male reproductive cancers and non-malignant conditions including incontinence, urinary tract infections, erectile dysfunction and kidney stones. We are committed to improving outcomes, quality of life and saving lives through investing in cuttingedge urology research; providing and supporting education and training programmes for the medical and scientific urology community; and achieving impact through awareness raising, improving understanding and driving change through policy and campaigns. Working with researchers, urologists, nurses and allied healthcare professionals, influencers and decision makers, patients and their families and those with an interest in urological diseases, we are leading the fight against urology disease.
https://www.theurologyfoundation. org/
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Management of BRCA in Men
BRCA stands for BReast CAncer gene. BRCA1 and BRCA2 are tumour suppressor genes which means that they stop the cells in our body from growing and dividing out of control and becoming cancer. People who inherit harmful variants in one of these genes have increased risks of several cancers—most notably breast and ovarian cancer, but also several additional types of cancer. People who have inherited a harmful variant in BRCA1 and BRCA2 also tend to develop cancer at younger ages than people who do not have such a variant.
A lot of people still think that this is a ‘Female or Woman’s’ gene, but the truth is that a BRCA1 or BRCA2 alteration/fault can be inherited from a person’s mother or father. If you carry a genetic alteration, each of your children (male or female), and each of your siblings (male or female) have a 50% (1 in 2) risk of inheriting the same alteration.
Faulty BRCA1 and BRCA2 genes are rare. Around 1 in every 400 people have a faulty BRCA1 or BRCA2 gene. Men who have inherited a fault in their BRCA1 or BRCA2 gene also have a higher risk of developing certain types of cancers, including prostate, pancreatic, and even breast cancers.
While breast cancer is rare in men, it can happen. The average male has a 0.1 percent lifetime risk of developing breast cancer, but in men with BRCA alteration, the risk is much higher: 1 to 5
Written by Bernie Carter, Assistant Director of Nursing, Marie Keating Foundation
percent lifetime risk for men with BRCA1 alteration and 5 to 10 percent lifetime risk for men with BRCA2 alteration.
However, most men are probably more worried about prostate cancer than breast cancer, with good reason: the lifetime risk for prostate cancer for an average male is 14 percent. In Ireland, after non-melanoma skin cancer, prostate cancer is the most common cancer in men. It accounts for almost one-third of all invasive cancers in men. 1:9 Irish men will develop prostate cancer (to the age of 75) and 1:6 in their life time. An average of 3,980 men are diagnosed each year in Ireland with prostate cancer and
623 deaths occur due to prostate cancer. However, the 5 year survival rate for prostate cancer is increasing all the time and it is now up to 93%!
For men with BRCA1/2 alterations, the risk of developing prostate cancer is higher than for the general public and if prostate cancer does develop, it may be more aggressive. The risk is higher for people born male with an alteration in the BRCA2 gene than in the BRCA1. Men who carry a BRCA2 alteration have a 27% risk of developing prostate cancer by the time they are 80 years old, more than double the rate compared to non-carriers and may be diagnosed at a younger age.
Men with BRCA alteration are also at increased risk for pancreatic cancer: 2 to 3 percent lifetime risk for those with BRCA1 alteration and 3 to 5 percent lifetime risk for those with BRCA2 alteration, compared to just 1 percent lifetime risk in the general population.
BRCA2 alteration are also associated with a higher risk of melanoma in males.
Patients should talk to their GP if they think they could have inherited any of these faulty genes or if they have a strong family history of cancer especially breast, ovarian and or prostate cancer. A strong family history of cancer means multiple close family members on the same side of the family who have the same cancer or related cancer types. Unfortunately, there's currently no reliable screening test for prostate cancer. Some research suggests that perhaps annual PSA tests for prostate cancer may benefit men who carry the faulty BRCA2 gene.
BRCA: The Breast Cancer Gene - BRCA Mutations & Risks (nationalbreastcancer.org)
Predictive genetic tests for cancer risk genes - NHS (www.nhs.uk)
BRCA Gene Mutations: Cancer Risk and Genetic Testing Fact Sheet - NCI
What Men Need to Know About BRCA and Other Gene Mutations | Breast Cancer Research Foundation (bcrf.org)
Cialis for men® Now Available OTC
Clonmel Healthcare, in conjunction with Opella, Sanofi’s consumer healthcare business unit are pleased to announce that Cialis for men® 10mg film-coated tablets tadalafil is now available over the counter (OTC), without prescription in Irish pharmacies for the treatment of erectile dysfunction (ED). This marks a significant development in the management of ED, providing an accessible, pharmacist-supervised alternative to previous OTC treatments.
Cialis for men® offers a new OTC approach to managing ED with its active ingredient, tadalafil, which increases blood flow to the penis, helping men achieve and maintain an erection when sexually aroused. Its effect, lasting up to 36 hours, allows for greater flexibility and reduces the pressure on timing, thereby improving patient experience and satisfaction. Available exclusively in pharmacies throughout Ireland from today, Cialis for men® requires pharmacist oversight to ensure patient safety and suitability, providing guidance on the proper use of the medication.
Recent research highlights the prevalence of ED in Ireland, with nearly 3 in 10 Irish men reporting experiences with the
Pictured at the launch of Cialis for men OTC at Boots Pharmacy on Dawson Street is Pharmacist
Said Danishani, Regulatory Affairs
Manager Boots Ireland, Olivia Reilly Marketing Manager at Clonmel Healthcare and Barry Fitzpatrick, Director of Sales at Clonmel Healthcare
condition. Despite the availability of treatments, awareness of over-the-counter options remains low, with 50% of men unaware of such solutions. The launch of Cialis for men® directly addresses this gap, offering a longer-lasting, accessible treatment that does not require a prescription, thereby removing barriers that may prevent men from seeking help.
The availability of Cialis for men® in pharmacies positions pharmacists at the forefront of men's health, enabling them to play a critical role in supporting patients experiencing ED. As trusted healthcare professionals, pharmacists can provide discreet advice and support, ensuring that men receive accurate information and appropriate treatment.
Longford-based Pharmacist Paula Reilly comments: “With
medications like Cialis for men® now available directly through pharmacies, men no longer need to visit their GP for treatment, which has removed a significant barrier to seeking help. This ease of access is paving the way to make a real difference in promoting better health outcomes for men and their partners."
The research also revealed critical insights into the state of men's sexual health in Ireland. More than 7 in 10 men believe there is still a significant stigma surrounding the discussion of men's sexual
health, however, making treatment options more accessible and raising awareness about the commonality of these conditions can help reduce that stigma. The study also highlights the impact of social media and online content, including pornography, on men's perceptions of sexual performance. It found that 31% of men feel that social media has influenced their expectations, with nearly half (47%) of men aged 18-34 admitting to regularly comparing their sexual experiences to these oftenunrealistic portrayals.
Abstract: Assessing our adherence to bone protection standards in metastatic prostate cancer in the largest Irish center: Are we falling behind?
Written by Razia Aslam, Danial Hadi, Syed Muhammad Bilal Shah, and Emma Barron, St James’s Hospital, Dublin
Background: Prostate cancer ranks as the second most prevalent cancer in men globally, often necessitating androgen deprivation therapy (ADT) as part of its treatment. While ADT effectively diminishes testosterone levels, a vital factor in prostate cancer cell growth, it concurrently poses a notable side effect – an accelerated rate of bone loss. This heightened bone loss elevates the vulnerability of patients to osteoporosis and fractures. The optimization of bone health entails early identification of patients susceptible to osteoporosis and fractures, the implementation of preventative measures, and prompt interventions to mitigate bone loss and fracture risks.
Methods: The audit aims to evaluate adherence to established guidelines, such as those outlined
by the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO), concerning the assessment and optimization of bone health. A retrospective analysis was performed on the medical records of prostate cancer patients who underwent Androgen Deprivation Therapy (ADT) at St James Hospital in Dublin. Pertinent data, encompassing patient demographics, duration of ADT, documentation of bone health assessment, frequency of Bone Mineral Density (BMD) testing, utilization of preventive measures (e.g., calcium and vitamin D supplementation), and any interventions for bone health optimization (such as bisphosphonate therapy and denosumab), was systematically collected.
Results: A comprehensive review encompassed 57 patients, revealing that 38 patients (67%) exhibited metastatic disease. Among them, 42 patients (74%) presented with castrate-sensitive disease. Out of the total, 24 patients (42%) underwent a baseline Dual-Energy X-ray Absorptiometry (DEXA) scan. Results indicated that 12 patients were diagnosed with Osteoporosis, 9 with Osteopenia, and 3 with normal Bone Mineral Density (BMD). At baseline, 26 patients (46%) initiated Calcium and Vitamin D supplements, while 12 patients (21%) commenced Bisphosphonates/Denosumab based on DEXA scan outcomes. Notably, 8 (14%) patients experienced a skeletal/bonerelated event which is much higher than reported in literature.
Conclusions: The findings are intended to guide healthcare professionals in optimizing bone health strategies, with the ultimate goal of improving patients' quality of life and minimizing the risk of fractures and related complications. Identified areas for improvement in clinical practices will be addressed by implementing recommended recommendations, aiming to enhance patient care, decrease the risk of osteoporosis and fractures, and overall improve patient outcomes. A re-audit is planned to monitor ongoing adherence to guidelines and assess the impact of interventions implemented as a result of this study.
This is an ASCO Meeting Abstract from the 2024 ASCO Annual Meeting I. This abstract does not include a full text component.
Why are fewer men being treated for this disease of obesity?
Written by Faisal Almohaileb and Carel W le Roux, Diabetes Complications Research Centre, University College Dublin, Ireland
Obesity was historically viewed as the fault of the person because of their poor lifestyle choices, while being linked to lower social and economic strata in wealthy societies. Previously, clinicians thought that risk factors for obesity included dietary habits, physical inactivity, environmental influences, psychosocial aspects, and genetic predispositions. Most diseases thought to cause obesity are considered neurobiological.i While specific genetic diseases cause syndromes like PraderWilli or Bardett Biedl, most other obesity diseases result from complex polygenic interactions influenced by environmental factors.ii, iii Thus, the latest science has changed our perspective on obesity as experts now recognize obesity as a chronic, complex biological disease.
Obesity remains a global health concern, with prevalence still increasing in all socioeconomic groups and regions. The World Health Organisation’s definition of excessive adipose tissue resulting in a deterioration of health moves the focus away from the widely held idea that an imbalance between caloric intake and energy expenditure is the cause of the disease. Obesity has a specific pathophysiology, and most current research is focused on the links between the brain, gut, and adipose tissue. Genetic, environmental, and behavioral factors contribute to obesity.ii iii A step change is expected after the latest studies
suggesting that obesity is not one disease but most likely the result of multiple diseases. This will allow us to understand our clinical observations regarding the heterogeneity of risk of obesity complications, and response to obesity treatment.iv
Obesity is associated with more than 220 complications; thus, medical students are now taught: “if you know obesity, you know medicine.” There are very few medical specialties not impacted by obesity-related complications such as cardiovascular disease, type 2 diabetes, dyslipidemia, gastroesophageal reflux disease, metabolic dysfunctional associated steatohepatitis, gallbladder diseases, musculoskeletal disorders like low back pain, obstructive sleep apnea, and increased risk for certain cancers. Furthermore, obesity can have profound psychological effects, thought to be in part related to stigma suffered by patients, leading to higher rates of depression and anxiety. Reproductive health issues are also more common, with increased incidences of infertility, polycystic ovarian syndrome, and complicated pregnancies such as gestational diabetes and preeclampsia.
Despite experts recognising obesity as a disease, most clinical services and research centers are treating or recruiting vastly fewer males. Recognising that men are undertreated may be the first step to ensure fair healthcare strategies.
Men and women respond similarly to various obesity treatments, including lifestyle modifications and bariatric surgery. The response to pharmacotherapy is also similar when weight loss is corrected for plasma levels of the drug.v Weight loss outcomes and improvements in metabolic health after treatment are comparable between males and females, suggesting that treatment protocols should be adjusted to the individual rather than being sex-specific. However, men constitute only about 25% of participants in clinical studies, limiting the generalisability of research findings and the development of universally effective treatments.iii, vi
Reasons for fewer men benefiting from obesity treatment may include societal stigma, lack of awareness, and differences in health-seeking behaviors. Men are generally less aware of health risks, and traditional views of masculinity often emphasize selfreliance. Society may also place less emphasis on the appearance of men. Visits to doctors are less regular compared to women. Thus, missing routine check-ups may reduce obesity being identified, and interventions suggested. Finally, men might perceive weight loss programs as being tailored primarily for women, which discourages them to seek help. Addressing these barriers is crucial to ensuring equitable access to obesity treatment.iii, v, vii
To address these imbalances, funding bodies and ethical review boards must emphasise guidelines for equitable representation in clinical studies, mandating minimum male participation thresholds. Healthcare providers must be trained to recognise and treat obesity with a patientcentered approach that considers individual circumstances rather than the sex of the person. Public health campaigns aimed explicitly at men should be developed to raise awareness about obesity as a chronic disease, reduce stigma, and promote early intervention. Additionally, policy interventions should promote equality in healthcare access and research funding, facilitating the inclusion of men in obesity clinical trials and clinical treatment programs.viii
* Underrepresented groups: older participants, those with class 3 obesity (BMI ≥ 40.0 kg/m2), nonWhite, and male participants.
References
Purnell JQ, le Roux CW. Hypothalamic control of body fat mass by food intake: The key to understanding why obesity should be treated as a disease. Diabetes Obes Metab. 2024 Apr;26 Suppl 2:3-12. doi: 10.1111/dom.15478. Epub 2024 Feb 14. PMID: 38351898.
ii World Health Organization. (2022). Obesity and overweight. Retrieved from https://www.who.int/news-room/factsheets/detail/obesity-and-overweight. iii Schorr, M., Dichtel, L. E., Gerweck, A. V., Valera, R. D., Torriani, M., Miller, K. K., & Bredella, M. A. (2018). Sex differences in body composition and association with cardiometabolic risk. Biology of Sex Differences, 7(1), 1-8. iv Delfin C, Dragan I, Kuznetsov D, Tajes JF, Smit F, Coral DE, Farzaneh A, Haugg A, Hungele A, Niknejad A, Hall C, Jacobs D, Marek D, Fraser DP, Thuillier D, Ahmadizar F, Mehl F, Pattou F, Burdet F, Hawkes G, Arts ICW, Blanch J, Van Soest J, Fernández-Real JM, Boehl J, Fink K, van Greevenbroek MMJ, Kavousi M, Minten M, Prinz N, Ipsen N, Franks PW, Ramos R, Holl RW, Horban S, Duarte-Salles T, Tran VDT, Raverdy V, Leal Y, Lenart A, Pearson E, Sparsø T, Giordano GN, Ioannidis V, Soh K, Frayling TM, Le Roux CW, Ibberson M. A Federated Database for Obesity Research: An IMI-SOPHIA Study. Life (Basel). 2024 Feb 16;14(2):262. doi: 10.3390/life14020262. PMID: 38398771; PMCID: PMC10890572.
v Pi-Sunyer X, Astrup A, Fujioka K, Greenway F, Halpern A, Krempf M, Lau DC, le Roux CW, Violante Ortiz R, Jensen CB, Wilding JP; SCALE Obesity and Prediabetes NN80221839 Study Group. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management. N Engl J Med. 2015 Jul 2;373(1):11-22. doi: 10.1056/ NEJMoa1411892. PMID: 26132939.
vi Le Roux, C. W., Aylwin, S. J., Batterham, R. L., Borg, C. M., Coyle, D., Prasad, V., ... & Meeran, K. (2007). Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters. Annals of Surgery, 243(1), 108-114.
vii Al-Nimr, R. I., Al-Aqeel, S. A., & AlSebayel, M. I. (2020). Gender disparities in seeking treatment for obesity in Saudi Arabia: a cross-sectional study. International Journal of Environmental Research and Public Health, 17(4), 1324
viii Rubino, F., Puhl, R. M., Cummings, D. E., Eckel, R. H., Frühbeck, G., & Mingrone, G. (2020). Joint international consensus statement for ending stigma of obesity. Nature Medicine, 26(4), 485-497
Faisal Almohaileb
Carel W le Roux
Lung Cancer 41
Lung Cancer and Men
The Facts about Lung Cancer
• Lung cancer is very common. It is the third most common cancer in Ireland, excluding non-melanoma skin cancer1
• On average, 2,586 people are diagnosed with lung cancer each year in Ireland
• It affects both men & women
• It is the leading cause of cancer death in both males and females in Ireland and also worldwide1, 4
• Smoking tobacco is the most common cause of lung3
• However, approximately 10–15% of lung cancers in Western countries occur in non-smokers17
• Lung cancer starts in the windpipe (trachea), the main airway (bronchus) or the lung tissue2
• It is often diagnosed at a late stage (Stage IV) when the cancer has spread outside of the lungs and when treatment options are limited4
• The most recent report from the National Cancer Registry in Ireland documented that during the period 2014-2018, more than one third (39%) of lung cancers were diagnosed at stage IV for which 5-year net survival was only 4%1
• Lung cancer screening of high risk individuals has the potential to dramatically improve survival rates through early detection4
• Currently in Ireland, there is no publicly funded national lung cancer screening service but this may change in the future.
• Early detection of lung cancer can lead to better treatments and outcomes4
More men than women are diagnosed with lung cancer each year in Ireland. The most recent statistics from the National Cancer Registry Ireland (NCRI) documented that 1,386 men and 1,199 women get lung cancer each year in Ireland. It is the 3rd most common cancer in men in Ireland after non-melanoma skin cancer.1 The NCRI stated that the number of lung cancer cases is increasing and is expected to rise to 3713 cases (+131%) for males and 2313 (+105%) for females by 2045.32
Lung cancer is the leading cause of cancer death in both sexes, with an average of 1,946 deaths per year but more men die from lung cancer than women, 1,081 men versus 865 women.1
In recent years, lung cancer incidence has been 27% higher among males compared to females though both incidence and mortality are declining more rapidly in males than females. These trends are generally
attributed to differences in gendered smoking patterns.31
Risks and causes of lung cancer
• Age - About 7 in 10 people diagnosed with lung cancer in Ireland are age 65 and older. It's rare in people younger than 40 but it can occur6
• Smoking tobacco - Smoking tobacco is the leading cause of lung cancer, responsible for approximately 85% of all cases4
o Even light or occasional smoking increases the risk of lung cancer. But your risk increases the more you smoke and the longer you smoke7
o Using other types of tobacco products can increase your risk of lung cancer, e.g. cigars, pipe tobacco, snuff (a powdered form of tobacco) and chewing tobacco9, 10
Written by Bernie Carter, Assistant Director of Nursing, Marie Keating Foundation
o Primary prevention (such as tobacco control measures and reducing exposure to environmental risk factors) can reduce the incidence of lung cancer and save lives4
• Passive smoking - Adults who do not smoke and are exposed to second-hand smoke which increases their risk of developing lung cancer by 20–30%11
• Previous lung diseasesPrevious lung diseases can increase your risk of lung cancer. These risks are usually higher in smokers. Your risk of lung cancer is higher if you have Chronic Obstructive Pulmonary Disease (COPD). It is sometimes called emphysema or chronic bronchitis.
o Idiopathic pulmonary fibrosis (IPF) also increases the risk of lung cancer developing19
o Tuberculosis (TB) at a young age is a risk factor for lung cancer, regardless of the underlying disease or smoking history20
• Chemicals and workplace risks - Some substances which people are exposed to in the workplace can increase the risk of lung cancer. These include asbestos, silica, and diesel exhaust, arsenic, beryllium, cadmium, coal and coke fumes and nickel7, 10
• Exposure to radon - Radon gas is a naturally occurring radioactive gas that comes from tiny amounts of uranium present in all rocks and soils that can increase the risk of lung cancer. Parts of Ireland have high
amounts of radon. Your risk of getting lung cancer from radon is 25 times higher if you smoke than someone who has never smoked7, 10, 12
• Marijuana and lung cancerSmoking marijuana may raise your chances of lung cancer, but scientists aren't sure yet. Marijuana smoke has many of the same harmful substances as tobacco smoke, which could damage lung tissue and lead to cancer. Also most people who smoke cannabis mix it with tobacco, inhale more deeply and hold the smoke in their lungs for longer10, 13
• Family history - Your risk of lung cancer is higher if you have a close relative (such as a parent or sibling) who has had lung cancer7
• Genetics - Some experts estimate that a genetic predisposition to lung cancer contributes to approximately 8% of cases. Some of these genetic risk factors are inherited while others are not. Some studies suggests that an individual’s genes are more likely to contribute to an increased chance of lung cancer if they are young and have never smoked. However, lung cancer can also run in families because of shared environmental factors and lifestyle habits14
o Regardless of whether you carry a higher hereditary risk for lung cancer, doctors recommend that all people avoid tobacco smoke and other exposures that increase the risk of lung cancer15
Lung Cancer
Signs and Symptoms?
The most common symptoms of lung cancer are:
• having a new cough or a cough most of the time
• getting out of breath doing the things you used to do without a problem
• having an ache or pain in the chest or shoulder
• chest infections that keep coming back or a chest infection that doesn't get better
• feeling tired all the time (fatigue)
• losing your appetite
• losing weight
• coughing up phlegm (sputum) with blood in it21
Less common symptoms of lung cancer include:
• larger fingertips and curved nails (finger clubbing)
• finding it difficult to swallow (dysphagia) or feeling pain when swallowing
• wheezing
• hoarse voice
• swelling of your face or neck
• chest or shoulder pain that does not go away22
Some of these symptoms are very common and may not be caused
by cancer, but you should see your GP to be sure.
Types of lung cancer
Cancer that starts in the lung is called primary lung cancer. Cancer that spreads to your lungs from somewhere else in your body is called secondary lung cancer.
There are different types of primary lung cancer and they are divided into 2 main groups:
• small cell lung cancer (SCLC)
• non-small cell lung cancer (NSCLC)
The most common type is nonsmall cell lung cancer.(26) How lung cancer is diagnosed
If you experience any of the above symptoms, see your GP without delay. Your GP will ask you about your general health and may also examine you.
They may feel your lymph nodes (glands) in your neck and under your arms and they may listen to your chest and breathing with a stethoscope. They might also ask you to breathe into a small device called a spirometer. This device measures the amount of air you breathe in and out and also measures how quickly you breathe. This test is called spirometry. Your GP might arrange for you to have blood tests and a Chest X-ray. If your GP is concerned about your symptoms
and your test results they may refer you to a Rapid Access Lung clinic.23
The aim of this clinic is to quickly establish whether lung cancer is present, to determine the extent of the disease and to have a multidisciplinary team of experts discuss your individual case. Test carried out in the Rapid Access Lung clinic may include one or all of the following: chest X-ray, bronchoscopy and CT scans (CT or PET-CT). Commonly, a biopsy, or small piece of the lung tissue, will be obtained to confirm the diagnosis. Most often, this is obtained by a bronchoscopy or by a CT-guided biopsy.24
Treatment for lung cancer
Many hospitals have multidisciplinary teams (MDTs) that treat lung cancer. This team together will discuss and plan your treatment. Your treatment depends on several factors including the following:
• the type of lung cancer you have
• how big it is and whether it has spread (the stage)
• your age and general health
• if it is primary or secondary lung cancer
The most common types of treatment for lung cancer are:
• surgery
• radiotherapy
• chemotherapy
• immunotherapy
• targeted therapy
You may have a combination of treatments. You can also ask if you can take part in a clinical trial.29, 30
Smoking and lung cancer
Tobacco smoke contains more than 70 toxic substances that are carcinogenic (cancer-producing).
Your risk of developing lung cancer:
• is higher if you smoke or smoked
• gets higher the more you smoke
• gets higher the longer you smoke27
If you smoke, the best way to reduce your risk of lung cancer is to quit. Quitting can be hard but with the right help you can double your chances of success. The HSE offers free support and advice on the different options that help with nicotine withdrawal. Their team will support you every step of the way.
• Freephone 1800 201 203 for a free Quit plan
• Visit the HSE website to create your own Quit Smoking Plan Create your quit smoking planQuit.ie (hse.ie)28
References available on request
Enhancing Men’s Awareness of Testicular Disease
Testicular cancer is rare, but it’s the most common cancer in young men aged between 15 and 44. About 170 men are diagnosed with testicular cancer every year in Ireland.
Just this year, a new initiative has been launched in Ireland – ‘On the Ball’ which is an inclusive community-based campaign to promote testicular awareness.
We spoke with Dr Mohamad Saab who led the campaign to find out more.
Dr Mohamad Saab is Senior Lecturer and Vice Dean of Graduate Studies in the School of Nursing and Midwifery, University College Cork (UCC). He holds a PhD in Nursing from UCC, a PGDip and Cert in Teaching and Learning in Higher Education from UCC, MSc in Advanced Practice Nursing and BSc in Nursing from the American University of Beirut. Mohamad has over 100 research outputs and around ¤11 million in research funding.
His research is primarily focused on the use of virtual reality in several contexts, including raising young men’s awareness of testicular diseases, teaching simulation to nursing students, and teaching nursing and medical students about difficult conversations. Mohamad teaches across several interdisciplinary oncology, palliative care, research, and communication modules and supervises a number of MSc and PhD students.
What are the key considerations in evaluating the long-term impact of the "On The Ball" campaign, particularly regarding early detection of testicular diseases?
“On the Ball” is an inclusive community-based campaign aimed to raise young men’s awareness of testicular diseases including testicular cancer. Funded by the Health Research Board (HRB), “On the Ball” was co-designed and refined with 20 representatives of various community organisations. A soft launch of “On the Ball” took place with 411 students engaging with the campaign stand and receiving various campaign merchandise.
The projected long-term impact of “On the Ball” is increased “testicular awareness” which involves men being aware of
the normal look and feel of their own testes and seeking help for symptoms of concern. This would lead to early detection, less aggressive treatment, and improved survival and survivorship.
How do you anticipate the combination of online and offline media (e.g., social media, games, place-based advertising) will evolve in future health campaigns to address stigma around men’s health topics like testicular cancer?
Participants in the co-design and refinement of “On the Ball” discussed the importance of being inclusive. To this end, they recommended delivering “On the Ball” both, offline and online. Offline delivery would target men who do not necessarily use social media while online delivery, primarily using social media, would reach age groups at risk of testicular disease (i.e., young men and boys aged 15-39 years) who are the primary users of social media. The effect of multimodal campaigning is well documented in the wider literature and the recommendation to deliver “On the Ball” both online and offline ties in with existing literature on cancer awareness campaigns.
As for addressing stigma, indeed, in the past we found that men and boys with suspected testicular diseases delay medical helpseeking for symptoms of concern primarily due to the inherent limited contact with the healthcare system, embarrassment due to the sensitive nature of testicular diseases, and perceived threats to masculinity. We believe that the use of light-hearted messages and easy and accessible language in “On the Ball” would help overcome some of these barriers, leading to early detection and treatment of testicular diseases.
Given the higher engagement and satisfaction with the VR component of E-MAT, how do you see VR's role in future health interventions for younger male populations? What are its limitations?
E-MAT stands for “Enhancing Men’s Awareness of Testicular
Diseases.” This intervention, also funded by the HRB, uses VR gaming to engage young men with information on testicular diseases, improving their knowledge of what could go wrong with their testes and highlighting the importance of early help-seeking for symptoms of concern. We have successfully tested E-MAT with young GAA players in Co. Cork who are at high risk of testicular injury. We hope to seek future funding in order to test E-MAT in a larger population across Ireland.
VR is one of the most rapidly growing technologies in healthcare. Adolescents and young adults aged 15-39 years, including Millennials and Generation Z, are prominent users of VR. This population is increasingly using VR for educational purposes. Therefore, the use of VR technology in the context of raising awareness of testicular diseases is appropriate and timely.
As for limitations, there are no major adverse effects from VR and since E-MAT does not involve sudden movement or jumping. However, it is not advisable for individuals with severe motion sickness and/or uncontrolled seizures to use VR. Just to note that only 1 of the 142 participants in the three studies testing
E-MAT reported mild nausea that subsided immediately after taking off the VR headset. Another limitation could be the cost of equipment. Having said that, the rapid growth and adoption of VR has led to significant price drops and the development of user friendly, wireless, light, and affordable devices.
What factors do you believe contributed to the sustained knowledge of testicular diseases among participants three months after the intervention, and how do you plan to address potential drop-offs in awareness over longer periods?
E-MAT is underpinned by the Preconscious Awareness to Action theoretical framework that I have developed. This framework highlights the role of various types of memories in knowledge retention. Episodic memory involves recalling events of interest in specific spatial and temporal contexts (e.g., weddings and concerts). In the context of E-MAT, experiencing VR technology, particularly for first-time VR users, would create a long-lasting memorable episode of the intervention. Semantic memory pertains to factual knowledge and general information, such as scientific concepts learned
Dr Mohamad Saab
Testicular Disease
As for addressing stigma, indeed, in the past we found that men and boys with suspected testicular diseases delay medical help-seeking for symptoms of concern primarily due to the inherent limited contact with the healthcare system, embarrassment due to the sensitive nature of testicular diseases, and perceived threats to masculinity. We believe that the use of light-hearted messages and easy and accessible language in “On the Ball” would help overcome some of these barriers, leading to early detection and treatment of testicular diseases.
Co-Design and Launch of “On The Ball”: An Inclusive Community-Based Campaign to Promote Testicular Awareness
through education. In E-MAT, the use of clear and accessible information to educate young men about testicular diseases would facilitate the retention of scientific facts. Procedural memory is acquired through practice and repetition (e.g., riding a bicycle or typing). Engaging with VR technology including headsets and handheld devices would aid in developing procedural skills and memory. All these factors could have contributed to the sustained increase in knowledge of testicular diseases.
November 2023
This study was funded by the Health Research Board (HRB) Knowledge Translation Awards (KTA) 2022.
Drop-offs in awareness and knowledge over longer periods are inevitable, especially in interventions delivered once. This phenomenon is at times referred to as “knowledge decay.” We are constantly bombarded by information and more important life events tend to take precedence over information acquired within health promoting
interventions. This is one of the reasons why several organisations and researchers involved in health promotion tend to design new health promotion interventions periodically. VR is still a novel and evolving technology and its use in the context of raising awareness of testicular diseases is warranted. The VR market is growing, and VR devices are evolving. This would require iterations of the E-MAT intervention.
response [QR] codes via posters) was more efficient and cost effective for recruiting participants in E-MAT from various GAA clubs. We also aimed to determine if the recruitment method influenced retention in E-MAT.
level and understand the impact of individual characteristics on recruitment. Researchers lacked direct administrative access to club accounts, making it difficult to separate participant data from general club data. Also, many participants learned about the study through friends, complicating the tracking of recruitment sources. The analysis revealed that some individuals accessed links via text or WhatsApp, further obscuring the effectiveness of recruitment methods. Insights into optimal posting times indicated that X usage peaks at noon, 6 PM, and 9 PM on Tuesdays and Thursdays, while Facebook peaks at 8 AM and 8 PM on Fridays. All these lessons will be taken into consideration while planning wider testing of E-MAT.
Authors: Dr. Mohamad M. Saab 1, Ms. Varsha N. Shetty 1, Ms. Megan McCarthy 1 , Dr. Martin P. Davoren 2,3, Dr. Angela Flynn 1, Dr. Ann Kirby 4, Professor Steve Robertson 5 , Dr. Gillian W. Shorter 6, Mr. David Murphy 7, Dr. Michael J. Rovito 8, Dr. Frances Shiely 3,9 and Professor Josephine Hegarty 1
What specific lessons were learned from the SWAT about recruiting male participants in sports organisations, and how might these inform future recruitment strategies for health trials targeting young men?
The E-MAT intervention was accompanied by a Study Within A Trial (SWAT). The purpose of the SWAT was to determine which recruitment method (X, [formerly Twitter], Facebook, or quick
We found that participants mainly heard about the study through friends, with some engagement via social media platforms Facebook and X, and little to no engagement with the QR code. Primary outcomes were hindered by the inability to disaggregate data by GAA club. Economic outcomes revealed QR code as the costliest strategy, and while X was cheaper than Facebook in terms of the number of clicks, Facebook demonstrated better recruitment and retention and thus reduced the costs per participant.
1 Catherine McAuley School of Nursing and Midwifery, University College Cork, Cork, Ireland. | 2 Sexual Health Centre, Cork, Ireland. | 3 School of Public Health, University College Cork, Cork, Ireland. | 4 Department of Economics, Cork University Business School, University College Cork, Cork, Ireland. | 5 School of Allied Health Professions, Nursing & Midwifery, Faculty of Health, University of Sheffield, United Kingdom. | 6 Centre for Improving Health Related Quality of Life, School of Psychology, Queen’s University Belfast, Belfast, Northern Ireland, United Kingdom. | 7 School of Computer Science and Information Technology, University College Cork, Cork, Ireland. | 8 Department of Health Sciences, College of Health Professions and Sciences, University of Central Florida, Orlando, Florida, United States of America. | 9 Health Research Board Centre for Health and Diet Research, School of Public Health, University College Cork, Cork, Ireland.
The SWAT had some limitations (or lessons learned!) in evaluating recruitment strategies for GAA
The study found no significant difference in knowledge outcomes between VR and tablet-based interventions. Do you believe future iterations of E-MAT should focus more on enhancing interactivity, or should the emphasis shift toward accessibility and cost-effectiveness?
We compared the effect of E-MAT delivered using VR (E-MATVR) to E-MAT delivered electronically as plain text using a tablet (E-MATE) and found that, while knowledge improved in both E-MATVR and E-MATE groups, knowledge did not differ when E-MATVR was compared to E-MATE. This can be explained by the fact that the
E-MAT study was a feasibility trial with only 74 participants. A full trial with a larger sample size powered to detect the efficacy of E-MATVR is needed to establish efficacy.
As part of the E-MAT feasibility trial, we conducted a process evaluation to determine how to best deliver E-MAT in the future. Overall, participants were highly satisfied with E-MATVR. They made valuable recommendations to enhance interactivity, reduce cost, and improve access to VR. All these recommendations will be taken into consideration when developing and testing E-MAT in the future.
Dr Saab can be contacted on msaab@ucc.ie
Saab, M. M., McCarthy, M., Davoren, M. P., Shiely, F., Harrington, J. M., Shorter, G. W., ... & Dahly, D. (2024). Enhancing Men’s Awareness of Testicular Diseases (E-MAT) using virtual reality: A randomised pilot feasibility study and mixed method process evaluation. PLOS ONE, 19(7), e0307426. https:// doi.org/10.1371/journal. pone.0307426
Saab, M. M., Shetty, V. N., McCarthy, M., Davoren, M. P., Flynn, A., Kirby, A., ... & Hegarty, J. (2024). Codesign and Launch of ‘On the Ball’: An Inclusive Community- Based ‘Testicular Awareness’ Campaign. Health Expectations, 27(3), e14100. https://doi. org/10.1111/ hex.14100
NEWS - Gaps in Neuro-rehabilitation Care
People with neuro-rehabilitative needs living in the community have identified challenges, gaps and opportunities in neuro-rehabilitation care in Ireland.
A neuro-mapping project, led by the HSE, Disability Federation of Ireland and the Neurological Alliance of Ireland engaged with 56 people with neurological conditions and 137 service providers to establish the current picture of community neuro-rehabilitation services in Ireland. The voices of people with lived experience of neurological conditions are an important element of the neuro mapping project.
This mapping project has resulted in the Report on the Neuro-Mapping Project Phase 2 which recommends:
• Increasing knowledge and information on services that are available in the community for people with neurological conditions
• Improving how services work together
• Providing access to services based on need
• Funding and resourcing specialist services in the community
• Designing future services to support the continuum of care for people with neurological conditions.
The recommendations will be developed into actionable objectives under the National Neuro-Rehabilitation Strategy.
A similar project, engaging with people with neuro-rehabilitative needs and service providers, will take place in three years’ time to determine what progress has been made in community neuro-rehabilitation service provision.
Dr Emer Begley, Director of Advocacy, Disability Federation of Ireland said, “Disability Federation of Ireland (DFI) valued the partnership with the Neurological Alliance of Ireland and the HSE on this project to identify the service and support needs of people with neuro-rehabilitative, and to ascertain the challenges they face as they seek to maximise their independence. The frustrations expressed by those with lived experience who participated in the project give harsh insights into the challenges they face on a daily basis. DFI welcomes the comprehensive recommendations outlined in the report and we look forward to working collectively, and in partnership with all stakeholders to progress their implementation.”
Environment & Health
Trees and Health in a Changing World
ENVIRONMENTAL OVERVIEW
Background
I was thinking about climate change and whether there was any place for the medical profession (world-wide) to advocate for the people. I was looking for some up-to date article on the subject to try to briefly put into perspective the size of the problem, and whether the threats that have been expounded are real, and thus likely to make people die (like diseases that we try to prevent and treat). Well in a case of nearly perfect timing, the Guardian, not known for disinformation, in May, published an article where they had asked 380 top climate scientists what they felt about the future, and to be honest, it made scary reading. The climate crisis is already causing profound damage as the average global temperature has reached about 1.2C above the pre-industrial average over the last 4 years. Of the respondents 77% believe that global temperatures will reach at least 2.5C above preindustrial levels, and 44% believe that it will be more than 3C. Only 6% believe that the 1.5C limit (UN climate summit Paris 2015) will be achieved. A few pointers on these observations. Even just 1C of heating has supercharged the planets extreme weather, delivering searing heatwaves that would have been otherwise impossible. A world hotter by 2.5-3C takes us into truly unchartered territory, with everything from 2 billion people being pushed outside humanity’s climate niche, to Cities like Rio, Miami, Shanghai and the Hague ending up below sea level. “It is the greatest threat humanity has faced with the potential to wreck our social fabric and way of life. It has the potential to kill millions, if not billions, through starvation, war over resources, and displacement – none of us will be unaffected by the devastation”. Climate tipping
Written by Dr David Mulcahy, Consultant Cardiologist MD FRCPI FESC
points, where a tiny temperature rise tips crucial parts of the climate system into collapse, such as the Greenland Ice-sheet, the Amazon rain-forest, and key Atlantic currents, have also come into play. “Most people do not realise how big these risks are”.
So I (like the rest of the more than 19,000 practicing physicians in Ireland in 2023) am spending much of my life trying to improve the lot of my patients but I am beginning to feel that we have a very significant health issue here with climate change which, by and large, we are assiduously avoiding. I am aware that, as governments come and go, it is difficult for them to commit to often unpopular longterm strategies when their jobs are “on the line” after 4-5 years. So, as it seems climate change is a major health issue (clearly more of a one than many of the diseases that we successfully treat) perhaps the (global) medical profession should take climate change as a vital new disease to attempt to treat, either with personal actions or with lobbying as a way of advocating for our (8 billion) “patients”.
Action we can take
So, in Ireland, what can we do? Well, we can always encourage our government to do better, and to support initiatives which reduce our reliance on fossil fuels (Banks worldwide have apparently given
almost 7 Trillion dollars to fossil fuel firms since the Paris Accord). We can join the ranks of people who don’t ignore those who advocate for “green” initiatives, while questioning those who use “green” initiatives purely for money-making purposes, but who make no positive contribution to climate change. We can take personal action to try to
make even tiny contributions in mitigating against climate change, and while knowing that, whatever we do in Ireland is not going to change the global situation directly, it may generate a global effect (A la our cigarette ban), which might then lead to greater benefits. With these musings in mind – let's talk about trees!
1. Trees are the best way of increasing Carbon trapping
2. Planting trees is enormously helpful when trying to protect our natural world and increase biodiversity
3. Ireland has one of the lowest levels of afforestation in Europe (approx. 11.5%) with most trees being non-native conifers Trees. We just take them for granted. They are everywhere They have been in Ireland for eons. We live in the emerald Isle. We are inundated with trees – are we not ? Forest upon forest of – aah but they are dark green – imported from North America in the 1800’s, the Sitka Spruce now accounts for over half the tree population in
With photography by Martin Blake, Bailey and Blake Video productions
Figure 1 Figure 1: Commercial Spruce Forest, County Wicklow
and indeed most of the native tree planting done over this period has been done by private individuals over the past 40 years.
on
Ireland, with over 70% of all trees in Ireland composed of conifers. Great for investors and good for building, they have marched through the Irish landscape, killing all below them (ecological dead zone) (Figure 1); but a good investment, and very important for building etc. But why would
we worry, there are stacks of native trees in Ireland, are there not; everything from giant Oak to beautiful Irish Cherries. No !. Unfortunately Ireland is one of the least afforested countries in Europe, ranking 40thin 2020, at about 11.35% of land forested, and ahead of the Netherlands, Malta, Iceland and Monaco (Figure 2). Ireland has lost almost all of its native forests, with just 2% of the country being covered by native broadleaf trees. With it are going all the things, both plant and animal, that would have lived
in those native “hotels” (Figure 3). While most of Ireland was covered in trees 6000 years ago (80% coverage), by the end of the 19th Century only 1% of the country was forested, representing almost total destruction of our woodlands and forests, and resulting from multiple factors, ranging from mobile sawmills touring around the country, the destruction of anything standing in the way of the rush to increase agricultural land, to, understandably, tree felling for wood to keep the home fire burning. For a long time outside agencies were held responsible for the loss of the native tree, one of the emeralds of our Isle, but in the over 100 years where we have been able to directly impact on this issue ourselves, little has been done to address the loss of such a vital cog in our natural world,
Government incentives in the past have only tended to aggravate the problem of afforestation in Ireland. Grants were available to plant forests, but once forests were planted, that land could not be used for any other purpose again into the future (described as a “negative nudge” for landowners). Furthermore the grants were only for 15-20 years, and so this provided a strong financial incentive to plant fast-growing non-native species, which when harvested would disturb wildlife, release carbon, damage water quality, and leave the landscape “scarred”. It is argued that if we really wanted people to grow native forests (predominantly slow growing) there should be a subsidy to reflect long-term ecosystem support, and subsidies should of course also reflect the value of any action as a public good.
Figure 2
Figure 3: Native Oak Forest at Tomnafinnoge, County Wicklow
Figure 4: Benefits of Urban Mini-forests
Figure 4 Benefits of Urban mini-forests
Environment & Health
Example of 2000 Tree native miniforest planted December 2022 (Tinturn Abbey) and photgraphed 19 months later.
How do you get the public on board?
change. Trees hugely benefit wildlife, and trees improve physical and mental health (Figure 4).
Figure 5: Example of 2000 Tree native miniforest planted December 2022 (Tinturn Abbey) and photgraphed 19 months later
But what does any of that matter to people, especially as many don’t really feel any personal responsibility for the protection of nature and the environment, and as we continue to strive for the inexorable expansion of the human’s world. Are trees actually any use for humans, and indeed do they have any health benefits. Well, yes actually, they do. To mention a few, trees help clean our air. Trees help reduce noise. Trees help reduce storm water and run-off. Trees provide cooling. Trees help clean our drinking water. Trees provide us with oxygen. Trees increase our property values and apparently help reduce crime. Trees help us save energy. Trees help us reduce the effects of climate
Private individuals and communities need to “seize the moment” to address the afforestation issue for the benefit of our environment, and to attempt to mitigate, in whatever small way, against climate change. Most importantly we need to think about our birds, our bees, our insects and our wildlife, none of which we can afford to lose, but who we have given scant regard to. As of 2022, 63% of Irelands bird species are in serious trouble. More than half of Irelands bee species have undergone substantial declines since the 1980’s, in part due to loss of the natural abundance of flora due to increased land use, and habitat destruction.
Insectageddon is probably an exaggeration, but it is suggested that there is a loss of insect biomass at a rate of 2.5% per annum in some cases.
Example of 2000 Tree native miniforest planted December 2022 (Tinturn Abbey) and photgraphed 19 months later.
How do we move forwards together?
So what can we do ? well we have set up a community driven programme, the 100 million tree project (www.100milliontreeproject. ie), with the aim of planting 100 million native trees in a 10 year period. We call it community driven because we need philanthropists to help us pay for the trees; we need the tree growers to upscale, knowing that we will buy their native trees, and that they don’t have to be exported (or imported); we need Forestry services to upscale on tree planters to deal
with the exponential increase in tree planting over time, and most importantly we need people, and institutions to give of their land for the benefit of all, so that native trees can be grown – these of course would be their trees, their mini-forests, with no restriction to future use of the land, while hoping of course that the forest would be allowed to flourish with all the attendant benefits, from birdsong to the buzzing of bees, pleasures often absent in our modern world. And how much land would have to be used ? A quarter acre would allow the planting of 2500 native trees of 14-15 different varieties, with everything from Oak to Alder and Birch to Hawthorne, Scots pine to Irish Cherry, Rowan to Hazel to Holly and many more. The intensive planting (Miyawaki method, also referred to as crowdforesting), allows for rapid growth, increased density, increased biodiversity, and the development of a very rapid carbon sink. Evidence suggests that trees prefer being planted close together, and do well when species are mixed in close quarters. Finally, maintenance is simple with occasional trampling down of weeds for the first couple of years, and then the rapidly growing forests look after themselves. The
Examples of 10 different miniforest sites planted December 2022 to March 2024 at:
Fairyhouse racecourse
Tintern Abbey
Glenstal Abbey
Powerscourt Estate
Ballymun kickhams GAA
IDA Site Athlone
Figure 6: Examples of 10 different miniforest sites planted December 2022 to March 2024 at:
Fairyhouse racecourse
Tintern Abbey
Glenstal Abbey
Powerscourt Estate
Ballymun kickhams GAA
IDA Site Athlone
Ballybritt Racecourse Galway
Bride Street Church Wexford
Waterford Airport
University College Dublin
Ballybritt Racecourse Galway
Bride Street Church Wexford
Waterford Airport
University College Dublin
argument over what type of trees to plant on the 450,000 hectares of land needing to be planted if the government wishes to achieve its aim of 18% of Ireland covered in forestry by 2050 should be mute – if most of this land needs to be planted with fast growing sitka forests in order to protect the building and manufacturing industry into the future, then more land should be made available for native tree planting, thus protecting the wood production for building while significantly increasing our afforestation and biodiversity, and eliminating substantial penalties for failing to achieve our environmental goals. In the meantime, we, the people, should be doing as much as we can ourselves.
In our “trial” year (Nov 22 – Apr 23 (bare-root planting season)) we developed a comprehensive website and planted just over 20,000 native trees in 18 different sites throughout the country, funded by an Irish Philanthropist living in the US, (figure 5) and in our first “full” planting season (Nov 23- May24) we planted just over 200,000 native trees in 83 different sites, funded almost entirely by Uniphar. Most of the sites were of a 1/4 acre size with 2500 native trees being planted
in each one. A few landowners wanted more than one 1/4 acre site (up to 3 in one case). Unlike many countries where the soil is not rich, and requires preparation prior to planting, Ireland should be an ideal climate for tree planting, and preparation simply involves ploughing the site, and rotivating it to loosen the soil to about 8 inches so that the saplings can be easily (and quickly) planted, and this also gives tree saplings an early breathing space where they don’t have to contend with grass or weeds. If there are rabbits or hares around then appropriate fencing will be required, and of course if there are deer, then deer fencing is essential. While this (fencing) requires some expenditure, it will be well worth it when your own native forest is flourishing. A normal mini-forest should take a few hours to plant with proper preparation and professional planters (also provided) (Figure) The benefits of mini-forests are not simply confined to the actual planting of thousands of small areas of carbon capture and biodiversity. Intense planting means that the forests will be impenetrable to natures biggest threat, the human, after a couple of years: Because only 1 native tree
is a conifer, excellent undergrowth areas of biodiversity can develop within the mini-forests; Also having 40,000 miniforests (100,000,000 trees) means that destructive forest fires are not a worry (Canada lost 4 times the total tree stock of Ireland last summer in extensive forest fires). Finally it is likely that little or none of the 10,000 acres used to intensively plant the 100 million trees would have been considered for tree planting under any national plan, as it almost entirely consists of small allotments of private land. To plant a similar number of native trees with “normal” planting of 1000 trees per acre, 100,000 acres of land would need to be acquired. Thus the contribution of the 100 million tree project should be very much a win-win situation for both citizens and state.
In summary
So, if the medical profession in Ireland decided to get stuck into tree planting, as part of our overall management of the “health of the nation”, and say 500 (5%) had a site to turn into a native mini-forest, or knew someone who had one, this would add 500 new areas of biodiversity and 1,250,000 native trees, with all the attendant benefits of same
(at 5 to 8 years you can assume that 1.25 million trees will be sequestering about 17,500 tonnes of Carbon per year). All that is needed is a quarter acre of land and we will supply and plant a 2500 tree native mini-forest for you (or you and your friends can plant or help plant it). At present we have enough philanthropic support to plant 550,000 native trees for the upcoming (2024 –25) season, and over 120 people or institutions have prebooked mini-forests. If people choose, they can pay for a 2500 tree native mini-forest (works out as 2 euro/ tree), and we will video the whole project for them: any money left from the tree growers and tree planters goes back into the system to pay for future trees. As mentioned before, if we can get a commitment to significant funding, we can commit to supporting our tree growers, who will be able to expand their growth and supply of native trees, thereby reducing and, hopefully eventually eliminating, the requirement to import native species from abroad. Ideally government should support our tree growers to exponentially expand their productivity.
Do we believe that climate change is, as they would say in the movies, an existential threat to mankind. If we do, let us as Doctors, Nurses and allied Professionals get more generally involved in treating it – a good way to help treat would be to plant, or support the planting of trees, while also setting an example for all our colleagues internationally.
Osteoporosis
World Osteoporosis Day – Time for a Check
Day – Time for a Check
Written by Michele O'Brien, CEO, Irish Osteoporosis Society
Written by Michele O'Brien, CEO, Irish Osteoporosis Society
people living in Ireland. This is to help prevent people at high risk ending up disfigured, losing their independence and their care costing far more than the ¤120 to do a DXA scan on them.
young children but due to back pain was unable to work, was refused a follow up DXA scan. He ended up paying privately for one and the DXA scan showed his results had declined, was sadly he told to “come back when you have fractured”.
Research shows that most fractures happen between a T score of -1. 5 to -2.49 which is the moderate to marked Osteopenia range. If a patient with bone loss is refused a DXA scan and/or a treatment and then fractures, who is responsible for them fracturing and possibly losing their independence?
World Osteoporosis having taken place on 20th October, the Irish Osteoporosis Society are asking everyone to check to see if they have risk factors for bone loss.
on 20th October, the Irish
Society are
everyone to check to see if they have risk factors for bone loss.
Why prevention of Fractures is common sense as well as economical
Worldwide, up to 37 million fragility fractures occur annually in people over 55, the equivalent of 70 fractures per minute. A fragility fracture is a broken bone from a trip and fall that if the persons bones were healthy, the fracture would not have occurred.
1 in 2 women over age 50 will experience osteoporosis fractures, and 1 in 4 men aged over 50, even though research shows that most fractures are preventable. A recent survey in Ireland showed that over one third of Irish adults over 40, had experienced a fragility fracture. The level of fractures in the survey would generally be expected/assumed by most people to be amongst the older age groups.
A person knowing they are high risk for vertebral fractures which will leave them with skeletal damage that are not reversible, is at risk for high cortisol levels and anti-depressants, which many cause bone loss, which results in further bone loss, see figure 1 below.
prevention of Fractures is common sense as well as economical
Research shows that most fractures happen between a T score of -1. 5 to -2.49 moderate to marked Osteopenia range. If a patient with bone loss is refused a DXA and/or a treatment and then fractures, who is responsible for them fracturing and losing their independence?
Osteoporosis Society on 20th October, the Irish Osteoporosis if they have risk factors for bone loss. sense as well as economical occur annually in people over 55, the fragility fracture is a broken bone from a trip and fall fracture would not have occurred.
Normal bone Image
The Irish Osteoporosis Society who are the National experts in Osteoporosis (IOS) find that a person who is high risk to fracture and especially those who have witnessed a family member who suffered from Osteoporosis, are usually the most proactive about their bone health. There was a person in Ireland who sadly committed suicide and in the note that was left, the person said that they could no longer live with the pain they were in. We are not a third world country and the fact that treatments are available this type of situation should never occur.
Worldwide, up to 37 million fragility fractures occur annually in people over 55, the equivalent of 70 fractures per minute. A fragility fracture is a broken bone from a trip and the persons bones were healthy, the fracture would not have occurred.
There are some in Ireland who believe that DXA scans should only be done on those 65 and older, as they are the highest risk group. Considering the rate of fragility fractures in this survey was highest amongst 40 to 54-year-olds shows that prevention of fractures not only is common sense, but financially for our health service and for the overall wellbeing of
The Irish Osteoporosis Society who are the leading experts in Osteoporosis recommend anyone who has one or more risk factors for bone loss, be referred for a DXA scan, as many will more than likely already have bone loss. Prevention is much cheaper for our health service and certainly less painful for patients then to treat them for fractures, which we all know in the first place can be life threatening. 20% of Irish
A person knowing they are high risk for vertebral fractures which will leave them damage that are not reversible, is at risk for high cortisol levels and anti-depressants many cause bone loss, which results in further bone loss
Bone
There is no other disease in the world that the IOS are aware off, where patients are discouraged from being proactive in preventing a disease. Recently a 33 year old male with T scores of -3.4, -3.6, -3.4 and -2.6 in his spine, with
image with bone loss
Figure 1: The images show the progression of vertebral fractures that are not reversible
The images show the progression of vertebral fractures that are not reversible
Bone image with bone loss
women over age 50 will experience osteoporosis fractures, a men aged over even though research shows that most fractures are preventable recent survey in Ireland showed that over one third of Irish adults over 40, had experienced a fragility fracture in the survey would generally be expected/assumed by most people to be
here are some in Ireland who believe that DXA scans should only be done on those
as they are the highest risk group. Considering the rate of fragility fractures in this
Bone image with bone loss World Osteoporosis
Normal bone Image
With World Osteoporosis having taken place
Osteoporosis
asking
people who fracture their hip will die within 6 to 12 months, 50% will lose the their independence, why would anyone not take preventing fractures more seriously.
Using the World Health Organization definition of osteoporosis, the disease affects approximately 6.3% of men over the age of 50 and 21.2% of women over the same age range globally. Based on the world population of men and women, this suggests that approximately 500 million men and women worldwide may be affected.
Across Europe in 2019 (European Union, plus Switzerland & the UK) 32 million individuals age 50+ are estimated to have osteoporosis, which is equivalent to 5.6% of the total European population age +50, or approximately 25.5 million women (22.1% of women aged +50) and 6.5 million men (6.6% of men aged +50).
These statistics are why prevention of bone loss and earlier diagnosis is crucial not only so that people in Ireland age gracefully but also in order that billions is not used to treat fractures, when a fraction of that cost could be used to prevent them in the first place.
By 2050, the worldwide incidence of hip fracture is projected to increase by 310% in men and 240% in women, compared to rates in 1990. The greatest number of hip fractures occur between 75 and 79 years of age for both sexes. For all other fractures, the highest number occur between 50-59 years which is why the IOS believe that not preventing fractures is not acceptable in this day and age.
Hip fractures cause chronic pain, reduced mobility, disability, loss of independence and in 20% of cases in Ireland premature death. The secondary effects of a hip fracture are a blood clot, pneumonia or infection. Less than half those who survive the hip fracture regain their previous level of function.
In Caucasian women worldwide, the lifetime risk of hip fracture is 1 in 6, compared with a 1 in 9 risk of a breast cancer diagnosis.
Vertebral fractures are the most common osteoporotic fractures that occur. A woman 65 years of age with one vertebral fracture has a one in four chance of another fracture over 5 years, which can be reduced to one in eight by them being investigated and placed on an Osteoporosis treatment. Prescribed Osteoporosis treatments have been shown to significantly reduce patients risk of fractures, which is why it is such a shame that the diagnosis rate is so poor not only in Ireland but worldwide.
Vertebral fractures can lead to back pain, loss of height, irreversible deformity of the skeleton, immobility, increased number of bed days, reduced pulmonary function and premature death. Their impact on quality of life can be profound as a result of loss of self-esteem, distorted body image and depression. Vertebral fractures significantly impact the person’s ability to be able to wash and dress themselves and even to be able to look up see where they are actually walking in order to prevent themselves from falling. Dowagers hump place them at higher risk of falling as their centre of gravity has altered and skeletal changes from vertebral fractures can cause the person to avoid socializing as they are embarrassed regarding how they now look.
Vertebral fractures are associated with an increased risk of further vertebral fractures but also nonvertebral fractures. Women who develop a vertebral fracture are at substantial risk for additional fracture within the following 1-2 years.
It is estimated that only one third of vertebral fractures are actually diagnosed and under diagnosis of vertebral fracture is not just in Ireland it is a worldwide issue. The proportion of vertebral fractures that go undiagnosed, during the assessment of a thoracolumbar lateral radiograph, is as high as 46% in Latin America, 45% in North America, and 29% in Europe/South Africa/Australia.
The incidence of vertebral fractures increases with age in males and females. Most studies indicate that the prevalence of vertebral fracture in men is similar
women, the mortality rate in men after hip fracture increases with age and is highest in the first year after a fracture. Over the first 6 months, the mortality rate in men approximately doubled that in similarly aged women.
A forearm fracture is an early indicator of male skeletal fragility. In aging men, wrist fractures carry a much higher risk for a hip fracture than spinal fractures in comparison to women. These statistics are why not only women in Ireland need to be proactive regarding their bone health, but men need to be more proactive and should be discouraged from doing so.
Personal and Economic affects of Osteoporosis
to, or even greater than, that seen in women up to age 50 to 60. Research shows that over 55% of patients with hip fractures have evidence of a prior vertebral fracture, which is why screening of people for signs and symptoms of undiagnosed bone loss as well as for risk factors for bone loss is essential.
When a decline in bone loss occurs on a DXA scan it is crucial that the causes of why the decline has occurred is investigated and addressed, not assumed. Changing their treatment without investigating the cause/s is not the solution, as 10% loss of bone mass in the vertebrae can double the risk of vertebral fractures. Why are women affected by bone loss more than men?
There are many reasons why women are more at risk, one of the main reasons is that women tend to have more hormonal issues, as they have ovaries and go through the menopause, when significant bone loss occurs.
So what about Men?
Bone loss is one disease that men are at a significant disadvantage as it is considered by most people to be “An old woman’s disease”. This is a myth as it is estimated that men’s lifetime risk of a fragility fracture is greater than developing prostate cancer. The overall number of fragility fractures is higher in women, but men generally have higher rates of fracture related mortality.
Research shows that more men die then women post hip fractures and that Men account for 25% of hip fractures occurring in the over 50 population. Similar to
In Europe, the disability due to osteoporosis is greater than that caused by all cancers, except lung cancer. It is comparable or greater than that lost to a variety of chronic noncommunicable diseases, such as rheumatoid arthritis, asthma and high blood pressure related heart diseases.
Fragility fractures are the fourth leading cause of chronic disease morbidity in Europe. The only ones preceding are ischemic heart disease, dementia and lung cancer. Finding causes of bone loss
The Irish Osteoporosis Society recommends that everyone fill in a risk factor boen loss questionnaire, which is available from the charity by emailing info@irishsoteporosis.ie causes of bone loss are found by
How is bone loss (Osteoporosis /Osteopenia) screened for or diagnosed?
• A DXA scan is the only test the Irish Osteoporosis Society recommend to screen or diagnosis Osteoporosis
• A DXA scan takes approximately 15 minutes
• A DXA scan is painless
• A DXA scan is not claustrophobic
• A DXA scan costs approximately ¤120
Repeat DXA scanning is important to monitor your bone health
• If you are losing bone, you will not feel bone loss
• A DXA scan does NOT contain excessive radiation
• A DXA scan contains 10% radiation of a regular Chest X-Ray
• A person flying from Dublin to New York is exposed to more radiation than a DXA scan
Osteoporosis
Did you know there are approximately 200 causes of bone loss?
The Irish Osteoporosis Society, the National experts in Osteoporosis, believe that every woman and man need to make their bone health a major priority. Research shows that fractures are preventable in most people, which is why the IOS believe people should not neglect their bone health, as you need healthy bones to sit up and walk.
Can senior citizens actually improve their bone health? YES
The woman below had become wheelchair bound due to vertebral fractures when her son phoned the Irish Osteoporosis Society. Sadly her son had been told that nothing could be done to help his mother.
To the Irish Osteoporosis Society Charity
I wanted to thank your organisation for the help and guidance I received from you regarding my mum’s Osteoporosis.
Touching
A person can look perfectly fine on the outside and have severe bone loss inside their bones
• Postural change - Your head starting to protrude forward from your body
What weight bearing exercises are safe for you should be based on the following:
The improvement has been substantial and together with the practical steps we took to adapt her house, her quality of life has improved substantially to the point that she is mobile and active again. We recently took her to Bath, UK to celebrate her 90th birthday and she will go on a Mediterranean cruise with my sister next month!
My Mum and I are extremely grateful for your guidance that has truly given her a new lease of life.
Well done and keep up the great work.
Best Regards, Vincent C
What are the signs and symptoms of Bone Loss?
There are NO signs or symptoms (warning signs) prior to a person fracturing.
NOTE: A person can exercise daily and have a healthy diet, but still develop or have bone loss. Only 19% of people with bone loss are diagnosed, are you or a loved one or any of your customers in the 81% undiagnosed?
• Postural change - A hump developing on your back.
What type of exercise is recommended for bone health?
Are there Signs and Symptoms of Undiagnosed Osteoporosis?
• Your body shape changingExample a pot belly developing
• You are losing height
your toes while in the sitting position or standing position, excessive bells, yoga, jumping off boxes, stopping your feet when walking, trampolines
Yes, if you or a loved one have one or more of the following signs/symptoms, you may have undiagnosed bone loss
The image above (figure 2) shows the irreversible changes that occur when a person develops bone loss and is not diagnosed or treated.
If you have already broken bones or are high risk to break bones, your age, the results from your DXA scan report, your medical history and your fitness level. It is much safer to slowly build up your bone strength, then take the risk of breaking bones.
A person with bone loss should be individually assessed by a chartered physiotherapist a special interest in bone health, to see what exercises are safe and appropriate do. Please contact the Irish Osteoporosis Society as there appears to be many issues area.
What type of exercise is recommended for bone health?
• A broken bone/s (fracture) from a trip and fall or less, even if on ice or cement
• Upper, middle or low back pain, intermittent or constant back pain
THOSE WHO HAVE BONE LOSS NEED TO BE VERY CAREFUL WHAT EXERCISES THEY DO AS THEIR MUSCLES MAY BE STRONG, BUT WHEN A STRONG MUSCLE PULLS ON A WEAK BONE, IT CAN FRACTURE.
What weight bearing exercises are safe for you should be based on the following:
• Postural changes - Your shoulders starting to become rounded
A person with bone loss should be individually assessed by a chartered physiotherapist with a special interest in bone health, to see what exercises are safe and appropriate for them to do. Please contact the Irish Osteoporosis Society as there appears to be many issues in this area.
As mentioned already, research shows that most broken bones occur in the Osteopenia range. This is why the Irish Osteoporosis Society recommend that senior citizens who have never lifted weights, start out actively without them and slowly build up to lifting
If you have already broken bones or are high risk to break bones, your age, the results your DXA scan report, your medical history and your fitness level. It is much safer
THOSE WHO HAVE BONE LOSS NEED TO BE VERY CAREFUL WHAT EXERCISES THEY DO AS THEIR MUSCLES MAY BE STRONG, BUT WHEN A STRONG MUSCLE
As mentioned already, research shows that most broken bones occur in the Osteopenia
This is why the Irish Osteoporosis Society recommend that senior citizens never lifted weights, start out actively without them and slowly build up to lifting weights. do not end up really sore or with fractures. Those that prior diagnosis had lifted weights should start out with low weights and slowly build up,
The following are some of the many exercises the Irish Osteoporosis Society recommend for those with bone loss:
Figure 2
weights. This is to ensure that they do not end up really sore or with fractures. Those that prior to their diagnosis had lifted weights should start out with low weights and slowly build up, as it is not worth the risk of the person fracturing. At the foot of the page are some of the many exercises the Irish Osteoporosis Society do not recommend for those with bone loss:
Touching your toes while in the sitting position or standing position, excessive weights, kettle bells, yoga, jumping off boxes, stopping your feet when walking, trampolines or swiss balls.
Did you know that all senior citizens need to ensure that they make their homes safe to reduce their risk of falling in their home?
It is very important that throw rugs are removed from floors, that people wear a good pair of walking shoes in their home versus slippers as many give no support. A handrail should be placed on steps into homes and handrails on both side of your stairs can make it much easier and safer for you. Clothes should be between hip and eye level in cupboards and any clothes that have not been worn in 5 years should be donated. The reason being that if you or a loved one has trouble finding clothes or when trying to pull an item out, you have difficulty, you have too many items. There are so many people who are not in this position and would be forever grateful to receive clothing. There have been multiple incidences where senior citizens with bone loss have actually fractured vertebrae while attempting to manoeuvre clothes out of a wardrobe.
More than one out of four older people fall each year, but less than half actually tell their doctor. The Irish Osteoporosis Society believe from feedback this is due to embarrassment and also many are concerned they may be sent to a nursing home. Research shows that falling once doubles the person’s risk of falling again and that more than 95% of hip fractures are caused by falling, usually by falling sideways.
What makes walking with a cane or rollator much more difficult?
One of the major issues with those who use canes or rollators is that they are adjusted to high. If either are too high, they can cause, neck, shoulder and back pain and make it more difficult for a person to walk.
How to check if your cane or rollator is too high – you will need someone to help you
A person needs to stand up as straight as they can, with their arms down by their sides, preferable with a chair behind them in case they need to sit down. It is important that the person looks straight ahead because if they look down to see what the person is doing their arm will lengthen. The handle of the cane or rollator should be level with the small bone on your wrist.
Did you know that there are major advances in the area of incontinence?
75% of people can completely recover and the other 25% can significantly improve the issue. This is so important because most people when they begin to have leakage of urine (or bowel), they start to reduce the amount of fluids they drink because they
do not want to have an accident. Most people area not aware of the consequences of decreasing fluid intake.
Reducing the amount of fluids you drink can place you at risk of falls for several reasons.
• Slipping and falling from rushing to the bathroom or having an accident while trying to get there, can cause fractures.
• If you ever feel thirsty studies show that you only need to be 1% dehydrated to experience a 5% decrease in cognitive function, which can place a person at risk of falling. A 2% decrease in brain hydration can result in short term memory loss.
• You can develop kidney issues which can affect your overall health but also can affect the ability for a person to take some Osteoporosis treatments.
How much fluids should you drink?
8 regular glasses of fluids. Your body is made up of water, so it is essential for your overall health. By including fortified milk with Vitamin D, not only are you helping your bone health but also your overall health as Vitamin D is essential for your immune system. You should reduce caffeine intake to 2 a day.
Treatments for Bone Loss
The patient’s treatment plan should be based on
• The patient’s risk of fracture or re-fracture
• The results of their DXA scan of the spine and hips.
• The cause/s of why they developed low bone density
• Their age
• Their lifestyle
• Their medical history
Treatments available are the following
Bisphosphonates - Weekly or monthly tablets. A person should only take for maximum 5 years, not 5 years on different ones.
HRT - HRT is appropriate for menopausal symptoms but should not be taken just to protect bone, except in certain cases in premenopausal women.
Denosumab, brand name
Prolia - Twice yearly injection. Should not be stopped without closing off the action of it with a bisphosphonate to prevent significant bone loss occurring.
Zoledronic Acid, brand name Aclasta - once a year IV bisphosphonate
Teriparatide – Daily injection for severe Osteoporosis.
Summary as to why everyone should be checking to see if they have risk factors for bone loss!
It is very important that everyone take their bone health seriously if they want to stay independent as they age, as a prior fracture is associated with an 86% increased risk of a further fracture occurring. The risk of a subsequent fracture is particularly increased in the first two years after an initial fracture. Research evidence suggests that many women who sustain a fragility fracture are not appropriately diagnosed and treated for osteoporosis. The great majority of individuals at high risk (possibly 80%), who have already had at least one osteoporosis fracture, are neither identified nor treated.
An IOF survey, conducted in 11 countries, showed denial of personal risk by postmenopausal women, lack of dialogue about osteoporosis with their doctor, and restricted access to diagnosis and treatment before the first fracture resulting in under diagnosis and under treatment of the disease.
A second hip fracture occurs in approximately one in four patients after any previous osteoporotic fracture, and in one in three patients who have sustained a hip fracture, on average within one and a half years.
For additional information, you can check our website at www.irishosteoporosis.ie
Or Email info@irishosteoporosis.ie
Nutrition and Cancer Survivorship Nutrition
Introduction
In Ireland, there are more than 200,000 people who are living with or beyond cancer. This is equivalent to nearly 4% of the total population (Mullen & Hanan, 2019). In the next 25 years, the number of Irish cancer survivors is expected to double due to demographics, earlier detection, and improved treatment outcomes (Mullen et al., 2020). Cancer survivorship is now recognised as a distinct phase of the cancer journey with its own distinct health implications brought about by the cancer itself, the treatment received as well as a potentially impaired nutrition and physical status, these are discussed below.
National reviews and strategies
The National Cancer Registry of Ireland and the Irish Cancer Society recently published a review titled; ‘The Unmet Needs of Cancer Survivors in Ireland’ (O’ Connor et al., 2019). It highlights that the needs of cancer survivors have not been prioritised, with little support available for the management of treatment side-effects. A study included in this review, which focused on breast cancer survivors specifically, found a significant lack of nutritional information being made available during survivorship care (Power & Hegarty, 2010). A more recent survey of Irish cancer survivors found a lack of nutrition support being provided also (O’Sullivan et al., 2020).
Following the review, the Irish Cancer Society’s strategy for 2020-2025 includes ‘Living Well After Treatment’ as one of its five priorities, emphasising the importance of research in helping to improve the quality of life of cancer survivors by uncovering their unmet needs. Moreover, the HSE’s National Cancer Control Programme has placed significant
Written by Laura Keaver, Registered Dietitian, Lecturer in Human Nutrition and Dietetics and Programme Director, Department of Health and Nutritional Science, Atlantic Technological University Sligo
importance on the wellbeing of survivors in its recent ‘National Cancer Survivorship Needs Assessment’ report (Hegarty et al., 2018). A cancer survivor’s quality of life can be profoundly impacted by the burden of symptoms including nutritional symptoms (Hegarty et al., 2018). One of the most common symptoms encountered by Irish healthcare professionals working with adult survivors in the acute sector were nutritional symptoms (Hegarty et al., 2018; Mullen & Hanan, 2019). It is therefore important that healthcare professionals are aware of the nutritional issues faced by cancer survivors and are familiar with the current guidelines for nutrition for this group.
Nutrition-related issues
Survivors may become at risk of weight loss/gain, malnutrition, decreased intake of food and quality of life, should they not receive follow-up care long-term. Therefore, doctors, nurses and dietitians should regularly monitor and manage these symptoms into survivorship (Crowder et al., 2018).
Weight
Weight management in those with cancer has routinely been dominated by concerns about unintentional weight loss, however, many cancer survivors can be at increased risk for weight gain. As this can be associated with an increased risk of developing cancer, maintaining a healthy weight and body composition is important in survivorship (Reeves et al., 2014). This is reflected in the World Cancer Research Fund guidelines for cancer prevention (Table 1). This is further endorsed by European and American bodies where survivors are recommended to aim to achieve and maintain a healthy body weight and that weight loss should be modest (5-10% of total body weight) (El-Shami et al., 2015; Arends et al., 2017, WCRF/AICR 2018).
Residual impact symptoms
Cancer treatment can result in a variety of side effects. These side
effects can, in turn, affect the food intake, nutrition status and quality of life of the individual.
Recent Irish data (O’Callaghan et al., 2021) has shown that these impact symptoms can persist into survivorship. In this cohort of 169 Irish cancer survivors, who were at least six months post-treatment. Fatigue was still being experienced by the majority (76%). Other common impact symptoms were decreased energy levels (51.5%); pain (36.1%); constipation (33%); dry mouth (26%) and diarrhoea (16.6%). This is similar to findings in other countries where, fatigue, difficulty sleeping and pain are commonly reported in survivors (Strollo et al., 2020; Bower 2008).
Cardiovascular disease
After cancer recurrence, cardiovascular disease is the secondary cause of mortality in cancer survivors. This is a long-term complication of cancer therapies (Okwuosa et al., 2017). The risk of cardiovascular morbidity is actually higher than that of cancer recurrence (Schultz et al., 2003; Oeffinger et al., 2006). These morbidities include hypertension, dyslipidaemia, obesity and type 2 diabetes (Schultz et al., 2003; Oeffinger et
al., 2006). Screening is important as is the promotion of lifestyle modifications such as increasing physical activity, consuming a healthy balanced diet and maintaining a healthy weight (Okwuosa et al., 2017). The WCRF recommendations in Table 1 should be promoted.
Nutrition related behaviours of survivors
While some studies have shown that cancer survivors are more likely to adopt healthy behaviours than those without a history of cancer (Park et al., 2015; Oh et al., 2013), there are many studies that have highlighted poor fruit and vegetable intakes (Kanera et al., 2016) as well as non-adherence to recommendations for alcohol intake (Iyer et al,2016; Underwood et al., 2009 Cortés-Ibáñez et al., 2020); and Body Mass Index (BMI) (Underwood et al., 2009; Cortes). Compared to those without cancer, cancer survivors in the USA have a higher consumption of foods containing added sugars, solid fats and alcohol and lower intakes of fibre, calcium, vitamin D and vitamin E (Zhang et al., 2015).
Nutrition advice
Survivors have consistently indicated a desire for nutrition
support (Hardcastle et al., 2017; Matsell et al., 2020.; Puller and Jackson 2012), particularly from healthcare professionals (Matsell et al.,2020). Survivors currently report receiving no or conflicting nutrition advice (Hardcastle et al., 2017; Matsell et al.; Puller and Jackson 2012). In the absence of advice from healthcare professionals, survivors source nutrition and physical activity advice from online sources (Keaver et al., 2020; Matsell et al., 2020), which are largely unregulated and often present conflicting or nonevidence-based advice (Keaver et al., 2019). Currently only 11% of Irish cancer survivors report receiving nutrition advice from a dietitian (O’Callaghan et al., 2021).
Current guidelines and recommendations
A UK survey of specialist nurses, clinicians, surgeons and allied health professionals showed only half were aware of diet as part of lifestyle guidelines for those who had completed treatment (Murphy et al., 2021).
The World Cancer Research Fund recommends that in the absence of survivor specific evidence, cancer survivors should follow their guidelines for cancer prevention. These have been outlined in Table 1 below. Similar guidelines have been promoted by the American Institute for Cancer Research.
Unfortunately, adherence to these
Table 1: World Cancer Research Fund Guidelines for Cancer Prevention
Be a Healthy Weight
Be Physically Active
Eat a Diet Rich in Wholegrains, Vegetables, Fruits and Beans
Limit Consumption of ‘Fast Foods’ and Other Processed Foods High in Fat, Starches or Sugars
Limit Consumption of Red and Processed Meat
Limit Consumption of Sugar Sweetened Drinks
Limit Alcohol Consumption
Do Not Use Supplements for Cancer Prevention
For Mothers: Breastfeed Your Baby, If You Can
After A Cancer Diagnosis: Follow Our Recommendations, If You Can
recommendations is poor (Winkels 2016) and baseline knowledge of general or specific risk factors is low in some populations (Anderson, 2015)
Better adherence to these recommendations has been positively associated with global health status, most functioning scales and less fatigue among 1096 colorectal cancer survivors in the Netherlands (van Veen et al., 2019), with improvements in health-related quality of life also being observed in elderly female cancer survivors from the Iowa Women's Health Study (Inoue-Choi et al., 2013) and Chinese breast cancer survivors (Yei et al., 2018). Greater adherence has also been associated with improved survival in those with colorectal cancer (Song et al., 2021).
Results from a global survey of breast cancer survivors (Keaver et al., 2020) reported that fatigue (reported by 72.1% of respondents); followed by stress, depression or reduced mental function (69.5%); changes in taste preference during or after cancer treatment (48.6%); craving unhealthy food (42.5%); loss of appetite (31.4%); healthy food costing too much (30.5%); and lack of time to prepare healthy foods (34.3%) as the main barriers to healthy eating. Fatigue was also the main barrier to being physically active. To support
positive behaviour changes we need to consider these barriers moving forward.
Future
There is a need for research into the nutrition specific needs of cancer survivors as well as the impact of diet on longer term cancer recurrence and survival. This will help inform the development of more specific guidelines and practices for cancer survivors. There is also a need to determine how best to integrate nutrition into survivorship care. Survivors have a desire for individualised and specific advice relating to their nutritional problems (Matsell et al., 2020). Providing individualized nutritional advice could improve dietary intake and potentially prevent weight loss or weight gain, as well as vitamin and mineral deficiencies.
So, what can you do?
Monitoring weight and nutrition related impact symptoms and signposting to nutrition resources such as the WCRF guidelines or breakthrough cancer research cookbooks https:// breakthroughcancerresearch.ie/ cancer-diet/for specific impact symptoms and healthy eating and referring to a dietitian where appropriate could make a big impact to the health and health related quality of life of cancer survivors.
References available on request
56 Honours
Honours Red Carpet
Over 550 hospital professionals and industry leaders were in attendance as winners across 15 categories were announced at the annual Hospital Professional Honours.
Each year Hospital Professional News, Ireland’s only independent monthly publication for hospital professionals, celebrates and acknowledges the achievements of teams and individuals within the profession.
The Honours took place on Saturday, September 14th; hosted by Marty Whelan, the Honours ceremony took place in the Radisson Blu Hotel, Dublin.
The Hospital Professional Honours recognise the achievements of individuals and teams working in the hospital sector; their dedication and innovation which positions the profession at the forefront of healthcare, improving the lives of people across the country.
Pictured are some of those who attended.
1. Athlone Pharmaceuticals 2. The team from the Department of Mental Health, CHI Temple Street 3. The team from St James’s Hospital
4. Colleagues from St James’s Hospital 5. The team from MedFind Solutions 6. Staff and colleagues from Midland Regional Hospital, Portlaoise
1. Blackrock Clinic team 2. Joe and Martyna Ega, Myfeet.ie 3. The team from Blackrock Health, Hermitage Clinic 4. Midland Regional Hospital, Tullamore
5. The Pain Management Centre team, Croom Orthopaedic Hospital, ULHG 6. Nuala Kenny and Rosemary King, Blackrock Health
1. Blackrock Health Hermitage Clinic 2. Grace Walsh, Cassie Doyle and Denise Byrne, Mater Misericordiae University Hospital 3. The team from St James’s Hospital 4. The team from MSD 5. Colleagues from Pharmasource, Uniphar and Sligo Hospital 6. Caroline Conlon and Liz Devlin, Medisource
1. Dr Jason McGrath, RCSI and Aoife Tremere 2. Katie Butler and Kevin Fahy, St James’s Hospital 3. Munaza Wajahat, Dr Muhammed Raheel Khan (Tallaght University Hospital), Ciara Keany Sheehan and Patrice Kearney Sheehan - St James Testicular Team 4. Emma Mahon, Jayne Tuthill and Sarah Tuthill, Mater Misericordiae University Hospital 5. Ninv and Sangeetha, Blackrock Health Hermitage Clinic 6. Dr Laura Sahm, Dr Sarah O’Dwyer, Dr Ita Fitzgerald, Dr Cathy Breen and Dr Jean O’Connell
Clinical R&D
CRITICAL NEW STUDY CONFIRMS IRISH INCIDENCE OF SUDDEN UNEXPECTED DEATH IN EPILEPSY (SUDEP)
New research has revealed the firstever national data on the incidence of Sudden Unexpected Death in Epilepsy (SUDEP) in Ireland.
SUDEP is the sudden, unexpected death of someone with epilepsy, where no other cause of death can be found.
The study, led by Dr. Yvonne Langan of St. James’s Hospital Dublin & Trinity College Dublin, together with the HRB, examined data from all deaths referred to coroners in 2019, identifying those with a history of epilepsy. The research identified 33 cases of definite SUDEP in 2019, representing an incidence rate of 1:1400 per annum among people living with epilepsy. Of the 33 cases, 21 were men and 12 were women, with ages ranging from 9 to 81.
Speaking on the importance of identifying Irish specific data, lead investigator Dr. Yvonne Langan said the study will shape the treatment of epilepsy patients in future.
She said: “Ireland-specific data is vital in shaping effective healthcare policies. The findings will help raise awareness of SUDEP within both the patient and medical community and I hope will support tailored interventions to reduce risk for patients in the future.”
While the exact reasons for SUDEP occurring in some people with epilepsy is unknown, previous research has shown that having uncontrolled or untreated tonic-clonic seizures is the biggest risk factor. Epilepsy Ireland believes that with targeted action to improve access to specialist care, the incidence of SUDEP can be decreased.
Peter Murphy, CEO of Epilepsy Ireland, said not enough is known about SUDEP, even within the Irish epilepsy community.
He said: "This study is a significant step forward in our understanding of the extent of SUDEP in Ireland.
“SUDEP is the most devastating consequence of epilepsy and over the years, we have met with far too many bereaved families who were not aware of SUDEP until their loved one passed away.
“We know that at least some of these deaths can be prevented by ensuring that more people with epilepsy become seizure-free and remain that way. This can be achieved through faster access to diagnosis and treatment, improved dialogue between healthcare professionals and patients, and through enhanced efforts to improve education and selfmanagement about known SUDEP risk factors which are modifiable.
“To date, much of the action around SUDEP in Ireland has come from Epilepsy Ireland, supported by the fundraising efforts of bereaved families.
“The epilepsy community should not have to depend on the fundraising efforts of bereaved families to target this serious issue. This study tells us that a national, government-led strategy with input from clinicians and patients is urgently required and it is vital that these calls will be taken seriously by Government, the HSE and Department of Health.”
Continuing Research
While this study has established the incidence SUDEP in Ireland for the first time, ongoing research will focus on identifying the total number of epilepsy-related deaths, including causes such as status epilepticus (prolonged seizures) and seizure-related injuries. It is currently estimated that over 130 epilepsy-related deaths occur annually in Ireland (including those from SUDEP). This data is expected to be published in the coming months and according to Epilepsy Ireland, will further highlight the urgent need to develop a new strategy to reduce SUDEP and epilepsyrelated deaths.
The study’s findings have been released to coincide with SUDEP Action Day 2024 – a day in which awareness is raised of SUDEP and epilepsy risks internationally, as well as remembering those who have passed away.
Epilepsy Ireland is appealing to people with epilepsy and their families to visit www.epilepsy.ie to learn more about the risks of SUDEP and measures which can potentially be taken to reduce them
LIBTAYO® (CEMIPLIMAB) APPROVED FOR REIMBURSEMENT IN IRELAND FOR THE TREATMENT OF ADVANCED CUTANEOUS SQUAMOUS CELL CARCINOMA
Regeneron Ireland DAC has announced that Libtayo® (cemiplimab) has been reimbursed by the Ireland Health Service Executive (HSE) for use as monotherapy treatment for adults with metastatic or locally advanced cutaneous squamous cell carcinoma (mCSCC or laCSCC) who are not candidates for curative surgery or curative radiation. Cemiplimab is a fully human monoclonal antibody targeting the immune checkpoint receptor PD-1 (programmed cell death protein-1) and is the first and only systemic treatment available on the HSE in Ireland to treat advanced CSCC.
When CSCC invades deeper layers of the skin or adjacent tissues, it is categorised as locally advanced. Once it spreads to other distant parts of the body, it is considered metastatic. Advanced disease is associated with a poor prognosis and can have a significant impact on quality of life. Currently, people with CSCC too advanced for surgery or radiation have a median survival of approximately one year. In Ireland, approximately 120 people each year will be impacted by advanced CSCC.
“CSCC is the second most common skin cancer, but compared to melanoma, treatment advances have been scarce,” said James Winterman, Regeneron UK and Ireland Country Manager, Oncology. “This acceptance of cemiplimab by the HSE marks the first targeted treatment for advanced CSCC in Ireland and a significant advance for people who until now have only had chemotherapy as an option. We are pleased to be able to bring this treatment to patients in Ireland.”
About Cemiplimab
Cemiplimab is a fully human monoclonal antibody targeting the immune checkpoint receptor PD-1 on T cells and was invented using Regeneron's proprietary VelocImmune® technology.10 By binding to PD-1, cemiplimab has been shown to block cancer cells from using the PD-1 pathway to suppress T-cell activation.10
Reimbursement approval is based on data from the pivotal, open-label, multi-centre, nonrandomised Phase 2 trial known as EMPOWER-CSCC 1 (Study 1540). Patients within the study (n=193) were assigned to three cohort groups (Groups 1, 2 and 3). The primary endpoint was confirmed objective response rate (ORR) by
independent review committee. With a median duration of followup of 18.5 months (Group 1, n=59), 15.5 months (Group 2, n=78) and 17 months (Group 3, n=56), the ORR was respectively 51% for metastatic CSCC patients (Group 1), 45% for locally advanced CSCC patients (Group 2) treated with weight-based dosing, and 46% for metastatic CSCC patients (Group 3) treated with the licensed dose of 350 mg every three weeks.
The safety of cemiplimab has been evaluated in 1,281 patients with advanced solid malignancies who received cemiplimab monotherapy in five clinical studies. Immune-mediated adverse reactions occurred in 21% of patients treated with cemiplimab and led to permanent discontinuation in 5% of patients. The most common immunemediated adverse reactions were hypothyroidism (7%), hyperthyroidism (3%), pneumonitis (3%), hepatitis (2%), colitis (2%) and skin adverse reactions (2%). Adverse reactions were serious in 32% of patients and led to permanent discontinuation in 9% of patients. Grade 3 or higher adverse reactions occurring in >1% of patients were anaemia (5%), hypertension (3%), fatigue (3%), urinary tract infection (2%), hepatitis (2%), musculoskeletal pain (2%), rash (2%), dyspnoea (1%) and pneumonitis (1%).
HEALTH CAMPAIGNERS URGE PUBLIC NOT TO DELAY STARTING CPR
The public has been urged not to be afraid of starting cardio pulmonary resuscitation (CPR) in cases of a cardiac arrest –after figures showed 240 people survived because someone started CPR or used a defibrillator.
The Irish Heart Foundation has said almost 70% of cardiac arrests happen at home, making it more
likely that CPR will have to be performed on a family member instead of a stranger. It highlighted the importance of CPR training to coincide with World Restart a Heart Day on Wednesday. (Oct16)
“By starting CPR and using an AED (defibrillator), you can double a person’s chance of survival,” said Brigid Sinnott, the charity’s Resuscitation Manager.
“For every minute without CPR or defibrillation, the chance of survival decreases by 10% per minute.
“What we want people to understand is that you can do no harm - it’s better to do CPR on someone who doesn’t need it than not to do CPR on someone who does.
“Ireland has a high bystander CPR rate (where someone who witnesses cardiac arrest steps in to provide CPR) at 85% but it is important to remember that it is more likely to be a family member’s life you could save.”
Bystander CPR in cases of outof-hospital cardiac arrest in this country increased from 60% to 85% between 2012 and 2023, according to the Out of Hospital Cardiac Arrest Register report 2023 from the HSE National Ambulance Service, published last week.
The Irish Heart Foundation aims to create a nation of lifesavers through its CPR courses, provided to the public through Affiliated Training Sites all around the country, and its free CPR 4 Schools programme.
The programme for post-primary schools trains students to perform the skill, respond in a cardiac emergency and use an AED.
A person who learns CPR even once in their life is ten times more likely to respond in an emergency than someone who has not.
“Our CPR 4 Schools programme has a reach of over 350,000 students in Ireland, thanks to the generosity of our supporters and the public - without their continued support, it just wouldn’t be possible,” said Ms Sinnott.
“The school programme means students will have learned CPR skills a number of times before they leave school, which will help to build a nation of lifesavers.
“Not everyone will survive a cardiac arrest but by performing CPR, you are giving people the best chance.
“I always equate it to riding a bike - you might be a bit rusty but with a small bit of practice, it’s easy to get back into it.”
To learn more about World Restart a Heart Day and to learn the crucial steps of CPR, visit: irishheart.ie
ILLUMINATING HEART HEALTH ON WORLD HEART DAY
Croí, the heart and stroke charity, was delighted to collaborate with some of the most iconic and historic buildings, organisations and landmarks throughout the west region to celebrate World Heart Day.
The illuminations are organised in support of the World Heart Federation’s (WHF) campaign urging all countries to have a ‘National Cardiovascular Action Plan’ to tackle heart disease, the world’s number one killer. Marking this year’s World Heart Day with the launch of a global online petition, the WHF hopes the call to action will inspire a more robust and coordinated response to cardiovascular disease (CVD), which is responsible for more than 20.5 million deaths every year.
The staggering number of deaths from heart disease combined with scarce plans to tackle the disease, highlights the urgent need for countries to develop tailored strategies to address cardiovascular disease.
For over two decades, WHF has been leading the World Heart Day movement, which is celebrated every year on 29 September –raising awareness about CVD, calling for better healthcare policies and more funding for heart health research. To sign the global petition visit www.worldheartfederation.org
To mark their commitment in promoting the importance of Heart Heath, the following buildings and landmarks were illuminated red on World Heart Day:
ATU Mayo.
ATU Connemara.
ATU Donegal.
Ashford Castle.
The Mall Bridge, Westport.
Castlebar Garda Station.
Roscommon Town Garda Station.
Sligo Town Garda Station.
Garda North Western Regional Headquarters, Renmore, Galway.
Galway Hookers, Claddagh Basin.
PRECISIONBIOTICS LAUNCHES ‘WOMEN’S FLORA’ AND ‘GOOD BACTERIA’
The Portershed Galway.
Bon Secours Hospital Galway.
Kylemore Abbey.
The illumination campaign draws a close on the many events organised by Croí throughout September in recognition of World Heart Month. Details of events can be found on www.croi.ie
Croí not only encourages people to ensure their heart health is a priority, but also those around them, friends, family, and colleagues. Croí’s aim is to educate and empower individuals, families, and communities to take control of their heart health and to make and maintain the changes that can lead to a longer and healthier life.
Croí would like to extend thanks to the public, the many healthcare professionals, organisations, and volunteers who worked to ensure World Heart Month was an outstanding success.
PrecisionBiotics has launched two new products in the Irish market. The products are ‘Women’s Flora,’ which supports a healthy vaginal microbiome and ‘Good Bacteria,’ a daily bacterial supplement. Both are now available in pharmacies around the country.
The latest products mark an expansion of the range of supplements the company sells in the Irish market. Current products include Alflorex and Zenflore.
PrecisionBiotics has its origins in UCC, Co Cork where more than 20 years ago scientists began researching thousands of bacterial cultures, together with experts from one of the world’s leading centres of microbiome research, the APC Microbiome Institute in UCC. Since then, they’ve discovered hundreds of different bacterial cultures and they’ve put each one through rigorous scientific tests. Amongst these hundreds are a handful of special bacteria that stand out because of the precise and significant impact they make to human gut health.
In 2020 Novozymes acquired the PrecisionBiotics Group, with an office located at the Cork Airport Business Park, and R&D labs based at the food hub in Teagasc, Fermoy. In January of this year, Novoymes merged with Chr. Hansen, a company established in 1984 to supply cultures and enzymes to the Irish dairy industry, to form Novonesis Ireland. With an emphasis on efficiency and sustainability, Novonesis creates scientifically researched and clinically tested biosolutions which include prebiotics, probiotics, enzymes, novel vitamins and proteins.
'Women’s Flora' is designed for women who are actively seeking to maintain a healthy vaginal balance. The product has been formulated with scientifically tested
Clinical R&D
bacterial strains prevalent in a healthy vaginal microbiome. Most women will experience vaginal bacterial or yeast imbalance in their lifetime, and over half will recur within 12 months. Common vaginal conditions and issues are often caused by an unbalanced microbiome. Symptoms include itching, discharge and odour, which can have a negative effect on both physical and mental health.
'Good Bacteria' was developed for those seeking a daily bacteria supplement, particularly during and after a course of antibiotics. Research has shown that over one in three people experience negative side effects while taking antibiotics, due to a disruption to the natural gut flora. These side effects commonly include diarrhoea.
The product aims to address the fact that diet and antibiotics can impact the delicate balance of gut microbiome. 'Good Bacteria'
combines scientifically tested bacterial strains and fibres.
Commenting on the new products, Marketing Manager Ireland with PrecisionBiotics Shirley O’Regan said: “We have pioneered the field of gut health research for decades now, creating unique solutions for the gut microbiome and gut / brain health, through products like Alflorex and Zenflore. We are extremely proud to now launch a product that promotes a healthy vaginal microbiome, which has its own universe of bacteria. It’s a largely unexplored area of women’s health and through rigorous trials and world class scientific research, we have created 'Women’s Flora,' which is a groundbreaking product. Similarly, 'Good Bacteria' addresses the very common but often ignored side effects of taking antibiotics. Our scientists have formulated a unique combination of bacterial strains to help balance tummy issues when people are on a course of antibiotics.”
'Women’s Flora' and 'Good Bacteria 'are available through pharmacies nationwide. For more information visit www.precisionbiotics.ie
HONOURS FOR DIABETES PATIENTS
On Wednesday, 02 October at a special awards ceremony in Croí, Diabetes Ireland honoured twelve people living with type 1 diabetes with special 50 and 65-year achievement medals in recognition of their courage and endurance in living with diabetes.
The Five women and seven men from across Galway, Mayo, Roscommon and Clare who attend Diabetes Outpatient Clinics in University Hospital Galway and Roscommon University Hospital, received either a 50-year or 65year achievement medal. (Two recipients of a 65-year medal and ten recipients of a 50-year medal).
Currently, there are approximately 308,000 people living with diabetes in Ireland. Professor Tim O Brien, Clinical Director of Saolta’s Medicine MCAN said, “I am delighted to be able to attend and share this time with these very special people. I have been working in diabetes care for 40 years and have witnessed the significant advances in care over that time but acknowledge the challenges that these patients have dealt with. It is a privilege for us in healthcare professions to be able to help in whatever way we can but the celebration tonight is an acknowledgment of the achievements of these incredible individuals who serve as role models to all of us.”
Speaking about this momentous occasion, Tomás Griffin, Consultant Physician/Diabetologist between University Hospital Galway, Roscommon University Hospital and Community Healthcare West said, “We are deeply honoured to celebrate this extraordinary group of individuals who have lived with diabetes for 50 years or more.
“Their resilience and determination inspires us all, showing that it is
not only possible but empowering to lead active, healthy, and fulfilling lives with diabetes. We also recognize the invaluable support of their families and caregivers – this milestone is a shared achievement, shaped by the dedication of many.
“It is a true privilege to stand alongside these individuals and their loved ones as we celebrate this remarkable journey. Over the past 50 years, people living with diabetes have witnessed incredible technological advancements, from the early days of urine testing and rigid insulin regimens to the introduction of continuous glucose monitors, insulin pumps, and now hybrid closed-loop systems. The progress has been nothing short of transformative.”
Kieran O’Leary, CEO, Diabetes Ireland said, ‘Our Living Well With Diabetes’ ceremony celebrates life with diabetes and it’s an honour and a privilege to present medals to people with diabetes who have lived over 50 years managing their condition and adapting to the many changes in treatment over the years.
“This group of recipients are among a special group of 289 people who have received a medal.”
Diabetes Ireland honouring twelve people living with type 1 diabetes with special 50 and 65-year achievement medals in recognition of their courage and endurance in living with diabetes
MATER PRIVATE NETWORK WINS AWARD FOR BEST PRIVATE HOSPITAL IN IRELAND
Mater Private Network is proud to announce its success at the recent Private Healthcare Awards, where it received two accolades: the Overall Excellence Award and the Best Private Hospital Award. These awards recognise Mater Private Network’s commitment to providing world-class healthcare, and underscores its dedication to innovation, clinical excellence, and patient-centred care.
The awards also reflect a range of significant achievements across the network, including the retention of Joint Commission International (JCI) Gold Standard Accreditation, a 91% customer satisfaction rating from the Voice of the Patient survey, and exemplary outcomes in patient safety metrics. Mater Private Network is also the only hospital network in Ireland to participate in the internationally recognised HCAHPS survey, benchmarking itself against leading global healthcare providers, and achieving a strong ranking in the 81st percentile.
John Hurley, CEO of Mater Private Network, commenting on last night’s awards, said: "This recognition is a testament to the collective effort and commitment of our staff across all care centres in the Mater Private Network. From delivering seamless, patient-focused care, to driving forward our digital transformation programme, every member of our team plays a crucial role in making these standards of excellence
possible. We remain dedicated to providing the best possible healthcare to our patients, and this recognition further motivates us to continue raising the standard of care for people that come through our doors."
Mater Private Network places a key focus on innovation, particularly through its Digital Transformation Programme. This implementation has been instrumental in enhancing patient care by improving access to services, streamlining the patient experience, and ensuring continuity of care across the network. In addition, Mater Private Network has demonstrated a strong commitment to clinical governance and compliance in 2024. This includes regular internal and external audits, continuous professional development programmes, and a robust framework ensuring adherence to regulatory standards. This focus has helped to foster a culture of safety, transparency, and accountability, contributing to the high standards of care that are recognised by these awards.
HEALTH INNOVATION HUB IRELAND, HSE, IRISH COLLEGE OF GPS LAUNCH NATIONAL GREENTECH HEALTHCARE CALL
In a national first, Health Innovation Hub Ireland (HIHI), with the HSE and Irish College of GPs is launching the GreenTech in healthcare call. The three leading healthcare organisations are searching for innovative products and services that promote environmental sustainability in both
Mater Private Network team at the 2024 Private Healthcare Awards. In attendance - Hugh Healy, Director of Cancer, Fionnuala Kennedy, Pharmacy Executive Manager, Carl Galliers, Director of Nursing, Carmel McBride, Quality & Safety Manager, Kathryn McBride, Human Resources Manager, Audrey Doyle, Group Director of Quality and Patient Experience, Angela Moynihan, Quality Dept, Kieran McNamara, Quality and Risk Manager, Sandra Daly, Chief Executive Officer, Edel Murphy Assistant Director of Nursing, Nikki Kane, Chief Operations Officer, Garry McCabe, Group Chief People Officer, Lana Kane - Managing Director of Medforce
primary and secondary healthcare. The Irish healthcare sector is responsible for an estimated 5 per cent of the country's Global Greenhouse Gas (GHG) emissions. Additionally, the sector uses a high volume of single use products, adding to resource use and waste. The national GreenTech in healthcare call is focussed on three key areas:
1. Production: Single-use medical products often involve resourceintensive processes, using plastics and other materials that require significant energy inputs. This results in substantial greenhouse gas emissions.
2. Disposal: Many healthcare items are designed for single use and create a constant stream of waste. The disposal process, whether it involves incineration (which can release harmful emissions and substances) or landfilling (which leads to issues like leachate, soil contamination, and methane emissions), adds to the environmental and health burden.
3. Decontamination: The combination of processes including cleaning, disinfection and sterilisation used to render reusable invasive medical devices safe for handling by staff and for service users. Effective decontamination of reusable invasive medical devices is an essential component in the prevention of healthcare associated infections.
The focus areas are informed by HIHI Clinical Sustainability Advisors (CSA) from across Ireland who work on the frontline and are committed to sustainability in Irish healthcare. These clinical experts have also highlighted a particular need to develop and test alternatives in the following areas: Syringes/sharps, bottles, packaging, cutlery and crockery, nappies and sanitary products, medical textiles (including surgical gowns, theatre drapes, aprons, masks, hats accessories).
CSAs include: Dr Lisa McNamee, Irish College of GPs, Dr Cathy Burke, Cork University Maternity Hospital (CUMH), Dr Ana Rakovac Tallaght University Hospital (TUH) and Michael Duane, University Hospital Galway (UHG).
Through the call, HIHI, HSE and the ICGP will stimulate and support the development and testing of innovative products and services that promote environmental sustainability in the three focus areas. Health Innovation Hub Ireland, will test and evaluate the winning submissions. HIHI is a joint government initiative of the Department of Health and the
Department of Enterprise Trade and Employment, which is delivered through a national HSE and Enterprise Ireland partnership.
HIHI National Director Dr Tanya Mulcahy said: “GreenTech in healthcare represents a growing movement within the global health industry to adopt technologies and practices that are environmentally sustainable, aiming to improve health outcomes while minimising ecological footprints.
“HIHI is committed to the development of innovative sustainable products and services for Irish healthcare. Through engaging national partners, the HSE and ICG we are taking a significant step to begin delivery of this. Crucial to getting the right focus for this call in Irish healthcare is the expertise and guidance our Clinical Sustainability Advisors (CSAs) on the frontline.”
Dr Philip Crowley National Director HSE Climate and Global Health said, “As Ireland’s largest Public Body with a core objective to improve, promote and protect the health and welfare of the public, we recognise we have a significant role to play in tackling the climate crisis. The healthcare sector is a notable contributor to global greenhouse gas (GHG) emissions. We are committed to dealing with the growing health impacts of climate change and curbing our own emissions.
“The HSE Climate Strategy, launched in June 2023, represented a step-change in intent on climate change and sustainability and this national Greentech call builds on this and actively engages committed clinical personnel to inform our focus.”
Dr Diarmuid Quinlan, Medical Director of the Irish College of GPs said, “The Irish College of GPs supports this call for gathering proposals for innovative ways to improve processes in GP healthcare that will contribute positively to sustainability in healthcare. Irish GPs, GP Nurses and Practice teams, deliver “first point of care” healthcare to the national population, and are wellplaced to generate ideas for new ways of working in primary care that can help HSE and HIHI deliver the HSE Climate strategy.”
The call is open to all companies, organisations, researchers, institutions regardless of size or origin.Applications will be reviewed in two stages. Stage one comprises review of all applications. Aoolcianst that progress to stage two will be invited to pitch before a panel of experts. For full submission details, timelines and how to apply please visit: hihi.ie.
Generic Product Launch
Ferric Carboxymaltose Teva
50 mg iron/mL
Dispersion for Injection/Infusion iron as ferric carboxymaltose
Indications
Ferric Carboxymaltose Teva is indicated for the treatment of iron deficiency when: oral iron preparations are ineffective. oral iron preparations cannot be used. there is a clinical need to deliver iron rapidly.
The diagnosis of iron deficiency must be based on laboratory tests.
Presentation: One ml of dispersion contains 50mg of iron (as ferric carboxymaltose). Indications: Ferric Carboxymaltose Teva is indicated for the treatment of iron deficiency when: oral iron preparations are ineffective; oral iron preparations cannot be used; there is a clinical need to deliver iron rapidly. The diagnosis of iron deficiency must be based on laboratory tests. Dosage and administration: For intravenous administration only by injection, infusion or during a haemodialysis session. Ferric Carboxymaltose Teva should only be administered when staff trained to evaluate and manage anaphylactic reactions is immediately available, in an environment where full resuscitation facilities can be assured. The patient should be observed for adverse effects for at least 30 minutes following each Ferric Carboxymaltose Teva administration. Adults and Adolescents (aged 14 years and older): A single Ferric Carboxymaltose Teva administration should not exceed: 15mg iron/kg body weight (for administration by intravenous injection) or 20mg iron/kg body weight (for administration by intravenous infusion); 1000mg of iron (20ml Ferric Carboxymaltose Teva). Children and Adolescents (aged 1 to 13 years): A single Ferric Carboxymaltose Teva administration should not exceed: 15mg iron/kg body weight; 750mg of iron (15 mL Ferric Carboxymaltose Teva). Children below 1 year of age: Not recommended for use. Hepatic and Renal impairment: In patients with liver dysfunction, parenteral iron should only be administered after careful benefit/risk assessment. Parenteral iron administration should be avoided in patients with hepatic dysfunction where iron overload is a precipitating factor, in particular Porphyria Cutanea Tarda (PCT). Careful monitoring of iron status is recommended to avoid iron overload. No safety data on haemodialysis-dependent chronic kidney disease patients receiving single doses of more than 200mg iron are available. Contraindications: Hypersensitivity to the active substance, to Ferric Carboxymaltose Teva or to any of the excipients. Known serious hypersensitivity to other parenteral iron products. Anaemia not attributed to iron deficiency, e.g. other microcytic anaemia. Evidence of iron overload or disturbances in the utilisation of iron. Precautions and warnings: Parenterally administered iron preparations can cause hypersensitivity reactions including serious and potentially fatal anaphylactic reactions. Hypersensitivity reactions have also been reported after previously uneventful doses of parenteral iron complexes. There have been reports of hypersensitivity reactions which progressed to Kounis syndrome (acute allergic coronary arteriospasm that can result in myocardial infarction). The risk is enhanced for patients with known allergies including drug allergies, including patients with a history of severe asthma, eczema or other atopic allergy. There is also an increased risk of hypersensitivity reactions to parenteral iron complexes in patients with immune or inflammatory conditions (e.g. systemic lupus erythematosus, rheumatoid arthritis). If hypersensitivity reactions or signs of intolerance occur during
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Freephone: 1800 - 201 700 | Email: info@teva.ie
Prescription Only Medicine.
administration, the treatment must be stopped immediately. Facilities for cardiorespiratory resuscitation and equipment for handling acute anaphylactic reactions should be available, including an injectable 1:1000 adrenaline solution. Additional treatment with antihistamines and/or corticosteroids should be given as appropriate. Symptomatic hypophosphataemia leading to osteomalacia and fractures requiring clinical intervention including surgery has been reported in the post marketing setting. Patients should be asked to seek medical advice if they experience worsening fatigue with myalgias or bone pain. Serum phosphate should be monitored in patients who receive multiple administrations at higher doses or long-term treatment, and those with existing risk factors for hypophosphataemia. In case of persisting hypophosphataemia, treatment with ferric carboxymaltose should be re-evaluated. Parenteral iron must be used with caution in case of acute or chronic infection, asthma, eczema or atopic allergies. It is recommended that the treatment with Ferric Carboxymaltose Teva is stopped in patients with ongoing bacteraemia. Therefore, in patients with chronic infection a benefit/risk evaluation has to be performed, taking into account the suppression of erythropoiesis. Caution should be exercised to avoid paravenous leakage when administering Ferric Carboxymaltose Teva Paravenous leakage of Ferric Carboxymaltose Teva at the administration site may lead to irritation of the skin and potentially long lasting brown discolouration at the site of administration. In case of paravenous leakage, the administration of Ferric Carboxymaltose Teva must be stopped immediately. Interactions: The absorption of oral iron is reduced when administered concomitantly with parenteral iron preparations. Therefore, if required, oral iron therapy should not be started for at least 5 days after the last administration of Ferric Carboxymaltose Teva. Pregnancy and lactation: A careful benefit/risk evaluation is required before use during pregnancy and Ferric Carboxymaltose Teva should not be used during pregnancy unless clearly necessary. Based on limited data on breast-feeding patients it is unlikely that ferric carboxymaltose represents a risk to the breast-fed child. Effects on ability to drive and use machines: Ferric Carboxymaltose Teva is unlikely to impair the ability to drive and use machines. Adverse reactions: Hypersensitivity, anaphylactic reactions, loss of consciousness, phlebitis, syncope, angioedema, hypophosphataemic osteomalacia. Common: Hypophosphataemia, headache, dizziness, flushing, hypertensions, nausea, injection/infusion site reactions. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: Administration of in quantities exceeding the amount needed to correct iron deficit at the time of administration may lead to accumulation of iron in storage sites eventually leading to haemosiderosis. Monitoring of iron parameters such as serum ferritin and transferrin saturation (TSAT) may assist in recognising iron accumulation. If iron accumulation has occurred, treat according to standard medical practice, e.g. consider the use of an iron chelator. Legal category: POM. Marketing Authorisation Number: PA1986/124/001. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00082. Date of Preparation: July 2024
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie.
Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Date of Preparation: July 2024 | Job Code: GEN-IE-00092
Further information is available on request or in the SmPC. Product Information also available on the HPRA website.